User login
Commentary: Enthesitis, synovitis, spondyloarthritis, and PsA, June 2023

The relationship between enthesitis and synovitis is of considerable interest to both clinicians and researchers. This relationship is best evaluated using imaging, particularly ultrasonography, and could provide pathophysiologic insights. Balulu and colleagues recruited 158 patients with PsA who underwent sonographic assessment of 52 joints, 40 tendons, and 14 entheses as well as clinical evaluation. Overall, total sonographic enthesitis scores were significantly associated with total sonographic synovitis and sonographic tenosynovitis scores and also with older age, male sex, swollen joint count, C-reactive protein, physical occupation, and patient-reported outcomes. The association between enthesitis and synovitis was also demonstrated at the elbows, knees, and ankles. This study demonstrates that psoriatic enthesitis and synovitis are closely related and thus may share pathophysiologic mechanisms. Longitudinal studies in very early PsA using ultrasound might provide clues to confirm the hypothesis that psoriatic synovitis is secondary to enthesitis.
Another important domain that is increasingly studied is axial PsA. Currently, the evidence for treatment of axial PsA is extrapolated from that for axial spondyloarthritis (SpA), in the belief that the two diseases are pathophysiologically similar. However, there is increasing evidence for differences between axial PsA and axial SpA that might influence the choice of treatment. In a recent study, de Hooge and colleagues demonstrated that patients with axial PsA have lower severity of damage to the spine compared with those with axial SpA. Using data from 312 patients with PsA and 213 patients with SpA who underwent radiographic imaging assessment in the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) and the Ghent and Belgian Inflammatory Arthritis and Spondylitis (Be-GIANT) study, respectively, they show that the proportion of patients with PsA vs SpA having spinal damage was comparable. Patients with SpA and spinal damage had higher modified Stoke Ankylosing Spondylitis Spine Scores, indicating more severe damage. These results are consistent with other published studies and indicate that patients with PsA have less severe spinal disease compared with other patients with axial SpA. Randomized controlled trials (RCTs) specifically investigating the treatment of axial PsA are currently underway. Nevertheless, post hoc analyses of data from PsA RCTs indicate that most drugs efficacious for PsA overall also provide benefit in axial disease.
In a recent report, Baraliakos and colleagues analyzed data from the SELECT-PsA 1 and SELECT-PsA 2 trials that evaluated the efficacy of upadacitinib in PsA. They show that, compared with placebo, 15 mg upadacitinib led to a greater improvement in axial symptoms. The improvement in overall Bath Ankylosing Spondylitis Disease Activity Index score at week 24 was significantly higher with 15 mg upadacitinib compared with placebo in both trials. However, these results are not definitive because there is yet no consensus on the definition of and outcome measures for axial PsA.
The relationship between enthesitis and synovitis is of considerable interest to both clinicians and researchers. This relationship is best evaluated using imaging, particularly ultrasonography, and could provide pathophysiologic insights. Balulu and colleagues recruited 158 patients with PsA who underwent sonographic assessment of 52 joints, 40 tendons, and 14 entheses as well as clinical evaluation. Overall, total sonographic enthesitis scores were significantly associated with total sonographic synovitis and sonographic tenosynovitis scores and also with older age, male sex, swollen joint count, C-reactive protein, physical occupation, and patient-reported outcomes. The association between enthesitis and synovitis was also demonstrated at the elbows, knees, and ankles. This study demonstrates that psoriatic enthesitis and synovitis are closely related and thus may share pathophysiologic mechanisms. Longitudinal studies in very early PsA using ultrasound might provide clues to confirm the hypothesis that psoriatic synovitis is secondary to enthesitis.
Another important domain that is increasingly studied is axial PsA. Currently, the evidence for treatment of axial PsA is extrapolated from that for axial spondyloarthritis (SpA), in the belief that the two diseases are pathophysiologically similar. However, there is increasing evidence for differences between axial PsA and axial SpA that might influence the choice of treatment. In a recent study, de Hooge and colleagues demonstrated that patients with axial PsA have lower severity of damage to the spine compared with those with axial SpA. Using data from 312 patients with PsA and 213 patients with SpA who underwent radiographic imaging assessment in the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) and the Ghent and Belgian Inflammatory Arthritis and Spondylitis (Be-GIANT) study, respectively, they show that the proportion of patients with PsA vs SpA having spinal damage was comparable. Patients with SpA and spinal damage had higher modified Stoke Ankylosing Spondylitis Spine Scores, indicating more severe damage. These results are consistent with other published studies and indicate that patients with PsA have less severe spinal disease compared with other patients with axial SpA. Randomized controlled trials (RCTs) specifically investigating the treatment of axial PsA are currently underway. Nevertheless, post hoc analyses of data from PsA RCTs indicate that most drugs efficacious for PsA overall also provide benefit in axial disease.
In a recent report, Baraliakos and colleagues analyzed data from the SELECT-PsA 1 and SELECT-PsA 2 trials that evaluated the efficacy of upadacitinib in PsA. They show that, compared with placebo, 15 mg upadacitinib led to a greater improvement in axial symptoms. The improvement in overall Bath Ankylosing Spondylitis Disease Activity Index score at week 24 was significantly higher with 15 mg upadacitinib compared with placebo in both trials. However, these results are not definitive because there is yet no consensus on the definition of and outcome measures for axial PsA.
The relationship between enthesitis and synovitis is of considerable interest to both clinicians and researchers. This relationship is best evaluated using imaging, particularly ultrasonography, and could provide pathophysiologic insights. Balulu and colleagues recruited 158 patients with PsA who underwent sonographic assessment of 52 joints, 40 tendons, and 14 entheses as well as clinical evaluation. Overall, total sonographic enthesitis scores were significantly associated with total sonographic synovitis and sonographic tenosynovitis scores and also with older age, male sex, swollen joint count, C-reactive protein, physical occupation, and patient-reported outcomes. The association between enthesitis and synovitis was also demonstrated at the elbows, knees, and ankles. This study demonstrates that psoriatic enthesitis and synovitis are closely related and thus may share pathophysiologic mechanisms. Longitudinal studies in very early PsA using ultrasound might provide clues to confirm the hypothesis that psoriatic synovitis is secondary to enthesitis.
Another important domain that is increasingly studied is axial PsA. Currently, the evidence for treatment of axial PsA is extrapolated from that for axial spondyloarthritis (SpA), in the belief that the two diseases are pathophysiologically similar. However, there is increasing evidence for differences between axial PsA and axial SpA that might influence the choice of treatment. In a recent study, de Hooge and colleagues demonstrated that patients with axial PsA have lower severity of damage to the spine compared with those with axial SpA. Using data from 312 patients with PsA and 213 patients with SpA who underwent radiographic imaging assessment in the Belgian Epidemiological Psoriatic Arthritis Study (BEPAS) and the Ghent and Belgian Inflammatory Arthritis and Spondylitis (Be-GIANT) study, respectively, they show that the proportion of patients with PsA vs SpA having spinal damage was comparable. Patients with SpA and spinal damage had higher modified Stoke Ankylosing Spondylitis Spine Scores, indicating more severe damage. These results are consistent with other published studies and indicate that patients with PsA have less severe spinal disease compared with other patients with axial SpA. Randomized controlled trials (RCTs) specifically investigating the treatment of axial PsA are currently underway. Nevertheless, post hoc analyses of data from PsA RCTs indicate that most drugs efficacious for PsA overall also provide benefit in axial disease.
In a recent report, Baraliakos and colleagues analyzed data from the SELECT-PsA 1 and SELECT-PsA 2 trials that evaluated the efficacy of upadacitinib in PsA. They show that, compared with placebo, 15 mg upadacitinib led to a greater improvement in axial symptoms. The improvement in overall Bath Ankylosing Spondylitis Disease Activity Index score at week 24 was significantly higher with 15 mg upadacitinib compared with placebo in both trials. However, these results are not definitive because there is yet no consensus on the definition of and outcome measures for axial PsA.
Commentary: Pregnancy, neoadjuvant treatment, and sexual function after BC diagnosis, June 2023

The advantages of neoadjuvant therapy (NAT), including the downstaging of the primary tumor/nodal burden and assessment of the tumor biology via response to chemotherapy, can have prognostic and therapeutic implications in the adjuvant setting. Additionally, trials in the neoadjuvant space allow rapid assessment of new agents that can help patients gain access to these therapies in an expedited fashion. Three-year outcomes from the neoadjuvant I-SPY2 trial have shown that achievement of pathologic complete response (pCR) after NAT is associated with an approximately 80% reduction in recurrence rate, regardless of molecular subtype or treatment regimen (including various novel therapy combinations).3 An analysis of individual data from 3710 patients with human epidermal growth factor receptor 2 (HER2)–positive early BC from 11 neoadjuvant trials evaluated additional prognostic factors to better characterize pCR (van Mackelenbergh et al). A total of 1497 patients (40%) had pCR, and these patients had improved event-free survival (hazard ratio 0.39; P < .001) and overall survival (hazard ratio 0.32 P < .001) compared to those with residual disease after NAT. Among patients who had pCR, tumor size at presentation (cT1-2 vs cT3-4) and nodal status (cN0 vs cN+) were independent prognostic factors for event-free survival (hazard ratio 0.67 [P = .007] and 0.72 [P = .039], respectively). These data support the role of pCR as an indicator of outcome post-NAT and, furthermore, identify additional features beyond pCR that can affect recurrence risk. It is valuable to take these other factors into account when considering patients for adjuvant therapies, even in the context of pCR.
Advances in detection modalities and treatments have led to improved survival after BC diagnosis, and as a result, more women in the survivorship setting are experiencing side effects that affect quality of life. The prevalence of sexual dysfunction is variable, perhaps owing to how this variable is defined and reported, and includes symptoms of low libido, dyspareunia, vaginal dryness, and anorgasmia.4 Chang and colleagues performed a population-based study evaluating sexual dysfunction among a cohort of 19,709 BC survivors ≥ 18 years of age from the Utah Cancer Registry and 93,389 cancer-free women matched by age and birth state from the general population. BC survivors had a higher risk for sexual dysfunction (hazard ratio 1.60; 95% CI 1.51-1.70) compared with the general population, and this effect was more prominent within 1-5 years after diagnosis (hazard ratio 2.05; 95% CI 1.89-2.22) and in those < 50 years of age (hazard ratio 3.05; 95% CI 2.65-3.51). Furthermore, BC survivors who received chemotherapy and ET had an increased risk for sexual dysfunction (hazard ratio 1.16 and 1.46, respectively). These findings underscore the importance of recognition and communication regarding survivorship issues, such as sexual health, which can affect medication adherence, quality of life, and outcomes for patients.
