User login
From Beirut to frontline hematology research
“If we start treatment earlier, in the smoldering phase, maybe there is a chance of actually curing the disease and completely getting rid of it,” said Dr. Mouhieddine, 31, a research fellow at the Icahn School of Medicine at Mount Sinai, in New York. “We haven’t proven that yet, and it’s going to take years before we’re able to prove it. I’m hoping to be one of those spearheading the initiative.”

As he develops clinical trials, the young physician scientist has another focus: A deeply personal connection to the very disease he’s trying to cure. Last year Dr. Mouhieddine diagnosed his aunt back in Lebanon with multiple myeloma. “I have always been close to her, and I’m like her son,” he said, and her situation is especially scary because she lives in a country where treatment options are limited.
Dr. Mouhieddine was born and raised in Beirut, the son of a sports journalist father and a mother who worked in a bank. Lebanon’s civil war ended in 1990, shortly before his birth, but political instability returned when he was a child.
“Everything was a disaster,” he recalled. “There was a period of time when there were bombs throughout the city because certain politicians were being targeted. I remember when groups of people would have gunfights in the street.”
Dr. Mouhieddine attended the American University of Beirut, then after college and medical school there, he headed to the United States.
“I wanted to make a difference in medicine. And I knew that if I stayed back home, I wouldn’t be able to,” he said. Fortunately, “everybody has made me feel that I really belong here, and I’ve never felt like I’m an outsider.”
Early on, as he went through fellowships and residency, he developed an interest in multiple myeloma.
Ajai Chari, MD, a colleague of Dr. Mouhieddine’s at Icahn School of Medicine, said in an interview, “I remember meeting him at a conference before he had even started an internal medicine residency, let alone a hematology oncology fellowship. He was already certain he wanted to work in multiple myeloma, due to his work at Dana-Farber Cancer Institute.”
Myeloma was especially intriguing to Dr. Mouhieddine because of the rapid rate of progress in treating the disease. “Over the past 10 years, the myeloma field has advanced at such an extremely fast pace, more than any other cancer,” he said. “Maybe 15 years ago, you would tell someone with newly diagnosed myeloma that they had a chance for an average of another 2 years. Now, we tell patients they have 10 years to live on average, which means you could live 15 or 20 years. That alone was astounding to me and piqued my interest in myeloma.”
At the same time, smoldering myeloma – which can be discovered during routine blood work – remains little understood. As the National Cancer Institute explains, “smoldering myeloma is a precancerous condition that alters certain proteins in blood and/or increases plasma cells in bone marrow, but it does not cause symptoms of disease. About half of those diagnosed with the condition, however, will develop multiple myeloma within 5 years.”
“If we understand what drives smoldering myeloma, we may be able to prevent it from progressing to its active form,” said hematologist oncologist Samir Parekh, MD, who works with Dr. Mouhieddine at Icahn School of Medicine. “Or at the minimum, we could better predict who will progress so we can tailor therapy for high-risk patients and minimize toxicity by not overtreating patients who may not need therapy.”
Dr. Mouhieddine’s current work is focusing on developing clinical trials to test whether immunotherapy can snuff out myeloma when it’s at the smoldering stage, “before anything bad happens.
“If a myeloma patient comes in with renal failure, and we treat the myeloma at that stage, it doesn’t mean that the patient’s kidneys are gonna go back to normal. A lot of the damage can be permanent,” he said. “Even when you treat multiple myeloma, and it goes into remission, it ends up coming back. And you just have to go from one therapy to the other.”
In contrast, a successful treatment for smoldering myeloma would prevent progression to the full disease. In other words, it would be a cure – which is now elusive.
Specifically, Dr. Mouhieddine hopes to test whether bispecific antibodies, a type of immunotherapy that enlists the body’s T cells to kill myeloma cells, will be effective in the smoldering phase. Bispecific antibodies are now being explored as treatments for full multiple myeloma when the immune system is weaker, he said, and they may be even more effective earlier, when the body is better equipped to fight off the disease.
Dr. Mouhieddine hopes better treatments for multiple myeloma itself will help save his 64-year-old aunt Hassana, back in Beirut. He diagnosed her in 2022 after she told him that she felt tired all the time and underwent various tests. The woman he calls his “second mom” is doing well, despite struggles to buy medication due to the lack of access to bank funds in Lebanon.

“I’m always going to be afraid that the disease is going to progress or come back at some point,” he said. “Lebanon doesn’t have as many options as people in the U.S. do. Once you exhaust your first option, and maybe your second option, then you don’t have any other options. Here, we have outpatients who exhaust option number 15 and go to option number 16. That’s definitely not the case over there.”
For now, Dr. Mouhieddine is treating patients and working to launch clinical trials into smoldering myeloma. “His work ethic is incredible,” said his colleague, Dr. Chari. “He has seen multiple projects to publication, and he develops deep connections with his patients and follows up on their care whether or not he is in clinic on a particular day.”
Dr. Parekh, another colleague, said Dr. Mouhieddine can even be a role model. “Other trainees may benefit from thinking about their career early on and exploring both lab and clinical research projects, so that they can develop the necessary experience to be competitive in academia later on.”
His workload can a burden for Dr. Mouhieddine, who is Muslim. He expressed regret that his busy schedule does not always permit him to fast during Ramadan. On a nonmedical front, his recent efforts have paid off. In March 2023 Dr. Mouhieddine became a U.S. citizen.
“It’s surreal,” he said, “but also a dream come true. I feel very grateful, like it’s like an appreciation of who I am, what I’ve done, and what I can do for this country.”
“If we start treatment earlier, in the smoldering phase, maybe there is a chance of actually curing the disease and completely getting rid of it,” said Dr. Mouhieddine, 31, a research fellow at the Icahn School of Medicine at Mount Sinai, in New York. “We haven’t proven that yet, and it’s going to take years before we’re able to prove it. I’m hoping to be one of those spearheading the initiative.”
As he develops clinical trials, the young physician scientist has another focus: A deeply personal connection to the very disease he’s trying to cure. Last year Dr. Mouhieddine diagnosed his aunt back in Lebanon with multiple myeloma. “I have always been close to her, and I’m like her son,” he said, and her situation is especially scary because she lives in a country where treatment options are limited.
Dr. Mouhieddine was born and raised in Beirut, the son of a sports journalist father and a mother who worked in a bank. Lebanon’s civil war ended in 1990, shortly before his birth, but political instability returned when he was a child.
“Everything was a disaster,” he recalled. “There was a period of time when there were bombs throughout the city because certain politicians were being targeted. I remember when groups of people would have gunfights in the street.”
Dr. Mouhieddine attended the American University of Beirut, then after college and medical school there, he headed to the United States.
“I wanted to make a difference in medicine. And I knew that if I stayed back home, I wouldn’t be able to,” he said. Fortunately, “everybody has made me feel that I really belong here, and I’ve never felt like I’m an outsider.”
Early on, as he went through fellowships and residency, he developed an interest in multiple myeloma.
Ajai Chari, MD, a colleague of Dr. Mouhieddine’s at Icahn School of Medicine, said in an interview, “I remember meeting him at a conference before he had even started an internal medicine residency, let alone a hematology oncology fellowship. He was already certain he wanted to work in multiple myeloma, due to his work at Dana-Farber Cancer Institute.”
Myeloma was especially intriguing to Dr. Mouhieddine because of the rapid rate of progress in treating the disease. “Over the past 10 years, the myeloma field has advanced at such an extremely fast pace, more than any other cancer,” he said. “Maybe 15 years ago, you would tell someone with newly diagnosed myeloma that they had a chance for an average of another 2 years. Now, we tell patients they have 10 years to live on average, which means you could live 15 or 20 years. That alone was astounding to me and piqued my interest in myeloma.”
At the same time, smoldering myeloma – which can be discovered during routine blood work – remains little understood. As the National Cancer Institute explains, “smoldering myeloma is a precancerous condition that alters certain proteins in blood and/or increases plasma cells in bone marrow, but it does not cause symptoms of disease. About half of those diagnosed with the condition, however, will develop multiple myeloma within 5 years.”
“If we understand what drives smoldering myeloma, we may be able to prevent it from progressing to its active form,” said hematologist oncologist Samir Parekh, MD, who works with Dr. Mouhieddine at Icahn School of Medicine. “Or at the minimum, we could better predict who will progress so we can tailor therapy for high-risk patients and minimize toxicity by not overtreating patients who may not need therapy.”
Dr. Mouhieddine’s current work is focusing on developing clinical trials to test whether immunotherapy can snuff out myeloma when it’s at the smoldering stage, “before anything bad happens.
“If a myeloma patient comes in with renal failure, and we treat the myeloma at that stage, it doesn’t mean that the patient’s kidneys are gonna go back to normal. A lot of the damage can be permanent,” he said. “Even when you treat multiple myeloma, and it goes into remission, it ends up coming back. And you just have to go from one therapy to the other.”
In contrast, a successful treatment for smoldering myeloma would prevent progression to the full disease. In other words, it would be a cure – which is now elusive.
Specifically, Dr. Mouhieddine hopes to test whether bispecific antibodies, a type of immunotherapy that enlists the body’s T cells to kill myeloma cells, will be effective in the smoldering phase. Bispecific antibodies are now being explored as treatments for full multiple myeloma when the immune system is weaker, he said, and they may be even more effective earlier, when the body is better equipped to fight off the disease.
Dr. Mouhieddine hopes better treatments for multiple myeloma itself will help save his 64-year-old aunt Hassana, back in Beirut. He diagnosed her in 2022 after she told him that she felt tired all the time and underwent various tests. The woman he calls his “second mom” is doing well, despite struggles to buy medication due to the lack of access to bank funds in Lebanon.
“I’m always going to be afraid that the disease is going to progress or come back at some point,” he said. “Lebanon doesn’t have as many options as people in the U.S. do. Once you exhaust your first option, and maybe your second option, then you don’t have any other options. Here, we have outpatients who exhaust option number 15 and go to option number 16. That’s definitely not the case over there.”
For now, Dr. Mouhieddine is treating patients and working to launch clinical trials into smoldering myeloma. “His work ethic is incredible,” said his colleague, Dr. Chari. “He has seen multiple projects to publication, and he develops deep connections with his patients and follows up on their care whether or not he is in clinic on a particular day.”
Dr. Parekh, another colleague, said Dr. Mouhieddine can even be a role model. “Other trainees may benefit from thinking about their career early on and exploring both lab and clinical research projects, so that they can develop the necessary experience to be competitive in academia later on.”
His workload can a burden for Dr. Mouhieddine, who is Muslim. He expressed regret that his busy schedule does not always permit him to fast during Ramadan. On a nonmedical front, his recent efforts have paid off. In March 2023 Dr. Mouhieddine became a U.S. citizen.
“It’s surreal,” he said, “but also a dream come true. I feel very grateful, like it’s like an appreciation of who I am, what I’ve done, and what I can do for this country.”
“If we start treatment earlier, in the smoldering phase, maybe there is a chance of actually curing the disease and completely getting rid of it,” said Dr. Mouhieddine, 31, a research fellow at the Icahn School of Medicine at Mount Sinai, in New York. “We haven’t proven that yet, and it’s going to take years before we’re able to prove it. I’m hoping to be one of those spearheading the initiative.”
As he develops clinical trials, the young physician scientist has another focus: A deeply personal connection to the very disease he’s trying to cure. Last year Dr. Mouhieddine diagnosed his aunt back in Lebanon with multiple myeloma. “I have always been close to her, and I’m like her son,” he said, and her situation is especially scary because she lives in a country where treatment options are limited.
Dr. Mouhieddine was born and raised in Beirut, the son of a sports journalist father and a mother who worked in a bank. Lebanon’s civil war ended in 1990, shortly before his birth, but political instability returned when he was a child.
“Everything was a disaster,” he recalled. “There was a period of time when there were bombs throughout the city because certain politicians were being targeted. I remember when groups of people would have gunfights in the street.”
Dr. Mouhieddine attended the American University of Beirut, then after college and medical school there, he headed to the United States.
“I wanted to make a difference in medicine. And I knew that if I stayed back home, I wouldn’t be able to,” he said. Fortunately, “everybody has made me feel that I really belong here, and I’ve never felt like I’m an outsider.”
Early on, as he went through fellowships and residency, he developed an interest in multiple myeloma.
Ajai Chari, MD, a colleague of Dr. Mouhieddine’s at Icahn School of Medicine, said in an interview, “I remember meeting him at a conference before he had even started an internal medicine residency, let alone a hematology oncology fellowship. He was already certain he wanted to work in multiple myeloma, due to his work at Dana-Farber Cancer Institute.”
Myeloma was especially intriguing to Dr. Mouhieddine because of the rapid rate of progress in treating the disease. “Over the past 10 years, the myeloma field has advanced at such an extremely fast pace, more than any other cancer,” he said. “Maybe 15 years ago, you would tell someone with newly diagnosed myeloma that they had a chance for an average of another 2 years. Now, we tell patients they have 10 years to live on average, which means you could live 15 or 20 years. That alone was astounding to me and piqued my interest in myeloma.”
At the same time, smoldering myeloma – which can be discovered during routine blood work – remains little understood. As the National Cancer Institute explains, “smoldering myeloma is a precancerous condition that alters certain proteins in blood and/or increases plasma cells in bone marrow, but it does not cause symptoms of disease. About half of those diagnosed with the condition, however, will develop multiple myeloma within 5 years.”
“If we understand what drives smoldering myeloma, we may be able to prevent it from progressing to its active form,” said hematologist oncologist Samir Parekh, MD, who works with Dr. Mouhieddine at Icahn School of Medicine. “Or at the minimum, we could better predict who will progress so we can tailor therapy for high-risk patients and minimize toxicity by not overtreating patients who may not need therapy.”
Dr. Mouhieddine’s current work is focusing on developing clinical trials to test whether immunotherapy can snuff out myeloma when it’s at the smoldering stage, “before anything bad happens.
“If a myeloma patient comes in with renal failure, and we treat the myeloma at that stage, it doesn’t mean that the patient’s kidneys are gonna go back to normal. A lot of the damage can be permanent,” he said. “Even when you treat multiple myeloma, and it goes into remission, it ends up coming back. And you just have to go from one therapy to the other.”
In contrast, a successful treatment for smoldering myeloma would prevent progression to the full disease. In other words, it would be a cure – which is now elusive.
Specifically, Dr. Mouhieddine hopes to test whether bispecific antibodies, a type of immunotherapy that enlists the body’s T cells to kill myeloma cells, will be effective in the smoldering phase. Bispecific antibodies are now being explored as treatments for full multiple myeloma when the immune system is weaker, he said, and they may be even more effective earlier, when the body is better equipped to fight off the disease.
Dr. Mouhieddine hopes better treatments for multiple myeloma itself will help save his 64-year-old aunt Hassana, back in Beirut. He diagnosed her in 2022 after she told him that she felt tired all the time and underwent various tests. The woman he calls his “second mom” is doing well, despite struggles to buy medication due to the lack of access to bank funds in Lebanon.
“I’m always going to be afraid that the disease is going to progress or come back at some point,” he said. “Lebanon doesn’t have as many options as people in the U.S. do. Once you exhaust your first option, and maybe your second option, then you don’t have any other options. Here, we have outpatients who exhaust option number 15 and go to option number 16. That’s definitely not the case over there.”
For now, Dr. Mouhieddine is treating patients and working to launch clinical trials into smoldering myeloma. “His work ethic is incredible,” said his colleague, Dr. Chari. “He has seen multiple projects to publication, and he develops deep connections with his patients and follows up on their care whether or not he is in clinic on a particular day.”
Dr. Parekh, another colleague, said Dr. Mouhieddine can even be a role model. “Other trainees may benefit from thinking about their career early on and exploring both lab and clinical research projects, so that they can develop the necessary experience to be competitive in academia later on.”
His workload can a burden for Dr. Mouhieddine, who is Muslim. He expressed regret that his busy schedule does not always permit him to fast during Ramadan. On a nonmedical front, his recent efforts have paid off. In March 2023 Dr. Mouhieddine became a U.S. citizen.
“It’s surreal,” he said, “but also a dream come true. I feel very grateful, like it’s like an appreciation of who I am, what I’ve done, and what I can do for this country.”
Managing Type 2 Diabetes in Pediatric Patients
Type 2 diabetes (T2D) is associated with obesity and is increasing at an alarming rate in youth. Pediatric T2D disease progresses more rapidly than adult T2D and is harder to treat.
Dr Maria Redondo, a pediatric endocrinologist at Baylor College of Medicine in Houston, Texas, explains that insulin resistance is the major trigger of T2D, and beta-cell dysfunction is key to its development. In children, beta-cell dysfunction occurs more rapidly compared with adults. Children also have higher rates of complications and associated conditions, such as renal disease, cardiovascular disease, and nonalcoholic fatty liver disease.
Dr Redondo references evidence from the TODAY study, which indicates that treatment failure with first-line metformin is common in the pediatric population and affords minimal weight loss.
She then discusses GLP-1 receptor agonists as second-line therapy for children aged 10 years or older. There are currently two FDA-approved options: once-daily liraglutide and once-weekly exenatide. Both are given subcutaneously.
Finally, Dr Redondo highlights DPP-4 inhibitors, such as linagliptin, saxagliptin, and sitagliptin, as well as SGLT-2 inhibitors, such as dapagliflozin and canagliflozin, as emerging therapies currently in clinical trials.
