User login
When can your hypochondria help patients?
Hypochondria has been useful to my patients. I mean my own hypochondria. It may not take one to know one, but we hypochondriacs understand each other.

Hypochondriacs worry that we are sick, worry that our fears are foolish and that we will be mocked for worrying about nothing, and worry even more that this time, we finally worried about something after all. Reassurance leaves us sheepish, then elated. Elation soon fades, and a new worry appears. Worry, rinse, repeat. . Some folks are just needy. Soothing the needs of the needy can feel like trying to drain the seven seas with a teaspoon. Those who work with people must either find ways to cope with the spectrum of neediness, or find another kind of work to do.
Some patient needs call for diagnosis and treatment. Other needs go beyond the strictly medical. Beyond knowing whether they are ill, patients have questions like, “Will this get worse?” “Will I be ashamed to go out in public?” “Can I visit my grandchildren, or will my daughter-in-law throw me out as contagious?” “Is this the beginning of the end?” or, worst of all, “Am I losing my hair?”
The list of possible patient needs is long, though not endless. Lining them up one after the other can make them sound melodramatic, even silly. (Other people’s worries often sound silly; your own never do.) Can a small growth or slight itch really cause existential agitation? Anyone who deals with complaints like these knows that the answer is yes.
Hypochondriacs with medical degrees cannot reassure themselves, but we can bring useful experience to help other members of the worry club. Doing so means paying attention not just to what doctors worry about but what patients do.
Sometimes a patient is terrified, the doctor not at all. Gentle sympathy may be enough. But the reverse can also be true: The doctor is concerned, but the patient thinks there is no problem. Sometimes I am worried enough to ask a patient to call or email an update. Patients who have already stopped worrying may not bother to answer the phone or shoot back an email. Failure to respond may mean they are fine, or in intensive care. Silence is hard to interpret.
Skin doctors have one advantageous disadvantage: Few tests help us beyond a skin scraping, the odd blood test, or a biopsy. Otherwise, most of the time all we can do is look, and perhaps apply “tincture of time,” watching the clinical course. We cannot send patients for the complex and expensive tests our colleagues use “just to be sure,” because we have no such tests to send them for.
Practice and experience help us recognize needs and worries that patients might not express. For instance, a man may show up with pimples on his back. His concerns seem intense. “What worries you?” we ask. The patient whispers, “It couldn’t be ... shingles, could it?” No, it couldn’t be shingles, because it is bilateral and for many other reasons.
The question is not whether he has shingles but why he thinks he does. Maybe his aunt suggested it. Or an article told him to watch out for it. Or his pharmacy is promoting zoster vaccination by showing huge, full-color photos of shingles cases worthy of horror movies. (Shingles the 13th!) Because he wants to visit his grandkids and his daughter is in her fourth month of pregnancy. In other words, along with the fear of cancer, fear of shingles is just out there. There are other such public concerns. Over time, we come to recognize them.
Anyone can worry, but anxiety paralyzes some to such an extent that referral to a mental health professional seems reasonable. The problem with advising it is that patients who somaticize may take exception to suggestions, however delicately put, that make us sound dismissive, locating their concern “all in the head.” Over the years, my attempts to make such referrals have met with limited success.
Dealing with needs – and neediness – can take up more of a doctor’s day than making specific diagnoses and prescribing helpful treatments. Besides, addressing needs and neediness demands skills not always stressed at school.
Practice at noting neediness makes you better at it, but no doctor nails the true wellsprings of worry all the time. We hypochondriacs can be devilishly inventive.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His latest book, “Doctoring from the Outside In,” was recently published. Write to him at [email protected].
Hypochondria has been useful to my patients. I mean my own hypochondria. It may not take one to know one, but we hypochondriacs understand each other.
Hypochondriacs worry that we are sick, worry that our fears are foolish and that we will be mocked for worrying about nothing, and worry even more that this time, we finally worried about something after all. Reassurance leaves us sheepish, then elated. Elation soon fades, and a new worry appears. Worry, rinse, repeat. . Some folks are just needy. Soothing the needs of the needy can feel like trying to drain the seven seas with a teaspoon. Those who work with people must either find ways to cope with the spectrum of neediness, or find another kind of work to do.
Some patient needs call for diagnosis and treatment. Other needs go beyond the strictly medical. Beyond knowing whether they are ill, patients have questions like, “Will this get worse?” “Will I be ashamed to go out in public?” “Can I visit my grandchildren, or will my daughter-in-law throw me out as contagious?” “Is this the beginning of the end?” or, worst of all, “Am I losing my hair?”
The list of possible patient needs is long, though not endless. Lining them up one after the other can make them sound melodramatic, even silly. (Other people’s worries often sound silly; your own never do.) Can a small growth or slight itch really cause existential agitation? Anyone who deals with complaints like these knows that the answer is yes.
Hypochondriacs with medical degrees cannot reassure themselves, but we can bring useful experience to help other members of the worry club. Doing so means paying attention not just to what doctors worry about but what patients do.
Sometimes a patient is terrified, the doctor not at all. Gentle sympathy may be enough. But the reverse can also be true: The doctor is concerned, but the patient thinks there is no problem. Sometimes I am worried enough to ask a patient to call or email an update. Patients who have already stopped worrying may not bother to answer the phone or shoot back an email. Failure to respond may mean they are fine, or in intensive care. Silence is hard to interpret.
Skin doctors have one advantageous disadvantage: Few tests help us beyond a skin scraping, the odd blood test, or a biopsy. Otherwise, most of the time all we can do is look, and perhaps apply “tincture of time,” watching the clinical course. We cannot send patients for the complex and expensive tests our colleagues use “just to be sure,” because we have no such tests to send them for.
Practice and experience help us recognize needs and worries that patients might not express. For instance, a man may show up with pimples on his back. His concerns seem intense. “What worries you?” we ask. The patient whispers, “It couldn’t be ... shingles, could it?” No, it couldn’t be shingles, because it is bilateral and for many other reasons.
The question is not whether he has shingles but why he thinks he does. Maybe his aunt suggested it. Or an article told him to watch out for it. Or his pharmacy is promoting zoster vaccination by showing huge, full-color photos of shingles cases worthy of horror movies. (Shingles the 13th!) Because he wants to visit his grandkids and his daughter is in her fourth month of pregnancy. In other words, along with the fear of cancer, fear of shingles is just out there. There are other such public concerns. Over time, we come to recognize them.
Anyone can worry, but anxiety paralyzes some to such an extent that referral to a mental health professional seems reasonable. The problem with advising it is that patients who somaticize may take exception to suggestions, however delicately put, that make us sound dismissive, locating their concern “all in the head.” Over the years, my attempts to make such referrals have met with limited success.
Dealing with needs – and neediness – can take up more of a doctor’s day than making specific diagnoses and prescribing helpful treatments. Besides, addressing needs and neediness demands skills not always stressed at school.
Practice at noting neediness makes you better at it, but no doctor nails the true wellsprings of worry all the time. We hypochondriacs can be devilishly inventive.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His latest book, “Doctoring from the Outside In,” was recently published. Write to him at [email protected].
Hypochondria has been useful to my patients. I mean my own hypochondria. It may not take one to know one, but we hypochondriacs understand each other.
Hypochondriacs worry that we are sick, worry that our fears are foolish and that we will be mocked for worrying about nothing, and worry even more that this time, we finally worried about something after all. Reassurance leaves us sheepish, then elated. Elation soon fades, and a new worry appears. Worry, rinse, repeat. . Some folks are just needy. Soothing the needs of the needy can feel like trying to drain the seven seas with a teaspoon. Those who work with people must either find ways to cope with the spectrum of neediness, or find another kind of work to do.
Some patient needs call for diagnosis and treatment. Other needs go beyond the strictly medical. Beyond knowing whether they are ill, patients have questions like, “Will this get worse?” “Will I be ashamed to go out in public?” “Can I visit my grandchildren, or will my daughter-in-law throw me out as contagious?” “Is this the beginning of the end?” or, worst of all, “Am I losing my hair?”
The list of possible patient needs is long, though not endless. Lining them up one after the other can make them sound melodramatic, even silly. (Other people’s worries often sound silly; your own never do.) Can a small growth or slight itch really cause existential agitation? Anyone who deals with complaints like these knows that the answer is yes.
Hypochondriacs with medical degrees cannot reassure themselves, but we can bring useful experience to help other members of the worry club. Doing so means paying attention not just to what doctors worry about but what patients do.
Sometimes a patient is terrified, the doctor not at all. Gentle sympathy may be enough. But the reverse can also be true: The doctor is concerned, but the patient thinks there is no problem. Sometimes I am worried enough to ask a patient to call or email an update. Patients who have already stopped worrying may not bother to answer the phone or shoot back an email. Failure to respond may mean they are fine, or in intensive care. Silence is hard to interpret.
Skin doctors have one advantageous disadvantage: Few tests help us beyond a skin scraping, the odd blood test, or a biopsy. Otherwise, most of the time all we can do is look, and perhaps apply “tincture of time,” watching the clinical course. We cannot send patients for the complex and expensive tests our colleagues use “just to be sure,” because we have no such tests to send them for.
Practice and experience help us recognize needs and worries that patients might not express. For instance, a man may show up with pimples on his back. His concerns seem intense. “What worries you?” we ask. The patient whispers, “It couldn’t be ... shingles, could it?” No, it couldn’t be shingles, because it is bilateral and for many other reasons.
The question is not whether he has shingles but why he thinks he does. Maybe his aunt suggested it. Or an article told him to watch out for it. Or his pharmacy is promoting zoster vaccination by showing huge, full-color photos of shingles cases worthy of horror movies. (Shingles the 13th!) Because he wants to visit his grandkids and his daughter is in her fourth month of pregnancy. In other words, along with the fear of cancer, fear of shingles is just out there. There are other such public concerns. Over time, we come to recognize them.
Anyone can worry, but anxiety paralyzes some to such an extent that referral to a mental health professional seems reasonable. The problem with advising it is that patients who somaticize may take exception to suggestions, however delicately put, that make us sound dismissive, locating their concern “all in the head.” Over the years, my attempts to make such referrals have met with limited success.
Dealing with needs – and neediness – can take up more of a doctor’s day than making specific diagnoses and prescribing helpful treatments. Besides, addressing needs and neediness demands skills not always stressed at school.
Practice at noting neediness makes you better at it, but no doctor nails the true wellsprings of worry all the time. We hypochondriacs can be devilishly inventive.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His latest book, “Doctoring from the Outside In,” was recently published. Write to him at [email protected].
What’s my number? Do I really need $10 million to retire from my medical practice?
“What’s my number?” When I hear this from my financial planning clients, I know they mean: In my 20-year career, this “magic number” is by far the most common thing physicians want to know.

If you look online, articles may recommend having a portfolio valued at $2 million, $5 million, and not uncommonly $10 million or more to retire. Really? $10 million? You might be thinking that surely not everyone needs that amount. Luckily, that’s true.
There’s no magic number your portfolio should be – just your number.
It’s human nature to want a simple, clear target to shoot for. But unfortunately, there’s no generic answer when it comes to saving for retirement. Even after a comprehensive hour-long review of a client’s financial plan – including insurance, investments, estate planning, and other items – the most honest answer I can give is: “It depends.” Not satisfying, I know. But there are still too many holes to fill.
By far the most important factor in getting beyond “it depends” is having an accurate estimate of annual retirement expenses. I have clients who live comfortably on $50,000 a year in retirement and others who need $250,000 or more. Knowing how much you need – your personal number – depends on the individual’s unique dream for retirement and calculating what that dream will cost.
Form a guesstimate based on savings and anticipated expenses
The total portfolio value needed to sustain an annual expense of $50,000 a year in retirement spending versus the portfolio size needed for $250,000 or more, blows apart the fiction of a universal “magic number.” It’s just not that simple. While it’s hard to gauge exactly what you will need, the right information can lead to a logical guesstimate about what size portfolio will provide you with financial independence.
In the end, it’s up to you to determine your desired retirement lifestyle. Then, the only way to get there is to calculate how much it will cost and save up for it by following a well-informed financial plan. This plan will be based on strategy that shifts from the middle to the later stages of your medical career and into retirement.
Let’s see how it works.
Early to mid-career: Focus on building up retirement savings
We ultimately want to save enough to meet our retirement expenses. But figuring out how much to save when you’re in your 40s and 50s is difficult. A mid-career physician likely has significant family- and child-related expenses. When we become empty-nesters, those expenses will decline. In retirement they may disappear entirely, but new expenses may arise.
With large variations in expenses at different life stages, it’s hard to calculate exactly how much you will need to save. Early on, the most sensible thing is putting aside a “reasonable” percentage of gross income for retirement savings.
What is a ‘reasonable’ savings goal for retirement?
As is often the case with high-income earners, many of our clients don’t have a budget or a clear picture of their current expenses and spending habits. That’s alright as long as they are building up a reasonable nest egg for the future – which begs the question of what is reasonable.
For mid-career docs, a reasonable goal to aim for is putting aside 20% of gross income for retirement. What you spend the rest of your money on is less important than how much you’re saving.
This is quite different from how you’ll handle expenses during retirement, when you no longer have a steady stream of income; rather, you have a pot of money that needs to last you another 20, 30, or even 40 years. At that point, thinking about specific expenses becomes more important (more on this topic later). That said, if you’re a mid-career doctor who is not meeting this 20% savings goal, it’s time to make a plan that will free up cash for retirement savings and investments.
Later-career docs: Calculate your spending level in retirement
Financial success means having a portfolio that can support your retirement dreams – with the confidence that your money will last and you won’t need to watch every dollar you spend. As you near retirement, your focus will shift away from accumulating savings to calculating the annual expenses you will have to meet in retirement.
A good place to start is figuring out which expenses will be necessary and which will be more flexible. To do this, separate your anticipated spending into these two categories:
- Fixed expenses: You can confidently forecast your “must-have” fixed expenses – such as property taxes, property/casualty insurance, health care costs, utilities, and groceries – because they remain steady from month to month.
- Discretionary expenses: These “like-to-have” expenses vary from month to month. This makes them harder to predict but easier to control. They might include dining out, travel, and charitable contributions.
As a retiree, understanding your fixed and discretionary expenses can help you prepare for a bear market, when the stock market can decline by 20% or more. Your portfolio won’t consist entirely of stocks, so it shouldn’t drop to that degree. Still, it will decline significantly. You may need to cut back on spending for a year or 2 to allow your portfolio to recover, particularly if the portfolio declines early in retirement.
Are you ready for retirement?
During the long bull market preceding the great recession of 2007 and 2009, many physicians retired –only to return to their practices when their portfolio values plummeted. In the exuberance of the moment, many failed to heed the warnings of many economists and got caught flat-footed.
Right now it’s a bull market, but we’re seeing concerning signs, such as an out-of-control housing market and rumblings about inflation and rising consumer costs. Sound familiar? If you hope to retire soon, take the time to objectively look around the corner so you can plan appropriately – whether your goal is to retire completely, stay in practice part-time, or even take on a new opportunity.
In an “it-depends” world, don’t be lured by a fictitious magic number, no matter what comes up when you Google: “When can I retire?” Instead, save early, imagine your dream retirement, and calculate expenses later to see what’s possible.
Dr. Greenwald is a graduate of the Albert Einstein College of Medicine, New York. Dr. Greenwald completed his internal medicine residency at the University of Minnesota, Minneapolis. He practiced internal medicine in the Twin Cities for 11 years before making the transition to financial planning for physicians, beginning in 1998.
A version of this article first appeared on Medscape.com.
“What’s my number?” When I hear this from my financial planning clients, I know they mean: In my 20-year career, this “magic number” is by far the most common thing physicians want to know.
If you look online, articles may recommend having a portfolio valued at $2 million, $5 million, and not uncommonly $10 million or more to retire. Really? $10 million? You might be thinking that surely not everyone needs that amount. Luckily, that’s true.
There’s no magic number your portfolio should be – just your number.
It’s human nature to want a simple, clear target to shoot for. But unfortunately, there’s no generic answer when it comes to saving for retirement. Even after a comprehensive hour-long review of a client’s financial plan – including insurance, investments, estate planning, and other items – the most honest answer I can give is: “It depends.” Not satisfying, I know. But there are still too many holes to fill.
By far the most important factor in getting beyond “it depends” is having an accurate estimate of annual retirement expenses. I have clients who live comfortably on $50,000 a year in retirement and others who need $250,000 or more. Knowing how much you need – your personal number – depends on the individual’s unique dream for retirement and calculating what that dream will cost.
Form a guesstimate based on savings and anticipated expenses
The total portfolio value needed to sustain an annual expense of $50,000 a year in retirement spending versus the portfolio size needed for $250,000 or more, blows apart the fiction of a universal “magic number.” It’s just not that simple. While it’s hard to gauge exactly what you will need, the right information can lead to a logical guesstimate about what size portfolio will provide you with financial independence.
In the end, it’s up to you to determine your desired retirement lifestyle. Then, the only way to get there is to calculate how much it will cost and save up for it by following a well-informed financial plan. This plan will be based on strategy that shifts from the middle to the later stages of your medical career and into retirement.
Let’s see how it works.
Early to mid-career: Focus on building up retirement savings
We ultimately want to save enough to meet our retirement expenses. But figuring out how much to save when you’re in your 40s and 50s is difficult. A mid-career physician likely has significant family- and child-related expenses. When we become empty-nesters, those expenses will decline. In retirement they may disappear entirely, but new expenses may arise.
With large variations in expenses at different life stages, it’s hard to calculate exactly how much you will need to save. Early on, the most sensible thing is putting aside a “reasonable” percentage of gross income for retirement savings.
What is a ‘reasonable’ savings goal for retirement?
As is often the case with high-income earners, many of our clients don’t have a budget or a clear picture of their current expenses and spending habits. That’s alright as long as they are building up a reasonable nest egg for the future – which begs the question of what is reasonable.
For mid-career docs, a reasonable goal to aim for is putting aside 20% of gross income for retirement. What you spend the rest of your money on is less important than how much you’re saving.
This is quite different from how you’ll handle expenses during retirement, when you no longer have a steady stream of income; rather, you have a pot of money that needs to last you another 20, 30, or even 40 years. At that point, thinking about specific expenses becomes more important (more on this topic later). That said, if you’re a mid-career doctor who is not meeting this 20% savings goal, it’s time to make a plan that will free up cash for retirement savings and investments.
Later-career docs: Calculate your spending level in retirement
Financial success means having a portfolio that can support your retirement dreams – with the confidence that your money will last and you won’t need to watch every dollar you spend. As you near retirement, your focus will shift away from accumulating savings to calculating the annual expenses you will have to meet in retirement.
