User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Many doctors not advising on proper infant care
Many doctors have neglected to advise or have misinformed mothers on the proper infant care practices, according to a self-report study of mothers, with an oversampling of black and Hispanics.
“Advice received by mothers from potentially influential sources such as medical professionals, family, and the media represents a potentially important modifiable factor that may influence mothers’ choices about infant care practices,” wrote Dr. Staci R. Eisenberg of Boston Medical Center and her colleagues (Pediatrics 2015 [doi:10.1542/peds.2015-0551]). However, little is known about how regularly these mothers receive such advice and whether the advice given is consistent.
The researchers studied responses to survey questions on mothers’ knowledge of generally accepted practices regarding immunization, breastfeeding, sleep position, sleep location, and pacifier use. The survey probed mothers on what advice they received on caring for their infants and from whom they obtained such suggestions. Thirty-two U.S. hospitals administered the survey to approximately 1,000 mothers of infants aged 2-6 months.
Although survey participants most often reported receiving advice on infant care from doctors, approximately 20% of mothers said that they did not receive advice from doctors on breastfeeding and sleep positions, and more than 50% of survey participants said they received no advice about sleep location or pacifier use.
Incorrect advice on breastfeeding and pacifier use was received by 10%-15% of the mothers.
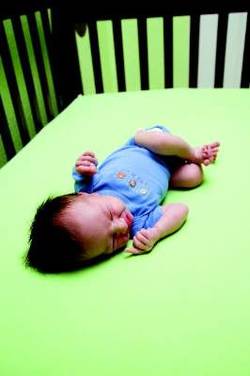
Additionally, more than 25% of the study’s participants were told to have their babies sleep in positions and locations that were “not consistent with recommendations,” a finding that Dr. Scott Krugman of MedStar Franklin Square Medical Center, Baltimore, and Carolyn J. Crumpsty-Fowler, Ph.D., of the Bloomberg School of Public Health, in Baltimore, said they found concerning in an accompanying editorial (Pediatrics 2015 [doi:10.1542/peds.2015-1826]).
This study “is a wake-up call for all pediatricians,” said Dr. Krugman and Dr. Crumpsty-Fowler. “We can and must do a better job of engaging fully in evidence-informed, culturally appropriate public discourse that transforms social norms about the necessity of providing a safe sleep environment for infants.
The survey participants also said they received advice on infant care practices from birth hospital nurses, family members, and the media. Nurses and doctors provided similar advice on most practices. The mothers report receiving advice from family members about 30%-60% of the time on the subjects surveyed, and “more than 20% of advice about breastfeeding, and roughly two-thirds of advice about sleep position, sleep location, and pacifier use was not consistent with recommendations,” the investigators said.
The media was reported as a source of advice less than half of the time on all practices, with the exception of breastfeeding; approximately 70% of mothers reported receiving advice on breastfeeding from this source, but the advice was inconsistent with “recommended infant care practices” about 20% of the time.
Another of the study’s findings was that black and Hispanic mothers were more likely than white mothers to report receiving advice consistent with generally accepted practices.
“For health care providers, our findings may suggest a need for increased attention not only to the content of advice delivered, but also to message clarity and delivery,” noted Dr. Staci R. Eisenberg and her colleagues. Understanding that advice provided often is “inconsistent with recommendations may help identify important targets for public health efforts to increase adherence.”
Read the full study in Pediatrics (doi:10.1542/peds.2015-0551).
Many doctors have neglected to advise or have misinformed mothers on the proper infant care practices, according to a self-report study of mothers, with an oversampling of black and Hispanics.
“Advice received by mothers from potentially influential sources such as medical professionals, family, and the media represents a potentially important modifiable factor that may influence mothers’ choices about infant care practices,” wrote Dr. Staci R. Eisenberg of Boston Medical Center and her colleagues (Pediatrics 2015 [doi:10.1542/peds.2015-0551]). However, little is known about how regularly these mothers receive such advice and whether the advice given is consistent.
The researchers studied responses to survey questions on mothers’ knowledge of generally accepted practices regarding immunization, breastfeeding, sleep position, sleep location, and pacifier use. The survey probed mothers on what advice they received on caring for their infants and from whom they obtained such suggestions. Thirty-two U.S. hospitals administered the survey to approximately 1,000 mothers of infants aged 2-6 months.
Although survey participants most often reported receiving advice on infant care from doctors, approximately 20% of mothers said that they did not receive advice from doctors on breastfeeding and sleep positions, and more than 50% of survey participants said they received no advice about sleep location or pacifier use.
Incorrect advice on breastfeeding and pacifier use was received by 10%-15% of the mothers.
Additionally, more than 25% of the study’s participants were told to have their babies sleep in positions and locations that were “not consistent with recommendations,” a finding that Dr. Scott Krugman of MedStar Franklin Square Medical Center, Baltimore, and Carolyn J. Crumpsty-Fowler, Ph.D., of the Bloomberg School of Public Health, in Baltimore, said they found concerning in an accompanying editorial (Pediatrics 2015 [doi:10.1542/peds.2015-1826]).
This study “is a wake-up call for all pediatricians,” said Dr. Krugman and Dr. Crumpsty-Fowler. “We can and must do a better job of engaging fully in evidence-informed, culturally appropriate public discourse that transforms social norms about the necessity of providing a safe sleep environment for infants.
The survey participants also said they received advice on infant care practices from birth hospital nurses, family members, and the media. Nurses and doctors provided similar advice on most practices. The mothers report receiving advice from family members about 30%-60% of the time on the subjects surveyed, and “more than 20% of advice about breastfeeding, and roughly two-thirds of advice about sleep position, sleep location, and pacifier use was not consistent with recommendations,” the investigators said.
The media was reported as a source of advice less than half of the time on all practices, with the exception of breastfeeding; approximately 70% of mothers reported receiving advice on breastfeeding from this source, but the advice was inconsistent with “recommended infant care practices” about 20% of the time.
Another of the study’s findings was that black and Hispanic mothers were more likely than white mothers to report receiving advice consistent with generally accepted practices.
“For health care providers, our findings may suggest a need for increased attention not only to the content of advice delivered, but also to message clarity and delivery,” noted Dr. Staci R. Eisenberg and her colleagues. Understanding that advice provided often is “inconsistent with recommendations may help identify important targets for public health efforts to increase adherence.”
Read the full study in Pediatrics (doi:10.1542/peds.2015-0551).
Many doctors have neglected to advise or have misinformed mothers on the proper infant care practices, according to a self-report study of mothers, with an oversampling of black and Hispanics.
“Advice received by mothers from potentially influential sources such as medical professionals, family, and the media represents a potentially important modifiable factor that may influence mothers’ choices about infant care practices,” wrote Dr. Staci R. Eisenberg of Boston Medical Center and her colleagues (Pediatrics 2015 [doi:10.1542/peds.2015-0551]). However, little is known about how regularly these mothers receive such advice and whether the advice given is consistent.
The researchers studied responses to survey questions on mothers’ knowledge of generally accepted practices regarding immunization, breastfeeding, sleep position, sleep location, and pacifier use. The survey probed mothers on what advice they received on caring for their infants and from whom they obtained such suggestions. Thirty-two U.S. hospitals administered the survey to approximately 1,000 mothers of infants aged 2-6 months.
Although survey participants most often reported receiving advice on infant care from doctors, approximately 20% of mothers said that they did not receive advice from doctors on breastfeeding and sleep positions, and more than 50% of survey participants said they received no advice about sleep location or pacifier use.
Incorrect advice on breastfeeding and pacifier use was received by 10%-15% of the mothers.
Additionally, more than 25% of the study’s participants were told to have their babies sleep in positions and locations that were “not consistent with recommendations,” a finding that Dr. Scott Krugman of MedStar Franklin Square Medical Center, Baltimore, and Carolyn J. Crumpsty-Fowler, Ph.D., of the Bloomberg School of Public Health, in Baltimore, said they found concerning in an accompanying editorial (Pediatrics 2015 [doi:10.1542/peds.2015-1826]).
This study “is a wake-up call for all pediatricians,” said Dr. Krugman and Dr. Crumpsty-Fowler. “We can and must do a better job of engaging fully in evidence-informed, culturally appropriate public discourse that transforms social norms about the necessity of providing a safe sleep environment for infants.
The survey participants also said they received advice on infant care practices from birth hospital nurses, family members, and the media. Nurses and doctors provided similar advice on most practices. The mothers report receiving advice from family members about 30%-60% of the time on the subjects surveyed, and “more than 20% of advice about breastfeeding, and roughly two-thirds of advice about sleep position, sleep location, and pacifier use was not consistent with recommendations,” the investigators said.
The media was reported as a source of advice less than half of the time on all practices, with the exception of breastfeeding; approximately 70% of mothers reported receiving advice on breastfeeding from this source, but the advice was inconsistent with “recommended infant care practices” about 20% of the time.
Another of the study’s findings was that black and Hispanic mothers were more likely than white mothers to report receiving advice consistent with generally accepted practices.
“For health care providers, our findings may suggest a need for increased attention not only to the content of advice delivered, but also to message clarity and delivery,” noted Dr. Staci R. Eisenberg and her colleagues. Understanding that advice provided often is “inconsistent with recommendations may help identify important targets for public health efforts to increase adherence.”
Read the full study in Pediatrics (doi:10.1542/peds.2015-0551).

First-time youth tobacco users turning to e-cigarettes
First-time youth tobacco users are turning to e-cigarettes, a survey showed.
Researchers examining the results of the survey of 2,084 11th- and 12th-grade participants in the Southern California Children’s Health Study during the spring of 2014 found that e-cigarettes were enjoying a “favorable social environment” among this group.
“This finding is a cause for concern because e-cigarettes were the dominant tobacco product used, and a substantial portion of e-cigarette users had no history of tobacco use,” Jessica L. Barrington-Trimis, Ph.D., a researcher at the University of Southern California’s department of preventive medicine, and her colleagues said in the August issue of Pediatrics (doi:10.1542/peds.2015-0639).

Twenty-four percent of teens reported any lifetime e-cigarette use; 10% were current users (past 30 days) and 14% were past users. “Notably, a lower proportion of adolescents (n = 390, 18.7%) had ever smoked a cigarette; 5.7% (n = 119) were current cigarette users and 10.0% (n = 271) were past cigarette smokers,” Dr. Barrington-Trimis and her associates reported.
The investigators suggested that because of a more favorable perception of e-cigarettes (for example, 43% of the adolescents predicted that their friends would react positively to their own e-cigarette use), they “could contribute to the ‘renormalization’ of tobacco products generally,” and called for more research in this area.
Research was funded by a grant from the National Cancer Institute and the Food and Drug Administration Center for Tobacco Products. The authors reported no relevant financial conflicts of interest.
First-time youth tobacco users are turning to e-cigarettes, a survey showed.
Researchers examining the results of the survey of 2,084 11th- and 12th-grade participants in the Southern California Children’s Health Study during the spring of 2014 found that e-cigarettes were enjoying a “favorable social environment” among this group.
“This finding is a cause for concern because e-cigarettes were the dominant tobacco product used, and a substantial portion of e-cigarette users had no history of tobacco use,” Jessica L. Barrington-Trimis, Ph.D., a researcher at the University of Southern California’s department of preventive medicine, and her colleagues said in the August issue of Pediatrics (doi:10.1542/peds.2015-0639).
Twenty-four percent of teens reported any lifetime e-cigarette use; 10% were current users (past 30 days) and 14% were past users. “Notably, a lower proportion of adolescents (n = 390, 18.7%) had ever smoked a cigarette; 5.7% (n = 119) were current cigarette users and 10.0% (n = 271) were past cigarette smokers,” Dr. Barrington-Trimis and her associates reported.
