User login
Cosmetic Corner: Dermatologists Weigh in on OTC Adult Acne Products
To improve patient care and outcomes, leading dermatologists offered their recommendations on adult acne products. Consideration must be given to:
- Bioclear Face Lotion and Face Cream
Jan Marini Skin Research, Inc
“These products contain a powerful combination of glycolic, salicylic, and azelaic acids to smooth and brighten acne-prone skin.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- Neutrogena Clear Pore Cleanser/Mask
Johnson & Johnson Consumer Inc
“This is a good daily product for acne-prone skin. It is formulated with benzoyl peroxide and can be used as a daily wash or mask.”—Anthony M. Rossi, MD, New York, New York
- Offects Sulfur Masque Acne Treatment
ZO Skin Health Inc
“This nonirritating mask reduces inflammation and oiliness and is safe to use in pregnancy.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- PanOxyl Acne Foaming Wash and Acne Creamy Wash
Stiefel, a GSK company
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments, as well as products for dry cuticles, hyperhidrosis, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on adult acne products. Consideration must be given to:
- Bioclear Face Lotion and Face Cream
Jan Marini Skin Research, Inc
“These products contain a powerful combination of glycolic, salicylic, and azelaic acids to smooth and brighten acne-prone skin.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- Neutrogena Clear Pore Cleanser/Mask
Johnson & Johnson Consumer Inc
“This is a good daily product for acne-prone skin. It is formulated with benzoyl peroxide and can be used as a daily wash or mask.”—Anthony M. Rossi, MD, New York, New York
- Offects Sulfur Masque Acne Treatment
ZO Skin Health Inc
“This nonirritating mask reduces inflammation and oiliness and is safe to use in pregnancy.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- PanOxyl Acne Foaming Wash and Acne Creamy Wash
Stiefel, a GSK company
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments, as well as products for dry cuticles, hyperhidrosis, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]
To improve patient care and outcomes, leading dermatologists offered their recommendations on adult acne products. Consideration must be given to:
- Bioclear Face Lotion and Face Cream
Jan Marini Skin Research, Inc
“These products contain a powerful combination of glycolic, salicylic, and azelaic acids to smooth and brighten acne-prone skin.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- Neutrogena Clear Pore Cleanser/Mask
Johnson & Johnson Consumer Inc
“This is a good daily product for acne-prone skin. It is formulated with benzoyl peroxide and can be used as a daily wash or mask.”—Anthony M. Rossi, MD, New York, New York
- Offects Sulfur Masque Acne Treatment
ZO Skin Health Inc
“This nonirritating mask reduces inflammation and oiliness and is safe to use in pregnancy.”—Larisa Ravitskiy, MD, Gahanna, Ohio
- PanOxyl Acne Foaming Wash and Acne Creamy Wash
Stiefel, a GSK company
Recommended by Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Athlete’s foot treatments, as well as products for dry cuticles, hyperhidrosis, and sensitive skin will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
[polldaddy:9711250]

VIDEO: Advances in noninvasive fat reduction include permanent effects
WAILEA, HAWAII – In the past few years, there have been “exciting” advances in noninvasive techniques to permanently remove fat, according to Suzanne Kilmer, MD, of the department of dermatology, University of California, Davis.
There are devices now available to reduce fat “in a permanent way that’s not injurious, it’s not uncomfortable – patients love it,” Dr. Kilmer said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Currently, the three noninvasive modalities she considers most effective for reducing fat are cryolipolysis, the 1,060-nm laser, and focused pulsed ultrasound. In the interview, she discussed the ways these treatments work and their safety.
With all three, “the fat that goes away stays away,” said Dr. Kilmer, who is director of the Laser and Skin Surgery Center of Northern California, Sacramento. Treatment results in release of fat, which is “cleared like it is as if you ate a cheeseburger,” she added. Interestingly, she said, trials that have looked at whether the fat reduction is accompanied by weight loss have found that, in most cases, the patient’s weight remains stable.
Dr. Kilmer’s disclosures included serving as a consultant and/or researcher for Allergan, Cutera, Cynosure, Cytrellis, Kythera, Lumenis, Merz, Miramar, Sebacia, Sienna Labs, Solta, Zeltiq, and Zift.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – In the past few years, there have been “exciting” advances in noninvasive techniques to permanently remove fat, according to Suzanne Kilmer, MD, of the department of dermatology, University of California, Davis.
There are devices now available to reduce fat “in a permanent way that’s not injurious, it’s not uncomfortable – patients love it,” Dr. Kilmer said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Currently, the three noninvasive modalities she considers most effective for reducing fat are cryolipolysis, the 1,060-nm laser, and focused pulsed ultrasound. In the interview, she discussed the ways these treatments work and their safety.
With all three, “the fat that goes away stays away,” said Dr. Kilmer, who is director of the Laser and Skin Surgery Center of Northern California, Sacramento. Treatment results in release of fat, which is “cleared like it is as if you ate a cheeseburger,” she added. Interestingly, she said, trials that have looked at whether the fat reduction is accompanied by weight loss have found that, in most cases, the patient’s weight remains stable.
Dr. Kilmer’s disclosures included serving as a consultant and/or researcher for Allergan, Cutera, Cynosure, Cytrellis, Kythera, Lumenis, Merz, Miramar, Sebacia, Sienna Labs, Solta, Zeltiq, and Zift.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – In the past few years, there have been “exciting” advances in noninvasive techniques to permanently remove fat, according to Suzanne Kilmer, MD, of the department of dermatology, University of California, Davis.
There are devices now available to reduce fat “in a permanent way that’s not injurious, it’s not uncomfortable – patients love it,” Dr. Kilmer said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Currently, the three noninvasive modalities she considers most effective for reducing fat are cryolipolysis, the 1,060-nm laser, and focused pulsed ultrasound. In the interview, she discussed the ways these treatments work and their safety.
With all three, “the fat that goes away stays away,” said Dr. Kilmer, who is director of the Laser and Skin Surgery Center of Northern California, Sacramento. Treatment results in release of fat, which is “cleared like it is as if you ate a cheeseburger,” she added. Interestingly, she said, trials that have looked at whether the fat reduction is accompanied by weight loss have found that, in most cases, the patient’s weight remains stable.
