User login
50 years of pediatric residency: What has changed?
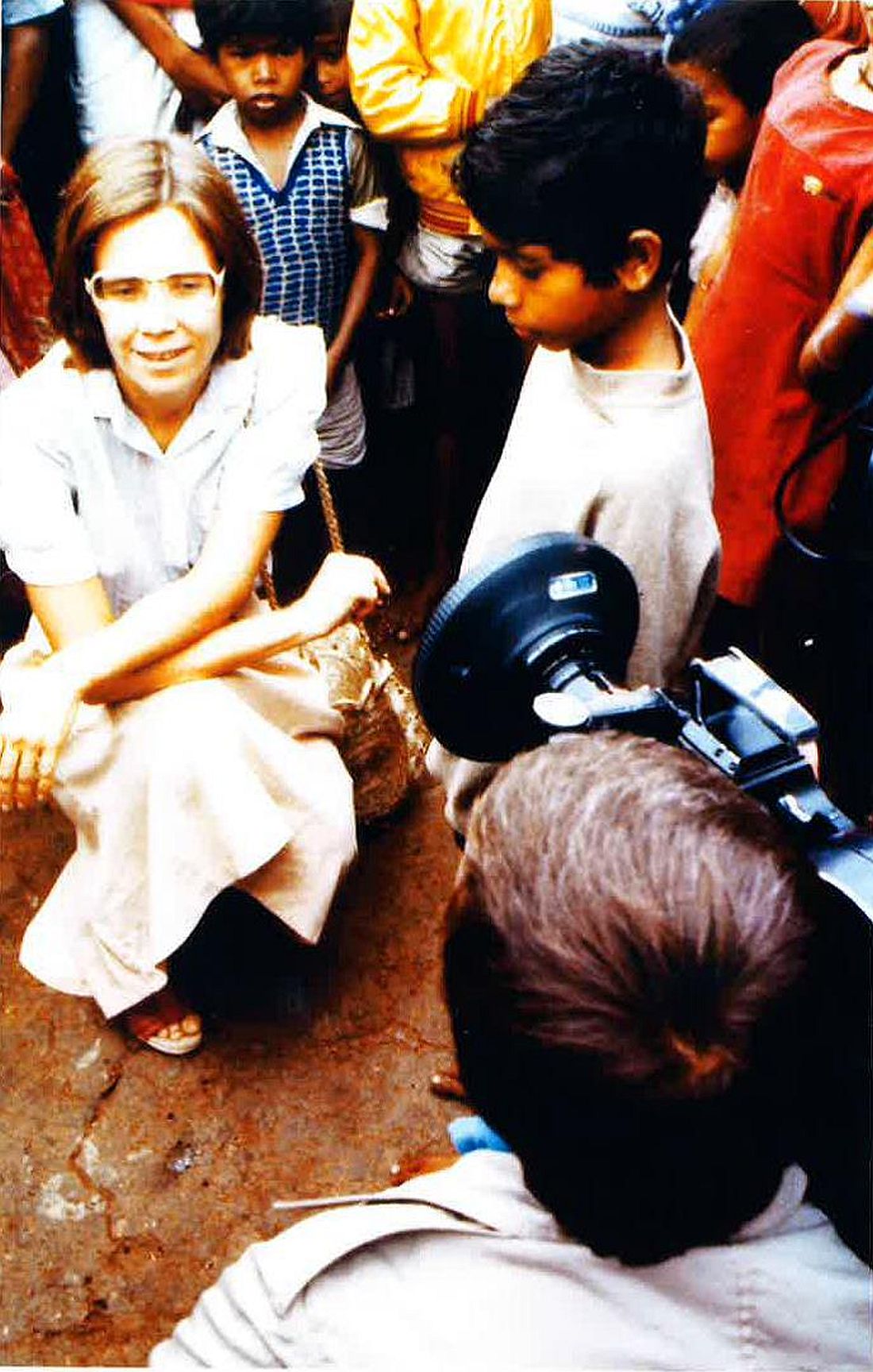
When Eileen Ouellette, MD, graduated from Boston’s Harvard Medical School in 1962, she was one of seven women in her class of 141 students. She went on to become one of only three women in pediatric residency at Massachusetts General Hospital later that year.
Free room and board was included in the program, Dr. Ouellette recalled, but her cramped room was poorly insulated and so small that she had to kneel on the bed to open her chest of drawers. The young doctor also soon learned that the women residents made less money than their male counterparts.

Dr. Ouellette, 79, now can laugh at the memory of her tiny room and tinier paycheck. The pediatric residents of today are entering a vastly different environment, she said. For starters, the average pay for medical residents in 2017 is $54,107. Women pediatric residents today far outnumber male residents. And most residents enjoy standard-sized rooms or apartments when completing their residencies.

Technology, for instance, greatly aids pediatric residents in their education today, said Renee Jenkins, MD, a professor at Howard University in Washington and a past AAP president.

Fewer hours, more hand-offs
During Dr. Ouellette’s residency from 1962 to 1965, sleep became a luxury. Of 168 hours in a week, residents were sometimes off for only 26 of them, she said.
“That was absolutely brutal,” she said. “You could not think of anything other than sleep. That became the primary focus of your whole life.”

“It didn’t seem crazy at the time,” said Dr. Stanton, founding dean of Seton Hall University Hackensack Meridian School of Medicine, South Orange, N.J. ”You developed the kind of bond with these families that it wouldn’t occur to you to go home.”
In the 1960s, there were no explicit limits on duty hours, according to Susan White, director of external communications for the Accreditation Council of Graduate Medical Education (ACGME). A “Guide for Residency Programs in Pediatrics,” published in 1968, recommended that “time off should be taken only when the service needs of the patients are assured and that “night and weekend duty provides a valuable educational experience. ... Duty of this type every second or third night and weekend is desirable.”
The guide predates the existence of the ACGME – established in 1981 – but it originated from a committee approved by the American Academy of Pediatrics, the American Board of Pediatrics, and the Council on Medical Education of the American Medical Association, according to Ms. White. While some residency programs changed their work hours over the years, the first mandated requirements for duty hours came in 1990 when ACGME set an 80-hour work week for four specialties: internal medicine, dermatology, ophthalmology, and preventive medicine. The council also limited on-call to every third night that year. In 2003, ACGME put in place duty hour requirements for all specialties.
“The pediatric requirements currently in effect provide safeguards for the resident, guidelines for educational programs, specific competencies and medical knowledge, as well as communication skills, professionalism requirements, and standardized assessment,” Ms. White said.
Current limitations for duty hours are beneficial in terms of resident safety, but the restrictions can be a double-edged sword, Dr. Jenkins said.
A changing gender demographic
By the time Dr. Stanton graduated from Yale in 1976, about 15% of her class were women, a marked shift from just a few years earlier, she said.
“In my residency program, women made up a quarter of our group,” she recalled. “That was a big change.”
The number of women going into pediatric residency has steadily increased in the last 5 decades, now far surpassing the number of men. Of 8,933 pediatric residents from 2015 to 2016, 67% were female and 25% were male, (with 8% not reporting), according to ACGME data.
“

Pediatrics is a natural selection for women, especially for those who plan to raise families, said Antoinette Eaton, MD, a retired pediatrician who completed her residency in the late 1950s at what is now Nationwide Children’s Hospital in Columbus, Ohio. Pediatrics is a prime specialty for career and family balance, she said.
“I worked part time a lot during my career,” said Dr. Eaton, a past AAP president. “Always being responsible as a mother and to the house were very high priorities.”
Dr. Stanton agrees that pediatric practices are much more tolerant of part time work, allowing women to better juggle children and career. However, she notes that the decline of male pediatricians also can be negative for the field overall.

New focus, growing debt
The curriculum focus for pediatric residency, meanwhile, has changed significantly over the years, pediatricians say. Dr. Eaton recalls her residency being almost entirely focused on inpatient care. In fact, insurance companies often refused to pay for outpatient care in sharp contrast to today, she said.
“You had to admit the patient if you wanted insurance to pay for it,” she said. “For example, if you had a patient with cerebral palsy or special needs, I had to admit that patient for 3, 4, 5 days. It was really different than what you have today.”
As time has passed, pediatric requirements have changed to emphasize the need for balance between inpatient and outpatient care, with a focus on continuity of care in either setting, Ms. White said. Newer additions to the requirements include the competencies of professionalism, communication, and life-long learning.
“Over the years these setting have expanded to include inpatients in hospitals, clinics, emergency centers, intensive care units, and in the community, [including] schools and other settings,” she said. “The requirements have always emphasized the importance of having high-quality, board-certified faculty to provide bedside teaching and deliver lectures at conferences.”
Another marked change for pediatric residents is the accumulation of debt. After her medical education, Dr. Jenkins owed about $1,500, she recalls.
“Today, that’s a drop in the bucket,” she said. “For the most part, you stayed out of [debt] trouble. It was nothing compared to that kids have to pay now.”
In 2014, the average medical school student graduated with a median debt of $180,000, according to data from the Association of American Medical Colleges. The wide debt differences are attributed to more expensive medical education today, Dr. Jenkins said.
While debt has risen, clinical responsibilities for residents have dropped as physician extenders and advanced equipment have become commonplace.
When Dr. Ouellette was a resident in the 1960s, there were few technicians to assist and no CT scans or MRIs for imaging. Residents drew blood from and gave blood to patients themselves. They took x-rays and developed them, she said.
“We had to use our brains and figure out what was going on,” she said. “People don’t think so much now. They send x-rays or scans to someone else, rather than figuring out the answer. Medicine may not be as much fun now as it was back then.”
Dr. Eaton added that residents have more technical demands today, more regulations to follow, and more paperwork to complete than the residents of the past. However, she believes pediatrics remains a worthwhile medical path. Three of her four children became doctors, one of whom went into pediatrics.
“I’m very disturbed when people try to convince children not to go into medicine,” she said. “I think it’s still a wonderful and rewarding career.”
[email protected]
On Twitter @legal_med
*Clarification made on 4/21/17
When Eileen Ouellette, MD, graduated from Boston’s Harvard Medical School in 1962, she was one of seven women in her class of 141 students. She went on to become one of only three women in pediatric residency at Massachusetts General Hospital later that year.
Free room and board was included in the program, Dr. Ouellette recalled, but her cramped room was poorly insulated and so small that she had to kneel on the bed to open her chest of drawers. The young doctor also soon learned that the women residents made less money than their male counterparts.
Dr. Ouellette, 79, now can laugh at the memory of her tiny room and tinier paycheck. The pediatric residents of today are entering a vastly different environment, she said. For starters, the average pay for medical residents in 2017 is $54,107. Women pediatric residents today far outnumber male residents. And most residents enjoy standard-sized rooms or apartments when completing their residencies.
Technology, for instance, greatly aids pediatric residents in their education today, said Renee Jenkins, MD, a professor at Howard University in Washington and a past AAP president.
Fewer hours, more hand-offs
During Dr. Ouellette’s residency from 1962 to 1965, sleep became a luxury. Of 168 hours in a week, residents were sometimes off for only 26 of them, she said.
“That was absolutely brutal,” she said. “You could not think of anything other than sleep. That became the primary focus of your whole life.”
“It didn’t seem crazy at the time,” said Dr. Stanton, founding dean of Seton Hall University Hackensack Meridian School of Medicine, South Orange, N.J. ”You developed the kind of bond with these families that it wouldn’t occur to you to go home.”
In the 1960s, there were no explicit limits on duty hours, according to Susan White, director of external communications for the Accreditation Council of Graduate Medical Education (ACGME). A “Guide for Residency Programs in Pediatrics,” published in 1968, recommended that “time off should be taken only when the service needs of the patients are assured and that “night and weekend duty provides a valuable educational experience. ... Duty of this type every second or third night and weekend is desirable.”
The guide predates the existence of the ACGME – established in 1981 – but it originated from a committee approved by the American Academy of Pediatrics, the American Board of Pediatrics, and the Council on Medical Education of the American Medical Association, according to Ms. White. While some residency programs changed their work hours over the years, the first mandated requirements for duty hours came in 1990 when ACGME set an 80-hour work week for four specialties: internal medicine, dermatology, ophthalmology, and preventive medicine. The council also limited on-call to every third night that year. In 2003, ACGME put in place duty hour requirements for all specialties.
“The pediatric requirements currently in effect provide safeguards for the resident, guidelines for educational programs, specific competencies and medical knowledge, as well as communication skills, professionalism requirements, and standardized assessment,” Ms. White said.
Current limitations for duty hours are beneficial in terms of resident safety, but the restrictions can be a double-edged sword, Dr. Jenkins said.
A changing gender demographic
By the time Dr. Stanton graduated from Yale in 1976, about 15% of her class were women, a marked shift from just a few years earlier, she said.
“In my residency program, women made up a quarter of our group,” she recalled. “That was a big change.”
The number of women going into pediatric residency has steadily increased in the last 5 decades, now far surpassing the number of men. Of 8,933 pediatric residents from 2015 to 2016, 67% were female and 25% were male, (with 8% not reporting), according to ACGME data.
“
Pediatrics is a natural selection for women, especially for those who plan to raise families, said Antoinette Eaton, MD, a retired pediatrician who completed her residency in the late 1950s at what is now Nationwide Children’s Hospital in Columbus, Ohio. Pediatrics is a prime specialty for career and family balance, she said.
“I worked part time a lot during my career,” said Dr. Eaton, a past AAP president. “Always being responsible as a mother and to the house were very high priorities.”
Dr. Stanton agrees that pediatric practices are much more tolerant of part time work, allowing women to better juggle children and career. However, she notes that the decline of male pediatricians also can be negative for the field overall.
New focus, growing debt
The curriculum focus for pediatric residency, meanwhile, has changed significantly over the years, pediatricians say. Dr. Eaton recalls her residency being almost entirely focused on inpatient care. In fact, insurance companies often refused to pay for outpatient care in sharp contrast to today, she said.
“You had to admit the patient if you wanted insurance to pay for it,” she said. “For example, if you had a patient with cerebral palsy or special needs, I had to admit that patient for 3, 4, 5 days. It was really different than what you have today.”
As time has passed, pediatric requirements have changed to emphasize the need for balance between inpatient and outpatient care, with a focus on continuity of care in either setting, Ms. White said. Newer additions to the requirements include the competencies of professionalism, communication, and life-long learning.
“Over the years these setting have expanded to include inpatients in hospitals, clinics, emergency centers, intensive care units, and in the community, [including] schools and other settings,” she said. “The requirements have always emphasized the importance of having high-quality, board-certified faculty to provide bedside teaching and deliver lectures at conferences.”
Another marked change for pediatric residents is the accumulation of debt. After her medical education, Dr. Jenkins owed about $1,500, she recalls.
“Today, that’s a drop in the bucket,” she said. “For the most part, you stayed out of [debt] trouble. It was nothing compared to that kids have to pay now.”
In 2014, the average medical school student graduated with a median debt of $180,000, according to data from the Association of American Medical Colleges. The wide debt differences are attributed to more expensive medical education today, Dr. Jenkins said.
While debt has risen, clinical responsibilities for residents have dropped as physician extenders and advanced equipment have become commonplace.
When Dr. Ouellette was a resident in the 1960s, there were few technicians to assist and no CT scans or MRIs for imaging. Residents drew blood from and gave blood to patients themselves. They took x-rays and developed them, she said.
“We had to use our brains and figure out what was going on,” she said. “People don’t think so much now. They send x-rays or scans to someone else, rather than figuring out the answer. Medicine may not be as much fun now as it was back then.”
Dr. Eaton added that residents have more technical demands today, more regulations to follow, and more paperwork to complete than the residents of the past. However, she believes pediatrics remains a worthwhile medical path. Three of her four children became doctors, one of whom went into pediatrics.
“I’m very disturbed when people try to convince children not to go into medicine,” she said. “I think it’s still a wonderful and rewarding career.”
[email protected]
On Twitter @legal_med
*Clarification made on 4/21/17
When Eileen Ouellette, MD, graduated from Boston’s Harvard Medical School in 1962, she was one of seven women in her class of 141 students. She went on to become one of only three women in pediatric residency at Massachusetts General Hospital later that year.
Free room and board was included in the program, Dr. Ouellette recalled, but her cramped room was poorly insulated and so small that she had to kneel on the bed to open her chest of drawers. The young doctor also soon learned that the women residents made less money than their male counterparts.
Dr. Ouellette, 79, now can laugh at the memory of her tiny room and tinier paycheck. The pediatric residents of today are entering a vastly different environment, she said. For starters, the average pay for medical residents in 2017 is $54,107. Women pediatric residents today far outnumber male residents. And most residents enjoy standard-sized rooms or apartments when completing their residencies.
Technology, for instance, greatly aids pediatric residents in their education today, said Renee Jenkins, MD, a professor at Howard University in Washington and a past AAP president.
Fewer hours, more hand-offs
During Dr. Ouellette’s residency from 1962 to 1965, sleep became a luxury. Of 168 hours in a week, residents were sometimes off for only 26 of them, she said.
“That was absolutely brutal,” she said. “You could not think of anything other than sleep. That became the primary focus of your whole life.”
“It didn’t seem crazy at the time,” said Dr. Stanton, founding dean of Seton Hall University Hackensack Meridian School of Medicine, South Orange, N.J. ”You developed the kind of bond with these families that it wouldn’t occur to you to go home.”
In the 1960s, there were no explicit limits on duty hours, according to Susan White, director of external communications for the Accreditation Council of Graduate Medical Education (ACGME). A “Guide for Residency Programs in Pediatrics,” published in 1968, recommended that “time off should be taken only when the service needs of the patients are assured and that “night and weekend duty provides a valuable educational experience. ... Duty of this type every second or third night and weekend is desirable.”
The guide predates the existence of the ACGME – established in 1981 – but it originated from a committee approved by the American Academy of Pediatrics, the American Board of Pediatrics, and the Council on Medical Education of the American Medical Association, according to Ms. White. While some residency programs changed their work hours over the years, the first mandated requirements for duty hours came in 1990 when ACGME set an 80-hour work week for four specialties: internal medicine, dermatology, ophthalmology, and preventive medicine. The council also limited on-call to every third night that year. In 2003, ACGME put in place duty hour requirements for all specialties.
“The pediatric requirements currently in effect provide safeguards for the resident, guidelines for educational programs, specific competencies and medical knowledge, as well as communication skills, professionalism requirements, and standardized assessment,” Ms. White said.
Current limitations for duty hours are beneficial in terms of resident safety, but the restrictions can be a double-edged sword, Dr. Jenkins said.
A changing gender demographic
By the time Dr. Stanton graduated from Yale in 1976, about 15% of her class were women, a marked shift from just a few years earlier, she said.
“In my residency program, women made up a quarter of our group,” she recalled. “That was a big change.”
The number of women going into pediatric residency has steadily increased in the last 5 decades, now far surpassing the number of men. Of 8,933 pediatric residents from 2015 to 2016, 67% were female and 25% were male, (with 8% not reporting), according to ACGME data.
“
Pediatrics is a natural selection for women, especially for those who plan to raise families, said Antoinette Eaton, MD, a retired pediatrician who completed her residency in the late 1950s at what is now Nationwide Children’s Hospital in Columbus, Ohio. Pediatrics is a prime specialty for career and family balance, she said.
“I worked part time a lot during my career,” said Dr. Eaton, a past AAP president. “Always being responsible as a mother and to the house were very high priorities.”
Dr. Stanton agrees that pediatric practices are much more tolerant of part time work, allowing women to better juggle children and career. However, she notes that the decline of male pediatricians also can be negative for the field overall.
New focus, growing debt
The curriculum focus for pediatric residency, meanwhile, has changed significantly over the years, pediatricians say. Dr. Eaton recalls her residency being almost entirely focused on inpatient care. In fact, insurance companies often refused to pay for outpatient care in sharp contrast to today, she said.
“You had to admit the patient if you wanted insurance to pay for it,” she said. “For example, if you had a patient with cerebral palsy or special needs, I had to admit that patient for 3, 4, 5 days. It was really different than what you have today.”
As time has passed, pediatric requirements have changed to emphasize the need for balance between inpatient and outpatient care, with a focus on continuity of care in either setting, Ms. White said. Newer additions to the requirements include the competencies of professionalism, communication, and life-long learning.
“Over the years these setting have expanded to include inpatients in hospitals, clinics, emergency centers, intensive care units, and in the community, [including] schools and other settings,” she said. “The requirements have always emphasized the importance of having high-quality, board-certified faculty to provide bedside teaching and deliver lectures at conferences.”
Another marked change for pediatric residents is the accumulation of debt. After her medical education, Dr. Jenkins owed about $1,500, she recalls.
“Today, that’s a drop in the bucket,” she said. “For the most part, you stayed out of [debt] trouble. It was nothing compared to that kids have to pay now.”
In 2014, the average medical school student graduated with a median debt of $180,000, according to data from the Association of American Medical Colleges. The wide debt differences are attributed to more expensive medical education today, Dr. Jenkins said.
While debt has risen, clinical responsibilities for residents have dropped as physician extenders and advanced equipment have become commonplace.
When Dr. Ouellette was a resident in the 1960s, there were few technicians to assist and no CT scans or MRIs for imaging. Residents drew blood from and gave blood to patients themselves. They took x-rays and developed them, she said.
“We had to use our brains and figure out what was going on,” she said. “People don’t think so much now. They send x-rays or scans to someone else, rather than figuring out the answer. Medicine may not be as much fun now as it was back then.”
Dr. Eaton added that residents have more technical demands today, more regulations to follow, and more paperwork to complete than the residents of the past. However, she believes pediatrics remains a worthwhile medical path. Three of her four children became doctors, one of whom went into pediatrics.
“I’m very disturbed when people try to convince children not to go into medicine,” she said. “I think it’s still a wonderful and rewarding career.”
[email protected]
On Twitter @legal_med
*Clarification made on 4/21/17
Psychiatry Innovation Lab aimed at transforming mental health
“Often, innovation is a product of desperation. I have seen too many of my patients die from opioid overdoses, and I’ve decided to create something that can stop this.”
This is the opening description of an innovative idea that Joseph Insler, MD, an early–career psychiatrist in Boston, pitched to the judges last October.
As one of the judges, this is how I described the item: “It’s like a Fitbit for people addicted to opioids, who are at risk of overdose. But, instead of tracking your footsteps and your sleep movements, it tracks your blood oxygen level, heart rate, and lack of movement. Based on an algorithm tuned to identify signs of an overdose, the Opioid Overdose Recovery Bracelet would give you a shot of medicine in your wrist. If you have accidentally overdosed, it will give you a premeasured dose of naloxone from its reservoir, likely saving your life.”