The investigators suggested that because of a more favorable perception of e-cigarettes (for example, 43% of the adolescents predicted that their friends would react positively to their own e-cigarette use), they “could contribute to the ‘renormalization’ of tobacco products generally,” and called for more research in this area.
Research was funded by a grant from the National Cancer Institute and the Food and Drug Administration Center for Tobacco Products. The authors reported no relevant financial conflicts of interest.
First-time youth tobacco users are turning to e-cigarettes, a survey showed.
Researchers examining the results of the survey of 2,084 11th- and 12th-grade participants in the Southern California Children’s Health Study during the spring of 2014 found that e-cigarettes were enjoying a “favorable social environment” among this group.
“This finding is a cause for concern because e-cigarettes were the dominant tobacco product used, and a substantial portion of e-cigarette users had no history of tobacco use,” Jessica L. Barrington-Trimis, Ph.D., a researcher at the University of Southern California’s department of preventive medicine, and her colleagues said in the August issue of Pediatrics (doi:10.1542/peds.2015-0639).
Twenty-four percent of teens reported any lifetime e-cigarette use; 10% were current users (past 30 days) and 14% were past users. “Notably, a lower proportion of adolescents (n = 390, 18.7%) had ever smoked a cigarette; 5.7% (n = 119) were current cigarette users and 10.0% (n = 271) were past cigarette smokers,” Dr. Barrington-Trimis and her associates reported.
The investigators suggested that because of a more favorable perception of e-cigarettes (for example, 43% of the adolescents predicted that their friends would react positively to their own e-cigarette use), they “could contribute to the ‘renormalization’ of tobacco products generally,” and called for more research in this area.
Research was funded by a grant from the National Cancer Institute and the Food and Drug Administration Center for Tobacco Products. The authors reported no relevant financial conflicts of interest.
FROM PEDIATRICS

Home VTE treatment with rivaroxaban safe and effective
Home treatment with rivaroxaban for patients with a low-risk first deep vein thrombosis or pulmonary embolism is associated with low rates of thrombosis recurrence or major bleeding, according to data from a prospective observational study.
The study enrolled 71 patients with low-risk deep vein thrombosis (DVT), 30 with pulmonary embolism, and five with both, all of whom were discharged with prescriptions for 15mg of rivaroxaban twice a day for 21 days and then 20 mg once per day for a further month.

There were no cases of thrombosis recurrence within the treatment period – although three patients had a recurrent DVT after stopping treatment – and no incidents of major or clinically relevant bleeding while on the therapy, as was reported in the July edition of Academic Emergency Medicine.
“This preliminary report provides data to support the initial outpatient treatment of low-risk ED patients with deep vein thrombosis and pulmonary embolism,” wrote Dr. Daren M. Beam and colleagues from the Indiana University School of Medicine (Academic Emergency Medicine 2015, 22:789–795 [doi:10.1111/acem.12711]).
The study was partly supported by the Lilly Physician Scientist Award. One author declared consultancies with Stago Diagnostica, Janssen, and Pfizer.
Home treatment with rivaroxaban for patients with a low-risk first deep vein thrombosis or pulmonary embolism is associated with low rates of thrombosis recurrence or major bleeding, according to data from a prospective observational study.
The study enrolled 71 patients with low-risk deep vein thrombosis (DVT), 30 with pulmonary embolism, and five with both, all of whom were discharged with prescriptions for 15mg of rivaroxaban twice a day for 21 days and then 20 mg once per day for a further month.
There were no cases of thrombosis recurrence within the treatment period – although three patients had a recurrent DVT after stopping treatment – and no incidents of major or clinically relevant bleeding while on the therapy, as was reported in the July edition of Academic Emergency Medicine.
“This preliminary report provides data to support the initial outpatient treatment of low-risk ED patients with deep vein thrombosis and pulmonary embolism,” wrote Dr. Daren M. Beam and colleagues from the Indiana University School of Medicine (Academic Emergency Medicine 2015, 22:789–795 [doi:10.1111/acem.12711]).
The study was partly supported by the Lilly Physician Scientist Award. One author declared consultancies with Stago Diagnostica, Janssen, and Pfizer.
Home treatment with rivaroxaban for patients with a low-risk first deep vein thrombosis or pulmonary embolism is associated with low rates of thrombosis recurrence or major bleeding, according to data from a prospective observational study.
The study enrolled 71 patients with low-risk deep vein thrombosis (DVT), 30 with pulmonary embolism, and five with both, all of whom were discharged with prescriptions for 15mg of rivaroxaban twice a day for 21 days and then 20 mg once per day for a further month.
There were no cases of thrombosis recurrence within the treatment period – although three patients had a recurrent DVT after stopping treatment – and no incidents of major or clinically relevant bleeding while on the therapy, as was reported in the July edition of Academic Emergency Medicine.
“This preliminary report provides data to support the initial outpatient treatment of low-risk ED patients with deep vein thrombosis and pulmonary embolism,” wrote Dr. Daren M. Beam and colleagues from the Indiana University School of Medicine (Academic Emergency Medicine 2015, 22:789–795 [doi:10.1111/acem.12711]).
The study was partly supported by the Lilly Physician Scientist Award. One author declared consultancies with Stago Diagnostica, Janssen, and Pfizer.
FROM ACADEMIC EMERGENCY MEDICINE
Key clinical point: Home treatment with rivaroxaban for patients with a low-risk first deep vein thrombosis or pulmonary embolism is safe and effective.
Major finding: Patients treated at home with rivaroxaban reported no cases of recurrent VTE or major bleeding during the treatment period.
Data source: A prospective observational study in 106 patients with deep vein thrombosis or pulmonary embolism.
Disclosures: The study was partly supported by the Lilly Physician Scientist Award. One author declared consultancies with Stago Diagnostica, Janssen, and Pfizer.

Why, oh why, won’t she go to bed?!
To weary parents, the fact that their child does not want to go to bed at night is both puzzling and exasperating. No matter what age, it is important to have a healthy bedtime for the child’s well-being as well as their caregiver’s!
Sleep, like the “canary in the mine,” is vulnerable to disruption by anything from minor illness to changes in schedule, things viewed on media, or emotions in the home, to life changes such as a new sibling, toilet training, or a new school year. In patients on stimulant medicine resisting bedtime, consider the need to finally eat. Asking about these specifically will help you plan an appropriate time to successfully address bedtime conflicts.

Knowing some basic principles about falling asleep can help your counseling. “Sleep drive” builds up over the day like a coiled spring, making falling asleep easier initially than for wakings later in the night. It also means that a nap too close to bedtime reduces the drive. Avoiding any naps (after age 4 years) and naps lasting past 4 p.m. for children under 4, even in car rides, is crucial. Beware of teens “having trouble falling asleep” who have sneaked in a nap after school!
To optimize sleep drive, calculate age-related sleep needs and, ideally, ask parents to keep a sleep diary for 1-2 weeks, especially checking on naps at daycare. Updated sleep duration standards (preschool 10-13 hours; school age 9-11 hours; teens 8-10 hours (see sleepfoundation.org) show that ranges of total sleep are remarkably stable, but may not meet parents’ ideals for time “off duty.”
If placed in bed when not yet tired, anyone will have trouble falling asleep (phase shift). For a child, lying awake in the dark alone is time for active imaginations to conjure fear of separation (> 4-6 months), monsters (for preschoolers), burglars (for anxious school-aged children), or the next day’s social or academic stresses (for school-aged children to teens). Children with anxiety disorders even worry that they may not get enough sleep! A soothing routine with a story in their bed (not media), a spritzing of “monster spray” or a “bedtime ticket” to cash in for “one more thing” (for those who beg) will usually suffice for preschoolers. A “magic flashlight” lends the child some control to check for monsters, but an “exorcism ritual” by the all-powerful parent can be added if needed. Teens are never too old for a chance to talk or even a story read by the parent (but they won’t ask for this).
A secret to managing bedtime struggles is to start the routine at the time the child is now falling asleep to avoid resistance, and keeping wake-up time appropriate to the new schedule. Once falling asleep within 10 minutes, move bedtime 15 minutes earlier each night to reach the schedule, then maintain 7 days per week (or within 1 hour) to prevent resetting the biological clock. Sorry, no movie nights until 2 a.m. or “sleeping in” on weekends! Teens who resist bedtime may be napping, socializing at the “only time” peers are up, addicted to media, or avoiding family. Their cooperation must be engaged to make a change by staying up all night once, then setting a new schedule, or staying up 1 hour later each night until the desired bedtime is reached.

Because sleep includes being paralyzed (REM stages), evolution encourages animals to sleep together to protect from predators. Sleeping alone requires a great deal of reassurance, such as from a friendly atmosphere, favorite stuffed toy, and familiar routine that implies safety. Children could use a toy, pet, or even a sibling to feel safe. While body contact is the most reassuring, children may not return to sleep from the many normal night wakings without it. Most can be weaned from this dependence by the parent sitting by the bed silently, moving one foot closer to the door each night. A promise to “check on you” in 5 minutes also helps.
Other factors making sleep easier include avoiding caffeine, stimulating medicines, or nicotine as well as exciting games, media, or exercise within 2 hours of bedtime. A quiet, dark, cool but not damp location used only for sleeping is helpful, but not always possible. A white noise generator, fan, or radio on static can help.
Many parents strangely expect their child to give up the pleasures of the day and take themselves to bed! As for other kinds of limit setting, parental company is typically needed for brushing teeth, pajamas, and a story. Ideally, it can be fun as a race or with songs, not a yelling match, which undermines the sense of safety. Setting rules about no electronics in the bedroom, even for charging, after a certain hour is often the only solution (even for adults) to the common struggle over ending media.
Often the bedtime complaint is “curtain calls” after being settled in bed. For children who call out, advise parents wait a few moments before responding, then reassure verbally without entering their room, waiting longer each time. For the child getting out of bed, one parent should lead them back without talking at all as many times as necessary. A reward for staying in bed without calling or coming out can be an extra story the next night and/or a morning reward. Alternatively, close the door and turn off the light if they come out or call out. After a few moments in the dark, give a “second chance” as long as they are quietly in bed. Gating the doorway works well for toddlers – sleeping on the floor is not dangerous!
Families often are ambivalent about asking for bedtime advice, thinking your solutions might be stressful, harmful to their relationship, or will take up their own precious sleep. For many, a prolonged bedtime is the best part of their day. Special Time earlier is often key to enforcing a healthy bedtime. Reassure them that these solutions usually take less than 3 weeks!
For the child, bedtime means giving up on fun but, more importantly, separation from the parent. This separation is harder if negative emotions are left from a day of behavior struggles or parents are even subtly angry at each other. For parents, bedtime means separating from their main pleasure in life. They also may be regretting their interactions during the day. Ambivalence about parting also may come from fears of being alone with their partner due to marital discord, intimate partner violence, chronic arguing, substance use, or simply depression. When simple advice fails, it is important to explore these meanings with families, encourage positive daytime behavior management methods, and avoid conflict in front of the children to resolve bedtime struggles.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
To weary parents, the fact that their child does not want to go to bed at night is both puzzling and exasperating. No matter what age, it is important to have a healthy bedtime for the child’s well-being as well as their caregiver’s!
Sleep, like the “canary in the mine,” is vulnerable to disruption by anything from minor illness to changes in schedule, things viewed on media, or emotions in the home, to life changes such as a new sibling, toilet training, or a new school year. In patients on stimulant medicine resisting bedtime, consider the need to finally eat. Asking about these specifically will help you plan an appropriate time to successfully address bedtime conflicts.
Knowing some basic principles about falling asleep can help your counseling. “Sleep drive” builds up over the day like a coiled spring, making falling asleep easier initially than for wakings later in the night. It also means that a nap too close to bedtime reduces the drive. Avoiding any naps (after age 4 years) and naps lasting past 4 p.m. for children under 4, even in car rides, is crucial. Beware of teens “having trouble falling asleep” who have sneaked in a nap after school!
