User login
Duration of VTE Risk in Medically Ill Patients
Patients who are hospitalized for acute medical illness are at an increased risk of developing venous thromboembolism (VTE), which comprises deep‐vein thrombosis (DVT) and pulmonary embolism (PE).13 In a recent real‐world study of 158,325 US medical patients by Spyropoulos et al,4 4.0% of patients developed DVT, 1.5% developed PE, and 0.2% developed both DVT and PE. Furthermore, results from a population‐based case‐control study indicate that hospitalization for medical illness accounted for a proportion of VTE events similar to that of hospitalization for surgery (22% and 24%, respectively).5
Thromboprophylaxis reduces VTE incidence in at‐risk medical patients and is recommended according to evidence‐based guidelines from the American College of Chest Physicians (ACCP).1 The ACCP guidelines advocate that acutely ill medical patients admitted to the hospital with congestive heart failure (CHF) or severe lung disease/chronic obstructive pulmonary disease (COPD) or those who are confined to bed and have one or more additional risk factors (including active cancer, previous VTE, sepsis, acute neurologic disease, or inflammatory bowel disease) receive pharmacological prophylaxis with lowmolecular weight heparin (LMWH), low‐dose unfractionated heparin (UFH), or fondaparinux.1 Although guidelines provide recommendations for the duration of prophylaxis after major orthopedic surgery, such recommendations are unavailable for medical patients. In clinical trials of acutely ill medical patients, prophylaxis regimens found to be effective were provided for a duration of hospitalization of 6‐14 days.68 The mean length of hospital stay for medical illnesses is decreasing and is currently shorter than 6‐14 days.9, 10
In clinical practice, the duration of VTE risk during and after hospitalization is not well understood in medical patients, particularly in the context of shortening hospital stays. Such information could, however, provide insight into whether current thromboprophylaxis practices reflect real‐world need. To gain a greater understanding of the period during which patients are at risk of VTE, this retrospective, observational study assessed the incidence and time course of symptomatic VTE events during and after hospitalization in a large population of US medical patients.
METHODS
Data and Patient Selection
This study employed linked administrative claims data and hospital billing data contained in the Thomson Reuters MarketScan Inpatient Drug Link File. This combines longitudinal patient‐level inpatient and outpatient medical and pharmaceutical claims data from the MarketScan Commercial claims data from the MarketScan Commercial Claims and Encounters (Commercial) and Medicare Supplemental and Coordination of Benefits (Medicare Supplemental) databases, with hospital discharge records detailing services used and drugs administered during a hospitalization, which are included in the Hospital Drug Database. The linked data sources enable analysis of a patient's experience before, during, and after a hospitalization. The present study was not designed to obtain bleeding rates.
The study cohort comprised patients considered to be at‐risk for VTE as a result of a medical hospitalization occurring between January 1, 2005, and December 31, 2008. At‐risk medical hospitalizations were those for which the primary diagnosis was for cancer, CHF, severe lung disease/COPD, or infectious disease (see Supporting Information, Appendix I, for International Classification of Diseases, 9th Revision, Clinical Modification [ICD‐9‐CM] codes used to identify patients with medical illnesses). Included patients were required to be at least 18 years of age at the time of admission and were required to be continuously enrolled in their insurance benefits for at least 12 months before admission (the baseline period) and for at least 180 days after the admission date (the evaluation period) to ensure that all administrative claims data during that period were captured. Patients who died in‐hospital from any cause were exempted from the continuous enrollment criterion, as long as they had been continuously enrolled prior to inpatient death. Patients transferred from or discharged to another acute‐care facility were excluded because of the possibility for incomplete inpatient data capture. For patients who had multiple medical hospitalizations between January 1, 2005, and December 31, 2008, the hospitalization around which the analysis focused was randomly selected from the set of potential medical hospitalizations.
Prophylaxis
Pharmacological prophylaxis was identified via charge codes during hospitalization or via pharmacy claims after discharge for UFH, enoxaparin, dalteparin, warfarin, and fondaparinux. All dosages of a pharmacological agent were considered prophylactic only if there was no evidence of VTE during the admission, with the exception of warfarin (Supporting Information, Appendix II). Post‐discharge use of anticoagulation therapy was measured for up to 35 days after discharge from the hospital. Use of mechanical prophylaxis during hospitalization was identified via charge codes for graduated compression stockings and charge codes indicating use of intermittent pneumatic compression devices and/or venous foot pumps. The appropriateness of prophylaxis was not assessed.
Analysis
The risk of VTE was estimated across an evaluation period of 180 days by measuring VTE occurrence and person‐time exposure. Inpatient VTE occurrence was defined as any nonprimary diagnosis of DVT and/or PE during the at‐risk hospitalization. VTE after discharge was defined as an ICD‐9‐CM diagnosis code, whether primary or secondary, for DVT or PE in the evaluation period during an emergency room or inpatient admission, or on an outpatient claim with 1 or more of the following confirmatory events: an emergency room or inpatient admission for VTE within 2 days of the outpatient diagnosis; a prescription claim for enoxaparin, fondaparinux, or UFH within 15 days after diagnosis; or a prescription claim for warfarin within 15 days after diagnosis and no evidence of atrial fibrillation or atrial flutter in the 6 months before the outpatient diagnosis for DVT or PE. Person‐time exposure was measured as the number of days from the hospital admission date to the first occurrence of VTE, or censoring at a subsequent at‐risk hospitalization, death, or 180 days after admission.
Cumulative risk of VTE over the 180‐day evaluation period was calculated by the Kaplan‐Meier product limit method of survival analysis and displayed for deciles of cumulative risk at 180 days after the hospital admission date. The risk of VTE at each point of time during the evaluation period (the hazard function) was first calculated on a daily basis and then smoothed via LOESS regression, a locally weighted regression procedure.
RESULTS
Patient Demographics
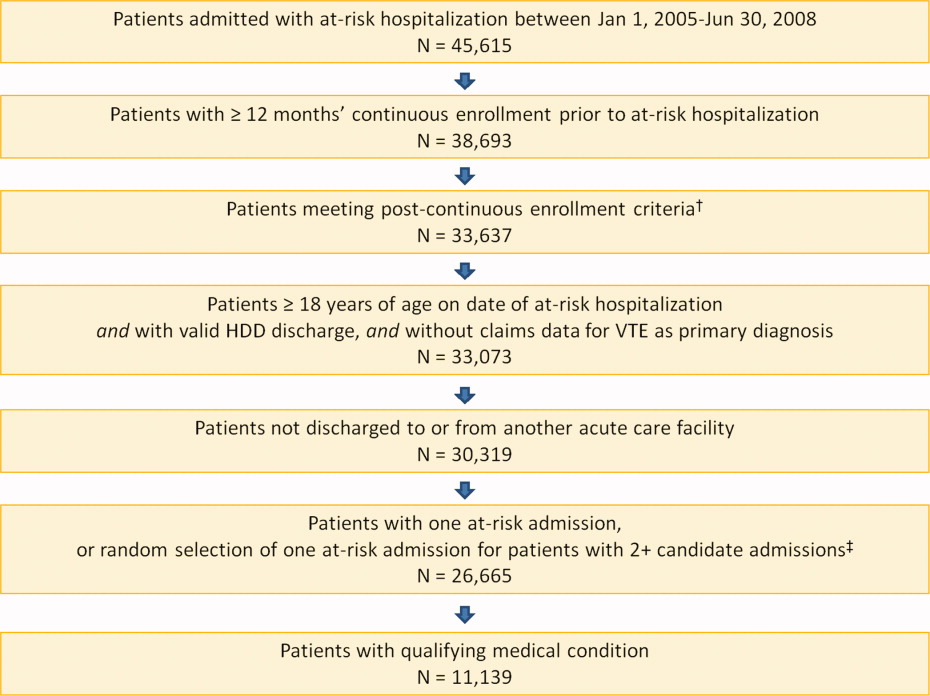
A total of 11,139 medical patients were included in the analysis (Figure 1), with a mean standard deviation (SD) age of 67.6 13.9 years, and 51.6% were women (Table 1). Of the reasons for admission to the hospital, 51.5% of patients were admitted for severe lung disease/COPD, 20.1% were admitted for cancer, 15.3% were admitted for CHF, and 13.1% were admitted for severe infectious disease. Most patients were treated in an urban hospital (87.5%), in a hospital without teaching status (87.9%), and in the South Census region (74.1%). The majority of patients were treated in medium‐sized to large care facilities. Risk factors for VTE during the baseline period included hospitalization for a medical condition with a high risk for VTE (75.6%), a prior at‐risk hospitalization (18.6%), cancer therapy (10.0% of all medical patients combined and 18.5% of cancer patients), trauma (9.2%), and previous VTE (4.3%).
| Characteristic | Medical Patients (N = 11,139) |
|---|---|
| |
| Gender | |
| Men | 5389 (48.4) |
| Women | 5750 (51.6) |
| Reason for hospitalization | |
| Cancer | 2243 (20.1) |
| CHF | 1705 (15.3) |
| Severe lung disease/COPD | 5736 (51.5) |
| Severe infectious disease | 1455 (13.1) |
| Age group, years | |
| 1834 | 230 (2.1) |
| 3544 | 442 (4.0) |
| 4554 | 1188 (10.7) |
| 5564 | 2644 (23.7) |
| 6574 | 2657 (23.9) |
| 7584 | 2969 (26.7) |
| 85 years | 1009 (9.1) |
| Median age SD, years | 67.6 13.9 |
| Primary payer* | |
| Medicare | 6819 (61.2) |
| Commercial | 4320 (38.8) |
| Geographical area | |
| Northeast | 122 (1.1) |
| North Central | 2649 (23.8) |
| South | 8258 (74.1) |
| West | 110 (1.0) |
| Urban location | 9743 (87.5) |
| Teaching hospital | 1345 (12.1) |
| Licensed bed size | |
| 1199 | 1621 (14.6) |
| 200299 | 2869 (25.8) |
| 300499 | 4005 (36.0) |
| 500 | 2644 (23.7) |
VTE Prophylaxis
Patients stayed in hospital for a mean SD duration of 5.3 5.3 days, varying from 4.6 3.9 days in patients with CHF to 6.7 6.5 days in patients with infectious disease, during which 46.7% of patients received pharmacological VTE prophylaxis. Inpatient pharmacological prophylaxis rates ranged from 64.1% in patients with CHF to 30.7% in patients with cancer (Table 2). Overall, the most commonly used form of inpatient pharmacological prophylaxis was enoxaparin (26.8% of all patients), followed by UFH (13.5% of all patients). Mechanical prophylaxis was received by 12.2% of all patients. Mean SD VTE prophylaxis duration during hospitalization was 5.0 4.7 days, varying from 4.2 4.0 days in patients with cancer to 6.2 5.5 days in patients with infectious disease.
| n (%) | Infectious Disease (n = 1455) | CHF (n = 1705) | Severe Lung Disease/COPD (n = 5736) | Cancer (n = 2243) | Any Medical (N = 11,139) |
|---|---|---|---|---|---|
| |||||
| Pharmacological prophylaxis during hospitalization* | 599 (41.2) | 1093 (64.1) | 2820 (49.2) | 688 (30.7) | 5200 (46.7) |
| Enoxaparin | 362 (24.9) | 466 (27.3) | 1877 (32.7) | 282 (12.6) | 2987 (26.8) |
| UFH | 191 (13.1) | 400 (23.5) | 527 (9.2) | 383 (17.1) | 1501 (13.5) |
| Warfarin | 135 (9.3) | 498 (29.2) | 622 (10.8) | 95 (4.2) | 1350 (12.1) |
| Dalteparin | 16 (1.1) | 21 (1.2) | 109 (1.9) | 16 (0.7) | 162 (1.5) |
| Fondaparinux | 5 (0.3) | 4 (0.2) | 22 (0.4) | 2 (0.1) | 33 (0.3) |
| Mechanical prophylaxis in hospital | 148 (10.2) | 65 (3.8) | 343 (6.0) | 803 (35.8) | 1359 (12.2) |
| Anticoagulation within 35 days after discharge | 104 (7.1) | 315 (18.5) | 397 (6.9) | 166 (7.4) | 982 (8.8) |
| Enoxaparin | 15 (1.0) | 14 (0.8) | 32 (0.6) | 25 (1.1) | 86 (0.8) |
| UFH | 17 (1.2) | 10 (0.6) | 23 (0.4) | 35 (1.6) | 85 (0.8) |
| Warfarin | 79 (5.4) | 302 (17.7) | 357 (6.2) | 116 (5.2) | 854 (7.7) |
| Dalteparin | 0 | 0 | 2 (<0.1) | 1 (<0.1) | 3 (<0.1) |
| Fondaparinux | 1 (0.1) | 0 | 0 | 2 (0.1) | 3 (<0.1) |
| Antiplatelet therapy within 35 days after discharge | 72 (4.9) | 217 (12.7) | 351 (6.1) | 53 (2.4) | 693 (6.2) |
In the 35 days after discharge, 8.8% of patients received anticoagulation therapy, most commonly warfarin (7.7%). The rate of outpatient prophylaxis was highest in patients hospitalized for CHF (18.5%) compared with other medical conditions (7%).
Time Course of VTE Risk and Hazard Function
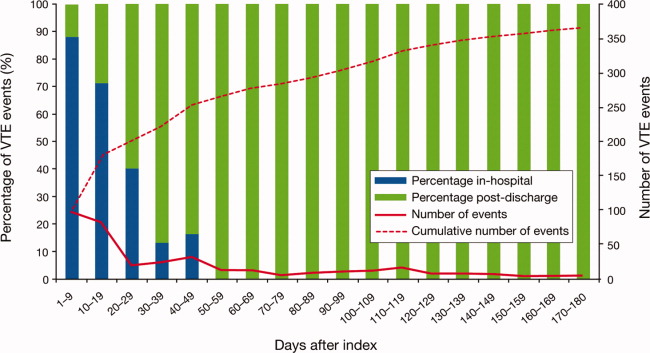
Overall, there were 366 symptomatic VTE events, representing a VTE rate of 3.3%. These events comprised 241 DVT‐only events, 98 PE‐only events, and 27 events with evidence of both DVT and PE. In total, 43.4% of events occurred during hospitalization (Figure 2). The VTE rate was 5.7% in patients with cancer (30.5% of events occurring in hospital), 4.3% with infectious disease (61.9% in hospital), 3.1% with CHF (54.7% in hospital), and 2.1% with severe lung disease/COPD (42.6% in hospital). The highest number of VTE events, 97 events (62 DVT only, 26 PE only, and 9 events both DVT and PE), occurred in the first 9 days after the hospital admission date, of which 87.6% were during hospitalization. During days 10‐19, there were 82 VTE events (50 DVT only, 24 PE only, and 8 both DVT and PE), 70.7% of which occurred in the hospital. Over the following 10‐day periods, VTE incidence gradually declined (Figure 2) and fluctuated at a background level of 4‐8 events during each 10‐day interval from 120 to 180 days.
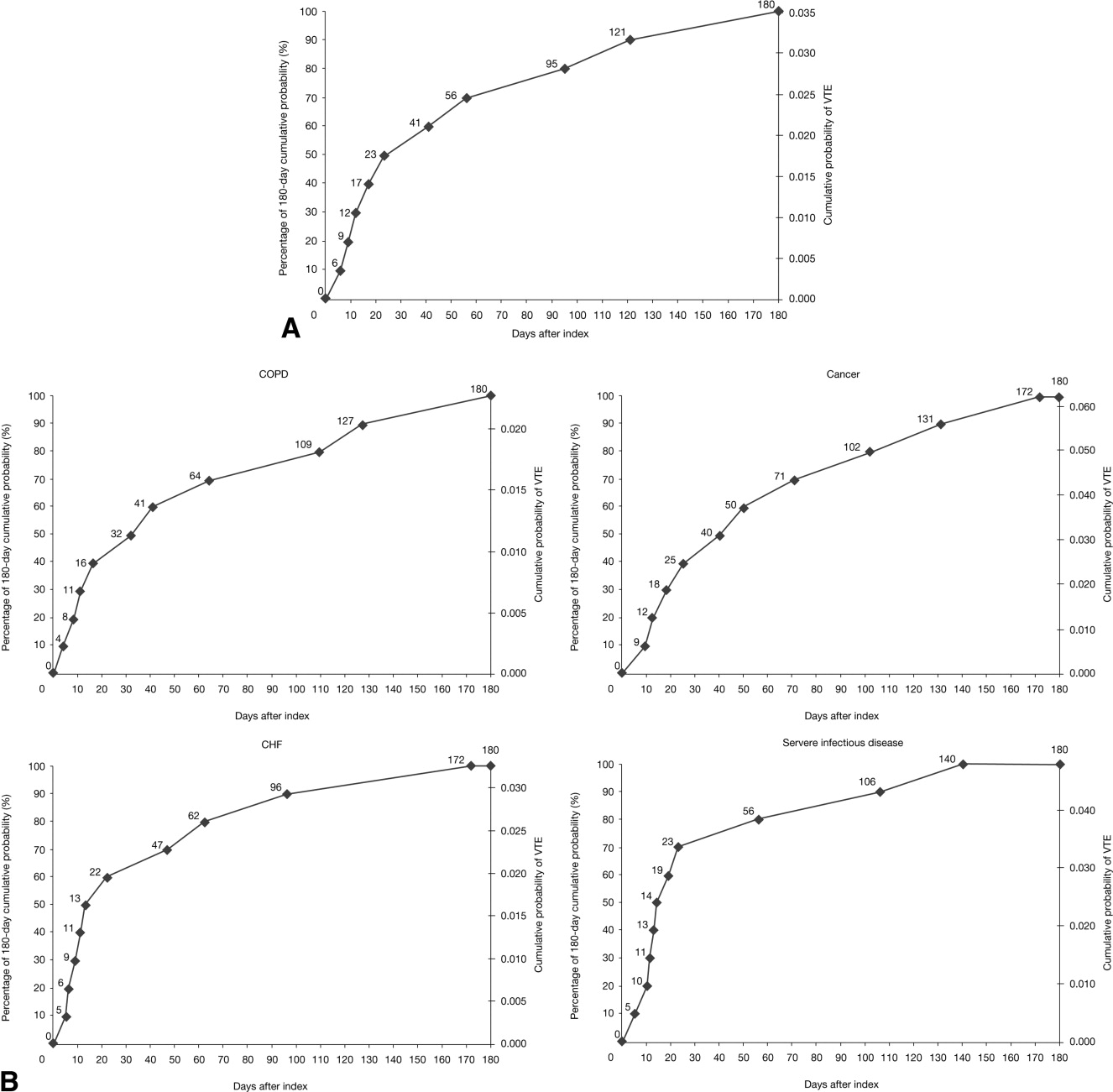
The cumulative probability of VTE among all patients was 0.035 (Figure 3A). Half of the VTE risk had accumulated by day 23, and 75% had accumulated by day 71. By day 30, the proportion of cumulative risk was 52.6% overall, and ranged from 41.9% with cancer to 72.9% with infectious disease (Figure 3).
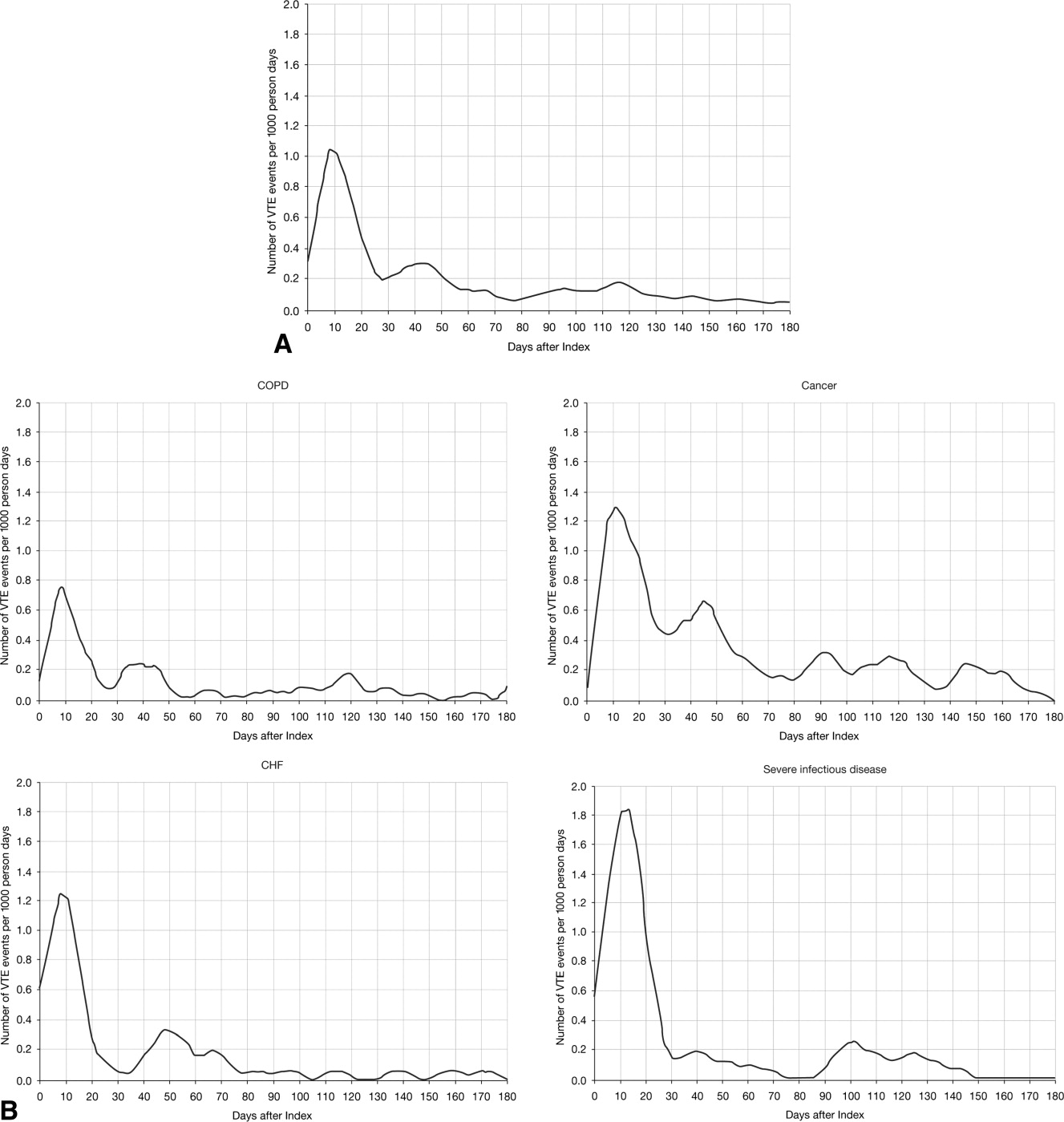
The VTE hazard peaked at approximately 1.05 VTE events per 1000 person‐days on day 8 after the hospital admission date overall (Figure 4A). The cumulative hazard at the peak day was 18.2% of the total VTE hazard over the 180‐day evaluation period. The hazard peak ranged from day 7 in patients with severe lung disease/COPD to day 12 in patients with infectious disease (Figure 4B). The cumulative hazard at the peak day was 39.7% for patients with infectious disease, 29.2% for patients with CHF, and approximately 19% for cancer or severe lung disease/COPD. After the peak risk day, the VTE hazard function decreased until the curve reached an inflection point, at day 28, when the cumulative risk was 51.8% (Figure 4A). After the inflection point, the VTE hazard increased to 0.3 VTE events per 1000 person‐days at approximately day 40‐45 and then decreased to <0.2 events per 1000 person‐days. The timing of the inflection varied by approximately 1 week across the medical illnesses (ranging from day 25 for severe lung disease/COPD to day 33 for CHF), with the cumulative risk at the inflection point ranging from 41.9% with cancer to 72.9% with infectious disease.
DISCUSSION
The results from this large, real‐world study provide new insights into the duration of risk of symptomatic VTE in medical patients and demonstrate that the number of VTE events was highest during days 0‐19, with the peak of VTE hazard at day 8. Half of the total 180‐day cumulative risk had been incurred by day 23 after hospital admission, and the period of greatest increased risk extended up to at least 30 days. Importantly, more than half of VTE events occurred after discharge (56.6%). A particularly high proportion of VTE events (69.5%) had occurred after discharge in patients with cancer. Although it was assumed that most VTE events that could be reasonably attributed to an at‐risk hospitalization would occur within 90 days as shown previously,4, 11 the 180‐day evaluation period was used to examine whether there was a prolonged period of continually diminished VTE risk from 90 to 180 days. Thus, events occurring within the later portions of the evaluation period may or may not have been attributable to the index hospitalization, potentially reflecting a background rate of VTE as noted above. Although these events are included in our estimate of the 180‐day cumulative risk of VTE, interpretation of the study results excluding such events is possible by examining the cumulative risk that had been incurred at each time point during the evaluation period.
Few other studies have assessed the duration of VTE risk in hospitalized medical patients. In a study by Spyropoulos et al,4 the median time to a DVT and/or PE event was 74 days, ranging from 62 days in severe infectious disease to 126 days in CHF. In another observational study that included patients who had recently been hospitalized but had not undergone surgery, 66.9% of patients who experienced DVT and/or PE events were diagnosed with DVT and/or PE within the first month after hospital discharge; 19.9% between months 1 and 2, and 13.2% between months 2 and 3.12
Fewer than half of the patients in the present study received thromboprophylaxis, which is consistent with other studies demonstrating the low prophylaxis rates in medical inpatients.9, 1315 In a recently published US study of discharge records that included 22,455 medical inpatients, prophylaxis rates were 59.4% in patients with CHF, 52.3% with cancer, 45.8% with severe lung disease/COPD, and 40.4% with infectious disease.14 Fewer than 10% of patients in the present study received prophylaxis after discharge, a result that is consistent with other studies.4, 9
The effect of extended prophylaxis in acutely ill medical patients with the LMWH enoxaparin beyond 6‐14 days has been investigated in the EXCLAIM study.16 This trial included approximately 5800 acutely ill medical patients at significant risk of developing VTE due to a recent reduction in mobility. Patients in the extended prophylaxis group had a lower risk of VTE (2.5% vs 4% for placebo; absolute risk reduction 1.5% [95.8% confidence interval 2.54% to 0.52%]), but had increased major bleeding events (0.8% vs 0.3% for placebo; absolute risk difference favoring placebo, 0.51% [95% confidence interval, 0.12% to 0.89%]). The patient populations with most benefit from an additional 28 days prophylaxis with enoxaparin, in addition to the usual short‐term prophylaxis of 10 days, were patients with restricted mobility (level 1; total bed rest/sedentary), elderly patients (age >75 years), and women. A limitation of the EXCLAIM trial is that estimates of efficacy and safety are difficult to interpret: after an interim analysis of adjudicated efficacy and safety outcomes, amendments were made to the original study protocol by changing eligibility criteria for patients with level 2 immobility (level 1 with bathroom privileges).16
The optimal duration of prophylaxis for medical patients has not been determined; prophylaxis is generally administered to at‐risk medical patients for the duration of hospitalization. In the current study, mean length of stay was 5.3 5.3 days overall. As hospital stays shorten, many medical patients who are prescribed inpatient prophylaxis alone are unlikely to receive the standard 6‐14 days of prophylaxis shown to be effective in clinical trials.68 Furthermore, the extended period of VTE risk in the present study and the finding that 56.6% of events occurred after discharge also suggest that current practices for inpatient prophylaxis alone may need to be evaluated.
This study reports real‐world data from a large, well‐defined population and obtains the incidence of symptomatic VTE events. Even though certain demographic data deviate from the national averagefor example, 74.1% of patients were treated in the South Census region, whereas this region is served by 37.6% of US hospitals17; 87.5% of hospitals had an urban location (compared with 60.1% of US hospitals18), and 85.4% of hospitals had a licensed bed size of at least 200 beds (compared with 28.2% of US hospitals, with the average US hospital having fewer than 100 beds19)these data may be beneficial in guiding policy and health care strategies for gaining understanding of the duration of risk for VTE.
Limitations of the study include characterization of the VTE risk period through examination of the cumulative risk and hazard of VTE across time, as the actual VTE risk period cannot be determined with exact precision. We used ICD‐9‐CM diagnosis coding to identify VTE. Since many cases of PE are asymptomatic and detected at autopsy,20 our approach may have missed such cases, as they would not have been recorded within the database. Furthermore, validation studies suggest that suboptimal specificity exists for ICD‐9‐CM diagnosis codes used to identify VTE.21 In an attempt to improve the specificity of our VTE identification algorithm, we required that post‐discharge VTE was recorded either during an emergency room or subsequent inpatient admission (which would be indicative of acute care for VTE) or on an outpatient claim with subsequent evidence of treatment for VTE. The true sensitivity and specificity of the VTE identification algorithms used for this study remain unknown, however, so the study findings should be interpreted in light of this limitation. The databases used for the analysis may not be representative of the US population as a whole; for example, this study used claims data from commercial and Medicare supplemental databases, which do not include Medicaid patients. Another limitation was that outpatient mechanical prophylaxis, such as graded compression stockings, was not captured due to over‐the‐counter availability. In addition, appropriateness of prophylaxis was not determined in this study, because these data could not be obtained from the claims database used. Further studies are warranted to obtain information on the incidence of VTE after hospitalization for medical illness in patients who received appropriate prophylaxis during hospitalization.
