User login
Guidelines issued on radiation-induced heart disease
Cancer patients undergoing radiation therapy need to have baseline studies of cardiac function and routine screening for heart disease, according to recommendations from the European Society of Cardiology and the American Society of Echocardiography published July 16 in the European Heart Journal–Cardiovascular Imaging.
The groups recommend baseline preradiation echocardiography along with a cardiac exam as well as screening for risk factors. An annual cardiac history and physical should be performed to check for new-onset heart problems.
Within 10 years of treatment, 10%-30% of patients who undergo radiation therapy develop radiation-induced heart diseases (RIHD), including chronic pericarditis, myocardial fibrosis, coronary artery disease, aortic calcification, and valve regurgitation or stenosis. The hope of screening is to catch early RIHD, but screening is not currently routine.
"We wrote the expert consensus to raise the alarm that the risks of radiation-induced heart disease should not be ignored. The prevalence ... is increasing because the rate of cancer survival has improved," said Dr. Patrizio Lancellotti, who is a professor of cardiology at the University Hospital of Liège, Belgium, and led the recommendations task force.
Radiotherapy is given in more targeted form and at lower doses than it once was, but "patients are still at increased risk of RIHD, particularly when the heart is in the radiation field. This applies to patients treated for lymphoma, breast cancer, and esophageal cancer. Patients who receive radiotherapy for neck cancer are also at risk because lesions can develop on the carotid artery and increase the risk of stroke," Dr. Lancellotti said in a statement.
Using targeted radiation and alternate radiation fields, with avoidance and shielding of the heart, remain "the most important interventions to prevent" cardiac complications, the authors noted.
The task force advises that high-risk patients without evidence of heart disease on history and physical should have screening echocardiography every 5 years and noninvasive stress testing every 5-10 years; low-risk patients should have screening echocardiography every 10 years. If heart disorders are detected, routine monitoring should include echocardiography, cardiac magnetic resonance imaging, or carotid ultrasound as appropriate.
High-risk patients include those who received radiotherapy at younger ages; those who have cardiovascular risk factors or preexisting heart disease; and those who receive high-dose radiation (greater than 30 Gy), concomitant chemotherapy, radiation without shielding, or anterior or left chest radiation (Eur. Heart J. Cardiovasc. Imaging 2013;14:721-40).
The recommendations are based on an extensive literature review and analysis by Dr. Lancellotti and other specialists.
The authors reported no financial conflicts or outside funding for their work.
Cancer patients undergoing radiation therapy need to have baseline studies of cardiac function and routine screening for heart disease, according to recommendations from the European Society of Cardiology and the American Society of Echocardiography published July 16 in the European Heart Journal–Cardiovascular Imaging.
The groups recommend baseline preradiation echocardiography along with a cardiac exam as well as screening for risk factors. An annual cardiac history and physical should be performed to check for new-onset heart problems.
Within 10 years of treatment, 10%-30% of patients who undergo radiation therapy develop radiation-induced heart diseases (RIHD), including chronic pericarditis, myocardial fibrosis, coronary artery disease, aortic calcification, and valve regurgitation or stenosis. The hope of screening is to catch early RIHD, but screening is not currently routine.
"We wrote the expert consensus to raise the alarm that the risks of radiation-induced heart disease should not be ignored. The prevalence ... is increasing because the rate of cancer survival has improved," said Dr. Patrizio Lancellotti, who is a professor of cardiology at the University Hospital of Liège, Belgium, and led the recommendations task force.
Radiotherapy is given in more targeted form and at lower doses than it once was, but "patients are still at increased risk of RIHD, particularly when the heart is in the radiation field. This applies to patients treated for lymphoma, breast cancer, and esophageal cancer. Patients who receive radiotherapy for neck cancer are also at risk because lesions can develop on the carotid artery and increase the risk of stroke," Dr. Lancellotti said in a statement.
Using targeted radiation and alternate radiation fields, with avoidance and shielding of the heart, remain "the most important interventions to prevent" cardiac complications, the authors noted.
The task force advises that high-risk patients without evidence of heart disease on history and physical should have screening echocardiography every 5 years and noninvasive stress testing every 5-10 years; low-risk patients should have screening echocardiography every 10 years. If heart disorders are detected, routine monitoring should include echocardiography, cardiac magnetic resonance imaging, or carotid ultrasound as appropriate.
High-risk patients include those who received radiotherapy at younger ages; those who have cardiovascular risk factors or preexisting heart disease; and those who receive high-dose radiation (greater than 30 Gy), concomitant chemotherapy, radiation without shielding, or anterior or left chest radiation (Eur. Heart J. Cardiovasc. Imaging 2013;14:721-40).
The recommendations are based on an extensive literature review and analysis by Dr. Lancellotti and other specialists.
The authors reported no financial conflicts or outside funding for their work.
Cancer patients undergoing radiation therapy need to have baseline studies of cardiac function and routine screening for heart disease, according to recommendations from the European Society of Cardiology and the American Society of Echocardiography published July 16 in the European Heart Journal–Cardiovascular Imaging.
The groups recommend baseline preradiation echocardiography along with a cardiac exam as well as screening for risk factors. An annual cardiac history and physical should be performed to check for new-onset heart problems.
Within 10 years of treatment, 10%-30% of patients who undergo radiation therapy develop radiation-induced heart diseases (RIHD), including chronic pericarditis, myocardial fibrosis, coronary artery disease, aortic calcification, and valve regurgitation or stenosis. The hope of screening is to catch early RIHD, but screening is not currently routine.
"We wrote the expert consensus to raise the alarm that the risks of radiation-induced heart disease should not be ignored. The prevalence ... is increasing because the rate of cancer survival has improved," said Dr. Patrizio Lancellotti, who is a professor of cardiology at the University Hospital of Liège, Belgium, and led the recommendations task force.
Radiotherapy is given in more targeted form and at lower doses than it once was, but "patients are still at increased risk of RIHD, particularly when the heart is in the radiation field. This applies to patients treated for lymphoma, breast cancer, and esophageal cancer. Patients who receive radiotherapy for neck cancer are also at risk because lesions can develop on the carotid artery and increase the risk of stroke," Dr. Lancellotti said in a statement.
Using targeted radiation and alternate radiation fields, with avoidance and shielding of the heart, remain "the most important interventions to prevent" cardiac complications, the authors noted.
The task force advises that high-risk patients without evidence of heart disease on history and physical should have screening echocardiography every 5 years and noninvasive stress testing every 5-10 years; low-risk patients should have screening echocardiography every 10 years. If heart disorders are detected, routine monitoring should include echocardiography, cardiac magnetic resonance imaging, or carotid ultrasound as appropriate.
High-risk patients include those who received radiotherapy at younger ages; those who have cardiovascular risk factors or preexisting heart disease; and those who receive high-dose radiation (greater than 30 Gy), concomitant chemotherapy, radiation without shielding, or anterior or left chest radiation (Eur. Heart J. Cardiovasc. Imaging 2013;14:721-40).
The recommendations are based on an extensive literature review and analysis by Dr. Lancellotti and other specialists.
The authors reported no financial conflicts or outside funding for their work.
FROM THE EUROPEAN HEART JOURNAL – CARDIOVASCULAR IMAGING
How Can Tumor Lysis Syndrome Be Prevented and Managed in Cancer Patients?
Case
A 25-year-old male with HIV/AIDS and a CD4 count of 65 cells/μL presents to the ED with intractable nausea and vomiting for one week. Laboratory evaluation revealed a white blood cell of 67,000 cells/mm3. An extended chemistry panel reveals creatinine 3.5 mg/dL, potassium 3.0 mmol/L, LDH 250 IU/L, and uric acid 5mg/dL. Calcium and phosphorus were both normal. The patient was admitted for further evaluation and management, and was later diagnosed with Burkitt’s lymphoma.
Overview
Tumor lysis syndrome (TLS) is an acute cell lysis of tumor cells with the release of cell content into circulation either spontaneously or in response to therapy, leading to hyperurecemia, hyperkalemia, hyperphosphatemia, and hypocalcemia.1-3
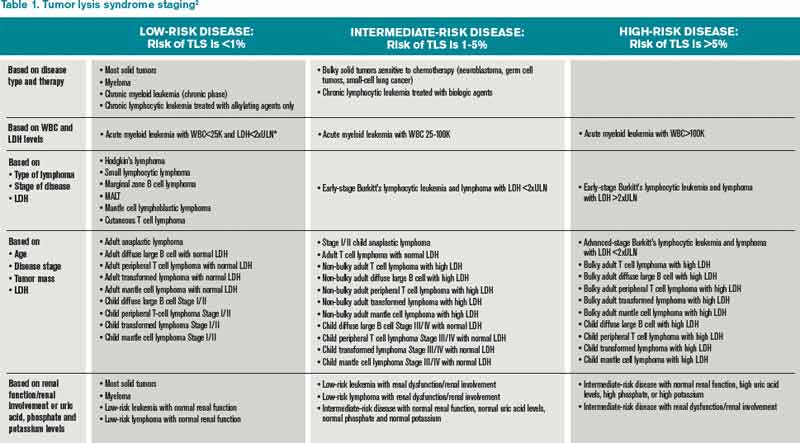
TLS is one of the most common oncology emergencies encountered by hospitalists caring for patients with hematologic malignancies. The incidence and severity of TLS depend on the cell burden, cell proliferation rate, potential for cell lysis or chemo sensitivity, baseline clinical characteristics, and preventive measures taken (see Table 1).2,4
TLS is classified as laboratory or clinical. Laboratory TLS is described as the presence of two or more of the following serum abnormalities at the same time, present within three days before or seven days after the start of therapy.5
- Uric acid >8 mg/dL (475.8 micromole/L) or 25% increase;
- Potassium >6 mEq/L (6 mmol/L) or 25% increase;
- Phosphorus >6.5 mg/dL (2.1 mmol/L) for children or >4.5 mg/dl (1.45 mmol/L) for adults or 25% increase; and
- Calcium >7 mg/dL (1.75 mmol/L) or 25% increase.
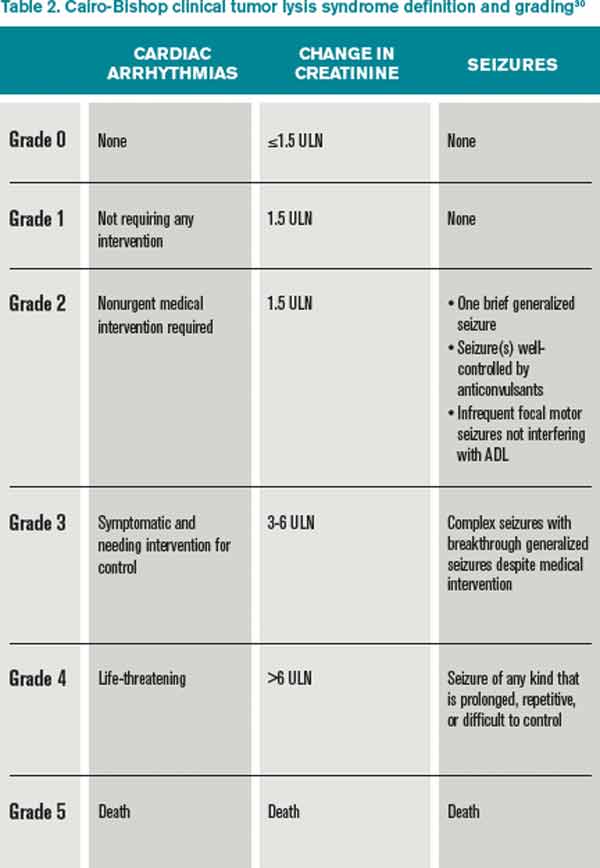
Clinical TLS is defined as laboratory TLS in association with increased creatinine levels, seizures, cardiac arrhythmias, or death (see Table 2).5
Pathogenesis
Tumor cell lysis releases DNA, cytokines, phosphate, and potassium. DNA is metabolized into adenosine and guanosine, which are then converted into xanthines. Xanthines are oxidized by xanthine oxidase into uric acid, which is then excreted through the kidneys.
TLS develops when the accumulation of xanthine, uric acid, potassium, and phosphorus exceeds the kidney’s capacity to excrete them. Cytokines cause hypotension, inflammation, and kidney injury, and worsen the kidney’s excretory capacity. Damage to the kidneys also occurs by renal precipitation of uric acid, xanthine, and calcium phosphate.4
Phosphorus concentrations in tumor cells are four times higher than in normal cells. When the calcium phosphorus product exceeds 60 mg2/dL2, there is an increased risk of calcium phosphate precipitation in the kidney tubules, which could lead to kidney failure. Accumulation of calcium phosphate product may also be cardiotoxic and can lead to cardiac arrhythmias. In addition, hyperphosphatemia can cause secondary hypocalcemia, which may lead to parasthesias, tetany, and cardiac arrhythmias.2,4
TLS is most common in tumors with high proliferative rates and high tumor burden, such as acute lymphoblastic leukemia and Burkitt’s lymphoma, but it can occur with other hematologic malignancies, such as T-cell precursor acute lymphocytic leukemia (ALL), B-cell precursor ALL, acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), anaplastic large cell lymphoma, and plasma cell disorders (e.g. multiple myeloma and plasmacytoma).6,7 TLS has also been reported with the treatment of solid organ nonhematologic tumors (see Table 3).
In hematologic tumors, TLS frequently is associated with cytotoxic chemotherapy, and less frequently with glucocorticoid treatment, monoclonal antibodies (eg, rituximab, bortezomab, imatinib), and radiation therapy.25-29
Patient factors, such as baseline kidney disease or lack of prophylactic/preventive measures for TLS, also increase the risk.4 TLS, however, can develop in patients classified as low risk (see Table 1.
TLS Prevention
Intravenous fluids. Every patient at intermediate or high risk of TLS should receive intravenous fluids (IVF) prior to cancer treatment; those at low risk may receive IVF based on the provider’s clinical judgment.30 The purpose of administering IVF is to generate high urine output to reduce the risk of precipitation of uric acid in the renal tubules.30 Both adults and children should receive approximately 2 to 3 L/m2 per day of IVF,30 and urine output should be maintained at 2 ml/kg/hr (or 4 to 6 ml/kg/hr for children <10kg).30 IVF should be cautiously administered in patients with renal insufficiency or heart failure, and diuretics may be used to maintain goal urine output. Recommended initial fluids are D51/4 normal saline, or normal saline for patients who are dehydrated or hyponatremic.30
Allopurinol. Allopurinol is usually also administered to patients at risk for developing TLS.30 Allopurinol inhibits the metabolism of hypoxanthine and xanthine to uric acid, which decreases the accumulation of uric acid in the renal tubules, thus preventing obstructive renal disease from precipitation of uric acid.4 The recommended dose of allopurinol is 100 mg/m2 every eight hours, and should not exceed 800 mg per day in adults. It should be started one to two days prior to induction chemotherapy and continued for three to seven days after the treatment and until uric acid levels and other electrolyte levels have returned to normal. The dose is adjusted to 50 mg/m2 every eight hours in patients with kidney failure.30
In some cases, allopurinol can lead to increased levels of xanthine crystals in the renal tubules, leading to acute kidney injury. Also, allopurinol does not have any effect on uric acid that has already been formed, so patients with elevated uric acid levels prior to the initiation of cancer therapy will not have any reduction in the levels of uric acid. Allopurinol reduces the degradation of other purines, so it can cause toxicity in patients on azathioprine and 6-mercaptopurine if the doses of these medications are not adjusted.
Rasburicase. Rasburicase is a recombinant urate oxidase, derived from aspergillus favus, which catalyzes the breakdown of uric acid to allantoin, which is a water-soluble product. Rasburicase is recommended as a first-line treatment for patients at high risk for clinical TLS.30 Rasburicase has an earlier onset than allopurinol and rapidly decreases serum levels of uric acid within four hours of administration.30,31 The recommended dose is 0.10 to 0.20 mg/kg once a day for five days in adults.30
A Phase III trial compared the efficiency and safety of rasburicase to rasburicase with allopurinol or allopurinol alone.32 A significantly higher normalization of uric acid was found in patients on rasburicase compared to allopurinol alone. The incidence of laboratory TLS was also significantly lower with rasburicase alone compared to allopurinol alone, and was even lower with allopurinol plus rasburicase. The incidence of acute kidney injury was the same with rasburicase alone or allopurinol alone but was higher with rasburicase plus allopurinol.
Serum uric acid, phosphorus, potassium, and calcium need to be monitored every four hours for 24 hours after the completion of chemotherapy in patients on rasburicase.4 The sample of blood drawn to check the uric acid levels has to be placed on ice and processed within four hours in order to avoid falsely lower levels of uric acid due to the conversion of uric acid to allantoin. Rasburicase is contraindicated in patients with G6PD deficiency and pregnant women, because one of the byproducts of uric acid breakdown is hydrogen peroxide, which can cause severe hemolysis and the formation of methemoglobin in these patients.30
Rasburicase has been approved for use in both children and adults, but there is more evidence for the use in children. Rasburicase has a black-box label for patients with anaphylaxis, methemoglobinemia, hemolysis, and hemoglobinuria, and there is a recommendation to check G6PD deficiency before use in high-risk patients.30
TLS Treatment
Alkalinization. Alkalinization of urine is controversial in the management of TLS. Urine alkalinization increases uric acid solubility but causes hyperphosphatemia and decreases calcium phosphate solubility, which can then deposit in the kidney once cancer treatment starts. Of note, hyperphosphatemia is much more difficult to correct than high levels of uric acid, and there are no clinical trials proving the superiority of urine alkalinization over normal saline.
Normalization of electrolytes. Electrolyte abnormalities should be corrected to avoid arrhythmias and seizures. Phosphorus levels >6.5 mg/dl (2.1 mmol/L) should be managed by restricting phosphorus intake, and by the use of phosphate binders (calcium acetate, calcium carbonate, sevelamer, lanthanum, or aluminum hydroxide). Aluminum hydroxide should be avoided in patients with renal insufficiency. In severe cases of hyperphosphatemia, dialysis should be considered.
Symptomatic hypocalcemia should be treated with calcium gluconate if changes are present on the electrocardiography (ECG). Hypocalcemia in the presence of hyperphosphatemia should be treated only in patients with tetany or cardiac arrhythmias; otherwise, hypocalcemia should not be treated until hyperphosphatemia has been corrected.
In cases of hyperkalemia, patients should be placed on a cardiac monitor and stabilized with calcium gluconate; kayexalate should be administered to reduce total body potassium. Other interventions, such as intravenous insulin given with dextrose, sodium bicarbonate, and albuterol, have a temporary effect on hyperkalemia and can be used as adjunct treatments in patients with severe hyperkalemia (>7). Hemodialysis should be strongly considered in severe cases of hyperkalemia, particularly in patients with persistently elevated potassium levels despite other treatments.
Back to the Case
Our patient was started on IVFs with close monitoring of his urine output. He was considered intermediate risk for developing TLS. Allopurinol, renally dosed, was administered for two days prior to initiating treatment with rituximab plus chemotherapy. His chemistry panel was monitored daily and he did not develop any form of TLS.
Bottom Line
TLS is a common oncology emergency in patients with hematologic malignancies. Preventative measures include starting IVF prior to cancer treatment, and administering allopurinol and/or rasburicase to patients at risk of developing TLS. Treatment should include normalizing electrolytes to avoid arrhythmias and seizures.
Dr. Akwe is assistant professor of medicine at the Emory University School of Medicine and a clinical instructor of medicine at the Morehouse School of Medicine, both in Atlanta. Dr. Smith is an assistant director for education in the division of hospital medicine at Emory. Both work as hospitalists at the Atlanta VA Medical Center.
References
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55:Suppl 3:S1-S13.
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578-586.
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179-180.
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med. 2011;364:1844.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127:3.
- Wössmann W, Schrappe M, Meyer U, et al. Incidence of tumor lysis syndrome in children with advanced stage Burkitt’s lymphoma/leukemia before and after introduction of prophylactic use of urate oxidase. Ann Hematol. 2003;82:160.
- Hussain K, Mazza JJ, Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy Gemici C. Tumor lysis syndrome in solid tumors. J Clin Oncol. 2009;27:2738-2739
- Rostom AY, El-Hussainy G, Kandil A, Allam A. Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer. Ann Oncol. 2000;11:1349.
- Drakos P, Bar-Ziv J, Catane R. Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature. Am J Clin Oncol. 1994;17:502.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51:187.
- Kalemkerian GP, Darwish B, Varterasian ML. Tumor lysis syndrome in small cell carcinoma and other solid tumors. Am J Med. 1997;103:363.
- Noh GY, Choe DH, Kim CH, Lee JC. Fatal tumor lysis syndrome during radiotherapy for non-small-cell lung cancer. J Clin Oncol. 2008;26:6005-6006.
- Pentheroudakis G, O’Neill VJ, Vasey P, Kaye SB. Spontaneous acute tumour lysis syndrome in patients with metastatic germ cell tumours. Report of two cases. Support Care Cancer. 2001;9:554.
- Joshita S, Yoshizawa K, Sano K, et al., A patient with advanced hepatocellular carcinoma treated with sorafenib tosylate showed massive tumor lysis with avoidance of tumor lysis syndrome. Intern Med. 2010;49:991-994.
- Huang WS, Yang CH. Sorafenib-induced tumor lysis syndrome in an advanced hepatocellular carcinoma patient. World J Gastroenterol. 2009;15:4464-4466.
- Bilgrami SF, Fallon BG. Tumor lysis syndrome after combination chemotherapy for ovarian cancer. Med Pediatr Oncol. 1993;21:521.
- Chan JK, Lin SS, McMeekin DS, Berman ML. Patients with malignancy requiring urgent therapy: CASE 3. Tumor lysis syndrome associated with chemotherapy in ovarian cancer. J Clin Oncol. 2005;23:6794.
- Godoy H, Kesterson JP, Lele S. Tumor lysis syndrome associated with carboplatin and paclitaxel in a woman with recurrent endometrial cancer. Int J Gynaecol Obstet. 2010;109:254.
- Shamseddine AI, Khalil AM, Wehbeh MH. Acute tumor lysis syndrome with squamous cell carcinoma of the vulva. Gynecol Oncol 1993;51:258
- Pinder EM, Atwal GS, Ayantunde AA, et al. Tumour lysis syndrome occurring in a patient with metastatic gastrointestinal stromal tumour treated with Glivec (imatinib mesylate, Gleevec, STI571). Sarcoma. 2007;2007:82012.
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406-2408.
- Oztop I, Demirkan B, Yaren A, et al. Rapid tumor lysis syndrome in a patient with metastatic colon cancer as a complication of treatment with 5-fluorouracil/leucoverin and irinotecan. Tumori. 2004;90:514.
- Lin CJ, Lim KH, Cheng YC, et al. Tumor lysis syndrome after treatment with gemcitabine for metastatic transitional cell carcinoma. Med Oncol. 2007;24:455.
- Malik IA, Abubakar S, Alam F, Khan A. Dexamethasone-induced tumor lysis syndrome in high-grade non-Hodgkin’s lymphoma. South Med J. 1994;87:409.
- Jabr FI. Acute tumor lysis syndrome induced by rituximab in diffuse large B-cell lymphoma. Int J Hematol. 2005;82:312.
- Sezer O, Vesole DH, Singhal S, et al. Bortezomib-induced tumor lysis syndrome in multiple myeloma. Clin Lymphoma Myeloma. 2006;7:233.
- Jensen M, Winkler U, Manzke O, et al. Rapid tumor lysis in a patient with B-cell chronic lymphocytic leukemia and lymphocytosis treated with an anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab). Ann Hematol. 1998;77:89.
- Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysis syndrome immediately after 4 Gy fractionated TBI as part of reduced intensity preparative regimen in a patient with T-ALL with high tumor burden. Bone Marrow Transplant. 2003;31:935.
- Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008;26(16):2767-2778. [Erratum, J Clin Oncol. 2010;28:708.]
- Cheuk DK, Chiang AK, Chan GC, Ha SY. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database Syst Rev. 2010;(6):CD006945.
- Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol. 2010;28:4207.
Case
A 25-year-old male with HIV/AIDS and a CD4 count of 65 cells/μL presents to the ED with intractable nausea and vomiting for one week. Laboratory evaluation revealed a white blood cell of 67,000 cells/mm3. An extended chemistry panel reveals creatinine 3.5 mg/dL, potassium 3.0 mmol/L, LDH 250 IU/L, and uric acid 5mg/dL. Calcium and phosphorus were both normal. The patient was admitted for further evaluation and management, and was later diagnosed with Burkitt’s lymphoma.
Overview
Tumor lysis syndrome (TLS) is an acute cell lysis of tumor cells with the release of cell content into circulation either spontaneously or in response to therapy, leading to hyperurecemia, hyperkalemia, hyperphosphatemia, and hypocalcemia.1-3
TLS is one of the most common oncology emergencies encountered by hospitalists caring for patients with hematologic malignancies. The incidence and severity of TLS depend on the cell burden, cell proliferation rate, potential for cell lysis or chemo sensitivity, baseline clinical characteristics, and preventive measures taken (see Table 1).2,4
TLS is classified as laboratory or clinical. Laboratory TLS is described as the presence of two or more of the following serum abnormalities at the same time, present within three days before or seven days after the start of therapy.5
- Uric acid >8 mg/dL (475.8 micromole/L) or 25% increase;
- Potassium >6 mEq/L (6 mmol/L) or 25% increase;
- Phosphorus >6.5 mg/dL (2.1 mmol/L) for children or >4.5 mg/dl (1.45 mmol/L) for adults or 25% increase; and
- Calcium >7 mg/dL (1.75 mmol/L) or 25% increase.
Clinical TLS is defined as laboratory TLS in association with increased creatinine levels, seizures, cardiac arrhythmias, or death (see Table 2).5
Pathogenesis
Tumor cell lysis releases DNA, cytokines, phosphate, and potassium. DNA is metabolized into adenosine and guanosine, which are then converted into xanthines. Xanthines are oxidized by xanthine oxidase into uric acid, which is then excreted through the kidneys.
TLS develops when the accumulation of xanthine, uric acid, potassium, and phosphorus exceeds the kidney’s capacity to excrete them. Cytokines cause hypotension, inflammation, and kidney injury, and worsen the kidney’s excretory capacity. Damage to the kidneys also occurs by renal precipitation of uric acid, xanthine, and calcium phosphate.4
Phosphorus concentrations in tumor cells are four times higher than in normal cells. When the calcium phosphorus product exceeds 60 mg2/dL2, there is an increased risk of calcium phosphate precipitation in the kidney tubules, which could lead to kidney failure. Accumulation of calcium phosphate product may also be cardiotoxic and can lead to cardiac arrhythmias. In addition, hyperphosphatemia can cause secondary hypocalcemia, which may lead to parasthesias, tetany, and cardiac arrhythmias.2,4
TLS is most common in tumors with high proliferative rates and high tumor burden, such as acute lymphoblastic leukemia and Burkitt’s lymphoma, but it can occur with other hematologic malignancies, such as T-cell precursor acute lymphocytic leukemia (ALL), B-cell precursor ALL, acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), anaplastic large cell lymphoma, and plasma cell disorders (e.g. multiple myeloma and plasmacytoma).6,7 TLS has also been reported with the treatment of solid organ nonhematologic tumors (see Table 3).
In hematologic tumors, TLS frequently is associated with cytotoxic chemotherapy, and less frequently with glucocorticoid treatment, monoclonal antibodies (eg, rituximab, bortezomab, imatinib), and radiation therapy.25-29
Patient factors, such as baseline kidney disease or lack of prophylactic/preventive measures for TLS, also increase the risk.4 TLS, however, can develop in patients classified as low risk (see Table 1.
TLS Prevention
Intravenous fluids. Every patient at intermediate or high risk of TLS should receive intravenous fluids (IVF) prior to cancer treatment; those at low risk may receive IVF based on the provider’s clinical judgment.30 The purpose of administering IVF is to generate high urine output to reduce the risk of precipitation of uric acid in the renal tubules.30 Both adults and children should receive approximately 2 to 3 L/m2 per day of IVF,30 and urine output should be maintained at 2 ml/kg/hr (or 4 to 6 ml/kg/hr for children <10kg).30 IVF should be cautiously administered in patients with renal insufficiency or heart failure, and diuretics may be used to maintain goal urine output. Recommended initial fluids are D51/4 normal saline, or normal saline for patients who are dehydrated or hyponatremic.30
Allopurinol. Allopurinol is usually also administered to patients at risk for developing TLS.30 Allopurinol inhibits the metabolism of hypoxanthine and xanthine to uric acid, which decreases the accumulation of uric acid in the renal tubules, thus preventing obstructive renal disease from precipitation of uric acid.4 The recommended dose of allopurinol is 100 mg/m2 every eight hours, and should not exceed 800 mg per day in adults. It should be started one to two days prior to induction chemotherapy and continued for three to seven days after the treatment and until uric acid levels and other electrolyte levels have returned to normal. The dose is adjusted to 50 mg/m2 every eight hours in patients with kidney failure.30
In some cases, allopurinol can lead to increased levels of xanthine crystals in the renal tubules, leading to acute kidney injury. Also, allopurinol does not have any effect on uric acid that has already been formed, so patients with elevated uric acid levels prior to the initiation of cancer therapy will not have any reduction in the levels of uric acid. Allopurinol reduces the degradation of other purines, so it can cause toxicity in patients on azathioprine and 6-mercaptopurine if the doses of these medications are not adjusted.
Rasburicase. Rasburicase is a recombinant urate oxidase, derived from aspergillus favus, which catalyzes the breakdown of uric acid to allantoin, which is a water-soluble product. Rasburicase is recommended as a first-line treatment for patients at high risk for clinical TLS.30 Rasburicase has an earlier onset than allopurinol and rapidly decreases serum levels of uric acid within four hours of administration.30,31 The recommended dose is 0.10 to 0.20 mg/kg once a day for five days in adults.30
A Phase III trial compared the efficiency and safety of rasburicase to rasburicase with allopurinol or allopurinol alone.32 A significantly higher normalization of uric acid was found in patients on rasburicase compared to allopurinol alone. The incidence of laboratory TLS was also significantly lower with rasburicase alone compared to allopurinol alone, and was even lower with allopurinol plus rasburicase. The incidence of acute kidney injury was the same with rasburicase alone or allopurinol alone but was higher with rasburicase plus allopurinol.
Serum uric acid, phosphorus, potassium, and calcium need to be monitored every four hours for 24 hours after the completion of chemotherapy in patients on rasburicase.4 The sample of blood drawn to check the uric acid levels has to be placed on ice and processed within four hours in order to avoid falsely lower levels of uric acid due to the conversion of uric acid to allantoin. Rasburicase is contraindicated in patients with G6PD deficiency and pregnant women, because one of the byproducts of uric acid breakdown is hydrogen peroxide, which can cause severe hemolysis and the formation of methemoglobin in these patients.30
Rasburicase has been approved for use in both children and adults, but there is more evidence for the use in children. Rasburicase has a black-box label for patients with anaphylaxis, methemoglobinemia, hemolysis, and hemoglobinuria, and there is a recommendation to check G6PD deficiency before use in high-risk patients.30
TLS Treatment
Alkalinization. Alkalinization of urine is controversial in the management of TLS. Urine alkalinization increases uric acid solubility but causes hyperphosphatemia and decreases calcium phosphate solubility, which can then deposit in the kidney once cancer treatment starts. Of note, hyperphosphatemia is much more difficult to correct than high levels of uric acid, and there are no clinical trials proving the superiority of urine alkalinization over normal saline.
Normalization of electrolytes. Electrolyte abnormalities should be corrected to avoid arrhythmias and seizures. Phosphorus levels >6.5 mg/dl (2.1 mmol/L) should be managed by restricting phosphorus intake, and by the use of phosphate binders (calcium acetate, calcium carbonate, sevelamer, lanthanum, or aluminum hydroxide). Aluminum hydroxide should be avoided in patients with renal insufficiency. In severe cases of hyperphosphatemia, dialysis should be considered.
Symptomatic hypocalcemia should be treated with calcium gluconate if changes are present on the electrocardiography (ECG). Hypocalcemia in the presence of hyperphosphatemia should be treated only in patients with tetany or cardiac arrhythmias; otherwise, hypocalcemia should not be treated until hyperphosphatemia has been corrected.
In cases of hyperkalemia, patients should be placed on a cardiac monitor and stabilized with calcium gluconate; kayexalate should be administered to reduce total body potassium. Other interventions, such as intravenous insulin given with dextrose, sodium bicarbonate, and albuterol, have a temporary effect on hyperkalemia and can be used as adjunct treatments in patients with severe hyperkalemia (>7). Hemodialysis should be strongly considered in severe cases of hyperkalemia, particularly in patients with persistently elevated potassium levels despite other treatments.
Back to the Case
Our patient was started on IVFs with close monitoring of his urine output. He was considered intermediate risk for developing TLS. Allopurinol, renally dosed, was administered for two days prior to initiating treatment with rituximab plus chemotherapy. His chemistry panel was monitored daily and he did not develop any form of TLS.
Bottom Line
TLS is a common oncology emergency in patients with hematologic malignancies. Preventative measures include starting IVF prior to cancer treatment, and administering allopurinol and/or rasburicase to patients at risk of developing TLS. Treatment should include normalizing electrolytes to avoid arrhythmias and seizures.
Dr. Akwe is assistant professor of medicine at the Emory University School of Medicine and a clinical instructor of medicine at the Morehouse School of Medicine, both in Atlanta. Dr. Smith is an assistant director for education in the division of hospital medicine at Emory. Both work as hospitalists at the Atlanta VA Medical Center.
References
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55:Suppl 3:S1-S13.
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578-586.
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179-180.
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med. 2011;364:1844.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127:3.
- Wössmann W, Schrappe M, Meyer U, et al. Incidence of tumor lysis syndrome in children with advanced stage Burkitt’s lymphoma/leukemia before and after introduction of prophylactic use of urate oxidase. Ann Hematol. 2003;82:160.
- Hussain K, Mazza JJ, Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy Gemici C. Tumor lysis syndrome in solid tumors. J Clin Oncol. 2009;27:2738-2739
- Rostom AY, El-Hussainy G, Kandil A, Allam A. Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer. Ann Oncol. 2000;11:1349.
- Drakos P, Bar-Ziv J, Catane R. Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature. Am J Clin Oncol. 1994;17:502.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51:187.
- Kalemkerian GP, Darwish B, Varterasian ML. Tumor lysis syndrome in small cell carcinoma and other solid tumors. Am J Med. 1997;103:363.
- Noh GY, Choe DH, Kim CH, Lee JC. Fatal tumor lysis syndrome during radiotherapy for non-small-cell lung cancer. J Clin Oncol. 2008;26:6005-6006.
- Pentheroudakis G, O’Neill VJ, Vasey P, Kaye SB. Spontaneous acute tumour lysis syndrome in patients with metastatic germ cell tumours. Report of two cases. Support Care Cancer. 2001;9:554.
- Joshita S, Yoshizawa K, Sano K, et al., A patient with advanced hepatocellular carcinoma treated with sorafenib tosylate showed massive tumor lysis with avoidance of tumor lysis syndrome. Intern Med. 2010;49:991-994.
- Huang WS, Yang CH. Sorafenib-induced tumor lysis syndrome in an advanced hepatocellular carcinoma patient. World J Gastroenterol. 2009;15:4464-4466.
- Bilgrami SF, Fallon BG. Tumor lysis syndrome after combination chemotherapy for ovarian cancer. Med Pediatr Oncol. 1993;21:521.
- Chan JK, Lin SS, McMeekin DS, Berman ML. Patients with malignancy requiring urgent therapy: CASE 3. Tumor lysis syndrome associated with chemotherapy in ovarian cancer. J Clin Oncol. 2005;23:6794.
- Godoy H, Kesterson JP, Lele S. Tumor lysis syndrome associated with carboplatin and paclitaxel in a woman with recurrent endometrial cancer. Int J Gynaecol Obstet. 2010;109:254.
- Shamseddine AI, Khalil AM, Wehbeh MH. Acute tumor lysis syndrome with squamous cell carcinoma of the vulva. Gynecol Oncol 1993;51:258
- Pinder EM, Atwal GS, Ayantunde AA, et al. Tumour lysis syndrome occurring in a patient with metastatic gastrointestinal stromal tumour treated with Glivec (imatinib mesylate, Gleevec, STI571). Sarcoma. 2007;2007:82012.
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406-2408.
- Oztop I, Demirkan B, Yaren A, et al. Rapid tumor lysis syndrome in a patient with metastatic colon cancer as a complication of treatment with 5-fluorouracil/leucoverin and irinotecan. Tumori. 2004;90:514.
- Lin CJ, Lim KH, Cheng YC, et al. Tumor lysis syndrome after treatment with gemcitabine for metastatic transitional cell carcinoma. Med Oncol. 2007;24:455.
- Malik IA, Abubakar S, Alam F, Khan A. Dexamethasone-induced tumor lysis syndrome in high-grade non-Hodgkin’s lymphoma. South Med J. 1994;87:409.
- Jabr FI. Acute tumor lysis syndrome induced by rituximab in diffuse large B-cell lymphoma. Int J Hematol. 2005;82:312.
- Sezer O, Vesole DH, Singhal S, et al. Bortezomib-induced tumor lysis syndrome in multiple myeloma. Clin Lymphoma Myeloma. 2006;7:233.
- Jensen M, Winkler U, Manzke O, et al. Rapid tumor lysis in a patient with B-cell chronic lymphocytic leukemia and lymphocytosis treated with an anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab). Ann Hematol. 1998;77:89.
- Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysis syndrome immediately after 4 Gy fractionated TBI as part of reduced intensity preparative regimen in a patient with T-ALL with high tumor burden. Bone Marrow Transplant. 2003;31:935.
- Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008;26(16):2767-2778. [Erratum, J Clin Oncol. 2010;28:708.]
- Cheuk DK, Chiang AK, Chan GC, Ha SY. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database Syst Rev. 2010;(6):CD006945.
- Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol. 2010;28:4207.
Case
A 25-year-old male with HIV/AIDS and a CD4 count of 65 cells/μL presents to the ED with intractable nausea and vomiting for one week. Laboratory evaluation revealed a white blood cell of 67,000 cells/mm3. An extended chemistry panel reveals creatinine 3.5 mg/dL, potassium 3.0 mmol/L, LDH 250 IU/L, and uric acid 5mg/dL. Calcium and phosphorus were both normal. The patient was admitted for further evaluation and management, and was later diagnosed with Burkitt’s lymphoma.
Overview
Tumor lysis syndrome (TLS) is an acute cell lysis of tumor cells with the release of cell content into circulation either spontaneously or in response to therapy, leading to hyperurecemia, hyperkalemia, hyperphosphatemia, and hypocalcemia.1-3
TLS is one of the most common oncology emergencies encountered by hospitalists caring for patients with hematologic malignancies. The incidence and severity of TLS depend on the cell burden, cell proliferation rate, potential for cell lysis or chemo sensitivity, baseline clinical characteristics, and preventive measures taken (see Table 1).2,4
TLS is classified as laboratory or clinical. Laboratory TLS is described as the presence of two or more of the following serum abnormalities at the same time, present within three days before or seven days after the start of therapy.5
- Uric acid >8 mg/dL (475.8 micromole/L) or 25% increase;
- Potassium >6 mEq/L (6 mmol/L) or 25% increase;
- Phosphorus >6.5 mg/dL (2.1 mmol/L) for children or >4.5 mg/dl (1.45 mmol/L) for adults or 25% increase; and
- Calcium >7 mg/dL (1.75 mmol/L) or 25% increase.
Clinical TLS is defined as laboratory TLS in association with increased creatinine levels, seizures, cardiac arrhythmias, or death (see Table 2).5
Pathogenesis
Tumor cell lysis releases DNA, cytokines, phosphate, and potassium. DNA is metabolized into adenosine and guanosine, which are then converted into xanthines. Xanthines are oxidized by xanthine oxidase into uric acid, which is then excreted through the kidneys.
TLS develops when the accumulation of xanthine, uric acid, potassium, and phosphorus exceeds the kidney’s capacity to excrete them. Cytokines cause hypotension, inflammation, and kidney injury, and worsen the kidney’s excretory capacity. Damage to the kidneys also occurs by renal precipitation of uric acid, xanthine, and calcium phosphate.4
Phosphorus concentrations in tumor cells are four times higher than in normal cells. When the calcium phosphorus product exceeds 60 mg2/dL2, there is an increased risk of calcium phosphate precipitation in the kidney tubules, which could lead to kidney failure. Accumulation of calcium phosphate product may also be cardiotoxic and can lead to cardiac arrhythmias. In addition, hyperphosphatemia can cause secondary hypocalcemia, which may lead to parasthesias, tetany, and cardiac arrhythmias.2,4
TLS is most common in tumors with high proliferative rates and high tumor burden, such as acute lymphoblastic leukemia and Burkitt’s lymphoma, but it can occur with other hematologic malignancies, such as T-cell precursor acute lymphocytic leukemia (ALL), B-cell precursor ALL, acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), anaplastic large cell lymphoma, and plasma cell disorders (e.g. multiple myeloma and plasmacytoma).6,7 TLS has also been reported with the treatment of solid organ nonhematologic tumors (see Table 3).
In hematologic tumors, TLS frequently is associated with cytotoxic chemotherapy, and less frequently with glucocorticoid treatment, monoclonal antibodies (eg, rituximab, bortezomab, imatinib), and radiation therapy.25-29
Patient factors, such as baseline kidney disease or lack of prophylactic/preventive measures for TLS, also increase the risk.4 TLS, however, can develop in patients classified as low risk (see Table 1.
TLS Prevention
Intravenous fluids. Every patient at intermediate or high risk of TLS should receive intravenous fluids (IVF) prior to cancer treatment; those at low risk may receive IVF based on the provider’s clinical judgment.30 The purpose of administering IVF is to generate high urine output to reduce the risk of precipitation of uric acid in the renal tubules.30 Both adults and children should receive approximately 2 to 3 L/m2 per day of IVF,30 and urine output should be maintained at 2 ml/kg/hr (or 4 to 6 ml/kg/hr for children <10kg).30 IVF should be cautiously administered in patients with renal insufficiency or heart failure, and diuretics may be used to maintain goal urine output. Recommended initial fluids are D51/4 normal saline, or normal saline for patients who are dehydrated or hyponatremic.30
Allopurinol. Allopurinol is usually also administered to patients at risk for developing TLS.30 Allopurinol inhibits the metabolism of hypoxanthine and xanthine to uric acid, which decreases the accumulation of uric acid in the renal tubules, thus preventing obstructive renal disease from precipitation of uric acid.4 The recommended dose of allopurinol is 100 mg/m2 every eight hours, and should not exceed 800 mg per day in adults. It should be started one to two days prior to induction chemotherapy and continued for three to seven days after the treatment and until uric acid levels and other electrolyte levels have returned to normal. The dose is adjusted to 50 mg/m2 every eight hours in patients with kidney failure.30
In some cases, allopurinol can lead to increased levels of xanthine crystals in the renal tubules, leading to acute kidney injury. Also, allopurinol does not have any effect on uric acid that has already been formed, so patients with elevated uric acid levels prior to the initiation of cancer therapy will not have any reduction in the levels of uric acid. Allopurinol reduces the degradation of other purines, so it can cause toxicity in patients on azathioprine and 6-mercaptopurine if the doses of these medications are not adjusted.
Rasburicase. Rasburicase is a recombinant urate oxidase, derived from aspergillus favus, which catalyzes the breakdown of uric acid to allantoin, which is a water-soluble product. Rasburicase is recommended as a first-line treatment for patients at high risk for clinical TLS.30 Rasburicase has an earlier onset than allopurinol and rapidly decreases serum levels of uric acid within four hours of administration.30,31 The recommended dose is 0.10 to 0.20 mg/kg once a day for five days in adults.30
A Phase III trial compared the efficiency and safety of rasburicase to rasburicase with allopurinol or allopurinol alone.32 A significantly higher normalization of uric acid was found in patients on rasburicase compared to allopurinol alone. The incidence of laboratory TLS was also significantly lower with rasburicase alone compared to allopurinol alone, and was even lower with allopurinol plus rasburicase. The incidence of acute kidney injury was the same with rasburicase alone or allopurinol alone but was higher with rasburicase plus allopurinol.
Serum uric acid, phosphorus, potassium, and calcium need to be monitored every four hours for 24 hours after the completion of chemotherapy in patients on rasburicase.4 The sample of blood drawn to check the uric acid levels has to be placed on ice and processed within four hours in order to avoid falsely lower levels of uric acid due to the conversion of uric acid to allantoin. Rasburicase is contraindicated in patients with G6PD deficiency and pregnant women, because one of the byproducts of uric acid breakdown is hydrogen peroxide, which can cause severe hemolysis and the formation of methemoglobin in these patients.30
Rasburicase has been approved for use in both children and adults, but there is more evidence for the use in children. Rasburicase has a black-box label for patients with anaphylaxis, methemoglobinemia, hemolysis, and hemoglobinuria, and there is a recommendation to check G6PD deficiency before use in high-risk patients.30
TLS Treatment
Alkalinization. Alkalinization of urine is controversial in the management of TLS. Urine alkalinization increases uric acid solubility but causes hyperphosphatemia and decreases calcium phosphate solubility, which can then deposit in the kidney once cancer treatment starts. Of note, hyperphosphatemia is much more difficult to correct than high levels of uric acid, and there are no clinical trials proving the superiority of urine alkalinization over normal saline.
Normalization of electrolytes. Electrolyte abnormalities should be corrected to avoid arrhythmias and seizures. Phosphorus levels >6.5 mg/dl (2.1 mmol/L) should be managed by restricting phosphorus intake, and by the use of phosphate binders (calcium acetate, calcium carbonate, sevelamer, lanthanum, or aluminum hydroxide). Aluminum hydroxide should be avoided in patients with renal insufficiency. In severe cases of hyperphosphatemia, dialysis should be considered.
Symptomatic hypocalcemia should be treated with calcium gluconate if changes are present on the electrocardiography (ECG). Hypocalcemia in the presence of hyperphosphatemia should be treated only in patients with tetany or cardiac arrhythmias; otherwise, hypocalcemia should not be treated until hyperphosphatemia has been corrected.
In cases of hyperkalemia, patients should be placed on a cardiac monitor and stabilized with calcium gluconate; kayexalate should be administered to reduce total body potassium. Other interventions, such as intravenous insulin given with dextrose, sodium bicarbonate, and albuterol, have a temporary effect on hyperkalemia and can be used as adjunct treatments in patients with severe hyperkalemia (>7). Hemodialysis should be strongly considered in severe cases of hyperkalemia, particularly in patients with persistently elevated potassium levels despite other treatments.
Back to the Case
Our patient was started on IVFs with close monitoring of his urine output. He was considered intermediate risk for developing TLS. Allopurinol, renally dosed, was administered for two days prior to initiating treatment with rituximab plus chemotherapy. His chemistry panel was monitored daily and he did not develop any form of TLS.
Bottom Line
TLS is a common oncology emergency in patients with hematologic malignancies. Preventative measures include starting IVF prior to cancer treatment, and administering allopurinol and/or rasburicase to patients at risk of developing TLS. Treatment should include normalizing electrolytes to avoid arrhythmias and seizures.
Dr. Akwe is assistant professor of medicine at the Emory University School of Medicine and a clinical instructor of medicine at the Morehouse School of Medicine, both in Atlanta. Dr. Smith is an assistant director for education in the division of hospital medicine at Emory. Both work as hospitalists at the Atlanta VA Medical Center.
References
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55:Suppl 3:S1-S13.
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578-586.
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179-180.
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med. 2011;364:1844.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127:3.
- Wössmann W, Schrappe M, Meyer U, et al. Incidence of tumor lysis syndrome in children with advanced stage Burkitt’s lymphoma/leukemia before and after introduction of prophylactic use of urate oxidase. Ann Hematol. 2003;82:160.
- Hussain K, Mazza JJ, Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy Gemici C. Tumor lysis syndrome in solid tumors. J Clin Oncol. 2009;27:2738-2739
- Rostom AY, El-Hussainy G, Kandil A, Allam A. Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer. Ann Oncol. 2000;11:1349.
- Drakos P, Bar-Ziv J, Catane R. Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature. Am J Clin Oncol. 1994;17:502.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51:187.
- Kalemkerian GP, Darwish B, Varterasian ML. Tumor lysis syndrome in small cell carcinoma and other solid tumors. Am J Med. 1997;103:363.
- Noh GY, Choe DH, Kim CH, Lee JC. Fatal tumor lysis syndrome during radiotherapy for non-small-cell lung cancer. J Clin Oncol. 2008;26:6005-6006.
- Pentheroudakis G, O’Neill VJ, Vasey P, Kaye SB. Spontaneous acute tumour lysis syndrome in patients with metastatic germ cell tumours. Report of two cases. Support Care Cancer. 2001;9:554.
- Joshita S, Yoshizawa K, Sano K, et al., A patient with advanced hepatocellular carcinoma treated with sorafenib tosylate showed massive tumor lysis with avoidance of tumor lysis syndrome. Intern Med. 2010;49:991-994.
- Huang WS, Yang CH. Sorafenib-induced tumor lysis syndrome in an advanced hepatocellular carcinoma patient. World J Gastroenterol. 2009;15:4464-4466.
- Bilgrami SF, Fallon BG. Tumor lysis syndrome after combination chemotherapy for ovarian cancer. Med Pediatr Oncol. 1993;21:521.
- Chan JK, Lin SS, McMeekin DS, Berman ML. Patients with malignancy requiring urgent therapy: CASE 3. Tumor lysis syndrome associated with chemotherapy in ovarian cancer. J Clin Oncol. 2005;23:6794.
- Godoy H, Kesterson JP, Lele S. Tumor lysis syndrome associated with carboplatin and paclitaxel in a woman with recurrent endometrial cancer. Int J Gynaecol Obstet. 2010;109:254.
- Shamseddine AI, Khalil AM, Wehbeh MH. Acute tumor lysis syndrome with squamous cell carcinoma of the vulva. Gynecol Oncol 1993;51:258
- Pinder EM, Atwal GS, Ayantunde AA, et al. Tumour lysis syndrome occurring in a patient with metastatic gastrointestinal stromal tumour treated with Glivec (imatinib mesylate, Gleevec, STI571). Sarcoma. 2007;2007:82012.
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406-2408.
- Oztop I, Demirkan B, Yaren A, et al. Rapid tumor lysis syndrome in a patient with metastatic colon cancer as a complication of treatment with 5-fluorouracil/leucoverin and irinotecan. Tumori. 2004;90:514.
- Lin CJ, Lim KH, Cheng YC, et al. Tumor lysis syndrome after treatment with gemcitabine for metastatic transitional cell carcinoma. Med Oncol. 2007;24:455.
- Malik IA, Abubakar S, Alam F, Khan A. Dexamethasone-induced tumor lysis syndrome in high-grade non-Hodgkin’s lymphoma. South Med J. 1994;87:409.
- Jabr FI. Acute tumor lysis syndrome induced by rituximab in diffuse large B-cell lymphoma. Int J Hematol. 2005;82:312.
- Sezer O, Vesole DH, Singhal S, et al. Bortezomib-induced tumor lysis syndrome in multiple myeloma. Clin Lymphoma Myeloma. 2006;7:233.
- Jensen M, Winkler U, Manzke O, et al. Rapid tumor lysis in a patient with B-cell chronic lymphocytic leukemia and lymphocytosis treated with an anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab). Ann Hematol. 1998;77:89.
- Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysis syndrome immediately after 4 Gy fractionated TBI as part of reduced intensity preparative regimen in a patient with T-ALL with high tumor burden. Bone Marrow Transplant. 2003;31:935.
- Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008;26(16):2767-2778. [Erratum, J Clin Oncol. 2010;28:708.]
- Cheuk DK, Chiang AK, Chan GC, Ha SY. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database Syst Rev. 2010;(6):CD006945.
- Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol. 2010;28:4207.
Hospital ICUs Chart Progress in Preventing Central-Line-Associated Bloodstream Infections
New CDC research published in the June issue of Infection Control and Hospital Epidemiology estimates that as many as 200,000 central-line-associated bloodstream infections (CLABSIs) in ICUs nationally have been prevented since 1990.3 The report indicates much of the success is due to U.S. hospitals adopting successful prevention strategies, namely the dissemination of guideline-supported central-line insertion and maintenance best practices, infection-control treatment bundles, and widespread availability of alcohol-based hand rubs.
Between 462,000 and 636,000 CLABSIs occurred in non-neonatal ICU patients from 1990-2010, CDC estimates, about 104,000 to 198,000 less CLABSIs than would have occurred if rates had remained the same as they were in 1990.
“These findings suggest that technical innovations and dissemination of evidence-based CLABSI prevention practices have likely been effective on a national scale,” Matthew Wise, PhD, lead author of the study, said in a statement.
At the same time, a CLABSI-reduction intervention in a hospital in Hawaii found that while the costs of care were much higher for patients who developed a CLABSI, reimbursement and the hospital’s margin also were higher (margin of $54,906 vs. $6,506).4 The authors conclude that current reimbursement practices offer a perverse incentive for hospitals to have more line infections, “while an optimal reimbursement system would reward them for prevention rather than treating illness.”
Lead author Eugene Hsu, MD, MBA, of Johns Hopkins University School of Medicine said in an email that the study demonstrates how a quality initiative led by providers and funded by a major commercial insurer can save both lives and money. “Hospitalists, like all healthcare providers, must be aware of the distorted financial incentives that may affect how they provide care to patients,” Dr. Hsu said.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Stobbe, M. Germ-zapping “robots”: Hospitals combat superbugs. Associated Press website. Available at: http://bigstory.ap.org/article/hospitals-see-surge-superbug-fighting-products. Accessed June 7, 2013.
- Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6209a3.htm?s_cid=mm6209a3_w. Accessed June 7, 2013.
- Wise ME, Scott RD, Baggs JM, et al. National estimates of central line-associated bloodstream infections in critical care patients. Infect Control Hosp Epidemiol, 2013;34(6):547-554.
- Hsu E, Lin D, Evans SJ, et al. Doing well by doing good: assessing the cost savings of an intervention to reduce central line-associated bloodstream infections in a Hawaii hospital. Am J Med Qual, 2013 May 7 [Epub ahead of print].
- Association of American Medical Colleges. Medical school enrollment on pace to reach 30 percent increase by 2017. Association of American Medical Colleges website. Available at: https://www.aamc.org/newsroom/newsreleases/ 335244/050213.html. Accessed June 7, 2013.
New CDC research published in the June issue of Infection Control and Hospital Epidemiology estimates that as many as 200,000 central-line-associated bloodstream infections (CLABSIs) in ICUs nationally have been prevented since 1990.3 The report indicates much of the success is due to U.S. hospitals adopting successful prevention strategies, namely the dissemination of guideline-supported central-line insertion and maintenance best practices, infection-control treatment bundles, and widespread availability of alcohol-based hand rubs.
Between 462,000 and 636,000 CLABSIs occurred in non-neonatal ICU patients from 1990-2010, CDC estimates, about 104,000 to 198,000 less CLABSIs than would have occurred if rates had remained the same as they were in 1990.
“These findings suggest that technical innovations and dissemination of evidence-based CLABSI prevention practices have likely been effective on a national scale,” Matthew Wise, PhD, lead author of the study, said in a statement.
At the same time, a CLABSI-reduction intervention in a hospital in Hawaii found that while the costs of care were much higher for patients who developed a CLABSI, reimbursement and the hospital’s margin also were higher (margin of $54,906 vs. $6,506).4 The authors conclude that current reimbursement practices offer a perverse incentive for hospitals to have more line infections, “while an optimal reimbursement system would reward them for prevention rather than treating illness.”
Lead author Eugene Hsu, MD, MBA, of Johns Hopkins University School of Medicine said in an email that the study demonstrates how a quality initiative led by providers and funded by a major commercial insurer can save both lives and money. “Hospitalists, like all healthcare providers, must be aware of the distorted financial incentives that may affect how they provide care to patients,” Dr. Hsu said.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Stobbe, M. Germ-zapping “robots”: Hospitals combat superbugs. Associated Press website. Available at: http://bigstory.ap.org/article/hospitals-see-surge-superbug-fighting-products. Accessed June 7, 2013.
- Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6209a3.htm?s_cid=mm6209a3_w. Accessed June 7, 2013.
- Wise ME, Scott RD, Baggs JM, et al. National estimates of central line-associated bloodstream infections in critical care patients. Infect Control Hosp Epidemiol, 2013;34(6):547-554.
- Hsu E, Lin D, Evans SJ, et al. Doing well by doing good: assessing the cost savings of an intervention to reduce central line-associated bloodstream infections in a Hawaii hospital. Am J Med Qual, 2013 May 7 [Epub ahead of print].
- Association of American Medical Colleges. Medical school enrollment on pace to reach 30 percent increase by 2017. Association of American Medical Colleges website. Available at: https://www.aamc.org/newsroom/newsreleases/ 335244/050213.html. Accessed June 7, 2013.
New CDC research published in the June issue of Infection Control and Hospital Epidemiology estimates that as many as 200,000 central-line-associated bloodstream infections (CLABSIs) in ICUs nationally have been prevented since 1990.3 The report indicates much of the success is due to U.S. hospitals adopting successful prevention strategies, namely the dissemination of guideline-supported central-line insertion and maintenance best practices, infection-control treatment bundles, and widespread availability of alcohol-based hand rubs.
Between 462,000 and 636,000 CLABSIs occurred in non-neonatal ICU patients from 1990-2010, CDC estimates, about 104,000 to 198,000 less CLABSIs than would have occurred if rates had remained the same as they were in 1990.
“These findings suggest that technical innovations and dissemination of evidence-based CLABSI prevention practices have likely been effective on a national scale,” Matthew Wise, PhD, lead author of the study, said in a statement.
At the same time, a CLABSI-reduction intervention in a hospital in Hawaii found that while the costs of care were much higher for patients who developed a CLABSI, reimbursement and the hospital’s margin also were higher (margin of $54,906 vs. $6,506).4 The authors conclude that current reimbursement practices offer a perverse incentive for hospitals to have more line infections, “while an optimal reimbursement system would reward them for prevention rather than treating illness.”
Lead author Eugene Hsu, MD, MBA, of Johns Hopkins University School of Medicine said in an email that the study demonstrates how a quality initiative led by providers and funded by a major commercial insurer can save both lives and money. “Hospitalists, like all healthcare providers, must be aware of the distorted financial incentives that may affect how they provide care to patients,” Dr. Hsu said.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Stobbe, M. Germ-zapping “robots”: Hospitals combat superbugs. Associated Press website. Available at: http://bigstory.ap.org/article/hospitals-see-surge-superbug-fighting-products. Accessed June 7, 2013.
- Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6209a3.htm?s_cid=mm6209a3_w. Accessed June 7, 2013.
- Wise ME, Scott RD, Baggs JM, et al. National estimates of central line-associated bloodstream infections in critical care patients. Infect Control Hosp Epidemiol, 2013;34(6):547-554.
- Hsu E, Lin D, Evans SJ, et al. Doing well by doing good: assessing the cost savings of an intervention to reduce central line-associated bloodstream infections in a Hawaii hospital. Am J Med Qual, 2013 May 7 [Epub ahead of print].
- Association of American Medical Colleges. Medical school enrollment on pace to reach 30 percent increase by 2017. Association of American Medical Colleges website. Available at: https://www.aamc.org/newsroom/newsreleases/ 335244/050213.html. Accessed June 7, 2013.
Four Factors Physicians Should Consider Before Job Termination

