User login
Derail Behavioral Emergencies in Hospitals

Summary
Behavioral emergencies occur when a patient is physically aggressive or potentially harmful to himself/herself or others. Although they may be rare, behavioral emergencies are high-risk situations, and untrained staff might be uncomfortable dealing with these events.
Patients with underlying psychiatric or developmental disorders, those who have ingested substances, or those who have a medication side effect are at the highest risk for becoming violent. Triggers for these events could be pain, hunger, isolation, change in routine, or even the hospital’s physical environment. Early warning signs for a behavioral emergency can include verbal threats, yelling, or silence. Physical signs may include pacing, crossed arms, furrowed brow, or throwing objects.
The first response to a potential behavioral emergency is to try to de-escalate the situation. Speak in a quiet, calm voice; back off and give personal space. Try to reduce a source of discomfort, and use distractions or rewards. If de-escalation is not successful and a patient becomes violent, the provider’s first role is to be safe: Get away and get help. Hospitals should have—or should develop—a violent patient response team, which may then physically restrain the patient. Medications can be used to treat medical issues but should not be used solely for chemical restraint.
Once a patient is safely restrained, a number of Joint Commission on Accreditation of Healthcare Organizations-mandated actions must occur. The legal guardian and attending of record must be notified. A debrief must occur regarding the events; this must be documented in the medical record. Finally, a strategy must be formulated to enable the patient to be safely removed from restraints as soon as it is safe.
The presenters demonstrated various personal safety techniques to escape from a violent patient, as well as the use of physical restraints. Participants engaged in a mock behavioral emergency to experience the chaos of these events.
Summary
Behavioral emergencies occur when a patient is physically aggressive or potentially harmful to himself/herself or others. Although they may be rare, behavioral emergencies are high-risk situations, and untrained staff might be uncomfortable dealing with these events.
Patients with underlying psychiatric or developmental disorders, those who have ingested substances, or those who have a medication side effect are at the highest risk for becoming violent. Triggers for these events could be pain, hunger, isolation, change in routine, or even the hospital’s physical environment. Early warning signs for a behavioral emergency can include verbal threats, yelling, or silence. Physical signs may include pacing, crossed arms, furrowed brow, or throwing objects.
The first response to a potential behavioral emergency is to try to de-escalate the situation. Speak in a quiet, calm voice; back off and give personal space. Try to reduce a source of discomfort, and use distractions or rewards. If de-escalation is not successful and a patient becomes violent, the provider’s first role is to be safe: Get away and get help. Hospitals should have—or should develop—a violent patient response team, which may then physically restrain the patient. Medications can be used to treat medical issues but should not be used solely for chemical restraint.
Once a patient is safely restrained, a number of Joint Commission on Accreditation of Healthcare Organizations-mandated actions must occur. The legal guardian and attending of record must be notified. A debrief must occur regarding the events; this must be documented in the medical record. Finally, a strategy must be formulated to enable the patient to be safely removed from restraints as soon as it is safe.
The presenters demonstrated various personal safety techniques to escape from a violent patient, as well as the use of physical restraints. Participants engaged in a mock behavioral emergency to experience the chaos of these events.
Summary
Behavioral emergencies occur when a patient is physically aggressive or potentially harmful to himself/herself or others. Although they may be rare, behavioral emergencies are high-risk situations, and untrained staff might be uncomfortable dealing with these events.
Patients with underlying psychiatric or developmental disorders, those who have ingested substances, or those who have a medication side effect are at the highest risk for becoming violent. Triggers for these events could be pain, hunger, isolation, change in routine, or even the hospital’s physical environment. Early warning signs for a behavioral emergency can include verbal threats, yelling, or silence. Physical signs may include pacing, crossed arms, furrowed brow, or throwing objects.
The first response to a potential behavioral emergency is to try to de-escalate the situation. Speak in a quiet, calm voice; back off and give personal space. Try to reduce a source of discomfort, and use distractions or rewards. If de-escalation is not successful and a patient becomes violent, the provider’s first role is to be safe: Get away and get help. Hospitals should have—or should develop—a violent patient response team, which may then physically restrain the patient. Medications can be used to treat medical issues but should not be used solely for chemical restraint.
Once a patient is safely restrained, a number of Joint Commission on Accreditation of Healthcare Organizations-mandated actions must occur. The legal guardian and attending of record must be notified. A debrief must occur regarding the events; this must be documented in the medical record. Finally, a strategy must be formulated to enable the patient to be safely removed from restraints as soon as it is safe.
The presenters demonstrated various personal safety techniques to escape from a violent patient, as well as the use of physical restraints. Participants engaged in a mock behavioral emergency to experience the chaos of these events.
Hospitalist Program Building Blocks

Summary
“Master the basics of a good hospitalist program and keep revisiting your core values, and you will continue to have a high quality and sustainable program,” says Dr. Dan Hale at the PHM14 workshop “Building Blocks in the Evolution of a Successful Distributed Hospitalist Program.”
Dr. Elisabeth Schainker, chief of pediatric hospitalist medicine at The Floating Hospital for Children at Tufts Medical Center in Boston, and Dr. Hale, a hospitalist at The Floating Hospital and site director of the Lawrence General Hospital affiliated pediatric hospitalist program, allowed participants to share their experiences in program development.
This workshop reviewed the fundamentals programs should review before starting and also, periodically, after they’ve been established. Program changes should be made as needed. The workshop used an assessment tool to evaluate the basic elements of the participants’ programs. The February 2014 article “Key Principles and Characteristics of an Effective Hospital Medicine Group” in the Journal of Hospital Medicine was used as a starting point for program self-evaluation.
These “building blocks” include the following:
- Establish the rationale for the program and include all stakeholders;
- Determine financial expectations;
- Define scope of practice;
- Organize nursing and referral physician collaboration;
- Assess staffing and workload expectations;
- Establish referral base; and
- Ensure basic code and emergency preparedness.
Ongoing development elements of a program were discussed as well. These components help further integrate a hospitalist program with the hospital as a whole and help add value. These ongoing “building blocks” include:
- Communication and collaboration with other hospital departments (e.g. emergency, radiology, surgery);
- Newborn medicine care;
- Internal group clinical practice guidelines;
- Co-management of surgical or specialty patients;
- Transfers from other hospitals or continuing care from tertiary care centers;
- Pediatric code teams and rapid response teams;
- Advanced code and emergency preparedness and mock code training; and
- Nursing education.
These additive features may be different at each program. Not all of these components are applicable or needed at all hospitals. Thoughtful approaches and thorough planning can create synergy with other components of a program.
The essentials of a successful distributed network of multiple hospitalist program sites were also described.
After assuring that the fundamentals are present at each site, transparency and institutional alignment are imperative.
Summary
“Master the basics of a good hospitalist program and keep revisiting your core values, and you will continue to have a high quality and sustainable program,” says Dr. Dan Hale at the PHM14 workshop “Building Blocks in the Evolution of a Successful Distributed Hospitalist Program.”
Dr. Elisabeth Schainker, chief of pediatric hospitalist medicine at The Floating Hospital for Children at Tufts Medical Center in Boston, and Dr. Hale, a hospitalist at The Floating Hospital and site director of the Lawrence General Hospital affiliated pediatric hospitalist program, allowed participants to share their experiences in program development.
This workshop reviewed the fundamentals programs should review before starting and also, periodically, after they’ve been established. Program changes should be made as needed. The workshop used an assessment tool to evaluate the basic elements of the participants’ programs. The February 2014 article “Key Principles and Characteristics of an Effective Hospital Medicine Group” in the Journal of Hospital Medicine was used as a starting point for program self-evaluation.
These “building blocks” include the following:
- Establish the rationale for the program and include all stakeholders;
- Determine financial expectations;
- Define scope of practice;
- Organize nursing and referral physician collaboration;
- Assess staffing and workload expectations;
- Establish referral base; and
- Ensure basic code and emergency preparedness.
Ongoing development elements of a program were discussed as well. These components help further integrate a hospitalist program with the hospital as a whole and help add value. These ongoing “building blocks” include:
- Communication and collaboration with other hospital departments (e.g. emergency, radiology, surgery);
- Newborn medicine care;
- Internal group clinical practice guidelines;
- Co-management of surgical or specialty patients;
- Transfers from other hospitals or continuing care from tertiary care centers;
- Pediatric code teams and rapid response teams;
- Advanced code and emergency preparedness and mock code training; and
- Nursing education.
These additive features may be different at each program. Not all of these components are applicable or needed at all hospitals. Thoughtful approaches and thorough planning can create synergy with other components of a program.
The essentials of a successful distributed network of multiple hospitalist program sites were also described.
After assuring that the fundamentals are present at each site, transparency and institutional alignment are imperative.
Summary
“Master the basics of a good hospitalist program and keep revisiting your core values, and you will continue to have a high quality and sustainable program,” says Dr. Dan Hale at the PHM14 workshop “Building Blocks in the Evolution of a Successful Distributed Hospitalist Program.”
Dr. Elisabeth Schainker, chief of pediatric hospitalist medicine at The Floating Hospital for Children at Tufts Medical Center in Boston, and Dr. Hale, a hospitalist at The Floating Hospital and site director of the Lawrence General Hospital affiliated pediatric hospitalist program, allowed participants to share their experiences in program development.
This workshop reviewed the fundamentals programs should review before starting and also, periodically, after they’ve been established. Program changes should be made as needed. The workshop used an assessment tool to evaluate the basic elements of the participants’ programs. The February 2014 article “Key Principles and Characteristics of an Effective Hospital Medicine Group” in the Journal of Hospital Medicine was used as a starting point for program self-evaluation.
These “building blocks” include the following:
- Establish the rationale for the program and include all stakeholders;
- Determine financial expectations;
- Define scope of practice;
- Organize nursing and referral physician collaboration;
- Assess staffing and workload expectations;
- Establish referral base; and
- Ensure basic code and emergency preparedness.
Ongoing development elements of a program were discussed as well. These components help further integrate a hospitalist program with the hospital as a whole and help add value. These ongoing “building blocks” include:
- Communication and collaboration with other hospital departments (e.g. emergency, radiology, surgery);
- Newborn medicine care;
- Internal group clinical practice guidelines;
- Co-management of surgical or specialty patients;
- Transfers from other hospitals or continuing care from tertiary care centers;
- Pediatric code teams and rapid response teams;
- Advanced code and emergency preparedness and mock code training; and
- Nursing education.
These additive features may be different at each program. Not all of these components are applicable or needed at all hospitals. Thoughtful approaches and thorough planning can create synergy with other components of a program.
The essentials of a successful distributed network of multiple hospitalist program sites were also described.
After assuring that the fundamentals are present at each site, transparency and institutional alignment are imperative.
Pediatric Hospital Medicine 2014 Conference Draws Record-Setting Crowd

Surrounded by the bucolic grounds of the Disney Yacht and Beach Club Resort in Lake Buena Vista, Fla., more than 800 pediatric hospitalists gathered in July for Pediatric Hospital Medicine 2014 (PHM14). Preceded by the Society for Pediatric Sedation’s pre-course, PHM14 began in earnest with a warm welcome from Doug Carlson, MD, FAAP, chief of pediatric hospital medicine programs at St. Louis (Mo.) Children’s Hospital and chair of the PHM14 organizing committee.
The first day of the conference started with Patrick Conway, MD, MSc, FAAP, MHM, chief medical officer for the Centers for Medicare and Medicaid Services (CMS), who gave an update of ongoing reforms in the U.S. health delivery system, with a focus on pediatrics. With three years of experience as CMS’ top doc, Dr. Conway related the difficulties of going from an unsustainable fee-for-service system to a people-centered, outcomes-driven system.
“Pediatrics,” Dr. Conway said, “is a leader in patient and family engagement and population health.” This practice, he added, means that the six goals of the CMS Quality Strategy align well with ongoing efforts in PHM.
Despite the difficulties of instituting change in a system that handles $3 billion daily, Dr. Conway, formerly a pediatric hospitalist at Cincinnati Children’s Hospital, said he’s witnessed many signs of improvement in the CMS landscape. Preliminary data from 2012-2014, he said, have shown a 9% reduction in hospital-acquired conditions across all measures, and overall hospital utilization is “dropping like a rock.”
While “having a foot in the boat and a foot on the dock” has been difficult, the transition, through its alphabet soup of innovation programs, is now beginning to pay off. Giving providers a pathway through the changing landscape of risk, Dr. Conway said, is an ongoing priority.
Wrapping up the first day, three healthcare system CEOs took the stage to answer questions from the audience, with Mark Shen, MD, SFHM, president of Dell Children’s Medical Center of Central Texas in Austin, Texas, posing questions like a seasoned talk show host. Panel members included David J. Bailey, MD, MBA, president and CEO of the Nemours Foundation; Steve Narang, MD, MHCM, FAAP, CEO of Banner Good Samaritan Medical Center in Phoenix, Ariz.; and Jeff Sperring, MD, FAAP, president and CEO of Riley Hospital for Children at Indiana University Health in Indianapolis.
Questions were wide-ranging.
Q: How did you become a CEO?
“All I had to do was keep on saying ‘yes,’” Dr. Bailey said.
Q: What are you doing as a CEO to move from a fee-for-service system to a population-based system?
“We are still living in two different worlds. …It depends on ACO penetration, whether quality or volume will be the driver over the next three to five years,” Dr. Narang said.
Q: If PHM fellowship becomes a requirement, will your hospital fund them?
“It’s hard to define what we do, but we know there are core competencies. I don’t think we’re going to be at a point where certification will limit being a hospitalist anytime soon,” Dr. Shen said.
Q: What are the three most important things, from a CEO perspective, that a hospitalist should know?
“Know where your organization wants to go,” Dr. Sperring said.
The next day kicked off with an inspiring call to action by Steve Meuthing, MD, vice president for safety at Cincinnati Children’s Hospital Medical Center. He called on pediatric hospitalists to eliminate all serious harm from children’s hospitals in the U.S. As a part of the Children’s Hospitals’ Solutions for Patient Safety (SPS) network, an organization accounting for 25% of all children hospitalized in the U.S., Dr. Meuthing related the need to employ high reliability theory, along with operational and cultural changes, to improve reliability in patient safety.
“If you don’t standardize, the rest is just chaos,” he said. “We have to make it easy to do these things.”
Dr. Meuthing said improving process reliability is key to reducing adverse outcomes, and high reliability organizations have utilized this approach to reduce serious harm events across the 81 SPS hospitals. While prevention of patient harm is the goal, an additional benefit is cost savings. He estimated $27 million of cost savings was realized within SPS network hospitals in 2012-2013.
Oral abstract and conundrum presentations, concurrent with 23 sessions across nine tracks, kept attendees busy. Topics ranged from a PHM circumcision service to decreasing overuse of continuous pulse oximetry. The day’s talks wrapped up with the respective presidents of the meeting’s co-sponsors—the American Academy of Pediatrics, the American Pediatrics Association, and SHM—sharing their organizations’ visions of PHM’s future in a town hall format.
The second full day began with an update of the Joint Council of Pediatric Hospital Medicine’s efforts to further advance PHM as a field. The process of submitting a petition to the American Board of Pediatrics was reviewed, as were the current status and time course of the move toward Accreditation Council for Graduate Medical Education certification.
After lunch, the highly anticipated “Top Articles” session was presented by Robert Dudas, MD, medical director of the pediatric hospitalist program at Johns Hopkins Bayview Medical Center in Baltimore, and Karen Wilson, MD, MPH, section head for pediatric hospital medicine at Children’s Hospital Colorado in Aurora. The presenters reviewed literature from the past year on topics ranging from nebulized hypertonic saline for bronchiolitis to antibiotic prophylaxis in vesicoureteral reflux.
The final day commenced with a talk by Alberto Puig, MD, PhD, FACP, associate director of undergraduate education at Massachusetts General Hospital in Boston, whose experiences as an internist provided insight regarding the history of the physical examination, from the aphorisms of Hippocrates to the family-centered bedside rounding of today.
Dr. Chang is associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. He is pediatric editor of The Hospitalist.
Dr. O’Callaghan is a clinical assistant professor of pediatrics at the University of Washington and a member of Team Hospitalist.
Dr. Hale is a past member of Team Hospitalist and a pediatric hospitalist at the Floating Hospital for Children at Tufts Medical Center in Boston.
Dr. Pressel is a pediatric hospitalist and inpatient medical director at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and a member of Team Hospitalist.
Surrounded by the bucolic grounds of the Disney Yacht and Beach Club Resort in Lake Buena Vista, Fla., more than 800 pediatric hospitalists gathered in July for Pediatric Hospital Medicine 2014 (PHM14). Preceded by the Society for Pediatric Sedation’s pre-course, PHM14 began in earnest with a warm welcome from Doug Carlson, MD, FAAP, chief of pediatric hospital medicine programs at St. Louis (Mo.) Children’s Hospital and chair of the PHM14 organizing committee.
The first day of the conference started with Patrick Conway, MD, MSc, FAAP, MHM, chief medical officer for the Centers for Medicare and Medicaid Services (CMS), who gave an update of ongoing reforms in the U.S. health delivery system, with a focus on pediatrics. With three years of experience as CMS’ top doc, Dr. Conway related the difficulties of going from an unsustainable fee-for-service system to a people-centered, outcomes-driven system.
“Pediatrics,” Dr. Conway said, “is a leader in patient and family engagement and population health.” This practice, he added, means that the six goals of the CMS Quality Strategy align well with ongoing efforts in PHM.
Despite the difficulties of instituting change in a system that handles $3 billion daily, Dr. Conway, formerly a pediatric hospitalist at Cincinnati Children’s Hospital, said he’s witnessed many signs of improvement in the CMS landscape. Preliminary data from 2012-2014, he said, have shown a 9% reduction in hospital-acquired conditions across all measures, and overall hospital utilization is “dropping like a rock.”
While “having a foot in the boat and a foot on the dock” has been difficult, the transition, through its alphabet soup of innovation programs, is now beginning to pay off. Giving providers a pathway through the changing landscape of risk, Dr. Conway said, is an ongoing priority.
Wrapping up the first day, three healthcare system CEOs took the stage to answer questions from the audience, with Mark Shen, MD, SFHM, president of Dell Children’s Medical Center of Central Texas in Austin, Texas, posing questions like a seasoned talk show host. Panel members included David J. Bailey, MD, MBA, president and CEO of the Nemours Foundation; Steve Narang, MD, MHCM, FAAP, CEO of Banner Good Samaritan Medical Center in Phoenix, Ariz.; and Jeff Sperring, MD, FAAP, president and CEO of Riley Hospital for Children at Indiana University Health in Indianapolis.
Questions were wide-ranging.
Q: How did you become a CEO?
“All I had to do was keep on saying ‘yes,’” Dr. Bailey said.
Q: What are you doing as a CEO to move from a fee-for-service system to a population-based system?
“We are still living in two different worlds. …It depends on ACO penetration, whether quality or volume will be the driver over the next three to five years,” Dr. Narang said.
Q: If PHM fellowship becomes a requirement, will your hospital fund them?
“It’s hard to define what we do, but we know there are core competencies. I don’t think we’re going to be at a point where certification will limit being a hospitalist anytime soon,” Dr. Shen said.
Q: What are the three most important things, from a CEO perspective, that a hospitalist should know?
“Know where your organization wants to go,” Dr. Sperring said.
The next day kicked off with an inspiring call to action by Steve Meuthing, MD, vice president for safety at Cincinnati Children’s Hospital Medical Center. He called on pediatric hospitalists to eliminate all serious harm from children’s hospitals in the U.S. As a part of the Children’s Hospitals’ Solutions for Patient Safety (SPS) network, an organization accounting for 25% of all children hospitalized in the U.S., Dr. Meuthing related the need to employ high reliability theory, along with operational and cultural changes, to improve reliability in patient safety.
