User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
‘We just have to keep them alive’: Transitioning youth with type 1 diabetes
“No one has asked young people what they want,” said Tabitha Randell, MBChB, an endocrinologist with Nottingham (England) University Hospitals NHS Trust, who specializes in treating teenagers with type 1 diabetes as they transition to adult care.
Dr. Randell, who has set up a very successful specialist service in her hospital for such patients, said: “We consistently have the best, or the second best, outcomes in this country for our diabetes patients.” She believes this is one of the most important issues in modern endocrinology today.

Speaking at the Diabetes Professional Care conference in London at the end of 2021, and sharing her thoughts afterward with this news organization, she noted that in general there are “virtually no published outcomes” on how best to transition a patient with type 1 diabetes from pediatric to adult care.
“If you actually get them to transition – because some just drop out and disengage and there’s nothing you can do – none of them get lost. Some of them disengage in the adult clinic, but if you’re in the young diabetes service [in England] the rules are that if you miss a diabetes appointment you do not get discharged, as compared with the adult clinic, where if you miss an appointment, you are discharged.”
In the young diabetes clinic, doctors will “carry on trying to contact you, and get you back,” she explained. “And the patients do eventually come back in – it might be a year or 2, but they do come back. We’ve just got to keep them alive in the meantime!”
This issue needs tackling all over the world. Dr. Randell said she’s not aware of any one country – although there may be “pockets” of good care within a given country – that is doing this perfectly.
Across the pond, Grazia Aleppo, MD, division of endocrinology at Northwestern University, Chicago, agreed that transitioning pediatric patients with type 1 diabetes to adult care presents “unique challenges.”
Challenges when transitioning from pediatric to adult care
During childhood, type 1 diabetes management is largely supervised by patients’ parents and members of the pediatric diabetes care team, which may include diabetes educators, psychologists, or social workers, as well as pediatric endocrinologists.
When the patient with type 1 diabetes becomes a young adult and takes over management of their own health, Dr. Aleppo said, the care team may diminish along with the time spent in provider visits.
The adult endocrinology setting focuses more on self-management and autonomous functioning of the individual with diabetes.
Adult appointments are typically shorter, and the patient is usually expected to follow doctors’ suggestions independently, she noted. They are also expected to manage the practical aspects of their diabetes care, including prescriptions, diabetes supplies, laboratory tests, scheduling, and keeping appointments.
At the same time that the emerging adult needs to start asserting independence over their health care, they will also be going through a myriad of other important lifestyle changes, such as attending college, living on their own for the first time, and starting a career.
“With these fundamental differences and challenges, competing priorities, such as college, work and relationships, medical care may become of secondary importance and patients may become disengaged,” Dr. Aleppo explained.
As Dr. Randell has said, loss to follow-up is a big problem with this patient population, with disengagement from specialist services and worsening A1c across the transition, Dr. Aleppo noted. This makes addressing these patients’ specific needs extremely important.
Engage with kid, not disease; don’t palm them off on new recruits
“The really key thing these kids say is, ‘I do not want to be a disease,’” Dr. Randell said. “They want you to know that they are a person. Engage these kids!” she suggested. “Ask them: ‘How is your exam revision going?’ Find something positive to say, even if it’s just: ‘I’m glad you came today.’ ”
“If the first thing that you do is tell them off [for poor diabetes care], you are never going to see them again,” she cautioned.
Dr. Randell also said that role models with type 1 diabetes, such as Lila Moss – daughter of British supermodel Kate Moss – who was recently pictured wearing an insulin pump on her leg on the catwalk, are helping youngsters not feel so self-conscious about their diabetes.
“Let them know it’s not the end of the world, having [type 1] diabetes,” she emphasized.
And Partha Kar, MBBS, OBE, national specialty advisor, diabetes with NHS England, agreed wholeheartedly with Dr. Randall.
Reminiscing about his early days as a newly qualified endocrinologist, Dr. Kar, who works at Portsmouth (England) Hospital NHS Trust, noted that as a new member of staff he was given the youth with type 1 diabetes – those getting ready to transition to adult care – to look after.
But this is the exact opposite of what should be happening, he emphasized. “If you don’t think transition care is important, you shouldn’t be treating type 1 diabetes.”
He believes that every diabetes center “must have a young-adult team lead” and this job must not be given to the least experienced member of staff.
This lead “doesn’t need to be a doctor,” Dr. Kar stressed. “It can be a psychologist, or a diabetes nurse, or a pharmacist, or a dietician.”
In short, it must be someone experienced who loves working with this age group.
Dr. Randell agreed: “Make sure the team is interested in young people. It shouldn’t be the last person in who gets the job no one else wants.” Teens “are my favorite group to work with. They don’t take any nonsense.”
And she explained: “Young people like to get to know the person who’s going to take care of them. So, stay with them for their young adult years.” This can be “quite a fluid period,” with it normally extending to age 25, but in some cases, “it can be up to 32 years old.”
Preparing for the transition
To ease pediatric patients into the transition to adult care, Dr. Aleppo recommended that the pediatric diabetes team provide enough time so that any concerns the patient and their family may have can be addressed.
This should also include transferring management responsibilities to the young adult rather than their parent.
The pediatric provider should discuss with the patient available potential adult colleagues, personalizing these options to their needs, she said.
And the adult and pediatric clinicians should collaborate and provide important information beyond medical records or health summaries.
Adult providers should guide young adults on how to navigate the new practices, from scheduling follow-up appointments to policies regarding medication refills or supplies, to providing information about urgent numbers or email addresses for after-hours communications.
Dr. Kar reiterated that there are too few published outcomes in this patient group to guide the establishment of good transition services.
“Without data, we are dead on the ground. Without data, it’s all conjecture, anecdotes,” he said.
What he does know is that, in the latest national type 1 diabetes audit for England, “Diabetic ketoacidosis admissions ... are up in this age group,” which suggests these patients are not receiving adequate care.
Be a guide, not a gatekeeper
Dr. Kar stressed that, of the 8,760 hours in a year, the average patient with type 1 diabetes in the United Kingdom gets just “1-2 hours with you as a clinician, based on four appointments per year of 30 minutes each.”
“So you spend 0.02% of their time with individuals with type 1 diabetes. So, what’s the one thing you can do with that minimal contact? Be nice!”
Dr. Kar said he always has his email open to his adult patients and they are very respectful of his time. “They don’t email you at 1 a.m. That means every one of my patients has got support [from me]. Don’t be a barrier.”
“We have to fundamentally change the narrative. Doctors must have more empathy,” he said, stating that the one thing adolescents have constantly given feedback on has been, “Why don’t appointments start with: ‘How are you?’
“For a teenager, if you throw type 1 diabetes into the loop, it’s not easy,” he stressed. “Talk to them about something else. As a clinician, be a guide, not a gatekeeper. Give people the tools to self-manage better.”
Adult providers can meet these young adult patients “at their level,” Dr. Aleppo agreed.
“Pay attention to their immediate needs and focus on their present circumstances – whether how to get through their next semester in college, navigating job interviews, or handling having diabetes in the workplace.”
Paying attention to the mental health needs of these young patients is equally “paramount,” Dr. Aleppo said.
While access to mental health professionals may be challenging in the adult setting, providers should bring it up with their patients and offer counseling referrals.
“Diabetes impacts everything, and office appointments and conversations carry weight on these patients’ lives as a whole, not just on their diabetes,” she stressed. “A patient told me recently: ‘We’re learning to be adults,’ which can be hard enough, and with diabetes it can be even more challenging. Adult providers need to be aware of the patient’s ‘diabetes language’ in that often it is not what a patient is saying, rather how they are saying it that gives us information on what they truly need.
“As adult providers, we need to also train and teach our young patients to advocate for themselves on where to find resources that can help them navigate adulthood with diabetes,” she added.
One particularly helpful resource in the United States is the College Diabetes Network, a not-for-profit organization whose mission is to equip young adults with type 1 diabetes to successfully manage the challenging transition to independence at college and beyond.
“The sweetest thing that can happen to us as adult diabetes providers is when a patient – seen as an emerging adult during college – returns to your practice 10 years later after moving back and seeks you out for their diabetes care because of the relationship and trust you developed in those transitioning years,” Dr. Aleppo said.
Another resource is a freely available comic book series cocreated by Dr. Kar and colleague Mayank Patel, MBBS, an endocrinologist from University Hospital Southampton NHS Foundation Trust.
As detailed by this news organization in 2021, the series consists of three volumes: the first, Type 1: Origins, focuses on actual experiences of patients who have type 1 diabetes; the second, Type 1: Attack of the Ketones, is aimed at professionals who may provide care but have limited understanding of type 1 diabetes; and the third, Type 1 Mission 3: S.T.I.G.M.A., addresses the stigmas and misconceptions that patients with type 1 diabetes may face.
The idea for the first comic was inspired by a patient who compared having diabetes to being like the Marvel character The Hulk, said Dr. Kar, and has been expanded to include the additional volumes.
Dr. Kar and Dr. Patel have also just launched the fourth comic in the series, Type 1: Generations, to mark the 100-year anniversary since insulin was first given to a human.
“This is high priority”
Dr. Kar said the NHS in England has just appointed a national lead for type 1 diabetes in youth, Fulya Mehta, MD, of Alder Hey Children’s NHS Foundation Trust, Liverpool, England.
“If you have a plan, bring it to us,” he told the audience at the DPC conference, and “tell us, what is the one thing you would change? This is not a session we are doing just to tick a box. This is high priority.
“Encourage your colleagues to think about transition services. This is an absolute priority. We will be asking every center [in England] who is your transitioning lead?”
And he once again stressed that “a lead of transition service does not have to be a medic. This should be a multidisciplinary team. But they do need to be comfortable in that space. To that teenager, your job title means nothing. Give them time and space.”
Dr. Randell summed it up: “If we can work together, it’s only going to result in better outcomes. We need to blaze the trail for young people.”
Dr. Aleppo has reported serving as a consultant to Dexcom and Insulet and receiving support to Northwestern University from AstraZeneca, Dexcom, Eli Lilly, Fractyl Health, Insulet, and Novo Nordisk. Dr. Randell and Dr. Kar have no conflicts of interest.
A version of this article first appeared on Medscape.com.
“No one has asked young people what they want,” said Tabitha Randell, MBChB, an endocrinologist with Nottingham (England) University Hospitals NHS Trust, who specializes in treating teenagers with type 1 diabetes as they transition to adult care.
Dr. Randell, who has set up a very successful specialist service in her hospital for such patients, said: “We consistently have the best, or the second best, outcomes in this country for our diabetes patients.” She believes this is one of the most important issues in modern endocrinology today.
Speaking at the Diabetes Professional Care conference in London at the end of 2021, and sharing her thoughts afterward with this news organization, she noted that in general there are “virtually no published outcomes” on how best to transition a patient with type 1 diabetes from pediatric to adult care.
“If you actually get them to transition – because some just drop out and disengage and there’s nothing you can do – none of them get lost. Some of them disengage in the adult clinic, but if you’re in the young diabetes service [in England] the rules are that if you miss a diabetes appointment you do not get discharged, as compared with the adult clinic, where if you miss an appointment, you are discharged.”
In the young diabetes clinic, doctors will “carry on trying to contact you, and get you back,” she explained. “And the patients do eventually come back in – it might be a year or 2, but they do come back. We’ve just got to keep them alive in the meantime!”
This issue needs tackling all over the world. Dr. Randell said she’s not aware of any one country – although there may be “pockets” of good care within a given country – that is doing this perfectly.
Across the pond, Grazia Aleppo, MD, division of endocrinology at Northwestern University, Chicago, agreed that transitioning pediatric patients with type 1 diabetes to adult care presents “unique challenges.”
Challenges when transitioning from pediatric to adult care
During childhood, type 1 diabetes management is largely supervised by patients’ parents and members of the pediatric diabetes care team, which may include diabetes educators, psychologists, or social workers, as well as pediatric endocrinologists.
When the patient with type 1 diabetes becomes a young adult and takes over management of their own health, Dr. Aleppo said, the care team may diminish along with the time spent in provider visits.
The adult endocrinology setting focuses more on self-management and autonomous functioning of the individual with diabetes.
Adult appointments are typically shorter, and the patient is usually expected to follow doctors’ suggestions independently, she noted. They are also expected to manage the practical aspects of their diabetes care, including prescriptions, diabetes supplies, laboratory tests, scheduling, and keeping appointments.
At the same time that the emerging adult needs to start asserting independence over their health care, they will also be going through a myriad of other important lifestyle changes, such as attending college, living on their own for the first time, and starting a career.
“With these fundamental differences and challenges, competing priorities, such as college, work and relationships, medical care may become of secondary importance and patients may become disengaged,” Dr. Aleppo explained.
As Dr. Randell has said, loss to follow-up is a big problem with this patient population, with disengagement from specialist services and worsening A1c across the transition, Dr. Aleppo noted. This makes addressing these patients’ specific needs extremely important.
Engage with kid, not disease; don’t palm them off on new recruits
“The really key thing these kids say is, ‘I do not want to be a disease,’” Dr. Randell said. “They want you to know that they are a person. Engage these kids!” she suggested. “Ask them: ‘How is your exam revision going?’ Find something positive to say, even if it’s just: ‘I’m glad you came today.’ ”
“If the first thing that you do is tell them off [for poor diabetes care], you are never going to see them again,” she cautioned.
Dr. Randell also said that role models with type 1 diabetes, such as Lila Moss – daughter of British supermodel Kate Moss – who was recently pictured wearing an insulin pump on her leg on the catwalk, are helping youngsters not feel so self-conscious about their diabetes.
“Let them know it’s not the end of the world, having [type 1] diabetes,” she emphasized.
And Partha Kar, MBBS, OBE, national specialty advisor, diabetes with NHS England, agreed wholeheartedly with Dr. Randall.
Reminiscing about his early days as a newly qualified endocrinologist, Dr. Kar, who works at Portsmouth (England) Hospital NHS Trust, noted that as a new member of staff he was given the youth with type 1 diabetes – those getting ready to transition to adult care – to look after.
But this is the exact opposite of what should be happening, he emphasized. “If you don’t think transition care is important, you shouldn’t be treating type 1 diabetes.”
He believes that every diabetes center “must have a young-adult team lead” and this job must not be given to the least experienced member of staff.
This lead “doesn’t need to be a doctor,” Dr. Kar stressed. “It can be a psychologist, or a diabetes nurse, or a pharmacist, or a dietician.”
In short, it must be someone experienced who loves working with this age group.
Dr. Randell agreed: “Make sure the team is interested in young people. It shouldn’t be the last person in who gets the job no one else wants.” Teens “are my favorite group to work with. They don’t take any nonsense.”
And she explained: “Young people like to get to know the person who’s going to take care of them. So, stay with them for their young adult years.” This can be “quite a fluid period,” with it normally extending to age 25, but in some cases, “it can be up to 32 years old.”
Preparing for the transition
To ease pediatric patients into the transition to adult care, Dr. Aleppo recommended that the pediatric diabetes team provide enough time so that any concerns the patient and their family may have can be addressed.
This should also include transferring management responsibilities to the young adult rather than their parent.
The pediatric provider should discuss with the patient available potential adult colleagues, personalizing these options to their needs, she said.
And the adult and pediatric clinicians should collaborate and provide important information beyond medical records or health summaries.
Adult providers should guide young adults on how to navigate the new practices, from scheduling follow-up appointments to policies regarding medication refills or supplies, to providing information about urgent numbers or email addresses for after-hours communications.
Dr. Kar reiterated that there are too few published outcomes in this patient group to guide the establishment of good transition services.
“Without data, we are dead on the ground. Without data, it’s all conjecture, anecdotes,” he said.
What he does know is that, in the latest national type 1 diabetes audit for England, “Diabetic ketoacidosis admissions ... are up in this age group,” which suggests these patients are not receiving adequate care.
Be a guide, not a gatekeeper
Dr. Kar stressed that, of the 8,760 hours in a year, the average patient with type 1 diabetes in the United Kingdom gets just “1-2 hours with you as a clinician, based on four appointments per year of 30 minutes each.”
“So you spend 0.02% of their time with individuals with type 1 diabetes. So, what’s the one thing you can do with that minimal contact? Be nice!”
Dr. Kar said he always has his email open to his adult patients and they are very respectful of his time. “They don’t email you at 1 a.m. That means every one of my patients has got support [from me]. Don’t be a barrier.”
“We have to fundamentally change the narrative. Doctors must have more empathy,” he said, stating that the one thing adolescents have constantly given feedback on has been, “Why don’t appointments start with: ‘How are you?’
“For a teenager, if you throw type 1 diabetes into the loop, it’s not easy,” he stressed. “Talk to them about something else. As a clinician, be a guide, not a gatekeeper. Give people the tools to self-manage better.”
Adult providers can meet these young adult patients “at their level,” Dr. Aleppo agreed.
“Pay attention to their immediate needs and focus on their present circumstances – whether how to get through their next semester in college, navigating job interviews, or handling having diabetes in the workplace.”
Paying attention to the mental health needs of these young patients is equally “paramount,” Dr. Aleppo said.
While access to mental health professionals may be challenging in the adult setting, providers should bring it up with their patients and offer counseling referrals.
“Diabetes impacts everything, and office appointments and conversations carry weight on these patients’ lives as a whole, not just on their diabetes,” she stressed. “A patient told me recently: ‘We’re learning to be adults,’ which can be hard enough, and with diabetes it can be even more challenging. Adult providers need to be aware of the patient’s ‘diabetes language’ in that often it is not what a patient is saying, rather how they are saying it that gives us information on what they truly need.
“As adult providers, we need to also train and teach our young patients to advocate for themselves on where to find resources that can help them navigate adulthood with diabetes,” she added.
One particularly helpful resource in the United States is the College Diabetes Network, a not-for-profit organization whose mission is to equip young adults with type 1 diabetes to successfully manage the challenging transition to independence at college and beyond.
“The sweetest thing that can happen to us as adult diabetes providers is when a patient – seen as an emerging adult during college – returns to your practice 10 years later after moving back and seeks you out for their diabetes care because of the relationship and trust you developed in those transitioning years,” Dr. Aleppo said.
Another resource is a freely available comic book series cocreated by Dr. Kar and colleague Mayank Patel, MBBS, an endocrinologist from University Hospital Southampton NHS Foundation Trust.
As detailed by this news organization in 2021, the series consists of three volumes: the first, Type 1: Origins, focuses on actual experiences of patients who have type 1 diabetes; the second, Type 1: Attack of the Ketones, is aimed at professionals who may provide care but have limited understanding of type 1 diabetes; and the third, Type 1 Mission 3: S.T.I.G.M.A., addresses the stigmas and misconceptions that patients with type 1 diabetes may face.
The idea for the first comic was inspired by a patient who compared having diabetes to being like the Marvel character The Hulk, said Dr. Kar, and has been expanded to include the additional volumes.
Dr. Kar and Dr. Patel have also just launched the fourth comic in the series, Type 1: Generations, to mark the 100-year anniversary since insulin was first given to a human.
“This is high priority”
Dr. Kar said the NHS in England has just appointed a national lead for type 1 diabetes in youth, Fulya Mehta, MD, of Alder Hey Children’s NHS Foundation Trust, Liverpool, England.
“If you have a plan, bring it to us,” he told the audience at the DPC conference, and “tell us, what is the one thing you would change? This is not a session we are doing just to tick a box. This is high priority.
“Encourage your colleagues to think about transition services. This is an absolute priority. We will be asking every center [in England] who is your transitioning lead?”
And he once again stressed that “a lead of transition service does not have to be a medic. This should be a multidisciplinary team. But they do need to be comfortable in that space. To that teenager, your job title means nothing. Give them time and space.”
Dr. Randell summed it up: “If we can work together, it’s only going to result in better outcomes. We need to blaze the trail for young people.”
Dr. Aleppo has reported serving as a consultant to Dexcom and Insulet and receiving support to Northwestern University from AstraZeneca, Dexcom, Eli Lilly, Fractyl Health, Insulet, and Novo Nordisk. Dr. Randell and Dr. Kar have no conflicts of interest.
A version of this article first appeared on Medscape.com.
“No one has asked young people what they want,” said Tabitha Randell, MBChB, an endocrinologist with Nottingham (England) University Hospitals NHS Trust, who specializes in treating teenagers with type 1 diabetes as they transition to adult care.
Dr. Randell, who has set up a very successful specialist service in her hospital for such patients, said: “We consistently have the best, or the second best, outcomes in this country for our diabetes patients.” She believes this is one of the most important issues in modern endocrinology today.
Speaking at the Diabetes Professional Care conference in London at the end of 2021, and sharing her thoughts afterward with this news organization, she noted that in general there are “virtually no published outcomes” on how best to transition a patient with type 1 diabetes from pediatric to adult care.
“If you actually get them to transition – because some just drop out and disengage and there’s nothing you can do – none of them get lost. Some of them disengage in the adult clinic, but if you’re in the young diabetes service [in England] the rules are that if you miss a diabetes appointment you do not get discharged, as compared with the adult clinic, where if you miss an appointment, you are discharged.”
