User login
'JNC 8' guideline follows convoluted endgame
The federally funded program to produce a set of U.S. guidelines for hypertension management, a process more than 5 years in the making, came to an unusual end on December 18 when the members of what had already become the officially-disbanded JNC 8 panel published their conclusions and guideline.
No longer recognized or supported by the National Heart Lung and Blood Institute (NHLBI), the Federal agency that had organized the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) panel in 2008, and unwilling to work with potential collaborating groups like the American Heart Association (AHA), the American College of Cardiology (ACC), or the American Society of Hypertension (ASH), the 17-person group that wound up identifying themselves as the “panel members appointed to the Eighth Joint National Committee (JNC 8).”
Call them JNC Ain’t.

The U.S. hypertension guidelines began veering off on an unexpected course last June, when Dr. Gary H. Gibbons, NHLBI director, announced that the agency was withdrawing from issuing guidelines itself and would instead collaborate with “partner organizations.”
In August, Dr. Gibbons, said that the AHA and ACC had reached an agreement with the agency to “spearhead” development of three sets of practice guidelines, for hypertension, cholesterol, and obesity. This agreement led to the release in November of the cholesterol and obesity guidelines under the auspices of the AHA and ACC, but instead of also releasing hypertension guidelines, the AHA and ACC as well as the NHLBI said that the process had fallen through and failed to produce guidelines.
According to Dr. Paul A. James, co-chair of the former JNC 8 panel and professor of family medicine at the University of Iowa in Iowa City, that’s because the panel members decided they weren’t comfortable with “the idea of shopping our guideline around prior to publication and getting an endorsement.” Now that the panel’s conclusions have been published “we hope to get active public review of our work; we invite people to analyze our process, and hopefully organizations will endorse our findings,” he said in an interview. “Our belief is that the approach we took, the transparent nature of our guideline development, and our release of it through JAMA will increase the credibility of our work.”
But others said that the panel’s break with the NHLBI and its inability to partner with any organization will inevitably affect how people view these recommendations, especially because parts are also clinically controversial.
“There was clear controversy when this guideline was circulated” while under review, said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. “The biggest problem this committee has is that many experts with a very significant stake in the recommendations were excluded from the process of generating the guideline. That limits buy-in from key opinion leaders, which will be needed for the uptake of this guideline into clinical practice,” he said in an interview.
“Unlike the previous JNC reports, this one will be seen as interesting, but not as persuasive,” said Dr. Michael A. Weber, professor of medicine at the State University of New York Downstate Medical Center in Brooklyn. “I believe the AHA, ACC, and ASH had hoped to endorse these guidelines, but that wasn’t possible.”

ASH leaders had discussions with the JNC 8 panel last summer, but the two groups could not reach an agreement on how to use the panel’s work for management recommendations, said Dr. William B. White, ASH president and chief of hypertension and clinical pharmacology at the University of Connecticut in Farmington.
What ASH has since agreed to do is join with the AHA and ACC to produce evidence-based hypertension guidelines using NHLBI materials, Dr. White said in an interview. The planned guidelines will “use some of the evidence derived by the NHLBI’s methodology, but adding to it other clinical issues,” including blood pressure measurement. These groups also hope the guidelines development will receive participation from a primary-care society such as the American College of Physicians, he said.
“The ACC/AHA Task Force on Practice Guidelines has begun the process of developing the collaborative model to update the national hypertensive guidelines in partnership with the NHLBI, which will provide an updated systematic review informed by the relevant critical clinical questions. We are seeking appropriate partners to begin this work in early 2014. The writing group will draft recommendations, followed by a peer and stakeholder review process. Once the review process is complete the ACC/AHA and partnering organizations will publish the guidelines in 2015 for clinicians to follow as the national standard for hypertension prevention and treatment,” said a spokeswoman for the American College of Cardiology in a statement released on December 18.
Leaders from the AHA and ACC said that once it became clear several weeks ago that they would not be able to collaborate with the JNC 8 panel, they felt compelled to immediately develop some form of updated guidance on hypertensive management. That led to an AHA-ACC Science Advisory (J. Am. Coll. Card. 2013;doi:10.1016/j.jacc.2013.11.007) released on Nov. 15 in collaboration with the Centers for Disease Control and Prevention that endorsed the use of treatment algorithms when managing patients with hypertension.

“Because the JNC 8 panel chose not to be part of the AHA-ACC structure, we felt we needed to go forward to make sure that we had guidance that reflected the evidence,” said Dr. Kim A. Williams Sr., professor and head of cardiology at Rush University in Chicago, vice president of the ACC, and a member of the group that wrote the advisory. “We felt the need to have risk covered as best we could, and have some hypertension guidance out there, even if it is not a guideline,” he said in an interview.
“We felt that after the enormous progress forward with the other four guidelines” released on Nov. 12 by the AHA and ACC (Circulation 2013 [doi: 10.1161/01.cir.0000437738.63853.7a; doi: 10.1161/01.cir.0000437739.71477.ee; doi: 10.1161/01.cir.0000437740.48606.d1; doi: 10.1161/01.cir.0000437741.48606.98]) “there was some urgency” to provide guidance for hypertension too, said Dr. Mariell Jessup, professor and medical director of the Penn Heart and Vascular Center at the University of Pennsylvania in Philadelphia and president of the AHA, during a session on the new guidelines at the AHA Scientific Sessions in Dallas in November.

The potential this now presents for the AHA and ACC to produce unified U.S. guidelines for all aspects of cardiovascular disease risk, integrating the assessment and treatment of hypertension, cholesterol, and obesity, is a positive development, said Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. He was also hopeful that this new collaboration will draw in groups like ASH and the American College of Physicians to represent the interests of subspecialists and primary-care physicians. “Ideally you want consensus on where you’re trying to get blood pressure” that cuts across all strata of U.S. medicine, he said.
Dr. James, Dr. White, Dr. Jessup, Dr. Williams and Dr. Peterson said that they had no disclosures. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest.
[email protected]
On Twitter @mitchelzoler
**UPDATED Jan. 4, 2014
The federally funded program to produce a set of U.S. guidelines for hypertension management, a process more than 5 years in the making, came to an unusual end on December 18 when the members of what had already become the officially-disbanded JNC 8 panel published their conclusions and guideline.
No longer recognized or supported by the National Heart Lung and Blood Institute (NHLBI), the Federal agency that had organized the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) panel in 2008, and unwilling to work with potential collaborating groups like the American Heart Association (AHA), the American College of Cardiology (ACC), or the American Society of Hypertension (ASH), the 17-person group that wound up identifying themselves as the “panel members appointed to the Eighth Joint National Committee (JNC 8).”
Call them JNC Ain’t.
The U.S. hypertension guidelines began veering off on an unexpected course last June, when Dr. Gary H. Gibbons, NHLBI director, announced that the agency was withdrawing from issuing guidelines itself and would instead collaborate with “partner organizations.”
In August, Dr. Gibbons, said that the AHA and ACC had reached an agreement with the agency to “spearhead” development of three sets of practice guidelines, for hypertension, cholesterol, and obesity. This agreement led to the release in November of the cholesterol and obesity guidelines under the auspices of the AHA and ACC, but instead of also releasing hypertension guidelines, the AHA and ACC as well as the NHLBI said that the process had fallen through and failed to produce guidelines.
According to Dr. Paul A. James, co-chair of the former JNC 8 panel and professor of family medicine at the University of Iowa in Iowa City, that’s because the panel members decided they weren’t comfortable with “the idea of shopping our guideline around prior to publication and getting an endorsement.” Now that the panel’s conclusions have been published “we hope to get active public review of our work; we invite people to analyze our process, and hopefully organizations will endorse our findings,” he said in an interview. “Our belief is that the approach we took, the transparent nature of our guideline development, and our release of it through JAMA will increase the credibility of our work.”
But others said that the panel’s break with the NHLBI and its inability to partner with any organization will inevitably affect how people view these recommendations, especially because parts are also clinically controversial.
“There was clear controversy when this guideline was circulated” while under review, said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. “The biggest problem this committee has is that many experts with a very significant stake in the recommendations were excluded from the process of generating the guideline. That limits buy-in from key opinion leaders, which will be needed for the uptake of this guideline into clinical practice,” he said in an interview.
“Unlike the previous JNC reports, this one will be seen as interesting, but not as persuasive,” said Dr. Michael A. Weber, professor of medicine at the State University of New York Downstate Medical Center in Brooklyn. “I believe the AHA, ACC, and ASH had hoped to endorse these guidelines, but that wasn’t possible.”
ASH leaders had discussions with the JNC 8 panel last summer, but the two groups could not reach an agreement on how to use the panel’s work for management recommendations, said Dr. William B. White, ASH president and chief of hypertension and clinical pharmacology at the University of Connecticut in Farmington.
What ASH has since agreed to do is join with the AHA and ACC to produce evidence-based hypertension guidelines using NHLBI materials, Dr. White said in an interview. The planned guidelines will “use some of the evidence derived by the NHLBI’s methodology, but adding to it other clinical issues,” including blood pressure measurement. These groups also hope the guidelines development will receive participation from a primary-care society such as the American College of Physicians, he said.
“The ACC/AHA Task Force on Practice Guidelines has begun the process of developing the collaborative model to update the national hypertensive guidelines in partnership with the NHLBI, which will provide an updated systematic review informed by the relevant critical clinical questions. We are seeking appropriate partners to begin this work in early 2014. The writing group will draft recommendations, followed by a peer and stakeholder review process. Once the review process is complete the ACC/AHA and partnering organizations will publish the guidelines in 2015 for clinicians to follow as the national standard for hypertension prevention and treatment,” said a spokeswoman for the American College of Cardiology in a statement released on December 18.
Leaders from the AHA and ACC said that once it became clear several weeks ago that they would not be able to collaborate with the JNC 8 panel, they felt compelled to immediately develop some form of updated guidance on hypertensive management. That led to an AHA-ACC Science Advisory (J. Am. Coll. Card. 2013;doi:10.1016/j.jacc.2013.11.007) released on Nov. 15 in collaboration with the Centers for Disease Control and Prevention that endorsed the use of treatment algorithms when managing patients with hypertension.
“Because the JNC 8 panel chose not to be part of the AHA-ACC structure, we felt we needed to go forward to make sure that we had guidance that reflected the evidence,” said Dr. Kim A. Williams Sr., professor and head of cardiology at Rush University in Chicago, vice president of the ACC, and a member of the group that wrote the advisory. “We felt the need to have risk covered as best we could, and have some hypertension guidance out there, even if it is not a guideline,” he said in an interview.
“We felt that after the enormous progress forward with the other four guidelines” released on Nov. 12 by the AHA and ACC (Circulation 2013 [doi: 10.1161/01.cir.0000437738.63853.7a; doi: 10.1161/01.cir.0000437739.71477.ee; doi: 10.1161/01.cir.0000437740.48606.d1; doi: 10.1161/01.cir.0000437741.48606.98]) “there was some urgency” to provide guidance for hypertension too, said Dr. Mariell Jessup, professor and medical director of the Penn Heart and Vascular Center at the University of Pennsylvania in Philadelphia and president of the AHA, during a session on the new guidelines at the AHA Scientific Sessions in Dallas in November.
The potential this now presents for the AHA and ACC to produce unified U.S. guidelines for all aspects of cardiovascular disease risk, integrating the assessment and treatment of hypertension, cholesterol, and obesity, is a positive development, said Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. He was also hopeful that this new collaboration will draw in groups like ASH and the American College of Physicians to represent the interests of subspecialists and primary-care physicians. “Ideally you want consensus on where you’re trying to get blood pressure” that cuts across all strata of U.S. medicine, he said.
Dr. James, Dr. White, Dr. Jessup, Dr. Williams and Dr. Peterson said that they had no disclosures. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest.
[email protected]
On Twitter @mitchelzoler
**UPDATED Jan. 4, 2014
The federally funded program to produce a set of U.S. guidelines for hypertension management, a process more than 5 years in the making, came to an unusual end on December 18 when the members of what had already become the officially-disbanded JNC 8 panel published their conclusions and guideline.
No longer recognized or supported by the National Heart Lung and Blood Institute (NHLBI), the Federal agency that had organized the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) panel in 2008, and unwilling to work with potential collaborating groups like the American Heart Association (AHA), the American College of Cardiology (ACC), or the American Society of Hypertension (ASH), the 17-person group that wound up identifying themselves as the “panel members appointed to the Eighth Joint National Committee (JNC 8).”
Call them JNC Ain’t.
The U.S. hypertension guidelines began veering off on an unexpected course last June, when Dr. Gary H. Gibbons, NHLBI director, announced that the agency was withdrawing from issuing guidelines itself and would instead collaborate with “partner organizations.”
In August, Dr. Gibbons, said that the AHA and ACC had reached an agreement with the agency to “spearhead” development of three sets of practice guidelines, for hypertension, cholesterol, and obesity. This agreement led to the release in November of the cholesterol and obesity guidelines under the auspices of the AHA and ACC, but instead of also releasing hypertension guidelines, the AHA and ACC as well as the NHLBI said that the process had fallen through and failed to produce guidelines.
According to Dr. Paul A. James, co-chair of the former JNC 8 panel and professor of family medicine at the University of Iowa in Iowa City, that’s because the panel members decided they weren’t comfortable with “the idea of shopping our guideline around prior to publication and getting an endorsement.” Now that the panel’s conclusions have been published “we hope to get active public review of our work; we invite people to analyze our process, and hopefully organizations will endorse our findings,” he said in an interview. “Our belief is that the approach we took, the transparent nature of our guideline development, and our release of it through JAMA will increase the credibility of our work.”
But others said that the panel’s break with the NHLBI and its inability to partner with any organization will inevitably affect how people view these recommendations, especially because parts are also clinically controversial.
“There was clear controversy when this guideline was circulated” while under review, said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. “The biggest problem this committee has is that many experts with a very significant stake in the recommendations were excluded from the process of generating the guideline. That limits buy-in from key opinion leaders, which will be needed for the uptake of this guideline into clinical practice,” he said in an interview.
“Unlike the previous JNC reports, this one will be seen as interesting, but not as persuasive,” said Dr. Michael A. Weber, professor of medicine at the State University of New York Downstate Medical Center in Brooklyn. “I believe the AHA, ACC, and ASH had hoped to endorse these guidelines, but that wasn’t possible.”
ASH leaders had discussions with the JNC 8 panel last summer, but the two groups could not reach an agreement on how to use the panel’s work for management recommendations, said Dr. William B. White, ASH president and chief of hypertension and clinical pharmacology at the University of Connecticut in Farmington.
What ASH has since agreed to do is join with the AHA and ACC to produce evidence-based hypertension guidelines using NHLBI materials, Dr. White said in an interview. The planned guidelines will “use some of the evidence derived by the NHLBI’s methodology, but adding to it other clinical issues,” including blood pressure measurement. These groups also hope the guidelines development will receive participation from a primary-care society such as the American College of Physicians, he said.
“The ACC/AHA Task Force on Practice Guidelines has begun the process of developing the collaborative model to update the national hypertensive guidelines in partnership with the NHLBI, which will provide an updated systematic review informed by the relevant critical clinical questions. We are seeking appropriate partners to begin this work in early 2014. The writing group will draft recommendations, followed by a peer and stakeholder review process. Once the review process is complete the ACC/AHA and partnering organizations will publish the guidelines in 2015 for clinicians to follow as the national standard for hypertension prevention and treatment,” said a spokeswoman for the American College of Cardiology in a statement released on December 18.
Leaders from the AHA and ACC said that once it became clear several weeks ago that they would not be able to collaborate with the JNC 8 panel, they felt compelled to immediately develop some form of updated guidance on hypertensive management. That led to an AHA-ACC Science Advisory (J. Am. Coll. Card. 2013;doi:10.1016/j.jacc.2013.11.007) released on Nov. 15 in collaboration with the Centers for Disease Control and Prevention that endorsed the use of treatment algorithms when managing patients with hypertension.
“Because the JNC 8 panel chose not to be part of the AHA-ACC structure, we felt we needed to go forward to make sure that we had guidance that reflected the evidence,” said Dr. Kim A. Williams Sr., professor and head of cardiology at Rush University in Chicago, vice president of the ACC, and a member of the group that wrote the advisory. “We felt the need to have risk covered as best we could, and have some hypertension guidance out there, even if it is not a guideline,” he said in an interview.
“We felt that after the enormous progress forward with the other four guidelines” released on Nov. 12 by the AHA and ACC (Circulation 2013 [doi: 10.1161/01.cir.0000437738.63853.7a; doi: 10.1161/01.cir.0000437739.71477.ee; doi: 10.1161/01.cir.0000437740.48606.d1; doi: 10.1161/01.cir.0000437741.48606.98]) “there was some urgency” to provide guidance for hypertension too, said Dr. Mariell Jessup, professor and medical director of the Penn Heart and Vascular Center at the University of Pennsylvania in Philadelphia and president of the AHA, during a session on the new guidelines at the AHA Scientific Sessions in Dallas in November.
The potential this now presents for the AHA and ACC to produce unified U.S. guidelines for all aspects of cardiovascular disease risk, integrating the assessment and treatment of hypertension, cholesterol, and obesity, is a positive development, said Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. He was also hopeful that this new collaboration will draw in groups like ASH and the American College of Physicians to represent the interests of subspecialists and primary-care physicians. “Ideally you want consensus on where you’re trying to get blood pressure” that cuts across all strata of U.S. medicine, he said.
Dr. James, Dr. White, Dr. Jessup, Dr. Williams and Dr. Peterson said that they had no disclosures. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest.
[email protected]
On Twitter @mitchelzoler
**UPDATED Jan. 4, 2014

Evidence and expertise in writing medical guidelines
With timing that defies coincidence, the American Society of Hypertension (ASH) and International Society of Hypertension (ISH) posted on Dec. 17 new guidelines for hypertension diagnosis and treatment, and on Dec. 18 guidelines addressing the same topic were issued by the group of experts who had previously been called the Eighth Joint National Committee (JNC 8).
The big disagreement between the two was target systolic blood pressure (SBP) for hypertensive patients aged 60 or older. Guidelines from the former JNC 8 panel created an SBP target of less than 150 mm Hg, concluding that no high-quality evidence existed to justify treating these patients to a lower pressure. The ASH-ISH guidelines called for a target SBP of less than 140 mm Hg in patients aged 79 or younger, and they did not present any formal literature review to justify their choice. Their most clearly articulated reason for picking less than 140/90 mm Hg? "Guidelines tend to use 140/90 mm Hg for all adults (up to 80 years)."