--
Maria J. Redondo, MD, PhD, MPH, Professor, Department of Pediatrics, Baylor College of Medicine; Staff Physician, Texas Children's Hospital, Houston, Texas
Maria J. Redondo, MD, PhD, MPH, has disclosed the following relevant financial relationships:
Received research grant from: NIH; NIDDK
Type 2 diabetes (T2D) is associated with obesity and is increasing at an alarming rate in youth. Pediatric T2D disease progresses more rapidly than adult T2D and is harder to treat.
Dr Maria Redondo, a pediatric endocrinologist at Baylor College of Medicine in Houston, Texas, explains that insulin resistance is the major trigger of T2D, and beta-cell dysfunction is key to its development. In children, beta-cell dysfunction occurs more rapidly compared with adults. Children also have higher rates of complications and associated conditions, such as renal disease, cardiovascular disease, and nonalcoholic fatty liver disease.
Dr Redondo references evidence from the TODAY study, which indicates that treatment failure with first-line metformin is common in the pediatric population and affords minimal weight loss.
She then discusses GLP-1 receptor agonists as second-line therapy for children aged 10 years or older. There are currently two FDA-approved options: once-daily liraglutide and once-weekly exenatide. Both are given subcutaneously.
Finally, Dr Redondo highlights DPP-4 inhibitors, such as linagliptin, saxagliptin, and sitagliptin, as well as SGLT-2 inhibitors, such as dapagliflozin and canagliflozin, as emerging therapies currently in clinical trials.
--
Maria J. Redondo, MD, PhD, MPH, Professor, Department of Pediatrics, Baylor College of Medicine; Staff Physician, Texas Children's Hospital, Houston, Texas
Maria J. Redondo, MD, PhD, MPH, has disclosed the following relevant financial relationships:
Received research grant from: NIH; NIDDK
Type 2 diabetes (T2D) is associated with obesity and is increasing at an alarming rate in youth. Pediatric T2D disease progresses more rapidly than adult T2D and is harder to treat.
Dr Maria Redondo, a pediatric endocrinologist at Baylor College of Medicine in Houston, Texas, explains that insulin resistance is the major trigger of T2D, and beta-cell dysfunction is key to its development. In children, beta-cell dysfunction occurs more rapidly compared with adults. Children also have higher rates of complications and associated conditions, such as renal disease, cardiovascular disease, and nonalcoholic fatty liver disease.
Dr Redondo references evidence from the TODAY study, which indicates that treatment failure with first-line metformin is common in the pediatric population and affords minimal weight loss.
She then discusses GLP-1 receptor agonists as second-line therapy for children aged 10 years or older. There are currently two FDA-approved options: once-daily liraglutide and once-weekly exenatide. Both are given subcutaneously.
Finally, Dr Redondo highlights DPP-4 inhibitors, such as linagliptin, saxagliptin, and sitagliptin, as well as SGLT-2 inhibitors, such as dapagliflozin and canagliflozin, as emerging therapies currently in clinical trials.
--
Maria J. Redondo, MD, PhD, MPH, Professor, Department of Pediatrics, Baylor College of Medicine; Staff Physician, Texas Children's Hospital, Houston, Texas
Maria J. Redondo, MD, PhD, MPH, has disclosed the following relevant financial relationships:
Received research grant from: NIH; NIDDK

Living the introvert’s dream: Alone for 500 days, but never lonely
Beating the allegory of the cave
When Beatriz Flamini spoke with reporters on April 14, she knew nothing of the previous 18 months. The Russian invasion of Ukraine? Nope. The death of Queen Elizabeth? Also no. But before you make fun of her, she has an excuse. She’s been living under a rock.
As part of an experiment to test how social isolation and disorientation affect a person’s mind, sense of time, and sleeping patterns, Ms. Flamini lived in a 70-meter-deep cave in southern Spain for 500 days, starting in November 2021. Alone. No outside communication with the outside world in any way, though she was constantly monitored by a team of researchers. She also had multiple cameras filming her for an upcoming documentary.
This is a massive step up from the previous record for time spent underground for science: A team of 15 spent 50 days underground in 2021 to similar study of isolation and how it affected circadian rhythms. It’s also almost certainly a world record for time spent underground.
All that time alone certainly sounds like some sort of medieval torture, but Ms. Flamini had access to food, water, and a library of books. Which she made liberal use of, reading at least 60 books during her stay. She also had a panic button in case the isolation became too much or an emergency developed, but she never considered using it.
She lost track of time after 2 months, flies invaded the cave on occasion, and maintaining coherence was occasionally a struggle, but she kept things together very well. In fact, she didn’t even want to leave when her team came for her. She wasn’t even finished with her 61st book.
When she spoke with gathered reporters after the ordeal, words were obviously difficult to come by for her, having not spoken in nearly 18 months, but her mind was clearly still sharp and she had a very important question for everyone gathered around her.
Who’s buying the beer?
We approve of this request.
Staphylococcus and the speed of evolution
Bacteria, we know, are tough little buggers that are hard to see and even harder to get rid of. So hard, actually, that human bodies eventually gave up on the task and decided to just incorporate them into our organ systems. But why are bacteria so hard to eliminate?

Two words: rapid evolution. How rapid? For the first time, scientists have directly observed adaptive evolution by Staphylococcus aureus in a single person’s skin microbiome. That’s how rapid.
For their study, the researchers collected samples from the nostrils, backs of knees, insides of elbows, and forearms of 23 children with eczema. They eventually cultured almost 1,500 unique colonies of S. aureus cells from those samples and sequenced the cells’ genomes.
All that sampling and culturing and sequencing showed that it was rare for a new S. aureus strain to come in and replace the existing strain. “Despite the stability at the lineage level, we see a lot of dynamics at the whole genome level, where new mutations are constantly arising in these bacteria and then spreading throughout the entire body,” Tami D. Lieberman, PhD, of the Massachusetts Institute of Technology, Cambridge, said in a written statement from MIT.
One frequent mutation involved a gene called capD, which encodes an enzyme necessary for synthesizing the capsular polysaccharide – a coating that protects S. aureus from recognition by immune cells. In one patient, four different mutations of capD arose independently in different samples before one variant became dominant and spread over the entire microbiome, MIT reported.
The mutation, which actually results in the loss of the polysaccharide capsule, may allow cells to grow faster than those without the mutation because they have more fuel to power their own growth, the researchers suggested. It’s also possible that loss of the capsule allows S. aureus cells to stick to the skin better because proteins that allow them to adhere to the skin are more exposed.
Dr. Lieberman and her associates hope that these variant-containing cells could be a new target for eczema treatments, but we’re never optimistic when it comes to bacteria. That’s because some of us are old enough to remember evolutionary biologist Stephen Jay Gould, who wrote in his book “Full House”: “Our planet has always been in the ‘Age of Bacteria,’ ever since the first fossils – bacteria, of course – were entombed in rocks more than 3 billion years ago. On any possible, reasonable or fair criterion, bacteria are – and always have been – the dominant forms of life on Earth.”
In the distant future, long after humans have left the scene, the bacteria will be laughing at the last rats and cockroaches scurrying across the landscape. Wanna bet?
The height of genetic prediction
Genetics are practically a DNA Scrabble bag. Traits like eye color and hair texture are chosen in the same fashion, based on what gets pulled from our own genetic bag of letters, but what about height? Researchers may now have a way to predict adult height and make it more than just an educated guess.
How? By looking at the genes in our growth plates. The cartilage on the ends of our bones hardens as we age, eventually deciding an individual’s stature. In a recently published study, a research team looked at 600 million cartilage cells linked to maturation and cell growth in mice. Because everything starts with rodents.
After that search identified 145 genes linked to growth plate maturation and formation of the bones, they compared the mouse genes with data from genome-wide association studies (GWAS) of human height to look for hotspots where the height genes exist in human DNA.
The results showed which genes play a role in deciding height, and the GWAS data also suggested that genetic changes affecting cartilage cell maturation may strongly influence adult height, said the investigators, who hope that earlier interventions can improve outcomes in patients with conditions such as skeletal dysplasia.
So, yeah, you may want to be a little taller or shorter, but the outcome of that particular Scrabble game was determined when your parents, you know, dropped the letters in the bag.
Beating the allegory of the cave
When Beatriz Flamini spoke with reporters on April 14, she knew nothing of the previous 18 months. The Russian invasion of Ukraine? Nope. The death of Queen Elizabeth? Also no. But before you make fun of her, she has an excuse. She’s been living under a rock.
As part of an experiment to test how social isolation and disorientation affect a person’s mind, sense of time, and sleeping patterns, Ms. Flamini lived in a 70-meter-deep cave in southern Spain for 500 days, starting in November 2021. Alone. No outside communication with the outside world in any way, though she was constantly monitored by a team of researchers. She also had multiple cameras filming her for an upcoming documentary.
This is a massive step up from the previous record for time spent underground for science: A team of 15 spent 50 days underground in 2021 to similar study of isolation and how it affected circadian rhythms. It’s also almost certainly a world record for time spent underground.
All that time alone certainly sounds like some sort of medieval torture, but Ms. Flamini had access to food, water, and a library of books. Which she made liberal use of, reading at least 60 books during her stay. She also had a panic button in case the isolation became too much or an emergency developed, but she never considered using it.
She lost track of time after 2 months, flies invaded the cave on occasion, and maintaining coherence was occasionally a struggle, but she kept things together very well. In fact, she didn’t even want to leave when her team came for her. She wasn’t even finished with her 61st book.
When she spoke with gathered reporters after the ordeal, words were obviously difficult to come by for her, having not spoken in nearly 18 months, but her mind was clearly still sharp and she had a very important question for everyone gathered around her.
Who’s buying the beer?
We approve of this request.
Staphylococcus and the speed of evolution
Bacteria, we know, are tough little buggers that are hard to see and even harder to get rid of. So hard, actually, that human bodies eventually gave up on the task and decided to just incorporate them into our organ systems. But why are bacteria so hard to eliminate?
Two words: rapid evolution. How rapid? For the first time, scientists have directly observed adaptive evolution by Staphylococcus aureus in a single person’s skin microbiome. That’s how rapid.
For their study, the researchers collected samples from the nostrils, backs of knees, insides of elbows, and forearms of 23 children with eczema. They eventually cultured almost 1,500 unique colonies of S. aureus cells from those samples and sequenced the cells’ genomes.
All that sampling and culturing and sequencing showed that it was rare for a new S. aureus strain to come in and replace the existing strain. “Despite the stability at the lineage level, we see a lot of dynamics at the whole genome level, where new mutations are constantly arising in these bacteria and then spreading throughout the entire body,” Tami D. Lieberman, PhD, of the Massachusetts Institute of Technology, Cambridge, said in a written statement from MIT.
One frequent mutation involved a gene called capD, which encodes an enzyme necessary for synthesizing the capsular polysaccharide – a coating that protects S. aureus from recognition by immune cells. In one patient, four different mutations of capD arose independently in different samples before one variant became dominant and spread over the entire microbiome, MIT reported.
The mutation, which actually results in the loss of the polysaccharide capsule, may allow cells to grow faster than those without the mutation because they have more fuel to power their own growth, the researchers suggested. It’s also possible that loss of the capsule allows S. aureus cells to stick to the skin better because proteins that allow them to adhere to the skin are more exposed.
Dr. Lieberman and her associates hope that these variant-containing cells could be a new target for eczema treatments, but we’re never optimistic when it comes to bacteria. That’s because some of us are old enough to remember evolutionary biologist Stephen Jay Gould, who wrote in his book “Full House”: “Our planet has always been in the ‘Age of Bacteria,’ ever since the first fossils – bacteria, of course – were entombed in rocks more than 3 billion years ago. On any possible, reasonable or fair criterion, bacteria are – and always have been – the dominant forms of life on Earth.”
In the distant future, long after humans have left the scene, the bacteria will be laughing at the last rats and cockroaches scurrying across the landscape. Wanna bet?
The height of genetic prediction
Genetics are practically a DNA Scrabble bag. Traits like eye color and hair texture are chosen in the same fashion, based on what gets pulled from our own genetic bag of letters, but what about height? Researchers may now have a way to predict adult height and make it more than just an educated guess.
How? By looking at the genes in our growth plates. The cartilage on the ends of our bones hardens as we age, eventually deciding an individual’s stature. In a recently published study, a research team looked at 600 million cartilage cells linked to maturation and cell growth in mice. Because everything starts with rodents.
After that search identified 145 genes linked to growth plate maturation and formation of the bones, they compared the mouse genes with data from genome-wide association studies (GWAS) of human height to look for hotspots where the height genes exist in human DNA.
The results showed which genes play a role in deciding height, and the GWAS data also suggested that genetic changes affecting cartilage cell maturation may strongly influence adult height, said the investigators, who hope that earlier interventions can improve outcomes in patients with conditions such as skeletal dysplasia.
So, yeah, you may want to be a little taller or shorter, but the outcome of that particular Scrabble game was determined when your parents, you know, dropped the letters in the bag.
Beating the allegory of the cave
When Beatriz Flamini spoke with reporters on April 14, she knew nothing of the previous 18 months. The Russian invasion of Ukraine? Nope. The death of Queen Elizabeth? Also no. But before you make fun of her, she has an excuse. She’s been living under a rock.
As part of an experiment to test how social isolation and disorientation affect a person’s mind, sense of time, and sleeping patterns, Ms. Flamini lived in a 70-meter-deep cave in southern Spain for 500 days, starting in November 2021. Alone. No outside communication with the outside world in any way, though she was constantly monitored by a team of researchers. She also had multiple cameras filming her for an upcoming documentary.
This is a massive step up from the previous record for time spent underground for science: A team of 15 spent 50 days underground in 2021 to similar study of isolation and how it affected circadian rhythms. It’s also almost certainly a world record for time spent underground.
All that time alone certainly sounds like some sort of medieval torture, but Ms. Flamini had access to food, water, and a library of books. Which she made liberal use of, reading at least 60 books during her stay. She also had a panic button in case the isolation became too much or an emergency developed, but she never considered using it.
She lost track of time after 2 months, flies invaded the cave on occasion, and maintaining coherence was occasionally a struggle, but she kept things together very well. In fact, she didn’t even want to leave when her team came for her. She wasn’t even finished with her 61st book.
When she spoke with gathered reporters after the ordeal, words were obviously difficult to come by for her, having not spoken in nearly 18 months, but her mind was clearly still sharp and she had a very important question for everyone gathered around her.
Who’s buying the beer?
We approve of this request.
Staphylococcus and the speed of evolution
Bacteria, we know, are tough little buggers that are hard to see and even harder to get rid of. So hard, actually, that human bodies eventually gave up on the task and decided to just incorporate them into our organ systems. But why are bacteria so hard to eliminate?
Two words: rapid evolution. How rapid? For the first time, scientists have directly observed adaptive evolution by Staphylococcus aureus in a single person’s skin microbiome. That’s how rapid.
For their study, the researchers collected samples from the nostrils, backs of knees, insides of elbows, and forearms of 23 children with eczema. They eventually cultured almost 1,500 unique colonies of S. aureus cells from those samples and sequenced the cells’ genomes.
All that sampling and culturing and sequencing showed that it was rare for a new S. aureus strain to come in and replace the existing strain. “Despite the stability at the lineage level, we see a lot of dynamics at the whole genome level, where new mutations are constantly arising in these bacteria and then spreading throughout the entire body,” Tami D. Lieberman, PhD, of the Massachusetts Institute of Technology, Cambridge, said in a written statement from MIT.
One frequent mutation involved a gene called capD, which encodes an enzyme necessary for synthesizing the capsular polysaccharide – a coating that protects S. aureus from recognition by immune cells. In one patient, four different mutations of capD arose independently in different samples before one variant became dominant and spread over the entire microbiome, MIT reported.
The mutation, which actually results in the loss of the polysaccharide capsule, may allow cells to grow faster than those without the mutation because they have more fuel to power their own growth, the researchers suggested. It’s also possible that loss of the capsule allows S. aureus cells to stick to the skin better because proteins that allow them to adhere to the skin are more exposed.
Dr. Lieberman and her associates hope that these variant-containing cells could be a new target for eczema treatments, but we’re never optimistic when it comes to bacteria. That’s because some of us are old enough to remember evolutionary biologist Stephen Jay Gould, who wrote in his book “Full House”: “Our planet has always been in the ‘Age of Bacteria,’ ever since the first fossils – bacteria, of course – were entombed in rocks more than 3 billion years ago. On any possible, reasonable or fair criterion, bacteria are – and always have been – the dominant forms of life on Earth.”
In the distant future, long after humans have left the scene, the bacteria will be laughing at the last rats and cockroaches scurrying across the landscape. Wanna bet?
The height of genetic prediction
Genetics are practically a DNA Scrabble bag. Traits like eye color and hair texture are chosen in the same fashion, based on what gets pulled from our own genetic bag of letters, but what about height? Researchers may now have a way to predict adult height and make it more than just an educated guess.
How? By looking at the genes in our growth plates. The cartilage on the ends of our bones hardens as we age, eventually deciding an individual’s stature. In a recently published study, a research team looked at 600 million cartilage cells linked to maturation and cell growth in mice. Because everything starts with rodents.
After that search identified 145 genes linked to growth plate maturation and formation of the bones, they compared the mouse genes with data from genome-wide association studies (GWAS) of human height to look for hotspots where the height genes exist in human DNA.
The results showed which genes play a role in deciding height, and the GWAS data also suggested that genetic changes affecting cartilage cell maturation may strongly influence adult height, said the investigators, who hope that earlier interventions can improve outcomes in patients with conditions such as skeletal dysplasia.