Additional References
- Lambertini M, Blondeaux E, Bruzzone M, et al. Pregnancy after breast cancer: a systematic review and meta-analysis. J Clin Oncol. 2021;39:3293-3305. doi: 10.1200/JCO.200535
- Anderson RA, Lambertini M, Hall PS, et al. Survival after breast cancer in women with a subsequent live birth: Influence of age at diagnosis and interval to subsequent pregnancy. Eur J Cancer. 2022;173:113-12 doi: 10.1016/j.ejca.20206.048
- I-SPY2 Trial Consortium. Association of event-free and distant recurrence-free survival with individual-level pathologic complete response in neoadjuvant treatment of stages 2 and 3 breast cancer: three-year follow-up analysis for the I-SPY2 adaptively randomized clinical trial. JAMA Oncol. 2020;6:1355-1362. doi: 10.1001/jamaoncol.2020.2535
- Panjari M, Bell RJ, Davis SR. Sexual function after breast cancer. J Sex Med. 2011;8:294-302. doi: 10.1111/j.1743-6109.2010.0203x
The advantages of neoadjuvant therapy (NAT), including the downstaging of the primary tumor/nodal burden and assessment of the tumor biology via response to chemotherapy, can have prognostic and therapeutic implications in the adjuvant setting. Additionally, trials in the neoadjuvant space allow rapid assessment of new agents that can help patients gain access to these therapies in an expedited fashion. Three-year outcomes from the neoadjuvant I-SPY2 trial have shown that achievement of pathologic complete response (pCR) after NAT is associated with an approximately 80% reduction in recurrence rate, regardless of molecular subtype or treatment regimen (including various novel therapy combinations).3 An analysis of individual data from 3710 patients with human epidermal growth factor receptor 2 (HER2)–positive early BC from 11 neoadjuvant trials evaluated additional prognostic factors to better characterize pCR (van Mackelenbergh et al). A total of 1497 patients (40%) had pCR, and these patients had improved event-free survival (hazard ratio 0.39; P < .001) and overall survival (hazard ratio 0.32 P < .001) compared to those with residual disease after NAT. Among patients who had pCR, tumor size at presentation (cT1-2 vs cT3-4) and nodal status (cN0 vs cN+) were independent prognostic factors for event-free survival (hazard ratio 0.67 [P = .007] and 0.72 [P = .039], respectively). These data support the role of pCR as an indicator of outcome post-NAT and, furthermore, identify additional features beyond pCR that can affect recurrence risk. It is valuable to take these other factors into account when considering patients for adjuvant therapies, even in the context of pCR.
Advances in detection modalities and treatments have led to improved survival after BC diagnosis, and as a result, more women in the survivorship setting are experiencing side effects that affect quality of life. The prevalence of sexual dysfunction is variable, perhaps owing to how this variable is defined and reported, and includes symptoms of low libido, dyspareunia, vaginal dryness, and anorgasmia.4 Chang and colleagues performed a population-based study evaluating sexual dysfunction among a cohort of 19,709 BC survivors ≥ 18 years of age from the Utah Cancer Registry and 93,389 cancer-free women matched by age and birth state from the general population. BC survivors had a higher risk for sexual dysfunction (hazard ratio 1.60; 95% CI 1.51-1.70) compared with the general population, and this effect was more prominent within 1-5 years after diagnosis (hazard ratio 2.05; 95% CI 1.89-2.22) and in those < 50 years of age (hazard ratio 3.05; 95% CI 2.65-3.51). Furthermore, BC survivors who received chemotherapy and ET had an increased risk for sexual dysfunction (hazard ratio 1.16 and 1.46, respectively). These findings underscore the importance of recognition and communication regarding survivorship issues, such as sexual health, which can affect medication adherence, quality of life, and outcomes for patients.
Additional References
- Lambertini M, Blondeaux E, Bruzzone M, et al. Pregnancy after breast cancer: a systematic review and meta-analysis. J Clin Oncol. 2021;39:3293-3305. doi: 10.1200/JCO.200535
- Anderson RA, Lambertini M, Hall PS, et al. Survival after breast cancer in women with a subsequent live birth: Influence of age at diagnosis and interval to subsequent pregnancy. Eur J Cancer. 2022;173:113-12 doi: 10.1016/j.ejca.20206.048
- I-SPY2 Trial Consortium. Association of event-free and distant recurrence-free survival with individual-level pathologic complete response in neoadjuvant treatment of stages 2 and 3 breast cancer: three-year follow-up analysis for the I-SPY2 adaptively randomized clinical trial. JAMA Oncol. 2020;6:1355-1362. doi: 10.1001/jamaoncol.2020.2535
- Panjari M, Bell RJ, Davis SR. Sexual function after breast cancer. J Sex Med. 2011;8:294-302. doi: 10.1111/j.1743-6109.2010.0203x
The advantages of neoadjuvant therapy (NAT), including the downstaging of the primary tumor/nodal burden and assessment of the tumor biology via response to chemotherapy, can have prognostic and therapeutic implications in the adjuvant setting. Additionally, trials in the neoadjuvant space allow rapid assessment of new agents that can help patients gain access to these therapies in an expedited fashion. Three-year outcomes from the neoadjuvant I-SPY2 trial have shown that achievement of pathologic complete response (pCR) after NAT is associated with an approximately 80% reduction in recurrence rate, regardless of molecular subtype or treatment regimen (including various novel therapy combinations).3 An analysis of individual data from 3710 patients with human epidermal growth factor receptor 2 (HER2)–positive early BC from 11 neoadjuvant trials evaluated additional prognostic factors to better characterize pCR (van Mackelenbergh et al). A total of 1497 patients (40%) had pCR, and these patients had improved event-free survival (hazard ratio 0.39; P < .001) and overall survival (hazard ratio 0.32 P < .001) compared to those with residual disease after NAT. Among patients who had pCR, tumor size at presentation (cT1-2 vs cT3-4) and nodal status (cN0 vs cN+) were independent prognostic factors for event-free survival (hazard ratio 0.67 [P = .007] and 0.72 [P = .039], respectively). These data support the role of pCR as an indicator of outcome post-NAT and, furthermore, identify additional features beyond pCR that can affect recurrence risk. It is valuable to take these other factors into account when considering patients for adjuvant therapies, even in the context of pCR.
Advances in detection modalities and treatments have led to improved survival after BC diagnosis, and as a result, more women in the survivorship setting are experiencing side effects that affect quality of life. The prevalence of sexual dysfunction is variable, perhaps owing to how this variable is defined and reported, and includes symptoms of low libido, dyspareunia, vaginal dryness, and anorgasmia.4 Chang and colleagues performed a population-based study evaluating sexual dysfunction among a cohort of 19,709 BC survivors ≥ 18 years of age from the Utah Cancer Registry and 93,389 cancer-free women matched by age and birth state from the general population. BC survivors had a higher risk for sexual dysfunction (hazard ratio 1.60; 95% CI 1.51-1.70) compared with the general population, and this effect was more prominent within 1-5 years after diagnosis (hazard ratio 2.05; 95% CI 1.89-2.22) and in those < 50 years of age (hazard ratio 3.05; 95% CI 2.65-3.51). Furthermore, BC survivors who received chemotherapy and ET had an increased risk for sexual dysfunction (hazard ratio 1.16 and 1.46, respectively). These findings underscore the importance of recognition and communication regarding survivorship issues, such as sexual health, which can affect medication adherence, quality of life, and outcomes for patients.
Additional References
- Lambertini M, Blondeaux E, Bruzzone M, et al. Pregnancy after breast cancer: a systematic review and meta-analysis. J Clin Oncol. 2021;39:3293-3305. doi: 10.1200/JCO.200535
- Anderson RA, Lambertini M, Hall PS, et al. Survival after breast cancer in women with a subsequent live birth: Influence of age at diagnosis and interval to subsequent pregnancy. Eur J Cancer. 2022;173:113-12 doi: 10.1016/j.ejca.20206.048
- I-SPY2 Trial Consortium. Association of event-free and distant recurrence-free survival with individual-level pathologic complete response in neoadjuvant treatment of stages 2 and 3 breast cancer: three-year follow-up analysis for the I-SPY2 adaptively randomized clinical trial. JAMA Oncol. 2020;6:1355-1362. doi: 10.1001/jamaoncol.2020.2535
- Panjari M, Bell RJ, Davis SR. Sexual function after breast cancer. J Sex Med. 2011;8:294-302. doi: 10.1111/j.1743-6109.2010.0203x
CardioMEMS boosts QoL, curbs HF hospitalizations: MONITOR-HF
In the first randomized clinical trial of remote pulmonary artery pressure–guided monitoring and management of chronic heart failure (HF) in Europe, the intervention “substantially” improved quality of life (QoL) and reduced HF hospitalizations, new data show.
The CardioMEMS-HF system (Abbot Laboratories) used in the trial, called MONITOR-HF, remotely monitors changes in pulmonary artery pressure and provides an early warning of worsening HF.
Jasper Brugts, MD, PhD, of Erasmus MC University Medical Centre, Rotterdam, the Netherlands, said in an interview, “The concordance on outcomes of the three CardioMEMS trials across different eras, evolving GDMT [guideline-directed medical therapy], different conditions (pandemic), and different health care systems is reassuring and supportive of technologies such as CardioMEMS to improve patient monitoring to prevent HF hospitalizations and improve QoL.”
Dr. Brugts presented the study at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions.
(11 vs. 17), in comparison with standard of care, Dr. Brugts told meeting attendees.
Furthermore, CardioMEMS monitors hypervolemia as well as hypovolemia, enabling “fine-tuning of diuretics.”
The presentation drew such applause that one chairperson described it as “close to a standing ovation.” The study was published simultaneously in The Lancet.
Aggregate evidence
Early clinical evidence of the benefits of remote monitoring with the CardioMEMS-HF system was provided by the CHAMPION trial, which included patients with New York Heart Association (NYHA) class III heart failure.
Results of the subsequent GUIDE-HF trial, which aimed to test a broader population of patients with NYHA class II–IV heart failure and either increased N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentrations or hospitalization, were inconclusive.
However, a pre–COVID-19 impact analysis of GUIDE-HF indicated a possible benefit, which was primarily driven by a lower HF hospitalization rate, compared with the control group. That finding was the basis for an expanded indication for the system from the U.S. Food and Drug Administration.
The 2022 FDA indication permits the use of CardioMEMS for patients with NYHA class II HF and for those with worsening HF, as assessed by elevated natriuretic peptide levels.
From United States to Europe
Aware that most CardioMEMS data came from U.S. trials, the investigators embarked on the current trial, MONITOR-HF, an open-label, randomized trial in 25 centers in the Netherlands. Eligible patients had chronic NYHA class III HF, irrespective of ejection fraction, and had previously undergone hospitalization for HF.
A total of 348 patients were randomly assigned to either CardioMEMS-HF or standard of care (SoC) between 2019 and 2022.The median age of the patients was 69 years, and the median ejection fraction was 30%.
All patients were scheduled to be seen by their clinician at 3 months, 6 months, and every 6 months thereafter for up to 48 months.
The primary endpoint was the mean difference in the Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score at 12 months
That difference between groups was 7.13 (+7.05 in the CardioMEMS group and –0.08 in the SoC group).
In the responder analysis, the odds ratio of an improvement of at least 5 points in the KCCQ overall summary score was 1.69 in the CardioMEMS group vs. the SoC group; the OR of a deterioration of at least 5 points was 0.45.
Subgroup analyses showed no relevant heterogeneity in the treatment effect on total HF hospitalizations and, notably, no significant interaction in patients with an EF below 40% and an EF above 40%.
There was a significant reduction in the median NT-proBNP change from baseline only in the remote monitoring group (800 pg/mL) and a smaller, nonsignificant difference with SoC.
Both groups received highly appropriate background guideline–directed medical therapy throughout the study. There were no significant between-group differences at 12 months.
Freedom from device-related or system-related complications and sensor failure were 97.7% and 98.8%, respectively.
Two sensor failures occurred during a mean follow-up 1.8 years. The percentage of failures was comparable to CHAMPION and GUIDE-HF trials.
The trial was not powered to assess a mortality benefit.
Pick the right patients
“As in the U.S. trials, there will be side effects, so select the right patients, because [remote monitoring] is not without risk,” Dr. Brugts told meeting attendees.
That point also was made by Christiane E. Angermann of University and University Hospital Würzburg, Germany, in a related editorial in The Lancet.