Finally, all dosages of a pharmacological agent were considered prophylactic only if a VTE event did not occur, with the exception of warfarin; any dose of warfarin was considered for prophylaxis, regardless of a VTE diagnosis. Warfarin may be used for purposes other than VTE prophylaxis (eg, prophylaxis for a thromboembolic cerebrovascular accident). The data source does not allow for identifying the exact reason for anticoagulation therapy with warfarin. Nonetheless, warfarin therapy will confer a decreased risk of VTE regardless of its purpose.
Results from this large cohort of medical patients indicate that symptomatic VTE risk is highest within the first 19 days after hospital admission (a period that may encompass both the duration of hospitalization as well as the period after discharge) with a considerable risk of VTE extending into the period after discharge. Receiving appropriate prophylaxis in‐hospital remains of great importance to prevent inpatient and likely post‐discharge VTE in patients with acute medical illness. In addition, given the time course of VTE events, with VTE incidence peaking at 8 days but with increased risk extending to 30 days, and the number of out‐of‐hospital VTE events incurred, the results of this study suggest that future research is warranted to investigate the risks and benefits of improving thromboprophylaxis practices in the period after hospitalization.
Acknowledgements
Funding Source: sanofi‐aventis U.S. provided funding to Thomson Reuters to perform this study. The authors received editorial/writing support from Tessa Hartog of Excerpta Medica in the preparation of the manuscript funded by sanofi‐aventis U.S.
Disclosure: Alpesh Amin has received research honorarium and is on the speakers bureau for sanofi‐aventis U.S. Otsuka Pharmaceutical, and Boehringer‐Ingelheim. Helen Varker, Nicole Princic, and Stephen Johnston are employees at Thomson Reuters, which received funding from sanofi‐aventis U.S. Jay Lin is an employee of Novosys Health, which received funding from sanofi‐aventis U.S. Stephen Thompson is an employee of sanofi‐aventis U.S.
- , , , et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):381S–453S.
- , , , , , . Risk factors for deep vein thrombosis and pulmonary embolism: a population‐based case‐control study. Arch Intern Med. 2000;160:809–815.
- . The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008;28:370–372.
- , , , . Rates of venous thromboembolism occurrence in medical patients among the insured population. Thromb Haemost. 2009;102:951–957.
- , , , et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population‐based study. Arch Intern Med. 2002;162:1245–1248.
- , , , et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999;341:793–800.
- , , , et al. Randomized, placebo‐controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004;110:874–879.
- , , , et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006;332:325–329.
- , , . Lack of thromboprophylaxis across the care continuum in US medical patients. Hosp Pract (Minneap). 2010;38:17–25.
- HCUP NIS Related Reports. Healthcare Cost and Utilization Project (HCUP), September 2008. Available at: www.hcup‐us.ahrq.gov/db/nation/nis/nisrelatedreports.jsp. Accessed June 2011.
- , . Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13:475–486.
- , , , , . Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167:1471–1475.
- , , , . Inpatient thromboprophylaxis use in U.S. hospitals: adherence to the seventh American College of Chest Physician's recommendations for at‐risk medical and surgical patients. J Hosp Med. 2009;4:E15–E21.
- , , , et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE start). J Thromb Thrombolysis. 2010;29:326–339.
- , , , et al. Venous thromboembolism risk and prophylaxis in hospitalised medically ill patients. The ENDORSE Global Survey. Thromb Haemost. 2010;103:736–748.
- , , , et al. Extended‐duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153:8–18.
- American Society for Healthcare Engineering of the American Hospital Association. Overview of the Hospital Market, 2009. Available from: www.ashe.org/e2c/pdfs/energy/heg_ch2_background.pdf. Accessed June 2011.
- American Hospital Association. Fast Facts on US Hospitals, 2009. Available at: http://www.aha.org/aha/resource‐center/Statistics‐and‐Studies/fast‐facts.html. Accessed June 2011.
- American Hospital Association. AHA Annual Survey of Hospitals Database, 2009. Available from: http://www.ahadata.com/ahadata_app/index.jsp. Accessed June 2011.
- . The epidemiology of venous thromboembolism. Circulation. 2003;107(23 suppl 1):I4–I8.
- , , , et al. How valid is the ICD‐9‐CM based AHRQ patient safety indicator for postoperative venous thromboembolism? Med Care. 2009;47:1237–1243.
Patients who are hospitalized for acute medical illness are at an increased risk of developing venous thromboembolism (VTE), which comprises deep‐vein thrombosis (DVT) and pulmonary embolism (PE).13 In a recent real‐world study of 158,325 US medical patients by Spyropoulos et al,4 4.0% of patients developed DVT, 1.5% developed PE, and 0.2% developed both DVT and PE. Furthermore, results from a population‐based case‐control study indicate that hospitalization for medical illness accounted for a proportion of VTE events similar to that of hospitalization for surgery (22% and 24%, respectively).5
Thromboprophylaxis reduces VTE incidence in at‐risk medical patients and is recommended according to evidence‐based guidelines from the American College of Chest Physicians (ACCP).1 The ACCP guidelines advocate that acutely ill medical patients admitted to the hospital with congestive heart failure (CHF) or severe lung disease/chronic obstructive pulmonary disease (COPD) or those who are confined to bed and have one or more additional risk factors (including active cancer, previous VTE, sepsis, acute neurologic disease, or inflammatory bowel disease) receive pharmacological prophylaxis with lowmolecular weight heparin (LMWH), low‐dose unfractionated heparin (UFH), or fondaparinux.1 Although guidelines provide recommendations for the duration of prophylaxis after major orthopedic surgery, such recommendations are unavailable for medical patients. In clinical trials of acutely ill medical patients, prophylaxis regimens found to be effective were provided for a duration of hospitalization of 6‐14 days.68 The mean length of hospital stay for medical illnesses is decreasing and is currently shorter than 6‐14 days.9, 10
In clinical practice, the duration of VTE risk during and after hospitalization is not well understood in medical patients, particularly in the context of shortening hospital stays. Such information could, however, provide insight into whether current thromboprophylaxis practices reflect real‐world need. To gain a greater understanding of the period during which patients are at risk of VTE, this retrospective, observational study assessed the incidence and time course of symptomatic VTE events during and after hospitalization in a large population of US medical patients.
METHODS
Data and Patient Selection
This study employed linked administrative claims data and hospital billing data contained in the Thomson Reuters MarketScan Inpatient Drug Link File. This combines longitudinal patient‐level inpatient and outpatient medical and pharmaceutical claims data from the MarketScan Commercial claims data from the MarketScan Commercial Claims and Encounters (Commercial) and Medicare Supplemental and Coordination of Benefits (Medicare Supplemental) databases, with hospital discharge records detailing services used and drugs administered during a hospitalization, which are included in the Hospital Drug Database. The linked data sources enable analysis of a patient's experience before, during, and after a hospitalization. The present study was not designed to obtain bleeding rates.
The study cohort comprised patients considered to be at‐risk for VTE as a result of a medical hospitalization occurring between January 1, 2005, and December 31, 2008. At‐risk medical hospitalizations were those for which the primary diagnosis was for cancer, CHF, severe lung disease/COPD, or infectious disease (see Supporting Information, Appendix I, for International Classification of Diseases, 9th Revision, Clinical Modification [ICD‐9‐CM] codes used to identify patients with medical illnesses). Included patients were required to be at least 18 years of age at the time of admission and were required to be continuously enrolled in their insurance benefits for at least 12 months before admission (the baseline period) and for at least 180 days after the admission date (the evaluation period) to ensure that all administrative claims data during that period were captured. Patients who died in‐hospital from any cause were exempted from the continuous enrollment criterion, as long as they had been continuously enrolled prior to inpatient death. Patients transferred from or discharged to another acute‐care facility were excluded because of the possibility for incomplete inpatient data capture. For patients who had multiple medical hospitalizations between January 1, 2005, and December 31, 2008, the hospitalization around which the analysis focused was randomly selected from the set of potential medical hospitalizations.
Prophylaxis
Pharmacological prophylaxis was identified via charge codes during hospitalization or via pharmacy claims after discharge for UFH, enoxaparin, dalteparin, warfarin, and fondaparinux. All dosages of a pharmacological agent were considered prophylactic only if there was no evidence of VTE during the admission, with the exception of warfarin (Supporting Information, Appendix II). Post‐discharge use of anticoagulation therapy was measured for up to 35 days after discharge from the hospital. Use of mechanical prophylaxis during hospitalization was identified via charge codes for graduated compression stockings and charge codes indicating use of intermittent pneumatic compression devices and/or venous foot pumps. The appropriateness of prophylaxis was not assessed.
Analysis
The risk of VTE was estimated across an evaluation period of 180 days by measuring VTE occurrence and person‐time exposure. Inpatient VTE occurrence was defined as any nonprimary diagnosis of DVT and/or PE during the at‐risk hospitalization. VTE after discharge was defined as an ICD‐9‐CM diagnosis code, whether primary or secondary, for DVT or PE in the evaluation period during an emergency room or inpatient admission, or on an outpatient claim with 1 or more of the following confirmatory events: an emergency room or inpatient admission for VTE within 2 days of the outpatient diagnosis; a prescription claim for enoxaparin, fondaparinux, or UFH within 15 days after diagnosis; or a prescription claim for warfarin within 15 days after diagnosis and no evidence of atrial fibrillation or atrial flutter in the 6 months before the outpatient diagnosis for DVT or PE. Person‐time exposure was measured as the number of days from the hospital admission date to the first occurrence of VTE, or censoring at a subsequent at‐risk hospitalization, death, or 180 days after admission.
Cumulative risk of VTE over the 180‐day evaluation period was calculated by the Kaplan‐Meier product limit method of survival analysis and displayed for deciles of cumulative risk at 180 days after the hospital admission date. The risk of VTE at each point of time during the evaluation period (the hazard function) was first calculated on a daily basis and then smoothed via LOESS regression, a locally weighted regression procedure.
RESULTS
Patient Demographics
A total of 11,139 medical patients were included in the analysis (Figure 1), with a mean standard deviation (SD) age of 67.6 13.9 years, and 51.6% were women (Table 1). Of the reasons for admission to the hospital, 51.5% of patients were admitted for severe lung disease/COPD, 20.1% were admitted for cancer, 15.3% were admitted for CHF, and 13.1% were admitted for severe infectious disease. Most patients were treated in an urban hospital (87.5%), in a hospital without teaching status (87.9%), and in the South Census region (74.1%). The majority of patients were treated in medium‐sized to large care facilities. Risk factors for VTE during the baseline period included hospitalization for a medical condition with a high risk for VTE (75.6%), a prior at‐risk hospitalization (18.6%), cancer therapy (10.0% of all medical patients combined and 18.5% of cancer patients), trauma (9.2%), and previous VTE (4.3%).
| Characteristic | Medical Patients (N = 11,139) |
|---|---|
| |
| Gender | |
| Men | 5389 (48.4) |
| Women | 5750 (51.6) |
| Reason for hospitalization | |
| Cancer | 2243 (20.1) |
| CHF | 1705 (15.3) |
| Severe lung disease/COPD | 5736 (51.5) |
| Severe infectious disease | 1455 (13.1) |
| Age group, years | |
| 1834 | 230 (2.1) |
| 3544 | 442 (4.0) |
| 4554 | 1188 (10.7) |
| 5564 | 2644 (23.7) |
| 6574 | 2657 (23.9) |
| 7584 | 2969 (26.7) |
| 85 years | 1009 (9.1) |
| Median age SD, years | 67.6 13.9 |
| Primary payer* | |
| Medicare | 6819 (61.2) |
| Commercial | 4320 (38.8) |
| Geographical area | |
| Northeast | 122 (1.1) |
| North Central | 2649 (23.8) |
| South | 8258 (74.1) |
| West | 110 (1.0) |
| Urban location | 9743 (87.5) |
| Teaching hospital | 1345 (12.1) |
| Licensed bed size | |
| 1199 | 1621 (14.6) |
| 200299 | 2869 (25.8) |
| 300499 | 4005 (36.0) |
| 500 | 2644 (23.7) |
VTE Prophylaxis
Patients stayed in hospital for a mean SD duration of 5.3 5.3 days, varying from 4.6 3.9 days in patients with CHF to 6.7 6.5 days in patients with infectious disease, during which 46.7% of patients received pharmacological VTE prophylaxis. Inpatient pharmacological prophylaxis rates ranged from 64.1% in patients with CHF to 30.7% in patients with cancer (Table 2). Overall, the most commonly used form of inpatient pharmacological prophylaxis was enoxaparin (26.8% of all patients), followed by UFH (13.5% of all patients). Mechanical prophylaxis was received by 12.2% of all patients. Mean SD VTE prophylaxis duration during hospitalization was 5.0 4.7 days, varying from 4.2 4.0 days in patients with cancer to 6.2 5.5 days in patients with infectious disease.
| n (%) | Infectious Disease (n = 1455) | CHF (n = 1705) | Severe Lung Disease/COPD (n = 5736) | Cancer (n = 2243) | Any Medical (N = 11,139) |
|---|---|---|---|---|---|
| |||||
| Pharmacological prophylaxis during hospitalization* | 599 (41.2) | 1093 (64.1) | 2820 (49.2) | 688 (30.7) | 5200 (46.7) |
| Enoxaparin | 362 (24.9) | 466 (27.3) | 1877 (32.7) | 282 (12.6) | 2987 (26.8) |
| UFH | 191 (13.1) | 400 (23.5) | 527 (9.2) | 383 (17.1) | 1501 (13.5) |
| Warfarin | 135 (9.3) | 498 (29.2) | 622 (10.8) | 95 (4.2) | 1350 (12.1) |
| Dalteparin | 16 (1.1) | 21 (1.2) | 109 (1.9) | 16 (0.7) | 162 (1.5) |
| Fondaparinux | 5 (0.3) | 4 (0.2) | 22 (0.4) | 2 (0.1) | 33 (0.3) |
| Mechanical prophylaxis in hospital | 148 (10.2) | 65 (3.8) | 343 (6.0) | 803 (35.8) | 1359 (12.2) |
| Anticoagulation within 35 days after discharge | 104 (7.1) | 315 (18.5) | 397 (6.9) | 166 (7.4) | 982 (8.8) |
| Enoxaparin | 15 (1.0) | 14 (0.8) | 32 (0.6) | 25 (1.1) | 86 (0.8) |
| UFH | 17 (1.2) | 10 (0.6) | 23 (0.4) | 35 (1.6) | 85 (0.8) |
| Warfarin | 79 (5.4) | 302 (17.7) | 357 (6.2) | 116 (5.2) | 854 (7.7) |
| Dalteparin | 0 | 0 | 2 (<0.1) | 1 (<0.1) | 3 (<0.1) |
| Fondaparinux | 1 (0.1) | 0 | 0 | 2 (0.1) | 3 (<0.1) |
| Antiplatelet therapy within 35 days after discharge | 72 (4.9) | 217 (12.7) | 351 (6.1) | 53 (2.4) | 693 (6.2) |
In the 35 days after discharge, 8.8% of patients received anticoagulation therapy, most commonly warfarin (7.7%). The rate of outpatient prophylaxis was highest in patients hospitalized for CHF (18.5%) compared with other medical conditions (7%).
Time Course of VTE Risk and Hazard Function
Overall, there were 366 symptomatic VTE events, representing a VTE rate of 3.3%. These events comprised 241 DVT‐only events, 98 PE‐only events, and 27 events with evidence of both DVT and PE. In total, 43.4% of events occurred during hospitalization (Figure 2). The VTE rate was 5.7% in patients with cancer (30.5% of events occurring in hospital), 4.3% with infectious disease (61.9% in hospital), 3.1% with CHF (54.7% in hospital), and 2.1% with severe lung disease/COPD (42.6% in hospital). The highest number of VTE events, 97 events (62 DVT only, 26 PE only, and 9 events both DVT and PE), occurred in the first 9 days after the hospital admission date, of which 87.6% were during hospitalization. During days 10‐19, there were 82 VTE events (50 DVT only, 24 PE only, and 8 both DVT and PE), 70.7% of which occurred in the hospital. Over the following 10‐day periods, VTE incidence gradually declined (Figure 2) and fluctuated at a background level of 4‐8 events during each 10‐day interval from 120 to 180 days.
The cumulative probability of VTE among all patients was 0.035 (Figure 3A). Half of the VTE risk had accumulated by day 23, and 75% had accumulated by day 71. By day 30, the proportion of cumulative risk was 52.6% overall, and ranged from 41.9% with cancer to 72.9% with infectious disease (Figure 3).
The VTE hazard peaked at approximately 1.05 VTE events per 1000 person‐days on day 8 after the hospital admission date overall (Figure 4A). The cumulative hazard at the peak day was 18.2% of the total VTE hazard over the 180‐day evaluation period. The hazard peak ranged from day 7 in patients with severe lung disease/COPD to day 12 in patients with infectious disease (Figure 4B). The cumulative hazard at the peak day was 39.7% for patients with infectious disease, 29.2% for patients with CHF, and approximately 19% for cancer or severe lung disease/COPD. After the peak risk day, the VTE hazard function decreased until the curve reached an inflection point, at day 28, when the cumulative risk was 51.8% (Figure 4A). After the inflection point, the VTE hazard increased to 0.3 VTE events per 1000 person‐days at approximately day 40‐45 and then decreased to <0.2 events per 1000 person‐days. The timing of the inflection varied by approximately 1 week across the medical illnesses (ranging from day 25 for severe lung disease/COPD to day 33 for CHF), with the cumulative risk at the inflection point ranging from 41.9% with cancer to 72.9% with infectious disease.
DISCUSSION
The results from this large, real‐world study provide new insights into the duration of risk of symptomatic VTE in medical patients and demonstrate that the number of VTE events was highest during days 0‐19, with the peak of VTE hazard at day 8. Half of the total 180‐day cumulative risk had been incurred by day 23 after hospital admission, and the period of greatest increased risk extended up to at least 30 days. Importantly, more than half of VTE events occurred after discharge (56.6%). A particularly high proportion of VTE events (69.5%) had occurred after discharge in patients with cancer. Although it was assumed that most VTE events that could be reasonably attributed to an at‐risk hospitalization would occur within 90 days as shown previously,4, 11 the 180‐day evaluation period was used to examine whether there was a prolonged period of continually diminished VTE risk from 90 to 180 days. Thus, events occurring within the later portions of the evaluation period may or may not have been attributable to the index hospitalization, potentially reflecting a background rate of VTE as noted above. Although these events are included in our estimate of the 180‐day cumulative risk of VTE, interpretation of the study results excluding such events is possible by examining the cumulative risk that had been incurred at each time point during the evaluation period.
Few other studies have assessed the duration of VTE risk in hospitalized medical patients. In a study by Spyropoulos et al,4 the median time to a DVT and/or PE event was 74 days, ranging from 62 days in severe infectious disease to 126 days in CHF. In another observational study that included patients who had recently been hospitalized but had not undergone surgery, 66.9% of patients who experienced DVT and/or PE events were diagnosed with DVT and/or PE within the first month after hospital discharge; 19.9% between months 1 and 2, and 13.2% between months 2 and 3.12
Fewer than half of the patients in the present study received thromboprophylaxis, which is consistent with other studies demonstrating the low prophylaxis rates in medical inpatients.9, 1315 In a recently published US study of discharge records that included 22,455 medical inpatients, prophylaxis rates were 59.4% in patients with CHF, 52.3% with cancer, 45.8% with severe lung disease/COPD, and 40.4% with infectious disease.14 Fewer than 10% of patients in the present study received prophylaxis after discharge, a result that is consistent with other studies.4, 9
The effect of extended prophylaxis in acutely ill medical patients with the LMWH enoxaparin beyond 6‐14 days has been investigated in the EXCLAIM study.16 This trial included approximately 5800 acutely ill medical patients at significant risk of developing VTE due to a recent reduction in mobility. Patients in the extended prophylaxis group had a lower risk of VTE (2.5% vs 4% for placebo; absolute risk reduction 1.5% [95.8% confidence interval 2.54% to 0.52%]), but had increased major bleeding events (0.8% vs 0.3% for placebo; absolute risk difference favoring placebo, 0.51% [95% confidence interval, 0.12% to 0.89%]). The patient populations with most benefit from an additional 28 days prophylaxis with enoxaparin, in addition to the usual short‐term prophylaxis of 10 days, were patients with restricted mobility (level 1; total bed rest/sedentary), elderly patients (age >75 years), and women. A limitation of the EXCLAIM trial is that estimates of efficacy and safety are difficult to interpret: after an interim analysis of adjudicated efficacy and safety outcomes, amendments were made to the original study protocol by changing eligibility criteria for patients with level 2 immobility (level 1 with bathroom privileges).16
The optimal duration of prophylaxis for medical patients has not been determined; prophylaxis is generally administered to at‐risk medical patients for the duration of hospitalization. In the current study, mean length of stay was 5.3 5.3 days overall. As hospital stays shorten, many medical patients who are prescribed inpatient prophylaxis alone are unlikely to receive the standard 6‐14 days of prophylaxis shown to be effective in clinical trials.68 Furthermore, the extended period of VTE risk in the present study and the finding that 56.6% of events occurred after discharge also suggest that current practices for inpatient prophylaxis alone may need to be evaluated.
This study reports real‐world data from a large, well‐defined population and obtains the incidence of symptomatic VTE events. Even though certain demographic data deviate from the national averagefor example, 74.1% of patients were treated in the South Census region, whereas this region is served by 37.6% of US hospitals17; 87.5% of hospitals had an urban location (compared with 60.1% of US hospitals18), and 85.4% of hospitals had a licensed bed size of at least 200 beds (compared with 28.2% of US hospitals, with the average US hospital having fewer than 100 beds19)these data may be beneficial in guiding policy and health care strategies for gaining understanding of the duration of risk for VTE.
Limitations of the study include characterization of the VTE risk period through examination of the cumulative risk and hazard of VTE across time, as the actual VTE risk period cannot be determined with exact precision. We used ICD‐9‐CM diagnosis coding to identify VTE. Since many cases of PE are asymptomatic and detected at autopsy,20 our approach may have missed such cases, as they would not have been recorded within the database. Furthermore, validation studies suggest that suboptimal specificity exists for ICD‐9‐CM diagnosis codes used to identify VTE.21 In an attempt to improve the specificity of our VTE identification algorithm, we required that post‐discharge VTE was recorded either during an emergency room or subsequent inpatient admission (which would be indicative of acute care for VTE) or on an outpatient claim with subsequent evidence of treatment for VTE. The true sensitivity and specificity of the VTE identification algorithms used for this study remain unknown, however, so the study findings should be interpreted in light of this limitation. The databases used for the analysis may not be representative of the US population as a whole; for example, this study used claims data from commercial and Medicare supplemental databases, which do not include Medicaid patients. Another limitation was that outpatient mechanical prophylaxis, such as graded compression stockings, was not captured due to over‐the‐counter availability. In addition, appropriateness of prophylaxis was not determined in this study, because these data could not be obtained from the claims database used. Further studies are warranted to obtain information on the incidence of VTE after hospitalization for medical illness in patients who received appropriate prophylaxis during hospitalization.
Finally, all dosages of a pharmacological agent were considered prophylactic only if a VTE event did not occur, with the exception of warfarin; any dose of warfarin was considered for prophylaxis, regardless of a VTE diagnosis. Warfarin may be used for purposes other than VTE prophylaxis (eg, prophylaxis for a thromboembolic cerebrovascular accident). The data source does not allow for identifying the exact reason for anticoagulation therapy with warfarin. Nonetheless, warfarin therapy will confer a decreased risk of VTE regardless of its purpose.
Results from this large cohort of medical patients indicate that symptomatic VTE risk is highest within the first 19 days after hospital admission (a period that may encompass both the duration of hospitalization as well as the period after discharge) with a considerable risk of VTE extending into the period after discharge. Receiving appropriate prophylaxis in‐hospital remains of great importance to prevent inpatient and likely post‐discharge VTE in patients with acute medical illness. In addition, given the time course of VTE events, with VTE incidence peaking at 8 days but with increased risk extending to 30 days, and the number of out‐of‐hospital VTE events incurred, the results of this study suggest that future research is warranted to investigate the risks and benefits of improving thromboprophylaxis practices in the period after hospitalization.
Acknowledgements
Funding Source: sanofi‐aventis U.S. provided funding to Thomson Reuters to perform this study. The authors received editorial/writing support from Tessa Hartog of Excerpta Medica in the preparation of the manuscript funded by sanofi‐aventis U.S.
Disclosure: Alpesh Amin has received research honorarium and is on the speakers bureau for sanofi‐aventis U.S. Otsuka Pharmaceutical, and Boehringer‐Ingelheim. Helen Varker, Nicole Princic, and Stephen Johnston are employees at Thomson Reuters, which received funding from sanofi‐aventis U.S. Jay Lin is an employee of Novosys Health, which received funding from sanofi‐aventis U.S. Stephen Thompson is an employee of sanofi‐aventis U.S.
Patients who are hospitalized for acute medical illness are at an increased risk of developing venous thromboembolism (VTE), which comprises deep‐vein thrombosis (DVT) and pulmonary embolism (PE).13 In a recent real‐world study of 158,325 US medical patients by Spyropoulos et al,4 4.0% of patients developed DVT, 1.5% developed PE, and 0.2% developed both DVT and PE. Furthermore, results from a population‐based case‐control study indicate that hospitalization for medical illness accounted for a proportion of VTE events similar to that of hospitalization for surgery (22% and 24%, respectively).5
Thromboprophylaxis reduces VTE incidence in at‐risk medical patients and is recommended according to evidence‐based guidelines from the American College of Chest Physicians (ACCP).1 The ACCP guidelines advocate that acutely ill medical patients admitted to the hospital with congestive heart failure (CHF) or severe lung disease/chronic obstructive pulmonary disease (COPD) or those who are confined to bed and have one or more additional risk factors (including active cancer, previous VTE, sepsis, acute neurologic disease, or inflammatory bowel disease) receive pharmacological prophylaxis with lowmolecular weight heparin (LMWH), low‐dose unfractionated heparin (UFH), or fondaparinux.1 Although guidelines provide recommendations for the duration of prophylaxis after major orthopedic surgery, such recommendations are unavailable for medical patients. In clinical trials of acutely ill medical patients, prophylaxis regimens found to be effective were provided for a duration of hospitalization of 6‐14 days.68 The mean length of hospital stay for medical illnesses is decreasing and is currently shorter than 6‐14 days.9, 10
In clinical practice, the duration of VTE risk during and after hospitalization is not well understood in medical patients, particularly in the context of shortening hospital stays. Such information could, however, provide insight into whether current thromboprophylaxis practices reflect real‐world need. To gain a greater understanding of the period during which patients are at risk of VTE, this retrospective, observational study assessed the incidence and time course of symptomatic VTE events during and after hospitalization in a large population of US medical patients.
METHODS
Data and Patient Selection
This study employed linked administrative claims data and hospital billing data contained in the Thomson Reuters MarketScan Inpatient Drug Link File. This combines longitudinal patient‐level inpatient and outpatient medical and pharmaceutical claims data from the MarketScan Commercial claims data from the MarketScan Commercial Claims and Encounters (Commercial) and Medicare Supplemental and Coordination of Benefits (Medicare Supplemental) databases, with hospital discharge records detailing services used and drugs administered during a hospitalization, which are included in the Hospital Drug Database. The linked data sources enable analysis of a patient's experience before, during, and after a hospitalization. The present study was not designed to obtain bleeding rates.
The study cohort comprised patients considered to be at‐risk for VTE as a result of a medical hospitalization occurring between January 1, 2005, and December 31, 2008. At‐risk medical hospitalizations were those for which the primary diagnosis was for cancer, CHF, severe lung disease/COPD, or infectious disease (see Supporting Information, Appendix I, for International Classification of Diseases, 9th Revision, Clinical Modification [ICD‐9‐CM] codes used to identify patients with medical illnesses). Included patients were required to be at least 18 years of age at the time of admission and were required to be continuously enrolled in their insurance benefits for at least 12 months before admission (the baseline period) and for at least 180 days after the admission date (the evaluation period) to ensure that all administrative claims data during that period were captured. Patients who died in‐hospital from any cause were exempted from the continuous enrollment criterion, as long as they had been continuously enrolled prior to inpatient death. Patients transferred from or discharged to another acute‐care facility were excluded because of the possibility for incomplete inpatient data capture. For patients who had multiple medical hospitalizations between January 1, 2005, and December 31, 2008, the hospitalization around which the analysis focused was randomly selected from the set of potential medical hospitalizations.
