User login
Tips for avoiding, taming most postlaser complications
SAN DIEGO – Do not use the fractional laser on tanned skin or skin that will be getting sun exposure soon after the treatment, Tina Alster, MD, advised as one of her cardinal rules for avoiding hyperpigmentation complications.
Melanocytes are already activated and ready to deposit pigment in such patients. Also, use strict posttreatment sun protection with a mineral sunscreen, she said.

Fractional lasers – both ablative and nonablative – are remarkably safe, said Dr. Alster of Georgetown University Medical Center, Washington.
Her own 2008 study found side effects and complications in just 7.6% of 961 patients. The most frequent were acneiform eruptions (1.8%) and herpes simplex virus outbreaks (1.7%).
A more recent study comprising 730 patients treated with three different fractional lasers found an even lower complication rate of 4%. Complications included 5 herpes simplex virus breakouts, 13 acne eruptions, one abrasion, one bacterial infection, 9 cases of dermatitis, one drug eruption, 4 cases of prolonged erythema, one case of hyperpigmentation, one case of increased swelling and one of telangiectasia.
“We consistently find these very low incidences of less than 10%, and most of these I would term ‘side effects’ and not true complications,” Dr. Alster said at the annual meeting of the American Academy of Dermatology.
Still, if a clinician performs enough laser procedures, these outcomes will eventually occur. Dr. Alster gave her “top tips” for dealing with them when they do arise.
Tip #1: Adequate preoperative assessment
“You must be thorough in assessing all of these things: the type and location of the lesion, the Fitzpatrick skin phototype, any prior treatments the patient has had for the condition (and many have had them). We need to know of any pre-existing medical conditions, particularly autoimmune, and whether the patient has a history of scarring or delayed wound healing.”
Another part of this assessment is managing patient expectations upfront to avoid postprocedural dissatisfaction. “If someone comes to me and says ‘I want you to get rid of every acne scar on my face,’ I tell them right there, ‘I can’t do that,’” she said.
Tip #2: Prepare the patient for the expected – and the unexpected
“The overall risk of even the most common side effects, like prolonged erythema, is relatively small. But they can happen and patients need to be prepared for them.” The most common are prolonged erythema of more than 4 days for nonablative fractional lasers and more than a month for ablative lasers. But dermatitis may appear, as well as reactivation of acne, especially in patients who are having acne scars removed. There is also always the risk of infection and pigmentary alteration.”
Tip #3: Proper technique and close follow-up
The most expensive laser in the world still relies on good technique during deployment, she said. “I always stress, do not ‘pulse stack.’ Use side-by-side, nonoverlapping passes.”
Another key for success is to avoid using the laser on any tanned skin, or skin that will soon have sun exposure. “Any skin phototype with recent sun exposure has activated melanocytes and will have a higher tendency to develop postinflammatory hyperpigmentation. The cells are already activated and in the presence of any other damage – including a laser – they are programmed to produce more pigment.”
Individualize your treatment plan, she advised. “Do additional passes on the most severe areas, like cheek scars and perioral rhytides, and fewer passes and lower density on scar-prone areas, like the infraorbital area, mandible neck, and chest.”
Tip #4: Recognize and address complications
“Complications run the full spectrum from mild erythema to disseminated infections. I am always careful to figure out if it’s a true complication or an expected side effect. The greatest risk profiles are patients with darker skin phototypes, treatments in more sensitive areas, and patients with predisposing medical conditions like collagen or vascular diseases. You don’t need to avoid treating them, just be prepared for the higher risks.”
Dr. Alster also shared her techniques for managing some of the more common adverse events following a fractional laser procedure.
Prolonged erythema isn’t clinically serious, but it really bothers patients. They should be counseled to avoid putting any potentially irritating or allergenic product on their face, and that includes chemical sunscreens. A mineral sunscreen is a much better choice. “For management, postoperative cooling with ice packs is important. A mild topical corticosteroid and a nonsteroidal anti-inflammatory can help, too.”
Acne exacerbation is not uncommon, especially among patients being treated for acne scars. “In people who are prone to acne, I write a script for doxycycline. They don’t have to take it unless they break out. And I always avoid laser skin resurfacing in active acne.”
If a breakout does happen, stick to the well-trodden path, she advised. “We know how to treat acne. Discontinue any occlusive topical, start the patent on an antibiotic, treat topically with a clay masque to help dry things out.”
Infections can be alarming but are manageable when promptly treated. “The main thing is to diagnose and treat early. In those patients who are proven to have herpes simplex virus, I give an antiviral, like valacyclovir. I give 1 gram twice a day for a week, starting on the day of the procedure. I think a bigger question is, ‘Does everyone need a prophylactic antibiotic?’ There is probably no reason to start one routinely, and in fact, there is some evidence that if you do, you may get a more pathogenic organism if you do get an infection.”
Hyperpigmentation is always a concern. Dr Alster repeated her cardinal rule: Do not use the fractional laser on tanned skin or skin that will be getting sun exposure soon after the treatment, as melanocytes are already activated and ready to deposit pigment. Use strict posttreatment sun protection with a mineral sunscreen. While she is not “a big fan” of hydroquinone, Dr. Alster does employ other bleaching agents for postoperative hyperpigmentation, including alpha hydroxyl acid, retinoic acid, kojic acid, and lignin peroxidase.
Good technique and aftercare reduce the risk of hypertrophic scarring. This means avoiding excessive fluences and aggressive lasering techniques and early treatment of any suspected infection. “My main treatment is the 585nm pulsed dye laser, but the main thing is to avoid aggressive techniques with overlapping or stacking of pulses, strict wound care, and early treatment of any infections.”
Dr. Alster disclosed that she is a consultant to L’Oréal USA, an investigator for Revance Therapeutics and Sente Labs, and a medical advisor to Merz Aesthetics, and has investments/commercial interests in Home Skinovations.
SOURCE: Alster, T. et al, PREVENTION & MANAGEMENT OF
SAN DIEGO – Do not use the fractional laser on tanned skin or skin that will be getting sun exposure soon after the treatment, Tina Alster, MD, advised as one of her cardinal rules for avoiding hyperpigmentation complications.
Melanocytes are already activated and ready to deposit pigment in such patients. Also, use strict posttreatment sun protection with a mineral sunscreen, she said.
Fractional lasers – both ablative and nonablative – are remarkably safe, said Dr. Alster of Georgetown University Medical Center, Washington.
Her own 2008 study found side effects and complications in just 7.6% of 961 patients. The most frequent were acneiform eruptions (1.8%) and herpes simplex virus outbreaks (1.7%).
A more recent study comprising 730 patients treated with three different fractional lasers found an even lower complication rate of 4%. Complications included 5 herpes simplex virus breakouts, 13 acne eruptions, one abrasion, one bacterial infection, 9 cases of dermatitis, one drug eruption, 4 cases of prolonged erythema, one case of hyperpigmentation, one case of increased swelling and one of telangiectasia.
“We consistently find these very low incidences of less than 10%, and most of these I would term ‘side effects’ and not true complications,” Dr. Alster said at the annual meeting of the American Academy of Dermatology.
Still, if a clinician performs enough laser procedures, these outcomes will eventually occur. Dr. Alster gave her “top tips” for dealing with them when they do arise.
Tip #1: Adequate preoperative assessment
“You must be thorough in assessing all of these things: the type and location of the lesion, the Fitzpatrick skin phototype, any prior treatments the patient has had for the condition (and many have had them). We need to know of any pre-existing medical conditions, particularly autoimmune, and whether the patient has a history of scarring or delayed wound healing.”
Another part of this assessment is managing patient expectations upfront to avoid postprocedural dissatisfaction. “If someone comes to me and says ‘I want you to get rid of every acne scar on my face,’ I tell them right there, ‘I can’t do that,’” she said.
Tip #2: Prepare the patient for the expected – and the unexpected
“The overall risk of even the most common side effects, like prolonged erythema, is relatively small. But they can happen and patients need to be prepared for them.” The most common are prolonged erythema of more than 4 days for nonablative fractional lasers and more than a month for ablative lasers. But dermatitis may appear, as well as reactivation of acne, especially in patients who are having acne scars removed. There is also always the risk of infection and pigmentary alteration.”
Tip #3: Proper technique and close follow-up
The most expensive laser in the world still relies on good technique during deployment, she said. “I always stress, do not ‘pulse stack.’ Use side-by-side, nonoverlapping passes.”
Another key for success is to avoid using the laser on any tanned skin, or skin that will soon have sun exposure. “Any skin phototype with recent sun exposure has activated melanocytes and will have a higher tendency to develop postinflammatory hyperpigmentation. The cells are already activated and in the presence of any other damage – including a laser – they are programmed to produce more pigment.”
Individualize your treatment plan, she advised. “Do additional passes on the most severe areas, like cheek scars and perioral rhytides, and fewer passes and lower density on scar-prone areas, like the infraorbital area, mandible neck, and chest.”
Tip #4: Recognize and address complications
“Complications run the full spectrum from mild erythema to disseminated infections. I am always careful to figure out if it’s a true complication or an expected side effect. The greatest risk profiles are patients with darker skin phototypes, treatments in more sensitive areas, and patients with predisposing medical conditions like collagen or vascular diseases. You don’t need to avoid treating them, just be prepared for the higher risks.”
Dr. Alster also shared her techniques for managing some of the more common adverse events following a fractional laser procedure.
Prolonged erythema isn’t clinically serious, but it really bothers patients. They should be counseled to avoid putting any potentially irritating or allergenic product on their face, and that includes chemical sunscreens. A mineral sunscreen is a much better choice. “For management, postoperative cooling with ice packs is important. A mild topical corticosteroid and a nonsteroidal anti-inflammatory can help, too.”
Acne exacerbation is not uncommon, especially among patients being treated for acne scars. “In people who are prone to acne, I write a script for doxycycline. They don’t have to take it unless they break out. And I always avoid laser skin resurfacing in active acne.”
If a breakout does happen, stick to the well-trodden path, she advised. “We know how to treat acne. Discontinue any occlusive topical, start the patent on an antibiotic, treat topically with a clay masque to help dry things out.”
Infections can be alarming but are manageable when promptly treated. “The main thing is to diagnose and treat early. In those patients who are proven to have herpes simplex virus, I give an antiviral, like valacyclovir. I give 1 gram twice a day for a week, starting on the day of the procedure. I think a bigger question is, ‘Does everyone need a prophylactic antibiotic?’ There is probably no reason to start one routinely, and in fact, there is some evidence that if you do, you may get a more pathogenic organism if you do get an infection.”
Hyperpigmentation is always a concern. Dr Alster repeated her cardinal rule: Do not use the fractional laser on tanned skin or skin that will be getting sun exposure soon after the treatment, as melanocytes are already activated and ready to deposit pigment. Use strict posttreatment sun protection with a mineral sunscreen. While she is not “a big fan” of hydroquinone, Dr. Alster does employ other bleaching agents for postoperative hyperpigmentation, including alpha hydroxyl acid, retinoic acid, kojic acid, and lignin peroxidase.
Good technique and aftercare reduce the risk of hypertrophic scarring. This means avoiding excessive fluences and aggressive lasering techniques and early treatment of any suspected infection. “My main treatment is the 585nm pulsed dye laser, but the main thing is to avoid aggressive techniques with overlapping or stacking of pulses, strict wound care, and early treatment of any infections.”
Dr. Alster disclosed that she is a consultant to L’Oréal USA, an investigator for Revance Therapeutics and Sente Labs, and a medical advisor to Merz Aesthetics, and has investments/commercial interests in Home Skinovations.
SOURCE: Alster, T. et al, PREVENTION & MANAGEMENT OF
SAN DIEGO – Do not use the fractional laser on tanned skin or skin that will be getting sun exposure soon after the treatment, Tina Alster, MD, advised as one of her cardinal rules for avoiding hyperpigmentation complications.
Melanocytes are already activated and ready to deposit pigment in such patients. Also, use strict posttreatment sun protection with a mineral sunscreen, she said.
Fractional lasers – both ablative and nonablative – are remarkably safe, said Dr. Alster of Georgetown University Medical Center, Washington.
Her own 2008 study found side effects and complications in just 7.6% of 961 patients. The most frequent were acneiform eruptions (1.8%) and herpes simplex virus outbreaks (1.7%).
A more recent study comprising 730 patients treated with three different fractional lasers found an even lower complication rate of 4%. Complications included 5 herpes simplex virus breakouts, 13 acne eruptions, one abrasion, one bacterial infection, 9 cases of dermatitis, one drug eruption, 4 cases of prolonged erythema, one case of hyperpigmentation, one case of increased swelling and one of telangiectasia.
“We consistently find these very low incidences of less than 10%, and most of these I would term ‘side effects’ and not true complications,” Dr. Alster said at the annual meeting of the American Academy of Dermatology.
Still, if a clinician performs enough laser procedures, these outcomes will eventually occur. Dr. Alster gave her “top tips” for dealing with them when they do arise.
Tip #1: Adequate preoperative assessment
“You must be thorough in assessing all of these things: the type and location of the lesion, the Fitzpatrick skin phototype, any prior treatments the patient has had for the condition (and many have had them). We need to know of any pre-existing medical conditions, particularly autoimmune, and whether the patient has a history of scarring or delayed wound healing.”
Another part of this assessment is managing patient expectations upfront to avoid postprocedural dissatisfaction. “If someone comes to me and says ‘I want you to get rid of every acne scar on my face,’ I tell them right there, ‘I can’t do that,’” she said.
Tip #2: Prepare the patient for the expected – and the unexpected
“The overall risk of even the most common side effects, like prolonged erythema, is relatively small. But they can happen and patients need to be prepared for them.” The most common are prolonged erythema of more than 4 days for nonablative fractional lasers and more than a month for ablative lasers. But dermatitis may appear, as well as reactivation of acne, especially in patients who are having acne scars removed. There is also always the risk of infection and pigmentary alteration.”
Tip #3: Proper technique and close follow-up
The most expensive laser in the world still relies on good technique during deployment, she said. “I always stress, do not ‘pulse stack.’ Use side-by-side, nonoverlapping passes.”
Another key for success is to avoid using the laser on any tanned skin, or skin that will soon have sun exposure. “Any skin phototype with recent sun exposure has activated melanocytes and will have a higher tendency to develop postinflammatory hyperpigmentation. The cells are already activated and in the presence of any other damage – including a laser – they are programmed to produce more pigment.”
Individualize your treatment plan, she advised. “Do additional passes on the most severe areas, like cheek scars and perioral rhytides, and fewer passes and lower density on scar-prone areas, like the infraorbital area, mandible neck, and chest.”
Tip #4: Recognize and address complications
“Complications run the full spectrum from mild erythema to disseminated infections. I am always careful to figure out if it’s a true complication or an expected side effect. The greatest risk profiles are patients with darker skin phototypes, treatments in more sensitive areas, and patients with predisposing medical conditions like collagen or vascular diseases. You don’t need to avoid treating them, just be prepared for the higher risks.”
Dr. Alster also shared her techniques for managing some of the more common adverse events following a fractional laser procedure.
Prolonged erythema isn’t clinically serious, but it really bothers patients. They should be counseled to avoid putting any potentially irritating or allergenic product on their face, and that includes chemical sunscreens. A mineral sunscreen is a much better choice. “For management, postoperative cooling with ice packs is important. A mild topical corticosteroid and a nonsteroidal anti-inflammatory can help, too.”
Acne exacerbation is not uncommon, especially among patients being treated for acne scars. “In people who are prone to acne, I write a script for doxycycline. They don’t have to take it unless they break out. And I always avoid laser skin resurfacing in active acne.”
If a breakout does happen, stick to the well-trodden path, she advised. “We know how to treat acne. Discontinue any occlusive topical, start the patent on an antibiotic, treat topically with a clay masque to help dry things out.”
Infections can be alarming but are manageable when promptly treated. “The main thing is to diagnose and treat early. In those patients who are proven to have herpes simplex virus, I give an antiviral, like valacyclovir. I give 1 gram twice a day for a week, starting on the day of the procedure. I think a bigger question is, ‘Does everyone need a prophylactic antibiotic?’ There is probably no reason to start one routinely, and in fact, there is some evidence that if you do, you may get a more pathogenic organism if you do get an infection.”
Hyperpigmentation is always a concern. Dr Alster repeated her cardinal rule: Do not use the fractional laser on tanned skin or skin that will be getting sun exposure soon after the treatment, as melanocytes are already activated and ready to deposit pigment. Use strict posttreatment sun protection with a mineral sunscreen. While she is not “a big fan” of hydroquinone, Dr. Alster does employ other bleaching agents for postoperative hyperpigmentation, including alpha hydroxyl acid, retinoic acid, kojic acid, and lignin peroxidase.
Good technique and aftercare reduce the risk of hypertrophic scarring. This means avoiding excessive fluences and aggressive lasering techniques and early treatment of any suspected infection. “My main treatment is the 585nm pulsed dye laser, but the main thing is to avoid aggressive techniques with overlapping or stacking of pulses, strict wound care, and early treatment of any infections.”
Dr. Alster disclosed that she is a consultant to L’Oréal USA, an investigator for Revance Therapeutics and Sente Labs, and a medical advisor to Merz Aesthetics, and has investments/commercial interests in Home Skinovations.
SOURCE: Alster, T. et al, PREVENTION & MANAGEMENT OF
EXPERT ANALYSIS AT AAD 18

Set realistic expectations prior to perioral rejuvenation procedures
MIAMI – The success of perioral rejuvenation depends in large part on setting realistic expectations. But there are also tips and tricks to individualizing the technique for each patient that can lead to better outcomes and greater satisfaction – whether patients receive injections into the fine lines above the lip, full-field erbium laser resurfacing, neuromodulator treatment, or a combination approach, according to Joel L. Cohen, MD.
When a patient presents with major lines in the perioral area, an “orange peel” texture, and/or elastotic changes, laser resurfacing can be an appropriate option. “Full field erbium laser resurfacing can give patients a nice improvement of upper lip lines and even a nice contraction of oral commissure,” Dr. Cohen said at the Orlando Dermatology Aesthetic and Clinical Conference.

