User login
HAC Diagnosis Code and MS‐DRG Assignment
One financial incentive to improve quality of care is the Centers for Medicare and Medicaid Services' (CMS) policy to not pay additionally for certain adverse events that are classified as hospital‐acquired conditions (HACs).[1, 2, 3] HACs are specific conditions that occur during the hospital stay and presumably could have been prevented.[4, 5, 6] Under the CMS policy, if an HAC occurs during a patient's stay, that condition is not included in the Medicare Severity Diagnosis‐Related Group (MS‐DRG) assignment.
The MS‐DRG assigned to a patient discharge determines reimbursement. Each MS‐DRG is assigned a weight, which is used to adjust for the fact that the treatment of different conditions consume different resources and have difference costs. Groups of patients who are expected to require above‐average resources have a higher weight than those who require fewer resources, and higher‐weighted MS‐DRG assignment results in a higher payment. In some cases, the inclusion of the diagnosis code of an HAC in the determination of the MS‐DRG results in a higher complexity level and higher DRG weight. The policy is designed to shift the incremental costs associated with treating the HAC to the hospital. As of October 2009, there were 10 HACs included in the CMS nonpayment program (see Supporting Table 1 in the online version of this article). CMS expanded the list of HACs to include 13 conditions in 2013.
| Variable | MS‐DRG Change, No. (%) or MSD, N=980 | No MS‐DRG Change, No. (%) or MSD, N=6,047 | P Value |
|---|---|---|---|
| |||
| Patient sociodemographic characteristics | |||
| Age, y | 62.718.9 | 57.521.9 | <0.001 |
| Race | |||
| White | 687 (70.1) | 4,006 (66.3) | 0.024 |
| Black | 166 (16.9) | 1,100 (18.2) | |
| Hispanic | 45 (4.6) | 416 (6.9) | |
| Other | 82 (8.4) | 525 (8.7) | |
| Sex | <0.001 | ||
| Male | 441 (45.0) | 3,298 (54.5) | |
| Female | 539 (55.0) | 2,749 (45.5) | |
| Payer | <0.001 | ||
| Commercial | 279 (28.5) | 1,609 (26.6) | |
| Medicaid | 88 (9.0) | 910 (15.1) | |
| Medicare | 532 (54.3) | 3,003 (49.7) | |
| Self‐pay/charity | 52 (5.3) | 331 (5.5) | |
| Other | 29 (3.0) | 194 (3.2) | |
| Severity of illness | <0.001 | ||
| Minor | 50 (5.1) | 71 (1.2) | |
| Moderate | 216 (22.0) | 359 (5.9) | |
| Major | 599 (61.1) | 1,318 (21.8) | |
| Extreme | 115 (11.7) | 4,299 (71.1) | |
| Patient clinical characteristics | |||
| Number of ICD‐9 diagnosis codes per patient | 13.76.0 | 20.26.6 | <0.001 |
| MS‐DRG weight | 2.92.1 | 5.96.1 | <0.001 |
| Hospital characteristics | |||
| Mean number of ICD‐9 diagnosis codes per patient per hospital | 8.51.4 | 8.61.4 | 0.280 |
| Total hospital discharges | 15,9576,553 | 16,8576,634 | <0.001 |
| HACs per 1,000 discharges | 9.83.7 | 10.23.7 | <0.001 |
| Hospital‐acquired condition | |||
| Type of HAC | <0.001 | ||
| Pressure ulcer | 334 (34.1) | 1,599 (26.4) | |
| Falls/trauma | 96 (9.8) | 440 (7.3) | |
| Catheter‐associated UTI | 19 (1.9) | 215 (3.6) | |
| Vascular catheter infection | 26 (2.7) | 1,179 (19.5) | |
| DVT/pulmonary embolism | 448 (45.7) | 2,145 (35.5) | |
| Other conditions | 57 (5.8) | 469 (7.8) | |
| HAC position | <0.001 | ||
| 2nd code | 850 (86.7) | 697 (11.5) | |
| 3rd code | 45 (4.6) | 739 (12.2) | |
| 4th code | 30 (3.1) | 641 (10.6) | |
| 5th code | 15 (1.5) | 569 (9.4) | |
| 6th code or higher | 40 (4.1) | 3,401 (56.2) | |
Withholding additional reimbursement for an HAC has been controversial. One area of debate is that the assignment of an HAC may be imprecise, in part due to the variation in how physicians document in the medical record.[1, 2, 6, 7, 8, 9] Coding is derived from documentation in physician notes and is the primary mechanism for assigning International Classification of Diseases, 9th Revision, Clinical Modification (ICD‐9) diagnosis codes to the patient's encounter. The coding process begins with health information technicians (ie, medical record coders) reviewing all medical record documentation to assign diagnosis and procedure codes using the ICD‐9 codes.[10] Primary and secondary diagnoses are determined by certain definitions in the hospital setting. Secondary diagnoses can be further separated into complications or comorbidities in the MS‐DRG system, which can affect reimbursement. The MS‐DRG is then determined using these diagnosis and procedure codes. Physician documentation is the principal source of data for hospital billing, because health information technicians (ie, medical record coders) must assign a code based on what is documented in the chart. If key medical detail is missing or language is ambiguous, then coding can be inaccurate, which may lead to inappropriate compensation.[11]
Accurate and complete ICD‐9 diagnosis and procedure coding is essential for correct MS‐DRG assignment and reimbursement.[12] Physicians may influence coding prioritization by either over‐emphasizing a patient diagnosis or by downplaying the significance of new findings. In addition, unless the physician uses specific, accurate, and accepted terminology, the diagnosis may not even appear in the list of diagnosis codes. Medical records with nonstandard abbreviations may result in coder‐omission of key diagnoses. Finally, when clinicians use qualified diagnoses such as rule‐out or probable, the final diagnosis coded may not be accurate.[10]
Although the CMS policy creates a financial incentive for hospitals to improve quality, the extent to which the policy actually impacts reimbursement across multiple HACs has not been quantified. Additionally, if HACsas a policy initiativereflect actual quality of care, then the position of the ICD‐9 code should not affect MS‐DRG assignment. In this study we evaluated the extent to which MS‐DRG assignment would have been influenced by the presence of an HAC and tested the association of the position of an HAC in the list of ICD‐9 diagnosis codes with changes in MS‐DRG assignment.