Dr. Kilmer’s disclosures included serving as a consultant and/or researcher for Allergan, Cutera, Cynosure, Cytrellis, Kythera, Lumenis, Merz, Miramar, Sebacia, Sienna Labs, Solta, Zeltiq, and Zift.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

Laser resurfacing can effectively minimize post surgery scars
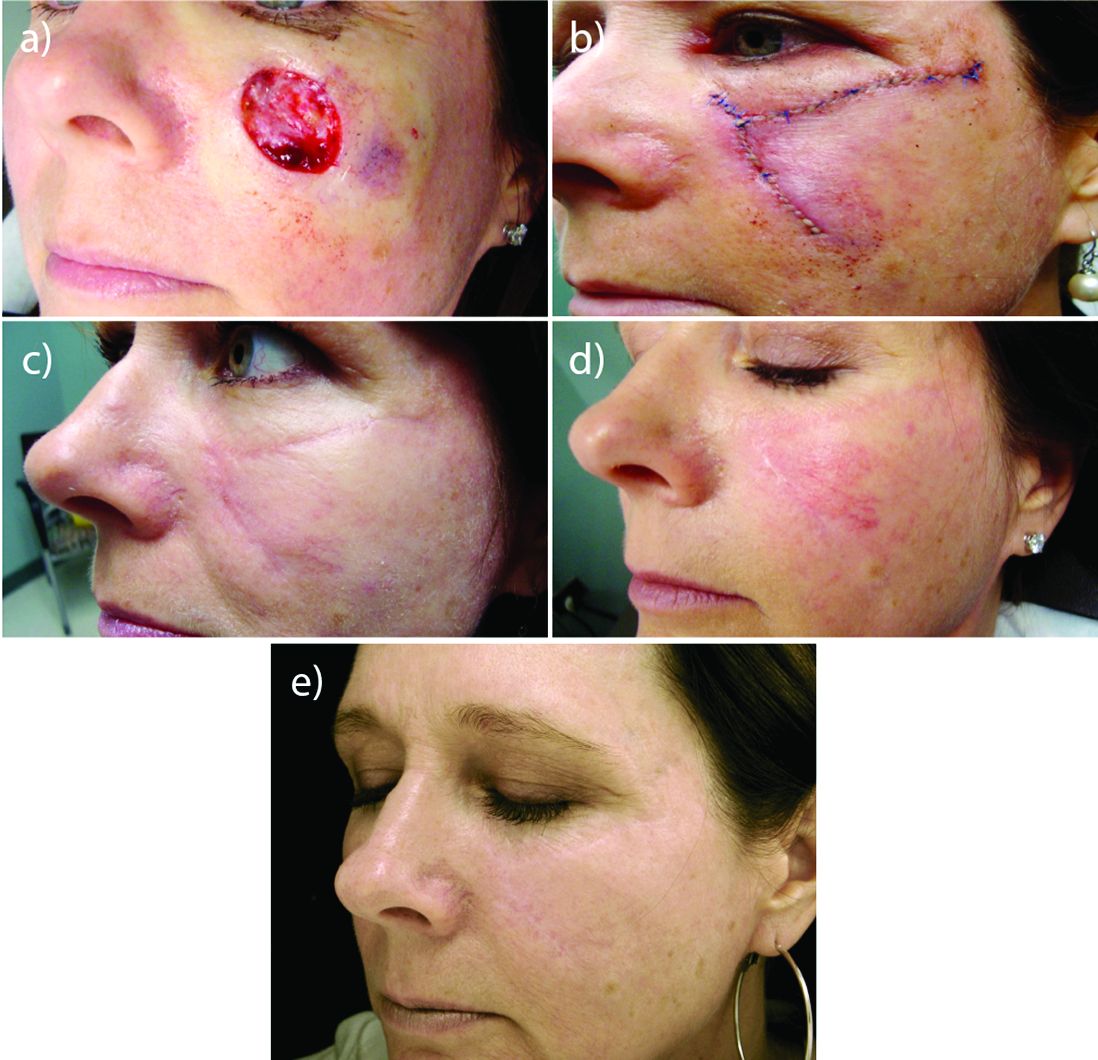
MIAMI – In his practice, Joel L. Cohen, MD, spends a good part of his day doing Mohs surgery, “with the goal of cancer removal, and after surgery, having the patient look good,” he said at the Orlando Dermatology Aesthetic and Clinical Conference.
“Having resurfacing in my practice has allowed me to treat not only wrinkles and etched lines, but also help skin cancer patients by blending and minimizing their skin cancer scars,” said Dr. Cohen, an aesthetic dermatologist and Mohs surgeon in private practice in Denver.

Resurfacing in his practice using a variety of lasers is very helpful, Dr. Cohen said. He published a study in November that compared pulse dye laser, CO2 ablative fractional lasers, or a combination of both for modification of scars following Mohs surgery (J Drugs Dermatol. 2016 Nov 1;15[11]:1315-9).
The prospective, multicenter study revealed that although both monotherapy approaches were safe and effective, the combination of pulse dye laser and fractional ablative laser offered some synergy that was preferred by patients.
Perioral resurfacing possible
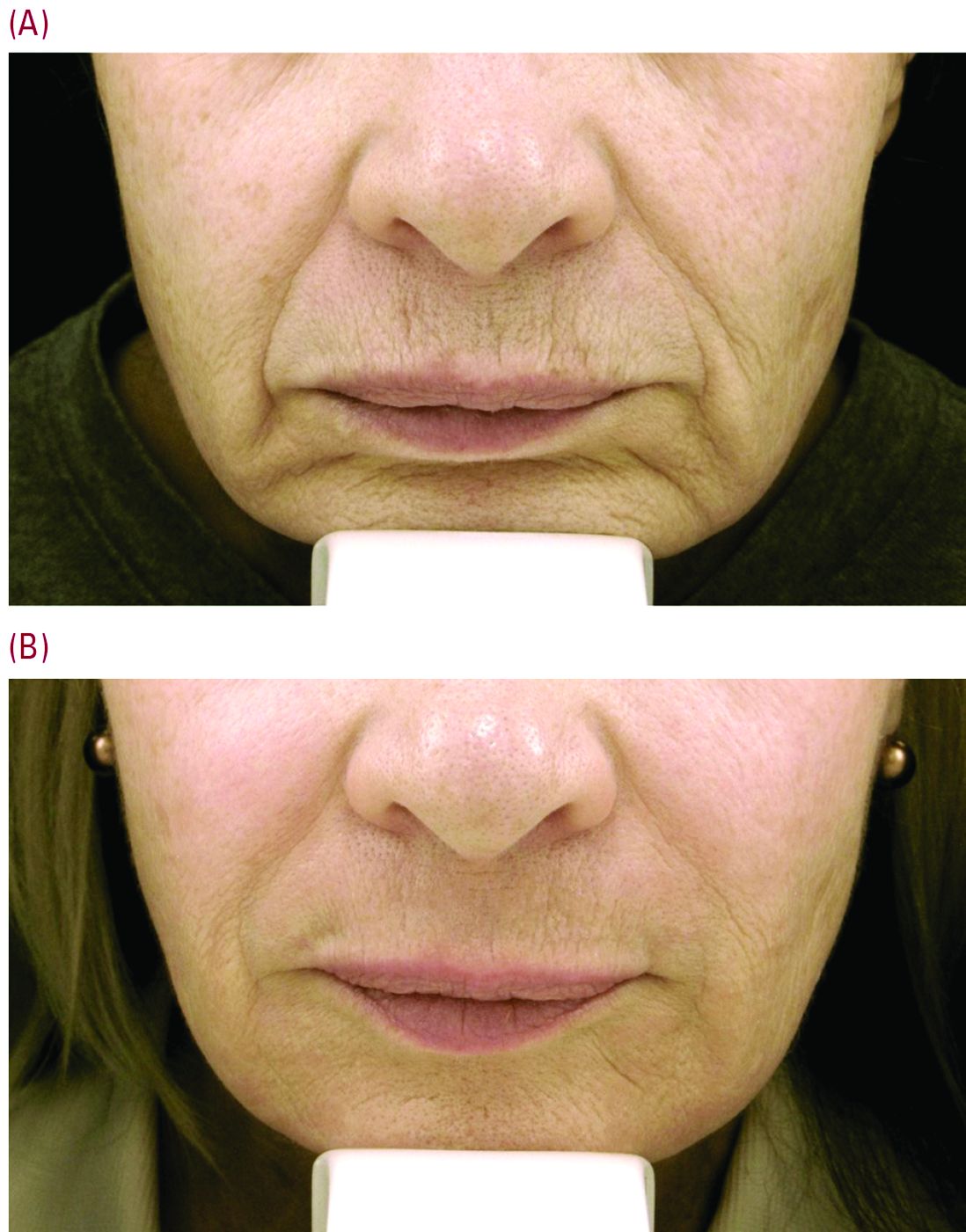
Beyond the world of treating scars, a typical cosmetic patient in Dr. Cohen’s practice presents with numerous lines around the perioral area. “When people think about rejuvenation of the lips, they only think of fillers. But fillers are not the only way to rejuvenate this area, and it is really about choosing the right tool for the right job – where resurfacing lasers are needed.”
Set realistic expectations
Setting the right expectations for people is extremely important, Dr. Cohen said. “You can educate the patient that if you’re putting the needle into the lines, you’re only treating the larger lines that you can get a 30-g needle into, but there are often a host of other lines in that area – many of which are too small to get a needle into.”
As a starting point, neuromodulators can have a role in trying to prevent or delay etched-in lines from forming around the mouth in the first place. “These are the lines between the musculature, the ones you see when you ask the patient to purse their lips,” Dr. Cohen said. He typically injects a medium dose of one of three neuromodulators – such as 6-10 U of onabotulinumtoxinA (Botox), 6-10 U of incobotulinumtoxinA (Xeomin) or 14-18 U of abobotulinumtoxinA (Dysport). “Then somewhere between week 8 and 10, there is an attenuation of the effect, and I often will see patients back then for additional treatment with a neuromodulator,” he added.