Prophylaxis
Pharmacological prophylaxis was identified via charge codes during hospitalization or via pharmacy claims after discharge for UFH, enoxaparin, dalteparin, warfarin, and fondaparinux. All dosages of a pharmacological agent were considered prophylactic only if there was no evidence of VTE during the admission, with the exception of warfarin (Supporting Information, Appendix II). Post‐discharge use of anticoagulation therapy was measured for up to 35 days after discharge from the hospital. Use of mechanical prophylaxis during hospitalization was identified via charge codes for graduated compression stockings and charge codes indicating use of intermittent pneumatic compression devices and/or venous foot pumps. The appropriateness of prophylaxis was not assessed.
Analysis
The risk of VTE was estimated across an evaluation period of 180 days by measuring VTE occurrence and person‐time exposure. Inpatient VTE occurrence was defined as any nonprimary diagnosis of DVT and/or PE during the at‐risk hospitalization. VTE after discharge was defined as an ICD‐9‐CM diagnosis code, whether primary or secondary, for DVT or PE in the evaluation period during an emergency room or inpatient admission, or on an outpatient claim with 1 or more of the following confirmatory events: an emergency room or inpatient admission for VTE within 2 days of the outpatient diagnosis; a prescription claim for enoxaparin, fondaparinux, or UFH within 15 days after diagnosis; or a prescription claim for warfarin within 15 days after diagnosis and no evidence of atrial fibrillation or atrial flutter in the 6 months before the outpatient diagnosis for DVT or PE. Person‐time exposure was measured as the number of days from the hospital admission date to the first occurrence of VTE, or censoring at a subsequent at‐risk hospitalization, death, or 180 days after admission.
Cumulative risk of VTE over the 180‐day evaluation period was calculated by the Kaplan‐Meier product limit method of survival analysis and displayed for deciles of cumulative risk at 180 days after the hospital admission date. The risk of VTE at each point of time during the evaluation period (the hazard function) was first calculated on a daily basis and then smoothed via LOESS regression, a locally weighted regression procedure.
RESULTS
Patient Demographics
A total of 11,139 medical patients were included in the analysis (Figure 1), with a mean standard deviation (SD) age of 67.6 13.9 years, and 51.6% were women (Table 1). Of the reasons for admission to the hospital, 51.5% of patients were admitted for severe lung disease/COPD, 20.1% were admitted for cancer, 15.3% were admitted for CHF, and 13.1% were admitted for severe infectious disease. Most patients were treated in an urban hospital (87.5%), in a hospital without teaching status (87.9%), and in the South Census region (74.1%). The majority of patients were treated in medium‐sized to large care facilities. Risk factors for VTE during the baseline period included hospitalization for a medical condition with a high risk for VTE (75.6%), a prior at‐risk hospitalization (18.6%), cancer therapy (10.0% of all medical patients combined and 18.5% of cancer patients), trauma (9.2%), and previous VTE (4.3%).
| Characteristic | Medical Patients (N = 11,139) |
|---|---|
| |
| Gender | |
| Men | 5389 (48.4) |
| Women | 5750 (51.6) |
| Reason for hospitalization | |
| Cancer | 2243 (20.1) |
| CHF | 1705 (15.3) |
| Severe lung disease/COPD | 5736 (51.5) |
| Severe infectious disease | 1455 (13.1) |
| Age group, years | |
| 1834 | 230 (2.1) |
| 3544 | 442 (4.0) |
| 4554 | 1188 (10.7) |
| 5564 | 2644 (23.7) |
| 6574 | 2657 (23.9) |
| 7584 | 2969 (26.7) |
| 85 years | 1009 (9.1) |
| Median age SD, years | 67.6 13.9 |
| Primary payer* | |
| Medicare | 6819 (61.2) |
| Commercial | 4320 (38.8) |
| Geographical area | |
| Northeast | 122 (1.1) |
| North Central | 2649 (23.8) |
| South | 8258 (74.1) |
| West | 110 (1.0) |
| Urban location | 9743 (87.5) |
| Teaching hospital | 1345 (12.1) |
| Licensed bed size | |
| 1199 | 1621 (14.6) |
| 200299 | 2869 (25.8) |
| 300499 | 4005 (36.0) |
| 500 | 2644 (23.7) |
VTE Prophylaxis
Patients stayed in hospital for a mean SD duration of 5.3 5.3 days, varying from 4.6 3.9 days in patients with CHF to 6.7 6.5 days in patients with infectious disease, during which 46.7% of patients received pharmacological VTE prophylaxis. Inpatient pharmacological prophylaxis rates ranged from 64.1% in patients with CHF to 30.7% in patients with cancer (Table 2). Overall, the most commonly used form of inpatient pharmacological prophylaxis was enoxaparin (26.8% of all patients), followed by UFH (13.5% of all patients). Mechanical prophylaxis was received by 12.2% of all patients. Mean SD VTE prophylaxis duration during hospitalization was 5.0 4.7 days, varying from 4.2 4.0 days in patients with cancer to 6.2 5.5 days in patients with infectious disease.
| n (%) | Infectious Disease (n = 1455) | CHF (n = 1705) | Severe Lung Disease/COPD (n = 5736) | Cancer (n = 2243) | Any Medical (N = 11,139) |
|---|---|---|---|---|---|
| |||||
| Pharmacological prophylaxis during hospitalization* | 599 (41.2) | 1093 (64.1) | 2820 (49.2) | 688 (30.7) | 5200 (46.7) |
| Enoxaparin | 362 (24.9) | 466 (27.3) | 1877 (32.7) | 282 (12.6) | 2987 (26.8) |
| UFH | 191 (13.1) | 400 (23.5) | 527 (9.2) | 383 (17.1) | 1501 (13.5) |
| Warfarin | 135 (9.3) | 498 (29.2) | 622 (10.8) | 95 (4.2) | 1350 (12.1) |
| Dalteparin | 16 (1.1) | 21 (1.2) | 109 (1.9) | 16 (0.7) | 162 (1.5) |
| Fondaparinux | 5 (0.3) | 4 (0.2) | 22 (0.4) | 2 (0.1) | 33 (0.3) |
| Mechanical prophylaxis in hospital | 148 (10.2) | 65 (3.8) | 343 (6.0) | 803 (35.8) | 1359 (12.2) |
| Anticoagulation within 35 days after discharge | 104 (7.1) | 315 (18.5) | 397 (6.9) | 166 (7.4) | 982 (8.8) |
| Enoxaparin | 15 (1.0) | 14 (0.8) | 32 (0.6) | 25 (1.1) | 86 (0.8) |
| UFH | 17 (1.2) | 10 (0.6) | 23 (0.4) | 35 (1.6) | 85 (0.8) |
| Warfarin | 79 (5.4) | 302 (17.7) | 357 (6.2) | 116 (5.2) | 854 (7.7) |
| Dalteparin | 0 | 0 | 2 (<0.1) | 1 (<0.1) | 3 (<0.1) |
| Fondaparinux | 1 (0.1) | 0 | 0 | 2 (0.1) | 3 (<0.1) |
| Antiplatelet therapy within 35 days after discharge | 72 (4.9) | 217 (12.7) | 351 (6.1) | 53 (2.4) | 693 (6.2) |
In the 35 days after discharge, 8.8% of patients received anticoagulation therapy, most commonly warfarin (7.7%). The rate of outpatient prophylaxis was highest in patients hospitalized for CHF (18.5%) compared with other medical conditions (7%).
Time Course of VTE Risk and Hazard Function
Overall, there were 366 symptomatic VTE events, representing a VTE rate of 3.3%. These events comprised 241 DVT‐only events, 98 PE‐only events, and 27 events with evidence of both DVT and PE. In total, 43.4% of events occurred during hospitalization (Figure 2). The VTE rate was 5.7% in patients with cancer (30.5% of events occurring in hospital), 4.3% with infectious disease (61.9% in hospital), 3.1% with CHF (54.7% in hospital), and 2.1% with severe lung disease/COPD (42.6% in hospital). The highest number of VTE events, 97 events (62 DVT only, 26 PE only, and 9 events both DVT and PE), occurred in the first 9 days after the hospital admission date, of which 87.6% were during hospitalization. During days 10‐19, there were 82 VTE events (50 DVT only, 24 PE only, and 8 both DVT and PE), 70.7% of which occurred in the hospital. Over the following 10‐day periods, VTE incidence gradually declined (Figure 2) and fluctuated at a background level of 4‐8 events during each 10‐day interval from 120 to 180 days.
The cumulative probability of VTE among all patients was 0.035 (Figure 3A). Half of the VTE risk had accumulated by day 23, and 75% had accumulated by day 71. By day 30, the proportion of cumulative risk was 52.6% overall, and ranged from 41.9% with cancer to 72.9% with infectious disease (Figure 3).
The VTE hazard peaked at approximately 1.05 VTE events per 1000 person‐days on day 8 after the hospital admission date overall (Figure 4A). The cumulative hazard at the peak day was 18.2% of the total VTE hazard over the 180‐day evaluation period. The hazard peak ranged from day 7 in patients with severe lung disease/COPD to day 12 in patients with infectious disease (Figure 4B). The cumulative hazard at the peak day was 39.7% for patients with infectious disease, 29.2% for patients with CHF, and approximately 19% for cancer or severe lung disease/COPD. After the peak risk day, the VTE hazard function decreased until the curve reached an inflection point, at day 28, when the cumulative risk was 51.8% (Figure 4A). After the inflection point, the VTE hazard increased to 0.3 VTE events per 1000 person‐days at approximately day 40‐45 and then decreased to <0.2 events per 1000 person‐days. The timing of the inflection varied by approximately 1 week across the medical illnesses (ranging from day 25 for severe lung disease/COPD to day 33 for CHF), with the cumulative risk at the inflection point ranging from 41.9% with cancer to 72.9% with infectious disease.
DISCUSSION
The results from this large, real‐world study provide new insights into the duration of risk of symptomatic VTE in medical patients and demonstrate that the number of VTE events was highest during days 0‐19, with the peak of VTE hazard at day 8. Half of the total 180‐day cumulative risk had been incurred by day 23 after hospital admission, and the period of greatest increased risk extended up to at least 30 days. Importantly, more than half of VTE events occurred after discharge (56.6%). A particularly high proportion of VTE events (69.5%) had occurred after discharge in patients with cancer. Although it was assumed that most VTE events that could be reasonably attributed to an at‐risk hospitalization would occur within 90 days as shown previously,4, 11 the 180‐day evaluation period was used to examine whether there was a prolonged period of continually diminished VTE risk from 90 to 180 days. Thus, events occurring within the later portions of the evaluation period may or may not have been attributable to the index hospitalization, potentially reflecting a background rate of VTE as noted above. Although these events are included in our estimate of the 180‐day cumulative risk of VTE, interpretation of the study results excluding such events is possible by examining the cumulative risk that had been incurred at each time point during the evaluation period.
Few other studies have assessed the duration of VTE risk in hospitalized medical patients. In a study by Spyropoulos et al,4 the median time to a DVT and/or PE event was 74 days, ranging from 62 days in severe infectious disease to 126 days in CHF. In another observational study that included patients who had recently been hospitalized but had not undergone surgery, 66.9% of patients who experienced DVT and/or PE events were diagnosed with DVT and/or PE within the first month after hospital discharge; 19.9% between months 1 and 2, and 13.2% between months 2 and 3.12
Fewer than half of the patients in the present study received thromboprophylaxis, which is consistent with other studies demonstrating the low prophylaxis rates in medical inpatients.9, 1315 In a recently published US study of discharge records that included 22,455 medical inpatients, prophylaxis rates were 59.4% in patients with CHF, 52.3% with cancer, 45.8% with severe lung disease/COPD, and 40.4% with infectious disease.14 Fewer than 10% of patients in the present study received prophylaxis after discharge, a result that is consistent with other studies.4, 9
The effect of extended prophylaxis in acutely ill medical patients with the LMWH enoxaparin beyond 6‐14 days has been investigated in the EXCLAIM study.16 This trial included approximately 5800 acutely ill medical patients at significant risk of developing VTE due to a recent reduction in mobility. Patients in the extended prophylaxis group had a lower risk of VTE (2.5% vs 4% for placebo; absolute risk reduction 1.5% [95.8% confidence interval 2.54% to 0.52%]), but had increased major bleeding events (0.8% vs 0.3% for placebo; absolute risk difference favoring placebo, 0.51% [95% confidence interval, 0.12% to 0.89%]). The patient populations with most benefit from an additional 28 days prophylaxis with enoxaparin, in addition to the usual short‐term prophylaxis of 10 days, were patients with restricted mobility (level 1; total bed rest/sedentary), elderly patients (age >75 years), and women. A limitation of the EXCLAIM trial is that estimates of efficacy and safety are difficult to interpret: after an interim analysis of adjudicated efficacy and safety outcomes, amendments were made to the original study protocol by changing eligibility criteria for patients with level 2 immobility (level 1 with bathroom privileges).16
The optimal duration of prophylaxis for medical patients has not been determined; prophylaxis is generally administered to at‐risk medical patients for the duration of hospitalization. In the current study, mean length of stay was 5.3 5.3 days overall. As hospital stays shorten, many medical patients who are prescribed inpatient prophylaxis alone are unlikely to receive the standard 6‐14 days of prophylaxis shown to be effective in clinical trials.68 Furthermore, the extended period of VTE risk in the present study and the finding that 56.6% of events occurred after discharge also suggest that current practices for inpatient prophylaxis alone may need to be evaluated.
This study reports real‐world data from a large, well‐defined population and obtains the incidence of symptomatic VTE events. Even though certain demographic data deviate from the national averagefor example, 74.1% of patients were treated in the South Census region, whereas this region is served by 37.6% of US hospitals17; 87.5% of hospitals had an urban location (compared with 60.1% of US hospitals18), and 85.4% of hospitals had a licensed bed size of at least 200 beds (compared with 28.2% of US hospitals, with the average US hospital having fewer than 100 beds19)these data may be beneficial in guiding policy and health care strategies for gaining understanding of the duration of risk for VTE.
Limitations of the study include characterization of the VTE risk period through examination of the cumulative risk and hazard of VTE across time, as the actual VTE risk period cannot be determined with exact precision. We used ICD‐9‐CM diagnosis coding to identify VTE. Since many cases of PE are asymptomatic and detected at autopsy,20 our approach may have missed such cases, as they would not have been recorded within the database. Furthermore, validation studies suggest that suboptimal specificity exists for ICD‐9‐CM diagnosis codes used to identify VTE.21 In an attempt to improve the specificity of our VTE identification algorithm, we required that post‐discharge VTE was recorded either during an emergency room or subsequent inpatient admission (which would be indicative of acute care for VTE) or on an outpatient claim with subsequent evidence of treatment for VTE. The true sensitivity and specificity of the VTE identification algorithms used for this study remain unknown, however, so the study findings should be interpreted in light of this limitation. The databases used for the analysis may not be representative of the US population as a whole; for example, this study used claims data from commercial and Medicare supplemental databases, which do not include Medicaid patients. Another limitation was that outpatient mechanical prophylaxis, such as graded compression stockings, was not captured due to over‐the‐counter availability. In addition, appropriateness of prophylaxis was not determined in this study, because these data could not be obtained from the claims database used. Further studies are warranted to obtain information on the incidence of VTE after hospitalization for medical illness in patients who received appropriate prophylaxis during hospitalization.
Finally, all dosages of a pharmacological agent were considered prophylactic only if a VTE event did not occur, with the exception of warfarin; any dose of warfarin was considered for prophylaxis, regardless of a VTE diagnosis. Warfarin may be used for purposes other than VTE prophylaxis (eg, prophylaxis for a thromboembolic cerebrovascular accident). The data source does not allow for identifying the exact reason for anticoagulation therapy with warfarin. Nonetheless, warfarin therapy will confer a decreased risk of VTE regardless of its purpose.
Results from this large cohort of medical patients indicate that symptomatic VTE risk is highest within the first 19 days after hospital admission (a period that may encompass both the duration of hospitalization as well as the period after discharge) with a considerable risk of VTE extending into the period after discharge. Receiving appropriate prophylaxis in‐hospital remains of great importance to prevent inpatient and likely post‐discharge VTE in patients with acute medical illness. In addition, given the time course of VTE events, with VTE incidence peaking at 8 days but with increased risk extending to 30 days, and the number of out‐of‐hospital VTE events incurred, the results of this study suggest that future research is warranted to investigate the risks and benefits of improving thromboprophylaxis practices in the period after hospitalization.
Acknowledgements
Funding Source: sanofi‐aventis U.S. provided funding to Thomson Reuters to perform this study. The authors received editorial/writing support from Tessa Hartog of Excerpta Medica in the preparation of the manuscript funded by sanofi‐aventis U.S.
Disclosure: Alpesh Amin has received research honorarium and is on the speakers bureau for sanofi‐aventis U.S. Otsuka Pharmaceutical, and Boehringer‐Ingelheim. Helen Varker, Nicole Princic, and Stephen Johnston are employees at Thomson Reuters, which received funding from sanofi‐aventis U.S. Jay Lin is an employee of Novosys Health, which received funding from sanofi‐aventis U.S. Stephen Thompson is an employee of sanofi‐aventis U.S.
- , , , et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):381S–453S.
- , , , , , . Risk factors for deep vein thrombosis and pulmonary embolism: a population‐based case‐control study. Arch Intern Med. 2000;160:809–815.
- . The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008;28:370–372.
- , , , . Rates of venous thromboembolism occurrence in medical patients among the insured population. Thromb Haemost. 2009;102:951–957.
- , , , et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population‐based study. Arch Intern Med. 2002;162:1245–1248.
- , , , et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999;341:793–800.
- , , , et al. Randomized, placebo‐controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004;110:874–879.
- , , , et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006;332:325–329.
- , , . Lack of thromboprophylaxis across the care continuum in US medical patients. Hosp Pract (Minneap). 2010;38:17–25.
- HCUP NIS Related Reports. Healthcare Cost and Utilization Project (HCUP), September 2008. Available at: www.hcup‐us.ahrq.gov/db/nation/nis/nisrelatedreports.jsp. Accessed June 2011.
- , . Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13:475–486.
- , , , , . Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167:1471–1475.
- , , , . Inpatient thromboprophylaxis use in U.S. hospitals: adherence to the seventh American College of Chest Physician's recommendations for at‐risk medical and surgical patients. J Hosp Med. 2009;4:E15–E21.
- , , , et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE start). J Thromb Thrombolysis. 2010;29:326–339.
- , , , et al. Venous thromboembolism risk and prophylaxis in hospitalised medically ill patients. The ENDORSE Global Survey. Thromb Haemost. 2010;103:736–748.
- , , , et al. Extended‐duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153:8–18.
- American Society for Healthcare Engineering of the American Hospital Association. Overview of the Hospital Market, 2009. Available from: www.ashe.org/e2c/pdfs/energy/heg_ch2_background.pdf. Accessed June 2011.
- American Hospital Association. Fast Facts on US Hospitals, 2009. Available at: http://www.aha.org/aha/resource‐center/Statistics‐and‐Studies/fast‐facts.html. Accessed June 2011.
- American Hospital Association. AHA Annual Survey of Hospitals Database, 2009. Available from: http://www.ahadata.com/ahadata_app/index.jsp. Accessed June 2011.
- . The epidemiology of venous thromboembolism. Circulation. 2003;107(23 suppl 1):I4–I8.
- , , , et al. How valid is the ICD‐9‐CM based AHRQ patient safety indicator for postoperative venous thromboembolism? Med Care. 2009;47:1237–1243.
- , , , et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):381S–453S.
- , , , , , . Risk factors for deep vein thrombosis and pulmonary embolism: a population‐based case‐control study. Arch Intern Med. 2000;160:809–815.
- . The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008;28:370–372.
- , , , . Rates of venous thromboembolism occurrence in medical patients among the insured population. Thromb Haemost. 2009;102:951–957.
- , , , et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population‐based study. Arch Intern Med. 2002;162:1245–1248.
- , , , et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med. 1999;341:793–800.
- , , , et al. Randomized, placebo‐controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004;110:874–879.
- , , , et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ. 2006;332:325–329.
- , , . Lack of thromboprophylaxis across the care continuum in US medical patients. Hosp Pract (Minneap). 2010;38:17–25.
- HCUP NIS Related Reports. Healthcare Cost and Utilization Project (HCUP), September 2008. Available at: www.hcup‐us.ahrq.gov/db/nation/nis/nisrelatedreports.jsp. Accessed June 2011.
- , . Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13:475–486.
- , , , , . Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167:1471–1475.
- , , , . Inpatient thromboprophylaxis use in U.S. hospitals: adherence to the seventh American College of Chest Physician's recommendations for at‐risk medical and surgical patients. J Hosp Med. 2009;4:E15–E21.
- , , , et al. Are hospitals delivering appropriate VTE prevention? The venous thromboembolism study to assess the rate of thromboprophylaxis (VTE start). J Thromb Thrombolysis. 2010;29:326–339.
- , , , et al. Venous thromboembolism risk and prophylaxis in hospitalised medically ill patients. The ENDORSE Global Survey. Thromb Haemost. 2010;103:736–748.
- , , , et al. Extended‐duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153:8–18.
- American Society for Healthcare Engineering of the American Hospital Association. Overview of the Hospital Market, 2009. Available from: www.ashe.org/e2c/pdfs/energy/heg_ch2_background.pdf. Accessed June 2011.
- American Hospital Association. Fast Facts on US Hospitals, 2009. Available at: http://www.aha.org/aha/resource‐center/Statistics‐and‐Studies/fast‐facts.html. Accessed June 2011.
- American Hospital Association. AHA Annual Survey of Hospitals Database, 2009. Available from: http://www.ahadata.com/ahadata_app/index.jsp. Accessed June 2011.
- . The epidemiology of venous thromboembolism. Circulation. 2003;107(23 suppl 1):I4–I8.
- , , , et al. How valid is the ICD‐9‐CM based AHRQ patient safety indicator for postoperative venous thromboembolism? Med Care. 2009;47:1237–1243.
Copyright © 2011 Society of Hospital Medicine
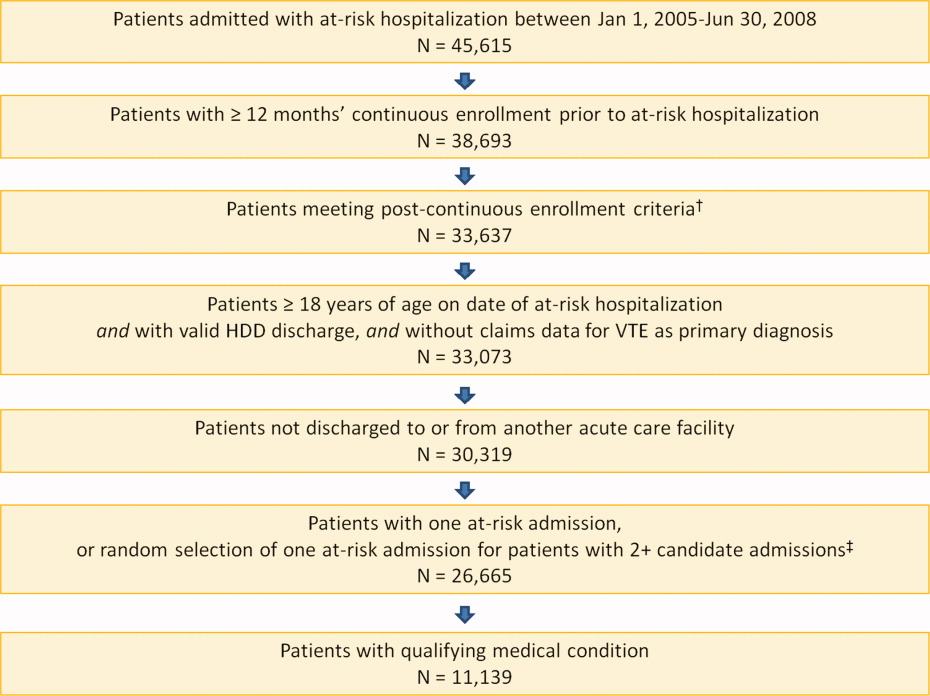
Nominal Group Technique
Pain is considered the fifth vital sign, and the appropriate management of pain is fundamental for patient care. Uncontrolled pain has adverse negative physiological consequences,14 and better pain control in hospitalized patients has been associated with decreased length of stay and improved recovery and physical comfort.36 However, many patients fail to receive state‐of‐the‐art pain relief7; for example, in a study of 176 hospitalized patients with cancer, 46% reported severe pain at the time of the interview.8 The prevalence of pain in hospitalized patients with other diagnoses besides cancer likewise remains high.9
Over the last 2 decades, the quality of care in pain management has gained increasing attention. In 2000, the Joint Commission unveiled an official statement for the purpose of improving the quality of pain management.10 The Joint Commission's 6 core principles include the right of pain assessment and treatment, institution of organizational procedures to assess pain, provision of care of persons with pain, general education, continuity of pain management after hospital discharge, and inclusion of pain management as a performance measure. Pain management is now a hospital accountability indicator. Although multiple initiatives have been undertaken to improve pain control, however, challenges still remain. Effective strategies for consensus development are still needed to prioritize interventions.
The nominal group technique (NGT) is a brainstorming tool for quality improvement; NGT is a highly structured small group discussion used to elicit and prioritize a list of answers to a specific question.1115 We conducted an NGT session to identify the multiple challenges, barriers, and perspectives of healthcare providers in managing pain among hospitalized patients. The ultimate goals were to identify potential areas for pain management improvement, build consensus among caregivers, and introduce the NGT as a tool to elicit caregivers' ideas for quality improvement.
METHODS
In a multistep process, we first identified areas for quality improvement interventions in pain management by using the NGT in hospitalized patients, then organized the information by using an iterative consensus development process, and finally displayed the main findings using a Fishbone diagram.
Setting and Participants
At a large university hospital, we targeted 3 inpatient services based on pain management performance data. We obtained the data from patient satisfaction and the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. They included 1 medical, 1 medical‐surgical, and 1 surgical hospital unit at a large academic medical center.
Within these units we recruited participants from a convenience sample of nurses, resident physicians, patient care technicians, and unit clerks. We included patient care technicians and unit clerks as they often interface between patients and providers. To maintain anonymity of the responses, we did not record participant composition during the session. Participation was voluntary and no incentives were provided. The institutional review board at the University of Alabama at Birmingham approved the use of existing quality improvement data.
Nominal Group Technique
During 2009, we conducted an NGT session within each of the 3 inpatient units. Two of the authors (MB, DS) developed the question posed to each group: What causes uncontrolled pain in your unit? The NGT supports equal participation, controls the extraneous discussion that frequently occurs when groups are convened, minimizes real or perceived power differentials among members, and, in the aggregate, minimizes the process loss that exists in unstructured focus group meetings.1116 Thus, the ideas generated by this process provide a valid reflection of the implicit prioritized views held by the group. The NGT also provides concise written documentation summarizing participants' responses, rendering audiotape recording and transcription unnecessary.13, 17
Each NGT session, lasting 1 hour, followed the following steps.13 First, after a brief introduction of the purpose of the session and general instructions, the moderators (MB, DS) posed the question: What causes uncontrolled pain in your unit? Second, in response to the standard question, each participant in the group silently and individually generated a list of ideas and wrote them down. Third, using a round‐robin approach (1 person at a time mentions the idea), each idea was concisely transcribed by the facilitator onto a flip‐chart for all participants to see; debate was not allowed during this step. Fourth, each recorded idea was then discussed for the sole purpose of clarification, and not for evaluation or argument as to the relative importance. The proposer of the idea did not need to defend the idea. During this step, participants were prompted to combine those ideas that were perceived to be substantively similar. Finally, during the voting phase, participants privately selected what they considered to be the 3 most important reasons for uncontrolled pain in their unit. Each participant prioritized their choices on their own and without discussing with other participants, giving a rank of 3 to the most important idea and 1 to the least important idea. The moderator recorded the votes onto the flip‐chart in front of all participants and then tallied the votes for each idea. We discarded a small number of idiosyncratic suggestions, which is a standard procedure in the nominal group technique. The main results were the top 5 suggestions identified within each group; the secondary results were all other suggestions. A more detailed description of the NGT steps is available elsewhere.11
Ishikawa (Fishbone) Diagram
Fishbone diagrams are designed to organize contributing factors to a particular outcome in a pictorial display. This is a common tool used to identify areas for improvement by facilitating brainstorming and graphically displaying the relationship of the causes to the effect. Through an iterative process, 3 of the authors (AP, MB, CAE) categorized all of the generated ideas into common themes until consensus was reached. The top 5 and all other suggestions within each service were organized into the Fishbone diagram.