The two guidelines differed just as starkly in their approach. In fact, one interpretation is that the difference in approach largely drove the difference in systolic targets. The former JNC 8 panel said that they focused on high-quality evidence from randomized clinical trials. They spell out their dissection of the evidence in a 300-page supplement to their JAMA paper that includes hundreds of references. The ASH-ISH guideline document has no evidence review, and includes a taut 25 citations as "suggested reading."
"Our group was very evidence based," said Dr. Paul A. James, a family medicine professor at the University of Iowa, Iowa City, and cochair of the former JNC 8 panel.
"To my mind, the purpose of a guideline is for a group of experts to go as far as they can guided by the evidence, and then to use their experience and judgment to make recommendations in the best interests of patients," said Dr. Michael A. Weber, professor of medicine at SUNY Downstate Medical Center, New York, and chair of the ASH-ISH guideline panel.
Was the former JNC 8 panel consistently objective in drawing conclusions from the evidence, or lack of evidence? An editorial that accompanied the former JNC 8 panel’s report noted, "In older populations the majority of the panel interpreted the lack of definitive benefit from RCTs (randomized controlled trials) as grounds to raise the SBP treatment goal recommendation to 150 mm Hg; however, for patients younger than 60 years, the paucity of any trial evidence provided no reason for the panel to change the existing treatment goal at 140 mm Hg."
As Dr. John M. Flack, chief of medicine at Wayne State University in Detroit, told me: "The committee was selective in what they considered could be justified."
"It’s astounding that we don’t have the evidence to say what the right treatment thresholds are even though hypertension is the No. 1 modifiable risk factor" for cardiovascular disease, observed Dr. Eric D. Peterson, the Duke University cardiologist who was lead author on the editorial.
Once concluding that not enough evidence existed to pinpoint a treatment target, the former JNC 8 panel still needed to choose a target. In their JAMA paper they acknowledged the panel’s minority view: "Some members recommended continuing the JNC 7 SBP goal of lower than 140 mm Hg for individuals older than 60 years based on expert opinion" and because "the evidence was insufficient to raise the SBP target from lower than 140 mm Hg to lower than 150 mm Hg in high-risk groups."
But a majority opted for a more controversial target instead.
On Twitter @mitchelzoler
With timing that defies coincidence, the American Society of Hypertension (ASH) and International Society of Hypertension (ISH) posted on Dec. 17 new guidelines for hypertension diagnosis and treatment, and on Dec. 18 guidelines addressing the same topic were issued by the group of experts who had previously been called the Eighth Joint National Committee (JNC 8).
The big disagreement between the two was target systolic blood pressure (SBP) for hypertensive patients aged 60 or older. Guidelines from the former JNC 8 panel created an SBP target of less than 150 mm Hg, concluding that no high-quality evidence existed to justify treating these patients to a lower pressure. The ASH-ISH guidelines called for a target SBP of less than 140 mm Hg in patients aged 79 or younger, and they did not present any formal literature review to justify their choice. Their most clearly articulated reason for picking less than 140/90 mm Hg? "Guidelines tend to use 140/90 mm Hg for all adults (up to 80 years)."
The two guidelines differed just as starkly in their approach. In fact, one interpretation is that the difference in approach largely drove the difference in systolic targets. The former JNC 8 panel said that they focused on high-quality evidence from randomized clinical trials. They spell out their dissection of the evidence in a 300-page supplement to their JAMA paper that includes hundreds of references. The ASH-ISH guideline document has no evidence review, and includes a taut 25 citations as "suggested reading."
"Our group was very evidence based," said Dr. Paul A. James, a family medicine professor at the University of Iowa, Iowa City, and cochair of the former JNC 8 panel.
"To my mind, the purpose of a guideline is for a group of experts to go as far as they can guided by the evidence, and then to use their experience and judgment to make recommendations in the best interests of patients," said Dr. Michael A. Weber, professor of medicine at SUNY Downstate Medical Center, New York, and chair of the ASH-ISH guideline panel.
Was the former JNC 8 panel consistently objective in drawing conclusions from the evidence, or lack of evidence? An editorial that accompanied the former JNC 8 panel’s report noted, "In older populations the majority of the panel interpreted the lack of definitive benefit from RCTs (randomized controlled trials) as grounds to raise the SBP treatment goal recommendation to 150 mm Hg; however, for patients younger than 60 years, the paucity of any trial evidence provided no reason for the panel to change the existing treatment goal at 140 mm Hg."
As Dr. John M. Flack, chief of medicine at Wayne State University in Detroit, told me: "The committee was selective in what they considered could be justified."
"It’s astounding that we don’t have the evidence to say what the right treatment thresholds are even though hypertension is the No. 1 modifiable risk factor" for cardiovascular disease, observed Dr. Eric D. Peterson, the Duke University cardiologist who was lead author on the editorial.
Once concluding that not enough evidence existed to pinpoint a treatment target, the former JNC 8 panel still needed to choose a target. In their JAMA paper they acknowledged the panel’s minority view: "Some members recommended continuing the JNC 7 SBP goal of lower than 140 mm Hg for individuals older than 60 years based on expert opinion" and because "the evidence was insufficient to raise the SBP target from lower than 140 mm Hg to lower than 150 mm Hg in high-risk groups."
But a majority opted for a more controversial target instead.
On Twitter @mitchelzoler
With timing that defies coincidence, the American Society of Hypertension (ASH) and International Society of Hypertension (ISH) posted on Dec. 17 new guidelines for hypertension diagnosis and treatment, and on Dec. 18 guidelines addressing the same topic were issued by the group of experts who had previously been called the Eighth Joint National Committee (JNC 8).
The big disagreement between the two was target systolic blood pressure (SBP) for hypertensive patients aged 60 or older. Guidelines from the former JNC 8 panel created an SBP target of less than 150 mm Hg, concluding that no high-quality evidence existed to justify treating these patients to a lower pressure. The ASH-ISH guidelines called for a target SBP of less than 140 mm Hg in patients aged 79 or younger, and they did not present any formal literature review to justify their choice. Their most clearly articulated reason for picking less than 140/90 mm Hg? "Guidelines tend to use 140/90 mm Hg for all adults (up to 80 years)."
The two guidelines differed just as starkly in their approach. In fact, one interpretation is that the difference in approach largely drove the difference in systolic targets. The former JNC 8 panel said that they focused on high-quality evidence from randomized clinical trials. They spell out their dissection of the evidence in a 300-page supplement to their JAMA paper that includes hundreds of references. The ASH-ISH guideline document has no evidence review, and includes a taut 25 citations as "suggested reading."
"Our group was very evidence based," said Dr. Paul A. James, a family medicine professor at the University of Iowa, Iowa City, and cochair of the former JNC 8 panel.
"To my mind, the purpose of a guideline is for a group of experts to go as far as they can guided by the evidence, and then to use their experience and judgment to make recommendations in the best interests of patients," said Dr. Michael A. Weber, professor of medicine at SUNY Downstate Medical Center, New York, and chair of the ASH-ISH guideline panel.
Was the former JNC 8 panel consistently objective in drawing conclusions from the evidence, or lack of evidence? An editorial that accompanied the former JNC 8 panel’s report noted, "In older populations the majority of the panel interpreted the lack of definitive benefit from RCTs (randomized controlled trials) as grounds to raise the SBP treatment goal recommendation to 150 mm Hg; however, for patients younger than 60 years, the paucity of any trial evidence provided no reason for the panel to change the existing treatment goal at 140 mm Hg."
As Dr. John M. Flack, chief of medicine at Wayne State University in Detroit, told me: "The committee was selective in what they considered could be justified."
"It’s astounding that we don’t have the evidence to say what the right treatment thresholds are even though hypertension is the No. 1 modifiable risk factor" for cardiovascular disease, observed Dr. Eric D. Peterson, the Duke University cardiologist who was lead author on the editorial.
Once concluding that not enough evidence existed to pinpoint a treatment target, the former JNC 8 panel still needed to choose a target. In their JAMA paper they acknowledged the panel’s minority view: "Some members recommended continuing the JNC 7 SBP goal of lower than 140 mm Hg for individuals older than 60 years based on expert opinion" and because "the evidence was insufficient to raise the SBP target from lower than 140 mm Hg to lower than 150 mm Hg in high-risk groups."
But a majority opted for a more controversial target instead.
On Twitter @mitchelzoler

‘JNC 8’ relaxes elderly systolic target below 150 mm Hg
The group of experts who had constituted the JNC 8 panel, a team assembled in 2008 by the National Heart, Lung, and Blood Institute to update official U.S. hypertension management guidelines, set the target blood pressure for the general population aged 60 years or older to less than 150/90 mm Hg, a major break from long-standing practice to treat such patients to a target systolic pressure of less than 140 mm Hg.
This decision, which the panel contends was driven by lack of clear evidence for extra benefit from the below–140 mm Hg target, will surely prove controversial, along with the panel’s relaxing of target blood pressures for patients with diabetes or chronic kidney disease to less than 140/90 mm Hg (increased from 130/80 mm Hg in the prior, JNC 7 guidelines). That controversy would be a fitting final curtain for the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), a project that courted controversy by running years longer than anticipated and then generating several plot twists during the final months leading up to Dec. 18, when the former JNC 8 panel published its hypertension-management guideline (JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284427]).

The new target of a systolic pressure of less than 150 mm Hg for hypertensive patients aged 60 or older without diabetes or chronic kidney disease "is definitely controversial," said Dr. Paul A. James, cochairman of the panel and professor of family medicine at the University of Iowa in Iowa City. "There is A-level evidence that getting blood pressure below 150 mm Hg results in improved outcomes that really matter, but we have no evidence at this time to support going lower," to less than 140 mm Hg. "The good news is that the panel is comfortable that we don’t do harm," by treating patients to less than 140 mm Hg. "But why put patients at increased risk for medication adverse events when we don’t have strong evidence of benefit?" he said in an interview.
He stressed that his group released their conclusions and guideline on their own, identifying themselves as "the panel members appointed to the Eighth Joint National Committee (JNC 8)." Leaders from the National Heart, Lung, and Blood Institute announced last June that the agency was pulling out of the business of issuing cardiovascular-disease management guidelines, and would instead fund evidence reviews and partner with other organizations to issue guidelines. The NHLBI arranged for its cholesterol, obesity, and lifestyle guidelines to be released through the American Heart Association and American College of Cardiology, but no similar arrangement worked out for the JNC 8 panel, which became the former panel when the NHLBI officially dissolved it by late summer.
The former JNC 8 panel applied "a very narrow interpretation" of the clinical evidence where the evidence is very incomplete, commented Dr. Michael A. Weber, professor of medicine at State University of New York, Brooklyn. "The purpose of guidelines is for a group of experts to be guided as far as they can by the evidence, and then use their judgment and experience to make recommendations that in the best interests of patients." He cited findings from the ACCOMPLISH, INVEST, and VALUE trials that show benefits from treating patients older than 60 years to a systolic pressure of less than 140 mm Hg, though he admitted that in each of these studies the findings did not come from primary, prespecified analyses.

Dr. Weber led a panel organized by the American Society of Hypertension and International Society of Hypertension that released its own set of hypertension diagnosis and management guidelines a day earlier, on Dec. 17 (J. Clin. Hypertension 2013 [doi:10.1111/ch.1223]). Where they overlap, the guidelines from ASH/ISH and from the former JNC 8 panel are mostly the same, with the systolic target for the general population aged 60-79 years being the main area of contention, Dr. Weber said. The ASH/ISH guideline set a systolic target of less than 150 mm Hg for the general hypertensive population aged 80 years or older.
The former-JNC 8 panel also qualified their 150 mm Hg–target by adding that if general population patients aged 60 years or older are on stable, well-tolerated antihypertensive treatment and have a systolic pressure of less than 140 mm Hg, changing treatment and aiming for a higher systolic pressure is not recommended.
The target of less than 150 mm Hg for these patients also had defenders. "They made a reasonable recommendation for the elderly based on the evidence," said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. But he took the JNC 8 panel to task for relaxing the systolic and diastolic pressure targets for patients with either diabetes or chronic kidney disease from the prior target of less than 130/80 mm Hg to new targets of less than 140/90 mm Hg. "Relaxing blood pressure targets in high-risk groups when so much progress has been made over the last decade is going to be very controversial," he said in an interview. The new ASH-ISH hypertension guideline also set a blood pressure target of less than 140/90 mm Hg for patients with diabetes or chronic kidney disease.
The guideline from the former JNC 8 panel "will produce a lot of discussion, and the main target will be whether the 150 mm Hg target is right or not," commented Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. In an editorial that accompanied the published guideline, Dr. Peterson and his associates also noted that the hypertension goals specified in authoritative guidelines had a magnified importance these days because they often are incorporated into "performance measures" to which physicians can be often held rigidly accountable.(JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284430]).
"I chair the ACC/AHA Task Force on Performance Measures, and we will be in a bind because the current performance measures call for a blood pressure target of less than 140/90 mm Hg," he said in an interview. The ACC/AHA task force is one of the main contributors of performance measures for cardiovascular disease to the U.S. clearing house for performance measures, the National Quality Forum. "The Task Force will need to respond to this guideline in some way," he said, but the Task Force takes into account the range of current guidelines that exist and their backup evidence, so how it will decide on this issue remains uncertain.
"My concern is not so much with the number they came up with as with how it will be used by physicians in the community," Dr. Peterson said. On one hand, you don’t want physicians to get carried away and feel they need to treat all their patients to below some magical number." As he pointed out in his editorial, the counterbalancing problem is that there is always a gap between the hypertension treatment goals and what is often achieved in practice. If that relationship remains and the accepted goal for patients aged 60-79 years becomes less than 150 mm Hg, then many U.S. patients in this group may end up treated but with systolic pressures above 150 mm Hg.
Dr. James and Dr. Peterson said that they had no disclosures. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic.
On Twitter @mitchelzoler
The group of experts who had constituted the JNC 8 panel, a team assembled in 2008 by the National Heart, Lung, and Blood Institute to update official U.S. hypertension management guidelines, set the target blood pressure for the general population aged 60 years or older to less than 150/90 mm Hg, a major break from long-standing practice to treat such patients to a target systolic pressure of less than 140 mm Hg.
This decision, which the panel contends was driven by lack of clear evidence for extra benefit from the below–140 mm Hg target, will surely prove controversial, along with the panel’s relaxing of target blood pressures for patients with diabetes or chronic kidney disease to less than 140/90 mm Hg (increased from 130/80 mm Hg in the prior, JNC 7 guidelines). That controversy would be a fitting final curtain for the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), a project that courted controversy by running years longer than anticipated and then generating several plot twists during the final months leading up to Dec. 18, when the former JNC 8 panel published its hypertension-management guideline (JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284427]).
The new target of a systolic pressure of less than 150 mm Hg for hypertensive patients aged 60 or older without diabetes or chronic kidney disease "is definitely controversial," said Dr. Paul A. James, cochairman of the panel and professor of family medicine at the University of Iowa in Iowa City. "There is A-level evidence that getting blood pressure below 150 mm Hg results in improved outcomes that really matter, but we have no evidence at this time to support going lower," to less than 140 mm Hg. "The good news is that the panel is comfortable that we don’t do harm," by treating patients to less than 140 mm Hg. "But why put patients at increased risk for medication adverse events when we don’t have strong evidence of benefit?" he said in an interview.
He stressed that his group released their conclusions and guideline on their own, identifying themselves as "the panel members appointed to the Eighth Joint National Committee (JNC 8)." Leaders from the National Heart, Lung, and Blood Institute announced last June that the agency was pulling out of the business of issuing cardiovascular-disease management guidelines, and would instead fund evidence reviews and partner with other organizations to issue guidelines. The NHLBI arranged for its cholesterol, obesity, and lifestyle guidelines to be released through the American Heart Association and American College of Cardiology, but no similar arrangement worked out for the JNC 8 panel, which became the former panel when the NHLBI officially dissolved it by late summer.
The former JNC 8 panel applied "a very narrow interpretation" of the clinical evidence where the evidence is very incomplete, commented Dr. Michael A. Weber, professor of medicine at State University of New York, Brooklyn. "The purpose of guidelines is for a group of experts to be guided as far as they can by the evidence, and then use their judgment and experience to make recommendations that in the best interests of patients." He cited findings from the ACCOMPLISH, INVEST, and VALUE trials that show benefits from treating patients older than 60 years to a systolic pressure of less than 140 mm Hg, though he admitted that in each of these studies the findings did not come from primary, prespecified analyses.
Dr. Weber led a panel organized by the American Society of Hypertension and International Society of Hypertension that released its own set of hypertension diagnosis and management guidelines a day earlier, on Dec. 17 (J. Clin. Hypertension 2013 [doi:10.1111/ch.1223]). Where they overlap, the guidelines from ASH/ISH and from the former JNC 8 panel are mostly the same, with the systolic target for the general population aged 60-79 years being the main area of contention, Dr. Weber said. The ASH/ISH guideline set a systolic target of less than 150 mm Hg for the general hypertensive population aged 80 years or older.
The former-JNC 8 panel also qualified their 150 mm Hg–target by adding that if general population patients aged 60 years or older are on stable, well-tolerated antihypertensive treatment and have a systolic pressure of less than 140 mm Hg, changing treatment and aiming for a higher systolic pressure is not recommended.
The target of less than 150 mm Hg for these patients also had defenders. "They made a reasonable recommendation for the elderly based on the evidence," said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. But he took the JNC 8 panel to task for relaxing the systolic and diastolic pressure targets for patients with either diabetes or chronic kidney disease from the prior target of less than 130/80 mm Hg to new targets of less than 140/90 mm Hg. "Relaxing blood pressure targets in high-risk groups when so much progress has been made over the last decade is going to be very controversial," he said in an interview. The new ASH-ISH hypertension guideline also set a blood pressure target of less than 140/90 mm Hg for patients with diabetes or chronic kidney disease.
The guideline from the former JNC 8 panel "will produce a lot of discussion, and the main target will be whether the 150 mm Hg target is right or not," commented Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. In an editorial that accompanied the published guideline, Dr. Peterson and his associates also noted that the hypertension goals specified in authoritative guidelines had a magnified importance these days because they often are incorporated into "performance measures" to which physicians can be often held rigidly accountable.(JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284430]).
"I chair the ACC/AHA Task Force on Performance Measures, and we will be in a bind because the current performance measures call for a blood pressure target of less than 140/90 mm Hg," he said in an interview. The ACC/AHA task force is one of the main contributors of performance measures for cardiovascular disease to the U.S. clearing house for performance measures, the National Quality Forum. "The Task Force will need to respond to this guideline in some way," he said, but the Task Force takes into account the range of current guidelines that exist and their backup evidence, so how it will decide on this issue remains uncertain.
"My concern is not so much with the number they came up with as with how it will be used by physicians in the community," Dr. Peterson said. On one hand, you don’t want physicians to get carried away and feel they need to treat all their patients to below some magical number." As he pointed out in his editorial, the counterbalancing problem is that there is always a gap between the hypertension treatment goals and what is often achieved in practice. If that relationship remains and the accepted goal for patients aged 60-79 years becomes less than 150 mm Hg, then many U.S. patients in this group may end up treated but with systolic pressures above 150 mm Hg.
Dr. James and Dr. Peterson said that they had no disclosures. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic.
On Twitter @mitchelzoler
The group of experts who had constituted the JNC 8 panel, a team assembled in 2008 by the National Heart, Lung, and Blood Institute to update official U.S. hypertension management guidelines, set the target blood pressure for the general population aged 60 years or older to less than 150/90 mm Hg, a major break from long-standing practice to treat such patients to a target systolic pressure of less than 140 mm Hg.
This decision, which the panel contends was driven by lack of clear evidence for extra benefit from the below–140 mm Hg target, will surely prove controversial, along with the panel’s relaxing of target blood pressures for patients with diabetes or chronic kidney disease to less than 140/90 mm Hg (increased from 130/80 mm Hg in the prior, JNC 7 guidelines). That controversy would be a fitting final curtain for the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), a project that courted controversy by running years longer than anticipated and then generating several plot twists during the final months leading up to Dec. 18, when the former JNC 8 panel published its hypertension-management guideline (JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284427]).
The new target of a systolic pressure of less than 150 mm Hg for hypertensive patients aged 60 or older without diabetes or chronic kidney disease "is definitely controversial," said Dr. Paul A. James, cochairman of the panel and professor of family medicine at the University of Iowa in Iowa City. "There is A-level evidence that getting blood pressure below 150 mm Hg results in improved outcomes that really matter, but we have no evidence at this time to support going lower," to less than 140 mm Hg. "The good news is that the panel is comfortable that we don’t do harm," by treating patients to less than 140 mm Hg. "But why put patients at increased risk for medication adverse events when we don’t have strong evidence of benefit?" he said in an interview.
He stressed that his group released their conclusions and guideline on their own, identifying themselves as "the panel members appointed to the Eighth Joint National Committee (JNC 8)." Leaders from the National Heart, Lung, and Blood Institute announced last June that the agency was pulling out of the business of issuing cardiovascular-disease management guidelines, and would instead fund evidence reviews and partner with other organizations to issue guidelines. The NHLBI arranged for its cholesterol, obesity, and lifestyle guidelines to be released through the American Heart Association and American College of Cardiology, but no similar arrangement worked out for the JNC 8 panel, which became the former panel when the NHLBI officially dissolved it by late summer.
The former JNC 8 panel applied "a very narrow interpretation" of the clinical evidence where the evidence is very incomplete, commented Dr. Michael A. Weber, professor of medicine at State University of New York, Brooklyn. "The purpose of guidelines is for a group of experts to be guided as far as they can by the evidence, and then use their judgment and experience to make recommendations that in the best interests of patients." He cited findings from the ACCOMPLISH, INVEST, and VALUE trials that show benefits from treating patients older than 60 years to a systolic pressure of less than 140 mm Hg, though he admitted that in each of these studies the findings did not come from primary, prespecified analyses.
Dr. Weber led a panel organized by the American Society of Hypertension and International Society of Hypertension that released its own set of hypertension diagnosis and management guidelines a day earlier, on Dec. 17 (J. Clin. Hypertension 2013 [doi:10.1111/ch.1223]). Where they overlap, the guidelines from ASH/ISH and from the former JNC 8 panel are mostly the same, with the systolic target for the general population aged 60-79 years being the main area of contention, Dr. Weber said. The ASH/ISH guideline set a systolic target of less than 150 mm Hg for the general hypertensive population aged 80 years or older.
The former-JNC 8 panel also qualified their 150 mm Hg–target by adding that if general population patients aged 60 years or older are on stable, well-tolerated antihypertensive treatment and have a systolic pressure of less than 140 mm Hg, changing treatment and aiming for a higher systolic pressure is not recommended.
The target of less than 150 mm Hg for these patients also had defenders. "They made a reasonable recommendation for the elderly based on the evidence," said Dr. John M. Flack, professor and chief of medicine at Wayne State University in Detroit. But he took the JNC 8 panel to task for relaxing the systolic and diastolic pressure targets for patients with either diabetes or chronic kidney disease from the prior target of less than 130/80 mm Hg to new targets of less than 140/90 mm Hg. "Relaxing blood pressure targets in high-risk groups when so much progress has been made over the last decade is going to be very controversial," he said in an interview. The new ASH-ISH hypertension guideline also set a blood pressure target of less than 140/90 mm Hg for patients with diabetes or chronic kidney disease.
The guideline from the former JNC 8 panel "will produce a lot of discussion, and the main target will be whether the 150 mm Hg target is right or not," commented Dr. Eric D. Peterson, professor of medicine at Duke University in Durham, N.C. In an editorial that accompanied the published guideline, Dr. Peterson and his associates also noted that the hypertension goals specified in authoritative guidelines had a magnified importance these days because they often are incorporated into "performance measures" to which physicians can be often held rigidly accountable.(JAMA 2013 Dec. 18 [doi:10.1001/jama.2013.284430]).
"I chair the ACC/AHA Task Force on Performance Measures, and we will be in a bind because the current performance measures call for a blood pressure target of less than 140/90 mm Hg," he said in an interview. The ACC/AHA task force is one of the main contributors of performance measures for cardiovascular disease to the U.S. clearing house for performance measures, the National Quality Forum. "The Task Force will need to respond to this guideline in some way," he said, but the Task Force takes into account the range of current guidelines that exist and their backup evidence, so how it will decide on this issue remains uncertain.
"My concern is not so much with the number they came up with as with how it will be used by physicians in the community," Dr. Peterson said. On one hand, you don’t want physicians to get carried away and feel they need to treat all their patients to below some magical number." As he pointed out in his editorial, the counterbalancing problem is that there is always a gap between the hypertension treatment goals and what is often achieved in practice. If that relationship remains and the accepted goal for patients aged 60-79 years becomes less than 150 mm Hg, then many U.S. patients in this group may end up treated but with systolic pressures above 150 mm Hg.
Dr. James and Dr. Peterson said that they had no disclosures. Dr. Weber said that he has been a consultant to Novartis, Takeda, and Forest. Dr. Flack said that he has been a consultant to Novartis, Medtronic, and Back Beat Hypertension and received funding from Novartis and Medtronic.
On Twitter @mitchelzoler
FROM JAMA