The goal of the Psychiatry Innovation Lab is to catalyze the formation of innovative ventures to transform mental health. “We nurture early stage ideas and ventures by investing in them with mentorship, education, funding, and collaboration opportunities with our community of mental health innovators,” Dr. Vasan said. At its core, the lab is an interactive exercise in experiential learning, where participants learn how to develop and pitch an entrepreneurial idea and then work together with experts in real time to improve their idea so that they leave with a solid plan for improving mental health. A panel of judges and leaders in innovation collaborate by providing feedback and mentoring. The competition event uses a “Shark Tank” style of winnowing out competitors but is a friendlier format than that of the TV show.
“There’s been a real call to action for using entrepreneurship to change the future, and the Psychiatry Innovation Lab is our answer to that call,” Dr. Vasan said. “We’ve had finalists ranging from high school students to emeritus professors. We’ve seen ideas for [anything from] advancing human rights all the way to using technology to improve access to care.”
Access to mental health and addiction care is one of the driving forces behind a recent wave of investment in behavioral health. There is a lot of interest now in how newer technologies can be leveraged in to improve access, screening, prevention, analytics, and treatments. Younger people coming into the field now have a much shorter path between idea and action. “Think of the lab as a place where people turn their idealism into impact. They learn how to create change that reflects our values: effective, measurable, collaborative, affordable, and sustainable.”

New lab will set records
On May 21, at the APA annual meeting in San Diego, the third Innovation Lab event will take place with record sponsorship and funding. More than $30,000 in prizes will be awarded to winning teams in the following categories: Grand Prize, Audience Choice, Outstanding Progress, Most Promising Innovation, and Most Disruptive Innovation. New this year, the Accelerator Prize will be awarded to the alumni team that has made the most progress since its participation in a previous Innovation Lab. A special prize from Google, worth $20,000, will be given to the innovation that best uses the potential of Cloud services, including Web applications, software, and machine learning.

Also, on May 21, the live Innovation Lab event will begin with the seven finalists giving initial pitches about their innovative ideas for improving mental health care delivery and how psychiatrists are diagnosing, treating, or managing patients. In addition, 10 semifinalists will be selected to deliver rapid pitches. Audience members will then vote from their devices, and the top semifinalist will proceed as a finalist. The event will end with an evening networking session aimed at building community and collaborations among mental health innovators, including clinicians, entrepreneurs, engineers, investors, and patients.
To learn more or watch videos about these innovators, go to www.psychiatryinnovation.com, or search for “APA innovation lab.”
Dr. Daviss is the chief medical informatics officer at M3 Information and chairs the American Psychiatric Association’s Committee on Mental Health Information Technology.
Psychiatry Innovation Lab alumni
Entrepreneurs from the October 2016 competition created products that addressed addiction, autism, Alzheimer’s, posttraumatic stress disorder, and other mental disorders.
Finalists
- Overdose Recovery Bracelet – “A novel solution to the opioid epidemic” – Joseph Insler
- Spectrum – “An app to encourage facial processing and emotion recognition in autism spectrum disorder” – Swathi Krishna
- Spring – “Enabling personalized behavioral healthcare using machine learning and big data” – April Koh
- Alzhelp – “Using augmented reality and intelligent personal assistant software to keep Alzheimer’s patients safe” – Akanksha Jain, Michelle Koh, and Priscilla Siow
- MiHelper – “Identifying patterns of distress and determining optimal periods for real time mental health interventions” – Kammarauche Isuzu and Mackenzie Drazan
- WEmbrace – “A mobile application for foreign-background psychiatric patients to effectively provide critical care” – Ellen Oh
Semifinalists
- Broadleaf Mental Health –“Reaching school-aged children in the rural eastern Himalayas” – Michael Matergia
- TechLink – “Connecting students and tech” – Akanksha Jain, Michelle Koh, and Priscilla Siow
- Beacon – “Smarter therapy. Together” – Shrenik Jain and Ravi Shah
- Muse – “Assisted meditation in mental health” – Graeme Moffat
- MiResource – “Helping adolescents find the right therapeutic fit” – Gabriela Asturias and Mackenzie Drazen
- BraVe Reality – “Virtual treatment for PTSD patients” – Monica Kullar
- SKNR – “A user-centric psychotherapy tool for the digital age” – Hyun-Hee Kim
- We2Link – “Connect better” – Michael Malone PRISM – “Helping patients gain insight through digital art mobile app” – Kenechi Ejebe and Whitney McFadden
SOURCE: Dr. Daviss
“Often, innovation is a product of desperation. I have seen too many of my patients die from opioid overdoses, and I’ve decided to create something that can stop this.”
This is the opening description of an innovative idea that Joseph Insler, MD, an early–career psychiatrist in Boston, pitched to the judges last October.
As one of the judges, this is how I described the item: “It’s like a Fitbit for people addicted to opioids, who are at risk of overdose. But, instead of tracking your footsteps and your sleep movements, it tracks your blood oxygen level, heart rate, and lack of movement. Based on an algorithm tuned to identify signs of an overdose, the Opioid Overdose Recovery Bracelet would give you a shot of medicine in your wrist. If you have accidentally overdosed, it will give you a premeasured dose of naloxone from its reservoir, likely saving your life.”
The goal of the Psychiatry Innovation Lab is to catalyze the formation of innovative ventures to transform mental health. “We nurture early stage ideas and ventures by investing in them with mentorship, education, funding, and collaboration opportunities with our community of mental health innovators,” Dr. Vasan said. At its core, the lab is an interactive exercise in experiential learning, where participants learn how to develop and pitch an entrepreneurial idea and then work together with experts in real time to improve their idea so that they leave with a solid plan for improving mental health. A panel of judges and leaders in innovation collaborate by providing feedback and mentoring. The competition event uses a “Shark Tank” style of winnowing out competitors but is a friendlier format than that of the TV show.
“There’s been a real call to action for using entrepreneurship to change the future, and the Psychiatry Innovation Lab is our answer to that call,” Dr. Vasan said. “We’ve had finalists ranging from high school students to emeritus professors. We’ve seen ideas for [anything from] advancing human rights all the way to using technology to improve access to care.”
Access to mental health and addiction care is one of the driving forces behind a recent wave of investment in behavioral health. There is a lot of interest now in how newer technologies can be leveraged in to improve access, screening, prevention, analytics, and treatments. Younger people coming into the field now have a much shorter path between idea and action. “Think of the lab as a place where people turn their idealism into impact. They learn how to create change that reflects our values: effective, measurable, collaborative, affordable, and sustainable.”
New lab will set records
On May 21, at the APA annual meeting in San Diego, the third Innovation Lab event will take place with record sponsorship and funding. More than $30,000 in prizes will be awarded to winning teams in the following categories: Grand Prize, Audience Choice, Outstanding Progress, Most Promising Innovation, and Most Disruptive Innovation. New this year, the Accelerator Prize will be awarded to the alumni team that has made the most progress since its participation in a previous Innovation Lab. A special prize from Google, worth $20,000, will be given to the innovation that best uses the potential of Cloud services, including Web applications, software, and machine learning.
Also, on May 21, the live Innovation Lab event will begin with the seven finalists giving initial pitches about their innovative ideas for improving mental health care delivery and how psychiatrists are diagnosing, treating, or managing patients. In addition, 10 semifinalists will be selected to deliver rapid pitches. Audience members will then vote from their devices, and the top semifinalist will proceed as a finalist. The event will end with an evening networking session aimed at building community and collaborations among mental health innovators, including clinicians, entrepreneurs, engineers, investors, and patients.
To learn more or watch videos about these innovators, go to www.psychiatryinnovation.com, or search for “APA innovation lab.”
Dr. Daviss is the chief medical informatics officer at M3 Information and chairs the American Psychiatric Association’s Committee on Mental Health Information Technology.
Psychiatry Innovation Lab alumni
Entrepreneurs from the October 2016 competition created products that addressed addiction, autism, Alzheimer’s, posttraumatic stress disorder, and other mental disorders.
Finalists
- Overdose Recovery Bracelet – “A novel solution to the opioid epidemic” – Joseph Insler
- Spectrum – “An app to encourage facial processing and emotion recognition in autism spectrum disorder” – Swathi Krishna
- Spring – “Enabling personalized behavioral healthcare using machine learning and big data” – April Koh
- Alzhelp – “Using augmented reality and intelligent personal assistant software to keep Alzheimer’s patients safe” – Akanksha Jain, Michelle Koh, and Priscilla Siow
- MiHelper – “Identifying patterns of distress and determining optimal periods for real time mental health interventions” – Kammarauche Isuzu and Mackenzie Drazan
- WEmbrace – “A mobile application for foreign-background psychiatric patients to effectively provide critical care” – Ellen Oh
Semifinalists
- Broadleaf Mental Health –“Reaching school-aged children in the rural eastern Himalayas” – Michael Matergia
- TechLink – “Connecting students and tech” – Akanksha Jain, Michelle Koh, and Priscilla Siow
- Beacon – “Smarter therapy. Together” – Shrenik Jain and Ravi Shah
- Muse – “Assisted meditation in mental health” – Graeme Moffat
- MiResource – “Helping adolescents find the right therapeutic fit” – Gabriela Asturias and Mackenzie Drazen
- BraVe Reality – “Virtual treatment for PTSD patients” – Monica Kullar
- SKNR – “A user-centric psychotherapy tool for the digital age” – Hyun-Hee Kim
- We2Link – “Connect better” – Michael Malone PRISM – “Helping patients gain insight through digital art mobile app” – Kenechi Ejebe and Whitney McFadden
SOURCE: Dr. Daviss
“Often, innovation is a product of desperation. I have seen too many of my patients die from opioid overdoses, and I’ve decided to create something that can stop this.”
This is the opening description of an innovative idea that Joseph Insler, MD, an early–career psychiatrist in Boston, pitched to the judges last October.
As one of the judges, this is how I described the item: “It’s like a Fitbit for people addicted to opioids, who are at risk of overdose. But, instead of tracking your footsteps and your sleep movements, it tracks your blood oxygen level, heart rate, and lack of movement. Based on an algorithm tuned to identify signs of an overdose, the Opioid Overdose Recovery Bracelet would give you a shot of medicine in your wrist. If you have accidentally overdosed, it will give you a premeasured dose of naloxone from its reservoir, likely saving your life.”
The goal of the Psychiatry Innovation Lab is to catalyze the formation of innovative ventures to transform mental health. “We nurture early stage ideas and ventures by investing in them with mentorship, education, funding, and collaboration opportunities with our community of mental health innovators,” Dr. Vasan said. At its core, the lab is an interactive exercise in experiential learning, where participants learn how to develop and pitch an entrepreneurial idea and then work together with experts in real time to improve their idea so that they leave with a solid plan for improving mental health. A panel of judges and leaders in innovation collaborate by providing feedback and mentoring. The competition event uses a “Shark Tank” style of winnowing out competitors but is a friendlier format than that of the TV show.
“There’s been a real call to action for using entrepreneurship to change the future, and the Psychiatry Innovation Lab is our answer to that call,” Dr. Vasan said. “We’ve had finalists ranging from high school students to emeritus professors. We’ve seen ideas for [anything from] advancing human rights all the way to using technology to improve access to care.”
Access to mental health and addiction care is one of the driving forces behind a recent wave of investment in behavioral health. There is a lot of interest now in how newer technologies can be leveraged in to improve access, screening, prevention, analytics, and treatments. Younger people coming into the field now have a much shorter path between idea and action. “Think of the lab as a place where people turn their idealism into impact. They learn how to create change that reflects our values: effective, measurable, collaborative, affordable, and sustainable.”
New lab will set records
On May 21, at the APA annual meeting in San Diego, the third Innovation Lab event will take place with record sponsorship and funding. More than $30,000 in prizes will be awarded to winning teams in the following categories: Grand Prize, Audience Choice, Outstanding Progress, Most Promising Innovation, and Most Disruptive Innovation. New this year, the Accelerator Prize will be awarded to the alumni team that has made the most progress since its participation in a previous Innovation Lab. A special prize from Google, worth $20,000, will be given to the innovation that best uses the potential of Cloud services, including Web applications, software, and machine learning.
Also, on May 21, the live Innovation Lab event will begin with the seven finalists giving initial pitches about their innovative ideas for improving mental health care delivery and how psychiatrists are diagnosing, treating, or managing patients. In addition, 10 semifinalists will be selected to deliver rapid pitches. Audience members will then vote from their devices, and the top semifinalist will proceed as a finalist. The event will end with an evening networking session aimed at building community and collaborations among mental health innovators, including clinicians, entrepreneurs, engineers, investors, and patients.
To learn more or watch videos about these innovators, go to www.psychiatryinnovation.com, or search for “APA innovation lab.”
Dr. Daviss is the chief medical informatics officer at M3 Information and chairs the American Psychiatric Association’s Committee on Mental Health Information Technology.
Psychiatry Innovation Lab alumni
Entrepreneurs from the October 2016 competition created products that addressed addiction, autism, Alzheimer’s, posttraumatic stress disorder, and other mental disorders.
Finalists
- Overdose Recovery Bracelet – “A novel solution to the opioid epidemic” – Joseph Insler
- Spectrum – “An app to encourage facial processing and emotion recognition in autism spectrum disorder” – Swathi Krishna
- Spring – “Enabling personalized behavioral healthcare using machine learning and big data” – April Koh
- Alzhelp – “Using augmented reality and intelligent personal assistant software to keep Alzheimer’s patients safe” – Akanksha Jain, Michelle Koh, and Priscilla Siow
- MiHelper – “Identifying patterns of distress and determining optimal periods for real time mental health interventions” – Kammarauche Isuzu and Mackenzie Drazan
- WEmbrace – “A mobile application for foreign-background psychiatric patients to effectively provide critical care” – Ellen Oh
Semifinalists
- Broadleaf Mental Health –“Reaching school-aged children in the rural eastern Himalayas” – Michael Matergia
- TechLink – “Connecting students and tech” – Akanksha Jain, Michelle Koh, and Priscilla Siow
- Beacon – “Smarter therapy. Together” – Shrenik Jain and Ravi Shah
- Muse – “Assisted meditation in mental health” – Graeme Moffat
- MiResource – “Helping adolescents find the right therapeutic fit” – Gabriela Asturias and Mackenzie Drazen
- BraVe Reality – “Virtual treatment for PTSD patients” – Monica Kullar
- SKNR – “A user-centric psychotherapy tool for the digital age” – Hyun-Hee Kim
- We2Link – “Connect better” – Michael Malone PRISM – “Helping patients gain insight through digital art mobile app” – Kenechi Ejebe and Whitney McFadden
SOURCE: Dr. Daviss
Managing family differences
What is it about families that makes our patients so upset? Why can our patients not just walk away from conflict? Why do they get so bent out of shape when family members do not say or do what they expect them to do? We all have families that are less than ideal and struggle with how to manage difference.
This column gives psychiatrists a framework for thinking with families about the universal dilemma of managing difference. This dilemma can be viewed from the perspectives of the individual, the family, and society: Identity is formed in the crucible of the family, where parental introjects become a model for the child’s development and can be rejected as an adolescent or adult as individuals shape their own identity. Processes within the family shape family members’ relationships and, therefore, their expectations of one another. Strong boundaries provide safety for those inside the family versus those outside the family.
Individual perspective
Family members’ perspective and expectations of others depend on their family position. Children or young adults want to please the parent, and to be accepted and recognized for who they are. They want their unique qualities to be valued, they want to be loved, and they want to feel that they belong.

