User login
Participatory pharmacotherapy: 10 strategies for enhancing adherence
Psychiatric patients stand to benefit greatly from adhering to prescribed pharmacotherapy, but many patients typically do not follow their medication regimens.1,2 Three months after pharmacotherapy is initiated, approximately 50% of patients with major depressive disorder (MDD) do not take their prescribed antidepressants.3 Adherence rates in patients with schizophrenia range from 50% to 60%, and patients with bipolar disorder have adherence rates as low as 35%.4-6 One possible explanation for “treatment-resistant” depression, schizophrenia, and bipolar disorder may simply be nonadherence to prescribed pharmacotherapy.
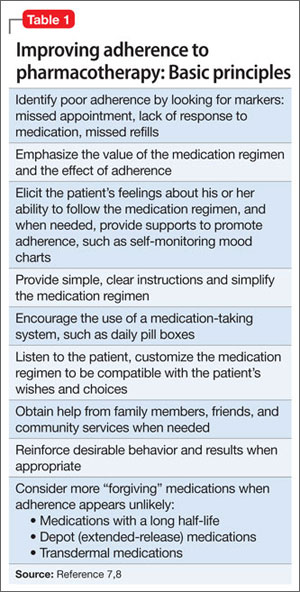
Several strategies have been used to address this vexing problem (Table 1).7,8 They include individual and family psychoeducation,9,10 cognitive-behavioral therapy,11 interpersonal and social rhythm therapy, and family-focused therapy. This article describes an additional strategy I call “participatory pharmacotherapy.” In this model, the patient becomes a partner in the process of treatment choices and decision-making. This encourages patients to provide their own opinions and points of view regarding medication use. The prescribing clinician makes the patient feel that he or she has been listened to and understood. This and other techniques emphasize forming a therapeutic alliance with the patient before initiating pharmacotherapy. The patient provides information on his or her family history, medical and psychiatric history, and experience with previous medications, with a specific focus on which medications worked best for the patient and family members diagnosed with a similar condition.
Getting patients to participate
One of the fundamental tasks is to encourage patients to accept a participatory role, determine their underlying diagnosis, and co-create a treatment plan that will be most compatible with their illness and their personality. There are 10 components of establishing and practicing participatory pharmacotherapy.
1. Encourage patients to share their opinion of what a desirable treatment outcome should be. Some patients have unrealistic expectations about what medications can achieve. Clarify with patients what would be a realistic expectation of pharmacotherapy, and modify the patient’s beliefs to be compatible with a more probable outcome. For example, Ms. D, a 46-year-old mother of 2, is diagnosed with MDD, recurrent type without psychotic features. She states she expects pharmacotherapy will alleviate all symptoms and allow her to achieve a new healthy, happy state in which she will be able to laugh, socialize, and have fun every day for the rest of her life. Although achieving remission is a realistic and desirable treatment goal, Ms. D’s expectations are idealistic. Helping Ms. D accept and agree to realistic and achievable outcomes will improve her adherence to prescribed medications.
2. Encourage patients to share their ideas of how a desirable outcome can be accomplished. Similar to their expectations of outcomes, some patients have an unrealistic understanding of how treatment is conducted. Some patients expect treatment to be limited to prescribed medications or a one-time injection of a curative drug. Others prefer to use herbs and supplements and want to avoid prescribed medications. Understanding the patient’s expectations of how treatment is carried out will allow clinicians to provide patients with a rational view of treatment and establish a partnership based on realistic expectations.
3. Engage patients in choosing the best medication for them. Many patients have preconceived ideas about medications and which medicine would be best for them. They get this information from various sources, including family members and friends who benefitted from a specific drug, personal experience with medications, and exposure to drug advertising.
Understanding the patient’s preference for a specific medication and why he or she made such a choice is critical because doing so can take advantage of the patient’s self-fulfilling prophecies and improve the chances of obtaining a better outcome. For example, Mr. O, a 52-year-old father of 3, has been experiencing recurrent episodes of severe panic attacks. His clinician asked him to describe medications that in his opinion were most helpful in the past. He said he preferred clonazepam because it had helped him control the panic attacks and had minimal side effects, but he discontinued it after a previous psychotherapist told him he would become addicted to it. Obtaining this information was valuable because the clinician was able to clarify guidelines for clonazepam use without the risk of dependence. Mr. O is prescribed clonazepam, which he takes consistently and responds to excellently.
4. Involve patients in setting treatment goals and targeting symptoms to be relieved. Actively listen when patients describe their symptoms, discomforts, and past experiences with treatments. I invite patients to speak uninterrupted for 5 to 10 minutes, even if they talk about issues that seem irrelevant. I then summarize the patient’s major points and ask, “And what else?” After he or she says, “That’s it,” I ask the patient to assign a priority to alleviating each symptom.
For example, Ms. J, a 38-year-old married mother of 2, was diagnosed with bipolar II disorder. She listed her highest priority as controlling her impulsive shopping rather than alleviating depression, insomnia, or overeating. She had been forced to declare bankruptcy twice, and she was determined to never do so again. She also wanted to regain her husband’s trust and her ability to manage her finances. Ensuring that Ms. J felt understood regarding this issue increased the chances of establishing a solid treatment partnership. Providing Ms. J with a menu of treatment choices and asking her to describe her previous experiences with medications helped her and the clinician choose a medication that is compatible with her desire to control her impulsive shopping.
5. Engage patients in choosing the best delivery system for the prescribed medication. For many medications, clinicians can choose from a variety of delivery systems, including pills, transdermal patches, rectal or vaginal suppositories, creams, ointments, orally disintegrating tablets, liquids, and intramuscular injections. Patients have varying beliefs about the efficacy of particular delivery systems, based on personal experiences or what they have learned from the media, their family and friends, or the Internet. For example, Ms. S, age 28, experienced recurrent, disabling anxiety attacks. When asked about the best way of providing medication to relieve her symptoms, she chose gluteal injections because, as a child, her pediatrician had treated her for an unspecified illness by injecting medication in her buttock, which rapidly relieved her symptoms. This left her with the impression that injectable medications were the best therapeutic delivery system. After discussing the practicalities and availability of fast-acting medications to control panic attacks, we agreed to use orally disintegrating clonazepam, which is absorbed swiftly and provides fast symptom relief. Ms. S reported favorable results and was pleased with the process of developing this strategy with her clinician.
6. Involve patients in choosing the times and frequency of medication administration. The timing and frequency of medication administration can be used to enhance desirable therapeutic effects. For example, an antidepressant that causes sedation and somnolence could be taken at bedtime to help alleviate insomnia. Some studies have shown that taking a medication once a day improves adherence compared with taking the same medication in divided doses.13 Other patients may wish to take a medication several times a day so they can keep the medication in their purse or briefcase and feel confident that if they need a medication for immediate symptom relief, it will be readily available.
7. Teach patients to self-monitor changes and improvements in target symptoms. Engaging patients in a system of self-monitoring improves their chances of achieving successful treatment outcomes.14 Instruct patients to create a list of symptoms and monitor the intensity of each symptom using a rating scale of 1 to 5, where 1 represents the lowest intensity and 5 represents the highest. As for frequency, patients can rate each symptom from “not present” to “present most of the time.”
Self-monitoring allows patients to observe which daily behaviors and lifestyle choices make symptoms better and which make them worse. For example, Mrs. P, a 38-year-old married mother of 2, had anxiety and panic attacks associated with low self-esteem and chronic depression. Her clinician instructed her to use a 1-page form to monitor the frequency and intensity of her anxiety and panic symptoms by focusing on the physical manifestations, such as rapid heartbeat, shortness of breath, nausea, tremors, dry mouth, frequent urination, and diarrhea to see if there was any correlation between her behaviors and her symptoms.
8. Instruct patients to call you to report any changes, including minor successes. Early in my career, toward the end of each appointment after I’d prescribed medications I’d tell patients, “Please call me if you have a problem.” Frequently, patients would call with a list of problems and side effects that they believed were caused by the newly prescribed medication. Later, I realized that I may have inadvertently encouraged patients to develop problems so they would have a reason to call me. To achieve a more favorable outcome I changed the way I communicate. I now say, “Please call me next week, even if you begin to feel better with this new medication.” The phone call is now associated with the idea that they will “get better,” and internalizing such a suggestion allows patients to talk with the clinician and report favorable treatment results.
9. Tell patients to monitor their successes by relabeling and reframing their symptoms. Mr. B, age 28, has MDD and reports irritability, insomnia, short temper, and restlessness. After reviewing his desired treatment outcome, we discuss the benefits of pharmacotherapy. I tell him the new medication will improve the quality and length of his sleep, which will allow his body and mind to recharge his “internal batteries” and restore health and energy. When we discuss side effects, I tell him to expect a dry mouth, which will be his signal that the medication is working. This discussion helps patients reframe side effects and improves their ability to tolerate side effects and adhere to pharmacotherapy.
10. Harness the placebo effect and the power of suggestion to increase chances of achieving the best treatment outcomes. In a previous article,12 I reviewed the principles of recognizing and enhancing the placebo effect and the power of suggestion to improve the chances of achieving better pharmacotherapy outcomes. When practicing participatory pharmacotherapy, clinicians are consciously aware of the power embedded in their words and are careful to use language that enhances the placebo effect and the power of suggestion when prescribing medications. Use the patient’s own language as a way of pacing yourself to the patient’s description of his or her distress. For example, Ms. R, a 42-year-old mother of 3, describes her experiences seeking help for her anxiety and depression, stating that she has not yet found the right combination of medications that provide benefits with tolerable side effects. Her clinician responds by focusing on the word “yet” (pacing) stating, “even though you have not yet found the right combination of medications to provide the most desirable benefit of beginning healing and restoring your hope, I promise to work with you and together we will try to achieve an improvement in your overall health and well-being.” This response includes several positive words and suggestions of future success, which are referred to as leading.
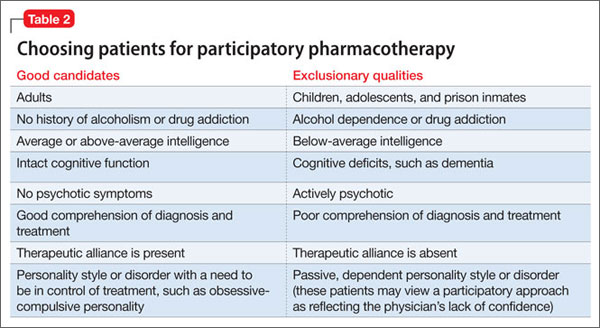
Not all patients will respond to participatory pharmacotherapy. Some factors will make patients good candidates for this approach, and others should be considered exclusionary qualities (Table 2).
Bottom Line
“Participatory pharmacotherapy” involves identifying patients as partners in the process of treatment choice and decision-making, encouraging them to provide their opinions regarding medication use, and making patients feel they have been heard and understood. This technique emphasizes forming a therapeutic alliance with the patient to improve patients’ adherence to pharmacotherapy and optimize treatment outcomes.
Related Resources
- Haynes RB, Ackloo E, Sahota N, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;16(2);CD000011.
- Mahone IH. Shared decision making and serious mental illness. Arch Psychiatr Nurs. 2008;22(6):334-343.
- Russel CL, Ruppar TM, Metteson M. Improving medication adherence: moving from intention and motivation to a personal systems approach. Nurs Clin North Am. 2011;46(3):271-281.
- Tibaldi G, Salvador-Carulla L, Garcia-Gutierrez JC. From treatment adherence to advanced shared decision making: New professional strategies and attitudes in mental health care. Curr Clin Pharmacol. 2011;6(2):91-99.
Drug Brand Name
Clonazepam • Klonopin
Disclosure
Dr. Torem reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Zygmunt A, Olfson M, Boyer CA, et al. Interventions to improve medication adherence in schizophrenia. Am J Psychiatry. 2002;159:1653-1664.
2. Nosé M, Barbui C, Gray R, et al. Clinical interventions for treatment non-adherence in psychosis: meta-analysis. Br J Psychiatry. 2003;183:197-206.
3. Vergouwen AC, van Hout HP, Bakker A. Methods to improve patient compliance in the use of antidepressants. Ned Tijdschr Geneeskd. 2002;146:204-207.
4. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature.
J Clin Psychiatry. 2002;63:892-909.
5. Perkins DO. Predictors of noncompliance in patients with schizophrenia. J Clin Psychiatry. 2002;63:1121-1128.
6. Colom F, Vieta E, Martinez-Aran A, et al. Clinical factors associated with treatment noncompliance in euthymic bipolar patients. J Clin Psychiatry. 2000;61:549-555.
7. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487-497.
8. Osterberg LG, Rudd R. Medication adherence for antihypertensive therapy. In: Oparil S, Weber MA, eds. Hypertension: a companion to Brenner and Rector’s the kidney. 2nd ed. Philadelphia. PA: Elsevier Saunders; 2005:848.
9. Velligan DI, Weiden PJ, Sajatovic M, et al. Strategies for addressing adherence problems in patients with serious and persistent mental illness: recommendations from expert consensus guidelines. J Psychiatr Pract. 2010;16:306-324.
10. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008; 165:1408-1419.
11. Szentagotai A, David D. The efficacy of cognitive-behavioral therapy in bipolar disorder: a quantitative meta-analysis. J Clin Psychiatry. 2010;71:66-72.
12. Torem MS. Words to the wise: 4 secrets of successful pharmacotherapy. Current Psychiatry. 2008;7(12):19-24.
13. Medic G, Higashi K, Littlewood KJ, et al. Dosing frequency and adherence in chronic psychiatric disease: systematic review and meta-analysis. Neuropsychiatr Dis Treat. 2013; 9:119-131.
14. Virdi N, Daskiran M, Nigam S, et al. The association of self-monitoring of blood glucose use with medication adherence and glycemic control in patients with type 2 diabetes initiating non-insulin treatment. Diabetes Technol Ther. 2012;14(9):790-798.
Psychiatric patients stand to benefit greatly from adhering to prescribed pharmacotherapy, but many patients typically do not follow their medication regimens.1,2 Three months after pharmacotherapy is initiated, approximately 50% of patients with major depressive disorder (MDD) do not take their prescribed antidepressants.3 Adherence rates in patients with schizophrenia range from 50% to 60%, and patients with bipolar disorder have adherence rates as low as 35%.4-6 One possible explanation for “treatment-resistant” depression, schizophrenia, and bipolar disorder may simply be nonadherence to prescribed pharmacotherapy.
Several strategies have been used to address this vexing problem (Table 1).7,8 They include individual and family psychoeducation,9,10 cognitive-behavioral therapy,11 interpersonal and social rhythm therapy, and family-focused therapy. This article describes an additional strategy I call “participatory pharmacotherapy.” In this model, the patient becomes a partner in the process of treatment choices and decision-making. This encourages patients to provide their own opinions and points of view regarding medication use. The prescribing clinician makes the patient feel that he or she has been listened to and understood. This and other techniques emphasize forming a therapeutic alliance with the patient before initiating pharmacotherapy. The patient provides information on his or her family history, medical and psychiatric history, and experience with previous medications, with a specific focus on which medications worked best for the patient and family members diagnosed with a similar condition.
Getting patients to participate
One of the fundamental tasks is to encourage patients to accept a participatory role, determine their underlying diagnosis, and co-create a treatment plan that will be most compatible with their illness and their personality. There are 10 components of establishing and practicing participatory pharmacotherapy.
1. Encourage patients to share their opinion of what a desirable treatment outcome should be. Some patients have unrealistic expectations about what medications can achieve. Clarify with patients what would be a realistic expectation of pharmacotherapy, and modify the patient’s beliefs to be compatible with a more probable outcome. For example, Ms. D, a 46-year-old mother of 2, is diagnosed with MDD, recurrent type without psychotic features. She states she expects pharmacotherapy will alleviate all symptoms and allow her to achieve a new healthy, happy state in which she will be able to laugh, socialize, and have fun every day for the rest of her life. Although achieving remission is a realistic and desirable treatment goal, Ms. D’s expectations are idealistic. Helping Ms. D accept and agree to realistic and achievable outcomes will improve her adherence to prescribed medications.
2. Encourage patients to share their ideas of how a desirable outcome can be accomplished. Similar to their expectations of outcomes, some patients have an unrealistic understanding of how treatment is conducted. Some patients expect treatment to be limited to prescribed medications or a one-time injection of a curative drug. Others prefer to use herbs and supplements and want to avoid prescribed medications. Understanding the patient’s expectations of how treatment is carried out will allow clinicians to provide patients with a rational view of treatment and establish a partnership based on realistic expectations.
3. Engage patients in choosing the best medication for them. Many patients have preconceived ideas about medications and which medicine would be best for them. They get this information from various sources, including family members and friends who benefitted from a specific drug, personal experience with medications, and exposure to drug advertising.
Understanding the patient’s preference for a specific medication and why he or she made such a choice is critical because doing so can take advantage of the patient’s self-fulfilling prophecies and improve the chances of obtaining a better outcome. For example, Mr. O, a 52-year-old father of 3, has been experiencing recurrent episodes of severe panic attacks. His clinician asked him to describe medications that in his opinion were most helpful in the past. He said he preferred clonazepam because it had helped him control the panic attacks and had minimal side effects, but he discontinued it after a previous psychotherapist told him he would become addicted to it. Obtaining this information was valuable because the clinician was able to clarify guidelines for clonazepam use without the risk of dependence. Mr. O is prescribed clonazepam, which he takes consistently and responds to excellently.
4. Involve patients in setting treatment goals and targeting symptoms to be relieved. Actively listen when patients describe their symptoms, discomforts, and past experiences with treatments. I invite patients to speak uninterrupted for 5 to 10 minutes, even if they talk about issues that seem irrelevant. I then summarize the patient’s major points and ask, “And what else?” After he or she says, “That’s it,” I ask the patient to assign a priority to alleviating each symptom.
For example, Ms. J, a 38-year-old married mother of 2, was diagnosed with bipolar II disorder. She listed her highest priority as controlling her impulsive shopping rather than alleviating depression, insomnia, or overeating. She had been forced to declare bankruptcy twice, and she was determined to never do so again. She also wanted to regain her husband’s trust and her ability to manage her finances. Ensuring that Ms. J felt understood regarding this issue increased the chances of establishing a solid treatment partnership. Providing Ms. J with a menu of treatment choices and asking her to describe her previous experiences with medications helped her and the clinician choose a medication that is compatible with her desire to control her impulsive shopping.
5. Engage patients in choosing the best delivery system for the prescribed medication. For many medications, clinicians can choose from a variety of delivery systems, including pills, transdermal patches, rectal or vaginal suppositories, creams, ointments, orally disintegrating tablets, liquids, and intramuscular injections. Patients have varying beliefs about the efficacy of particular delivery systems, based on personal experiences or what they have learned from the media, their family and friends, or the Internet. For example, Ms. S, age 28, experienced recurrent, disabling anxiety attacks. When asked about the best way of providing medication to relieve her symptoms, she chose gluteal injections because, as a child, her pediatrician had treated her for an unspecified illness by injecting medication in her buttock, which rapidly relieved her symptoms. This left her with the impression that injectable medications were the best therapeutic delivery system. After discussing the practicalities and availability of fast-acting medications to control panic attacks, we agreed to use orally disintegrating clonazepam, which is absorbed swiftly and provides fast symptom relief. Ms. S reported favorable results and was pleased with the process of developing this strategy with her clinician.
6. Involve patients in choosing the times and frequency of medication administration. The timing and frequency of medication administration can be used to enhance desirable therapeutic effects. For example, an antidepressant that causes sedation and somnolence could be taken at bedtime to help alleviate insomnia. Some studies have shown that taking a medication once a day improves adherence compared with taking the same medication in divided doses.13 Other patients may wish to take a medication several times a day so they can keep the medication in their purse or briefcase and feel confident that if they need a medication for immediate symptom relief, it will be readily available.
7. Teach patients to self-monitor changes and improvements in target symptoms. Engaging patients in a system of self-monitoring improves their chances of achieving successful treatment outcomes.14 Instruct patients to create a list of symptoms and monitor the intensity of each symptom using a rating scale of 1 to 5, where 1 represents the lowest intensity and 5 represents the highest. As for frequency, patients can rate each symptom from “not present” to “present most of the time.”
Self-monitoring allows patients to observe which daily behaviors and lifestyle choices make symptoms better and which make them worse. For example, Mrs. P, a 38-year-old married mother of 2, had anxiety and panic attacks associated with low self-esteem and chronic depression. Her clinician instructed her to use a 1-page form to monitor the frequency and intensity of her anxiety and panic symptoms by focusing on the physical manifestations, such as rapid heartbeat, shortness of breath, nausea, tremors, dry mouth, frequent urination, and diarrhea to see if there was any correlation between her behaviors and her symptoms.
8. Instruct patients to call you to report any changes, including minor successes. Early in my career, toward the end of each appointment after I’d prescribed medications I’d tell patients, “Please call me if you have a problem.” Frequently, patients would call with a list of problems and side effects that they believed were caused by the newly prescribed medication. Later, I realized that I may have inadvertently encouraged patients to develop problems so they would have a reason to call me. To achieve a more favorable outcome I changed the way I communicate. I now say, “Please call me next week, even if you begin to feel better with this new medication.” The phone call is now associated with the idea that they will “get better,” and internalizing such a suggestion allows patients to talk with the clinician and report favorable treatment results.
9. Tell patients to monitor their successes by relabeling and reframing their symptoms. Mr. B, age 28, has MDD and reports irritability, insomnia, short temper, and restlessness. After reviewing his desired treatment outcome, we discuss the benefits of pharmacotherapy. I tell him the new medication will improve the quality and length of his sleep, which will allow his body and mind to recharge his “internal batteries” and restore health and energy. When we discuss side effects, I tell him to expect a dry mouth, which will be his signal that the medication is working. This discussion helps patients reframe side effects and improves their ability to tolerate side effects and adhere to pharmacotherapy.
10. Harness the placebo effect and the power of suggestion to increase chances of achieving the best treatment outcomes. In a previous article,12 I reviewed the principles of recognizing and enhancing the placebo effect and the power of suggestion to improve the chances of achieving better pharmacotherapy outcomes. When practicing participatory pharmacotherapy, clinicians are consciously aware of the power embedded in their words and are careful to use language that enhances the placebo effect and the power of suggestion when prescribing medications. Use the patient’s own language as a way of pacing yourself to the patient’s description of his or her distress. For example, Ms. R, a 42-year-old mother of 3, describes her experiences seeking help for her anxiety and depression, stating that she has not yet found the right combination of medications that provide benefits with tolerable side effects. Her clinician responds by focusing on the word “yet” (pacing) stating, “even though you have not yet found the right combination of medications to provide the most desirable benefit of beginning healing and restoring your hope, I promise to work with you and together we will try to achieve an improvement in your overall health and well-being.” This response includes several positive words and suggestions of future success, which are referred to as leading.
Not all patients will respond to participatory pharmacotherapy. Some factors will make patients good candidates for this approach, and others should be considered exclusionary qualities (Table 2).
Bottom Line
“Participatory pharmacotherapy” involves identifying patients as partners in the process of treatment choice and decision-making, encouraging them to provide their opinions regarding medication use, and making patients feel they have been heard and understood. This technique emphasizes forming a therapeutic alliance with the patient to improve patients’ adherence to pharmacotherapy and optimize treatment outcomes.
Related Resources
- Haynes RB, Ackloo E, Sahota N, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;16(2);CD000011.
- Mahone IH. Shared decision making and serious mental illness. Arch Psychiatr Nurs. 2008;22(6):334-343.
- Russel CL, Ruppar TM, Metteson M. Improving medication adherence: moving from intention and motivation to a personal systems approach. Nurs Clin North Am. 2011;46(3):271-281.
- Tibaldi G, Salvador-Carulla L, Garcia-Gutierrez JC. From treatment adherence to advanced shared decision making: New professional strategies and attitudes in mental health care. Curr Clin Pharmacol. 2011;6(2):91-99.
Drug Brand Name
Clonazepam • Klonopin
Disclosure
Dr. Torem reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Psychiatric patients stand to benefit greatly from adhering to prescribed pharmacotherapy, but many patients typically do not follow their medication regimens.1,2 Three months after pharmacotherapy is initiated, approximately 50% of patients with major depressive disorder (MDD) do not take their prescribed antidepressants.3 Adherence rates in patients with schizophrenia range from 50% to 60%, and patients with bipolar disorder have adherence rates as low as 35%.4-6 One possible explanation for “treatment-resistant” depression, schizophrenia, and bipolar disorder may simply be nonadherence to prescribed pharmacotherapy.
