User login
Probiotic LGG doesn’t lessen eczema, asthma, or rhinitis risk by age 7
Giving the probiotic supplement Lactobacillus rhamnosus GG (LGG) to high-risk infants in the first 6 months of life is not effective in lessening incidence of eczema, asthma, or rhinitis in later childhood, researchers have found.
The researchers, led by Michael D. Cabana, MD, MPH, with the Children’s Hospital of Montefiore, New York, said they cannot support its use in this population of children at high risk for allergic disease. Findings were published in Pediatrics.
Jonathan Spergel, MD, PhD, chief of the allergy program at Children’s Hospital of Philadelphia, who was not part of the study, said the “small, but very interesting study adds to the literature indicating that allergy prevention needs to be a multifactorial approach and simply adding LGG in a select population makes no difference.”
He noted that the study of probiotics for allergic conditions is complex as it depends on many factors, such as the child’s environment, including exposure to pets and pollution, and whether the child was delivered vaginally or by cesarean section.
Study builds on previous work
The new study builds on the same researchers’ randomized, double-masked, parallel-arm, controlled Trial of Infant Probiotic Supplementation (TIPS). That study investigated whether daily administration of LGG in the first 6 months to children at high risk for allergic disease because of asthma in a parent, could decrease their cumulative incidence of eczema. Investigators found LGG had no effect.
These additional results included participants at least 7 years old and also included physician-diagnosed asthma and physician-diagnosed rhinitis as secondary outcomes.
Retention rate over the 7-year follow-up was 56%; 49 (53%) of 92 in the intervention group and 54 (59%) of 92 in the control group.
The researchers performed modified intention-to-treat analyses with all children who received treatment in the study arm to which they had been randomized.
Eczema was diagnosed in 78 participants, asthma in 32, and rhinitis in 15. Incidence of eczema was high in infancy, but low thereafter. Incidence rates for asthma and rhinitis were constant throughout childhood.
The researchers used modeling to compare the incidence of each outcome between the intervention and control groups, adjusting for mode of delivery and how long a child was breastfed.
Cesarean delivery was linked to a greater incidence of rhinitis, with a hazard ratio of 3.33 (95% confidence interval, 1.21-9.21).
Finding the right strain
Heather Cassell, MD, a pediatric allergist and immunologist at University of Arizona, Tucson, who was not part of the study, said in an interview that many researchers, including those at her institution, are trying to find which strain of probiotic might be beneficial in lowering risk for allergic disease.
Though it appears LGG doesn’t have an effect, she said, another strain might be successful and this helps zero in on the right one.
The TIPS trial showed that there were no significant side effects from giving LGG early, which is good information to have as the search resumes for the right strain, she said.
“We know that there’s probably some immune dysregulation in kids with asthma, eczema, other allergies, but we don’t fully know the extent of it,” she said, adding that it may be that skin flora or respiratory flora and microbiomes in other parts of the body play a role.
“We don’t have bacteria just in our guts,” she noted. “It may be a combination of strains or a combination of bacteria.”
The authors, Dr. Spergel, and Dr. Cassell reported no relevant financial relationships.
Giving the probiotic supplement Lactobacillus rhamnosus GG (LGG) to high-risk infants in the first 6 months of life is not effective in lessening incidence of eczema, asthma, or rhinitis in later childhood, researchers have found.
The researchers, led by Michael D. Cabana, MD, MPH, with the Children’s Hospital of Montefiore, New York, said they cannot support its use in this population of children at high risk for allergic disease. Findings were published in Pediatrics.
Jonathan Spergel, MD, PhD, chief of the allergy program at Children’s Hospital of Philadelphia, who was not part of the study, said the “small, but very interesting study adds to the literature indicating that allergy prevention needs to be a multifactorial approach and simply adding LGG in a select population makes no difference.”
He noted that the study of probiotics for allergic conditions is complex as it depends on many factors, such as the child’s environment, including exposure to pets and pollution, and whether the child was delivered vaginally or by cesarean section.
Study builds on previous work
The new study builds on the same researchers’ randomized, double-masked, parallel-arm, controlled Trial of Infant Probiotic Supplementation (TIPS). That study investigated whether daily administration of LGG in the first 6 months to children at high risk for allergic disease because of asthma in a parent, could decrease their cumulative incidence of eczema. Investigators found LGG had no effect.
These additional results included participants at least 7 years old and also included physician-diagnosed asthma and physician-diagnosed rhinitis as secondary outcomes.
Retention rate over the 7-year follow-up was 56%; 49 (53%) of 92 in the intervention group and 54 (59%) of 92 in the control group.
The researchers performed modified intention-to-treat analyses with all children who received treatment in the study arm to which they had been randomized.
Eczema was diagnosed in 78 participants, asthma in 32, and rhinitis in 15. Incidence of eczema was high in infancy, but low thereafter. Incidence rates for asthma and rhinitis were constant throughout childhood.
The researchers used modeling to compare the incidence of each outcome between the intervention and control groups, adjusting for mode of delivery and how long a child was breastfed.
Cesarean delivery was linked to a greater incidence of rhinitis, with a hazard ratio of 3.33 (95% confidence interval, 1.21-9.21).
Finding the right strain
Heather Cassell, MD, a pediatric allergist and immunologist at University of Arizona, Tucson, who was not part of the study, said in an interview that many researchers, including those at her institution, are trying to find which strain of probiotic might be beneficial in lowering risk for allergic disease.
Though it appears LGG doesn’t have an effect, she said, another strain might be successful and this helps zero in on the right one.
The TIPS trial showed that there were no significant side effects from giving LGG early, which is good information to have as the search resumes for the right strain, she said.
“We know that there’s probably some immune dysregulation in kids with asthma, eczema, other allergies, but we don’t fully know the extent of it,” she said, adding that it may be that skin flora or respiratory flora and microbiomes in other parts of the body play a role.
“We don’t have bacteria just in our guts,” she noted. “It may be a combination of strains or a combination of bacteria.”
The authors, Dr. Spergel, and Dr. Cassell reported no relevant financial relationships.
Giving the probiotic supplement Lactobacillus rhamnosus GG (LGG) to high-risk infants in the first 6 months of life is not effective in lessening incidence of eczema, asthma, or rhinitis in later childhood, researchers have found.
The researchers, led by Michael D. Cabana, MD, MPH, with the Children’s Hospital of Montefiore, New York, said they cannot support its use in this population of children at high risk for allergic disease. Findings were published in Pediatrics.
Jonathan Spergel, MD, PhD, chief of the allergy program at Children’s Hospital of Philadelphia, who was not part of the study, said the “small, but very interesting study adds to the literature indicating that allergy prevention needs to be a multifactorial approach and simply adding LGG in a select population makes no difference.”
He noted that the study of probiotics for allergic conditions is complex as it depends on many factors, such as the child’s environment, including exposure to pets and pollution, and whether the child was delivered vaginally or by cesarean section.
Study builds on previous work
The new study builds on the same researchers’ randomized, double-masked, parallel-arm, controlled Trial of Infant Probiotic Supplementation (TIPS). That study investigated whether daily administration of LGG in the first 6 months to children at high risk for allergic disease because of asthma in a parent, could decrease their cumulative incidence of eczema. Investigators found LGG had no effect.
These additional results included participants at least 7 years old and also included physician-diagnosed asthma and physician-diagnosed rhinitis as secondary outcomes.
Retention rate over the 7-year follow-up was 56%; 49 (53%) of 92 in the intervention group and 54 (59%) of 92 in the control group.
The researchers performed modified intention-to-treat analyses with all children who received treatment in the study arm to which they had been randomized.
Eczema was diagnosed in 78 participants, asthma in 32, and rhinitis in 15. Incidence of eczema was high in infancy, but low thereafter. Incidence rates for asthma and rhinitis were constant throughout childhood.
The researchers used modeling to compare the incidence of each outcome between the intervention and control groups, adjusting for mode of delivery and how long a child was breastfed.
Cesarean delivery was linked to a greater incidence of rhinitis, with a hazard ratio of 3.33 (95% confidence interval, 1.21-9.21).
Finding the right strain
Heather Cassell, MD, a pediatric allergist and immunologist at University of Arizona, Tucson, who was not part of the study, said in an interview that many researchers, including those at her institution, are trying to find which strain of probiotic might be beneficial in lowering risk for allergic disease.
Though it appears LGG doesn’t have an effect, she said, another strain might be successful and this helps zero in on the right one.
The TIPS trial showed that there were no significant side effects from giving LGG early, which is good information to have as the search resumes for the right strain, she said.
“We know that there’s probably some immune dysregulation in kids with asthma, eczema, other allergies, but we don’t fully know the extent of it,” she said, adding that it may be that skin flora or respiratory flora and microbiomes in other parts of the body play a role.
“We don’t have bacteria just in our guts,” she noted. “It may be a combination of strains or a combination of bacteria.”
The authors, Dr. Spergel, and Dr. Cassell reported no relevant financial relationships.
FROM PEDIATRICS
Treat or refer? New primary care flow diagrams for allergy patients
Most patients with allergy problems first see PCPs, not allergists, the authors write in Allergy. The new flow diagrams help PCPs treat anaphylaxis, asthma, drug allergy, food allergy, and urticaria.
“The European Academy of Allergy and Clinical Immunology established the Logogram Task Force to create a set of simple flow diagrams to assist allergy nonspecialist, generalist, and primary care teams in the diagnosis of five common allergic diseases encountered in primary care,” lead author Dermot Ryan, MB BCh, BAO, FRGCP, of the University of Edinburgh told this news organization.
“The source documents were mainstream guidelines coupled with ancillary literature,” he added in an email. “A multi-disciplinary taskforce ... distilled these guidelines into accessible, comprehensible, usable, and context-specific flow diagrams.”
The flow diagrams developed in Europe can be used by providers in the United States and elsewhere
“These diagrams are consistent with practices in the U.S.,” Christina E. Ciaccio, MD, an associate professor of pediatrics and the section chief of pediatric allergy and immunology at the University of Chicago Medicine, said in an email. “They will prove helpful to PCPs in the U.S. and elsewhere, particularly to young physicians new to practice.
“Treating allergies is part of the ‘bread-and-butter’ practice of primary care physicians in the U.S.,” Dr. Ciaccio, who was not involved in developing the flow diagrams, explained. “Up to 30% of Americans are atopic, and the vast majority seek treatment advice from their PCP first.”
The flow diagrams can help providers in developing countries, where allergic diseases are common, provide the best patient care possible, she said.
At some point, a PCP may need to think beyond flow diagrams and refer the patient to an allergist
“If the treatment plan for a patient falls outside first- or second-line medications, or if a diagnosis is unclear with preliminary testing, a PCP may reach out to an allergy/immunology specialist to assist in providing care,” Dr. Ciaccio advised. “Allergists may provide treatment options, such as immunotherapy, that the PCP does not offer. PCPs also often reach out to allergy team members for help with patients whose allergies are not ‘run-of-the-mill.’
“The flow diagrams are complex and may not be practical in the middle of a busy clinic,” she cautioned. “However, when a patient comes into a primary care clinic with an atypical presentation of an allergic disease, the diagrams are likely to help a physician feel confident that an allergist is the right physician for consultation.”
Patricia Lynne Lugar, MD, an associate professor of medicine in pulmonary, allergy, and critical care medicine at Duke University in Durham, N.C., noted that providers in the U.S. can use the flow diagrams because the definitions, differential diagnosis, and treatments for the conditions they cover are similar.
“The flow diagrams are comprehensive, and they attempt to condense a great deal of information into summary points. They are very useful in the U.S., and not just for generalists,” Dr. Lugar, who also was not involved in the project, said. “Even emergency rooms would benefit from these flow diagrams, especially regarding the recognition of symptoms and differential diagnosis.”
Asthma and seasonal and environmental allergies are often managed by PCPs, and the flow diagrams would help them decide when to refer their patients to an allergist, she added in an email.
Dr. Lugar advises PCPs to “recognize the symptoms of an allergic condition, offer treatment based on confidence the diagnosis is correct, and offer a referral for testing to confirm the allergy.
“Because 50% or more of asthmatics are allergic, all asthmatics should be offered an allergy evaluation to determine their allergies and avoid exacerbating the asthma,” she added. “I do not see the flow diagrams as comprehensive enough to manage chronic urticaria, asthma, venom allergy, and drug allergy.”
With food allergy, environmental allergy, venom allergy, or anaphylaxis, “allergists are experts at considering the differential diagnosis and providing the next steps in the diagnostic workup,” Dr. Lugar said. “Allergists can also provide special treatments, such as allergen-specific immunotherapy or desensitization.”
The flow diagrams guide nonspecialists in diagnosis and treatment of their patients with allergy, with supplementary information as needed. The diagrams recommend referral to a specialist when appropriate, as in cases of anaphylaxis, or chronic urticaria.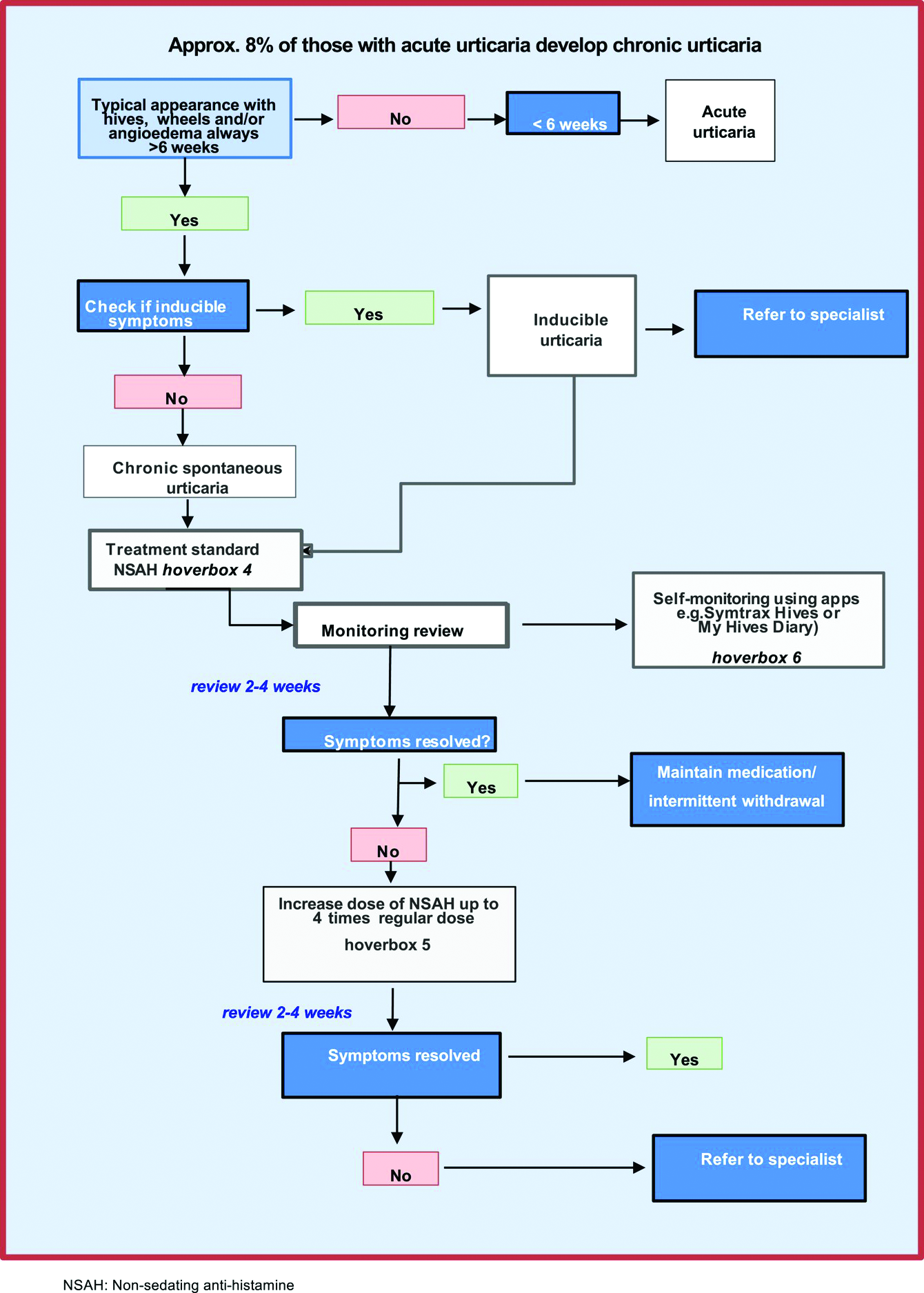
The task force was funded by EAACI. Dr. Ryan and several other authors report financial relationships with pharmaceutical companies. Dr. Ciaccio and Dr. Lugar report no such relationships.
A version of this article first appeared on Medscape.com.
Most patients with allergy problems first see PCPs, not allergists, the authors write in Allergy. The new flow diagrams help PCPs treat anaphylaxis, asthma, drug allergy, food allergy, and urticaria.