Although each treatment is individualized to the patient, “I tend to do full field erbium resurfacing around the mouth and eyes, and fractional ablative resurfacing around the rest of the face,” said Dr. Cohen, an aesthetic dermatologist and Mohs surgeon in private practice in metropolitan Denver.
More downtime is associated with laser resurfacing compared with fillers or neuromodulator injections, but long-term patient satisfaction, even with improvement in quality of life for some patients (who become less anxious about these lines and more self-confident), can make this approach worthwhile. During his presentation, Dr. Cohen showed photos of many of his treated patients, including one woman whose grandchildren he said had been commenting about the “orange peel texture of her upper lip,” until she completed the resurfacing treatment.
Keep expectations realistic
Dr. Cohen recommended counseling patients about the potential benefits – and the caveats – associated with full-field erbium heavier resurfacing. “Make sure people understand they will look terrible for several days after heavy resurfacing, usually taking about 10-12 days to re-epithelialize,” he said. “We need to tell patients that the perioral area typically manifests more lines than other areas, so we need treat this area differently than just ablative fractional resurfacing in many cases.”
He explained that with heavier resurfacing procedures, it helps to show patients what is expected over the days to weeks in the healing process. They need to understand and see photos that show that the full-field erbium areas will have a yellow fibrinous healing response for the first week or so, which looks very different from the fractional ablative-treated areas (which are more typically red, weepy, and swollen).
He encourages these patients to come back a few days after the procedure to check their healing and review wound-care instructions, especially for patients who have deeper full-field perioral erbium resurfacing (those who are treated with 450-700 microns). Another tip he provided is to have these postresurfacing patients enter/exit through a separate entrance and also sit in a separate cosmetic waiting room at off-hours.
Re-epithelialization generally takes about 10-12 days for most people, with a maximal improvement at approximately 3 months, Dr. Cohen said. “Some patients can see not only significant improvement of upper lip lines, but often a nice contraction of the oral commissure even before fillers are performed to buttress the marionette area and oral commissure,” he said.
With full-field ablative resurfacing in specific areas, rather than simply fractional ablative resurfacing, it is also important to educate patients that some postinflammatory erythema is expected, which, in some cases, may persist for a few months. “In my experience, topical vasoconstrictors don’t seem to help minimize prolonged redness in the full-field erbium areas, but potent topical steroids can be beneficial,” Dr. Cohen said.
More tips for success
Injected local anesthesia is warranted prior to heavier laser resurfacing to keep patients as comfortable as possible. An infraorbital block with an added submucosal/sulcus block with plain lidocaine can be a good approach, he noted. Different perioral and facial areas have different degrees of lines, requiring different laser settings. He prefers to use plain lidocaine perioral blocks, “so that I can theoretically best see the endpoint pinpoint bleeding,” he said, adding that “significant pinpoint bleeding is a good place to stop.”
Typically, he uses a neuromodulator a week or two before full-field perioral erbium resurfacing. “I choose not to give a neuromodulator on the same day as I am concerned about swelling or manipulation of the skin causing unwanted spread to adjacent musculature,” Dr. Cohen said.
Another tip is to take photos with more than one device. “Standardized photos may lose detail of etched lines; we take both iPad and standardized camera system photos,” he said, adding that it is important that clinic staff are proficient at taking proper before-and-after photos, making sure, for example, that the patient does not have confounding makeup or lipstick on for photos, and patient positioning is consistent.
He said it is imperative to emphasize the importance of diligent sun protection for several months after the laser procedure. “Every patient reassures us they use sunscreen, but we often don’t know what sunscreen they are using or how frequently they are using it,” Dr. Cohen said. “If they don’t follow our specific instructions to use a physical block sunscreen, they will significantly increase their risk of developing postinflammatory hyperpigmentation. This caveat applies all year round, and isn’t just for those that go to the beach or play golf, but is also especially important for those patients that ski or hike at higher altitudes.”
Depending on the degree of etched-in lines in the perioral area, one perioral full-field laser resurfacing treatment is generally sufficient for most patients to see significant improvement. For those with more severe etched lines and/or bigger goals for improvement, additional treatments can be performed – but he generally waits about 3 months to see the overall effect of the initial treatment session.
If patients have just a few discrete etched-lines on each side of the upper lip, fillers can be helpful. But, the number and caliber of fine lines on the cutaneous lip limit how much a dermatologist can realistically treat. “So for people with many, many etched-in lines on the cutaneous lip, I explain that fillers are not the right tool for the job – and that they need heavier laser resurfacing.” And those patients really concerned about downtime need to understand that the bruising that can occur with fillers for several days can lead to some degree of social downtime as well.
Options to treat perioral lines not ‘etched in’
Sometimes younger patients, those in their late 20s to early 40s, present with concerns about their perioral appearance. Although they do not have lines at rest yet, they can be unhappy with the muscle columns that appear above their lips with animation that begin to cause lines at rest imprinted in the skin. And many of these women complain that their lipstick bleeds into this area,” Dr. Cohen said. “These patients without etched lines can be treated with a neuromodulator alone to soften the mechanical action of the orbicularis oris muscle,” he pointed out.
Dr. Cohen disclosed having participated in clinical trials and/or having served as a consultant for Merz, Allergan, Galderma, Suneva, Sciton, and Lutronic.
MIAMI – The success of perioral rejuvenation depends in large part on setting realistic expectations. But there are also tips and tricks to individualizing the technique for each patient that can lead to better outcomes and greater satisfaction – whether patients receive injections into the fine lines above the lip, full-field erbium laser resurfacing, neuromodulator treatment, or a combination approach, according to Joel L. Cohen, MD.
When a patient presents with major lines in the perioral area, an “orange peel” texture, and/or elastotic changes, laser resurfacing can be an appropriate option. “Full field erbium laser resurfacing can give patients a nice improvement of upper lip lines and even a nice contraction of oral commissure,” Dr. Cohen said at the Orlando Dermatology Aesthetic and Clinical Conference.
Although each treatment is individualized to the patient, “I tend to do full field erbium resurfacing around the mouth and eyes, and fractional ablative resurfacing around the rest of the face,” said Dr. Cohen, an aesthetic dermatologist and Mohs surgeon in private practice in metropolitan Denver.
More downtime is associated with laser resurfacing compared with fillers or neuromodulator injections, but long-term patient satisfaction, even with improvement in quality of life for some patients (who become less anxious about these lines and more self-confident), can make this approach worthwhile. During his presentation, Dr. Cohen showed photos of many of his treated patients, including one woman whose grandchildren he said had been commenting about the “orange peel texture of her upper lip,” until she completed the resurfacing treatment.
Keep expectations realistic
Dr. Cohen recommended counseling patients about the potential benefits – and the caveats – associated with full-field erbium heavier resurfacing. “Make sure people understand they will look terrible for several days after heavy resurfacing, usually taking about 10-12 days to re-epithelialize,” he said. “We need to tell patients that the perioral area typically manifests more lines than other areas, so we need treat this area differently than just ablative fractional resurfacing in many cases.”
He explained that with heavier resurfacing procedures, it helps to show patients what is expected over the days to weeks in the healing process. They need to understand and see photos that show that the full-field erbium areas will have a yellow fibrinous healing response for the first week or so, which looks very different from the fractional ablative-treated areas (which are more typically red, weepy, and swollen).
He encourages these patients to come back a few days after the procedure to check their healing and review wound-care instructions, especially for patients who have deeper full-field perioral erbium resurfacing (those who are treated with 450-700 microns). Another tip he provided is to have these postresurfacing patients enter/exit through a separate entrance and also sit in a separate cosmetic waiting room at off-hours.
Re-epithelialization generally takes about 10-12 days for most people, with a maximal improvement at approximately 3 months, Dr. Cohen said. “Some patients can see not only significant improvement of upper lip lines, but often a nice contraction of the oral commissure even before fillers are performed to buttress the marionette area and oral commissure,” he said.
With full-field ablative resurfacing in specific areas, rather than simply fractional ablative resurfacing, it is also important to educate patients that some postinflammatory erythema is expected, which, in some cases, may persist for a few months. “In my experience, topical vasoconstrictors don’t seem to help minimize prolonged redness in the full-field erbium areas, but potent topical steroids can be beneficial,” Dr. Cohen said.
More tips for success
Injected local anesthesia is warranted prior to heavier laser resurfacing to keep patients as comfortable as possible. An infraorbital block with an added submucosal/sulcus block with plain lidocaine can be a good approach, he noted. Different perioral and facial areas have different degrees of lines, requiring different laser settings. He prefers to use plain lidocaine perioral blocks, “so that I can theoretically best see the endpoint pinpoint bleeding,” he said, adding that “significant pinpoint bleeding is a good place to stop.”
Typically, he uses a neuromodulator a week or two before full-field perioral erbium resurfacing. “I choose not to give a neuromodulator on the same day as I am concerned about swelling or manipulation of the skin causing unwanted spread to adjacent musculature,” Dr. Cohen said.
Another tip is to take photos with more than one device. “Standardized photos may lose detail of etched lines; we take both iPad and standardized camera system photos,” he said, adding that it is important that clinic staff are proficient at taking proper before-and-after photos, making sure, for example, that the patient does not have confounding makeup or lipstick on for photos, and patient positioning is consistent.
He said it is imperative to emphasize the importance of diligent sun protection for several months after the laser procedure. “Every patient reassures us they use sunscreen, but we often don’t know what sunscreen they are using or how frequently they are using it,” Dr. Cohen said. “If they don’t follow our specific instructions to use a physical block sunscreen, they will significantly increase their risk of developing postinflammatory hyperpigmentation. This caveat applies all year round, and isn’t just for those that go to the beach or play golf, but is also especially important for those patients that ski or hike at higher altitudes.”
Depending on the degree of etched-in lines in the perioral area, one perioral full-field laser resurfacing treatment is generally sufficient for most patients to see significant improvement. For those with more severe etched lines and/or bigger goals for improvement, additional treatments can be performed – but he generally waits about 3 months to see the overall effect of the initial treatment session.
If patients have just a few discrete etched-lines on each side of the upper lip, fillers can be helpful. But, the number and caliber of fine lines on the cutaneous lip limit how much a dermatologist can realistically treat. “So for people with many, many etched-in lines on the cutaneous lip, I explain that fillers are not the right tool for the job – and that they need heavier laser resurfacing.” And those patients really concerned about downtime need to understand that the bruising that can occur with fillers for several days can lead to some degree of social downtime as well.
Options to treat perioral lines not ‘etched in’
Sometimes younger patients, those in their late 20s to early 40s, present with concerns about their perioral appearance. Although they do not have lines at rest yet, they can be unhappy with the muscle columns that appear above their lips with animation that begin to cause lines at rest imprinted in the skin. And many of these women complain that their lipstick bleeds into this area,” Dr. Cohen said. “These patients without etched lines can be treated with a neuromodulator alone to soften the mechanical action of the orbicularis oris muscle,” he pointed out.
Dr. Cohen disclosed having participated in clinical trials and/or having served as a consultant for Merz, Allergan, Galderma, Suneva, Sciton, and Lutronic.
MIAMI – The success of perioral rejuvenation depends in large part on setting realistic expectations. But there are also tips and tricks to individualizing the technique for each patient that can lead to better outcomes and greater satisfaction – whether patients receive injections into the fine lines above the lip, full-field erbium laser resurfacing, neuromodulator treatment, or a combination approach, according to Joel L. Cohen, MD.
When a patient presents with major lines in the perioral area, an “orange peel” texture, and/or elastotic changes, laser resurfacing can be an appropriate option. “Full field erbium laser resurfacing can give patients a nice improvement of upper lip lines and even a nice contraction of oral commissure,” Dr. Cohen said at the Orlando Dermatology Aesthetic and Clinical Conference.
Although each treatment is individualized to the patient, “I tend to do full field erbium resurfacing around the mouth and eyes, and fractional ablative resurfacing around the rest of the face,” said Dr. Cohen, an aesthetic dermatologist and Mohs surgeon in private practice in metropolitan Denver.
More downtime is associated with laser resurfacing compared with fillers or neuromodulator injections, but long-term patient satisfaction, even with improvement in quality of life for some patients (who become less anxious about these lines and more self-confident), can make this approach worthwhile. During his presentation, Dr. Cohen showed photos of many of his treated patients, including one woman whose grandchildren he said had been commenting about the “orange peel texture of her upper lip,” until she completed the resurfacing treatment.
Keep expectations realistic
Dr. Cohen recommended counseling patients about the potential benefits – and the caveats – associated with full-field erbium heavier resurfacing. “Make sure people understand they will look terrible for several days after heavy resurfacing, usually taking about 10-12 days to re-epithelialize,” he said. “We need to tell patients that the perioral area typically manifests more lines than other areas, so we need treat this area differently than just ablative fractional resurfacing in many cases.”
He explained that with heavier resurfacing procedures, it helps to show patients what is expected over the days to weeks in the healing process. They need to understand and see photos that show that the full-field erbium areas will have a yellow fibrinous healing response for the first week or so, which looks very different from the fractional ablative-treated areas (which are more typically red, weepy, and swollen).
He encourages these patients to come back a few days after the procedure to check their healing and review wound-care instructions, especially for patients who have deeper full-field perioral erbium resurfacing (those who are treated with 450-700 microns). Another tip he provided is to have these postresurfacing patients enter/exit through a separate entrance and also sit in a separate cosmetic waiting room at off-hours.
Re-epithelialization generally takes about 10-12 days for most people, with a maximal improvement at approximately 3 months, Dr. Cohen said. “Some patients can see not only significant improvement of upper lip lines, but often a nice contraction of the oral commissure even before fillers are performed to buttress the marionette area and oral commissure,” he said.
With full-field ablative resurfacing in specific areas, rather than simply fractional ablative resurfacing, it is also important to educate patients that some postinflammatory erythema is expected, which, in some cases, may persist for a few months. “In my experience, topical vasoconstrictors don’t seem to help minimize prolonged redness in the full-field erbium areas, but potent topical steroids can be beneficial,” Dr. Cohen said.
More tips for success
Injected local anesthesia is warranted prior to heavier laser resurfacing to keep patients as comfortable as possible. An infraorbital block with an added submucosal/sulcus block with plain lidocaine can be a good approach, he noted. Different perioral and facial areas have different degrees of lines, requiring different laser settings. He prefers to use plain lidocaine perioral blocks, “so that I can theoretically best see the endpoint pinpoint bleeding,” he said, adding that “significant pinpoint bleeding is a good place to stop.”
Typically, he uses a neuromodulator a week or two before full-field perioral erbium resurfacing. “I choose not to give a neuromodulator on the same day as I am concerned about swelling or manipulation of the skin causing unwanted spread to adjacent musculature,” Dr. Cohen said.
Another tip is to take photos with more than one device. “Standardized photos may lose detail of etched lines; we take both iPad and standardized camera system photos,” he said, adding that it is important that clinic staff are proficient at taking proper before-and-after photos, making sure, for example, that the patient does not have confounding makeup or lipstick on for photos, and patient positioning is consistent.
He said it is imperative to emphasize the importance of diligent sun protection for several months after the laser procedure. “Every patient reassures us they use sunscreen, but we often don’t know what sunscreen they are using or how frequently they are using it,” Dr. Cohen said. “If they don’t follow our specific instructions to use a physical block sunscreen, they will significantly increase their risk of developing postinflammatory hyperpigmentation. This caveat applies all year round, and isn’t just for those that go to the beach or play golf, but is also especially important for those patients that ski or hike at higher altitudes.”
Depending on the degree of etched-in lines in the perioral area, one perioral full-field laser resurfacing treatment is generally sufficient for most patients to see significant improvement. For those with more severe etched lines and/or bigger goals for improvement, additional treatments can be performed – but he generally waits about 3 months to see the overall effect of the initial treatment session.
If patients have just a few discrete etched-lines on each side of the upper lip, fillers can be helpful. But, the number and caliber of fine lines on the cutaneous lip limit how much a dermatologist can realistically treat. “So for people with many, many etched-in lines on the cutaneous lip, I explain that fillers are not the right tool for the job – and that they need heavier laser resurfacing.” And those patients really concerned about downtime need to understand that the bruising that can occur with fillers for several days can lead to some degree of social downtime as well.
Options to treat perioral lines not ‘etched in’
Sometimes younger patients, those in their late 20s to early 40s, present with concerns about their perioral appearance. Although they do not have lines at rest yet, they can be unhappy with the muscle columns that appear above their lips with animation that begin to cause lines at rest imprinted in the skin. And many of these women complain that their lipstick bleeds into this area,” Dr. Cohen said. “These patients without etched lines can be treated with a neuromodulator alone to soften the mechanical action of the orbicularis oris muscle,” he pointed out.
Dr. Cohen disclosed having participated in clinical trials and/or having served as a consultant for Merz, Allergan, Galderma, Suneva, Sciton, and Lutronic.
EXPERT ANALYSIS FROM ODAC 2018
Oral treatment for menorrhagia shows promise for melasma
SAN DIEGO – The use of , according to Amit Pandya, MD.
Tranexamic acid is also used to treat intraoperative hemorrhage, is available over the counter in some countries, and is used widely for treating melasma in East Asia, Dr. Pandya said at a meeting of the Skin of Color Society, held the day before the annual meeting of the American Academy of Dermatology.

Dr. Pandya, professor of dermatology at the University of Texas Southwestern, Dallas, described a woman with a 20-year history of melasma who had been treated with triple combination creams, chemical peels, and Fraxel lasers “to no avail,” similar to patients he sees in his practice every week. But after 3 months of treatment with 325 mg of tranexamic acid twice daily, triple combination cream, and visible light sunscreen, she was clearer than she had been for some time, he said.
Tranexamic acid “ blocks keratinocytes from causing plasminogen to go into plasmin,” and plasmin stimulates fibroblast growth factor production, which is “one of the most potent stimulants of melanin,” he explained.