“For our every day patient complaining of lots of etched perioral lines, we have laser resurfacing,” Dr. Cohen noted. He is a bigger proponent of full-field erbium treatment versus fractional ablative laser resurfacing for these prominent upper cutaneous lip lines because the results are much more impressive with a single treatment. He added that dermatologists could do fractional treatment around the rest of the face, and reserve the erbium resurfacing to improve the appearance of lines around the mouth and prominent creping skin around the eyes.
Realistic postprocedure expectations are especially essential in the days after erbium laser resurfacing – as it is a tough downtime procedure for patients, often taking 7-9 days to re-epithelialize. “Having photos to show patients what they will look like is really helpful,” Dr. Cohen said. He suggested showing patients a chronologic set of photos of the downtime period as well as the results – so they realize improvement occurs slowly over time. “Getting people to understand they are gong to look terrible for 1.5-2 weeks is superimportant.”
“I like to have them back in the office for a postprocedure check a few days after the bigger laser resurfacing procedures are done, just to check on them,” Dr. Cohen said. “A lot of hand holding is often needed, as there is significantly more healing time with the full-field ablative resurfacing than there is with fractional. Full-field resurfacing patients will experience postprocedure erythema for a few weeks or even months,” Dr. Cohen said. A prescription of topical steroids, and sometimes some brimonidine topical gel (Mirvaso) as well can help reduce the redness.
Toxin injection then laser resurfacing
For some patients, injection of a neuromodulator a week or 2 before laser resurfacing treatment can decrease some of the movement and contraction of the muscle, “and hopefully give them better results,” Dr. Cohen said.
Timing is important. “You don’t want to use neuromodulators on the same day of treatment,” he advised. “The thinking is swelling could potentially cause the neuromodulators to spread to unwanted adjacent muscles.”
Safety first
Another tip for the postprocedure period is to supply patients with very specific written instructions. “I wish they would follow them. Patients don’t always listen to what we advise, demonstrate, and also have written down for them,” he commented. For example, one patient had resurfacing several weeks before leaving on an undisclosed kayaking trip. Despite instructions to use sunscreen, she said she wore a hat for sun protection and developed postinflammatory hyperpigmentation around the mouth that lasted for several months, Dr. Cohen said.*
With heavy resurfacing and ablative resurfacing in general, it is advised to always give patients an antiviral prophylaxis course such as valacyclovir, but it is unfortunate that not all patients will adhere to the recommended regimen, he added.
Another patient had an adverse reaction after resurfacing because she did not follow instructions to apply white petrolatum to her chest following laser resurfacing, Dr. Cohen said. She used Neosporin, “even though in all our paperwork we say never use Neosporin and just use the petrolatum. She had a big contact dermatitis reaction to the Neosporin.”
“So you really need to caution people about the importance of following instructions very carefully,” he emphasized.
Dr. Cohen is a consultant for Sciton and for companies that manufacture injectables, including Allergan, Galderma, and Merz.
Correction 2/24/17: An earlier version of this article mischaracterized the type of pigmentation disorder that the patient developed.
MIAMI – In his practice, Joel L. Cohen, MD, spends a good part of his day doing Mohs surgery, “with the goal of cancer removal, and after surgery, having the patient look good,” he said at the Orlando Dermatology Aesthetic and Clinical Conference.
“Having resurfacing in my practice has allowed me to treat not only wrinkles and etched lines, but also help skin cancer patients by blending and minimizing their skin cancer scars,” said Dr. Cohen, an aesthetic dermatologist and Mohs surgeon in private practice in Denver.
Resurfacing in his practice using a variety of lasers is very helpful, Dr. Cohen said. He published a study in November that compared pulse dye laser, CO2 ablative fractional lasers, or a combination of both for modification of scars following Mohs surgery (J Drugs Dermatol. 2016 Nov 1;15[11]:1315-9).
The prospective, multicenter study revealed that although both monotherapy approaches were safe and effective, the combination of pulse dye laser and fractional ablative laser offered some synergy that was preferred by patients.
Perioral resurfacing possible
Beyond the world of treating scars, a typical cosmetic patient in Dr. Cohen’s practice presents with numerous lines around the perioral area. “When people think about rejuvenation of the lips, they only think of fillers. But fillers are not the only way to rejuvenate this area, and it is really about choosing the right tool for the right job – where resurfacing lasers are needed.”
Set realistic expectations
Setting the right expectations for people is extremely important, Dr. Cohen said. “You can educate the patient that if you’re putting the needle into the lines, you’re only treating the larger lines that you can get a 30-g needle into, but there are often a host of other lines in that area – many of which are too small to get a needle into.”
As a starting point, neuromodulators can have a role in trying to prevent or delay etched-in lines from forming around the mouth in the first place. “These are the lines between the musculature, the ones you see when you ask the patient to purse their lips,” Dr. Cohen said. He typically injects a medium dose of one of three neuromodulators – such as 6-10 U of onabotulinumtoxinA (Botox), 6-10 U of incobotulinumtoxinA (Xeomin) or 14-18 U of abobotulinumtoxinA (Dysport). “Then somewhere between week 8 and 10, there is an attenuation of the effect, and I often will see patients back then for additional treatment with a neuromodulator,” he added.
“For our every day patient complaining of lots of etched perioral lines, we have laser resurfacing,” Dr. Cohen noted. He is a bigger proponent of full-field erbium treatment versus fractional ablative laser resurfacing for these prominent upper cutaneous lip lines because the results are much more impressive with a single treatment. He added that dermatologists could do fractional treatment around the rest of the face, and reserve the erbium resurfacing to improve the appearance of lines around the mouth and prominent creping skin around the eyes.
Realistic postprocedure expectations are especially essential in the days after erbium laser resurfacing – as it is a tough downtime procedure for patients, often taking 7-9 days to re-epithelialize. “Having photos to show patients what they will look like is really helpful,” Dr. Cohen said. He suggested showing patients a chronologic set of photos of the downtime period as well as the results – so they realize improvement occurs slowly over time. “Getting people to understand they are gong to look terrible for 1.5-2 weeks is superimportant.”
“I like to have them back in the office for a postprocedure check a few days after the bigger laser resurfacing procedures are done, just to check on them,” Dr. Cohen said. “A lot of hand holding is often needed, as there is significantly more healing time with the full-field ablative resurfacing than there is with fractional. Full-field resurfacing patients will experience postprocedure erythema for a few weeks or even months,” Dr. Cohen said. A prescription of topical steroids, and sometimes some brimonidine topical gel (Mirvaso) as well can help reduce the redness.
Toxin injection then laser resurfacing
For some patients, injection of a neuromodulator a week or 2 before laser resurfacing treatment can decrease some of the movement and contraction of the muscle, “and hopefully give them better results,” Dr. Cohen said.
Timing is important. “You don’t want to use neuromodulators on the same day of treatment,” he advised. “The thinking is swelling could potentially cause the neuromodulators to spread to unwanted adjacent muscles.”
Safety first
Another tip for the postprocedure period is to supply patients with very specific written instructions. “I wish they would follow them. Patients don’t always listen to what we advise, demonstrate, and also have written down for them,” he commented. For example, one patient had resurfacing several weeks before leaving on an undisclosed kayaking trip. Despite instructions to use sunscreen, she said she wore a hat for sun protection and developed postinflammatory hyperpigmentation around the mouth that lasted for several months, Dr. Cohen said.*
With heavy resurfacing and ablative resurfacing in general, it is advised to always give patients an antiviral prophylaxis course such as valacyclovir, but it is unfortunate that not all patients will adhere to the recommended regimen, he added.
Another patient had an adverse reaction after resurfacing because she did not follow instructions to apply white petrolatum to her chest following laser resurfacing, Dr. Cohen said. She used Neosporin, “even though in all our paperwork we say never use Neosporin and just use the petrolatum. She had a big contact dermatitis reaction to the Neosporin.”