“The European Academy of Allergy and Clinical Immunology established the Logogram Task Force to create a set of simple flow diagrams to assist allergy nonspecialist, generalist, and primary care teams in the diagnosis of five common allergic diseases encountered in primary care,” lead author Dermot Ryan, MB BCh, BAO, FRGCP, of the University of Edinburgh told this news organization.
“The source documents were mainstream guidelines coupled with ancillary literature,” he added in an email. “A multi-disciplinary taskforce ... distilled these guidelines into accessible, comprehensible, usable, and context-specific flow diagrams.”
The flow diagrams developed in Europe can be used by providers in the United States and elsewhere
“These diagrams are consistent with practices in the U.S.,” Christina E. Ciaccio, MD, an associate professor of pediatrics and the section chief of pediatric allergy and immunology at the University of Chicago Medicine, said in an email. “They will prove helpful to PCPs in the U.S. and elsewhere, particularly to young physicians new to practice.
“Treating allergies is part of the ‘bread-and-butter’ practice of primary care physicians in the U.S.,” Dr. Ciaccio, who was not involved in developing the flow diagrams, explained. “Up to 30% of Americans are atopic, and the vast majority seek treatment advice from their PCP first.”
The flow diagrams can help providers in developing countries, where allergic diseases are common, provide the best patient care possible, she said.
At some point, a PCP may need to think beyond flow diagrams and refer the patient to an allergist
“If the treatment plan for a patient falls outside first- or second-line medications, or if a diagnosis is unclear with preliminary testing, a PCP may reach out to an allergy/immunology specialist to assist in providing care,” Dr. Ciaccio advised. “Allergists may provide treatment options, such as immunotherapy, that the PCP does not offer. PCPs also often reach out to allergy team members for help with patients whose allergies are not ‘run-of-the-mill.’
“The flow diagrams are complex and may not be practical in the middle of a busy clinic,” she cautioned. “However, when a patient comes into a primary care clinic with an atypical presentation of an allergic disease, the diagrams are likely to help a physician feel confident that an allergist is the right physician for consultation.”
Patricia Lynne Lugar, MD, an associate professor of medicine in pulmonary, allergy, and critical care medicine at Duke University in Durham, N.C., noted that providers in the U.S. can use the flow diagrams because the definitions, differential diagnosis, and treatments for the conditions they cover are similar.
“The flow diagrams are comprehensive, and they attempt to condense a great deal of information into summary points. They are very useful in the U.S., and not just for generalists,” Dr. Lugar, who also was not involved in the project, said. “Even emergency rooms would benefit from these flow diagrams, especially regarding the recognition of symptoms and differential diagnosis.”
Asthma and seasonal and environmental allergies are often managed by PCPs, and the flow diagrams would help them decide when to refer their patients to an allergist, she added in an email.
Dr. Lugar advises PCPs to “recognize the symptoms of an allergic condition, offer treatment based on confidence the diagnosis is correct, and offer a referral for testing to confirm the allergy.
“Because 50% or more of asthmatics are allergic, all asthmatics should be offered an allergy evaluation to determine their allergies and avoid exacerbating the asthma,” she added. “I do not see the flow diagrams as comprehensive enough to manage chronic urticaria, asthma, venom allergy, and drug allergy.”
With food allergy, environmental allergy, venom allergy, or anaphylaxis, “allergists are experts at considering the differential diagnosis and providing the next steps in the diagnostic workup,” Dr. Lugar said. “Allergists can also provide special treatments, such as allergen-specific immunotherapy or desensitization.”
The flow diagrams guide nonspecialists in diagnosis and treatment of their patients with allergy, with supplementary information as needed. The diagrams recommend referral to a specialist when appropriate, as in cases of anaphylaxis, or chronic urticaria.
The task force was funded by EAACI. Dr. Ryan and several other authors report financial relationships with pharmaceutical companies. Dr. Ciaccio and Dr. Lugar report no such relationships.
A version of this article first appeared on Medscape.com.
Most patients with allergy problems first see PCPs, not allergists, the authors write in Allergy. The new flow diagrams help PCPs treat anaphylaxis, asthma, drug allergy, food allergy, and urticaria.
“The European Academy of Allergy and Clinical Immunology established the Logogram Task Force to create a set of simple flow diagrams to assist allergy nonspecialist, generalist, and primary care teams in the diagnosis of five common allergic diseases encountered in primary care,” lead author Dermot Ryan, MB BCh, BAO, FRGCP, of the University of Edinburgh told this news organization.
“The source documents were mainstream guidelines coupled with ancillary literature,” he added in an email. “A multi-disciplinary taskforce ... distilled these guidelines into accessible, comprehensible, usable, and context-specific flow diagrams.”
The flow diagrams developed in Europe can be used by providers in the United States and elsewhere
“These diagrams are consistent with practices in the U.S.,” Christina E. Ciaccio, MD, an associate professor of pediatrics and the section chief of pediatric allergy and immunology at the University of Chicago Medicine, said in an email. “They will prove helpful to PCPs in the U.S. and elsewhere, particularly to young physicians new to practice.
“Treating allergies is part of the ‘bread-and-butter’ practice of primary care physicians in the U.S.,” Dr. Ciaccio, who was not involved in developing the flow diagrams, explained. “Up to 30% of Americans are atopic, and the vast majority seek treatment advice from their PCP first.”
The flow diagrams can help providers in developing countries, where allergic diseases are common, provide the best patient care possible, she said.
At some point, a PCP may need to think beyond flow diagrams and refer the patient to an allergist
“If the treatment plan for a patient falls outside first- or second-line medications, or if a diagnosis is unclear with preliminary testing, a PCP may reach out to an allergy/immunology specialist to assist in providing care,” Dr. Ciaccio advised. “Allergists may provide treatment options, such as immunotherapy, that the PCP does not offer. PCPs also often reach out to allergy team members for help with patients whose allergies are not ‘run-of-the-mill.’
“The flow diagrams are complex and may not be practical in the middle of a busy clinic,” she cautioned. “However, when a patient comes into a primary care clinic with an atypical presentation of an allergic disease, the diagrams are likely to help a physician feel confident that an allergist is the right physician for consultation.”
Patricia Lynne Lugar, MD, an associate professor of medicine in pulmonary, allergy, and critical care medicine at Duke University in Durham, N.C., noted that providers in the U.S. can use the flow diagrams because the definitions, differential diagnosis, and treatments for the conditions they cover are similar.
“The flow diagrams are comprehensive, and they attempt to condense a great deal of information into summary points. They are very useful in the U.S., and not just for generalists,” Dr. Lugar, who also was not involved in the project, said. “Even emergency rooms would benefit from these flow diagrams, especially regarding the recognition of symptoms and differential diagnosis.”
Asthma and seasonal and environmental allergies are often managed by PCPs, and the flow diagrams would help them decide when to refer their patients to an allergist, she added in an email.
Dr. Lugar advises PCPs to “recognize the symptoms of an allergic condition, offer treatment based on confidence the diagnosis is correct, and offer a referral for testing to confirm the allergy.
“Because 50% or more of asthmatics are allergic, all asthmatics should be offered an allergy evaluation to determine their allergies and avoid exacerbating the asthma,” she added. “I do not see the flow diagrams as comprehensive enough to manage chronic urticaria, asthma, venom allergy, and drug allergy.”
With food allergy, environmental allergy, venom allergy, or anaphylaxis, “allergists are experts at considering the differential diagnosis and providing the next steps in the diagnostic workup,” Dr. Lugar said. “Allergists can also provide special treatments, such as allergen-specific immunotherapy or desensitization.”
The flow diagrams guide nonspecialists in diagnosis and treatment of their patients with allergy, with supplementary information as needed. The diagrams recommend referral to a specialist when appropriate, as in cases of anaphylaxis, or chronic urticaria.
The task force was funded by EAACI. Dr. Ryan and several other authors report financial relationships with pharmaceutical companies. Dr. Ciaccio and Dr. Lugar report no such relationships.
A version of this article first appeared on Medscape.com.
FROM ALLERGY
Gaps in follow-up care put kids with asthma at risk of severe recurrence
Jo Ward’s twin boys have been to the emergency department for respiratory problems about as many times as the dozen years they’ve been alive. Both have asthma and bronchopulmonary dysplasia, a form of chronic airway damage that can occur in children born premature, as the twins were. But each time Ms. Ward took them in for treatment during an acute bout of breathing distress, the staff told her to schedule a follow-up visit for the children with their physician only if they didn’t get better, not regardless of the outcome – as medical guidelines recommend.
“They asked questions, they did the exams, but they really didn’t give you a lot of information to help you at home,” Ms. Ward told this news organization. If they had, she doesn’t think she’d have needed to take them in for emergency care so often.
A new study, published in Academic Pediatrics, suggests she’s right.
Current clinical guidelines for asthma recommend that patients who visit the ED for an asthma-related problem should have a follow-up appointment within a month after the visit, independent of how well they have recovered once home, according to Naomi S. Bardach, MD, a professor of pediatrics and health policy at the University of California, San Francisco, who led the new study.
Her research found that children who have a follow-up appointment within 2 weeks of such a visit are less likely to come back again the next year. Yet the study also found that only about one in five youth had a follow-up visit within that 2-week window.
“The emergency department visit is probably a sign that they need some additional attention for their asthma,” Dr. Bardach said. “We know we can prevent emergency department visits if they get the right kind of medication or if they figure out how to avoid the things that are going to cause an asthma exacerbation or flare.”
For the study, Dr. Bardach and colleagues analyzed data from California, Vermont, and Massachusetts for all asthma-related emergency visits for patients aged 3-21 years between 2013 and 2016.
Out of the 90,267 such visits they identified, 22.6% of patients had a follow-up within 2 weeks, more often by patients who were younger, had commercial insurance, had evidence of prior asthma, or had complex chronic conditions.
Whereas 5.7% of patients who had follow-up visits returned to the ED within 60 days, 6.4% of those who didn’t came back – a 12% difference (P < .001). The gap was larger a year out, with 25% of those with follow-ups returning to the ED, compared with 28.3% of those without follow-ups returning (P < .001), according to the researchers.
Overall, Dr. Bardach’s group estimates that for every 30 children who have follow-up visits with a physician, one would avoid a return trip to the emergency department for asthma within a year.
But given the sheer number of asthma-related trips to the ED each year – 164,145 for kids age 1-17 years in the United States in 2016 alone – that translates into big numbers of kids not going back to the hospital: approximately 72,000 such trips avoided at a savings to the health care system of at least $8.6 million annually.
Missed opportunities
Had Ms. Ward’s boys been among the one in five to receive follow-up care earlier in their lives, she might have saved a significant amount of time, money, anxiety, and heartache. When the twins were 9 years old, she took them to a new pediatric pulmonologist. That changed everything. In that first visit, “they gave me way more information than I ever had in the first 9 years,” she said.
The doctor told Ms. Ward to keep steroids on hand, gave her a prescription for extra doses of the powerful medication, and explained that they needed to be used within 24 hours of the first sign of a breathing problem.
“She said if you give them the steroids right away, it keeps them out of the emergency room, and that’s actually worked,” Ms. Ward said. “She made sure we had care plans every visit and asked me each time if I still had it or we needed to rewrite it. They gave me signs to look for, for when to go to hospital visits. I think that when you go to the doctor, they should be telling you stuff like that.”
Dr. Bardach said visits with a primary care doctor or asthma specialist offer families a chance to receive information to keep the condition from becoming critical.
“Going to that follow-up visit, they can get access to education from the provider about how to avoid things that trigger asthma, and there’s medication that kids can take that keeps the lungs calm and less likely to have a big asthma reaction, so getting access to that medication can be really helpful,” she said.
That was the case for Amy Davenport, of Chapel Hill, N.C., whose 6-year-old son has been to the ED twice for his asthma.
The first time, when he was 3, he was having trouble breathing with a respiratory tract infection and received nebulizer treatment – although he received it in the ED since no beds were available in the ICU. The staff did tell Ms. Davenport to follow up with her primary care provider, but her son’s pediatrician was reluctant to diagnose him with asthma at such a young age and didn’t prescribe any maintenance medications.
A few months later, Ms. Davenport and her son found themselves back in the hospital, and an ICU bed was open this time. The critical care staff referred Davenport to a pediatric pulmonary specialist, and they haven’t been back to the hospital since. Ms. Davenport said she believes if they’d received a maintenance medication after the first visit, it likely would have prevented the second one.
“I’ve definitely seen now that, after the second admission, we got an asthma action plan and it said exactly what to do,” she said. “I felt like we had really good follow-up. We had that action plan on our refrigerator for a long time, and it helped us as parents with three small children to manage.”
Of course, follow-up care takes time – time away from work and school that not all families can spare, the researchers acknowledged. Telehealth may be an option, especially after its use expanded during the COVID-19 pandemic.
“We know that health systems have a hard time being flexible enough to actually have a kid be able to make an appointment within a short period of time, and we also know it’s hard for families sometimes to go back into a clinical setting within a certain period of time,” Dr. Bardach said. The urgency for the appointment may wane for those whose children seem to be doing better.
When the researchers adjusted their calculations for socioeconomic status, the results didn’t change much. But the study did find that patients with private insurance were about twice as likely to have follow-up visits as those on Medicaid (43.7% vs. 21.7%). And “the content and conduct” of the follow-up visit makes a difference as well.
Ms. Ward, whose boys are insured through Medicaid, recalled several visits to the ED where she had to push the staff to get the care her children needed. In one case, when one of her boys was a year old and struggling to breathe, the emergency doctor handed her a prescription and recommended she fill it at a neighborhood drugstore that would be cheaper than the hospital’s pharmacy. Then a nurse came in to begin the discharge process.
“I said no, ‘we’re not ready yet. Look at him,’” Ms. Ward said. The nurse took a pulse oximeter reading that showed the boy’s oxygen levels were at 84%, dangerously low. “If I wasn’t so knowledgeable and paid attention when they were born, since they were preemies, if it would have been somebody else, they probably would’ve went home and he’d have died.”
With the pediatric pulmonologist the boys have now, Ms. Ward said she feels more capable of managing their asthma and knowing how to reduce the likelihood that they’ll need to visit the ED.
“Part of what we’re seeing here is that having an existing and trusting relationship with a clinician can be helpful to kids with asthma,” Dr. Bardach said. “If we help establish and maintain those connections, and explain how important that connection can be, that can also help somebody with asthma overall.”
The research was funded by the Agency for Healthcare Research and Quality. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jo Ward’s twin boys have been to the emergency department for respiratory problems about as many times as the dozen years they’ve been alive. Both have asthma and bronchopulmonary dysplasia, a form of chronic airway damage that can occur in children born premature, as the twins were. But each time Ms. Ward took them in for treatment during an acute bout of breathing distress, the staff told her to schedule a follow-up visit for the children with their physician only if they didn’t get better, not regardless of the outcome – as medical guidelines recommend.
“They asked questions, they did the exams, but they really didn’t give you a lot of information to help you at home,” Ms. Ward told this news organization. If they had, she doesn’t think she’d have needed to take them in for emergency care so often.
A new study, published in Academic Pediatrics, suggests she’s right.
Current clinical guidelines for asthma recommend that patients who visit the ED for an asthma-related problem should have a follow-up appointment within a month after the visit, independent of how well they have recovered once home, according to Naomi S. Bardach, MD, a professor of pediatrics and health policy at the University of California, San Francisco, who led the new study.
Her research found that children who have a follow-up appointment within 2 weeks of such a visit are less likely to come back again the next year. Yet the study also found that only about one in five youth had a follow-up visit within that 2-week window.
“The emergency department visit is probably a sign that they need some additional attention for their asthma,” Dr. Bardach said. “We know we can prevent emergency department visits if they get the right kind of medication or if they figure out how to avoid the things that are going to cause an asthma exacerbation or flare.”
For the study, Dr. Bardach and colleagues analyzed data from California, Vermont, and Massachusetts for all asthma-related emergency visits for patients aged 3-21 years between 2013 and 2016.
Out of the 90,267 such visits they identified, 22.6% of patients had a follow-up within 2 weeks, more often by patients who were younger, had commercial insurance, had evidence of prior asthma, or had complex chronic conditions.
Whereas 5.7% of patients who had follow-up visits returned to the ED within 60 days, 6.4% of those who didn’t came back – a 12% difference (P < .001). The gap was larger a year out, with 25% of those with follow-ups returning to the ED, compared with 28.3% of those without follow-ups returning (P < .001), according to the researchers.
Overall, Dr. Bardach’s group estimates that for every 30 children who have follow-up visits with a physician, one would avoid a return trip to the emergency department for asthma within a year.
But given the sheer number of asthma-related trips to the ED each year – 164,145 for kids age 1-17 years in the United States in 2016 alone – that translates into big numbers of kids not going back to the hospital: approximately 72,000 such trips avoided at a savings to the health care system of at least $8.6 million annually.