In a retrospective study published in 2016, conducted by investigators at the National Skin Center in Singapore, 561 patients with melasma were treated with oral tranexamic acid for a median of 4 months, almost 90% of the patients improved. There was one serious adverse event, a deep vein thrombosis (J Am Acad Dermatol. 2016 Aug;75[2]:385-92). The other adverse effects were mild. When Dr. Pandya spoke with the investigators about this patient, he was told that the patient had not disclosed her true medical history, which included protein S deficiency and a strong family history of thrombotic events, which would have excluded her from treatment.
Of 2,000 published cases of melasma treated with tranexamic acid to date, “this is the only severe event ever seen with tranexamic acid,” he noted.
Dr. Pandya and his associates recently published the results of a study evaluating tranexamic acid in 44 Latino women with moderate to severe melasma, which he said was the first study of tranexamic acid in the Western hemisphere. For 3 months, the women were treated with 250 mg of tranexamic acid or placebo in combination with sunscreen in both groups, then sunscreen only for 3 months in both groups. The primary outcome was the change in the modified Melasma Area and Severity Index (mMASI) score.
“Results were spectacular,” he said. At 3 months, the mMASI score had improved by 49% among those in the tranexamic acid group, compared with 18% among those on placebo and sunscreen. After 3 months on sunscreen only, there was a 26% reduction in the mMASI score from baseline among those treated with tranexamic acid, compared with 19% in the placebo group. None of the patients in either group had severe adverse events (J Am Acad Dermatol. 2018 Feb;78[2]:363-9). Side effects include GI upset, reduced menstrual flow, myalgias, and headache.
Rebound after cessation of therapy is an issue, however, and was worse in the treated group “because more melanocytes are actually created when you reduce melanin. So once you stop the tranexamic acid, it rebounds,” Dr. Pandya said. Patients should use triple combination cream when they stop taking tranexamic acid, he advised.
However, he said that patients have called him within 1 month of stopping tranexamic acid, asking to restart treatment. He has had patients on tranexamic acid for 1 year or longer, without any side effects.
Women who are pregnant or nursing, have had two or more spontaneous abortions, are on oral contraceptives or other hormone-based birth control, have a history of thrombosis, are on blood thinners, are smokers, or have significant cardiovascular or respiratory disease, subarachnoid hemorrhage, any DVT, or a strong family history of thromboembolic events should not be treated with tranexamic acid.
Dr. Pandya pointed out that the 250-mg dose used in the study is not available in the United States, where only the 650-mg dose is available. So he writes a prescription for 650 mg a day, and tells patients to cut the pill in half and take a 325-mg dose twice a day (half in the morning and half at night).
At the Skin of Color Society meeting, Nahla Shihab, MD, of Universitas Indonesia, Jakarta, presented the results of a randomized, placebo-controlled study evaluating oral tranexamic acid plus hydroquinone cream in patients with moderate to severe melasma, in collaboration with UT Southwestern and Dr. Pandya. Patients were randomized to treatment with topical hydroquinone 4% cream, sunscreen, and tranexamic acid (250 mg twice a day), or hydroquinone 4% cream, sunscreen, and placebo for 3 months, followed by 3 months of sunscreen only.
At 12 weeks, those in the tranexamic acid group had a 55% decrease in the mMASI score, compared with 10.9% in the control group. After stopping treatment, some patients experienced relapses, similar to what has been observed in other studies, but “the severity was still lower than baseline,” Dr. Shihab reported.
In addition, the improvement in the mMASI score was higher than that seen in other studies, which could be due to a synergistic effect of the fibrin inhibitor with hydroquinone, she added. Another important finding was that improvements were noticeable after 2 weeks of treatment, “which suggests that the combination of oral tranexamic acid and hydroquinone has a rapid onset of action,” she said.
In both groups, 6% of the patients experienced erythema and pruritus, which resolved with continued use of hydroquinone, and one woman on tranexamic acid had menstrual cycle changes. Further studies should evaluate a longer duration of treatment and follow-up, with tranexamic acid and hydroquinone, and in combination with other treatments, Dr. Shihab said.
Dr. Pandya reported that he is a consultant to Aclaris Therapeutics and Pfizer, and has received grants/research funding from Incyte Corp. Dr. Shihab had no disclosures.
SAN DIEGO – The use of , according to Amit Pandya, MD.
Tranexamic acid is also used to treat intraoperative hemorrhage, is available over the counter in some countries, and is used widely for treating melasma in East Asia, Dr. Pandya said at a meeting of the Skin of Color Society, held the day before the annual meeting of the American Academy of Dermatology.
Dr. Pandya, professor of dermatology at the University of Texas Southwestern, Dallas, described a woman with a 20-year history of melasma who had been treated with triple combination creams, chemical peels, and Fraxel lasers “to no avail,” similar to patients he sees in his practice every week. But after 3 months of treatment with 325 mg of tranexamic acid twice daily, triple combination cream, and visible light sunscreen, she was clearer than she had been for some time, he said.
Tranexamic acid “ blocks keratinocytes from causing plasminogen to go into plasmin,” and plasmin stimulates fibroblast growth factor production, which is “one of the most potent stimulants of melanin,” he explained.
In a retrospective study published in 2016, conducted by investigators at the National Skin Center in Singapore, 561 patients with melasma were treated with oral tranexamic acid for a median of 4 months, almost 90% of the patients improved. There was one serious adverse event, a deep vein thrombosis (J Am Acad Dermatol. 2016 Aug;75[2]:385-92). The other adverse effects were mild. When Dr. Pandya spoke with the investigators about this patient, he was told that the patient had not disclosed her true medical history, which included protein S deficiency and a strong family history of thrombotic events, which would have excluded her from treatment.
Of 2,000 published cases of melasma treated with tranexamic acid to date, “this is the only severe event ever seen with tranexamic acid,” he noted.
Dr. Pandya and his associates recently published the results of a study evaluating tranexamic acid in 44 Latino women with moderate to severe melasma, which he said was the first study of tranexamic acid in the Western hemisphere. For 3 months, the women were treated with 250 mg of tranexamic acid or placebo in combination with sunscreen in both groups, then sunscreen only for 3 months in both groups. The primary outcome was the change in the modified Melasma Area and Severity Index (mMASI) score.
“Results were spectacular,” he said. At 3 months, the mMASI score had improved by 49% among those in the tranexamic acid group, compared with 18% among those on placebo and sunscreen. After 3 months on sunscreen only, there was a 26% reduction in the mMASI score from baseline among those treated with tranexamic acid, compared with 19% in the placebo group. None of the patients in either group had severe adverse events (J Am Acad Dermatol. 2018 Feb;78[2]:363-9). Side effects include GI upset, reduced menstrual flow, myalgias, and headache.
Rebound after cessation of therapy is an issue, however, and was worse in the treated group “because more melanocytes are actually created when you reduce melanin. So once you stop the tranexamic acid, it rebounds,” Dr. Pandya said. Patients should use triple combination cream when they stop taking tranexamic acid, he advised.
However, he said that patients have called him within 1 month of stopping tranexamic acid, asking to restart treatment. He has had patients on tranexamic acid for 1 year or longer, without any side effects.
Women who are pregnant or nursing, have had two or more spontaneous abortions, are on oral contraceptives or other hormone-based birth control, have a history of thrombosis, are on blood thinners, are smokers, or have significant cardiovascular or respiratory disease, subarachnoid hemorrhage, any DVT, or a strong family history of thromboembolic events should not be treated with tranexamic acid.
Dr. Pandya pointed out that the 250-mg dose used in the study is not available in the United States, where only the 650-mg dose is available. So he writes a prescription for 650 mg a day, and tells patients to cut the pill in half and take a 325-mg dose twice a day (half in the morning and half at night).
At the Skin of Color Society meeting, Nahla Shihab, MD, of Universitas Indonesia, Jakarta, presented the results of a randomized, placebo-controlled study evaluating oral tranexamic acid plus hydroquinone cream in patients with moderate to severe melasma, in collaboration with UT Southwestern and Dr. Pandya. Patients were randomized to treatment with topical hydroquinone 4% cream, sunscreen, and tranexamic acid (250 mg twice a day), or hydroquinone 4% cream, sunscreen, and placebo for 3 months, followed by 3 months of sunscreen only.
At 12 weeks, those in the tranexamic acid group had a 55% decrease in the mMASI score, compared with 10.9% in the control group. After stopping treatment, some patients experienced relapses, similar to what has been observed in other studies, but “the severity was still lower than baseline,” Dr. Shihab reported.
In addition, the improvement in the mMASI score was higher than that seen in other studies, which could be due to a synergistic effect of the fibrin inhibitor with hydroquinone, she added. Another important finding was that improvements were noticeable after 2 weeks of treatment, “which suggests that the combination of oral tranexamic acid and hydroquinone has a rapid onset of action,” she said.
In both groups, 6% of the patients experienced erythema and pruritus, which resolved with continued use of hydroquinone, and one woman on tranexamic acid had menstrual cycle changes. Further studies should evaluate a longer duration of treatment and follow-up, with tranexamic acid and hydroquinone, and in combination with other treatments, Dr. Shihab said.
Dr. Pandya reported that he is a consultant to Aclaris Therapeutics and Pfizer, and has received grants/research funding from Incyte Corp. Dr. Shihab had no disclosures.
SAN DIEGO – The use of , according to Amit Pandya, MD.
Tranexamic acid is also used to treat intraoperative hemorrhage, is available over the counter in some countries, and is used widely for treating melasma in East Asia, Dr. Pandya said at a meeting of the Skin of Color Society, held the day before the annual meeting of the American Academy of Dermatology.
Dr. Pandya, professor of dermatology at the University of Texas Southwestern, Dallas, described a woman with a 20-year history of melasma who had been treated with triple combination creams, chemical peels, and Fraxel lasers “to no avail,” similar to patients he sees in his practice every week. But after 3 months of treatment with 325 mg of tranexamic acid twice daily, triple combination cream, and visible light sunscreen, she was clearer than she had been for some time, he said.
Tranexamic acid “ blocks keratinocytes from causing plasminogen to go into plasmin,” and plasmin stimulates fibroblast growth factor production, which is “one of the most potent stimulants of melanin,” he explained.
In a retrospective study published in 2016, conducted by investigators at the National Skin Center in Singapore, 561 patients with melasma were treated with oral tranexamic acid for a median of 4 months, almost 90% of the patients improved. There was one serious adverse event, a deep vein thrombosis (J Am Acad Dermatol. 2016 Aug;75[2]:385-92). The other adverse effects were mild. When Dr. Pandya spoke with the investigators about this patient, he was told that the patient had not disclosed her true medical history, which included protein S deficiency and a strong family history of thrombotic events, which would have excluded her from treatment.
Of 2,000 published cases of melasma treated with tranexamic acid to date, “this is the only severe event ever seen with tranexamic acid,” he noted.
Dr. Pandya and his associates recently published the results of a study evaluating tranexamic acid in 44 Latino women with moderate to severe melasma, which he said was the first study of tranexamic acid in the Western hemisphere. For 3 months, the women were treated with 250 mg of tranexamic acid or placebo in combination with sunscreen in both groups, then sunscreen only for 3 months in both groups. The primary outcome was the change in the modified Melasma Area and Severity Index (mMASI) score.
“Results were spectacular,” he said. At 3 months, the mMASI score had improved by 49% among those in the tranexamic acid group, compared with 18% among those on placebo and sunscreen. After 3 months on sunscreen only, there was a 26% reduction in the mMASI score from baseline among those treated with tranexamic acid, compared with 19% in the placebo group. None of the patients in either group had severe adverse events (J Am Acad Dermatol. 2018 Feb;78[2]:363-9). Side effects include GI upset, reduced menstrual flow, myalgias, and headache.
Rebound after cessation of therapy is an issue, however, and was worse in the treated group “because more melanocytes are actually created when you reduce melanin. So once you stop the tranexamic acid, it rebounds,” Dr. Pandya said. Patients should use triple combination cream when they stop taking tranexamic acid, he advised.
However, he said that patients have called him within 1 month of stopping tranexamic acid, asking to restart treatment. He has had patients on tranexamic acid for 1 year or longer, without any side effects.
Women who are pregnant or nursing, have had two or more spontaneous abortions, are on oral contraceptives or other hormone-based birth control, have a history of thrombosis, are on blood thinners, are smokers, or have significant cardiovascular or respiratory disease, subarachnoid hemorrhage, any DVT, or a strong family history of thromboembolic events should not be treated with tranexamic acid.
Dr. Pandya pointed out that the 250-mg dose used in the study is not available in the United States, where only the 650-mg dose is available. So he writes a prescription for 650 mg a day, and tells patients to cut the pill in half and take a 325-mg dose twice a day (half in the morning and half at night).
At the Skin of Color Society meeting, Nahla Shihab, MD, of Universitas Indonesia, Jakarta, presented the results of a randomized, placebo-controlled study evaluating oral tranexamic acid plus hydroquinone cream in patients with moderate to severe melasma, in collaboration with UT Southwestern and Dr. Pandya. Patients were randomized to treatment with topical hydroquinone 4% cream, sunscreen, and tranexamic acid (250 mg twice a day), or hydroquinone 4% cream, sunscreen, and placebo for 3 months, followed by 3 months of sunscreen only.
At 12 weeks, those in the tranexamic acid group had a 55% decrease in the mMASI score, compared with 10.9% in the control group. After stopping treatment, some patients experienced relapses, similar to what has been observed in other studies, but “the severity was still lower than baseline,” Dr. Shihab reported.
In addition, the improvement in the mMASI score was higher than that seen in other studies, which could be due to a synergistic effect of the fibrin inhibitor with hydroquinone, she added. Another important finding was that improvements were noticeable after 2 weeks of treatment, “which suggests that the combination of oral tranexamic acid and hydroquinone has a rapid onset of action,” she said.
In both groups, 6% of the patients experienced erythema and pruritus, which resolved with continued use of hydroquinone, and one woman on tranexamic acid had menstrual cycle changes. Further studies should evaluate a longer duration of treatment and follow-up, with tranexamic acid and hydroquinone, and in combination with other treatments, Dr. Shihab said.
Dr. Pandya reported that he is a consultant to Aclaris Therapeutics and Pfizer, and has received grants/research funding from Incyte Corp. Dr. Shihab had no disclosures.
REPORTING FROM THE SKIN OF COLOR SOCIETY SCIENTIFIC SYMPOSIUM
VIDEO: Parabens named ‘nonallergen’ of the year
SAN DIEGO – With propylene glycol already declared 2018 Allergen of the Year in a published journal article, the news at the Allergen of the Year session of the American Contact Dermatitis Society was announcement of the 2019 pick, parabens.
From a skin perspective, parabens are “perhaps the safest” preservative, but despite that they have a bad public reputation Donald V. Belsito, MD, said in his Allergen of the Year talk during the Society’s annual meeting held the day before the annual meeting of the American Academy of Dermatology.
There is an unfounded public perception that parabens cause endocrine disruption. Naming parabens the “nonallergen” of the year for 2019 is an effort to dispel this myth, Dr. Belsito said in a video interview.
The public prejudice against parabens, exacerbated by many products that tout being paraben free, has helped cause a crisis because preservative systems in general have been under attack and facing restrictions. Dr. Belsito cited European limitations on the preservative methylisothiazolinone (Allergen of the Year in 2013) and withdrawal of formaldehyde (2015 Allergen of the Year) from many products.
Dr. Belsito also highlighted why propylene glycol received the nod as 2018’s Allergen of the Year (Dermatitis. 2018 Jan/Feb;29[1]:3-5). Propylene glycol is a very ubiquitous emulsifier found in cosmetics, foods, and both topical and oral medications. Caution is needed when running a patch test on the agent to distinguish an irritation reaction from an allergic reaction. Interpreting the test result correctly is very important, said Dr. Belsito, professor of dermatology at Columbia University in New York.
Parabens is the 20th Allergen of the Year named by the Society, an annual event since 2000.
Dr. Belsito has participated in the program since its start.
SAN DIEGO – With propylene glycol already declared 2018 Allergen of the Year in a published journal article, the news at the Allergen of the Year session of the American Contact Dermatitis Society was announcement of the 2019 pick, parabens.
From a skin perspective, parabens are “perhaps the safest” preservative, but despite that they have a bad public reputation Donald V. Belsito, MD, said in his Allergen of the Year talk during the Society’s annual meeting held the day before the annual meeting of the American Academy of Dermatology.
There is an unfounded public perception that parabens cause endocrine disruption. Naming parabens the “nonallergen” of the year for 2019 is an effort to dispel this myth, Dr. Belsito said in a video interview.
The public prejudice against parabens, exacerbated by many products that tout being paraben free, has helped cause a crisis because preservative systems in general have been under attack and facing restrictions. Dr. Belsito cited European limitations on the preservative methylisothiazolinone (Allergen of the Year in 2013) and withdrawal of formaldehyde (2015 Allergen of the Year) from many products.
Dr. Belsito also highlighted why propylene glycol received the nod as 2018’s Allergen of the Year (Dermatitis. 2018 Jan/Feb;29[1]:3-5). Propylene glycol is a very ubiquitous emulsifier found in cosmetics, foods, and both topical and oral medications. Caution is needed when running a patch test on the agent to distinguish an irritation reaction from an allergic reaction. Interpreting the test result correctly is very important, said Dr. Belsito, professor of dermatology at Columbia University in New York.
Parabens is the 20th Allergen of the Year named by the Society, an annual event since 2000.
Dr. Belsito has participated in the program since its start.
SAN DIEGO – With propylene glycol already declared 2018 Allergen of the Year in a published journal article, the news at the Allergen of the Year session of the American Contact Dermatitis Society was announcement of the 2019 pick, parabens.
From a skin perspective, parabens are “perhaps the safest” preservative, but despite that they have a bad public reputation Donald V. Belsito, MD, said in his Allergen of the Year talk during the Society’s annual meeting held the day before the annual meeting of the American Academy of Dermatology.
There is an unfounded public perception that parabens cause endocrine disruption. Naming parabens the “nonallergen” of the year for 2019 is an effort to dispel this myth, Dr. Belsito said in a video interview.