Leaving a job is never an easy decision, whether it is made voluntarily or not. A physician terminating a relationship with an employer may face emotionally charged conversations, difficult financial considerations, and long-term legal consequences. As you plan your exit strategy, it is critical for you to be aware of these issues and address them proactively with your employer. This can minimize hard feelings and surprises down the road for you, your former employer, and your colleagues.
In today’s competitive climate, a physician might work for several employers during the length of his or her career. With the tighter financial medical market and pressures from managed care mounting, employers are less likely to tolerate a nonproductive employee. Interoffice or personality conflicts may become intolerable for an unhappy or stressed physician. Physician turnover is a more common occurrence, and if not handled properly, it can be disruptive for all parties involved.
The following steps are meant for physicians contemplating leaving their place of employment or who may be asked to leave in the near future.
Step 1: Consider the Employment Agreement
Ideally, physician-separation matters are addressed preemptively when the physician enters the employer-employee relationship and signs an employment agreement. Thus, before contemplating a move, you should always start by reviewing the terms of your current employment agreement. A well-drafted employment agreement should specify the grounds for termination, both for cause (i.e. a specific set of reasons for immediate termination) and without cause (i.e. either party may terminate voluntarily). The agreement should specify the parties’ rights and obligations following a termination. These rights and obligations likely will vary depending on the basis for termination.
Typically, an employer will provide malpractice insurance for its physicians during the term of employment. However, physicians may be responsible for the cost of “tail coverage” upon the termination of employment. This is designed to protect the departing physician’s professional acts after leaving the employ of an employer with claims-made coverage. Because the coverage can be quite costly, a well-drafted employment agreement often will set forth which party is responsible for the procurement and payment of tail coverage. It is prudent for a departing physician to review the employment agreement to identify who has the affirmative obligation to provide the tail coverage, as it can be a costly surprise at termination.
The employment agreement also must be reviewed to determine the proper method to provide notice of termination (such as first-class mail, overnight courier, or hand delivery). Often, employment agreements will include a clause titled “Notice” that outlines the delivery method for proper notice to the employer.
Step 2: Consider a Termination/Separation Agreement
Entering into a termination agreement (sometimes referred to as a separation agreement) between the departing physician and the employer may address and resolve many of the outstanding issues that are not otherwise addressed in the employment agreement. A termination agreement may avoid unnecessary problems down the road and potentially acrimonious and costly litigation.
The termination agreement can fill in the gaps where the employment agreement is silent (or if an employment agreement does not exist). The key elements of a termination agreement often include:
- The effective date of the separation as well as what exactly is ending (e.g. employment, co-ownership, board membership, medical staff privileges);
- Payment and buyout terms;
- The physician’s removal from any management or administrative position (e.g. member of the governing board);
- Deferred compensation payments or severance pay that may need to be calculated and distributed;
- Employer obligations (if any) to provide the departing physician’s fringe benefits and business expenses, including retirement-plan contributions, health insurance, life insurance, medical dues, etc.; and
- Unused vacation days, bonuses, or expenses due.
If previously addressed in the employment agreement, the parties should reaffirm their respective rights and obligations regarding medical records, confidential information, noncompetition and nonsolicitation provisions. Otherwise, the termination agreement should identify the physician’s competitive and solicitation activities post-termination.
A noncompetition provision should include the geographic territory in which and the time period during which the departing physician cannot compete with the former employer. It is important to remember courts will render these provisions as unenforceable and invalid if improperly drafted or overly broad. It is common to see nondisparagement provisions, whereby each party agrees to refrain from making any negative or false statements regarding the other. Nondisclosure provisions are common as well with regards to what may be disclosed to third parties.
The separation agreement also should address the return of company property, including office key, credit card, computer, cell phone, and beeper. Patient records and charts should be completed and returned to the employer. Often, the departing physician will still be allowed reasonable access to patient records post-termination for certain authorized purposes (e.g. defending disciplinary actions, malpractice claims, and billing/payer claims and audits), usually at the physician’s own expense.
The termination agreement may also outline how patients will be notified about the physician’s departure. If a patient wishes to continue treatment with the departing physician, the former employer must be ready to transition the patient.
A well-written termination agreement will provide for mutual releases. However, there are often exclusions from the mutual releases, such as pre-termination date liabilities; medical malpractice claims resulting from the physician’s misconduct; or taxes, interests, and penalties covering the pre-termination date.
Step 3: Severance Pay
Depending on the circumstances surrounding the termination and employment agreements, a physician may be entitled to severance payments beginning on the date of termination and/or for a period of time post-termination. The departing physician should determine whether severance is appropriate and whether he or she is willing to forego severance payments in exchange for other benefits. Depending on the dollar amount and the physician’s career objectives, it may be worthwhile to sacrifice severance payments for a less onerous noncompete provision, for example.
Step 4: Take the High Road
Because you never know when your paths might cross with former coworkers or employers, it is always sensible to remain discreet and level-headed during this trying period. Although it is natural to discuss an impending move with others, a prudent physician will avoid water-cooler gossip.
In the event conflicts arise, limit the public disclosure of these disputes. Neither side wins the public relations battle, and often, both sides lose. This is a circumstance where experienced legal counsel can be invaluable as you navigate these potentially rocky waters. You would be well served to seek legal advice to discuss your intentions before making an actual move.
As always, remember conversations you have with counsel are typically protected by attorney-client privilege. It is always advisable to secure legal counsel to review the terms of an employment agreement, negotiate a fair termination/separation agreement, and serve as an advocate during this challenging career move.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Leaving a job is never an easy decision, whether it is made voluntarily or not. A physician terminating a relationship with an employer may face emotionally charged conversations, difficult financial considerations, and long-term legal consequences. As you plan your exit strategy, it is critical for you to be aware of these issues and address them proactively with your employer. This can minimize hard feelings and surprises down the road for you, your former employer, and your colleagues.
In today’s competitive climate, a physician might work for several employers during the length of his or her career. With the tighter financial medical market and pressures from managed care mounting, employers are less likely to tolerate a nonproductive employee. Interoffice or personality conflicts may become intolerable for an unhappy or stressed physician. Physician turnover is a more common occurrence, and if not handled properly, it can be disruptive for all parties involved.
The following steps are meant for physicians contemplating leaving their place of employment or who may be asked to leave in the near future.
Step 1: Consider the Employment Agreement
Ideally, physician-separation matters are addressed preemptively when the physician enters the employer-employee relationship and signs an employment agreement. Thus, before contemplating a move, you should always start by reviewing the terms of your current employment agreement. A well-drafted employment agreement should specify the grounds for termination, both for cause (i.e. a specific set of reasons for immediate termination) and without cause (i.e. either party may terminate voluntarily). The agreement should specify the parties’ rights and obligations following a termination. These rights and obligations likely will vary depending on the basis for termination.
Typically, an employer will provide malpractice insurance for its physicians during the term of employment. However, physicians may be responsible for the cost of “tail coverage” upon the termination of employment. This is designed to protect the departing physician’s professional acts after leaving the employ of an employer with claims-made coverage. Because the coverage can be quite costly, a well-drafted employment agreement often will set forth which party is responsible for the procurement and payment of tail coverage. It is prudent for a departing physician to review the employment agreement to identify who has the affirmative obligation to provide the tail coverage, as it can be a costly surprise at termination.
The employment agreement also must be reviewed to determine the proper method to provide notice of termination (such as first-class mail, overnight courier, or hand delivery). Often, employment agreements will include a clause titled “Notice” that outlines the delivery method for proper notice to the employer.
Step 2: Consider a Termination/Separation Agreement
Entering into a termination agreement (sometimes referred to as a separation agreement) between the departing physician and the employer may address and resolve many of the outstanding issues that are not otherwise addressed in the employment agreement. A termination agreement may avoid unnecessary problems down the road and potentially acrimonious and costly litigation.
The termination agreement can fill in the gaps where the employment agreement is silent (or if an employment agreement does not exist). The key elements of a termination agreement often include:
- The effective date of the separation as well as what exactly is ending (e.g. employment, co-ownership, board membership, medical staff privileges);
- Payment and buyout terms;
- The physician’s removal from any management or administrative position (e.g. member of the governing board);
- Deferred compensation payments or severance pay that may need to be calculated and distributed;
- Employer obligations (if any) to provide the departing physician’s fringe benefits and business expenses, including retirement-plan contributions, health insurance, life insurance, medical dues, etc.; and
- Unused vacation days, bonuses, or expenses due.
If previously addressed in the employment agreement, the parties should reaffirm their respective rights and obligations regarding medical records, confidential information, noncompetition and nonsolicitation provisions. Otherwise, the termination agreement should identify the physician’s competitive and solicitation activities post-termination.
A noncompetition provision should include the geographic territory in which and the time period during which the departing physician cannot compete with the former employer. It is important to remember courts will render these provisions as unenforceable and invalid if improperly drafted or overly broad. It is common to see nondisparagement provisions, whereby each party agrees to refrain from making any negative or false statements regarding the other. Nondisclosure provisions are common as well with regards to what may be disclosed to third parties.
The separation agreement also should address the return of company property, including office key, credit card, computer, cell phone, and beeper. Patient records and charts should be completed and returned to the employer. Often, the departing physician will still be allowed reasonable access to patient records post-termination for certain authorized purposes (e.g. defending disciplinary actions, malpractice claims, and billing/payer claims and audits), usually at the physician’s own expense.
The termination agreement may also outline how patients will be notified about the physician’s departure. If a patient wishes to continue treatment with the departing physician, the former employer must be ready to transition the patient.
A well-written termination agreement will provide for mutual releases. However, there are often exclusions from the mutual releases, such as pre-termination date liabilities; medical malpractice claims resulting from the physician’s misconduct; or taxes, interests, and penalties covering the pre-termination date.
Step 3: Severance Pay
Depending on the circumstances surrounding the termination and employment agreements, a physician may be entitled to severance payments beginning on the date of termination and/or for a period of time post-termination. The departing physician should determine whether severance is appropriate and whether he or she is willing to forego severance payments in exchange for other benefits. Depending on the dollar amount and the physician’s career objectives, it may be worthwhile to sacrifice severance payments for a less onerous noncompete provision, for example.
Step 4: Take the High Road
Because you never know when your paths might cross with former coworkers or employers, it is always sensible to remain discreet and level-headed during this trying period. Although it is natural to discuss an impending move with others, a prudent physician will avoid water-cooler gossip.
In the event conflicts arise, limit the public disclosure of these disputes. Neither side wins the public relations battle, and often, both sides lose. This is a circumstance where experienced legal counsel can be invaluable as you navigate these potentially rocky waters. You would be well served to seek legal advice to discuss your intentions before making an actual move.
As always, remember conversations you have with counsel are typically protected by attorney-client privilege. It is always advisable to secure legal counsel to review the terms of an employment agreement, negotiate a fair termination/separation agreement, and serve as an advocate during this challenging career move.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Leaving a job is never an easy decision, whether it is made voluntarily or not. A physician terminating a relationship with an employer may face emotionally charged conversations, difficult financial considerations, and long-term legal consequences. As you plan your exit strategy, it is critical for you to be aware of these issues and address them proactively with your employer. This can minimize hard feelings and surprises down the road for you, your former employer, and your colleagues.
In today’s competitive climate, a physician might work for several employers during the length of his or her career. With the tighter financial medical market and pressures from managed care mounting, employers are less likely to tolerate a nonproductive employee. Interoffice or personality conflicts may become intolerable for an unhappy or stressed physician. Physician turnover is a more common occurrence, and if not handled properly, it can be disruptive for all parties involved.
The following steps are meant for physicians contemplating leaving their place of employment or who may be asked to leave in the near future.
Step 1: Consider the Employment Agreement
Ideally, physician-separation matters are addressed preemptively when the physician enters the employer-employee relationship and signs an employment agreement. Thus, before contemplating a move, you should always start by reviewing the terms of your current employment agreement. A well-drafted employment agreement should specify the grounds for termination, both for cause (i.e. a specific set of reasons for immediate termination) and without cause (i.e. either party may terminate voluntarily). The agreement should specify the parties’ rights and obligations following a termination. These rights and obligations likely will vary depending on the basis for termination.
Typically, an employer will provide malpractice insurance for its physicians during the term of employment. However, physicians may be responsible for the cost of “tail coverage” upon the termination of employment. This is designed to protect the departing physician’s professional acts after leaving the employ of an employer with claims-made coverage. Because the coverage can be quite costly, a well-drafted employment agreement often will set forth which party is responsible for the procurement and payment of tail coverage. It is prudent for a departing physician to review the employment agreement to identify who has the affirmative obligation to provide the tail coverage, as it can be a costly surprise at termination.
The employment agreement also must be reviewed to determine the proper method to provide notice of termination (such as first-class mail, overnight courier, or hand delivery). Often, employment agreements will include a clause titled “Notice” that outlines the delivery method for proper notice to the employer.
Step 2: Consider a Termination/Separation Agreement
Entering into a termination agreement (sometimes referred to as a separation agreement) between the departing physician and the employer may address and resolve many of the outstanding issues that are not otherwise addressed in the employment agreement. A termination agreement may avoid unnecessary problems down the road and potentially acrimonious and costly litigation.
The termination agreement can fill in the gaps where the employment agreement is silent (or if an employment agreement does not exist). The key elements of a termination agreement often include:
- The effective date of the separation as well as what exactly is ending (e.g. employment, co-ownership, board membership, medical staff privileges);
- Payment and buyout terms;
- The physician’s removal from any management or administrative position (e.g. member of the governing board);
- Deferred compensation payments or severance pay that may need to be calculated and distributed;
- Employer obligations (if any) to provide the departing physician’s fringe benefits and business expenses, including retirement-plan contributions, health insurance, life insurance, medical dues, etc.; and
- Unused vacation days, bonuses, or expenses due.
If previously addressed in the employment agreement, the parties should reaffirm their respective rights and obligations regarding medical records, confidential information, noncompetition and nonsolicitation provisions. Otherwise, the termination agreement should identify the physician’s competitive and solicitation activities post-termination.
A noncompetition provision should include the geographic territory in which and the time period during which the departing physician cannot compete with the former employer. It is important to remember courts will render these provisions as unenforceable and invalid if improperly drafted or overly broad. It is common to see nondisparagement provisions, whereby each party agrees to refrain from making any negative or false statements regarding the other. Nondisclosure provisions are common as well with regards to what may be disclosed to third parties.
The separation agreement also should address the return of company property, including office key, credit card, computer, cell phone, and beeper. Patient records and charts should be completed and returned to the employer. Often, the departing physician will still be allowed reasonable access to patient records post-termination for certain authorized purposes (e.g. defending disciplinary actions, malpractice claims, and billing/payer claims and audits), usually at the physician’s own expense.
The termination agreement may also outline how patients will be notified about the physician’s departure. If a patient wishes to continue treatment with the departing physician, the former employer must be ready to transition the patient.
A well-written termination agreement will provide for mutual releases. However, there are often exclusions from the mutual releases, such as pre-termination date liabilities; medical malpractice claims resulting from the physician’s misconduct; or taxes, interests, and penalties covering the pre-termination date.
Step 3: Severance Pay
Depending on the circumstances surrounding the termination and employment agreements, a physician may be entitled to severance payments beginning on the date of termination and/or for a period of time post-termination. The departing physician should determine whether severance is appropriate and whether he or she is willing to forego severance payments in exchange for other benefits. Depending on the dollar amount and the physician’s career objectives, it may be worthwhile to sacrifice severance payments for a less onerous noncompete provision, for example.
Step 4: Take the High Road
Because you never know when your paths might cross with former coworkers or employers, it is always sensible to remain discreet and level-headed during this trying period. Although it is natural to discuss an impending move with others, a prudent physician will avoid water-cooler gossip.
In the event conflicts arise, limit the public disclosure of these disputes. Neither side wins the public relations battle, and often, both sides lose. This is a circumstance where experienced legal counsel can be invaluable as you navigate these potentially rocky waters. You would be well served to seek legal advice to discuss your intentions before making an actual move.
As always, remember conversations you have with counsel are typically protected by attorney-client privilege. It is always advisable to secure legal counsel to review the terms of an employment agreement, negotiate a fair termination/separation agreement, and serve as an advocate during this challenging career move.
Steven M. Harris, Esq., is a nationally recognized healthcare attorney and a member of the law firm McDonald Hopkins LLC in Chicago. Write to him at [email protected].
Upcoming guidelines on inherited arrhythmias contain surprises
DENVER – Major new guidelines on the diagnosis and management of patients with inherited primary arrhythmia syndromes have been jointly issued by the Heart Rhythm Society and its European and Asian counterparts.
The guidelines were sorely needed, according to Dr. Silvia G. Priori, cochair of the expert consensus panel writing group.
The field of inherited arrhythmias is rapidly evolving, with new pathogenic genetic mutations being found all the time. Much has changed in the 7 years since issuance of the last major guidelines: the American College of Cardiology/American Heart Association/European Society of Cardiology guidelines on prevention of sudden cardiac death (Circulation 2006;114:e385-484), noted Dr. Priori of the University of Pavia (Italy).