Missed opportunities
Had Ms. Ward’s boys been among the one in five to receive follow-up care earlier in their lives, she might have saved a significant amount of time, money, anxiety, and heartache. When the twins were 9 years old, she took them to a new pediatric pulmonologist. That changed everything. In that first visit, “they gave me way more information than I ever had in the first 9 years,” she said.
The doctor told Ms. Ward to keep steroids on hand, gave her a prescription for extra doses of the powerful medication, and explained that they needed to be used within 24 hours of the first sign of a breathing problem.
“She said if you give them the steroids right away, it keeps them out of the emergency room, and that’s actually worked,” Ms. Ward said. “She made sure we had care plans every visit and asked me each time if I still had it or we needed to rewrite it. They gave me signs to look for, for when to go to hospital visits. I think that when you go to the doctor, they should be telling you stuff like that.”
Dr. Bardach said visits with a primary care doctor or asthma specialist offer families a chance to receive information to keep the condition from becoming critical.
“Going to that follow-up visit, they can get access to education from the provider about how to avoid things that trigger asthma, and there’s medication that kids can take that keeps the lungs calm and less likely to have a big asthma reaction, so getting access to that medication can be really helpful,” she said.
That was the case for Amy Davenport, of Chapel Hill, N.C., whose 6-year-old son has been to the ED twice for his asthma.
The first time, when he was 3, he was having trouble breathing with a respiratory tract infection and received nebulizer treatment – although he received it in the ED since no beds were available in the ICU. The staff did tell Ms. Davenport to follow up with her primary care provider, but her son’s pediatrician was reluctant to diagnose him with asthma at such a young age and didn’t prescribe any maintenance medications.
A few months later, Ms. Davenport and her son found themselves back in the hospital, and an ICU bed was open this time. The critical care staff referred Davenport to a pediatric pulmonary specialist, and they haven’t been back to the hospital since. Ms. Davenport said she believes if they’d received a maintenance medication after the first visit, it likely would have prevented the second one.
“I’ve definitely seen now that, after the second admission, we got an asthma action plan and it said exactly what to do,” she said. “I felt like we had really good follow-up. We had that action plan on our refrigerator for a long time, and it helped us as parents with three small children to manage.”
Of course, follow-up care takes time – time away from work and school that not all families can spare, the researchers acknowledged. Telehealth may be an option, especially after its use expanded during the COVID-19 pandemic.
“We know that health systems have a hard time being flexible enough to actually have a kid be able to make an appointment within a short period of time, and we also know it’s hard for families sometimes to go back into a clinical setting within a certain period of time,” Dr. Bardach said. The urgency for the appointment may wane for those whose children seem to be doing better.
When the researchers adjusted their calculations for socioeconomic status, the results didn’t change much. But the study did find that patients with private insurance were about twice as likely to have follow-up visits as those on Medicaid (43.7% vs. 21.7%). And “the content and conduct” of the follow-up visit makes a difference as well.
Ms. Ward, whose boys are insured through Medicaid, recalled several visits to the ED where she had to push the staff to get the care her children needed. In one case, when one of her boys was a year old and struggling to breathe, the emergency doctor handed her a prescription and recommended she fill it at a neighborhood drugstore that would be cheaper than the hospital’s pharmacy. Then a nurse came in to begin the discharge process.
“I said no, ‘we’re not ready yet. Look at him,’” Ms. Ward said. The nurse took a pulse oximeter reading that showed the boy’s oxygen levels were at 84%, dangerously low. “If I wasn’t so knowledgeable and paid attention when they were born, since they were preemies, if it would have been somebody else, they probably would’ve went home and he’d have died.”
With the pediatric pulmonologist the boys have now, Ms. Ward said she feels more capable of managing their asthma and knowing how to reduce the likelihood that they’ll need to visit the ED.
“Part of what we’re seeing here is that having an existing and trusting relationship with a clinician can be helpful to kids with asthma,” Dr. Bardach said. “If we help establish and maintain those connections, and explain how important that connection can be, that can also help somebody with asthma overall.”
The research was funded by the Agency for Healthcare Research and Quality. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Jo Ward’s twin boys have been to the emergency department for respiratory problems about as many times as the dozen years they’ve been alive. Both have asthma and bronchopulmonary dysplasia, a form of chronic airway damage that can occur in children born premature, as the twins were. But each time Ms. Ward took them in for treatment during an acute bout of breathing distress, the staff told her to schedule a follow-up visit for the children with their physician only if they didn’t get better, not regardless of the outcome – as medical guidelines recommend.
“They asked questions, they did the exams, but they really didn’t give you a lot of information to help you at home,” Ms. Ward told this news organization. If they had, she doesn’t think she’d have needed to take them in for emergency care so often.
A new study, published in Academic Pediatrics, suggests she’s right.
Current clinical guidelines for asthma recommend that patients who visit the ED for an asthma-related problem should have a follow-up appointment within a month after the visit, independent of how well they have recovered once home, according to Naomi S. Bardach, MD, a professor of pediatrics and health policy at the University of California, San Francisco, who led the new study.
Her research found that children who have a follow-up appointment within 2 weeks of such a visit are less likely to come back again the next year. Yet the study also found that only about one in five youth had a follow-up visit within that 2-week window.
“The emergency department visit is probably a sign that they need some additional attention for their asthma,” Dr. Bardach said. “We know we can prevent emergency department visits if they get the right kind of medication or if they figure out how to avoid the things that are going to cause an asthma exacerbation or flare.”
For the study, Dr. Bardach and colleagues analyzed data from California, Vermont, and Massachusetts for all asthma-related emergency visits for patients aged 3-21 years between 2013 and 2016.
Out of the 90,267 such visits they identified, 22.6% of patients had a follow-up within 2 weeks, more often by patients who were younger, had commercial insurance, had evidence of prior asthma, or had complex chronic conditions.
Whereas 5.7% of patients who had follow-up visits returned to the ED within 60 days, 6.4% of those who didn’t came back – a 12% difference (P < .001). The gap was larger a year out, with 25% of those with follow-ups returning to the ED, compared with 28.3% of those without follow-ups returning (P < .001), according to the researchers.
Overall, Dr. Bardach’s group estimates that for every 30 children who have follow-up visits with a physician, one would avoid a return trip to the emergency department for asthma within a year.
But given the sheer number of asthma-related trips to the ED each year – 164,145 for kids age 1-17 years in the United States in 2016 alone – that translates into big numbers of kids not going back to the hospital: approximately 72,000 such trips avoided at a savings to the health care system of at least $8.6 million annually.
Missed opportunities
Had Ms. Ward’s boys been among the one in five to receive follow-up care earlier in their lives, she might have saved a significant amount of time, money, anxiety, and heartache. When the twins were 9 years old, she took them to a new pediatric pulmonologist. That changed everything. In that first visit, “they gave me way more information than I ever had in the first 9 years,” she said.
The doctor told Ms. Ward to keep steroids on hand, gave her a prescription for extra doses of the powerful medication, and explained that they needed to be used within 24 hours of the first sign of a breathing problem.
“She said if you give them the steroids right away, it keeps them out of the emergency room, and that’s actually worked,” Ms. Ward said. “She made sure we had care plans every visit and asked me each time if I still had it or we needed to rewrite it. They gave me signs to look for, for when to go to hospital visits. I think that when you go to the doctor, they should be telling you stuff like that.”
Dr. Bardach said visits with a primary care doctor or asthma specialist offer families a chance to receive information to keep the condition from becoming critical.
“Going to that follow-up visit, they can get access to education from the provider about how to avoid things that trigger asthma, and there’s medication that kids can take that keeps the lungs calm and less likely to have a big asthma reaction, so getting access to that medication can be really helpful,” she said.
That was the case for Amy Davenport, of Chapel Hill, N.C., whose 6-year-old son has been to the ED twice for his asthma.
The first time, when he was 3, he was having trouble breathing with a respiratory tract infection and received nebulizer treatment – although he received it in the ED since no beds were available in the ICU. The staff did tell Ms. Davenport to follow up with her primary care provider, but her son’s pediatrician was reluctant to diagnose him with asthma at such a young age and didn’t prescribe any maintenance medications.
A few months later, Ms. Davenport and her son found themselves back in the hospital, and an ICU bed was open this time. The critical care staff referred Davenport to a pediatric pulmonary specialist, and they haven’t been back to the hospital since. Ms. Davenport said she believes if they’d received a maintenance medication after the first visit, it likely would have prevented the second one.
“I’ve definitely seen now that, after the second admission, we got an asthma action plan and it said exactly what to do,” she said. “I felt like we had really good follow-up. We had that action plan on our refrigerator for a long time, and it helped us as parents with three small children to manage.”
Of course, follow-up care takes time – time away from work and school that not all families can spare, the researchers acknowledged. Telehealth may be an option, especially after its use expanded during the COVID-19 pandemic.
“We know that health systems have a hard time being flexible enough to actually have a kid be able to make an appointment within a short period of time, and we also know it’s hard for families sometimes to go back into a clinical setting within a certain period of time,” Dr. Bardach said. The urgency for the appointment may wane for those whose children seem to be doing better.
When the researchers adjusted their calculations for socioeconomic status, the results didn’t change much. But the study did find that patients with private insurance were about twice as likely to have follow-up visits as those on Medicaid (43.7% vs. 21.7%). And “the content and conduct” of the follow-up visit makes a difference as well.
Ms. Ward, whose boys are insured through Medicaid, recalled several visits to the ED where she had to push the staff to get the care her children needed. In one case, when one of her boys was a year old and struggling to breathe, the emergency doctor handed her a prescription and recommended she fill it at a neighborhood drugstore that would be cheaper than the hospital’s pharmacy. Then a nurse came in to begin the discharge process.
“I said no, ‘we’re not ready yet. Look at him,’” Ms. Ward said. The nurse took a pulse oximeter reading that showed the boy’s oxygen levels were at 84%, dangerously low. “If I wasn’t so knowledgeable and paid attention when they were born, since they were preemies, if it would have been somebody else, they probably would’ve went home and he’d have died.”
With the pediatric pulmonologist the boys have now, Ms. Ward said she feels more capable of managing their asthma and knowing how to reduce the likelihood that they’ll need to visit the ED.
“Part of what we’re seeing here is that having an existing and trusting relationship with a clinician can be helpful to kids with asthma,” Dr. Bardach said. “If we help establish and maintain those connections, and explain how important that connection can be, that can also help somebody with asthma overall.”
The research was funded by the Agency for Healthcare Research and Quality. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACADEMIC PEDIATRICS
Denosumab boosts bone strength in glucocorticoid users
Bone strength and microarchitecture remained stronger at 24 months after treatment with denosumab compared to risedronate, in a study of 110 adults using glucocorticoids.
Patients using glucocorticoids are at increased risk for vertebral and nonvertebral fractures at both the start of treatment or as treatment continues, wrote Piet Geusens, MD, of Maastricht University, the Netherlands, and colleagues.

Imaging data collected via high-resolution peripheral quantitative computed tomography (HR-pQCT) allow for the assessment of bone microarchitecture and strength, but specific data comparing the impact of bone treatment in patients using glucocorticoids are lacking, they said.
In a study published in the Journal of Bone and Mineral Research, the researchers identified a subset of 56 patients randomized to denosumab and 54 to risedronate patients out of a total of 590 patients who were enrolled in a phase 3 randomized, controlled trial of denosumab vs. risedronate for bone mineral density. The main results of the larger trial – presented at EULAR 2018 – showed greater increases in bone strength with denosumab over risedronate in patients receiving glucocorticoids.
In the current study, the researchers reviewed HR-pQCT scans of the distal radius and tibia at baseline, 12 months, and 24 months. Bone strength and microarchitecture were defined in terms of failure load (FL) as a primary outcome. Patients also were divided into subpopulations of those initiating glucocorticoid treatment (GC-I) and continuing treatment (GC-C).
Baseline characteristics were mainly balanced among the treatment groups within the GC-I and GC-C categories.
Among the GC-I patients, in the denosumab group, FL increased significantly from baseline to 12 months at the radius at tibia (1.8% and 1.7%, respectively) but did not change significantly in the risedronate group, which translated to a significant treatment difference between the drugs of 3.3% for radius and 2.5% for tibia.
At 24 months, the radius measure of FL was unchanged from baseline in denosumab patients but significantly decreased in risedronate patients, with a difference of –4.1%, which translated to a significant between-treatment difference at the radius of 5.6% (P < .001). Changes at the tibia were not significantly different between the groups at 24 months.
Among the GC-C patients, FL was unchanged from baseline to 12 months for both the denosumab and risedronate groups. However, FL significantly increased with denosumab (4.3%) and remained unchanged in the risedronate group.
The researchers also found significant differences between denosumab and risedronate in percentage changes in cortical bone mineral density, and less prominent changes and differences in trabecular bone mineral density.
The study findings were limited by several factors including the use of the HR-pQCT scanner, which limits the measurement of trabecular microarchitecture, and the use of only standard HR-pQCT parameters, which do not allow insight into endosteal changes, and the inability to correct for multiplicity of data, the researchers noted.
However, the results support the superiority of denosumab over risedronate for preventing FL and total bone mineral density loss at the radius and tibia in new glucocorticoid users, and for increasing FL and total bone mineral density at the radius in long-term glucocorticoid users, they said.
Denosumab therefore could be a useful therapeutic option and could inform decision-making in patients initiating GC-therapy or on long-term GC-therapy, they concluded.
The study was supported by Amgen. Dr. Geusens disclosed grants from Amgen, Celgene, Lilly, Merck, Pfizer, Roche, UCB, Fresenius, Mylan, and Sandoz, and grants and other funding from AbbVie, outside the current study.
Bone strength and microarchitecture remained stronger at 24 months after treatment with denosumab compared to risedronate, in a study of 110 adults using glucocorticoids.
Patients using glucocorticoids are at increased risk for vertebral and nonvertebral fractures at both the start of treatment or as treatment continues, wrote Piet Geusens, MD, of Maastricht University, the Netherlands, and colleagues.
Imaging data collected via high-resolution peripheral quantitative computed tomography (HR-pQCT) allow for the assessment of bone microarchitecture and strength, but specific data comparing the impact of bone treatment in patients using glucocorticoids are lacking, they said.
In a study published in the Journal of Bone and Mineral Research, the researchers identified a subset of 56 patients randomized to denosumab and 54 to risedronate patients out of a total of 590 patients who were enrolled in a phase 3 randomized, controlled trial of denosumab vs. risedronate for bone mineral density. The main results of the larger trial – presented at EULAR 2018 – showed greater increases in bone strength with denosumab over risedronate in patients receiving glucocorticoids.
In the current study, the researchers reviewed HR-pQCT scans of the distal radius and tibia at baseline, 12 months, and 24 months. Bone strength and microarchitecture were defined in terms of failure load (FL) as a primary outcome. Patients also were divided into subpopulations of those initiating glucocorticoid treatment (GC-I) and continuing treatment (GC-C).
Baseline characteristics were mainly balanced among the treatment groups within the GC-I and GC-C categories.
Among the GC-I patients, in the denosumab group, FL increased significantly from baseline to 12 months at the radius at tibia (1.8% and 1.7%, respectively) but did not change significantly in the risedronate group, which translated to a significant treatment difference between the drugs of 3.3% for radius and 2.5% for tibia.
At 24 months, the radius measure of FL was unchanged from baseline in denosumab patients but significantly decreased in risedronate patients, with a difference of –4.1%, which translated to a significant between-treatment difference at the radius of 5.6% (P < .001). Changes at the tibia were not significantly different between the groups at 24 months.
Among the GC-C patients, FL was unchanged from baseline to 12 months for both the denosumab and risedronate groups. However, FL significantly increased with denosumab (4.3%) and remained unchanged in the risedronate group.
The researchers also found significant differences between denosumab and risedronate in percentage changes in cortical bone mineral density, and less prominent changes and differences in trabecular bone mineral density.
The study findings were limited by several factors including the use of the HR-pQCT scanner, which limits the measurement of trabecular microarchitecture, and the use of only standard HR-pQCT parameters, which do not allow insight into endosteal changes, and the inability to correct for multiplicity of data, the researchers noted.
However, the results support the superiority of denosumab over risedronate for preventing FL and total bone mineral density loss at the radius and tibia in new glucocorticoid users, and for increasing FL and total bone mineral density at the radius in long-term glucocorticoid users, they said.
Denosumab therefore could be a useful therapeutic option and could inform decision-making in patients initiating GC-therapy or on long-term GC-therapy, they concluded.
The study was supported by Amgen. Dr. Geusens disclosed grants from Amgen, Celgene, Lilly, Merck, Pfizer, Roche, UCB, Fresenius, Mylan, and Sandoz, and grants and other funding from AbbVie, outside the current study.
Bone strength and microarchitecture remained stronger at 24 months after treatment with denosumab compared to risedronate, in a study of 110 adults using glucocorticoids.