RESULTS
The 27 health workers representing the 3 units completing the nominal group sessions generated a total of 94 ideas. The Fishbone diagram shown in Figure 1 shows each service's top 5 rankings of the elements perceived contributing most to uncontrolled pain; the elements were organized into 3 main factors and 7 priority themes identified during the iterative process.
The main categories illustrate system factors (timeliness, communication, pain assessment; Figure 1, top portion), human factors (knowledge and experience, provider bias, patient factors; Figure 1, bottom portion), and an interface between system and human factors (standardization; Figure 1, center left). The remaining 79 ideas, non‐top 5 for each unit, fell into the following priority themes: provider bias (n = 6), knowledge and experience (n = 12), pain assessment (n = 7), communication (n = 10), timeliness (n = 14), standardization (or policies and practice variation) (n = 13), and patient factors (n = 17); the ideas and representative examples are shown in Figure 2.
DISCUSSION
Using a brainstorming tool for idea generation (NGT) in quality improvement, we identified almost 100 causes of uncontrolled pain management in hospital units. We identified 7 priority themes along 3 main factors: system factors, human factors, and an interface of system and human factors. Timeliness and education emerged from 2 of the 3 services as top priorities, though they were unique and specific to the providers and patient populations within each service. The third service yielded surprisingly different priorities, with patient issues and provider bias foremost in the minds of the staff caring for these patients.
In the decade since To Err Is Human was released by the Institute of Medicine,18 healthcare improvement work has become commonplace and routine. Projects start by soliciting staff views about possible areas for improvement, usually during group meetings; however, this process is informal and not systematic. Unstructured group meetings and brainstorming have some limitations when used to uncover creative ideas for healthcare improvement.19 The literature has consistently reported that groups produce fewer ideas than an equivalent number of individuals working alone.20 In a meta‐analysis, Mullen et al21 found that interacting groups usually produced ideas of poorer quality than did nominal groups. Interpersonal interactions in a multidisciplinary team may be influenced by perceived roles and dominant personalities, and can impede a collaborative, critical discourse.22
In contrast, in NGT sessions, the weight of each member's opinion is the same, and it appears that process loss is less likely to occur.17 Moreover, the highly structured format of NGT provides an opportunity for group members to achieve a substantial amount of work in a relatively short time. Another advantage of NGT is the deliberate avoidance of interference or interpretation from a moderator or facilitator who, in the case of NGT, has the responsibility to explore but not interfere with or influence the members of the group.13 However, the NGT has some limitations. The composition and representativeness of participants may limit the generalizability of the findings. Also, it requires training and preparation, restricts the discussion to a single topic, and may not allow further elaboration of other ideas.13 Despite its potential benefits, NGT is relatively underutilized in quality improvement initiatives. To the best of our knowledge, this is the first study that has utilized NGT to elicit ideas about potential areas for pain control improvement. NGT is a good method for achieving local solutions to local problems; teams of healthcare providers should consider using NGT to address their own challenges and barriers.
In our study, timeliness, knowledge, and experience were considered the top priorities to improve pain management. Our findings are similar to a Canadian study, where delay of more than an hour to administer analgesia was considered one of the most important factors to provide good pain control management.23 Also our findings are coherent with a recent survey of 225 hospitals in the United Kingdom, where perceived lack of training was a highly ranked contributing factor for suboptimal postoperative pain management.24
Our study also identified other interesting observations that deserve comment. Examining the top priorities among the 3 services, there is some dissonance of reasoning underlying the inadequate pain control. We can speculate several reasons. First, pain control management, like any other condition, happens within a specific context with unique problems or barriers that prevent the delivery of the best care for each service. The other possible explanation is a silo effect. It is possible that workers of the same service represent a relatively homogenous social group despite differing training and backgrounds; they live the same experiences and face similar problems. Workers of one silo may work in parallel but do not interact with members of another silo, so they do not have opportunities to share their experiences or compare their beliefs. Finally, it is possible that the greater number of groups used in this study resulted in a broader array of issues. Studies have confirmed that the presence of several groups using NGT can produce a larger pool of issues, with more variation.16 Thus, the ideas generated in our NGT can be easily grouped into 2 broader categories: human factors (knowledge, experience, provider bias, and patient factors) and system factors (timeliness, communication, and pain assessment).
Our study has some limitations. The study was conducted in a single institution and in a limited number of inpatient units. The list of potential areas for improvement generated in this study may require further confirmation and validation at other institutions and with other sources of information (actual pain assessments, timeliness, knowledge, patient satisfaction). Importantly, the study design only involved healthcare providers and did not involve other stakeholders such as the patients or their families.
Despite these limitations, we propose that the NGT is a good alternative to unstructured brainstorming to systematically identify, characterize, categorize, and prioritize ideas behind inadequate pain management. The NGT is a valuable tool in conducting a robust formative assessment to better understand the multiple challenges, barriers, and perspectives of healthcare providers in guiding quality improvement interventions in a systematic and less biased manner.
CONCLUSIONS
In conclusion, healthcare workers have clear ideas about potential areas for improvement in pain management. Using the NGT, we identified 7 potential areas for improvement encompassed within human and system factors. Knowledge and timeliness emerged from 2 of the 3 clinical services as top priorities, whereas the third group identified disparate concerns suggesting provider bias and patient issues. We believe the nominal group technique is an efficient tool to uncover general and context‐specific priorities and to guide quality improvement work.
- .Success stories: how hospitals are improving care.Am Heart J.2004;148(5 suppl):S52–S55.
- ,.Acute pain.Lancet.1999;353(9169):2051–2058.
- ,,, et al.Improving the management of pain in hospitalized adults.Arch Intern Med.2006;166(9):1033–1039.
- ,,.Pain and satisfaction with pain control in hospitalized medical patients: no such thing as low risk.Arch Intern Med.2004;164(2):175–180.
- ,,,.Pain prevalence study in a large Canadian teaching hospital. Round 2: lessons learned?Pain Manag Nurs.2010;11(1):45–55.
- ,,,,.Pain prevalence study in a large Canadian teaching hospital.Pain Manag Nurs.2008;9(3):104–112.
- Institute of Medicine.Crossing the Quality Chasm: A New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- .Pain intensity and pain interference in hospitalized patients with cancer.Oncol Nurs Forum.2000;27(6):985–991.
- ,.Incidence and characteristics of pain in a sample of hospitalized cancer patients.Cancer Nurs.1987;10(2):85–92.
- .JCAHO pain management standards are unveiled. Joint Commission on Accreditation of Healthcare Organizations.JAMA.2000;284(4):428–429.
- ,,,,.A pilot study using nominal group technique to assess residents' perceptions of successful attending rounds.J Gen Intern Med.2008;23(7):1060–1065.
- ,,, et al.What should we include in a cultural competence curriculum? An emerging formative evaluation process to foster curriculum development.Acad Med.2011;86(3):333–341.
- Brief 7. Gaining Consensus Among Stakeholders Through the Nominal Group Technique. Available at: http://www.cdc.gov/HealthyYouth/evaluation/pdf/brief7.pdf. Accessed October 19,2011.
- ,.The nominal group as a research instrument for exploratory health studies.Am J Public Health.1972;62(3):337–342.
- ,,, et al.Reasons for not intensifying medications: differentiating “clinical inertia” from appropriate care.J Gen Intern Med.2007;22(12):1648–1655.
- ,,,.Nominal group technique: a process for identifying diabetes self‐care issues among patients and caregivers.Diabetes Educ.2000;26(2):305–310,312,314.
- ,,,,.The nominal group technique: a research tool for general practice?Fam Pract.1993;10(1):76–81.
- Institute of Medicine.To Err Is Human. Building a Safer Health System.Washington, DC:National Academy Press;2000.
- ,,.Quality by Design: A Clinical Microsystems Approach.San Francisco, CA:Jossey‐Bass Wiley;2007.
- ,.Group versus individual performance on tasks requiring ideational proficiency (brainstorming): a review.Eur J Soc Psychol.1973;3(4):361–388.
- ,,.Productivity loss in brainstorming groups: a meta‐analytic integration.Basic Appl Soc Psychol.1991;12:3–23.
- ,.Productivity loss in brainstorming groups: toward the solution of a riddle.J Pers Soc Psychol.1987;53:497–509.
- ,,.An interventional study to improve the quality of analgesia in the emergency department.CJEM.2008;10(5):435–439.
- ,,,.Pain assessment and management in medical wards: an area of unmet need.Postgrad Med J.2010;86(1015):279–284.
Pain is considered the fifth vital sign, and the appropriate management of pain is fundamental for patient care. Uncontrolled pain has adverse negative physiological consequences,14 and better pain control in hospitalized patients has been associated with decreased length of stay and improved recovery and physical comfort.36 However, many patients fail to receive state‐of‐the‐art pain relief7; for example, in a study of 176 hospitalized patients with cancer, 46% reported severe pain at the time of the interview.8 The prevalence of pain in hospitalized patients with other diagnoses besides cancer likewise remains high.9
Over the last 2 decades, the quality of care in pain management has gained increasing attention. In 2000, the Joint Commission unveiled an official statement for the purpose of improving the quality of pain management.10 The Joint Commission's 6 core principles include the right of pain assessment and treatment, institution of organizational procedures to assess pain, provision of care of persons with pain, general education, continuity of pain management after hospital discharge, and inclusion of pain management as a performance measure. Pain management is now a hospital accountability indicator. Although multiple initiatives have been undertaken to improve pain control, however, challenges still remain. Effective strategies for consensus development are still needed to prioritize interventions.
The nominal group technique (NGT) is a brainstorming tool for quality improvement; NGT is a highly structured small group discussion used to elicit and prioritize a list of answers to a specific question.1115 We conducted an NGT session to identify the multiple challenges, barriers, and perspectives of healthcare providers in managing pain among hospitalized patients. The ultimate goals were to identify potential areas for pain management improvement, build consensus among caregivers, and introduce the NGT as a tool to elicit caregivers' ideas for quality improvement.
METHODS
In a multistep process, we first identified areas for quality improvement interventions in pain management by using the NGT in hospitalized patients, then organized the information by using an iterative consensus development process, and finally displayed the main findings using a Fishbone diagram.
Setting and Participants
At a large university hospital, we targeted 3 inpatient services based on pain management performance data. We obtained the data from patient satisfaction and the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. They included 1 medical, 1 medical‐surgical, and 1 surgical hospital unit at a large academic medical center.
Within these units we recruited participants from a convenience sample of nurses, resident physicians, patient care technicians, and unit clerks. We included patient care technicians and unit clerks as they often interface between patients and providers. To maintain anonymity of the responses, we did not record participant composition during the session. Participation was voluntary and no incentives were provided. The institutional review board at the University of Alabama at Birmingham approved the use of existing quality improvement data.
Nominal Group Technique
During 2009, we conducted an NGT session within each of the 3 inpatient units. Two of the authors (MB, DS) developed the question posed to each group: What causes uncontrolled pain in your unit? The NGT supports equal participation, controls the extraneous discussion that frequently occurs when groups are convened, minimizes real or perceived power differentials among members, and, in the aggregate, minimizes the process loss that exists in unstructured focus group meetings.1116 Thus, the ideas generated by this process provide a valid reflection of the implicit prioritized views held by the group. The NGT also provides concise written documentation summarizing participants' responses, rendering audiotape recording and transcription unnecessary.13, 17
Each NGT session, lasting 1 hour, followed the following steps.13 First, after a brief introduction of the purpose of the session and general instructions, the moderators (MB, DS) posed the question: What causes uncontrolled pain in your unit? Second, in response to the standard question, each participant in the group silently and individually generated a list of ideas and wrote them down. Third, using a round‐robin approach (1 person at a time mentions the idea), each idea was concisely transcribed by the facilitator onto a flip‐chart for all participants to see; debate was not allowed during this step. Fourth, each recorded idea was then discussed for the sole purpose of clarification, and not for evaluation or argument as to the relative importance. The proposer of the idea did not need to defend the idea. During this step, participants were prompted to combine those ideas that were perceived to be substantively similar. Finally, during the voting phase, participants privately selected what they considered to be the 3 most important reasons for uncontrolled pain in their unit. Each participant prioritized their choices on their own and without discussing with other participants, giving a rank of 3 to the most important idea and 1 to the least important idea. The moderator recorded the votes onto the flip‐chart in front of all participants and then tallied the votes for each idea. We discarded a small number of idiosyncratic suggestions, which is a standard procedure in the nominal group technique. The main results were the top 5 suggestions identified within each group; the secondary results were all other suggestions. A more detailed description of the NGT steps is available elsewhere.11
Ishikawa (Fishbone) Diagram
Fishbone diagrams are designed to organize contributing factors to a particular outcome in a pictorial display. This is a common tool used to identify areas for improvement by facilitating brainstorming and graphically displaying the relationship of the causes to the effect. Through an iterative process, 3 of the authors (AP, MB, CAE) categorized all of the generated ideas into common themes until consensus was reached. The top 5 and all other suggestions within each service were organized into the Fishbone diagram.
RESULTS
The 27 health workers representing the 3 units completing the nominal group sessions generated a total of 94 ideas. The Fishbone diagram shown in Figure 1 shows each service's top 5 rankings of the elements perceived contributing most to uncontrolled pain; the elements were organized into 3 main factors and 7 priority themes identified during the iterative process.
The main categories illustrate system factors (timeliness, communication, pain assessment; Figure 1, top portion), human factors (knowledge and experience, provider bias, patient factors; Figure 1, bottom portion), and an interface between system and human factors (standardization; Figure 1, center left). The remaining 79 ideas, non‐top 5 for each unit, fell into the following priority themes: provider bias (n = 6), knowledge and experience (n = 12), pain assessment (n = 7), communication (n = 10), timeliness (n = 14), standardization (or policies and practice variation) (n = 13), and patient factors (n = 17); the ideas and representative examples are shown in Figure 2.
DISCUSSION
Using a brainstorming tool for idea generation (NGT) in quality improvement, we identified almost 100 causes of uncontrolled pain management in hospital units. We identified 7 priority themes along 3 main factors: system factors, human factors, and an interface of system and human factors. Timeliness and education emerged from 2 of the 3 services as top priorities, though they were unique and specific to the providers and patient populations within each service. The third service yielded surprisingly different priorities, with patient issues and provider bias foremost in the minds of the staff caring for these patients.
In the decade since To Err Is Human was released by the Institute of Medicine,18 healthcare improvement work has become commonplace and routine. Projects start by soliciting staff views about possible areas for improvement, usually during group meetings; however, this process is informal and not systematic. Unstructured group meetings and brainstorming have some limitations when used to uncover creative ideas for healthcare improvement.19 The literature has consistently reported that groups produce fewer ideas than an equivalent number of individuals working alone.20 In a meta‐analysis, Mullen et al21 found that interacting groups usually produced ideas of poorer quality than did nominal groups. Interpersonal interactions in a multidisciplinary team may be influenced by perceived roles and dominant personalities, and can impede a collaborative, critical discourse.22
In contrast, in NGT sessions, the weight of each member's opinion is the same, and it appears that process loss is less likely to occur.17 Moreover, the highly structured format of NGT provides an opportunity for group members to achieve a substantial amount of work in a relatively short time. Another advantage of NGT is the deliberate avoidance of interference or interpretation from a moderator or facilitator who, in the case of NGT, has the responsibility to explore but not interfere with or influence the members of the group.13 However, the NGT has some limitations. The composition and representativeness of participants may limit the generalizability of the findings. Also, it requires training and preparation, restricts the discussion to a single topic, and may not allow further elaboration of other ideas.13 Despite its potential benefits, NGT is relatively underutilized in quality improvement initiatives. To the best of our knowledge, this is the first study that has utilized NGT to elicit ideas about potential areas for pain control improvement. NGT is a good method for achieving local solutions to local problems; teams of healthcare providers should consider using NGT to address their own challenges and barriers.
In our study, timeliness, knowledge, and experience were considered the top priorities to improve pain management. Our findings are similar to a Canadian study, where delay of more than an hour to administer analgesia was considered one of the most important factors to provide good pain control management.23 Also our findings are coherent with a recent survey of 225 hospitals in the United Kingdom, where perceived lack of training was a highly ranked contributing factor for suboptimal postoperative pain management.24
Our study also identified other interesting observations that deserve comment. Examining the top priorities among the 3 services, there is some dissonance of reasoning underlying the inadequate pain control. We can speculate several reasons. First, pain control management, like any other condition, happens within a specific context with unique problems or barriers that prevent the delivery of the best care for each service. The other possible explanation is a silo effect. It is possible that workers of the same service represent a relatively homogenous social group despite differing training and backgrounds; they live the same experiences and face similar problems. Workers of one silo may work in parallel but do not interact with members of another silo, so they do not have opportunities to share their experiences or compare their beliefs. Finally, it is possible that the greater number of groups used in this study resulted in a broader array of issues. Studies have confirmed that the presence of several groups using NGT can produce a larger pool of issues, with more variation.16 Thus, the ideas generated in our NGT can be easily grouped into 2 broader categories: human factors (knowledge, experience, provider bias, and patient factors) and system factors (timeliness, communication, and pain assessment).
Our study has some limitations. The study was conducted in a single institution and in a limited number of inpatient units. The list of potential areas for improvement generated in this study may require further confirmation and validation at other institutions and with other sources of information (actual pain assessments, timeliness, knowledge, patient satisfaction). Importantly, the study design only involved healthcare providers and did not involve other stakeholders such as the patients or their families.
Despite these limitations, we propose that the NGT is a good alternative to unstructured brainstorming to systematically identify, characterize, categorize, and prioritize ideas behind inadequate pain management. The NGT is a valuable tool in conducting a robust formative assessment to better understand the multiple challenges, barriers, and perspectives of healthcare providers in guiding quality improvement interventions in a systematic and less biased manner.
CONCLUSIONS
In conclusion, healthcare workers have clear ideas about potential areas for improvement in pain management. Using the NGT, we identified 7 potential areas for improvement encompassed within human and system factors. Knowledge and timeliness emerged from 2 of the 3 clinical services as top priorities, whereas the third group identified disparate concerns suggesting provider bias and patient issues. We believe the nominal group technique is an efficient tool to uncover general and context‐specific priorities and to guide quality improvement work.
Pain is considered the fifth vital sign, and the appropriate management of pain is fundamental for patient care. Uncontrolled pain has adverse negative physiological consequences,14 and better pain control in hospitalized patients has been associated with decreased length of stay and improved recovery and physical comfort.36 However, many patients fail to receive state‐of‐the‐art pain relief7; for example, in a study of 176 hospitalized patients with cancer, 46% reported severe pain at the time of the interview.8 The prevalence of pain in hospitalized patients with other diagnoses besides cancer likewise remains high.9
Over the last 2 decades, the quality of care in pain management has gained increasing attention. In 2000, the Joint Commission unveiled an official statement for the purpose of improving the quality of pain management.10 The Joint Commission's 6 core principles include the right of pain assessment and treatment, institution of organizational procedures to assess pain, provision of care of persons with pain, general education, continuity of pain management after hospital discharge, and inclusion of pain management as a performance measure. Pain management is now a hospital accountability indicator. Although multiple initiatives have been undertaken to improve pain control, however, challenges still remain. Effective strategies for consensus development are still needed to prioritize interventions.
The nominal group technique (NGT) is a brainstorming tool for quality improvement; NGT is a highly structured small group discussion used to elicit and prioritize a list of answers to a specific question.1115 We conducted an NGT session to identify the multiple challenges, barriers, and perspectives of healthcare providers in managing pain among hospitalized patients. The ultimate goals were to identify potential areas for pain management improvement, build consensus among caregivers, and introduce the NGT as a tool to elicit caregivers' ideas for quality improvement.
METHODS
In a multistep process, we first identified areas for quality improvement interventions in pain management by using the NGT in hospitalized patients, then organized the information by using an iterative consensus development process, and finally displayed the main findings using a Fishbone diagram.
Setting and Participants
At a large university hospital, we targeted 3 inpatient services based on pain management performance data. We obtained the data from patient satisfaction and the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. They included 1 medical, 1 medical‐surgical, and 1 surgical hospital unit at a large academic medical center.
Within these units we recruited participants from a convenience sample of nurses, resident physicians, patient care technicians, and unit clerks. We included patient care technicians and unit clerks as they often interface between patients and providers. To maintain anonymity of the responses, we did not record participant composition during the session. Participation was voluntary and no incentives were provided. The institutional review board at the University of Alabama at Birmingham approved the use of existing quality improvement data.
Nominal Group Technique
During 2009, we conducted an NGT session within each of the 3 inpatient units. Two of the authors (MB, DS) developed the question posed to each group: What causes uncontrolled pain in your unit? The NGT supports equal participation, controls the extraneous discussion that frequently occurs when groups are convened, minimizes real or perceived power differentials among members, and, in the aggregate, minimizes the process loss that exists in unstructured focus group meetings.1116 Thus, the ideas generated by this process provide a valid reflection of the implicit prioritized views held by the group. The NGT also provides concise written documentation summarizing participants' responses, rendering audiotape recording and transcription unnecessary.13, 17
Each NGT session, lasting 1 hour, followed the following steps.13 First, after a brief introduction of the purpose of the session and general instructions, the moderators (MB, DS) posed the question: What causes uncontrolled pain in your unit? Second, in response to the standard question, each participant in the group silently and individually generated a list of ideas and wrote them down. Third, using a round‐robin approach (1 person at a time mentions the idea), each idea was concisely transcribed by the facilitator onto a flip‐chart for all participants to see; debate was not allowed during this step. Fourth, each recorded idea was then discussed for the sole purpose of clarification, and not for evaluation or argument as to the relative importance. The proposer of the idea did not need to defend the idea. During this step, participants were prompted to combine those ideas that were perceived to be substantively similar. Finally, during the voting phase, participants privately selected what they considered to be the 3 most important reasons for uncontrolled pain in their unit. Each participant prioritized their choices on their own and without discussing with other participants, giving a rank of 3 to the most important idea and 1 to the least important idea. The moderator recorded the votes onto the flip‐chart in front of all participants and then tallied the votes for each idea. We discarded a small number of idiosyncratic suggestions, which is a standard procedure in the nominal group technique. The main results were the top 5 suggestions identified within each group; the secondary results were all other suggestions. A more detailed description of the NGT steps is available elsewhere.11
Ishikawa (Fishbone) Diagram
Fishbone diagrams are designed to organize contributing factors to a particular outcome in a pictorial display. This is a common tool used to identify areas for improvement by facilitating brainstorming and graphically displaying the relationship of the causes to the effect. Through an iterative process, 3 of the authors (AP, MB, CAE) categorized all of the generated ideas into common themes until consensus was reached. The top 5 and all other suggestions within each service were organized into the Fishbone diagram.
RESULTS
The 27 health workers representing the 3 units completing the nominal group sessions generated a total of 94 ideas. The Fishbone diagram shown in Figure 1 shows each service's top 5 rankings of the elements perceived contributing most to uncontrolled pain; the elements were organized into 3 main factors and 7 priority themes identified during the iterative process.
The main categories illustrate system factors (timeliness, communication, pain assessment; Figure 1, top portion), human factors (knowledge and experience, provider bias, patient factors; Figure 1, bottom portion), and an interface between system and human factors (standardization; Figure 1, center left). The remaining 79 ideas, non‐top 5 for each unit, fell into the following priority themes: provider bias (n = 6), knowledge and experience (n = 12), pain assessment (n = 7), communication (n = 10), timeliness (n = 14), standardization (or policies and practice variation) (n = 13), and patient factors (n = 17); the ideas and representative examples are shown in Figure 2.
DISCUSSION
Using a brainstorming tool for idea generation (NGT) in quality improvement, we identified almost 100 causes of uncontrolled pain management in hospital units. We identified 7 priority themes along 3 main factors: system factors, human factors, and an interface of system and human factors. Timeliness and education emerged from 2 of the 3 services as top priorities, though they were unique and specific to the providers and patient populations within each service. The third service yielded surprisingly different priorities, with patient issues and provider bias foremost in the minds of the staff caring for these patients.
In the decade since To Err Is Human was released by the Institute of Medicine,18 healthcare improvement work has become commonplace and routine. Projects start by soliciting staff views about possible areas for improvement, usually during group meetings; however, this process is informal and not systematic. Unstructured group meetings and brainstorming have some limitations when used to uncover creative ideas for healthcare improvement.19 The literature has consistently reported that groups produce fewer ideas than an equivalent number of individuals working alone.20 In a meta‐analysis, Mullen et al21 found that interacting groups usually produced ideas of poorer quality than did nominal groups. Interpersonal interactions in a multidisciplinary team may be influenced by perceived roles and dominant personalities, and can impede a collaborative, critical discourse.22
In contrast, in NGT sessions, the weight of each member's opinion is the same, and it appears that process loss is less likely to occur.17 Moreover, the highly structured format of NGT provides an opportunity for group members to achieve a substantial amount of work in a relatively short time. Another advantage of NGT is the deliberate avoidance of interference or interpretation from a moderator or facilitator who, in the case of NGT, has the responsibility to explore but not interfere with or influence the members of the group.13 However, the NGT has some limitations. The composition and representativeness of participants may limit the generalizability of the findings. Also, it requires training and preparation, restricts the discussion to a single topic, and may not allow further elaboration of other ideas.13 Despite its potential benefits, NGT is relatively underutilized in quality improvement initiatives. To the best of our knowledge, this is the first study that has utilized NGT to elicit ideas about potential areas for pain control improvement. NGT is a good method for achieving local solutions to local problems; teams of healthcare providers should consider using NGT to address their own challenges and barriers.
In our study, timeliness, knowledge, and experience were considered the top priorities to improve pain management. Our findings are similar to a Canadian study, where delay of more than an hour to administer analgesia was considered one of the most important factors to provide good pain control management.23 Also our findings are coherent with a recent survey of 225 hospitals in the United Kingdom, where perceived lack of training was a highly ranked contributing factor for suboptimal postoperative pain management.24
Our study also identified other interesting observations that deserve comment. Examining the top priorities among the 3 services, there is some dissonance of reasoning underlying the inadequate pain control. We can speculate several reasons. First, pain control management, like any other condition, happens within a specific context with unique problems or barriers that prevent the delivery of the best care for each service. The other possible explanation is a silo effect. It is possible that workers of the same service represent a relatively homogenous social group despite differing training and backgrounds; they live the same experiences and face similar problems. Workers of one silo may work in parallel but do not interact with members of another silo, so they do not have opportunities to share their experiences or compare their beliefs. Finally, it is possible that the greater number of groups used in this study resulted in a broader array of issues. Studies have confirmed that the presence of several groups using NGT can produce a larger pool of issues, with more variation.16 Thus, the ideas generated in our NGT can be easily grouped into 2 broader categories: human factors (knowledge, experience, provider bias, and patient factors) and system factors (timeliness, communication, and pain assessment).
Our study has some limitations. The study was conducted in a single institution and in a limited number of inpatient units. The list of potential areas for improvement generated in this study may require further confirmation and validation at other institutions and with other sources of information (actual pain assessments, timeliness, knowledge, patient satisfaction). Importantly, the study design only involved healthcare providers and did not involve other stakeholders such as the patients or their families.
Despite these limitations, we propose that the NGT is a good alternative to unstructured brainstorming to systematically identify, characterize, categorize, and prioritize ideas behind inadequate pain management. The NGT is a valuable tool in conducting a robust formative assessment to better understand the multiple challenges, barriers, and perspectives of healthcare providers in guiding quality improvement interventions in a systematic and less biased manner.
CONCLUSIONS
In conclusion, healthcare workers have clear ideas about potential areas for improvement in pain management. Using the NGT, we identified 7 potential areas for improvement encompassed within human and system factors. Knowledge and timeliness emerged from 2 of the 3 clinical services as top priorities, whereas the third group identified disparate concerns suggesting provider bias and patient issues. We believe the nominal group technique is an efficient tool to uncover general and context‐specific priorities and to guide quality improvement work.
- .Success stories: how hospitals are improving care.Am Heart J.2004;148(5 suppl):S52–S55.
- ,.Acute pain.Lancet.1999;353(9169):2051–2058.
- ,,, et al.Improving the management of pain in hospitalized adults.Arch Intern Med.2006;166(9):1033–1039.
- ,,.Pain and satisfaction with pain control in hospitalized medical patients: no such thing as low risk.Arch Intern Med.2004;164(2):175–180.
- ,,,.Pain prevalence study in a large Canadian teaching hospital. Round 2: lessons learned?Pain Manag Nurs.2010;11(1):45–55.
- ,,,,.Pain prevalence study in a large Canadian teaching hospital.Pain Manag Nurs.2008;9(3):104–112.
- Institute of Medicine.Crossing the Quality Chasm: A New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- .Pain intensity and pain interference in hospitalized patients with cancer.Oncol Nurs Forum.2000;27(6):985–991.