“To reproduce these results on a large scale in real-life health care, diligent patient selection should identify those at high risk of heart failure–related hospitalization who agree with the concept of daily data collection and are able and motivated to comply with treatment recommendations even if asymptomatic,” Dr. Angermann writes.
“Without direct interaction between health care providers and patients, and timely treatment modification triggered by abnormal monitoring results, the care cycle might break and the potential benefits from early detection of decompensation would be lost.”
Val Rakita, MD, assistant professor of medicine at Temple University, Philadelphia, a specialist in advanced heart failure and main implanter of the CardioMEMS device at Temple University Hospital, commented on the study for this article.
“This study confirms the previous data that the device is very safe and effective in preventing HF hospitalizations and improving patients’ quality of life, even in a different population with more modern background guideline-directed medical therapy.”
Nevertheless, he noted, “Studies have yet to confirm a mortality benefit, despite logic telling us that preventing heart failure hospitalizations should also improve patient survival. More studies are needed to see if a survival benefit can be proven over a longer follow-up period.”
Overall, he said, “Remote monitoring allows more precise management of medications, prevention of hospitalizations, and improvement in quality of life, and I am an advocate for it in my practice.”
Not everyone is an advocate, however. In a commentary published last year, John M. Mandrola, MD, a cardiac electrophysiologist at Baptist Medical Associates in Louisville, Ky., said the expanded FDA indication for the device is the result of “dubious trial analysis, spin, lax regulation, and the growth of low-value care.”
Others also have questioned the device’s value in the clinic.
But at least for now, as Dr. Angermann writes, “Scientific evidence supports the use of the CardioMEMS-HF system to enhance remote patient management in heart failure care. For more widespread application, technological advancements are desirable to provide more comfort for patients and reusable external device components, thereby improving care experience and saving resources.”
The MONITOR-HF trial is funded by the Dutch Ministry of Health and Health Care institute. Dr. Brugts has an independent research grant from Abbott (investigator-sponsored study) and has had speaker engagements or has participated in advisory boards for Abbott and other pharmaceutical companies. Dr. Angermann has received personal fees from Abbott for serving as chair of the steering committee for the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF) and consulting fees, honoraria, and travel costs from Abbott. Dr. Rakita has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In the first randomized clinical trial of remote pulmonary artery pressure–guided monitoring and management of chronic heart failure (HF) in Europe, the intervention “substantially” improved quality of life (QoL) and reduced HF hospitalizations, new data show.
The CardioMEMS-HF system (Abbot Laboratories) used in the trial, called MONITOR-HF, remotely monitors changes in pulmonary artery pressure and provides an early warning of worsening HF.
Jasper Brugts, MD, PhD, of Erasmus MC University Medical Centre, Rotterdam, the Netherlands, said in an interview, “The concordance on outcomes of the three CardioMEMS trials across different eras, evolving GDMT [guideline-directed medical therapy], different conditions (pandemic), and different health care systems is reassuring and supportive of technologies such as CardioMEMS to improve patient monitoring to prevent HF hospitalizations and improve QoL.”
Dr. Brugts presented the study at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions.
(11 vs. 17), in comparison with standard of care, Dr. Brugts told meeting attendees.
Furthermore, CardioMEMS monitors hypervolemia as well as hypovolemia, enabling “fine-tuning of diuretics.”
The presentation drew such applause that one chairperson described it as “close to a standing ovation.” The study was published simultaneously in The Lancet.
Aggregate evidence
Early clinical evidence of the benefits of remote monitoring with the CardioMEMS-HF system was provided by the CHAMPION trial, which included patients with New York Heart Association (NYHA) class III heart failure.
Results of the subsequent GUIDE-HF trial, which aimed to test a broader population of patients with NYHA class II–IV heart failure and either increased N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentrations or hospitalization, were inconclusive.
However, a pre–COVID-19 impact analysis of GUIDE-HF indicated a possible benefit, which was primarily driven by a lower HF hospitalization rate, compared with the control group. That finding was the basis for an expanded indication for the system from the U.S. Food and Drug Administration.
The 2022 FDA indication permits the use of CardioMEMS for patients with NYHA class II HF and for those with worsening HF, as assessed by elevated natriuretic peptide levels.
From United States to Europe
Aware that most CardioMEMS data came from U.S. trials, the investigators embarked on the current trial, MONITOR-HF, an open-label, randomized trial in 25 centers in the Netherlands. Eligible patients had chronic NYHA class III HF, irrespective of ejection fraction, and had previously undergone hospitalization for HF.
A total of 348 patients were randomly assigned to either CardioMEMS-HF or standard of care (SoC) between 2019 and 2022.The median age of the patients was 69 years, and the median ejection fraction was 30%.
All patients were scheduled to be seen by their clinician at 3 months, 6 months, and every 6 months thereafter for up to 48 months.
The primary endpoint was the mean difference in the Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score at 12 months
That difference between groups was 7.13 (+7.05 in the CardioMEMS group and –0.08 in the SoC group).
In the responder analysis, the odds ratio of an improvement of at least 5 points in the KCCQ overall summary score was 1.69 in the CardioMEMS group vs. the SoC group; the OR of a deterioration of at least 5 points was 0.45.
Subgroup analyses showed no relevant heterogeneity in the treatment effect on total HF hospitalizations and, notably, no significant interaction in patients with an EF below 40% and an EF above 40%.
There was a significant reduction in the median NT-proBNP change from baseline only in the remote monitoring group (800 pg/mL) and a smaller, nonsignificant difference with SoC.
Both groups received highly appropriate background guideline–directed medical therapy throughout the study. There were no significant between-group differences at 12 months.
Freedom from device-related or system-related complications and sensor failure were 97.7% and 98.8%, respectively.
Two sensor failures occurred during a mean follow-up 1.8 years. The percentage of failures was comparable to CHAMPION and GUIDE-HF trials.
The trial was not powered to assess a mortality benefit.
Pick the right patients
“As in the U.S. trials, there will be side effects, so select the right patients, because [remote monitoring] is not without risk,” Dr. Brugts told meeting attendees.
That point also was made by Christiane E. Angermann of University and University Hospital Würzburg, Germany, in a related editorial in The Lancet.
“To reproduce these results on a large scale in real-life health care, diligent patient selection should identify those at high risk of heart failure–related hospitalization who agree with the concept of daily data collection and are able and motivated to comply with treatment recommendations even if asymptomatic,” Dr. Angermann writes.
“Without direct interaction between health care providers and patients, and timely treatment modification triggered by abnormal monitoring results, the care cycle might break and the potential benefits from early detection of decompensation would be lost.”
Val Rakita, MD, assistant professor of medicine at Temple University, Philadelphia, a specialist in advanced heart failure and main implanter of the CardioMEMS device at Temple University Hospital, commented on the study for this article.
“This study confirms the previous data that the device is very safe and effective in preventing HF hospitalizations and improving patients’ quality of life, even in a different population with more modern background guideline-directed medical therapy.”
Nevertheless, he noted, “Studies have yet to confirm a mortality benefit, despite logic telling us that preventing heart failure hospitalizations should also improve patient survival. More studies are needed to see if a survival benefit can be proven over a longer follow-up period.”
Overall, he said, “Remote monitoring allows more precise management of medications, prevention of hospitalizations, and improvement in quality of life, and I am an advocate for it in my practice.”
Not everyone is an advocate, however. In a commentary published last year, John M. Mandrola, MD, a cardiac electrophysiologist at Baptist Medical Associates in Louisville, Ky., said the expanded FDA indication for the device is the result of “dubious trial analysis, spin, lax regulation, and the growth of low-value care.”
Others also have questioned the device’s value in the clinic.
But at least for now, as Dr. Angermann writes, “Scientific evidence supports the use of the CardioMEMS-HF system to enhance remote patient management in heart failure care. For more widespread application, technological advancements are desirable to provide more comfort for patients and reusable external device components, thereby improving care experience and saving resources.”
The MONITOR-HF trial is funded by the Dutch Ministry of Health and Health Care institute. Dr. Brugts has an independent research grant from Abbott (investigator-sponsored study) and has had speaker engagements or has participated in advisory boards for Abbott and other pharmaceutical companies. Dr. Angermann has received personal fees from Abbott for serving as chair of the steering committee for the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF) and consulting fees, honoraria, and travel costs from Abbott. Dr. Rakita has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
In the first randomized clinical trial of remote pulmonary artery pressure–guided monitoring and management of chronic heart failure (HF) in Europe, the intervention “substantially” improved quality of life (QoL) and reduced HF hospitalizations, new data show.
The CardioMEMS-HF system (Abbot Laboratories) used in the trial, called MONITOR-HF, remotely monitors changes in pulmonary artery pressure and provides an early warning of worsening HF.
Jasper Brugts, MD, PhD, of Erasmus MC University Medical Centre, Rotterdam, the Netherlands, said in an interview, “The concordance on outcomes of the three CardioMEMS trials across different eras, evolving GDMT [guideline-directed medical therapy], different conditions (pandemic), and different health care systems is reassuring and supportive of technologies such as CardioMEMS to improve patient monitoring to prevent HF hospitalizations and improve QoL.”
Dr. Brugts presented the study at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions.
(11 vs. 17), in comparison with standard of care, Dr. Brugts told meeting attendees.
Furthermore, CardioMEMS monitors hypervolemia as well as hypovolemia, enabling “fine-tuning of diuretics.”
The presentation drew such applause that one chairperson described it as “close to a standing ovation.” The study was published simultaneously in The Lancet.
Aggregate evidence
Early clinical evidence of the benefits of remote monitoring with the CardioMEMS-HF system was provided by the CHAMPION trial, which included patients with New York Heart Association (NYHA) class III heart failure.
Results of the subsequent GUIDE-HF trial, which aimed to test a broader population of patients with NYHA class II–IV heart failure and either increased N-terminal-pro-B-type natriuretic peptide (NT-proBNP) concentrations or hospitalization, were inconclusive.
However, a pre–COVID-19 impact analysis of GUIDE-HF indicated a possible benefit, which was primarily driven by a lower HF hospitalization rate, compared with the control group. That finding was the basis for an expanded indication for the system from the U.S. Food and Drug Administration.
The 2022 FDA indication permits the use of CardioMEMS for patients with NYHA class II HF and for those with worsening HF, as assessed by elevated natriuretic peptide levels.
From United States to Europe
Aware that most CardioMEMS data came from U.S. trials, the investigators embarked on the current trial, MONITOR-HF, an open-label, randomized trial in 25 centers in the Netherlands. Eligible patients had chronic NYHA class III HF, irrespective of ejection fraction, and had previously undergone hospitalization for HF.
A total of 348 patients were randomly assigned to either CardioMEMS-HF or standard of care (SoC) between 2019 and 2022.The median age of the patients was 69 years, and the median ejection fraction was 30%.
All patients were scheduled to be seen by their clinician at 3 months, 6 months, and every 6 months thereafter for up to 48 months.
The primary endpoint was the mean difference in the Kansas City Cardiomyopathy Questionnaire (KCCQ) summary score at 12 months
That difference between groups was 7.13 (+7.05 in the CardioMEMS group and –0.08 in the SoC group).
In the responder analysis, the odds ratio of an improvement of at least 5 points in the KCCQ overall summary score was 1.69 in the CardioMEMS group vs. the SoC group; the OR of a deterioration of at least 5 points was 0.45.
Subgroup analyses showed no relevant heterogeneity in the treatment effect on total HF hospitalizations and, notably, no significant interaction in patients with an EF below 40% and an EF above 40%.
There was a significant reduction in the median NT-proBNP change from baseline only in the remote monitoring group (800 pg/mL) and a smaller, nonsignificant difference with SoC.
