User login
The role of defensins in treating skin aging
Most skin-aging treatments work by prodding old fibroblasts and keratinocytes to accelerate the production of important cellular components. For example, retinoids act on retinoic acid receptors to activate collagen genes and deactivate collagenase genes. Glycolic acid, ascorbic acid, and certain growth factors stimulate synthesis of collagen by fibroblasts. Older fibroblasts and keratinocytes are sluggish for many reasons; they do not “hear” signals as well as younger cells do. Glycosaminoglycans such as heparan sulfate can help cells hear these signals. Heparan sulfate, for example, assists in the delivery of growth factors to cells, stabilizes them, and presents them to the receptors on the keratinocytes and fibroblasts, and amplifies cellular response to these factors.
A new angle in antiaging skin care is to create new keratinocytes rather than to stimulate old cells. For the last decade, personal care companies have touted the benefit of putting stem cells in cosmeceuticals, claiming that these cells would rejuvenate skin. However, this proved to be unsubstantiated marketing hype because the stem cells were plant derived (often from apples), had poor shelf life, and could not intercalate between the native skin cells and work with them to have any effect. Stems cells in cosmeceuticals became a point of disdain for savvy scientists.

Stem cells
Wounding the skin stimulates LGR6+ stem cells. This occurs when neutrophils in the immune system release defensins in response to injury, and, in turn, defensins activate LGR6+ stem cells. Situated above the follicular bulge, these cells are reported to have the capacity to synthesize all cutaneous cell lineages, including sebaceous gland and interfollicular epidermal cells.1,2 There are no specific studies that show that the LGR6+ cells generate new fibroblasts, but it seems likely. Transplantation of LGR6+ stem cells into the skin results in increased wound healing, hair follicle genesis, and angiogenesis.3 LGR6+ stem cells repopulate the epidermis by creating new basal stem cells. In regards to skin rejuvenation, it is clear that activated LGR6+ stems cells produce new, younger-acting keratinocytes in the epidermis.
Peptides
Defensin is a peptide. Peptides are short amino acid chains. These important substances are challenging to incorporate into topical formulations for various reasons, including stabilization difficulty, interaction with other molecules, and poor penetration (greater than 500 Dalton molecular weight). For these reasons, many peptide-containing formulations do not have efficacy. Attempts are underway to better develop or modify peptide products to enhance solubility, achieve better penetration, and target increased receptor activity. Defensins are peptides, which makes them difficult to formulate in a topical product. Special steps must be taken in the formulation process to stabilize defensin and allow penetration into the hair follicle where the LGR6+ cells reside. Fortunately, it is easier for a peptide to target the hair follicle because it can traverse through the “pore” – than it is to get a peptide to reach the fibroblasts in the dermis.
Defensins
Defensins, or human beta-defensins, are host defense peptides that exhibit antimicrobial activities against numerous bacteria.4 LGR6+ stem cells, which are dormant until they are activated to respond to damage, are stimulated by defensins. Defensins have been shown to stimulate keratinocyte proliferation, migration, and wound healing. (3) **Human alpha-defensin 5 peptide has also been shown to enhance wound healing, increasing LGR5+ and LGR6+ stem cell migration in the wound bed.(1)***
When formulated in a manner that allows for stability and penetration into the hair follicle where the LGR6+ stem cells reside, defensin formulations can be applied topically. A product sold as DefenAge uses a patented formulation that uses albumin, a large and stable protein, to stabilize defensin and act as a carrier molecule while helping the defensin maintain its integrity and extend shelf life in the serum base. The albumin/defensin complex is incorporated into liposomes to prevent other ingredients in the cosmetic base from interacting with the peptide and to enhance delivery to the LGR6+ target cell.
The role of defensins in treating skin aging
- Old fibroblast and keratinocytes are sluggish and lazy.
- Old cells do not “hear” signals as well as younger cells.
- LGR6+ stem cells repopulate the epidermis with new, young keratinocytes.
- Defensin stimulates LGR6+ stem cells.
- The defensin/LGR6+ pathway plays a role in keratinization.
- Using topical defensin can improve the skin’s appearance.
Studying DefenAge
At this time, there is only one small multicenter, double-blind, placebo-controlled clinical study completed at three locations by investigators who are stockholders in the company and an independent dermatologic histopathologist who has no relation with the company; results have been reported in aesthetic dermatology industry newsletters. Each site had 15 patients for a total of 45 patients; all were women, aged 41-70 years (average age, 60 years), with little or no history of “quality” skin care. The study regimen used a system that contained alpha- and beta-defensins developed by Progenitor Biologics. Thirty patients used the three products in the DefenAge line: the 2-Minute Reveal Masque Exfoliator, 24/7 Barrier Balance Cream, and 8-in-1 BioSerum. The remaining patients received a three-part placebo system. Baseline biopsies were obtained to evaluate underlying conditions in the patients’ skin, and their skin was evaluated at 6 and 12 weeks, when additional biopsies were taken. Data analysis indicated that patients using DefenAge experienced significant improvement in coarse and fine wrinkles, pigmentation, pore prominence, epidermal thickness, as well as skin texture and evenness.
My personal opinion
I have never been a fan of formulations containing stem cells or peptides for the reasons listed above. DefenAge is unique in the way it has been stabilized, by penetrating the hair follicle rather than through the dermis and because defensin has very well-documented effects on the important LGR6+ stem cells. The effects of defensin on LGR6+ stem cells intrigue me. I do not intend to stop recommending retinoids for antiaging, but rather will add DefenAge to the antiaging regimen. In the past year, I have used DefenAge on many patients and have had many observations. I do not recommend starting retinoids and DefenAge at the same time because I have seen increased retinoid dermatitis. I suggest starting one the first month and then introducing the other product during the second month. Although no studies have been performed on this, my impression is that the DefenAge gives a quick result that helps improve patient compliance with the entire skin care regimen, but the effects reach a point at which no further improvement is seen. Combining DefenAge with a skin care regimen (targeted specifically to their Baumann Skin Type of course!) that includes a retinoid will increase efficacy. For wrinkle-prone skin types, I combine DefenAge with a retinoid, vitamin C, and heparan sulfate. After cleansing in the morning, I have them apply vitamin C followed by the DefenAge and an SPF. In the evening after cleansing, I have them apply a retinoid followed by a heparan sulfate analogue.
Conclusion
DefenAge offers a new approach to skin aging. At this time, there is much basic science research about the benefits of LGR6+ and that uses defensin to stimulate these stem cells; however, only one small clinical trial using defensin topically for antiaging has been published. It is doubtful that many studies will be performed because cosmetic companies are not allowed to make biologic claims so they have little incentive to demonstrate biologic changes. For this reason, we have to rely upon anecdotal reports from physicians such as the information that I have shared here.
Conflict of interest note: I have no financial relationship (no honorarium, stocks, or research funding) with Progenitor Biologics. I was asked to lecture in a DefenAge Symposium at the Vegas Cosmetic Surgery meeting but received no compensation. DefenAge products are sold through doctors, with my company, Skin Type Solutions Franchise Systems, as are heparan sulfate analogues, multiple brands of retinol, and 40 other product brands.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Lough D et al. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
2. Snippert HJ et al. Science. 2010 Mar 12;327(5971):1385-9.
3. Lough DM et al. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
4. Kiatsurayanon C et al. J Invest Dermatol. 2014 Aug;134(8):2163-73.
Most skin-aging treatments work by prodding old fibroblasts and keratinocytes to accelerate the production of important cellular components. For example, retinoids act on retinoic acid receptors to activate collagen genes and deactivate collagenase genes. Glycolic acid, ascorbic acid, and certain growth factors stimulate synthesis of collagen by fibroblasts. Older fibroblasts and keratinocytes are sluggish for many reasons; they do not “hear” signals as well as younger cells do. Glycosaminoglycans such as heparan sulfate can help cells hear these signals. Heparan sulfate, for example, assists in the delivery of growth factors to cells, stabilizes them, and presents them to the receptors on the keratinocytes and fibroblasts, and amplifies cellular response to these factors.
A new angle in antiaging skin care is to create new keratinocytes rather than to stimulate old cells. For the last decade, personal care companies have touted the benefit of putting stem cells in cosmeceuticals, claiming that these cells would rejuvenate skin. However, this proved to be unsubstantiated marketing hype because the stem cells were plant derived (often from apples), had poor shelf life, and could not intercalate between the native skin cells and work with them to have any effect. Stems cells in cosmeceuticals became a point of disdain for savvy scientists.
Stem cells
Wounding the skin stimulates LGR6+ stem cells. This occurs when neutrophils in the immune system release defensins in response to injury, and, in turn, defensins activate LGR6+ stem cells. Situated above the follicular bulge, these cells are reported to have the capacity to synthesize all cutaneous cell lineages, including sebaceous gland and interfollicular epidermal cells.1,2 There are no specific studies that show that the LGR6+ cells generate new fibroblasts, but it seems likely. Transplantation of LGR6+ stem cells into the skin results in increased wound healing, hair follicle genesis, and angiogenesis.3 LGR6+ stem cells repopulate the epidermis by creating new basal stem cells. In regards to skin rejuvenation, it is clear that activated LGR6+ stems cells produce new, younger-acting keratinocytes in the epidermis.
Peptides
Defensin is a peptide. Peptides are short amino acid chains. These important substances are challenging to incorporate into topical formulations for various reasons, including stabilization difficulty, interaction with other molecules, and poor penetration (greater than 500 Dalton molecular weight). For these reasons, many peptide-containing formulations do not have efficacy. Attempts are underway to better develop or modify peptide products to enhance solubility, achieve better penetration, and target increased receptor activity. Defensins are peptides, which makes them difficult to formulate in a topical product. Special steps must be taken in the formulation process to stabilize defensin and allow penetration into the hair follicle where the LGR6+ cells reside. Fortunately, it is easier for a peptide to target the hair follicle because it can traverse through the “pore” – than it is to get a peptide to reach the fibroblasts in the dermis.
Defensins
Defensins, or human beta-defensins, are host defense peptides that exhibit antimicrobial activities against numerous bacteria.4 LGR6+ stem cells, which are dormant until they are activated to respond to damage, are stimulated by defensins. Defensins have been shown to stimulate keratinocyte proliferation, migration, and wound healing. (3) **Human alpha-defensin 5 peptide has also been shown to enhance wound healing, increasing LGR5+ and LGR6+ stem cell migration in the wound bed.(1)***
When formulated in a manner that allows for stability and penetration into the hair follicle where the LGR6+ stem cells reside, defensin formulations can be applied topically. A product sold as DefenAge uses a patented formulation that uses albumin, a large and stable protein, to stabilize defensin and act as a carrier molecule while helping the defensin maintain its integrity and extend shelf life in the serum base. The albumin/defensin complex is incorporated into liposomes to prevent other ingredients in the cosmetic base from interacting with the peptide and to enhance delivery to the LGR6+ target cell.
The role of defensins in treating skin aging
- Old fibroblast and keratinocytes are sluggish and lazy.
- Old cells do not “hear” signals as well as younger cells.
- LGR6+ stem cells repopulate the epidermis with new, young keratinocytes.
- Defensin stimulates LGR6+ stem cells.
- The defensin/LGR6+ pathway plays a role in keratinization.
- Using topical defensin can improve the skin’s appearance.
Studying DefenAge
At this time, there is only one small multicenter, double-blind, placebo-controlled clinical study completed at three locations by investigators who are stockholders in the company and an independent dermatologic histopathologist who has no relation with the company; results have been reported in aesthetic dermatology industry newsletters. Each site had 15 patients for a total of 45 patients; all were women, aged 41-70 years (average age, 60 years), with little or no history of “quality” skin care. The study regimen used a system that contained alpha- and beta-defensins developed by Progenitor Biologics. Thirty patients used the three products in the DefenAge line: the 2-Minute Reveal Masque Exfoliator, 24/7 Barrier Balance Cream, and 8-in-1 BioSerum. The remaining patients received a three-part placebo system. Baseline biopsies were obtained to evaluate underlying conditions in the patients’ skin, and their skin was evaluated at 6 and 12 weeks, when additional biopsies were taken. Data analysis indicated that patients using DefenAge experienced significant improvement in coarse and fine wrinkles, pigmentation, pore prominence, epidermal thickness, as well as skin texture and evenness.
My personal opinion
I have never been a fan of formulations containing stem cells or peptides for the reasons listed above. DefenAge is unique in the way it has been stabilized, by penetrating the hair follicle rather than through the dermis and because defensin has very well-documented effects on the important LGR6+ stem cells. The effects of defensin on LGR6+ stem cells intrigue me. I do not intend to stop recommending retinoids for antiaging, but rather will add DefenAge to the antiaging regimen. In the past year, I have used DefenAge on many patients and have had many observations. I do not recommend starting retinoids and DefenAge at the same time because I have seen increased retinoid dermatitis. I suggest starting one the first month and then introducing the other product during the second month. Although no studies have been performed on this, my impression is that the DefenAge gives a quick result that helps improve patient compliance with the entire skin care regimen, but the effects reach a point at which no further improvement is seen. Combining DefenAge with a skin care regimen (targeted specifically to their Baumann Skin Type of course!) that includes a retinoid will increase efficacy. For wrinkle-prone skin types, I combine DefenAge with a retinoid, vitamin C, and heparan sulfate. After cleansing in the morning, I have them apply vitamin C followed by the DefenAge and an SPF. In the evening after cleansing, I have them apply a retinoid followed by a heparan sulfate analogue.
Conclusion
DefenAge offers a new approach to skin aging. At this time, there is much basic science research about the benefits of LGR6+ and that uses defensin to stimulate these stem cells; however, only one small clinical trial using defensin topically for antiaging has been published. It is doubtful that many studies will be performed because cosmetic companies are not allowed to make biologic claims so they have little incentive to demonstrate biologic changes. For this reason, we have to rely upon anecdotal reports from physicians such as the information that I have shared here.
Conflict of interest note: I have no financial relationship (no honorarium, stocks, or research funding) with Progenitor Biologics. I was asked to lecture in a DefenAge Symposium at the Vegas Cosmetic Surgery meeting but received no compensation. DefenAge products are sold through doctors, with my company, Skin Type Solutions Franchise Systems, as are heparan sulfate analogues, multiple brands of retinol, and 40 other product brands.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Lough D et al. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
2. Snippert HJ et al. Science. 2010 Mar 12;327(5971):1385-9.
3. Lough DM et al. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
4. Kiatsurayanon C et al. J Invest Dermatol. 2014 Aug;134(8):2163-73.
Most skin-aging treatments work by prodding old fibroblasts and keratinocytes to accelerate the production of important cellular components. For example, retinoids act on retinoic acid receptors to activate collagen genes and deactivate collagenase genes. Glycolic acid, ascorbic acid, and certain growth factors stimulate synthesis of collagen by fibroblasts. Older fibroblasts and keratinocytes are sluggish for many reasons; they do not “hear” signals as well as younger cells do. Glycosaminoglycans such as heparan sulfate can help cells hear these signals. Heparan sulfate, for example, assists in the delivery of growth factors to cells, stabilizes them, and presents them to the receptors on the keratinocytes and fibroblasts, and amplifies cellular response to these factors.