Several strategies have been used to address this vexing problem (Table 1).7,8 They include individual and family psychoeducation,9,10 cognitive-behavioral therapy,11 interpersonal and social rhythm therapy, and family-focused therapy. This article describes an additional strategy I call “participatory pharmacotherapy.” In this model, the patient becomes a partner in the process of treatment choices and decision-making. This encourages patients to provide their own opinions and points of view regarding medication use. The prescribing clinician makes the patient feel that he or she has been listened to and understood. This and other techniques emphasize forming a therapeutic alliance with the patient before initiating pharmacotherapy. The patient provides information on his or her family history, medical and psychiatric history, and experience with previous medications, with a specific focus on which medications worked best for the patient and family members diagnosed with a similar condition.
Getting patients to participate
One of the fundamental tasks is to encourage patients to accept a participatory role, determine their underlying diagnosis, and co-create a treatment plan that will be most compatible with their illness and their personality. There are 10 components of establishing and practicing participatory pharmacotherapy.
1. Encourage patients to share their opinion of what a desirable treatment outcome should be. Some patients have unrealistic expectations about what medications can achieve. Clarify with patients what would be a realistic expectation of pharmacotherapy, and modify the patient’s beliefs to be compatible with a more probable outcome. For example, Ms. D, a 46-year-old mother of 2, is diagnosed with MDD, recurrent type without psychotic features. She states she expects pharmacotherapy will alleviate all symptoms and allow her to achieve a new healthy, happy state in which she will be able to laugh, socialize, and have fun every day for the rest of her life. Although achieving remission is a realistic and desirable treatment goal, Ms. D’s expectations are idealistic. Helping Ms. D accept and agree to realistic and achievable outcomes will improve her adherence to prescribed medications.
2. Encourage patients to share their ideas of how a desirable outcome can be accomplished. Similar to their expectations of outcomes, some patients have an unrealistic understanding of how treatment is conducted. Some patients expect treatment to be limited to prescribed medications or a one-time injection of a curative drug. Others prefer to use herbs and supplements and want to avoid prescribed medications. Understanding the patient’s expectations of how treatment is carried out will allow clinicians to provide patients with a rational view of treatment and establish a partnership based on realistic expectations.
3. Engage patients in choosing the best medication for them. Many patients have preconceived ideas about medications and which medicine would be best for them. They get this information from various sources, including family members and friends who benefitted from a specific drug, personal experience with medications, and exposure to drug advertising.
Understanding the patient’s preference for a specific medication and why he or she made such a choice is critical because doing so can take advantage of the patient’s self-fulfilling prophecies and improve the chances of obtaining a better outcome. For example, Mr. O, a 52-year-old father of 3, has been experiencing recurrent episodes of severe panic attacks. His clinician asked him to describe medications that in his opinion were most helpful in the past. He said he preferred clonazepam because it had helped him control the panic attacks and had minimal side effects, but he discontinued it after a previous psychotherapist told him he would become addicted to it. Obtaining this information was valuable because the clinician was able to clarify guidelines for clonazepam use without the risk of dependence. Mr. O is prescribed clonazepam, which he takes consistently and responds to excellently.
4. Involve patients in setting treatment goals and targeting symptoms to be relieved. Actively listen when patients describe their symptoms, discomforts, and past experiences with treatments. I invite patients to speak uninterrupted for 5 to 10 minutes, even if they talk about issues that seem irrelevant. I then summarize the patient’s major points and ask, “And what else?” After he or she says, “That’s it,” I ask the patient to assign a priority to alleviating each symptom.
For example, Ms. J, a 38-year-old married mother of 2, was diagnosed with bipolar II disorder. She listed her highest priority as controlling her impulsive shopping rather than alleviating depression, insomnia, or overeating. She had been forced to declare bankruptcy twice, and she was determined to never do so again. She also wanted to regain her husband’s trust and her ability to manage her finances. Ensuring that Ms. J felt understood regarding this issue increased the chances of establishing a solid treatment partnership. Providing Ms. J with a menu of treatment choices and asking her to describe her previous experiences with medications helped her and the clinician choose a medication that is compatible with her desire to control her impulsive shopping.
5. Engage patients in choosing the best delivery system for the prescribed medication. For many medications, clinicians can choose from a variety of delivery systems, including pills, transdermal patches, rectal or vaginal suppositories, creams, ointments, orally disintegrating tablets, liquids, and intramuscular injections. Patients have varying beliefs about the efficacy of particular delivery systems, based on personal experiences or what they have learned from the media, their family and friends, or the Internet. For example, Ms. S, age 28, experienced recurrent, disabling anxiety attacks. When asked about the best way of providing medication to relieve her symptoms, she chose gluteal injections because, as a child, her pediatrician had treated her for an unspecified illness by injecting medication in her buttock, which rapidly relieved her symptoms. This left her with the impression that injectable medications were the best therapeutic delivery system. After discussing the practicalities and availability of fast-acting medications to control panic attacks, we agreed to use orally disintegrating clonazepam, which is absorbed swiftly and provides fast symptom relief. Ms. S reported favorable results and was pleased with the process of developing this strategy with her clinician.
6. Involve patients in choosing the times and frequency of medication administration. The timing and frequency of medication administration can be used to enhance desirable therapeutic effects. For example, an antidepressant that causes sedation and somnolence could be taken at bedtime to help alleviate insomnia. Some studies have shown that taking a medication once a day improves adherence compared with taking the same medication in divided doses.13 Other patients may wish to take a medication several times a day so they can keep the medication in their purse or briefcase and feel confident that if they need a medication for immediate symptom relief, it will be readily available.
7. Teach patients to self-monitor changes and improvements in target symptoms. Engaging patients in a system of self-monitoring improves their chances of achieving successful treatment outcomes.14 Instruct patients to create a list of symptoms and monitor the intensity of each symptom using a rating scale of 1 to 5, where 1 represents the lowest intensity and 5 represents the highest. As for frequency, patients can rate each symptom from “not present” to “present most of the time.”
Self-monitoring allows patients to observe which daily behaviors and lifestyle choices make symptoms better and which make them worse. For example, Mrs. P, a 38-year-old married mother of 2, had anxiety and panic attacks associated with low self-esteem and chronic depression. Her clinician instructed her to use a 1-page form to monitor the frequency and intensity of her anxiety and panic symptoms by focusing on the physical manifestations, such as rapid heartbeat, shortness of breath, nausea, tremors, dry mouth, frequent urination, and diarrhea to see if there was any correlation between her behaviors and her symptoms.
8. Instruct patients to call you to report any changes, including minor successes. Early in my career, toward the end of each appointment after I’d prescribed medications I’d tell patients, “Please call me if you have a problem.” Frequently, patients would call with a list of problems and side effects that they believed were caused by the newly prescribed medication. Later, I realized that I may have inadvertently encouraged patients to develop problems so they would have a reason to call me. To achieve a more favorable outcome I changed the way I communicate. I now say, “Please call me next week, even if you begin to feel better with this new medication.” The phone call is now associated with the idea that they will “get better,” and internalizing such a suggestion allows patients to talk with the clinician and report favorable treatment results.
9. Tell patients to monitor their successes by relabeling and reframing their symptoms. Mr. B, age 28, has MDD and reports irritability, insomnia, short temper, and restlessness. After reviewing his desired treatment outcome, we discuss the benefits of pharmacotherapy. I tell him the new medication will improve the quality and length of his sleep, which will allow his body and mind to recharge his “internal batteries” and restore health and energy. When we discuss side effects, I tell him to expect a dry mouth, which will be his signal that the medication is working. This discussion helps patients reframe side effects and improves their ability to tolerate side effects and adhere to pharmacotherapy.
10. Harness the placebo effect and the power of suggestion to increase chances of achieving the best treatment outcomes. In a previous article,12 I reviewed the principles of recognizing and enhancing the placebo effect and the power of suggestion to improve the chances of achieving better pharmacotherapy outcomes. When practicing participatory pharmacotherapy, clinicians are consciously aware of the power embedded in their words and are careful to use language that enhances the placebo effect and the power of suggestion when prescribing medications. Use the patient’s own language as a way of pacing yourself to the patient’s description of his or her distress. For example, Ms. R, a 42-year-old mother of 3, describes her experiences seeking help for her anxiety and depression, stating that she has not yet found the right combination of medications that provide benefits with tolerable side effects. Her clinician responds by focusing on the word “yet” (pacing) stating, “even though you have not yet found the right combination of medications to provide the most desirable benefit of beginning healing and restoring your hope, I promise to work with you and together we will try to achieve an improvement in your overall health and well-being.” This response includes several positive words and suggestions of future success, which are referred to as leading.
Not all patients will respond to participatory pharmacotherapy. Some factors will make patients good candidates for this approach, and others should be considered exclusionary qualities (Table 2).
Bottom Line
“Participatory pharmacotherapy” involves identifying patients as partners in the process of treatment choice and decision-making, encouraging them to provide their opinions regarding medication use, and making patients feel they have been heard and understood. This technique emphasizes forming a therapeutic alliance with the patient to improve patients’ adherence to pharmacotherapy and optimize treatment outcomes.
Related Resources
- Haynes RB, Ackloo E, Sahota N, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;16(2);CD000011.
- Mahone IH. Shared decision making and serious mental illness. Arch Psychiatr Nurs. 2008;22(6):334-343.
- Russel CL, Ruppar TM, Metteson M. Improving medication adherence: moving from intention and motivation to a personal systems approach. Nurs Clin North Am. 2011;46(3):271-281.
- Tibaldi G, Salvador-Carulla L, Garcia-Gutierrez JC. From treatment adherence to advanced shared decision making: New professional strategies and attitudes in mental health care. Curr Clin Pharmacol. 2011;6(2):91-99.
Drug Brand Name
Clonazepam • Klonopin
Disclosure
Dr. Torem reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Zygmunt A, Olfson M, Boyer CA, et al. Interventions to improve medication adherence in schizophrenia. Am J Psychiatry. 2002;159:1653-1664.
2. Nosé M, Barbui C, Gray R, et al. Clinical interventions for treatment non-adherence in psychosis: meta-analysis. Br J Psychiatry. 2003;183:197-206.
3. Vergouwen AC, van Hout HP, Bakker A. Methods to improve patient compliance in the use of antidepressants. Ned Tijdschr Geneeskd. 2002;146:204-207.
4. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature.
J Clin Psychiatry. 2002;63:892-909.
5. Perkins DO. Predictors of noncompliance in patients with schizophrenia. J Clin Psychiatry. 2002;63:1121-1128.
6. Colom F, Vieta E, Martinez-Aran A, et al. Clinical factors associated with treatment noncompliance in euthymic bipolar patients. J Clin Psychiatry. 2000;61:549-555.
7. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487-497.
8. Osterberg LG, Rudd R. Medication adherence for antihypertensive therapy. In: Oparil S, Weber MA, eds. Hypertension: a companion to Brenner and Rector’s the kidney. 2nd ed. Philadelphia. PA: Elsevier Saunders; 2005:848.
9. Velligan DI, Weiden PJ, Sajatovic M, et al. Strategies for addressing adherence problems in patients with serious and persistent mental illness: recommendations from expert consensus guidelines. J Psychiatr Pract. 2010;16:306-324.
10. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008; 165:1408-1419.
11. Szentagotai A, David D. The efficacy of cognitive-behavioral therapy in bipolar disorder: a quantitative meta-analysis. J Clin Psychiatry. 2010;71:66-72.
12. Torem MS. Words to the wise: 4 secrets of successful pharmacotherapy. Current Psychiatry. 2008;7(12):19-24.
13. Medic G, Higashi K, Littlewood KJ, et al. Dosing frequency and adherence in chronic psychiatric disease: systematic review and meta-analysis. Neuropsychiatr Dis Treat. 2013; 9:119-131.
14. Virdi N, Daskiran M, Nigam S, et al. The association of self-monitoring of blood glucose use with medication adherence and glycemic control in patients with type 2 diabetes initiating non-insulin treatment. Diabetes Technol Ther. 2012;14(9):790-798.
1. Zygmunt A, Olfson M, Boyer CA, et al. Interventions to improve medication adherence in schizophrenia. Am J Psychiatry. 2002;159:1653-1664.
2. Nosé M, Barbui C, Gray R, et al. Clinical interventions for treatment non-adherence in psychosis: meta-analysis. Br J Psychiatry. 2003;183:197-206.
3. Vergouwen AC, van Hout HP, Bakker A. Methods to improve patient compliance in the use of antidepressants. Ned Tijdschr Geneeskd. 2002;146:204-207.
4. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature.
J Clin Psychiatry. 2002;63:892-909.
5. Perkins DO. Predictors of noncompliance in patients with schizophrenia. J Clin Psychiatry. 2002;63:1121-1128.
6. Colom F, Vieta E, Martinez-Aran A, et al. Clinical factors associated with treatment noncompliance in euthymic bipolar patients. J Clin Psychiatry. 2000;61:549-555.
7. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487-497.
8. Osterberg LG, Rudd R. Medication adherence for antihypertensive therapy. In: Oparil S, Weber MA, eds. Hypertension: a companion to Brenner and Rector’s the kidney. 2nd ed. Philadelphia. PA: Elsevier Saunders; 2005:848.
9. Velligan DI, Weiden PJ, Sajatovic M, et al. Strategies for addressing adherence problems in patients with serious and persistent mental illness: recommendations from expert consensus guidelines. J Psychiatr Pract. 2010;16:306-324.
10. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008; 165:1408-1419.
11. Szentagotai A, David D. The efficacy of cognitive-behavioral therapy in bipolar disorder: a quantitative meta-analysis. J Clin Psychiatry. 2010;71:66-72.
12. Torem MS. Words to the wise: 4 secrets of successful pharmacotherapy. Current Psychiatry. 2008;7(12):19-24.
13. Medic G, Higashi K, Littlewood KJ, et al. Dosing frequency and adherence in chronic psychiatric disease: systematic review and meta-analysis. Neuropsychiatr Dis Treat. 2013; 9:119-131.
14. Virdi N, Daskiran M, Nigam S, et al. The association of self-monitoring of blood glucose use with medication adherence and glycemic control in patients with type 2 diabetes initiating non-insulin treatment. Diabetes Technol Ther. 2012;14(9):790-798.

Neuropsychiatric impairment in a septic shock survivor
The effect of sepsis survivorship on cognition is a substantially under-recognized public health problem.1 Sepsis survivorship has implications for patients’ families and the health care system.2 Research has demonstrated that older patients may develop impaired cognition and functional capacity after severe sepsis3; limited evidence shows neurocognitive decline in non-geriatric patients.3 There are no reports of exacerbation of psychiatric illness after severe sepsis or septic shock, and existing literature indicates that the causative factors, epidemiology, and predisposition that may worsen psychiatric illness after septic shock are poorly defined.
Case: Sepsis-induced cognitive decline?
Following an intensive care admission for septic shock, Mr. J, age 49, presents to the outpatient behavioral medicine department with worsening mood, lethargy, agitation, suicidal ideations, hallucinations, and poor work performance for 10 months. He was diagnosed with major depressive disorder 13 years prior, but has no history of hospitalization for psychiatric illness. His depressive symptoms respond well to paroxetine, 60 mg/d. Subsequently, Mr. J becomes delusional, has intense command hallucinations, and attempts suicide, resulting in hospitalization. Neuropsychological testing reveals dementia and significant psychiatric distress, including elevated levels of depression and suicidal ideation. He is stabilized with duloxetine, 90 mg/d, and quetiapine, 50 mg/d. Two years later, Mr. J still exhibits cognitive and psychiatric disturbances.
Long-term results
The underlying mechanism of septic shock on the brain may be similar to the mechanisms that exacerbate psychiatric illnesses. This case validates the use of neuropsychological testing in septic shock survivors and encourages recognition of the effect septic shock has on neuropsychiatric illness.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers
of competing products.
References
1. Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794.
2. Safdieh J. Cognition after sepsis. Neurology Alert. 2010; 29(4):30-31.
3. Williams GS. Older severe sepsis survivors are at risk for cognitive and developmental disability. Pulmonary Reviews. 2010;15(12):17-18.
The effect of sepsis survivorship on cognition is a substantially under-recognized public health problem.1 Sepsis survivorship has implications for patients’ families and the health care system.2 Research has demonstrated that older patients may develop impaired cognition and functional capacity after severe sepsis3; limited evidence shows neurocognitive decline in non-geriatric patients.3 There are no reports of exacerbation of psychiatric illness after severe sepsis or septic shock, and existing literature indicates that the causative factors, epidemiology, and predisposition that may worsen psychiatric illness after septic shock are poorly defined.
Case: Sepsis-induced cognitive decline?
Following an intensive care admission for septic shock, Mr. J, age 49, presents to the outpatient behavioral medicine department with worsening mood, lethargy, agitation, suicidal ideations, hallucinations, and poor work performance for 10 months. He was diagnosed with major depressive disorder 13 years prior, but has no history of hospitalization for psychiatric illness. His depressive symptoms respond well to paroxetine, 60 mg/d. Subsequently, Mr. J becomes delusional, has intense command hallucinations, and attempts suicide, resulting in hospitalization. Neuropsychological testing reveals dementia and significant psychiatric distress, including elevated levels of depression and suicidal ideation. He is stabilized with duloxetine, 90 mg/d, and quetiapine, 50 mg/d. Two years later, Mr. J still exhibits cognitive and psychiatric disturbances.
Long-term results
The underlying mechanism of septic shock on the brain may be similar to the mechanisms that exacerbate psychiatric illnesses. This case validates the use of neuropsychological testing in septic shock survivors and encourages recognition of the effect septic shock has on neuropsychiatric illness.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers
of competing products.
References
1. Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794.
2. Safdieh J. Cognition after sepsis. Neurology Alert. 2010; 29(4):30-31.
3. Williams GS. Older severe sepsis survivors are at risk for cognitive and developmental disability. Pulmonary Reviews. 2010;15(12):17-18.
The effect of sepsis survivorship on cognition is a substantially under-recognized public health problem.1 Sepsis survivorship has implications for patients’ families and the health care system.2 Research has demonstrated that older patients may develop impaired cognition and functional capacity after severe sepsis3; limited evidence shows neurocognitive decline in non-geriatric patients.3 There are no reports of exacerbation of psychiatric illness after severe sepsis or septic shock, and existing literature indicates that the causative factors, epidemiology, and predisposition that may worsen psychiatric illness after septic shock are poorly defined.
Case: Sepsis-induced cognitive decline?
Following an intensive care admission for septic shock, Mr. J, age 49, presents to the outpatient behavioral medicine department with worsening mood, lethargy, agitation, suicidal ideations, hallucinations, and poor work performance for 10 months. He was diagnosed with major depressive disorder 13 years prior, but has no history of hospitalization for psychiatric illness. His depressive symptoms respond well to paroxetine, 60 mg/d. Subsequently, Mr. J becomes delusional, has intense command hallucinations, and attempts suicide, resulting in hospitalization. Neuropsychological testing reveals dementia and significant psychiatric distress, including elevated levels of depression and suicidal ideation. He is stabilized with duloxetine, 90 mg/d, and quetiapine, 50 mg/d. Two years later, Mr. J still exhibits cognitive and psychiatric disturbances.
Long-term results
The underlying mechanism of septic shock on the brain may be similar to the mechanisms that exacerbate psychiatric illnesses. This case validates the use of neuropsychological testing in septic shock survivors and encourages recognition of the effect septic shock has on neuropsychiatric illness.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers
of competing products.
References
1. Iwashyna TJ, Ely EW, Smith DM, et al. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304(16):1787-1794.
2. Safdieh J. Cognition after sepsis. Neurology Alert. 2010; 29(4):30-31.
3. Williams GS. Older severe sepsis survivors are at risk for cognitive and developmental disability. Pulmonary Reviews. 2010;15(12):17-18.
The Affordable Care Act and the drive for electronic health records: Are small practices being squeezed?
Two years ago, I zeroed in on the pressures straining small ObGyn practices in an article entitled, “Is private ObGyn practice on its way out?”1 The pressures haven’t eased in the interim. Today, small practices are still feeling squeezed to keep up with the many demands of modern specialty care. The push for electronic health records (EHRs), in particular, can profoundly affect physicians in private practice.
In this article, I outline some of the challenges facing small practices when they set out to implement EHRs, as well as the potential benefits they stand to gain a little farther down the road. Before we begin, however, let’s look at the latest trends in ObGyn practice, as they are related, in part, to the need to implement EHRs.
The exodus from private practice continues
A 2012 Accenture Physicians Alignment Survey shows an accelerating increase in physician employment. In 2000, 57% of all physicians were in independent practice; by the end of 2013, only 36% of physicians are projected to remain independent.2
The ObGyn specialty is a clear part of this trend, with both seasoned and incoming physicians finding hospital or other employment an attractive alternative to private practice. Fully one-third of ObGyn residents entering practice today sign hospital employment contracts. ObGyns who have made the switch from private to hospital practice, or who have become ObGyn hospitalists, often point to the difficulties of maintaining a solvent private practice, especially given the push toward EHRs and increasing regulatory and administrative burdens, as justification for their move.
The main reasons for the shift to employment. Top concerns influencing physicians’ decisions to opt for employment include:
- business expenses (87%)
- the dominance of managed care (61%)
- the requirement for EHRs (53%)
- the need to maintain and manage staff (53%)
- the increasing number of patients needed to break even (39%).2
A 2008 socioeconomic survey from ACOG revealed that 23.6% of ObGyn practices are solo practices, and 27.1% are single-specialty group practices. Many ObGyns—especially those in solo or small practices—are hesitant to make the large capital investment that is necessary to adopt EHRs.
EHRs offer benefits—and real costs
The system-wide benefits of health information technology (HIT), including EHRs, are many. Insurers stand to save money by reducing unnecessary tests, and patients will benefit from better coordination of their care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices. Instead, physicians face payment cuts from Medicare and private insurance.
Although there’s wide agreement that HIT can improve quality of care and reduce health-care costs, fewer than one-quarter (22%) of office-based physicians had adopted EHRs by 2009. We know the main reasons why:
- upfront cost and maintenance expense
- uncertain return on investment
- fragmented business model in a high proportion of small and solo practices
- changing and inconsistent information technology (IT) systems.
What can a practice expect to fork over?
In 2011, the Agency for Healthcare Research and Quality (AHRQ) found that the “real-life” cost of implementing EHRs “in an average five-physician primary care practice, operating within a large physician network committed to network-wide implementation of electronic health records, is about $162,000, with an additional $85,500 in maintenance expenses during the first year.”3
These figures include an average of 134 hours needed per physician to prepare to use EHRs during patient visits.3
Fleming and colleagues investigated the cost associated with implementing EHRs within 26 primary care practices in Texas. They found the cost to be $32,409 per physician through the first 60 days after the EHR system was launched, with one-time costs for hardware of $25,000 per practice and an additional $7,000 per physician for personal computers, printers, and scanners. The annual cost of software and maintenance was approximately $17,100 per physician.4
Why physicians should hold out for the return on their investment
Despite these considerable expenses, EHRs hold promise over the long term. The Medical Group Management Association reported, through a 2009 survey of about 1,300 primary care and specialty practice members using EHRs, that efficiency gains from the elimination of paper charts, as well as transcription savings, better charge capturing, and reduced billing errors, resulted in a median revenue increase of $49,916 per full-time physician after operating costs.
After 5 years of EHR use, practices reported a median operating margin 10.1% higher than that of practices in the first year of EHR use.5
Trends in the adoption of EHRs
Private practice. An article in Health Affairs showed that, by 2011, only one in six office-based physicians was using an EHR system robust enough to approach “meaningful use”—that is, the use of EHRs to measurably improve the quality of health care.6 These robust systems offered physicians the ability to record information on patient demographics, view laboratory and imaging results, maintain patients’ problem lists, compile clinical notes, and manage prescription ordering. EHR adoption lagged among non−primary care physicians, physicians aged 55 and older, and physicians in small (1–2 providers) practices and physician-owned practices.6 (ObGyns were considered primary care providers in this survey.)