A good place to start is figuring out which expenses will be necessary and which will be more flexible. To do this, separate your anticipated spending into these two categories:
- Fixed expenses: You can confidently forecast your “must-have” fixed expenses – such as property taxes, property/casualty insurance, health care costs, utilities, and groceries – because they remain steady from month to month.
- Discretionary expenses: These “like-to-have” expenses vary from month to month. This makes them harder to predict but easier to control. They might include dining out, travel, and charitable contributions.
As a retiree, understanding your fixed and discretionary expenses can help you prepare for a bear market, when the stock market can decline by 20% or more. Your portfolio won’t consist entirely of stocks, so it shouldn’t drop to that degree. Still, it will decline significantly. You may need to cut back on spending for a year or 2 to allow your portfolio to recover, particularly if the portfolio declines early in retirement.
Are you ready for retirement?
During the long bull market preceding the great recession of 2007 and 2009, many physicians retired –only to return to their practices when their portfolio values plummeted. In the exuberance of the moment, many failed to heed the warnings of many economists and got caught flat-footed.
Right now it’s a bull market, but we’re seeing concerning signs, such as an out-of-control housing market and rumblings about inflation and rising consumer costs. Sound familiar? If you hope to retire soon, take the time to objectively look around the corner so you can plan appropriately – whether your goal is to retire completely, stay in practice part-time, or even take on a new opportunity.
In an “it-depends” world, don’t be lured by a fictitious magic number, no matter what comes up when you Google: “When can I retire?” Instead, save early, imagine your dream retirement, and calculate expenses later to see what’s possible.
Dr. Greenwald is a graduate of the Albert Einstein College of Medicine, New York. Dr. Greenwald completed his internal medicine residency at the University of Minnesota, Minneapolis. He practiced internal medicine in the Twin Cities for 11 years before making the transition to financial planning for physicians, beginning in 1998.
A version of this article first appeared on Medscape.com.
“What’s my number?” When I hear this from my financial planning clients, I know they mean: In my 20-year career, this “magic number” is by far the most common thing physicians want to know.
If you look online, articles may recommend having a portfolio valued at $2 million, $5 million, and not uncommonly $10 million or more to retire. Really? $10 million? You might be thinking that surely not everyone needs that amount. Luckily, that’s true.
There’s no magic number your portfolio should be – just your number.
It’s human nature to want a simple, clear target to shoot for. But unfortunately, there’s no generic answer when it comes to saving for retirement. Even after a comprehensive hour-long review of a client’s financial plan – including insurance, investments, estate planning, and other items – the most honest answer I can give is: “It depends.” Not satisfying, I know. But there are still too many holes to fill.
By far the most important factor in getting beyond “it depends” is having an accurate estimate of annual retirement expenses. I have clients who live comfortably on $50,000 a year in retirement and others who need $250,000 or more. Knowing how much you need – your personal number – depends on the individual’s unique dream for retirement and calculating what that dream will cost.
Form a guesstimate based on savings and anticipated expenses
The total portfolio value needed to sustain an annual expense of $50,000 a year in retirement spending versus the portfolio size needed for $250,000 or more, blows apart the fiction of a universal “magic number.” It’s just not that simple. While it’s hard to gauge exactly what you will need, the right information can lead to a logical guesstimate about what size portfolio will provide you with financial independence.
In the end, it’s up to you to determine your desired retirement lifestyle. Then, the only way to get there is to calculate how much it will cost and save up for it by following a well-informed financial plan. This plan will be based on strategy that shifts from the middle to the later stages of your medical career and into retirement.
Let’s see how it works.
Early to mid-career: Focus on building up retirement savings
We ultimately want to save enough to meet our retirement expenses. But figuring out how much to save when you’re in your 40s and 50s is difficult. A mid-career physician likely has significant family- and child-related expenses. When we become empty-nesters, those expenses will decline. In retirement they may disappear entirely, but new expenses may arise.
With large variations in expenses at different life stages, it’s hard to calculate exactly how much you will need to save. Early on, the most sensible thing is putting aside a “reasonable” percentage of gross income for retirement savings.
What is a ‘reasonable’ savings goal for retirement?
As is often the case with high-income earners, many of our clients don’t have a budget or a clear picture of their current expenses and spending habits. That’s alright as long as they are building up a reasonable nest egg for the future – which begs the question of what is reasonable.
For mid-career docs, a reasonable goal to aim for is putting aside 20% of gross income for retirement. What you spend the rest of your money on is less important than how much you’re saving.
This is quite different from how you’ll handle expenses during retirement, when you no longer have a steady stream of income; rather, you have a pot of money that needs to last you another 20, 30, or even 40 years. At that point, thinking about specific expenses becomes more important (more on this topic later). That said, if you’re a mid-career doctor who is not meeting this 20% savings goal, it’s time to make a plan that will free up cash for retirement savings and investments.
Later-career docs: Calculate your spending level in retirement
Financial success means having a portfolio that can support your retirement dreams – with the confidence that your money will last and you won’t need to watch every dollar you spend. As you near retirement, your focus will shift away from accumulating savings to calculating the annual expenses you will have to meet in retirement.
A good place to start is figuring out which expenses will be necessary and which will be more flexible. To do this, separate your anticipated spending into these two categories:
- Fixed expenses: You can confidently forecast your “must-have” fixed expenses – such as property taxes, property/casualty insurance, health care costs, utilities, and groceries – because they remain steady from month to month.
- Discretionary expenses: These “like-to-have” expenses vary from month to month. This makes them harder to predict but easier to control. They might include dining out, travel, and charitable contributions.
As a retiree, understanding your fixed and discretionary expenses can help you prepare for a bear market, when the stock market can decline by 20% or more. Your portfolio won’t consist entirely of stocks, so it shouldn’t drop to that degree. Still, it will decline significantly. You may need to cut back on spending for a year or 2 to allow your portfolio to recover, particularly if the portfolio declines early in retirement.
Are you ready for retirement?
During the long bull market preceding the great recession of 2007 and 2009, many physicians retired –only to return to their practices when their portfolio values plummeted. In the exuberance of the moment, many failed to heed the warnings of many economists and got caught flat-footed.
Right now it’s a bull market, but we’re seeing concerning signs, such as an out-of-control housing market and rumblings about inflation and rising consumer costs. Sound familiar? If you hope to retire soon, take the time to objectively look around the corner so you can plan appropriately – whether your goal is to retire completely, stay in practice part-time, or even take on a new opportunity.
In an “it-depends” world, don’t be lured by a fictitious magic number, no matter what comes up when you Google: “When can I retire?” Instead, save early, imagine your dream retirement, and calculate expenses later to see what’s possible.
Dr. Greenwald is a graduate of the Albert Einstein College of Medicine, New York. Dr. Greenwald completed his internal medicine residency at the University of Minnesota, Minneapolis. He practiced internal medicine in the Twin Cities for 11 years before making the transition to financial planning for physicians, beginning in 1998.
A version of this article first appeared on Medscape.com.
A pediatrician wonders about the influence of an unhappy teacher
You are seeing a third-grader who has been experiencing some difficulty in school and his parents are wondering if he might have attention-deficit/hyperactivity disorder. In addition to interviewing his parents and doing a complete physical exam, you solicit information from his teacher, whose report confirms his struggles and also raises the possibility of an attention-deficit disorder. While the child has never been a model student, his parents have not voiced concerns at any of his previous health maintenance visits.

The child’s mother mentions that she has heard from another mother whose son and several other boys in the class have been struggling and misbehaving. Math seems to have been a particular problem. You don’t recall seeing any other third-graders whose parents have reported recent-onset school problems. But you practice in a large community with several grade schools spread out over a large county and may not be aware of a cluster.
As you get to know this child and his family better, you decide this doesn’t feel like a textbook case of ADHD, if indeed there is such a thing. You wonder if something is going on at school but you haven’t elicited any history that suggests bullying.
The parents have not expressed any concerns about the teacher, but you are beginning to wonder whether it’s time to consider the teacher’s role in this scenario. You recall reading about an article recently published in the journal Child Development that describes a study of more than 1,500 Head Start students in which the researchers found that teachers’ self-reported depressive symptoms were directly associated with lower math skills acquisition over the academic year.
There has been little published previously on an association between depressive symptoms in a teacher and academic achievement; however, the most quoted article I could find is from 2015 in which researchers studied 523 third-graders and 17 teachers at eight Florida school districts. The investigators found that in classes taught by teachers at increased risk for depression there was a decrease in the “quality of the learning environment” as determined by trained observers who watched classroom videos. It is interesting that a new math curriculum had been introduced during the academic year in which these observations were made.
Teaching can be a tough job and I guess we shouldn’t be surprised that the Rand Corporation has reported that teachers are nearly twice as likely to experience job stress and almost three times as likely to experience depression than is the general adult population.
Even if you have a strong suspicion that a depressed teacher is contributing to your patient’s academic struggles and maybe those of his classmates, what are your options? You don’t have enough information, nor would privacy concerns allow you to speak to the school administration. Your best approach would probably be to share with the child’s parents your concern that “something” in the school environment maybe contributing to the changes they are seeing, being careful to avoid singling out the teacher as the culprit because you really have nothing more than a suspicion. If the situation worsens and more parents share their stories, some of them may be bold enough to speak to the school administration.
I have always thought that here is a role for the principal. He or she may be aware of the teacher’s fragility and may be taking steps to correct the problem – but at a minimum, a visit to the classroom to get a sense for the “quality of the learning environment” would be in order.
Unfortunately, because mental health diagnoses continue to carry a stigma, it is very unlikely that a situation like this will resolve quickly to the benefit of the teacher or your patient and his classmates.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
You are seeing a third-grader who has been experiencing some difficulty in school and his parents are wondering if he might have attention-deficit/hyperactivity disorder. In addition to interviewing his parents and doing a complete physical exam, you solicit information from his teacher, whose report confirms his struggles and also raises the possibility of an attention-deficit disorder. While the child has never been a model student, his parents have not voiced concerns at any of his previous health maintenance visits.
The child’s mother mentions that she has heard from another mother whose son and several other boys in the class have been struggling and misbehaving. Math seems to have been a particular problem. You don’t recall seeing any other third-graders whose parents have reported recent-onset school problems. But you practice in a large community with several grade schools spread out over a large county and may not be aware of a cluster.
As you get to know this child and his family better, you decide this doesn’t feel like a textbook case of ADHD, if indeed there is such a thing. You wonder if something is going on at school but you haven’t elicited any history that suggests bullying.
The parents have not expressed any concerns about the teacher, but you are beginning to wonder whether it’s time to consider the teacher’s role in this scenario. You recall reading about an article recently published in the journal Child Development that describes a study of more than 1,500 Head Start students in which the researchers found that teachers’ self-reported depressive symptoms were directly associated with lower math skills acquisition over the academic year.
There has been little published previously on an association between depressive symptoms in a teacher and academic achievement; however, the most quoted article I could find is from 2015 in which researchers studied 523 third-graders and 17 teachers at eight Florida school districts. The investigators found that in classes taught by teachers at increased risk for depression there was a decrease in the “quality of the learning environment” as determined by trained observers who watched classroom videos. It is interesting that a new math curriculum had been introduced during the academic year in which these observations were made.
Teaching can be a tough job and I guess we shouldn’t be surprised that the Rand Corporation has reported that teachers are nearly twice as likely to experience job stress and almost three times as likely to experience depression than is the general adult population.
Even if you have a strong suspicion that a depressed teacher is contributing to your patient’s academic struggles and maybe those of his classmates, what are your options? You don’t have enough information, nor would privacy concerns allow you to speak to the school administration. Your best approach would probably be to share with the child’s parents your concern that “something” in the school environment maybe contributing to the changes they are seeing, being careful to avoid singling out the teacher as the culprit because you really have nothing more than a suspicion. If the situation worsens and more parents share their stories, some of them may be bold enough to speak to the school administration.
I have always thought that here is a role for the principal. He or she may be aware of the teacher’s fragility and may be taking steps to correct the problem – but at a minimum, a visit to the classroom to get a sense for the “quality of the learning environment” would be in order.
Unfortunately, because mental health diagnoses continue to carry a stigma, it is very unlikely that a situation like this will resolve quickly to the benefit of the teacher or your patient and his classmates.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
You are seeing a third-grader who has been experiencing some difficulty in school and his parents are wondering if he might have attention-deficit/hyperactivity disorder. In addition to interviewing his parents and doing a complete physical exam, you solicit information from his teacher, whose report confirms his struggles and also raises the possibility of an attention-deficit disorder. While the child has never been a model student, his parents have not voiced concerns at any of his previous health maintenance visits.
The child’s mother mentions that she has heard from another mother whose son and several other boys in the class have been struggling and misbehaving. Math seems to have been a particular problem. You don’t recall seeing any other third-graders whose parents have reported recent-onset school problems. But you practice in a large community with several grade schools spread out over a large county and may not be aware of a cluster.
As you get to know this child and his family better, you decide this doesn’t feel like a textbook case of ADHD, if indeed there is such a thing. You wonder if something is going on at school but you haven’t elicited any history that suggests bullying.
The parents have not expressed any concerns about the teacher, but you are beginning to wonder whether it’s time to consider the teacher’s role in this scenario. You recall reading about an article recently published in the journal Child Development that describes a study of more than 1,500 Head Start students in which the researchers found that teachers’ self-reported depressive symptoms were directly associated with lower math skills acquisition over the academic year.
There has been little published previously on an association between depressive symptoms in a teacher and academic achievement; however, the most quoted article I could find is from 2015 in which researchers studied 523 third-graders and 17 teachers at eight Florida school districts. The investigators found that in classes taught by teachers at increased risk for depression there was a decrease in the “quality of the learning environment” as determined by trained observers who watched classroom videos. It is interesting that a new math curriculum had been introduced during the academic year in which these observations were made.
Teaching can be a tough job and I guess we shouldn’t be surprised that the Rand Corporation has reported that teachers are nearly twice as likely to experience job stress and almost three times as likely to experience depression than is the general adult population.
Even if you have a strong suspicion that a depressed teacher is contributing to your patient’s academic struggles and maybe those of his classmates, what are your options? You don’t have enough information, nor would privacy concerns allow you to speak to the school administration. Your best approach would probably be to share with the child’s parents your concern that “something” in the school environment maybe contributing to the changes they are seeing, being careful to avoid singling out the teacher as the culprit because you really have nothing more than a suspicion. If the situation worsens and more parents share their stories, some of them may be bold enough to speak to the school administration.
I have always thought that here is a role for the principal. He or she may be aware of the teacher’s fragility and may be taking steps to correct the problem – but at a minimum, a visit to the classroom to get a sense for the “quality of the learning environment” would be in order.
Unfortunately, because mental health diagnoses continue to carry a stigma, it is very unlikely that a situation like this will resolve quickly to the benefit of the teacher or your patient and his classmates.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
The challenge of poverty to health and success: What should pediatricians do?
Some days it feels like more than half of the journal articles I encounter report data suggesting that poverty is associated with some disease entity. I realize that young postgraduates are under some pressure to publish, but I’m ready for a break. I and most pediatricians already know, or at least have assumed, that in general and with few exceptions unwellness and poverty are closely linked. Whether that association is causal or not is a more interesting question. The answer, I suspect, depends on which health condition we are talking about. For the moment I think we should assume that poverty is more likely a major contributor and not merely a fellow traveler of poor health.
Some other questions: What are we as pediatricians expected to do about poverty? Is awareness sufficient? Should I be content with having an elevated awareness that a certain patient has a given disease because I know his family is economically challenged? Or, conversely, should I be satisfied that I have asked about a family’s economic distress when I have just diagnosed a child with asthma? The answer to those questions is a very personal one for each of us to ponder and may depend on where we feel we can best invest our time and skill set.
Like me, you may feel that the focus of your professional life is better spent diagnosing and treating the collateral damage of poverty and addressing economic inequities in your philanthropic activities and your choices at the polls. On the other hand, you may choose to use your public persona as a physician to more actively address poverty whether it is on a local, national, or global stage. There is no correct answer and a hybrid may work best for you.
On the other hand, while you agree that there is some link between poverty and unwellness, perhaps the issue is overblown and we should pay more attention to other factors such as the sad state of the family in both disadvantaged and advantaged populations. Maybe if we worked harder to foster and support two-parent families the drag of economic disadvantage would be reduced.
I recently encountered a study that explores this very question. Christina Cross, PhD, a postdoctoral fellow in the department of sociology at Harvard University, reports on her soon-to-be-published study of a nationally representative sample in which she found that, using a selection of academic metrics including earned grades, likelihood of grade repetition, and rates of suspension, in low-income families there was no difference in achievement between Black youth raised in single-parent households and Black youth raised in two-parent households. However, in well-off families, Black youth raised in two-parent households had better academic metrics. (“Why living in a two-parent home isn’t a cure-all for Black students.” Christina Cross. The Harvard Gazette. 2021 Jun 3).
I guess few of us are surprised that living in a two-parent household can provide a child with some advantages. However, it is disappointing and again not surprising that poverty can rob a child of these advantages. While it may make us feel like we are doing something when we offer counseling that promotes two-family households, this may be no more valuable than supporting apple pie and motherhood. Dr. Cross concludes that President Biden’s proposed American Families Plan is more likely to succeed than those focused on counseling because it will offer direct financial support with its tax credits and subsidies.*
Let’s hope she is correct.
* This story was updated on July 6, 2021.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Some days it feels like more than half of the journal articles I encounter report data suggesting that poverty is associated with some disease entity. I realize that young postgraduates are under some pressure to publish, but I’m ready for a break. I and most pediatricians already know, or at least have assumed, that in general and with few exceptions unwellness and poverty are closely linked. Whether that association is causal or not is a more interesting question. The answer, I suspect, depends on which health condition we are talking about. For the moment I think we should assume that poverty is more likely a major contributor and not merely a fellow traveler of poor health.
Some other questions: What are we as pediatricians expected to do about poverty? Is awareness sufficient? Should I be content with having an elevated awareness that a certain patient has a given disease because I know his family is economically challenged? Or, conversely, should I be satisfied that I have asked about a family’s economic distress when I have just diagnosed a child with asthma? The answer to those questions is a very personal one for each of us to ponder and may depend on where we feel we can best invest our time and skill set.
Like me, you may feel that the focus of your professional life is better spent diagnosing and treating the collateral damage of poverty and addressing economic inequities in your philanthropic activities and your choices at the polls. On the other hand, you may choose to use your public persona as a physician to more actively address poverty whether it is on a local, national, or global stage. There is no correct answer and a hybrid may work best for you.