Her cochair, Dr. Arthur A. Wilde of the University of Amsterdam pointed out that the new 69-page report is the first major document to address some of the newer inherited arrhythmia syndromes, including catecholaminergic polymorphic ventricular tachycardia (CPVT), short QT syndrome, early repolarization, and progressive cardiac conduction disease (PCCD). In addition, the new report proposes major changes in the diagnostic criteria for the two most common primary arrhythmia syndromes: long QT syndrome (LQTS) and Brugada syndrome.
"Many of our colleagues in the field will be surprised," Dr. Priori predicted.
Here are the highlights:
• LQTS: With an estimated prevalence of roughly 1 per 2,000 live births worldwide, this is the most common of the inherited arrhythmia syndromes. What is likely to come as a surprise to many physicians is the expert consensus panel’s recommendation that the diagnosis of LQTS requires either the finding of an unequivocally causative mutation in one of the LQTS genes or, in the absence of such a defect, either a QTc interval of 480-499 ms in repeated 12-lead ECGs in a patient with unexplained syncope or a QTc of 500 ms in repeated ECGs in the absence of a secondary cause for QT prolongation in a nonsyncopal patient.
"A single ECG reading 10 ms above the upper limit of normal is not enough to establish the diagnosis. That’s quite different from what’s being done in common practice. Many of the patients who are referred to the centers of expertise on inherited arrhythmias are borderline patients in whom maybe one ECG was abnormal, and yet because of that they’ve been labeled as being affected by a genetic disease even if the genetic studies were negative. A single abnormal QTc measurement in a patient with negative genetic testing is not enough," Dr. Priori declared.
Dr. Wilde said the new guidelines loosen up the guidance on participation in competitive sports. The blanket prohibition of the past has been replaced by a case-by-case approach, with a Class I recommendation for routine referral to a clinical expert for evaluation of the risk posed by athletic activity. For example, although swimming is a very-high-risk activity for patients with the LQTS1 genotype, that’s not true for those who have LQTS2 or -3.
"It’s clear that if a patient with long QT syndrome has exercise-related syncopal events, that patient should not participate in competitive sports. But if the patient is asymptomatic and has minor QT prolongation, there’s probably not much reason for concern," he said.