In the young diabetes clinic, doctors will “carry on trying to contact you, and get you back,” she explained. “And the patients do eventually come back in – it might be a year or 2, but they do come back. We’ve just got to keep them alive in the meantime!”
This issue needs tackling all over the world. Dr. Randell said she’s not aware of any one country – although there may be “pockets” of good care within a given country – that is doing this perfectly.
Across the pond, Grazia Aleppo, MD, division of endocrinology at Northwestern University, Chicago, agreed that transitioning pediatric patients with type 1 diabetes to adult care presents “unique challenges.”
Challenges when transitioning from pediatric to adult care
During childhood, type 1 diabetes management is largely supervised by patients’ parents and members of the pediatric diabetes care team, which may include diabetes educators, psychologists, or social workers, as well as pediatric endocrinologists.
When the patient with type 1 diabetes becomes a young adult and takes over management of their own health, Dr. Aleppo said, the care team may diminish along with the time spent in provider visits.
The adult endocrinology setting focuses more on self-management and autonomous functioning of the individual with diabetes.
Adult appointments are typically shorter, and the patient is usually expected to follow doctors’ suggestions independently, she noted. They are also expected to manage the practical aspects of their diabetes care, including prescriptions, diabetes supplies, laboratory tests, scheduling, and keeping appointments.
At the same time that the emerging adult needs to start asserting independence over their health care, they will also be going through a myriad of other important lifestyle changes, such as attending college, living on their own for the first time, and starting a career.
“With these fundamental differences and challenges, competing priorities, such as college, work and relationships, medical care may become of secondary importance and patients may become disengaged,” Dr. Aleppo explained.
As Dr. Randell has said, loss to follow-up is a big problem with this patient population, with disengagement from specialist services and worsening A1c across the transition, Dr. Aleppo noted. This makes addressing these patients’ specific needs extremely important.
Engage with kid, not disease; don’t palm them off on new recruits
“The really key thing these kids say is, ‘I do not want to be a disease,’” Dr. Randell said. “They want you to know that they are a person. Engage these kids!” she suggested. “Ask them: ‘How is your exam revision going?’ Find something positive to say, even if it’s just: ‘I’m glad you came today.’ ”
“If the first thing that you do is tell them off [for poor diabetes care], you are never going to see them again,” she cautioned.
Dr. Randell also said that role models with type 1 diabetes, such as Lila Moss – daughter of British supermodel Kate Moss – who was recently pictured wearing an insulin pump on her leg on the catwalk, are helping youngsters not feel so self-conscious about their diabetes.
“Let them know it’s not the end of the world, having [type 1] diabetes,” she emphasized.
And Partha Kar, MBBS, OBE, national specialty advisor, diabetes with NHS England, agreed wholeheartedly with Dr. Randall.
Reminiscing about his early days as a newly qualified endocrinologist, Dr. Kar, who works at Portsmouth (England) Hospital NHS Trust, noted that as a new member of staff he was given the youth with type 1 diabetes – those getting ready to transition to adult care – to look after.
But this is the exact opposite of what should be happening, he emphasized. “If you don’t think transition care is important, you shouldn’t be treating type 1 diabetes.”
He believes that every diabetes center “must have a young-adult team lead” and this job must not be given to the least experienced member of staff.
This lead “doesn’t need to be a doctor,” Dr. Kar stressed. “It can be a psychologist, or a diabetes nurse, or a pharmacist, or a dietician.”
In short, it must be someone experienced who loves working with this age group.
Dr. Randell agreed: “Make sure the team is interested in young people. It shouldn’t be the last person in who gets the job no one else wants.” Teens “are my favorite group to work with. They don’t take any nonsense.”
And she explained: “Young people like to get to know the person who’s going to take care of them. So, stay with them for their young adult years.” This can be “quite a fluid period,” with it normally extending to age 25, but in some cases, “it can be up to 32 years old.”
Preparing for the transition
To ease pediatric patients into the transition to adult care, Dr. Aleppo recommended that the pediatric diabetes team provide enough time so that any concerns the patient and their family may have can be addressed.
This should also include transferring management responsibilities to the young adult rather than their parent.
The pediatric provider should discuss with the patient available potential adult colleagues, personalizing these options to their needs, she said.
And the adult and pediatric clinicians should collaborate and provide important information beyond medical records or health summaries.
Adult providers should guide young adults on how to navigate the new practices, from scheduling follow-up appointments to policies regarding medication refills or supplies, to providing information about urgent numbers or email addresses for after-hours communications.
Dr. Kar reiterated that there are too few published outcomes in this patient group to guide the establishment of good transition services.
“Without data, we are dead on the ground. Without data, it’s all conjecture, anecdotes,” he said.
What he does know is that, in the latest national type 1 diabetes audit for England, “Diabetic ketoacidosis admissions ... are up in this age group,” which suggests these patients are not receiving adequate care.
Be a guide, not a gatekeeper
Dr. Kar stressed that, of the 8,760 hours in a year, the average patient with type 1 diabetes in the United Kingdom gets just “1-2 hours with you as a clinician, based on four appointments per year of 30 minutes each.”
“So you spend 0.02% of their time with individuals with type 1 diabetes. So, what’s the one thing you can do with that minimal contact? Be nice!”
Dr. Kar said he always has his email open to his adult patients and they are very respectful of his time. “They don’t email you at 1 a.m. That means every one of my patients has got support [from me]. Don’t be a barrier.”
“We have to fundamentally change the narrative. Doctors must have more empathy,” he said, stating that the one thing adolescents have constantly given feedback on has been, “Why don’t appointments start with: ‘How are you?’
“For a teenager, if you throw type 1 diabetes into the loop, it’s not easy,” he stressed. “Talk to them about something else. As a clinician, be a guide, not a gatekeeper. Give people the tools to self-manage better.”
Adult providers can meet these young adult patients “at their level,” Dr. Aleppo agreed.
“Pay attention to their immediate needs and focus on their present circumstances – whether how to get through their next semester in college, navigating job interviews, or handling having diabetes in the workplace.”
Paying attention to the mental health needs of these young patients is equally “paramount,” Dr. Aleppo said.
While access to mental health professionals may be challenging in the adult setting, providers should bring it up with their patients and offer counseling referrals.
“Diabetes impacts everything, and office appointments and conversations carry weight on these patients’ lives as a whole, not just on their diabetes,” she stressed. “A patient told me recently: ‘We’re learning to be adults,’ which can be hard enough, and with diabetes it can be even more challenging. Adult providers need to be aware of the patient’s ‘diabetes language’ in that often it is not what a patient is saying, rather how they are saying it that gives us information on what they truly need.
“As adult providers, we need to also train and teach our young patients to advocate for themselves on where to find resources that can help them navigate adulthood with diabetes,” she added.
One particularly helpful resource in the United States is the College Diabetes Network, a not-for-profit organization whose mission is to equip young adults with type 1 diabetes to successfully manage the challenging transition to independence at college and beyond.
“The sweetest thing that can happen to us as adult diabetes providers is when a patient – seen as an emerging adult during college – returns to your practice 10 years later after moving back and seeks you out for their diabetes care because of the relationship and trust you developed in those transitioning years,” Dr. Aleppo said.
Another resource is a freely available comic book series cocreated by Dr. Kar and colleague Mayank Patel, MBBS, an endocrinologist from University Hospital Southampton NHS Foundation Trust.
As detailed by this news organization in 2021, the series consists of three volumes: the first, Type 1: Origins, focuses on actual experiences of patients who have type 1 diabetes; the second, Type 1: Attack of the Ketones, is aimed at professionals who may provide care but have limited understanding of type 1 diabetes; and the third, Type 1 Mission 3: S.T.I.G.M.A., addresses the stigmas and misconceptions that patients with type 1 diabetes may face.
The idea for the first comic was inspired by a patient who compared having diabetes to being like the Marvel character The Hulk, said Dr. Kar, and has been expanded to include the additional volumes.
Dr. Kar and Dr. Patel have also just launched the fourth comic in the series, Type 1: Generations, to mark the 100-year anniversary since insulin was first given to a human.
“This is high priority”
Dr. Kar said the NHS in England has just appointed a national lead for type 1 diabetes in youth, Fulya Mehta, MD, of Alder Hey Children’s NHS Foundation Trust, Liverpool, England.
“If you have a plan, bring it to us,” he told the audience at the DPC conference, and “tell us, what is the one thing you would change? This is not a session we are doing just to tick a box. This is high priority.
“Encourage your colleagues to think about transition services. This is an absolute priority. We will be asking every center [in England] who is your transitioning lead?”
And he once again stressed that “a lead of transition service does not have to be a medic. This should be a multidisciplinary team. But they do need to be comfortable in that space. To that teenager, your job title means nothing. Give them time and space.”
Dr. Randell summed it up: “If we can work together, it’s only going to result in better outcomes. We need to blaze the trail for young people.”
Dr. Aleppo has reported serving as a consultant to Dexcom and Insulet and receiving support to Northwestern University from AstraZeneca, Dexcom, Eli Lilly, Fractyl Health, Insulet, and Novo Nordisk. Dr. Randell and Dr. Kar have no conflicts of interest.
A version of this article first appeared on Medscape.com.
Learning a growth mindset
“Turns out smarter kids are made, not born.” The headline of the article leapt off the computer screen. Although I realize that it has limits when it comes to dissuading vaccine refusers, I believe that education is a critical element in the success of individuals and the societies they inhabit. However, I must admit to a bias based on my observations that, in general, cognitive skill is inherited. This is an opinion I suspect I share with most folks. You can understand why the article I discovered describing a recent study by several Harvard-based researchers caught my attention.
The study involved 33 mothers and their 1-year-old children. The researchers found that infants whose mothers were stressed and had a “fixed mindset” had lower brain activity than the infants of stressed mothers who held a “growth mindset.” You may be on top of the education literature but I had to do some heavy Googling to learn what was up with growth and fixed mindsets. Was this just a new riff on the whole mindfulness thing?

I quickly learned that in 2006 Carol Dweck, PhD, a psychologist now at Stanford, published a book titled “Mindset” (New York: Penguin Random House) in which she described individuals with a “fixed mindset” who believe that their personality or intelligence will not change over time. On the other hand, individuals with a “growth mindset” view their intelligence and personality as malleable. Her observations have spread across the education and self-help literature like a wildfire that has somehow been roaring along under my radar. I guess I have noticed a subtle change in emphasis when I hear some parents and educators praising a child’s effort in situations in which I might have expected them to say, “You’re so smart.” But, in general I have been clueless.
My initial impression was that this mindset stuff was just coining new buzz words to differentiate optimists from pessimists. But, here I am again revealing a fixed mindset bias. I probably should have said that someone demonstrating a growth mindset approach is “exercising optimism” instead of implying that they were simply born with a sunny disposition.
The growth mindset revolution has not been without skeptics and critics, which is not surprising because educators have a history of jumping on bandwagons before all the wheels have been completely tightened. However, the mindset approach does have some merit, especially for individuals in the center of the bell-shaped curve. We all know of individuals who have failed to meet or have exceeded what would seem to be rational expectations. It is likely that the degree to which a growth mindset approach was applied may be the explanation.
Which brings me to the question of whether we as pediatricians should be more careful of how we choose our words when talking to patients and parents. If the results of the study that alerted me to the growth mindset are reproducible, maybe we should be spending more time with new parents (all of whom are stressed by definition), helping them discover ways in which they can improve the situation they find themselves in by praising them for their efforts at parenting.
Should we be modeling growth mindset language by using it when we interact with our patients? For example, not just complimenting a child on the acquisition of a skill but adding that we were even more impressed by the effort required to acquire it. When we hear a parent clearly expressing a fixed mindset in describing their child should we correct them on the spot or make an appointment to discuss how adopting a growth mindset might help their child meet or exceed his or her potential?
Most smart children may be born that way, but there are always opportunities for improvement, and our patients and their parents need to believe that.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
“Turns out smarter kids are made, not born.” The headline of the article leapt off the computer screen. Although I realize that it has limits when it comes to dissuading vaccine refusers, I believe that education is a critical element in the success of individuals and the societies they inhabit. However, I must admit to a bias based on my observations that, in general, cognitive skill is inherited. This is an opinion I suspect I share with most folks. You can understand why the article I discovered describing a recent study by several Harvard-based researchers caught my attention.
The study involved 33 mothers and their 1-year-old children. The researchers found that infants whose mothers were stressed and had a “fixed mindset” had lower brain activity than the infants of stressed mothers who held a “growth mindset.” You may be on top of the education literature but I had to do some heavy Googling to learn what was up with growth and fixed mindsets. Was this just a new riff on the whole mindfulness thing?
I quickly learned that in 2006 Carol Dweck, PhD, a psychologist now at Stanford, published a book titled “Mindset” (New York: Penguin Random House) in which she described individuals with a “fixed mindset” who believe that their personality or intelligence will not change over time. On the other hand, individuals with a “growth mindset” view their intelligence and personality as malleable. Her observations have spread across the education and self-help literature like a wildfire that has somehow been roaring along under my radar. I guess I have noticed a subtle change in emphasis when I hear some parents and educators praising a child’s effort in situations in which I might have expected them to say, “You’re so smart.” But, in general I have been clueless.
My initial impression was that this mindset stuff was just coining new buzz words to differentiate optimists from pessimists. But, here I am again revealing a fixed mindset bias. I probably should have said that someone demonstrating a growth mindset approach is “exercising optimism” instead of implying that they were simply born with a sunny disposition.
The growth mindset revolution has not been without skeptics and critics, which is not surprising because educators have a history of jumping on bandwagons before all the wheels have been completely tightened. However, the mindset approach does have some merit, especially for individuals in the center of the bell-shaped curve. We all know of individuals who have failed to meet or have exceeded what would seem to be rational expectations. It is likely that the degree to which a growth mindset approach was applied may be the explanation.
Which brings me to the question of whether we as pediatricians should be more careful of how we choose our words when talking to patients and parents. If the results of the study that alerted me to the growth mindset are reproducible, maybe we should be spending more time with new parents (all of whom are stressed by definition), helping them discover ways in which they can improve the situation they find themselves in by praising them for their efforts at parenting.
Should we be modeling growth mindset language by using it when we interact with our patients? For example, not just complimenting a child on the acquisition of a skill but adding that we were even more impressed by the effort required to acquire it. When we hear a parent clearly expressing a fixed mindset in describing their child should we correct them on the spot or make an appointment to discuss how adopting a growth mindset might help their child meet or exceed his or her potential?
Most smart children may be born that way, but there are always opportunities for improvement, and our patients and their parents need to believe that.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
“Turns out smarter kids are made, not born.” The headline of the article leapt off the computer screen. Although I realize that it has limits when it comes to dissuading vaccine refusers, I believe that education is a critical element in the success of individuals and the societies they inhabit. However, I must admit to a bias based on my observations that, in general, cognitive skill is inherited. This is an opinion I suspect I share with most folks. You can understand why the article I discovered describing a recent study by several Harvard-based researchers caught my attention.
The study involved 33 mothers and their 1-year-old children. The researchers found that infants whose mothers were stressed and had a “fixed mindset” had lower brain activity than the infants of stressed mothers who held a “growth mindset.” You may be on top of the education literature but I had to do some heavy Googling to learn what was up with growth and fixed mindsets. Was this just a new riff on the whole mindfulness thing?
I quickly learned that in 2006 Carol Dweck, PhD, a psychologist now at Stanford, published a book titled “Mindset” (New York: Penguin Random House) in which she described individuals with a “fixed mindset” who believe that their personality or intelligence will not change over time. On the other hand, individuals with a “growth mindset” view their intelligence and personality as malleable. Her observations have spread across the education and self-help literature like a wildfire that has somehow been roaring along under my radar. I guess I have noticed a subtle change in emphasis when I hear some parents and educators praising a child’s effort in situations in which I might have expected them to say, “You’re so smart.” But, in general I have been clueless.
My initial impression was that this mindset stuff was just coining new buzz words to differentiate optimists from pessimists. But, here I am again revealing a fixed mindset bias. I probably should have said that someone demonstrating a growth mindset approach is “exercising optimism” instead of implying that they were simply born with a sunny disposition.
The growth mindset revolution has not been without skeptics and critics, which is not surprising because educators have a history of jumping on bandwagons before all the wheels have been completely tightened. However, the mindset approach does have some merit, especially for individuals in the center of the bell-shaped curve. We all know of individuals who have failed to meet or have exceeded what would seem to be rational expectations. It is likely that the degree to which a growth mindset approach was applied may be the explanation.
Which brings me to the question of whether we as pediatricians should be more careful of how we choose our words when talking to patients and parents. If the results of the study that alerted me to the growth mindset are reproducible, maybe we should be spending more time with new parents (all of whom are stressed by definition), helping them discover ways in which they can improve the situation they find themselves in by praising them for their efforts at parenting.
Should we be modeling growth mindset language by using it when we interact with our patients? For example, not just complimenting a child on the acquisition of a skill but adding that we were even more impressed by the effort required to acquire it. When we hear a parent clearly expressing a fixed mindset in describing their child should we correct them on the spot or make an appointment to discuss how adopting a growth mindset might help their child meet or exceed his or her potential?
Most smart children may be born that way, but there are always opportunities for improvement, and our patients and their parents need to believe that.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
100 coauthored papers, 10 years: Cancer transplant pioneers model 'team science'
On July 29, 2021, Sergio Giralt, MD, deputy division head of the division of hematologic malignancies and Miguel-Angel Perales, MD, chief of the adult bone marrow transplant service at MSKCC, published their 100th peer-reviewed paper as coauthors. Listing hundreds of such articles on a CV is standard for top-tier physicians, but the pair had gone one better: 100 publications written together in 10 years.
Their centenary article hit scientific newsstands almost exactly a decade after their first joint paper, which appeared in September 2011, not long after they met.
Born in Cuba, Dr. Giralt grew up in Venezuela. From the age of 14, he knew that medicine was his path, and in 1984 he earned a medical degree from the Universidad Central de Venezuela, Caracas. Next came a research position at Harvard Medical School, a residency at the Good Samaritan Hospital, Cincinnati, and a fellowship at the University of Texas MD Anderson Cancer Center, Houston. Dr. Giralt arrived at MSKCC in 2010 as the new chief of the adult bone marrow transplant service. There he was introduced to a new colleague, Dr. Perales. They soon learned that in addition to expertise in hematology, they had second language in common: Spanish.
Dr. Giralt said: “We both have a Spanish background and in a certain sense, there was an affinity there. ... We both have shared experiences.”
Dr. Perales was brought up in Belgium, a European nation with three official languages: French, Dutch, and German. He speaks five tongues in all and learned Spanish from his father, who came from Spain.
Fluency in Spanish enables both physicians to take care of the many New Yorkers who are more comfortable in that language – especially when navigating cancer treatment. However, both Dr. Giralt and Dr. Perales said that a second language is more than a professional tool. They described the enjoyable change of persona that happens when they switch to Spanish.
“People who are multilingual have different roles [as much as] different languages,” said Dr. Perales. “When I’m in Spanish, part of my brain is [thinking back to] summer vacations and hanging out with my cousins.”
When it comes to clinical science, however, English is the language of choice.
Global leaders in HSCT
Dr. Giralt and Dr. Perales are known worldwide in the field of allogeneic HSCT, a potentially curative treatment for an elongating list of both malignant and nonmalignant diseases.
In 1973, MSKCC conducted the first bone-marrow transplant from an unrelated donor. Fifty years on, medical oncologists in the United States conduct approximately 8,500 allogeneic transplants each year, 72% to treat acute leukemias or myelodysplastic syndrome (MDS).
However, stripping the immune system with intensive chemotherapy ‘conditioning,’ then rebuilding it with non-diseased donor hematopoietic cells is a hazardous undertaking. Older patients are less likely to survive the intensive conditioning, so historically have missed out. Also, even with a good human leukocyte antigen (HLA) match, the recipient needs often brutal immunosuppression.
Since Dr. Giralt and Dr. Perales began their partnership in 2010, the goals of their work have not changed: to develop safer, lower-intensity transplantation suitable for older, more vulnerable patients and reduce fearsome posttransplant sequelae such as graft-versus-host disease (GVHD).
Dr. Giralt’s publication list spans more than 600 peer-reviewed papers, articles and book chapters, almost exclusively on HSCT. Dr. Perales has more than 300 publication credits on the topic.
The two paired up on their first paper just months after Dr. Giralt arrived at MSKCC. That article, published in Biology of Blood and Marrow Transplantation, compared umbilical cord blood for HSCT with donor blood in 367 people with a variety of hematologic malignancies, including acute and chronic leukemias, MDS, and lymphoma.

The MSKCC team found that transplant-related mortality in the first 180 days was higher for the cord blood (21%), but thereafter mortality and relapse were much lower than for donated blood, with the result that 2-year progression-free survival of 55% was similar. Dr. Perales, Dr. Giralt and their coauthors concluded that the data provided “strong support” for further work on cord blood as an alternative stem-cell source.
