User login
Clinical Guidelines Updated for Surviving Sepsis in Hospitals
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
Bariatric surgery advancement spurs guideline update
Weight loss surgery patients should get routine copper supplements along with other vitamins and minerals, according to newly updated bariatric surgery guidelines from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery.
The groups call for 2 mg/day to offset the potential for surgery to cause a deficiency. Although routine copper screening isn’t necessary after the procedure, copper levels should be assessed and treated as needed in patients with anemia, neutropenia, myeloneuropathy, and impaired wound healing.
The copper recommendations are new since the guidelines were last published in 2008. Other recommendations – there are 74 in all – have been revised to incorporate new advances in weight loss surgery and an improved evidence base. Changes are pointed out where they’ve been made, and the level of evidence cited for each assertion. Pre- and postoperative bariatric surgery checklists have been added as well, to help avoid errors.
"This is actually a very unique collaboration among the internists represented by the endocrinologists and the obesity people and the surgeons. We actually agreed on all these things. The main intent is to assist with clinical decision making," including selecting patients and procedures and perioperative management, said lead author Dr. Jeffrey Mechanick, president-elect of the American Association of Clinical Endocrinologists and director of metabolic support at the Mt. Sinai School of Medicine in New York.
"We scrutinized every recommendation one by one in the context of the new data. In many cases the recommendations changed," he said in an interview.
Another new recommendation is for patients to be followed by their primary care physicians and screened for cancer prior to surgery, as appropriate for age and risk. Dr. Mechanick and his colleagues have also given more attention to consent, behavioral, and psychiatric issues as well as weight loss surgery in patients with type 2 diabetes.
There’s more information on sleeve gastrectomy, as well. Considered experimental in 2008, it’s now "approved and being done more widely. There are some very nice data about its metabolic effects, independent from just the weight loss effect, effects on glycemic control, and cardiovascular risk. It was very important to devote a fair amount of time" to the procedure, he said.
The guidelines note that "sleeve gastrectomy has demonstrated benefits comparable to other bariatric procedures. ... A national risk-adjusted database positions [it] between the laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass in terms of weight loss, co-morbidity resolution, and complications."
"We [also] addressed two issues which were quite controversial, and are still rather unsettled. The first is the use of the lap band for mild obesity. The second is the use of these weight loss procedures specifically for patients with type 2 diabetes for glycemic control. Since 2008, there’ve been a lot more data" about the issues, he said, just as there’ve been more data about the need for copper supplementation.
As in 2008, the guidelines do not recommend bariatric surgery solely for glycemic control. "We still don’t have an absolute indication for ‘diabetes surgery,’ but we do recognize the existence of the salutary effects on glycemic control when these procedures are done for weight loss. It was important for the reader to be exposed to this information," Dr. Mechanick said.
Regarding surgery in the mildly obese, the guidelines note that patients with a body mass index of 30-34.9 kg/m2 with diabetes or metabolic syndrome "may also be offered a bariatric procedure, although current evidence is limited by the number of subjects studied and lack of long-term data demonstrating net benefit."
The guidelines will be published in the March/April 2013 issue of Endocrine Practice and March 2013 issue of Surgery for Obesity and Related Diseases.
Dr. Mechanick disclosed compensation from Abbott Nutrition for lectures and program development.
From preoperative evaluation through bariatric
surgery and onward through long-term postoperative health management, weight
loss surgery and the medical care associated with it is, obligatorily, a
thoroughly interdisciplinary effort. Endocrinologists and internists on the
bariatrics team spearhead lifestyle management, medical weight loss, and
long-term postoperative care and efforts to maintain durable weight loss.
Surgeons, endocrinologists, and internists work together to select patients
appropriate for bariatric surgery, to choose the weight-loss surgery best
suited to each individual patient, and to provide the proper preoperative
evaluation. Surgeons perform the appropriate bariatric operation and oversee
immediate postoperative and short-term perioperative care, and, frequently in
concert with gastroenterologists, internists, and endocrinologists, manage
complications that can result from bariatric surgery. Finally, long-term
continuity of medical care and durable maintenance of weight loss is again
directed by the endocrinologist and internist.
Thus, given that the entire bariatric care schema is
such an interdisciplinary effort, clinical practice guidelines for the
management of bariatric surgical patients must also be the product of an
analogous interdisciplinary effort. It is with this aim and in this spirit that
the American Association of Clinical Endocrinologists (AACE), The Obesity
Society (TOS), and American Society for Metabolic and Bariatric Surgery (AAMBS)
published their initial Medical Guidelines for Clinical Practice for the Perioperative
Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery
Patient in 2008. The same cooperating societies have just published their
sequel with numerous substantive additions, changes, and refinements. The
Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and
Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update: Cosponsored
by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery was published jointly in
the March issue of Surgery for Obesity and Related Disease, and in the
March/April issue of Endocrine Practice.
Clearly, much has changed in the bariatric landscape
in the intervening half-decade. Laparoscopic gastric band surgery has declined,
while sleeve gastrectomy has gained traction as a restrictive bariatric
operation with more robust weight loss and glycemic effects. The
increasingly recognized impact of Roux-en-Y gastric bypass surgery not only on
weight loss, but also on glycemic control and other endocrinologic endpoints
has prompted studies to determine if such benefits might also result from
restrictive-only bariatric surgeries such as sleeve gastrectomy, and initial
results appear encouraging. The arrival of more and higher-quality data with
longer-term follow up of a greater variety of endpoints has led to the ability
of these updated guidelines to provide an increasing number of more specific,
data-driven recommendations related to the broader spectrum of bariatric
surgical procedures and anatomies managed by clinicians today. They cover every
aspect of the bariatric surgical patient, from preoperative evaluation through
surgery, to postoperative management, all with more solidly outcomes-based
recommendations from over 400 references, with user-friendly and more
error-proof preoperative and postoperative care checklists, while still
arriving at such expert guidelines through interdisciplinary study and
agreement in this timely update.
John A. Martin, M.D., is associate
professor of medicine and surgery and director of endoscopy, Northwestern
University Feinberg School of Medicine, Chicago.
From preoperative evaluation through bariatric
surgery and onward through long-term postoperative health management, weight
loss surgery and the medical care associated with it is, obligatorily, a
thoroughly interdisciplinary effort. Endocrinologists and internists on the
bariatrics team spearhead lifestyle management, medical weight loss, and
long-term postoperative care and efforts to maintain durable weight loss.
Surgeons, endocrinologists, and internists work together to select patients
appropriate for bariatric surgery, to choose the weight-loss surgery best
suited to each individual patient, and to provide the proper preoperative
evaluation. Surgeons perform the appropriate bariatric operation and oversee
immediate postoperative and short-term perioperative care, and, frequently in
concert with gastroenterologists, internists, and endocrinologists, manage
complications that can result from bariatric surgery. Finally, long-term
continuity of medical care and durable maintenance of weight loss is again
directed by the endocrinologist and internist.
Thus, given that the entire bariatric care schema is
such an interdisciplinary effort, clinical practice guidelines for the
management of bariatric surgical patients must also be the product of an
analogous interdisciplinary effort. It is with this aim and in this spirit that
the American Association of Clinical Endocrinologists (AACE), The Obesity
Society (TOS), and American Society for Metabolic and Bariatric Surgery (AAMBS)
published their initial Medical Guidelines for Clinical Practice for the Perioperative
Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery
Patient in 2008. The same cooperating societies have just published their
sequel with numerous substantive additions, changes, and refinements. The
Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and
Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update: Cosponsored
by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery was published jointly in
the March issue of Surgery for Obesity and Related Disease, and in the
March/April issue of Endocrine Practice.
Clearly, much has changed in the bariatric landscape
in the intervening half-decade. Laparoscopic gastric band surgery has declined,
while sleeve gastrectomy has gained traction as a restrictive bariatric
operation with more robust weight loss and glycemic effects. The
increasingly recognized impact of Roux-en-Y gastric bypass surgery not only on
weight loss, but also on glycemic control and other endocrinologic endpoints
has prompted studies to determine if such benefits might also result from
restrictive-only bariatric surgeries such as sleeve gastrectomy, and initial
results appear encouraging. The arrival of more and higher-quality data with
longer-term follow up of a greater variety of endpoints has led to the ability
of these updated guidelines to provide an increasing number of more specific,
data-driven recommendations related to the broader spectrum of bariatric
surgical procedures and anatomies managed by clinicians today. They cover every
aspect of the bariatric surgical patient, from preoperative evaluation through
surgery, to postoperative management, all with more solidly outcomes-based
recommendations from over 400 references, with user-friendly and more
error-proof preoperative and postoperative care checklists, while still
arriving at such expert guidelines through interdisciplinary study and
agreement in this timely update.
John A. Martin, M.D., is associate
professor of medicine and surgery and director of endoscopy, Northwestern
University Feinberg School of Medicine, Chicago.
From preoperative evaluation through bariatric
surgery and onward through long-term postoperative health management, weight
loss surgery and the medical care associated with it is, obligatorily, a
thoroughly interdisciplinary effort. Endocrinologists and internists on the
bariatrics team spearhead lifestyle management, medical weight loss, and
long-term postoperative care and efforts to maintain durable weight loss.
Surgeons, endocrinologists, and internists work together to select patients
appropriate for bariatric surgery, to choose the weight-loss surgery best
suited to each individual patient, and to provide the proper preoperative
evaluation. Surgeons perform the appropriate bariatric operation and oversee
immediate postoperative and short-term perioperative care, and, frequently in
concert with gastroenterologists, internists, and endocrinologists, manage
complications that can result from bariatric surgery. Finally, long-term
continuity of medical care and durable maintenance of weight loss is again
directed by the endocrinologist and internist.
Thus, given that the entire bariatric care schema is
such an interdisciplinary effort, clinical practice guidelines for the
management of bariatric surgical patients must also be the product of an
analogous interdisciplinary effort. It is with this aim and in this spirit that
the American Association of Clinical Endocrinologists (AACE), The Obesity
Society (TOS), and American Society for Metabolic and Bariatric Surgery (AAMBS)
published their initial Medical Guidelines for Clinical Practice for the Perioperative
Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery
Patient in 2008. The same cooperating societies have just published their
sequel with numerous substantive additions, changes, and refinements. The
Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and
Nonsurgical Support of the Bariatric Surgery Patient – 2013 Update: Cosponsored
by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery was published jointly in
the March issue of Surgery for Obesity and Related Disease, and in the
March/April issue of Endocrine Practice.
Clearly, much has changed in the bariatric landscape
in the intervening half-decade. Laparoscopic gastric band surgery has declined,
while sleeve gastrectomy has gained traction as a restrictive bariatric
operation with more robust weight loss and glycemic effects. The
increasingly recognized impact of Roux-en-Y gastric bypass surgery not only on
weight loss, but also on glycemic control and other endocrinologic endpoints
has prompted studies to determine if such benefits might also result from
restrictive-only bariatric surgeries such as sleeve gastrectomy, and initial
results appear encouraging. The arrival of more and higher-quality data with
longer-term follow up of a greater variety of endpoints has led to the ability
of these updated guidelines to provide an increasing number of more specific,
data-driven recommendations related to the broader spectrum of bariatric
surgical procedures and anatomies managed by clinicians today. They cover every
aspect of the bariatric surgical patient, from preoperative evaluation through
surgery, to postoperative management, all with more solidly outcomes-based
recommendations from over 400 references, with user-friendly and more
error-proof preoperative and postoperative care checklists, while still
arriving at such expert guidelines through interdisciplinary study and
agreement in this timely update.
John A. Martin, M.D., is associate
professor of medicine and surgery and director of endoscopy, Northwestern
University Feinberg School of Medicine, Chicago.
Weight loss surgery patients should get routine copper supplements along with other vitamins and minerals, according to newly updated bariatric surgery guidelines from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery.
The groups call for 2 mg/day to offset the potential for surgery to cause a deficiency. Although routine copper screening isn’t necessary after the procedure, copper levels should be assessed and treated as needed in patients with anemia, neutropenia, myeloneuropathy, and impaired wound healing.