"This is a sharp departure," Dr. Priori observed. "In several European countries, if you have the diagnosis of long QT syndrome, sports participation is not permitted, even if your physician clears you. So we hope with this document to slowly, carefully, begin to allow patients with this condition to do sports safely. We wanted to lift the ban so that a physician who feels a specific patient would have a low risk in the proper environment could make that recommendation."
• Brugada syndrome: Far more common in Asia than the western world, Brugada syndrome is 8- to 10-fold more frequent in males than females. The big change in the new guidelines is that the diagnosis no longer requires specific ECG changes plus clinical manifestations. Now, Brugada syndrome, like LQTS, is a pure ECG diagnosis. It is made definitively when a type 1 ST-segment elevation is noted either spontaneously or after administration of an intravenous sodium channel-blocking agent; the ST finding has to be observed in at least one right precordial lead placed in a standard or superior position up to the second intercostal space.
An implantable cardioverter-defibrillator is clearly indicated in a Brugada syndrome patient with a prior cardiac arrest or documented ventricular arrhythmias. The controversy lies in how to manage the asymptomatic patient. The guidelines give ICD implantation a weak Class IIb recommendation – meaning it "may be considered" – when such patients exhibit inducible ventricular arrhythmias during programmed electrical stimulation in the electrophysiology lab.
• Catecholaminergic polymorphic ventricular tachycardia: The prevalence of CPVT is unclear, but it has been estimated at 1 per 5,000 live births, according to Dr. Wilde. This highly malignant condition is diagnosed in patients with a known pathogenic mutation, or in the presence of a structurally normal heart, a normal resting ECG, and unexplained exercise- or catecholamine-induced bidirectional VT of polymorphic ventricular premature beats or VT before age 40 years. First-line therapy is a long-acting beta-blocker such as nadolol, coupled with exercise restriction. ICD therapy is problematic because the inevitable inappropriate shocks increase sympathetic tone, triggering true shockable arrhythmias in a vicious cycle.
• Short QT syndrome: This is a rare channelopathy. It is diagnosed on the basis of a QTc of 330 ms or less, or a QTc of less than 360 ms in the presence of a pathogenic mutation, family history of sudden death before age 40 years, cardiac arrest in the absence of structural heart disease, or a family history of short QT syndrome.
• Progressive cardiac conduction disease: Still incompletely understood, PCCD is diagnosed in individuals under age 50 years who have unexplained progressive conduction abnormalities and a structurally normal heart with no skeletal myopathies. Pacemaker implantation is the most useful therapy.
• Early repolarization: The first report linking this extremely common ECG finding to sudden death came less than 5 years ago. Early repolarization, as characterized by J-point and ST-segment elevation in two or more contiguous leads, is present in up to 10% of normal individuals. In preparticipation athletic screening programs, it can be found in up to 15%-20% of subjects.
"There’s no reason for concern if that’s the only thing you find. It’s something you shouldn’t even communicate if there is no other issue. If a patient with early repolarization has no symptoms and no family history of premature sudden death, just leave it," Dr. Wilde advised.
On the other hand, if a patient with the early repolarization ECG pattern in two or more contiguous inferior and/or lateral leads experiences exercise-induced syncopal symptoms, further evaluation is warranted. Given how common and generally benign the early repolarization ECG pattern is, the expert panel recommended a conservative approach to diagnosis, urging that the formal diagnosis of early repolarization syndrome be restricted largely to those with the characteristic ECG findings who in addition have been resuscitated from unexplained ventricular fibrillation or polymorphic VT.
Dr. Priori emphasized that the guidelines have as a Class I recommendation that patients with a diagnosed or suspected inherited arrhythmia syndrome that can result in sudden cardiac death – and their first-degree relatives, as well – should be evaluated in a specialized multidisciplinary inherited arrhythmia clinic. Such clinics are more common in Europe than the United States; however, thought leaders in American electrophysiology now recognize that the increasing complexity of the field requires that more of these dedicated clinics be created in the United States, she said.
The expert consensus statement was a joint project of the Heart Rhythm Society, the European Heart Rhythm Association, and the Asia Pacific Heart Rhythm Society. The document is available at the HRS website and will be published this fall in Heart Rhythm, EP Europace, and the Journal of Arrhythmias.
Dr. Priori reported serving as a consultant to Medtronic, Boston Scientific, Biotronic, and Transgenomic. Dr. Wilde disclosed serving as a consultant to Sorin.
inherited primary arrhythmia, Dr. Silvia G. Priori, arrythmia guidelines, Arthur Wilde
DENVER – Major new guidelines on the diagnosis and management of patients with inherited primary arrhythmia syndromes have been jointly issued by the Heart Rhythm Society and its European and Asian counterparts.
The guidelines were sorely needed, according to Dr. Silvia G. Priori, cochair of the expert consensus panel writing group.
The field of inherited arrhythmias is rapidly evolving, with new pathogenic genetic mutations being found all the time. Much has changed in the 7 years since issuance of the last major guidelines: the American College of Cardiology/American Heart Association/European Society of Cardiology guidelines on prevention of sudden cardiac death (Circulation 2006;114:e385-484), noted Dr. Priori of the University of Pavia (Italy).
Her cochair, Dr. Arthur A. Wilde of the University of Amsterdam pointed out that the new 69-page report is the first major document to address some of the newer inherited arrhythmia syndromes, including catecholaminergic polymorphic ventricular tachycardia (CPVT), short QT syndrome, early repolarization, and progressive cardiac conduction disease (PCCD). In addition, the new report proposes major changes in the diagnostic criteria for the two most common primary arrhythmia syndromes: long QT syndrome (LQTS) and Brugada syndrome.
"Many of our colleagues in the field will be surprised," Dr. Priori predicted.
Here are the highlights:
• LQTS: With an estimated prevalence of roughly 1 per 2,000 live births worldwide, this is the most common of the inherited arrhythmia syndromes. What is likely to come as a surprise to many physicians is the expert consensus panel’s recommendation that the diagnosis of LQTS requires either the finding of an unequivocally causative mutation in one of the LQTS genes or, in the absence of such a defect, either a QTc interval of 480-499 ms in repeated 12-lead ECGs in a patient with unexplained syncope or a QTc of 500 ms in repeated ECGs in the absence of a secondary cause for QT prolongation in a nonsyncopal patient.
"A single ECG reading 10 ms above the upper limit of normal is not enough to establish the diagnosis. That’s quite different from what’s being done in common practice. Many of the patients who are referred to the centers of expertise on inherited arrhythmias are borderline patients in whom maybe one ECG was abnormal, and yet because of that they’ve been labeled as being affected by a genetic disease even if the genetic studies were negative. A single abnormal QTc measurement in a patient with negative genetic testing is not enough," Dr. Priori declared.
Dr. Wilde said the new guidelines loosen up the guidance on participation in competitive sports. The blanket prohibition of the past has been replaced by a case-by-case approach, with a Class I recommendation for routine referral to a clinical expert for evaluation of the risk posed by athletic activity. For example, although swimming is a very-high-risk activity for patients with the LQTS1 genotype, that’s not true for those who have LQTS2 or -3.
"It’s clear that if a patient with long QT syndrome has exercise-related syncopal events, that patient should not participate in competitive sports. But if the patient is asymptomatic and has minor QT prolongation, there’s probably not much reason for concern," he said.
"This is a sharp departure," Dr. Priori observed. "In several European countries, if you have the diagnosis of long QT syndrome, sports participation is not permitted, even if your physician clears you. So we hope with this document to slowly, carefully, begin to allow patients with this condition to do sports safely. We wanted to lift the ban so that a physician who feels a specific patient would have a low risk in the proper environment could make that recommendation."
• Brugada syndrome: Far more common in Asia than the western world, Brugada syndrome is 8- to 10-fold more frequent in males than females. The big change in the new guidelines is that the diagnosis no longer requires specific ECG changes plus clinical manifestations. Now, Brugada syndrome, like LQTS, is a pure ECG diagnosis. It is made definitively when a type 1 ST-segment elevation is noted either spontaneously or after administration of an intravenous sodium channel-blocking agent; the ST finding has to be observed in at least one right precordial lead placed in a standard or superior position up to the second intercostal space.
An implantable cardioverter-defibrillator is clearly indicated in a Brugada syndrome patient with a prior cardiac arrest or documented ventricular arrhythmias. The controversy lies in how to manage the asymptomatic patient. The guidelines give ICD implantation a weak Class IIb recommendation – meaning it "may be considered" – when such patients exhibit inducible ventricular arrhythmias during programmed electrical stimulation in the electrophysiology lab.
• Catecholaminergic polymorphic ventricular tachycardia: The prevalence of CPVT is unclear, but it has been estimated at 1 per 5,000 live births, according to Dr. Wilde. This highly malignant condition is diagnosed in patients with a known pathogenic mutation, or in the presence of a structurally normal heart, a normal resting ECG, and unexplained exercise- or catecholamine-induced bidirectional VT of polymorphic ventricular premature beats or VT before age 40 years. First-line therapy is a long-acting beta-blocker such as nadolol, coupled with exercise restriction. ICD therapy is problematic because the inevitable inappropriate shocks increase sympathetic tone, triggering true shockable arrhythmias in a vicious cycle.
• Short QT syndrome: This is a rare channelopathy. It is diagnosed on the basis of a QTc of 330 ms or less, or a QTc of less than 360 ms in the presence of a pathogenic mutation, family history of sudden death before age 40 years, cardiac arrest in the absence of structural heart disease, or a family history of short QT syndrome.
• Progressive cardiac conduction disease: Still incompletely understood, PCCD is diagnosed in individuals under age 50 years who have unexplained progressive conduction abnormalities and a structurally normal heart with no skeletal myopathies. Pacemaker implantation is the most useful therapy.
• Early repolarization: The first report linking this extremely common ECG finding to sudden death came less than 5 years ago. Early repolarization, as characterized by J-point and ST-segment elevation in two or more contiguous leads, is present in up to 10% of normal individuals. In preparticipation athletic screening programs, it can be found in up to 15%-20% of subjects.
"There’s no reason for concern if that’s the only thing you find. It’s something you shouldn’t even communicate if there is no other issue. If a patient with early repolarization has no symptoms and no family history of premature sudden death, just leave it," Dr. Wilde advised.
On the other hand, if a patient with the early repolarization ECG pattern in two or more contiguous inferior and/or lateral leads experiences exercise-induced syncopal symptoms, further evaluation is warranted. Given how common and generally benign the early repolarization ECG pattern is, the expert panel recommended a conservative approach to diagnosis, urging that the formal diagnosis of early repolarization syndrome be restricted largely to those with the characteristic ECG findings who in addition have been resuscitated from unexplained ventricular fibrillation or polymorphic VT.
Dr. Priori emphasized that the guidelines have as a Class I recommendation that patients with a diagnosed or suspected inherited arrhythmia syndrome that can result in sudden cardiac death – and their first-degree relatives, as well – should be evaluated in a specialized multidisciplinary inherited arrhythmia clinic. Such clinics are more common in Europe than the United States; however, thought leaders in American electrophysiology now recognize that the increasing complexity of the field requires that more of these dedicated clinics be created in the United States, she said.
The expert consensus statement was a joint project of the Heart Rhythm Society, the European Heart Rhythm Association, and the Asia Pacific Heart Rhythm Society. The document is available at the HRS website and will be published this fall in Heart Rhythm, EP Europace, and the Journal of Arrhythmias.
Dr. Priori reported serving as a consultant to Medtronic, Boston Scientific, Biotronic, and Transgenomic. Dr. Wilde disclosed serving as a consultant to Sorin.
DENVER – Major new guidelines on the diagnosis and management of patients with inherited primary arrhythmia syndromes have been jointly issued by the Heart Rhythm Society and its European and Asian counterparts.
The guidelines were sorely needed, according to Dr. Silvia G. Priori, cochair of the expert consensus panel writing group.
The field of inherited arrhythmias is rapidly evolving, with new pathogenic genetic mutations being found all the time. Much has changed in the 7 years since issuance of the last major guidelines: the American College of Cardiology/American Heart Association/European Society of Cardiology guidelines on prevention of sudden cardiac death (Circulation 2006;114:e385-484), noted Dr. Priori of the University of Pavia (Italy).
Her cochair, Dr. Arthur A. Wilde of the University of Amsterdam pointed out that the new 69-page report is the first major document to address some of the newer inherited arrhythmia syndromes, including catecholaminergic polymorphic ventricular tachycardia (CPVT), short QT syndrome, early repolarization, and progressive cardiac conduction disease (PCCD). In addition, the new report proposes major changes in the diagnostic criteria for the two most common primary arrhythmia syndromes: long QT syndrome (LQTS) and Brugada syndrome.
"Many of our colleagues in the field will be surprised," Dr. Priori predicted.
Here are the highlights:
• LQTS: With an estimated prevalence of roughly 1 per 2,000 live births worldwide, this is the most common of the inherited arrhythmia syndromes. What is likely to come as a surprise to many physicians is the expert consensus panel’s recommendation that the diagnosis of LQTS requires either the finding of an unequivocally causative mutation in one of the LQTS genes or, in the absence of such a defect, either a QTc interval of 480-499 ms in repeated 12-lead ECGs in a patient with unexplained syncope or a QTc of 500 ms in repeated ECGs in the absence of a secondary cause for QT prolongation in a nonsyncopal patient.
"A single ECG reading 10 ms above the upper limit of normal is not enough to establish the diagnosis. That’s quite different from what’s being done in common practice. Many of the patients who are referred to the centers of expertise on inherited arrhythmias are borderline patients in whom maybe one ECG was abnormal, and yet because of that they’ve been labeled as being affected by a genetic disease even if the genetic studies were negative. A single abnormal QTc measurement in a patient with negative genetic testing is not enough," Dr. Priori declared.
Dr. Wilde said the new guidelines loosen up the guidance on participation in competitive sports. The blanket prohibition of the past has been replaced by a case-by-case approach, with a Class I recommendation for routine referral to a clinical expert for evaluation of the risk posed by athletic activity. For example, although swimming is a very-high-risk activity for patients with the LQTS1 genotype, that’s not true for those who have LQTS2 or -3.
"It’s clear that if a patient with long QT syndrome has exercise-related syncopal events, that patient should not participate in competitive sports. But if the patient is asymptomatic and has minor QT prolongation, there’s probably not much reason for concern," he said.
"This is a sharp departure," Dr. Priori observed. "In several European countries, if you have the diagnosis of long QT syndrome, sports participation is not permitted, even if your physician clears you. So we hope with this document to slowly, carefully, begin to allow patients with this condition to do sports safely. We wanted to lift the ban so that a physician who feels a specific patient would have a low risk in the proper environment could make that recommendation."
• Brugada syndrome: Far more common in Asia than the western world, Brugada syndrome is 8- to 10-fold more frequent in males than females. The big change in the new guidelines is that the diagnosis no longer requires specific ECG changes plus clinical manifestations. Now, Brugada syndrome, like LQTS, is a pure ECG diagnosis. It is made definitively when a type 1 ST-segment elevation is noted either spontaneously or after administration of an intravenous sodium channel-blocking agent; the ST finding has to be observed in at least one right precordial lead placed in a standard or superior position up to the second intercostal space.
An implantable cardioverter-defibrillator is clearly indicated in a Brugada syndrome patient with a prior cardiac arrest or documented ventricular arrhythmias. The controversy lies in how to manage the asymptomatic patient. The guidelines give ICD implantation a weak Class IIb recommendation – meaning it "may be considered" – when such patients exhibit inducible ventricular arrhythmias during programmed electrical stimulation in the electrophysiology lab.
• Catecholaminergic polymorphic ventricular tachycardia: The prevalence of CPVT is unclear, but it has been estimated at 1 per 5,000 live births, according to Dr. Wilde. This highly malignant condition is diagnosed in patients with a known pathogenic mutation, or in the presence of a structurally normal heart, a normal resting ECG, and unexplained exercise- or catecholamine-induced bidirectional VT of polymorphic ventricular premature beats or VT before age 40 years. First-line therapy is a long-acting beta-blocker such as nadolol, coupled with exercise restriction. ICD therapy is problematic because the inevitable inappropriate shocks increase sympathetic tone, triggering true shockable arrhythmias in a vicious cycle.
• Short QT syndrome: This is a rare channelopathy. It is diagnosed on the basis of a QTc of 330 ms or less, or a QTc of less than 360 ms in the presence of a pathogenic mutation, family history of sudden death before age 40 years, cardiac arrest in the absence of structural heart disease, or a family history of short QT syndrome.
• Progressive cardiac conduction disease: Still incompletely understood, PCCD is diagnosed in individuals under age 50 years who have unexplained progressive conduction abnormalities and a structurally normal heart with no skeletal myopathies. Pacemaker implantation is the most useful therapy.
• Early repolarization: The first report linking this extremely common ECG finding to sudden death came less than 5 years ago. Early repolarization, as characterized by J-point and ST-segment elevation in two or more contiguous leads, is present in up to 10% of normal individuals. In preparticipation athletic screening programs, it can be found in up to 15%-20% of subjects.
"There’s no reason for concern if that’s the only thing you find. It’s something you shouldn’t even communicate if there is no other issue. If a patient with early repolarization has no symptoms and no family history of premature sudden death, just leave it," Dr. Wilde advised.
On the other hand, if a patient with the early repolarization ECG pattern in two or more contiguous inferior and/or lateral leads experiences exercise-induced syncopal symptoms, further evaluation is warranted. Given how common and generally benign the early repolarization ECG pattern is, the expert panel recommended a conservative approach to diagnosis, urging that the formal diagnosis of early repolarization syndrome be restricted largely to those with the characteristic ECG findings who in addition have been resuscitated from unexplained ventricular fibrillation or polymorphic VT.
Dr. Priori emphasized that the guidelines have as a Class I recommendation that patients with a diagnosed or suspected inherited arrhythmia syndrome that can result in sudden cardiac death – and their first-degree relatives, as well – should be evaluated in a specialized multidisciplinary inherited arrhythmia clinic. Such clinics are more common in Europe than the United States; however, thought leaders in American electrophysiology now recognize that the increasing complexity of the field requires that more of these dedicated clinics be created in the United States, she said.
The expert consensus statement was a joint project of the Heart Rhythm Society, the European Heart Rhythm Association, and the Asia Pacific Heart Rhythm Society. The document is available at the HRS website and will be published this fall in Heart Rhythm, EP Europace, and the Journal of Arrhythmias.
Dr. Priori reported serving as a consultant to Medtronic, Boston Scientific, Biotronic, and Transgenomic. Dr. Wilde disclosed serving as a consultant to Sorin.
inherited primary arrhythmia, Dr. Silvia G. Priori, arrythmia guidelines, Arthur Wilde
inherited primary arrhythmia, Dr. Silvia G. Priori, arrythmia guidelines, Arthur Wilde
AT HEART RHYTHM 2013