Patients using glucocorticoids are at increased risk for vertebral and nonvertebral fractures at both the start of treatment or as treatment continues, wrote Piet Geusens, MD, of Maastricht University, the Netherlands, and colleagues.
Imaging data collected via high-resolution peripheral quantitative computed tomography (HR-pQCT) allow for the assessment of bone microarchitecture and strength, but specific data comparing the impact of bone treatment in patients using glucocorticoids are lacking, they said.
In a study published in the Journal of Bone and Mineral Research, the researchers identified a subset of 56 patients randomized to denosumab and 54 to risedronate patients out of a total of 590 patients who were enrolled in a phase 3 randomized, controlled trial of denosumab vs. risedronate for bone mineral density. The main results of the larger trial – presented at EULAR 2018 – showed greater increases in bone strength with denosumab over risedronate in patients receiving glucocorticoids.
In the current study, the researchers reviewed HR-pQCT scans of the distal radius and tibia at baseline, 12 months, and 24 months. Bone strength and microarchitecture were defined in terms of failure load (FL) as a primary outcome. Patients also were divided into subpopulations of those initiating glucocorticoid treatment (GC-I) and continuing treatment (GC-C).
Baseline characteristics were mainly balanced among the treatment groups within the GC-I and GC-C categories.
Among the GC-I patients, in the denosumab group, FL increased significantly from baseline to 12 months at the radius at tibia (1.8% and 1.7%, respectively) but did not change significantly in the risedronate group, which translated to a significant treatment difference between the drugs of 3.3% for radius and 2.5% for tibia.
At 24 months, the radius measure of FL was unchanged from baseline in denosumab patients but significantly decreased in risedronate patients, with a difference of –4.1%, which translated to a significant between-treatment difference at the radius of 5.6% (P < .001). Changes at the tibia were not significantly different between the groups at 24 months.
Among the GC-C patients, FL was unchanged from baseline to 12 months for both the denosumab and risedronate groups. However, FL significantly increased with denosumab (4.3%) and remained unchanged in the risedronate group.
The researchers also found significant differences between denosumab and risedronate in percentage changes in cortical bone mineral density, and less prominent changes and differences in trabecular bone mineral density.
The study findings were limited by several factors including the use of the HR-pQCT scanner, which limits the measurement of trabecular microarchitecture, and the use of only standard HR-pQCT parameters, which do not allow insight into endosteal changes, and the inability to correct for multiplicity of data, the researchers noted.
However, the results support the superiority of denosumab over risedronate for preventing FL and total bone mineral density loss at the radius and tibia in new glucocorticoid users, and for increasing FL and total bone mineral density at the radius in long-term glucocorticoid users, they said.
Denosumab therefore could be a useful therapeutic option and could inform decision-making in patients initiating GC-therapy or on long-term GC-therapy, they concluded.
The study was supported by Amgen. Dr. Geusens disclosed grants from Amgen, Celgene, Lilly, Merck, Pfizer, Roche, UCB, Fresenius, Mylan, and Sandoz, and grants and other funding from AbbVie, outside the current study.
FROM THE JOURNAL OF BONE AND MINERAL RESEARCH
Step test signals exercise capacity in asthma patients
The incremental step test is a highly reliable measure of exercise capacity in patients with moderate to severe asthma, based on data from 50 individuals.
Asthma patients often limit their physical exercise to avoid respiratory symptoms, which creates a downward spiral of reduced exercise capacity and ability to perform activities of daily living, wrote Renata Cléia Claudino Barbosa of the University of Sao Paulo and colleagues. “However, exercise training has been shown to be an important adjunctive therapy for asthma treatment that improves exercise capacity and health-related quality of life,” they wrote.
Step tests have been identified as a simpler, less costly alternative to cardiopulmonary exercise tests to measure exercise capacity in patients with chronic obstructive pulmonary disease, but their effectiveness for asthma patients has not investigated, the researchers said.
In a study published in Pulmonology, the researchers recruited 50 adults with moderate or severe asthma during routine care at a university hospital. The participants had been clinically stable for at least 6 months, with no hospitalizations, emergency care, or medication changes in the past 30 days. All participants received short-acting and long-acting bronchodilators and inhaled corticosteroids. The patients ranged in age from 18 to 60 years, with body mass index measures from 20 kg/m2 to 40 kg/m2.
Participants were randomized to tests on 2 nonconsecutive days at least 48 hours apart. On the first day, patients completed asthma control questionnaires and lung function tests, then performed either a cardiopulmonary exercise test (CPET) or two incremental step tests (IST-1 and IST-2). On the second day, they performed the other test. Participants were instructed to use bronchodilators 15 minutes before each test.
The step test involved stepping up and down on a 20-cm high wooden bench.
Overall, the peak oxygen uptakes were 27.6 mL/kg per minute for the CPET, 22.3 mL/kg per minute for the first IST, and 23.3 mL/kg per minute for the second IST.
“The IST with better performance regarding the peak VO2 value was called the best IST (b-IST),” and these values were used for validity and interpretability analyses, the researchers wrote.
In a reliability analysis, the intraclass correlation coefficient (ICC) was 0.93, the measurement error was 2.5%, and the construct validity for peak VO2 was significantly more reliable than the CPET (P < 0.001), the researchers said. The ICC for total number of steps was 0.88.
Notably, “the present study also demonstrated that IST is not interchangeable with the CPET since the subjects with moderate to severe asthma did not reach the maximal exercise capacity,” the researchers said. However, “we believe that the IST is superior to walking tests in subjects with asthma because it is an activity that requires greater ventilation in a subject’s daily life,” they said.
The study findings were limited by several factors including the relatively small study population and the small number of male patients, which may limit generalizability to males with asthma or other asthma endotypes, the researchers said. However, the results were strengthened by the randomized design, and support the value of the IST as a cost-effective option for assessing exercise capacity, preferably with two step tests to minimize the learning effect, they said. Additional research is needed to determine whether IST can assess responsiveness to pharmacological and nonpharmalogical treatments in asthma patients, they noted.
The study was supported by the Sao Paulo Research Foundation, Conselho Nacional de Pesquisa, and Coordination of Improvement of Higher Level Personnel--Brazil. The researchers had no financial conflicts to disclose.
The incremental step test is a highly reliable measure of exercise capacity in patients with moderate to severe asthma, based on data from 50 individuals.
Asthma patients often limit their physical exercise to avoid respiratory symptoms, which creates a downward spiral of reduced exercise capacity and ability to perform activities of daily living, wrote Renata Cléia Claudino Barbosa of the University of Sao Paulo and colleagues. “However, exercise training has been shown to be an important adjunctive therapy for asthma treatment that improves exercise capacity and health-related quality of life,” they wrote.
Step tests have been identified as a simpler, less costly alternative to cardiopulmonary exercise tests to measure exercise capacity in patients with chronic obstructive pulmonary disease, but their effectiveness for asthma patients has not investigated, the researchers said.
In a study published in Pulmonology, the researchers recruited 50 adults with moderate or severe asthma during routine care at a university hospital. The participants had been clinically stable for at least 6 months, with no hospitalizations, emergency care, or medication changes in the past 30 days. All participants received short-acting and long-acting bronchodilators and inhaled corticosteroids. The patients ranged in age from 18 to 60 years, with body mass index measures from 20 kg/m2 to 40 kg/m2.
Participants were randomized to tests on 2 nonconsecutive days at least 48 hours apart. On the first day, patients completed asthma control questionnaires and lung function tests, then performed either a cardiopulmonary exercise test (CPET) or two incremental step tests (IST-1 and IST-2). On the second day, they performed the other test. Participants were instructed to use bronchodilators 15 minutes before each test.
The step test involved stepping up and down on a 20-cm high wooden bench.
Overall, the peak oxygen uptakes were 27.6 mL/kg per minute for the CPET, 22.3 mL/kg per minute for the first IST, and 23.3 mL/kg per minute for the second IST.
“The IST with better performance regarding the peak VO2 value was called the best IST (b-IST),” and these values were used for validity and interpretability analyses, the researchers wrote.
In a reliability analysis, the intraclass correlation coefficient (ICC) was 0.93, the measurement error was 2.5%, and the construct validity for peak VO2 was significantly more reliable than the CPET (P < 0.001), the researchers said. The ICC for total number of steps was 0.88.
Notably, “the present study also demonstrated that IST is not interchangeable with the CPET since the subjects with moderate to severe asthma did not reach the maximal exercise capacity,” the researchers said. However, “we believe that the IST is superior to walking tests in subjects with asthma because it is an activity that requires greater ventilation in a subject’s daily life,” they said.
The study findings were limited by several factors including the relatively small study population and the small number of male patients, which may limit generalizability to males with asthma or other asthma endotypes, the researchers said. However, the results were strengthened by the randomized design, and support the value of the IST as a cost-effective option for assessing exercise capacity, preferably with two step tests to minimize the learning effect, they said. Additional research is needed to determine whether IST can assess responsiveness to pharmacological and nonpharmalogical treatments in asthma patients, they noted.
The study was supported by the Sao Paulo Research Foundation, Conselho Nacional de Pesquisa, and Coordination of Improvement of Higher Level Personnel--Brazil. The researchers had no financial conflicts to disclose.
The incremental step test is a highly reliable measure of exercise capacity in patients with moderate to severe asthma, based on data from 50 individuals.
Asthma patients often limit their physical exercise to avoid respiratory symptoms, which creates a downward spiral of reduced exercise capacity and ability to perform activities of daily living, wrote Renata Cléia Claudino Barbosa of the University of Sao Paulo and colleagues. “However, exercise training has been shown to be an important adjunctive therapy for asthma treatment that improves exercise capacity and health-related quality of life,” they wrote.
Step tests have been identified as a simpler, less costly alternative to cardiopulmonary exercise tests to measure exercise capacity in patients with chronic obstructive pulmonary disease, but their effectiveness for asthma patients has not investigated, the researchers said.
In a study published in Pulmonology, the researchers recruited 50 adults with moderate or severe asthma during routine care at a university hospital. The participants had been clinically stable for at least 6 months, with no hospitalizations, emergency care, or medication changes in the past 30 days. All participants received short-acting and long-acting bronchodilators and inhaled corticosteroids. The patients ranged in age from 18 to 60 years, with body mass index measures from 20 kg/m2 to 40 kg/m2.
Participants were randomized to tests on 2 nonconsecutive days at least 48 hours apart. On the first day, patients completed asthma control questionnaires and lung function tests, then performed either a cardiopulmonary exercise test (CPET) or two incremental step tests (IST-1 and IST-2). On the second day, they performed the other test. Participants were instructed to use bronchodilators 15 minutes before each test.
The step test involved stepping up and down on a 20-cm high wooden bench.
Overall, the peak oxygen uptakes were 27.6 mL/kg per minute for the CPET, 22.3 mL/kg per minute for the first IST, and 23.3 mL/kg per minute for the second IST.
“The IST with better performance regarding the peak VO2 value was called the best IST (b-IST),” and these values were used for validity and interpretability analyses, the researchers wrote.
In a reliability analysis, the intraclass correlation coefficient (ICC) was 0.93, the measurement error was 2.5%, and the construct validity for peak VO2 was significantly more reliable than the CPET (P < 0.001), the researchers said. The ICC for total number of steps was 0.88.
Notably, “the present study also demonstrated that IST is not interchangeable with the CPET since the subjects with moderate to severe asthma did not reach the maximal exercise capacity,” the researchers said. However, “we believe that the IST is superior to walking tests in subjects with asthma because it is an activity that requires greater ventilation in a subject’s daily life,” they said.
The study findings were limited by several factors including the relatively small study population and the small number of male patients, which may limit generalizability to males with asthma or other asthma endotypes, the researchers said. However, the results were strengthened by the randomized design, and support the value of the IST as a cost-effective option for assessing exercise capacity, preferably with two step tests to minimize the learning effect, they said. Additional research is needed to determine whether IST can assess responsiveness to pharmacological and nonpharmalogical treatments in asthma patients, they noted.
The study was supported by the Sao Paulo Research Foundation, Conselho Nacional de Pesquisa, and Coordination of Improvement of Higher Level Personnel--Brazil. The researchers had no financial conflicts to disclose.
FROM PULMONOLOGY
Obesity linked to combined OSA syndrome and severe asthma
Almost all patients with both obstructive sleep apnea syndrome and severe asthma fell into the obesity phenotype, not the allergy phenotype, based on data from nearly 1,500 adults.
Both asthma and sleep-disordered breathing are common conditions worldwide, and previous research suggests that obstructive sleep apnea syndrome (OSAS) and severe asthma in particular could be associated, wrote Laurent Portel, MD, of Centre Hospitalier de Libourne, France, and colleagues.
“Even if the underlying mechanisms are not well established, it is clear that both OSAS and obesity act to aggravate existing asthma, making it more difficult to control,” they said. However, the pathology of this relationship is not well-understood, and data on severe asthma phenotypes and OSAS are limited, they said.
In a study published in Respiratory Medicine and Research, the investigators reviewed data from 1,465 patients older than 18 years with severe asthma who were part of a larger, prospective multicenter study of the management of asthma patients. The larger study, developed by the Collège des Pneumologues des Hôpitaux Généraux (CPHG) is known as the FASE-CPHG (France Asthme SEvère-CPHG) and includes 104 nonacademic hospitals in France.
Diagnosis of OSAS was reported by physicians; diagnosis of severe asthma was based on the Global Initiative for Asthma criteria. The average age of the patients was 54.4 years, 63% were women, and 60% were nonsmokers.
A total of 161 patients were diagnosed with OSAS. The researchers conducted a cluster analysis on 1,424 patients, including 156 of the OSAS patients. They identified five clusters: early-onset atopic asthma (690 patients), obese asthma (153 patients), late-onset asthma (299 patients), eosinophilic asthma (143 patients), and aspirin sensitivity asthma (139 patients).
All 153 patients in the obese asthma cluster had OSAS, by contrast, none of the patients in the early atopic asthma cluster had OSAS.
Overall, obesity, male sex, high blood pressure, depression, late-onset asthma, and early-onset atopic asthma were independently associated with OSAS, with odds ratios of 5.782, 3.047, 2.875, 2.552, 1.789, and 0.622, respectively.
Notably, OSAS patients were more frequently treated with long-term oral corticosteroids than those without OSAS (30% vs. 15%, P < .0001), the researchers said. “It is possible that this treatment may be responsible for obesity, and it represents a well-known risk factor for developing OSAS,” they wrote.
Uncontrolled asthma was significantly more common in OSAS patients than in those without OSAS (77.7% vs. 69%, P = .03), and significantly more OSAS patients reported no or occasional physical activity (79.8% vs. 68.2%, P ≤ .001).
The study findings were limited by several factors including the lack of patients from primary care or university hospitals, which may limit the generalizability of the results, the reliance on physician statements for diagnosis of OSAS, and the lack of data on OSAS severity or treatment, the researchers noted.
However, the results fill a needed gap in the literature because of the limited data on severe asthma patients in real life, and identifying severe asthma patients by phenotype may help identify those at greatest risk for OSAS, they said.
“Identified patients could more easily benefit from specific examinations such as poly(somno)graphy and, consequently, could benefit from a better management of both asthma and OSAS,” they emphasized.
The larger FASE-CPHG study was supported in part by ALK, AstraZeneca, Boehringer Ingelheim, GSK, and Le Nouveau Souffle. The researchers had no financial conflicts to disclose.
Almost all patients with both obstructive sleep apnea syndrome and severe asthma fell into the obesity phenotype, not the allergy phenotype, based on data from nearly 1,500 adults.
Both asthma and sleep-disordered breathing are common conditions worldwide, and previous research suggests that obstructive sleep apnea syndrome (OSAS) and severe asthma in particular could be associated, wrote Laurent Portel, MD, of Centre Hospitalier de Libourne, France, and colleagues.
“Even if the underlying mechanisms are not well established, it is clear that both OSAS and obesity act to aggravate existing asthma, making it more difficult to control,” they said. However, the pathology of this relationship is not well-understood, and data on severe asthma phenotypes and OSAS are limited, they said.
In a study published in Respiratory Medicine and Research, the investigators reviewed data from 1,465 patients older than 18 years with severe asthma who were part of a larger, prospective multicenter study of the management of asthma patients. The larger study, developed by the Collège des Pneumologues des Hôpitaux Généraux (CPHG) is known as the FASE-CPHG (France Asthme SEvère-CPHG) and includes 104 nonacademic hospitals in France.
Diagnosis of OSAS was reported by physicians; diagnosis of severe asthma was based on the Global Initiative for Asthma criteria. The average age of the patients was 54.4 years, 63% were women, and 60% were nonsmokers.
A total of 161 patients were diagnosed with OSAS. The researchers conducted a cluster analysis on 1,424 patients, including 156 of the OSAS patients. They identified five clusters: early-onset atopic asthma (690 patients), obese asthma (153 patients), late-onset asthma (299 patients), eosinophilic asthma (143 patients), and aspirin sensitivity asthma (139 patients).