To optimize sleep drive, calculate age-related sleep needs and, ideally, ask parents to keep a sleep diary for 1-2 weeks, especially checking on naps at daycare. Updated sleep duration standards (preschool 10-13 hours; school age 9-11 hours; teens 8-10 hours (see sleepfoundation.org) show that ranges of total sleep are remarkably stable, but may not meet parents’ ideals for time “off duty.”
If placed in bed when not yet tired, anyone will have trouble falling asleep (phase shift). For a child, lying awake in the dark alone is time for active imaginations to conjure fear of separation (> 4-6 months), monsters (for preschoolers), burglars (for anxious school-aged children), or the next day’s social or academic stresses (for school-aged children to teens). Children with anxiety disorders even worry that they may not get enough sleep! A soothing routine with a story in their bed (not media), a spritzing of “monster spray” or a “bedtime ticket” to cash in for “one more thing” (for those who beg) will usually suffice for preschoolers. A “magic flashlight” lends the child some control to check for monsters, but an “exorcism ritual” by the all-powerful parent can be added if needed. Teens are never too old for a chance to talk or even a story read by the parent (but they won’t ask for this).
A secret to managing bedtime struggles is to start the routine at the time the child is now falling asleep to avoid resistance, and keeping wake-up time appropriate to the new schedule. Once falling asleep within 10 minutes, move bedtime 15 minutes earlier each night to reach the schedule, then maintain 7 days per week (or within 1 hour) to prevent resetting the biological clock. Sorry, no movie nights until 2 a.m. or “sleeping in” on weekends! Teens who resist bedtime may be napping, socializing at the “only time” peers are up, addicted to media, or avoiding family. Their cooperation must be engaged to make a change by staying up all night once, then setting a new schedule, or staying up 1 hour later each night until the desired bedtime is reached.
Because sleep includes being paralyzed (REM stages), evolution encourages animals to sleep together to protect from predators. Sleeping alone requires a great deal of reassurance, such as from a friendly atmosphere, favorite stuffed toy, and familiar routine that implies safety. Children could use a toy, pet, or even a sibling to feel safe. While body contact is the most reassuring, children may not return to sleep from the many normal night wakings without it. Most can be weaned from this dependence by the parent sitting by the bed silently, moving one foot closer to the door each night. A promise to “check on you” in 5 minutes also helps.
Other factors making sleep easier include avoiding caffeine, stimulating medicines, or nicotine as well as exciting games, media, or exercise within 2 hours of bedtime. A quiet, dark, cool but not damp location used only for sleeping is helpful, but not always possible. A white noise generator, fan, or radio on static can help.
Many parents strangely expect their child to give up the pleasures of the day and take themselves to bed! As for other kinds of limit setting, parental company is typically needed for brushing teeth, pajamas, and a story. Ideally, it can be fun as a race or with songs, not a yelling match, which undermines the sense of safety. Setting rules about no electronics in the bedroom, even for charging, after a certain hour is often the only solution (even for adults) to the common struggle over ending media.
Often the bedtime complaint is “curtain calls” after being settled in bed. For children who call out, advise parents wait a few moments before responding, then reassure verbally without entering their room, waiting longer each time. For the child getting out of bed, one parent should lead them back without talking at all as many times as necessary. A reward for staying in bed without calling or coming out can be an extra story the next night and/or a morning reward. Alternatively, close the door and turn off the light if they come out or call out. After a few moments in the dark, give a “second chance” as long as they are quietly in bed. Gating the doorway works well for toddlers – sleeping on the floor is not dangerous!
Families often are ambivalent about asking for bedtime advice, thinking your solutions might be stressful, harmful to their relationship, or will take up their own precious sleep. For many, a prolonged bedtime is the best part of their day. Special Time earlier is often key to enforcing a healthy bedtime. Reassure them that these solutions usually take less than 3 weeks!
For the child, bedtime means giving up on fun but, more importantly, separation from the parent. This separation is harder if negative emotions are left from a day of behavior struggles or parents are even subtly angry at each other. For parents, bedtime means separating from their main pleasure in life. They also may be regretting their interactions during the day. Ambivalence about parting also may come from fears of being alone with their partner due to marital discord, intimate partner violence, chronic arguing, substance use, or simply depression. When simple advice fails, it is important to explore these meanings with families, encourage positive daytime behavior management methods, and avoid conflict in front of the children to resolve bedtime struggles.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
To weary parents, the fact that their child does not want to go to bed at night is both puzzling and exasperating. No matter what age, it is important to have a healthy bedtime for the child’s well-being as well as their caregiver’s!
Sleep, like the “canary in the mine,” is vulnerable to disruption by anything from minor illness to changes in schedule, things viewed on media, or emotions in the home, to life changes such as a new sibling, toilet training, or a new school year. In patients on stimulant medicine resisting bedtime, consider the need to finally eat. Asking about these specifically will help you plan an appropriate time to successfully address bedtime conflicts.
Knowing some basic principles about falling asleep can help your counseling. “Sleep drive” builds up over the day like a coiled spring, making falling asleep easier initially than for wakings later in the night. It also means that a nap too close to bedtime reduces the drive. Avoiding any naps (after age 4 years) and naps lasting past 4 p.m. for children under 4, even in car rides, is crucial. Beware of teens “having trouble falling asleep” who have sneaked in a nap after school!
To optimize sleep drive, calculate age-related sleep needs and, ideally, ask parents to keep a sleep diary for 1-2 weeks, especially checking on naps at daycare. Updated sleep duration standards (preschool 10-13 hours; school age 9-11 hours; teens 8-10 hours (see sleepfoundation.org) show that ranges of total sleep are remarkably stable, but may not meet parents’ ideals for time “off duty.”
If placed in bed when not yet tired, anyone will have trouble falling asleep (phase shift). For a child, lying awake in the dark alone is time for active imaginations to conjure fear of separation (> 4-6 months), monsters (for preschoolers), burglars (for anxious school-aged children), or the next day’s social or academic stresses (for school-aged children to teens). Children with anxiety disorders even worry that they may not get enough sleep! A soothing routine with a story in their bed (not media), a spritzing of “monster spray” or a “bedtime ticket” to cash in for “one more thing” (for those who beg) will usually suffice for preschoolers. A “magic flashlight” lends the child some control to check for monsters, but an “exorcism ritual” by the all-powerful parent can be added if needed. Teens are never too old for a chance to talk or even a story read by the parent (but they won’t ask for this).
A secret to managing bedtime struggles is to start the routine at the time the child is now falling asleep to avoid resistance, and keeping wake-up time appropriate to the new schedule. Once falling asleep within 10 minutes, move bedtime 15 minutes earlier each night to reach the schedule, then maintain 7 days per week (or within 1 hour) to prevent resetting the biological clock. Sorry, no movie nights until 2 a.m. or “sleeping in” on weekends! Teens who resist bedtime may be napping, socializing at the “only time” peers are up, addicted to media, or avoiding family. Their cooperation must be engaged to make a change by staying up all night once, then setting a new schedule, or staying up 1 hour later each night until the desired bedtime is reached.
Because sleep includes being paralyzed (REM stages), evolution encourages animals to sleep together to protect from predators. Sleeping alone requires a great deal of reassurance, such as from a friendly atmosphere, favorite stuffed toy, and familiar routine that implies safety. Children could use a toy, pet, or even a sibling to feel safe. While body contact is the most reassuring, children may not return to sleep from the many normal night wakings without it. Most can be weaned from this dependence by the parent sitting by the bed silently, moving one foot closer to the door each night. A promise to “check on you” in 5 minutes also helps.
Other factors making sleep easier include avoiding caffeine, stimulating medicines, or nicotine as well as exciting games, media, or exercise within 2 hours of bedtime. A quiet, dark, cool but not damp location used only for sleeping is helpful, but not always possible. A white noise generator, fan, or radio on static can help.
Many parents strangely expect their child to give up the pleasures of the day and take themselves to bed! As for other kinds of limit setting, parental company is typically needed for brushing teeth, pajamas, and a story. Ideally, it can be fun as a race or with songs, not a yelling match, which undermines the sense of safety. Setting rules about no electronics in the bedroom, even for charging, after a certain hour is often the only solution (even for adults) to the common struggle over ending media.
Often the bedtime complaint is “curtain calls” after being settled in bed. For children who call out, advise parents wait a few moments before responding, then reassure verbally without entering their room, waiting longer each time. For the child getting out of bed, one parent should lead them back without talking at all as many times as necessary. A reward for staying in bed without calling or coming out can be an extra story the next night and/or a morning reward. Alternatively, close the door and turn off the light if they come out or call out. After a few moments in the dark, give a “second chance” as long as they are quietly in bed. Gating the doorway works well for toddlers – sleeping on the floor is not dangerous!
Families often are ambivalent about asking for bedtime advice, thinking your solutions might be stressful, harmful to their relationship, or will take up their own precious sleep. For many, a prolonged bedtime is the best part of their day. Special Time earlier is often key to enforcing a healthy bedtime. Reassure them that these solutions usually take less than 3 weeks!
For the child, bedtime means giving up on fun but, more importantly, separation from the parent. This separation is harder if negative emotions are left from a day of behavior struggles or parents are even subtly angry at each other. For parents, bedtime means separating from their main pleasure in life. They also may be regretting their interactions during the day. Ambivalence about parting also may come from fears of being alone with their partner due to marital discord, intimate partner violence, chronic arguing, substance use, or simply depression. When simple advice fails, it is important to explore these meanings with families, encourage positive daytime behavior management methods, and avoid conflict in front of the children to resolve bedtime struggles.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].

Dicloxacillin may cut INR levels in warfarin users
The antibiotic dicloxacillin appears to markedly decrease INR levels in patients taking warfarin, reducing the mean INR to subtherapeutic ranges in the majority who take both drugs concomitantly, according to a research letter to the editor published online July 20 in JAMA.
Adverse interactions between warfarin and other drugs are often suspected, but solid data are lacking. Case reports have suggested that the commonly used antibiotic dicloxacillin reduces warfarin’s anticoagulant effects, but no studies have examined the issue, said Anton Pottegård, Ph.D., of the department of clinical pharmacology, University of Southern Denmark, Odense, and his associates (JAMA 2015;314:296-7).
To further investigate that possibility, the investigators analyzed information in an anticoagulant database covering 7,400 patients treated by three outpatient clinics and 50 general practitioners during a 15-year period. They focused on weekly INR levels recorded for 236 patients (median age, 68 years), most of whom took warfarin because of atrial fibrillation or heart valve replacement.
The mean INR level before dicloxacillin exposure was 2.59, compared with 1.97 after dicloxacillin exposure (P < .001). A total of 144 patients (61%) had subtherapeutic INR levels (< 2.0) during the 2-4 weeks following a course of dicloxacillin, Dr. Pottegård and his associates said.
A similar but less drastic decrease was observed among the 64 patients taking a different anticoagulant, phenprocoumon, who were given dicloxacillin. Mean INR levels dropped from 2.61 before exposure to 2.30 afterward (P = .003), and 41% of the group had subtherapeutic INR levels after taking the antibiotic.
No sponsor was reported for this study. Dr. Pottegård and his associates reported having no relevant financial disclosures.
The antibiotic dicloxacillin appears to markedly decrease INR levels in patients taking warfarin, reducing the mean INR to subtherapeutic ranges in the majority who take both drugs concomitantly, according to a research letter to the editor published online July 20 in JAMA.
Adverse interactions between warfarin and other drugs are often suspected, but solid data are lacking. Case reports have suggested that the commonly used antibiotic dicloxacillin reduces warfarin’s anticoagulant effects, but no studies have examined the issue, said Anton Pottegård, Ph.D., of the department of clinical pharmacology, University of Southern Denmark, Odense, and his associates (JAMA 2015;314:296-7).