Parents want their young adult to reach what they consider a successful life, and to be fulfilled and healthy. When their child strikes out on his or her own, the parent may not understand, and may feel let down or angry. The parent may say: “She married him to get back at me.” “Why is my son so rejecting of the business our family spent generations to build?” “How can my child reject our family values that we brought from the old country?” “How did it happen that my son is gay?”
Siblings have an idea of who their sibling should be, and this idea often is fixed and immutable. They may ask, “Why won’t my sister help me out?” “Why can’t she be a good sister?” “Why is my brother so jealous of me?”
Family elders may wonder why their adult children do not want to return home to care for them or why they want their parents to go into a nursing home.
These dilemmas are easy to understand as conscious expectations. More difficult to understand are the unconscious projections that tangle up families.
Unconscious psychological processes
The two main unconscious psychological processes that tangle up families are projection and projective identification. Projective identification is an unconscious process in which aspects of the self are split off and projected onto another person. In 1946, Melanie Klein introduced the term “projective identification” as follows: “Much of the hatred against parts of the self is now directed toward the mother. This leads to a particular form of identification which establishes the prototype of an aggressive object-relation. I suggest for these processes the term ‘projective identification’ ” (Int J Psychoanal. 1946;27[pt 3-4]:99-110).
Mutual projective processes can occur in committed relationships. The following scenario helps illustrate this: Ms. A. projects onto her husband her own feared and unwanted aggressive, dominating aspects of herself. The result is that she fears and respects him. He, in turn, comes to feel aggressive and dominating toward her, not only because of his own resources but because of her projections, which she forces onto him. He may, in turn, despise and disown timid and fearful aspects of his own personality and by a similar mechanism of projective identification force these unwanted aspects of himself onto his wife. Ms. A. is then composed of timid unaggressive parts of herself as well as his projections, and she carries these feelings as her part in the relationship. Some couples, like Mr. and Ms. A., live in such locked systems, dominated by mutual projections, with each not truly married to the other person but to the unwanted, split-off, and projected parts of themselves.
In this scenario, the husband becomes dominant and cruel, and the wife becomes stupidly timid and respectful. These marriages are stable, because each partner needs the other for narcissistic pathologic purposes (see “Some Psychodynamics of Large Groups” in “The Large Group: Dynamics and Therapy” [London: Karnac Books, 1975] and “The Ailment and Other Psychoanalytic Essays” [London: Free Association Books, 2015]).
Marriage offers an opportunity for individuals to work out these types of issues, or, in the case of Mr. and Ms. A, not work through them. Instead, they exist in tight mutual projections.
Family process perspective
Families function as a system or unit, and each person in the family has a role or function. When change occurs, basic rules of systems theory apply. For example, if the mother functions as the emotional barometer, no one else needs to pay attention to emotions, as that is the mother’s job. If she leaves or becomes ill, someone else will take on that role or the family will fall apart. If the father becomes depressed and unable to function in his role as a parent, the oldest child may have to step up to become the parent. When he gets better and his depression resolves, there may be tension – as the older child may not want to give up that role. There may be a disagreement in the family vision.
When the children grow and develop their own identities and lifestyles, the family has to adjust to include the adult children or cut them off. Individuals also may cut themselves off from the family if there are significant disagreements. There are variations, such as “semi-cutoffs,” where there is little contact except at ritualized holidays and significant family events. Therefore, tensions arise most clearly at these times when family members come together.
Boundaries protect the family
A family functions like a pack. As with most species, families and parents protect the young until they are able to care for themselves. The marriage contract specifies that spouses care for each other but additionally that they join extended families together. Family cares for family before caring for strangers. It is the elder’s role and responsibility to keep the family together, or the family members may drift apart or be subsumed into other family groups.
A clan is made up of related families that form a larger extended family unit. Historically, strong alliances, as in clans or family dynasties, become dominant socially. In recent history, the idea of clans has become less attractive as the idea of individualism has become the American ideal.
Modern families tend to be individually oriented and do not need their families for protection as much as primitive tribes did. Modern families have fairly loose boundaries, and problems can arise when the family tries to define boundaries and values.
Families also change composition with the impact of sociocultural influences, such as migration. However, the primitive social drive still forces us to form families and clans. This drive can explain much of the need for identifying people as “in or out” of the family. The Amish intentionally address this dilemma. At adolescence, the ritual of Rumspringa allows the young person to experience 1 year out of Amish life in Western life. The adolescent can then decide to be in or out. If the adolescent decides to be in, conformity to Amish lifestyle is required (“Serving the Amish,” Baltimore: Johns Hopkins University Press, 2014).
Lastly, our families provide memories of where we have come from and where we are going, both as individuals and as a clan. Powerful stories serve the next generation with a sense of belonging and a specific orientation to the world. The studies of third-generation Holocaust survivors attest to the power of family narratives. Individuals can choose to embrace the family narrative or alter it to allow individual growth.
Explaining families to families
When helping patients work through issues with their families, it is helpful to provide them with context. Among the important points we can make are:
● Families came into existence as a way to protect our young; this is true across the animal kingdom. Humans congregated into clans or tribes that demanded conformity and obedience to the chief. There was a clear sense of who was in and who was out. Many of the difficulties that we experience are tied to the primitive tension of needing to decide who is in and who is out. This is a normal function of families.
● These days, families have much looser boundaries, and individuals have the freedom to strike out on their own. Families have to grapple with their collective identity only when they get together at holiday times or transitional events like marriages, births, and deaths. So, is it worth getting upset about this? If so, ask patients what they would like to change – and why.
● With this background, the family can dive deeper. Ask your patients, “Is the issue a problem with roles within the family? Has there been a role transition? Has there been a death, serious illness, or birth? Has someone left, retired, or joined the family? How would you as a family like to proceed?”
● Lastly, is there a complicated tangled web or relationship that might be explained by mutual projective identifications? If so, refer to a colleague with family therapy skills.
Key points to keep in mind
1. Families should be placed in the context of clans and tribes.
2. Transitions and family events cause families to question their family identity, boundaries, and values.
3. Patients should explore their individual expectations about what families should do. This conversation can be extensive, and include cultural and generational flash points.
4. If there is a tangled web that makes no sense to you, refer to a colleague with family therapy skills.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
What is it about families that makes our patients so upset? Why can our patients not just walk away from conflict? Why do they get so bent out of shape when family members do not say or do what they expect them to do? We all have families that are less than ideal and struggle with how to manage difference.
This column gives psychiatrists a framework for thinking with families about the universal dilemma of managing difference. This dilemma can be viewed from the perspectives of the individual, the family, and society: Identity is formed in the crucible of the family, where parental introjects become a model for the child’s development and can be rejected as an adolescent or adult as individuals shape their own identity. Processes within the family shape family members’ relationships and, therefore, their expectations of one another. Strong boundaries provide safety for those inside the family versus those outside the family.
Individual perspective
Family members’ perspective and expectations of others depend on their family position. Children or young adults want to please the parent, and to be accepted and recognized for who they are. They want their unique qualities to be valued, they want to be loved, and they want to feel that they belong.
Parents want their young adult to reach what they consider a successful life, and to be fulfilled and healthy. When their child strikes out on his or her own, the parent may not understand, and may feel let down or angry. The parent may say: “She married him to get back at me.” “Why is my son so rejecting of the business our family spent generations to build?” “How can my child reject our family values that we brought from the old country?” “How did it happen that my son is gay?”
Siblings have an idea of who their sibling should be, and this idea often is fixed and immutable. They may ask, “Why won’t my sister help me out?” “Why can’t she be a good sister?” “Why is my brother so jealous of me?”
Family elders may wonder why their adult children do not want to return home to care for them or why they want their parents to go into a nursing home.
These dilemmas are easy to understand as conscious expectations. More difficult to understand are the unconscious projections that tangle up families.
Unconscious psychological processes
The two main unconscious psychological processes that tangle up families are projection and projective identification. Projective identification is an unconscious process in which aspects of the self are split off and projected onto another person. In 1946, Melanie Klein introduced the term “projective identification” as follows: “Much of the hatred against parts of the self is now directed toward the mother. This leads to a particular form of identification which establishes the prototype of an aggressive object-relation. I suggest for these processes the term ‘projective identification’ ” (Int J Psychoanal. 1946;27[pt 3-4]:99-110).
Mutual projective processes can occur in committed relationships. The following scenario helps illustrate this: Ms. A. projects onto her husband her own feared and unwanted aggressive, dominating aspects of herself. The result is that she fears and respects him. He, in turn, comes to feel aggressive and dominating toward her, not only because of his own resources but because of her projections, which she forces onto him. He may, in turn, despise and disown timid and fearful aspects of his own personality and by a similar mechanism of projective identification force these unwanted aspects of himself onto his wife. Ms. A. is then composed of timid unaggressive parts of herself as well as his projections, and she carries these feelings as her part in the relationship. Some couples, like Mr. and Ms. A., live in such locked systems, dominated by mutual projections, with each not truly married to the other person but to the unwanted, split-off, and projected parts of themselves.
In this scenario, the husband becomes dominant and cruel, and the wife becomes stupidly timid and respectful. These marriages are stable, because each partner needs the other for narcissistic pathologic purposes (see “Some Psychodynamics of Large Groups” in “The Large Group: Dynamics and Therapy” [London: Karnac Books, 1975] and “The Ailment and Other Psychoanalytic Essays” [London: Free Association Books, 2015]).
Marriage offers an opportunity for individuals to work out these types of issues, or, in the case of Mr. and Ms. A, not work through them. Instead, they exist in tight mutual projections.
Family process perspective
Families function as a system or unit, and each person in the family has a role or function. When change occurs, basic rules of systems theory apply. For example, if the mother functions as the emotional barometer, no one else needs to pay attention to emotions, as that is the mother’s job. If she leaves or becomes ill, someone else will take on that role or the family will fall apart. If the father becomes depressed and unable to function in his role as a parent, the oldest child may have to step up to become the parent. When he gets better and his depression resolves, there may be tension – as the older child may not want to give up that role. There may be a disagreement in the family vision.
When the children grow and develop their own identities and lifestyles, the family has to adjust to include the adult children or cut them off. Individuals also may cut themselves off from the family if there are significant disagreements. There are variations, such as “semi-cutoffs,” where there is little contact except at ritualized holidays and significant family events. Therefore, tensions arise most clearly at these times when family members come together.
Boundaries protect the family
A family functions like a pack. As with most species, families and parents protect the young until they are able to care for themselves. The marriage contract specifies that spouses care for each other but additionally that they join extended families together. Family cares for family before caring for strangers. It is the elder’s role and responsibility to keep the family together, or the family members may drift apart or be subsumed into other family groups.
A clan is made up of related families that form a larger extended family unit. Historically, strong alliances, as in clans or family dynasties, become dominant socially. In recent history, the idea of clans has become less attractive as the idea of individualism has become the American ideal.
Modern families tend to be individually oriented and do not need their families for protection as much as primitive tribes did. Modern families have fairly loose boundaries, and problems can arise when the family tries to define boundaries and values.
Families also change composition with the impact of sociocultural influences, such as migration. However, the primitive social drive still forces us to form families and clans. This drive can explain much of the need for identifying people as “in or out” of the family. The Amish intentionally address this dilemma. At adolescence, the ritual of Rumspringa allows the young person to experience 1 year out of Amish life in Western life. The adolescent can then decide to be in or out. If the adolescent decides to be in, conformity to Amish lifestyle is required (“Serving the Amish,” Baltimore: Johns Hopkins University Press, 2014).
Lastly, our families provide memories of where we have come from and where we are going, both as individuals and as a clan. Powerful stories serve the next generation with a sense of belonging and a specific orientation to the world. The studies of third-generation Holocaust survivors attest to the power of family narratives. Individuals can choose to embrace the family narrative or alter it to allow individual growth.
Explaining families to families
When helping patients work through issues with their families, it is helpful to provide them with context. Among the important points we can make are:
● Families came into existence as a way to protect our young; this is true across the animal kingdom. Humans congregated into clans or tribes that demanded conformity and obedience to the chief. There was a clear sense of who was in and who was out. Many of the difficulties that we experience are tied to the primitive tension of needing to decide who is in and who is out. This is a normal function of families.
● These days, families have much looser boundaries, and individuals have the freedom to strike out on their own. Families have to grapple with their collective identity only when they get together at holiday times or transitional events like marriages, births, and deaths. So, is it worth getting upset about this? If so, ask patients what they would like to change – and why.
● With this background, the family can dive deeper. Ask your patients, “Is the issue a problem with roles within the family? Has there been a role transition? Has there been a death, serious illness, or birth? Has someone left, retired, or joined the family? How would you as a family like to proceed?”
● Lastly, is there a complicated tangled web or relationship that might be explained by mutual projective identifications? If so, refer to a colleague with family therapy skills.
Key points to keep in mind
1. Families should be placed in the context of clans and tribes.
2. Transitions and family events cause families to question their family identity, boundaries, and values.
3. Patients should explore their individual expectations about what families should do. This conversation can be extensive, and include cultural and generational flash points.
4. If there is a tangled web that makes no sense to you, refer to a colleague with family therapy skills.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
What is it about families that makes our patients so upset? Why can our patients not just walk away from conflict? Why do they get so bent out of shape when family members do not say or do what they expect them to do? We all have families that are less than ideal and struggle with how to manage difference.
This column gives psychiatrists a framework for thinking with families about the universal dilemma of managing difference. This dilemma can be viewed from the perspectives of the individual, the family, and society: Identity is formed in the crucible of the family, where parental introjects become a model for the child’s development and can be rejected as an adolescent or adult as individuals shape their own identity. Processes within the family shape family members’ relationships and, therefore, their expectations of one another. Strong boundaries provide safety for those inside the family versus those outside the family.
Individual perspective
Family members’ perspective and expectations of others depend on their family position. Children or young adults want to please the parent, and to be accepted and recognized for who they are. They want their unique qualities to be valued, they want to be loved, and they want to feel that they belong.
Parents want their young adult to reach what they consider a successful life, and to be fulfilled and healthy. When their child strikes out on his or her own, the parent may not understand, and may feel let down or angry. The parent may say: “She married him to get back at me.” “Why is my son so rejecting of the business our family spent generations to build?” “How can my child reject our family values that we brought from the old country?” “How did it happen that my son is gay?”
Siblings have an idea of who their sibling should be, and this idea often is fixed and immutable. They may ask, “Why won’t my sister help me out?” “Why can’t she be a good sister?” “Why is my brother so jealous of me?”
Family elders may wonder why their adult children do not want to return home to care for them or why they want their parents to go into a nursing home.
These dilemmas are easy to understand as conscious expectations. More difficult to understand are the unconscious projections that tangle up families.
Unconscious psychological processes
The two main unconscious psychological processes that tangle up families are projection and projective identification. Projective identification is an unconscious process in which aspects of the self are split off and projected onto another person. In 1946, Melanie Klein introduced the term “projective identification” as follows: “Much of the hatred against parts of the self is now directed toward the mother. This leads to a particular form of identification which establishes the prototype of an aggressive object-relation. I suggest for these processes the term ‘projective identification’ ” (Int J Psychoanal. 1946;27[pt 3-4]:99-110).
Mutual projective processes can occur in committed relationships. The following scenario helps illustrate this: Ms. A. projects onto her husband her own feared and unwanted aggressive, dominating aspects of herself. The result is that she fears and respects him. He, in turn, comes to feel aggressive and dominating toward her, not only because of his own resources but because of her projections, which she forces onto him. He may, in turn, despise and disown timid and fearful aspects of his own personality and by a similar mechanism of projective identification force these unwanted aspects of himself onto his wife. Ms. A. is then composed of timid unaggressive parts of herself as well as his projections, and she carries these feelings as her part in the relationship. Some couples, like Mr. and Ms. A., live in such locked systems, dominated by mutual projections, with each not truly married to the other person but to the unwanted, split-off, and projected parts of themselves.
In this scenario, the husband becomes dominant and cruel, and the wife becomes stupidly timid and respectful. These marriages are stable, because each partner needs the other for narcissistic pathologic purposes (see “Some Psychodynamics of Large Groups” in “The Large Group: Dynamics and Therapy” [London: Karnac Books, 1975] and “The Ailment and Other Psychoanalytic Essays” [London: Free Association Books, 2015]).
Marriage offers an opportunity for individuals to work out these types of issues, or, in the case of Mr. and Ms. A, not work through them. Instead, they exist in tight mutual projections.
Family process perspective
Families function as a system or unit, and each person in the family has a role or function. When change occurs, basic rules of systems theory apply. For example, if the mother functions as the emotional barometer, no one else needs to pay attention to emotions, as that is the mother’s job. If she leaves or becomes ill, someone else will take on that role or the family will fall apart. If the father becomes depressed and unable to function in his role as a parent, the oldest child may have to step up to become the parent. When he gets better and his depression resolves, there may be tension – as the older child may not want to give up that role. There may be a disagreement in the family vision.
When the children grow and develop their own identities and lifestyles, the family has to adjust to include the adult children or cut them off. Individuals also may cut themselves off from the family if there are significant disagreements. There are variations, such as “semi-cutoffs,” where there is little contact except at ritualized holidays and significant family events. Therefore, tensions arise most clearly at these times when family members come together.
Boundaries protect the family
A family functions like a pack. As with most species, families and parents protect the young until they are able to care for themselves. The marriage contract specifies that spouses care for each other but additionally that they join extended families together. Family cares for family before caring for strangers. It is the elder’s role and responsibility to keep the family together, or the family members may drift apart or be subsumed into other family groups.
A clan is made up of related families that form a larger extended family unit. Historically, strong alliances, as in clans or family dynasties, become dominant socially. In recent history, the idea of clans has become less attractive as the idea of individualism has become the American ideal.
Modern families tend to be individually oriented and do not need their families for protection as much as primitive tribes did. Modern families have fairly loose boundaries, and problems can arise when the family tries to define boundaries and values.
Families also change composition with the impact of sociocultural influences, such as migration. However, the primitive social drive still forces us to form families and clans. This drive can explain much of the need for identifying people as “in or out” of the family. The Amish intentionally address this dilemma. At adolescence, the ritual of Rumspringa allows the young person to experience 1 year out of Amish life in Western life. The adolescent can then decide to be in or out. If the adolescent decides to be in, conformity to Amish lifestyle is required (“Serving the Amish,” Baltimore: Johns Hopkins University Press, 2014).
Lastly, our families provide memories of where we have come from and where we are going, both as individuals and as a clan. Powerful stories serve the next generation with a sense of belonging and a specific orientation to the world. The studies of third-generation Holocaust survivors attest to the power of family narratives. Individuals can choose to embrace the family narrative or alter it to allow individual growth.
Explaining families to families
When helping patients work through issues with their families, it is helpful to provide them with context. Among the important points we can make are:
● Families came into existence as a way to protect our young; this is true across the animal kingdom. Humans congregated into clans or tribes that demanded conformity and obedience to the chief. There was a clear sense of who was in and who was out. Many of the difficulties that we experience are tied to the primitive tension of needing to decide who is in and who is out. This is a normal function of families.
● These days, families have much looser boundaries, and individuals have the freedom to strike out on their own. Families have to grapple with their collective identity only when they get together at holiday times or transitional events like marriages, births, and deaths. So, is it worth getting upset about this? If so, ask patients what they would like to change – and why.
● With this background, the family can dive deeper. Ask your patients, “Is the issue a problem with roles within the family? Has there been a role transition? Has there been a death, serious illness, or birth? Has someone left, retired, or joined the family? How would you as a family like to proceed?”
● Lastly, is there a complicated tangled web or relationship that might be explained by mutual projective identifications? If so, refer to a colleague with family therapy skills.
Key points to keep in mind
1. Families should be placed in the context of clans and tribes.
2. Transitions and family events cause families to question their family identity, boundaries, and values.
3. Patients should explore their individual expectations about what families should do. This conversation can be extensive, and include cultural and generational flash points.
4. If there is a tangled web that makes no sense to you, refer to a colleague with family therapy skills.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
Well-child care: Steady growth in breadth and content
Fifty years ago in 1967, the American Academy of Pediatrics published a “Suggested Schedule for Preventive Child Health Care.” It was, in essence, the first periodicity schedule for well-child visits.
Described by AAP officials at the time as an “amalgamation of schedules used in various clinics and private offices,” it charted out the frequency and basic content of visits from 1 month through 6 years of age, and offered a simple list of items to be considered for guidance and discussion in all visits from 6 years on.
It is updated in real time, and is accompanied by an expansive package of Bright Futures recommendations, guidelines, and tools (including forms, handouts, and questionnaires) for health promotion and guidance. Together, the Periodicity Schedule and Bright Futures guidance reflect decades of steady change in the breadth and content of well-child care – and more recently, in some of its processes.
“When I started practicing [in 1979], developmental surveillance meant asking a few questions about developmental milestones, observing, and maybe lifting a few questions from the Denver Scale [the Denver Developmental Screening Test] to support our surveillance,” said Joseph F. Hagan, Jr., MD, a pediatrician in Burlington, Vt., and coeditor of Bright Futures.

Jack Swanson, MD, a pediatrician in Ames, Iowa, and a member of the Bright Futures Steering Committee, has similar recollections of well-child care in the early 1970s. “The developmental milestones were just questions and nothing more formal. Nutrition was a big [anticipatory guidance] issue, and some safety,” he recalled.
In early pediatric visits, “parents were interested in Dr. [Benjamin] Spock’s recommendations about feeding and raising their baby… and we used to make our own [anticipatory guidance] handouts,” he said. And in the later years, “an adolescent visit used to be every 2 or 3 years.”

“During the Vietnam War, there weren’t enough people who were healthy enough, physically fit enough, to be mustered into the Army,” said Peter Rappo, MD, a pediatrician in Brockton, Mass., who chaired the AAP’s Committee on Practice and Ambulatory Medicine in the late 1990s.
Dr. Rappo became interested in the history of preventive pediatric care after discovering a Children’s Year Campaign (1918-1919) poster in an antiques market. The poster’s message – “The Health of the Child is the Power of the Nation” – remained relevant through the Vietnam War. “I’d like to think that [childhood preventive services] were all about the kids,” he said, “but at the end of the day, it was about military issues too.”
Still, interest in the 1960s in the long-term implications of early-life development fed research that eventually led to an explosion of new science in the 1990s on the importance of early brain development and early life experiences. This scientific literature combined with greater societal interest in school readiness helped drive development of research-based instruments for developmental screening, said pediatrician Edward L. Schor, MD, formerly a vice president at the Commonwealth Fund and now a senior vice president for programs and partnerships at Lucile Packard Foundation for Children’s Health.
“Development was the first topic … of screening instruments,” he said. The tools have “not only increased the quality of care, they also have increased the efficiency of care, because the time to ask and answer these questions was shifted to the waiting room.”
Their use is far from universal, but increasing. Results of the Periodic Surveys administered to a national random sample of AAP members show that pediatricians’ use of at least one formal screening instrument to identify children through 36 months of age at risk for developmental delay increased from 23% in 2002 to 45% in 2009 and 63% in 2016. (And in 2016, 81% reported “always/almost always” using at least one formal screening tool for autism.) The data was presented at the annual meeting of the Society of Developmental and Behavioral Pediatrics September 2016.
For Dr. Rappo’s practice in Massachusetts, the adoption of developmental and behavioral health screening questionnaires for all ages was spurred by a 2007 mandate requiring formal screening for children and adolescents in MassHealth, the state’s combined Medicaid–Children’s Health Insurance Program.
“We all knew intuitively this is what we should be doing, so we also sat down with insurers to talk about why this is important for kids,” he said. Reimbursement improved, and most importantly, he said, use of the tools “has tremendously improved our opportunities for opening up discussions with parents about developmental-behavioral issues.”
The well-child visit of 50 years ago was much more of “a physician-generated, physician-led visit,” said Dr. Swanson. “The pediatrician knew what was needed, and at the end, we’d ask if there were any questions. Today, the first question recommended by Bright Futures is ‘Do you have any questions for the visit?’”
According to a 2009 focus group study involving 282 pediatricians and 41 nurse-practitioners, clinicians agree that eliciting and prioritizing parent concerns is a top priority in well-child care. Yet there’s also some unease. Some said in the focus group discussions that they feel constrained by the Periodicity Schedule, for instance, or feel tension between inviting parents’ concerns while simultaneously addressing the content recommended by professional guidelines (Pediatrics. 2009 Sep;124[3]:849-57).
Indeed, policies and recommendations for health promotion and anticipatory guidance (some consensus-based, some evidence-based or evidence-informed) mushroomed throughout the 1980s and 1990s, Dr. Swanson said. Combined with the increase in recommended screenings through the 1990s and 2000s – and in recent years, the increasing need for discussions to address vaccine concerns, mental and behavioral health issues, and obesity and overweight problems – there are real pulls and tugs.
The time allotted to well-child visits may have increased slightly for some pediatricians – to just over 20 minutes – but overall, visit length hasn’t changed much over the past few decades. “It has pretty much stayed the same, averaging between 15 and 20 minutes,” said Dr. Schor.
Offering guidance to clinicians in prioritizing questions and issues has been a goal in the last two editions (2008 and 2016) of the Bright Futures recommendations – formally called the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. “The joke was that if you did a Bright Futures well-child visit according to the old Bright Futures, you’d do one in the morning and one in the afternoon,” said Dr. Hagan.
The first edition came out in 1994, after a multidisciplinary group convened by the Maternal and Child Health Bureau at the Health Resources and Services Administration, and the Medicaid Bureau (then part of the Health Care Financing Administration) established the Bright Futures Children’s Health Charter to improve children’s health. The second edition was released in 2000 and updated in 2002, at which point the AAP established the Bright Futures National Center.
Previsit screening tools included in the new edition are aimed at assessing and prioritizing anticipatory guidance issues, Dr. Hagan said, noting too that the Periodicity Schedule and Bright Futures recommendations make distinctions between universal and selective screening. “By design,” he emphasized, “there’s more anticipatory guidance than you might ever accomplish in one visit, because we want to be thorough enough to provide a context – a schema – to deal with the issues.”
Oftentimes, he said, “what parents want to talk about is what you want to talk about.” And pediatricians “develop a skill set to temporize, to figure out what needs to be covered today, and what can be dealt with better at a later time,” Dr. Hagan said. “If you tell kids, for instance, ‘I can help you with this, I just have to get more information,’ they hear that there’s help on the way. Then you follow through.”