METHODS
Study Population
This study was a retrospective analysis of all patients discharged from hospital members of the University HealthSystem Consortium's (UHC) Clinical Data Base between October 2007 and April 2008. The data set was limited to patient discharge records with at least 1 of 10 HACs for which CMS no longer provides additional reimbursement (see Supporting Table 1 in the online version of this article). The presence of an HAC was indicated by the corresponding diagnosis code using the ICD‐9 diagnosis and procedure codes.
Data Source
UHC's Clinical Data Base is a database of patient discharge‐level administrative data used primarily for billing purposes. UHC's Clinical Data Base provides comparative data for in‐hospital healthcare outcomes using encounter‐level and line‐item transactional information from each member organization. UHC is a nonprofit alliance of 116 academic medical centers and 276 of their affiliated hospitals.
Dependent Variable: Change in MS‐DRG Assignment
The dependent variable was a change in MS‐DRG assignment. MS‐DRG assignment was calculated by comparing the MS‐DRG assigned when the HAC's ICD‐9 diagnosis code was considered a no‐payment event and was not included in the determination (ie, post‐policy DRG) with the MS‐DRG that would have been assigned when the HAC was not included in the determination (ie, pre‐policy DRG). The list of ICD‐9 diagnosis codes was entered into MS‐DRG grouping software with the ICD‐9 diagnosis code for each HAC in the identical position presented to CMS. Up to 29 secondary ICD‐9 diagnosis and procedure codes were entered, but the analyses of association on the position of the HAC used the first 9 diagnosis and 6 procedure codes processed by CMS, as only codes in these positions would have changed the MS‐DRG assigned during the study time period. If the 2 MS‐DRGs (pre‐policy DRG and post‐policy DRG) did not match, the case was classified as having a change in MS‐DRG assignment (MS‐DRG change).
Independent variables included in this analysis were coding variables and patient characteristics. Coding variables included the total number of ICD‐9 diagnosis codes recorded in the discharge record, absolute position of the HAC ICD‐9 diagnosis code in the order of all diagnosis codes, weight for the actual MS‐DRG, and specific type of HAC. The absolute position of the HAC was included in the analysis as a categorical variable (second position, third, fourth, fifth, and sixth position and higher). In addition, patient‐level characteristics including sociodemographic characteristics, clinical factors and severity of illness (minor, moderate, major, extreme),[6] and hospital‐level characteristics.
Statistical Analysis
Means and standard deviations or frequencies and percentages were used to describe the variables. A 2 test was used to test for differences in the absolute position of the HAC with change in MS‐DRG assignment (change/no change). In addition, 2 tests were used to test for differences in each of the other categorical independent variables with change in MS‐DRG assignment; t tests were used to test for differences in the continuous variables with change in MS‐DRG assignment.
Two multivariable binary logistic regression models were fit to test the relationship between change in MS‐DRG assignment with the absolute position of the HAC, adjusting for coding variables, patient characteristics, and hospital characteristics that were associated with change in MS‐DRG assignment in the bivariate analysis. The first model tested the relationship between change in MS‐DRG and position of the HAC, without accounting for the specific type of HAC, and the second tested the relationship including both position and the specific type of HAC. Receiver operating characteristic (ROC) curves were developed for each model to evaluate the predictive accuracy. Additionally, analyses were stratified by severity of illness, and the areas under the ROC curves for 3 models were compared to determine whether the predictive accuracy increased with the inclusion of variables other than HAC position. The first model included HAC position only, the second model added type of HAC, and the third model added other coding variables and patient‐ and hospital‐level variables.
Two sensitivity analyses were performed to test the robustness of the results. The first analysis tested the sensitivity of the results to the specification of comorbid disease burden, as measured by number of diagnosis codes. We used Elixhauser's method[13] for identifying comorbid conditions to create binary variables indicating the presence or absence of 29 distinct comorbid conditions, then calculated the total number of comorbid conditions. The binary logistic regression model was refit, with the total number of comorbid conditions in place of the number of diagnosis codes. An additional binary logistic regression model was fit that included the individual comorbid conditions that were associated with change in MS‐DRG assignment in a bivariate analysis (P<0.05). The second sensitivity analysis evaluated whether hospital‐level variation in coding practices explained change in MS‐DRG assignment using a hierarchical binary logistic regression model that included hospital as a random effect.
All statistical analyses were conducted using the SAS version 9.2 statistical software package (SAS Institute Inc., Cary, NC). The Rush University Medical Center Institutional Review Board approved the study protocol.
RESULTS
Of the 954,946 discharges from UHC academic medical centers, 7027 patients (0.7%) had an HAC. Of the patients with an HAC, 6047 did not change MS‐DRG assignment, whereas 980 patients (13.8%) had a change in MS‐DRG assignment. Patients with a change in MS‐DRG assignment were significantly different from those without a change in MS‐DRG assignment on all patient‐level characteristics and all but 1 hospital characteristic (Table 1). The variable with the largest absolute difference between those with and without a change in MS‐DRG was the actual position of the HAC; 86.7% of those with an MS‐DRG change had their HAC in the second position, whereas those without a change had only 11.5% in the second position.
After controlling for patient and hospital characteristics, an HAC in the second position in the list of ICD‐9 codes was associated with the greatest likelihood of a change in MS‐DRG assignment (P<0.001) (Table 2). Each additional ICD‐9 code decreased the odds of an MS‐DRG change (P=0.004), demonstrating that having more secondary diagnosis codes was associated with a lesser likelihood of an MS‐DRG change. After including the individual HACs in the regression model, the second position remained associated with the likelihood of a change in MS‐DRG assignment (results not shown). The predictive accuracy of our model did not improve, however, with the addition of type of HAC. The area under the ROC curve was 0.94 in both models, indicating high predictive power.