“If you don’t standardize, the rest is just chaos,” he said. “We have to make it easy to do these things.”
Dr. Meuthing said improving process reliability is key to reducing adverse outcomes, and high reliability organizations have utilized this approach to reduce serious harm events across the 81 SPS hospitals. While prevention of patient harm is the goal, an additional benefit is cost savings. He estimated $27 million of cost savings was realized within SPS network hospitals in 2012-2013.
Oral abstract and conundrum presentations, concurrent with 23 sessions across nine tracks, kept attendees busy. Topics ranged from a PHM circumcision service to decreasing overuse of continuous pulse oximetry. The day’s talks wrapped up with the respective presidents of the meeting’s co-sponsors—the American Academy of Pediatrics, the American Pediatrics Association, and SHM—sharing their organizations’ visions of PHM’s future in a town hall format.
The second full day began with an update of the Joint Council of Pediatric Hospital Medicine’s efforts to further advance PHM as a field. The process of submitting a petition to the American Board of Pediatrics was reviewed, as were the current status and time course of the move toward Accreditation Council for Graduate Medical Education certification.
After lunch, the highly anticipated “Top Articles” session was presented by Robert Dudas, MD, medical director of the pediatric hospitalist program at Johns Hopkins Bayview Medical Center in Baltimore, and Karen Wilson, MD, MPH, section head for pediatric hospital medicine at Children’s Hospital Colorado in Aurora. The presenters reviewed literature from the past year on topics ranging from nebulized hypertonic saline for bronchiolitis to antibiotic prophylaxis in vesicoureteral reflux.
The final day commenced with a talk by Alberto Puig, MD, PhD, FACP, associate director of undergraduate education at Massachusetts General Hospital in Boston, whose experiences as an internist provided insight regarding the history of the physical examination, from the aphorisms of Hippocrates to the family-centered bedside rounding of today.
Dr. Chang is associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. He is pediatric editor of The Hospitalist.
Dr. O’Callaghan is a clinical assistant professor of pediatrics at the University of Washington and a member of Team Hospitalist.
Dr. Hale is a past member of Team Hospitalist and a pediatric hospitalist at the Floating Hospital for Children at Tufts Medical Center in Boston.
Dr. Pressel is a pediatric hospitalist and inpatient medical director at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and a member of Team Hospitalist.
Surrounded by the bucolic grounds of the Disney Yacht and Beach Club Resort in Lake Buena Vista, Fla., more than 800 pediatric hospitalists gathered in July for Pediatric Hospital Medicine 2014 (PHM14). Preceded by the Society for Pediatric Sedation’s pre-course, PHM14 began in earnest with a warm welcome from Doug Carlson, MD, FAAP, chief of pediatric hospital medicine programs at St. Louis (Mo.) Children’s Hospital and chair of the PHM14 organizing committee.
The first day of the conference started with Patrick Conway, MD, MSc, FAAP, MHM, chief medical officer for the Centers for Medicare and Medicaid Services (CMS), who gave an update of ongoing reforms in the U.S. health delivery system, with a focus on pediatrics. With three years of experience as CMS’ top doc, Dr. Conway related the difficulties of going from an unsustainable fee-for-service system to a people-centered, outcomes-driven system.
“Pediatrics,” Dr. Conway said, “is a leader in patient and family engagement and population health.” This practice, he added, means that the six goals of the CMS Quality Strategy align well with ongoing efforts in PHM.
Despite the difficulties of instituting change in a system that handles $3 billion daily, Dr. Conway, formerly a pediatric hospitalist at Cincinnati Children’s Hospital, said he’s witnessed many signs of improvement in the CMS landscape. Preliminary data from 2012-2014, he said, have shown a 9% reduction in hospital-acquired conditions across all measures, and overall hospital utilization is “dropping like a rock.”
While “having a foot in the boat and a foot on the dock” has been difficult, the transition, through its alphabet soup of innovation programs, is now beginning to pay off. Giving providers a pathway through the changing landscape of risk, Dr. Conway said, is an ongoing priority.
Wrapping up the first day, three healthcare system CEOs took the stage to answer questions from the audience, with Mark Shen, MD, SFHM, president of Dell Children’s Medical Center of Central Texas in Austin, Texas, posing questions like a seasoned talk show host. Panel members included David J. Bailey, MD, MBA, president and CEO of the Nemours Foundation; Steve Narang, MD, MHCM, FAAP, CEO of Banner Good Samaritan Medical Center in Phoenix, Ariz.; and Jeff Sperring, MD, FAAP, president and CEO of Riley Hospital for Children at Indiana University Health in Indianapolis.
Questions were wide-ranging.
Q: How did you become a CEO?
“All I had to do was keep on saying ‘yes,’” Dr. Bailey said.
Q: What are you doing as a CEO to move from a fee-for-service system to a population-based system?
“We are still living in two different worlds. …It depends on ACO penetration, whether quality or volume will be the driver over the next three to five years,” Dr. Narang said.
Q: If PHM fellowship becomes a requirement, will your hospital fund them?
“It’s hard to define what we do, but we know there are core competencies. I don’t think we’re going to be at a point where certification will limit being a hospitalist anytime soon,” Dr. Shen said.
Q: What are the three most important things, from a CEO perspective, that a hospitalist should know?
“Know where your organization wants to go,” Dr. Sperring said.
The next day kicked off with an inspiring call to action by Steve Meuthing, MD, vice president for safety at Cincinnati Children’s Hospital Medical Center. He called on pediatric hospitalists to eliminate all serious harm from children’s hospitals in the U.S. As a part of the Children’s Hospitals’ Solutions for Patient Safety (SPS) network, an organization accounting for 25% of all children hospitalized in the U.S., Dr. Meuthing related the need to employ high reliability theory, along with operational and cultural changes, to improve reliability in patient safety.
“If you don’t standardize, the rest is just chaos,” he said. “We have to make it easy to do these things.”
Dr. Meuthing said improving process reliability is key to reducing adverse outcomes, and high reliability organizations have utilized this approach to reduce serious harm events across the 81 SPS hospitals. While prevention of patient harm is the goal, an additional benefit is cost savings. He estimated $27 million of cost savings was realized within SPS network hospitals in 2012-2013.
Oral abstract and conundrum presentations, concurrent with 23 sessions across nine tracks, kept attendees busy. Topics ranged from a PHM circumcision service to decreasing overuse of continuous pulse oximetry. The day’s talks wrapped up with the respective presidents of the meeting’s co-sponsors—the American Academy of Pediatrics, the American Pediatrics Association, and SHM—sharing their organizations’ visions of PHM’s future in a town hall format.
The second full day began with an update of the Joint Council of Pediatric Hospital Medicine’s efforts to further advance PHM as a field. The process of submitting a petition to the American Board of Pediatrics was reviewed, as were the current status and time course of the move toward Accreditation Council for Graduate Medical Education certification.
After lunch, the highly anticipated “Top Articles” session was presented by Robert Dudas, MD, medical director of the pediatric hospitalist program at Johns Hopkins Bayview Medical Center in Baltimore, and Karen Wilson, MD, MPH, section head for pediatric hospital medicine at Children’s Hospital Colorado in Aurora. The presenters reviewed literature from the past year on topics ranging from nebulized hypertonic saline for bronchiolitis to antibiotic prophylaxis in vesicoureteral reflux.
The final day commenced with a talk by Alberto Puig, MD, PhD, FACP, associate director of undergraduate education at Massachusetts General Hospital in Boston, whose experiences as an internist provided insight regarding the history of the physical examination, from the aphorisms of Hippocrates to the family-centered bedside rounding of today.
Dr. Chang is associate clinical professor of medicine and pediatrics at the University of California at San Diego School of Medicine and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. He is pediatric editor of The Hospitalist.
Dr. O’Callaghan is a clinical assistant professor of pediatrics at the University of Washington and a member of Team Hospitalist.
Dr. Hale is a past member of Team Hospitalist and a pediatric hospitalist at the Floating Hospital for Children at Tufts Medical Center in Boston.
Dr. Pressel is a pediatric hospitalist and inpatient medical director at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and a member of Team Hospitalist.
Specially-Trained Hospitalists Spearhead SHM’s Quality Improvement Programs

When SHM received the Joint Commission’s John M. Eisenberg Patient Safety and Quality Award for 2011 for innovation in patient safety and quality at the national level, the award represented national recognition for the society’s three major hospital quality improvement initiatives. Moreover, it highlighted the integral role mentors play in each of the programs, helping physicians and hospitals make accelerated progress on important patient safety and quality issues.
Mentored implementation assigns a physician expert to train, guide, and work with the participating facilities’ hospitalist-led, multidisciplinary team through the life cycle of a QI initiative. The three programs focus on VTE prevention, glycemic control, and transitions of care. The first hospital cohort for VTE prevention—the VTE Prevention Collaborative—was in 2007. The care transitions program, known as Project BOOST, started in 2008. The Glycemic Control Mentored Implementation (GCMI) Program began in 2009. A fourth SHM mentored implementation program is MARQUIS, the Multi-Center Medication Reconciliation Quality Improvement Study.
In basic terms, mentoring is “coaching from a physician who has expertise both in the clinical subject matter and in implementing the processes and tools of quality improvement—usually because they’ve done it themselves,” says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement and a co-founder of two of its mentored implementation programs.
Mentors typically are paired with one or two participating hospitals for 12 to 18 months, conducting monthly conference calls with the team, sharing tools and resources from SHM’s online library, and offering advice on how to navigate the treacherous currents of culture change within a hospital. BOOST mentors also make in-person site visits. They are well versed in protocol and order set design and quality measurement strategies, and they know how to engage frontline professionals and institutional leadership, Dr. Maynard says.
Some mentors have received formal QI training, and many have attended Mentor University, a 1-1/2 day intensive training course offered by SHM that reinforces the nuances of coaching, the contents of SHM’s quality toolkits, and ideas for overcoming common barriers to improvement. SHM’s mentor support provides continuous professional development for the mentors, pairing new mentors with senior mentors to coach them in the process and hosting an online community with other mentors.
“What’s telling to me is that many of the people who have been mentored by SHM’s programs in one topic go on to become mentors in another topic, taking those portable skills and principles and applying them in other quality areas,” Dr. Maynard says. “We’re fostering leadership and quality improvement skills among hospitalists; that’s really one of our main goals. People learn the skill and then spread it within their system.”
Mark Williams, MD, FACP, MHM, Project BOOST principal investigator and a veteran SHM mentor, says that just providing educational materials to health professionals often isn’t enough for them to overcome the barriers to change.
“I’ve seen many large-scale quality projects that didn’t work, as they were simply disseminating information, content, or knowledge,” he says. Mentored implementation as practiced by SHM is “a model for disseminating quality improvement nationally,” he adds. “Pretty much any quality improvement project can be done this way.”
Key to the mentored implementation program’s success is the personalized approach and customized solutions.
“You directly meet with the team in their own setting and begin to see what’s going on,” Dr. Williams says. “You also meet with the hospital’s senior leadership. That’s when you start to see change.”
The Hospitalist connected with eight SHM mentors. The following are snapshots of their work in the mentorship program and some of the lessons they taught—and learned—from the program.

Christine Lum Lung, MD, SFHM
Title: Medical director, Northern Colorado Hospitalists, Fort Collins
Program: VTE Prevention Collaborative
Background: As a practicing hospitalist and medical director of the HM group for a two-hospital system, Dr. Lum Lung chaired its quality committee for VTE protocol development. “It was obvious at our hospitals that we needed to do better at VTE prevention,” she explains.
Dr. Lum Lung’s team received VTE mentorship from Dr. Maynard, who later asked her to become a VTE mentor. She also attended all three levels of SHM’s Leadership Academy and has since become a mentor for the new HP3 (Hospitalist Program Peak Performance) mentored implementation program, a one-year collaboration among SHM, Northwestern University, Blue Cross/Blue Shield of Illinois, and the Illinois Hospital Association that is designed to help hospitalist groups optimize their programs and build healthy group culture.
Teachable moment: The essential qualities of a good mentee, Dr. Lum Lung says, are drive and dedication. “You believe strongly about it, so you can sell it to others. You also need a thick skin to face the adversities that come up. When my mentor gave me tasks and deadlines, I met those deadlines.”
Success story: “I’ve been impressed with how hard groups and individuals can work.” Most of the teams she has worked with were facing significant external stressors—starting a new program, moving into a new hospital, rolling out a new EHR, becoming part of a growing medical group. “Yet each of them has been incredibly engaged in the process and dedicated to completing their projects.”
Lessons learned: “That we all have something to learn from each other. While I am officially the mentor, I have learned a lot about processes, teamwork, and flow issues from the sites that could potentially be incorporated in our program.”
Advice: Working on a project as a team can be very powerful, she says. Even seemingly ‘small’ projects have allowed teams to learn how to work better together on day-to-day issues. With the victory of a small project behind them, they make lists of the next thing that they want to tackle.
“Our profession is constantly changing. We need to be thinking ahead for how we will face those challenges,” Dr. Lum Lung says. “A team that works well together will have an advantage in this new environment. Even if you have people who are new to quality improvement, their participation can still be important.”

Jordan Messler, MD, SFHM
Title: Medical director, Morton Plant Hospitalists, Clearwater, Fla.
Program: GCMI; Project BOOST
Background: Dr. Messler’s interest in QI led him to work with colleagues in SHM who are national leaders in quality. “A couple of years ago, I enrolled in Emory’s Quality Academy, a sister course to Intermountain Health’s course on quality. Then I enrolled our hospital in both the GCMI Program and Project BOOST. My mentors for those programs were terrific guides, which led to my interest in seeing their side of the program as a mentor myself.”
Teachable moment: One program had difficulty implementing a VTE prevention tool and couldn’t get nursing support as it had expected, largely due to lack of nursing engagement on the project team, he says. “We started talking about the history of the projects, and prior interventions. In addition, we talked to the different disciplines separately. It seems there used to be an excellent system where nursing helped out on the project team for risk assessment.”
As VTE prevention became more of a priority, some physicians separately created a new tool to replace the nursing tool without involving the whole team. “And they couldn’t understand why nursing wasn’t buying into the new process.”
Success story: There are similar themes to success and failure. Sites that have strong administrative support (i.e., C-suite representation on the QI team), that have “accountability structure and stick to the basics of QI, with clear goals, ability to gather and report data, and use of a QI model [such as PDSA or Six Sigma] are the ones that succeed,” Dr. Messler says. “And the reverse is consistently true. Sustainable QI needs to be multidisciplinary, involving every voice, considering prior interventions and understanding of the culture.”
Lessons learned: “As mentors, we all continue to say we learn as much or more from these sites as they, hopefully, are learning from us. This collaboration and sharing of ideas has been instrumental to the success of the program.”
Advice: Get started today, and don’t give up. Follow the road map of QI projects, gather support, and get started. You will learn as much from your failures as your successes.
Dr. Messler says hospitals are looking for physician leaders to improve quality, and hospitalists are perfectly positioned to be those QI leaders. These big projects can last for years, so quality teams and hospitals need to be prepared to take the long view.
—Jennifer Quartarolo, MD, SFHM

Stephanie Rennke, MD
Title: Associate clinical professor of medicine, co-director of faculty development, division of hospital medicine, University of California San Francisco Medical Center.
Program: Project BOOST
Background: “When I started as a hospitalist right out of residency, QI had not been part of my training. But I noticed that quality was at the forefront of the academic interests of all the hospitalists at UCSF. I was personally interested in transitions of care. I still do home visits after hours for at-risk patients when they leave the hospital.”
Dr. Rennke started in QI as a member of UCSF’s BOOST team in 2008. “I worked with other faculty in the division who had previous experience in quality improvement and transitions in care. One of the co-principal investigators for BOOST, Dr. Arpana Vidyarthi, suggested that it would be a really rewarding experience to mentor—and it was.”
Teachable moment: “I’ve been so impressed by the diversity of what’s out there. No hospitalist program or hospital is the same. There is no one-size-fits-all for quality improvement or transitions of care, so it is incredibly important that the mentor takes the time to get to know both the team and the hospital.”
Success story: “During a site visit, I had an opportunity to watch one of the nurses, who had received training from a competency-based Teach Back program, practice Teach Back with a patient at the bedside,” Dr. Rennke says. “I was doing a tour of the floor and went into the room of a patient about to be discharged. A young float nurse, not long out of school, sat down with the patient and went through the medications and discharge plan using Teach Back. It didn’t take more time, but the time was spent more constructively, with interaction back and forth. I remember that ‘aha’ moment for the patient and the look in her eyes. For me, as a mentor, it was exciting to think that something I had tried to bring to them had been incorporated by the site and was really working.”
Lessons learned: “I have learned that, while at a large institution like UCSF we tend to work in silos, smaller sites are often more integrated with the various disciplines. You can walk down the hall to the clinical pharmacist or have lunch with the charge nurse. So I’ve tried to bring back home a commitment to really get to know professional colleagues and have them feel that I’m interested in their perspectives.”
Advice: “Work in teams. You cannot do this alone. Include frontline staff. And don’t forget to advertise to others that the program exists. Get the word out—let people know.”

Jennifer Quartarolo, MD, SFHM
Title: Medical director, clinical resource management; associate clinical professor, division of hospital medicine, University of California San Diego Health System
Program: Project BOOST
Background: Dr. Quartarolo has 11 years of clinical experience as an academic hospitalist at two different medical centers, and she completed a training program in healthcare delivery and improvement through the Institute for Health Care Delivery Research in Salt Lake City, Utah. “At my own institution, I had been involved in multiple QI projects,” she says. “Since joining the faculty, I worked with our care transitions team for five years before becoming a mentor. We incorporated many elements from Project BOOST as we worked to improve our care transitions process,” which led to an invitation to be a mentor.
Teachable moment: “I had one site that I worked with that had a great new form they had developed to incorporate into their transition process; however, when they decided to implement the form, they got a lot of pushback from nursing,” she says. “Then they realized that they had not involved any frontline nurses in their planning. This example points out how important it is to have all the key players involved on your team, as improving transitions of care is a complex process requiring multidisciplinary collaboration.”
Success story: Dr. Quartarolo says she has worked with several hospitals that have seen significant improvement in their readmission rates after participating in Project BOOST and implementing its tools.
Lessons learned: “I am constantly impressed by the innovative ideas that teams come up with to deal with the challenges that their hospitals face,” she says. Every hospital is unique and needs to do self-evaluation before deciding what to focus on. “I have also worked with many sites that have challenges getting physicians engaged in their efforts, particularly if they do not have a hospitalist program.”
Advice: “We are in a unique role as hospitalists to identify systems issues and improve quality of care in the inpatient setting, and this is particularly useful in improving care transitions and decreasing readmissions rates.”

Rich Balaban, MD
Title: Medical director, Hospital-to-Home Community Collaboration Program, Cambridge Health Alliance; assistant professor of medicine, Harvard Medical School, Boston
Program: Project BOOST
Background: Dr. Balaban has worked clinically in both the inpatient setting as a hospitalist and the outpatient setting as a primary care doctor. “I have seen hospital discharges as both a receiver and a sender, so [I] have been able to appreciate the challenges facing doctors, nurses, case managers, and patients involved in the care transition process,” he says.
Dr. Balaban also conducted a randomized controlled trial that demonstrated the benefits of engaging nurses at a patient’s primary care site to make outreach phone calls immediately after hospital discharge. Dr. Williams asked him to present on the study.
“It was a great opportunity for me to share the results of our work and for Mark to see my presentation skills,” he says. “When I asked if there were opportunities to get more involved in care transitions work, he invited me to consider becoming a BOOST mentor.”