During their first decade of collaboration, Dr. Giralt and Dr. Perales worked on any promising avenue that could improve outcomes and the experience of HSCT recipients, including reduced-intensity conditioning regimens to allow older adults to benefit from curative HSCT and donor T-cell depletion by CD34 selection, to reduce graft-versus-host disease (GVHD).
The CD34 protein is typically found on the surface of early stage and highly active stem cell types. Selecting these cell types using a range of techniques can eliminate many other potentially interfering or inactive cells. This enriches the transplant population with the most effective cells and can lower the risk of GVHD.
The 100th paper on which Dr. Giralt and Dr. Perales were coauthors was published in Blood Advances on July 27, 2021. The retrospective study examined the fate of 58 MSKCC patients with a rare form of chronic lymphocytic leukemia, CLL with Richter’s transformation (CLL-RT). It was the largest such study to date of this rare disease.
M.D. Anderson Cancer Center had shown in 2006 that, despite chemotherapy, overall survival in patients with CLL-RT was approximately 8 months. HSCT improved survival dramatically (75% at 3 years; n = 7). However, with the advent of novel targeted drugs for CLL such as ibrutinib (Imbruvica), venetoclax (Venclexta), or idelalisib (Zydelig), the MSKCC team asked themselves: What was the role of reduced-intensive conditioning HSCT? Was it even safe? Among other findings, Dr. Giralt and Dr. Perales’ 100th paper showed that reduced-intensity HSCT remained a viable alternative after a CLL-RT patient progressed on a novel agent.
Impact of the pandemic
When COVID-19 hit, the team lost many research staff and developed a huge backlog, said Dr. Giralt. He and Dr. Perales realized that they needed to be “thoughtful and careful” about which studies to continue. “For example, the CD-34 selection trials we did not close because these are our workhorse trials,” Dr. Giralt said. “We have people we need to treat, and some of the patients that we need to treat can only be treated on trial.”
The team was also able to pivot some of their work into COVID 19 itself, and they collected crucial information on HSCT in recovered COVID-19 patients, as an example.
“We were living through a critical time, but that doesn’t mean we [aren’t] obligated to continue our mission, our research mission,” said Dr. Giralt. “It really is team science. The way we look at it ... there’s a common thread: We both like to do allogeneic transplant, and we both believe in trying to make CD-34 selection better. So we’re both very much [working on] how can we improve what we call ‘the Memorial way’ of doing transplants. Where we separate is, Miguel does primarily lymphoma. He doesn’t do myeloma [like me]. So in those two areas, we’re helping develop the junior faculty in a different way.”
Something more in common
Right from the start, Dr. Perales and Dr. Giralt also shared a commitment to mentoring. Since 2010, Dr. Perales has mentored 22 up-and-coming junior faculty, including 10 from Europe (8 from Spain) and 2 from Latin America.
“[It makes] the research enterprise much more productive but [these young scientists] really increase the visibility of the program,” said Dr. Giralt.
He cited Dr. Perales’ track record of mentoring as one of the reasons for his promotion to chief of the adult bone marrow transplant service. In March 2020, Dr. Perales seamlessly stepped into Dr. Giralt’s shoes, while Dr. Giralt moved on to his present role as deputy division head of the division of hematologic malignancies.
Dr. Perales said: “The key aspect [of these promotions] is the fantastic working relationship that we’ve had over the years. ... I consider Sergio my mentor, but also a good friend and colleague. And so I think it’s this ability that we’ve had to work together and that relationship of trust, which has been key.”
“Sergio is somebody who lifts people up,” Dr. Perales added. “Many people will tell you that Sergio has helped them in their career. ... And I think that’s a lesson I’ve learned from him: training the next generation. And [that’s] not just in the U.S., but outside. I think that’s a key role that we have. And our responsibility.”
Asked to comment on their 100th-paper milestone, Dr. Perales firmly turned the spotlight from himself and Dr. Giralt to the junior investigators who have passed through the doors of the bone-marrow transplant program: “This body of work represents not just our collaboration but also the many contributions of our team at MSK ... and beyond MSK.”
This article was updated 1/26/22.
On July 29, 2021, Sergio Giralt, MD, deputy division head of the division of hematologic malignancies and Miguel-Angel Perales, MD, chief of the adult bone marrow transplant service at MSKCC, published their 100th peer-reviewed paper as coauthors. Listing hundreds of such articles on a CV is standard for top-tier physicians, but the pair had gone one better: 100 publications written together in 10 years.
Their centenary article hit scientific newsstands almost exactly a decade after their first joint paper, which appeared in September 2011, not long after they met.
Born in Cuba, Dr. Giralt grew up in Venezuela. From the age of 14, he knew that medicine was his path, and in 1984 he earned a medical degree from the Universidad Central de Venezuela, Caracas. Next came a research position at Harvard Medical School, a residency at the Good Samaritan Hospital, Cincinnati, and a fellowship at the University of Texas MD Anderson Cancer Center, Houston. Dr. Giralt arrived at MSKCC in 2010 as the new chief of the adult bone marrow transplant service. There he was introduced to a new colleague, Dr. Perales. They soon learned that in addition to expertise in hematology, they had second language in common: Spanish.
Dr. Giralt said: “We both have a Spanish background and in a certain sense, there was an affinity there. ... We both have shared experiences.”
Dr. Perales was brought up in Belgium, a European nation with three official languages: French, Dutch, and German. He speaks five tongues in all and learned Spanish from his father, who came from Spain.
Fluency in Spanish enables both physicians to take care of the many New Yorkers who are more comfortable in that language – especially when navigating cancer treatment. However, both Dr. Giralt and Dr. Perales said that a second language is more than a professional tool. They described the enjoyable change of persona that happens when they switch to Spanish.
“People who are multilingual have different roles [as much as] different languages,” said Dr. Perales. “When I’m in Spanish, part of my brain is [thinking back to] summer vacations and hanging out with my cousins.”
When it comes to clinical science, however, English is the language of choice.
Global leaders in HSCT
Dr. Giralt and Dr. Perales are known worldwide in the field of allogeneic HSCT, a potentially curative treatment for an elongating list of both malignant and nonmalignant diseases.
In 1973, MSKCC conducted the first bone-marrow transplant from an unrelated donor. Fifty years on, medical oncologists in the United States conduct approximately 8,500 allogeneic transplants each year, 72% to treat acute leukemias or myelodysplastic syndrome (MDS).
However, stripping the immune system with intensive chemotherapy ‘conditioning,’ then rebuilding it with non-diseased donor hematopoietic cells is a hazardous undertaking. Older patients are less likely to survive the intensive conditioning, so historically have missed out. Also, even with a good human leukocyte antigen (HLA) match, the recipient needs often brutal immunosuppression.
Since Dr. Giralt and Dr. Perales began their partnership in 2010, the goals of their work have not changed: to develop safer, lower-intensity transplantation suitable for older, more vulnerable patients and reduce fearsome posttransplant sequelae such as graft-versus-host disease (GVHD).
Dr. Giralt’s publication list spans more than 600 peer-reviewed papers, articles and book chapters, almost exclusively on HSCT. Dr. Perales has more than 300 publication credits on the topic.
The two paired up on their first paper just months after Dr. Giralt arrived at MSKCC. That article, published in Biology of Blood and Marrow Transplantation, compared umbilical cord blood for HSCT with donor blood in 367 people with a variety of hematologic malignancies, including acute and chronic leukemias, MDS, and lymphoma.
The MSKCC team found that transplant-related mortality in the first 180 days was higher for the cord blood (21%), but thereafter mortality and relapse were much lower than for donated blood, with the result that 2-year progression-free survival of 55% was similar. Dr. Perales, Dr. Giralt and their coauthors concluded that the data provided “strong support” for further work on cord blood as an alternative stem-cell source.
During their first decade of collaboration, Dr. Giralt and Dr. Perales worked on any promising avenue that could improve outcomes and the experience of HSCT recipients, including reduced-intensity conditioning regimens to allow older adults to benefit from curative HSCT and donor T-cell depletion by CD34 selection, to reduce graft-versus-host disease (GVHD).
The CD34 protein is typically found on the surface of early stage and highly active stem cell types. Selecting these cell types using a range of techniques can eliminate many other potentially interfering or inactive cells. This enriches the transplant population with the most effective cells and can lower the risk of GVHD.
The 100th paper on which Dr. Giralt and Dr. Perales were coauthors was published in Blood Advances on July 27, 2021. The retrospective study examined the fate of 58 MSKCC patients with a rare form of chronic lymphocytic leukemia, CLL with Richter’s transformation (CLL-RT). It was the largest such study to date of this rare disease.
M.D. Anderson Cancer Center had shown in 2006 that, despite chemotherapy, overall survival in patients with CLL-RT was approximately 8 months. HSCT improved survival dramatically (75% at 3 years; n = 7). However, with the advent of novel targeted drugs for CLL such as ibrutinib (Imbruvica), venetoclax (Venclexta), or idelalisib (Zydelig), the MSKCC team asked themselves: What was the role of reduced-intensive conditioning HSCT? Was it even safe? Among other findings, Dr. Giralt and Dr. Perales’ 100th paper showed that reduced-intensity HSCT remained a viable alternative after a CLL-RT patient progressed on a novel agent.
Impact of the pandemic
When COVID-19 hit, the team lost many research staff and developed a huge backlog, said Dr. Giralt. He and Dr. Perales realized that they needed to be “thoughtful and careful” about which studies to continue. “For example, the CD-34 selection trials we did not close because these are our workhorse trials,” Dr. Giralt said. “We have people we need to treat, and some of the patients that we need to treat can only be treated on trial.”
The team was also able to pivot some of their work into COVID 19 itself, and they collected crucial information on HSCT in recovered COVID-19 patients, as an example.
“We were living through a critical time, but that doesn’t mean we [aren’t] obligated to continue our mission, our research mission,” said Dr. Giralt. “It really is team science. The way we look at it ... there’s a common thread: We both like to do allogeneic transplant, and we both believe in trying to make CD-34 selection better. So we’re both very much [working on] how can we improve what we call ‘the Memorial way’ of doing transplants. Where we separate is, Miguel does primarily lymphoma. He doesn’t do myeloma [like me]. So in those two areas, we’re helping develop the junior faculty in a different way.”
Something more in common
Right from the start, Dr. Perales and Dr. Giralt also shared a commitment to mentoring. Since 2010, Dr. Perales has mentored 22 up-and-coming junior faculty, including 10 from Europe (8 from Spain) and 2 from Latin America.
“[It makes] the research enterprise much more productive but [these young scientists] really increase the visibility of the program,” said Dr. Giralt.
He cited Dr. Perales’ track record of mentoring as one of the reasons for his promotion to chief of the adult bone marrow transplant service. In March 2020, Dr. Perales seamlessly stepped into Dr. Giralt’s shoes, while Dr. Giralt moved on to his present role as deputy division head of the division of hematologic malignancies.
Dr. Perales said: “The key aspect [of these promotions] is the fantastic working relationship that we’ve had over the years. ... I consider Sergio my mentor, but also a good friend and colleague. And so I think it’s this ability that we’ve had to work together and that relationship of trust, which has been key.”
“Sergio is somebody who lifts people up,” Dr. Perales added. “Many people will tell you that Sergio has helped them in their career. ... And I think that’s a lesson I’ve learned from him: training the next generation. And [that’s] not just in the U.S., but outside. I think that’s a key role that we have. And our responsibility.”
Asked to comment on their 100th-paper milestone, Dr. Perales firmly turned the spotlight from himself and Dr. Giralt to the junior investigators who have passed through the doors of the bone-marrow transplant program: “This body of work represents not just our collaboration but also the many contributions of our team at MSK ... and beyond MSK.”
This article was updated 1/26/22.
On July 29, 2021, Sergio Giralt, MD, deputy division head of the division of hematologic malignancies and Miguel-Angel Perales, MD, chief of the adult bone marrow transplant service at MSKCC, published their 100th peer-reviewed paper as coauthors. Listing hundreds of such articles on a CV is standard for top-tier physicians, but the pair had gone one better: 100 publications written together in 10 years.
Their centenary article hit scientific newsstands almost exactly a decade after their first joint paper, which appeared in September 2011, not long after they met.
Born in Cuba, Dr. Giralt grew up in Venezuela. From the age of 14, he knew that medicine was his path, and in 1984 he earned a medical degree from the Universidad Central de Venezuela, Caracas. Next came a research position at Harvard Medical School, a residency at the Good Samaritan Hospital, Cincinnati, and a fellowship at the University of Texas MD Anderson Cancer Center, Houston. Dr. Giralt arrived at MSKCC in 2010 as the new chief of the adult bone marrow transplant service. There he was introduced to a new colleague, Dr. Perales. They soon learned that in addition to expertise in hematology, they had second language in common: Spanish.
Dr. Giralt said: “We both have a Spanish background and in a certain sense, there was an affinity there. ... We both have shared experiences.”
Dr. Perales was brought up in Belgium, a European nation with three official languages: French, Dutch, and German. He speaks five tongues in all and learned Spanish from his father, who came from Spain.
Fluency in Spanish enables both physicians to take care of the many New Yorkers who are more comfortable in that language – especially when navigating cancer treatment. However, both Dr. Giralt and Dr. Perales said that a second language is more than a professional tool. They described the enjoyable change of persona that happens when they switch to Spanish.
“People who are multilingual have different roles [as much as] different languages,” said Dr. Perales. “When I’m in Spanish, part of my brain is [thinking back to] summer vacations and hanging out with my cousins.”
When it comes to clinical science, however, English is the language of choice.
Global leaders in HSCT
Dr. Giralt and Dr. Perales are known worldwide in the field of allogeneic HSCT, a potentially curative treatment for an elongating list of both malignant and nonmalignant diseases.
In 1973, MSKCC conducted the first bone-marrow transplant from an unrelated donor. Fifty years on, medical oncologists in the United States conduct approximately 8,500 allogeneic transplants each year, 72% to treat acute leukemias or myelodysplastic syndrome (MDS).
However, stripping the immune system with intensive chemotherapy ‘conditioning,’ then rebuilding it with non-diseased donor hematopoietic cells is a hazardous undertaking. Older patients are less likely to survive the intensive conditioning, so historically have missed out. Also, even with a good human leukocyte antigen (HLA) match, the recipient needs often brutal immunosuppression.
Since Dr. Giralt and Dr. Perales began their partnership in 2010, the goals of their work have not changed: to develop safer, lower-intensity transplantation suitable for older, more vulnerable patients and reduce fearsome posttransplant sequelae such as graft-versus-host disease (GVHD).
Dr. Giralt’s publication list spans more than 600 peer-reviewed papers, articles and book chapters, almost exclusively on HSCT. Dr. Perales has more than 300 publication credits on the topic.
The two paired up on their first paper just months after Dr. Giralt arrived at MSKCC. That article, published in Biology of Blood and Marrow Transplantation, compared umbilical cord blood for HSCT with donor blood in 367 people with a variety of hematologic malignancies, including acute and chronic leukemias, MDS, and lymphoma.
The MSKCC team found that transplant-related mortality in the first 180 days was higher for the cord blood (21%), but thereafter mortality and relapse were much lower than for donated blood, with the result that 2-year progression-free survival of 55% was similar. Dr. Perales, Dr. Giralt and their coauthors concluded that the data provided “strong support” for further work on cord blood as an alternative stem-cell source.
During their first decade of collaboration, Dr. Giralt and Dr. Perales worked on any promising avenue that could improve outcomes and the experience of HSCT recipients, including reduced-intensity conditioning regimens to allow older adults to benefit from curative HSCT and donor T-cell depletion by CD34 selection, to reduce graft-versus-host disease (GVHD).
The CD34 protein is typically found on the surface of early stage and highly active stem cell types. Selecting these cell types using a range of techniques can eliminate many other potentially interfering or inactive cells. This enriches the transplant population with the most effective cells and can lower the risk of GVHD.
The 100th paper on which Dr. Giralt and Dr. Perales were coauthors was published in Blood Advances on July 27, 2021. The retrospective study examined the fate of 58 MSKCC patients with a rare form of chronic lymphocytic leukemia, CLL with Richter’s transformation (CLL-RT). It was the largest such study to date of this rare disease.
M.D. Anderson Cancer Center had shown in 2006 that, despite chemotherapy, overall survival in patients with CLL-RT was approximately 8 months. HSCT improved survival dramatically (75% at 3 years; n = 7). However, with the advent of novel targeted drugs for CLL such as ibrutinib (Imbruvica), venetoclax (Venclexta), or idelalisib (Zydelig), the MSKCC team asked themselves: What was the role of reduced-intensive conditioning HSCT? Was it even safe? Among other findings, Dr. Giralt and Dr. Perales’ 100th paper showed that reduced-intensity HSCT remained a viable alternative after a CLL-RT patient progressed on a novel agent.
Impact of the pandemic
When COVID-19 hit, the team lost many research staff and developed a huge backlog, said Dr. Giralt. He and Dr. Perales realized that they needed to be “thoughtful and careful” about which studies to continue. “For example, the CD-34 selection trials we did not close because these are our workhorse trials,” Dr. Giralt said. “We have people we need to treat, and some of the patients that we need to treat can only be treated on trial.”
The team was also able to pivot some of their work into COVID 19 itself, and they collected crucial information on HSCT in recovered COVID-19 patients, as an example.
“We were living through a critical time, but that doesn’t mean we [aren’t] obligated to continue our mission, our research mission,” said Dr. Giralt. “It really is team science. The way we look at it ... there’s a common thread: We both like to do allogeneic transplant, and we both believe in trying to make CD-34 selection better. So we’re both very much [working on] how can we improve what we call ‘the Memorial way’ of doing transplants. Where we separate is, Miguel does primarily lymphoma. He doesn’t do myeloma [like me]. So in those two areas, we’re helping develop the junior faculty in a different way.”
Something more in common
Right from the start, Dr. Perales and Dr. Giralt also shared a commitment to mentoring. Since 2010, Dr. Perales has mentored 22 up-and-coming junior faculty, including 10 from Europe (8 from Spain) and 2 from Latin America.
“[It makes] the research enterprise much more productive but [these young scientists] really increase the visibility of the program,” said Dr. Giralt.
He cited Dr. Perales’ track record of mentoring as one of the reasons for his promotion to chief of the adult bone marrow transplant service. In March 2020, Dr. Perales seamlessly stepped into Dr. Giralt’s shoes, while Dr. Giralt moved on to his present role as deputy division head of the division of hematologic malignancies.
Dr. Perales said: “The key aspect [of these promotions] is the fantastic working relationship that we’ve had over the years. ... I consider Sergio my mentor, but also a good friend and colleague. And so I think it’s this ability that we’ve had to work together and that relationship of trust, which has been key.”
“Sergio is somebody who lifts people up,” Dr. Perales added. “Many people will tell you that Sergio has helped them in their career. ... And I think that’s a lesson I’ve learned from him: training the next generation. And [that’s] not just in the U.S., but outside. I think that’s a key role that we have. And our responsibility.”
Asked to comment on their 100th-paper milestone, Dr. Perales firmly turned the spotlight from himself and Dr. Giralt to the junior investigators who have passed through the doors of the bone-marrow transplant program: “This body of work represents not just our collaboration but also the many contributions of our team at MSK ... and beyond MSK.”
This article was updated 1/26/22.
Peanut oral immunotherapy is safe and effective in toddlers in large placebo-controlled trial
In a large, blinded study of peanut-allergic toddlers published in The Lancet, 71% of treated participants could safely consume 5,000 mg of peanut protein – equivalent to nearly 17 peanuts – after 2½ years on oral immunotherapy. Even after stopping maintenance dosing for the next 6 months, more than 1 in 5 maintained that level of protection, and nearly 3 in 5 still met the 600-mg benchmark (about 2 peanuts) set by the phase 3 PALISADE trial of the FDA-approved peanut-flour product, Palforzia.
About 2% of children in the United States are allergic to peanuts, and most will not outgrow this allergy. In addition, other research suggests that the immune system is more malleable during early childhood.
Consistent with this idea, prior research showed that toddlers can succeed with peanut oral immunotherapy (OIT) – a regimen that builds tolerance through small amounts of the allergen consumed daily for months. However, that trial (DEVIL) was small, was conducted at a single site, and had no placebo group.
In contrast, the Peanut Oral Immunotherapy in Children Trial (IMPACT) enrolled 146 children aged 1-3 years at five academic medical centers in the United States – the first placebo-controlled study of OIT in this younger age group.
“This is a well done study,” Jaclyn Bjelac, MD, associate director of the Food Allergy Center of Excellence at the Cleveland Clinic, told this news organization. “We have seen improved outcomes in OIT, both in our own experience and other published studies, so while this is no surprise, the outcomes and large number of participants contribute to this being a really exciting publication.”