So, yeah, you may want to be a little taller or shorter, but the outcome of that particular Scrabble game was determined when your parents, you know, dropped the letters in the bag.
PARP/ATR inhibitor combo shows hints of promise in children with tumors
The small phase 1 trial also identified some molecular signatures in responders that may inform future clinical trials.
The results, presented at the annual meeting of the American Association of Cancer Research, came from a single arm of the European Proof-of-Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory Tumors (ESMART) trial. This trial matches pediatric, adolescent, and young adult cancer patients with treatment regimens based on the molecular profile of their tumors.
In over 220 children to date, the trial has investigated 15 different treatment regimens, most of which are combination therapies.
In adults, PARP) inhibitors have been shown to be effective in tumors with deficiencies in homologous repair, which is a DNA repair mechanism, with notable successes in patients carrying the BRCA1 and BRCA2 mutations. But BRCA1 and BRCA2 mutations are rare in pediatric cancer, and there is a belief that there may be primary resistance to PARP inhibitors in pediatric tumors, according to Susanne Gatz, MD, PhD, who presented the research at the meeting.
Previous research identified alterations in pediatric tumors that are candidates for patient selection. “These tumors have alterations which could potentially cause this resistance effect [against PARP inhibitors] and [also cause] sensitivity to ataxia telangiectasia–mutated Rad3-related inhibitors. This is how this arm [of the ESMART trial] was born,” said Dr. Gatz.
The phase 1 portion of the study included 18 pediatric and young adult patients with relapsed or treatment-refractory tumors. There were eight sarcomas, five central nervous system tumors, four neuroblastomas, and one carcinoma. Each had mutations thought to lead to HR deficiency or replication stress. The study included three dose levels of twice-daily oral olaparib that was given continuously, and ceralasertib, which was given day 1-14 of each 28-day cycle.
Patients underwent a median of 3.5 cycles of treatment. There were dose-limiting adverse events of thrombocytopenia and neutropenia in five patients, two of which occurred at the dose that was recommended for phase 2.
There were some positive clinical signs, including one partial response in a pineoblastoma patient who received treatment for 11 cycles. A neuroblastoma patient had stable disease until cycle 9 of treatment, and then converted to a partial response and is currently in cycle 12. Two other patients remain in treatment at cycle 8 and one is in treatment at cycle 15. None of the patients who experienced clinical benefit had BRCA mutations.
An important goal of the study was to understand molecular signature that might predict response to the drug combination. Although no firm conclusions could be drawn, there were some interesting patterns. In particular, five of the six worst responders had TP53 mutations. “It is striking ... so we need to learn what TP53 in this setting means if it’s mutated, and if it could be a resistance factor,” said Dr. Gatz, an associate clinical professor in pediatric oncology at the Institute of Cancer and Genomic Sciences of the University of Birmingham, during her talk.
Although the study is too small and included too many tumor types to identify tumor-based patterns of response, it did provide some hints as to biomarkers that could inform future studies, according to Julia Glade Bender, MD, who served as a discussant following the presentation and is a pediatric oncologist at Memorial Sloan Kettering Cancer Center, New York.
“The pediatric frequency of the common DNA damage repair biomarkers that have been [identified in] the adult literature – that is to say, BRCA1 and 2 and [ataxia-telangiectasia mutation] – are exceedingly rare in pediatrics,” said Dr. Bender during the session while serving as a discussant. She highlighted the following findings: Loss of the 11q region on chromosome 11 is common among the patients and that region contains three genes involved in the DNA damage response, along with a gene involved in homologous recombination, telomere maintenance, and double strand break repair.
She added that 11q deletion is also found in up to 40% of neuroblastomas, and is associated with poor prognosis, and the patients have multiple segmental chromosomal abnormalities. “That begs the question [of] whether chromosomal instability is another biomarker for pediatric cancer,” said Dr. Bender.
“The research highlights the complexity of pediatric cancers, whose distinct biology could make them more vulnerable to ATR [kinase], [checkpoint kinase 1], and WEE1 pathway inhibition with a PARP inhibitor used to induce replication stress and be the sensitizer. The biomarker profiles are going to be complex, context-dependent, and likely to reflect a constellation of findings that would be signatures or algorithms, rather than single gene alterations. The post hoc iterative analysis of responders and nonresponders is going to be absolutely critical to understanding those biomarkers and the role of DNA damage response inhibitors in pediatrics. Given the rarity of these diagnoses, and then the molecular subclasses, I think collaboration across ages and geography is absolutely critical, and I really congratulate the ESMART consortium for doing just that in Europe,” said Dr. Bender.
The study is limited by its small sample size and the fact that it was not randomized.
The study received funding from French Institut National de Cancer, Imagine for Margo, Fondation ARC, AstraZeneca France, AstraZeneca Global R&D, AstraZeneca UK, Cancer Research UK, Fondation Gustave Roussy, and Little Princess Trust/Children’s Cancer and Leukaemia Group. Dr. Gatz has no relevant financial disclosures. Dr. Bender has done paid consulting for Jazz Pharmaceuticals and has done unpaid work for Bristol-Myers Squibb, Eisai, Springworks Therapeutics, Merck Sharp & Dohme, and Pfizer. She has received research support from Eli Lilly, Loxo-oncology, Eisai, Cellectar, Bayer, Amgen, and Jazz Pharmaceuticals.
From American Association for Cancer Research (AACR) Annual Meeting 2023: Abstract CT019. Presented Tuesday, April 18.
The small phase 1 trial also identified some molecular signatures in responders that may inform future clinical trials.
The results, presented at the annual meeting of the American Association of Cancer Research, came from a single arm of the European Proof-of-Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory Tumors (ESMART) trial. This trial matches pediatric, adolescent, and young adult cancer patients with treatment regimens based on the molecular profile of their tumors.
In over 220 children to date, the trial has investigated 15 different treatment regimens, most of which are combination therapies.
In adults, PARP) inhibitors have been shown to be effective in tumors with deficiencies in homologous repair, which is a DNA repair mechanism, with notable successes in patients carrying the BRCA1 and BRCA2 mutations. But BRCA1 and BRCA2 mutations are rare in pediatric cancer, and there is a belief that there may be primary resistance to PARP inhibitors in pediatric tumors, according to Susanne Gatz, MD, PhD, who presented the research at the meeting.
Previous research identified alterations in pediatric tumors that are candidates for patient selection. “These tumors have alterations which could potentially cause this resistance effect [against PARP inhibitors] and [also cause] sensitivity to ataxia telangiectasia–mutated Rad3-related inhibitors. This is how this arm [of the ESMART trial] was born,” said Dr. Gatz.
The phase 1 portion of the study included 18 pediatric and young adult patients with relapsed or treatment-refractory tumors. There were eight sarcomas, five central nervous system tumors, four neuroblastomas, and one carcinoma. Each had mutations thought to lead to HR deficiency or replication stress. The study included three dose levels of twice-daily oral olaparib that was given continuously, and ceralasertib, which was given day 1-14 of each 28-day cycle.
Patients underwent a median of 3.5 cycles of treatment. There were dose-limiting adverse events of thrombocytopenia and neutropenia in five patients, two of which occurred at the dose that was recommended for phase 2.
There were some positive clinical signs, including one partial response in a pineoblastoma patient who received treatment for 11 cycles. A neuroblastoma patient had stable disease until cycle 9 of treatment, and then converted to a partial response and is currently in cycle 12. Two other patients remain in treatment at cycle 8 and one is in treatment at cycle 15. None of the patients who experienced clinical benefit had BRCA mutations.
An important goal of the study was to understand molecular signature that might predict response to the drug combination. Although no firm conclusions could be drawn, there were some interesting patterns. In particular, five of the six worst responders had TP53 mutations. “It is striking ... so we need to learn what TP53 in this setting means if it’s mutated, and if it could be a resistance factor,” said Dr. Gatz, an associate clinical professor in pediatric oncology at the Institute of Cancer and Genomic Sciences of the University of Birmingham, during her talk.
Although the study is too small and included too many tumor types to identify tumor-based patterns of response, it did provide some hints as to biomarkers that could inform future studies, according to Julia Glade Bender, MD, who served as a discussant following the presentation and is a pediatric oncologist at Memorial Sloan Kettering Cancer Center, New York.
“The pediatric frequency of the common DNA damage repair biomarkers that have been [identified in] the adult literature – that is to say, BRCA1 and 2 and [ataxia-telangiectasia mutation] – are exceedingly rare in pediatrics,” said Dr. Bender during the session while serving as a discussant. She highlighted the following findings: Loss of the 11q region on chromosome 11 is common among the patients and that region contains three genes involved in the DNA damage response, along with a gene involved in homologous recombination, telomere maintenance, and double strand break repair.
She added that 11q deletion is also found in up to 40% of neuroblastomas, and is associated with poor prognosis, and the patients have multiple segmental chromosomal abnormalities. “That begs the question [of] whether chromosomal instability is another biomarker for pediatric cancer,” said Dr. Bender.
“The research highlights the complexity of pediatric cancers, whose distinct biology could make them more vulnerable to ATR [kinase], [checkpoint kinase 1], and WEE1 pathway inhibition with a PARP inhibitor used to induce replication stress and be the sensitizer. The biomarker profiles are going to be complex, context-dependent, and likely to reflect a constellation of findings that would be signatures or algorithms, rather than single gene alterations. The post hoc iterative analysis of responders and nonresponders is going to be absolutely critical to understanding those biomarkers and the role of DNA damage response inhibitors in pediatrics. Given the rarity of these diagnoses, and then the molecular subclasses, I think collaboration across ages and geography is absolutely critical, and I really congratulate the ESMART consortium for doing just that in Europe,” said Dr. Bender.
The study is limited by its small sample size and the fact that it was not randomized.
The study received funding from French Institut National de Cancer, Imagine for Margo, Fondation ARC, AstraZeneca France, AstraZeneca Global R&D, AstraZeneca UK, Cancer Research UK, Fondation Gustave Roussy, and Little Princess Trust/Children’s Cancer and Leukaemia Group. Dr. Gatz has no relevant financial disclosures. Dr. Bender has done paid consulting for Jazz Pharmaceuticals and has done unpaid work for Bristol-Myers Squibb, Eisai, Springworks Therapeutics, Merck Sharp & Dohme, and Pfizer. She has received research support from Eli Lilly, Loxo-oncology, Eisai, Cellectar, Bayer, Amgen, and Jazz Pharmaceuticals.
From American Association for Cancer Research (AACR) Annual Meeting 2023: Abstract CT019. Presented Tuesday, April 18.
The small phase 1 trial also identified some molecular signatures in responders that may inform future clinical trials.
The results, presented at the annual meeting of the American Association of Cancer Research, came from a single arm of the European Proof-of-Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory Tumors (ESMART) trial. This trial matches pediatric, adolescent, and young adult cancer patients with treatment regimens based on the molecular profile of their tumors.
In over 220 children to date, the trial has investigated 15 different treatment regimens, most of which are combination therapies.
In adults, PARP) inhibitors have been shown to be effective in tumors with deficiencies in homologous repair, which is a DNA repair mechanism, with notable successes in patients carrying the BRCA1 and BRCA2 mutations. But BRCA1 and BRCA2 mutations are rare in pediatric cancer, and there is a belief that there may be primary resistance to PARP inhibitors in pediatric tumors, according to Susanne Gatz, MD, PhD, who presented the research at the meeting.
Previous research identified alterations in pediatric tumors that are candidates for patient selection. “These tumors have alterations which could potentially cause this resistance effect [against PARP inhibitors] and [also cause] sensitivity to ataxia telangiectasia–mutated Rad3-related inhibitors. This is how this arm [of the ESMART trial] was born,” said Dr. Gatz.
The phase 1 portion of the study included 18 pediatric and young adult patients with relapsed or treatment-refractory tumors. There were eight sarcomas, five central nervous system tumors, four neuroblastomas, and one carcinoma. Each had mutations thought to lead to HR deficiency or replication stress. The study included three dose levels of twice-daily oral olaparib that was given continuously, and ceralasertib, which was given day 1-14 of each 28-day cycle.
Patients underwent a median of 3.5 cycles of treatment. There were dose-limiting adverse events of thrombocytopenia and neutropenia in five patients, two of which occurred at the dose that was recommended for phase 2.
There were some positive clinical signs, including one partial response in a pineoblastoma patient who received treatment for 11 cycles. A neuroblastoma patient had stable disease until cycle 9 of treatment, and then converted to a partial response and is currently in cycle 12. Two other patients remain in treatment at cycle 8 and one is in treatment at cycle 15. None of the patients who experienced clinical benefit had BRCA mutations.
An important goal of the study was to understand molecular signature that might predict response to the drug combination. Although no firm conclusions could be drawn, there were some interesting patterns. In particular, five of the six worst responders had TP53 mutations. “It is striking ... so we need to learn what TP53 in this setting means if it’s mutated, and if it could be a resistance factor,” said Dr. Gatz, an associate clinical professor in pediatric oncology at the Institute of Cancer and Genomic Sciences of the University of Birmingham, during her talk.
Although the study is too small and included too many tumor types to identify tumor-based patterns of response, it did provide some hints as to biomarkers that could inform future studies, according to Julia Glade Bender, MD, who served as a discussant following the presentation and is a pediatric oncologist at Memorial Sloan Kettering Cancer Center, New York.
“The pediatric frequency of the common DNA damage repair biomarkers that have been [identified in] the adult literature – that is to say, BRCA1 and 2 and [ataxia-telangiectasia mutation] – are exceedingly rare in pediatrics,” said Dr. Bender during the session while serving as a discussant. She highlighted the following findings: Loss of the 11q region on chromosome 11 is common among the patients and that region contains three genes involved in the DNA damage response, along with a gene involved in homologous recombination, telomere maintenance, and double strand break repair.
She added that 11q deletion is also found in up to 40% of neuroblastomas, and is associated with poor prognosis, and the patients have multiple segmental chromosomal abnormalities. “That begs the question [of] whether chromosomal instability is another biomarker for pediatric cancer,” said Dr. Bender.
“The research highlights the complexity of pediatric cancers, whose distinct biology could make them more vulnerable to ATR [kinase], [checkpoint kinase 1], and WEE1 pathway inhibition with a PARP inhibitor used to induce replication stress and be the sensitizer. The biomarker profiles are going to be complex, context-dependent, and likely to reflect a constellation of findings that would be signatures or algorithms, rather than single gene alterations. The post hoc iterative analysis of responders and nonresponders is going to be absolutely critical to understanding those biomarkers and the role of DNA damage response inhibitors in pediatrics. Given the rarity of these diagnoses, and then the molecular subclasses, I think collaboration across ages and geography is absolutely critical, and I really congratulate the ESMART consortium for doing just that in Europe,” said Dr. Bender.
The study is limited by its small sample size and the fact that it was not randomized.
The study received funding from French Institut National de Cancer, Imagine for Margo, Fondation ARC, AstraZeneca France, AstraZeneca Global R&D, AstraZeneca UK, Cancer Research UK, Fondation Gustave Roussy, and Little Princess Trust/Children’s Cancer and Leukaemia Group. Dr. Gatz has no relevant financial disclosures. Dr. Bender has done paid consulting for Jazz Pharmaceuticals and has done unpaid work for Bristol-Myers Squibb, Eisai, Springworks Therapeutics, Merck Sharp & Dohme, and Pfizer. She has received research support from Eli Lilly, Loxo-oncology, Eisai, Cellectar, Bayer, Amgen, and Jazz Pharmaceuticals.
From American Association for Cancer Research (AACR) Annual Meeting 2023: Abstract CT019. Presented Tuesday, April 18.
FROM AACR 2023
Circulating DNA has promise for cancer detection, but faces challenges
Cancer screening remains challenging. There are screens available for a handful of solid tumors, but uptake is low caused in part by health care access barriers as well as the potential for unnecessary follow-up procedures, according to Phillip Febbo, MD.
These issues could threaten efforts like that of President Joe Biden’s Cancer Moonshot initiative, which aims to reduce cancer mortality by 50%. Advances in circulating tumor (ct) DNA analysis could help address these problems, but a lack of diversity among study participants needs to be addressed to ensure it has broad utility, continued Dr. Febbo, during his presentation at the annual meeting of the American Association for Cancer Research.
The problem is particularly acute among African American, Hispanic, and other underserved populations who often face health care barriers that can exacerbate the issue, said Dr. Febbo, who is chief medical officer for Illumina. The lack of access is compounded by the fact that there are only currently screens for lung, breast, colorectal, cervical, and prostate cancer, leaving a vast unmet need.
“We still do not have screening tests for 70% of the deaths that are due to cancer,” he said.
ctDNA released from dying cancer cells has the potential to reveal a wide range of cancer types and reduce barriers to access, because it is based on a blood test. It can be analyzed for various factors, including mutations, chromosomal rearrangements, methylation patterns, and other characteristics that hint at the presence of cancer. However, it can’t be successful without sufficient inclusion in research studies, Dr. Febbo explained.
“We have to ensure we have the right representation [of] populations when we develop these tests, when we go through the clinical trials, and as we bring these into communities,” he said.
During his presentation, Dr. Febbo shared a slide showing that about 78% of participants in published gene-association studies were White.
ctDNA showed promise in at least on recent study. Dr. Febbo discussed the ECLIPSE trial, which used the Guardant Health SHIELD assay for colorectal cancer (CRC). About 13% of its approximately 20,000 participants were Black or African American, 15% were Hispanic, and 7% were Asian Americans. It also included both urban and rural individuals. In results announced in December 2022, the researchers found a sensitivity of 83%, which was lower than the 92.3% found in standard CRC screening, but above the 74% threshold set by the Food and Drug Administration. The specificity was 90%.