A new angle in antiaging skin care is to create new keratinocytes rather than to stimulate old cells. For the last decade, personal care companies have touted the benefit of putting stem cells in cosmeceuticals, claiming that these cells would rejuvenate skin. However, this proved to be unsubstantiated marketing hype because the stem cells were plant derived (often from apples), had poor shelf life, and could not intercalate between the native skin cells and work with them to have any effect. Stems cells in cosmeceuticals became a point of disdain for savvy scientists.
Stem cells
Wounding the skin stimulates LGR6+ stem cells. This occurs when neutrophils in the immune system release defensins in response to injury, and, in turn, defensins activate LGR6+ stem cells. Situated above the follicular bulge, these cells are reported to have the capacity to synthesize all cutaneous cell lineages, including sebaceous gland and interfollicular epidermal cells.1,2 There are no specific studies that show that the LGR6+ cells generate new fibroblasts, but it seems likely. Transplantation of LGR6+ stem cells into the skin results in increased wound healing, hair follicle genesis, and angiogenesis.3 LGR6+ stem cells repopulate the epidermis by creating new basal stem cells. In regards to skin rejuvenation, it is clear that activated LGR6+ stems cells produce new, younger-acting keratinocytes in the epidermis.
Peptides
Defensin is a peptide. Peptides are short amino acid chains. These important substances are challenging to incorporate into topical formulations for various reasons, including stabilization difficulty, interaction with other molecules, and poor penetration (greater than 500 Dalton molecular weight). For these reasons, many peptide-containing formulations do not have efficacy. Attempts are underway to better develop or modify peptide products to enhance solubility, achieve better penetration, and target increased receptor activity. Defensins are peptides, which makes them difficult to formulate in a topical product. Special steps must be taken in the formulation process to stabilize defensin and allow penetration into the hair follicle where the LGR6+ cells reside. Fortunately, it is easier for a peptide to target the hair follicle because it can traverse through the “pore” – than it is to get a peptide to reach the fibroblasts in the dermis.
Defensins
Defensins, or human beta-defensins, are host defense peptides that exhibit antimicrobial activities against numerous bacteria.4 LGR6+ stem cells, which are dormant until they are activated to respond to damage, are stimulated by defensins. Defensins have been shown to stimulate keratinocyte proliferation, migration, and wound healing. (3) **Human alpha-defensin 5 peptide has also been shown to enhance wound healing, increasing LGR5+ and LGR6+ stem cell migration in the wound bed.(1)***
When formulated in a manner that allows for stability and penetration into the hair follicle where the LGR6+ stem cells reside, defensin formulations can be applied topically. A product sold as DefenAge uses a patented formulation that uses albumin, a large and stable protein, to stabilize defensin and act as a carrier molecule while helping the defensin maintain its integrity and extend shelf life in the serum base. The albumin/defensin complex is incorporated into liposomes to prevent other ingredients in the cosmetic base from interacting with the peptide and to enhance delivery to the LGR6+ target cell.
The role of defensins in treating skin aging
- Old fibroblast and keratinocytes are sluggish and lazy.
- Old cells do not “hear” signals as well as younger cells.
- LGR6+ stem cells repopulate the epidermis with new, young keratinocytes.
- Defensin stimulates LGR6+ stem cells.
- The defensin/LGR6+ pathway plays a role in keratinization.
- Using topical defensin can improve the skin’s appearance.
Studying DefenAge
At this time, there is only one small multicenter, double-blind, placebo-controlled clinical study completed at three locations by investigators who are stockholders in the company and an independent dermatologic histopathologist who has no relation with the company; results have been reported in aesthetic dermatology industry newsletters. Each site had 15 patients for a total of 45 patients; all were women, aged 41-70 years (average age, 60 years), with little or no history of “quality” skin care. The study regimen used a system that contained alpha- and beta-defensins developed by Progenitor Biologics. Thirty patients used the three products in the DefenAge line: the 2-Minute Reveal Masque Exfoliator, 24/7 Barrier Balance Cream, and 8-in-1 BioSerum. The remaining patients received a three-part placebo system. Baseline biopsies were obtained to evaluate underlying conditions in the patients’ skin, and their skin was evaluated at 6 and 12 weeks, when additional biopsies were taken. Data analysis indicated that patients using DefenAge experienced significant improvement in coarse and fine wrinkles, pigmentation, pore prominence, epidermal thickness, as well as skin texture and evenness.
My personal opinion
I have never been a fan of formulations containing stem cells or peptides for the reasons listed above. DefenAge is unique in the way it has been stabilized, by penetrating the hair follicle rather than through the dermis and because defensin has very well-documented effects on the important LGR6+ stem cells. The effects of defensin on LGR6+ stem cells intrigue me. I do not intend to stop recommending retinoids for antiaging, but rather will add DefenAge to the antiaging regimen. In the past year, I have used DefenAge on many patients and have had many observations. I do not recommend starting retinoids and DefenAge at the same time because I have seen increased retinoid dermatitis. I suggest starting one the first month and then introducing the other product during the second month. Although no studies have been performed on this, my impression is that the DefenAge gives a quick result that helps improve patient compliance with the entire skin care regimen, but the effects reach a point at which no further improvement is seen. Combining DefenAge with a skin care regimen (targeted specifically to their Baumann Skin Type of course!) that includes a retinoid will increase efficacy. For wrinkle-prone skin types, I combine DefenAge with a retinoid, vitamin C, and heparan sulfate. After cleansing in the morning, I have them apply vitamin C followed by the DefenAge and an SPF. In the evening after cleansing, I have them apply a retinoid followed by a heparan sulfate analogue.
Conclusion
DefenAge offers a new approach to skin aging. At this time, there is much basic science research about the benefits of LGR6+ and that uses defensin to stimulate these stem cells; however, only one small clinical trial using defensin topically for antiaging has been published. It is doubtful that many studies will be performed because cosmetic companies are not allowed to make biologic claims so they have little incentive to demonstrate biologic changes. For this reason, we have to rely upon anecdotal reports from physicians such as the information that I have shared here.
Conflict of interest note: I have no financial relationship (no honorarium, stocks, or research funding) with Progenitor Biologics. I was asked to lecture in a DefenAge Symposium at the Vegas Cosmetic Surgery meeting but received no compensation. DefenAge products are sold through doctors, with my company, Skin Type Solutions Franchise Systems, as are heparan sulfate analogues, multiple brands of retinol, and 40 other product brands.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Lough D et al. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
2. Snippert HJ et al. Science. 2010 Mar 12;327(5971):1385-9.
3. Lough DM et al. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
4. Kiatsurayanon C et al. J Invest Dermatol. 2014 Aug;134(8):2163-73.

Laser tattoo removal clinic closures: Are patients getting scammed?
A patient came into my office recently and informed me that a well-known laser tattoo removal clinic in Los Angeles that she had gone to for years had suddenly shut down. All locations closed. No one answered the phone. No information about the remainder of the money in the package she bought. After researching online, she found that the Better Business Bureau did not yet have much information but doubted she would get her money back. This particular patient had not gone to the clinic in more than a year but had a residual tattoo and had looked into returning for more treatments and using the remainder of her package. She was one of the lucky ones. Other online discussion groups had entries from numerous patients who paid for packages (some costing thousands of dollars) for multiple laser treatments. Some had paid recently and had not yet received a single treatment and were left with no information about their options or where their money had gone.

It turns out in Southern California and Texas. No notification was given to the patients in advance. Nor was any notification given to some of the staff members, who complained online that they suddenly lost their jobs. Ironically, the same clinics had posted a letter online several years ago honoring discounted first treatments and packages for patients of a different laser tattoo clinic that had suddenly shut down.
So how often is this happening? Are all these clinics owned by the same people? And what can our specialty do to protect patients from being scammed and, for that matter, receiving treatment from professionals who may not be properly trained or experienced to provide that treatment?
In a world in which insurance reimbursements keep getting cut, more and more medical professionals – physicians and nonphysicians alike – are looking to fee-for-service procedures and practice models for increasing income. Sometimes, this may involve physicians delegating procedures to nonphysicians. Franchised clinics open up with a physician to “oversee” the clinic, while extenders often perform the procedures (many times without the physician present). Physicians who are neither trained nor specialized to do certain cosmetic procedures start to perform them. Patients get used to receiving treatments from nonphysicians or from physicians who are not specialized to perform cosmetic procedures, and then may devalue the procedure, feeling it’s unnecessary for a physician or a specialized physician to perform it.


Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
A patient came into my office recently and informed me that a well-known laser tattoo removal clinic in Los Angeles that she had gone to for years had suddenly shut down. All locations closed. No one answered the phone. No information about the remainder of the money in the package she bought. After researching online, she found that the Better Business Bureau did not yet have much information but doubted she would get her money back. This particular patient had not gone to the clinic in more than a year but had a residual tattoo and had looked into returning for more treatments and using the remainder of her package. She was one of the lucky ones. Other online discussion groups had entries from numerous patients who paid for packages (some costing thousands of dollars) for multiple laser treatments. Some had paid recently and had not yet received a single treatment and were left with no information about their options or where their money had gone.
It turns out in Southern California and Texas. No notification was given to the patients in advance. Nor was any notification given to some of the staff members, who complained online that they suddenly lost their jobs. Ironically, the same clinics had posted a letter online several years ago honoring discounted first treatments and packages for patients of a different laser tattoo clinic that had suddenly shut down.
So how often is this happening? Are all these clinics owned by the same people? And what can our specialty do to protect patients from being scammed and, for that matter, receiving treatment from professionals who may not be properly trained or experienced to provide that treatment?
In a world in which insurance reimbursements keep getting cut, more and more medical professionals – physicians and nonphysicians alike – are looking to fee-for-service procedures and practice models for increasing income. Sometimes, this may involve physicians delegating procedures to nonphysicians. Franchised clinics open up with a physician to “oversee” the clinic, while extenders often perform the procedures (many times without the physician present). Physicians who are neither trained nor specialized to do certain cosmetic procedures start to perform them. Patients get used to receiving treatments from nonphysicians or from physicians who are not specialized to perform cosmetic procedures, and then may devalue the procedure, feeling it’s unnecessary for a physician or a specialized physician to perform it.
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
A patient came into my office recently and informed me that a well-known laser tattoo removal clinic in Los Angeles that she had gone to for years had suddenly shut down. All locations closed. No one answered the phone. No information about the remainder of the money in the package she bought. After researching online, she found that the Better Business Bureau did not yet have much information but doubted she would get her money back. This particular patient had not gone to the clinic in more than a year but had a residual tattoo and had looked into returning for more treatments and using the remainder of her package. She was one of the lucky ones. Other online discussion groups had entries from numerous patients who paid for packages (some costing thousands of dollars) for multiple laser treatments. Some had paid recently and had not yet received a single treatment and were left with no information about their options or where their money had gone.
It turns out in Southern California and Texas. No notification was given to the patients in advance. Nor was any notification given to some of the staff members, who complained online that they suddenly lost their jobs. Ironically, the same clinics had posted a letter online several years ago honoring discounted first treatments and packages for patients of a different laser tattoo clinic that had suddenly shut down.
So how often is this happening? Are all these clinics owned by the same people? And what can our specialty do to protect patients from being scammed and, for that matter, receiving treatment from professionals who may not be properly trained or experienced to provide that treatment?
In a world in which insurance reimbursements keep getting cut, more and more medical professionals – physicians and nonphysicians alike – are looking to fee-for-service procedures and practice models for increasing income. Sometimes, this may involve physicians delegating procedures to nonphysicians. Franchised clinics open up with a physician to “oversee” the clinic, while extenders often perform the procedures (many times without the physician present). Physicians who are neither trained nor specialized to do certain cosmetic procedures start to perform them. Patients get used to receiving treatments from nonphysicians or from physicians who are not specialized to perform cosmetic procedures, and then may devalue the procedure, feeling it’s unnecessary for a physician or a specialized physician to perform it.
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at [email protected]. They had no relevant disclosures.
Less vacuum may reduce post–cryolipolysis adipose hyperplasia
KAUAI, HAWAII – Gentler vacuum pressure seems to reduce the risk of paradoxical adipose hyperplasia after cryolipolysis, according to Suzanne Kilmer, MD, director of the Laser and Skin Surgery Center of Northern California, Sacramento.
She and her colleagues have noticed a reduction with the newer CoolAdvantage applicators from Zeltiq Aesthetics, the manufacturer of CoolSculpting equipment. CoolAdvantage runs colder and with less suction than earlier applicators. “It seems to work equally as well,” but with shorter treatment times, less bruising, and less discomfort. Although paradoxical adipose hyperplasia (PAH) “is incredibly rare, it is something we want to reduce, and we do see decreased incidence with these new applicators,” Dr. Kilmer said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.

Typically, one CoolSculpting session will get rid of about 20%-25% of the fat sucked up into the cryolipolysis cup. There can be some discomfort, for instance, when ice crystals are massaged afterward. To ensure patient satisfaction, “you really need to be realistic about what they can expect. It’s likely to be more than one session,” she said.
Another newer option from the manufacturer is the CoolMini applicator for submental fat. Dr. Kilmer generally does two overlapping applications with the CoolMini in the same session, in order to cover as much chin fat as possible. There will be what looks like a stick of butter under the chin when the applicators are removed; it goes away after a few minutes of massage. Patient satisfaction is high, but there can be unveiling of the platysmal bands, which is “something you want to talk to patients about ahead of time,” she said.
She sometimes uses the CoolMini first, followed by the other recently available option for submental fat, deoxycholic acid (Kybella). “We shrink down everything we can with CoolSculpting, and then come back with Kybella to clean up whatever’s left.” Using this approach, patients are injected with less deoxycholic acid, with less inflammation, she said.
“I think you get more fat loss out of a given CoolSculpting treatment than you do with Kybella,” said Dr. Kilmer, who noted that deoxycholic acid is also an option for PAH.
As for going off label with CoolSculpting for jowls, “we’ve done it, and I tell everybody there’s a chance of a 2-3 month palsy. All you are really doing is demyelinating the nerve, not injuring it. If you do liposuction, you actually have a little bit of risk of actually injuring it. You can use a nerve stimulator to map out the nerves beforehand,” she said.
Dr. Kilmer is a consultant for Zeltiq Aesthetics, and an investigator on many of the company’s development trials. She’s also a consultant for Allergan, manufacturer of Kybella, which recently acquired Zeltiq. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Gentler vacuum pressure seems to reduce the risk of paradoxical adipose hyperplasia after cryolipolysis, according to Suzanne Kilmer, MD, director of the Laser and Skin Surgery Center of Northern California, Sacramento.
She and her colleagues have noticed a reduction with the newer CoolAdvantage applicators from Zeltiq Aesthetics, the manufacturer of CoolSculpting equipment. CoolAdvantage runs colder and with less suction than earlier applicators. “It seems to work equally as well,” but with shorter treatment times, less bruising, and less discomfort. Although paradoxical adipose hyperplasia (PAH) “is incredibly rare, it is something we want to reduce, and we do see decreased incidence with these new applicators,” Dr. Kilmer said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Typically, one CoolSculpting session will get rid of about 20%-25% of the fat sucked up into the cryolipolysis cup. There can be some discomfort, for instance, when ice crystals are massaged afterward. To ensure patient satisfaction, “you really need to be realistic about what they can expect. It’s likely to be more than one session,” she said.