The trial was long and demanding for families. Toddlers who reacted to 500 mg or less of peanut protein in an entry food challenge were randomized in a 2:1 ratio to receive daily peanut flour or oat flour placebo. After initial dose escalation (from 0.1 mg to 6 mg) and biweekly buildup to a 2,000-mg target dose by week 30, participants continued with 20,00-mg daily maintenance dosing through week 134 – at which point they underwent a food challenge. They then went off treatment for 26 weeks and had another food challenge (week 160). In addition, participants came in for skin-prick and blood tests at baseline and at weeks 30, 82, 134, and 160.
In the placebo group, only 23 of 50 participants (46%) completed the study. “If you did 2½ years of this and then bombed the food challenge, you probably can guess that you were not on the real thing. And they were still asked to come back in 6 months and do it again. So, sure enough, a big chunk of those people chose not to continue, and you can’t blame them,” said Lancet co-author Edwin Kim, MD, in an interview. Dr. Kim directs the UNC Food Allergy Initiative at the University of North Carolina School of Medicine, Chapel Hill.
There was attrition in the treatment group as well. Among 96 children initially assigned to this arm, 68 (71%) passed the 5,000-mg peanut challenge at week 134 – but 11 withdrew in the study’s off-treatment phase. “It was a very tough decision. How much do you give toward science?” said Dr. Kim. “When push came to shove, some of the families couldn’t pull the trigger to potentially give up what they worked so hard for.”
In the intention-to-treat analysis, 20 of 96 treated participants (21%) could still tolerate 5,000 mg of peanut protein after going off therapy for 6 months. That translates to a 29% remission rate in the per-protocol subset (n = 70) who completed the study. Forty (57%) of these completers safely consumed at least 1,755 mg of peanut (cumulative dose). By comparison, the PALISADE trial of Palforzia used a 10,430-mg cumulative peanut dose to measure treatment efficacy.
On safety, 98% of treated participants – but also 80% of the placebo group – reported reactions, of which 35 were treated with epinephrine in 21 children receiving peanut OIT.
While some have noted that epinephrine use seemed high, Dr. Kim said, “we’re actually OK with that, because we’d much rather they overtreat and make sure that 1-year-old is safe than take any chances.” Overall, the safety profile looks similar to prior OIT studies of older children. “I think it suggests that, yeah, side effects will happen, [but] they’re all manageable, and people are not anaphylaxing left and right.”
On remission and immunologic parameters, benefits seemed stronger in the youngest subset (12 to 24 months), particularly those with lower peanut-specific IgE at baseline. These trends require further analyses, though, given the limited number of participants under 24 months.
Another noteworthy observation from longitudinal peanut-specific IgE trends in the placebo group: “Avoidance may not be benign,” Dr. Kim said. “If you look at their labs, they don’t stay flat. They actually go up.” The results jibe with the long-held idea of an early window of opportunity while a child’s immune system is maturing. “If you can grab this kid when his IgE is 10, versus next year when it might be 50, maybe you’ll get a different treatment effect,” Dr. Kim said. “We don’t know that for sure, but the placebo labs kind of point toward that.”
Beyond the science, there are practical advantages to starting OIT early. “Trying to convince a 9-year-old who’s been petrified of peanuts for their whole life to start doing this every day is not an easy task,” whereas with a 1- or 2-year-old, “you build it into their routine,” Dr. Kim said.
Plus, some say there’s no need for families to wait for regulatory approval of additional commercial products for very young children. Though some have advocated against the use of “grocery store” products, most peanut OIT research “has used the same 12% light roast defatted peanut flour used in IMPACT,” noted Marcus S. Shaker, MD, professor of pediatrics and of medicine at the Dartmouth Geisel School of Medicine and a physician at the Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. The commercial product (Palforzia) and grocery-store products “come from the exact same source in the U.S.,” he said in an interview. “Both are an option for parents to consider, but a commercial product is not, nor has [it] ever been, a necessity.”
Dr. Bjelac reports no relevant financial relationships. Dr. Kim reports consultancy with Aimmune Therapeutics, Allako, AllerGenis, Belhaven Pharma, DBV Technologies, Duke Clinical Research Institute, and Nutricia; advisory board membership with ALK, DBV Technologies, Kenota Health, and Ukko; and grant support from the NIH’s National Institute of Allergy and Infectious Diseases, National Center for Complementary and Integrative Health and Immune Tolerance Network, Food Allergy Research and Education, and the Wallace Research Foundation. Dr. Shaker has participated in research funded by DBV, is cochair of the AAAAI/ACAAI Joint Task Force on Practice Parameters, is an associate editor at the Annals of Allergy, Asthma, and Immunology, and is an editorial board member of the Journal of Allergy and Clinical Immunology in Practice.
A version of this article first appeared on Medscape.com.
In a large, blinded study of peanut-allergic toddlers published in The Lancet, 71% of treated participants could safely consume 5,000 mg of peanut protein – equivalent to nearly 17 peanuts – after 2½ years on oral immunotherapy. Even after stopping maintenance dosing for the next 6 months, more than 1 in 5 maintained that level of protection, and nearly 3 in 5 still met the 600-mg benchmark (about 2 peanuts) set by the phase 3 PALISADE trial of the FDA-approved peanut-flour product, Palforzia.
About 2% of children in the United States are allergic to peanuts, and most will not outgrow this allergy. In addition, other research suggests that the immune system is more malleable during early childhood.
Consistent with this idea, prior research showed that toddlers can succeed with peanut oral immunotherapy (OIT) – a regimen that builds tolerance through small amounts of the allergen consumed daily for months. However, that trial (DEVIL) was small, was conducted at a single site, and had no placebo group.
In contrast, the Peanut Oral Immunotherapy in Children Trial (IMPACT) enrolled 146 children aged 1-3 years at five academic medical centers in the United States – the first placebo-controlled study of OIT in this younger age group.
“This is a well done study,” Jaclyn Bjelac, MD, associate director of the Food Allergy Center of Excellence at the Cleveland Clinic, told this news organization. “We have seen improved outcomes in OIT, both in our own experience and other published studies, so while this is no surprise, the outcomes and large number of participants contribute to this being a really exciting publication.”
The trial was long and demanding for families. Toddlers who reacted to 500 mg or less of peanut protein in an entry food challenge were randomized in a 2:1 ratio to receive daily peanut flour or oat flour placebo. After initial dose escalation (from 0.1 mg to 6 mg) and biweekly buildup to a 2,000-mg target dose by week 30, participants continued with 20,00-mg daily maintenance dosing through week 134 – at which point they underwent a food challenge. They then went off treatment for 26 weeks and had another food challenge (week 160). In addition, participants came in for skin-prick and blood tests at baseline and at weeks 30, 82, 134, and 160.
In the placebo group, only 23 of 50 participants (46%) completed the study. “If you did 2½ years of this and then bombed the food challenge, you probably can guess that you were not on the real thing. And they were still asked to come back in 6 months and do it again. So, sure enough, a big chunk of those people chose not to continue, and you can’t blame them,” said Lancet co-author Edwin Kim, MD, in an interview. Dr. Kim directs the UNC Food Allergy Initiative at the University of North Carolina School of Medicine, Chapel Hill.
There was attrition in the treatment group as well. Among 96 children initially assigned to this arm, 68 (71%) passed the 5,000-mg peanut challenge at week 134 – but 11 withdrew in the study’s off-treatment phase. “It was a very tough decision. How much do you give toward science?” said Dr. Kim. “When push came to shove, some of the families couldn’t pull the trigger to potentially give up what they worked so hard for.”
In the intention-to-treat analysis, 20 of 96 treated participants (21%) could still tolerate 5,000 mg of peanut protein after going off therapy for 6 months. That translates to a 29% remission rate in the per-protocol subset (n = 70) who completed the study. Forty (57%) of these completers safely consumed at least 1,755 mg of peanut (cumulative dose). By comparison, the PALISADE trial of Palforzia used a 10,430-mg cumulative peanut dose to measure treatment efficacy.
On safety, 98% of treated participants – but also 80% of the placebo group – reported reactions, of which 35 were treated with epinephrine in 21 children receiving peanut OIT.
While some have noted that epinephrine use seemed high, Dr. Kim said, “we’re actually OK with that, because we’d much rather they overtreat and make sure that 1-year-old is safe than take any chances.” Overall, the safety profile looks similar to prior OIT studies of older children. “I think it suggests that, yeah, side effects will happen, [but] they’re all manageable, and people are not anaphylaxing left and right.”
On remission and immunologic parameters, benefits seemed stronger in the youngest subset (12 to 24 months), particularly those with lower peanut-specific IgE at baseline. These trends require further analyses, though, given the limited number of participants under 24 months.
Another noteworthy observation from longitudinal peanut-specific IgE trends in the placebo group: “Avoidance may not be benign,” Dr. Kim said. “If you look at their labs, they don’t stay flat. They actually go up.” The results jibe with the long-held idea of an early window of opportunity while a child’s immune system is maturing. “If you can grab this kid when his IgE is 10, versus next year when it might be 50, maybe you’ll get a different treatment effect,” Dr. Kim said. “We don’t know that for sure, but the placebo labs kind of point toward that.”
Beyond the science, there are practical advantages to starting OIT early. “Trying to convince a 9-year-old who’s been petrified of peanuts for their whole life to start doing this every day is not an easy task,” whereas with a 1- or 2-year-old, “you build it into their routine,” Dr. Kim said.
Plus, some say there’s no need for families to wait for regulatory approval of additional commercial products for very young children. Though some have advocated against the use of “grocery store” products, most peanut OIT research “has used the same 12% light roast defatted peanut flour used in IMPACT,” noted Marcus S. Shaker, MD, professor of pediatrics and of medicine at the Dartmouth Geisel School of Medicine and a physician at the Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. The commercial product (Palforzia) and grocery-store products “come from the exact same source in the U.S.,” he said in an interview. “Both are an option for parents to consider, but a commercial product is not, nor has [it] ever been, a necessity.”
Dr. Bjelac reports no relevant financial relationships. Dr. Kim reports consultancy with Aimmune Therapeutics, Allako, AllerGenis, Belhaven Pharma, DBV Technologies, Duke Clinical Research Institute, and Nutricia; advisory board membership with ALK, DBV Technologies, Kenota Health, and Ukko; and grant support from the NIH’s National Institute of Allergy and Infectious Diseases, National Center for Complementary and Integrative Health and Immune Tolerance Network, Food Allergy Research and Education, and the Wallace Research Foundation. Dr. Shaker has participated in research funded by DBV, is cochair of the AAAAI/ACAAI Joint Task Force on Practice Parameters, is an associate editor at the Annals of Allergy, Asthma, and Immunology, and is an editorial board member of the Journal of Allergy and Clinical Immunology in Practice.
A version of this article first appeared on Medscape.com.
In a large, blinded study of peanut-allergic toddlers published in The Lancet, 71% of treated participants could safely consume 5,000 mg of peanut protein – equivalent to nearly 17 peanuts – after 2½ years on oral immunotherapy. Even after stopping maintenance dosing for the next 6 months, more than 1 in 5 maintained that level of protection, and nearly 3 in 5 still met the 600-mg benchmark (about 2 peanuts) set by the phase 3 PALISADE trial of the FDA-approved peanut-flour product, Palforzia.
About 2% of children in the United States are allergic to peanuts, and most will not outgrow this allergy. In addition, other research suggests that the immune system is more malleable during early childhood.
Consistent with this idea, prior research showed that toddlers can succeed with peanut oral immunotherapy (OIT) – a regimen that builds tolerance through small amounts of the allergen consumed daily for months. However, that trial (DEVIL) was small, was conducted at a single site, and had no placebo group.
In contrast, the Peanut Oral Immunotherapy in Children Trial (IMPACT) enrolled 146 children aged 1-3 years at five academic medical centers in the United States – the first placebo-controlled study of OIT in this younger age group.
“This is a well done study,” Jaclyn Bjelac, MD, associate director of the Food Allergy Center of Excellence at the Cleveland Clinic, told this news organization. “We have seen improved outcomes in OIT, both in our own experience and other published studies, so while this is no surprise, the outcomes and large number of participants contribute to this being a really exciting publication.”
The trial was long and demanding for families. Toddlers who reacted to 500 mg or less of peanut protein in an entry food challenge were randomized in a 2:1 ratio to receive daily peanut flour or oat flour placebo. After initial dose escalation (from 0.1 mg to 6 mg) and biweekly buildup to a 2,000-mg target dose by week 30, participants continued with 20,00-mg daily maintenance dosing through week 134 – at which point they underwent a food challenge. They then went off treatment for 26 weeks and had another food challenge (week 160). In addition, participants came in for skin-prick and blood tests at baseline and at weeks 30, 82, 134, and 160.
In the placebo group, only 23 of 50 participants (46%) completed the study. “If you did 2½ years of this and then bombed the food challenge, you probably can guess that you were not on the real thing. And they were still asked to come back in 6 months and do it again. So, sure enough, a big chunk of those people chose not to continue, and you can’t blame them,” said Lancet co-author Edwin Kim, MD, in an interview. Dr. Kim directs the UNC Food Allergy Initiative at the University of North Carolina School of Medicine, Chapel Hill.
There was attrition in the treatment group as well. Among 96 children initially assigned to this arm, 68 (71%) passed the 5,000-mg peanut challenge at week 134 – but 11 withdrew in the study’s off-treatment phase. “It was a very tough decision. How much do you give toward science?” said Dr. Kim. “When push came to shove, some of the families couldn’t pull the trigger to potentially give up what they worked so hard for.”
In the intention-to-treat analysis, 20 of 96 treated participants (21%) could still tolerate 5,000 mg of peanut protein after going off therapy for 6 months. That translates to a 29% remission rate in the per-protocol subset (n = 70) who completed the study. Forty (57%) of these completers safely consumed at least 1,755 mg of peanut (cumulative dose). By comparison, the PALISADE trial of Palforzia used a 10,430-mg cumulative peanut dose to measure treatment efficacy.
On safety, 98% of treated participants – but also 80% of the placebo group – reported reactions, of which 35 were treated with epinephrine in 21 children receiving peanut OIT.
While some have noted that epinephrine use seemed high, Dr. Kim said, “we’re actually OK with that, because we’d much rather they overtreat and make sure that 1-year-old is safe than take any chances.” Overall, the safety profile looks similar to prior OIT studies of older children. “I think it suggests that, yeah, side effects will happen, [but] they’re all manageable, and people are not anaphylaxing left and right.”
On remission and immunologic parameters, benefits seemed stronger in the youngest subset (12 to 24 months), particularly those with lower peanut-specific IgE at baseline. These trends require further analyses, though, given the limited number of participants under 24 months.
Another noteworthy observation from longitudinal peanut-specific IgE trends in the placebo group: “Avoidance may not be benign,” Dr. Kim said. “If you look at their labs, they don’t stay flat. They actually go up.” The results jibe with the long-held idea of an early window of opportunity while a child’s immune system is maturing. “If you can grab this kid when his IgE is 10, versus next year when it might be 50, maybe you’ll get a different treatment effect,” Dr. Kim said. “We don’t know that for sure, but the placebo labs kind of point toward that.”
Beyond the science, there are practical advantages to starting OIT early. “Trying to convince a 9-year-old who’s been petrified of peanuts for their whole life to start doing this every day is not an easy task,” whereas with a 1- or 2-year-old, “you build it into their routine,” Dr. Kim said.
Plus, some say there’s no need for families to wait for regulatory approval of additional commercial products for very young children. Though some have advocated against the use of “grocery store” products, most peanut OIT research “has used the same 12% light roast defatted peanut flour used in IMPACT,” noted Marcus S. Shaker, MD, professor of pediatrics and of medicine at the Dartmouth Geisel School of Medicine and a physician at the Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. The commercial product (Palforzia) and grocery-store products “come from the exact same source in the U.S.,” he said in an interview. “Both are an option for parents to consider, but a commercial product is not, nor has [it] ever been, a necessity.”
Dr. Bjelac reports no relevant financial relationships. Dr. Kim reports consultancy with Aimmune Therapeutics, Allako, AllerGenis, Belhaven Pharma, DBV Technologies, Duke Clinical Research Institute, and Nutricia; advisory board membership with ALK, DBV Technologies, Kenota Health, and Ukko; and grant support from the NIH’s National Institute of Allergy and Infectious Diseases, National Center for Complementary and Integrative Health and Immune Tolerance Network, Food Allergy Research and Education, and the Wallace Research Foundation. Dr. Shaker has participated in research funded by DBV, is cochair of the AAAAI/ACAAI Joint Task Force on Practice Parameters, is an associate editor at the Annals of Allergy, Asthma, and Immunology, and is an editorial board member of the Journal of Allergy and Clinical Immunology in Practice.
A version of this article first appeared on Medscape.com.
Rituximab and COVID-19 vaccines: Studies begin to answer key questions
Rituximab has presented something of a conundrum for patients taking the monoclonal antibody during the COVID-19 pandemic.
Used to manage a variety of autoimmune diseases and cancers, rituximab acts against CD20 proteins expressed on the surface of B cells, causing B-cell depletion. However, it is this B-cell depletion that may put these patients at greater risk of COVID-19 development, progression to more severe disease, and in-hospital mortality. Evidence for this appears to be mixed, with studies showing both that patients using rituximab to manage various diseases are and are not at increased risk for SARS-CoV-2 infection, COVID-19 progression, and mortality.
As COVID-19 vaccine rollouts take place across the world, more questions have been raised about the relationship between B-cell depletion from anti-CD20 therapies and COVID-19 vaccines. Do rituximab and other anti-CD20 therapies affect a patient’s response to COVID-19 vaccines? If this is the case, does the timing of anti-CD20 treatment matter to maximize B-cell levels and improve the vaccine’s effectiveness? And how do COVID-19 vaccine booster doses factor into the equation?
Humoral and cell-mediated responses following COVID-19 vaccination
First, the bad news: The vaccine is unquestionably safe to administer in patients taking rituximab, but one thing that has been well established is that antibody response to COVID-19 vaccination in these individuals does is reduced. This isn’t entirely unprecedented, as previous studies have shown a weakened immune response to pneumococcal polysaccharide and keyhole limpet hemocyanin vaccines among patients taking rituximab.

“Compromised immunogenicity to the SARS-CoV-2 vaccines has been demonstrated in rituximab-treated patients, which is of particular concern given the observation that B-cell–depleting therapies may be associated with worse COVID outcomes,” Robert F. Spiera, MD, director of the Scleroderma, Vasculitis, and Myositis Center at the Hospital for Special Surgery in New York, said in an interview.
For example, in a recent study from the Medical University of Vienna, 29 (39%) of 74 patients receiving rituximab (43% as monotherapy, 57% with conventional-synthetic disease-modifying antirheumatic drugs) who were vaccinated with either the Comirnaty (Pfizer-BioNTech) or Spikevax (Moderna) COVID-19 vaccine achieved seroconversion, compared with 100% of patients in a healthy control group, and all but 1 patient without detectable CD19+ peripheral B cells did not develop anti–SARS-CoV-2 receptor-binding domain antibodies.
“There is an increasing number of studies in this field, and they confirm that patients treated with rituximab and other anti-CD20 agents have severely reduced serological responses to COVID-19 vaccines,” Ingrid Jyssum, MD, of the division of rheumatology and research at Diakonhjemmet Hospital in Oslo, said in an interview.

One silver lining is that patients treated with anti-CD20 therapies appear to have a cell-mediated response following vaccination even if they don’t develop SARS-CoV-2 antibodies. “Studies that also investigate T-cell responses are starting to emerge, and so far, they show that, even if the patients do not have antibodies, they may have T-cell responses,” Dr. Jyssum said.
One study of 24 patients with autoimmune diseases taking rituximab that evaluated humoral and T-cell responses following vaccination with the Comirnaty vaccine found that none had a humoral response to the vaccine, but the T-cell response from that group did not significantly differ from 35 patients receiving other immunosuppressants and 26 patients in a healthy control group. In another study of rituximab- or ocrelizumab-treated patients who received mRNA-based COVID-19 vaccines, 69.4% developed SARS-CoV-2–specific antibodies, compared with a control group, but 96.2% of patients taking ocrelizumab and 81.8% of patients taking rituximab mounted a spike-specific CD8+ T-cell response, compared with 66.7% in the control group, and there were comparable rates (85%-90%) of spike-specific CD4+ T cells in all groups. In the study from the Medical University of Vienna, T-cell response was detected in rituximab-treated patients who both did and did not mount an antibody response.
The clinical relevance of how a blunted humoral immune response but a respectable T-cell response to COVID-19 vaccines affects patients treated with anti-CD20 therapies isn’t currently known, Dr. Jyssum said.
While these data are reassuring, they’re also incomplete, Dr. Spiera noted. “The ultimate outcome of relevance to assess vaccine efficacy is protection from COVID and from severe outcomes of COVID infection (i.e., hospitalization, mechanical ventilation, death). That data will require assessment of very large numbers of rituximab-treated vaccinated patients to be compared with rituximab-treated unvaccinated patients, and is unlikely to be forthcoming in the very near future.
“In the meantime, however, achieving serologic positivity, meaning having evidence of serologic as well as cellular immunity following vaccination, is a desired outcome, and likely implies more robust immunity.”