Both groups received highly appropriate background guideline–directed medical therapy throughout the study. There were no significant between-group differences at 12 months.
Freedom from device-related or system-related complications and sensor failure were 97.7% and 98.8%, respectively.
Two sensor failures occurred during a mean follow-up 1.8 years. The percentage of failures was comparable to CHAMPION and GUIDE-HF trials.
The trial was not powered to assess a mortality benefit.
Pick the right patients
“As in the U.S. trials, there will be side effects, so select the right patients, because [remote monitoring] is not without risk,” Dr. Brugts told meeting attendees.
That point also was made by Christiane E. Angermann of University and University Hospital Würzburg, Germany, in a related editorial in The Lancet.
“To reproduce these results on a large scale in real-life health care, diligent patient selection should identify those at high risk of heart failure–related hospitalization who agree with the concept of daily data collection and are able and motivated to comply with treatment recommendations even if asymptomatic,” Dr. Angermann writes.
“Without direct interaction between health care providers and patients, and timely treatment modification triggered by abnormal monitoring results, the care cycle might break and the potential benefits from early detection of decompensation would be lost.”
Val Rakita, MD, assistant professor of medicine at Temple University, Philadelphia, a specialist in advanced heart failure and main implanter of the CardioMEMS device at Temple University Hospital, commented on the study for this article.
“This study confirms the previous data that the device is very safe and effective in preventing HF hospitalizations and improving patients’ quality of life, even in a different population with more modern background guideline-directed medical therapy.”
Nevertheless, he noted, “Studies have yet to confirm a mortality benefit, despite logic telling us that preventing heart failure hospitalizations should also improve patient survival. More studies are needed to see if a survival benefit can be proven over a longer follow-up period.”
Overall, he said, “Remote monitoring allows more precise management of medications, prevention of hospitalizations, and improvement in quality of life, and I am an advocate for it in my practice.”
Not everyone is an advocate, however. In a commentary published last year, John M. Mandrola, MD, a cardiac electrophysiologist at Baptist Medical Associates in Louisville, Ky., said the expanded FDA indication for the device is the result of “dubious trial analysis, spin, lax regulation, and the growth of low-value care.”
Others also have questioned the device’s value in the clinic.
But at least for now, as Dr. Angermann writes, “Scientific evidence supports the use of the CardioMEMS-HF system to enhance remote patient management in heart failure care. For more widespread application, technological advancements are desirable to provide more comfort for patients and reusable external device components, thereby improving care experience and saving resources.”
The MONITOR-HF trial is funded by the Dutch Ministry of Health and Health Care institute. Dr. Brugts has an independent research grant from Abbott (investigator-sponsored study) and has had speaker engagements or has participated in advisory boards for Abbott and other pharmaceutical companies. Dr. Angermann has received personal fees from Abbott for serving as chair of the steering committee for the CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF) and consulting fees, honoraria, and travel costs from Abbott. Dr. Rakita has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ESC HEART FAILURE 2023
Losing weight may bolster AFib ablation’s chances for success: LEAF interim results
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.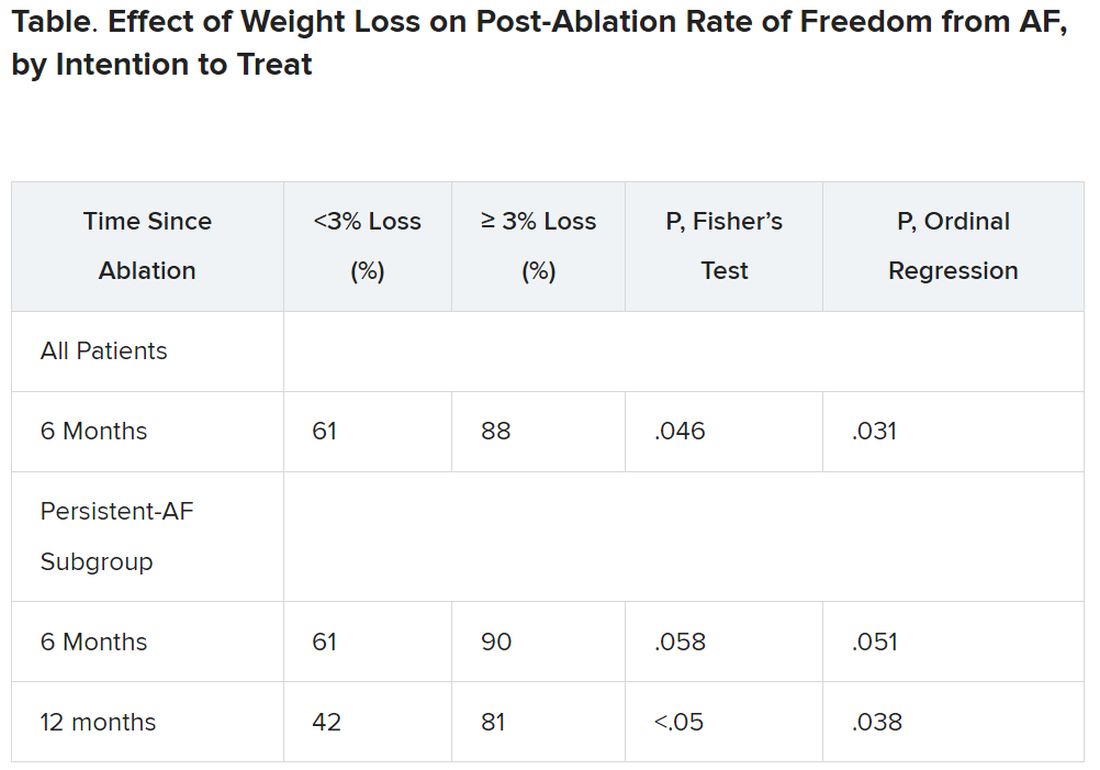
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new analysis suggests.
The finding comes from a small study that entered such patients with paroxysmal and especially persistent AFib who were candidates for ablation. Those shedding at least 3% of body weight in the months before the procedure while engaged in a structured risk-factor modification (RFM) program were “dramatically” more likely to be AFib-free 6 months later.
The improved ablation efficacy, compared with results in similar patients who didn’t lose as much weight, was most pronounced among those whose AFib had been the persistent form, reported investigators at the annual scientific sessions of the Heart Rhythm Society, held in New Orleans.
Of note, ablations in the study were consistently limited, as much as possible, to standard pulmonary-vein isolation (PVI).
Associations between AFib and obesity and other behavioral and lifestyle-related risk factors are well recognized, but the limited studies of their effect on AFib ablation success have been inconsistent. The current analysis, the group says, points specifically to preablation weight loss as means to improving AFib-ablation outcomes.
“Adjunctive therapy focused on weight loss should be incorporated in the treatment plan for obese patients undergoing ablation for atrial fibrillation,” Jeffrey J. Goldberger, MD, MBA, of the University of Miami, said when presenting the new results at the HRS sessions.
Such a plan is entirely consistent with recent guidelines and especially a 2020 American Heart Association (AHA) consensus statement, but is inconsistently and perhaps even seldom realized in clinical practice.
Dramatic increase in success
Even modest weight loss before ablation may help, proposed Dr. Goldberger, who directs his institution’s Center for Atrial Fibrillation. Decreases for the greater-weight-loss group actually averaged less than 6% of baseline body weight.
Yet it was apparently enough to improve ablation outcomes significantly: Eighty-eight percent were free of AFib 6 months after the procedure, compared with 61% for patients who lost less than 3% of their preablation weight.
For improving ablation success, he said, “We’re talking about a moderate amount of weight loss. These patients are not going from being obese to being thin. They’re still quite overweight.”
In an analysis limited to the four-fifths of patients with persistent AFib, “we saw the same pattern,” Dr. Goldberger said at a media presentation prior to his formal report at the HRS sessions.
Moreover, that subgroup’s benefit persisted out to 12 months, at which time 42% and 81% of patients with less and greater weight loss, respectively, were free of AFib. That represents, he said, “a really tremendous – dramatic, actually – increase in success of pulmonary vein isolation in those who lost weight.”
“We’ve known for a long time that weight loss is important for preventing atrial fibrillation or increasing the success rates of the different treatments we use,” Cynthia M. Tracy, MD, said in an interview. “Probably in some studies, weight loss has been as effective as antiarrhythmics.”
A loss of 3% body weight “is not a lot,” she said. In the current analysis, “It’s notable that it made that much difference with even a fairly modest amount of weight loss.”
Now when asked, “ ‘How much do I have to lose before you’ll consider doing my ablation?’ we have a bit more concrete data to give patients and doctors as to what amount might be beneficial,” said Dr. Tracy of George Washington University Hospital, Washington, who is not associated with the study.
Evolving view of AFib
The findings are emblematic of the profession’s evolving view of AFib and its management, Dr. Goldberger observed at the press conference. Should clinicians think of AFib as similar to “a disease like Wolff-Parkinson-White syndrome,” in which the patient usually has a successful ablation, and then “we expect that to last in perpetuity with no further interventions?”
Or, he said, “is atrial fibrillation more a disease like coronary artery disease, where even if they have an intervention, the disease process is still ongoing and requires long-term disease management? I think it’s pretty clear that we’re dealing with the latter case.”
Dr. Goldberger’s report was an interim analysis of an ongoing randomized trial called LEAF (Liraglutide Effect on Atrial Fibrillation), which is comparing patients with AFib assigned to “take” vs. “not take” the GLP-1 receptor agonist liraglutide, an antidiabetic (Victoza) and weight-loss (Saxenda) drug. The trial aims to assess the drug’s apparent ability to shrink atrial epicardial adipose tissue which, Dr. Goldberger said, is thought to contribute to AFib development and influence AFib-ablation outcomes.
It’s unknown and a limitation of the current analysis, he said, whether the observed link between improved preablation–weight ablation success “is specifically related to weight loss, liraglutide treatment, or both.”
As the invited discussant for Dr. Goldberger’s presentation, David Frankel, MD, observed that studies have been inconsistent on whether substantial weight loss may improve the results of AFib rhythm-control therapy.
Those finding such an association, including LEAF and the influential LEGACY study, differed from others showing a null effect by including “a comprehensive risk factor management” program, observed Dr. Frankel, of the Hospital of the University of Pennsylvania and Penn Heart and Vascular Center, Philadelphia.
Rather than focusing solely on weight loss or sleep apnea as AFib risk factors, he said, the studies linking weight loss to AFib rhythm control also included “hypertension, diabetes, hyperlipidemia, smoking cessation, and alcohol reduction,” Dr. Frankel said. “So it seems clear that to significantly impact AF recurrence, we need to focus on all these contributors to metabolic syndrome.”
Comprehensive risk-factor management
LEAF entered patients with AFib, 79% of whom had persistent AF and the rest paroxysmal AF, who followed the RFM program and were randomly assigned also to take liraglutide or placebo. The “nurse-practitioner-led” RFM program, conducted both in-clinic and online, featured “established goals for each patient” using AHA diet and lifestyle recommendations, an exercise prescription, dietary counseling, evaluation and treatment of sleep apnea, and measures to control any diabetes, hyperlipidemia, or hypertension, Dr. Goldberger said. And patients “were counseled on alcohol reduction and smoking cessation as necessary.”
After 3 months, 29 and 30 patients – regardless of randomization assignment – had lost < 3% and at least 3% of baseline body weight, respectively.
Catheter ablation achieved PVI in all patients. A 3-month blanking period followed, after which they went off antiarrhythmic meds.