Overall, his well-child visits “have gotten much more involved with the emotional well-being of children.” Given that emotional issues and behavioral issues “tend to take a longer time to discuss and unravel,” he sets aside consultation times near the end of the day for families who need to discuss these issues.
And he routinely devotes time – starting at the 2-month visit – to discuss screen time and media use. “I believe that technology is making our children sick,” he said, noting that in his nearly 17 years of practice he has seen increasing numbers of children and adolescents with depression, anxiety, anger, and attention deficit/hyperactivity disorder. “The AAP has done a pretty good job of raising the point, but I don’t think it has hit home with parents yet.”
For Dr. Chung, electronic medical records and systems have enabled him to better flag issues for follow-up over the course of well-child visits, leading to “better longitudinal care.”
Surveys and questionnaires filled out by parents in his practice’s waiting room are scanned into charts, he noted, and adolescents can mark answers on a proprietary confidential risk questionnaire that subsequently gets scrambled so that no one but the provider can understand the responses.
Other potential impacts of electronic systems have yet to be realized, he and others said. Some pediatric practices, Dr. Schor said, have begun engaging with families ahead of well-child visits through the use of a computerized questionnaire that elicits areas and issues of interest. Such outreach may help families feel more invested and committed to attending the visits, particularly those that don’t involve immunizations or school/sport forms, he said.
Families are “not [always] buying what we’re selling [for well-child care],” said Dr. Schor, who has served on AAP committees and has written several well-cited articles on preventive pediatrics care.
Insurance coverage for well-child care got a boost in 2010 when Bright Futures was cited in the Affordable Care Act as the standard of what well-child care should accomplish, and its recommended screenings and services were required to be covered by insurers without cost-sharing.
In the long-run, he said, rethinking the roles of nonphysicians in anticipatory guidance and developmental and psychosocial screening – in interpreting results of questionnaires, for instance – may be essential for well-child care. Outside of large health care systems, “the use of personnel [has been] pretty much been unchanged over the years,” he said. “We need to ask, how can we use each individual’s skills and training most efficiently? How can we retrain and reorganize our patient flow?”
This may be especially important as well-child care increasingly considers family psychosocial issues such as housing, food insecurity, family violence, and other family social stressors. Maternal depression screening made its way into the Periodicity Schedule in February 2016, and Dr. Schor predicts that the schedule will include “family psychosocial risk screening” in another several years.
For now, the newly revised Bright Futures guidelines – and much of well-child care – places an increased emphasis on the social determinants of health, which Dr. Hagan said reflects the “long-standing, logical conclusion that we reached back in the 1990s – that if families are healthy, kids will be healthy … and that family health is also linked to community health.”
Fifty years ago in 1967, the American Academy of Pediatrics published a “Suggested Schedule for Preventive Child Health Care.” It was, in essence, the first periodicity schedule for well-child visits.
Described by AAP officials at the time as an “amalgamation of schedules used in various clinics and private offices,” it charted out the frequency and basic content of visits from 1 month through 6 years of age, and offered a simple list of items to be considered for guidance and discussion in all visits from 6 years on.
It is updated in real time, and is accompanied by an expansive package of Bright Futures recommendations, guidelines, and tools (including forms, handouts, and questionnaires) for health promotion and guidance. Together, the Periodicity Schedule and Bright Futures guidance reflect decades of steady change in the breadth and content of well-child care – and more recently, in some of its processes.
“When I started practicing [in 1979], developmental surveillance meant asking a few questions about developmental milestones, observing, and maybe lifting a few questions from the Denver Scale [the Denver Developmental Screening Test] to support our surveillance,” said Joseph F. Hagan, Jr., MD, a pediatrician in Burlington, Vt., and coeditor of Bright Futures.
Jack Swanson, MD, a pediatrician in Ames, Iowa, and a member of the Bright Futures Steering Committee, has similar recollections of well-child care in the early 1970s. “The developmental milestones were just questions and nothing more formal. Nutrition was a big [anticipatory guidance] issue, and some safety,” he recalled.
In early pediatric visits, “parents were interested in Dr. [Benjamin] Spock’s recommendations about feeding and raising their baby… and we used to make our own [anticipatory guidance] handouts,” he said. And in the later years, “an adolescent visit used to be every 2 or 3 years.”
“During the Vietnam War, there weren’t enough people who were healthy enough, physically fit enough, to be mustered into the Army,” said Peter Rappo, MD, a pediatrician in Brockton, Mass., who chaired the AAP’s Committee on Practice and Ambulatory Medicine in the late 1990s.
Dr. Rappo became interested in the history of preventive pediatric care after discovering a Children’s Year Campaign (1918-1919) poster in an antiques market. The poster’s message – “The Health of the Child is the Power of the Nation” – remained relevant through the Vietnam War. “I’d like to think that [childhood preventive services] were all about the kids,” he said, “but at the end of the day, it was about military issues too.”
Still, interest in the 1960s in the long-term implications of early-life development fed research that eventually led to an explosion of new science in the 1990s on the importance of early brain development and early life experiences. This scientific literature combined with greater societal interest in school readiness helped drive development of research-based instruments for developmental screening, said pediatrician Edward L. Schor, MD, formerly a vice president at the Commonwealth Fund and now a senior vice president for programs and partnerships at Lucile Packard Foundation for Children’s Health.
“Development was the first topic … of screening instruments,” he said. The tools have “not only increased the quality of care, they also have increased the efficiency of care, because the time to ask and answer these questions was shifted to the waiting room.”
Their use is far from universal, but increasing. Results of the Periodic Surveys administered to a national random sample of AAP members show that pediatricians’ use of at least one formal screening instrument to identify children through 36 months of age at risk for developmental delay increased from 23% in 2002 to 45% in 2009 and 63% in 2016. (And in 2016, 81% reported “always/almost always” using at least one formal screening tool for autism.) The data was presented at the annual meeting of the Society of Developmental and Behavioral Pediatrics September 2016.
For Dr. Rappo’s practice in Massachusetts, the adoption of developmental and behavioral health screening questionnaires for all ages was spurred by a 2007 mandate requiring formal screening for children and adolescents in MassHealth, the state’s combined Medicaid–Children’s Health Insurance Program.
“We all knew intuitively this is what we should be doing, so we also sat down with insurers to talk about why this is important for kids,” he said. Reimbursement improved, and most importantly, he said, use of the tools “has tremendously improved our opportunities for opening up discussions with parents about developmental-behavioral issues.”
The well-child visit of 50 years ago was much more of “a physician-generated, physician-led visit,” said Dr. Swanson. “The pediatrician knew what was needed, and at the end, we’d ask if there were any questions. Today, the first question recommended by Bright Futures is ‘Do you have any questions for the visit?’”
According to a 2009 focus group study involving 282 pediatricians and 41 nurse-practitioners, clinicians agree that eliciting and prioritizing parent concerns is a top priority in well-child care. Yet there’s also some unease. Some said in the focus group discussions that they feel constrained by the Periodicity Schedule, for instance, or feel tension between inviting parents’ concerns while simultaneously addressing the content recommended by professional guidelines (Pediatrics. 2009 Sep;124[3]:849-57).
Indeed, policies and recommendations for health promotion and anticipatory guidance (some consensus-based, some evidence-based or evidence-informed) mushroomed throughout the 1980s and 1990s, Dr. Swanson said. Combined with the increase in recommended screenings through the 1990s and 2000s – and in recent years, the increasing need for discussions to address vaccine concerns, mental and behavioral health issues, and obesity and overweight problems – there are real pulls and tugs.
The time allotted to well-child visits may have increased slightly for some pediatricians – to just over 20 minutes – but overall, visit length hasn’t changed much over the past few decades. “It has pretty much stayed the same, averaging between 15 and 20 minutes,” said Dr. Schor.
Offering guidance to clinicians in prioritizing questions and issues has been a goal in the last two editions (2008 and 2016) of the Bright Futures recommendations – formally called the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. “The joke was that if you did a Bright Futures well-child visit according to the old Bright Futures, you’d do one in the morning and one in the afternoon,” said Dr. Hagan.
The first edition came out in 1994, after a multidisciplinary group convened by the Maternal and Child Health Bureau at the Health Resources and Services Administration, and the Medicaid Bureau (then part of the Health Care Financing Administration) established the Bright Futures Children’s Health Charter to improve children’s health. The second edition was released in 2000 and updated in 2002, at which point the AAP established the Bright Futures National Center.
Previsit screening tools included in the new edition are aimed at assessing and prioritizing anticipatory guidance issues, Dr. Hagan said, noting too that the Periodicity Schedule and Bright Futures recommendations make distinctions between universal and selective screening. “By design,” he emphasized, “there’s more anticipatory guidance than you might ever accomplish in one visit, because we want to be thorough enough to provide a context – a schema – to deal with the issues.”
Oftentimes, he said, “what parents want to talk about is what you want to talk about.” And pediatricians “develop a skill set to temporize, to figure out what needs to be covered today, and what can be dealt with better at a later time,” Dr. Hagan said. “If you tell kids, for instance, ‘I can help you with this, I just have to get more information,’ they hear that there’s help on the way. Then you follow through.”
Overall, his well-child visits “have gotten much more involved with the emotional well-being of children.” Given that emotional issues and behavioral issues “tend to take a longer time to discuss and unravel,” he sets aside consultation times near the end of the day for families who need to discuss these issues.
And he routinely devotes time – starting at the 2-month visit – to discuss screen time and media use. “I believe that technology is making our children sick,” he said, noting that in his nearly 17 years of practice he has seen increasing numbers of children and adolescents with depression, anxiety, anger, and attention deficit/hyperactivity disorder. “The AAP has done a pretty good job of raising the point, but I don’t think it has hit home with parents yet.”
For Dr. Chung, electronic medical records and systems have enabled him to better flag issues for follow-up over the course of well-child visits, leading to “better longitudinal care.”
Surveys and questionnaires filled out by parents in his practice’s waiting room are scanned into charts, he noted, and adolescents can mark answers on a proprietary confidential risk questionnaire that subsequently gets scrambled so that no one but the provider can understand the responses.
Other potential impacts of electronic systems have yet to be realized, he and others said. Some pediatric practices, Dr. Schor said, have begun engaging with families ahead of well-child visits through the use of a computerized questionnaire that elicits areas and issues of interest. Such outreach may help families feel more invested and committed to attending the visits, particularly those that don’t involve immunizations or school/sport forms, he said.
Families are “not [always] buying what we’re selling [for well-child care],” said Dr. Schor, who has served on AAP committees and has written several well-cited articles on preventive pediatrics care.
Insurance coverage for well-child care got a boost in 2010 when Bright Futures was cited in the Affordable Care Act as the standard of what well-child care should accomplish, and its recommended screenings and services were required to be covered by insurers without cost-sharing.
In the long-run, he said, rethinking the roles of nonphysicians in anticipatory guidance and developmental and psychosocial screening – in interpreting results of questionnaires, for instance – may be essential for well-child care. Outside of large health care systems, “the use of personnel [has been] pretty much been unchanged over the years,” he said. “We need to ask, how can we use each individual’s skills and training most efficiently? How can we retrain and reorganize our patient flow?”
This may be especially important as well-child care increasingly considers family psychosocial issues such as housing, food insecurity, family violence, and other family social stressors. Maternal depression screening made its way into the Periodicity Schedule in February 2016, and Dr. Schor predicts that the schedule will include “family psychosocial risk screening” in another several years.
For now, the newly revised Bright Futures guidelines – and much of well-child care – places an increased emphasis on the social determinants of health, which Dr. Hagan said reflects the “long-standing, logical conclusion that we reached back in the 1990s – that if families are healthy, kids will be healthy … and that family health is also linked to community health.”
Fifty years ago in 1967, the American Academy of Pediatrics published a “Suggested Schedule for Preventive Child Health Care.” It was, in essence, the first periodicity schedule for well-child visits.
Described by AAP officials at the time as an “amalgamation of schedules used in various clinics and private offices,” it charted out the frequency and basic content of visits from 1 month through 6 years of age, and offered a simple list of items to be considered for guidance and discussion in all visits from 6 years on.
It is updated in real time, and is accompanied by an expansive package of Bright Futures recommendations, guidelines, and tools (including forms, handouts, and questionnaires) for health promotion and guidance. Together, the Periodicity Schedule and Bright Futures guidance reflect decades of steady change in the breadth and content of well-child care – and more recently, in some of its processes.
“When I started practicing [in 1979], developmental surveillance meant asking a few questions about developmental milestones, observing, and maybe lifting a few questions from the Denver Scale [the Denver Developmental Screening Test] to support our surveillance,” said Joseph F. Hagan, Jr., MD, a pediatrician in Burlington, Vt., and coeditor of Bright Futures.
Jack Swanson, MD, a pediatrician in Ames, Iowa, and a member of the Bright Futures Steering Committee, has similar recollections of well-child care in the early 1970s. “The developmental milestones were just questions and nothing more formal. Nutrition was a big [anticipatory guidance] issue, and some safety,” he recalled.
In early pediatric visits, “parents were interested in Dr. [Benjamin] Spock’s recommendations about feeding and raising their baby… and we used to make our own [anticipatory guidance] handouts,” he said. And in the later years, “an adolescent visit used to be every 2 or 3 years.”
“During the Vietnam War, there weren’t enough people who were healthy enough, physically fit enough, to be mustered into the Army,” said Peter Rappo, MD, a pediatrician in Brockton, Mass., who chaired the AAP’s Committee on Practice and Ambulatory Medicine in the late 1990s.
Dr. Rappo became interested in the history of preventive pediatric care after discovering a Children’s Year Campaign (1918-1919) poster in an antiques market. The poster’s message – “The Health of the Child is the Power of the Nation” – remained relevant through the Vietnam War. “I’d like to think that [childhood preventive services] were all about the kids,” he said, “but at the end of the day, it was about military issues too.”
Still, interest in the 1960s in the long-term implications of early-life development fed research that eventually led to an explosion of new science in the 1990s on the importance of early brain development and early life experiences. This scientific literature combined with greater societal interest in school readiness helped drive development of research-based instruments for developmental screening, said pediatrician Edward L. Schor, MD, formerly a vice president at the Commonwealth Fund and now a senior vice president for programs and partnerships at Lucile Packard Foundation for Children’s Health.
“Development was the first topic … of screening instruments,” he said. The tools have “not only increased the quality of care, they also have increased the efficiency of care, because the time to ask and answer these questions was shifted to the waiting room.”
Their use is far from universal, but increasing. Results of the Periodic Surveys administered to a national random sample of AAP members show that pediatricians’ use of at least one formal screening instrument to identify children through 36 months of age at risk for developmental delay increased from 23% in 2002 to 45% in 2009 and 63% in 2016. (And in 2016, 81% reported “always/almost always” using at least one formal screening tool for autism.) The data was presented at the annual meeting of the Society of Developmental and Behavioral Pediatrics September 2016.
For Dr. Rappo’s practice in Massachusetts, the adoption of developmental and behavioral health screening questionnaires for all ages was spurred by a 2007 mandate requiring formal screening for children and adolescents in MassHealth, the state’s combined Medicaid–Children’s Health Insurance Program.
“We all knew intuitively this is what we should be doing, so we also sat down with insurers to talk about why this is important for kids,” he said. Reimbursement improved, and most importantly, he said, use of the tools “has tremendously improved our opportunities for opening up discussions with parents about developmental-behavioral issues.”
The well-child visit of 50 years ago was much more of “a physician-generated, physician-led visit,” said Dr. Swanson. “The pediatrician knew what was needed, and at the end, we’d ask if there were any questions. Today, the first question recommended by Bright Futures is ‘Do you have any questions for the visit?’”
According to a 2009 focus group study involving 282 pediatricians and 41 nurse-practitioners, clinicians agree that eliciting and prioritizing parent concerns is a top priority in well-child care. Yet there’s also some unease. Some said in the focus group discussions that they feel constrained by the Periodicity Schedule, for instance, or feel tension between inviting parents’ concerns while simultaneously addressing the content recommended by professional guidelines (Pediatrics. 2009 Sep;124[3]:849-57).
Indeed, policies and recommendations for health promotion and anticipatory guidance (some consensus-based, some evidence-based or evidence-informed) mushroomed throughout the 1980s and 1990s, Dr. Swanson said. Combined with the increase in recommended screenings through the 1990s and 2000s – and in recent years, the increasing need for discussions to address vaccine concerns, mental and behavioral health issues, and obesity and overweight problems – there are real pulls and tugs.
The time allotted to well-child visits may have increased slightly for some pediatricians – to just over 20 minutes – but overall, visit length hasn’t changed much over the past few decades. “It has pretty much stayed the same, averaging between 15 and 20 minutes,” said Dr. Schor.
Offering guidance to clinicians in prioritizing questions and issues has been a goal in the last two editions (2008 and 2016) of the Bright Futures recommendations – formally called the Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. “The joke was that if you did a Bright Futures well-child visit according to the old Bright Futures, you’d do one in the morning and one in the afternoon,” said Dr. Hagan.
The first edition came out in 1994, after a multidisciplinary group convened by the Maternal and Child Health Bureau at the Health Resources and Services Administration, and the Medicaid Bureau (then part of the Health Care Financing Administration) established the Bright Futures Children’s Health Charter to improve children’s health. The second edition was released in 2000 and updated in 2002, at which point the AAP established the Bright Futures National Center.
Previsit screening tools included in the new edition are aimed at assessing and prioritizing anticipatory guidance issues, Dr. Hagan said, noting too that the Periodicity Schedule and Bright Futures recommendations make distinctions between universal and selective screening. “By design,” he emphasized, “there’s more anticipatory guidance than you might ever accomplish in one visit, because we want to be thorough enough to provide a context – a schema – to deal with the issues.”
Oftentimes, he said, “what parents want to talk about is what you want to talk about.” And pediatricians “develop a skill set to temporize, to figure out what needs to be covered today, and what can be dealt with better at a later time,” Dr. Hagan said. “If you tell kids, for instance, ‘I can help you with this, I just have to get more information,’ they hear that there’s help on the way. Then you follow through.”
Overall, his well-child visits “have gotten much more involved with the emotional well-being of children.” Given that emotional issues and behavioral issues “tend to take a longer time to discuss and unravel,” he sets aside consultation times near the end of the day for families who need to discuss these issues.
And he routinely devotes time – starting at the 2-month visit – to discuss screen time and media use. “I believe that technology is making our children sick,” he said, noting that in his nearly 17 years of practice he has seen increasing numbers of children and adolescents with depression, anxiety, anger, and attention deficit/hyperactivity disorder. “The AAP has done a pretty good job of raising the point, but I don’t think it has hit home with parents yet.”
For Dr. Chung, electronic medical records and systems have enabled him to better flag issues for follow-up over the course of well-child visits, leading to “better longitudinal care.”
Surveys and questionnaires filled out by parents in his practice’s waiting room are scanned into charts, he noted, and adolescents can mark answers on a proprietary confidential risk questionnaire that subsequently gets scrambled so that no one but the provider can understand the responses.
Other potential impacts of electronic systems have yet to be realized, he and others said. Some pediatric practices, Dr. Schor said, have begun engaging with families ahead of well-child visits through the use of a computerized questionnaire that elicits areas and issues of interest. Such outreach may help families feel more invested and committed to attending the visits, particularly those that don’t involve immunizations or school/sport forms, he said.
Families are “not [always] buying what we’re selling [for well-child care],” said Dr. Schor, who has served on AAP committees and has written several well-cited articles on preventive pediatrics care.
Insurance coverage for well-child care got a boost in 2010 when Bright Futures was cited in the Affordable Care Act as the standard of what well-child care should accomplish, and its recommended screenings and services were required to be covered by insurers without cost-sharing.
In the long-run, he said, rethinking the roles of nonphysicians in anticipatory guidance and developmental and psychosocial screening – in interpreting results of questionnaires, for instance – may be essential for well-child care. Outside of large health care systems, “the use of personnel [has been] pretty much been unchanged over the years,” he said. “We need to ask, how can we use each individual’s skills and training most efficiently? How can we retrain and reorganize our patient flow?”
This may be especially important as well-child care increasingly considers family psychosocial issues such as housing, food insecurity, family violence, and other family social stressors. Maternal depression screening made its way into the Periodicity Schedule in February 2016, and Dr. Schor predicts that the schedule will include “family psychosocial risk screening” in another several years.
For now, the newly revised Bright Futures guidelines – and much of well-child care – places an increased emphasis on the social determinants of health, which Dr. Hagan said reflects the “long-standing, logical conclusion that we reached back in the 1990s – that if families are healthy, kids will be healthy … and that family health is also linked to community health.”
50 years of child psychiatry, developmental-behavioral pediatrics
The 50th anniversary of Pediatric News prompts us to look back on the past 50 years in child psychiatry and developmental-behavioral pediatrics, and reflect on the evolution of the field. This includes the approach to diagnosis, the thinking about development and family, and the approach and access to treatment during this dynamic period.
While some historians identify the establishment of the first juvenile court in Chicago in 1899 and the work to help judges evaluate juvenile delinquency as the origin of child psychiatry in the United States, it was not until after World War II that the field really began to take root here, largely based on psychiatrists fleeing Europe and the seminal work of Anna Freud. Some of the earliest connections between pediatrics and child psychiatry were based on the work in England of Donald W. Winnicott, a practicing pediatrician and child psychiatrist, Albert J. Solnit, MD, at the Yale Child Study Center, and psychologically informed work of pediatrician Benjamin M. Spock, MD.
The first Diagnostic and Statistical Manual (DSM) was published in 1952, based on a codification of mental disorders established by the Navy during WWII. The American Academy of Child & Adolescent Psychiatry was established in 1953, the same year that the first “tranquilizer,” chlorpromazine (Thorazine) was introduced (in France), marking the start of a revolution in psychiatric care. In 1959, the first candidates sat for a licensing examination in child psychiatry. The Section on Developmental and Behavioral Pediatrics was established as part of the American Academy of Pediatrics in 1960 to support training in this area. The AACAP established a journal in 1961. Child guidance clinics started affiliating with hospitals and universities in the 1960’s, after the Community Mental Health Act of 1963. Then, in 1965, Julius B. Richmond, MD, (a pediatrician) and Uri Bronfenbrenner, PhD, (a developmental psychologist), recognizing the importance of ecological systems to child development, were involved in the creation of Head Start, and the first Joint Commission on Mental Health for Children was established by federal legislation in 1965. The field was truly coalescing into a distinct discipline of medicine, one that bridged pediatrics, psychiatry, and neurology with nonmedical disciplines such as justice and education.
The decade between 1967 and 1977 was a period of transition from the focus on psychoanalytic concepts typical of the first half of the century to a more systematic approach to diagnosis. Children in psychiatric treatment had commonly been seen for extended individual treatments, and those with more disruptive disorders often were hospitalized for long periods. Psychoanalysis focused on the unconscious (theoretical drives and conflicts) to guide treatment. Treatment often focused on the role (causal) of parents, and family treatment was common, even on inpatient units. The second edition of the DSM (DSM-II) was published in 1968, with its first distinct section for disorders of childhood and adolescence, and an overarching focus on psychodynamics. In 1974, the decision was made to publish a new edition of the DSM that would establish a multiaxial assessment system (separating “biological” mental health problems from personality disorders, medical illnesses, and psychosocial stressors) and research-oriented diagnostic criteria that would attempt to facilitate reliable diagnoses based on common clusters of symptoms. Field trials sponsored by the National Institute of Mental Health began in 1977 to establish the reliability of the new diagnoses.
The year 1977 saw the first Apple computer, the New York City blackout, the release of the first “Star Wars” movie, and also the start of a momentous decade in general and child psychiatry. The third edition of the DSM (DSM-III) was published in 1980, the beginning of a revolution in psychiatric diagnosis and treatments. It created reliable, reproducible diagnostic constructs to serve as the basis for studies on epidemiology and treatment. Implications of causality were replaced by description; for example, hyperkinetic reaction of childhood was redefined and labeled attention-deficit disorder. Recognizing the importance of research and training in this rapidly changing field, W.T. Grant Foundation funded 11 fellowship programs in 1977, and the Society for Developmental and Behavioral Pediatrics was founded in 1982 by the leaders of those programs.
In 1983, The AACAP published “Child Psychiatry: A Plan for the Coming Decades.” It was the result of 5 years’ work by 100 child psychiatrists, general psychiatrists, pediatricians, epidemiologists, nurses, leaders of the NIMH, and various child advocates. This report laid out a challenge for child psychiatry to develop research strategies that would allow evidence-based understanding and treatment of the mental illnesses of children. The established focus on individual experience and anecdotal data, particularly about social and psychodynamic influences, would shift towards a more scientific approach to diagnosis and treatment. This decade started an explosion in epidemiologic research, medication trials, and controlled studies of nonbiological treatments in child psychiatry. At the same time, the political landscape changed, and an ascendant conservatism began the process of closing publicly funded residential treatment centers that had offered care to the more chronically mentally ill and children with profound developmental disorders. This would accelerate the shift towards outpatient psychiatric care of children. Ironically, as research would accelerate in child psychiatry, access to effective treatments would become more difficult.
