User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Delta whiplash: How the new surge is affecting mental health
Thanks to the rollout of the COVID-19 vaccines, more than just flowers were blooming this past spring. People came out of lockdown like bears emerging from hibernation, making plans to reunite with friends and loved ones they hadn’t seen in months. But with the tremendous surge in cases brought by the Delta variant, this summer has been anything but sunny and carefree. Case counts have once more reached prevaccination levels. In a repeat of last summer, people are canceling travel plans, and the lead-up to the new school year has become fraught and stressful.
“This whiplash is causing people to feel a variety of emotions: disappointment, uncertainty, anxiety, possibly anger and frustration,” says Vaile Wright, Ph.D., senior director of health care innovation at the American Psychological Association. “When it seemed like there was a light at the end of the tunnel, and we have the tools to overcome [the virus], and we’re not really using them, it can be hard for people to understand.”
The importance of hope
For decades, researchers have been digging into the crucial role hopefulness plays in mental health. The vaccine rollout, earlier than anticipated, provided a much needed burst of hope after months of bad news.
“It was a feeling of almost euphoria in June: ‘We’re going to see everybody!’” says Rachel Goldenberg, a rabbi in Jackson Heights, NY. “We have a theme for our High Holidays, and this year’s is very hopeful: Sow in tears, reap in joy. It felt like the sowing in tears part was behind us, and we were looking forward to reaping in joy. Slowly but surely, with Delta, everything has turned upside down.”
For Roxanne Hawn, a writer in Golden, Colo., vaccination offered a glimpse of something like normal life.
“I wore cute clothes. I stopped and got takeout for lunch. I bought myself flowers. I even had a little uplifting soundtrack for that time of hope and relief,” she says. “With the Delta variant, it feels like that window of normalcy closed quickly.”
Having that little bit of hope dashed can wear down even the sturdiest spirits, says Marissa King, PhD, author of “Social Chemistry: Decoding the Elements of Human Connection”.
“There was a moment when we were able to reconnect, to experience joy and the hope of being able to revitalize relationships,” she says. “The loss of that hope and the fear of being isolated again is causing so much distress.”
A new kind of loneliness
When the pandemic started, mom of three Julie Schwietert Collazo formed a WhatsApp group with several friends who were taking lockdown seriously. They got each other through months of isolation and celebrated the idea of reopening. Then Ms. Collazo’s oldest got COVID, just 5 weeks before her 12th birthday, and their family went back into quarantine. Her moms’ group is no longer on the same page about precautions.
“Last year we were doing it together, and it made it feel a bit easier,” she says. “As things started to normalize, everybody started thinking and moving in different directions. It feels like we’re not working through the same issues collectively like before.”
Dr. King says the feeling Ms. Collazo describes is quite common these days.
“A profound sense of loneliness comes from feeling like you’re the only one,” she says. “There’s such disagreement about the best path forward, it can feel lonely just because you think differently.”
An epidemic of anxiety
As the Delta variant drives case numbers back up again, worries increase as well.
“Is this ever going to end?” asks Ms. Collazo. “Is this our new reality, constantly having to order our lives around COVID?”
This uneasiness affects our well-being.
The National Center for Health Statistics and the Census Bureau have monitored the nation’s mental health via the ongoing Household Pulse Survey during the pandemic. It asks participants about their symptoms of either anxiety or depression. Throughout, more people have reported feeling anxious than depressed.
Anxiety peaked around Thanksgiving and Christmas, with nearly 38% of people reporting symptoms. The first vaccines began to roll out around that time, and anxiety levels steadily went down through the spring and early summer, dipping below 25% in late June. But those numbers have begun to creep back up – the most recent data, which goes through Aug. 2, found 27% of Americans reporting symptoms of anxiety.
“Nervous is the new normal,” says Vivian Pender, MD, president of the American Psychiatric Association. “Uncertainty makes people feel anxious.”
Empathy vs. anger
The way politics play into basic measures like mask-wearing and vaccination adds its own layer of stress. Physical altercations have resulted: In Los Angeles, a participant was stabbed at an antivaccination protest. At an Austin, Tex., elementary school, angry parents physically and verbally assaulted teachers who wore masks. Things have gotten so heated, the Department of Homeland Security issued a National Terrorism Advisory System bulletin last week. It warns that extremists could use new COVID-driven public health restrictions as an excuse to commit domestic terrorism.
Anger goes in the opposite direction, too, with people who’ve been following recommended procedures becoming increasingly fed up with those who flout them. Those intense emotions may not lead to violence, but they do make it harder for us to feel secure.
“It’s a public health crisis, and it’s turned into something different. When we get into us/them situations, we start to lose empathy. Empathy is important to identify solutions and work together as a community,” says Dr. Wright. “That’s what sparks the anger: the sense of ‘You aren’t doing what you’re supposed to be doing.’”
How to cope
Loneliness, anxiety, and anger may be swirling all around you right now. But that doesn’t make you powerless to boost your mental health. These suggestions may help:
- Trust your gut. If your community is reopening faster than feels comfortable to you, do whatever makes your family feel safe. “Ask yourself how you’re feeling, and use your feelings to guide your decisions,” says Dr. Pender. “Get more information, then follow the science.”
- Stop judging yourself. If you’re feeling lonely or mourning the losses COVID has brought, don’t fight it, says Wright. “Let it be an emotion that comes and goes, and try to find ways to feel connected to other people.”
- Practice self-care. It may sound simplistic, but eating healthy foods, exercising, and getting a good night’s sleep can all contribute to a more positive
- Try to ease anxiety. Meditation, calming self-talk, and soothing music can all lift your spirits. Or try diaphragmatic breathing: Breathe in for 5 seconds, hold for 2, and breathe out for 5. Even squeezing a stress ball can give you a tangible sense of
- Take action. Both Rabbi Goldenberg and Ms. Collazo, who runs a nonprofit that works to reunite immigrant families, say helping their community helps them feel better. “To sing and lead Shabbat services, even on Zoom, to see the faces of my people, it’s very healing,” says Rabbi Goldenberg. One small thing you can do: If you have family or friends who are hesitant about vaccination, Dr. Wright suggests having gentle conversations to convince them. “You can be way more influential than a celebrity,” she says.
- Remember you’re not alone. Whether you’re physically isolated from others or just feel like nobody else is following the same protocols as you, there are ways to feel connected. “Reach out to people you’ve been close with in the past, but you may have lost touch,” says Dr. King. “It gives you an opportunity to rekindle joy. Particularly in this moment, when a lot of people are so afraid, it’s easier to reach out to those you already know than try to meet new people.” Dr. King’s research has found it takes as few as two close connections to make people feel supported.
- Stay in the present. Instead of stressing over what’s already happened or worrying about what might still come, just think about today. “We’ve learned a lot about the coronavirus, and we’re still learning more,” says Dr. Wright. “We don’t know what the future looks like, but it won’t be like this forever.”
A version of this article first appeared on WebMD.com.
Thanks to the rollout of the COVID-19 vaccines, more than just flowers were blooming this past spring. People came out of lockdown like bears emerging from hibernation, making plans to reunite with friends and loved ones they hadn’t seen in months. But with the tremendous surge in cases brought by the Delta variant, this summer has been anything but sunny and carefree. Case counts have once more reached prevaccination levels. In a repeat of last summer, people are canceling travel plans, and the lead-up to the new school year has become fraught and stressful.
“This whiplash is causing people to feel a variety of emotions: disappointment, uncertainty, anxiety, possibly anger and frustration,” says Vaile Wright, Ph.D., senior director of health care innovation at the American Psychological Association. “When it seemed like there was a light at the end of the tunnel, and we have the tools to overcome [the virus], and we’re not really using them, it can be hard for people to understand.”
The importance of hope
For decades, researchers have been digging into the crucial role hopefulness plays in mental health. The vaccine rollout, earlier than anticipated, provided a much needed burst of hope after months of bad news.
“It was a feeling of almost euphoria in June: ‘We’re going to see everybody!’” says Rachel Goldenberg, a rabbi in Jackson Heights, NY. “We have a theme for our High Holidays, and this year’s is very hopeful: Sow in tears, reap in joy. It felt like the sowing in tears part was behind us, and we were looking forward to reaping in joy. Slowly but surely, with Delta, everything has turned upside down.”
For Roxanne Hawn, a writer in Golden, Colo., vaccination offered a glimpse of something like normal life.
“I wore cute clothes. I stopped and got takeout for lunch. I bought myself flowers. I even had a little uplifting soundtrack for that time of hope and relief,” she says. “With the Delta variant, it feels like that window of normalcy closed quickly.”
Having that little bit of hope dashed can wear down even the sturdiest spirits, says Marissa King, PhD, author of “Social Chemistry: Decoding the Elements of Human Connection”.
“There was a moment when we were able to reconnect, to experience joy and the hope of being able to revitalize relationships,” she says. “The loss of that hope and the fear of being isolated again is causing so much distress.”
A new kind of loneliness
When the pandemic started, mom of three Julie Schwietert Collazo formed a WhatsApp group with several friends who were taking lockdown seriously. They got each other through months of isolation and celebrated the idea of reopening. Then Ms. Collazo’s oldest got COVID, just 5 weeks before her 12th birthday, and their family went back into quarantine. Her moms’ group is no longer on the same page about precautions.
“Last year we were doing it together, and it made it feel a bit easier,” she says. “As things started to normalize, everybody started thinking and moving in different directions. It feels like we’re not working through the same issues collectively like before.”
Dr. King says the feeling Ms. Collazo describes is quite common these days.
“A profound sense of loneliness comes from feeling like you’re the only one,” she says. “There’s such disagreement about the best path forward, it can feel lonely just because you think differently.”
An epidemic of anxiety
As the Delta variant drives case numbers back up again, worries increase as well.
“Is this ever going to end?” asks Ms. Collazo. “Is this our new reality, constantly having to order our lives around COVID?”
This uneasiness affects our well-being.
The National Center for Health Statistics and the Census Bureau have monitored the nation’s mental health via the ongoing Household Pulse Survey during the pandemic. It asks participants about their symptoms of either anxiety or depression. Throughout, more people have reported feeling anxious than depressed.
Anxiety peaked around Thanksgiving and Christmas, with nearly 38% of people reporting symptoms. The first vaccines began to roll out around that time, and anxiety levels steadily went down through the spring and early summer, dipping below 25% in late June. But those numbers have begun to creep back up – the most recent data, which goes through Aug. 2, found 27% of Americans reporting symptoms of anxiety.
“Nervous is the new normal,” says Vivian Pender, MD, president of the American Psychiatric Association. “Uncertainty makes people feel anxious.”
Empathy vs. anger
The way politics play into basic measures like mask-wearing and vaccination adds its own layer of stress. Physical altercations have resulted: In Los Angeles, a participant was stabbed at an antivaccination protest. At an Austin, Tex., elementary school, angry parents physically and verbally assaulted teachers who wore masks. Things have gotten so heated, the Department of Homeland Security issued a National Terrorism Advisory System bulletin last week. It warns that extremists could use new COVID-driven public health restrictions as an excuse to commit domestic terrorism.
Anger goes in the opposite direction, too, with people who’ve been following recommended procedures becoming increasingly fed up with those who flout them. Those intense emotions may not lead to violence, but they do make it harder for us to feel secure.
“It’s a public health crisis, and it’s turned into something different. When we get into us/them situations, we start to lose empathy. Empathy is important to identify solutions and work together as a community,” says Dr. Wright. “That’s what sparks the anger: the sense of ‘You aren’t doing what you’re supposed to be doing.’”
How to cope
Loneliness, anxiety, and anger may be swirling all around you right now. But that doesn’t make you powerless to boost your mental health. These suggestions may help:
- Trust your gut. If your community is reopening faster than feels comfortable to you, do whatever makes your family feel safe. “Ask yourself how you’re feeling, and use your feelings to guide your decisions,” says Dr. Pender. “Get more information, then follow the science.”
- Stop judging yourself. If you’re feeling lonely or mourning the losses COVID has brought, don’t fight it, says Wright. “Let it be an emotion that comes and goes, and try to find ways to feel connected to other people.”
- Practice self-care. It may sound simplistic, but eating healthy foods, exercising, and getting a good night’s sleep can all contribute to a more positive
- Try to ease anxiety. Meditation, calming self-talk, and soothing music can all lift your spirits. Or try diaphragmatic breathing: Breathe in for 5 seconds, hold for 2, and breathe out for 5. Even squeezing a stress ball can give you a tangible sense of
- Take action. Both Rabbi Goldenberg and Ms. Collazo, who runs a nonprofit that works to reunite immigrant families, say helping their community helps them feel better. “To sing and lead Shabbat services, even on Zoom, to see the faces of my people, it’s very healing,” says Rabbi Goldenberg. One small thing you can do: If you have family or friends who are hesitant about vaccination, Dr. Wright suggests having gentle conversations to convince them. “You can be way more influential than a celebrity,” she says.
- Remember you’re not alone. Whether you’re physically isolated from others or just feel like nobody else is following the same protocols as you, there are ways to feel connected. “Reach out to people you’ve been close with in the past, but you may have lost touch,” says Dr. King. “It gives you an opportunity to rekindle joy. Particularly in this moment, when a lot of people are so afraid, it’s easier to reach out to those you already know than try to meet new people.” Dr. King’s research has found it takes as few as two close connections to make people feel supported.
- Stay in the present. Instead of stressing over what’s already happened or worrying about what might still come, just think about today. “We’ve learned a lot about the coronavirus, and we’re still learning more,” says Dr. Wright. “We don’t know what the future looks like, but it won’t be like this forever.”
A version of this article first appeared on WebMD.com.
Thanks to the rollout of the COVID-19 vaccines, more than just flowers were blooming this past spring. People came out of lockdown like bears emerging from hibernation, making plans to reunite with friends and loved ones they hadn’t seen in months. But with the tremendous surge in cases brought by the Delta variant, this summer has been anything but sunny and carefree. Case counts have once more reached prevaccination levels. In a repeat of last summer, people are canceling travel plans, and the lead-up to the new school year has become fraught and stressful.
“This whiplash is causing people to feel a variety of emotions: disappointment, uncertainty, anxiety, possibly anger and frustration,” says Vaile Wright, Ph.D., senior director of health care innovation at the American Psychological Association. “When it seemed like there was a light at the end of the tunnel, and we have the tools to overcome [the virus], and we’re not really using them, it can be hard for people to understand.”
The importance of hope
For decades, researchers have been digging into the crucial role hopefulness plays in mental health. The vaccine rollout, earlier than anticipated, provided a much needed burst of hope after months of bad news.
“It was a feeling of almost euphoria in June: ‘We’re going to see everybody!’” says Rachel Goldenberg, a rabbi in Jackson Heights, NY. “We have a theme for our High Holidays, and this year’s is very hopeful: Sow in tears, reap in joy. It felt like the sowing in tears part was behind us, and we were looking forward to reaping in joy. Slowly but surely, with Delta, everything has turned upside down.”
For Roxanne Hawn, a writer in Golden, Colo., vaccination offered a glimpse of something like normal life.
“I wore cute clothes. I stopped and got takeout for lunch. I bought myself flowers. I even had a little uplifting soundtrack for that time of hope and relief,” she says. “With the Delta variant, it feels like that window of normalcy closed quickly.”
Having that little bit of hope dashed can wear down even the sturdiest spirits, says Marissa King, PhD, author of “Social Chemistry: Decoding the Elements of Human Connection”.
“There was a moment when we were able to reconnect, to experience joy and the hope of being able to revitalize relationships,” she says. “The loss of that hope and the fear of being isolated again is causing so much distress.”
A new kind of loneliness
When the pandemic started, mom of three Julie Schwietert Collazo formed a WhatsApp group with several friends who were taking lockdown seriously. They got each other through months of isolation and celebrated the idea of reopening. Then Ms. Collazo’s oldest got COVID, just 5 weeks before her 12th birthday, and their family went back into quarantine. Her moms’ group is no longer on the same page about precautions.
“Last year we were doing it together, and it made it feel a bit easier,” she says. “As things started to normalize, everybody started thinking and moving in different directions. It feels like we’re not working through the same issues collectively like before.”
Dr. King says the feeling Ms. Collazo describes is quite common these days.
“A profound sense of loneliness comes from feeling like you’re the only one,” she says. “There’s such disagreement about the best path forward, it can feel lonely just because you think differently.”
An epidemic of anxiety
As the Delta variant drives case numbers back up again, worries increase as well.
“Is this ever going to end?” asks Ms. Collazo. “Is this our new reality, constantly having to order our lives around COVID?”