The copper recommendations are new since the guidelines were last published in 2008. Other recommendations – there are 74 in all – have been revised to incorporate new advances in weight loss surgery and an improved evidence base. Changes are pointed out where they’ve been made, and the level of evidence cited for each assertion. Pre- and postoperative bariatric surgery checklists have been added as well, to help avoid errors.
"This is actually a very unique collaboration among the internists represented by the endocrinologists and the obesity people and the surgeons. We actually agreed on all these things. The main intent is to assist with clinical decision making," including selecting patients and procedures and perioperative management, said lead author Dr. Jeffrey Mechanick, president-elect of the American Association of Clinical Endocrinologists and director of metabolic support at the Mt. Sinai School of Medicine in New York.
"We scrutinized every recommendation one by one in the context of the new data. In many cases the recommendations changed," he said in an interview.
Another new recommendation is for patients to be followed by their primary care physicians and screened for cancer prior to surgery, as appropriate for age and risk. Dr. Mechanick and his colleagues have also given more attention to consent, behavioral, and psychiatric issues as well as weight loss surgery in patients with type 2 diabetes.
There’s more information on sleeve gastrectomy, as well. Considered experimental in 2008, it’s now "approved and being done more widely. There are some very nice data about its metabolic effects, independent from just the weight loss effect, effects on glycemic control, and cardiovascular risk. It was very important to devote a fair amount of time" to the procedure, he said.
The guidelines note that "sleeve gastrectomy has demonstrated benefits comparable to other bariatric procedures. ... A national risk-adjusted database positions [it] between the laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass in terms of weight loss, co-morbidity resolution, and complications."
"We [also] addressed two issues which were quite controversial, and are still rather unsettled. The first is the use of the lap band for mild obesity. The second is the use of these weight loss procedures specifically for patients with type 2 diabetes for glycemic control. Since 2008, there’ve been a lot more data" about the issues, he said, just as there’ve been more data about the need for copper supplementation.
As in 2008, the guidelines do not recommend bariatric surgery solely for glycemic control. "We still don’t have an absolute indication for ‘diabetes surgery,’ but we do recognize the existence of the salutary effects on glycemic control when these procedures are done for weight loss. It was important for the reader to be exposed to this information," Dr. Mechanick said.
Regarding surgery in the mildly obese, the guidelines note that patients with a body mass index of 30-34.9 kg/m2 with diabetes or metabolic syndrome "may also be offered a bariatric procedure, although current evidence is limited by the number of subjects studied and lack of long-term data demonstrating net benefit."
The guidelines will be published in the March/April 2013 issue of Endocrine Practice and March 2013 issue of Surgery for Obesity and Related Diseases.
Dr. Mechanick disclosed compensation from Abbott Nutrition for lectures and program development.
Weight loss surgery patients should get routine copper supplements along with other vitamins and minerals, according to newly updated bariatric surgery guidelines from the American Association of Clinical Endocrinologists, the Obesity Society, and the American Society for Metabolic and Bariatric Surgery.
The groups call for 2 mg/day to offset the potential for surgery to cause a deficiency. Although routine copper screening isn’t necessary after the procedure, copper levels should be assessed and treated as needed in patients with anemia, neutropenia, myeloneuropathy, and impaired wound healing.
The copper recommendations are new since the guidelines were last published in 2008. Other recommendations – there are 74 in all – have been revised to incorporate new advances in weight loss surgery and an improved evidence base. Changes are pointed out where they’ve been made, and the level of evidence cited for each assertion. Pre- and postoperative bariatric surgery checklists have been added as well, to help avoid errors.
"This is actually a very unique collaboration among the internists represented by the endocrinologists and the obesity people and the surgeons. We actually agreed on all these things. The main intent is to assist with clinical decision making," including selecting patients and procedures and perioperative management, said lead author Dr. Jeffrey Mechanick, president-elect of the American Association of Clinical Endocrinologists and director of metabolic support at the Mt. Sinai School of Medicine in New York.
"We scrutinized every recommendation one by one in the context of the new data. In many cases the recommendations changed," he said in an interview.
Another new recommendation is for patients to be followed by their primary care physicians and screened for cancer prior to surgery, as appropriate for age and risk. Dr. Mechanick and his colleagues have also given more attention to consent, behavioral, and psychiatric issues as well as weight loss surgery in patients with type 2 diabetes.
There’s more information on sleeve gastrectomy, as well. Considered experimental in 2008, it’s now "approved and being done more widely. There are some very nice data about its metabolic effects, independent from just the weight loss effect, effects on glycemic control, and cardiovascular risk. It was very important to devote a fair amount of time" to the procedure, he said.
The guidelines note that "sleeve gastrectomy has demonstrated benefits comparable to other bariatric procedures. ... A national risk-adjusted database positions [it] between the laparoscopic adjustable gastric band and laparoscopic Roux-en-Y gastric bypass in terms of weight loss, co-morbidity resolution, and complications."
"We [also] addressed two issues which were quite controversial, and are still rather unsettled. The first is the use of the lap band for mild obesity. The second is the use of these weight loss procedures specifically for patients with type 2 diabetes for glycemic control. Since 2008, there’ve been a lot more data" about the issues, he said, just as there’ve been more data about the need for copper supplementation.
As in 2008, the guidelines do not recommend bariatric surgery solely for glycemic control. "We still don’t have an absolute indication for ‘diabetes surgery,’ but we do recognize the existence of the salutary effects on glycemic control when these procedures are done for weight loss. It was important for the reader to be exposed to this information," Dr. Mechanick said.
Regarding surgery in the mildly obese, the guidelines note that patients with a body mass index of 30-34.9 kg/m2 with diabetes or metabolic syndrome "may also be offered a bariatric procedure, although current evidence is limited by the number of subjects studied and lack of long-term data demonstrating net benefit."
The guidelines will be published in the March/April 2013 issue of Endocrine Practice and March 2013 issue of Surgery for Obesity and Related Diseases.
Dr. Mechanick disclosed compensation from Abbott Nutrition for lectures and program development.
Ten Clinical Decisions to Eliminate Wasteful Healthcare Spending
Have you ever prescribed stress ulcer prophylaxis therapy to patients at low risk for gastrointestinal complications? Have you ever repeated CBC or chemistry testing in the face of clinical and lab stability? Have you once or twice ordered bronchodilators for children with bronchiolitis?
If you answered “yes” to any of those questions, you might want to reconsider some of your practices. That’s the message hospitalist leaders have for adult and pediatric HM practitioners interested in curbing wasteful healthcare spending.
SHM has joined the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign, a multiyear effort to spark national dialogue about waste in the healthcare system and the kinds of common treatments that doctors and patients should think twice about before deciding to pursue. Ad hoc subcommittees of SHM’s Hospital Quality and Patient Safety Committee created lists of five adult and five pediatric treatments that hospitalists and their patients should question. Those lists were shared alongside 15 other medical specialty societies at a Feb. 21 news conference in Washington, D.C.

Choosing Wisely (www.choosingwisely.org) has been recognized by the professional and consumer media in a big way, says Daniel Wolfson, executive vice president and chief operating officer of the ABIM Foundation, which is affiliated with but distinct from the American Board of Internal Medicine (www.abim.org). “The conversation about overuse is now on the table, and people recognize that it’s an important subject to talk about—without the kind of hysterics that we’ve seen previously around, for example, rationing,” he says. “We’re talking about treatments that are not beneficial and potentially are harmful to patients … things that are ordered for many patients when the benefit does not exceed the risk. These are not absolutes; there are times when a treatment might be indicated because of a certain history or clinical finding. But be clear on what those circumstances are.”
SHM is excited to be a partner in the Choosing Wisely campaign, says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Healthcare Improvement and Innovation. With its broad professional and consumer outreach and emphasis on informing and engaging the consumer, the Choosing Wisely effort meshes well with the center’s QI and patient safety goals.
“We acknowledge that there is waste in our system. We also believe that if you have an engaged, empowered patient, together you will make better choices, have less waste, and probably also reduce costs,” Dr. Maynard says.
Developing SHM’s “think twice” lists under a tight deadline was a challenge, says John Bulger, DO, FACP, SFHM, chief quality officer at Geisinger Medical Center in Danville, Pa., and chair of the adult committee. It was especially difficult trying to encourage the broadest possible input from experts in the field. SHM board and committee members were asked for suggested treatments that should be targeted as wasteful, and a preliminary list of 100 was grouped, whittled down, and sent to SHM members to vote on. The committee conducted two blind votes and sent a list of seven recommendations to the SHM board, which made the final choices for submission to the ABIM Foundation.
“The ABIM Foundation has fairly strict guidelines for Choosing Wisely,” Dr. Bulger says. The process was meant to be transparent and well documented, and the SHM committees will publish an article in the Journal of Hospital Medicine describing how its lists were compiled. Choices were to be made based on the evidence for treatments that lie within the specialty’s purview. “Because our practice is so diverse, you can find many core treatments that hospitalists impact on a daily basis and that are unique to the work of hospital medicine,” Dr. Bulger adds.
Fourteen pediatric hospitalists followed a similar process in developing its five suggestions.
“While this issue has been addressed in adult settings, in pediatrics, discussions about waste are almost nonexistent,” says Ricardo Quinonez, MD, FHM, a pediatric hospitalist at Texas Children’s Hospital in Houston and chair of the pediatric ad-hoc committee. “I don’t think anyone was too surprised by our list, which is heavy on respiratory illnesses. That’s what kids get admitted to the hospital for.”

Dr. Quinonez suggests pediatric hospitalists use the list to engage with their specialist colleagues about appropriate treatment choices. “If you want to improve quality, here’s a place to start,” he says.

Dr. Bulger encourages hospitalists to stop and take a long look at the lists and think about ways to improve their own practice. He encourages hospitalists to take the recommendations to their hospitals’ quality-improvement (QI) committees and start collecting baseline data, he says, adding that “we should be able to come back a year from now and show that we’ve been able to change practice using these lists.”
A full-day pre-course, “QI for High Value Healthcare: Making the ABIM Foundation’s Choosing Wisely Campaign a Reality,” co-led by Dr. Bulger and Ian Jenkins, MD, of the University of California at San Diego, is planned for HM13 in Washington, D.C., in May (www.hospitalmedicine2013.org).
“[The pre-course] will feature the Choosing Wisely list and how you can both implement and improve on it,” Dr. Maynard says. Longer-term, SHM hopes to compile protocols, order sets, checklists, and other tools for posting on its technical assistance web pages. “Eventually, there may be a mentored implementation program and toolkit, based on best practices from the field. … Lots of people have done bits and pieces of this in their local settings. What’s lacking is a cohesive, portable approach, and that’s what we have our eyes on.”
Wolfson says the ABIM Foundation plans to conduct surveys in the next six months to gauge whether physicians think they should be stewards of healthcare resources. “I think you’ll start to see at leading institutions where it’s no longer just ‘Why didn’t you order this test?’ But ‘Why did you—and what were you hoping to learn from it?’” he says. “Just asking that question is a good start—and saying to yourself: Am I choosing wisely?”
Larry Beresford is a freelance writer in Oakland, Calif.
Have you ever prescribed stress ulcer prophylaxis therapy to patients at low risk for gastrointestinal complications? Have you ever repeated CBC or chemistry testing in the face of clinical and lab stability? Have you once or twice ordered bronchodilators for children with bronchiolitis?
If you answered “yes” to any of those questions, you might want to reconsider some of your practices. That’s the message hospitalist leaders have for adult and pediatric HM practitioners interested in curbing wasteful healthcare spending.
SHM has joined the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign, a multiyear effort to spark national dialogue about waste in the healthcare system and the kinds of common treatments that doctors and patients should think twice about before deciding to pursue. Ad hoc subcommittees of SHM’s Hospital Quality and Patient Safety Committee created lists of five adult and five pediatric treatments that hospitalists and their patients should question. Those lists were shared alongside 15 other medical specialty societies at a Feb. 21 news conference in Washington, D.C.