“Big” practice. By comparison, in 2011, 99% of physicians in health maintenance organizations, or HMOs, and 73% in academic health centers and other hospitals used EHR systems.6 The number of physicians in these practice settings is small but growing.
In 2011, only 17% of physicians were in large practices of 10 or more physicians; 40% were in practices of one or two physicians.6
Primary care. These practices lead others in the adoption of EHRs, in part because of federal assistance, including a nationwide system of regional HIT assistance centers established by the Health Information Technology for Economic and Clinical Health (HITECH) Act to help providers located in rural areas participate in the Centers for Medicare and Medicaid Services (CMS) programs in EHR. The goal of these programs is to provide HIT support to at least 100,000 primary care providers, including ObGyns, by 2014.
The numbers cited in the Health Affairs article largely mirror data developed by other research organizations, including the Deloitte Center for Health Solutions.6
The EHR incentive
The drive for EHRs started long before the Affordable Care Act (ACA) was passed in 2010. The US Congress took a first stab at encouraging the health-care community to embrace HIT in 1996, when it passed the Health Insurance Portability and Accountability Act (HIPAA). HIPAA created an electronic data interchange that health plans, health-care clearinghouses, and certain health-care providers, including pharmacists, are required to use for electronic transactions, including:
- claims and encounter information
- payment and remittance advice
- claims status
- eligibility
- enrollment and disenrollment
- referrals and authorizations
- coordination of benefits
- premium payment.
Congress stepped up its game in 2009, when it offered higher Medicare and Medicaid payments to physicians who adopt and “meaningfully use” EHRs. The HITECH Act included $30 billion in new Medicare and Medicaid incentive payments—as much as $44,000 under Medicare and $63,750 under Medicaid—as well as $500 million for states to develop health information exchanges.
The Act also established a government-led process for certification of electronic health records through a $35 billion appropriation for the Office of the National Coordinator for Health IT, housed in CMS.
Other programs designed to encourage use of EHRs
Other federal programs include the Physician Quality Reporting System (PQRS), which, when created in 2006, was a voluntary physician electronic reporting program. Under the ACA, however, it has become a mandate. Starting in 2015, Medicare payments will be reduced for nonparticipating physicians.
The Electronic Prescribing (eRx) Incentive Program, created in 2008 under the Medicare Improvements for Patients and Providers Act, provides incentives for eligible physicians who e-prescribe Medicare Part D medications through a qualified system. This program converted to a penalty program last year for physicians who don’t use eRx.
Grants were also provided under the HITECH Act to fund an HIT infrastructure and low-interest HIT loans. The AHRQ has awarded $300 million in federal grant money to more than 200 projects in 48 states to promote access to and encourage HIT adoption. Over $150 million in Medicaid transformation grants have been awarded to three states and territories for HIT in the Medicaid program under the 2005 Deficit Reduction Act.
The ACA carried these initiatives even further by establishing uniform standards that HIT systems must meet, including:
- automatic reconciliation of electronic fund transfers and HIPAA payment and remittance
- improved claims payment process
- consistent methods of health plan enrollment and claim edits
- simplified and improved routing of health-care transactions
- electronic claims attachments.
Clearly, a lot of effort and taxpayer dollars have been dedicated to drive efficient use of HIT and EHRs in the hopes that they can:
- help make sense of our increasingly fragmented health-care system
- improve patient safety
- increase efficiency
- reduce paperwork
- reduce unnecessary tests
- better coordinate patient care.
To see which providers are cashing in on the government’s incentives for EHRs, see “Some physicians are more likely to seek incentives for meaningful use of EHRs” on page 37.
The long view
HIT and EHRs are here to stay. Products are maturing and improving. Acceptance by large and small practices has gained traction. Are small practices being squeezed? No doubt.
In 2011, I urged all ObGyns—especially those in private practice—to read an article written by President Barack Obama’s health-reform deputies on how physicians can be successful under the ACA.1 It reads, in part:
To realize the full benefits of the Affordable Care Act, physicians will need to embrace rather than resist change. The economic forces put in motion by the Act are likely to lead to vertical organization of providers and accelerate physician employment by hospitals and aggregation into larger physician groups. The most successful physicians will be those who most effectively collaborate with other providers to improve outcomes, care productivity, and patient experience.7
1. DiVenere L, Yates J. Is private ObGyn practice on its way out? OBG Manage. 2011;23(10):42–54.
2. More US doctors leaving private practice due to rising costs and technology mandates, Accenture report finds [news release]. Arlington, Virginia: Accenture Newsroom; October 31, 2012. http://newsroom.accenture.com/news/more-us-doctors-leaving-private-practice-due-to-rising-costs-and-technology-mandates-accenture-report-finds.htm. Accessed June 5, 2013.
3. Study identifies costs of implementing electronic health records in network of physician practices: Research Activities October 2011, No. 374. Rockville, MD: Agency for Healthcare Research and Quality. http://www.ahrq.gov/news/newsletters/research-activities/oct11/1011RA15.html. Accessed June 5, 2013.
5. MGMA survey: Medical groups with EHRs report better financial performance than practices with paper medical records [news release]. New Orleans, Louisiana: Medical Group Management Association; October 25, 2010. http://www.mgma.com/press/default.aspx?id=39824. Accessed June 6, 2013.
8. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicaid Incentive Payments for 2011. GAO-13-146R. December 13, 2012. http://www.gao.gov/products/GAO-13-146R. Accessed June 6, 2013.
9. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicare Incentive Payments for 2011. GAO-12-778R. July 26, 2012. http://www.gao.gov/products/GAO-12-778R. Accessed June 6, 2013.
10. US Department of Health and Human Services. Doctors’ and hospitals’ use of health IT more than doubles since 2012 [news release]. Washington, DC: HHS.gov; May 22, 2013. http://www.hhs.gov/news/press/2013pres/05/20130522a.html. Accessed June 6, 2013.

Two years ago, I zeroed in on the pressures straining small ObGyn practices in an article entitled, “Is private ObGyn practice on its way out?”1 The pressures haven’t eased in the interim. Today, small practices are still feeling squeezed to keep up with the many demands of modern specialty care. The push for electronic health records (EHRs), in particular, can profoundly affect physicians in private practice.
In this article, I outline some of the challenges facing small practices when they set out to implement EHRs, as well as the potential benefits they stand to gain a little farther down the road. Before we begin, however, let’s look at the latest trends in ObGyn practice, as they are related, in part, to the need to implement EHRs.
The exodus from private practice continues
A 2012 Accenture Physicians Alignment Survey shows an accelerating increase in physician employment. In 2000, 57% of all physicians were in independent practice; by the end of 2013, only 36% of physicians are projected to remain independent.2
The ObGyn specialty is a clear part of this trend, with both seasoned and incoming physicians finding hospital or other employment an attractive alternative to private practice. Fully one-third of ObGyn residents entering practice today sign hospital employment contracts. ObGyns who have made the switch from private to hospital practice, or who have become ObGyn hospitalists, often point to the difficulties of maintaining a solvent private practice, especially given the push toward EHRs and increasing regulatory and administrative burdens, as justification for their move.
The main reasons for the shift to employment. Top concerns influencing physicians’ decisions to opt for employment include:
- business expenses (87%)
- the dominance of managed care (61%)
- the requirement for EHRs (53%)
- the need to maintain and manage staff (53%)
- the increasing number of patients needed to break even (39%).2
A 2008 socioeconomic survey from ACOG revealed that 23.6% of ObGyn practices are solo practices, and 27.1% are single-specialty group practices. Many ObGyns—especially those in solo or small practices—are hesitant to make the large capital investment that is necessary to adopt EHRs.
EHRs offer benefits—and real costs
The system-wide benefits of health information technology (HIT), including EHRs, are many. Insurers stand to save money by reducing unnecessary tests, and patients will benefit from better coordination of their care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices. Instead, physicians face payment cuts from Medicare and private insurance.
Although there’s wide agreement that HIT can improve quality of care and reduce health-care costs, fewer than one-quarter (22%) of office-based physicians had adopted EHRs by 2009. We know the main reasons why:
- upfront cost and maintenance expense
- uncertain return on investment
- fragmented business model in a high proportion of small and solo practices
- changing and inconsistent information technology (IT) systems.
What can a practice expect to fork over?
In 2011, the Agency for Healthcare Research and Quality (AHRQ) found that the “real-life” cost of implementing EHRs “in an average five-physician primary care practice, operating within a large physician network committed to network-wide implementation of electronic health records, is about $162,000, with an additional $85,500 in maintenance expenses during the first year.”3
These figures include an average of 134 hours needed per physician to prepare to use EHRs during patient visits.3
Fleming and colleagues investigated the cost associated with implementing EHRs within 26 primary care practices in Texas. They found the cost to be $32,409 per physician through the first 60 days after the EHR system was launched, with one-time costs for hardware of $25,000 per practice and an additional $7,000 per physician for personal computers, printers, and scanners. The annual cost of software and maintenance was approximately $17,100 per physician.4
Why physicians should hold out for the return on their investment
Despite these considerable expenses, EHRs hold promise over the long term. The Medical Group Management Association reported, through a 2009 survey of about 1,300 primary care and specialty practice members using EHRs, that efficiency gains from the elimination of paper charts, as well as transcription savings, better charge capturing, and reduced billing errors, resulted in a median revenue increase of $49,916 per full-time physician after operating costs.
After 5 years of EHR use, practices reported a median operating margin 10.1% higher than that of practices in the first year of EHR use.5
Trends in the adoption of EHRs
Private practice. An article in Health Affairs showed that, by 2011, only one in six office-based physicians was using an EHR system robust enough to approach “meaningful use”—that is, the use of EHRs to measurably improve the quality of health care.6 These robust systems offered physicians the ability to record information on patient demographics, view laboratory and imaging results, maintain patients’ problem lists, compile clinical notes, and manage prescription ordering. EHR adoption lagged among non−primary care physicians, physicians aged 55 and older, and physicians in small (1–2 providers) practices and physician-owned practices.6 (ObGyns were considered primary care providers in this survey.)
“Big” practice. By comparison, in 2011, 99% of physicians in health maintenance organizations, or HMOs, and 73% in academic health centers and other hospitals used EHR systems.6 The number of physicians in these practice settings is small but growing.
In 2011, only 17% of physicians were in large practices of 10 or more physicians; 40% were in practices of one or two physicians.6
Primary care. These practices lead others in the adoption of EHRs, in part because of federal assistance, including a nationwide system of regional HIT assistance centers established by the Health Information Technology for Economic and Clinical Health (HITECH) Act to help providers located in rural areas participate in the Centers for Medicare and Medicaid Services (CMS) programs in EHR. The goal of these programs is to provide HIT support to at least 100,000 primary care providers, including ObGyns, by 2014.
The numbers cited in the Health Affairs article largely mirror data developed by other research organizations, including the Deloitte Center for Health Solutions.6
The EHR incentive
The drive for EHRs started long before the Affordable Care Act (ACA) was passed in 2010. The US Congress took a first stab at encouraging the health-care community to embrace HIT in 1996, when it passed the Health Insurance Portability and Accountability Act (HIPAA). HIPAA created an electronic data interchange that health plans, health-care clearinghouses, and certain health-care providers, including pharmacists, are required to use for electronic transactions, including:
- claims and encounter information
- payment and remittance advice
- claims status
- eligibility
- enrollment and disenrollment
- referrals and authorizations
- coordination of benefits
- premium payment.
Congress stepped up its game in 2009, when it offered higher Medicare and Medicaid payments to physicians who adopt and “meaningfully use” EHRs. The HITECH Act included $30 billion in new Medicare and Medicaid incentive payments—as much as $44,000 under Medicare and $63,750 under Medicaid—as well as $500 million for states to develop health information exchanges.
The Act also established a government-led process for certification of electronic health records through a $35 billion appropriation for the Office of the National Coordinator for Health IT, housed in CMS.
Other programs designed to encourage use of EHRs
Other federal programs include the Physician Quality Reporting System (PQRS), which, when created in 2006, was a voluntary physician electronic reporting program. Under the ACA, however, it has become a mandate. Starting in 2015, Medicare payments will be reduced for nonparticipating physicians.
The Electronic Prescribing (eRx) Incentive Program, created in 2008 under the Medicare Improvements for Patients and Providers Act, provides incentives for eligible physicians who e-prescribe Medicare Part D medications through a qualified system. This program converted to a penalty program last year for physicians who don’t use eRx.
Grants were also provided under the HITECH Act to fund an HIT infrastructure and low-interest HIT loans. The AHRQ has awarded $300 million in federal grant money to more than 200 projects in 48 states to promote access to and encourage HIT adoption. Over $150 million in Medicaid transformation grants have been awarded to three states and territories for HIT in the Medicaid program under the 2005 Deficit Reduction Act.
The ACA carried these initiatives even further by establishing uniform standards that HIT systems must meet, including:
- automatic reconciliation of electronic fund transfers and HIPAA payment and remittance
- improved claims payment process
- consistent methods of health plan enrollment and claim edits
- simplified and improved routing of health-care transactions
- electronic claims attachments.
Clearly, a lot of effort and taxpayer dollars have been dedicated to drive efficient use of HIT and EHRs in the hopes that they can:
- help make sense of our increasingly fragmented health-care system
- improve patient safety
- increase efficiency
- reduce paperwork
- reduce unnecessary tests
- better coordinate patient care.
To see which providers are cashing in on the government’s incentives for EHRs, see “Some physicians are more likely to seek incentives for meaningful use of EHRs” on page 37.
The long view
HIT and EHRs are here to stay. Products are maturing and improving. Acceptance by large and small practices has gained traction. Are small practices being squeezed? No doubt.
In 2011, I urged all ObGyns—especially those in private practice—to read an article written by President Barack Obama’s health-reform deputies on how physicians can be successful under the ACA.1 It reads, in part:
To realize the full benefits of the Affordable Care Act, physicians will need to embrace rather than resist change. The economic forces put in motion by the Act are likely to lead to vertical organization of providers and accelerate physician employment by hospitals and aggregation into larger physician groups. The most successful physicians will be those who most effectively collaborate with other providers to improve outcomes, care productivity, and patient experience.7
Two years ago, I zeroed in on the pressures straining small ObGyn practices in an article entitled, “Is private ObGyn practice on its way out?”1 The pressures haven’t eased in the interim. Today, small practices are still feeling squeezed to keep up with the many demands of modern specialty care. The push for electronic health records (EHRs), in particular, can profoundly affect physicians in private practice.
In this article, I outline some of the challenges facing small practices when they set out to implement EHRs, as well as the potential benefits they stand to gain a little farther down the road. Before we begin, however, let’s look at the latest trends in ObGyn practice, as they are related, in part, to the need to implement EHRs.
The exodus from private practice continues
A 2012 Accenture Physicians Alignment Survey shows an accelerating increase in physician employment. In 2000, 57% of all physicians were in independent practice; by the end of 2013, only 36% of physicians are projected to remain independent.2
The ObGyn specialty is a clear part of this trend, with both seasoned and incoming physicians finding hospital or other employment an attractive alternative to private practice. Fully one-third of ObGyn residents entering practice today sign hospital employment contracts. ObGyns who have made the switch from private to hospital practice, or who have become ObGyn hospitalists, often point to the difficulties of maintaining a solvent private practice, especially given the push toward EHRs and increasing regulatory and administrative burdens, as justification for their move.
The main reasons for the shift to employment. Top concerns influencing physicians’ decisions to opt for employment include:
- business expenses (87%)
- the dominance of managed care (61%)
- the requirement for EHRs (53%)
- the need to maintain and manage staff (53%)
- the increasing number of patients needed to break even (39%).2
A 2008 socioeconomic survey from ACOG revealed that 23.6% of ObGyn practices are solo practices, and 27.1% are single-specialty group practices. Many ObGyns—especially those in solo or small practices—are hesitant to make the large capital investment that is necessary to adopt EHRs.
EHRs offer benefits—and real costs
The system-wide benefits of health information technology (HIT), including EHRs, are many. Insurers stand to save money by reducing unnecessary tests, and patients will benefit from better coordination of their care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices. Instead, physicians face payment cuts from Medicare and private insurance.
Although there’s wide agreement that HIT can improve quality of care and reduce health-care costs, fewer than one-quarter (22%) of office-based physicians had adopted EHRs by 2009. We know the main reasons why:
- upfront cost and maintenance expense
- uncertain return on investment
- fragmented business model in a high proportion of small and solo practices
- changing and inconsistent information technology (IT) systems.
What can a practice expect to fork over?
In 2011, the Agency for Healthcare Research and Quality (AHRQ) found that the “real-life” cost of implementing EHRs “in an average five-physician primary care practice, operating within a large physician network committed to network-wide implementation of electronic health records, is about $162,000, with an additional $85,500 in maintenance expenses during the first year.”3
These figures include an average of 134 hours needed per physician to prepare to use EHRs during patient visits.3
Fleming and colleagues investigated the cost associated with implementing EHRs within 26 primary care practices in Texas. They found the cost to be $32,409 per physician through the first 60 days after the EHR system was launched, with one-time costs for hardware of $25,000 per practice and an additional $7,000 per physician for personal computers, printers, and scanners. The annual cost of software and maintenance was approximately $17,100 per physician.4
Why physicians should hold out for the return on their investment
Despite these considerable expenses, EHRs hold promise over the long term. The Medical Group Management Association reported, through a 2009 survey of about 1,300 primary care and specialty practice members using EHRs, that efficiency gains from the elimination of paper charts, as well as transcription savings, better charge capturing, and reduced billing errors, resulted in a median revenue increase of $49,916 per full-time physician after operating costs.
After 5 years of EHR use, practices reported a median operating margin 10.1% higher than that of practices in the first year of EHR use.5
Trends in the adoption of EHRs
Private practice. An article in Health Affairs showed that, by 2011, only one in six office-based physicians was using an EHR system robust enough to approach “meaningful use”—that is, the use of EHRs to measurably improve the quality of health care.6 These robust systems offered physicians the ability to record information on patient demographics, view laboratory and imaging results, maintain patients’ problem lists, compile clinical notes, and manage prescription ordering. EHR adoption lagged among non−primary care physicians, physicians aged 55 and older, and physicians in small (1–2 providers) practices and physician-owned practices.6 (ObGyns were considered primary care providers in this survey.)
“Big” practice. By comparison, in 2011, 99% of physicians in health maintenance organizations, or HMOs, and 73% in academic health centers and other hospitals used EHR systems.6 The number of physicians in these practice settings is small but growing.
In 2011, only 17% of physicians were in large practices of 10 or more physicians; 40% were in practices of one or two physicians.6
Primary care. These practices lead others in the adoption of EHRs, in part because of federal assistance, including a nationwide system of regional HIT assistance centers established by the Health Information Technology for Economic and Clinical Health (HITECH) Act to help providers located in rural areas participate in the Centers for Medicare and Medicaid Services (CMS) programs in EHR. The goal of these programs is to provide HIT support to at least 100,000 primary care providers, including ObGyns, by 2014.
The numbers cited in the Health Affairs article largely mirror data developed by other research organizations, including the Deloitte Center for Health Solutions.6
The EHR incentive
The drive for EHRs started long before the Affordable Care Act (ACA) was passed in 2010. The US Congress took a first stab at encouraging the health-care community to embrace HIT in 1996, when it passed the Health Insurance Portability and Accountability Act (HIPAA). HIPAA created an electronic data interchange that health plans, health-care clearinghouses, and certain health-care providers, including pharmacists, are required to use for electronic transactions, including:
- claims and encounter information
- payment and remittance advice
- claims status
- eligibility
- enrollment and disenrollment
- referrals and authorizations
- coordination of benefits
- premium payment.
Congress stepped up its game in 2009, when it offered higher Medicare and Medicaid payments to physicians who adopt and “meaningfully use” EHRs. The HITECH Act included $30 billion in new Medicare and Medicaid incentive payments—as much as $44,000 under Medicare and $63,750 under Medicaid—as well as $500 million for states to develop health information exchanges.
The Act also established a government-led process for certification of electronic health records through a $35 billion appropriation for the Office of the National Coordinator for Health IT, housed in CMS.
Other programs designed to encourage use of EHRs
Other federal programs include the Physician Quality Reporting System (PQRS), which, when created in 2006, was a voluntary physician electronic reporting program. Under the ACA, however, it has become a mandate. Starting in 2015, Medicare payments will be reduced for nonparticipating physicians.
The Electronic Prescribing (eRx) Incentive Program, created in 2008 under the Medicare Improvements for Patients and Providers Act, provides incentives for eligible physicians who e-prescribe Medicare Part D medications through a qualified system. This program converted to a penalty program last year for physicians who don’t use eRx.
Grants were also provided under the HITECH Act to fund an HIT infrastructure and low-interest HIT loans. The AHRQ has awarded $300 million in federal grant money to more than 200 projects in 48 states to promote access to and encourage HIT adoption. Over $150 million in Medicaid transformation grants have been awarded to three states and territories for HIT in the Medicaid program under the 2005 Deficit Reduction Act.
The ACA carried these initiatives even further by establishing uniform standards that HIT systems must meet, including:
- automatic reconciliation of electronic fund transfers and HIPAA payment and remittance
- improved claims payment process
- consistent methods of health plan enrollment and claim edits
- simplified and improved routing of health-care transactions
- electronic claims attachments.
Clearly, a lot of effort and taxpayer dollars have been dedicated to drive efficient use of HIT and EHRs in the hopes that they can:
- help make sense of our increasingly fragmented health-care system
- improve patient safety
- increase efficiency
- reduce paperwork
- reduce unnecessary tests
- better coordinate patient care.
To see which providers are cashing in on the government’s incentives for EHRs, see “Some physicians are more likely to seek incentives for meaningful use of EHRs” on page 37.
The long view
HIT and EHRs are here to stay. Products are maturing and improving. Acceptance by large and small practices has gained traction. Are small practices being squeezed? No doubt.
In 2011, I urged all ObGyns—especially those in private practice—to read an article written by President Barack Obama’s health-reform deputies on how physicians can be successful under the ACA.1 It reads, in part:
To realize the full benefits of the Affordable Care Act, physicians will need to embrace rather than resist change. The economic forces put in motion by the Act are likely to lead to vertical organization of providers and accelerate physician employment by hospitals and aggregation into larger physician groups. The most successful physicians will be those who most effectively collaborate with other providers to improve outcomes, care productivity, and patient experience.7
1. DiVenere L, Yates J. Is private ObGyn practice on its way out? OBG Manage. 2011;23(10):42–54.
2. More US doctors leaving private practice due to rising costs and technology mandates, Accenture report finds [news release]. Arlington, Virginia: Accenture Newsroom; October 31, 2012. http://newsroom.accenture.com/news/more-us-doctors-leaving-private-practice-due-to-rising-costs-and-technology-mandates-accenture-report-finds.htm. Accessed June 5, 2013.
3. Study identifies costs of implementing electronic health records in network of physician practices: Research Activities October 2011, No. 374. Rockville, MD: Agency for Healthcare Research and Quality. http://www.ahrq.gov/news/newsletters/research-activities/oct11/1011RA15.html. Accessed June 5, 2013.
5. MGMA survey: Medical groups with EHRs report better financial performance than practices with paper medical records [news release]. New Orleans, Louisiana: Medical Group Management Association; October 25, 2010. http://www.mgma.com/press/default.aspx?id=39824. Accessed June 6, 2013.
8. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicaid Incentive Payments for 2011. GAO-13-146R. December 13, 2012. http://www.gao.gov/products/GAO-13-146R. Accessed June 6, 2013.
9. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicare Incentive Payments for 2011. GAO-12-778R. July 26, 2012. http://www.gao.gov/products/GAO-12-778R. Accessed June 6, 2013.
10. US Department of Health and Human Services. Doctors’ and hospitals’ use of health IT more than doubles since 2012 [news release]. Washington, DC: HHS.gov; May 22, 2013. http://www.hhs.gov/news/press/2013pres/05/20130522a.html. Accessed June 6, 2013.
1. DiVenere L, Yates J. Is private ObGyn practice on its way out? OBG Manage. 2011;23(10):42–54.
2. More US doctors leaving private practice due to rising costs and technology mandates, Accenture report finds [news release]. Arlington, Virginia: Accenture Newsroom; October 31, 2012. http://newsroom.accenture.com/news/more-us-doctors-leaving-private-practice-due-to-rising-costs-and-technology-mandates-accenture-report-finds.htm. Accessed June 5, 2013.