| Intercept | Odds Ratio | P Value |
|---|---|---|
| ||
| Minor severity of illness | 6.80 | <0.001 |
| Moderate severity of illness | 5.52 | <0.001 |
| Major severity of illness | 8.02 | <0.001 |
| Number of ICD‐9 diagnosis codes per patient | 0.97 | 0.004 |
| HAC ICD‐9 diagnosis code in 2nd position | 40.52 | <0.001 |
| HAC ICD‐9 diagnosis code in 3rd position | 1.82 | 0.009 |
| HAC ICD‐9 diagnosis code in 4th position | 1.72 | 0.032 |
| HAC ICD‐9 diagnosis code in 5th position | 1.15 | 0.662 |
| Area under the ROC curve | 0.94 | <0.001* |
| Area under the ROC curve, model with patient socio‐demographic characteristics only | 0.85 | |
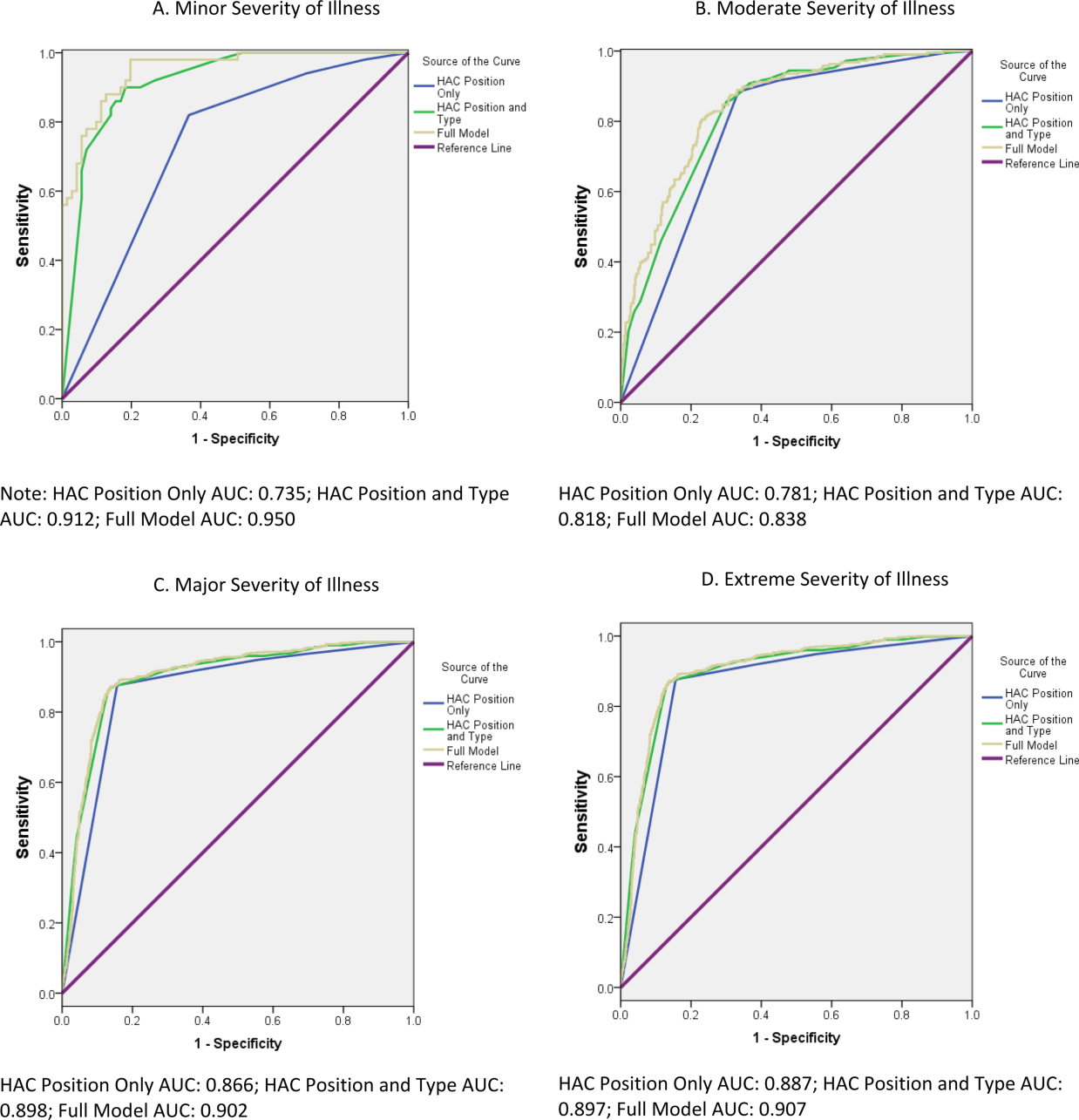
The proportion of cases with a change in MS‐DRG by severity of illness is reported in Table 3. The largest proportion of cases with a change in MS‐DRG was in the minor severity of illness category (41.3%), whereas only 2.6% of cases with an extreme severity of illness had a change in MS‐DRG. Figure 1 shows ROC curves stratified by severity of illness. Figure 1A illustrates the ROC curves for the 121 (1.7%) patients with minor severity of illness. The area under the ROC curve for the model including HAC position only was 0.74, indicating moderate predictive power. The inclusion of HAC type increased the predictive power to 0.91, and inclusion of sociodemographic characteristics further increased the predictive power to 0.95. Figure 1BD illustrates the ROC curves for moderate, major, and extreme severities of illness. For more severe illnesses, the predictive accuracy of the models with only HAC position were similar to the full models, demonstrating that HAC position alone had a high predictive power for change in MS‐DRG assignment.
| Variable | No. | Within Category Percent With MS‐DRG Change |
|---|---|---|
| ||
| Severity of illness | ||
| Minor | 121 | 41.3 |
| Moderate | 575 | 37.6 |
| Major | 1,917 | 31.3 |
| Extreme | 4,414 | 2.6 |
In a sensitivity analysis that evaluated the robustness of our results to the specification of disease burden, inclusion of the number of comorbid conditions did not improve the predictive accuracy of the model. Although inclusion of individual comorbid conditions rather than number of diagnosis codes attenuated the odds ratio (OR) for HAC position (OR: 40.5 in the original model vs OR: 32.9 in the model with individual comorbid conditions), the improvement of the predictive accuracy of the model was small (area under the ROC curve=0.936 in the original model vs 0.943 in the model with individual conditions, P<0.001) (results not shown). In a sensitivity analysis using a hierarchical logistic regression model that included hospital random effects, hospital‐level variation in coding practices did not attenuate the relationship between HAC position and MS‐DRG change (results not shown).