Does treatment timing impact COVID-19 vaccine response?
Given enough time, B-cell reconstitution will occur in patients taking rituximab. With that in mind, is it beneficial to wait a certain amount of time after a patient has stopped rituximab therapy or time since their last dose before giving them a COVID-19 vaccine? In their guidance on COVID-19 vaccines for patients with rheumatic and musculoskeletal diseases, the American College of Rheumatology said there is moderate evidence to consider “optimal timing of dosing and vaccination with the rheumatology provider before proceeding.”
“Guidelines and preliminary studies of serologic response to COVID vaccine in rituximab-treated patients have suggested that longer time from last rituximab exposure is associated with a greater likelihood of a serologic response,” Dr. Spiera said.
In a brief report published in Arthritis & Rheumatology, Dr. Spiera and colleagues performed a retrospective chart review of 56 patients with varying levels of last exposure to rituximab who received a COVID-19 vaccine. Their results showed that, when patients were vaccinated 6-12 months after the last rituximab dose, 55% were seronegative, and when this was more than 12 months, only 13% were seronegative, compared with seronegativity in 86% who were vaccinated less than 6 months after their last rituximab dose.
The RituxiVac trial, conducted by researchers in Switzerland, also examined vaccine responses of 96 rituximab-treated patients who received Comirnaty or Spikevax; results recently published in The Lancet Rheumatology showed findings similar to other studies, with reduced humoral and cell-mediated responses. In the RituxiVac trial, the median time to last anti-CD20 treatment was 1.07 years.
“The typical interval between rituximab doses [for treatment of rheumatoid arthritis, as well as for remission maintenance in antineutrophil cytoplasmic antibody–associated vasculitis] is typically 6 months, and this has become widely used as the interval from last rituximab to time of COVID vaccination, with a recommendation to wait 4 weeks (if possible) from time of vaccination until the next rituximab administration,” Dr. Spiera explained. However, this window seems to vary depending on the study.
Recent research published in Arthritis & Rheumatology indicates B-cell levels could be a relevant indicator for humoral and cell-mediated response in patients with rheumatic diseases treated with rituximab, with a level of 10 B cells/mcL (0.4% of lymphocytes) identified as one potential marker for likely seroconversion following COVID-19 vaccination.
“In some smaller case series, it has been further recognized that rituximab-treated patients who were beginning to reconstitute peripheral B cells were most likely to respond serologically. Our present study confirmed those findings, demonstrating that the presence of detectable B cells was strongly associated with vaccine responsiveness, and affords complementary information to time from last [rituximab dose] in informing the likelihood of a vaccine response,” Dr. Spiera said.
However, the literature is limited in this area, and an exact cutoff for B-cell counts in these patients isn’t currently known, Dr. Jyssum said. A better metric is time away from anti-CD20 therapies, with CD19 cell count being highly correlated with last infusion.
Dr. Spiera agreed that there is no consistent B-cell percentage that works as a cutoff. “In our study, we looked at it as a binary variable, although we did find that a higher percentage of B cells in the peripheral lymphocyte population was associated with a higher likelihood of seroconversion. We did not, however, identify a ‘threshold’ for vaccine serologic responsiveness.”
Should clinicians measure antibodies?
The Food and Drug Administration and the Centers for Disease Control and Prevention have recommended that health care providers and the public not use COVID-19 antibody tests as a way to gauge immunity after exposure to SARS-CoV-2 and after receiving a COVID-19 vaccination. The ACR’s guidance on COVID-19 vaccination for patients with rheumatic and musculoskeletal diseases strongly recommends against ordering antibody tests for patients with autoimmune inflammatory rheumatic diseases as a way to measure immunity.
“Generally, such measurements are not recommended as the clinical correlate of various antibody levels are not known,” Dr. Jyssum said. “With regular infusions of rituximab or other anti-CD20 agents, one cannot expect that these patients will develop significant levels of antibodies.”
However, she said there might be situations where it’s useful to know whether a patient has developed antibodies at all. “Assessing the significance of specific antibody levels is difficult, and the subject of scientific studies. Patients lacking a humoral vaccine response are left to rely on their T-cell responses and on infectious control measures to prevent disease.”
Dr. Spiera said he disagreed with guidelines recommending against checking antibody levels after vaccination, “particularly in patients treated with immunosuppressive medications that might be expected to blunt their serologic response to the vaccines.
“Although we cannot be sure what level of measurable antibodies offer what level of protection, most clinicians would agree that patients who demonstrate no detectable antibodies (which is a common finding in rituximab-treated patients) should be considered at higher risk,” he said. “Indeed, recommendations regarding booster vaccine administration in general was initially based on the observation of declining antibody levels with longer time from vaccination.”
Do COVID-19 vaccine boosters help patients on anti-CD20 therapy?
As of January 2022, the FDA and CDC have recommended a third primary series shot of COVID-19 vaccines for some moderately to severely immunocompromised patients as young as 5 years old (for Comirnaty vaccine) or a booster shot of either Comirnaty or Spikevax for everyone aged 12 years and older, including immunocompromised people, while the ACR goes into more detail and recommends clinicians time a patient’s booster shot with temporary treatment interruption.
In The Lancet Rheumatology, Dr. Jyssum and colleagues recently published results from the prospective Nor-vaC study examining the humoral and cell-mediated immune responses of 87 patients with RA being treated with rituximab who received the Comirnaty, Spikevax, or Vaxzevria (AstraZeneca) COVID-19 vaccines; of these, 49 patients received a booster dose at a median of 70 days after completing their primary series. The results showed 19 patients (28.1%) had a serologic response after their primary series, while 8 of 49 patients (16.3%) who received their booster dose had a serologic response.
All patients who received a third dose in the study had a T-cell response, Dr. Jyssum said. “This is reassuring for patients and clinicians. T cells have been found to be important in countering COVID-19 disease, but whether we can rely on the T-cell response alone in the absence of antibodies to protect patients from infection or from serious COVID disease is still not determined,” she said.
When asked if she would recommend COVID-19 vaccine booster doses for patients on rituximab, Dr. Jyssum replied: “Absolutely.”
Another study, recently published in Annals of the Rheumatic Diseases, examined heterologous and homologous booster doses for 60 patients receiving rituximab without seroconversion after their COVID-19 vaccine primary series. The results showed no significant difference in new seroconversion at 4 weeks based on whether the patient received a vector or mRNA vaccine (22% vs. 32%), but all patients who received a booster dose with a vector vaccine had specific T-cell responses, compared with 81% of patients who received an mRNA vaccine booster. There was a new humoral and/or cellular response in 9 of 11 patients (82%), and most patients with peripheral B cells (12 of 18 patients; 67%) achieved seroconversion.
“Our data show that a cellular and/or humoral immune response can be achieved on a third COVID-19 vaccination in most of the patients who initially developed neither a humoral nor a cellular immune response,” the researchers concluded. “The efficacy data together with the safety data seen in our trial provide a favorable risk/benefit ratio and support the implementation of a third vaccination for nonseroconverted high-risk autoimmune disease patients treated with B-cell–depleting agents.”
Dr. Spiera said booster doses are an important part of the equation, and “it is important to consider factors that would be associated with a greater likelihood of achieving a serologic response, particularly in those patients who did not demonstrate a serologic response to the initial vaccines series.
“Preliminary data shows that the beginnings of B-cell reconstitution is also associated with a positive serologic response following a booster of the COVID-19 vaccine,” he said.
The authors of the cited studies reported numerous relevant financial disclosures. Dr. Spiera and Dr. Jyssum reported no relevant financial disclosures.
Rituximab has presented something of a conundrum for patients taking the monoclonal antibody during the COVID-19 pandemic.
Used to manage a variety of autoimmune diseases and cancers, rituximab acts against CD20 proteins expressed on the surface of B cells, causing B-cell depletion. However, it is this B-cell depletion that may put these patients at greater risk of COVID-19 development, progression to more severe disease, and in-hospital mortality. Evidence for this appears to be mixed, with studies showing both that patients using rituximab to manage various diseases are and are not at increased risk for SARS-CoV-2 infection, COVID-19 progression, and mortality.
As COVID-19 vaccine rollouts take place across the world, more questions have been raised about the relationship between B-cell depletion from anti-CD20 therapies and COVID-19 vaccines. Do rituximab and other anti-CD20 therapies affect a patient’s response to COVID-19 vaccines? If this is the case, does the timing of anti-CD20 treatment matter to maximize B-cell levels and improve the vaccine’s effectiveness? And how do COVID-19 vaccine booster doses factor into the equation?
Humoral and cell-mediated responses following COVID-19 vaccination
First, the bad news: The vaccine is unquestionably safe to administer in patients taking rituximab, but one thing that has been well established is that antibody response to COVID-19 vaccination in these individuals does is reduced. This isn’t entirely unprecedented, as previous studies have shown a weakened immune response to pneumococcal polysaccharide and keyhole limpet hemocyanin vaccines among patients taking rituximab.
“Compromised immunogenicity to the SARS-CoV-2 vaccines has been demonstrated in rituximab-treated patients, which is of particular concern given the observation that B-cell–depleting therapies may be associated with worse COVID outcomes,” Robert F. Spiera, MD, director of the Scleroderma, Vasculitis, and Myositis Center at the Hospital for Special Surgery in New York, said in an interview.
For example, in a recent study from the Medical University of Vienna, 29 (39%) of 74 patients receiving rituximab (43% as monotherapy, 57% with conventional-synthetic disease-modifying antirheumatic drugs) who were vaccinated with either the Comirnaty (Pfizer-BioNTech) or Spikevax (Moderna) COVID-19 vaccine achieved seroconversion, compared with 100% of patients in a healthy control group, and all but 1 patient without detectable CD19+ peripheral B cells did not develop anti–SARS-CoV-2 receptor-binding domain antibodies.
“There is an increasing number of studies in this field, and they confirm that patients treated with rituximab and other anti-CD20 agents have severely reduced serological responses to COVID-19 vaccines,” Ingrid Jyssum, MD, of the division of rheumatology and research at Diakonhjemmet Hospital in Oslo, said in an interview.
One silver lining is that patients treated with anti-CD20 therapies appear to have a cell-mediated response following vaccination even if they don’t develop SARS-CoV-2 antibodies. “Studies that also investigate T-cell responses are starting to emerge, and so far, they show that, even if the patients do not have antibodies, they may have T-cell responses,” Dr. Jyssum said.
One study of 24 patients with autoimmune diseases taking rituximab that evaluated humoral and T-cell responses following vaccination with the Comirnaty vaccine found that none had a humoral response to the vaccine, but the T-cell response from that group did not significantly differ from 35 patients receiving other immunosuppressants and 26 patients in a healthy control group. In another study of rituximab- or ocrelizumab-treated patients who received mRNA-based COVID-19 vaccines, 69.4% developed SARS-CoV-2–specific antibodies, compared with a control group, but 96.2% of patients taking ocrelizumab and 81.8% of patients taking rituximab mounted a spike-specific CD8+ T-cell response, compared with 66.7% in the control group, and there were comparable rates (85%-90%) of spike-specific CD4+ T cells in all groups. In the study from the Medical University of Vienna, T-cell response was detected in rituximab-treated patients who both did and did not mount an antibody response.
The clinical relevance of how a blunted humoral immune response but a respectable T-cell response to COVID-19 vaccines affects patients treated with anti-CD20 therapies isn’t currently known, Dr. Jyssum said.
While these data are reassuring, they’re also incomplete, Dr. Spiera noted. “The ultimate outcome of relevance to assess vaccine efficacy is protection from COVID and from severe outcomes of COVID infection (i.e., hospitalization, mechanical ventilation, death). That data will require assessment of very large numbers of rituximab-treated vaccinated patients to be compared with rituximab-treated unvaccinated patients, and is unlikely to be forthcoming in the very near future.
“In the meantime, however, achieving serologic positivity, meaning having evidence of serologic as well as cellular immunity following vaccination, is a desired outcome, and likely implies more robust immunity.”
Does treatment timing impact COVID-19 vaccine response?
Given enough time, B-cell reconstitution will occur in patients taking rituximab. With that in mind, is it beneficial to wait a certain amount of time after a patient has stopped rituximab therapy or time since their last dose before giving them a COVID-19 vaccine? In their guidance on COVID-19 vaccines for patients with rheumatic and musculoskeletal diseases, the American College of Rheumatology said there is moderate evidence to consider “optimal timing of dosing and vaccination with the rheumatology provider before proceeding.”
“Guidelines and preliminary studies of serologic response to COVID vaccine in rituximab-treated patients have suggested that longer time from last rituximab exposure is associated with a greater likelihood of a serologic response,” Dr. Spiera said.
In a brief report published in Arthritis & Rheumatology, Dr. Spiera and colleagues performed a retrospective chart review of 56 patients with varying levels of last exposure to rituximab who received a COVID-19 vaccine. Their results showed that, when patients were vaccinated 6-12 months after the last rituximab dose, 55% were seronegative, and when this was more than 12 months, only 13% were seronegative, compared with seronegativity in 86% who were vaccinated less than 6 months after their last rituximab dose.
The RituxiVac trial, conducted by researchers in Switzerland, also examined vaccine responses of 96 rituximab-treated patients who received Comirnaty or Spikevax; results recently published in The Lancet Rheumatology showed findings similar to other studies, with reduced humoral and cell-mediated responses. In the RituxiVac trial, the median time to last anti-CD20 treatment was 1.07 years.
“The typical interval between rituximab doses [for treatment of rheumatoid arthritis, as well as for remission maintenance in antineutrophil cytoplasmic antibody–associated vasculitis] is typically 6 months, and this has become widely used as the interval from last rituximab to time of COVID vaccination, with a recommendation to wait 4 weeks (if possible) from time of vaccination until the next rituximab administration,” Dr. Spiera explained. However, this window seems to vary depending on the study.
Recent research published in Arthritis & Rheumatology indicates B-cell levels could be a relevant indicator for humoral and cell-mediated response in patients with rheumatic diseases treated with rituximab, with a level of 10 B cells/mcL (0.4% of lymphocytes) identified as one potential marker for likely seroconversion following COVID-19 vaccination.
“In some smaller case series, it has been further recognized that rituximab-treated patients who were beginning to reconstitute peripheral B cells were most likely to respond serologically. Our present study confirmed those findings, demonstrating that the presence of detectable B cells was strongly associated with vaccine responsiveness, and affords complementary information to time from last [rituximab dose] in informing the likelihood of a vaccine response,” Dr. Spiera said.
However, the literature is limited in this area, and an exact cutoff for B-cell counts in these patients isn’t currently known, Dr. Jyssum said. A better metric is time away from anti-CD20 therapies, with CD19 cell count being highly correlated with last infusion.
Dr. Spiera agreed that there is no consistent B-cell percentage that works as a cutoff. “In our study, we looked at it as a binary variable, although we did find that a higher percentage of B cells in the peripheral lymphocyte population was associated with a higher likelihood of seroconversion. We did not, however, identify a ‘threshold’ for vaccine serologic responsiveness.”
Should clinicians measure antibodies?
The Food and Drug Administration and the Centers for Disease Control and Prevention have recommended that health care providers and the public not use COVID-19 antibody tests as a way to gauge immunity after exposure to SARS-CoV-2 and after receiving a COVID-19 vaccination. The ACR’s guidance on COVID-19 vaccination for patients with rheumatic and musculoskeletal diseases strongly recommends against ordering antibody tests for patients with autoimmune inflammatory rheumatic diseases as a way to measure immunity.
“Generally, such measurements are not recommended as the clinical correlate of various antibody levels are not known,” Dr. Jyssum said. “With regular infusions of rituximab or other anti-CD20 agents, one cannot expect that these patients will develop significant levels of antibodies.”
However, she said there might be situations where it’s useful to know whether a patient has developed antibodies at all. “Assessing the significance of specific antibody levels is difficult, and the subject of scientific studies. Patients lacking a humoral vaccine response are left to rely on their T-cell responses and on infectious control measures to prevent disease.”
Dr. Spiera said he disagreed with guidelines recommending against checking antibody levels after vaccination, “particularly in patients treated with immunosuppressive medications that might be expected to blunt their serologic response to the vaccines.
“Although we cannot be sure what level of measurable antibodies offer what level of protection, most clinicians would agree that patients who demonstrate no detectable antibodies (which is a common finding in rituximab-treated patients) should be considered at higher risk,” he said. “Indeed, recommendations regarding booster vaccine administration in general was initially based on the observation of declining antibody levels with longer time from vaccination.”
Do COVID-19 vaccine boosters help patients on anti-CD20 therapy?
As of January 2022, the FDA and CDC have recommended a third primary series shot of COVID-19 vaccines for some moderately to severely immunocompromised patients as young as 5 years old (for Comirnaty vaccine) or a booster shot of either Comirnaty or Spikevax for everyone aged 12 years and older, including immunocompromised people, while the ACR goes into more detail and recommends clinicians time a patient’s booster shot with temporary treatment interruption.
In The Lancet Rheumatology, Dr. Jyssum and colleagues recently published results from the prospective Nor-vaC study examining the humoral and cell-mediated immune responses of 87 patients with RA being treated with rituximab who received the Comirnaty, Spikevax, or Vaxzevria (AstraZeneca) COVID-19 vaccines; of these, 49 patients received a booster dose at a median of 70 days after completing their primary series. The results showed 19 patients (28.1%) had a serologic response after their primary series, while 8 of 49 patients (16.3%) who received their booster dose had a serologic response.
All patients who received a third dose in the study had a T-cell response, Dr. Jyssum said. “This is reassuring for patients and clinicians. T cells have been found to be important in countering COVID-19 disease, but whether we can rely on the T-cell response alone in the absence of antibodies to protect patients from infection or from serious COVID disease is still not determined,” she said.
When asked if she would recommend COVID-19 vaccine booster doses for patients on rituximab, Dr. Jyssum replied: “Absolutely.”
Another study, recently published in Annals of the Rheumatic Diseases, examined heterologous and homologous booster doses for 60 patients receiving rituximab without seroconversion after their COVID-19 vaccine primary series. The results showed no significant difference in new seroconversion at 4 weeks based on whether the patient received a vector or mRNA vaccine (22% vs. 32%), but all patients who received a booster dose with a vector vaccine had specific T-cell responses, compared with 81% of patients who received an mRNA vaccine booster. There was a new humoral and/or cellular response in 9 of 11 patients (82%), and most patients with peripheral B cells (12 of 18 patients; 67%) achieved seroconversion.
“Our data show that a cellular and/or humoral immune response can be achieved on a third COVID-19 vaccination in most of the patients who initially developed neither a humoral nor a cellular immune response,” the researchers concluded. “The efficacy data together with the safety data seen in our trial provide a favorable risk/benefit ratio and support the implementation of a third vaccination for nonseroconverted high-risk autoimmune disease patients treated with B-cell–depleting agents.”
Dr. Spiera said booster doses are an important part of the equation, and “it is important to consider factors that would be associated with a greater likelihood of achieving a serologic response, particularly in those patients who did not demonstrate a serologic response to the initial vaccines series.
“Preliminary data shows that the beginnings of B-cell reconstitution is also associated with a positive serologic response following a booster of the COVID-19 vaccine,” he said.
The authors of the cited studies reported numerous relevant financial disclosures. Dr. Spiera and Dr. Jyssum reported no relevant financial disclosures.
Rituximab has presented something of a conundrum for patients taking the monoclonal antibody during the COVID-19 pandemic.
Used to manage a variety of autoimmune diseases and cancers, rituximab acts against CD20 proteins expressed on the surface of B cells, causing B-cell depletion. However, it is this B-cell depletion that may put these patients at greater risk of COVID-19 development, progression to more severe disease, and in-hospital mortality. Evidence for this appears to be mixed, with studies showing both that patients using rituximab to manage various diseases are and are not at increased risk for SARS-CoV-2 infection, COVID-19 progression, and mortality.
As COVID-19 vaccine rollouts take place across the world, more questions have been raised about the relationship between B-cell depletion from anti-CD20 therapies and COVID-19 vaccines. Do rituximab and other anti-CD20 therapies affect a patient’s response to COVID-19 vaccines? If this is the case, does the timing of anti-CD20 treatment matter to maximize B-cell levels and improve the vaccine’s effectiveness? And how do COVID-19 vaccine booster doses factor into the equation?
Humoral and cell-mediated responses following COVID-19 vaccination
First, the bad news: The vaccine is unquestionably safe to administer in patients taking rituximab, but one thing that has been well established is that antibody response to COVID-19 vaccination in these individuals does is reduced. This isn’t entirely unprecedented, as previous studies have shown a weakened immune response to pneumococcal polysaccharide and keyhole limpet hemocyanin vaccines among patients taking rituximab.
“Compromised immunogenicity to the SARS-CoV-2 vaccines has been demonstrated in rituximab-treated patients, which is of particular concern given the observation that B-cell–depleting therapies may be associated with worse COVID outcomes,” Robert F. Spiera, MD, director of the Scleroderma, Vasculitis, and Myositis Center at the Hospital for Special Surgery in New York, said in an interview.