3. Study identifies costs of implementing electronic health records in network of physician practices: Research Activities October 2011, No. 374. Rockville, MD: Agency for Healthcare Research and Quality. http://www.ahrq.gov/news/newsletters/research-activities/oct11/1011RA15.html. Accessed June 5, 2013.
5. MGMA survey: Medical groups with EHRs report better financial performance than practices with paper medical records [news release]. New Orleans, Louisiana: Medical Group Management Association; October 25, 2010. http://www.mgma.com/press/default.aspx?id=39824. Accessed June 6, 2013.
8. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicaid Incentive Payments for 2011. GAO-13-146R. December 13, 2012. http://www.gao.gov/products/GAO-13-146R. Accessed June 6, 2013.
9. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicare Incentive Payments for 2011. GAO-12-778R. July 26, 2012. http://www.gao.gov/products/GAO-12-778R. Accessed June 6, 2013.
10. US Department of Health and Human Services. Doctors’ and hospitals’ use of health IT more than doubles since 2012 [news release]. Washington, DC: HHS.gov; May 22, 2013. http://www.hhs.gov/news/press/2013pres/05/20130522a.html. Accessed June 6, 2013.
Mean income for ObGyns increased in 2012
ObGyns’ 2012 mean income was $242,000, up from a mean of $220,000 in 2011, although almost half (45%) of ObGyns reported their 2012 income to be the same as their 2011 income. In 2012, about 25% of ObGyns reported earnings of $300,000 or more, and 10% said they earn less than $100,000.1 The newest salary data are based on Medscape’s 2013 Compensation Report, a survey of 21,878 US physicians across 25 specialties.
Forty-three percent of ObGyns were satisfied with their 2012 compensation levels; 48% of all physicians were satisfied.1,2
Other Findings
Men still make more than women. In 2012, male ObGyns reported earning 14% more than female ObGyns. This pay gap is smaller for ObGyns than for all physicians, however; overall, male physicians earn 30% more than females. One contributing factor to the closer pay gap for ObGyns is that there are fewer women in the higher-paying specialties, such as orthopedics (only 9% of orthopedic respondents were female). Response rates also matter: of those who responded to the overall Medscape poll, 31% were female; of the ObGyn respondents, 43% were female.1,2
ObGyn compensation varies by region. Highest earnings were found in the South Central region (mean: $250,000 in 2012); lowest earnings were found in the Northeast (mean: $213,000).1
Work setting counts. When ranked by job setting, in 2012, ObGyns employed by health-care organizations were the top earners (mean income: $272,000). This figure rose considerably from the 2011 mean of $239,000. Additional mean earnings of ObGyns ranked by work setting in 2012 were1:
single-specialty (office-based) group practices: $264,000
multispecialty (office-based) group practices: $252,000
hospitals: $216,000
academic: $212,000
solo practices (office-based): $208,000
outpatient clinics: $206,000.
When ranked by work situation, partners beat all other situations at $268,000 (mean). Employed ObGyns earned more than owners of solo practices (mean: $241,000 vs $204,000, respectively). Independent contractors came in the lowest at $198,000 (mean).1
Satisfaction with career choice and practice setting showed a slight dip from 2011. When all physicians were asked if they would choose medicine again, 53% would do so in 2012, versus 55% in 2011. Among the ObGyns who said they would choose medicine again, 37% said they would choose the same specialty (the same as in 2011). In 2012, 18% of ObGyns said they would choose the same practice setting, compared with 23% in 2011.1,2
What’s most rewarding? In 2012, 42% of ObGyns ranked their relationships with patients as the most satisfying part of their job, compared with 31% of all physicians. While 34% of all physicians said that being good at the practice of medicine was their primary reward, 28% of ObGyns listed that first.1,2
FINDINGS ON HOW YOU MAKE AND DISCUSS MONEY
Where does your income come from? In the 2011 report, only 4% of ObGyns either participated in or planned to join an accountable care organization (ACO). In 2012, that figure jumped to 25%. Only 1% of ObGyns opted for concierge medical practices in 2012 and 2011, and only 3% chose cash-only practices in 2012 and 2011.1,2
What about Medicare and Medicaid? More physicians were concerned with the potential for reduced Medicare reimbursement in 2012 than in 2011. The current report indicated that 15% of ObGyns plan to stop taking new Medicare or Medicaid patients, 3% plan to stop seeing current Medicare or Medicaid patients, and 28% are undecided. However, 53% of ObGyns are not conflicted and will continue to see current patients and take on new Medicare and Medicaid patients. In 2012, 59% of all physicians planned to treat new Medicare and Medicaid patients.1,2
What about insurance company payments? Practice management experts often recommend that physicians review their annual payments from insurers and drop those who pay the worst or create the most trouble. In 2012, 26% of ObGyns reported that they already do that or are planning to take that advice. However, 29% will keep all insurers because they feel that even poor payers still represent income. About 15% felt that dropping insurers was inappropriate behavior.1
Do you provide ancillary services? When asked if they would offer additional medical services to increase income, 21% of ObGyns said yes. Nineteen percent of all physicians said they had begun to do that.1,2
Do you discuss cost with your patients? In larger practices and hospital settings, treatment costs are often discussed by a staff member responsible for billing and payment, rather than by the physician. As physicians move toward these larger organizations, the trend is becoming more apparent1:
In 2011, 41% of ObGyns reported that they regularly discuss the cost of services with their patients; 48% said they occasionally discuss cost if the patient brings it up (89% total).
In 2012, 35% of ObGyns said they regularly discuss cost with their patients; 41% said they occasionally discuss cost (76% total).
In 2011, 84% of all physicians either regularly or occasionally discussed the cost of treatment with patients. In 2012, 68% of all physicians regularly discussed cost of treatment (30%) or did so if the patient asked (38%), and 6% reported that it was inappropriate to discuss cost with patients.1,2
Findings on how you spend your time
How many hours do you work? The number of hours in a workweek remained approximately the same for the last 2 years: in 2012, 11% of ObGyns worked 41–45 h/w; 13% worked 46–50 h/w; 4% worked 51–55 h/w; and 9% worked 56–60 h/w. Approximately 20% of ObGyns reported working less than 30 h/w.1
How much time do you spend with patients? In 2012, most ObGyns spent 16 minutes or less per patient visit. Thirty percent of ObGyns spent 13–16 minutes with a patient, and another 30% spent less than 13 minutes. Some indicated longer patient visits—17% saw patients for 21 minutes or more.1
Demographics of the survey
Respondents to the Medscape survey totaled 21,878 US physicians and ranged in age from 28 years to older than 70; 66% were aged 40 to 64 years; 31% were female; 69% were male; and 89% were board certified.
Of the overall survey respondents, 5% (n = 1094) were ObGyns. Of these respondents, 71% were aged 40 to 64; 43% were female; 57% were male; and 92% were board certified.1,2
- Medscape News. Ob/Gyn Compensation Report 2013. Medscape Today Web site. http://www.medscape.com/features/slideshow/compensation/2013/womenshealth. Accessed June 30, 2013.
- Medscape News. Physician Compensation Report 2013. Medscape Today Web site. http://www.medscape.com/features/slideshow/compensation/2013/public. Accessed June 30, 2013.
ObGyns’ 2012 mean income was $242,000, up from a mean of $220,000 in 2011, although almost half (45%) of ObGyns reported their 2012 income to be the same as their 2011 income. In 2012, about 25% of ObGyns reported earnings of $300,000 or more, and 10% said they earn less than $100,000.1 The newest salary data are based on Medscape’s 2013 Compensation Report, a survey of 21,878 US physicians across 25 specialties.
Forty-three percent of ObGyns were satisfied with their 2012 compensation levels; 48% of all physicians were satisfied.1,2
Other Findings
Men still make more than women. In 2012, male ObGyns reported earning 14% more than female ObGyns. This pay gap is smaller for ObGyns than for all physicians, however; overall, male physicians earn 30% more than females. One contributing factor to the closer pay gap for ObGyns is that there are fewer women in the higher-paying specialties, such as orthopedics (only 9% of orthopedic respondents were female). Response rates also matter: of those who responded to the overall Medscape poll, 31% were female; of the ObGyn respondents, 43% were female.1,2
ObGyn compensation varies by region. Highest earnings were found in the South Central region (mean: $250,000 in 2012); lowest earnings were found in the Northeast (mean: $213,000).1
Work setting counts. When ranked by job setting, in 2012, ObGyns employed by health-care organizations were the top earners (mean income: $272,000). This figure rose considerably from the 2011 mean of $239,000. Additional mean earnings of ObGyns ranked by work setting in 2012 were1:
single-specialty (office-based) group practices: $264,000
multispecialty (office-based) group practices: $252,000
hospitals: $216,000
academic: $212,000
solo practices (office-based): $208,000
outpatient clinics: $206,000.
When ranked by work situation, partners beat all other situations at $268,000 (mean). Employed ObGyns earned more than owners of solo practices (mean: $241,000 vs $204,000, respectively). Independent contractors came in the lowest at $198,000 (mean).1
Satisfaction with career choice and practice setting showed a slight dip from 2011. When all physicians were asked if they would choose medicine again, 53% would do so in 2012, versus 55% in 2011. Among the ObGyns who said they would choose medicine again, 37% said they would choose the same specialty (the same as in 2011). In 2012, 18% of ObGyns said they would choose the same practice setting, compared with 23% in 2011.1,2
What’s most rewarding? In 2012, 42% of ObGyns ranked their relationships with patients as the most satisfying part of their job, compared with 31% of all physicians. While 34% of all physicians said that being good at the practice of medicine was their primary reward, 28% of ObGyns listed that first.1,2
FINDINGS ON HOW YOU MAKE AND DISCUSS MONEY
Where does your income come from? In the 2011 report, only 4% of ObGyns either participated in or planned to join an accountable care organization (ACO). In 2012, that figure jumped to 25%. Only 1% of ObGyns opted for concierge medical practices in 2012 and 2011, and only 3% chose cash-only practices in 2012 and 2011.1,2
What about Medicare and Medicaid? More physicians were concerned with the potential for reduced Medicare reimbursement in 2012 than in 2011. The current report indicated that 15% of ObGyns plan to stop taking new Medicare or Medicaid patients, 3% plan to stop seeing current Medicare or Medicaid patients, and 28% are undecided. However, 53% of ObGyns are not conflicted and will continue to see current patients and take on new Medicare and Medicaid patients. In 2012, 59% of all physicians planned to treat new Medicare and Medicaid patients.1,2
What about insurance company payments? Practice management experts often recommend that physicians review their annual payments from insurers and drop those who pay the worst or create the most trouble. In 2012, 26% of ObGyns reported that they already do that or are planning to take that advice. However, 29% will keep all insurers because they feel that even poor payers still represent income. About 15% felt that dropping insurers was inappropriate behavior.1
Do you provide ancillary services? When asked if they would offer additional medical services to increase income, 21% of ObGyns said yes. Nineteen percent of all physicians said they had begun to do that.1,2
Do you discuss cost with your patients? In larger practices and hospital settings, treatment costs are often discussed by a staff member responsible for billing and payment, rather than by the physician. As physicians move toward these larger organizations, the trend is becoming more apparent1:
In 2011, 41% of ObGyns reported that they regularly discuss the cost of services with their patients; 48% said they occasionally discuss cost if the patient brings it up (89% total).
In 2012, 35% of ObGyns said they regularly discuss cost with their patients; 41% said they occasionally discuss cost (76% total).
In 2011, 84% of all physicians either regularly or occasionally discussed the cost of treatment with patients. In 2012, 68% of all physicians regularly discussed cost of treatment (30%) or did so if the patient asked (38%), and 6% reported that it was inappropriate to discuss cost with patients.1,2
Findings on how you spend your time
How many hours do you work? The number of hours in a workweek remained approximately the same for the last 2 years: in 2012, 11% of ObGyns worked 41–45 h/w; 13% worked 46–50 h/w; 4% worked 51–55 h/w; and 9% worked 56–60 h/w. Approximately 20% of ObGyns reported working less than 30 h/w.1
How much time do you spend with patients? In 2012, most ObGyns spent 16 minutes or less per patient visit. Thirty percent of ObGyns spent 13–16 minutes with a patient, and another 30% spent less than 13 minutes. Some indicated longer patient visits—17% saw patients for 21 minutes or more.1
Demographics of the survey
Respondents to the Medscape survey totaled 21,878 US physicians and ranged in age from 28 years to older than 70; 66% were aged 40 to 64 years; 31% were female; 69% were male; and 89% were board certified.
Of the overall survey respondents, 5% (n = 1094) were ObGyns. Of these respondents, 71% were aged 40 to 64; 43% were female; 57% were male; and 92% were board certified.1,2
ObGyns’ 2012 mean income was $242,000, up from a mean of $220,000 in 2011, although almost half (45%) of ObGyns reported their 2012 income to be the same as their 2011 income. In 2012, about 25% of ObGyns reported earnings of $300,000 or more, and 10% said they earn less than $100,000.1 The newest salary data are based on Medscape’s 2013 Compensation Report, a survey of 21,878 US physicians across 25 specialties.
Forty-three percent of ObGyns were satisfied with their 2012 compensation levels; 48% of all physicians were satisfied.1,2
Other Findings
Men still make more than women. In 2012, male ObGyns reported earning 14% more than female ObGyns. This pay gap is smaller for ObGyns than for all physicians, however; overall, male physicians earn 30% more than females. One contributing factor to the closer pay gap for ObGyns is that there are fewer women in the higher-paying specialties, such as orthopedics (only 9% of orthopedic respondents were female). Response rates also matter: of those who responded to the overall Medscape poll, 31% were female; of the ObGyn respondents, 43% were female.1,2
ObGyn compensation varies by region. Highest earnings were found in the South Central region (mean: $250,000 in 2012); lowest earnings were found in the Northeast (mean: $213,000).1
Work setting counts. When ranked by job setting, in 2012, ObGyns employed by health-care organizations were the top earners (mean income: $272,000). This figure rose considerably from the 2011 mean of $239,000. Additional mean earnings of ObGyns ranked by work setting in 2012 were1:
single-specialty (office-based) group practices: $264,000
multispecialty (office-based) group practices: $252,000
hospitals: $216,000
academic: $212,000
solo practices (office-based): $208,000
outpatient clinics: $206,000.
When ranked by work situation, partners beat all other situations at $268,000 (mean). Employed ObGyns earned more than owners of solo practices (mean: $241,000 vs $204,000, respectively). Independent contractors came in the lowest at $198,000 (mean).1
Satisfaction with career choice and practice setting showed a slight dip from 2011. When all physicians were asked if they would choose medicine again, 53% would do so in 2012, versus 55% in 2011. Among the ObGyns who said they would choose medicine again, 37% said they would choose the same specialty (the same as in 2011). In 2012, 18% of ObGyns said they would choose the same practice setting, compared with 23% in 2011.1,2
What’s most rewarding? In 2012, 42% of ObGyns ranked their relationships with patients as the most satisfying part of their job, compared with 31% of all physicians. While 34% of all physicians said that being good at the practice of medicine was their primary reward, 28% of ObGyns listed that first.1,2
FINDINGS ON HOW YOU MAKE AND DISCUSS MONEY
Where does your income come from? In the 2011 report, only 4% of ObGyns either participated in or planned to join an accountable care organization (ACO). In 2012, that figure jumped to 25%. Only 1% of ObGyns opted for concierge medical practices in 2012 and 2011, and only 3% chose cash-only practices in 2012 and 2011.1,2
What about Medicare and Medicaid? More physicians were concerned with the potential for reduced Medicare reimbursement in 2012 than in 2011. The current report indicated that 15% of ObGyns plan to stop taking new Medicare or Medicaid patients, 3% plan to stop seeing current Medicare or Medicaid patients, and 28% are undecided. However, 53% of ObGyns are not conflicted and will continue to see current patients and take on new Medicare and Medicaid patients. In 2012, 59% of all physicians planned to treat new Medicare and Medicaid patients.1,2
What about insurance company payments? Practice management experts often recommend that physicians review their annual payments from insurers and drop those who pay the worst or create the most trouble. In 2012, 26% of ObGyns reported that they already do that or are planning to take that advice. However, 29% will keep all insurers because they feel that even poor payers still represent income. About 15% felt that dropping insurers was inappropriate behavior.1
Do you provide ancillary services? When asked if they would offer additional medical services to increase income, 21% of ObGyns said yes. Nineteen percent of all physicians said they had begun to do that.1,2
Do you discuss cost with your patients? In larger practices and hospital settings, treatment costs are often discussed by a staff member responsible for billing and payment, rather than by the physician. As physicians move toward these larger organizations, the trend is becoming more apparent1:
In 2011, 41% of ObGyns reported that they regularly discuss the cost of services with their patients; 48% said they occasionally discuss cost if the patient brings it up (89% total).
In 2012, 35% of ObGyns said they regularly discuss cost with their patients; 41% said they occasionally discuss cost (76% total).
In 2011, 84% of all physicians either regularly or occasionally discussed the cost of treatment with patients. In 2012, 68% of all physicians regularly discussed cost of treatment (30%) or did so if the patient asked (38%), and 6% reported that it was inappropriate to discuss cost with patients.1,2
Findings on how you spend your time
How many hours do you work? The number of hours in a workweek remained approximately the same for the last 2 years: in 2012, 11% of ObGyns worked 41–45 h/w; 13% worked 46–50 h/w; 4% worked 51–55 h/w; and 9% worked 56–60 h/w. Approximately 20% of ObGyns reported working less than 30 h/w.1
How much time do you spend with patients? In 2012, most ObGyns spent 16 minutes or less per patient visit. Thirty percent of ObGyns spent 13–16 minutes with a patient, and another 30% spent less than 13 minutes. Some indicated longer patient visits—17% saw patients for 21 minutes or more.1
Demographics of the survey
Respondents to the Medscape survey totaled 21,878 US physicians and ranged in age from 28 years to older than 70; 66% were aged 40 to 64 years; 31% were female; 69% were male; and 89% were board certified.
Of the overall survey respondents, 5% (n = 1094) were ObGyns. Of these respondents, 71% were aged 40 to 64; 43% were female; 57% were male; and 92% were board certified.1,2
- Medscape News. Ob/Gyn Compensation Report 2013. Medscape Today Web site. http://www.medscape.com/features/slideshow/compensation/2013/womenshealth. Accessed June 30, 2013.
- Medscape News. Physician Compensation Report 2013. Medscape Today Web site. http://www.medscape.com/features/slideshow/compensation/2013/public. Accessed June 30, 2013.
- Medscape News. Ob/Gyn Compensation Report 2013. Medscape Today Web site. http://www.medscape.com/features/slideshow/compensation/2013/womenshealth. Accessed June 30, 2013.
- Medscape News. Physician Compensation Report 2013. Medscape Today Web site. http://www.medscape.com/features/slideshow/compensation/2013/public. Accessed June 30, 2013.
Should have used other dystocia maneuvers first
gb
AN OBGYN ENCOUNTERED SHOULDER DYSTOCIA. He used fundal pressure and downward lateral traction to free the baby’s shoulder. The child has a brachial plexus injury of the right shoulder, including nerve avulsion, a fractured clavicle, and permanent disfigurement. She underwent surgery; physical and occupational therapy will continue.
PARENTS' CLAIM The standard sequence of maneuvers should have been attempted before fundal pressure and lateral traction were used—the baby was sufficiently oxygenated to allow time for these maneuvers. Excessive lateral traction caused the injury.
DEFENDANTS' DEFENSE The injuries occurred in utero before or while the fetus progressed down the birth canal, and were due to the maternal forces of labor.
VERDICT A $3,070,000 Michigan verdict was returned against the hospital, ObGyn, and ObGyn group.
WHAT IS THE STANDARD SEQUENCE OF MANEUVERS FOR SHOULDER DYSTOCIA?
Read Dr. Robert L. Barbieri’s May Editorial, You are the second responder to a shoulder dystocia emergency. What do you do first? and Dr. Ronald T. Burkman’s March Stop/Start article, Stop all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Meconium aspiration leads to brain injury
LATE IN HER PREGNANCY, a woman went to the emergency department (ED) with hypertension; she was discharged the same day. She saw her ObGyns, Dr. A and Dr. B, three times in the next 2 weeks. A day after her last visit, she returned to the ED in active labor. Dr. B assumed her care. Fetal monitoring indicated a nonreassuring heart rate with decelerations. Dr. B administered oxytocin and labor continued.
The baby was born by cesarean delivery after 25 minutes of fetal bradycardia. She was covered in meconium, with a low heart rate and irregular, labored respirations. The baby was transferred to another hospital, where she was treated for pulmonary hypertension, meconium aspiration, and seizures. The child is totally disabled, and will require constant care for life.
PARENTS' CLAIM The mother’s hypertension was not properly treated. Dr. B and the nurse waited too long to perform a cesarean delivery.
DEFENDANTS' DEFENSE Proper prenatal care was provided. There was no reason for additional testing; fetal heart tones at the mother’s last office visit were reactive. There were no clinical signs of a hematoma or cord varix during office visits. An unpredictable, unpreventable umbilical cord hematoma caused ischemia and hypoxia, and the subsequent brain injury. Meconium had been in the amniotic fluid for at least 10 hours due to the ischemic/hypoxic episode. The hematoma formed between her last office visit and when the mother came to the hospital the next day.
VERDICT Settlements were reached with Dr. A and the hospital. An Arkansas defense verdict was returned for Dr. B and the nurse.
14 months' recovery after mass removed
A GYNECOLOGIC ONCOLOGIST operated on a woman in her 50s to remove a large, noncancerous pelvic mass. The patient, discharged on postoperative day 2, was readmitted the next day with a fever (temperature, 103ºF), nausea, vomiting, and abdominal pain. Four days later, the oncologist repaired a perforated bowel and created an ileostomy. Other procedures were needed to drain abscesses and repair fistulas, and resect a large portion of colon due to continuing infection. Treatment lasted 14 months.
PATIENT'S CLAIM The gynecologic oncologist was negligent in failing to timely diagnose and treat the bowel perforation. Earlier repair would have curtailed development of the abscesses and fistulae.
PHYSICIAN'S DEFENSE Any complications the patient experienced were unrelated to any delay in treatment.
VERDICT A $612,237 Michigan verdict was returned.
Colon perforated during abdominal access
WHEN A MORBIDLY OBESE 37-YEAR-OLD WOMAN reported chronic pelvic pain, her gynecologist suspected endometriosis. Conservative treatment failed and the gynecologist offered laparoscopic hysterectomy.
After abdominal insufflation was unsuccessfully attempted twice using a Veress needle, the gynecologist entered the abdomen with a Visiport optical trocar, and continued the procedure. The gynecologist inspected the abdomen before closing but found no injuries.
The patient did not do well after surgery. CT scan detected a bowel perforation on postoperative day 6. During exploratory laparotomy, a through-and-through “bayonet” colon perforation was repaired. Because of the extensive infection, the patient’s surgical wound was left open and several “washouts” were performed; the wound was closed several weeks later. The patient also underwent two adhesiolysis procedures.
PATIENT'S CLAIM Access to the abdomen was not properly performed and caused colon perforation. The injury should have been found and treated earlier.
PHYSICIAN'S DEFENSE The case was settled before trial.
VERDICT A $750,000 Virginia settlement was reached.
READ How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy, by Michael Baggish, MD (Surgical Techniques, October 2012) What caused this C. diff infection after hysterectomy?
AFTER A HYSTERECTOMY, a 42-year-old woman developed a persistent fever and increased white blood cell count. The gynecologist prescribed ciprofloxacin for a urinary tract infection, and discharged the patient from the hospital on postoperative day 4. She returned to the gynecologist’s office with severe abdominal pain and vomiting 4 days after discharge. The gynecologist prescribed an antacid and told her to continue taking ciprofloxacin.
The patient was taken to the ED by ambulance 3 days later. Testing revealed a Clostridium dificule (C. diff) infection. During emergency surgery, a large portion of her colon was resected, and a colostomy was performed. The colostomy was reversed 6 months later. The patient developed an incisional hernia and has abdominal scarring.
PATIENT'S CLAIM Prophylactic antibiotics should have been prescribed before surgery.