The decade from 1987 to 1997 was a period of dramatic growth in medication use in child psychiatry. Prozac was approved by the Food and Drug Administration for use in the United States in 1988 and soon followed by other selective serotonin reuptake inhibitors (Zoloft in 1991 and Paxil in 1992). The journal of the AACAP began to publish more randomized controlled trials of medication treatments in children with DSM-codified diagnoses, and clinicians became more comfortable using stimulants, antidepressants, and even antipsychotic medications in the outpatient setting. This trend was enhanced by the emergence of managed care and the denial of coverage for alleged “nonbiological” diagnoses and for many psychiatric treatments. Loss of reimbursement led to a significant decline in resources, particularly inpatient child psychiatry beds and specialized clinics. This, in turn, contributed to the growing emphasis on medication treatments for children’s mental health problems. For-profit managed care companies underbid each other to provide mental health coverage and incentivized medication visits. Of note, the medical budgets, not the mental health carve outs, were billed for the medication prescribed.
The Americans with Disabilities Act was passed in 1990, increasing the funding for school-based mental health resources for children, and in 1996, Congress passed the Mental Health Parity Act, the first of several legislative attempts to ensure parity between insurance coverage for medical and psychiatric illnesses – legislation that to this day has not achieved parity of access to care. As pediatricians took on more of mental health care, a multidisciplinary team created a primary care version of DSM IV, the DSM-IV-PC, in 1995, to assist with defining levels of symptoms less than disorder to facilitate earlier intervention. A formal subspecialty of developmental-behavioral pediatrics was established in 1999 to educate leaders. Pediatric residents have had required training in developmental-behavioral pediatrics since 2008.
The year 1997 saw the first nationwide survey of parents about attention-deficit/hyperactivity disorder, kicking off what could be called the decade of ADHD, in which prevalence rates steadily climbed, from 5.7% in 1997 to 9.5% in 2007. The prevalence of stimulant treatment in children skyrocketed in this period. According to the NIMH, stimulants were prescribed to 4.2% of 6- to 12-year-olds in 1996, and that number grew to 5.1% in 2008. For 13- to 18-year-olds, the rate more than doubled during this time, from 2.3% in 1996 to 4.9% in 2008. The prevalence of autism also grew dramatically during this time, from 1.9 per 1,000 in 1997-1999 to 7.4 per 1,000 in 2006-2008, probably based on an evolving understanding of the disorder and this diagnosis providing special access to resources in schools.
Research during this decade became increasingly focused on imaging studies of children (and adults), as leaders in the field were trying to move from symptom clusters to anatomic and physiologic correlates of psychiatric illness. The great increase in medication use in children hit a speed bump in October 2004, when the Food and Drug Administration issued a controversial public warning about an increased risk of suicidal thoughts or behaviors in youth being treated with SSRI antidepressants. As access to child psychiatric treatment had become more difficult over the preceding decades, pediatricians had assumed much of the medication treatment of common psychiatric problems. The FDA’s black box warning complicated pediatricians’ efforts to fill this void.
The last decade has been the decade of genetics and efforts to improve access to care. It started in 2007 with the FDA expanding its SSRI warning to acknowledge that depression itself increased the risk for suicide, in an effort to not discourage needed depression treatment in young people. But studies demonstrated that the rates of diagnosing and treating depression dropped dramatically in the years following the warning: Diagnoses of depression declined by as much as 42% in children, and the rate of antidepressant treatment in adolescents dropped by as much as 32% in the 2 years following the warning (N Engl J Med. 2014 Oct 30;371(18):1666-8). There was no compensatory increase in utilization of other kinds of treatments. While suicide rates in young people had been stubbornly steady from the mid-1970’s to the mid-1990’s, they began to decline in 1996, according to the Centers for Disease Control and Prevention. But that trend was broken in 2004, with a jump in attempted and completed suicides in young people. The rate stabilized later in the decade, but has never returned to the lows that were being achieved prior to the warning.
This decade was marked by the passage of the Affordable Care Act, including – again – an unfulfilled mandate for mental health parity for any insurance plans in the marketplace. Although diagnosis is still symptom based, the effort to define psychiatric disorders based on brain anatomy, neurotransmitters, and genomics continues to intensify. There is growing evidence that psychiatric disorders are not nature or nurture, but nature and nurture. Epigenetic findings show that environment impacts gene expression and brain functioning. These findings promise to deepen our understanding of the critical role of early experiences (consider Adverse Childhood Experiences [ACE] scores) and the promise of protective relationships, in schools and parenting.
And what will come next? We believe that silos – medical, psychiatric, parenting, school, environment – will be bridged to understand the many factors that impact behavior and treatment, but the need to advocate for policies that support funding for the education and mental health care of children and the training of professionals to provide that care is never ending. As our knowledge of the genome marches forward, we may discover effective strategies for preventing the emergence of mental illness in children or create individualized treatments. We may learn more about the role of nutrition and the microbiome in health and disease, about autoimmunity and mental illness. Our focus may return to parents, not as culprits, but as the mediators of health from the prenatal period on. Technology may enable us to improve access to effective treatments, with teens monitoring their sleep and mood, and accessing therapy on their smart phones. And our understanding of development and vulnerability may help us stem the rise in autism or collaborate with educators so that education could better put every child on their healthiest possible path. We look forward to experiencing it – and writing about it – with you!
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. They said they had no relevant financial disclosures. Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email them at [email protected].
The 50th anniversary of Pediatric News prompts us to look back on the past 50 years in child psychiatry and developmental-behavioral pediatrics, and reflect on the evolution of the field. This includes the approach to diagnosis, the thinking about development and family, and the approach and access to treatment during this dynamic period.
While some historians identify the establishment of the first juvenile court in Chicago in 1899 and the work to help judges evaluate juvenile delinquency as the origin of child psychiatry in the United States, it was not until after World War II that the field really began to take root here, largely based on psychiatrists fleeing Europe and the seminal work of Anna Freud. Some of the earliest connections between pediatrics and child psychiatry were based on the work in England of Donald W. Winnicott, a practicing pediatrician and child psychiatrist, Albert J. Solnit, MD, at the Yale Child Study Center, and psychologically informed work of pediatrician Benjamin M. Spock, MD.
The first Diagnostic and Statistical Manual (DSM) was published in 1952, based on a codification of mental disorders established by the Navy during WWII. The American Academy of Child & Adolescent Psychiatry was established in 1953, the same year that the first “tranquilizer,” chlorpromazine (Thorazine) was introduced (in France), marking the start of a revolution in psychiatric care. In 1959, the first candidates sat for a licensing examination in child psychiatry. The Section on Developmental and Behavioral Pediatrics was established as part of the American Academy of Pediatrics in 1960 to support training in this area. The AACAP established a journal in 1961. Child guidance clinics started affiliating with hospitals and universities in the 1960’s, after the Community Mental Health Act of 1963. Then, in 1965, Julius B. Richmond, MD, (a pediatrician) and Uri Bronfenbrenner, PhD, (a developmental psychologist), recognizing the importance of ecological systems to child development, were involved in the creation of Head Start, and the first Joint Commission on Mental Health for Children was established by federal legislation in 1965. The field was truly coalescing into a distinct discipline of medicine, one that bridged pediatrics, psychiatry, and neurology with nonmedical disciplines such as justice and education.
The decade between 1967 and 1977 was a period of transition from the focus on psychoanalytic concepts typical of the first half of the century to a more systematic approach to diagnosis. Children in psychiatric treatment had commonly been seen for extended individual treatments, and those with more disruptive disorders often were hospitalized for long periods. Psychoanalysis focused on the unconscious (theoretical drives and conflicts) to guide treatment. Treatment often focused on the role (causal) of parents, and family treatment was common, even on inpatient units. The second edition of the DSM (DSM-II) was published in 1968, with its first distinct section for disorders of childhood and adolescence, and an overarching focus on psychodynamics. In 1974, the decision was made to publish a new edition of the DSM that would establish a multiaxial assessment system (separating “biological” mental health problems from personality disorders, medical illnesses, and psychosocial stressors) and research-oriented diagnostic criteria that would attempt to facilitate reliable diagnoses based on common clusters of symptoms. Field trials sponsored by the National Institute of Mental Health began in 1977 to establish the reliability of the new diagnoses.
The year 1977 saw the first Apple computer, the New York City blackout, the release of the first “Star Wars” movie, and also the start of a momentous decade in general and child psychiatry. The third edition of the DSM (DSM-III) was published in 1980, the beginning of a revolution in psychiatric diagnosis and treatments. It created reliable, reproducible diagnostic constructs to serve as the basis for studies on epidemiology and treatment. Implications of causality were replaced by description; for example, hyperkinetic reaction of childhood was redefined and labeled attention-deficit disorder. Recognizing the importance of research and training in this rapidly changing field, W.T. Grant Foundation funded 11 fellowship programs in 1977, and the Society for Developmental and Behavioral Pediatrics was founded in 1982 by the leaders of those programs.
In 1983, The AACAP published “Child Psychiatry: A Plan for the Coming Decades.” It was the result of 5 years’ work by 100 child psychiatrists, general psychiatrists, pediatricians, epidemiologists, nurses, leaders of the NIMH, and various child advocates. This report laid out a challenge for child psychiatry to develop research strategies that would allow evidence-based understanding and treatment of the mental illnesses of children. The established focus on individual experience and anecdotal data, particularly about social and psychodynamic influences, would shift towards a more scientific approach to diagnosis and treatment. This decade started an explosion in epidemiologic research, medication trials, and controlled studies of nonbiological treatments in child psychiatry. At the same time, the political landscape changed, and an ascendant conservatism began the process of closing publicly funded residential treatment centers that had offered care to the more chronically mentally ill and children with profound developmental disorders. This would accelerate the shift towards outpatient psychiatric care of children. Ironically, as research would accelerate in child psychiatry, access to effective treatments would become more difficult.
The decade from 1987 to 1997 was a period of dramatic growth in medication use in child psychiatry. Prozac was approved by the Food and Drug Administration for use in the United States in 1988 and soon followed by other selective serotonin reuptake inhibitors (Zoloft in 1991 and Paxil in 1992). The journal of the AACAP began to publish more randomized controlled trials of medication treatments in children with DSM-codified diagnoses, and clinicians became more comfortable using stimulants, antidepressants, and even antipsychotic medications in the outpatient setting. This trend was enhanced by the emergence of managed care and the denial of coverage for alleged “nonbiological” diagnoses and for many psychiatric treatments. Loss of reimbursement led to a significant decline in resources, particularly inpatient child psychiatry beds and specialized clinics. This, in turn, contributed to the growing emphasis on medication treatments for children’s mental health problems. For-profit managed care companies underbid each other to provide mental health coverage and incentivized medication visits. Of note, the medical budgets, not the mental health carve outs, were billed for the medication prescribed.
The Americans with Disabilities Act was passed in 1990, increasing the funding for school-based mental health resources for children, and in 1996, Congress passed the Mental Health Parity Act, the first of several legislative attempts to ensure parity between insurance coverage for medical and psychiatric illnesses – legislation that to this day has not achieved parity of access to care. As pediatricians took on more of mental health care, a multidisciplinary team created a primary care version of DSM IV, the DSM-IV-PC, in 1995, to assist with defining levels of symptoms less than disorder to facilitate earlier intervention. A formal subspecialty of developmental-behavioral pediatrics was established in 1999 to educate leaders. Pediatric residents have had required training in developmental-behavioral pediatrics since 2008.
The year 1997 saw the first nationwide survey of parents about attention-deficit/hyperactivity disorder, kicking off what could be called the decade of ADHD, in which prevalence rates steadily climbed, from 5.7% in 1997 to 9.5% in 2007. The prevalence of stimulant treatment in children skyrocketed in this period. According to the NIMH, stimulants were prescribed to 4.2% of 6- to 12-year-olds in 1996, and that number grew to 5.1% in 2008. For 13- to 18-year-olds, the rate more than doubled during this time, from 2.3% in 1996 to 4.9% in 2008. The prevalence of autism also grew dramatically during this time, from 1.9 per 1,000 in 1997-1999 to 7.4 per 1,000 in 2006-2008, probably based on an evolving understanding of the disorder and this diagnosis providing special access to resources in schools.
Research during this decade became increasingly focused on imaging studies of children (and adults), as leaders in the field were trying to move from symptom clusters to anatomic and physiologic correlates of psychiatric illness. The great increase in medication use in children hit a speed bump in October 2004, when the Food and Drug Administration issued a controversial public warning about an increased risk of suicidal thoughts or behaviors in youth being treated with SSRI antidepressants. As access to child psychiatric treatment had become more difficult over the preceding decades, pediatricians had assumed much of the medication treatment of common psychiatric problems. The FDA’s black box warning complicated pediatricians’ efforts to fill this void.
The last decade has been the decade of genetics and efforts to improve access to care. It started in 2007 with the FDA expanding its SSRI warning to acknowledge that depression itself increased the risk for suicide, in an effort to not discourage needed depression treatment in young people. But studies demonstrated that the rates of diagnosing and treating depression dropped dramatically in the years following the warning: Diagnoses of depression declined by as much as 42% in children, and the rate of antidepressant treatment in adolescents dropped by as much as 32% in the 2 years following the warning (N Engl J Med. 2014 Oct 30;371(18):1666-8). There was no compensatory increase in utilization of other kinds of treatments. While suicide rates in young people had been stubbornly steady from the mid-1970’s to the mid-1990’s, they began to decline in 1996, according to the Centers for Disease Control and Prevention. But that trend was broken in 2004, with a jump in attempted and completed suicides in young people. The rate stabilized later in the decade, but has never returned to the lows that were being achieved prior to the warning.
This decade was marked by the passage of the Affordable Care Act, including – again – an unfulfilled mandate for mental health parity for any insurance plans in the marketplace. Although diagnosis is still symptom based, the effort to define psychiatric disorders based on brain anatomy, neurotransmitters, and genomics continues to intensify. There is growing evidence that psychiatric disorders are not nature or nurture, but nature and nurture. Epigenetic findings show that environment impacts gene expression and brain functioning. These findings promise to deepen our understanding of the critical role of early experiences (consider Adverse Childhood Experiences [ACE] scores) and the promise of protective relationships, in schools and parenting.
And what will come next? We believe that silos – medical, psychiatric, parenting, school, environment – will be bridged to understand the many factors that impact behavior and treatment, but the need to advocate for policies that support funding for the education and mental health care of children and the training of professionals to provide that care is never ending. As our knowledge of the genome marches forward, we may discover effective strategies for preventing the emergence of mental illness in children or create individualized treatments. We may learn more about the role of nutrition and the microbiome in health and disease, about autoimmunity and mental illness. Our focus may return to parents, not as culprits, but as the mediators of health from the prenatal period on. Technology may enable us to improve access to effective treatments, with teens monitoring their sleep and mood, and accessing therapy on their smart phones. And our understanding of development and vulnerability may help us stem the rise in autism or collaborate with educators so that education could better put every child on their healthiest possible path. We look forward to experiencing it – and writing about it – with you!
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. They said they had no relevant financial disclosures. Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email them at [email protected].
The 50th anniversary of Pediatric News prompts us to look back on the past 50 years in child psychiatry and developmental-behavioral pediatrics, and reflect on the evolution of the field. This includes the approach to diagnosis, the thinking about development and family, and the approach and access to treatment during this dynamic period.
While some historians identify the establishment of the first juvenile court in Chicago in 1899 and the work to help judges evaluate juvenile delinquency as the origin of child psychiatry in the United States, it was not until after World War II that the field really began to take root here, largely based on psychiatrists fleeing Europe and the seminal work of Anna Freud. Some of the earliest connections between pediatrics and child psychiatry were based on the work in England of Donald W. Winnicott, a practicing pediatrician and child psychiatrist, Albert J. Solnit, MD, at the Yale Child Study Center, and psychologically informed work of pediatrician Benjamin M. Spock, MD.
The first Diagnostic and Statistical Manual (DSM) was published in 1952, based on a codification of mental disorders established by the Navy during WWII. The American Academy of Child & Adolescent Psychiatry was established in 1953, the same year that the first “tranquilizer,” chlorpromazine (Thorazine) was introduced (in France), marking the start of a revolution in psychiatric care. In 1959, the first candidates sat for a licensing examination in child psychiatry. The Section on Developmental and Behavioral Pediatrics was established as part of the American Academy of Pediatrics in 1960 to support training in this area. The AACAP established a journal in 1961. Child guidance clinics started affiliating with hospitals and universities in the 1960’s, after the Community Mental Health Act of 1963. Then, in 1965, Julius B. Richmond, MD, (a pediatrician) and Uri Bronfenbrenner, PhD, (a developmental psychologist), recognizing the importance of ecological systems to child development, were involved in the creation of Head Start, and the first Joint Commission on Mental Health for Children was established by federal legislation in 1965. The field was truly coalescing into a distinct discipline of medicine, one that bridged pediatrics, psychiatry, and neurology with nonmedical disciplines such as justice and education.
The decade between 1967 and 1977 was a period of transition from the focus on psychoanalytic concepts typical of the first half of the century to a more systematic approach to diagnosis. Children in psychiatric treatment had commonly been seen for extended individual treatments, and those with more disruptive disorders often were hospitalized for long periods. Psychoanalysis focused on the unconscious (theoretical drives and conflicts) to guide treatment. Treatment often focused on the role (causal) of parents, and family treatment was common, even on inpatient units. The second edition of the DSM (DSM-II) was published in 1968, with its first distinct section for disorders of childhood and adolescence, and an overarching focus on psychodynamics. In 1974, the decision was made to publish a new edition of the DSM that would establish a multiaxial assessment system (separating “biological” mental health problems from personality disorders, medical illnesses, and psychosocial stressors) and research-oriented diagnostic criteria that would attempt to facilitate reliable diagnoses based on common clusters of symptoms. Field trials sponsored by the National Institute of Mental Health began in 1977 to establish the reliability of the new diagnoses.
The year 1977 saw the first Apple computer, the New York City blackout, the release of the first “Star Wars” movie, and also the start of a momentous decade in general and child psychiatry. The third edition of the DSM (DSM-III) was published in 1980, the beginning of a revolution in psychiatric diagnosis and treatments. It created reliable, reproducible diagnostic constructs to serve as the basis for studies on epidemiology and treatment. Implications of causality were replaced by description; for example, hyperkinetic reaction of childhood was redefined and labeled attention-deficit disorder. Recognizing the importance of research and training in this rapidly changing field, W.T. Grant Foundation funded 11 fellowship programs in 1977, and the Society for Developmental and Behavioral Pediatrics was founded in 1982 by the leaders of those programs.
In 1983, The AACAP published “Child Psychiatry: A Plan for the Coming Decades.” It was the result of 5 years’ work by 100 child psychiatrists, general psychiatrists, pediatricians, epidemiologists, nurses, leaders of the NIMH, and various child advocates. This report laid out a challenge for child psychiatry to develop research strategies that would allow evidence-based understanding and treatment of the mental illnesses of children. The established focus on individual experience and anecdotal data, particularly about social and psychodynamic influences, would shift towards a more scientific approach to diagnosis and treatment. This decade started an explosion in epidemiologic research, medication trials, and controlled studies of nonbiological treatments in child psychiatry. At the same time, the political landscape changed, and an ascendant conservatism began the process of closing publicly funded residential treatment centers that had offered care to the more chronically mentally ill and children with profound developmental disorders. This would accelerate the shift towards outpatient psychiatric care of children. Ironically, as research would accelerate in child psychiatry, access to effective treatments would become more difficult.
The decade from 1987 to 1997 was a period of dramatic growth in medication use in child psychiatry. Prozac was approved by the Food and Drug Administration for use in the United States in 1988 and soon followed by other selective serotonin reuptake inhibitors (Zoloft in 1991 and Paxil in 1992). The journal of the AACAP began to publish more randomized controlled trials of medication treatments in children with DSM-codified diagnoses, and clinicians became more comfortable using stimulants, antidepressants, and even antipsychotic medications in the outpatient setting. This trend was enhanced by the emergence of managed care and the denial of coverage for alleged “nonbiological” diagnoses and for many psychiatric treatments. Loss of reimbursement led to a significant decline in resources, particularly inpatient child psychiatry beds and specialized clinics. This, in turn, contributed to the growing emphasis on medication treatments for children’s mental health problems. For-profit managed care companies underbid each other to provide mental health coverage and incentivized medication visits. Of note, the medical budgets, not the mental health carve outs, were billed for the medication prescribed.
The Americans with Disabilities Act was passed in 1990, increasing the funding for school-based mental health resources for children, and in 1996, Congress passed the Mental Health Parity Act, the first of several legislative attempts to ensure parity between insurance coverage for medical and psychiatric illnesses – legislation that to this day has not achieved parity of access to care. As pediatricians took on more of mental health care, a multidisciplinary team created a primary care version of DSM IV, the DSM-IV-PC, in 1995, to assist with defining levels of symptoms less than disorder to facilitate earlier intervention. A formal subspecialty of developmental-behavioral pediatrics was established in 1999 to educate leaders. Pediatric residents have had required training in developmental-behavioral pediatrics since 2008.
The year 1997 saw the first nationwide survey of parents about attention-deficit/hyperactivity disorder, kicking off what could be called the decade of ADHD, in which prevalence rates steadily climbed, from 5.7% in 1997 to 9.5% in 2007. The prevalence of stimulant treatment in children skyrocketed in this period. According to the NIMH, stimulants were prescribed to 4.2% of 6- to 12-year-olds in 1996, and that number grew to 5.1% in 2008. For 13- to 18-year-olds, the rate more than doubled during this time, from 2.3% in 1996 to 4.9% in 2008. The prevalence of autism also grew dramatically during this time, from 1.9 per 1,000 in 1997-1999 to 7.4 per 1,000 in 2006-2008, probably based on an evolving understanding of the disorder and this diagnosis providing special access to resources in schools.
Research during this decade became increasingly focused on imaging studies of children (and adults), as leaders in the field were trying to move from symptom clusters to anatomic and physiologic correlates of psychiatric illness. The great increase in medication use in children hit a speed bump in October 2004, when the Food and Drug Administration issued a controversial public warning about an increased risk of suicidal thoughts or behaviors in youth being treated with SSRI antidepressants. As access to child psychiatric treatment had become more difficult over the preceding decades, pediatricians had assumed much of the medication treatment of common psychiatric problems. The FDA’s black box warning complicated pediatricians’ efforts to fill this void.
The last decade has been the decade of genetics and efforts to improve access to care. It started in 2007 with the FDA expanding its SSRI warning to acknowledge that depression itself increased the risk for suicide, in an effort to not discourage needed depression treatment in young people. But studies demonstrated that the rates of diagnosing and treating depression dropped dramatically in the years following the warning: Diagnoses of depression declined by as much as 42% in children, and the rate of antidepressant treatment in adolescents dropped by as much as 32% in the 2 years following the warning (N Engl J Med. 2014 Oct 30;371(18):1666-8). There was no compensatory increase in utilization of other kinds of treatments. While suicide rates in young people had been stubbornly steady from the mid-1970’s to the mid-1990’s, they began to decline in 1996, according to the Centers for Disease Control and Prevention. But that trend was broken in 2004, with a jump in attempted and completed suicides in young people. The rate stabilized later in the decade, but has never returned to the lows that were being achieved prior to the warning.
This decade was marked by the passage of the Affordable Care Act, including – again – an unfulfilled mandate for mental health parity for any insurance plans in the marketplace. Although diagnosis is still symptom based, the effort to define psychiatric disorders based on brain anatomy, neurotransmitters, and genomics continues to intensify. There is growing evidence that psychiatric disorders are not nature or nurture, but nature and nurture. Epigenetic findings show that environment impacts gene expression and brain functioning. These findings promise to deepen our understanding of the critical role of early experiences (consider Adverse Childhood Experiences [ACE] scores) and the promise of protective relationships, in schools and parenting.
And what will come next? We believe that silos – medical, psychiatric, parenting, school, environment – will be bridged to understand the many factors that impact behavior and treatment, but the need to advocate for policies that support funding for the education and mental health care of children and the training of professionals to provide that care is never ending. As our knowledge of the genome marches forward, we may discover effective strategies for preventing the emergence of mental illness in children or create individualized treatments. We may learn more about the role of nutrition and the microbiome in health and disease, about autoimmunity and mental illness. Our focus may return to parents, not as culprits, but as the mediators of health from the prenatal period on. Technology may enable us to improve access to effective treatments, with teens monitoring their sleep and mood, and accessing therapy on their smart phones. And our understanding of development and vulnerability may help us stem the rise in autism or collaborate with educators so that education could better put every child on their healthiest possible path. We look forward to experiencing it – and writing about it – with you!
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. They said they had no relevant financial disclosures. Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email them at [email protected].
CMS makes economics of primary care ACOs more appealing
As you may have read, accountable care organizations have met uneven success over the last several years. But, when they are broken down into categories, physician-sponsored ACOs have done better, particularly those with a strong primary care core.
This is true for several reasons.
In this transition period from a fee-for-service payment system that rewards volume and expensive inpatient care to a pay-for-value system, some ACOs set up by health systems or specialists envisioned the savings coming through lower utilization of their services. They had an inherent impediment to fully committing to keeping people well and avoiding acute care. In contrast, primary care providers are free to be all in with population health value-based programs.