On the other hand, while you agree that there is some link between poverty and unwellness, perhaps the issue is overblown and we should pay more attention to other factors such as the sad state of the family in both disadvantaged and advantaged populations. Maybe if we worked harder to foster and support two-parent families the drag of economic disadvantage would be reduced.
I recently encountered a study that explores this very question. Christina Cross, PhD, a postdoctoral fellow in the department of sociology at Harvard University, reports on her soon-to-be-published study of a nationally representative sample in which she found that, using a selection of academic metrics including earned grades, likelihood of grade repetition, and rates of suspension, in low-income families there was no difference in achievement between Black youth raised in single-parent households and Black youth raised in two-parent households. However, in well-off families, Black youth raised in two-parent households had better academic metrics. (“Why living in a two-parent home isn’t a cure-all for Black students.” Christina Cross. The Harvard Gazette. 2021 Jun 3).
I guess few of us are surprised that living in a two-parent household can provide a child with some advantages. However, it is disappointing and again not surprising that poverty can rob a child of these advantages. While it may make us feel like we are doing something when we offer counseling that promotes two-family households, this may be no more valuable than supporting apple pie and motherhood. Dr. Cross concludes that President Biden’s proposed American Families Plan is more likely to succeed than those focused on counseling because it will offer direct financial support with its tax credits and subsidies.*
Let’s hope she is correct.
* This story was updated on July 6, 2021.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Some days it feels like more than half of the journal articles I encounter report data suggesting that poverty is associated with some disease entity. I realize that young postgraduates are under some pressure to publish, but I’m ready for a break. I and most pediatricians already know, or at least have assumed, that in general and with few exceptions unwellness and poverty are closely linked. Whether that association is causal or not is a more interesting question. The answer, I suspect, depends on which health condition we are talking about. For the moment I think we should assume that poverty is more likely a major contributor and not merely a fellow traveler of poor health.
Some other questions: What are we as pediatricians expected to do about poverty? Is awareness sufficient? Should I be content with having an elevated awareness that a certain patient has a given disease because I know his family is economically challenged? Or, conversely, should I be satisfied that I have asked about a family’s economic distress when I have just diagnosed a child with asthma? The answer to those questions is a very personal one for each of us to ponder and may depend on where we feel we can best invest our time and skill set.
Like me, you may feel that the focus of your professional life is better spent diagnosing and treating the collateral damage of poverty and addressing economic inequities in your philanthropic activities and your choices at the polls. On the other hand, you may choose to use your public persona as a physician to more actively address poverty whether it is on a local, national, or global stage. There is no correct answer and a hybrid may work best for you.
On the other hand, while you agree that there is some link between poverty and unwellness, perhaps the issue is overblown and we should pay more attention to other factors such as the sad state of the family in both disadvantaged and advantaged populations. Maybe if we worked harder to foster and support two-parent families the drag of economic disadvantage would be reduced.
I recently encountered a study that explores this very question. Christina Cross, PhD, a postdoctoral fellow in the department of sociology at Harvard University, reports on her soon-to-be-published study of a nationally representative sample in which she found that, using a selection of academic metrics including earned grades, likelihood of grade repetition, and rates of suspension, in low-income families there was no difference in achievement between Black youth raised in single-parent households and Black youth raised in two-parent households. However, in well-off families, Black youth raised in two-parent households had better academic metrics. (“Why living in a two-parent home isn’t a cure-all for Black students.” Christina Cross. The Harvard Gazette. 2021 Jun 3).
I guess few of us are surprised that living in a two-parent household can provide a child with some advantages. However, it is disappointing and again not surprising that poverty can rob a child of these advantages. While it may make us feel like we are doing something when we offer counseling that promotes two-family households, this may be no more valuable than supporting apple pie and motherhood. Dr. Cross concludes that President Biden’s proposed American Families Plan is more likely to succeed than those focused on counseling because it will offer direct financial support with its tax credits and subsidies.*
Let’s hope she is correct.
* This story was updated on July 6, 2021.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
The challenge of ‘holding space’ while holding the pager
At morning shift change a few months ago on my consultation-liaison rotation, I thanked the night float resident who had been called to a case that was not at all psychiatrically acute. When I told my colleague I was sorry she had had such a “soft consult” during a busy shift, she graciously replied that the patient had been exceedingly pleasant. She said, “Sometimes we just offer our presence, and you know what? I’m glad I’m in that kind of field. The ‘being-present’ kind of field.”
As mental health professionals, we pride ourselves on being present for our patients and our colleagues alike. Winnicott1 originally coined the psychoanalytic term “holding” to denote one of the earliest stages of parental care, wherein an environment of both physical and emotional reliability allows a child to develop their sense of self. The complementary concept of “containing,” developed by Bion,2 indicates a parental figure’s receiving the child’s emotions, however difficult, and then processing them into a more tolerable form. I am frequently struck by how often our role as psychiatrists is not necessarily to offer a specific diagnosis or medication recommendation, but instead to “hold” by listening, “contain” whatever emotions emerge, and offer a sense of validation and perhaps a biopsychosocial formulation for the patient’s experience.3-5 In the consultation-liaison setting, we might assess the contribution of sleep cycle disturbance, postoperative opioids, and anticholinergic medications on a patient’s mental status. Just as important, we might help the patient and their primary team understand that the patient’s history of childhood trauma could, under stressful conditions such as a prolonged hospitalization, lead to affective dysregulation and result in projective identification through which the team felt just as frustrated and helpless as the patient.
The relentless pursuit of efficiency vs time spent with patients
In inpatient work, I may serve as short-term psychotherapist for the patient, their family members, or a consulting team, and I treasure the time spent in those roles. But I concurrently hold various other responsibilities during my shift, including the roles of triage clinician, medical ethicist, and psychopharmacology expert (or, in the case of a newly-third-year resident such as myself, a nonexpert trying to build her knowledge base). I am also literally holding a pager, which intrudes—with aggressive cacophony, vibration, or both—upon the sanctity of any space. The pager is a reminder of a myriad of tasks: calling collateral, answering questions from team members, pre-charting, note-writing, ordering labs, checking labs, updating the handoff, reconciling medication lists, filling out legal paperwork, triaging the next consult. These are unavoidable and generally necessary parts of clinical work, but sometimes they veer into sheer drudgery.
As a medical student, learning to complete tasks is a substantial part of each clinical rotation, and task completion provides plenty of dopaminergic reinforcements that could masquerade as job satisfaction. Through my first year and a half of residency, I pushed hard to build “efficiency” in my workflow, but eventually, task completion stopped providing sufficient inherent satisfaction. It has been a relief to find that amid the stream of checkboxes, the true work of psychiatric care (the interactions with patients, their clinical presentations, and considering their differential diagnoses and treatment options) feels deeply meaningful and ever more fascinating.
At times, I am angered by the reality of limited clinician bandwidth. This frustration motivates me to seek system-level improvements that can enable us to deliver quality psychiatric care while mitigating the risk of clinician burnout. What ends up shortchanged in the relentless pursuit of efficiency is the time spent with patients. This is never more apparent than during a busy inpatient shift, when I often need to compress patient interactions and focus only on the most acute clinical questions. When I have to apologize for stepping out of the interview room to answer yet another page, I marvel at seeing attending psychiatrists who—with apparent ease—make patients feel as if they have all the time in the world, and I wonder when I will be able to do the same.
And yet, there are other times when my pager stays blessedly quiet, time can slow down in the room, and I can make a patient feel heard, held, and contained. In those moments, I also hold my own need for connection with the patient, and can recall what my colleague reminded me: what a privilege it is to be in the “being-present” kind of field.
1. Winnicott DW. The theory of the parent-infant relationship. Int J Psychoanal. 1961;41:585-595.
2. Bion WR. Learning from experience. William Heinemann Medical Books; 1962.
3. Green SA. Psychotherapeutic principles and techniques: principles of medical psychotherapy. In: Fogel BS, Greenberg DB, eds. Psychiatric care of the medical patient. 3rd ed. Oxford University Press; 2015:191-204.
4. Griffith JL, Gaby L. Brief psychotherapy at the bedside: countering demoralization from medical illness. Psychosomatics. 2005;46(2):109-116. doi:10.1176/appi.psy.46.2.109
5. Nash SS, Kent LK, Muskin PR. Psychodynamics in medically ill patients. Harv Rev Psychiatry. 2009;17(6):389-397. doi:10.3109/10673220903465726
At morning shift change a few months ago on my consultation-liaison rotation, I thanked the night float resident who had been called to a case that was not at all psychiatrically acute. When I told my colleague I was sorry she had had such a “soft consult” during a busy shift, she graciously replied that the patient had been exceedingly pleasant. She said, “Sometimes we just offer our presence, and you know what? I’m glad I’m in that kind of field. The ‘being-present’ kind of field.”
As mental health professionals, we pride ourselves on being present for our patients and our colleagues alike. Winnicott1 originally coined the psychoanalytic term “holding” to denote one of the earliest stages of parental care, wherein an environment of both physical and emotional reliability allows a child to develop their sense of self. The complementary concept of “containing,” developed by Bion,2 indicates a parental figure’s receiving the child’s emotions, however difficult, and then processing them into a more tolerable form. I am frequently struck by how often our role as psychiatrists is not necessarily to offer a specific diagnosis or medication recommendation, but instead to “hold” by listening, “contain” whatever emotions emerge, and offer a sense of validation and perhaps a biopsychosocial formulation for the patient’s experience.3-5 In the consultation-liaison setting, we might assess the contribution of sleep cycle disturbance, postoperative opioids, and anticholinergic medications on a patient’s mental status. Just as important, we might help the patient and their primary team understand that the patient’s history of childhood trauma could, under stressful conditions such as a prolonged hospitalization, lead to affective dysregulation and result in projective identification through which the team felt just as frustrated and helpless as the patient.
The relentless pursuit of efficiency vs time spent with patients
In inpatient work, I may serve as short-term psychotherapist for the patient, their family members, or a consulting team, and I treasure the time spent in those roles. But I concurrently hold various other responsibilities during my shift, including the roles of triage clinician, medical ethicist, and psychopharmacology expert (or, in the case of a newly-third-year resident such as myself, a nonexpert trying to build her knowledge base). I am also literally holding a pager, which intrudes—with aggressive cacophony, vibration, or both—upon the sanctity of any space. The pager is a reminder of a myriad of tasks: calling collateral, answering questions from team members, pre-charting, note-writing, ordering labs, checking labs, updating the handoff, reconciling medication lists, filling out legal paperwork, triaging the next consult. These are unavoidable and generally necessary parts of clinical work, but sometimes they veer into sheer drudgery.
As a medical student, learning to complete tasks is a substantial part of each clinical rotation, and task completion provides plenty of dopaminergic reinforcements that could masquerade as job satisfaction. Through my first year and a half of residency, I pushed hard to build “efficiency” in my workflow, but eventually, task completion stopped providing sufficient inherent satisfaction. It has been a relief to find that amid the stream of checkboxes, the true work of psychiatric care (the interactions with patients, their clinical presentations, and considering their differential diagnoses and treatment options) feels deeply meaningful and ever more fascinating.
At times, I am angered by the reality of limited clinician bandwidth. This frustration motivates me to seek system-level improvements that can enable us to deliver quality psychiatric care while mitigating the risk of clinician burnout. What ends up shortchanged in the relentless pursuit of efficiency is the time spent with patients. This is never more apparent than during a busy inpatient shift, when I often need to compress patient interactions and focus only on the most acute clinical questions. When I have to apologize for stepping out of the interview room to answer yet another page, I marvel at seeing attending psychiatrists who—with apparent ease—make patients feel as if they have all the time in the world, and I wonder when I will be able to do the same.
And yet, there are other times when my pager stays blessedly quiet, time can slow down in the room, and I can make a patient feel heard, held, and contained. In those moments, I also hold my own need for connection with the patient, and can recall what my colleague reminded me: what a privilege it is to be in the “being-present” kind of field.
At morning shift change a few months ago on my consultation-liaison rotation, I thanked the night float resident who had been called to a case that was not at all psychiatrically acute. When I told my colleague I was sorry she had had such a “soft consult” during a busy shift, she graciously replied that the patient had been exceedingly pleasant. She said, “Sometimes we just offer our presence, and you know what? I’m glad I’m in that kind of field. The ‘being-present’ kind of field.”
As mental health professionals, we pride ourselves on being present for our patients and our colleagues alike. Winnicott1 originally coined the psychoanalytic term “holding” to denote one of the earliest stages of parental care, wherein an environment of both physical and emotional reliability allows a child to develop their sense of self. The complementary concept of “containing,” developed by Bion,2 indicates a parental figure’s receiving the child’s emotions, however difficult, and then processing them into a more tolerable form. I am frequently struck by how often our role as psychiatrists is not necessarily to offer a specific diagnosis or medication recommendation, but instead to “hold” by listening, “contain” whatever emotions emerge, and offer a sense of validation and perhaps a biopsychosocial formulation for the patient’s experience.3-5 In the consultation-liaison setting, we might assess the contribution of sleep cycle disturbance, postoperative opioids, and anticholinergic medications on a patient’s mental status. Just as important, we might help the patient and their primary team understand that the patient’s history of childhood trauma could, under stressful conditions such as a prolonged hospitalization, lead to affective dysregulation and result in projective identification through which the team felt just as frustrated and helpless as the patient.
The relentless pursuit of efficiency vs time spent with patients
In inpatient work, I may serve as short-term psychotherapist for the patient, their family members, or a consulting team, and I treasure the time spent in those roles. But I concurrently hold various other responsibilities during my shift, including the roles of triage clinician, medical ethicist, and psychopharmacology expert (or, in the case of a newly-third-year resident such as myself, a nonexpert trying to build her knowledge base). I am also literally holding a pager, which intrudes—with aggressive cacophony, vibration, or both—upon the sanctity of any space. The pager is a reminder of a myriad of tasks: calling collateral, answering questions from team members, pre-charting, note-writing, ordering labs, checking labs, updating the handoff, reconciling medication lists, filling out legal paperwork, triaging the next consult. These are unavoidable and generally necessary parts of clinical work, but sometimes they veer into sheer drudgery.
As a medical student, learning to complete tasks is a substantial part of each clinical rotation, and task completion provides plenty of dopaminergic reinforcements that could masquerade as job satisfaction. Through my first year and a half of residency, I pushed hard to build “efficiency” in my workflow, but eventually, task completion stopped providing sufficient inherent satisfaction. It has been a relief to find that amid the stream of checkboxes, the true work of psychiatric care (the interactions with patients, their clinical presentations, and considering their differential diagnoses and treatment options) feels deeply meaningful and ever more fascinating.
At times, I am angered by the reality of limited clinician bandwidth. This frustration motivates me to seek system-level improvements that can enable us to deliver quality psychiatric care while mitigating the risk of clinician burnout. What ends up shortchanged in the relentless pursuit of efficiency is the time spent with patients. This is never more apparent than during a busy inpatient shift, when I often need to compress patient interactions and focus only on the most acute clinical questions. When I have to apologize for stepping out of the interview room to answer yet another page, I marvel at seeing attending psychiatrists who—with apparent ease—make patients feel as if they have all the time in the world, and I wonder when I will be able to do the same.
And yet, there are other times when my pager stays blessedly quiet, time can slow down in the room, and I can make a patient feel heard, held, and contained. In those moments, I also hold my own need for connection with the patient, and can recall what my colleague reminded me: what a privilege it is to be in the “being-present” kind of field.
1. Winnicott DW. The theory of the parent-infant relationship. Int J Psychoanal. 1961;41:585-595.
2. Bion WR. Learning from experience. William Heinemann Medical Books; 1962.
3. Green SA. Psychotherapeutic principles and techniques: principles of medical psychotherapy. In: Fogel BS, Greenberg DB, eds. Psychiatric care of the medical patient. 3rd ed. Oxford University Press; 2015:191-204.
4. Griffith JL, Gaby L. Brief psychotherapy at the bedside: countering demoralization from medical illness. Psychosomatics. 2005;46(2):109-116. doi:10.1176/appi.psy.46.2.109
5. Nash SS, Kent LK, Muskin PR. Psychodynamics in medically ill patients. Harv Rev Psychiatry. 2009;17(6):389-397. doi:10.3109/10673220903465726
1. Winnicott DW. The theory of the parent-infant relationship. Int J Psychoanal. 1961;41:585-595.
2. Bion WR. Learning from experience. William Heinemann Medical Books; 1962.
3. Green SA. Psychotherapeutic principles and techniques: principles of medical psychotherapy. In: Fogel BS, Greenberg DB, eds. Psychiatric care of the medical patient. 3rd ed. Oxford University Press; 2015:191-204.
4. Griffith JL, Gaby L. Brief psychotherapy at the bedside: countering demoralization from medical illness. Psychosomatics. 2005;46(2):109-116. doi:10.1176/appi.psy.46.2.109
5. Nash SS, Kent LK, Muskin PR. Psychodynamics in medically ill patients. Harv Rev Psychiatry. 2009;17(6):389-397. doi:10.3109/10673220903465726

From ideology to articles of faith: The ‘religification’ of political beliefs
Man is a political animal.
— Aristotle, Politics , Book 1, Section 1253a
Religion is the opium of the people.
— Karl Marx, A contribution to the critique of Hegel’s philosophy of right , introduction
Beliefs are at the core of psychiatric practice. Our patients are often shackled by their anomalous beliefs, which are not reality-based. These beliefs are often the primary targets of psychiatric treatment. Consider a day at the office of a psychiatrist who may see several patients impaired by false beliefs, such as:
- My neighbor is reading my mind remotely and is plotting to kill me
- If I ride on a plane, it will crash and I will die
- I am a failure, a worthless person, and a burden on my family
- I am hopeless and helpless; life is too painful and not worth living anymore
- I am a prophet with supernatural gifts, and I can predict the future
- Whenever I take this substance, I feel I can jump out of a window and fly
- If I do not shower 5 times in a row every night before going to bed, something terrible will happen to my family.
Patients with false beliefs obviously need psychiatric care. However, a large number of religious individuals harbor “unusual” beliefs involving angels and devils and hell and paradise after death. Those people of faith are not considered to have a DSM-5 psychiatric disorder. Billions of people around the world belong to one of the approximately 4,300 religions, which they celebrate using one of the more than 6,800 living languages. Psychiatrists encourage patients to have a faith because it can be quite comforting to its adherents, enhancing their social relations and providing them with hope and resilience during the darkest days of life. Regular attendance at a house of worship is a measure of the strong roots of one’s faith.