Addressing The Joint Commission's Concern About Opioid-Induced Respiratory Depression
The recent article by Susan Kreimer, “Serious Complications from Opioid Overuse in Hospitalized Patients Prompts Nationwide Alert” (February 2013, p. 34) highlights a very important patient safety issue—opioid-induced respiratory depression.
Post-operative patients often manage their pain with patient-controlled analgesia (PCA) pumps. An estimated 14 million patients use PCA annually.1 As the article points out, PCA “offers built-in safety features—if patients become too sedated, they can’t push a button for extra doses—but that isn’t always the case.”
As Dr. Jason McKeown says, “While PCA may be the safest mode of opioid delivery, it is true that regardless of the route of administration, respiratory depression may still occur. To help prevent such incidents from happening, it should be remembered that some of the most significant strides in medicine and surgery are directly attributable to anesthesiology’s advances in patient monitoring.”
With the goal of helping to reduce adverse events and deaths with PCA pumps, the Physician-Patient Alliance for Health & Safety (PPAHS) recently released a safety checklist that reminds caregivers of the essential steps needed to be taken to initiate PCA with a patient, and to continue to assess that patient’s use of PCA. This checklist was developed after consultation with a group of 19 renowned health experts and is a free download at www.ppahs.org.
The checklist provides five recommended steps to have been completed when initiating PCA:
- Risk factors that increase risk of respiratory depression have been considered.
- Pre-procedural cognitive assessment has determined patient is capable of participating in pain management.
However, it should be noted that these first two steps are not an attempt at risk stratification. In reviewing current approaches to address failure-to-rescue, Dr. Andreas Taenzer and his colleagues showed that these current approaches are not able to predict which patients are at risk and at which point the crisis can be detected.
- Patient has been provided with information on proper patient use of PCA pump (other recipients of information—family/visitors) and purpose of monitoring.
The Institute for Safe Medical Practice (www.ismp.org) cautions against PCA proxy and stresses the importance of patient education. The safe use of PCA includes making sure the patient controlling the device actually knows how to use it and the importance of the monitoring used to continuously assess their status.
- Two health-care providers have independently double-checked: patient ID; allergies; drug selection and concentration; dosage adjustments; pump settings; and line attachment to patient and tubing insertion.
Error prevention is critical. The Pennsylvania Patient Safety Authority recently released its analysis of medication errors and adverse drug reactions involving intravenous fentanyl that were reported to them. Researchers found 2,319 events between June 2004 to March 2012; that’s almost 25 events per month. Although one error a day may seem high, their analysis is confined to reports that were made to the authority and only include fentanyl, a potent, synthetic narcotic analgesic with a rapid onset and short duration of action.
- Patient is electronically monitored with both pulse oximetry and capnography.
As Dr. Robert Stoelting, president of the Anesthesia Patient Safety Foundation, recently stated: “The conclusions and recommendations of APSF are that intermittent ‘spot checks’ of [pulse oximetry] and ventilation are not adequate for reliably recognizing clinically significant, evolving, drug-induced, respiratory depression in the postoperative period....APSF recommends that monitoring be continuous and not intermittent, and that continuous electronic monitoring with both pulse oximetry for oxygenation and capnography for the adequacy of ventilation be considered for all patients.”
Frank Federico, a member of the Patient Safety Advisory Group at The Joint Commission and executive director at the Institute for Healthcare Improvement, concurs: “Although nurse spot checks on patients are advisable, pulse oximetry and capnography are essential risk prevention tools in any pain management plan.”
PPAHS encourages all hospitals and health-care facilities to download and utilize the PCA Safety Checklist.
The recent article by Susan Kreimer, “Serious Complications from Opioid Overuse in Hospitalized Patients Prompts Nationwide Alert” (February 2013, p. 34) highlights a very important patient safety issue—opioid-induced respiratory depression.
Post-operative patients often manage their pain with patient-controlled analgesia (PCA) pumps. An estimated 14 million patients use PCA annually.1 As the article points out, PCA “offers built-in safety features—if patients become too sedated, they can’t push a button for extra doses—but that isn’t always the case.”
As Dr. Jason McKeown says, “While PCA may be the safest mode of opioid delivery, it is true that regardless of the route of administration, respiratory depression may still occur. To help prevent such incidents from happening, it should be remembered that some of the most significant strides in medicine and surgery are directly attributable to anesthesiology’s advances in patient monitoring.”
With the goal of helping to reduce adverse events and deaths with PCA pumps, the Physician-Patient Alliance for Health & Safety (PPAHS) recently released a safety checklist that reminds caregivers of the essential steps needed to be taken to initiate PCA with a patient, and to continue to assess that patient’s use of PCA. This checklist was developed after consultation with a group of 19 renowned health experts and is a free download at www.ppahs.org.
The checklist provides five recommended steps to have been completed when initiating PCA:
- Risk factors that increase risk of respiratory depression have been considered.
- Pre-procedural cognitive assessment has determined patient is capable of participating in pain management.
However, it should be noted that these first two steps are not an attempt at risk stratification. In reviewing current approaches to address failure-to-rescue, Dr. Andreas Taenzer and his colleagues showed that these current approaches are not able to predict which patients are at risk and at which point the crisis can be detected.
- Patient has been provided with information on proper patient use of PCA pump (other recipients of information—family/visitors) and purpose of monitoring.
The Institute for Safe Medical Practice (www.ismp.org) cautions against PCA proxy and stresses the importance of patient education. The safe use of PCA includes making sure the patient controlling the device actually knows how to use it and the importance of the monitoring used to continuously assess their status.
- Two health-care providers have independently double-checked: patient ID; allergies; drug selection and concentration; dosage adjustments; pump settings; and line attachment to patient and tubing insertion.
Error prevention is critical. The Pennsylvania Patient Safety Authority recently released its analysis of medication errors and adverse drug reactions involving intravenous fentanyl that were reported to them. Researchers found 2,319 events between June 2004 to March 2012; that’s almost 25 events per month. Although one error a day may seem high, their analysis is confined to reports that were made to the authority and only include fentanyl, a potent, synthetic narcotic analgesic with a rapid onset and short duration of action.
- Patient is electronically monitored with both pulse oximetry and capnography.
As Dr. Robert Stoelting, president of the Anesthesia Patient Safety Foundation, recently stated: “The conclusions and recommendations of APSF are that intermittent ‘spot checks’ of [pulse oximetry] and ventilation are not adequate for reliably recognizing clinically significant, evolving, drug-induced, respiratory depression in the postoperative period....APSF recommends that monitoring be continuous and not intermittent, and that continuous electronic monitoring with both pulse oximetry for oxygenation and capnography for the adequacy of ventilation be considered for all patients.”
Frank Federico, a member of the Patient Safety Advisory Group at The Joint Commission and executive director at the Institute for Healthcare Improvement, concurs: “Although nurse spot checks on patients are advisable, pulse oximetry and capnography are essential risk prevention tools in any pain management plan.”
PPAHS encourages all hospitals and health-care facilities to download and utilize the PCA Safety Checklist.
The recent article by Susan Kreimer, “Serious Complications from Opioid Overuse in Hospitalized Patients Prompts Nationwide Alert” (February 2013, p. 34) highlights a very important patient safety issue—opioid-induced respiratory depression.
Post-operative patients often manage their pain with patient-controlled analgesia (PCA) pumps. An estimated 14 million patients use PCA annually.1 As the article points out, PCA “offers built-in safety features—if patients become too sedated, they can’t push a button for extra doses—but that isn’t always the case.”
As Dr. Jason McKeown says, “While PCA may be the safest mode of opioid delivery, it is true that regardless of the route of administration, respiratory depression may still occur. To help prevent such incidents from happening, it should be remembered that some of the most significant strides in medicine and surgery are directly attributable to anesthesiology’s advances in patient monitoring.”
With the goal of helping to reduce adverse events and deaths with PCA pumps, the Physician-Patient Alliance for Health & Safety (PPAHS) recently released a safety checklist that reminds caregivers of the essential steps needed to be taken to initiate PCA with a patient, and to continue to assess that patient’s use of PCA. This checklist was developed after consultation with a group of 19 renowned health experts and is a free download at www.ppahs.org.
The checklist provides five recommended steps to have been completed when initiating PCA:
- Risk factors that increase risk of respiratory depression have been considered.
- Pre-procedural cognitive assessment has determined patient is capable of participating in pain management.
However, it should be noted that these first two steps are not an attempt at risk stratification. In reviewing current approaches to address failure-to-rescue, Dr. Andreas Taenzer and his colleagues showed that these current approaches are not able to predict which patients are at risk and at which point the crisis can be detected.
- Patient has been provided with information on proper patient use of PCA pump (other recipients of information—family/visitors) and purpose of monitoring.
The Institute for Safe Medical Practice (www.ismp.org) cautions against PCA proxy and stresses the importance of patient education. The safe use of PCA includes making sure the patient controlling the device actually knows how to use it and the importance of the monitoring used to continuously assess their status.
- Two health-care providers have independently double-checked: patient ID; allergies; drug selection and concentration; dosage adjustments; pump settings; and line attachment to patient and tubing insertion.
Error prevention is critical. The Pennsylvania Patient Safety Authority recently released its analysis of medication errors and adverse drug reactions involving intravenous fentanyl that were reported to them. Researchers found 2,319 events between June 2004 to March 2012; that’s almost 25 events per month. Although one error a day may seem high, their analysis is confined to reports that were made to the authority and only include fentanyl, a potent, synthetic narcotic analgesic with a rapid onset and short duration of action.
- Patient is electronically monitored with both pulse oximetry and capnography.
As Dr. Robert Stoelting, president of the Anesthesia Patient Safety Foundation, recently stated: “The conclusions and recommendations of APSF are that intermittent ‘spot checks’ of [pulse oximetry] and ventilation are not adequate for reliably recognizing clinically significant, evolving, drug-induced, respiratory depression in the postoperative period....APSF recommends that monitoring be continuous and not intermittent, and that continuous electronic monitoring with both pulse oximetry for oxygenation and capnography for the adequacy of ventilation be considered for all patients.”
Frank Federico, a member of the Patient Safety Advisory Group at The Joint Commission and executive director at the Institute for Healthcare Improvement, concurs: “Although nurse spot checks on patients are advisable, pulse oximetry and capnography are essential risk prevention tools in any pain management plan.”
PPAHS encourages all hospitals and health-care facilities to download and utilize the PCA Safety Checklist.
Surviving Sepsis Campaign 2012 Guidelines: Updates For the Hospitalist
Background
Sepsis is a clinical syndrome with systemic effects that can progress to severe sepsis and/or septic shock. The incidence of severe sepsis and septic shock is rising in the United States, and these syndromes are associated with significant morbidity and a mortality rate as high as 25% to 35%.1 In fact, sepsis is one of the 10 leading causes of death in the U.S., accounting for 2% of hospital admissions but 17% of in-hospital deaths.1
The main principles of effective treatment for severe sepsis and septic shock are timely recognition and early aggressive therapy. Launched in 2002, the Surviving Sepsis Campaign (SSC) was the result of a collaboration of three professional societies. The goal of the SSC collaborative was to reduce mortality from severe sepsis and septic shock by 25%. To that end, the SSC convened representatives from several international societies to develop a set of evidence-based guidelines as a means of guiding clinicians in optimizing management of patients with severe sepsis and septic shock. Since the original publication of the SSC guidelines in 2004, there have been two updates—one in 2008 and one in February 2013.2
Guideline Updates
Quantitative, protocol-driven initial resuscitation in the first six hours for patients with severe sepsis and septic shock remains a high-level recommendation, but SSC has added normalization of the lactate level as a resuscitation goal. This new suggestion is based on two studies published since the 2008 SCC guidelines that showed noninferiority to previously established goals and absolute mortality benefit.3,4
There is a new focus on screening for sepsis and the use of hospital-based performance-improvement programs, which were not previously addressed in the 2008 SCC guidelines. Patients with suspected infections and who are seriously ill should be screened in order to identify sepsis early during the hospital course. Additionally, it is recommended that hospitals implement performance-improvement measures by which multidisciplinary teams can address treatment of sepsis by improving compliance with the SSC bundles, citing their own data as the model but ultimately leaving this recommendation as ungradable in regards to the quality of available supporting evidence.5
Cultures drawn before antibiotics and early imaging to confirm potential sources are still recommended, but the committee has added the use of one: 3 beta D-glucan and the mannan antigen and anti-mannan antibody assays when considering invasive candidiasis as your infective agent. They do note the known risk of false positive results with these assays and warn that they should be used with caution.
Early, broad-spectrum antibiotic administration within the first hour of presentation was upgraded for severe sepsis and downgraded for septic shock. The decision to initiate double coverage for suspected gram-negative infection is not recommended specifically but can be considered in situations when highly antibiotic resistant pathogens are potentially present. Daily assessment of the appropriate antibiotic regimen remains an important tenet, and the use of low procalcitonin levels as a tool to assist in the decision to discontinue antibiotics has been introduced. Source control is still strongly recommended in the first 12 hours of treatment.
The SSC 2012 guidelines specifically address the rate of fluid administered and the type of fluid that should be used. It is now recommended that a fluid challenge of 30 mL/kg be used for initial resuscitation, but the guidelines leave it up to the clinician to give more fluid if needed. There is a strong push for use of crystalloids rather than colloids during initial resuscitation and thereafter. Disfavor for colloids stemmed from trials showing increased mortality when comparing resuscitation with hydroxyethyl starch versus crystalloid for patients in septic shock.6,7 Albumin, on the other hand, is recommended to resuscitate patients with severe sepsis and septic shock in cases for which large amounts of crystalloid are required.
The 2012 SSC guidelines recommend norepinephrine (NE) alone as the first-line vasopressor in sepsis and no longer include dopamine in this category. In fact, the use of dopamine in septic shock has been downgraded and should only to be considered in patients at low risk of tachyarrhythmia and in bradycardia syndromes. Epinephrine is now favored as the second agent or as a substitute to NE. Phenylephrine is no longer recommended unless there is contraindication to using NE, the patient has a high cardiac output, or it is used as a salvage therapy. Vasopressin is considered only an adjunctive agent to NE and should never be used alone.
Recommendations regarding corticosteroid therapy remain largely unchanged from 2008 SCC guidelines, which only support their use when adequate volume resuscitation and vasopressor support has failed to achieve hemodynamic stability. Glucose control is recommended but at the new target of achieving a level of <180 mg/dL, up from a previous target of <150 mg/dL.
Notably, recombinant human activated protein C was completely omitted from the 2012 guidelines, prompted by the voluntary removal of the drug by the manufacturer after failing to show benefit. Use of selenium and intravenous immunoglobulin received comment, but there is insufficient evidence supporting their benefit at the current time. They also encourage clinicians to incorporate goals of care and end-of-life issues into the treatment plan and discuss this with patients and/or surrogates early in treatment.
Guideline Analysis
Prior versions of the SSC guidelines have been met with a fair amount of skepticism.8 Much of the criticism is based on the industry sponsorship of the 2004 version, the lack of transparency regarding potential conflicts of interest of the committee members, and that the bundle recommendations largely were based on only one trial and, therefore, not evidenced-based.9 The 2012 SSC committee seems to have addressed these issues as the guidelines are free of commercial sponsorship in the 2008 and current versions. They also rigorously applied the GRADE system to methodically assess the strength and quality of supporting evidence. The result is a set of guidelines that are partially evidence-based and partially based on expert opinion, but this is clearly delineated in these newest guidelines. This provides clinicians with a clear and concise recommended approach to the patient with severe sepsis and septic shock.
The guidelines continue to place a heavy emphasis on three- and six-hour treatment bundles, and with the assistance of the Institute for Health Care Improvement efforts to improve implementation of the bundle, they are already are widespread with an eye to expand across the country. The components of the three-hour treatment bundle (lactate measurement, blood cultures prior to initiation of antibiotics, broad-spectrum antibiotics, and IV crystalloids for hypotension or for a lactate of >4 mmol/L) recommended by the SSC have not changed substantially since 2008. The one exception is the rate at which IV crystalloid should be administered of 30 mL/kg, which is up from 20 mL/kg. Only time will tell how this change will affect bundle compliance or reduce mortality. But this does pose a significant challenge to quality and performance improvement groups accustomed to tracking compliance with IV fluid administration under the old standard and the educational campaigns associated with a change.
It appears that the SSC is here to stay, now in its third iteration. The lasting legacy of the SSC guidelines might not rest with the content of the guidelines, per se, but in raising awareness of severe sepsis and septic shock in a way that had not previously been considered.
HM Takeaways
The revised 2012 SCC updates bring some new tools to the clinician for early recognition and effective management of patients with sepsis. The push for institutions to adopt screening and performance measures reflects a general trend in health care to create high-performance systems. As these new guidelines are put into practice, there are several changes that might require augmentation of quality metrics being tracked at institutions nationally and internationally.
Dr. Pendharker is assistant professor of medicine in the division of hospital medicine at the University of California San Francisco and San Francisco General Hospital. Dr. Gomez is assistant professor of medicine in the division of pulmonary and critical care medicine at UCSF and San Francisco General Hospital.
References
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011:1-8.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580-637.
- Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-761.
- Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010;303:739-746.
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367-374.
- Guidet B, Martinet O, Boulain T, et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:R94.
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124-134.
- Marik PE. Surviving sepsis: going beyond the guidelines. Ann Intensive Care. 2011;1:17.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
Background
Sepsis is a clinical syndrome with systemic effects that can progress to severe sepsis and/or septic shock. The incidence of severe sepsis and septic shock is rising in the United States, and these syndromes are associated with significant morbidity and a mortality rate as high as 25% to 35%.1 In fact, sepsis is one of the 10 leading causes of death in the U.S., accounting for 2% of hospital admissions but 17% of in-hospital deaths.1
The main principles of effective treatment for severe sepsis and septic shock are timely recognition and early aggressive therapy. Launched in 2002, the Surviving Sepsis Campaign (SSC) was the result of a collaboration of three professional societies. The goal of the SSC collaborative was to reduce mortality from severe sepsis and septic shock by 25%. To that end, the SSC convened representatives from several international societies to develop a set of evidence-based guidelines as a means of guiding clinicians in optimizing management of patients with severe sepsis and septic shock. Since the original publication of the SSC guidelines in 2004, there have been two updates—one in 2008 and one in February 2013.2
Guideline Updates
Quantitative, protocol-driven initial resuscitation in the first six hours for patients with severe sepsis and septic shock remains a high-level recommendation, but SSC has added normalization of the lactate level as a resuscitation goal. This new suggestion is based on two studies published since the 2008 SCC guidelines that showed noninferiority to previously established goals and absolute mortality benefit.3,4
There is a new focus on screening for sepsis and the use of hospital-based performance-improvement programs, which were not previously addressed in the 2008 SCC guidelines. Patients with suspected infections and who are seriously ill should be screened in order to identify sepsis early during the hospital course. Additionally, it is recommended that hospitals implement performance-improvement measures by which multidisciplinary teams can address treatment of sepsis by improving compliance with the SSC bundles, citing their own data as the model but ultimately leaving this recommendation as ungradable in regards to the quality of available supporting evidence.5
Cultures drawn before antibiotics and early imaging to confirm potential sources are still recommended, but the committee has added the use of one: 3 beta D-glucan and the mannan antigen and anti-mannan antibody assays when considering invasive candidiasis as your infective agent. They do note the known risk of false positive results with these assays and warn that they should be used with caution.
Early, broad-spectrum antibiotic administration within the first hour of presentation was upgraded for severe sepsis and downgraded for septic shock. The decision to initiate double coverage for suspected gram-negative infection is not recommended specifically but can be considered in situations when highly antibiotic resistant pathogens are potentially present. Daily assessment of the appropriate antibiotic regimen remains an important tenet, and the use of low procalcitonin levels as a tool to assist in the decision to discontinue antibiotics has been introduced. Source control is still strongly recommended in the first 12 hours of treatment.
The SSC 2012 guidelines specifically address the rate of fluid administered and the type of fluid that should be used. It is now recommended that a fluid challenge of 30 mL/kg be used for initial resuscitation, but the guidelines leave it up to the clinician to give more fluid if needed. There is a strong push for use of crystalloids rather than colloids during initial resuscitation and thereafter. Disfavor for colloids stemmed from trials showing increased mortality when comparing resuscitation with hydroxyethyl starch versus crystalloid for patients in septic shock.6,7 Albumin, on the other hand, is recommended to resuscitate patients with severe sepsis and septic shock in cases for which large amounts of crystalloid are required.
The 2012 SSC guidelines recommend norepinephrine (NE) alone as the first-line vasopressor in sepsis and no longer include dopamine in this category. In fact, the use of dopamine in septic shock has been downgraded and should only to be considered in patients at low risk of tachyarrhythmia and in bradycardia syndromes. Epinephrine is now favored as the second agent or as a substitute to NE. Phenylephrine is no longer recommended unless there is contraindication to using NE, the patient has a high cardiac output, or it is used as a salvage therapy. Vasopressin is considered only an adjunctive agent to NE and should never be used alone.
Recommendations regarding corticosteroid therapy remain largely unchanged from 2008 SCC guidelines, which only support their use when adequate volume resuscitation and vasopressor support has failed to achieve hemodynamic stability. Glucose control is recommended but at the new target of achieving a level of <180 mg/dL, up from a previous target of <150 mg/dL.
Notably, recombinant human activated protein C was completely omitted from the 2012 guidelines, prompted by the voluntary removal of the drug by the manufacturer after failing to show benefit. Use of selenium and intravenous immunoglobulin received comment, but there is insufficient evidence supporting their benefit at the current time. They also encourage clinicians to incorporate goals of care and end-of-life issues into the treatment plan and discuss this with patients and/or surrogates early in treatment.
Guideline Analysis
Prior versions of the SSC guidelines have been met with a fair amount of skepticism.8 Much of the criticism is based on the industry sponsorship of the 2004 version, the lack of transparency regarding potential conflicts of interest of the committee members, and that the bundle recommendations largely were based on only one trial and, therefore, not evidenced-based.9 The 2012 SSC committee seems to have addressed these issues as the guidelines are free of commercial sponsorship in the 2008 and current versions. They also rigorously applied the GRADE system to methodically assess the strength and quality of supporting evidence. The result is a set of guidelines that are partially evidence-based and partially based on expert opinion, but this is clearly delineated in these newest guidelines. This provides clinicians with a clear and concise recommended approach to the patient with severe sepsis and septic shock.
The guidelines continue to place a heavy emphasis on three- and six-hour treatment bundles, and with the assistance of the Institute for Health Care Improvement efforts to improve implementation of the bundle, they are already are widespread with an eye to expand across the country. The components of the three-hour treatment bundle (lactate measurement, blood cultures prior to initiation of antibiotics, broad-spectrum antibiotics, and IV crystalloids for hypotension or for a lactate of >4 mmol/L) recommended by the SSC have not changed substantially since 2008. The one exception is the rate at which IV crystalloid should be administered of 30 mL/kg, which is up from 20 mL/kg. Only time will tell how this change will affect bundle compliance or reduce mortality. But this does pose a significant challenge to quality and performance improvement groups accustomed to tracking compliance with IV fluid administration under the old standard and the educational campaigns associated with a change.
It appears that the SSC is here to stay, now in its third iteration. The lasting legacy of the SSC guidelines might not rest with the content of the guidelines, per se, but in raising awareness of severe sepsis and septic shock in a way that had not previously been considered.
HM Takeaways
The revised 2012 SCC updates bring some new tools to the clinician for early recognition and effective management of patients with sepsis. The push for institutions to adopt screening and performance measures reflects a general trend in health care to create high-performance systems. As these new guidelines are put into practice, there are several changes that might require augmentation of quality metrics being tracked at institutions nationally and internationally.
Dr. Pendharker is assistant professor of medicine in the division of hospital medicine at the University of California San Francisco and San Francisco General Hospital. Dr. Gomez is assistant professor of medicine in the division of pulmonary and critical care medicine at UCSF and San Francisco General Hospital.
References
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011:1-8.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580-637.
- Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-761.
- Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010;303:739-746.
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367-374.
- Guidet B, Martinet O, Boulain T, et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:R94.
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124-134.
- Marik PE. Surviving sepsis: going beyond the guidelines. Ann Intensive Care. 2011;1:17.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
Background
Sepsis is a clinical syndrome with systemic effects that can progress to severe sepsis and/or septic shock. The incidence of severe sepsis and septic shock is rising in the United States, and these syndromes are associated with significant morbidity and a mortality rate as high as 25% to 35%.1 In fact, sepsis is one of the 10 leading causes of death in the U.S., accounting for 2% of hospital admissions but 17% of in-hospital deaths.1
The main principles of effective treatment for severe sepsis and septic shock are timely recognition and early aggressive therapy. Launched in 2002, the Surviving Sepsis Campaign (SSC) was the result of a collaboration of three professional societies. The goal of the SSC collaborative was to reduce mortality from severe sepsis and septic shock by 25%. To that end, the SSC convened representatives from several international societies to develop a set of evidence-based guidelines as a means of guiding clinicians in optimizing management of patients with severe sepsis and septic shock. Since the original publication of the SSC guidelines in 2004, there have been two updates—one in 2008 and one in February 2013.2
Guideline Updates
Quantitative, protocol-driven initial resuscitation in the first six hours for patients with severe sepsis and septic shock remains a high-level recommendation, but SSC has added normalization of the lactate level as a resuscitation goal. This new suggestion is based on two studies published since the 2008 SCC guidelines that showed noninferiority to previously established goals and absolute mortality benefit.3,4
There is a new focus on screening for sepsis and the use of hospital-based performance-improvement programs, which were not previously addressed in the 2008 SCC guidelines. Patients with suspected infections and who are seriously ill should be screened in order to identify sepsis early during the hospital course. Additionally, it is recommended that hospitals implement performance-improvement measures by which multidisciplinary teams can address treatment of sepsis by improving compliance with the SSC bundles, citing their own data as the model but ultimately leaving this recommendation as ungradable in regards to the quality of available supporting evidence.5
Cultures drawn before antibiotics and early imaging to confirm potential sources are still recommended, but the committee has added the use of one: 3 beta D-glucan and the mannan antigen and anti-mannan antibody assays when considering invasive candidiasis as your infective agent. They do note the known risk of false positive results with these assays and warn that they should be used with caution.
Early, broad-spectrum antibiotic administration within the first hour of presentation was upgraded for severe sepsis and downgraded for septic shock. The decision to initiate double coverage for suspected gram-negative infection is not recommended specifically but can be considered in situations when highly antibiotic resistant pathogens are potentially present. Daily assessment of the appropriate antibiotic regimen remains an important tenet, and the use of low procalcitonin levels as a tool to assist in the decision to discontinue antibiotics has been introduced. Source control is still strongly recommended in the first 12 hours of treatment.
The SSC 2012 guidelines specifically address the rate of fluid administered and the type of fluid that should be used. It is now recommended that a fluid challenge of 30 mL/kg be used for initial resuscitation, but the guidelines leave it up to the clinician to give more fluid if needed. There is a strong push for use of crystalloids rather than colloids during initial resuscitation and thereafter. Disfavor for colloids stemmed from trials showing increased mortality when comparing resuscitation with hydroxyethyl starch versus crystalloid for patients in septic shock.6,7 Albumin, on the other hand, is recommended to resuscitate patients with severe sepsis and septic shock in cases for which large amounts of crystalloid are required.
The 2012 SSC guidelines recommend norepinephrine (NE) alone as the first-line vasopressor in sepsis and no longer include dopamine in this category. In fact, the use of dopamine in septic shock has been downgraded and should only to be considered in patients at low risk of tachyarrhythmia and in bradycardia syndromes. Epinephrine is now favored as the second agent or as a substitute to NE. Phenylephrine is no longer recommended unless there is contraindication to using NE, the patient has a high cardiac output, or it is used as a salvage therapy. Vasopressin is considered only an adjunctive agent to NE and should never be used alone.
Recommendations regarding corticosteroid therapy remain largely unchanged from 2008 SCC guidelines, which only support their use when adequate volume resuscitation and vasopressor support has failed to achieve hemodynamic stability. Glucose control is recommended but at the new target of achieving a level of <180 mg/dL, up from a previous target of <150 mg/dL.
Notably, recombinant human activated protein C was completely omitted from the 2012 guidelines, prompted by the voluntary removal of the drug by the manufacturer after failing to show benefit. Use of selenium and intravenous immunoglobulin received comment, but there is insufficient evidence supporting their benefit at the current time. They also encourage clinicians to incorporate goals of care and end-of-life issues into the treatment plan and discuss this with patients and/or surrogates early in treatment.
Guideline Analysis
Prior versions of the SSC guidelines have been met with a fair amount of skepticism.8 Much of the criticism is based on the industry sponsorship of the 2004 version, the lack of transparency regarding potential conflicts of interest of the committee members, and that the bundle recommendations largely were based on only one trial and, therefore, not evidenced-based.9 The 2012 SSC committee seems to have addressed these issues as the guidelines are free of commercial sponsorship in the 2008 and current versions. They also rigorously applied the GRADE system to methodically assess the strength and quality of supporting evidence. The result is a set of guidelines that are partially evidence-based and partially based on expert opinion, but this is clearly delineated in these newest guidelines. This provides clinicians with a clear and concise recommended approach to the patient with severe sepsis and septic shock.
The guidelines continue to place a heavy emphasis on three- and six-hour treatment bundles, and with the assistance of the Institute for Health Care Improvement efforts to improve implementation of the bundle, they are already are widespread with an eye to expand across the country. The components of the three-hour treatment bundle (lactate measurement, blood cultures prior to initiation of antibiotics, broad-spectrum antibiotics, and IV crystalloids for hypotension or for a lactate of >4 mmol/L) recommended by the SSC have not changed substantially since 2008. The one exception is the rate at which IV crystalloid should be administered of 30 mL/kg, which is up from 20 mL/kg. Only time will tell how this change will affect bundle compliance or reduce mortality. But this does pose a significant challenge to quality and performance improvement groups accustomed to tracking compliance with IV fluid administration under the old standard and the educational campaigns associated with a change.
It appears that the SSC is here to stay, now in its third iteration. The lasting legacy of the SSC guidelines might not rest with the content of the guidelines, per se, but in raising awareness of severe sepsis and septic shock in a way that had not previously been considered.
HM Takeaways
The revised 2012 SCC updates bring some new tools to the clinician for early recognition and effective management of patients with sepsis. The push for institutions to adopt screening and performance measures reflects a general trend in health care to create high-performance systems. As these new guidelines are put into practice, there are several changes that might require augmentation of quality metrics being tracked at institutions nationally and internationally.
Dr. Pendharker is assistant professor of medicine in the division of hospital medicine at the University of California San Francisco and San Francisco General Hospital. Dr. Gomez is assistant professor of medicine in the division of pulmonary and critical care medicine at UCSF and San Francisco General Hospital.
References
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011:1-8.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580-637.
- Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-761.
- Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010;303:739-746.
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367-374.
- Guidet B, Martinet O, Boulain T, et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:R94.
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124-134.
- Marik PE. Surviving sepsis: going beyond the guidelines. Ann Intensive Care. 2011;1:17.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
15 Things Dermatologists Think Hospitalists Need to Know