Teachable moment: “Wearing my primary care hat, I believe that while it is very important to structure an effective discharge for the patient while in the hospital, success or failure ultimately is determined by what happens in the outpatient setting,” Dr. Balaban says. Even if a ‘perfect discharge’ occurs in the hospital, it can all quickly unravel once the patient arrives at home.
Success story: “At several sites, I have encouraged the inpatient care team to invite the outpatient care team to become part of the care transitions team. This has frequently brought an important viewpoint and voice to the care transitions table. While hospitalists have initiated the discussion about care transitions, they need an effective outpatient partner to create a truly effective process.”
Lessons learned: “I have learned to hold judgment until seeing with my own eyes,” Dr. Balaban says. “One of the first sites I visited had developed a post-discharge clinic, which they were excited to show me. From my point of view, I thought that after discharge, patient care should be assumed by the primary care office as soon as possible, and a post-discharge clinic would only delay that process.
“To my great surprise, their post-discharge clinic provided an ideal bridge between the hospital and primary care. The post-discharge clinic really worked and provided patients with a wonderful resource. … I’ve learned that there are many ways to solve problems, often based on the available resources at a specific site.”
Advice: In order to best understand the challenges of hospital discharge, it is critical that you understand what happens to patients after they leave the hospital. Make a home visit to a recently discharged patient to really understand the challenges that patients face when they return home.

Amitkumar R. Patel, MD, MBA, FACP, SFHM
Title: Clinical instructor in hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Program: Project BOOST; also working with critical access hospitals in Illinois through PREP (Preventing Readmissions through Effective Partnerships)
Background: Although he now works in an urban teaching hospital, Dr. Patel also did private practice as a community hospitalist and has pursued formal healthcare management-focused training.
“I became a mentor because my experience and interest in quality improvement fit well with Project BOOST,” he says. “I enjoy coaching teams as they face challenges in quality improvement, especially in relation to readmissions reduction. My work with critical access hospitals is the result of my first year as a mentor with the PREP collaborative in Illinois.”
PREP, a collaborative initiative of SHM and the Illinois Hospital Association that is funded by Blue Cross/Blue Shield of Illinois, aims to help hospitals focus on quality initiatives, including BOOST.
Teachable moment/success story: One of Dr. Patel’s BOOST sites believed the team included all appropriate personnel to obtain discharge appointments prior to patients’ discharges. But as they began to work through the process of making sure each appointment was appropriately documented, the various team members assigned to this process could not consistently complete the task within their workflow.
The pilot unit secretaries were not part of the BOOST team initially but saw that they could fulfill this role quickly and easily. They knew who to call at the physicians’ offices to avoid getting stuck in the phone menu trees, and they used this knowledge to reach the schedulers directly. The BOOST team quickly realized the unit secretaries were the most appropriate personnel to capture this information and work with the patients or their families/caregivers to obtain the most convenient appointments. This role was added to the team, and the unit secretaries took ownership of this process. Other teams may also want to look beyond the customary team members to roles that may not be thought of as quality team members.
Lessons learned: “The biggest take-away for me involves the unique culture that exists in many of our urban and rural communities,” he says. Every BOOST site implements the project’s elements in its own unique way, and what works well in one location may not fit the needs of another. The role of the mentor is to balance the need for community-specific advice with unique attributes of the facility and the elements of Project BOOST. “Often, we use our mentor calls to brainstorm solutions, and the teams are teaching me what will work best in their environment.”
Advice: “Responsibility for hospital change management should not be abdicated to administrators or quality improvement staff members,” he says. “QI is not a sometime thing for some staff; it’s an all-the-time process for every staff member, including physicians, to participate in and actively manage.”
—Christopher Kim, MD, MBA, SFHM

Cheryl O’Malley, MD, FHM
Title: Internal medicine residency program director, Banner Good Samaritan Medical Center, Phoenix
Program: GCMI
Background: Banner Good Samaritan has participated in the BOOST, VTE, and GCMI programs. Dr. O’Malley brought her experience from developing, implementing, and leading local glycemic control efforts to mentoring others.
“When I first started working on our hospital’s process, I had so many questions and asked one of my mentors from residency, Dr. Greg Maynard,” she says. “He helped me to see that people around the country were asking the same questions and invited me to join SHM’s glycemic control work group. When the GCMI program started, I was asked to be a mentor.”
Teachable moment: “When I was a new attending on the wards after residency, my patients would ask me why their blood sugars were so much better controlled at home than in the hospital. Usually, the answer was that they were put on a sliding scale when they came into the hospital,” she says, noting that what was done at home wasn’t going to work in the hospital. Patients needed a different regimen—a more proactive approach than just the customary sliding scale.
“I started to learn more about basal rates, nutrition, and correction insulin regimens in the hospital, but I realized that to really have adequate safety and direction for the nursing staff, it would require a formal order set and systematic approach,” she says.
Success story: “One of my sites invited me to come and present grand rounds at the hospital, and the local physician team leader invited the whole quality team to her home. It was a very exciting team and had achieved a lot. Fifteen or 20 of us spent the evening talking about the project but also just enjoying the collegiality,” Dr. O’Malley says. “Even though we had never seen one another, I instantly knew everyone by voice from spending so much time on the phone. And we knew a lot about one another’s personal lives and careers.”
Lessons learned: “Hearing a program describe what they are doing and knowing that they were far ahead of my own hospital in many ways but still being able to provide an insight or a perspective to help them achieve their own next steps. Everyone has something to learn from another hospital or another discipline. We can all leverage our experiences to improve patient care.”
Advice: “Be patient. This is a really long process of constant improvements. I have been working on glycemic control for 10 years now and still feel like we have many opportunities to further improve.”

Christopher Kim, MD, MBA, SFHM
Title: Clinical associate professor of internal medicine and assistant professor of pediatrics, University of Michigan Health System, Ann Arbor
Program: Project BOOST; Michigan Transitions of Care Collaborative (M-TC2)
Background: Dr. Kim brings clinical, quality improvement, leadership, collaborative learning, and discussion facilitation skills to his work as program director of M-TC2 and as mentor to the sites he works with.
The collaborative is part of a set of state collaborative quality initiatives funded by Blue Cross Blue Shield of Michigan. One of those initiatives is focused on improving care transitions between the hospital setting and ambulatory care providers, using Project BOOST tools—expanded to integrate more closely with primary care providers, physician organizations, and ambulatory care. The eight Michigan-based mentors for M-TC2 have all attended SHM’s Mentor University.
Teachable moment: There are local challenges and there are general challenges—those that are commonly shared by most hospitals, Dr. Kim explains. Both need to be overcome when working on an improvement project such as transitions of care. The local hospitalist brings expertise about the former—which are often more difficult to understand and overcome. The mentor brings knowledge and experience of the universal challenges, as well as the benefit of having seen or heard about what other programs have done. Together, they can work to help the organization become better equipped to improve the initiative at hand.
Success story: “One hospital in the collaborative realized that it could roll out the Teach Back concept to both nurses and physicians,” he says. They started to teach residents how to interact with patients and began using this approach in physician-nurse teams. Subsequently, the team shared with the collaborative how physicians have embraced the concept.
Lessons learned: Every site has its successes and challenges, he says. Sharing both sides of the story can only advance the mission of the collaborative, as each organization learns from the successes and failures of the others.
Mentored implementation really does what it’s intended to do—helping to support the sites and keeping an organization on track and accountable for the work it does, because someone external to the organization is working with it and providing information about what other sites are doing.
Advice: Talk with different disciplines and find out how much they long to work with other care providers, and then have discussions about how to make interdisciplinary practice happen. “At our collaborative meetings over time, many of the 24 participating sites have shared their progress—the good things and the struggles,” Dr. Kim says.
Larry Beresford is a freelance writer in Alameda, Calif.
When SHM received the Joint Commission’s John M. Eisenberg Patient Safety and Quality Award for 2011 for innovation in patient safety and quality at the national level, the award represented national recognition for the society’s three major hospital quality improvement initiatives. Moreover, it highlighted the integral role mentors play in each of the programs, helping physicians and hospitals make accelerated progress on important patient safety and quality issues.
Mentored implementation assigns a physician expert to train, guide, and work with the participating facilities’ hospitalist-led, multidisciplinary team through the life cycle of a QI initiative. The three programs focus on VTE prevention, glycemic control, and transitions of care. The first hospital cohort for VTE prevention—the VTE Prevention Collaborative—was in 2007. The care transitions program, known as Project BOOST, started in 2008. The Glycemic Control Mentored Implementation (GCMI) Program began in 2009. A fourth SHM mentored implementation program is MARQUIS, the Multi-Center Medication Reconciliation Quality Improvement Study.
In basic terms, mentoring is “coaching from a physician who has expertise both in the clinical subject matter and in implementing the processes and tools of quality improvement—usually because they’ve done it themselves,” says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement and a co-founder of two of its mentored implementation programs.
Mentors typically are paired with one or two participating hospitals for 12 to 18 months, conducting monthly conference calls with the team, sharing tools and resources from SHM’s online library, and offering advice on how to navigate the treacherous currents of culture change within a hospital. BOOST mentors also make in-person site visits. They are well versed in protocol and order set design and quality measurement strategies, and they know how to engage frontline professionals and institutional leadership, Dr. Maynard says.
Some mentors have received formal QI training, and many have attended Mentor University, a 1-1/2 day intensive training course offered by SHM that reinforces the nuances of coaching, the contents of SHM’s quality toolkits, and ideas for overcoming common barriers to improvement. SHM’s mentor support provides continuous professional development for the mentors, pairing new mentors with senior mentors to coach them in the process and hosting an online community with other mentors.
“What’s telling to me is that many of the people who have been mentored by SHM’s programs in one topic go on to become mentors in another topic, taking those portable skills and principles and applying them in other quality areas,” Dr. Maynard says. “We’re fostering leadership and quality improvement skills among hospitalists; that’s really one of our main goals. People learn the skill and then spread it within their system.”
Mark Williams, MD, FACP, MHM, Project BOOST principal investigator and a veteran SHM mentor, says that just providing educational materials to health professionals often isn’t enough for them to overcome the barriers to change.
“I’ve seen many large-scale quality projects that didn’t work, as they were simply disseminating information, content, or knowledge,” he says. Mentored implementation as practiced by SHM is “a model for disseminating quality improvement nationally,” he adds. “Pretty much any quality improvement project can be done this way.”
Key to the mentored implementation program’s success is the personalized approach and customized solutions.
“You directly meet with the team in their own setting and begin to see what’s going on,” Dr. Williams says. “You also meet with the hospital’s senior leadership. That’s when you start to see change.”
The Hospitalist connected with eight SHM mentors. The following are snapshots of their work in the mentorship program and some of the lessons they taught—and learned—from the program.
Christine Lum Lung, MD, SFHM
Title: Medical director, Northern Colorado Hospitalists, Fort Collins
Program: VTE Prevention Collaborative
Background: As a practicing hospitalist and medical director of the HM group for a two-hospital system, Dr. Lum Lung chaired its quality committee for VTE protocol development. “It was obvious at our hospitals that we needed to do better at VTE prevention,” she explains.
Dr. Lum Lung’s team received VTE mentorship from Dr. Maynard, who later asked her to become a VTE mentor. She also attended all three levels of SHM’s Leadership Academy and has since become a mentor for the new HP3 (Hospitalist Program Peak Performance) mentored implementation program, a one-year collaboration among SHM, Northwestern University, Blue Cross/Blue Shield of Illinois, and the Illinois Hospital Association that is designed to help hospitalist groups optimize their programs and build healthy group culture.
Teachable moment: The essential qualities of a good mentee, Dr. Lum Lung says, are drive and dedication. “You believe strongly about it, so you can sell it to others. You also need a thick skin to face the adversities that come up. When my mentor gave me tasks and deadlines, I met those deadlines.”
Success story: “I’ve been impressed with how hard groups and individuals can work.” Most of the teams she has worked with were facing significant external stressors—starting a new program, moving into a new hospital, rolling out a new EHR, becoming part of a growing medical group. “Yet each of them has been incredibly engaged in the process and dedicated to completing their projects.”
Lessons learned: “That we all have something to learn from each other. While I am officially the mentor, I have learned a lot about processes, teamwork, and flow issues from the sites that could potentially be incorporated in our program.”
Advice: Working on a project as a team can be very powerful, she says. Even seemingly ‘small’ projects have allowed teams to learn how to work better together on day-to-day issues. With the victory of a small project behind them, they make lists of the next thing that they want to tackle.
“Our profession is constantly changing. We need to be thinking ahead for how we will face those challenges,” Dr. Lum Lung says. “A team that works well together will have an advantage in this new environment. Even if you have people who are new to quality improvement, their participation can still be important.”
Jordan Messler, MD, SFHM
Title: Medical director, Morton Plant Hospitalists, Clearwater, Fla.
Program: GCMI; Project BOOST
Background: Dr. Messler’s interest in QI led him to work with colleagues in SHM who are national leaders in quality. “A couple of years ago, I enrolled in Emory’s Quality Academy, a sister course to Intermountain Health’s course on quality. Then I enrolled our hospital in both the GCMI Program and Project BOOST. My mentors for those programs were terrific guides, which led to my interest in seeing their side of the program as a mentor myself.”
Teachable moment: One program had difficulty implementing a VTE prevention tool and couldn’t get nursing support as it had expected, largely due to lack of nursing engagement on the project team, he says. “We started talking about the history of the projects, and prior interventions. In addition, we talked to the different disciplines separately. It seems there used to be an excellent system where nursing helped out on the project team for risk assessment.”
As VTE prevention became more of a priority, some physicians separately created a new tool to replace the nursing tool without involving the whole team. “And they couldn’t understand why nursing wasn’t buying into the new process.”
Success story: There are similar themes to success and failure. Sites that have strong administrative support (i.e., C-suite representation on the QI team), that have “accountability structure and stick to the basics of QI, with clear goals, ability to gather and report data, and use of a QI model [such as PDSA or Six Sigma] are the ones that succeed,” Dr. Messler says. “And the reverse is consistently true. Sustainable QI needs to be multidisciplinary, involving every voice, considering prior interventions and understanding of the culture.”
Lessons learned: “As mentors, we all continue to say we learn as much or more from these sites as they, hopefully, are learning from us. This collaboration and sharing of ideas has been instrumental to the success of the program.”
Advice: Get started today, and don’t give up. Follow the road map of QI projects, gather support, and get started. You will learn as much from your failures as your successes.
Dr. Messler says hospitals are looking for physician leaders to improve quality, and hospitalists are perfectly positioned to be those QI leaders. These big projects can last for years, so quality teams and hospitals need to be prepared to take the long view.
—Jennifer Quartarolo, MD, SFHM
Stephanie Rennke, MD
Title: Associate clinical professor of medicine, co-director of faculty development, division of hospital medicine, University of California San Francisco Medical Center.
Program: Project BOOST
Background: “When I started as a hospitalist right out of residency, QI had not been part of my training. But I noticed that quality was at the forefront of the academic interests of all the hospitalists at UCSF. I was personally interested in transitions of care. I still do home visits after hours for at-risk patients when they leave the hospital.”
Dr. Rennke started in QI as a member of UCSF’s BOOST team in 2008. “I worked with other faculty in the division who had previous experience in quality improvement and transitions in care. One of the co-principal investigators for BOOST, Dr. Arpana Vidyarthi, suggested that it would be a really rewarding experience to mentor—and it was.”
Teachable moment: “I’ve been so impressed by the diversity of what’s out there. No hospitalist program or hospital is the same. There is no one-size-fits-all for quality improvement or transitions of care, so it is incredibly important that the mentor takes the time to get to know both the team and the hospital.”
Success story: “During a site visit, I had an opportunity to watch one of the nurses, who had received training from a competency-based Teach Back program, practice Teach Back with a patient at the bedside,” Dr. Rennke says. “I was doing a tour of the floor and went into the room of a patient about to be discharged. A young float nurse, not long out of school, sat down with the patient and went through the medications and discharge plan using Teach Back. It didn’t take more time, but the time was spent more constructively, with interaction back and forth. I remember that ‘aha’ moment for the patient and the look in her eyes. For me, as a mentor, it was exciting to think that something I had tried to bring to them had been incorporated by the site and was really working.”
Lessons learned: “I have learned that, while at a large institution like UCSF we tend to work in silos, smaller sites are often more integrated with the various disciplines. You can walk down the hall to the clinical pharmacist or have lunch with the charge nurse. So I’ve tried to bring back home a commitment to really get to know professional colleagues and have them feel that I’m interested in their perspectives.”
Advice: “Work in teams. You cannot do this alone. Include frontline staff. And don’t forget to advertise to others that the program exists. Get the word out—let people know.”
Jennifer Quartarolo, MD, SFHM
Title: Medical director, clinical resource management; associate clinical professor, division of hospital medicine, University of California San Diego Health System
Program: Project BOOST
Background: Dr. Quartarolo has 11 years of clinical experience as an academic hospitalist at two different medical centers, and she completed a training program in healthcare delivery and improvement through the Institute for Health Care Delivery Research in Salt Lake City, Utah. “At my own institution, I had been involved in multiple QI projects,” she says. “Since joining the faculty, I worked with our care transitions team for five years before becoming a mentor. We incorporated many elements from Project BOOST as we worked to improve our care transitions process,” which led to an invitation to be a mentor.
Teachable moment: “I had one site that I worked with that had a great new form they had developed to incorporate into their transition process; however, when they decided to implement the form, they got a lot of pushback from nursing,” she says. “Then they realized that they had not involved any frontline nurses in their planning. This example points out how important it is to have all the key players involved on your team, as improving transitions of care is a complex process requiring multidisciplinary collaboration.”
Success story: Dr. Quartarolo says she has worked with several hospitals that have seen significant improvement in their readmission rates after participating in Project BOOST and implementing its tools.
Lessons learned: “I am constantly impressed by the innovative ideas that teams come up with to deal with the challenges that their hospitals face,” she says. Every hospital is unique and needs to do self-evaluation before deciding what to focus on. “I have also worked with many sites that have challenges getting physicians engaged in their efforts, particularly if they do not have a hospitalist program.”
Advice: “We are in a unique role as hospitalists to identify systems issues and improve quality of care in the inpatient setting, and this is particularly useful in improving care transitions and decreasing readmissions rates.”
Rich Balaban, MD
Title: Medical director, Hospital-to-Home Community Collaboration Program, Cambridge Health Alliance; assistant professor of medicine, Harvard Medical School, Boston
Program: Project BOOST
Background: Dr. Balaban has worked clinically in both the inpatient setting as a hospitalist and the outpatient setting as a primary care doctor. “I have seen hospital discharges as both a receiver and a sender, so [I] have been able to appreciate the challenges facing doctors, nurses, case managers, and patients involved in the care transition process,” he says.
Dr. Balaban also conducted a randomized controlled trial that demonstrated the benefits of engaging nurses at a patient’s primary care site to make outreach phone calls immediately after hospital discharge. Dr. Williams asked him to present on the study.
“It was a great opportunity for me to share the results of our work and for Mark to see my presentation skills,” he says. “When I asked if there were opportunities to get more involved in care transitions work, he invited me to consider becoming a BOOST mentor.”
Teachable moment: “Wearing my primary care hat, I believe that while it is very important to structure an effective discharge for the patient while in the hospital, success or failure ultimately is determined by what happens in the outpatient setting,” Dr. Balaban says. Even if a ‘perfect discharge’ occurs in the hospital, it can all quickly unravel once the patient arrives at home.