It’s very difficult for patients to lose 10% or more of body weight, “and it would not happen overnight,” Dr. Tracy observed. “These are symptomatic patients, for the most part, if they get referred to an electrophysiologist. So you don’t want to defer them indefinitely.”
The current findings, she said, point to “a more realistic target,” suggesting that weight loss of at least 3% should improve AFib ablation’s chances for success.
Dr. Goldberger disclosed ties to Medtronic. Dr. Frankel disclosed ties to Medtronic, Stryker, Biosense Webster, and Boston Scientific. Dr. Tracy reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HEART RHYTHM 2023
AI & U
Since the November 2022 release of a much-discussed artificial intelligence (AI)-based chatbot, I have been curious what all the buzz is about. I decided to engage my well-connected software-savvy son-in-law to hear where he thought things were going.
He started by suggesting that I pose a question to the chatbot about something of which I had some current knowledge. I had recently researched the concept of primal beliefs and so we asked the chatbot to write a short essay about when an individual develops his/her primal beliefs.

In a matter of seconds the “machine” spit out a very readable document that included all the information that had taken me several hours to unearth and digest. And ... it included the references that I had determined to be valid and appropriate. It was an impressive performance to say the least.
Obviously, a technological development with this capability is sending tremors through the educational establishment. One can easily think of several human skills that an AI like this might eventually make superfluous. It will also make it increasingly difficult for educators to determine a students’ true abilities – research, synthesis, and writing to name just a few. But, of course, one could question whether we will need to teach and then test for these skills that the chatbot can perform more quickly. I’m going to leave it to the educators to struggle with that question.
In the long term you and I may find that AI is a serious threat to our existence as health care providers. In the meantime
My first thought is that if I were having trouble arriving at a diagnosis, I might appreciate having a chatbot to ask for help. Of course this would require that I had already taken a history, done a good exam, and ordered some obvious lab and imaging studies. It would also mean that I had decent knowledge and understanding of basic pathophysiology and was capable of thinking broadly enough to ask a question that would give me the greatest chance of getting the correct answer.
Knowing how to ask the right question is a skill that can be taught. For example, my wife is a successful and experienced online shopper but she acknowledges that when we have medical questions, I can often find the answer more quickly than she can. My relative success usually hinges on my choice of the key word(s) to begin the search, clearly the result of my medical training.
Once I have received a list of possible diagnoses from the chatbot, I must then be able to evaluate the validity and applicability of the references it has supplied. That too is a skill that can be taught. And, for the moment the critical importance of having these two skills suggests that graduating from medical school will continue to give us some job security in the face of expanding AI.
The same process I could used to coax the chatbot to arrive at a diagnosis could be applied when faced with a therapeutic question. Is surgery better than a pharmacological approach? If I need help with a dosage regimen, I could find this information online now. But, wouldn’t it be quicker and maybe better if I asked the chatbot to do the research for me and print a short essay on the pros and cons of different management approaches?
Once I’ve made the diagnosis, crafted a management plan, and now want to hand the patient a document in his/her primary language and at his/her reading skill level describing the diagnosis and giving detailed instructions to follow, this would seem to be a piece of cake for a chatbot given the appropriate commands. Hopefully I would remember to include the disclaimer that “This document was created with the help of a chatbot.”
Clearly, there is nothing to prevent our patients from asking the chatbot the same questions I have posed. And, no doubt, this will happen. It is already happening in a more cumbersome fashion when patients research their own symptoms. However, in the short term I believe we will retain the upper hand.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Since the November 2022 release of a much-discussed artificial intelligence (AI)-based chatbot, I have been curious what all the buzz is about. I decided to engage my well-connected software-savvy son-in-law to hear where he thought things were going.
He started by suggesting that I pose a question to the chatbot about something of which I had some current knowledge. I had recently researched the concept of primal beliefs and so we asked the chatbot to write a short essay about when an individual develops his/her primal beliefs.
In a matter of seconds the “machine” spit out a very readable document that included all the information that had taken me several hours to unearth and digest. And ... it included the references that I had determined to be valid and appropriate. It was an impressive performance to say the least.
Obviously, a technological development with this capability is sending tremors through the educational establishment. One can easily think of several human skills that an AI like this might eventually make superfluous. It will also make it increasingly difficult for educators to determine a students’ true abilities – research, synthesis, and writing to name just a few. But, of course, one could question whether we will need to teach and then test for these skills that the chatbot can perform more quickly. I’m going to leave it to the educators to struggle with that question.
In the long term you and I may find that AI is a serious threat to our existence as health care providers. In the meantime
My first thought is that if I were having trouble arriving at a diagnosis, I might appreciate having a chatbot to ask for help. Of course this would require that I had already taken a history, done a good exam, and ordered some obvious lab and imaging studies. It would also mean that I had decent knowledge and understanding of basic pathophysiology and was capable of thinking broadly enough to ask a question that would give me the greatest chance of getting the correct answer.
Knowing how to ask the right question is a skill that can be taught. For example, my wife is a successful and experienced online shopper but she acknowledges that when we have medical questions, I can often find the answer more quickly than she can. My relative success usually hinges on my choice of the key word(s) to begin the search, clearly the result of my medical training.
Once I have received a list of possible diagnoses from the chatbot, I must then be able to evaluate the validity and applicability of the references it has supplied. That too is a skill that can be taught. And, for the moment the critical importance of having these two skills suggests that graduating from medical school will continue to give us some job security in the face of expanding AI.
The same process I could used to coax the chatbot to arrive at a diagnosis could be applied when faced with a therapeutic question. Is surgery better than a pharmacological approach? If I need help with a dosage regimen, I could find this information online now. But, wouldn’t it be quicker and maybe better if I asked the chatbot to do the research for me and print a short essay on the pros and cons of different management approaches?
Once I’ve made the diagnosis, crafted a management plan, and now want to hand the patient a document in his/her primary language and at his/her reading skill level describing the diagnosis and giving detailed instructions to follow, this would seem to be a piece of cake for a chatbot given the appropriate commands. Hopefully I would remember to include the disclaimer that “This document was created with the help of a chatbot.”
Clearly, there is nothing to prevent our patients from asking the chatbot the same questions I have posed. And, no doubt, this will happen. It is already happening in a more cumbersome fashion when patients research their own symptoms. However, in the short term I believe we will retain the upper hand.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Since the November 2022 release of a much-discussed artificial intelligence (AI)-based chatbot, I have been curious what all the buzz is about. I decided to engage my well-connected software-savvy son-in-law to hear where he thought things were going.
He started by suggesting that I pose a question to the chatbot about something of which I had some current knowledge. I had recently researched the concept of primal beliefs and so we asked the chatbot to write a short essay about when an individual develops his/her primal beliefs.
In a matter of seconds the “machine” spit out a very readable document that included all the information that had taken me several hours to unearth and digest. And ... it included the references that I had determined to be valid and appropriate. It was an impressive performance to say the least.
Obviously, a technological development with this capability is sending tremors through the educational establishment. One can easily think of several human skills that an AI like this might eventually make superfluous. It will also make it increasingly difficult for educators to determine a students’ true abilities – research, synthesis, and writing to name just a few. But, of course, one could question whether we will need to teach and then test for these skills that the chatbot can perform more quickly. I’m going to leave it to the educators to struggle with that question.
In the long term you and I may find that AI is a serious threat to our existence as health care providers. In the meantime
My first thought is that if I were having trouble arriving at a diagnosis, I might appreciate having a chatbot to ask for help. Of course this would require that I had already taken a history, done a good exam, and ordered some obvious lab and imaging studies. It would also mean that I had decent knowledge and understanding of basic pathophysiology and was capable of thinking broadly enough to ask a question that would give me the greatest chance of getting the correct answer.
Knowing how to ask the right question is a skill that can be taught. For example, my wife is a successful and experienced online shopper but she acknowledges that when we have medical questions, I can often find the answer more quickly than she can. My relative success usually hinges on my choice of the key word(s) to begin the search, clearly the result of my medical training.
Once I have received a list of possible diagnoses from the chatbot, I must then be able to evaluate the validity and applicability of the references it has supplied. That too is a skill that can be taught. And, for the moment the critical importance of having these two skills suggests that graduating from medical school will continue to give us some job security in the face of expanding AI.
The same process I could used to coax the chatbot to arrive at a diagnosis could be applied when faced with a therapeutic question. Is surgery better than a pharmacological approach? If I need help with a dosage regimen, I could find this information online now. But, wouldn’t it be quicker and maybe better if I asked the chatbot to do the research for me and print a short essay on the pros and cons of different management approaches?
Once I’ve made the diagnosis, crafted a management plan, and now want to hand the patient a document in his/her primary language and at his/her reading skill level describing the diagnosis and giving detailed instructions to follow, this would seem to be a piece of cake for a chatbot given the appropriate commands. Hopefully I would remember to include the disclaimer that “This document was created with the help of a chatbot.”
Clearly, there is nothing to prevent our patients from asking the chatbot the same questions I have posed. And, no doubt, this will happen. It is already happening in a more cumbersome fashion when patients research their own symptoms. However, in the short term I believe we will retain the upper hand.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Safety remains top parent concern for HPV vaccine
, according to a study published online in Pediatrics.
“Although HPV vaccination rates in the United States have steadily improved over the past decade, a sizable subset of parents remains highly hesitant about administering the vaccine to their adolescent children,” wrote Eric Adjei Boakye, PhD, of the departments of public health sciences and otolaryngology–head and neck surgery at the Henry Ford Health System, Detroit, and associates. But a silver lining in the study is the downward trend in parents not vaccinating their children against HPV because the child’s provider did not recommend it.
“Provider recommendation has been shown to be the single best predictor of HPV vaccine uptake and vaccine acceptability,” the authors wrote. They noted one previous study finding that provider recommendations for the vaccine had increased from 27% in 2012 to 49.3% in 2018.
Safety concerns increased while other concerns decreased
The findings were not surprising to Robert A. Bednarczyk, PhD, associate professor of global health at Emory University Rollins School of Public Health, Atlanta, who specializes in HPV vaccine research.
“We have seen over the years that vaccine safety concerns have been on the increase, notably recently in the context of the COVID-19 pandemic and vaccination program, but HPV vaccine safety, though well established, continues to be a major concern for parents,” Dr. Bednarczyk said in an interview. But he found it striking that parents’ other reasons for turning down the vaccine had declined. “This shows that the outreach around the need for HPV vaccination and efforts to improve provider recommendation strategies is likely having positive impacts on HPV vaccine attitudes.”
Top five reasons for not vaccinating
The researchers analyzed data from the National Immunization Survey–Teen for the years 2010 through 2020 to track the annual changes in the top five reasons cited for not planning to get the HPV vaccine. The data covered 119,695 teens aged 13-17.
The researchers identified parents’ five most commonly cited reasons for not planning to vaccinate their children against HPV: “not necessary,” “safety concerns,” “lack of recommendation,” “lack of knowledge,” and “not sexually active.”
Parents’ HPV vaccine hesitancy decreased by 5.5% each year from 2010 to 2012, but then it stagnated for the remaining years through 2020. Across most of that time, from 2010 to 2018, parents’ concerns about the vaccine’s safety and side effects increased by 15.6%. A major reason for this increase, the authors suggested, may include the widespread distribution of online misinformation, particularly given the 7.8 million increase in antivaccine social media accounts since 2019.
“Fear tactics are often used by antivaccine campaigners to dissuade parents from vaccinating their children. There have been several myths propagated about vaccines causing adverse reactions,” the authors wrote. “Although these myths have been scientifically debunked, they continue to circulate.”