DISCUSSION
This study investigated the association of a change in MS‐DRG assignment and position of the ICD‐9 diagnosis codes for HACs in a sample of patients discharged from US academic medical centers. We found that only 14% of the MS‐DRGs for patients with an HAC would have experienced a change in DRG assignment. Our results are consistent with those of Teufack et al.,[14] who estimated the economic impact of CMS' HAC policy for neurosurgery services at a single hospital to be 0.007% of overall net revenues. Nevertheless, the majority of hospitals have increased their efforts to prevent HACs that are included in CMS' policy.[15] At the same time, most hospitals have not increased their budgets for preventing HACs, and instead have reallocated resources from nontargeted HACs to those included in CMS' policy.
The low proportion of records that are impacted by the policy may be partially explained by the fact that CMS' policy only has an impact on reimbursement for MS‐DRGs with multiple levels. For example, heart failure has 3 levels of reimbursement in the MS‐DRG system (Table 4). Prior to CMS' policy, a heart failure patient with an air embolism as an HAC would have been classified in the most severe MS‐DRG (291), whereas after implementation the patient would be classified in the least severe MS‐DRG, if no other complication or comorbidity (CC) or a major complication or comorbidity (MCC) were present. Chest pain has only 1 level, and reimbursement for a patient with an HAC and classified in the chest pain MS‐DRG would not be impacted by CMS' policy. Most hospitalized patients are complicated, and the proportion of patients who are complicated will continue to increase over time as less complex care shifts to the ambulatory setting. The relative effectiveness of CMS' policy is likely to diminish with the continued shift of care to the ambulatory setting.
| Variable | MS‐DRG | DRG Weight |
|---|---|---|
| ||
| Heart failure and shock | ||
| With major complications and comorbidities (MS‐DRG 291) | 291 | 1.5062 |
| With complications and comorbidities | 292 | 0.9952 |
| Without major complications or comorbidities | 293 | 0.6718 |
| Chest pain | 313 | 0.5992 |
Patient discharges with a diagnosis code for as HAC in the second position were substantially more likely to have a change in MS‐DRG assignment compared to cases with an HAC listed lower in the final list of diagnosis codes. Perhaps it is not surprising that MS‐DRG assignment is most likely to change when the HAC is in the second position, because an ICD‐9 diagnosis code in this position is more likely to be a major complication or comorbidity. For HACs listed in a lower position of the list of ICD‐9 diagnosis codes, it is likely that the patient had another major complication or comorbidity listed in the second position that would have maintained classification in the same MS‐DRG. Our results suggest that physicians and hospitals caring for patients with lower complexity of illness will sustain a higher financial burden as a result of an HAC under CMS' policy compared to providers whose patients sustain the exact same HAC but have underlying medical care of greater complexity.
These results raise further concerns about the ability of CMS' payment policy to improve quality. One criticism of CMS' policy is that all HACs are not universally preventable. If they are not preventable, payment reductions promulgated via the policy would be punitive rather than incentivizing. In their study of central catheter‐associated bloodstream infections and catheter‐associated urinary tract infections, for example, Lee et al. found no change in infection rates after implementation of CMS' policy.[16] As such, some have suggested HACs should not be used to determine reimbursement, and CMS should abandon its current nonpayment policy.[4, 17] Our findings echo this criticism given that the financial penalty for an HAC depends on whether a patient is more or less complex.
Because coding emanates from physician documentation, a uniform documentation process must exist to ensure nonvariable coding practices.[1, 2, 7, 9] This is not the case, however, and some hospitals comanage documentation to refine or maximize the number of ICD‐9 diagnosis and procedure codes. Furthermore, there are certain differences in the documentation practices of individual physicians. If physician documentation and coding variation leads to fewer ICD‐9 codes during an encounter, the chance that an HAC will influence MS‐DRG change increases.
Another source of variation in coding practices found in this study was code sequencing. Although guidelines for appropriate ICD‐9 diagnosis coding currently exist, individual subjectivity remains. The most essential step in the coding process is identifying the principal diagnosis by extrapolating from physician documentation and clinical data. For example, when a patient is admitted for chest pain, and after some evaluation it is determined that the patient experienced a myocardial infarction, then myocardial infarction becomes the principal diagnosis. Based on that principal diagnosis, coders must select the relevant secondary diagnoses. The process involves a series of steps that must be followed exactly in order to ensure accurate coding.[12] There are no guidelines by which coding personnel must follow to sequence secondary diagnoses, with the exception of listed MCCs and CCs prior to other secondary diagnoses. Ultimately, the order by which these codes are assigned may result in unfavorable variation in MS‐DRG assignment.[1, 2, 4, 7, 8, 9, 17]
There are a number of limitations to this study. First, our cohort included only UHC‐affiliated academic medical centers, which may not represent all acute‐care hospitals and their coding practices. Although our data are for discharges prior to implementation of the policy, we were able to analyze the anticipated impact of the policy prior to any direct or indirect changes in coding that may have occurred in response to CMS' policy. Additionally, the number of diagnosis codes accepted by CMS was expanded from 9 to 25 in 2011. Future analyses that include MS‐DRG classifications with the expanded number of diagnosis codes should be conducted to validate our findings and determine whether any changes have occurred over time. It is not known whether low illness severity scores signify patient or hospital characteristics. If they represent patient characteristics, then CMS' policy will disproportionately affect hospitals taking care of less severely ill patients. Alternatively, if hospital coding practice explains more of the variation in the number of ICD‐9 codes (and thus severity of illness), then the system of adjudicating reimbursement via HACs to incentivize quality of care will be flawed, as there is no standard position for HACs on a more lengthy diagnosis list. Finally, we did not evaluate the change in DRG weight with the reassignment of MS‐DRG if the HAC had been included in the calculation. Future work should evaluate whether there is a differential impact of the policy by change in MS‐DRG weight.
CONCLUSION
Under CMS' current policy, hospitals and physicians caring for patients with lower severity of illness and have an HAC will be penalized by CMS disproportionately more than those caring for more complex, sicker patients with the identical HAC. If, in fact, HACs are indicators of a hospital's quality of care, then the CMS policy will likely do little to foster improved quality unless there is a reduction in coding practice variation and modifications to ensure that the policy impacts reimbursement, independent of severity of illness.