So why have there been so many religious wars over centuries of recorded history? Why have millions of people died during conflicts among religions? Why does one religious group adamantly believe that theirs is the real God, while the god of other religions is fake? And why have people who withdrew from or refused to adopt a certain religious belief been persecuted; labeled as “heretic,” “infidel,” “heathen,” or “apostate”; and burned at the stake or beheaded? Perhaps religion is not always a kinder, gentler belief system.
Continue to: Recent statistics...
Recent statistics show a precipitous decline in religious observance in the United States.1 So what happens to a society that gradually abandons its previously entrenched religious beliefs and becomes secular? This trend is spreading widely in Europe and North America. But widely held beliefs with powerful personal meaning don’t just fizzle away: they re-emerge in another form. The substantial energy of religious faith must be invested elsewhere and manifested in an alternative form with similar dynamics.
Enter politics!
It seems that humans’ need to uphold a strong belief is so powerful that they either incorporate political doctrines side-by-side with their religious beliefs (if the 2 are compatible) or adopt a strong political belief if they abandon their religion and become secular. This does not have to be an intellectually wrenching change because there are many similarities between hyper-religiosity and fanatic political beliefs (Table).

The toxic hyperpartisanship that has dominated the United States over the past several years may be the culmination of an intensified “religification” of politics. The incendiary mix of religious zealotry and political fanaticism is conducive to intensified loathing, hostility, and animus to those with an opposing political ideology.
So it all boils down to the human imperative of harboring a strong personal belief. What is the origin of beliefs, religious, political, or otherwise? Why does the human species have the overwhelming need to uphold a belief? Research suggests that it is the result of evolution and the phylogenetic enlargement of the brain, including the parietal and medial frontal cortex in humans.2 And according to many studies, abnormal and delusional beliefs encountered in psychiatric practice appear to be caused by altered perception and/or misattribution of aversive meaning.3 Lesions in the right hemisphere have been reported to play an important role in generating delusional beliefs.4 A healthy right hemisphere plays an important role in:
- pragmatic communications
- perceptual integration
- attentional surveillance and anomaly novelty detection
- belief updating.4
Right hemispheric pathology disrupts those functions and can lead to false beliefs such as delusions, or, on a milder scale, strongly held superstitions.
One wonders how the structure and function of the right hemisphere generates and perpetuates a belief in a religion or political ideology that ultimately shapes one’s life. Religiosity and politics are an inherent part of human nature, and they can replace each other or merge together. If one is to believe what Durkheim5 proposed more than a century ago, the existence of belief systems is essential for societal stability. He posited that the absence of stable belief systems can lead to what he labeled “anomie,” leading to a surge of suicide and crime. If that is true, then the coexistence of religious and political beliefs may have a significant upside, but also with a palpable downside when either or both of those belief systems become excessively antagonistic or extreme. Three cheers for religious and political moderation that allows them to peacefully coexist.
1. Jones JM. U.S. church membership falls below majority for first time. Gallup. March 29, 2021. Accessed June 7, 2021. https://news.gallup.com/poll/341963/church-membership-falls-below-majority-first-time.aspx
2. Seitz RJ, Angel HF. Belief formation—a driving force for brain evolution. Brain Cogn. 2020;140:105548. doi: 10.1016/j.bandc.2020.105548
3. Seitz RJ. Beliefs: a challenge in neuropsychological disorders. J Neuropsychol. 2021. doi: 10.1111/jnp.12249
4. Gurin L, Blum S. Delusions and the right hemisphere: a review of the case for the right hemisphere as a mediator of reality-based belief. J Neuropsychiatry Clin Neurosci. 2017;29(3):225-235. doi: 10.1176/appi.neuropsych.16060118
5. Durkheim E. Suicide: a study in sociology. The Free Press; 1951.
Man is a political animal.
— Aristotle, Politics , Book 1, Section 1253a
Religion is the opium of the people.
— Karl Marx, A contribution to the critique of Hegel’s philosophy of right , introduction
Beliefs are at the core of psychiatric practice. Our patients are often shackled by their anomalous beliefs, which are not reality-based. These beliefs are often the primary targets of psychiatric treatment. Consider a day at the office of a psychiatrist who may see several patients impaired by false beliefs, such as:
- My neighbor is reading my mind remotely and is plotting to kill me
- If I ride on a plane, it will crash and I will die
- I am a failure, a worthless person, and a burden on my family
- I am hopeless and helpless; life is too painful and not worth living anymore
- I am a prophet with supernatural gifts, and I can predict the future
- Whenever I take this substance, I feel I can jump out of a window and fly
- If I do not shower 5 times in a row every night before going to bed, something terrible will happen to my family.
Patients with false beliefs obviously need psychiatric care. However, a large number of religious individuals harbor “unusual” beliefs involving angels and devils and hell and paradise after death. Those people of faith are not considered to have a DSM-5 psychiatric disorder. Billions of people around the world belong to one of the approximately 4,300 religions, which they celebrate using one of the more than 6,800 living languages. Psychiatrists encourage patients to have a faith because it can be quite comforting to its adherents, enhancing their social relations and providing them with hope and resilience during the darkest days of life. Regular attendance at a house of worship is a measure of the strong roots of one’s faith.
So why have there been so many religious wars over centuries of recorded history? Why have millions of people died during conflicts among religions? Why does one religious group adamantly believe that theirs is the real God, while the god of other religions is fake? And why have people who withdrew from or refused to adopt a certain religious belief been persecuted; labeled as “heretic,” “infidel,” “heathen,” or “apostate”; and burned at the stake or beheaded? Perhaps religion is not always a kinder, gentler belief system.
Continue to: Recent statistics...
Recent statistics show a precipitous decline in religious observance in the United States.1 So what happens to a society that gradually abandons its previously entrenched religious beliefs and becomes secular? This trend is spreading widely in Europe and North America. But widely held beliefs with powerful personal meaning don’t just fizzle away: they re-emerge in another form. The substantial energy of religious faith must be invested elsewhere and manifested in an alternative form with similar dynamics.
Enter politics!
It seems that humans’ need to uphold a strong belief is so powerful that they either incorporate political doctrines side-by-side with their religious beliefs (if the 2 are compatible) or adopt a strong political belief if they abandon their religion and become secular. This does not have to be an intellectually wrenching change because there are many similarities between hyper-religiosity and fanatic political beliefs (Table).
The toxic hyperpartisanship that has dominated the United States over the past several years may be the culmination of an intensified “religification” of politics. The incendiary mix of religious zealotry and political fanaticism is conducive to intensified loathing, hostility, and animus to those with an opposing political ideology.
So it all boils down to the human imperative of harboring a strong personal belief. What is the origin of beliefs, religious, political, or otherwise? Why does the human species have the overwhelming need to uphold a belief? Research suggests that it is the result of evolution and the phylogenetic enlargement of the brain, including the parietal and medial frontal cortex in humans.2 And according to many studies, abnormal and delusional beliefs encountered in psychiatric practice appear to be caused by altered perception and/or misattribution of aversive meaning.3 Lesions in the right hemisphere have been reported to play an important role in generating delusional beliefs.4 A healthy right hemisphere plays an important role in:
- pragmatic communications
- perceptual integration
- attentional surveillance and anomaly novelty detection
- belief updating.4
Right hemispheric pathology disrupts those functions and can lead to false beliefs such as delusions, or, on a milder scale, strongly held superstitions.
One wonders how the structure and function of the right hemisphere generates and perpetuates a belief in a religion or political ideology that ultimately shapes one’s life. Religiosity and politics are an inherent part of human nature, and they can replace each other or merge together. If one is to believe what Durkheim5 proposed more than a century ago, the existence of belief systems is essential for societal stability. He posited that the absence of stable belief systems can lead to what he labeled “anomie,” leading to a surge of suicide and crime. If that is true, then the coexistence of religious and political beliefs may have a significant upside, but also with a palpable downside when either or both of those belief systems become excessively antagonistic or extreme. Three cheers for religious and political moderation that allows them to peacefully coexist.
Man is a political animal.
— Aristotle, Politics , Book 1, Section 1253a
Religion is the opium of the people.
— Karl Marx, A contribution to the critique of Hegel’s philosophy of right , introduction
Beliefs are at the core of psychiatric practice. Our patients are often shackled by their anomalous beliefs, which are not reality-based. These beliefs are often the primary targets of psychiatric treatment. Consider a day at the office of a psychiatrist who may see several patients impaired by false beliefs, such as:
- My neighbor is reading my mind remotely and is plotting to kill me
- If I ride on a plane, it will crash and I will die
- I am a failure, a worthless person, and a burden on my family
- I am hopeless and helpless; life is too painful and not worth living anymore
- I am a prophet with supernatural gifts, and I can predict the future
- Whenever I take this substance, I feel I can jump out of a window and fly
- If I do not shower 5 times in a row every night before going to bed, something terrible will happen to my family.
Patients with false beliefs obviously need psychiatric care. However, a large number of religious individuals harbor “unusual” beliefs involving angels and devils and hell and paradise after death. Those people of faith are not considered to have a DSM-5 psychiatric disorder. Billions of people around the world belong to one of the approximately 4,300 religions, which they celebrate using one of the more than 6,800 living languages. Psychiatrists encourage patients to have a faith because it can be quite comforting to its adherents, enhancing their social relations and providing them with hope and resilience during the darkest days of life. Regular attendance at a house of worship is a measure of the strong roots of one’s faith.
So why have there been so many religious wars over centuries of recorded history? Why have millions of people died during conflicts among religions? Why does one religious group adamantly believe that theirs is the real God, while the god of other religions is fake? And why have people who withdrew from or refused to adopt a certain religious belief been persecuted; labeled as “heretic,” “infidel,” “heathen,” or “apostate”; and burned at the stake or beheaded? Perhaps religion is not always a kinder, gentler belief system.
Continue to: Recent statistics...
Recent statistics show a precipitous decline in religious observance in the United States.1 So what happens to a society that gradually abandons its previously entrenched religious beliefs and becomes secular? This trend is spreading widely in Europe and North America. But widely held beliefs with powerful personal meaning don’t just fizzle away: they re-emerge in another form. The substantial energy of religious faith must be invested elsewhere and manifested in an alternative form with similar dynamics.
Enter politics!
It seems that humans’ need to uphold a strong belief is so powerful that they either incorporate political doctrines side-by-side with their religious beliefs (if the 2 are compatible) or adopt a strong political belief if they abandon their religion and become secular. This does not have to be an intellectually wrenching change because there are many similarities between hyper-religiosity and fanatic political beliefs (Table).
The toxic hyperpartisanship that has dominated the United States over the past several years may be the culmination of an intensified “religification” of politics. The incendiary mix of religious zealotry and political fanaticism is conducive to intensified loathing, hostility, and animus to those with an opposing political ideology.
So it all boils down to the human imperative of harboring a strong personal belief. What is the origin of beliefs, religious, political, or otherwise? Why does the human species have the overwhelming need to uphold a belief? Research suggests that it is the result of evolution and the phylogenetic enlargement of the brain, including the parietal and medial frontal cortex in humans.2 And according to many studies, abnormal and delusional beliefs encountered in psychiatric practice appear to be caused by altered perception and/or misattribution of aversive meaning.3 Lesions in the right hemisphere have been reported to play an important role in generating delusional beliefs.4 A healthy right hemisphere plays an important role in:
- pragmatic communications
- perceptual integration
- attentional surveillance and anomaly novelty detection
- belief updating.4
Right hemispheric pathology disrupts those functions and can lead to false beliefs such as delusions, or, on a milder scale, strongly held superstitions.
One wonders how the structure and function of the right hemisphere generates and perpetuates a belief in a religion or political ideology that ultimately shapes one’s life. Religiosity and politics are an inherent part of human nature, and they can replace each other or merge together. If one is to believe what Durkheim5 proposed more than a century ago, the existence of belief systems is essential for societal stability. He posited that the absence of stable belief systems can lead to what he labeled “anomie,” leading to a surge of suicide and crime. If that is true, then the coexistence of religious and political beliefs may have a significant upside, but also with a palpable downside when either or both of those belief systems become excessively antagonistic or extreme. Three cheers for religious and political moderation that allows them to peacefully coexist.
1. Jones JM. U.S. church membership falls below majority for first time. Gallup. March 29, 2021. Accessed June 7, 2021. https://news.gallup.com/poll/341963/church-membership-falls-below-majority-first-time.aspx
2. Seitz RJ, Angel HF. Belief formation—a driving force for brain evolution. Brain Cogn. 2020;140:105548. doi: 10.1016/j.bandc.2020.105548
3. Seitz RJ. Beliefs: a challenge in neuropsychological disorders. J Neuropsychol. 2021. doi: 10.1111/jnp.12249
4. Gurin L, Blum S. Delusions and the right hemisphere: a review of the case for the right hemisphere as a mediator of reality-based belief. J Neuropsychiatry Clin Neurosci. 2017;29(3):225-235. doi: 10.1176/appi.neuropsych.16060118
5. Durkheim E. Suicide: a study in sociology. The Free Press; 1951.
1. Jones JM. U.S. church membership falls below majority for first time. Gallup. March 29, 2021. Accessed June 7, 2021. https://news.gallup.com/poll/341963/church-membership-falls-below-majority-first-time.aspx
2. Seitz RJ, Angel HF. Belief formation—a driving force for brain evolution. Brain Cogn. 2020;140:105548. doi: 10.1016/j.bandc.2020.105548
3. Seitz RJ. Beliefs: a challenge in neuropsychological disorders. J Neuropsychol. 2021. doi: 10.1111/jnp.12249
4. Gurin L, Blum S. Delusions and the right hemisphere: a review of the case for the right hemisphere as a mediator of reality-based belief. J Neuropsychiatry Clin Neurosci. 2017;29(3):225-235. doi: 10.1176/appi.neuropsych.16060118
5. Durkheim E. Suicide: a study in sociology. The Free Press; 1951.

More on long-acting injectable antipsychotics
Benefits of early LAI use
I want to thank Dr. Nasrallah for his editorial calling for more frequent and earlier use of long-acting injectable antipsychotics (LAIs) in schizophrenia (From the Editor,
In addition to the neuroprotective biologic effects of early LAI usage, I’ve found that many of my FEP patients find great psychological comfort from incorporating LAIs into their treatment plan. The first psychotic break is generally when a person (and their family) feels the most afraid about the future and is in desperate need of hope that they can have a full life—with educational opportunities, sustained employment, meaningful relationships, and more. Just as society has seen the COVID-19 vaccines as a symbol of hope and the first step in overcoming the oppression of living in fear of an uncertain future, we need to help people experiencing FEP find hope in a needle.
Craig Chepke, MD, FAPA
Excel Psychiatric Associates
Huntersville, North Carolina
Reference
1. Chepke C. Drive-up pharmacotherapy during the COVID-19 pandemic. Current Psychiatry. 2020;19(5):29-30.
Dr. Nasrallah responds
Thank you, Dr. Chepke, for your letter confirming full support for using LAIs in schizophrenia. I like the phrase you coined: “hope in a needle.” The early use of LAIs in schizophrenia can provide the same type of hope that the vaccines against the life-threatening COVID-19 virus have generated in our society. Based on my direct observations, I also agree with you that the longer patients with schizophrenia remain on LAIs, the more engaged and happy they are with their progress and the quality of their lives. It is tragic that many patients never had the opportunity to return to their baseline with the early use of LAIs immediately following their first psychotic episode, instead of relapsing again and again due to their inability to adhere completely to their oral medications.
Henry A. Nasrallah, MD
Editor-In-Chief
Continue to: LAIs as the standard of care
LAIs as the standard of care
Thank you, Dr. Nasrallah, for reiterating the importance of compliance with pharmacologic management of schizophrenia after FEP (From the Editor,
As you point out in your editorial, the facts are powerful, well-known, undisputed, and yet not adopted in the United States, when in other countries LAIs are first-line care. Yes, LAIs are expensive, but not nearly as expensive as the disabilities caused by noncompliance are to society.
Why isn’t LAI use the standard of care here in the United States? In the United States, there is advocacy for treatment because there’s money in it. There is no good advocacy for preventive care because there’s no immediate money in it. We have another good example of this in the United States: private, for-profit prisons. They have a vested interest in keeping prisons full and building new ones. Patients with FEP are most often treated in the hospital, where a standard of care could easily be established that mandates LAIs as first-tier care. Why is that not so? Who is pushing for it? Who is resisting?
Your editorial inspired me to advocate more strongly. Do you have advice about how to effect policy change? I know administrators respond when we talk dollars and cents, not quality of care. What is the dollar cost of not using LAIs as the standard of care after FEP? Who cares? Who would listen to the numbers?
Edward A. Major, MD, LFAPA
Clinical Professor of Psychiatry
Upstate Medical Center
Syracuse, New York
Dr. Nasrallah responds
Dr. Major, thanks for your message. Establishing a standard of care for the use of LAIs (or any other therapy) is not that simple. It requires well-coordinated collaboration among several stakeholders (clinicians, researchers, payors, advocacy groups, and a national organization such as the American Psychiatric Association). The cost issue is certainly powerful, but the equation works in favor of LAIs because 1 psychiatric hospitalization due to a psychotic relapse costs up to 3 times the annual cost of an LAI medication that can prevent that rehospitalization. In addition, disability comprises the lion’s share of the large indirect costs of schizophrenia (disability payments, lifetime room and board, incarceration and legal costs, and loss of work and generation of taxes). LAIs can save both lives and expenditures, and a lot of suffering by patients and their families. I, too, long to see the emergence of a rational standard of care for schizophrenia using LAIs right after the initial psychotic episode. Oncology and cardiology have standards of care, so why not psychiatry?
Henry A. Nasrallah, MD
Editor-In-Chief
Continue to: Psychosis and epilepsy
Psychosis and epilepsy
I just read your editorial regarding the devastating consequences of psychotic relapses (From the Editor,
I work in the spheres of psychiatry, epileptology, and whole genome sequencing, and have experienced a psychotic episode myself (in 2013, after temporal lobe resection and overdose). I now consider myself even more lucky to be out the other side! As Governor for South London and Maudsley NHS Foundation Trust (SLaM) and Trustee for Epilepsy Action, many of our patients have psychosis. Some patients with epilepsy even experience postictal psychosis. Just yesterday, we had a call at SLaM regarding patients from a secure unit, and a psychiatric nurse spoke about patients at risk to themselves and others because of their psychotic illness, and how crucial effective long-term care was.