All 153 patients in the obese asthma cluster had OSAS, by contrast, none of the patients in the early atopic asthma cluster had OSAS.
Overall, obesity, male sex, high blood pressure, depression, late-onset asthma, and early-onset atopic asthma were independently associated with OSAS, with odds ratios of 5.782, 3.047, 2.875, 2.552, 1.789, and 0.622, respectively.
Notably, OSAS patients were more frequently treated with long-term oral corticosteroids than those without OSAS (30% vs. 15%, P < .0001), the researchers said. “It is possible that this treatment may be responsible for obesity, and it represents a well-known risk factor for developing OSAS,” they wrote.
Uncontrolled asthma was significantly more common in OSAS patients than in those without OSAS (77.7% vs. 69%, P = .03), and significantly more OSAS patients reported no or occasional physical activity (79.8% vs. 68.2%, P ≤ .001).
The study findings were limited by several factors including the lack of patients from primary care or university hospitals, which may limit the generalizability of the results, the reliance on physician statements for diagnosis of OSAS, and the lack of data on OSAS severity or treatment, the researchers noted.
However, the results fill a needed gap in the literature because of the limited data on severe asthma patients in real life, and identifying severe asthma patients by phenotype may help identify those at greatest risk for OSAS, they said.
“Identified patients could more easily benefit from specific examinations such as poly(somno)graphy and, consequently, could benefit from a better management of both asthma and OSAS,” they emphasized.
The larger FASE-CPHG study was supported in part by ALK, AstraZeneca, Boehringer Ingelheim, GSK, and Le Nouveau Souffle. The researchers had no financial conflicts to disclose.
Almost all patients with both obstructive sleep apnea syndrome and severe asthma fell into the obesity phenotype, not the allergy phenotype, based on data from nearly 1,500 adults.
Both asthma and sleep-disordered breathing are common conditions worldwide, and previous research suggests that obstructive sleep apnea syndrome (OSAS) and severe asthma in particular could be associated, wrote Laurent Portel, MD, of Centre Hospitalier de Libourne, France, and colleagues.
“Even if the underlying mechanisms are not well established, it is clear that both OSAS and obesity act to aggravate existing asthma, making it more difficult to control,” they said. However, the pathology of this relationship is not well-understood, and data on severe asthma phenotypes and OSAS are limited, they said.
In a study published in Respiratory Medicine and Research, the investigators reviewed data from 1,465 patients older than 18 years with severe asthma who were part of a larger, prospective multicenter study of the management of asthma patients. The larger study, developed by the Collège des Pneumologues des Hôpitaux Généraux (CPHG) is known as the FASE-CPHG (France Asthme SEvère-CPHG) and includes 104 nonacademic hospitals in France.
Diagnosis of OSAS was reported by physicians; diagnosis of severe asthma was based on the Global Initiative for Asthma criteria. The average age of the patients was 54.4 years, 63% were women, and 60% were nonsmokers.
A total of 161 patients were diagnosed with OSAS. The researchers conducted a cluster analysis on 1,424 patients, including 156 of the OSAS patients. They identified five clusters: early-onset atopic asthma (690 patients), obese asthma (153 patients), late-onset asthma (299 patients), eosinophilic asthma (143 patients), and aspirin sensitivity asthma (139 patients).
All 153 patients in the obese asthma cluster had OSAS, by contrast, none of the patients in the early atopic asthma cluster had OSAS.
Overall, obesity, male sex, high blood pressure, depression, late-onset asthma, and early-onset atopic asthma were independently associated with OSAS, with odds ratios of 5.782, 3.047, 2.875, 2.552, 1.789, and 0.622, respectively.
Notably, OSAS patients were more frequently treated with long-term oral corticosteroids than those without OSAS (30% vs. 15%, P < .0001), the researchers said. “It is possible that this treatment may be responsible for obesity, and it represents a well-known risk factor for developing OSAS,” they wrote.
Uncontrolled asthma was significantly more common in OSAS patients than in those without OSAS (77.7% vs. 69%, P = .03), and significantly more OSAS patients reported no or occasional physical activity (79.8% vs. 68.2%, P ≤ .001).
The study findings were limited by several factors including the lack of patients from primary care or university hospitals, which may limit the generalizability of the results, the reliance on physician statements for diagnosis of OSAS, and the lack of data on OSAS severity or treatment, the researchers noted.
However, the results fill a needed gap in the literature because of the limited data on severe asthma patients in real life, and identifying severe asthma patients by phenotype may help identify those at greatest risk for OSAS, they said.
“Identified patients could more easily benefit from specific examinations such as poly(somno)graphy and, consequently, could benefit from a better management of both asthma and OSAS,” they emphasized.
The larger FASE-CPHG study was supported in part by ALK, AstraZeneca, Boehringer Ingelheim, GSK, and Le Nouveau Souffle. The researchers had no financial conflicts to disclose.
FROM RESPIRATORY MEDICINE AND RESEARCH
Dealing with life-threatening asthma attacks
In assessing and managing patients presenting with acute, life-threatening asthma, if the exacerbation does not resolve relatively quickly, clinicians need to start looking for other causes of the patient’s respiratory distress, a review of the literature suggests.
“I think one of the most important points of this review is that asthma is a self-limiting disease, and it’s important to understand that with appropriate treatment and immediate response to it, exacerbations will get better with time,” Orlando Garner, MD, Baylor College of Medicine, Houston, said in an interview.
“So I think one of the key points is, if these exacerbations do not resolve within 24-48 hours, clinicians need to start thinking: ‘This could be something else,’ and not get stuck in the diagnosis that this is an asthmatic patient who is having an exacerbation. If the distress doesn’t resolve within 48 hours, it’s time to look for other clues,” he stressed.
The study was published online in the journal CHEST®.
Appropriate triage
Appropriate triage is key in the management of acute asthma, Dr. Garner and colleagues pointed out. A simplified severity score for the evaluation of asthma in the ED can help in this regard. Depending on the presence or absence of a number of key signs and symptoms, patients can be readily categorized as having mild, moderate, or severe asthma. “Static assessments and dynamic assessments of acute asthma exacerbation in the ED can also help triage patients,” the authors added.
Static assessment involves assessing the severity at presentation, which in turn determines the aggressiveness of initial treatment. Objective static assessments include the measurement of peak expiratory flow (PEF) or forced expiratory volume in 1 second (FEV1). A severe exacerbation is usually defined as a PEF or an FEV1 of less than 50%-60% of predicted normal values, the authors noted.
Dynamic assessment is more helpful than static assessment because it gauges response to treatment. “A lack of improvement in expiratory flow rates after initial bronchodilator therapy with continuous or worsening symptoms suggests need for hospitalization,” Dr. Garner and colleagues observed. The main treatment goals for patients with acute asthma are reversal of bronchospasm and correction of hypoxemia.
These are achieved at least initially with conventional agents, such as repeated doses of inhaled short-acting beta2-agonists, inhaled short-acting anticholinergics, systemic corticosteroids, and occasionally intravenous magnesium sulfate. If there is concomitant hypoxemia, oxygen therapy should be initiated as well. Patients who have evidence of hypercapnic respiratory failure or diaphragmatic fatigue need to be admitted to the intensive care unit, the authors indicated.
For these patients, clinicians need to remember that there are therapies other than inhalers, such as epinephrine and systemic terbutaline. During a life-threatening asthma episode, airflow in the medium and small airways often becomes turbulent, increasing the work of breathing, the researchers pointed out.
Heliox, a combination of helium and oxygen, reduces turbulent flow, they noted, although FiO2 requirements need to be less than 30% in order for it to work. “Heliox can be used in patients with severe bronchospasm who do not respond to the conventional therapies,” the authors noted, “[but] therapy should be abandoned if there is no clinical improvement after 15 minutes of use.”
Although none of the biologics such as dupilumab (Dupixent) has yet been approved for the treatment of acute exacerbations, Dr. Garner predicts they will become the “future of medicine” for patients with severe asthma as well.
Ventilation in life-threatening asthma
Rapid sequence intubation is generally recommended for patients who require mechanical ventilation, but as an alternative, “we are advocating a slower approach, where we get patients to slow down their breathing and relax them with something like ketamine infusions and wait before we given them a paralytic to see if the work of breathing improves,” Dr. Garner said. Bag-mask ventilation should be avoided because it can worsen dynamic hyperinflation or cause barotrauma.
Salvage therapies such as the use of bronchoscopy with N-acetylcysteine instilled directly into the airway is another option in cases in which mucus plugging is considered to be the main driver of airflow limitation.
Asked to comment, Brit Long, MD, an emergency medicine physician at the Brooke Army Medical Center in San Antonio, Tex., felt the review was extremely useful and well done.
“We see these patients very frequently, and being able to assess them right away and get an accurate picture of what’s going on is very important,” he said in an interview. The one thing that is often more difficult, at least in the ED, is obtaining a PEF or the FEV1 – “both very helpful if the patient can do them, but if the patient is critically ill, it’s more likely you will not be able to get those assessments, and if patients are speaking in one-word sentences and are working really hard to breathe, that’s a severe exacerbation, and they need immediate intervention.” Dr. Long also liked all the essential treatments the authors recommended that patients be given immediately, although he noted that Heliox is not going to be available in most EDs.
On the other hand, he agreed with the authors’ recommendation to take a slower approach to mechanical ventilation, if it is needed at all. “I try my best to absolutely avoid intubating these patients – you are not fixing the issue with mechanical ventilation, you are just creating further problems.
“And while I see the entire spectrum of asthma patients from very mild to severe patients, these authors did a good job in explaining what the goals of treatment are and what to do with the severe ones,” he said.
Dr. Garner and Dr. Long disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In assessing and managing patients presenting with acute, life-threatening asthma, if the exacerbation does not resolve relatively quickly, clinicians need to start looking for other causes of the patient’s respiratory distress, a review of the literature suggests.
“I think one of the most important points of this review is that asthma is a self-limiting disease, and it’s important to understand that with appropriate treatment and immediate response to it, exacerbations will get better with time,” Orlando Garner, MD, Baylor College of Medicine, Houston, said in an interview.
“So I think one of the key points is, if these exacerbations do not resolve within 24-48 hours, clinicians need to start thinking: ‘This could be something else,’ and not get stuck in the diagnosis that this is an asthmatic patient who is having an exacerbation. If the distress doesn’t resolve within 48 hours, it’s time to look for other clues,” he stressed.
The study was published online in the journal CHEST®.
Appropriate triage
Appropriate triage is key in the management of acute asthma, Dr. Garner and colleagues pointed out. A simplified severity score for the evaluation of asthma in the ED can help in this regard. Depending on the presence or absence of a number of key signs and symptoms, patients can be readily categorized as having mild, moderate, or severe asthma. “Static assessments and dynamic assessments of acute asthma exacerbation in the ED can also help triage patients,” the authors added.
Static assessment involves assessing the severity at presentation, which in turn determines the aggressiveness of initial treatment. Objective static assessments include the measurement of peak expiratory flow (PEF) or forced expiratory volume in 1 second (FEV1). A severe exacerbation is usually defined as a PEF or an FEV1 of less than 50%-60% of predicted normal values, the authors noted.
Dynamic assessment is more helpful than static assessment because it gauges response to treatment. “A lack of improvement in expiratory flow rates after initial bronchodilator therapy with continuous or worsening symptoms suggests need for hospitalization,” Dr. Garner and colleagues observed. The main treatment goals for patients with acute asthma are reversal of bronchospasm and correction of hypoxemia.
These are achieved at least initially with conventional agents, such as repeated doses of inhaled short-acting beta2-agonists, inhaled short-acting anticholinergics, systemic corticosteroids, and occasionally intravenous magnesium sulfate. If there is concomitant hypoxemia, oxygen therapy should be initiated as well. Patients who have evidence of hypercapnic respiratory failure or diaphragmatic fatigue need to be admitted to the intensive care unit, the authors indicated.
For these patients, clinicians need to remember that there are therapies other than inhalers, such as epinephrine and systemic terbutaline. During a life-threatening asthma episode, airflow in the medium and small airways often becomes turbulent, increasing the work of breathing, the researchers pointed out.
Heliox, a combination of helium and oxygen, reduces turbulent flow, they noted, although FiO2 requirements need to be less than 30% in order for it to work. “Heliox can be used in patients with severe bronchospasm who do not respond to the conventional therapies,” the authors noted, “[but] therapy should be abandoned if there is no clinical improvement after 15 minutes of use.”
Although none of the biologics such as dupilumab (Dupixent) has yet been approved for the treatment of acute exacerbations, Dr. Garner predicts they will become the “future of medicine” for patients with severe asthma as well.
Ventilation in life-threatening asthma
Rapid sequence intubation is generally recommended for patients who require mechanical ventilation, but as an alternative, “we are advocating a slower approach, where we get patients to slow down their breathing and relax them with something like ketamine infusions and wait before we given them a paralytic to see if the work of breathing improves,” Dr. Garner said. Bag-mask ventilation should be avoided because it can worsen dynamic hyperinflation or cause barotrauma.
Salvage therapies such as the use of bronchoscopy with N-acetylcysteine instilled directly into the airway is another option in cases in which mucus plugging is considered to be the main driver of airflow limitation.
Asked to comment, Brit Long, MD, an emergency medicine physician at the Brooke Army Medical Center in San Antonio, Tex., felt the review was extremely useful and well done.
“We see these patients very frequently, and being able to assess them right away and get an accurate picture of what’s going on is very important,” he said in an interview. The one thing that is often more difficult, at least in the ED, is obtaining a PEF or the FEV1 – “both very helpful if the patient can do them, but if the patient is critically ill, it’s more likely you will not be able to get those assessments, and if patients are speaking in one-word sentences and are working really hard to breathe, that’s a severe exacerbation, and they need immediate intervention.” Dr. Long also liked all the essential treatments the authors recommended that patients be given immediately, although he noted that Heliox is not going to be available in most EDs.
On the other hand, he agreed with the authors’ recommendation to take a slower approach to mechanical ventilation, if it is needed at all. “I try my best to absolutely avoid intubating these patients – you are not fixing the issue with mechanical ventilation, you are just creating further problems.
“And while I see the entire spectrum of asthma patients from very mild to severe patients, these authors did a good job in explaining what the goals of treatment are and what to do with the severe ones,” he said.
Dr. Garner and Dr. Long disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In assessing and managing patients presenting with acute, life-threatening asthma, if the exacerbation does not resolve relatively quickly, clinicians need to start looking for other causes of the patient’s respiratory distress, a review of the literature suggests.
“I think one of the most important points of this review is that asthma is a self-limiting disease, and it’s important to understand that with appropriate treatment and immediate response to it, exacerbations will get better with time,” Orlando Garner, MD, Baylor College of Medicine, Houston, said in an interview.
“So I think one of the key points is, if these exacerbations do not resolve within 24-48 hours, clinicians need to start thinking: ‘This could be something else,’ and not get stuck in the diagnosis that this is an asthmatic patient who is having an exacerbation. If the distress doesn’t resolve within 48 hours, it’s time to look for other clues,” he stressed.
The study was published online in the journal CHEST®.
Appropriate triage
Appropriate triage is key in the management of acute asthma, Dr. Garner and colleagues pointed out. A simplified severity score for the evaluation of asthma in the ED can help in this regard. Depending on the presence or absence of a number of key signs and symptoms, patients can be readily categorized as having mild, moderate, or severe asthma. “Static assessments and dynamic assessments of acute asthma exacerbation in the ED can also help triage patients,” the authors added.
Static assessment involves assessing the severity at presentation, which in turn determines the aggressiveness of initial treatment. Objective static assessments include the measurement of peak expiratory flow (PEF) or forced expiratory volume in 1 second (FEV1). A severe exacerbation is usually defined as a PEF or an FEV1 of less than 50%-60% of predicted normal values, the authors noted.
Dynamic assessment is more helpful than static assessment because it gauges response to treatment. “A lack of improvement in expiratory flow rates after initial bronchodilator therapy with continuous or worsening symptoms suggests need for hospitalization,” Dr. Garner and colleagues observed. The main treatment goals for patients with acute asthma are reversal of bronchospasm and correction of hypoxemia.
These are achieved at least initially with conventional agents, such as repeated doses of inhaled short-acting beta2-agonists, inhaled short-acting anticholinergics, systemic corticosteroids, and occasionally intravenous magnesium sulfate. If there is concomitant hypoxemia, oxygen therapy should be initiated as well. Patients who have evidence of hypercapnic respiratory failure or diaphragmatic fatigue need to be admitted to the intensive care unit, the authors indicated.
For these patients, clinicians need to remember that there are therapies other than inhalers, such as epinephrine and systemic terbutaline. During a life-threatening asthma episode, airflow in the medium and small airways often becomes turbulent, increasing the work of breathing, the researchers pointed out.