Success story: “At several sites, I have encouraged the inpatient care team to invite the outpatient care team to become part of the care transitions team. This has frequently brought an important viewpoint and voice to the care transitions table. While hospitalists have initiated the discussion about care transitions, they need an effective outpatient partner to create a truly effective process.”
Lessons learned: “I have learned to hold judgment until seeing with my own eyes,” Dr. Balaban says. “One of the first sites I visited had developed a post-discharge clinic, which they were excited to show me. From my point of view, I thought that after discharge, patient care should be assumed by the primary care office as soon as possible, and a post-discharge clinic would only delay that process.
“To my great surprise, their post-discharge clinic provided an ideal bridge between the hospital and primary care. The post-discharge clinic really worked and provided patients with a wonderful resource. … I’ve learned that there are many ways to solve problems, often based on the available resources at a specific site.”
Advice: In order to best understand the challenges of hospital discharge, it is critical that you understand what happens to patients after they leave the hospital. Make a home visit to a recently discharged patient to really understand the challenges that patients face when they return home.
Amitkumar R. Patel, MD, MBA, FACP, SFHM
Title: Clinical instructor in hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Program: Project BOOST; also working with critical access hospitals in Illinois through PREP (Preventing Readmissions through Effective Partnerships)
Background: Although he now works in an urban teaching hospital, Dr. Patel also did private practice as a community hospitalist and has pursued formal healthcare management-focused training.
“I became a mentor because my experience and interest in quality improvement fit well with Project BOOST,” he says. “I enjoy coaching teams as they face challenges in quality improvement, especially in relation to readmissions reduction. My work with critical access hospitals is the result of my first year as a mentor with the PREP collaborative in Illinois.”
PREP, a collaborative initiative of SHM and the Illinois Hospital Association that is funded by Blue Cross/Blue Shield of Illinois, aims to help hospitals focus on quality initiatives, including BOOST.
Teachable moment/success story: One of Dr. Patel’s BOOST sites believed the team included all appropriate personnel to obtain discharge appointments prior to patients’ discharges. But as they began to work through the process of making sure each appointment was appropriately documented, the various team members assigned to this process could not consistently complete the task within their workflow.
The pilot unit secretaries were not part of the BOOST team initially but saw that they could fulfill this role quickly and easily. They knew who to call at the physicians’ offices to avoid getting stuck in the phone menu trees, and they used this knowledge to reach the schedulers directly. The BOOST team quickly realized the unit secretaries were the most appropriate personnel to capture this information and work with the patients or their families/caregivers to obtain the most convenient appointments. This role was added to the team, and the unit secretaries took ownership of this process. Other teams may also want to look beyond the customary team members to roles that may not be thought of as quality team members.
Lessons learned: “The biggest take-away for me involves the unique culture that exists in many of our urban and rural communities,” he says. Every BOOST site implements the project’s elements in its own unique way, and what works well in one location may not fit the needs of another. The role of the mentor is to balance the need for community-specific advice with unique attributes of the facility and the elements of Project BOOST. “Often, we use our mentor calls to brainstorm solutions, and the teams are teaching me what will work best in their environment.”
Advice: “Responsibility for hospital change management should not be abdicated to administrators or quality improvement staff members,” he says. “QI is not a sometime thing for some staff; it’s an all-the-time process for every staff member, including physicians, to participate in and actively manage.”
—Christopher Kim, MD, MBA, SFHM
Cheryl O’Malley, MD, FHM
Title: Internal medicine residency program director, Banner Good Samaritan Medical Center, Phoenix
Program: GCMI
Background: Banner Good Samaritan has participated in the BOOST, VTE, and GCMI programs. Dr. O’Malley brought her experience from developing, implementing, and leading local glycemic control efforts to mentoring others.
“When I first started working on our hospital’s process, I had so many questions and asked one of my mentors from residency, Dr. Greg Maynard,” she says. “He helped me to see that people around the country were asking the same questions and invited me to join SHM’s glycemic control work group. When the GCMI program started, I was asked to be a mentor.”
Teachable moment: “When I was a new attending on the wards after residency, my patients would ask me why their blood sugars were so much better controlled at home than in the hospital. Usually, the answer was that they were put on a sliding scale when they came into the hospital,” she says, noting that what was done at home wasn’t going to work in the hospital. Patients needed a different regimen—a more proactive approach than just the customary sliding scale.
“I started to learn more about basal rates, nutrition, and correction insulin regimens in the hospital, but I realized that to really have adequate safety and direction for the nursing staff, it would require a formal order set and systematic approach,” she says.
Success story: “One of my sites invited me to come and present grand rounds at the hospital, and the local physician team leader invited the whole quality team to her home. It was a very exciting team and had achieved a lot. Fifteen or 20 of us spent the evening talking about the project but also just enjoying the collegiality,” Dr. O’Malley says. “Even though we had never seen one another, I instantly knew everyone by voice from spending so much time on the phone. And we knew a lot about one another’s personal lives and careers.”
Lessons learned: “Hearing a program describe what they are doing and knowing that they were far ahead of my own hospital in many ways but still being able to provide an insight or a perspective to help them achieve their own next steps. Everyone has something to learn from another hospital or another discipline. We can all leverage our experiences to improve patient care.”
Advice: “Be patient. This is a really long process of constant improvements. I have been working on glycemic control for 10 years now and still feel like we have many opportunities to further improve.”
Christopher Kim, MD, MBA, SFHM
Title: Clinical associate professor of internal medicine and assistant professor of pediatrics, University of Michigan Health System, Ann Arbor
Program: Project BOOST; Michigan Transitions of Care Collaborative (M-TC2)
Background: Dr. Kim brings clinical, quality improvement, leadership, collaborative learning, and discussion facilitation skills to his work as program director of M-TC2 and as mentor to the sites he works with.
The collaborative is part of a set of state collaborative quality initiatives funded by Blue Cross Blue Shield of Michigan. One of those initiatives is focused on improving care transitions between the hospital setting and ambulatory care providers, using Project BOOST tools—expanded to integrate more closely with primary care providers, physician organizations, and ambulatory care. The eight Michigan-based mentors for M-TC2 have all attended SHM’s Mentor University.
Teachable moment: There are local challenges and there are general challenges—those that are commonly shared by most hospitals, Dr. Kim explains. Both need to be overcome when working on an improvement project such as transitions of care. The local hospitalist brings expertise about the former—which are often more difficult to understand and overcome. The mentor brings knowledge and experience of the universal challenges, as well as the benefit of having seen or heard about what other programs have done. Together, they can work to help the organization become better equipped to improve the initiative at hand.
Success story: “One hospital in the collaborative realized that it could roll out the Teach Back concept to both nurses and physicians,” he says. They started to teach residents how to interact with patients and began using this approach in physician-nurse teams. Subsequently, the team shared with the collaborative how physicians have embraced the concept.
Lessons learned: Every site has its successes and challenges, he says. Sharing both sides of the story can only advance the mission of the collaborative, as each organization learns from the successes and failures of the others.
Mentored implementation really does what it’s intended to do—helping to support the sites and keeping an organization on track and accountable for the work it does, because someone external to the organization is working with it and providing information about what other sites are doing.
Advice: Talk with different disciplines and find out how much they long to work with other care providers, and then have discussions about how to make interdisciplinary practice happen. “At our collaborative meetings over time, many of the 24 participating sites have shared their progress—the good things and the struggles,” Dr. Kim says.
Larry Beresford is a freelance writer in Alameda, Calif.
When SHM received the Joint Commission’s John M. Eisenberg Patient Safety and Quality Award for 2011 for innovation in patient safety and quality at the national level, the award represented national recognition for the society’s three major hospital quality improvement initiatives. Moreover, it highlighted the integral role mentors play in each of the programs, helping physicians and hospitals make accelerated progress on important patient safety and quality issues.
Mentored implementation assigns a physician expert to train, guide, and work with the participating facilities’ hospitalist-led, multidisciplinary team through the life cycle of a QI initiative. The three programs focus on VTE prevention, glycemic control, and transitions of care. The first hospital cohort for VTE prevention—the VTE Prevention Collaborative—was in 2007. The care transitions program, known as Project BOOST, started in 2008. The Glycemic Control Mentored Implementation (GCMI) Program began in 2009. A fourth SHM mentored implementation program is MARQUIS, the Multi-Center Medication Reconciliation Quality Improvement Study.
In basic terms, mentoring is “coaching from a physician who has expertise both in the clinical subject matter and in implementing the processes and tools of quality improvement—usually because they’ve done it themselves,” says Gregory Maynard, MD, MSc, SFHM, senior vice president of SHM’s Center for Hospital Innovation and Improvement and a co-founder of two of its mentored implementation programs.
Mentors typically are paired with one or two participating hospitals for 12 to 18 months, conducting monthly conference calls with the team, sharing tools and resources from SHM’s online library, and offering advice on how to navigate the treacherous currents of culture change within a hospital. BOOST mentors also make in-person site visits. They are well versed in protocol and order set design and quality measurement strategies, and they know how to engage frontline professionals and institutional leadership, Dr. Maynard says.
Some mentors have received formal QI training, and many have attended Mentor University, a 1-1/2 day intensive training course offered by SHM that reinforces the nuances of coaching, the contents of SHM’s quality toolkits, and ideas for overcoming common barriers to improvement. SHM’s mentor support provides continuous professional development for the mentors, pairing new mentors with senior mentors to coach them in the process and hosting an online community with other mentors.
“What’s telling to me is that many of the people who have been mentored by SHM’s programs in one topic go on to become mentors in another topic, taking those portable skills and principles and applying them in other quality areas,” Dr. Maynard says. “We’re fostering leadership and quality improvement skills among hospitalists; that’s really one of our main goals. People learn the skill and then spread it within their system.”
Mark Williams, MD, FACP, MHM, Project BOOST principal investigator and a veteran SHM mentor, says that just providing educational materials to health professionals often isn’t enough for them to overcome the barriers to change.
“I’ve seen many large-scale quality projects that didn’t work, as they were simply disseminating information, content, or knowledge,” he says. Mentored implementation as practiced by SHM is “a model for disseminating quality improvement nationally,” he adds. “Pretty much any quality improvement project can be done this way.”
Key to the mentored implementation program’s success is the personalized approach and customized solutions.
“You directly meet with the team in their own setting and begin to see what’s going on,” Dr. Williams says. “You also meet with the hospital’s senior leadership. That’s when you start to see change.”
The Hospitalist connected with eight SHM mentors. The following are snapshots of their work in the mentorship program and some of the lessons they taught—and learned—from the program.
Christine Lum Lung, MD, SFHM
Title: Medical director, Northern Colorado Hospitalists, Fort Collins
Program: VTE Prevention Collaborative
Background: As a practicing hospitalist and medical director of the HM group for a two-hospital system, Dr. Lum Lung chaired its quality committee for VTE protocol development. “It was obvious at our hospitals that we needed to do better at VTE prevention,” she explains.
Dr. Lum Lung’s team received VTE mentorship from Dr. Maynard, who later asked her to become a VTE mentor. She also attended all three levels of SHM’s Leadership Academy and has since become a mentor for the new HP3 (Hospitalist Program Peak Performance) mentored implementation program, a one-year collaboration among SHM, Northwestern University, Blue Cross/Blue Shield of Illinois, and the Illinois Hospital Association that is designed to help hospitalist groups optimize their programs and build healthy group culture.
Teachable moment: The essential qualities of a good mentee, Dr. Lum Lung says, are drive and dedication. “You believe strongly about it, so you can sell it to others. You also need a thick skin to face the adversities that come up. When my mentor gave me tasks and deadlines, I met those deadlines.”
Success story: “I’ve been impressed with how hard groups and individuals can work.” Most of the teams she has worked with were facing significant external stressors—starting a new program, moving into a new hospital, rolling out a new EHR, becoming part of a growing medical group. “Yet each of them has been incredibly engaged in the process and dedicated to completing their projects.”
Lessons learned: “That we all have something to learn from each other. While I am officially the mentor, I have learned a lot about processes, teamwork, and flow issues from the sites that could potentially be incorporated in our program.”
Advice: Working on a project as a team can be very powerful, she says. Even seemingly ‘small’ projects have allowed teams to learn how to work better together on day-to-day issues. With the victory of a small project behind them, they make lists of the next thing that they want to tackle.
“Our profession is constantly changing. We need to be thinking ahead for how we will face those challenges,” Dr. Lum Lung says. “A team that works well together will have an advantage in this new environment. Even if you have people who are new to quality improvement, their participation can still be important.”
Jordan Messler, MD, SFHM
Title: Medical director, Morton Plant Hospitalists, Clearwater, Fla.
Program: GCMI; Project BOOST
Background: Dr. Messler’s interest in QI led him to work with colleagues in SHM who are national leaders in quality. “A couple of years ago, I enrolled in Emory’s Quality Academy, a sister course to Intermountain Health’s course on quality. Then I enrolled our hospital in both the GCMI Program and Project BOOST. My mentors for those programs were terrific guides, which led to my interest in seeing their side of the program as a mentor myself.”
Teachable moment: One program had difficulty implementing a VTE prevention tool and couldn’t get nursing support as it had expected, largely due to lack of nursing engagement on the project team, he says. “We started talking about the history of the projects, and prior interventions. In addition, we talked to the different disciplines separately. It seems there used to be an excellent system where nursing helped out on the project team for risk assessment.”
As VTE prevention became more of a priority, some physicians separately created a new tool to replace the nursing tool without involving the whole team. “And they couldn’t understand why nursing wasn’t buying into the new process.”
Success story: There are similar themes to success and failure. Sites that have strong administrative support (i.e., C-suite representation on the QI team), that have “accountability structure and stick to the basics of QI, with clear goals, ability to gather and report data, and use of a QI model [such as PDSA or Six Sigma] are the ones that succeed,” Dr. Messler says. “And the reverse is consistently true. Sustainable QI needs to be multidisciplinary, involving every voice, considering prior interventions and understanding of the culture.”
Lessons learned: “As mentors, we all continue to say we learn as much or more from these sites as they, hopefully, are learning from us. This collaboration and sharing of ideas has been instrumental to the success of the program.”
Advice: Get started today, and don’t give up. Follow the road map of QI projects, gather support, and get started. You will learn as much from your failures as your successes.
Dr. Messler says hospitals are looking for physician leaders to improve quality, and hospitalists are perfectly positioned to be those QI leaders. These big projects can last for years, so quality teams and hospitals need to be prepared to take the long view.
—Jennifer Quartarolo, MD, SFHM
Stephanie Rennke, MD
Title: Associate clinical professor of medicine, co-director of faculty development, division of hospital medicine, University of California San Francisco Medical Center.
Program: Project BOOST
Background: “When I started as a hospitalist right out of residency, QI had not been part of my training. But I noticed that quality was at the forefront of the academic interests of all the hospitalists at UCSF. I was personally interested in transitions of care. I still do home visits after hours for at-risk patients when they leave the hospital.”
Dr. Rennke started in QI as a member of UCSF’s BOOST team in 2008. “I worked with other faculty in the division who had previous experience in quality improvement and transitions in care. One of the co-principal investigators for BOOST, Dr. Arpana Vidyarthi, suggested that it would be a really rewarding experience to mentor—and it was.”
Teachable moment: “I’ve been so impressed by the diversity of what’s out there. No hospitalist program or hospital is the same. There is no one-size-fits-all for quality improvement or transitions of care, so it is incredibly important that the mentor takes the time to get to know both the team and the hospital.”
Success story: “During a site visit, I had an opportunity to watch one of the nurses, who had received training from a competency-based Teach Back program, practice Teach Back with a patient at the bedside,” Dr. Rennke says. “I was doing a tour of the floor and went into the room of a patient about to be discharged. A young float nurse, not long out of school, sat down with the patient and went through the medications and discharge plan using Teach Back. It didn’t take more time, but the time was spent more constructively, with interaction back and forth. I remember that ‘aha’ moment for the patient and the look in her eyes. For me, as a mentor, it was exciting to think that something I had tried to bring to them had been incorporated by the site and was really working.”
Lessons learned: “I have learned that, while at a large institution like UCSF we tend to work in silos, smaller sites are often more integrated with the various disciplines. You can walk down the hall to the clinical pharmacist or have lunch with the charge nurse. So I’ve tried to bring back home a commitment to really get to know professional colleagues and have them feel that I’m interested in their perspectives.”
Advice: “Work in teams. You cannot do this alone. Include frontline staff. And don’t forget to advertise to others that the program exists. Get the word out—let people know.”
Jennifer Quartarolo, MD, SFHM
Title: Medical director, clinical resource management; associate clinical professor, division of hospital medicine, University of California San Diego Health System
Program: Project BOOST
Background: Dr. Quartarolo has 11 years of clinical experience as an academic hospitalist at two different medical centers, and she completed a training program in healthcare delivery and improvement through the Institute for Health Care Delivery Research in Salt Lake City, Utah. “At my own institution, I had been involved in multiple QI projects,” she says. “Since joining the faculty, I worked with our care transitions team for five years before becoming a mentor. We incorporated many elements from Project BOOST as we worked to improve our care transitions process,” which led to an invitation to be a mentor.
Teachable moment: “I had one site that I worked with that had a great new form they had developed to incorporate into their transition process; however, when they decided to implement the form, they got a lot of pushback from nursing,” she says. “Then they realized that they had not involved any frontline nurses in their planning. This example points out how important it is to have all the key players involved on your team, as improving transitions of care is a complex process requiring multidisciplinary collaboration.”
Success story: Dr. Quartarolo says she has worked with several hospitals that have seen significant improvement in their readmission rates after participating in Project BOOST and implementing its tools.
Lessons learned: “I am constantly impressed by the innovative ideas that teams come up with to deal with the challenges that their hospitals face,” she says. Every hospital is unique and needs to do self-evaluation before deciding what to focus on. “I have also worked with many sites that have challenges getting physicians engaged in their efforts, particularly if they do not have a hospitalist program.”
Advice: “We are in a unique role as hospitalists to identify systems issues and improve quality of care in the inpatient setting, and this is particularly useful in improving care transitions and decreasing readmissions rates.”
Rich Balaban, MD
Title: Medical director, Hospital-to-Home Community Collaboration Program, Cambridge Health Alliance; assistant professor of medicine, Harvard Medical School, Boston
Program: Project BOOST
Background: Dr. Balaban has worked clinically in both the inpatient setting as a hospitalist and the outpatient setting as a primary care doctor. “I have seen hospital discharges as both a receiver and a sender, so [I] have been able to appreciate the challenges facing doctors, nurses, case managers, and patients involved in the care transition process,” he says.
Dr. Balaban also conducted a randomized controlled trial that demonstrated the benefits of engaging nurses at a patient’s primary care site to make outreach phone calls immediately after hospital discharge. Dr. Williams asked him to present on the study.
“It was a great opportunity for me to share the results of our work and for Mark to see my presentation skills,” he says. “When I asked if there were opportunities to get more involved in care transitions work, he invited me to consider becoming a BOOST mentor.”
Teachable moment: “Wearing my primary care hat, I believe that while it is very important to structure an effective discharge for the patient while in the hospital, success or failure ultimately is determined by what happens in the outpatient setting,” Dr. Balaban says. Even if a ‘perfect discharge’ occurs in the hospital, it can all quickly unravel once the patient arrives at home.
Success story: “At several sites, I have encouraged the inpatient care team to invite the outpatient care team to become part of the care transitions team. This has frequently brought an important viewpoint and voice to the care transitions table. While hospitalists have initiated the discussion about care transitions, they need an effective outpatient partner to create a truly effective process.”
Lessons learned: “I have learned to hold judgment until seeing with my own eyes,” Dr. Balaban says. “One of the first sites I visited had developed a post-discharge clinic, which they were excited to show me. From my point of view, I thought that after discharge, patient care should be assumed by the primary care office as soon as possible, and a post-discharge clinic would only delay that process.