The public prejudice against parabens, exacerbated by many products that tout being paraben free, has helped cause a crisis because preservative systems in general have been under attack and facing restrictions. Dr. Belsito cited European limitations on the preservative methylisothiazolinone (Allergen of the Year in 2013) and withdrawal of formaldehyde (2015 Allergen of the Year) from many products.
Dr. Belsito also highlighted why propylene glycol received the nod as 2018’s Allergen of the Year (Dermatitis. 2018 Jan/Feb;29[1]:3-5). Propylene glycol is a very ubiquitous emulsifier found in cosmetics, foods, and both topical and oral medications. Caution is needed when running a patch test on the agent to distinguish an irritation reaction from an allergic reaction. Interpreting the test result correctly is very important, said Dr. Belsito, professor of dermatology at Columbia University in New York.
Parabens is the 20th Allergen of the Year named by the Society, an annual event since 2000.
Dr. Belsito has participated in the program since its start.
FROM ACDS 18

Choosing noninvasive tightening treatments wisely
We all have one priority with all of our facial rejuvenation patients: Having happy, satisfied patients. With this in mind, I find I am torn by the armamentarium of noninvasive tightening devices to choose from. What are the critical factors in choosing a platform for your practice? Most practices look at pain, downtime, cost, and the number of treatments necessary to reach the expected outcome.

The treatment options are varied and include radio-frequency, ultrasound, and fractional resurfacing. There are numerous devices on the market that deliver energy into the dermis thereby causing collagen contraction and neocollagenesis. In my experience, the more “invasive” procedures or surgical tissue-tightening procedures provide the most reliable and immediate results. The radio-frequency and ultrasound devices that are “noninvasive” have little down-time, but multiple treatments are often needed and have inconsistent outcomes.
The technology for noninvasive modalities has improved over the last decade, but there are still no longterm clinical data, and results are highly varied. The difference in protocols and outcomes depends on proper patient selection, method of energy delivery, and sequential treatments.

We believe the optimal way to utilize these devices is as a combination approach with other procedures to optimize skin tightening and improvement in tone and texture. Tissue-tightening devices should be used with fractional ablative or nonablative resurfacing, fillers, and toxins. Often, we recommend starting with fillers and resurfacing treatments first to get the immediate “wow” factor and achieve immediate patient satisfaction. If patients want to then add skin tightening, this can be useful as an adjunct treatment and can even be used as a maintenance approach once per year. Actinic damage is also highly predictive of the degree of tissue laxity. Treating both the dermis and epidermis together delivers more immediate results. Using a fractional resurfacing device provides tissue tightening, improved skin color, decreased discoloration, and a reduction in the number of brown spots and freckles. Patients usually only need one to two treatments, there is minimal downtime, and satisfaction is very high.

In my practice, I choose fractional resurfacing treatments first. If patients want additional tissue tightening, radio-frequency is used as an adjunct treatment. This keeps costs lower, patients happier, and results more attainable.
When choosing devices for my practice, I follow a simple mantra: highest satisfaction per patient dollar spent. Happy patients build trust and integrity for the provider and practice. Don’t just buy a device because others are using it, and don’t just recommend a device because you have it.
Dr. Lily Talakoub and Dr. Naissan Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They have no relevant disclosures.
We all have one priority with all of our facial rejuvenation patients: Having happy, satisfied patients. With this in mind, I find I am torn by the armamentarium of noninvasive tightening devices to choose from. What are the critical factors in choosing a platform for your practice? Most practices look at pain, downtime, cost, and the number of treatments necessary to reach the expected outcome.
The treatment options are varied and include radio-frequency, ultrasound, and fractional resurfacing. There are numerous devices on the market that deliver energy into the dermis thereby causing collagen contraction and neocollagenesis. In my experience, the more “invasive” procedures or surgical tissue-tightening procedures provide the most reliable and immediate results. The radio-frequency and ultrasound devices that are “noninvasive” have little down-time, but multiple treatments are often needed and have inconsistent outcomes.
The technology for noninvasive modalities has improved over the last decade, but there are still no longterm clinical data, and results are highly varied. The difference in protocols and outcomes depends on proper patient selection, method of energy delivery, and sequential treatments.
We believe the optimal way to utilize these devices is as a combination approach with other procedures to optimize skin tightening and improvement in tone and texture. Tissue-tightening devices should be used with fractional ablative or nonablative resurfacing, fillers, and toxins. Often, we recommend starting with fillers and resurfacing treatments first to get the immediate “wow” factor and achieve immediate patient satisfaction. If patients want to then add skin tightening, this can be useful as an adjunct treatment and can even be used as a maintenance approach once per year. Actinic damage is also highly predictive of the degree of tissue laxity. Treating both the dermis and epidermis together delivers more immediate results. Using a fractional resurfacing device provides tissue tightening, improved skin color, decreased discoloration, and a reduction in the number of brown spots and freckles. Patients usually only need one to two treatments, there is minimal downtime, and satisfaction is very high.
In my practice, I choose fractional resurfacing treatments first. If patients want additional tissue tightening, radio-frequency is used as an adjunct treatment. This keeps costs lower, patients happier, and results more attainable.
When choosing devices for my practice, I follow a simple mantra: highest satisfaction per patient dollar spent. Happy patients build trust and integrity for the provider and practice. Don’t just buy a device because others are using it, and don’t just recommend a device because you have it.
Dr. Lily Talakoub and Dr. Naissan Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They have no relevant disclosures.
We all have one priority with all of our facial rejuvenation patients: Having happy, satisfied patients. With this in mind, I find I am torn by the armamentarium of noninvasive tightening devices to choose from. What are the critical factors in choosing a platform for your practice? Most practices look at pain, downtime, cost, and the number of treatments necessary to reach the expected outcome.
The treatment options are varied and include radio-frequency, ultrasound, and fractional resurfacing. There are numerous devices on the market that deliver energy into the dermis thereby causing collagen contraction and neocollagenesis. In my experience, the more “invasive” procedures or surgical tissue-tightening procedures provide the most reliable and immediate results. The radio-frequency and ultrasound devices that are “noninvasive” have little down-time, but multiple treatments are often needed and have inconsistent outcomes.
The technology for noninvasive modalities has improved over the last decade, but there are still no longterm clinical data, and results are highly varied. The difference in protocols and outcomes depends on proper patient selection, method of energy delivery, and sequential treatments.
We believe the optimal way to utilize these devices is as a combination approach with other procedures to optimize skin tightening and improvement in tone and texture. Tissue-tightening devices should be used with fractional ablative or nonablative resurfacing, fillers, and toxins. Often, we recommend starting with fillers and resurfacing treatments first to get the immediate “wow” factor and achieve immediate patient satisfaction. If patients want to then add skin tightening, this can be useful as an adjunct treatment and can even be used as a maintenance approach once per year. Actinic damage is also highly predictive of the degree of tissue laxity. Treating both the dermis and epidermis together delivers more immediate results. Using a fractional resurfacing device provides tissue tightening, improved skin color, decreased discoloration, and a reduction in the number of brown spots and freckles. Patients usually only need one to two treatments, there is minimal downtime, and satisfaction is very high.
In my practice, I choose fractional resurfacing treatments first. If patients want additional tissue tightening, radio-frequency is used as an adjunct treatment. This keeps costs lower, patients happier, and results more attainable.
When choosing devices for my practice, I follow a simple mantra: highest satisfaction per patient dollar spent. Happy patients build trust and integrity for the provider and practice. Don’t just buy a device because others are using it, and don’t just recommend a device because you have it.
Dr. Lily Talakoub and Dr. Naissan Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at [email protected]. They have no relevant disclosures.
Multisite, same-day cryolipolysis treatments don’t skew lipids, liver enzymes
Multiple, same-day cryolipolysis treatments don’t adversely affect serum lipids or liver enzymes, either acutely or after 12 weeks.
Among all the lipids measured, only triglycerides showed a significant increase, jumping from a mean 77 mg/dL to 83.4 mg/dL. The just over 6 mg/dL increase was “clinically trivial” and driven by a single patient in the 35-subject study, Kenneth B. Klein, MD, and his colleagues reported in Lasers in Surgery and Medicine.
Results of the small, prospective study are reassuring, if not surprising, the authors wrote. Even four flank treatments, as performed in this cohort, release only about 160 g of fat, at a rate of less than 2 g/day. “To put this figure in perspective, the typical American diet contains at least 75 g of fat per day. Moreover, it has been shown that consuming as much as 261 grams of fat per day causes no ill effects or laboratory abnormalities.”
The study included 35 men and women with a mean age of 45 years but a range of 20-67 years. The mean body mass index was 24.7 kg/m2, although the range was quite wide, at 18-29.7 kg/m2. All subjects underwent cryolipolysis of the lower abdomen and both flanks. Blood was drawn for analysis at baseline and at weeks 1, 4, and 14 after treatment. One patient didn’t complete the treatment because it was impossible to draw enough flank tissue into the applicator.
Patients experienced the expected procedural side effects of erythema, numbness, and edema, with a few reports of tingling and bruising. All of these resolved spontaneously. Immediately after the procedure, the mean pain score was 4 on a 1-10 scale; by week 12, there were no reports of pain.
Other than the triglyceride change in the single patient, there were no statistically or clinically significant changes from baseline to week 12 in total cholesterol (mean 186.5 mg/dL vs. 189.2 mg/dL), HDL cholesterol (71 mg/dL vs. 73.8 mg/dL), LDL cholesterol (100 mg/dL vs. 102.5 mg/dL), or very low-density cholesterol (15.7 mg/dL vs. 16.8 mg/dL). Although the mean triglyceride change was statistically significant, the final measurement was still well below the upper limit of reference (150 mg/dL).
The only liver enzyme change of note occurred in one patient, who had one sharp increase in aminotransferase. That was related to alcohol consumption the night before the week 12 blood draw.
The study was sponsored by Zeltiq Aesthetics, which manufactures the device used in the trial. Dr. Klein is a consultant to Zeltiq. All three coauthors were paid investigators; in addition, one of them, Eric P. Bachelor, MD, is on the Zeltiq speakers’ bureau.
SOURCE: Klein KB et al. Lasers Surg Med. 2017 Sep;49(7):640-4.
Multiple, same-day cryolipolysis treatments don’t adversely affect serum lipids or liver enzymes, either acutely or after 12 weeks.
Among all the lipids measured, only triglycerides showed a significant increase, jumping from a mean 77 mg/dL to 83.4 mg/dL. The just over 6 mg/dL increase was “clinically trivial” and driven by a single patient in the 35-subject study, Kenneth B. Klein, MD, and his colleagues reported in Lasers in Surgery and Medicine.
Results of the small, prospective study are reassuring, if not surprising, the authors wrote. Even four flank treatments, as performed in this cohort, release only about 160 g of fat, at a rate of less than 2 g/day. “To put this figure in perspective, the typical American diet contains at least 75 g of fat per day. Moreover, it has been shown that consuming as much as 261 grams of fat per day causes no ill effects or laboratory abnormalities.”
The study included 35 men and women with a mean age of 45 years but a range of 20-67 years. The mean body mass index was 24.7 kg/m2, although the range was quite wide, at 18-29.7 kg/m2. All subjects underwent cryolipolysis of the lower abdomen and both flanks. Blood was drawn for analysis at baseline and at weeks 1, 4, and 14 after treatment. One patient didn’t complete the treatment because it was impossible to draw enough flank tissue into the applicator.
Patients experienced the expected procedural side effects of erythema, numbness, and edema, with a few reports of tingling and bruising. All of these resolved spontaneously. Immediately after the procedure, the mean pain score was 4 on a 1-10 scale; by week 12, there were no reports of pain.
Other than the triglyceride change in the single patient, there were no statistically or clinically significant changes from baseline to week 12 in total cholesterol (mean 186.5 mg/dL vs. 189.2 mg/dL), HDL cholesterol (71 mg/dL vs. 73.8 mg/dL), LDL cholesterol (100 mg/dL vs. 102.5 mg/dL), or very low-density cholesterol (15.7 mg/dL vs. 16.8 mg/dL). Although the mean triglyceride change was statistically significant, the final measurement was still well below the upper limit of reference (150 mg/dL).
The only liver enzyme change of note occurred in one patient, who had one sharp increase in aminotransferase. That was related to alcohol consumption the night before the week 12 blood draw.
The study was sponsored by Zeltiq Aesthetics, which manufactures the device used in the trial. Dr. Klein is a consultant to Zeltiq. All three coauthors were paid investigators; in addition, one of them, Eric P. Bachelor, MD, is on the Zeltiq speakers’ bureau.
SOURCE: Klein KB et al. Lasers Surg Med. 2017 Sep;49(7):640-4.
Multiple, same-day cryolipolysis treatments don’t adversely affect serum lipids or liver enzymes, either acutely or after 12 weeks.
Among all the lipids measured, only triglycerides showed a significant increase, jumping from a mean 77 mg/dL to 83.4 mg/dL. The just over 6 mg/dL increase was “clinically trivial” and driven by a single patient in the 35-subject study, Kenneth B. Klein, MD, and his colleagues reported in Lasers in Surgery and Medicine.
Results of the small, prospective study are reassuring, if not surprising, the authors wrote. Even four flank treatments, as performed in this cohort, release only about 160 g of fat, at a rate of less than 2 g/day. “To put this figure in perspective, the typical American diet contains at least 75 g of fat per day. Moreover, it has been shown that consuming as much as 261 grams of fat per day causes no ill effects or laboratory abnormalities.”
The study included 35 men and women with a mean age of 45 years but a range of 20-67 years. The mean body mass index was 24.7 kg/m2, although the range was quite wide, at 18-29.7 kg/m2. All subjects underwent cryolipolysis of the lower abdomen and both flanks. Blood was drawn for analysis at baseline and at weeks 1, 4, and 14 after treatment. One patient didn’t complete the treatment because it was impossible to draw enough flank tissue into the applicator.
Patients experienced the expected procedural side effects of erythema, numbness, and edema, with a few reports of tingling and bruising. All of these resolved spontaneously. Immediately after the procedure, the mean pain score was 4 on a 1-10 scale; by week 12, there were no reports of pain.
Other than the triglyceride change in the single patient, there were no statistically or clinically significant changes from baseline to week 12 in total cholesterol (mean 186.5 mg/dL vs. 189.2 mg/dL), HDL cholesterol (71 mg/dL vs. 73.8 mg/dL), LDL cholesterol (100 mg/dL vs. 102.5 mg/dL), or very low-density cholesterol (15.7 mg/dL vs. 16.8 mg/dL). Although the mean triglyceride change was statistically significant, the final measurement was still well below the upper limit of reference (150 mg/dL).
The only liver enzyme change of note occurred in one patient, who had one sharp increase in aminotransferase. That was related to alcohol consumption the night before the week 12 blood draw.
The study was sponsored by Zeltiq Aesthetics, which manufactures the device used in the trial. Dr. Klein is a consultant to Zeltiq. All three coauthors were paid investigators; in addition, one of them, Eric P. Bachelor, MD, is on the Zeltiq speakers’ bureau.
SOURCE: Klein KB et al. Lasers Surg Med. 2017 Sep;49(7):640-4.
FROM LASERS IN SURGERY AND MEDICINE
Key clinical point:
Major finding: There were no statistically or clinically significant changes from baseline to week 12 in total cholesterol (mean 186.5 mg/dL vs. 189.2 mg/dL), HDL cholesterol (71 mg/dL vs. 73.8 mg/dL), LDL cholesterol (100 mg/dL vs. 102.5 mg/dL), or VLDL cholesterol (15.7 mg/dL vs. 16.8 mg/dL).
Data source: A small prospective study of 35 men and women who underwent cryolipolysis of the lower abdomen and both flanks.
Disclosures: The study was sponsored by Zeltiq Aesthetics, which manufactures the device used in the trial. Dr. Klein is a consultant for Zeltiq. All three coauthors were paid investigators; in addition, one of them, Eric Bachelor, MD, is on the Zeltiq speakers’ bureau.
Source: Klein KB et al. Lasers Surg Med. 2017 Sep;49(7):640-4.
Mobile Medical Apps for Patient Education: A Graded Review of Available Dermatology Apps
According to industry estimates, roughly 64% of US adults were smartphone users in 2015.1 Smartphones enable users to utilize mobile applications (apps) that can perform a variety of functions in many categories, including business, music, photography, entertainment, education, social networking, travel, and lifestyle. The widespread adoption and use of mobile apps has implications for medical practice. Mobile apps have the capability to serve as information sources for patients, educational tools for students, and diagnostic aids for physicians.2 Consequently, a number of medical and health care–oriented apps have already been developed3 and are increasingly utilized by patients and providers.4
Given its visual nature, dermatology is particularly amenable to the integration of mobile medical apps. A study by Brewer et al5 identified more than 229 dermatology-related apps in categories ranging from general dermatology reference, self-surveillance and diagnosis, disease guides, educational aids, sunscreen and UV recommendations, and teledermatology. Patients served as the target audience and principal consumers of more than half of these dermatology apps.5
Mobile medical and health care apps demonstrate great potential for serving as valuable information sources for patients with dermatologic conditions; however, the content, functions, accuracy, and educational value of dermatology mobile apps are not well characterized, making it difficult for patients and health care providers to select and recommend appropriate apps.6 In this study, we created a rubric to objectively grade 44 publicly available mobile dermatology apps with the primary focus of patient education.
Methods
We conducted a search of dermatology-related educational mobile apps that were publicly available via the App Store (Apple Inc) from January 2016 to November 2016. (The pricing, availability, and other features of these apps may have changed since the study period.) The following search terms were used: dermatology, dermoscopy, melanoma, skin cancer, psoriasis, rosacea, acne, eczema, dermal fillers, and Mohs surgery. We excluded apps that were not in English; had a solely commercial focus; were mobile textbooks or scientific journals; were used to provide teledermatology services with no educational purpose; were solely focused on homeopathic, alternative, and/or complementary medicine; or were intended primarily as a reference for students or health care professionals. Our search yielded 44 apps with patient education as a primary objective. The apps were divided into 6 categories based on their focus: general dermatology, cosmetic dermatology, acne, eczema, psoriasis, and skin cancer.