Heliox, a combination of helium and oxygen, reduces turbulent flow, they noted, although FiO2 requirements need to be less than 30% in order for it to work. “Heliox can be used in patients with severe bronchospasm who do not respond to the conventional therapies,” the authors noted, “[but] therapy should be abandoned if there is no clinical improvement after 15 minutes of use.”
Although none of the biologics such as dupilumab (Dupixent) has yet been approved for the treatment of acute exacerbations, Dr. Garner predicts they will become the “future of medicine” for patients with severe asthma as well.
Ventilation in life-threatening asthma
Rapid sequence intubation is generally recommended for patients who require mechanical ventilation, but as an alternative, “we are advocating a slower approach, where we get patients to slow down their breathing and relax them with something like ketamine infusions and wait before we given them a paralytic to see if the work of breathing improves,” Dr. Garner said. Bag-mask ventilation should be avoided because it can worsen dynamic hyperinflation or cause barotrauma.
Salvage therapies such as the use of bronchoscopy with N-acetylcysteine instilled directly into the airway is another option in cases in which mucus plugging is considered to be the main driver of airflow limitation.
Asked to comment, Brit Long, MD, an emergency medicine physician at the Brooke Army Medical Center in San Antonio, Tex., felt the review was extremely useful and well done.
“We see these patients very frequently, and being able to assess them right away and get an accurate picture of what’s going on is very important,” he said in an interview. The one thing that is often more difficult, at least in the ED, is obtaining a PEF or the FEV1 – “both very helpful if the patient can do them, but if the patient is critically ill, it’s more likely you will not be able to get those assessments, and if patients are speaking in one-word sentences and are working really hard to breathe, that’s a severe exacerbation, and they need immediate intervention.” Dr. Long also liked all the essential treatments the authors recommended that patients be given immediately, although he noted that Heliox is not going to be available in most EDs.
On the other hand, he agreed with the authors’ recommendation to take a slower approach to mechanical ventilation, if it is needed at all. “I try my best to absolutely avoid intubating these patients – you are not fixing the issue with mechanical ventilation, you are just creating further problems.
“And while I see the entire spectrum of asthma patients from very mild to severe patients, these authors did a good job in explaining what the goals of treatment are and what to do with the severe ones,” he said.
Dr. Garner and Dr. Long disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CHEST
FDA approves generic Symbicort for asthma, COPD
The U.S. Food and Drug Administration approved the first generic of Symbicort (budesonide and formoterol fumarate dihydrate) inhalation aerosol for the treatment of asthma in patients 6 years of age and older and for the maintenance treatment of patients with chronic obstructive pulmonary disease (COPD), including chronic bronchitis and/or emphysema.
The approval was given for a complex generic drug-device combination product – a metered-dose inhaler that contains both budesonide (a corticosteroid that reduces inflammation) and formoterol (a long-acting bronchodilator that relaxes muscles in the airways to improve breathing). It is intended to be used as two inhalations, two times a day (usually morning and night, about 12 hours apart), to treat both diseases by preventing symptoms, such as wheezing for those with asthma and for improved breathing for patients with COPD.
The inhaler is approved at two strengths (160/4.5 mcg/actuation and 80/4.5 mcg/actuation), according to the March 15 FDA announcement. The device is not intended for the treatment of acute asthma.
“Today’s approval of the first generic for one of the most commonly prescribed complex drug-device combination products to treat asthma and COPD is another step forward in our commitment to bring generic copies of complex drugs to the market, which can improve quality of life and help reduce the cost of treatment,” said Sally Choe, PhD, director of the Office of Generic Drugs in the FDA’s Center for Drug Evaluation and Research.
The most common side effects associated with budesonide and formoterol fumarate dihydrate oral inhalation aerosol for those with asthma are nasopharyngitis pain, sinusitis, influenza, back pain, nasal congestion, stomach discomfort, vomiting, and oral candidiasis (thrush). For those with COPD, the most common side effects are nasopharyngitis, oral candidiasis, bronchitis, sinusitis, and upper respiratory tract infection, the FDA reported.
The approval of this generic drug-device combination was granted to Mylan Pharmaceuticals.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration approved the first generic of Symbicort (budesonide and formoterol fumarate dihydrate) inhalation aerosol for the treatment of asthma in patients 6 years of age and older and for the maintenance treatment of patients with chronic obstructive pulmonary disease (COPD), including chronic bronchitis and/or emphysema.
The approval was given for a complex generic drug-device combination product – a metered-dose inhaler that contains both budesonide (a corticosteroid that reduces inflammation) and formoterol (a long-acting bronchodilator that relaxes muscles in the airways to improve breathing). It is intended to be used as two inhalations, two times a day (usually morning and night, about 12 hours apart), to treat both diseases by preventing symptoms, such as wheezing for those with asthma and for improved breathing for patients with COPD.
The inhaler is approved at two strengths (160/4.5 mcg/actuation and 80/4.5 mcg/actuation), according to the March 15 FDA announcement. The device is not intended for the treatment of acute asthma.
“Today’s approval of the first generic for one of the most commonly prescribed complex drug-device combination products to treat asthma and COPD is another step forward in our commitment to bring generic copies of complex drugs to the market, which can improve quality of life and help reduce the cost of treatment,” said Sally Choe, PhD, director of the Office of Generic Drugs in the FDA’s Center for Drug Evaluation and Research.
The most common side effects associated with budesonide and formoterol fumarate dihydrate oral inhalation aerosol for those with asthma are nasopharyngitis pain, sinusitis, influenza, back pain, nasal congestion, stomach discomfort, vomiting, and oral candidiasis (thrush). For those with COPD, the most common side effects are nasopharyngitis, oral candidiasis, bronchitis, sinusitis, and upper respiratory tract infection, the FDA reported.
The approval of this generic drug-device combination was granted to Mylan Pharmaceuticals.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration approved the first generic of Symbicort (budesonide and formoterol fumarate dihydrate) inhalation aerosol for the treatment of asthma in patients 6 years of age and older and for the maintenance treatment of patients with chronic obstructive pulmonary disease (COPD), including chronic bronchitis and/or emphysema.
The approval was given for a complex generic drug-device combination product – a metered-dose inhaler that contains both budesonide (a corticosteroid that reduces inflammation) and formoterol (a long-acting bronchodilator that relaxes muscles in the airways to improve breathing). It is intended to be used as two inhalations, two times a day (usually morning and night, about 12 hours apart), to treat both diseases by preventing symptoms, such as wheezing for those with asthma and for improved breathing for patients with COPD.
The inhaler is approved at two strengths (160/4.5 mcg/actuation and 80/4.5 mcg/actuation), according to the March 15 FDA announcement. The device is not intended for the treatment of acute asthma.
“Today’s approval of the first generic for one of the most commonly prescribed complex drug-device combination products to treat asthma and COPD is another step forward in our commitment to bring generic copies of complex drugs to the market, which can improve quality of life and help reduce the cost of treatment,” said Sally Choe, PhD, director of the Office of Generic Drugs in the FDA’s Center for Drug Evaluation and Research.
The most common side effects associated with budesonide and formoterol fumarate dihydrate oral inhalation aerosol for those with asthma are nasopharyngitis pain, sinusitis, influenza, back pain, nasal congestion, stomach discomfort, vomiting, and oral candidiasis (thrush). For those with COPD, the most common side effects are nasopharyngitis, oral candidiasis, bronchitis, sinusitis, and upper respiratory tract infection, the FDA reported.
The approval of this generic drug-device combination was granted to Mylan Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Digital monitors can relieve asthma burden by boosting medication adherence and inhaler technique
PHOENIX – Before considering oral steroids or biologic therapies, many people with difficult-to-control asthma can reduce symptoms by addressing medication adherence and inhaler technique – and digital monitoring devices can play a key role.
Often physicians “will approach a patient about a biologic if they’re not responding to standard therapy. But we need to sometimes go back to those basic building blocks, like, are you taking the standard therapy?” William C. Anderson, MD, codirector of the multidisciplinary asthma clinic at Children’s Hospital Colorado, Aurora, said in an interview.
At the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and others presented data highlighting the diagnostic and therapeutic potential of digital monitoring devices for difficult-to-control asthma, the theme of the 2022s meeting.
The Global Initiative for Asthma (GINA) defines asthma as “difficult to control” if it remains uncontrolled despite medium- or high-dose inhaled corticosteroids with a second controller or with maintenance oral steroids, or if the asthma requires high-dose treatment to curb symptoms and exacerbations. About 17% of adult asthma patients have difficult-to-control asthma, according to the 2021 GINA report.
However, correcting for inhaling technique and adherence cuts the 17% down to just 3.7%, Giselle Mosnaim, MD, an allergist at NorthShore University HealthSystem outside Chicago and AAAAI immediate past president, told attendees at a Feb. 25 session on digital technologies for asthma management.
The CRITIKAL study, which reviewed data from more than 5,000 asthma patients, “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” Dr. Mosnaim said. Sadly, it also shows that, from 1975 to 2014, despite new devices and new technologies, “we still have poor inhaler technique.”
As for ways to measure adherence, physician judgments tend to be inaccurate, patient self-reporting has proved unreliable, and prescription refill data doesn’t indicate whether patients actually used the medications. “The ideal measure of adherence should be objective, accurate and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Tracking adherence
A closing afternoon session featured three presentations on research tracking adherence and outcomes in difficult-to-treat asthma patients – two pediatric cohorts and one across all ages. All studies used the Propeller Health sensor, a Food and Drug Administration–cleared device that attaches to the patient’s inhaler and automatically collects information on where, when, and how often they use their medication. The sensor then sends that information to a data cloud accessible to the patient and their health care professional.
Dr. Anderson’s team scoured a nationwide Propeller Health database for 8,000 patients using the digital monitors with controller therapies for asthma or chronic obstructive pulmonary disease (COPD). The study explored whether adherence differed for once-daily versus twice-daily medications, and if adherence differed based on patient age (4-60+ years).
For both asthma and COPD patients, those on once-daily regimens had higher medication adherence, compared with those who were prescribed twice-daily therapies. Plus, a greater proportion of once-daily patients met the prespecified 80% adherence threshold.
Looking across ages, medication use in the youngest group (aged 4-11 years) looked comparable with 30-somethings, “probably because parents are the ones giving the drug,” Dr. Anderson said. Mirroring patterns from other studies, adherence levels dipped in adolescents and young adults, relative to other age subsets.
Since this population-level analysis didn’t include individualized data on exacerbations or asthma control, “we can’t relate this to outcomes,” Dr. Anderson noted. But he said the data correlating medication use with adherence suggest that once-daily formulations may be the better option.
In one of the two pediatric studies, Matt McCulloch, MD, an allergy and immunology fellow working with Dr. Anderson, and colleagues reviewed charts of 40 children who received care at the Colorado Children’s multidisciplinary asthma clinic between 2018 and 2021. Half of these patients used Propeller Health sensors with their daily inhaled controller; the other patients were matched for age, ethnicity, sex, medication level, and disease control and severity – but had no electronic monitoring device.
On the whole, children who used digital monitoring for 12 months did not fare much better than matched controls on lung function (judged by forced expiratory volume) or asthma control (measured by Asthma Control Test scores).
However, within the digital monitoring group, patients who stayed on the Propeller system for 12 months did have better asthma control, fewer exacerbations, and improved asthma severity scores (measured by the Composite Asthma Severity Index), compared with when they first began digital monitoring. These children had all received care at the clinic for a while before their families opted for the electronic sensor, so “the effect wouldn’t have just been from starting in the clinic,” Dr. McCulloch said in an interview.
The gains came despite waning medication adherence. Similar to other digital monitoring studies, use of daily controller therapies in this retrospective analysis began at 50%-80% but dropped considerably during the first 4-5 months before settling into the 20%-30% range by 1 year.
Rachelle Ramsey, PhD, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center, presented data from 20 children with difficult-to-treat asthma who received 8 weeks of a digital adherence intervention during a 12-month treatment period. They analyzed three subsets – each with interventions based on how well the patients were managing daily controller therapy at baseline.
One patient with high (>80%) baseline adherence just received digital monitoring. The seven patients who began the study with intermediate (50%-80%) adherence received digital monitoring plus prescriptive text messaging. And the 12 children with poorest (<50%) baseline adherence received digital monitoring and a telehealth session in which a behavioral health specialist helped them set goals and create strategies to overcome barriers – for example, keeping the inhaler near their toothbrush in order to pair medication use with a daily habit.
“Overall, we found that matching Propeller with a behavioral intervention really improved adherence,” Dr. Ramsey said in an interview. While patients were receiving the intervention, adherence averaged across all groups increased from 39% to 76%. However, once the intervention period ended, the group’s adherence regressed toward baseline (36%).
Although adherence did not associate with clinical gains in this small study, the use of digital monitoring to improve medication adherence has translated to better outcomes in other recent efforts.
Remote monitoring
In a quality improvement project in the United Kingdom, nurses asked difficult-to-control asthma patients if they understood how to use their corticosteroid/long-acting beta2-agonist (LABA) inhalers and if they were adhering to treatment guidelines.
Those who answered yes to these questions were invited to a 28-day study that involved swapping their steroid/LABA inhalers for a different controller/bronchodilator (fluticasone/salmeterol) with INCA (Inhaler Compliance Assessment), a device that not only tracks adherence but also uses acoustics to gauge inhaler technique.
Among the 23 patients who participated, many had better clinical outcomes after 28 days of INCA monitoring. As Dr. Mosnaim told attendees, “what was amazing is so many of the patients that had been these difficult-to-control asthmatics who would have gone on to oral steroids or perhaps a biologic – lo and behold, you put them on a digital inhaler, and what do you see?” In two-thirds of the patients, “you see FeNo [a test that measures airway inflammation by detecting nitric oxide in exhalations] goes down. You see spirometry improve. You see the asthma control questionnaire improve. You see blood eosinophils go down.”
And in a 2020 randomized trial, Dr. Mosnaim and colleagues recruited 100 adults with uncontrolled asthma who had prescriptions for a daily inhaled corticosteroid and a short-acting beta-agonist (SABA) inhaler. Participants received Propeller sensors for their steroid and SABA inhalers. After a 2-week run-in period to calculate baseline corticosteroid adherence and SABA use for all participants, half the participants were randomly assigned to the control group, which had the app and sensor in silent mode, merely to collect data on medication use – whereas the treatment group received reminders, alerts, and monthly phone calls from providers who gave feedback on adherence and technique.
After 3 months of digital monitoring, patients didn’t use their rescue medication quite as often – as judged by a rise in the percentage of SABA-free days, compared with when they began the study. But the change in SABA-free days relative to baseline was more pronounced in the treatment group (19%) than in the control group (6%).
As seen in the other digital monitoring studies, adherence to daily corticosteroids fell with time, but the drop was milder in treated participants (2%) versus the control group (17%). So in this study, digital monitoring plus mobile app reminders and clinician feedback “prevented against fall in adherence to inhaled steroids over time,” Dr. Mosnaim said.
These results are “very encouraging” and offer “proof of concept that this type of remote monitoring could work,” Thanai Pongdee, MD, an allergist-immunologist with the Mayo Clinic in Rochester, Minn., said in an interview. One limitation was that the study was too short to measure exacerbation rates. A yearlong analysis would be “really fascinating because you’d catch all the seasons of the year – all the pollen seasons, all these things that could exacerbate you. Some people’s asthma can be quite seasonal.”
More important, the clinical utility of digital sensors will depend on how physicians choose to use them. If the doctor puts out a “blanket recommendation for using it but doesn’t ask you about it or doesn’t use the data to inform your care, then I think people just lose engagement and lose excitement over it,” Dr. Ramsey said. But if the health care team “asks you about the data or looks at the data with you or shows you how valuable this can be to your care, then I think that changes things.”
Building these analyses and interactions into the clinic workflow isn’t trivial. “If you have this wealth of data coming in, how are you going to look at it? Are you going to have an individual person assigned to this role? How are you going to respond to alerts?” Dr. Anderson asked.
In addition, because some digital monitors issue alerts when a patient’s asthma is not well controlled, some providers worry about liability if “something bad were to happen if you had that data but didn’t act upon it,” he said. Yet he noted that remote data monitoring is already used routinely in other areas of medicine, such as managing diabetes and heart conditions, “and it’s not like people are getting dinged for that stuff.”
Another issue is cost. Insurance only covers digital monitors in select cases, but it’s a bit of a catch-22. Insurers “don’t want to cover it until they get the data, but you can’t get the data until insurance covers it,” said Dr. Anderson, who added that “this year we finally got CPT reimbursement codes for monitoring devices.”
On the whole, studies of digital medication monitors suggest that better outcomes require “a good partnership between the health care provider and the patient,” Dr. Pongdee said. “It wasn’t like you could just put these things on and expect them to help. You still need that personal relationship to get the optimal results. We can have all this technology, but you still can’t take the people out of it.”