Another newer option from the manufacturer is the CoolMini applicator for submental fat. Dr. Kilmer generally does two overlapping applications with the CoolMini in the same session, in order to cover as much chin fat as possible. There will be what looks like a stick of butter under the chin when the applicators are removed; it goes away after a few minutes of massage. Patient satisfaction is high, but there can be unveiling of the platysmal bands, which is “something you want to talk to patients about ahead of time,” she said.
She sometimes uses the CoolMini first, followed by the other recently available option for submental fat, deoxycholic acid (Kybella). “We shrink down everything we can with CoolSculpting, and then come back with Kybella to clean up whatever’s left.” Using this approach, patients are injected with less deoxycholic acid, with less inflammation, she said.
“I think you get more fat loss out of a given CoolSculpting treatment than you do with Kybella,” said Dr. Kilmer, who noted that deoxycholic acid is also an option for PAH.
As for going off label with CoolSculpting for jowls, “we’ve done it, and I tell everybody there’s a chance of a 2-3 month palsy. All you are really doing is demyelinating the nerve, not injuring it. If you do liposuction, you actually have a little bit of risk of actually injuring it. You can use a nerve stimulator to map out the nerves beforehand,” she said.
Dr. Kilmer is a consultant for Zeltiq Aesthetics, and an investigator on many of the company’s development trials. She’s also a consultant for Allergan, manufacturer of Kybella, which recently acquired Zeltiq. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Gentler vacuum pressure seems to reduce the risk of paradoxical adipose hyperplasia after cryolipolysis, according to Suzanne Kilmer, MD, director of the Laser and Skin Surgery Center of Northern California, Sacramento.
She and her colleagues have noticed a reduction with the newer CoolAdvantage applicators from Zeltiq Aesthetics, the manufacturer of CoolSculpting equipment. CoolAdvantage runs colder and with less suction than earlier applicators. “It seems to work equally as well,” but with shorter treatment times, less bruising, and less discomfort. Although paradoxical adipose hyperplasia (PAH) “is incredibly rare, it is something we want to reduce, and we do see decreased incidence with these new applicators,” Dr. Kilmer said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Education Foundation.
Typically, one CoolSculpting session will get rid of about 20%-25% of the fat sucked up into the cryolipolysis cup. There can be some discomfort, for instance, when ice crystals are massaged afterward. To ensure patient satisfaction, “you really need to be realistic about what they can expect. It’s likely to be more than one session,” she said.
Another newer option from the manufacturer is the CoolMini applicator for submental fat. Dr. Kilmer generally does two overlapping applications with the CoolMini in the same session, in order to cover as much chin fat as possible. There will be what looks like a stick of butter under the chin when the applicators are removed; it goes away after a few minutes of massage. Patient satisfaction is high, but there can be unveiling of the platysmal bands, which is “something you want to talk to patients about ahead of time,” she said.
She sometimes uses the CoolMini first, followed by the other recently available option for submental fat, deoxycholic acid (Kybella). “We shrink down everything we can with CoolSculpting, and then come back with Kybella to clean up whatever’s left.” Using this approach, patients are injected with less deoxycholic acid, with less inflammation, she said.
“I think you get more fat loss out of a given CoolSculpting treatment than you do with Kybella,” said Dr. Kilmer, who noted that deoxycholic acid is also an option for PAH.
As for going off label with CoolSculpting for jowls, “we’ve done it, and I tell everybody there’s a chance of a 2-3 month palsy. All you are really doing is demyelinating the nerve, not injuring it. If you do liposuction, you actually have a little bit of risk of actually injuring it. You can use a nerve stimulator to map out the nerves beforehand,” she said.
Dr. Kilmer is a consultant for Zeltiq Aesthetics, and an investigator on many of the company’s development trials. She’s also a consultant for Allergan, manufacturer of Kybella, which recently acquired Zeltiq. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Review finds some evidence of efficacy for nonpharmacological acne therapies
A systematic review of 33 studies evaluating nonpharmacological treatments for acne provided what was described as “circumstantial” evidence of efficacy by the authors who conducted the analysis.
The 33 studies evaluated three types of treatments: laser-based and light-based treatments (20), chemical peels (11), and fractional microneedling radiofrequency (2); most were associated with significant reductions in acne lesions in the studies. The evidence for efficacy was “strong” for glycolic acid at concentrations from 10% to 40%, and “moderate” for amino fruit acids at concentrations of 20%-60%, for intense pulsed light (IPL: 400-700 and 870-1,200 nm), and for the diode laser 1450 nm, according to F.M.C. de Vries, MD, of the department of dermatology, Radboud University, Nijmegen, the Netherlands, and coauthors.
However, they added, “although a high rate of statistically significant results was found in most of the studies, indicating efficacy of nonpharmacological therapies, the low methodological quality of the included studies made it difficult to draw clear conclusions.” Most of the studies were limited by factors that included a small number of enrolled participants, short follow-up, and lack of or possibly inadequate blinding in participants and/or clinicians.
Their review of three electronic databases (MEDLINE, Cochrane library, CINAHL) identified the 33 studies evaluating these treatments in 1,404 participants with acne, published between January 2000 and May 2017, which met their inclusion criteria.
Most of the studies on laser- and light-based treatments found a “significant reduction in acne lesions,” including eight that had a control group. However, with two exceptions, “suboptimal methodologic quality of the majority of these studies resulted in limited evidence of efficacy,” they added. The exceptions were two studies that were the basis of their “moderate” rating for IPL and the diode laser: a randomized study of IPL (40-700 and 870-1,200 nm, 100 ms, 20 J/cm2, 20 ms, 18 J/cm2), which found that treatment with IPL resulted in a significant reduction in papules, pustules, and comedones, compared with controls; and a randomized controlled study that found that treatment with a diode laser (1,450 nm, 9.5-11.0 J/cm2, 29-30 ms) resulted in reductions in inflammatory acne that were statistically significant.

The agents studied in the 11 chemical peel trials included salicylic acid, glycolic acid, Jessner solution, trichloroacetic acid, mandelic acid, amino fruit acid, and lipohydroxy acids. “Strong evidence of efficacy” was evident in two studies of glycolic acid (10% and 40% concentrations), which were double-blind, randomized, placebo-controlled studies that were of “high methodological quality,” the authors wrote.
Both studies of fractional microneedling radiofrequency, which were split-face randomized controlled studies, found statistically significant effects of treatment on inflammatory and noninflammatory acne in one study, and a “substantial” reduction in papules and pustules, compared with baseline in the other study. But this evidence was considered limited, because of the “suboptimal methodological quality” of both studies, they noted.
Erythema, pain (described as “tolerable”), purpura, edema, and hyperpigmentation were among the most common adverse effects associated with the nonpharmacological treatments and were described as mild and transient in most cases.
The review provided “circumstantial evidence for nonpharmacological therapies in the treatment of acne vulgaris” and “has created order and structure in resulting outcomes in which a first step towards future research is generated,” the authors concluded. “The large amount of studies performed in the area of acne treatment and the frequent application of these therapies in daily practice indicates a great interest in this topic and the urgent demand for effective nonpharmacological treatment options for acne in addition to the use of conventional therapies,” they added.
The authors had no disclosures. Of the six authors, Dr. de Vries and three other authors are affiliated with HU University of Applied Sciences, Utrecht, the Netherlands, which funded the study.
SOURCE: de Vries FMC et al. J Eur Acad Dermatol Venereol. 2018 Feb 14. doi: 10.1111/jdv.14881.
A systematic review of 33 studies evaluating nonpharmacological treatments for acne provided what was described as “circumstantial” evidence of efficacy by the authors who conducted the analysis.
The 33 studies evaluated three types of treatments: laser-based and light-based treatments (20), chemical peels (11), and fractional microneedling radiofrequency (2); most were associated with significant reductions in acne lesions in the studies. The evidence for efficacy was “strong” for glycolic acid at concentrations from 10% to 40%, and “moderate” for amino fruit acids at concentrations of 20%-60%, for intense pulsed light (IPL: 400-700 and 870-1,200 nm), and for the diode laser 1450 nm, according to F.M.C. de Vries, MD, of the department of dermatology, Radboud University, Nijmegen, the Netherlands, and coauthors.
However, they added, “although a high rate of statistically significant results was found in most of the studies, indicating efficacy of nonpharmacological therapies, the low methodological quality of the included studies made it difficult to draw clear conclusions.” Most of the studies were limited by factors that included a small number of enrolled participants, short follow-up, and lack of or possibly inadequate blinding in participants and/or clinicians.
Their review of three electronic databases (MEDLINE, Cochrane library, CINAHL) identified the 33 studies evaluating these treatments in 1,404 participants with acne, published between January 2000 and May 2017, which met their inclusion criteria.
Most of the studies on laser- and light-based treatments found a “significant reduction in acne lesions,” including eight that had a control group. However, with two exceptions, “suboptimal methodologic quality of the majority of these studies resulted in limited evidence of efficacy,” they added. The exceptions were two studies that were the basis of their “moderate” rating for IPL and the diode laser: a randomized study of IPL (40-700 and 870-1,200 nm, 100 ms, 20 J/cm2, 20 ms, 18 J/cm2), which found that treatment with IPL resulted in a significant reduction in papules, pustules, and comedones, compared with controls; and a randomized controlled study that found that treatment with a diode laser (1,450 nm, 9.5-11.0 J/cm2, 29-30 ms) resulted in reductions in inflammatory acne that were statistically significant.
The agents studied in the 11 chemical peel trials included salicylic acid, glycolic acid, Jessner solution, trichloroacetic acid, mandelic acid, amino fruit acid, and lipohydroxy acids. “Strong evidence of efficacy” was evident in two studies of glycolic acid (10% and 40% concentrations), which were double-blind, randomized, placebo-controlled studies that were of “high methodological quality,” the authors wrote.
Both studies of fractional microneedling radiofrequency, which were split-face randomized controlled studies, found statistically significant effects of treatment on inflammatory and noninflammatory acne in one study, and a “substantial” reduction in papules and pustules, compared with baseline in the other study. But this evidence was considered limited, because of the “suboptimal methodological quality” of both studies, they noted.
Erythema, pain (described as “tolerable”), purpura, edema, and hyperpigmentation were among the most common adverse effects associated with the nonpharmacological treatments and were described as mild and transient in most cases.
The review provided “circumstantial evidence for nonpharmacological therapies in the treatment of acne vulgaris” and “has created order and structure in resulting outcomes in which a first step towards future research is generated,” the authors concluded. “The large amount of studies performed in the area of acne treatment and the frequent application of these therapies in daily practice indicates a great interest in this topic and the urgent demand for effective nonpharmacological treatment options for acne in addition to the use of conventional therapies,” they added.
The authors had no disclosures. Of the six authors, Dr. de Vries and three other authors are affiliated with HU University of Applied Sciences, Utrecht, the Netherlands, which funded the study.
SOURCE: de Vries FMC et al. J Eur Acad Dermatol Venereol. 2018 Feb 14. doi: 10.1111/jdv.14881.
A systematic review of 33 studies evaluating nonpharmacological treatments for acne provided what was described as “circumstantial” evidence of efficacy by the authors who conducted the analysis.
The 33 studies evaluated three types of treatments: laser-based and light-based treatments (20), chemical peels (11), and fractional microneedling radiofrequency (2); most were associated with significant reductions in acne lesions in the studies. The evidence for efficacy was “strong” for glycolic acid at concentrations from 10% to 40%, and “moderate” for amino fruit acids at concentrations of 20%-60%, for intense pulsed light (IPL: 400-700 and 870-1,200 nm), and for the diode laser 1450 nm, according to F.M.C. de Vries, MD, of the department of dermatology, Radboud University, Nijmegen, the Netherlands, and coauthors.
However, they added, “although a high rate of statistically significant results was found in most of the studies, indicating efficacy of nonpharmacological therapies, the low methodological quality of the included studies made it difficult to draw clear conclusions.” Most of the studies were limited by factors that included a small number of enrolled participants, short follow-up, and lack of or possibly inadequate blinding in participants and/or clinicians.
Their review of three electronic databases (MEDLINE, Cochrane library, CINAHL) identified the 33 studies evaluating these treatments in 1,404 participants with acne, published between January 2000 and May 2017, which met their inclusion criteria.
Most of the studies on laser- and light-based treatments found a “significant reduction in acne lesions,” including eight that had a control group. However, with two exceptions, “suboptimal methodologic quality of the majority of these studies resulted in limited evidence of efficacy,” they added. The exceptions were two studies that were the basis of their “moderate” rating for IPL and the diode laser: a randomized study of IPL (40-700 and 870-1,200 nm, 100 ms, 20 J/cm2, 20 ms, 18 J/cm2), which found that treatment with IPL resulted in a significant reduction in papules, pustules, and comedones, compared with controls; and a randomized controlled study that found that treatment with a diode laser (1,450 nm, 9.5-11.0 J/cm2, 29-30 ms) resulted in reductions in inflammatory acne that were statistically significant.
The agents studied in the 11 chemical peel trials included salicylic acid, glycolic acid, Jessner solution, trichloroacetic acid, mandelic acid, amino fruit acid, and lipohydroxy acids. “Strong evidence of efficacy” was evident in two studies of glycolic acid (10% and 40% concentrations), which were double-blind, randomized, placebo-controlled studies that were of “high methodological quality,” the authors wrote.
Both studies of fractional microneedling radiofrequency, which were split-face randomized controlled studies, found statistically significant effects of treatment on inflammatory and noninflammatory acne in one study, and a “substantial” reduction in papules and pustules, compared with baseline in the other study. But this evidence was considered limited, because of the “suboptimal methodological quality” of both studies, they noted.
Erythema, pain (described as “tolerable”), purpura, edema, and hyperpigmentation were among the most common adverse effects associated with the nonpharmacological treatments and were described as mild and transient in most cases.
The review provided “circumstantial evidence for nonpharmacological therapies in the treatment of acne vulgaris” and “has created order and structure in resulting outcomes in which a first step towards future research is generated,” the authors concluded. “The large amount of studies performed in the area of acne treatment and the frequent application of these therapies in daily practice indicates a great interest in this topic and the urgent demand for effective nonpharmacological treatment options for acne in addition to the use of conventional therapies,” they added.
The authors had no disclosures. Of the six authors, Dr. de Vries and three other authors are affiliated with HU University of Applied Sciences, Utrecht, the Netherlands, which funded the study.
SOURCE: de Vries FMC et al. J Eur Acad Dermatol Venereol. 2018 Feb 14. doi: 10.1111/jdv.14881.
FROM THE JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Key clinical point: Certain nonpharmacological acne treatments are effective but better data are needed.
Major finding: There is moderate to strong evidence of efficacy for glycolic acid, IPL, and the diode laser in treating acne.
Study details: A systematic review of 33 studies evaluating nonpharmacological treatments in 1,404 participants with acne.
Disclosures: The authors had no disclosures; three of the six authors are affiliated with HU University of Applied Sciences, Utrecht, which funded the study.
Source: de Vries FMC et al. J Eur Acad Dermatol Venereol. 2018 Feb 14. doi: 10.1111/jdv.14881.
