User login
Anticoagulant Rivaroxaban Clears FDA Panel Hurdle
An FDA advisory panel has recommended the approval of rivaroxaban (Xarelto) for stroke prevention in patients with non-valvular atrial fibrillation, but the panelists raised questions about the methodology of the trial that compared the drug to the gold standard, warfarin (Coumadin).
A final decision on the drug is expected in November.
Rivaroxaban has been developed as a once-a-day oral medication that prevents clotting by inhibiting factor Xa, a key component in the generation of thrombin. It is one medication in a line of drugs trying to position themselves to replace warfarin, which has many contraindications and requires frequent blood draws for monitoring; the new drugs would not require frequent blood draws.
Panelists questioned whether ROCKET-AF—the trial that compared rivaroxaban to warfarin—was sufficient to show noninferiority, as only 55% of the patients on warfarin had international normalized ratio (INR) levels needed for stroke prevention.
Ian Jenkins, MD, assistant professor in the division of hospital medicine at the University of California at San Diego, says that rivaroxaban “will be an option for AF, but probably not my first choice.”
Another oral warfarin alternative—dabigatran, which inhibits thrombin—is already available, he notes. And dabigatran was found to be superior to warfarin, while rivaroxaban was only found to be noninferior. But Dr. Jenkins also notes that dabigatran and rivaroxaban have not been compared head-to-head.
“The low percent of therapeutic INRs in ROCKET-AF does concern me,” Dr. Jenkins adds, “but we have to remember that the patients who will benefit the most from these medications are the ones with difficult-to-control INRs anyway.”
He also explains that patients now doing well on warfarin don’t have a “great reason” to boost their costs by trying another drug.
An FDA advisory panel has recommended the approval of rivaroxaban (Xarelto) for stroke prevention in patients with non-valvular atrial fibrillation, but the panelists raised questions about the methodology of the trial that compared the drug to the gold standard, warfarin (Coumadin).
A final decision on the drug is expected in November.
Rivaroxaban has been developed as a once-a-day oral medication that prevents clotting by inhibiting factor Xa, a key component in the generation of thrombin. It is one medication in a line of drugs trying to position themselves to replace warfarin, which has many contraindications and requires frequent blood draws for monitoring; the new drugs would not require frequent blood draws.
Panelists questioned whether ROCKET-AF—the trial that compared rivaroxaban to warfarin—was sufficient to show noninferiority, as only 55% of the patients on warfarin had international normalized ratio (INR) levels needed for stroke prevention.
Ian Jenkins, MD, assistant professor in the division of hospital medicine at the University of California at San Diego, says that rivaroxaban “will be an option for AF, but probably not my first choice.”
Another oral warfarin alternative—dabigatran, which inhibits thrombin—is already available, he notes. And dabigatran was found to be superior to warfarin, while rivaroxaban was only found to be noninferior. But Dr. Jenkins also notes that dabigatran and rivaroxaban have not been compared head-to-head.
“The low percent of therapeutic INRs in ROCKET-AF does concern me,” Dr. Jenkins adds, “but we have to remember that the patients who will benefit the most from these medications are the ones with difficult-to-control INRs anyway.”
He also explains that patients now doing well on warfarin don’t have a “great reason” to boost their costs by trying another drug.
An FDA advisory panel has recommended the approval of rivaroxaban (Xarelto) for stroke prevention in patients with non-valvular atrial fibrillation, but the panelists raised questions about the methodology of the trial that compared the drug to the gold standard, warfarin (Coumadin).
A final decision on the drug is expected in November.
Rivaroxaban has been developed as a once-a-day oral medication that prevents clotting by inhibiting factor Xa, a key component in the generation of thrombin. It is one medication in a line of drugs trying to position themselves to replace warfarin, which has many contraindications and requires frequent blood draws for monitoring; the new drugs would not require frequent blood draws.
Panelists questioned whether ROCKET-AF—the trial that compared rivaroxaban to warfarin—was sufficient to show noninferiority, as only 55% of the patients on warfarin had international normalized ratio (INR) levels needed for stroke prevention.
Ian Jenkins, MD, assistant professor in the division of hospital medicine at the University of California at San Diego, says that rivaroxaban “will be an option for AF, but probably not my first choice.”
Another oral warfarin alternative—dabigatran, which inhibits thrombin—is already available, he notes. And dabigatran was found to be superior to warfarin, while rivaroxaban was only found to be noninferior. But Dr. Jenkins also notes that dabigatran and rivaroxaban have not been compared head-to-head.
“The low percent of therapeutic INRs in ROCKET-AF does concern me,” Dr. Jenkins adds, “but we have to remember that the patients who will benefit the most from these medications are the ones with difficult-to-control INRs anyway.”
He also explains that patients now doing well on warfarin don’t have a “great reason” to boost their costs by trying another drug.
Continuous Glucose Monitor Accurate Post-Cardiac Surgery
LISBON – Although microcirculation in cardiac surgery patients is impaired during the first few hours of admission to the intensive care unit, the degree of impairment was not great enough to affect the accuracy of continuous glucose monitors in a prospective, observational study of 60 patients.
Hyperglycemia, hypoglycemia, and glucose hypervariability are all associated with increased mortality in critically ill patients following cardiac surgery. Continuous glucose monitoring (CGM) is a potential alternative to frequent, time-consuming fingerstick glucose measurements, and can provide more information about glucose trends. However, the accuracy of these systems in critically ill patients has been uncertain, said Dr. J. Hans DeVries, an endocrinologist at the University of Amsterdam.

Now, "these results support CGM use in cardiac surgery patients, with quite good sensor accuracy in patients with a low severity of illness," he said at the annual meeting of the European Association for the Study of Diabetes (EASD).
The patients had a mean age of 65 years, and 48 of the 60 were male. Nearly a third (27%) had diabetes. Thirty-two (53%) of the patients were undergoing only coronary artery bypass surgery, 16 (27%) were having just valve surgery, and 12 (20%) had both procedures. Their APACHE score predicting mortality was low, 0.01. Total ICU stay was 23 hours. Hemodynamic parameters were fairly good, with a microcirculatory function index of 2.8 (out of 3.0). The proportion of perfused vessels was high, 0.97. However, the patients’ peripheral temperature was low, 32.8 °C.
Two sensors – the Medtronic Guardian REAL-Time and the Abbott FreeStyle Navigator – were placed subcutaneously in the abdominal wall of each patient prior to surgery. The Navigator performed slightly better than did the Guardian. Microcirculation was measured by microvascular flow index (MFI), perfused vessel density (PVD), and proportion of perfused vessels (PPV) using sublingual sidestream dark-field (SDF) imaging; and tissue oxygenation (StO2) was obtained with near-infrared spectroscopy.
While StO2 and PVD were impaired in the first hours after surgery, at no point were any microcirculatory parameters significantly associated with sensor accuracy. For the Navigator CGM, lower peripheral temperature and higher APACHE IV scores were significantly associated with decreased sensor accuracy (P values of .003 and less than .001, respectively). For the Guardian, lower peripheral temperature was significantly associated with decreased sensor accuracy (P = .048).
"Further studies are needed to assess the influence of microcirculation on sensor accuracy in more severely ill patients, such as those with sepsis," Dr. DeVries concluded.
The study was supported by the EASD’s European Foundation for the Study of Diabetes. Dr. DeVries has received research support from, and is on the speakers’ bureau for Dexcom, Abbott, and Medtronic.
LISBON – Although microcirculation in cardiac surgery patients is impaired during the first few hours of admission to the intensive care unit, the degree of impairment was not great enough to affect the accuracy of continuous glucose monitors in a prospective, observational study of 60 patients.
Hyperglycemia, hypoglycemia, and glucose hypervariability are all associated with increased mortality in critically ill patients following cardiac surgery. Continuous glucose monitoring (CGM) is a potential alternative to frequent, time-consuming fingerstick glucose measurements, and can provide more information about glucose trends. However, the accuracy of these systems in critically ill patients has been uncertain, said Dr. J. Hans DeVries, an endocrinologist at the University of Amsterdam.
Now, "these results support CGM use in cardiac surgery patients, with quite good sensor accuracy in patients with a low severity of illness," he said at the annual meeting of the European Association for the Study of Diabetes (EASD).
The patients had a mean age of 65 years, and 48 of the 60 were male. Nearly a third (27%) had diabetes. Thirty-two (53%) of the patients were undergoing only coronary artery bypass surgery, 16 (27%) were having just valve surgery, and 12 (20%) had both procedures. Their APACHE score predicting mortality was low, 0.01. Total ICU stay was 23 hours. Hemodynamic parameters were fairly good, with a microcirculatory function index of 2.8 (out of 3.0). The proportion of perfused vessels was high, 0.97. However, the patients’ peripheral temperature was low, 32.8 °C.
Two sensors – the Medtronic Guardian REAL-Time and the Abbott FreeStyle Navigator – were placed subcutaneously in the abdominal wall of each patient prior to surgery. The Navigator performed slightly better than did the Guardian. Microcirculation was measured by microvascular flow index (MFI), perfused vessel density (PVD), and proportion of perfused vessels (PPV) using sublingual sidestream dark-field (SDF) imaging; and tissue oxygenation (StO2) was obtained with near-infrared spectroscopy.
While StO2 and PVD were impaired in the first hours after surgery, at no point were any microcirculatory parameters significantly associated with sensor accuracy. For the Navigator CGM, lower peripheral temperature and higher APACHE IV scores were significantly associated with decreased sensor accuracy (P values of .003 and less than .001, respectively). For the Guardian, lower peripheral temperature was significantly associated with decreased sensor accuracy (P = .048).
"Further studies are needed to assess the influence of microcirculation on sensor accuracy in more severely ill patients, such as those with sepsis," Dr. DeVries concluded.
The study was supported by the EASD’s European Foundation for the Study of Diabetes. Dr. DeVries has received research support from, and is on the speakers’ bureau for Dexcom, Abbott, and Medtronic.
LISBON – Although microcirculation in cardiac surgery patients is impaired during the first few hours of admission to the intensive care unit, the degree of impairment was not great enough to affect the accuracy of continuous glucose monitors in a prospective, observational study of 60 patients.
Hyperglycemia, hypoglycemia, and glucose hypervariability are all associated with increased mortality in critically ill patients following cardiac surgery. Continuous glucose monitoring (CGM) is a potential alternative to frequent, time-consuming fingerstick glucose measurements, and can provide more information about glucose trends. However, the accuracy of these systems in critically ill patients has been uncertain, said Dr. J. Hans DeVries, an endocrinologist at the University of Amsterdam.
Now, "these results support CGM use in cardiac surgery patients, with quite good sensor accuracy in patients with a low severity of illness," he said at the annual meeting of the European Association for the Study of Diabetes (EASD).
The patients had a mean age of 65 years, and 48 of the 60 were male. Nearly a third (27%) had diabetes. Thirty-two (53%) of the patients were undergoing only coronary artery bypass surgery, 16 (27%) were having just valve surgery, and 12 (20%) had both procedures. Their APACHE score predicting mortality was low, 0.01. Total ICU stay was 23 hours. Hemodynamic parameters were fairly good, with a microcirculatory function index of 2.8 (out of 3.0). The proportion of perfused vessels was high, 0.97. However, the patients’ peripheral temperature was low, 32.8 °C.
Two sensors – the Medtronic Guardian REAL-Time and the Abbott FreeStyle Navigator – were placed subcutaneously in the abdominal wall of each patient prior to surgery. The Navigator performed slightly better than did the Guardian. Microcirculation was measured by microvascular flow index (MFI), perfused vessel density (PVD), and proportion of perfused vessels (PPV) using sublingual sidestream dark-field (SDF) imaging; and tissue oxygenation (StO2) was obtained with near-infrared spectroscopy.
While StO2 and PVD were impaired in the first hours after surgery, at no point were any microcirculatory parameters significantly associated with sensor accuracy. For the Navigator CGM, lower peripheral temperature and higher APACHE IV scores were significantly associated with decreased sensor accuracy (P values of .003 and less than .001, respectively). For the Guardian, lower peripheral temperature was significantly associated with decreased sensor accuracy (P = .048).
"Further studies are needed to assess the influence of microcirculation on sensor accuracy in more severely ill patients, such as those with sepsis," Dr. DeVries concluded.
The study was supported by the EASD’s European Foundation for the Study of Diabetes. Dr. DeVries has received research support from, and is on the speakers’ bureau for Dexcom, Abbott, and Medtronic.
FROM THE ANNUAL MEETING OF THE EUROPEAN ASSOCIATION FOR THE STUDY OF DIABETES (EASD)
Major Finding: While StO2 and PVD were impaired in the first hours after surgery, at no point were any microcirculatory parameters significantly associated with sensor accuracy.
Data Source: Prospective, observational study of 60 patients undergoing cardiac surgery.
Disclosures: The study was supported by the EASD’s European Foundation for the Study of Diabetes. Dr. DeVries has received research support from, and is on the speakers’ bureau for Dexcom, Abbott, and Medtronic.
Household Medicine Cabinet Source of Most Pediatric Poisonings
Approximately 95% of visits related to medication poisoning in children younger than 5 years are caused by self-ingestion, based on data from nearly 500,000 emergency visits during 2001-2008, according to a study published online Sept. 16 in the Journal of Pediatrics.
"If we are to make progress in reducing childhood injury from pharmaceutical poisoning, we need to better understand the epidemic," said Dr. G. Randall Bond of the University of Cincinnati and colleagues.
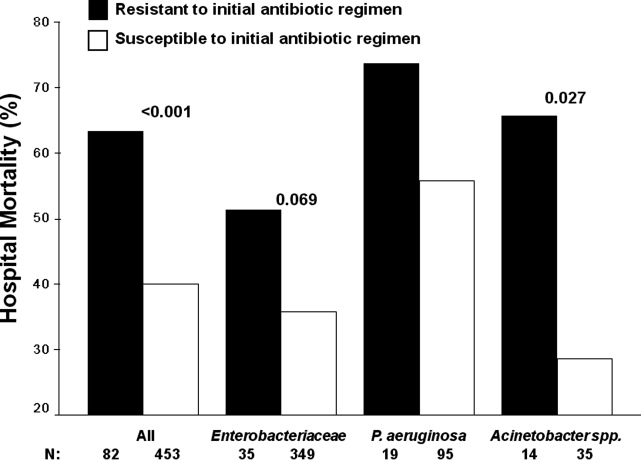
The researchers reviewed case information from 453,599 children aged 5 years and younger who visited emergency departments due to possible medication poisoning via ingestion of a single product. Data were taken from the American Association of Poison Control Centers’ National Poison Data System, an electronic database of all calls to the organization’s member centers (J. Pediatr. 2011 Sept. 16 [doi:10.1016/j.jpeds.2011.07.042]).

Of the self-ingested poisonings, prescription products accounted for the largest percentage of ED visits (55%), hospital admissions (76%), and significant injuries (71%).
Opioid analgesics had the greatest increase in impact on health care resources during the study period – ED visits increased by 101%, injury rates increased by 92%, and hospital admission rates increased by 86%.
The findings were limited by the self-reported nature of the cases, but they support data from previous studies on the increasing numbers of emergency department visits by young children due to medication poisoning, Dr. Bond and his coauthors said. "The most likely explanation for these observations is a rise in the number of medications in the environment of small children," they noted.
These medications may be more accessible to children in the home because the number of opioid analgesic prescriptions has increased, according to data from the U.S. Drug Enforcement Administration’s database, the researchers noted.
When it comes to preventing medication poisonings, "the results of this study suggest that focus should shift to self-ingestion and prescription products," the researchers said. "The largest potential benefits would come from a shift in attention to packaging design changes that reduce the quantity a child could quickly and easily access in a self-ingestion episode," they added.
Of 90 unintentional deaths recorded in the database, 66 were ingestion related. Of these, opioid analgesic and cough medicines accounted for the most deaths (20).
Another recent study by Dr. Gary M. Vilke of the University of California, San Diego and colleagues provided a breakdown of more than 40,000 paramedic transport calls related to poisonings in children younger than 5 years between 2000 and 2007 (J. Emerg. Med. 2011;41:265-9).
In this retrospective study, more than half of the poisonings were due to ingestion of prescription or over-the-counter medications (56%). In addition, medications made up a majority of the poisonings in each age group: less than 1 year (40%), 1 year (46%), 2 years (66%), 3 years (68%), and 4 years (60%). The researchers also noted that 10% of the poisonings were caused by cosmetics. This study was limited by the use of a preexisting database and the inclusion only of cases in which poisoning was the chief complaint.
However, the findings reinforce the need for better education about the poisoning potential of household medications, as shown in the study by Dr. Bond and colleagues.
None of the researchers in either study had any financial conflicts to disclose.
Approximately 95% of visits related to medication poisoning in children younger than 5 years are caused by self-ingestion, based on data from nearly 500,000 emergency visits during 2001-2008, according to a study published online Sept. 16 in the Journal of Pediatrics.
"If we are to make progress in reducing childhood injury from pharmaceutical poisoning, we need to better understand the epidemic," said Dr. G. Randall Bond of the University of Cincinnati and colleagues.
The researchers reviewed case information from 453,599 children aged 5 years and younger who visited emergency departments due to possible medication poisoning via ingestion of a single product. Data were taken from the American Association of Poison Control Centers’ National Poison Data System, an electronic database of all calls to the organization’s member centers (J. Pediatr. 2011 Sept. 16 [doi:10.1016/j.jpeds.2011.07.042]).
Of the self-ingested poisonings, prescription products accounted for the largest percentage of ED visits (55%), hospital admissions (76%), and significant injuries (71%).
Opioid analgesics had the greatest increase in impact on health care resources during the study period – ED visits increased by 101%, injury rates increased by 92%, and hospital admission rates increased by 86%.
The findings were limited by the self-reported nature of the cases, but they support data from previous studies on the increasing numbers of emergency department visits by young children due to medication poisoning, Dr. Bond and his coauthors said. "The most likely explanation for these observations is a rise in the number of medications in the environment of small children," they noted.
These medications may be more accessible to children in the home because the number of opioid analgesic prescriptions has increased, according to data from the U.S. Drug Enforcement Administration’s database, the researchers noted.
When it comes to preventing medication poisonings, "the results of this study suggest that focus should shift to self-ingestion and prescription products," the researchers said. "The largest potential benefits would come from a shift in attention to packaging design changes that reduce the quantity a child could quickly and easily access in a self-ingestion episode," they added.
Of 90 unintentional deaths recorded in the database, 66 were ingestion related. Of these, opioid analgesic and cough medicines accounted for the most deaths (20).
Another recent study by Dr. Gary M. Vilke of the University of California, San Diego and colleagues provided a breakdown of more than 40,000 paramedic transport calls related to poisonings in children younger than 5 years between 2000 and 2007 (J. Emerg. Med. 2011;41:265-9).
In this retrospective study, more than half of the poisonings were due to ingestion of prescription or over-the-counter medications (56%). In addition, medications made up a majority of the poisonings in each age group: less than 1 year (40%), 1 year (46%), 2 years (66%), 3 years (68%), and 4 years (60%). The researchers also noted that 10% of the poisonings were caused by cosmetics. This study was limited by the use of a preexisting database and the inclusion only of cases in which poisoning was the chief complaint.
However, the findings reinforce the need for better education about the poisoning potential of household medications, as shown in the study by Dr. Bond and colleagues.
None of the researchers in either study had any financial conflicts to disclose.
Approximately 95% of visits related to medication poisoning in children younger than 5 years are caused by self-ingestion, based on data from nearly 500,000 emergency visits during 2001-2008, according to a study published online Sept. 16 in the Journal of Pediatrics.
"If we are to make progress in reducing childhood injury from pharmaceutical poisoning, we need to better understand the epidemic," said Dr. G. Randall Bond of the University of Cincinnati and colleagues.
The researchers reviewed case information from 453,599 children aged 5 years and younger who visited emergency departments due to possible medication poisoning via ingestion of a single product. Data were taken from the American Association of Poison Control Centers’ National Poison Data System, an electronic database of all calls to the organization’s member centers (J. Pediatr. 2011 Sept. 16 [doi:10.1016/j.jpeds.2011.07.042]).
Of the self-ingested poisonings, prescription products accounted for the largest percentage of ED visits (55%), hospital admissions (76%), and significant injuries (71%).
Opioid analgesics had the greatest increase in impact on health care resources during the study period – ED visits increased by 101%, injury rates increased by 92%, and hospital admission rates increased by 86%.
The findings were limited by the self-reported nature of the cases, but they support data from previous studies on the increasing numbers of emergency department visits by young children due to medication poisoning, Dr. Bond and his coauthors said. "The most likely explanation for these observations is a rise in the number of medications in the environment of small children," they noted.
These medications may be more accessible to children in the home because the number of opioid analgesic prescriptions has increased, according to data from the U.S. Drug Enforcement Administration’s database, the researchers noted.
When it comes to preventing medication poisonings, "the results of this study suggest that focus should shift to self-ingestion and prescription products," the researchers said. "The largest potential benefits would come from a shift in attention to packaging design changes that reduce the quantity a child could quickly and easily access in a self-ingestion episode," they added.
Of 90 unintentional deaths recorded in the database, 66 were ingestion related. Of these, opioid analgesic and cough medicines accounted for the most deaths (20).
Another recent study by Dr. Gary M. Vilke of the University of California, San Diego and colleagues provided a breakdown of more than 40,000 paramedic transport calls related to poisonings in children younger than 5 years between 2000 and 2007 (J. Emerg. Med. 2011;41:265-9).
In this retrospective study, more than half of the poisonings were due to ingestion of prescription or over-the-counter medications (56%). In addition, medications made up a majority of the poisonings in each age group: less than 1 year (40%), 1 year (46%), 2 years (66%), 3 years (68%), and 4 years (60%). The researchers also noted that 10% of the poisonings were caused by cosmetics. This study was limited by the use of a preexisting database and the inclusion only of cases in which poisoning was the chief complaint.
However, the findings reinforce the need for better education about the poisoning potential of household medications, as shown in the study by Dr. Bond and colleagues.
None of the researchers in either study had any financial conflicts to disclose.
FROM THE JOURNAL OF PEDIATRICS
Major Finding: Prescription medications accounted for 55% of emergency department visits for poisoning in children aged 5 years and younger.
Data Source: Data on 453,599 cases from the American Association of Poison Control Centers’ National Poison Data System, 2001-2008.
Disclosures: None of the researchers in either study had any financial conflicts to disclose.
Court Upholds Doctors' Right to Discuss Firearms
A U.S. District Court judge has granted a preliminary injunction that stops Florida from enforcing a new law barring physicians from asking their patients about firearms ownership, saying that the law may be unconstitutional and has a good chance of being overturned.
The injunction, granted Sept. 14 by Judge Marcia Cooke, immediately prevents the state from pursuing disciplinary action against physicians who inquire about firearms in the home and counsel on firearms-injury prevention.
The decision won praise from the American Academy of Pediatrics, which has fought the law.
"The AAP is pleased the court recognized the confidential nature of the physician-patient relationship and the critical importance of this counseling, which is a cornerstone of pediatric care," Dr. O. Marion Burton, AAP president, said in a statement. "Today’s court victory ensures that important conversations about firearm safety can continue to take place between doctors and patients."
The Florida law, passed last spring and signed by Gov. Rick Scott (R) in June, forbids licensed health care practitioners from asking about gun ownership unless the practitioner believes "in good faith" that the information is relevant to patients’ and family members’ medical care or safety. Under the law, physicians and other health care practitioners also cannot record information on firearms in patients’ medical records.
Violators of the law could be subject to state medical board disciplinary action and sanctions.
The Florida chapters of the AAP, the American College of Physicians, and the American Academy of Family Physicians, along with six individual Florida physicians, filed suit in June against the law, saying it substantially curtails their First Amendment rights to exchange information with patients about gun safety. The judge agreed.
"Plaintiffs state that, as a result of the law, they are no longer (i) asking patients about firearm ownership, (ii) following up on routine questions regarding firearm ownership, (iii) providing patient intake questionnaires that include questions about firearms, or (iv) orally counseling patients about firearm safety," Judge Cooke wrote in her injunction.
Proponents of the Florida law have argued that it represents a Second Amendment issue involving the right to bear arms. However, Judge Cooke disagreed, calling it a First Amendment – or freedom of speech – issue instead.
"A practitioner who counsels a patient on firearm safety, even when entirely irrelevant to medical care or safety, does not affect nor interfere with the patient’s right to continue to own, possess, or use firearms," she wrote.
A U.S. District Court judge has granted a preliminary injunction that stops Florida from enforcing a new law barring physicians from asking their patients about firearms ownership, saying that the law may be unconstitutional and has a good chance of being overturned.
The injunction, granted Sept. 14 by Judge Marcia Cooke, immediately prevents the state from pursuing disciplinary action against physicians who inquire about firearms in the home and counsel on firearms-injury prevention.
The decision won praise from the American Academy of Pediatrics, which has fought the law.
"The AAP is pleased the court recognized the confidential nature of the physician-patient relationship and the critical importance of this counseling, which is a cornerstone of pediatric care," Dr. O. Marion Burton, AAP president, said in a statement. "Today’s court victory ensures that important conversations about firearm safety can continue to take place between doctors and patients."
The Florida law, passed last spring and signed by Gov. Rick Scott (R) in June, forbids licensed health care practitioners from asking about gun ownership unless the practitioner believes "in good faith" that the information is relevant to patients’ and family members’ medical care or safety. Under the law, physicians and other health care practitioners also cannot record information on firearms in patients’ medical records.
Violators of the law could be subject to state medical board disciplinary action and sanctions.
The Florida chapters of the AAP, the American College of Physicians, and the American Academy of Family Physicians, along with six individual Florida physicians, filed suit in June against the law, saying it substantially curtails their First Amendment rights to exchange information with patients about gun safety. The judge agreed.
"Plaintiffs state that, as a result of the law, they are no longer (i) asking patients about firearm ownership, (ii) following up on routine questions regarding firearm ownership, (iii) providing patient intake questionnaires that include questions about firearms, or (iv) orally counseling patients about firearm safety," Judge Cooke wrote in her injunction.
Proponents of the Florida law have argued that it represents a Second Amendment issue involving the right to bear arms. However, Judge Cooke disagreed, calling it a First Amendment – or freedom of speech – issue instead.
"A practitioner who counsels a patient on firearm safety, even when entirely irrelevant to medical care or safety, does not affect nor interfere with the patient’s right to continue to own, possess, or use firearms," she wrote.
A U.S. District Court judge has granted a preliminary injunction that stops Florida from enforcing a new law barring physicians from asking their patients about firearms ownership, saying that the law may be unconstitutional and has a good chance of being overturned.
The injunction, granted Sept. 14 by Judge Marcia Cooke, immediately prevents the state from pursuing disciplinary action against physicians who inquire about firearms in the home and counsel on firearms-injury prevention.
The decision won praise from the American Academy of Pediatrics, which has fought the law.
"The AAP is pleased the court recognized the confidential nature of the physician-patient relationship and the critical importance of this counseling, which is a cornerstone of pediatric care," Dr. O. Marion Burton, AAP president, said in a statement. "Today’s court victory ensures that important conversations about firearm safety can continue to take place between doctors and patients."
The Florida law, passed last spring and signed by Gov. Rick Scott (R) in June, forbids licensed health care practitioners from asking about gun ownership unless the practitioner believes "in good faith" that the information is relevant to patients’ and family members’ medical care or safety. Under the law, physicians and other health care practitioners also cannot record information on firearms in patients’ medical records.
Violators of the law could be subject to state medical board disciplinary action and sanctions.
The Florida chapters of the AAP, the American College of Physicians, and the American Academy of Family Physicians, along with six individual Florida physicians, filed suit in June against the law, saying it substantially curtails their First Amendment rights to exchange information with patients about gun safety. The judge agreed.
"Plaintiffs state that, as a result of the law, they are no longer (i) asking patients about firearm ownership, (ii) following up on routine questions regarding firearm ownership, (iii) providing patient intake questionnaires that include questions about firearms, or (iv) orally counseling patients about firearm safety," Judge Cooke wrote in her injunction.