Dr. Mosnaim reported receiving current research grant support from GlaxoSmithKline, Novartis, Sanofi-Regeneron, and Teva; and past research grant support from AstraZeneca, Alk-Abello, and Genentech. She is immediate past president of the AAAAI, and directs the board of directors for the American Board of Allergy and Immunology. Dr. Anderson has served as a consultant for Regeneron, GlaxoSmithKline, and AstraZeneca, and has received research support from Colorado Medicaid. Dr. McCulloch and Dr. Ramsey disclosed no relevant financial relationships. Dr. Pongdee serves as an at-large director on the American Academy of Allergy, Asthma and Immunology board of directors. He receives grant funding from GlaxoSmithKline, and the Mayo Clinic is a trial site for GlaxoSmithKline and AstraZeneca.
A version of this article first appeared on Medscape.com.
PHOENIX – Before considering oral steroids or biologic therapies, many people with difficult-to-control asthma can reduce symptoms by addressing medication adherence and inhaler technique – and digital monitoring devices can play a key role.
Often physicians “will approach a patient about a biologic if they’re not responding to standard therapy. But we need to sometimes go back to those basic building blocks, like, are you taking the standard therapy?” William C. Anderson, MD, codirector of the multidisciplinary asthma clinic at Children’s Hospital Colorado, Aurora, said in an interview.
At the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and others presented data highlighting the diagnostic and therapeutic potential of digital monitoring devices for difficult-to-control asthma, the theme of the 2022s meeting.
The Global Initiative for Asthma (GINA) defines asthma as “difficult to control” if it remains uncontrolled despite medium- or high-dose inhaled corticosteroids with a second controller or with maintenance oral steroids, or if the asthma requires high-dose treatment to curb symptoms and exacerbations. About 17% of adult asthma patients have difficult-to-control asthma, according to the 2021 GINA report.
However, correcting for inhaling technique and adherence cuts the 17% down to just 3.7%, Giselle Mosnaim, MD, an allergist at NorthShore University HealthSystem outside Chicago and AAAAI immediate past president, told attendees at a Feb. 25 session on digital technologies for asthma management.
The CRITIKAL study, which reviewed data from more than 5,000 asthma patients, “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” Dr. Mosnaim said. Sadly, it also shows that, from 1975 to 2014, despite new devices and new technologies, “we still have poor inhaler technique.”
As for ways to measure adherence, physician judgments tend to be inaccurate, patient self-reporting has proved unreliable, and prescription refill data doesn’t indicate whether patients actually used the medications. “The ideal measure of adherence should be objective, accurate and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Tracking adherence
A closing afternoon session featured three presentations on research tracking adherence and outcomes in difficult-to-treat asthma patients – two pediatric cohorts and one across all ages. All studies used the Propeller Health sensor, a Food and Drug Administration–cleared device that attaches to the patient’s inhaler and automatically collects information on where, when, and how often they use their medication. The sensor then sends that information to a data cloud accessible to the patient and their health care professional.
Dr. Anderson’s team scoured a nationwide Propeller Health database for 8,000 patients using the digital monitors with controller therapies for asthma or chronic obstructive pulmonary disease (COPD). The study explored whether adherence differed for once-daily versus twice-daily medications, and if adherence differed based on patient age (4-60+ years).
For both asthma and COPD patients, those on once-daily regimens had higher medication adherence, compared with those who were prescribed twice-daily therapies. Plus, a greater proportion of once-daily patients met the prespecified 80% adherence threshold.
Looking across ages, medication use in the youngest group (aged 4-11 years) looked comparable with 30-somethings, “probably because parents are the ones giving the drug,” Dr. Anderson said. Mirroring patterns from other studies, adherence levels dipped in adolescents and young adults, relative to other age subsets.
Since this population-level analysis didn’t include individualized data on exacerbations or asthma control, “we can’t relate this to outcomes,” Dr. Anderson noted. But he said the data correlating medication use with adherence suggest that once-daily formulations may be the better option.
In one of the two pediatric studies, Matt McCulloch, MD, an allergy and immunology fellow working with Dr. Anderson, and colleagues reviewed charts of 40 children who received care at the Colorado Children’s multidisciplinary asthma clinic between 2018 and 2021. Half of these patients used Propeller Health sensors with their daily inhaled controller; the other patients were matched for age, ethnicity, sex, medication level, and disease control and severity – but had no electronic monitoring device.
On the whole, children who used digital monitoring for 12 months did not fare much better than matched controls on lung function (judged by forced expiratory volume) or asthma control (measured by Asthma Control Test scores).
However, within the digital monitoring group, patients who stayed on the Propeller system for 12 months did have better asthma control, fewer exacerbations, and improved asthma severity scores (measured by the Composite Asthma Severity Index), compared with when they first began digital monitoring. These children had all received care at the clinic for a while before their families opted for the electronic sensor, so “the effect wouldn’t have just been from starting in the clinic,” Dr. McCulloch said in an interview.
The gains came despite waning medication adherence. Similar to other digital monitoring studies, use of daily controller therapies in this retrospective analysis began at 50%-80% but dropped considerably during the first 4-5 months before settling into the 20%-30% range by 1 year.
Rachelle Ramsey, PhD, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center, presented data from 20 children with difficult-to-treat asthma who received 8 weeks of a digital adherence intervention during a 12-month treatment period. They analyzed three subsets – each with interventions based on how well the patients were managing daily controller therapy at baseline.
One patient with high (>80%) baseline adherence just received digital monitoring. The seven patients who began the study with intermediate (50%-80%) adherence received digital monitoring plus prescriptive text messaging. And the 12 children with poorest (<50%) baseline adherence received digital monitoring and a telehealth session in which a behavioral health specialist helped them set goals and create strategies to overcome barriers – for example, keeping the inhaler near their toothbrush in order to pair medication use with a daily habit.
“Overall, we found that matching Propeller with a behavioral intervention really improved adherence,” Dr. Ramsey said in an interview. While patients were receiving the intervention, adherence averaged across all groups increased from 39% to 76%. However, once the intervention period ended, the group’s adherence regressed toward baseline (36%).
Although adherence did not associate with clinical gains in this small study, the use of digital monitoring to improve medication adherence has translated to better outcomes in other recent efforts.
Remote monitoring
In a quality improvement project in the United Kingdom, nurses asked difficult-to-control asthma patients if they understood how to use their corticosteroid/long-acting beta2-agonist (LABA) inhalers and if they were adhering to treatment guidelines.
Those who answered yes to these questions were invited to a 28-day study that involved swapping their steroid/LABA inhalers for a different controller/bronchodilator (fluticasone/salmeterol) with INCA (Inhaler Compliance Assessment), a device that not only tracks adherence but also uses acoustics to gauge inhaler technique.
Among the 23 patients who participated, many had better clinical outcomes after 28 days of INCA monitoring. As Dr. Mosnaim told attendees, “what was amazing is so many of the patients that had been these difficult-to-control asthmatics who would have gone on to oral steroids or perhaps a biologic – lo and behold, you put them on a digital inhaler, and what do you see?” In two-thirds of the patients, “you see FeNo [a test that measures airway inflammation by detecting nitric oxide in exhalations] goes down. You see spirometry improve. You see the asthma control questionnaire improve. You see blood eosinophils go down.”
And in a 2020 randomized trial, Dr. Mosnaim and colleagues recruited 100 adults with uncontrolled asthma who had prescriptions for a daily inhaled corticosteroid and a short-acting beta-agonist (SABA) inhaler. Participants received Propeller sensors for their steroid and SABA inhalers. After a 2-week run-in period to calculate baseline corticosteroid adherence and SABA use for all participants, half the participants were randomly assigned to the control group, which had the app and sensor in silent mode, merely to collect data on medication use – whereas the treatment group received reminders, alerts, and monthly phone calls from providers who gave feedback on adherence and technique.
After 3 months of digital monitoring, patients didn’t use their rescue medication quite as often – as judged by a rise in the percentage of SABA-free days, compared with when they began the study. But the change in SABA-free days relative to baseline was more pronounced in the treatment group (19%) than in the control group (6%).
As seen in the other digital monitoring studies, adherence to daily corticosteroids fell with time, but the drop was milder in treated participants (2%) versus the control group (17%). So in this study, digital monitoring plus mobile app reminders and clinician feedback “prevented against fall in adherence to inhaled steroids over time,” Dr. Mosnaim said.
These results are “very encouraging” and offer “proof of concept that this type of remote monitoring could work,” Thanai Pongdee, MD, an allergist-immunologist with the Mayo Clinic in Rochester, Minn., said in an interview. One limitation was that the study was too short to measure exacerbation rates. A yearlong analysis would be “really fascinating because you’d catch all the seasons of the year – all the pollen seasons, all these things that could exacerbate you. Some people’s asthma can be quite seasonal.”
More important, the clinical utility of digital sensors will depend on how physicians choose to use them. If the doctor puts out a “blanket recommendation for using it but doesn’t ask you about it or doesn’t use the data to inform your care, then I think people just lose engagement and lose excitement over it,” Dr. Ramsey said. But if the health care team “asks you about the data or looks at the data with you or shows you how valuable this can be to your care, then I think that changes things.”
Building these analyses and interactions into the clinic workflow isn’t trivial. “If you have this wealth of data coming in, how are you going to look at it? Are you going to have an individual person assigned to this role? How are you going to respond to alerts?” Dr. Anderson asked.
In addition, because some digital monitors issue alerts when a patient’s asthma is not well controlled, some providers worry about liability if “something bad were to happen if you had that data but didn’t act upon it,” he said. Yet he noted that remote data monitoring is already used routinely in other areas of medicine, such as managing diabetes and heart conditions, “and it’s not like people are getting dinged for that stuff.”
Another issue is cost. Insurance only covers digital monitors in select cases, but it’s a bit of a catch-22. Insurers “don’t want to cover it until they get the data, but you can’t get the data until insurance covers it,” said Dr. Anderson, who added that “this year we finally got CPT reimbursement codes for monitoring devices.”
On the whole, studies of digital medication monitors suggest that better outcomes require “a good partnership between the health care provider and the patient,” Dr. Pongdee said. “It wasn’t like you could just put these things on and expect them to help. You still need that personal relationship to get the optimal results. We can have all this technology, but you still can’t take the people out of it.”
Dr. Mosnaim reported receiving current research grant support from GlaxoSmithKline, Novartis, Sanofi-Regeneron, and Teva; and past research grant support from AstraZeneca, Alk-Abello, and Genentech. She is immediate past president of the AAAAI, and directs the board of directors for the American Board of Allergy and Immunology. Dr. Anderson has served as a consultant for Regeneron, GlaxoSmithKline, and AstraZeneca, and has received research support from Colorado Medicaid. Dr. McCulloch and Dr. Ramsey disclosed no relevant financial relationships. Dr. Pongdee serves as an at-large director on the American Academy of Allergy, Asthma and Immunology board of directors. He receives grant funding from GlaxoSmithKline, and the Mayo Clinic is a trial site for GlaxoSmithKline and AstraZeneca.
A version of this article first appeared on Medscape.com.
PHOENIX – Before considering oral steroids or biologic therapies, many people with difficult-to-control asthma can reduce symptoms by addressing medication adherence and inhaler technique – and digital monitoring devices can play a key role.
Often physicians “will approach a patient about a biologic if they’re not responding to standard therapy. But we need to sometimes go back to those basic building blocks, like, are you taking the standard therapy?” William C. Anderson, MD, codirector of the multidisciplinary asthma clinic at Children’s Hospital Colorado, Aurora, said in an interview.
At the annual meeting of the American Academy of Allergy, Asthma, and Immunology, he and others presented data highlighting the diagnostic and therapeutic potential of digital monitoring devices for difficult-to-control asthma, the theme of the 2022s meeting.
The Global Initiative for Asthma (GINA) defines asthma as “difficult to control” if it remains uncontrolled despite medium- or high-dose inhaled corticosteroids with a second controller or with maintenance oral steroids, or if the asthma requires high-dose treatment to curb symptoms and exacerbations. About 17% of adult asthma patients have difficult-to-control asthma, according to the 2021 GINA report.
However, correcting for inhaling technique and adherence cuts the 17% down to just 3.7%, Giselle Mosnaim, MD, an allergist at NorthShore University HealthSystem outside Chicago and AAAAI immediate past president, told attendees at a Feb. 25 session on digital technologies for asthma management.
The CRITIKAL study, which reviewed data from more than 5,000 asthma patients, “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” Dr. Mosnaim said. Sadly, it also shows that, from 1975 to 2014, despite new devices and new technologies, “we still have poor inhaler technique.”
As for ways to measure adherence, physician judgments tend to be inaccurate, patient self-reporting has proved unreliable, and prescription refill data doesn’t indicate whether patients actually used the medications. “The ideal measure of adherence should be objective, accurate and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Tracking adherence
A closing afternoon session featured three presentations on research tracking adherence and outcomes in difficult-to-treat asthma patients – two pediatric cohorts and one across all ages. All studies used the Propeller Health sensor, a Food and Drug Administration–cleared device that attaches to the patient’s inhaler and automatically collects information on where, when, and how often they use their medication. The sensor then sends that information to a data cloud accessible to the patient and their health care professional.
Dr. Anderson’s team scoured a nationwide Propeller Health database for 8,000 patients using the digital monitors with controller therapies for asthma or chronic obstructive pulmonary disease (COPD). The study explored whether adherence differed for once-daily versus twice-daily medications, and if adherence differed based on patient age (4-60+ years).
For both asthma and COPD patients, those on once-daily regimens had higher medication adherence, compared with those who were prescribed twice-daily therapies. Plus, a greater proportion of once-daily patients met the prespecified 80% adherence threshold.
Looking across ages, medication use in the youngest group (aged 4-11 years) looked comparable with 30-somethings, “probably because parents are the ones giving the drug,” Dr. Anderson said. Mirroring patterns from other studies, adherence levels dipped in adolescents and young adults, relative to other age subsets.
Since this population-level analysis didn’t include individualized data on exacerbations or asthma control, “we can’t relate this to outcomes,” Dr. Anderson noted. But he said the data correlating medication use with adherence suggest that once-daily formulations may be the better option.
In one of the two pediatric studies, Matt McCulloch, MD, an allergy and immunology fellow working with Dr. Anderson, and colleagues reviewed charts of 40 children who received care at the Colorado Children’s multidisciplinary asthma clinic between 2018 and 2021. Half of these patients used Propeller Health sensors with their daily inhaled controller; the other patients were matched for age, ethnicity, sex, medication level, and disease control and severity – but had no electronic monitoring device.
On the whole, children who used digital monitoring for 12 months did not fare much better than matched controls on lung function (judged by forced expiratory volume) or asthma control (measured by Asthma Control Test scores).
However, within the digital monitoring group, patients who stayed on the Propeller system for 12 months did have better asthma control, fewer exacerbations, and improved asthma severity scores (measured by the Composite Asthma Severity Index), compared with when they first began digital monitoring. These children had all received care at the clinic for a while before their families opted for the electronic sensor, so “the effect wouldn’t have just been from starting in the clinic,” Dr. McCulloch said in an interview.
The gains came despite waning medication adherence. Similar to other digital monitoring studies, use of daily controller therapies in this retrospective analysis began at 50%-80% but dropped considerably during the first 4-5 months before settling into the 20%-30% range by 1 year.
Rachelle Ramsey, PhD, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center, presented data from 20 children with difficult-to-treat asthma who received 8 weeks of a digital adherence intervention during a 12-month treatment period. They analyzed three subsets – each with interventions based on how well the patients were managing daily controller therapy at baseline.
One patient with high (>80%) baseline adherence just received digital monitoring. The seven patients who began the study with intermediate (50%-80%) adherence received digital monitoring plus prescriptive text messaging. And the 12 children with poorest (<50%) baseline adherence received digital monitoring and a telehealth session in which a behavioral health specialist helped them set goals and create strategies to overcome barriers – for example, keeping the inhaler near their toothbrush in order to pair medication use with a daily habit.
“Overall, we found that matching Propeller with a behavioral intervention really improved adherence,” Dr. Ramsey said in an interview. While patients were receiving the intervention, adherence averaged across all groups increased from 39% to 76%. However, once the intervention period ended, the group’s adherence regressed toward baseline (36%).
Although adherence did not associate with clinical gains in this small study, the use of digital monitoring to improve medication adherence has translated to better outcomes in other recent efforts.
Remote monitoring
In a quality improvement project in the United Kingdom, nurses asked difficult-to-control asthma patients if they understood how to use their corticosteroid/long-acting beta2-agonist (LABA) inhalers and if they were adhering to treatment guidelines.
Those who answered yes to these questions were invited to a 28-day study that involved swapping their steroid/LABA inhalers for a different controller/bronchodilator (fluticasone/salmeterol) with INCA (Inhaler Compliance Assessment), a device that not only tracks adherence but also uses acoustics to gauge inhaler technique.