- ,.Incidence and characteristics of pain in a sample of hospitalized cancer patients.Cancer Nurs.1987;10(2):85–92.
- .JCAHO pain management standards are unveiled. Joint Commission on Accreditation of Healthcare Organizations.JAMA.2000;284(4):428–429.
- ,,,,.A pilot study using nominal group technique to assess residents' perceptions of successful attending rounds.J Gen Intern Med.2008;23(7):1060–1065.
- ,,, et al.What should we include in a cultural competence curriculum? An emerging formative evaluation process to foster curriculum development.Acad Med.2011;86(3):333–341.
- Brief 7. Gaining Consensus Among Stakeholders Through the Nominal Group Technique. Available at: http://www.cdc.gov/HealthyYouth/evaluation/pdf/brief7.pdf. Accessed October 19,2011.
- ,.The nominal group as a research instrument for exploratory health studies.Am J Public Health.1972;62(3):337–342.
- ,,, et al.Reasons for not intensifying medications: differentiating “clinical inertia” from appropriate care.J Gen Intern Med.2007;22(12):1648–1655.
- ,,,.Nominal group technique: a process for identifying diabetes self‐care issues among patients and caregivers.Diabetes Educ.2000;26(2):305–310,312,314.
- ,,,,.The nominal group technique: a research tool for general practice?Fam Pract.1993;10(1):76–81.
- Institute of Medicine.To Err Is Human. Building a Safer Health System.Washington, DC:National Academy Press;2000.
- ,,.Quality by Design: A Clinical Microsystems Approach.San Francisco, CA:Jossey‐Bass Wiley;2007.
- ,.Group versus individual performance on tasks requiring ideational proficiency (brainstorming): a review.Eur J Soc Psychol.1973;3(4):361–388.
- ,,.Productivity loss in brainstorming groups: a meta‐analytic integration.Basic Appl Soc Psychol.1991;12:3–23.
- ,.Productivity loss in brainstorming groups: toward the solution of a riddle.J Pers Soc Psychol.1987;53:497–509.
- ,,.An interventional study to improve the quality of analgesia in the emergency department.CJEM.2008;10(5):435–439.
- ,,,.Pain assessment and management in medical wards: an area of unmet need.Postgrad Med J.2010;86(1015):279–284.
- .Success stories: how hospitals are improving care.Am Heart J.2004;148(5 suppl):S52–S55.
- ,.Acute pain.Lancet.1999;353(9169):2051–2058.
- ,,, et al.Improving the management of pain in hospitalized adults.Arch Intern Med.2006;166(9):1033–1039.
- ,,.Pain and satisfaction with pain control in hospitalized medical patients: no such thing as low risk.Arch Intern Med.2004;164(2):175–180.
- ,,,.Pain prevalence study in a large Canadian teaching hospital. Round 2: lessons learned?Pain Manag Nurs.2010;11(1):45–55.
- ,,,,.Pain prevalence study in a large Canadian teaching hospital.Pain Manag Nurs.2008;9(3):104–112.
- Institute of Medicine.Crossing the Quality Chasm: A New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- .Pain intensity and pain interference in hospitalized patients with cancer.Oncol Nurs Forum.2000;27(6):985–991.
- ,.Incidence and characteristics of pain in a sample of hospitalized cancer patients.Cancer Nurs.1987;10(2):85–92.
- .JCAHO pain management standards are unveiled. Joint Commission on Accreditation of Healthcare Organizations.JAMA.2000;284(4):428–429.
- ,,,,.A pilot study using nominal group technique to assess residents' perceptions of successful attending rounds.J Gen Intern Med.2008;23(7):1060–1065.
- ,,, et al.What should we include in a cultural competence curriculum? An emerging formative evaluation process to foster curriculum development.Acad Med.2011;86(3):333–341.
- Brief 7. Gaining Consensus Among Stakeholders Through the Nominal Group Technique. Available at: http://www.cdc.gov/HealthyYouth/evaluation/pdf/brief7.pdf. Accessed October 19,2011.
- ,.The nominal group as a research instrument for exploratory health studies.Am J Public Health.1972;62(3):337–342.
- ,,, et al.Reasons for not intensifying medications: differentiating “clinical inertia” from appropriate care.J Gen Intern Med.2007;22(12):1648–1655.
- ,,,.Nominal group technique: a process for identifying diabetes self‐care issues among patients and caregivers.Diabetes Educ.2000;26(2):305–310,312,314.
- ,,,,.The nominal group technique: a research tool for general practice?Fam Pract.1993;10(1):76–81.
- Institute of Medicine.To Err Is Human. Building a Safer Health System.Washington, DC:National Academy Press;2000.
- ,,.Quality by Design: A Clinical Microsystems Approach.San Francisco, CA:Jossey‐Bass Wiley;2007.
- ,.Group versus individual performance on tasks requiring ideational proficiency (brainstorming): a review.Eur J Soc Psychol.1973;3(4):361–388.
- ,,.Productivity loss in brainstorming groups: a meta‐analytic integration.Basic Appl Soc Psychol.1991;12:3–23.
- ,.Productivity loss in brainstorming groups: toward the solution of a riddle.J Pers Soc Psychol.1987;53:497–509.
- ,,.An interventional study to improve the quality of analgesia in the emergency department.CJEM.2008;10(5):435–439.
- ,,,.Pain assessment and management in medical wards: an area of unmet need.Postgrad Med J.2010;86(1015):279–284.
Copyright © 2011 Society of Hospital Medicine
Inappropriate Prescribing of PPIs
Proton pump inhibitors (PPIs) are the third most commonly prescribed class of medication in the United States, with $13.6 billion in yearly sales.1 Despite their effectiveness in treating acid reflux2 and their mortality benefit in the treatment of patients with gastrointestinal bleeding,3 recent literature has identified a number of risks associated with PPIs, including an increased incidence of Clostridium difficile infection,4 decreased effectiveness of clopidogrel in patients with acute coronary syndrome,5 increased risk of community‐ and hospital‐acquired pneumonia, and an increased risk of hip fracture.69 Additionally, in March of 2011, the US Food and Drug Administration (FDA) issued a warning regarding the potential for PPIs to cause low magnesium levels which can, in turn, cause muscle spasms, an irregular heartbeat, and convulsions.10
Inappropriate PPI prescription practice has been demonstrated in the primary care setting,11 as well as in small studies conducted in the hospital setting.1216 We hypothesized that many hospitalized patients receive these medications without having an accepted indication, and examined 2 populations of hospitalized patients, including administrative data from 6.5 million discharges from US university hospitals, to look for appropriate diagnoses justifying their use.
METHODS
We performed a retrospective review of administrative data collected between January 1, 2008 and December 31, 2009 from 2 patient populations: (a) those discharged from Denver Health (DH), a university‐affiliated public safety net hospital in Denver, CO; and (b) patients discharged from 112 academic health centers and 256 of their affiliated hospitals that participate in the University HealthSystem Consortium (UHC). The Colorado Multiple Institution Review Board reviewed and approved the conduct of this study.
Inclusion criteria for both populations were age >18 or <90 years, and hospitalization on a Medicine service. Prisoners and women known to be pregnant were excluded. In both cohorts, if patients had more than 1 admission during the 2‐year study period, only data from the first admission were used.
We recorded demographics, admitting diagnosis, and discharge diagnoses together with information pertaining to the name, route, and duration of administration of all PPIs (ie, omeprazole, lansoprazole, esomeprazole, pantoprazole, rabeprazole). We created a broadly inclusive set of valid indications for PPIs by incorporating diagnoses that could be identified by International Classification of Diseases, Ninth Revision.
(ICD‐9) codes from a number of previously published sources including the National Institute of Clinical Excellence (NICE) guidelines issued by the National Health Service (NHS) of the United Kingdom in 200012, 1721 (Table 1).
| Indication | ICD‐9 Code |
|---|---|
| |
| Helicobacter pylori | 041.86 |
| Abnormality of secretion of gastrin | 251.5 |
| Esophageal varices with bleeding | 456.0 |
| Esophageal varices without mention of bleeding | 456.1 |
| Esophageal varices in diseases classified elsewhere | 456.2 |
| Esophagitis | 530.10530.19 |
| Perforation of esophagus | 530.4 |
| Gastroesophageal laceration‐hemorrhage syndrome | 530.7 |
| Esophageal reflux | 530.81 |
| Barrett's esophagus | 530.85 |
| Gastric ulcer | 531.0031.91 |
| Duodenal ulcer | 532.00532.91 |
| Peptic ulcer, site unspecified | 533.00533.91 |
| Gastritis and duodenitis | 535.00535.71 |
| Gastroparesis | 536.3 |
| Dyspepsia and other specified disorders of function of stomach | 536.8 |
| Hemorrhage of gastrointestinal tract, unspecified | 578.9 |
To assess the accuracy of the administrative data from DH, we also reviewed the Emergency Department histories, admission histories, progress notes, electronic pharmacy records, endoscopy reports, and discharge summaries of 123 patients randomly selected (ie, a 5% sample) from the group of patients identified by administrative data to have received a PPI without a valid indication, looking for any accepted indication that might have been missed in the administrative data.
All analyses were performed using SAS Enterprise Guide 4.1 (SAS Institute, Cary, NC). A Student t test was used to compare continuous variables and a chi‐square test was used to compare categorical variables. Bonferroni corrections were used for multiple comparisons, such that P values less than 0.01 were considered to be significant for categorical variables.
RESULTS
Inclusion criteria were met by 9875 patients in the Denver Health database and 6,592,100 patients in the UHC database. The demographics and primary discharge diagnoses for these patients are summarized in Table 2.
| DH (N = 9875) | UHC (N = 6,592,100) | ||||
|---|---|---|---|---|---|
| Received a PPI | No PPI | Received a PPI | No PPI | ||
| |||||
| No. (%) | 3962 (40) | 5913 (60) | 918,474 (14) | 5,673,626 (86) | |
| Age (mean SD) | 53 15 | 51 16 | 59 17 | 55 18 | |
| Gender (% male) | 2197 (55) | 3438 (58) | 464,552 (51) | 2,882,577 (51) | |
| Race (% white) | 1610 (41) | 2425 (41) | 619,571 (67) | 3,670,450 (65) | |
| Top 5 primary discharge diagnoses | |||||
| Chest pain | 229 (6) | 462 (8) | Coronary atherosclerosis | 35,470 (4) | 186,321 (3) |
| Alcohol withdrawal | 147 (4) | 174 (3) | Acute myocardial infarction | 26,507 (3) | 132,159 (2) |
| Pneumonia, organism unspecified | 142 (4) | 262 (4) | Heart failure | 21,143 (2) | 103,751 (2) |
| Acute pancreatitis | 132 (3) | 106 (2) | Septicemia | 20,345 (2) | 64,915 (1) |
| Obstructive chronic bronchitis with (acute) exacerbation | 89 (2) | 154 (3) | Chest pain | 16,936 (2) | 107,497 (2) |
Only 39% and 27% of the patients in the DH and UHC databases, respectively, had a valid indication for PPIs on the basis of discharge diagnoses (Table 3). In the DH data, if admission ICD‐9 codes were also inspected for valid PPI indications, 1579 (40%) of patients receiving PPIs had a valid indication (admission ICD‐9 codes were not available for patients in the UHC database). Thirty‐one percent of Denver Health patients spent time in the intensive care unit (ICU) during their hospital stay and 65% of those patients received a PPI without a valid indication, as compared to 59% of patients who remained on the General Medicine ward (Table 3).
| DH (N = 9875) | UHC (N = 6,592,100) | |
|---|---|---|
| ||
| Patients receiving PPIs (% of total) | 3962 (40) | 918,474 (14) |
| Any ICU stay, N (% of all patients) | 1238 (31) | |
| General Medicine ward only, N (% of all patients) | 2724 (69) | |
| Patients with indication for PPI (% of all patients receiving PPIs)* | 1540 (39) | 247,142 (27) |
| Any ICU stay, N (% of all ICU patients) | 434 (35) | |
| General Medicine ward only, N (% of all ward patients) | 1106 (41) | |
| Patients without indication for PPI (% of those receiving PPIs)* | 2422 (61) | 671,332 (73) |
| Any ICU stay, N (% of all ICU patients) | 804 (65) | |
| General Medicine ward only, N (% of all ward patients) | 1618 (59) | |
Higher rates of concurrent C. difficile infections were observed in patients receiving PPIs in both databases; a higher rate of concurrent diagnosis of pneumonia was seen in patients receiving PPIs in the UHC population, with a nonsignificant trend towards the same finding in DH patients (Table 4).
| Denver Health | UHC | |||||
|---|---|---|---|---|---|---|
| Concurrent diagnosis | (+) PPI 3962 | () PPI 5913 | P | (+) PPI 918,474 | () PPI 5,673,626 | P |
| ||||||
| C. difficile | 46 (1.16) | 26 (0.44) | <0.0001 | 12,113 (1.32) | 175 (0.0031) | <0.0001 |
| Pneumonia | 400 (10.1) | 517 (8.7) | 0.0232 | 75,274 (8.2) | 300,557 (5.3) | <0.0001 |
Chart review in the DH population found valid indications for PPIs in 19% of patients who were thought not have a valid indication on the basis of the administrative data (Table 5). For 56% of those in whom no valid indication was confirmed, physicians identified prophylaxis as the justification.
| Characteristic | N (%) |
|---|---|
| |
| Valid indication found on chart review only | 23 (19) |
| No valid indication after chart review | 100 (81) |
| Written indication: prophylaxis | 56 (56) |
| No written documentation of indication present in the chart | 33 (33) |
| Written indication: continue home medication | 9 (9) |
| Intubated with or without written indication of prophylaxis | 16 (16) |
DISCUSSION
The important finding of this study was that the majority of patients in 2 large groups of Medicine patients hospitalized in university‐affiliated hospitals received PPIs without having a valid indication. To our knowledge, the more than 900,000 UHC patients who received a PPI during their hospitalization represent the largest inpatient population evaluated for appropriateness of PPI prescriptions.
Our finding that 41% of the patients admitted to the DH Medicine service received a PPI during their hospital stay is similar to what has been observed by others.9, 14, 22 The rate of PPI prescription was lower in the UHC population (14%) for unclear reasons. By our definition, 61% lacked an adequate diagnosis to justify the prescription of the PPI. After performing a chart review on a randomly selected 5% of these records, we found that the DH administrative database had failed to identify 19% of patients who had a valid indication for receiving a PPI. Adjusting the administrative data accordingly still resulted in 50% of DH patients not having a valid indication for receiving a PPI. This is consistent with the 54% recorded by Batuwitage and colleagues11 in the outpatient setting by direct chart review, as well as a range of 60%‐75% for hospitalized patients in other studies.12, 13, 15, 23, 24
Stomach acidity is believed to provide an important host defense against lower gastrointestinal tract infections including Salmonella, Campylobacter, and Clostridium difficile.25 A recent study by Howell et al26 showed a doseresponse effect between PPI use and C. difficile infection, supporting a causal connection between loss of stomach acidity and development of Clostridium difficile‐associated diarrhea (CDAD). We found that C. difficile infection was more common in both populations of patients receiving PPIs (although the relative risk was much higher in the UHC database) (Table 5). The rate of CDAD in DH patients who received PPIs was 2.6 times higher than in patients who did not receive these acid suppressive agents.
The role of acid suppression in increasing risk for community‐acquired pneumonia is not entirely clear. Theories regarding the loss of an important host defense and bacterial proliferation head the list.6, 8, 27 Gastric and duodenal bacterial overgrowth is significantly more common in patients receiving PPIs than in patients receiving histamine type‐2 (H2) blockers.28 Previous studies have identified an increased rate of hospital‐acquired pneumonia and recurrent community‐acquired pneumonia27 in patients receiving any form of acid suppression therapy, but the risk appears to be greater in patients receiving PPIs than in those receiving H2 receptor antagonists (H2RAs).9 Significantly more patients in the UHC population who were taking PPIs had a concurrent diagnosis of pneumonia, consistent with previous studies alerting to this association6, 8, 9, 27 and consistent with the nonsignificant trend observed in the DH population.
Our study has a number of limitations. Our database comes from a single university‐affiliated public hospital with residents and hospitalists writing orders for all medications. The hospitals in the UHC are also teaching hospitals. Accordingly, our results might not generalize to other settings or reflect prescribing patterns in private, nonteaching hospital environments. Because our study was retrospective, we could not confirm the decision‐making process supporting the prescription of PPIs. Similarly, we could not temporarily relate the existence of the indication with the time the PPI was prescribed. Our list of appropriate indications for prescribing PPIs was developed by reviewing a number of references, and other studies have used slightly different lists (albeit the more commonly recognized indications are the same), but it may be argued that the list either includes or misses diagnoses in error.
While there is considerable debate about the use of PPIs for stress ulcer prophylaxis,29 we specifically chose not to include this as one of our valid indications for PPIs for 4 reasons. First, the American Society of Health‐System Pharmacists (ASHP) Report does not recommend prophylaxis for non‐ICU patients, and only recommends prophylaxis for those ICU patients with a coagulopathy, those requiring mechanical ventilation for more than 48 hours, those with a history of gastrointestinal ulceration or bleeding in the year prior to admission, and those with 2 or more of the following indications: sepsis, ICU stay >1 week, occult bleeding lasting 6 or more days, receiving high‐dose corticosteroids, and selected surgical situations.30 At the time the guideline was written, the authors note that there was insufficient data on PPIs to make any recommendations on their use, but no subsequent guidelines have been issued.30 Second, a review by Mohebbi and Hesch published in 2009, and a meta‐analysis by Lin and colleagues published in 2010, summarize subsequent randomized trials that suggest that PPIs and H2 blockers are, at best, similarly effective at preventing upper gastrointestinal (GI) bleeding among critically ill patients.31, 32 Third, the NICE guidelines do not include stress ulcer prophylaxis as an appropriate indication for PPIs except in the prevention and treatment of NSAID [non‐steroidal anti‐inflammatory drug]‐associated ulcers.19 Finally, H2RAs are currently the only medications with an FDA‐approved indication for stress ulcer prophylaxis. We acknowledge that PPIs may be a reasonable and acceptable choice for stress ulcer prophylaxis in patients who meet indications, but we were unable to identify such patients in either of our administrative databases.
In our Denver Health population, only 31% of our patients spent any time in the intensive care unit, and only a fraction of these would have both an accepted indication for stress ulcer prophylaxis by the ASHP guidelines and an intolerance or contraindication to an H2RA or sulcralfate. While our administrative database lacked the detail necessary to identify this small group of patients, the number of patients who might have been misclassified as not having a valid PPI indication was likely very small. Similar to the findings of previous studies,15, 18, 23, 29 prophylaxis against gastrointestinal bleeding was the stated justification for prescribing the PPI in 56% of the DH patient charts reviewed. It is impossible for us to estimate the number of patients in our administrative database for whom stress ulcer prophylaxis was justified by existing guidelines, as it would be necessary to gather a number of specific clinical details for each patient including: 1) ICU stay; 2) presence of coagulopathy; 3) duration of mechanical ventilation; 4) presence of sepsis; 5) duration of ICU stay; 6) presence of occult bleeding for >6 days; and 7) use of high‐dose corticosteroids. This level of clinical detail would likely only be available through a prospective study design, as has been suggested by other authors.33 Further research into the use, safety, and effectiveness of PPIs specifically for stress ulcer prophylaxis is warranted.
In conclusion, we found that 73% of nearly 1 million Medicine patients discharged from academic medical centers received a PPI without a valid indication during their hospitalization. The implications of our findings are broad. PPIs are more expensive31 than H2RAs and there is increasing evidence that they have significant side effects. In both databases we examined, the rate of C. difficile infection was higher in patients receiving PPIs than others. The prescribing habits of physicians in these university hospital settings appear to be far out of line with published guidelines and evidence‐based practice. Reducing inappropriate prescribing of PPIs would be an important educational and quality assurance project in most institutions.
- IMS Health Web site. Available at: http://www.imshealth.com/deployedfiles/ims/Global/Content/Corporate/Press%20Room/Top‐line%20Market%20Data/2009%20Top‐line%20Market%20Data/Top%20Therapy%20Classes%20by%20U.S.Sales.pdf. Accessed May 1,2011.
- ,, , et al.Comparison of omeprazole and cimetidine in reflux oesophagitis: symptomatic, endoscopic, and histological evaluations.Gut.1990;31(9):968–972.
- ,,, et al.Omeprazole before endoscopy in patients with gastrointestinal bleeding.N Engl J Med.2007;356(16):1631–1640.
- ,,,.Use of gastric acid‐suppressive agents and the risk of community‐acquired Clostridium difficile‐associated disease.JAMA.2005;294(23):2989–2995.
- ,,, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome.JAMA.2009;301(9):937–944.
- ,,,,,.Risk of community‐acquired pneumonia and use of gastric acid‐suppressive drugs.JAMA.2004;292(16):1955–1960.
- ,,,.Long‐term proton pump inhibitor therapy and risk of hip fracture.JAMA2006;296(24):2947–2953.
- ,,,,,.Use of proton pump inhibitors and the risk of community‐acquired pneumonia: a population‐based case‐control study.Arch Intern Med.2007;167(9):950–955.
- ,,,.Acid‐suppressive medication use and the risk for hospital‐acquired pneumonia.JAMA.2009;301(20):2120–2128.
- US Food and Drug Administration (FDA) Website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsfor HumanMedicalProducts/ucm245275.htm. Accessed March 2,2011.
- ,,,.Inappropriate prescribing of proton pump inhibitors in primary care.Postgrad Med J.2007;83(975):66–68.
- ,.Stress ulcer prophylaxis in hospitalized patients not in intensive care units.Am J Health Syst Pharm.2007;64(13):1396–1400.
- ,,,.Predictors of inappropriate utilization of intravenous proton pump inhibitors.Aliment Pharmacol Ther.2007;25(5):609–615.
- ,,.Overuse of acid‐suppressive therapy in hospitalized patients.Am J Gastroenterol.2000;95(11):3118–3122.
- ,,,,,.Patterns and predictors of proton pump inhibitor overuse among academic and non‐academic hospitalists.Intern Med2010;49(23):2561–2568.
- ,,, et al.Hospital use of acid‐suppressive medications and its fall‐out on prescribing in general practice: a 1‐month survey.Aliment Pharmacol Ther.2003;17(12):1503–1506.
- ,,.Overuse and inappropriate prescribing of proton pump inhibitors in patients with Clostridium difficile‐associated disease.QJM.2008;101(6):445–448.
- ,,,.Acid suppressive therapy use on an inpatient internal medicine service.Ann Pharmacother.2006;40(7–8):1261–1266.
- National Institute of Clinical Excellence (NICE), National Health Service (NHS), Dyspepsia: Management of dyspepsia in adults in primary care. Web site. Available at: http://www.nice.org.uk/nicemedia/live/10950/29460/29460.pdf. Accessed May 1,2011.
- ,,.When should stress ulcer prophylaxis be used in the ICU?Curr Opin Crit Care.2009;15(2):139–143.
- ,.An evaluation of the use of proton pump inhibitors.Pharm World Sci2001;23(3):116–117.
- ,,.Overuse of proton pump inhibitors.J Clin Pharm Ther.2000;25(5):333–340.
- ,,,.Pattern of intravenous proton pump inhibitors use in ICU and non‐ICU setting: a prospective observational study.Saudi J Gastroenterol.2010;16(4):275–279.
- ,,, et al.Overuse of PPIs in patients at admission, during treatment, and at discharge in a tertiary Spanish hospital.Curr Clin Pharmacol.2010;5(4):288–297.
- ,,.Systematic review of the risk of enteric infection in patients taking acid suppression.Am J Gastroenterol.2007;102(9):2047–2056.
- ,,, et al.Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection.Arch Intern Med.2010;170(9):784–790.
- ,,,,.Recurrent community‐acquired pneumonia in patients starting acid‐suppressing drugs.Am J Med.2010;123(1):47–53.
- ,,, et al.Bacterial overgrowth during treatment with omeprazole compared with cimetidine: a prospective randomised double blind study.Gut.1996;39(1):54–59.
- ,,,.Why do physicians prescribe stress ulcer prophylaxis to general medicine patients?South Med J2010;103(11):1103–1110.
- ASHP therapeutic guidelines on stress ulcer prophylaxis.ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998.Am J Health Syst Pharm.1999;56(4):347–379.
- ,.Stress ulcer prophylaxis in the intensive care unit.Proc (Bayl Univ Med Cent).2009;22(4):373–376.
- ,,,,.The efficacy and safety of proton pump inhibitors vs histamine‐2 receptor antagonists for stress ulcer bleeding prophylaxis among critical care patients: a meta‐analysis.Crit Care Med.2010;38(4):1197–1205.
- ,,.Proton pump inhibitors for the prevention of stress‐related mucosal disease in critically‐ill patients: a meta‐analysis.J Med Assoc Thai.2009;92(5):632–637.
- ,,,.Proton pump inhibitors for prophylaxis of nosocomial upper gastrointestinal tract bleeding: effect of standardized guidelines on prescribing practice.Arch Intern Med.2010;170(9):779–783.
Proton pump inhibitors (PPIs) are the third most commonly prescribed class of medication in the United States, with $13.6 billion in yearly sales.1 Despite their effectiveness in treating acid reflux2 and their mortality benefit in the treatment of patients with gastrointestinal bleeding,3 recent literature has identified a number of risks associated with PPIs, including an increased incidence of Clostridium difficile infection,4 decreased effectiveness of clopidogrel in patients with acute coronary syndrome,5 increased risk of community‐ and hospital‐acquired pneumonia, and an increased risk of hip fracture.69 Additionally, in March of 2011, the US Food and Drug Administration (FDA) issued a warning regarding the potential for PPIs to cause low magnesium levels which can, in turn, cause muscle spasms, an irregular heartbeat, and convulsions.10
Inappropriate PPI prescription practice has been demonstrated in the primary care setting,11 as well as in small studies conducted in the hospital setting.1216 We hypothesized that many hospitalized patients receive these medications without having an accepted indication, and examined 2 populations of hospitalized patients, including administrative data from 6.5 million discharges from US university hospitals, to look for appropriate diagnoses justifying their use.
METHODS
We performed a retrospective review of administrative data collected between January 1, 2008 and December 31, 2009 from 2 patient populations: (a) those discharged from Denver Health (DH), a university‐affiliated public safety net hospital in Denver, CO; and (b) patients discharged from 112 academic health centers and 256 of their affiliated hospitals that participate in the University HealthSystem Consortium (UHC). The Colorado Multiple Institution Review Board reviewed and approved the conduct of this study.
Inclusion criteria for both populations were age >18 or <90 years, and hospitalization on a Medicine service. Prisoners and women known to be pregnant were excluded. In both cohorts, if patients had more than 1 admission during the 2‐year study period, only data from the first admission were used.
We recorded demographics, admitting diagnosis, and discharge diagnoses together with information pertaining to the name, route, and duration of administration of all PPIs (ie, omeprazole, lansoprazole, esomeprazole, pantoprazole, rabeprazole). We created a broadly inclusive set of valid indications for PPIs by incorporating diagnoses that could be identified by International Classification of Diseases, Ninth Revision.
(ICD‐9) codes from a number of previously published sources including the National Institute of Clinical Excellence (NICE) guidelines issued by the National Health Service (NHS) of the United Kingdom in 200012, 1721 (Table 1).
| Indication | ICD‐9 Code |
|---|---|
| |
| Helicobacter pylori | 041.86 |
| Abnormality of secretion of gastrin | 251.5 |
| Esophageal varices with bleeding | 456.0 |
| Esophageal varices without mention of bleeding | 456.1 |
| Esophageal varices in diseases classified elsewhere | 456.2 |
| Esophagitis | 530.10530.19 |
| Perforation of esophagus | 530.4 |
| Gastroesophageal laceration‐hemorrhage syndrome | 530.7 |
| Esophageal reflux | 530.81 |
| Barrett's esophagus | 530.85 |
| Gastric ulcer | 531.0031.91 |
| Duodenal ulcer | 532.00532.91 |
| Peptic ulcer, site unspecified | 533.00533.91 |
| Gastritis and duodenitis | 535.00535.71 |
| Gastroparesis | 536.3 |
| Dyspepsia and other specified disorders of function of stomach | 536.8 |
| Hemorrhage of gastrointestinal tract, unspecified | 578.9 |
To assess the accuracy of the administrative data from DH, we also reviewed the Emergency Department histories, admission histories, progress notes, electronic pharmacy records, endoscopy reports, and discharge summaries of 123 patients randomly selected (ie, a 5% sample) from the group of patients identified by administrative data to have received a PPI without a valid indication, looking for any accepted indication that might have been missed in the administrative data.
All analyses were performed using SAS Enterprise Guide 4.1 (SAS Institute, Cary, NC). A Student t test was used to compare continuous variables and a chi‐square test was used to compare categorical variables. Bonferroni corrections were used for multiple comparisons, such that P values less than 0.01 were considered to be significant for categorical variables.