Each app was reviewed using a quantified grading rubric developed by the researchers. In a prior evaluation, Handel7 reviewed 35 health and wellness mobile apps utilizing the categories of ease of use, reliability, quality, scope of information, and aesthetics.4 These criteria were modified and adapted for the purposes of this study, and a 4-point scale was applied to each criterion. The final criteria were (1) educational objectives, (2) content, (3) accuracy, (4) design, and (5) conflict of interest. The quantified grading rubric is described in Table 1.
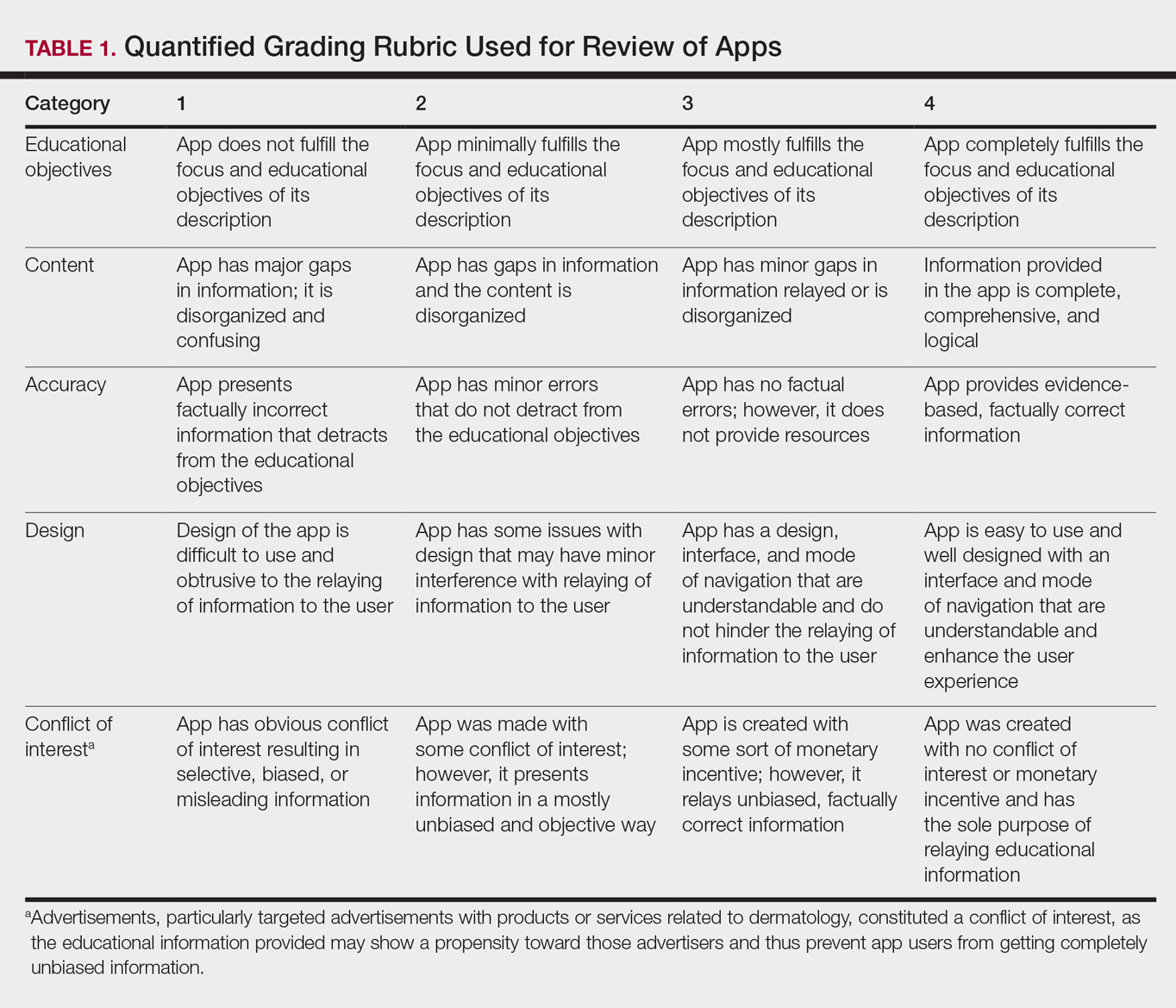
Results
The possible range of scores based on the grading rubric was 5 to 20. The actual range of scores was 8 to 19 (Table 2). The 44 reviewed apps were categorized by topic as acne, cosmetic dermatology, eczema, general dermatology, psoriasis, or skin cancer. A sample of 15 apps selected to represent the distribution of scores and their grading on the rubric are presented in Table 3.
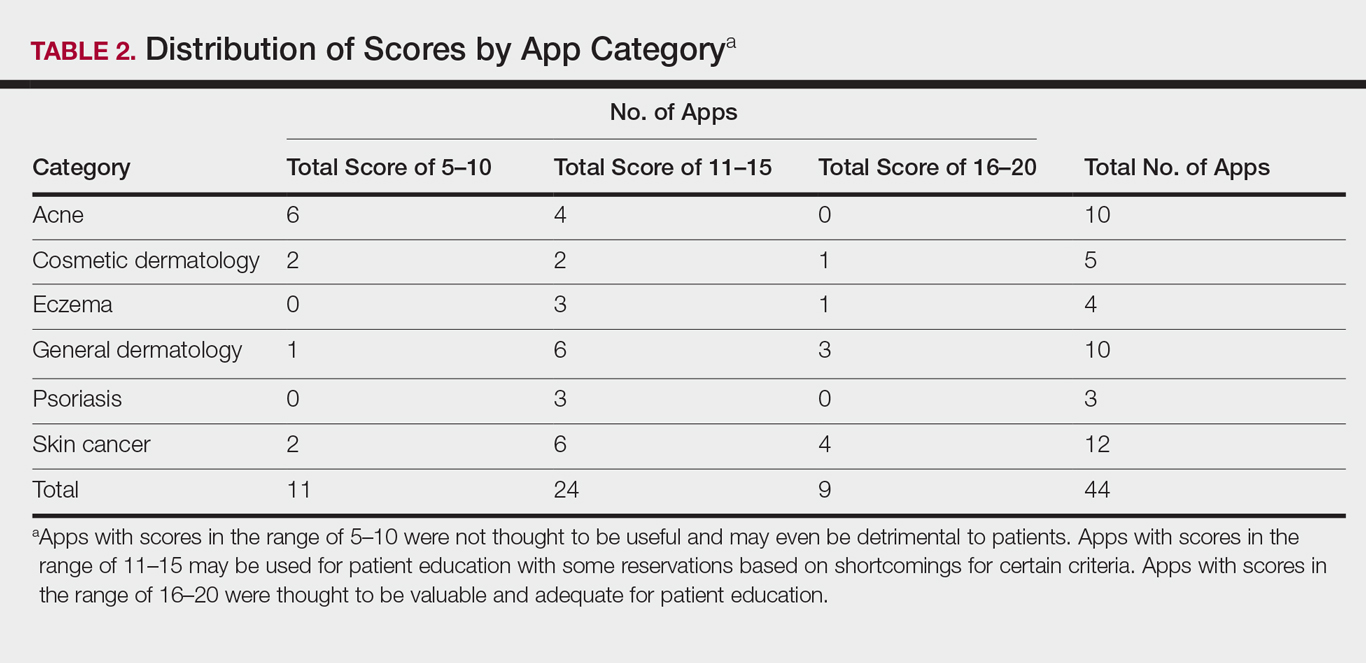
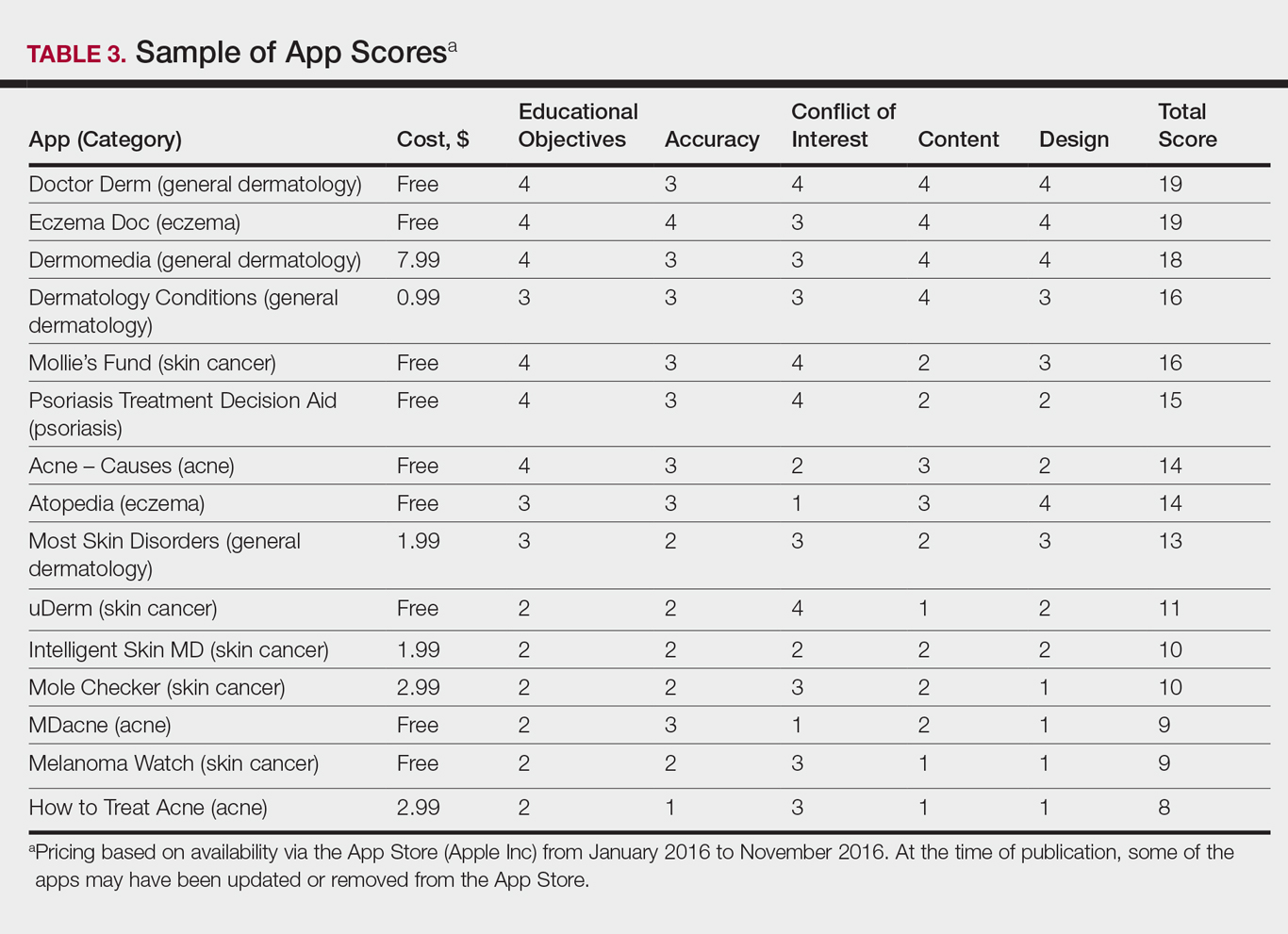
Comment
The number of dermatology-related apps available to mobile users continues to grow at an increasing rate.8 The apps vary in many aspects, including their purpose, scope, intended audience, and goals of the app publisher. In turn, more individuals are turning to mobile apps for medical information,4 especially in dermatology, thus it is necessary to create a systematic way to evaluate the quality and utility of each app to assist users in making informed decisions about which apps will best meet their needs in the midst of a wide array of choices.
For the purpose of this study, an objective rubric was created that can be used to evaluate the quality of medical apps for patient education in dermatology. An app’s adequacy and usefulness for patient education was thought to depend on 3 possible score ranges into which the app could fall based on the grading rubric. An app with a total score in the range of 5 to 10 was not thought to be useful and may even be detrimental to patients. An app with a total score in the range of 11 to 15 may be used for patient education with some reservations based on shortcomings for certain criteria. An app with a score in the range of 16 to 20 was thought to be valuable and adequate for patient education. For example, the How to Treat Acne app received a total score of 8 and therefore would not be recommended to patients based on the grading rubric used in this study. This particular app provided sparse and sometimes inaccurate information, had a confusing user interface, and contained many obstructive advertisements. In contrast, the Eczema Doc app received a total score of 19, which indicates a quality app deemed to be useful for patient information based on the established rubric. This app met all the objectives that it advertised, contained accurate information with verified citation of sources, and was very easy for users to navigate.
Of the 44 graded apps, only 9 (20.5%) received scores in the highest range of 16 to 20, which indicates a need for improvements in mobile dermatology apps intended for patient education. Adopting the grading rubric developed in this study as a standard in the creation of medical apps could have beneficial implications in disseminating accurate, safe, unbiased, and easy-to-understand information to patients.
- Smith A. U.S. smartphone use in 2015. Pew Research Center website. http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015. Published April 1, 2015. Accessed August 29, 2017.
- Nilsen W, Kumar S, Shar A, et al. Advancing the science of mHealth. J Health Commun. 2012;17(suppl 1):5-10.
- West DM. How mobile devices are transforming healthcare issues in technology innovation. Issues Technol Innov. 2012;18:1-14.
- Boudreaux ED, Waring ME, Hayes RB, et al. Evaluating and selecting mobile health apps: strategies for healthcare providers and healthcare organizations. Transl Behav Med. 2014;4:363-371.
- Brewer AC, Endly DC, Henley J, et al. Mobile applications in dermatology. JAMA Dermatol. 2013;149:1300-1304.
- Cummings E, Borycki E, Roehrer E. Issues and considerations for healthcare consumers using mobile applications. Stud Health Technol Inform. 2013;183:227-231.
- Handel MJ. mHealth (mobile health)-using apps for health and wellness. Explore. 2011;7:256-261.
- Boulos MN, Brewer AC, Karimkhani C, et al. Mobile medical and health apps: state of the art, concerns, regulatory control and certification. Online J Public Health Inform. 2014;5:229.
According to industry estimates, roughly 64% of US adults were smartphone users in 2015.1 Smartphones enable users to utilize mobile applications (apps) that can perform a variety of functions in many categories, including business, music, photography, entertainment, education, social networking, travel, and lifestyle. The widespread adoption and use of mobile apps has implications for medical practice. Mobile apps have the capability to serve as information sources for patients, educational tools for students, and diagnostic aids for physicians.2 Consequently, a number of medical and health care–oriented apps have already been developed3 and are increasingly utilized by patients and providers.4
Given its visual nature, dermatology is particularly amenable to the integration of mobile medical apps. A study by Brewer et al5 identified more than 229 dermatology-related apps in categories ranging from general dermatology reference, self-surveillance and diagnosis, disease guides, educational aids, sunscreen and UV recommendations, and teledermatology. Patients served as the target audience and principal consumers of more than half of these dermatology apps.5
Mobile medical and health care apps demonstrate great potential for serving as valuable information sources for patients with dermatologic conditions; however, the content, functions, accuracy, and educational value of dermatology mobile apps are not well characterized, making it difficult for patients and health care providers to select and recommend appropriate apps.6 In this study, we created a rubric to objectively grade 44 publicly available mobile dermatology apps with the primary focus of patient education.
Methods
We conducted a search of dermatology-related educational mobile apps that were publicly available via the App Store (Apple Inc) from January 2016 to November 2016. (The pricing, availability, and other features of these apps may have changed since the study period.) The following search terms were used: dermatology, dermoscopy, melanoma, skin cancer, psoriasis, rosacea, acne, eczema, dermal fillers, and Mohs surgery. We excluded apps that were not in English; had a solely commercial focus; were mobile textbooks or scientific journals; were used to provide teledermatology services with no educational purpose; were solely focused on homeopathic, alternative, and/or complementary medicine; or were intended primarily as a reference for students or health care professionals. Our search yielded 44 apps with patient education as a primary objective. The apps were divided into 6 categories based on their focus: general dermatology, cosmetic dermatology, acne, eczema, psoriasis, and skin cancer.
Each app was reviewed using a quantified grading rubric developed by the researchers. In a prior evaluation, Handel7 reviewed 35 health and wellness mobile apps utilizing the categories of ease of use, reliability, quality, scope of information, and aesthetics.4 These criteria were modified and adapted for the purposes of this study, and a 4-point scale was applied to each criterion. The final criteria were (1) educational objectives, (2) content, (3) accuracy, (4) design, and (5) conflict of interest. The quantified grading rubric is described in Table 1.
Results
The possible range of scores based on the grading rubric was 5 to 20. The actual range of scores was 8 to 19 (Table 2). The 44 reviewed apps were categorized by topic as acne, cosmetic dermatology, eczema, general dermatology, psoriasis, or skin cancer. A sample of 15 apps selected to represent the distribution of scores and their grading on the rubric are presented in Table 3.
Comment
The number of dermatology-related apps available to mobile users continues to grow at an increasing rate.8 The apps vary in many aspects, including their purpose, scope, intended audience, and goals of the app publisher. In turn, more individuals are turning to mobile apps for medical information,4 especially in dermatology, thus it is necessary to create a systematic way to evaluate the quality and utility of each app to assist users in making informed decisions about which apps will best meet their needs in the midst of a wide array of choices.
For the purpose of this study, an objective rubric was created that can be used to evaluate the quality of medical apps for patient education in dermatology. An app’s adequacy and usefulness for patient education was thought to depend on 3 possible score ranges into which the app could fall based on the grading rubric. An app with a total score in the range of 5 to 10 was not thought to be useful and may even be detrimental to patients. An app with a total score in the range of 11 to 15 may be used for patient education with some reservations based on shortcomings for certain criteria. An app with a score in the range of 16 to 20 was thought to be valuable and adequate for patient education. For example, the How to Treat Acne app received a total score of 8 and therefore would not be recommended to patients based on the grading rubric used in this study. This particular app provided sparse and sometimes inaccurate information, had a confusing user interface, and contained many obstructive advertisements. In contrast, the Eczema Doc app received a total score of 19, which indicates a quality app deemed to be useful for patient information based on the established rubric. This app met all the objectives that it advertised, contained accurate information with verified citation of sources, and was very easy for users to navigate.