Disclosures
The authors acknowledge the financial support for data acquisition from the Rush University College of Health Sciences. The authors report no conflicts of interest.
- Centers for Medicare and Medicaid Services. Hospital‐acquired conditions (present on admission indicator). Available at: http://www.cms.hhs.gov/HospitalAcqCond/05_Coding.asp#TopOfPage. Updated 2012. Accessed September 20, 2012.
- Centers for Medicare and Medicaid Services. Hospital‐acquired conditions: coding. Available at: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/HospitalAcqCond/Coding.html. Updated 2012. Accessed February 2, 2012.
- ICD‐9‐CM 2009 Coders' Desk Reference for Procedures. Eden Prairie, MN: Ingenix; 2009.
- , , , . Hospital complications: linking payment reduction to preventability. Jt Comm J Qual Patient Saf. 2009;35(5):283–285.
- , , , et al. Change in MS‐DRG assignment and hospital reimbursement as a result of Centers for Medicare
One financial incentive to improve quality of care is the Centers for Medicare and Medicaid Services' (CMS) policy to not pay additionally for certain adverse events that are classified as hospital‐acquired conditions (HACs).[1, 2, 3] HACs are specific conditions that occur during the hospital stay and presumably could have been prevented.[4, 5, 6] Under the CMS policy, if an HAC occurs during a patient's stay, that condition is not included in the Medicare Severity Diagnosis‐Related Group (MS‐DRG) assignment.
The MS‐DRG assigned to a patient discharge determines reimbursement. Each MS‐DRG is assigned a weight, which is used to adjust for the fact that the treatment of different conditions consume different resources and have difference costs. Groups of patients who are expected to require above‐average resources have a higher weight than those who require fewer resources, and higher‐weighted MS‐DRG assignment results in a higher payment. In some cases, the inclusion of the diagnosis code of an HAC in the determination of the MS‐DRG results in a higher complexity level and higher DRG weight. The policy is designed to shift the incremental costs associated with treating the HAC to the hospital. As of October 2009, there were 10 HACs included in the CMS nonpayment program (see Supporting Table 1 in the online version of this article). CMS expanded the list of HACs to include 13 conditions in 2013.
| Variable | MS‐DRG Change, No. (%) or MSD, N=980 | No MS‐DRG Change, No. (%) or MSD, N=6,047 | P Value |
|---|---|---|---|
| |||
| Patient sociodemographic characteristics | |||
| Age, y | 62.718.9 | 57.521.9 | <0.001 |
| Race | |||
| White | 687 (70.1) | 4,006 (66.3) | 0.024 |
| Black | 166 (16.9) | 1,100 (18.2) | |
| Hispanic | 45 (4.6) | 416 (6.9) | |
| Other | 82 (8.4) | 525 (8.7) | |
| Sex | <0.001 | ||
| Male | 441 (45.0) | 3,298 (54.5) | |
| Female | 539 (55.0) | 2,749 (45.5) | |
| Payer | <0.001 | ||
| Commercial | 279 (28.5) | 1,609 (26.6) | |
| Medicaid | 88 (9.0) | 910 (15.1) | |
| Medicare | 532 (54.3) | 3,003 (49.7) | |
| Self‐pay/charity | 52 (5.3) | 331 (5.5) | |
| Other | 29 (3.0) | 194 (3.2) | |
| Severity of illness | <0.001 | ||
| Minor | 50 (5.1) | 71 (1.2) | |
| Moderate | 216 (22.0) | 359 (5.9) | |
| Major | 599 (61.1) | 1,318 (21.8) | |
| Extreme | 115 (11.7) | 4,299 (71.1) | |
| Patient clinical characteristics | |||
| Number of ICD‐9 diagnosis codes per patient | 13.76.0 | 20.26.6 | <0.001 |
| MS‐DRG weight | 2.92.1 | 5.96.1 | <0.001 |
| Hospital characteristics | |||
| Mean number of ICD‐9 diagnosis codes per patient per hospital | 8.51.4 | 8.61.4 | 0.280 |
| Total hospital discharges | 15,9576,553 | 16,8576,634 | <0.001 |
| HACs per 1,000 discharges | 9.83.7 | 10.23.7 | <0.001 |
| Hospital‐acquired condition | |||
| Type of HAC | <0.001 | ||
| Pressure ulcer | 334 (34.1) | 1,599 (26.4) | |
| Falls/trauma | 96 (9.8) | 440 (7.3) | |
| Catheter‐associated UTI | 19 (1.9) | 215 (3.6) | |
| Vascular catheter infection | 26 (2.7) | 1,179 (19.5) | |
| DVT/pulmonary embolism | 448 (45.7) | 2,145 (35.5) | |
| Other conditions | 57 (5.8) | 469 (7.8) | |
| HAC position | <0.001 | ||
| 2nd code | 850 (86.7) | 697 (11.5) | |
| 3rd code | 45 (4.6) | 739 (12.2) | |
| 4th code | 30 (3.1) | 641 (10.6) | |
| 5th code | 15 (1.5) | 569 (9.4) | |
| 6th code or higher | 40 (4.1) | 3,401 (56.2) | |
Withholding additional reimbursement for an HAC has been controversial. One area of debate is that the assignment of an HAC may be imprecise, in part due to the variation in how physicians document in the medical record.[1, 2, 6, 7, 8, 9] Coding is derived from documentation in physician notes and is the primary mechanism for assigning International Classification of Diseases, 9th Revision, Clinical Modification (ICD‐9) diagnosis codes to the patient's encounter. The coding process begins with health information technicians (ie, medical record coders) reviewing all medical record documentation to assign diagnosis and procedure codes using the ICD‐9 codes.[10] Primary and secondary diagnoses are determined by certain definitions in the hospital setting. Secondary diagnoses can be further separated into complications or comorbidities in the MS‐DRG system, which can affect reimbursement. The MS‐DRG is then determined using these diagnosis and procedure codes. Physician documentation is the principal source of data for hospital billing, because health information technicians (ie, medical record coders) must assign a code based on what is documented in the chart. If key medical detail is missing or language is ambiguous, then coding can be inaccurate, which may lead to inappropriate compensation.[11]
Accurate and complete ICD‐9 diagnosis and procedure coding is essential for correct MS‐DRG assignment and reimbursement.[12] Physicians may influence coding prioritization by either over‐emphasizing a patient diagnosis or by downplaying the significance of new findings. In addition, unless the physician uses specific, accurate, and accepted terminology, the diagnosis may not even appear in the list of diagnosis codes. Medical records with nonstandard abbreviations may result in coder‐omission of key diagnoses. Finally, when clinicians use qualified diagnoses such as rule‐out or probable, the final diagnosis coded may not be accurate.[10]
Although the CMS policy creates a financial incentive for hospitals to improve quality, the extent to which the policy actually impacts reimbursement across multiple HACs has not been quantified. Additionally, if HACsas a policy initiativereflect actual quality of care, then the position of the ICD‐9 code should not affect MS‐DRG assignment. In this study we evaluated the extent to which MS‐DRG assignment would have been influenced by the presence of an HAC and tested the association of the position of an HAC in the list of ICD‐9 diagnosis codes with changes in MS‐DRG assignment.