“So you really need to caution people about the importance of following instructions very carefully,” he emphasized.
Dr. Cohen is a consultant for Sciton and for companies that manufacture injectables, including Allergan, Galderma, and Merz.
Correction 2/24/17: An earlier version of this article mischaracterized the type of pigmentation disorder that the patient developed.
MIAMI – In his practice, Joel L. Cohen, MD, spends a good part of his day doing Mohs surgery, “with the goal of cancer removal, and after surgery, having the patient look good,” he said at the Orlando Dermatology Aesthetic and Clinical Conference.
“Having resurfacing in my practice has allowed me to treat not only wrinkles and etched lines, but also help skin cancer patients by blending and minimizing their skin cancer scars,” said Dr. Cohen, an aesthetic dermatologist and Mohs surgeon in private practice in Denver.
Resurfacing in his practice using a variety of lasers is very helpful, Dr. Cohen said. He published a study in November that compared pulse dye laser, CO2 ablative fractional lasers, or a combination of both for modification of scars following Mohs surgery (J Drugs Dermatol. 2016 Nov 1;15[11]:1315-9).
The prospective, multicenter study revealed that although both monotherapy approaches were safe and effective, the combination of pulse dye laser and fractional ablative laser offered some synergy that was preferred by patients.
Perioral resurfacing possible
Beyond the world of treating scars, a typical cosmetic patient in Dr. Cohen’s practice presents with numerous lines around the perioral area. “When people think about rejuvenation of the lips, they only think of fillers. But fillers are not the only way to rejuvenate this area, and it is really about choosing the right tool for the right job – where resurfacing lasers are needed.”
Set realistic expectations
Setting the right expectations for people is extremely important, Dr. Cohen said. “You can educate the patient that if you’re putting the needle into the lines, you’re only treating the larger lines that you can get a 30-g needle into, but there are often a host of other lines in that area – many of which are too small to get a needle into.”
As a starting point, neuromodulators can have a role in trying to prevent or delay etched-in lines from forming around the mouth in the first place. “These are the lines between the musculature, the ones you see when you ask the patient to purse their lips,” Dr. Cohen said. He typically injects a medium dose of one of three neuromodulators – such as 6-10 U of onabotulinumtoxinA (Botox), 6-10 U of incobotulinumtoxinA (Xeomin) or 14-18 U of abobotulinumtoxinA (Dysport). “Then somewhere between week 8 and 10, there is an attenuation of the effect, and I often will see patients back then for additional treatment with a neuromodulator,” he added.
“For our every day patient complaining of lots of etched perioral lines, we have laser resurfacing,” Dr. Cohen noted. He is a bigger proponent of full-field erbium treatment versus fractional ablative laser resurfacing for these prominent upper cutaneous lip lines because the results are much more impressive with a single treatment. He added that dermatologists could do fractional treatment around the rest of the face, and reserve the erbium resurfacing to improve the appearance of lines around the mouth and prominent creping skin around the eyes.
Realistic postprocedure expectations are especially essential in the days after erbium laser resurfacing – as it is a tough downtime procedure for patients, often taking 7-9 days to re-epithelialize. “Having photos to show patients what they will look like is really helpful,” Dr. Cohen said. He suggested showing patients a chronologic set of photos of the downtime period as well as the results – so they realize improvement occurs slowly over time. “Getting people to understand they are gong to look terrible for 1.5-2 weeks is superimportant.”
“I like to have them back in the office for a postprocedure check a few days after the bigger laser resurfacing procedures are done, just to check on them,” Dr. Cohen said. “A lot of hand holding is often needed, as there is significantly more healing time with the full-field ablative resurfacing than there is with fractional. Full-field resurfacing patients will experience postprocedure erythema for a few weeks or even months,” Dr. Cohen said. A prescription of topical steroids, and sometimes some brimonidine topical gel (Mirvaso) as well can help reduce the redness.
Toxin injection then laser resurfacing
For some patients, injection of a neuromodulator a week or 2 before laser resurfacing treatment can decrease some of the movement and contraction of the muscle, “and hopefully give them better results,” Dr. Cohen said.
Timing is important. “You don’t want to use neuromodulators on the same day of treatment,” he advised. “The thinking is swelling could potentially cause the neuromodulators to spread to unwanted adjacent muscles.”
Safety first
Another tip for the postprocedure period is to supply patients with very specific written instructions. “I wish they would follow them. Patients don’t always listen to what we advise, demonstrate, and also have written down for them,” he commented. For example, one patient had resurfacing several weeks before leaving on an undisclosed kayaking trip. Despite instructions to use sunscreen, she said she wore a hat for sun protection and developed postinflammatory hyperpigmentation around the mouth that lasted for several months, Dr. Cohen said.*
With heavy resurfacing and ablative resurfacing in general, it is advised to always give patients an antiviral prophylaxis course such as valacyclovir, but it is unfortunate that not all patients will adhere to the recommended regimen, he added.
Another patient had an adverse reaction after resurfacing because she did not follow instructions to apply white petrolatum to her chest following laser resurfacing, Dr. Cohen said. She used Neosporin, “even though in all our paperwork we say never use Neosporin and just use the petrolatum. She had a big contact dermatitis reaction to the Neosporin.”
“So you really need to caution people about the importance of following instructions very carefully,” he emphasized.
Dr. Cohen is a consultant for Sciton and for companies that manufacture injectables, including Allergan, Galderma, and Merz.
Correction 2/24/17: An earlier version of this article mischaracterized the type of pigmentation disorder that the patient developed.
EXPERT ANALYSIS FROM THE ODAC CONFERENCE
Consider plumes from laser hair removal a biohazard
The plume of burning hair occurring during laser hair removal should be considered a biohazard, reported Gary S. Chuang, MD, of Harvard Medical School, Boston and his coauthors.
Use of smoke evacuators, good ventilation, and respiratory protection are warranted, especially for health care workers exposed to the plume for extended periods, they said.

While the laser was treating the hair, the particle counters recorded a eightfold increase in ultrafine-particle concentrations, compared with ambient room baseline; this occurred even with a smoke evacuator within 5 cm of the procedure site. When a smoke evacuator was turned off for 30 seconds, the increase was 26-fold, Dr. Chuang and his associates reported.
Read more at JAMA Dermatology (2016;152[12]:1320-6).
The plume of burning hair occurring during laser hair removal should be considered a biohazard, reported Gary S. Chuang, MD, of Harvard Medical School, Boston and his coauthors.
Use of smoke evacuators, good ventilation, and respiratory protection are warranted, especially for health care workers exposed to the plume for extended periods, they said.
While the laser was treating the hair, the particle counters recorded a eightfold increase in ultrafine-particle concentrations, compared with ambient room baseline; this occurred even with a smoke evacuator within 5 cm of the procedure site. When a smoke evacuator was turned off for 30 seconds, the increase was 26-fold, Dr. Chuang and his associates reported.
Read more at JAMA Dermatology (2016;152[12]:1320-6).
The plume of burning hair occurring during laser hair removal should be considered a biohazard, reported Gary S. Chuang, MD, of Harvard Medical School, Boston and his coauthors.
Use of smoke evacuators, good ventilation, and respiratory protection are warranted, especially for health care workers exposed to the plume for extended periods, they said.
While the laser was treating the hair, the particle counters recorded a eightfold increase in ultrafine-particle concentrations, compared with ambient room baseline; this occurred even with a smoke evacuator within 5 cm of the procedure site. When a smoke evacuator was turned off for 30 seconds, the increase was 26-fold, Dr. Chuang and his associates reported.
Read more at JAMA Dermatology (2016;152[12]:1320-6).
FROM JAMA DERMATOLOGY
Picosecond alexandrite laser with lens modification effective for wrinkles
reported Robert A. Weiss, MD, of the MD Laser and Vein Institute, Baltimore, and his associates.