Proponents of the Florida law have argued that it represents a Second Amendment issue involving the right to bear arms. However, Judge Cooke disagreed, calling it a First Amendment – or freedom of speech – issue instead.
"A practitioner who counsels a patient on firearm safety, even when entirely irrelevant to medical care or safety, does not affect nor interfere with the patient’s right to continue to own, possess, or use firearms," she wrote.
Mount Sinai Team Reduces LOS, Costs with Mobile ACE Approach

With our aging population, the challenges of meeting the unique needs of frail elderly patients will continue to mount. In the current issue of the Journal of Hospital Medicine, authors from Mount Sinai Medical Center in New York City report on their adaptation of the acute care for the elderly, or ACE, approach.1 They found that by bringing geriatrics-focused, team-based care to the patient (instead of locating the patient only in the ACE unit), they were able to reduce costs by an average of $4,943 per patient.
And, beginning in year two of the study, when the team incorporated hospitalists into their model, the ACE team decreased length of stay (LOS) by 1.6 days per patient.
From ACE to MACE
Since the mid-1990s, studies have shown that the ACE unit model can be effective in meeting the unique needs of frail, elderly patients. But even at institutions where these geriatric-focused units have been established, hospitals might not have enough dedicated beds for every elderly patient.
“A geographically based unit is difficult to accomplish when you have high occupancy rates in the hospital,” says lead author Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile ACE Service at Mount Sinai.
Dr. Farber and his colleagues began their mobile ACE (MACE) approach in 2007. Their retrospective cohort study compared outcomes of 8,094 hospitalized elderly patients cared for in the traditional ACE, the general medical service, or the MACE over a three-year period. To compare ACE and MACE patient outcomes, they limited their study sample to patients who already had been seen as part of their outpatient geriatrics service. Besides the shorter LOS, the MACE model also realized a net savings of $2,081 in direct hospital costs, $9,37 in nursing costs, and $223 in pharmacy costs in year two.
The MACE team, comprised of a geriatrician-hospitalist, geriatric medicine fellow, social worker, and nurse coordinator, met daily or twice a day. The nurse coordinator identified and resolved complex family and living situations, and daily check-ins with the patients’ caregivers or family members ensured that care plans and discharge plans were clearly understood before the patient left the hospital, Dr. Farber explains.

—Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine, director, Mobile ACE Service, Mount Sinai Medical Center, New York City
Gathering pre-hospitalization history is facilitated by the linkage of the hospital’s electronic health record with that of the Mount Sinai outpatient geriatrics practice and the hospital’s affiliated nursing home. Dr. Farber admits the integrated system confers an advantage to the geriatrics service. But community-based hospitalists can increase their odds of having accurate pre-hospitalization information by concerted outreach to referral sources in their community, he says.
Commenting on the study’s results, Heidi Wald, MD, MSPH, associate professor of medicine in the division of healthcare policy research at the University of Colorado Denver School of Medicine, notes that “hospitalists are great at providing efficient care, and geriatricians are good at preserving function and mitigating harm, so it was only logical that hybrids of the two models might achieve both sets of aims.”
One model that she and her UC Denver colleagues have studied utilizes “geriatricized” hospitalists (through focused geriatrics and CME programs), which allows the physicians to feel comfortable managing the unique needs of these patients. She says that functional outcomes warrant attention in the next generation of studies in this area.
Dr. Farber’s colleague, William Hung, MD, is analyzing the data of a prospective, longitudinal study focusing on functional status and post-hospitalization follow-up.
Gretchen Henkel is a freelance writer based in southern California.
Reference
1. Farber JI, Korc-Grodzicki B, Du Q, Leipzig, RM, Siu, AL. Operational and quality outcomes of a mobile acute care for the elderly service. J Hosp Med. 2011;6(6):358-363.
With our aging population, the challenges of meeting the unique needs of frail elderly patients will continue to mount. In the current issue of the Journal of Hospital Medicine, authors from Mount Sinai Medical Center in New York City report on their adaptation of the acute care for the elderly, or ACE, approach.1 They found that by bringing geriatrics-focused, team-based care to the patient (instead of locating the patient only in the ACE unit), they were able to reduce costs by an average of $4,943 per patient.
And, beginning in year two of the study, when the team incorporated hospitalists into their model, the ACE team decreased length of stay (LOS) by 1.6 days per patient.
From ACE to MACE
Since the mid-1990s, studies have shown that the ACE unit model can be effective in meeting the unique needs of frail, elderly patients. But even at institutions where these geriatric-focused units have been established, hospitals might not have enough dedicated beds for every elderly patient.
“A geographically based unit is difficult to accomplish when you have high occupancy rates in the hospital,” says lead author Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile ACE Service at Mount Sinai.
Dr. Farber and his colleagues began their mobile ACE (MACE) approach in 2007. Their retrospective cohort study compared outcomes of 8,094 hospitalized elderly patients cared for in the traditional ACE, the general medical service, or the MACE over a three-year period. To compare ACE and MACE patient outcomes, they limited their study sample to patients who already had been seen as part of their outpatient geriatrics service. Besides the shorter LOS, the MACE model also realized a net savings of $2,081 in direct hospital costs, $9,37 in nursing costs, and $223 in pharmacy costs in year two.
The MACE team, comprised of a geriatrician-hospitalist, geriatric medicine fellow, social worker, and nurse coordinator, met daily or twice a day. The nurse coordinator identified and resolved complex family and living situations, and daily check-ins with the patients’ caregivers or family members ensured that care plans and discharge plans were clearly understood before the patient left the hospital, Dr. Farber explains.
—Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine, director, Mobile ACE Service, Mount Sinai Medical Center, New York City
Gathering pre-hospitalization history is facilitated by the linkage of the hospital’s electronic health record with that of the Mount Sinai outpatient geriatrics practice and the hospital’s affiliated nursing home. Dr. Farber admits the integrated system confers an advantage to the geriatrics service. But community-based hospitalists can increase their odds of having accurate pre-hospitalization information by concerted outreach to referral sources in their community, he says.
Commenting on the study’s results, Heidi Wald, MD, MSPH, associate professor of medicine in the division of healthcare policy research at the University of Colorado Denver School of Medicine, notes that “hospitalists are great at providing efficient care, and geriatricians are good at preserving function and mitigating harm, so it was only logical that hybrids of the two models might achieve both sets of aims.”
One model that she and her UC Denver colleagues have studied utilizes “geriatricized” hospitalists (through focused geriatrics and CME programs), which allows the physicians to feel comfortable managing the unique needs of these patients. She says that functional outcomes warrant attention in the next generation of studies in this area.
Dr. Farber’s colleague, William Hung, MD, is analyzing the data of a prospective, longitudinal study focusing on functional status and post-hospitalization follow-up.
Gretchen Henkel is a freelance writer based in southern California.
Reference
1. Farber JI, Korc-Grodzicki B, Du Q, Leipzig, RM, Siu, AL. Operational and quality outcomes of a mobile acute care for the elderly service. J Hosp Med. 2011;6(6):358-363.
With our aging population, the challenges of meeting the unique needs of frail elderly patients will continue to mount. In the current issue of the Journal of Hospital Medicine, authors from Mount Sinai Medical Center in New York City report on their adaptation of the acute care for the elderly, or ACE, approach.1 They found that by bringing geriatrics-focused, team-based care to the patient (instead of locating the patient only in the ACE unit), they were able to reduce costs by an average of $4,943 per patient.
And, beginning in year two of the study, when the team incorporated hospitalists into their model, the ACE team decreased length of stay (LOS) by 1.6 days per patient.
From ACE to MACE
Since the mid-1990s, studies have shown that the ACE unit model can be effective in meeting the unique needs of frail, elderly patients. But even at institutions where these geriatric-focused units have been established, hospitals might not have enough dedicated beds for every elderly patient.
“A geographically based unit is difficult to accomplish when you have high occupancy rates in the hospital,” says lead author Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine and director of the Mobile ACE Service at Mount Sinai.
Dr. Farber and his colleagues began their mobile ACE (MACE) approach in 2007. Their retrospective cohort study compared outcomes of 8,094 hospitalized elderly patients cared for in the traditional ACE, the general medical service, or the MACE over a three-year period. To compare ACE and MACE patient outcomes, they limited their study sample to patients who already had been seen as part of their outpatient geriatrics service. Besides the shorter LOS, the MACE model also realized a net savings of $2,081 in direct hospital costs, $9,37 in nursing costs, and $223 in pharmacy costs in year two.
The MACE team, comprised of a geriatrician-hospitalist, geriatric medicine fellow, social worker, and nurse coordinator, met daily or twice a day. The nurse coordinator identified and resolved complex family and living situations, and daily check-ins with the patients’ caregivers or family members ensured that care plans and discharge plans were clearly understood before the patient left the hospital, Dr. Farber explains.
—Jeffrey Farber, MD, assistant professor of geriatrics and palliative medicine, director, Mobile ACE Service, Mount Sinai Medical Center, New York City
Gathering pre-hospitalization history is facilitated by the linkage of the hospital’s electronic health record with that of the Mount Sinai outpatient geriatrics practice and the hospital’s affiliated nursing home. Dr. Farber admits the integrated system confers an advantage to the geriatrics service. But community-based hospitalists can increase their odds of having accurate pre-hospitalization information by concerted outreach to referral sources in their community, he says.
Commenting on the study’s results, Heidi Wald, MD, MSPH, associate professor of medicine in the division of healthcare policy research at the University of Colorado Denver School of Medicine, notes that “hospitalists are great at providing efficient care, and geriatricians are good at preserving function and mitigating harm, so it was only logical that hybrids of the two models might achieve both sets of aims.”
One model that she and her UC Denver colleagues have studied utilizes “geriatricized” hospitalists (through focused geriatrics and CME programs), which allows the physicians to feel comfortable managing the unique needs of these patients. She says that functional outcomes warrant attention in the next generation of studies in this area.
Dr. Farber’s colleague, William Hung, MD, is analyzing the data of a prospective, longitudinal study focusing on functional status and post-hospitalization follow-up.
Gretchen Henkel is a freelance writer based in southern California.
Reference
1. Farber JI, Korc-Grodzicki B, Du Q, Leipzig, RM, Siu, AL. Operational and quality outcomes of a mobile acute care for the elderly service. J Hosp Med. 2011;6(6):358-363.
Showtime for Patient Education
Hospitalist Andrea Peterson, MD, of Norwalk Hospital in Norwalk, Conn., whose job involves educating hospitalized patients about their personal health, has found an additional channel for teaching health concepts: She cohosts "Health Talk," a half-hour local cable television show in Fairfield County.
Dr. Peterson, who started working at Norwalk in 2002 as the hospital's fourth hospitalist, cohosts "Health Talk" with the hospital's vice president and chief medical officer, Eric Mazur, MD. She first appeared on the show as a guest, discussing subjects of professional interest, such as end-of-life care, ethics, patient safety, and spirituality in medicine, then served later as fill-in host before becoming the permanent cohost.
"It's really fun. It's totally different than my day job," she says. "It can also be fatiguing—you have to be bright and energetic on a sustained basis."
Conversations on the air are different than interactions with patients, as the dead space of TV can be deadly, she says. "I had to learn, with the help of a media coach, to start asking the next question while the person is finishing the previous answer. But I've gotten to interact with colleagues in totally different ways and to meet patients with inspiring stories," she says.
The program tapes four shows one day a month. Each program is broadcast several times over the course of a week. Interview subjects are both doctors and patients, and most of the interactions are unscripted.
"Both Eric and I feel it is very important to have topics and discussions that are real and meaningful to people's health, bread-and-butter issues like diabetes, colon-cancer screening, strokes and MI, and medication safety," Dr. Peterson says. "We continually do smoking education. We're always telling people: Talk to your family about what's important to you. Appoint a healthcare surrogate. These are the same messages I give to my patients in the hospital," she says.
Think you may be interesting in hosting your own patient education program? Click here for a list of community and public access TV sites.
Hospitalist Andrea Peterson, MD, of Norwalk Hospital in Norwalk, Conn., whose job involves educating hospitalized patients about their personal health, has found an additional channel for teaching health concepts: She cohosts "Health Talk," a half-hour local cable television show in Fairfield County.
Dr. Peterson, who started working at Norwalk in 2002 as the hospital's fourth hospitalist, cohosts "Health Talk" with the hospital's vice president and chief medical officer, Eric Mazur, MD. She first appeared on the show as a guest, discussing subjects of professional interest, such as end-of-life care, ethics, patient safety, and spirituality in medicine, then served later as fill-in host before becoming the permanent cohost.
"It's really fun. It's totally different than my day job," she says. "It can also be fatiguing—you have to be bright and energetic on a sustained basis."
Conversations on the air are different than interactions with patients, as the dead space of TV can be deadly, she says. "I had to learn, with the help of a media coach, to start asking the next question while the person is finishing the previous answer. But I've gotten to interact with colleagues in totally different ways and to meet patients with inspiring stories," she says.
The program tapes four shows one day a month. Each program is broadcast several times over the course of a week. Interview subjects are both doctors and patients, and most of the interactions are unscripted.
"Both Eric and I feel it is very important to have topics and discussions that are real and meaningful to people's health, bread-and-butter issues like diabetes, colon-cancer screening, strokes and MI, and medication safety," Dr. Peterson says. "We continually do smoking education. We're always telling people: Talk to your family about what's important to you. Appoint a healthcare surrogate. These are the same messages I give to my patients in the hospital," she says.
Think you may be interesting in hosting your own patient education program? Click here for a list of community and public access TV sites.
Hospitalist Andrea Peterson, MD, of Norwalk Hospital in Norwalk, Conn., whose job involves educating hospitalized patients about their personal health, has found an additional channel for teaching health concepts: She cohosts "Health Talk," a half-hour local cable television show in Fairfield County.
Dr. Peterson, who started working at Norwalk in 2002 as the hospital's fourth hospitalist, cohosts "Health Talk" with the hospital's vice president and chief medical officer, Eric Mazur, MD. She first appeared on the show as a guest, discussing subjects of professional interest, such as end-of-life care, ethics, patient safety, and spirituality in medicine, then served later as fill-in host before becoming the permanent cohost.
"It's really fun. It's totally different than my day job," she says. "It can also be fatiguing—you have to be bright and energetic on a sustained basis."
Conversations on the air are different than interactions with patients, as the dead space of TV can be deadly, she says. "I had to learn, with the help of a media coach, to start asking the next question while the person is finishing the previous answer. But I've gotten to interact with colleagues in totally different ways and to meet patients with inspiring stories," she says.
The program tapes four shows one day a month. Each program is broadcast several times over the course of a week. Interview subjects are both doctors and patients, and most of the interactions are unscripted.
"Both Eric and I feel it is very important to have topics and discussions that are real and meaningful to people's health, bread-and-butter issues like diabetes, colon-cancer screening, strokes and MI, and medication safety," Dr. Peterson says. "We continually do smoking education. We're always telling people: Talk to your family about what's important to you. Appoint a healthcare surrogate. These are the same messages I give to my patients in the hospital," she says.
Think you may be interesting in hosting your own patient education program? Click here for a list of community and public access TV sites.
In the Literature: Research You Need to Know
Clinical question: Is transcatheter aortic-valve replacement comparable to surgical valve replacement in high-operative-risk patients?
Background: In the randomized Placement of Aortic Transcatheter Valves (PARTNER) trial, patients who were not surgical candidates underwent transcatheter aortic-valve replacement, resulting in reduced symptoms and 20% improvement in one-year survival rates. Transcatheter valve replacement has not been compared to surgical replacement in high-operative-risk patients who remain candidates for surgical replacement.
Study design: Randomized controlled trial powered for noninferiority.
Setting: Twenty-five centers in the U.S., Canada, and Germany.
Synopsis: Six-hundred ninety-nine high-operative-risk patients with severe aortic stenosis were randomized to undergo transcatheter aortic-valve replacement or surgical replacement. In the intention-to-treat analysis, all-cause mortality rates were 3.4% in the transcatheter group and 6.5% in the surgical group at 30 days (P=0.07) and 24.2% vs. 26.8% at one year (P=0.44). Rates of major stroke were 3.8% in the transcatheter group compared with 2.1% in the surgical group at 30 days (P=0.20) and 5.1% vs. 2.4% at one year (P=0.07).
The transcatheter group had a significantly higher rate of major vascular complications, but had lower rates of major bleeding and new onset-atrial fibrillation. At one year, improvement in cardiac symptoms and the six-minute-walk distance were not significantly different in the two groups.
Bottom line: In high-operative-risk patients with severe aortic stenosis, transcatheter and surgical aortic-valve replacement had similar mortality at 30 days and one year, but there were a few significant differences in periprocedural risks.
Citation: Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
For more physician reviews of HM-related literature, visit our website.
Clinical question: Is transcatheter aortic-valve replacement comparable to surgical valve replacement in high-operative-risk patients?
Background: In the randomized Placement of Aortic Transcatheter Valves (PARTNER) trial, patients who were not surgical candidates underwent transcatheter aortic-valve replacement, resulting in reduced symptoms and 20% improvement in one-year survival rates. Transcatheter valve replacement has not been compared to surgical replacement in high-operative-risk patients who remain candidates for surgical replacement.
Study design: Randomized controlled trial powered for noninferiority.
Setting: Twenty-five centers in the U.S., Canada, and Germany.
Synopsis: Six-hundred ninety-nine high-operative-risk patients with severe aortic stenosis were randomized to undergo transcatheter aortic-valve replacement or surgical replacement. In the intention-to-treat analysis, all-cause mortality rates were 3.4% in the transcatheter group and 6.5% in the surgical group at 30 days (P=0.07) and 24.2% vs. 26.8% at one year (P=0.44). Rates of major stroke were 3.8% in the transcatheter group compared with 2.1% in the surgical group at 30 days (P=0.20) and 5.1% vs. 2.4% at one year (P=0.07).
The transcatheter group had a significantly higher rate of major vascular complications, but had lower rates of major bleeding and new onset-atrial fibrillation. At one year, improvement in cardiac symptoms and the six-minute-walk distance were not significantly different in the two groups.
Bottom line: In high-operative-risk patients with severe aortic stenosis, transcatheter and surgical aortic-valve replacement had similar mortality at 30 days and one year, but there were a few significant differences in periprocedural risks.
Citation: Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
For more physician reviews of HM-related literature, visit our website.
Clinical question: Is transcatheter aortic-valve replacement comparable to surgical valve replacement in high-operative-risk patients?
Background: In the randomized Placement of Aortic Transcatheter Valves (PARTNER) trial, patients who were not surgical candidates underwent transcatheter aortic-valve replacement, resulting in reduced symptoms and 20% improvement in one-year survival rates. Transcatheter valve replacement has not been compared to surgical replacement in high-operative-risk patients who remain candidates for surgical replacement.
Study design: Randomized controlled trial powered for noninferiority.
Setting: Twenty-five centers in the U.S., Canada, and Germany.
Synopsis: Six-hundred ninety-nine high-operative-risk patients with severe aortic stenosis were randomized to undergo transcatheter aortic-valve replacement or surgical replacement. In the intention-to-treat analysis, all-cause mortality rates were 3.4% in the transcatheter group and 6.5% in the surgical group at 30 days (P=0.07) and 24.2% vs. 26.8% at one year (P=0.44). Rates of major stroke were 3.8% in the transcatheter group compared with 2.1% in the surgical group at 30 days (P=0.20) and 5.1% vs. 2.4% at one year (P=0.07).
The transcatheter group had a significantly higher rate of major vascular complications, but had lower rates of major bleeding and new onset-atrial fibrillation. At one year, improvement in cardiac symptoms and the six-minute-walk distance were not significantly different in the two groups.
Bottom line: In high-operative-risk patients with severe aortic stenosis, transcatheter and surgical aortic-valve replacement had similar mortality at 30 days and one year, but there were a few significant differences in periprocedural risks.
Citation: Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-2198.
For more physician reviews of HM-related literature, visit our website.
International Hospital Medicine Scene
In the 15 years since Wachter and Goldman coined the term hospitalists, the specialty of Hospital Medicine grew faster than any other in the history of American medicine.1 The early drivers for growth were largely economic: There were significant reductions in resource use, with a 13% decrease in hospital costs and a 16% decrease in hospital lengths of stay (LOS).2 Hospitalist clinician‐educators increased the satisfaction of residents and medical students in academic settings.2 Patient satisfaction and hospital mortality did not suffer.2
Recent growth of Hospital Medicine revolves around 3 drivers: 1) improving quality and safety of hospitalized patientsowing in large part to the Institute of Medicine's 2 compelling reports, To Err Is Human3 and Crossing the Quality Chasm4; 2) hospitalist and specialist (surgeon) comanagement; and 3) the effects of duty hours restrictions imposed by the Accreditation Council for Graduate Medical Education affecting United States (US) teaching hospitals.5
In this issue of the Journal of Hospital Medicine, Shu and colleagues6 report on the performance of a hospitalist program in Taiwan. To the best of our knowledge, this report from Asia is the first published report of a successful hospitalist model with measurable patient outcomes outside of North America. Specifically, over a year, the authors found that patients admitted by hospitalists had a shorter LOS and lower cost per case, with no difference in in‐hospital mortality and 30‐day readmission. These results were obtained despite the fact that the cohort of patients admitted to the hospitalist team was older, sicker, and had worse functional capacity. Additionally, the patients admitted to the hospitalist team, and who died during hospitalization, were more likely to have a do‐not‐resuscitate (DNR) order signed, when compared with those patients admitted to the general internal medicine teaching service. Comparing LOS with North America may be problematic. As Shu and colleagues6 point out, there are cultural and economic issues that affect the behavior of patients and physicians in Taiwan.
The healthcare system in Taiwan has similarities to the healthcare systems in the United Kingdom (UK) and the US. In 1995, Taiwan implemented a national health insurance system. The UK has had a National Health Service for many years that provides most services for free. The Taiwanese system requires modest copayments for services. The implementation of the national health insurance system in Taiwan increased healthcare access from 57% of the population to 98%.7 The increase in insurance across the population with modest copayments has made it possible for a larger percentage of the population to access the healthcare system.7 According to the authors, this has resulted in increased hospital admissions (35% in the decade since the introduction of national health insurance), resulting in a shortage of Hospital Medicine physicians and hospital beds.7 Compounding the stressors on this system is that the diagnosis related group (DRG) reimbursement model, similar to the American DRG reimbursement model, will soon take effect in Taiwan. As a result, our colleagues in Taiwan are experiencing issues commonly faced by mature hospitalist programs in the US: increased needs in efficiency to improve patient flow and decrease emergency room overcrowding and LOS; and concerns with safe discharges of high‐risk patients while ensuring outpatient follow‐up. This is a scenario with which US hospitalists are all too familiar.
The next step for Taiwan might be to implement a culturally specific patient education program regarding the discharge process. The first step would be a needs assessment survey of patients in Taiwan, inquiring about concerns regarding readiness for discharge. They might inquire about patient beliefs regarding understanding indications for inpatient hospitalization versus discharge to home, home with home services, or skilled nursing facilities. They might be able to drill down to the root cause of refusal to be discharged home. These data could help our colleagues in Taiwan create their own discharge program to drive down LOS closer to that of the US and other Western countries, in order to reap financial benefits and improve resource utilization.
What do we know about the growth of Hospital Medicine around the world? The Society of Hospital Medicine (SHM) reports international members from 26 countries around the world. In North America, SHM members are found in the US, Canada, and Bermuda. In Europe, SHM members are found in England, Ireland, Scotland, Spain, Belgium, Portugal, Italy, and Germany. In South America, SHM members are found in Brazil, Chile, Colombia, and Argentina. In Asia and the Middle East, SHM has members in Saudi Arabia, Israel, United Arab Emirates, Pakistan, Japan, China, the Philippines, and Singapore. In Oceania, SHM has members in Australia, and New Zealand. In Africa, 1 SHM member is from Nigeria (Society of Hospital Medicine Data, 2011). In fact, the International Hospitalists Section of SHM is 1 of only 2 sections that the Society recognizes.
Hospitalists are organizing themselves abroad as well. In Canada, the Canadian Society of Hospital Medicine was founded in 2001 and has had 8 national conferences to date.8 There are roughly 1,000 Canadian hospitalists (Wilton D, personal communication, 2011). Whereas most US hospitalists are internists or pediatricians, in Canada, most hospitalists are family physicians. In the US, hospitalists are more likely to perform the following services: consultation, intensive care unit patient care, rapid response team service, surgical comanagement, and evening on‐site coverage. Canadian hospitalists are more likely to provide pediatric care and psychiatry inpatient comanagement.9
In the UK, the professional organization of physicians most similar to US hospitalists, acute physicians, is called SAM (The Society for Acute Medicine). It was founded in 2000.10 In the UK, general practitioners (GPs) never care for inpatients; at the time, GPs referred all admissions to organ‐specific specialists (eg, cardiologists). Acute medicine was created due to the realization that medical inpatients were too complex to have specialists managing them. Training programs were set up circa 2003 to create this specialty and address this need. Acute physicians staff geographically localized acute medicine units near emergency departments. These patients stay 1 to 3 days in an effort to concentrate services and resources to these patients, to prevent longer stays once fully admitted (Smith R, personal communication, April 23, 2011). Acute medicine units in the UK, Ireland, and Australia have led to positive benefits on patient outcomes. A review article by Scott and colleagues revealed reductions in LOS, inpatient mortality, and emergency department LOS, without increased 30‐day readmission rates. They found increased staff and patient satisfaction, and more medical patients discharged directly to home from acute medical units.11 The development of acute medicine in Australia and New Zealand began around 2005 and derives from the geographic localization of the UK model. Whereas the UK model has a focus on the first 72 hours of hospitalization, the model in Australia and New Zealand is more similar to the US model of following patients through their entire admission.12 Unlike the UK, Australia does not have dedicated acute medicine training programs.
PASHA, the Pan‐American Society of Hospitalists, is a loose affiliation of hospitalists largely in South America, linking with their North American colleagues. PASHA grew out of SOBRAMH, Sociedade Brasileira de Medicina Hospitalarthe first Hospital Medicine Society in South America, tracing its roots to 2004. To date, PASHA has had 1 international conference, but there have been 2 national conferences each in Brazil and Chile, and 1 in Colombia. The concept and advantages of Hospital Medicine have been presented at a conference in Panama. Argentina has its first Hospital Medicine Congress scheduled for September 2011, in concert with PASHA.
Two Hospital Medicine programs abroad deserve special mention. Both started in 2005 and have instituted the full hospitalist package, including multiple evidence‐based order sets at both sites (eg, deep vein thrombosis [DVT] prophylaxis and hyperglycemia management). At the Pontificia Universidad Catlica in Santiago, Chile, they have been awarded national grants to study hyperglycemia in hospitalized patients, and they have sent their faculty to the US for additional training in patient safety, quality improvement, leadership, and medical informatics. They have succeeded in decreasing LOS and improved the exam grades of their learners. Their faculty has published in national journals and is now beginning to submit their work for publication in US‐based journals (Rojas L, personal communication, April 22, 2011). The Clnica Universidad de Navarra (CUN) in Pamplona, Spain is a Joint Commission certified facility with a full electronic medical record. Hospitalists there are looking at ways in which hospitalist‐staffed intermediate care units can benefit patient outcomes. Additionally, they have comanagement arrangements with nearly all surgical subspecialties. The Management of the Hospitalized Patient symposium was organized by CUN hospitalists in 2007the first Hospital Medicine Congress, to our knowledge, in continental Europe. At any one time, 30% of all residents in all specialties rotate with CUN hospitalists (Lucena F, personal communication, April 22, 2011).
The specialty of Hospital Medicine is truly global. Our colleagues around the world employing the hospitalist model of care are now producing outcomes similar to the published models in North America and to the acute medicine models in Europe and Australia. According to the Society of Hospital Medicine, there are over 30,000 hospitalists in the US. There could be well over 50,000 hospitalists around the world. In 5 years, the world may have 100,000 hospitalists. The same drivers are fueling the growth of Hospital Medicine around the world. The evidence is building that the hospitalist model of care has financial and quality benefits that transcend borders. We forecast that the hospitalist model of care will become an increasingly larger part of the solution around the world to fix these international healthcare systems.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335(7):514–517.