METHODS
Study Population
This study was a retrospective analysis of all patients discharged from hospital members of the University HealthSystem Consortium's (UHC) Clinical Data Base between October 2007 and April 2008. The data set was limited to patient discharge records with at least 1 of 10 HACs for which CMS no longer provides additional reimbursement (see Supporting Table 1 in the online version of this article). The presence of an HAC was indicated by the corresponding diagnosis code using the ICD‐9 diagnosis and procedure codes.
Data Source
UHC's Clinical Data Base is a database of patient discharge‐level administrative data used primarily for billing purposes. UHC's Clinical Data Base provides comparative data for in‐hospital healthcare outcomes using encounter‐level and line‐item transactional information from each member organization. UHC is a nonprofit alliance of 116 academic medical centers and 276 of their affiliated hospitals.
Dependent Variable: Change in MS‐DRG Assignment
The dependent variable was a change in MS‐DRG assignment. MS‐DRG assignment was calculated by comparing the MS‐DRG assigned when the HAC's ICD‐9 diagnosis code was considered a no‐payment event and was not included in the determination (ie, post‐policy DRG) with the MS‐DRG that would have been assigned when the HAC was not included in the determination (ie, pre‐policy DRG). The list of ICD‐9 diagnosis codes was entered into MS‐DRG grouping software with the ICD‐9 diagnosis code for each HAC in the identical position presented to CMS. Up to 29 secondary ICD‐9 diagnosis and procedure codes were entered, but the analyses of association on the position of the HAC used the first 9 diagnosis and 6 procedure codes processed by CMS, as only codes in these positions would have changed the MS‐DRG assigned during the study time period. If the 2 MS‐DRGs (pre‐policy DRG and post‐policy DRG) did not match, the case was classified as having a change in MS‐DRG assignment (MS‐DRG change).
Independent variables included in this analysis were coding variables and patient characteristics. Coding variables included the total number of ICD‐9 diagnosis codes recorded in the discharge record, absolute position of the HAC ICD‐9 diagnosis code in the order of all diagnosis codes, weight for the actual MS‐DRG, and specific type of HAC. The absolute position of the HAC was included in the analysis as a categorical variable (second position, third, fourth, fifth, and sixth position and higher). In addition, patient‐level characteristics including sociodemographic characteristics, clinical factors and severity of illness (minor, moderate, major, extreme),[6] and hospital‐level characteristics.
Statistical Analysis
Means and standard deviations or frequencies and percentages were used to describe the variables. A 2 test was used to test for differences in the absolute position of the HAC with change in MS‐DRG assignment (change/no change). In addition, 2 tests were used to test for differences in each of the other categorical independent variables with change in MS‐DRG assignment; t tests were used to test for differences in the continuous variables with change in MS‐DRG assignment.
Two multivariable binary logistic regression models were fit to test the relationship between change in MS‐DRG assignment with the absolute position of the HAC, adjusting for coding variables, patient characteristics, and hospital characteristics that were associated with change in MS‐DRG assignment in the bivariate analysis. The first model tested the relationship between change in MS‐DRG and position of the HAC, without accounting for the specific type of HAC, and the second tested the relationship including both position and the specific type of HAC. Receiver operating characteristic (ROC) curves were developed for each model to evaluate the predictive accuracy. Additionally, analyses were stratified by severity of illness, and the areas under the ROC curves for 3 models were compared to determine whether the predictive accuracy increased with the inclusion of variables other than HAC position. The first model included HAC position only, the second model added type of HAC, and the third model added other coding variables and patient‐ and hospital‐level variables.
Two sensitivity analyses were performed to test the robustness of the results. The first analysis tested the sensitivity of the results to the specification of comorbid disease burden, as measured by number of diagnosis codes. We used Elixhauser's method[13] for identifying comorbid conditions to create binary variables indicating the presence or absence of 29 distinct comorbid conditions, then calculated the total number of comorbid conditions. The binary logistic regression model was refit, with the total number of comorbid conditions in place of the number of diagnosis codes. An additional binary logistic regression model was fit that included the individual comorbid conditions that were associated with change in MS‐DRG assignment in a bivariate analysis (P<0.05). The second sensitivity analysis evaluated whether hospital‐level variation in coding practices explained change in MS‐DRG assignment using a hierarchical binary logistic regression model that included hospital as a random effect.
All statistical analyses were conducted using the SAS version 9.2 statistical software package (SAS Institute Inc., Cary, NC). The Rush University Medical Center Institutional Review Board approved the study protocol.
RESULTS
Of the 954,946 discharges from UHC academic medical centers, 7027 patients (0.7%) had an HAC. Of the patients with an HAC, 6047 did not change MS‐DRG assignment, whereas 980 patients (13.8%) had a change in MS‐DRG assignment. Patients with a change in MS‐DRG assignment were significantly different from those without a change in MS‐DRG assignment on all patient‐level characteristics and all but 1 hospital characteristic (Table 1). The variable with the largest absolute difference between those with and without a change in MS‐DRG was the actual position of the HAC; 86.7% of those with an MS‐DRG change had their HAC in the second position, whereas those without a change had only 11.5% in the second position.