In contrast to parents’ concerns, a study in 2021 found a downward trend in reports of nonserious adverse effects and no change in reports of serious adverse effects from the HPV vaccine between 2015 and 2018. Further, more than 95% of the adverse effect reports to the Vaccine Adverse Event Reporting System after HPV vaccination were nonserious.
Reducing perceived barriers
Meanwhile, however, parents’ other reasons for avoiding the vaccine became less prevalent throughout most of the study period. For each year between 2013 and 2020, the proportion of parents saying they didn’t intend to get their children the HPV vaccine because it was “not recommended” decreased by 6.8%.
Similarly, avoiding the vaccine due to “lack of knowledge” declined 9.9%, and avoidance because the child was “not sexually active” declined 5.9% each year from 2013 to 2020. No difference occurred during that time period regarding how frequently parents cited that the vaccine was “not necessary.”
“Decreases in the percentage of parents/guardians citing lack of provider recommendation, lack of knowledge, and child ‘not sexually active’ as the main reason for HPV vaccine hesitancy ... are encouraging and suggest that interventions have been successful in reducing perceived barriers to HPV vaccination,” the authors wrote.
Dr. Bednarczyk agreed that these findings were encouraging, underscoring that outreach and support for health care providers to give strong recommendations for the vaccine need to continue.
“But additionally, we need to find better ways to communicate about vaccine safety,” Dr. Bednarczyk said. “Seeing that the number of parents citing safety concerns as the primary barrier has not changed much between 2016 and 2020, but that the percent of parents having those concerns increased, likely means there is a stable part of the population with these safety concerns, and as more adolescents are getting vaccinated against HPV, the relative contribution of safety concerns is increasing.” A key way to address those concerns includes “engaging with our trusted community partners and giving them the tools to discuss the safety of HPV vaccination with members of the community,” he said.
Debunking misinformation
Like the authors, Dr. Bednarczyk pointed out several conditions that parents erroneously worry could be caused by the HPV vaccine, but he emphasized that simply telling parents those misconceptions are untrue is insufficient to allay fears.
“It’s important for both clinicians and community partners to recognize we cannot just present a list of facts and figures and statistics to parents to reassure them and hope that this works,” Dr. Bednarczyk said. “Effective communication, strong narratives to illustrate this knowledge, and engagement with not just clinicians but community partners and other trusted sources is needed.” Dr. Bednarczyk continues to support the evidence-based model of presumptive recommendations, which does not remove parental autonomy but simplifies vaccine messaging about what’s recommended, “but clinicians need to be prepared with both the data and effective ways to communicate it to address questions if they come up after the presumptive recommendation is given,” he added.
The researchers pointed out that their study data were collected before the pandemic, so “it is reasonable to expect that HPV vaccine–related safety concerns may continue to rise because of the plethora of misinformation surrounding coronavirus disease 2019 vaccination.”
Dr. Bednarczyk said it will be important to see in future research whether shifts in beliefs about the HPV vaccine have occurred in the midst of the pandemic and afterward.
“As the authors stated, it’s important to remember that HPV vaccination has consistently been shown to be safe and effective,” Dr. Bednarczyk said. “But those research findings are not seeming to resonate with parents, highlighting how we need to improve our outreach and communication work.”
The research did not receive external funding. A coauthor is a scientific adviser to Navigating Cancer. The other authors and Dr. Bednarczyk had no disclosures.
, according to a study published online in Pediatrics.
“Although HPV vaccination rates in the United States have steadily improved over the past decade, a sizable subset of parents remains highly hesitant about administering the vaccine to their adolescent children,” wrote Eric Adjei Boakye, PhD, of the departments of public health sciences and otolaryngology–head and neck surgery at the Henry Ford Health System, Detroit, and associates. But a silver lining in the study is the downward trend in parents not vaccinating their children against HPV because the child’s provider did not recommend it.
“Provider recommendation has been shown to be the single best predictor of HPV vaccine uptake and vaccine acceptability,” the authors wrote. They noted one previous study finding that provider recommendations for the vaccine had increased from 27% in 2012 to 49.3% in 2018.
Safety concerns increased while other concerns decreased
The findings were not surprising to Robert A. Bednarczyk, PhD, associate professor of global health at Emory University Rollins School of Public Health, Atlanta, who specializes in HPV vaccine research.
“We have seen over the years that vaccine safety concerns have been on the increase, notably recently in the context of the COVID-19 pandemic and vaccination program, but HPV vaccine safety, though well established, continues to be a major concern for parents,” Dr. Bednarczyk said in an interview. But he found it striking that parents’ other reasons for turning down the vaccine had declined. “This shows that the outreach around the need for HPV vaccination and efforts to improve provider recommendation strategies is likely having positive impacts on HPV vaccine attitudes.”
Top five reasons for not vaccinating
The researchers analyzed data from the National Immunization Survey–Teen for the years 2010 through 2020 to track the annual changes in the top five reasons cited for not planning to get the HPV vaccine. The data covered 119,695 teens aged 13-17.
The researchers identified parents’ five most commonly cited reasons for not planning to vaccinate their children against HPV: “not necessary,” “safety concerns,” “lack of recommendation,” “lack of knowledge,” and “not sexually active.”
Parents’ HPV vaccine hesitancy decreased by 5.5% each year from 2010 to 2012, but then it stagnated for the remaining years through 2020. Across most of that time, from 2010 to 2018, parents’ concerns about the vaccine’s safety and side effects increased by 15.6%. A major reason for this increase, the authors suggested, may include the widespread distribution of online misinformation, particularly given the 7.8 million increase in antivaccine social media accounts since 2019.
“Fear tactics are often used by antivaccine campaigners to dissuade parents from vaccinating their children. There have been several myths propagated about vaccines causing adverse reactions,” the authors wrote. “Although these myths have been scientifically debunked, they continue to circulate.”
In contrast to parents’ concerns, a study in 2021 found a downward trend in reports of nonserious adverse effects and no change in reports of serious adverse effects from the HPV vaccine between 2015 and 2018. Further, more than 95% of the adverse effect reports to the Vaccine Adverse Event Reporting System after HPV vaccination were nonserious.
Reducing perceived barriers
Meanwhile, however, parents’ other reasons for avoiding the vaccine became less prevalent throughout most of the study period. For each year between 2013 and 2020, the proportion of parents saying they didn’t intend to get their children the HPV vaccine because it was “not recommended” decreased by 6.8%.
Similarly, avoiding the vaccine due to “lack of knowledge” declined 9.9%, and avoidance because the child was “not sexually active” declined 5.9% each year from 2013 to 2020. No difference occurred during that time period regarding how frequently parents cited that the vaccine was “not necessary.”
“Decreases in the percentage of parents/guardians citing lack of provider recommendation, lack of knowledge, and child ‘not sexually active’ as the main reason for HPV vaccine hesitancy ... are encouraging and suggest that interventions have been successful in reducing perceived barriers to HPV vaccination,” the authors wrote.
Dr. Bednarczyk agreed that these findings were encouraging, underscoring that outreach and support for health care providers to give strong recommendations for the vaccine need to continue.
“But additionally, we need to find better ways to communicate about vaccine safety,” Dr. Bednarczyk said. “Seeing that the number of parents citing safety concerns as the primary barrier has not changed much between 2016 and 2020, but that the percent of parents having those concerns increased, likely means there is a stable part of the population with these safety concerns, and as more adolescents are getting vaccinated against HPV, the relative contribution of safety concerns is increasing.” A key way to address those concerns includes “engaging with our trusted community partners and giving them the tools to discuss the safety of HPV vaccination with members of the community,” he said.
Debunking misinformation
Like the authors, Dr. Bednarczyk pointed out several conditions that parents erroneously worry could be caused by the HPV vaccine, but he emphasized that simply telling parents those misconceptions are untrue is insufficient to allay fears.
“It’s important for both clinicians and community partners to recognize we cannot just present a list of facts and figures and statistics to parents to reassure them and hope that this works,” Dr. Bednarczyk said. “Effective communication, strong narratives to illustrate this knowledge, and engagement with not just clinicians but community partners and other trusted sources is needed.” Dr. Bednarczyk continues to support the evidence-based model of presumptive recommendations, which does not remove parental autonomy but simplifies vaccine messaging about what’s recommended, “but clinicians need to be prepared with both the data and effective ways to communicate it to address questions if they come up after the presumptive recommendation is given,” he added.
The researchers pointed out that their study data were collected before the pandemic, so “it is reasonable to expect that HPV vaccine–related safety concerns may continue to rise because of the plethora of misinformation surrounding coronavirus disease 2019 vaccination.”
Dr. Bednarczyk said it will be important to see in future research whether shifts in beliefs about the HPV vaccine have occurred in the midst of the pandemic and afterward.
“As the authors stated, it’s important to remember that HPV vaccination has consistently been shown to be safe and effective,” Dr. Bednarczyk said. “But those research findings are not seeming to resonate with parents, highlighting how we need to improve our outreach and communication work.”
The research did not receive external funding. A coauthor is a scientific adviser to Navigating Cancer. The other authors and Dr. Bednarczyk had no disclosures.
, according to a study published online in Pediatrics.
“Although HPV vaccination rates in the United States have steadily improved over the past decade, a sizable subset of parents remains highly hesitant about administering the vaccine to their adolescent children,” wrote Eric Adjei Boakye, PhD, of the departments of public health sciences and otolaryngology–head and neck surgery at the Henry Ford Health System, Detroit, and associates. But a silver lining in the study is the downward trend in parents not vaccinating their children against HPV because the child’s provider did not recommend it.
“Provider recommendation has been shown to be the single best predictor of HPV vaccine uptake and vaccine acceptability,” the authors wrote. They noted one previous study finding that provider recommendations for the vaccine had increased from 27% in 2012 to 49.3% in 2018.
Safety concerns increased while other concerns decreased
The findings were not surprising to Robert A. Bednarczyk, PhD, associate professor of global health at Emory University Rollins School of Public Health, Atlanta, who specializes in HPV vaccine research.
“We have seen over the years that vaccine safety concerns have been on the increase, notably recently in the context of the COVID-19 pandemic and vaccination program, but HPV vaccine safety, though well established, continues to be a major concern for parents,” Dr. Bednarczyk said in an interview. But he found it striking that parents’ other reasons for turning down the vaccine had declined. “This shows that the outreach around the need for HPV vaccination and efforts to improve provider recommendation strategies is likely having positive impacts on HPV vaccine attitudes.”
Top five reasons for not vaccinating
The researchers analyzed data from the National Immunization Survey–Teen for the years 2010 through 2020 to track the annual changes in the top five reasons cited for not planning to get the HPV vaccine. The data covered 119,695 teens aged 13-17.
The researchers identified parents’ five most commonly cited reasons for not planning to vaccinate their children against HPV: “not necessary,” “safety concerns,” “lack of recommendation,” “lack of knowledge,” and “not sexually active.”
Parents’ HPV vaccine hesitancy decreased by 5.5% each year from 2010 to 2012, but then it stagnated for the remaining years through 2020. Across most of that time, from 2010 to 2018, parents’ concerns about the vaccine’s safety and side effects increased by 15.6%. A major reason for this increase, the authors suggested, may include the widespread distribution of online misinformation, particularly given the 7.8 million increase in antivaccine social media accounts since 2019.
“Fear tactics are often used by antivaccine campaigners to dissuade parents from vaccinating their children. There have been several myths propagated about vaccines causing adverse reactions,” the authors wrote. “Although these myths have been scientifically debunked, they continue to circulate.”
In contrast to parents’ concerns, a study in 2021 found a downward trend in reports of nonserious adverse effects and no change in reports of serious adverse effects from the HPV vaccine between 2015 and 2018. Further, more than 95% of the adverse effect reports to the Vaccine Adverse Event Reporting System after HPV vaccination were nonserious.