Two possible scenarios were presented: 1) A bowel injury occurred during surgery, and ciprofloxacin likely worsened the infection caused by the bowel injury; or 2) ciprofloxacin triggered the C. diff infection that caused leaking colon perforations and subsequent peritonitis.
The colon perforations could have been avoided if the gynecologist had diagnosed and treated the C. diff infection in a timely manner.
PHYSICIAN'S DEFENSE The patient’s symptoms did not suggest a C. diff infection; testing was not necessary. Ciprofloxacin might have allowed the proliferation of the C. diff infection, but the use of the drug was not negligent. The infection was not preventable and could not have been diagnosed earlier.
VERDICT A $776,000 New York verdict was returned.
Brain injury and cerebral palsy: When did this occur?
DURING LABOR AND DELIVERY, there were periods when the fetal heart-rate tracings were nonreassuring with variable decelerations and fetal tachycardia; some variables were severe. The child suffered anoxic encephalopathy that caused neurologic injury and cerebral palsy.
PARENTS' CLAIM The infant suffered numerous hypoxic incidents before cesarean delivery was performed. An earlier cesarean delivery could have prevented the injury.
PHYSICIAN'S DEFENSE The newborn had a normal blood cord gas level of 7.2 pH and Apgar scores of 9 and 10, at 1 and 5 minutes, respectively. Fetal heart-rate tracings did not show evidence of fetal hypoxia. The brain injury likely occurred prior to the onset of labor and was possibly related to a viral encephalopathy.
VERDICT A Virginia defense verdict was returned. These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
gb
AN OBGYN ENCOUNTERED SHOULDER DYSTOCIA. He used fundal pressure and downward lateral traction to free the baby’s shoulder. The child has a brachial plexus injury of the right shoulder, including nerve avulsion, a fractured clavicle, and permanent disfigurement. She underwent surgery; physical and occupational therapy will continue.
PARENTS' CLAIM The standard sequence of maneuvers should have been attempted before fundal pressure and lateral traction were used—the baby was sufficiently oxygenated to allow time for these maneuvers. Excessive lateral traction caused the injury.
DEFENDANTS' DEFENSE The injuries occurred in utero before or while the fetus progressed down the birth canal, and were due to the maternal forces of labor.
VERDICT A $3,070,000 Michigan verdict was returned against the hospital, ObGyn, and ObGyn group.
WHAT IS THE STANDARD SEQUENCE OF MANEUVERS FOR SHOULDER DYSTOCIA?
Read Dr. Robert L. Barbieri’s May Editorial, You are the second responder to a shoulder dystocia emergency. What do you do first? and Dr. Ronald T. Burkman’s March Stop/Start article, Stop all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Meconium aspiration leads to brain injury
LATE IN HER PREGNANCY, a woman went to the emergency department (ED) with hypertension; she was discharged the same day. She saw her ObGyns, Dr. A and Dr. B, three times in the next 2 weeks. A day after her last visit, she returned to the ED in active labor. Dr. B assumed her care. Fetal monitoring indicated a nonreassuring heart rate with decelerations. Dr. B administered oxytocin and labor continued.
The baby was born by cesarean delivery after 25 minutes of fetal bradycardia. She was covered in meconium, with a low heart rate and irregular, labored respirations. The baby was transferred to another hospital, where she was treated for pulmonary hypertension, meconium aspiration, and seizures. The child is totally disabled, and will require constant care for life.
PARENTS' CLAIM The mother’s hypertension was not properly treated. Dr. B and the nurse waited too long to perform a cesarean delivery.
DEFENDANTS' DEFENSE Proper prenatal care was provided. There was no reason for additional testing; fetal heart tones at the mother’s last office visit were reactive. There were no clinical signs of a hematoma or cord varix during office visits. An unpredictable, unpreventable umbilical cord hematoma caused ischemia and hypoxia, and the subsequent brain injury. Meconium had been in the amniotic fluid for at least 10 hours due to the ischemic/hypoxic episode. The hematoma formed between her last office visit and when the mother came to the hospital the next day.
VERDICT Settlements were reached with Dr. A and the hospital. An Arkansas defense verdict was returned for Dr. B and the nurse.
14 months' recovery after mass removed
A GYNECOLOGIC ONCOLOGIST operated on a woman in her 50s to remove a large, noncancerous pelvic mass. The patient, discharged on postoperative day 2, was readmitted the next day with a fever (temperature, 103ºF), nausea, vomiting, and abdominal pain. Four days later, the oncologist repaired a perforated bowel and created an ileostomy. Other procedures were needed to drain abscesses and repair fistulas, and resect a large portion of colon due to continuing infection. Treatment lasted 14 months.
PATIENT'S CLAIM The gynecologic oncologist was negligent in failing to timely diagnose and treat the bowel perforation. Earlier repair would have curtailed development of the abscesses and fistulae.
PHYSICIAN'S DEFENSE Any complications the patient experienced were unrelated to any delay in treatment.
VERDICT A $612,237 Michigan verdict was returned.
Colon perforated during abdominal access
WHEN A MORBIDLY OBESE 37-YEAR-OLD WOMAN reported chronic pelvic pain, her gynecologist suspected endometriosis. Conservative treatment failed and the gynecologist offered laparoscopic hysterectomy.
After abdominal insufflation was unsuccessfully attempted twice using a Veress needle, the gynecologist entered the abdomen with a Visiport optical trocar, and continued the procedure. The gynecologist inspected the abdomen before closing but found no injuries.
The patient did not do well after surgery. CT scan detected a bowel perforation on postoperative day 6. During exploratory laparotomy, a through-and-through “bayonet” colon perforation was repaired. Because of the extensive infection, the patient’s surgical wound was left open and several “washouts” were performed; the wound was closed several weeks later. The patient also underwent two adhesiolysis procedures.
PATIENT'S CLAIM Access to the abdomen was not properly performed and caused colon perforation. The injury should have been found and treated earlier.
PHYSICIAN'S DEFENSE The case was settled before trial.
VERDICT A $750,000 Virginia settlement was reached.
READ How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy, by Michael Baggish, MD (Surgical Techniques, October 2012) What caused this C. diff infection after hysterectomy?
AFTER A HYSTERECTOMY, a 42-year-old woman developed a persistent fever and increased white blood cell count. The gynecologist prescribed ciprofloxacin for a urinary tract infection, and discharged the patient from the hospital on postoperative day 4. She returned to the gynecologist’s office with severe abdominal pain and vomiting 4 days after discharge. The gynecologist prescribed an antacid and told her to continue taking ciprofloxacin.
The patient was taken to the ED by ambulance 3 days later. Testing revealed a Clostridium dificule (C. diff) infection. During emergency surgery, a large portion of her colon was resected, and a colostomy was performed. The colostomy was reversed 6 months later. The patient developed an incisional hernia and has abdominal scarring.
PATIENT'S CLAIM Prophylactic antibiotics should have been prescribed before surgery.
Two possible scenarios were presented: 1) A bowel injury occurred during surgery, and ciprofloxacin likely worsened the infection caused by the bowel injury; or 2) ciprofloxacin triggered the C. diff infection that caused leaking colon perforations and subsequent peritonitis.
The colon perforations could have been avoided if the gynecologist had diagnosed and treated the C. diff infection in a timely manner.
PHYSICIAN'S DEFENSE The patient’s symptoms did not suggest a C. diff infection; testing was not necessary. Ciprofloxacin might have allowed the proliferation of the C. diff infection, but the use of the drug was not negligent. The infection was not preventable and could not have been diagnosed earlier.
VERDICT A $776,000 New York verdict was returned.
Brain injury and cerebral palsy: When did this occur?
DURING LABOR AND DELIVERY, there were periods when the fetal heart-rate tracings were nonreassuring with variable decelerations and fetal tachycardia; some variables were severe. The child suffered anoxic encephalopathy that caused neurologic injury and cerebral palsy.
PARENTS' CLAIM The infant suffered numerous hypoxic incidents before cesarean delivery was performed. An earlier cesarean delivery could have prevented the injury.
PHYSICIAN'S DEFENSE The newborn had a normal blood cord gas level of 7.2 pH and Apgar scores of 9 and 10, at 1 and 5 minutes, respectively. Fetal heart-rate tracings did not show evidence of fetal hypoxia. The brain injury likely occurred prior to the onset of labor and was possibly related to a viral encephalopathy.
VERDICT A Virginia defense verdict was returned. These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
gb
AN OBGYN ENCOUNTERED SHOULDER DYSTOCIA. He used fundal pressure and downward lateral traction to free the baby’s shoulder. The child has a brachial plexus injury of the right shoulder, including nerve avulsion, a fractured clavicle, and permanent disfigurement. She underwent surgery; physical and occupational therapy will continue.
PARENTS' CLAIM The standard sequence of maneuvers should have been attempted before fundal pressure and lateral traction were used—the baby was sufficiently oxygenated to allow time for these maneuvers. Excessive lateral traction caused the injury.
DEFENDANTS' DEFENSE The injuries occurred in utero before or while the fetus progressed down the birth canal, and were due to the maternal forces of labor.
VERDICT A $3,070,000 Michigan verdict was returned against the hospital, ObGyn, and ObGyn group.
WHAT IS THE STANDARD SEQUENCE OF MANEUVERS FOR SHOULDER DYSTOCIA?
Read Dr. Robert L. Barbieri’s May Editorial, You are the second responder to a shoulder dystocia emergency. What do you do first? and Dr. Ronald T. Burkman’s March Stop/Start article, Stop all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Meconium aspiration leads to brain injury
LATE IN HER PREGNANCY, a woman went to the emergency department (ED) with hypertension; she was discharged the same day. She saw her ObGyns, Dr. A and Dr. B, three times in the next 2 weeks. A day after her last visit, she returned to the ED in active labor. Dr. B assumed her care. Fetal monitoring indicated a nonreassuring heart rate with decelerations. Dr. B administered oxytocin and labor continued.
The baby was born by cesarean delivery after 25 minutes of fetal bradycardia. She was covered in meconium, with a low heart rate and irregular, labored respirations. The baby was transferred to another hospital, where she was treated for pulmonary hypertension, meconium aspiration, and seizures. The child is totally disabled, and will require constant care for life.
PARENTS' CLAIM The mother’s hypertension was not properly treated. Dr. B and the nurse waited too long to perform a cesarean delivery.
DEFENDANTS' DEFENSE Proper prenatal care was provided. There was no reason for additional testing; fetal heart tones at the mother’s last office visit were reactive. There were no clinical signs of a hematoma or cord varix during office visits. An unpredictable, unpreventable umbilical cord hematoma caused ischemia and hypoxia, and the subsequent brain injury. Meconium had been in the amniotic fluid for at least 10 hours due to the ischemic/hypoxic episode. The hematoma formed between her last office visit and when the mother came to the hospital the next day.
VERDICT Settlements were reached with Dr. A and the hospital. An Arkansas defense verdict was returned for Dr. B and the nurse.
14 months' recovery after mass removed
A GYNECOLOGIC ONCOLOGIST operated on a woman in her 50s to remove a large, noncancerous pelvic mass. The patient, discharged on postoperative day 2, was readmitted the next day with a fever (temperature, 103ºF), nausea, vomiting, and abdominal pain. Four days later, the oncologist repaired a perforated bowel and created an ileostomy. Other procedures were needed to drain abscesses and repair fistulas, and resect a large portion of colon due to continuing infection. Treatment lasted 14 months.
PATIENT'S CLAIM The gynecologic oncologist was negligent in failing to timely diagnose and treat the bowel perforation. Earlier repair would have curtailed development of the abscesses and fistulae.
PHYSICIAN'S DEFENSE Any complications the patient experienced were unrelated to any delay in treatment.
VERDICT A $612,237 Michigan verdict was returned.
Colon perforated during abdominal access
WHEN A MORBIDLY OBESE 37-YEAR-OLD WOMAN reported chronic pelvic pain, her gynecologist suspected endometriosis. Conservative treatment failed and the gynecologist offered laparoscopic hysterectomy.
After abdominal insufflation was unsuccessfully attempted twice using a Veress needle, the gynecologist entered the abdomen with a Visiport optical trocar, and continued the procedure. The gynecologist inspected the abdomen before closing but found no injuries.
The patient did not do well after surgery. CT scan detected a bowel perforation on postoperative day 6. During exploratory laparotomy, a through-and-through “bayonet” colon perforation was repaired. Because of the extensive infection, the patient’s surgical wound was left open and several “washouts” were performed; the wound was closed several weeks later. The patient also underwent two adhesiolysis procedures.
PATIENT'S CLAIM Access to the abdomen was not properly performed and caused colon perforation. The injury should have been found and treated earlier.
PHYSICIAN'S DEFENSE The case was settled before trial.
VERDICT A $750,000 Virginia settlement was reached.
READ How to avoid intestinal and urinary tract injuries during gynecologic laparoscopy, by Michael Baggish, MD (Surgical Techniques, October 2012) What caused this C. diff infection after hysterectomy?
AFTER A HYSTERECTOMY, a 42-year-old woman developed a persistent fever and increased white blood cell count. The gynecologist prescribed ciprofloxacin for a urinary tract infection, and discharged the patient from the hospital on postoperative day 4. She returned to the gynecologist’s office with severe abdominal pain and vomiting 4 days after discharge. The gynecologist prescribed an antacid and told her to continue taking ciprofloxacin.
The patient was taken to the ED by ambulance 3 days later. Testing revealed a Clostridium dificule (C. diff) infection. During emergency surgery, a large portion of her colon was resected, and a colostomy was performed. The colostomy was reversed 6 months later. The patient developed an incisional hernia and has abdominal scarring.
PATIENT'S CLAIM Prophylactic antibiotics should have been prescribed before surgery.
Two possible scenarios were presented: 1) A bowel injury occurred during surgery, and ciprofloxacin likely worsened the infection caused by the bowel injury; or 2) ciprofloxacin triggered the C. diff infection that caused leaking colon perforations and subsequent peritonitis.
The colon perforations could have been avoided if the gynecologist had diagnosed and treated the C. diff infection in a timely manner.
PHYSICIAN'S DEFENSE The patient’s symptoms did not suggest a C. diff infection; testing was not necessary. Ciprofloxacin might have allowed the proliferation of the C. diff infection, but the use of the drug was not negligent. The infection was not preventable and could not have been diagnosed earlier.
VERDICT A $776,000 New York verdict was returned.
Brain injury and cerebral palsy: When did this occur?
DURING LABOR AND DELIVERY, there were periods when the fetal heart-rate tracings were nonreassuring with variable decelerations and fetal tachycardia; some variables were severe. The child suffered anoxic encephalopathy that caused neurologic injury and cerebral palsy.
PARENTS' CLAIM The infant suffered numerous hypoxic incidents before cesarean delivery was performed. An earlier cesarean delivery could have prevented the injury.
PHYSICIAN'S DEFENSE The newborn had a normal blood cord gas level of 7.2 pH and Apgar scores of 9 and 10, at 1 and 5 minutes, respectively. Fetal heart-rate tracings did not show evidence of fetal hypoxia. The brain injury likely occurred prior to the onset of labor and was possibly related to a viral encephalopathy.
VERDICT A Virginia defense verdict was returned. These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.

Practical considerations in the delivery of genetic counseling and testing services for inherited cancer predisposition
Many professional entities endorse the need to deliver cancer genetics risk assessment (CGRA) services through a multidisciplinary team that includes trained genetics professionals. However, market forces, a lack of regulation of genetic testing, patent laws, cost barriers, and a limited workforce in genetics have resulted in an increasing number of community practitioners who order and interpret genetic testing. In addition, varying state-level laws and licensure requirements for genetic counselors may contribute to the nonuniform delivery of CGRA services across the United States. Those who perform genetic testing without having adequate training or expertise may incur liability risks. Moreover, the patient might not enjoy the maximum benefit of testing at the hands of an inadequately trained individual. In the setting of a limited number of professional who are trained in CGRA and a dearth of education and training resources, it is a challenge to integrate genetic testing services into clinical care. With advances in genomics and the implementation of personalized medicine, the problem will only be magnified, and it is critical that there are more opportunities for high quality education and training in clinical cancer genetics free of commercial bias. Successful strategies for delivering comprehensive CGRA services include academic-community partnerships that focus on collaboration with nongenetics providers or the inclusion of a genetics professional in the community setting as part of multidisciplinary patient care. These approaches can leverage the expertise of genetics professionals while allowing patients to remain in their community and enjoy better access to resources for long-term follow-up care.
*Click on the link to the left for a PDF of the full article.
Many professional entities endorse the need to deliver cancer genetics risk assessment (CGRA) services through a multidisciplinary team that includes trained genetics professionals. However, market forces, a lack of regulation of genetic testing, patent laws, cost barriers, and a limited workforce in genetics have resulted in an increasing number of community practitioners who order and interpret genetic testing. In addition, varying state-level laws and licensure requirements for genetic counselors may contribute to the nonuniform delivery of CGRA services across the United States. Those who perform genetic testing without having adequate training or expertise may incur liability risks. Moreover, the patient might not enjoy the maximum benefit of testing at the hands of an inadequately trained individual. In the setting of a limited number of professional who are trained in CGRA and a dearth of education and training resources, it is a challenge to integrate genetic testing services into clinical care. With advances in genomics and the implementation of personalized medicine, the problem will only be magnified, and it is critical that there are more opportunities for high quality education and training in clinical cancer genetics free of commercial bias. Successful strategies for delivering comprehensive CGRA services include academic-community partnerships that focus on collaboration with nongenetics providers or the inclusion of a genetics professional in the community setting as part of multidisciplinary patient care. These approaches can leverage the expertise of genetics professionals while allowing patients to remain in their community and enjoy better access to resources for long-term follow-up care.
*Click on the link to the left for a PDF of the full article.
Many professional entities endorse the need to deliver cancer genetics risk assessment (CGRA) services through a multidisciplinary team that includes trained genetics professionals. However, market forces, a lack of regulation of genetic testing, patent laws, cost barriers, and a limited workforce in genetics have resulted in an increasing number of community practitioners who order and interpret genetic testing. In addition, varying state-level laws and licensure requirements for genetic counselors may contribute to the nonuniform delivery of CGRA services across the United States. Those who perform genetic testing without having adequate training or expertise may incur liability risks. Moreover, the patient might not enjoy the maximum benefit of testing at the hands of an inadequately trained individual. In the setting of a limited number of professional who are trained in CGRA and a dearth of education and training resources, it is a challenge to integrate genetic testing services into clinical care. With advances in genomics and the implementation of personalized medicine, the problem will only be magnified, and it is critical that there are more opportunities for high quality education and training in clinical cancer genetics free of commercial bias. Successful strategies for delivering comprehensive CGRA services include academic-community partnerships that focus on collaboration with nongenetics providers or the inclusion of a genetics professional in the community setting as part of multidisciplinary patient care. These approaches can leverage the expertise of genetics professionals while allowing patients to remain in their community and enjoy better access to resources for long-term follow-up care.
*Click on the link to the left for a PDF of the full article.
Ensuring optimal adherence to BCR-ABL1 tyrosine kinase inhibitor therapy for chronic myeloid leukemia
The advent of BCR-ABL1 tyrosine kinase inhibitors (TKIs) for the treatment of chronic myeloid leukemia (CML) has dramatically changed the management of patients with CML. With continuous long-term TKI therapy, CML can be managed like a chronic condition, and most patients can expect to have a normal life expectancy. Given the prospect of lifelong therapy, however, issues related to adherence become particularly important and warrant greater attention since attainment of favorable long-term survival depends in large part on consistent, appropriate treatment administration over years, if not decades. As the multidisciplinary care team approach to cancer care has gained traction at academic centers and community practices, midlevel providers, including nurse practitioners and physician assistants, have taken on greater patient-related responsibilities. Midlevel providers have the potential to foster and maintain meaningful provider-patient relationships that may span years, and are well positioned to recognize and manage problems that patients may have with adherence. Here we discuss the importance of achieving and maintaining responses to TKI therapy, describe the clinical consequences of poor adherence to TKI therapy in CML, and outline factors behind poor adherence. We also share strategies that we use at our center to improve adherence to long-term TKI therapy for CML.
*Click on the link to the left for a PDF of the full article.
The advent of BCR-ABL1 tyrosine kinase inhibitors (TKIs) for the treatment of chronic myeloid leukemia (CML) has dramatically changed the management of patients with CML. With continuous long-term TKI therapy, CML can be managed like a chronic condition, and most patients can expect to have a normal life expectancy. Given the prospect of lifelong therapy, however, issues related to adherence become particularly important and warrant greater attention since attainment of favorable long-term survival depends in large part on consistent, appropriate treatment administration over years, if not decades. As the multidisciplinary care team approach to cancer care has gained traction at academic centers and community practices, midlevel providers, including nurse practitioners and physician assistants, have taken on greater patient-related responsibilities. Midlevel providers have the potential to foster and maintain meaningful provider-patient relationships that may span years, and are well positioned to recognize and manage problems that patients may have with adherence. Here we discuss the importance of achieving and maintaining responses to TKI therapy, describe the clinical consequences of poor adherence to TKI therapy in CML, and outline factors behind poor adherence. We also share strategies that we use at our center to improve adherence to long-term TKI therapy for CML.
*Click on the link to the left for a PDF of the full article.
The advent of BCR-ABL1 tyrosine kinase inhibitors (TKIs) for the treatment of chronic myeloid leukemia (CML) has dramatically changed the management of patients with CML. With continuous long-term TKI therapy, CML can be managed like a chronic condition, and most patients can expect to have a normal life expectancy. Given the prospect of lifelong therapy, however, issues related to adherence become particularly important and warrant greater attention since attainment of favorable long-term survival depends in large part on consistent, appropriate treatment administration over years, if not decades. As the multidisciplinary care team approach to cancer care has gained traction at academic centers and community practices, midlevel providers, including nurse practitioners and physician assistants, have taken on greater patient-related responsibilities. Midlevel providers have the potential to foster and maintain meaningful provider-patient relationships that may span years, and are well positioned to recognize and manage problems that patients may have with adherence. Here we discuss the importance of achieving and maintaining responses to TKI therapy, describe the clinical consequences of poor adherence to TKI therapy in CML, and outline factors behind poor adherence. We also share strategies that we use at our center to improve adherence to long-term TKI therapy for CML.
*Click on the link to the left for a PDF of the full article.
Atypical antipsychotics during pregnancy
Although clinicians and patients generally are cautious when prescribing or using antipsychotics during pregnancy, inadequately controlled psychiatric illness poses risks to both mother and child. Calculating the risks and benefits of antipsychotic use during pregnancy is limited by an incomplete understanding of the true effectiveness and full spectrum of risks of these medications. Ethical principles prohibit the type of rigorous research that would be needed to achieve clarity on this issue. This article reviews studies that might help guide clinicians who are considering prescribing an atypical antipsychotic to manage psychiatric illness in a pregnant woman.
Antipsychotic efficacy in pregnancy
All atypical antipsychotics available in the United States are FDA-approved for treating schizophrenia; some also have been approved for treating bipolar disorder, unipolar depression, or symptoms associated with autism (Table 1). Atypical antipsychotics frequently are used off-label for these and other categories of psychiatric illness, including unipolar depression, generalized anxiety disorder, and obsessive-compulsive disorder.
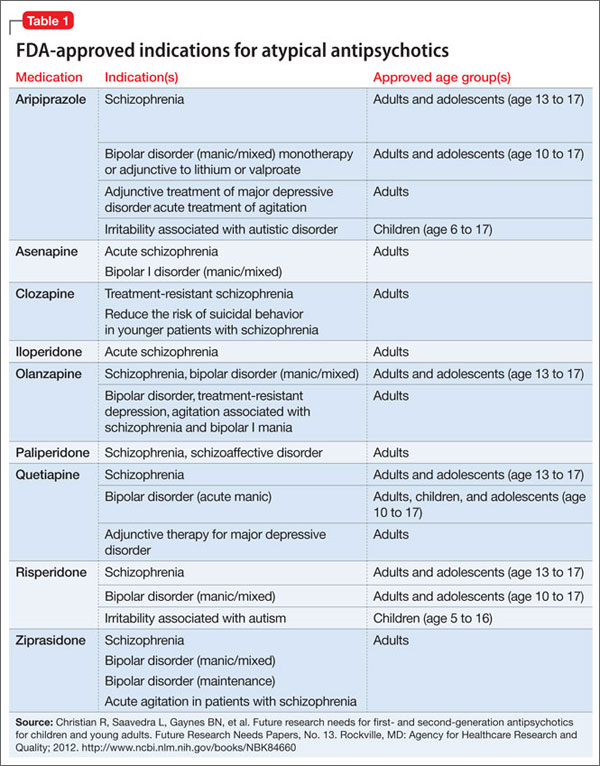
Studies of pharmacotherapy in pregnant women tend to focus more on safety rather than efficacy. Clinical decisions for an individual patient are best made based on knowledge about which medications have been effective for that patient in the past (Algorithm).