Choosing Wisely (www.choosingwisely.org) has been recognized by the professional and consumer media in a big way, says Daniel Wolfson, executive vice president and chief operating officer of the ABIM Foundation, which is affiliated with but distinct from the American Board of Internal Medicine (www.abim.org). “The conversation about overuse is now on the table, and people recognize that it’s an important subject to talk about—without the kind of hysterics that we’ve seen previously around, for example, rationing,” he says. “We’re talking about treatments that are not beneficial and potentially are harmful to patients … things that are ordered for many patients when the benefit does not exceed the risk. These are not absolutes; there are times when a treatment might be indicated because of a certain history or clinical finding. But be clear on what those circumstances are.”
SHM is excited to be a partner in the Choosing Wisely campaign, says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Healthcare Improvement and Innovation. With its broad professional and consumer outreach and emphasis on informing and engaging the consumer, the Choosing Wisely effort meshes well with the center’s QI and patient safety goals.
“We acknowledge that there is waste in our system. We also believe that if you have an engaged, empowered patient, together you will make better choices, have less waste, and probably also reduce costs,” Dr. Maynard says.
Developing SHM’s “think twice” lists under a tight deadline was a challenge, says John Bulger, DO, FACP, SFHM, chief quality officer at Geisinger Medical Center in Danville, Pa., and chair of the adult committee. It was especially difficult trying to encourage the broadest possible input from experts in the field. SHM board and committee members were asked for suggested treatments that should be targeted as wasteful, and a preliminary list of 100 was grouped, whittled down, and sent to SHM members to vote on. The committee conducted two blind votes and sent a list of seven recommendations to the SHM board, which made the final choices for submission to the ABIM Foundation.
“The ABIM Foundation has fairly strict guidelines for Choosing Wisely,” Dr. Bulger says. The process was meant to be transparent and well documented, and the SHM committees will publish an article in the Journal of Hospital Medicine describing how its lists were compiled. Choices were to be made based on the evidence for treatments that lie within the specialty’s purview. “Because our practice is so diverse, you can find many core treatments that hospitalists impact on a daily basis and that are unique to the work of hospital medicine,” Dr. Bulger adds.
Fourteen pediatric hospitalists followed a similar process in developing its five suggestions.
“While this issue has been addressed in adult settings, in pediatrics, discussions about waste are almost nonexistent,” says Ricardo Quinonez, MD, FHM, a pediatric hospitalist at Texas Children’s Hospital in Houston and chair of the pediatric ad-hoc committee. “I don’t think anyone was too surprised by our list, which is heavy on respiratory illnesses. That’s what kids get admitted to the hospital for.”
Dr. Quinonez suggests pediatric hospitalists use the list to engage with their specialist colleagues about appropriate treatment choices. “If you want to improve quality, here’s a place to start,” he says.
Dr. Bulger encourages hospitalists to stop and take a long look at the lists and think about ways to improve their own practice. He encourages hospitalists to take the recommendations to their hospitals’ quality-improvement (QI) committees and start collecting baseline data, he says, adding that “we should be able to come back a year from now and show that we’ve been able to change practice using these lists.”
A full-day pre-course, “QI for High Value Healthcare: Making the ABIM Foundation’s Choosing Wisely Campaign a Reality,” co-led by Dr. Bulger and Ian Jenkins, MD, of the University of California at San Diego, is planned for HM13 in Washington, D.C., in May (www.hospitalmedicine2013.org).
“[The pre-course] will feature the Choosing Wisely list and how you can both implement and improve on it,” Dr. Maynard says. Longer-term, SHM hopes to compile protocols, order sets, checklists, and other tools for posting on its technical assistance web pages. “Eventually, there may be a mentored implementation program and toolkit, based on best practices from the field. … Lots of people have done bits and pieces of this in their local settings. What’s lacking is a cohesive, portable approach, and that’s what we have our eyes on.”
Wolfson says the ABIM Foundation plans to conduct surveys in the next six months to gauge whether physicians think they should be stewards of healthcare resources. “I think you’ll start to see at leading institutions where it’s no longer just ‘Why didn’t you order this test?’ But ‘Why did you—and what were you hoping to learn from it?’” he says. “Just asking that question is a good start—and saying to yourself: Am I choosing wisely?”
Larry Beresford is a freelance writer in Oakland, Calif.
Have you ever prescribed stress ulcer prophylaxis therapy to patients at low risk for gastrointestinal complications? Have you ever repeated CBC or chemistry testing in the face of clinical and lab stability? Have you once or twice ordered bronchodilators for children with bronchiolitis?
If you answered “yes” to any of those questions, you might want to reconsider some of your practices. That’s the message hospitalist leaders have for adult and pediatric HM practitioners interested in curbing wasteful healthcare spending.
SHM has joined the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign, a multiyear effort to spark national dialogue about waste in the healthcare system and the kinds of common treatments that doctors and patients should think twice about before deciding to pursue. Ad hoc subcommittees of SHM’s Hospital Quality and Patient Safety Committee created lists of five adult and five pediatric treatments that hospitalists and their patients should question. Those lists were shared alongside 15 other medical specialty societies at a Feb. 21 news conference in Washington, D.C.
Choosing Wisely (www.choosingwisely.org) has been recognized by the professional and consumer media in a big way, says Daniel Wolfson, executive vice president and chief operating officer of the ABIM Foundation, which is affiliated with but distinct from the American Board of Internal Medicine (www.abim.org). “The conversation about overuse is now on the table, and people recognize that it’s an important subject to talk about—without the kind of hysterics that we’ve seen previously around, for example, rationing,” he says. “We’re talking about treatments that are not beneficial and potentially are harmful to patients … things that are ordered for many patients when the benefit does not exceed the risk. These are not absolutes; there are times when a treatment might be indicated because of a certain history or clinical finding. But be clear on what those circumstances are.”
SHM is excited to be a partner in the Choosing Wisely campaign, says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Healthcare Improvement and Innovation. With its broad professional and consumer outreach and emphasis on informing and engaging the consumer, the Choosing Wisely effort meshes well with the center’s QI and patient safety goals.
“We acknowledge that there is waste in our system. We also believe that if you have an engaged, empowered patient, together you will make better choices, have less waste, and probably also reduce costs,” Dr. Maynard says.
Developing SHM’s “think twice” lists under a tight deadline was a challenge, says John Bulger, DO, FACP, SFHM, chief quality officer at Geisinger Medical Center in Danville, Pa., and chair of the adult committee. It was especially difficult trying to encourage the broadest possible input from experts in the field. SHM board and committee members were asked for suggested treatments that should be targeted as wasteful, and a preliminary list of 100 was grouped, whittled down, and sent to SHM members to vote on. The committee conducted two blind votes and sent a list of seven recommendations to the SHM board, which made the final choices for submission to the ABIM Foundation.
“The ABIM Foundation has fairly strict guidelines for Choosing Wisely,” Dr. Bulger says. The process was meant to be transparent and well documented, and the SHM committees will publish an article in the Journal of Hospital Medicine describing how its lists were compiled. Choices were to be made based on the evidence for treatments that lie within the specialty’s purview. “Because our practice is so diverse, you can find many core treatments that hospitalists impact on a daily basis and that are unique to the work of hospital medicine,” Dr. Bulger adds.
Fourteen pediatric hospitalists followed a similar process in developing its five suggestions.
“While this issue has been addressed in adult settings, in pediatrics, discussions about waste are almost nonexistent,” says Ricardo Quinonez, MD, FHM, a pediatric hospitalist at Texas Children’s Hospital in Houston and chair of the pediatric ad-hoc committee. “I don’t think anyone was too surprised by our list, which is heavy on respiratory illnesses. That’s what kids get admitted to the hospital for.”
Dr. Quinonez suggests pediatric hospitalists use the list to engage with their specialist colleagues about appropriate treatment choices. “If you want to improve quality, here’s a place to start,” he says.
Dr. Bulger encourages hospitalists to stop and take a long look at the lists and think about ways to improve their own practice. He encourages hospitalists to take the recommendations to their hospitals’ quality-improvement (QI) committees and start collecting baseline data, he says, adding that “we should be able to come back a year from now and show that we’ve been able to change practice using these lists.”
A full-day pre-course, “QI for High Value Healthcare: Making the ABIM Foundation’s Choosing Wisely Campaign a Reality,” co-led by Dr. Bulger and Ian Jenkins, MD, of the University of California at San Diego, is planned for HM13 in Washington, D.C., in May (www.hospitalmedicine2013.org).
“[The pre-course] will feature the Choosing Wisely list and how you can both implement and improve on it,” Dr. Maynard says. Longer-term, SHM hopes to compile protocols, order sets, checklists, and other tools for posting on its technical assistance web pages. “Eventually, there may be a mentored implementation program and toolkit, based on best practices from the field. … Lots of people have done bits and pieces of this in their local settings. What’s lacking is a cohesive, portable approach, and that’s what we have our eyes on.”
Wolfson says the ABIM Foundation plans to conduct surveys in the next six months to gauge whether physicians think they should be stewards of healthcare resources. “I think you’ll start to see at leading institutions where it’s no longer just ‘Why didn’t you order this test?’ But ‘Why did you—and what were you hoping to learn from it?’” he says. “Just asking that question is a good start—and saying to yourself: Am I choosing wisely?”
Larry Beresford is a freelance writer in Oakland, Calif.
Hospital Medicine Guidelines for Management of Diabetic Foot Infections
Background
In the U.S. alone, there are an estimated 25.8 million people with diabetes, or about 8.3% of the population. Due to comorbidities of peripheral neuropathy and peripheral vascular disease associated with diabetes, these patients are at higher risk for developing foot infections. Among the myriad diabetes complications, diabetic foot infections (DFI) are the main reason for diabetes-related hospitalizations and lower-extremity amputations. U.S. hospitals admit roughly 5,700 patients per year for DFI; 71,000 lower-extremity amputations are attributed to diabetes.1,2
Studies have demonstrated that DFI management according to guidelines improves survival, reduces complications, and is cost-effective with a major clinical outcome of reduced amputations.3 But prospective observational studies have shown that, in practice, guidelines often are not followed and can lead to poor outcomes.4 Studies suggest a need for more simple, straightforward guidelines.
Guidelines Update
In June 2012, the Infectious Diseases Society of America (IDSA) updated its 2004 guidelines on the management of diabetic foot infections.5 Although IDSA made no major changes to its recommendations, the 2012 guidelines were revised to be more simple and clear. These new guidelines have been reviewed and endorsed by SHM.
Specific recommendations include:
- All patients with suspected DFI should be assessed on three levels: the patient, the extremity involved, and the wound. Patients should be assessed for signs of systemic illness or metabolic derangements. The extremity should be examined for peripheral arterial disease (PAD) using the Ankle-Brachial Index (ABI), and those with an ABI <0.4 should be evaluated by a vascular surgeon.
- Uninfected wounds should be distinguished from infected wounds based on the presence of two or more classic signs of inflammation and purulence. All wounds should be classified based on validated systems, such as those established by IDSA or the International Working Group on the Diabetic Foot (IWGDF). The IDSA classification of wounds as uninfected, mild, moderate, and severe correlate well with the IWGDF’s PEDIS (Perfusion, Extent, Depth, Infection and Sensation) Grades 1, 2, 3, and 4. Wounds are distinguished by size (more or less than 2 cm in width), extent (depth of tissue involvement), and the presence of two or more signs of systemic inflammatory response syndrome.
- Whenever possible, management of DFI should involve multidisciplinary teams that include a microbiologist or ID expert, surgeon/podiatrist familiar with debridement of foot infections, and wound care experts familiar with dressings that provide pressure off-loading.
- All wounds should be debrided, and cultures should be sent from deep tissue via biopsy or curettage (scraping of the base of the ulcer). Wound surface swabs should not be sent for culture, as they often are inaccurate.
- All patients with severe infections and some patients with moderate infections with complicating features (i.e. severe PAD or inability to manage outpatient treatment due to psychosocial reasons) should be admitted. Those with mild infection or some moderate infections without complicating features can be managed as outpatients.