One approach that could dramatically change the landscape of cancer screening is a multicancer early detection (MCED) test, according to Dr. Febbo. The CancerSeek MCED test, developed by Johns Hopkins Kimmel Cancer Center researchers, uses a series of genetic and protein biomarkers to detect all cancers, with the exception of leukemia, skin cancer, and central nervous system tumors. Among 10,006 women aged between 65 and 75 years with no history of cancer, it had a sensitivity of 27.1% and a specificity of 98.9%, with a positive predictive value of 19.4%. The study’s population was 95% non-Hispanic White.
He also discussed the Pathfinder study, sponsored by the Illumina subsidiary Grail, which included 6,662 individuals age 50 and over from seven sites in the United States, and grouped them into normal and increased risk; 92% were non-Hispanic White. It used the Galleri MCED test, which performed with a sensitivity of 29%, specificity of 99.1%, and a positive predictive value of 38.0%. False positives produced to limited burden, with 93% undergoing imaging, 28% nonsurgical invasive procedures, and 2% undergoing fruitless invasive surgical procedures.
Dr. Febbo touted the potential for such tests to greatly reduce cancer mortality, but only if there is adequate uptake of screening procedures, particularly in underserved groups. He put up a slide of a model showing that MCED has the potential to reduce cancer mortality by 20%, but only if the screen is widely accepted among all groups. “I’ve had my team model this. If we accept the current use of screening tests, and we don’t address disparities, and we don’t ensure everybody feels included and participates actively – not only in the research, but also in the testing and adoption, you would cut that potential benefit in half. That would be hundreds of thousands of lives lost because we didn’t address disparities.”
Successful recruiting of African Americans for research
Following Dr. Febbo’s talk, Karriem Watson, MS, spoke about some potential solutions to the issue, including his own experiences and success stories in recruiting African Americans to play active roles in research. He is chief engagement officer for the National Institute of Health’s All of Us Research Program, which aims to gather health data on at least 1 million residents of the United States. Mr. Watson has spent time reaching out to people living in communities in the Chicago area to encourage participation in breast cancer screening. An event at his church inspired his own sister to get a mammogram, and she was diagnosed with early-stage breast cancer.
“I’m a living witness that early engagement can lead to early detection,” said Mr. Watson during his talk.
He reported that the All of Us research program has succeeded in creating diversity within its data collection, as 46.7% of participants identify as racial and ethnic minorities.
Mr. Watson took issue with the common perception that underrepresented communities may be hard to reach.
“I want to challenge us to think outside the box and really ask ourselves: Are populations hard to reach, or are there opportunities for us to do better and more intentional engagement?” He went on to describe a program to recruit African American men as citizen scientists. He and his colleagues developed a network that included barbers, faith leaders, and fraternity and civic organization members to help recruit participants for a prostate cancer screening project. They exceeded their initial recruitment goal.
They went on to develop a network of barbers in the south and west sides of Chicago to recruit individuals to participate in studies of protein methylation and lung cancer screening, as well as a project that investigated associations between neighborhood of residence and lung cancer. The results of those efforts have also informed other projects, including a smoking cessation study. “We’ve not only included African American men in our research, but we’ve included them as part of our research team,” said Mr. Watson.
Dr. Febbo is also a stockholder of Illumina. Mr. Watson has no relevant financial disclosures.
From American Association for Cancer Research (AACR) Annual Meeting 2023: Improving cancer outcomes through equitable access to cfDNA tests. Presented Monday, April 17, 2023.
Cancer screening remains challenging. There are screens available for a handful of solid tumors, but uptake is low caused in part by health care access barriers as well as the potential for unnecessary follow-up procedures, according to Phillip Febbo, MD.
These issues could threaten efforts like that of President Joe Biden’s Cancer Moonshot initiative, which aims to reduce cancer mortality by 50%. Advances in circulating tumor (ct) DNA analysis could help address these problems, but a lack of diversity among study participants needs to be addressed to ensure it has broad utility, continued Dr. Febbo, during his presentation at the annual meeting of the American Association for Cancer Research.
The problem is particularly acute among African American, Hispanic, and other underserved populations who often face health care barriers that can exacerbate the issue, said Dr. Febbo, who is chief medical officer for Illumina. The lack of access is compounded by the fact that there are only currently screens for lung, breast, colorectal, cervical, and prostate cancer, leaving a vast unmet need.
“We still do not have screening tests for 70% of the deaths that are due to cancer,” he said.
ctDNA released from dying cancer cells has the potential to reveal a wide range of cancer types and reduce barriers to access, because it is based on a blood test. It can be analyzed for various factors, including mutations, chromosomal rearrangements, methylation patterns, and other characteristics that hint at the presence of cancer. However, it can’t be successful without sufficient inclusion in research studies, Dr. Febbo explained.
“We have to ensure we have the right representation [of] populations when we develop these tests, when we go through the clinical trials, and as we bring these into communities,” he said.
During his presentation, Dr. Febbo shared a slide showing that about 78% of participants in published gene-association studies were White.
ctDNA showed promise in at least on recent study. Dr. Febbo discussed the ECLIPSE trial, which used the Guardant Health SHIELD assay for colorectal cancer (CRC). About 13% of its approximately 20,000 participants were Black or African American, 15% were Hispanic, and 7% were Asian Americans. It also included both urban and rural individuals. In results announced in December 2022, the researchers found a sensitivity of 83%, which was lower than the 92.3% found in standard CRC screening, but above the 74% threshold set by the Food and Drug Administration. The specificity was 90%.
One approach that could dramatically change the landscape of cancer screening is a multicancer early detection (MCED) test, according to Dr. Febbo. The CancerSeek MCED test, developed by Johns Hopkins Kimmel Cancer Center researchers, uses a series of genetic and protein biomarkers to detect all cancers, with the exception of leukemia, skin cancer, and central nervous system tumors. Among 10,006 women aged between 65 and 75 years with no history of cancer, it had a sensitivity of 27.1% and a specificity of 98.9%, with a positive predictive value of 19.4%. The study’s population was 95% non-Hispanic White.
He also discussed the Pathfinder study, sponsored by the Illumina subsidiary Grail, which included 6,662 individuals age 50 and over from seven sites in the United States, and grouped them into normal and increased risk; 92% were non-Hispanic White. It used the Galleri MCED test, which performed with a sensitivity of 29%, specificity of 99.1%, and a positive predictive value of 38.0%. False positives produced to limited burden, with 93% undergoing imaging, 28% nonsurgical invasive procedures, and 2% undergoing fruitless invasive surgical procedures.
Dr. Febbo touted the potential for such tests to greatly reduce cancer mortality, but only if there is adequate uptake of screening procedures, particularly in underserved groups. He put up a slide of a model showing that MCED has the potential to reduce cancer mortality by 20%, but only if the screen is widely accepted among all groups. “I’ve had my team model this. If we accept the current use of screening tests, and we don’t address disparities, and we don’t ensure everybody feels included and participates actively – not only in the research, but also in the testing and adoption, you would cut that potential benefit in half. That would be hundreds of thousands of lives lost because we didn’t address disparities.”
Successful recruiting of African Americans for research
Following Dr. Febbo’s talk, Karriem Watson, MS, spoke about some potential solutions to the issue, including his own experiences and success stories in recruiting African Americans to play active roles in research. He is chief engagement officer for the National Institute of Health’s All of Us Research Program, which aims to gather health data on at least 1 million residents of the United States. Mr. Watson has spent time reaching out to people living in communities in the Chicago area to encourage participation in breast cancer screening. An event at his church inspired his own sister to get a mammogram, and she was diagnosed with early-stage breast cancer.
“I’m a living witness that early engagement can lead to early detection,” said Mr. Watson during his talk.
He reported that the All of Us research program has succeeded in creating diversity within its data collection, as 46.7% of participants identify as racial and ethnic minorities.
Mr. Watson took issue with the common perception that underrepresented communities may be hard to reach.
“I want to challenge us to think outside the box and really ask ourselves: Are populations hard to reach, or are there opportunities for us to do better and more intentional engagement?” He went on to describe a program to recruit African American men as citizen scientists. He and his colleagues developed a network that included barbers, faith leaders, and fraternity and civic organization members to help recruit participants for a prostate cancer screening project. They exceeded their initial recruitment goal.
They went on to develop a network of barbers in the south and west sides of Chicago to recruit individuals to participate in studies of protein methylation and lung cancer screening, as well as a project that investigated associations between neighborhood of residence and lung cancer. The results of those efforts have also informed other projects, including a smoking cessation study. “We’ve not only included African American men in our research, but we’ve included them as part of our research team,” said Mr. Watson.
Dr. Febbo is also a stockholder of Illumina. Mr. Watson has no relevant financial disclosures.
From American Association for Cancer Research (AACR) Annual Meeting 2023: Improving cancer outcomes through equitable access to cfDNA tests. Presented Monday, April 17, 2023.
Cancer screening remains challenging. There are screens available for a handful of solid tumors, but uptake is low caused in part by health care access barriers as well as the potential for unnecessary follow-up procedures, according to Phillip Febbo, MD.
These issues could threaten efforts like that of President Joe Biden’s Cancer Moonshot initiative, which aims to reduce cancer mortality by 50%. Advances in circulating tumor (ct) DNA analysis could help address these problems, but a lack of diversity among study participants needs to be addressed to ensure it has broad utility, continued Dr. Febbo, during his presentation at the annual meeting of the American Association for Cancer Research.
The problem is particularly acute among African American, Hispanic, and other underserved populations who often face health care barriers that can exacerbate the issue, said Dr. Febbo, who is chief medical officer for Illumina. The lack of access is compounded by the fact that there are only currently screens for lung, breast, colorectal, cervical, and prostate cancer, leaving a vast unmet need.
“We still do not have screening tests for 70% of the deaths that are due to cancer,” he said.
ctDNA released from dying cancer cells has the potential to reveal a wide range of cancer types and reduce barriers to access, because it is based on a blood test. It can be analyzed for various factors, including mutations, chromosomal rearrangements, methylation patterns, and other characteristics that hint at the presence of cancer. However, it can’t be successful without sufficient inclusion in research studies, Dr. Febbo explained.
“We have to ensure we have the right representation [of] populations when we develop these tests, when we go through the clinical trials, and as we bring these into communities,” he said.
During his presentation, Dr. Febbo shared a slide showing that about 78% of participants in published gene-association studies were White.
ctDNA showed promise in at least on recent study. Dr. Febbo discussed the ECLIPSE trial, which used the Guardant Health SHIELD assay for colorectal cancer (CRC). About 13% of its approximately 20,000 participants were Black or African American, 15% were Hispanic, and 7% were Asian Americans. It also included both urban and rural individuals. In results announced in December 2022, the researchers found a sensitivity of 83%, which was lower than the 92.3% found in standard CRC screening, but above the 74% threshold set by the Food and Drug Administration. The specificity was 90%.
One approach that could dramatically change the landscape of cancer screening is a multicancer early detection (MCED) test, according to Dr. Febbo. The CancerSeek MCED test, developed by Johns Hopkins Kimmel Cancer Center researchers, uses a series of genetic and protein biomarkers to detect all cancers, with the exception of leukemia, skin cancer, and central nervous system tumors. Among 10,006 women aged between 65 and 75 years with no history of cancer, it had a sensitivity of 27.1% and a specificity of 98.9%, with a positive predictive value of 19.4%. The study’s population was 95% non-Hispanic White.
He also discussed the Pathfinder study, sponsored by the Illumina subsidiary Grail, which included 6,662 individuals age 50 and over from seven sites in the United States, and grouped them into normal and increased risk; 92% were non-Hispanic White. It used the Galleri MCED test, which performed with a sensitivity of 29%, specificity of 99.1%, and a positive predictive value of 38.0%. False positives produced to limited burden, with 93% undergoing imaging, 28% nonsurgical invasive procedures, and 2% undergoing fruitless invasive surgical procedures.
Dr. Febbo touted the potential for such tests to greatly reduce cancer mortality, but only if there is adequate uptake of screening procedures, particularly in underserved groups. He put up a slide of a model showing that MCED has the potential to reduce cancer mortality by 20%, but only if the screen is widely accepted among all groups. “I’ve had my team model this. If we accept the current use of screening tests, and we don’t address disparities, and we don’t ensure everybody feels included and participates actively – not only in the research, but also in the testing and adoption, you would cut that potential benefit in half. That would be hundreds of thousands of lives lost because we didn’t address disparities.”
Successful recruiting of African Americans for research
Following Dr. Febbo’s talk, Karriem Watson, MS, spoke about some potential solutions to the issue, including his own experiences and success stories in recruiting African Americans to play active roles in research. He is chief engagement officer for the National Institute of Health’s All of Us Research Program, which aims to gather health data on at least 1 million residents of the United States. Mr. Watson has spent time reaching out to people living in communities in the Chicago area to encourage participation in breast cancer screening. An event at his church inspired his own sister to get a mammogram, and she was diagnosed with early-stage breast cancer.
“I’m a living witness that early engagement can lead to early detection,” said Mr. Watson during his talk.
He reported that the All of Us research program has succeeded in creating diversity within its data collection, as 46.7% of participants identify as racial and ethnic minorities.
Mr. Watson took issue with the common perception that underrepresented communities may be hard to reach.
“I want to challenge us to think outside the box and really ask ourselves: Are populations hard to reach, or are there opportunities for us to do better and more intentional engagement?” He went on to describe a program to recruit African American men as citizen scientists. He and his colleagues developed a network that included barbers, faith leaders, and fraternity and civic organization members to help recruit participants for a prostate cancer screening project. They exceeded their initial recruitment goal.
They went on to develop a network of barbers in the south and west sides of Chicago to recruit individuals to participate in studies of protein methylation and lung cancer screening, as well as a project that investigated associations between neighborhood of residence and lung cancer. The results of those efforts have also informed other projects, including a smoking cessation study. “We’ve not only included African American men in our research, but we’ve included them as part of our research team,” said Mr. Watson.
Dr. Febbo is also a stockholder of Illumina. Mr. Watson has no relevant financial disclosures.
From American Association for Cancer Research (AACR) Annual Meeting 2023: Improving cancer outcomes through equitable access to cfDNA tests. Presented Monday, April 17, 2023.
FROM AACR 2023
Endometriosis and Abnormal Uterine Bleeding
What is the link between endometriosis and abnormal uterine bleeding?
Dr. Lager: This is an important question because when people first learn about endometriosis, common symptoms include pain with periods, pelvic pain, but not necessarily abnormal uterine bleeding. However, many patients do complain of abnormal uterine bleeding when presenting with endometriosis.
There are a couple of reasons why abnormal uterine bleeding is important to consider. Within the spectrum of endometriosis, vaginal endometriosis can contribute to abnormal vaginal bleeding, most commonly cyclic or postcoital. The bleeding could be rectal due to deeply infiltrative endometriosis, although gastrointestinal etiologies should be included in the differential. Another link is coexisting diagnoses such as fibroids, adenomyosis, and endometrial polyps. In fact, the rates for coexisting conditions with endometriosis can be high and vary from study to study.
As an example, some studies show rates between 7% and 11%, where adenomyosis coexists with endometriosis. Other studies look at magnetic resonance imaging for adenomyosis and deep infiltrative endometriosis and find that women younger than 36 years have rates as high as 90% for coexisting diagnoses, and 79% for all women, regardless of the diagnosis.
The overlap is high. When I think particularly about adenomyosis and endometriosis, in some ways, the conditions are along a spectrum where adenomyosis involves ectopic endometrial glands in the myometrium, whereas endometriosis involves ectopic tissue outside of the uterus, predominantly in reproductive organs, but can be anywhere outside of the endometrium. So, when I think about abnormal uterine bleeding particularly associated with dysmenorrhea or pelvic pain, this can often be included in the constellation of symptoms for endometriosis.
Furthermore, it is important to rule out other causes of abnormal uterine bleeding because they would potentially change the treatment.
What are the current treatment options for endometriosis and abnormal uterine bleeding?
Dr. Lager: Treatments for endometriosis are inclusive of any overlapping conditions and we use a multidisciplinary approach to address symptoms. Medical treatments include hormonal management, including birth control pills, etonogestrel implants (Nexplanon), levonorgestrel-releasing intrauterine devices, progestin-only pills, gonadotropin-releasing hormone (GnRH) agonists, GnRH antagonists, and combination medications. Some medications do overlap and work for both, such as combined GnRH antagonists, estradiol, and progesterone.
Surgical management includes diagnostic laparoscopy with excision of endometriosis. If there is another coexisting diagnosis that is structural in nature, such as endometrial polyps, adenomyosis, or fibroids, surgical management may include hysteroscopy, myomectomy, or hysterectomy as indicated. When we consider surgical and nonsurgical approaches, it is important to be clear on the etiology of abnormal uterine bleeding to appropriately counsel patients for what the surgery could entail.
Have you found there to be any age or racial disparities in endometriosis treatment?
Dr. Lager: One of the things that is important about endometriosis, and in medicine in general, is to really think about how we approach race as a social construct. In the past, medicine has included race as a risk factor for certain medical conditions. And physicians in training were taught to use these risk factors to determine a differential diagnosis. However, this strategy has limited us in understanding how historical and structural racism affected patient diagnosis and treatment.