- Maintain a broader range of differential diagnoses before ruling in or out something more concrete.
- Attend dermatology lectures as part of primary care’s continuing medical education courses.
- Review a good basic dermatology atlas from time to time.
- Learn to correctly describe lesions to a dermatologist by phone.
- Don’t assume that groin rashes are all fungal.
- Don’t mistakenly associate a drug-related reaction with a medication given one to two days before the onset of a rash.
- Consider involving a dermatologist to help manage open skin lesions, particularly if you’re unsure of the cause.
- Prescribe an adequate quantity of topical corticosteroids for the duration of treatment.
- Beware of painful or blistering rashes, especially if they involve the mucosa of the mouth, eyes, or genitals.
- Watch out for zoster, widespread herpes, pemphigus, and pemphigoid.
- Pay attention to itching in the wrists, genital region, and web spaces of fingers and toes.
- Be mindful of the rapid onset of purpuric lesions on the skin.
- Avoid consults for improving rashes and seborrheic keratosis, as well as nonurgent outpatient issues, such as psoriasis, rosacea, or a history of skin cancer.
- Don’t prescribe combined betamethasone/clotrimazole, also known as Lotrisone, for chronic scaly hands, feet, or groin.
- Encourage patients to follow up with a dermatologist on an outpatient basis.
Dermatologic diseases tend to receive little attention at most U.S. medical schools—typically only several days of lectures or a few weeks of clinical exposure.
“Not surprisingly, many general practitioners may feel unprepared to address hospitalized patients with challenging dermatologic findings,” says R. Samuel Hopkins, MD, assistant professor of dermatology and assistant residency program director at Oregon Health & Science University in Portland.
Few studies have examined the quality of inpatient dermatologic care. One study, a retrospective chart review at a Midwestern university hospital, found that the primary ward team submitted an accurate dermatologic diagnosis in only 23.9% of cases. Meanwhile, consultation with a dermatologist led to a change or addition to treatment in 77% of patients (Dermatol Online J. 2010;16(2):12).
“Given that medical schools may not be able to dedicate more time to managing dermatologic conditions, the burden of education may fall on post-graduate programs and continuing medical education to fill this gap,” Dr. Hopkins says. To further complicate matters, “it is difficult in many hospitals to obtain a dermatology consult on an inpatient, reflecting the limited access hospitalists often have to dermatologists.”

The most frequently encountered dermatologic conditions in the hospital setting are drug eruptions and skin infections. Dermatitis is the most misdiagnosed condition by nondermatologists in hospitals, says Russell Vinik, MD, co-director of the hospitalist group at the University of Utah Health Care in Salt Lake City.
The majority of skin issues don’t require a dermatologist’s input, but some do. “Clearly, there’s also the rash that we just don’t know what it is,” Dr. Vinik says. When in doubt, it’s best to err on the safe side and call the specialist.
Here’s how to assess whether to manage a dermatologic case yourself, or how to involve a dermatologist for appropriate diagnosis and treatment. In general, Dr. Hopkins says, “Whether one can handle a case on their own or not is a case-by-case decision by the hospitalist based on their comfort with their diagnosis and management.”
Maintain a broader range of differential diagnoses before ruling in or out something more concrete.
“Very often, patients with skin diseases are given a specific diagnosis without consideration of mimickers,” says Daniela Kroshinsky, MD, MPH, assistant professor of dermatology at Harvard Medical School in Boston.
“Cellulitis is a great example. People will come in with hot, red skin and be diagnosed with and treated for cellulitis but really have stasis dermatitis, Lyme [disease], gout, et cetera,” says Dr. Kroshinsky, who also is director of pediatric dermatology and director of inpatient dermatology, education, and research at Massachusetts General Hospital.
“The clinical picture of warm, red, tender skin can fit many conditions but is most often called cellulitis by nondermatologists,” she explains. “It’s not clear why, but I would suspect this is because cellulitis is one of the few dermatologic conditions taught in medical school, while the mimickers get less attention.”
Attend dermatology lectures as part of primary care’s continuing medical education courses.
This would increase your knowledge of skin conditions affecting hospitalized patients, Dr. Kroshinsky says. If there is a dermatologic consultant for your hospital, work closely with this specialist until you feel comfortable making diagnoses and incorporating treatment plans.
Similarly, if you are a resident who is interested in a career in hospital medicine, consider doing a rotation in dermatology.
Review a good basic dermatology atlas from time to time.
This keeps your mind open to differential diagnoses for a given situation that you may encounter in the hospital setting. A more comprehensive book or online reference can be helpful to peruse after seeing a patient with a particular rash, Dr. Kroshinsky says.
Learn to correctly describe lesions to a dermatologist by phone.
When a specialist isn’t available on site, the phone communication is vital to the specialist. This includes familiarizing yourself with some of the more life-threatening dermatologic problems, such as drug-induced hypersensitivity reactions. It will be easier to recognize when an urgent dermatologic consultation is required. Sometimes this is necessary when a patient doesn’t respond to treatment for a reasonable and presumed diagnosis—when one condition seems to mimic the symptoms of another, says Lindy Fox, MD, associate professor of clinical dermatology at the University of California at San Francisco and director of its hospital dermatology consultation service.
Don’t assume that groin rashes are all fungal.
In fact, there is a very large differential diagnosis for intertriginous eruptions, Dr. Fox says. Perform a KOH test (potassium hydroxide) and fungal cultures on intertriginous eruptions. If no fungus is identified or the patient is not responding appropriately to therapy, call for a dermatologic consultation.
Don’t mistakenly associate a drug-related reaction with a medication given one to two days before the onset of a rash.
It is typically seven to 10 days post-exposure that a drug eruption develops, Dr. Fox says. He suggests making a drug chart to highlight dates of medication administration. This helps pinpoint the most likely culprit based on timing and the probability that a certain drug may induce cutaneous eruptions. Correct identification of the type of drug eruption (e.g. simple drug eruption vs. hypersensitivity vs. potentially deadly Stevens-Johnson syndrome) is important.
Consider involving a dermatologist to help manage open skin lesions, particularly if you’re unsure of the cause.
There are many different causes of skin ulcers. Trauma, infections, and even malignancies can present as open wounds. Leg ulcers may be due to venous stasis, but they also can be caused by arterial insufficiency, vasculitis, and other conditions. A dermatologist might opt to perform a skin biopsy to help diagnose the lesion.

“Wound-care nurses can be very helpful in managing skin lesions, but they do not always have the experience needed to correctly diagnose the underlying problem,” says Kathryn Schwarzenberger, MD, professor of medicine at the University of Vermont College of Medicine in Burlington. “If you’re thinking of calling the wound-care nurse, think of calling the dermatologist first.”
Prescribe an adequate quantity of topical corticosteroids for the duration of treatment.
“It’s really important to provide enough medicine,” Dr. Schwarzenberger says. Typically, a patient will receive a small tube, apply the contents, and find that “it’s enough medicine to cover their body once. This doesn’t work if you intended to have the patient apply it all over for two weeks.”
It takes, on average, 30 g of a topical medication to cover the body once. With topical steroids, prescribing an insufficient quantity “dooms your therapy to failure.”
Allergic reactions from these medications are rare, and some insurance companies charge the same regardless of the size. Prescribing a small amount initially might incur an additional expense for the patient.
Beware of painful or blistering rashes, especially if they involve the mucosa of the mouth, eyes, or genitals.
“These symptoms can be associated with potentially deadly toxic epidermal necrolysis,” says Daniel Aires, MD, JD, director of the division of dermatology at the University of Kansas School of Medicine in Kansas City, Kan. “Consult dermatology immediately. The sooner treatment is begun, the better the odds of survival.”
If a rash involves the eye, call an ophthalmologist and a dermatologist. “Eyes are more likely than skin to develop chronic complications after resolution of an acute condition,” he says.
For a rash involving primarily the mouth, call an otolaryngologist, a dentist, or both, as well as a dermatologist. These specialists are more skilled in visualizing and treating oral conditions.
Watch out for zoster, widespread herpes, pemphigus, and pemphigoid.
These blistering conditions require urgent diagnosis and treatment, so a dermatologist’s expertise is needed quickly, Dr. Aires says. Even without the presence of blisters, a single region of the skin or “dermatome” gives pause for concern.

“This could be a sign of zoster, which is especially dangerous in immunosuppressed or otherwise debilitated patients,” he cautions. “Either perform a culture and begin treatment, or consult dermatology, or do both.”
Pay attention to itching in the wrists, genital region, and web spaces of fingers and toes.
This may be due to scabies infestation. “Scabies can spread rapidly throughout a hospital ward,” Dr. Aires says. What to do: Scrape for scabies, consider a trial of topical treatment, and consult a dermatologist if you’re unsure.
Be mindful of the rapid onset of purpuric lesionscon the skin.
They warrant suspicion of such conditions as vasculitis, hypercoaguable states, and disseminated angiotropic infections, says Dr. Hopkins of Oregon Health & Science University. “The shape and size of purpuric skin lesions help determine the etiology. A few characteristic examples include papular purpura and retiform purpura. Papular purpura [raised purpuric papules] may suggest vasculitis. Purpura that forms net-like patches is called retiform purpura and suggests a vaso-occlusive process, such as from a hypercoaguable state, embolic phenomena, or calciphylaxis.”
13 Avoid consults for improving rashes and seborrheic keratosis, as well as nonurgent outpatient issues, such as psoriasis, rosacea, or a history of skin cancer. These conditions “are more easily addressed in a clinic, as opposed to in a hospital, where the patient is lying in a bed feeling ill with IV tubes in place,” Dr. Aires says. “It also reflects respect for the dermatologist’s time. Inpatient dermatology can be pretty busy, so it’s preferable to consult primarily for urgent skin issues.” Consultations can be costly, too, and most patients would rather avoid additional medical bills.
Don’t prescribe combined betamethasone/clotrimazole, also known as Lotrisone, for chronic scaly hands, feet, or groin.
Although it is not harmful, “it is not usually a great choice for typical ‘dermatophyte’ fungal infections, such as athlete’s foot and ‘jock itch,’” Dr. Aires says. “Over-the-counter Lamisil is better, particularly following daily use of 10-minute soaks in 50-50 vinegar-water. Even for yeast infections, miconazole is better than clotrimazole.”
As for betamethasone, this “component is way too strong for the groin area and can cause atrophy or worse,” he says.