Among the 23 patients who participated, many had better clinical outcomes after 28 days of INCA monitoring. As Dr. Mosnaim told attendees, “what was amazing is so many of the patients that had been these difficult-to-control asthmatics who would have gone on to oral steroids or perhaps a biologic – lo and behold, you put them on a digital inhaler, and what do you see?” In two-thirds of the patients, “you see FeNo [a test that measures airway inflammation by detecting nitric oxide in exhalations] goes down. You see spirometry improve. You see the asthma control questionnaire improve. You see blood eosinophils go down.”
And in a 2020 randomized trial, Dr. Mosnaim and colleagues recruited 100 adults with uncontrolled asthma who had prescriptions for a daily inhaled corticosteroid and a short-acting beta-agonist (SABA) inhaler. Participants received Propeller sensors for their steroid and SABA inhalers. After a 2-week run-in period to calculate baseline corticosteroid adherence and SABA use for all participants, half the participants were randomly assigned to the control group, which had the app and sensor in silent mode, merely to collect data on medication use – whereas the treatment group received reminders, alerts, and monthly phone calls from providers who gave feedback on adherence and technique.
After 3 months of digital monitoring, patients didn’t use their rescue medication quite as often – as judged by a rise in the percentage of SABA-free days, compared with when they began the study. But the change in SABA-free days relative to baseline was more pronounced in the treatment group (19%) than in the control group (6%).
As seen in the other digital monitoring studies, adherence to daily corticosteroids fell with time, but the drop was milder in treated participants (2%) versus the control group (17%). So in this study, digital monitoring plus mobile app reminders and clinician feedback “prevented against fall in adherence to inhaled steroids over time,” Dr. Mosnaim said.
These results are “very encouraging” and offer “proof of concept that this type of remote monitoring could work,” Thanai Pongdee, MD, an allergist-immunologist with the Mayo Clinic in Rochester, Minn., said in an interview. One limitation was that the study was too short to measure exacerbation rates. A yearlong analysis would be “really fascinating because you’d catch all the seasons of the year – all the pollen seasons, all these things that could exacerbate you. Some people’s asthma can be quite seasonal.”
More important, the clinical utility of digital sensors will depend on how physicians choose to use them. If the doctor puts out a “blanket recommendation for using it but doesn’t ask you about it or doesn’t use the data to inform your care, then I think people just lose engagement and lose excitement over it,” Dr. Ramsey said. But if the health care team “asks you about the data or looks at the data with you or shows you how valuable this can be to your care, then I think that changes things.”
Building these analyses and interactions into the clinic workflow isn’t trivial. “If you have this wealth of data coming in, how are you going to look at it? Are you going to have an individual person assigned to this role? How are you going to respond to alerts?” Dr. Anderson asked.
In addition, because some digital monitors issue alerts when a patient’s asthma is not well controlled, some providers worry about liability if “something bad were to happen if you had that data but didn’t act upon it,” he said. Yet he noted that remote data monitoring is already used routinely in other areas of medicine, such as managing diabetes and heart conditions, “and it’s not like people are getting dinged for that stuff.”
Another issue is cost. Insurance only covers digital monitors in select cases, but it’s a bit of a catch-22. Insurers “don’t want to cover it until they get the data, but you can’t get the data until insurance covers it,” said Dr. Anderson, who added that “this year we finally got CPT reimbursement codes for monitoring devices.”
On the whole, studies of digital medication monitors suggest that better outcomes require “a good partnership between the health care provider and the patient,” Dr. Pongdee said. “It wasn’t like you could just put these things on and expect them to help. You still need that personal relationship to get the optimal results. We can have all this technology, but you still can’t take the people out of it.”
Dr. Mosnaim reported receiving current research grant support from GlaxoSmithKline, Novartis, Sanofi-Regeneron, and Teva; and past research grant support from AstraZeneca, Alk-Abello, and Genentech. She is immediate past president of the AAAAI, and directs the board of directors for the American Board of Allergy and Immunology. Dr. Anderson has served as a consultant for Regeneron, GlaxoSmithKline, and AstraZeneca, and has received research support from Colorado Medicaid. Dr. McCulloch and Dr. Ramsey disclosed no relevant financial relationships. Dr. Pongdee serves as an at-large director on the American Academy of Allergy, Asthma and Immunology board of directors. He receives grant funding from GlaxoSmithKline, and the Mayo Clinic is a trial site for GlaxoSmithKline and AstraZeneca.
A version of this article first appeared on Medscape.com.
AT AAAAI
New gene signals for asthma-COPD overlap identified
A large-scale analysis of the genetic underpinnings of the overlap between asthma and chronic obstructive pulmonary disease (COPD) has identified eight novel signals that may be linked to inflammation and worse asthma outcomes, according to an international team of investigators.
They conducted a genome-wide association study (GWAS) of 8,068 individuals with asthma-COPD overlap (ACO) and 40,360 controls with either asthma or COPD alone and identified genetic variants that could predispose patients to ACO.
The findings by Catherine John, MBBChir, from the University of Leicester, England, and colleagues from Europe, the United States, and Canada were published online in Chest.
“Our study contributes to understanding the genetic landscape of asthma and COPD at the population level,” explained coauthor Lystra P. Hayden, MD, from Brigham and Women’s Hospital and Harvard Medical School, Boston, in an email.
“It provides evidence for shared genetic influence ranging from variants implicated in asthma to those implicated in fixed airflow obstruction and specifically those which influence an intermediate phenotype with features of both, which was the focus of this investigation,” she wrote.
Although the study does not provide sufficient evidence to support patient-level genetic testing for these variants, “it does suggest potential common biological mechanisms underpinning both asthma and COPD, which in the future could inform treatments of people displaying features of both conditions,” Dr. Hayden said.
Asthma and COPD are distinct conditions but share certain features, such as airflow obstruction, inflammation, and cytokine profiles. Recent studies have suggested that patients with features of both conditions – ACO – have worse outcomes than those with either condition alone.
The authors note that recent guidelines from the Global Initiative for Chronic Obstructive Lung Disease “emphasize that asthma and COPD are different conditions but may coexist in the same patient.”
“One of the things that genetics can do is to see if there is a genetic basis to the etiology of both of these conditions,” said coauthor Sina A. Gharib, MD, professor of pulmonary, critical care, and sleep medicine at the University of Washington, Seattle.
“Are these both just the same disease manifesting differently, or are they two really different diseases? That’s an ongoing controversy, and I don’t think this paper or any other paper that I’ve seen really settles this,” he said in an interview.
He noted that most genetic studies of asthma tend to exclude patients with COPD, and vice versa, because the complexity of the respective phenotypes can make it difficult to draw strong conclusions about genetic contributions to disease etiology.
Dr. Gharib’s group contributed data for the validation portion of the study.
Genetic study
The authors first drew data on the patients with ACO and controls from the UK Biobank and conducted a GWAS using a cutoff P value of less than 5x10-6 to identify “promising” signals that remained significant in analyses comparing patients with ACO with those with asthma alone and with COPD alone.
They then analyzed the variants in 12 independent cohorts and identified 31 variants they deemed to be worth a closer look.
“These signals suggest a spectrum of shared genetic influences, some predominantly influencing asthma (FAM105A, GLB1, PHB, TSLP), others predominantly influencing fixed airflow obstruction (IL17RD, C5orf56, HLA-DQB1). One intergenic signal on chromosome 5 had not been previously associated with asthma, COPD or lung function,” they write.
The investigators also performed subgroup analyses stratified by age of asthma onset and by smoking status.
“We found that for the 31 ACO signals of interest examined, the effect sizes amongst cases with childhood-onset asthma were highly correlated to those with adult onset. Effect sizes in ever- and never-smokers were also closely correlated. Our study suggests that ACO is not due solely to smoking in people with asthma,” Dr. Hayden said.
In addition, they tested variants across a wide range of phenotypes and found that traits of eosinophil counts, atopy, and asthma were prominent.
“Our findings suggest a spectrum of shared genetic influences, from variants predominantly influencing asthma to those predominantly influencing fixed airflow obstruction. We focus on variants that tend towards an intermediate phenotype with features of both asthma and fixed airflow obstruction with pathways implicating innate and adaptive immunity and potentially bone development and signals for which the biology remains unclear,” they write.
While it’s still unclear whether ACO is a distinct entity unto itself, “we do seem to find some signals that seem to be uniquely displayed in this population that has diagnosis of asthma but also has a reduction in lung function that’s not reversible, which is what we see in COPD,” Dr. Gharib said.
Further exploration of the biology of ACO could lead to development of methods to prevent fixed airflow obstruction in patients with asthma, the authors conclude.
The study was supported by BREATHE, the Health Data Research Hub for Respiratory Health in partnership with SAIL Databank. Dr. Hayden and Dr. Gharib reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large-scale analysis of the genetic underpinnings of the overlap between asthma and chronic obstructive pulmonary disease (COPD) has identified eight novel signals that may be linked to inflammation and worse asthma outcomes, according to an international team of investigators.
They conducted a genome-wide association study (GWAS) of 8,068 individuals with asthma-COPD overlap (ACO) and 40,360 controls with either asthma or COPD alone and identified genetic variants that could predispose patients to ACO.
The findings by Catherine John, MBBChir, from the University of Leicester, England, and colleagues from Europe, the United States, and Canada were published online in Chest.
“Our study contributes to understanding the genetic landscape of asthma and COPD at the population level,” explained coauthor Lystra P. Hayden, MD, from Brigham and Women’s Hospital and Harvard Medical School, Boston, in an email.
“It provides evidence for shared genetic influence ranging from variants implicated in asthma to those implicated in fixed airflow obstruction and specifically those which influence an intermediate phenotype with features of both, which was the focus of this investigation,” she wrote.
Although the study does not provide sufficient evidence to support patient-level genetic testing for these variants, “it does suggest potential common biological mechanisms underpinning both asthma and COPD, which in the future could inform treatments of people displaying features of both conditions,” Dr. Hayden said.
Asthma and COPD are distinct conditions but share certain features, such as airflow obstruction, inflammation, and cytokine profiles. Recent studies have suggested that patients with features of both conditions – ACO – have worse outcomes than those with either condition alone.
The authors note that recent guidelines from the Global Initiative for Chronic Obstructive Lung Disease “emphasize that asthma and COPD are different conditions but may coexist in the same patient.”
“One of the things that genetics can do is to see if there is a genetic basis to the etiology of both of these conditions,” said coauthor Sina A. Gharib, MD, professor of pulmonary, critical care, and sleep medicine at the University of Washington, Seattle.
“Are these both just the same disease manifesting differently, or are they two really different diseases? That’s an ongoing controversy, and I don’t think this paper or any other paper that I’ve seen really settles this,” he said in an interview.
He noted that most genetic studies of asthma tend to exclude patients with COPD, and vice versa, because the complexity of the respective phenotypes can make it difficult to draw strong conclusions about genetic contributions to disease etiology.
Dr. Gharib’s group contributed data for the validation portion of the study.
Genetic study
The authors first drew data on the patients with ACO and controls from the UK Biobank and conducted a GWAS using a cutoff P value of less than 5x10-6 to identify “promising” signals that remained significant in analyses comparing patients with ACO with those with asthma alone and with COPD alone.
They then analyzed the variants in 12 independent cohorts and identified 31 variants they deemed to be worth a closer look.
“These signals suggest a spectrum of shared genetic influences, some predominantly influencing asthma (FAM105A, GLB1, PHB, TSLP), others predominantly influencing fixed airflow obstruction (IL17RD, C5orf56, HLA-DQB1). One intergenic signal on chromosome 5 had not been previously associated with asthma, COPD or lung function,” they write.
The investigators also performed subgroup analyses stratified by age of asthma onset and by smoking status.
“We found that for the 31 ACO signals of interest examined, the effect sizes amongst cases with childhood-onset asthma were highly correlated to those with adult onset. Effect sizes in ever- and never-smokers were also closely correlated. Our study suggests that ACO is not due solely to smoking in people with asthma,” Dr. Hayden said.
In addition, they tested variants across a wide range of phenotypes and found that traits of eosinophil counts, atopy, and asthma were prominent.
“Our findings suggest a spectrum of shared genetic influences, from variants predominantly influencing asthma to those predominantly influencing fixed airflow obstruction. We focus on variants that tend towards an intermediate phenotype with features of both asthma and fixed airflow obstruction with pathways implicating innate and adaptive immunity and potentially bone development and signals for which the biology remains unclear,” they write.
While it’s still unclear whether ACO is a distinct entity unto itself, “we do seem to find some signals that seem to be uniquely displayed in this population that has diagnosis of asthma but also has a reduction in lung function that’s not reversible, which is what we see in COPD,” Dr. Gharib said.
Further exploration of the biology of ACO could lead to development of methods to prevent fixed airflow obstruction in patients with asthma, the authors conclude.
The study was supported by BREATHE, the Health Data Research Hub for Respiratory Health in partnership with SAIL Databank. Dr. Hayden and Dr. Gharib reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large-scale analysis of the genetic underpinnings of the overlap between asthma and chronic obstructive pulmonary disease (COPD) has identified eight novel signals that may be linked to inflammation and worse asthma outcomes, according to an international team of investigators.
They conducted a genome-wide association study (GWAS) of 8,068 individuals with asthma-COPD overlap (ACO) and 40,360 controls with either asthma or COPD alone and identified genetic variants that could predispose patients to ACO.
The findings by Catherine John, MBBChir, from the University of Leicester, England, and colleagues from Europe, the United States, and Canada were published online in Chest.
“Our study contributes to understanding the genetic landscape of asthma and COPD at the population level,” explained coauthor Lystra P. Hayden, MD, from Brigham and Women’s Hospital and Harvard Medical School, Boston, in an email.
“It provides evidence for shared genetic influence ranging from variants implicated in asthma to those implicated in fixed airflow obstruction and specifically those which influence an intermediate phenotype with features of both, which was the focus of this investigation,” she wrote.
Although the study does not provide sufficient evidence to support patient-level genetic testing for these variants, “it does suggest potential common biological mechanisms underpinning both asthma and COPD, which in the future could inform treatments of people displaying features of both conditions,” Dr. Hayden said.
Asthma and COPD are distinct conditions but share certain features, such as airflow obstruction, inflammation, and cytokine profiles. Recent studies have suggested that patients with features of both conditions – ACO – have worse outcomes than those with either condition alone.
The authors note that recent guidelines from the Global Initiative for Chronic Obstructive Lung Disease “emphasize that asthma and COPD are different conditions but may coexist in the same patient.”
“One of the things that genetics can do is to see if there is a genetic basis to the etiology of both of these conditions,” said coauthor Sina A. Gharib, MD, professor of pulmonary, critical care, and sleep medicine at the University of Washington, Seattle.
“Are these both just the same disease manifesting differently, or are they two really different diseases? That’s an ongoing controversy, and I don’t think this paper or any other paper that I’ve seen really settles this,” he said in an interview.
He noted that most genetic studies of asthma tend to exclude patients with COPD, and vice versa, because the complexity of the respective phenotypes can make it difficult to draw strong conclusions about genetic contributions to disease etiology.
Dr. Gharib’s group contributed data for the validation portion of the study.
Genetic study
The authors first drew data on the patients with ACO and controls from the UK Biobank and conducted a GWAS using a cutoff P value of less than 5x10-6 to identify “promising” signals that remained significant in analyses comparing patients with ACO with those with asthma alone and with COPD alone.
They then analyzed the variants in 12 independent cohorts and identified 31 variants they deemed to be worth a closer look.
“These signals suggest a spectrum of shared genetic influences, some predominantly influencing asthma (FAM105A, GLB1, PHB, TSLP), others predominantly influencing fixed airflow obstruction (IL17RD, C5orf56, HLA-DQB1). One intergenic signal on chromosome 5 had not been previously associated with asthma, COPD or lung function,” they write.
The investigators also performed subgroup analyses stratified by age of asthma onset and by smoking status.
“We found that for the 31 ACO signals of interest examined, the effect sizes amongst cases with childhood-onset asthma were highly correlated to those with adult onset. Effect sizes in ever- and never-smokers were also closely correlated. Our study suggests that ACO is not due solely to smoking in people with asthma,” Dr. Hayden said.
In addition, they tested variants across a wide range of phenotypes and found that traits of eosinophil counts, atopy, and asthma were prominent.
“Our findings suggest a spectrum of shared genetic influences, from variants predominantly influencing asthma to those predominantly influencing fixed airflow obstruction. We focus on variants that tend towards an intermediate phenotype with features of both asthma and fixed airflow obstruction with pathways implicating innate and adaptive immunity and potentially bone development and signals for which the biology remains unclear,” they write.
While it’s still unclear whether ACO is a distinct entity unto itself, “we do seem to find some signals that seem to be uniquely displayed in this population that has diagnosis of asthma but also has a reduction in lung function that’s not reversible, which is what we see in COPD,” Dr. Gharib said.
Further exploration of the biology of ACO could lead to development of methods to prevent fixed airflow obstruction in patients with asthma, the authors conclude.
The study was supported by BREATHE, the Health Data Research Hub for Respiratory Health in partnership with SAIL Databank. Dr. Hayden and Dr. Gharib reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.