Of the 44 graded apps, only 9 (20.5%) received scores in the highest range of 16 to 20, which indicates a need for improvements in mobile dermatology apps intended for patient education. Adopting the grading rubric developed in this study as a standard in the creation of medical apps could have beneficial implications in disseminating accurate, safe, unbiased, and easy-to-understand information to patients.
According to industry estimates, roughly 64% of US adults were smartphone users in 2015.1 Smartphones enable users to utilize mobile applications (apps) that can perform a variety of functions in many categories, including business, music, photography, entertainment, education, social networking, travel, and lifestyle. The widespread adoption and use of mobile apps has implications for medical practice. Mobile apps have the capability to serve as information sources for patients, educational tools for students, and diagnostic aids for physicians.2 Consequently, a number of medical and health care–oriented apps have already been developed3 and are increasingly utilized by patients and providers.4
Given its visual nature, dermatology is particularly amenable to the integration of mobile medical apps. A study by Brewer et al5 identified more than 229 dermatology-related apps in categories ranging from general dermatology reference, self-surveillance and diagnosis, disease guides, educational aids, sunscreen and UV recommendations, and teledermatology. Patients served as the target audience and principal consumers of more than half of these dermatology apps.5
Mobile medical and health care apps demonstrate great potential for serving as valuable information sources for patients with dermatologic conditions; however, the content, functions, accuracy, and educational value of dermatology mobile apps are not well characterized, making it difficult for patients and health care providers to select and recommend appropriate apps.6 In this study, we created a rubric to objectively grade 44 publicly available mobile dermatology apps with the primary focus of patient education.
Methods
We conducted a search of dermatology-related educational mobile apps that were publicly available via the App Store (Apple Inc) from January 2016 to November 2016. (The pricing, availability, and other features of these apps may have changed since the study period.) The following search terms were used: dermatology, dermoscopy, melanoma, skin cancer, psoriasis, rosacea, acne, eczema, dermal fillers, and Mohs surgery. We excluded apps that were not in English; had a solely commercial focus; were mobile textbooks or scientific journals; were used to provide teledermatology services with no educational purpose; were solely focused on homeopathic, alternative, and/or complementary medicine; or were intended primarily as a reference for students or health care professionals. Our search yielded 44 apps with patient education as a primary objective. The apps were divided into 6 categories based on their focus: general dermatology, cosmetic dermatology, acne, eczema, psoriasis, and skin cancer.
Each app was reviewed using a quantified grading rubric developed by the researchers. In a prior evaluation, Handel7 reviewed 35 health and wellness mobile apps utilizing the categories of ease of use, reliability, quality, scope of information, and aesthetics.4 These criteria were modified and adapted for the purposes of this study, and a 4-point scale was applied to each criterion. The final criteria were (1) educational objectives, (2) content, (3) accuracy, (4) design, and (5) conflict of interest. The quantified grading rubric is described in Table 1.
Results
The possible range of scores based on the grading rubric was 5 to 20. The actual range of scores was 8 to 19 (Table 2). The 44 reviewed apps were categorized by topic as acne, cosmetic dermatology, eczema, general dermatology, psoriasis, or skin cancer. A sample of 15 apps selected to represent the distribution of scores and their grading on the rubric are presented in Table 3.
Comment
The number of dermatology-related apps available to mobile users continues to grow at an increasing rate.8 The apps vary in many aspects, including their purpose, scope, intended audience, and goals of the app publisher. In turn, more individuals are turning to mobile apps for medical information,4 especially in dermatology, thus it is necessary to create a systematic way to evaluate the quality and utility of each app to assist users in making informed decisions about which apps will best meet their needs in the midst of a wide array of choices.
For the purpose of this study, an objective rubric was created that can be used to evaluate the quality of medical apps for patient education in dermatology. An app’s adequacy and usefulness for patient education was thought to depend on 3 possible score ranges into which the app could fall based on the grading rubric. An app with a total score in the range of 5 to 10 was not thought to be useful and may even be detrimental to patients. An app with a total score in the range of 11 to 15 may be used for patient education with some reservations based on shortcomings for certain criteria. An app with a score in the range of 16 to 20 was thought to be valuable and adequate for patient education. For example, the How to Treat Acne app received a total score of 8 and therefore would not be recommended to patients based on the grading rubric used in this study. This particular app provided sparse and sometimes inaccurate information, had a confusing user interface, and contained many obstructive advertisements. In contrast, the Eczema Doc app received a total score of 19, which indicates a quality app deemed to be useful for patient information based on the established rubric. This app met all the objectives that it advertised, contained accurate information with verified citation of sources, and was very easy for users to navigate.
Of the 44 graded apps, only 9 (20.5%) received scores in the highest range of 16 to 20, which indicates a need for improvements in mobile dermatology apps intended for patient education. Adopting the grading rubric developed in this study as a standard in the creation of medical apps could have beneficial implications in disseminating accurate, safe, unbiased, and easy-to-understand information to patients.
- Smith A. U.S. smartphone use in 2015. Pew Research Center website. http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015. Published April 1, 2015. Accessed August 29, 2017.
- Nilsen W, Kumar S, Shar A, et al. Advancing the science of mHealth. J Health Commun. 2012;17(suppl 1):5-10.
- West DM. How mobile devices are transforming healthcare issues in technology innovation. Issues Technol Innov. 2012;18:1-14.
- Boudreaux ED, Waring ME, Hayes RB, et al. Evaluating and selecting mobile health apps: strategies for healthcare providers and healthcare organizations. Transl Behav Med. 2014;4:363-371.
- Brewer AC, Endly DC, Henley J, et al. Mobile applications in dermatology. JAMA Dermatol. 2013;149:1300-1304.
- Cummings E, Borycki E, Roehrer E. Issues and considerations for healthcare consumers using mobile applications. Stud Health Technol Inform. 2013;183:227-231.
- Handel MJ. mHealth (mobile health)-using apps for health and wellness. Explore. 2011;7:256-261.
- Boulos MN, Brewer AC, Karimkhani C, et al. Mobile medical and health apps: state of the art, concerns, regulatory control and certification. Online J Public Health Inform. 2014;5:229.
- Smith A. U.S. smartphone use in 2015. Pew Research Center website. http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015. Published April 1, 2015. Accessed August 29, 2017.
- Nilsen W, Kumar S, Shar A, et al. Advancing the science of mHealth. J Health Commun. 2012;17(suppl 1):5-10.
- West DM. How mobile devices are transforming healthcare issues in technology innovation. Issues Technol Innov. 2012;18:1-14.
- Boudreaux ED, Waring ME, Hayes RB, et al. Evaluating and selecting mobile health apps: strategies for healthcare providers and healthcare organizations. Transl Behav Med. 2014;4:363-371.
- Brewer AC, Endly DC, Henley J, et al. Mobile applications in dermatology. JAMA Dermatol. 2013;149:1300-1304.
- Cummings E, Borycki E, Roehrer E. Issues and considerations for healthcare consumers using mobile applications. Stud Health Technol Inform. 2013;183:227-231.
- Handel MJ. mHealth (mobile health)-using apps for health and wellness. Explore. 2011;7:256-261.
- Boulos MN, Brewer AC, Karimkhani C, et al. Mobile medical and health apps: state of the art, concerns, regulatory control and certification. Online J Public Health Inform. 2014;5:229.
Practice Points
- Mobile dermatology apps for educational purposes should be objectively reviewed before being used by patients.
- In our study, only 9 (20.5%) of the 44 dermatology apps evaluated were considered adequate for patient information based on our grading criteria.
Using oral and topical cosmeceuticals to prevent and treat skin aging, Part II
This month’s column resumes my review of prevention and treatment strategies for aging skin using oral and topical cosmeceutical agents.
Preventing and treating inflammation
Skin aging can result from inflammation through several mechanisms, including the formation of reactive oxygen species. Inflammation itself arises from myriad etiologic pathways, with multiple inflammatory mediators potentially involved, including histamines, cytokines, eicosanoids (for example, prostaglandins, thromboxanes, and leukotrienes), complement cascade components, kinins, fibrinopeptide enzymes, nuclear factor–kappa B, and free radicals.

Topically applied argan oil, caffeine, chamomile, feverfew, green tea, licorice extract, aloe, linoleic acid (found in high concentrations in argan oil and safflower oil), and niacinamide are among the anti-inflammatory ingredients that have been used successfully in topical skin care to reduce inflammation. The Food and Drug Administration does not allow cosmetics to make “anti-inflammatory” claims. For this reason, these products will state they have “soothing” effects or imply they improve of redness.
Oral polypodium leucotomos has been demonstrated to suppress the effect of UV radiation on COX-2 expression.2 Also, glycolic acid has exhibited the capacity to inhibit COX-2 signaling and other inflammatory mediators.3
Preventing and treating glycation
Glycation is produced by the Maillard reaction, a chemical reaction – particularly well known in cooking – between an amino acid and a sugar molecule that typically requires heat. This reaction was first described by Louis Camille Maillard in 1912 when he noted that amino acids can react with sugar to yield brown or golden-brown substances. It took until the 1980s for scientists to understand the importance of glycation in health.
When glycation occurs, sugar molecules attach to proteins, creating cross-linked proteins known as advanced glycation end products (or AGEs) and causing a series of chemical reactions. Glycation occurs in collagen fibers and results in the formation of cross-links that bind collagen fibers to each other, which leaves the skin stiffer. Glycosylated collagen is believed to be a factor in the appearance of aged skin.4 Glycation also can affect elastin: Recent research suggests that glycation can engender elastosis, which is elastin that is abnormally clumped together and presents more frequently in aged skin.
Several antiaging skin care products claim to treat glycation, but – unfortunately – glycation is not a reversible reaction. It must be prevented in the first place. Some studies suggest that antioxidants can prevent glycation, but it is more likely that they just divert the process down a different pathway that still leads to glycation. Reducing serum glucose levels is the optimum method of preventing glycation.5 Dietary intervention and oral metformin are recommended for lowering glycation.
REVERSING SKIN CELL AGING
Epidermal keratinocytes in aging
Young basal stem cells synthesize a plethora of new keratinocytes at a pace that leads to fast cell turnover and vigorous production of protective epidermal constituents. Old keratinocytes display less energy, show reduced responsiveness to cellular signals, and do not synthesize these protective components.6,7 Keratinocyte stem cell function declines over time while damage accumulates, as seen in a diminished response to growth factors, decreased keratinization, and impaired function.8
Dermal fibroblasts in cutaneous aging
Young fibroblasts produce key cellular constituents, including collagen, elastin, hyaluronic acid, and heparan sulfate. This production declines in older fibroblasts. Like aging keratinocytes, old fibroblasts lose energy and responsiveness to growth factors and other cellular signals.6,7
Rejuvenating aged skin with cosmeceuticals
Gene expression, growth factors, cytokines, chemokines, and receptor activation guide the function of keratinocytes and fibroblasts. To reverse or slow cellular skin aging, old keratinocytes and fibroblasts must be galvanized to respond to such signals or the signals must be enhanced.
Stimulating old keratinocytes and fibroblasts
Essential steps in stimulating aged keratinocytes and fibroblasts include: activating gene expression, adding growth factors, activating cytokines and chemokines, turning on receptors, and making cells more responsive to signals.
Influencing gene expression
Retinoids are known to affect collagen genes and increase activity of procollagen genes, thereby reducing the production of collagenase. Many studies have shown the efficacy of retinoids in treating aged skin and preventing cutaneous aging in both areas frequently exposed to the sun but also those that aren’t.9,10 Prescription retinoids (tretinoin, adapalene, tazarotene) and over-the-counter retinoids (retinol) are first-line options to treat and prevent aging by stimulating old keratinocytes and fibroblasts.10,11 However, exposing retinoic acid receptors to retinoids almost invariably leads to erythema and flaking in the first few weeks. Therefore, retinoids should be titrated slowly. Note that retinoid esters, such as retinyl palmitate and retinyl linoleate, do not penetrate well into the dermis;12 they also are not as effective as retinol, tretinoin, adapalene, and tazarotene. Compliance with retinoids is always an issue with patients. They should receive printed educational material about how to begin use and why it is important to use these products consistently.

Growth factors
The use of cosmetic formulations that contain growth factors can contribute to skin rejuvenation. There are various types of growth factors that have the capacity to stimulate old keratinocytes and fibroblasts to enhance function.17 Growth factors, which are inactive or vulnerable to degradation in their native, soluble form, can directly energize genes or act as a signaling mechanism. To exert their quintessential functions, growth factors must be transferred to the correct receptor site in order for the cell to respond to their signal.18
Heparan sulfate
Heparan sulfate (HS) plays a primary role in cell-to-cell communications. It increases cellular response to growth factors by facilitating the response of old, lazy fibroblasts to the cellular signals.18 HS binds, stores, and protects growth factors, which allows them to complete movement to their targets, and then presents them to the appropriate binding site.18,19 A topically applied analogue of HS has been demonstrated to rejuvenate aged skin.20
Stem cells
Stem cells included and pointedly marketed in cosmeceutical products are usually plant derived, are too large to penetrate the stratum corneum, display short shelf lives, and do not behave as human stem cells would. As a result, stem cells in cosmeceutical agents are essentially useless.
However, novel technologies have revealed ingredients that can incite native stem cells to repopulate the epidermis and dermis with young cells. Stem cells in skin include basal stem cells and 10 varieties of hair follicle stem cells. The LGR6+ hair follicle cells play a pivotal role in repopulating the epidermis after wounding has occurred.21,22 Aesthetic physicians have known for several years that inducing skin wounding with lasers, needles, and acidic peels leads to improvement in its appearance. Researchers have provided new data showing that wounding the skin prompts LGR6+ stem cells to repopulate the epidermis. Once wounding occurs, neutrophils release the peptide defensin, which stimulates the LGR6+ stem cells to repopulate the epidermis.23 Topical defensin that has been formulated to penetrate into hair follicles, where the LGR6+ stem cells reside, has been demonstrated to render a smoother, more youthful appearance to the skin.
Conclusion
It is important for practitioners to identify patients at risk for premature skin aging as early as possible and start them on an appropriate and consistent skin care regimen. This typically will include at least a daily sunscreen with an SPF 15 or higher, a nightly topical retinoid, and oral and topical antioxidants. The patient’s additional skin type proclivities (for example, dryness, inflammation, melanocyte activity) should guide the physician as to how to combine these baseline product types with cleansers, moisturizers, and formulations with hydroxy acids, growth factors, heparan sulfate, and defensin.
Several studies have revealed that patients exhibit poor compliance with recommended regimens.24 Informing patients about the need for skin protection and providing printed instructions can help to improve compliance.25 This can promote healthy lifestyle habits and compliance with scientifically proven antiaging therapies.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
1. Arch Dermatol Res. 2010 Jan;302(1):5-17.
2. Am J Pathol. 2009 Nov;175(5):1952-61.
3. J Dermatol Sci. 2017 Jun;86(3):238-48.
4. Eur J Dermatol. 2007 Jan-Feb;17(1):12-20.
5. “Advanced Glycation End Products (AGEs): Emerging Mediators of Skin Aging,” in Textbook of Aging Skin (Berlin: Springer, 2017, pp. 1675-86).
6. Mech Ageing Dev. 1986 Jul;35(2):185-98.
7. Exp Cell Res. 1996 Sep 15;227(2):252-5.
8. J Cutan Pathol. 2003 Jul;30(6):351-7.
9. PLoS One. 2015 Feb 6;10(2):e0117491.
10. Arch Dermatol. 2007 May;143(5):606-12.
11. JAMA. 1988 Jan 22-29;259(4):527-32.
12. J Invest Dermatol. 1997 Sep;109(3):301-5.
13. J Am Acad Dermatol. 1996 Feb;34(2 Pt 1):187-95.
14. J Am Acad Dermatol. 1996 Sep;35(3 Pt 1):388-91.
15. Dermatol Surg. 2001 May;27(5):429-33.
16. J Invest Dermatol. 1994 Aug;103(2):228-32.
17. Clin Cosmet Investig Dermatol. 2016 Nov 9;9:411-9.
18. Chem Biol Drug Des. 2008 Dec;72(6):455-82.
19. Front Immunol. 2013 Dec 18;4:470.
20. J Drugs Dermatol. 2015 Jul;14(7):669-74.
21. Science. 2010 Mar 12;327(5971):1385-9.
22. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
23. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
24. J Am Acad Dermatol. 2008 Jul;59(1):27-33.
25. J Am Acad Dermatol. 2013 Mar;68(3):364.e1-10.
This month’s column resumes my review of prevention and treatment strategies for aging skin using oral and topical cosmeceutical agents.
Preventing and treating inflammation
Skin aging can result from inflammation through several mechanisms, including the formation of reactive oxygen species. Inflammation itself arises from myriad etiologic pathways, with multiple inflammatory mediators potentially involved, including histamines, cytokines, eicosanoids (for example, prostaglandins, thromboxanes, and leukotrienes), complement cascade components, kinins, fibrinopeptide enzymes, nuclear factor–kappa B, and free radicals.
Topically applied argan oil, caffeine, chamomile, feverfew, green tea, licorice extract, aloe, linoleic acid (found in high concentrations in argan oil and safflower oil), and niacinamide are among the anti-inflammatory ingredients that have been used successfully in topical skin care to reduce inflammation. The Food and Drug Administration does not allow cosmetics to make “anti-inflammatory” claims. For this reason, these products will state they have “soothing” effects or imply they improve of redness.
Oral polypodium leucotomos has been demonstrated to suppress the effect of UV radiation on COX-2 expression.2 Also, glycolic acid has exhibited the capacity to inhibit COX-2 signaling and other inflammatory mediators.3
Preventing and treating glycation
Glycation is produced by the Maillard reaction, a chemical reaction – particularly well known in cooking – between an amino acid and a sugar molecule that typically requires heat. This reaction was first described by Louis Camille Maillard in 1912 when he noted that amino acids can react with sugar to yield brown or golden-brown substances. It took until the 1980s for scientists to understand the importance of glycation in health.