- All patients with suspected DFI should have plain radiographs of the affected limb to evaluate for bony abnormalities, soft-tissue gas, or foreign bodies, but they are only 54% sensitive and 68% specific for osteomyelitis. MRI is more sensitive (90%) and specific (up to 90%) for detecting osteomyelitis. When MRI is contraindicated, a bone scan coupled with a tagged white-blood count scan is the next best test for detecting osteomyelitis.
- Osteomyelitis, which is found in as many as 20% of mild to moderate DFI cases and as many as 50% of severe DFI cases, should be suspected in any patient with large (>2 cm square), deep, or chronic (>six weeks) wounds, as well as those who have wounds overlying a bony prominence or have a positive probe-to-bone (PTB) test. The most definitive diagnosis of osteomyelitis is via bone biopsy for culture and histology. Patients with osteomyelitis can be managed surgically with resection or medically with prolonged antibiotics (>four weeks). If surgical resection removes the infected bone with clean margins, the antibiotic course can be shortened to two to five days post-operatively.
- Effective treatment includes both wound care as well as antibiotic therapy. Antibiotics should be started after cultures are sent. Empiric antibiotics for mild to moderate infections in patients who have not been recently treated can be directed at gram-positive cocci (GPC), as Staphylococcus is the most common causal organism identified. Patients with severe infection can be started empirically on parenteral broad-spectrum antibiotics covering for GPC (particularly methicillin-resistant Staphylococcus aureus in at-risk patients), gram-negative bacteria, and obligate anaerobes. Antibiotics should be tailored once culture and sensitivity results are available. Generally, mild infections should be treated for one to two weeks and moderate to severe infections for two to three weeks, if there is no suspicion of osteomyelitis.
Analysis
The United Kingdom National Institute for Clinical Excellence (NICE) guideline development group published guidelines for inpatient management of diabetic foot problems in 2011.6 The NICE guidelines are largely similar to the 2012 IDSA guidelines. NICE guidelines call for each hospital to have a care pathway for all patients who present with a diabetic foot problem, and that these patients should be cared for by a multidisciplinary team, including appropriate wound care and debridement, assessment of vascular function, imaging with plain radiographs and MRI if osteomyelitis is suspected, and directed antibiotic therapy.
HM Takeaways
Diabetic foot infections are a common occurrence, and the guidelines for their management demonstrate how coordinated clinical care is important for improving patient care and outcomes. As health reimbursement moves toward a model of bundled payments for treatment and a greater emphasis on measureable outcomes, hospitalists are well positioned to be managers of such organized approaches with multidisciplinary teams.
Dr. Ly is a hospitalist in the division of hospital medicine at the University of California at San Francisco.
References
- Centers for Disease Control and Prevention. Age-Adjusted Hospital Discharge Rates for Peripheral Arterial Disease (PAD), Ulcer/Inflammation/Infection (ULCER), or Neuropathy as First-Listed Diagnosis per 1,000 Diabetic Population, United States, 1988–2007. CDC website. Available at: http://www.cdc.gov/diabetes/statistics/hosplea/diabetes_complications/fig2_pop.htm. Accessed Jan. 28, 2013.
- Centers for Disease Control and Prevention. Number (in thousands) of hospital discharges for nontraumatic lower extremity amputation with diabetes as a listed diagnosis, 1988-2006. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/diabetes/statistics/lea/fig1.htm. Accessed Jan. 28, 2013.
- Ortegon MM, Redekop WK, Niessen LW. Cost-effectiveness of prevention and treatment of the diabetic foot: a Markov analysis. Diabetes Care. 2004;27:901-907.Prompers L, Huijberts M, Apelqvist J, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18-25.
- Lipsky BA, Berendt AR, Comia PB, et al. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):132-173.
- Tan T, Shaw EJ, Siddiqui F, Kandaswamy P, Barry PW, Baker M. Inpatient management of diabetic foot problems: summary of NICE guidance. BMJ. 2011;342:d1280.
Background
In the U.S. alone, there are an estimated 25.8 million people with diabetes, or about 8.3% of the population. Due to comorbidities of peripheral neuropathy and peripheral vascular disease associated with diabetes, these patients are at higher risk for developing foot infections. Among the myriad diabetes complications, diabetic foot infections (DFI) are the main reason for diabetes-related hospitalizations and lower-extremity amputations. U.S. hospitals admit roughly 5,700 patients per year for DFI; 71,000 lower-extremity amputations are attributed to diabetes.1,2
Studies have demonstrated that DFI management according to guidelines improves survival, reduces complications, and is cost-effective with a major clinical outcome of reduced amputations.3 But prospective observational studies have shown that, in practice, guidelines often are not followed and can lead to poor outcomes.4 Studies suggest a need for more simple, straightforward guidelines.
Guidelines Update
In June 2012, the Infectious Diseases Society of America (IDSA) updated its 2004 guidelines on the management of diabetic foot infections.5 Although IDSA made no major changes to its recommendations, the 2012 guidelines were revised to be more simple and clear. These new guidelines have been reviewed and endorsed by SHM.
Specific recommendations include:
- All patients with suspected DFI should be assessed on three levels: the patient, the extremity involved, and the wound. Patients should be assessed for signs of systemic illness or metabolic derangements. The extremity should be examined for peripheral arterial disease (PAD) using the Ankle-Brachial Index (ABI), and those with an ABI <0.4 should be evaluated by a vascular surgeon.
- Uninfected wounds should be distinguished from infected wounds based on the presence of two or more classic signs of inflammation and purulence. All wounds should be classified based on validated systems, such as those established by IDSA or the International Working Group on the Diabetic Foot (IWGDF). The IDSA classification of wounds as uninfected, mild, moderate, and severe correlate well with the IWGDF’s PEDIS (Perfusion, Extent, Depth, Infection and Sensation) Grades 1, 2, 3, and 4. Wounds are distinguished by size (more or less than 2 cm in width), extent (depth of tissue involvement), and the presence of two or more signs of systemic inflammatory response syndrome.
- Whenever possible, management of DFI should involve multidisciplinary teams that include a microbiologist or ID expert, surgeon/podiatrist familiar with debridement of foot infections, and wound care experts familiar with dressings that provide pressure off-loading.
- All wounds should be debrided, and cultures should be sent from deep tissue via biopsy or curettage (scraping of the base of the ulcer). Wound surface swabs should not be sent for culture, as they often are inaccurate.
- All patients with severe infections and some patients with moderate infections with complicating features (i.e. severe PAD or inability to manage outpatient treatment due to psychosocial reasons) should be admitted. Those with mild infection or some moderate infections without complicating features can be managed as outpatients.
- All patients with suspected DFI should have plain radiographs of the affected limb to evaluate for bony abnormalities, soft-tissue gas, or foreign bodies, but they are only 54% sensitive and 68% specific for osteomyelitis. MRI is more sensitive (90%) and specific (up to 90%) for detecting osteomyelitis. When MRI is contraindicated, a bone scan coupled with a tagged white-blood count scan is the next best test for detecting osteomyelitis.
- Osteomyelitis, which is found in as many as 20% of mild to moderate DFI cases and as many as 50% of severe DFI cases, should be suspected in any patient with large (>2 cm square), deep, or chronic (>six weeks) wounds, as well as those who have wounds overlying a bony prominence or have a positive probe-to-bone (PTB) test. The most definitive diagnosis of osteomyelitis is via bone biopsy for culture and histology. Patients with osteomyelitis can be managed surgically with resection or medically with prolonged antibiotics (>four weeks). If surgical resection removes the infected bone with clean margins, the antibiotic course can be shortened to two to five days post-operatively.
- Effective treatment includes both wound care as well as antibiotic therapy. Antibiotics should be started after cultures are sent. Empiric antibiotics for mild to moderate infections in patients who have not been recently treated can be directed at gram-positive cocci (GPC), as Staphylococcus is the most common causal organism identified. Patients with severe infection can be started empirically on parenteral broad-spectrum antibiotics covering for GPC (particularly methicillin-resistant Staphylococcus aureus in at-risk patients), gram-negative bacteria, and obligate anaerobes. Antibiotics should be tailored once culture and sensitivity results are available. Generally, mild infections should be treated for one to two weeks and moderate to severe infections for two to three weeks, if there is no suspicion of osteomyelitis.
Analysis
The United Kingdom National Institute for Clinical Excellence (NICE) guideline development group published guidelines for inpatient management of diabetic foot problems in 2011.6 The NICE guidelines are largely similar to the 2012 IDSA guidelines. NICE guidelines call for each hospital to have a care pathway for all patients who present with a diabetic foot problem, and that these patients should be cared for by a multidisciplinary team, including appropriate wound care and debridement, assessment of vascular function, imaging with plain radiographs and MRI if osteomyelitis is suspected, and directed antibiotic therapy.
HM Takeaways
Diabetic foot infections are a common occurrence, and the guidelines for their management demonstrate how coordinated clinical care is important for improving patient care and outcomes. As health reimbursement moves toward a model of bundled payments for treatment and a greater emphasis on measureable outcomes, hospitalists are well positioned to be managers of such organized approaches with multidisciplinary teams.
Dr. Ly is a hospitalist in the division of hospital medicine at the University of California at San Francisco.
References
- Centers for Disease Control and Prevention. Age-Adjusted Hospital Discharge Rates for Peripheral Arterial Disease (PAD), Ulcer/Inflammation/Infection (ULCER), or Neuropathy as First-Listed Diagnosis per 1,000 Diabetic Population, United States, 1988–2007. CDC website. Available at: http://www.cdc.gov/diabetes/statistics/hosplea/diabetes_complications/fig2_pop.htm. Accessed Jan. 28, 2013.
- Centers for Disease Control and Prevention. Number (in thousands) of hospital discharges for nontraumatic lower extremity amputation with diabetes as a listed diagnosis, 1988-2006. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/diabetes/statistics/lea/fig1.htm. Accessed Jan. 28, 2013.
- Ortegon MM, Redekop WK, Niessen LW. Cost-effectiveness of prevention and treatment of the diabetic foot: a Markov analysis. Diabetes Care. 2004;27:901-907.Prompers L, Huijberts M, Apelqvist J, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18-25.
- Lipsky BA, Berendt AR, Comia PB, et al. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):132-173.
- Tan T, Shaw EJ, Siddiqui F, Kandaswamy P, Barry PW, Baker M. Inpatient management of diabetic foot problems: summary of NICE guidance. BMJ. 2011;342:d1280.
Background
In the U.S. alone, there are an estimated 25.8 million people with diabetes, or about 8.3% of the population. Due to comorbidities of peripheral neuropathy and peripheral vascular disease associated with diabetes, these patients are at higher risk for developing foot infections. Among the myriad diabetes complications, diabetic foot infections (DFI) are the main reason for diabetes-related hospitalizations and lower-extremity amputations. U.S. hospitals admit roughly 5,700 patients per year for DFI; 71,000 lower-extremity amputations are attributed to diabetes.1,2
Studies have demonstrated that DFI management according to guidelines improves survival, reduces complications, and is cost-effective with a major clinical outcome of reduced amputations.3 But prospective observational studies have shown that, in practice, guidelines often are not followed and can lead to poor outcomes.4 Studies suggest a need for more simple, straightforward guidelines.
Guidelines Update
In June 2012, the Infectious Diseases Society of America (IDSA) updated its 2004 guidelines on the management of diabetic foot infections.5 Although IDSA made no major changes to its recommendations, the 2012 guidelines were revised to be more simple and clear. These new guidelines have been reviewed and endorsed by SHM.
Specific recommendations include:
- All patients with suspected DFI should be assessed on three levels: the patient, the extremity involved, and the wound. Patients should be assessed for signs of systemic illness or metabolic derangements. The extremity should be examined for peripheral arterial disease (PAD) using the Ankle-Brachial Index (ABI), and those with an ABI <0.4 should be evaluated by a vascular surgeon.