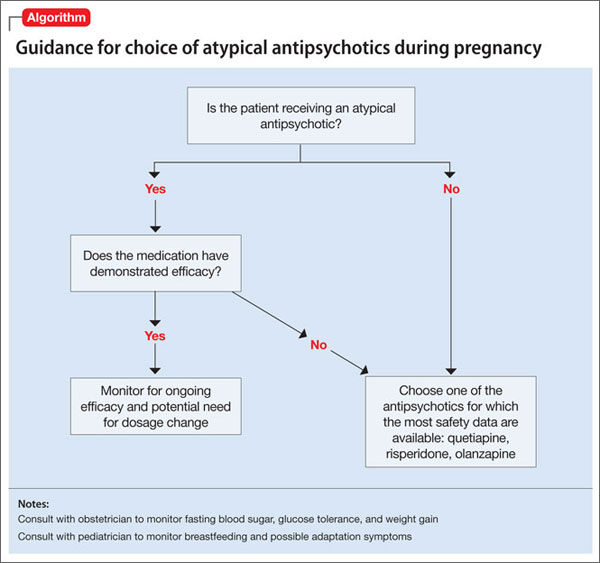
However, safety concerns in pregnancy may require modifying an existing regimen. In other cases, new symptoms arise during pregnancy and necessitate new medications. Additionally, a drug’s effectiveness may be affected by physiologic changes of pregnancy that can alter drug metabolism,1 potentially necessitating dose changes (Box 1).
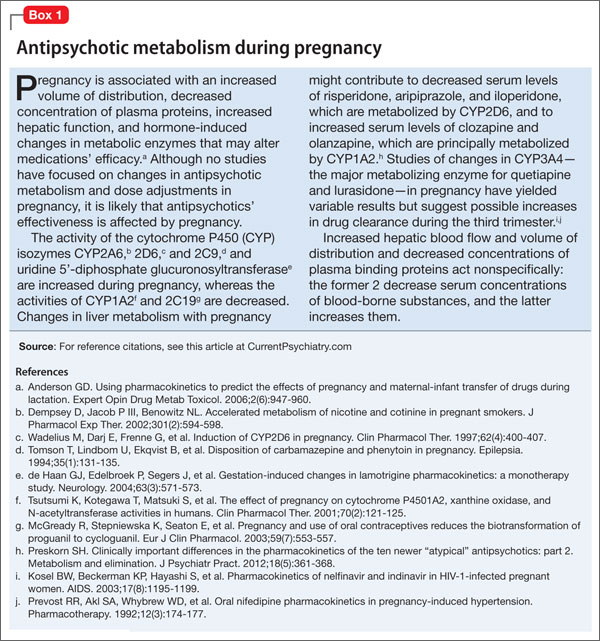
Risks of treatment vs illness
Complete safety data on the use of any psychotropic medication during pregnancy are not available. To date, studies of atypical antipsychotics do not support any increased risk for congenital malformations large enough to be detected in medium-sized samples,2-4 although it is possible that there are increases in risk that are below the detection limit of these studies. Data regarding delivery outcomes are conflicting and difficult to interpret.
Several studies2-4 have yielded inconsistent results, including:
• risks for increased birth weight and large for gestational age3
• risks for low birth weight and small for gestational age2
• no significant differences from controls.4
Atypical antipsychotics increase the risk of gestational diabetes, whereas typical antipsychotics do not appear to increase this risk.4
Until recently, research has been limited by difficulties in separating the effects of treatment from the effects of psychiatric illness, which include intrauterine growth retardation, prematurity, preterm birth, low Apgar scores, and congenital defects.5 In addition, most studies address early and easily measurable outcomes such as preterm labor, birth weight, and congenital malformations. Researchers are just beginning to investigate more subtle and long-term potential behavioral effects.
Several recent studies have explored outcomes associated with antipsychotic use during pregnancy while attempting to separate the effects of treatment from those of disease (Box 2).

Data on atypicals
Aripiprazole. Case reports of aripiprazole use during pregnancy have reported difficulties including transient unexplained fetal tachycardia that required emergent caesarean section6 and transient respiratory distress.7 Several small case series were not powered to detect risks related to aripiprazole.8,9
Animal data suggest teratogenic potential at dosages 3 and 10 times the maximum recommended human dose.10,11 Two studies7,12 that measured placental transfer of aripiprazole found cord-to-maternal serum concentration ratios ranging from 0.47 to 0.63, which is similar to the ratios for quetiapine and risperidone and lower than those for olanzapine and haloperidol.13
There are insufficient data to identify risks related to aripiprazole compared with other drugs in its class, and fewer reports are available than for other atypical antipsychotics such as quetiapine and olanzapine. Placental transfer appears to be on the lower end of the spectrum for drugs in this class. Aripiprazole would be an acceptable choice for a woman who had a history of response to aripiprazole but likely would not be a first choice for a woman requiring a new medication during pregnancy.
Clozapine. In case reports, adverse effects associated with clozapine exposure during pregnancy include major malformations, gestational metabolic complications, poor pregnancy outcome, and perinatal adverse reactions. In one case, neonatal plasma clozapine concentrations were found to be twice that found in maternal plasma.14 Animal data have shown no evidence of increased teratogenicity at 2 to 4 times the maximum recommended human dosages.15 Boden et al8 found an increased risk for gestational diabetes and macrocephaly with clozapine (11 exposures). Four other series2-4,16 were underpowered to detect concerns related specifically to clozapine.
There are insufficient data to identify risks related specifically to clozapine use during pregnancy. However, the rare but severe adverse effects associated with clozapine in other patient populations—including agranulocytosis and severe constipation17—could be devastating in a pregnant patient, which suggests this medication would not be a first-line treatment.
Olanzapine. In postmarketing surveillance studies and case reports, there have been have anecdotal cases of fetal malformations related to olanzapine use during pregnancy. Several larger studies2-4,8,16 did not find higher rates of congenital malformations or any pattern of malformation types, although none were designed or powered to examine rare events. Animal data show no evidence of teratogenicity.18 A study comparing rates of placental passage of antipsychotics13 found higher rates for olanzapine than for quetiapine and risperidone, as well as higher prevalence of low birth weight and perinatal complications. A neonatal withdrawal syndrome has also been reported.19 Boden et al8 found an increased risk for gestational diabetes and macrocephaly with olanzapine.
Data suggest that olanzapine may be associated with somewhat higher rates of the adverse effects attributable to atypical antipsychotics (gestational diabetes and possibly macrocephaly), which could be related to olanzapine’s relatively higher rate of placental passage. Olanzapine could be a reasonable choice in a woman who had a history of good response to this medication, but would be lower priority than quetiapine when a new drug is indicated during pregnancy.
Quetiapine. In clinical trials, quetiapine had lower rates of placental passage compared with risperidone and olanzapine.13 One case report found only small changes in quetiapine serum levels during pregnancy.20 Prospective studies (90 exposures,8 36 exposures,2 7 exposures,16 4 exposures,3 and 4 exposures4) show no increase in fetal malformations or adverse neonatal health outcomes related to quetiapine, and manufacturer safety data reveal no teratogenic effect, although delays in fetal skeletal ossification were seen in rats and rabbits at doses comparable to the recommended human range.21
Quetiapine is a reasonable first choice when a new atypical antipsychotic is indicated for a pregnant patient.
Risperidone. Rates of placental passage of risperidone are higher compared with quetiapine.13 Postmarketing surveillance data (265 exposures22 and 10 exposures23) and prospective studies (including 72 exposures,8 49 exposures,2 51 exposures,4 16 exposures,16 and 5 exposures3) suggest risperidone has no major teratogenic effect. When malformations were present, they were similar to expected rates and types of malformations, and no specific malformation type was overrepresented. However, in some cases, researchers noted a withdrawal-emergent syndrome that included various combinations of tremors, irritability, poor feeding, and somnolence.22 Animal data are similarly reassuring, although increases in early fetal mortality and (potentially related) changes in maternal behavior have been observed in rats.24,25 A major caveat with risperidone is its propensity to cause hyperprolactinemia, which is detrimental to efforts to conceive and maintain a pregnancy.26,27
Risperidone is not associated with higher rates of adverse events in pregnancy than other atypical antipsychotics. It would not be a first choice for a woman trying to conceive or in the early stages of pregnancy, but would be a reasonable choice for a woman already well into pregnancy.
Ziprasidone. Available reports are few and generally do not report findings on ziprasidone separately.8,28 Manufacturer data includes 5 spontaneous abortions, one malformation, and one stillbirth among 57 exposures,4 and available animal data suggest significant developmental toxicity and impaired fertility.29 In pregnant rats, ziprasidone dosed as low as 0.5 times the maximum human recommended dose resulted in delayed fetal skeletal ossification, increased stillbirths, and decreased fetal weight and postnatal survival, and ziprasidone dosed as low as 0.2 times the maximum recommended human dose resulted in developmental delays and neurobehavioral impairments in offspring. In pregnant rabbits, ziprasidone dosed at 3 times the maximum recommended human dose resulted in cardiac and renal malformations.29
Although available data are too sparse to draw reliable conclusions, the small amount of human data plus animal data suggest that ziprasidone should be less preferred than other atypical antipsychotics during pregnancy.
Lurasidone. No data addressing lurasidone use in humans during pregnancy are available. Material submitted to the FDA includes no evidence of teratogenicity or embryo-fetal toxicity in rat and rabbit studies using 3 and 12 times the maximum recommended human dose (80 mg) based on a body surface area comparison.30
Asenapine. No data specifically addressing asenapine use in humans during pregnancy are available. Studies in rats and rabbits found no increase in teratogenicity, but did find increases in postimplantation loss and decreases in pup survival and weight gain with maternal doses equivalent to less than the maximum recommended human dose.31
Iloperidone. No data specifically addressing iloperidone use in humans during pregnancy are available. Animal studies of iloperidone found multiple developmental toxicities when iloperidone was administered during gestation.32 In one study, pregnant rats were given up to 26 times the maximum recommended human dose of 24 mg/d during the period of organogenesis. The highest dose caused increased early intrauterine deaths, decreased fetal weight and length, decreased fetal skeletal ossification, and increased minor fetal skeletal anomalies and variations. In a similar study using pregnant rabbits, the highest dose caused increased early intrauterine deaths and decreased fetal viability at term.
Paliperidone. In animal studies, there were no increases in fetal abnormalities when pregnant rats and rabbits were treated with up to 8 times the maximum recommended human dose of paliperidone during the period of organogenesis.33
A single case report34 measured levels of risperidone and its 9-hydroxy metabolite, paliperidone, in the breast milk of a mother who had taken risperidone during pregnancy and in the serum of her child. 9-OH-risperidone dose in breast milk was calculated as 4.7% of the weight-adjusted maternal dose, and serum levels in the infant were undetectable. No ill effects on the child were observed.
It is not possible to draw solid conclusions about atypical antipsychotics’ potential effects on human development from animal studies. Because of the lack of human data for the newer atypical antipsychotics—asenapine, iloperidone, lurasidone, paliperidone—in general these agents would not be advisable as first-line medications for treating pregnant women.
A few caveats
All atypical antipsychotics share the propensity to trigger or worsen glucose intolerance, which can have significant negative consequences in a pregnant patient. When deciding to use an atypical antipsychotic during pregnancy, blood glucose should be monitored carefully and regularly.
Because all atypical antipsychotics (except clozapine) are FDA pregnancy class C—indicating that animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks—the decision to use these medications must be based on an individualized assessment of risks and benefits. Patients and their providers together should make a fully informed decision.
There is an urgent need for larger and better-designed investigations that will be sufficiently powered to detect differences in outcomes—particularly major malformations, preterm delivery, adverse events in labor and delivery, metabolic and anthropometric effects on the newborn, and neurodevelopmental and psychiatric outcomes for individuals exposed in utero—between women without mental illness, untreated women with mental illness, and women receiving atypical antipsychotics during pregnancy. Further research into the pharmacokinetics and clinical efficacy of antipsychotics in pregnant women also would be useful. Clinicians can assist with these efforts by submitting their patient data to a pregnancy registry maintained by the Massachusetts General Hospital (see Related Resources).
Bottom Line
Treatment with atypical antipsychotics during pregnancy may increase the risk of adverse birth outcomes, but inadequately controlled mental illness also carries some degree of risk. The decision to use any atypical antipsychotic during pregnancy must be based on an individualized assessment of risks and benefits and made by the pregnant patient and her provider.
Related Resources
- Gentile S. Antipsychotic therapy during early and late pregnancy. A systematic review. Schizophr Bull. 2010;36(3):518-544. www.ncbi.nlm.nih.gov/pmc/articles/PMC2879689.
- Massachusetts General Hospital National Pregnancy Registry for Atypical Antipsychotics. www.womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry.
Drug Brand Names
Aripiprazole • Abilify Olanzapine • Zyprexa
Asenapine • Saphris Paliperidone • Invega
Clozapine • Clozaril Quetiapine • Seroquel
Haloperidol • Haldol Risperidone • Risperdal
Iloperidone • Fanapt Ziprasidone • Geodon
Lurasidone • Latuda
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Chang J, Streitman D. Physiologic adaptations to pregnancy. Neurol Clin. 2012;30(3):781-789.
2. McKenna K, Koren G, Tetelbaum M, et al. Pregnancy outcome of women using atypical antipsychotic drugs: a prospective comparative study. J Clin Psychiatry. 2005;66(4): 444-449; quiz 546.
3. Newham JJ, Thomas SH, MacRitchie K, et al. Birth weight of infants after maternal exposure to typical and atypical antipsychotics: prospective comparison study. Br J Psychiatry. 2008;192(5):333-337.
4. Reis M, Kallen B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
5. Matevosyan NR. Pregnancy and postpartum specifics in women with schizophrenia: a meta-study. Arch Gynecol Obstet. 2011;283(2):141-147.
6. Mendhekar DN, Sunder KR, Andrade C. Aripiprazole use in a pregnant schizoaffective woman. Bipolar Disord. 2006;8(3):299-300.
7. Watanabe N, Kasahara M, Sugibayashi R, et al. Perinatal use of aripiprazole: a case report. J Clin Psychopharmacol. 2011;31(3):377-379.
8. Bodén R, Lundgren M, Brandt L, et al. Antipsychotics during pregnancy: relation to fetal and maternal metabolic effects. Arch Gen Psychiatry. 2012;69(7):715-721.
9. Maáková E, Hubicˇková L. Antidepressant drug exposure during pregnancy. CZTIS small prospective study. Neuro Endocrinol Lett. 2011;32(suppl 1):53-56.
10. Bristol-Myers Squibb (Ed.). Aripiprazole: Drugdex drug evaluations, 1974-2003. Princeton, NJ: Thomson Micromedex; 2003.
11. U.S. Food and Drug Administration. FDA datasheet: Aripiprazole. http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/21436slr006_abilify_lbl.pdf. Accessed April 8, 2013.
12. Nguyen T, Teoh S, Hackett LP, et al. Placental transfer of aripiprazole. Aust N Z J Psychiatry. 2011;45(6):500-501.
13. Newport DJ, Calamaras MR, DeVane CL, et al. Atypical antipsychotic administration during late pregnancy: placental passage and obstetrical outcomes. Am J Psychiatry. 2007;164(8):1214-1220.
14. Barnas C, Bergant A, Hummer M, et al. Clozapine concentrations in maternal and fetal plasma, amniotic fluid, and breast milk. Am J Psychiatry. 1994;151(6):945.
15. Clozaril [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2013.
16. Lin H, Chen I, Chen Y, et al. Maternal schizophrenia and pregnancy outcome: does the use of antipsychotics make a difference? Schizophr Res. 2010;116(1):55-60.
17. Young CR, Bowers MB Jr, Mazure CM. Management of the adverse effects of clozapine. Schizophr Bull. 1998;24(3):
381-390.
18. Zyprexa [package insert]. Indianapolis, IN: Eli Lilly and Company; 1997.
19. Gilad O, Merlob P, Stahl B, et al. Outcome of infants exposed to olanzapine during breastfeeding. Breastfeed Med. 2011;6(2):55-58.
20. Klier CM, Mossaheb N, Saria A, et al. Pharmacokinetics and elimination of quetiapine, venlafaxine, and trazodone during pregnancy and postpartum. J Clin Psychopharmacol. 2007;27(6):720-722.
21. U.S. Food and Drug Administration. FDA datasheet: quetiapine. http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/20639se1-017,016_seroquel_lbl.pdf. Accessed April 11, 2013.
22. Coppola D, Russo LJ, Kwarta RF Jr, et al. Evaluating the postmarketing experience of risperidone use during pregnancy: pregnancy and neonatal outcomes. Drug Saf. 2007;30(3):247-264.
23. Mackay FJ, Wilton LV, Pearce GL, et al. The safety of risperidone: a post-marketing study on 7,684 patients. Hum Psychopharmacol. 1998;13(6):413-418.
24. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2012.
25. U.S. Food and Drug Administration. FDA datasheet: risperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020272s056,020588s044,021346s033,021444s03lbl.pdf. Accessed April 11, 2013.
26. Katz E, Adashi EY. Hyperprolactinemic disorders. Clin Obstet Gynecol. 1990;33(3):622-639.
27. Davis JR. Prolactin and reproductive medicine. Curr Opin Obstet Gynecol. 2004;16(4):331-337.
28. Johnson KC, Laprairie JL, Brennan PA, et al. Prenatal antipsychotic exposure and neuromotor performance during infancy. Arch Gen Psychiatry. 2012;69(8):787-794. doi: 10.1001/archgenpsychiatry.2012.160.
29. U.S. Food and Drug Administration. FDA datasheet: ziprasidone. http://www.fda.gov/downloads/Advisory
Committees/CommitteesMeetingMaterials/Pediatric AdvisoryCommittee/UCM191883.pdf. Accessed March 15, 2013.
30. U.S. Food and Drug Administration. FDA datasheet: lurasidone. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/200603Orig1s000PharmR.pdf. Accessed March 15, 2013.
31. U.S. Food and Drug Administration. FDA datasheet: asenapine. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022117s000_OtherR.pdf. Accessed March 15, 2013.
32. U.S. Food and Drug Administration. FDA datasheet: iloperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022192lbl.pdf. Accessed March 15, 2013.
33. U.S. Food and Drug Administration. FDA datasheet: paliperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021999s018lbl.pdf. Accessed March 15, 2013.
34. Weggelaar NM, Keijer WJ, Janssen PK. A case report of risperidone distribution and excretion into human milk: how to give good advice if you have not enough data available. J Clin Psychopharmacol. 2011;31(1):129-131.
Although clinicians and patients generally are cautious when prescribing or using antipsychotics during pregnancy, inadequately controlled psychiatric illness poses risks to both mother and child. Calculating the risks and benefits of antipsychotic use during pregnancy is limited by an incomplete understanding of the true effectiveness and full spectrum of risks of these medications. Ethical principles prohibit the type of rigorous research that would be needed to achieve clarity on this issue. This article reviews studies that might help guide clinicians who are considering prescribing an atypical antipsychotic to manage psychiatric illness in a pregnant woman.
Antipsychotic efficacy in pregnancy
All atypical antipsychotics available in the United States are FDA-approved for treating schizophrenia; some also have been approved for treating bipolar disorder, unipolar depression, or symptoms associated with autism (Table 1). Atypical antipsychotics frequently are used off-label for these and other categories of psychiatric illness, including unipolar depression, generalized anxiety disorder, and obsessive-compulsive disorder.
Studies of pharmacotherapy in pregnant women tend to focus more on safety rather than efficacy. Clinical decisions for an individual patient are best made based on knowledge about which medications have been effective for that patient in the past (Algorithm).
However, safety concerns in pregnancy may require modifying an existing regimen. In other cases, new symptoms arise during pregnancy and necessitate new medications. Additionally, a drug’s effectiveness may be affected by physiologic changes of pregnancy that can alter drug metabolism,1 potentially necessitating dose changes (Box 1).
Risks of treatment vs illness
Complete safety data on the use of any psychotropic medication during pregnancy are not available. To date, studies of atypical antipsychotics do not support any increased risk for congenital malformations large enough to be detected in medium-sized samples,2-4 although it is possible that there are increases in risk that are below the detection limit of these studies. Data regarding delivery outcomes are conflicting and difficult to interpret.
Several studies2-4 have yielded inconsistent results, including:
• risks for increased birth weight and large for gestational age3
• risks for low birth weight and small for gestational age2
• no significant differences from controls.4
Atypical antipsychotics increase the risk of gestational diabetes, whereas typical antipsychotics do not appear to increase this risk.4
Until recently, research has been limited by difficulties in separating the effects of treatment from the effects of psychiatric illness, which include intrauterine growth retardation, prematurity, preterm birth, low Apgar scores, and congenital defects.5 In addition, most studies address early and easily measurable outcomes such as preterm labor, birth weight, and congenital malformations. Researchers are just beginning to investigate more subtle and long-term potential behavioral effects.
Several recent studies have explored outcomes associated with antipsychotic use during pregnancy while attempting to separate the effects of treatment from those of disease (Box 2).
Data on atypicals
Aripiprazole. Case reports of aripiprazole use during pregnancy have reported difficulties including transient unexplained fetal tachycardia that required emergent caesarean section6 and transient respiratory distress.7 Several small case series were not powered to detect risks related to aripiprazole.8,9
Animal data suggest teratogenic potential at dosages 3 and 10 times the maximum recommended human dose.10,11 Two studies7,12 that measured placental transfer of aripiprazole found cord-to-maternal serum concentration ratios ranging from 0.47 to 0.63, which is similar to the ratios for quetiapine and risperidone and lower than those for olanzapine and haloperidol.13
There are insufficient data to identify risks related to aripiprazole compared with other drugs in its class, and fewer reports are available than for other atypical antipsychotics such as quetiapine and olanzapine. Placental transfer appears to be on the lower end of the spectrum for drugs in this class. Aripiprazole would be an acceptable choice for a woman who had a history of response to aripiprazole but likely would not be a first choice for a woman requiring a new medication during pregnancy.
Clozapine. In case reports, adverse effects associated with clozapine exposure during pregnancy include major malformations, gestational metabolic complications, poor pregnancy outcome, and perinatal adverse reactions. In one case, neonatal plasma clozapine concentrations were found to be twice that found in maternal plasma.14 Animal data have shown no evidence of increased teratogenicity at 2 to 4 times the maximum recommended human dosages.15 Boden et al8 found an increased risk for gestational diabetes and macrocephaly with clozapine (11 exposures). Four other series2-4,16 were underpowered to detect concerns related specifically to clozapine.
There are insufficient data to identify risks related specifically to clozapine use during pregnancy. However, the rare but severe adverse effects associated with clozapine in other patient populations—including agranulocytosis and severe constipation17—could be devastating in a pregnant patient, which suggests this medication would not be a first-line treatment.
Olanzapine. In postmarketing surveillance studies and case reports, there have been have anecdotal cases of fetal malformations related to olanzapine use during pregnancy. Several larger studies2-4,8,16 did not find higher rates of congenital malformations or any pattern of malformation types, although none were designed or powered to examine rare events. Animal data show no evidence of teratogenicity.18 A study comparing rates of placental passage of antipsychotics13 found higher rates for olanzapine than for quetiapine and risperidone, as well as higher prevalence of low birth weight and perinatal complications. A neonatal withdrawal syndrome has also been reported.19 Boden et al8 found an increased risk for gestational diabetes and macrocephaly with olanzapine.
Data suggest that olanzapine may be associated with somewhat higher rates of the adverse effects attributable to atypical antipsychotics (gestational diabetes and possibly macrocephaly), which could be related to olanzapine’s relatively higher rate of placental passage. Olanzapine could be a reasonable choice in a woman who had a history of good response to this medication, but would be lower priority than quetiapine when a new drug is indicated during pregnancy.