When glycation occurs, sugar molecules attach to proteins, creating cross-linked proteins known as advanced glycation end products (or AGEs) and causing a series of chemical reactions. Glycation occurs in collagen fibers and results in the formation of cross-links that bind collagen fibers to each other, which leaves the skin stiffer. Glycosylated collagen is believed to be a factor in the appearance of aged skin.4 Glycation also can affect elastin: Recent research suggests that glycation can engender elastosis, which is elastin that is abnormally clumped together and presents more frequently in aged skin.
Several antiaging skin care products claim to treat glycation, but – unfortunately – glycation is not a reversible reaction. It must be prevented in the first place. Some studies suggest that antioxidants can prevent glycation, but it is more likely that they just divert the process down a different pathway that still leads to glycation. Reducing serum glucose levels is the optimum method of preventing glycation.5 Dietary intervention and oral metformin are recommended for lowering glycation.
REVERSING SKIN CELL AGING
Epidermal keratinocytes in aging
Young basal stem cells synthesize a plethora of new keratinocytes at a pace that leads to fast cell turnover and vigorous production of protective epidermal constituents. Old keratinocytes display less energy, show reduced responsiveness to cellular signals, and do not synthesize these protective components.6,7 Keratinocyte stem cell function declines over time while damage accumulates, as seen in a diminished response to growth factors, decreased keratinization, and impaired function.8
Dermal fibroblasts in cutaneous aging
Young fibroblasts produce key cellular constituents, including collagen, elastin, hyaluronic acid, and heparan sulfate. This production declines in older fibroblasts. Like aging keratinocytes, old fibroblasts lose energy and responsiveness to growth factors and other cellular signals.6,7
Rejuvenating aged skin with cosmeceuticals
Gene expression, growth factors, cytokines, chemokines, and receptor activation guide the function of keratinocytes and fibroblasts. To reverse or slow cellular skin aging, old keratinocytes and fibroblasts must be galvanized to respond to such signals or the signals must be enhanced.
Stimulating old keratinocytes and fibroblasts
Essential steps in stimulating aged keratinocytes and fibroblasts include: activating gene expression, adding growth factors, activating cytokines and chemokines, turning on receptors, and making cells more responsive to signals.
Influencing gene expression
Retinoids are known to affect collagen genes and increase activity of procollagen genes, thereby reducing the production of collagenase. Many studies have shown the efficacy of retinoids in treating aged skin and preventing cutaneous aging in both areas frequently exposed to the sun but also those that aren’t.9,10 Prescription retinoids (tretinoin, adapalene, tazarotene) and over-the-counter retinoids (retinol) are first-line options to treat and prevent aging by stimulating old keratinocytes and fibroblasts.10,11 However, exposing retinoic acid receptors to retinoids almost invariably leads to erythema and flaking in the first few weeks. Therefore, retinoids should be titrated slowly. Note that retinoid esters, such as retinyl palmitate and retinyl linoleate, do not penetrate well into the dermis;12 they also are not as effective as retinol, tretinoin, adapalene, and tazarotene. Compliance with retinoids is always an issue with patients. They should receive printed educational material about how to begin use and why it is important to use these products consistently.
Growth factors
The use of cosmetic formulations that contain growth factors can contribute to skin rejuvenation. There are various types of growth factors that have the capacity to stimulate old keratinocytes and fibroblasts to enhance function.17 Growth factors, which are inactive or vulnerable to degradation in their native, soluble form, can directly energize genes or act as a signaling mechanism. To exert their quintessential functions, growth factors must be transferred to the correct receptor site in order for the cell to respond to their signal.18
Heparan sulfate
Heparan sulfate (HS) plays a primary role in cell-to-cell communications. It increases cellular response to growth factors by facilitating the response of old, lazy fibroblasts to the cellular signals.18 HS binds, stores, and protects growth factors, which allows them to complete movement to their targets, and then presents them to the appropriate binding site.18,19 A topically applied analogue of HS has been demonstrated to rejuvenate aged skin.20
Stem cells
Stem cells included and pointedly marketed in cosmeceutical products are usually plant derived, are too large to penetrate the stratum corneum, display short shelf lives, and do not behave as human stem cells would. As a result, stem cells in cosmeceutical agents are essentially useless.
However, novel technologies have revealed ingredients that can incite native stem cells to repopulate the epidermis and dermis with young cells. Stem cells in skin include basal stem cells and 10 varieties of hair follicle stem cells. The LGR6+ hair follicle cells play a pivotal role in repopulating the epidermis after wounding has occurred.21,22 Aesthetic physicians have known for several years that inducing skin wounding with lasers, needles, and acidic peels leads to improvement in its appearance. Researchers have provided new data showing that wounding the skin prompts LGR6+ stem cells to repopulate the epidermis. Once wounding occurs, neutrophils release the peptide defensin, which stimulates the LGR6+ stem cells to repopulate the epidermis.23 Topical defensin that has been formulated to penetrate into hair follicles, where the LGR6+ stem cells reside, has been demonstrated to render a smoother, more youthful appearance to the skin.
Conclusion
It is important for practitioners to identify patients at risk for premature skin aging as early as possible and start them on an appropriate and consistent skin care regimen. This typically will include at least a daily sunscreen with an SPF 15 or higher, a nightly topical retinoid, and oral and topical antioxidants. The patient’s additional skin type proclivities (for example, dryness, inflammation, melanocyte activity) should guide the physician as to how to combine these baseline product types with cleansers, moisturizers, and formulations with hydroxy acids, growth factors, heparan sulfate, and defensin.
Several studies have revealed that patients exhibit poor compliance with recommended regimens.24 Informing patients about the need for skin protection and providing printed instructions can help to improve compliance.25 This can promote healthy lifestyle habits and compliance with scientifically proven antiaging therapies.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
1. Arch Dermatol Res. 2010 Jan;302(1):5-17.
2. Am J Pathol. 2009 Nov;175(5):1952-61.
3. J Dermatol Sci. 2017 Jun;86(3):238-48.
4. Eur J Dermatol. 2007 Jan-Feb;17(1):12-20.
5. “Advanced Glycation End Products (AGEs): Emerging Mediators of Skin Aging,” in Textbook of Aging Skin (Berlin: Springer, 2017, pp. 1675-86).
6. Mech Ageing Dev. 1986 Jul;35(2):185-98.
7. Exp Cell Res. 1996 Sep 15;227(2):252-5.
8. J Cutan Pathol. 2003 Jul;30(6):351-7.
9. PLoS One. 2015 Feb 6;10(2):e0117491.
10. Arch Dermatol. 2007 May;143(5):606-12.
11. JAMA. 1988 Jan 22-29;259(4):527-32.
12. J Invest Dermatol. 1997 Sep;109(3):301-5.
13. J Am Acad Dermatol. 1996 Feb;34(2 Pt 1):187-95.
14. J Am Acad Dermatol. 1996 Sep;35(3 Pt 1):388-91.
15. Dermatol Surg. 2001 May;27(5):429-33.
16. J Invest Dermatol. 1994 Aug;103(2):228-32.
17. Clin Cosmet Investig Dermatol. 2016 Nov 9;9:411-9.
18. Chem Biol Drug Des. 2008 Dec;72(6):455-82.
19. Front Immunol. 2013 Dec 18;4:470.
20. J Drugs Dermatol. 2015 Jul;14(7):669-74.
21. Science. 2010 Mar 12;327(5971):1385-9.
22. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
23. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
24. J Am Acad Dermatol. 2008 Jul;59(1):27-33.
25. J Am Acad Dermatol. 2013 Mar;68(3):364.e1-10.
This month’s column resumes my review of prevention and treatment strategies for aging skin using oral and topical cosmeceutical agents.
Preventing and treating inflammation
Skin aging can result from inflammation through several mechanisms, including the formation of reactive oxygen species. Inflammation itself arises from myriad etiologic pathways, with multiple inflammatory mediators potentially involved, including histamines, cytokines, eicosanoids (for example, prostaglandins, thromboxanes, and leukotrienes), complement cascade components, kinins, fibrinopeptide enzymes, nuclear factor–kappa B, and free radicals.
Topically applied argan oil, caffeine, chamomile, feverfew, green tea, licorice extract, aloe, linoleic acid (found in high concentrations in argan oil and safflower oil), and niacinamide are among the anti-inflammatory ingredients that have been used successfully in topical skin care to reduce inflammation. The Food and Drug Administration does not allow cosmetics to make “anti-inflammatory” claims. For this reason, these products will state they have “soothing” effects or imply they improve of redness.
Oral polypodium leucotomos has been demonstrated to suppress the effect of UV radiation on COX-2 expression.2 Also, glycolic acid has exhibited the capacity to inhibit COX-2 signaling and other inflammatory mediators.3
Preventing and treating glycation
Glycation is produced by the Maillard reaction, a chemical reaction – particularly well known in cooking – between an amino acid and a sugar molecule that typically requires heat. This reaction was first described by Louis Camille Maillard in 1912 when he noted that amino acids can react with sugar to yield brown or golden-brown substances. It took until the 1980s for scientists to understand the importance of glycation in health.
When glycation occurs, sugar molecules attach to proteins, creating cross-linked proteins known as advanced glycation end products (or AGEs) and causing a series of chemical reactions. Glycation occurs in collagen fibers and results in the formation of cross-links that bind collagen fibers to each other, which leaves the skin stiffer. Glycosylated collagen is believed to be a factor in the appearance of aged skin.4 Glycation also can affect elastin: Recent research suggests that glycation can engender elastosis, which is elastin that is abnormally clumped together and presents more frequently in aged skin.
Several antiaging skin care products claim to treat glycation, but – unfortunately – glycation is not a reversible reaction. It must be prevented in the first place. Some studies suggest that antioxidants can prevent glycation, but it is more likely that they just divert the process down a different pathway that still leads to glycation. Reducing serum glucose levels is the optimum method of preventing glycation.5 Dietary intervention and oral metformin are recommended for lowering glycation.
REVERSING SKIN CELL AGING
Epidermal keratinocytes in aging
Young basal stem cells synthesize a plethora of new keratinocytes at a pace that leads to fast cell turnover and vigorous production of protective epidermal constituents. Old keratinocytes display less energy, show reduced responsiveness to cellular signals, and do not synthesize these protective components.6,7 Keratinocyte stem cell function declines over time while damage accumulates, as seen in a diminished response to growth factors, decreased keratinization, and impaired function.8
Dermal fibroblasts in cutaneous aging
Young fibroblasts produce key cellular constituents, including collagen, elastin, hyaluronic acid, and heparan sulfate. This production declines in older fibroblasts. Like aging keratinocytes, old fibroblasts lose energy and responsiveness to growth factors and other cellular signals.6,7
Rejuvenating aged skin with cosmeceuticals
Gene expression, growth factors, cytokines, chemokines, and receptor activation guide the function of keratinocytes and fibroblasts. To reverse or slow cellular skin aging, old keratinocytes and fibroblasts must be galvanized to respond to such signals or the signals must be enhanced.
Stimulating old keratinocytes and fibroblasts
Essential steps in stimulating aged keratinocytes and fibroblasts include: activating gene expression, adding growth factors, activating cytokines and chemokines, turning on receptors, and making cells more responsive to signals.
Influencing gene expression
Retinoids are known to affect collagen genes and increase activity of procollagen genes, thereby reducing the production of collagenase. Many studies have shown the efficacy of retinoids in treating aged skin and preventing cutaneous aging in both areas frequently exposed to the sun but also those that aren’t.9,10 Prescription retinoids (tretinoin, adapalene, tazarotene) and over-the-counter retinoids (retinol) are first-line options to treat and prevent aging by stimulating old keratinocytes and fibroblasts.10,11 However, exposing retinoic acid receptors to retinoids almost invariably leads to erythema and flaking in the first few weeks. Therefore, retinoids should be titrated slowly. Note that retinoid esters, such as retinyl palmitate and retinyl linoleate, do not penetrate well into the dermis;12 they also are not as effective as retinol, tretinoin, adapalene, and tazarotene. Compliance with retinoids is always an issue with patients. They should receive printed educational material about how to begin use and why it is important to use these products consistently.
Growth factors
The use of cosmetic formulations that contain growth factors can contribute to skin rejuvenation. There are various types of growth factors that have the capacity to stimulate old keratinocytes and fibroblasts to enhance function.17 Growth factors, which are inactive or vulnerable to degradation in their native, soluble form, can directly energize genes or act as a signaling mechanism. To exert their quintessential functions, growth factors must be transferred to the correct receptor site in order for the cell to respond to their signal.18
Heparan sulfate
Heparan sulfate (HS) plays a primary role in cell-to-cell communications. It increases cellular response to growth factors by facilitating the response of old, lazy fibroblasts to the cellular signals.18 HS binds, stores, and protects growth factors, which allows them to complete movement to their targets, and then presents them to the appropriate binding site.18,19 A topically applied analogue of HS has been demonstrated to rejuvenate aged skin.20
Stem cells
Stem cells included and pointedly marketed in cosmeceutical products are usually plant derived, are too large to penetrate the stratum corneum, display short shelf lives, and do not behave as human stem cells would. As a result, stem cells in cosmeceutical agents are essentially useless.
However, novel technologies have revealed ingredients that can incite native stem cells to repopulate the epidermis and dermis with young cells. Stem cells in skin include basal stem cells and 10 varieties of hair follicle stem cells. The LGR6+ hair follicle cells play a pivotal role in repopulating the epidermis after wounding has occurred.21,22 Aesthetic physicians have known for several years that inducing skin wounding with lasers, needles, and acidic peels leads to improvement in its appearance. Researchers have provided new data showing that wounding the skin prompts LGR6+ stem cells to repopulate the epidermis. Once wounding occurs, neutrophils release the peptide defensin, which stimulates the LGR6+ stem cells to repopulate the epidermis.23 Topical defensin that has been formulated to penetrate into hair follicles, where the LGR6+ stem cells reside, has been demonstrated to render a smoother, more youthful appearance to the skin.
Conclusion
It is important for practitioners to identify patients at risk for premature skin aging as early as possible and start them on an appropriate and consistent skin care regimen. This typically will include at least a daily sunscreen with an SPF 15 or higher, a nightly topical retinoid, and oral and topical antioxidants. The patient’s additional skin type proclivities (for example, dryness, inflammation, melanocyte activity) should guide the physician as to how to combine these baseline product types with cleansers, moisturizers, and formulations with hydroxy acids, growth factors, heparan sulfate, and defensin.
Several studies have revealed that patients exhibit poor compliance with recommended regimens.24 Informing patients about the need for skin protection and providing printed instructions can help to improve compliance.25 This can promote healthy lifestyle habits and compliance with scientifically proven antiaging therapies.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
1. Arch Dermatol Res. 2010 Jan;302(1):5-17.
2. Am J Pathol. 2009 Nov;175(5):1952-61.
3. J Dermatol Sci. 2017 Jun;86(3):238-48.
4. Eur J Dermatol. 2007 Jan-Feb;17(1):12-20.
5. “Advanced Glycation End Products (AGEs): Emerging Mediators of Skin Aging,” in Textbook of Aging Skin (Berlin: Springer, 2017, pp. 1675-86).
6. Mech Ageing Dev. 1986 Jul;35(2):185-98.
7. Exp Cell Res. 1996 Sep 15;227(2):252-5.
8. J Cutan Pathol. 2003 Jul;30(6):351-7.
9. PLoS One. 2015 Feb 6;10(2):e0117491.
10. Arch Dermatol. 2007 May;143(5):606-12.
11. JAMA. 1988 Jan 22-29;259(4):527-32.
12. J Invest Dermatol. 1997 Sep;109(3):301-5.
13. J Am Acad Dermatol. 1996 Feb;34(2 Pt 1):187-95.
14. J Am Acad Dermatol. 1996 Sep;35(3 Pt 1):388-91.
15. Dermatol Surg. 2001 May;27(5):429-33.
16. J Invest Dermatol. 1994 Aug;103(2):228-32.
17. Clin Cosmet Investig Dermatol. 2016 Nov 9;9:411-9.
18. Chem Biol Drug Des. 2008 Dec;72(6):455-82.
19. Front Immunol. 2013 Dec 18;4:470.
20. J Drugs Dermatol. 2015 Jul;14(7):669-74.
21. Science. 2010 Mar 12;327(5971):1385-9.
22. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
23. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
24. J Am Acad Dermatol. 2008 Jul;59(1):27-33.
25. J Am Acad Dermatol. 2013 Mar;68(3):364.e1-10.
Cosmetic Corner: Dermatologists Weigh in on Bar Soaps
To improve patient care and outcomes, leading dermatologists offered their recommendations on bar soaps. Consideration must be given to:
- Avène Cold Cream Ultra-Rich Cleansing Bar
Pierre Fabre Dermo-Cosmetique USA
“This gentle cleansing bar is not only hypoallergenic, soap free, and lanolin free, it also has Avène’s soothing Thermal Spring Water, plus white beeswax and a noncomedogenic, pharmaceutical-grade paraffin oil to protect the skin.”—Jeannette Graf, MD, Great Neck, New York
- Hydrating Cleanser Bar
CeraVe
Recommended by Shari Lipner, MD, PhD, New York, New York
- Vanicream Cleansing Bar
Pharmaceutical Specialties, Inc
“This is a great option for patients with eczema or dry, sensitive skin.”—Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Lip plumpers, shaving lotions for men, and night creams will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on bar soaps. Consideration must be given to:
- Avène Cold Cream Ultra-Rich Cleansing Bar
Pierre Fabre Dermo-Cosmetique USA
“This gentle cleansing bar is not only hypoallergenic, soap free, and lanolin free, it also has Avène’s soothing Thermal Spring Water, plus white beeswax and a noncomedogenic, pharmaceutical-grade paraffin oil to protect the skin.”—Jeannette Graf, MD, Great Neck, New York
- Hydrating Cleanser Bar
CeraVe
Recommended by Shari Lipner, MD, PhD, New York, New York
- Vanicream Cleansing Bar
Pharmaceutical Specialties, Inc
“This is a great option for patients with eczema or dry, sensitive skin.”—Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Lip plumpers, shaving lotions for men, and night creams will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.