In a prospective, blinded study of perioral and periocular wrinkles in 40 healthy women (average age 58 years) who were nonsmokers, a 6-mm spot size diffractive lens array delivered a fluence of 0.71 J/cm2 at each focal point using 10-Hz pulse repetition at a pulse duration of 750 picoseconds. During each treatment, four passes of the 755-nm alexandrite laser (Picosure) for a total of 5,000 pulses were delivered. At 6 months follow-up, the mean Fitzpatrick wrinkle score had improved to 3.47 from the baseline average of 5.48 (P less than .05), with an overall average change in score of 1.97. Adverse events were mild, and all resolved, most within 24 hours (Lasers Surg Med. 2017 Jan;49[1]:40-44).
At 1 and 6 months, physician satisfaction ratings were 97.4% and 89.5% (extremely satisfied or satisfied), respectively. At 1 month, 42.1% of the patients were extremely satisfied, and 47.4% were satisfied. At 6 months, 42.1% were extremely likely to recommend the treatment, and 44.7% were likely to recommend the treatment.
The picosecond 755-nm alexandrite laser has been reported to be effective for tattoo removal, compared with the nanosecond domain lasers, they noted.
Dr. Weiss and a coauthor are consultants, researchers, and speakers for Cynosure, manufacturer of PicoSure. The other authors had no financial disclosures.
reported Robert A. Weiss, MD, of the MD Laser and Vein Institute, Baltimore, and his associates.
In a prospective, blinded study of perioral and periocular wrinkles in 40 healthy women (average age 58 years) who were nonsmokers, a 6-mm spot size diffractive lens array delivered a fluence of 0.71 J/cm2 at each focal point using 10-Hz pulse repetition at a pulse duration of 750 picoseconds. During each treatment, four passes of the 755-nm alexandrite laser (Picosure) for a total of 5,000 pulses were delivered. At 6 months follow-up, the mean Fitzpatrick wrinkle score had improved to 3.47 from the baseline average of 5.48 (P less than .05), with an overall average change in score of 1.97. Adverse events were mild, and all resolved, most within 24 hours (Lasers Surg Med. 2017 Jan;49[1]:40-44).
At 1 and 6 months, physician satisfaction ratings were 97.4% and 89.5% (extremely satisfied or satisfied), respectively. At 1 month, 42.1% of the patients were extremely satisfied, and 47.4% were satisfied. At 6 months, 42.1% were extremely likely to recommend the treatment, and 44.7% were likely to recommend the treatment.
The picosecond 755-nm alexandrite laser has been reported to be effective for tattoo removal, compared with the nanosecond domain lasers, they noted.
Dr. Weiss and a coauthor are consultants, researchers, and speakers for Cynosure, manufacturer of PicoSure. The other authors had no financial disclosures.
reported Robert A. Weiss, MD, of the MD Laser and Vein Institute, Baltimore, and his associates.
In a prospective, blinded study of perioral and periocular wrinkles in 40 healthy women (average age 58 years) who were nonsmokers, a 6-mm spot size diffractive lens array delivered a fluence of 0.71 J/cm2 at each focal point using 10-Hz pulse repetition at a pulse duration of 750 picoseconds. During each treatment, four passes of the 755-nm alexandrite laser (Picosure) for a total of 5,000 pulses were delivered. At 6 months follow-up, the mean Fitzpatrick wrinkle score had improved to 3.47 from the baseline average of 5.48 (P less than .05), with an overall average change in score of 1.97. Adverse events were mild, and all resolved, most within 24 hours (Lasers Surg Med. 2017 Jan;49[1]:40-44).
At 1 and 6 months, physician satisfaction ratings were 97.4% and 89.5% (extremely satisfied or satisfied), respectively. At 1 month, 42.1% of the patients were extremely satisfied, and 47.4% were satisfied. At 6 months, 42.1% were extremely likely to recommend the treatment, and 44.7% were likely to recommend the treatment.
The picosecond 755-nm alexandrite laser has been reported to be effective for tattoo removal, compared with the nanosecond domain lasers, they noted.
Dr. Weiss and a coauthor are consultants, researchers, and speakers for Cynosure, manufacturer of PicoSure. The other authors had no financial disclosures.
FROM LASERS IN SURGERY AND MEDICINE
Dual fractional laser offers advantages for facial rejuvenation
MIAMI – A device that combines nonablative and ablative laser energies can promote mild to moderate facial photo rejuvenation and improve the appearance of fine lines and wrinkles, according to Jason Pozner, MD.
Clinicians can tailor the depth for the 1470 nm nonablative diode and the 2940 nm Er:YAG lasers for each individual patient, Dr. Pozner said at the Orlando Dermatology Aesthetic and Clinical Conference. Advantages of resurfacing with the device, the HALO laser, include a cost-effective disposable tip and the ability to combine treatment with other therapies, he noted.
Before treatment begins, clinicians use the device to take facial measurements. Many patients find this precision reassuring, Dr. Pozner said during a live patient demonstration. Also, the device uses the information to help clinicians deliver the appropriate duration of therapy.
At this stage, it is a simple procedure, said Dr. Pozner, a plastic surgeon in a group practice in Boca Raton, Fla. Suction is turned on and the probe is then slowly advanced back and forth until the zone is finished, and “the laser beeps at you and you know you’re done,” he explained.
The HALO laser is useful for rejuvenation with little downtime. Most women treated with the device can wear makeup the same day, although more aggressively treated patients generally wait 1 additional day, Dr. Pozner said.
“I’ve never seen anything in our practice that gives this good a clinical result with this little downtime,” he added. He initially expected results to fall in between those associated with typical nonablative and ablative fractional laser treatments. But “in our experience, we get better results than ablative fractional [laser therapy], a story of one plus one equals three,” he said. “No matter what laser setting you use, patients are better by 5 days.”
When combined with intense pulsed light (IPL) treatment you can get a “double whammy effect,” Dr. Pozner said.
A meeting attendee asked about the appropriate order of IPL and HALO treatments. “When you combine the BBL (IPL) and HALO, yes, you do the IPL first,” Joel L. Cohen, MD, a private practice aesthetic dermatologist and Mohs surgeon in Denver who moderated the session at the meeting and also gave his own lecture on resurfacing options for the face.
Aside from the laser itself, the HALO system contains two tubes integrated into the handpiece, one of which is a Zimmer to deliver cooling during the procedure and the other is an air evacuator, he explained. “By having all of this integrated into the handpiece itself, it makes it much easier for the nurse who is circulating in the room to assist.”
Patients may feel warm for about 90 minutes post procedure, Dr. Cohen said. Make sure patients’ hands are clean and that the circulating nurse has given them an ice pack to minimize discomfort. “Even though I practice in Denver, where it is freezing cold right now, I’ve had patients drive home with the air conditioning on – just to try to cool down in the hour or so immediately following the laser treatment.”
Dr. Pozner said that a decrease in pore counts was an unexpected effect of HALO treatment, and he estimated that patients end up with about 20% fewer pores in treated areas, which can be advantage because “nothing else works on pores.” In his experience, most of the pore reduction persists over time.
A HALO disposal tip costs approximately $50, which he said was inexpensive, compared with other devices.
Dr. Cohen said that in his practice, using HALO, “We can give patients a significant improvement in overall photodamage and mild improvement in wrinkles with only about 5 days of redness and swelling, and on the last few days, some coffee-ground appearance.” The nonablative component can promote coagulation, so there is less bleeding when you turn up the erbium component, “offering synergistic results for the patient,” he added.
Dr. Pozner has received equipment, consulting fees, and honoraria from Halo manufacturer Sciton and is a member of the company’s advisory board and speakers bureau. Dr. Cohen is a consultant for Sciton.
MIAMI – A device that combines nonablative and ablative laser energies can promote mild to moderate facial photo rejuvenation and improve the appearance of fine lines and wrinkles, according to Jason Pozner, MD.
Clinicians can tailor the depth for the 1470 nm nonablative diode and the 2940 nm Er:YAG lasers for each individual patient, Dr. Pozner said at the Orlando Dermatology Aesthetic and Clinical Conference. Advantages of resurfacing with the device, the HALO laser, include a cost-effective disposable tip and the ability to combine treatment with other therapies, he noted.