- ,.The hospitalist movement 5 years later.JAMA.2002;287(4):487–494.
- ,,.To Err Is Human: Building a Safer Health System; Institute of Medicine Committee on Quality of Health Care in America.Washington, DC:National Academy Press;2000.
- ,,.Crossing the Quality Chasm: A New Health System for the 21st Century; Institute of Medicine Committee of Health Care in America.Washington, DC:National Academy Press;2001.
- .The state of hospital medicine in 2008.Med Clin North Am.2008;92:265–273.
- et al.J Hosp Med.2011;6:378–382.
- ,,.A 10‐year experience with universal health insurance in Taiwan: measuring changes in health and health disparity.Ann Intern Med.2008;148(4):258–267.
- Canadian Hospitalist: Canadian Society of Hospital Medicine Web site. Available at: http://canadianhospitalist.ca/. Accessed April 15,2011.
- ,,,,,.Characteristics of hospitalists and hospitalist programs in the United States and Canada.J Clin Outcomes Manage.2009;16(2):69–74.
- The Society for Acute Medicine Web site. Available at: www.acutemedicine.org.uk. Accessed April 14,2011.
- ,,.Effectiveness of acute medical units in hospitals: a systematic review.Int J Qual Health Care.2009;21(6):397–407.
- .Acute and general medicine on opposite sides of the world.Acute Med.2011;10(2):67–68.
In the 15 years since Wachter and Goldman coined the term hospitalists, the specialty of Hospital Medicine grew faster than any other in the history of American medicine.1 The early drivers for growth were largely economic: There were significant reductions in resource use, with a 13% decrease in hospital costs and a 16% decrease in hospital lengths of stay (LOS).2 Hospitalist clinician‐educators increased the satisfaction of residents and medical students in academic settings.2 Patient satisfaction and hospital mortality did not suffer.2
Recent growth of Hospital Medicine revolves around 3 drivers: 1) improving quality and safety of hospitalized patientsowing in large part to the Institute of Medicine's 2 compelling reports, To Err Is Human3 and Crossing the Quality Chasm4; 2) hospitalist and specialist (surgeon) comanagement; and 3) the effects of duty hours restrictions imposed by the Accreditation Council for Graduate Medical Education affecting United States (US) teaching hospitals.5
In this issue of the Journal of Hospital Medicine, Shu and colleagues6 report on the performance of a hospitalist program in Taiwan. To the best of our knowledge, this report from Asia is the first published report of a successful hospitalist model with measurable patient outcomes outside of North America. Specifically, over a year, the authors found that patients admitted by hospitalists had a shorter LOS and lower cost per case, with no difference in in‐hospital mortality and 30‐day readmission. These results were obtained despite the fact that the cohort of patients admitted to the hospitalist team was older, sicker, and had worse functional capacity. Additionally, the patients admitted to the hospitalist team, and who died during hospitalization, were more likely to have a do‐not‐resuscitate (DNR) order signed, when compared with those patients admitted to the general internal medicine teaching service. Comparing LOS with North America may be problematic. As Shu and colleagues6 point out, there are cultural and economic issues that affect the behavior of patients and physicians in Taiwan.
The healthcare system in Taiwan has similarities to the healthcare systems in the United Kingdom (UK) and the US. In 1995, Taiwan implemented a national health insurance system. The UK has had a National Health Service for many years that provides most services for free. The Taiwanese system requires modest copayments for services. The implementation of the national health insurance system in Taiwan increased healthcare access from 57% of the population to 98%.7 The increase in insurance across the population with modest copayments has made it possible for a larger percentage of the population to access the healthcare system.7 According to the authors, this has resulted in increased hospital admissions (35% in the decade since the introduction of national health insurance), resulting in a shortage of Hospital Medicine physicians and hospital beds.7 Compounding the stressors on this system is that the diagnosis related group (DRG) reimbursement model, similar to the American DRG reimbursement model, will soon take effect in Taiwan. As a result, our colleagues in Taiwan are experiencing issues commonly faced by mature hospitalist programs in the US: increased needs in efficiency to improve patient flow and decrease emergency room overcrowding and LOS; and concerns with safe discharges of high‐risk patients while ensuring outpatient follow‐up. This is a scenario with which US hospitalists are all too familiar.
The next step for Taiwan might be to implement a culturally specific patient education program regarding the discharge process. The first step would be a needs assessment survey of patients in Taiwan, inquiring about concerns regarding readiness for discharge. They might inquire about patient beliefs regarding understanding indications for inpatient hospitalization versus discharge to home, home with home services, or skilled nursing facilities. They might be able to drill down to the root cause of refusal to be discharged home. These data could help our colleagues in Taiwan create their own discharge program to drive down LOS closer to that of the US and other Western countries, in order to reap financial benefits and improve resource utilization.
What do we know about the growth of Hospital Medicine around the world? The Society of Hospital Medicine (SHM) reports international members from 26 countries around the world. In North America, SHM members are found in the US, Canada, and Bermuda. In Europe, SHM members are found in England, Ireland, Scotland, Spain, Belgium, Portugal, Italy, and Germany. In South America, SHM members are found in Brazil, Chile, Colombia, and Argentina. In Asia and the Middle East, SHM has members in Saudi Arabia, Israel, United Arab Emirates, Pakistan, Japan, China, the Philippines, and Singapore. In Oceania, SHM has members in Australia, and New Zealand. In Africa, 1 SHM member is from Nigeria (Society of Hospital Medicine Data, 2011). In fact, the International Hospitalists Section of SHM is 1 of only 2 sections that the Society recognizes.
Hospitalists are organizing themselves abroad as well. In Canada, the Canadian Society of Hospital Medicine was founded in 2001 and has had 8 national conferences to date.8 There are roughly 1,000 Canadian hospitalists (Wilton D, personal communication, 2011). Whereas most US hospitalists are internists or pediatricians, in Canada, most hospitalists are family physicians. In the US, hospitalists are more likely to perform the following services: consultation, intensive care unit patient care, rapid response team service, surgical comanagement, and evening on‐site coverage. Canadian hospitalists are more likely to provide pediatric care and psychiatry inpatient comanagement.9
In the UK, the professional organization of physicians most similar to US hospitalists, acute physicians, is called SAM (The Society for Acute Medicine). It was founded in 2000.10 In the UK, general practitioners (GPs) never care for inpatients; at the time, GPs referred all admissions to organ‐specific specialists (eg, cardiologists). Acute medicine was created due to the realization that medical inpatients were too complex to have specialists managing them. Training programs were set up circa 2003 to create this specialty and address this need. Acute physicians staff geographically localized acute medicine units near emergency departments. These patients stay 1 to 3 days in an effort to concentrate services and resources to these patients, to prevent longer stays once fully admitted (Smith R, personal communication, April 23, 2011). Acute medicine units in the UK, Ireland, and Australia have led to positive benefits on patient outcomes. A review article by Scott and colleagues revealed reductions in LOS, inpatient mortality, and emergency department LOS, without increased 30‐day readmission rates. They found increased staff and patient satisfaction, and more medical patients discharged directly to home from acute medical units.11 The development of acute medicine in Australia and New Zealand began around 2005 and derives from the geographic localization of the UK model. Whereas the UK model has a focus on the first 72 hours of hospitalization, the model in Australia and New Zealand is more similar to the US model of following patients through their entire admission.12 Unlike the UK, Australia does not have dedicated acute medicine training programs.
PASHA, the Pan‐American Society of Hospitalists, is a loose affiliation of hospitalists largely in South America, linking with their North American colleagues. PASHA grew out of SOBRAMH, Sociedade Brasileira de Medicina Hospitalarthe first Hospital Medicine Society in South America, tracing its roots to 2004. To date, PASHA has had 1 international conference, but there have been 2 national conferences each in Brazil and Chile, and 1 in Colombia. The concept and advantages of Hospital Medicine have been presented at a conference in Panama. Argentina has its first Hospital Medicine Congress scheduled for September 2011, in concert with PASHA.
Two Hospital Medicine programs abroad deserve special mention. Both started in 2005 and have instituted the full hospitalist package, including multiple evidence‐based order sets at both sites (eg, deep vein thrombosis [DVT] prophylaxis and hyperglycemia management). At the Pontificia Universidad Catlica in Santiago, Chile, they have been awarded national grants to study hyperglycemia in hospitalized patients, and they have sent their faculty to the US for additional training in patient safety, quality improvement, leadership, and medical informatics. They have succeeded in decreasing LOS and improved the exam grades of their learners. Their faculty has published in national journals and is now beginning to submit their work for publication in US‐based journals (Rojas L, personal communication, April 22, 2011). The Clnica Universidad de Navarra (CUN) in Pamplona, Spain is a Joint Commission certified facility with a full electronic medical record. Hospitalists there are looking at ways in which hospitalist‐staffed intermediate care units can benefit patient outcomes. Additionally, they have comanagement arrangements with nearly all surgical subspecialties. The Management of the Hospitalized Patient symposium was organized by CUN hospitalists in 2007the first Hospital Medicine Congress, to our knowledge, in continental Europe. At any one time, 30% of all residents in all specialties rotate with CUN hospitalists (Lucena F, personal communication, April 22, 2011).
The specialty of Hospital Medicine is truly global. Our colleagues around the world employing the hospitalist model of care are now producing outcomes similar to the published models in North America and to the acute medicine models in Europe and Australia. According to the Society of Hospital Medicine, there are over 30,000 hospitalists in the US. There could be well over 50,000 hospitalists around the world. In 5 years, the world may have 100,000 hospitalists. The same drivers are fueling the growth of Hospital Medicine around the world. The evidence is building that the hospitalist model of care has financial and quality benefits that transcend borders. We forecast that the hospitalist model of care will become an increasingly larger part of the solution around the world to fix these international healthcare systems.
In the 15 years since Wachter and Goldman coined the term hospitalists, the specialty of Hospital Medicine grew faster than any other in the history of American medicine.1 The early drivers for growth were largely economic: There were significant reductions in resource use, with a 13% decrease in hospital costs and a 16% decrease in hospital lengths of stay (LOS).2 Hospitalist clinician‐educators increased the satisfaction of residents and medical students in academic settings.2 Patient satisfaction and hospital mortality did not suffer.2
Recent growth of Hospital Medicine revolves around 3 drivers: 1) improving quality and safety of hospitalized patientsowing in large part to the Institute of Medicine's 2 compelling reports, To Err Is Human3 and Crossing the Quality Chasm4; 2) hospitalist and specialist (surgeon) comanagement; and 3) the effects of duty hours restrictions imposed by the Accreditation Council for Graduate Medical Education affecting United States (US) teaching hospitals.5
In this issue of the Journal of Hospital Medicine, Shu and colleagues6 report on the performance of a hospitalist program in Taiwan. To the best of our knowledge, this report from Asia is the first published report of a successful hospitalist model with measurable patient outcomes outside of North America. Specifically, over a year, the authors found that patients admitted by hospitalists had a shorter LOS and lower cost per case, with no difference in in‐hospital mortality and 30‐day readmission. These results were obtained despite the fact that the cohort of patients admitted to the hospitalist team was older, sicker, and had worse functional capacity. Additionally, the patients admitted to the hospitalist team, and who died during hospitalization, were more likely to have a do‐not‐resuscitate (DNR) order signed, when compared with those patients admitted to the general internal medicine teaching service. Comparing LOS with North America may be problematic. As Shu and colleagues6 point out, there are cultural and economic issues that affect the behavior of patients and physicians in Taiwan.
The healthcare system in Taiwan has similarities to the healthcare systems in the United Kingdom (UK) and the US. In 1995, Taiwan implemented a national health insurance system. The UK has had a National Health Service for many years that provides most services for free. The Taiwanese system requires modest copayments for services. The implementation of the national health insurance system in Taiwan increased healthcare access from 57% of the population to 98%.7 The increase in insurance across the population with modest copayments has made it possible for a larger percentage of the population to access the healthcare system.7 According to the authors, this has resulted in increased hospital admissions (35% in the decade since the introduction of national health insurance), resulting in a shortage of Hospital Medicine physicians and hospital beds.7 Compounding the stressors on this system is that the diagnosis related group (DRG) reimbursement model, similar to the American DRG reimbursement model, will soon take effect in Taiwan. As a result, our colleagues in Taiwan are experiencing issues commonly faced by mature hospitalist programs in the US: increased needs in efficiency to improve patient flow and decrease emergency room overcrowding and LOS; and concerns with safe discharges of high‐risk patients while ensuring outpatient follow‐up. This is a scenario with which US hospitalists are all too familiar.
The next step for Taiwan might be to implement a culturally specific patient education program regarding the discharge process. The first step would be a needs assessment survey of patients in Taiwan, inquiring about concerns regarding readiness for discharge. They might inquire about patient beliefs regarding understanding indications for inpatient hospitalization versus discharge to home, home with home services, or skilled nursing facilities. They might be able to drill down to the root cause of refusal to be discharged home. These data could help our colleagues in Taiwan create their own discharge program to drive down LOS closer to that of the US and other Western countries, in order to reap financial benefits and improve resource utilization.
What do we know about the growth of Hospital Medicine around the world? The Society of Hospital Medicine (SHM) reports international members from 26 countries around the world. In North America, SHM members are found in the US, Canada, and Bermuda. In Europe, SHM members are found in England, Ireland, Scotland, Spain, Belgium, Portugal, Italy, and Germany. In South America, SHM members are found in Brazil, Chile, Colombia, and Argentina. In Asia and the Middle East, SHM has members in Saudi Arabia, Israel, United Arab Emirates, Pakistan, Japan, China, the Philippines, and Singapore. In Oceania, SHM has members in Australia, and New Zealand. In Africa, 1 SHM member is from Nigeria (Society of Hospital Medicine Data, 2011). In fact, the International Hospitalists Section of SHM is 1 of only 2 sections that the Society recognizes.
Hospitalists are organizing themselves abroad as well. In Canada, the Canadian Society of Hospital Medicine was founded in 2001 and has had 8 national conferences to date.8 There are roughly 1,000 Canadian hospitalists (Wilton D, personal communication, 2011). Whereas most US hospitalists are internists or pediatricians, in Canada, most hospitalists are family physicians. In the US, hospitalists are more likely to perform the following services: consultation, intensive care unit patient care, rapid response team service, surgical comanagement, and evening on‐site coverage. Canadian hospitalists are more likely to provide pediatric care and psychiatry inpatient comanagement.9
In the UK, the professional organization of physicians most similar to US hospitalists, acute physicians, is called SAM (The Society for Acute Medicine). It was founded in 2000.10 In the UK, general practitioners (GPs) never care for inpatients; at the time, GPs referred all admissions to organ‐specific specialists (eg, cardiologists). Acute medicine was created due to the realization that medical inpatients were too complex to have specialists managing them. Training programs were set up circa 2003 to create this specialty and address this need. Acute physicians staff geographically localized acute medicine units near emergency departments. These patients stay 1 to 3 days in an effort to concentrate services and resources to these patients, to prevent longer stays once fully admitted (Smith R, personal communication, April 23, 2011). Acute medicine units in the UK, Ireland, and Australia have led to positive benefits on patient outcomes. A review article by Scott and colleagues revealed reductions in LOS, inpatient mortality, and emergency department LOS, without increased 30‐day readmission rates. They found increased staff and patient satisfaction, and more medical patients discharged directly to home from acute medical units.11 The development of acute medicine in Australia and New Zealand began around 2005 and derives from the geographic localization of the UK model. Whereas the UK model has a focus on the first 72 hours of hospitalization, the model in Australia and New Zealand is more similar to the US model of following patients through their entire admission.12 Unlike the UK, Australia does not have dedicated acute medicine training programs.
PASHA, the Pan‐American Society of Hospitalists, is a loose affiliation of hospitalists largely in South America, linking with their North American colleagues. PASHA grew out of SOBRAMH, Sociedade Brasileira de Medicina Hospitalarthe first Hospital Medicine Society in South America, tracing its roots to 2004. To date, PASHA has had 1 international conference, but there have been 2 national conferences each in Brazil and Chile, and 1 in Colombia. The concept and advantages of Hospital Medicine have been presented at a conference in Panama. Argentina has its first Hospital Medicine Congress scheduled for September 2011, in concert with PASHA.
Two Hospital Medicine programs abroad deserve special mention. Both started in 2005 and have instituted the full hospitalist package, including multiple evidence‐based order sets at both sites (eg, deep vein thrombosis [DVT] prophylaxis and hyperglycemia management). At the Pontificia Universidad Catlica in Santiago, Chile, they have been awarded national grants to study hyperglycemia in hospitalized patients, and they have sent their faculty to the US for additional training in patient safety, quality improvement, leadership, and medical informatics. They have succeeded in decreasing LOS and improved the exam grades of their learners. Their faculty has published in national journals and is now beginning to submit their work for publication in US‐based journals (Rojas L, personal communication, April 22, 2011). The Clnica Universidad de Navarra (CUN) in Pamplona, Spain is a Joint Commission certified facility with a full electronic medical record. Hospitalists there are looking at ways in which hospitalist‐staffed intermediate care units can benefit patient outcomes. Additionally, they have comanagement arrangements with nearly all surgical subspecialties. The Management of the Hospitalized Patient symposium was organized by CUN hospitalists in 2007the first Hospital Medicine Congress, to our knowledge, in continental Europe. At any one time, 30% of all residents in all specialties rotate with CUN hospitalists (Lucena F, personal communication, April 22, 2011).
The specialty of Hospital Medicine is truly global. Our colleagues around the world employing the hospitalist model of care are now producing outcomes similar to the published models in North America and to the acute medicine models in Europe and Australia. According to the Society of Hospital Medicine, there are over 30,000 hospitalists in the US. There could be well over 50,000 hospitalists around the world. In 5 years, the world may have 100,000 hospitalists. The same drivers are fueling the growth of Hospital Medicine around the world. The evidence is building that the hospitalist model of care has financial and quality benefits that transcend borders. We forecast that the hospitalist model of care will become an increasingly larger part of the solution around the world to fix these international healthcare systems.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335(7):514–517.
- ,.The hospitalist movement 5 years later.JAMA.2002;287(4):487–494.
- ,,.To Err Is Human: Building a Safer Health System; Institute of Medicine Committee on Quality of Health Care in America.Washington, DC:National Academy Press;2000.
- ,,.Crossing the Quality Chasm: A New Health System for the 21st Century; Institute of Medicine Committee of Health Care in America.Washington, DC:National Academy Press;2001.
- .The state of hospital medicine in 2008.Med Clin North Am.2008;92:265–273.
- et al.J Hosp Med.2011;6:378–382.
- ,,.A 10‐year experience with universal health insurance in Taiwan: measuring changes in health and health disparity.Ann Intern Med.2008;148(4):258–267.
- Canadian Hospitalist: Canadian Society of Hospital Medicine Web site. Available at: http://canadianhospitalist.ca/. Accessed April 15,2011.
- ,,,,,.Characteristics of hospitalists and hospitalist programs in the United States and Canada.J Clin Outcomes Manage.2009;16(2):69–74.
- The Society for Acute Medicine Web site. Available at: www.acutemedicine.org.uk. Accessed April 14,2011.
- ,,.Effectiveness of acute medical units in hospitals: a systematic review.Int J Qual Health Care.2009;21(6):397–407.
- .Acute and general medicine on opposite sides of the world.Acute Med.2011;10(2):67–68.
- ,.The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335(7):514–517.
- ,.The hospitalist movement 5 years later.JAMA.2002;287(4):487–494.
- ,,.To Err Is Human: Building a Safer Health System; Institute of Medicine Committee on Quality of Health Care in America.Washington, DC:National Academy Press;2000.
- ,,.Crossing the Quality Chasm: A New Health System for the 21st Century; Institute of Medicine Committee of Health Care in America.Washington, DC:National Academy Press;2001.
- .The state of hospital medicine in 2008.Med Clin North Am.2008;92:265–273.
- et al.J Hosp Med.2011;6:378–382.
- ,,.A 10‐year experience with universal health insurance in Taiwan: measuring changes in health and health disparity.Ann Intern Med.2008;148(4):258–267.
- Canadian Hospitalist: Canadian Society of Hospital Medicine Web site. Available at: http://canadianhospitalist.ca/. Accessed April 15,2011.
- ,,,,,.Characteristics of hospitalists and hospitalist programs in the United States and Canada.J Clin Outcomes Manage.2009;16(2):69–74.
- The Society for Acute Medicine Web site. Available at: www.acutemedicine.org.uk. Accessed April 14,2011.
- ,,.Effectiveness of acute medical units in hospitals: a systematic review.Int J Qual Health Care.2009;21(6):397–407.
- .Acute and general medicine on opposite sides of the world.Acute Med.2011;10(2):67–68.
Quantifying Resident Clinical Experience
Internal medicine residency training continues to evolve as competency‐based and with education organized around patient care.13 Making the patient the center of resident education provides an opportunity for experiential learning in which learning can be organized around the clinical conditions that residents encounter. Despite the renewed emphasis on using patient experience as the basis for residency education, little is known regarding what specific diagnostic conditions are seen by internal medicine residents throughout their training. Attempts have been made to quantify resident clinical experience in various fields, using approaches such as review of medical records, case logs, and prescription profiles, but to date, we lack systematic methods to obtain clinical experience data for internal medicine residents.47
While residency curricula in internal medicine typically outlines specific rotations in various clinical areas such as general medical wards, cardiology services, and intensive care units, time spent on such rotations does not necessarily provide quantitative data on the actual clinical conditions that residents encounter, nor does it ensure consistent clinical experience between residents. It is plausible that there may be substantial variability in clinical experience between residents within the same program, and that the overall spectrum of clinical disorders seen by residents in a program may or may not be consistent with a desired optimum, though this is yet to be defined.
If residency education in internal medicine is to progressively incorporate more experiential learning, detailed knowledge of the clinical conditions seen by residents should be useful, not only for overall curriculum design, but this might also allow for various educational interventions to be made when there are variations in clinical experience between residents. Our program has been interested in the application of electronic resources for the improvement of patient care, such as through the handoff process and the use of personal digital assistants.8 We previously did a small analysis of clinical conditions seen by residents through non‐International Classification of Diseases, Ninth Revision (ICD‐9)‐based data they entered onto personal digital assistants. This suggested to us that electronic resources used by residents might serve as a venue by which they could enter diagnostic information which we could use to generate a more detailed analysis of the clinical conditions that they see. Here we describe a method by which we have attempted to quantify resident clinical experience in internal medicine using a modification of an electronic handoff system.
METHODS
The study was conducted within the Internal Medicine Residency Program at the Long Island Jewish Medical Center in New Hyde Park, New York, part of the North ShoreLong Island Jewish Health System, and was approved by the Institutional Review Board. This work was carried out as part of our participation in the Educational Innovation Project of the Residency Review Committee for Internal Medicine. A central objective of our proposal was to develop a method to assess residents' clinical experience on an individual and an aggregate basis. A group of faculty and residents in our residency program developed an electronic handoff tool which residents use for rapid access to key clinical data for their patients and for the handoff of clinical information for on call coverage. This handoff tool was developed with the technical assistance of MedTech Notes LLC which owns Patient Data Transfer System (PDTS) HandOff Note. We modified the handoff tool to include a section in which residents were required to enter a primary diagnosis for each of their patients (a hard stop design). We chose to use the ICD‐9 system for standardization and created two methods to select the code: 1) an organ system‐based dropdown list containing frequently used codes and 2) a search box allowing for searching of the complete ICD‐9 database. For the organ‐based dropdown list, selection of that organ system would reveal a brief list of frequently used codes to make it easier for residents to find them. Prior to using the handoff tool with the ICD‐9based primary diagnosis coding system, training sessions with the residents were conducted by 3 of the investigators along with 3 chief medical residents. These sessions included training not only in technical aspects of how to find diagnosis codes, but also how to make decisions regarding what the primary diagnosis should be. We also instructed our postgraduate year (PGY)‐1s to update their diagnostic selections during the course of the hospital stay.
Each data point represents a resident caring for a patient with a specific diagnostic entity, and is counted once for that resident's period of taking care of that patient. Thirty‐three PGY‐1s were studied and, on the internal medicine service, they were supervised by either hospitalist faculty or voluntary faculty in comparable proportions. If the patient's care is taken over by another resident, that second resident was also recorded as having had a diagnostic encounter with that patient, hence 1 patient could provide experience with the same diagnostic entity for 1 or more residents. Using this method, the denominator is not patients seen, but residentpatient diagnostic encounters that have taken place. The ICD‐9 diagnostic conditions entered by the residents were grouped using the ICD‐9 system. Individual diagnostic profiles for each resident, as well as an aggregate profile for all residents to reflect the residency program as a whole, were generated. We also carried out an analysis of the ICD‐9 codes entered by 6 consecutive PGY‐1s to assess how the diagnostic spectrum might vary among a small sampling of PGY‐1s. In order to evaluate the accuracy of the residents' diagnostic selections, we carried out a validation assessment using a tool used by the residents' supervising hospitalists (who were the attendings of record for those patients). This was carried out on a subset of patients and could be done at any time during the hospital stay. The hospitalists were asked to review their residents' ICD‐9 codes and indicate whether they agreed or disagreed.