If we think back to literature that was published in the 1950s or the 1970s, Dr. Meeks was one of the physicians who described a set of characteristics of patients with endometriosis. He commented that typical patients were women who were goal-oriented, had private insurance, and experienced delayed marriage, among other traits.
The problem with this characterization was that patients would then present with symptoms of endometriosis who did not fit the original phenotype as historically described and they would be misdiagnosed and thus treated incorrectly. This incorrect treatment further reinforced incorrect stereotypes of patient presentations. These misdiagnoses could lead to unfortunate consequences in their activities of daily living as well as reproductive outcomes. We do not have data on how many patients may have been misdiagnosed and treated for pelvic inflammatory disease because they were not White, did not have private insurance, or had children early. This is an example of areas where we need to recognize systemic racism and classism and work hard to simply do better for our patients.
Although misdiagnosing based on stereotypes has decreased over time, I still think that original thinking can certainly affect patient referrals. When we look at the data of patients who are diagnosed with endometriosis, we find a higher rate of White patients (17%) compared to Black (10.1%), Asian (11.3%), and Hispanic patients (7.4%). Ensuring that all of our patients are getting appropriate referrals and diagnosis should be a priority.
When we think about the timing to initial diagnosis, globally, we know that there is a delay in diagnosis anywhere from 7 to 12 years, and then on top of that, those social constructs decrease the rate of diagnosis for certain patient populations. Misdiagnosis based on social constructs is unacceptable and one aspect that I think is very important to point out.
In a more recent study of 12,000 patients in 2022, the rate of surgical complications associated with endometriosis surgery was higher in women who were Black, Asian and Pacific Islander, and Native American/American Indian than in women who were White. These groups have a much higher rate of complications and higher rates of laparotomy—an open procedure—versus laparoscopy. In younger women, there is a higher rate of oophorectomy at the time of surgery for endometriosis than in older women.
Are there any best practices you would like to share with your peers?
Dr. Lager: For patients with abnormal uterine bleeding, it is important to consider other diagnoses and not assume that abnormal bleeding is solely related to endometriosis, while considering deeply infiltrative endometriosis in the differential.
When patients do present with cyclical bleeding, especially, for example, after hysterectomy, it is important to examine for either vaginal or vaginal cuff endometriosis because there can be other reasons that patients will have abnormal uterine bleeding related to atypical endometriosis.
It is important to know the patient’s history and focus on each patient’s level of pain, how it affects their day-to-day activities, and how they are experiencing that pain.
We all should be working to improve our understanding of social history and systemic racism as best as we can and make sure all patients are getting the right care that they deserve.
What is the link between endometriosis and abnormal uterine bleeding?
Dr. Lager: This is an important question because when people first learn about endometriosis, common symptoms include pain with periods, pelvic pain, but not necessarily abnormal uterine bleeding. However, many patients do complain of abnormal uterine bleeding when presenting with endometriosis.
There are a couple of reasons why abnormal uterine bleeding is important to consider. Within the spectrum of endometriosis, vaginal endometriosis can contribute to abnormal vaginal bleeding, most commonly cyclic or postcoital. The bleeding could be rectal due to deeply infiltrative endometriosis, although gastrointestinal etiologies should be included in the differential. Another link is coexisting diagnoses such as fibroids, adenomyosis, and endometrial polyps. In fact, the rates for coexisting conditions with endometriosis can be high and vary from study to study.
As an example, some studies show rates between 7% and 11%, where adenomyosis coexists with endometriosis. Other studies look at magnetic resonance imaging for adenomyosis and deep infiltrative endometriosis and find that women younger than 36 years have rates as high as 90% for coexisting diagnoses, and 79% for all women, regardless of the diagnosis.
The overlap is high. When I think particularly about adenomyosis and endometriosis, in some ways, the conditions are along a spectrum where adenomyosis involves ectopic endometrial glands in the myometrium, whereas endometriosis involves ectopic tissue outside of the uterus, predominantly in reproductive organs, but can be anywhere outside of the endometrium. So, when I think about abnormal uterine bleeding particularly associated with dysmenorrhea or pelvic pain, this can often be included in the constellation of symptoms for endometriosis.
Furthermore, it is important to rule out other causes of abnormal uterine bleeding because they would potentially change the treatment.
What are the current treatment options for endometriosis and abnormal uterine bleeding?
Dr. Lager: Treatments for endometriosis are inclusive of any overlapping conditions and we use a multidisciplinary approach to address symptoms. Medical treatments include hormonal management, including birth control pills, etonogestrel implants (Nexplanon), levonorgestrel-releasing intrauterine devices, progestin-only pills, gonadotropin-releasing hormone (GnRH) agonists, GnRH antagonists, and combination medications. Some medications do overlap and work for both, such as combined GnRH antagonists, estradiol, and progesterone.
Surgical management includes diagnostic laparoscopy with excision of endometriosis. If there is another coexisting diagnosis that is structural in nature, such as endometrial polyps, adenomyosis, or fibroids, surgical management may include hysteroscopy, myomectomy, or hysterectomy as indicated. When we consider surgical and nonsurgical approaches, it is important to be clear on the etiology of abnormal uterine bleeding to appropriately counsel patients for what the surgery could entail.
Have you found there to be any age or racial disparities in endometriosis treatment?
Dr. Lager: One of the things that is important about endometriosis, and in medicine in general, is to really think about how we approach race as a social construct. In the past, medicine has included race as a risk factor for certain medical conditions. And physicians in training were taught to use these risk factors to determine a differential diagnosis. However, this strategy has limited us in understanding how historical and structural racism affected patient diagnosis and treatment.
If we think back to literature that was published in the 1950s or the 1970s, Dr. Meeks was one of the physicians who described a set of characteristics of patients with endometriosis. He commented that typical patients were women who were goal-oriented, had private insurance, and experienced delayed marriage, among other traits.
The problem with this characterization was that patients would then present with symptoms of endometriosis who did not fit the original phenotype as historically described and they would be misdiagnosed and thus treated incorrectly. This incorrect treatment further reinforced incorrect stereotypes of patient presentations. These misdiagnoses could lead to unfortunate consequences in their activities of daily living as well as reproductive outcomes. We do not have data on how many patients may have been misdiagnosed and treated for pelvic inflammatory disease because they were not White, did not have private insurance, or had children early. This is an example of areas where we need to recognize systemic racism and classism and work hard to simply do better for our patients.
Although misdiagnosing based on stereotypes has decreased over time, I still think that original thinking can certainly affect patient referrals. When we look at the data of patients who are diagnosed with endometriosis, we find a higher rate of White patients (17%) compared to Black (10.1%), Asian (11.3%), and Hispanic patients (7.4%). Ensuring that all of our patients are getting appropriate referrals and diagnosis should be a priority.
When we think about the timing to initial diagnosis, globally, we know that there is a delay in diagnosis anywhere from 7 to 12 years, and then on top of that, those social constructs decrease the rate of diagnosis for certain patient populations. Misdiagnosis based on social constructs is unacceptable and one aspect that I think is very important to point out.
In a more recent study of 12,000 patients in 2022, the rate of surgical complications associated with endometriosis surgery was higher in women who were Black, Asian and Pacific Islander, and Native American/American Indian than in women who were White. These groups have a much higher rate of complications and higher rates of laparotomy—an open procedure—versus laparoscopy. In younger women, there is a higher rate of oophorectomy at the time of surgery for endometriosis than in older women.
Are there any best practices you would like to share with your peers?
Dr. Lager: For patients with abnormal uterine bleeding, it is important to consider other diagnoses and not assume that abnormal bleeding is solely related to endometriosis, while considering deeply infiltrative endometriosis in the differential.
When patients do present with cyclical bleeding, especially, for example, after hysterectomy, it is important to examine for either vaginal or vaginal cuff endometriosis because there can be other reasons that patients will have abnormal uterine bleeding related to atypical endometriosis.
It is important to know the patient’s history and focus on each patient’s level of pain, how it affects their day-to-day activities, and how they are experiencing that pain.
We all should be working to improve our understanding of social history and systemic racism as best as we can and make sure all patients are getting the right care that they deserve.
What is the link between endometriosis and abnormal uterine bleeding?
Dr. Lager: This is an important question because when people first learn about endometriosis, common symptoms include pain with periods, pelvic pain, but not necessarily abnormal uterine bleeding. However, many patients do complain of abnormal uterine bleeding when presenting with endometriosis.
There are a couple of reasons why abnormal uterine bleeding is important to consider. Within the spectrum of endometriosis, vaginal endometriosis can contribute to abnormal vaginal bleeding, most commonly cyclic or postcoital. The bleeding could be rectal due to deeply infiltrative endometriosis, although gastrointestinal etiologies should be included in the differential. Another link is coexisting diagnoses such as fibroids, adenomyosis, and endometrial polyps. In fact, the rates for coexisting conditions with endometriosis can be high and vary from study to study.
As an example, some studies show rates between 7% and 11%, where adenomyosis coexists with endometriosis. Other studies look at magnetic resonance imaging for adenomyosis and deep infiltrative endometriosis and find that women younger than 36 years have rates as high as 90% for coexisting diagnoses, and 79% for all women, regardless of the diagnosis.
The overlap is high. When I think particularly about adenomyosis and endometriosis, in some ways, the conditions are along a spectrum where adenomyosis involves ectopic endometrial glands in the myometrium, whereas endometriosis involves ectopic tissue outside of the uterus, predominantly in reproductive organs, but can be anywhere outside of the endometrium. So, when I think about abnormal uterine bleeding particularly associated with dysmenorrhea or pelvic pain, this can often be included in the constellation of symptoms for endometriosis.
Furthermore, it is important to rule out other causes of abnormal uterine bleeding because they would potentially change the treatment.
What are the current treatment options for endometriosis and abnormal uterine bleeding?
Dr. Lager: Treatments for endometriosis are inclusive of any overlapping conditions and we use a multidisciplinary approach to address symptoms. Medical treatments include hormonal management, including birth control pills, etonogestrel implants (Nexplanon), levonorgestrel-releasing intrauterine devices, progestin-only pills, gonadotropin-releasing hormone (GnRH) agonists, GnRH antagonists, and combination medications. Some medications do overlap and work for both, such as combined GnRH antagonists, estradiol, and progesterone.
Surgical management includes diagnostic laparoscopy with excision of endometriosis. If there is another coexisting diagnosis that is structural in nature, such as endometrial polyps, adenomyosis, or fibroids, surgical management may include hysteroscopy, myomectomy, or hysterectomy as indicated. When we consider surgical and nonsurgical approaches, it is important to be clear on the etiology of abnormal uterine bleeding to appropriately counsel patients for what the surgery could entail.
Have you found there to be any age or racial disparities in endometriosis treatment?
Dr. Lager: One of the things that is important about endometriosis, and in medicine in general, is to really think about how we approach race as a social construct. In the past, medicine has included race as a risk factor for certain medical conditions. And physicians in training were taught to use these risk factors to determine a differential diagnosis. However, this strategy has limited us in understanding how historical and structural racism affected patient diagnosis and treatment.
If we think back to literature that was published in the 1950s or the 1970s, Dr. Meeks was one of the physicians who described a set of characteristics of patients with endometriosis. He commented that typical patients were women who were goal-oriented, had private insurance, and experienced delayed marriage, among other traits.
The problem with this characterization was that patients would then present with symptoms of endometriosis who did not fit the original phenotype as historically described and they would be misdiagnosed and thus treated incorrectly. This incorrect treatment further reinforced incorrect stereotypes of patient presentations. These misdiagnoses could lead to unfortunate consequences in their activities of daily living as well as reproductive outcomes. We do not have data on how many patients may have been misdiagnosed and treated for pelvic inflammatory disease because they were not White, did not have private insurance, or had children early. This is an example of areas where we need to recognize systemic racism and classism and work hard to simply do better for our patients.
Although misdiagnosing based on stereotypes has decreased over time, I still think that original thinking can certainly affect patient referrals. When we look at the data of patients who are diagnosed with endometriosis, we find a higher rate of White patients (17%) compared to Black (10.1%), Asian (11.3%), and Hispanic patients (7.4%). Ensuring that all of our patients are getting appropriate referrals and diagnosis should be a priority.
When we think about the timing to initial diagnosis, globally, we know that there is a delay in diagnosis anywhere from 7 to 12 years, and then on top of that, those social constructs decrease the rate of diagnosis for certain patient populations. Misdiagnosis based on social constructs is unacceptable and one aspect that I think is very important to point out.
In a more recent study of 12,000 patients in 2022, the rate of surgical complications associated with endometriosis surgery was higher in women who were Black, Asian and Pacific Islander, and Native American/American Indian than in women who were White. These groups have a much higher rate of complications and higher rates of laparotomy—an open procedure—versus laparoscopy. In younger women, there is a higher rate of oophorectomy at the time of surgery for endometriosis than in older women.
Are there any best practices you would like to share with your peers?
Dr. Lager: For patients with abnormal uterine bleeding, it is important to consider other diagnoses and not assume that abnormal bleeding is solely related to endometriosis, while considering deeply infiltrative endometriosis in the differential.
When patients do present with cyclical bleeding, especially, for example, after hysterectomy, it is important to examine for either vaginal or vaginal cuff endometriosis because there can be other reasons that patients will have abnormal uterine bleeding related to atypical endometriosis.
It is important to know the patient’s history and focus on each patient’s level of pain, how it affects their day-to-day activities, and how they are experiencing that pain.
We all should be working to improve our understanding of social history and systemic racism as best as we can and make sure all patients are getting the right care that they deserve.
The Prediabetes Debate: Should the Diabetes Diagnostic Threshold Be Lowered, Allowing Clinicians to Intervene Earlier?
I believe that the diagnosis of type 2 diabetes mellitus (T2DM) should be broadened to match the glycemic thresholds currently used for prediabetes. This would eliminate the need for a separate category, the “prediabetes” nomenclature, and allow for earlier therapeutic intervention in patients. Current diabetes diagnostic thresholds do not reflect the latest advancements in T2DM understanding. The latest in T2DM research suggests that intervening and treating prediabetes earlier could potentially offer better clinical outcomes and enhance patients’ quality of life, as cell and tissue damage occurs early and leads to dysfunction prior to a diabetes diagnosis.1 T2DM is a highly complex disease with multifactorial causes beyond hyperglycemia that should be considered, such as hyperlipidemia, insulin resistance, hyperinsulinemia, and autoimmune inflammatory mechanisms that lead to β-cell dysfunction or failure, which results in hyperglycemia.
Prediabetes is associated with micro- and macrovascular complications that can occur early in the progression to frank disease state.1,2 This phase of diabetes also includes insulin resistance, impaired incretin action, insulin hypersecretion, increased lipolysis, and ectopic lipid storage—all of which damage β cells. These dysfunctions are also present in the frank diabetic disease state.3,4 Furthermore, diabetic retinopathy occurs in 8% to 12% of patients with prediabetes, and retinopathy begins earlier than previously thought, with neuroinflammation occurring even before vascular damage.5,6 Unfortunately, these neuro-inflammatory lesions cannot be detected with the typical instruments used in an ophthalmologist’s office.
It is believed that, through the principle of metabolic memory, even a moderate increase or episodic spikes in blood glucose can lead to negative effects in prediabetic patients who are susceptible to T2DM.1,5 Therefore, a lower diabetes diagnostic threshold could allow for earlier, more precise, and personalized therapies based on each patient’s individual risk factors and biomarkers. With a diagnosis of T2DM at the current prediabetes threshold, patients could receive treatment covered by health insurance while in the “prediabetic” state—treatment that would not have been previously approved. Patients should be treated earlier and on an individual basis with counseling on diet and lifestyle changes and antidiabetic agents to reduce glycemic levels, preserve β cells, and reduce cardiovascular [CV] or renal risk, among other complications.6,7
Moreover, the newer agents for treating diabetes such as glucagon-like pepetide-1 receptor agonists and sodium-glucose cotransporter 2 inhibitors, which are also associated with reduction in adverse CV and/or renal outcomes, could be beneficial if administered early in the prediabetic stage of disease.8,9
Early lifestyle and pharmacologic interventions can reduce the rate of progression from prediabetes to diabetes as well as complications and associated conditions, and even potentially result in remission or a full reversal of diabetes. These “side benefits” of lowering the diabetes diagnostic threshold (over and above glycemic control) make any cost-effectiveness calculations all the more advantageous to individual patients as well as to society.
Given the numerous benefits of earlier intervention for diabetes treatment, I believe a call to re-evaluate the current diabetes diagnostic threshold is in order, as it will do a great service for all patients who are currently at risk for developing T2DM.
Armato JP, DeFronzo RA, Abdul-Ghani M, Ruby RJ. Successful treatment of prediabetes in clinical practice using physiological assessment (STOP DIABETES). Lancet Diabetes Endocrinol. 2018;6:781-789.
Schwartz SS, Epstein S, Corkey BE, et al. A unified pathophysiological construct of diabetes and its complications. Trends Endocrinol Metab. 2017;28:645-655.
American Diabetes Association. Standards of Medical Care in Diabetes – 2021. Diabetes Care. 2021;44(S15–S39):S111-S124.
Brannick B, Wynn A, Dagogo-Jack S. Prediabetes as a toxic environment for the initiation of microvascular and macrovascular complications. Exp Biol Med (Maywood). 2016;241:1323-1331.
Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 1997;20:1183-1197.
Sinclair SH, Schwartz SS. Diabetic retinopathy–an underdiagnosed and undertreated inflammatory, neuro-vascular complication of diabetes. Front Endocrinol (Lausanne). 2019;10:843.