This uneasiness affects our well-being.
The National Center for Health Statistics and the Census Bureau have monitored the nation’s mental health via the ongoing Household Pulse Survey during the pandemic. It asks participants about their symptoms of either anxiety or depression. Throughout, more people have reported feeling anxious than depressed.
Anxiety peaked around Thanksgiving and Christmas, with nearly 38% of people reporting symptoms. The first vaccines began to roll out around that time, and anxiety levels steadily went down through the spring and early summer, dipping below 25% in late June. But those numbers have begun to creep back up – the most recent data, which goes through Aug. 2, found 27% of Americans reporting symptoms of anxiety.
“Nervous is the new normal,” says Vivian Pender, MD, president of the American Psychiatric Association. “Uncertainty makes people feel anxious.”
Empathy vs. anger
The way politics play into basic measures like mask-wearing and vaccination adds its own layer of stress. Physical altercations have resulted: In Los Angeles, a participant was stabbed at an antivaccination protest. At an Austin, Tex., elementary school, angry parents physically and verbally assaulted teachers who wore masks. Things have gotten so heated, the Department of Homeland Security issued a National Terrorism Advisory System bulletin last week. It warns that extremists could use new COVID-driven public health restrictions as an excuse to commit domestic terrorism.
Anger goes in the opposite direction, too, with people who’ve been following recommended procedures becoming increasingly fed up with those who flout them. Those intense emotions may not lead to violence, but they do make it harder for us to feel secure.
“It’s a public health crisis, and it’s turned into something different. When we get into us/them situations, we start to lose empathy. Empathy is important to identify solutions and work together as a community,” says Dr. Wright. “That’s what sparks the anger: the sense of ‘You aren’t doing what you’re supposed to be doing.’”
How to cope
Loneliness, anxiety, and anger may be swirling all around you right now. But that doesn’t make you powerless to boost your mental health. These suggestions may help:
- Trust your gut. If your community is reopening faster than feels comfortable to you, do whatever makes your family feel safe. “Ask yourself how you’re feeling, and use your feelings to guide your decisions,” says Dr. Pender. “Get more information, then follow the science.”
- Stop judging yourself. If you’re feeling lonely or mourning the losses COVID has brought, don’t fight it, says Wright. “Let it be an emotion that comes and goes, and try to find ways to feel connected to other people.”
- Practice self-care. It may sound simplistic, but eating healthy foods, exercising, and getting a good night’s sleep can all contribute to a more positive
- Try to ease anxiety. Meditation, calming self-talk, and soothing music can all lift your spirits. Or try diaphragmatic breathing: Breathe in for 5 seconds, hold for 2, and breathe out for 5. Even squeezing a stress ball can give you a tangible sense of
- Take action. Both Rabbi Goldenberg and Ms. Collazo, who runs a nonprofit that works to reunite immigrant families, say helping their community helps them feel better. “To sing and lead Shabbat services, even on Zoom, to see the faces of my people, it’s very healing,” says Rabbi Goldenberg. One small thing you can do: If you have family or friends who are hesitant about vaccination, Dr. Wright suggests having gentle conversations to convince them. “You can be way more influential than a celebrity,” she says.
- Remember you’re not alone. Whether you’re physically isolated from others or just feel like nobody else is following the same protocols as you, there are ways to feel connected. “Reach out to people you’ve been close with in the past, but you may have lost touch,” says Dr. King. “It gives you an opportunity to rekindle joy. Particularly in this moment, when a lot of people are so afraid, it’s easier to reach out to those you already know than try to meet new people.” Dr. King’s research has found it takes as few as two close connections to make people feel supported.
- Stay in the present. Instead of stressing over what’s already happened or worrying about what might still come, just think about today. “We’ve learned a lot about the coronavirus, and we’re still learning more,” says Dr. Wright. “We don’t know what the future looks like, but it won’t be like this forever.”
A version of this article first appeared on WebMD.com.
How to pick the best face masks for children, according to the experts
One essential back-to-school item for children this fall is a face mask – the Centers for Disease Control and Prevention and the American Academy of Pediatrics both recommend them – but finding one that’s actually protective for a child is not a straightforward task, as many parents can attest.
There’s little in the way of official guidance or research to inform evidence-based recommendations on what type of face masks works best for children.
Search for children’s face masks on Amazon and you’ll run into a smorgasbord of options: masks with three, four, or five layers, different designs, and different materials. There’s one company selling a mask it calls an m95 model, a term the company devised.
It’s almost impossible to verify many of the claims being made by the manufacturers, or to know if they will fit your child’s face until you order some, which can get expensive.
But it’s worth looking for a good mask. A large study of more than 1 million people being conducted online by Facebook and Carnegie Mellon University found that students who wore face masks in school had a reduced risk for testing positive for the virus and getting sick with COVID-19 symptoms. The study was published in June in the journal Science.
Delta more contagious
The Delta variant of the new coronavirus is much more contagious than previous versions of the virus. Studies have shown that infected people carry 1,000 times more virus in their noses and throats than with the viruses that circulated last winter and spring. They shed more viral particles into the air when they talk or yell or sing, making this COVID-19–causing virus much more transmissible than in the past.
What that means, says Kimberly Prather, PhD, an aerosol scientist and distinguished professor at the Scripps Institution of Oceanography in La Jolla, California, is that if it once took about 15 minutes of proximity to an infected person to catch the infection, that window of risk is now much shorter.
“If you believe the 15-minute magical number, now if you take 1,000 times the viral load, basically in 1 second you could inhale that same amount of virus. So it’s gone from 15 minutes to 1 second,” Dr. Prather said in an online seminar on school safety she helped to organize.
A better mask
What that means is that we need to upgrade our face masks, switching away from ill-fitting fabric masks, which can offer varying degrees of protection depending on the number of layers and type of fabric that’s used, to more highly protective surgical masks or better yet, N95 respirators, which provide the highest level of filtration.
That’s harder to do for children, who have much smaller faces.
Any masks that gapes around the edges isn’t going to work well, no matter how well it filters.
“N95s are not made to fit kids. They do not come in kid sizes, so I do not recommend N95s for kids,” said Linsey Marr, an environmental engineer at Virginia Tech, who tests face masks in her lab.
Ms. Marr says parents need to consider the attributes masks in this order of priority:
Comfort: “If your kid won’t wear it, it’s not helping at all,” she said.
Fit: “Leaks around the sides are like having a hole in your mask and aerosols carrying the virus can get right through,” Ms. Marr said.
Filtration: How well the mask blocks small particles.
One option to improve fit is to layer a fabric mask over a surgical mask. The fabric mask helps to hold the edges of the surgical mask more tightly to a person’s face. The surgical mask creates better filtration.
Ms. Marr said KN94 or KN95 masks, which are being manufactured in China and Korea, are good choices. They offer nearly the same degree of filtration as an N95, and they fit closely to the face, to minimize leaks.
Check for counterfeits
The KN94 and KN95 masks for children are widely available, but Ms. Marr said parents do need to watch out for counterfeits, which don’t perform as well.
The National Institute for Occupational Safety and Health gives examples of counterfeit products here.
There’s also a type of cloth mask that has a built-in, edge-to-edge filter layer that is made for children.
“Some of these filter out more than 99% of particles and those can be very effective, if they fit well,” Ms. Marr said.
She has compiled and publicly posted a list of her recommendations for masks for children.
There’s also a new standard for face masks. It’s called ASTM F3502-21, and it’s published by an international organization that sets voluntary standards for thousands of products. To claim that a mask meets this standard, a manufacturer has to have its mask tested and demonstrate that it provides a certain level of filtration and breathability.
A version of this article first appeared on Medscape.com.
One essential back-to-school item for children this fall is a face mask – the Centers for Disease Control and Prevention and the American Academy of Pediatrics both recommend them – but finding one that’s actually protective for a child is not a straightforward task, as many parents can attest.
There’s little in the way of official guidance or research to inform evidence-based recommendations on what type of face masks works best for children.
Search for children’s face masks on Amazon and you’ll run into a smorgasbord of options: masks with three, four, or five layers, different designs, and different materials. There’s one company selling a mask it calls an m95 model, a term the company devised.
It’s almost impossible to verify many of the claims being made by the manufacturers, or to know if they will fit your child’s face until you order some, which can get expensive.
But it’s worth looking for a good mask. A large study of more than 1 million people being conducted online by Facebook and Carnegie Mellon University found that students who wore face masks in school had a reduced risk for testing positive for the virus and getting sick with COVID-19 symptoms. The study was published in June in the journal Science.
Delta more contagious
The Delta variant of the new coronavirus is much more contagious than previous versions of the virus. Studies have shown that infected people carry 1,000 times more virus in their noses and throats than with the viruses that circulated last winter and spring. They shed more viral particles into the air when they talk or yell or sing, making this COVID-19–causing virus much more transmissible than in the past.
What that means, says Kimberly Prather, PhD, an aerosol scientist and distinguished professor at the Scripps Institution of Oceanography in La Jolla, California, is that if it once took about 15 minutes of proximity to an infected person to catch the infection, that window of risk is now much shorter.
“If you believe the 15-minute magical number, now if you take 1,000 times the viral load, basically in 1 second you could inhale that same amount of virus. So it’s gone from 15 minutes to 1 second,” Dr. Prather said in an online seminar on school safety she helped to organize.
A better mask
What that means is that we need to upgrade our face masks, switching away from ill-fitting fabric masks, which can offer varying degrees of protection depending on the number of layers and type of fabric that’s used, to more highly protective surgical masks or better yet, N95 respirators, which provide the highest level of filtration.
That’s harder to do for children, who have much smaller faces.
Any masks that gapes around the edges isn’t going to work well, no matter how well it filters.
“N95s are not made to fit kids. They do not come in kid sizes, so I do not recommend N95s for kids,” said Linsey Marr, an environmental engineer at Virginia Tech, who tests face masks in her lab.
Ms. Marr says parents need to consider the attributes masks in this order of priority:
Comfort: “If your kid won’t wear it, it’s not helping at all,” she said.
Fit: “Leaks around the sides are like having a hole in your mask and aerosols carrying the virus can get right through,” Ms. Marr said.
Filtration: How well the mask blocks small particles.
One option to improve fit is to layer a fabric mask over a surgical mask. The fabric mask helps to hold the edges of the surgical mask more tightly to a person’s face. The surgical mask creates better filtration.
Ms. Marr said KN94 or KN95 masks, which are being manufactured in China and Korea, are good choices. They offer nearly the same degree of filtration as an N95, and they fit closely to the face, to minimize leaks.
Check for counterfeits
The KN94 and KN95 masks for children are widely available, but Ms. Marr said parents do need to watch out for counterfeits, which don’t perform as well.
The National Institute for Occupational Safety and Health gives examples of counterfeit products here.
There’s also a type of cloth mask that has a built-in, edge-to-edge filter layer that is made for children.
“Some of these filter out more than 99% of particles and those can be very effective, if they fit well,” Ms. Marr said.
She has compiled and publicly posted a list of her recommendations for masks for children.
There’s also a new standard for face masks. It’s called ASTM F3502-21, and it’s published by an international organization that sets voluntary standards for thousands of products. To claim that a mask meets this standard, a manufacturer has to have its mask tested and demonstrate that it provides a certain level of filtration and breathability.
A version of this article first appeared on Medscape.com.
One essential back-to-school item for children this fall is a face mask – the Centers for Disease Control and Prevention and the American Academy of Pediatrics both recommend them – but finding one that’s actually protective for a child is not a straightforward task, as many parents can attest.
There’s little in the way of official guidance or research to inform evidence-based recommendations on what type of face masks works best for children.
Search for children’s face masks on Amazon and you’ll run into a smorgasbord of options: masks with three, four, or five layers, different designs, and different materials. There’s one company selling a mask it calls an m95 model, a term the company devised.
It’s almost impossible to verify many of the claims being made by the manufacturers, or to know if they will fit your child’s face until you order some, which can get expensive.
But it’s worth looking for a good mask. A large study of more than 1 million people being conducted online by Facebook and Carnegie Mellon University found that students who wore face masks in school had a reduced risk for testing positive for the virus and getting sick with COVID-19 symptoms. The study was published in June in the journal Science.
Delta more contagious
The Delta variant of the new coronavirus is much more contagious than previous versions of the virus. Studies have shown that infected people carry 1,000 times more virus in their noses and throats than with the viruses that circulated last winter and spring. They shed more viral particles into the air when they talk or yell or sing, making this COVID-19–causing virus much more transmissible than in the past.
What that means, says Kimberly Prather, PhD, an aerosol scientist and distinguished professor at the Scripps Institution of Oceanography in La Jolla, California, is that if it once took about 15 minutes of proximity to an infected person to catch the infection, that window of risk is now much shorter.
“If you believe the 15-minute magical number, now if you take 1,000 times the viral load, basically in 1 second you could inhale that same amount of virus. So it’s gone from 15 minutes to 1 second,” Dr. Prather said in an online seminar on school safety she helped to organize.
A better mask
What that means is that we need to upgrade our face masks, switching away from ill-fitting fabric masks, which can offer varying degrees of protection depending on the number of layers and type of fabric that’s used, to more highly protective surgical masks or better yet, N95 respirators, which provide the highest level of filtration.
That’s harder to do for children, who have much smaller faces.
Any masks that gapes around the edges isn’t going to work well, no matter how well it filters.
“N95s are not made to fit kids. They do not come in kid sizes, so I do not recommend N95s for kids,” said Linsey Marr, an environmental engineer at Virginia Tech, who tests face masks in her lab.
Ms. Marr says parents need to consider the attributes masks in this order of priority:
Comfort: “If your kid won’t wear it, it’s not helping at all,” she said.
Fit: “Leaks around the sides are like having a hole in your mask and aerosols carrying the virus can get right through,” Ms. Marr said.
Filtration: How well the mask blocks small particles.
One option to improve fit is to layer a fabric mask over a surgical mask. The fabric mask helps to hold the edges of the surgical mask more tightly to a person’s face. The surgical mask creates better filtration.
Ms. Marr said KN94 or KN95 masks, which are being manufactured in China and Korea, are good choices. They offer nearly the same degree of filtration as an N95, and they fit closely to the face, to minimize leaks.
Check for counterfeits
The KN94 and KN95 masks for children are widely available, but Ms. Marr said parents do need to watch out for counterfeits, which don’t perform as well.
The National Institute for Occupational Safety and Health gives examples of counterfeit products here.
There’s also a type of cloth mask that has a built-in, edge-to-edge filter layer that is made for children.
“Some of these filter out more than 99% of particles and those can be very effective, if they fit well,” Ms. Marr said.
She has compiled and publicly posted a list of her recommendations for masks for children.
There’s also a new standard for face masks. It’s called ASTM F3502-21, and it’s published by an international organization that sets voluntary standards for thousands of products. To claim that a mask meets this standard, a manufacturer has to have its mask tested and demonstrate that it provides a certain level of filtration and breathability.
A version of this article first appeared on Medscape.com.
Tocilizumab shortage continues as pandemic wears on
With worldwide supplies of tocilizumab dwindling as the COVID-19 pandemic rages on, a shortage of the agent will persist “for at least the next several weeks,” according to Genentech, the Roche unit that manufactures tocilizumab under the trade name Actemra IV.
The World Health Organization and Unitaid have called on Genentech to guarantee equitable distribution of the biologic agent globally and to ease up on technology transfer restrictions to make the treatment more accessible.
At this point, supplies of tocilizumab for subcutaneous use to treat rheumatoid arthritis and its other approved indications for inflammatory conditions aren’t as dire, but Genentech is watching them as well, the company says.
In June, the Food and Drug Administration issued an emergency use authorization for intravenous tocilizumab for hospitalized COVID-19 patients. Since then, it has been included in the WHO Therapeutics and COVID-19: living guideline. And on the same day Genentech and Roche reported the tocilizumab shortage, the European Medicines Agency posted a statement that it had started evaluating RoActemra, the European brand name for tocilizumab, for hospitalized COVID-19 patients.
The FDA authorization has caused an unprecedented run on supplies for the biologic agent, which is FDA approved to treat RA, giant cell arteritis, systemic sclerosis–associated interstitial lung disease, polyarticular juvenile idiopathic arthritis, systemic juvenile idiopathic arthritis, and cytokine release syndrome.
Depleted stocks
In the United States, stocks of the 200- and 400-mg units were unavailable, according to an FDA update in mid-August on its website, and the 80-mg/4-mL unit is available by drop ship only. Supplies of 80-mg units were expected to be depleted by the end of the third week in August, Genentech said in a press release.