After controlling for patient and hospital characteristics, an HAC in the second position in the list of ICD‐9 codes was associated with the greatest likelihood of a change in MS‐DRG assignment (P<0.001) (Table 2). Each additional ICD‐9 code decreased the odds of an MS‐DRG change (P=0.004), demonstrating that having more secondary diagnosis codes was associated with a lesser likelihood of an MS‐DRG change. After including the individual HACs in the regression model, the second position remained associated with the likelihood of a change in MS‐DRG assignment (results not shown). The predictive accuracy of our model did not improve, however, with the addition of type of HAC. The area under the ROC curve was 0.94 in both models, indicating high predictive power.
| Intercept | Odds Ratio | P Value |
|---|---|---|
| ||
| Minor severity of illness | 6.80 | <0.001 |
| Moderate severity of illness | 5.52 | <0.001 |
| Major severity of illness | 8.02 | <0.001 |
| Number of ICD‐9 diagnosis codes per patient | 0.97 | 0.004 |
| HAC ICD‐9 diagnosis code in 2nd position | 40.52 | <0.001 |
| HAC ICD‐9 diagnosis code in 3rd position | 1.82 | 0.009 |
| HAC ICD‐9 diagnosis code in 4th position | 1.72 | 0.032 |
| HAC ICD‐9 diagnosis code in 5th position | 1.15 | 0.662 |
| Area under the ROC curve | 0.94 | <0.001* |
| Area under the ROC curve, model with patient socio‐demographic characteristics only | 0.85 | |
The proportion of cases with a change in MS‐DRG by severity of illness is reported in Table 3. The largest proportion of cases with a change in MS‐DRG was in the minor severity of illness category (41.3%), whereas only 2.6% of cases with an extreme severity of illness had a change in MS‐DRG. Figure 1 shows ROC curves stratified by severity of illness. Figure 1A illustrates the ROC curves for the 121 (1.7%) patients with minor severity of illness. The area under the ROC curve for the model including HAC position only was 0.74, indicating moderate predictive power. The inclusion of HAC type increased the predictive power to 0.91, and inclusion of sociodemographic characteristics further increased the predictive power to 0.95. Figure 1BD illustrates the ROC curves for moderate, major, and extreme severities of illness. For more severe illnesses, the predictive accuracy of the models with only HAC position were similar to the full models, demonstrating that HAC position alone had a high predictive power for change in MS‐DRG assignment.
| Variable | No. | Within Category Percent With MS‐DRG Change |
|---|---|---|
| ||
| Severity of illness | ||
| Minor | 121 | 41.3 |
| Moderate | 575 | 37.6 |
| Major | 1,917 | 31.3 |
| Extreme | 4,414 | 2.6 |
In a sensitivity analysis that evaluated the robustness of our results to the specification of disease burden, inclusion of the number of comorbid conditions did not improve the predictive accuracy of the model. Although inclusion of individual comorbid conditions rather than number of diagnosis codes attenuated the odds ratio (OR) for HAC position (OR: 40.5 in the original model vs OR: 32.9 in the model with individual comorbid conditions), the improvement of the predictive accuracy of the model was small (area under the ROC curve=0.936 in the original model vs 0.943 in the model with individual conditions, P<0.001) (results not shown). In a sensitivity analysis using a hierarchical logistic regression model that included hospital random effects, hospital‐level variation in coding practices did not attenuate the relationship between HAC position and MS‐DRG change (results not shown).
DISCUSSION
This study investigated the association of a change in MS‐DRG assignment and position of the ICD‐9 diagnosis codes for HACs in a sample of patients discharged from US academic medical centers. We found that only 14% of the MS‐DRGs for patients with an HAC would have experienced a change in DRG assignment. Our results are consistent with those of Teufack et al.,[14] who estimated the economic impact of CMS' HAC policy for neurosurgery services at a single hospital to be 0.007% of overall net revenues. Nevertheless, the majority of hospitals have increased their efforts to prevent HACs that are included in CMS' policy.[15] At the same time, most hospitals have not increased their budgets for preventing HACs, and instead have reallocated resources from nontargeted HACs to those included in CMS' policy.
The low proportion of records that are impacted by the policy may be partially explained by the fact that CMS' policy only has an impact on reimbursement for MS‐DRGs with multiple levels. For example, heart failure has 3 levels of reimbursement in the MS‐DRG system (Table 4). Prior to CMS' policy, a heart failure patient with an air embolism as an HAC would have been classified in the most severe MS‐DRG (291), whereas after implementation the patient would be classified in the least severe MS‐DRG, if no other complication or comorbidity (CC) or a major complication or comorbidity (MCC) were present. Chest pain has only 1 level, and reimbursement for a patient with an HAC and classified in the chest pain MS‐DRG would not be impacted by CMS' policy. Most hospitalized patients are complicated, and the proportion of patients who are complicated will continue to increase over time as less complex care shifts to the ambulatory setting. The relative effectiveness of CMS' policy is likely to diminish with the continued shift of care to the ambulatory setting.
| Variable | MS‐DRG | DRG Weight |
|---|---|---|
| ||
| Heart failure and shock | ||
| With major complications and comorbidities (MS‐DRG 291) | 291 | 1.5062 |
| With complications and comorbidities | 292 | 0.9952 |
| Without major complications or comorbidities | 293 | 0.6718 |
| Chest pain | 313 | 0.5992 |
Patient discharges with a diagnosis code for as HAC in the second position were substantially more likely to have a change in MS‐DRG assignment compared to cases with an HAC listed lower in the final list of diagnosis codes. Perhaps it is not surprising that MS‐DRG assignment is most likely to change when the HAC is in the second position, because an ICD‐9 diagnosis code in this position is more likely to be a major complication or comorbidity. For HACs listed in a lower position of the list of ICD‐9 diagnosis codes, it is likely that the patient had another major complication or comorbidity listed in the second position that would have maintained classification in the same MS‐DRG. Our results suggest that physicians and hospitals caring for patients with lower complexity of illness will sustain a higher financial burden as a result of an HAC under CMS' policy compared to providers whose patients sustain the exact same HAC but have underlying medical care of greater complexity.