RESULTS
A total of 7562 residentpatient diagnostic encounters were studied from July 1, 2007 through June 1, 2008. Mean patient age was 66 19.4 years. The age distribution is given in Table 1 and reveals that 65% of diagnostic encounters were with patients age 60 years or greater. Twelve housestaff teams were studied, each consisting of 2 PGY‐1s and a supervising PGY‐2 or PGY‐3 resident. All ICD‐9 codes were selected by categorical and preliminary internal medicine PGY‐1s on medical ward and intensive care unit rotations. Residents from other departments doing rotations on the medical service were excluded. A validation assessment of 341 patients indicated 83.3% agreement by the supervising hospitalist with the primary ICD‐9 code selected. ICD‐9 codes were then grouped and categorized using ICD‐9 nomenclature with the distribution provided in Table 2. A wide spectrum of clinical conditions is apparent including symptoms and ill‐defined conditions, circulatory disorders, respiratory disorders, neoplasms, genitourinary disorders, digestive disorders, diseases of the blood/blood forming organs, endocrinologic/nutritional/metabolic/emmmune disorders, and disorders of the skin and subcutaneous tissue, overall accounting for about 86% of resident clinical experience.
| Age Category | No. | Percent of Total |
|---|---|---|
| 1829 | 441 | 5.83 |
| 3039 | 455 | 6.02 |
| 4049 | 705 | 9.32 |
| 5059 | 1,010 | 13.36 |
| 6069 | 1,218 | 16.11 |
| 7079 | 1,465 | 19.37 |
| 8089 | 1,673 | 22.12 |
| 90110 | 595 | 7.87 |
| ICD‐9 Category Description | Frequency | Percent |
|---|---|---|
| ||
| Symptoms/Ill‐Defined Conditions | 1,475 | 19.51 |
| Circulatory System | 1,381 | 18.26 |
| Respiratory System | 939 | 12.42 |
| Neoplasms | 572 | 7.56 |
| Genitourinary System | 502 | 6.64 |
| Digestive System | 464 | 6.14 |
| Blood/Blood‐Forming Organs | 444 | 5.87 |
| Endo/Nutritional/Metabolic/Immunity | 393 | 5.20 |
| Skin and Subcutaneous Tissue | 380 | 5.03 |
| Injury and Poisoning | 222 | 2.94 |
| Musculoskeletal/Connective Tissue | 199 | 2.63 |
| Infectious/Parasitic | 194 | 2.57 |
| Mental Disorders | 166 | 2.20 |
| Nervous System/Sense Organs | 125 | 1.65 |
| Health Status/Contact with Health Services | 81 | 1.07 |
| Pregnancy/Childbirth/Puerperium | 14 | 0.19 |
We also examined the most common diagnostic conditions within each of these categories. The 3 most common ICD‐9 codes entered by residents within each category are provided in Table 3. Symptoms and ill‐defined conditions represent a sizable portion of resident clinical experience (19.51%). Within this category, the most common conditions were fever; abdominal pain (unspecified site); and chest pain, unspecified. Disorders of the circulatory and respiratory systems were the next most common categories of conditions seen by residents, comprising 18.26% and 12.42%, respectively, of resident clinical experience. Within the category of circulatory disorders, congestive heart failure and acute myocardial infarction were the most common conditions seen; for respiratory disorders, pneumonia, chronic airway obstruction, and asthma were most commonly encountered. In aggregate, symptoms and ill‐defined conditions, and disorders of the circulatory and respiratory systems accounted for 50% of resident clinical experience.
| ICD‐9 Category Description | ICD‐9 Code | Code Description | Frequency | Percent |
|---|---|---|---|---|
| ||||
| Symptoms/Ill‐Defined Conditions | 780.6 | Fever | 190 | 2.51 |
| 789 | Abdominal pain; unspecified site | 149 | 1.97 | |
| 786.5 | Chest pain, unspecified | 140 | 1.85 | |
| Circulatory System | 428 | Congestive heart failure, unspecified | 346 | 4.58 |
| 410.9 | Acute myocardial infarction; unspecified site; unspecified episode of care | 135 | 1.79 | |
| 410.1 | Acute myocardial infarction; other anterior wall; unspecified episode of care | 106 | 1.40 | |
| Respiratory System | 486 | Pneumonia, organism unspecified | 363 | 4.80 |
| 496 | Chronic airway obstruction, not elsewhere classified | 162 | 2.14 | |
| 493.9 | Asthma, unspecified; unspecified | 96 | 1.27 | |
| Neoplasms | 199.1 | Malignant neoplasm without specification of site; other | 86 | 1.14 |
| 162.9 | Malignant neoplasm; bronchus lung; unspecified | 73 | 0.97 | |
| 202.8 | Other lymphomas; unspecified site, extranodal and solid organ sites | 71 | 0.94 | |
| Genitourinary System | 599 | Urinary tract infection, site not specified | 247 | 3.27 |
| 584.9 | Acute renal failure, unspecified | 91 | 1.20 | |
| 585.6 | End stage renal disease | 40 | 0.53 | |
| Digestive System | 578.9 | Hemorrhage of gastrointestinal tract, unspecified | 119 | 1.57 |
| 558.9 | Other and unspecified noninfectious gastroenteritis and colitis | 69 | 0.91 | |
| 577 | Acute pancreatitis | 36 | 0.48 | |
| Blood/Blood‐Forming Organs | 285.9 | Anemia, unspecified | 127 | 1.68 |
| 282.64 | Sickle‐cell/Hb‐C disease with crisis | 80 | 1.06 | |
| 282.6 | Sickle‐cell disease, unspecified | 73 | 0.97 | |
| Endo/Nutritional/Metabolic/Immunity | 276.1 | Hypoosmolality and/or hyponatremia | 57 | 0.75 |
| 251.2 | Hypoglycemia, unspecified | 56 | 0.74 | |
| 250.1 | Diabetes with ketoacidosis; type II, not stated as uncontrolled | 50 | 0.66 | |
| Skin and Subcutaneous Tissue | 682.9 | Other cellulitis and abscess; unspecified site | 256 | 3.39 |
| 682.5 | Other cellulitis and abscess; buttock | 37 | 0.49 | |
| 686.9 | Unspecified local infection of skin and subcutaneous tissue | 23 | 0.30 | |
| Injury and Poisoning | 848.9 | Unspecified site of sprain and strain | 32 | 0.42 |
| 977.9 | Poisoning by unspecified drug or medicinal substance | 32 | 0.42 | |
| 829 | Fracture; unspecified bone, closed | 22 | 0.29 | |
| Musculoskeletal/Connective Tissue | 730.2 | Unspecified osteomyelitis; site unspecified | 33 | 0.44 |
| 710 | Systemic lupus erythematosus | 25 | 0.33 | |
| 728.87 | Muscle weakness (generalized) | 19 | 0.25 | |
| Infectious/Parasitic | 38.9 | Unspecified septicemia | 58 | 0.77 |
| 8.45 | Intestinal infection/clostridium difficile | 54 | 0.71 | |
| 9.1 | Colitis, enteritis, and gastroenteritis of presumed infectious organ | 15 | 0.20 | |
| Mental Disorders | 291.81 | Alcohol withdrawal | 43 | 0.57 |
| 307.9 | Other and unspecified special symptoms or syndromes, not elsewhere classified | 35 | 0.46 | |
| 294.8 | Other persistent mental disorders due to conditions classified elsewhere | 20 | 0.26 | |
| Nervous System/Sense Organs | 322.9 | Meningitis, unspecified | 30 | 0.40 |
| 331 | Alzheimer's disease | 14 | 0.19 | |
| 340 | Multiple sclerosis | 6 | 0.08 | |
| Health Status/Contact with Health Services | 885.9 | Accidental fall from other slipping tripping or stumbling | 18 | 0.24 |
| 884.4 | Accidental fall from bed | 7 | 0.09 | |
| V13.02 | Personal history of urinary (tract) infection | 4 | 0.05 | |
| Pregnancy/Childbirth/Puerperium | 673.8 | Other pulmonary embolism; unspecified episode of care | 9 | 0.12 |
| 665 | Rupture of uterus before onset of labor; unspecified episode of care | 1 | 0.01 | |
| 665.7 | Pelvic hematoma, unspecified episode of care | 1 | 0.01 | |
Individual resident clinical experience varied as well. As shown in Table 4, for a group of 6 PGY‐1s, there was substantial variability in the ICD‐9 diagnostic categories. For example, the percentages of codes falling into the cardiovascular disease category ranged from 15.27% to 27.91%, and for respiratory disease ranged from 8.22% to 18.55%. These data suggest that there may be sizable differences in the proportions of various clinical conditions seen by residents over a year of training.
| ICD‐9 Category Description | Mean | SD | Min | Max |
|---|---|---|---|---|
| ||||
| Symptoms/Ill‐Defined Conditions | 21.43 | 5.07 | 15.50 | 29.90 |
| Circulatory System | 21.84 | 4.38 | 15.27 | 27.91 |
| Respiratory System | 12.43 | 3.83 | 8.22 | 18.55 |
| Neoplasms | 8.47 | 2.64 | 4.12 | 11.80 |
| Genitourinary System | 5.26 | 1.09 | 4.03 | 6.98 |
| Digestive System | 4.53 | 0.96 | 3.09 | 5.65 |
| Blood/Blood‐Forming Organs | 4.64 | 2.73 | 3.05 | 10.05 |
| Endo/Nutritional/Metabolic/Immunity | 5.64 | 1.68 | 3.11 | 7.22 |
| Skin and Subcutaneous Tissue | 4.28 | 1.63 | 2.42 | 6.19 |
| Injury and Poisoning | 3.90 | 1.01 | 3.09 | 5.43 |
| Musculoskeletal/Connective Tissue | 2.86 | 1.36 | 1.55 | 4.58 |
| Infectious/Parasitic | 3.86 | 2.62 | 2.42 | 8.53 |
| Mental Disorders | 1.47 | 0.62 | 0.81 | 2.28 |
| Nervous System/Sense Organs | 1.49 | 0.87 | 0.62 | 3.09 |
DISCUSSION
Years ago, residency training transitioned from a predominantly bedside experience to a curriculum with a large didactic, non‐bedside component, following parameters defined by organizations such as the Accreditation Council for Graduate Medical Education. Residency training is undergoing substantial change to become competency‐based and to organize learning around patient care experiences.2, 3, 9 The Educational Innovation Project of the Residency Review Committee for Internal Medicine is one such endeavor to help develop new methods by which to accomplish this.1 Effective incorporation of innovative experiential learning methods, based on the core competencies, will require a detailed knowledge of resident clinical experience during the course of their training, yet such data have been sparse in internal medicine. Sequist et al. analyzed data from an electronic medical record to assess resident clinical experience in the outpatient setting.4 Bachur and Nagler have used an electronic patient tracking system to assess the clinical experience of pediatric emergency medicine fellows.5, 6 Most attempts to describe resident clinical experience have relied upon extracting diagnostic information from medical records, case logs, etc, though in another approach, Rohrbaugh et al. reviewed psychiatric resident prescription profiles,7 which might provide some indirect data on clinical experience if applied to internal medicine.
In this study, we attempted to quantify resident clinical experience using resident‐selected ICD‐9 codes, in contrast to other methods that have relied upon medical record review and other resident‐independent approaches. There are various strengths and limitations to this approach. Using the ICD‐9 system provides a number of strengths, a major one being standardization, allowing comparisons between different programs and perhaps even facilitating the development of guidelines for resident clinical experience. In addition, this approach using the ICD‐9 system could be readily implemented at any institution and does not require any specific technology. While we chose to do this through our handoff system, an institution could use any of a variety of other systems to accomplish this. For example, resident‐entered ICD‐9 coding systems could be incorporated into electronic discharge summaries, history and physicals, or progress notes. There may also be some practical benefits to having residents learn how to use the ICD‐9 system at this stage of their careers.
There are limitations to this approach as well. The ICD‐9 system was not intended to be used for medical education purposes. There are features of it that can make finding the best diagnosis difficult, and routes to it may at times seem counterintuitive. While we did not carry out resident surveys, a number of residents anecdotally mentioned that it took time to become comfortable using the system, and it could be challenging at times to find a diagnosis description that best fit what they were looking for. To make diagnosis selection easier, we created an organ system‐based dropdown list in the handoff tool so that when residents select an organ system, another list opens up containing commonly used ICD‐9 codes. This grouping is based on organ system alone and does not necessarily follow the ICD‐9 grouping (in contrast, our reported data in this article are all based on ICD‐9 grouping). A search tool to allow searching the entire ICD‐9 database was also made available on the handoff tool. Other factors that could limit diagnosis code accuracy could be lack of clinical knowledge, and error as a result of pressure to come up with a diagnosis because of the hard stop design of our system, in which residents were required to enter a primary diagnosis, potentially causing alert fatigue. A validation assessment that we carried out revealed fairly good agreement with the specific ICD‐9 codes chosen by the resident, but greater accuracy would be desirable. Further education on diagnosis selection and refinements to the handoff tool should help facilitate this. We are currently addressing this by ongoing education on diagnosis selection and by having the hospitalists share the handoff tool with the residents, allowing them to provide direct feedback on diagnostic selections.
More than 19% of the diagnoses selected by residents fell into the category of symptoms and ill‐defined conditions. This raises a number of potential educational issues. One of those is that if residents do, in fact, encounter such entities at such a high frequency, then the internal medicine curriculum must be structured in such a way as to complement this clinical experience with a comprehensive learning program. However, we must also consider the possibility that, in many such instances, a more definitive diagnosis became evident by the time of discharge and this may not have been reflected in the ICD‐9 code that the resident chose. Hence, the category of symptoms and ill‐defined conditions may actually be somewhat smaller than our findings would suggest.
Many issues will need to be addressed as programs obtain more data on their residents' clinical experience. While there may be many reasons to use the ICD‐9 system for selecting diagnoses including those listed above, the system by which ICD‐9 groups diagnoses might not provide ideal educational information, again as the ICD‐9 system was not designed for this purpose. While in this article we have reported the residents' diagnostic encounters grouped according to the ICD‐9 grouping system to provide an initial standardized description, grouping according to another diagnostic system that is felt to be more educationally meaningful may be preferred.
While one might assume that a higher frequency of exposure to certain clinical conditions should enhance competency, that relationship may not be straightforward in internal medicine. For surgical procedures, there are, in fact, data to show improved outcomes for surgeons with higher operative volumes for those procedures,10 but in internal medicine, we do not have data to demonstrate that competence of a resident caring for a particular condition is enhanced by experience alone. Therefore, as programs obtain more data on clinical experience, it will be important that the focus be kept on quality as opposed to quantity.
Obtaining data on resident clinical experience might greatly facilitate experiential learning approaches. For example, as residents go through training and encounter specific diagnostic conditions, those experiences could be supplemented by various learning innovations to make those experiences more meaningful and, hopefully, more likely to result in the development of competence, though that will require measurement. In our program, for example, we have incorporated an approach using illness scenarios, in that when residents have had a certain level of clinical experience with a given clinical condition, they are assembled in small groups and competency‐based case discussions are carried out with a preceptor. In addition, for those instances in which an individual resident may lack direct clinical experience in a certain area, this might be addressed by interventions to increase their contact with those conditions and/or targeted learning interventions to help develop competence. A resident found to be lacking in clinical experience in a certain area could be assigned to the care of more patients with that condition, or to spending more time in a venue in which that condition is more likely to be encountered. Various learning activities including didactics, case discussions, simulation, self‐directed learning, and others could also be used to compensate for such variability. Furthermore, if a residency program's aggregate clinical experience is divergent from some desirable standard yet to be determined, a detailed knowledge of this could help guide that program's curriculum revision. For example, for residents in a program in which there is relatively low exposure to patients with oncological issues, this could be compensated for by external rotations to achieve more clinical experience in oncology, as well as supplementation of the curriculum with additional learning activities in oncology, which could include small group discussions, self‐directed learning activities, case discussions, and others. While at present there are no defined standards for clinical experience and it remains to be seen if there would be a correlation with development of competence, no such standard would serve a purpose if programs did not have reliable and practical means of clinical experience assessment.
In summary, resident‐selected ICD‐9 codes may be a useful means to obtain data regarding resident clinical experience in internal medicine. Such data may be useful to residency training programs in developing new curricula based on experiential learning.
- ,,.Internal medicine's Educational Innovations Project: improving health care and learning.Am J Med.2009;122:398–404.
- ,,,,.Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144:920–926.
- ,,for the Education Committee of the American College of Physicians.Redesigning training for internal medicine.Ann Intern Med.2006;144:927–932.
- ,,,,.Use of an electronic medical record to profile the continuity clinic experiences of primary care residents.Acad Med.2005;80:390–394.
- ,,.An automated electronic case log: using electronic information systems to assess training in emergency medicine.Acad Emerg Med.2006;13:733–739.
- ,.Use of an automated electronic case log to assess fellowship training: tracking the pediatric emergency medicine experience.Pediatr Emerg Care.2008;24:75–82.
- ,,,.Utilizing VA information technology to develop psychiatric resident prescription profiles.Acad Psychiatry.2009;33:27–30.
- ,,, et al.Personal digital assistants (PDAs): a review of their application in graduate medical education.Am J Med Qual.2005;20:262–267.
- ,,, et al.Redesigning residency training in internal medicine: the consensus report of the Alliance for Academic Internal Medicine Education Redesign Task Force.Acad Med.2007;82:1211–1219.
- ,,,,,.Surgeon volume and operative mortality in the United States.N Engl J Med.2003;349:2117–2127.
Internal medicine residency training continues to evolve as competency‐based and with education organized around patient care.13 Making the patient the center of resident education provides an opportunity for experiential learning in which learning can be organized around the clinical conditions that residents encounter. Despite the renewed emphasis on using patient experience as the basis for residency education, little is known regarding what specific diagnostic conditions are seen by internal medicine residents throughout their training. Attempts have been made to quantify resident clinical experience in various fields, using approaches such as review of medical records, case logs, and prescription profiles, but to date, we lack systematic methods to obtain clinical experience data for internal medicine residents.47
While residency curricula in internal medicine typically outlines specific rotations in various clinical areas such as general medical wards, cardiology services, and intensive care units, time spent on such rotations does not necessarily provide quantitative data on the actual clinical conditions that residents encounter, nor does it ensure consistent clinical experience between residents. It is plausible that there may be substantial variability in clinical experience between residents within the same program, and that the overall spectrum of clinical disorders seen by residents in a program may or may not be consistent with a desired optimum, though this is yet to be defined.
If residency education in internal medicine is to progressively incorporate more experiential learning, detailed knowledge of the clinical conditions seen by residents should be useful, not only for overall curriculum design, but this might also allow for various educational interventions to be made when there are variations in clinical experience between residents. Our program has been interested in the application of electronic resources for the improvement of patient care, such as through the handoff process and the use of personal digital assistants.8 We previously did a small analysis of clinical conditions seen by residents through non‐International Classification of Diseases, Ninth Revision (ICD‐9)‐based data they entered onto personal digital assistants. This suggested to us that electronic resources used by residents might serve as a venue by which they could enter diagnostic information which we could use to generate a more detailed analysis of the clinical conditions that they see. Here we describe a method by which we have attempted to quantify resident clinical experience in internal medicine using a modification of an electronic handoff system.
METHODS
The study was conducted within the Internal Medicine Residency Program at the Long Island Jewish Medical Center in New Hyde Park, New York, part of the North ShoreLong Island Jewish Health System, and was approved by the Institutional Review Board. This work was carried out as part of our participation in the Educational Innovation Project of the Residency Review Committee for Internal Medicine. A central objective of our proposal was to develop a method to assess residents' clinical experience on an individual and an aggregate basis. A group of faculty and residents in our residency program developed an electronic handoff tool which residents use for rapid access to key clinical data for their patients and for the handoff of clinical information for on call coverage. This handoff tool was developed with the technical assistance of MedTech Notes LLC which owns Patient Data Transfer System (PDTS) HandOff Note. We modified the handoff tool to include a section in which residents were required to enter a primary diagnosis for each of their patients (a hard stop design). We chose to use the ICD‐9 system for standardization and created two methods to select the code: 1) an organ system‐based dropdown list containing frequently used codes and 2) a search box allowing for searching of the complete ICD‐9 database. For the organ‐based dropdown list, selection of that organ system would reveal a brief list of frequently used codes to make it easier for residents to find them. Prior to using the handoff tool with the ICD‐9based primary diagnosis coding system, training sessions with the residents were conducted by 3 of the investigators along with 3 chief medical residents. These sessions included training not only in technical aspects of how to find diagnosis codes, but also how to make decisions regarding what the primary diagnosis should be. We also instructed our postgraduate year (PGY)‐1s to update their diagnostic selections during the course of the hospital stay.
Each data point represents a resident caring for a patient with a specific diagnostic entity, and is counted once for that resident's period of taking care of that patient. Thirty‐three PGY‐1s were studied and, on the internal medicine service, they were supervised by either hospitalist faculty or voluntary faculty in comparable proportions. If the patient's care is taken over by another resident, that second resident was also recorded as having had a diagnostic encounter with that patient, hence 1 patient could provide experience with the same diagnostic entity for 1 or more residents. Using this method, the denominator is not patients seen, but residentpatient diagnostic encounters that have taken place. The ICD‐9 diagnostic conditions entered by the residents were grouped using the ICD‐9 system. Individual diagnostic profiles for each resident, as well as an aggregate profile for all residents to reflect the residency program as a whole, were generated. We also carried out an analysis of the ICD‐9 codes entered by 6 consecutive PGY‐1s to assess how the diagnostic spectrum might vary among a small sampling of PGY‐1s. In order to evaluate the accuracy of the residents' diagnostic selections, we carried out a validation assessment using a tool used by the residents' supervising hospitalists (who were the attendings of record for those patients). This was carried out on a subset of patients and could be done at any time during the hospital stay. The hospitalists were asked to review their residents' ICD‐9 codes and indicate whether they agreed or disagreed.
RESULTS
A total of 7562 residentpatient diagnostic encounters were studied from July 1, 2007 through June 1, 2008. Mean patient age was 66 19.4 years. The age distribution is given in Table 1 and reveals that 65% of diagnostic encounters were with patients age 60 years or greater. Twelve housestaff teams were studied, each consisting of 2 PGY‐1s and a supervising PGY‐2 or PGY‐3 resident. All ICD‐9 codes were selected by categorical and preliminary internal medicine PGY‐1s on medical ward and intensive care unit rotations. Residents from other departments doing rotations on the medical service were excluded. A validation assessment of 341 patients indicated 83.3% agreement by the supervising hospitalist with the primary ICD‐9 code selected. ICD‐9 codes were then grouped and categorized using ICD‐9 nomenclature with the distribution provided in Table 2. A wide spectrum of clinical conditions is apparent including symptoms and ill‐defined conditions, circulatory disorders, respiratory disorders, neoplasms, genitourinary disorders, digestive disorders, diseases of the blood/blood forming organs, endocrinologic/nutritional/metabolic/emmmune disorders, and disorders of the skin and subcutaneous tissue, overall accounting for about 86% of resident clinical experience.
| Age Category | No. | Percent of Total |
|---|---|---|
| 1829 | 441 | 5.83 |
| 3039 | 455 | 6.02 |
| 4049 | 705 | 9.32 |
| 5059 | 1,010 | 13.36 |
| 6069 | 1,218 | 16.11 |
| 7079 | 1,465 | 19.37 |
| 8089 | 1,673 | 22.12 |
| 90110 | 595 | 7.87 |
| ICD‐9 Category Description | Frequency | Percent |
|---|---|---|
| ||
| Symptoms/Ill‐Defined Conditions | 1,475 | 19.51 |
| Circulatory System | 1,381 | 18.26 |
| Respiratory System | 939 | 12.42 |
| Neoplasms | 572 | 7.56 |
| Genitourinary System | 502 | 6.64 |
| Digestive System | 464 | 6.14 |
| Blood/Blood‐Forming Organs | 444 | 5.87 |
| Endo/Nutritional/Metabolic/Immunity | 393 | 5.20 |
| Skin and Subcutaneous Tissue | 380 | 5.03 |
| Injury and Poisoning | 222 | 2.94 |
| Musculoskeletal/Connective Tissue | 199 | 2.63 |
| Infectious/Parasitic | 194 | 2.57 |
| Mental Disorders | 166 | 2.20 |
| Nervous System/Sense Organs | 125 | 1.65 |
| Health Status/Contact with Health Services | 81 | 1.07 |
| Pregnancy/Childbirth/Puerperium | 14 | 0.19 |
We also examined the most common diagnostic conditions within each of these categories. The 3 most common ICD‐9 codes entered by residents within each category are provided in Table 3. Symptoms and ill‐defined conditions represent a sizable portion of resident clinical experience (19.51%). Within this category, the most common conditions were fever; abdominal pain (unspecified site); and chest pain, unspecified. Disorders of the circulatory and respiratory systems were the next most common categories of conditions seen by residents, comprising 18.26% and 12.42%, respectively, of resident clinical experience. Within the category of circulatory disorders, congestive heart failure and acute myocardial infarction were the most common conditions seen; for respiratory disorders, pneumonia, chronic airway obstruction, and asthma were most commonly encountered. In aggregate, symptoms and ill‐defined conditions, and disorders of the circulatory and respiratory systems accounted for 50% of resident clinical experience.
| ICD‐9 Category Description | ICD‐9 Code | Code Description | Frequency | Percent |
|---|---|---|---|---|
| ||||
| Symptoms/Ill‐Defined Conditions | 780.6 | Fever | 190 | 2.51 |
| 789 | Abdominal pain; unspecified site | 149 | 1.97 | |
| 786.5 | Chest pain, unspecified | 140 | 1.85 | |
| Circulatory System | 428 | Congestive heart failure, unspecified | 346 | 4.58 |
| 410.9 | Acute myocardial infarction; unspecified site; unspecified episode of care | 135 | 1.79 | |
| 410.1 | Acute myocardial infarction; other anterior wall; unspecified episode of care | 106 | 1.40 | |
| Respiratory System | 486 | Pneumonia, organism unspecified | 363 | 4.80 |
| 496 | Chronic airway obstruction, not elsewhere classified | 162 | 2.14 | |
| 493.9 | Asthma, unspecified; unspecified | 96 | 1.27 | |
| Neoplasms | 199.1 | Malignant neoplasm without specification of site; other | 86 | 1.14 |
| 162.9 | Malignant neoplasm; bronchus lung; unspecified | 73 | 0.97 | |
| 202.8 | Other lymphomas; unspecified site, extranodal and solid organ sites | 71 | 0.94 | |
| Genitourinary System | 599 | Urinary tract infection, site not specified | 247 | 3.27 |
| 584.9 | Acute renal failure, unspecified | 91 | 1.20 | |
| 585.6 | End stage renal disease | 40 | 0.53 | |
| Digestive System | 578.9 | Hemorrhage of gastrointestinal tract, unspecified | 119 | 1.57 |
| 558.9 | Other and unspecified noninfectious gastroenteritis and colitis | 69 | 0.91 | |
| 577 | Acute pancreatitis | 36 | 0.48 | |
| Blood/Blood‐Forming Organs | 285.9 | Anemia, unspecified | 127 | 1.68 |
| 282.64 | Sickle‐cell/Hb‐C disease with crisis | 80 | 1.06 | |
| 282.6 | Sickle‐cell disease, unspecified | 73 | 0.97 | |
| Endo/Nutritional/Metabolic/Immunity | 276.1 | Hypoosmolality and/or hyponatremia | 57 | 0.75 |
| 251.2 | Hypoglycemia, unspecified | 56 | 0.74 | |
| 250.1 | Diabetes with ketoacidosis; type II, not stated as uncontrolled | 50 | 0.66 | |
| Skin and Subcutaneous Tissue | 682.9 | Other cellulitis and abscess; unspecified site | 256 | 3.39 |
| 682.5 | Other cellulitis and abscess; buttock | 37 | 0.49 | |
| 686.9 | Unspecified local infection of skin and subcutaneous tissue | 23 | 0.30 | |
| Injury and Poisoning | 848.9 | Unspecified site of sprain and strain | 32 | 0.42 |
| 977.9 | Poisoning by unspecified drug or medicinal substance | 32 | 0.42 | |
| 829 | Fracture; unspecified bone, closed | 22 | 0.29 | |
| Musculoskeletal/Connective Tissue | 730.2 | Unspecified osteomyelitis; site unspecified | 33 | 0.44 |
| 710 | Systemic lupus erythematosus | 25 | 0.33 | |
| 728.87 | Muscle weakness (generalized) | 19 | 0.25 | |
| Infectious/Parasitic | 38.9 | Unspecified septicemia | 58 | 0.77 |
| 8.45 | Intestinal infection/clostridium difficile | 54 | 0.71 | |
| 9.1 | Colitis, enteritis, and gastroenteritis of presumed infectious organ | 15 | 0.20 | |
| Mental Disorders | 291.81 | Alcohol withdrawal | 43 | 0.57 |
| 307.9 | Other and unspecified special symptoms or syndromes, not elsewhere classified | 35 | 0.46 | |
| 294.8 | Other persistent mental disorders due to conditions classified elsewhere | 20 | 0.26 | |
| Nervous System/Sense Organs | 322.9 | Meningitis, unspecified | 30 | 0.40 |
| 331 | Alzheimer's disease | 14 | 0.19 | |
| 340 | Multiple sclerosis | 6 | 0.08 | |
| Health Status/Contact with Health Services | 885.9 | Accidental fall from other slipping tripping or stumbling | 18 | 0.24 |
| 884.4 | Accidental fall from bed | 7 | 0.09 | |
| V13.02 | Personal history of urinary (tract) infection | 4 | 0.05 | |
| Pregnancy/Childbirth/Puerperium | 673.8 | Other pulmonary embolism; unspecified episode of care | 9 | 0.12 |
| 665 | Rupture of uterus before onset of labor; unspecified episode of care | 1 | 0.01 | |
| 665.7 | Pelvic hematoma, unspecified episode of care | 1 | 0.01 | |
Individual resident clinical experience varied as well. As shown in Table 4, for a group of 6 PGY‐1s, there was substantial variability in the ICD‐9 diagnostic categories. For example, the percentages of codes falling into the cardiovascular disease category ranged from 15.27% to 27.91%, and for respiratory disease ranged from 8.22% to 18.55%. These data suggest that there may be sizable differences in the proportions of various clinical conditions seen by residents over a year of training.
| ICD‐9 Category Description | Mean | SD | Min | Max |
|---|---|---|---|---|
| ||||
| Symptoms/Ill‐Defined Conditions | 21.43 | 5.07 | 15.50 | 29.90 |
| Circulatory System | 21.84 | 4.38 | 15.27 | 27.91 |
| Respiratory System | 12.43 | 3.83 | 8.22 | 18.55 |
| Neoplasms | 8.47 | 2.64 | 4.12 | 11.80 |
| Genitourinary System | 5.26 | 1.09 | 4.03 | 6.98 |
| Digestive System | 4.53 | 0.96 | 3.09 | 5.65 |
| Blood/Blood‐Forming Organs | 4.64 | 2.73 | 3.05 | 10.05 |
| Endo/Nutritional/Metabolic/Immunity | 5.64 | 1.68 | 3.11 | 7.22 |
| Skin and Subcutaneous Tissue | 4.28 | 1.63 | 2.42 | 6.19 |
| Injury and Poisoning | 3.90 | 1.01 | 3.09 | 5.43 |
| Musculoskeletal/Connective Tissue | 2.86 | 1.36 | 1.55 | 4.58 |
| Infectious/Parasitic | 3.86 | 2.62 | 2.42 | 8.53 |
| Mental Disorders | 1.47 | 0.62 | 0.81 | 2.28 |
| Nervous System/Sense Organs | 1.49 | 0.87 | 0.62 | 3.09 |
DISCUSSION
Years ago, residency training transitioned from a predominantly bedside experience to a curriculum with a large didactic, non‐bedside component, following parameters defined by organizations such as the Accreditation Council for Graduate Medical Education. Residency training is undergoing substantial change to become competency‐based and to organize learning around patient care experiences.2, 3, 9 The Educational Innovation Project of the Residency Review Committee for Internal Medicine is one such endeavor to help develop new methods by which to accomplish this.1 Effective incorporation of innovative experiential learning methods, based on the core competencies, will require a detailed knowledge of resident clinical experience during the course of their training, yet such data have been sparse in internal medicine. Sequist et al. analyzed data from an electronic medical record to assess resident clinical experience in the outpatient setting.4 Bachur and Nagler have used an electronic patient tracking system to assess the clinical experience of pediatric emergency medicine fellows.5, 6 Most attempts to describe resident clinical experience have relied upon extracting diagnostic information from medical records, case logs, etc, though in another approach, Rohrbaugh et al. reviewed psychiatric resident prescription profiles,7 which might provide some indirect data on clinical experience if applied to internal medicine.