Torie Robinson
CEO, Epilepsy Sparks
Dr. Nasrallah responds
Ms. Robinson, thank you for sharing your story. It is important to note that the neurobiology of the psychosis that may occur with epilepsy may not be as neurodegenerative as the psychosis of schizophrenia. Many neurologic conditions can be associated with psychotic episodes, not only epilepsy. I am glad you overcame your post-temporal lobectomy psychotic episode and have had a very good outcome with high functioning.
Henry A. Nasrallah, MD
Editor-In-Chief
Disclosures
Dr. Chepke is a consultant to and speaker for Janssen Pharmaceuticals, Otsuka Pharmaceuticals, and Alkermes. The other authors report no financial relationships with any companies whose products are mentioned in their letters, or with manufacturers of competing products.
Benefits of early LAI use
I want to thank Dr. Nasrallah for his editorial calling for more frequent and earlier use of long-acting injectable antipsychotics (LAIs) in schizophrenia (From the Editor,
In addition to the neuroprotective biologic effects of early LAI usage, I’ve found that many of my FEP patients find great psychological comfort from incorporating LAIs into their treatment plan. The first psychotic break is generally when a person (and their family) feels the most afraid about the future and is in desperate need of hope that they can have a full life—with educational opportunities, sustained employment, meaningful relationships, and more. Just as society has seen the COVID-19 vaccines as a symbol of hope and the first step in overcoming the oppression of living in fear of an uncertain future, we need to help people experiencing FEP find hope in a needle.
Craig Chepke, MD, FAPA
Excel Psychiatric Associates
Huntersville, North Carolina
Reference
1. Chepke C. Drive-up pharmacotherapy during the COVID-19 pandemic. Current Psychiatry. 2020;19(5):29-30.
Dr. Nasrallah responds
Thank you, Dr. Chepke, for your letter confirming full support for using LAIs in schizophrenia. I like the phrase you coined: “hope in a needle.” The early use of LAIs in schizophrenia can provide the same type of hope that the vaccines against the life-threatening COVID-19 virus have generated in our society. Based on my direct observations, I also agree with you that the longer patients with schizophrenia remain on LAIs, the more engaged and happy they are with their progress and the quality of their lives. It is tragic that many patients never had the opportunity to return to their baseline with the early use of LAIs immediately following their first psychotic episode, instead of relapsing again and again due to their inability to adhere completely to their oral medications.
Henry A. Nasrallah, MD
Editor-In-Chief
Continue to: LAIs as the standard of care
LAIs as the standard of care
Thank you, Dr. Nasrallah, for reiterating the importance of compliance with pharmacologic management of schizophrenia after FEP (From the Editor,
As you point out in your editorial, the facts are powerful, well-known, undisputed, and yet not adopted in the United States, when in other countries LAIs are first-line care. Yes, LAIs are expensive, but not nearly as expensive as the disabilities caused by noncompliance are to society.
Why isn’t LAI use the standard of care here in the United States? In the United States, there is advocacy for treatment because there’s money in it. There is no good advocacy for preventive care because there’s no immediate money in it. We have another good example of this in the United States: private, for-profit prisons. They have a vested interest in keeping prisons full and building new ones. Patients with FEP are most often treated in the hospital, where a standard of care could easily be established that mandates LAIs as first-tier care. Why is that not so? Who is pushing for it? Who is resisting?
Your editorial inspired me to advocate more strongly. Do you have advice about how to effect policy change? I know administrators respond when we talk dollars and cents, not quality of care. What is the dollar cost of not using LAIs as the standard of care after FEP? Who cares? Who would listen to the numbers?
Edward A. Major, MD, LFAPA
Clinical Professor of Psychiatry
Upstate Medical Center
Syracuse, New York
Dr. Nasrallah responds
Dr. Major, thanks for your message. Establishing a standard of care for the use of LAIs (or any other therapy) is not that simple. It requires well-coordinated collaboration among several stakeholders (clinicians, researchers, payors, advocacy groups, and a national organization such as the American Psychiatric Association). The cost issue is certainly powerful, but the equation works in favor of LAIs because 1 psychiatric hospitalization due to a psychotic relapse costs up to 3 times the annual cost of an LAI medication that can prevent that rehospitalization. In addition, disability comprises the lion’s share of the large indirect costs of schizophrenia (disability payments, lifetime room and board, incarceration and legal costs, and loss of work and generation of taxes). LAIs can save both lives and expenditures, and a lot of suffering by patients and their families. I, too, long to see the emergence of a rational standard of care for schizophrenia using LAIs right after the initial psychotic episode. Oncology and cardiology have standards of care, so why not psychiatry?
Henry A. Nasrallah, MD
Editor-In-Chief
Continue to: Psychosis and epilepsy
Psychosis and epilepsy
I just read your editorial regarding the devastating consequences of psychotic relapses (From the Editor,
I work in the spheres of psychiatry, epileptology, and whole genome sequencing, and have experienced a psychotic episode myself (in 2013, after temporal lobe resection and overdose). I now consider myself even more lucky to be out the other side! As Governor for South London and Maudsley NHS Foundation Trust (SLaM) and Trustee for Epilepsy Action, many of our patients have psychosis. Some patients with epilepsy even experience postictal psychosis. Just yesterday, we had a call at SLaM regarding patients from a secure unit, and a psychiatric nurse spoke about patients at risk to themselves and others because of their psychotic illness, and how crucial effective long-term care was.
Torie Robinson
CEO, Epilepsy Sparks
Dr. Nasrallah responds
Ms. Robinson, thank you for sharing your story. It is important to note that the neurobiology of the psychosis that may occur with epilepsy may not be as neurodegenerative as the psychosis of schizophrenia. Many neurologic conditions can be associated with psychotic episodes, not only epilepsy. I am glad you overcame your post-temporal lobectomy psychotic episode and have had a very good outcome with high functioning.
Henry A. Nasrallah, MD
Editor-In-Chief
Disclosures
Dr. Chepke is a consultant to and speaker for Janssen Pharmaceuticals, Otsuka Pharmaceuticals, and Alkermes. The other authors report no financial relationships with any companies whose products are mentioned in their letters, or with manufacturers of competing products.
Benefits of early LAI use
I want to thank Dr. Nasrallah for his editorial calling for more frequent and earlier use of long-acting injectable antipsychotics (LAIs) in schizophrenia (From the Editor,
In addition to the neuroprotective biologic effects of early LAI usage, I’ve found that many of my FEP patients find great psychological comfort from incorporating LAIs into their treatment plan. The first psychotic break is generally when a person (and their family) feels the most afraid about the future and is in desperate need of hope that they can have a full life—with educational opportunities, sustained employment, meaningful relationships, and more. Just as society has seen the COVID-19 vaccines as a symbol of hope and the first step in overcoming the oppression of living in fear of an uncertain future, we need to help people experiencing FEP find hope in a needle.
Craig Chepke, MD, FAPA
Excel Psychiatric Associates
Huntersville, North Carolina
Reference
1. Chepke C. Drive-up pharmacotherapy during the COVID-19 pandemic. Current Psychiatry. 2020;19(5):29-30.
Dr. Nasrallah responds
Thank you, Dr. Chepke, for your letter confirming full support for using LAIs in schizophrenia. I like the phrase you coined: “hope in a needle.” The early use of LAIs in schizophrenia can provide the same type of hope that the vaccines against the life-threatening COVID-19 virus have generated in our society. Based on my direct observations, I also agree with you that the longer patients with schizophrenia remain on LAIs, the more engaged and happy they are with their progress and the quality of their lives. It is tragic that many patients never had the opportunity to return to their baseline with the early use of LAIs immediately following their first psychotic episode, instead of relapsing again and again due to their inability to adhere completely to their oral medications.
Henry A. Nasrallah, MD
Editor-In-Chief
Continue to: LAIs as the standard of care
LAIs as the standard of care
Thank you, Dr. Nasrallah, for reiterating the importance of compliance with pharmacologic management of schizophrenia after FEP (From the Editor,
As you point out in your editorial, the facts are powerful, well-known, undisputed, and yet not adopted in the United States, when in other countries LAIs are first-line care. Yes, LAIs are expensive, but not nearly as expensive as the disabilities caused by noncompliance are to society.
Why isn’t LAI use the standard of care here in the United States? In the United States, there is advocacy for treatment because there’s money in it. There is no good advocacy for preventive care because there’s no immediate money in it. We have another good example of this in the United States: private, for-profit prisons. They have a vested interest in keeping prisons full and building new ones. Patients with FEP are most often treated in the hospital, where a standard of care could easily be established that mandates LAIs as first-tier care. Why is that not so? Who is pushing for it? Who is resisting?
Your editorial inspired me to advocate more strongly. Do you have advice about how to effect policy change? I know administrators respond when we talk dollars and cents, not quality of care. What is the dollar cost of not using LAIs as the standard of care after FEP? Who cares? Who would listen to the numbers?
Edward A. Major, MD, LFAPA
Clinical Professor of Psychiatry
Upstate Medical Center
Syracuse, New York
Dr. Nasrallah responds
Dr. Major, thanks for your message. Establishing a standard of care for the use of LAIs (or any other therapy) is not that simple. It requires well-coordinated collaboration among several stakeholders (clinicians, researchers, payors, advocacy groups, and a national organization such as the American Psychiatric Association). The cost issue is certainly powerful, but the equation works in favor of LAIs because 1 psychiatric hospitalization due to a psychotic relapse costs up to 3 times the annual cost of an LAI medication that can prevent that rehospitalization. In addition, disability comprises the lion’s share of the large indirect costs of schizophrenia (disability payments, lifetime room and board, incarceration and legal costs, and loss of work and generation of taxes). LAIs can save both lives and expenditures, and a lot of suffering by patients and their families. I, too, long to see the emergence of a rational standard of care for schizophrenia using LAIs right after the initial psychotic episode. Oncology and cardiology have standards of care, so why not psychiatry?
Henry A. Nasrallah, MD
Editor-In-Chief
Continue to: Psychosis and epilepsy
Psychosis and epilepsy
I just read your editorial regarding the devastating consequences of psychotic relapses (From the Editor,
I work in the spheres of psychiatry, epileptology, and whole genome sequencing, and have experienced a psychotic episode myself (in 2013, after temporal lobe resection and overdose). I now consider myself even more lucky to be out the other side! As Governor for South London and Maudsley NHS Foundation Trust (SLaM) and Trustee for Epilepsy Action, many of our patients have psychosis. Some patients with epilepsy even experience postictal psychosis. Just yesterday, we had a call at SLaM regarding patients from a secure unit, and a psychiatric nurse spoke about patients at risk to themselves and others because of their psychotic illness, and how crucial effective long-term care was.
Torie Robinson
CEO, Epilepsy Sparks
Dr. Nasrallah responds
Ms. Robinson, thank you for sharing your story. It is important to note that the neurobiology of the psychosis that may occur with epilepsy may not be as neurodegenerative as the psychosis of schizophrenia. Many neurologic conditions can be associated with psychotic episodes, not only epilepsy. I am glad you overcame your post-temporal lobectomy psychotic episode and have had a very good outcome with high functioning.
Henry A. Nasrallah, MD
Editor-In-Chief
Disclosures
Dr. Chepke is a consultant to and speaker for Janssen Pharmaceuticals, Otsuka Pharmaceuticals, and Alkermes. The other authors report no financial relationships with any companies whose products are mentioned in their letters, or with manufacturers of competing products.
Does MELD need an update?
Dear colleagues and friends,
The Perspectives series continues! There are few issues in our discipline that are as challenging, and controversial, as liver transplant prioritization. The Model for End-Stage Liver Disease (MELD) has been the mainstay for organ allocation for nearly 2 decades, and there has been vigorous debate as to whether it should remain so. In this issue, Dr. Jasmohan Bajaj and Dr. Julie Heimbach discuss the strengths and limitations of MELD and provide a vision of upcoming developments. As always, I welcome your feedback and suggestions for future topics at [email protected].
Charles J. Kahi, MD, MS, AGAF, is professor of medicine at Indiana University, Indianapolis. He is an associate editor for GI & Hepatology News.
Yes, it’s time for an update
BY JASMOHAN S. BAJAJ, MD, AGAF
Since February 2002, the U.S.-based liver transplant system has adopted the MELD score for transplant priority. Initially developed to predict outcomes after transjugular intrahepatic porto-systemic shunt, it was modified to exclude etiology for the purpose of listing patients.1

There were several advantages with MELD including objectivity, ease of calculation using a website, and over time, a burgeoning experience nationwide that extended even beyond transplant. Moreover, it focused on “sickest-first,” did away with the extremely “manipulable” waiting list, and left off hepatic encephalopathy (HE) and ascites severity.1 However, even earlier on, there were concerns regarding not capturing hepatocellular cancer (HCC) and some complications of cirrhosis that required exceptions. The points awarded to all these exceptions also changed with time, with lower priority and reincorporation of the waiting list time for HCC. Over time, the addition of serum sodium led it to be converted to “MELD-Na,” which now remains the primary method for transplant listing priority.
But the population with cirrhosis that existed 20 years ago has shifted radically. Patients with cirrhosis currently tend to either be much older with more comorbid conditions that predispose them to chronic kidney disease and cerebrovascular and cardiovascular compromise or be younger with an earlier presentation of alcohol-associated hepatitis. Moreover, the widespread availability of hepatitis C virus (HCV) eradication has changed the landscape and stopped the progression of cirrhosis organically by virtually removing that etiology. This is relevant because a recent United Network for Organ Sharing (UNOS) analysis showed that the concordance between MELD score and 90-day mortality was the lowest in the rapidly increasing population with alcohol-related and nonalcoholic fatty liver disease etiologies, but conversely, this concordance was the highest in the population with hepatitis C–related cirrhosis.2 These demographic shifts in age and changes in etiology likely lessen the predictive power of the current MELD score iteration.
There is also increasing evidence that MELD is “stuck in the middle.” This means that both patients at low MELD score and those with organ failures may be underserved with respect to transplant listing with the current MELD score iteration.
Among patients with a MELD score disproportionately lower than their complications of cirrhosis several studies demonstrate the improvement in prognostication with addition of covert HE, history of overt HE, frailty, and sarcopenia indices. These are independently prognostic variables that affect daily function, affect patient-reported outcomes, and can influence readmissions. The burden of impending falls, readmissions, infections, and overall ill health is not captured even though relatively objective methods such as cognitive tests and documented admissions for overt HE can be utilized.3 This relative mistrust in including HE and covariables likely harkens back to a dramatic reduction in grade III/IV HE severity seen the year after MELD introduction, when compared with the year before, during which that designation was added to the listing priority.4 However, objective additions to the MELD score that capture the distress of patients and their families with multiple readmissions for HE worsened by sarcopenia are desperately needed (see table).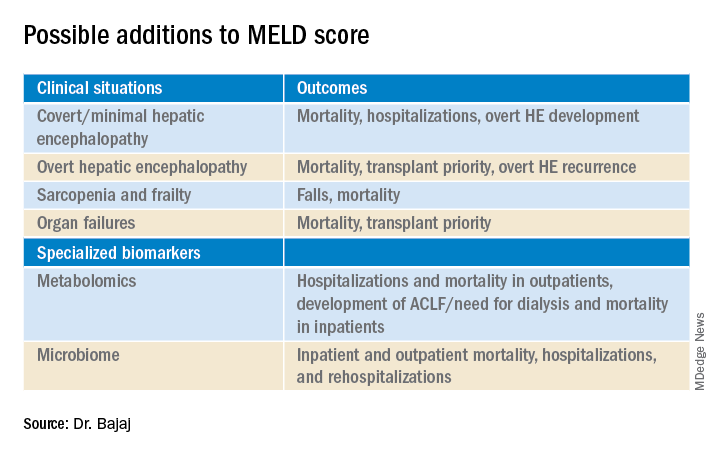
On the other extreme, there is an increasing recognition of acute-on-chronic liver failure (ACLF) and higher acceptability for transplanting alcohol-associated hepatitis (AAH).5 Prognostic variables in AAH have relied on Maddrey’s score and MELD score as well as the dynamic Lille score. The ability of MELD to predict outcomes is variable, but it is still required for listing these critical patients. A relatively newer entity, ACLF is defined variably across the world. In retrospective studies of the UNOS database in which patients were listed based on native MELD score rather than ACLF grades, there was a cut-off beyond which transplant was not useful. However, there is evidence that organ failures that do not involve creatinine or INR can influence survival independent of the MELD score.5 The rapidly increasing burden of critical illness may force a rethink of allocation policies, but a recent survey among U.S.-based transplant providers found little appetite to do so currently.
Objectivity is a major strength of the MELD score, but several systemic issues, including creatinine variability by sex, interlaboratory inconsistencies in laboratory results, and lack of accounting for international normalized ratio (INR) changes in those on warfarin or other INR-prolonging medications, to name a few that still exist.6 However, in our zeal to list patients and get the maximum chance for organ offers, there is a tendency to maximize or inflate the listing scores. This hope to provide the best care for patients under our specific care could come at the expense of patients listed elsewhere, but no score, however objective, is going to completely eliminate this possibility.
So, does this mean MELD-Na should be abandoned?
Absolutely not. An ecosystem of practitioners has now grown up under this system in the U.S., and it is rapidly being exported to other parts of the world. As with everything else, we need to keep up with the times, and for the popular MELD score, it needs to be responsive to issues at both extremes of cirrhosis severity. Studies on specialized markers such as serum, urine, and stool metabolomics as well as microbiome could be an objective addition to MELD score, but further studies are needed. It is also likely that artificial intelligence approaches could be used to not only improve access but also geographic equity that has plagued liver transplant in the U.S.
In the immortal words of Bob Dylan, “The times, they are a-changin’ …” We have to make sure the MELD score does too.
Jasmohan S. Bajaj, MD, AGAF, is with the division of gastroenterology, hepatology, and nutrition at Virginia Commonwealth University, Richmond, and Richmond VA Medical Center. He has no conflicts of interest.