To further investigate that possibility, the investigators analyzed information in an anticoagulant database covering 7,400 patients treated by three outpatient clinics and 50 general practitioners during a 15-year period. They focused on weekly INR levels recorded for 236 patients (median age, 68 years), most of whom took warfarin because of atrial fibrillation or heart valve replacement.
The mean INR level before dicloxacillin exposure was 2.59, compared with 1.97 after dicloxacillin exposure (P < .001). A total of 144 patients (61%) had subtherapeutic INR levels (< 2.0) during the 2-4 weeks following a course of dicloxacillin, Dr. Pottegård and his associates said.
A similar but less drastic decrease was observed among the 64 patients taking a different anticoagulant, phenprocoumon, who were given dicloxacillin. Mean INR levels dropped from 2.61 before exposure to 2.30 afterward (P = .003), and 41% of the group had subtherapeutic INR levels after taking the antibiotic.
No sponsor was reported for this study. Dr. Pottegård and his associates reported having no relevant financial disclosures.
The antibiotic dicloxacillin appears to markedly decrease INR levels in patients taking warfarin, reducing the mean INR to subtherapeutic ranges in the majority who take both drugs concomitantly, according to a research letter to the editor published online July 20 in JAMA.
Adverse interactions between warfarin and other drugs are often suspected, but solid data are lacking. Case reports have suggested that the commonly used antibiotic dicloxacillin reduces warfarin’s anticoagulant effects, but no studies have examined the issue, said Anton Pottegård, Ph.D., of the department of clinical pharmacology, University of Southern Denmark, Odense, and his associates (JAMA 2015;314:296-7).
To further investigate that possibility, the investigators analyzed information in an anticoagulant database covering 7,400 patients treated by three outpatient clinics and 50 general practitioners during a 15-year period. They focused on weekly INR levels recorded for 236 patients (median age, 68 years), most of whom took warfarin because of atrial fibrillation or heart valve replacement.
The mean INR level before dicloxacillin exposure was 2.59, compared with 1.97 after dicloxacillin exposure (P < .001). A total of 144 patients (61%) had subtherapeutic INR levels (< 2.0) during the 2-4 weeks following a course of dicloxacillin, Dr. Pottegård and his associates said.
A similar but less drastic decrease was observed among the 64 patients taking a different anticoagulant, phenprocoumon, who were given dicloxacillin. Mean INR levels dropped from 2.61 before exposure to 2.30 afterward (P = .003), and 41% of the group had subtherapeutic INR levels after taking the antibiotic.
No sponsor was reported for this study. Dr. Pottegård and his associates reported having no relevant financial disclosures.
FROM JAMA
Key clinical point: The antibiotic dicloxacillin appears to markedly decrease INR levels in patients using warfarin.
Major finding: 144 patients taking warfarin (61%) had subtherapeutic international normalized ratio levels during the 2-4 weeks following a course of dicloxacillin.
Data source: An analysis of INR levels before and after antibiotic use from a Danish database of 7,400 patients taking anticoagulants.
Disclosures: No sponsor was reported for this study. Dr. Pottegard and his associates reported having no relevant financial disclosures.
Water woes: Recognizing and treating recreational water illness
Most of our patients have been or will be exposed to water in a recreational setting this summer. As health care providers, we might not routinely consider illnesses associated with recreational water exposure or discuss preventive strategies; however, the Centers for Disease Control and Prevention has been actively promoting awareness about recreational water illnesses for years. May 18-24, 2015, was the 11th annual observance of Healthy and Safe Swimming Week, formerly known as Recreational Illness and Injury Prevention Week. The focus for 2015 was promoting the role of swimmers, residential pool owners, public health officials, and beach staff in the prevention of drownings, chemical injuries, and outbreaks of illness. One goal was for the swimmer to take a more active role in protecting themselves and preventing the spread of infections to others. For our colleagues, that means educating both parents and children.

To begin our discussion, let’s define recreational water illnesses (RWI). RWIs are caused by a variety of infectious pathogens transmitted by ingestion, inhalation of aerosols or mists, or having contact with contaminated water from both treated (swimming pools, hot tubs, water parks, and fountains) and untreated (lakes, rivers, and oceans) sources of water in recreational venues. RWIs also can be caused by chemicals that have evaporated from water leading to poor indoor air quality. However, I am focusing on the infectious etiologies.
A broad spectrum of infections are associated with RWIs, including infections of the gastrointestinal tract, ear, skin, eye, central nervous system, and wounds. Diarrhea is the most common infection. Implicated pathogens include Giardia, Shigella, norovirus, and Escherichia coli O157:H7, but it is Cryptosporidium that has emerged as the pathogen implicated most often in swimming pool–related outbreaks. Recently published data from the CDC revealed that in 2011-2012, there were 90 recreational-associated outbreaks reported from 32 states and Puerto Rico resulting in 1,788 infections, with 69 outbreaks occurring in treated water venues. Of these, 36 (51%) were caused by Cryptosporidium. Among 21 outbreaks occurring in untreated recreational water, E. coli was responsible for 7 (33%) (MMWR Morb. Mortal. Wkly Rep. 2015;64:668-72)
It’s no surprise diarrhea is the most common illness. Infection can easily occur after swallowing contaminated water. Many erroneously think chlorine kills all pathogens. Cryptosporidium is chlorine tolerant and can persist in treated water with the current recommended levels of chlorine for more than 10 days (J. Water Health 2008;6:513-20). For chlorine-sensitive pathogens, maintenance of the disinfection process must remain intact. What role do swimmers play? Most people have about 0.4 g of feces on their bottoms that can contaminate water when rinsed off. How many people enter a pool with a diarrheal illness? How many may go swimming after having recently recovered from a diarrheal illness and may have asymptomatic shedding? We all have cringed when we see a diapered child in the water. All of these are potential ways for the swimmer to contaminate an adequately treated pool. Additionally, while Cryptosporidium infections are usually self-limited, some individuals, including the immunocompromised host and especially those with advanced HIV and those who are solid organ transplant recipients, may have a protracted course of profuse diarrhea if infected.
While diarrhea maybe the most common RWI, it is not the only one. Acute otitis externa (AOE), more commonly known as “swimmer’s ear,” is one of the most frequent reasons for summer health care encounters. It has been estimated that in the United States in 2007, 2.4 million health care visits resulted in the diagnosis of AOE (MMWR Morb. Mortal. Wkly. Rep. 2011;60:605-9). Visits were highest among children aged 5-9 years; however, adults accounted for 53% of the encounters. Inflammation and infection of the external auditory canal is usually caused by bacteria. Pseudomonas aeruginosa or Staphylococcus aureus are the two most common etiologies. Water is easily introduced into the external auditory canal with recreational water activities, leading to maceration and subsequent infection of the canal. Simply reminding parents to thoroughly dry their child’s ears after water exposure can help prevent AOE.

P. aeruginosa also is the agent causing the self-limiting conditions hot tub folliculitis and hot-foot syndrome. Hot tub folliculitis is characterized by the development of tender, pruritic papules and papulopustules on the hips, buttocks, and axillae, usually developing 8-48 hours after exposure to water that has been contaminated because of inadequate chlorination. Hot-foot syndrome is characterized by painful planter nodules (N. Engl. J. Med. 2001;345:335).
Serious diseases are encountered infrequently, but there are some that require more urgent interventions. Primary amebic meningoencephalitis (PAM) is an extremely rare, progressive, and almost always fatal infection of the brain caused by Naegleria fowleri. The pathogen is found in warm freshwater including lakes, rivers, streams, and hot springs. It enters the body through the nose and travels via the olfactory nerve to the brain. Infection usually occurs when individuals swim or dive in warm freshwater. Most cases have been reported in children from Southern states. In 2010, the first case in a northern state was reported from Minnesota, and three additional cases have since been reported in Kansas and Indiana (J. Ped. Infect. Dis. 2014 [doi: 10.1093/jpids/piu103]). Cases also have been reported in two individuals who were regular users of neti pots for sinus irrigation because the irrigating solution was prepared with contaminated tap water (Clin. Infect. Dis. 2012;55:e79-85). Clinical presentation is similar to bacterial meningitis. Helpful diagnostic clues may come from obtaining a history of swimming in freshwater within the 2 weeks prior to presentation, especially during the summer, or the use of nasal or sinus irrigation with untreated tap water. Consultation with an infectious disease specialist is recommended.
Acanthamoeba keratitis is a potentially blinding infection of the cornea that primarily occurs in individuals who wear contact lenses. Risk factors for the infection include swimming, showering, and use of hot tubs while wearing contact lenses. Improper storage and cleansing contacts with tap water are other risk factors. Anyone with corneal trauma and similar water exposures also would be at risk. Clinically, the history combined with a foreign-body sensation, pain, and decreased visual acuity should make one include this infection in the differential diagnosis. Referral to an ophthalmologist is required.
Finally, swimming with an open wound is a portal of entry for Vibrio vulnificus. It usually is associated with consumption of contaminated seafood, especially oysters. In immunocompromised individuals, especially those with chronic liver disease, this bacteria can cause a life-threatening illness leading to bacteremia, septic shock, and development of blistering skin lesions. Infections are fatal in approximately 50% of cases.
The goal of this brief review was not to discourage swimming, but to make your patients and their families healthy swimmers. Here are a few things the CDC is recommending to help them achieve that goal:
• Shower prior to going swimming.
• Do not swallow or drink pool water.
• Take bathroom breaks every hour and rinse off before going back into the water.
• Do not swim if you have diarrhea.
• Wait at least 2 weeks to go swimming if you have had diarrhea.
• Change swim diapers frequently and away from the water.
• Suggest patients download the free CDC app Healthy Swimming for more detailed information and suggest they visit cdc.gov/healthywater/swimming.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Write to Dr. Word at [email protected].
Most of our patients have been or will be exposed to water in a recreational setting this summer. As health care providers, we might not routinely consider illnesses associated with recreational water exposure or discuss preventive strategies; however, the Centers for Disease Control and Prevention has been actively promoting awareness about recreational water illnesses for years. May 18-24, 2015, was the 11th annual observance of Healthy and Safe Swimming Week, formerly known as Recreational Illness and Injury Prevention Week. The focus for 2015 was promoting the role of swimmers, residential pool owners, public health officials, and beach staff in the prevention of drownings, chemical injuries, and outbreaks of illness. One goal was for the swimmer to take a more active role in protecting themselves and preventing the spread of infections to others. For our colleagues, that means educating both parents and children.
To begin our discussion, let’s define recreational water illnesses (RWI). RWIs are caused by a variety of infectious pathogens transmitted by ingestion, inhalation of aerosols or mists, or having contact with contaminated water from both treated (swimming pools, hot tubs, water parks, and fountains) and untreated (lakes, rivers, and oceans) sources of water in recreational venues. RWIs also can be caused by chemicals that have evaporated from water leading to poor indoor air quality. However, I am focusing on the infectious etiologies.