The company expects to resupply stocks by the end of August. “However,” the Genentech statement added, “if the pandemic continues to spread at its current pace, we anticipate additional periods of stockout in the weeks and months ahead.”
For patients with RA or other approved indications taking the subcutaneous formulation – pens and prefilled syringes – supplies continue to be available, but, the company added, “the supply situation continues to evolve.” The subcutaneous formulations aren’t authorized for use in COVID-19 patients. However, the American Society of Health-System Pharmacists’ website lists the 162-mg/0.9-mL prefilled syringe as one of the products affected by the shortage.
In a separate statement, Roche said that demand for tocilizumab increased 300% in developing countries over prepandemic orders, and that U.S. demand spiked more than 400% in the first 2 weeks of August.
Roche laid out four reasons for the shortage: global manufacturing capacity limits; raw material shortages; the overall complex process of manufacturing biologic agents; and “the dynamically evolving nature of the pandemic.”
The Roche statement noted the company ramped up manufacturing of tocilizumab more than 100% over prepandemic capacity.
With regard to issues WHO and Unitaid raised in their statement, Roche stated that about 60% of its COVID-19 supplies have gone to developing countries, and that Roche and partner Chugai – both of whom hold tocilizumab-related patents – won’t assert any patents over its use for COVID-19 in low- and middle-income countries (LMICs) during the pandemic.
“Roche is in the midst of discussions with WHO and we are committed to support access in LMICs as much as we can,” a Roche spokesperson said in an interview.
Blair Solow, MD, chair of the American College of Rheumatology’s government affairs committee, said the organization supports the equitable distribution of tocilizumab. “We will work to ensure that our patients continue to have access to the medications they need,” she said. “We will continue to engage with the FDA and others to address shortages and ensure patient access to critical therapies.”
The ACR said that any health care professionals having difficulty getting tocilizumab IV or any other COVID-19-related issues can contact the organization at [email protected].
A version of this article first appeared on Medscape.com.
With worldwide supplies of tocilizumab dwindling as the COVID-19 pandemic rages on, a shortage of the agent will persist “for at least the next several weeks,” according to Genentech, the Roche unit that manufactures tocilizumab under the trade name Actemra IV.
The World Health Organization and Unitaid have called on Genentech to guarantee equitable distribution of the biologic agent globally and to ease up on technology transfer restrictions to make the treatment more accessible.
At this point, supplies of tocilizumab for subcutaneous use to treat rheumatoid arthritis and its other approved indications for inflammatory conditions aren’t as dire, but Genentech is watching them as well, the company says.
In June, the Food and Drug Administration issued an emergency use authorization for intravenous tocilizumab for hospitalized COVID-19 patients. Since then, it has been included in the WHO Therapeutics and COVID-19: living guideline. And on the same day Genentech and Roche reported the tocilizumab shortage, the European Medicines Agency posted a statement that it had started evaluating RoActemra, the European brand name for tocilizumab, for hospitalized COVID-19 patients.
The FDA authorization has caused an unprecedented run on supplies for the biologic agent, which is FDA approved to treat RA, giant cell arteritis, systemic sclerosis–associated interstitial lung disease, polyarticular juvenile idiopathic arthritis, systemic juvenile idiopathic arthritis, and cytokine release syndrome.
Depleted stocks
In the United States, stocks of the 200- and 400-mg units were unavailable, according to an FDA update in mid-August on its website, and the 80-mg/4-mL unit is available by drop ship only. Supplies of 80-mg units were expected to be depleted by the end of the third week in August, Genentech said in a press release.
The company expects to resupply stocks by the end of August. “However,” the Genentech statement added, “if the pandemic continues to spread at its current pace, we anticipate additional periods of stockout in the weeks and months ahead.”
For patients with RA or other approved indications taking the subcutaneous formulation – pens and prefilled syringes – supplies continue to be available, but, the company added, “the supply situation continues to evolve.” The subcutaneous formulations aren’t authorized for use in COVID-19 patients. However, the American Society of Health-System Pharmacists’ website lists the 162-mg/0.9-mL prefilled syringe as one of the products affected by the shortage.
In a separate statement, Roche said that demand for tocilizumab increased 300% in developing countries over prepandemic orders, and that U.S. demand spiked more than 400% in the first 2 weeks of August.
Roche laid out four reasons for the shortage: global manufacturing capacity limits; raw material shortages; the overall complex process of manufacturing biologic agents; and “the dynamically evolving nature of the pandemic.”
The Roche statement noted the company ramped up manufacturing of tocilizumab more than 100% over prepandemic capacity.
With regard to issues WHO and Unitaid raised in their statement, Roche stated that about 60% of its COVID-19 supplies have gone to developing countries, and that Roche and partner Chugai – both of whom hold tocilizumab-related patents – won’t assert any patents over its use for COVID-19 in low- and middle-income countries (LMICs) during the pandemic.
“Roche is in the midst of discussions with WHO and we are committed to support access in LMICs as much as we can,” a Roche spokesperson said in an interview.
Blair Solow, MD, chair of the American College of Rheumatology’s government affairs committee, said the organization supports the equitable distribution of tocilizumab. “We will work to ensure that our patients continue to have access to the medications they need,” she said. “We will continue to engage with the FDA and others to address shortages and ensure patient access to critical therapies.”
The ACR said that any health care professionals having difficulty getting tocilizumab IV or any other COVID-19-related issues can contact the organization at [email protected].
A version of this article first appeared on Medscape.com.
With worldwide supplies of tocilizumab dwindling as the COVID-19 pandemic rages on, a shortage of the agent will persist “for at least the next several weeks,” according to Genentech, the Roche unit that manufactures tocilizumab under the trade name Actemra IV.
The World Health Organization and Unitaid have called on Genentech to guarantee equitable distribution of the biologic agent globally and to ease up on technology transfer restrictions to make the treatment more accessible.
At this point, supplies of tocilizumab for subcutaneous use to treat rheumatoid arthritis and its other approved indications for inflammatory conditions aren’t as dire, but Genentech is watching them as well, the company says.
In June, the Food and Drug Administration issued an emergency use authorization for intravenous tocilizumab for hospitalized COVID-19 patients. Since then, it has been included in the WHO Therapeutics and COVID-19: living guideline. And on the same day Genentech and Roche reported the tocilizumab shortage, the European Medicines Agency posted a statement that it had started evaluating RoActemra, the European brand name for tocilizumab, for hospitalized COVID-19 patients.
The FDA authorization has caused an unprecedented run on supplies for the biologic agent, which is FDA approved to treat RA, giant cell arteritis, systemic sclerosis–associated interstitial lung disease, polyarticular juvenile idiopathic arthritis, systemic juvenile idiopathic arthritis, and cytokine release syndrome.
Depleted stocks
In the United States, stocks of the 200- and 400-mg units were unavailable, according to an FDA update in mid-August on its website, and the 80-mg/4-mL unit is available by drop ship only. Supplies of 80-mg units were expected to be depleted by the end of the third week in August, Genentech said in a press release.
The company expects to resupply stocks by the end of August. “However,” the Genentech statement added, “if the pandemic continues to spread at its current pace, we anticipate additional periods of stockout in the weeks and months ahead.”
For patients with RA or other approved indications taking the subcutaneous formulation – pens and prefilled syringes – supplies continue to be available, but, the company added, “the supply situation continues to evolve.” The subcutaneous formulations aren’t authorized for use in COVID-19 patients. However, the American Society of Health-System Pharmacists’ website lists the 162-mg/0.9-mL prefilled syringe as one of the products affected by the shortage.
In a separate statement, Roche said that demand for tocilizumab increased 300% in developing countries over prepandemic orders, and that U.S. demand spiked more than 400% in the first 2 weeks of August.
Roche laid out four reasons for the shortage: global manufacturing capacity limits; raw material shortages; the overall complex process of manufacturing biologic agents; and “the dynamically evolving nature of the pandemic.”
The Roche statement noted the company ramped up manufacturing of tocilizumab more than 100% over prepandemic capacity.
With regard to issues WHO and Unitaid raised in their statement, Roche stated that about 60% of its COVID-19 supplies have gone to developing countries, and that Roche and partner Chugai – both of whom hold tocilizumab-related patents – won’t assert any patents over its use for COVID-19 in low- and middle-income countries (LMICs) during the pandemic.
“Roche is in the midst of discussions with WHO and we are committed to support access in LMICs as much as we can,” a Roche spokesperson said in an interview.
Blair Solow, MD, chair of the American College of Rheumatology’s government affairs committee, said the organization supports the equitable distribution of tocilizumab. “We will work to ensure that our patients continue to have access to the medications they need,” she said. “We will continue to engage with the FDA and others to address shortages and ensure patient access to critical therapies.”
The ACR said that any health care professionals having difficulty getting tocilizumab IV or any other COVID-19-related issues can contact the organization at [email protected].
A version of this article first appeared on Medscape.com.
Vax campaign averted nearly 140,000 U.S. deaths through early May: Study
New York had 11.7 fewer COVID-19 deaths per 10,000 adults, and Hawaii had 1.1 fewer deaths per 10,000 than would have occurred without vaccinations, the study shows. The rest of the states fell somewhere in between, with the average state experiencing five fewer COVID-19 deaths per 10,000 adults.
At a national level, this means that instead of the 550,000 COVID-19 deaths that occurred by early May, there would have been 709,000 deaths in the absence of a vaccination campaign, according to the study.
Researchers from RAND and Indiana University created models to estimate the number of COVID-19 deaths that would have happened without vaccinations. The difference between the actual number of deaths and those estimates provides a measure of the number of COVID-19 deaths averted by the vaccination campaign.
Information about vaccine doses administered in each state came from the Bloomberg COVID-19 Vaccine Tracker, and data on COVID-19 deaths for each state came from The New York Times’ Coronavirus (COVID-19) Data in the United States database.
The study spanned the period from Dec. 21, 2020 to May 9, 2021. The U.S. Food and Drug Administration issued its first emergency use authorization (EUA) for a COVID-19 vaccine to Pfizer/BioNTech on December 11, followed by an EUA for the Moderna vaccine on December 18 and one for Johnson & Johnson’s vaccine on Feb. 27, 2021.
Varied by state
There were wide variations in the speed and extent of the vaccination campaigns in various states, the researchers found. For example, West Virginia was the first state to reach 10 doses per 100 adults, reaching that goal on Jan. 16, 2021, and Idaho was the last state to hit that mark, on Feb. 4, 2021. Alaska was the first to reach 20 doses per 100 adults, on January 29, and Alabama was the last to do it, on February 21.
On May 6, California was the first state to administer 120 doses per 100 adults, but many states have still not reached that milestone.
The median number of days between the milestones of 10 and 20 doses per 100 adults was 19 days, and the median number of days between 20 and 40 doses per 100 adults was 24 days.
Hard to establish causality
The researchers emphasized that “establishment of causality is challenging” in comparing individual states’ vaccination levels with their COVID-19 mortality rates.
Aside from the study being observational, they pointed out, the analysis “relied on variation in the administration of COVID-19 vaccines across states … Vaccine administration patterns may be associated with declining mortality because of vaccine prevention of deaths and severe complications as state-level vaccine campaigns allocated initial doses to the highest-risk populations with the aim of immediately reducing COVID-19 deaths.”
Nevertheless, the authors note, “clinical trial evidence has shown that COVID-19 vaccines have high efficacy. Our study provides support for policies that further expand vaccine administration, which will enable larger populations to benefit.”
Study confirms vaccine benefit
Aaron Glatt, MD, chair of medicine at Mount Sinai South Nassau in Oceanside, New York, and a spokesman for the Infectious Disease Society of America, said in an interview that the study is important because it confirms the benefit of COVID-19 vaccination.
Regardless of whether the study’s results are statistically valid, he said, “I don’t think anyone can argue the benefit isn’t there. It’s a question of how important the benefit is.”
Dr. Glatt is not surprised that there are variations across states in the number of COVID-19 deaths averted through vaccination. “Clearly, in states where there was a lot of disease, a significant amount of vaccination is going to impact that tremendously.”
The authors note that their paper has some limitations. For one thing, they couldn’t determine what share of the estimated reduction in COVID-19 deaths was a result of the proportion of the population that was vaccinated or had antibodies and what share was a result of lower population-level risk for COVID-19 transmission.
Vaccination versus natural immunity
In addition, the researchers weren’t able to identify the roles of vaccination, natural immunity, and changes in mobility in the numbers of COVID-19 deaths.
Dr. Glatt says that’s understandable, since this was a retrospective study, and the researchers didn’t know how many people had been infected with COVID-19 at some point. Moreover, he adds, scientists don’t know how strong natural immunity from prior infection is, how long it endures, or how robust it is against new variants.
“It’s clear to me that there’s a benefit in preventing the second episode of COVID in people who had a first episode of COVID,” he said. “What we don’t know is how much that benefit is and how long it will last.”
The researchers also didn’t know how many people had gotten both doses of the Pfizer or the Moderna vaccine and how many of them had received only one. This is an important piece of information, Dr. Glatt said, but the lack of it doesn’t impair the study’s overall finding.
“Every vaccine potentially prevents death,” he stressed. “The more we vaccinate, the more deaths we’ll prevent. We’re starting to see increased vaccinations again. There were a million of them yesterday. So people are recognizing that COVID hasn’t gone away, and we need to vaccinate more people. The benefit from the vaccination hasn’t decreased. The more we vaccinate, the more the benefit will be.”
A version of this article first appeared on Medscape.com.
New York had 11.7 fewer COVID-19 deaths per 10,000 adults, and Hawaii had 1.1 fewer deaths per 10,000 than would have occurred without vaccinations, the study shows. The rest of the states fell somewhere in between, with the average state experiencing five fewer COVID-19 deaths per 10,000 adults.
At a national level, this means that instead of the 550,000 COVID-19 deaths that occurred by early May, there would have been 709,000 deaths in the absence of a vaccination campaign, according to the study.
Researchers from RAND and Indiana University created models to estimate the number of COVID-19 deaths that would have happened without vaccinations. The difference between the actual number of deaths and those estimates provides a measure of the number of COVID-19 deaths averted by the vaccination campaign.
Information about vaccine doses administered in each state came from the Bloomberg COVID-19 Vaccine Tracker, and data on COVID-19 deaths for each state came from The New York Times’ Coronavirus (COVID-19) Data in the United States database.
The study spanned the period from Dec. 21, 2020 to May 9, 2021. The U.S. Food and Drug Administration issued its first emergency use authorization (EUA) for a COVID-19 vaccine to Pfizer/BioNTech on December 11, followed by an EUA for the Moderna vaccine on December 18 and one for Johnson & Johnson’s vaccine on Feb. 27, 2021.
Varied by state
There were wide variations in the speed and extent of the vaccination campaigns in various states, the researchers found. For example, West Virginia was the first state to reach 10 doses per 100 adults, reaching that goal on Jan. 16, 2021, and Idaho was the last state to hit that mark, on Feb. 4, 2021. Alaska was the first to reach 20 doses per 100 adults, on January 29, and Alabama was the last to do it, on February 21.
On May 6, California was the first state to administer 120 doses per 100 adults, but many states have still not reached that milestone.
The median number of days between the milestones of 10 and 20 doses per 100 adults was 19 days, and the median number of days between 20 and 40 doses per 100 adults was 24 days.
Hard to establish causality
The researchers emphasized that “establishment of causality is challenging” in comparing individual states’ vaccination levels with their COVID-19 mortality rates.
Aside from the study being observational, they pointed out, the analysis “relied on variation in the administration of COVID-19 vaccines across states … Vaccine administration patterns may be associated with declining mortality because of vaccine prevention of deaths and severe complications as state-level vaccine campaigns allocated initial doses to the highest-risk populations with the aim of immediately reducing COVID-19 deaths.”
Nevertheless, the authors note, “clinical trial evidence has shown that COVID-19 vaccines have high efficacy. Our study provides support for policies that further expand vaccine administration, which will enable larger populations to benefit.”
Study confirms vaccine benefit
Aaron Glatt, MD, chair of medicine at Mount Sinai South Nassau in Oceanside, New York, and a spokesman for the Infectious Disease Society of America, said in an interview that the study is important because it confirms the benefit of COVID-19 vaccination.
Regardless of whether the study’s results are statistically valid, he said, “I don’t think anyone can argue the benefit isn’t there. It’s a question of how important the benefit is.”