References
1. Kamath PS and Kim WR. Hepatology. 2007;45:797-805.
2. Godfrey EL et al. Am J Transplant. 2019;19:3299-307.
3. Acharya C and Bajaj JS. Liver Transpl. 2021 May 21. doi:10.1002/lt.26099.
4. Bajaj JS and Saeian K. Dig Dis Sci 2005;50:753-6.
5. Artru F and Samuel D. JHEP Rep 2019 May;1(1):53-65.
6. Bernardi M et al. J Hepatol 2010 Dec 9;54:1297-306.
Maybe, but take it slow
BY JULIE K. HEIMBACH, MD
Even though 2020 was another record year for organ donation in the United States, a truly remarkable feat considering the profound impact of COVID-19 on health care as well as the population at large, there remains a critical shortage of available liver allografts.1 Last year in the U.S., of the approximately 13,000 patients waiting for a liver transplant, just under 9,000 patients underwent liver transplantation from a deceased or a living donor, while 2,345 either died waiting on the list or were removed for being too sick, and the rest remained waiting.1 In a perfect system, we would transplant every wait-listed patient at a time that would provide them the greatest benefit with the least amount of distress. However, because of the shortage of available organs for transplantation, an allocation system to rank wait-listed candidates is required. Because organ transplantation relies on the incredible altruism of individuals and their family members who make this ultimate gift on their behalf, it is crucial both for donor families and for waiting recipients that organ allocation be transparent, as fair and equitable as possible, and compliant with federal law, which is currently determined by the “Final Rule” that states that organ allocation be based in order of urgency.2

Since February 2002, U.S. liver allocation policy has been based on MELD.3 Prior to that time, liver allocation was based in part on the Child-Turcot-Pugh classification of liver disease, which included subjective components (ascites and encephalopathy) that are difficult to measure, as well as increased priority based on admission to the intensive care unit, also subjective and open to interpretation or abuse. Most crucially, the system defaulted to length of waiting time with large numbers of patients in the same category, which led to higher death rates for patients whose disease progressed more quickly or who were referred very late in their disease course.
MELD relies on a simple set of laboratory values that are easily obtained at any clinical lab and are already being routinely monitored as part of standard care for patients with end-stage liver disease.3 MELD initially required just three variables (bilirubin, creatinine, INR) and was updated to include just four variables with the adoption of MELD-Na in 2016, which added sodium levels. The MELD- and MELD-Na–based approach is a highly reliable, accurate way to rank patients who are most at risk of death in the next 3 months, with a C statistic of approximately 0.83-0.84.3,4 Perhaps the greatest testament to the strength of MELD is that, following the adoption of MELD-based liver allocation, MELD has gradually been adopted as the system of liver allocation by most countries around the world.
With the adoption of MELD and subsequently MELD-Na, which prioritize deceased donor liver allografts to the sickest patients first and is therefore compliant with the Final Rule, outcomes for patients waiting for liver transplant have steadily improved.3,4 In addition, MELD has provided an easily obtainable, objective measure to guide decisions about timing of liver transplant, especially in the setting of potential living donor liver transplantation. MELD is also predictive of outcome for patients undergoing nontransplant elective and emergent surgical procedures, and because of the ease in calculating the score, it allows for an objective comparison of patients with cirrhosis across a variety of clinical and research settings.
The MELD system has many additional strengths, though perhaps the most important is that it is adaptable. While the MELD score accurately predicts death from chronic liver disease, the MELD score is not able to predict mortality or risk of wait-list dropout due to disease progression from certain complications of chronic liver disease such as the development of HCC or hepatopulmonary syndrome, in which access to timely transplantation has been proven to be beneficial. This has required an adaption to the system whereby candidates with conditions, such as HCC, that meet specific criteria receive an assigned MELD score, rather than a calculated score. Determining which patients should qualify for MELD exceptions, as well as what the assigned priority score should be, has required careful analysis and ongoing revision. An additional issue for MELD, which was identified more than a decade ago and is overdue for adjustment, is the disparity in access to transplant for women who continue to experience a lower transplant rate (14.4% according to the most recent analysis) and approximately 8.6% higher death rate than men with the same MELD score.5 This is due, in part, to the use of creatinine in the MELD equation, which as a by-product of muscle metabolism, underestimates the degree of renal dysfunction in women and thus underestimates their risk of wait-list mortality.5 A potential modification to the MELD-Na score that corrects for this sex-based disparity is currently being studied by the OPTN Liver-Intestine committee, which is further evidence of the strength and adaptability of a MELD-based allocation system.
While it is tempting to conclude that a system that requires on-going monitoring and revision is best discarded in favor of a new model such as an artificial intelligence–based solution, policy development requires a tremendous amount of time for consensus-building, as well as effort to ensure that unexpected negative effects are not created. Whereas a novel system could be identified and determined to be superior down the road, the amount of effort and expense that would be needed to build consensus around such a new model should not be underestimated. Considering the challenges to health care and the population at large that are already occurring as we emerge from the COVID pandemic, as well as the short-term need to monitor the impact from the recent adoption of the acuity circle model which went live in February 2020 and allocates according to MELD but over a broader geographic area based on a circle around the donor hospital, building consensus around incremental changes to a MELD-based allocation system likely represents the best option in our continued quest for the optimal liver allocation system.
Julie K. Heimbach, MD, is a transplant surgeon and the surgical director of liver transplantation at Mayo Clinic in Rochester, Minn. She has no conflicts to report.
References
1. Organ Procurement and Transplantation Network data. Available at https://optn.transplant.hrsa.gov/data/view-data-reports/national-data. Accessed May 1, 2021.
2. Organ Procurement and Transplantation Network. Final rule. Available at https://optn.transplant.hrsa.gov/governance/about-the-optn/final-rule. Accessed May 1, 2021.
3. Wiesner R et al; United Network for Organ Sharing Liver Disease Severity Score Committee. Gastroenterology. 2003 Jan;124(1):91-6.
4. Nagai S et al. Gastroenterology. 2018 Nov;155(5):1451-62.e3.
5. Locke JE et al. JAMA Surg. 2020 Jul 1;155(7):e201129.
Dear colleagues and friends,
The Perspectives series continues! There are few issues in our discipline that are as challenging, and controversial, as liver transplant prioritization. The Model for End-Stage Liver Disease (MELD) has been the mainstay for organ allocation for nearly 2 decades, and there has been vigorous debate as to whether it should remain so. In this issue, Dr. Jasmohan Bajaj and Dr. Julie Heimbach discuss the strengths and limitations of MELD and provide a vision of upcoming developments. As always, I welcome your feedback and suggestions for future topics at [email protected].
Charles J. Kahi, MD, MS, AGAF, is professor of medicine at Indiana University, Indianapolis. He is an associate editor for GI & Hepatology News.
Yes, it’s time for an update
BY JASMOHAN S. BAJAJ, MD, AGAF
Since February 2002, the U.S.-based liver transplant system has adopted the MELD score for transplant priority. Initially developed to predict outcomes after transjugular intrahepatic porto-systemic shunt, it was modified to exclude etiology for the purpose of listing patients.1
There were several advantages with MELD including objectivity, ease of calculation using a website, and over time, a burgeoning experience nationwide that extended even beyond transplant. Moreover, it focused on “sickest-first,” did away with the extremely “manipulable” waiting list, and left off hepatic encephalopathy (HE) and ascites severity.1 However, even earlier on, there were concerns regarding not capturing hepatocellular cancer (HCC) and some complications of cirrhosis that required exceptions. The points awarded to all these exceptions also changed with time, with lower priority and reincorporation of the waiting list time for HCC. Over time, the addition of serum sodium led it to be converted to “MELD-Na,” which now remains the primary method for transplant listing priority.
But the population with cirrhosis that existed 20 years ago has shifted radically. Patients with cirrhosis currently tend to either be much older with more comorbid conditions that predispose them to chronic kidney disease and cerebrovascular and cardiovascular compromise or be younger with an earlier presentation of alcohol-associated hepatitis. Moreover, the widespread availability of hepatitis C virus (HCV) eradication has changed the landscape and stopped the progression of cirrhosis organically by virtually removing that etiology. This is relevant because a recent United Network for Organ Sharing (UNOS) analysis showed that the concordance between MELD score and 90-day mortality was the lowest in the rapidly increasing population with alcohol-related and nonalcoholic fatty liver disease etiologies, but conversely, this concordance was the highest in the population with hepatitis C–related cirrhosis.2 These demographic shifts in age and changes in etiology likely lessen the predictive power of the current MELD score iteration.
There is also increasing evidence that MELD is “stuck in the middle.” This means that both patients at low MELD score and those with organ failures may be underserved with respect to transplant listing with the current MELD score iteration.
Among patients with a MELD score disproportionately lower than their complications of cirrhosis several studies demonstrate the improvement in prognostication with addition of covert HE, history of overt HE, frailty, and sarcopenia indices. These are independently prognostic variables that affect daily function, affect patient-reported outcomes, and can influence readmissions. The burden of impending falls, readmissions, infections, and overall ill health is not captured even though relatively objective methods such as cognitive tests and documented admissions for overt HE can be utilized.3 This relative mistrust in including HE and covariables likely harkens back to a dramatic reduction in grade III/IV HE severity seen the year after MELD introduction, when compared with the year before, during which that designation was added to the listing priority.4 However, objective additions to the MELD score that capture the distress of patients and their families with multiple readmissions for HE worsened by sarcopenia are desperately needed (see table).
On the other extreme, there is an increasing recognition of acute-on-chronic liver failure (ACLF) and higher acceptability for transplanting alcohol-associated hepatitis (AAH).5 Prognostic variables in AAH have relied on Maddrey’s score and MELD score as well as the dynamic Lille score. The ability of MELD to predict outcomes is variable, but it is still required for listing these critical patients. A relatively newer entity, ACLF is defined variably across the world. In retrospective studies of the UNOS database in which patients were listed based on native MELD score rather than ACLF grades, there was a cut-off beyond which transplant was not useful. However, there is evidence that organ failures that do not involve creatinine or INR can influence survival independent of the MELD score.5 The rapidly increasing burden of critical illness may force a rethink of allocation policies, but a recent survey among U.S.-based transplant providers found little appetite to do so currently.
Objectivity is a major strength of the MELD score, but several systemic issues, including creatinine variability by sex, interlaboratory inconsistencies in laboratory results, and lack of accounting for international normalized ratio (INR) changes in those on warfarin or other INR-prolonging medications, to name a few that still exist.6 However, in our zeal to list patients and get the maximum chance for organ offers, there is a tendency to maximize or inflate the listing scores. This hope to provide the best care for patients under our specific care could come at the expense of patients listed elsewhere, but no score, however objective, is going to completely eliminate this possibility.
So, does this mean MELD-Na should be abandoned?
Absolutely not. An ecosystem of practitioners has now grown up under this system in the U.S., and it is rapidly being exported to other parts of the world. As with everything else, we need to keep up with the times, and for the popular MELD score, it needs to be responsive to issues at both extremes of cirrhosis severity. Studies on specialized markers such as serum, urine, and stool metabolomics as well as microbiome could be an objective addition to MELD score, but further studies are needed. It is also likely that artificial intelligence approaches could be used to not only improve access but also geographic equity that has plagued liver transplant in the U.S.
In the immortal words of Bob Dylan, “The times, they are a-changin’ …” We have to make sure the MELD score does too.
Jasmohan S. Bajaj, MD, AGAF, is with the division of gastroenterology, hepatology, and nutrition at Virginia Commonwealth University, Richmond, and Richmond VA Medical Center. He has no conflicts of interest.
References
1. Kamath PS and Kim WR. Hepatology. 2007;45:797-805.
2. Godfrey EL et al. Am J Transplant. 2019;19:3299-307.
3. Acharya C and Bajaj JS. Liver Transpl. 2021 May 21. doi:10.1002/lt.26099.
4. Bajaj JS and Saeian K. Dig Dis Sci 2005;50:753-6.
5. Artru F and Samuel D. JHEP Rep 2019 May;1(1):53-65.
6. Bernardi M et al. J Hepatol 2010 Dec 9;54:1297-306.
Maybe, but take it slow
BY JULIE K. HEIMBACH, MD
Even though 2020 was another record year for organ donation in the United States, a truly remarkable feat considering the profound impact of COVID-19 on health care as well as the population at large, there remains a critical shortage of available liver allografts.1 Last year in the U.S., of the approximately 13,000 patients waiting for a liver transplant, just under 9,000 patients underwent liver transplantation from a deceased or a living donor, while 2,345 either died waiting on the list or were removed for being too sick, and the rest remained waiting.1 In a perfect system, we would transplant every wait-listed patient at a time that would provide them the greatest benefit with the least amount of distress. However, because of the shortage of available organs for transplantation, an allocation system to rank wait-listed candidates is required. Because organ transplantation relies on the incredible altruism of individuals and their family members who make this ultimate gift on their behalf, it is crucial both for donor families and for waiting recipients that organ allocation be transparent, as fair and equitable as possible, and compliant with federal law, which is currently determined by the “Final Rule” that states that organ allocation be based in order of urgency.2
Since February 2002, U.S. liver allocation policy has been based on MELD.3 Prior to that time, liver allocation was based in part on the Child-Turcot-Pugh classification of liver disease, which included subjective components (ascites and encephalopathy) that are difficult to measure, as well as increased priority based on admission to the intensive care unit, also subjective and open to interpretation or abuse. Most crucially, the system defaulted to length of waiting time with large numbers of patients in the same category, which led to higher death rates for patients whose disease progressed more quickly or who were referred very late in their disease course.
MELD relies on a simple set of laboratory values that are easily obtained at any clinical lab and are already being routinely monitored as part of standard care for patients with end-stage liver disease.3 MELD initially required just three variables (bilirubin, creatinine, INR) and was updated to include just four variables with the adoption of MELD-Na in 2016, which added sodium levels. The MELD- and MELD-Na–based approach is a highly reliable, accurate way to rank patients who are most at risk of death in the next 3 months, with a C statistic of approximately 0.83-0.84.3,4 Perhaps the greatest testament to the strength of MELD is that, following the adoption of MELD-based liver allocation, MELD has gradually been adopted as the system of liver allocation by most countries around the world.
With the adoption of MELD and subsequently MELD-Na, which prioritize deceased donor liver allografts to the sickest patients first and is therefore compliant with the Final Rule, outcomes for patients waiting for liver transplant have steadily improved.3,4 In addition, MELD has provided an easily obtainable, objective measure to guide decisions about timing of liver transplant, especially in the setting of potential living donor liver transplantation. MELD is also predictive of outcome for patients undergoing nontransplant elective and emergent surgical procedures, and because of the ease in calculating the score, it allows for an objective comparison of patients with cirrhosis across a variety of clinical and research settings.
The MELD system has many additional strengths, though perhaps the most important is that it is adaptable. While the MELD score accurately predicts death from chronic liver disease, the MELD score is not able to predict mortality or risk of wait-list dropout due to disease progression from certain complications of chronic liver disease such as the development of HCC or hepatopulmonary syndrome, in which access to timely transplantation has been proven to be beneficial. This has required an adaption to the system whereby candidates with conditions, such as HCC, that meet specific criteria receive an assigned MELD score, rather than a calculated score. Determining which patients should qualify for MELD exceptions, as well as what the assigned priority score should be, has required careful analysis and ongoing revision. An additional issue for MELD, which was identified more than a decade ago and is overdue for adjustment, is the disparity in access to transplant for women who continue to experience a lower transplant rate (14.4% according to the most recent analysis) and approximately 8.6% higher death rate than men with the same MELD score.5 This is due, in part, to the use of creatinine in the MELD equation, which as a by-product of muscle metabolism, underestimates the degree of renal dysfunction in women and thus underestimates their risk of wait-list mortality.5 A potential modification to the MELD-Na score that corrects for this sex-based disparity is currently being studied by the OPTN Liver-Intestine committee, which is further evidence of the strength and adaptability of a MELD-based allocation system.
While it is tempting to conclude that a system that requires on-going monitoring and revision is best discarded in favor of a new model such as an artificial intelligence–based solution, policy development requires a tremendous amount of time for consensus-building, as well as effort to ensure that unexpected negative effects are not created. Whereas a novel system could be identified and determined to be superior down the road, the amount of effort and expense that would be needed to build consensus around such a new model should not be underestimated. Considering the challenges to health care and the population at large that are already occurring as we emerge from the COVID pandemic, as well as the short-term need to monitor the impact from the recent adoption of the acuity circle model which went live in February 2020 and allocates according to MELD but over a broader geographic area based on a circle around the donor hospital, building consensus around incremental changes to a MELD-based allocation system likely represents the best option in our continued quest for the optimal liver allocation system.
Julie K. Heimbach, MD, is a transplant surgeon and the surgical director of liver transplantation at Mayo Clinic in Rochester, Minn. She has no conflicts to report.
References
1. Organ Procurement and Transplantation Network data. Available at https://optn.transplant.hrsa.gov/data/view-data-reports/national-data. Accessed May 1, 2021.
2. Organ Procurement and Transplantation Network. Final rule. Available at https://optn.transplant.hrsa.gov/governance/about-the-optn/final-rule. Accessed May 1, 2021.
3. Wiesner R et al; United Network for Organ Sharing Liver Disease Severity Score Committee. Gastroenterology. 2003 Jan;124(1):91-6.
4. Nagai S et al. Gastroenterology. 2018 Nov;155(5):1451-62.e3.
5. Locke JE et al. JAMA Surg. 2020 Jul 1;155(7):e201129.
Dear colleagues and friends,
The Perspectives series continues! There are few issues in our discipline that are as challenging, and controversial, as liver transplant prioritization. The Model for End-Stage Liver Disease (MELD) has been the mainstay for organ allocation for nearly 2 decades, and there has been vigorous debate as to whether it should remain so. In this issue, Dr. Jasmohan Bajaj and Dr. Julie Heimbach discuss the strengths and limitations of MELD and provide a vision of upcoming developments. As always, I welcome your feedback and suggestions for future topics at [email protected].
Charles J. Kahi, MD, MS, AGAF, is professor of medicine at Indiana University, Indianapolis. He is an associate editor for GI & Hepatology News.
Yes, it’s time for an update
BY JASMOHAN S. BAJAJ, MD, AGAF
Since February 2002, the U.S.-based liver transplant system has adopted the MELD score for transplant priority. Initially developed to predict outcomes after transjugular intrahepatic porto-systemic shunt, it was modified to exclude etiology for the purpose of listing patients.1
There were several advantages with MELD including objectivity, ease of calculation using a website, and over time, a burgeoning experience nationwide that extended even beyond transplant. Moreover, it focused on “sickest-first,” did away with the extremely “manipulable” waiting list, and left off hepatic encephalopathy (HE) and ascites severity.1 However, even earlier on, there were concerns regarding not capturing hepatocellular cancer (HCC) and some complications of cirrhosis that required exceptions. The points awarded to all these exceptions also changed with time, with lower priority and reincorporation of the waiting list time for HCC. Over time, the addition of serum sodium led it to be converted to “MELD-Na,” which now remains the primary method for transplant listing priority.