A broad spectrum of infections are associated with RWIs, including infections of the gastrointestinal tract, ear, skin, eye, central nervous system, and wounds. Diarrhea is the most common infection. Implicated pathogens include Giardia, Shigella, norovirus, and Escherichia coli O157:H7, but it is Cryptosporidium that has emerged as the pathogen implicated most often in swimming pool–related outbreaks. Recently published data from the CDC revealed that in 2011-2012, there were 90 recreational-associated outbreaks reported from 32 states and Puerto Rico resulting in 1,788 infections, with 69 outbreaks occurring in treated water venues. Of these, 36 (51%) were caused by Cryptosporidium. Among 21 outbreaks occurring in untreated recreational water, E. coli was responsible for 7 (33%) (MMWR Morb. Mortal. Wkly Rep. 2015;64:668-72)
It’s no surprise diarrhea is the most common illness. Infection can easily occur after swallowing contaminated water. Many erroneously think chlorine kills all pathogens. Cryptosporidium is chlorine tolerant and can persist in treated water with the current recommended levels of chlorine for more than 10 days (J. Water Health 2008;6:513-20). For chlorine-sensitive pathogens, maintenance of the disinfection process must remain intact. What role do swimmers play? Most people have about 0.4 g of feces on their bottoms that can contaminate water when rinsed off. How many people enter a pool with a diarrheal illness? How many may go swimming after having recently recovered from a diarrheal illness and may have asymptomatic shedding? We all have cringed when we see a diapered child in the water. All of these are potential ways for the swimmer to contaminate an adequately treated pool. Additionally, while Cryptosporidium infections are usually self-limited, some individuals, including the immunocompromised host and especially those with advanced HIV and those who are solid organ transplant recipients, may have a protracted course of profuse diarrhea if infected.
While diarrhea maybe the most common RWI, it is not the only one. Acute otitis externa (AOE), more commonly known as “swimmer’s ear,” is one of the most frequent reasons for summer health care encounters. It has been estimated that in the United States in 2007, 2.4 million health care visits resulted in the diagnosis of AOE (MMWR Morb. Mortal. Wkly. Rep. 2011;60:605-9). Visits were highest among children aged 5-9 years; however, adults accounted for 53% of the encounters. Inflammation and infection of the external auditory canal is usually caused by bacteria. Pseudomonas aeruginosa or Staphylococcus aureus are the two most common etiologies. Water is easily introduced into the external auditory canal with recreational water activities, leading to maceration and subsequent infection of the canal. Simply reminding parents to thoroughly dry their child’s ears after water exposure can help prevent AOE.
P. aeruginosa also is the agent causing the self-limiting conditions hot tub folliculitis and hot-foot syndrome. Hot tub folliculitis is characterized by the development of tender, pruritic papules and papulopustules on the hips, buttocks, and axillae, usually developing 8-48 hours after exposure to water that has been contaminated because of inadequate chlorination. Hot-foot syndrome is characterized by painful planter nodules (N. Engl. J. Med. 2001;345:335).
Serious diseases are encountered infrequently, but there are some that require more urgent interventions. Primary amebic meningoencephalitis (PAM) is an extremely rare, progressive, and almost always fatal infection of the brain caused by Naegleria fowleri. The pathogen is found in warm freshwater including lakes, rivers, streams, and hot springs. It enters the body through the nose and travels via the olfactory nerve to the brain. Infection usually occurs when individuals swim or dive in warm freshwater. Most cases have been reported in children from Southern states. In 2010, the first case in a northern state was reported from Minnesota, and three additional cases have since been reported in Kansas and Indiana (J. Ped. Infect. Dis. 2014 [doi: 10.1093/jpids/piu103]). Cases also have been reported in two individuals who were regular users of neti pots for sinus irrigation because the irrigating solution was prepared with contaminated tap water (Clin. Infect. Dis. 2012;55:e79-85). Clinical presentation is similar to bacterial meningitis. Helpful diagnostic clues may come from obtaining a history of swimming in freshwater within the 2 weeks prior to presentation, especially during the summer, or the use of nasal or sinus irrigation with untreated tap water. Consultation with an infectious disease specialist is recommended.
Acanthamoeba keratitis is a potentially blinding infection of the cornea that primarily occurs in individuals who wear contact lenses. Risk factors for the infection include swimming, showering, and use of hot tubs while wearing contact lenses. Improper storage and cleansing contacts with tap water are other risk factors. Anyone with corneal trauma and similar water exposures also would be at risk. Clinically, the history combined with a foreign-body sensation, pain, and decreased visual acuity should make one include this infection in the differential diagnosis. Referral to an ophthalmologist is required.
Finally, swimming with an open wound is a portal of entry for Vibrio vulnificus. It usually is associated with consumption of contaminated seafood, especially oysters. In immunocompromised individuals, especially those with chronic liver disease, this bacteria can cause a life-threatening illness leading to bacteremia, septic shock, and development of blistering skin lesions. Infections are fatal in approximately 50% of cases.
The goal of this brief review was not to discourage swimming, but to make your patients and their families healthy swimmers. Here are a few things the CDC is recommending to help them achieve that goal:
• Shower prior to going swimming.
• Do not swallow or drink pool water.
• Take bathroom breaks every hour and rinse off before going back into the water.
• Do not swim if you have diarrhea.
• Wait at least 2 weeks to go swimming if you have had diarrhea.
• Change swim diapers frequently and away from the water.
• Suggest patients download the free CDC app Healthy Swimming for more detailed information and suggest they visit cdc.gov/healthywater/swimming.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Write to Dr. Word at [email protected].
Most of our patients have been or will be exposed to water in a recreational setting this summer. As health care providers, we might not routinely consider illnesses associated with recreational water exposure or discuss preventive strategies; however, the Centers for Disease Control and Prevention has been actively promoting awareness about recreational water illnesses for years. May 18-24, 2015, was the 11th annual observance of Healthy and Safe Swimming Week, formerly known as Recreational Illness and Injury Prevention Week. The focus for 2015 was promoting the role of swimmers, residential pool owners, public health officials, and beach staff in the prevention of drownings, chemical injuries, and outbreaks of illness. One goal was for the swimmer to take a more active role in protecting themselves and preventing the spread of infections to others. For our colleagues, that means educating both parents and children.
To begin our discussion, let’s define recreational water illnesses (RWI). RWIs are caused by a variety of infectious pathogens transmitted by ingestion, inhalation of aerosols or mists, or having contact with contaminated water from both treated (swimming pools, hot tubs, water parks, and fountains) and untreated (lakes, rivers, and oceans) sources of water in recreational venues. RWIs also can be caused by chemicals that have evaporated from water leading to poor indoor air quality. However, I am focusing on the infectious etiologies.
A broad spectrum of infections are associated with RWIs, including infections of the gastrointestinal tract, ear, skin, eye, central nervous system, and wounds. Diarrhea is the most common infection. Implicated pathogens include Giardia, Shigella, norovirus, and Escherichia coli O157:H7, but it is Cryptosporidium that has emerged as the pathogen implicated most often in swimming pool–related outbreaks. Recently published data from the CDC revealed that in 2011-2012, there were 90 recreational-associated outbreaks reported from 32 states and Puerto Rico resulting in 1,788 infections, with 69 outbreaks occurring in treated water venues. Of these, 36 (51%) were caused by Cryptosporidium. Among 21 outbreaks occurring in untreated recreational water, E. coli was responsible for 7 (33%) (MMWR Morb. Mortal. Wkly Rep. 2015;64:668-72)
It’s no surprise diarrhea is the most common illness. Infection can easily occur after swallowing contaminated water. Many erroneously think chlorine kills all pathogens. Cryptosporidium is chlorine tolerant and can persist in treated water with the current recommended levels of chlorine for more than 10 days (J. Water Health 2008;6:513-20). For chlorine-sensitive pathogens, maintenance of the disinfection process must remain intact. What role do swimmers play? Most people have about 0.4 g of feces on their bottoms that can contaminate water when rinsed off. How many people enter a pool with a diarrheal illness? How many may go swimming after having recently recovered from a diarrheal illness and may have asymptomatic shedding? We all have cringed when we see a diapered child in the water. All of these are potential ways for the swimmer to contaminate an adequately treated pool. Additionally, while Cryptosporidium infections are usually self-limited, some individuals, including the immunocompromised host and especially those with advanced HIV and those who are solid organ transplant recipients, may have a protracted course of profuse diarrhea if infected.
While diarrhea maybe the most common RWI, it is not the only one. Acute otitis externa (AOE), more commonly known as “swimmer’s ear,” is one of the most frequent reasons for summer health care encounters. It has been estimated that in the United States in 2007, 2.4 million health care visits resulted in the diagnosis of AOE (MMWR Morb. Mortal. Wkly. Rep. 2011;60:605-9). Visits were highest among children aged 5-9 years; however, adults accounted for 53% of the encounters. Inflammation and infection of the external auditory canal is usually caused by bacteria. Pseudomonas aeruginosa or Staphylococcus aureus are the two most common etiologies. Water is easily introduced into the external auditory canal with recreational water activities, leading to maceration and subsequent infection of the canal. Simply reminding parents to thoroughly dry their child’s ears after water exposure can help prevent AOE.
P. aeruginosa also is the agent causing the self-limiting conditions hot tub folliculitis and hot-foot syndrome. Hot tub folliculitis is characterized by the development of tender, pruritic papules and papulopustules on the hips, buttocks, and axillae, usually developing 8-48 hours after exposure to water that has been contaminated because of inadequate chlorination. Hot-foot syndrome is characterized by painful planter nodules (N. Engl. J. Med. 2001;345:335).
Serious diseases are encountered infrequently, but there are some that require more urgent interventions. Primary amebic meningoencephalitis (PAM) is an extremely rare, progressive, and almost always fatal infection of the brain caused by Naegleria fowleri. The pathogen is found in warm freshwater including lakes, rivers, streams, and hot springs. It enters the body through the nose and travels via the olfactory nerve to the brain. Infection usually occurs when individuals swim or dive in warm freshwater. Most cases have been reported in children from Southern states. In 2010, the first case in a northern state was reported from Minnesota, and three additional cases have since been reported in Kansas and Indiana (J. Ped. Infect. Dis. 2014 [doi: 10.1093/jpids/piu103]). Cases also have been reported in two individuals who were regular users of neti pots for sinus irrigation because the irrigating solution was prepared with contaminated tap water (Clin. Infect. Dis. 2012;55:e79-85). Clinical presentation is similar to bacterial meningitis. Helpful diagnostic clues may come from obtaining a history of swimming in freshwater within the 2 weeks prior to presentation, especially during the summer, or the use of nasal or sinus irrigation with untreated tap water. Consultation with an infectious disease specialist is recommended.
Acanthamoeba keratitis is a potentially blinding infection of the cornea that primarily occurs in individuals who wear contact lenses. Risk factors for the infection include swimming, showering, and use of hot tubs while wearing contact lenses. Improper storage and cleansing contacts with tap water are other risk factors. Anyone with corneal trauma and similar water exposures also would be at risk. Clinically, the history combined with a foreign-body sensation, pain, and decreased visual acuity should make one include this infection in the differential diagnosis. Referral to an ophthalmologist is required.
Finally, swimming with an open wound is a portal of entry for Vibrio vulnificus. It usually is associated with consumption of contaminated seafood, especially oysters. In immunocompromised individuals, especially those with chronic liver disease, this bacteria can cause a life-threatening illness leading to bacteremia, septic shock, and development of blistering skin lesions. Infections are fatal in approximately 50% of cases.
The goal of this brief review was not to discourage swimming, but to make your patients and their families healthy swimmers. Here are a few things the CDC is recommending to help them achieve that goal:
• Shower prior to going swimming.
• Do not swallow or drink pool water.
• Take bathroom breaks every hour and rinse off before going back into the water.
• Do not swim if you have diarrhea.
• Wait at least 2 weeks to go swimming if you have had diarrhea.
• Change swim diapers frequently and away from the water.
• Suggest patients download the free CDC app Healthy Swimming for more detailed information and suggest they visit cdc.gov/healthywater/swimming.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Write to Dr. Word at [email protected].

CAP shifting to viral disease as vaccines knock out bacterial causes
Viral infections appear to be the primary cause of pneumonia that results in hospitalization, according to a Centers for Disease Control and Prevention study of five urban hospitals in Chicago and Nashville, Tenn.
The study was published online July 14 in the New England Journal of Medicine.