Edwards CM, Cusi K. Prediabetes: a worldwide epidemic. Endocrinol Metab Clin N Am. 2016;45:751-764.
Kanat M, DeFronzo RA, Abdul-Ghani MA. Treatment of prediabetes. World J Diabetes. 2015;6:1207-1222.
Dankner R, Roth J. The personalized approach for detecting prediabetes and diabetes. Curr Diabetes Rev. 2016;12:58-65.
I believe that the diagnosis of type 2 diabetes mellitus (T2DM) should be broadened to match the glycemic thresholds currently used for prediabetes. This would eliminate the need for a separate category, the “prediabetes” nomenclature, and allow for earlier therapeutic intervention in patients. Current diabetes diagnostic thresholds do not reflect the latest advancements in T2DM understanding. The latest in T2DM research suggests that intervening and treating prediabetes earlier could potentially offer better clinical outcomes and enhance patients’ quality of life, as cell and tissue damage occurs early and leads to dysfunction prior to a diabetes diagnosis.1 T2DM is a highly complex disease with multifactorial causes beyond hyperglycemia that should be considered, such as hyperlipidemia, insulin resistance, hyperinsulinemia, and autoimmune inflammatory mechanisms that lead to β-cell dysfunction or failure, which results in hyperglycemia.
Prediabetes is associated with micro- and macrovascular complications that can occur early in the progression to frank disease state.1,2 This phase of diabetes also includes insulin resistance, impaired incretin action, insulin hypersecretion, increased lipolysis, and ectopic lipid storage—all of which damage β cells. These dysfunctions are also present in the frank diabetic disease state.3,4 Furthermore, diabetic retinopathy occurs in 8% to 12% of patients with prediabetes, and retinopathy begins earlier than previously thought, with neuroinflammation occurring even before vascular damage.5,6 Unfortunately, these neuro-inflammatory lesions cannot be detected with the typical instruments used in an ophthalmologist’s office.
It is believed that, through the principle of metabolic memory, even a moderate increase or episodic spikes in blood glucose can lead to negative effects in prediabetic patients who are susceptible to T2DM.1,5 Therefore, a lower diabetes diagnostic threshold could allow for earlier, more precise, and personalized therapies based on each patient’s individual risk factors and biomarkers. With a diagnosis of T2DM at the current prediabetes threshold, patients could receive treatment covered by health insurance while in the “prediabetic” state—treatment that would not have been previously approved. Patients should be treated earlier and on an individual basis with counseling on diet and lifestyle changes and antidiabetic agents to reduce glycemic levels, preserve β cells, and reduce cardiovascular [CV] or renal risk, among other complications.6,7
Moreover, the newer agents for treating diabetes such as glucagon-like pepetide-1 receptor agonists and sodium-glucose cotransporter 2 inhibitors, which are also associated with reduction in adverse CV and/or renal outcomes, could be beneficial if administered early in the prediabetic stage of disease.8,9
Early lifestyle and pharmacologic interventions can reduce the rate of progression from prediabetes to diabetes as well as complications and associated conditions, and even potentially result in remission or a full reversal of diabetes. These “side benefits” of lowering the diabetes diagnostic threshold (over and above glycemic control) make any cost-effectiveness calculations all the more advantageous to individual patients as well as to society.
Given the numerous benefits of earlier intervention for diabetes treatment, I believe a call to re-evaluate the current diabetes diagnostic threshold is in order, as it will do a great service for all patients who are currently at risk for developing T2DM.
I believe that the diagnosis of type 2 diabetes mellitus (T2DM) should be broadened to match the glycemic thresholds currently used for prediabetes. This would eliminate the need for a separate category, the “prediabetes” nomenclature, and allow for earlier therapeutic intervention in patients. Current diabetes diagnostic thresholds do not reflect the latest advancements in T2DM understanding. The latest in T2DM research suggests that intervening and treating prediabetes earlier could potentially offer better clinical outcomes and enhance patients’ quality of life, as cell and tissue damage occurs early and leads to dysfunction prior to a diabetes diagnosis.1 T2DM is a highly complex disease with multifactorial causes beyond hyperglycemia that should be considered, such as hyperlipidemia, insulin resistance, hyperinsulinemia, and autoimmune inflammatory mechanisms that lead to β-cell dysfunction or failure, which results in hyperglycemia.
Prediabetes is associated with micro- and macrovascular complications that can occur early in the progression to frank disease state.1,2 This phase of diabetes also includes insulin resistance, impaired incretin action, insulin hypersecretion, increased lipolysis, and ectopic lipid storage—all of which damage β cells. These dysfunctions are also present in the frank diabetic disease state.3,4 Furthermore, diabetic retinopathy occurs in 8% to 12% of patients with prediabetes, and retinopathy begins earlier than previously thought, with neuroinflammation occurring even before vascular damage.5,6 Unfortunately, these neuro-inflammatory lesions cannot be detected with the typical instruments used in an ophthalmologist’s office.
It is believed that, through the principle of metabolic memory, even a moderate increase or episodic spikes in blood glucose can lead to negative effects in prediabetic patients who are susceptible to T2DM.1,5 Therefore, a lower diabetes diagnostic threshold could allow for earlier, more precise, and personalized therapies based on each patient’s individual risk factors and biomarkers. With a diagnosis of T2DM at the current prediabetes threshold, patients could receive treatment covered by health insurance while in the “prediabetic” state—treatment that would not have been previously approved. Patients should be treated earlier and on an individual basis with counseling on diet and lifestyle changes and antidiabetic agents to reduce glycemic levels, preserve β cells, and reduce cardiovascular [CV] or renal risk, among other complications.6,7
Moreover, the newer agents for treating diabetes such as glucagon-like pepetide-1 receptor agonists and sodium-glucose cotransporter 2 inhibitors, which are also associated with reduction in adverse CV and/or renal outcomes, could be beneficial if administered early in the prediabetic stage of disease.8,9
Early lifestyle and pharmacologic interventions can reduce the rate of progression from prediabetes to diabetes as well as complications and associated conditions, and even potentially result in remission or a full reversal of diabetes. These “side benefits” of lowering the diabetes diagnostic threshold (over and above glycemic control) make any cost-effectiveness calculations all the more advantageous to individual patients as well as to society.
Given the numerous benefits of earlier intervention for diabetes treatment, I believe a call to re-evaluate the current diabetes diagnostic threshold is in order, as it will do a great service for all patients who are currently at risk for developing T2DM.
Armato JP, DeFronzo RA, Abdul-Ghani M, Ruby RJ. Successful treatment of prediabetes in clinical practice using physiological assessment (STOP DIABETES). Lancet Diabetes Endocrinol. 2018;6:781-789.
Schwartz SS, Epstein S, Corkey BE, et al. A unified pathophysiological construct of diabetes and its complications. Trends Endocrinol Metab. 2017;28:645-655.
American Diabetes Association. Standards of Medical Care in Diabetes – 2021. Diabetes Care. 2021;44(S15–S39):S111-S124.
Brannick B, Wynn A, Dagogo-Jack S. Prediabetes as a toxic environment for the initiation of microvascular and macrovascular complications. Exp Biol Med (Maywood). 2016;241:1323-1331.
Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 1997;20:1183-1197.
Sinclair SH, Schwartz SS. Diabetic retinopathy–an underdiagnosed and undertreated inflammatory, neuro-vascular complication of diabetes. Front Endocrinol (Lausanne). 2019;10:843.
Edwards CM, Cusi K. Prediabetes: a worldwide epidemic. Endocrinol Metab Clin N Am. 2016;45:751-764.
Kanat M, DeFronzo RA, Abdul-Ghani MA. Treatment of prediabetes. World J Diabetes. 2015;6:1207-1222.
Dankner R, Roth J. The personalized approach for detecting prediabetes and diabetes. Curr Diabetes Rev. 2016;12:58-65.
Armato JP, DeFronzo RA, Abdul-Ghani M, Ruby RJ. Successful treatment of prediabetes in clinical practice using physiological assessment (STOP DIABETES). Lancet Diabetes Endocrinol. 2018;6:781-789.
Schwartz SS, Epstein S, Corkey BE, et al. A unified pathophysiological construct of diabetes and its complications. Trends Endocrinol Metab. 2017;28:645-655.
American Diabetes Association. Standards of Medical Care in Diabetes – 2021. Diabetes Care. 2021;44(S15–S39):S111-S124.
Brannick B, Wynn A, Dagogo-Jack S. Prediabetes as a toxic environment for the initiation of microvascular and macrovascular complications. Exp Biol Med (Maywood). 2016;241:1323-1331.
Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 1997;20:1183-1197.
Sinclair SH, Schwartz SS. Diabetic retinopathy–an underdiagnosed and undertreated inflammatory, neuro-vascular complication of diabetes. Front Endocrinol (Lausanne). 2019;10:843.
Edwards CM, Cusi K. Prediabetes: a worldwide epidemic. Endocrinol Metab Clin N Am. 2016;45:751-764.
Kanat M, DeFronzo RA, Abdul-Ghani MA. Treatment of prediabetes. World J Diabetes. 2015;6:1207-1222.
Dankner R, Roth J. The personalized approach for detecting prediabetes and diabetes. Curr Diabetes Rev. 2016;12:58-65.
Green Mediterranean diet may relieve aortic stiffness
A green adaptation to the traditional Mediterranean diet improves proximal aortic stiffness (PAS), a distinct marker of vascular aging and increased cardiovascular risk, according to an exploratory post hoc analysis of the DIRECT-PLUS randomized clinical trial.
The green Mediterranean diet is distinct from the traditional Mediterranean diet because of its more abundant dietary polyphenols, from green tea and a Wolffia globosa (Mankai) plant green shake, and lower intake of red or processed meat.
Independent of weight loss, the modified green Mediterranean diet regressed PAS by 15%, the traditional Mediterranean diet by 7.3%, and the healthy dietary guideline–based diet by 4.8%, the study team observed.
“The DIRECT-PLUS trial research team was the first to introduce the concept of the green-Mediterranean/high polyphenols diet,” lead researcher Iris Shai, RD, PhD, with Ben-Gurion University of the Negev, Be’er-Sheva, Israel, told this news organization.
This diet promoted “dramatic proximal aortic de-stiffening” as assessed by MRI over 18 months in roughly 300 participants with abdominal obesity/dyslipidemia. “To date, no dietary strategies have been shown to impact vascular aging physiology,” Dr. Shai said.
The analysis was published online in the Journal of the American College of Cardiology.
Not all healthy diets are equal
Of the 294 participants, 281 had valid PAS measurements at baseline. The baseline PAS (6.1 m/s) was similar across intervention groups (P = .20). Increased PAS was associated with aging, hypertension, dyslipidemia, diabetes, and visceral adiposity (P < .05).
After 18 months’ intervention (retention rate 89.8%), all diet groups showed significant PAS reductions: –0.05 m/s with the standard healthy diet (4.8%), –0.08 m/s with the traditional Mediterranean diet (7.3%) and –0.15 the green Mediterranean diet (15%).
In the multivariable model, the green Mediterranean dieters had greater PAS reduction than did the healthy-diet and Mediterranean dieters (P = .003 and P = .032, respectively).
The researchers caution that DIRECT-PLUS had multiple endpoints and this exploratory post hoc analysis might be sensitive to type I statistical error and should be considered “hypothesis-generating.”
High-quality study, believable results
Reached for comment on the study, Deepak L. Bhatt, MD, MPH, director of Mount Sinai Heart in New York, said, “There is not a lot of high-quality research on diet, and I would call this high-quality research in as much as they used randomization which most dietary studies don’t do.
“The greener Mediterranean diet seemed to be the best one on the surrogate marker of MRI-defined aortic stiffness,” Dr. Bhatt, professor of cardiovascular medicine, Icahn School of Medicine at Mount Sinai, who wasn’t involved in the study, told this news organization.
“It makes sense that a diet that has more green in it, more polyphenols, would be healthier. This has been shown in some other studies, that these plant-based polyphenols might have various cardiovascular protective aspects to them,” Dr. Bhatt said.
Overall, he said the results are “quite believable, with the caveat that it would be nice to see the results reproduced in a more diverse and larger sample.”
“There is emerging evidence that diets that are higher in fresh fruits and vegetables and whole grains and lower in overall caloric intake, in general, seem to be good diets to reduce cardiovascular risk factors and maybe even reduce actual cardiovascular risk,” Dr. Bhatt added.
The study was funded by grants from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), the Rosetrees Trust, Israel Ministry of Health, Israel Ministry of Science and Technology, and the California Walnuts Commission. Dr. Shai and Dr. Bhatt have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A green adaptation to the traditional Mediterranean diet improves proximal aortic stiffness (PAS), a distinct marker of vascular aging and increased cardiovascular risk, according to an exploratory post hoc analysis of the DIRECT-PLUS randomized clinical trial.
The green Mediterranean diet is distinct from the traditional Mediterranean diet because of its more abundant dietary polyphenols, from green tea and a Wolffia globosa (Mankai) plant green shake, and lower intake of red or processed meat.
Independent of weight loss, the modified green Mediterranean diet regressed PAS by 15%, the traditional Mediterranean diet by 7.3%, and the healthy dietary guideline–based diet by 4.8%, the study team observed.
“The DIRECT-PLUS trial research team was the first to introduce the concept of the green-Mediterranean/high polyphenols diet,” lead researcher Iris Shai, RD, PhD, with Ben-Gurion University of the Negev, Be’er-Sheva, Israel, told this news organization.
This diet promoted “dramatic proximal aortic de-stiffening” as assessed by MRI over 18 months in roughly 300 participants with abdominal obesity/dyslipidemia. “To date, no dietary strategies have been shown to impact vascular aging physiology,” Dr. Shai said.
The analysis was published online in the Journal of the American College of Cardiology.
Not all healthy diets are equal
Of the 294 participants, 281 had valid PAS measurements at baseline. The baseline PAS (6.1 m/s) was similar across intervention groups (P = .20). Increased PAS was associated with aging, hypertension, dyslipidemia, diabetes, and visceral adiposity (P < .05).
After 18 months’ intervention (retention rate 89.8%), all diet groups showed significant PAS reductions: –0.05 m/s with the standard healthy diet (4.8%), –0.08 m/s with the traditional Mediterranean diet (7.3%) and –0.15 the green Mediterranean diet (15%).
In the multivariable model, the green Mediterranean dieters had greater PAS reduction than did the healthy-diet and Mediterranean dieters (P = .003 and P = .032, respectively).
The researchers caution that DIRECT-PLUS had multiple endpoints and this exploratory post hoc analysis might be sensitive to type I statistical error and should be considered “hypothesis-generating.”
High-quality study, believable results
Reached for comment on the study, Deepak L. Bhatt, MD, MPH, director of Mount Sinai Heart in New York, said, “There is not a lot of high-quality research on diet, and I would call this high-quality research in as much as they used randomization which most dietary studies don’t do.
“The greener Mediterranean diet seemed to be the best one on the surrogate marker of MRI-defined aortic stiffness,” Dr. Bhatt, professor of cardiovascular medicine, Icahn School of Medicine at Mount Sinai, who wasn’t involved in the study, told this news organization.
“It makes sense that a diet that has more green in it, more polyphenols, would be healthier. This has been shown in some other studies, that these plant-based polyphenols might have various cardiovascular protective aspects to them,” Dr. Bhatt said.
Overall, he said the results are “quite believable, with the caveat that it would be nice to see the results reproduced in a more diverse and larger sample.”
“There is emerging evidence that diets that are higher in fresh fruits and vegetables and whole grains and lower in overall caloric intake, in general, seem to be good diets to reduce cardiovascular risk factors and maybe even reduce actual cardiovascular risk,” Dr. Bhatt added.
The study was funded by grants from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), the Rosetrees Trust, Israel Ministry of Health, Israel Ministry of Science and Technology, and the California Walnuts Commission. Dr. Shai and Dr. Bhatt have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
A green adaptation to the traditional Mediterranean diet improves proximal aortic stiffness (PAS), a distinct marker of vascular aging and increased cardiovascular risk, according to an exploratory post hoc analysis of the DIRECT-PLUS randomized clinical trial.
The green Mediterranean diet is distinct from the traditional Mediterranean diet because of its more abundant dietary polyphenols, from green tea and a Wolffia globosa (Mankai) plant green shake, and lower intake of red or processed meat.
Independent of weight loss, the modified green Mediterranean diet regressed PAS by 15%, the traditional Mediterranean diet by 7.3%, and the healthy dietary guideline–based diet by 4.8%, the study team observed.
“The DIRECT-PLUS trial research team was the first to introduce the concept of the green-Mediterranean/high polyphenols diet,” lead researcher Iris Shai, RD, PhD, with Ben-Gurion University of the Negev, Be’er-Sheva, Israel, told this news organization.
This diet promoted “dramatic proximal aortic de-stiffening” as assessed by MRI over 18 months in roughly 300 participants with abdominal obesity/dyslipidemia. “To date, no dietary strategies have been shown to impact vascular aging physiology,” Dr. Shai said.
The analysis was published online in the Journal of the American College of Cardiology.
Not all healthy diets are equal
Of the 294 participants, 281 had valid PAS measurements at baseline. The baseline PAS (6.1 m/s) was similar across intervention groups (P = .20). Increased PAS was associated with aging, hypertension, dyslipidemia, diabetes, and visceral adiposity (P < .05).