For example, in a recent study from the Medical University of Vienna, 29 (39%) of 74 patients receiving rituximab (43% as monotherapy, 57% with conventional-synthetic disease-modifying antirheumatic drugs) who were vaccinated with either the Comirnaty (Pfizer-BioNTech) or Spikevax (Moderna) COVID-19 vaccine achieved seroconversion, compared with 100% of patients in a healthy control group, and all but 1 patient without detectable CD19+ peripheral B cells did not develop anti–SARS-CoV-2 receptor-binding domain antibodies.
“There is an increasing number of studies in this field, and they confirm that patients treated with rituximab and other anti-CD20 agents have severely reduced serological responses to COVID-19 vaccines,” Ingrid Jyssum, MD, of the division of rheumatology and research at Diakonhjemmet Hospital in Oslo, said in an interview.
One silver lining is that patients treated with anti-CD20 therapies appear to have a cell-mediated response following vaccination even if they don’t develop SARS-CoV-2 antibodies. “Studies that also investigate T-cell responses are starting to emerge, and so far, they show that, even if the patients do not have antibodies, they may have T-cell responses,” Dr. Jyssum said.
One study of 24 patients with autoimmune diseases taking rituximab that evaluated humoral and T-cell responses following vaccination with the Comirnaty vaccine found that none had a humoral response to the vaccine, but the T-cell response from that group did not significantly differ from 35 patients receiving other immunosuppressants and 26 patients in a healthy control group. In another study of rituximab- or ocrelizumab-treated patients who received mRNA-based COVID-19 vaccines, 69.4% developed SARS-CoV-2–specific antibodies, compared with a control group, but 96.2% of patients taking ocrelizumab and 81.8% of patients taking rituximab mounted a spike-specific CD8+ T-cell response, compared with 66.7% in the control group, and there were comparable rates (85%-90%) of spike-specific CD4+ T cells in all groups. In the study from the Medical University of Vienna, T-cell response was detected in rituximab-treated patients who both did and did not mount an antibody response.
The clinical relevance of how a blunted humoral immune response but a respectable T-cell response to COVID-19 vaccines affects patients treated with anti-CD20 therapies isn’t currently known, Dr. Jyssum said.
While these data are reassuring, they’re also incomplete, Dr. Spiera noted. “The ultimate outcome of relevance to assess vaccine efficacy is protection from COVID and from severe outcomes of COVID infection (i.e., hospitalization, mechanical ventilation, death). That data will require assessment of very large numbers of rituximab-treated vaccinated patients to be compared with rituximab-treated unvaccinated patients, and is unlikely to be forthcoming in the very near future.
“In the meantime, however, achieving serologic positivity, meaning having evidence of serologic as well as cellular immunity following vaccination, is a desired outcome, and likely implies more robust immunity.”
Does treatment timing impact COVID-19 vaccine response?
Given enough time, B-cell reconstitution will occur in patients taking rituximab. With that in mind, is it beneficial to wait a certain amount of time after a patient has stopped rituximab therapy or time since their last dose before giving them a COVID-19 vaccine? In their guidance on COVID-19 vaccines for patients with rheumatic and musculoskeletal diseases, the American College of Rheumatology said there is moderate evidence to consider “optimal timing of dosing and vaccination with the rheumatology provider before proceeding.”
“Guidelines and preliminary studies of serologic response to COVID vaccine in rituximab-treated patients have suggested that longer time from last rituximab exposure is associated with a greater likelihood of a serologic response,” Dr. Spiera said.
In a brief report published in Arthritis & Rheumatology, Dr. Spiera and colleagues performed a retrospective chart review of 56 patients with varying levels of last exposure to rituximab who received a COVID-19 vaccine. Their results showed that, when patients were vaccinated 6-12 months after the last rituximab dose, 55% were seronegative, and when this was more than 12 months, only 13% were seronegative, compared with seronegativity in 86% who were vaccinated less than 6 months after their last rituximab dose.
The RituxiVac trial, conducted by researchers in Switzerland, also examined vaccine responses of 96 rituximab-treated patients who received Comirnaty or Spikevax; results recently published in The Lancet Rheumatology showed findings similar to other studies, with reduced humoral and cell-mediated responses. In the RituxiVac trial, the median time to last anti-CD20 treatment was 1.07 years.
“The typical interval between rituximab doses [for treatment of rheumatoid arthritis, as well as for remission maintenance in antineutrophil cytoplasmic antibody–associated vasculitis] is typically 6 months, and this has become widely used as the interval from last rituximab to time of COVID vaccination, with a recommendation to wait 4 weeks (if possible) from time of vaccination until the next rituximab administration,” Dr. Spiera explained. However, this window seems to vary depending on the study.
Recent research published in Arthritis & Rheumatology indicates B-cell levels could be a relevant indicator for humoral and cell-mediated response in patients with rheumatic diseases treated with rituximab, with a level of 10 B cells/mcL (0.4% of lymphocytes) identified as one potential marker for likely seroconversion following COVID-19 vaccination.
“In some smaller case series, it has been further recognized that rituximab-treated patients who were beginning to reconstitute peripheral B cells were most likely to respond serologically. Our present study confirmed those findings, demonstrating that the presence of detectable B cells was strongly associated with vaccine responsiveness, and affords complementary information to time from last [rituximab dose] in informing the likelihood of a vaccine response,” Dr. Spiera said.
However, the literature is limited in this area, and an exact cutoff for B-cell counts in these patients isn’t currently known, Dr. Jyssum said. A better metric is time away from anti-CD20 therapies, with CD19 cell count being highly correlated with last infusion.
Dr. Spiera agreed that there is no consistent B-cell percentage that works as a cutoff. “In our study, we looked at it as a binary variable, although we did find that a higher percentage of B cells in the peripheral lymphocyte population was associated with a higher likelihood of seroconversion. We did not, however, identify a ‘threshold’ for vaccine serologic responsiveness.”
Should clinicians measure antibodies?
The Food and Drug Administration and the Centers for Disease Control and Prevention have recommended that health care providers and the public not use COVID-19 antibody tests as a way to gauge immunity after exposure to SARS-CoV-2 and after receiving a COVID-19 vaccination. The ACR’s guidance on COVID-19 vaccination for patients with rheumatic and musculoskeletal diseases strongly recommends against ordering antibody tests for patients with autoimmune inflammatory rheumatic diseases as a way to measure immunity.
“Generally, such measurements are not recommended as the clinical correlate of various antibody levels are not known,” Dr. Jyssum said. “With regular infusions of rituximab or other anti-CD20 agents, one cannot expect that these patients will develop significant levels of antibodies.”
However, she said there might be situations where it’s useful to know whether a patient has developed antibodies at all. “Assessing the significance of specific antibody levels is difficult, and the subject of scientific studies. Patients lacking a humoral vaccine response are left to rely on their T-cell responses and on infectious control measures to prevent disease.”
Dr. Spiera said he disagreed with guidelines recommending against checking antibody levels after vaccination, “particularly in patients treated with immunosuppressive medications that might be expected to blunt their serologic response to the vaccines.
“Although we cannot be sure what level of measurable antibodies offer what level of protection, most clinicians would agree that patients who demonstrate no detectable antibodies (which is a common finding in rituximab-treated patients) should be considered at higher risk,” he said. “Indeed, recommendations regarding booster vaccine administration in general was initially based on the observation of declining antibody levels with longer time from vaccination.”
Do COVID-19 vaccine boosters help patients on anti-CD20 therapy?
As of January 2022, the FDA and CDC have recommended a third primary series shot of COVID-19 vaccines for some moderately to severely immunocompromised patients as young as 5 years old (for Comirnaty vaccine) or a booster shot of either Comirnaty or Spikevax for everyone aged 12 years and older, including immunocompromised people, while the ACR goes into more detail and recommends clinicians time a patient’s booster shot with temporary treatment interruption.
In The Lancet Rheumatology, Dr. Jyssum and colleagues recently published results from the prospective Nor-vaC study examining the humoral and cell-mediated immune responses of 87 patients with RA being treated with rituximab who received the Comirnaty, Spikevax, or Vaxzevria (AstraZeneca) COVID-19 vaccines; of these, 49 patients received a booster dose at a median of 70 days after completing their primary series. The results showed 19 patients (28.1%) had a serologic response after their primary series, while 8 of 49 patients (16.3%) who received their booster dose had a serologic response.
All patients who received a third dose in the study had a T-cell response, Dr. Jyssum said. “This is reassuring for patients and clinicians. T cells have been found to be important in countering COVID-19 disease, but whether we can rely on the T-cell response alone in the absence of antibodies to protect patients from infection or from serious COVID disease is still not determined,” she said.
When asked if she would recommend COVID-19 vaccine booster doses for patients on rituximab, Dr. Jyssum replied: “Absolutely.”
Another study, recently published in Annals of the Rheumatic Diseases, examined heterologous and homologous booster doses for 60 patients receiving rituximab without seroconversion after their COVID-19 vaccine primary series. The results showed no significant difference in new seroconversion at 4 weeks based on whether the patient received a vector or mRNA vaccine (22% vs. 32%), but all patients who received a booster dose with a vector vaccine had specific T-cell responses, compared with 81% of patients who received an mRNA vaccine booster. There was a new humoral and/or cellular response in 9 of 11 patients (82%), and most patients with peripheral B cells (12 of 18 patients; 67%) achieved seroconversion.
“Our data show that a cellular and/or humoral immune response can be achieved on a third COVID-19 vaccination in most of the patients who initially developed neither a humoral nor a cellular immune response,” the researchers concluded. “The efficacy data together with the safety data seen in our trial provide a favorable risk/benefit ratio and support the implementation of a third vaccination for nonseroconverted high-risk autoimmune disease patients treated with B-cell–depleting agents.”
Dr. Spiera said booster doses are an important part of the equation, and “it is important to consider factors that would be associated with a greater likelihood of achieving a serologic response, particularly in those patients who did not demonstrate a serologic response to the initial vaccines series.
“Preliminary data shows that the beginnings of B-cell reconstitution is also associated with a positive serologic response following a booster of the COVID-19 vaccine,” he said.
The authors of the cited studies reported numerous relevant financial disclosures. Dr. Spiera and Dr. Jyssum reported no relevant financial disclosures.
Antimicrobial resistance linked to 1.2 million global deaths in 2019
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
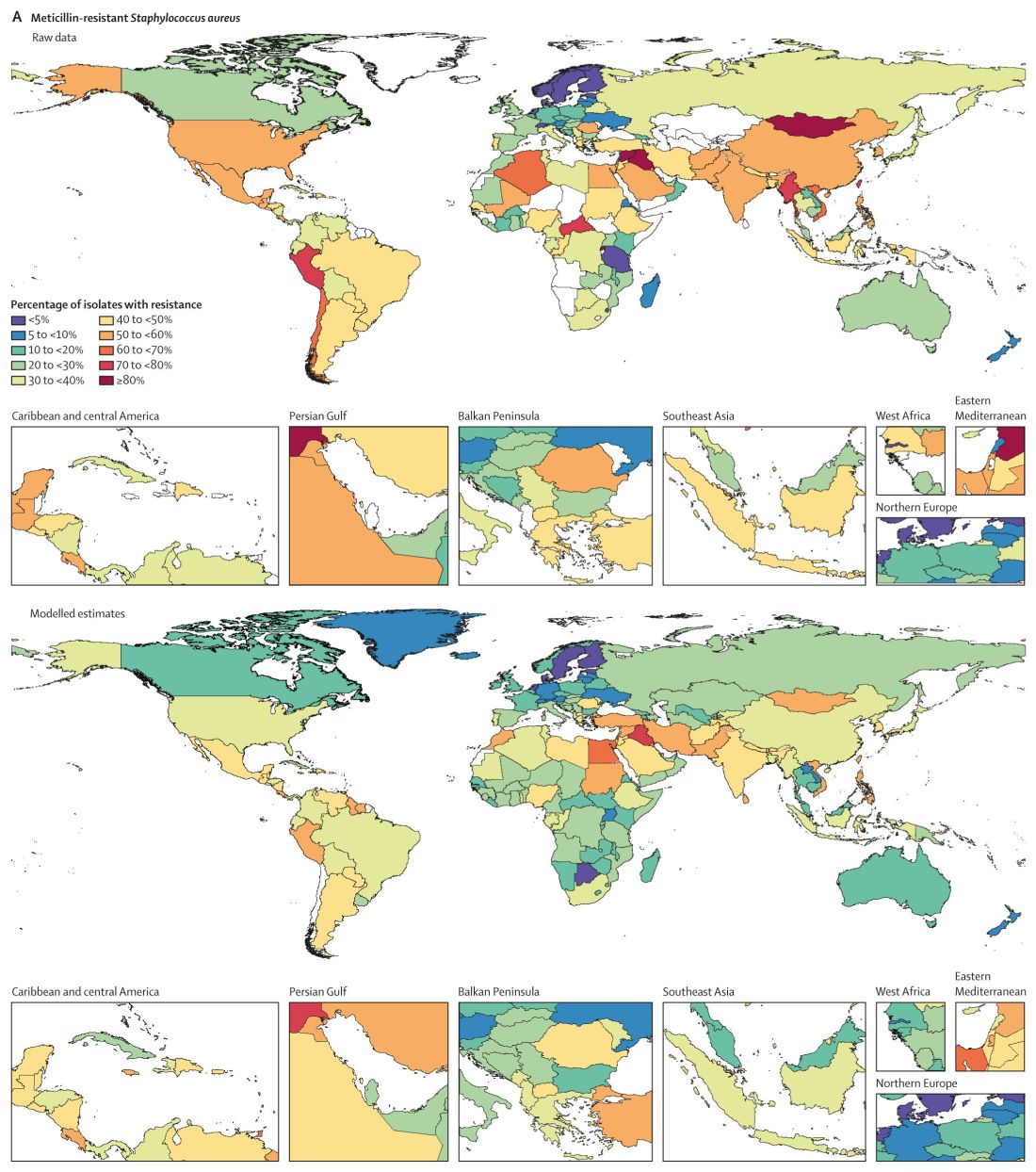
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
More than HIV, more than malaria.
In terms of preventable deaths, 1.27 million people could have been saved if drug-resistant infections were replaced with infections susceptible to current antibiotics. Furthermore, 4.95 million fewer people would have died if drug-resistant infections were replaced by no infections, researchers estimated.
Although the COVID-19 pandemic took some focus off the AMR burden worldwide over the past 2 years, the urgency to address risk to public health did not ebb. In fact, based on the findings, the researchers noted that AMR is now a leading cause of death worldwide.
“If left unchecked, the spread of AMR could make many bacterial pathogens much more lethal in the future than they are today,” the researchers noted in the study, published online Jan. 20, 2022, in The Lancet.
“These findings are a warning signal that antibiotic resistance is placing pressure on health care systems and leading to significant health loss,” study author Kevin Ikuta, MD, MPH, told this news organization.
“We need to continue to adhere to and support infection prevention and control programs, be thoughtful about our antibiotic use, and advocate for increased funding to vaccine discovery and the antibiotic development pipeline,” added Dr. Ikuta, health sciences assistant clinical professor of medicine at the University of California, Los Angeles.
Although many investigators have studied AMR, this study is the largest in scope, covering 204 countries and territories and incorporating data on a comprehensive range of pathogens and pathogen-drug combinations.
Dr. Ikuta, lead author Christopher J.L. Murray, DPhil, and colleagues estimated the global burden of AMR using the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. They specifically looked at rates of death directly attributed to and separately those associated with resistance.
Regional differences
Broken down by 21 regions, Australasia had 6.5 deaths per 100,000 people attributable to AMR, the lowest rate reported. This region also had 28 deaths per 100,000 associated with AMR.
Researchers found the highest rates in western sub-Saharan Africa. Deaths attributable to AMR were 27.3 per 100,000 and associated death rate was 114.8 per 100,000.
Lower- and middle-income regions had the highest AMR death rates, although resistance remains a high-priority issue for high-income countries as well.
“It’s important to take a global perspective on resistant infections because we can learn about regions and countries that are experiencing the greatest burden, information that was previously unknown,” Dr. Ikuta said. “With these estimates policy makers can prioritize regions that are hotspots and would most benefit from additional interventions.”
Furthermore, the study emphasized the global nature of AMR. “We’ve seen over the last 2 years with COVID-19 that this sort of problem doesn’t respect country borders, and high rates of resistance in one location can spread across a region or spread globally pretty quickly,” Dr. Ikuta said.
Leading resistant infections
Lower respiratory and thorax infections, bloodstream infections, and intra-abdominal infections together accounted for almost 79% of such deaths linked to AMR.
The six leading pathogens are likely household names among infectious disease specialists. The researchers found Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa, each responsible for more than 250,000 AMR-associated deaths.
The study also revealed that resistance to several first-line antibiotic agents often used empirically to treat infections accounted for more than 70% of the AMR-attributable deaths. These included fluoroquinolones and beta-lactam antibiotics such as carbapenems, cephalosporins, and penicillins.
Consistent with previous studies, MRSA stood out as a major cause of mortality. Of 88 different pathogen-drug combinations evaluated, MRSA was responsible for the most mortality: more than 100,000 deaths and 3·5 million disability-adjusted life-years.
The current study findings on MRSA “being a particularly nasty culprit” in AMR infections validates previous work that reported similar results, Vance Fowler, MD, told this news organization when asked to comment on the research. “That is reassuring.”
Potential solutions offered
Dr. Murray and colleagues outlined five strategies to address the challenge of bacterial AMR:
- Infection prevention and control remain paramount in minimizing infections in general and AMR infections in particular.
- More vaccines are needed to reduce the need for antibiotics. “Vaccines are available for only one of the six leading pathogens (S. pneumoniae), although new vaccine programs are underway for S. aureus, E. coli, and others,” the researchers wrote.
- Reduce antibiotic use unrelated to treatment of human disease.
- Avoid using antibiotics for viral infections and other unnecessary indications.
- Invest in new antibiotic development and ensure access to second-line agents in areas without widespread access.
“Identifying strategies that can work to reduce the burden of bacterial AMR – either across a wide range of settings or those that are specifically tailored to the resources available and leading pathogen-drug combinations in a particular setting – is an urgent priority,” the researchers noted.
Admirable AMR research
The results of the study are “startling, but not surprising,” said Dr. Fowler, professor of medicine at Duke University, Durham, N.C.
The authors did a “nice job” of addressing both deaths attributable and associated with AMR, Dr. Fowler added. “Those two categories unlock applications, not just in terms of how you interpret it but also what you do about it.”
The deaths attributable to AMR show that there is more work to be done regarding infection control and prevention, Dr. Fowler said, including in areas of the world like lower- and middle-income countries where infection resistance is most pronounced.
The deaths associated with AMR can be more challenging to calculate – people with infections can die for multiple reasons. However, Dr. Fowler applauded the researchers for doing “as good a job as you can” in estimating the extent of associated mortality.
‘The overlooked pandemic of antimicrobial resistance’
In an accompanying editorial in The Lancet, Ramanan Laxminarayan, PhD, MPH, wrote: “As COVID-19 rages on, the pandemic of antimicrobial resistance continues in the shadows. The toll taken by AMR on patients and their families is largely invisible but is reflected in prolonged bacterial infections that extend hospital stays and cause needless deaths.”
Dr. Laxminarayan pointed out an irony with AMR in different regions. Some of the AMR burden in sub-Saharan Africa is “probably due to inadequate access to antibiotics and high infection levels, albeit at low levels of resistance, whereas in south Asia and Latin America, it is because of high resistance even with good access to antibiotics.”
More funding to address AMR is needed, Dr. Laxminarayan noted. “Even the lower end of 911,000 deaths estimated by Murray and colleagues is higher than the number of deaths from HIV, which attracts close to U.S. $50 billion each year. However, global spending on addressing AMR is probably much lower than that.” Dr. Laxminarayan is an economist and epidemiologist affiliated with the Center for Disease Dynamics, Economics & Policy in Washington, D.C., and the Global Antibiotic Research and Development Partnership in Geneva.
An overlap with COVID-19
The Lancet report is likely “to bring more attention to AMR, especially since so many people have been distracted by COVID, and rightly so,” Dr. Fowler predicted. “The world has had its hands full with COVID.”
The two infections interact in direct ways, Dr. Fowler added. For example, some people hospitalized for COVID-19 for an extended time could develop progressively drug-resistant bacteria – leading to a superinfection.
The overlap could be illustrated by a Venn diagram, he said. A yellow circle could illustrate people with COVID-19 who are asymptomatic or who remain outpatients. Next to that would be a blue circle showing people who develop AMR infections. Where the two circles overlap would be green for those hospitalized who – because of receiving steroids, being on a ventilator, or getting a central line – develop a superinfection.
Official guidance continues
The study comes in the context of recent guidance and federal action on AMR. For example, the Infectious Diseases Society of America released new guidelines for AMR in November 2021 as part of ongoing advice on prevention and treatment of this “ongoing crisis.”