Dr. Glatt is not surprised that there are variations across states in the number of COVID-19 deaths averted through vaccination. “Clearly, in states where there was a lot of disease, a significant amount of vaccination is going to impact that tremendously.”
The authors note that their paper has some limitations. For one thing, they couldn’t determine what share of the estimated reduction in COVID-19 deaths was a result of the proportion of the population that was vaccinated or had antibodies and what share was a result of lower population-level risk for COVID-19 transmission.
Vaccination versus natural immunity
In addition, the researchers weren’t able to identify the roles of vaccination, natural immunity, and changes in mobility in the numbers of COVID-19 deaths.
Dr. Glatt says that’s understandable, since this was a retrospective study, and the researchers didn’t know how many people had been infected with COVID-19 at some point. Moreover, he adds, scientists don’t know how strong natural immunity from prior infection is, how long it endures, or how robust it is against new variants.
“It’s clear to me that there’s a benefit in preventing the second episode of COVID in people who had a first episode of COVID,” he said. “What we don’t know is how much that benefit is and how long it will last.”
The researchers also didn’t know how many people had gotten both doses of the Pfizer or the Moderna vaccine and how many of them had received only one. This is an important piece of information, Dr. Glatt said, but the lack of it doesn’t impair the study’s overall finding.
“Every vaccine potentially prevents death,” he stressed. “The more we vaccinate, the more deaths we’ll prevent. We’re starting to see increased vaccinations again. There were a million of them yesterday. So people are recognizing that COVID hasn’t gone away, and we need to vaccinate more people. The benefit from the vaccination hasn’t decreased. The more we vaccinate, the more the benefit will be.”
A version of this article first appeared on Medscape.com.
New York had 11.7 fewer COVID-19 deaths per 10,000 adults, and Hawaii had 1.1 fewer deaths per 10,000 than would have occurred without vaccinations, the study shows. The rest of the states fell somewhere in between, with the average state experiencing five fewer COVID-19 deaths per 10,000 adults.
At a national level, this means that instead of the 550,000 COVID-19 deaths that occurred by early May, there would have been 709,000 deaths in the absence of a vaccination campaign, according to the study.
Researchers from RAND and Indiana University created models to estimate the number of COVID-19 deaths that would have happened without vaccinations. The difference between the actual number of deaths and those estimates provides a measure of the number of COVID-19 deaths averted by the vaccination campaign.
Information about vaccine doses administered in each state came from the Bloomberg COVID-19 Vaccine Tracker, and data on COVID-19 deaths for each state came from The New York Times’ Coronavirus (COVID-19) Data in the United States database.
The study spanned the period from Dec. 21, 2020 to May 9, 2021. The U.S. Food and Drug Administration issued its first emergency use authorization (EUA) for a COVID-19 vaccine to Pfizer/BioNTech on December 11, followed by an EUA for the Moderna vaccine on December 18 and one for Johnson & Johnson’s vaccine on Feb. 27, 2021.
Varied by state
There were wide variations in the speed and extent of the vaccination campaigns in various states, the researchers found. For example, West Virginia was the first state to reach 10 doses per 100 adults, reaching that goal on Jan. 16, 2021, and Idaho was the last state to hit that mark, on Feb. 4, 2021. Alaska was the first to reach 20 doses per 100 adults, on January 29, and Alabama was the last to do it, on February 21.
On May 6, California was the first state to administer 120 doses per 100 adults, but many states have still not reached that milestone.
The median number of days between the milestones of 10 and 20 doses per 100 adults was 19 days, and the median number of days between 20 and 40 doses per 100 adults was 24 days.
Hard to establish causality
The researchers emphasized that “establishment of causality is challenging” in comparing individual states’ vaccination levels with their COVID-19 mortality rates.
Aside from the study being observational, they pointed out, the analysis “relied on variation in the administration of COVID-19 vaccines across states … Vaccine administration patterns may be associated with declining mortality because of vaccine prevention of deaths and severe complications as state-level vaccine campaigns allocated initial doses to the highest-risk populations with the aim of immediately reducing COVID-19 deaths.”
Nevertheless, the authors note, “clinical trial evidence has shown that COVID-19 vaccines have high efficacy. Our study provides support for policies that further expand vaccine administration, which will enable larger populations to benefit.”
Study confirms vaccine benefit
Aaron Glatt, MD, chair of medicine at Mount Sinai South Nassau in Oceanside, New York, and a spokesman for the Infectious Disease Society of America, said in an interview that the study is important because it confirms the benefit of COVID-19 vaccination.
Regardless of whether the study’s results are statistically valid, he said, “I don’t think anyone can argue the benefit isn’t there. It’s a question of how important the benefit is.”
Dr. Glatt is not surprised that there are variations across states in the number of COVID-19 deaths averted through vaccination. “Clearly, in states where there was a lot of disease, a significant amount of vaccination is going to impact that tremendously.”
The authors note that their paper has some limitations. For one thing, they couldn’t determine what share of the estimated reduction in COVID-19 deaths was a result of the proportion of the population that was vaccinated or had antibodies and what share was a result of lower population-level risk for COVID-19 transmission.
Vaccination versus natural immunity
In addition, the researchers weren’t able to identify the roles of vaccination, natural immunity, and changes in mobility in the numbers of COVID-19 deaths.
Dr. Glatt says that’s understandable, since this was a retrospective study, and the researchers didn’t know how many people had been infected with COVID-19 at some point. Moreover, he adds, scientists don’t know how strong natural immunity from prior infection is, how long it endures, or how robust it is against new variants.
“It’s clear to me that there’s a benefit in preventing the second episode of COVID in people who had a first episode of COVID,” he said. “What we don’t know is how much that benefit is and how long it will last.”
The researchers also didn’t know how many people had gotten both doses of the Pfizer or the Moderna vaccine and how many of them had received only one. This is an important piece of information, Dr. Glatt said, but the lack of it doesn’t impair the study’s overall finding.
“Every vaccine potentially prevents death,” he stressed. “The more we vaccinate, the more deaths we’ll prevent. We’re starting to see increased vaccinations again. There were a million of them yesterday. So people are recognizing that COVID hasn’t gone away, and we need to vaccinate more people. The benefit from the vaccination hasn’t decreased. The more we vaccinate, the more the benefit will be.”
A version of this article first appeared on Medscape.com.
Medicinal liquor and edited mosquitoes
Drink to your health?
Whether you drink or not, most of us can agree that liquor is not the first thing that comes to mind when looking to make health improvements. But researchers have found a small exception in something traditional.

We’ve added buckwheat to pancakes, bread, and other baked goodies we made during the height of quarantine, but it’s also used to create a traditional liquor in some East Asian countries, where it is used medicinally.
Investigators have found that extracts in the Tartary buckwheat used to make the liquor induce autophagy, a process cells go through to remove proteins that are damaged or not needed anymore – sort of like a cellular spring cleaning.
To test this, the researchers treated liver and skin cells with Tartary buckwheat extract and looked to see how the cells responded with fluorescent markers. The results were clear.
“Treating cells with the extract stimulated the formation of autophagosomes, specialized cellular structures that carry out autophagy, and altered the location of proteins involved in regulating autophagy,” said senior author Takeshi Noda of Osaka (Japan) University.
Looking deeper, the researchers found that quercetin, a component of the buckwheat extract, had the same autophagic effect. And both the buckwheat and the quercetin gave the green light for liver cells to induce aggrephagy, the process of cleaning up protein aggregates.
Those protein aggregates in liver cells are closely linked to alcoholic liver disease, suggesting that quercetin could be a game changer in its treatment. In other words, liquor could help fix the problem that liquor started. Go figure.
From hospital bills to X-rated
Ralph Puglisi was an accounting manager for the University Medical Service Association (UMSA), a nonprofit that supports the massive University of South Florida health system. The association took in over $300 million in revenue in the 2019-2020 fiscal year, which is a rather large sum of money, but we’ll glide over the ethics of a “nonprofit” making a few hundred million for now.

Mr. Puglisi was in very close proximity to the money, generated from patient care, and he pled guilty to stealing it using UMSA credit cards. Now, that wouldn’t be LOTME worthy on its own, but what elevates this above garden-variety embezzlement is how the intrepid Mr. Puglisi chose to spend the millions he stole from the university health system: Adult entertainment.
And before you ask, he didn’t spend $11.5 million on something most people so inclined can find for free with judicious Google searches. What Mr. Puglisi actually did was invest in a website providing adult content through individual user profiles, one of which is believed to belong to his stepson’s fiancée, which brings a whole new level of sleaze to this enterprise. Over the course of 2 years, he visited her profile 2,800 times, an amount some might view as excessive.
While the vast majority of the embezzled money went to the adult website, Mr. Puglisi also used thousands of UMSA dollars to pay for travel, household improvements, rent, the works. Almost $44,000 was spent at a resort sometimes known as the happiest place on earth.
Then there’s Mr. Puglisi’s wife. Oh yes, this guy is married. He poured over $600,000 into a company he and his wife owned, which is a lot, but how much do you think went to the woman he married? Probably quite a bit. Go ahead, try to think of a number. It’s not like it was his money.
Did you guess $100 went into his wife’s PayPal account? No? Clearly you don’t understand the criminal mind. His stepson’s fiancée got millions, and his wife got a hundred. Now there are some priorities.
Step 1: Sit at desk. Step 2: Get in shape
Being a physician is not really a desk job, but doctors must spend a fair share of their time sitting, yes? Dealing with recalcitrant EHRs or talking on the phone to insurers or PBMs? If you are one of these physicians, or if you have patients who spend a lot of time sitting at their desks and might need to get a bit of exercise, then we’ve got a multitasking tip for you.

It came to us via one of our favorite websites, Sad and Useless. It’s the site that declares itself “the most depressive humor site on the Internet” and they’re offering up the “12 Best Exercises To Do At Your Desk.” It may not sound like much, but we think that the gang at Dunder-Mifflin would approve. And besides, who couldn’t stand to burn a few calories without having to leave the chair?
We won’t spoil your fun by going through all 12 – each one comes with step-by-step instructions and a helpful illustration or GIF – but here are just a few:
- Bending over backwards: “Agree to do something you don’t want to do. Spend twice as long as expected doing that thing. Hate yourself.”
- Fake laughter: “Hear a joke that isn’t even remotely funny. Open your mouth and make laughing sounds.”
- Bang your head: Feel the “pointlessness of your job overwhelm you” and then “bring your head forcefully down to your desk.”
Now, we here at LOTME are, of course [Bang!], highly skilled, professional wordsmithing humorists [Bang!], so when we tell you that this is a great workout [Bang!] … that this is a great workout [Bang!] … it’s great … uggh.
Wooooo. Feel the burn.
One order of mosquitoes, extra Crispr
What would it be like to have a barbecue in your backyard on a humid summer night and not get eaten alive by mosquitoes? If you’re like us, you probably thought you’d never see that day.

Mosquitoes cause itchy bites, but, more importantly, they can carry dengue, malaria, yellow fever, and Zika virus. New research shows that protection from these diseases may be possible with use of the Crispr-Cas9 gene-editing tool, which could make humans invisible to mosquitoes by taking away their light-sensing abilities and, thus, their ability to find us.
“The better we understand how they sense the human, the better we can control the mosquito in an eco-friendly manner,” Yinpeng Zhan, a postdoctoral researcher at the University of California, Santa Barbara, and the study’s lead author, told the New York Times.
After studying the mosquitoes and figuring out their hunting patterns, the researchers found that mosquitoes are attracted to dark spots more than white spots and used this to their advantage. After knocking out two of the proteins that mosquitoes need for vision – via Crispr – the little suckers could not distinguish the difference between the white and dark spots.
We’re sure mosquitoes don’t mean any harm – they’re just trying to survive and reproduce like any other species – but thanks to this new tool, gone might be the days of having to douse yourself in bug spray that smells like a mix of chemicals and melon.
Drink to your health?
Whether you drink or not, most of us can agree that liquor is not the first thing that comes to mind when looking to make health improvements. But researchers have found a small exception in something traditional.
We’ve added buckwheat to pancakes, bread, and other baked goodies we made during the height of quarantine, but it’s also used to create a traditional liquor in some East Asian countries, where it is used medicinally.
Investigators have found that extracts in the Tartary buckwheat used to make the liquor induce autophagy, a process cells go through to remove proteins that are damaged or not needed anymore – sort of like a cellular spring cleaning.
To test this, the researchers treated liver and skin cells with Tartary buckwheat extract and looked to see how the cells responded with fluorescent markers. The results were clear.
“Treating cells with the extract stimulated the formation of autophagosomes, specialized cellular structures that carry out autophagy, and altered the location of proteins involved in regulating autophagy,” said senior author Takeshi Noda of Osaka (Japan) University.
Looking deeper, the researchers found that quercetin, a component of the buckwheat extract, had the same autophagic effect. And both the buckwheat and the quercetin gave the green light for liver cells to induce aggrephagy, the process of cleaning up protein aggregates.
Those protein aggregates in liver cells are closely linked to alcoholic liver disease, suggesting that quercetin could be a game changer in its treatment. In other words, liquor could help fix the problem that liquor started. Go figure.
From hospital bills to X-rated
Ralph Puglisi was an accounting manager for the University Medical Service Association (UMSA), a nonprofit that supports the massive University of South Florida health system. The association took in over $300 million in revenue in the 2019-2020 fiscal year, which is a rather large sum of money, but we’ll glide over the ethics of a “nonprofit” making a few hundred million for now.
Mr. Puglisi was in very close proximity to the money, generated from patient care, and he pled guilty to stealing it using UMSA credit cards. Now, that wouldn’t be LOTME worthy on its own, but what elevates this above garden-variety embezzlement is how the intrepid Mr. Puglisi chose to spend the millions he stole from the university health system: Adult entertainment.
And before you ask, he didn’t spend $11.5 million on something most people so inclined can find for free with judicious Google searches. What Mr. Puglisi actually did was invest in a website providing adult content through individual user profiles, one of which is believed to belong to his stepson’s fiancée, which brings a whole new level of sleaze to this enterprise. Over the course of 2 years, he visited her profile 2,800 times, an amount some might view as excessive.
While the vast majority of the embezzled money went to the adult website, Mr. Puglisi also used thousands of UMSA dollars to pay for travel, household improvements, rent, the works. Almost $44,000 was spent at a resort sometimes known as the happiest place on earth.
Then there’s Mr. Puglisi’s wife. Oh yes, this guy is married. He poured over $600,000 into a company he and his wife owned, which is a lot, but how much do you think went to the woman he married? Probably quite a bit. Go ahead, try to think of a number. It’s not like it was his money.
Did you guess $100 went into his wife’s PayPal account? No? Clearly you don’t understand the criminal mind. His stepson’s fiancée got millions, and his wife got a hundred. Now there are some priorities.
Step 1: Sit at desk. Step 2: Get in shape
Being a physician is not really a desk job, but doctors must spend a fair share of their time sitting, yes? Dealing with recalcitrant EHRs or talking on the phone to insurers or PBMs? If you are one of these physicians, or if you have patients who spend a lot of time sitting at their desks and might need to get a bit of exercise, then we’ve got a multitasking tip for you.
It came to us via one of our favorite websites, Sad and Useless. It’s the site that declares itself “the most depressive humor site on the Internet” and they’re offering up the “12 Best Exercises To Do At Your Desk.” It may not sound like much, but we think that the gang at Dunder-Mifflin would approve. And besides, who couldn’t stand to burn a few calories without having to leave the chair?
We won’t spoil your fun by going through all 12 – each one comes with step-by-step instructions and a helpful illustration or GIF – but here are just a few:
- Bending over backwards: “Agree to do something you don’t want to do. Spend twice as long as expected doing that thing. Hate yourself.”
- Fake laughter: “Hear a joke that isn’t even remotely funny. Open your mouth and make laughing sounds.”
- Bang your head: Feel the “pointlessness of your job overwhelm you” and then “bring your head forcefully down to your desk.”
Now, we here at LOTME are, of course [Bang!], highly skilled, professional wordsmithing humorists [Bang!], so when we tell you that this is a great workout [Bang!] … that this is a great workout [Bang!] … it’s great … uggh.
Wooooo. Feel the burn.
One order of mosquitoes, extra Crispr
What would it be like to have a barbecue in your backyard on a humid summer night and not get eaten alive by mosquitoes? If you’re like us, you probably thought you’d never see that day.
Mosquitoes cause itchy bites, but, more importantly, they can carry dengue, malaria, yellow fever, and Zika virus. New research shows that protection from these diseases may be possible with use of the Crispr-Cas9 gene-editing tool, which could make humans invisible to mosquitoes by taking away their light-sensing abilities and, thus, their ability to find us.