RESULTS
Inclusion criteria were met by 9875 patients in the Denver Health database and 6,592,100 patients in the UHC database. The demographics and primary discharge diagnoses for these patients are summarized in Table 2.
| DH (N = 9875) | UHC (N = 6,592,100) | ||||
|---|---|---|---|---|---|
| Received a PPI | No PPI | Received a PPI | No PPI | ||
| |||||
| No. (%) | 3962 (40) | 5913 (60) | 918,474 (14) | 5,673,626 (86) | |
| Age (mean SD) | 53 15 | 51 16 | 59 17 | 55 18 | |
| Gender (% male) | 2197 (55) | 3438 (58) | 464,552 (51) | 2,882,577 (51) | |
| Race (% white) | 1610 (41) | 2425 (41) | 619,571 (67) | 3,670,450 (65) | |
| Top 5 primary discharge diagnoses | |||||
| Chest pain | 229 (6) | 462 (8) | Coronary atherosclerosis | 35,470 (4) | 186,321 (3) |
| Alcohol withdrawal | 147 (4) | 174 (3) | Acute myocardial infarction | 26,507 (3) | 132,159 (2) |
| Pneumonia, organism unspecified | 142 (4) | 262 (4) | Heart failure | 21,143 (2) | 103,751 (2) |
| Acute pancreatitis | 132 (3) | 106 (2) | Septicemia | 20,345 (2) | 64,915 (1) |
| Obstructive chronic bronchitis with (acute) exacerbation | 89 (2) | 154 (3) | Chest pain | 16,936 (2) | 107,497 (2) |
Only 39% and 27% of the patients in the DH and UHC databases, respectively, had a valid indication for PPIs on the basis of discharge diagnoses (Table 3). In the DH data, if admission ICD‐9 codes were also inspected for valid PPI indications, 1579 (40%) of patients receiving PPIs had a valid indication (admission ICD‐9 codes were not available for patients in the UHC database). Thirty‐one percent of Denver Health patients spent time in the intensive care unit (ICU) during their hospital stay and 65% of those patients received a PPI without a valid indication, as compared to 59% of patients who remained on the General Medicine ward (Table 3).
| DH (N = 9875) | UHC (N = 6,592,100) | |
|---|---|---|
| ||
| Patients receiving PPIs (% of total) | 3962 (40) | 918,474 (14) |
| Any ICU stay, N (% of all patients) | 1238 (31) | |
| General Medicine ward only, N (% of all patients) | 2724 (69) | |
| Patients with indication for PPI (% of all patients receiving PPIs)* | 1540 (39) | 247,142 (27) |
| Any ICU stay, N (% of all ICU patients) | 434 (35) | |
| General Medicine ward only, N (% of all ward patients) | 1106 (41) | |
| Patients without indication for PPI (% of those receiving PPIs)* | 2422 (61) | 671,332 (73) |
| Any ICU stay, N (% of all ICU patients) | 804 (65) | |
| General Medicine ward only, N (% of all ward patients) | 1618 (59) | |
Higher rates of concurrent C. difficile infections were observed in patients receiving PPIs in both databases; a higher rate of concurrent diagnosis of pneumonia was seen in patients receiving PPIs in the UHC population, with a nonsignificant trend towards the same finding in DH patients (Table 4).
| Denver Health | UHC | |||||
|---|---|---|---|---|---|---|
| Concurrent diagnosis | (+) PPI 3962 | () PPI 5913 | P | (+) PPI 918,474 | () PPI 5,673,626 | P |
| ||||||
| C. difficile | 46 (1.16) | 26 (0.44) | <0.0001 | 12,113 (1.32) | 175 (0.0031) | <0.0001 |
| Pneumonia | 400 (10.1) | 517 (8.7) | 0.0232 | 75,274 (8.2) | 300,557 (5.3) | <0.0001 |
Chart review in the DH population found valid indications for PPIs in 19% of patients who were thought not have a valid indication on the basis of the administrative data (Table 5). For 56% of those in whom no valid indication was confirmed, physicians identified prophylaxis as the justification.
| Characteristic | N (%) |
|---|---|
| |
| Valid indication found on chart review only | 23 (19) |
| No valid indication after chart review | 100 (81) |
| Written indication: prophylaxis | 56 (56) |
| No written documentation of indication present in the chart | 33 (33) |
| Written indication: continue home medication | 9 (9) |
| Intubated with or without written indication of prophylaxis | 16 (16) |
DISCUSSION
The important finding of this study was that the majority of patients in 2 large groups of Medicine patients hospitalized in university‐affiliated hospitals received PPIs without having a valid indication. To our knowledge, the more than 900,000 UHC patients who received a PPI during their hospitalization represent the largest inpatient population evaluated for appropriateness of PPI prescriptions.
Our finding that 41% of the patients admitted to the DH Medicine service received a PPI during their hospital stay is similar to what has been observed by others.9, 14, 22 The rate of PPI prescription was lower in the UHC population (14%) for unclear reasons. By our definition, 61% lacked an adequate diagnosis to justify the prescription of the PPI. After performing a chart review on a randomly selected 5% of these records, we found that the DH administrative database had failed to identify 19% of patients who had a valid indication for receiving a PPI. Adjusting the administrative data accordingly still resulted in 50% of DH patients not having a valid indication for receiving a PPI. This is consistent with the 54% recorded by Batuwitage and colleagues11 in the outpatient setting by direct chart review, as well as a range of 60%‐75% for hospitalized patients in other studies.12, 13, 15, 23, 24
Stomach acidity is believed to provide an important host defense against lower gastrointestinal tract infections including Salmonella, Campylobacter, and Clostridium difficile.25 A recent study by Howell et al26 showed a doseresponse effect between PPI use and C. difficile infection, supporting a causal connection between loss of stomach acidity and development of Clostridium difficile‐associated diarrhea (CDAD). We found that C. difficile infection was more common in both populations of patients receiving PPIs (although the relative risk was much higher in the UHC database) (Table 5). The rate of CDAD in DH patients who received PPIs was 2.6 times higher than in patients who did not receive these acid suppressive agents.
The role of acid suppression in increasing risk for community‐acquired pneumonia is not entirely clear. Theories regarding the loss of an important host defense and bacterial proliferation head the list.6, 8, 27 Gastric and duodenal bacterial overgrowth is significantly more common in patients receiving PPIs than in patients receiving histamine type‐2 (H2) blockers.28 Previous studies have identified an increased rate of hospital‐acquired pneumonia and recurrent community‐acquired pneumonia27 in patients receiving any form of acid suppression therapy, but the risk appears to be greater in patients receiving PPIs than in those receiving H2 receptor antagonists (H2RAs).9 Significantly more patients in the UHC population who were taking PPIs had a concurrent diagnosis of pneumonia, consistent with previous studies alerting to this association6, 8, 9, 27 and consistent with the nonsignificant trend observed in the DH population.
Our study has a number of limitations. Our database comes from a single university‐affiliated public hospital with residents and hospitalists writing orders for all medications. The hospitals in the UHC are also teaching hospitals. Accordingly, our results might not generalize to other settings or reflect prescribing patterns in private, nonteaching hospital environments. Because our study was retrospective, we could not confirm the decision‐making process supporting the prescription of PPIs. Similarly, we could not temporarily relate the existence of the indication with the time the PPI was prescribed. Our list of appropriate indications for prescribing PPIs was developed by reviewing a number of references, and other studies have used slightly different lists (albeit the more commonly recognized indications are the same), but it may be argued that the list either includes or misses diagnoses in error.
While there is considerable debate about the use of PPIs for stress ulcer prophylaxis,29 we specifically chose not to include this as one of our valid indications for PPIs for 4 reasons. First, the American Society of Health‐System Pharmacists (ASHP) Report does not recommend prophylaxis for non‐ICU patients, and only recommends prophylaxis for those ICU patients with a coagulopathy, those requiring mechanical ventilation for more than 48 hours, those with a history of gastrointestinal ulceration or bleeding in the year prior to admission, and those with 2 or more of the following indications: sepsis, ICU stay >1 week, occult bleeding lasting 6 or more days, receiving high‐dose corticosteroids, and selected surgical situations.30 At the time the guideline was written, the authors note that there was insufficient data on PPIs to make any recommendations on their use, but no subsequent guidelines have been issued.30 Second, a review by Mohebbi and Hesch published in 2009, and a meta‐analysis by Lin and colleagues published in 2010, summarize subsequent randomized trials that suggest that PPIs and H2 blockers are, at best, similarly effective at preventing upper gastrointestinal (GI) bleeding among critically ill patients.31, 32 Third, the NICE guidelines do not include stress ulcer prophylaxis as an appropriate indication for PPIs except in the prevention and treatment of NSAID [non‐steroidal anti‐inflammatory drug]‐associated ulcers.19 Finally, H2RAs are currently the only medications with an FDA‐approved indication for stress ulcer prophylaxis. We acknowledge that PPIs may be a reasonable and acceptable choice for stress ulcer prophylaxis in patients who meet indications, but we were unable to identify such patients in either of our administrative databases.
In our Denver Health population, only 31% of our patients spent any time in the intensive care unit, and only a fraction of these would have both an accepted indication for stress ulcer prophylaxis by the ASHP guidelines and an intolerance or contraindication to an H2RA or sulcralfate. While our administrative database lacked the detail necessary to identify this small group of patients, the number of patients who might have been misclassified as not having a valid PPI indication was likely very small. Similar to the findings of previous studies,15, 18, 23, 29 prophylaxis against gastrointestinal bleeding was the stated justification for prescribing the PPI in 56% of the DH patient charts reviewed. It is impossible for us to estimate the number of patients in our administrative database for whom stress ulcer prophylaxis was justified by existing guidelines, as it would be necessary to gather a number of specific clinical details for each patient including: 1) ICU stay; 2) presence of coagulopathy; 3) duration of mechanical ventilation; 4) presence of sepsis; 5) duration of ICU stay; 6) presence of occult bleeding for >6 days; and 7) use of high‐dose corticosteroids. This level of clinical detail would likely only be available through a prospective study design, as has been suggested by other authors.33 Further research into the use, safety, and effectiveness of PPIs specifically for stress ulcer prophylaxis is warranted.
In conclusion, we found that 73% of nearly 1 million Medicine patients discharged from academic medical centers received a PPI without a valid indication during their hospitalization. The implications of our findings are broad. PPIs are more expensive31 than H2RAs and there is increasing evidence that they have significant side effects. In both databases we examined, the rate of C. difficile infection was higher in patients receiving PPIs than others. The prescribing habits of physicians in these university hospital settings appear to be far out of line with published guidelines and evidence‐based practice. Reducing inappropriate prescribing of PPIs would be an important educational and quality assurance project in most institutions.
Proton pump inhibitors (PPIs) are the third most commonly prescribed class of medication in the United States, with $13.6 billion in yearly sales.1 Despite their effectiveness in treating acid reflux2 and their mortality benefit in the treatment of patients with gastrointestinal bleeding,3 recent literature has identified a number of risks associated with PPIs, including an increased incidence of Clostridium difficile infection,4 decreased effectiveness of clopidogrel in patients with acute coronary syndrome,5 increased risk of community‐ and hospital‐acquired pneumonia, and an increased risk of hip fracture.69 Additionally, in March of 2011, the US Food and Drug Administration (FDA) issued a warning regarding the potential for PPIs to cause low magnesium levels which can, in turn, cause muscle spasms, an irregular heartbeat, and convulsions.10
Inappropriate PPI prescription practice has been demonstrated in the primary care setting,11 as well as in small studies conducted in the hospital setting.1216 We hypothesized that many hospitalized patients receive these medications without having an accepted indication, and examined 2 populations of hospitalized patients, including administrative data from 6.5 million discharges from US university hospitals, to look for appropriate diagnoses justifying their use.
METHODS
We performed a retrospective review of administrative data collected between January 1, 2008 and December 31, 2009 from 2 patient populations: (a) those discharged from Denver Health (DH), a university‐affiliated public safety net hospital in Denver, CO; and (b) patients discharged from 112 academic health centers and 256 of their affiliated hospitals that participate in the University HealthSystem Consortium (UHC). The Colorado Multiple Institution Review Board reviewed and approved the conduct of this study.
Inclusion criteria for both populations were age >18 or <90 years, and hospitalization on a Medicine service. Prisoners and women known to be pregnant were excluded. In both cohorts, if patients had more than 1 admission during the 2‐year study period, only data from the first admission were used.
We recorded demographics, admitting diagnosis, and discharge diagnoses together with information pertaining to the name, route, and duration of administration of all PPIs (ie, omeprazole, lansoprazole, esomeprazole, pantoprazole, rabeprazole). We created a broadly inclusive set of valid indications for PPIs by incorporating diagnoses that could be identified by International Classification of Diseases, Ninth Revision.
(ICD‐9) codes from a number of previously published sources including the National Institute of Clinical Excellence (NICE) guidelines issued by the National Health Service (NHS) of the United Kingdom in 200012, 1721 (Table 1).
| Indication | ICD‐9 Code |
|---|---|
| |
| Helicobacter pylori | 041.86 |
| Abnormality of secretion of gastrin | 251.5 |
| Esophageal varices with bleeding | 456.0 |
| Esophageal varices without mention of bleeding | 456.1 |
| Esophageal varices in diseases classified elsewhere | 456.2 |
| Esophagitis | 530.10530.19 |
| Perforation of esophagus | 530.4 |
| Gastroesophageal laceration‐hemorrhage syndrome | 530.7 |
| Esophageal reflux | 530.81 |
| Barrett's esophagus | 530.85 |
| Gastric ulcer | 531.0031.91 |
| Duodenal ulcer | 532.00532.91 |
| Peptic ulcer, site unspecified | 533.00533.91 |
| Gastritis and duodenitis | 535.00535.71 |
| Gastroparesis | 536.3 |
| Dyspepsia and other specified disorders of function of stomach | 536.8 |
| Hemorrhage of gastrointestinal tract, unspecified | 578.9 |
To assess the accuracy of the administrative data from DH, we also reviewed the Emergency Department histories, admission histories, progress notes, electronic pharmacy records, endoscopy reports, and discharge summaries of 123 patients randomly selected (ie, a 5% sample) from the group of patients identified by administrative data to have received a PPI without a valid indication, looking for any accepted indication that might have been missed in the administrative data.
All analyses were performed using SAS Enterprise Guide 4.1 (SAS Institute, Cary, NC). A Student t test was used to compare continuous variables and a chi‐square test was used to compare categorical variables. Bonferroni corrections were used for multiple comparisons, such that P values less than 0.01 were considered to be significant for categorical variables.
RESULTS
Inclusion criteria were met by 9875 patients in the Denver Health database and 6,592,100 patients in the UHC database. The demographics and primary discharge diagnoses for these patients are summarized in Table 2.
| DH (N = 9875) | UHC (N = 6,592,100) | ||||
|---|---|---|---|---|---|
| Received a PPI | No PPI | Received a PPI | No PPI | ||
| |||||
| No. (%) | 3962 (40) | 5913 (60) | 918,474 (14) | 5,673,626 (86) | |
| Age (mean SD) | 53 15 | 51 16 | 59 17 | 55 18 | |
| Gender (% male) | 2197 (55) | 3438 (58) | 464,552 (51) | 2,882,577 (51) | |
| Race (% white) | 1610 (41) | 2425 (41) | 619,571 (67) | 3,670,450 (65) | |
| Top 5 primary discharge diagnoses | |||||
| Chest pain | 229 (6) | 462 (8) | Coronary atherosclerosis | 35,470 (4) | 186,321 (3) |
| Alcohol withdrawal | 147 (4) | 174 (3) | Acute myocardial infarction | 26,507 (3) | 132,159 (2) |
| Pneumonia, organism unspecified | 142 (4) | 262 (4) | Heart failure | 21,143 (2) | 103,751 (2) |
| Acute pancreatitis | 132 (3) | 106 (2) | Septicemia | 20,345 (2) | 64,915 (1) |
| Obstructive chronic bronchitis with (acute) exacerbation | 89 (2) | 154 (3) | Chest pain | 16,936 (2) | 107,497 (2) |
Only 39% and 27% of the patients in the DH and UHC databases, respectively, had a valid indication for PPIs on the basis of discharge diagnoses (Table 3). In the DH data, if admission ICD‐9 codes were also inspected for valid PPI indications, 1579 (40%) of patients receiving PPIs had a valid indication (admission ICD‐9 codes were not available for patients in the UHC database). Thirty‐one percent of Denver Health patients spent time in the intensive care unit (ICU) during their hospital stay and 65% of those patients received a PPI without a valid indication, as compared to 59% of patients who remained on the General Medicine ward (Table 3).
| DH (N = 9875) | UHC (N = 6,592,100) | |
|---|---|---|
| ||
| Patients receiving PPIs (% of total) | 3962 (40) | 918,474 (14) |
| Any ICU stay, N (% of all patients) | 1238 (31) | |
| General Medicine ward only, N (% of all patients) | 2724 (69) | |
| Patients with indication for PPI (% of all patients receiving PPIs)* | 1540 (39) | 247,142 (27) |
| Any ICU stay, N (% of all ICU patients) | 434 (35) | |
| General Medicine ward only, N (% of all ward patients) | 1106 (41) | |
| Patients without indication for PPI (% of those receiving PPIs)* | 2422 (61) | 671,332 (73) |
| Any ICU stay, N (% of all ICU patients) | 804 (65) | |
| General Medicine ward only, N (% of all ward patients) | 1618 (59) | |
Higher rates of concurrent C. difficile infections were observed in patients receiving PPIs in both databases; a higher rate of concurrent diagnosis of pneumonia was seen in patients receiving PPIs in the UHC population, with a nonsignificant trend towards the same finding in DH patients (Table 4).
| Denver Health | UHC | |||||
|---|---|---|---|---|---|---|
| Concurrent diagnosis | (+) PPI 3962 | () PPI 5913 | P | (+) PPI 918,474 | () PPI 5,673,626 | P |
| ||||||
| C. difficile | 46 (1.16) | 26 (0.44) | <0.0001 | 12,113 (1.32) | 175 (0.0031) | <0.0001 |
| Pneumonia | 400 (10.1) | 517 (8.7) | 0.0232 | 75,274 (8.2) | 300,557 (5.3) | <0.0001 |
Chart review in the DH population found valid indications for PPIs in 19% of patients who were thought not have a valid indication on the basis of the administrative data (Table 5). For 56% of those in whom no valid indication was confirmed, physicians identified prophylaxis as the justification.
| Characteristic | N (%) |
|---|---|
| |
| Valid indication found on chart review only | 23 (19) |
| No valid indication after chart review | 100 (81) |
| Written indication: prophylaxis | 56 (56) |
| No written documentation of indication present in the chart | 33 (33) |
| Written indication: continue home medication | 9 (9) |
| Intubated with or without written indication of prophylaxis | 16 (16) |
DISCUSSION
The important finding of this study was that the majority of patients in 2 large groups of Medicine patients hospitalized in university‐affiliated hospitals received PPIs without having a valid indication. To our knowledge, the more than 900,000 UHC patients who received a PPI during their hospitalization represent the largest inpatient population evaluated for appropriateness of PPI prescriptions.
Our finding that 41% of the patients admitted to the DH Medicine service received a PPI during their hospital stay is similar to what has been observed by others.9, 14, 22 The rate of PPI prescription was lower in the UHC population (14%) for unclear reasons. By our definition, 61% lacked an adequate diagnosis to justify the prescription of the PPI. After performing a chart review on a randomly selected 5% of these records, we found that the DH administrative database had failed to identify 19% of patients who had a valid indication for receiving a PPI. Adjusting the administrative data accordingly still resulted in 50% of DH patients not having a valid indication for receiving a PPI. This is consistent with the 54% recorded by Batuwitage and colleagues11 in the outpatient setting by direct chart review, as well as a range of 60%‐75% for hospitalized patients in other studies.12, 13, 15, 23, 24
Stomach acidity is believed to provide an important host defense against lower gastrointestinal tract infections including Salmonella, Campylobacter, and Clostridium difficile.25 A recent study by Howell et al26 showed a doseresponse effect between PPI use and C. difficile infection, supporting a causal connection between loss of stomach acidity and development of Clostridium difficile‐associated diarrhea (CDAD). We found that C. difficile infection was more common in both populations of patients receiving PPIs (although the relative risk was much higher in the UHC database) (Table 5). The rate of CDAD in DH patients who received PPIs was 2.6 times higher than in patients who did not receive these acid suppressive agents.
The role of acid suppression in increasing risk for community‐acquired pneumonia is not entirely clear. Theories regarding the loss of an important host defense and bacterial proliferation head the list.6, 8, 27 Gastric and duodenal bacterial overgrowth is significantly more common in patients receiving PPIs than in patients receiving histamine type‐2 (H2) blockers.28 Previous studies have identified an increased rate of hospital‐acquired pneumonia and recurrent community‐acquired pneumonia27 in patients receiving any form of acid suppression therapy, but the risk appears to be greater in patients receiving PPIs than in those receiving H2 receptor antagonists (H2RAs).9 Significantly more patients in the UHC population who were taking PPIs had a concurrent diagnosis of pneumonia, consistent with previous studies alerting to this association6, 8, 9, 27 and consistent with the nonsignificant trend observed in the DH population.
Our study has a number of limitations. Our database comes from a single university‐affiliated public hospital with residents and hospitalists writing orders for all medications. The hospitals in the UHC are also teaching hospitals. Accordingly, our results might not generalize to other settings or reflect prescribing patterns in private, nonteaching hospital environments. Because our study was retrospective, we could not confirm the decision‐making process supporting the prescription of PPIs. Similarly, we could not temporarily relate the existence of the indication with the time the PPI was prescribed. Our list of appropriate indications for prescribing PPIs was developed by reviewing a number of references, and other studies have used slightly different lists (albeit the more commonly recognized indications are the same), but it may be argued that the list either includes or misses diagnoses in error.
While there is considerable debate about the use of PPIs for stress ulcer prophylaxis,29 we specifically chose not to include this as one of our valid indications for PPIs for 4 reasons. First, the American Society of Health‐System Pharmacists (ASHP) Report does not recommend prophylaxis for non‐ICU patients, and only recommends prophylaxis for those ICU patients with a coagulopathy, those requiring mechanical ventilation for more than 48 hours, those with a history of gastrointestinal ulceration or bleeding in the year prior to admission, and those with 2 or more of the following indications: sepsis, ICU stay >1 week, occult bleeding lasting 6 or more days, receiving high‐dose corticosteroids, and selected surgical situations.30 At the time the guideline was written, the authors note that there was insufficient data on PPIs to make any recommendations on their use, but no subsequent guidelines have been issued.30 Second, a review by Mohebbi and Hesch published in 2009, and a meta‐analysis by Lin and colleagues published in 2010, summarize subsequent randomized trials that suggest that PPIs and H2 blockers are, at best, similarly effective at preventing upper gastrointestinal (GI) bleeding among critically ill patients.31, 32 Third, the NICE guidelines do not include stress ulcer prophylaxis as an appropriate indication for PPIs except in the prevention and treatment of NSAID [non‐steroidal anti‐inflammatory drug]‐associated ulcers.19 Finally, H2RAs are currently the only medications with an FDA‐approved indication for stress ulcer prophylaxis. We acknowledge that PPIs may be a reasonable and acceptable choice for stress ulcer prophylaxis in patients who meet indications, but we were unable to identify such patients in either of our administrative databases.
In our Denver Health population, only 31% of our patients spent any time in the intensive care unit, and only a fraction of these would have both an accepted indication for stress ulcer prophylaxis by the ASHP guidelines and an intolerance or contraindication to an H2RA or sulcralfate. While our administrative database lacked the detail necessary to identify this small group of patients, the number of patients who might have been misclassified as not having a valid PPI indication was likely very small. Similar to the findings of previous studies,15, 18, 23, 29 prophylaxis against gastrointestinal bleeding was the stated justification for prescribing the PPI in 56% of the DH patient charts reviewed. It is impossible for us to estimate the number of patients in our administrative database for whom stress ulcer prophylaxis was justified by existing guidelines, as it would be necessary to gather a number of specific clinical details for each patient including: 1) ICU stay; 2) presence of coagulopathy; 3) duration of mechanical ventilation; 4) presence of sepsis; 5) duration of ICU stay; 6) presence of occult bleeding for >6 days; and 7) use of high‐dose corticosteroids. This level of clinical detail would likely only be available through a prospective study design, as has been suggested by other authors.33 Further research into the use, safety, and effectiveness of PPIs specifically for stress ulcer prophylaxis is warranted.
In conclusion, we found that 73% of nearly 1 million Medicine patients discharged from academic medical centers received a PPI without a valid indication during their hospitalization. The implications of our findings are broad. PPIs are more expensive31 than H2RAs and there is increasing evidence that they have significant side effects. In both databases we examined, the rate of C. difficile infection was higher in patients receiving PPIs than others. The prescribing habits of physicians in these university hospital settings appear to be far out of line with published guidelines and evidence‐based practice. Reducing inappropriate prescribing of PPIs would be an important educational and quality assurance project in most institutions.
- IMS Health Web site. Available at: http://www.imshealth.com/deployedfiles/ims/Global/Content/Corporate/Press%20Room/Top‐line%20Market%20Data/2009%20Top‐line%20Market%20Data/Top%20Therapy%20Classes%20by%20U.S.Sales.pdf. Accessed May 1,2011.
- ,, , et al.Comparison of omeprazole and cimetidine in reflux oesophagitis: symptomatic, endoscopic, and histological evaluations.Gut.1990;31(9):968–972.
- ,,, et al.Omeprazole before endoscopy in patients with gastrointestinal bleeding.N Engl J Med.2007;356(16):1631–1640.
- ,,,.Use of gastric acid‐suppressive agents and the risk of community‐acquired Clostridium difficile‐associated disease.JAMA.2005;294(23):2989–2995.
- ,,, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome.JAMA.2009;301(9):937–944.
- ,,,,,.Risk of community‐acquired pneumonia and use of gastric acid‐suppressive drugs.JAMA.2004;292(16):1955–1960.
- ,,,.Long‐term proton pump inhibitor therapy and risk of hip fracture.JAMA2006;296(24):2947–2953.
- ,,,,,.Use of proton pump inhibitors and the risk of community‐acquired pneumonia: a population‐based case‐control study.Arch Intern Med.2007;167(9):950–955.
- ,,,.Acid‐suppressive medication use and the risk for hospital‐acquired pneumonia.JAMA.2009;301(20):2120–2128.
- US Food and Drug Administration (FDA) Website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsfor HumanMedicalProducts/ucm245275.htm. Accessed March 2,2011.
- ,,,.Inappropriate prescribing of proton pump inhibitors in primary care.Postgrad Med J.2007;83(975):66–68.
- ,.Stress ulcer prophylaxis in hospitalized patients not in intensive care units.Am J Health Syst Pharm.2007;64(13):1396–1400.
- ,,,.Predictors of inappropriate utilization of intravenous proton pump inhibitors.Aliment Pharmacol Ther.2007;25(5):609–615.
- ,,.Overuse of acid‐suppressive therapy in hospitalized patients.Am J Gastroenterol.2000;95(11):3118–3122.
- ,,,,,.Patterns and predictors of proton pump inhibitor overuse among academic and non‐academic hospitalists.Intern Med2010;49(23):2561–2568.
- ,,, et al.Hospital use of acid‐suppressive medications and its fall‐out on prescribing in general practice: a 1‐month survey.Aliment Pharmacol Ther.2003;17(12):1503–1506.
- ,,.Overuse and inappropriate prescribing of proton pump inhibitors in patients with Clostridium difficile‐associated disease.QJM.2008;101(6):445–448.
- ,,,.Acid suppressive therapy use on an inpatient internal medicine service.Ann Pharmacother.2006;40(7–8):1261–1266.
- National Institute of Clinical Excellence (NICE), National Health Service (NHS), Dyspepsia: Management of dyspepsia in adults in primary care. Web site. Available at: http://www.nice.org.uk/nicemedia/live/10950/29460/29460.pdf. Accessed May 1,2011.
- ,,.When should stress ulcer prophylaxis be used in the ICU?Curr Opin Crit Care.2009;15(2):139–143.
- ,.An evaluation of the use of proton pump inhibitors.Pharm World Sci2001;23(3):116–117.
- ,,.Overuse of proton pump inhibitors.J Clin Pharm Ther.2000;25(5):333–340.
- ,,,.Pattern of intravenous proton pump inhibitors use in ICU and non‐ICU setting: a prospective observational study.Saudi J Gastroenterol.2010;16(4):275–279.
- ,,, et al.Overuse of PPIs in patients at admission, during treatment, and at discharge in a tertiary Spanish hospital.Curr Clin Pharmacol.2010;5(4):288–297.