Deepithelialized Flaps and Grafts: Applications in Dermatologic Surgery
Deepithelialized flaps and grafts have been widely used by reconstructive surgeons in a diverse range of medical specialties since the early 20th century. 1 These reconstructive modalities have more recently been applied to dermatologic surgery. Deepithelialized flaps and grafts involve removal of the epidermis from the dermis for a variety of surgical purposes. Although these techniques play an important role in dermatologic surgery, reports of application of deepithelialized flaps and grafts in the dermatology literature is limited. This article includes a presentation of the applications of deepithelialized flaps and grafts in procedural dermatology.
DEEPITHELIALIZATION TECHNIQUES
There are a variety of techniques for deepithelialization, although sharp deepithelialization generally is preferred by dermatologic surgeons. The scalpel technique can be accomplished by making an intradermal incision with a No. 15 blade. Traction is an essential component of the deepthelialization process and facilitates sharp removal of the epidermis and superficial dermis in an even plane. The peeling orange technique, which has been described in reduction mammoplasty, is a variant of the scalpel technique used for creating a large area of deepithelialized tissue.2 A No. 10 blade is used to make multiple partial-thickness intradermal incisions 1 to 2 cm apart along the pedicle. Traction facilitates rapid deepithelialization of the skin strips on the pedicle. A sharp curette is an alternative option for sharply removing the epithelium from a small area. Electric dermatome, laser, and electrocautery techniques for deepithelialization also can be considered.2,3
APPLICATION OF DEEPITHELIALIZED FLAPS
Deepithelialized flaps may be considered for single-stage reconstruction with tunneled interpolation flaps, reconstruction requiring contour preservation, and reconstruction involving free margins.4-17
Reconstruction With Single-Stage Tunneled Interpolated Flaps
Alar Base
A partially deepithelialized tunneled interpolated flap is an elegant reconstructive option for defects involving the upper cutaneous lip and alar base. The flap is elevated from the ipsilateral nasolabial fold, deepithelialized proximally, and tunneled under the intact portion of the cutaneous upper lip and ala. The flap is then deepithelialized superiorly to bolster the alar base and inset at the recipient site.4
Nasal Ala
The tunneled interpolated flap is useful for reconstruction of defects of the nasal ala. A flap with a superior deepithelialized pedicle and an anticipated inferior Burow triangle is designed along the axis of the nasolabial fold. The inferior Burow triangle and central flap are elevated at the level of the superficial subcutaneous fat and the pedicle is dissected. The donor and recipient sites are widely undermined, and the flap and pedicle pass through the tunnel. The donor site is closed primarily, the inferior Burow triangle is trimmed, and the flap is sutured into the defect.5 This flap allows for preservation of free margins and favorable placement of incision lines. Furthermore, pincushioning of the flap helps to recreate the rounded shape of the lateral ala.6
Nasal Tip
Nasal tip defects can be repaired with a retroangular flap, centered on the angular artery. The flap is elevated along the axis of the nasolabial fold, deepithelialized at its proximal base, and transferred through a subcutaneous tunnel to the nasal tip. The angular artery is ligated at the inferior aspect of the flap.7
Nasal Sidewall
A deepithelialized tunneled interpolated forehead flap, similar to the classic paramedian forehead flap, can be used to reconstruct nasal sidewall defects. A flap is elevated on the contralateral forehead and the proximal portion is deepithelialized. A tunnel is then bluntly dissected just above the periosteum, and the flap is introduced into the defect through the tunnel and inset. This flap has the advantages of being a single-stage procedure, restoring volume to the defect area, and maintaining excellent vascular supply.8
Eyelid
A tunneled interpolated forehead flap also can be used to repair medial canthal defects and for anterior lamellar repair of lower eyelid defects. In a study of 9 patients receiving a tunneled interpolated forehead flap in these anatomic locations, all flaps demonstrated viability, protection of the globe, and preservation of the concave architecture of the medial canthus.9
Earlobe
Earlobe defects may be repaired with a pull-through interpolated preauricular flap. A flap is elevated superiorly in the preauricular region and the proximal aspect of the flap is deepithelialized. The flap is pulled through a tunnel and inset at the anterior earlobe defect. The donor site is closed primarily.10,11
Concha
Reconstruction of anterior conchal defects with exposed cartilage can be accomplished with a pull-through interpolated postauricular flap based on the auriculomastoid fossa. The postauricular flap is elevated, the base is deepithelialized, an incision is made in the medial aspect of the defect, and the flap is moved through a tunnel between the posterior and anterior surfaces of the ear. The flap is secured to the anterior surface of the concha.12
Reconstruction Requiring Contour Preservation
Central Face
The hinge flap is optimal for reconstruction of deep central facial defects (Figure 1). The hinge flap is planned at a site contiguous with a margin of the defect and can include the dermis, subcutaneous tissue, muscle, or a combination of these. The desired tissue is folded over on the pedicle to fill the defect. Cutaneous coverage is accomplished through a primary closure, separate flap, or skin graft. In addition to restoring contour and therefore the cosmetic subunit, the hinge flap is performed in a single stage, resists wound contracture, and provides a well-vascularized wound bed resulting in a low incidence of graft failure.13,14 Muscular hinge flaps have been described for reconstruction of forehead defects with exposed bone based on the frontalis muscle.15
Lower Lip
A variant of a V-Y advancement flap has been described for reconstruction of defects greater than one-third the length of the lower lip. The top of the “V” is deepithelialized and the flap is advanced such that the top of the “V” abuts the inferior border of the defect. The “V” flap is inset at its advanced position, converting the “V”-shaped wound into a “Y.” An overlying buccal mucosal graft provides reconstruction of the lower red lip and labial mucosa.16
Helix of the Ear
Large defects of the scapha and helix of the ear can be reconstructed with the use of a staged interpolated postauricular flap. The postauricular flap is elevated into a subcutaneous plane. A full-thickness incision is made medial to the helical rim, and the flap is tunneled through and sutured into place. The pedicle is later divided, and the distal aspect of the flap is deepithelialized and inset into the helical rim for volume restoration.17
Reconstruction Involving Free Margins
Nasal Ala
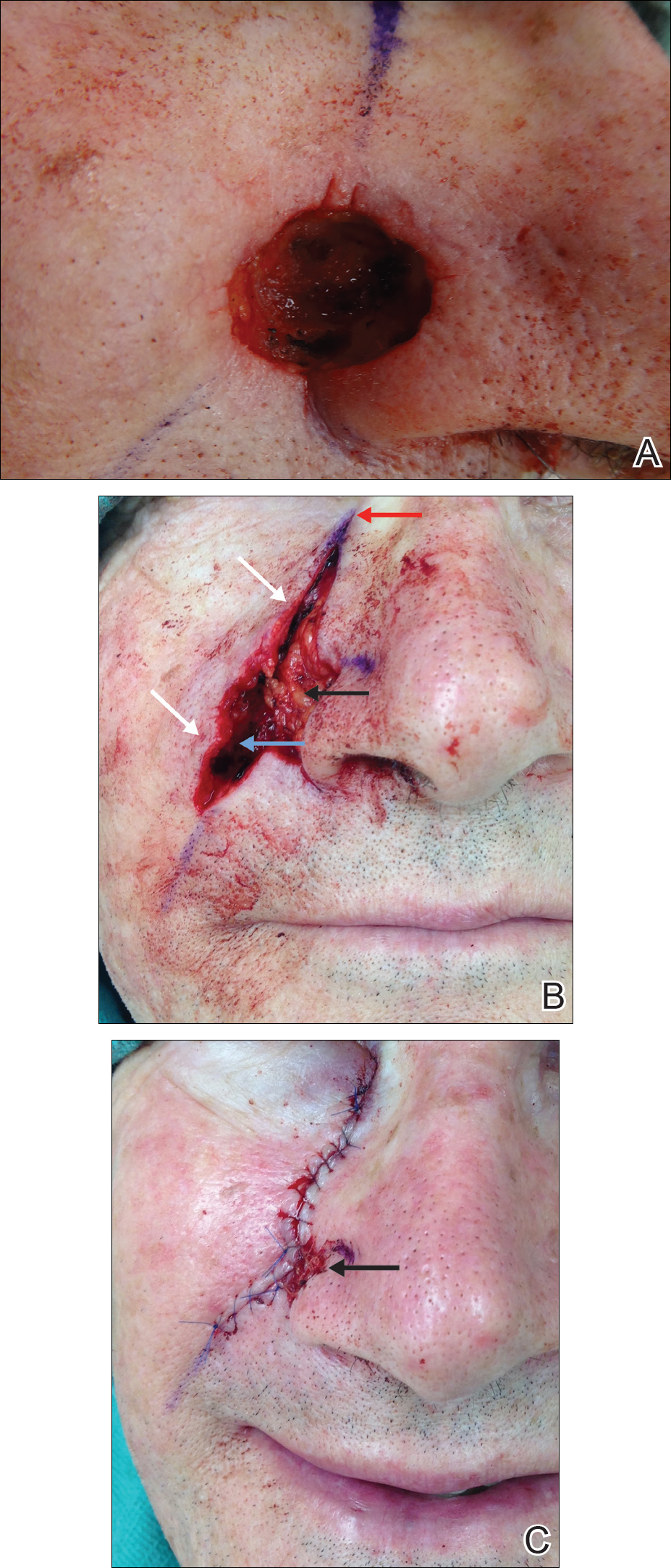
For large defects involving the upper cutaneous lip with adjacent alar base involvement, a partially deepithelialized V-Y flap is a useful reconstructive option (Figure 2).

Infraorbital Region
A deepithelialized variant of a V-Y advancement flap can be used for closure of infraorbital defects. The limbs of the V-Y flap are deepithelialized and anchored to the medial and lateral canthal tendons or periosteum. Ectropion prevention is the primary advantage of this flap.18
APPLICATION OF DEEPITHELIALIZED GRAFTS
Deepithelialized grafts may be considered for volume replacement, reconstruction requiring contour preservation, and restoration of mechanical integrity in areas of high mechanical tension.3,19-21
Reconstruction Requiring Contour Preservation
Deepithelialized grafts are used to improve depressed nasal scars and restore volume in deep nasal wounds. One method involves deepithelialization of 2 postauricular punch biopsies. An 18-gauge needle is used to make a small hole in the depressed nasal scar, the dermal grafts are inserted, and the defect is closed primarily.19 Dermal grafts may be harvested from excess full-thickness skin grafts (FTSGs) or dog-ear tissue. When used under flaps, the dermal graft is trimmed to the size of the defect. When used under FTSGs, thin dermal graft strips are placed in a gridlike pattern to allow for revascularization. A study of 15 patients with contour deformities reconstructed with dermal graft insertions demonstrated that 14 (94%) patients had no significant complications and improvement of scar depression was achieved.20
Reconstruction in Areas of High Mechanical Tension
Plantar Foot
A combined dermal and full-thickness sandwich graft has been described for reconstruction of plantar foot defects.3 The graft is created by obtaining a FTSG twice the size of the wound defect and deepithelializing half of the graft. The graft is then defatted and the deepithelialized portion is folded beneath the other half, allowing the papillary dermis to make contact with the wound surface.
Scalp
Dermal graft reconstruction for scalp defects may be accomplished with a split-thickness skin flap. The flap is harvested using an electronic dermatome that ensures the proximal aspect is still attached to adjacent skin. The dermis is removed from the area underneath the back-folded split-thickness skin flap. The dermal graft is meshed and sutured into the recipient site. The split-thickness skin flap is replaced over the donor site. Meshed reversed dermal grafts have excellent survival rates, even with direct placement on bone without periosteum. Querings et al21 reported graft survival with no complications in 19 of 21 (90.4%) patients undergoing scalp or plantar sole reconstruction.
CONCLUSION
With the widespread adoption of the fresh-tissue technique for Mohs micrographic surgery and the establishment of the American Society for Dermatologic Surgery in 1970, the depth and scope of techniques used by dermatologic surgeons has dramatically expanded. Although the use of dermal flaps and grafts is not as widespread in dermatology as other reconstructive techniques, their unique advantages should be considered. Deepithelialized flaps and grafts should be considered when the following reconstructive goals are desired: (1) conversion of a 2-stage interpolation flap to a single-stage tunneled flap, (2) contour and cosmetic subunit preservation of deep defects through volume augmentation, (3) reconstruction in areas of high mechanical tension, and (4) free margin preservation. The multiple applications of deepithelialized flaps and grafts as described in this review demonstrate their continued applicability in dermatologic surgery.
- Straatsma CR. Use of the dermal graft in the repairs of small saddle defects of the nose. Arch Otolaryngol. 1932;16:506-509.
- Cydeli A, Hunter J. Peeling orange: rapid deepithelialization in reduction mammoplasty. J Aesthet Surg. 2004;24:580-581.
- Bechara F, Sand M, Radenhausen M, et al. Erbium:YAG laser-assisted preparation of a combined dermal/full thickness sandwich skin graft. Dermatol Surg. 2006;32:353-358.
- Cook JL. Tunneled and transposed island flaps in facial reconstructive surgery. Dermatol Surg. 2014;40(suppl 9):S16-S29.
- Krishnan RS, Clark DP. Tunneled transposition flap for reconstruction of defects of the nasal ala. Dermatol Surg. 2007;33:1496-1501.
- Mahlberg M. Tunneled melolabial pedicle flap for small but deep lateral alar rim defect. Dermatol Surg. 2013;39:1527-1529.
- Ascari-Raccagni A, Balderi U. The retroangular flap used in the surgery of nasal tip defects. Dermatol Surg. 2004;30:1131-1137.
- Hollmig ST, Leach BC, Cook J. Single-staged interpolation flaps in facial reconstruction. Dermatol Surg. 2014;40(suppl 9):S62-S70.
- Mombaerts I, Gillis A. The tunneled forehead flap in medial canthal and eyelid reconstruction. Dermatol Surg. 2010:36:1118-1125.
- Wang SQ, Goldberg LH, Kimyah-Asadi A. Tunneled island pedicle flap for an earlobe defect. Dermatol Surg. 2007;33:835-838.
- Hatoko M, Kuwahara M, Shiba A, et al. Earlobe reconstruction using a subcutaneous island pedicle flap after resection of “earlobe keloid.” Dermatol Surg. 1998;24:257-261.
- Alder N, Ad-El D, Azaria R. Reconstruction of nonhelical auricular defects with local flaps. Dermatol Surg. 2008;34:501-507.
- Fader DJ, Wang TS, Johnson TM. Nasal reconstruction utilizing a muscle hinge flap with overlying FTSG. J Am Acad Dermatol. 2000;43:837-840.
- Braun MA, Cook J. Hinge flaps in facial reconstruction. Dermatol Surg. 2007;33:213-221.
- Salmon PL, Mortimer NL, Hill SE. Muscular hinge flaps: utility and technique in facial reconstructive surgery. Dermatol Surg. 2010;36:227-234.
- Seo Y, Song S, Choi Y, et al. A lower lip reconstruction. Dermatol Surg. 2015;41:505-507.
- Malone CH, Wagner RF. Partially de-epithelialized postauricular flap for ear reconstruction. J Am Acad Dermatol. 2015;73:E219-E220.
- Yildrim S, Akoz T, Akan M, et al. Nasolabial V-Y advancement for closure of the midface defects. Dermatol Surg. 2001;27:656-662.
- Jensen DJ, Cohen JL. Nasal tip revision using a dermal graft. Dermatol Surg. 2014;40:1140-1142.