“To my great surprise, their post-discharge clinic provided an ideal bridge between the hospital and primary care. The post-discharge clinic really worked and provided patients with a wonderful resource. … I’ve learned that there are many ways to solve problems, often based on the available resources at a specific site.”
Advice: In order to best understand the challenges of hospital discharge, it is critical that you understand what happens to patients after they leave the hospital. Make a home visit to a recently discharged patient to really understand the challenges that patients face when they return home.
Amitkumar R. Patel, MD, MBA, FACP, SFHM
Title: Clinical instructor in hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Program: Project BOOST; also working with critical access hospitals in Illinois through PREP (Preventing Readmissions through Effective Partnerships)
Background: Although he now works in an urban teaching hospital, Dr. Patel also did private practice as a community hospitalist and has pursued formal healthcare management-focused training.
“I became a mentor because my experience and interest in quality improvement fit well with Project BOOST,” he says. “I enjoy coaching teams as they face challenges in quality improvement, especially in relation to readmissions reduction. My work with critical access hospitals is the result of my first year as a mentor with the PREP collaborative in Illinois.”
PREP, a collaborative initiative of SHM and the Illinois Hospital Association that is funded by Blue Cross/Blue Shield of Illinois, aims to help hospitals focus on quality initiatives, including BOOST.
Teachable moment/success story: One of Dr. Patel’s BOOST sites believed the team included all appropriate personnel to obtain discharge appointments prior to patients’ discharges. But as they began to work through the process of making sure each appointment was appropriately documented, the various team members assigned to this process could not consistently complete the task within their workflow.
The pilot unit secretaries were not part of the BOOST team initially but saw that they could fulfill this role quickly and easily. They knew who to call at the physicians’ offices to avoid getting stuck in the phone menu trees, and they used this knowledge to reach the schedulers directly. The BOOST team quickly realized the unit secretaries were the most appropriate personnel to capture this information and work with the patients or their families/caregivers to obtain the most convenient appointments. This role was added to the team, and the unit secretaries took ownership of this process. Other teams may also want to look beyond the customary team members to roles that may not be thought of as quality team members.
Lessons learned: “The biggest take-away for me involves the unique culture that exists in many of our urban and rural communities,” he says. Every BOOST site implements the project’s elements in its own unique way, and what works well in one location may not fit the needs of another. The role of the mentor is to balance the need for community-specific advice with unique attributes of the facility and the elements of Project BOOST. “Often, we use our mentor calls to brainstorm solutions, and the teams are teaching me what will work best in their environment.”
Advice: “Responsibility for hospital change management should not be abdicated to administrators or quality improvement staff members,” he says. “QI is not a sometime thing for some staff; it’s an all-the-time process for every staff member, including physicians, to participate in and actively manage.”
—Christopher Kim, MD, MBA, SFHM
Cheryl O’Malley, MD, FHM
Title: Internal medicine residency program director, Banner Good Samaritan Medical Center, Phoenix
Program: GCMI
Background: Banner Good Samaritan has participated in the BOOST, VTE, and GCMI programs. Dr. O’Malley brought her experience from developing, implementing, and leading local glycemic control efforts to mentoring others.
“When I first started working on our hospital’s process, I had so many questions and asked one of my mentors from residency, Dr. Greg Maynard,” she says. “He helped me to see that people around the country were asking the same questions and invited me to join SHM’s glycemic control work group. When the GCMI program started, I was asked to be a mentor.”
Teachable moment: “When I was a new attending on the wards after residency, my patients would ask me why their blood sugars were so much better controlled at home than in the hospital. Usually, the answer was that they were put on a sliding scale when they came into the hospital,” she says, noting that what was done at home wasn’t going to work in the hospital. Patients needed a different regimen—a more proactive approach than just the customary sliding scale.
“I started to learn more about basal rates, nutrition, and correction insulin regimens in the hospital, but I realized that to really have adequate safety and direction for the nursing staff, it would require a formal order set and systematic approach,” she says.
Success story: “One of my sites invited me to come and present grand rounds at the hospital, and the local physician team leader invited the whole quality team to her home. It was a very exciting team and had achieved a lot. Fifteen or 20 of us spent the evening talking about the project but also just enjoying the collegiality,” Dr. O’Malley says. “Even though we had never seen one another, I instantly knew everyone by voice from spending so much time on the phone. And we knew a lot about one another’s personal lives and careers.”
Lessons learned: “Hearing a program describe what they are doing and knowing that they were far ahead of my own hospital in many ways but still being able to provide an insight or a perspective to help them achieve their own next steps. Everyone has something to learn from another hospital or another discipline. We can all leverage our experiences to improve patient care.”
Advice: “Be patient. This is a really long process of constant improvements. I have been working on glycemic control for 10 years now and still feel like we have many opportunities to further improve.”
Christopher Kim, MD, MBA, SFHM
Title: Clinical associate professor of internal medicine and assistant professor of pediatrics, University of Michigan Health System, Ann Arbor
Program: Project BOOST; Michigan Transitions of Care Collaborative (M-TC2)
Background: Dr. Kim brings clinical, quality improvement, leadership, collaborative learning, and discussion facilitation skills to his work as program director of M-TC2 and as mentor to the sites he works with.
The collaborative is part of a set of state collaborative quality initiatives funded by Blue Cross Blue Shield of Michigan. One of those initiatives is focused on improving care transitions between the hospital setting and ambulatory care providers, using Project BOOST tools—expanded to integrate more closely with primary care providers, physician organizations, and ambulatory care. The eight Michigan-based mentors for M-TC2 have all attended SHM’s Mentor University.
Teachable moment: There are local challenges and there are general challenges—those that are commonly shared by most hospitals, Dr. Kim explains. Both need to be overcome when working on an improvement project such as transitions of care. The local hospitalist brings expertise about the former—which are often more difficult to understand and overcome. The mentor brings knowledge and experience of the universal challenges, as well as the benefit of having seen or heard about what other programs have done. Together, they can work to help the organization become better equipped to improve the initiative at hand.
Success story: “One hospital in the collaborative realized that it could roll out the Teach Back concept to both nurses and physicians,” he says. They started to teach residents how to interact with patients and began using this approach in physician-nurse teams. Subsequently, the team shared with the collaborative how physicians have embraced the concept.
Lessons learned: Every site has its successes and challenges, he says. Sharing both sides of the story can only advance the mission of the collaborative, as each organization learns from the successes and failures of the others.
Mentored implementation really does what it’s intended to do—helping to support the sites and keeping an organization on track and accountable for the work it does, because someone external to the organization is working with it and providing information about what other sites are doing.
Advice: Talk with different disciplines and find out how much they long to work with other care providers, and then have discussions about how to make interdisciplinary practice happen. “At our collaborative meetings over time, many of the 24 participating sites have shared their progress—the good things and the struggles,” Dr. Kim says.
Larry Beresford is a freelance writer in Alameda, Calif.
Do oral contraceptives put women with a family history of breast cancer at increased risk?
No. Modern combined oral contraceptive pills (OCPs) don’t increase breast cancer risk in women with a family history (strength of recommendation [SOR]: B, systematic review of cohort, case-control studies). However, older, higher-dose OCPs (in use before 1975) did increase breast cancer risk in these women (SOR: C, case-control study).
Similarly, modern OCPs don’t raise breast cancer risk in women with BRCA1/2 mutations, although higher-dose, pre-1975 OCPs did (SOR: B and C, a meta-analysis of cohort and case-control studies).
EVIDENCE SUMMARY
A systematic review of the effect of combined OCPs on women with a family history of breast cancer found no additional increase in risk.1 Investigators identified 3 retrospective cohort studies (N=66,500, with 8500 cases) and 7 case-control studies (total 10,500 cases) from the past 40 years, most including women from the United States and Canada, but one including women from 5 continents.
In most trials, women of reproductive age using combined OCPs had 1 or more first-degree female relatives with breast cancer, although a few trials also included second-degree relatives. Women ranged in age from 20 to 79 years at diagnosis, and most trials controlled for age, parity, menstrual and menopausal history, duration of OCP exposure, and age at first use. Follow-up intervals for the retrospective cohort studies ranged from 5 to 16 years. Investigators were unable to combine results because of heterogenous populations.
Three of the cohort studies found no significant difference in breast cancer risk between OCP users and nonusers, regardless of age or duration of use. One cohort study found an increased risk in women taking older, higher-dose OCPs from before 1975 (relative risk [RR]=3.3; 95% confidence interval [CI], 1.5-7.2). All of the case-control studies found no significant difference in breast cancer risk for any age of starting, duration of OCP use, or degree of relative with breast cancer.
A meta-analysis of 54 case-control studies (6757 cases), comprising approximately 90% of the epidemiologic information on this topic, also found no significant difference in breast cancer risk related to OCP use among women with one or more first-degree relatives with breast cancer.2 Investigators found that neither recent OCP use (<10 years, RR=0.77; 95% CI, 0.54-1.11) nor past OCP use (>10 years, RR=1.01; 95% CI, 0.80-1.28) affected risk of developing breast cancer.
Three additional case-control studies involving women with a family history of breast cancer also found no significant association for breast cancer incidence among OCP users compared with nonusers.3-5
Modern combined OCPs don’t raise risk in women with BRCA1/2 mutations
A meta-analysis of 5 studies (one retrospective cohort, 4 case-control, with a total of 2855 breast cancer cases and 2944 controls) evaluated whether combined OCPs increased the risk of breast cancer in women, all of whom were carrying BRCA1/2 mutations.6
Using modern combined OCPs didn’t raise the risk of breast cancer in BRCA1/2 carriers overall (RR=1.13; 95% CI, 0.88-1.45) or separately in BRCA1 carriers (5 studies, RR=1.09; 95% CI, 0.77-1.54) or BRCA2 carriers (3 studies, RR=1.15; 95% CI, 0.88-1.45).
However, pre-1975 (higher dose) combined OCPs produced significantly increased risk (RR=1.47; 95% CI, 1.06-2.04). Similarly, women who had used combined OCPs >10 years before the study (older women, likely to have been using pre-1975 OCPs) also had significantly increased risk (RR=1.46; 95% CI, 1.07-2.07).
A bit of good news: Combined OCPs reduce ovarian cancer risk
The analysis also determined that combined OCPs significantly reduced the risk of ovarian cancer in women carrying BRCA1/2 mutations (RR=0.50; 95% CI, 0.33-0.75), with an additional linear decrease in risk for each 10 years of OCP use (RR=0.64; 95% CI, 0.53-0.78).
RECOMMENDATIONS
The World Health Organization guidelines outlining criteria for contraceptive use state that OCPs don’t alter the risk of breast cancer among women with either a family history of breast cancer or breast cancer susceptibility genes.7
The American College of Obstetricians and Gynecologists (ACOG) says that a positive family history of breast cancer shouldn’t be regarded as a contraindication to OCP use.8 ACOG also says that women with the BRCA1 mutation have an increased risk of breast cancer if they used OCPs for longer than 5 years before age 30, but this risk may be more than balanced by the benefit of a greatly reduced risk of ovarian cancer.
1. Gaffield ME, Culwell KR, Ravi A. Oral contraceptives and family history of breast cancer. Contraception. 2009;80:372-380.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative re-analysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet. 1996;347:1713-1727.
3. Jernström H, Loman N, Johannsson OT, et al. Impact of teenage oral contraceptive use in a population-based series of early-onset breast cancer cases who have undergone BRCA mutation testing. Eur J Cancer. 2005;41:2312-2320.
4. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Human Reprod Update. 2010;16: 631-650.
5. Long-term oral contraceptive use and the risk of breast cancer. The Centers for Disease Control Cancer and Steroid Hormone Study. JAMA. 1983;249:1591-1595.
6. Iodice S, Barile M, Rotmensz N, et al. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer. 2010;46:2275-2284.
7. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. 4th ed. Geneva, Switzerland: World Health Organization; 2009. World Health Organization Web site. Available at: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed September 24, 2013.
8. ACOG Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107:1453-1472.
No. Modern combined oral contraceptive pills (OCPs) don’t increase breast cancer risk in women with a family history (strength of recommendation [SOR]: B, systematic review of cohort, case-control studies). However, older, higher-dose OCPs (in use before 1975) did increase breast cancer risk in these women (SOR: C, case-control study).
Similarly, modern OCPs don’t raise breast cancer risk in women with BRCA1/2 mutations, although higher-dose, pre-1975 OCPs did (SOR: B and C, a meta-analysis of cohort and case-control studies).
EVIDENCE SUMMARY
A systematic review of the effect of combined OCPs on women with a family history of breast cancer found no additional increase in risk.1 Investigators identified 3 retrospective cohort studies (N=66,500, with 8500 cases) and 7 case-control studies (total 10,500 cases) from the past 40 years, most including women from the United States and Canada, but one including women from 5 continents.
In most trials, women of reproductive age using combined OCPs had 1 or more first-degree female relatives with breast cancer, although a few trials also included second-degree relatives. Women ranged in age from 20 to 79 years at diagnosis, and most trials controlled for age, parity, menstrual and menopausal history, duration of OCP exposure, and age at first use. Follow-up intervals for the retrospective cohort studies ranged from 5 to 16 years. Investigators were unable to combine results because of heterogenous populations.
Three of the cohort studies found no significant difference in breast cancer risk between OCP users and nonusers, regardless of age or duration of use. One cohort study found an increased risk in women taking older, higher-dose OCPs from before 1975 (relative risk [RR]=3.3; 95% confidence interval [CI], 1.5-7.2). All of the case-control studies found no significant difference in breast cancer risk for any age of starting, duration of OCP use, or degree of relative with breast cancer.
A meta-analysis of 54 case-control studies (6757 cases), comprising approximately 90% of the epidemiologic information on this topic, also found no significant difference in breast cancer risk related to OCP use among women with one or more first-degree relatives with breast cancer.2 Investigators found that neither recent OCP use (<10 years, RR=0.77; 95% CI, 0.54-1.11) nor past OCP use (>10 years, RR=1.01; 95% CI, 0.80-1.28) affected risk of developing breast cancer.
Three additional case-control studies involving women with a family history of breast cancer also found no significant association for breast cancer incidence among OCP users compared with nonusers.3-5
Modern combined OCPs don’t raise risk in women with BRCA1/2 mutations
A meta-analysis of 5 studies (one retrospective cohort, 4 case-control, with a total of 2855 breast cancer cases and 2944 controls) evaluated whether combined OCPs increased the risk of breast cancer in women, all of whom were carrying BRCA1/2 mutations.6
Using modern combined OCPs didn’t raise the risk of breast cancer in BRCA1/2 carriers overall (RR=1.13; 95% CI, 0.88-1.45) or separately in BRCA1 carriers (5 studies, RR=1.09; 95% CI, 0.77-1.54) or BRCA2 carriers (3 studies, RR=1.15; 95% CI, 0.88-1.45).
However, pre-1975 (higher dose) combined OCPs produced significantly increased risk (RR=1.47; 95% CI, 1.06-2.04). Similarly, women who had used combined OCPs >10 years before the study (older women, likely to have been using pre-1975 OCPs) also had significantly increased risk (RR=1.46; 95% CI, 1.07-2.07).
A bit of good news: Combined OCPs reduce ovarian cancer risk
The analysis also determined that combined OCPs significantly reduced the risk of ovarian cancer in women carrying BRCA1/2 mutations (RR=0.50; 95% CI, 0.33-0.75), with an additional linear decrease in risk for each 10 years of OCP use (RR=0.64; 95% CI, 0.53-0.78).
RECOMMENDATIONS
The World Health Organization guidelines outlining criteria for contraceptive use state that OCPs don’t alter the risk of breast cancer among women with either a family history of breast cancer or breast cancer susceptibility genes.7
The American College of Obstetricians and Gynecologists (ACOG) says that a positive family history of breast cancer shouldn’t be regarded as a contraindication to OCP use.8 ACOG also says that women with the BRCA1 mutation have an increased risk of breast cancer if they used OCPs for longer than 5 years before age 30, but this risk may be more than balanced by the benefit of a greatly reduced risk of ovarian cancer.
No. Modern combined oral contraceptive pills (OCPs) don’t increase breast cancer risk in women with a family history (strength of recommendation [SOR]: B, systematic review of cohort, case-control studies). However, older, higher-dose OCPs (in use before 1975) did increase breast cancer risk in these women (SOR: C, case-control study).
Similarly, modern OCPs don’t raise breast cancer risk in women with BRCA1/2 mutations, although higher-dose, pre-1975 OCPs did (SOR: B and C, a meta-analysis of cohort and case-control studies).
EVIDENCE SUMMARY
A systematic review of the effect of combined OCPs on women with a family history of breast cancer found no additional increase in risk.1 Investigators identified 3 retrospective cohort studies (N=66,500, with 8500 cases) and 7 case-control studies (total 10,500 cases) from the past 40 years, most including women from the United States and Canada, but one including women from 5 continents.
In most trials, women of reproductive age using combined OCPs had 1 or more first-degree female relatives with breast cancer, although a few trials also included second-degree relatives. Women ranged in age from 20 to 79 years at diagnosis, and most trials controlled for age, parity, menstrual and menopausal history, duration of OCP exposure, and age at first use. Follow-up intervals for the retrospective cohort studies ranged from 5 to 16 years. Investigators were unable to combine results because of heterogenous populations.
Three of the cohort studies found no significant difference in breast cancer risk between OCP users and nonusers, regardless of age or duration of use. One cohort study found an increased risk in women taking older, higher-dose OCPs from before 1975 (relative risk [RR]=3.3; 95% confidence interval [CI], 1.5-7.2). All of the case-control studies found no significant difference in breast cancer risk for any age of starting, duration of OCP use, or degree of relative with breast cancer.
A meta-analysis of 54 case-control studies (6757 cases), comprising approximately 90% of the epidemiologic information on this topic, also found no significant difference in breast cancer risk related to OCP use among women with one or more first-degree relatives with breast cancer.2 Investigators found that neither recent OCP use (<10 years, RR=0.77; 95% CI, 0.54-1.11) nor past OCP use (>10 years, RR=1.01; 95% CI, 0.80-1.28) affected risk of developing breast cancer.
Three additional case-control studies involving women with a family history of breast cancer also found no significant association for breast cancer incidence among OCP users compared with nonusers.3-5
Modern combined OCPs don’t raise risk in women with BRCA1/2 mutations
A meta-analysis of 5 studies (one retrospective cohort, 4 case-control, with a total of 2855 breast cancer cases and 2944 controls) evaluated whether combined OCPs increased the risk of breast cancer in women, all of whom were carrying BRCA1/2 mutations.6
Using modern combined OCPs didn’t raise the risk of breast cancer in BRCA1/2 carriers overall (RR=1.13; 95% CI, 0.88-1.45) or separately in BRCA1 carriers (5 studies, RR=1.09; 95% CI, 0.77-1.54) or BRCA2 carriers (3 studies, RR=1.15; 95% CI, 0.88-1.45).
However, pre-1975 (higher dose) combined OCPs produced significantly increased risk (RR=1.47; 95% CI, 1.06-2.04). Similarly, women who had used combined OCPs >10 years before the study (older women, likely to have been using pre-1975 OCPs) also had significantly increased risk (RR=1.46; 95% CI, 1.07-2.07).
A bit of good news: Combined OCPs reduce ovarian cancer risk
The analysis also determined that combined OCPs significantly reduced the risk of ovarian cancer in women carrying BRCA1/2 mutations (RR=0.50; 95% CI, 0.33-0.75), with an additional linear decrease in risk for each 10 years of OCP use (RR=0.64; 95% CI, 0.53-0.78).