- Uninfected wounds should be distinguished from infected wounds based on the presence of two or more classic signs of inflammation and purulence. All wounds should be classified based on validated systems, such as those established by IDSA or the International Working Group on the Diabetic Foot (IWGDF). The IDSA classification of wounds as uninfected, mild, moderate, and severe correlate well with the IWGDF’s PEDIS (Perfusion, Extent, Depth, Infection and Sensation) Grades 1, 2, 3, and 4. Wounds are distinguished by size (more or less than 2 cm in width), extent (depth of tissue involvement), and the presence of two or more signs of systemic inflammatory response syndrome.
- Whenever possible, management of DFI should involve multidisciplinary teams that include a microbiologist or ID expert, surgeon/podiatrist familiar with debridement of foot infections, and wound care experts familiar with dressings that provide pressure off-loading.
- All wounds should be debrided, and cultures should be sent from deep tissue via biopsy or curettage (scraping of the base of the ulcer). Wound surface swabs should not be sent for culture, as they often are inaccurate.
- All patients with severe infections and some patients with moderate infections with complicating features (i.e. severe PAD or inability to manage outpatient treatment due to psychosocial reasons) should be admitted. Those with mild infection or some moderate infections without complicating features can be managed as outpatients.
- All patients with suspected DFI should have plain radiographs of the affected limb to evaluate for bony abnormalities, soft-tissue gas, or foreign bodies, but they are only 54% sensitive and 68% specific for osteomyelitis. MRI is more sensitive (90%) and specific (up to 90%) for detecting osteomyelitis. When MRI is contraindicated, a bone scan coupled with a tagged white-blood count scan is the next best test for detecting osteomyelitis.
- Osteomyelitis, which is found in as many as 20% of mild to moderate DFI cases and as many as 50% of severe DFI cases, should be suspected in any patient with large (>2 cm square), deep, or chronic (>six weeks) wounds, as well as those who have wounds overlying a bony prominence or have a positive probe-to-bone (PTB) test. The most definitive diagnosis of osteomyelitis is via bone biopsy for culture and histology. Patients with osteomyelitis can be managed surgically with resection or medically with prolonged antibiotics (>four weeks). If surgical resection removes the infected bone with clean margins, the antibiotic course can be shortened to two to five days post-operatively.
- Effective treatment includes both wound care as well as antibiotic therapy. Antibiotics should be started after cultures are sent. Empiric antibiotics for mild to moderate infections in patients who have not been recently treated can be directed at gram-positive cocci (GPC), as Staphylococcus is the most common causal organism identified. Patients with severe infection can be started empirically on parenteral broad-spectrum antibiotics covering for GPC (particularly methicillin-resistant Staphylococcus aureus in at-risk patients), gram-negative bacteria, and obligate anaerobes. Antibiotics should be tailored once culture and sensitivity results are available. Generally, mild infections should be treated for one to two weeks and moderate to severe infections for two to three weeks, if there is no suspicion of osteomyelitis.
Analysis
The United Kingdom National Institute for Clinical Excellence (NICE) guideline development group published guidelines for inpatient management of diabetic foot problems in 2011.6 The NICE guidelines are largely similar to the 2012 IDSA guidelines. NICE guidelines call for each hospital to have a care pathway for all patients who present with a diabetic foot problem, and that these patients should be cared for by a multidisciplinary team, including appropriate wound care and debridement, assessment of vascular function, imaging with plain radiographs and MRI if osteomyelitis is suspected, and directed antibiotic therapy.
HM Takeaways
Diabetic foot infections are a common occurrence, and the guidelines for their management demonstrate how coordinated clinical care is important for improving patient care and outcomes. As health reimbursement moves toward a model of bundled payments for treatment and a greater emphasis on measureable outcomes, hospitalists are well positioned to be managers of such organized approaches with multidisciplinary teams.
Dr. Ly is a hospitalist in the division of hospital medicine at the University of California at San Francisco.
References
- Centers for Disease Control and Prevention. Age-Adjusted Hospital Discharge Rates for Peripheral Arterial Disease (PAD), Ulcer/Inflammation/Infection (ULCER), or Neuropathy as First-Listed Diagnosis per 1,000 Diabetic Population, United States, 1988–2007. CDC website. Available at: http://www.cdc.gov/diabetes/statistics/hosplea/diabetes_complications/fig2_pop.htm. Accessed Jan. 28, 2013.
- Centers for Disease Control and Prevention. Number (in thousands) of hospital discharges for nontraumatic lower extremity amputation with diabetes as a listed diagnosis, 1988-2006. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/diabetes/statistics/lea/fig1.htm. Accessed Jan. 28, 2013.
- Ortegon MM, Redekop WK, Niessen LW. Cost-effectiveness of prevention and treatment of the diabetic foot: a Markov analysis. Diabetes Care. 2004;27:901-907.Prompers L, Huijberts M, Apelqvist J, et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia. 2007;50:18-25.
- Lipsky BA, Berendt AR, Comia PB, et al. 2012 Infectious Diseases Society of America Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. Clin Infect Dis. 2012;54(12):132-173.
- Tan T, Shaw EJ, Siddiqui F, Kandaswamy P, Barry PW, Baker M. Inpatient management of diabetic foot problems: summary of NICE guidance. BMJ. 2011;342:d1280.
New Anticoagulation Website Offers Guidelines, Self-Assessment Tools
In January, the Anticoagulation Forum, a nonprofit in Newton, Mass., launched “Anti-Coagulation Centers of Excellence,” a searchable resource center of guidelines and tools, including up-to-date information on novel oral anticoagulants, examples of excellence submitted by other providers, and an online self-assessment tool of anticoagulation programs’ performance. In its first month, the site (www.excellence.acforum.org) had 1,200 visitors, with about 10% of visitors attempting the self-assessment. Participating centers tend to be hospital-based outpatient clinics for patients receiving anti-thrombotic medications.
In January, the Anticoagulation Forum, a nonprofit in Newton, Mass., launched “Anti-Coagulation Centers of Excellence,” a searchable resource center of guidelines and tools, including up-to-date information on novel oral anticoagulants, examples of excellence submitted by other providers, and an online self-assessment tool of anticoagulation programs’ performance. In its first month, the site (www.excellence.acforum.org) had 1,200 visitors, with about 10% of visitors attempting the self-assessment. Participating centers tend to be hospital-based outpatient clinics for patients receiving anti-thrombotic medications.
In January, the Anticoagulation Forum, a nonprofit in Newton, Mass., launched “Anti-Coagulation Centers of Excellence,” a searchable resource center of guidelines and tools, including up-to-date information on novel oral anticoagulants, examples of excellence submitted by other providers, and an online self-assessment tool of anticoagulation programs’ performance. In its first month, the site (www.excellence.acforum.org) had 1,200 visitors, with about 10% of visitors attempting the self-assessment. Participating centers tend to be hospital-based outpatient clinics for patients receiving anti-thrombotic medications.
Society for Hospital Medicine Compiles List of Don'ts for Hospitalists
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
In hospital medicine, what a hospitalist doesn’t do can be just as important as what he or she does do.
That’s why SHM and hospitalist experts from across the country collaborated with the American Board of Internal Medicine Foundation on its groundbreaking Choosing Wisely campaign to publish 10 procedures that hospitalists should think twice about before conducting. Together, with more than a dozen medical specialties, SHM will announce the list of procedures in Washington, D.C., on Feb. 21.
Of the medical specialties contributing lists to Choosing Wisely, SHM is unique in that it will publish two lists (each with five recommendations): one for adult HM and another for pediatric HM.
Once the recommendations have been made public, hospitalists will have multiple ways of learning about them. SHM will publish the recommendations online, via email, and in The Hospitalist. Details about the unique process of developing the Choosing Wisely lists—and the impact they will have on everyday hospitalist practice—will be published in the Journal of Hospital Medicine.
Others in healthcare, including patients and family members, will have a chance to learn about Choosing Wisely through a partnership with Consumer Reports and the public dialogue that the campaign hopes to generate.
SHM President Shaun Frost, MD, SFHM, has been unequivocal in his support for the campaign and has urged all hospitalists to support it as well. “Attention to care affordability and experience are essential to reforming our broken healthcare system, so let’s lead the charge in these areas and help others who are doing the same,” Dr. Frost wrote in the November 2012 issue of The Hospitalist.
To get more involved with this industry-changing campaign, visit www.choosingwisely.org and check out the upcoming Choosing Wisely pre-course at SHM’s annual meeting at www.hospitalmedicine2013.org.
When Should an Abdominal Aortic Aneurysm Be Treated?
Case
A generally healthy, 74-year-old man presents with sudden-onset abdominal pain due to acute pancreatitis. Computed tomography (CT) of his abdomen shows pancreatic inflammation and an incidental finding of a 4.5-cm abdominal aortic aneurysm. He had never had any imaging of his abdomen prior to this study and described no prior episodes of abdominal pain.
When should his abdominal aortic aneurysm be treated?
Overview
An abdominal aortic aneurysm (AAA) is an abnormal dilation of the abdominal aorta between the diaphragm and the aortic bifurcation of the iliac arteries. An AAA is usually defined as a dilatation with a diameter of >3 cm or 50% greater than the typical diameter. Most AAAs are located in the infrarenal aorta, proximal to the iliac bifurcation.
Population screening programs show a prevalence of AAA of 4% to 8% in men aged 65 to 80 years.1 AAA prevalence is approximately six times greater in men than women, though the prevalence in women might be increasing.1 AAA is most common in white men, with black men and those of Asian heritage having lower risk. A combination of genetic predisposition and environmental and physiologic factors lead to initiation and progression of AAAs; family history, male sex, advanced age, and history of smoking are major risk factors.
Mortality after AAA rupture is high. Approximately 62% of patients die prior to hospital arrival.2 Of those who undergo emergent AAA surgery, 50% will die.1
Aortic repair with a prosthetic vascular graft reduces morbidity and mortality from rupture, but the risks of repair are not trivial.2
Review of the Data
Risk of rupture. An AAA should be repaired when the risk of rupture outweighs the risks of surgical repair. Symptomatic aneurysms—such as those causing back or abdominal pain—have a higher risk of rupture than asymptomatic aneurysms. Most AAAs are asymptomatic and, in the absence of imaging, not identified until the time of rupture. Given the significant mortality associated with rupture, there is benefit to intervening on asymptomatic aneurysms before rupture.
The risk of AAA rupture has been studied in patients who either have been unfit for surgical repair or uninterested in intervention. Risk of rupture increases substantially with aneurysm size. Lederle et al estimated a two-year aneurysm rupture risk of 22.1% for AAA with a diameter of 5.0 to 5.9 cm, 18.9% for 6.0 to 6.9 cm, and 43.4% for a diameter ≥7.0 cm.3 In another study of 476 patients, the average risks of rupture in male and female patients with an AAA of 5.0 to 5.9 cm were 1.0% and 3.9% per year, respectively. For male and female patients with ≥6.0 cm AAAs, risks of rupture were 14.1% and 22.3% per year.4 Women with AAA have been found to have a higher risk of rupture in all studies in which female patients were included.
Because rupture risk increases with size, predicting the rate of growth is clinically important. Powell et al conducted a systematic review of growth rates of small AAAs.5 In 15 studies that examined 7,630 patients, the growth rate for a 3.5-cm aneurysm was estimated at 1.9 mm/year and for a 4.5-cm aneurysm was 3.5 mm/year. Given an exponentially increasing aneurysm diameter, this suggests an elapsed time of 6.2 years for a 3.5-cm aneurysm to grow to 5.5 cm, and 2.3 years for a 4.5-cm AAA to grow to 5.5 cm. This prediction does not account for individual variability in growth rate. Some AAAs grow quickly, others erratically, and others not at all. This growth variability is influenced by individual characteristics including cigarette smoking, sex, age, and other factors.