10 Things Urologists Think Hospitalists Should Know
10 Things: At A Glance
- Take out urinary catheters as soon as possible.
- But don’t carry the Choosing Wisely directive on urinary catheters—and in-house protocols—too far.
- Beware certain types of medications in vulnerable patients.
- Don’t discharge patients who are having difficulty voiding.
- Broach sensitive topics, but do so gently.
- Call in a urologist, or someone with more experience, when you have difficulty placing a catheter.
- Diabetic patients require extra attention.
- Practice good antibiotic stewardship.
- Determine whether the patient can be seen as an outpatient.
- Embrace your role as eyes and ears.
1: Intravenous Haloperidol Does Not Prevent ICU Delirium
Urology is an area in which hospitalists might not have much formal training, but because many of these patients undergo highly complicated surgical procedures with great potential for complications, hospitalists can be vital for good outcomes, urologists say.
The use of urinary catheters is a prime area of concern when it comes to quality and safety, making hospitalists’ role in the care of urological patients even more crucial.
The Hospitalist spoke with a half dozen urologists and well-versed HM clinicians about caring for patients with urological disorders. Here are the best nuggets of guidance for hospitalists.
Take out urinary catheters as soon as possible.
John Bulger, DO, FACOI, FACP, SFHM, a hospitalist and chief quality officer at Geisinger Health System in Pennsylvania, says that, all too often, urinary catheters are left in too long. “There’s pretty good data to suggest that there’s a very direct relationship with the length of time the catheter’s in and the chance of it getting infected,” he says. “Upwards to half of the urinary catheters that are in in hospitals right now wouldn’t meet the guidelines of having a urinary catheter in.”
Dr. Bulger is chair of SHM’s Choosing Wisely subcommittee. One of SHM’s Choosing Wisely recommendations warns physicians not to place, or leave in place, catheters for incontinence, convenience, or monitoring of non-critically ill patients.1
2: But don’t carry the Choosing Wisely directive on urinary catheters—and in-house protocols—too far.
William Steers, MD, chair of urology at the University of Virginia and editor of the Journal of Urology, says there are risks associated with taking catheters out when it’s not appropriate, especially in patients who’ve undergone surgery.
“We’ve seen situations where we’re called into the operating room by another team,” Dr. Steers says. “Let’s say there was a bladder injury of another service. We’ve repaired the bladder with a catheter in for seven to 10 days. It’s taken out day one; the bladder fills and has the potential of causing harm.”
Early removal before the bladder wall heals can cause bladder rupture, requiring emergency surgery.
“So the devil’s in the details,” he says.
Mark Austenfeld, MD, FACS, president of the American Association of Clinical Urologists, which is dedicated to political action, advocacy, and best practice parameters, says catheters should remain in place for patients with mental status changes, or those who are debilitated in some way and can’t get out of bed or don’t have the wherewithal to ask for help from a nurse.
He says he realizes hospitalists are following pay-for-performance protocols, but he adds a caveat.
“Many times these protocols cannot take into account all of these specialized situations,” says Dr. Austenfeld, a urologist with Kansas City Urology Care. He stresses, though, that the hospitalists he’s worked with do high-quality work.
Sanjay Saint, MD, MPH, FHM, hospitalist and professor of internal medicine at the University of Michigan in Ann Arbor, says that even with these issues, early removal should remain a priority when appropriate.
“There’s going to be anecdotal evidence that in some particular patients, when the catheter is removed, it needs to be reinserted when they haven’t urinated for a while,” Dr. Saint explains. “But I think, in general, the studies that have looked at reinsertion have not found a statistically significant increase in reinsertion of the catheter after some type of a stop-order or nurse initiative, protocol, or urinary catheter reminder system has been put in place.”2
Dr. Steers says most agree that urinary catheters are often “overutilized.”
“You do want to get them out as soon as possible,” he says. “But if it’s ever in doubt, there should be communication with the urology team.”
3: Beware certain types of medications in vulnerable patients.
Hospitalists should tread carefully with medications that might be difficult to handle for patients with kidney issues, like stones or obstructive disease, Dr. Bulger says.
“If they only have one kidney that works well, you have to pay particular attention to drugs that are toxic to the kidneys,” he says. He notes that the nature of the patient’s health “will change the doses of some drugs, as well, depending on what the function of their kidney is.”
Dr. Austenfeld says that drugs with anticholinergic side effects, including some cold remedies such as Benadryl, should possibly be avoided in patients who are having trouble emptying their bladders, because they might make it more difficult for a patient to urinate. Some sedatives, such as amitriptyline, have similar effects and should be used cautiously in these patients, Dr. Austenfeld points out.
“That class of drugs—sometimes I see patients on them for a long time, or placed on them, and they do have a little trouble emptying their bladders,” he says.
4: Don’t discharge patients who are having difficulty voiding.
“If patients are in the hospital and they’ve been taking narcotics post-surgically, or they’re a diabetic patient and they’ve had urinary catheter infections, we should be very careful that these patients are emptying their bladders,” says Dennis Pessis, professor of urology at Rush University Medical Center in Chicago and immediate past president of the American Urological Association. “You can do a very simple ultrasound of the bladder to be sure that they’re emptying. Because if they’re not emptying well, and if they’re going to go home, they may not empty their bladders well and may colonize bacteria.”
Dr. Pessis says it’s not common, but it does happen.
“It’s something that’s of concern,” he says. “It happens often enough that we should be very alert to watching for those problems.”
5: Broach sensitive topics, but do so gently.
“Sexual dysfunction is a significant issue,” Dr. Bulger says. “I think that it’s in the best interest of the patient to address that up front. Generally, urologists are pretty good at that as well. Because you’re co-managing with them, they’re going to help out with that. But it’s important to always remember what’s going to concern the patient.”
Incontinence can be similarly sensitive but important to discuss.
“I think it helps sometimes if the physician brings it up in an appropriate way and kind of opens the door to be able to have the discussion,” Dr. Bulger said.

—Dennis Pessis, professor of urology, Rush University Medical Center, Chicago, immediate past president, American Urological Association
6: Call in a urologist, or someone with more experience, when you have difficulty placing a catheter.
One rule of thumb is, if you try twice to put in a urinary catheter without success, call in someone else to do it.
“You don’t want what we call ‘false passages,’” Dr. Pessis says. “If you are having difficulty inserting the catheter, if it’s not moving down the channel well, then you should back off and either consult someone that has more experience in catheterizing or contact the urologist.”
Two reasons the placement might be difficult: strictures like old scar formations, within the urethra, or an enlarged prostate.

John Danella, MD, FACS, head of urology for the Geisinger Health System, says a coudé catheter, with a curved tip to help it navigate around the prostate, should be tried on male patients over 50.
“If that’s not successful, then I think you need to call the urologist,” he says. “It’s better to call them before there’s been trauma to the urethra than afterwards.”
Dr. Danella says he understands that attempts by hospitalists in the face of difficulty are made with “best intentions” to save the urologist the time. But when injuries happen, “often times you’re forced to take that patient to the operating room for cystoscopy.”
7: Diabetic patients require extra attention.
“They may have what we call a diabetic type of neuropathy for the bladder, which means that they don’t have the sensation and they may not empty their bladders,” Dr. Pessis explains. “They’re also susceptible to a higher incidence of bladder infection. So if you do have a diabetic patient, be sure they’re not infected before they leave. And be sure they’re emptying their bladders well.”
8: Practice good antibiotic stewardship.
After 72 hours, almost all urine cultures from a catheterized patient are positive. That doesn’t mean they all need antibiotics, Dr. Steers says.
“Unless the patient’s symptomatic, we don’t treat until a catheter comes out,” he says. “The constant use of antibiotics in somebody with an in-dwelling catheter is creating tremendous problems with resistance and biofilms, etc.”
Dr. Steers says hospitalists can be an educational resource for care teams, using the latest infectious disease literature to say, “Hey, this antibiotic should be stopped. You don’t need to continue this many days.”
“One of the problems we’re having with guidelines is every specialty has their own antibiotic prophylaxis guidelines,” he adds. “So it can be very confusing for the hospitalist.”
9: Determine whether the patient can be seen as an outpatient.
Dr. Danella says that determination often is not made carefully enough. After initial treatment, follow-up with the urologist often can be done on an outpatient basis.
“Sometimes, they’re waiting around all day before we’re free and we can come see them. So I think in many cases, at least in our system, it would be helpful if folks could just place a phone call or just send a message and say, ‘Do you need to see this patient or can we send them home?’” Dr. Danella says. “I think it’s better for everybody if we can do that.”
One common example is an elderly patient who comes to the hospital, is put into a bed, and can’t void. Often, the patient would respond to a catheter and an alpha-blocker (if no contraindication), he says. But, that day, there’s nothing the urologist will be able to do to help make them void immediately, he says.
Another example is a patient with a small kidney stone, less than 5 mm, who probably would respond to medical therapy and won’t need an intervention, Dr. Danella says.