—Daniela Kroshinsky, MD, MPH, director of inpatient dermatology, education, and research, Massachusetts General Hospital, Boston
Encourage patients to follow up with a dermatologist on an outpatient basis.
By heeding this advice, patients are less likely to return to the ED for skin conditions that can be managed in an office, says Kirsten Flynn, MD, a dermatologist at Banner Health Center in Sun City West, Ariz. Inpatient admissions by dermatologists have been decreasing over the years. Most patients with skin diseases or cutaneous manifestations of systemic illnesses are admitted to hospitals by other physicians.
“Many dermatologists are happy to fit in urgent consults in their clinics. Drug eruptions are by far the most common consultation request,” says Dr. Flynn, who notes that high-dose IV steroids can cause complications, such as gastrointestinal bleeding, bowel perforation, opportunistic infections, and exacerbation of underlying diseases. “In most cases, removing the offending agent and providing supportive care is the best option.”
Susan Kreimer is a freelance writer in New York.
- Maintain a broader range of differential diagnoses before ruling in or out something more concrete.
- Attend dermatology lectures as part of primary care’s continuing medical education courses.
- Review a good basic dermatology atlas from time to time.
- Learn to correctly describe lesions to a dermatologist by phone.
- Don’t assume that groin rashes are all fungal.
- Don’t mistakenly associate a drug-related reaction with a medication given one to two days before the onset of a rash.
- Consider involving a dermatologist to help manage open skin lesions, particularly if you’re unsure of the cause.
- Prescribe an adequate quantity of topical corticosteroids for the duration of treatment.
- Beware of painful or blistering rashes, especially if they involve the mucosa of the mouth, eyes, or genitals.
- Watch out for zoster, widespread herpes, pemphigus, and pemphigoid.
- Pay attention to itching in the wrists, genital region, and web spaces of fingers and toes.
- Be mindful of the rapid onset of purpuric lesions on the skin.
- Avoid consults for improving rashes and seborrheic keratosis, as well as nonurgent outpatient issues, such as psoriasis, rosacea, or a history of skin cancer.
- Don’t prescribe combined betamethasone/clotrimazole, also known as Lotrisone, for chronic scaly hands, feet, or groin.
- Encourage patients to follow up with a dermatologist on an outpatient basis.
Dermatologic diseases tend to receive little attention at most U.S. medical schools—typically only several days of lectures or a few weeks of clinical exposure.
“Not surprisingly, many general practitioners may feel unprepared to address hospitalized patients with challenging dermatologic findings,” says R. Samuel Hopkins, MD, assistant professor of dermatology and assistant residency program director at Oregon Health & Science University in Portland.
Few studies have examined the quality of inpatient dermatologic care. One study, a retrospective chart review at a Midwestern university hospital, found that the primary ward team submitted an accurate dermatologic diagnosis in only 23.9% of cases. Meanwhile, consultation with a dermatologist led to a change or addition to treatment in 77% of patients (Dermatol Online J. 2010;16(2):12).
“Given that medical schools may not be able to dedicate more time to managing dermatologic conditions, the burden of education may fall on post-graduate programs and continuing medical education to fill this gap,” Dr. Hopkins says. To further complicate matters, “it is difficult in many hospitals to obtain a dermatology consult on an inpatient, reflecting the limited access hospitalists often have to dermatologists.”
The most frequently encountered dermatologic conditions in the hospital setting are drug eruptions and skin infections. Dermatitis is the most misdiagnosed condition by nondermatologists in hospitals, says Russell Vinik, MD, co-director of the hospitalist group at the University of Utah Health Care in Salt Lake City.
The majority of skin issues don’t require a dermatologist’s input, but some do. “Clearly, there’s also the rash that we just don’t know what it is,” Dr. Vinik says. When in doubt, it’s best to err on the safe side and call the specialist.
Here’s how to assess whether to manage a dermatologic case yourself, or how to involve a dermatologist for appropriate diagnosis and treatment. In general, Dr. Hopkins says, “Whether one can handle a case on their own or not is a case-by-case decision by the hospitalist based on their comfort with their diagnosis and management.”
Maintain a broader range of differential diagnoses before ruling in or out something more concrete.
“Very often, patients with skin diseases are given a specific diagnosis without consideration of mimickers,” says Daniela Kroshinsky, MD, MPH, assistant professor of dermatology at Harvard Medical School in Boston.
“Cellulitis is a great example. People will come in with hot, red skin and be diagnosed with and treated for cellulitis but really have stasis dermatitis, Lyme [disease], gout, et cetera,” says Dr. Kroshinsky, who also is director of pediatric dermatology and director of inpatient dermatology, education, and research at Massachusetts General Hospital.
“The clinical picture of warm, red, tender skin can fit many conditions but is most often called cellulitis by nondermatologists,” she explains. “It’s not clear why, but I would suspect this is because cellulitis is one of the few dermatologic conditions taught in medical school, while the mimickers get less attention.”
Attend dermatology lectures as part of primary care’s continuing medical education courses.
This would increase your knowledge of skin conditions affecting hospitalized patients, Dr. Kroshinsky says. If there is a dermatologic consultant for your hospital, work closely with this specialist until you feel comfortable making diagnoses and incorporating treatment plans.
Similarly, if you are a resident who is interested in a career in hospital medicine, consider doing a rotation in dermatology.
Review a good basic dermatology atlas from time to time.
This keeps your mind open to differential diagnoses for a given situation that you may encounter in the hospital setting. A more comprehensive book or online reference can be helpful to peruse after seeing a patient with a particular rash, Dr. Kroshinsky says.
Learn to correctly describe lesions to a dermatologist by phone.
When a specialist isn’t available on site, the phone communication is vital to the specialist. This includes familiarizing yourself with some of the more life-threatening dermatologic problems, such as drug-induced hypersensitivity reactions. It will be easier to recognize when an urgent dermatologic consultation is required. Sometimes this is necessary when a patient doesn’t respond to treatment for a reasonable and presumed diagnosis—when one condition seems to mimic the symptoms of another, says Lindy Fox, MD, associate professor of clinical dermatology at the University of California at San Francisco and director of its hospital dermatology consultation service.
Don’t assume that groin rashes are all fungal.
In fact, there is a very large differential diagnosis for intertriginous eruptions, Dr. Fox says. Perform a KOH test (potassium hydroxide) and fungal cultures on intertriginous eruptions. If no fungus is identified or the patient is not responding appropriately to therapy, call for a dermatologic consultation.
Don’t mistakenly associate a drug-related reaction with a medication given one to two days before the onset of a rash.
It is typically seven to 10 days post-exposure that a drug eruption develops, Dr. Fox says. He suggests making a drug chart to highlight dates of medication administration. This helps pinpoint the most likely culprit based on timing and the probability that a certain drug may induce cutaneous eruptions. Correct identification of the type of drug eruption (e.g. simple drug eruption vs. hypersensitivity vs. potentially deadly Stevens-Johnson syndrome) is important.
Consider involving a dermatologist to help manage open skin lesions, particularly if you’re unsure of the cause.
There are many different causes of skin ulcers. Trauma, infections, and even malignancies can present as open wounds. Leg ulcers may be due to venous stasis, but they also can be caused by arterial insufficiency, vasculitis, and other conditions. A dermatologist might opt to perform a skin biopsy to help diagnose the lesion.
“Wound-care nurses can be very helpful in managing skin lesions, but they do not always have the experience needed to correctly diagnose the underlying problem,” says Kathryn Schwarzenberger, MD, professor of medicine at the University of Vermont College of Medicine in Burlington. “If you’re thinking of calling the wound-care nurse, think of calling the dermatologist first.”
Prescribe an adequate quantity of topical corticosteroids for the duration of treatment.
“It’s really important to provide enough medicine,” Dr. Schwarzenberger says. Typically, a patient will receive a small tube, apply the contents, and find that “it’s enough medicine to cover their body once. This doesn’t work if you intended to have the patient apply it all over for two weeks.”
It takes, on average, 30 g of a topical medication to cover the body once. With topical steroids, prescribing an insufficient quantity “dooms your therapy to failure.”
Allergic reactions from these medications are rare, and some insurance companies charge the same regardless of the size. Prescribing a small amount initially might incur an additional expense for the patient.
Beware of painful or blistering rashes, especially if they involve the mucosa of the mouth, eyes, or genitals.
“These symptoms can be associated with potentially deadly toxic epidermal necrolysis,” says Daniel Aires, MD, JD, director of the division of dermatology at the University of Kansas School of Medicine in Kansas City, Kan. “Consult dermatology immediately. The sooner treatment is begun, the better the odds of survival.”
If a rash involves the eye, call an ophthalmologist and a dermatologist. “Eyes are more likely than skin to develop chronic complications after resolution of an acute condition,” he says.
For a rash involving primarily the mouth, call an otolaryngologist, a dentist, or both, as well as a dermatologist. These specialists are more skilled in visualizing and treating oral conditions.
Watch out for zoster, widespread herpes, pemphigus, and pemphigoid.
These blistering conditions require urgent diagnosis and treatment, so a dermatologist’s expertise is needed quickly, Dr. Aires says. Even without the presence of blisters, a single region of the skin or “dermatome” gives pause for concern.
“This could be a sign of zoster, which is especially dangerous in immunosuppressed or otherwise debilitated patients,” he cautions. “Either perform a culture and begin treatment, or consult dermatology, or do both.”
Pay attention to itching in the wrists, genital region, and web spaces of fingers and toes.
This may be due to scabies infestation. “Scabies can spread rapidly throughout a hospital ward,” Dr. Aires says. What to do: Scrape for scabies, consider a trial of topical treatment, and consult a dermatologist if you’re unsure.
Be mindful of the rapid onset of purpuric lesionscon the skin.
They warrant suspicion of such conditions as vasculitis, hypercoaguable states, and disseminated angiotropic infections, says Dr. Hopkins of Oregon Health & Science University. “The shape and size of purpuric skin lesions help determine the etiology. A few characteristic examples include papular purpura and retiform purpura. Papular purpura [raised purpuric papules] may suggest vasculitis. Purpura that forms net-like patches is called retiform purpura and suggests a vaso-occlusive process, such as from a hypercoaguable state, embolic phenomena, or calciphylaxis.”
13 Avoid consults for improving rashes and seborrheic keratosis, as well as nonurgent outpatient issues, such as psoriasis, rosacea, or a history of skin cancer. These conditions “are more easily addressed in a clinic, as opposed to in a hospital, where the patient is lying in a bed feeling ill with IV tubes in place,” Dr. Aires says. “It also reflects respect for the dermatologist’s time. Inpatient dermatology can be pretty busy, so it’s preferable to consult primarily for urgent skin issues.” Consultations can be costly, too, and most patients would rather avoid additional medical bills.
Don’t prescribe combined betamethasone/clotrimazole, also known as Lotrisone, for chronic scaly hands, feet, or groin.
Although it is not harmful, “it is not usually a great choice for typical ‘dermatophyte’ fungal infections, such as athlete’s foot and ‘jock itch,’” Dr. Aires says. “Over-the-counter Lamisil is better, particularly following daily use of 10-minute soaks in 50-50 vinegar-water. Even for yeast infections, miconazole is better than clotrimazole.”
As for betamethasone, this “component is way too strong for the groin area and can cause atrophy or worse,” he says.
—Daniela Kroshinsky, MD, MPH, director of inpatient dermatology, education, and research, Massachusetts General Hospital, Boston
Encourage patients to follow up with a dermatologist on an outpatient basis.
By heeding this advice, patients are less likely to return to the ED for skin conditions that can be managed in an office, says Kirsten Flynn, MD, a dermatologist at Banner Health Center in Sun City West, Ariz. Inpatient admissions by dermatologists have been decreasing over the years. Most patients with skin diseases or cutaneous manifestations of systemic illnesses are admitted to hospitals by other physicians.
“Many dermatologists are happy to fit in urgent consults in their clinics. Drug eruptions are by far the most common consultation request,” says Dr. Flynn, who notes that high-dose IV steroids can cause complications, such as gastrointestinal bleeding, bowel perforation, opportunistic infections, and exacerbation of underlying diseases. “In most cases, removing the offending agent and providing supportive care is the best option.”
Susan Kreimer is a freelance writer in New York.
- Maintain a broader range of differential diagnoses before ruling in or out something more concrete.
- Attend dermatology lectures as part of primary care’s continuing medical education courses.
- Review a good basic dermatology atlas from time to time.
- Learn to correctly describe lesions to a dermatologist by phone.
- Don’t assume that groin rashes are all fungal.
- Don’t mistakenly associate a drug-related reaction with a medication given one to two days before the onset of a rash.
- Consider involving a dermatologist to help manage open skin lesions, particularly if you’re unsure of the cause.
- Prescribe an adequate quantity of topical corticosteroids for the duration of treatment.
- Beware of painful or blistering rashes, especially if they involve the mucosa of the mouth, eyes, or genitals.
- Watch out for zoster, widespread herpes, pemphigus, and pemphigoid.
- Pay attention to itching in the wrists, genital region, and web spaces of fingers and toes.
- Be mindful of the rapid onset of purpuric lesions on the skin.
- Avoid consults for improving rashes and seborrheic keratosis, as well as nonurgent outpatient issues, such as psoriasis, rosacea, or a history of skin cancer.
- Don’t prescribe combined betamethasone/clotrimazole, also known as Lotrisone, for chronic scaly hands, feet, or groin.
- Encourage patients to follow up with a dermatologist on an outpatient basis.
Dermatologic diseases tend to receive little attention at most U.S. medical schools—typically only several days of lectures or a few weeks of clinical exposure.
“Not surprisingly, many general practitioners may feel unprepared to address hospitalized patients with challenging dermatologic findings,” says R. Samuel Hopkins, MD, assistant professor of dermatology and assistant residency program director at Oregon Health & Science University in Portland.
Few studies have examined the quality of inpatient dermatologic care. One study, a retrospective chart review at a Midwestern university hospital, found that the primary ward team submitted an accurate dermatologic diagnosis in only 23.9% of cases. Meanwhile, consultation with a dermatologist led to a change or addition to treatment in 77% of patients (Dermatol Online J. 2010;16(2):12).
“Given that medical schools may not be able to dedicate more time to managing dermatologic conditions, the burden of education may fall on post-graduate programs and continuing medical education to fill this gap,” Dr. Hopkins says. To further complicate matters, “it is difficult in many hospitals to obtain a dermatology consult on an inpatient, reflecting the limited access hospitalists often have to dermatologists.”
The most frequently encountered dermatologic conditions in the hospital setting are drug eruptions and skin infections. Dermatitis is the most misdiagnosed condition by nondermatologists in hospitals, says Russell Vinik, MD, co-director of the hospitalist group at the University of Utah Health Care in Salt Lake City.
The majority of skin issues don’t require a dermatologist’s input, but some do. “Clearly, there’s also the rash that we just don’t know what it is,” Dr. Vinik says. When in doubt, it’s best to err on the safe side and call the specialist.
Here’s how to assess whether to manage a dermatologic case yourself, or how to involve a dermatologist for appropriate diagnosis and treatment. In general, Dr. Hopkins says, “Whether one can handle a case on their own or not is a case-by-case decision by the hospitalist based on their comfort with their diagnosis and management.”
Maintain a broader range of differential diagnoses before ruling in or out something more concrete.
“Very often, patients with skin diseases are given a specific diagnosis without consideration of mimickers,” says Daniela Kroshinsky, MD, MPH, assistant professor of dermatology at Harvard Medical School in Boston.
“Cellulitis is a great example. People will come in with hot, red skin and be diagnosed with and treated for cellulitis but really have stasis dermatitis, Lyme [disease], gout, et cetera,” says Dr. Kroshinsky, who also is director of pediatric dermatology and director of inpatient dermatology, education, and research at Massachusetts General Hospital.
“The clinical picture of warm, red, tender skin can fit many conditions but is most often called cellulitis by nondermatologists,” she explains. “It’s not clear why, but I would suspect this is because cellulitis is one of the few dermatologic conditions taught in medical school, while the mimickers get less attention.”
Attend dermatology lectures as part of primary care’s continuing medical education courses.
This would increase your knowledge of skin conditions affecting hospitalized patients, Dr. Kroshinsky says. If there is a dermatologic consultant for your hospital, work closely with this specialist until you feel comfortable making diagnoses and incorporating treatment plans.
Similarly, if you are a resident who is interested in a career in hospital medicine, consider doing a rotation in dermatology.
Review a good basic dermatology atlas from time to time.
This keeps your mind open to differential diagnoses for a given situation that you may encounter in the hospital setting. A more comprehensive book or online reference can be helpful to peruse after seeing a patient with a particular rash, Dr. Kroshinsky says.
Learn to correctly describe lesions to a dermatologist by phone.
When a specialist isn’t available on site, the phone communication is vital to the specialist. This includes familiarizing yourself with some of the more life-threatening dermatologic problems, such as drug-induced hypersensitivity reactions. It will be easier to recognize when an urgent dermatologic consultation is required. Sometimes this is necessary when a patient doesn’t respond to treatment for a reasonable and presumed diagnosis—when one condition seems to mimic the symptoms of another, says Lindy Fox, MD, associate professor of clinical dermatology at the University of California at San Francisco and director of its hospital dermatology consultation service.
Don’t assume that groin rashes are all fungal.
In fact, there is a very large differential diagnosis for intertriginous eruptions, Dr. Fox says. Perform a KOH test (potassium hydroxide) and fungal cultures on intertriginous eruptions. If no fungus is identified or the patient is not responding appropriately to therapy, call for a dermatologic consultation.
Don’t mistakenly associate a drug-related reaction with a medication given one to two days before the onset of a rash.
It is typically seven to 10 days post-exposure that a drug eruption develops, Dr. Fox says. He suggests making a drug chart to highlight dates of medication administration. This helps pinpoint the most likely culprit based on timing and the probability that a certain drug may induce cutaneous eruptions. Correct identification of the type of drug eruption (e.g. simple drug eruption vs. hypersensitivity vs. potentially deadly Stevens-Johnson syndrome) is important.
Consider involving a dermatologist to help manage open skin lesions, particularly if you’re unsure of the cause.
There are many different causes of skin ulcers. Trauma, infections, and even malignancies can present as open wounds. Leg ulcers may be due to venous stasis, but they also can be caused by arterial insufficiency, vasculitis, and other conditions. A dermatologist might opt to perform a skin biopsy to help diagnose the lesion.
“Wound-care nurses can be very helpful in managing skin lesions, but they do not always have the experience needed to correctly diagnose the underlying problem,” says Kathryn Schwarzenberger, MD, professor of medicine at the University of Vermont College of Medicine in Burlington. “If you’re thinking of calling the wound-care nurse, think of calling the dermatologist first.”
Prescribe an adequate quantity of topical corticosteroids for the duration of treatment.
“It’s really important to provide enough medicine,” Dr. Schwarzenberger says. Typically, a patient will receive a small tube, apply the contents, and find that “it’s enough medicine to cover their body once. This doesn’t work if you intended to have the patient apply it all over for two weeks.”
It takes, on average, 30 g of a topical medication to cover the body once. With topical steroids, prescribing an insufficient quantity “dooms your therapy to failure.”
Allergic reactions from these medications are rare, and some insurance companies charge the same regardless of the size. Prescribing a small amount initially might incur an additional expense for the patient.
Beware of painful or blistering rashes, especially if they involve the mucosa of the mouth, eyes, or genitals.
“These symptoms can be associated with potentially deadly toxic epidermal necrolysis,” says Daniel Aires, MD, JD, director of the division of dermatology at the University of Kansas School of Medicine in Kansas City, Kan. “Consult dermatology immediately. The sooner treatment is begun, the better the odds of survival.”
If a rash involves the eye, call an ophthalmologist and a dermatologist. “Eyes are more likely than skin to develop chronic complications after resolution of an acute condition,” he says.
For a rash involving primarily the mouth, call an otolaryngologist, a dentist, or both, as well as a dermatologist. These specialists are more skilled in visualizing and treating oral conditions.
Watch out for zoster, widespread herpes, pemphigus, and pemphigoid.
These blistering conditions require urgent diagnosis and treatment, so a dermatologist’s expertise is needed quickly, Dr. Aires says. Even without the presence of blisters, a single region of the skin or “dermatome” gives pause for concern.
“This could be a sign of zoster, which is especially dangerous in immunosuppressed or otherwise debilitated patients,” he cautions. “Either perform a culture and begin treatment, or consult dermatology, or do both.”
Pay attention to itching in the wrists, genital region, and web spaces of fingers and toes.
This may be due to scabies infestation. “Scabies can spread rapidly throughout a hospital ward,” Dr. Aires says. What to do: Scrape for scabies, consider a trial of topical treatment, and consult a dermatologist if you’re unsure.
Be mindful of the rapid onset of purpuric lesionscon the skin.
They warrant suspicion of such conditions as vasculitis, hypercoaguable states, and disseminated angiotropic infections, says Dr. Hopkins of Oregon Health & Science University. “The shape and size of purpuric skin lesions help determine the etiology. A few characteristic examples include papular purpura and retiform purpura. Papular purpura [raised purpuric papules] may suggest vasculitis. Purpura that forms net-like patches is called retiform purpura and suggests a vaso-occlusive process, such as from a hypercoaguable state, embolic phenomena, or calciphylaxis.”
13 Avoid consults for improving rashes and seborrheic keratosis, as well as nonurgent outpatient issues, such as psoriasis, rosacea, or a history of skin cancer. These conditions “are more easily addressed in a clinic, as opposed to in a hospital, where the patient is lying in a bed feeling ill with IV tubes in place,” Dr. Aires says. “It also reflects respect for the dermatologist’s time. Inpatient dermatology can be pretty busy, so it’s preferable to consult primarily for urgent skin issues.” Consultations can be costly, too, and most patients would rather avoid additional medical bills.
Don’t prescribe combined betamethasone/clotrimazole, also known as Lotrisone, for chronic scaly hands, feet, or groin.
Although it is not harmful, “it is not usually a great choice for typical ‘dermatophyte’ fungal infections, such as athlete’s foot and ‘jock itch,’” Dr. Aires says. “Over-the-counter Lamisil is better, particularly following daily use of 10-minute soaks in 50-50 vinegar-water. Even for yeast infections, miconazole is better than clotrimazole.”
As for betamethasone, this “component is way too strong for the groin area and can cause atrophy or worse,” he says.
—Daniela Kroshinsky, MD, MPH, director of inpatient dermatology, education, and research, Massachusetts General Hospital, Boston
Encourage patients to follow up with a dermatologist on an outpatient basis.
By heeding this advice, patients are less likely to return to the ED for skin conditions that can be managed in an office, says Kirsten Flynn, MD, a dermatologist at Banner Health Center in Sun City West, Ariz. Inpatient admissions by dermatologists have been decreasing over the years. Most patients with skin diseases or cutaneous manifestations of systemic illnesses are admitted to hospitals by other physicians.
“Many dermatologists are happy to fit in urgent consults in their clinics. Drug eruptions are by far the most common consultation request,” says Dr. Flynn, who notes that high-dose IV steroids can cause complications, such as gastrointestinal bleeding, bowel perforation, opportunistic infections, and exacerbation of underlying diseases. “In most cases, removing the offending agent and providing supportive care is the best option.”
Susan Kreimer is a freelance writer in New York.
AMA Report Offers Nine Steps to Help PCPs Prevent Readmissions
The American Medical Association recently released a report developed by a 21-member expert panel proposing a nine-step plan for primary-care-physician (PCP) practices to play an integral role in improving care transitions and preventing avoidable rehospitalizations.2 The report recommends focusing on more than just the hospital-admitting diagnosis, conducting a thorough patient health assessment, clarifying the patient’s short- and long-term goals, and coordinating care with other care settings.
With simultaneous research in JAMA concluding that the vast majority of readmissions are for reasons unrelated to the previous hospital stay, coordination between the inpatient and outpatient teams is crucial to successful transitions of care.3 Moreover, a recent survey showed that nearly 30% of PCPs say they miss alerts about patients’ test results from an electronic health record (EHR) notification system.4 According to the survey by Hardeep Singh, MD, MPH, and colleagues from the Michael E. DeBakey VA Medical Center in Houston, the doctors received on average 63 such alerts per day. Seventy percent reported that they cannot effectively manage the alerts, and more than half said that the current EHR notification system makes it possible to miss test results.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
The American Medical Association recently released a report developed by a 21-member expert panel proposing a nine-step plan for primary-care-physician (PCP) practices to play an integral role in improving care transitions and preventing avoidable rehospitalizations.2 The report recommends focusing on more than just the hospital-admitting diagnosis, conducting a thorough patient health assessment, clarifying the patient’s short- and long-term goals, and coordinating care with other care settings.
With simultaneous research in JAMA concluding that the vast majority of readmissions are for reasons unrelated to the previous hospital stay, coordination between the inpatient and outpatient teams is crucial to successful transitions of care.3 Moreover, a recent survey showed that nearly 30% of PCPs say they miss alerts about patients’ test results from an electronic health record (EHR) notification system.4 According to the survey by Hardeep Singh, MD, MPH, and colleagues from the Michael E. DeBakey VA Medical Center in Houston, the doctors received on average 63 such alerts per day. Seventy percent reported that they cannot effectively manage the alerts, and more than half said that the current EHR notification system makes it possible to miss test results.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
The American Medical Association recently released a report developed by a 21-member expert panel proposing a nine-step plan for primary-care-physician (PCP) practices to play an integral role in improving care transitions and preventing avoidable rehospitalizations.2 The report recommends focusing on more than just the hospital-admitting diagnosis, conducting a thorough patient health assessment, clarifying the patient’s short- and long-term goals, and coordinating care with other care settings.
With simultaneous research in JAMA concluding that the vast majority of readmissions are for reasons unrelated to the previous hospital stay, coordination between the inpatient and outpatient teams is crucial to successful transitions of care.3 Moreover, a recent survey showed that nearly 30% of PCPs say they miss alerts about patients’ test results from an electronic health record (EHR) notification system.4 According to the survey by Hardeep Singh, MD, MPH, and colleagues from the Michael E. DeBakey VA Medical Center in Houston, the doctors received on average 63 such alerts per day. Seventy percent reported that they cannot effectively manage the alerts, and more than half said that the current EHR notification system makes it possible to miss test results.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
20 Things Psychiatrists Think Hospitalists Need to Know
20 Things At A Glance
- Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
- Secure patient consent before consulting a psychiatrist.
- Present the psychiatrist’s anticipated insight as a benefit to the patient.
- Ask the patient if it’s all right to discuss their health status and needs with family members.
- Recognize that psychiatric illness is real, not imaginary.
- Realize that not all sadness constitutes depression.
- Don’t gloss over the possibility of delirium.
- Take the time to really listen.
- Always remain conscious of alcohol and substance abuse.
- Monitor patients’ vital signs for autonomic instability.
- Avoid arguments and power struggles with difficult or demanding patients.
- Adapt your vocabulary to the patient’s and family’s level of understanding.
- Be mindful of your nonverbal cues.
- Always take suicide risk seriously.
- Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
- Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
- Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
- Listen to your instincts.
- Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
- Extend genuine compassion to your patients.
Patients can be hospitalized with chest pain, a kidney infection, pneumonia, or myriad other medical conditions. Hospital stays on occasion upend a patient’s mental state, with upcoming tests, surgery, or other procedures triggering anxiety or other conditions.
That doesn’t mean these patients have psychiatric or psychological problems, but some of them might. Hospitalists walk a fine line in deciding when to consult a psychiatrist in certain cases.

“A common mistake, when it comes to psychiatry, for hospitalists is to either think they know too much or they know too little,” says Philip R. Muskin, MD, professor of clinical psychiatry at Columbia University College of Physicians & Surgeons in New York City. “Sometimes they’re too quick to call a psychiatrist, and sometimes they’re too slow to call a specialist because they don’t think it’s a psychiatric problem.”
The Hospitalist asked more than half a dozen specialists in psychiatry and hospital medicine to shed light on when to seek additional expertise—and how to inform patients about your request to do so. “If I say, ‘You need to see a psychiatrist,’ it carries some stigma,” says Dr. Muskin, who is the chief of consultation for liaison psychiatry at New York-Presbyterian Medical Center’s Columbia campus. “We have to be sensitive to that.”
So how can you more comfortably approach psychiatric or psychological issues in the hospital setting?
1. Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
“Because of the overwhelming comorbidity between psychiatric illness and medical illness, it’s important to have some communication between the emergency room, caregiver, the hospitalist, and the psychiatrist,” says Ken Duckworth, MD, medical director of the National Alliance on Mental Illness (NAMI) and an assistant clinical professor of psychiatry at Harvard Medical School in Boston. “We know that people with mental health vulnerabilities consume a much higher amount of medical services. That’s a well-known phenomenon.”
2. Secure patient consent before consulting a psychiatrist.

“You need the patient’s permission,” Dr. Duckworth says. “That’s an important piece of the equation.” There are exceptions in emergencies, and the laws pertaining to this vary by state. Verbal consent may suffice if written authorization is already on file. If a patient declines, a hospitalist has to respect those wishes.
3. Present the psychiatrist’s anticipated insight as a benefit to the patient.

Physicians sometimes are uncomfortable informing their patients that they’re asking for a psychiatric consultation. They fear a bad reaction, such as “You think I’m crazy?” The consultation will be more useful if the patient is open and accepting of the process. For example, tell your patient at the outset: “I’d really like you to talk to one of my colleagues, whom I trust a great deal. He/she is an expert in the overlapping area between the body and the brain. I need their help so that I can take better care of you,’” says Linda L.M. Worley, MD, FAPM, professor of psychiatry and obstetrics and gynecology at the University of Arkansas for Medical Sciences in Little Rock.
4. Ask the patient if it’s all right to discuss their health status and needs with family members.
Get to know their names. Identify the medical expert in the family and be certain to involve them in overall discussions and the decision-making process, Dr. Worley says.
5. Recognize that psychiatric illness is real, not imaginary.
The illness “should be placed in exactly the same arena as other medical problems,” Dr. Muskin says. Patients with psychiatric conditions are “not weak. They’re not dumb. It’s not all in their head.” Their mental health “deserves the same attention as their heart, stomach, or kidneys.”
6. Realize that not all sadness constitutes depression.

“There are many reasons why people cry or feel down, and most are not psychiatric illnesses. Depression is often overdiagnosed, leading to wasted time and inappropriate medications,” says Robert Boland, MD, professor of psychiatry and human behavior at Brown University’s Warren Alpert School of Medicine in Providence, R.I. “Unfortunately, the opposite is also true. Depression is often missed in the hospital.”
So how does a hospitalist reconcile those extremes? First, consider depression in any patient who is predisposed, then rely on a consistent way of working it up. The Diagnostic and Statistical Manual of Mental Disorders (DSM, http://www.dsm5.org) offers a conservative approach, so you usually can’t go wrong by following it.
7. Don’t gloss over the possibility of delirium.
It is probably the most frequently missed diagnosis in the general hospital. “We usually recognize it when patients are agitated, but most patients aren’t,” Dr. Boland says. “If anything, they are hypoactive or change throughout the day. When a patient seems confused, we want to find a cause, but that cause isn’t always obvious.”
These situations are particularly true in fragile patients (e.g. the very old or those with dementia). Sometimes medical problems that seem very minor can “push them over the edge,” he adds. When you do expect dementia, the main treatments revolve around medically stabilizing the patient, and psychiatric medications are a minor part of the management, if at all.
8. Take the time to really listen.
Patients’ biggest complaint is that physicians don’t listen. “The best doctors in any specialty know how to communicate with patients,” Dr. Boland says. “It doesn’t take longer—in fact, good communication usually saves time. But it does take attention and focus to let the patient try and explain what is going on with them. It always pays off in the end.”
9. Always remain conscious of alcohol and substance abuse.
Although it might not be the reason patients are hospitalized, it is one of the more common underlying causes. When this is the case, don’t be nihilistic. Many patients improve with treatment, and some get better simply because a physician explained how damaging substance abuse can be to their health, Dr. Boland says.
For those in complete remission from a past addiction to alcohol, benzodiazepines, opiates, or a combination thereof, beware that prescribing certain medications puts them at substantially increased risk for relapse. Use alternative treatments whenever possible; if clinically indicated, be certain that these patients have a safety net to prevent relapse. Patients with severe pain need effective relief.
“If a patient has been exposed to significant dosages of pain medications in the past, their neurotransmitters will have physically adapted,” says Dr. Worley, president-elect of the Academy of Psychosomatic Medicine. “They will require higher doses than normal for effective pain relief.”

—Gregory Ruhnke, MD, assistant professor in the section of hospital medicine, University of Chicago Pritzker School of Medicine
10. Monitor patients’ vital signs for autonomic instability.
“Patients in withdrawal from physiologically addictive medications may have forgotten to tell you that they were taking these medications,” Dr. Worley says. “Abrupt discontinuation can cause incapacitating anxiety and life-threatening delirium.”
11. Avoid arguments and power struggles with difficult or demanding patients.
Put on your thick skin. Don’t take insults or slights personally. And resist the urge to flee or counterattack. Instead, Dr. Worley suggests hospitalists stay calm and focused on providing the best medical care that they can. “Chronically noncompliant patients can be excruciatingly frustrating to care for when they don’t follow through on what they are repeatedly advised to do, but lecturing more vigorously at them won’t help,” she says. “It only makes them shut down more and feel more helpless and you more exhausted. Shift to more of a listening mode and inquire about what they hope to accomplish by coming to you for help.”
12. Adapt your vocabulary to the patient’s and family’s level of understanding.
After your explanation, ask them, “Do me a favor and explain back to me in your words what I said. I want to be sure I got across what I wanted to say.” Then ask whether they have any questions. Also know that all too often patients are so anxious and upset that they are “emotionally flooded” and unable to hear much of what you communicated. You can save a lot of time if they understand you in the first place.
13. Be mindful of your nonverbal cues.
A majority of communication is nonverbal, and your facial expressions, gestures, and body posture speak volumes to patients and family members. “The innocent tilt of a chin upwards while peering through bifocals can be misperceived as arrogance,” Dr. Worley says. “The thoughtful furled brow of contemplation may be misconstrued as irritability or disapproval.”
14. Always take suicide risk seriously.
It’s better to call a psychiatrist unnecessarily than to overlook a patient at risk for suicide. Benzodiazepines, alcohol, or a combination of the two might reduce inhibition and increase the likelihood of a suicide attempt. Be sure to assess suicidal ideation, intent, and lethality of suicide attempt.
“Hopelessness about the future correlates with completed suicide,” says Gregory Ruhnke, MD, assistant professor in the section of hospital medicine at the University of Chicago Pritzker School of Medicine. “Additionally, it is helpful to ask about the four H’s: Hate, humiliation, hostility, handguns.”
15. Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
“The patient may become angry and engage in splitting, whereby he or she emphatically expresses the view that certain caregivers are all good or all bad. This may reflect such [a] patient’s desire to divide the caregivers into opposing factions. It’s a maladaptive way of coping,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the Pritzker School of Medicine. This can be very time-consuming, and it can breed hostility among colleagues. “Communication between caregivers is really important in creating a unified treatment plan that is coherently presented to the patient in a single voice.”
Fortunately, she says, “even though these situations can arise, they are the exception rather than the rule.”

—Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist, University of Chicago Pritzker School of Medicine
16. Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
For example, Dr. Ruhnke says, if a patient complains of hemoptysis and hematochezia with negative endoscopies, talk to the nurse about the patient’s diet, and be suspicious if it includes only red foods and liquids. The most common symptoms among patients who come to medical attention because of factitious disorders are diarrhea, fever of unknown origin, gastrointestinal bleeding, hematuria, seizures, and hypoglycemia.
17. Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
A patient with schizophrenia or bipolar disorder could experience a severe psychiatric episode without psychiatric medication. An appropriate alternative, perhaps administered intravenously if necessary, “can make all the difference in the world,” says Christopher Dobbelstein, MD, assistant professor of psychiatry at the University of Pittsburgh School of Medicine.
18. Listen to your instincts.
Medical teams can handle many psychiatric issues. Straightforward delirium is a good example. The bigger question, which takes experience and confidence, is to recognize when a line has been crossed. “The decision to consult psychiatry is not formulaic,” Dr. Dobbelstein says.
Sometimes a patient is acting strangely, and the team can’t explain why a psychiatrist could offer sound advice. “That’s when they should trust their instincts and consult us,” he says, “because the patient likely does have something more complex going on.”
19. Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
Sometimes psychiatric medications are started without good oversight. Suicide risk is highest during the weeks following an inpatient psychiatric admission, so a patient should see an outpatient mental health provider within seven days after hospital discharge, says NAMI’s Dr. Duckworth.
20. Extend genuine compassion to your patients.
“This is the secret to achieving a lifelong rewarding career in medicine,” Dr. Worley says, “and is the most important ingredient in positive outcomes.”
Susan Kreimer is a freelance writer in New York.
Survival Tips
- Pull up a chair and sit down.
- Ask what name your patient likes to go by. Be respectful and use correct titles when appropriate. One size doesn’t fit all. “Mrs. X” might be a mother-in-law.
- Appreciate how terrifying it can be as a patient—ill, in pain, having no control, with a loss of privacy and at times dignity.
- Remember that any one of us in the role of a patient regresses and copes in different ways. Some become demanding and express a strong need for control, while others want and need information from their physician.
- Privacy is important. Close the door. Don’t ask sensitive questions within earshot of other patients or visitors.
20 Things At A Glance
- Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
- Secure patient consent before consulting a psychiatrist.
- Present the psychiatrist’s anticipated insight as a benefit to the patient.
- Ask the patient if it’s all right to discuss their health status and needs with family members.
- Recognize that psychiatric illness is real, not imaginary.
- Realize that not all sadness constitutes depression.
- Don’t gloss over the possibility of delirium.
- Take the time to really listen.
- Always remain conscious of alcohol and substance abuse.
- Monitor patients’ vital signs for autonomic instability.
- Avoid arguments and power struggles with difficult or demanding patients.
- Adapt your vocabulary to the patient’s and family’s level of understanding.
- Be mindful of your nonverbal cues.
- Always take suicide risk seriously.
- Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
- Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
- Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
- Listen to your instincts.
- Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
- Extend genuine compassion to your patients.
Patients can be hospitalized with chest pain, a kidney infection, pneumonia, or myriad other medical conditions. Hospital stays on occasion upend a patient’s mental state, with upcoming tests, surgery, or other procedures triggering anxiety or other conditions.
That doesn’t mean these patients have psychiatric or psychological problems, but some of them might. Hospitalists walk a fine line in deciding when to consult a psychiatrist in certain cases.
“A common mistake, when it comes to psychiatry, for hospitalists is to either think they know too much or they know too little,” says Philip R. Muskin, MD, professor of clinical psychiatry at Columbia University College of Physicians & Surgeons in New York City. “Sometimes they’re too quick to call a psychiatrist, and sometimes they’re too slow to call a specialist because they don’t think it’s a psychiatric problem.”
The Hospitalist asked more than half a dozen specialists in psychiatry and hospital medicine to shed light on when to seek additional expertise—and how to inform patients about your request to do so. “If I say, ‘You need to see a psychiatrist,’ it carries some stigma,” says Dr. Muskin, who is the chief of consultation for liaison psychiatry at New York-Presbyterian Medical Center’s Columbia campus. “We have to be sensitive to that.”
So how can you more comfortably approach psychiatric or psychological issues in the hospital setting?
1. Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
“Because of the overwhelming comorbidity between psychiatric illness and medical illness, it’s important to have some communication between the emergency room, caregiver, the hospitalist, and the psychiatrist,” says Ken Duckworth, MD, medical director of the National Alliance on Mental Illness (NAMI) and an assistant clinical professor of psychiatry at Harvard Medical School in Boston. “We know that people with mental health vulnerabilities consume a much higher amount of medical services. That’s a well-known phenomenon.”
2. Secure patient consent before consulting a psychiatrist.
“You need the patient’s permission,” Dr. Duckworth says. “That’s an important piece of the equation.” There are exceptions in emergencies, and the laws pertaining to this vary by state. Verbal consent may suffice if written authorization is already on file. If a patient declines, a hospitalist has to respect those wishes.
3. Present the psychiatrist’s anticipated insight as a benefit to the patient.
Physicians sometimes are uncomfortable informing their patients that they’re asking for a psychiatric consultation. They fear a bad reaction, such as “You think I’m crazy?” The consultation will be more useful if the patient is open and accepting of the process. For example, tell your patient at the outset: “I’d really like you to talk to one of my colleagues, whom I trust a great deal. He/she is an expert in the overlapping area between the body and the brain. I need their help so that I can take better care of you,’” says Linda L.M. Worley, MD, FAPM, professor of psychiatry and obstetrics and gynecology at the University of Arkansas for Medical Sciences in Little Rock.
4. Ask the patient if it’s all right to discuss their health status and needs with family members.
Get to know their names. Identify the medical expert in the family and be certain to involve them in overall discussions and the decision-making process, Dr. Worley says.
5. Recognize that psychiatric illness is real, not imaginary.
The illness “should be placed in exactly the same arena as other medical problems,” Dr. Muskin says. Patients with psychiatric conditions are “not weak. They’re not dumb. It’s not all in their head.” Their mental health “deserves the same attention as their heart, stomach, or kidneys.”
6. Realize that not all sadness constitutes depression.
“There are many reasons why people cry or feel down, and most are not psychiatric illnesses. Depression is often overdiagnosed, leading to wasted time and inappropriate medications,” says Robert Boland, MD, professor of psychiatry and human behavior at Brown University’s Warren Alpert School of Medicine in Providence, R.I. “Unfortunately, the opposite is also true. Depression is often missed in the hospital.”
So how does a hospitalist reconcile those extremes? First, consider depression in any patient who is predisposed, then rely on a consistent way of working it up. The Diagnostic and Statistical Manual of Mental Disorders (DSM, http://www.dsm5.org) offers a conservative approach, so you usually can’t go wrong by following it.
7. Don’t gloss over the possibility of delirium.
It is probably the most frequently missed diagnosis in the general hospital. “We usually recognize it when patients are agitated, but most patients aren’t,” Dr. Boland says. “If anything, they are hypoactive or change throughout the day. When a patient seems confused, we want to find a cause, but that cause isn’t always obvious.”
These situations are particularly true in fragile patients (e.g. the very old or those with dementia). Sometimes medical problems that seem very minor can “push them over the edge,” he adds. When you do expect dementia, the main treatments revolve around medically stabilizing the patient, and psychiatric medications are a minor part of the management, if at all.
8. Take the time to really listen.
Patients’ biggest complaint is that physicians don’t listen. “The best doctors in any specialty know how to communicate with patients,” Dr. Boland says. “It doesn’t take longer—in fact, good communication usually saves time. But it does take attention and focus to let the patient try and explain what is going on with them. It always pays off in the end.”
9. Always remain conscious of alcohol and substance abuse.
Although it might not be the reason patients are hospitalized, it is one of the more common underlying causes. When this is the case, don’t be nihilistic. Many patients improve with treatment, and some get better simply because a physician explained how damaging substance abuse can be to their health, Dr. Boland says.
For those in complete remission from a past addiction to alcohol, benzodiazepines, opiates, or a combination thereof, beware that prescribing certain medications puts them at substantially increased risk for relapse. Use alternative treatments whenever possible; if clinically indicated, be certain that these patients have a safety net to prevent relapse. Patients with severe pain need effective relief.
“If a patient has been exposed to significant dosages of pain medications in the past, their neurotransmitters will have physically adapted,” says Dr. Worley, president-elect of the Academy of Psychosomatic Medicine. “They will require higher doses than normal for effective pain relief.”
—Gregory Ruhnke, MD, assistant professor in the section of hospital medicine, University of Chicago Pritzker School of Medicine
10. Monitor patients’ vital signs for autonomic instability.
“Patients in withdrawal from physiologically addictive medications may have forgotten to tell you that they were taking these medications,” Dr. Worley says. “Abrupt discontinuation can cause incapacitating anxiety and life-threatening delirium.”
11. Avoid arguments and power struggles with difficult or demanding patients.
Put on your thick skin. Don’t take insults or slights personally. And resist the urge to flee or counterattack. Instead, Dr. Worley suggests hospitalists stay calm and focused on providing the best medical care that they can. “Chronically noncompliant patients can be excruciatingly frustrating to care for when they don’t follow through on what they are repeatedly advised to do, but lecturing more vigorously at them won’t help,” she says. “It only makes them shut down more and feel more helpless and you more exhausted. Shift to more of a listening mode and inquire about what they hope to accomplish by coming to you for help.”
12. Adapt your vocabulary to the patient’s and family’s level of understanding.
After your explanation, ask them, “Do me a favor and explain back to me in your words what I said. I want to be sure I got across what I wanted to say.” Then ask whether they have any questions. Also know that all too often patients are so anxious and upset that they are “emotionally flooded” and unable to hear much of what you communicated. You can save a lot of time if they understand you in the first place.
13. Be mindful of your nonverbal cues.
A majority of communication is nonverbal, and your facial expressions, gestures, and body posture speak volumes to patients and family members. “The innocent tilt of a chin upwards while peering through bifocals can be misperceived as arrogance,” Dr. Worley says. “The thoughtful furled brow of contemplation may be misconstrued as irritability or disapproval.”
14. Always take suicide risk seriously.
It’s better to call a psychiatrist unnecessarily than to overlook a patient at risk for suicide. Benzodiazepines, alcohol, or a combination of the two might reduce inhibition and increase the likelihood of a suicide attempt. Be sure to assess suicidal ideation, intent, and lethality of suicide attempt.
“Hopelessness about the future correlates with completed suicide,” says Gregory Ruhnke, MD, assistant professor in the section of hospital medicine at the University of Chicago Pritzker School of Medicine. “Additionally, it is helpful to ask about the four H’s: Hate, humiliation, hostility, handguns.”
15. Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
“The patient may become angry and engage in splitting, whereby he or she emphatically expresses the view that certain caregivers are all good or all bad. This may reflect such [a] patient’s desire to divide the caregivers into opposing factions. It’s a maladaptive way of coping,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the Pritzker School of Medicine. This can be very time-consuming, and it can breed hostility among colleagues. “Communication between caregivers is really important in creating a unified treatment plan that is coherently presented to the patient in a single voice.”
Fortunately, she says, “even though these situations can arise, they are the exception rather than the rule.”
—Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist, University of Chicago Pritzker School of Medicine
16. Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
For example, Dr. Ruhnke says, if a patient complains of hemoptysis and hematochezia with negative endoscopies, talk to the nurse about the patient’s diet, and be suspicious if it includes only red foods and liquids. The most common symptoms among patients who come to medical attention because of factitious disorders are diarrhea, fever of unknown origin, gastrointestinal bleeding, hematuria, seizures, and hypoglycemia.
17. Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
A patient with schizophrenia or bipolar disorder could experience a severe psychiatric episode without psychiatric medication. An appropriate alternative, perhaps administered intravenously if necessary, “can make all the difference in the world,” says Christopher Dobbelstein, MD, assistant professor of psychiatry at the University of Pittsburgh School of Medicine.
18. Listen to your instincts.
Medical teams can handle many psychiatric issues. Straightforward delirium is a good example. The bigger question, which takes experience and confidence, is to recognize when a line has been crossed. “The decision to consult psychiatry is not formulaic,” Dr. Dobbelstein says.
Sometimes a patient is acting strangely, and the team can’t explain why a psychiatrist could offer sound advice. “That’s when they should trust their instincts and consult us,” he says, “because the patient likely does have something more complex going on.”
19. Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
Sometimes psychiatric medications are started without good oversight. Suicide risk is highest during the weeks following an inpatient psychiatric admission, so a patient should see an outpatient mental health provider within seven days after hospital discharge, says NAMI’s Dr. Duckworth.
20. Extend genuine compassion to your patients.
“This is the secret to achieving a lifelong rewarding career in medicine,” Dr. Worley says, “and is the most important ingredient in positive outcomes.”
Susan Kreimer is a freelance writer in New York.
Survival Tips
- Pull up a chair and sit down.
- Ask what name your patient likes to go by. Be respectful and use correct titles when appropriate. One size doesn’t fit all. “Mrs. X” might be a mother-in-law.
- Appreciate how terrifying it can be as a patient—ill, in pain, having no control, with a loss of privacy and at times dignity.
- Remember that any one of us in the role of a patient regresses and copes in different ways. Some become demanding and express a strong need for control, while others want and need information from their physician.
- Privacy is important. Close the door. Don’t ask sensitive questions within earshot of other patients or visitors.
20 Things At A Glance
- Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
- Secure patient consent before consulting a psychiatrist.
- Present the psychiatrist’s anticipated insight as a benefit to the patient.
- Ask the patient if it’s all right to discuss their health status and needs with family members.
- Recognize that psychiatric illness is real, not imaginary.
- Realize that not all sadness constitutes depression.
- Don’t gloss over the possibility of delirium.
- Take the time to really listen.
- Always remain conscious of alcohol and substance abuse.
- Monitor patients’ vital signs for autonomic instability.
- Avoid arguments and power struggles with difficult or demanding patients.
- Adapt your vocabulary to the patient’s and family’s level of understanding.
- Be mindful of your nonverbal cues.
- Always take suicide risk seriously.
- Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
- Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
- Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
- Listen to your instincts.
- Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
- Extend genuine compassion to your patients.
Patients can be hospitalized with chest pain, a kidney infection, pneumonia, or myriad other medical conditions. Hospital stays on occasion upend a patient’s mental state, with upcoming tests, surgery, or other procedures triggering anxiety or other conditions.
That doesn’t mean these patients have psychiatric or psychological problems, but some of them might. Hospitalists walk a fine line in deciding when to consult a psychiatrist in certain cases.
“A common mistake, when it comes to psychiatry, for hospitalists is to either think they know too much or they know too little,” says Philip R. Muskin, MD, professor of clinical psychiatry at Columbia University College of Physicians & Surgeons in New York City. “Sometimes they’re too quick to call a psychiatrist, and sometimes they’re too slow to call a specialist because they don’t think it’s a psychiatric problem.”
The Hospitalist asked more than half a dozen specialists in psychiatry and hospital medicine to shed light on when to seek additional expertise—and how to inform patients about your request to do so. “If I say, ‘You need to see a psychiatrist,’ it carries some stigma,” says Dr. Muskin, who is the chief of consultation for liaison psychiatry at New York-Presbyterian Medical Center’s Columbia campus. “We have to be sensitive to that.”
So how can you more comfortably approach psychiatric or psychological issues in the hospital setting?
1. Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
“Because of the overwhelming comorbidity between psychiatric illness and medical illness, it’s important to have some communication between the emergency room, caregiver, the hospitalist, and the psychiatrist,” says Ken Duckworth, MD, medical director of the National Alliance on Mental Illness (NAMI) and an assistant clinical professor of psychiatry at Harvard Medical School in Boston. “We know that people with mental health vulnerabilities consume a much higher amount of medical services. That’s a well-known phenomenon.”
2. Secure patient consent before consulting a psychiatrist.
“You need the patient’s permission,” Dr. Duckworth says. “That’s an important piece of the equation.” There are exceptions in emergencies, and the laws pertaining to this vary by state. Verbal consent may suffice if written authorization is already on file. If a patient declines, a hospitalist has to respect those wishes.
3. Present the psychiatrist’s anticipated insight as a benefit to the patient.
Physicians sometimes are uncomfortable informing their patients that they’re asking for a psychiatric consultation. They fear a bad reaction, such as “You think I’m crazy?” The consultation will be more useful if the patient is open and accepting of the process. For example, tell your patient at the outset: “I’d really like you to talk to one of my colleagues, whom I trust a great deal. He/she is an expert in the overlapping area between the body and the brain. I need their help so that I can take better care of you,’” says Linda L.M. Worley, MD, FAPM, professor of psychiatry and obstetrics and gynecology at the University of Arkansas for Medical Sciences in Little Rock.
4. Ask the patient if it’s all right to discuss their health status and needs with family members.
Get to know their names. Identify the medical expert in the family and be certain to involve them in overall discussions and the decision-making process, Dr. Worley says.
5. Recognize that psychiatric illness is real, not imaginary.
The illness “should be placed in exactly the same arena as other medical problems,” Dr. Muskin says. Patients with psychiatric conditions are “not weak. They’re not dumb. It’s not all in their head.” Their mental health “deserves the same attention as their heart, stomach, or kidneys.”
6. Realize that not all sadness constitutes depression.
“There are many reasons why people cry or feel down, and most are not psychiatric illnesses. Depression is often overdiagnosed, leading to wasted time and inappropriate medications,” says Robert Boland, MD, professor of psychiatry and human behavior at Brown University’s Warren Alpert School of Medicine in Providence, R.I. “Unfortunately, the opposite is also true. Depression is often missed in the hospital.”
So how does a hospitalist reconcile those extremes? First, consider depression in any patient who is predisposed, then rely on a consistent way of working it up. The Diagnostic and Statistical Manual of Mental Disorders (DSM, http://www.dsm5.org) offers a conservative approach, so you usually can’t go wrong by following it.
7. Don’t gloss over the possibility of delirium.
It is probably the most frequently missed diagnosis in the general hospital. “We usually recognize it when patients are agitated, but most patients aren’t,” Dr. Boland says. “If anything, they are hypoactive or change throughout the day. When a patient seems confused, we want to find a cause, but that cause isn’t always obvious.”
These situations are particularly true in fragile patients (e.g. the very old or those with dementia). Sometimes medical problems that seem very minor can “push them over the edge,” he adds. When you do expect dementia, the main treatments revolve around medically stabilizing the patient, and psychiatric medications are a minor part of the management, if at all.
8. Take the time to really listen.
Patients’ biggest complaint is that physicians don’t listen. “The best doctors in any specialty know how to communicate with patients,” Dr. Boland says. “It doesn’t take longer—in fact, good communication usually saves time. But it does take attention and focus to let the patient try and explain what is going on with them. It always pays off in the end.”
9. Always remain conscious of alcohol and substance abuse.
Although it might not be the reason patients are hospitalized, it is one of the more common underlying causes. When this is the case, don’t be nihilistic. Many patients improve with treatment, and some get better simply because a physician explained how damaging substance abuse can be to their health, Dr. Boland says.
For those in complete remission from a past addiction to alcohol, benzodiazepines, opiates, or a combination thereof, beware that prescribing certain medications puts them at substantially increased risk for relapse. Use alternative treatments whenever possible; if clinically indicated, be certain that these patients have a safety net to prevent relapse. Patients with severe pain need effective relief.
“If a patient has been exposed to significant dosages of pain medications in the past, their neurotransmitters will have physically adapted,” says Dr. Worley, president-elect of the Academy of Psychosomatic Medicine. “They will require higher doses than normal for effective pain relief.”
—Gregory Ruhnke, MD, assistant professor in the section of hospital medicine, University of Chicago Pritzker School of Medicine
10. Monitor patients’ vital signs for autonomic instability.
“Patients in withdrawal from physiologically addictive medications may have forgotten to tell you that they were taking these medications,” Dr. Worley says. “Abrupt discontinuation can cause incapacitating anxiety and life-threatening delirium.”
11. Avoid arguments and power struggles with difficult or demanding patients.
Put on your thick skin. Don’t take insults or slights personally. And resist the urge to flee or counterattack. Instead, Dr. Worley suggests hospitalists stay calm and focused on providing the best medical care that they can. “Chronically noncompliant patients can be excruciatingly frustrating to care for when they don’t follow through on what they are repeatedly advised to do, but lecturing more vigorously at them won’t help,” she says. “It only makes them shut down more and feel more helpless and you more exhausted. Shift to more of a listening mode and inquire about what they hope to accomplish by coming to you for help.”
12. Adapt your vocabulary to the patient’s and family’s level of understanding.
After your explanation, ask them, “Do me a favor and explain back to me in your words what I said. I want to be sure I got across what I wanted to say.” Then ask whether they have any questions. Also know that all too often patients are so anxious and upset that they are “emotionally flooded” and unable to hear much of what you communicated. You can save a lot of time if they understand you in the first place.
13. Be mindful of your nonverbal cues.
A majority of communication is nonverbal, and your facial expressions, gestures, and body posture speak volumes to patients and family members. “The innocent tilt of a chin upwards while peering through bifocals can be misperceived as arrogance,” Dr. Worley says. “The thoughtful furled brow of contemplation may be misconstrued as irritability or disapproval.”
14. Always take suicide risk seriously.
It’s better to call a psychiatrist unnecessarily than to overlook a patient at risk for suicide. Benzodiazepines, alcohol, or a combination of the two might reduce inhibition and increase the likelihood of a suicide attempt. Be sure to assess suicidal ideation, intent, and lethality of suicide attempt.
“Hopelessness about the future correlates with completed suicide,” says Gregory Ruhnke, MD, assistant professor in the section of hospital medicine at the University of Chicago Pritzker School of Medicine. “Additionally, it is helpful to ask about the four H’s: Hate, humiliation, hostility, handguns.”
15. Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
“The patient may become angry and engage in splitting, whereby he or she emphatically expresses the view that certain caregivers are all good or all bad. This may reflect such [a] patient’s desire to divide the caregivers into opposing factions. It’s a maladaptive way of coping,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the Pritzker School of Medicine. This can be very time-consuming, and it can breed hostility among colleagues. “Communication between caregivers is really important in creating a unified treatment plan that is coherently presented to the patient in a single voice.”
Fortunately, she says, “even though these situations can arise, they are the exception rather than the rule.”
—Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist, University of Chicago Pritzker School of Medicine
16. Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
For example, Dr. Ruhnke says, if a patient complains of hemoptysis and hematochezia with negative endoscopies, talk to the nurse about the patient’s diet, and be suspicious if it includes only red foods and liquids. The most common symptoms among patients who come to medical attention because of factitious disorders are diarrhea, fever of unknown origin, gastrointestinal bleeding, hematuria, seizures, and hypoglycemia.
17. Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
A patient with schizophrenia or bipolar disorder could experience a severe psychiatric episode without psychiatric medication. An appropriate alternative, perhaps administered intravenously if necessary, “can make all the difference in the world,” says Christopher Dobbelstein, MD, assistant professor of psychiatry at the University of Pittsburgh School of Medicine.
18. Listen to your instincts.
Medical teams can handle many psychiatric issues. Straightforward delirium is a good example. The bigger question, which takes experience and confidence, is to recognize when a line has been crossed. “The decision to consult psychiatry is not formulaic,” Dr. Dobbelstein says.
Sometimes a patient is acting strangely, and the team can’t explain why a psychiatrist could offer sound advice. “That’s when they should trust their instincts and consult us,” he says, “because the patient likely does have something more complex going on.”
19. Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
Sometimes psychiatric medications are started without good oversight. Suicide risk is highest during the weeks following an inpatient psychiatric admission, so a patient should see an outpatient mental health provider within seven days after hospital discharge, says NAMI’s Dr. Duckworth.
20. Extend genuine compassion to your patients.
“This is the secret to achieving a lifelong rewarding career in medicine,” Dr. Worley says, “and is the most important ingredient in positive outcomes.”
Susan Kreimer is a freelance writer in New York.
Survival Tips
- Pull up a chair and sit down.
- Ask what name your patient likes to go by. Be respectful and use correct titles when appropriate. One size doesn’t fit all. “Mrs. X” might be a mother-in-law.
- Appreciate how terrifying it can be as a patient—ill, in pain, having no control, with a loss of privacy and at times dignity.
- Remember that any one of us in the role of a patient regresses and copes in different ways. Some become demanding and express a strong need for control, while others want and need information from their physician.
- Privacy is important. Close the door. Don’t ask sensitive questions within earshot of other patients or visitors.