From January 2010 through June 2012, 2,259 patients hospitalized for community-acquired pneumonia (CAP) had both radiographic evidence of disease and specimens for bacterial and viral testing. A pathogen was detected in just 853 (38%). One or more viruses were detected in 530 (23%), bacteria in 247 (11%), bacterial and viral pathogens in 59 (3%), and fungal or mycobacterial pathogens in 17 (1%). The findings indicate the annual incidence of community-acquired pneumonia requiring hospitalization is about 25 cases per 10,000 adults, with the highest rates among adults 65-79 years old (63 cases per 10,000) and 80 years or older (164 cases per 10,000).
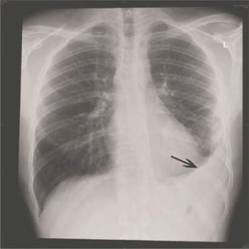
The most common pathogens were rhinovirus in 9% of patients, influenza virus in 6%, and Streptococcus pneumoniae in 5%, which was the most commonly detected bacterium (N. Engl. J. Med. 14 July 2015 [doi:10.1056/NEJMoa1500245]).
CAP is thought to be caused most often by S. pneumoniae and other bacteria; the fact that viruses were more frequently detected “probably reflects the direct and indirect benefit of bacterial vaccines,” but also “relatively insensitive diagnostic tests,” said the investigators, led by CDC medical epidemiologist Dr. Seema Jain.
The project, dubbed the Etiology of Pneumonia in the Community (EPIC) study, “adds to the growing evidence of the contribution of viruses to hospitalizations of adults.” It also suggests “that improving the coverage and effectiveness of recommended influenza and pneumococcal vaccines and developing effective vaccines and treatments for human metapneumovirus, respiratory syncytial virus, and parainfluenza virus” – also found in study patients – “could reduce the burden of pneumonia among adults,” the researchers said.
The work matters because “the last U.S. population–based incidence estimates of hospitalization due to community-acquired pneumonia were made in the 1990s, before the availability of the pneumococcal conjugate vaccine and more sensitive molecular and antigen-based laboratory diagnostic tests. Thus, contemporary population-based etiologic studies involving U.S. adults with pneumonia are needed,” they noted.
Blood, urine, and respiratory cultures; serologic testing; antigen detection; molecular diagnostics, and chest x-rays were all used to find the cause of disease. The fact that infections were found in just 38% of the patients could have something to do with the team’s “inability to obtain lower respiratory tract specimens, antibiotic use before specimen collection, [and] insensitive diagnostic tests for known pathogens,” among other problems, they said.
There was a low prevalence of Enterobacteriaceae (1%) and other gram-negative bacteria, probably because patients with recent hospitalizations and severe immunosuppression were excluded. Subjects were on average 60 years old.
The CDC’s National Center for Immunizations and Respiratory Diseases funded the work. Several of the authors disclosed ties to industry, including GlaxoSmithKline, Abbvie, and Pfizer.
Viral infections appear to be the primary cause of pneumonia that results in hospitalization, according to a Centers for Disease Control and Prevention study of five urban hospitals in Chicago and Nashville, Tenn.
The study was published online July 14 in the New England Journal of Medicine.
From January 2010 through June 2012, 2,259 patients hospitalized for community-acquired pneumonia (CAP) had both radiographic evidence of disease and specimens for bacterial and viral testing. A pathogen was detected in just 853 (38%). One or more viruses were detected in 530 (23%), bacteria in 247 (11%), bacterial and viral pathogens in 59 (3%), and fungal or mycobacterial pathogens in 17 (1%). The findings indicate the annual incidence of community-acquired pneumonia requiring hospitalization is about 25 cases per 10,000 adults, with the highest rates among adults 65-79 years old (63 cases per 10,000) and 80 years or older (164 cases per 10,000).
The most common pathogens were rhinovirus in 9% of patients, influenza virus in 6%, and Streptococcus pneumoniae in 5%, which was the most commonly detected bacterium (N. Engl. J. Med. 14 July 2015 [doi:10.1056/NEJMoa1500245]).
CAP is thought to be caused most often by S. pneumoniae and other bacteria; the fact that viruses were more frequently detected “probably reflects the direct and indirect benefit of bacterial vaccines,” but also “relatively insensitive diagnostic tests,” said the investigators, led by CDC medical epidemiologist Dr. Seema Jain.
The project, dubbed the Etiology of Pneumonia in the Community (EPIC) study, “adds to the growing evidence of the contribution of viruses to hospitalizations of adults.” It also suggests “that improving the coverage and effectiveness of recommended influenza and pneumococcal vaccines and developing effective vaccines and treatments for human metapneumovirus, respiratory syncytial virus, and parainfluenza virus” – also found in study patients – “could reduce the burden of pneumonia among adults,” the researchers said.
The work matters because “the last U.S. population–based incidence estimates of hospitalization due to community-acquired pneumonia were made in the 1990s, before the availability of the pneumococcal conjugate vaccine and more sensitive molecular and antigen-based laboratory diagnostic tests. Thus, contemporary population-based etiologic studies involving U.S. adults with pneumonia are needed,” they noted.
Blood, urine, and respiratory cultures; serologic testing; antigen detection; molecular diagnostics, and chest x-rays were all used to find the cause of disease. The fact that infections were found in just 38% of the patients could have something to do with the team’s “inability to obtain lower respiratory tract specimens, antibiotic use before specimen collection, [and] insensitive diagnostic tests for known pathogens,” among other problems, they said.
There was a low prevalence of Enterobacteriaceae (1%) and other gram-negative bacteria, probably because patients with recent hospitalizations and severe immunosuppression were excluded. Subjects were on average 60 years old.
The CDC’s National Center for Immunizations and Respiratory Diseases funded the work. Several of the authors disclosed ties to industry, including GlaxoSmithKline, Abbvie, and Pfizer.
Viral infections appear to be the primary cause of pneumonia that results in hospitalization, according to a Centers for Disease Control and Prevention study of five urban hospitals in Chicago and Nashville, Tenn.
The study was published online July 14 in the New England Journal of Medicine.
From January 2010 through June 2012, 2,259 patients hospitalized for community-acquired pneumonia (CAP) had both radiographic evidence of disease and specimens for bacterial and viral testing. A pathogen was detected in just 853 (38%). One or more viruses were detected in 530 (23%), bacteria in 247 (11%), bacterial and viral pathogens in 59 (3%), and fungal or mycobacterial pathogens in 17 (1%). The findings indicate the annual incidence of community-acquired pneumonia requiring hospitalization is about 25 cases per 10,000 adults, with the highest rates among adults 65-79 years old (63 cases per 10,000) and 80 years or older (164 cases per 10,000).
The most common pathogens were rhinovirus in 9% of patients, influenza virus in 6%, and Streptococcus pneumoniae in 5%, which was the most commonly detected bacterium (N. Engl. J. Med. 14 July 2015 [doi:10.1056/NEJMoa1500245]).
CAP is thought to be caused most often by S. pneumoniae and other bacteria; the fact that viruses were more frequently detected “probably reflects the direct and indirect benefit of bacterial vaccines,” but also “relatively insensitive diagnostic tests,” said the investigators, led by CDC medical epidemiologist Dr. Seema Jain.
The project, dubbed the Etiology of Pneumonia in the Community (EPIC) study, “adds to the growing evidence of the contribution of viruses to hospitalizations of adults.” It also suggests “that improving the coverage and effectiveness of recommended influenza and pneumococcal vaccines and developing effective vaccines and treatments for human metapneumovirus, respiratory syncytial virus, and parainfluenza virus” – also found in study patients – “could reduce the burden of pneumonia among adults,” the researchers said.
The work matters because “the last U.S. population–based incidence estimates of hospitalization due to community-acquired pneumonia were made in the 1990s, before the availability of the pneumococcal conjugate vaccine and more sensitive molecular and antigen-based laboratory diagnostic tests. Thus, contemporary population-based etiologic studies involving U.S. adults with pneumonia are needed,” they noted.
Blood, urine, and respiratory cultures; serologic testing; antigen detection; molecular diagnostics, and chest x-rays were all used to find the cause of disease. The fact that infections were found in just 38% of the patients could have something to do with the team’s “inability to obtain lower respiratory tract specimens, antibiotic use before specimen collection, [and] insensitive diagnostic tests for known pathogens,” among other problems, they said.
There was a low prevalence of Enterobacteriaceae (1%) and other gram-negative bacteria, probably because patients with recent hospitalizations and severe immunosuppression were excluded. Subjects were on average 60 years old.
The CDC’s National Center for Immunizations and Respiratory Diseases funded the work. Several of the authors disclosed ties to industry, including GlaxoSmithKline, Abbvie, and Pfizer.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Viral infections may be on the rise as a cause of community-acquired pneumonia.
Major finding: Among more than 2,000 patients hospitalized for CAP, one or more viruses were detected in 23%, and bacteria in 11%.
Data source: Prospective surveillance study at five urban hospitals.
Disclosures: The CDC’s National Center for Immunizations and Respiratory Diseases funded the work. Several of the authors disclosed ties to industry.

WCD: Pramocaine is a common contact sensitizer
VANCOUVER – Pramocaine, a topical anesthetic long used in many OTC anti-itch preparations, turns out to itself be a common cause of contact sensitization, Dr. Mariam Abbas reported at the World Congress of Dermatology.
Pramocaine, also known as pramoxine, is an ingredient in Gold Bond cream, some forms of calamine lotion, hemorrhoid relief products, and other OTC antipruritic agents. It’s not available in commercial patch test kits, so Dr. Abbas created a test material comprised of 2% pramocaine in petrolatum.
Seven of 232 patients (3%) referred to a university patch test clinic and who underwent testing to pramocaine along with recognized contact sensitizers showed a clear positive response to pramocaine at 96 hours. The reactions were clinically relevant, according to Dr. Abbas of the University of Alberta, Edmonton.
That 3% positive rate is in the range of published figures for such well-known problem contact sensitizers as neomycin, thiuram mix, and Balsam of Peru.
Dr. Mariam Abbas reported having no financial conflicts regarding this study, conducted free of commercial support.
VANCOUVER – Pramocaine, a topical anesthetic long used in many OTC anti-itch preparations, turns out to itself be a common cause of contact sensitization, Dr. Mariam Abbas reported at the World Congress of Dermatology.
Pramocaine, also known as pramoxine, is an ingredient in Gold Bond cream, some forms of calamine lotion, hemorrhoid relief products, and other OTC antipruritic agents. It’s not available in commercial patch test kits, so Dr. Abbas created a test material comprised of 2% pramocaine in petrolatum.
Seven of 232 patients (3%) referred to a university patch test clinic and who underwent testing to pramocaine along with recognized contact sensitizers showed a clear positive response to pramocaine at 96 hours. The reactions were clinically relevant, according to Dr. Abbas of the University of Alberta, Edmonton.
That 3% positive rate is in the range of published figures for such well-known problem contact sensitizers as neomycin, thiuram mix, and Balsam of Peru.
Dr. Mariam Abbas reported having no financial conflicts regarding this study, conducted free of commercial support.
VANCOUVER – Pramocaine, a topical anesthetic long used in many OTC anti-itch preparations, turns out to itself be a common cause of contact sensitization, Dr. Mariam Abbas reported at the World Congress of Dermatology.
Pramocaine, also known as pramoxine, is an ingredient in Gold Bond cream, some forms of calamine lotion, hemorrhoid relief products, and other OTC antipruritic agents. It’s not available in commercial patch test kits, so Dr. Abbas created a test material comprised of 2% pramocaine in petrolatum.
Seven of 232 patients (3%) referred to a university patch test clinic and who underwent testing to pramocaine along with recognized contact sensitizers showed a clear positive response to pramocaine at 96 hours. The reactions were clinically relevant, according to Dr. Abbas of the University of Alberta, Edmonton.