“The better we understand how they sense the human, the better we can control the mosquito in an eco-friendly manner,” Yinpeng Zhan, a postdoctoral researcher at the University of California, Santa Barbara, and the study’s lead author, told the New York Times.
After studying the mosquitoes and figuring out their hunting patterns, the researchers found that mosquitoes are attracted to dark spots more than white spots and used this to their advantage. After knocking out two of the proteins that mosquitoes need for vision – via Crispr – the little suckers could not distinguish the difference between the white and dark spots.
We’re sure mosquitoes don’t mean any harm – they’re just trying to survive and reproduce like any other species – but thanks to this new tool, gone might be the days of having to douse yourself in bug spray that smells like a mix of chemicals and melon.
Drink to your health?
Whether you drink or not, most of us can agree that liquor is not the first thing that comes to mind when looking to make health improvements. But researchers have found a small exception in something traditional.
We’ve added buckwheat to pancakes, bread, and other baked goodies we made during the height of quarantine, but it’s also used to create a traditional liquor in some East Asian countries, where it is used medicinally.
Investigators have found that extracts in the Tartary buckwheat used to make the liquor induce autophagy, a process cells go through to remove proteins that are damaged or not needed anymore – sort of like a cellular spring cleaning.
To test this, the researchers treated liver and skin cells with Tartary buckwheat extract and looked to see how the cells responded with fluorescent markers. The results were clear.
“Treating cells with the extract stimulated the formation of autophagosomes, specialized cellular structures that carry out autophagy, and altered the location of proteins involved in regulating autophagy,” said senior author Takeshi Noda of Osaka (Japan) University.
Looking deeper, the researchers found that quercetin, a component of the buckwheat extract, had the same autophagic effect. And both the buckwheat and the quercetin gave the green light for liver cells to induce aggrephagy, the process of cleaning up protein aggregates.
Those protein aggregates in liver cells are closely linked to alcoholic liver disease, suggesting that quercetin could be a game changer in its treatment. In other words, liquor could help fix the problem that liquor started. Go figure.
From hospital bills to X-rated
Ralph Puglisi was an accounting manager for the University Medical Service Association (UMSA), a nonprofit that supports the massive University of South Florida health system. The association took in over $300 million in revenue in the 2019-2020 fiscal year, which is a rather large sum of money, but we’ll glide over the ethics of a “nonprofit” making a few hundred million for now.
Mr. Puglisi was in very close proximity to the money, generated from patient care, and he pled guilty to stealing it using UMSA credit cards. Now, that wouldn’t be LOTME worthy on its own, but what elevates this above garden-variety embezzlement is how the intrepid Mr. Puglisi chose to spend the millions he stole from the university health system: Adult entertainment.
And before you ask, he didn’t spend $11.5 million on something most people so inclined can find for free with judicious Google searches. What Mr. Puglisi actually did was invest in a website providing adult content through individual user profiles, one of which is believed to belong to his stepson’s fiancée, which brings a whole new level of sleaze to this enterprise. Over the course of 2 years, he visited her profile 2,800 times, an amount some might view as excessive.
While the vast majority of the embezzled money went to the adult website, Mr. Puglisi also used thousands of UMSA dollars to pay for travel, household improvements, rent, the works. Almost $44,000 was spent at a resort sometimes known as the happiest place on earth.
Then there’s Mr. Puglisi’s wife. Oh yes, this guy is married. He poured over $600,000 into a company he and his wife owned, which is a lot, but how much do you think went to the woman he married? Probably quite a bit. Go ahead, try to think of a number. It’s not like it was his money.
Did you guess $100 went into his wife’s PayPal account? No? Clearly you don’t understand the criminal mind. His stepson’s fiancée got millions, and his wife got a hundred. Now there are some priorities.
Step 1: Sit at desk. Step 2: Get in shape
Being a physician is not really a desk job, but doctors must spend a fair share of their time sitting, yes? Dealing with recalcitrant EHRs or talking on the phone to insurers or PBMs? If you are one of these physicians, or if you have patients who spend a lot of time sitting at their desks and might need to get a bit of exercise, then we’ve got a multitasking tip for you.
It came to us via one of our favorite websites, Sad and Useless. It’s the site that declares itself “the most depressive humor site on the Internet” and they’re offering up the “12 Best Exercises To Do At Your Desk.” It may not sound like much, but we think that the gang at Dunder-Mifflin would approve. And besides, who couldn’t stand to burn a few calories without having to leave the chair?
We won’t spoil your fun by going through all 12 – each one comes with step-by-step instructions and a helpful illustration or GIF – but here are just a few:
- Bending over backwards: “Agree to do something you don’t want to do. Spend twice as long as expected doing that thing. Hate yourself.”
- Fake laughter: “Hear a joke that isn’t even remotely funny. Open your mouth and make laughing sounds.”
- Bang your head: Feel the “pointlessness of your job overwhelm you” and then “bring your head forcefully down to your desk.”
Now, we here at LOTME are, of course [Bang!], highly skilled, professional wordsmithing humorists [Bang!], so when we tell you that this is a great workout [Bang!] … that this is a great workout [Bang!] … it’s great … uggh.
Wooooo. Feel the burn.
One order of mosquitoes, extra Crispr
What would it be like to have a barbecue in your backyard on a humid summer night and not get eaten alive by mosquitoes? If you’re like us, you probably thought you’d never see that day.
Mosquitoes cause itchy bites, but, more importantly, they can carry dengue, malaria, yellow fever, and Zika virus. New research shows that protection from these diseases may be possible with use of the Crispr-Cas9 gene-editing tool, which could make humans invisible to mosquitoes by taking away their light-sensing abilities and, thus, their ability to find us.
“The better we understand how they sense the human, the better we can control the mosquito in an eco-friendly manner,” Yinpeng Zhan, a postdoctoral researcher at the University of California, Santa Barbara, and the study’s lead author, told the New York Times.
After studying the mosquitoes and figuring out their hunting patterns, the researchers found that mosquitoes are attracted to dark spots more than white spots and used this to their advantage. After knocking out two of the proteins that mosquitoes need for vision – via Crispr – the little suckers could not distinguish the difference between the white and dark spots.
We’re sure mosquitoes don’t mean any harm – they’re just trying to survive and reproduce like any other species – but thanks to this new tool, gone might be the days of having to douse yourself in bug spray that smells like a mix of chemicals and melon.
COVID-19 booster shots to start in September: Officials
at a press briefing August 18.
Those who received the Pfizer-BioNTech and Moderna vaccines would be eligible to get a booster shot 8 months after they received the second dose of those vaccines, officials said. Information on boosters for those who got the one-dose Johnson & Johnson vaccine will be forthcoming.
“We anticipate a booster will [also] likely be needed,” said U.S. Surgeon General Vivek Murthy, MD. The J&J vaccine was not available in the U.S. until March, he said, and ‘’we expect more data on J&J in the coming weeks, so that plan is coming.”
The plan for boosters for the two mRNA vaccines is pending the FDA’s conducting of an independent review and authorizing the third dose of the Moderna and Pfizer-BioNTech vaccines, as well as an advisory committee of the CDC making the recommendation.
“We know that even highly effective vaccines become less effective over time,” Dr. Murthy said. “Having reviewed the most current data, it is now our clinical judgment that the time to lay out a plan for the COVID-19 boosters is now.”
Research released Aug. 18 shows waning effectiveness of the two mRNA vaccines.
At the briefing, Dr. Murthy and others continually reassured listeners that while effectiveness against infection declines, the vaccines continue to protect against severe infections, hospitalizations, and death.
“If you are fully vaccinated, you still have a high degree of protection against the worst outcomes,” Dr. Murthy said.
Data driving the plan
CDC Director Rochelle Walensky, MD, cited three research studies published Aug. 18 in the CDC’s Morbidity and Mortality Weekly Report that helped to drive the decision to recommend boosters.
Analysis of nursing home COVID-19 data from the CDC’s National Healthcare Safety Network showed a significant decline in the effectiveness of the full mRNA vaccine against lab-confirmed COVID-19 infection, from 74.7% before the Delta variant (March 1-May 9, 2021) to 53% when the Delta variant became predominant in the United States. The analysis during the Delta dominant period included 85,000 weekly reports from nearly 15,000 facilities.
Another study looked at more than 10 million New York adults who had been fully vaccinated with either the Moderna, Pfizer, or J&J vaccine by July 25. During the period from May 3 to July 25, overall, the age-adjusted vaccine effectiveness against infection decreased from 91.7% to 79.8%.
Vaccine effectiveness against hospitalization remains high, another study found. An analysis of 1,129 patients who had gotten two doses of an mRNA vaccine showed vaccine effectiveness against hospitalization after 24 weeks. It was 86% at weeks 2-12 and 84% at weeks 13-24.
Immunologic facts
Immunologic information also points to the need for a booster, said Anthony Fauci, MD, the chief medical advisor to the president and director of the National Institute of Allergy and Infectious Diseases.
“Antibody levels decline over time,” he said, “and higher antibody levels are associated with higher efficacy of the vaccine. Higher levels of antibody may be needed to protect against Delta.”
A booster increased antibody levels by ‘’at least tenfold and possibly more,” he said. And higher levels of antibody may be required to protect against Delta. Taken together, he said, the data support the use of a booster to increase the overall level of protection.
Booster details
“We will make sure it is convenient and easy to get the booster shot,” said Jeff Zients, the White House COVID-19 response coordinator. As with the previous immunization, he said, the booster will be free, and no one will be asked about immigration status.
The plan for booster shots is an attempt to stay ahead of the virus, officials stressed
Big picture
Not everyone agrees with the booster dose idea. At a World Health Organization briefing Aug. 18, WHO’s Chief Scientist Soumya Swaminathan, MD, an Indian pediatrician, said that the right thing to do right now ‘’is to wait for the science to tell us when boosters, which groups of people, and which vaccines need boosters.”
Like others, she also broached the ‘’moral and ethical argument of giving people third doses, when they’re already well protected and while the rest of the world is waiting for their primary immunization.”
Dr. Swaminathan does see a role for boosters to protect immunocompromised people but noted that ‘’that’s a small number of people.” Widespread boosters ‘’will only lead to more variants, to more escape variants, and perhaps we’re heading into more dire situations.”
A version of this article first appeared on WebMD.com.
at a press briefing August 18.
Those who received the Pfizer-BioNTech and Moderna vaccines would be eligible to get a booster shot 8 months after they received the second dose of those vaccines, officials said. Information on boosters for those who got the one-dose Johnson & Johnson vaccine will be forthcoming.
“We anticipate a booster will [also] likely be needed,” said U.S. Surgeon General Vivek Murthy, MD. The J&J vaccine was not available in the U.S. until March, he said, and ‘’we expect more data on J&J in the coming weeks, so that plan is coming.”
The plan for boosters for the two mRNA vaccines is pending the FDA’s conducting of an independent review and authorizing the third dose of the Moderna and Pfizer-BioNTech vaccines, as well as an advisory committee of the CDC making the recommendation.
“We know that even highly effective vaccines become less effective over time,” Dr. Murthy said. “Having reviewed the most current data, it is now our clinical judgment that the time to lay out a plan for the COVID-19 boosters is now.”
Research released Aug. 18 shows waning effectiveness of the two mRNA vaccines.
At the briefing, Dr. Murthy and others continually reassured listeners that while effectiveness against infection declines, the vaccines continue to protect against severe infections, hospitalizations, and death.
“If you are fully vaccinated, you still have a high degree of protection against the worst outcomes,” Dr. Murthy said.
Data driving the plan
CDC Director Rochelle Walensky, MD, cited three research studies published Aug. 18 in the CDC’s Morbidity and Mortality Weekly Report that helped to drive the decision to recommend boosters.
Analysis of nursing home COVID-19 data from the CDC’s National Healthcare Safety Network showed a significant decline in the effectiveness of the full mRNA vaccine against lab-confirmed COVID-19 infection, from 74.7% before the Delta variant (March 1-May 9, 2021) to 53% when the Delta variant became predominant in the United States. The analysis during the Delta dominant period included 85,000 weekly reports from nearly 15,000 facilities.
Another study looked at more than 10 million New York adults who had been fully vaccinated with either the Moderna, Pfizer, or J&J vaccine by July 25. During the period from May 3 to July 25, overall, the age-adjusted vaccine effectiveness against infection decreased from 91.7% to 79.8%.
Vaccine effectiveness against hospitalization remains high, another study found. An analysis of 1,129 patients who had gotten two doses of an mRNA vaccine showed vaccine effectiveness against hospitalization after 24 weeks. It was 86% at weeks 2-12 and 84% at weeks 13-24.
Immunologic facts
Immunologic information also points to the need for a booster, said Anthony Fauci, MD, the chief medical advisor to the president and director of the National Institute of Allergy and Infectious Diseases.
“Antibody levels decline over time,” he said, “and higher antibody levels are associated with higher efficacy of the vaccine. Higher levels of antibody may be needed to protect against Delta.”
A booster increased antibody levels by ‘’at least tenfold and possibly more,” he said. And higher levels of antibody may be required to protect against Delta. Taken together, he said, the data support the use of a booster to increase the overall level of protection.
Booster details
“We will make sure it is convenient and easy to get the booster shot,” said Jeff Zients, the White House COVID-19 response coordinator. As with the previous immunization, he said, the booster will be free, and no one will be asked about immigration status.
The plan for booster shots is an attempt to stay ahead of the virus, officials stressed
Big picture
Not everyone agrees with the booster dose idea. At a World Health Organization briefing Aug. 18, WHO’s Chief Scientist Soumya Swaminathan, MD, an Indian pediatrician, said that the right thing to do right now ‘’is to wait for the science to tell us when boosters, which groups of people, and which vaccines need boosters.”
Like others, she also broached the ‘’moral and ethical argument of giving people third doses, when they’re already well protected and while the rest of the world is waiting for their primary immunization.”
Dr. Swaminathan does see a role for boosters to protect immunocompromised people but noted that ‘’that’s a small number of people.” Widespread boosters ‘’will only lead to more variants, to more escape variants, and perhaps we’re heading into more dire situations.”
A version of this article first appeared on WebMD.com.
at a press briefing August 18.
Those who received the Pfizer-BioNTech and Moderna vaccines would be eligible to get a booster shot 8 months after they received the second dose of those vaccines, officials said. Information on boosters for those who got the one-dose Johnson & Johnson vaccine will be forthcoming.
“We anticipate a booster will [also] likely be needed,” said U.S. Surgeon General Vivek Murthy, MD. The J&J vaccine was not available in the U.S. until March, he said, and ‘’we expect more data on J&J in the coming weeks, so that plan is coming.”
The plan for boosters for the two mRNA vaccines is pending the FDA’s conducting of an independent review and authorizing the third dose of the Moderna and Pfizer-BioNTech vaccines, as well as an advisory committee of the CDC making the recommendation.
“We know that even highly effective vaccines become less effective over time,” Dr. Murthy said. “Having reviewed the most current data, it is now our clinical judgment that the time to lay out a plan for the COVID-19 boosters is now.”
Research released Aug. 18 shows waning effectiveness of the two mRNA vaccines.
At the briefing, Dr. Murthy and others continually reassured listeners that while effectiveness against infection declines, the vaccines continue to protect against severe infections, hospitalizations, and death.
“If you are fully vaccinated, you still have a high degree of protection against the worst outcomes,” Dr. Murthy said.
Data driving the plan
CDC Director Rochelle Walensky, MD, cited three research studies published Aug. 18 in the CDC’s Morbidity and Mortality Weekly Report that helped to drive the decision to recommend boosters.
Analysis of nursing home COVID-19 data from the CDC’s National Healthcare Safety Network showed a significant decline in the effectiveness of the full mRNA vaccine against lab-confirmed COVID-19 infection, from 74.7% before the Delta variant (March 1-May 9, 2021) to 53% when the Delta variant became predominant in the United States. The analysis during the Delta dominant period included 85,000 weekly reports from nearly 15,000 facilities.
Another study looked at more than 10 million New York adults who had been fully vaccinated with either the Moderna, Pfizer, or J&J vaccine by July 25. During the period from May 3 to July 25, overall, the age-adjusted vaccine effectiveness against infection decreased from 91.7% to 79.8%.
Vaccine effectiveness against hospitalization remains high, another study found. An analysis of 1,129 patients who had gotten two doses of an mRNA vaccine showed vaccine effectiveness against hospitalization after 24 weeks. It was 86% at weeks 2-12 and 84% at weeks 13-24.