Quetiapine. In clinical trials, quetiapine had lower rates of placental passage compared with risperidone and olanzapine.13 One case report found only small changes in quetiapine serum levels during pregnancy.20 Prospective studies (90 exposures,8 36 exposures,2 7 exposures,16 4 exposures,3 and 4 exposures4) show no increase in fetal malformations or adverse neonatal health outcomes related to quetiapine, and manufacturer safety data reveal no teratogenic effect, although delays in fetal skeletal ossification were seen in rats and rabbits at doses comparable to the recommended human range.21
Quetiapine is a reasonable first choice when a new atypical antipsychotic is indicated for a pregnant patient.
Risperidone. Rates of placental passage of risperidone are higher compared with quetiapine.13 Postmarketing surveillance data (265 exposures22 and 10 exposures23) and prospective studies (including 72 exposures,8 49 exposures,2 51 exposures,4 16 exposures,16 and 5 exposures3) suggest risperidone has no major teratogenic effect. When malformations were present, they were similar to expected rates and types of malformations, and no specific malformation type was overrepresented. However, in some cases, researchers noted a withdrawal-emergent syndrome that included various combinations of tremors, irritability, poor feeding, and somnolence.22 Animal data are similarly reassuring, although increases in early fetal mortality and (potentially related) changes in maternal behavior have been observed in rats.24,25 A major caveat with risperidone is its propensity to cause hyperprolactinemia, which is detrimental to efforts to conceive and maintain a pregnancy.26,27
Risperidone is not associated with higher rates of adverse events in pregnancy than other atypical antipsychotics. It would not be a first choice for a woman trying to conceive or in the early stages of pregnancy, but would be a reasonable choice for a woman already well into pregnancy.
Ziprasidone. Available reports are few and generally do not report findings on ziprasidone separately.8,28 Manufacturer data includes 5 spontaneous abortions, one malformation, and one stillbirth among 57 exposures,4 and available animal data suggest significant developmental toxicity and impaired fertility.29 In pregnant rats, ziprasidone dosed as low as 0.5 times the maximum human recommended dose resulted in delayed fetal skeletal ossification, increased stillbirths, and decreased fetal weight and postnatal survival, and ziprasidone dosed as low as 0.2 times the maximum recommended human dose resulted in developmental delays and neurobehavioral impairments in offspring. In pregnant rabbits, ziprasidone dosed at 3 times the maximum recommended human dose resulted in cardiac and renal malformations.29
Although available data are too sparse to draw reliable conclusions, the small amount of human data plus animal data suggest that ziprasidone should be less preferred than other atypical antipsychotics during pregnancy.
Lurasidone. No data addressing lurasidone use in humans during pregnancy are available. Material submitted to the FDA includes no evidence of teratogenicity or embryo-fetal toxicity in rat and rabbit studies using 3 and 12 times the maximum recommended human dose (80 mg) based on a body surface area comparison.30
Asenapine. No data specifically addressing asenapine use in humans during pregnancy are available. Studies in rats and rabbits found no increase in teratogenicity, but did find increases in postimplantation loss and decreases in pup survival and weight gain with maternal doses equivalent to less than the maximum recommended human dose.31
Iloperidone. No data specifically addressing iloperidone use in humans during pregnancy are available. Animal studies of iloperidone found multiple developmental toxicities when iloperidone was administered during gestation.32 In one study, pregnant rats were given up to 26 times the maximum recommended human dose of 24 mg/d during the period of organogenesis. The highest dose caused increased early intrauterine deaths, decreased fetal weight and length, decreased fetal skeletal ossification, and increased minor fetal skeletal anomalies and variations. In a similar study using pregnant rabbits, the highest dose caused increased early intrauterine deaths and decreased fetal viability at term.
Paliperidone. In animal studies, there were no increases in fetal abnormalities when pregnant rats and rabbits were treated with up to 8 times the maximum recommended human dose of paliperidone during the period of organogenesis.33
A single case report34 measured levels of risperidone and its 9-hydroxy metabolite, paliperidone, in the breast milk of a mother who had taken risperidone during pregnancy and in the serum of her child. 9-OH-risperidone dose in breast milk was calculated as 4.7% of the weight-adjusted maternal dose, and serum levels in the infant were undetectable. No ill effects on the child were observed.
It is not possible to draw solid conclusions about atypical antipsychotics’ potential effects on human development from animal studies. Because of the lack of human data for the newer atypical antipsychotics—asenapine, iloperidone, lurasidone, paliperidone—in general these agents would not be advisable as first-line medications for treating pregnant women.
A few caveats
All atypical antipsychotics share the propensity to trigger or worsen glucose intolerance, which can have significant negative consequences in a pregnant patient. When deciding to use an atypical antipsychotic during pregnancy, blood glucose should be monitored carefully and regularly.
Because all atypical antipsychotics (except clozapine) are FDA pregnancy class C—indicating that animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks—the decision to use these medications must be based on an individualized assessment of risks and benefits. Patients and their providers together should make a fully informed decision.
There is an urgent need for larger and better-designed investigations that will be sufficiently powered to detect differences in outcomes—particularly major malformations, preterm delivery, adverse events in labor and delivery, metabolic and anthropometric effects on the newborn, and neurodevelopmental and psychiatric outcomes for individuals exposed in utero—between women without mental illness, untreated women with mental illness, and women receiving atypical antipsychotics during pregnancy. Further research into the pharmacokinetics and clinical efficacy of antipsychotics in pregnant women also would be useful. Clinicians can assist with these efforts by submitting their patient data to a pregnancy registry maintained by the Massachusetts General Hospital (see Related Resources).
Bottom Line
Treatment with atypical antipsychotics during pregnancy may increase the risk of adverse birth outcomes, but inadequately controlled mental illness also carries some degree of risk. The decision to use any atypical antipsychotic during pregnancy must be based on an individualized assessment of risks and benefits and made by the pregnant patient and her provider.
Related Resources
- Gentile S. Antipsychotic therapy during early and late pregnancy. A systematic review. Schizophr Bull. 2010;36(3):518-544. www.ncbi.nlm.nih.gov/pmc/articles/PMC2879689.
- Massachusetts General Hospital National Pregnancy Registry for Atypical Antipsychotics. www.womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry.
Drug Brand Names
Aripiprazole • Abilify Olanzapine • Zyprexa
Asenapine • Saphris Paliperidone • Invega
Clozapine • Clozaril Quetiapine • Seroquel
Haloperidol • Haldol Risperidone • Risperdal
Iloperidone • Fanapt Ziprasidone • Geodon
Lurasidone • Latuda
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Although clinicians and patients generally are cautious when prescribing or using antipsychotics during pregnancy, inadequately controlled psychiatric illness poses risks to both mother and child. Calculating the risks and benefits of antipsychotic use during pregnancy is limited by an incomplete understanding of the true effectiveness and full spectrum of risks of these medications. Ethical principles prohibit the type of rigorous research that would be needed to achieve clarity on this issue. This article reviews studies that might help guide clinicians who are considering prescribing an atypical antipsychotic to manage psychiatric illness in a pregnant woman.
Antipsychotic efficacy in pregnancy
All atypical antipsychotics available in the United States are FDA-approved for treating schizophrenia; some also have been approved for treating bipolar disorder, unipolar depression, or symptoms associated with autism (Table 1). Atypical antipsychotics frequently are used off-label for these and other categories of psychiatric illness, including unipolar depression, generalized anxiety disorder, and obsessive-compulsive disorder.
Studies of pharmacotherapy in pregnant women tend to focus more on safety rather than efficacy. Clinical decisions for an individual patient are best made based on knowledge about which medications have been effective for that patient in the past (Algorithm).
However, safety concerns in pregnancy may require modifying an existing regimen. In other cases, new symptoms arise during pregnancy and necessitate new medications. Additionally, a drug’s effectiveness may be affected by physiologic changes of pregnancy that can alter drug metabolism,1 potentially necessitating dose changes (Box 1).
Risks of treatment vs illness
Complete safety data on the use of any psychotropic medication during pregnancy are not available. To date, studies of atypical antipsychotics do not support any increased risk for congenital malformations large enough to be detected in medium-sized samples,2-4 although it is possible that there are increases in risk that are below the detection limit of these studies. Data regarding delivery outcomes are conflicting and difficult to interpret.
Several studies2-4 have yielded inconsistent results, including:
• risks for increased birth weight and large for gestational age3
• risks for low birth weight and small for gestational age2
• no significant differences from controls.4
Atypical antipsychotics increase the risk of gestational diabetes, whereas typical antipsychotics do not appear to increase this risk.4
Until recently, research has been limited by difficulties in separating the effects of treatment from the effects of psychiatric illness, which include intrauterine growth retardation, prematurity, preterm birth, low Apgar scores, and congenital defects.5 In addition, most studies address early and easily measurable outcomes such as preterm labor, birth weight, and congenital malformations. Researchers are just beginning to investigate more subtle and long-term potential behavioral effects.
Several recent studies have explored outcomes associated with antipsychotic use during pregnancy while attempting to separate the effects of treatment from those of disease (Box 2).
Data on atypicals
Aripiprazole. Case reports of aripiprazole use during pregnancy have reported difficulties including transient unexplained fetal tachycardia that required emergent caesarean section6 and transient respiratory distress.7 Several small case series were not powered to detect risks related to aripiprazole.8,9
Animal data suggest teratogenic potential at dosages 3 and 10 times the maximum recommended human dose.10,11 Two studies7,12 that measured placental transfer of aripiprazole found cord-to-maternal serum concentration ratios ranging from 0.47 to 0.63, which is similar to the ratios for quetiapine and risperidone and lower than those for olanzapine and haloperidol.13
There are insufficient data to identify risks related to aripiprazole compared with other drugs in its class, and fewer reports are available than for other atypical antipsychotics such as quetiapine and olanzapine. Placental transfer appears to be on the lower end of the spectrum for drugs in this class. Aripiprazole would be an acceptable choice for a woman who had a history of response to aripiprazole but likely would not be a first choice for a woman requiring a new medication during pregnancy.
Clozapine. In case reports, adverse effects associated with clozapine exposure during pregnancy include major malformations, gestational metabolic complications, poor pregnancy outcome, and perinatal adverse reactions. In one case, neonatal plasma clozapine concentrations were found to be twice that found in maternal plasma.14 Animal data have shown no evidence of increased teratogenicity at 2 to 4 times the maximum recommended human dosages.15 Boden et al8 found an increased risk for gestational diabetes and macrocephaly with clozapine (11 exposures). Four other series2-4,16 were underpowered to detect concerns related specifically to clozapine.
There are insufficient data to identify risks related specifically to clozapine use during pregnancy. However, the rare but severe adverse effects associated with clozapine in other patient populations—including agranulocytosis and severe constipation17—could be devastating in a pregnant patient, which suggests this medication would not be a first-line treatment.
Olanzapine. In postmarketing surveillance studies and case reports, there have been have anecdotal cases of fetal malformations related to olanzapine use during pregnancy. Several larger studies2-4,8,16 did not find higher rates of congenital malformations or any pattern of malformation types, although none were designed or powered to examine rare events. Animal data show no evidence of teratogenicity.18 A study comparing rates of placental passage of antipsychotics13 found higher rates for olanzapine than for quetiapine and risperidone, as well as higher prevalence of low birth weight and perinatal complications. A neonatal withdrawal syndrome has also been reported.19 Boden et al8 found an increased risk for gestational diabetes and macrocephaly with olanzapine.
Data suggest that olanzapine may be associated with somewhat higher rates of the adverse effects attributable to atypical antipsychotics (gestational diabetes and possibly macrocephaly), which could be related to olanzapine’s relatively higher rate of placental passage. Olanzapine could be a reasonable choice in a woman who had a history of good response to this medication, but would be lower priority than quetiapine when a new drug is indicated during pregnancy.
Quetiapine. In clinical trials, quetiapine had lower rates of placental passage compared with risperidone and olanzapine.13 One case report found only small changes in quetiapine serum levels during pregnancy.20 Prospective studies (90 exposures,8 36 exposures,2 7 exposures,16 4 exposures,3 and 4 exposures4) show no increase in fetal malformations or adverse neonatal health outcomes related to quetiapine, and manufacturer safety data reveal no teratogenic effect, although delays in fetal skeletal ossification were seen in rats and rabbits at doses comparable to the recommended human range.21
Quetiapine is a reasonable first choice when a new atypical antipsychotic is indicated for a pregnant patient.
Risperidone. Rates of placental passage of risperidone are higher compared with quetiapine.13 Postmarketing surveillance data (265 exposures22 and 10 exposures23) and prospective studies (including 72 exposures,8 49 exposures,2 51 exposures,4 16 exposures,16 and 5 exposures3) suggest risperidone has no major teratogenic effect. When malformations were present, they were similar to expected rates and types of malformations, and no specific malformation type was overrepresented. However, in some cases, researchers noted a withdrawal-emergent syndrome that included various combinations of tremors, irritability, poor feeding, and somnolence.22 Animal data are similarly reassuring, although increases in early fetal mortality and (potentially related) changes in maternal behavior have been observed in rats.24,25 A major caveat with risperidone is its propensity to cause hyperprolactinemia, which is detrimental to efforts to conceive and maintain a pregnancy.26,27
Risperidone is not associated with higher rates of adverse events in pregnancy than other atypical antipsychotics. It would not be a first choice for a woman trying to conceive or in the early stages of pregnancy, but would be a reasonable choice for a woman already well into pregnancy.
Ziprasidone. Available reports are few and generally do not report findings on ziprasidone separately.8,28 Manufacturer data includes 5 spontaneous abortions, one malformation, and one stillbirth among 57 exposures,4 and available animal data suggest significant developmental toxicity and impaired fertility.29 In pregnant rats, ziprasidone dosed as low as 0.5 times the maximum human recommended dose resulted in delayed fetal skeletal ossification, increased stillbirths, and decreased fetal weight and postnatal survival, and ziprasidone dosed as low as 0.2 times the maximum recommended human dose resulted in developmental delays and neurobehavioral impairments in offspring. In pregnant rabbits, ziprasidone dosed at 3 times the maximum recommended human dose resulted in cardiac and renal malformations.29
Although available data are too sparse to draw reliable conclusions, the small amount of human data plus animal data suggest that ziprasidone should be less preferred than other atypical antipsychotics during pregnancy.
Lurasidone. No data addressing lurasidone use in humans during pregnancy are available. Material submitted to the FDA includes no evidence of teratogenicity or embryo-fetal toxicity in rat and rabbit studies using 3 and 12 times the maximum recommended human dose (80 mg) based on a body surface area comparison.30
Asenapine. No data specifically addressing asenapine use in humans during pregnancy are available. Studies in rats and rabbits found no increase in teratogenicity, but did find increases in postimplantation loss and decreases in pup survival and weight gain with maternal doses equivalent to less than the maximum recommended human dose.31
Iloperidone. No data specifically addressing iloperidone use in humans during pregnancy are available. Animal studies of iloperidone found multiple developmental toxicities when iloperidone was administered during gestation.32 In one study, pregnant rats were given up to 26 times the maximum recommended human dose of 24 mg/d during the period of organogenesis. The highest dose caused increased early intrauterine deaths, decreased fetal weight and length, decreased fetal skeletal ossification, and increased minor fetal skeletal anomalies and variations. In a similar study using pregnant rabbits, the highest dose caused increased early intrauterine deaths and decreased fetal viability at term.
Paliperidone. In animal studies, there were no increases in fetal abnormalities when pregnant rats and rabbits were treated with up to 8 times the maximum recommended human dose of paliperidone during the period of organogenesis.33
A single case report34 measured levels of risperidone and its 9-hydroxy metabolite, paliperidone, in the breast milk of a mother who had taken risperidone during pregnancy and in the serum of her child. 9-OH-risperidone dose in breast milk was calculated as 4.7% of the weight-adjusted maternal dose, and serum levels in the infant were undetectable. No ill effects on the child were observed.
It is not possible to draw solid conclusions about atypical antipsychotics’ potential effects on human development from animal studies. Because of the lack of human data for the newer atypical antipsychotics—asenapine, iloperidone, lurasidone, paliperidone—in general these agents would not be advisable as first-line medications for treating pregnant women.
A few caveats
All atypical antipsychotics share the propensity to trigger or worsen glucose intolerance, which can have significant negative consequences in a pregnant patient. When deciding to use an atypical antipsychotic during pregnancy, blood glucose should be monitored carefully and regularly.
Because all atypical antipsychotics (except clozapine) are FDA pregnancy class C—indicating that animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks—the decision to use these medications must be based on an individualized assessment of risks and benefits. Patients and their providers together should make a fully informed decision.
There is an urgent need for larger and better-designed investigations that will be sufficiently powered to detect differences in outcomes—particularly major malformations, preterm delivery, adverse events in labor and delivery, metabolic and anthropometric effects on the newborn, and neurodevelopmental and psychiatric outcomes for individuals exposed in utero—between women without mental illness, untreated women with mental illness, and women receiving atypical antipsychotics during pregnancy. Further research into the pharmacokinetics and clinical efficacy of antipsychotics in pregnant women also would be useful. Clinicians can assist with these efforts by submitting their patient data to a pregnancy registry maintained by the Massachusetts General Hospital (see Related Resources).
Bottom Line
Treatment with atypical antipsychotics during pregnancy may increase the risk of adverse birth outcomes, but inadequately controlled mental illness also carries some degree of risk. The decision to use any atypical antipsychotic during pregnancy must be based on an individualized assessment of risks and benefits and made by the pregnant patient and her provider.
Related Resources
- Gentile S. Antipsychotic therapy during early and late pregnancy. A systematic review. Schizophr Bull. 2010;36(3):518-544. www.ncbi.nlm.nih.gov/pmc/articles/PMC2879689.
- Massachusetts General Hospital National Pregnancy Registry for Atypical Antipsychotics. www.womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry.
Drug Brand Names
Aripiprazole • Abilify Olanzapine • Zyprexa
Asenapine • Saphris Paliperidone • Invega
Clozapine • Clozaril Quetiapine • Seroquel
Haloperidol • Haldol Risperidone • Risperdal
Iloperidone • Fanapt Ziprasidone • Geodon
Lurasidone • Latuda
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Chang J, Streitman D. Physiologic adaptations to pregnancy. Neurol Clin. 2012;30(3):781-789.
2. McKenna K, Koren G, Tetelbaum M, et al. Pregnancy outcome of women using atypical antipsychotic drugs: a prospective comparative study. J Clin Psychiatry. 2005;66(4): 444-449; quiz 546.
3. Newham JJ, Thomas SH, MacRitchie K, et al. Birth weight of infants after maternal exposure to typical and atypical antipsychotics: prospective comparison study. Br J Psychiatry. 2008;192(5):333-337.
4. Reis M, Kallen B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
5. Matevosyan NR. Pregnancy and postpartum specifics in women with schizophrenia: a meta-study. Arch Gynecol Obstet. 2011;283(2):141-147.
6. Mendhekar DN, Sunder KR, Andrade C. Aripiprazole use in a pregnant schizoaffective woman. Bipolar Disord. 2006;8(3):299-300.
7. Watanabe N, Kasahara M, Sugibayashi R, et al. Perinatal use of aripiprazole: a case report. J Clin Psychopharmacol. 2011;31(3):377-379.
8. Bodén R, Lundgren M, Brandt L, et al. Antipsychotics during pregnancy: relation to fetal and maternal metabolic effects. Arch Gen Psychiatry. 2012;69(7):715-721.
9. Maáková E, Hubicˇková L. Antidepressant drug exposure during pregnancy. CZTIS small prospective study. Neuro Endocrinol Lett. 2011;32(suppl 1):53-56.
10. Bristol-Myers Squibb (Ed.). Aripiprazole: Drugdex drug evaluations, 1974-2003. Princeton, NJ: Thomson Micromedex; 2003.
11. U.S. Food and Drug Administration. FDA datasheet: Aripiprazole. http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/21436slr006_abilify_lbl.pdf. Accessed April 8, 2013.
12. Nguyen T, Teoh S, Hackett LP, et al. Placental transfer of aripiprazole. Aust N Z J Psychiatry. 2011;45(6):500-501.
13. Newport DJ, Calamaras MR, DeVane CL, et al. Atypical antipsychotic administration during late pregnancy: placental passage and obstetrical outcomes. Am J Psychiatry. 2007;164(8):1214-1220.
14. Barnas C, Bergant A, Hummer M, et al. Clozapine concentrations in maternal and fetal plasma, amniotic fluid, and breast milk. Am J Psychiatry. 1994;151(6):945.
15. Clozaril [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2013.
16. Lin H, Chen I, Chen Y, et al. Maternal schizophrenia and pregnancy outcome: does the use of antipsychotics make a difference? Schizophr Res. 2010;116(1):55-60.
17. Young CR, Bowers MB Jr, Mazure CM. Management of the adverse effects of clozapine. Schizophr Bull. 1998;24(3):
381-390.
18. Zyprexa [package insert]. Indianapolis, IN: Eli Lilly and Company; 1997.
19. Gilad O, Merlob P, Stahl B, et al. Outcome of infants exposed to olanzapine during breastfeeding. Breastfeed Med. 2011;6(2):55-58.
20. Klier CM, Mossaheb N, Saria A, et al. Pharmacokinetics and elimination of quetiapine, venlafaxine, and trazodone during pregnancy and postpartum. J Clin Psychopharmacol. 2007;27(6):720-722.
21. U.S. Food and Drug Administration. FDA datasheet: quetiapine. http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/20639se1-017,016_seroquel_lbl.pdf. Accessed April 11, 2013.
22. Coppola D, Russo LJ, Kwarta RF Jr, et al. Evaluating the postmarketing experience of risperidone use during pregnancy: pregnancy and neonatal outcomes. Drug Saf. 2007;30(3):247-264.
23. Mackay FJ, Wilton LV, Pearce GL, et al. The safety of risperidone: a post-marketing study on 7,684 patients. Hum Psychopharmacol. 1998;13(6):413-418.
24. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2012.
25. U.S. Food and Drug Administration. FDA datasheet: risperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020272s056,020588s044,021346s033,021444s03lbl.pdf. Accessed April 11, 2013.
26. Katz E, Adashi EY. Hyperprolactinemic disorders. Clin Obstet Gynecol. 1990;33(3):622-639.
27. Davis JR. Prolactin and reproductive medicine. Curr Opin Obstet Gynecol. 2004;16(4):331-337.
28. Johnson KC, Laprairie JL, Brennan PA, et al. Prenatal antipsychotic exposure and neuromotor performance during infancy. Arch Gen Psychiatry. 2012;69(8):787-794. doi: 10.1001/archgenpsychiatry.2012.160.
29. U.S. Food and Drug Administration. FDA datasheet: ziprasidone. http://www.fda.gov/downloads/Advisory
Committees/CommitteesMeetingMaterials/Pediatric AdvisoryCommittee/UCM191883.pdf. Accessed March 15, 2013.
30. U.S. Food and Drug Administration. FDA datasheet: lurasidone. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/200603Orig1s000PharmR.pdf. Accessed March 15, 2013.
31. U.S. Food and Drug Administration. FDA datasheet: asenapine. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022117s000_OtherR.pdf. Accessed March 15, 2013.
32. U.S. Food and Drug Administration. FDA datasheet: iloperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022192lbl.pdf. Accessed March 15, 2013.
33. U.S. Food and Drug Administration. FDA datasheet: paliperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021999s018lbl.pdf. Accessed March 15, 2013.
34. Weggelaar NM, Keijer WJ, Janssen PK. A case report of risperidone distribution and excretion into human milk: how to give good advice if you have not enough data available. J Clin Psychopharmacol. 2011;31(1):129-131.
1. Chang J, Streitman D. Physiologic adaptations to pregnancy. Neurol Clin. 2012;30(3):781-789.
2. McKenna K, Koren G, Tetelbaum M, et al. Pregnancy outcome of women using atypical antipsychotic drugs: a prospective comparative study. J Clin Psychiatry. 2005;66(4): 444-449; quiz 546.