After 18 months’ intervention (retention rate 89.8%), all diet groups showed significant PAS reductions: –0.05 m/s with the standard healthy diet (4.8%), –0.08 m/s with the traditional Mediterranean diet (7.3%) and –0.15 the green Mediterranean diet (15%).
In the multivariable model, the green Mediterranean dieters had greater PAS reduction than did the healthy-diet and Mediterranean dieters (P = .003 and P = .032, respectively).
The researchers caution that DIRECT-PLUS had multiple endpoints and this exploratory post hoc analysis might be sensitive to type I statistical error and should be considered “hypothesis-generating.”
High-quality study, believable results
Reached for comment on the study, Deepak L. Bhatt, MD, MPH, director of Mount Sinai Heart in New York, said, “There is not a lot of high-quality research on diet, and I would call this high-quality research in as much as they used randomization which most dietary studies don’t do.
“The greener Mediterranean diet seemed to be the best one on the surrogate marker of MRI-defined aortic stiffness,” Dr. Bhatt, professor of cardiovascular medicine, Icahn School of Medicine at Mount Sinai, who wasn’t involved in the study, told this news organization.
“It makes sense that a diet that has more green in it, more polyphenols, would be healthier. This has been shown in some other studies, that these plant-based polyphenols might have various cardiovascular protective aspects to them,” Dr. Bhatt said.
Overall, he said the results are “quite believable, with the caveat that it would be nice to see the results reproduced in a more diverse and larger sample.”
“There is emerging evidence that diets that are higher in fresh fruits and vegetables and whole grains and lower in overall caloric intake, in general, seem to be good diets to reduce cardiovascular risk factors and maybe even reduce actual cardiovascular risk,” Dr. Bhatt added.
The study was funded by grants from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation), the Rosetrees Trust, Israel Ministry of Health, Israel Ministry of Science and Technology, and the California Walnuts Commission. Dr. Shai and Dr. Bhatt have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Mediterranean diet improves cognition in MS
due to a potential neuroprotective mechanism, according to findings of a study that was released early, ahead of presentation at the annual meting of the American Academy of Neurology.
“We were most surprised by the magnitude of the results,” said Ilana Katz Sand, MD, associate professor of neurology at the Corinne Goldsmith Dickinson Center for MS at Mount Sinai in New York. “We hypothesized a significant association between Mediterranean diet and cognition in MS, but we did not anticipate the 20% absolute difference, particularly because we rigorously controlled the demographic and health-related factors, like socioeconomic status, body mass index, and exercise habits.”

The Mediterranean diet consists of predominately vegetables, fruits, legumes, fish, and healthy fats while minimizing the consumption of dairy products, meats, and saturated acids. Previous literature has drawn an association between diet and MS symptomology, notably with regard to the Mediterranean diet. These studies indicated a connection between thalamic volume in patients with early MS as well as objectively captured MS-related disability. In this study, researchers have continued their investigation by exploring how the Mediterranean diet affects cognition.
In this cross-sectional observational study, investigators evaluated 563 people with MS ranging in age from 18 to 65 years (n = 563; 71% women; aged 44.2 ± 11.3 years). To accomplish this task, researchers conducted a retrospective chart review capturing data from patients with MS who had undergone neurobehavioral screenings. Qualifying subjects completed the Mediterranean Diet Adherence Screener (MEDAS) to determine the extent to which they adhered to the Mediterranean diet. A 14-item questionnaire, MEDAS assess a person’s usual intake of healthful foods such as vegetables and olive oil, as well as minimization of unhealthy foods such as butter and red meat. They also completed an analogue of the CICMAS cognitive battery comprised of a composite of Symbol Digit Modalities Test, Hopkins Verbal Learning Test, Revised, and CANTAB Paired Associate Learning.
Researchers evaluated patient-reported outcomes adjusted based on demographics (i.e., age, sex, race, ethnicity, and socioeconomic status) and health-related factors. These elements included body mass index, exercise, sleep disturbance, hypertension, diabetes, hyperlipidemia, and smoking.
The study excluded patients who had another primary neurological condition in addition to MS (n = 24), serious psychiatric illness such as schizophrenia (n = 5) or clinical relapse within 6 weeks (n = 2), or missing data (n = 13).
Based on the diet scores, investigators stratified participants into four groups. Those with the scores ranging from 0 to 4 were classified into the lowest group, while scores of 9 or greater qualified participants for the high group.
Investigators observed a significant association between a higher Mediterranean diet score and condition in the population sampled. They found a mean z-score of –0.67 (0.95). In addition, a higher MEDAS proved an independent indicator of better cognition (B = 0.08 [95% confidence interval (CI), 0.05, 0.11], beta = 0.20, P < .001). In fact, a high MEDAS independently correlated to a 20% lower risk for cognitive impairment (odds ratio [OR] = .80 {95% CI, 0.73, 0.89}, P < .001). Ultimately, the study’s findings demonstrated MEDAS served as the strongest health-related indicator of z-score and cognitive impairment. Moreover, dietary modification based on effect suggested stronger associations between diet and cognition with progressive disease as opposed to relapsing disease, as noted by the relationship between the z-score and cognition.
“Further research is needed,” Dr. Katz Sand said. “But because the progressive phenotype reflects more prominent neurodegeneration, the greater observed effect size in those with progressive MS suggests a potential neuroprotective mechanism.”
This study was funded in part by an Irma T. Hirschl/Monique Weill-Caulier Research Award to Dr. Katz Sand. Dr. Katz Sand and coauthors also received funding from the National Multiple Sclerosis Society.
due to a potential neuroprotective mechanism, according to findings of a study that was released early, ahead of presentation at the annual meting of the American Academy of Neurology.
“We were most surprised by the magnitude of the results,” said Ilana Katz Sand, MD, associate professor of neurology at the Corinne Goldsmith Dickinson Center for MS at Mount Sinai in New York. “We hypothesized a significant association between Mediterranean diet and cognition in MS, but we did not anticipate the 20% absolute difference, particularly because we rigorously controlled the demographic and health-related factors, like socioeconomic status, body mass index, and exercise habits.”
The Mediterranean diet consists of predominately vegetables, fruits, legumes, fish, and healthy fats while minimizing the consumption of dairy products, meats, and saturated acids. Previous literature has drawn an association between diet and MS symptomology, notably with regard to the Mediterranean diet. These studies indicated a connection between thalamic volume in patients with early MS as well as objectively captured MS-related disability. In this study, researchers have continued their investigation by exploring how the Mediterranean diet affects cognition.
In this cross-sectional observational study, investigators evaluated 563 people with MS ranging in age from 18 to 65 years (n = 563; 71% women; aged 44.2 ± 11.3 years). To accomplish this task, researchers conducted a retrospective chart review capturing data from patients with MS who had undergone neurobehavioral screenings. Qualifying subjects completed the Mediterranean Diet Adherence Screener (MEDAS) to determine the extent to which they adhered to the Mediterranean diet. A 14-item questionnaire, MEDAS assess a person’s usual intake of healthful foods such as vegetables and olive oil, as well as minimization of unhealthy foods such as butter and red meat. They also completed an analogue of the CICMAS cognitive battery comprised of a composite of Symbol Digit Modalities Test, Hopkins Verbal Learning Test, Revised, and CANTAB Paired Associate Learning.
Researchers evaluated patient-reported outcomes adjusted based on demographics (i.e., age, sex, race, ethnicity, and socioeconomic status) and health-related factors. These elements included body mass index, exercise, sleep disturbance, hypertension, diabetes, hyperlipidemia, and smoking.
The study excluded patients who had another primary neurological condition in addition to MS (n = 24), serious psychiatric illness such as schizophrenia (n = 5) or clinical relapse within 6 weeks (n = 2), or missing data (n = 13).
Based on the diet scores, investigators stratified participants into four groups. Those with the scores ranging from 0 to 4 were classified into the lowest group, while scores of 9 or greater qualified participants for the high group.
Investigators observed a significant association between a higher Mediterranean diet score and condition in the population sampled. They found a mean z-score of –0.67 (0.95). In addition, a higher MEDAS proved an independent indicator of better cognition (B = 0.08 [95% confidence interval (CI), 0.05, 0.11], beta = 0.20, P < .001). In fact, a high MEDAS independently correlated to a 20% lower risk for cognitive impairment (odds ratio [OR] = .80 {95% CI, 0.73, 0.89}, P < .001). Ultimately, the study’s findings demonstrated MEDAS served as the strongest health-related indicator of z-score and cognitive impairment. Moreover, dietary modification based on effect suggested stronger associations between diet and cognition with progressive disease as opposed to relapsing disease, as noted by the relationship between the z-score and cognition.
“Further research is needed,” Dr. Katz Sand said. “But because the progressive phenotype reflects more prominent neurodegeneration, the greater observed effect size in those with progressive MS suggests a potential neuroprotective mechanism.”
This study was funded in part by an Irma T. Hirschl/Monique Weill-Caulier Research Award to Dr. Katz Sand. Dr. Katz Sand and coauthors also received funding from the National Multiple Sclerosis Society.
due to a potential neuroprotective mechanism, according to findings of a study that was released early, ahead of presentation at the annual meting of the American Academy of Neurology.
“We were most surprised by the magnitude of the results,” said Ilana Katz Sand, MD, associate professor of neurology at the Corinne Goldsmith Dickinson Center for MS at Mount Sinai in New York. “We hypothesized a significant association between Mediterranean diet and cognition in MS, but we did not anticipate the 20% absolute difference, particularly because we rigorously controlled the demographic and health-related factors, like socioeconomic status, body mass index, and exercise habits.”
The Mediterranean diet consists of predominately vegetables, fruits, legumes, fish, and healthy fats while minimizing the consumption of dairy products, meats, and saturated acids. Previous literature has drawn an association between diet and MS symptomology, notably with regard to the Mediterranean diet. These studies indicated a connection between thalamic volume in patients with early MS as well as objectively captured MS-related disability. In this study, researchers have continued their investigation by exploring how the Mediterranean diet affects cognition.
In this cross-sectional observational study, investigators evaluated 563 people with MS ranging in age from 18 to 65 years (n = 563; 71% women; aged 44.2 ± 11.3 years). To accomplish this task, researchers conducted a retrospective chart review capturing data from patients with MS who had undergone neurobehavioral screenings. Qualifying subjects completed the Mediterranean Diet Adherence Screener (MEDAS) to determine the extent to which they adhered to the Mediterranean diet. A 14-item questionnaire, MEDAS assess a person’s usual intake of healthful foods such as vegetables and olive oil, as well as minimization of unhealthy foods such as butter and red meat. They also completed an analogue of the CICMAS cognitive battery comprised of a composite of Symbol Digit Modalities Test, Hopkins Verbal Learning Test, Revised, and CANTAB Paired Associate Learning.
Researchers evaluated patient-reported outcomes adjusted based on demographics (i.e., age, sex, race, ethnicity, and socioeconomic status) and health-related factors. These elements included body mass index, exercise, sleep disturbance, hypertension, diabetes, hyperlipidemia, and smoking.
The study excluded patients who had another primary neurological condition in addition to MS (n = 24), serious psychiatric illness such as schizophrenia (n = 5) or clinical relapse within 6 weeks (n = 2), or missing data (n = 13).
Based on the diet scores, investigators stratified participants into four groups. Those with the scores ranging from 0 to 4 were classified into the lowest group, while scores of 9 or greater qualified participants for the high group.
Investigators observed a significant association between a higher Mediterranean diet score and condition in the population sampled. They found a mean z-score of –0.67 (0.95). In addition, a higher MEDAS proved an independent indicator of better cognition (B = 0.08 [95% confidence interval (CI), 0.05, 0.11], beta = 0.20, P < .001). In fact, a high MEDAS independently correlated to a 20% lower risk for cognitive impairment (odds ratio [OR] = .80 {95% CI, 0.73, 0.89}, P < .001). Ultimately, the study’s findings demonstrated MEDAS served as the strongest health-related indicator of z-score and cognitive impairment. Moreover, dietary modification based on effect suggested stronger associations between diet and cognition with progressive disease as opposed to relapsing disease, as noted by the relationship between the z-score and cognition.
“Further research is needed,” Dr. Katz Sand said. “But because the progressive phenotype reflects more prominent neurodegeneration, the greater observed effect size in those with progressive MS suggests a potential neuroprotective mechanism.”
This study was funded in part by an Irma T. Hirschl/Monique Weill-Caulier Research Award to Dr. Katz Sand. Dr. Katz Sand and coauthors also received funding from the National Multiple Sclerosis Society.
FROM AAN 2023

Rabies: How to respond to parents’ questions
When most families hear the word rabies, they envision a dog foaming at the mouth and think about receiving multiple painful, often intra-abdominal injections. However, the epidemiology of rabies has changed in the United States. Postexposure prophylaxis (PEP) may not always be indicated and for certain persons preexposure prophylaxis (PrEP) is available and recommended.
Rabies is a Lyssavirus that is transmitted through saliva most often from the bite or scratch of an infected animal. Sometimes it’s via direct contact with mucous membranes. Although rare, cases have been described in which an undiagnosed donor passed the virus via transplant to recipients and four cases of aerosolized transmission were documented in two spelunkers and two laboratory technicians working with the virus. Worldwide it’s estimated that rabies causes 59,000 deaths annually.
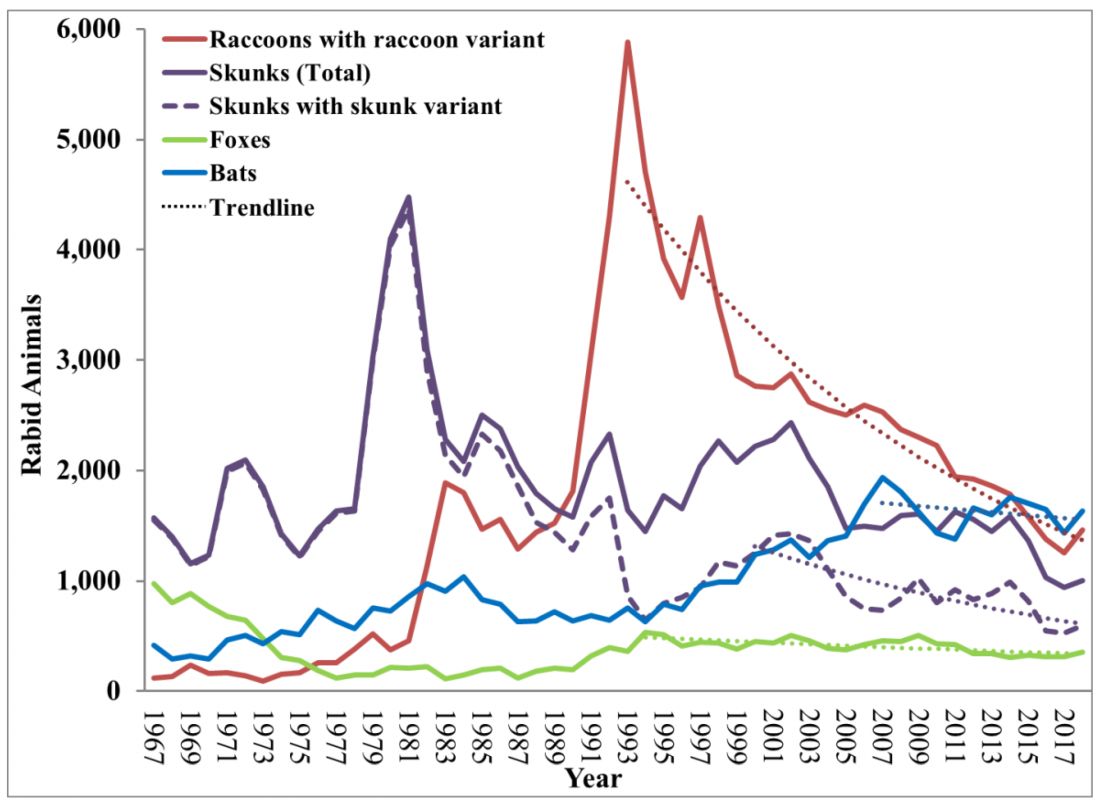
Most cases (98%) are secondary to canine rabies. Prior to 1960, dogs were the major reservoir in the United States; however, after introduction of leash laws and animal vaccination in 1947, there was a drastic decline in cases caused by the canine rabies virus variant (CRVV). By 2004, CRVV was eliminated in the United States.
However, the proportion of strains associated with wildlife including raccoons, skunks, foxes, bats, coyotes, and mongoose now account for most of the cases in humans. Wildlife rabies is found in all states except Hawaii. Between 1960 and 2018, 89 cases were acquired in the United States and 62 (70%) were from bat exposure. Dog bites acquired during international travel were the cause of 36 cases.
Once signs and symptoms of disease develop there is no treatment. Regardless of the species variant, rabies virus infection is fatal in over 99% of cases. However, disease can be prevented with prompt initiation of PEP, which includes administration of rabies immune globulin (RIG) and rabies vaccine. Let’s look at a few different scenarios.
1. A delivery person is bitten by your neighbor’s dog while making a delivery. He was told to get rabies vaccine. What should we advise?
Canine rabies has been eliminated in the United States. However, unvaccinated canines can acquire rabies from wildlife. In this situation, you can determine the immunization status of the dog. Contact your local/state health department to assist with enforcement and management. Bites by cats and ferrets should be managed similarly.
Healthy dog:
1. Observe for 10 days.
2. PEP is not indicated unless the animal develops signs/symptoms of rabies. Then euthanize and begin PEP.
Dog appears rabid or suspected to be rabid:
1. Begin PEP.
2. Animal should be euthanized. If immunofluorescent test is negative discontinue PEP.
Dog unavailable:
Contact local/state health department. They are more familiar with rabies surveillance data.