Before treatment begins, clinicians use the device to take facial measurements. Many patients find this precision reassuring, Dr. Pozner said during a live patient demonstration. Also, the device uses the information to help clinicians deliver the appropriate duration of therapy.
At this stage, it is a simple procedure, said Dr. Pozner, a plastic surgeon in a group practice in Boca Raton, Fla. Suction is turned on and the probe is then slowly advanced back and forth until the zone is finished, and “the laser beeps at you and you know you’re done,” he explained.
The HALO laser is useful for rejuvenation with little downtime. Most women treated with the device can wear makeup the same day, although more aggressively treated patients generally wait 1 additional day, Dr. Pozner said.
“I’ve never seen anything in our practice that gives this good a clinical result with this little downtime,” he added. He initially expected results to fall in between those associated with typical nonablative and ablative fractional laser treatments. But “in our experience, we get better results than ablative fractional [laser therapy], a story of one plus one equals three,” he said. “No matter what laser setting you use, patients are better by 5 days.”
When combined with intense pulsed light (IPL) treatment you can get a “double whammy effect,” Dr. Pozner said.
A meeting attendee asked about the appropriate order of IPL and HALO treatments. “When you combine the BBL (IPL) and HALO, yes, you do the IPL first,” Joel L. Cohen, MD, a private practice aesthetic dermatologist and Mohs surgeon in Denver who moderated the session at the meeting and also gave his own lecture on resurfacing options for the face.
Aside from the laser itself, the HALO system contains two tubes integrated into the handpiece, one of which is a Zimmer to deliver cooling during the procedure and the other is an air evacuator, he explained. “By having all of this integrated into the handpiece itself, it makes it much easier for the nurse who is circulating in the room to assist.”
Patients may feel warm for about 90 minutes post procedure, Dr. Cohen said. Make sure patients’ hands are clean and that the circulating nurse has given them an ice pack to minimize discomfort. “Even though I practice in Denver, where it is freezing cold right now, I’ve had patients drive home with the air conditioning on – just to try to cool down in the hour or so immediately following the laser treatment.”
Dr. Pozner said that a decrease in pore counts was an unexpected effect of HALO treatment, and he estimated that patients end up with about 20% fewer pores in treated areas, which can be advantage because “nothing else works on pores.” In his experience, most of the pore reduction persists over time.
A HALO disposal tip costs approximately $50, which he said was inexpensive, compared with other devices.
Dr. Cohen said that in his practice, using HALO, “We can give patients a significant improvement in overall photodamage and mild improvement in wrinkles with only about 5 days of redness and swelling, and on the last few days, some coffee-ground appearance.” The nonablative component can promote coagulation, so there is less bleeding when you turn up the erbium component, “offering synergistic results for the patient,” he added.
Dr. Pozner has received equipment, consulting fees, and honoraria from Halo manufacturer Sciton and is a member of the company’s advisory board and speakers bureau. Dr. Cohen is a consultant for Sciton.
MIAMI – A device that combines nonablative and ablative laser energies can promote mild to moderate facial photo rejuvenation and improve the appearance of fine lines and wrinkles, according to Jason Pozner, MD.
Clinicians can tailor the depth for the 1470 nm nonablative diode and the 2940 nm Er:YAG lasers for each individual patient, Dr. Pozner said at the Orlando Dermatology Aesthetic and Clinical Conference. Advantages of resurfacing with the device, the HALO laser, include a cost-effective disposable tip and the ability to combine treatment with other therapies, he noted.
Before treatment begins, clinicians use the device to take facial measurements. Many patients find this precision reassuring, Dr. Pozner said during a live patient demonstration. Also, the device uses the information to help clinicians deliver the appropriate duration of therapy.
At this stage, it is a simple procedure, said Dr. Pozner, a plastic surgeon in a group practice in Boca Raton, Fla. Suction is turned on and the probe is then slowly advanced back and forth until the zone is finished, and “the laser beeps at you and you know you’re done,” he explained.
The HALO laser is useful for rejuvenation with little downtime. Most women treated with the device can wear makeup the same day, although more aggressively treated patients generally wait 1 additional day, Dr. Pozner said.
“I’ve never seen anything in our practice that gives this good a clinical result with this little downtime,” he added. He initially expected results to fall in between those associated with typical nonablative and ablative fractional laser treatments. But “in our experience, we get better results than ablative fractional [laser therapy], a story of one plus one equals three,” he said. “No matter what laser setting you use, patients are better by 5 days.”
When combined with intense pulsed light (IPL) treatment you can get a “double whammy effect,” Dr. Pozner said.
A meeting attendee asked about the appropriate order of IPL and HALO treatments. “When you combine the BBL (IPL) and HALO, yes, you do the IPL first,” Joel L. Cohen, MD, a private practice aesthetic dermatologist and Mohs surgeon in Denver who moderated the session at the meeting and also gave his own lecture on resurfacing options for the face.
Aside from the laser itself, the HALO system contains two tubes integrated into the handpiece, one of which is a Zimmer to deliver cooling during the procedure and the other is an air evacuator, he explained. “By having all of this integrated into the handpiece itself, it makes it much easier for the nurse who is circulating in the room to assist.”
Patients may feel warm for about 90 minutes post procedure, Dr. Cohen said. Make sure patients’ hands are clean and that the circulating nurse has given them an ice pack to minimize discomfort. “Even though I practice in Denver, where it is freezing cold right now, I’ve had patients drive home with the air conditioning on – just to try to cool down in the hour or so immediately following the laser treatment.”
Dr. Pozner said that a decrease in pore counts was an unexpected effect of HALO treatment, and he estimated that patients end up with about 20% fewer pores in treated areas, which can be advantage because “nothing else works on pores.” In his experience, most of the pore reduction persists over time.
A HALO disposal tip costs approximately $50, which he said was inexpensive, compared with other devices.
Dr. Cohen said that in his practice, using HALO, “We can give patients a significant improvement in overall photodamage and mild improvement in wrinkles with only about 5 days of redness and swelling, and on the last few days, some coffee-ground appearance.” The nonablative component can promote coagulation, so there is less bleeding when you turn up the erbium component, “offering synergistic results for the patient,” he added.
Dr. Pozner has received equipment, consulting fees, and honoraria from Halo manufacturer Sciton and is a member of the company’s advisory board and speakers bureau. Dr. Cohen is a consultant for Sciton.
AT THE ODAC CONFERENCE
Microneedling With Platelet-Rich Plasma


Tips to maximize minimally invasive lower facial lift procedure
MIAMI – Lifting the lower face using minimally invasive barbed sutures can yield rejuvenation results that last 12-18 months, providing an option for patients who do not wish to undergo full facelift surgery, according to a presentation at ODAC 2017.
“We have something new in our toolbox. The Silhouette InstaLift is a “good new thing to consider adding to your practice. It works really nice for me in combination with other facial rejuvenation strategies,” said Susan Weinkle, MD, a private practice Mohs surgeon and aesthetic dermatologist in Bradenton, Fla.
“Now we can reposition the skin. It works quite nicely in skin of color also,” Dr. Weinkle said during a lecture and live demonstration at the Orlando Dermatology Aesthetic and Clinical Conference.
Procedure tips
Begin by marking where on the patient’s face you intend to place the sutures. The proper vector is a straight lift back toward the upper ear in many cases. Also, take a photo before you start, so you know the location of the sutures in case the patient comes back for more, Dr. Weinkle recommended.
“What I like to do next is to sit the patient up and look at them head-on,” Dr. Weinkle said. “It helps to tweak the placement of the suture markings.” If a patient’s face appears asymmetrical, the dermatologist can place more sutures on one side than the other. Also, when there are neck issues, you can put an exit point for the sutures 1.5 cm below the mandible, she added.
Be patient after you anesthetize the entry and exit points because the epinephrine does not work immediately, Dr. Weinkle advised.
She does not anesthetize along the entire suture tract because the aim is to thread the sutures through the subcutaneous tissue. “You do not want to anesthetize the tract area between entry and exit points. If the patient feels it, you’re probably too superficial and you’re in the dermis.”