—Sanjay Saint, MD, MPH, FHM, hospitalist, professor of internal medicine, University of Michigan, Ann Arbor
10: Embrace your role as eyes and ears.
If a surgical patient’s note isn’t changed in three or four days, the hospitalist needs to ask the surgical team about what has changed in the case, Dr. Steers says.
“At the end of the day, it’s communication with urologists and surgeons,” he says. “And most would appreciate that. I think the [attitude from the] old days of ‘untold command of my patient, I want no other input,’ is really short-sighted.”
Hospitalist vigilance is especially important for complicated patients, such as those who’ve undergone radical cystectomy for bladder cancer. That’s the procedure with the highest mortality rate in urology, as patients are generally older, smoke, and often are obese. And they have high readmission rates—nearly 30 percent.3
Dr. Steers says hospitalists are needed to look for early warning signs in these patients.
“We look for that sort of input, especially when it comes to being the early eyes and ears of potential problems or somebody helping in discharge planning,” he says. “It might be a little too early to go home, and being readmitted is not very good for the hospital as a whole, but, more importantly, the patient.”
Tom Collins is a freelance writer in South Florida.
References
- Society of Hospital Medicine. Five things physicians and patients should question. SHM website. Available at: http://www.hospitalmedicine.org/AM/pdf/SHM-Adult_5things_List_Web.pdf. Accessed October 24, 2013.
- Loeb M, Hunt D, O’Halloran K, Carusone SC, Dafoe N, Walter SD. Stop orders to reduce inappropriate urinary catheterization in hospitalized patients: a randomized controlled trial. J Gen Intern Med. 2008;23(6):816-820.
- Stimson CJ, Chang SS, Barocas DA, et al. Early and late perioperative outcomes following radical cystectomy: 90-day readmissions, morbidity and mortality in a contemporary series. J Urol. 2010;184(4):1296-1300.
- Saint S, Lipsky BA, Goold SD. Indwelling urinary catheters: a one-point restraint? Ann Intern Med. 2002;137(2):125-127.
10 Things: At A Glance
- Take out urinary catheters as soon as possible.
- But don’t carry the Choosing Wisely directive on urinary catheters—and in-house protocols—too far.
- Beware certain types of medications in vulnerable patients.
- Don’t discharge patients who are having difficulty voiding.
- Broach sensitive topics, but do so gently.
- Call in a urologist, or someone with more experience, when you have difficulty placing a catheter.
- Diabetic patients require extra attention.
- Practice good antibiotic stewardship.
- Determine whether the patient can be seen as an outpatient.
- Embrace your role as eyes and ears.
1: Intravenous Haloperidol Does Not Prevent ICU Delirium
Urology is an area in which hospitalists might not have much formal training, but because many of these patients undergo highly complicated surgical procedures with great potential for complications, hospitalists can be vital for good outcomes, urologists say.
The use of urinary catheters is a prime area of concern when it comes to quality and safety, making hospitalists’ role in the care of urological patients even more crucial.
The Hospitalist spoke with a half dozen urologists and well-versed HM clinicians about caring for patients with urological disorders. Here are the best nuggets of guidance for hospitalists.
Take out urinary catheters as soon as possible.
John Bulger, DO, FACOI, FACP, SFHM, a hospitalist and chief quality officer at Geisinger Health System in Pennsylvania, says that, all too often, urinary catheters are left in too long. “There’s pretty good data to suggest that there’s a very direct relationship with the length of time the catheter’s in and the chance of it getting infected,” he says. “Upwards to half of the urinary catheters that are in in hospitals right now wouldn’t meet the guidelines of having a urinary catheter in.”
Dr. Bulger is chair of SHM’s Choosing Wisely subcommittee. One of SHM’s Choosing Wisely recommendations warns physicians not to place, or leave in place, catheters for incontinence, convenience, or monitoring of non-critically ill patients.1
2: But don’t carry the Choosing Wisely directive on urinary catheters—and in-house protocols—too far.
William Steers, MD, chair of urology at the University of Virginia and editor of the Journal of Urology, says there are risks associated with taking catheters out when it’s not appropriate, especially in patients who’ve undergone surgery.
“We’ve seen situations where we’re called into the operating room by another team,” Dr. Steers says. “Let’s say there was a bladder injury of another service. We’ve repaired the bladder with a catheter in for seven to 10 days. It’s taken out day one; the bladder fills and has the potential of causing harm.”
Early removal before the bladder wall heals can cause bladder rupture, requiring emergency surgery.
“So the devil’s in the details,” he says.
Mark Austenfeld, MD, FACS, president of the American Association of Clinical Urologists, which is dedicated to political action, advocacy, and best practice parameters, says catheters should remain in place for patients with mental status changes, or those who are debilitated in some way and can’t get out of bed or don’t have the wherewithal to ask for help from a nurse.
He says he realizes hospitalists are following pay-for-performance protocols, but he adds a caveat.
“Many times these protocols cannot take into account all of these specialized situations,” says Dr. Austenfeld, a urologist with Kansas City Urology Care. He stresses, though, that the hospitalists he’s worked with do high-quality work.
Sanjay Saint, MD, MPH, FHM, hospitalist and professor of internal medicine at the University of Michigan in Ann Arbor, says that even with these issues, early removal should remain a priority when appropriate.
“There’s going to be anecdotal evidence that in some particular patients, when the catheter is removed, it needs to be reinserted when they haven’t urinated for a while,” Dr. Saint explains. “But I think, in general, the studies that have looked at reinsertion have not found a statistically significant increase in reinsertion of the catheter after some type of a stop-order or nurse initiative, protocol, or urinary catheter reminder system has been put in place.”2
Dr. Steers says most agree that urinary catheters are often “overutilized.”
“You do want to get them out as soon as possible,” he says. “But if it’s ever in doubt, there should be communication with the urology team.”
3: Beware certain types of medications in vulnerable patients.
Hospitalists should tread carefully with medications that might be difficult to handle for patients with kidney issues, like stones or obstructive disease, Dr. Bulger says.
“If they only have one kidney that works well, you have to pay particular attention to drugs that are toxic to the kidneys,” he says. He notes that the nature of the patient’s health “will change the doses of some drugs, as well, depending on what the function of their kidney is.”
Dr. Austenfeld says that drugs with anticholinergic side effects, including some cold remedies such as Benadryl, should possibly be avoided in patients who are having trouble emptying their bladders, because they might make it more difficult for a patient to urinate. Some sedatives, such as amitriptyline, have similar effects and should be used cautiously in these patients, Dr. Austenfeld points out.
“That class of drugs—sometimes I see patients on them for a long time, or placed on them, and they do have a little trouble emptying their bladders,” he says.
4: Don’t discharge patients who are having difficulty voiding.
“If patients are in the hospital and they’ve been taking narcotics post-surgically, or they’re a diabetic patient and they’ve had urinary catheter infections, we should be very careful that these patients are emptying their bladders,” says Dennis Pessis, professor of urology at Rush University Medical Center in Chicago and immediate past president of the American Urological Association. “You can do a very simple ultrasound of the bladder to be sure that they’re emptying. Because if they’re not emptying well, and if they’re going to go home, they may not empty their bladders well and may colonize bacteria.”
Dr. Pessis says it’s not common, but it does happen.
“It’s something that’s of concern,” he says. “It happens often enough that we should be very alert to watching for those problems.”
5: Broach sensitive topics, but do so gently.
“Sexual dysfunction is a significant issue,” Dr. Bulger says. “I think that it’s in the best interest of the patient to address that up front. Generally, urologists are pretty good at that as well. Because you’re co-managing with them, they’re going to help out with that. But it’s important to always remember what’s going to concern the patient.”
Incontinence can be similarly sensitive but important to discuss.
“I think it helps sometimes if the physician brings it up in an appropriate way and kind of opens the door to be able to have the discussion,” Dr. Bulger said.
—Dennis Pessis, professor of urology, Rush University Medical Center, Chicago, immediate past president, American Urological Association
6: Call in a urologist, or someone with more experience, when you have difficulty placing a catheter.
One rule of thumb is, if you try twice to put in a urinary catheter without success, call in someone else to do it.
“You don’t want what we call ‘false passages,’” Dr. Pessis says. “If you are having difficulty inserting the catheter, if it’s not moving down the channel well, then you should back off and either consult someone that has more experience in catheterizing or contact the urologist.”
Two reasons the placement might be difficult: strictures like old scar formations, within the urethra, or an enlarged prostate.
John Danella, MD, FACS, head of urology for the Geisinger Health System, says a coudé catheter, with a curved tip to help it navigate around the prostate, should be tried on male patients over 50.
“If that’s not successful, then I think you need to call the urologist,” he says. “It’s better to call them before there’s been trauma to the urethra than afterwards.”
Dr. Danella says he understands that attempts by hospitalists in the face of difficulty are made with “best intentions” to save the urologist the time. But when injuries happen, “often times you’re forced to take that patient to the operating room for cystoscopy.”
7: Diabetic patients require extra attention.
“They may have what we call a diabetic type of neuropathy for the bladder, which means that they don’t have the sensation and they may not empty their bladders,” Dr. Pessis explains. “They’re also susceptible to a higher incidence of bladder infection. So if you do have a diabetic patient, be sure they’re not infected before they leave. And be sure they’re emptying their bladders well.”
8: Practice good antibiotic stewardship.
After 72 hours, almost all urine cultures from a catheterized patient are positive. That doesn’t mean they all need antibiotics, Dr. Steers says.
“Unless the patient’s symptomatic, we don’t treat until a catheter comes out,” he says. “The constant use of antibiotics in somebody with an in-dwelling catheter is creating tremendous problems with resistance and biofilms, etc.”
Dr. Steers says hospitalists can be an educational resource for care teams, using the latest infectious disease literature to say, “Hey, this antibiotic should be stopped. You don’t need to continue this many days.”
“One of the problems we’re having with guidelines is every specialty has their own antibiotic prophylaxis guidelines,” he adds. “So it can be very confusing for the hospitalist.”
9: Determine whether the patient can be seen as an outpatient.
Dr. Danella says that determination often is not made carefully enough. After initial treatment, follow-up with the urologist often can be done on an outpatient basis.
“Sometimes, they’re waiting around all day before we’re free and we can come see them. So I think in many cases, at least in our system, it would be helpful if folks could just place a phone call or just send a message and say, ‘Do you need to see this patient or can we send them home?’” Dr. Danella says. “I think it’s better for everybody if we can do that.”
One common example is an elderly patient who comes to the hospital, is put into a bed, and can’t void. Often, the patient would respond to a catheter and an alpha-blocker (if no contraindication), he says. But, that day, there’s nothing the urologist will be able to do to help make them void immediately, he says.
Another example is a patient with a small kidney stone, less than 5 mm, who probably would respond to medical therapy and won’t need an intervention, Dr. Danella says.
—Sanjay Saint, MD, MPH, FHM, hospitalist, professor of internal medicine, University of Michigan, Ann Arbor
10: Embrace your role as eyes and ears.
If a surgical patient’s note isn’t changed in three or four days, the hospitalist needs to ask the surgical team about what has changed in the case, Dr. Steers says.
“At the end of the day, it’s communication with urologists and surgeons,” he says. “And most would appreciate that. I think the [attitude from the] old days of ‘untold command of my patient, I want no other input,’ is really short-sighted.”
Hospitalist vigilance is especially important for complicated patients, such as those who’ve undergone radical cystectomy for bladder cancer. That’s the procedure with the highest mortality rate in urology, as patients are generally older, smoke, and often are obese. And they have high readmission rates—nearly 30 percent.3
Dr. Steers says hospitalists are needed to look for early warning signs in these patients.
“We look for that sort of input, especially when it comes to being the early eyes and ears of potential problems or somebody helping in discharge planning,” he says. “It might be a little too early to go home, and being readmitted is not very good for the hospital as a whole, but, more importantly, the patient.”
Tom Collins is a freelance writer in South Florida.
References
- Society of Hospital Medicine. Five things physicians and patients should question. SHM website. Available at: http://www.hospitalmedicine.org/AM/pdf/SHM-Adult_5things_List_Web.pdf. Accessed October 24, 2013.
- Loeb M, Hunt D, O’Halloran K, Carusone SC, Dafoe N, Walter SD. Stop orders to reduce inappropriate urinary catheterization in hospitalized patients: a randomized controlled trial. J Gen Intern Med. 2008;23(6):816-820.
- Stimson CJ, Chang SS, Barocas DA, et al. Early and late perioperative outcomes following radical cystectomy: 90-day readmissions, morbidity and mortality in a contemporary series. J Urol. 2010;184(4):1296-1300.
- Saint S, Lipsky BA, Goold SD. Indwelling urinary catheters: a one-point restraint? Ann Intern Med. 2002;137(2):125-127.
10 Things: At A Glance
- Take out urinary catheters as soon as possible.
- But don’t carry the Choosing Wisely directive on urinary catheters—and in-house protocols—too far.
- Beware certain types of medications in vulnerable patients.
- Don’t discharge patients who are having difficulty voiding.
- Broach sensitive topics, but do so gently.
- Call in a urologist, or someone with more experience, when you have difficulty placing a catheter.
- Diabetic patients require extra attention.
- Practice good antibiotic stewardship.
- Determine whether the patient can be seen as an outpatient.
- Embrace your role as eyes and ears.
1: Intravenous Haloperidol Does Not Prevent ICU Delirium
Urology is an area in which hospitalists might not have much formal training, but because many of these patients undergo highly complicated surgical procedures with great potential for complications, hospitalists can be vital for good outcomes, urologists say.
The use of urinary catheters is a prime area of concern when it comes to quality and safety, making hospitalists’ role in the care of urological patients even more crucial.
The Hospitalist spoke with a half dozen urologists and well-versed HM clinicians about caring for patients with urological disorders. Here are the best nuggets of guidance for hospitalists.
Take out urinary catheters as soon as possible.
John Bulger, DO, FACOI, FACP, SFHM, a hospitalist and chief quality officer at Geisinger Health System in Pennsylvania, says that, all too often, urinary catheters are left in too long. “There’s pretty good data to suggest that there’s a very direct relationship with the length of time the catheter’s in and the chance of it getting infected,” he says. “Upwards to half of the urinary catheters that are in in hospitals right now wouldn’t meet the guidelines of having a urinary catheter in.”
Dr. Bulger is chair of SHM’s Choosing Wisely subcommittee. One of SHM’s Choosing Wisely recommendations warns physicians not to place, or leave in place, catheters for incontinence, convenience, or monitoring of non-critically ill patients.1
2: But don’t carry the Choosing Wisely directive on urinary catheters—and in-house protocols—too far.
William Steers, MD, chair of urology at the University of Virginia and editor of the Journal of Urology, says there are risks associated with taking catheters out when it’s not appropriate, especially in patients who’ve undergone surgery.
“We’ve seen situations where we’re called into the operating room by another team,” Dr. Steers says. “Let’s say there was a bladder injury of another service. We’ve repaired the bladder with a catheter in for seven to 10 days. It’s taken out day one; the bladder fills and has the potential of causing harm.”
Early removal before the bladder wall heals can cause bladder rupture, requiring emergency surgery.
“So the devil’s in the details,” he says.
Mark Austenfeld, MD, FACS, president of the American Association of Clinical Urologists, which is dedicated to political action, advocacy, and best practice parameters, says catheters should remain in place for patients with mental status changes, or those who are debilitated in some way and can’t get out of bed or don’t have the wherewithal to ask for help from a nurse.
He says he realizes hospitalists are following pay-for-performance protocols, but he adds a caveat.
“Many times these protocols cannot take into account all of these specialized situations,” says Dr. Austenfeld, a urologist with Kansas City Urology Care. He stresses, though, that the hospitalists he’s worked with do high-quality work.
Sanjay Saint, MD, MPH, FHM, hospitalist and professor of internal medicine at the University of Michigan in Ann Arbor, says that even with these issues, early removal should remain a priority when appropriate.
“There’s going to be anecdotal evidence that in some particular patients, when the catheter is removed, it needs to be reinserted when they haven’t urinated for a while,” Dr. Saint explains. “But I think, in general, the studies that have looked at reinsertion have not found a statistically significant increase in reinsertion of the catheter after some type of a stop-order or nurse initiative, protocol, or urinary catheter reminder system has been put in place.”2
Dr. Steers says most agree that urinary catheters are often “overutilized.”
“You do want to get them out as soon as possible,” he says. “But if it’s ever in doubt, there should be communication with the urology team.”
3: Beware certain types of medications in vulnerable patients.
Hospitalists should tread carefully with medications that might be difficult to handle for patients with kidney issues, like stones or obstructive disease, Dr. Bulger says.
“If they only have one kidney that works well, you have to pay particular attention to drugs that are toxic to the kidneys,” he says. He notes that the nature of the patient’s health “will change the doses of some drugs, as well, depending on what the function of their kidney is.”
Dr. Austenfeld says that drugs with anticholinergic side effects, including some cold remedies such as Benadryl, should possibly be avoided in patients who are having trouble emptying their bladders, because they might make it more difficult for a patient to urinate. Some sedatives, such as amitriptyline, have similar effects and should be used cautiously in these patients, Dr. Austenfeld points out.
“That class of drugs—sometimes I see patients on them for a long time, or placed on them, and they do have a little trouble emptying their bladders,” he says.
4: Don’t discharge patients who are having difficulty voiding.
“If patients are in the hospital and they’ve been taking narcotics post-surgically, or they’re a diabetic patient and they’ve had urinary catheter infections, we should be very careful that these patients are emptying their bladders,” says Dennis Pessis, professor of urology at Rush University Medical Center in Chicago and immediate past president of the American Urological Association. “You can do a very simple ultrasound of the bladder to be sure that they’re emptying. Because if they’re not emptying well, and if they’re going to go home, they may not empty their bladders well and may colonize bacteria.”
Dr. Pessis says it’s not common, but it does happen.
“It’s something that’s of concern,” he says. “It happens often enough that we should be very alert to watching for those problems.”
5: Broach sensitive topics, but do so gently.
“Sexual dysfunction is a significant issue,” Dr. Bulger says. “I think that it’s in the best interest of the patient to address that up front. Generally, urologists are pretty good at that as well. Because you’re co-managing with them, they’re going to help out with that. But it’s important to always remember what’s going to concern the patient.”
Incontinence can be similarly sensitive but important to discuss.
“I think it helps sometimes if the physician brings it up in an appropriate way and kind of opens the door to be able to have the discussion,” Dr. Bulger said.
—Dennis Pessis, professor of urology, Rush University Medical Center, Chicago, immediate past president, American Urological Association
6: Call in a urologist, or someone with more experience, when you have difficulty placing a catheter.
One rule of thumb is, if you try twice to put in a urinary catheter without success, call in someone else to do it.
“You don’t want what we call ‘false passages,’” Dr. Pessis says. “If you are having difficulty inserting the catheter, if it’s not moving down the channel well, then you should back off and either consult someone that has more experience in catheterizing or contact the urologist.”
Two reasons the placement might be difficult: strictures like old scar formations, within the urethra, or an enlarged prostate.
John Danella, MD, FACS, head of urology for the Geisinger Health System, says a coudé catheter, with a curved tip to help it navigate around the prostate, should be tried on male patients over 50.
“If that’s not successful, then I think you need to call the urologist,” he says. “It’s better to call them before there’s been trauma to the urethra than afterwards.”
Dr. Danella says he understands that attempts by hospitalists in the face of difficulty are made with “best intentions” to save the urologist the time. But when injuries happen, “often times you’re forced to take that patient to the operating room for cystoscopy.”
7: Diabetic patients require extra attention.
“They may have what we call a diabetic type of neuropathy for the bladder, which means that they don’t have the sensation and they may not empty their bladders,” Dr. Pessis explains. “They’re also susceptible to a higher incidence of bladder infection. So if you do have a diabetic patient, be sure they’re not infected before they leave. And be sure they’re emptying their bladders well.”
8: Practice good antibiotic stewardship.
After 72 hours, almost all urine cultures from a catheterized patient are positive. That doesn’t mean they all need antibiotics, Dr. Steers says.
“Unless the patient’s symptomatic, we don’t treat until a catheter comes out,” he says. “The constant use of antibiotics in somebody with an in-dwelling catheter is creating tremendous problems with resistance and biofilms, etc.”
Dr. Steers says hospitalists can be an educational resource for care teams, using the latest infectious disease literature to say, “Hey, this antibiotic should be stopped. You don’t need to continue this many days.”
“One of the problems we’re having with guidelines is every specialty has their own antibiotic prophylaxis guidelines,” he adds. “So it can be very confusing for the hospitalist.”
9: Determine whether the patient can be seen as an outpatient.
Dr. Danella says that determination often is not made carefully enough. After initial treatment, follow-up with the urologist often can be done on an outpatient basis.
“Sometimes, they’re waiting around all day before we’re free and we can come see them. So I think in many cases, at least in our system, it would be helpful if folks could just place a phone call or just send a message and say, ‘Do you need to see this patient or can we send them home?’” Dr. Danella says. “I think it’s better for everybody if we can do that.”
One common example is an elderly patient who comes to the hospital, is put into a bed, and can’t void. Often, the patient would respond to a catheter and an alpha-blocker (if no contraindication), he says. But, that day, there’s nothing the urologist will be able to do to help make them void immediately, he says.
Another example is a patient with a small kidney stone, less than 5 mm, who probably would respond to medical therapy and won’t need an intervention, Dr. Danella says.
—Sanjay Saint, MD, MPH, FHM, hospitalist, professor of internal medicine, University of Michigan, Ann Arbor
10: Embrace your role as eyes and ears.
If a surgical patient’s note isn’t changed in three or four days, the hospitalist needs to ask the surgical team about what has changed in the case, Dr. Steers says.
“At the end of the day, it’s communication with urologists and surgeons,” he says. “And most would appreciate that. I think the [attitude from the] old days of ‘untold command of my patient, I want no other input,’ is really short-sighted.”
Hospitalist vigilance is especially important for complicated patients, such as those who’ve undergone radical cystectomy for bladder cancer. That’s the procedure with the highest mortality rate in urology, as patients are generally older, smoke, and often are obese. And they have high readmission rates—nearly 30 percent.3
Dr. Steers says hospitalists are needed to look for early warning signs in these patients.
“We look for that sort of input, especially when it comes to being the early eyes and ears of potential problems or somebody helping in discharge planning,” he says. “It might be a little too early to go home, and being readmitted is not very good for the hospital as a whole, but, more importantly, the patient.”
Tom Collins is a freelance writer in South Florida.
References
- Society of Hospital Medicine. Five things physicians and patients should question. SHM website. Available at: http://www.hospitalmedicine.org/AM/pdf/SHM-Adult_5things_List_Web.pdf. Accessed October 24, 2013.
- Loeb M, Hunt D, O’Halloran K, Carusone SC, Dafoe N, Walter SD. Stop orders to reduce inappropriate urinary catheterization in hospitalized patients: a randomized controlled trial. J Gen Intern Med. 2008;23(6):816-820.
- Stimson CJ, Chang SS, Barocas DA, et al. Early and late perioperative outcomes following radical cystectomy: 90-day readmissions, morbidity and mortality in a contemporary series. J Urol. 2010;184(4):1296-1300.
- Saint S, Lipsky BA, Goold SD. Indwelling urinary catheters: a one-point restraint? Ann Intern Med. 2002;137(2):125-127.
NHLBI hands off hypertension guidelines to ACC, AHA
The two U.S. groups most active in issuing guidelines and recommendations for cardiovascular disease diagnosis and management, the American College of Cardiology and American Heart Association, received a surprise in June when the National Heart, Lung, and Blood Institute suddenly announced that it would shift to these and other "partner organizations" primary responsibility for the next updates of U.S. hypertension guidelines, national cholesterol-management guidelines, and the other cardiovascular disease–related management recommendations that the institute has had in the works.
The NHLBI launched "a collaborative relationship with the ACC, AHA, and other organizations because they said they are not in a position to endorse guidelines, they must be endorsed by other organizations," said Dr. Sidney C. Smith Jr., professor of medicine at the University of North Carolina in Chapel Hill. Dr. Smith is a member of the panel that’s been writing the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), and has been active for a long time in the ACC and AHA guidelines-development process.
On June 19, Dr. Gary H. Gibbons, NHLBI director, and his associates announced that effective immediately the institute was getting out of the guidelines-issuing business (Circulation 2013; doi: 10.1161/CIRCULATIONAHA.113.004587).
"Just over the past couple of months we began to look at how this will be done. Everyone wants the process to move quickly. How quickly can these organizations put it together? That’s the limiting factor right now," Dr. Smith said in an interview in early September.
While the ACC and AHA have on record some 20 sets of practice guidelines that cover most facets of cardiology, their list omits areas that the NHLBI covered in the past, notably hypertension and hypercholesterolemia assessment and management.
"The ACC and AHA guideline process is very expensive, and we wouldn’t dream of duplicating something when people you trust were commissioned by someone else [NHLBI] to do the work," said Dr. Kim Allan Williams Sr. of Wayne State University, Detroit. Dr. Williams will take the position of professor of medicine and chief of cardiovascular services at Rush University Medical Center in Chicago on Nov. 1. He serves as vice-president of the ACC. "We have all been under the impression that JNC 8 was being put together and getting published soon," he said in an interview.
Dr. Williams stressed that he and other ACC officials have pledged not to talk about the JNC 8 process until transition from the NHLBI works itself out, but he offered this succinct observation: The ACC "has made a commitment to go forward with the JNC process. There will be a publication from that panel, although it may not have that name."
Dr. Smith and Dr. Williams said that they had no relevant disclosures.
On Twitter @mitchelzoler
The two U.S. groups most active in issuing guidelines and recommendations for cardiovascular disease diagnosis and management, the American College of Cardiology and American Heart Association, received a surprise in June when the National Heart, Lung, and Blood Institute suddenly announced that it would shift to these and other "partner organizations" primary responsibility for the next updates of U.S. hypertension guidelines, national cholesterol-management guidelines, and the other cardiovascular disease–related management recommendations that the institute has had in the works.