- ,,.Systematic review of the risk of enteric infection in patients taking acid suppression.Am J Gastroenterol.2007;102(9):2047–2056.
- ,,, et al.Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection.Arch Intern Med.2010;170(9):784–790.
- ,,,,.Recurrent community‐acquired pneumonia in patients starting acid‐suppressing drugs.Am J Med.2010;123(1):47–53.
- ,,, et al.Bacterial overgrowth during treatment with omeprazole compared with cimetidine: a prospective randomised double blind study.Gut.1996;39(1):54–59.
- ,,,.Why do physicians prescribe stress ulcer prophylaxis to general medicine patients?South Med J2010;103(11):1103–1110.
- ASHP therapeutic guidelines on stress ulcer prophylaxis.ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998.Am J Health Syst Pharm.1999;56(4):347–379.
- ,.Stress ulcer prophylaxis in the intensive care unit.Proc (Bayl Univ Med Cent).2009;22(4):373–376.
- ,,,,.The efficacy and safety of proton pump inhibitors vs histamine‐2 receptor antagonists for stress ulcer bleeding prophylaxis among critical care patients: a meta‐analysis.Crit Care Med.2010;38(4):1197–1205.
- ,,.Proton pump inhibitors for the prevention of stress‐related mucosal disease in critically‐ill patients: a meta‐analysis.J Med Assoc Thai.2009;92(5):632–637.
- ,,,.Proton pump inhibitors for prophylaxis of nosocomial upper gastrointestinal tract bleeding: effect of standardized guidelines on prescribing practice.Arch Intern Med.2010;170(9):779–783.
- IMS Health Web site. Available at: http://www.imshealth.com/deployedfiles/ims/Global/Content/Corporate/Press%20Room/Top‐line%20Market%20Data/2009%20Top‐line%20Market%20Data/Top%20Therapy%20Classes%20by%20U.S.Sales.pdf. Accessed May 1,2011.
- ,, , et al.Comparison of omeprazole and cimetidine in reflux oesophagitis: symptomatic, endoscopic, and histological evaluations.Gut.1990;31(9):968–972.
- ,,, et al.Omeprazole before endoscopy in patients with gastrointestinal bleeding.N Engl J Med.2007;356(16):1631–1640.
- ,,,.Use of gastric acid‐suppressive agents and the risk of community‐acquired Clostridium difficile‐associated disease.JAMA.2005;294(23):2989–2995.
- ,,, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome.JAMA.2009;301(9):937–944.
- ,,,,,.Risk of community‐acquired pneumonia and use of gastric acid‐suppressive drugs.JAMA.2004;292(16):1955–1960.
- ,,,.Long‐term proton pump inhibitor therapy and risk of hip fracture.JAMA2006;296(24):2947–2953.
- ,,,,,.Use of proton pump inhibitors and the risk of community‐acquired pneumonia: a population‐based case‐control study.Arch Intern Med.2007;167(9):950–955.
- ,,,.Acid‐suppressive medication use and the risk for hospital‐acquired pneumonia.JAMA.2009;301(20):2120–2128.
- US Food and Drug Administration (FDA) Website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsfor HumanMedicalProducts/ucm245275.htm. Accessed March 2,2011.
- ,,,.Inappropriate prescribing of proton pump inhibitors in primary care.Postgrad Med J.2007;83(975):66–68.
- ,.Stress ulcer prophylaxis in hospitalized patients not in intensive care units.Am J Health Syst Pharm.2007;64(13):1396–1400.
- ,,,.Predictors of inappropriate utilization of intravenous proton pump inhibitors.Aliment Pharmacol Ther.2007;25(5):609–615.
- ,,.Overuse of acid‐suppressive therapy in hospitalized patients.Am J Gastroenterol.2000;95(11):3118–3122.
- ,,,,,.Patterns and predictors of proton pump inhibitor overuse among academic and non‐academic hospitalists.Intern Med2010;49(23):2561–2568.
- ,,, et al.Hospital use of acid‐suppressive medications and its fall‐out on prescribing in general practice: a 1‐month survey.Aliment Pharmacol Ther.2003;17(12):1503–1506.
- ,,.Overuse and inappropriate prescribing of proton pump inhibitors in patients with Clostridium difficile‐associated disease.QJM.2008;101(6):445–448.
- ,,,.Acid suppressive therapy use on an inpatient internal medicine service.Ann Pharmacother.2006;40(7–8):1261–1266.
- National Institute of Clinical Excellence (NICE), National Health Service (NHS), Dyspepsia: Management of dyspepsia in adults in primary care. Web site. Available at: http://www.nice.org.uk/nicemedia/live/10950/29460/29460.pdf. Accessed May 1,2011.
- ,,.When should stress ulcer prophylaxis be used in the ICU?Curr Opin Crit Care.2009;15(2):139–143.
- ,.An evaluation of the use of proton pump inhibitors.Pharm World Sci2001;23(3):116–117.
- ,,.Overuse of proton pump inhibitors.J Clin Pharm Ther.2000;25(5):333–340.
- ,,,.Pattern of intravenous proton pump inhibitors use in ICU and non‐ICU setting: a prospective observational study.Saudi J Gastroenterol.2010;16(4):275–279.
- ,,, et al.Overuse of PPIs in patients at admission, during treatment, and at discharge in a tertiary Spanish hospital.Curr Clin Pharmacol.2010;5(4):288–297.
- ,,.Systematic review of the risk of enteric infection in patients taking acid suppression.Am J Gastroenterol.2007;102(9):2047–2056.
- ,,, et al.Iatrogenic gastric acid suppression and the risk of nosocomial Clostridium difficile infection.Arch Intern Med.2010;170(9):784–790.
- ,,,,.Recurrent community‐acquired pneumonia in patients starting acid‐suppressing drugs.Am J Med.2010;123(1):47–53.
- ,,, et al.Bacterial overgrowth during treatment with omeprazole compared with cimetidine: a prospective randomised double blind study.Gut.1996;39(1):54–59.
- ,,,.Why do physicians prescribe stress ulcer prophylaxis to general medicine patients?South Med J2010;103(11):1103–1110.
- ASHP therapeutic guidelines on stress ulcer prophylaxis.ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998.Am J Health Syst Pharm.1999;56(4):347–379.
- ,.Stress ulcer prophylaxis in the intensive care unit.Proc (Bayl Univ Med Cent).2009;22(4):373–376.
- ,,,,.The efficacy and safety of proton pump inhibitors vs histamine‐2 receptor antagonists for stress ulcer bleeding prophylaxis among critical care patients: a meta‐analysis.Crit Care Med.2010;38(4):1197–1205.
- ,,.Proton pump inhibitors for the prevention of stress‐related mucosal disease in critically‐ill patients: a meta‐analysis.J Med Assoc Thai.2009;92(5):632–637.
- ,,,.Proton pump inhibitors for prophylaxis of nosocomial upper gastrointestinal tract bleeding: effect of standardized guidelines on prescribing practice.Arch Intern Med.2010;170(9):779–783.
Copyright © 2011 Society of Hospital Medicine
Program Targets "Frequent Fliers"
A new Michigan clinic for a hospital system's ED "frequent fliers" is a chance for HM to help streamline care delivery, a hospitalist involved in the effort says.
Doug Apple, MD, hospitalist division chief for Spectrum Health in Grand Rapids, Mich., says the Spectrum Health Medical Group Center for Integrative Medicine will help deal with patients who have used the ED at least 10 times in the past year. In the past, many of the patients would be admitted to the hospital, becoming part of a hospitalist's census. Often, they will have nonspecific conditions, such as chronic abdominal pain.
"Patients get admitted, they might not see the same hospitalist, they may not see the same surgical specialist or GI specialist," Dr. Apple says. "And so every time they get admitted, there's a different plan, there's a different diagnosis or idea. … The intent is to figure out how are these individuals able to get better care, more appropriate care, in an environment that allows them to actually have somebody that pays strict attention to what their needs are?"
Dr. Apple, who worked on the conceptual planning of the clinic, says hospitalists will have no hands-on role with its initial operation, other than referrals. But he says hospitalists who proactively identify patients best cared for via the clinic could save themselves readmissions and ensure better transitions of care.
"We're trying to figure out how we make these transitions, either into a hospital, or out of a hospital, or between an ED and back to the clinic," he adds. "We're trying to make sure these transitions do not become gaps in healthcare."
A new Michigan clinic for a hospital system's ED "frequent fliers" is a chance for HM to help streamline care delivery, a hospitalist involved in the effort says.
Doug Apple, MD, hospitalist division chief for Spectrum Health in Grand Rapids, Mich., says the Spectrum Health Medical Group Center for Integrative Medicine will help deal with patients who have used the ED at least 10 times in the past year. In the past, many of the patients would be admitted to the hospital, becoming part of a hospitalist's census. Often, they will have nonspecific conditions, such as chronic abdominal pain.
"Patients get admitted, they might not see the same hospitalist, they may not see the same surgical specialist or GI specialist," Dr. Apple says. "And so every time they get admitted, there's a different plan, there's a different diagnosis or idea. … The intent is to figure out how are these individuals able to get better care, more appropriate care, in an environment that allows them to actually have somebody that pays strict attention to what their needs are?"
Dr. Apple, who worked on the conceptual planning of the clinic, says hospitalists will have no hands-on role with its initial operation, other than referrals. But he says hospitalists who proactively identify patients best cared for via the clinic could save themselves readmissions and ensure better transitions of care.
"We're trying to figure out how we make these transitions, either into a hospital, or out of a hospital, or between an ED and back to the clinic," he adds. "We're trying to make sure these transitions do not become gaps in healthcare."
A new Michigan clinic for a hospital system's ED "frequent fliers" is a chance for HM to help streamline care delivery, a hospitalist involved in the effort says.
Doug Apple, MD, hospitalist division chief for Spectrum Health in Grand Rapids, Mich., says the Spectrum Health Medical Group Center for Integrative Medicine will help deal with patients who have used the ED at least 10 times in the past year. In the past, many of the patients would be admitted to the hospital, becoming part of a hospitalist's census. Often, they will have nonspecific conditions, such as chronic abdominal pain.
"Patients get admitted, they might not see the same hospitalist, they may not see the same surgical specialist or GI specialist," Dr. Apple says. "And so every time they get admitted, there's a different plan, there's a different diagnosis or idea. … The intent is to figure out how are these individuals able to get better care, more appropriate care, in an environment that allows them to actually have somebody that pays strict attention to what their needs are?"
Dr. Apple, who worked on the conceptual planning of the clinic, says hospitalists will have no hands-on role with its initial operation, other than referrals. But he says hospitalists who proactively identify patients best cared for via the clinic could save themselves readmissions and ensure better transitions of care.
"We're trying to figure out how we make these transitions, either into a hospital, or out of a hospital, or between an ED and back to the clinic," he adds. "We're trying to make sure these transitions do not become gaps in healthcare."
In the Literature: Research You Need to Know
Clinical question: Can the aortic dissection detection (ADD) risk score be used to screen patients for acute aortic dissection at the bedside?
Background: AAD, a life-threatening condition, often is missed due to relatively low incidence, varied presentation, and need for advanced imaging studies. The American Heart Association and the American College of Cardiology have published guidelines on thoracic aortic disease from which the ADD risk score has been adapted to identify high-risk patients and to suggest additional testing based on pretest probability of disease.
Study design: Retrospective application of ADD risk score to the International Registry of Acute Aortic Dissection (IRAD) database.
Setting: Multinational medical registry compiled from 24 medical centers.
Synopsis: A total of 2,538 patients with confirmed ADD were reviewed. The number of patients presenting with one or more of 12 proposed clinical risk markers was determined. An ADD risk score of 0 to 3 was calculated based on the number of risk categories (high-risk predisposing conditions, pain features, examination features) in which patients met criteria.
Among 108 (4.3%) patients found to be low-risk (ADD score 0), 72 had a chest X-ray, 35 of which were found to have a widened mediastinum. High-risk features (ADD score 2 or 3) were found in 1,503 (59.2%) patients, and the remaining 927 (36.5%) patients had intermediate risk (ADD score 1).
The guidelines recommend further imaging for all intermediate- and high-risk patients and for low-risk patients with a wide mediastinum resulting in very good sensitivity.
Bottom line: The ADD risk score is a sensitive bedside screening tool for aortic dissection, ensuring that more than 95% patients with true dissection undergo further investigation, but it may lead to overinvestigation due to unknown specificity.
Citation: Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circ. 2011;123:2213-2218.
For more physician reviews of HM-related literature, visit our website and search "Literature."
Clinical question: Can the aortic dissection detection (ADD) risk score be used to screen patients for acute aortic dissection at the bedside?
Background: AAD, a life-threatening condition, often is missed due to relatively low incidence, varied presentation, and need for advanced imaging studies. The American Heart Association and the American College of Cardiology have published guidelines on thoracic aortic disease from which the ADD risk score has been adapted to identify high-risk patients and to suggest additional testing based on pretest probability of disease.
Study design: Retrospective application of ADD risk score to the International Registry of Acute Aortic Dissection (IRAD) database.
Setting: Multinational medical registry compiled from 24 medical centers.
Synopsis: A total of 2,538 patients with confirmed ADD were reviewed. The number of patients presenting with one or more of 12 proposed clinical risk markers was determined. An ADD risk score of 0 to 3 was calculated based on the number of risk categories (high-risk predisposing conditions, pain features, examination features) in which patients met criteria.
Among 108 (4.3%) patients found to be low-risk (ADD score 0), 72 had a chest X-ray, 35 of which were found to have a widened mediastinum. High-risk features (ADD score 2 or 3) were found in 1,503 (59.2%) patients, and the remaining 927 (36.5%) patients had intermediate risk (ADD score 1).
The guidelines recommend further imaging for all intermediate- and high-risk patients and for low-risk patients with a wide mediastinum resulting in very good sensitivity.
Bottom line: The ADD risk score is a sensitive bedside screening tool for aortic dissection, ensuring that more than 95% patients with true dissection undergo further investigation, but it may lead to overinvestigation due to unknown specificity.
Citation: Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circ. 2011;123:2213-2218.
For more physician reviews of HM-related literature, visit our website and search "Literature."
Clinical question: Can the aortic dissection detection (ADD) risk score be used to screen patients for acute aortic dissection at the bedside?
Background: AAD, a life-threatening condition, often is missed due to relatively low incidence, varied presentation, and need for advanced imaging studies. The American Heart Association and the American College of Cardiology have published guidelines on thoracic aortic disease from which the ADD risk score has been adapted to identify high-risk patients and to suggest additional testing based on pretest probability of disease.
Study design: Retrospective application of ADD risk score to the International Registry of Acute Aortic Dissection (IRAD) database.
Setting: Multinational medical registry compiled from 24 medical centers.
Synopsis: A total of 2,538 patients with confirmed ADD were reviewed. The number of patients presenting with one or more of 12 proposed clinical risk markers was determined. An ADD risk score of 0 to 3 was calculated based on the number of risk categories (high-risk predisposing conditions, pain features, examination features) in which patients met criteria.
Among 108 (4.3%) patients found to be low-risk (ADD score 0), 72 had a chest X-ray, 35 of which were found to have a widened mediastinum. High-risk features (ADD score 2 or 3) were found in 1,503 (59.2%) patients, and the remaining 927 (36.5%) patients had intermediate risk (ADD score 1).
The guidelines recommend further imaging for all intermediate- and high-risk patients and for low-risk patients with a wide mediastinum resulting in very good sensitivity.
Bottom line: The ADD risk score is a sensitive bedside screening tool for aortic dissection, ensuring that more than 95% patients with true dissection undergo further investigation, but it may lead to overinvestigation due to unknown specificity.
Citation: Rogers AM, Hermann LK, Booher AM, et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circ. 2011;123:2213-2218.
For more physician reviews of HM-related literature, visit our website and search "Literature."
NPs Improve Discharges, Not Readmissions
Adding a nurse practitioner (NP) to a resident physician team improves the efficiency of the discharge process but does nothing to decrease readmissions, according to a study in this month's Journal of Hospital Medicine.
In a randomized controlled trial at Massachusetts General Hospital (MGH) in Boston, NP use resulted in more discharge summaries completed within 24 hours when compared to a control group (67% vs 47%, P<0.001), according to the report, "Improving the Discharge Process by Embedding a Discharge Facilitator in a Resident Team." The study reported more follow-up appointments scheduled (62% vs. 36%, P<0.0001) scheduled and better attendance at those appointments within two weeks (36% vs. 23%, P<0.0002).
But for all the benefits, study author Kathleen Finn MD, MPhil, FACP, FHM, expresses disappointment in the fact that there was no significant difference between the groups in 30-day ED visits or 30-day readmissions.
"The literature suggests if we improve the discharge process, make it safer, and make sure patients have appropriate follow-ups in a timely fashion, we should be able to reduce readmissions," she says. "When we took a general medical population and did all that, we didn't get those results. However, its a single study, with one nurse, so its hard to say. But that was a little disappointing."
The study's results were enough to prompt the expansion of the program from one resident team to three. In the long term, Dr. Finn wants physician educators who are interested in limiting work hours and admissions to view the discharge process as just as important.
"We don't consider the discharge process as time-consuming, but it does take almost as much time as an admission does and yet patients are being discharged, even on admitting days,” she says. "The discharge is a very vulnerable time as the literature keeps showing. We need to rethink the discharge process."
Adding a nurse practitioner (NP) to a resident physician team improves the efficiency of the discharge process but does nothing to decrease readmissions, according to a study in this month's Journal of Hospital Medicine.
In a randomized controlled trial at Massachusetts General Hospital (MGH) in Boston, NP use resulted in more discharge summaries completed within 24 hours when compared to a control group (67% vs 47%, P<0.001), according to the report, "Improving the Discharge Process by Embedding a Discharge Facilitator in a Resident Team." The study reported more follow-up appointments scheduled (62% vs. 36%, P<0.0001) scheduled and better attendance at those appointments within two weeks (36% vs. 23%, P<0.0002).
But for all the benefits, study author Kathleen Finn MD, MPhil, FACP, FHM, expresses disappointment in the fact that there was no significant difference between the groups in 30-day ED visits or 30-day readmissions.
"The literature suggests if we improve the discharge process, make it safer, and make sure patients have appropriate follow-ups in a timely fashion, we should be able to reduce readmissions," she says. "When we took a general medical population and did all that, we didn't get those results. However, its a single study, with one nurse, so its hard to say. But that was a little disappointing."
The study's results were enough to prompt the expansion of the program from one resident team to three. In the long term, Dr. Finn wants physician educators who are interested in limiting work hours and admissions to view the discharge process as just as important.
"We don't consider the discharge process as time-consuming, but it does take almost as much time as an admission does and yet patients are being discharged, even on admitting days,” she says. "The discharge is a very vulnerable time as the literature keeps showing. We need to rethink the discharge process."
Adding a nurse practitioner (NP) to a resident physician team improves the efficiency of the discharge process but does nothing to decrease readmissions, according to a study in this month's Journal of Hospital Medicine.
In a randomized controlled trial at Massachusetts General Hospital (MGH) in Boston, NP use resulted in more discharge summaries completed within 24 hours when compared to a control group (67% vs 47%, P<0.001), according to the report, "Improving the Discharge Process by Embedding a Discharge Facilitator in a Resident Team." The study reported more follow-up appointments scheduled (62% vs. 36%, P<0.0001) scheduled and better attendance at those appointments within two weeks (36% vs. 23%, P<0.0002).
But for all the benefits, study author Kathleen Finn MD, MPhil, FACP, FHM, expresses disappointment in the fact that there was no significant difference between the groups in 30-day ED visits or 30-day readmissions.
"The literature suggests if we improve the discharge process, make it safer, and make sure patients have appropriate follow-ups in a timely fashion, we should be able to reduce readmissions," she says. "When we took a general medical population and did all that, we didn't get those results. However, its a single study, with one nurse, so its hard to say. But that was a little disappointing."
The study's results were enough to prompt the expansion of the program from one resident team to three. In the long term, Dr. Finn wants physician educators who are interested in limiting work hours and admissions to view the discharge process as just as important.
"We don't consider the discharge process as time-consuming, but it does take almost as much time as an admission does and yet patients are being discharged, even on admitting days,” she says. "The discharge is a very vulnerable time as the literature keeps showing. We need to rethink the discharge process."
Debunking the "Holiday Blues" Myth
Around the winter holidays—for reasons as varied as weather, grieving, holiday stress, or just plain Scrooge-liness—people are more susceptible to the "holiday blues." But Timothy Lineberry, MD, psychiatric hospitalist and medical director of Mayo Psychiatric Hospital and board chair of the American Association of Suicidology, points out that depression and associated suicide risk are year-round issues.
"The holidays aren't necessarily the worst. Depression and suicide are important all year long," Dr. Lineberry says.
In fact, a 2010 Annenberg Public Policy Center study (PDF) found that the rate of suicide in the U.S. is lowest in December. Suicide actually peaks in the spring and fall, a pattern that has not changed in recent years according to the same study.
Physicians write 60% of prescriptions for anti-depressants. And because depression and other mental health issues remain a taboo topic to many Americans, many patients visit their physician instead of a mental health clinician. As such, hospitalists need to be able to accurately assess depression and suicide risk.
Dr. Lineberry suggests the following steps for hospitalists who diagnose patients with depression:
- Consider using the holidays to renew or update systems of practice to better identify depression;
- Use the PHQ-9 questionnaire with patients who display symptoms of depression; and
- Ask direct and clear questions about suicidal thoughts and behaviors. Keep substance abuse as a risk factor in mind.
Around the winter holidays—for reasons as varied as weather, grieving, holiday stress, or just plain Scrooge-liness—people are more susceptible to the "holiday blues." But Timothy Lineberry, MD, psychiatric hospitalist and medical director of Mayo Psychiatric Hospital and board chair of the American Association of Suicidology, points out that depression and associated suicide risk are year-round issues.
"The holidays aren't necessarily the worst. Depression and suicide are important all year long," Dr. Lineberry says.
In fact, a 2010 Annenberg Public Policy Center study (PDF) found that the rate of suicide in the U.S. is lowest in December. Suicide actually peaks in the spring and fall, a pattern that has not changed in recent years according to the same study.
Physicians write 60% of prescriptions for anti-depressants. And because depression and other mental health issues remain a taboo topic to many Americans, many patients visit their physician instead of a mental health clinician. As such, hospitalists need to be able to accurately assess depression and suicide risk.
Dr. Lineberry suggests the following steps for hospitalists who diagnose patients with depression:
- Consider using the holidays to renew or update systems of practice to better identify depression;
- Use the PHQ-9 questionnaire with patients who display symptoms of depression; and
- Ask direct and clear questions about suicidal thoughts and behaviors. Keep substance abuse as a risk factor in mind.
Around the winter holidays—for reasons as varied as weather, grieving, holiday stress, or just plain Scrooge-liness—people are more susceptible to the "holiday blues." But Timothy Lineberry, MD, psychiatric hospitalist and medical director of Mayo Psychiatric Hospital and board chair of the American Association of Suicidology, points out that depression and associated suicide risk are year-round issues.
"The holidays aren't necessarily the worst. Depression and suicide are important all year long," Dr. Lineberry says.
In fact, a 2010 Annenberg Public Policy Center study (PDF) found that the rate of suicide in the U.S. is lowest in December. Suicide actually peaks in the spring and fall, a pattern that has not changed in recent years according to the same study.
Physicians write 60% of prescriptions for anti-depressants. And because depression and other mental health issues remain a taboo topic to many Americans, many patients visit their physician instead of a mental health clinician. As such, hospitalists need to be able to accurately assess depression and suicide risk.
Dr. Lineberry suggests the following steps for hospitalists who diagnose patients with depression:
- Consider using the holidays to renew or update systems of practice to better identify depression;
- Use the PHQ-9 questionnaire with patients who display symptoms of depression; and
- Ask direct and clear questions about suicidal thoughts and behaviors. Keep substance abuse as a risk factor in mind.
Second-Cancer Signal Affirmed After Lenalidomide for Myeloma
SAN DIEGO – The risk of a secondary malignancy doubled in patients with newly diagnosed multiple myeloma treated with melphalan plus thalidomide or lenalidomide in a retrospective, pooled analysis of 2,283 patients.
Incidence rates per 100 persons per year of follow-up were 0.95 with high-dose melphalan (Alkeran) followed by lenalidomide (Revlimid) maintenance and 1.05 with melphalan and thalidomide. In comparison, rates were 0.40 with cyclophosphamide, lenalidomide, and dexamethasone and 0.42 with melphalan and no immunomodulatory drugs, Dr. Antonio Palumbo reported at the annual meeting of the American Society of Hematology (ASH).

At 4 years of follow-up, second cancers were diagnosed in 48 (2.1%) of the 2,283 patients enrolled in nine experimental trials of the European Myeloma Network. There was consistent evidence of an increase in late events over time.
"I do not want to underestimate the issue," Dr. Palumbo said. "There is a signal, but the first conclusion is caution. When you come to 48 cancers versus 2,200 patients, by chance many things may happen."
He noted that the risk of multiple myeloma progression is between 10 and 15 times higher than the diagnosis of a second cancer, and suggested that the emphasis on second cancers may be overshadowing the risk of death due to toxic effects and infections.
Of the 48 secondary cancers, 8 of the 10 hematologic malignancies and 8 of the 38 solid tumors were fatal. In contrast, there were 124 toxic deaths (8.6%) and 49 infective deaths (3.4%) among 1,435 patients given the combination of melphalan-prednisone-thalidomide or bortezomib (Velcade)-melphalan-prednisone, said Dr. Palumbo, chief of the myeloma unit at the University of Torino (Italy).
"We take it for granted that with chemo we have some toxic effects," he said in an interview. "We should increase our alert of our combinations, and not focus solely on the second cancers."
Session co-moderator Dr. Meral Beksac, with Ankara (Turkey) University, said the Italian data suggest caution and greater vigilance regarding routine cancer screenings among multiple myeloma patients, but would not change her treatment approach.
"Dr. Palumbo has shown very beautifully that the benefits you achieve in terms of the long-term myeloma effect outweigh the risk of secondary malignancies," she said in an interview. "Personally, I think we must plan to avoid alkylating agents when we now have these better agents."
Preliminary data from three trials showing a fourfold increase in secondary cancers in multiple myeloma patients treated with lenalidomide as maintenance therapy or in combination with melphalan prompted investigations into the safety of lenalidomide in the United States and Europe in 2011.
The European Medicines Agency concluded in September that the benefits of lenalidomide continue to outweigh the risks within the approved setting of relapsed multiple myeloma, but recommended that a warning be added on the risk of second cancers. The U.S. Food and Drug Administration review is ongoing, and includes the risk for thalidomide, since lenalidomide is an analogue of thalidomide.
Although the development of acute myeloid leukemia (AML) following multiple myeloma was observed decades ago, the underlying mechanisms remain unclear. Swedish researchers recently reported that the risk of AML and myelodysplastic syndromes is 11.5-fold higher in multiple myeloma patients than in the general population, even before the introduction of novel agents (Blood 2011;118:4086-92). In addition, the risk of AML/MDS was eightfold higher in patients with monoclonal gammopathy of undetermined significance (MGUS), even though none of the MGUS patients developed multiple myeloma, according to session co-moderator Dr. Sigurdur Y. Kristinsson, who was a coauthor of the Swedish study.
"Even those people that never develop the disease have an increased risk of AML and MDS, so it shows that it’s not only the treatment that we’re giving, but it’s also an inherent susceptibility," Dr. Kristinsson, with the Karolinska Hospital and Institute in Stockholm, said in an interview.
Work is ongoing to identify multiple myeloma patients at an increased risk of second cancers, thereby allowing clinicians to tailor therapy to reduce risks. A separate poster presentation at the ASH meeting reported that higher risk of second cancers was associated with older age, male sex, and radiation and/or surgery among roughly 29,250 multiple myeloma patients in the Surveillance, Epidemiology, and End Results (SEER) database.
Subgroup analysis of the pooled Italian data did not identify specific subgroups at greater risk, Dr. Palumbo said. The incidence rate was higher at 1.13 per 100 person-years for patients given melphalan-lenalidomide vs. 0.76 per 100 person-years for patients treated with autologous stem cell transplantation and lenalidomide (median age 68 years vs. 59 years, respectively).
Speaking on behalf of the investigators, Dr. Palumbo reported employment with, serving as a consultant and on the speakers bureau of, having equity ownership in, and receiving research funding, patent royalties, and honoraria from Celgene, maker of lenalidomide. Dr. Beksac reported honoraria and speakers bureau activity with Celgene and Janssen Cilag. Dr. Kristinsson reported no conflicts of interest.
SAN DIEGO – The risk of a secondary malignancy doubled in patients with newly diagnosed multiple myeloma treated with melphalan plus thalidomide or lenalidomide in a retrospective, pooled analysis of 2,283 patients.