But the population with cirrhosis that existed 20 years ago has shifted radically. Patients with cirrhosis currently tend to either be much older with more comorbid conditions that predispose them to chronic kidney disease and cerebrovascular and cardiovascular compromise or be younger with an earlier presentation of alcohol-associated hepatitis. Moreover, the widespread availability of hepatitis C virus (HCV) eradication has changed the landscape and stopped the progression of cirrhosis organically by virtually removing that etiology. This is relevant because a recent United Network for Organ Sharing (UNOS) analysis showed that the concordance between MELD score and 90-day mortality was the lowest in the rapidly increasing population with alcohol-related and nonalcoholic fatty liver disease etiologies, but conversely, this concordance was the highest in the population with hepatitis C–related cirrhosis.2 These demographic shifts in age and changes in etiology likely lessen the predictive power of the current MELD score iteration.
There is also increasing evidence that MELD is “stuck in the middle.” This means that both patients at low MELD score and those with organ failures may be underserved with respect to transplant listing with the current MELD score iteration.
Among patients with a MELD score disproportionately lower than their complications of cirrhosis several studies demonstrate the improvement in prognostication with addition of covert HE, history of overt HE, frailty, and sarcopenia indices. These are independently prognostic variables that affect daily function, affect patient-reported outcomes, and can influence readmissions. The burden of impending falls, readmissions, infections, and overall ill health is not captured even though relatively objective methods such as cognitive tests and documented admissions for overt HE can be utilized.3 This relative mistrust in including HE and covariables likely harkens back to a dramatic reduction in grade III/IV HE severity seen the year after MELD introduction, when compared with the year before, during which that designation was added to the listing priority.4 However, objective additions to the MELD score that capture the distress of patients and their families with multiple readmissions for HE worsened by sarcopenia are desperately needed (see table).
On the other extreme, there is an increasing recognition of acute-on-chronic liver failure (ACLF) and higher acceptability for transplanting alcohol-associated hepatitis (AAH).5 Prognostic variables in AAH have relied on Maddrey’s score and MELD score as well as the dynamic Lille score. The ability of MELD to predict outcomes is variable, but it is still required for listing these critical patients. A relatively newer entity, ACLF is defined variably across the world. In retrospective studies of the UNOS database in which patients were listed based on native MELD score rather than ACLF grades, there was a cut-off beyond which transplant was not useful. However, there is evidence that organ failures that do not involve creatinine or INR can influence survival independent of the MELD score.5 The rapidly increasing burden of critical illness may force a rethink of allocation policies, but a recent survey among U.S.-based transplant providers found little appetite to do so currently.
Objectivity is a major strength of the MELD score, but several systemic issues, including creatinine variability by sex, interlaboratory inconsistencies in laboratory results, and lack of accounting for international normalized ratio (INR) changes in those on warfarin or other INR-prolonging medications, to name a few that still exist.6 However, in our zeal to list patients and get the maximum chance for organ offers, there is a tendency to maximize or inflate the listing scores. This hope to provide the best care for patients under our specific care could come at the expense of patients listed elsewhere, but no score, however objective, is going to completely eliminate this possibility.
So, does this mean MELD-Na should be abandoned?
Absolutely not. An ecosystem of practitioners has now grown up under this system in the U.S., and it is rapidly being exported to other parts of the world. As with everything else, we need to keep up with the times, and for the popular MELD score, it needs to be responsive to issues at both extremes of cirrhosis severity. Studies on specialized markers such as serum, urine, and stool metabolomics as well as microbiome could be an objective addition to MELD score, but further studies are needed. It is also likely that artificial intelligence approaches could be used to not only improve access but also geographic equity that has plagued liver transplant in the U.S.
In the immortal words of Bob Dylan, “The times, they are a-changin’ …” We have to make sure the MELD score does too.
Jasmohan S. Bajaj, MD, AGAF, is with the division of gastroenterology, hepatology, and nutrition at Virginia Commonwealth University, Richmond, and Richmond VA Medical Center. He has no conflicts of interest.
References
1. Kamath PS and Kim WR. Hepatology. 2007;45:797-805.
2. Godfrey EL et al. Am J Transplant. 2019;19:3299-307.
3. Acharya C and Bajaj JS. Liver Transpl. 2021 May 21. doi:10.1002/lt.26099.
4. Bajaj JS and Saeian K. Dig Dis Sci 2005;50:753-6.
5. Artru F and Samuel D. JHEP Rep 2019 May;1(1):53-65.
6. Bernardi M et al. J Hepatol 2010 Dec 9;54:1297-306.
Maybe, but take it slow
BY JULIE K. HEIMBACH, MD
Even though 2020 was another record year for organ donation in the United States, a truly remarkable feat considering the profound impact of COVID-19 on health care as well as the population at large, there remains a critical shortage of available liver allografts.1 Last year in the U.S., of the approximately 13,000 patients waiting for a liver transplant, just under 9,000 patients underwent liver transplantation from a deceased or a living donor, while 2,345 either died waiting on the list or were removed for being too sick, and the rest remained waiting.1 In a perfect system, we would transplant every wait-listed patient at a time that would provide them the greatest benefit with the least amount of distress. However, because of the shortage of available organs for transplantation, an allocation system to rank wait-listed candidates is required. Because organ transplantation relies on the incredible altruism of individuals and their family members who make this ultimate gift on their behalf, it is crucial both for donor families and for waiting recipients that organ allocation be transparent, as fair and equitable as possible, and compliant with federal law, which is currently determined by the “Final Rule” that states that organ allocation be based in order of urgency.2
Since February 2002, U.S. liver allocation policy has been based on MELD.3 Prior to that time, liver allocation was based in part on the Child-Turcot-Pugh classification of liver disease, which included subjective components (ascites and encephalopathy) that are difficult to measure, as well as increased priority based on admission to the intensive care unit, also subjective and open to interpretation or abuse. Most crucially, the system defaulted to length of waiting time with large numbers of patients in the same category, which led to higher death rates for patients whose disease progressed more quickly or who were referred very late in their disease course.
MELD relies on a simple set of laboratory values that are easily obtained at any clinical lab and are already being routinely monitored as part of standard care for patients with end-stage liver disease.3 MELD initially required just three variables (bilirubin, creatinine, INR) and was updated to include just four variables with the adoption of MELD-Na in 2016, which added sodium levels. The MELD- and MELD-Na–based approach is a highly reliable, accurate way to rank patients who are most at risk of death in the next 3 months, with a C statistic of approximately 0.83-0.84.3,4 Perhaps the greatest testament to the strength of MELD is that, following the adoption of MELD-based liver allocation, MELD has gradually been adopted as the system of liver allocation by most countries around the world.
With the adoption of MELD and subsequently MELD-Na, which prioritize deceased donor liver allografts to the sickest patients first and is therefore compliant with the Final Rule, outcomes for patients waiting for liver transplant have steadily improved.3,4 In addition, MELD has provided an easily obtainable, objective measure to guide decisions about timing of liver transplant, especially in the setting of potential living donor liver transplantation. MELD is also predictive of outcome for patients undergoing nontransplant elective and emergent surgical procedures, and because of the ease in calculating the score, it allows for an objective comparison of patients with cirrhosis across a variety of clinical and research settings.
The MELD system has many additional strengths, though perhaps the most important is that it is adaptable. While the MELD score accurately predicts death from chronic liver disease, the MELD score is not able to predict mortality or risk of wait-list dropout due to disease progression from certain complications of chronic liver disease such as the development of HCC or hepatopulmonary syndrome, in which access to timely transplantation has been proven to be beneficial. This has required an adaption to the system whereby candidates with conditions, such as HCC, that meet specific criteria receive an assigned MELD score, rather than a calculated score. Determining which patients should qualify for MELD exceptions, as well as what the assigned priority score should be, has required careful analysis and ongoing revision. An additional issue for MELD, which was identified more than a decade ago and is overdue for adjustment, is the disparity in access to transplant for women who continue to experience a lower transplant rate (14.4% according to the most recent analysis) and approximately 8.6% higher death rate than men with the same MELD score.5 This is due, in part, to the use of creatinine in the MELD equation, which as a by-product of muscle metabolism, underestimates the degree of renal dysfunction in women and thus underestimates their risk of wait-list mortality.5 A potential modification to the MELD-Na score that corrects for this sex-based disparity is currently being studied by the OPTN Liver-Intestine committee, which is further evidence of the strength and adaptability of a MELD-based allocation system.
While it is tempting to conclude that a system that requires on-going monitoring and revision is best discarded in favor of a new model such as an artificial intelligence–based solution, policy development requires a tremendous amount of time for consensus-building, as well as effort to ensure that unexpected negative effects are not created. Whereas a novel system could be identified and determined to be superior down the road, the amount of effort and expense that would be needed to build consensus around such a new model should not be underestimated. Considering the challenges to health care and the population at large that are already occurring as we emerge from the COVID pandemic, as well as the short-term need to monitor the impact from the recent adoption of the acuity circle model which went live in February 2020 and allocates according to MELD but over a broader geographic area based on a circle around the donor hospital, building consensus around incremental changes to a MELD-based allocation system likely represents the best option in our continued quest for the optimal liver allocation system.
Julie K. Heimbach, MD, is a transplant surgeon and the surgical director of liver transplantation at Mayo Clinic in Rochester, Minn. She has no conflicts to report.
References
1. Organ Procurement and Transplantation Network data. Available at https://optn.transplant.hrsa.gov/data/view-data-reports/national-data. Accessed May 1, 2021.
2. Organ Procurement and Transplantation Network. Final rule. Available at https://optn.transplant.hrsa.gov/governance/about-the-optn/final-rule. Accessed May 1, 2021.
3. Wiesner R et al; United Network for Organ Sharing Liver Disease Severity Score Committee. Gastroenterology. 2003 Jan;124(1):91-6.
4. Nagai S et al. Gastroenterology. 2018 Nov;155(5):1451-62.e3.
5. Locke JE et al. JAMA Surg. 2020 Jul 1;155(7):e201129.
Artificial intelligence, COVID-19, and the future of pandemics
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
Artificial intelligence (AI) has proven of value in the COVID-19 pandemic and shows promise for mitigating future health care crises. During the pandemic’s first wave in New York, for example, Mount Sinai Health System used an algorithm to help identify patients ready for discharge. Such systems can help overburdened hospitals manage personnel and the flow of supplies in a medical crisis so they can continue to provide superior patient care.1

Pandemic applications have demonstrated AI’s potential not only to lift administrative burdens, but also to give physicians back what Eric Topol, MD, founder and director of Scripps Research Translational Institute and author of Deep Medicine, calls “the gift of time.”2 More time with patients contributes to clear communication and positive relationships, which lower the odds of medical errors, enhance patient safety, and potentially reduce physicians’ risks of certain types of litigation.3
However, physicians and health systems will need to approach AI with caution. Many unknowns remain – including potential liability risks and the potential for worsening preexisting bias. The law will need to evolve to account for AI-related liability scenarios, some of which are yet to be imagined.
Like any emerging technology, AI brings risk, but its promise of benefit should outweigh the probability of negative consequences – provided we remain aware of and mitigate the potential for AI-induced adverse events.
AI’s pandemic success limited due to fragmented data
Innovation is the key to success in any crisis, and many health care providers have shown their ability to innovate with AI during the pandemic. For example, researchers at the University of California, San Diego, health system who were designing an AI program to help doctors spot pneumonia on a chest x-ray retooled their application to assist physicians fighting coronavirus.4
Meanwhile, AI has been used to distinguish COVID-19–specific symptoms: It was a computer sifting medical records that took anosmia, loss of the sense of smell, from an anecdotal connection to an officially recognized early symptom of the virus.5 This information now helps physicians distinguish COVID-19 from influenza.
However, holding back more innovation is the fragmentation of health care data in the United States. Most AI applications for medicine rely on machine learning; that is, they train on historical patient data to recognize patterns. Therefore, “Everything that we’re doing gets better with a lot more annotated datasets,” Dr. Topol says. Unfortunately, because of our disparate systems, we don’t have centralized data.6 And even if our data were centralized, researchers lack enough reliable COVID-19 data to perfect algorithms in the short term.
Or, put in bleaker terms by the Washington Post: “One of the biggest challenges has been that much data remains siloed inside incompatible computer systems, hoarded by business interests and tangled in geopolitics.”7
The good news is that machine learning and data science platform Kaggle is hosting the COVID-19 Open Research Dataset, or CORD-19, which contains well over 100,000 scholarly articles on COVID-19, SARS, and other relevant infections.8 In lieu of a true central repository of anonymized health data, such large datasets can help train new AI applications in search of new diagnostic tools and therapies.
AI introduces new questions around liability
While AI may eventually be assigned legal personhood, it is not, in fact, a person: It is a tool wielded by individual clinicians, by teams, by health systems, even multiple systems collaborating. Our current liability laws are not ready for the era of digital medicine.
AI algorithms are not perfect. Because we know that diagnostic error is already a major allegation in malpractice claims, we must ask: What happens when a patient alleges that diagnostic error occurred because a physician or physicians leaned too heavily on AI?
In the United States, testing delays have threatened the safety of patients, physicians, and the public by delaying diagnosis of COVID-19. But again, health care providers have applied real innovation – generating novel and useful ideas and applying those ideas – to this problem. For example, researchers at Mount Sinai became the first in the country to combine AI with imaging and clinical data to produce an algorithm that can detect COVID-19 based on computed tomography scans of the chest, in combination with patient information and exposure history.9
AI in health care can help mitigate bias – or worsen it
Machine learning is only as good as the information provided to train the machine. Models trained on partial datasets can skew toward demographics that turned up more often in the data – for example, White race or men over 60. There is concern that “analyses based on faulty or biased algorithms could exacerbate existing racial gaps and other disparities in health care.”10 Already during the pandemic’s first waves, multiple AI systems used to classify x-rays have been found to show racial, gender, and socioeconomic biases.11
Such bias could create high potential for poor recommendations, including false positives and false negatives. It’s critical that system builders are able to explain and qualify their training data and that those who best understand AI-related system risks are the ones who influence health care systems or alter applications to mitigate AI-related harms.12
AI can help spot the next outbreak
More than a week before the World Health Organization released its first warning about a novel coronavirus, the AI platform BlueDot, created in Toronto, spotted an unusual cluster of pneumonia cases in Wuhan, China. Meanwhile, at Boston Children’s Hospital, the AI application Healthmap was scanning social media and news sites for signs of disease cluster, and it, too, flagged the first signs of what would become the COVID-19 outbreak – days before the WHO’s first formal alert.13
These innovative applications of AI in health care demonstrate real promise in detecting future outbreaks of new viruses early. This will allow health care providers and public health officials to get information out sooner, reducing the load on health systems, and ultimately, saving lives.
Dr. Anderson is chairman and chief executive officer, The Doctors Company and TDC Group.
References
1. Gold A. “Coronavirus tests the value of artificial intelligence in medicine” Fierce Biotech. 2020 May 22.
2. Topol E. “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again” (New York: Hachette Book Group; 2019:285).
3. The Doctors Company. “The Algorithm Will See You Now: How AI’s Healthcare Potential Outweighs Its Risk” 2020 Jan.
4. Gold A. Coronavirus tests the value of artificial intelligence in medicine. Fierce Biotech. 2020 May 22.
5. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
6. Reuter E. Hundreds of AI solutions proposed for pandemic, but few are proven. MedCity News. 2020 May 28.
7. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
8. Lee K. COVID-19 will accelerate the AI health care revolution. Wired. 2020 May 22.
9. Mei X et al. Artificial intelligence–enabled rapid diagnosis of patients with COVID-19. Nat Med. 2020 May 19;26:1224-8. doi: 10.1038/s41591-020-0931-3.
10. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
11. Wiggers K. Researchers find evidence of racial, gender, and socioeconomic bias in chest X-ray classifiers. The Machine: Making Sense of AI. 2020 Oct 21.
12. The Doctors Company. “The Algorithm Will See You Now: How AI’s Healthcare Potential Outweighs Its Risk” 2020 Jan.
13. Sewalk K. Innovative disease surveillance platforms detected early warning signs for novel coronavirus outbreak (nCoV-2019). The Disease Daily. 2020 Jan 31.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
Artificial intelligence (AI) has proven of value in the COVID-19 pandemic and shows promise for mitigating future health care crises. During the pandemic’s first wave in New York, for example, Mount Sinai Health System used an algorithm to help identify patients ready for discharge. Such systems can help overburdened hospitals manage personnel and the flow of supplies in a medical crisis so they can continue to provide superior patient care.1
Pandemic applications have demonstrated AI’s potential not only to lift administrative burdens, but also to give physicians back what Eric Topol, MD, founder and director of Scripps Research Translational Institute and author of Deep Medicine, calls “the gift of time.”2 More time with patients contributes to clear communication and positive relationships, which lower the odds of medical errors, enhance patient safety, and potentially reduce physicians’ risks of certain types of litigation.3
However, physicians and health systems will need to approach AI with caution. Many unknowns remain – including potential liability risks and the potential for worsening preexisting bias. The law will need to evolve to account for AI-related liability scenarios, some of which are yet to be imagined.
Like any emerging technology, AI brings risk, but its promise of benefit should outweigh the probability of negative consequences – provided we remain aware of and mitigate the potential for AI-induced adverse events.
AI’s pandemic success limited due to fragmented data
Innovation is the key to success in any crisis, and many health care providers have shown their ability to innovate with AI during the pandemic. For example, researchers at the University of California, San Diego, health system who were designing an AI program to help doctors spot pneumonia on a chest x-ray retooled their application to assist physicians fighting coronavirus.4
Meanwhile, AI has been used to distinguish COVID-19–specific symptoms: It was a computer sifting medical records that took anosmia, loss of the sense of smell, from an anecdotal connection to an officially recognized early symptom of the virus.5 This information now helps physicians distinguish COVID-19 from influenza.
However, holding back more innovation is the fragmentation of health care data in the United States. Most AI applications for medicine rely on machine learning; that is, they train on historical patient data to recognize patterns. Therefore, “Everything that we’re doing gets better with a lot more annotated datasets,” Dr. Topol says. Unfortunately, because of our disparate systems, we don’t have centralized data.6 And even if our data were centralized, researchers lack enough reliable COVID-19 data to perfect algorithms in the short term.
Or, put in bleaker terms by the Washington Post: “One of the biggest challenges has been that much data remains siloed inside incompatible computer systems, hoarded by business interests and tangled in geopolitics.”7
The good news is that machine learning and data science platform Kaggle is hosting the COVID-19 Open Research Dataset, or CORD-19, which contains well over 100,000 scholarly articles on COVID-19, SARS, and other relevant infections.8 In lieu of a true central repository of anonymized health data, such large datasets can help train new AI applications in search of new diagnostic tools and therapies.