- Meyers S, Rohrer T. Use of dermal grafts in reconstructing deep nasal defects and shaping the ala nasi. Dermatol Surg. 2001;27:300-305.
- Querings K, Bachter D, Balda B. Meshed reversed dermal graft in patients with surgical defects of sole and scalp: technique and long-term results. Dermatol Surg. 2002;28:122-126.
Deepithelialized flaps and grafts have been widely used by reconstructive surgeons in a diverse range of medical specialties since the early 20th century. 1 These reconstructive modalities have more recently been applied to dermatologic surgery. Deepithelialized flaps and grafts involve removal of the epidermis from the dermis for a variety of surgical purposes. Although these techniques play an important role in dermatologic surgery, reports of application of deepithelialized flaps and grafts in the dermatology literature is limited. This article includes a presentation of the applications of deepithelialized flaps and grafts in procedural dermatology.
DEEPITHELIALIZATION TECHNIQUES
There are a variety of techniques for deepithelialization, although sharp deepithelialization generally is preferred by dermatologic surgeons. The scalpel technique can be accomplished by making an intradermal incision with a No. 15 blade. Traction is an essential component of the deepthelialization process and facilitates sharp removal of the epidermis and superficial dermis in an even plane. The peeling orange technique, which has been described in reduction mammoplasty, is a variant of the scalpel technique used for creating a large area of deepithelialized tissue.2 A No. 10 blade is used to make multiple partial-thickness intradermal incisions 1 to 2 cm apart along the pedicle. Traction facilitates rapid deepithelialization of the skin strips on the pedicle. A sharp curette is an alternative option for sharply removing the epithelium from a small area. Electric dermatome, laser, and electrocautery techniques for deepithelialization also can be considered.2,3
APPLICATION OF DEEPITHELIALIZED FLAPS
Deepithelialized flaps may be considered for single-stage reconstruction with tunneled interpolation flaps, reconstruction requiring contour preservation, and reconstruction involving free margins.4-17
Reconstruction With Single-Stage Tunneled Interpolated Flaps
Alar Base
A partially deepithelialized tunneled interpolated flap is an elegant reconstructive option for defects involving the upper cutaneous lip and alar base. The flap is elevated from the ipsilateral nasolabial fold, deepithelialized proximally, and tunneled under the intact portion of the cutaneous upper lip and ala. The flap is then deepithelialized superiorly to bolster the alar base and inset at the recipient site.4
Nasal Ala
The tunneled interpolated flap is useful for reconstruction of defects of the nasal ala. A flap with a superior deepithelialized pedicle and an anticipated inferior Burow triangle is designed along the axis of the nasolabial fold. The inferior Burow triangle and central flap are elevated at the level of the superficial subcutaneous fat and the pedicle is dissected. The donor and recipient sites are widely undermined, and the flap and pedicle pass through the tunnel. The donor site is closed primarily, the inferior Burow triangle is trimmed, and the flap is sutured into the defect.5 This flap allows for preservation of free margins and favorable placement of incision lines. Furthermore, pincushioning of the flap helps to recreate the rounded shape of the lateral ala.6
Nasal Tip
Nasal tip defects can be repaired with a retroangular flap, centered on the angular artery. The flap is elevated along the axis of the nasolabial fold, deepithelialized at its proximal base, and transferred through a subcutaneous tunnel to the nasal tip. The angular artery is ligated at the inferior aspect of the flap.7
Nasal Sidewall
A deepithelialized tunneled interpolated forehead flap, similar to the classic paramedian forehead flap, can be used to reconstruct nasal sidewall defects. A flap is elevated on the contralateral forehead and the proximal portion is deepithelialized. A tunnel is then bluntly dissected just above the periosteum, and the flap is introduced into the defect through the tunnel and inset. This flap has the advantages of being a single-stage procedure, restoring volume to the defect area, and maintaining excellent vascular supply.8
Eyelid
A tunneled interpolated forehead flap also can be used to repair medial canthal defects and for anterior lamellar repair of lower eyelid defects. In a study of 9 patients receiving a tunneled interpolated forehead flap in these anatomic locations, all flaps demonstrated viability, protection of the globe, and preservation of the concave architecture of the medial canthus.9
Earlobe
Earlobe defects may be repaired with a pull-through interpolated preauricular flap. A flap is elevated superiorly in the preauricular region and the proximal aspect of the flap is deepithelialized. The flap is pulled through a tunnel and inset at the anterior earlobe defect. The donor site is closed primarily.10,11
Concha
Reconstruction of anterior conchal defects with exposed cartilage can be accomplished with a pull-through interpolated postauricular flap based on the auriculomastoid fossa. The postauricular flap is elevated, the base is deepithelialized, an incision is made in the medial aspect of the defect, and the flap is moved through a tunnel between the posterior and anterior surfaces of the ear. The flap is secured to the anterior surface of the concha.12
Reconstruction Requiring Contour Preservation
Central Face
The hinge flap is optimal for reconstruction of deep central facial defects (Figure 1). The hinge flap is planned at a site contiguous with a margin of the defect and can include the dermis, subcutaneous tissue, muscle, or a combination of these. The desired tissue is folded over on the pedicle to fill the defect. Cutaneous coverage is accomplished through a primary closure, separate flap, or skin graft. In addition to restoring contour and therefore the cosmetic subunit, the hinge flap is performed in a single stage, resists wound contracture, and provides a well-vascularized wound bed resulting in a low incidence of graft failure.13,14 Muscular hinge flaps have been described for reconstruction of forehead defects with exposed bone based on the frontalis muscle.15
Lower Lip
A variant of a V-Y advancement flap has been described for reconstruction of defects greater than one-third the length of the lower lip. The top of the “V” is deepithelialized and the flap is advanced such that the top of the “V” abuts the inferior border of the defect. The “V” flap is inset at its advanced position, converting the “V”-shaped wound into a “Y.” An overlying buccal mucosal graft provides reconstruction of the lower red lip and labial mucosa.16
Helix of the Ear
Large defects of the scapha and helix of the ear can be reconstructed with the use of a staged interpolated postauricular flap. The postauricular flap is elevated into a subcutaneous plane. A full-thickness incision is made medial to the helical rim, and the flap is tunneled through and sutured into place. The pedicle is later divided, and the distal aspect of the flap is deepithelialized and inset into the helical rim for volume restoration.17
Reconstruction Involving Free Margins
Nasal Ala
For large defects involving the upper cutaneous lip with adjacent alar base involvement, a partially deepithelialized V-Y flap is a useful reconstructive option (Figure 2).
Infraorbital Region
A deepithelialized variant of a V-Y advancement flap can be used for closure of infraorbital defects. The limbs of the V-Y flap are deepithelialized and anchored to the medial and lateral canthal tendons or periosteum. Ectropion prevention is the primary advantage of this flap.18
APPLICATION OF DEEPITHELIALIZED GRAFTS
Deepithelialized grafts may be considered for volume replacement, reconstruction requiring contour preservation, and restoration of mechanical integrity in areas of high mechanical tension.3,19-21
Reconstruction Requiring Contour Preservation
Deepithelialized grafts are used to improve depressed nasal scars and restore volume in deep nasal wounds. One method involves deepithelialization of 2 postauricular punch biopsies. An 18-gauge needle is used to make a small hole in the depressed nasal scar, the dermal grafts are inserted, and the defect is closed primarily.19 Dermal grafts may be harvested from excess full-thickness skin grafts (FTSGs) or dog-ear tissue. When used under flaps, the dermal graft is trimmed to the size of the defect. When used under FTSGs, thin dermal graft strips are placed in a gridlike pattern to allow for revascularization. A study of 15 patients with contour deformities reconstructed with dermal graft insertions demonstrated that 14 (94%) patients had no significant complications and improvement of scar depression was achieved.20
Reconstruction in Areas of High Mechanical Tension
Plantar Foot
A combined dermal and full-thickness sandwich graft has been described for reconstruction of plantar foot defects.3 The graft is created by obtaining a FTSG twice the size of the wound defect and deepithelializing half of the graft. The graft is then defatted and the deepithelialized portion is folded beneath the other half, allowing the papillary dermis to make contact with the wound surface.
Scalp
Dermal graft reconstruction for scalp defects may be accomplished with a split-thickness skin flap. The flap is harvested using an electronic dermatome that ensures the proximal aspect is still attached to adjacent skin. The dermis is removed from the area underneath the back-folded split-thickness skin flap. The dermal graft is meshed and sutured into the recipient site. The split-thickness skin flap is replaced over the donor site. Meshed reversed dermal grafts have excellent survival rates, even with direct placement on bone without periosteum. Querings et al21 reported graft survival with no complications in 19 of 21 (90.4%) patients undergoing scalp or plantar sole reconstruction.
CONCLUSION
With the widespread adoption of the fresh-tissue technique for Mohs micrographic surgery and the establishment of the American Society for Dermatologic Surgery in 1970, the depth and scope of techniques used by dermatologic surgeons has dramatically expanded. Although the use of dermal flaps and grafts is not as widespread in dermatology as other reconstructive techniques, their unique advantages should be considered. Deepithelialized flaps and grafts should be considered when the following reconstructive goals are desired: (1) conversion of a 2-stage interpolation flap to a single-stage tunneled flap, (2) contour and cosmetic subunit preservation of deep defects through volume augmentation, (3) reconstruction in areas of high mechanical tension, and (4) free margin preservation. The multiple applications of deepithelialized flaps and grafts as described in this review demonstrate their continued applicability in dermatologic surgery.
Deepithelialized flaps and grafts have been widely used by reconstructive surgeons in a diverse range of medical specialties since the early 20th century. 1 These reconstructive modalities have more recently been applied to dermatologic surgery. Deepithelialized flaps and grafts involve removal of the epidermis from the dermis for a variety of surgical purposes. Although these techniques play an important role in dermatologic surgery, reports of application of deepithelialized flaps and grafts in the dermatology literature is limited. This article includes a presentation of the applications of deepithelialized flaps and grafts in procedural dermatology.
DEEPITHELIALIZATION TECHNIQUES
There are a variety of techniques for deepithelialization, although sharp deepithelialization generally is preferred by dermatologic surgeons. The scalpel technique can be accomplished by making an intradermal incision with a No. 15 blade. Traction is an essential component of the deepthelialization process and facilitates sharp removal of the epidermis and superficial dermis in an even plane. The peeling orange technique, which has been described in reduction mammoplasty, is a variant of the scalpel technique used for creating a large area of deepithelialized tissue.2 A No. 10 blade is used to make multiple partial-thickness intradermal incisions 1 to 2 cm apart along the pedicle. Traction facilitates rapid deepithelialization of the skin strips on the pedicle. A sharp curette is an alternative option for sharply removing the epithelium from a small area. Electric dermatome, laser, and electrocautery techniques for deepithelialization also can be considered.2,3
APPLICATION OF DEEPITHELIALIZED FLAPS
Deepithelialized flaps may be considered for single-stage reconstruction with tunneled interpolation flaps, reconstruction requiring contour preservation, and reconstruction involving free margins.4-17
Reconstruction With Single-Stage Tunneled Interpolated Flaps
Alar Base
A partially deepithelialized tunneled interpolated flap is an elegant reconstructive option for defects involving the upper cutaneous lip and alar base. The flap is elevated from the ipsilateral nasolabial fold, deepithelialized proximally, and tunneled under the intact portion of the cutaneous upper lip and ala. The flap is then deepithelialized superiorly to bolster the alar base and inset at the recipient site.4
Nasal Ala
The tunneled interpolated flap is useful for reconstruction of defects of the nasal ala. A flap with a superior deepithelialized pedicle and an anticipated inferior Burow triangle is designed along the axis of the nasolabial fold. The inferior Burow triangle and central flap are elevated at the level of the superficial subcutaneous fat and the pedicle is dissected. The donor and recipient sites are widely undermined, and the flap and pedicle pass through the tunnel. The donor site is closed primarily, the inferior Burow triangle is trimmed, and the flap is sutured into the defect.5 This flap allows for preservation of free margins and favorable placement of incision lines. Furthermore, pincushioning of the flap helps to recreate the rounded shape of the lateral ala.6
Nasal Tip
Nasal tip defects can be repaired with a retroangular flap, centered on the angular artery. The flap is elevated along the axis of the nasolabial fold, deepithelialized at its proximal base, and transferred through a subcutaneous tunnel to the nasal tip. The angular artery is ligated at the inferior aspect of the flap.7
Nasal Sidewall
A deepithelialized tunneled interpolated forehead flap, similar to the classic paramedian forehead flap, can be used to reconstruct nasal sidewall defects. A flap is elevated on the contralateral forehead and the proximal portion is deepithelialized. A tunnel is then bluntly dissected just above the periosteum, and the flap is introduced into the defect through the tunnel and inset. This flap has the advantages of being a single-stage procedure, restoring volume to the defect area, and maintaining excellent vascular supply.8
Eyelid
A tunneled interpolated forehead flap also can be used to repair medial canthal defects and for anterior lamellar repair of lower eyelid defects. In a study of 9 patients receiving a tunneled interpolated forehead flap in these anatomic locations, all flaps demonstrated viability, protection of the globe, and preservation of the concave architecture of the medial canthus.9
Earlobe
Earlobe defects may be repaired with a pull-through interpolated preauricular flap. A flap is elevated superiorly in the preauricular region and the proximal aspect of the flap is deepithelialized. The flap is pulled through a tunnel and inset at the anterior earlobe defect. The donor site is closed primarily.10,11
Concha
Reconstruction of anterior conchal defects with exposed cartilage can be accomplished with a pull-through interpolated postauricular flap based on the auriculomastoid fossa. The postauricular flap is elevated, the base is deepithelialized, an incision is made in the medial aspect of the defect, and the flap is moved through a tunnel between the posterior and anterior surfaces of the ear. The flap is secured to the anterior surface of the concha.12
Reconstruction Requiring Contour Preservation
Central Face
The hinge flap is optimal for reconstruction of deep central facial defects (Figure 1). The hinge flap is planned at a site contiguous with a margin of the defect and can include the dermis, subcutaneous tissue, muscle, or a combination of these. The desired tissue is folded over on the pedicle to fill the defect. Cutaneous coverage is accomplished through a primary closure, separate flap, or skin graft. In addition to restoring contour and therefore the cosmetic subunit, the hinge flap is performed in a single stage, resists wound contracture, and provides a well-vascularized wound bed resulting in a low incidence of graft failure.13,14 Muscular hinge flaps have been described for reconstruction of forehead defects with exposed bone based on the frontalis muscle.15
Lower Lip
A variant of a V-Y advancement flap has been described for reconstruction of defects greater than one-third the length of the lower lip. The top of the “V” is deepithelialized and the flap is advanced such that the top of the “V” abuts the inferior border of the defect. The “V” flap is inset at its advanced position, converting the “V”-shaped wound into a “Y.” An overlying buccal mucosal graft provides reconstruction of the lower red lip and labial mucosa.16
Helix of the Ear
Large defects of the scapha and helix of the ear can be reconstructed with the use of a staged interpolated postauricular flap. The postauricular flap is elevated into a subcutaneous plane. A full-thickness incision is made medial to the helical rim, and the flap is tunneled through and sutured into place. The pedicle is later divided, and the distal aspect of the flap is deepithelialized and inset into the helical rim for volume restoration.17
Reconstruction Involving Free Margins
Nasal Ala
For large defects involving the upper cutaneous lip with adjacent alar base involvement, a partially deepithelialized V-Y flap is a useful reconstructive option (Figure 2).