The next step is using an 18G needle to form an entry point for the 23G needle. “Pinch the skin, insert and stretch the skin just a bit. If you don’t pinch at the entry point, the cones can be difficult to pop in.” Dr. Weinkle said. Also, if you establish all entry points before inserting the sutures, it can save time.
Dr. Weinkle generally uses a number 8 InstaLift suture, but it also comes in sizes 12 and 16. After you open the package, gently pull the suture to tighten the knots between the cones. “Don’t pull hard from both ends – you can break the suture.”
When inserting the long needle to place the suture, it’s “almost like playing the violin with a bow.” As the clinician advances along tract line, he or she should run the needle between thumb and forefinger to check the positioning. Once the suture is placed and the needle removed, pull medially on the suture until the cones audibly “pop” – they are self anchoring. “I’ve seen some people break the sutures. You can pull them out and start again,” she noted.
“InstaLift is a bit of a misnomer,” Dr. Weinkle said. “Fibroblast stimulation and collagen improves final result over the next 2-3 months.” Improvements can last 12-18 months – it’s not permanent. “I think I would make a great candidate,” she joked. “Unfortunately, this is one thing I cannot do myself.”
There is minimal bruising after the procedure in Dr. Weinkle’s experience. Potential complications include swelling, dimpling at entry points, misplacement, and ecchymosis.
Dr. Weinkle is a consultant and principal investigator for Sinclair Pharma, manufacturer of InstaLift.
MIAMI – Lifting the lower face using minimally invasive barbed sutures can yield rejuvenation results that last 12-18 months, providing an option for patients who do not wish to undergo full facelift surgery, according to a presentation at ODAC 2017.
“We have something new in our toolbox. The Silhouette InstaLift is a “good new thing to consider adding to your practice. It works really nice for me in combination with other facial rejuvenation strategies,” said Susan Weinkle, MD, a private practice Mohs surgeon and aesthetic dermatologist in Bradenton, Fla.
“Now we can reposition the skin. It works quite nicely in skin of color also,” Dr. Weinkle said during a lecture and live demonstration at the Orlando Dermatology Aesthetic and Clinical Conference.
Procedure tips
Begin by marking where on the patient’s face you intend to place the sutures. The proper vector is a straight lift back toward the upper ear in many cases. Also, take a photo before you start, so you know the location of the sutures in case the patient comes back for more, Dr. Weinkle recommended.
“What I like to do next is to sit the patient up and look at them head-on,” Dr. Weinkle said. “It helps to tweak the placement of the suture markings.” If a patient’s face appears asymmetrical, the dermatologist can place more sutures on one side than the other. Also, when there are neck issues, you can put an exit point for the sutures 1.5 cm below the mandible, she added.
Be patient after you anesthetize the entry and exit points because the epinephrine does not work immediately, Dr. Weinkle advised.
She does not anesthetize along the entire suture tract because the aim is to thread the sutures through the subcutaneous tissue. “You do not want to anesthetize the tract area between entry and exit points. If the patient feels it, you’re probably too superficial and you’re in the dermis.”
The next step is using an 18G needle to form an entry point for the 23G needle. “Pinch the skin, insert and stretch the skin just a bit. If you don’t pinch at the entry point, the cones can be difficult to pop in.” Dr. Weinkle said. Also, if you establish all entry points before inserting the sutures, it can save time.
Dr. Weinkle generally uses a number 8 InstaLift suture, but it also comes in sizes 12 and 16. After you open the package, gently pull the suture to tighten the knots between the cones. “Don’t pull hard from both ends – you can break the suture.”
When inserting the long needle to place the suture, it’s “almost like playing the violin with a bow.” As the clinician advances along tract line, he or she should run the needle between thumb and forefinger to check the positioning. Once the suture is placed and the needle removed, pull medially on the suture until the cones audibly “pop” – they are self anchoring. “I’ve seen some people break the sutures. You can pull them out and start again,” she noted.
“InstaLift is a bit of a misnomer,” Dr. Weinkle said. “Fibroblast stimulation and collagen improves final result over the next 2-3 months.” Improvements can last 12-18 months – it’s not permanent. “I think I would make a great candidate,” she joked. “Unfortunately, this is one thing I cannot do myself.”
There is minimal bruising after the procedure in Dr. Weinkle’s experience. Potential complications include swelling, dimpling at entry points, misplacement, and ecchymosis.
Dr. Weinkle is a consultant and principal investigator for Sinclair Pharma, manufacturer of InstaLift.
MIAMI – Lifting the lower face using minimally invasive barbed sutures can yield rejuvenation results that last 12-18 months, providing an option for patients who do not wish to undergo full facelift surgery, according to a presentation at ODAC 2017.
“We have something new in our toolbox. The Silhouette InstaLift is a “good new thing to consider adding to your practice. It works really nice for me in combination with other facial rejuvenation strategies,” said Susan Weinkle, MD, a private practice Mohs surgeon and aesthetic dermatologist in Bradenton, Fla.
“Now we can reposition the skin. It works quite nicely in skin of color also,” Dr. Weinkle said during a lecture and live demonstration at the Orlando Dermatology Aesthetic and Clinical Conference.
Procedure tips
Begin by marking where on the patient’s face you intend to place the sutures. The proper vector is a straight lift back toward the upper ear in many cases. Also, take a photo before you start, so you know the location of the sutures in case the patient comes back for more, Dr. Weinkle recommended.
“What I like to do next is to sit the patient up and look at them head-on,” Dr. Weinkle said. “It helps to tweak the placement of the suture markings.” If a patient’s face appears asymmetrical, the dermatologist can place more sutures on one side than the other. Also, when there are neck issues, you can put an exit point for the sutures 1.5 cm below the mandible, she added.
Be patient after you anesthetize the entry and exit points because the epinephrine does not work immediately, Dr. Weinkle advised.
She does not anesthetize along the entire suture tract because the aim is to thread the sutures through the subcutaneous tissue. “You do not want to anesthetize the tract area between entry and exit points. If the patient feels it, you’re probably too superficial and you’re in the dermis.”
The next step is using an 18G needle to form an entry point for the 23G needle. “Pinch the skin, insert and stretch the skin just a bit. If you don’t pinch at the entry point, the cones can be difficult to pop in.” Dr. Weinkle said. Also, if you establish all entry points before inserting the sutures, it can save time.
Dr. Weinkle generally uses a number 8 InstaLift suture, but it also comes in sizes 12 and 16. After you open the package, gently pull the suture to tighten the knots between the cones. “Don’t pull hard from both ends – you can break the suture.”
When inserting the long needle to place the suture, it’s “almost like playing the violin with a bow.” As the clinician advances along tract line, he or she should run the needle between thumb and forefinger to check the positioning. Once the suture is placed and the needle removed, pull medially on the suture until the cones audibly “pop” – they are self anchoring. “I’ve seen some people break the sutures. You can pull them out and start again,” she noted.
“InstaLift is a bit of a misnomer,” Dr. Weinkle said. “Fibroblast stimulation and collagen improves final result over the next 2-3 months.” Improvements can last 12-18 months – it’s not permanent. “I think I would make a great candidate,” she joked. “Unfortunately, this is one thing I cannot do myself.”
There is minimal bruising after the procedure in Dr. Weinkle’s experience. Potential complications include swelling, dimpling at entry points, misplacement, and ecchymosis.
Dr. Weinkle is a consultant and principal investigator for Sinclair Pharma, manufacturer of InstaLift.
EXPERT ANALYSIS AT ODAC 2017
Beauty sleep: Sleep deprivation and the skin
There are many, many, short-term and long-term consequences of sleep deprivation. The most clinically apparent ones – swollen, sunken eyes; dark circles; and pale, dehydrated skin – are obvious. However the subclinical consequences are not so obvious. Sleep deprivation affects wound healing, collagen growth, skin hydration, and skin texture. Inflammation is also higher in sleep-deprived patients, causing outbreaks of acne, eczema, psoriasis, and skin allergies.