RECOMMENDATIONS
The World Health Organization guidelines outlining criteria for contraceptive use state that OCPs don’t alter the risk of breast cancer among women with either a family history of breast cancer or breast cancer susceptibility genes.7
The American College of Obstetricians and Gynecologists (ACOG) says that a positive family history of breast cancer shouldn’t be regarded as a contraindication to OCP use.8 ACOG also says that women with the BRCA1 mutation have an increased risk of breast cancer if they used OCPs for longer than 5 years before age 30, but this risk may be more than balanced by the benefit of a greatly reduced risk of ovarian cancer.
1. Gaffield ME, Culwell KR, Ravi A. Oral contraceptives and family history of breast cancer. Contraception. 2009;80:372-380.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative re-analysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet. 1996;347:1713-1727.
3. Jernström H, Loman N, Johannsson OT, et al. Impact of teenage oral contraceptive use in a population-based series of early-onset breast cancer cases who have undergone BRCA mutation testing. Eur J Cancer. 2005;41:2312-2320.
4. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Human Reprod Update. 2010;16: 631-650.
5. Long-term oral contraceptive use and the risk of breast cancer. The Centers for Disease Control Cancer and Steroid Hormone Study. JAMA. 1983;249:1591-1595.
6. Iodice S, Barile M, Rotmensz N, et al. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer. 2010;46:2275-2284.
7. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. 4th ed. Geneva, Switzerland: World Health Organization; 2009. World Health Organization Web site. Available at: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed September 24, 2013.
8. ACOG Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107:1453-1472.
1. Gaffield ME, Culwell KR, Ravi A. Oral contraceptives and family history of breast cancer. Contraception. 2009;80:372-380.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative re-analysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet. 1996;347:1713-1727.
3. Jernström H, Loman N, Johannsson OT, et al. Impact of teenage oral contraceptive use in a population-based series of early-onset breast cancer cases who have undergone BRCA mutation testing. Eur J Cancer. 2005;41:2312-2320.
4. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Human Reprod Update. 2010;16: 631-650.
5. Long-term oral contraceptive use and the risk of breast cancer. The Centers for Disease Control Cancer and Steroid Hormone Study. JAMA. 1983;249:1591-1595.
6. Iodice S, Barile M, Rotmensz N, et al. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer. 2010;46:2275-2284.
7. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. 4th ed. Geneva, Switzerland: World Health Organization; 2009. World Health Organization Web site. Available at: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed September 24, 2013.
8. ACOG Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107:1453-1472.
Evidence-based answers from the Family Physicians Inquiries Network
LISTEN NOW: Mark Williams, MD, MHM, Discusses SHM's Mentored Implementation Programs
Click here to listen to excerpts of our interview with Dr. Williams
Click here to listen to excerpts of our interview with Dr. Williams
Click here to listen to excerpts of our interview with Dr. Williams
Surgery for persistent knee pain? Not so fast
Do not refer patients with a degenerative medial meniscus tear for arthroscopic partial meniscectomy because outcomes are no better than those of conservative treatment.1
Strength of recommendation
B: Based on a single high-quality randomized control trial.
Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
Illustrative case
A 40-year-old man comes to your office for follow-up of medial left knee pain he’s had for 3 months that hasn’t responded to conservative treatment. The pain developed gradually, without a history of trauma. The patient has no signs of degenerative joint disease on x-ray but magnetic resonance imaging (MRI) reveals a tear of the medial meniscus. Should you refer him for meniscectomy?
Patients and doctors alike tend to look for a treatment that will “fix” the problem, which may be why we have continued to use arthroscopic partial meniscectomy to attempt to relieve symptoms of meniscal tears despite a lack of evidence to support the practice.
Guidelines from the American Academy of Orthopaedic Surgeons state that the evidence for medial meniscectomy in patients with a torn meniscus and osteoarthritis (OA) is inconclusive; the organization offers no guidelines for patients with a torn meniscus who don’t have OA.2 The American College of Occupational and Environmental Medicine states that there is insufficient evidence to support arthroscopic partial meniscectomy for symptomatic, torn medial menisci for select patients and “the vast majority of patients [with medial meniscal tears] do not require surgery.”3 Previous studies have concluded that arthroscopic surgery for OA of the knee provides no additional benefit to optimized physical and medical therapy.4 Furthermore, research by Katz et al5 shows that meniscectomy provides no benefit over conservative treatment in functional status at 6 months in patients with OA and a medial meniscal tear.
That said, arthroscopic partial meniscectomy is still the most common orthopedic procedure in the United States.1 Although its use has decreased over the last 15 years, it is performed nearly 700,000 times annually at a cost of approximately $4 billion.1,6,7 Like any surgical procedure, meniscectomy carries a risk of complications. In the double-blind, randomized trial reported on here, Sihvonen et al1 compared meniscectomy to a sham procedure for patients with knee pain, but not OA.
STUDY SUMMARY: Meniscectomy and sham surgery are equally effective
Sihvonen et al1 conducted a randomized, double-blind, sham-controlled trial at 5 orthopedic clinics in Finland. Patients ages 35 to 65 years were enrolled if they had clinical findings of a medial meniscus tear and knee pain for >3 months that wasn’t relieved by conservative treatment. The trial excluded patients who had an obvious traumatic onset of symptoms; clinical or radiological evidence of knee OA; a locked knee that could not be straightened; knee instability or decreased range of motion; previous surgery on the affected knee; fracture within the past 12 months on the affected limb; or other notable pathology on MRI or during arthroscopy.
Before randomization, 160 patients underwent diagnostic arthroscopy. Fourteen patients were excluded: 6 because they did not actually have a medial meniscal tear, one because he also had a lateral meniscus tear, 3 due to a major chondral flap, 2 who had already undergone meniscal repair, and 2 due to an osteochondral microfracture.
At the end of the diagnostic arthroscopy, each patient was blindly randomized to arthroscopic partial meniscectomy or sham surgery. To simulate the meniscectomy procedure, the surgeon similarly manipulated the knee, made comparable noise and vibration using tools and suction, and ensured that the patient was kept in the operating room (OR) for a comparable time. Only the orthopedic surgeon and OR staff were aware of which surgery the patient underwent, and these staff members were not included in further treatment or follow-up. After the procedure, all patients received the same walking aids and instructions for a graduated exercise program.
The 70 patients in the meniscectomy group and the 76 in the sham surgery group were similar in age (mean: 52 years), sex, body mass index, and duration of pain (mean: 10 months). Patients in both groups also had similar tears noted on arthroscopy.
Three primary outcomes were measured before surgery and at 12 months: knee pain, knee symptoms and function, and quality of life. Knee pain after exercise was evaluated on a 0 to 10 scale, with 0 indicating no pain. The validated Lysholm knee score was used to assess knee symptoms and function and the Western Ontario Meniscal Evaluation Tool (WOMET) was utilized to evaluate quality of life; both are 100-point scales in which lower scores indicate more severe symptoms.
Both groups had marked improvement in pain and function from baseline to 12 months, and there was no significant difference between the 2 groups. Knee pain scores improved by 3.1 in the meniscectomy group and 3.3 in the sham surgery group.
Lysholm symptom and function scores improved 21.7 points in the meniscectomy group and 23.3 points in the sham surgery group (a change of 11.5 points would have been considered clinically significant). The mean between-group difference was -1.6 points (95% confidence interval [CI], -7.2 to 4.0).
WOMET quality of life scores improved 24.6 points in the meniscectomy group and 27.1 points in the sham surgery (a change of 15.5 points would have been considered clinically significant). The mean between-group difference was -2.5 points (95% CI, -9.2 to 4.1).
There were no significant between-group differences in serious adverse events or number of patients who required subsequent knee surgery. Similar proportions in each group thought they had sham surgery, which confirmed the effectiveness of the blinding. Ninety-six percent of patients in the sham procedure group and 93% in the meniscectomy group reported they would be willing to repeat the procedure.
WHAT'S NEW: Recommend physical therapy, exercise instead of surgery
Previous studies of arthroscopic partial meniscectomy to treat degenerative meniscal tears in patients with knee OA found no benefit.6,8 This study specifically examined patients without OA and found arthroscopic partial meniscectomy offered no benefit over sham surgery.
In addition to fewer referrals for meniscectomy, these findings could lead to another change in practice: Physicians may be less likely to order an MRI to confirm the diagnosis of a medial meniscal tear, since doing so will not change their therapeutic approach. This approach centers on recommending that patients with a degenerative meniscal tear start and stick with physical therapy and their designated exercise regimen.
CAVEATS: Surgery might be effective for more active patients
This study, as well as previous research, did not look at surgery for an acute medial meniscus tear following a traumatic incident, such as a fall or direct blow. Additionally, these results are based on improved outcomes in activities of daily living, and may not extend to patients who engage in high-level functioning, such as sports or strenuous work. The sham surgery group received lavage, which could be considered an active treatment, although a previous trial found lavage had no benefit over conservative treatment in patients with knee OA.4
CHALLENGES TO IMPLEMENTATION: It might be hard to convince patients they don’t need surgery
Some patients expect immediate intervention with surgery. It may be difficult to convince such patients that active participation in physical therapy can lead to the same outcomes as surgery. Spending time with your patient to explain the injury, what happens during surgery, and the evidence that shows a lack of difference in outcomes can lead to fewer surgeries. Most patients and physicians will want to do an MRI after 3 months of persistent pain to determine the diagnosis, although some may be comfortable with continuing conservative treatment.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
2. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
3. Knee disorders. In: Hegmann KT, ed. Occupational Medicine Practice Guidelines. Evaluation and Management of Common Health Problems and Functional Recovery in Workers. 3rd ed. Elk Grove Village, IL: American College of Occupational and Environmental Medicine; 2011:1-503.
4. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial for arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359:1097-1107.
5. Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368:1675-1684.
6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health State Report. 2009;11:1-25.
7. Salzler MJ, Lin A, Miller CD, et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014;42:292-296.
8. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347:81-88.
Do not refer patients with a degenerative medial meniscus tear for arthroscopic partial meniscectomy because outcomes are no better than those of conservative treatment.1
Strength of recommendation
B: Based on a single high-quality randomized control trial.
Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
Illustrative case
A 40-year-old man comes to your office for follow-up of medial left knee pain he’s had for 3 months that hasn’t responded to conservative treatment. The pain developed gradually, without a history of trauma. The patient has no signs of degenerative joint disease on x-ray but magnetic resonance imaging (MRI) reveals a tear of the medial meniscus. Should you refer him for meniscectomy?
Patients and doctors alike tend to look for a treatment that will “fix” the problem, which may be why we have continued to use arthroscopic partial meniscectomy to attempt to relieve symptoms of meniscal tears despite a lack of evidence to support the practice.
Guidelines from the American Academy of Orthopaedic Surgeons state that the evidence for medial meniscectomy in patients with a torn meniscus and osteoarthritis (OA) is inconclusive; the organization offers no guidelines for patients with a torn meniscus who don’t have OA.2 The American College of Occupational and Environmental Medicine states that there is insufficient evidence to support arthroscopic partial meniscectomy for symptomatic, torn medial menisci for select patients and “the vast majority of patients [with medial meniscal tears] do not require surgery.”3 Previous studies have concluded that arthroscopic surgery for OA of the knee provides no additional benefit to optimized physical and medical therapy.4 Furthermore, research by Katz et al5 shows that meniscectomy provides no benefit over conservative treatment in functional status at 6 months in patients with OA and a medial meniscal tear.
That said, arthroscopic partial meniscectomy is still the most common orthopedic procedure in the United States.1 Although its use has decreased over the last 15 years, it is performed nearly 700,000 times annually at a cost of approximately $4 billion.1,6,7 Like any surgical procedure, meniscectomy carries a risk of complications. In the double-blind, randomized trial reported on here, Sihvonen et al1 compared meniscectomy to a sham procedure for patients with knee pain, but not OA.
STUDY SUMMARY: Meniscectomy and sham surgery are equally effective
Sihvonen et al1 conducted a randomized, double-blind, sham-controlled trial at 5 orthopedic clinics in Finland. Patients ages 35 to 65 years were enrolled if they had clinical findings of a medial meniscus tear and knee pain for >3 months that wasn’t relieved by conservative treatment. The trial excluded patients who had an obvious traumatic onset of symptoms; clinical or radiological evidence of knee OA; a locked knee that could not be straightened; knee instability or decreased range of motion; previous surgery on the affected knee; fracture within the past 12 months on the affected limb; or other notable pathology on MRI or during arthroscopy.
Before randomization, 160 patients underwent diagnostic arthroscopy. Fourteen patients were excluded: 6 because they did not actually have a medial meniscal tear, one because he also had a lateral meniscus tear, 3 due to a major chondral flap, 2 who had already undergone meniscal repair, and 2 due to an osteochondral microfracture.
At the end of the diagnostic arthroscopy, each patient was blindly randomized to arthroscopic partial meniscectomy or sham surgery. To simulate the meniscectomy procedure, the surgeon similarly manipulated the knee, made comparable noise and vibration using tools and suction, and ensured that the patient was kept in the operating room (OR) for a comparable time. Only the orthopedic surgeon and OR staff were aware of which surgery the patient underwent, and these staff members were not included in further treatment or follow-up. After the procedure, all patients received the same walking aids and instructions for a graduated exercise program.
The 70 patients in the meniscectomy group and the 76 in the sham surgery group were similar in age (mean: 52 years), sex, body mass index, and duration of pain (mean: 10 months). Patients in both groups also had similar tears noted on arthroscopy.
Three primary outcomes were measured before surgery and at 12 months: knee pain, knee symptoms and function, and quality of life. Knee pain after exercise was evaluated on a 0 to 10 scale, with 0 indicating no pain. The validated Lysholm knee score was used to assess knee symptoms and function and the Western Ontario Meniscal Evaluation Tool (WOMET) was utilized to evaluate quality of life; both are 100-point scales in which lower scores indicate more severe symptoms.
Both groups had marked improvement in pain and function from baseline to 12 months, and there was no significant difference between the 2 groups. Knee pain scores improved by 3.1 in the meniscectomy group and 3.3 in the sham surgery group.
Lysholm symptom and function scores improved 21.7 points in the meniscectomy group and 23.3 points in the sham surgery group (a change of 11.5 points would have been considered clinically significant). The mean between-group difference was -1.6 points (95% confidence interval [CI], -7.2 to 4.0).
WOMET quality of life scores improved 24.6 points in the meniscectomy group and 27.1 points in the sham surgery (a change of 15.5 points would have been considered clinically significant). The mean between-group difference was -2.5 points (95% CI, -9.2 to 4.1).
There were no significant between-group differences in serious adverse events or number of patients who required subsequent knee surgery. Similar proportions in each group thought they had sham surgery, which confirmed the effectiveness of the blinding. Ninety-six percent of patients in the sham procedure group and 93% in the meniscectomy group reported they would be willing to repeat the procedure.
WHAT'S NEW: Recommend physical therapy, exercise instead of surgery
Previous studies of arthroscopic partial meniscectomy to treat degenerative meniscal tears in patients with knee OA found no benefit.6,8 This study specifically examined patients without OA and found arthroscopic partial meniscectomy offered no benefit over sham surgery.
In addition to fewer referrals for meniscectomy, these findings could lead to another change in practice: Physicians may be less likely to order an MRI to confirm the diagnosis of a medial meniscal tear, since doing so will not change their therapeutic approach. This approach centers on recommending that patients with a degenerative meniscal tear start and stick with physical therapy and their designated exercise regimen.
CAVEATS: Surgery might be effective for more active patients
This study, as well as previous research, did not look at surgery for an acute medial meniscus tear following a traumatic incident, such as a fall or direct blow. Additionally, these results are based on improved outcomes in activities of daily living, and may not extend to patients who engage in high-level functioning, such as sports or strenuous work. The sham surgery group received lavage, which could be considered an active treatment, although a previous trial found lavage had no benefit over conservative treatment in patients with knee OA.4
CHALLENGES TO IMPLEMENTATION: It might be hard to convince patients they don’t need surgery
Some patients expect immediate intervention with surgery. It may be difficult to convince such patients that active participation in physical therapy can lead to the same outcomes as surgery. Spending time with your patient to explain the injury, what happens during surgery, and the evidence that shows a lack of difference in outcomes can lead to fewer surgeries. Most patients and physicians will want to do an MRI after 3 months of persistent pain to determine the diagnosis, although some may be comfortable with continuing conservative treatment.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Do not refer patients with a degenerative medial meniscus tear for arthroscopic partial meniscectomy because outcomes are no better than those of conservative treatment.1
Strength of recommendation
B: Based on a single high-quality randomized control trial.
Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
Illustrative case
A 40-year-old man comes to your office for follow-up of medial left knee pain he’s had for 3 months that hasn’t responded to conservative treatment. The pain developed gradually, without a history of trauma. The patient has no signs of degenerative joint disease on x-ray but magnetic resonance imaging (MRI) reveals a tear of the medial meniscus. Should you refer him for meniscectomy?
Patients and doctors alike tend to look for a treatment that will “fix” the problem, which may be why we have continued to use arthroscopic partial meniscectomy to attempt to relieve symptoms of meniscal tears despite a lack of evidence to support the practice.
Guidelines from the American Academy of Orthopaedic Surgeons state that the evidence for medial meniscectomy in patients with a torn meniscus and osteoarthritis (OA) is inconclusive; the organization offers no guidelines for patients with a torn meniscus who don’t have OA.2 The American College of Occupational and Environmental Medicine states that there is insufficient evidence to support arthroscopic partial meniscectomy for symptomatic, torn medial menisci for select patients and “the vast majority of patients [with medial meniscal tears] do not require surgery.”3 Previous studies have concluded that arthroscopic surgery for OA of the knee provides no additional benefit to optimized physical and medical therapy.4 Furthermore, research by Katz et al5 shows that meniscectomy provides no benefit over conservative treatment in functional status at 6 months in patients with OA and a medial meniscal tear.
That said, arthroscopic partial meniscectomy is still the most common orthopedic procedure in the United States.1 Although its use has decreased over the last 15 years, it is performed nearly 700,000 times annually at a cost of approximately $4 billion.1,6,7 Like any surgical procedure, meniscectomy carries a risk of complications. In the double-blind, randomized trial reported on here, Sihvonen et al1 compared meniscectomy to a sham procedure for patients with knee pain, but not OA.
STUDY SUMMARY: Meniscectomy and sham surgery are equally effective
Sihvonen et al1 conducted a randomized, double-blind, sham-controlled trial at 5 orthopedic clinics in Finland. Patients ages 35 to 65 years were enrolled if they had clinical findings of a medial meniscus tear and knee pain for >3 months that wasn’t relieved by conservative treatment. The trial excluded patients who had an obvious traumatic onset of symptoms; clinical or radiological evidence of knee OA; a locked knee that could not be straightened; knee instability or decreased range of motion; previous surgery on the affected knee; fracture within the past 12 months on the affected limb; or other notable pathology on MRI or during arthroscopy.
Before randomization, 160 patients underwent diagnostic arthroscopy. Fourteen patients were excluded: 6 because they did not actually have a medial meniscal tear, one because he also had a lateral meniscus tear, 3 due to a major chondral flap, 2 who had already undergone meniscal repair, and 2 due to an osteochondral microfracture.
At the end of the diagnostic arthroscopy, each patient was blindly randomized to arthroscopic partial meniscectomy or sham surgery. To simulate the meniscectomy procedure, the surgeon similarly manipulated the knee, made comparable noise and vibration using tools and suction, and ensured that the patient was kept in the operating room (OR) for a comparable time. Only the orthopedic surgeon and OR staff were aware of which surgery the patient underwent, and these staff members were not included in further treatment or follow-up. After the procedure, all patients received the same walking aids and instructions for a graduated exercise program.