That 3% positive rate is in the range of published figures for such well-known problem contact sensitizers as neomycin, thiuram mix, and Balsam of Peru.
Dr. Mariam Abbas reported having no financial conflicts regarding this study, conducted free of commercial support.
AT WCD 2015
Key clinical point: Pramocaine, a topical anesthetic that’s an ingredient in many widely used OTC anti-itch products, turns out to be a common cause of contact sensitization.
Major finding: Seven of 232 patients (3%) referred to a patch test clinic showed a clinically relevant positive test to pramocaine.
Data source: A prospective study of 232 patients referred to a patch test clinic.
Disclosures: Dr. Mariam Abbas reported having no financial conflicts regarding this study, conducted free of commercial support.
Routine screening sufficient for detecting occult cancer in patients with VTE
TORONTO – The prevalence of occult cancer is low in patients with a first unprovoked venous thromboembolism, according to results from a multicenter, randomized study presented at the International Society on Thrombosis and Haemostasis congress.
In addition, routine screening with the addition of a comprehensive CT scan of the abdomen and pelvis was no better than routine screening alone in detecting occult cancer in this population.

Those are key findings that Dr. Marc Carrier of the University of Ottawa presented from the Screening for Occult Malignancy in Patients with Idiopathic Venous Thromboembolism (SOME) trial, a multicenter, open-label, randomized controlled trial that compared the efficacy of conventional screening with or without comprehensive CT of the abdomen/pelvis for detecting occult cancers in patients with unprovoked venous thromboembolism (VTE). The results of this study were published the same day as his presentation in the New England Journal of Medicine.
“It has been described that up to 10% of patients with unprovoked VTE are diagnosed with cancer in the year following their VTE diagnosis,” Dr. Carrier said. “Therefore, it’s appealing for clinicians to screen these patients for occult cancer but it has led to a lot of great diversity in practices. Some clinicians prefer to use a limited screening strategy that would include a history, physical examination, routine blood tests, and a chest X-ray. Other clinicians prefer to use the limited screening strategy in combination with additional tests. That could be CT of the abdomen and pelvis, ultrasound, or tumor marker, or [computed axial tomography] scan. It’s hard for a physician to know what to use.”
For the SOME trial, a total of 854 patients with unprovoked VTE were randomized to two groups: 431 to limited occult cancer screening (basic blood work, chest X-ray, and breast/cervical/prostate cancer screening) and 423 to limited screening in combination with a comprehensive CT of the abdomen/pelvis. The comprehensive CT included a virtual colonoscopy and gastroscopy, a biphasic enhanced CT, a parenchymal pancreatogram, and a uniphasic enhanced CT of distended bladder. The primary outcome was confirmed cancer that was missed by the screening strategy and detected by the end of the 1-year follow-up period.
Dr. Carrier reported that 33 patients (3.9%) had a new diagnosis of cancer in the interval between randomization and 1-year follow-up: 14 in the limited-screening group and 19 in the limited-screening-plus-CT group, a difference that was not statistically significant (P = .28). In addition, the number of occult cancers missed by the end of the 1-year follow-up period was similar between the two groups: four in the limited-screening group and five in the limited-screening-plus-CT group.
He and his associates also found no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%, respectively; P = .37), in overall mortality (1.4% vs. 1.2%; P > 0.99), or in cancer-related mortality (1.4% vs. 0.95%; P = .75).
“Occult cancers are not nearly as common as we thought they were, which is reassuring for clinicians and patients because then we don’t have to do a lot of investigations to try and find them, and often scare patients and expose them to radiation and additional procedures,” Dr. Carrier said in an interview. “Limited screening alone, which is what is recommended in Canada and in the United States for age- and gender-specific screening, is more than reasonable for these patients.”
The SOME trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier had no relevant financial conflicts to disclose.
Therese Borden contributed to this article.
TORONTO – The prevalence of occult cancer is low in patients with a first unprovoked venous thromboembolism, according to results from a multicenter, randomized study presented at the International Society on Thrombosis and Haemostasis congress.
In addition, routine screening with the addition of a comprehensive CT scan of the abdomen and pelvis was no better than routine screening alone in detecting occult cancer in this population.
Those are key findings that Dr. Marc Carrier of the University of Ottawa presented from the Screening for Occult Malignancy in Patients with Idiopathic Venous Thromboembolism (SOME) trial, a multicenter, open-label, randomized controlled trial that compared the efficacy of conventional screening with or without comprehensive CT of the abdomen/pelvis for detecting occult cancers in patients with unprovoked venous thromboembolism (VTE). The results of this study were published the same day as his presentation in the New England Journal of Medicine.
“It has been described that up to 10% of patients with unprovoked VTE are diagnosed with cancer in the year following their VTE diagnosis,” Dr. Carrier said. “Therefore, it’s appealing for clinicians to screen these patients for occult cancer but it has led to a lot of great diversity in practices. Some clinicians prefer to use a limited screening strategy that would include a history, physical examination, routine blood tests, and a chest X-ray. Other clinicians prefer to use the limited screening strategy in combination with additional tests. That could be CT of the abdomen and pelvis, ultrasound, or tumor marker, or [computed axial tomography] scan. It’s hard for a physician to know what to use.”
For the SOME trial, a total of 854 patients with unprovoked VTE were randomized to two groups: 431 to limited occult cancer screening (basic blood work, chest X-ray, and breast/cervical/prostate cancer screening) and 423 to limited screening in combination with a comprehensive CT of the abdomen/pelvis. The comprehensive CT included a virtual colonoscopy and gastroscopy, a biphasic enhanced CT, a parenchymal pancreatogram, and a uniphasic enhanced CT of distended bladder. The primary outcome was confirmed cancer that was missed by the screening strategy and detected by the end of the 1-year follow-up period.
Dr. Carrier reported that 33 patients (3.9%) had a new diagnosis of cancer in the interval between randomization and 1-year follow-up: 14 in the limited-screening group and 19 in the limited-screening-plus-CT group, a difference that was not statistically significant (P = .28). In addition, the number of occult cancers missed by the end of the 1-year follow-up period was similar between the two groups: four in the limited-screening group and five in the limited-screening-plus-CT group.
He and his associates also found no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%, respectively; P = .37), in overall mortality (1.4% vs. 1.2%; P > 0.99), or in cancer-related mortality (1.4% vs. 0.95%; P = .75).
“Occult cancers are not nearly as common as we thought they were, which is reassuring for clinicians and patients because then we don’t have to do a lot of investigations to try and find them, and often scare patients and expose them to radiation and additional procedures,” Dr. Carrier said in an interview. “Limited screening alone, which is what is recommended in Canada and in the United States for age- and gender-specific screening, is more than reasonable for these patients.”
The SOME trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier had no relevant financial conflicts to disclose.
Therese Borden contributed to this article.
TORONTO – The prevalence of occult cancer is low in patients with a first unprovoked venous thromboembolism, according to results from a multicenter, randomized study presented at the International Society on Thrombosis and Haemostasis congress.
In addition, routine screening with the addition of a comprehensive CT scan of the abdomen and pelvis was no better than routine screening alone in detecting occult cancer in this population.
Those are key findings that Dr. Marc Carrier of the University of Ottawa presented from the Screening for Occult Malignancy in Patients with Idiopathic Venous Thromboembolism (SOME) trial, a multicenter, open-label, randomized controlled trial that compared the efficacy of conventional screening with or without comprehensive CT of the abdomen/pelvis for detecting occult cancers in patients with unprovoked venous thromboembolism (VTE). The results of this study were published the same day as his presentation in the New England Journal of Medicine.
“It has been described that up to 10% of patients with unprovoked VTE are diagnosed with cancer in the year following their VTE diagnosis,” Dr. Carrier said. “Therefore, it’s appealing for clinicians to screen these patients for occult cancer but it has led to a lot of great diversity in practices. Some clinicians prefer to use a limited screening strategy that would include a history, physical examination, routine blood tests, and a chest X-ray. Other clinicians prefer to use the limited screening strategy in combination with additional tests. That could be CT of the abdomen and pelvis, ultrasound, or tumor marker, or [computed axial tomography] scan. It’s hard for a physician to know what to use.”
For the SOME trial, a total of 854 patients with unprovoked VTE were randomized to two groups: 431 to limited occult cancer screening (basic blood work, chest X-ray, and breast/cervical/prostate cancer screening) and 423 to limited screening in combination with a comprehensive CT of the abdomen/pelvis. The comprehensive CT included a virtual colonoscopy and gastroscopy, a biphasic enhanced CT, a parenchymal pancreatogram, and a uniphasic enhanced CT of distended bladder. The primary outcome was confirmed cancer that was missed by the screening strategy and detected by the end of the 1-year follow-up period.
Dr. Carrier reported that 33 patients (3.9%) had a new diagnosis of cancer in the interval between randomization and 1-year follow-up: 14 in the limited-screening group and 19 in the limited-screening-plus-CT group, a difference that was not statistically significant (P = .28). In addition, the number of occult cancers missed by the end of the 1-year follow-up period was similar between the two groups: four in the limited-screening group and five in the limited-screening-plus-CT group.
He and his associates also found no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%, respectively; P = .37), in overall mortality (1.4% vs. 1.2%; P > 0.99), or in cancer-related mortality (1.4% vs. 0.95%; P = .75).
“Occult cancers are not nearly as common as we thought they were, which is reassuring for clinicians and patients because then we don’t have to do a lot of investigations to try and find them, and often scare patients and expose them to radiation and additional procedures,” Dr. Carrier said in an interview. “Limited screening alone, which is what is recommended in Canada and in the United States for age- and gender-specific screening, is more than reasonable for these patients.”
The SOME trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier had no relevant financial conflicts to disclose.
Therese Borden contributed to this article.
AT THE 2015 ISTH CONGRESS
Key clinical point: Occult cancers in patients with a first unprovoked VTE are not nearly as common as previously thought, and limited screening for such cancers is appropriate.
Major finding: There were no significant differences between the limited-screening group and the limited-screening-plus-CT group in the rate of detection of early cancers (0.23% vs. 0.71%); in overall mortality (1.4% vs. 1.2%), or in cancer-related mortality (1.4% vs. 0.95%).
Data source: A multicenter, open-label, randomized controlled trial of 854 patients with unprovoked VTE.
Disclosures: The trial was funded by the Heart and Stroke Foundation of Canada. Dr. Carrier reported having no financial disclosures.

Bipolar disorder patients may underestimate their sleep quality
MIAMI BEACH – Patients with active bipolar disorder significantly underestimated the quality of their sleep, despite having sleep quality comparable to that of healthy controls.
Sleep complaints are common among individuals with bipolar disorder, and addressing disruptive and troubling sleep problems can be an important component of treating bipolar disorder, noted Dr. Venkatesh Krishnamurthy and his collaborators at Penn State University (Hershey, Pa.).
“Mood state may affect perception of sleep, and the impact of mood state on subjective-objective differences of sleep parameters needs to be further explored,” the researchers noted.
They reported their comparison of subjective and objective measures of sleep for symptomatic patients with bipolar disorder in a poster presentation at a meeting of the American Society for Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
The study researchers evaluated 30 individuals with symptomatic bipolar disorder, compared with 31 healthy controls, reported Dr. Krishnamurthy, assistant professor at the department of psychiatry’s Sleep Research and Treatment Center at Penn State’s Milton S. Hershey Medical Center. Patients with bipolar disorder were inpatients or in a partial hospitalization program; 11 patients had bipolar depression, 18 had mixed-state bipolar disorder, and 1 had bipolar disorder with a manic episode, Dr. Krishnamurthy said in an interview.
To compare subjective and objective measures of sleep in the two groups, the researchers administered a sleep-quality questionnaire and used actigraphy to document sleep objectively.