The NHLBI launched "a collaborative relationship with the ACC, AHA, and other organizations because they said they are not in a position to endorse guidelines, they must be endorsed by other organizations," said Dr. Sidney C. Smith Jr., professor of medicine at the University of North Carolina in Chapel Hill. Dr. Smith is a member of the panel that’s been writing the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), and has been active for a long time in the ACC and AHA guidelines-development process.
On June 19, Dr. Gary H. Gibbons, NHLBI director, and his associates announced that effective immediately the institute was getting out of the guidelines-issuing business (Circulation 2013; doi: 10.1161/CIRCULATIONAHA.113.004587).
"Just over the past couple of months we began to look at how this will be done. Everyone wants the process to move quickly. How quickly can these organizations put it together? That’s the limiting factor right now," Dr. Smith said in an interview in early September.
While the ACC and AHA have on record some 20 sets of practice guidelines that cover most facets of cardiology, their list omits areas that the NHLBI covered in the past, notably hypertension and hypercholesterolemia assessment and management.
"The ACC and AHA guideline process is very expensive, and we wouldn’t dream of duplicating something when people you trust were commissioned by someone else [NHLBI] to do the work," said Dr. Kim Allan Williams Sr. of Wayne State University, Detroit. Dr. Williams will take the position of professor of medicine and chief of cardiovascular services at Rush University Medical Center in Chicago on Nov. 1. He serves as vice-president of the ACC. "We have all been under the impression that JNC 8 was being put together and getting published soon," he said in an interview.
Dr. Williams stressed that he and other ACC officials have pledged not to talk about the JNC 8 process until transition from the NHLBI works itself out, but he offered this succinct observation: The ACC "has made a commitment to go forward with the JNC process. There will be a publication from that panel, although it may not have that name."
Dr. Smith and Dr. Williams said that they had no relevant disclosures.
On Twitter @mitchelzoler
The two U.S. groups most active in issuing guidelines and recommendations for cardiovascular disease diagnosis and management, the American College of Cardiology and American Heart Association, received a surprise in June when the National Heart, Lung, and Blood Institute suddenly announced that it would shift to these and other "partner organizations" primary responsibility for the next updates of U.S. hypertension guidelines, national cholesterol-management guidelines, and the other cardiovascular disease–related management recommendations that the institute has had in the works.
The NHLBI launched "a collaborative relationship with the ACC, AHA, and other organizations because they said they are not in a position to endorse guidelines, they must be endorsed by other organizations," said Dr. Sidney C. Smith Jr., professor of medicine at the University of North Carolina in Chapel Hill. Dr. Smith is a member of the panel that’s been writing the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8), and has been active for a long time in the ACC and AHA guidelines-development process.
On June 19, Dr. Gary H. Gibbons, NHLBI director, and his associates announced that effective immediately the institute was getting out of the guidelines-issuing business (Circulation 2013; doi: 10.1161/CIRCULATIONAHA.113.004587).
"Just over the past couple of months we began to look at how this will be done. Everyone wants the process to move quickly. How quickly can these organizations put it together? That’s the limiting factor right now," Dr. Smith said in an interview in early September.
While the ACC and AHA have on record some 20 sets of practice guidelines that cover most facets of cardiology, their list omits areas that the NHLBI covered in the past, notably hypertension and hypercholesterolemia assessment and management.
"The ACC and AHA guideline process is very expensive, and we wouldn’t dream of duplicating something when people you trust were commissioned by someone else [NHLBI] to do the work," said Dr. Kim Allan Williams Sr. of Wayne State University, Detroit. Dr. Williams will take the position of professor of medicine and chief of cardiovascular services at Rush University Medical Center in Chicago on Nov. 1. He serves as vice-president of the ACC. "We have all been under the impression that JNC 8 was being put together and getting published soon," he said in an interview.
Dr. Williams stressed that he and other ACC officials have pledged not to talk about the JNC 8 process until transition from the NHLBI works itself out, but he offered this succinct observation: The ACC "has made a commitment to go forward with the JNC process. There will be a publication from that panel, although it may not have that name."
Dr. Smith and Dr. Williams said that they had no relevant disclosures.
On Twitter @mitchelzoler
ACCF/AHA 2013 Guidelines for Managing Heart Failure
Background
Heart failure (HF) is the No. 1 cause of both hospitalization and readmission among Americans 65 years and older.1 Hospitalizations in the HF population are associated with poor patient outcomes (30% mortality in the following year) and high costs, accounting for approximately 70% of the $32 billion spent on HF care annually in the United States.1 In 2009, the Centers for Medicare & Medicaid Services (CMS) introduced the 30-day, risk-standardized, all-cause readmission for HF as an indicator of quality and efficiency of care, which has since been incorporated into Medicare’s value-based purchasing program.2
HF is a complex syndrome that is associated with multiple comorbidities. Appropriate to these issues, management is multifaceted and involves care across the spectrum of disease:
- Diagnosing and treating underlying causes;
- Minimizing exacerbants;
- Optimizing management of comorbidities;
- Addressing psychosocial and environmental issues beyond the hospital; and
- Confronting end-of-life care.
In order to address this continuum of disease management, the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) simultaneously released a new Guideline for the Management of HF in June in the Journal of the American College of Cardiology and Circulation.3,4 This update was developed in collaboration with the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and the International Society for Heart and Lung Transplantation. The goals of the document are to improve quality of care, optimize patient outcomes, and advance the efficient use of healthcare resources. The guideline includes important recommendations for overall care, but particularly for hospital-based care and transitions of care that are largely the purview of hospitalists.
Guideline Update
The 2013 guideline is the third revision of the original guideline that was released in 2000. Despite being a complete rewrite of the 2009 HF guideline, the updated document contains relatively few changes to the recommendations that are Class I (should be performed) and III (no benefit or harm). The most significant randomized controlled trials in HF patients that have been published since the 2009 guideline include EMPHASIS-HF5 and MADIT-CRT/RAFT, which expand indications for aldosterone antagonists (AA) and cardiac resyncronization therapy (CRT), respectively, to patients with mild symptoms.5,6,7 Additionally, the WARCEF trial was published, which failed to demonstrate a significant difference in death, ischemic stroke, or intracerebral hemorrhage between treatment with warfarin or aspirin in patients with HF and reduced left ventricular ejection fraction (LVEF) in sinus rhythm.8
The most notable updates from the 2009 guideline include (* = Class I and III indications):
- The definition of HF has been revised to include: 1) HF with reduced ejection fraction (HFrEF; LVEF ≤40%), 2) HF failure with preserved ejection fraction (HFpEF; LVEF ≥50%), 3) HFpEF, borderline (LVEF 41-49%), and 4) HFpEF, improved (LVEF >40%).
- In the hospitalized patient, measurement of brain natriuretic peptide (BNP) or NT-proBNP is useful to support clinical judgment for the diagnosis of acutely decompensated HF, especially in the setting of uncertainty for the diagnosis.*
- AA should be used in patients with New York Heart Association (NYHA) functional Class II-IV and LVEF ≤35% unless contraindicated (creatinine ≤2.5 mg/dL in men, ≤2.0 mg/dL in women, and potassium <5.0 mEq/L).*
- CRT is indicated for patients who have LVEF of 35% or less, sinus rhythm, left bundle-branch block with a QRS duration of ³150 ms, and NYHA functional Class II-IV on guideline-directed medical therapy (GDMT).*
- Anticoagulation should not be used in patients with chronic HFrEF without atrial fibrillation, prior thromboembolic event, or cardioembolic source.*
- Transitions of care and GDMT can be improved by employing the following: 1) use of performance-improvement systems to identify HF patients, 2) development of multidisciplinary HF disease-management programs for patients at high risk of readmission, and 3) placing phone calls to the patient within three days of discharge and scheduling a follow-up visit within seven to 14 days.
Analysis
Overall, the new guideline provides a thorough reassessment and expert analysis on the diagnosis and management of HF for both inpatient and outpatient care. The authors introduce the phrase “guideline-directed medical therapy” (GDMT) to emphasize the smaller set of recommendations that constitute optimal medical therapy for HF patients. This designation, encompassing primarily Class I recommendations, helps providers rapidly determine the optimal treatment course for an individual patient. The mainstay of GDMT in HFrEF patients remains angiotensin-converting enzyme inhibitors (ACE-I), angiotensin receptor blockers (ARB) when ACE-I-intolerant, beta-blockers, and, in select patients, AA, hydralazine-nitrates, and diuretics.
A major shift in focus is seen in the new guideline with a greater emphasis on improved patient-centered outcomes across the spectrum of the disease. HF requires a continuum of care, from screening and genetic testing of family members of patients with idiopathic cardiomyopathy to conversations about palliative care and hospice. To this end, the authors highlight quality of life, shared decision-making, care coordination, transitions of care, and appropriateness of palliative care in a chronic disease state.
Further, the guideline expands upon previous recommendations for compliance with performance and quality metrics. Quality of care and adherence to performance measures of HF patients are becoming increasingly recognized, particularly in the hospital setting. The guideline offers recommendations for transitions of care in the hospitalized patient, which utilize systems of care coordination to ensure an evidence-based plan of care that includes the achievement of GDMT goals, effective management of comorbid conditions, timely follow-up, and appropriate dietary and physical activities.
HM Takeaways
HF is one of the most common, most challenging diseases managed by hospitalists. The 2013 ACCF/AHA Guideline for the Management of HF, while providing a comprehensive summary of evidence with recommendations for the totality of care for these patients throughout the course of the disease, places heavy emphasis on management during hospitalization and transitions. This includes repositioning of performance measures involving GDMT to better ensure optimal use of proven therapies in HFrEF, evidence-based steps to reduce readmissions, and greater recognition of the role of palliative care for patients with advanced disease.
Drs. McIlvennan and Allen are cardiologists in the Department of Medicine at the University of Colorado School of Medicine in Denver. Dr. Allen also works in the Colorado Health Outcomes Program.
References available at the-hospitalist.org.
Background
Heart failure (HF) is the No. 1 cause of both hospitalization and readmission among Americans 65 years and older.1 Hospitalizations in the HF population are associated with poor patient outcomes (30% mortality in the following year) and high costs, accounting for approximately 70% of the $32 billion spent on HF care annually in the United States.1 In 2009, the Centers for Medicare & Medicaid Services (CMS) introduced the 30-day, risk-standardized, all-cause readmission for HF as an indicator of quality and efficiency of care, which has since been incorporated into Medicare’s value-based purchasing program.2
HF is a complex syndrome that is associated with multiple comorbidities. Appropriate to these issues, management is multifaceted and involves care across the spectrum of disease:
- Diagnosing and treating underlying causes;
- Minimizing exacerbants;
- Optimizing management of comorbidities;
- Addressing psychosocial and environmental issues beyond the hospital; and
- Confronting end-of-life care.
In order to address this continuum of disease management, the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) simultaneously released a new Guideline for the Management of HF in June in the Journal of the American College of Cardiology and Circulation.3,4 This update was developed in collaboration with the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and the International Society for Heart and Lung Transplantation. The goals of the document are to improve quality of care, optimize patient outcomes, and advance the efficient use of healthcare resources. The guideline includes important recommendations for overall care, but particularly for hospital-based care and transitions of care that are largely the purview of hospitalists.
Guideline Update
The 2013 guideline is the third revision of the original guideline that was released in 2000. Despite being a complete rewrite of the 2009 HF guideline, the updated document contains relatively few changes to the recommendations that are Class I (should be performed) and III (no benefit or harm). The most significant randomized controlled trials in HF patients that have been published since the 2009 guideline include EMPHASIS-HF5 and MADIT-CRT/RAFT, which expand indications for aldosterone antagonists (AA) and cardiac resyncronization therapy (CRT), respectively, to patients with mild symptoms.5,6,7 Additionally, the WARCEF trial was published, which failed to demonstrate a significant difference in death, ischemic stroke, or intracerebral hemorrhage between treatment with warfarin or aspirin in patients with HF and reduced left ventricular ejection fraction (LVEF) in sinus rhythm.8
The most notable updates from the 2009 guideline include (* = Class I and III indications):
- The definition of HF has been revised to include: 1) HF with reduced ejection fraction (HFrEF; LVEF ≤40%), 2) HF failure with preserved ejection fraction (HFpEF; LVEF ≥50%), 3) HFpEF, borderline (LVEF 41-49%), and 4) HFpEF, improved (LVEF >40%).
- In the hospitalized patient, measurement of brain natriuretic peptide (BNP) or NT-proBNP is useful to support clinical judgment for the diagnosis of acutely decompensated HF, especially in the setting of uncertainty for the diagnosis.*
- AA should be used in patients with New York Heart Association (NYHA) functional Class II-IV and LVEF ≤35% unless contraindicated (creatinine ≤2.5 mg/dL in men, ≤2.0 mg/dL in women, and potassium <5.0 mEq/L).*
- CRT is indicated for patients who have LVEF of 35% or less, sinus rhythm, left bundle-branch block with a QRS duration of ³150 ms, and NYHA functional Class II-IV on guideline-directed medical therapy (GDMT).*
- Anticoagulation should not be used in patients with chronic HFrEF without atrial fibrillation, prior thromboembolic event, or cardioembolic source.*
- Transitions of care and GDMT can be improved by employing the following: 1) use of performance-improvement systems to identify HF patients, 2) development of multidisciplinary HF disease-management programs for patients at high risk of readmission, and 3) placing phone calls to the patient within three days of discharge and scheduling a follow-up visit within seven to 14 days.
Analysis
Overall, the new guideline provides a thorough reassessment and expert analysis on the diagnosis and management of HF for both inpatient and outpatient care. The authors introduce the phrase “guideline-directed medical therapy” (GDMT) to emphasize the smaller set of recommendations that constitute optimal medical therapy for HF patients. This designation, encompassing primarily Class I recommendations, helps providers rapidly determine the optimal treatment course for an individual patient. The mainstay of GDMT in HFrEF patients remains angiotensin-converting enzyme inhibitors (ACE-I), angiotensin receptor blockers (ARB) when ACE-I-intolerant, beta-blockers, and, in select patients, AA, hydralazine-nitrates, and diuretics.
A major shift in focus is seen in the new guideline with a greater emphasis on improved patient-centered outcomes across the spectrum of the disease. HF requires a continuum of care, from screening and genetic testing of family members of patients with idiopathic cardiomyopathy to conversations about palliative care and hospice. To this end, the authors highlight quality of life, shared decision-making, care coordination, transitions of care, and appropriateness of palliative care in a chronic disease state.
Further, the guideline expands upon previous recommendations for compliance with performance and quality metrics. Quality of care and adherence to performance measures of HF patients are becoming increasingly recognized, particularly in the hospital setting. The guideline offers recommendations for transitions of care in the hospitalized patient, which utilize systems of care coordination to ensure an evidence-based plan of care that includes the achievement of GDMT goals, effective management of comorbid conditions, timely follow-up, and appropriate dietary and physical activities.
HM Takeaways
HF is one of the most common, most challenging diseases managed by hospitalists. The 2013 ACCF/AHA Guideline for the Management of HF, while providing a comprehensive summary of evidence with recommendations for the totality of care for these patients throughout the course of the disease, places heavy emphasis on management during hospitalization and transitions. This includes repositioning of performance measures involving GDMT to better ensure optimal use of proven therapies in HFrEF, evidence-based steps to reduce readmissions, and greater recognition of the role of palliative care for patients with advanced disease.
Drs. McIlvennan and Allen are cardiologists in the Department of Medicine at the University of Colorado School of Medicine in Denver. Dr. Allen also works in the Colorado Health Outcomes Program.
References available at the-hospitalist.org.
Background
Heart failure (HF) is the No. 1 cause of both hospitalization and readmission among Americans 65 years and older.1 Hospitalizations in the HF population are associated with poor patient outcomes (30% mortality in the following year) and high costs, accounting for approximately 70% of the $32 billion spent on HF care annually in the United States.1 In 2009, the Centers for Medicare & Medicaid Services (CMS) introduced the 30-day, risk-standardized, all-cause readmission for HF as an indicator of quality and efficiency of care, which has since been incorporated into Medicare’s value-based purchasing program.2
HF is a complex syndrome that is associated with multiple comorbidities. Appropriate to these issues, management is multifaceted and involves care across the spectrum of disease:
- Diagnosing and treating underlying causes;
- Minimizing exacerbants;
- Optimizing management of comorbidities;
- Addressing psychosocial and environmental issues beyond the hospital; and
- Confronting end-of-life care.
In order to address this continuum of disease management, the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) simultaneously released a new Guideline for the Management of HF in June in the Journal of the American College of Cardiology and Circulation.3,4 This update was developed in collaboration with the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and the International Society for Heart and Lung Transplantation. The goals of the document are to improve quality of care, optimize patient outcomes, and advance the efficient use of healthcare resources. The guideline includes important recommendations for overall care, but particularly for hospital-based care and transitions of care that are largely the purview of hospitalists.
Guideline Update
The 2013 guideline is the third revision of the original guideline that was released in 2000. Despite being a complete rewrite of the 2009 HF guideline, the updated document contains relatively few changes to the recommendations that are Class I (should be performed) and III (no benefit or harm). The most significant randomized controlled trials in HF patients that have been published since the 2009 guideline include EMPHASIS-HF5 and MADIT-CRT/RAFT, which expand indications for aldosterone antagonists (AA) and cardiac resyncronization therapy (CRT), respectively, to patients with mild symptoms.5,6,7 Additionally, the WARCEF trial was published, which failed to demonstrate a significant difference in death, ischemic stroke, or intracerebral hemorrhage between treatment with warfarin or aspirin in patients with HF and reduced left ventricular ejection fraction (LVEF) in sinus rhythm.8
The most notable updates from the 2009 guideline include (* = Class I and III indications):
- The definition of HF has been revised to include: 1) HF with reduced ejection fraction (HFrEF; LVEF ≤40%), 2) HF failure with preserved ejection fraction (HFpEF; LVEF ≥50%), 3) HFpEF, borderline (LVEF 41-49%), and 4) HFpEF, improved (LVEF >40%).
- In the hospitalized patient, measurement of brain natriuretic peptide (BNP) or NT-proBNP is useful to support clinical judgment for the diagnosis of acutely decompensated HF, especially in the setting of uncertainty for the diagnosis.*
- AA should be used in patients with New York Heart Association (NYHA) functional Class II-IV and LVEF ≤35% unless contraindicated (creatinine ≤2.5 mg/dL in men, ≤2.0 mg/dL in women, and potassium <5.0 mEq/L).*
- CRT is indicated for patients who have LVEF of 35% or less, sinus rhythm, left bundle-branch block with a QRS duration of ³150 ms, and NYHA functional Class II-IV on guideline-directed medical therapy (GDMT).*
- Anticoagulation should not be used in patients with chronic HFrEF without atrial fibrillation, prior thromboembolic event, or cardioembolic source.*
- Transitions of care and GDMT can be improved by employing the following: 1) use of performance-improvement systems to identify HF patients, 2) development of multidisciplinary HF disease-management programs for patients at high risk of readmission, and 3) placing phone calls to the patient within three days of discharge and scheduling a follow-up visit within seven to 14 days.
Analysis
Overall, the new guideline provides a thorough reassessment and expert analysis on the diagnosis and management of HF for both inpatient and outpatient care. The authors introduce the phrase “guideline-directed medical therapy” (GDMT) to emphasize the smaller set of recommendations that constitute optimal medical therapy for HF patients. This designation, encompassing primarily Class I recommendations, helps providers rapidly determine the optimal treatment course for an individual patient. The mainstay of GDMT in HFrEF patients remains angiotensin-converting enzyme inhibitors (ACE-I), angiotensin receptor blockers (ARB) when ACE-I-intolerant, beta-blockers, and, in select patients, AA, hydralazine-nitrates, and diuretics.
A major shift in focus is seen in the new guideline with a greater emphasis on improved patient-centered outcomes across the spectrum of the disease. HF requires a continuum of care, from screening and genetic testing of family members of patients with idiopathic cardiomyopathy to conversations about palliative care and hospice. To this end, the authors highlight quality of life, shared decision-making, care coordination, transitions of care, and appropriateness of palliative care in a chronic disease state.
Further, the guideline expands upon previous recommendations for compliance with performance and quality metrics. Quality of care and adherence to performance measures of HF patients are becoming increasingly recognized, particularly in the hospital setting. The guideline offers recommendations for transitions of care in the hospitalized patient, which utilize systems of care coordination to ensure an evidence-based plan of care that includes the achievement of GDMT goals, effective management of comorbid conditions, timely follow-up, and appropriate dietary and physical activities.
HM Takeaways
HF is one of the most common, most challenging diseases managed by hospitalists. The 2013 ACCF/AHA Guideline for the Management of HF, while providing a comprehensive summary of evidence with recommendations for the totality of care for these patients throughout the course of the disease, places heavy emphasis on management during hospitalization and transitions. This includes repositioning of performance measures involving GDMT to better ensure optimal use of proven therapies in HFrEF, evidence-based steps to reduce readmissions, and greater recognition of the role of palliative care for patients with advanced disease.
Drs. McIlvennan and Allen are cardiologists in the Department of Medicine at the University of Colorado School of Medicine in Denver. Dr. Allen also works in the Colorado Health Outcomes Program.
References available at the-hospitalist.org.
Nine Things Chronic-Pain Specialists Think Hospitalists Need To Know
In This Edition
9 Things: At a Glance
An occasional series providing specialty-specific advice for hospitalists from experts in the field.
- Recognize the differential diagnosis for pain exacerbation in a chronic opioid therapy (COT) patient/chronic pain patient.
- Know where the opioids are going.
- Sometimes stopping pills, rather than adding them, can cure pain.
- Take time to educate patients about methadone and its risk of mortality if not used as prescribed.
- A little local anesthetic (and some steroid) goes a long way.
- Addiction to opioids is not rare.
- Safely changing opioid regimens requires good math and good judgment.
- For a low-risk chronic pain patient on low-dose opioids, don’t change the regimen, even if the indication for opioids isn’t clear.
- If a patient has pain all the time, they need to be on a medication that works all the time.
The differential diagnosis for pain exacerbation in a chronic opioid therapy (COT) patient/chronic pain patient is:
- Worsening medical problem;
- New medical problem;
- Nonopioid problem (side effect);
- Opioid problem (resistance/tolerance/side effect); and
- Opioid-induced hyperalgesia.
The search for an etiology and treatment for chronic pain should not end, even if a patient is labeled with “chronic pain syndrome.” The patient could simply be chronically undiagnosed or on an incorrect therapy.
Know where the opioids are going.
Whether it’s auditing a prescription-monitoring program (PMP), checking a urine drug screen, or calling a pharmacist, try to ensure that chronic pain patients are taking the opioids as prescribed. A phone call to the primary opioid prescriber or chronic pain provider could save a busy hospitalist a lot of time.
Using PMP data can consume a lot of time. Typically, only prescribing providers can access PMPs, so delegating this responsibility to someone else is not possible. If your state PMP does not help, simply call the patient’s pharmacy and ask for the last three fill dates on an opioid prescription. This also works well in case the patient’s pharmacy doesn’t participate in a PMP or is delayed in uploading recent prescriber data. Many COT patients have an opioid treatment agreement with their prescriber and must use only one pharmacy to fill opioids.
In January 2013, the University of North Carolina Injury Prevention Center published an analysis of three years of North Carolina PMP data.1 Patients followed by providers who consistently used the state PMP were five times more likely to receive treatment for opioid dependence compared with patients of providers who never used the state PMP.1
Why go through all this trouble if a chronic pain specialist is also doing it? It’s good documentation and good care, like monitoring levels of transplant meds or making sure hemoglobin A1Cs are up to date and trending toward goal. It may only take one misused or diverted opioid pill to result in a serious adverse event.
Sometimes stopping pills, rather than adding them, can cure pain.
Many chronic pain patients accumulate a patchwork of pills (e.g. benzodiazepines, opioids, muscle relaxants, and antidepressants). Many interpret noxious symptoms associated with the drug burden as “uncontrolled pain.” Two conditions that might afflict the pain sufferer who takes multiple medications are opioid-induced hyperalgesia (OIH) and medication-overuse headaches (MOH). They are uncommon but should be on a hospitalist’s differential for difficult-to-control chronic pain. Opioids commonly are implicated in causing MOH, a chronic headache occurring at least 15 days a month, four hours a day if untreated, and for at least three consecutive months. OIH is a nociceptive sensitization caused by opioids that can occur suddenly or insidiously.
If a drug isn’t absolutely necessary, stop it. If you and the patient start by agreeing to the shared goal of improving health, the conversation should go better. An axiom we learned from mentors at the University of Washington is: “There is no pain that cannot be made worse with inappropriate therapy.”
Take time to educate patients about methadone and its risk of mortality if not used as prescribed.
Methadone is less frequently prescribed than other opioids, yet it is more frequently associated with death from overdose. Though there is a risk of overdose and death with any opioid, managing methadone is more difficult. A desperate chronic pain patient may self-escalate their methadone without proper insight into the consequences.
Remember the logarithmic relationship methadone doses have with their morphine equivalency. The following highlights how deceiving the numbers are: 50 mg of methadone is about 100 mg of morphine-equivalent, but 100 mg of methadone is about 1,000 mg of morphine-equivalent, or 10 times as strong.
From 1999 to 2005, methadone-related deaths increased by 468%.2 If the patient doesn’t seem to understand these risks, they are not a good candidate for methadone treatment.
A little local anesthetic (and some steroid) goes a long way.
Hospitalists should offer an assortment of diagnostic and therapeutic injections to chronic pain patients. First, be sure you’ve done your due diligence:
- What procedures do you have privileges to do?
- Do you need to be proctored first?
- How do your local specialists feel about you doing injections?
In light of these considerations, hospitalists should be able to train and be credentialed to offer such procedures as trigger-point injections, joint injections (knees, shoulders), or even a peripheral nerve injection (e.g. lateral femoral cutaneous nerve or ilioinguinal nerve injection). Some hospitalists might even want to learn ultrasound-guided sacroiliac joint injections for chronic unexplained back pain.