Reducing perceived barriers
Meanwhile, however, parents’ other reasons for avoiding the vaccine became less prevalent throughout most of the study period. For each year between 2013 and 2020, the proportion of parents saying they didn’t intend to get their children the HPV vaccine because it was “not recommended” decreased by 6.8%.
Similarly, avoiding the vaccine due to “lack of knowledge” declined 9.9%, and avoidance because the child was “not sexually active” declined 5.9% each year from 2013 to 2020. No difference occurred during that time period regarding how frequently parents cited that the vaccine was “not necessary.”
“Decreases in the percentage of parents/guardians citing lack of provider recommendation, lack of knowledge, and child ‘not sexually active’ as the main reason for HPV vaccine hesitancy ... are encouraging and suggest that interventions have been successful in reducing perceived barriers to HPV vaccination,” the authors wrote.
Dr. Bednarczyk agreed that these findings were encouraging, underscoring that outreach and support for health care providers to give strong recommendations for the vaccine need to continue.
“But additionally, we need to find better ways to communicate about vaccine safety,” Dr. Bednarczyk said. “Seeing that the number of parents citing safety concerns as the primary barrier has not changed much between 2016 and 2020, but that the percent of parents having those concerns increased, likely means there is a stable part of the population with these safety concerns, and as more adolescents are getting vaccinated against HPV, the relative contribution of safety concerns is increasing.” A key way to address those concerns includes “engaging with our trusted community partners and giving them the tools to discuss the safety of HPV vaccination with members of the community,” he said.
Debunking misinformation
Like the authors, Dr. Bednarczyk pointed out several conditions that parents erroneously worry could be caused by the HPV vaccine, but he emphasized that simply telling parents those misconceptions are untrue is insufficient to allay fears.
“It’s important for both clinicians and community partners to recognize we cannot just present a list of facts and figures and statistics to parents to reassure them and hope that this works,” Dr. Bednarczyk said. “Effective communication, strong narratives to illustrate this knowledge, and engagement with not just clinicians but community partners and other trusted sources is needed.” Dr. Bednarczyk continues to support the evidence-based model of presumptive recommendations, which does not remove parental autonomy but simplifies vaccine messaging about what’s recommended, “but clinicians need to be prepared with both the data and effective ways to communicate it to address questions if they come up after the presumptive recommendation is given,” he added.
The researchers pointed out that their study data were collected before the pandemic, so “it is reasonable to expect that HPV vaccine–related safety concerns may continue to rise because of the plethora of misinformation surrounding coronavirus disease 2019 vaccination.”
Dr. Bednarczyk said it will be important to see in future research whether shifts in beliefs about the HPV vaccine have occurred in the midst of the pandemic and afterward.
“As the authors stated, it’s important to remember that HPV vaccination has consistently been shown to be safe and effective,” Dr. Bednarczyk said. “But those research findings are not seeming to resonate with parents, highlighting how we need to improve our outreach and communication work.”
The research did not receive external funding. A coauthor is a scientific adviser to Navigating Cancer. The other authors and Dr. Bednarczyk had no disclosures.
FROM PEDIATRICS
AxSpA effects may be more severe for Black patients
CLEVELAND – Documenting the prevalence of axial spondyloarthritis (axSpA) among Black Americans has been difficult because of little published data, but new research suggests that when Black Americans do have the disease, it seems to be more severe.
Iman Abutineh, MD, of the University of Tennessee, Memphis, discussed her team’s work at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
A total of 244 patients with axSpA were identified, including 168 (69%) males, 78 (32%) Black patients, and 143 (59%) White patients.
Average age of onset for patients overall was 27.7 years, and age at diagnosis was 36.1 years with a 7-year delay in diagnosis. Sixty-six (27%) patients had nonradiographic axSpA, 83% were on tumor necrosis factor inhibitors, and 38% were prescribed glucocorticoids.
The researchers found several differences by race.
White patients were more likely to be HLA-B27 positive (77% vs. 59%; P = .010). White patients also had higher prevalence of psoriasis, coronary artery disease, and family history of SpA. White females had a higher prevalence of inflammatory bowel disease, fibromyalgia, depression, and lower grades of sacroiliitis.
Black patients had more hip involvement
A higher percentage of Black patients had elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hip involvement. In comparing hip involvement, the researchers found that 39 (39%) White males had hip involvement as did 9 (21%) White females. In comparison, 22 (45%) Black men in the study and 14 (54%) Black women showed hip involvement (P = .035).
After adjustment for age, sex, HLA-B27, and insurance status, Black patients had higher grades of sacroiliitis with an odds ratio of 2.32 (95% confidence interval, 1.23-4.44). Black patients had a numerically longer delay in diagnosis, compared with Whites (7.93 vs. 6.64 years), but this did not achieve statistical significance (P = .454), the researchers wrote.
Study addresses racial disparities
“Traditionally we think of axial spondyloarthritis largely in Caucasian males who are HLA-B27 positive,” Dr. Abutineh said, “and we found that there is still a significant portion of patients who don’t meet the criteria that do have disease that is very significant.”
Although actual prevalence was not clear from this study, Dr. Abutineh said their data suggest a 3-to-1 ratio of White-to-Black patients with spondyloarthritis, “but of the Black patients who are diagnosed, their disease is almost always more severe. That points to why it’s important to have a high index of suspicion for this disease in that patient population because if you miss it, it could be detrimental to the patients.”
Swetha Alexander, MD, a rheumatology fellow at the University of Utah, Salt Lake City, who was not part of the study, said in an interview, “It is an excellent and timely study addressing the racial disparities and inequities surrounding axSpA diagnosis. It highlights the delay in diagnosis and increased burden of disease among Black Americans.”
She said the study may prompt a further look into barriers to care for Black Americans and their beliefs regarding seeking health care for their pain.
Higher rates of nonradiographic axSpA among Black patients
The rate of nonradiographic axSpA among Black Americans was more than twice that of their White counterparts, which, Dr. Alexander noted, could make it more difficult to diagnose axSpA in that population.
The odds ratio for Black patients having nonradiographic axSpA, compared with Whites, was 2.265 (95% CI, 1.082-4.999; P = .035), after adjustment for age, sex, and HLA-B27 status.
Adult patients with axSpA were identified from rheumatology clinics at four major hospital systems and one private clinic in Shelby County, Tenn., between 2011 and 2021. Patients met modified New York (mNY) or Assessment of Spondyloarthritis International Society (ASAS) criteria as assessed by reviewers.
The authors and Dr. Alexander reported no relevant financial relationships.
CLEVELAND – Documenting the prevalence of axial spondyloarthritis (axSpA) among Black Americans has been difficult because of little published data, but new research suggests that when Black Americans do have the disease, it seems to be more severe.
Iman Abutineh, MD, of the University of Tennessee, Memphis, discussed her team’s work at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
A total of 244 patients with axSpA were identified, including 168 (69%) males, 78 (32%) Black patients, and 143 (59%) White patients.
Average age of onset for patients overall was 27.7 years, and age at diagnosis was 36.1 years with a 7-year delay in diagnosis. Sixty-six (27%) patients had nonradiographic axSpA, 83% were on tumor necrosis factor inhibitors, and 38% were prescribed glucocorticoids.
The researchers found several differences by race.
White patients were more likely to be HLA-B27 positive (77% vs. 59%; P = .010). White patients also had higher prevalence of psoriasis, coronary artery disease, and family history of SpA. White females had a higher prevalence of inflammatory bowel disease, fibromyalgia, depression, and lower grades of sacroiliitis.
Black patients had more hip involvement
A higher percentage of Black patients had elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hip involvement. In comparing hip involvement, the researchers found that 39 (39%) White males had hip involvement as did 9 (21%) White females. In comparison, 22 (45%) Black men in the study and 14 (54%) Black women showed hip involvement (P = .035).
After adjustment for age, sex, HLA-B27, and insurance status, Black patients had higher grades of sacroiliitis with an odds ratio of 2.32 (95% confidence interval, 1.23-4.44). Black patients had a numerically longer delay in diagnosis, compared with Whites (7.93 vs. 6.64 years), but this did not achieve statistical significance (P = .454), the researchers wrote.
Study addresses racial disparities
“Traditionally we think of axial spondyloarthritis largely in Caucasian males who are HLA-B27 positive,” Dr. Abutineh said, “and we found that there is still a significant portion of patients who don’t meet the criteria that do have disease that is very significant.”
Although actual prevalence was not clear from this study, Dr. Abutineh said their data suggest a 3-to-1 ratio of White-to-Black patients with spondyloarthritis, “but of the Black patients who are diagnosed, their disease is almost always more severe. That points to why it’s important to have a high index of suspicion for this disease in that patient population because if you miss it, it could be detrimental to the patients.”
Swetha Alexander, MD, a rheumatology fellow at the University of Utah, Salt Lake City, who was not part of the study, said in an interview, “It is an excellent and timely study addressing the racial disparities and inequities surrounding axSpA diagnosis. It highlights the delay in diagnosis and increased burden of disease among Black Americans.”
She said the study may prompt a further look into barriers to care for Black Americans and their beliefs regarding seeking health care for their pain.
Higher rates of nonradiographic axSpA among Black patients
The rate of nonradiographic axSpA among Black Americans was more than twice that of their White counterparts, which, Dr. Alexander noted, could make it more difficult to diagnose axSpA in that population.
The odds ratio for Black patients having nonradiographic axSpA, compared with Whites, was 2.265 (95% CI, 1.082-4.999; P = .035), after adjustment for age, sex, and HLA-B27 status.
Adult patients with axSpA were identified from rheumatology clinics at four major hospital systems and one private clinic in Shelby County, Tenn., between 2011 and 2021. Patients met modified New York (mNY) or Assessment of Spondyloarthritis International Society (ASAS) criteria as assessed by reviewers.
The authors and Dr. Alexander reported no relevant financial relationships.
CLEVELAND – Documenting the prevalence of axial spondyloarthritis (axSpA) among Black Americans has been difficult because of little published data, but new research suggests that when Black Americans do have the disease, it seems to be more severe.
Iman Abutineh, MD, of the University of Tennessee, Memphis, discussed her team’s work at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN).
A total of 244 patients with axSpA were identified, including 168 (69%) males, 78 (32%) Black patients, and 143 (59%) White patients.
Average age of onset for patients overall was 27.7 years, and age at diagnosis was 36.1 years with a 7-year delay in diagnosis. Sixty-six (27%) patients had nonradiographic axSpA, 83% were on tumor necrosis factor inhibitors, and 38% were prescribed glucocorticoids.
The researchers found several differences by race.
White patients were more likely to be HLA-B27 positive (77% vs. 59%; P = .010). White patients also had higher prevalence of psoriasis, coronary artery disease, and family history of SpA. White females had a higher prevalence of inflammatory bowel disease, fibromyalgia, depression, and lower grades of sacroiliitis.
Black patients had more hip involvement
A higher percentage of Black patients had elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and hip involvement. In comparing hip involvement, the researchers found that 39 (39%) White males had hip involvement as did 9 (21%) White females. In comparison, 22 (45%) Black men in the study and 14 (54%) Black women showed hip involvement (P = .035).
After adjustment for age, sex, HLA-B27, and insurance status, Black patients had higher grades of sacroiliitis with an odds ratio of 2.32 (95% confidence interval, 1.23-4.44). Black patients had a numerically longer delay in diagnosis, compared with Whites (7.93 vs. 6.64 years), but this did not achieve statistical significance (P = .454), the researchers wrote.