The 70 patients in the meniscectomy group and the 76 in the sham surgery group were similar in age (mean: 52 years), sex, body mass index, and duration of pain (mean: 10 months). Patients in both groups also had similar tears noted on arthroscopy.
Three primary outcomes were measured before surgery and at 12 months: knee pain, knee symptoms and function, and quality of life. Knee pain after exercise was evaluated on a 0 to 10 scale, with 0 indicating no pain. The validated Lysholm knee score was used to assess knee symptoms and function and the Western Ontario Meniscal Evaluation Tool (WOMET) was utilized to evaluate quality of life; both are 100-point scales in which lower scores indicate more severe symptoms.
Both groups had marked improvement in pain and function from baseline to 12 months, and there was no significant difference between the 2 groups. Knee pain scores improved by 3.1 in the meniscectomy group and 3.3 in the sham surgery group.
Lysholm symptom and function scores improved 21.7 points in the meniscectomy group and 23.3 points in the sham surgery group (a change of 11.5 points would have been considered clinically significant). The mean between-group difference was -1.6 points (95% confidence interval [CI], -7.2 to 4.0).
WOMET quality of life scores improved 24.6 points in the meniscectomy group and 27.1 points in the sham surgery (a change of 15.5 points would have been considered clinically significant). The mean between-group difference was -2.5 points (95% CI, -9.2 to 4.1).
There were no significant between-group differences in serious adverse events or number of patients who required subsequent knee surgery. Similar proportions in each group thought they had sham surgery, which confirmed the effectiveness of the blinding. Ninety-six percent of patients in the sham procedure group and 93% in the meniscectomy group reported they would be willing to repeat the procedure.
WHAT'S NEW: Recommend physical therapy, exercise instead of surgery
Previous studies of arthroscopic partial meniscectomy to treat degenerative meniscal tears in patients with knee OA found no benefit.6,8 This study specifically examined patients without OA and found arthroscopic partial meniscectomy offered no benefit over sham surgery.
In addition to fewer referrals for meniscectomy, these findings could lead to another change in practice: Physicians may be less likely to order an MRI to confirm the diagnosis of a medial meniscal tear, since doing so will not change their therapeutic approach. This approach centers on recommending that patients with a degenerative meniscal tear start and stick with physical therapy and their designated exercise regimen.
CAVEATS: Surgery might be effective for more active patients
This study, as well as previous research, did not look at surgery for an acute medial meniscus tear following a traumatic incident, such as a fall or direct blow. Additionally, these results are based on improved outcomes in activities of daily living, and may not extend to patients who engage in high-level functioning, such as sports or strenuous work. The sham surgery group received lavage, which could be considered an active treatment, although a previous trial found lavage had no benefit over conservative treatment in patients with knee OA.4
CHALLENGES TO IMPLEMENTATION: It might be hard to convince patients they don’t need surgery
Some patients expect immediate intervention with surgery. It may be difficult to convince such patients that active participation in physical therapy can lead to the same outcomes as surgery. Spending time with your patient to explain the injury, what happens during surgery, and the evidence that shows a lack of difference in outcomes can lead to fewer surgeries. Most patients and physicians will want to do an MRI after 3 months of persistent pain to determine the diagnosis, although some may be comfortable with continuing conservative treatment.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
2. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
3. Knee disorders. In: Hegmann KT, ed. Occupational Medicine Practice Guidelines. Evaluation and Management of Common Health Problems and Functional Recovery in Workers. 3rd ed. Elk Grove Village, IL: American College of Occupational and Environmental Medicine; 2011:1-503.
4. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial for arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359:1097-1107.
5. Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368:1675-1684.
6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health State Report. 2009;11:1-25.
7. Salzler MJ, Lin A, Miller CD, et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014;42:292-296.
8. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347:81-88.
1. Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
2. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
3. Knee disorders. In: Hegmann KT, ed. Occupational Medicine Practice Guidelines. Evaluation and Management of Common Health Problems and Functional Recovery in Workers. 3rd ed. Elk Grove Village, IL: American College of Occupational and Environmental Medicine; 2011:1-503.
4. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial for arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359:1097-1107.
5. Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368:1675-1684.
6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health State Report. 2009;11:1-25.
7. Salzler MJ, Lin A, Miller CD, et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014;42:292-296.
8. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347:81-88.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
LISTEN NOW: Highlights of the September 2014 issue of The Hospitalist newsmagazine
In the September issue of The Hospitalist, we look at SHM’s award-winning quality improvement (QI) programs in our cover story, “Mentored Implementation.” Dr. Mark Williams, professor of medicine at the University of Kentucky and principal investigator for SHM’s Project BOOST, outlines what mentored implementation really means and explains how site visits became a central feature. Dr. Gregory Maynard, director of the UC San Diego Center for Innovation and Improvement Science and senior vice president of SHM’s Center for Hospital Innovation and Improvement, talks about how mentored implementation of QI programs works. Also featured in this issue, we recap key sessions from the 2014 Pediatric Hospital Medicine conference held last month, and launch into part one of our two-part series on using electronic health record systems to reduce readmissions. This issue also features a write-up on The Hospitalist’s latest editorial award: an APEX Grand Award for Magazines, Journals, and Tabloids!
In the September issue of The Hospitalist, we look at SHM’s award-winning quality improvement (QI) programs in our cover story, “Mentored Implementation.” Dr. Mark Williams, professor of medicine at the University of Kentucky and principal investigator for SHM’s Project BOOST, outlines what mentored implementation really means and explains how site visits became a central feature. Dr. Gregory Maynard, director of the UC San Diego Center for Innovation and Improvement Science and senior vice president of SHM’s Center for Hospital Innovation and Improvement, talks about how mentored implementation of QI programs works. Also featured in this issue, we recap key sessions from the 2014 Pediatric Hospital Medicine conference held last month, and launch into part one of our two-part series on using electronic health record systems to reduce readmissions. This issue also features a write-up on The Hospitalist’s latest editorial award: an APEX Grand Award for Magazines, Journals, and Tabloids!
In the September issue of The Hospitalist, we look at SHM’s award-winning quality improvement (QI) programs in our cover story, “Mentored Implementation.” Dr. Mark Williams, professor of medicine at the University of Kentucky and principal investigator for SHM’s Project BOOST, outlines what mentored implementation really means and explains how site visits became a central feature. Dr. Gregory Maynard, director of the UC San Diego Center for Innovation and Improvement Science and senior vice president of SHM’s Center for Hospital Innovation and Improvement, talks about how mentored implementation of QI programs works. Also featured in this issue, we recap key sessions from the 2014 Pediatric Hospital Medicine conference held last month, and launch into part one of our two-part series on using electronic health record systems to reduce readmissions. This issue also features a write-up on The Hospitalist’s latest editorial award: an APEX Grand Award for Magazines, Journals, and Tabloids!
The 2014-2015 influenza season: What you need to know
As physicians and the Centers for Disease Control and Prevention (CDC) prepare for the upcoming influenza season, many of the recommendations remain unchanged from last season. Vaccination continues to be recommended for everyone 6 months of age and older. However, for the first time, a specific vaccine is preferred for children ages 2 through 8 years. Here’s what you need to know about this change, as well as how to handle vaccination in patients who are, or might be, allergic to eggs.
Use LAIV for kids ages 2 through 8 (if available)
For the first time, the CDC’s Advisory Committee on Immunization Practices (ACIP) has stated a preference for a specific influenza vaccine for a specific age group. It recommends using the live attenuated influenza vaccine (LAIV), which is a nasal spray, for children ages 2 through 8 years.1
A systematic review found evidence of increased efficacy of LAIV compared to inactivated influenza vaccine (IIV) in this age group; both types of vaccine have similar rates of adverse reactions.2 This increased effectiveness results in 46 fewer cases of confirmed influenza per 1000 children vaccinated (number needed to treat=24). Although the evidence of LAIV’s increased effectiveness was found for children ages 2 to 6 years, ACIP extended this recommendation through age 8 because this is the age through which physicians need to consider 2 doses of vaccine for a child previously unvaccinated with the influenza vaccine. Children younger than age 2 should receive IIV3 or IIV4.3
ACIP realizes that due to programmatic constraints it would be difficult to vaccinate all children with LAIV this year and is emphasizing that it should be implemented when feasible this year but no later than the 2015 to 2016 influenza season. IIV is effective in children and should be given if LAIV is not available or is contraindicated. Vaccine should not be delayed in the hopes of receiving LAIV if IIV is available.1
LAIV should not be used in children <2 years or adults >49. This vaccine is contraindicated in children and adolescents who are taking chronic aspirin therapy, pregnant women, those who are immunosuppressed, those with a history of egg allergy, or those who have taken influenza antiviral medications in the past 48 hours.1 LAIV also is not recommended for children ages 2 through 4 years who have asthma or had a wheezing episode in the past 12 months.1
There are precautions for the use of LAIV in patients with chronic medical conditions that can place them at high risk for complications from influenza, such as chronic lung, heart, renal, neurologic, liver, blood, or metabolic disorders, including asthma and diabetes.1
Which vaccine for patients who are allergic to eggs?
Two influenza vaccines are now available that are not prepared in embryonated eggs: recombinant influenza vaccine (RIV3) and cell culture-based inactivated influenza vaccine (ccIIV3). Both are trivalent products that contain antigens from 2 influenza A viruses and one influenza B virus and were introduced in time for the 2013 to 2014 flu season. The RIV3 is considered egg-free but ccIIV3 is not, although the amount of egg protein in it is miniscule, estimated at 5 × 10-8 mcg/0.5 mL dose.1 Neither product is licensed for children younger than 18 years and RIV3 is licensed only for those ages 18 through 49 years.
Patients who experience only hives after egg exposure can receive any of the flu vaccines except LAIV, and only because of a lack of data on this product, not because it has been shown to be less safe than the other vaccines. Patients who are unsure if they have an egg allergy or only get hives when they eat eggs should be observed for at least 30 minutes1 following injection as a precaution. Those ages 18 through 49 who have a history of severe reactions to eggs should receive RIV3. Patients younger than 18 years of age and older than 49 years of age can receive IIV vaccines approved for their specific age group. Any patient who is severely allergic and who cannot receive an egg-free vaccine should be vaccinated by a physician with experience managing severe allergic conditions.
Although severe, anaphylactic reactions to influenza vaccine are very rare, physicians should be equipped and prepared to respond to a severe allergic reaction after providing influenza vaccine to anyone with a history of an egg allergy.
Additional tips and resources
In addition to the LAIV, RIV3, and ccIIV3 vaccines described here, 10 other vaccines are available, including 5 egg-based IIV3 products in standard-dose form, 1 IIV3 vaccine for intradermal use, 1 high-dose IIV3 product for patients ages 65 or older, and 3 standard-dose IIV4 products. More details on each of these vaccines are available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6207a1.htm?_%20cid=rr6207a1_w#Tab1.
Regardless of which type of flu vaccine they receive, children 6 months through 8 years should receive 2 doses, at least 4 weeks apart, unless they received:
- 1 dose in 2013 to 2014, or
- 2 or more doses of seasonal influenza vaccine since July 2010, or
- 2 or more doses of seasonal influenza vaccine before July 2010 and ≥1 dose of monovalent H1N1 vaccine, or
- at least 1 dose of seasonal influenza vaccine prior to July 2010 and ≥1 after.
Vaccine effectiveness. The CDC estimated that vaccine effectiveness during the 2013 to 2014 flu season was 66%.3 While this degree of effectiveness is important for minimizing the morbidity and mortality from influenza each year, it’s important to appreciate the limitations of the vaccine and not rely on it as the only prevention intervention.
Other forms of prevention. We need to advise and practice good respiratory hygiene, frequent hand washing, self-isolation when sick, effective infection control practices at health care facilities, targeted early treatment with antivirals, and targeted pre- and post-exposure antiviral chemoprevention. Details on each of these interventions, including recommendations on the use of antiviral medications, can be found on the CDC Web site at http://www.cdc.gov/flu.
1. Grohskopf LA, Olsen SJ, Sokolow LZ, et al; Influenza Division, National Center for Immunization and Respiratory Diseases, CDC. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States 2014-2015 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63:691-697.
2. Grohskopf L, Olsen S, Sokolow L. Effectiveness of live-attenuated vs inactivated influenza vaccines for healthy children. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/05-Flu-Grohskopf.pdf. Accessed August 6, 2014.
3. Flannery B. Interim estimates of 2013-14 seasonal influenza vaccine effectiveness. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/04-Flu-Flannery.pdf. Accessed August 6, 2014.
As physicians and the Centers for Disease Control and Prevention (CDC) prepare for the upcoming influenza season, many of the recommendations remain unchanged from last season. Vaccination continues to be recommended for everyone 6 months of age and older. However, for the first time, a specific vaccine is preferred for children ages 2 through 8 years. Here’s what you need to know about this change, as well as how to handle vaccination in patients who are, or might be, allergic to eggs.
Use LAIV for kids ages 2 through 8 (if available)
For the first time, the CDC’s Advisory Committee on Immunization Practices (ACIP) has stated a preference for a specific influenza vaccine for a specific age group. It recommends using the live attenuated influenza vaccine (LAIV), which is a nasal spray, for children ages 2 through 8 years.1
A systematic review found evidence of increased efficacy of LAIV compared to inactivated influenza vaccine (IIV) in this age group; both types of vaccine have similar rates of adverse reactions.2 This increased effectiveness results in 46 fewer cases of confirmed influenza per 1000 children vaccinated (number needed to treat=24). Although the evidence of LAIV’s increased effectiveness was found for children ages 2 to 6 years, ACIP extended this recommendation through age 8 because this is the age through which physicians need to consider 2 doses of vaccine for a child previously unvaccinated with the influenza vaccine. Children younger than age 2 should receive IIV3 or IIV4.3
ACIP realizes that due to programmatic constraints it would be difficult to vaccinate all children with LAIV this year and is emphasizing that it should be implemented when feasible this year but no later than the 2015 to 2016 influenza season. IIV is effective in children and should be given if LAIV is not available or is contraindicated. Vaccine should not be delayed in the hopes of receiving LAIV if IIV is available.1
LAIV should not be used in children <2 years or adults >49. This vaccine is contraindicated in children and adolescents who are taking chronic aspirin therapy, pregnant women, those who are immunosuppressed, those with a history of egg allergy, or those who have taken influenza antiviral medications in the past 48 hours.1 LAIV also is not recommended for children ages 2 through 4 years who have asthma or had a wheezing episode in the past 12 months.1
There are precautions for the use of LAIV in patients with chronic medical conditions that can place them at high risk for complications from influenza, such as chronic lung, heart, renal, neurologic, liver, blood, or metabolic disorders, including asthma and diabetes.1
Which vaccine for patients who are allergic to eggs?
Two influenza vaccines are now available that are not prepared in embryonated eggs: recombinant influenza vaccine (RIV3) and cell culture-based inactivated influenza vaccine (ccIIV3). Both are trivalent products that contain antigens from 2 influenza A viruses and one influenza B virus and were introduced in time for the 2013 to 2014 flu season. The RIV3 is considered egg-free but ccIIV3 is not, although the amount of egg protein in it is miniscule, estimated at 5 × 10-8 mcg/0.5 mL dose.1 Neither product is licensed for children younger than 18 years and RIV3 is licensed only for those ages 18 through 49 years.
Patients who experience only hives after egg exposure can receive any of the flu vaccines except LAIV, and only because of a lack of data on this product, not because it has been shown to be less safe than the other vaccines. Patients who are unsure if they have an egg allergy or only get hives when they eat eggs should be observed for at least 30 minutes1 following injection as a precaution. Those ages 18 through 49 who have a history of severe reactions to eggs should receive RIV3. Patients younger than 18 years of age and older than 49 years of age can receive IIV vaccines approved for their specific age group. Any patient who is severely allergic and who cannot receive an egg-free vaccine should be vaccinated by a physician with experience managing severe allergic conditions.
Although severe, anaphylactic reactions to influenza vaccine are very rare, physicians should be equipped and prepared to respond to a severe allergic reaction after providing influenza vaccine to anyone with a history of an egg allergy.
Additional tips and resources
In addition to the LAIV, RIV3, and ccIIV3 vaccines described here, 10 other vaccines are available, including 5 egg-based IIV3 products in standard-dose form, 1 IIV3 vaccine for intradermal use, 1 high-dose IIV3 product for patients ages 65 or older, and 3 standard-dose IIV4 products. More details on each of these vaccines are available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6207a1.htm?_%20cid=rr6207a1_w#Tab1.
Regardless of which type of flu vaccine they receive, children 6 months through 8 years should receive 2 doses, at least 4 weeks apart, unless they received:
- 1 dose in 2013 to 2014, or
- 2 or more doses of seasonal influenza vaccine since July 2010, or
- 2 or more doses of seasonal influenza vaccine before July 2010 and ≥1 dose of monovalent H1N1 vaccine, or
- at least 1 dose of seasonal influenza vaccine prior to July 2010 and ≥1 after.
Vaccine effectiveness. The CDC estimated that vaccine effectiveness during the 2013 to 2014 flu season was 66%.3 While this degree of effectiveness is important for minimizing the morbidity and mortality from influenza each year, it’s important to appreciate the limitations of the vaccine and not rely on it as the only prevention intervention.
Other forms of prevention. We need to advise and practice good respiratory hygiene, frequent hand washing, self-isolation when sick, effective infection control practices at health care facilities, targeted early treatment with antivirals, and targeted pre- and post-exposure antiviral chemoprevention. Details on each of these interventions, including recommendations on the use of antiviral medications, can be found on the CDC Web site at http://www.cdc.gov/flu.
As physicians and the Centers for Disease Control and Prevention (CDC) prepare for the upcoming influenza season, many of the recommendations remain unchanged from last season. Vaccination continues to be recommended for everyone 6 months of age and older. However, for the first time, a specific vaccine is preferred for children ages 2 through 8 years. Here’s what you need to know about this change, as well as how to handle vaccination in patients who are, or might be, allergic to eggs.
Use LAIV for kids ages 2 through 8 (if available)
For the first time, the CDC’s Advisory Committee on Immunization Practices (ACIP) has stated a preference for a specific influenza vaccine for a specific age group. It recommends using the live attenuated influenza vaccine (LAIV), which is a nasal spray, for children ages 2 through 8 years.1
A systematic review found evidence of increased efficacy of LAIV compared to inactivated influenza vaccine (IIV) in this age group; both types of vaccine have similar rates of adverse reactions.2 This increased effectiveness results in 46 fewer cases of confirmed influenza per 1000 children vaccinated (number needed to treat=24). Although the evidence of LAIV’s increased effectiveness was found for children ages 2 to 6 years, ACIP extended this recommendation through age 8 because this is the age through which physicians need to consider 2 doses of vaccine for a child previously unvaccinated with the influenza vaccine. Children younger than age 2 should receive IIV3 or IIV4.3
ACIP realizes that due to programmatic constraints it would be difficult to vaccinate all children with LAIV this year and is emphasizing that it should be implemented when feasible this year but no later than the 2015 to 2016 influenza season. IIV is effective in children and should be given if LAIV is not available or is contraindicated. Vaccine should not be delayed in the hopes of receiving LAIV if IIV is available.1
LAIV should not be used in children <2 years or adults >49. This vaccine is contraindicated in children and adolescents who are taking chronic aspirin therapy, pregnant women, those who are immunosuppressed, those with a history of egg allergy, or those who have taken influenza antiviral medications in the past 48 hours.1 LAIV also is not recommended for children ages 2 through 4 years who have asthma or had a wheezing episode in the past 12 months.1
There are precautions for the use of LAIV in patients with chronic medical conditions that can place them at high risk for complications from influenza, such as chronic lung, heart, renal, neurologic, liver, blood, or metabolic disorders, including asthma and diabetes.1
Which vaccine for patients who are allergic to eggs?