In this study, we attempted to quantify resident clinical experience using resident‐selected ICD‐9 codes, in contrast to other methods that have relied upon medical record review and other resident‐independent approaches. There are various strengths and limitations to this approach. Using the ICD‐9 system provides a number of strengths, a major one being standardization, allowing comparisons between different programs and perhaps even facilitating the development of guidelines for resident clinical experience. In addition, this approach using the ICD‐9 system could be readily implemented at any institution and does not require any specific technology. While we chose to do this through our handoff system, an institution could use any of a variety of other systems to accomplish this. For example, resident‐entered ICD‐9 coding systems could be incorporated into electronic discharge summaries, history and physicals, or progress notes. There may also be some practical benefits to having residents learn how to use the ICD‐9 system at this stage of their careers.
There are limitations to this approach as well. The ICD‐9 system was not intended to be used for medical education purposes. There are features of it that can make finding the best diagnosis difficult, and routes to it may at times seem counterintuitive. While we did not carry out resident surveys, a number of residents anecdotally mentioned that it took time to become comfortable using the system, and it could be challenging at times to find a diagnosis description that best fit what they were looking for. To make diagnosis selection easier, we created an organ system‐based dropdown list in the handoff tool so that when residents select an organ system, another list opens up containing commonly used ICD‐9 codes. This grouping is based on organ system alone and does not necessarily follow the ICD‐9 grouping (in contrast, our reported data in this article are all based on ICD‐9 grouping). A search tool to allow searching the entire ICD‐9 database was also made available on the handoff tool. Other factors that could limit diagnosis code accuracy could be lack of clinical knowledge, and error as a result of pressure to come up with a diagnosis because of the hard stop design of our system, in which residents were required to enter a primary diagnosis, potentially causing alert fatigue. A validation assessment that we carried out revealed fairly good agreement with the specific ICD‐9 codes chosen by the resident, but greater accuracy would be desirable. Further education on diagnosis selection and refinements to the handoff tool should help facilitate this. We are currently addressing this by ongoing education on diagnosis selection and by having the hospitalists share the handoff tool with the residents, allowing them to provide direct feedback on diagnostic selections.
More than 19% of the diagnoses selected by residents fell into the category of symptoms and ill‐defined conditions. This raises a number of potential educational issues. One of those is that if residents do, in fact, encounter such entities at such a high frequency, then the internal medicine curriculum must be structured in such a way as to complement this clinical experience with a comprehensive learning program. However, we must also consider the possibility that, in many such instances, a more definitive diagnosis became evident by the time of discharge and this may not have been reflected in the ICD‐9 code that the resident chose. Hence, the category of symptoms and ill‐defined conditions may actually be somewhat smaller than our findings would suggest.
Many issues will need to be addressed as programs obtain more data on their residents' clinical experience. While there may be many reasons to use the ICD‐9 system for selecting diagnoses including those listed above, the system by which ICD‐9 groups diagnoses might not provide ideal educational information, again as the ICD‐9 system was not designed for this purpose. While in this article we have reported the residents' diagnostic encounters grouped according to the ICD‐9 grouping system to provide an initial standardized description, grouping according to another diagnostic system that is felt to be more educationally meaningful may be preferred.
While one might assume that a higher frequency of exposure to certain clinical conditions should enhance competency, that relationship may not be straightforward in internal medicine. For surgical procedures, there are, in fact, data to show improved outcomes for surgeons with higher operative volumes for those procedures,10 but in internal medicine, we do not have data to demonstrate that competence of a resident caring for a particular condition is enhanced by experience alone. Therefore, as programs obtain more data on clinical experience, it will be important that the focus be kept on quality as opposed to quantity.
Obtaining data on resident clinical experience might greatly facilitate experiential learning approaches. For example, as residents go through training and encounter specific diagnostic conditions, those experiences could be supplemented by various learning innovations to make those experiences more meaningful and, hopefully, more likely to result in the development of competence, though that will require measurement. In our program, for example, we have incorporated an approach using illness scenarios, in that when residents have had a certain level of clinical experience with a given clinical condition, they are assembled in small groups and competency‐based case discussions are carried out with a preceptor. In addition, for those instances in which an individual resident may lack direct clinical experience in a certain area, this might be addressed by interventions to increase their contact with those conditions and/or targeted learning interventions to help develop competence. A resident found to be lacking in clinical experience in a certain area could be assigned to the care of more patients with that condition, or to spending more time in a venue in which that condition is more likely to be encountered. Various learning activities including didactics, case discussions, simulation, self‐directed learning, and others could also be used to compensate for such variability. Furthermore, if a residency program's aggregate clinical experience is divergent from some desirable standard yet to be determined, a detailed knowledge of this could help guide that program's curriculum revision. For example, for residents in a program in which there is relatively low exposure to patients with oncological issues, this could be compensated for by external rotations to achieve more clinical experience in oncology, as well as supplementation of the curriculum with additional learning activities in oncology, which could include small group discussions, self‐directed learning activities, case discussions, and others. While at present there are no defined standards for clinical experience and it remains to be seen if there would be a correlation with development of competence, no such standard would serve a purpose if programs did not have reliable and practical means of clinical experience assessment.
In summary, resident‐selected ICD‐9 codes may be a useful means to obtain data regarding resident clinical experience in internal medicine. Such data may be useful to residency training programs in developing new curricula based on experiential learning.
Internal medicine residency training continues to evolve as competency‐based and with education organized around patient care.13 Making the patient the center of resident education provides an opportunity for experiential learning in which learning can be organized around the clinical conditions that residents encounter. Despite the renewed emphasis on using patient experience as the basis for residency education, little is known regarding what specific diagnostic conditions are seen by internal medicine residents throughout their training. Attempts have been made to quantify resident clinical experience in various fields, using approaches such as review of medical records, case logs, and prescription profiles, but to date, we lack systematic methods to obtain clinical experience data for internal medicine residents.47
While residency curricula in internal medicine typically outlines specific rotations in various clinical areas such as general medical wards, cardiology services, and intensive care units, time spent on such rotations does not necessarily provide quantitative data on the actual clinical conditions that residents encounter, nor does it ensure consistent clinical experience between residents. It is plausible that there may be substantial variability in clinical experience between residents within the same program, and that the overall spectrum of clinical disorders seen by residents in a program may or may not be consistent with a desired optimum, though this is yet to be defined.
If residency education in internal medicine is to progressively incorporate more experiential learning, detailed knowledge of the clinical conditions seen by residents should be useful, not only for overall curriculum design, but this might also allow for various educational interventions to be made when there are variations in clinical experience between residents. Our program has been interested in the application of electronic resources for the improvement of patient care, such as through the handoff process and the use of personal digital assistants.8 We previously did a small analysis of clinical conditions seen by residents through non‐International Classification of Diseases, Ninth Revision (ICD‐9)‐based data they entered onto personal digital assistants. This suggested to us that electronic resources used by residents might serve as a venue by which they could enter diagnostic information which we could use to generate a more detailed analysis of the clinical conditions that they see. Here we describe a method by which we have attempted to quantify resident clinical experience in internal medicine using a modification of an electronic handoff system.
METHODS
The study was conducted within the Internal Medicine Residency Program at the Long Island Jewish Medical Center in New Hyde Park, New York, part of the North ShoreLong Island Jewish Health System, and was approved by the Institutional Review Board. This work was carried out as part of our participation in the Educational Innovation Project of the Residency Review Committee for Internal Medicine. A central objective of our proposal was to develop a method to assess residents' clinical experience on an individual and an aggregate basis. A group of faculty and residents in our residency program developed an electronic handoff tool which residents use for rapid access to key clinical data for their patients and for the handoff of clinical information for on call coverage. This handoff tool was developed with the technical assistance of MedTech Notes LLC which owns Patient Data Transfer System (PDTS) HandOff Note. We modified the handoff tool to include a section in which residents were required to enter a primary diagnosis for each of their patients (a hard stop design). We chose to use the ICD‐9 system for standardization and created two methods to select the code: 1) an organ system‐based dropdown list containing frequently used codes and 2) a search box allowing for searching of the complete ICD‐9 database. For the organ‐based dropdown list, selection of that organ system would reveal a brief list of frequently used codes to make it easier for residents to find them. Prior to using the handoff tool with the ICD‐9based primary diagnosis coding system, training sessions with the residents were conducted by 3 of the investigators along with 3 chief medical residents. These sessions included training not only in technical aspects of how to find diagnosis codes, but also how to make decisions regarding what the primary diagnosis should be. We also instructed our postgraduate year (PGY)‐1s to update their diagnostic selections during the course of the hospital stay.
Each data point represents a resident caring for a patient with a specific diagnostic entity, and is counted once for that resident's period of taking care of that patient. Thirty‐three PGY‐1s were studied and, on the internal medicine service, they were supervised by either hospitalist faculty or voluntary faculty in comparable proportions. If the patient's care is taken over by another resident, that second resident was also recorded as having had a diagnostic encounter with that patient, hence 1 patient could provide experience with the same diagnostic entity for 1 or more residents. Using this method, the denominator is not patients seen, but residentpatient diagnostic encounters that have taken place. The ICD‐9 diagnostic conditions entered by the residents were grouped using the ICD‐9 system. Individual diagnostic profiles for each resident, as well as an aggregate profile for all residents to reflect the residency program as a whole, were generated. We also carried out an analysis of the ICD‐9 codes entered by 6 consecutive PGY‐1s to assess how the diagnostic spectrum might vary among a small sampling of PGY‐1s. In order to evaluate the accuracy of the residents' diagnostic selections, we carried out a validation assessment using a tool used by the residents' supervising hospitalists (who were the attendings of record for those patients). This was carried out on a subset of patients and could be done at any time during the hospital stay. The hospitalists were asked to review their residents' ICD‐9 codes and indicate whether they agreed or disagreed.
RESULTS
A total of 7562 residentpatient diagnostic encounters were studied from July 1, 2007 through June 1, 2008. Mean patient age was 66 19.4 years. The age distribution is given in Table 1 and reveals that 65% of diagnostic encounters were with patients age 60 years or greater. Twelve housestaff teams were studied, each consisting of 2 PGY‐1s and a supervising PGY‐2 or PGY‐3 resident. All ICD‐9 codes were selected by categorical and preliminary internal medicine PGY‐1s on medical ward and intensive care unit rotations. Residents from other departments doing rotations on the medical service were excluded. A validation assessment of 341 patients indicated 83.3% agreement by the supervising hospitalist with the primary ICD‐9 code selected. ICD‐9 codes were then grouped and categorized using ICD‐9 nomenclature with the distribution provided in Table 2. A wide spectrum of clinical conditions is apparent including symptoms and ill‐defined conditions, circulatory disorders, respiratory disorders, neoplasms, genitourinary disorders, digestive disorders, diseases of the blood/blood forming organs, endocrinologic/nutritional/metabolic/emmmune disorders, and disorders of the skin and subcutaneous tissue, overall accounting for about 86% of resident clinical experience.
| Age Category | No. | Percent of Total |
|---|---|---|
| 1829 | 441 | 5.83 |
| 3039 | 455 | 6.02 |
| 4049 | 705 | 9.32 |
| 5059 | 1,010 | 13.36 |
| 6069 | 1,218 | 16.11 |
| 7079 | 1,465 | 19.37 |
| 8089 | 1,673 | 22.12 |
| 90110 | 595 | 7.87 |
| ICD‐9 Category Description | Frequency | Percent |
|---|---|---|
| ||
| Symptoms/Ill‐Defined Conditions | 1,475 | 19.51 |
| Circulatory System | 1,381 | 18.26 |
| Respiratory System | 939 | 12.42 |
| Neoplasms | 572 | 7.56 |
| Genitourinary System | 502 | 6.64 |
| Digestive System | 464 | 6.14 |
| Blood/Blood‐Forming Organs | 444 | 5.87 |
| Endo/Nutritional/Metabolic/Immunity | 393 | 5.20 |
| Skin and Subcutaneous Tissue | 380 | 5.03 |
| Injury and Poisoning | 222 | 2.94 |
| Musculoskeletal/Connective Tissue | 199 | 2.63 |
| Infectious/Parasitic | 194 | 2.57 |
| Mental Disorders | 166 | 2.20 |
| Nervous System/Sense Organs | 125 | 1.65 |
| Health Status/Contact with Health Services | 81 | 1.07 |
| Pregnancy/Childbirth/Puerperium | 14 | 0.19 |
We also examined the most common diagnostic conditions within each of these categories. The 3 most common ICD‐9 codes entered by residents within each category are provided in Table 3. Symptoms and ill‐defined conditions represent a sizable portion of resident clinical experience (19.51%). Within this category, the most common conditions were fever; abdominal pain (unspecified site); and chest pain, unspecified. Disorders of the circulatory and respiratory systems were the next most common categories of conditions seen by residents, comprising 18.26% and 12.42%, respectively, of resident clinical experience. Within the category of circulatory disorders, congestive heart failure and acute myocardial infarction were the most common conditions seen; for respiratory disorders, pneumonia, chronic airway obstruction, and asthma were most commonly encountered. In aggregate, symptoms and ill‐defined conditions, and disorders of the circulatory and respiratory systems accounted for 50% of resident clinical experience.
| ICD‐9 Category Description | ICD‐9 Code | Code Description | Frequency | Percent |
|---|---|---|---|---|
| ||||
| Symptoms/Ill‐Defined Conditions | 780.6 | Fever | 190 | 2.51 |
| 789 | Abdominal pain; unspecified site | 149 | 1.97 | |
| 786.5 | Chest pain, unspecified | 140 | 1.85 | |
| Circulatory System | 428 | Congestive heart failure, unspecified | 346 | 4.58 |
| 410.9 | Acute myocardial infarction; unspecified site; unspecified episode of care | 135 | 1.79 | |
| 410.1 | Acute myocardial infarction; other anterior wall; unspecified episode of care | 106 | 1.40 | |
| Respiratory System | 486 | Pneumonia, organism unspecified | 363 | 4.80 |
| 496 | Chronic airway obstruction, not elsewhere classified | 162 | 2.14 | |
| 493.9 | Asthma, unspecified; unspecified | 96 | 1.27 | |
| Neoplasms | 199.1 | Malignant neoplasm without specification of site; other | 86 | 1.14 |
| 162.9 | Malignant neoplasm; bronchus lung; unspecified | 73 | 0.97 | |
| 202.8 | Other lymphomas; unspecified site, extranodal and solid organ sites | 71 | 0.94 | |
| Genitourinary System | 599 | Urinary tract infection, site not specified | 247 | 3.27 |
| 584.9 | Acute renal failure, unspecified | 91 | 1.20 | |
| 585.6 | End stage renal disease | 40 | 0.53 | |
| Digestive System | 578.9 | Hemorrhage of gastrointestinal tract, unspecified | 119 | 1.57 |
| 558.9 | Other and unspecified noninfectious gastroenteritis and colitis | 69 | 0.91 | |
| 577 | Acute pancreatitis | 36 | 0.48 | |
| Blood/Blood‐Forming Organs | 285.9 | Anemia, unspecified | 127 | 1.68 |
| 282.64 | Sickle‐cell/Hb‐C disease with crisis | 80 | 1.06 | |
| 282.6 | Sickle‐cell disease, unspecified | 73 | 0.97 | |
| Endo/Nutritional/Metabolic/Immunity | 276.1 | Hypoosmolality and/or hyponatremia | 57 | 0.75 |
| 251.2 | Hypoglycemia, unspecified | 56 | 0.74 | |
| 250.1 | Diabetes with ketoacidosis; type II, not stated as uncontrolled | 50 | 0.66 | |
| Skin and Subcutaneous Tissue | 682.9 | Other cellulitis and abscess; unspecified site | 256 | 3.39 |
| 682.5 | Other cellulitis and abscess; buttock | 37 | 0.49 | |
| 686.9 | Unspecified local infection of skin and subcutaneous tissue | 23 | 0.30 | |
| Injury and Poisoning | 848.9 | Unspecified site of sprain and strain | 32 | 0.42 |
| 977.9 | Poisoning by unspecified drug or medicinal substance | 32 | 0.42 | |
| 829 | Fracture; unspecified bone, closed | 22 | 0.29 | |
| Musculoskeletal/Connective Tissue | 730.2 | Unspecified osteomyelitis; site unspecified | 33 | 0.44 |
| 710 | Systemic lupus erythematosus | 25 | 0.33 | |
| 728.87 | Muscle weakness (generalized) | 19 | 0.25 | |
| Infectious/Parasitic | 38.9 | Unspecified septicemia | 58 | 0.77 |
| 8.45 | Intestinal infection/clostridium difficile | 54 | 0.71 | |
| 9.1 | Colitis, enteritis, and gastroenteritis of presumed infectious organ | 15 | 0.20 | |
| Mental Disorders | 291.81 | Alcohol withdrawal | 43 | 0.57 |
| 307.9 | Other and unspecified special symptoms or syndromes, not elsewhere classified | 35 | 0.46 | |
| 294.8 | Other persistent mental disorders due to conditions classified elsewhere | 20 | 0.26 | |
| Nervous System/Sense Organs | 322.9 | Meningitis, unspecified | 30 | 0.40 |
| 331 | Alzheimer's disease | 14 | 0.19 | |
| 340 | Multiple sclerosis | 6 | 0.08 | |
| Health Status/Contact with Health Services | 885.9 | Accidental fall from other slipping tripping or stumbling | 18 | 0.24 |
| 884.4 | Accidental fall from bed | 7 | 0.09 | |
| V13.02 | Personal history of urinary (tract) infection | 4 | 0.05 | |
| Pregnancy/Childbirth/Puerperium | 673.8 | Other pulmonary embolism; unspecified episode of care | 9 | 0.12 |
| 665 | Rupture of uterus before onset of labor; unspecified episode of care | 1 | 0.01 | |
| 665.7 | Pelvic hematoma, unspecified episode of care | 1 | 0.01 | |
Individual resident clinical experience varied as well. As shown in Table 4, for a group of 6 PGY‐1s, there was substantial variability in the ICD‐9 diagnostic categories. For example, the percentages of codes falling into the cardiovascular disease category ranged from 15.27% to 27.91%, and for respiratory disease ranged from 8.22% to 18.55%. These data suggest that there may be sizable differences in the proportions of various clinical conditions seen by residents over a year of training.
| ICD‐9 Category Description | Mean | SD | Min | Max |
|---|---|---|---|---|
| ||||
| Symptoms/Ill‐Defined Conditions | 21.43 | 5.07 | 15.50 | 29.90 |
| Circulatory System | 21.84 | 4.38 | 15.27 | 27.91 |
| Respiratory System | 12.43 | 3.83 | 8.22 | 18.55 |
| Neoplasms | 8.47 | 2.64 | 4.12 | 11.80 |
| Genitourinary System | 5.26 | 1.09 | 4.03 | 6.98 |
| Digestive System | 4.53 | 0.96 | 3.09 | 5.65 |
| Blood/Blood‐Forming Organs | 4.64 | 2.73 | 3.05 | 10.05 |
| Endo/Nutritional/Metabolic/Immunity | 5.64 | 1.68 | 3.11 | 7.22 |
| Skin and Subcutaneous Tissue | 4.28 | 1.63 | 2.42 | 6.19 |
| Injury and Poisoning | 3.90 | 1.01 | 3.09 | 5.43 |
| Musculoskeletal/Connective Tissue | 2.86 | 1.36 | 1.55 | 4.58 |
| Infectious/Parasitic | 3.86 | 2.62 | 2.42 | 8.53 |
| Mental Disorders | 1.47 | 0.62 | 0.81 | 2.28 |
| Nervous System/Sense Organs | 1.49 | 0.87 | 0.62 | 3.09 |
DISCUSSION
Years ago, residency training transitioned from a predominantly bedside experience to a curriculum with a large didactic, non‐bedside component, following parameters defined by organizations such as the Accreditation Council for Graduate Medical Education. Residency training is undergoing substantial change to become competency‐based and to organize learning around patient care experiences.2, 3, 9 The Educational Innovation Project of the Residency Review Committee for Internal Medicine is one such endeavor to help develop new methods by which to accomplish this.1 Effective incorporation of innovative experiential learning methods, based on the core competencies, will require a detailed knowledge of resident clinical experience during the course of their training, yet such data have been sparse in internal medicine. Sequist et al. analyzed data from an electronic medical record to assess resident clinical experience in the outpatient setting.4 Bachur and Nagler have used an electronic patient tracking system to assess the clinical experience of pediatric emergency medicine fellows.5, 6 Most attempts to describe resident clinical experience have relied upon extracting diagnostic information from medical records, case logs, etc, though in another approach, Rohrbaugh et al. reviewed psychiatric resident prescription profiles,7 which might provide some indirect data on clinical experience if applied to internal medicine.
In this study, we attempted to quantify resident clinical experience using resident‐selected ICD‐9 codes, in contrast to other methods that have relied upon medical record review and other resident‐independent approaches. There are various strengths and limitations to this approach. Using the ICD‐9 system provides a number of strengths, a major one being standardization, allowing comparisons between different programs and perhaps even facilitating the development of guidelines for resident clinical experience. In addition, this approach using the ICD‐9 system could be readily implemented at any institution and does not require any specific technology. While we chose to do this through our handoff system, an institution could use any of a variety of other systems to accomplish this. For example, resident‐entered ICD‐9 coding systems could be incorporated into electronic discharge summaries, history and physicals, or progress notes. There may also be some practical benefits to having residents learn how to use the ICD‐9 system at this stage of their careers.
There are limitations to this approach as well. The ICD‐9 system was not intended to be used for medical education purposes. There are features of it that can make finding the best diagnosis difficult, and routes to it may at times seem counterintuitive. While we did not carry out resident surveys, a number of residents anecdotally mentioned that it took time to become comfortable using the system, and it could be challenging at times to find a diagnosis description that best fit what they were looking for. To make diagnosis selection easier, we created an organ system‐based dropdown list in the handoff tool so that when residents select an organ system, another list opens up containing commonly used ICD‐9 codes. This grouping is based on organ system alone and does not necessarily follow the ICD‐9 grouping (in contrast, our reported data in this article are all based on ICD‐9 grouping). A search tool to allow searching the entire ICD‐9 database was also made available on the handoff tool. Other factors that could limit diagnosis code accuracy could be lack of clinical knowledge, and error as a result of pressure to come up with a diagnosis because of the hard stop design of our system, in which residents were required to enter a primary diagnosis, potentially causing alert fatigue. A validation assessment that we carried out revealed fairly good agreement with the specific ICD‐9 codes chosen by the resident, but greater accuracy would be desirable. Further education on diagnosis selection and refinements to the handoff tool should help facilitate this. We are currently addressing this by ongoing education on diagnosis selection and by having the hospitalists share the handoff tool with the residents, allowing them to provide direct feedback on diagnostic selections.
More than 19% of the diagnoses selected by residents fell into the category of symptoms and ill‐defined conditions. This raises a number of potential educational issues. One of those is that if residents do, in fact, encounter such entities at such a high frequency, then the internal medicine curriculum must be structured in such a way as to complement this clinical experience with a comprehensive learning program. However, we must also consider the possibility that, in many such instances, a more definitive diagnosis became evident by the time of discharge and this may not have been reflected in the ICD‐9 code that the resident chose. Hence, the category of symptoms and ill‐defined conditions may actually be somewhat smaller than our findings would suggest.
Many issues will need to be addressed as programs obtain more data on their residents' clinical experience. While there may be many reasons to use the ICD‐9 system for selecting diagnoses including those listed above, the system by which ICD‐9 groups diagnoses might not provide ideal educational information, again as the ICD‐9 system was not designed for this purpose. While in this article we have reported the residents' diagnostic encounters grouped according to the ICD‐9 grouping system to provide an initial standardized description, grouping according to another diagnostic system that is felt to be more educationally meaningful may be preferred.
While one might assume that a higher frequency of exposure to certain clinical conditions should enhance competency, that relationship may not be straightforward in internal medicine. For surgical procedures, there are, in fact, data to show improved outcomes for surgeons with higher operative volumes for those procedures,10 but in internal medicine, we do not have data to demonstrate that competence of a resident caring for a particular condition is enhanced by experience alone. Therefore, as programs obtain more data on clinical experience, it will be important that the focus be kept on quality as opposed to quantity.
Obtaining data on resident clinical experience might greatly facilitate experiential learning approaches. For example, as residents go through training and encounter specific diagnostic conditions, those experiences could be supplemented by various learning innovations to make those experiences more meaningful and, hopefully, more likely to result in the development of competence, though that will require measurement. In our program, for example, we have incorporated an approach using illness scenarios, in that when residents have had a certain level of clinical experience with a given clinical condition, they are assembled in small groups and competency‐based case discussions are carried out with a preceptor. In addition, for those instances in which an individual resident may lack direct clinical experience in a certain area, this might be addressed by interventions to increase their contact with those conditions and/or targeted learning interventions to help develop competence. A resident found to be lacking in clinical experience in a certain area could be assigned to the care of more patients with that condition, or to spending more time in a venue in which that condition is more likely to be encountered. Various learning activities including didactics, case discussions, simulation, self‐directed learning, and others could also be used to compensate for such variability. Furthermore, if a residency program's aggregate clinical experience is divergent from some desirable standard yet to be determined, a detailed knowledge of this could help guide that program's curriculum revision. For example, for residents in a program in which there is relatively low exposure to patients with oncological issues, this could be compensated for by external rotations to achieve more clinical experience in oncology, as well as supplementation of the curriculum with additional learning activities in oncology, which could include small group discussions, self‐directed learning activities, case discussions, and others. While at present there are no defined standards for clinical experience and it remains to be seen if there would be a correlation with development of competence, no such standard would serve a purpose if programs did not have reliable and practical means of clinical experience assessment.
In summary, resident‐selected ICD‐9 codes may be a useful means to obtain data regarding resident clinical experience in internal medicine. Such data may be useful to residency training programs in developing new curricula based on experiential learning.
- ,,.Internal medicine's Educational Innovations Project: improving health care and learning.Am J Med.2009;122:398–404.