However, because the fee-for-service system has historically left primary care physicians at the bottom of the compensation food chain, we have a “can’t get there from here” dilemma. It is a cruel irony that the group best suited to stretch America’s health care dollar and benefit both professionally and financially usually does not have the capital to create and operate an ACO for the roughly 18 months before shared savings are distributed.
The Centers for Medicare & Medicaid Services has tried to mitigate this by offering financial support for small, non–health system ACOs, particularly those in rural areas. Some of those enrolled ACOs are primary care driven and have been among the most successful in the MSSP.
Nonetheless, the upfront costs, paired with the long delay for the sole economic return on the investment – shared savings – have combined to be deal killers for many promising would-be primary care ACOs.
New upfront payments are game changers
A successful ACO will be assigned one or more patient populations and be given a minimum of 50% of the savings for the overall costs for those populations, if the quality of their health is maintained or improved.
To excise avoidable waste, the ACO looks at gaps in care for those populations – frequent emergency department use for nonemergencies, avoidably high levels of diabetes and obesity, too-high readmission rates, unnecessarily high postacute care costs, etc. They then use evidence-based best team care practices – from patient self care and prevention, to multispecialty coordination and PCMH care management.
Why? Because these proved to give the highest impact on quality and reducing costs. To achieve significant shared savings, the costs are usually measured for a calendar year, then it takes about 6 months for the claims to be reported and paid. Thus, the shared savings check to the ACO will arrive about 18 months after all this is started.
The CMS has also figured out that primary care physician care coordination and management drive quality and savings. The agency knows that incentivizing this type of care, the very type calculated to create ACO success, will net significant savings to the Medicare program.
For example, the pilot project for preventing diabetes will be expanded, because Medicare hopes to save several thousand dollars a year per beneficiary in health care costs.
In a blog entry the day the expanded population health management codes were announced, the CMS acting administrator wrote that, “Over time, if the clinicians qualified to provide these services were to fully provide these services to all eligible beneficiaries, the increase would be as much as $4 billion or more in additional support for care coordination and patient-centered care.”
CMS revenue streams to support ACO success-driving activities include:
• Value-based screening and counseling codes to decrease downstream costs.
• Upward adjustment of evaluation and management reimbursement for assessment of care and care plan development for mobility-impaired patients.
• Annual wellness visits.
• Prolonged E&M services that accrue outside of a patient visit.
• Collaboration with mental health specialists.
• Comprehensive assessment and care planning for patients with cognitive impairment.
• Expansion of the diabetes prevention pilot program; diabetes prevention and diabetes education are two separate services.
• Transitional care management for high-risk patients post discharge.
• Structured obesity management.
The 2017 Medicare fee schedule smoothed some of the bumps in administering and being paid for chronic care management (CCM) services, and it added codes with increased reimbursement aligned with increased complexity of comorbidities/illness.
Perhaps the biggest new payment boost for primary care to engage in ACO high-value activities is actually the Merit-Based Incentive Payment System (MIPS) under MACRA, the Medicare Access and CHIP Reauthorization Act of 2015.
Under MACRA, all Medicare compensation for physicians will be determined by relative delivery of quality and efficient care. Experts are recommending that primary care physicians participate in non–risk-taking ACOs to optimize MIPS value scoring, while also reducing administrative burdens of compliance. Use an ACO’s analytics to support collaborative care and provide the reports required under MIPS.
Let’s be smart about it
According to Gordon Wilhoit, MD, a practicing physician and chief medical officer of an all–primary-care-physician ACO in South Carolina, “This is a no brainer. Start first with your MSSP ACO high-value game plan, then align the complementary care coordination codes, CCM, MIPS, and other revenue stream and reporting activities with it. Now, primary care physicians can finance their ACO and MIPS care coordination efforts with a stream of ongoing payments from these care management codes.
“One of my colleagues saw a 27% increase in revenues in 6 months just from providing and billing for this type of care,” Dr. Wilhoit explained. “And, not counting shared savings or MIPS incentive payments, our office’s reimbursement from these care management codes now exceeds our fee-for-service income, which has not decreased.”
Even with these payments, the CMS will reduce overall net expenditures. Your impact on health care will be more powerful as a manager of the team addressing patients’ overall health than reacting to patient sickness one at a time. The patients you impact the most may be ones you don’t actually see. Your empowerment to practice medicine the right way will continue to grow.
Now, finally, you may start getting compensation that takes away the last big hurdle to creating the infrastructure you need to succeed.
Mr. Bobbitt is a head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of, and Dr. Wilhoit is a consultant with, Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at either [email protected] or 919-906-4054.
As you may have read, accountable care organizations have met uneven success over the last several years. But, when they are broken down into categories, physician-sponsored ACOs have done better, particularly those with a strong primary care core.
This is true for several reasons.
In this transition period from a fee-for-service payment system that rewards volume and expensive inpatient care to a pay-for-value system, some ACOs set up by health systems or specialists envisioned the savings coming through lower utilization of their services. They had an inherent impediment to fully committing to keeping people well and avoiding acute care. In contrast, primary care providers are free to be all in with population health value-based programs.
However, because the fee-for-service system has historically left primary care physicians at the bottom of the compensation food chain, we have a “can’t get there from here” dilemma. It is a cruel irony that the group best suited to stretch America’s health care dollar and benefit both professionally and financially usually does not have the capital to create and operate an ACO for the roughly 18 months before shared savings are distributed.
The Centers for Medicare & Medicaid Services has tried to mitigate this by offering financial support for small, non–health system ACOs, particularly those in rural areas. Some of those enrolled ACOs are primary care driven and have been among the most successful in the MSSP.
Nonetheless, the upfront costs, paired with the long delay for the sole economic return on the investment – shared savings – have combined to be deal killers for many promising would-be primary care ACOs.
New upfront payments are game changers
A successful ACO will be assigned one or more patient populations and be given a minimum of 50% of the savings for the overall costs for those populations, if the quality of their health is maintained or improved.
To excise avoidable waste, the ACO looks at gaps in care for those populations – frequent emergency department use for nonemergencies, avoidably high levels of diabetes and obesity, too-high readmission rates, unnecessarily high postacute care costs, etc. They then use evidence-based best team care practices – from patient self care and prevention, to multispecialty coordination and PCMH care management.
Why? Because these proved to give the highest impact on quality and reducing costs. To achieve significant shared savings, the costs are usually measured for a calendar year, then it takes about 6 months for the claims to be reported and paid. Thus, the shared savings check to the ACO will arrive about 18 months after all this is started.
The CMS has also figured out that primary care physician care coordination and management drive quality and savings. The agency knows that incentivizing this type of care, the very type calculated to create ACO success, will net significant savings to the Medicare program.
For example, the pilot project for preventing diabetes will be expanded, because Medicare hopes to save several thousand dollars a year per beneficiary in health care costs.
In a blog entry the day the expanded population health management codes were announced, the CMS acting administrator wrote that, “Over time, if the clinicians qualified to provide these services were to fully provide these services to all eligible beneficiaries, the increase would be as much as $4 billion or more in additional support for care coordination and patient-centered care.”
CMS revenue streams to support ACO success-driving activities include:
• Value-based screening and counseling codes to decrease downstream costs.
• Upward adjustment of evaluation and management reimbursement for assessment of care and care plan development for mobility-impaired patients.
• Annual wellness visits.
• Prolonged E&M services that accrue outside of a patient visit.
• Collaboration with mental health specialists.
• Comprehensive assessment and care planning for patients with cognitive impairment.
• Expansion of the diabetes prevention pilot program; diabetes prevention and diabetes education are two separate services.
• Transitional care management for high-risk patients post discharge.
• Structured obesity management.
The 2017 Medicare fee schedule smoothed some of the bumps in administering and being paid for chronic care management (CCM) services, and it added codes with increased reimbursement aligned with increased complexity of comorbidities/illness.
Perhaps the biggest new payment boost for primary care to engage in ACO high-value activities is actually the Merit-Based Incentive Payment System (MIPS) under MACRA, the Medicare Access and CHIP Reauthorization Act of 2015.
Under MACRA, all Medicare compensation for physicians will be determined by relative delivery of quality and efficient care. Experts are recommending that primary care physicians participate in non–risk-taking ACOs to optimize MIPS value scoring, while also reducing administrative burdens of compliance. Use an ACO’s analytics to support collaborative care and provide the reports required under MIPS.
Let’s be smart about it
According to Gordon Wilhoit, MD, a practicing physician and chief medical officer of an all–primary-care-physician ACO in South Carolina, “This is a no brainer. Start first with your MSSP ACO high-value game plan, then align the complementary care coordination codes, CCM, MIPS, and other revenue stream and reporting activities with it. Now, primary care physicians can finance their ACO and MIPS care coordination efforts with a stream of ongoing payments from these care management codes.
“One of my colleagues saw a 27% increase in revenues in 6 months just from providing and billing for this type of care,” Dr. Wilhoit explained. “And, not counting shared savings or MIPS incentive payments, our office’s reimbursement from these care management codes now exceeds our fee-for-service income, which has not decreased.”
Even with these payments, the CMS will reduce overall net expenditures. Your impact on health care will be more powerful as a manager of the team addressing patients’ overall health than reacting to patient sickness one at a time. The patients you impact the most may be ones you don’t actually see. Your empowerment to practice medicine the right way will continue to grow.
Now, finally, you may start getting compensation that takes away the last big hurdle to creating the infrastructure you need to succeed.
Mr. Bobbitt is a head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of, and Dr. Wilhoit is a consultant with, Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at either [email protected] or 919-906-4054.
As you may have read, accountable care organizations have met uneven success over the last several years. But, when they are broken down into categories, physician-sponsored ACOs have done better, particularly those with a strong primary care core.
This is true for several reasons.
In this transition period from a fee-for-service payment system that rewards volume and expensive inpatient care to a pay-for-value system, some ACOs set up by health systems or specialists envisioned the savings coming through lower utilization of their services. They had an inherent impediment to fully committing to keeping people well and avoiding acute care. In contrast, primary care providers are free to be all in with population health value-based programs.
However, because the fee-for-service system has historically left primary care physicians at the bottom of the compensation food chain, we have a “can’t get there from here” dilemma. It is a cruel irony that the group best suited to stretch America’s health care dollar and benefit both professionally and financially usually does not have the capital to create and operate an ACO for the roughly 18 months before shared savings are distributed.
The Centers for Medicare & Medicaid Services has tried to mitigate this by offering financial support for small, non–health system ACOs, particularly those in rural areas. Some of those enrolled ACOs are primary care driven and have been among the most successful in the MSSP.
Nonetheless, the upfront costs, paired with the long delay for the sole economic return on the investment – shared savings – have combined to be deal killers for many promising would-be primary care ACOs.
New upfront payments are game changers
A successful ACO will be assigned one or more patient populations and be given a minimum of 50% of the savings for the overall costs for those populations, if the quality of their health is maintained or improved.
To excise avoidable waste, the ACO looks at gaps in care for those populations – frequent emergency department use for nonemergencies, avoidably high levels of diabetes and obesity, too-high readmission rates, unnecessarily high postacute care costs, etc. They then use evidence-based best team care practices – from patient self care and prevention, to multispecialty coordination and PCMH care management.
Why? Because these proved to give the highest impact on quality and reducing costs. To achieve significant shared savings, the costs are usually measured for a calendar year, then it takes about 6 months for the claims to be reported and paid. Thus, the shared savings check to the ACO will arrive about 18 months after all this is started.
The CMS has also figured out that primary care physician care coordination and management drive quality and savings. The agency knows that incentivizing this type of care, the very type calculated to create ACO success, will net significant savings to the Medicare program.
For example, the pilot project for preventing diabetes will be expanded, because Medicare hopes to save several thousand dollars a year per beneficiary in health care costs.
In a blog entry the day the expanded population health management codes were announced, the CMS acting administrator wrote that, “Over time, if the clinicians qualified to provide these services were to fully provide these services to all eligible beneficiaries, the increase would be as much as $4 billion or more in additional support for care coordination and patient-centered care.”
CMS revenue streams to support ACO success-driving activities include:
• Value-based screening and counseling codes to decrease downstream costs.
• Upward adjustment of evaluation and management reimbursement for assessment of care and care plan development for mobility-impaired patients.
• Annual wellness visits.
• Prolonged E&M services that accrue outside of a patient visit.
• Collaboration with mental health specialists.
• Comprehensive assessment and care planning for patients with cognitive impairment.
• Expansion of the diabetes prevention pilot program; diabetes prevention and diabetes education are two separate services.
• Transitional care management for high-risk patients post discharge.
• Structured obesity management.
The 2017 Medicare fee schedule smoothed some of the bumps in administering and being paid for chronic care management (CCM) services, and it added codes with increased reimbursement aligned with increased complexity of comorbidities/illness.
Perhaps the biggest new payment boost for primary care to engage in ACO high-value activities is actually the Merit-Based Incentive Payment System (MIPS) under MACRA, the Medicare Access and CHIP Reauthorization Act of 2015.
Under MACRA, all Medicare compensation for physicians will be determined by relative delivery of quality and efficient care. Experts are recommending that primary care physicians participate in non–risk-taking ACOs to optimize MIPS value scoring, while also reducing administrative burdens of compliance. Use an ACO’s analytics to support collaborative care and provide the reports required under MIPS.
Let’s be smart about it
According to Gordon Wilhoit, MD, a practicing physician and chief medical officer of an all–primary-care-physician ACO in South Carolina, “This is a no brainer. Start first with your MSSP ACO high-value game plan, then align the complementary care coordination codes, CCM, MIPS, and other revenue stream and reporting activities with it. Now, primary care physicians can finance their ACO and MIPS care coordination efforts with a stream of ongoing payments from these care management codes.
“One of my colleagues saw a 27% increase in revenues in 6 months just from providing and billing for this type of care,” Dr. Wilhoit explained. “And, not counting shared savings or MIPS incentive payments, our office’s reimbursement from these care management codes now exceeds our fee-for-service income, which has not decreased.”
Even with these payments, the CMS will reduce overall net expenditures. Your impact on health care will be more powerful as a manager of the team addressing patients’ overall health than reacting to patient sickness one at a time. The patients you impact the most may be ones you don’t actually see. Your empowerment to practice medicine the right way will continue to grow.
Now, finally, you may start getting compensation that takes away the last big hurdle to creating the infrastructure you need to succeed.
Mr. Bobbitt is a head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of, and Dr. Wilhoit is a consultant with, Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at either [email protected] or 919-906-4054.