Immunologic facts
Immunologic information also points to the need for a booster, said Anthony Fauci, MD, the chief medical advisor to the president and director of the National Institute of Allergy and Infectious Diseases.
“Antibody levels decline over time,” he said, “and higher antibody levels are associated with higher efficacy of the vaccine. Higher levels of antibody may be needed to protect against Delta.”
A booster increased antibody levels by ‘’at least tenfold and possibly more,” he said. And higher levels of antibody may be required to protect against Delta. Taken together, he said, the data support the use of a booster to increase the overall level of protection.
Booster details
“We will make sure it is convenient and easy to get the booster shot,” said Jeff Zients, the White House COVID-19 response coordinator. As with the previous immunization, he said, the booster will be free, and no one will be asked about immigration status.
The plan for booster shots is an attempt to stay ahead of the virus, officials stressed
Big picture
Not everyone agrees with the booster dose idea. At a World Health Organization briefing Aug. 18, WHO’s Chief Scientist Soumya Swaminathan, MD, an Indian pediatrician, said that the right thing to do right now ‘’is to wait for the science to tell us when boosters, which groups of people, and which vaccines need boosters.”
Like others, she also broached the ‘’moral and ethical argument of giving people third doses, when they’re already well protected and while the rest of the world is waiting for their primary immunization.”
Dr. Swaminathan does see a role for boosters to protect immunocompromised people but noted that ‘’that’s a small number of people.” Widespread boosters ‘’will only lead to more variants, to more escape variants, and perhaps we’re heading into more dire situations.”
A version of this article first appeared on WebMD.com.
Latest data show increase in breakthrough COVID-19 cases
Breakthrough cases accounted for about one in five newly diagnosed cases in six of the states, according to the New York Times. Hospitalizations and deaths among vaccinated people may be higher than previously thought as well.
“Remember when the early vaccine studies came out, it was like nobody gets hospitalized, nobody dies,” Robert Wachter, MD, chairman of the department of medicine at the University of California, San Francisco, said in an interview. “That clearly is not true.”
The New York Times analyzed data in seven states – California, Colorado, Massachusetts, Oregon, Utah, Vermont, and Virginia – that are tracking the most detailed information. The trends in these states may not reflect the numbers throughout the country, the newspaper reported.
Even still, the numbers back up the idea that vaccinated people may need booster shots this fall to support their earlier vaccine doses. Federal health officials are scheduled to approve the extra shots in coming weeks, potentially in September. The first people to receive booster shots will likely be health care workers and nursing home residents who took the first vaccines in December and January.
“If the chances of a breakthrough infection have gone up considerably, and I think the evidence is clear that they have, and the level of protection against severe illness is no longer as robust as it was, I think the case for boosters goes up pretty quickly,” Dr. Wachter said.
Previous analyses of breakthrough cases included data from June and earlier, the newspaper reported. But since July, COVID-19 cases have soared again because of the Delta variant, and the most recent numbers show an uptick among vaccinated people. In Los Angeles County, for instance, fully vaccinated people account for 20% of new COVID-19 cases, which is up from 11% in May, 5% in April, and 2% in March, according to a late July report from the Los Angeles County Department of Public Health.
What’s more, breakthrough infections in the seven states accounted for 12%-24% of COVID-19 hospitalizations in those states. About 8,000 breakthrough hospitalizations have been reported to the CDC. Still, the overall numbers remain low – in California, for instance, about 1,615 people have been hospitalized with breakthrough infections, which accounts for 0.007% of the state’s 22 million vaccinated people, the Times reported.
The breakthrough infections appear to be more severe among vaccinated people who are older or have weakened immune systems. About 74% of breakthrough cases are among adults 65 or older, the CDC reported.
The increase may shift how vaccinated people see their risks for infection and interact with loved ones. Public health officials have suggested that people follow some COVID-19 safety protocols again, such as wearing masks in public indoor spaces regardless of vaccination status.
As the Delta variant continues to circulate this fall, public health researchers will be researching more about breakthrough cases among vaccinated people, including whether they have prolonged symptoms and how easily they may pass the virus to others.
“I think some of us have been challenged by the numbers of clusters that we’ve seen,” Michael Osterholm, PhD, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, told this news organization.
“I think that really needs to be examined more,” he said.
A version of this article first appeared on WebMD.com.
Breakthrough cases accounted for about one in five newly diagnosed cases in six of the states, according to the New York Times. Hospitalizations and deaths among vaccinated people may be higher than previously thought as well.
“Remember when the early vaccine studies came out, it was like nobody gets hospitalized, nobody dies,” Robert Wachter, MD, chairman of the department of medicine at the University of California, San Francisco, said in an interview. “That clearly is not true.”
The New York Times analyzed data in seven states – California, Colorado, Massachusetts, Oregon, Utah, Vermont, and Virginia – that are tracking the most detailed information. The trends in these states may not reflect the numbers throughout the country, the newspaper reported.
Even still, the numbers back up the idea that vaccinated people may need booster shots this fall to support their earlier vaccine doses. Federal health officials are scheduled to approve the extra shots in coming weeks, potentially in September. The first people to receive booster shots will likely be health care workers and nursing home residents who took the first vaccines in December and January.
“If the chances of a breakthrough infection have gone up considerably, and I think the evidence is clear that they have, and the level of protection against severe illness is no longer as robust as it was, I think the case for boosters goes up pretty quickly,” Dr. Wachter said.
Previous analyses of breakthrough cases included data from June and earlier, the newspaper reported. But since July, COVID-19 cases have soared again because of the Delta variant, and the most recent numbers show an uptick among vaccinated people. In Los Angeles County, for instance, fully vaccinated people account for 20% of new COVID-19 cases, which is up from 11% in May, 5% in April, and 2% in March, according to a late July report from the Los Angeles County Department of Public Health.
What’s more, breakthrough infections in the seven states accounted for 12%-24% of COVID-19 hospitalizations in those states. About 8,000 breakthrough hospitalizations have been reported to the CDC. Still, the overall numbers remain low – in California, for instance, about 1,615 people have been hospitalized with breakthrough infections, which accounts for 0.007% of the state’s 22 million vaccinated people, the Times reported.
The breakthrough infections appear to be more severe among vaccinated people who are older or have weakened immune systems. About 74% of breakthrough cases are among adults 65 or older, the CDC reported.
The increase may shift how vaccinated people see their risks for infection and interact with loved ones. Public health officials have suggested that people follow some COVID-19 safety protocols again, such as wearing masks in public indoor spaces regardless of vaccination status.
As the Delta variant continues to circulate this fall, public health researchers will be researching more about breakthrough cases among vaccinated people, including whether they have prolonged symptoms and how easily they may pass the virus to others.
“I think some of us have been challenged by the numbers of clusters that we’ve seen,” Michael Osterholm, PhD, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, told this news organization.
“I think that really needs to be examined more,” he said.
A version of this article first appeared on WebMD.com.
Breakthrough cases accounted for about one in five newly diagnosed cases in six of the states, according to the New York Times. Hospitalizations and deaths among vaccinated people may be higher than previously thought as well.
“Remember when the early vaccine studies came out, it was like nobody gets hospitalized, nobody dies,” Robert Wachter, MD, chairman of the department of medicine at the University of California, San Francisco, said in an interview. “That clearly is not true.”
The New York Times analyzed data in seven states – California, Colorado, Massachusetts, Oregon, Utah, Vermont, and Virginia – that are tracking the most detailed information. The trends in these states may not reflect the numbers throughout the country, the newspaper reported.
Even still, the numbers back up the idea that vaccinated people may need booster shots this fall to support their earlier vaccine doses. Federal health officials are scheduled to approve the extra shots in coming weeks, potentially in September. The first people to receive booster shots will likely be health care workers and nursing home residents who took the first vaccines in December and January.
“If the chances of a breakthrough infection have gone up considerably, and I think the evidence is clear that they have, and the level of protection against severe illness is no longer as robust as it was, I think the case for boosters goes up pretty quickly,” Dr. Wachter said.
Previous analyses of breakthrough cases included data from June and earlier, the newspaper reported. But since July, COVID-19 cases have soared again because of the Delta variant, and the most recent numbers show an uptick among vaccinated people. In Los Angeles County, for instance, fully vaccinated people account for 20% of new COVID-19 cases, which is up from 11% in May, 5% in April, and 2% in March, according to a late July report from the Los Angeles County Department of Public Health.
What’s more, breakthrough infections in the seven states accounted for 12%-24% of COVID-19 hospitalizations in those states. About 8,000 breakthrough hospitalizations have been reported to the CDC. Still, the overall numbers remain low – in California, for instance, about 1,615 people have been hospitalized with breakthrough infections, which accounts for 0.007% of the state’s 22 million vaccinated people, the Times reported.
The breakthrough infections appear to be more severe among vaccinated people who are older or have weakened immune systems. About 74% of breakthrough cases are among adults 65 or older, the CDC reported.
The increase may shift how vaccinated people see their risks for infection and interact with loved ones. Public health officials have suggested that people follow some COVID-19 safety protocols again, such as wearing masks in public indoor spaces regardless of vaccination status.
As the Delta variant continues to circulate this fall, public health researchers will be researching more about breakthrough cases among vaccinated people, including whether they have prolonged symptoms and how easily they may pass the virus to others.
“I think some of us have been challenged by the numbers of clusters that we’ve seen,” Michael Osterholm, PhD, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, told this news organization.
“I think that really needs to be examined more,” he said.
A version of this article first appeared on WebMD.com.
Preterm and early term birth linked to an increased risk of autism
Preterm and early birth is associated with an increased risk of autism independent of genetic or environmental factors, according to new research published in Pediatrics.
Although previous studies have linked preterm births to an increased risk of autism – one 2017 study published in Cerebral Cortex found that 27.4% of the children born extremely preterm were diagnosed with autism – Casey Crump, MD, PhD, said potential causality, sex-specific differences, and association with early-term births were still unclear.
“Preterm birth had previously been linked with higher risk of autism; however, several important questions remained unanswered,” said Dr. Crump, professor and vice chair for research at the department of family medicine and community health and professor of epidemiology in the department of population health science and policy at Icahn School of Medicine at Mount Sinai New York. “To our knowledge, [our study] is the largest to date of gestational age at birth in relation to autism, and one of the first to investigate sex-specific differences, early term birth, or the influence of shared familial factors.”
Dr. Crump and colleagues examined data from more than 4 million infants born in Sweden between 1973 and 2013 who were followed-up for autism spectrum disorder identified from nationwide outpatient and inpatient diagnoses through December 2015. Children born between 22 and 27 weeks were considered extremely preterm, those born between 28 and 33 week were characterized as very to moderate preterm, and those born between 34 and 36 weeks were considered late preterm. Early-term births are characterized as infants born between 37 and 38 weeks and children born between 39 and 41 weeks were considered term births.
They found that 6.1% of those born extremely preterm were diagnosed with autism. Meanwhile, autism spectrum disorder prevalences were 2.6% for very to moderate preterm, 1.9% for late preterm, 2.1% for all preterm, and 1.6% for early term, compared with 1.4% for term birth.
The researchers’ analysis showed that preterm and early birth were associated with a significantly increased risk of autism in males and females. Children who were born extremely preterm had an approximately fourfold increased risk of autism. Researchers also found that each additional week of gestation was associated with a 5% lower prevalence of autism spectrum disorder (ASD) on average.
“The elevated risk even in [late preterm] infants is not completely surprising because a number of investigators have shown higher incidences of early cognitive, language motor and impairment, and school problems ... and psychiatric disorders, some of which may extend to adulthood,” Elisabeth McGowan, MD, who was not involved in the study, said in a solicited editorial commentary about the study.
Dr. Crump believes the association between preterm birth and autism may be because of increased inflammatory marker levels. A 2009 study published in Reproductive Sciences found that increased proinflammatory cytokine levels have been associated with the timing and initiation of preterm birth, and also have been detected in the brain and cerebrospinal fluid of individuals with autism “and may play a key role in its pathogenesis,” Dr. Crump said.
“Inflammatory-driven alteration of neuronal connections during critical periods of brain development may be central to the development of autism,” Dr. Crump explained.
However, Dr. Crump said that, although the relative risks of autism were higher in those born preterm, the absolute risk of the condition is low.
“The report by Crump is in many ways a definitive accounting of the elevated rates of ASD in preterm infants,” said Dr. McGowan, associate professor of pediatrics at the Women and Infants Hospital, Providence, R.I. “And although the impact of prematurity on brain development may be part of the causal chain resulting in ASD (or other neurodevelopmental outcomes), these factors are operating in a complex biological landscape, with pathways to ASD outcomes that can be expected to be heterogeneous.”
ASD is a developmental condition that affects about 1 in 54 children, according to the Centers for Disease Control and Prevention. Many children are not diagnosed with ASD until later in childhood, which in some cases delays treatment and early intervention. ASD may be detected as early as 18 months, but the average age of diagnosis for ASD is 4.3 years, according to the CDC.
“Children born prematurely need early evaluation and long-term follow-up to facilitate timely detection and treatment of autism, especially those born at the earliest gestational ages,” Dr. Crump said in an interview. “In patients of all ages, gestational age at birth should be routinely included in history-taking and medical records to help identify in clinical practice those born preterm or early term. Such information can provide additional valuable context for understanding patients’ health and may facilitate earlier evaluation for autism and other neurodevelopmental conditions in those born prematurely.”
Dr. Crump and colleagues said more research is needed to understand the biologic mechanisms linking preterm birth with higher risks of autism, which “may reveal new targets for intervention at critical windows of neurodevelopment to improve the disease trajectory.”
Experts interviewed did not disclose any relevant financial relationships.
Preterm and early birth is associated with an increased risk of autism independent of genetic or environmental factors, according to new research published in Pediatrics.
Although previous studies have linked preterm births to an increased risk of autism – one 2017 study published in Cerebral Cortex found that 27.4% of the children born extremely preterm were diagnosed with autism – Casey Crump, MD, PhD, said potential causality, sex-specific differences, and association with early-term births were still unclear.
“Preterm birth had previously been linked with higher risk of autism; however, several important questions remained unanswered,” said Dr. Crump, professor and vice chair for research at the department of family medicine and community health and professor of epidemiology in the department of population health science and policy at Icahn School of Medicine at Mount Sinai New York. “To our knowledge, [our study] is the largest to date of gestational age at birth in relation to autism, and one of the first to investigate sex-specific differences, early term birth, or the influence of shared familial factors.”
Dr. Crump and colleagues examined data from more than 4 million infants born in Sweden between 1973 and 2013 who were followed-up for autism spectrum disorder identified from nationwide outpatient and inpatient diagnoses through December 2015. Children born between 22 and 27 weeks were considered extremely preterm, those born between 28 and 33 week were characterized as very to moderate preterm, and those born between 34 and 36 weeks were considered late preterm. Early-term births are characterized as infants born between 37 and 38 weeks and children born between 39 and 41 weeks were considered term births.
They found that 6.1% of those born extremely preterm were diagnosed with autism. Meanwhile, autism spectrum disorder prevalences were 2.6% for very to moderate preterm, 1.9% for late preterm, 2.1% for all preterm, and 1.6% for early term, compared with 1.4% for term birth.
The researchers’ analysis showed that preterm and early birth were associated with a significantly increased risk of autism in males and females. Children who were born extremely preterm had an approximately fourfold increased risk of autism. Researchers also found that each additional week of gestation was associated with a 5% lower prevalence of autism spectrum disorder (ASD) on average.
“The elevated risk even in [late preterm] infants is not completely surprising because a number of investigators have shown higher incidences of early cognitive, language motor and impairment, and school problems ... and psychiatric disorders, some of which may extend to adulthood,” Elisabeth McGowan, MD, who was not involved in the study, said in a solicited editorial commentary about the study.
Dr. Crump believes the association between preterm birth and autism may be because of increased inflammatory marker levels. A 2009 study published in Reproductive Sciences found that increased proinflammatory cytokine levels have been associated with the timing and initiation of preterm birth, and also have been detected in the brain and cerebrospinal fluid of individuals with autism “and may play a key role in its pathogenesis,” Dr. Crump said.
“Inflammatory-driven alteration of neuronal connections during critical periods of brain development may be central to the development of autism,” Dr. Crump explained.
However, Dr. Crump said that, although the relative risks of autism were higher in those born preterm, the absolute risk of the condition is low.