- ,,,,.Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144:920–926.
- ,,for the Education Committee of the American College of Physicians.Redesigning training for internal medicine.Ann Intern Med.2006;144:927–932.
- ,,,,.Use of an electronic medical record to profile the continuity clinic experiences of primary care residents.Acad Med.2005;80:390–394.
- ,,.An automated electronic case log: using electronic information systems to assess training in emergency medicine.Acad Emerg Med.2006;13:733–739.
- ,.Use of an automated electronic case log to assess fellowship training: tracking the pediatric emergency medicine experience.Pediatr Emerg Care.2008;24:75–82.
- ,,,.Utilizing VA information technology to develop psychiatric resident prescription profiles.Acad Psychiatry.2009;33:27–30.
- ,,, et al.Personal digital assistants (PDAs): a review of their application in graduate medical education.Am J Med Qual.2005;20:262–267.
- ,,, et al.Redesigning residency training in internal medicine: the consensus report of the Alliance for Academic Internal Medicine Education Redesign Task Force.Acad Med.2007;82:1211–1219.
- ,,,,,.Surgeon volume and operative mortality in the United States.N Engl J Med.2003;349:2117–2127.
- ,,.Internal medicine's Educational Innovations Project: improving health care and learning.Am J Med.2009;122:398–404.
- ,,,,.Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144:920–926.
- ,,for the Education Committee of the American College of Physicians.Redesigning training for internal medicine.Ann Intern Med.2006;144:927–932.
- ,,,,.Use of an electronic medical record to profile the continuity clinic experiences of primary care residents.Acad Med.2005;80:390–394.
- ,,.An automated electronic case log: using electronic information systems to assess training in emergency medicine.Acad Emerg Med.2006;13:733–739.
- ,.Use of an automated electronic case log to assess fellowship training: tracking the pediatric emergency medicine experience.Pediatr Emerg Care.2008;24:75–82.
- ,,,.Utilizing VA information technology to develop psychiatric resident prescription profiles.Acad Psychiatry.2009;33:27–30.
- ,,, et al.Personal digital assistants (PDAs): a review of their application in graduate medical education.Am J Med Qual.2005;20:262–267.
- ,,, et al.Redesigning residency training in internal medicine: the consensus report of the Alliance for Academic Internal Medicine Education Redesign Task Force.Acad Med.2007;82:1211–1219.
- ,,,,,.Surgeon volume and operative mortality in the United States.N Engl J Med.2003;349:2117–2127.
Copyright © 2011 Society of Hospital Medicine
Severe Sepsis
Severe sepsis and septic shock are associated with excess mortality when inappropriate initial antimicrobial therapy, defined as an antimicrobial regimen that lacks in vitro activity against the isolated organism(s) responsible for the infection, is administered.14 Unfortunately, bacterial resistance to antibiotics is increasing and creates a therapeutic challenge for clinicians when treating patients with serious infections, such as severe sepsis. Increasing rates of bacterial resistance leads many clinicians to empirically treat critically ill patients with broad‐spectrum antibiotics, which can perpetuate the cycle of increasing resistance.5, 6 Conversely, inappropriate initial antimicrobial therapy can lead to treatment failures and adverse patient outcomes.7 Individuals with severe sepsis appear to be at particularly high risk of excess mortality when inappropriate initial antimicrobial therapy is administered.8, 9
The most recent Surviving Sepsis Guidelines recommend empiric combination therapy targeting Gram‐negative bacteria, particularly for patients with known or suspected Pseudomonas infections, as a means to decrease the likelihood of administering inappropriate initial antimicrobial therapy.10 However, the selection of an antimicrobial regimen that is active against the causative pathogen(s) is problematic, as the treating physician usually does not know the susceptibilities of the pathogen(s) for the selected empiric antibiotics. Therefore, we performed a study with the main goal of determining whether resistance to the initially prescribed antimicrobial regimen was associated with clinical outcome in patients with severe sepsis attributed to Gram‐negative bacteremia.
Materials and Methods
Study Location and Patients
This study was conducted at a university‐affiliated, urban teaching hospital: Barnes‐Jewish Hospital (1200 beds). During a 6‐year period (January 2002 to December 2007), all hospitalized patients with a positive blood culture for Gram‐negative bacteria, with antimicrobial susceptibility testing performed for the blood isolate(s), were eligible for this investigation. This study was approved by the Washington University School of Medicine Human Studies Committee.
Study Design and Data Collection
A retrospective cohort study design was employed. Two investigators (J.A.D., R.M.R.) identified potential study patients by the presence of a positive blood culture for Pseudomonas aeruginosa, Acinetobacter species, or Enterobacteriaceae (Escherichia coli, Klebsiella species, Enterobacter species) combined with primary or secondary International Classification of Diseases (ICD‐9‐CM) codes indicative of acute organ dysfunction, at least two criteria from the systemic inflammatory response syndrome (SIRS),10 and initial antibiotic treatment with either cefepime, piperacillin‐tazobactam, or a carbapenem (imipenem or meropenem). These antimicrobials represent the primary agents employed for the treatment of Gram‐negative infections at Barnes‐Jewish Hospital during the study period, and had to be administered within 12 hours of having the subsequently positive blood cultures drawn. Based on the initial study database construction, 3 investigators (E.C.W., J.K., M.P.) merged patient‐specific data from the automated hospital medical records, microbiology database, and pharmacy database of Barnes‐Jewish Hospital to complete the clinical database under the auspices of the definitions described below.
The baseline characteristics collected by the study investigators included: age, gender, race, the presence of congestive heart failure, chronic obstructive pulmonary disease, diabetes mellitus, chronic liver disease, underlying malignancy, and end‐stage renal disease requiring renal replacement therapy. All cause hospital mortality was evaluated as the primary outcome variable. Secondary outcomes included acquired organ dysfunction and hospital length of stay. The Acute Physiology and Chronic Health Evaluation (APACHE) II11 and Charlson co‐morbidity scores were also calculated during the 24 hours after the positive blood cultures were drawn. This was done because we included patients with community‐acquired infections who only had clinical data available after blood cultures were drawn.
Definitions
All definitions were selected prospectively as part of the original study design. Cases of Gram‐negative bacteremia were classified into mutually exclusive groups comprised of either community‐acquired or healthcare‐associated infection. Patients with healthcare‐associated bacteremia were categorized as community‐onset or hospital‐onset, as previously described.12 In brief, patients with healthcare‐associated community‐onset bacteremia had the positive culture obtained within the first 48 hours of hospital admission in combination with one or more of the following risk factors: (1) residence in a nursing home, rehabilitation hospital, or other long‐term nursing facility; (2) previous hospitalization within the immediately preceding 12 months; (3) receiving outpatient hemodialysis, peritoneal dialysis, wound care, or infusion therapy necessitating regular visits to a hospital‐based clinic; and (4) having an immune‐compromised state. Patients were classified as having healthcare‐associated hospital‐onset bacteremia when the culture was obtained 48 hours or more after admission. Community‐acquired bacteremia occurred in patients without healthcare risk factors and a positive blood culture within the first 48 hours of admission. Prior antibiotic exposure was defined as having occurred within the previous 30 days from the onset of severe sepsis.
To be included in the analysis, patients had to meet criteria for severe sepsis based on discharge ICD‐9‐CM codes for acute organ dysfunction, as previously described.13 The organs of interest included the heart, lungs, kidneys, bone marrow (hematologic), brain, and liver. Patients were classified as having septic shock if vasopressors (norepinephrine, dopamine, epinephrine, phenylephrine, or vasopressin) were initiated within 24 hours of the blood culture collection date and time. Empiric antimicrobial treatment was classified as being appropriate if the initially prescribed antibiotic regimen was active against the identified pathogen(s) based on in vitro susceptibility testing and administered within 12 hours following blood culture collection. Appropriate antimicrobial treatment also had to be prescribed for at least 24 hours. However, the total duration of antimicrobial therapy was at the discretion of the treating physicians. The Charlson co‐morbidity score was calculated using ICD‐9‐CM codes abstracted from the index hospitalization employing MS‐DRG Grouper version 26.
Antimicrobial Monitoring
From January 2002 through the present, Barnes‐Jewish Hospital utilized an antibiotic control program to help guide antimicrobial therapy. During this time, the use of cefepime and gentamicin was unrestricted. However, initiation of intravenous ciprofloxacin, imipenem/cilastatin, meropenem, or piperacillin/tazobactam was restricted and required preauthorization from either a clinical pharmacist or infectious diseases physician. Each intensive care unit (ICU) had a clinical pharmacist who reviewed all antibiotic orders to insure that dosing and interval of antibiotic administration was adequate for individual patients based on body size, renal function, and the resuscitation status of the patient. After daytime hours, the on‐call clinical pharmacist reviewed and approved the antibiotic orders. The initial antibiotic dosages for the antibiotics employed for the treatment of Gram‐negative infections at Barnes‐Jewish Hospital were as follows: cefepime, 1 to 2 grams every eight hours; pipercillin‐tazobactam, 4.5 grams every six hours; imipenem, 0.5 grams every six hours; meropenem, 1 gram every eight hours; ciprofloxacin, 400 mg every eight hours; gentamicin, 5 mg/kg once daily.
Starting in June 2005, a sepsis order set was implemented in the emergency department, general medical wards, and the intensive care units with the intent of standardizing empiric antibiotic selection for patients with sepsis based on the infection type (ie, community‐acquired pneumonia, healthcare‐associated pneumonia, intra‐abdominal infection, etc) and the hospital's antibiogram.14, 15 However, antimicrobial selection, dosing, and de‐escalation of therapy were still optimized by clinical pharmacists in these clinical areas.
Antimicrobial Susceptibility Testing
The microbiology laboratory performed antimicrobial susceptibility testing of the Gram‐negative blood isolates using the disk diffusion method according to guidelines and breakpoints established by the Clinical Laboratory and Standards Institute (CLSI) and published during the inclusive years of the study.16, 17 Zone diameters obtained by disk diffusion testing were converted to minimum inhibitory concentrations (MICs in mg/L) by linear regression analysis for each antimicrobial agent using the BIOMIC V3 antimicrobial susceptibility system (Giles Scientific, Inc., Santa Barbara, CA). Linear regression algorithms contained in the software of this system were determined by comparative studies correlating microbroth dilution‐determined MIC values with zone sizes obtained by disk diffusion testing.18
Data Analysis
Continuous variables were reported as mean the standard deviation, or median and quartiles. The Student's t test was used when comparing normally distributed data, and the MannWhitney U test was employed to analyze nonnormally distributed data. Categorical data were expressed as frequency distributions and the Chi‐squared test was used to determine if differences existed between groups. We performed multiple logistic regression analysis to identify clinical risk factors that were associated with hospital mortality (SPSS, Inc., Chicago, IL). All risk factors from Table 1, as well as the individual pathogens examined, were included in the corresponding multivariable analysis with the exception of acquired organ dysfunction (considered a secondary outcome). All tests were two‐tailed, and a P value <0.05 was determined to represent statistical significance.
| Variable | Hospital Survivors (n = 302) | Hospital Nonsurvivors (n = 233) | P value |
|---|---|---|---|
| |||
| Age, years | 57.9 16.2 | 60.3 15.8 | 0.091 |
| Male | 156 (51.7) | 132 (56.7) | 0.250 |
| Infection onset source | |||
| Community‐acquired | 31 (10.3) | 15 (6.4) | 0.005 |
| Healthcare‐associated community‐onset | 119 (39.4) | 68 (29.2) | |
| Healthcare‐associated hospital‐onset | 152 (50.3) | 150 (64.4) | |
| Underlying co‐morbidities | |||
| CHF | 43 (14.2) | 53 (22.7) | 0.011 |
| COPD | 42 (13.9) | 56 (24.0) | 0.003 |
| Chronic kidney disease | 31 (10.3) | 41 (17.6) | 0.014 |
| Liver disease | 34 (11.3) | 31 (13.3) | 0.473 |
| Active malignancy | 100 (33.1) | 83 (35.6) | 0.544 |
| Diabetes | 68 (22.5) | 50 (21.5) | 0.770 |
| Charlson co‐morbidity score | 4.5 3.5 | 5.2 3.9 | 0.041 |
| APACHE II score | 21.8 6.1 | 27.1 6.2 | <0.001 |
| ICU admission | 221 (73.2) | 216 (92.7) | <0.001 |
| Vasopressors | 137 (45.4) | 197 (84.5) | <0.001 |
| Mechanical ventilation | 124 (41.1) | 183 (78.5) | <0.001 |
| Drotrecogin alfa (activated) | 6 (2.0) | 21 (9.0) | <0.001 |
| Dysfunctional acquired organ systems | |||
| Cardiovascular | 149 (49.3) | 204 (87.6) | <0.001 |
| Respiratory | 141 (46.7) | 202 (86.7) | <0.001 |
| Renal | 145 (48.0) | 136 (58.4) | 0.017 |
| Hepatic | 13 (4.3) | 27 (11.6) | 0.001 |
| Hematologic | 103 (34.1) | 63 (27.0) | 0.080 |
| Neurologic | 11 (3.6) | 19 (8.2) | 0.024 |
| 2 Dysfunctional acquired organ systems | 164 (54.3) | 213 (91.4) | <0.001 |
| Source of bloodstream infection | |||
| Lungs | 95 (31.5) | 127 (54.5) | <0.001 |
| Urinary tract | 92 (30.5) | 45 (19.3) | |
| Central venous catheter | 30 (9.9) | 16 (6.9) | |
| Intra‐abdominal | 63 (20.9) | 33 (14.2) | |
| Unknown | 22 (7.3) | 12 (5.2) | |
| Prior antibiotics* | 103 (34.1) | 110 (47.2) | 0.002 |
Results
Patient Characteristics
Included in the study were 535 consecutive patients with severe sepsis attributed to Pseudomonas aeruginosa, Acinetobacter species, or Enterobacteriaceae bacteremia, of whom 233 (43.6%) died during their hospitalization. The mean age was 58.9 16.0 years (range, 18 to 96 years) with 288 (53.8%) males and 247 (46.2%) females. The infection sources included community‐acquired (n = 46, 8.6%), healthcare‐associated community‐onset (n = 187, 35.0%), and healthcare‐associated hospital‐onset (n = 302, 56.4%). Hospital nonsurvivors were statistically more likely to have a healthcare‐associated hospital‐onset infection, congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease, ICU admission, need for mechanical ventilation and/or vasopressors, administration of drotrecogin alfa (activated), prior antibiotic administration, the lungs as the source of infection, acquired dysfunction of the cardiovascular, respiratory, renal, hepatic, and neurologic organ systems, and greater APACHE II and Charlson co‐morbidity scores compared to hospital survivors (Table 1). Hospital nonsurvivors were also statistically less likely to have a healthcare‐associated community‐onset infection and a urinary source of infection compared to hospital survivors (Table 1).
Microbiology
Among the 547 Gram‐negative bacteria isolated from blood, the most common were Enterobacteriaceae (Escherichia coli, Klebsiella species, Enterobacter species) (70.2%) followed by Pseudomonas aeruginosa (20.8%) and Acinetobacter species (9.0%) (Table 2). Nine patients had two different Enterobacteriaceae species isolated from their blood cultures, and three patients had an Enterobacteriaceae species and Pseudomonas aeruginosa isolated from their blood cultures. Hospital nonsurvivors were statistically more likely to be infected with Pseudomonas aeruginosa and less likely to be infected with Enterobacteriaceae. The pathogen‐specific hospital mortality rate was significantly greater for Pseudomonas aeruginosa and Acinetobacter species compared to Enterobacteriaceae (P < 0.001 and P = 0.008, respectively).
| Bacteria | Hospital Survivors (n = 302) | Hospital Nonsurvivors (n = 233) | P value* | Percent Resistant | Pathogen‐ Specific Mortality Rate |
|---|---|---|---|---|---|
| |||||
| Enterobacteriaceae | 241 (79.8) | 143 (61.4) | <0.001 | 9.1 | 37.2 |
| Pseudomonas aeruginosa | 47 (15.6) | 67 (28.8) | <0.001 | 16.7 | 58.8 |
| Acinetobacter species | 22 (7.3) | 27 (11.6) | 0.087 | 71.4 | 55.1 |
Antimicrobial Treatment and Resistance
Among the study patients, 358 (66.9%) received cefepime, 102 (19.1%) received piperacillin‐tazobactam, and 75 (14.0%) received a carbapenem (meropenem or imipenem) as their initial antibiotic treatment. There were 169 (31.6%) patients who received initial combination therapy with either an aminoglycoside (n = 99, 58.6%) or ciprofloxacin (n = 70, 41.4%). Eighty‐two (15.3%) patients were infected with a pathogen that was resistant to the initial antibiotic treatment regimen [cefepime (n = 41; 50.0%), piperacillin‐tazobactam (n = 25; 30.5%), or imipenem/meropenem (n = 16; 19.5%), plus either an aminoglycoside or ciprofloxacin (n = 28; 34.1%)], and were classified as receiving inappropriate initial antibiotic therapy. Among the 453 (84.7%) patients infected with a pathogen that was susceptible to the initial antibiotic regimen, there was no relationship identified between minimum inhibitory concentration values and hospital mortality.
Patients infected with a pathogen resistant to the initial antibiotic regimen had significantly greater risk of hospital mortality (63.4% vs 40.0%; P < 0.001) (Figure 1). For the 82 individuals infected with a pathogen that was resistant to the initial antibiotic regimen, no difference in hospital mortality was observed among those prescribed initial combination treatment with an aminoglycoside (n = 17) (64.7% vs 61.1%; P = 0.790) or ciprofloxacin (n = 11) (72.7% vs 61.1%; P = 0.733) compared to monotherapy (n = 54). Similarly, among the patients infected with a pathogen that was susceptible to the initial antibiotic regimen, there was no difference in hospital mortality among those whose bloodstream isolate was only susceptible to the prescribed aminoglycoside (n = 12) compared to patients with isolates that were susceptible to the prescribed beta‐lactam antibiotic (n = 441) (41.7% vs 39.9%; P = 0.902).
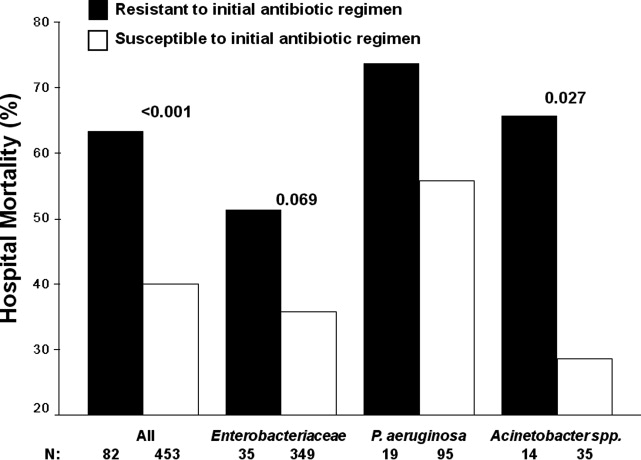
Logistic regression analysis identified infection with a pathogen resistant to the initial antibiotic regimen [adjusted odds ratio (AOR), 2.28; 95% confidence interval (CI), 1.69‐3.08; P = 0.006], increasing APACHE II scores (1‐point increments) (AOR, 1.13; 95% CI, 1.10‐1.15; P < 0.001), the need for vasopressors (AOR, 2.57; 95% CI, 2.15‐3.53; P < 0.001), the need for mechanical ventilation (AOR, 2.54; 95% CI, 2.19‐3.47; P < 0.001), healthcare‐associated hospital‐onset infection (AOR, 1.67; 95% CI, 1.32‐2.10; P =0.027), and infection with Pseudomonas aeruginosa (AOR, 2.21; 95% CI, 1.74‐2.86; P =0.002) as independent risk factors for hospital mortality (Hosmer‐Lemeshow goodness‐of‐fit test = 0.305). The model explained between 29.7% (Cox and Snell R square) and 39.8% (Nagelkerke R squared) of the variance in hospital mortality, and correctly classified 75.3% of cases.
Secondary Outcomes
Two or more acquired organ system derangements occurred significantly more often among patients with a pathogen resistant to the initial antibiotic regimen compared to those infected with susceptible isolates (84.1% vs 68.0%; P = 0.003). Hospital length of stay was significantly longer for patients infected with a pathogen resistant to the initial antibiotic regimen compared to those infected with susceptible isolates [39.9 50.6 days (median 27 days; quartiles 12 days and 45.5 days) vs 21.6 22.0 days (median 15 days; quartiles 7 days and 30 days); P < 0.001].
Discussion
Our study demonstrated that hospital nonsurvivors with severe sepsis attributed to Gram‐negative bacteremia had significantly greater rates of resistance to their initially prescribed antibiotic regimen compared to hospital survivors. This observation was confirmed in a multivariate analysis controlling for severity of illness and other potential confounding variables. Additionally, acquired organ system derangements and hospital length of stay were greater for patients infected with Gram‐negative pathogens resistant to the empiric antibiotic regimen. We also observed no survival advantage with the use of combination antimicrobial therapy for the subgroup of patients whose pathogens were resistant to the initially prescribed antibiotic regimen. Lastly, no difference in mortality was observed for patients with bacterial isolates that were susceptible only to the prescribed aminoglycoside compared to those with isolates susceptible to the prescribed beta‐lactam antibiotic.
Several previous investigators have linked antibiotic resistance and outcome in patients with serious infections attributed to Gram‐negative bacteria. Tam et al. examined 34 patients with Pseudomonas aeruginosa bacteremia having elevated MICs to piperacillin‐tazobactam (32 g/mL) that were reported as susceptible.19 In seven of these cases, piperacillin‐tazobactam was prescribed empirically, whereas other agents directed against Gram‐negative bacteria were employed in the other patients (carbapenems, aminoglycosides). Thirty‐day mortality was significantly greater for the patients treated with piperacillin‐tazobactam (85.7% vs 22.2%; P = 0.004), and a multivariate analysis found treatment with piperacillin‐tazobactam to be independently associated with 30‐day mortality. Similarly, Bhat et al. examined 204 episodes of bacteremia caused by Gram‐negative bacteria for which patients received cefepime.20 Patients infected with a Gram‐negative bacteria having an MIC to cefepime greater than, or equal to, 8 g/mL had a significantly greater 28‐day mortality compared to patients infected with isolates having an MIC to cefepime that was less than 8 g/mL (54.8% vs 24.1%; P = 0.001).
Our findings are consistent with earlier studies of patients with serious Gram‐negative infections including bacteremia and nosocomial pneumonia. Micek et al. showed that patients with Pseudomonas aeruginosa bacteremia who received inappropriate initial antimicrobial therapy had a greater risk of hospital mortality compared to patients initially treated with an antimicrobial regimen having activity for the Pseudomonas isolate based on in vitro susceptibility testing.21 Similarly, Trouillet et al.,22 Beardsley et al.,23 and Heyland et al.24 found that combination antimicrobial regimens directed against Gram‐negative bacteria in patients with nosocomial pneumonia were more likely to be appropriate based on the antimicrobial susceptibility patterns of the organisms compared to monotherapy. In a more recent study, Micek et al. demonstrated that combination antimicrobial therapy directed against severe sepsis attributed to Gram‐negative bacteria was associated with improved outcomes compared to monotherapy, especially when the combination agent was an aminoglycoside.25 However, empiric combination therapy that included an aminoglycoside was also associated with increased nephrotoxicity which makes the empiric use of aminoglycosides in all patients with suspected Gram‐negative severe sepsis problematic.25, 26 Nevertheless, the use of combination therapy represents a potential strategy to maximize the administration of appropriate treatment for serious Gram‐negative bacterial infections.
Rapid assessment of antimicrobial susceptibility is another strategy that offers the possibility of identifying the resistance pattern of Gram‐negative pathogens quickly in order to provide more appropriate treatment. Bouza et al. found that use of a rapid E‐test on the respiratory specimens of patients with ventilator‐associated pneumonia was associated with fewer days of fever, fewer days of antibiotic administration until resolution of the episode of ventilator‐associated pneumonia, decreased antibiotic consumption, less Clostridium difficile‐associated diarrhea, lower costs of antimicrobial agents, and fewer days receiving mechanical ventilation.27 Other methods for the rapid identification of resistant bacteria include real‐time polymerase chain reaction assays based on hybridization probes to identify specific resistance mechanisms in bacteria.28 Application of such methods for identification of broad categories of resistance mechanisms in Gram‐negative bacteria offer the possibility of tailoring initial antimicrobial regimens in order to provide appropriate therapy in a more timely manner.
Our study has several important limitations that should be noted. First, the study was performed at a single center and the results may not be generalizable to other institutions. However, the findings from other investigators corroborate the importance of antimicrobial resistance as a predictor of outcome for patients with serious Gram‐negative infections.19, 20 Additionally, a similar association has been observed in patients with methicillin‐resistant Staphylococcus aureus bacteremia, supporting the more general importance of antimicrobial resistance as an outcome predictor.29 Second, the method employed for determining MICs was a literature‐based linear regression method correlating disk diffusion diameters with broth dilution MIC determinations. Therefore, the lack of correlation we observed between MIC values and outcome for susceptible Gram‐negative isolates associated with severe sepsis requires further confirmation. Third, we only examined 3 antibiotics, or antibiotic classes, so our results may not be applicable to other agents. This also applies to doripenem, as we did not have that specific carbapenem available at the time this investigation took place.
Another important limitation of our study is the relatively small number of individuals infected with a pathogen that was resistant to the initial treatment regimen, or only susceptible to the aminoglycoside when combination therapy was prescribed. This limited our ability to detect meaningful associations in these subgroups of patients, to include whether or not combination therapy influenced their clinical outcome. Finally, we did not examine the exact timing of antibiotic therapy relative to the onset of severe sepsis. Instead we used a 12‐hour window from when subsequently positive blood cultures were drawn to the administration of initial antibiotic therapy. Other investigators have shown that delays in initial appropriate therapy of more than one hour for patients with septic shock increases the risk of death.9, 30 Failure to include the exact timing of therapy could have resulted in a final multivariate model that includes prediction variables that would not otherwise have been incorporated.
In summary, we demonstrated that resistance to the initial antibiotic treatment regimen was associated with a greater risk of hospital mortality in patients with severe sepsis attributed to Gram‐negative bacteremia. These findings imply that more rapid assessment of antimicrobial susceptibility could result in improved prescription of antibiotics in order to maximize initial administration of appropriate therapy. Future studies are required to address whether rapid determination of antimicrobial susceptibility can result in more effective administration of appropriate therapy, and if this can result in improved patient outcomes.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.The clinical evaluation committee in a large multicenter phase 3 trial of drotrecogin alfa (activated) in patients with severe sepsis (PROWESS): role, methodology, and results.Crit Care Med.2003;31:2291–2301.
- ,,,,,.Impact of adequate empical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis.Crit Care Med.2003;31:2742–2751.
- ,,,,,.Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med.2003;115:529–535.
- ,.Antibiotic‐resistant bugs in the 21st century—a clinical super‐challenge.N Engl J Med.2009;360:439–443.
- ,,, et al.Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America.Clin Infect Dis.2009;48:1–12.
- .Broad‐spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front.Clin Infect Dis.2008;47:S3–S13.
- ,,, et al.Bundled care for septic shock: an analysis of clinical trials.Crit Care Med.2010;38:668–678.
- ,,, et al.Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study.Am J Respir Crit Care Med.2009;180:861–866.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36:296–327.
- ,,,.APACHE II: a severity of disease classification system.Crit Care Med.1985;13:818–829.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,,,,.Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29:1303–1310.
- ,,,,,.Hospital‐wide impact of a standardized order set for the management of bacteremic severe sepsis.Crit Care Med.2009;37:819–824.
- ,,, et al.Before‐after study of a standardized hospital order set for the management of septic shock.Crit Care Med.2007;34:2707–2713.
- National Committee for Clinical Laboratory Standards.Performance Standards for Antimicrobial Susceptibility Testing: Twelfth Informational Supplement. M100‐S12.Wayne, PA:National Committee for Clinical Laboratory Standards;2002.