The Pittsburgh Sleep Quality Index (PSQI), the instrument used for subjective assessment, is a self-reporting tool that asks patients to report on aspects of sleep quality, usual sleep duration, daytime sleepiness, and sleep medication use over the past month.
The actigraphs used in the study used accelerometers to measure patient movement at a per-second level, and were worn around the clock for the week of the study. These devices, said Dr. Krishnamurthy, give sleep data that correlate well with polysomnography, the gold standard for sleep assessment.
For both patient groups, Dr. Krishnamurthy and his colleagues reported sleep latency, sleep duration, sleep dysfunction, sleep efficiency in percentage, sleep quality, and medication need as assessed by the PSQI, as well as the overall PSQI score.
The group with bipolar disorder reported a mean time to falling asleep of 61 minutes, compared with 14 minutes for the control group (P = 0.00064). Total sleep duration from the PSQI was 6.2 hours in the bipolar disorder patients, compared with 7.4 hours in the control group (P = 0.017). All other subjective measures of sleep quality were significantly worse for the patients with bipolar disorder, and the overall score on the PSQI was also much higher (worse), compared with the control group (11.7 vs 3.3, P = 1 x 10-11).
Actigraphy was used for a 1-week period to measure sleep latency, total sleep time, sleep efficiency, and number and length of awakenings for both groups. When measured objectively, there was no significant difference in the time it took to fall asleep between the patients with bipolar disorder and the healthy controls (14.64 minutes vs. 13.15 minutes), nor was there a significant difference in total sleep time (400.7 minutes vs. 413 minutes). Overall sleep efficiency was similar between groups.
The absolute difference in sleep duration, latency, and efficiency between subjective and objective measures was compared between groups. There was significantly less difference between objective and subjective ratings of all three sleep measures in the healthy subjects than in those with bipolar disorder.
Overall, the patients with bipolar disorder exhibited a strong perception of poor sleep quality, daytime impairment, and insufficient sleep, as shown by the PSQI scores for this group in comparison with the healthy controls. However, these perceptions did not correlate with objective sleep measures for sleep latency, total sleep duration, or sleep efficiency.
Patients with bipolar disorder were significantly more likely to lack employment and to be smokers or use illicit substances; their body mass index was also significantly higher on average than their healthy counterparts.
The bipolar disorder patients may have altered circadian rhythms, cognitive dysfunction because of the illness, and dysfunctional sleep beliefs, which may have independent effects on subjective perceptions of sleep that were not accounted for in the study, said Dr. Krishnamurthy.
The study’s findings mean that clinicians may wish to consider incorporating objective assessments of sleep, such as actigraphy, into care of individuals with bipolar disorder and sleep disturbances, Dr. Krishnamurthy said in an interview. In addition, “behavioral methods to address sleep misperception may be helpful in bipolar subjects.”
The Penn State Hershey College of Medicine funded the study. The authors reported no relevant disclosures.
MIAMI BEACH – Patients with active bipolar disorder significantly underestimated the quality of their sleep, despite having sleep quality comparable to that of healthy controls.
Sleep complaints are common among individuals with bipolar disorder, and addressing disruptive and troubling sleep problems can be an important component of treating bipolar disorder, noted Dr. Venkatesh Krishnamurthy and his collaborators at Penn State University (Hershey, Pa.).
“Mood state may affect perception of sleep, and the impact of mood state on subjective-objective differences of sleep parameters needs to be further explored,” the researchers noted.
They reported their comparison of subjective and objective measures of sleep for symptomatic patients with bipolar disorder in a poster presentation at a meeting of the American Society for Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
The study researchers evaluated 30 individuals with symptomatic bipolar disorder, compared with 31 healthy controls, reported Dr. Krishnamurthy, assistant professor at the department of psychiatry’s Sleep Research and Treatment Center at Penn State’s Milton S. Hershey Medical Center. Patients with bipolar disorder were inpatients or in a partial hospitalization program; 11 patients had bipolar depression, 18 had mixed-state bipolar disorder, and 1 had bipolar disorder with a manic episode, Dr. Krishnamurthy said in an interview.
To compare subjective and objective measures of sleep in the two groups, the researchers administered a sleep-quality questionnaire and used actigraphy to document sleep objectively.
The Pittsburgh Sleep Quality Index (PSQI), the instrument used for subjective assessment, is a self-reporting tool that asks patients to report on aspects of sleep quality, usual sleep duration, daytime sleepiness, and sleep medication use over the past month.
The actigraphs used in the study used accelerometers to measure patient movement at a per-second level, and were worn around the clock for the week of the study. These devices, said Dr. Krishnamurthy, give sleep data that correlate well with polysomnography, the gold standard for sleep assessment.
For both patient groups, Dr. Krishnamurthy and his colleagues reported sleep latency, sleep duration, sleep dysfunction, sleep efficiency in percentage, sleep quality, and medication need as assessed by the PSQI, as well as the overall PSQI score.
The group with bipolar disorder reported a mean time to falling asleep of 61 minutes, compared with 14 minutes for the control group (P = 0.00064). Total sleep duration from the PSQI was 6.2 hours in the bipolar disorder patients, compared with 7.4 hours in the control group (P = 0.017). All other subjective measures of sleep quality were significantly worse for the patients with bipolar disorder, and the overall score on the PSQI was also much higher (worse), compared with the control group (11.7 vs 3.3, P = 1 x 10-11).
Actigraphy was used for a 1-week period to measure sleep latency, total sleep time, sleep efficiency, and number and length of awakenings for both groups. When measured objectively, there was no significant difference in the time it took to fall asleep between the patients with bipolar disorder and the healthy controls (14.64 minutes vs. 13.15 minutes), nor was there a significant difference in total sleep time (400.7 minutes vs. 413 minutes). Overall sleep efficiency was similar between groups.
The absolute difference in sleep duration, latency, and efficiency between subjective and objective measures was compared between groups. There was significantly less difference between objective and subjective ratings of all three sleep measures in the healthy subjects than in those with bipolar disorder.
Overall, the patients with bipolar disorder exhibited a strong perception of poor sleep quality, daytime impairment, and insufficient sleep, as shown by the PSQI scores for this group in comparison with the healthy controls. However, these perceptions did not correlate with objective sleep measures for sleep latency, total sleep duration, or sleep efficiency.
Patients with bipolar disorder were significantly more likely to lack employment and to be smokers or use illicit substances; their body mass index was also significantly higher on average than their healthy counterparts.
The bipolar disorder patients may have altered circadian rhythms, cognitive dysfunction because of the illness, and dysfunctional sleep beliefs, which may have independent effects on subjective perceptions of sleep that were not accounted for in the study, said Dr. Krishnamurthy.
The study’s findings mean that clinicians may wish to consider incorporating objective assessments of sleep, such as actigraphy, into care of individuals with bipolar disorder and sleep disturbances, Dr. Krishnamurthy said in an interview. In addition, “behavioral methods to address sleep misperception may be helpful in bipolar subjects.”
The Penn State Hershey College of Medicine funded the study. The authors reported no relevant disclosures.
MIAMI BEACH – Patients with active bipolar disorder significantly underestimated the quality of their sleep, despite having sleep quality comparable to that of healthy controls.
Sleep complaints are common among individuals with bipolar disorder, and addressing disruptive and troubling sleep problems can be an important component of treating bipolar disorder, noted Dr. Venkatesh Krishnamurthy and his collaborators at Penn State University (Hershey, Pa.).
“Mood state may affect perception of sleep, and the impact of mood state on subjective-objective differences of sleep parameters needs to be further explored,” the researchers noted.
They reported their comparison of subjective and objective measures of sleep for symptomatic patients with bipolar disorder in a poster presentation at a meeting of the American Society for Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
The study researchers evaluated 30 individuals with symptomatic bipolar disorder, compared with 31 healthy controls, reported Dr. Krishnamurthy, assistant professor at the department of psychiatry’s Sleep Research and Treatment Center at Penn State’s Milton S. Hershey Medical Center. Patients with bipolar disorder were inpatients or in a partial hospitalization program; 11 patients had bipolar depression, 18 had mixed-state bipolar disorder, and 1 had bipolar disorder with a manic episode, Dr. Krishnamurthy said in an interview.
To compare subjective and objective measures of sleep in the two groups, the researchers administered a sleep-quality questionnaire and used actigraphy to document sleep objectively.
The Pittsburgh Sleep Quality Index (PSQI), the instrument used for subjective assessment, is a self-reporting tool that asks patients to report on aspects of sleep quality, usual sleep duration, daytime sleepiness, and sleep medication use over the past month.
The actigraphs used in the study used accelerometers to measure patient movement at a per-second level, and were worn around the clock for the week of the study. These devices, said Dr. Krishnamurthy, give sleep data that correlate well with polysomnography, the gold standard for sleep assessment.
For both patient groups, Dr. Krishnamurthy and his colleagues reported sleep latency, sleep duration, sleep dysfunction, sleep efficiency in percentage, sleep quality, and medication need as assessed by the PSQI, as well as the overall PSQI score.
The group with bipolar disorder reported a mean time to falling asleep of 61 minutes, compared with 14 minutes for the control group (P = 0.00064). Total sleep duration from the PSQI was 6.2 hours in the bipolar disorder patients, compared with 7.4 hours in the control group (P = 0.017). All other subjective measures of sleep quality were significantly worse for the patients with bipolar disorder, and the overall score on the PSQI was also much higher (worse), compared with the control group (11.7 vs 3.3, P = 1 x 10-11).
Actigraphy was used for a 1-week period to measure sleep latency, total sleep time, sleep efficiency, and number and length of awakenings for both groups. When measured objectively, there was no significant difference in the time it took to fall asleep between the patients with bipolar disorder and the healthy controls (14.64 minutes vs. 13.15 minutes), nor was there a significant difference in total sleep time (400.7 minutes vs. 413 minutes). Overall sleep efficiency was similar between groups.
The absolute difference in sleep duration, latency, and efficiency between subjective and objective measures was compared between groups. There was significantly less difference between objective and subjective ratings of all three sleep measures in the healthy subjects than in those with bipolar disorder.
Overall, the patients with bipolar disorder exhibited a strong perception of poor sleep quality, daytime impairment, and insufficient sleep, as shown by the PSQI scores for this group in comparison with the healthy controls. However, these perceptions did not correlate with objective sleep measures for sleep latency, total sleep duration, or sleep efficiency.
Patients with bipolar disorder were significantly more likely to lack employment and to be smokers or use illicit substances; their body mass index was also significantly higher on average than their healthy counterparts.
The bipolar disorder patients may have altered circadian rhythms, cognitive dysfunction because of the illness, and dysfunctional sleep beliefs, which may have independent effects on subjective perceptions of sleep that were not accounted for in the study, said Dr. Krishnamurthy.
The study’s findings mean that clinicians may wish to consider incorporating objective assessments of sleep, such as actigraphy, into care of individuals with bipolar disorder and sleep disturbances, Dr. Krishnamurthy said in an interview. In addition, “behavioral methods to address sleep misperception may be helpful in bipolar subjects.”
The Penn State Hershey College of Medicine funded the study. The authors reported no relevant disclosures.
AT THE ASCP Annual Meeting
Key clinical point: Subjective assessment of sleep efficiency and duration varied significantly from actigraphy in active bipolar disorder.
Major finding: Individuals with active bipolar disorder greatly overestimated sleep latency and underestimated sleep duration, reporting significantly worse sleep than healthy subjects, who were more accurate in subjective sleep assessment.
Data source: Subjective assessment via Pittsburgh Sleep Quality Index and objective measurement via actigraphy of 1 week of sleep for 30 individuals with active bipolar disorder (inpatients or partial hospitalization patients), compared with 31 healthy controls.
Disclosures: The Penn State Hershey College of Medicine funded the study. The authors reported no relevant disclosures.