“The report by Crump is in many ways a definitive accounting of the elevated rates of ASD in preterm infants,” said Dr. McGowan, associate professor of pediatrics at the Women and Infants Hospital, Providence, R.I. “And although the impact of prematurity on brain development may be part of the causal chain resulting in ASD (or other neurodevelopmental outcomes), these factors are operating in a complex biological landscape, with pathways to ASD outcomes that can be expected to be heterogeneous.”
ASD is a developmental condition that affects about 1 in 54 children, according to the Centers for Disease Control and Prevention. Many children are not diagnosed with ASD until later in childhood, which in some cases delays treatment and early intervention. ASD may be detected as early as 18 months, but the average age of diagnosis for ASD is 4.3 years, according to the CDC.
“Children born prematurely need early evaluation and long-term follow-up to facilitate timely detection and treatment of autism, especially those born at the earliest gestational ages,” Dr. Crump said in an interview. “In patients of all ages, gestational age at birth should be routinely included in history-taking and medical records to help identify in clinical practice those born preterm or early term. Such information can provide additional valuable context for understanding patients’ health and may facilitate earlier evaluation for autism and other neurodevelopmental conditions in those born prematurely.”
Dr. Crump and colleagues said more research is needed to understand the biologic mechanisms linking preterm birth with higher risks of autism, which “may reveal new targets for intervention at critical windows of neurodevelopment to improve the disease trajectory.”
Experts interviewed did not disclose any relevant financial relationships.
Preterm and early birth is associated with an increased risk of autism independent of genetic or environmental factors, according to new research published in Pediatrics.
Although previous studies have linked preterm births to an increased risk of autism – one 2017 study published in Cerebral Cortex found that 27.4% of the children born extremely preterm were diagnosed with autism – Casey Crump, MD, PhD, said potential causality, sex-specific differences, and association with early-term births were still unclear.
“Preterm birth had previously been linked with higher risk of autism; however, several important questions remained unanswered,” said Dr. Crump, professor and vice chair for research at the department of family medicine and community health and professor of epidemiology in the department of population health science and policy at Icahn School of Medicine at Mount Sinai New York. “To our knowledge, [our study] is the largest to date of gestational age at birth in relation to autism, and one of the first to investigate sex-specific differences, early term birth, or the influence of shared familial factors.”
Dr. Crump and colleagues examined data from more than 4 million infants born in Sweden between 1973 and 2013 who were followed-up for autism spectrum disorder identified from nationwide outpatient and inpatient diagnoses through December 2015. Children born between 22 and 27 weeks were considered extremely preterm, those born between 28 and 33 week were characterized as very to moderate preterm, and those born between 34 and 36 weeks were considered late preterm. Early-term births are characterized as infants born between 37 and 38 weeks and children born between 39 and 41 weeks were considered term births.
They found that 6.1% of those born extremely preterm were diagnosed with autism. Meanwhile, autism spectrum disorder prevalences were 2.6% for very to moderate preterm, 1.9% for late preterm, 2.1% for all preterm, and 1.6% for early term, compared with 1.4% for term birth.
The researchers’ analysis showed that preterm and early birth were associated with a significantly increased risk of autism in males and females. Children who were born extremely preterm had an approximately fourfold increased risk of autism. Researchers also found that each additional week of gestation was associated with a 5% lower prevalence of autism spectrum disorder (ASD) on average.
“The elevated risk even in [late preterm] infants is not completely surprising because a number of investigators have shown higher incidences of early cognitive, language motor and impairment, and school problems ... and psychiatric disorders, some of which may extend to adulthood,” Elisabeth McGowan, MD, who was not involved in the study, said in a solicited editorial commentary about the study.
Dr. Crump believes the association between preterm birth and autism may be because of increased inflammatory marker levels. A 2009 study published in Reproductive Sciences found that increased proinflammatory cytokine levels have been associated with the timing and initiation of preterm birth, and also have been detected in the brain and cerebrospinal fluid of individuals with autism “and may play a key role in its pathogenesis,” Dr. Crump said.
“Inflammatory-driven alteration of neuronal connections during critical periods of brain development may be central to the development of autism,” Dr. Crump explained.
However, Dr. Crump said that, although the relative risks of autism were higher in those born preterm, the absolute risk of the condition is low.
“The report by Crump is in many ways a definitive accounting of the elevated rates of ASD in preterm infants,” said Dr. McGowan, associate professor of pediatrics at the Women and Infants Hospital, Providence, R.I. “And although the impact of prematurity on brain development may be part of the causal chain resulting in ASD (or other neurodevelopmental outcomes), these factors are operating in a complex biological landscape, with pathways to ASD outcomes that can be expected to be heterogeneous.”
ASD is a developmental condition that affects about 1 in 54 children, according to the Centers for Disease Control and Prevention. Many children are not diagnosed with ASD until later in childhood, which in some cases delays treatment and early intervention. ASD may be detected as early as 18 months, but the average age of diagnosis for ASD is 4.3 years, according to the CDC.
“Children born prematurely need early evaluation and long-term follow-up to facilitate timely detection and treatment of autism, especially those born at the earliest gestational ages,” Dr. Crump said in an interview. “In patients of all ages, gestational age at birth should be routinely included in history-taking and medical records to help identify in clinical practice those born preterm or early term. Such information can provide additional valuable context for understanding patients’ health and may facilitate earlier evaluation for autism and other neurodevelopmental conditions in those born prematurely.”
Dr. Crump and colleagues said more research is needed to understand the biologic mechanisms linking preterm birth with higher risks of autism, which “may reveal new targets for intervention at critical windows of neurodevelopment to improve the disease trajectory.”
Experts interviewed did not disclose any relevant financial relationships.
FROM PEDIATRICS
‘Reassuring’ findings for second-generation antipsychotics during pregnancy
Second-generation antipsychotics (SGAs) taken by pregnant women are linked to a low rate of adverse effects in their children, new research suggests.

Data from a large registry study of almost 2,000 women showed that 2.5% of the live births in a group that had been exposed to antipsychotics had confirmed major malformations compared with 2% of the live births in a non-exposed group. This translated into an estimated odds ratio of 1.5 for major malformations.
“The 2.5% absolute risk for major malformations is consistent with the estimates of the Centers for Disease Control and Prevention’s national baseline rate of major malformations in the general population,” lead author Adele Viguera, MD, MPH, director of research for women’s mental health, Cleveland Clinic Neurological Institute, told this news organization.
“Our results are reassuring and suggest that second-generation antipsychotics, as a class, do not substantially increase the risk of major malformations,” Dr. Viguera said.
The findings were published online August 3 in the Journal of Clinical Psychiatry.
Safety data scarce
Despite the increasing use of SGAs to treat a “spectrum of psychiatric disorders,” relatively little data are available on the reproductive safety of these agents, Dr. Viguera said.
The National Pregnancy Registry for Atypical Antipsychotics (NPRAA) was established in 2008 to determine risk for major malformation among infants exposed to these medications during the first trimester, relative to a comparison group of unexposed infants of mothers with histories of psychiatric morbidity.
The NPRAA follows pregnant women (aged 18 to 45 years) with psychiatric illness who are exposed or unexposed to SGAs during pregnancy. Participants are recruited through nationwide provider referral, self-referral, and advertisement through the Massachusetts General Hospital Center for Women’s Mental Health website.
Specific data collected are shown in the following table.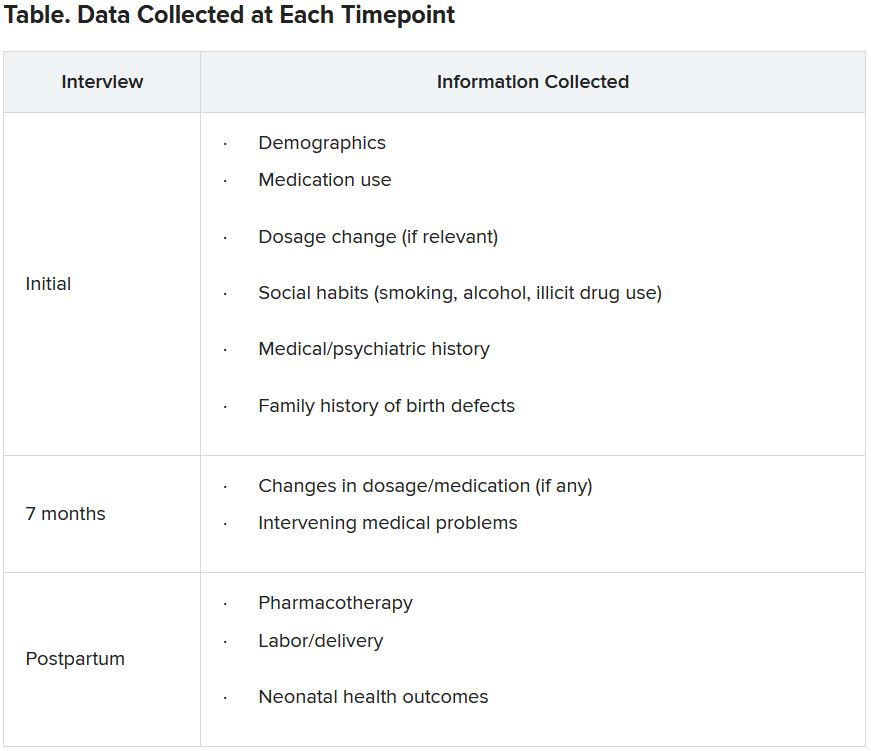
Since publication of the first results in 2015, the sample size for the trial has increased – and the absolute and relative risk for major malformations observed in the study population are “more precise,” the investigators note. The current study presented updated previous findings.
Demographic differences
Of the 1,906 women who enrolled as of April 2020, 1,311 (mean age, 32.6 years; 81.3% White) completed the study and were eligible for inclusion in the analysis.
Although the groups had a virtually identical mean age, fewer women in the exposure group were married compared with those in the non-exposure group (77% vs. 90%, respectively) and fewer had a college education (71.2% vs. 87.8%). There was also a higher percentage of first-trimester cigarette smokers in the exposure group (18.4% vs. 5.1%).
On the other hand, more women in the non-exposure group used alcohol than in the exposure group (28.6% vs. 21.4%, respectively).
The most frequent psychiatric disorder in the exposure group was bipolar disorder (63.9%), followed by major depression (12.9%), anxiety (5.8%), and schizophrenia (4.5%). Only 11.4% of women in the non-exposure group were diagnosed with bipolar disorder, whereas 34.1% were diagnosed with major depression, 31.3% with anxiety, and none with schizophrenia.
Notably, a large percentage of women in both groups had a history of postpartum depression and/or psychosis (41.4% and 35.5%, respectively).
The most frequently used SGAs in the exposure group were quetiapine (Seroquel), aripiprazole (Abilify), and lurasidone (Latuda).
Participants in the exposure group had a higher age at initial onset of primary psychiatric diagnosis and a lower proportion of lifetime illness compared with those in the non-exposure group.
Major clinical implication?
Among 640 live births in the exposure group, which included 17 twin pregnancies and 1 triplet pregnancy, 2.5% reported major malformations. Among 704 live births in the control group, which included 14 twin pregnancies, 1.99% reported major malformations.
The estimated OR for major malformations comparing exposed and unexposed infants was 1.48 (95% confidence interval, 0.625-3.517).
The authors note that their findings were consistent with one of the largest studies to date, which included a nationwide sample of more than 1 million women. Its results showed that, among infants exposed to SGAs versus those who were not exposed, the estimated risk ratio after adjusting for psychiatric conditions was 1.05 (95% CI, 0.96-1.16).
Additionally, “a hallmark of a teratogen is that it tends to cause a specific type or pattern of malformations, and we found no preponderance of one single type of major malformation or specific pattern of malformations among the exposed and unexposed groups,” Dr. Viguera said
“A major clinical implication of these findings is that for women with major mood and/or psychotic disorders, treatment with an atypical antipsychotic during pregnancy may be the most prudent clinical decision, much as continued treatment is recommended for pregnant women with other serious and chronic medical conditions, such as epilepsy,” she added.
The concept of ‘satisficing’
Commenting on the study, Vivien Burt, MD, PhD, founder and director/consultant of the Women’s Life Center at the Resnick University of California, Los Angeles (UCLA) Neuropsychiatric Hospital, called the findings “reassuring.”
The results “support the conclusion that in pregnant women with serious psychiatric illnesses, the use of SGAs is often a better option than avoiding these medications and exposing both the women and their offspring to the adverse consequences of maternal mental illness,” she said.
An accompanying editorial co-authored by Dr. Burt and colleague Sonya Rasminsky, MD, introduced the concept of “satisficing” – a term coined by Herbert Simon, a behavioral economist and Nobel Laureate. “Satisficing” is a “decision-making strategy that aims for a satisfactory (‘good enough’) outcome rather than a perfect one.”
The concept applies to decision-making beyond the field of economics “and is critical to how physicians help patients make decisions when they are faced with multiple treatment options,” said Dr. Burt, a professor emeritus of psychiatry at UCLA.
“The goal of ‘satisficing’ is to plan for the most satisfactory outcome, knowing that there are always unknowns, so in an uncertain world, clinicians should carefully help their patients make decisions that will allow them to achieve an outcome they can best live with,” she noted.
The investigators note that their findings may not be generalizable to the larger population of women taking SGAs, given that their participants were “overwhelmingly White, married, and well-educated women.”
They add that enrollment into the NPRAA registry is ongoing and larger sample sizes will “further narrow the confidence interval around the risk estimates and allow for adjustment of likely sources of confounding.”
The NPRAA is supported by Alkermes, Johnson & Johnson/Janssen Pharmaceuticals, Otsuka America Pharmaceutical, Sunovion Pharmaceuticals, SAGE Therapeutics, Teva Pharmaceuticals, and Aurobindo Pharma. Past sponsors of the NPRAA are listed in the original paper. Dr. Viguera receives research support from the NPRAA, Alkermes Biopharmaceuticals, Aurobindo Pharma, Janssen Pharmaceuticals, Otsuka Pharmaceutical, Sunovion Pharmaceuticals, Teva Pharmaceuticals, and SAGE Therapeutics and receives adviser/consulting fees from Up-to-Date. Dr. Burt has been a consultant/speaker for Sage Therapeutics. Dr. Rasminsky has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Second-generation antipsychotics (SGAs) taken by pregnant women are linked to a low rate of adverse effects in their children, new research suggests.
Data from a large registry study of almost 2,000 women showed that 2.5% of the live births in a group that had been exposed to antipsychotics had confirmed major malformations compared with 2% of the live births in a non-exposed group. This translated into an estimated odds ratio of 1.5 for major malformations.
“The 2.5% absolute risk for major malformations is consistent with the estimates of the Centers for Disease Control and Prevention’s national baseline rate of major malformations in the general population,” lead author Adele Viguera, MD, MPH, director of research for women’s mental health, Cleveland Clinic Neurological Institute, told this news organization.
“Our results are reassuring and suggest that second-generation antipsychotics, as a class, do not substantially increase the risk of major malformations,” Dr. Viguera said.
The findings were published online August 3 in the Journal of Clinical Psychiatry.
Safety data scarce
Despite the increasing use of SGAs to treat a “spectrum of psychiatric disorders,” relatively little data are available on the reproductive safety of these agents, Dr. Viguera said.
The National Pregnancy Registry for Atypical Antipsychotics (NPRAA) was established in 2008 to determine risk for major malformation among infants exposed to these medications during the first trimester, relative to a comparison group of unexposed infants of mothers with histories of psychiatric morbidity.
The NPRAA follows pregnant women (aged 18 to 45 years) with psychiatric illness who are exposed or unexposed to SGAs during pregnancy. Participants are recruited through nationwide provider referral, self-referral, and advertisement through the Massachusetts General Hospital Center for Women’s Mental Health website.
Specific data collected are shown in the following table.
Since publication of the first results in 2015, the sample size for the trial has increased – and the absolute and relative risk for major malformations observed in the study population are “more precise,” the investigators note. The current study presented updated previous findings.
Demographic differences
Of the 1,906 women who enrolled as of April 2020, 1,311 (mean age, 32.6 years; 81.3% White) completed the study and were eligible for inclusion in the analysis.
Although the groups had a virtually identical mean age, fewer women in the exposure group were married compared with those in the non-exposure group (77% vs. 90%, respectively) and fewer had a college education (71.2% vs. 87.8%). There was also a higher percentage of first-trimester cigarette smokers in the exposure group (18.4% vs. 5.1%).
On the other hand, more women in the non-exposure group used alcohol than in the exposure group (28.6% vs. 21.4%, respectively).