- Clinical Laboratory Standards Institute.Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement. M100‐S17.Wayne, PA:Clinical Laboratory Standards Institute;2007.
- ,,, et al.Evaluation of the BIOGRAM antimicrobial susceptibility test system.J Clin Microbiol.1985;22:793–798.
- ,,, et al.Outcomes of bacteremia due to Pseudomonas aeruginosa with reduced susceptibility to piperacillin‐tazobactam: implications on the appropriateness of the resistance breakpoint.Clin Infect Dis.2008;46:862–867.
- ,,, et al.Failure of current cefepime breakpoints to predict clinical outcomes of bacteremia caused by Gram‐negative organisms.Antimicrob Agents Chemother.2007;51:4390–4395.
- ,,,,,.Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment.Antimicrob Agents Chemother.2005;49:1306–1311.
- ,,.Ventilator‐associated pneumonia caused by potentially drug‐resistant bacteria.Am J Respir Crit Care Med.1998;157:531–539.
- ,,,,,.Using local microbiologic data to develop institution‐specific guidelines for the treatment of hospital‐acquired pneumonia.Chest.2006;130:787–793.
- ,,, et al.Randomized trial of combination versus monotherapy for the empiric treatment of suspected ventilator‐associated pneumonia.Crit Care Med.2008;36:737–744.
- ,,, et al.Empiric combination antibiotic therapy is associated with improved outcome in Gram‐negative sepsis: a retrospective analysis.Antimicrob Agents Chemother.2010;54:1742–1748.
- ,,, et al.Monotherapy versus beta‐lactam‐aminoglycoside combination treatment for Gram‐negative bacteremia: a prospective, observational study.Antimicrob Agents Chemother.1997;41:1127–1133.
- ,,, et al.Direct E‐test (AB Biodisk) of respiratory samples improves antimicrobial use in ventilator‐associated pneumonia.Clin Infect Dis.2007;44:382–387.
- ,,, et al.Rapid detection of CTX‐M‐producing Enterobacteriaceae in urine samples.J Antimicrob Chemother.2009;64:986–989.
- ,,, et al.Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46:193–200.
- ,,, et al.Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock.Crit Care Med.2006;34:1589–1596.
Severe sepsis and septic shock are associated with excess mortality when inappropriate initial antimicrobial therapy, defined as an antimicrobial regimen that lacks in vitro activity against the isolated organism(s) responsible for the infection, is administered.14 Unfortunately, bacterial resistance to antibiotics is increasing and creates a therapeutic challenge for clinicians when treating patients with serious infections, such as severe sepsis. Increasing rates of bacterial resistance leads many clinicians to empirically treat critically ill patients with broad‐spectrum antibiotics, which can perpetuate the cycle of increasing resistance.5, 6 Conversely, inappropriate initial antimicrobial therapy can lead to treatment failures and adverse patient outcomes.7 Individuals with severe sepsis appear to be at particularly high risk of excess mortality when inappropriate initial antimicrobial therapy is administered.8, 9
The most recent Surviving Sepsis Guidelines recommend empiric combination therapy targeting Gram‐negative bacteria, particularly for patients with known or suspected Pseudomonas infections, as a means to decrease the likelihood of administering inappropriate initial antimicrobial therapy.10 However, the selection of an antimicrobial regimen that is active against the causative pathogen(s) is problematic, as the treating physician usually does not know the susceptibilities of the pathogen(s) for the selected empiric antibiotics. Therefore, we performed a study with the main goal of determining whether resistance to the initially prescribed antimicrobial regimen was associated with clinical outcome in patients with severe sepsis attributed to Gram‐negative bacteremia.
Materials and Methods
Study Location and Patients
This study was conducted at a university‐affiliated, urban teaching hospital: Barnes‐Jewish Hospital (1200 beds). During a 6‐year period (January 2002 to December 2007), all hospitalized patients with a positive blood culture for Gram‐negative bacteria, with antimicrobial susceptibility testing performed for the blood isolate(s), were eligible for this investigation. This study was approved by the Washington University School of Medicine Human Studies Committee.
Study Design and Data Collection
A retrospective cohort study design was employed. Two investigators (J.A.D., R.M.R.) identified potential study patients by the presence of a positive blood culture for Pseudomonas aeruginosa, Acinetobacter species, or Enterobacteriaceae (Escherichia coli, Klebsiella species, Enterobacter species) combined with primary or secondary International Classification of Diseases (ICD‐9‐CM) codes indicative of acute organ dysfunction, at least two criteria from the systemic inflammatory response syndrome (SIRS),10 and initial antibiotic treatment with either cefepime, piperacillin‐tazobactam, or a carbapenem (imipenem or meropenem). These antimicrobials represent the primary agents employed for the treatment of Gram‐negative infections at Barnes‐Jewish Hospital during the study period, and had to be administered within 12 hours of having the subsequently positive blood cultures drawn. Based on the initial study database construction, 3 investigators (E.C.W., J.K., M.P.) merged patient‐specific data from the automated hospital medical records, microbiology database, and pharmacy database of Barnes‐Jewish Hospital to complete the clinical database under the auspices of the definitions described below.
The baseline characteristics collected by the study investigators included: age, gender, race, the presence of congestive heart failure, chronic obstructive pulmonary disease, diabetes mellitus, chronic liver disease, underlying malignancy, and end‐stage renal disease requiring renal replacement therapy. All cause hospital mortality was evaluated as the primary outcome variable. Secondary outcomes included acquired organ dysfunction and hospital length of stay. The Acute Physiology and Chronic Health Evaluation (APACHE) II11 and Charlson co‐morbidity scores were also calculated during the 24 hours after the positive blood cultures were drawn. This was done because we included patients with community‐acquired infections who only had clinical data available after blood cultures were drawn.
Definitions
All definitions were selected prospectively as part of the original study design. Cases of Gram‐negative bacteremia were classified into mutually exclusive groups comprised of either community‐acquired or healthcare‐associated infection. Patients with healthcare‐associated bacteremia were categorized as community‐onset or hospital‐onset, as previously described.12 In brief, patients with healthcare‐associated community‐onset bacteremia had the positive culture obtained within the first 48 hours of hospital admission in combination with one or more of the following risk factors: (1) residence in a nursing home, rehabilitation hospital, or other long‐term nursing facility; (2) previous hospitalization within the immediately preceding 12 months; (3) receiving outpatient hemodialysis, peritoneal dialysis, wound care, or infusion therapy necessitating regular visits to a hospital‐based clinic; and (4) having an immune‐compromised state. Patients were classified as having healthcare‐associated hospital‐onset bacteremia when the culture was obtained 48 hours or more after admission. Community‐acquired bacteremia occurred in patients without healthcare risk factors and a positive blood culture within the first 48 hours of admission. Prior antibiotic exposure was defined as having occurred within the previous 30 days from the onset of severe sepsis.
To be included in the analysis, patients had to meet criteria for severe sepsis based on discharge ICD‐9‐CM codes for acute organ dysfunction, as previously described.13 The organs of interest included the heart, lungs, kidneys, bone marrow (hematologic), brain, and liver. Patients were classified as having septic shock if vasopressors (norepinephrine, dopamine, epinephrine, phenylephrine, or vasopressin) were initiated within 24 hours of the blood culture collection date and time. Empiric antimicrobial treatment was classified as being appropriate if the initially prescribed antibiotic regimen was active against the identified pathogen(s) based on in vitro susceptibility testing and administered within 12 hours following blood culture collection. Appropriate antimicrobial treatment also had to be prescribed for at least 24 hours. However, the total duration of antimicrobial therapy was at the discretion of the treating physicians. The Charlson co‐morbidity score was calculated using ICD‐9‐CM codes abstracted from the index hospitalization employing MS‐DRG Grouper version 26.
Antimicrobial Monitoring
From January 2002 through the present, Barnes‐Jewish Hospital utilized an antibiotic control program to help guide antimicrobial therapy. During this time, the use of cefepime and gentamicin was unrestricted. However, initiation of intravenous ciprofloxacin, imipenem/cilastatin, meropenem, or piperacillin/tazobactam was restricted and required preauthorization from either a clinical pharmacist or infectious diseases physician. Each intensive care unit (ICU) had a clinical pharmacist who reviewed all antibiotic orders to insure that dosing and interval of antibiotic administration was adequate for individual patients based on body size, renal function, and the resuscitation status of the patient. After daytime hours, the on‐call clinical pharmacist reviewed and approved the antibiotic orders. The initial antibiotic dosages for the antibiotics employed for the treatment of Gram‐negative infections at Barnes‐Jewish Hospital were as follows: cefepime, 1 to 2 grams every eight hours; pipercillin‐tazobactam, 4.5 grams every six hours; imipenem, 0.5 grams every six hours; meropenem, 1 gram every eight hours; ciprofloxacin, 400 mg every eight hours; gentamicin, 5 mg/kg once daily.
Starting in June 2005, a sepsis order set was implemented in the emergency department, general medical wards, and the intensive care units with the intent of standardizing empiric antibiotic selection for patients with sepsis based on the infection type (ie, community‐acquired pneumonia, healthcare‐associated pneumonia, intra‐abdominal infection, etc) and the hospital's antibiogram.14, 15 However, antimicrobial selection, dosing, and de‐escalation of therapy were still optimized by clinical pharmacists in these clinical areas.
Antimicrobial Susceptibility Testing
The microbiology laboratory performed antimicrobial susceptibility testing of the Gram‐negative blood isolates using the disk diffusion method according to guidelines and breakpoints established by the Clinical Laboratory and Standards Institute (CLSI) and published during the inclusive years of the study.16, 17 Zone diameters obtained by disk diffusion testing were converted to minimum inhibitory concentrations (MICs in mg/L) by linear regression analysis for each antimicrobial agent using the BIOMIC V3 antimicrobial susceptibility system (Giles Scientific, Inc., Santa Barbara, CA). Linear regression algorithms contained in the software of this system were determined by comparative studies correlating microbroth dilution‐determined MIC values with zone sizes obtained by disk diffusion testing.18
Data Analysis
Continuous variables were reported as mean the standard deviation, or median and quartiles. The Student's t test was used when comparing normally distributed data, and the MannWhitney U test was employed to analyze nonnormally distributed data. Categorical data were expressed as frequency distributions and the Chi‐squared test was used to determine if differences existed between groups. We performed multiple logistic regression analysis to identify clinical risk factors that were associated with hospital mortality (SPSS, Inc., Chicago, IL). All risk factors from Table 1, as well as the individual pathogens examined, were included in the corresponding multivariable analysis with the exception of acquired organ dysfunction (considered a secondary outcome). All tests were two‐tailed, and a P value <0.05 was determined to represent statistical significance.
| Variable | Hospital Survivors (n = 302) | Hospital Nonsurvivors (n = 233) | P value |
|---|---|---|---|
| |||
| Age, years | 57.9 16.2 | 60.3 15.8 | 0.091 |
| Male | 156 (51.7) | 132 (56.7) | 0.250 |
| Infection onset source | |||
| Community‐acquired | 31 (10.3) | 15 (6.4) | 0.005 |
| Healthcare‐associated community‐onset | 119 (39.4) | 68 (29.2) | |
| Healthcare‐associated hospital‐onset | 152 (50.3) | 150 (64.4) | |
| Underlying co‐morbidities | |||
| CHF | 43 (14.2) | 53 (22.7) | 0.011 |
| COPD | 42 (13.9) | 56 (24.0) | 0.003 |
| Chronic kidney disease | 31 (10.3) | 41 (17.6) | 0.014 |
| Liver disease | 34 (11.3) | 31 (13.3) | 0.473 |
| Active malignancy | 100 (33.1) | 83 (35.6) | 0.544 |
| Diabetes | 68 (22.5) | 50 (21.5) | 0.770 |
| Charlson co‐morbidity score | 4.5 3.5 | 5.2 3.9 | 0.041 |
| APACHE II score | 21.8 6.1 | 27.1 6.2 | <0.001 |
| ICU admission | 221 (73.2) | 216 (92.7) | <0.001 |
| Vasopressors | 137 (45.4) | 197 (84.5) | <0.001 |
| Mechanical ventilation | 124 (41.1) | 183 (78.5) | <0.001 |
| Drotrecogin alfa (activated) | 6 (2.0) | 21 (9.0) | <0.001 |
| Dysfunctional acquired organ systems | |||
| Cardiovascular | 149 (49.3) | 204 (87.6) | <0.001 |
| Respiratory | 141 (46.7) | 202 (86.7) | <0.001 |
| Renal | 145 (48.0) | 136 (58.4) | 0.017 |
| Hepatic | 13 (4.3) | 27 (11.6) | 0.001 |
| Hematologic | 103 (34.1) | 63 (27.0) | 0.080 |
| Neurologic | 11 (3.6) | 19 (8.2) | 0.024 |
| 2 Dysfunctional acquired organ systems | 164 (54.3) | 213 (91.4) | <0.001 |
| Source of bloodstream infection | |||
| Lungs | 95 (31.5) | 127 (54.5) | <0.001 |
| Urinary tract | 92 (30.5) | 45 (19.3) | |
| Central venous catheter | 30 (9.9) | 16 (6.9) | |
| Intra‐abdominal | 63 (20.9) | 33 (14.2) | |
| Unknown | 22 (7.3) | 12 (5.2) | |
| Prior antibiotics* | 103 (34.1) | 110 (47.2) | 0.002 |
Results
Patient Characteristics
Included in the study were 535 consecutive patients with severe sepsis attributed to Pseudomonas aeruginosa, Acinetobacter species, or Enterobacteriaceae bacteremia, of whom 233 (43.6%) died during their hospitalization. The mean age was 58.9 16.0 years (range, 18 to 96 years) with 288 (53.8%) males and 247 (46.2%) females. The infection sources included community‐acquired (n = 46, 8.6%), healthcare‐associated community‐onset (n = 187, 35.0%), and healthcare‐associated hospital‐onset (n = 302, 56.4%). Hospital nonsurvivors were statistically more likely to have a healthcare‐associated hospital‐onset infection, congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease, ICU admission, need for mechanical ventilation and/or vasopressors, administration of drotrecogin alfa (activated), prior antibiotic administration, the lungs as the source of infection, acquired dysfunction of the cardiovascular, respiratory, renal, hepatic, and neurologic organ systems, and greater APACHE II and Charlson co‐morbidity scores compared to hospital survivors (Table 1). Hospital nonsurvivors were also statistically less likely to have a healthcare‐associated community‐onset infection and a urinary source of infection compared to hospital survivors (Table 1).
Microbiology
Among the 547 Gram‐negative bacteria isolated from blood, the most common were Enterobacteriaceae (Escherichia coli, Klebsiella species, Enterobacter species) (70.2%) followed by Pseudomonas aeruginosa (20.8%) and Acinetobacter species (9.0%) (Table 2). Nine patients had two different Enterobacteriaceae species isolated from their blood cultures, and three patients had an Enterobacteriaceae species and Pseudomonas aeruginosa isolated from their blood cultures. Hospital nonsurvivors were statistically more likely to be infected with Pseudomonas aeruginosa and less likely to be infected with Enterobacteriaceae. The pathogen‐specific hospital mortality rate was significantly greater for Pseudomonas aeruginosa and Acinetobacter species compared to Enterobacteriaceae (P < 0.001 and P = 0.008, respectively).
| Bacteria | Hospital Survivors (n = 302) | Hospital Nonsurvivors (n = 233) | P value* | Percent Resistant | Pathogen‐ Specific Mortality Rate |
|---|---|---|---|---|---|
| |||||
| Enterobacteriaceae | 241 (79.8) | 143 (61.4) | <0.001 | 9.1 | 37.2 |
| Pseudomonas aeruginosa | 47 (15.6) | 67 (28.8) | <0.001 | 16.7 | 58.8 |
| Acinetobacter species | 22 (7.3) | 27 (11.6) | 0.087 | 71.4 | 55.1 |
Antimicrobial Treatment and Resistance
Among the study patients, 358 (66.9%) received cefepime, 102 (19.1%) received piperacillin‐tazobactam, and 75 (14.0%) received a carbapenem (meropenem or imipenem) as their initial antibiotic treatment. There were 169 (31.6%) patients who received initial combination therapy with either an aminoglycoside (n = 99, 58.6%) or ciprofloxacin (n = 70, 41.4%). Eighty‐two (15.3%) patients were infected with a pathogen that was resistant to the initial antibiotic treatment regimen [cefepime (n = 41; 50.0%), piperacillin‐tazobactam (n = 25; 30.5%), or imipenem/meropenem (n = 16; 19.5%), plus either an aminoglycoside or ciprofloxacin (n = 28; 34.1%)], and were classified as receiving inappropriate initial antibiotic therapy. Among the 453 (84.7%) patients infected with a pathogen that was susceptible to the initial antibiotic regimen, there was no relationship identified between minimum inhibitory concentration values and hospital mortality.
Patients infected with a pathogen resistant to the initial antibiotic regimen had significantly greater risk of hospital mortality (63.4% vs 40.0%; P < 0.001) (Figure 1). For the 82 individuals infected with a pathogen that was resistant to the initial antibiotic regimen, no difference in hospital mortality was observed among those prescribed initial combination treatment with an aminoglycoside (n = 17) (64.7% vs 61.1%; P = 0.790) or ciprofloxacin (n = 11) (72.7% vs 61.1%; P = 0.733) compared to monotherapy (n = 54). Similarly, among the patients infected with a pathogen that was susceptible to the initial antibiotic regimen, there was no difference in hospital mortality among those whose bloodstream isolate was only susceptible to the prescribed aminoglycoside (n = 12) compared to patients with isolates that were susceptible to the prescribed beta‐lactam antibiotic (n = 441) (41.7% vs 39.9%; P = 0.902).
Logistic regression analysis identified infection with a pathogen resistant to the initial antibiotic regimen [adjusted odds ratio (AOR), 2.28; 95% confidence interval (CI), 1.69‐3.08; P = 0.006], increasing APACHE II scores (1‐point increments) (AOR, 1.13; 95% CI, 1.10‐1.15; P < 0.001), the need for vasopressors (AOR, 2.57; 95% CI, 2.15‐3.53; P < 0.001), the need for mechanical ventilation (AOR, 2.54; 95% CI, 2.19‐3.47; P < 0.001), healthcare‐associated hospital‐onset infection (AOR, 1.67; 95% CI, 1.32‐2.10; P =0.027), and infection with Pseudomonas aeruginosa (AOR, 2.21; 95% CI, 1.74‐2.86; P =0.002) as independent risk factors for hospital mortality (Hosmer‐Lemeshow goodness‐of‐fit test = 0.305). The model explained between 29.7% (Cox and Snell R square) and 39.8% (Nagelkerke R squared) of the variance in hospital mortality, and correctly classified 75.3% of cases.
Secondary Outcomes
Two or more acquired organ system derangements occurred significantly more often among patients with a pathogen resistant to the initial antibiotic regimen compared to those infected with susceptible isolates (84.1% vs 68.0%; P = 0.003). Hospital length of stay was significantly longer for patients infected with a pathogen resistant to the initial antibiotic regimen compared to those infected with susceptible isolates [39.9 50.6 days (median 27 days; quartiles 12 days and 45.5 days) vs 21.6 22.0 days (median 15 days; quartiles 7 days and 30 days); P < 0.001].
Discussion
Our study demonstrated that hospital nonsurvivors with severe sepsis attributed to Gram‐negative bacteremia had significantly greater rates of resistance to their initially prescribed antibiotic regimen compared to hospital survivors. This observation was confirmed in a multivariate analysis controlling for severity of illness and other potential confounding variables. Additionally, acquired organ system derangements and hospital length of stay were greater for patients infected with Gram‐negative pathogens resistant to the empiric antibiotic regimen. We also observed no survival advantage with the use of combination antimicrobial therapy for the subgroup of patients whose pathogens were resistant to the initially prescribed antibiotic regimen. Lastly, no difference in mortality was observed for patients with bacterial isolates that were susceptible only to the prescribed aminoglycoside compared to those with isolates susceptible to the prescribed beta‐lactam antibiotic.
Several previous investigators have linked antibiotic resistance and outcome in patients with serious infections attributed to Gram‐negative bacteria. Tam et al. examined 34 patients with Pseudomonas aeruginosa bacteremia having elevated MICs to piperacillin‐tazobactam (32 g/mL) that were reported as susceptible.19 In seven of these cases, piperacillin‐tazobactam was prescribed empirically, whereas other agents directed against Gram‐negative bacteria were employed in the other patients (carbapenems, aminoglycosides). Thirty‐day mortality was significantly greater for the patients treated with piperacillin‐tazobactam (85.7% vs 22.2%; P = 0.004), and a multivariate analysis found treatment with piperacillin‐tazobactam to be independently associated with 30‐day mortality. Similarly, Bhat et al. examined 204 episodes of bacteremia caused by Gram‐negative bacteria for which patients received cefepime.20 Patients infected with a Gram‐negative bacteria having an MIC to cefepime greater than, or equal to, 8 g/mL had a significantly greater 28‐day mortality compared to patients infected with isolates having an MIC to cefepime that was less than 8 g/mL (54.8% vs 24.1%; P = 0.001).
Our findings are consistent with earlier studies of patients with serious Gram‐negative infections including bacteremia and nosocomial pneumonia. Micek et al. showed that patients with Pseudomonas aeruginosa bacteremia who received inappropriate initial antimicrobial therapy had a greater risk of hospital mortality compared to patients initially treated with an antimicrobial regimen having activity for the Pseudomonas isolate based on in vitro susceptibility testing.21 Similarly, Trouillet et al.,22 Beardsley et al.,23 and Heyland et al.24 found that combination antimicrobial regimens directed against Gram‐negative bacteria in patients with nosocomial pneumonia were more likely to be appropriate based on the antimicrobial susceptibility patterns of the organisms compared to monotherapy. In a more recent study, Micek et al. demonstrated that combination antimicrobial therapy directed against severe sepsis attributed to Gram‐negative bacteria was associated with improved outcomes compared to monotherapy, especially when the combination agent was an aminoglycoside.25 However, empiric combination therapy that included an aminoglycoside was also associated with increased nephrotoxicity which makes the empiric use of aminoglycosides in all patients with suspected Gram‐negative severe sepsis problematic.25, 26 Nevertheless, the use of combination therapy represents a potential strategy to maximize the administration of appropriate treatment for serious Gram‐negative bacterial infections.
Rapid assessment of antimicrobial susceptibility is another strategy that offers the possibility of identifying the resistance pattern of Gram‐negative pathogens quickly in order to provide more appropriate treatment. Bouza et al. found that use of a rapid E‐test on the respiratory specimens of patients with ventilator‐associated pneumonia was associated with fewer days of fever, fewer days of antibiotic administration until resolution of the episode of ventilator‐associated pneumonia, decreased antibiotic consumption, less Clostridium difficile‐associated diarrhea, lower costs of antimicrobial agents, and fewer days receiving mechanical ventilation.27 Other methods for the rapid identification of resistant bacteria include real‐time polymerase chain reaction assays based on hybridization probes to identify specific resistance mechanisms in bacteria.28 Application of such methods for identification of broad categories of resistance mechanisms in Gram‐negative bacteria offer the possibility of tailoring initial antimicrobial regimens in order to provide appropriate therapy in a more timely manner.
Our study has several important limitations that should be noted. First, the study was performed at a single center and the results may not be generalizable to other institutions. However, the findings from other investigators corroborate the importance of antimicrobial resistance as a predictor of outcome for patients with serious Gram‐negative infections.19, 20 Additionally, a similar association has been observed in patients with methicillin‐resistant Staphylococcus aureus bacteremia, supporting the more general importance of antimicrobial resistance as an outcome predictor.29 Second, the method employed for determining MICs was a literature‐based linear regression method correlating disk diffusion diameters with broth dilution MIC determinations. Therefore, the lack of correlation we observed between MIC values and outcome for susceptible Gram‐negative isolates associated with severe sepsis requires further confirmation. Third, we only examined 3 antibiotics, or antibiotic classes, so our results may not be applicable to other agents. This also applies to doripenem, as we did not have that specific carbapenem available at the time this investigation took place.
Another important limitation of our study is the relatively small number of individuals infected with a pathogen that was resistant to the initial treatment regimen, or only susceptible to the aminoglycoside when combination therapy was prescribed. This limited our ability to detect meaningful associations in these subgroups of patients, to include whether or not combination therapy influenced their clinical outcome. Finally, we did not examine the exact timing of antibiotic therapy relative to the onset of severe sepsis. Instead we used a 12‐hour window from when subsequently positive blood cultures were drawn to the administration of initial antibiotic therapy. Other investigators have shown that delays in initial appropriate therapy of more than one hour for patients with septic shock increases the risk of death.9, 30 Failure to include the exact timing of therapy could have resulted in a final multivariate model that includes prediction variables that would not otherwise have been incorporated.
In summary, we demonstrated that resistance to the initial antibiotic treatment regimen was associated with a greater risk of hospital mortality in patients with severe sepsis attributed to Gram‐negative bacteremia. These findings imply that more rapid assessment of antimicrobial susceptibility could result in improved prescription of antibiotics in order to maximize initial administration of appropriate therapy. Future studies are required to address whether rapid determination of antimicrobial susceptibility can result in more effective administration of appropriate therapy, and if this can result in improved patient outcomes.
Severe sepsis and septic shock are associated with excess mortality when inappropriate initial antimicrobial therapy, defined as an antimicrobial regimen that lacks in vitro activity against the isolated organism(s) responsible for the infection, is administered.14 Unfortunately, bacterial resistance to antibiotics is increasing and creates a therapeutic challenge for clinicians when treating patients with serious infections, such as severe sepsis. Increasing rates of bacterial resistance leads many clinicians to empirically treat critically ill patients with broad‐spectrum antibiotics, which can perpetuate the cycle of increasing resistance.5, 6 Conversely, inappropriate initial antimicrobial therapy can lead to treatment failures and adverse patient outcomes.7 Individuals with severe sepsis appear to be at particularly high risk of excess mortality when inappropriate initial antimicrobial therapy is administered.8, 9
The most recent Surviving Sepsis Guidelines recommend empiric combination therapy targeting Gram‐negative bacteria, particularly for patients with known or suspected Pseudomonas infections, as a means to decrease the likelihood of administering inappropriate initial antimicrobial therapy.10 However, the selection of an antimicrobial regimen that is active against the causative pathogen(s) is problematic, as the treating physician usually does not know the susceptibilities of the pathogen(s) for the selected empiric antibiotics. Therefore, we performed a study with the main goal of determining whether resistance to the initially prescribed antimicrobial regimen was associated with clinical outcome in patients with severe sepsis attributed to Gram‐negative bacteremia.
Materials and Methods
Study Location and Patients
This study was conducted at a university‐affiliated, urban teaching hospital: Barnes‐Jewish Hospital (1200 beds). During a 6‐year period (January 2002 to December 2007), all hospitalized patients with a positive blood culture for Gram‐negative bacteria, with antimicrobial susceptibility testing performed for the blood isolate(s), were eligible for this investigation. This study was approved by the Washington University School of Medicine Human Studies Committee.
Study Design and Data Collection
A retrospective cohort study design was employed. Two investigators (J.A.D., R.M.R.) identified potential study patients by the presence of a positive blood culture for Pseudomonas aeruginosa, Acinetobacter species, or Enterobacteriaceae (Escherichia coli, Klebsiella species, Enterobacter species) combined with primary or secondary International Classification of Diseases (ICD‐9‐CM) codes indicative of acute organ dysfunction, at least two criteria from the systemic inflammatory response syndrome (SIRS),10 and initial antibiotic treatment with either cefepime, piperacillin‐tazobactam, or a carbapenem (imipenem or meropenem). These antimicrobials represent the primary agents employed for the treatment of Gram‐negative infections at Barnes‐Jewish Hospital during the study period, and had to be administered within 12 hours of having the subsequently positive blood cultures drawn. Based on the initial study database construction, 3 investigators (E.C.W., J.K., M.P.) merged patient‐specific data from the automated hospital medical records, microbiology database, and pharmacy database of Barnes‐Jewish Hospital to complete the clinical database under the auspices of the definitions described below.