Offering an indicated and effective injection is a good nonopioid option. And local anesthetic injections can help hospitalists establish an elusive diagnosis. For example, many patients spend years getting worked up for head and neck pain when dry-needling with a small volume (1 cc) of local anesthetic into a neck muscle trigger point can break their pain generator, eliminating their pain.
Addiction to opioids is not rare.
The use, misuse, and diversion of opioids and all the associated complications have appropriately received considerable media attention. A seminal paper by Porter and Jick titled “Addiction Is Rare in Patients Treated with Narcotics” is one of many tipping points associated with the boom in opioid prescribing.3 Whether it’s a three-day supply of hydrocodone, 24 hours on a PCA, or an opioid rotation, any exposure to opioids can put a patient on the runway to addiction.
There are only 3,071 board-certified addiction specialists certified by the American Board of Addiction Medicine, so access to an addiction specialist might be difficult.4
Nonetheless, do not become complacent and just continue the opioid therapy in a difficult opioid-addicted patient. Express your concerns to the primary opioid prescriber, or help patients who don’t have an opioid prescriber get access and treatment. Otherwise, you have no choice but to taper the opioids.
Ideally, chronic pain management should be delivered in the outpatient arena where long-term monitoring can take place.
Safely changing opioid regimens requires good math and good judgment.
During training and practice, hospitalists become accustomed to rapidly analyze objective data, such as ABGs, ECGs, anion gaps, and vent settings. A hospitalist should become similarly efficient at calculating morphine equivalencies (cautiously with methadone and fentanyl), making dose reductions, and rotating opioids. The more comfortable you are with morphine equivalencies, the faster and safer you will be at rotating opioids. Whatever morphine-equivalence table you feel comfortable with is the one you should use consistently.
We see many providers who unwittingly take, for example, a patient who has become resistant to hydrocodone/acetaminophen 10/325 mg PO TID (30 mg of morphine) and convert them to oxycodone/acetaminophen 10/325 mg PO QID (60 mg of morphine—a doubling), when doubling could cause respiratory depression or a faster path to addiction and dependency.
But there are cases in which judgment should trump math, such as when converting from an IV to an oral regimen. We frequently see patients in the clinic requesting refills for more than 100 mg of hydromorphone because “that’s what I was on when I was hospitalized and on the pump.” If the IV-to-oral conversion leaves you prescribing high doses of oral opioids, plan for a rapid taper and a smooth handoff to the outpatient setting.
One strategy to decrease an error in math and judgment is to use IV PCAs as infrequently as possible if a patient isn’t post-operative and they are able to take oral meds. And never hesitate to consult with your inpatient pharmacist or a chronic pain specialist.
For a low-risk chronic pain patient on low-dose opioids, don’t change the regimen, even if the indication for opioids isn’t clear.
Although it is tempting to become an opioid prohibitionist, if a patient has been taking an opioid for years and is functioning, working, compliant, and has no risk factors for complications from COT, it is likely fine to continue their current regimen. Touch base with the primary opioid prescriber, and if you’re concerned, use some of the monitoring instruments described earlier (PMP, urine drug screen, opioid treatment agreement, pill counts).
If a patient has pain all the time, they need to be on a medication that works all the time.
A good pain history followed by a good neurological and mental health assessment is of incalculable value, especially because physicians often underestimate a patient’s pain intensity and its impact on a patient’s quality of life.5,6 A patient’s pain intensity, quality of life, and function can be dramatically improved by starting a long-acting medication for “constant pain.”
If a patient hurts “24 hours a day” and cannot function on hydrocodone/acetaminophen 10/325 QID, it’s probably because they are constantly reacting to spikes in pain and using a “some of the time” medicine to treat “all the time” pain. Switching to a long-acting medication—and it doesn’t have to be an opioid—could improve control and decrease how much narcotic the patient needs.
If you choose a long-acting opioid (in this case, you could try morphine sulphate extended-release 15 mg BID and satisfy 50% of the hydrocodone need), then you could titrate slowly upwards to where the patient would not need hydrocodone. If the patient still had uncontrolled pain, then either morphine is the wrong compound for them or they are benefiting from the “nonanalgesic properties” of the opioids.
Give the patient the benefit of the doubt; because of genetic polymorphisms, a patient may need several opioid rotations before the right opioid compound is found.
Dr. Schultz is a hospitalist and assistant professor in the department of internal medicine at the University of Miami Miller School of Medicine. She is board-certified in hospice and palliative care and specializes in chronic pain management. Dr. Ajam is a hospitalist and a clinical assistant professor in the department of anesthesiology at Wake Forest University Baptist Medical Center and the Carolinas Pain Institute. He is board-certified in chronic pain management.
References
- Garrettson M, Ringwalt C. An evaluation of the North Carolina controlled substances reporting system: part II impact evaluation, January 2013. PDMP Center of Excellence website. Available at: http://pdmpexcellence.org/sites/all/pdfs/NC_control_sub_eval_pt_2.pdf. Accessed Sept. 3, 2013.
- Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: Final data for 2005, national vital statistics reports; Vol. 56 No. 10. Hyattsville, Md.: National Center for Health Statistics; 2008.
- Porter J, Jick H. Addiction rare in patients treated with narcotics. N Engl J Med. 1980;302(2):123.
- American Society of Addiction Medicine; personal communication, 2013.
- Mäntyselkä P, Kumpusalo E, Ahonen R, Takala J. Patients’ versus general practitioners’ assessments of pain intensity in primary care patients with non-cancer pain. Br J Gen Pract. 2001;51(473):995-997.
- Petersen MA, Larsen H, Pedersen L, Sonne N, Groenvold M. Assessing health-related quality of life in palliative care: comparing patient and physician assessments. Eur J Cancer. 2006;42(8):1159-1166.
In This Edition
9 Things: At a Glance
An occasional series providing specialty-specific advice for hospitalists from experts in the field.
- Recognize the differential diagnosis for pain exacerbation in a chronic opioid therapy (COT) patient/chronic pain patient.
- Know where the opioids are going.
- Sometimes stopping pills, rather than adding them, can cure pain.
- Take time to educate patients about methadone and its risk of mortality if not used as prescribed.
- A little local anesthetic (and some steroid) goes a long way.
- Addiction to opioids is not rare.
- Safely changing opioid regimens requires good math and good judgment.
- For a low-risk chronic pain patient on low-dose opioids, don’t change the regimen, even if the indication for opioids isn’t clear.
- If a patient has pain all the time, they need to be on a medication that works all the time.
The differential diagnosis for pain exacerbation in a chronic opioid therapy (COT) patient/chronic pain patient is:
- Worsening medical problem;
- New medical problem;
- Nonopioid problem (side effect);
- Opioid problem (resistance/tolerance/side effect); and
- Opioid-induced hyperalgesia.
The search for an etiology and treatment for chronic pain should not end, even if a patient is labeled with “chronic pain syndrome.” The patient could simply be chronically undiagnosed or on an incorrect therapy.
Know where the opioids are going.
Whether it’s auditing a prescription-monitoring program (PMP), checking a urine drug screen, or calling a pharmacist, try to ensure that chronic pain patients are taking the opioids as prescribed. A phone call to the primary opioid prescriber or chronic pain provider could save a busy hospitalist a lot of time.
Using PMP data can consume a lot of time. Typically, only prescribing providers can access PMPs, so delegating this responsibility to someone else is not possible. If your state PMP does not help, simply call the patient’s pharmacy and ask for the last three fill dates on an opioid prescription. This also works well in case the patient’s pharmacy doesn’t participate in a PMP or is delayed in uploading recent prescriber data. Many COT patients have an opioid treatment agreement with their prescriber and must use only one pharmacy to fill opioids.
In January 2013, the University of North Carolina Injury Prevention Center published an analysis of three years of North Carolina PMP data.1 Patients followed by providers who consistently used the state PMP were five times more likely to receive treatment for opioid dependence compared with patients of providers who never used the state PMP.1
Why go through all this trouble if a chronic pain specialist is also doing it? It’s good documentation and good care, like monitoring levels of transplant meds or making sure hemoglobin A1Cs are up to date and trending toward goal. It may only take one misused or diverted opioid pill to result in a serious adverse event.
Sometimes stopping pills, rather than adding them, can cure pain.
Many chronic pain patients accumulate a patchwork of pills (e.g. benzodiazepines, opioids, muscle relaxants, and antidepressants). Many interpret noxious symptoms associated with the drug burden as “uncontrolled pain.” Two conditions that might afflict the pain sufferer who takes multiple medications are opioid-induced hyperalgesia (OIH) and medication-overuse headaches (MOH). They are uncommon but should be on a hospitalist’s differential for difficult-to-control chronic pain. Opioids commonly are implicated in causing MOH, a chronic headache occurring at least 15 days a month, four hours a day if untreated, and for at least three consecutive months. OIH is a nociceptive sensitization caused by opioids that can occur suddenly or insidiously.
If a drug isn’t absolutely necessary, stop it. If you and the patient start by agreeing to the shared goal of improving health, the conversation should go better. An axiom we learned from mentors at the University of Washington is: “There is no pain that cannot be made worse with inappropriate therapy.”
Take time to educate patients about methadone and its risk of mortality if not used as prescribed.
Methadone is less frequently prescribed than other opioids, yet it is more frequently associated with death from overdose. Though there is a risk of overdose and death with any opioid, managing methadone is more difficult. A desperate chronic pain patient may self-escalate their methadone without proper insight into the consequences.
Remember the logarithmic relationship methadone doses have with their morphine equivalency. The following highlights how deceiving the numbers are: 50 mg of methadone is about 100 mg of morphine-equivalent, but 100 mg of methadone is about 1,000 mg of morphine-equivalent, or 10 times as strong.
From 1999 to 2005, methadone-related deaths increased by 468%.2 If the patient doesn’t seem to understand these risks, they are not a good candidate for methadone treatment.
A little local anesthetic (and some steroid) goes a long way.
Hospitalists should offer an assortment of diagnostic and therapeutic injections to chronic pain patients. First, be sure you’ve done your due diligence:
- What procedures do you have privileges to do?
- Do you need to be proctored first?
- How do your local specialists feel about you doing injections?
In light of these considerations, hospitalists should be able to train and be credentialed to offer such procedures as trigger-point injections, joint injections (knees, shoulders), or even a peripheral nerve injection (e.g. lateral femoral cutaneous nerve or ilioinguinal nerve injection). Some hospitalists might even want to learn ultrasound-guided sacroiliac joint injections for chronic unexplained back pain.
Offering an indicated and effective injection is a good nonopioid option. And local anesthetic injections can help hospitalists establish an elusive diagnosis. For example, many patients spend years getting worked up for head and neck pain when dry-needling with a small volume (1 cc) of local anesthetic into a neck muscle trigger point can break their pain generator, eliminating their pain.
Addiction to opioids is not rare.
The use, misuse, and diversion of opioids and all the associated complications have appropriately received considerable media attention. A seminal paper by Porter and Jick titled “Addiction Is Rare in Patients Treated with Narcotics” is one of many tipping points associated with the boom in opioid prescribing.3 Whether it’s a three-day supply of hydrocodone, 24 hours on a PCA, or an opioid rotation, any exposure to opioids can put a patient on the runway to addiction.
There are only 3,071 board-certified addiction specialists certified by the American Board of Addiction Medicine, so access to an addiction specialist might be difficult.4
Nonetheless, do not become complacent and just continue the opioid therapy in a difficult opioid-addicted patient. Express your concerns to the primary opioid prescriber, or help patients who don’t have an opioid prescriber get access and treatment. Otherwise, you have no choice but to taper the opioids.
Ideally, chronic pain management should be delivered in the outpatient arena where long-term monitoring can take place.
Safely changing opioid regimens requires good math and good judgment.
During training and practice, hospitalists become accustomed to rapidly analyze objective data, such as ABGs, ECGs, anion gaps, and vent settings. A hospitalist should become similarly efficient at calculating morphine equivalencies (cautiously with methadone and fentanyl), making dose reductions, and rotating opioids. The more comfortable you are with morphine equivalencies, the faster and safer you will be at rotating opioids. Whatever morphine-equivalence table you feel comfortable with is the one you should use consistently.
We see many providers who unwittingly take, for example, a patient who has become resistant to hydrocodone/acetaminophen 10/325 mg PO TID (30 mg of morphine) and convert them to oxycodone/acetaminophen 10/325 mg PO QID (60 mg of morphine—a doubling), when doubling could cause respiratory depression or a faster path to addiction and dependency.
But there are cases in which judgment should trump math, such as when converting from an IV to an oral regimen. We frequently see patients in the clinic requesting refills for more than 100 mg of hydromorphone because “that’s what I was on when I was hospitalized and on the pump.” If the IV-to-oral conversion leaves you prescribing high doses of oral opioids, plan for a rapid taper and a smooth handoff to the outpatient setting.
One strategy to decrease an error in math and judgment is to use IV PCAs as infrequently as possible if a patient isn’t post-operative and they are able to take oral meds. And never hesitate to consult with your inpatient pharmacist or a chronic pain specialist.
For a low-risk chronic pain patient on low-dose opioids, don’t change the regimen, even if the indication for opioids isn’t clear.
Although it is tempting to become an opioid prohibitionist, if a patient has been taking an opioid for years and is functioning, working, compliant, and has no risk factors for complications from COT, it is likely fine to continue their current regimen. Touch base with the primary opioid prescriber, and if you’re concerned, use some of the monitoring instruments described earlier (PMP, urine drug screen, opioid treatment agreement, pill counts).
If a patient has pain all the time, they need to be on a medication that works all the time.
A good pain history followed by a good neurological and mental health assessment is of incalculable value, especially because physicians often underestimate a patient’s pain intensity and its impact on a patient’s quality of life.5,6 A patient’s pain intensity, quality of life, and function can be dramatically improved by starting a long-acting medication for “constant pain.”
If a patient hurts “24 hours a day” and cannot function on hydrocodone/acetaminophen 10/325 QID, it’s probably because they are constantly reacting to spikes in pain and using a “some of the time” medicine to treat “all the time” pain. Switching to a long-acting medication—and it doesn’t have to be an opioid—could improve control and decrease how much narcotic the patient needs.
If you choose a long-acting opioid (in this case, you could try morphine sulphate extended-release 15 mg BID and satisfy 50% of the hydrocodone need), then you could titrate slowly upwards to where the patient would not need hydrocodone. If the patient still had uncontrolled pain, then either morphine is the wrong compound for them or they are benefiting from the “nonanalgesic properties” of the opioids.
Give the patient the benefit of the doubt; because of genetic polymorphisms, a patient may need several opioid rotations before the right opioid compound is found.
Dr. Schultz is a hospitalist and assistant professor in the department of internal medicine at the University of Miami Miller School of Medicine. She is board-certified in hospice and palliative care and specializes in chronic pain management. Dr. Ajam is a hospitalist and a clinical assistant professor in the department of anesthesiology at Wake Forest University Baptist Medical Center and the Carolinas Pain Institute. He is board-certified in chronic pain management.
References
- Garrettson M, Ringwalt C. An evaluation of the North Carolina controlled substances reporting system: part II impact evaluation, January 2013. PDMP Center of Excellence website. Available at: http://pdmpexcellence.org/sites/all/pdfs/NC_control_sub_eval_pt_2.pdf. Accessed Sept. 3, 2013.
- Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: Final data for 2005, national vital statistics reports; Vol. 56 No. 10. Hyattsville, Md.: National Center for Health Statistics; 2008.
- Porter J, Jick H. Addiction rare in patients treated with narcotics. N Engl J Med. 1980;302(2):123.
- American Society of Addiction Medicine; personal communication, 2013.
- Mäntyselkä P, Kumpusalo E, Ahonen R, Takala J. Patients’ versus general practitioners’ assessments of pain intensity in primary care patients with non-cancer pain. Br J Gen Pract. 2001;51(473):995-997.
- Petersen MA, Larsen H, Pedersen L, Sonne N, Groenvold M. Assessing health-related quality of life in palliative care: comparing patient and physician assessments. Eur J Cancer. 2006;42(8):1159-1166.
In This Edition
9 Things: At a Glance
An occasional series providing specialty-specific advice for hospitalists from experts in the field.
- Recognize the differential diagnosis for pain exacerbation in a chronic opioid therapy (COT) patient/chronic pain patient.
- Know where the opioids are going.
- Sometimes stopping pills, rather than adding them, can cure pain.
- Take time to educate patients about methadone and its risk of mortality if not used as prescribed.
- A little local anesthetic (and some steroid) goes a long way.
- Addiction to opioids is not rare.
- Safely changing opioid regimens requires good math and good judgment.
- For a low-risk chronic pain patient on low-dose opioids, don’t change the regimen, even if the indication for opioids isn’t clear.
- If a patient has pain all the time, they need to be on a medication that works all the time.
The differential diagnosis for pain exacerbation in a chronic opioid therapy (COT) patient/chronic pain patient is:
- Worsening medical problem;
- New medical problem;
- Nonopioid problem (side effect);
- Opioid problem (resistance/tolerance/side effect); and
- Opioid-induced hyperalgesia.
The search for an etiology and treatment for chronic pain should not end, even if a patient is labeled with “chronic pain syndrome.” The patient could simply be chronically undiagnosed or on an incorrect therapy.
Know where the opioids are going.
Whether it’s auditing a prescription-monitoring program (PMP), checking a urine drug screen, or calling a pharmacist, try to ensure that chronic pain patients are taking the opioids as prescribed. A phone call to the primary opioid prescriber or chronic pain provider could save a busy hospitalist a lot of time.
Using PMP data can consume a lot of time. Typically, only prescribing providers can access PMPs, so delegating this responsibility to someone else is not possible. If your state PMP does not help, simply call the patient’s pharmacy and ask for the last three fill dates on an opioid prescription. This also works well in case the patient’s pharmacy doesn’t participate in a PMP or is delayed in uploading recent prescriber data. Many COT patients have an opioid treatment agreement with their prescriber and must use only one pharmacy to fill opioids.
In January 2013, the University of North Carolina Injury Prevention Center published an analysis of three years of North Carolina PMP data.1 Patients followed by providers who consistently used the state PMP were five times more likely to receive treatment for opioid dependence compared with patients of providers who never used the state PMP.1
Why go through all this trouble if a chronic pain specialist is also doing it? It’s good documentation and good care, like monitoring levels of transplant meds or making sure hemoglobin A1Cs are up to date and trending toward goal. It may only take one misused or diverted opioid pill to result in a serious adverse event.
Sometimes stopping pills, rather than adding them, can cure pain.
Many chronic pain patients accumulate a patchwork of pills (e.g. benzodiazepines, opioids, muscle relaxants, and antidepressants). Many interpret noxious symptoms associated with the drug burden as “uncontrolled pain.” Two conditions that might afflict the pain sufferer who takes multiple medications are opioid-induced hyperalgesia (OIH) and medication-overuse headaches (MOH). They are uncommon but should be on a hospitalist’s differential for difficult-to-control chronic pain. Opioids commonly are implicated in causing MOH, a chronic headache occurring at least 15 days a month, four hours a day if untreated, and for at least three consecutive months. OIH is a nociceptive sensitization caused by opioids that can occur suddenly or insidiously.
If a drug isn’t absolutely necessary, stop it. If you and the patient start by agreeing to the shared goal of improving health, the conversation should go better. An axiom we learned from mentors at the University of Washington is: “There is no pain that cannot be made worse with inappropriate therapy.”
Take time to educate patients about methadone and its risk of mortality if not used as prescribed.
Methadone is less frequently prescribed than other opioids, yet it is more frequently associated with death from overdose. Though there is a risk of overdose and death with any opioid, managing methadone is more difficult. A desperate chronic pain patient may self-escalate their methadone without proper insight into the consequences.
Remember the logarithmic relationship methadone doses have with their morphine equivalency. The following highlights how deceiving the numbers are: 50 mg of methadone is about 100 mg of morphine-equivalent, but 100 mg of methadone is about 1,000 mg of morphine-equivalent, or 10 times as strong.
From 1999 to 2005, methadone-related deaths increased by 468%.2 If the patient doesn’t seem to understand these risks, they are not a good candidate for methadone treatment.
A little local anesthetic (and some steroid) goes a long way.
Hospitalists should offer an assortment of diagnostic and therapeutic injections to chronic pain patients. First, be sure you’ve done your due diligence:
- What procedures do you have privileges to do?
- Do you need to be proctored first?
- How do your local specialists feel about you doing injections?
In light of these considerations, hospitalists should be able to train and be credentialed to offer such procedures as trigger-point injections, joint injections (knees, shoulders), or even a peripheral nerve injection (e.g. lateral femoral cutaneous nerve or ilioinguinal nerve injection). Some hospitalists might even want to learn ultrasound-guided sacroiliac joint injections for chronic unexplained back pain.
Offering an indicated and effective injection is a good nonopioid option. And local anesthetic injections can help hospitalists establish an elusive diagnosis. For example, many patients spend years getting worked up for head and neck pain when dry-needling with a small volume (1 cc) of local anesthetic into a neck muscle trigger point can break their pain generator, eliminating their pain.
Addiction to opioids is not rare.
The use, misuse, and diversion of opioids and all the associated complications have appropriately received considerable media attention. A seminal paper by Porter and Jick titled “Addiction Is Rare in Patients Treated with Narcotics” is one of many tipping points associated with the boom in opioid prescribing.3 Whether it’s a three-day supply of hydrocodone, 24 hours on a PCA, or an opioid rotation, any exposure to opioids can put a patient on the runway to addiction.
There are only 3,071 board-certified addiction specialists certified by the American Board of Addiction Medicine, so access to an addiction specialist might be difficult.4
Nonetheless, do not become complacent and just continue the opioid therapy in a difficult opioid-addicted patient. Express your concerns to the primary opioid prescriber, or help patients who don’t have an opioid prescriber get access and treatment. Otherwise, you have no choice but to taper the opioids.
Ideally, chronic pain management should be delivered in the outpatient arena where long-term monitoring can take place.
Safely changing opioid regimens requires good math and good judgment.
During training and practice, hospitalists become accustomed to rapidly analyze objective data, such as ABGs, ECGs, anion gaps, and vent settings. A hospitalist should become similarly efficient at calculating morphine equivalencies (cautiously with methadone and fentanyl), making dose reductions, and rotating opioids. The more comfortable you are with morphine equivalencies, the faster and safer you will be at rotating opioids. Whatever morphine-equivalence table you feel comfortable with is the one you should use consistently.
We see many providers who unwittingly take, for example, a patient who has become resistant to hydrocodone/acetaminophen 10/325 mg PO TID (30 mg of morphine) and convert them to oxycodone/acetaminophen 10/325 mg PO QID (60 mg of morphine—a doubling), when doubling could cause respiratory depression or a faster path to addiction and dependency.
But there are cases in which judgment should trump math, such as when converting from an IV to an oral regimen. We frequently see patients in the clinic requesting refills for more than 100 mg of hydromorphone because “that’s what I was on when I was hospitalized and on the pump.” If the IV-to-oral conversion leaves you prescribing high doses of oral opioids, plan for a rapid taper and a smooth handoff to the outpatient setting.
One strategy to decrease an error in math and judgment is to use IV PCAs as infrequently as possible if a patient isn’t post-operative and they are able to take oral meds. And never hesitate to consult with your inpatient pharmacist or a chronic pain specialist.
For a low-risk chronic pain patient on low-dose opioids, don’t change the regimen, even if the indication for opioids isn’t clear.
Although it is tempting to become an opioid prohibitionist, if a patient has been taking an opioid for years and is functioning, working, compliant, and has no risk factors for complications from COT, it is likely fine to continue their current regimen. Touch base with the primary opioid prescriber, and if you’re concerned, use some of the monitoring instruments described earlier (PMP, urine drug screen, opioid treatment agreement, pill counts).
If a patient has pain all the time, they need to be on a medication that works all the time.
A good pain history followed by a good neurological and mental health assessment is of incalculable value, especially because physicians often underestimate a patient’s pain intensity and its impact on a patient’s quality of life.5,6 A patient’s pain intensity, quality of life, and function can be dramatically improved by starting a long-acting medication for “constant pain.”
If a patient hurts “24 hours a day” and cannot function on hydrocodone/acetaminophen 10/325 QID, it’s probably because they are constantly reacting to spikes in pain and using a “some of the time” medicine to treat “all the time” pain. Switching to a long-acting medication—and it doesn’t have to be an opioid—could improve control and decrease how much narcotic the patient needs.
If you choose a long-acting opioid (in this case, you could try morphine sulphate extended-release 15 mg BID and satisfy 50% of the hydrocodone need), then you could titrate slowly upwards to where the patient would not need hydrocodone. If the patient still had uncontrolled pain, then either morphine is the wrong compound for them or they are benefiting from the “nonanalgesic properties” of the opioids.
Give the patient the benefit of the doubt; because of genetic polymorphisms, a patient may need several opioid rotations before the right opioid compound is found.
Dr. Schultz is a hospitalist and assistant professor in the department of internal medicine at the University of Miami Miller School of Medicine. She is board-certified in hospice and palliative care and specializes in chronic pain management. Dr. Ajam is a hospitalist and a clinical assistant professor in the department of anesthesiology at Wake Forest University Baptist Medical Center and the Carolinas Pain Institute. He is board-certified in chronic pain management.
References
- Garrettson M, Ringwalt C. An evaluation of the North Carolina controlled substances reporting system: part II impact evaluation, January 2013. PDMP Center of Excellence website. Available at: http://pdmpexcellence.org/sites/all/pdfs/NC_control_sub_eval_pt_2.pdf. Accessed Sept. 3, 2013.
- Kung HC, Hoyert DL, Xu JQ, Murphy SL. Deaths: Final data for 2005, national vital statistics reports; Vol. 56 No. 10. Hyattsville, Md.: National Center for Health Statistics; 2008.
- Porter J, Jick H. Addiction rare in patients treated with narcotics. N Engl J Med. 1980;302(2):123.
- American Society of Addiction Medicine; personal communication, 2013.
- Mäntyselkä P, Kumpusalo E, Ahonen R, Takala J. Patients’ versus general practitioners’ assessments of pain intensity in primary care patients with non-cancer pain. Br J Gen Pract. 2001;51(473):995-997.
- Petersen MA, Larsen H, Pedersen L, Sonne N, Groenvold M. Assessing health-related quality of life in palliative care: comparing patient and physician assessments. Eur J Cancer. 2006;42(8):1159-1166.
What Are the Indications for a Blood Transfusion?

Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
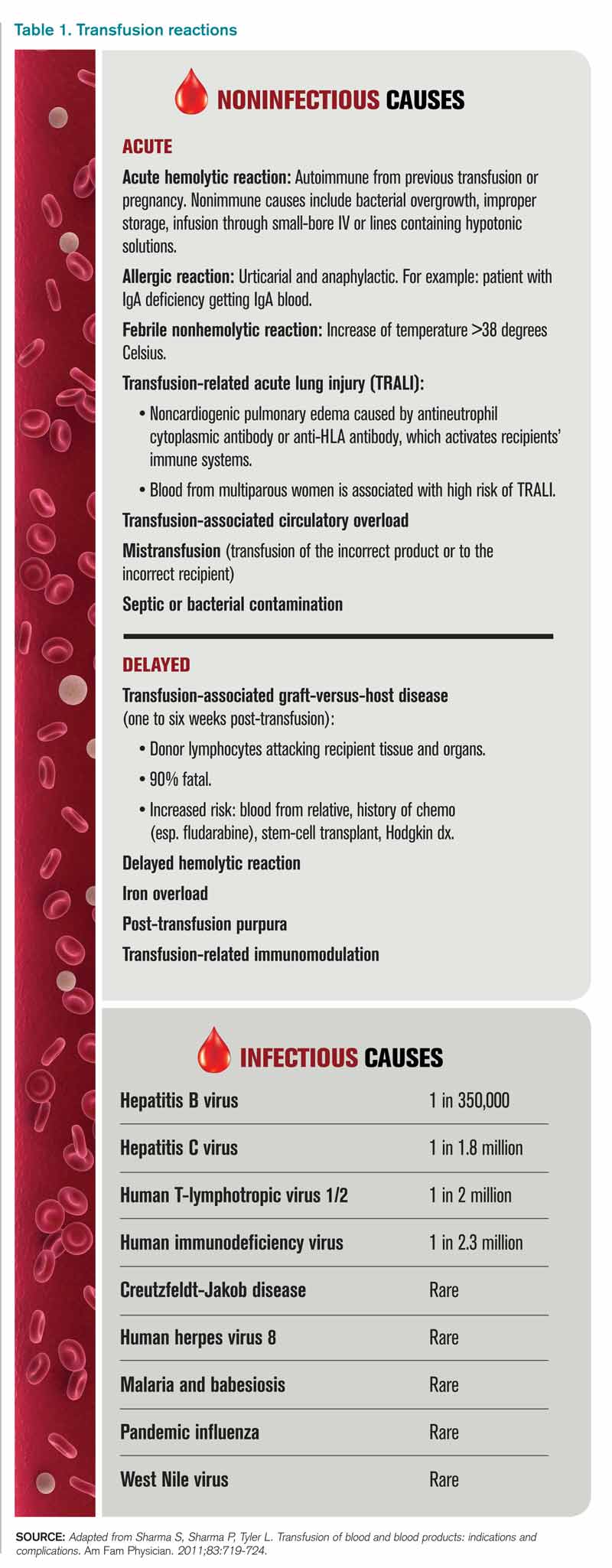
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
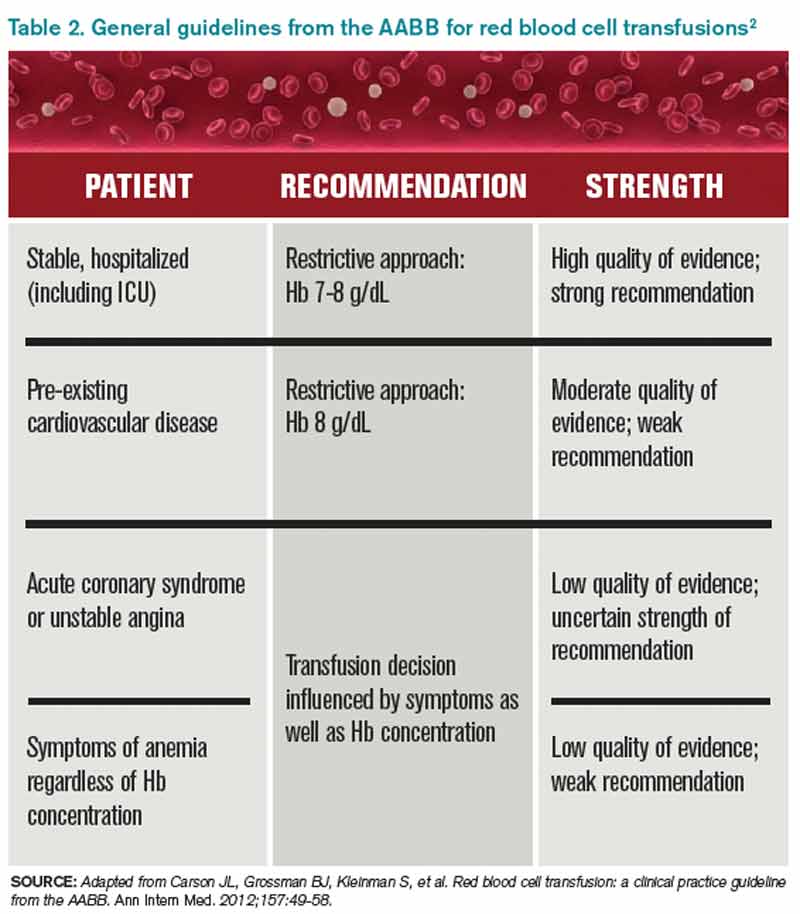
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
Case
A 65-year-old man with a history of coronary artery disease (CAD) presents to the ED after a mechanical fall. He was found to have a hip fracture, admitted to orthopedic service, and underwent an uneventful hip repair. His post-operative course was uncomplicated, except for his hemoglobin level of 7.5 g/dL, which had decreased from his pre-operative hemoglobin of 11.2 g/dL. The patient was without cardiac symptoms, was ambulating with assistance, had normal vital signs, and was otherwise having an unremarkable recovery. The orthopedic surgeon, who recently heard that you do not have to transfuse patients unless their hemoglobin is less than 7 g/dL, consulted the hospitalist to help make the decision. What would your recommendation be?
Overview
Blood transfusions are a common medical procedure routinely given in the hospital.1 An estimated 15 million red blood cell (RBC) units are transfused each year in the United States.2 Despite its common use, the clinical indications for transfusion continue to be the subject of considerable debate. Most clinicians would agree that treating a patient with a low hemoglobin level and symptoms of anemia is reasonable.1,3 However, in the absence of overt symptoms, there is debate about when transfusions are appropriate.2,3
Because tissue oxygen delivery is dependent on hemoglobin and cardiac output, past medical practice has supported the use of the “golden 10/30 rule,” by which patients are transfused to a hemoglobin concentration of 10 g/dL or a hematocrit of 30%, regardless of symptoms. The rationale for this approach is based on physiologic evidence that cardiac output increases when hemoglobin falls below 7 g/dl. In patients with cardiac disease, the ability to increase cardiac output is compromised. Therefore, in order to reduce strain on the heart, hemoglobin levels historically have been kept higher than this threshold.
However, several studies have forced us to re-evaluate this old paradigm, including increasing concern for the infectious and noninfectious complications associated with blood transfusions and the need for cost containment (see Table 1).1,2,4 Due to improved blood screening, infectious complications from transfusions have been greatly reduced; noninfectious complications are 1,000 times more likely than infectious ones.
Review of Data
Although a number of studies have been performed on the indications for blood transfusions, many of the trials conducted in the past were too small to substantiate a certain practice. However, three trials with a large number of participants have allowed for a more evidence-based approach to blood transfusions. The studies address different patient populations to help broaden the restrictive transfusion approach to a larger range of patients.
TRICC trial: critically ill patients5. The TRICC trial was the first major study that compared a liberal transfusion strategy (transfuse when Hb <10 g/dL) to a more conservative approach (transfuse when Hb <7 g/dL). In this multicenter, randomized controlled trial, Hébert et al enrolled 418 critically ill patients and found that there was no significant difference in 30-day all-cause mortality between the restrictive-strategy group (18.7%) and the liberal-strategy group (23.3%).
However, in the pre-determined subgroup analysis, patients who were less severely ill (APACHE II scores of <20) had 30-day all-cause mortality of 8.7%, compared with 16.1% in the liberal-strategy group. Interestingly, there were more cardiac complications (pulmonary edema, angina, MI, and cardiac arrest) in the liberal-strategy group (21%) compared with the restrictive-strategy group (13%). Despite this finding, 30-day mortality was not significantly different in patients with clinically significant cardiac disease (primary or secondary diagnosis of cardiac disease [20.5% restrictive versus 22.9% liberal]).
An average of 2.6 units of RBCs per patient were given in the restrictive group, while 5.6 units were given to patients in the liberal group. This reflects a 54% decrease in the number of transfusions used in the conservative group. All the patients in the liberal group received transfusions, while 33% of the restrictive group’s patients received no blood at all.
The results of this trial suggested that there is no clinical advantage in transfusing ICU patients to Hb values above 9 g/dL, even if they have a history of cardiac disease. In fact, it may be harmful to practice a liberal transfusion strategy in critically ill younger patients (<55 years old) and those who are less severely ill (APACHE II <20).5
FOCUS trial: hip surgery and history of cardiac disease6. The FOCUS trial is a recent study that looked at the optimal hemoglobin level at which an RBC transfusion is beneficial for patients undergoing hip surgery. This study enrolled patients aged 50 or older who had a history or risk factors for cardiovascular disease (clinical evidence of cardiovascular disease: h/o ischemic heart disease, EKG evidence of previous MI, h/o CHF/PVD, h/o stroke/TIA, h/o HTN, DM, hyperlipidemia (TC >200/LDL >130), current tobacco use, or Cr>2.0), who were undergoing primary surgical repair of a hip fracture, and who had Hb <10g/dL within three days after surgery.
More than 2,000 patients were assigned randomly to a liberal-strategy group (transfuse to maintain a Hb >10g/dL) or a restrictive strategy group (transfuse to maintain Hg >8g/dl or for symptoms or signs of anemia). These signs/symptoms included chest pain that was possibly cardiac-related, congestive heart failure, tachycardia, and unresponsive hypotension. The primary outcomes were mortality or inability to walk 10 feet without assistance at 60-day follow-up.
The FOCUS trial found no statistically significant difference in mortality rate (7.6% in the liberal group versus 6.6% in the restrictive group) or in the ability to walk at 60 days (35.2% in the liberal group versus 34.7% in the restrictive group). There were no significant differences in the rates of in-hospital acute MI, unstable angina, or death between the two groups.
Patients in the restrictive-strategy group received 65% fewer units of blood than the liberal group, with 59% receiving no blood after surgery compared with 3% of the liberal group. Overall, the liberal group received 1,866 units of blood, compared with 652 units in the restrictive group.
This trial helps support the findings in previous trials, such as TRICC, by showing that a restrictive transfusion strategy using a trigger point of 8 g/dl does not increase mortality or cardiovascular complications and does not decrease functional ability after orthopedic surgery.
TRAC trial: patients after cardiac surgery7. The TRAC trial was a prospective randomized trial in 502 patients undergoing cardiac surgery that assigned 253 patients to the liberal-transfusion-strategy group (Hb >10g/dl) and 249 to the restrictive-strategy group (Hb >8 g/dl). In this study, the primary endpoint of all-cause 30-day mortality occurred in 10% of the liberal group and 11% of the restrictive group. This difference was not significant.
Subanalysis showed that blood transfusion in both groups was an independent risk factor for the occurrence of respiratory, cardiac, renal, and infectious complications, in addition to the composite end point of 30-day mortality—again highlighting the risk involved in of blood transfusions.
These results support the other trial conclusions that a restrictive transfusion strategy of maintaining a hematocrit of 24% (Hb 8 g/dL) is as safe as a more liberal strategy with a hematocrit of 30% (Hb 10 g/dL). It also offers further evidence of the risks of blood transfusions and supports the view that blood transfusions should never be given simply to correct low hemoglobin levels.
Cochrane Review. A recent Cochrane Review that comprised 19 trials with a combined total of 6,264 patients also supported a restrictive-strategy approach.8 In this review, no difference in mortality was established between the restrictive and liberal transfusion groups, with a trend toward decreased hospital mortality in the restrictive-transfusion group. The authors of the study felt that for most patients, blood transfusion is not necessary until hemoglobin levels drop below 7-8 g/dL but emphasized that this criteria should not be generalized to patients with an acute cardiac issue.
Back to the Case
In this case, the patient is doing well post-operatively and has no cardiac symptoms or hypotension. However, based on the new available data from the FOCUS trial, given the patient’s history of CAD, and the threshold of 8 g/dL used in the study, it was recommended that the patient be transfused.
Bottom Line
Current practice guidelines clearly support clinical judgment as the primary determinant in the decision to transfuse.2 However, current evidence is growing that our threshold for blood transfusions should be a hemoglobin level of 7-8 g/dl.
Dr. Chang is a hospitalist and assistant professor at Mount Sinai Medical Center in New York City, and is co-director of the medicine-geriatrics clerkship at the Icahn School of Medicine at Mount Sinai. Dr. Torgalkar is a hospitalist and assistant professor at Mount Sinai Medical Center.
References
- Sharma S, Sharma P, Tyler L. Transfusion of blood and blood products: indications and complications. Am Fam Physician. 2011;83:719-724.
- Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2012;157:49-58.
- Valeri CR, Crowley JP, Loscalzo J. The red cell transfusion trigger: has a sin of commission now become a sin of omission? Transfusion. 1998;38:602-610.
- Klein HG, Spahn DR, Carson JL. Red blood cell transfusion in clinical practice. Lancet. 2007;370(9585):415-426.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409-17.
- Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453-2462.
- Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA. 2010;304:1559-1567.
- Carson JL, Carless PA, Hébert PC. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 2012; 4:CD002042.
11 Things Neurologists Think Hospitalists Need To Know