This most recent IDSA guidance addresses three pathogens in particular: AmpC beta-lactamase–producing Enterobacterales, carbapenem-resistant A. baumannii, and Stenotrophomonas maltophilia.
Also in November, the World Health Organization released an updated fact sheet on antimicrobial resistance. The WHO declared AMR one of the world’s top 10 global public health threats. The agency emphasized that misuse and overuse of antimicrobials are the main drivers in the development of drug-resistant pathogens. The WHO also pointed out that lack of clean water and sanitation in many areas of the world contribute to spread of microbes, including those resistant to current treatment options.
In September 2021, the Biden administration acknowledged the threat of AMR with allocation of more than $2 billion of the American Rescue Plan money for prevention and treatment of these infections.
Asked if there are any reasons for hope or optimism at this point, Dr. Ikuta said: “Definitely. We know what needs to be done to combat the spread of resistance. COVID-19 has demonstrated the importance of global commitment to infection control measures, such as hand washing and surveillance, and rapid investments in treatments, which can all be applied to antimicrobial resistance.”
The Bill & Melinda Gates Foundation, the Wellcome Trust, and the U.K. Department of Health and Social Care using U.K. aid funding managed by the Fleming Fund and other organizations provided funding for the study. Dr. Ikuta and Dr. Laxminarayan have disclosed no relevant financial relationships. Dr. Fowler reported receiving grants or honoraria, as well as serving as a consultant, for numerous sources. He also reported a patent pending in sepsis diagnostics and serving as chair of the V710 Scientific Advisory Committee (Merck).
A version of this article first appeared on Medscape.com.
DKMS: Small nonprofit to world’s largest stem cell donor registry
When Mechtild Harf was diagnosed with acute leukemia in 1990, physicians told her and her husband Peter that a bone marrow transplant was her best hope for survival. Back then, her native Germany had only 3,000 registered donors, and none was a match.
“My dad just went crazy, you know, to save his wife,” recalled Katharina Harf, who was a young teen at the time of her mother’s diagnosis.
In the course of 1 year, the Harfs recruited more than 68,000 potential bone marrow donors, but their heroic efforts couldn’t save Mechtild.
“She unfortunately didn’t make it. She died because of leukemia,” Katharina said.
Although Mechtild Harf did not survive, her legacy lives on in the bone marrow and stem cell donor recruitment organization DKMS (Deutsche Knochenmarkspenderdatei, or German Bone Marrow Donor Center).
In May of 1991, Peter Harf and Gerhard Ehninger, MD, the hematologist who treated Mechtild, founded DKMS with the mission, as its website states, “to provide as many blood cancer patients as possible with a second chance at life.”
From its German roots, the nonprofit organization has extended its mission to the United States (where it was initially known as Delete Blood Cancer DKMS), Poland, the United Kingdom, Chile, and in 2021, to South Africa.
Three decades after her mother’s death, Katharina Harf serves as Executive Chairwoman of DKMS U.S., based in New York.
World’s largest registry
“DKMS has the largest number of unrelated donors of any organization in the world,” noted Richard E. Champlin, MD, chair of the department of stem cell transplantation and cellular therapy at the University of Texas MD Anderson Cancer Center in Houston.
“In a large fraction of our donor searches, we find matches that are in the DKMS registry,” he said in an interview,
Alexander Schmidt, MD, PhD, global chief medical officer for DKMS, said that approximately 25% of all registered donors worldwide were recruited by his organization, and 39% of all unrelated donor transplants are made with peripheral blood stem cell or bone marrow products, donated by volunteers who are recruited by DKMS.
Since its founding, DKMS has registered 7.1 million potential donors in Germany, who made a total of 80,000 stem cell donations. DKMS U.S., which began operations in 2004, has registered 1.1 million donors and enabled 4,700 donations.
Global partners
DKMS partners with donor centers and recruitment organizations in each country where it operates. In the United States, DKMS works with the National Marrow Donor Program (NMDP) and its “Be The Match” donor registry.
“DKMS donors, both those from DKMS in Germany and those from DKMS in the United States are also listed in the NMDP registry, to make it easier for US search coordinators to accept these donors,” Dr. Schmidt explained in an interview.
The international cooperation and coordination makes it possible for a donor in the UK, for example, to save a life of a patient in Germany, the U.S., Chile, India, or many other parts of the world – anywhere that can be reached in time for a patient in need to receive a stem cell donation.
Pandemic affects donations
But, as with just about every aspect of life, the COVID-19 pandemic has created enormous challenges for recruiters, donor centers, and stem cell transplant centers.
Dr. Schmidt said that decline in donations during the pandemic was less severe than initially feared, with a decrease of just 3.5% in 2020, compared with the prepandemic year of 2019. In contrast, though, the average annual growth rate for donations prior to the pandemic was about 4%.
“Nevertheless, at the beginning of the pandemic in March 2020, for a few days things looked quite terrible, because all the borders were closed and flights were canceled, and about 50% of all stem cell products go abroad, and between 20% and 25% go intercontinental,” Dr. Schmidt said.
However, close cooperation and coordination between donor centers and national health authorities soon resolved the problem and helped insure that the flow of life-saving donations could continue with minimal disruption, he noted.
“I don’t think we had any product that could not be delivered at the end of the day, due to the pandemic,” he told this news organization.
Workforce and clinical problems
Although the flow of donations within and between nations has continued, the COVID-19 pandemic has had profound negative effects on transplant centers, particularly during the wave of infections caused by the Omicron variant, according to a transplant expert.
“With this most recent strain and how transmissible it is, what we’re dealing with is mass workforce shortages,” said Yi-Bin Chen, MD, director of the bone marrow transplant program at Massachusetts General Hospital in Boston.
“On top of a short-staffed hospital, you then take a very transmissible variant and deplete it even more due to the need to quarantine,” he said in an interview.
Both Dr. Champlin and Dr. Chen said that on-again, off-again pandemic travel bans and donor illnesses have necessitated first obtaining products and cryopreserving them before starting the recipient on a conditioning regimen for the transplant.
“The problem is that, while you can preserve peripheral blood stem cells pretty reliably, cryopreserving bone marrow is a bit more difficult,” Dr. Chen said.
In addition, evidence from recent studies comparing stem cell sources suggest that outcomes are less good with cryopreserved products than with fresh products, and with peripheral blood stem cells compared with bone marrow.
“But you’ve got to make do. A transplant with a cryopreserved product is better than no transplant,” Dr. Chen said.
To make things even more frustrating, as the pandemic waxed and waned throughout 2020 and 2021, the recommendations from donor centers seesawed between using fresh or cryopreserved product, making it difficult to plan a transplant for an individual patient.
The Omicron wave has also resulted in a much higher rate of donor dropout than anticipated, making it that much harder to schedule a transplant, Dr. Chen noted.
‘Every patient saved’
The pandemic will eventually subside, however, while the need for stem cell transplantation to treat hematologic malignancies will continue.
DKMS recently launched special aid programs to improve access to stem cell transplants in developing nations by offering financial support, free HLA typing, and other services.
In addition to its core mission of recruiting donors, DKMS is dedicated to improving the quality and efficiency of stem cell transplants. For example, in 2017 scientists in DKMS’ Life Science Lab created an antibody test for donor cytomegalovirus (CMV) infection, using a simple buccal swab rather than a more invasive blood sample. CMV infections can compromise the integrity of stem cell grafts and could be fatal to immunocompromised transplant recipients.
The last word goes to Mechtild Harf’s daughter Katharina.
“My big dream is that every patient will be saved from blood cancer,” she said in a video posted on the DKMS website. “When they get sick, we have a solution for them, whether it’s because they need a donor, with research, building hospitals, providing them with the best medical care we can. I will just keep fighting and keep spreading the word, recruiting donors, raising money – all the things that it takes for us to delete blood cancer.”
“I have to believe that this dream will come true because otherwise, why dream, right?” she said.
Dr. Champlin was the recipient of a Mechtild Harf Science Award and is a member of the board of DKMS U.S. Dr. Schmidt is employed by DKMS. Dr. Chen reported having no relevant disclosures.
When Mechtild Harf was diagnosed with acute leukemia in 1990, physicians told her and her husband Peter that a bone marrow transplant was her best hope for survival. Back then, her native Germany had only 3,000 registered donors, and none was a match.
“My dad just went crazy, you know, to save his wife,” recalled Katharina Harf, who was a young teen at the time of her mother’s diagnosis.
In the course of 1 year, the Harfs recruited more than 68,000 potential bone marrow donors, but their heroic efforts couldn’t save Mechtild.
“She unfortunately didn’t make it. She died because of leukemia,” Katharina said.
Although Mechtild Harf did not survive, her legacy lives on in the bone marrow and stem cell donor recruitment organization DKMS (Deutsche Knochenmarkspenderdatei, or German Bone Marrow Donor Center).
In May of 1991, Peter Harf and Gerhard Ehninger, MD, the hematologist who treated Mechtild, founded DKMS with the mission, as its website states, “to provide as many blood cancer patients as possible with a second chance at life.”
From its German roots, the nonprofit organization has extended its mission to the United States (where it was initially known as Delete Blood Cancer DKMS), Poland, the United Kingdom, Chile, and in 2021, to South Africa.
Three decades after her mother’s death, Katharina Harf serves as Executive Chairwoman of DKMS U.S., based in New York.
World’s largest registry
“DKMS has the largest number of unrelated donors of any organization in the world,” noted Richard E. Champlin, MD, chair of the department of stem cell transplantation and cellular therapy at the University of Texas MD Anderson Cancer Center in Houston.
“In a large fraction of our donor searches, we find matches that are in the DKMS registry,” he said in an interview,
Alexander Schmidt, MD, PhD, global chief medical officer for DKMS, said that approximately 25% of all registered donors worldwide were recruited by his organization, and 39% of all unrelated donor transplants are made with peripheral blood stem cell or bone marrow products, donated by volunteers who are recruited by DKMS.
Since its founding, DKMS has registered 7.1 million potential donors in Germany, who made a total of 80,000 stem cell donations. DKMS U.S., which began operations in 2004, has registered 1.1 million donors and enabled 4,700 donations.
Global partners
DKMS partners with donor centers and recruitment organizations in each country where it operates. In the United States, DKMS works with the National Marrow Donor Program (NMDP) and its “Be The Match” donor registry.
“DKMS donors, both those from DKMS in Germany and those from DKMS in the United States are also listed in the NMDP registry, to make it easier for US search coordinators to accept these donors,” Dr. Schmidt explained in an interview.
The international cooperation and coordination makes it possible for a donor in the UK, for example, to save a life of a patient in Germany, the U.S., Chile, India, or many other parts of the world – anywhere that can be reached in time for a patient in need to receive a stem cell donation.
Pandemic affects donations
But, as with just about every aspect of life, the COVID-19 pandemic has created enormous challenges for recruiters, donor centers, and stem cell transplant centers.
Dr. Schmidt said that decline in donations during the pandemic was less severe than initially feared, with a decrease of just 3.5% in 2020, compared with the prepandemic year of 2019. In contrast, though, the average annual growth rate for donations prior to the pandemic was about 4%.
“Nevertheless, at the beginning of the pandemic in March 2020, for a few days things looked quite terrible, because all the borders were closed and flights were canceled, and about 50% of all stem cell products go abroad, and between 20% and 25% go intercontinental,” Dr. Schmidt said.
However, close cooperation and coordination between donor centers and national health authorities soon resolved the problem and helped insure that the flow of life-saving donations could continue with minimal disruption, he noted.
“I don’t think we had any product that could not be delivered at the end of the day, due to the pandemic,” he told this news organization.
Workforce and clinical problems
Although the flow of donations within and between nations has continued, the COVID-19 pandemic has had profound negative effects on transplant centers, particularly during the wave of infections caused by the Omicron variant, according to a transplant expert.
“With this most recent strain and how transmissible it is, what we’re dealing with is mass workforce shortages,” said Yi-Bin Chen, MD, director of the bone marrow transplant program at Massachusetts General Hospital in Boston.
“On top of a short-staffed hospital, you then take a very transmissible variant and deplete it even more due to the need to quarantine,” he said in an interview.
Both Dr. Champlin and Dr. Chen said that on-again, off-again pandemic travel bans and donor illnesses have necessitated first obtaining products and cryopreserving them before starting the recipient on a conditioning regimen for the transplant.
“The problem is that, while you can preserve peripheral blood stem cells pretty reliably, cryopreserving bone marrow is a bit more difficult,” Dr. Chen said.
In addition, evidence from recent studies comparing stem cell sources suggest that outcomes are less good with cryopreserved products than with fresh products, and with peripheral blood stem cells compared with bone marrow.
“But you’ve got to make do. A transplant with a cryopreserved product is better than no transplant,” Dr. Chen said.
To make things even more frustrating, as the pandemic waxed and waned throughout 2020 and 2021, the recommendations from donor centers seesawed between using fresh or cryopreserved product, making it difficult to plan a transplant for an individual patient.
The Omicron wave has also resulted in a much higher rate of donor dropout than anticipated, making it that much harder to schedule a transplant, Dr. Chen noted.
‘Every patient saved’
The pandemic will eventually subside, however, while the need for stem cell transplantation to treat hematologic malignancies will continue.
DKMS recently launched special aid programs to improve access to stem cell transplants in developing nations by offering financial support, free HLA typing, and other services.
In addition to its core mission of recruiting donors, DKMS is dedicated to improving the quality and efficiency of stem cell transplants. For example, in 2017 scientists in DKMS’ Life Science Lab created an antibody test for donor cytomegalovirus (CMV) infection, using a simple buccal swab rather than a more invasive blood sample. CMV infections can compromise the integrity of stem cell grafts and could be fatal to immunocompromised transplant recipients.
The last word goes to Mechtild Harf’s daughter Katharina.
“My big dream is that every patient will be saved from blood cancer,” she said in a video posted on the DKMS website. “When they get sick, we have a solution for them, whether it’s because they need a donor, with research, building hospitals, providing them with the best medical care we can. I will just keep fighting and keep spreading the word, recruiting donors, raising money – all the things that it takes for us to delete blood cancer.”
“I have to believe that this dream will come true because otherwise, why dream, right?” she said.
Dr. Champlin was the recipient of a Mechtild Harf Science Award and is a member of the board of DKMS U.S. Dr. Schmidt is employed by DKMS. Dr. Chen reported having no relevant disclosures.
When Mechtild Harf was diagnosed with acute leukemia in 1990, physicians told her and her husband Peter that a bone marrow transplant was her best hope for survival. Back then, her native Germany had only 3,000 registered donors, and none was a match.
“My dad just went crazy, you know, to save his wife,” recalled Katharina Harf, who was a young teen at the time of her mother’s diagnosis.
In the course of 1 year, the Harfs recruited more than 68,000 potential bone marrow donors, but their heroic efforts couldn’t save Mechtild.
“She unfortunately didn’t make it. She died because of leukemia,” Katharina said.
Although Mechtild Harf did not survive, her legacy lives on in the bone marrow and stem cell donor recruitment organization DKMS (Deutsche Knochenmarkspenderdatei, or German Bone Marrow Donor Center).
In May of 1991, Peter Harf and Gerhard Ehninger, MD, the hematologist who treated Mechtild, founded DKMS with the mission, as its website states, “to provide as many blood cancer patients as possible with a second chance at life.”
From its German roots, the nonprofit organization has extended its mission to the United States (where it was initially known as Delete Blood Cancer DKMS), Poland, the United Kingdom, Chile, and in 2021, to South Africa.
Three decades after her mother’s death, Katharina Harf serves as Executive Chairwoman of DKMS U.S., based in New York.
World’s largest registry
“DKMS has the largest number of unrelated donors of any organization in the world,” noted Richard E. Champlin, MD, chair of the department of stem cell transplantation and cellular therapy at the University of Texas MD Anderson Cancer Center in Houston.
“In a large fraction of our donor searches, we find matches that are in the DKMS registry,” he said in an interview,
Alexander Schmidt, MD, PhD, global chief medical officer for DKMS, said that approximately 25% of all registered donors worldwide were recruited by his organization, and 39% of all unrelated donor transplants are made with peripheral blood stem cell or bone marrow products, donated by volunteers who are recruited by DKMS.
Since its founding, DKMS has registered 7.1 million potential donors in Germany, who made a total of 80,000 stem cell donations. DKMS U.S., which began operations in 2004, has registered 1.1 million donors and enabled 4,700 donations.
Global partners
DKMS partners with donor centers and recruitment organizations in each country where it operates. In the United States, DKMS works with the National Marrow Donor Program (NMDP) and its “Be The Match” donor registry.
“DKMS donors, both those from DKMS in Germany and those from DKMS in the United States are also listed in the NMDP registry, to make it easier for US search coordinators to accept these donors,” Dr. Schmidt explained in an interview.
The international cooperation and coordination makes it possible for a donor in the UK, for example, to save a life of a patient in Germany, the U.S., Chile, India, or many other parts of the world – anywhere that can be reached in time for a patient in need to receive a stem cell donation.
Pandemic affects donations
But, as with just about every aspect of life, the COVID-19 pandemic has created enormous challenges for recruiters, donor centers, and stem cell transplant centers.
Dr. Schmidt said that decline in donations during the pandemic was less severe than initially feared, with a decrease of just 3.5% in 2020, compared with the prepandemic year of 2019. In contrast, though, the average annual growth rate for donations prior to the pandemic was about 4%.
“Nevertheless, at the beginning of the pandemic in March 2020, for a few days things looked quite terrible, because all the borders were closed and flights were canceled, and about 50% of all stem cell products go abroad, and between 20% and 25% go intercontinental,” Dr. Schmidt said.
However, close cooperation and coordination between donor centers and national health authorities soon resolved the problem and helped insure that the flow of life-saving donations could continue with minimal disruption, he noted.
“I don’t think we had any product that could not be delivered at the end of the day, due to the pandemic,” he told this news organization.
Workforce and clinical problems
Although the flow of donations within and between nations has continued, the COVID-19 pandemic has had profound negative effects on transplant centers, particularly during the wave of infections caused by the Omicron variant, according to a transplant expert.
“With this most recent strain and how transmissible it is, what we’re dealing with is mass workforce shortages,” said Yi-Bin Chen, MD, director of the bone marrow transplant program at Massachusetts General Hospital in Boston.
“On top of a short-staffed hospital, you then take a very transmissible variant and deplete it even more due to the need to quarantine,” he said in an interview.
Both Dr. Champlin and Dr. Chen said that on-again, off-again pandemic travel bans and donor illnesses have necessitated first obtaining products and cryopreserving them before starting the recipient on a conditioning regimen for the transplant.
“The problem is that, while you can preserve peripheral blood stem cells pretty reliably, cryopreserving bone marrow is a bit more difficult,” Dr. Chen said.
In addition, evidence from recent studies comparing stem cell sources suggest that outcomes are less good with cryopreserved products than with fresh products, and with peripheral blood stem cells compared with bone marrow.
“But you’ve got to make do. A transplant with a cryopreserved product is better than no transplant,” Dr. Chen said.
To make things even more frustrating, as the pandemic waxed and waned throughout 2020 and 2021, the recommendations from donor centers seesawed between using fresh or cryopreserved product, making it difficult to plan a transplant for an individual patient.
The Omicron wave has also resulted in a much higher rate of donor dropout than anticipated, making it that much harder to schedule a transplant, Dr. Chen noted.
‘Every patient saved’
The pandemic will eventually subside, however, while the need for stem cell transplantation to treat hematologic malignancies will continue.
DKMS recently launched special aid programs to improve access to stem cell transplants in developing nations by offering financial support, free HLA typing, and other services.
In addition to its core mission of recruiting donors, DKMS is dedicated to improving the quality and efficiency of stem cell transplants. For example, in 2017 scientists in DKMS’ Life Science Lab created an antibody test for donor cytomegalovirus (CMV) infection, using a simple buccal swab rather than a more invasive blood sample. CMV infections can compromise the integrity of stem cell grafts and could be fatal to immunocompromised transplant recipients.
The last word goes to Mechtild Harf’s daughter Katharina.
“My big dream is that every patient will be saved from blood cancer,” she said in a video posted on the DKMS website. “When they get sick, we have a solution for them, whether it’s because they need a donor, with research, building hospitals, providing them with the best medical care we can. I will just keep fighting and keep spreading the word, recruiting donors, raising money – all the things that it takes for us to delete blood cancer.”
“I have to believe that this dream will come true because otherwise, why dream, right?” she said.
Dr. Champlin was the recipient of a Mechtild Harf Science Award and is a member of the board of DKMS U.S. Dr. Schmidt is employed by DKMS. Dr. Chen reported having no relevant disclosures.
Five things you should know about ‘free’ at-home COVID tests
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Americans keep hearing that it is important to test frequently for COVID-19 at home. But just try to find an “at-home” rapid COVID test in a store and at a price that makes frequent tests affordable.
Testing, as well as mask-wearing, is an important measure if the country ever hopes to beat COVID, restore normal routines and get the economy running efficiently. To get Americans cheaper tests, the federal government now plans to have insurance companies pay for them.