The most frequent psychiatric disorder in the exposure group was bipolar disorder (63.9%), followed by major depression (12.9%), anxiety (5.8%), and schizophrenia (4.5%). Only 11.4% of women in the non-exposure group were diagnosed with bipolar disorder, whereas 34.1% were diagnosed with major depression, 31.3% with anxiety, and none with schizophrenia.
Notably, a large percentage of women in both groups had a history of postpartum depression and/or psychosis (41.4% and 35.5%, respectively).
The most frequently used SGAs in the exposure group were quetiapine (Seroquel), aripiprazole (Abilify), and lurasidone (Latuda).
Participants in the exposure group had a higher age at initial onset of primary psychiatric diagnosis and a lower proportion of lifetime illness compared with those in the non-exposure group.
Major clinical implication?
Among 640 live births in the exposure group, which included 17 twin pregnancies and 1 triplet pregnancy, 2.5% reported major malformations. Among 704 live births in the control group, which included 14 twin pregnancies, 1.99% reported major malformations.
The estimated OR for major malformations comparing exposed and unexposed infants was 1.48 (95% confidence interval, 0.625-3.517).
The authors note that their findings were consistent with one of the largest studies to date, which included a nationwide sample of more than 1 million women. Its results showed that, among infants exposed to SGAs versus those who were not exposed, the estimated risk ratio after adjusting for psychiatric conditions was 1.05 (95% CI, 0.96-1.16).
Additionally, “a hallmark of a teratogen is that it tends to cause a specific type or pattern of malformations, and we found no preponderance of one single type of major malformation or specific pattern of malformations among the exposed and unexposed groups,” Dr. Viguera said
“A major clinical implication of these findings is that for women with major mood and/or psychotic disorders, treatment with an atypical antipsychotic during pregnancy may be the most prudent clinical decision, much as continued treatment is recommended for pregnant women with other serious and chronic medical conditions, such as epilepsy,” she added.
The concept of ‘satisficing’
Commenting on the study, Vivien Burt, MD, PhD, founder and director/consultant of the Women’s Life Center at the Resnick University of California, Los Angeles (UCLA) Neuropsychiatric Hospital, called the findings “reassuring.”
The results “support the conclusion that in pregnant women with serious psychiatric illnesses, the use of SGAs is often a better option than avoiding these medications and exposing both the women and their offspring to the adverse consequences of maternal mental illness,” she said.
An accompanying editorial co-authored by Dr. Burt and colleague Sonya Rasminsky, MD, introduced the concept of “satisficing” – a term coined by Herbert Simon, a behavioral economist and Nobel Laureate. “Satisficing” is a “decision-making strategy that aims for a satisfactory (‘good enough’) outcome rather than a perfect one.”
The concept applies to decision-making beyond the field of economics “and is critical to how physicians help patients make decisions when they are faced with multiple treatment options,” said Dr. Burt, a professor emeritus of psychiatry at UCLA.
“The goal of ‘satisficing’ is to plan for the most satisfactory outcome, knowing that there are always unknowns, so in an uncertain world, clinicians should carefully help their patients make decisions that will allow them to achieve an outcome they can best live with,” she noted.
The investigators note that their findings may not be generalizable to the larger population of women taking SGAs, given that their participants were “overwhelmingly White, married, and well-educated women.”
They add that enrollment into the NPRAA registry is ongoing and larger sample sizes will “further narrow the confidence interval around the risk estimates and allow for adjustment of likely sources of confounding.”
The NPRAA is supported by Alkermes, Johnson & Johnson/Janssen Pharmaceuticals, Otsuka America Pharmaceutical, Sunovion Pharmaceuticals, SAGE Therapeutics, Teva Pharmaceuticals, and Aurobindo Pharma. Past sponsors of the NPRAA are listed in the original paper. Dr. Viguera receives research support from the NPRAA, Alkermes Biopharmaceuticals, Aurobindo Pharma, Janssen Pharmaceuticals, Otsuka Pharmaceutical, Sunovion Pharmaceuticals, Teva Pharmaceuticals, and SAGE Therapeutics and receives adviser/consulting fees from Up-to-Date. Dr. Burt has been a consultant/speaker for Sage Therapeutics. Dr. Rasminsky has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Second-generation antipsychotics (SGAs) taken by pregnant women are linked to a low rate of adverse effects in their children, new research suggests.
Data from a large registry study of almost 2,000 women showed that 2.5% of the live births in a group that had been exposed to antipsychotics had confirmed major malformations compared with 2% of the live births in a non-exposed group. This translated into an estimated odds ratio of 1.5 for major malformations.
“The 2.5% absolute risk for major malformations is consistent with the estimates of the Centers for Disease Control and Prevention’s national baseline rate of major malformations in the general population,” lead author Adele Viguera, MD, MPH, director of research for women’s mental health, Cleveland Clinic Neurological Institute, told this news organization.
“Our results are reassuring and suggest that second-generation antipsychotics, as a class, do not substantially increase the risk of major malformations,” Dr. Viguera said.
The findings were published online August 3 in the Journal of Clinical Psychiatry.
Safety data scarce
Despite the increasing use of SGAs to treat a “spectrum of psychiatric disorders,” relatively little data are available on the reproductive safety of these agents, Dr. Viguera said.
The National Pregnancy Registry for Atypical Antipsychotics (NPRAA) was established in 2008 to determine risk for major malformation among infants exposed to these medications during the first trimester, relative to a comparison group of unexposed infants of mothers with histories of psychiatric morbidity.
The NPRAA follows pregnant women (aged 18 to 45 years) with psychiatric illness who are exposed or unexposed to SGAs during pregnancy. Participants are recruited through nationwide provider referral, self-referral, and advertisement through the Massachusetts General Hospital Center for Women’s Mental Health website.
Specific data collected are shown in the following table.
Since publication of the first results in 2015, the sample size for the trial has increased – and the absolute and relative risk for major malformations observed in the study population are “more precise,” the investigators note. The current study presented updated previous findings.
Demographic differences
Of the 1,906 women who enrolled as of April 2020, 1,311 (mean age, 32.6 years; 81.3% White) completed the study and were eligible for inclusion in the analysis.
Although the groups had a virtually identical mean age, fewer women in the exposure group were married compared with those in the non-exposure group (77% vs. 90%, respectively) and fewer had a college education (71.2% vs. 87.8%). There was also a higher percentage of first-trimester cigarette smokers in the exposure group (18.4% vs. 5.1%).
On the other hand, more women in the non-exposure group used alcohol than in the exposure group (28.6% vs. 21.4%, respectively).
The most frequent psychiatric disorder in the exposure group was bipolar disorder (63.9%), followed by major depression (12.9%), anxiety (5.8%), and schizophrenia (4.5%). Only 11.4% of women in the non-exposure group were diagnosed with bipolar disorder, whereas 34.1% were diagnosed with major depression, 31.3% with anxiety, and none with schizophrenia.
Notably, a large percentage of women in both groups had a history of postpartum depression and/or psychosis (41.4% and 35.5%, respectively).
The most frequently used SGAs in the exposure group were quetiapine (Seroquel), aripiprazole (Abilify), and lurasidone (Latuda).
Participants in the exposure group had a higher age at initial onset of primary psychiatric diagnosis and a lower proportion of lifetime illness compared with those in the non-exposure group.
Major clinical implication?
Among 640 live births in the exposure group, which included 17 twin pregnancies and 1 triplet pregnancy, 2.5% reported major malformations. Among 704 live births in the control group, which included 14 twin pregnancies, 1.99% reported major malformations.
The estimated OR for major malformations comparing exposed and unexposed infants was 1.48 (95% confidence interval, 0.625-3.517).
The authors note that their findings were consistent with one of the largest studies to date, which included a nationwide sample of more than 1 million women. Its results showed that, among infants exposed to SGAs versus those who were not exposed, the estimated risk ratio after adjusting for psychiatric conditions was 1.05 (95% CI, 0.96-1.16).
Additionally, “a hallmark of a teratogen is that it tends to cause a specific type or pattern of malformations, and we found no preponderance of one single type of major malformation or specific pattern of malformations among the exposed and unexposed groups,” Dr. Viguera said
“A major clinical implication of these findings is that for women with major mood and/or psychotic disorders, treatment with an atypical antipsychotic during pregnancy may be the most prudent clinical decision, much as continued treatment is recommended for pregnant women with other serious and chronic medical conditions, such as epilepsy,” she added.
The concept of ‘satisficing’
Commenting on the study, Vivien Burt, MD, PhD, founder and director/consultant of the Women’s Life Center at the Resnick University of California, Los Angeles (UCLA) Neuropsychiatric Hospital, called the findings “reassuring.”
The results “support the conclusion that in pregnant women with serious psychiatric illnesses, the use of SGAs is often a better option than avoiding these medications and exposing both the women and their offspring to the adverse consequences of maternal mental illness,” she said.
An accompanying editorial co-authored by Dr. Burt and colleague Sonya Rasminsky, MD, introduced the concept of “satisficing” – a term coined by Herbert Simon, a behavioral economist and Nobel Laureate. “Satisficing” is a “decision-making strategy that aims for a satisfactory (‘good enough’) outcome rather than a perfect one.”
The concept applies to decision-making beyond the field of economics “and is critical to how physicians help patients make decisions when they are faced with multiple treatment options,” said Dr. Burt, a professor emeritus of psychiatry at UCLA.
“The goal of ‘satisficing’ is to plan for the most satisfactory outcome, knowing that there are always unknowns, so in an uncertain world, clinicians should carefully help their patients make decisions that will allow them to achieve an outcome they can best live with,” she noted.
The investigators note that their findings may not be generalizable to the larger population of women taking SGAs, given that their participants were “overwhelmingly White, married, and well-educated women.”
They add that enrollment into the NPRAA registry is ongoing and larger sample sizes will “further narrow the confidence interval around the risk estimates and allow for adjustment of likely sources of confounding.”
The NPRAA is supported by Alkermes, Johnson & Johnson/Janssen Pharmaceuticals, Otsuka America Pharmaceutical, Sunovion Pharmaceuticals, SAGE Therapeutics, Teva Pharmaceuticals, and Aurobindo Pharma. Past sponsors of the NPRAA are listed in the original paper. Dr. Viguera receives research support from the NPRAA, Alkermes Biopharmaceuticals, Aurobindo Pharma, Janssen Pharmaceuticals, Otsuka Pharmaceutical, Sunovion Pharmaceuticals, Teva Pharmaceuticals, and SAGE Therapeutics and receives adviser/consulting fees from Up-to-Date. Dr. Burt has been a consultant/speaker for Sage Therapeutics. Dr. Rasminsky has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.

AAP ‘silencing debate’ on gender dysphoria, says doctor group
The American Academy of Pediatrics (AAP) is at the center of a row with an international group of doctors who question whether hormone treatment is the most appropriate way to treat adolescents with gender dysphoria.
After initially accepting the application and payment from the Society for Evidence-Based Gender Medicine (SEGM) for the organization to have an information booth at the AAP annual meeting in October, the AAP did a U-turn earlier this month and canceled the registration, with no explanation as to why.
“Just days earlier,” says SEGM in a statement on its website, “over 80% of AAP members” had indicated they wanted more discussion on the topic of “addressing alternatives to the use of hormone therapies for gender dysphoric youth.”
“This rejection sends a strong signal that the AAP does not want to see any debate on what constitutes evidence-based care for gender-diverse youth,” they add.
Asked for an explanation as to why it accepted but later rescinded SEGM’s application for a booth, the AAP has given no response to date.
A Wall Street Journal article on the furor, published last week, has clocked up 785 comments to date.
There has been an exponential increase in the number of adolescents who identify as transgender – reporting discomfort with their birth sex – in Western countries, and the debate has been covered in detail, having intensified worldwide in the last 12 months, regarding how best to treat youth with gender dysphoria.
Although “affirmative” medical care, defined as treatment with puberty blockers and cross-sex hormones to transition to the opposite sex, is supported by the AAP and other medical organizations, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed, given that there are a number of irreversible changes associated with treatment. There is also a growing number of “detransitioners” – mostly young people who transitioned and then changed their minds, and “detransitioned” back to their birth sex.
“Because of the low quality of the available evidence and the marked change in the presentation of gender dysphoria in youth in the last several years (many more adolescents with recently emerging transgender identities and significant mental health comorbidities are presenting for care), what constitutes good health care for this patient group is far from clear,” notes SEGM.
“Quelling the debate will not help America’s pediatricians guide patients and their families based on best available evidence. The politicization of the field of gender medicine must end, if we care about gender-variant youth and their long-term health,” they conclude.
A version of this article first appeared on Medscape.com.
The American Academy of Pediatrics (AAP) is at the center of a row with an international group of doctors who question whether hormone treatment is the most appropriate way to treat adolescents with gender dysphoria.
After initially accepting the application and payment from the Society for Evidence-Based Gender Medicine (SEGM) for the organization to have an information booth at the AAP annual meeting in October, the AAP did a U-turn earlier this month and canceled the registration, with no explanation as to why.
“Just days earlier,” says SEGM in a statement on its website, “over 80% of AAP members” had indicated they wanted more discussion on the topic of “addressing alternatives to the use of hormone therapies for gender dysphoric youth.”
“This rejection sends a strong signal that the AAP does not want to see any debate on what constitutes evidence-based care for gender-diverse youth,” they add.
Asked for an explanation as to why it accepted but later rescinded SEGM’s application for a booth, the AAP has given no response to date.
A Wall Street Journal article on the furor, published last week, has clocked up 785 comments to date.
There has been an exponential increase in the number of adolescents who identify as transgender – reporting discomfort with their birth sex – in Western countries, and the debate has been covered in detail, having intensified worldwide in the last 12 months, regarding how best to treat youth with gender dysphoria.
Although “affirmative” medical care, defined as treatment with puberty blockers and cross-sex hormones to transition to the opposite sex, is supported by the AAP and other medical organizations, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed, given that there are a number of irreversible changes associated with treatment. There is also a growing number of “detransitioners” – mostly young people who transitioned and then changed their minds, and “detransitioned” back to their birth sex.
“Because of the low quality of the available evidence and the marked change in the presentation of gender dysphoria in youth in the last several years (many more adolescents with recently emerging transgender identities and significant mental health comorbidities are presenting for care), what constitutes good health care for this patient group is far from clear,” notes SEGM.
“Quelling the debate will not help America’s pediatricians guide patients and their families based on best available evidence. The politicization of the field of gender medicine must end, if we care about gender-variant youth and their long-term health,” they conclude.
A version of this article first appeared on Medscape.com.
The American Academy of Pediatrics (AAP) is at the center of a row with an international group of doctors who question whether hormone treatment is the most appropriate way to treat adolescents with gender dysphoria.
After initially accepting the application and payment from the Society for Evidence-Based Gender Medicine (SEGM) for the organization to have an information booth at the AAP annual meeting in October, the AAP did a U-turn earlier this month and canceled the registration, with no explanation as to why.
“Just days earlier,” says SEGM in a statement on its website, “over 80% of AAP members” had indicated they wanted more discussion on the topic of “addressing alternatives to the use of hormone therapies for gender dysphoric youth.”
“This rejection sends a strong signal that the AAP does not want to see any debate on what constitutes evidence-based care for gender-diverse youth,” they add.
Asked for an explanation as to why it accepted but later rescinded SEGM’s application for a booth, the AAP has given no response to date.
A Wall Street Journal article on the furor, published last week, has clocked up 785 comments to date.
There has been an exponential increase in the number of adolescents who identify as transgender – reporting discomfort with their birth sex – in Western countries, and the debate has been covered in detail, having intensified worldwide in the last 12 months, regarding how best to treat youth with gender dysphoria.
Although “affirmative” medical care, defined as treatment with puberty blockers and cross-sex hormones to transition to the opposite sex, is supported by the AAP and other medical organizations, there is growing concern among many doctors and other health care professionals as to whether this is, in fact, the best way to proceed, given that there are a number of irreversible changes associated with treatment. There is also a growing number of “detransitioners” – mostly young people who transitioned and then changed their minds, and “detransitioned” back to their birth sex.
“Because of the low quality of the available evidence and the marked change in the presentation of gender dysphoria in youth in the last several years (many more adolescents with recently emerging transgender identities and significant mental health comorbidities are presenting for care), what constitutes good health care for this patient group is far from clear,” notes SEGM.
“Quelling the debate will not help America’s pediatricians guide patients and their families based on best available evidence. The politicization of the field of gender medicine must end, if we care about gender-variant youth and their long-term health,” they conclude.
A version of this article first appeared on Medscape.com.