Incidence rates per 100 persons per year of follow-up were 0.95 with high-dose melphalan (Alkeran) followed by lenalidomide (Revlimid) maintenance and 1.05 with melphalan and thalidomide. In comparison, rates were 0.40 with cyclophosphamide, lenalidomide, and dexamethasone and 0.42 with melphalan and no immunomodulatory drugs, Dr. Antonio Palumbo reported at the annual meeting of the American Society of Hematology (ASH).
At 4 years of follow-up, second cancers were diagnosed in 48 (2.1%) of the 2,283 patients enrolled in nine experimental trials of the European Myeloma Network. There was consistent evidence of an increase in late events over time.
"I do not want to underestimate the issue," Dr. Palumbo said. "There is a signal, but the first conclusion is caution. When you come to 48 cancers versus 2,200 patients, by chance many things may happen."
He noted that the risk of multiple myeloma progression is between 10 and 15 times higher than the diagnosis of a second cancer, and suggested that the emphasis on second cancers may be overshadowing the risk of death due to toxic effects and infections.
Of the 48 secondary cancers, 8 of the 10 hematologic malignancies and 8 of the 38 solid tumors were fatal. In contrast, there were 124 toxic deaths (8.6%) and 49 infective deaths (3.4%) among 1,435 patients given the combination of melphalan-prednisone-thalidomide or bortezomib (Velcade)-melphalan-prednisone, said Dr. Palumbo, chief of the myeloma unit at the University of Torino (Italy).
"We take it for granted that with chemo we have some toxic effects," he said in an interview. "We should increase our alert of our combinations, and not focus solely on the second cancers."
Session co-moderator Dr. Meral Beksac, with Ankara (Turkey) University, said the Italian data suggest caution and greater vigilance regarding routine cancer screenings among multiple myeloma patients, but would not change her treatment approach.
"Dr. Palumbo has shown very beautifully that the benefits you achieve in terms of the long-term myeloma effect outweigh the risk of secondary malignancies," she said in an interview. "Personally, I think we must plan to avoid alkylating agents when we now have these better agents."
Preliminary data from three trials showing a fourfold increase in secondary cancers in multiple myeloma patients treated with lenalidomide as maintenance therapy or in combination with melphalan prompted investigations into the safety of lenalidomide in the United States and Europe in 2011.
The European Medicines Agency concluded in September that the benefits of lenalidomide continue to outweigh the risks within the approved setting of relapsed multiple myeloma, but recommended that a warning be added on the risk of second cancers. The U.S. Food and Drug Administration review is ongoing, and includes the risk for thalidomide, since lenalidomide is an analogue of thalidomide.
Although the development of acute myeloid leukemia (AML) following multiple myeloma was observed decades ago, the underlying mechanisms remain unclear. Swedish researchers recently reported that the risk of AML and myelodysplastic syndromes is 11.5-fold higher in multiple myeloma patients than in the general population, even before the introduction of novel agents (Blood 2011;118:4086-92). In addition, the risk of AML/MDS was eightfold higher in patients with monoclonal gammopathy of undetermined significance (MGUS), even though none of the MGUS patients developed multiple myeloma, according to session co-moderator Dr. Sigurdur Y. Kristinsson, who was a coauthor of the Swedish study.
"Even those people that never develop the disease have an increased risk of AML and MDS, so it shows that it’s not only the treatment that we’re giving, but it’s also an inherent susceptibility," Dr. Kristinsson, with the Karolinska Hospital and Institute in Stockholm, said in an interview.
Work is ongoing to identify multiple myeloma patients at an increased risk of second cancers, thereby allowing clinicians to tailor therapy to reduce risks. A separate poster presentation at the ASH meeting reported that higher risk of second cancers was associated with older age, male sex, and radiation and/or surgery among roughly 29,250 multiple myeloma patients in the Surveillance, Epidemiology, and End Results (SEER) database.
Subgroup analysis of the pooled Italian data did not identify specific subgroups at greater risk, Dr. Palumbo said. The incidence rate was higher at 1.13 per 100 person-years for patients given melphalan-lenalidomide vs. 0.76 per 100 person-years for patients treated with autologous stem cell transplantation and lenalidomide (median age 68 years vs. 59 years, respectively).
Speaking on behalf of the investigators, Dr. Palumbo reported employment with, serving as a consultant and on the speakers bureau of, having equity ownership in, and receiving research funding, patent royalties, and honoraria from Celgene, maker of lenalidomide. Dr. Beksac reported honoraria and speakers bureau activity with Celgene and Janssen Cilag. Dr. Kristinsson reported no conflicts of interest.
SAN DIEGO – The risk of a secondary malignancy doubled in patients with newly diagnosed multiple myeloma treated with melphalan plus thalidomide or lenalidomide in a retrospective, pooled analysis of 2,283 patients.
Incidence rates per 100 persons per year of follow-up were 0.95 with high-dose melphalan (Alkeran) followed by lenalidomide (Revlimid) maintenance and 1.05 with melphalan and thalidomide. In comparison, rates were 0.40 with cyclophosphamide, lenalidomide, and dexamethasone and 0.42 with melphalan and no immunomodulatory drugs, Dr. Antonio Palumbo reported at the annual meeting of the American Society of Hematology (ASH).
At 4 years of follow-up, second cancers were diagnosed in 48 (2.1%) of the 2,283 patients enrolled in nine experimental trials of the European Myeloma Network. There was consistent evidence of an increase in late events over time.
"I do not want to underestimate the issue," Dr. Palumbo said. "There is a signal, but the first conclusion is caution. When you come to 48 cancers versus 2,200 patients, by chance many things may happen."
He noted that the risk of multiple myeloma progression is between 10 and 15 times higher than the diagnosis of a second cancer, and suggested that the emphasis on second cancers may be overshadowing the risk of death due to toxic effects and infections.
Of the 48 secondary cancers, 8 of the 10 hematologic malignancies and 8 of the 38 solid tumors were fatal. In contrast, there were 124 toxic deaths (8.6%) and 49 infective deaths (3.4%) among 1,435 patients given the combination of melphalan-prednisone-thalidomide or bortezomib (Velcade)-melphalan-prednisone, said Dr. Palumbo, chief of the myeloma unit at the University of Torino (Italy).
"We take it for granted that with chemo we have some toxic effects," he said in an interview. "We should increase our alert of our combinations, and not focus solely on the second cancers."
Session co-moderator Dr. Meral Beksac, with Ankara (Turkey) University, said the Italian data suggest caution and greater vigilance regarding routine cancer screenings among multiple myeloma patients, but would not change her treatment approach.
"Dr. Palumbo has shown very beautifully that the benefits you achieve in terms of the long-term myeloma effect outweigh the risk of secondary malignancies," she said in an interview. "Personally, I think we must plan to avoid alkylating agents when we now have these better agents."
Preliminary data from three trials showing a fourfold increase in secondary cancers in multiple myeloma patients treated with lenalidomide as maintenance therapy or in combination with melphalan prompted investigations into the safety of lenalidomide in the United States and Europe in 2011.
The European Medicines Agency concluded in September that the benefits of lenalidomide continue to outweigh the risks within the approved setting of relapsed multiple myeloma, but recommended that a warning be added on the risk of second cancers. The U.S. Food and Drug Administration review is ongoing, and includes the risk for thalidomide, since lenalidomide is an analogue of thalidomide.
Although the development of acute myeloid leukemia (AML) following multiple myeloma was observed decades ago, the underlying mechanisms remain unclear. Swedish researchers recently reported that the risk of AML and myelodysplastic syndromes is 11.5-fold higher in multiple myeloma patients than in the general population, even before the introduction of novel agents (Blood 2011;118:4086-92). In addition, the risk of AML/MDS was eightfold higher in patients with monoclonal gammopathy of undetermined significance (MGUS), even though none of the MGUS patients developed multiple myeloma, according to session co-moderator Dr. Sigurdur Y. Kristinsson, who was a coauthor of the Swedish study.
"Even those people that never develop the disease have an increased risk of AML and MDS, so it shows that it’s not only the treatment that we’re giving, but it’s also an inherent susceptibility," Dr. Kristinsson, with the Karolinska Hospital and Institute in Stockholm, said in an interview.
Work is ongoing to identify multiple myeloma patients at an increased risk of second cancers, thereby allowing clinicians to tailor therapy to reduce risks. A separate poster presentation at the ASH meeting reported that higher risk of second cancers was associated with older age, male sex, and radiation and/or surgery among roughly 29,250 multiple myeloma patients in the Surveillance, Epidemiology, and End Results (SEER) database.
Subgroup analysis of the pooled Italian data did not identify specific subgroups at greater risk, Dr. Palumbo said. The incidence rate was higher at 1.13 per 100 person-years for patients given melphalan-lenalidomide vs. 0.76 per 100 person-years for patients treated with autologous stem cell transplantation and lenalidomide (median age 68 years vs. 59 years, respectively).
Speaking on behalf of the investigators, Dr. Palumbo reported employment with, serving as a consultant and on the speakers bureau of, having equity ownership in, and receiving research funding, patent royalties, and honoraria from Celgene, maker of lenalidomide. Dr. Beksac reported honoraria and speakers bureau activity with Celgene and Janssen Cilag. Dr. Kristinsson reported no conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: At 4 years of follow-up, second cancers were diagnosed in 2.1% of patients.
Data Source: Retrospective, pooled analysis of 2,283 patients who received lenalidomide for treatment of multiple myeloma in nine experimental trials.
Disclosures: Speaking on behalf of the investigators, Dr. Palumbo reported employment with, serving as a consultant and on the speakers bureau of, having equity ownership in, and receiving research funding, patent royalties, and honoraria from Celgene, maker of lenalidomide. Dr. Beksac reported honoraria and speakers bureau activity with Celgene and Janssen Cilag. Dr. Kristinsson reported no conflicts of interest.
AMA Policy Opposes Switch to ICD-10
On Nov. 10, the American Medical Association’s House of Delegates approved a policy opposing implementation of the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-CM) at a policy meeting in New Orleans. Following the vote, Robert M. Wah, MD, AMA board chair, stated, “The AMA will work vigorously to stop implementation of ICD-10, which will create a significant burden on the practice of medicine with no direct benefit to individual patients’ care.”
Organizations tied to hospitals, however, are fully supportive of the switch.
“We strongly support ICD-10 and the enhancements it will bring to the care that’s provided in hospitals,” says Don May, the American Hospital Association’s (AHA) vice president for policy. “The current coding system has really run its course in its ability to keep up with modern medicine.”
SHM has taken a “neutral” stance on this issue, for the time being, says SHM’s AMA delegate Bradley E. Flansbaum, DO, MPH, SFHM, director of hospitalist services at Lenox Hill Hospital in New York City. “But [SHM is] cautiously optimistic as the inpatient ecosystem evolves, hopefully, for the better.”
History of Opposition
In 2003, the AMA wrote to the National Committee on Vital and Health Statistics regarding plans to adopt ICD-10. The 55 signees of the letter (including the American College of Surgeons and other specialty societies) urged the committee to “confine your recommendation [to HHS] to the uses of ICD-10-PCS [the procedural codes portion] as a coding system for inpatient hospital services.” Another letter in 2006 to Bill Frist, then the U.S. Senate majority leader, expressed concern over a “rapid transition” from ICD-9 to ICD-10.
The AMA contends that switching to ICD-10 disproportionately burdens physicians in practice. “Depending on the size of a medical practice,” Dr. Wah says, “the total cost of impact of the ICD-10 mandate will range from $83,290 to more than $2.7 million. Physicians should not be expected to carry a disproportionate burden of the implementation costs when others in the health sector stand to reap the primary financial benefits.”
Upgrade: The Time Has Come
Organizations in support of the changeover, however, see the implementation of ICD-10 coding as a necessary step forward in improving patient care.
—Robert M. Wah, MD, board chair, American Medical Association
“It’s not unreasonable to replace a 30-year-old, out-of-date system,” says Sue Bowman, RHIA, CCS, director of coding policy and compliance with the American Health Information Management Association (AHIMA). Bowman says she is surprised that the AMA maintains the switch will not benefit patient care. “Everything nowadays has to do with healthcare data,” she says. “Without good data, you cannot measure quality of care, patient outcomes, or effectiveness of treatments. The expectation is that ICD-10 will better mirror the terminology already used in medical records.”
May agrees. “We understand the concerns,” he says, “but if you think about how much better we’ll be able to track disease and how it affects patients, there will be a much more rich data set at our disposal. This will help us develop evidence-based medicine and quality standards in a much more robust way than we can do today.”
In addition, May says, hospitalists may be able to function as a “huge resource” to their community physician colleagues, to help them understand the benefits of making the switch, and help them find the short cuts to manage the new system.
AHIMA is aware, Bowman notes, that some physician groups “were struggling with moving forward with ICD-10, but our message to the industry is for people to continue working toward implementation. CMS has made it pretty clear that there’s not going to be a delay or a grace period.”
In response to the AMA action, a spokesperson for CMS says, “Implementation of this new coding system will mean better information to improve the quality of healthcare, and more accurate payments to providers. CMS is giving significant transition time and flexibility to providers to switch over, and we will continue to work with the healthcare community to ensure successful compliance.”
Gretchen Henkel is a freelance writer based in California.
On Nov. 10, the American Medical Association’s House of Delegates approved a policy opposing implementation of the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-CM) at a policy meeting in New Orleans. Following the vote, Robert M. Wah, MD, AMA board chair, stated, “The AMA will work vigorously to stop implementation of ICD-10, which will create a significant burden on the practice of medicine with no direct benefit to individual patients’ care.”
Organizations tied to hospitals, however, are fully supportive of the switch.
“We strongly support ICD-10 and the enhancements it will bring to the care that’s provided in hospitals,” says Don May, the American Hospital Association’s (AHA) vice president for policy. “The current coding system has really run its course in its ability to keep up with modern medicine.”
SHM has taken a “neutral” stance on this issue, for the time being, says SHM’s AMA delegate Bradley E. Flansbaum, DO, MPH, SFHM, director of hospitalist services at Lenox Hill Hospital in New York City. “But [SHM is] cautiously optimistic as the inpatient ecosystem evolves, hopefully, for the better.”
History of Opposition
In 2003, the AMA wrote to the National Committee on Vital and Health Statistics regarding plans to adopt ICD-10. The 55 signees of the letter (including the American College of Surgeons and other specialty societies) urged the committee to “confine your recommendation [to HHS] to the uses of ICD-10-PCS [the procedural codes portion] as a coding system for inpatient hospital services.” Another letter in 2006 to Bill Frist, then the U.S. Senate majority leader, expressed concern over a “rapid transition” from ICD-9 to ICD-10.
The AMA contends that switching to ICD-10 disproportionately burdens physicians in practice. “Depending on the size of a medical practice,” Dr. Wah says, “the total cost of impact of the ICD-10 mandate will range from $83,290 to more than $2.7 million. Physicians should not be expected to carry a disproportionate burden of the implementation costs when others in the health sector stand to reap the primary financial benefits.”
Upgrade: The Time Has Come
Organizations in support of the changeover, however, see the implementation of ICD-10 coding as a necessary step forward in improving patient care.
—Robert M. Wah, MD, board chair, American Medical Association
“It’s not unreasonable to replace a 30-year-old, out-of-date system,” says Sue Bowman, RHIA, CCS, director of coding policy and compliance with the American Health Information Management Association (AHIMA). Bowman says she is surprised that the AMA maintains the switch will not benefit patient care. “Everything nowadays has to do with healthcare data,” she says. “Without good data, you cannot measure quality of care, patient outcomes, or effectiveness of treatments. The expectation is that ICD-10 will better mirror the terminology already used in medical records.”
May agrees. “We understand the concerns,” he says, “but if you think about how much better we’ll be able to track disease and how it affects patients, there will be a much more rich data set at our disposal. This will help us develop evidence-based medicine and quality standards in a much more robust way than we can do today.”
In addition, May says, hospitalists may be able to function as a “huge resource” to their community physician colleagues, to help them understand the benefits of making the switch, and help them find the short cuts to manage the new system.
AHIMA is aware, Bowman notes, that some physician groups “were struggling with moving forward with ICD-10, but our message to the industry is for people to continue working toward implementation. CMS has made it pretty clear that there’s not going to be a delay or a grace period.”
In response to the AMA action, a spokesperson for CMS says, “Implementation of this new coding system will mean better information to improve the quality of healthcare, and more accurate payments to providers. CMS is giving significant transition time and flexibility to providers to switch over, and we will continue to work with the healthcare community to ensure successful compliance.”
Gretchen Henkel is a freelance writer based in California.
On Nov. 10, the American Medical Association’s House of Delegates approved a policy opposing implementation of the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-CM) at a policy meeting in New Orleans. Following the vote, Robert M. Wah, MD, AMA board chair, stated, “The AMA will work vigorously to stop implementation of ICD-10, which will create a significant burden on the practice of medicine with no direct benefit to individual patients’ care.”
Organizations tied to hospitals, however, are fully supportive of the switch.
“We strongly support ICD-10 and the enhancements it will bring to the care that’s provided in hospitals,” says Don May, the American Hospital Association’s (AHA) vice president for policy. “The current coding system has really run its course in its ability to keep up with modern medicine.”
SHM has taken a “neutral” stance on this issue, for the time being, says SHM’s AMA delegate Bradley E. Flansbaum, DO, MPH, SFHM, director of hospitalist services at Lenox Hill Hospital in New York City. “But [SHM is] cautiously optimistic as the inpatient ecosystem evolves, hopefully, for the better.”
History of Opposition
In 2003, the AMA wrote to the National Committee on Vital and Health Statistics regarding plans to adopt ICD-10. The 55 signees of the letter (including the American College of Surgeons and other specialty societies) urged the committee to “confine your recommendation [to HHS] to the uses of ICD-10-PCS [the procedural codes portion] as a coding system for inpatient hospital services.” Another letter in 2006 to Bill Frist, then the U.S. Senate majority leader, expressed concern over a “rapid transition” from ICD-9 to ICD-10.
The AMA contends that switching to ICD-10 disproportionately burdens physicians in practice. “Depending on the size of a medical practice,” Dr. Wah says, “the total cost of impact of the ICD-10 mandate will range from $83,290 to more than $2.7 million. Physicians should not be expected to carry a disproportionate burden of the implementation costs when others in the health sector stand to reap the primary financial benefits.”
Upgrade: The Time Has Come
Organizations in support of the changeover, however, see the implementation of ICD-10 coding as a necessary step forward in improving patient care.
—Robert M. Wah, MD, board chair, American Medical Association
“It’s not unreasonable to replace a 30-year-old, out-of-date system,” says Sue Bowman, RHIA, CCS, director of coding policy and compliance with the American Health Information Management Association (AHIMA). Bowman says she is surprised that the AMA maintains the switch will not benefit patient care. “Everything nowadays has to do with healthcare data,” she says. “Without good data, you cannot measure quality of care, patient outcomes, or effectiveness of treatments. The expectation is that ICD-10 will better mirror the terminology already used in medical records.”
May agrees. “We understand the concerns,” he says, “but if you think about how much better we’ll be able to track disease and how it affects patients, there will be a much more rich data set at our disposal. This will help us develop evidence-based medicine and quality standards in a much more robust way than we can do today.”
In addition, May says, hospitalists may be able to function as a “huge resource” to their community physician colleagues, to help them understand the benefits of making the switch, and help them find the short cuts to manage the new system.
AHIMA is aware, Bowman notes, that some physician groups “were struggling with moving forward with ICD-10, but our message to the industry is for people to continue working toward implementation. CMS has made it pretty clear that there’s not going to be a delay or a grace period.”
In response to the AMA action, a spokesperson for CMS says, “Implementation of this new coding system will mean better information to improve the quality of healthcare, and more accurate payments to providers. CMS is giving significant transition time and flexibility to providers to switch over, and we will continue to work with the healthcare community to ensure successful compliance.”
Gretchen Henkel is a freelance writer based in California.

Return ED Visits by Sickle Cell Patients Common
SAN DIEGO – More than 40% of patients with sickle cell disease return for acute care within 14 days following an emergency department treat-and-release visit, with young adults and those with public insurance having the highest rates of return.
Those are key findings from a large analysis of data from the 2005 and 2006 State Emergency Department Databases and State Inpatient Databases managed by the Healthcare Cost and Utilization Project, a federal, state, and industry partnership sponsored by the Agency for Healthcare Research and Quality.

"Patients with sickle cell disease who are discharged from the hospital have higher rates of rehospitalization than [patients with] almost any other chronic disease," lead study author Dr. David C. Brousseau said at the annual meeting of the American Society of Hematology. "Because of the high rate of rehospitalizations, many hospitals have been developing programs to decrease rehospitalization rates for sickle cell disease. This effort is primarily driven by two factors: the recent federal emphasis on rehospitalizations, and a desire to improve care, with the belief that rehospitalizations represent a deficiency in care quality, or at least an opportunity to improve care."
Previous studies have shown that about half of ED visits made by patients with sickle cell disease result in inpatient hospitalization, he continued, "yet little emphasis has been placed on what happens after an ED treat-and-release visit."
Dr. Brousseau and his associates conducted a retrospective cohort study of all sickle cell disease–related ED visits and hospitalizations during 2005 and 2006 in the states of Arizona, California, Florida, Massachusetts, Missouri, New York, South Carolina, and Tennessee. "One-third of patients with sickle cell disease in the United States reside in these eight states," said Dr. Brousseau, of the pediatrics department at the Medical College of Wisconsin and an emergency medicine specialist at Children’s Hospital of Wisconsin, Milwaukee.
The researchers hypothesized that patients with sickle cell disease who were treated and released from an ED would have high rates of 14-day return visits to both the ED and an inpatient unit. A 14-day window was chosen "to more accurately reflect a time period ... where a revisit would not be due to a new crisis," he said.
During the 2-year study period, 12,109 people with sickle cell disease made 39,775 index ED visits. The 14-day return visit rate was 42.1%, "meaning that 42.1% of all ED treat-and-release visits were followed within 14 days by a return visit to either the ED or the inpatient unit," Dr. Brousseau said. A higher proportion of the return visits were to the ED than to the inpatient unit (25.4% vs. 16.7%, respectively).
Analysis of data by patient age and insurance provider revealed that the highest proportion of return visits within 14 days was made by patients aged 18-30 years (49%) and by those who carried public insurance (46.5%).
The 7-day return rate was 31.6%. Of these, 18.6% were to the ED and 13% were to the inpatient unit.
The 14-day revisit rate to the same hospital was 31.2%. Children were more likely than adults to make return visits to the same hospital (84.3% vs. 72.7%, respectively).
"We conclude that an ED treat-and-release visit should serve as a trigger to focus enhanced outpatient care to prevent subsequent inpatient visits and to improve patient care," Dr. Brousseau said.
Dr. Brousseau said he had no relevant financial disclosures.
SAN DIEGO – More than 40% of patients with sickle cell disease return for acute care within 14 days following an emergency department treat-and-release visit, with young adults and those with public insurance having the highest rates of return.
Those are key findings from a large analysis of data from the 2005 and 2006 State Emergency Department Databases and State Inpatient Databases managed by the Healthcare Cost and Utilization Project, a federal, state, and industry partnership sponsored by the Agency for Healthcare Research and Quality.
"Patients with sickle cell disease who are discharged from the hospital have higher rates of rehospitalization than [patients with] almost any other chronic disease," lead study author Dr. David C. Brousseau said at the annual meeting of the American Society of Hematology. "Because of the high rate of rehospitalizations, many hospitals have been developing programs to decrease rehospitalization rates for sickle cell disease. This effort is primarily driven by two factors: the recent federal emphasis on rehospitalizations, and a desire to improve care, with the belief that rehospitalizations represent a deficiency in care quality, or at least an opportunity to improve care."
Previous studies have shown that about half of ED visits made by patients with sickle cell disease result in inpatient hospitalization, he continued, "yet little emphasis has been placed on what happens after an ED treat-and-release visit."
Dr. Brousseau and his associates conducted a retrospective cohort study of all sickle cell disease–related ED visits and hospitalizations during 2005 and 2006 in the states of Arizona, California, Florida, Massachusetts, Missouri, New York, South Carolina, and Tennessee. "One-third of patients with sickle cell disease in the United States reside in these eight states," said Dr. Brousseau, of the pediatrics department at the Medical College of Wisconsin and an emergency medicine specialist at Children’s Hospital of Wisconsin, Milwaukee.
The researchers hypothesized that patients with sickle cell disease who were treated and released from an ED would have high rates of 14-day return visits to both the ED and an inpatient unit. A 14-day window was chosen "to more accurately reflect a time period ... where a revisit would not be due to a new crisis," he said.
During the 2-year study period, 12,109 people with sickle cell disease made 39,775 index ED visits. The 14-day return visit rate was 42.1%, "meaning that 42.1% of all ED treat-and-release visits were followed within 14 days by a return visit to either the ED or the inpatient unit," Dr. Brousseau said. A higher proportion of the return visits were to the ED than to the inpatient unit (25.4% vs. 16.7%, respectively).
Analysis of data by patient age and insurance provider revealed that the highest proportion of return visits within 14 days was made by patients aged 18-30 years (49%) and by those who carried public insurance (46.5%).
The 7-day return rate was 31.6%. Of these, 18.6% were to the ED and 13% were to the inpatient unit.
The 14-day revisit rate to the same hospital was 31.2%. Children were more likely than adults to make return visits to the same hospital (84.3% vs. 72.7%, respectively).
"We conclude that an ED treat-and-release visit should serve as a trigger to focus enhanced outpatient care to prevent subsequent inpatient visits and to improve patient care," Dr. Brousseau said.
Dr. Brousseau said he had no relevant financial disclosures.
SAN DIEGO – More than 40% of patients with sickle cell disease return for acute care within 14 days following an emergency department treat-and-release visit, with young adults and those with public insurance having the highest rates of return.
Those are key findings from a large analysis of data from the 2005 and 2006 State Emergency Department Databases and State Inpatient Databases managed by the Healthcare Cost and Utilization Project, a federal, state, and industry partnership sponsored by the Agency for Healthcare Research and Quality.
"Patients with sickle cell disease who are discharged from the hospital have higher rates of rehospitalization than [patients with] almost any other chronic disease," lead study author Dr. David C. Brousseau said at the annual meeting of the American Society of Hematology. "Because of the high rate of rehospitalizations, many hospitals have been developing programs to decrease rehospitalization rates for sickle cell disease. This effort is primarily driven by two factors: the recent federal emphasis on rehospitalizations, and a desire to improve care, with the belief that rehospitalizations represent a deficiency in care quality, or at least an opportunity to improve care."
Previous studies have shown that about half of ED visits made by patients with sickle cell disease result in inpatient hospitalization, he continued, "yet little emphasis has been placed on what happens after an ED treat-and-release visit."
Dr. Brousseau and his associates conducted a retrospective cohort study of all sickle cell disease–related ED visits and hospitalizations during 2005 and 2006 in the states of Arizona, California, Florida, Massachusetts, Missouri, New York, South Carolina, and Tennessee. "One-third of patients with sickle cell disease in the United States reside in these eight states," said Dr. Brousseau, of the pediatrics department at the Medical College of Wisconsin and an emergency medicine specialist at Children’s Hospital of Wisconsin, Milwaukee.
The researchers hypothesized that patients with sickle cell disease who were treated and released from an ED would have high rates of 14-day return visits to both the ED and an inpatient unit. A 14-day window was chosen "to more accurately reflect a time period ... where a revisit would not be due to a new crisis," he said.
During the 2-year study period, 12,109 people with sickle cell disease made 39,775 index ED visits. The 14-day return visit rate was 42.1%, "meaning that 42.1% of all ED treat-and-release visits were followed within 14 days by a return visit to either the ED or the inpatient unit," Dr. Brousseau said. A higher proportion of the return visits were to the ED than to the inpatient unit (25.4% vs. 16.7%, respectively).
Analysis of data by patient age and insurance provider revealed that the highest proportion of return visits within 14 days was made by patients aged 18-30 years (49%) and by those who carried public insurance (46.5%).
The 7-day return rate was 31.6%. Of these, 18.6% were to the ED and 13% were to the inpatient unit.
The 14-day revisit rate to the same hospital was 31.2%. Children were more likely than adults to make return visits to the same hospital (84.3% vs. 72.7%, respectively).
"We conclude that an ED treat-and-release visit should serve as a trigger to focus enhanced outpatient care to prevent subsequent inpatient visits and to improve patient care," Dr. Brousseau said.
Dr. Brousseau said he had no relevant financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN SOCIETY OF HEMATOLOGY
Major Finding: More than 40% of patients with sickle cell disease return for acute care following an ED treat-and-release visit.
Data Source: A study of 12,109 people with sickle cell disease in eight states who made 39,775 index ED visits in 2005 and 2006, based on Healthcare Cost and Utilization Project data.
Disclosures: Dr. Brousseau said he had no relevant financial disclosures.