Infraorbital Region
A deepithelialized variant of a V-Y advancement flap can be used for closure of infraorbital defects. The limbs of the V-Y flap are deepithelialized and anchored to the medial and lateral canthal tendons or periosteum. Ectropion prevention is the primary advantage of this flap.18
APPLICATION OF DEEPITHELIALIZED GRAFTS
Deepithelialized grafts may be considered for volume replacement, reconstruction requiring contour preservation, and restoration of mechanical integrity in areas of high mechanical tension.3,19-21
Reconstruction Requiring Contour Preservation
Deepithelialized grafts are used to improve depressed nasal scars and restore volume in deep nasal wounds. One method involves deepithelialization of 2 postauricular punch biopsies. An 18-gauge needle is used to make a small hole in the depressed nasal scar, the dermal grafts are inserted, and the defect is closed primarily.19 Dermal grafts may be harvested from excess full-thickness skin grafts (FTSGs) or dog-ear tissue. When used under flaps, the dermal graft is trimmed to the size of the defect. When used under FTSGs, thin dermal graft strips are placed in a gridlike pattern to allow for revascularization. A study of 15 patients with contour deformities reconstructed with dermal graft insertions demonstrated that 14 (94%) patients had no significant complications and improvement of scar depression was achieved.20
Reconstruction in Areas of High Mechanical Tension
Plantar Foot
A combined dermal and full-thickness sandwich graft has been described for reconstruction of plantar foot defects.3 The graft is created by obtaining a FTSG twice the size of the wound defect and deepithelializing half of the graft. The graft is then defatted and the deepithelialized portion is folded beneath the other half, allowing the papillary dermis to make contact with the wound surface.
Scalp
Dermal graft reconstruction for scalp defects may be accomplished with a split-thickness skin flap. The flap is harvested using an electronic dermatome that ensures the proximal aspect is still attached to adjacent skin. The dermis is removed from the area underneath the back-folded split-thickness skin flap. The dermal graft is meshed and sutured into the recipient site. The split-thickness skin flap is replaced over the donor site. Meshed reversed dermal grafts have excellent survival rates, even with direct placement on bone without periosteum. Querings et al21 reported graft survival with no complications in 19 of 21 (90.4%) patients undergoing scalp or plantar sole reconstruction.
CONCLUSION
With the widespread adoption of the fresh-tissue technique for Mohs micrographic surgery and the establishment of the American Society for Dermatologic Surgery in 1970, the depth and scope of techniques used by dermatologic surgeons has dramatically expanded. Although the use of dermal flaps and grafts is not as widespread in dermatology as other reconstructive techniques, their unique advantages should be considered. Deepithelialized flaps and grafts should be considered when the following reconstructive goals are desired: (1) conversion of a 2-stage interpolation flap to a single-stage tunneled flap, (2) contour and cosmetic subunit preservation of deep defects through volume augmentation, (3) reconstruction in areas of high mechanical tension, and (4) free margin preservation. The multiple applications of deepithelialized flaps and grafts as described in this review demonstrate their continued applicability in dermatologic surgery.
- Straatsma CR. Use of the dermal graft in the repairs of small saddle defects of the nose. Arch Otolaryngol. 1932;16:506-509.
- Cydeli A, Hunter J. Peeling orange: rapid deepithelialization in reduction mammoplasty. J Aesthet Surg. 2004;24:580-581.
- Bechara F, Sand M, Radenhausen M, et al. Erbium:YAG laser-assisted preparation of a combined dermal/full thickness sandwich skin graft. Dermatol Surg. 2006;32:353-358.
- Cook JL. Tunneled and transposed island flaps in facial reconstructive surgery. Dermatol Surg. 2014;40(suppl 9):S16-S29.
- Krishnan RS, Clark DP. Tunneled transposition flap for reconstruction of defects of the nasal ala. Dermatol Surg. 2007;33:1496-1501.
- Mahlberg M. Tunneled melolabial pedicle flap for small but deep lateral alar rim defect. Dermatol Surg. 2013;39:1527-1529.
- Ascari-Raccagni A, Balderi U. The retroangular flap used in the surgery of nasal tip defects. Dermatol Surg. 2004;30:1131-1137.
- Hollmig ST, Leach BC, Cook J. Single-staged interpolation flaps in facial reconstruction. Dermatol Surg. 2014;40(suppl 9):S62-S70.
- Mombaerts I, Gillis A. The tunneled forehead flap in medial canthal and eyelid reconstruction. Dermatol Surg. 2010:36:1118-1125.
- Wang SQ, Goldberg LH, Kimyah-Asadi A. Tunneled island pedicle flap for an earlobe defect. Dermatol Surg. 2007;33:835-838.
- Hatoko M, Kuwahara M, Shiba A, et al. Earlobe reconstruction using a subcutaneous island pedicle flap after resection of “earlobe keloid.” Dermatol Surg. 1998;24:257-261.
- Alder N, Ad-El D, Azaria R. Reconstruction of nonhelical auricular defects with local flaps. Dermatol Surg. 2008;34:501-507.
- Fader DJ, Wang TS, Johnson TM. Nasal reconstruction utilizing a muscle hinge flap with overlying FTSG. J Am Acad Dermatol. 2000;43:837-840.
- Braun MA, Cook J. Hinge flaps in facial reconstruction. Dermatol Surg. 2007;33:213-221.
- Salmon PL, Mortimer NL, Hill SE. Muscular hinge flaps: utility and technique in facial reconstructive surgery. Dermatol Surg. 2010;36:227-234.
- Seo Y, Song S, Choi Y, et al. A lower lip reconstruction. Dermatol Surg. 2015;41:505-507.
- Malone CH, Wagner RF. Partially de-epithelialized postauricular flap for ear reconstruction. J Am Acad Dermatol. 2015;73:E219-E220.
- Yildrim S, Akoz T, Akan M, et al. Nasolabial V-Y advancement for closure of the midface defects. Dermatol Surg. 2001;27:656-662.
- Jensen DJ, Cohen JL. Nasal tip revision using a dermal graft. Dermatol Surg. 2014;40:1140-1142.
- Meyers S, Rohrer T. Use of dermal grafts in reconstructing deep nasal defects and shaping the ala nasi. Dermatol Surg. 2001;27:300-305.
- Querings K, Bachter D, Balda B. Meshed reversed dermal graft in patients with surgical defects of sole and scalp: technique and long-term results. Dermatol Surg. 2002;28:122-126.
- Straatsma CR. Use of the dermal graft in the repairs of small saddle defects of the nose. Arch Otolaryngol. 1932;16:506-509.
- Cydeli A, Hunter J. Peeling orange: rapid deepithelialization in reduction mammoplasty. J Aesthet Surg. 2004;24:580-581.
- Bechara F, Sand M, Radenhausen M, et al. Erbium:YAG laser-assisted preparation of a combined dermal/full thickness sandwich skin graft. Dermatol Surg. 2006;32:353-358.
- Cook JL. Tunneled and transposed island flaps in facial reconstructive surgery. Dermatol Surg. 2014;40(suppl 9):S16-S29.
- Krishnan RS, Clark DP. Tunneled transposition flap for reconstruction of defects of the nasal ala. Dermatol Surg. 2007;33:1496-1501.
- Mahlberg M. Tunneled melolabial pedicle flap for small but deep lateral alar rim defect. Dermatol Surg. 2013;39:1527-1529.
- Ascari-Raccagni A, Balderi U. The retroangular flap used in the surgery of nasal tip defects. Dermatol Surg. 2004;30:1131-1137.
- Hollmig ST, Leach BC, Cook J. Single-staged interpolation flaps in facial reconstruction. Dermatol Surg. 2014;40(suppl 9):S62-S70.
- Mombaerts I, Gillis A. The tunneled forehead flap in medial canthal and eyelid reconstruction. Dermatol Surg. 2010:36:1118-1125.
- Wang SQ, Goldberg LH, Kimyah-Asadi A. Tunneled island pedicle flap for an earlobe defect. Dermatol Surg. 2007;33:835-838.
- Hatoko M, Kuwahara M, Shiba A, et al. Earlobe reconstruction using a subcutaneous island pedicle flap after resection of “earlobe keloid.” Dermatol Surg. 1998;24:257-261.
- Alder N, Ad-El D, Azaria R. Reconstruction of nonhelical auricular defects with local flaps. Dermatol Surg. 2008;34:501-507.
- Fader DJ, Wang TS, Johnson TM. Nasal reconstruction utilizing a muscle hinge flap with overlying FTSG. J Am Acad Dermatol. 2000;43:837-840.
- Braun MA, Cook J. Hinge flaps in facial reconstruction. Dermatol Surg. 2007;33:213-221.
- Salmon PL, Mortimer NL, Hill SE. Muscular hinge flaps: utility and technique in facial reconstructive surgery. Dermatol Surg. 2010;36:227-234.
- Seo Y, Song S, Choi Y, et al. A lower lip reconstruction. Dermatol Surg. 2015;41:505-507.
- Malone CH, Wagner RF. Partially de-epithelialized postauricular flap for ear reconstruction. J Am Acad Dermatol. 2015;73:E219-E220.
- Yildrim S, Akoz T, Akan M, et al. Nasolabial V-Y advancement for closure of the midface defects. Dermatol Surg. 2001;27:656-662.
- Jensen DJ, Cohen JL. Nasal tip revision using a dermal graft. Dermatol Surg. 2014;40:1140-1142.
- Meyers S, Rohrer T. Use of dermal grafts in reconstructing deep nasal defects and shaping the ala nasi. Dermatol Surg. 2001;27:300-305.
- Querings K, Bachter D, Balda B. Meshed reversed dermal graft in patients with surgical defects of sole and scalp: technique and long-term results. Dermatol Surg. 2002;28:122-126.
Practice Points
- Deepithelialized flaps should be considered for single-stage reconstruction with tunneled interpolation flaps, reconstruction requiring contour preservation, and reconstruction involving free margins.
- Deepithelialized grafts may be considered for volume replacement, reconstruction requiring contour preservation, and reconstruction in areas of high mechanical tension.

Facing the world
***
Edgar is 86. His COPD recently caught up with him, and he needs oxygen. The nasal prongs that deliver it are irritating, but what really bothers him about them is that he won’t attend any activities in his assisted living facility wearing nasal prongs and trailing a tank.
***
Brenda comes in with a large bandage on her forehead. She takes it off to show me a large, jagged, fully-healed scar. Four months ago she gashed her head on an appliance and didn’t get medical help in time to have the wound properly stitched.
“My bangs aren’t thick enough to cover it,” she says. “My daughter asks why I wear a Band-Aid all the time,” says Brenda. But Brenda would rather walk around with a large bandage on her forehead. Just as Edgar won’t let anyone see him sick and diminished, Brenda won’t let anyone see her face damaged.
***
Stella has lymphoma. While she was on chemotherapy, she stayed put at home and avoided crowds to avoid catching someone’s virus. Once chemo was done, she was able to fly to Tallahassee, Fla., to see her new granddaughter Genevieve.
Unfortunately, her lymphoma recurred sooner than she and her doctors had hoped. Now Stella is on a new drug. This seems to be helping, but it puts her back at risk for infections in crowds.
And on planes. “Will you be able to visit Genevieve in Florida?” I ask.
Her husband Ben interjects. “Her doctors say she can,” he said, “but she would have to wear a mask on the plane, and Stella won’t wear a mask.”
***
Malcolm comes in now and then for this and that. This time, he is here for a skin check. At each visit he brings me up to date on an endless family lawsuit over a contested estate. Its subplots could script a whole Netflix series.
When I’m done with the skin check, Malcolm says, “also, I’d like Botox on my forehead.”
“OK,” I say. I don’t ask why, but Malcolm answers anyway.
“The lawsuit is finally coming to a head,” he says. “One of the nephews contesting the will is flying in from Indonesia, and the trial gets underway in Kentucky next week. I never would have started this fight, but since my charming relatives did, I’m in it to win it.”
I wish him luck.
“That’s why I want Botox,” he says. “I’m going to testify, and I want to look my confident best.”
Go, Malcolm!
While we’re talking Botox, I recall Amy, a well-traveled consultant who gave lectures all over.
“I’m curious,” I once asked her. “What do people say to you after you get Botox? Do they notice?”
“That’s interesting,” she said. “When I speak to groups, my face is projected onto large screens. That makes my wrinkles look like the Grand Canyon.
“When I started doing Botox, a man came over to me after a lecture and said, ‘I’ve heard you before, but this time you were, somehow, more cogent and compelling.’
“I thanked him, of course,” said Amy with a smile. “But the speech he was praising was the exact same speech he’d heard the first time.”
***

The rest of us try to put on the best face we can, assisted (in descending order of importance) by: makers of cosmetics, estheticians, dentists, plastic surgeons, and – oh yes – even dermatologists.
Happy to assist!
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
***
Edgar is 86. His COPD recently caught up with him, and he needs oxygen. The nasal prongs that deliver it are irritating, but what really bothers him about them is that he won’t attend any activities in his assisted living facility wearing nasal prongs and trailing a tank.
***
Brenda comes in with a large bandage on her forehead. She takes it off to show me a large, jagged, fully-healed scar. Four months ago she gashed her head on an appliance and didn’t get medical help in time to have the wound properly stitched.
“My bangs aren’t thick enough to cover it,” she says. “My daughter asks why I wear a Band-Aid all the time,” says Brenda. But Brenda would rather walk around with a large bandage on her forehead. Just as Edgar won’t let anyone see him sick and diminished, Brenda won’t let anyone see her face damaged.
***
Stella has lymphoma. While she was on chemotherapy, she stayed put at home and avoided crowds to avoid catching someone’s virus. Once chemo was done, she was able to fly to Tallahassee, Fla., to see her new granddaughter Genevieve.
Unfortunately, her lymphoma recurred sooner than she and her doctors had hoped. Now Stella is on a new drug. This seems to be helping, but it puts her back at risk for infections in crowds.
And on planes. “Will you be able to visit Genevieve in Florida?” I ask.
Her husband Ben interjects. “Her doctors say she can,” he said, “but she would have to wear a mask on the plane, and Stella won’t wear a mask.”
***
Malcolm comes in now and then for this and that. This time, he is here for a skin check. At each visit he brings me up to date on an endless family lawsuit over a contested estate. Its subplots could script a whole Netflix series.
When I’m done with the skin check, Malcolm says, “also, I’d like Botox on my forehead.”
“OK,” I say. I don’t ask why, but Malcolm answers anyway.
“The lawsuit is finally coming to a head,” he says. “One of the nephews contesting the will is flying in from Indonesia, and the trial gets underway in Kentucky next week. I never would have started this fight, but since my charming relatives did, I’m in it to win it.”
I wish him luck.
“That’s why I want Botox,” he says. “I’m going to testify, and I want to look my confident best.”
Go, Malcolm!
While we’re talking Botox, I recall Amy, a well-traveled consultant who gave lectures all over.
“I’m curious,” I once asked her. “What do people say to you after you get Botox? Do they notice?”
“That’s interesting,” she said. “When I speak to groups, my face is projected onto large screens. That makes my wrinkles look like the Grand Canyon.