AI introduces new questions around liability
While AI may eventually be assigned legal personhood, it is not, in fact, a person: It is a tool wielded by individual clinicians, by teams, by health systems, even multiple systems collaborating. Our current liability laws are not ready for the era of digital medicine.
AI algorithms are not perfect. Because we know that diagnostic error is already a major allegation in malpractice claims, we must ask: What happens when a patient alleges that diagnostic error occurred because a physician or physicians leaned too heavily on AI?
In the United States, testing delays have threatened the safety of patients, physicians, and the public by delaying diagnosis of COVID-19. But again, health care providers have applied real innovation – generating novel and useful ideas and applying those ideas – to this problem. For example, researchers at Mount Sinai became the first in the country to combine AI with imaging and clinical data to produce an algorithm that can detect COVID-19 based on computed tomography scans of the chest, in combination with patient information and exposure history.9
AI in health care can help mitigate bias – or worsen it
Machine learning is only as good as the information provided to train the machine. Models trained on partial datasets can skew toward demographics that turned up more often in the data – for example, White race or men over 60. There is concern that “analyses based on faulty or biased algorithms could exacerbate existing racial gaps and other disparities in health care.”10 Already during the pandemic’s first waves, multiple AI systems used to classify x-rays have been found to show racial, gender, and socioeconomic biases.11
Such bias could create high potential for poor recommendations, including false positives and false negatives. It’s critical that system builders are able to explain and qualify their training data and that those who best understand AI-related system risks are the ones who influence health care systems or alter applications to mitigate AI-related harms.12
AI can help spot the next outbreak
More than a week before the World Health Organization released its first warning about a novel coronavirus, the AI platform BlueDot, created in Toronto, spotted an unusual cluster of pneumonia cases in Wuhan, China. Meanwhile, at Boston Children’s Hospital, the AI application Healthmap was scanning social media and news sites for signs of disease cluster, and it, too, flagged the first signs of what would become the COVID-19 outbreak – days before the WHO’s first formal alert.13
These innovative applications of AI in health care demonstrate real promise in detecting future outbreaks of new viruses early. This will allow health care providers and public health officials to get information out sooner, reducing the load on health systems, and ultimately, saving lives.
Dr. Anderson is chairman and chief executive officer, The Doctors Company and TDC Group.
References
1. Gold A. “Coronavirus tests the value of artificial intelligence in medicine” Fierce Biotech. 2020 May 22.
2. Topol E. “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again” (New York: Hachette Book Group; 2019:285).
3. The Doctors Company. “The Algorithm Will See You Now: How AI’s Healthcare Potential Outweighs Its Risk” 2020 Jan.
4. Gold A. Coronavirus tests the value of artificial intelligence in medicine. Fierce Biotech. 2020 May 22.
5. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
6. Reuter E. Hundreds of AI solutions proposed for pandemic, but few are proven. MedCity News. 2020 May 28.
7. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
8. Lee K. COVID-19 will accelerate the AI health care revolution. Wired. 2020 May 22.
9. Mei X et al. Artificial intelligence–enabled rapid diagnosis of patients with COVID-19. Nat Med. 2020 May 19;26:1224-8. doi: 10.1038/s41591-020-0931-3.
10. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
11. Wiggers K. Researchers find evidence of racial, gender, and socioeconomic bias in chest X-ray classifiers. The Machine: Making Sense of AI. 2020 Oct 21.
12. The Doctors Company. “The Algorithm Will See You Now: How AI’s Healthcare Potential Outweighs Its Risk” 2020 Jan.
13. Sewalk K. Innovative disease surveillance platforms detected early warning signs for novel coronavirus outbreak (nCoV-2019). The Disease Daily. 2020 Jan 31.
Editor’s note: This article has been provided by The Doctors Company, the exclusively endorsed medical malpractice carrier for the Society of Hospital Medicine.
Artificial intelligence (AI) has proven of value in the COVID-19 pandemic and shows promise for mitigating future health care crises. During the pandemic’s first wave in New York, for example, Mount Sinai Health System used an algorithm to help identify patients ready for discharge. Such systems can help overburdened hospitals manage personnel and the flow of supplies in a medical crisis so they can continue to provide superior patient care.1
Pandemic applications have demonstrated AI’s potential not only to lift administrative burdens, but also to give physicians back what Eric Topol, MD, founder and director of Scripps Research Translational Institute and author of Deep Medicine, calls “the gift of time.”2 More time with patients contributes to clear communication and positive relationships, which lower the odds of medical errors, enhance patient safety, and potentially reduce physicians’ risks of certain types of litigation.3
However, physicians and health systems will need to approach AI with caution. Many unknowns remain – including potential liability risks and the potential for worsening preexisting bias. The law will need to evolve to account for AI-related liability scenarios, some of which are yet to be imagined.
Like any emerging technology, AI brings risk, but its promise of benefit should outweigh the probability of negative consequences – provided we remain aware of and mitigate the potential for AI-induced adverse events.
AI’s pandemic success limited due to fragmented data
Innovation is the key to success in any crisis, and many health care providers have shown their ability to innovate with AI during the pandemic. For example, researchers at the University of California, San Diego, health system who were designing an AI program to help doctors spot pneumonia on a chest x-ray retooled their application to assist physicians fighting coronavirus.4
Meanwhile, AI has been used to distinguish COVID-19–specific symptoms: It was a computer sifting medical records that took anosmia, loss of the sense of smell, from an anecdotal connection to an officially recognized early symptom of the virus.5 This information now helps physicians distinguish COVID-19 from influenza.
However, holding back more innovation is the fragmentation of health care data in the United States. Most AI applications for medicine rely on machine learning; that is, they train on historical patient data to recognize patterns. Therefore, “Everything that we’re doing gets better with a lot more annotated datasets,” Dr. Topol says. Unfortunately, because of our disparate systems, we don’t have centralized data.6 And even if our data were centralized, researchers lack enough reliable COVID-19 data to perfect algorithms in the short term.
Or, put in bleaker terms by the Washington Post: “One of the biggest challenges has been that much data remains siloed inside incompatible computer systems, hoarded by business interests and tangled in geopolitics.”7
The good news is that machine learning and data science platform Kaggle is hosting the COVID-19 Open Research Dataset, or CORD-19, which contains well over 100,000 scholarly articles on COVID-19, SARS, and other relevant infections.8 In lieu of a true central repository of anonymized health data, such large datasets can help train new AI applications in search of new diagnostic tools and therapies.
AI introduces new questions around liability
While AI may eventually be assigned legal personhood, it is not, in fact, a person: It is a tool wielded by individual clinicians, by teams, by health systems, even multiple systems collaborating. Our current liability laws are not ready for the era of digital medicine.
AI algorithms are not perfect. Because we know that diagnostic error is already a major allegation in malpractice claims, we must ask: What happens when a patient alleges that diagnostic error occurred because a physician or physicians leaned too heavily on AI?
In the United States, testing delays have threatened the safety of patients, physicians, and the public by delaying diagnosis of COVID-19. But again, health care providers have applied real innovation – generating novel and useful ideas and applying those ideas – to this problem. For example, researchers at Mount Sinai became the first in the country to combine AI with imaging and clinical data to produce an algorithm that can detect COVID-19 based on computed tomography scans of the chest, in combination with patient information and exposure history.9
AI in health care can help mitigate bias – or worsen it
Machine learning is only as good as the information provided to train the machine. Models trained on partial datasets can skew toward demographics that turned up more often in the data – for example, White race or men over 60. There is concern that “analyses based on faulty or biased algorithms could exacerbate existing racial gaps and other disparities in health care.”10 Already during the pandemic’s first waves, multiple AI systems used to classify x-rays have been found to show racial, gender, and socioeconomic biases.11
Such bias could create high potential for poor recommendations, including false positives and false negatives. It’s critical that system builders are able to explain and qualify their training data and that those who best understand AI-related system risks are the ones who influence health care systems or alter applications to mitigate AI-related harms.12
AI can help spot the next outbreak
More than a week before the World Health Organization released its first warning about a novel coronavirus, the AI platform BlueDot, created in Toronto, spotted an unusual cluster of pneumonia cases in Wuhan, China. Meanwhile, at Boston Children’s Hospital, the AI application Healthmap was scanning social media and news sites for signs of disease cluster, and it, too, flagged the first signs of what would become the COVID-19 outbreak – days before the WHO’s first formal alert.13
These innovative applications of AI in health care demonstrate real promise in detecting future outbreaks of new viruses early. This will allow health care providers and public health officials to get information out sooner, reducing the load on health systems, and ultimately, saving lives.
Dr. Anderson is chairman and chief executive officer, The Doctors Company and TDC Group.
References
1. Gold A. “Coronavirus tests the value of artificial intelligence in medicine” Fierce Biotech. 2020 May 22.
2. Topol E. “Deep Medicine: How Artificial Intelligence Can Make Healthcare Human Again” (New York: Hachette Book Group; 2019:285).
3. The Doctors Company. “The Algorithm Will See You Now: How AI’s Healthcare Potential Outweighs Its Risk” 2020 Jan.
4. Gold A. Coronavirus tests the value of artificial intelligence in medicine. Fierce Biotech. 2020 May 22.
5. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
6. Reuter E. Hundreds of AI solutions proposed for pandemic, but few are proven. MedCity News. 2020 May 28.
7. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
8. Lee K. COVID-19 will accelerate the AI health care revolution. Wired. 2020 May 22.
9. Mei X et al. Artificial intelligence–enabled rapid diagnosis of patients with COVID-19. Nat Med. 2020 May 19;26:1224-8. doi: 10.1038/s41591-020-0931-3.
10. Cha AE. Artificial intelligence and COVID-19: Can the machines save us? Washington Post. 2020 Nov 1.
11. Wiggers K. Researchers find evidence of racial, gender, and socioeconomic bias in chest X-ray classifiers. The Machine: Making Sense of AI. 2020 Oct 21.
12. The Doctors Company. “The Algorithm Will See You Now: How AI’s Healthcare Potential Outweighs Its Risk” 2020 Jan.
13. Sewalk K. Innovative disease surveillance platforms detected early warning signs for novel coronavirus outbreak (nCoV-2019). The Disease Daily. 2020 Jan 31.
Few clinical guidelines exist for treating post-COVID symptoms
As doctors struggled through several surges of COVID-19 infections, most of what we learned was acquired through real-life experience. While many treatment options were promoted, most flat-out failed to be real therapeutics at all. Now that we have a safe and effective vaccine, we can prevent many infections from this virus. However, we are still left to manage the many post-COVID symptoms our patients continue to suffer with.

Symptoms following infection can last for months and range widely from “brain fog,” fatigue, dyspnea, chest pain, generalized weakness, depression, and a host of others. Patients may experience one or all of these symptoms, and there is currently no good way to predict who will go on to become a COVID “long hauler”.
Following the example of being educated by COVID as it happened, the same is true for managing post-COVID symptoms. The medical community still has a poor understanding of why some people develop it and there are few evidence-based studies to support any treatment modalities.
which they define as “new, recurring, or ongoing symptoms more than 4 weeks after infection, sometimes after initial symptom recovery.” It is important to note that these symptoms can occur in any degree of sickness during the acute infection, including in those who were asymptomatic. Even the actual name of this post-COVID syndrome is still being developed, with several other names being used for it as well.
While the guidelines are quite extensive, the actual clinical recommendations are still vague. For example, it is advised to let the patient know that post-COVID symptoms are still not well understood. While it is important to be transparent with patients, this does little to reassure them. Patients look to doctors, especially their primary care physicians, to guide them on the best treatment paths. Yet, we currently have none for post-COVID syndrome.
It is also advised to treat the patients’ symptoms and help improve functioning. For many diseases, doctors like to get to the root cause of the problem. Treating a symptom often masks an underlying condition. It may make the patient feel better and improve what they are capable of doing, which is important, but it also fails to unmask the real problem. It is also important to note that symptoms can be out of proportion to clinical findings and should not be dismissed: we just don’t have the answers yet.
One helpful recommendation is having a patient keep a diary of their symptoms. This will help both the patient and doctor learn what may be triggering factors. If it is, for example, exertion that induces breathlessness, perhaps the patient can gradually increase their level of activity to minimize symptoms. Additionally, a “comprehensive rehabilitation program” is also advised and this can greatly assist addressing all the issues a patient is experiencing, physically and medically.
It is also advised that management of underlying medical conditions be optimized. While this is very important, it is not something specific to post-COVID syndrome: All patients should have their underlying medical conditions well controlled. It might be that the patient is paying more attention to their overall health, which is a good thing. However, this does not necessarily reduce the current symptoms a patient is experiencing.
The CDC makes a good attempt to offer guidance in the frustrating management of post-COVID syndrome. However, their clinical guidelines fail to offer specific management tools specific to treating post-COVID patients. The recommendations offered are more helpful to health in general. The fact that more specific recommendations are lacking is simply caused by the lack of knowledge of this condition at present. As more research is conducted and more knowledge obtained, new guidelines should become more detailed.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
As doctors struggled through several surges of COVID-19 infections, most of what we learned was acquired through real-life experience. While many treatment options were promoted, most flat-out failed to be real therapeutics at all. Now that we have a safe and effective vaccine, we can prevent many infections from this virus. However, we are still left to manage the many post-COVID symptoms our patients continue to suffer with.
Symptoms following infection can last for months and range widely from “brain fog,” fatigue, dyspnea, chest pain, generalized weakness, depression, and a host of others. Patients may experience one or all of these symptoms, and there is currently no good way to predict who will go on to become a COVID “long hauler”.
Following the example of being educated by COVID as it happened, the same is true for managing post-COVID symptoms. The medical community still has a poor understanding of why some people develop it and there are few evidence-based studies to support any treatment modalities.
which they define as “new, recurring, or ongoing symptoms more than 4 weeks after infection, sometimes after initial symptom recovery.” It is important to note that these symptoms can occur in any degree of sickness during the acute infection, including in those who were asymptomatic. Even the actual name of this post-COVID syndrome is still being developed, with several other names being used for it as well.
While the guidelines are quite extensive, the actual clinical recommendations are still vague. For example, it is advised to let the patient know that post-COVID symptoms are still not well understood. While it is important to be transparent with patients, this does little to reassure them. Patients look to doctors, especially their primary care physicians, to guide them on the best treatment paths. Yet, we currently have none for post-COVID syndrome.
It is also advised to treat the patients’ symptoms and help improve functioning. For many diseases, doctors like to get to the root cause of the problem. Treating a symptom often masks an underlying condition. It may make the patient feel better and improve what they are capable of doing, which is important, but it also fails to unmask the real problem. It is also important to note that symptoms can be out of proportion to clinical findings and should not be dismissed: we just don’t have the answers yet.
One helpful recommendation is having a patient keep a diary of their symptoms. This will help both the patient and doctor learn what may be triggering factors. If it is, for example, exertion that induces breathlessness, perhaps the patient can gradually increase their level of activity to minimize symptoms. Additionally, a “comprehensive rehabilitation program” is also advised and this can greatly assist addressing all the issues a patient is experiencing, physically and medically.
It is also advised that management of underlying medical conditions be optimized. While this is very important, it is not something specific to post-COVID syndrome: All patients should have their underlying medical conditions well controlled. It might be that the patient is paying more attention to their overall health, which is a good thing. However, this does not necessarily reduce the current symptoms a patient is experiencing.
The CDC makes a good attempt to offer guidance in the frustrating management of post-COVID syndrome. However, their clinical guidelines fail to offer specific management tools specific to treating post-COVID patients. The recommendations offered are more helpful to health in general. The fact that more specific recommendations are lacking is simply caused by the lack of knowledge of this condition at present. As more research is conducted and more knowledge obtained, new guidelines should become more detailed.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
As doctors struggled through several surges of COVID-19 infections, most of what we learned was acquired through real-life experience. While many treatment options were promoted, most flat-out failed to be real therapeutics at all. Now that we have a safe and effective vaccine, we can prevent many infections from this virus. However, we are still left to manage the many post-COVID symptoms our patients continue to suffer with.
Symptoms following infection can last for months and range widely from “brain fog,” fatigue, dyspnea, chest pain, generalized weakness, depression, and a host of others. Patients may experience one or all of these symptoms, and there is currently no good way to predict who will go on to become a COVID “long hauler”.
Following the example of being educated by COVID as it happened, the same is true for managing post-COVID symptoms. The medical community still has a poor understanding of why some people develop it and there are few evidence-based studies to support any treatment modalities.
which they define as “new, recurring, or ongoing symptoms more than 4 weeks after infection, sometimes after initial symptom recovery.” It is important to note that these symptoms can occur in any degree of sickness during the acute infection, including in those who were asymptomatic. Even the actual name of this post-COVID syndrome is still being developed, with several other names being used for it as well.
While the guidelines are quite extensive, the actual clinical recommendations are still vague. For example, it is advised to let the patient know that post-COVID symptoms are still not well understood. While it is important to be transparent with patients, this does little to reassure them. Patients look to doctors, especially their primary care physicians, to guide them on the best treatment paths. Yet, we currently have none for post-COVID syndrome.
It is also advised to treat the patients’ symptoms and help improve functioning. For many diseases, doctors like to get to the root cause of the problem. Treating a symptom often masks an underlying condition. It may make the patient feel better and improve what they are capable of doing, which is important, but it also fails to unmask the real problem. It is also important to note that symptoms can be out of proportion to clinical findings and should not be dismissed: we just don’t have the answers yet.
One helpful recommendation is having a patient keep a diary of their symptoms. This will help both the patient and doctor learn what may be triggering factors. If it is, for example, exertion that induces breathlessness, perhaps the patient can gradually increase their level of activity to minimize symptoms. Additionally, a “comprehensive rehabilitation program” is also advised and this can greatly assist addressing all the issues a patient is experiencing, physically and medically.
It is also advised that management of underlying medical conditions be optimized. While this is very important, it is not something specific to post-COVID syndrome: All patients should have their underlying medical conditions well controlled. It might be that the patient is paying more attention to their overall health, which is a good thing. However, this does not necessarily reduce the current symptoms a patient is experiencing.
The CDC makes a good attempt to offer guidance in the frustrating management of post-COVID syndrome. However, their clinical guidelines fail to offer specific management tools specific to treating post-COVID patients. The recommendations offered are more helpful to health in general. The fact that more specific recommendations are lacking is simply caused by the lack of knowledge of this condition at present. As more research is conducted and more knowledge obtained, new guidelines should become more detailed.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].