11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.

Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.

Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians

The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
11 Things: At a Glance
- You might be overdiagnosing transient ischemic attacks (TIA).
- Early mobilization after a stroke might be better for some patients.
- MRI is the best tool to evaluate TIA patients.
- Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
- Tracking the time a hospitalized patient was last seen to be normal is crucial.
- Consider neuromuscular disorders when a patient presents with weakness.
- Urinary tract infections (UTIs) are not the only cause of altered mental status.
- Take care in distinguishing aphasia from general confusion.
- A simple checklist might eliminate the need to consult the neurologist.
- Calling a neurologist earlier is way better than calling later.
- Hire a neurohospitalist if your institution doesn’t have one already.
When a patient is admitted to the hospital with neurological symptoms, such as altered mental status, he or she might not be the only one who is confused. Hospitalists might be a little confused, too.
Of all the subspecialties to which hospitalists are exposed, none might make them more uncomfortable than neurology. Because of what often is a dearth of training in this area, and because of the vexing and sometimes fleeting nature of symptoms, hospitalists might be inclined to lean on neurologists more than other specialists.
The Hospitalist spoke with a half-dozen experts, gathering their words of guidance and clinical tips. Here’s hoping they give you a little extra confidence the next time you see a patient with altered mental status.
You might be overdiagnosing transient ischemic attacks (TIA).
Ira Chang, MD, a neurohospitalist with Blue Sky Neurology in Englewood, Colo., and assistant clinical professor at the University of Colorado Health Sciences Center in Denver, says TIA is all too commonly a go-to diagnosis, frequently when there’s another cause.
“I think that hospitalists, and maybe medical internists in general, are very quick to diagnose anything that has a neurologic symptom that comes and goes as a TIA,” she says. “Patients have to have specific neurologic symptoms that we think are due to arterial blood flow or ischemia problems.”
Near-fainting spells and dizzy spells involving confusion commonly are diagnosed as TIA when these symptoms could be due to “a number of other causes,” Dr. Chang adds.
Kevin Barrett, MD, assistant professor of neurology and a neurohospitalist at Mayo Clinic in Jacksonville, Fla., says the suspicion of a TIA should be greater if the patient is older or has traditional cardiovascular risk factors, such as hyptertension, diabetes, hyperlipidemia, or tobacco use.
A TIA typically causes symptoms referable to common arterial distributions. Carotid-distribution TIA often causes ipsilateral loss of vision and contralateral weakness or numbness. Posterior-circulation TIAs bring on symptoms such as ataxia, unilateral or bilateral limb weakness, diplopia, and slurred or slow speech.
TIA diagnoses can be tricky even for those trained in neurology, Dr. Barrett says.
“Even among fellowship-trained vascular neurologists, TIA can be a challenging diagnosis, often with poor inter-observer agreement,” he notes.
Early mobilization after a stroke might be better for some patients.
After receiving tissue plasminogen activator (tPA) therapy for stroke, patients historically were kept on bed rest for 24 hours to reduce the risk of hemorrhage. Evidence now is coming to light that some patients might benefit from getting out of bed sooner, Dr. Barrett says.1
“We’re learning that in selected patients, they can actually be mobilized at 12 hours,” he says. “In some cases, that would not only reduce the risk of complications related to immobilization like DVT but shorten length of stay. These are all important metrics for anybody who practices primarily within an inpatient setting.”
Early mobilization generally is more suitable for patients with less severe deficits and who are hemodynamically stable.
MRI is the best tool to evaluate TIA patients.
TIA patients who have transient symptoms and normal diffusion-weighted imaging (DWI) abnormalities on an MRI are at a very low risk. “Less than 1% of those patients have a stroke within the subsequent seven days,” Dr. Barrett says.2 “But those patients who do have a DWI abnormality, they’re at very high risk: 7.1% at seven days.
“The utility of MRI following TIA is becoming very much apparent. It is something that hospitalists should be aware of.”
Consider focal seizure or complex partial seizure as one of the possible causes of confusion or speech disturbance, or both.
Patients experiencing confusion or speech disturbance or altered mentation—particularly if they’re elderly or have dementia—could be having a partial seizure, Dr. Chang says. Dementia patients have a 10% to 15% incidence of complex partial seizures, she says.
“I see that underdiagnosed a lot,” she says. “They keep coming back, and everybody diagnoses them with TIAs. So they keep getting put on aspirin, and they get switched to Aggrenox [to prevent clotting]. They keep coming back with the same symptoms.”
Tracking the time a hospitalized patient was last seen to be normal is crucial.
About 10% to 15% of strokes occur in patients who are in the hospital.
“While a lot of those strokes are perioperative, there also are patients who are going to be on hospitalist services,” says Eric Adelman, MD, assistant professor of neurology at the University of Michigan in Ann Arbor.
Hospitalists should note that patients suffering strokes are found not just in the ED but also on the floor, where all the tools for treatment might not be as readily available. That makes those cases a challenge and makes forethought that much more important, Dr. Adelman says.
“It’s a matter of trying to track down last normal times,” he says. “If they’re eligible for tPA and they’re within the therapeutic window, we should be able to do that within a hospital.”
Establishing a neurological baseline is particularly important for patients who are at higher stroke risk, like those with atrial fibrillation and other cardiovascular risk factors.
“In case something does happen,” Dr. Adelman says, “at least you have a baseline so you can [know that] at time X, we knew they had full strength in their right arm, and now they don’t.”
Consider neuromuscular disorders when a patient presents with weakness.
It’s safe to say some hospitalists might miss a neuromuscular disorder, Dr. Chang says.
“A lot of disorders that are harder for hospitalists to diagnose and that tend to take longer to call a neurologist [on] are things that are due to myasthenia gravis [a breakdown between nerves and muscles leading to muscle fatigue], myopathy, or ALS,” she says. “Many patients present with weakness. I think a lot of times there will be a lot of tests on and a lot of treatment for general medical conditions that can cause weakness.”
And that might be a case of misdirected attention. Patients with weakness accompanied by persistent swallowing problems, slurred speech with no other obvious cause, or the inability to lift their head off the bed without an obvious cause may end up with a neuromuscular diagnosis, she says.
It would be helpful to have a neurologist’s input in these cases, she says, where “nothing’s getting better, and three, four, five days later, the patient’s still weak.
“I think a neurologist would be more in tune with something like that,” she adds.
Urinary tract infections (UTIs) are not the only cause of altered mental status.
That might seem obvious, but too often, a UTI can be pegged as the source of altered mental status when it should not be, Dr. Chang says.
“We get a lot of people who come in with confusion and they have a slightly abnormal urinalysis and they diagnose them with UTI,” Dr. Chang says. “And it turns out that they actually had a stroke or they had a seizure.”
Significantly altered mentation should show a significantly abnormal urine with a positive culture, she says. “They ought to have significant laboratory support for a urinary tract infection.”
Dr. Barrett says a neurologic review of systems, or at least a neurologic exam, should be the physician’s guide.
“Those are key parts of a hospitalist’s practice,” he says, “because that’s what’s truly going to guide them to consider primary neurological causes of altered mental status.”
Take care in distinguishing aphasia from general confusion.
If a patient is still talking and is fairly fluent, that doesn’t mean they aren’t suffering from certain types of aphasia, a disorder caused by damage to parts of the brain that control language, Dr. Adelman says.
“Oftentimes, when you’re dealing with a patient with confusion, you want to make sure that it’s confusion, or encephalopathy, rather than a focal neurologic problem like aphasia,” he says. “Frequently patients with aphasia will have other symptoms such as a facial drop or weakness in the arm, but stroke can present as isolated aphasia.”
A good habit to get into is to determine whether the patient can repeat a phrase, follow a command, or name objects, he says. If they can, they probably do not have aphasia.
“The thing that you worry about with aphasia, particularly acute onset aphasia, is an ischemic stroke,” Dr. Adelman says.
A simple checklist might eliminate the need to consult the neurologist.
When Edgar Kenton, MD, now director of the stroke program at Geisinger Health System in Danville, Pa., was at Emory University Hospital in Atlanta, he found he was getting snowed under with consults from hospitalists. There were about 15 hospitalists for just one or two neurologists.
“There was no way I was able to see these patients, particularly in follow-up, because you might get five consults every day,” he says. “By the middle of the week, that’s 15 consults. You don’t get a chance to go back and see the patients because you’re just going from one consult to the other.”
The situation improved with a checklist of things to consider when a patient presents with altered mental status. Before seeking a consult, neurologists suggested the hospitalists check the electrolytes, blood pressure, and urine, and use CT scans as a screening test. That might uncover the root of the patient’s problems. If those are clear, by all means get the neurologist involved, he says.
“We were able to educate the hospitalists so they knew when to call; they knew when it was beyond their expertise to take care of the patient, so we weren’t getting called for every patient with altered mental status when all they needed to do was to check the electrolytes,” Dr. Kenton says.
Calling a neurologist earlier is way better than calling later.
Once the decision is made to consult with a neurologist, the consult should be done right away, Dr. Kenton says, not after a few days when symptoms don’t appear to be improving.
“We’ll get the call on a Friday afternoon because they thought, finally, ‘Well, you know, we need to get neurology involved because we a) haven’t solved the problem and b) there may be some other tests we should be getting,’” he says of common situations. “That has been a problem. If you don’t have a neurohospitalist involved day by day, working with the patient and the general hospitalist, neurology becomes an afterthought.”
He says accurate and early diagnosis is paramount to the patient.
“If the diagnosis is delayed, obviously there’s more insult to the patients, more persistent insult,” he says, noting the timing is particularly important in neurological conditions “because things can get bad in a hurry.”
He strongly urges hospitalists to consult with a neurologist before ordering an entire battery of tests.
At Geisinger, neurologists are encouraging hospitalists to chat informally with neurosurgeons about cases for guidance at the outset rather than after several days.
Hire a neurohospitalist if your institution doesn’t have one already.
At the top of the list of Dr. Kenton’s suggestions on caring for hospitalized neurology patients is this declaration: “Get a neurohospitalist.”
“It’s important to have the neurologist involved from the time the patient’s admitted,” he says. “That’s the value of connecting the general hospitalist with neurologists.”
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says his colleagues are team players and improve patient care.
“Neurology consultations can be called very quickly, and a nice partnership can develop between internal medicine hospitalists and neurohospitalists to care for those patients who have those medical and neurologic problems,” he says.
He also says having a neurohospitalist on board can ease some of the tension.
“No longer if there’s a neurologic condition does a hospitalist have to think about, ‘Well, does this rise to the level of something that I need to get the neurologist to drive across the city to come see?’” he explains. “‘Or is this something we should try to manage ourselves?’”
Tom Collins is a freelance writer in South Florida.
“Neurophobia” a Challenge for Hospitalists, Other Physicians
The unease that many hospitalists, internal-medicine doctors, and other providers feel about treating neurologic conditions is so readily recognized that a term has been coined to describe it: “neurophobia.”
The term has been used in published literature for at least two decades. A 2010 survey found that medical students and residents felt that neurology was the specialty they had the least knowledge about and was the one that was the most difficult.3 And trainees had the least confidence in treating patients with neurological complaints.
S. Andrew Josephson, MD, director of the neurohospitalist program at the University of California at San Francisco, says internal-medicine hospitalists are “increasingly feeling uncomfortable with requests that they have to care for patients with a wide range of primary neurologic conditions in some instances.”
That has helped lead to the emergence of neurohospitalists, he says.
John Vazquez, MD, medical director of the division hospital medicine of Emory University Hospital in Atlanta, says neurophobia is real.
“Every hospitalist has different subspecialty areas that they’re less comfortable with, and I think neurology specifically is one that does scare a lot of hospitalists,” he says. “I think on one side there are hospitalists that might ignore a neurologic problem because they don’t really know what they don’t know. On the other side are the hospitalists who I think are just concerned that they don’t know the field very well and may not feel comfortable.”
Dr. Vazquez did rotations in nephrology, pulmonology, cardiology, and rheumatology but, like many hospitalists, not neurology.
“Neurology is not one that you have to go through,” he says.
He made these suggestions:
- Know what you don’t know and get guidance when necessary.
- Do your own neurologic assessment. Even if a neurologist decides confusion is due to a patient being elderly and having a urinary tract infection, that doesn’t mean that they didn’t actually have a stroke. So if something seems not quite right, be willing to challenge the neurologist.
- Use the resources available to widen your knowledge base.
“You can utilize the consultants for your own education if you have neurologists in your hospital, and many at least have some that rotate in,” Dr. Vazquez says. “You can pick their brain on what they would do with different strokes and what’s the newest thing and ongoing treatment and whatever it is you’re concerned about.”
—Thomas R. Collins
John Vazquez, MD, of Emory University Hospital talks about neurophobia and provides tips for adjusting to the discomfort of working with neurology patients.
References
- Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke. 2008;39;390-396.
- Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs. time-defined TIA: a multicenter study. Neurology. 2011;77(13):1222-1228.
- Zinchuk AV, Flanagan EP, Tubridy NJ, Miller WA, McCullough LD. Attitudes of US medical trainees towards neurology education: “Neurophobia”—a global issue. BMC Med Educ. 2010;10:49.
American College of Gastroenterology Releases C. Diff Recommendations
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.
Clostridium difficile infection (CDI) is a common and costly bacterial illness in hospitalized patients, involving 1% of U.S. hospital stays with an aggregate cost of $8.2 billion annually.1 The spore-forming, gram-positive bacillus is spread by the fecal-oral route; in health-care settings, it is often transmitted by hand carriage and contamination of environmental surfaces. C. diff produces toxins that can cause a spectrum of diseases, including asymptomatic carriage, mild to severe diarrhea, colitis, and pseudomembranous colitis, which in severe cases can lead to sepsis, colectomy, or death.
CDI is defined as the acute onset of diarrhea in a patient with documented toxigenic C. diff or C. diff toxin, without any other clear cause of diarrhea.2 In the past decade, CDI has increased in frequency and severity, with most experts thinking it is related to a particularly virulent strain known as BI/NAP1/027.3 Antibiotic exposure is the most significant and modifiable risk factor for CDI, with increasing age, gastric acid suppression, and immunocompromised states also placing patients at increased risk for developing infection.
Guideline Analysis
In February, the American College of Gastroenterology (ACG) released guidelines for diagnostic testing and pharmacologic therapy for CDI, management of complicated and recurrent disease, and infection control and prevention.2 Previous recommendations for the prevention, diagnosis, and treatment of CDI have been provided by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and a collaboration of the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA).4,5 Recommendations addressing CDI in infants and children are also available.6 The 2013 ACG guidelines are the first from this group to address CDI and are intended to supplement previously published guidelines.
Diagnostic testing. The ACG guidelines emphasize that only stools from patients with diarrhea be tested for C. diff and/or its toxin. Colonization with C. diff is common, and performing tests in asymptomatic patients may complicate clinical care. Rarely, patients with CDI will develop ileus, and in those cases, rectal swab may be performed, but in nearly all circumstances, only diarrheal stools warrant testing. The authors also strongly discourage repeat testing after a negative test and testing for cure following treatment and resolution of symptoms. All of these recommendations are consistent with the SHEA-IDSA guidelines and reflect moderate- to high-quality evidence.
Recognizing that diagnostic testing for C. diff continues to evolve, the ACG makes specific recommendations regarding the use of newer tests, such as nucleic acid amplification and glutamate dehydrogenase detection. These are favored over toxin A and B enzyme immunoassay testing due to higher sensitivity.
Management of mild, moderate, and severe CDI. As with prior guidelines, the 2013 ACG guidelines stratify treatment recommendations by disease severity. Mild to moderate disease, which includes diarrhea only (mild) or diarrhea with signs and symptoms not meeting criteria for severe or complicated CDI (moderate), should be treated with metronidazole 500 mg orally three times daily for 10 days. Oral vancomycin should only be used in patients with mild to moderate disease who fail to respond after five to seven days of metronidazole or in those who are intolerant to metronidazole, or pregnant or breastfeeding. Although fidaxomicin is FDA-approved to treat mild to moderate CDI, the ACG does not make a formal recommendation on its use, given its high cost and limited data to support its effectiveness.
The ACG defines severe disease as CDI in patients with albumin <3 g/dL, and either WBC ≥15,000 cells/mm3 or abdominal tenderness. Though this definition of severe disease differs from the ESCMID and SHEA-IDSA definitions, which include elevated creatinine (>50% greater than premorbid level) instead of low albumin, the treatment recommendation is the same: vancomycin 125 mg orally four times daily for 10 days. While vancomycin and metronidazole are equally effective in mild to moderate CDI, there is some evidence to suggest that vancomycin is more effective in severe disease.7
Regardless of disease severity, one of the strongest recommendations is to discontinue any inciting antibiotics. This point, along with the recommendation to avoid anti-peristaltic agents, has also been emphasized in prior guidelines. Additionally, the authors note that although providers commonly prescribe treatment for 14 days, there is no evidence to suggest that a 14-day treatment course is more efficacious than a 10-day course for either metronidazole or vancomycin.
Management of severe and complicated CDI. Severe and complicated disease refers to CDI in patients meeting at least one of the following criteria: admission to the ICU, hypotension, fever ≥38.5°C, ileus or significant abdominal distention, mental status changes, WBC ≥35,000 or <2,000 cells/mm3, serum lactate >2.2 mmol/L, or end-stage organ failure. This definition is more specific than the SHEA-IDSA guidelines, which categorize severe and complicated disease as situations where shock, ileus, or megacolon are present. The recommended treatment is combined therapy with oral vancomycin 125 mg four times daily, plus intravenous metronidazole 500 mg three times daily. Surgical consultation should be obtained in all patients with complicated CDI. Colectomy should be considered in patients with evidence of severe sepsis, leukocytosis of ≥50,000, lactate ≥5 mmol/L, and failure to improve with medical therapy.
Patients with ileus or history of bowel surgery in whom oral antibiotics may not reach the colon should have vancomycin per rectum (enema of 500 mg in 100 mL to 500 mL of normal saline every six hours) added to the above treatments, regardless of disease severity.
Management of recurrent CDI. Consistent with previously published guidelines, the ACG recommends that the first recurrence of CDI be treated with the same regimen that was used for the initial episode. Second recurrences should be treated with a pulsed oral vancomycin regimen. Data are lacking regarding specific taper regimens, but the ACG suggests vancomycin 125 mg four times daily for 10 days, followed by a 125 mg dose every three days for 10 doses. For additional recurrences, fecal microbiota transplant may be considered. Reports suggest that this practice is safe and effective, but data from randomized controlled trials are lacking.
There is limited evidence to support the use of other antibiotics (e.g. rifampin, rifamixin), probiotics, or immunotherapy in the prevention of recurrent CDI.
Management of CDI in patients with comorbid conditions. A unique feature of the 2013 ACG guidelines is the incorporation of recommendations for patient groups who are at elevated risk for developing CDI or associated complications. Patients with inflammatory bowel disease (IBD) are one such group, as they often have underlying colonic inflammation and ongoing immunosuppression. The authors recommend that patients presenting with IBD flares be tested for C. diff. Other immunocompromised populations, including patients with malignancy, exposure to chemotherapy or corticosteroids, organ transplantation, and cirrhosis, should also be tested for CDI when presenting with diarrheal illness. Similarly, pregnant and peripartum women are considered high-risk and should undergo early testing and prompt initiation of treatment for CDI in the setting of diarrhea.
Infection control and prevention. Like SHEA-IDSA, the ACG recommends a hospital-based infection control program, antibiotic stewardship, and strict use of contact precautions for patients with known or suspected CDI. Contact precautions should be continued at minimum for the duration of diarrhea. Patients should be placed in private rooms and disposable equipment should be used, when possible. Disinfection of environmental surfaces is critical, as the environment is a common source of nosocomial infection. Disinfectants should have an Environmental Protection Agency-registered C. diff sporicidal label claim or contain a minimum concentration of chlorine solution. Important: Hand-washing with soap and water is required, as alcohol-based antiseptics are not active against C. diff spores.
HM Takeaways
The 2013 ACG guidelines for the diagnosis, treatment, and prevention of CDI are generally consistent with previously published guidelines from ESCMID and SHEA-IDSA. Ongoing points of emphasis are the following:
- Only test patients with diarrhea;
- Do not repeat testing after a negative test or after completion of treatment;
- Promptly discontinue any inciting antibiotics;
- Avoid use of anti-peristaltic agents; and
- Treat based on disease severity.
Hospitalists should be aware of criteria that place patients into the severe and complicated category, and understand that initial treatment should be provided for a 10-day course. These guidelines also highlight the need for a high index of suspicion and low threshold for empiric treatment in immunocompromised patients.
Finally, hospitalists should be attentive to antibiotic stewardship and strictly adhere to contact precautions and hand hygiene with soap and water, as these behaviors have been shown to prevent and control CDI.
Dr. Cunningham Sponsler is a hospitalist in the section of hospital medicine at Vanderbilt University in Nashville, Tenn.
References 1. Lucado J, Gould C, Elixhauser A. Clostridium difficile infections (CDI) in hospital stays, 2009. Healthcare Cost and Utilization Project website. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb124.pdf. Accessed June 17, 2013.
2. Surawicz CM, Brandt LJ, Binion DJ, et al. Guidelines for diagnosis, treatment and prevention of Clostridium difficile infections. Am J Gastroenterol. 2013;108:478-498.
3. Freeman J, Bauer MP, Baines SD, et al. The changing epidemiology of Clostridium difficile infections. Clin Microbiol Rev. 2010;23:529-549.
4. Bauer MP, Kuijper EJ, van Dissel JT. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance for Clostridium difficile infection (CDI). Clin Microbiol Infect. 2009;15:1067-1079.
5. Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol. 2010;31:431-455.
6. Committee on Infectious Diseases. Clostridium difficile infection in infants and children. Pediatrics. 2013;131:196-200.
7. Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45:302-307.