Study addresses racial disparities
“Traditionally we think of axial spondyloarthritis largely in Caucasian males who are HLA-B27 positive,” Dr. Abutineh said, “and we found that there is still a significant portion of patients who don’t meet the criteria that do have disease that is very significant.”
Although actual prevalence was not clear from this study, Dr. Abutineh said their data suggest a 3-to-1 ratio of White-to-Black patients with spondyloarthritis, “but of the Black patients who are diagnosed, their disease is almost always more severe. That points to why it’s important to have a high index of suspicion for this disease in that patient population because if you miss it, it could be detrimental to the patients.”
Swetha Alexander, MD, a rheumatology fellow at the University of Utah, Salt Lake City, who was not part of the study, said in an interview, “It is an excellent and timely study addressing the racial disparities and inequities surrounding axSpA diagnosis. It highlights the delay in diagnosis and increased burden of disease among Black Americans.”
She said the study may prompt a further look into barriers to care for Black Americans and their beliefs regarding seeking health care for their pain.
Higher rates of nonradiographic axSpA among Black patients
The rate of nonradiographic axSpA among Black Americans was more than twice that of their White counterparts, which, Dr. Alexander noted, could make it more difficult to diagnose axSpA in that population.
The odds ratio for Black patients having nonradiographic axSpA, compared with Whites, was 2.265 (95% CI, 1.082-4.999; P = .035), after adjustment for age, sex, and HLA-B27 status.
Adult patients with axSpA were identified from rheumatology clinics at four major hospital systems and one private clinic in Shelby County, Tenn., between 2011 and 2021. Patients met modified New York (mNY) or Assessment of Spondyloarthritis International Society (ASAS) criteria as assessed by reviewers.
The authors and Dr. Alexander reported no relevant financial relationships.
AT SPARTAN 2023
Novel antibody safe, promising for ATTR in phase 1 trial
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Currently, the only drug approved to treat ATTR is tafamidis, which improves survival and reduces hospitalizations, but does not reverse disease symptoms, the authors noted.
NI006 is a recombinant human anti-ATTR antibody given by infusion that was developed to trigger removal of ATTR by the body’s phagocytic immune cells.
Use of the drug was not associated with serious drug-related adverse events, though mild and moderate adverse events did occur.
Median N-terminal pro–B-type natriuretic peptide (NT-proBNP) and troponin T levels also seemed to be reduced over the study period.
Given the success of the antibody in this initial 40-patient trial, a larger phase-3 placebo-controlled trial is planned and expected to launch in the second half of 2023, said lead author Pablo Garcia-Pavia, MD, of Hospital Universitario Puerta de Hierro and the Spanish National Cardiovascular Research Institute, Madrid.
However, “The design of appropriate phase-3 trials to demonstrate efficacy of drugs for ATTR-CM is becoming more complicated and challenging,” he said.
“Increased awareness of the disease and advances in cardiac imaging techniques have led to recognition of a larger number of patients with ATTR-CM who have a different clinical profile and a different prognosis than the patients who were diagnosed in previous years and were enrolled in the initial trials of stabilizers,” Dr. Garcia-Pavia added.
“Moreover, the availability of tafamidis, and hopefully soon other medications to treat ATTR-CM has complicated the design of new clinical trials because of the heterogenicity of treatments that patients might receive,” he said. “Therefore, it is critical to plan the design very well.”
Dr. Garcia-Pavia presented the findings on NI006 at the Heart Failure Association of the European Society of Cardiology (HFA-ESC) 2023 sessions. The study was published simultaneously in the New England Journal of Medicine.
No serious adverse events
For the phase-1, double-blind, multicenter study, the investigators randomly assigned (2:1 ratio) 40 patients (median age, 72 years; 98% men) with wild-type or variant ATTR cardiomyopathy and chronic heart failure to receive IV infusions of either NI006, at one of six doses ranging from 0.3 mg/kg to 60 mg/kg of body weight, or placebo every 4 weeks for 4 months.
After the four infusions, participants were enrolled in an open-label extension phase in which they received eight NI006 infusions with stepwise increases in the dose.
Participants had a confirmed diagnosis of ATTR-CM; left ventricular wall thickness of at least 14 mm; left ventricular ejection fraction of at least 40%; New York Heart Association class I, II, or III; estimated glomerular filtration rate of more than 30 mL/min per 1.73 m2; and an NT-proBNP level of 600 to 6,000 pg/mL.
Most (36) were receiving tafamidis, with a median treatment duration of 7 months; other ATTR-specific drugs were not permitted. Patients randomly assigned to receive NI006 seemed to have more advanced disease compared with those assigned to placebo.
Adherence to the trial protocol was high: Thirty-four patients received the four scheduled infusions during the ascending-dose phase, and 34 of 35 patients who completed this phase subsequently enrolled in the open-label extension.
No apparent drug-related serious adverse events were reported. However, during the ascending-dose phase, 38 patients had at least one adverse event, most of which were mild or moderate; of the 191 total events, 124 were grade 1 and 60 were grade 2 (most commonly heart failure and arrhythmias). Three patients had cytokine release syndrome; all three completed treatment through the extension phase.
Musculoskeletal events increased with ascending doses of NI006, which led two patients to withdraw from the trial.
At doses of at least 10 mg/kg, cardiac tracer uptake on scintigraphy and extracellular volume on cardiac MRI, both of which are imaging-based surrogate markers of cardiac amyloid load, appeared to be reduced over 12 months.
Because NI006 stimulates the patient’s own immune system to eliminate cardiac amyloid fibrils, one session chair at the meeting wondered whether NI006 represented the “rise of immunology in cardiology,” and whether biologics might follow.
Another questioned how removing amyloid might affect cardiac function. The echocardiographic findings gathered so far don’t indicate dysfunction, “but this is a small trial, and we need more data,” Dr. Garcia-Pavia said.
Tempered excitement
In a comment, Ronald Witteles, MD, professor of cardiovascular medicine, Stanford (Calif.) University, and founder/codirector of the Stanford Amyloid Center, said that “antibody-based amyloid removal strategies are not currently clinically available and represent a fundamentally different mechanism to treat the disease from what we currently have.
“While the data are encouraging and will generate excitement for later-phase studies, we’re talking about small numbers of patients and nothing definitive should be drawn from this data,” said Dr. Witteles, deputy editor of JACC: CardioOncology.
“The biggest caveat is that similar approaches of antibody removal of amyloid deposits for other forms of amyloidosis — most notably AL amyloidosis (amyloid light chain or primary amyloidosis) – have failed in late-phase trials. Although there is reason to believe that ATTR amyloidosis may be more amenable to improvements with amyloid fibril removal than AL amyloidosis, the unimpressive results in other forms of amyloidosis still do temper the excitement to a degree.”
Like Dr. Garcia-Pavia, Dr. Witteles said, “Ultimately, we are going to need to see a phase 3 clinical trial which shows that NI006 – on top of standard-of-care treatment – improves hard outcomes in the disease. As treatment options likely expand in the coming years, that is likely to be a harder and harder bar to reach.”
Furthermore, although the safety profile was favorable overall, it “wasn’t entirely clean,” given cytokine release syndrome in three patients, a lowering of platelet counts in a couple of patients, and musculoskeletal side effects that triggered two to withdraw from the study. “Unless that changes,” he said, “that will be a barrier for some patients.”
Overall, he noted, “With the vast majority of patients being able to be diagnosed noninvasively, and with treatment options now available, we have seen a true explosion in the number of patients being diagnosed.
“But we also know that the large majority ... are still not getting diagnosed or are having huge delays in diagnosis. As such, the biggest thing we can do for patients with the disease is to continue to educate people about it,” Dr. Witteles concluded.
The study was funded by Neurimmune. Dr. Garcia-Pavia disclosed ties to Alexion, Alnylam Pharmaceuticals, AstraZeneca, Attralus, BridgeBio, General Electric, Intellia, Ionis Pharmaceuticals, Neurimmune, Novo Nordisk, and Pfizer. Dr. Witteles reported ties to Alexion, Alnylam, AstraZeneca, BridgeBio, Intellia, Ionis, Janssen, Novo Nordisk, and Pfizer.
A version of this article first appeared on Medscape.com.
FROM ESC HEART FAILURE 2023
Alzheimer’s Disease Etiology
FDA approves autoinjector pen for Humira biosimilar, Cyltezo
The U.S. Food and Drug Administration on May 22 approved a new autoinjection option for adalimumab-adbm (Cyltezo), a biosimilar to AbbVie’s adalimumab (Humira), ahead of Cyltezo’s commercial launch on July 1, 2023.

Cyltezo was approved by the FDA in 2017 as a prefilled syringe and was the first biosimilar deemed to be interchangeable with Humira in 2021. It is indicated to treat multiple chronic inflammatory conditions, including rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and hidradenitis suppurativa. This new design, which features one-button, three-step activation, has been certified as an “Ease of Use” product by the Arthritis Foundation, Boehringer Ingelheim said in a press release. The 40-mg, prefilled Cyltezo Pen will be available in two-, four-, and six-pack options.
“The FDA approval of the Cyltezo Pen is great news for patients living with chronic inflammatory diseases who may prefer administering the medication needed to manage their conditions via an autoinjector,” said Stephen Pagnotta, the executive director and biosimilar commercial lead at Boehringer Ingelheim in a statement; “we’re excited to be able to offer the Cyltezo Pen as an additional option to patients at Cyltezo’s launch on July 1.”
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration on May 22 approved a new autoinjection option for adalimumab-adbm (Cyltezo), a biosimilar to AbbVie’s adalimumab (Humira), ahead of Cyltezo’s commercial launch on July 1, 2023.
Cyltezo was approved by the FDA in 2017 as a prefilled syringe and was the first biosimilar deemed to be interchangeable with Humira in 2021. It is indicated to treat multiple chronic inflammatory conditions, including rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and hidradenitis suppurativa. This new design, which features one-button, three-step activation, has been certified as an “Ease of Use” product by the Arthritis Foundation, Boehringer Ingelheim said in a press release. The 40-mg, prefilled Cyltezo Pen will be available in two-, four-, and six-pack options.
“The FDA approval of the Cyltezo Pen is great news for patients living with chronic inflammatory diseases who may prefer administering the medication needed to manage their conditions via an autoinjector,” said Stephen Pagnotta, the executive director and biosimilar commercial lead at Boehringer Ingelheim in a statement; “we’re excited to be able to offer the Cyltezo Pen as an additional option to patients at Cyltezo’s launch on July 1.”
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration on May 22 approved a new autoinjection option for adalimumab-adbm (Cyltezo), a biosimilar to AbbVie’s adalimumab (Humira), ahead of Cyltezo’s commercial launch on July 1, 2023.
Cyltezo was approved by the FDA in 2017 as a prefilled syringe and was the first biosimilar deemed to be interchangeable with Humira in 2021. It is indicated to treat multiple chronic inflammatory conditions, including rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and hidradenitis suppurativa. This new design, which features one-button, three-step activation, has been certified as an “Ease of Use” product by the Arthritis Foundation, Boehringer Ingelheim said in a press release. The 40-mg, prefilled Cyltezo Pen will be available in two-, four-, and six-pack options.
“The FDA approval of the Cyltezo Pen is great news for patients living with chronic inflammatory diseases who may prefer administering the medication needed to manage their conditions via an autoinjector,” said Stephen Pagnotta, the executive director and biosimilar commercial lead at Boehringer Ingelheim in a statement; “we’re excited to be able to offer the Cyltezo Pen as an additional option to patients at Cyltezo’s launch on July 1.”
A version of this article first appeared on Medscape.com.