“When I started doing Botox, a man came over to me after a lecture and said, ‘I’ve heard you before, but this time you were, somehow, more cogent and compelling.’
“I thanked him, of course,” said Amy with a smile. “But the speech he was praising was the exact same speech he’d heard the first time.”
***
The rest of us try to put on the best face we can, assisted (in descending order of importance) by: makers of cosmetics, estheticians, dentists, plastic surgeons, and – oh yes – even dermatologists.
Happy to assist!
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
***
Edgar is 86. His COPD recently caught up with him, and he needs oxygen. The nasal prongs that deliver it are irritating, but what really bothers him about them is that he won’t attend any activities in his assisted living facility wearing nasal prongs and trailing a tank.
***
Brenda comes in with a large bandage on her forehead. She takes it off to show me a large, jagged, fully-healed scar. Four months ago she gashed her head on an appliance and didn’t get medical help in time to have the wound properly stitched.
“My bangs aren’t thick enough to cover it,” she says. “My daughter asks why I wear a Band-Aid all the time,” says Brenda. But Brenda would rather walk around with a large bandage on her forehead. Just as Edgar won’t let anyone see him sick and diminished, Brenda won’t let anyone see her face damaged.
***
Stella has lymphoma. While she was on chemotherapy, she stayed put at home and avoided crowds to avoid catching someone’s virus. Once chemo was done, she was able to fly to Tallahassee, Fla., to see her new granddaughter Genevieve.
Unfortunately, her lymphoma recurred sooner than she and her doctors had hoped. Now Stella is on a new drug. This seems to be helping, but it puts her back at risk for infections in crowds.
And on planes. “Will you be able to visit Genevieve in Florida?” I ask.
Her husband Ben interjects. “Her doctors say she can,” he said, “but she would have to wear a mask on the plane, and Stella won’t wear a mask.”
***
Malcolm comes in now and then for this and that. This time, he is here for a skin check. At each visit he brings me up to date on an endless family lawsuit over a contested estate. Its subplots could script a whole Netflix series.
When I’m done with the skin check, Malcolm says, “also, I’d like Botox on my forehead.”
“OK,” I say. I don’t ask why, but Malcolm answers anyway.
“The lawsuit is finally coming to a head,” he says. “One of the nephews contesting the will is flying in from Indonesia, and the trial gets underway in Kentucky next week. I never would have started this fight, but since my charming relatives did, I’m in it to win it.”
I wish him luck.
“That’s why I want Botox,” he says. “I’m going to testify, and I want to look my confident best.”
Go, Malcolm!
While we’re talking Botox, I recall Amy, a well-traveled consultant who gave lectures all over.
“I’m curious,” I once asked her. “What do people say to you after you get Botox? Do they notice?”
“That’s interesting,” she said. “When I speak to groups, my face is projected onto large screens. That makes my wrinkles look like the Grand Canyon.
“When I started doing Botox, a man came over to me after a lecture and said, ‘I’ve heard you before, but this time you were, somehow, more cogent and compelling.’
“I thanked him, of course,” said Amy with a smile. “But the speech he was praising was the exact same speech he’d heard the first time.”
***
The rest of us try to put on the best face we can, assisted (in descending order of importance) by: makers of cosmetics, estheticians, dentists, plastic surgeons, and – oh yes – even dermatologists.
Happy to assist!
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
Aesthetic procedures becoming more popular in skin of color patients
in a presentation at the Caribbean Dermatology Symposium.
In 2015, ethnic minority patients accounted for 25% of aesthetic procedures in the United States, up from 20% in 2010, according to data from the American Society for Aesthetic Plastic Surgery, said Dr. Alexis, chair of dermatology and director of the Skin of Color Center at Mount Sinai St. Luke’s and Mount Sinai West hospitals in New York.

Chemical peels can be used successfully to treat a range of conditions in skin of color patients, including postinflammatory hyperpigmentation, acne, melasma, textural irregularities, and pseudofolliculitis barbae. They also can be used for skin brightening, said Dr. Alexis, who recommended a chemical peel protocol of salicylic acid, glycolic acid, or Jessner’s every 2-4 weeks. “Consider hydroquinone 4% concurrently to enhance efficacy for treating hyperpigmentation and to prevent postinflammatory hyperpigmentation,” he said. Patients on retinoids should discontinue them for 1 week prior to a chemical peel, he added.
Dr. Alexis shared several treatment pearls to promote successful peels in skin of color patients:
- Salicylic acid: Resist the urge to overapply and “titrate according to patient tolerability.” The endpoint of a salicylic acid peel is white precipitate, not frost; cool compresses can be used for patient comfort and for later removal of the white precipitate.
- Glycolic acid: Stick to a contact time of 2-4 minutes to avoid epidermolysis. “Completely neutralize all areas of application to avoid overpeeling.”
- Trichloroacetic acid (TCA): TCA carries a greater risk of dyspigmentation, and should be reserved for patients who have not been successfully treated with salicylic or glycolic acid; a 10%-15% concentration of TCA, applied conservatively, is recommended.
Regardless of the type of chemical, potential pitfalls of peels in patients of color include using too much product, allowing too long of an application time, and applying the chemical to an inflamed or excoriated area, Dr. Alexis said. Patients who don’t discontinue retinoids before a peel are at increased risk of developing erosions or crusting, he added.
Dr. Alexis disclosed relationships with Allergan, BioPharmX, Dermira, Galderma, Novan, Novartis, RXi, Unilever, and Valeant.
Global Academy and this news organization are owned by the same parent company.
in a presentation at the Caribbean Dermatology Symposium.
In 2015, ethnic minority patients accounted for 25% of aesthetic procedures in the United States, up from 20% in 2010, according to data from the American Society for Aesthetic Plastic Surgery, said Dr. Alexis, chair of dermatology and director of the Skin of Color Center at Mount Sinai St. Luke’s and Mount Sinai West hospitals in New York.
Chemical peels can be used successfully to treat a range of conditions in skin of color patients, including postinflammatory hyperpigmentation, acne, melasma, textural irregularities, and pseudofolliculitis barbae. They also can be used for skin brightening, said Dr. Alexis, who recommended a chemical peel protocol of salicylic acid, glycolic acid, or Jessner’s every 2-4 weeks. “Consider hydroquinone 4% concurrently to enhance efficacy for treating hyperpigmentation and to prevent postinflammatory hyperpigmentation,” he said. Patients on retinoids should discontinue them for 1 week prior to a chemical peel, he added.
Dr. Alexis shared several treatment pearls to promote successful peels in skin of color patients:
- Salicylic acid: Resist the urge to overapply and “titrate according to patient tolerability.” The endpoint of a salicylic acid peel is white precipitate, not frost; cool compresses can be used for patient comfort and for later removal of the white precipitate.
- Glycolic acid: Stick to a contact time of 2-4 minutes to avoid epidermolysis. “Completely neutralize all areas of application to avoid overpeeling.”
- Trichloroacetic acid (TCA): TCA carries a greater risk of dyspigmentation, and should be reserved for patients who have not been successfully treated with salicylic or glycolic acid; a 10%-15% concentration of TCA, applied conservatively, is recommended.
Regardless of the type of chemical, potential pitfalls of peels in patients of color include using too much product, allowing too long of an application time, and applying the chemical to an inflamed or excoriated area, Dr. Alexis said. Patients who don’t discontinue retinoids before a peel are at increased risk of developing erosions or crusting, he added.
Dr. Alexis disclosed relationships with Allergan, BioPharmX, Dermira, Galderma, Novan, Novartis, RXi, Unilever, and Valeant.
Global Academy and this news organization are owned by the same parent company.
in a presentation at the Caribbean Dermatology Symposium.
In 2015, ethnic minority patients accounted for 25% of aesthetic procedures in the United States, up from 20% in 2010, according to data from the American Society for Aesthetic Plastic Surgery, said Dr. Alexis, chair of dermatology and director of the Skin of Color Center at Mount Sinai St. Luke’s and Mount Sinai West hospitals in New York.
Chemical peels can be used successfully to treat a range of conditions in skin of color patients, including postinflammatory hyperpigmentation, acne, melasma, textural irregularities, and pseudofolliculitis barbae. They also can be used for skin brightening, said Dr. Alexis, who recommended a chemical peel protocol of salicylic acid, glycolic acid, or Jessner’s every 2-4 weeks. “Consider hydroquinone 4% concurrently to enhance efficacy for treating hyperpigmentation and to prevent postinflammatory hyperpigmentation,” he said. Patients on retinoids should discontinue them for 1 week prior to a chemical peel, he added.
Dr. Alexis shared several treatment pearls to promote successful peels in skin of color patients:
- Salicylic acid: Resist the urge to overapply and “titrate according to patient tolerability.” The endpoint of a salicylic acid peel is white precipitate, not frost; cool compresses can be used for patient comfort and for later removal of the white precipitate.
- Glycolic acid: Stick to a contact time of 2-4 minutes to avoid epidermolysis. “Completely neutralize all areas of application to avoid overpeeling.”
- Trichloroacetic acid (TCA): TCA carries a greater risk of dyspigmentation, and should be reserved for patients who have not been successfully treated with salicylic or glycolic acid; a 10%-15% concentration of TCA, applied conservatively, is recommended.
Regardless of the type of chemical, potential pitfalls of peels in patients of color include using too much product, allowing too long of an application time, and applying the chemical to an inflamed or excoriated area, Dr. Alexis said. Patients who don’t discontinue retinoids before a peel are at increased risk of developing erosions or crusting, he added.
Dr. Alexis disclosed relationships with Allergan, BioPharmX, Dermira, Galderma, Novan, Novartis, RXi, Unilever, and Valeant.
Global Academy and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE CARIBBEAN DERMATOLOGY SYMPOSIUM
Enhancing the effects of microfocused ultrasound with cosmeceuticals
The use of microfocused ultrasound (MFUS) emerged in dermatology in 2009 as a minimally invasive approach to treating mild to moderate facial and neck laxity. Microfocused ultrasound with visualization (MFU-V), as represented by the device Ultherapy, adds high-resolution ultrasound imaging so that the user can see the targets for MFUS energy. Visualization also allows the user to choose the appropriate treatment depth and transducer.1 Since its introduction, Ultherapy has been investigated for efficacy and safety in tightening, lifting, and wrinkle reduction beyond the face and neck, specifically including the décolletage, abdomen, arms/elbows, knees, medial thighs, and buttocks.1-8 This column will focus on using cosmeceuticals to improve the skin-tightening outcomes of microfocused ultrasound.

Two weeks before the procedure
Ingredients that should be used prior to MFU-V include retinoids, such as tretinoin and retinol. Various studies have demonstrated that pretreatment with tretinoin increases collagen production and speeds wound healing.12-14 Kligman et al. assessed wound healing after punch biopsy and found that arm wounds pretreated with tretinoin cream 0.05%-0.1% were significantly smaller by 35%-37% on days 1 and 4 and by 47%-50% on days 6, 8, and 11 than were wounds on the untreated arms.15 The majority of studies on the subject recommend a 2- to 4-week tretinoin pretreatment regimen because peak epidermal hypertrophy occurs after 7 days of tretinoin application and normalizes after 14 days of continued treatment.16,17 This time frame allows for the skin to recover from any retinoid dermatitis prior to the procedure. Adapalene should be started 5-6 weeks prior to procedures because it has a longer half-life and requires an earlier initiation period.18 Although studies have not been performed evaluating the efficacy of topical ascorbic acid and hydroxy acids, pretreating skin with them also may accelerate collagen production after procedures such as MFU-V.19,20

Postprocedure skin care
Because no incision or ablation occurs with MFUS, the use of ascorbic acid, hydroxy acids, and retinoids can and should be continued after the procedure in addition to before the procedure. The combination of topical Arnica montana and Rhododendron tomentosum in a gel pad has been shown to mitigate postoperative ecchymosis and edema after oculofacial surgery.24 Topical curcumin has been shown to facilitate wound healing in animals, but its smell and color make it difficult to use topically. I recommend adding turmeric to food pre- and postprocedure.25
Adverse events
Late in 2017, Friedmann et al. offered a report on the nature of the rare complications from MFUS, which have included mild and fleeting ecchymosis, edema, erythema, and nerve paralysis. In this retrospective multicenter case series of five patients seen in the authors’ practice who experienced serious adverse reactions to Ultherapy, the authors reported that single sessions of MFUS yielded blistering, erosion/ulceration, or cutaneous or subcutaneous tissue edema with resulting atrophy and/or cutaneous necrosis. The authors concluded that while serious adverse events following MFUS are rare, such reactions might be underreported and should be prepared for with early management to diminish inflammation.26 Other adverse events, which are transient and rare, may include discomfort and mild bruising.
Educating patients on pre- and postprocedure instructions can help minimize adverse events. Avoiding foods that decrease platelet function, like ginger, green tea, alcohol (red wine), salmon, and flax seeds, can reduce the risk of bruising. Use of topical and oral antioxidants before and after treatments also may help reduce inflammation and edema.
Conclusion
Please email me at [email protected] if you have any comments, suggestions, or anecdotal reports to share on using cosmeceuticals and nutraceuticals before and after procedures. I will share your responses on my LinkedIn account.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also wrote a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems.
References
1. Clin Cosmet Investig Dermatol. 2017 Oct 30;10:423-9.
2. J Am Acad Dermatol. 2013 Dec;69(6):965-71.
3. Dermatol Surg. 2015 Mar;41(3):327-35.
4. J Cosmet Dermatol Sci Appl. 2012;2(2A):108-16.
5. Dermatol Surg. 2015 Jul;41(7):821-6.
6. J Cosmet Laser Ther. 2014 Oct;16(5):225-9.
7. Dermatol Surg. 2012 May;38(5):754-9.
8. Dermatol Surg. 2014 Oct;40(10):1113-7.
9. Clin Cosmet Investig Dermatol. 2015; 8: 47-52.
10. Dermatol Surg. 2017 Sep 8. doi: 10.1097/DSS.0000000000001216. [Epub ahead of print]
11. Arch Dermatol. 2004 Feb;140(2):204-9.
12. Aesthetic Plast Surg. 1995 May-Jun;19(3):243-6.
13. Plast Reconstr Surg. 2011 Mar;127(3):1343-5.
14. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S79-81.
15. Popp C et al. Br J Dermatol. 1995 Jan;132(1):46-53.
16. J Am Acad Dermatol. 2004 Dec;51(6):940-6.
17. J Korean Med Sci. 1996 Aug;11(4):335-41.
18. Eur J Dermatol. 2002 Mar-Apr;12(2):145-8.
19. Proc Natl Acad Sci U S A. 1981 May; 78(5): 2879-82.
20. Exp Dermatol. 2003;12 Suppl 2:57-63.
21. Dermatol Surg. 2001 Feb;27(2):137-42.
22. Br J Dermatol. 1992 Sep;127(3):247-53.
23. J Invest Dermatol. 1991;96:587.
24. Ophthal Plast Reconstr Surg. 2017 Jan/Feb;33(1):47-52.
25. Wound Repair Regen. 1998 Mar-Apr;6(2):167-77.
26. Lasers Surg Med. 2018 Jan;50(1):13-9.
The use of microfocused ultrasound (MFUS) emerged in dermatology in 2009 as a minimally invasive approach to treating mild to moderate facial and neck laxity. Microfocused ultrasound with visualization (MFU-V), as represented by the device Ultherapy, adds high-resolution ultrasound imaging so that the user can see the targets for MFUS energy. Visualization also allows the user to choose the appropriate treatment depth and transducer.1 Since its introduction, Ultherapy has been investigated for efficacy and safety in tightening, lifting, and wrinkle reduction beyond the face and neck, specifically including the décolletage, abdomen, arms/elbows, knees, medial thighs, and buttocks.1-8 This column will focus on using cosmeceuticals to improve the skin-tightening outcomes of microfocused ultrasound.