The baseline characteristics collected by the study investigators included: age, gender, race, the presence of congestive heart failure, chronic obstructive pulmonary disease, diabetes mellitus, chronic liver disease, underlying malignancy, and end‐stage renal disease requiring renal replacement therapy. All cause hospital mortality was evaluated as the primary outcome variable. Secondary outcomes included acquired organ dysfunction and hospital length of stay. The Acute Physiology and Chronic Health Evaluation (APACHE) II11 and Charlson co‐morbidity scores were also calculated during the 24 hours after the positive blood cultures were drawn. This was done because we included patients with community‐acquired infections who only had clinical data available after blood cultures were drawn.
Definitions
All definitions were selected prospectively as part of the original study design. Cases of Gram‐negative bacteremia were classified into mutually exclusive groups comprised of either community‐acquired or healthcare‐associated infection. Patients with healthcare‐associated bacteremia were categorized as community‐onset or hospital‐onset, as previously described.12 In brief, patients with healthcare‐associated community‐onset bacteremia had the positive culture obtained within the first 48 hours of hospital admission in combination with one or more of the following risk factors: (1) residence in a nursing home, rehabilitation hospital, or other long‐term nursing facility; (2) previous hospitalization within the immediately preceding 12 months; (3) receiving outpatient hemodialysis, peritoneal dialysis, wound care, or infusion therapy necessitating regular visits to a hospital‐based clinic; and (4) having an immune‐compromised state. Patients were classified as having healthcare‐associated hospital‐onset bacteremia when the culture was obtained 48 hours or more after admission. Community‐acquired bacteremia occurred in patients without healthcare risk factors and a positive blood culture within the first 48 hours of admission. Prior antibiotic exposure was defined as having occurred within the previous 30 days from the onset of severe sepsis.
To be included in the analysis, patients had to meet criteria for severe sepsis based on discharge ICD‐9‐CM codes for acute organ dysfunction, as previously described.13 The organs of interest included the heart, lungs, kidneys, bone marrow (hematologic), brain, and liver. Patients were classified as having septic shock if vasopressors (norepinephrine, dopamine, epinephrine, phenylephrine, or vasopressin) were initiated within 24 hours of the blood culture collection date and time. Empiric antimicrobial treatment was classified as being appropriate if the initially prescribed antibiotic regimen was active against the identified pathogen(s) based on in vitro susceptibility testing and administered within 12 hours following blood culture collection. Appropriate antimicrobial treatment also had to be prescribed for at least 24 hours. However, the total duration of antimicrobial therapy was at the discretion of the treating physicians. The Charlson co‐morbidity score was calculated using ICD‐9‐CM codes abstracted from the index hospitalization employing MS‐DRG Grouper version 26.
Antimicrobial Monitoring
From January 2002 through the present, Barnes‐Jewish Hospital utilized an antibiotic control program to help guide antimicrobial therapy. During this time, the use of cefepime and gentamicin was unrestricted. However, initiation of intravenous ciprofloxacin, imipenem/cilastatin, meropenem, or piperacillin/tazobactam was restricted and required preauthorization from either a clinical pharmacist or infectious diseases physician. Each intensive care unit (ICU) had a clinical pharmacist who reviewed all antibiotic orders to insure that dosing and interval of antibiotic administration was adequate for individual patients based on body size, renal function, and the resuscitation status of the patient. After daytime hours, the on‐call clinical pharmacist reviewed and approved the antibiotic orders. The initial antibiotic dosages for the antibiotics employed for the treatment of Gram‐negative infections at Barnes‐Jewish Hospital were as follows: cefepime, 1 to 2 grams every eight hours; pipercillin‐tazobactam, 4.5 grams every six hours; imipenem, 0.5 grams every six hours; meropenem, 1 gram every eight hours; ciprofloxacin, 400 mg every eight hours; gentamicin, 5 mg/kg once daily.
Starting in June 2005, a sepsis order set was implemented in the emergency department, general medical wards, and the intensive care units with the intent of standardizing empiric antibiotic selection for patients with sepsis based on the infection type (ie, community‐acquired pneumonia, healthcare‐associated pneumonia, intra‐abdominal infection, etc) and the hospital's antibiogram.14, 15 However, antimicrobial selection, dosing, and de‐escalation of therapy were still optimized by clinical pharmacists in these clinical areas.
Antimicrobial Susceptibility Testing
The microbiology laboratory performed antimicrobial susceptibility testing of the Gram‐negative blood isolates using the disk diffusion method according to guidelines and breakpoints established by the Clinical Laboratory and Standards Institute (CLSI) and published during the inclusive years of the study.16, 17 Zone diameters obtained by disk diffusion testing were converted to minimum inhibitory concentrations (MICs in mg/L) by linear regression analysis for each antimicrobial agent using the BIOMIC V3 antimicrobial susceptibility system (Giles Scientific, Inc., Santa Barbara, CA). Linear regression algorithms contained in the software of this system were determined by comparative studies correlating microbroth dilution‐determined MIC values with zone sizes obtained by disk diffusion testing.18
Data Analysis
Continuous variables were reported as mean the standard deviation, or median and quartiles. The Student's t test was used when comparing normally distributed data, and the MannWhitney U test was employed to analyze nonnormally distributed data. Categorical data were expressed as frequency distributions and the Chi‐squared test was used to determine if differences existed between groups. We performed multiple logistic regression analysis to identify clinical risk factors that were associated with hospital mortality (SPSS, Inc., Chicago, IL). All risk factors from Table 1, as well as the individual pathogens examined, were included in the corresponding multivariable analysis with the exception of acquired organ dysfunction (considered a secondary outcome). All tests were two‐tailed, and a P value <0.05 was determined to represent statistical significance.
| Variable | Hospital Survivors (n = 302) | Hospital Nonsurvivors (n = 233) | P value |
|---|---|---|---|
| |||
| Age, years | 57.9 16.2 | 60.3 15.8 | 0.091 |
| Male | 156 (51.7) | 132 (56.7) | 0.250 |
| Infection onset source | |||
| Community‐acquired | 31 (10.3) | 15 (6.4) | 0.005 |
| Healthcare‐associated community‐onset | 119 (39.4) | 68 (29.2) | |
| Healthcare‐associated hospital‐onset | 152 (50.3) | 150 (64.4) | |
| Underlying co‐morbidities | |||
| CHF | 43 (14.2) | 53 (22.7) | 0.011 |
| COPD | 42 (13.9) | 56 (24.0) | 0.003 |
| Chronic kidney disease | 31 (10.3) | 41 (17.6) | 0.014 |
| Liver disease | 34 (11.3) | 31 (13.3) | 0.473 |
| Active malignancy | 100 (33.1) | 83 (35.6) | 0.544 |
| Diabetes | 68 (22.5) | 50 (21.5) | 0.770 |
| Charlson co‐morbidity score | 4.5 3.5 | 5.2 3.9 | 0.041 |
| APACHE II score | 21.8 6.1 | 27.1 6.2 | <0.001 |
| ICU admission | 221 (73.2) | 216 (92.7) | <0.001 |
| Vasopressors | 137 (45.4) | 197 (84.5) | <0.001 |
| Mechanical ventilation | 124 (41.1) | 183 (78.5) | <0.001 |
| Drotrecogin alfa (activated) | 6 (2.0) | 21 (9.0) | <0.001 |
| Dysfunctional acquired organ systems | |||
| Cardiovascular | 149 (49.3) | 204 (87.6) | <0.001 |
| Respiratory | 141 (46.7) | 202 (86.7) | <0.001 |
| Renal | 145 (48.0) | 136 (58.4) | 0.017 |
| Hepatic | 13 (4.3) | 27 (11.6) | 0.001 |
| Hematologic | 103 (34.1) | 63 (27.0) | 0.080 |
| Neurologic | 11 (3.6) | 19 (8.2) | 0.024 |
| 2 Dysfunctional acquired organ systems | 164 (54.3) | 213 (91.4) | <0.001 |
| Source of bloodstream infection | |||
| Lungs | 95 (31.5) | 127 (54.5) | <0.001 |
| Urinary tract | 92 (30.5) | 45 (19.3) | |
| Central venous catheter | 30 (9.9) | 16 (6.9) | |
| Intra‐abdominal | 63 (20.9) | 33 (14.2) | |
| Unknown | 22 (7.3) | 12 (5.2) | |
| Prior antibiotics* | 103 (34.1) | 110 (47.2) | 0.002 |
Results
Patient Characteristics
Included in the study were 535 consecutive patients with severe sepsis attributed to Pseudomonas aeruginosa, Acinetobacter species, or Enterobacteriaceae bacteremia, of whom 233 (43.6%) died during their hospitalization. The mean age was 58.9 16.0 years (range, 18 to 96 years) with 288 (53.8%) males and 247 (46.2%) females. The infection sources included community‐acquired (n = 46, 8.6%), healthcare‐associated community‐onset (n = 187, 35.0%), and healthcare‐associated hospital‐onset (n = 302, 56.4%). Hospital nonsurvivors were statistically more likely to have a healthcare‐associated hospital‐onset infection, congestive heart failure, chronic obstructive pulmonary disease, chronic kidney disease, ICU admission, need for mechanical ventilation and/or vasopressors, administration of drotrecogin alfa (activated), prior antibiotic administration, the lungs as the source of infection, acquired dysfunction of the cardiovascular, respiratory, renal, hepatic, and neurologic organ systems, and greater APACHE II and Charlson co‐morbidity scores compared to hospital survivors (Table 1). Hospital nonsurvivors were also statistically less likely to have a healthcare‐associated community‐onset infection and a urinary source of infection compared to hospital survivors (Table 1).
Microbiology
Among the 547 Gram‐negative bacteria isolated from blood, the most common were Enterobacteriaceae (Escherichia coli, Klebsiella species, Enterobacter species) (70.2%) followed by Pseudomonas aeruginosa (20.8%) and Acinetobacter species (9.0%) (Table 2). Nine patients had two different Enterobacteriaceae species isolated from their blood cultures, and three patients had an Enterobacteriaceae species and Pseudomonas aeruginosa isolated from their blood cultures. Hospital nonsurvivors were statistically more likely to be infected with Pseudomonas aeruginosa and less likely to be infected with Enterobacteriaceae. The pathogen‐specific hospital mortality rate was significantly greater for Pseudomonas aeruginosa and Acinetobacter species compared to Enterobacteriaceae (P < 0.001 and P = 0.008, respectively).
| Bacteria | Hospital Survivors (n = 302) | Hospital Nonsurvivors (n = 233) | P value* | Percent Resistant | Pathogen‐ Specific Mortality Rate |
|---|---|---|---|---|---|
| |||||
| Enterobacteriaceae | 241 (79.8) | 143 (61.4) | <0.001 | 9.1 | 37.2 |
| Pseudomonas aeruginosa | 47 (15.6) | 67 (28.8) | <0.001 | 16.7 | 58.8 |
| Acinetobacter species | 22 (7.3) | 27 (11.6) | 0.087 | 71.4 | 55.1 |
Antimicrobial Treatment and Resistance
Among the study patients, 358 (66.9%) received cefepime, 102 (19.1%) received piperacillin‐tazobactam, and 75 (14.0%) received a carbapenem (meropenem or imipenem) as their initial antibiotic treatment. There were 169 (31.6%) patients who received initial combination therapy with either an aminoglycoside (n = 99, 58.6%) or ciprofloxacin (n = 70, 41.4%). Eighty‐two (15.3%) patients were infected with a pathogen that was resistant to the initial antibiotic treatment regimen [cefepime (n = 41; 50.0%), piperacillin‐tazobactam (n = 25; 30.5%), or imipenem/meropenem (n = 16; 19.5%), plus either an aminoglycoside or ciprofloxacin (n = 28; 34.1%)], and were classified as receiving inappropriate initial antibiotic therapy. Among the 453 (84.7%) patients infected with a pathogen that was susceptible to the initial antibiotic regimen, there was no relationship identified between minimum inhibitory concentration values and hospital mortality.
Patients infected with a pathogen resistant to the initial antibiotic regimen had significantly greater risk of hospital mortality (63.4% vs 40.0%; P < 0.001) (Figure 1). For the 82 individuals infected with a pathogen that was resistant to the initial antibiotic regimen, no difference in hospital mortality was observed among those prescribed initial combination treatment with an aminoglycoside (n = 17) (64.7% vs 61.1%; P = 0.790) or ciprofloxacin (n = 11) (72.7% vs 61.1%; P = 0.733) compared to monotherapy (n = 54). Similarly, among the patients infected with a pathogen that was susceptible to the initial antibiotic regimen, there was no difference in hospital mortality among those whose bloodstream isolate was only susceptible to the prescribed aminoglycoside (n = 12) compared to patients with isolates that were susceptible to the prescribed beta‐lactam antibiotic (n = 441) (41.7% vs 39.9%; P = 0.902).
Logistic regression analysis identified infection with a pathogen resistant to the initial antibiotic regimen [adjusted odds ratio (AOR), 2.28; 95% confidence interval (CI), 1.69‐3.08; P = 0.006], increasing APACHE II scores (1‐point increments) (AOR, 1.13; 95% CI, 1.10‐1.15; P < 0.001), the need for vasopressors (AOR, 2.57; 95% CI, 2.15‐3.53; P < 0.001), the need for mechanical ventilation (AOR, 2.54; 95% CI, 2.19‐3.47; P < 0.001), healthcare‐associated hospital‐onset infection (AOR, 1.67; 95% CI, 1.32‐2.10; P =0.027), and infection with Pseudomonas aeruginosa (AOR, 2.21; 95% CI, 1.74‐2.86; P =0.002) as independent risk factors for hospital mortality (Hosmer‐Lemeshow goodness‐of‐fit test = 0.305). The model explained between 29.7% (Cox and Snell R square) and 39.8% (Nagelkerke R squared) of the variance in hospital mortality, and correctly classified 75.3% of cases.
Secondary Outcomes
Two or more acquired organ system derangements occurred significantly more often among patients with a pathogen resistant to the initial antibiotic regimen compared to those infected with susceptible isolates (84.1% vs 68.0%; P = 0.003). Hospital length of stay was significantly longer for patients infected with a pathogen resistant to the initial antibiotic regimen compared to those infected with susceptible isolates [39.9 50.6 days (median 27 days; quartiles 12 days and 45.5 days) vs 21.6 22.0 days (median 15 days; quartiles 7 days and 30 days); P < 0.001].
Discussion
Our study demonstrated that hospital nonsurvivors with severe sepsis attributed to Gram‐negative bacteremia had significantly greater rates of resistance to their initially prescribed antibiotic regimen compared to hospital survivors. This observation was confirmed in a multivariate analysis controlling for severity of illness and other potential confounding variables. Additionally, acquired organ system derangements and hospital length of stay were greater for patients infected with Gram‐negative pathogens resistant to the empiric antibiotic regimen. We also observed no survival advantage with the use of combination antimicrobial therapy for the subgroup of patients whose pathogens were resistant to the initially prescribed antibiotic regimen. Lastly, no difference in mortality was observed for patients with bacterial isolates that were susceptible only to the prescribed aminoglycoside compared to those with isolates susceptible to the prescribed beta‐lactam antibiotic.
Several previous investigators have linked antibiotic resistance and outcome in patients with serious infections attributed to Gram‐negative bacteria. Tam et al. examined 34 patients with Pseudomonas aeruginosa bacteremia having elevated MICs to piperacillin‐tazobactam (32 g/mL) that were reported as susceptible.19 In seven of these cases, piperacillin‐tazobactam was prescribed empirically, whereas other agents directed against Gram‐negative bacteria were employed in the other patients (carbapenems, aminoglycosides). Thirty‐day mortality was significantly greater for the patients treated with piperacillin‐tazobactam (85.7% vs 22.2%; P = 0.004), and a multivariate analysis found treatment with piperacillin‐tazobactam to be independently associated with 30‐day mortality. Similarly, Bhat et al. examined 204 episodes of bacteremia caused by Gram‐negative bacteria for which patients received cefepime.20 Patients infected with a Gram‐negative bacteria having an MIC to cefepime greater than, or equal to, 8 g/mL had a significantly greater 28‐day mortality compared to patients infected with isolates having an MIC to cefepime that was less than 8 g/mL (54.8% vs 24.1%; P = 0.001).
Our findings are consistent with earlier studies of patients with serious Gram‐negative infections including bacteremia and nosocomial pneumonia. Micek et al. showed that patients with Pseudomonas aeruginosa bacteremia who received inappropriate initial antimicrobial therapy had a greater risk of hospital mortality compared to patients initially treated with an antimicrobial regimen having activity for the Pseudomonas isolate based on in vitro susceptibility testing.21 Similarly, Trouillet et al.,22 Beardsley et al.,23 and Heyland et al.24 found that combination antimicrobial regimens directed against Gram‐negative bacteria in patients with nosocomial pneumonia were more likely to be appropriate based on the antimicrobial susceptibility patterns of the organisms compared to monotherapy. In a more recent study, Micek et al. demonstrated that combination antimicrobial therapy directed against severe sepsis attributed to Gram‐negative bacteria was associated with improved outcomes compared to monotherapy, especially when the combination agent was an aminoglycoside.25 However, empiric combination therapy that included an aminoglycoside was also associated with increased nephrotoxicity which makes the empiric use of aminoglycosides in all patients with suspected Gram‐negative severe sepsis problematic.25, 26 Nevertheless, the use of combination therapy represents a potential strategy to maximize the administration of appropriate treatment for serious Gram‐negative bacterial infections.
Rapid assessment of antimicrobial susceptibility is another strategy that offers the possibility of identifying the resistance pattern of Gram‐negative pathogens quickly in order to provide more appropriate treatment. Bouza et al. found that use of a rapid E‐test on the respiratory specimens of patients with ventilator‐associated pneumonia was associated with fewer days of fever, fewer days of antibiotic administration until resolution of the episode of ventilator‐associated pneumonia, decreased antibiotic consumption, less Clostridium difficile‐associated diarrhea, lower costs of antimicrobial agents, and fewer days receiving mechanical ventilation.27 Other methods for the rapid identification of resistant bacteria include real‐time polymerase chain reaction assays based on hybridization probes to identify specific resistance mechanisms in bacteria.28 Application of such methods for identification of broad categories of resistance mechanisms in Gram‐negative bacteria offer the possibility of tailoring initial antimicrobial regimens in order to provide appropriate therapy in a more timely manner.
Our study has several important limitations that should be noted. First, the study was performed at a single center and the results may not be generalizable to other institutions. However, the findings from other investigators corroborate the importance of antimicrobial resistance as a predictor of outcome for patients with serious Gram‐negative infections.19, 20 Additionally, a similar association has been observed in patients with methicillin‐resistant Staphylococcus aureus bacteremia, supporting the more general importance of antimicrobial resistance as an outcome predictor.29 Second, the method employed for determining MICs was a literature‐based linear regression method correlating disk diffusion diameters with broth dilution MIC determinations. Therefore, the lack of correlation we observed between MIC values and outcome for susceptible Gram‐negative isolates associated with severe sepsis requires further confirmation. Third, we only examined 3 antibiotics, or antibiotic classes, so our results may not be applicable to other agents. This also applies to doripenem, as we did not have that specific carbapenem available at the time this investigation took place.
Another important limitation of our study is the relatively small number of individuals infected with a pathogen that was resistant to the initial treatment regimen, or only susceptible to the aminoglycoside when combination therapy was prescribed. This limited our ability to detect meaningful associations in these subgroups of patients, to include whether or not combination therapy influenced their clinical outcome. Finally, we did not examine the exact timing of antibiotic therapy relative to the onset of severe sepsis. Instead we used a 12‐hour window from when subsequently positive blood cultures were drawn to the administration of initial antibiotic therapy. Other investigators have shown that delays in initial appropriate therapy of more than one hour for patients with septic shock increases the risk of death.9, 30 Failure to include the exact timing of therapy could have resulted in a final multivariate model that includes prediction variables that would not otherwise have been incorporated.
In summary, we demonstrated that resistance to the initial antibiotic treatment regimen was associated with a greater risk of hospital mortality in patients with severe sepsis attributed to Gram‐negative bacteremia. These findings imply that more rapid assessment of antimicrobial susceptibility could result in improved prescription of antibiotics in order to maximize initial administration of appropriate therapy. Future studies are required to address whether rapid determination of antimicrobial susceptibility can result in more effective administration of appropriate therapy, and if this can result in improved patient outcomes.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.The clinical evaluation committee in a large multicenter phase 3 trial of drotrecogin alfa (activated) in patients with severe sepsis (PROWESS): role, methodology, and results.Crit Care Med.2003;31:2291–2301.
- ,,,,,.Impact of adequate empical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis.Crit Care Med.2003;31:2742–2751.
- ,,,,,.Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med.2003;115:529–535.
- ,.Antibiotic‐resistant bugs in the 21st century—a clinical super‐challenge.N Engl J Med.2009;360:439–443.
- ,,, et al.Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America.Clin Infect Dis.2009;48:1–12.
- .Broad‐spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front.Clin Infect Dis.2008;47:S3–S13.
- ,,, et al.Bundled care for septic shock: an analysis of clinical trials.Crit Care Med.2010;38:668–678.
- ,,, et al.Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study.Am J Respir Crit Care Med.2009;180:861–866.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36:296–327.
- ,,,.APACHE II: a severity of disease classification system.Crit Care Med.1985;13:818–829.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,,,,.Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29:1303–1310.
- ,,,,,.Hospital‐wide impact of a standardized order set for the management of bacteremic severe sepsis.Crit Care Med.2009;37:819–824.
- ,,, et al.Before‐after study of a standardized hospital order set for the management of septic shock.Crit Care Med.2007;34:2707–2713.
- National Committee for Clinical Laboratory Standards.Performance Standards for Antimicrobial Susceptibility Testing: Twelfth Informational Supplement. M100‐S12.Wayne, PA:National Committee for Clinical Laboratory Standards;2002.
- Clinical Laboratory Standards Institute.Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement. M100‐S17.Wayne, PA:Clinical Laboratory Standards Institute;2007.
- ,,, et al.Evaluation of the BIOGRAM antimicrobial susceptibility test system.J Clin Microbiol.1985;22:793–798.
- ,,, et al.Outcomes of bacteremia due to Pseudomonas aeruginosa with reduced susceptibility to piperacillin‐tazobactam: implications on the appropriateness of the resistance breakpoint.Clin Infect Dis.2008;46:862–867.
- ,,, et al.Failure of current cefepime breakpoints to predict clinical outcomes of bacteremia caused by Gram‐negative organisms.Antimicrob Agents Chemother.2007;51:4390–4395.
- ,,,,,.Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment.Antimicrob Agents Chemother.2005;49:1306–1311.
- ,,.Ventilator‐associated pneumonia caused by potentially drug‐resistant bacteria.Am J Respir Crit Care Med.1998;157:531–539.
- ,,,,,.Using local microbiologic data to develop institution‐specific guidelines for the treatment of hospital‐acquired pneumonia.Chest.2006;130:787–793.
- ,,, et al.Randomized trial of combination versus monotherapy for the empiric treatment of suspected ventilator‐associated pneumonia.Crit Care Med.2008;36:737–744.
- ,,, et al.Empiric combination antibiotic therapy is associated with improved outcome in Gram‐negative sepsis: a retrospective analysis.Antimicrob Agents Chemother.2010;54:1742–1748.
- ,,, et al.Monotherapy versus beta‐lactam‐aminoglycoside combination treatment for Gram‐negative bacteremia: a prospective, observational study.Antimicrob Agents Chemother.1997;41:1127–1133.
- ,,, et al.Direct E‐test (AB Biodisk) of respiratory samples improves antimicrobial use in ventilator‐associated pneumonia.Clin Infect Dis.2007;44:382–387.
- ,,, et al.Rapid detection of CTX‐M‐producing Enterobacteriaceae in urine samples.J Antimicrob Chemother.2009;64:986–989.
- ,,, et al.Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46:193–200.
- ,,, et al.Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock.Crit Care Med.2006;34:1589–1596.
- ,,,.Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients.Chest.1999;115:462–474.
- ,,, et al.The clinical evaluation committee in a large multicenter phase 3 trial of drotrecogin alfa (activated) in patients with severe sepsis (PROWESS): role, methodology, and results.Crit Care Med.2003;31:2291–2301.
- ,,,,,.Impact of adequate empical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis.Crit Care Med.2003;31:2742–2751.
- ,,,,,.Inappropriate initial antimicrobial therapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med.2003;115:529–535.
- ,.Antibiotic‐resistant bugs in the 21st century—a clinical super‐challenge.N Engl J Med.2009;360:439–443.
- ,,, et al.Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America.Clin Infect Dis.2009;48:1–12.
- .Broad‐spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front.Clin Infect Dis.2008;47:S3–S13.
- ,,, et al.Bundled care for septic shock: an analysis of clinical trials.Crit Care Med.2010;38:668–678.
- ,,, et al.Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study.Am J Respir Crit Care Med.2009;180:861–866.
- ,,, et al.Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008.Crit Care Med.2008;36:296–327.
- ,,,.APACHE II: a severity of disease classification system.Crit Care Med.1985;13:818–829.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,,,,.Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med.2001;29:1303–1310.
- ,,,,,.Hospital‐wide impact of a standardized order set for the management of bacteremic severe sepsis.Crit Care Med.2009;37:819–824.
- ,,, et al.Before‐after study of a standardized hospital order set for the management of septic shock.Crit Care Med.2007;34:2707–2713.
- National Committee for Clinical Laboratory Standards.Performance Standards for Antimicrobial Susceptibility Testing: Twelfth Informational Supplement. M100‐S12.Wayne, PA:National Committee for Clinical Laboratory Standards;2002.
- Clinical Laboratory Standards Institute.Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement. M100‐S17.Wayne, PA:Clinical Laboratory Standards Institute;2007.
- ,,, et al.Evaluation of the BIOGRAM antimicrobial susceptibility test system.J Clin Microbiol.1985;22:793–798.
- ,,, et al.Outcomes of bacteremia due to Pseudomonas aeruginosa with reduced susceptibility to piperacillin‐tazobactam: implications on the appropriateness of the resistance breakpoint.Clin Infect Dis.2008;46:862–867.
- ,,, et al.Failure of current cefepime breakpoints to predict clinical outcomes of bacteremia caused by Gram‐negative organisms.Antimicrob Agents Chemother.2007;51:4390–4395.
- ,,,,,.Pseudomonas aeruginosa bloodstream infection: importance of appropriate initial antimicrobial treatment.Antimicrob Agents Chemother.2005;49:1306–1311.
- ,,.Ventilator‐associated pneumonia caused by potentially drug‐resistant bacteria.Am J Respir Crit Care Med.1998;157:531–539.
- ,,,,,.Using local microbiologic data to develop institution‐specific guidelines for the treatment of hospital‐acquired pneumonia.Chest.2006;130:787–793.
- ,,, et al.Randomized trial of combination versus monotherapy for the empiric treatment of suspected ventilator‐associated pneumonia.Crit Care Med.2008;36:737–744.
- ,,, et al.Empiric combination antibiotic therapy is associated with improved outcome in Gram‐negative sepsis: a retrospective analysis.Antimicrob Agents Chemother.2010;54:1742–1748.
- ,,, et al.Monotherapy versus beta‐lactam‐aminoglycoside combination treatment for Gram‐negative bacteremia: a prospective, observational study.Antimicrob Agents Chemother.1997;41:1127–1133.
- ,,, et al.Direct E‐test (AB Biodisk) of respiratory samples improves antimicrobial use in ventilator‐associated pneumonia.Clin Infect Dis.2007;44:382–387.
- ,,, et al.Rapid detection of CTX‐M‐producing Enterobacteriaceae in urine samples.J Antimicrob Chemother.2009;64:986–989.
- ,,, et al.Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin‐resistant Staphylococcus aureus bacteremia.Clin Infect Dis.2008;46:193–200.
- ,,, et al.Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock.Crit Care Med.2006;34:1589–1596.
Copyright © 2011 Society of Hospital Medicine