Medical prevention of progression and rupture. Studies have assessed whether modification of risk factors can delay progression of growth of AAAs. In a small aneurysm trial in the United Kingdom, self-reported smoking status was associated with an incrementally increased growth rate of 0.4 mm per year.5 Each year of smoking increases the relative risk of AAA by 4%, and continued smoking leads to more rapid AAA expansion.6 There is no clear relationship between cholesterol levels and AAA expansion rate. Observational studies suggest that aneurysm expansion decreases with statin use, but there is not sufficient evidence to recommend statin therapy for AAA alone.6
Many patients with AAA, however, are candidates for statins because of concomitant coronary artery or peripheral vascular disease. Small, randomized controlled trials have shown that macrolides and tetracycline antibiotics might inhibit AAA growth, but prescribing them for this purpose is not currently the standard of care.7 Elevated mean blood pressure has been associated with rupture, but there is not good evidence showing delay of progression with treatment of hypertension.6 Early observational studies suggested that beta-blocker use would decrease AAA progression, but further evidence has not supported their benefit in slowing progression of size.8 Likewise, use of angiotensin-converting enzyme inhibitors has also shown no growth inhibition.7 An ongoing Cochrane review is evaluating evidence for these medical treatments of AAA.9
Surgical prevention of rupture. There are two surgical methods of AAA repair: open repair and endovascular aneurysm repair (EVAR). Both involve use of a prosthetic graft to prevent the aneurysm from enlarging. The EVAR procedure typically involves entry at the femoral artery, with use of catheters and guide wires to advance a graft to the desired location and anchor it in place. Because this utilizes an endovascular approach, regional rather than general anesthesia can be used.
Multiple investigators have evaluated for differences in outcomes between the two methods of surgical AAA repair. Studies have shown increased 30-day postoperative mortality with open repair, as well as significantly higher rates of postoperative cardiac, pulmonary, and renal complications. One randomized controlled study found 30-day operative mortality of 1.8% in the EVAR group and 4.3% in the open repair group.10 However, after a median six-year follow-up of patients after EVAR or open repair, there is no difference in total mortality or aneurysm-related mortality.10 Compared with open repair, the need for long-term surveillance and re-intervention post-EVAR is higher, with endoleak and graft migration the most common complications. This accounts for the loss of early survival advantage in post-EVAR patients. By two years post-operation, complication after repair with either technique is not statistically different. De Bruin et al found that six years after randomization for repair type, cumulative survival rates were 69.9% for patients after open repair and 68.9% with EVAR.11
Studies also have focused on subgroups of patients with a higher operative risk and shorter life expectancy, such as the elderly.12 A pooled analysis of 13,419 patients aged ≥80 years from six observational studies showed 8.6% immediate mortality after open repair and 2.3% after EVAR (risk difference 6.2%, 95% CI 5.4-7.0%).13 Pooled analysis of three longer-term studies showed similar overall survival at three years after EVAR and open repair.13 When EVAR is not available, open repair has acceptable short- and long-term survival in patients aged ≥80 years with an AAA at high risk of rupture.14
Screening. A Cochrane review evaluated the effect of ultrasound screening of asymptomatic AAA on mortality. In 127,891 men and 9,342 women aged 65 to 79, researchers found a significant decrease in mortality in men aged 65 to 79 who were screened (odds ratio 0.6, 95% CI 0.47-0.78) but no benefit to screening of women.15 The current U.S. Preventive Services Task Force (USPSTF) guidelines recommend one-time ultrasound-guided (USG) screening for AAA in men aged 65 to 75 who have any history of tobacco use. For men in this age group who have never smoked, the balance between benefits and harms of screening is too close for the USPSTF to make recommendations. Because of the lower prevalence in women, the USPSTF recommends against screening women for AAA.18
Timing of repair. Early repair of small AAAs (4 cm to 5.5 cm) has no long-term survival benefit compared to ultrasound surveillance without repair.16,17 Therefore, AAAs <5.5 cm should be followed with regular ultrasound surveillance every six months, with referral to surgery if the diameter reaches 5.5 cm, or grows >1 cm a year. The size at which surgery should be performed might be lower in women, given that their risk of rupture is higher than men. A thoughtful discussion of individual risks should take place in every case, but in many patients, even the elderly, repair of a large asymptomatic AAA is indicated. 5
Back to the Case
Our patient should have repeat imaging of his AAA in six months and regular surveillance afterward to monitor for growth every six months. When the AAA is >5.5 cm or if it grows >1 cm a year, he should be evaluated for EVAR or open repair.
Bottom Line
The current USPSTF guidelines recommend one-time ultrasound-guided (USG) screening for AAA in men aged 65 to 75 with a history of smoking. If an AAA >3 cm is found, the patient should undergo regular USG screening every six months. The AAA should be repaired if >5.5 cm or symptomatic, via either an endoscopic or open approach.
Dr. Best is a hospitalist at University of Washington Medicine at Harborview and associate program director of the internal-medicine residency program at the University of Washington, Seattle. Dr. Carpenter is a fellow in the division of geriatrics at the University of California at San Franscisco.
References
- Nordon IM, Hinchliffe RJ, Loftus IM, Thompson MM. Pathophysiology and epidemiology of abdominal aortic aneurysms. Nat Rev Cardiol. 2011;8, 92-102.
- Ernst CB. Abdominal aortic aneurysm. N Engl J Med. 1993;328(16):1167-1172.
- Lederle FA, Johnson GR, Wilson SE, et al. Rupture rate of large abdominal aortic aneurysms in patients refusing or unfit for elective repair. JAMA. 2002;287:2968-2972
- Brown PM, Zelt DT, Sobolev B. The risk of rupture in untreated aneurysms: the impact of size, gender, and expansion rate. J Vasc Surg. 2003;37:280-284.
- Powell JT, Sweeting MJ, Brown LC, Gotensparre SM, Fowkes FG, Thompson SG. Systematic review and meta-analysis of growth rates of small abdominal aortic aneurysms. British Journal of Surgery. 2011;98:609-618.
- Brown LC, Powell JT. Risk factors for aneurysm rupture in patients kept under ultrasound surveillance. UK Small Aneurysm Trial Participants. Ann Surg. 1999;230(3):289-297.
- Baxter BT, Terrin MC, Dalman RL. Medical management of small abdominal aortic aneurysms. Circulation. 2008;117:1883-1889.
- The Propranolol Aneurysm Trial Investigators. Propranolol for small abdominal aortic aneurysms: results of a randomized trial. J Vasc Surg. 2002:35:72-79.
- Ruhani G, Robertson L, Clarke M. Medical treatment for small abdominal aortic aneurysms. Cochrane Database for Systematic Reviews 2012. Sep 12;9:CD009536. doi: 10.1002/14651858.
- The United Kingdom EVAR Trial Investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010; 362:1863-1871.
- De Bruin JL, Baas AF, Buth J, et al. Long-term outcome of open or endovascular repair of abdominal aortic aneurysm. N Engl J Med. 2010;362:1881-1889.
- Jackson RS, Chang DC, Freischlag JA. Comparison of long-term survival after open vs. endovascular repair of intact abdominal aortic aneurysm among Medicare beneficiaries. JAMA. 2012;307(15):1621-1628.
- Biancari F, Catania A, D’Andrea V. Elective endovascular vs. open repair of abdominal aortic aneurysm in patients aged 80 years and older: systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2011;42:571-576.
- Schermerhorn ML, O’Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358:464-474.
- Cosford PA, Leng GC, Tomas J. Screening for abdominal aortic aneurysm. Cochrane Database for Systematic Reviews 2007, Issue 2. Art. No.: CD002945. DOI: 10.1002/14651858.CD002945.pub2.
- Filardo G, Powell JT, Martinez MA, Ballard DJ. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database for Systematic Reviews 2012, Issue 3. Art. No.:CD001835. DOI: 10.1002/14651858.CD001835.pub3.
- The UK Small Aneurysm Trial Participants. Final 12-year follow-up of surgery versus surveillance in the UK small aneurysm trial. Brit J Surg. 2007;94:702-708.
- U.S. Preventive Services Task Force. Screening for Abdominal Aortic Aneurysm: Recommendation Statement. AHRQ Publication No. 05-0569-A, February 2005.
Case
A generally healthy, 74-year-old man presents with sudden-onset abdominal pain due to acute pancreatitis. Computed tomography (CT) of his abdomen shows pancreatic inflammation and an incidental finding of a 4.5-cm abdominal aortic aneurysm. He had never had any imaging of his abdomen prior to this study and described no prior episodes of abdominal pain.
When should his abdominal aortic aneurysm be treated?
Overview
An abdominal aortic aneurysm (AAA) is an abnormal dilation of the abdominal aorta between the diaphragm and the aortic bifurcation of the iliac arteries. An AAA is usually defined as a dilatation with a diameter of >3 cm or 50% greater than the typical diameter. Most AAAs are located in the infrarenal aorta, proximal to the iliac bifurcation.
Population screening programs show a prevalence of AAA of 4% to 8% in men aged 65 to 80 years.1 AAA prevalence is approximately six times greater in men than women, though the prevalence in women might be increasing.1 AAA is most common in white men, with black men and those of Asian heritage having lower risk. A combination of genetic predisposition and environmental and physiologic factors lead to initiation and progression of AAAs; family history, male sex, advanced age, and history of smoking are major risk factors.
Mortality after AAA rupture is high. Approximately 62% of patients die prior to hospital arrival.2 Of those who undergo emergent AAA surgery, 50% will die.1
Aortic repair with a prosthetic vascular graft reduces morbidity and mortality from rupture, but the risks of repair are not trivial.2
Review of the Data
Risk of rupture. An AAA should be repaired when the risk of rupture outweighs the risks of surgical repair. Symptomatic aneurysms—such as those causing back or abdominal pain—have a higher risk of rupture than asymptomatic aneurysms. Most AAAs are asymptomatic and, in the absence of imaging, not identified until the time of rupture. Given the significant mortality associated with rupture, there is benefit to intervening on asymptomatic aneurysms before rupture.
The risk of AAA rupture has been studied in patients who either have been unfit for surgical repair or uninterested in intervention. Risk of rupture increases substantially with aneurysm size. Lederle et al estimated a two-year aneurysm rupture risk of 22.1% for AAA with a diameter of 5.0 to 5.9 cm, 18.9% for 6.0 to 6.9 cm, and 43.4% for a diameter ≥7.0 cm.3 In another study of 476 patients, the average risks of rupture in male and female patients with an AAA of 5.0 to 5.9 cm were 1.0% and 3.9% per year, respectively. For male and female patients with ≥6.0 cm AAAs, risks of rupture were 14.1% and 22.3% per year.4 Women with AAA have been found to have a higher risk of rupture in all studies in which female patients were included.
Because rupture risk increases with size, predicting the rate of growth is clinically important. Powell et al conducted a systematic review of growth rates of small AAAs.5 In 15 studies that examined 7,630 patients, the growth rate for a 3.5-cm aneurysm was estimated at 1.9 mm/year and for a 4.5-cm aneurysm was 3.5 mm/year. Given an exponentially increasing aneurysm diameter, this suggests an elapsed time of 6.2 years for a 3.5-cm aneurysm to grow to 5.5 cm, and 2.3 years for a 4.5-cm AAA to grow to 5.5 cm. This prediction does not account for individual variability in growth rate. Some AAAs grow quickly, others erratically, and others not at all. This growth variability is influenced by individual characteristics including cigarette smoking, sex, age, and other factors.