Two weeks before the procedure
Ingredients that should be used prior to MFU-V include retinoids, such as tretinoin and retinol. Various studies have demonstrated that pretreatment with tretinoin increases collagen production and speeds wound healing.12-14 Kligman et al. assessed wound healing after punch biopsy and found that arm wounds pretreated with tretinoin cream 0.05%-0.1% were significantly smaller by 35%-37% on days 1 and 4 and by 47%-50% on days 6, 8, and 11 than were wounds on the untreated arms.15 The majority of studies on the subject recommend a 2- to 4-week tretinoin pretreatment regimen because peak epidermal hypertrophy occurs after 7 days of tretinoin application and normalizes after 14 days of continued treatment.16,17 This time frame allows for the skin to recover from any retinoid dermatitis prior to the procedure. Adapalene should be started 5-6 weeks prior to procedures because it has a longer half-life and requires an earlier initiation period.18 Although studies have not been performed evaluating the efficacy of topical ascorbic acid and hydroxy acids, pretreating skin with them also may accelerate collagen production after procedures such as MFU-V.19,20
Postprocedure skin care
Because no incision or ablation occurs with MFUS, the use of ascorbic acid, hydroxy acids, and retinoids can and should be continued after the procedure in addition to before the procedure. The combination of topical Arnica montana and Rhododendron tomentosum in a gel pad has been shown to mitigate postoperative ecchymosis and edema after oculofacial surgery.24 Topical curcumin has been shown to facilitate wound healing in animals, but its smell and color make it difficult to use topically. I recommend adding turmeric to food pre- and postprocedure.25
Adverse events
Late in 2017, Friedmann et al. offered a report on the nature of the rare complications from MFUS, which have included mild and fleeting ecchymosis, edema, erythema, and nerve paralysis. In this retrospective multicenter case series of five patients seen in the authors’ practice who experienced serious adverse reactions to Ultherapy, the authors reported that single sessions of MFUS yielded blistering, erosion/ulceration, or cutaneous or subcutaneous tissue edema with resulting atrophy and/or cutaneous necrosis. The authors concluded that while serious adverse events following MFUS are rare, such reactions might be underreported and should be prepared for with early management to diminish inflammation.26 Other adverse events, which are transient and rare, may include discomfort and mild bruising.
Educating patients on pre- and postprocedure instructions can help minimize adverse events. Avoiding foods that decrease platelet function, like ginger, green tea, alcohol (red wine), salmon, and flax seeds, can reduce the risk of bruising. Use of topical and oral antioxidants before and after treatments also may help reduce inflammation and edema.
Conclusion
Please email me at [email protected] if you have any comments, suggestions, or anecdotal reports to share on using cosmeceuticals and nutraceuticals before and after procedures. I will share your responses on my LinkedIn account.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also wrote a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems.
References
1. Clin Cosmet Investig Dermatol. 2017 Oct 30;10:423-9.
2. J Am Acad Dermatol. 2013 Dec;69(6):965-71.
3. Dermatol Surg. 2015 Mar;41(3):327-35.
4. J Cosmet Dermatol Sci Appl. 2012;2(2A):108-16.
5. Dermatol Surg. 2015 Jul;41(7):821-6.
6. J Cosmet Laser Ther. 2014 Oct;16(5):225-9.
7. Dermatol Surg. 2012 May;38(5):754-9.
8. Dermatol Surg. 2014 Oct;40(10):1113-7.
9. Clin Cosmet Investig Dermatol. 2015; 8: 47-52.
10. Dermatol Surg. 2017 Sep 8. doi: 10.1097/DSS.0000000000001216. [Epub ahead of print]
11. Arch Dermatol. 2004 Feb;140(2):204-9.
12. Aesthetic Plast Surg. 1995 May-Jun;19(3):243-6.
13. Plast Reconstr Surg. 2011 Mar;127(3):1343-5.
14. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S79-81.
15. Popp C et al. Br J Dermatol. 1995 Jan;132(1):46-53.
16. J Am Acad Dermatol. 2004 Dec;51(6):940-6.
17. J Korean Med Sci. 1996 Aug;11(4):335-41.
18. Eur J Dermatol. 2002 Mar-Apr;12(2):145-8.
19. Proc Natl Acad Sci U S A. 1981 May; 78(5): 2879-82.
20. Exp Dermatol. 2003;12 Suppl 2:57-63.
21. Dermatol Surg. 2001 Feb;27(2):137-42.
22. Br J Dermatol. 1992 Sep;127(3):247-53.
23. J Invest Dermatol. 1991;96:587.
24. Ophthal Plast Reconstr Surg. 2017 Jan/Feb;33(1):47-52.
25. Wound Repair Regen. 1998 Mar-Apr;6(2):167-77.
26. Lasers Surg Med. 2018 Jan;50(1):13-9.
The use of microfocused ultrasound (MFUS) emerged in dermatology in 2009 as a minimally invasive approach to treating mild to moderate facial and neck laxity. Microfocused ultrasound with visualization (MFU-V), as represented by the device Ultherapy, adds high-resolution ultrasound imaging so that the user can see the targets for MFUS energy. Visualization also allows the user to choose the appropriate treatment depth and transducer.1 Since its introduction, Ultherapy has been investigated for efficacy and safety in tightening, lifting, and wrinkle reduction beyond the face and neck, specifically including the décolletage, abdomen, arms/elbows, knees, medial thighs, and buttocks.1-8 This column will focus on using cosmeceuticals to improve the skin-tightening outcomes of microfocused ultrasound.
Two weeks before the procedure
Ingredients that should be used prior to MFU-V include retinoids, such as tretinoin and retinol. Various studies have demonstrated that pretreatment with tretinoin increases collagen production and speeds wound healing.12-14 Kligman et al. assessed wound healing after punch biopsy and found that arm wounds pretreated with tretinoin cream 0.05%-0.1% were significantly smaller by 35%-37% on days 1 and 4 and by 47%-50% on days 6, 8, and 11 than were wounds on the untreated arms.15 The majority of studies on the subject recommend a 2- to 4-week tretinoin pretreatment regimen because peak epidermal hypertrophy occurs after 7 days of tretinoin application and normalizes after 14 days of continued treatment.16,17 This time frame allows for the skin to recover from any retinoid dermatitis prior to the procedure. Adapalene should be started 5-6 weeks prior to procedures because it has a longer half-life and requires an earlier initiation period.18 Although studies have not been performed evaluating the efficacy of topical ascorbic acid and hydroxy acids, pretreating skin with them also may accelerate collagen production after procedures such as MFU-V.19,20
Postprocedure skin care
Because no incision or ablation occurs with MFUS, the use of ascorbic acid, hydroxy acids, and retinoids can and should be continued after the procedure in addition to before the procedure. The combination of topical Arnica montana and Rhododendron tomentosum in a gel pad has been shown to mitigate postoperative ecchymosis and edema after oculofacial surgery.24 Topical curcumin has been shown to facilitate wound healing in animals, but its smell and color make it difficult to use topically. I recommend adding turmeric to food pre- and postprocedure.25
Adverse events
Late in 2017, Friedmann et al. offered a report on the nature of the rare complications from MFUS, which have included mild and fleeting ecchymosis, edema, erythema, and nerve paralysis. In this retrospective multicenter case series of five patients seen in the authors’ practice who experienced serious adverse reactions to Ultherapy, the authors reported that single sessions of MFUS yielded blistering, erosion/ulceration, or cutaneous or subcutaneous tissue edema with resulting atrophy and/or cutaneous necrosis. The authors concluded that while serious adverse events following MFUS are rare, such reactions might be underreported and should be prepared for with early management to diminish inflammation.26 Other adverse events, which are transient and rare, may include discomfort and mild bruising.
Educating patients on pre- and postprocedure instructions can help minimize adverse events. Avoiding foods that decrease platelet function, like ginger, green tea, alcohol (red wine), salmon, and flax seeds, can reduce the risk of bruising. Use of topical and oral antioxidants before and after treatments also may help reduce inflammation and edema.
Conclusion
Please email me at [email protected] if you have any comments, suggestions, or anecdotal reports to share on using cosmeceuticals and nutraceuticals before and after procedures. I will share your responses on my LinkedIn account.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks, “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also wrote a New York Times Best Sellers book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance. She is the founder and CEO of Skin Type Solutions Franchise Systems.
References
1. Clin Cosmet Investig Dermatol. 2017 Oct 30;10:423-9.
2. J Am Acad Dermatol. 2013 Dec;69(6):965-71.
3. Dermatol Surg. 2015 Mar;41(3):327-35.
4. J Cosmet Dermatol Sci Appl. 2012;2(2A):108-16.
5. Dermatol Surg. 2015 Jul;41(7):821-6.
6. J Cosmet Laser Ther. 2014 Oct;16(5):225-9.
7. Dermatol Surg. 2012 May;38(5):754-9.
8. Dermatol Surg. 2014 Oct;40(10):1113-7.
9. Clin Cosmet Investig Dermatol. 2015; 8: 47-52.
10. Dermatol Surg. 2017 Sep 8. doi: 10.1097/DSS.0000000000001216. [Epub ahead of print]
11. Arch Dermatol. 2004 Feb;140(2):204-9.
12. Aesthetic Plast Surg. 1995 May-Jun;19(3):243-6.
13. Plast Reconstr Surg. 2011 Mar;127(3):1343-5.
14. J Am Acad Dermatol. 1998 Aug;39(2 Pt 3):S79-81.
15. Popp C et al. Br J Dermatol. 1995 Jan;132(1):46-53.
16. J Am Acad Dermatol. 2004 Dec;51(6):940-6.
17. J Korean Med Sci. 1996 Aug;11(4):335-41.
18. Eur J Dermatol. 2002 Mar-Apr;12(2):145-8.
19. Proc Natl Acad Sci U S A. 1981 May; 78(5): 2879-82.
20. Exp Dermatol. 2003;12 Suppl 2:57-63.
21. Dermatol Surg. 2001 Feb;27(2):137-42.
22. Br J Dermatol. 1992 Sep;127(3):247-53.
23. J Invest Dermatol. 1991;96:587.
24. Ophthal Plast Reconstr Surg. 2017 Jan/Feb;33(1):47-52.
25. Wound Repair Regen. 1998 Mar-Apr;6(2):167-77.
26. Lasers Surg Med. 2018 Jan;50(1):13-9.
Treatment of Melasma Using Tranexamic Acid: What’s Known and What’s Next
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
Resident Pearl
- Oral tranexamic acid is an antifibrinolytic agent that can be used off-label for the treatment of melasma.

Nd:YAG laser treatment improves the appearance of facial wrinkles
wrote Eric F. Bernstein, MD, a laser surgeon in private practice in Ardmore, Pa., and his associates.
In the study, two fractionated lasers were each combined with a specially designed “holographic beam-splitting optic” to treat mild to moderate facial wrinkles in 24 patients aged 18-75 years with Fitzpatrick skin types I-VI; 14 patients received five monthly treatments with the 1,064 nm laser, while the other 10 patients received four monthly treatments with the 532 nm laser.
Blinded evaluators assessed images taken at baseline and at 12 weeks after treatment. The evaluators found improvements of greater than 20% in 56.9% of the evaluated images, with no statistically significant difference between the two wavelengths. Of those treated with the 1,064 nm laser, 12 of 14 patients were “satisfied” or “very satisfied”; of those treated with the 532 nm laser, 8 of the 10 were “satisfied” or “very satisfied,” Dr. Bernstein and his colleagues wrote in the Journal of Drugs in Dermatology.
Patients experienced only mild to moderate discomfort during the laser treatment. Side effects were mild and were limited to erythema and edema in almost all patients; fewer than half the patients developed petechiae. Side effects generally resolved within a few days of treatment.
Dr. Bernstein and some of the other authors reported relationships with Syneron Candela, which provided funding for and loaned equipment used in the study.
Source: Bernstein EF et al. J Drugs Dermatol. 2017 Nov 1;16(11):1077-82.
wrote Eric F. Bernstein, MD, a laser surgeon in private practice in Ardmore, Pa., and his associates.
In the study, two fractionated lasers were each combined with a specially designed “holographic beam-splitting optic” to treat mild to moderate facial wrinkles in 24 patients aged 18-75 years with Fitzpatrick skin types I-VI; 14 patients received five monthly treatments with the 1,064 nm laser, while the other 10 patients received four monthly treatments with the 532 nm laser.
Blinded evaluators assessed images taken at baseline and at 12 weeks after treatment. The evaluators found improvements of greater than 20% in 56.9% of the evaluated images, with no statistically significant difference between the two wavelengths. Of those treated with the 1,064 nm laser, 12 of 14 patients were “satisfied” or “very satisfied”; of those treated with the 532 nm laser, 8 of the 10 were “satisfied” or “very satisfied,” Dr. Bernstein and his colleagues wrote in the Journal of Drugs in Dermatology.
Patients experienced only mild to moderate discomfort during the laser treatment. Side effects were mild and were limited to erythema and edema in almost all patients; fewer than half the patients developed petechiae. Side effects generally resolved within a few days of treatment.
Dr. Bernstein and some of the other authors reported relationships with Syneron Candela, which provided funding for and loaned equipment used in the study.
Source: Bernstein EF et al. J Drugs Dermatol. 2017 Nov 1;16(11):1077-82.
wrote Eric F. Bernstein, MD, a laser surgeon in private practice in Ardmore, Pa., and his associates.
In the study, two fractionated lasers were each combined with a specially designed “holographic beam-splitting optic” to treat mild to moderate facial wrinkles in 24 patients aged 18-75 years with Fitzpatrick skin types I-VI; 14 patients received five monthly treatments with the 1,064 nm laser, while the other 10 patients received four monthly treatments with the 532 nm laser.
Blinded evaluators assessed images taken at baseline and at 12 weeks after treatment. The evaluators found improvements of greater than 20% in 56.9% of the evaluated images, with no statistically significant difference between the two wavelengths. Of those treated with the 1,064 nm laser, 12 of 14 patients were “satisfied” or “very satisfied”; of those treated with the 532 nm laser, 8 of the 10 were “satisfied” or “very satisfied,” Dr. Bernstein and his colleagues wrote in the Journal of Drugs in Dermatology.
Patients experienced only mild to moderate discomfort during the laser treatment. Side effects were mild and were limited to erythema and edema in almost all patients; fewer than half the patients developed petechiae. Side effects generally resolved within a few days of treatment.
Dr. Bernstein and some of the other authors reported relationships with Syneron Candela, which provided funding for and loaned equipment used in the study.
Source: Bernstein EF et al. J Drugs Dermatol. 2017 Nov 1;16(11):1077-82.
FROM THE JOURNAL OF DRUGS IN DERMATOLOGY