50 years in pediatrics: ‘You have to get involved’
A few years before the launch of Pediatric News in 1967, Dr. Henry Kempe and his colleagues at the University of Colorado, Denver, published a groundbreaking report on child abuse, “The Battered Child Syndrome,” in JAMA.
It had a major impact on Calvin C.J. Sia, MD, a now-retired pediatrician in Hawaii, not only because it was pioneering work and one of the milestones of 20th century pediatrics, but also because Dr. Kempe was a close friend and mentor of Dr. Sia, going back to when Dr. Sia was a resident in the 1950s.
Dr. Kempe “alerted me to the battered child syndrome and taught me the importance of looking at the whole child within the context of the family, and he repeatedly reminded me of the importance of preventive care. He taught me how to make preventive change, with the emphasis on the first 3 years” of life, Dr. Sia said in an interview from his home in Honolulu.
To celebrate the 50th anniversary of Pediatric News, it seemed appropriate to turn to Dr. Sia. His practice, launched in 1958, not only spanned our 50 years, but also illustrated one of the major themes in pediatrics over the past half-century. With the old scourges of infectious disease, malnutrition, and infant mortality largely brought under control, pediatrics turned to the broader struggles of childhood, including learning, poverty, and abusive parenting.

Dr. Sia has been president of the Hawaii Medical Association; president of the Hawaii chapter of the American Academy of Pediatrics; chief of staff at the Kauikeolani Children’s Hospital, Honolulu (now the Kapi‘olani Medical Center for Women and Children); chair of the American Medical Association Pediatric Delegation; and founder of the AMA’s Section Council on Pediatrics.
Positions like these eventually led him to contacts with legislators willing to listen and fund child abuse prevention, immunization programs, and other initiatives to help children. It often meant lobbying politicians for money.
“It doesn’t occur overnight; it takes chance and dedication,” said Dr. Sia, whose name, as one of its earliest champions, is now nearly synonymous with the concept of the medical home – an ideal of cradling children in a physician, family, and social services safety net of coordinated care.
Dr. Sia’s career spanned all of the developments that Pediatric News has covered over its 50 years, including the increasing recognition of autism, the earlier survival of premature infants, and phenylketonuria and other screenings at birth. He remembers all of them, and took action on many at the state and federal level.
Taking a step took courage, even when he wasn’t quite sure what to do. “I recognized autism back in the 60s. Children looked normal, were born normal, but then had trouble. I didn’t know what to do with them. That’s how I got involved with learning disabilities. I didn’t know anything, but I got involved,” he said.
With the advice of Robert Cooke, MD, another mentor and an eventual founder of the Head Start program, Dr. Sia cofounded Honolulu’s Variety School for Learning Disabilities in 1967. It’s still in operation; Don Ho and other local “variety hour” entertainers helped with early fundraising.
Dr. Sia also helped launch Healthy Start, one of the nation’s first home visit programs for at-risk kids, and an amendment to the federal Education of the Handicapped Act to extend aid to children with family and developmental challenges.
He convinced Sen. Daniel Inouye, another personal friend, to introduce the Emergency Medical Services for Children Act in the 1980s, which funded states to develop emergency medical services for children. “It was really important because kids need special instruments, IVs, and medications. I had to lobby. It was under Reaganomics,” Dr. Sia said.
At 89 years of age and recovering from a recent heart attack and open heart bypass, he is still trying to help children. Dr. Sia, who was born in Beijing, has been promoting the medical home concept in Asia. Meanwhile, he said he is worried about the fragmentation of health care in the United States, and the likely cutback in federal and state spending on kids.
Even so, “I believe in the future. I see in the generation coming up much more awareness of the whole child. I think they are going to do a much better job than I did,” but they need to learn “how to work the system.” Young physicians also must be mentored to believe in themselves, and take up the torch, he said.
A few years before the launch of Pediatric News in 1967, Dr. Henry Kempe and his colleagues at the University of Colorado, Denver, published a groundbreaking report on child abuse, “The Battered Child Syndrome,” in JAMA.
It had a major impact on Calvin C.J. Sia, MD, a now-retired pediatrician in Hawaii, not only because it was pioneering work and one of the milestones of 20th century pediatrics, but also because Dr. Kempe was a close friend and mentor of Dr. Sia, going back to when Dr. Sia was a resident in the 1950s.
Dr. Kempe “alerted me to the battered child syndrome and taught me the importance of looking at the whole child within the context of the family, and he repeatedly reminded me of the importance of preventive care. He taught me how to make preventive change, with the emphasis on the first 3 years” of life, Dr. Sia said in an interview from his home in Honolulu.
To celebrate the 50th anniversary of Pediatric News, it seemed appropriate to turn to Dr. Sia. His practice, launched in 1958, not only spanned our 50 years, but also illustrated one of the major themes in pediatrics over the past half-century. With the old scourges of infectious disease, malnutrition, and infant mortality largely brought under control, pediatrics turned to the broader struggles of childhood, including learning, poverty, and abusive parenting.
Dr. Sia has been president of the Hawaii Medical Association; president of the Hawaii chapter of the American Academy of Pediatrics; chief of staff at the Kauikeolani Children’s Hospital, Honolulu (now the Kapi‘olani Medical Center for Women and Children); chair of the American Medical Association Pediatric Delegation; and founder of the AMA’s Section Council on Pediatrics.
Positions like these eventually led him to contacts with legislators willing to listen and fund child abuse prevention, immunization programs, and other initiatives to help children. It often meant lobbying politicians for money.
“It doesn’t occur overnight; it takes chance and dedication,” said Dr. Sia, whose name, as one of its earliest champions, is now nearly synonymous with the concept of the medical home – an ideal of cradling children in a physician, family, and social services safety net of coordinated care.
Dr. Sia’s career spanned all of the developments that Pediatric News has covered over its 50 years, including the increasing recognition of autism, the earlier survival of premature infants, and phenylketonuria and other screenings at birth. He remembers all of them, and took action on many at the state and federal level.
Taking a step took courage, even when he wasn’t quite sure what to do. “I recognized autism back in the 60s. Children looked normal, were born normal, but then had trouble. I didn’t know what to do with them. That’s how I got involved with learning disabilities. I didn’t know anything, but I got involved,” he said.
With the advice of Robert Cooke, MD, another mentor and an eventual founder of the Head Start program, Dr. Sia cofounded Honolulu’s Variety School for Learning Disabilities in 1967. It’s still in operation; Don Ho and other local “variety hour” entertainers helped with early fundraising.
Dr. Sia also helped launch Healthy Start, one of the nation’s first home visit programs for at-risk kids, and an amendment to the federal Education of the Handicapped Act to extend aid to children with family and developmental challenges.
He convinced Sen. Daniel Inouye, another personal friend, to introduce the Emergency Medical Services for Children Act in the 1980s, which funded states to develop emergency medical services for children. “It was really important because kids need special instruments, IVs, and medications. I had to lobby. It was under Reaganomics,” Dr. Sia said.
At 89 years of age and recovering from a recent heart attack and open heart bypass, he is still trying to help children. Dr. Sia, who was born in Beijing, has been promoting the medical home concept in Asia. Meanwhile, he said he is worried about the fragmentation of health care in the United States, and the likely cutback in federal and state spending on kids.
Even so, “I believe in the future. I see in the generation coming up much more awareness of the whole child. I think they are going to do a much better job than I did,” but they need to learn “how to work the system.” Young physicians also must be mentored to believe in themselves, and take up the torch, he said.
A few years before the launch of Pediatric News in 1967, Dr. Henry Kempe and his colleagues at the University of Colorado, Denver, published a groundbreaking report on child abuse, “The Battered Child Syndrome,” in JAMA.
It had a major impact on Calvin C.J. Sia, MD, a now-retired pediatrician in Hawaii, not only because it was pioneering work and one of the milestones of 20th century pediatrics, but also because Dr. Kempe was a close friend and mentor of Dr. Sia, going back to when Dr. Sia was a resident in the 1950s.
Dr. Kempe “alerted me to the battered child syndrome and taught me the importance of looking at the whole child within the context of the family, and he repeatedly reminded me of the importance of preventive care. He taught me how to make preventive change, with the emphasis on the first 3 years” of life, Dr. Sia said in an interview from his home in Honolulu.
To celebrate the 50th anniversary of Pediatric News, it seemed appropriate to turn to Dr. Sia. His practice, launched in 1958, not only spanned our 50 years, but also illustrated one of the major themes in pediatrics over the past half-century. With the old scourges of infectious disease, malnutrition, and infant mortality largely brought under control, pediatrics turned to the broader struggles of childhood, including learning, poverty, and abusive parenting.
Dr. Sia has been president of the Hawaii Medical Association; president of the Hawaii chapter of the American Academy of Pediatrics; chief of staff at the Kauikeolani Children’s Hospital, Honolulu (now the Kapi‘olani Medical Center for Women and Children); chair of the American Medical Association Pediatric Delegation; and founder of the AMA’s Section Council on Pediatrics.
Positions like these eventually led him to contacts with legislators willing to listen and fund child abuse prevention, immunization programs, and other initiatives to help children. It often meant lobbying politicians for money.
“It doesn’t occur overnight; it takes chance and dedication,” said Dr. Sia, whose name, as one of its earliest champions, is now nearly synonymous with the concept of the medical home – an ideal of cradling children in a physician, family, and social services safety net of coordinated care.
Dr. Sia’s career spanned all of the developments that Pediatric News has covered over its 50 years, including the increasing recognition of autism, the earlier survival of premature infants, and phenylketonuria and other screenings at birth. He remembers all of them, and took action on many at the state and federal level.
Taking a step took courage, even when he wasn’t quite sure what to do. “I recognized autism back in the 60s. Children looked normal, were born normal, but then had trouble. I didn’t know what to do with them. That’s how I got involved with learning disabilities. I didn’t know anything, but I got involved,” he said.
With the advice of Robert Cooke, MD, another mentor and an eventual founder of the Head Start program, Dr. Sia cofounded Honolulu’s Variety School for Learning Disabilities in 1967. It’s still in operation; Don Ho and other local “variety hour” entertainers helped with early fundraising.
Dr. Sia also helped launch Healthy Start, one of the nation’s first home visit programs for at-risk kids, and an amendment to the federal Education of the Handicapped Act to extend aid to children with family and developmental challenges.
He convinced Sen. Daniel Inouye, another personal friend, to introduce the Emergency Medical Services for Children Act in the 1980s, which funded states to develop emergency medical services for children. “It was really important because kids need special instruments, IVs, and medications. I had to lobby. It was under Reaganomics,” Dr. Sia said.
At 89 years of age and recovering from a recent heart attack and open heart bypass, he is still trying to help children. Dr. Sia, who was born in Beijing, has been promoting the medical home concept in Asia. Meanwhile, he said he is worried about the fragmentation of health care in the United States, and the likely cutback in federal and state spending on kids.
Even so, “I believe in the future. I see in the generation coming up much more awareness of the whole child. I think they are going to do a much better job than I did,” but they need to learn “how to work the system.” Young physicians also must be mentored to believe in themselves, and take up the torch, he said.
1967 at a glance
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.

• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
• The Early and Periodic Screening, Diagnostic and Treatment (EPSDT) program was enacted as the child health component of Medicaid. Children under 21 years enrolled in Medicaid are entitled to EPSDT benefits, and states must cover a “broad array of preventive and treatment services.”
• By 1967, all states had laws requiring that physicians report child abuse.
• Field trials of experimental respiratory syncytial virus vaccines were performed but stalled. Currently, 65 RSV vaccines are being studied, and 13 are in phase III trials.
• The World Health Association declared a war on smallpox with a worldwide vaccination campaign. Twelve years later the disease was eradicated.
• The Public Health Service issued the second Surgeon General’s report on the health consequences of smoking.
• The first heart transplant was performed by Christian Barnard.
A look back at 1967
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
As Pediatric News celebrates 50 years of publication, we’re taking a look back at our first year: 1967.
A review of the 1967 issues of the journal Pediatrics offers a snapshot of the state of the science and some surprising similarities with pediatric medicine today.
A commentary in the November issue entitled “Pediatrics at a Crossroad” described an accelerating trend toward pediatric group practice and noted that full-time hospital employment of pediatricians was an emerging pattern of pediatric practice. The author, Richard Smith, MD, of the University of Florida, Gainesville, expressed concern about certain practices, such as the wide employment of antibiotics for uncomplicated respiratory infections and “routine use of gamma globulin in community hospital nurseries supposedly to treat sepsis or its regular injection in putatively allergic children.” He also was concerned about a quality gap in pediatric specialty education (Pediatrics. 1967 Nov;40[5]:783-7).
Articles of interest in the infectious disease area included an article demonstrating the response of infants to trivalent polio vaccine (Dec;40[6]:980-5); a new antibody test for rubella (Dec;40[5]:787-8, 789-97); and a live attenuated mumps vaccine (Dec;40[5]:798-803). And as we deal with emerging infectious diseases on a large scale, a fatal case of dengue hemorrhagic fever was reported in an American child (Dec;40[5]:804-7).
In a commentary, Starkey D. Davis, MD, and Ralph J. Wedgwood, MD, of the University of Washington, Seattle, said that the annual tuberculosis infection rate was low and falling, and that new cases were decreasing. Sufficient beds were available to isolate infectious cases, and effective chemotherapy made most cases noninfectious quickly. Isoniazid was cheap and effective, and it decreased complications of asymptomatic primary tuberculosis in children by 85%. “Pediatricians can expect to see tuberculosis in children become a medical curiosity in this country as infection rates continue to fall, if isoniazid prophylaxis is energetically used,” they predicted (Jun;39[6]:809-10).
D. Holdaway of the Royal Victoria Infirmary in Newcastle Upon Tyne, England, and associates reported on 211 children with acute bronchiolitis and 295 controls with nonrespiratory illness. Of the children with bronchiolitis, 59% had respiratory syncytial virus (RSV), compared with 1% of the controls, which confirmed the etiological significance of RSV in bronchiolitis, the researchers said. They also maintained that “oxygen is vitally important in bronchiolitis and there is little conclusive evidence that any other therapy is consistently or even occasionally useful” (Jun;39[6]:924-8).
In a commentary, Leon Eisenberg, MD, of the division of child psychiatry at the Johns Hopkins Hospital, Baltimore, called for more training in child development for pediatricians (May;39[5];645-7). Today, pediatricians are calling for more training in child psychiatry.
A report by the American Academy of Pediatrics Committee on Nutrition on obesity in childhood was prescient. They said, despite much research, that “our ignorance concerning the etiology, pathogenesis, and treatment is remarkable” (Sep;40[3]:455-67). The committee acknowledged that morbidity and mortality for diabetes and cardiovascular disease were higher in obese adults than in those of average weight, and that obese children tended to remain obese as adults. The committee also wrote that no treatments had achieved more than minor success of weight reduction. It suggested prevention of weight gain as the likely best approach, with initiation by the pediatrician in high-risk families – advice that still holds true today 50 years later.
Throughout 2017, Pediatric News will celebrate its 50th anniversary with exclusive articles looking at the evolution of the specialty, including changes in child psychiatry, pediatric dermatology, and infectious disease medicine, changes in residency training, and the transformation of the well-child visit. Look for these articles and more special features on the pages of Pediatric News and here online.
Helping patients bring an end to domestic violence
As healers trained to address some of the psychosocial issues facing our patients, we need to understand various forms of domestic violence – and what we can do to stop it. One form, honor killings, remains pervasive across the globe.
In a sample of 856 ninth-grade students from 14 schools in Amman, Jordan, for example, about 40% of boys and 20% of girls believed that killing a daughter, sister, or wife who had dishonored the family was justified (Aggress Behav. 2013 Sep-Oct;39[5]:405-17). The schools were representative of students from different religions, socioeconomic statuses, and upbringings. The proportions are broadly in line with the religious affiliation of Jordanians, with 92% of the population identifying themselves as Muslims, 6% as Christians, and 2% as affiliated with other religions.1 However, researchers found that support for honor killings was more widespread among adolescents from poorer and more traditional family backgrounds.
What are honor killings?
According to Sally Elakkary, MD, and her colleagues, honor killings are “violence implicated against a female for the deviancy of her activities from the traditional cultural norms.”2 The perpetrators in these crimes are usually male relatives but may be other family members, including women. Males also can be victims of honor crimes. For example, a male can become a victim if he is the female’s lover in an extramarital relationship or if he is homosexual.
Most honor killings are reported from countries in the Maghreb region of North Africa; the Middle East (Palestine, Lebanon, Syria, Jordan, and Turkey); and Western and Central Asia (Iraq, Pakistan, Afghanistan, and India). However, honor killings also occur in countries with strong minorities from those origins. A report3 published in 2000 by the United Nations Population Fund estimated that 5,000 honor killings were carried out worldwide per year, with the largest absolute numbers reported for Pakistan and India (about 1,000 cases per year in each country).
Until the 1960s in the United States, penal codes in some states, such as Georgia, New Mexico, Texas, and Utah, justified a husband killing his wife’s lover. In those states, the law was formulated to protect the male’s honor. Honor killings are culture-based practices that are supported indirectly by that country’s legal system. In a recent New York Times op-ed4 piece, Bina Shah stated that “upending misogynistic tribal codes is the real key to finally ending the most egregious gender crime.” The Pakistan Parliament recently stiffened the punishment for honor killings. The new anti–honor killing law mandates a minimum lifetime jail sentence for perpetrators and closes a legal loophole that allowed an honor killer to walk free if the family of the victim forgave him.
However, in rural areas, a Pakistani woman accused of violating family or tribal honor can be sentenced to death by an informal village court or a gathering of tribal elders. Women have been killed by stoning, shooting, or being buried alive. Sometimes, the woman’s relatives condemn her to death without a trial. Women are killed for reasons such as wanting to marry of their own choice, divorcing abusive husbands, or speaking to a man or boy outside the family; “in one case, four young girls who were filmed dancing in a rain shower were executed by their cousin for immorality,” Ms. Shah said.
Range of behaviors
Abusive behavior can take many forms, including:
• Isolating a person from her friends and family.
• Depriving her of basic needs.
• Monitoring her time.
• Monitoring her use of online communication tools or spyware.
• Taking control over aspects of her everyday life, such as where she can go, whom she can see, what she can wear, and when she can sleep.
• Depriving her of access to support services, such as specialist support or medical services.
• Repeatedly putting her down, such as telling her that she is worthless.
• Enforcing rules and activities that humiliate, degrade, or dehumanize the victim.
• Forcing the victim to take part in criminal activity such as shoplifting, and neglecting or abusing children to encourage self-blame and prevent disclosure to authorities.
• Abusing finances, including controlling resources so that the person is allowed only a punitive allowance.
• Threatening to hurt or kill her.
• Threatening a child.
• Threatening to reveal or publish private information (for example, threatening to “out” someone).
• Assaulting the person.
• Causing criminal damage (such as destruction of household goods).
• Engaging in rape.
• Preventing a person from having access to transportation or from working.
New domestic violence law in the United Kingdom
Meanwhile, domestic violence laws in England and Wales now consider emotional and psychological abuse as legally actionable. The new legislation targets those who subject spouses, partners, and family members to psychological and emotional torment, but stop short of violence. The new law5 follows a Home Office consultation showing that 85% of participants said the existing law did not provide sufficient protection and a Citizens Advice report showing a 24% rise in people seeking advice for domestic abuse.
The new law falls under the Serious Crime Act 2015 of England and Wales. The act creates a new offense of “controlling or coercive behavior in intimate or familial relationships.” The act states: “The new offence closes a gap in the law around patterns of controlling or coercive behavior in an ongoing relationship between intimate partners or family members.”
Breaking the law carries a maximum sentence of 5 years’ imprisonment, a fine, or both. The behavior must have had a “serious effect” on the victim, meaning that it has caused the victim to fear violence will be used against them on “at least two occasions,” or it has had a “substantial adverse effect on the victim’s day to day activities.”
The alleged perpetrator must have known that his behavior would have a serious effect on the victim, or the behavior must have been such that he “ought to have known” it would have that effect.
The new law includes honor-based violence, female genital mutilation, and forced marriage. The law explicitly states that the victim may fear that the perpetrator has asked another person to commit violence against them, thus including family honor killings.
Gendered nature of domestic controlling or coercive behavior
While all legislation is gender neutral, women and girls are disproportionately affected by crimes of domestic violence and abuse. Women from black and minority ethnic backgrounds may experience barriers to reporting, such as a distrust of the police, concerns about racism, language barriers, concerns about family finding out, or fear of rejection by the wider community. A victim might be fearful about her children being taken away if she makes a report. Lesbian, gay, bisexual, and transgender individuals in relationships may be subjected to threats to reveal sexual orientation to family or others.
Interestingly, the U.K. guidelines state that victims of controlling or coercive behavior may not recognize themselves as victims. Therefore, it is important that the new offense be considered by the police and other authorities in attendance at all call-outs. Police are encouraged to ask questions about rules, decision making, norms, and fear in the relationship, rather than just what happened. The guidelines provide specific comments about handling perpetrators who are described as being “particularly adept” at manipulating professionals, agencies, and systems, and may use a range of tactics in relation to this offense, including targeting people who might be vulnerable (there may be evidence of this from previous relationships) and using the system against the victim by making false or vexatious allegations to agencies.
The Authorized Professional Practice on Investigating Domestic Abuse issued by the College of Policing states: “A manipulative perpetrator may be trying to draw the police into colluding with their coercive control of the victim. Police officers must avoid playing into the primary perpetrator’s hands and take account of all available evidence when making the decision to arrest.” Such evidence includes attempting to frustrate or interfere with the police investigation; making counterallegations against the victim; and using threats of manipulation against the victim – such as telling the victim that he will make a counterallegation against her, that the victim will not be believed by the police or other agencies, that he will inform social services, or that he will inform immigration officials where the victim does not have a right to remain.
How can psychiatrists raise awareness?
• Individual change. Abusive controlling behavior can have its origin in childhood psychological experiences, in the same way that honor killings and wife beating can have their roots in the perpetrator’s cultural experience. As a child, the adult perpetrator may have been a direct victim of violence or may have been a witness to domestic violence. Controlling abusive behavior also can occur as a choice in perpetrators with personality disorders unrelated to childhood experiences. It can occur in a person with both exposure and personality disorder. It is important to understand the origins and reasoning behind the behavior in order to understand how best to intervene.
If the behavior is based on the childhood experience of the prevailing sociocultural practice, the psychiatrist can explore values and beliefs, identifying those that are based on family and cultural factors. Beliefs that have been present during a person’s entire life can appear as the unexamined “background” of their lives. Bringing those beliefs to the fore can allow discussion. For example, does the individual hold the belief that women are possessions? What is the basis of holding such a belief? How does he account for the differences between societies?
• Family change. Individuals in the family may differ in their support of honor killings. Those who do not support honor killings may have difficulty speaking out for fear of becoming a future target. When we meet with families who have a belief in honor killings, we can discuss how patriarchal societies have encouraged families to maintain a firm hand on the behavior of their members. This practice encourages repression of women’s individuality and also may consider women to be possessions. Patriarchal societies control their populations by supporting values and beliefs in their citizens that support the patriarchal structure. In this way, they can exert social control easily by having members of the society act as enforcers. Open and clear discussion with families about the ways in which cultural practice affects individual behavior may allow families that are unsure to explore alternative new beliefs.
Families must understand that, under U.S. law, perpetrators of honor killings and domestic violence can be prosecuted.
• System change. According to the U.S. Justice Department, 9 out of 10 honor killings were victims who had become “too Westernized.” Leaders of the American Muslim community and members of the Council on American-Islamic Relations have condemned all honor killings, stating that the practice stems from sexism and tribal behavior that predates the religion. In February 2009, after the high-profile killing of Aasiya Zubair Hassan in New York, Muslim leaders began a nationwide effort entitled, “Imams Speak Out: Domestic Violence Will Not Be Tolerated in Our Communities,” asking all imams and religious leaders to discuss domestic violence in their weekly sermon or their Friday prayer services. The group, “Muslim Men Against Domestic Violence,” was founded soon after the murder, which came just a few days after she had filed for divorce. (After a 3-week trial, Mrs. Hassan’s estranged husband, Muzzammil “Mo” Hassan, was found guilty of second-degree murder and received a 25-year to life sentence).
Our laws reflect our values as a society. As citizens, we must actively work for the enforcement of domestic violence laws. Our mental health organizations can support the training of police and health agencies to identify victims and perpetrators.
References
1. The World Factbook, Central Intelligence Agency, 2009.
2 Forensic Sci Med Pathol. 2014;10(1):76-82.
3. “Lives Together, Worlds Apart: Men and Women in a Time of Change,” United Nations Population Fund report, 2000.
4. “Pakistan’s Honor-Killing Law Isn’t Enough,” The New York Times, Oct. 27, 2016.
5. “Controlling or Coercive Behaviour in an Intimate or Family Relationship,” Home Office, December 2015.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
As healers trained to address some of the psychosocial issues facing our patients, we need to understand various forms of domestic violence – and what we can do to stop it. One form, honor killings, remains pervasive across the globe.
In a sample of 856 ninth-grade students from 14 schools in Amman, Jordan, for example, about 40% of boys and 20% of girls believed that killing a daughter, sister, or wife who had dishonored the family was justified (Aggress Behav. 2013 Sep-Oct;39[5]:405-17). The schools were representative of students from different religions, socioeconomic statuses, and upbringings. The proportions are broadly in line with the religious affiliation of Jordanians, with 92% of the population identifying themselves as Muslims, 6% as Christians, and 2% as affiliated with other religions.1 However, researchers found that support for honor killings was more widespread among adolescents from poorer and more traditional family backgrounds.
What are honor killings?
According to Sally Elakkary, MD, and her colleagues, honor killings are “violence implicated against a female for the deviancy of her activities from the traditional cultural norms.”2 The perpetrators in these crimes are usually male relatives but may be other family members, including women. Males also can be victims of honor crimes. For example, a male can become a victim if he is the female’s lover in an extramarital relationship or if he is homosexual.
Most honor killings are reported from countries in the Maghreb region of North Africa; the Middle East (Palestine, Lebanon, Syria, Jordan, and Turkey); and Western and Central Asia (Iraq, Pakistan, Afghanistan, and India). However, honor killings also occur in countries with strong minorities from those origins. A report3 published in 2000 by the United Nations Population Fund estimated that 5,000 honor killings were carried out worldwide per year, with the largest absolute numbers reported for Pakistan and India (about 1,000 cases per year in each country).
Until the 1960s in the United States, penal codes in some states, such as Georgia, New Mexico, Texas, and Utah, justified a husband killing his wife’s lover. In those states, the law was formulated to protect the male’s honor. Honor killings are culture-based practices that are supported indirectly by that country’s legal system. In a recent New York Times op-ed4 piece, Bina Shah stated that “upending misogynistic tribal codes is the real key to finally ending the most egregious gender crime.” The Pakistan Parliament recently stiffened the punishment for honor killings. The new anti–honor killing law mandates a minimum lifetime jail sentence for perpetrators and closes a legal loophole that allowed an honor killer to walk free if the family of the victim forgave him.
However, in rural areas, a Pakistani woman accused of violating family or tribal honor can be sentenced to death by an informal village court or a gathering of tribal elders. Women have been killed by stoning, shooting, or being buried alive. Sometimes, the woman’s relatives condemn her to death without a trial. Women are killed for reasons such as wanting to marry of their own choice, divorcing abusive husbands, or speaking to a man or boy outside the family; “in one case, four young girls who were filmed dancing in a rain shower were executed by their cousin for immorality,” Ms. Shah said.
Range of behaviors
Abusive behavior can take many forms, including:
• Isolating a person from her friends and family.
• Depriving her of basic needs.
• Monitoring her time.
• Monitoring her use of online communication tools or spyware.
• Taking control over aspects of her everyday life, such as where she can go, whom she can see, what she can wear, and when she can sleep.
• Depriving her of access to support services, such as specialist support or medical services.
• Repeatedly putting her down, such as telling her that she is worthless.
• Enforcing rules and activities that humiliate, degrade, or dehumanize the victim.
• Forcing the victim to take part in criminal activity such as shoplifting, and neglecting or abusing children to encourage self-blame and prevent disclosure to authorities.
• Abusing finances, including controlling resources so that the person is allowed only a punitive allowance.
• Threatening to hurt or kill her.
• Threatening a child.
• Threatening to reveal or publish private information (for example, threatening to “out” someone).
• Assaulting the person.
• Causing criminal damage (such as destruction of household goods).
• Engaging in rape.
• Preventing a person from having access to transportation or from working.
New domestic violence law in the United Kingdom
Meanwhile, domestic violence laws in England and Wales now consider emotional and psychological abuse as legally actionable. The new legislation targets those who subject spouses, partners, and family members to psychological and emotional torment, but stop short of violence. The new law5 follows a Home Office consultation showing that 85% of participants said the existing law did not provide sufficient protection and a Citizens Advice report showing a 24% rise in people seeking advice for domestic abuse.
The new law falls under the Serious Crime Act 2015 of England and Wales. The act creates a new offense of “controlling or coercive behavior in intimate or familial relationships.” The act states: “The new offence closes a gap in the law around patterns of controlling or coercive behavior in an ongoing relationship between intimate partners or family members.”
Breaking the law carries a maximum sentence of 5 years’ imprisonment, a fine, or both. The behavior must have had a “serious effect” on the victim, meaning that it has caused the victim to fear violence will be used against them on “at least two occasions,” or it has had a “substantial adverse effect on the victim’s day to day activities.”
The alleged perpetrator must have known that his behavior would have a serious effect on the victim, or the behavior must have been such that he “ought to have known” it would have that effect.
The new law includes honor-based violence, female genital mutilation, and forced marriage. The law explicitly states that the victim may fear that the perpetrator has asked another person to commit violence against them, thus including family honor killings.
Gendered nature of domestic controlling or coercive behavior
While all legislation is gender neutral, women and girls are disproportionately affected by crimes of domestic violence and abuse. Women from black and minority ethnic backgrounds may experience barriers to reporting, such as a distrust of the police, concerns about racism, language barriers, concerns about family finding out, or fear of rejection by the wider community. A victim might be fearful about her children being taken away if she makes a report. Lesbian, gay, bisexual, and transgender individuals in relationships may be subjected to threats to reveal sexual orientation to family or others.
Interestingly, the U.K. guidelines state that victims of controlling or coercive behavior may not recognize themselves as victims. Therefore, it is important that the new offense be considered by the police and other authorities in attendance at all call-outs. Police are encouraged to ask questions about rules, decision making, norms, and fear in the relationship, rather than just what happened. The guidelines provide specific comments about handling perpetrators who are described as being “particularly adept” at manipulating professionals, agencies, and systems, and may use a range of tactics in relation to this offense, including targeting people who might be vulnerable (there may be evidence of this from previous relationships) and using the system against the victim by making false or vexatious allegations to agencies.
The Authorized Professional Practice on Investigating Domestic Abuse issued by the College of Policing states: “A manipulative perpetrator may be trying to draw the police into colluding with their coercive control of the victim. Police officers must avoid playing into the primary perpetrator’s hands and take account of all available evidence when making the decision to arrest.” Such evidence includes attempting to frustrate or interfere with the police investigation; making counterallegations against the victim; and using threats of manipulation against the victim – such as telling the victim that he will make a counterallegation against her, that the victim will not be believed by the police or other agencies, that he will inform social services, or that he will inform immigration officials where the victim does not have a right to remain.
How can psychiatrists raise awareness?
• Individual change. Abusive controlling behavior can have its origin in childhood psychological experiences, in the same way that honor killings and wife beating can have their roots in the perpetrator’s cultural experience. As a child, the adult perpetrator may have been a direct victim of violence or may have been a witness to domestic violence. Controlling abusive behavior also can occur as a choice in perpetrators with personality disorders unrelated to childhood experiences. It can occur in a person with both exposure and personality disorder. It is important to understand the origins and reasoning behind the behavior in order to understand how best to intervene.
If the behavior is based on the childhood experience of the prevailing sociocultural practice, the psychiatrist can explore values and beliefs, identifying those that are based on family and cultural factors. Beliefs that have been present during a person’s entire life can appear as the unexamined “background” of their lives. Bringing those beliefs to the fore can allow discussion. For example, does the individual hold the belief that women are possessions? What is the basis of holding such a belief? How does he account for the differences between societies?
• Family change. Individuals in the family may differ in their support of honor killings. Those who do not support honor killings may have difficulty speaking out for fear of becoming a future target. When we meet with families who have a belief in honor killings, we can discuss how patriarchal societies have encouraged families to maintain a firm hand on the behavior of their members. This practice encourages repression of women’s individuality and also may consider women to be possessions. Patriarchal societies control their populations by supporting values and beliefs in their citizens that support the patriarchal structure. In this way, they can exert social control easily by having members of the society act as enforcers. Open and clear discussion with families about the ways in which cultural practice affects individual behavior may allow families that are unsure to explore alternative new beliefs.
Families must understand that, under U.S. law, perpetrators of honor killings and domestic violence can be prosecuted.
• System change. According to the U.S. Justice Department, 9 out of 10 honor killings were victims who had become “too Westernized.” Leaders of the American Muslim community and members of the Council on American-Islamic Relations have condemned all honor killings, stating that the practice stems from sexism and tribal behavior that predates the religion. In February 2009, after the high-profile killing of Aasiya Zubair Hassan in New York, Muslim leaders began a nationwide effort entitled, “Imams Speak Out: Domestic Violence Will Not Be Tolerated in Our Communities,” asking all imams and religious leaders to discuss domestic violence in their weekly sermon or their Friday prayer services. The group, “Muslim Men Against Domestic Violence,” was founded soon after the murder, which came just a few days after she had filed for divorce. (After a 3-week trial, Mrs. Hassan’s estranged husband, Muzzammil “Mo” Hassan, was found guilty of second-degree murder and received a 25-year to life sentence).
Our laws reflect our values as a society. As citizens, we must actively work for the enforcement of domestic violence laws. Our mental health organizations can support the training of police and health agencies to identify victims and perpetrators.
References
1. The World Factbook, Central Intelligence Agency, 2009.
2 Forensic Sci Med Pathol. 2014;10(1):76-82.
3. “Lives Together, Worlds Apart: Men and Women in a Time of Change,” United Nations Population Fund report, 2000.
4. “Pakistan’s Honor-Killing Law Isn’t Enough,” The New York Times, Oct. 27, 2016.
5. “Controlling or Coercive Behaviour in an Intimate or Family Relationship,” Home Office, December 2015.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
As healers trained to address some of the psychosocial issues facing our patients, we need to understand various forms of domestic violence – and what we can do to stop it. One form, honor killings, remains pervasive across the globe.
In a sample of 856 ninth-grade students from 14 schools in Amman, Jordan, for example, about 40% of boys and 20% of girls believed that killing a daughter, sister, or wife who had dishonored the family was justified (Aggress Behav. 2013 Sep-Oct;39[5]:405-17). The schools were representative of students from different religions, socioeconomic statuses, and upbringings. The proportions are broadly in line with the religious affiliation of Jordanians, with 92% of the population identifying themselves as Muslims, 6% as Christians, and 2% as affiliated with other religions.1 However, researchers found that support for honor killings was more widespread among adolescents from poorer and more traditional family backgrounds.
What are honor killings?
According to Sally Elakkary, MD, and her colleagues, honor killings are “violence implicated against a female for the deviancy of her activities from the traditional cultural norms.”2 The perpetrators in these crimes are usually male relatives but may be other family members, including women. Males also can be victims of honor crimes. For example, a male can become a victim if he is the female’s lover in an extramarital relationship or if he is homosexual.
Most honor killings are reported from countries in the Maghreb region of North Africa; the Middle East (Palestine, Lebanon, Syria, Jordan, and Turkey); and Western and Central Asia (Iraq, Pakistan, Afghanistan, and India). However, honor killings also occur in countries with strong minorities from those origins. A report3 published in 2000 by the United Nations Population Fund estimated that 5,000 honor killings were carried out worldwide per year, with the largest absolute numbers reported for Pakistan and India (about 1,000 cases per year in each country).
Until the 1960s in the United States, penal codes in some states, such as Georgia, New Mexico, Texas, and Utah, justified a husband killing his wife’s lover. In those states, the law was formulated to protect the male’s honor. Honor killings are culture-based practices that are supported indirectly by that country’s legal system. In a recent New York Times op-ed4 piece, Bina Shah stated that “upending misogynistic tribal codes is the real key to finally ending the most egregious gender crime.” The Pakistan Parliament recently stiffened the punishment for honor killings. The new anti–honor killing law mandates a minimum lifetime jail sentence for perpetrators and closes a legal loophole that allowed an honor killer to walk free if the family of the victim forgave him.
However, in rural areas, a Pakistani woman accused of violating family or tribal honor can be sentenced to death by an informal village court or a gathering of tribal elders. Women have been killed by stoning, shooting, or being buried alive. Sometimes, the woman’s relatives condemn her to death without a trial. Women are killed for reasons such as wanting to marry of their own choice, divorcing abusive husbands, or speaking to a man or boy outside the family; “in one case, four young girls who were filmed dancing in a rain shower were executed by their cousin for immorality,” Ms. Shah said.
Range of behaviors
Abusive behavior can take many forms, including:
• Isolating a person from her friends and family.
• Depriving her of basic needs.
• Monitoring her time.
• Monitoring her use of online communication tools or spyware.
• Taking control over aspects of her everyday life, such as where she can go, whom she can see, what she can wear, and when she can sleep.
• Depriving her of access to support services, such as specialist support or medical services.
• Repeatedly putting her down, such as telling her that she is worthless.
• Enforcing rules and activities that humiliate, degrade, or dehumanize the victim.
• Forcing the victim to take part in criminal activity such as shoplifting, and neglecting or abusing children to encourage self-blame and prevent disclosure to authorities.
• Abusing finances, including controlling resources so that the person is allowed only a punitive allowance.
• Threatening to hurt or kill her.
• Threatening a child.
• Threatening to reveal or publish private information (for example, threatening to “out” someone).
• Assaulting the person.
• Causing criminal damage (such as destruction of household goods).
• Engaging in rape.
• Preventing a person from having access to transportation or from working.
New domestic violence law in the United Kingdom
Meanwhile, domestic violence laws in England and Wales now consider emotional and psychological abuse as legally actionable. The new legislation targets those who subject spouses, partners, and family members to psychological and emotional torment, but stop short of violence. The new law5 follows a Home Office consultation showing that 85% of participants said the existing law did not provide sufficient protection and a Citizens Advice report showing a 24% rise in people seeking advice for domestic abuse.
The new law falls under the Serious Crime Act 2015 of England and Wales. The act creates a new offense of “controlling or coercive behavior in intimate or familial relationships.” The act states: “The new offence closes a gap in the law around patterns of controlling or coercive behavior in an ongoing relationship between intimate partners or family members.”
Breaking the law carries a maximum sentence of 5 years’ imprisonment, a fine, or both. The behavior must have had a “serious effect” on the victim, meaning that it has caused the victim to fear violence will be used against them on “at least two occasions,” or it has had a “substantial adverse effect on the victim’s day to day activities.”
The alleged perpetrator must have known that his behavior would have a serious effect on the victim, or the behavior must have been such that he “ought to have known” it would have that effect.
The new law includes honor-based violence, female genital mutilation, and forced marriage. The law explicitly states that the victim may fear that the perpetrator has asked another person to commit violence against them, thus including family honor killings.
Gendered nature of domestic controlling or coercive behavior
While all legislation is gender neutral, women and girls are disproportionately affected by crimes of domestic violence and abuse. Women from black and minority ethnic backgrounds may experience barriers to reporting, such as a distrust of the police, concerns about racism, language barriers, concerns about family finding out, or fear of rejection by the wider community. A victim might be fearful about her children being taken away if she makes a report. Lesbian, gay, bisexual, and transgender individuals in relationships may be subjected to threats to reveal sexual orientation to family or others.
Interestingly, the U.K. guidelines state that victims of controlling or coercive behavior may not recognize themselves as victims. Therefore, it is important that the new offense be considered by the police and other authorities in attendance at all call-outs. Police are encouraged to ask questions about rules, decision making, norms, and fear in the relationship, rather than just what happened. The guidelines provide specific comments about handling perpetrators who are described as being “particularly adept” at manipulating professionals, agencies, and systems, and may use a range of tactics in relation to this offense, including targeting people who might be vulnerable (there may be evidence of this from previous relationships) and using the system against the victim by making false or vexatious allegations to agencies.
The Authorized Professional Practice on Investigating Domestic Abuse issued by the College of Policing states: “A manipulative perpetrator may be trying to draw the police into colluding with their coercive control of the victim. Police officers must avoid playing into the primary perpetrator’s hands and take account of all available evidence when making the decision to arrest.” Such evidence includes attempting to frustrate or interfere with the police investigation; making counterallegations against the victim; and using threats of manipulation against the victim – such as telling the victim that he will make a counterallegation against her, that the victim will not be believed by the police or other agencies, that he will inform social services, or that he will inform immigration officials where the victim does not have a right to remain.
How can psychiatrists raise awareness?
• Individual change. Abusive controlling behavior can have its origin in childhood psychological experiences, in the same way that honor killings and wife beating can have their roots in the perpetrator’s cultural experience. As a child, the adult perpetrator may have been a direct victim of violence or may have been a witness to domestic violence. Controlling abusive behavior also can occur as a choice in perpetrators with personality disorders unrelated to childhood experiences. It can occur in a person with both exposure and personality disorder. It is important to understand the origins and reasoning behind the behavior in order to understand how best to intervene.
If the behavior is based on the childhood experience of the prevailing sociocultural practice, the psychiatrist can explore values and beliefs, identifying those that are based on family and cultural factors. Beliefs that have been present during a person’s entire life can appear as the unexamined “background” of their lives. Bringing those beliefs to the fore can allow discussion. For example, does the individual hold the belief that women are possessions? What is the basis of holding such a belief? How does he account for the differences between societies?
• Family change. Individuals in the family may differ in their support of honor killings. Those who do not support honor killings may have difficulty speaking out for fear of becoming a future target. When we meet with families who have a belief in honor killings, we can discuss how patriarchal societies have encouraged families to maintain a firm hand on the behavior of their members. This practice encourages repression of women’s individuality and also may consider women to be possessions. Patriarchal societies control their populations by supporting values and beliefs in their citizens that support the patriarchal structure. In this way, they can exert social control easily by having members of the society act as enforcers. Open and clear discussion with families about the ways in which cultural practice affects individual behavior may allow families that are unsure to explore alternative new beliefs.
Families must understand that, under U.S. law, perpetrators of honor killings and domestic violence can be prosecuted.
• System change. According to the U.S. Justice Department, 9 out of 10 honor killings were victims who had become “too Westernized.” Leaders of the American Muslim community and members of the Council on American-Islamic Relations have condemned all honor killings, stating that the practice stems from sexism and tribal behavior that predates the religion. In February 2009, after the high-profile killing of Aasiya Zubair Hassan in New York, Muslim leaders began a nationwide effort entitled, “Imams Speak Out: Domestic Violence Will Not Be Tolerated in Our Communities,” asking all imams and religious leaders to discuss domestic violence in their weekly sermon or their Friday prayer services. The group, “Muslim Men Against Domestic Violence,” was founded soon after the murder, which came just a few days after she had filed for divorce. (After a 3-week trial, Mrs. Hassan’s estranged husband, Muzzammil “Mo” Hassan, was found guilty of second-degree murder and received a 25-year to life sentence).
Our laws reflect our values as a society. As citizens, we must actively work for the enforcement of domestic violence laws. Our mental health organizations can support the training of police and health agencies to identify victims and perpetrators.
References
1. The World Factbook, Central Intelligence Agency, 2009.
2 Forensic Sci Med Pathol. 2014;10(1):76-82.
3. “Lives Together, Worlds Apart: Men and Women in a Time of Change,” United Nations Population Fund report, 2000.
4. “Pakistan’s Honor-Killing Law Isn’t Enough,” The New York Times, Oct. 27, 2016.
5. “Controlling or Coercive Behaviour in an Intimate or Family Relationship,” Home Office, December 2015.
Dr. Heru is professor of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.