You can either get one without any out-of-pocket expense from retail pharmacies that are part of an insurance company’s network or buy it at any store and get reimbursed by the insurer.
Congress said private insurers must cover all COVID testing and any associated medical services when it passed the Families First Coronavirus Response Act and the Coronavirus Aid, Relief and Economic Security, or CARES, Act. The have-insurance-pay-for-it solution has been used frequently through the pandemic. Insurance companies have been told to pay for polymerase chain reaction tests, COVID treatments and the administration of vaccines. (Taxpayers are paying for the cost of the vaccines themselves.) It appears to be an elegant solution for a politician because it looks free and isn’t using taxpayer money.
1. Are the tests really free?
Well, no. As many an economist will tell you, there ain’t no such thing as a free lunch. Someone has to pick up the tab. Initially, the insurance companies bear the cost. Cynthia Cox, a vice president at KFF who studies the Affordable Care Act and private insurers, said the total bill could amount to billions of dollars. Exactly how much depends on “how easy it is to get them, and how many will be reimbursed,” she said.
2. Will the insurance company just swallow those imposed costs?
If companies draw from the time-tested insurance giants’ playbook, they’ll pass along those costs to customers. “This will put upward pressure on premiums,” said Emily Gee, vice president and coordinator for health policy at the Center for American Progress.
Major insurance companies like Cigna, Anthem, UnitedHealthcare, and Aetna did not respond to requests to discuss this issue.
3. If that’s the case, why haven’t I been hit with higher premiums already?
Insurance companies had the chance last year to raise premiums but, mostly, they did not.
Why? Perhaps because insurers have so far made so much money during the pandemic they didn’t need to. For example, the industry’s profits in 2020 increased 41% to $31 billion from $22 billion, according to the National Association of Insurance Commissioners. The NAIC said the industry has continued its “tremendous growth trend” that started before COVID emerged. Companies will be reporting 2021 results soon.
The reason behind these profits is clear. You were paying premiums based on projections your insurance company made about how much health care consumers would use that year. Because people stayed home, had fewer accidents, postponed surgeries and often avoided going to visit the doctor or the hospital, insurers paid out less. They rebated some of their earnings back to customers, but they pocketed a lot more.
As the companies’ actuaries work on predicting 2023 expenditures, premiums could go up if they foresee more claims and expenses. Paying for millions of rapid tests is something they would include in their calculations.
4. Regardless of my premiums, will the tests cost me money directly?
It’s quite possible. If your insurance company doesn’t have an arrangement with a retailer where you can simply pick up your allotted tests, you’ll have to pay for them – at whatever price the store sets. If that’s the case, you’ll need to fill out a form to request a reimbursement from the insurance company. How many times have you lost receipts or just plain neglected to mail in for rebates on something you bought? A lot, right?
Here’s another thing: The reimbursement is set at $12 per test. If you pay $30 for a test – and that is not unheard of – your insurer is only on the hook for $12. You eat the $18.
And by the way, people on Medicare will have to pay for their tests themselves. People who get their health care covered by Medicaid can obtain free test kits at community centers.
A few free tests are supposed to arrive at every American home via the U.S. Postal Service. And the Biden administration has activated a website where Americans can order free tests from a cache of a billion the federal government ordered.
5. Will this help bring down the costs of at-home tests and make them easier to find?
The free COVID tests are unlikely to have much immediate impact on general cost and availability. You will still need to search for them. The federal measures likely will stimulate the demand for tests, which in the short term may make them harder to find.
But the demand, and some government guarantees to manufacturers, may induce test makers to make more of them faster. The increased competition and supply theoretically could bring down the price. There is certainly room for prices to decline since the wholesale cost of the test is between $5 and $7, analysts estimate. “It’s a big step in the right direction,” Ms. Gee said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
‘Artificial pancreas’ life-changing in kids with type 1 diabetes
A semiautomated insulin delivery system improved glycemic control in young children with type 1 diabetes aged 1-7 years without increasing hypoglycemia.
“Hybrid closed-loop” systems – comprising an insulin pump, a continuous glucose monitor (CGM), and software enabling communication that semiautomates insulin delivery based on glucose levels – have been shown to improve glucose control in older children and adults.
The technology, also known as an artificial pancreas, has been less studied in very young children even though it may uniquely benefit them, said the authors of the new study, led by Julia Ware, MD, of the Wellcome Trust–Medical Research Council Institute of Metabolic Science and the University of Cambridge (England). The findings were published online Jan. 19, 2022, in the New England Journal of Medicine.
“Very young children are extremely vulnerable to changes in their blood sugar levels. High levels in particular can have potentially lasting consequences to their brain development. On top of that, diabetes is very challenging to manage in this age group, creating a huge burden for families,” she said in a University of Cambridge statement.
There is “high variability of insulin requirements, marked insulin sensitivity, and unpredictable eating and activity patterns,” Dr. Ware and colleagues noted.
“Caregiver fear of hypoglycemia, particularly overnight, is common and, coupled with young children’s unawareness that hypoglycemia is occurring, contributes to children not meeting the recommended glycemic targets or having difficulty maintaining recommended glycemic control unless caregivers can provide constant monitoring. These issues often lead to ... reduced quality of life for the whole family,” they added.
Except for mealtimes, device is fully automated
The new multicenter, randomized, crossover trial was conducted at seven centers across Austria, Germany, Luxembourg, and the United Kingdom in 2019-2020.
The trial compared the safety and efficacy of hybrid closed-loop therapy with sensor-augmented pump therapy (that is, without the device communication, as a control). All 74 children used the CamAPS FX hybrid closed-loop system for 16 weeks, and then used the control treatment for 16 weeks. The children were a mean age of 5.6 years and had a baseline hemoglobin A1c of 7.3% (56.6 mmol/mol).
The hybrid closed-loop system consisted of components that are commercially available in Europe: the Sooil insulin pump (Dana Diabecare RS) and the Dexcom G6 CGM, along with an unlocked Samsung Galaxy 8 smartphone housing an app (CamAPS FX, CamDiab) that runs the Cambridge proprietary model predictive control algorithm.
The smartphone communicates wirelessly with both the pump and the CGM transmitter and automatically adjusts the pump’s insulin delivery based on real-time sensor glucose readings. It also issues alarms if glucose levels fall below or rise above user-specified thresholds. This functionality was disabled during the study control periods.
Senior investigator Roman Hovorka, PhD, who developed the CamAPS FX app, explained in the University of Cambridge statement that the app “makes predictions about what it thinks is likely to happen next based on past experience. It learns how much insulin the child needs per day and how this changes at different times of the day.
“It then uses this [information] to adjust insulin levels to help achieve ideal blood sugar levels. Other than at mealtimes, it is fully automated, so parents do not need to continually monitor their child’s blood sugar levels.”
Indeed, the time spent in target glucose range (70-180 mg/dL) during the 16-week closed-loop period was 8.7 percentage points higher than during the control period (P < .001).
That difference translates to “a clinically meaningful 125 minutes per day,” and represented around three-quarters of their day (71.6%) in the target range, the investigators wrote.
The mean adjusted difference in time spent above 180 mg/dL was 8.5 percentage points lower with the closed-loop, also a significant difference (P < .001). Time spent below 70 mg/dL did not differ significantly between the two interventions (P = .74).
At the end of the study periods, the mean adjusted between-treatment difference in A1c was –0.4 percentage points, significantly lower following the closed-loop, compared with the control period (P < .001).
That percentage point difference (equivalent to 3.9 mmol/mol) “is important in a population of patients who had tight glycemic control at baseline. This result was observed without an increase in the time spent in a hypoglycemic state,” Dr. Ware and colleagues noted.
Median glucose sensor use was 99% during the closed-loop period and 96% during the control periods. During the closed-loop periods, the system was in closed-loop mode 95% of the time.
This finding supports longer-term usability in this age group and compares well with use in older children, they said.
One serious hypoglycemic episode, attributed to parental error rather than system malfunction, occurred during the closed-loop period. There were no episodes of diabetic ketoacidosis. Rates of other adverse events didn’t differ between the two periods.
“CamAPS FX led to improvements in several measures, including hyperglycemia and average blood sugar levels, without increasing the risk of hypos. This is likely to have important benefits for those children who use it,” Dr. Ware summarized.
Sleep quality could improve for children and caregivers
Reductions in time spent in hyperglycemia without increasing hypoglycemia could minimize the risk for neurocognitive deficits that have been reported among young children with type 1 diabetes, the authors speculated.
In addition, they noted that because 80% of overnight sensor readings were within target range and less than 3% were below 70 mg/dL, sleep quality could improve for both the children and their parents. This, in turn, “would confer associated quality of life benefits.”
“Parents have described our artificial pancreas as ‘life changing’ as it meant they were able to relax and spend less time worrying about their child’s blood sugar levels, particularly at nighttime. They tell us it gives them more time to do what any ‘normal’ family can do, to play and do fun things with their children,” observed Dr. Ware.
The CamAPS FX has been commercialized by CamDiab, a spin-out company set up by Dr. Hovorka. It is currently available through several NHS trusts across the United Kingdom, including Cambridge University Hospitals NHS Foundation Trust, and is expected to be more widely available soon.
The study was supported by the European Commission within the Horizon 2020 Framework Program, the NIHR Cambridge Biomedical Research Centre, and JDRF. Dr. Ware had no further disclosures. Dr. Hovorka has reported acting as consultant for Abbott Diabetes Care, BD, Dexcom, being a speaker for Novo Nordisk and Eli Lilly, and receiving royalty payments from B. Braun for software. He is director of CamDiab.
A version of this article first appeared on Medscape.com.
A semiautomated insulin delivery system improved glycemic control in young children with type 1 diabetes aged 1-7 years without increasing hypoglycemia.
“Hybrid closed-loop” systems – comprising an insulin pump, a continuous glucose monitor (CGM), and software enabling communication that semiautomates insulin delivery based on glucose levels – have been shown to improve glucose control in older children and adults.
The technology, also known as an artificial pancreas, has been less studied in very young children even though it may uniquely benefit them, said the authors of the new study, led by Julia Ware, MD, of the Wellcome Trust–Medical Research Council Institute of Metabolic Science and the University of Cambridge (England). The findings were published online Jan. 19, 2022, in the New England Journal of Medicine.
“Very young children are extremely vulnerable to changes in their blood sugar levels. High levels in particular can have potentially lasting consequences to their brain development. On top of that, diabetes is very challenging to manage in this age group, creating a huge burden for families,” she said in a University of Cambridge statement.
There is “high variability of insulin requirements, marked insulin sensitivity, and unpredictable eating and activity patterns,” Dr. Ware and colleagues noted.
“Caregiver fear of hypoglycemia, particularly overnight, is common and, coupled with young children’s unawareness that hypoglycemia is occurring, contributes to children not meeting the recommended glycemic targets or having difficulty maintaining recommended glycemic control unless caregivers can provide constant monitoring. These issues often lead to ... reduced quality of life for the whole family,” they added.
Except for mealtimes, device is fully automated
The new multicenter, randomized, crossover trial was conducted at seven centers across Austria, Germany, Luxembourg, and the United Kingdom in 2019-2020.
The trial compared the safety and efficacy of hybrid closed-loop therapy with sensor-augmented pump therapy (that is, without the device communication, as a control). All 74 children used the CamAPS FX hybrid closed-loop system for 16 weeks, and then used the control treatment for 16 weeks. The children were a mean age of 5.6 years and had a baseline hemoglobin A1c of 7.3% (56.6 mmol/mol).
The hybrid closed-loop system consisted of components that are commercially available in Europe: the Sooil insulin pump (Dana Diabecare RS) and the Dexcom G6 CGM, along with an unlocked Samsung Galaxy 8 smartphone housing an app (CamAPS FX, CamDiab) that runs the Cambridge proprietary model predictive control algorithm.
The smartphone communicates wirelessly with both the pump and the CGM transmitter and automatically adjusts the pump’s insulin delivery based on real-time sensor glucose readings. It also issues alarms if glucose levels fall below or rise above user-specified thresholds. This functionality was disabled during the study control periods.
Senior investigator Roman Hovorka, PhD, who developed the CamAPS FX app, explained in the University of Cambridge statement that the app “makes predictions about what it thinks is likely to happen next based on past experience. It learns how much insulin the child needs per day and how this changes at different times of the day.
“It then uses this [information] to adjust insulin levels to help achieve ideal blood sugar levels. Other than at mealtimes, it is fully automated, so parents do not need to continually monitor their child’s blood sugar levels.”
Indeed, the time spent in target glucose range (70-180 mg/dL) during the 16-week closed-loop period was 8.7 percentage points higher than during the control period (P < .001).
That difference translates to “a clinically meaningful 125 minutes per day,” and represented around three-quarters of their day (71.6%) in the target range, the investigators wrote.
The mean adjusted difference in time spent above 180 mg/dL was 8.5 percentage points lower with the closed-loop, also a significant difference (P < .001). Time spent below 70 mg/dL did not differ significantly between the two interventions (P = .74).
At the end of the study periods, the mean adjusted between-treatment difference in A1c was –0.4 percentage points, significantly lower following the closed-loop, compared with the control period (P < .001).
That percentage point difference (equivalent to 3.9 mmol/mol) “is important in a population of patients who had tight glycemic control at baseline. This result was observed without an increase in the time spent in a hypoglycemic state,” Dr. Ware and colleagues noted.
Median glucose sensor use was 99% during the closed-loop period and 96% during the control periods. During the closed-loop periods, the system was in closed-loop mode 95% of the time.
This finding supports longer-term usability in this age group and compares well with use in older children, they said.
One serious hypoglycemic episode, attributed to parental error rather than system malfunction, occurred during the closed-loop period. There were no episodes of diabetic ketoacidosis. Rates of other adverse events didn’t differ between the two periods.
“CamAPS FX led to improvements in several measures, including hyperglycemia and average blood sugar levels, without increasing the risk of hypos. This is likely to have important benefits for those children who use it,” Dr. Ware summarized.
Sleep quality could improve for children and caregivers
Reductions in time spent in hyperglycemia without increasing hypoglycemia could minimize the risk for neurocognitive deficits that have been reported among young children with type 1 diabetes, the authors speculated.
In addition, they noted that because 80% of overnight sensor readings were within target range and less than 3% were below 70 mg/dL, sleep quality could improve for both the children and their parents. This, in turn, “would confer associated quality of life benefits.”
“Parents have described our artificial pancreas as ‘life changing’ as it meant they were able to relax and spend less time worrying about their child’s blood sugar levels, particularly at nighttime. They tell us it gives them more time to do what any ‘normal’ family can do, to play and do fun things with their children,” observed Dr. Ware.
The CamAPS FX has been commercialized by CamDiab, a spin-out company set up by Dr. Hovorka. It is currently available through several NHS trusts across the United Kingdom, including Cambridge University Hospitals NHS Foundation Trust, and is expected to be more widely available soon.
The study was supported by the European Commission within the Horizon 2020 Framework Program, the NIHR Cambridge Biomedical Research Centre, and JDRF. Dr. Ware had no further disclosures. Dr. Hovorka has reported acting as consultant for Abbott Diabetes Care, BD, Dexcom, being a speaker for Novo Nordisk and Eli Lilly, and receiving royalty payments from B. Braun for software. He is director of CamDiab.
A version of this article first appeared on Medscape.com.
A semiautomated insulin delivery system improved glycemic control in young children with type 1 diabetes aged 1-7 years without increasing hypoglycemia.
“Hybrid closed-loop” systems – comprising an insulin pump, a continuous glucose monitor (CGM), and software enabling communication that semiautomates insulin delivery based on glucose levels – have been shown to improve glucose control in older children and adults.
The technology, also known as an artificial pancreas, has been less studied in very young children even though it may uniquely benefit them, said the authors of the new study, led by Julia Ware, MD, of the Wellcome Trust–Medical Research Council Institute of Metabolic Science and the University of Cambridge (England). The findings were published online Jan. 19, 2022, in the New England Journal of Medicine.
“Very young children are extremely vulnerable to changes in their blood sugar levels. High levels in particular can have potentially lasting consequences to their brain development. On top of that, diabetes is very challenging to manage in this age group, creating a huge burden for families,” she said in a University of Cambridge statement.
There is “high variability of insulin requirements, marked insulin sensitivity, and unpredictable eating and activity patterns,” Dr. Ware and colleagues noted.
“Caregiver fear of hypoglycemia, particularly overnight, is common and, coupled with young children’s unawareness that hypoglycemia is occurring, contributes to children not meeting the recommended glycemic targets or having difficulty maintaining recommended glycemic control unless caregivers can provide constant monitoring. These issues often lead to ... reduced quality of life for the whole family,” they added.
Except for mealtimes, device is fully automated
The new multicenter, randomized, crossover trial was conducted at seven centers across Austria, Germany, Luxembourg, and the United Kingdom in 2019-2020.
The trial compared the safety and efficacy of hybrid closed-loop therapy with sensor-augmented pump therapy (that is, without the device communication, as a control). All 74 children used the CamAPS FX hybrid closed-loop system for 16 weeks, and then used the control treatment for 16 weeks. The children were a mean age of 5.6 years and had a baseline hemoglobin A1c of 7.3% (56.6 mmol/mol).
The hybrid closed-loop system consisted of components that are commercially available in Europe: the Sooil insulin pump (Dana Diabecare RS) and the Dexcom G6 CGM, along with an unlocked Samsung Galaxy 8 smartphone housing an app (CamAPS FX, CamDiab) that runs the Cambridge proprietary model predictive control algorithm.
The smartphone communicates wirelessly with both the pump and the CGM transmitter and automatically adjusts the pump’s insulin delivery based on real-time sensor glucose readings. It also issues alarms if glucose levels fall below or rise above user-specified thresholds. This functionality was disabled during the study control periods.
Senior investigator Roman Hovorka, PhD, who developed the CamAPS FX app, explained in the University of Cambridge statement that the app “makes predictions about what it thinks is likely to happen next based on past experience. It learns how much insulin the child needs per day and how this changes at different times of the day.
“It then uses this [information] to adjust insulin levels to help achieve ideal blood sugar levels. Other than at mealtimes, it is fully automated, so parents do not need to continually monitor their child’s blood sugar levels.”
Indeed, the time spent in target glucose range (70-180 mg/dL) during the 16-week closed-loop period was 8.7 percentage points higher than during the control period (P < .001).
That difference translates to “a clinically meaningful 125 minutes per day,” and represented around three-quarters of their day (71.6%) in the target range, the investigators wrote.
The mean adjusted difference in time spent above 180 mg/dL was 8.5 percentage points lower with the closed-loop, also a significant difference (P < .001). Time spent below 70 mg/dL did not differ significantly between the two interventions (P = .74).
At the end of the study periods, the mean adjusted between-treatment difference in A1c was –0.4 percentage points, significantly lower following the closed-loop, compared with the control period (P < .001).
That percentage point difference (equivalent to 3.9 mmol/mol) “is important in a population of patients who had tight glycemic control at baseline. This result was observed without an increase in the time spent in a hypoglycemic state,” Dr. Ware and colleagues noted.
Median glucose sensor use was 99% during the closed-loop period and 96% during the control periods. During the closed-loop periods, the system was in closed-loop mode 95% of the time.
This finding supports longer-term usability in this age group and compares well with use in older children, they said.
One serious hypoglycemic episode, attributed to parental error rather than system malfunction, occurred during the closed-loop period. There were no episodes of diabetic ketoacidosis. Rates of other adverse events didn’t differ between the two periods.
“CamAPS FX led to improvements in several measures, including hyperglycemia and average blood sugar levels, without increasing the risk of hypos. This is likely to have important benefits for those children who use it,” Dr. Ware summarized.
Sleep quality could improve for children and caregivers
Reductions in time spent in hyperglycemia without increasing hypoglycemia could minimize the risk for neurocognitive deficits that have been reported among young children with type 1 diabetes, the authors speculated.
In addition, they noted that because 80% of overnight sensor readings were within target range and less than 3% were below 70 mg/dL, sleep quality could improve for both the children and their parents. This, in turn, “would confer associated quality of life benefits.”
“Parents have described our artificial pancreas as ‘life changing’ as it meant they were able to relax and spend less time worrying about their child’s blood sugar levels, particularly at nighttime. They tell us it gives them more time to do what any ‘normal’ family can do, to play and do fun things with their children,” observed Dr. Ware.
The CamAPS FX has been commercialized by CamDiab, a spin-out company set up by Dr. Hovorka. It is currently available through several NHS trusts across the United Kingdom, including Cambridge University Hospitals NHS Foundation Trust, and is expected to be more widely available soon.
The study was supported by the European Commission within the Horizon 2020 Framework Program, the NIHR Cambridge Biomedical Research Centre, and JDRF. Dr. Ware had no further disclosures. Dr. Hovorka has reported acting as consultant for Abbott Diabetes Care, BD, Dexcom, being a speaker for Novo Nordisk and Eli Lilly, and receiving royalty payments from B. Braun for software. He is director of CamDiab.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Two studies detail the dangers of COVID in pregnancy
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.