2. Patient relocating to Malaysia for 3-4 years. Rabies PrEP was recommended but the family wants your opinion before receiving the vaccine. What would you advise?
Canine rabies is felt to be the primary cause of rabies outside of the United States. Canines are not routinely vaccinated in many foreign destinations, and the availability of RIG and rabies vaccine is not guaranteed in developing countries. As noted above, dog bites during international travel accounted for 28% of U.S. cases between 1960 and 2018.

In May 2022 recommendations for a modified two-dose PrEP schedule was published that identifies five risk groups and includes specific timing for checking rabies titers. The third rabies dose can now be administered up until year 3 (Morb Mortal Wkly Rep. 2022 May 6;71[18]:619-27). For individuals relocating to countries where CRVV is present, I prefer the traditional three-dose PrEP schedule administered between 21 and 28 days. However, we now have options. If exposure occurs any time after completion of a three-dose PrEP series or within 3 years after completion of a two-dose PrEP series, RIG would not be required. All patients would receive two doses of rabies vaccine (days 0, 3). If exposure occurs after 3 years in a person who received two doses of PrEP who did not have documentation of a protective rabies titer (> 5 IU/mL), treatment will include RIG plus four doses of vaccine (days 0, 3, 7, 14).
For this relocating patient, supporting PrEP would be strongly recommended.
3. A mother tells you she sees bats flying around her home at night and a few have even gotten into the home. This morning she saw one in her child’s room. He was still sleeping. Is there anything she needs to do?
Bats have become the predominant source of rabies in the United States. In addition to the cases noted above, three fatal cases occurred between Sept. 28 and Nov. 10, 2021, after bat exposures in August 2021 (MMWR Morb Mortal Wkly Rep. 2022 Jan 7;71:31-2). All had recognized contact with a bat 3-7 weeks prior to onset of symptoms and died 2-3 weeks after symptom onset. One declined PEP and the other two did not realize the risk for rabies from their exposure or did not notice a scratch or bite. Bites from bats may be small and unnoticed. Exposure to a bat in a closed room while sleeping is considered an exposure. Hawaii is the only state not reporting rabid bats.
PEP is recommended for her child. She should identify potential areas bats may enter the home and seal them in addition to removal of any bat roosts.
4. A parent realizes a house guest has been feeding raccoons in the backyard. What’s your response?
While bat rabies is the predominant variant associated with disease in the United States, as illustrated in Figure 1, other species of wildlife including raccoons are a major source of rabies. The geographic spread of the raccoon variant of rabies has been limited by oral vaccination via bait. In the situation noted here, the raccoons have returned because food was being offered thus increasing the families chance of a potential rabies exposure. Wildlife including skunks, raccoons, coyotes, foxes, and mongooses are always considered rabid until proven negative by laboratory testing.
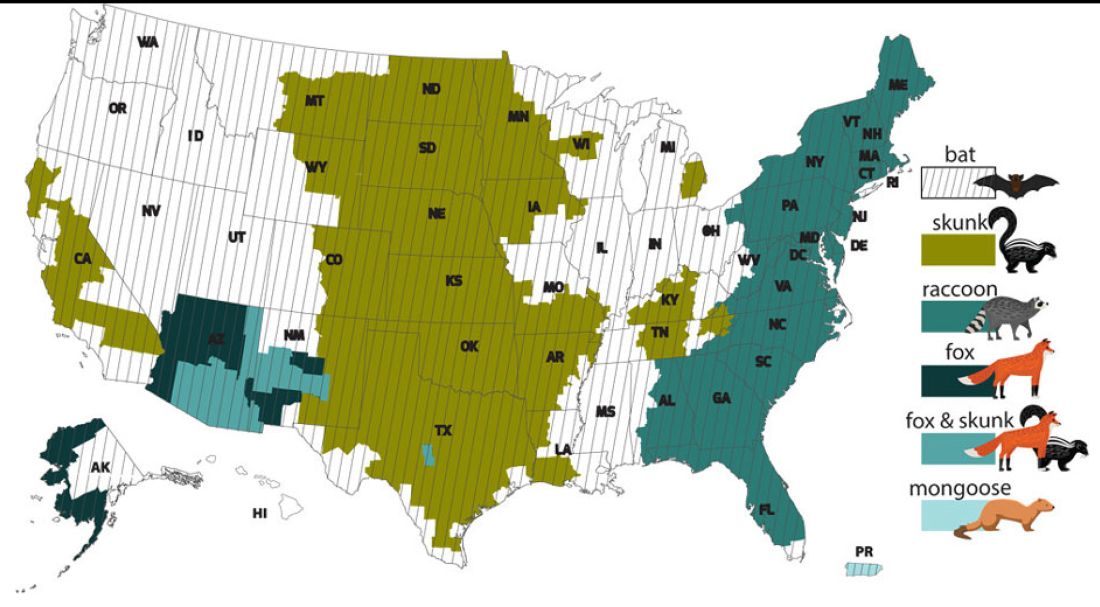
You recommend to stop feeding wildlife and never to approach them. Have them contact the local rabies control unit and/or state wildlife services to assist with removal of the raccoons. Depending on the locale, pest control may be required at the owners expense. Inform the family to seek PEP if anyone is bitten or scratched by the raccoons.
As per the Centers for Disease Control and Prevention, about 55,000 residents receive PEP annually with health-associated expenditures including diagnostics, prevention, and control estimated between $245 and $510 million annually. Rabies is one of the most fatal diseases that can be prevented by avoiding contact with wild animals, maintenance of high immunization rates in pets, and keeping people informed of potential sources including bats. One can’t determine if an animal has rabies by looking at it. Rabies remains an urgent disease that we have to remember to address with our patients and their families. For additional information go to www.CDC.gov/rabies.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She has no relevant financial disclosures.
When most families hear the word rabies, they envision a dog foaming at the mouth and think about receiving multiple painful, often intra-abdominal injections. However, the epidemiology of rabies has changed in the United States. Postexposure prophylaxis (PEP) may not always be indicated and for certain persons preexposure prophylaxis (PrEP) is available and recommended.
Rabies is a Lyssavirus that is transmitted through saliva most often from the bite or scratch of an infected animal. Sometimes it’s via direct contact with mucous membranes. Although rare, cases have been described in which an undiagnosed donor passed the virus via transplant to recipients and four cases of aerosolized transmission were documented in two spelunkers and two laboratory technicians working with the virus. Worldwide it’s estimated that rabies causes 59,000 deaths annually.
Most cases (98%) are secondary to canine rabies. Prior to 1960, dogs were the major reservoir in the United States; however, after introduction of leash laws and animal vaccination in 1947, there was a drastic decline in cases caused by the canine rabies virus variant (CRVV). By 2004, CRVV was eliminated in the United States.
However, the proportion of strains associated with wildlife including raccoons, skunks, foxes, bats, coyotes, and mongoose now account for most of the cases in humans. Wildlife rabies is found in all states except Hawaii. Between 1960 and 2018, 89 cases were acquired in the United States and 62 (70%) were from bat exposure. Dog bites acquired during international travel were the cause of 36 cases.
Once signs and symptoms of disease develop there is no treatment. Regardless of the species variant, rabies virus infection is fatal in over 99% of cases. However, disease can be prevented with prompt initiation of PEP, which includes administration of rabies immune globulin (RIG) and rabies vaccine. Let’s look at a few different scenarios.
1. A delivery person is bitten by your neighbor’s dog while making a delivery. He was told to get rabies vaccine. What should we advise?
Canine rabies has been eliminated in the United States. However, unvaccinated canines can acquire rabies from wildlife. In this situation, you can determine the immunization status of the dog. Contact your local/state health department to assist with enforcement and management. Bites by cats and ferrets should be managed similarly.
Healthy dog:
1. Observe for 10 days.
2. PEP is not indicated unless the animal develops signs/symptoms of rabies. Then euthanize and begin PEP.
Dog appears rabid or suspected to be rabid:
1. Begin PEP.
2. Animal should be euthanized. If immunofluorescent test is negative discontinue PEP.
Dog unavailable:
Contact local/state health department. They are more familiar with rabies surveillance data.
2. Patient relocating to Malaysia for 3-4 years. Rabies PrEP was recommended but the family wants your opinion before receiving the vaccine. What would you advise?
Canine rabies is felt to be the primary cause of rabies outside of the United States. Canines are not routinely vaccinated in many foreign destinations, and the availability of RIG and rabies vaccine is not guaranteed in developing countries. As noted above, dog bites during international travel accounted for 28% of U.S. cases between 1960 and 2018.
In May 2022 recommendations for a modified two-dose PrEP schedule was published that identifies five risk groups and includes specific timing for checking rabies titers. The third rabies dose can now be administered up until year 3 (Morb Mortal Wkly Rep. 2022 May 6;71[18]:619-27). For individuals relocating to countries where CRVV is present, I prefer the traditional three-dose PrEP schedule administered between 21 and 28 days. However, we now have options. If exposure occurs any time after completion of a three-dose PrEP series or within 3 years after completion of a two-dose PrEP series, RIG would not be required. All patients would receive two doses of rabies vaccine (days 0, 3). If exposure occurs after 3 years in a person who received two doses of PrEP who did not have documentation of a protective rabies titer (> 5 IU/mL), treatment will include RIG plus four doses of vaccine (days 0, 3, 7, 14).
For this relocating patient, supporting PrEP would be strongly recommended.
3. A mother tells you she sees bats flying around her home at night and a few have even gotten into the home. This morning she saw one in her child’s room. He was still sleeping. Is there anything she needs to do?
Bats have become the predominant source of rabies in the United States. In addition to the cases noted above, three fatal cases occurred between Sept. 28 and Nov. 10, 2021, after bat exposures in August 2021 (MMWR Morb Mortal Wkly Rep. 2022 Jan 7;71:31-2). All had recognized contact with a bat 3-7 weeks prior to onset of symptoms and died 2-3 weeks after symptom onset. One declined PEP and the other two did not realize the risk for rabies from their exposure or did not notice a scratch or bite. Bites from bats may be small and unnoticed. Exposure to a bat in a closed room while sleeping is considered an exposure. Hawaii is the only state not reporting rabid bats.
PEP is recommended for her child. She should identify potential areas bats may enter the home and seal them in addition to removal of any bat roosts.
4. A parent realizes a house guest has been feeding raccoons in the backyard. What’s your response?
While bat rabies is the predominant variant associated with disease in the United States, as illustrated in Figure 1, other species of wildlife including raccoons are a major source of rabies. The geographic spread of the raccoon variant of rabies has been limited by oral vaccination via bait. In the situation noted here, the raccoons have returned because food was being offered thus increasing the families chance of a potential rabies exposure. Wildlife including skunks, raccoons, coyotes, foxes, and mongooses are always considered rabid until proven negative by laboratory testing.
You recommend to stop feeding wildlife and never to approach them. Have them contact the local rabies control unit and/or state wildlife services to assist with removal of the raccoons. Depending on the locale, pest control may be required at the owners expense. Inform the family to seek PEP if anyone is bitten or scratched by the raccoons.
As per the Centers for Disease Control and Prevention, about 55,000 residents receive PEP annually with health-associated expenditures including diagnostics, prevention, and control estimated between $245 and $510 million annually. Rabies is one of the most fatal diseases that can be prevented by avoiding contact with wild animals, maintenance of high immunization rates in pets, and keeping people informed of potential sources including bats. One can’t determine if an animal has rabies by looking at it. Rabies remains an urgent disease that we have to remember to address with our patients and their families. For additional information go to www.CDC.gov/rabies.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She has no relevant financial disclosures.
When most families hear the word rabies, they envision a dog foaming at the mouth and think about receiving multiple painful, often intra-abdominal injections. However, the epidemiology of rabies has changed in the United States. Postexposure prophylaxis (PEP) may not always be indicated and for certain persons preexposure prophylaxis (PrEP) is available and recommended.
Rabies is a Lyssavirus that is transmitted through saliva most often from the bite or scratch of an infected animal. Sometimes it’s via direct contact with mucous membranes. Although rare, cases have been described in which an undiagnosed donor passed the virus via transplant to recipients and four cases of aerosolized transmission were documented in two spelunkers and two laboratory technicians working with the virus. Worldwide it’s estimated that rabies causes 59,000 deaths annually.
Most cases (98%) are secondary to canine rabies. Prior to 1960, dogs were the major reservoir in the United States; however, after introduction of leash laws and animal vaccination in 1947, there was a drastic decline in cases caused by the canine rabies virus variant (CRVV). By 2004, CRVV was eliminated in the United States.
However, the proportion of strains associated with wildlife including raccoons, skunks, foxes, bats, coyotes, and mongoose now account for most of the cases in humans. Wildlife rabies is found in all states except Hawaii. Between 1960 and 2018, 89 cases were acquired in the United States and 62 (70%) were from bat exposure. Dog bites acquired during international travel were the cause of 36 cases.
Once signs and symptoms of disease develop there is no treatment. Regardless of the species variant, rabies virus infection is fatal in over 99% of cases. However, disease can be prevented with prompt initiation of PEP, which includes administration of rabies immune globulin (RIG) and rabies vaccine. Let’s look at a few different scenarios.
1. A delivery person is bitten by your neighbor’s dog while making a delivery. He was told to get rabies vaccine. What should we advise?
Canine rabies has been eliminated in the United States. However, unvaccinated canines can acquire rabies from wildlife. In this situation, you can determine the immunization status of the dog. Contact your local/state health department to assist with enforcement and management. Bites by cats and ferrets should be managed similarly.
Healthy dog:
1. Observe for 10 days.
2. PEP is not indicated unless the animal develops signs/symptoms of rabies. Then euthanize and begin PEP.
Dog appears rabid or suspected to be rabid:
1. Begin PEP.
2. Animal should be euthanized. If immunofluorescent test is negative discontinue PEP.
Dog unavailable:
Contact local/state health department. They are more familiar with rabies surveillance data.
2. Patient relocating to Malaysia for 3-4 years. Rabies PrEP was recommended but the family wants your opinion before receiving the vaccine. What would you advise?
Canine rabies is felt to be the primary cause of rabies outside of the United States. Canines are not routinely vaccinated in many foreign destinations, and the availability of RIG and rabies vaccine is not guaranteed in developing countries. As noted above, dog bites during international travel accounted for 28% of U.S. cases between 1960 and 2018.
In May 2022 recommendations for a modified two-dose PrEP schedule was published that identifies five risk groups and includes specific timing for checking rabies titers. The third rabies dose can now be administered up until year 3 (Morb Mortal Wkly Rep. 2022 May 6;71[18]:619-27). For individuals relocating to countries where CRVV is present, I prefer the traditional three-dose PrEP schedule administered between 21 and 28 days. However, we now have options. If exposure occurs any time after completion of a three-dose PrEP series or within 3 years after completion of a two-dose PrEP series, RIG would not be required. All patients would receive two doses of rabies vaccine (days 0, 3). If exposure occurs after 3 years in a person who received two doses of PrEP who did not have documentation of a protective rabies titer (> 5 IU/mL), treatment will include RIG plus four doses of vaccine (days 0, 3, 7, 14).
For this relocating patient, supporting PrEP would be strongly recommended.
3. A mother tells you she sees bats flying around her home at night and a few have even gotten into the home. This morning she saw one in her child’s room. He was still sleeping. Is there anything she needs to do?
Bats have become the predominant source of rabies in the United States. In addition to the cases noted above, three fatal cases occurred between Sept. 28 and Nov. 10, 2021, after bat exposures in August 2021 (MMWR Morb Mortal Wkly Rep. 2022 Jan 7;71:31-2). All had recognized contact with a bat 3-7 weeks prior to onset of symptoms and died 2-3 weeks after symptom onset. One declined PEP and the other two did not realize the risk for rabies from their exposure or did not notice a scratch or bite. Bites from bats may be small and unnoticed. Exposure to a bat in a closed room while sleeping is considered an exposure. Hawaii is the only state not reporting rabid bats.
PEP is recommended for her child. She should identify potential areas bats may enter the home and seal them in addition to removal of any bat roosts.
4. A parent realizes a house guest has been feeding raccoons in the backyard. What’s your response?
While bat rabies is the predominant variant associated with disease in the United States, as illustrated in Figure 1, other species of wildlife including raccoons are a major source of rabies. The geographic spread of the raccoon variant of rabies has been limited by oral vaccination via bait. In the situation noted here, the raccoons have returned because food was being offered thus increasing the families chance of a potential rabies exposure. Wildlife including skunks, raccoons, coyotes, foxes, and mongooses are always considered rabid until proven negative by laboratory testing.
You recommend to stop feeding wildlife and never to approach them. Have them contact the local rabies control unit and/or state wildlife services to assist with removal of the raccoons. Depending on the locale, pest control may be required at the owners expense. Inform the family to seek PEP if anyone is bitten or scratched by the raccoons.
As per the Centers for Disease Control and Prevention, about 55,000 residents receive PEP annually with health-associated expenditures including diagnostics, prevention, and control estimated between $245 and $510 million annually. Rabies is one of the most fatal diseases that can be prevented by avoiding contact with wild animals, maintenance of high immunization rates in pets, and keeping people informed of potential sources including bats. One can’t determine if an animal has rabies by looking at it. Rabies remains an urgent disease that we have to remember to address with our patients and their families. For additional information go to www.CDC.gov/rabies.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She has no relevant financial disclosures.