To improve patient care and outcomes, leading dermatologists offered their recommendations on bar soaps. Consideration must be given to:
- Avène Cold Cream Ultra-Rich Cleansing Bar
Pierre Fabre Dermo-Cosmetique USA
“This gentle cleansing bar is not only hypoallergenic, soap free, and lanolin free, it also has Avène’s soothing Thermal Spring Water, plus white beeswax and a noncomedogenic, pharmaceutical-grade paraffin oil to protect the skin.”—Jeannette Graf, MD, Great Neck, New York
- Hydrating Cleanser Bar
CeraVe
Recommended by Shari Lipner, MD, PhD, New York, New York
- Vanicream Cleansing Bar
Pharmaceutical Specialties, Inc
“This is a great option for patients with eczema or dry, sensitive skin.”—Gary Goldenberg, MD, New York, New York
Cutis invites readers to send us their recommendations. Lip plumpers, shaving lotions for men, and night creams will be featured in upcoming editions of Cosmetic Corner. Please e-mail your recommendation(s) to the Editorial Office.
Disclaimer: Opinions expressed herein do not necessarily reflect those of Cutis or Frontline Medical Communications Inc. and shall not be used for product endorsement purposes. Any reference made to a specific commercial product does not indicate or imply that Cutis or Frontline Medical Communications Inc. endorses, recommends, or favors the product mentioned. No guarantee is given to the effects of recommended products.

Want to expand aesthetic dermatology business? Appeal to men
MIAMI – Bringing more men into an aesthetic dermatology practice can expand the patient population, increase business revenue, and pay long-term dividends in terms of patient loyalty and repeat business.
But men aren’t like women when it comes to aesthetic concerns, so the strategies used to market your aesthetic offerings to female patients might miss the mark with men, cautioned Terrence Keaney, MD.

“I spend more time explaining therapies and what might be best for them,” he noted. “I explain the scientific rationale and treatment mechanisms so they will be more comfortable.” Making sure they understand is important, because “men often nod and don’t ask questions.”
The extra effort up front can pay off.
“The beauty of men is when they get a great result and are happy with you, men are very physician loyal. Once they get a great result, they’re yours forever,” said Dr. Keaney, an assistant clinical professor of dermatology at George Washington University, Washington, and a private practice dermatologist in Arlington, Va.
Cost is the leading deterrent for men to embrace aesthetic procedures, a factor that also ranks first among women. Men are also concerned that results will not look natural and want information about safety and side effects, Dr. Keaney said. “These deterrents can be overcome with proper education and counseling.”
Marketing to men is different
Although growing a male anesthetic patient base is more difficult, Dr. Keaney recommends it, especially for dermatology practices in a competitive market.
This tactic of targeting untapped markets to grow a business, rather than competing on the same level as everyone else, is outlined in a book he recommends, “Blue Ocean Strategy,” by W. Chan Kim and Renée Mauborgne. “It’s about unlocking new demand, and I will argue that, in aesthetic medicine, it’s those male patients.”
“The male aesthetic market is truly untapped and shows tremendous growth potential,” Dr. Keaney said. “Particularly as millennials age, the demand for cosmetic procedures in men will only increase.”
A first step is to make male aesthetic patients feel welcome and comfortable. “Think about a reluctant male patient walking into your office; it can be intimidating if the staff and everyone in the waiting room is female,” Dr. Keaney said. “But you don’t need to put a keg in the corner, either.” He added more wood and changed the colors of his office, for example.
Don’t go overboard
Marketing aesthetic services to men is also different, a lesson Dr. Keaney learned from the outset.
“When I first started a practice, I wanted to attract more male cosmetic patients, and I decided to throw a male cosmetics seminar,” he recalled. “I thought it would be a great opportunity to educate them.”
He partnered with a plastic surgeon, rented a ballroom, sent out an e-blast, and mailed flyers. “We had zero RSVPs. We canceled it.”
He added, “Men are not sitting at the computer thinking, ‘I wish someone would throw a seminar on aesthetics.’”
A better strategy came the following year as a men’s health event with a broader scope. A urologist, internist, dermatologist, and plastic surgeon talked about a variety of health issues. “They were blown away by the options from the dermatologist and the plastic surgeon.”
A growing market
An American Society for Dermatologic Surgery annual survey reveals dermatologic surgeons performed nearly 10.5 million medically necessary and cosmetic procedures in 2016, the latest year for which results are available. The rate is up 5% from the year before, and up by more than 30%, compared with 2012.
“Within the growth of procedures performed, the male and millennial demographics’ interest in cosmetic treatments also continues to rise,” the survey authors noted. “In the last 5 years, men receiving wrinkle relaxers has increased 9%, and men using soft-tissue fillers grew from 2% to 9%.” The survey also reveals that patients younger than 30 years are seeking more cosmetic treatments. In fact, millennials’ use of wrinkle relaxers increased 20% from 2015, and 50% since 2012.
Address the top male aesthetic concerns
Men are interested in looking healthy, young, and staying fit, Dr. Keaney said, but there is often a disconnect in the male market. “I would argue the real rate limiter is education,” he explained, “and that both the industry and physicians are at fault.”
Most messages about aesthetic procedures have not been targeted toward men. For example, only 39% of 600 aesthetically inclined men knew about dermal fillers in a study Dr. Keaney co-authored (Dermatol Surg. 2016 Oct;42[10]:1155-63).
“I talk to men in my practice about dermal fillers, and most think they’re only for injection in the lips,” he said. The results of the online survey came from men “cosmetically on the cusp,” as he described them – men familiar with neuromodulators for facial rejuvenation, but who had never tried such a therapy.
Tear troughs, double chin, crow’s feet, and forehead lines were the most common concerns, in order, reported by study participants. Dr. Keaney said. “You’ll notice what is missing here: the cheeks, the nasolabial folds, and the lips. And what are those? The FDA-approved indications for dermal fillers.”
Even though it doesn’t top the list of men’s concerns in this study, overall, “if you’re looking to grow your male aesthetic patient population, the number one cosmetic concern among men remains hair loss,” noted Dr. Keaney. “You cannot ignore hair loss. It has a large psychosocial impact.”
During a full-body exam, Dr. Keaney recommends using a scalp exam as an opportunity to ask about any hair-loss concerns.
Encouraging signs from other industries
Other industries are showing a rise in the appearance-conscious male consumer, Dr. Keaney said. Men’s skin care, grooming, and luxury fashion industries are all growing, for example.
Worldwide, the personal care market for men is forecast to grow to $166 billion globally by 2022, according to a report from Allied Market Research. The compound average growth rate is expected to grow more than 5% each year between now and then.
“Men are spending money on their hair and skin,” Dr. Keaney said. “The question is, Why aren’t they spending money on their face? It’s how we interact with the world.”
Dr. Keaney has served on the advisory board of, consulted for, and was a speaker for Allergan. He was also a speaker for Eclipse, Sciton, and Syneron Candela, and served on the advisory boards for Aclaris and Merz.
MIAMI – Bringing more men into an aesthetic dermatology practice can expand the patient population, increase business revenue, and pay long-term dividends in terms of patient loyalty and repeat business.
But men aren’t like women when it comes to aesthetic concerns, so the strategies used to market your aesthetic offerings to female patients might miss the mark with men, cautioned Terrence Keaney, MD.
“I spend more time explaining therapies and what might be best for them,” he noted. “I explain the scientific rationale and treatment mechanisms so they will be more comfortable.” Making sure they understand is important, because “men often nod and don’t ask questions.”
The extra effort up front can pay off.
“The beauty of men is when they get a great result and are happy with you, men are very physician loyal. Once they get a great result, they’re yours forever,” said Dr. Keaney, an assistant clinical professor of dermatology at George Washington University, Washington, and a private practice dermatologist in Arlington, Va.
Cost is the leading deterrent for men to embrace aesthetic procedures, a factor that also ranks first among women. Men are also concerned that results will not look natural and want information about safety and side effects, Dr. Keaney said. “These deterrents can be overcome with proper education and counseling.”
Marketing to men is different
Although growing a male anesthetic patient base is more difficult, Dr. Keaney recommends it, especially for dermatology practices in a competitive market.
This tactic of targeting untapped markets to grow a business, rather than competing on the same level as everyone else, is outlined in a book he recommends, “Blue Ocean Strategy,” by W. Chan Kim and Renée Mauborgne. “It’s about unlocking new demand, and I will argue that, in aesthetic medicine, it’s those male patients.”
“The male aesthetic market is truly untapped and shows tremendous growth potential,” Dr. Keaney said. “Particularly as millennials age, the demand for cosmetic procedures in men will only increase.”
A first step is to make male aesthetic patients feel welcome and comfortable. “Think about a reluctant male patient walking into your office; it can be intimidating if the staff and everyone in the waiting room is female,” Dr. Keaney said. “But you don’t need to put a keg in the corner, either.” He added more wood and changed the colors of his office, for example.
Don’t go overboard
Marketing aesthetic services to men is also different, a lesson Dr. Keaney learned from the outset.
“When I first started a practice, I wanted to attract more male cosmetic patients, and I decided to throw a male cosmetics seminar,” he recalled. “I thought it would be a great opportunity to educate them.”
He partnered with a plastic surgeon, rented a ballroom, sent out an e-blast, and mailed flyers. “We had zero RSVPs. We canceled it.”
He added, “Men are not sitting at the computer thinking, ‘I wish someone would throw a seminar on aesthetics.’”
A better strategy came the following year as a men’s health event with a broader scope. A urologist, internist, dermatologist, and plastic surgeon talked about a variety of health issues. “They were blown away by the options from the dermatologist and the plastic surgeon.”
A growing market
An American Society for Dermatologic Surgery annual survey reveals dermatologic surgeons performed nearly 10.5 million medically necessary and cosmetic procedures in 2016, the latest year for which results are available. The rate is up 5% from the year before, and up by more than 30%, compared with 2012.
“Within the growth of procedures performed, the male and millennial demographics’ interest in cosmetic treatments also continues to rise,” the survey authors noted. “In the last 5 years, men receiving wrinkle relaxers has increased 9%, and men using soft-tissue fillers grew from 2% to 9%.” The survey also reveals that patients younger than 30 years are seeking more cosmetic treatments. In fact, millennials’ use of wrinkle relaxers increased 20% from 2015, and 50% since 2012.
Address the top male aesthetic concerns
Men are interested in looking healthy, young, and staying fit, Dr. Keaney said, but there is often a disconnect in the male market. “I would argue the real rate limiter is education,” he explained, “and that both the industry and physicians are at fault.”
Most messages about aesthetic procedures have not been targeted toward men. For example, only 39% of 600 aesthetically inclined men knew about dermal fillers in a study Dr. Keaney co-authored (Dermatol Surg. 2016 Oct;42[10]:1155-63).
“I talk to men in my practice about dermal fillers, and most think they’re only for injection in the lips,” he said. The results of the online survey came from men “cosmetically on the cusp,” as he described them – men familiar with neuromodulators for facial rejuvenation, but who had never tried such a therapy.
Tear troughs, double chin, crow’s feet, and forehead lines were the most common concerns, in order, reported by study participants. Dr. Keaney said. “You’ll notice what is missing here: the cheeks, the nasolabial folds, and the lips. And what are those? The FDA-approved indications for dermal fillers.”
Even though it doesn’t top the list of men’s concerns in this study, overall, “if you’re looking to grow your male aesthetic patient population, the number one cosmetic concern among men remains hair loss,” noted Dr. Keaney. “You cannot ignore hair loss. It has a large psychosocial impact.”
During a full-body exam, Dr. Keaney recommends using a scalp exam as an opportunity to ask about any hair-loss concerns.
Encouraging signs from other industries
Other industries are showing a rise in the appearance-conscious male consumer, Dr. Keaney said. Men’s skin care, grooming, and luxury fashion industries are all growing, for example.
Worldwide, the personal care market for men is forecast to grow to $166 billion globally by 2022, according to a report from Allied Market Research. The compound average growth rate is expected to grow more than 5% each year between now and then.
“Men are spending money on their hair and skin,” Dr. Keaney said. “The question is, Why aren’t they spending money on their face? It’s how we interact with the world.”
Dr. Keaney has served on the advisory board of, consulted for, and was a speaker for Allergan. He was also a speaker for Eclipse, Sciton, and Syneron Candela, and served on the advisory boards for Aclaris and Merz.
MIAMI – Bringing more men into an aesthetic dermatology practice can expand the patient population, increase business revenue, and pay long-term dividends in terms of patient loyalty and repeat business.
But men aren’t like women when it comes to aesthetic concerns, so the strategies used to market your aesthetic offerings to female patients might miss the mark with men, cautioned Terrence Keaney, MD.
“I spend more time explaining therapies and what might be best for them,” he noted. “I explain the scientific rationale and treatment mechanisms so they will be more comfortable.” Making sure they understand is important, because “men often nod and don’t ask questions.”
The extra effort up front can pay off.
“The beauty of men is when they get a great result and are happy with you, men are very physician loyal. Once they get a great result, they’re yours forever,” said Dr. Keaney, an assistant clinical professor of dermatology at George Washington University, Washington, and a private practice dermatologist in Arlington, Va.
Cost is the leading deterrent for men to embrace aesthetic procedures, a factor that also ranks first among women. Men are also concerned that results will not look natural and want information about safety and side effects, Dr. Keaney said. “These deterrents can be overcome with proper education and counseling.”
Marketing to men is different
Although growing a male anesthetic patient base is more difficult, Dr. Keaney recommends it, especially for dermatology practices in a competitive market.
This tactic of targeting untapped markets to grow a business, rather than competing on the same level as everyone else, is outlined in a book he recommends, “Blue Ocean Strategy,” by W. Chan Kim and Renée Mauborgne. “It’s about unlocking new demand, and I will argue that, in aesthetic medicine, it’s those male patients.”
“The male aesthetic market is truly untapped and shows tremendous growth potential,” Dr. Keaney said. “Particularly as millennials age, the demand for cosmetic procedures in men will only increase.”
A first step is to make male aesthetic patients feel welcome and comfortable. “Think about a reluctant male patient walking into your office; it can be intimidating if the staff and everyone in the waiting room is female,” Dr. Keaney said. “But you don’t need to put a keg in the corner, either.” He added more wood and changed the colors of his office, for example.
Don’t go overboard
Marketing aesthetic services to men is also different, a lesson Dr. Keaney learned from the outset.
“When I first started a practice, I wanted to attract more male cosmetic patients, and I decided to throw a male cosmetics seminar,” he recalled. “I thought it would be a great opportunity to educate them.”
He partnered with a plastic surgeon, rented a ballroom, sent out an e-blast, and mailed flyers. “We had zero RSVPs. We canceled it.”
He added, “Men are not sitting at the computer thinking, ‘I wish someone would throw a seminar on aesthetics.’”
A better strategy came the following year as a men’s health event with a broader scope. A urologist, internist, dermatologist, and plastic surgeon talked about a variety of health issues. “They were blown away by the options from the dermatologist and the plastic surgeon.”
A growing market
An American Society for Dermatologic Surgery annual survey reveals dermatologic surgeons performed nearly 10.5 million medically necessary and cosmetic procedures in 2016, the latest year for which results are available. The rate is up 5% from the year before, and up by more than 30%, compared with 2012.
“Within the growth of procedures performed, the male and millennial demographics’ interest in cosmetic treatments also continues to rise,” the survey authors noted. “In the last 5 years, men receiving wrinkle relaxers has increased 9%, and men using soft-tissue fillers grew from 2% to 9%.” The survey also reveals that patients younger than 30 years are seeking more cosmetic treatments. In fact, millennials’ use of wrinkle relaxers increased 20% from 2015, and 50% since 2012.
Address the top male aesthetic concerns
Men are interested in looking healthy, young, and staying fit, Dr. Keaney said, but there is often a disconnect in the male market. “I would argue the real rate limiter is education,” he explained, “and that both the industry and physicians are at fault.”
Most messages about aesthetic procedures have not been targeted toward men. For example, only 39% of 600 aesthetically inclined men knew about dermal fillers in a study Dr. Keaney co-authored (Dermatol Surg. 2016 Oct;42[10]:1155-63).
“I talk to men in my practice about dermal fillers, and most think they’re only for injection in the lips,” he said. The results of the online survey came from men “cosmetically on the cusp,” as he described them – men familiar with neuromodulators for facial rejuvenation, but who had never tried such a therapy.
Tear troughs, double chin, crow’s feet, and forehead lines were the most common concerns, in order, reported by study participants. Dr. Keaney said. “You’ll notice what is missing here: the cheeks, the nasolabial folds, and the lips. And what are those? The FDA-approved indications for dermal fillers.”
Even though it doesn’t top the list of men’s concerns in this study, overall, “if you’re looking to grow your male aesthetic patient population, the number one cosmetic concern among men remains hair loss,” noted Dr. Keaney. “You cannot ignore hair loss. It has a large psychosocial impact.”
During a full-body exam, Dr. Keaney recommends using a scalp exam as an opportunity to ask about any hair-loss concerns.
Encouraging signs from other industries
Other industries are showing a rise in the appearance-conscious male consumer, Dr. Keaney said. Men’s skin care, grooming, and luxury fashion industries are all growing, for example.
Worldwide, the personal care market for men is forecast to grow to $166 billion globally by 2022, according to a report from Allied Market Research. The compound average growth rate is expected to grow more than 5% each year between now and then.
“Men are spending money on their hair and skin,” Dr. Keaney said. “The question is, Why aren’t they spending money on their face? It’s how we interact with the world.”
Dr. Keaney has served on the advisory board of, consulted for, and was a speaker for Allergan. He was also a speaker for Eclipse, Sciton, and Syneron Candela, and served on the advisory boards for Aclaris and Merz.
REPORTING FROM ODAC 2018