Two influenza vaccines are now available that are not prepared in embryonated eggs: recombinant influenza vaccine (RIV3) and cell culture-based inactivated influenza vaccine (ccIIV3). Both are trivalent products that contain antigens from 2 influenza A viruses and one influenza B virus and were introduced in time for the 2013 to 2014 flu season. The RIV3 is considered egg-free but ccIIV3 is not, although the amount of egg protein in it is miniscule, estimated at 5 × 10-8 mcg/0.5 mL dose.1 Neither product is licensed for children younger than 18 years and RIV3 is licensed only for those ages 18 through 49 years.
Patients who experience only hives after egg exposure can receive any of the flu vaccines except LAIV, and only because of a lack of data on this product, not because it has been shown to be less safe than the other vaccines. Patients who are unsure if they have an egg allergy or only get hives when they eat eggs should be observed for at least 30 minutes1 following injection as a precaution. Those ages 18 through 49 who have a history of severe reactions to eggs should receive RIV3. Patients younger than 18 years of age and older than 49 years of age can receive IIV vaccines approved for their specific age group. Any patient who is severely allergic and who cannot receive an egg-free vaccine should be vaccinated by a physician with experience managing severe allergic conditions.
Although severe, anaphylactic reactions to influenza vaccine are very rare, physicians should be equipped and prepared to respond to a severe allergic reaction after providing influenza vaccine to anyone with a history of an egg allergy.
Additional tips and resources
In addition to the LAIV, RIV3, and ccIIV3 vaccines described here, 10 other vaccines are available, including 5 egg-based IIV3 products in standard-dose form, 1 IIV3 vaccine for intradermal use, 1 high-dose IIV3 product for patients ages 65 or older, and 3 standard-dose IIV4 products. More details on each of these vaccines are available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6207a1.htm?_%20cid=rr6207a1_w#Tab1.
Regardless of which type of flu vaccine they receive, children 6 months through 8 years should receive 2 doses, at least 4 weeks apart, unless they received:
- 1 dose in 2013 to 2014, or
- 2 or more doses of seasonal influenza vaccine since July 2010, or
- 2 or more doses of seasonal influenza vaccine before July 2010 and ≥1 dose of monovalent H1N1 vaccine, or
- at least 1 dose of seasonal influenza vaccine prior to July 2010 and ≥1 after.
Vaccine effectiveness. The CDC estimated that vaccine effectiveness during the 2013 to 2014 flu season was 66%.3 While this degree of effectiveness is important for minimizing the morbidity and mortality from influenza each year, it’s important to appreciate the limitations of the vaccine and not rely on it as the only prevention intervention.
Other forms of prevention. We need to advise and practice good respiratory hygiene, frequent hand washing, self-isolation when sick, effective infection control practices at health care facilities, targeted early treatment with antivirals, and targeted pre- and post-exposure antiviral chemoprevention. Details on each of these interventions, including recommendations on the use of antiviral medications, can be found on the CDC Web site at http://www.cdc.gov/flu.
1. Grohskopf LA, Olsen SJ, Sokolow LZ, et al; Influenza Division, National Center for Immunization and Respiratory Diseases, CDC. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States 2014-2015 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63:691-697.
2. Grohskopf L, Olsen S, Sokolow L. Effectiveness of live-attenuated vs inactivated influenza vaccines for healthy children. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/05-Flu-Grohskopf.pdf. Accessed August 6, 2014.
3. Flannery B. Interim estimates of 2013-14 seasonal influenza vaccine effectiveness. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/04-Flu-Flannery.pdf. Accessed August 6, 2014.
1. Grohskopf LA, Olsen SJ, Sokolow LZ, et al; Influenza Division, National Center for Immunization and Respiratory Diseases, CDC. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States 2014-2015 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63:691-697.
2. Grohskopf L, Olsen S, Sokolow L. Effectiveness of live-attenuated vs inactivated influenza vaccines for healthy children. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/05-Flu-Grohskopf.pdf. Accessed August 6, 2014.
3. Flannery B. Interim estimates of 2013-14 seasonal influenza vaccine effectiveness. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/04-Flu-Flannery.pdf. Accessed August 6, 2014.
Reticulated erythematous patch on teenager’s foot
An 18-year-old Caucasian male sought care for an ill-defined reticulated patch on his right plantar arch (FIGURE 1). The patient said that the lesion had gradually appeared 2 years earlier, had grown slowly, and was occasionally itchy. Physical exam revealed a lacy violaceous, hyperpigmented, reticulated patch that was blanchable and nontender to palpation.
Our patient denied having a history of trauma to the area or a coagulation or connective tissue disorder. The lesion didn’t vary with temperature or season, and there were no known triggers. The patient’s left plantar arch was unchanged.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Erythema ab igne
Upon further questioning, the patient acknowledged that he occasionally rested his bare feet around a portable heater under his desk while using his computer for a few hours each day (FIGURE 2). He often kept his right foot on the heater while he let his left foot rest on the ground. A punch biopsy was performed; the findings, when combined with the patient’s report of having exposed his foot to heat, supported the diagnosis of erythema ab igne (EAI).

EAI commonly presents as an asymptomatic reticulated erythematous to violaceous patch in an area of the body that has been in contact with heat.1 It originally was described on the bilateral anterior lower extremities after prolonged exposure to burning stoves or open fires.1 With the advent of central heating, these presentations have decreased, but there has been a resurgence of EAI with atypical distributions as a result of evolving technology and new heating sources. Reported causes of EAI include heating pads,1,2 laptop computers3 (FIGURE 3), car seat heaters,4 hot water bottles, popcorn bags, cell phones,5 and space heaters that have resulted in patches on the breast, thighs, arms, and, in our patient, foot.1-5
Blood work, biopsy can help narrow the differential
The differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectasia. Livedo reticularis can be associated with autoimmune conditions and coagulopathies. Livedo racemosa is a typical sign of Sneddon’s syndrome and can be seen in up to 70% of patients with antiphospholipid-antibody syndrome and systemic lupus erythematosus. Diagnosis of these conditions is confirmed by elevated coagulation factors, presence of autoimmune antibodies, or history of cerebrovascular accident.6 These tests would be normal in EAI.
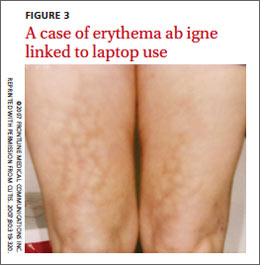
Histopathologic changes observed in EAI include an atrophic epidermis with an interface dermatitis, vasodilation, and dermal pigmentation. Necrotic keratinocytes and focal hyperkeratosis can be noted, along with squamous atypia. Although these changes are nonspecific, they can be used to confirm an EAI diagnosis in patients for whom the affected area has been exposed to a heat source.
Histologically, EAI is similar to actinic keratosis, with epidermal changes showing squamous atypia.2 Due to the similarities, these lesions are sometimes referred to as “thermal keratosis.” Some researchers have suggested that the thermal heat may induce epithelial changes in the same way that ultraviolet light produces epithelial changes.7
Rarely, EAI can turn into cancer. There have been a few reported cases of EAI transforming into squamous cell carcinoma or Merkel cell carcinoma; squamous cell carcinoma is more common, and tends to occur after a long latent period (up to 30 years).7-9 EAI lesions often begin as a chronic ulcer and tend not to heal. If the lesion continues to evolve (ie, ulcerate), a biopsy may be warranted to rule out a malignant transformation.
Eliminate heat exposure, consider a topical treatment
Treatment of acute EAI involves eliminating the offending heat source. The hyperpigmentation will slowly resolve over months to years.4 Persistent exposure to heat sources can lead to chronic EAI, which is more difficult to eliminate.
Because hyperpigmentation can be visually unappealing and emotionally distressing, some patients prefer active treatment. EAI has been effectively treated with 4% hydroquinone topical cream twice a day and tretinoin topical cream at night.2,10,11 Lesions that have epithelial atypia have improved with 5-fluorouracil topical cream.7
EAI also has been successfully treated with laser therapy with the 1064-nm Q-switched Nd:YAG laser with low fluence at 2-week intervals.9
Our patient declined topical therapy. He improved after a few months of avoiding the heater under his desk.
CORRESPONDENCE
Megan Morrison, DO, 5333 McAuley Drive Suite R-5003, Ypsilanti, MI 48197; [email protected]
1. Huynh N, Sarma D, Huerter C. Erythema ab igne: a case report and review of the literature. Cutis. 2011;88:290-292.
2. Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
3. Fu LW, Vender R. Erythema ab igne caused by laptop computer gaming—a case report. Int J Dermatol. 2012;51:716-717.
4. Brodell D, Mostow EN. Automobile seat heater-induced erythema ab igne. Arch Dermtol. 2012;148:264-265.
5. Dela Rosa K, Satter EK. Erythematous patches on the chest. Arch Dermatol. 2012;148:113-118.
6. Uthman IW, Khamashta MA. Livedo racemosa: a striking dermatological sign for antiphospholipid syndrome. J Rheumatol. 2006;33:2379-2382.
7. Bilic M, Adams B. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973-974.
8. Jones CS, Tyring SK, Lee PC, et al. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Arch Dermatol. 1998;124:110-113.
9. Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011;37:551-553.
10. Cardona LFC, Parsons AC, Sangueza OP. Erythematous lesions on the back of a man: challenge. Erythema ab igne. Am J Dermatopathol. 2011;33:185,199.
11. Sahl WJ, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. J Am Acad Dermatol. 1992;27:109-110.
An 18-year-old Caucasian male sought care for an ill-defined reticulated patch on his right plantar arch (FIGURE 1). The patient said that the lesion had gradually appeared 2 years earlier, had grown slowly, and was occasionally itchy. Physical exam revealed a lacy violaceous, hyperpigmented, reticulated patch that was blanchable and nontender to palpation.
Our patient denied having a history of trauma to the area or a coagulation or connective tissue disorder. The lesion didn’t vary with temperature or season, and there were no known triggers. The patient’s left plantar arch was unchanged.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Erythema ab igne
Upon further questioning, the patient acknowledged that he occasionally rested his bare feet around a portable heater under his desk while using his computer for a few hours each day (FIGURE 2). He often kept his right foot on the heater while he let his left foot rest on the ground. A punch biopsy was performed; the findings, when combined with the patient’s report of having exposed his foot to heat, supported the diagnosis of erythema ab igne (EAI).
EAI commonly presents as an asymptomatic reticulated erythematous to violaceous patch in an area of the body that has been in contact with heat.1 It originally was described on the bilateral anterior lower extremities after prolonged exposure to burning stoves or open fires.1 With the advent of central heating, these presentations have decreased, but there has been a resurgence of EAI with atypical distributions as a result of evolving technology and new heating sources. Reported causes of EAI include heating pads,1,2 laptop computers3 (FIGURE 3), car seat heaters,4 hot water bottles, popcorn bags, cell phones,5 and space heaters that have resulted in patches on the breast, thighs, arms, and, in our patient, foot.1-5
Blood work, biopsy can help narrow the differential
The differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectasia. Livedo reticularis can be associated with autoimmune conditions and coagulopathies. Livedo racemosa is a typical sign of Sneddon’s syndrome and can be seen in up to 70% of patients with antiphospholipid-antibody syndrome and systemic lupus erythematosus. Diagnosis of these conditions is confirmed by elevated coagulation factors, presence of autoimmune antibodies, or history of cerebrovascular accident.6 These tests would be normal in EAI.
Histopathologic changes observed in EAI include an atrophic epidermis with an interface dermatitis, vasodilation, and dermal pigmentation. Necrotic keratinocytes and focal hyperkeratosis can be noted, along with squamous atypia. Although these changes are nonspecific, they can be used to confirm an EAI diagnosis in patients for whom the affected area has been exposed to a heat source.
Histologically, EAI is similar to actinic keratosis, with epidermal changes showing squamous atypia.2 Due to the similarities, these lesions are sometimes referred to as “thermal keratosis.” Some researchers have suggested that the thermal heat may induce epithelial changes in the same way that ultraviolet light produces epithelial changes.7
Rarely, EAI can turn into cancer. There have been a few reported cases of EAI transforming into squamous cell carcinoma or Merkel cell carcinoma; squamous cell carcinoma is more common, and tends to occur after a long latent period (up to 30 years).7-9 EAI lesions often begin as a chronic ulcer and tend not to heal. If the lesion continues to evolve (ie, ulcerate), a biopsy may be warranted to rule out a malignant transformation.
Eliminate heat exposure, consider a topical treatment
Treatment of acute EAI involves eliminating the offending heat source. The hyperpigmentation will slowly resolve over months to years.4 Persistent exposure to heat sources can lead to chronic EAI, which is more difficult to eliminate.
Because hyperpigmentation can be visually unappealing and emotionally distressing, some patients prefer active treatment. EAI has been effectively treated with 4% hydroquinone topical cream twice a day and tretinoin topical cream at night.2,10,11 Lesions that have epithelial atypia have improved with 5-fluorouracil topical cream.7
EAI also has been successfully treated with laser therapy with the 1064-nm Q-switched Nd:YAG laser with low fluence at 2-week intervals.9
Our patient declined topical therapy. He improved after a few months of avoiding the heater under his desk.
CORRESPONDENCE
Megan Morrison, DO, 5333 McAuley Drive Suite R-5003, Ypsilanti, MI 48197; [email protected]
An 18-year-old Caucasian male sought care for an ill-defined reticulated patch on his right plantar arch (FIGURE 1). The patient said that the lesion had gradually appeared 2 years earlier, had grown slowly, and was occasionally itchy. Physical exam revealed a lacy violaceous, hyperpigmented, reticulated patch that was blanchable and nontender to palpation.
Our patient denied having a history of trauma to the area or a coagulation or connective tissue disorder. The lesion didn’t vary with temperature or season, and there were no known triggers. The patient’s left plantar arch was unchanged.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Erythema ab igne
Upon further questioning, the patient acknowledged that he occasionally rested his bare feet around a portable heater under his desk while using his computer for a few hours each day (FIGURE 2). He often kept his right foot on the heater while he let his left foot rest on the ground. A punch biopsy was performed; the findings, when combined with the patient’s report of having exposed his foot to heat, supported the diagnosis of erythema ab igne (EAI).
EAI commonly presents as an asymptomatic reticulated erythematous to violaceous patch in an area of the body that has been in contact with heat.1 It originally was described on the bilateral anterior lower extremities after prolonged exposure to burning stoves or open fires.1 With the advent of central heating, these presentations have decreased, but there has been a resurgence of EAI with atypical distributions as a result of evolving technology and new heating sources. Reported causes of EAI include heating pads,1,2 laptop computers3 (FIGURE 3), car seat heaters,4 hot water bottles, popcorn bags, cell phones,5 and space heaters that have resulted in patches on the breast, thighs, arms, and, in our patient, foot.1-5
Blood work, biopsy can help narrow the differential
The differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectasia. Livedo reticularis can be associated with autoimmune conditions and coagulopathies. Livedo racemosa is a typical sign of Sneddon’s syndrome and can be seen in up to 70% of patients with antiphospholipid-antibody syndrome and systemic lupus erythematosus. Diagnosis of these conditions is confirmed by elevated coagulation factors, presence of autoimmune antibodies, or history of cerebrovascular accident.6 These tests would be normal in EAI.
Histopathologic changes observed in EAI include an atrophic epidermis with an interface dermatitis, vasodilation, and dermal pigmentation. Necrotic keratinocytes and focal hyperkeratosis can be noted, along with squamous atypia. Although these changes are nonspecific, they can be used to confirm an EAI diagnosis in patients for whom the affected area has been exposed to a heat source.
Histologically, EAI is similar to actinic keratosis, with epidermal changes showing squamous atypia.2 Due to the similarities, these lesions are sometimes referred to as “thermal keratosis.” Some researchers have suggested that the thermal heat may induce epithelial changes in the same way that ultraviolet light produces epithelial changes.7
Rarely, EAI can turn into cancer. There have been a few reported cases of EAI transforming into squamous cell carcinoma or Merkel cell carcinoma; squamous cell carcinoma is more common, and tends to occur after a long latent period (up to 30 years).7-9 EAI lesions often begin as a chronic ulcer and tend not to heal. If the lesion continues to evolve (ie, ulcerate), a biopsy may be warranted to rule out a malignant transformation.
Eliminate heat exposure, consider a topical treatment
Treatment of acute EAI involves eliminating the offending heat source. The hyperpigmentation will slowly resolve over months to years.4 Persistent exposure to heat sources can lead to chronic EAI, which is more difficult to eliminate.
Because hyperpigmentation can be visually unappealing and emotionally distressing, some patients prefer active treatment. EAI has been effectively treated with 4% hydroquinone topical cream twice a day and tretinoin topical cream at night.2,10,11 Lesions that have epithelial atypia have improved with 5-fluorouracil topical cream.7
EAI also has been successfully treated with laser therapy with the 1064-nm Q-switched Nd:YAG laser with low fluence at 2-week intervals.9
Our patient declined topical therapy. He improved after a few months of avoiding the heater under his desk.
CORRESPONDENCE
Megan Morrison, DO, 5333 McAuley Drive Suite R-5003, Ypsilanti, MI 48197; [email protected]
1. Huynh N, Sarma D, Huerter C. Erythema ab igne: a case report and review of the literature. Cutis. 2011;88:290-292.
2. Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
3. Fu LW, Vender R. Erythema ab igne caused by laptop computer gaming—a case report. Int J Dermatol. 2012;51:716-717.
4. Brodell D, Mostow EN. Automobile seat heater-induced erythema ab igne. Arch Dermtol. 2012;148:264-265.
5. Dela Rosa K, Satter EK. Erythematous patches on the chest. Arch Dermatol. 2012;148:113-118.
6. Uthman IW, Khamashta MA. Livedo racemosa: a striking dermatological sign for antiphospholipid syndrome. J Rheumatol. 2006;33:2379-2382.
7. Bilic M, Adams B. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973-974.
8. Jones CS, Tyring SK, Lee PC, et al. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Arch Dermatol. 1998;124:110-113.
9. Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011;37:551-553.
10. Cardona LFC, Parsons AC, Sangueza OP. Erythematous lesions on the back of a man: challenge. Erythema ab igne. Am J Dermatopathol. 2011;33:185,199.
11. Sahl WJ, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. J Am Acad Dermatol. 1992;27:109-110.
1. Huynh N, Sarma D, Huerter C. Erythema ab igne: a case report and review of the literature. Cutis. 2011;88:290-292.
2. Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
3. Fu LW, Vender R. Erythema ab igne caused by laptop computer gaming—a case report. Int J Dermatol. 2012;51:716-717.
4. Brodell D, Mostow EN. Automobile seat heater-induced erythema ab igne. Arch Dermtol. 2012;148:264-265.
5. Dela Rosa K, Satter EK. Erythematous patches on the chest. Arch Dermatol. 2012;148:113-118.
6. Uthman IW, Khamashta MA. Livedo racemosa: a striking dermatological sign for antiphospholipid syndrome. J Rheumatol. 2006;33:2379-2382.
7. Bilic M, Adams B. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973-974.
8. Jones CS, Tyring SK, Lee PC, et al. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Arch Dermatol. 1998;124:110-113.
9. Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011;37:551-553.
10. Cardona LFC, Parsons AC, Sangueza OP. Erythematous lesions on the back of a man: challenge. Erythema ab igne. Am J Dermatopathol. 2011;33:185,199.
11. Sahl WJ, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. J Am Acad Dermatol. 1992;27:109-110.