Medical prevention of progression and rupture. Studies have assessed whether modification of risk factors can delay progression of growth of AAAs. In a small aneurysm trial in the United Kingdom, self-reported smoking status was associated with an incrementally increased growth rate of 0.4 mm per year.5 Each year of smoking increases the relative risk of AAA by 4%, and continued smoking leads to more rapid AAA expansion.6 There is no clear relationship between cholesterol levels and AAA expansion rate. Observational studies suggest that aneurysm expansion decreases with statin use, but there is not sufficient evidence to recommend statin therapy for AAA alone.6
Many patients with AAA, however, are candidates for statins because of concomitant coronary artery or peripheral vascular disease. Small, randomized controlled trials have shown that macrolides and tetracycline antibiotics might inhibit AAA growth, but prescribing them for this purpose is not currently the standard of care.7 Elevated mean blood pressure has been associated with rupture, but there is not good evidence showing delay of progression with treatment of hypertension.6 Early observational studies suggested that beta-blocker use would decrease AAA progression, but further evidence has not supported their benefit in slowing progression of size.8 Likewise, use of angiotensin-converting enzyme inhibitors has also shown no growth inhibition.7 An ongoing Cochrane review is evaluating evidence for these medical treatments of AAA.9
Surgical prevention of rupture. There are two surgical methods of AAA repair: open repair and endovascular aneurysm repair (EVAR). Both involve use of a prosthetic graft to prevent the aneurysm from enlarging. The EVAR procedure typically involves entry at the femoral artery, with use of catheters and guide wires to advance a graft to the desired location and anchor it in place. Because this utilizes an endovascular approach, regional rather than general anesthesia can be used.
Multiple investigators have evaluated for differences in outcomes between the two methods of surgical AAA repair. Studies have shown increased 30-day postoperative mortality with open repair, as well as significantly higher rates of postoperative cardiac, pulmonary, and renal complications. One randomized controlled study found 30-day operative mortality of 1.8% in the EVAR group and 4.3% in the open repair group.10 However, after a median six-year follow-up of patients after EVAR or open repair, there is no difference in total mortality or aneurysm-related mortality.10 Compared with open repair, the need for long-term surveillance and re-intervention post-EVAR is higher, with endoleak and graft migration the most common complications. This accounts for the loss of early survival advantage in post-EVAR patients. By two years post-operation, complication after repair with either technique is not statistically different. De Bruin et al found that six years after randomization for repair type, cumulative survival rates were 69.9% for patients after open repair and 68.9% with EVAR.11
Studies also have focused on subgroups of patients with a higher operative risk and shorter life expectancy, such as the elderly.12 A pooled analysis of 13,419 patients aged ≥80 years from six observational studies showed 8.6% immediate mortality after open repair and 2.3% after EVAR (risk difference 6.2%, 95% CI 5.4-7.0%).13 Pooled analysis of three longer-term studies showed similar overall survival at three years after EVAR and open repair.13 When EVAR is not available, open repair has acceptable short- and long-term survival in patients aged ≥80 years with an AAA at high risk of rupture.14
Screening. A Cochrane review evaluated the effect of ultrasound screening of asymptomatic AAA on mortality. In 127,891 men and 9,342 women aged 65 to 79, researchers found a significant decrease in mortality in men aged 65 to 79 who were screened (odds ratio 0.6, 95% CI 0.47-0.78) but no benefit to screening of women.15 The current U.S. Preventive Services Task Force (USPSTF) guidelines recommend one-time ultrasound-guided (USG) screening for AAA in men aged 65 to 75 who have any history of tobacco use. For men in this age group who have never smoked, the balance between benefits and harms of screening is too close for the USPSTF to make recommendations. Because of the lower prevalence in women, the USPSTF recommends against screening women for AAA.18
Timing of repair. Early repair of small AAAs (4 cm to 5.5 cm) has no long-term survival benefit compared to ultrasound surveillance without repair.16,17 Therefore, AAAs <5.5 cm should be followed with regular ultrasound surveillance every six months, with referral to surgery if the diameter reaches 5.5 cm, or grows >1 cm a year. The size at which surgery should be performed might be lower in women, given that their risk of rupture is higher than men. A thoughtful discussion of individual risks should take place in every case, but in many patients, even the elderly, repair of a large asymptomatic AAA is indicated. 5
Back to the Case
Our patient should have repeat imaging of his AAA in six months and regular surveillance afterward to monitor for growth every six months. When the AAA is >5.5 cm or if it grows >1 cm a year, he should be evaluated for EVAR or open repair.
Bottom Line
The current USPSTF guidelines recommend one-time ultrasound-guided (USG) screening for AAA in men aged 65 to 75 with a history of smoking. If an AAA >3 cm is found, the patient should undergo regular USG screening every six months. The AAA should be repaired if >5.5 cm or symptomatic, via either an endoscopic or open approach.
Dr. Best is a hospitalist at University of Washington Medicine at Harborview and associate program director of the internal-medicine residency program at the University of Washington, Seattle. Dr. Carpenter is a fellow in the division of geriatrics at the University of California at San Franscisco.
References
- Nordon IM, Hinchliffe RJ, Loftus IM, Thompson MM. Pathophysiology and epidemiology of abdominal aortic aneurysms. Nat Rev Cardiol. 2011;8, 92-102.
- Ernst CB. Abdominal aortic aneurysm. N Engl J Med. 1993;328(16):1167-1172.
- Lederle FA, Johnson GR, Wilson SE, et al. Rupture rate of large abdominal aortic aneurysms in patients refusing or unfit for elective repair. JAMA. 2002;287:2968-2972
- Brown PM, Zelt DT, Sobolev B. The risk of rupture in untreated aneurysms: the impact of size, gender, and expansion rate. J Vasc Surg. 2003;37:280-284.
- Powell JT, Sweeting MJ, Brown LC, Gotensparre SM, Fowkes FG, Thompson SG. Systematic review and meta-analysis of growth rates of small abdominal aortic aneurysms. British Journal of Surgery. 2011;98:609-618.
- Brown LC, Powell JT. Risk factors for aneurysm rupture in patients kept under ultrasound surveillance. UK Small Aneurysm Trial Participants. Ann Surg. 1999;230(3):289-297.
- Baxter BT, Terrin MC, Dalman RL. Medical management of small abdominal aortic aneurysms. Circulation. 2008;117:1883-1889.
- The Propranolol Aneurysm Trial Investigators. Propranolol for small abdominal aortic aneurysms: results of a randomized trial. J Vasc Surg. 2002:35:72-79.
- Ruhani G, Robertson L, Clarke M. Medical treatment for small abdominal aortic aneurysms. Cochrane Database for Systematic Reviews 2012. Sep 12;9:CD009536. doi: 10.1002/14651858.
- The United Kingdom EVAR Trial Investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010; 362:1863-1871.
- De Bruin JL, Baas AF, Buth J, et al. Long-term outcome of open or endovascular repair of abdominal aortic aneurysm. N Engl J Med. 2010;362:1881-1889.
- Jackson RS, Chang DC, Freischlag JA. Comparison of long-term survival after open vs. endovascular repair of intact abdominal aortic aneurysm among Medicare beneficiaries. JAMA. 2012;307(15):1621-1628.
- Biancari F, Catania A, D’Andrea V. Elective endovascular vs. open repair of abdominal aortic aneurysm in patients aged 80 years and older: systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2011;42:571-576.
- Schermerhorn ML, O’Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358:464-474.
- Cosford PA, Leng GC, Tomas J. Screening for abdominal aortic aneurysm. Cochrane Database for Systematic Reviews 2007, Issue 2. Art. No.: CD002945. DOI: 10.1002/14651858.CD002945.pub2.
- Filardo G, Powell JT, Martinez MA, Ballard DJ. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database for Systematic Reviews 2012, Issue 3. Art. No.:CD001835. DOI: 10.1002/14651858.CD001835.pub3.
- The UK Small Aneurysm Trial Participants. Final 12-year follow-up of surgery versus surveillance in the UK small aneurysm trial. Brit J Surg. 2007;94:702-708.
- U.S. Preventive Services Task Force. Screening for Abdominal Aortic Aneurysm: Recommendation Statement. AHRQ Publication No. 05-0569-A, February 2005.
Case
A generally healthy, 74-year-old man presents with sudden-onset abdominal pain due to acute pancreatitis. Computed tomography (CT) of his abdomen shows pancreatic inflammation and an incidental finding of a 4.5-cm abdominal aortic aneurysm. He had never had any imaging of his abdomen prior to this study and described no prior episodes of abdominal pain.
When should his abdominal aortic aneurysm be treated?
Overview
An abdominal aortic aneurysm (AAA) is an abnormal dilation of the abdominal aorta between the diaphragm and the aortic bifurcation of the iliac arteries. An AAA is usually defined as a dilatation with a diameter of >3 cm or 50% greater than the typical diameter. Most AAAs are located in the infrarenal aorta, proximal to the iliac bifurcation.
Population screening programs show a prevalence of AAA of 4% to 8% in men aged 65 to 80 years.1 AAA prevalence is approximately six times greater in men than women, though the prevalence in women might be increasing.1 AAA is most common in white men, with black men and those of Asian heritage having lower risk. A combination of genetic predisposition and environmental and physiologic factors lead to initiation and progression of AAAs; family history, male sex, advanced age, and history of smoking are major risk factors.
Mortality after AAA rupture is high. Approximately 62% of patients die prior to hospital arrival.2 Of those who undergo emergent AAA surgery, 50% will die.1
Aortic repair with a prosthetic vascular graft reduces morbidity and mortality from rupture, but the risks of repair are not trivial.2
Review of the Data
Risk of rupture. An AAA should be repaired when the risk of rupture outweighs the risks of surgical repair. Symptomatic aneurysms—such as those causing back or abdominal pain—have a higher risk of rupture than asymptomatic aneurysms. Most AAAs are asymptomatic and, in the absence of imaging, not identified until the time of rupture. Given the significant mortality associated with rupture, there is benefit to intervening on asymptomatic aneurysms before rupture.
The risk of AAA rupture has been studied in patients who either have been unfit for surgical repair or uninterested in intervention. Risk of rupture increases substantially with aneurysm size. Lederle et al estimated a two-year aneurysm rupture risk of 22.1% for AAA with a diameter of 5.0 to 5.9 cm, 18.9% for 6.0 to 6.9 cm, and 43.4% for a diameter ≥7.0 cm.3 In another study of 476 patients, the average risks of rupture in male and female patients with an AAA of 5.0 to 5.9 cm were 1.0% and 3.9% per year, respectively. For male and female patients with ≥6.0 cm AAAs, risks of rupture were 14.1% and 22.3% per year.4 Women with AAA have been found to have a higher risk of rupture in all studies in which female patients were included.
Because rupture risk increases with size, predicting the rate of growth is clinically important. Powell et al conducted a systematic review of growth rates of small AAAs.5 In 15 studies that examined 7,630 patients, the growth rate for a 3.5-cm aneurysm was estimated at 1.9 mm/year and for a 4.5-cm aneurysm was 3.5 mm/year. Given an exponentially increasing aneurysm diameter, this suggests an elapsed time of 6.2 years for a 3.5-cm aneurysm to grow to 5.5 cm, and 2.3 years for a 4.5-cm AAA to grow to 5.5 cm. This prediction does not account for individual variability in growth rate. Some AAAs grow quickly, others erratically, and others not at all. This growth variability is influenced by individual characteristics including cigarette smoking, sex, age, and other factors.
Medical prevention of progression and rupture. Studies have assessed whether modification of risk factors can delay progression of growth of AAAs. In a small aneurysm trial in the United Kingdom, self-reported smoking status was associated with an incrementally increased growth rate of 0.4 mm per year.5 Each year of smoking increases the relative risk of AAA by 4%, and continued smoking leads to more rapid AAA expansion.6 There is no clear relationship between cholesterol levels and AAA expansion rate. Observational studies suggest that aneurysm expansion decreases with statin use, but there is not sufficient evidence to recommend statin therapy for AAA alone.6
Many patients with AAA, however, are candidates for statins because of concomitant coronary artery or peripheral vascular disease. Small, randomized controlled trials have shown that macrolides and tetracycline antibiotics might inhibit AAA growth, but prescribing them for this purpose is not currently the standard of care.7 Elevated mean blood pressure has been associated with rupture, but there is not good evidence showing delay of progression with treatment of hypertension.6 Early observational studies suggested that beta-blocker use would decrease AAA progression, but further evidence has not supported their benefit in slowing progression of size.8 Likewise, use of angiotensin-converting enzyme inhibitors has also shown no growth inhibition.7 An ongoing Cochrane review is evaluating evidence for these medical treatments of AAA.9
Surgical prevention of rupture. There are two surgical methods of AAA repair: open repair and endovascular aneurysm repair (EVAR). Both involve use of a prosthetic graft to prevent the aneurysm from enlarging. The EVAR procedure typically involves entry at the femoral artery, with use of catheters and guide wires to advance a graft to the desired location and anchor it in place. Because this utilizes an endovascular approach, regional rather than general anesthesia can be used.