The reduction of sleep time affects the composition and integrity of the skin. Sleep deprivation increases glucocorticoid production. The elevation of cortisol inhibits fibroblast function and increases matrix metalloproteinases (collagenase, gelatinase). Matrix metalloproteinases accelerate collagen and elastin breakdown, which is essential to skin integrity, and hastens the aging process by increasing wrinkles, decreasing skin thickness, inhibiting growth factors, and decreasing skin elasticity.
Are there treatments to reverse these signs? Yes. Treatments to help increase skin collagen production include microneedling, radiofrequency devices, fractionated lasers, and topical agents such as retinoids. However, we cannot readily reverse the impact inflammatory processes, skin barrier dysfunction, or the disruption of the skin biome has on our skin. Beauty sleep is both necessary and irreplaceable.
References
1. Am J Physiol. 1993 Nov;265(5 Pt 2):R1148-54.
2. Am J Physiol Regul Integr Comp Physiol. 2000 Apr;278(4):R905-16.
3. Am J Physiol Regul Integr Comp Physiol. 2005 Feb;288(2):R374-83.
4. Am J Physiol Regul Integr Comp Physiol. 2007 Jul;293(1):R504-9.
5. Med Hypotheses. 2010 Dec;75(6):535-7.
6. Sleep. 2013 Sep 1;36(9):1355-60.
7. BMJ. 2010 Dec 14;341:c6614.
8. Brain Behav Immun. 2009 Nov;23(8):1089-95.
Dr. Talakoub and Dr. Wesley and are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected].
There are many, many, short-term and long-term consequences of sleep deprivation. The most clinically apparent ones – swollen, sunken eyes; dark circles; and pale, dehydrated skin – are obvious. However the subclinical consequences are not so obvious. Sleep deprivation affects wound healing, collagen growth, skin hydration, and skin texture. Inflammation is also higher in sleep-deprived patients, causing outbreaks of acne, eczema, psoriasis, and skin allergies.
The reduction of sleep time affects the composition and integrity of the skin. Sleep deprivation increases glucocorticoid production. The elevation of cortisol inhibits fibroblast function and increases matrix metalloproteinases (collagenase, gelatinase). Matrix metalloproteinases accelerate collagen and elastin breakdown, which is essential to skin integrity, and hastens the aging process by increasing wrinkles, decreasing skin thickness, inhibiting growth factors, and decreasing skin elasticity.
Are there treatments to reverse these signs? Yes. Treatments to help increase skin collagen production include microneedling, radiofrequency devices, fractionated lasers, and topical agents such as retinoids. However, we cannot readily reverse the impact inflammatory processes, skin barrier dysfunction, or the disruption of the skin biome has on our skin. Beauty sleep is both necessary and irreplaceable.
References
1. Am J Physiol. 1993 Nov;265(5 Pt 2):R1148-54.
2. Am J Physiol Regul Integr Comp Physiol. 2000 Apr;278(4):R905-16.
3. Am J Physiol Regul Integr Comp Physiol. 2005 Feb;288(2):R374-83.
4. Am J Physiol Regul Integr Comp Physiol. 2007 Jul;293(1):R504-9.
5. Med Hypotheses. 2010 Dec;75(6):535-7.
6. Sleep. 2013 Sep 1;36(9):1355-60.
7. BMJ. 2010 Dec 14;341:c6614.
8. Brain Behav Immun. 2009 Nov;23(8):1089-95.
Dr. Talakoub and Dr. Wesley and are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected].
There are many, many, short-term and long-term consequences of sleep deprivation. The most clinically apparent ones – swollen, sunken eyes; dark circles; and pale, dehydrated skin – are obvious. However the subclinical consequences are not so obvious. Sleep deprivation affects wound healing, collagen growth, skin hydration, and skin texture. Inflammation is also higher in sleep-deprived patients, causing outbreaks of acne, eczema, psoriasis, and skin allergies.
The reduction of sleep time affects the composition and integrity of the skin. Sleep deprivation increases glucocorticoid production. The elevation of cortisol inhibits fibroblast function and increases matrix metalloproteinases (collagenase, gelatinase). Matrix metalloproteinases accelerate collagen and elastin breakdown, which is essential to skin integrity, and hastens the aging process by increasing wrinkles, decreasing skin thickness, inhibiting growth factors, and decreasing skin elasticity.
Are there treatments to reverse these signs? Yes. Treatments to help increase skin collagen production include microneedling, radiofrequency devices, fractionated lasers, and topical agents such as retinoids. However, we cannot readily reverse the impact inflammatory processes, skin barrier dysfunction, or the disruption of the skin biome has on our skin. Beauty sleep is both necessary and irreplaceable.
References
1. Am J Physiol. 1993 Nov;265(5 Pt 2):R1148-54.
2. Am J Physiol Regul Integr Comp Physiol. 2000 Apr;278(4):R905-16.
3. Am J Physiol Regul Integr Comp Physiol. 2005 Feb;288(2):R374-83.
4. Am J Physiol Regul Integr Comp Physiol. 2007 Jul;293(1):R504-9.
5. Med Hypotheses. 2010 Dec;75(6):535-7.
6. Sleep. 2013 Sep 1;36(9):1355-60.
7. BMJ. 2010 Dec 14;341:c6614.
8. Brain Behav Immun. 2009 Nov;23(8):1089-95.
Dr. Talakoub and Dr. Wesley and are co-contributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected].
VIDEO: Dosing an important consideration when using neuromodulators in men
WAILEA, HAWAII – Using larger doses and avoiding overarching of the brows are among the considerations to keep in mind when using neuromodulators in men, advised Canadian dermatologist Katie Beleznay, MD.
In general, men have a very different anatomy with a different brow position, and have needs different from those of women, said Dr. Beleznay of the University of British Columbia, Vancouver.
One secret for successful injections of toxins in male patients: Dose matters. Men have stronger muscles in the face and need larger doses to overcome their muscular strength, Dr. Beleznay said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, “if you use 20-30 units in a female glabella, maybe you’d use 40-50, maybe even 60 units in a male patient,” she said. However, the volume depends on the strength of the muscles in the area, and some men may need less to avoid a frozen look. “You can always treat less and bring them back in a couple of weeks and add more,” especially with patients who are new to treatment, Dr. Beleznay noted.
She disclosed financial relationships with Allergan, Revance, Evolus, Galderma, and Zeltiq.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Using larger doses and avoiding overarching of the brows are among the considerations to keep in mind when using neuromodulators in men, advised Canadian dermatologist Katie Beleznay, MD.
In general, men have a very different anatomy with a different brow position, and have needs different from those of women, said Dr. Beleznay of the University of British Columbia, Vancouver.
One secret for successful injections of toxins in male patients: Dose matters. Men have stronger muscles in the face and need larger doses to overcome their muscular strength, Dr. Beleznay said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, “if you use 20-30 units in a female glabella, maybe you’d use 40-50, maybe even 60 units in a male patient,” she said. However, the volume depends on the strength of the muscles in the area, and some men may need less to avoid a frozen look. “You can always treat less and bring them back in a couple of weeks and add more,” especially with patients who are new to treatment, Dr. Beleznay noted.
She disclosed financial relationships with Allergan, Revance, Evolus, Galderma, and Zeltiq.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WAILEA, HAWAII – Using larger doses and avoiding overarching of the brows are among the considerations to keep in mind when using neuromodulators in men, advised Canadian dermatologist Katie Beleznay, MD.
In general, men have a very different anatomy with a different brow position, and have needs different from those of women, said Dr. Beleznay of the University of British Columbia, Vancouver.
One secret for successful injections of toxins in male patients: Dose matters. Men have stronger muscles in the face and need larger doses to overcome their muscular strength, Dr. Beleznay said in a video interview at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
On average, “if you use 20-30 units in a female glabella, maybe you’d use 40-50, maybe even 60 units in a male patient,” she said. However, the volume depends on the strength of the muscles in the area, and some men may need less to avoid a frozen look. “You can always treat less and bring them back in a couple of weeks and add more,” especially with patients who are new to treatment, Dr. Beleznay noted.
She disclosed financial relationships with Allergan, Revance, Evolus, Galderma, and Zeltiq.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF HAWAII DERMATOLOGY SEMINAR