3. Newham JJ, Thomas SH, MacRitchie K, et al. Birth weight of infants after maternal exposure to typical and atypical antipsychotics: prospective comparison study. Br J Psychiatry. 2008;192(5):333-337.
4. Reis M, Kallen B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
5. Matevosyan NR. Pregnancy and postpartum specifics in women with schizophrenia: a meta-study. Arch Gynecol Obstet. 2011;283(2):141-147.
6. Mendhekar DN, Sunder KR, Andrade C. Aripiprazole use in a pregnant schizoaffective woman. Bipolar Disord. 2006;8(3):299-300.
7. Watanabe N, Kasahara M, Sugibayashi R, et al. Perinatal use of aripiprazole: a case report. J Clin Psychopharmacol. 2011;31(3):377-379.
8. Bodén R, Lundgren M, Brandt L, et al. Antipsychotics during pregnancy: relation to fetal and maternal metabolic effects. Arch Gen Psychiatry. 2012;69(7):715-721.
9. Maáková E, Hubicˇková L. Antidepressant drug exposure during pregnancy. CZTIS small prospective study. Neuro Endocrinol Lett. 2011;32(suppl 1):53-56.
10. Bristol-Myers Squibb (Ed.). Aripiprazole: Drugdex drug evaluations, 1974-2003. Princeton, NJ: Thomson Micromedex; 2003.
11. U.S. Food and Drug Administration. FDA datasheet: Aripiprazole. http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/21436slr006_abilify_lbl.pdf. Accessed April 8, 2013.
12. Nguyen T, Teoh S, Hackett LP, et al. Placental transfer of aripiprazole. Aust N Z J Psychiatry. 2011;45(6):500-501.
13. Newport DJ, Calamaras MR, DeVane CL, et al. Atypical antipsychotic administration during late pregnancy: placental passage and obstetrical outcomes. Am J Psychiatry. 2007;164(8):1214-1220.
14. Barnas C, Bergant A, Hummer M, et al. Clozapine concentrations in maternal and fetal plasma, amniotic fluid, and breast milk. Am J Psychiatry. 1994;151(6):945.
15. Clozaril [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2013.
16. Lin H, Chen I, Chen Y, et al. Maternal schizophrenia and pregnancy outcome: does the use of antipsychotics make a difference? Schizophr Res. 2010;116(1):55-60.
17. Young CR, Bowers MB Jr, Mazure CM. Management of the adverse effects of clozapine. Schizophr Bull. 1998;24(3):
381-390.
18. Zyprexa [package insert]. Indianapolis, IN: Eli Lilly and Company; 1997.
19. Gilad O, Merlob P, Stahl B, et al. Outcome of infants exposed to olanzapine during breastfeeding. Breastfeed Med. 2011;6(2):55-58.
20. Klier CM, Mossaheb N, Saria A, et al. Pharmacokinetics and elimination of quetiapine, venlafaxine, and trazodone during pregnancy and postpartum. J Clin Psychopharmacol. 2007;27(6):720-722.
21. U.S. Food and Drug Administration. FDA datasheet: quetiapine. http://www.accessdata.fda.gov/drugsatfda_docs/label/2004/20639se1-017,016_seroquel_lbl.pdf. Accessed April 11, 2013.
22. Coppola D, Russo LJ, Kwarta RF Jr, et al. Evaluating the postmarketing experience of risperidone use during pregnancy: pregnancy and neonatal outcomes. Drug Saf. 2007;30(3):247-264.
23. Mackay FJ, Wilton LV, Pearce GL, et al. The safety of risperidone: a post-marketing study on 7,684 patients. Hum Psychopharmacol. 1998;13(6):413-418.
24. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; 2012.
25. U.S. Food and Drug Administration. FDA datasheet: risperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020272s056,020588s044,021346s033,021444s03lbl.pdf. Accessed April 11, 2013.
26. Katz E, Adashi EY. Hyperprolactinemic disorders. Clin Obstet Gynecol. 1990;33(3):622-639.
27. Davis JR. Prolactin and reproductive medicine. Curr Opin Obstet Gynecol. 2004;16(4):331-337.
28. Johnson KC, Laprairie JL, Brennan PA, et al. Prenatal antipsychotic exposure and neuromotor performance during infancy. Arch Gen Psychiatry. 2012;69(8):787-794. doi: 10.1001/archgenpsychiatry.2012.160.
29. U.S. Food and Drug Administration. FDA datasheet: ziprasidone. http://www.fda.gov/downloads/Advisory
Committees/CommitteesMeetingMaterials/Pediatric AdvisoryCommittee/UCM191883.pdf. Accessed March 15, 2013.
30. U.S. Food and Drug Administration. FDA datasheet: lurasidone. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/200603Orig1s000PharmR.pdf. Accessed March 15, 2013.
31. U.S. Food and Drug Administration. FDA datasheet: asenapine. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022117s000_OtherR.pdf. Accessed March 15, 2013.
32. U.S. Food and Drug Administration. FDA datasheet: iloperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/022192lbl.pdf. Accessed March 15, 2013.
33. U.S. Food and Drug Administration. FDA datasheet: paliperidone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021999s018lbl.pdf. Accessed March 15, 2013.
34. Weggelaar NM, Keijer WJ, Janssen PK. A case report of risperidone distribution and excretion into human milk: how to give good advice if you have not enough data available. J Clin Psychopharmacol. 2011;31(1):129-131.

Take CAUTION in emergency and inpatient psychiatric settings
Mental health care professionals are at increased risk of being assaulted by patients, especially in emergency and inpatient settings. Less experienced clinicians are at an even higher risk: Studies estimate that up to 56% percent of psychiatric residents have been physically assaulted by a patient.1 Some researchers have examined systematic approaches to improving violence risk assessment2; however, the assessment and interview process itself poses a risk to residents and medical students. We recommend using the mnemonic CAUTION to remind clinicians about safety considerations when working in psychiatric settings.
Communication. Talking about safety should be a priority during daily rounds. Routinely ask staff and other personnel about safety concerns. In inpatient settings, post a safety board where hospital staff can record aggressive behaviors and other safety issues displayed by patients. Notify staff whenever you plan to interact with patients at risk for aggression or when a patient seems agitated.
Attire. Follow proper dress codes to ensure personal safety and improve your ability to quickly assist others in need. Avoid wearing necklaces, ties, and high heels in inpatient psychiatric units. Valuable accessories (eg, expensive wrist watches) should not be worn because they may be broken during a “take down.”
Untreated symptoms. Be aware of patients with untreated or undertreated symptoms, including psychosis or substance intoxication. Emergency room patients or newly admitted inpatients often present the greatest risk because of their untreated symptoms (eg, patients with paranoid delusions).
Threats. Patients who express threats are at significantly increased risk of assaulting someone.3 Patients who have recently voiced threats should not be engaged alone or without adequate staff support. Inform all residents and students about specific patients who have voiced threats. Agitated and threatening patients can pose a risk to everyone in the unit, regardless of whether they have worked directly with the clinician.
Impulsivity. Approach impulsive and aggressive patients with particular caution. Until the aggression is controlled, these patients are at risk for sudden assaults when they feel provoked. Warning signs include punching a wall or breaking objects on the unit, facial muscle tightening, clenching of fists, and pacing. If a patient does not respond to redirection from staff, he or she may require seclusion, emergency medications, or both.
Options. Whenever possible, provide patients with choices, especially when a patient requests discharge or demands a particular medication. Avoid taking an authoritarian stance by clarifying reasons why the patient’s requests are being denied and by providing alternatives and options. For instance, if discharge is not indicated, direct a patient to contact the patients’ rights advocate. You also can give some agitated patients the option of taking a voluntary “timeout” or going to an isolated area to calm down.
Navigate safely. Identify potential exits from the room before the encounter. Residents and medical students should have a clear understanding of where to escape from a potential assault. Also, it is important to point out to patients where the door is should they feel threatened. Do not block the door when interviewing paranoid patients.
We suggest that less experienced clinicians refer to this mnemonic before starting work in emergency and inpatient psychiatric settings. Safety is an important consideration. By considering these basic concepts, we believe that safety can be improved.
1. Antonius D, Fuchs L, Herbert F, et al. Psychiatric assessment of aggressive patients: a violent attack on a resident. Am J Psychiatry. 2010;167(3):253-259.
2.Teo AR, Holley SR, Leary M, et al. The relationship between level of training and accuracy of violence risk assessment. Psychiatr Serv. 2012;63(11):1089-1094.
3. Maier GJ. Managing threatening behavior: the role of talk down and talk up. J Psychosoc Nurs Ment Health Serv. 1996;34(6):25-30.
Mental health care professionals are at increased risk of being assaulted by patients, especially in emergency and inpatient settings. Less experienced clinicians are at an even higher risk: Studies estimate that up to 56% percent of psychiatric residents have been physically assaulted by a patient.1 Some researchers have examined systematic approaches to improving violence risk assessment2; however, the assessment and interview process itself poses a risk to residents and medical students. We recommend using the mnemonic CAUTION to remind clinicians about safety considerations when working in psychiatric settings.
Communication. Talking about safety should be a priority during daily rounds. Routinely ask staff and other personnel about safety concerns. In inpatient settings, post a safety board where hospital staff can record aggressive behaviors and other safety issues displayed by patients. Notify staff whenever you plan to interact with patients at risk for aggression or when a patient seems agitated.
Attire. Follow proper dress codes to ensure personal safety and improve your ability to quickly assist others in need. Avoid wearing necklaces, ties, and high heels in inpatient psychiatric units. Valuable accessories (eg, expensive wrist watches) should not be worn because they may be broken during a “take down.”
Untreated symptoms. Be aware of patients with untreated or undertreated symptoms, including psychosis or substance intoxication. Emergency room patients or newly admitted inpatients often present the greatest risk because of their untreated symptoms (eg, patients with paranoid delusions).
Threats. Patients who express threats are at significantly increased risk of assaulting someone.3 Patients who have recently voiced threats should not be engaged alone or without adequate staff support. Inform all residents and students about specific patients who have voiced threats. Agitated and threatening patients can pose a risk to everyone in the unit, regardless of whether they have worked directly with the clinician.
Impulsivity. Approach impulsive and aggressive patients with particular caution. Until the aggression is controlled, these patients are at risk for sudden assaults when they feel provoked. Warning signs include punching a wall or breaking objects on the unit, facial muscle tightening, clenching of fists, and pacing. If a patient does not respond to redirection from staff, he or she may require seclusion, emergency medications, or both.
Options. Whenever possible, provide patients with choices, especially when a patient requests discharge or demands a particular medication. Avoid taking an authoritarian stance by clarifying reasons why the patient’s requests are being denied and by providing alternatives and options. For instance, if discharge is not indicated, direct a patient to contact the patients’ rights advocate. You also can give some agitated patients the option of taking a voluntary “timeout” or going to an isolated area to calm down.
Navigate safely. Identify potential exits from the room before the encounter. Residents and medical students should have a clear understanding of where to escape from a potential assault. Also, it is important to point out to patients where the door is should they feel threatened. Do not block the door when interviewing paranoid patients.
We suggest that less experienced clinicians refer to this mnemonic before starting work in emergency and inpatient psychiatric settings. Safety is an important consideration. By considering these basic concepts, we believe that safety can be improved.
Mental health care professionals are at increased risk of being assaulted by patients, especially in emergency and inpatient settings. Less experienced clinicians are at an even higher risk: Studies estimate that up to 56% percent of psychiatric residents have been physically assaulted by a patient.1 Some researchers have examined systematic approaches to improving violence risk assessment2; however, the assessment and interview process itself poses a risk to residents and medical students. We recommend using the mnemonic CAUTION to remind clinicians about safety considerations when working in psychiatric settings.
Communication. Talking about safety should be a priority during daily rounds. Routinely ask staff and other personnel about safety concerns. In inpatient settings, post a safety board where hospital staff can record aggressive behaviors and other safety issues displayed by patients. Notify staff whenever you plan to interact with patients at risk for aggression or when a patient seems agitated.
Attire. Follow proper dress codes to ensure personal safety and improve your ability to quickly assist others in need. Avoid wearing necklaces, ties, and high heels in inpatient psychiatric units. Valuable accessories (eg, expensive wrist watches) should not be worn because they may be broken during a “take down.”
Untreated symptoms. Be aware of patients with untreated or undertreated symptoms, including psychosis or substance intoxication. Emergency room patients or newly admitted inpatients often present the greatest risk because of their untreated symptoms (eg, patients with paranoid delusions).
Threats. Patients who express threats are at significantly increased risk of assaulting someone.3 Patients who have recently voiced threats should not be engaged alone or without adequate staff support. Inform all residents and students about specific patients who have voiced threats. Agitated and threatening patients can pose a risk to everyone in the unit, regardless of whether they have worked directly with the clinician.
Impulsivity. Approach impulsive and aggressive patients with particular caution. Until the aggression is controlled, these patients are at risk for sudden assaults when they feel provoked. Warning signs include punching a wall or breaking objects on the unit, facial muscle tightening, clenching of fists, and pacing. If a patient does not respond to redirection from staff, he or she may require seclusion, emergency medications, or both.
Options. Whenever possible, provide patients with choices, especially when a patient requests discharge or demands a particular medication. Avoid taking an authoritarian stance by clarifying reasons why the patient’s requests are being denied and by providing alternatives and options. For instance, if discharge is not indicated, direct a patient to contact the patients’ rights advocate. You also can give some agitated patients the option of taking a voluntary “timeout” or going to an isolated area to calm down.
Navigate safely. Identify potential exits from the room before the encounter. Residents and medical students should have a clear understanding of where to escape from a potential assault. Also, it is important to point out to patients where the door is should they feel threatened. Do not block the door when interviewing paranoid patients.
We suggest that less experienced clinicians refer to this mnemonic before starting work in emergency and inpatient psychiatric settings. Safety is an important consideration. By considering these basic concepts, we believe that safety can be improved.
1. Antonius D, Fuchs L, Herbert F, et al. Psychiatric assessment of aggressive patients: a violent attack on a resident. Am J Psychiatry. 2010;167(3):253-259.
2.Teo AR, Holley SR, Leary M, et al. The relationship between level of training and accuracy of violence risk assessment. Psychiatr Serv. 2012;63(11):1089-1094.
3. Maier GJ. Managing threatening behavior: the role of talk down and talk up. J Psychosoc Nurs Ment Health Serv. 1996;34(6):25-30.
1. Antonius D, Fuchs L, Herbert F, et al. Psychiatric assessment of aggressive patients: a violent attack on a resident. Am J Psychiatry. 2010;167(3):253-259.
2.Teo AR, Holley SR, Leary M, et al. The relationship between level of training and accuracy of violence risk assessment. Psychiatr Serv. 2012;63(11):1089-1094.
3. Maier GJ. Managing threatening behavior: the role of talk down and talk up. J Psychosoc Nurs Ment Health Serv. 1996;34(6):25-30.
Adoption by mentally ill individuals: What to recommend
Ms. T, age 28, wishes to adopt a child. She has a history of bipolar disorder, but has been stable for several years. She asks her psychiatrist if her diagnosis will disqualify her as a potential parent. She also wants to know how the psychiatrist can help with the adoption process because he has been treating her long-term and is familiar with her psychiatric history.
Many adults with a history of psychiatric illness prefer to adopt rather than have biological children. Their preference may be fueled by concerns regarding psychiatric destabilization during pregnancy or fear of psychotropic-induced fetal teratogenicity. Child adoption laws vary from state to state. Although some licensed adoption agencies sympathize with potential adoptive parents with a history of mental illness, the law usually considers the following factors:
• the potential adopter’s emotional ties to the child
• their parenting skills
• emotional needs of the child
• the potential adopter’s desire to maintain continuity of the child’s care
• permanence of the family unit of the proposed home
• the physical, moral, and mental fitness of the potential parent.
The psychiatrist’s role
So long as the adoptee’s well-being is the reason for adoption, and the adoption is in the “best interest of the child,”1 a history of mental illness does not necessarily exclude an individual from adopting a child. The psychiatrist needs to consider the potential adopter’s motives, intellectual capacity, and judgment with regards to caregiving. The psychiatrist needs to assess the degree to which the patient’s mental disorder may or may not interfere with their parenting. The clinician also needs to consider potential changes that may occur in the adopter’s personal life, work hours, recreational and social activities, and sleep patterns.
It also is important to estimate the changes that an adoption may cause in the potential adopter’s living arrangements, daily schedule, and life events such as family vacations. Based on knowledge of the patient’s psychiatric history, a clinician may need to consider whether adoption-related stress could destabilize or exacerbate the potential parent’s psychiatric condition.2 Other psychosocial factors of importance are the reliability of the adopter’s support system, their history of previous child-rearing success, care-taking arrangements, etc.1
What to consider
The potential adoptee’s unique needs also should be considered. Is the child physically handicapped or mentally challenged, and is your patient capable of handling these issues? Would there be a good temperament fit between the potential adoptive parent and child?
Because child adoption laws vary from state to state, there are no established criteria for determining the eligibility of an individual with a history of mental illness. The success of a child adoption by an individual with a history of mental illness will depend on state laws and the policy of the adoption agency. Some U.S. states and territories (Alaska, Arizona, California, Kentucky, North Dakota, and Puerto Rico) regard parental mental illness as “aggravated circumstances.”1
Although psychiatrists are not expected to be able to accurately predict the future, courts and adoption agencies may request a psychiatrist’s professional opinion on a specific adoption. See the Table for a list of suggested information to share when approached by an adoption agency or court.
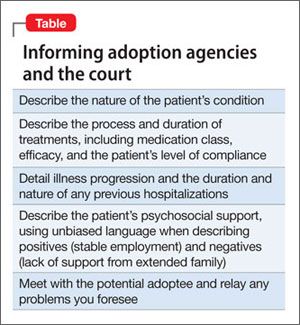
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bacani-Oropilla T, Lippmann SB, Turns DM. Should the mentally ill adopt children? How physicians can influence the decision. Postgrad Med. 1988;84(6):201-205.
2. Linn L. Clinical manifestations of psychiatric disorder: the Homes-Rahe scale of stress of adjusting to change. In: Fredman A, Kaplan H, Sadock B, eds. Modern synopsis of comprehensive textbook of psychiatry, II. 2nd ed. Baltimore, MD: Williams & Wilkins; 1976:785.
Ms. T, age 28, wishes to adopt a child. She has a history of bipolar disorder, but has been stable for several years. She asks her psychiatrist if her diagnosis will disqualify her as a potential parent. She also wants to know how the psychiatrist can help with the adoption process because he has been treating her long-term and is familiar with her psychiatric history.
Many adults with a history of psychiatric illness prefer to adopt rather than have biological children. Their preference may be fueled by concerns regarding psychiatric destabilization during pregnancy or fear of psychotropic-induced fetal teratogenicity. Child adoption laws vary from state to state. Although some licensed adoption agencies sympathize with potential adoptive parents with a history of mental illness, the law usually considers the following factors:
• the potential adopter’s emotional ties to the child
• their parenting skills
• emotional needs of the child
• the potential adopter’s desire to maintain continuity of the child’s care
• permanence of the family unit of the proposed home
• the physical, moral, and mental fitness of the potential parent.
The psychiatrist’s role
So long as the adoptee’s well-being is the reason for adoption, and the adoption is in the “best interest of the child,”1 a history of mental illness does not necessarily exclude an individual from adopting a child. The psychiatrist needs to consider the potential adopter’s motives, intellectual capacity, and judgment with regards to caregiving. The psychiatrist needs to assess the degree to which the patient’s mental disorder may or may not interfere with their parenting. The clinician also needs to consider potential changes that may occur in the adopter’s personal life, work hours, recreational and social activities, and sleep patterns.
It also is important to estimate the changes that an adoption may cause in the potential adopter’s living arrangements, daily schedule, and life events such as family vacations. Based on knowledge of the patient’s psychiatric history, a clinician may need to consider whether adoption-related stress could destabilize or exacerbate the potential parent’s psychiatric condition.2 Other psychosocial factors of importance are the reliability of the adopter’s support system, their history of previous child-rearing success, care-taking arrangements, etc.1
What to consider
The potential adoptee’s unique needs also should be considered. Is the child physically handicapped or mentally challenged, and is your patient capable of handling these issues? Would there be a good temperament fit between the potential adoptive parent and child?
Because child adoption laws vary from state to state, there are no established criteria for determining the eligibility of an individual with a history of mental illness. The success of a child adoption by an individual with a history of mental illness will depend on state laws and the policy of the adoption agency. Some U.S. states and territories (Alaska, Arizona, California, Kentucky, North Dakota, and Puerto Rico) regard parental mental illness as “aggravated circumstances.”1
Although psychiatrists are not expected to be able to accurately predict the future, courts and adoption agencies may request a psychiatrist’s professional opinion on a specific adoption. See the Table for a list of suggested information to share when approached by an adoption agency or court.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. T, age 28, wishes to adopt a child. She has a history of bipolar disorder, but has been stable for several years. She asks her psychiatrist if her diagnosis will disqualify her as a potential parent. She also wants to know how the psychiatrist can help with the adoption process because he has been treating her long-term and is familiar with her psychiatric history.
Many adults with a history of psychiatric illness prefer to adopt rather than have biological children. Their preference may be fueled by concerns regarding psychiatric destabilization during pregnancy or fear of psychotropic-induced fetal teratogenicity. Child adoption laws vary from state to state. Although some licensed adoption agencies sympathize with potential adoptive parents with a history of mental illness, the law usually considers the following factors:
• the potential adopter’s emotional ties to the child
• their parenting skills
• emotional needs of the child
• the potential adopter’s desire to maintain continuity of the child’s care
• permanence of the family unit of the proposed home
• the physical, moral, and mental fitness of the potential parent.
The psychiatrist’s role
So long as the adoptee’s well-being is the reason for adoption, and the adoption is in the “best interest of the child,”1 a history of mental illness does not necessarily exclude an individual from adopting a child. The psychiatrist needs to consider the potential adopter’s motives, intellectual capacity, and judgment with regards to caregiving. The psychiatrist needs to assess the degree to which the patient’s mental disorder may or may not interfere with their parenting. The clinician also needs to consider potential changes that may occur in the adopter’s personal life, work hours, recreational and social activities, and sleep patterns.
It also is important to estimate the changes that an adoption may cause in the potential adopter’s living arrangements, daily schedule, and life events such as family vacations. Based on knowledge of the patient’s psychiatric history, a clinician may need to consider whether adoption-related stress could destabilize or exacerbate the potential parent’s psychiatric condition.2 Other psychosocial factors of importance are the reliability of the adopter’s support system, their history of previous child-rearing success, care-taking arrangements, etc.1
What to consider
The potential adoptee’s unique needs also should be considered. Is the child physically handicapped or mentally challenged, and is your patient capable of handling these issues? Would there be a good temperament fit between the potential adoptive parent and child?
Because child adoption laws vary from state to state, there are no established criteria for determining the eligibility of an individual with a history of mental illness. The success of a child adoption by an individual with a history of mental illness will depend on state laws and the policy of the adoption agency. Some U.S. states and territories (Alaska, Arizona, California, Kentucky, North Dakota, and Puerto Rico) regard parental mental illness as “aggravated circumstances.”1
Although psychiatrists are not expected to be able to accurately predict the future, courts and adoption agencies may request a psychiatrist’s professional opinion on a specific adoption. See the Table for a list of suggested information to share when approached by an adoption agency or court.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Bacani-Oropilla T, Lippmann SB, Turns DM. Should the mentally ill adopt children? How physicians can influence the decision. Postgrad Med. 1988;84(6):201-205.
2. Linn L. Clinical manifestations of psychiatric disorder: the Homes-Rahe scale of stress of adjusting to change. In: Fredman A, Kaplan H, Sadock B, eds. Modern synopsis of comprehensive textbook of psychiatry, II. 2nd ed. Baltimore, MD: Williams & Wilkins; 1976:785.
1. Bacani-Oropilla T, Lippmann SB, Turns DM. Should the mentally ill adopt children? How physicians can influence the decision. Postgrad Med. 1988;84(6):201-205.
2. Linn L. Clinical manifestations of psychiatric disorder: the Homes-Rahe scale of stress of adjusting to change. In: Fredman A, Kaplan H, Sadock B, eds. Modern synopsis of comprehensive textbook of psychiatry, II. 2nd ed. Baltimore, MD: Williams & Wilkins; 1976:785.