Multiple investigators have evaluated for differences in outcomes between the two methods of surgical AAA repair. Studies have shown increased 30-day postoperative mortality with open repair, as well as significantly higher rates of postoperative cardiac, pulmonary, and renal complications. One randomized controlled study found 30-day operative mortality of 1.8% in the EVAR group and 4.3% in the open repair group.10 However, after a median six-year follow-up of patients after EVAR or open repair, there is no difference in total mortality or aneurysm-related mortality.10 Compared with open repair, the need for long-term surveillance and re-intervention post-EVAR is higher, with endoleak and graft migration the most common complications. This accounts for the loss of early survival advantage in post-EVAR patients. By two years post-operation, complication after repair with either technique is not statistically different. De Bruin et al found that six years after randomization for repair type, cumulative survival rates were 69.9% for patients after open repair and 68.9% with EVAR.11
Studies also have focused on subgroups of patients with a higher operative risk and shorter life expectancy, such as the elderly.12 A pooled analysis of 13,419 patients aged ≥80 years from six observational studies showed 8.6% immediate mortality after open repair and 2.3% after EVAR (risk difference 6.2%, 95% CI 5.4-7.0%).13 Pooled analysis of three longer-term studies showed similar overall survival at three years after EVAR and open repair.13 When EVAR is not available, open repair has acceptable short- and long-term survival in patients aged ≥80 years with an AAA at high risk of rupture.14
Screening. A Cochrane review evaluated the effect of ultrasound screening of asymptomatic AAA on mortality. In 127,891 men and 9,342 women aged 65 to 79, researchers found a significant decrease in mortality in men aged 65 to 79 who were screened (odds ratio 0.6, 95% CI 0.47-0.78) but no benefit to screening of women.15 The current U.S. Preventive Services Task Force (USPSTF) guidelines recommend one-time ultrasound-guided (USG) screening for AAA in men aged 65 to 75 who have any history of tobacco use. For men in this age group who have never smoked, the balance between benefits and harms of screening is too close for the USPSTF to make recommendations. Because of the lower prevalence in women, the USPSTF recommends against screening women for AAA.18
Timing of repair. Early repair of small AAAs (4 cm to 5.5 cm) has no long-term survival benefit compared to ultrasound surveillance without repair.16,17 Therefore, AAAs <5.5 cm should be followed with regular ultrasound surveillance every six months, with referral to surgery if the diameter reaches 5.5 cm, or grows >1 cm a year. The size at which surgery should be performed might be lower in women, given that their risk of rupture is higher than men. A thoughtful discussion of individual risks should take place in every case, but in many patients, even the elderly, repair of a large asymptomatic AAA is indicated. 5
Back to the Case
Our patient should have repeat imaging of his AAA in six months and regular surveillance afterward to monitor for growth every six months. When the AAA is >5.5 cm or if it grows >1 cm a year, he should be evaluated for EVAR or open repair.
Bottom Line
The current USPSTF guidelines recommend one-time ultrasound-guided (USG) screening for AAA in men aged 65 to 75 with a history of smoking. If an AAA >3 cm is found, the patient should undergo regular USG screening every six months. The AAA should be repaired if >5.5 cm or symptomatic, via either an endoscopic or open approach.
Dr. Best is a hospitalist at University of Washington Medicine at Harborview and associate program director of the internal-medicine residency program at the University of Washington, Seattle. Dr. Carpenter is a fellow in the division of geriatrics at the University of California at San Franscisco.
References
- Nordon IM, Hinchliffe RJ, Loftus IM, Thompson MM. Pathophysiology and epidemiology of abdominal aortic aneurysms. Nat Rev Cardiol. 2011;8, 92-102.
- Ernst CB. Abdominal aortic aneurysm. N Engl J Med. 1993;328(16):1167-1172.
- Lederle FA, Johnson GR, Wilson SE, et al. Rupture rate of large abdominal aortic aneurysms in patients refusing or unfit for elective repair. JAMA. 2002;287:2968-2972
- Brown PM, Zelt DT, Sobolev B. The risk of rupture in untreated aneurysms: the impact of size, gender, and expansion rate. J Vasc Surg. 2003;37:280-284.
- Powell JT, Sweeting MJ, Brown LC, Gotensparre SM, Fowkes FG, Thompson SG. Systematic review and meta-analysis of growth rates of small abdominal aortic aneurysms. British Journal of Surgery. 2011;98:609-618.
- Brown LC, Powell JT. Risk factors for aneurysm rupture in patients kept under ultrasound surveillance. UK Small Aneurysm Trial Participants. Ann Surg. 1999;230(3):289-297.
- Baxter BT, Terrin MC, Dalman RL. Medical management of small abdominal aortic aneurysms. Circulation. 2008;117:1883-1889.
- The Propranolol Aneurysm Trial Investigators. Propranolol for small abdominal aortic aneurysms: results of a randomized trial. J Vasc Surg. 2002:35:72-79.
- Ruhani G, Robertson L, Clarke M. Medical treatment for small abdominal aortic aneurysms. Cochrane Database for Systematic Reviews 2012. Sep 12;9:CD009536. doi: 10.1002/14651858.
- The United Kingdom EVAR Trial Investigators. Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med. 2010; 362:1863-1871.
- De Bruin JL, Baas AF, Buth J, et al. Long-term outcome of open or endovascular repair of abdominal aortic aneurysm. N Engl J Med. 2010;362:1881-1889.
- Jackson RS, Chang DC, Freischlag JA. Comparison of long-term survival after open vs. endovascular repair of intact abdominal aortic aneurysm among Medicare beneficiaries. JAMA. 2012;307(15):1621-1628.
- Biancari F, Catania A, D’Andrea V. Elective endovascular vs. open repair of abdominal aortic aneurysm in patients aged 80 years and older: systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2011;42:571-576.
- Schermerhorn ML, O’Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358:464-474.
- Cosford PA, Leng GC, Tomas J. Screening for abdominal aortic aneurysm. Cochrane Database for Systematic Reviews 2007, Issue 2. Art. No.: CD002945. DOI: 10.1002/14651858.CD002945.pub2.
- Filardo G, Powell JT, Martinez MA, Ballard DJ. Surgery for small asymptomatic abdominal aortic aneurysms. Cochrane Database for Systematic Reviews 2012, Issue 3. Art. No.:CD001835. DOI: 10.1002/14651858.CD001835.pub3.
- The UK Small Aneurysm Trial Participants. Final 12-year follow-up of surgery versus surveillance in the UK small aneurysm trial. Brit J Surg. 2007;94:702-708.
- U.S. Preventive Services Task Force. Screening for Abdominal Aortic Aneurysm: Recommendation Statement. AHRQ Publication No. 05-0569-A, February 2005.
Guidelines Help Hospitalists Manage Acute Coronary Syndrome Patients

Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
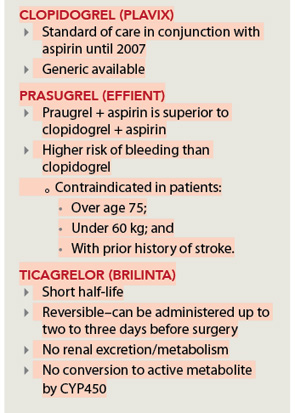
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Recommendations for Antithrombotic and Thrombolytic Therapy
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Off-Label Use of Antipsychotics for Dementia Patients Discouraged
Hospitalists can play a major role in reducing deaths that come as a result of off-label prescriptions for antipsychotic drugs being given to dementia patients, according to the Centers for Medicare & Medicaid Services (CMS) and SHM.
In a letter to hospitalist leaders, SHM encouraged hospitalists to “partner with others in your clinical work environment to reduce the use of antipsychotics for treating behavioral problems in patients with dementia. We believe that hospitalists have an important role to play in this initiative; hospital-based clinicians frequently care for patients with dementia and are responsible for medications prescribed during a patient’s hospitalization and at discharge.”
The joint education effort by CMS and SHM is based on an April 2011 report from the U.S. Department of Health and Human Services’ Office of Inspector General (OIG) that found that antipsychotic medications sometimes are used to treat patients with dementia for off-label reasons (e.g. “behaviors”) or against black-box warnings despite potential dangers to patients’ health.
An earlier warning from the FDA in 2008 outlined the potential dangers as:
- Increased risk (60% to 70%) of death in older adults with dementia;
- Prolongation of the QT interval on electrocardiogram, particularly with intravenous haloperidol use;
- Increased risk of stroke and TIAs; and
- Worsening cognitive function.
The letter to hospitalists noted the necessary changes and the need for collaboration between SHM, its members, and hospital leaders. “Increased prescriber training and system practice changes will help reduce unnecessary antipsychotic drug prescribing,” the letter stated. “SHM looks forward to an ongoing collaboration with members and hospital leaders on this important patient safety concern.”
Hospitalists can play a major role in reducing deaths that come as a result of off-label prescriptions for antipsychotic drugs being given to dementia patients, according to the Centers for Medicare & Medicaid Services (CMS) and SHM.
In a letter to hospitalist leaders, SHM encouraged hospitalists to “partner with others in your clinical work environment to reduce the use of antipsychotics for treating behavioral problems in patients with dementia. We believe that hospitalists have an important role to play in this initiative; hospital-based clinicians frequently care for patients with dementia and are responsible for medications prescribed during a patient’s hospitalization and at discharge.”
The joint education effort by CMS and SHM is based on an April 2011 report from the U.S. Department of Health and Human Services’ Office of Inspector General (OIG) that found that antipsychotic medications sometimes are used to treat patients with dementia for off-label reasons (e.g. “behaviors”) or against black-box warnings despite potential dangers to patients’ health.
An earlier warning from the FDA in 2008 outlined the potential dangers as:
- Increased risk (60% to 70%) of death in older adults with dementia;
- Prolongation of the QT interval on electrocardiogram, particularly with intravenous haloperidol use;
- Increased risk of stroke and TIAs; and
- Worsening cognitive function.
The letter to hospitalists noted the necessary changes and the need for collaboration between SHM, its members, and hospital leaders. “Increased prescriber training and system practice changes will help reduce unnecessary antipsychotic drug prescribing,” the letter stated. “SHM looks forward to an ongoing collaboration with members and hospital leaders on this important patient safety concern.”
Hospitalists can play a major role in reducing deaths that come as a result of off-label prescriptions for antipsychotic drugs being given to dementia patients, according to the Centers for Medicare & Medicaid Services (CMS) and SHM.
In a letter to hospitalist leaders, SHM encouraged hospitalists to “partner with others in your clinical work environment to reduce the use of antipsychotics for treating behavioral problems in patients with dementia. We believe that hospitalists have an important role to play in this initiative; hospital-based clinicians frequently care for patients with dementia and are responsible for medications prescribed during a patient’s hospitalization and at discharge.”
The joint education effort by CMS and SHM is based on an April 2011 report from the U.S. Department of Health and Human Services’ Office of Inspector General (OIG) that found that antipsychotic medications sometimes are used to treat patients with dementia for off-label reasons (e.g. “behaviors”) or against black-box warnings despite potential dangers to patients’ health.
An earlier warning from the FDA in 2008 outlined the potential dangers as:
- Increased risk (60% to 70%) of death in older adults with dementia;
- Prolongation of the QT interval on electrocardiogram, particularly with intravenous haloperidol use;
- Increased risk of stroke and TIAs; and
- Worsening cognitive function.
The letter to hospitalists noted the necessary changes and the need for collaboration between SHM, its members, and hospital leaders. “Increased prescriber training and system practice changes will help reduce unnecessary antipsychotic drug prescribing,” the letter stated. “SHM looks forward to an ongoing collaboration with members and hospital leaders on this important patient safety concern.”