These results raise further concerns about the ability of CMS' payment policy to improve quality. One criticism of CMS' policy is that all HACs are not universally preventable. If they are not preventable, payment reductions promulgated via the policy would be punitive rather than incentivizing. In their study of central catheter‐associated bloodstream infections and catheter‐associated urinary tract infections, for example, Lee et al. found no change in infection rates after implementation of CMS' policy.[16] As such, some have suggested HACs should not be used to determine reimbursement, and CMS should abandon its current nonpayment policy.[4, 17] Our findings echo this criticism given that the financial penalty for an HAC depends on whether a patient is more or less complex.
Because coding emanates from physician documentation, a uniform documentation process must exist to ensure nonvariable coding practices.[1, 2, 7, 9] This is not the case, however, and some hospitals comanage documentation to refine or maximize the number of ICD‐9 diagnosis and procedure codes. Furthermore, there are certain differences in the documentation practices of individual physicians. If physician documentation and coding variation leads to fewer ICD‐9 codes during an encounter, the chance that an HAC will influence MS‐DRG change increases.
Another source of variation in coding practices found in this study was code sequencing. Although guidelines for appropriate ICD‐9 diagnosis coding currently exist, individual subjectivity remains. The most essential step in the coding process is identifying the principal diagnosis by extrapolating from physician documentation and clinical data. For example, when a patient is admitted for chest pain, and after some evaluation it is determined that the patient experienced a myocardial infarction, then myocardial infarction becomes the principal diagnosis. Based on that principal diagnosis, coders must select the relevant secondary diagnoses. The process involves a series of steps that must be followed exactly in order to ensure accurate coding.[12] There are no guidelines by which coding personnel must follow to sequence secondary diagnoses, with the exception of listed MCCs and CCs prior to other secondary diagnoses. Ultimately, the order by which these codes are assigned may result in unfavorable variation in MS‐DRG assignment.[1, 2, 4, 7, 8, 9, 17]
There are a number of limitations to this study. First, our cohort included only UHC‐affiliated academic medical centers, which may not represent all acute‐care hospitals and their coding practices. Although our data are for discharges prior to implementation of the policy, we were able to analyze the anticipated impact of the policy prior to any direct or indirect changes in coding that may have occurred in response to CMS' policy. Additionally, the number of diagnosis codes accepted by CMS was expanded from 9 to 25 in 2011. Future analyses that include MS‐DRG classifications with the expanded number of diagnosis codes should be conducted to validate our findings and determine whether any changes have occurred over time. It is not known whether low illness severity scores signify patient or hospital characteristics. If they represent patient characteristics, then CMS' policy will disproportionately affect hospitals taking care of less severely ill patients. Alternatively, if hospital coding practice explains more of the variation in the number of ICD‐9 codes (and thus severity of illness), then the system of adjudicating reimbursement via HACs to incentivize quality of care will be flawed, as there is no standard position for HACs on a more lengthy diagnosis list. Finally, we did not evaluate the change in DRG weight with the reassignment of MS‐DRG if the HAC had been included in the calculation. Future work should evaluate whether there is a differential impact of the policy by change in MS‐DRG weight.
CONCLUSION
Under CMS' current policy, hospitals and physicians caring for patients with lower severity of illness and have an HAC will be penalized by CMS disproportionately more than those caring for more complex, sicker patients with the identical HAC. If, in fact, HACs are indicators of a hospital's quality of care, then the CMS policy will likely do little to foster improved quality unless there is a reduction in coding practice variation and modifications to ensure that the policy impacts reimbursement, independent of severity of illness.
Disclosures
The authors acknowledge the financial support for data acquisition from the Rush University College of Health Sciences. The authors report no conflicts of interest.
One financial incentive to improve quality of care is the Centers for Medicare and Medicaid Services' (CMS) policy to not pay additionally for certain adverse events that are classified as hospital‐acquired conditions (HACs).[1, 2, 3] HACs are specific conditions that occur during the hospital stay and presumably could have been prevented.[4, 5, 6] Under the CMS policy, if an HAC occurs during a patient's stay, that condition is not included in the Medicare Severity Diagnosis‐Related Group (MS‐DRG) assignment.
The MS‐DRG assigned to a patient discharge determines reimbursement. Each MS‐DRG is assigned a weight, which is used to adjust for the fact that the treatment of different conditions consume different resources and have difference costs. Groups of patients who are expected to require above‐average resources have a higher weight than those who require fewer resources, and higher‐weighted MS‐DRG assignment results in a higher payment. In some cases, the inclusion of the diagnosis code of an HAC in the determination of the MS‐DRG results in a higher complexity level and higher DRG weight. The policy is designed to shift the incremental costs associated with treating the HAC to the hospital. As of October 2009, there were 10 HACs included in the CMS nonpayment program (see Supporting Table 1 in the online version of this article). CMS expanded the list of HACs to include 13 conditions in 2013.
| Variable | MS‐DRG Change, No. (%) or MSD, N=980 | No MS‐DRG Change, No. (%) or MSD, N=6,047 | P Value |
|---|---|---|---|
| |||
| Patient sociodemographic characteristics | |||
| Age, y | 62.718.9 | 57.521.9 | <0.001 |
| Race | |||
| White | 687 (70.1) | 4,006 (66.3) | 0.024 |
| Black | 166 (16.9) | 1,100 (18.2) | |
| Hispanic | 45 (4.6) | 416 (6.9) | |
| Other | 82 (8.4) | 525 (8.7) | |
| Sex | <0.001 | ||
| Male | 441 (45.0) | 3,298 (54.5) | |
| Female | 539 (55.0) | 2,749 (45.5) | |
| Payer | <0.001 | ||
| Commercial | 279 (28.5) | 1,609 (26.6) | |
| Medicaid | 88 (9.0) | 910 (15.1) | |
| Medicare | 532 (54.3) | 3,003 (49.7) | |
| Self‐pay/charity | 52 (5.3) | 331 (5.5) | |
| Other | 29 (3.0) | 194 (3.2) | |
| Severity of illness | <0.001 | ||
| Minor | 50 (5.1) | 71 (1.2) | |
| Moderate | 216 (22.0) | 359 (5.9) | |
| Major | 599 (61.1) | 1,318 (21.8) | |
| Extreme | 115 (11.7) | 4,299 (71.1) | |
| Patient clinical characteristics | |||
| Number of ICD‐9 diagnosis codes per patient | 13.76.0 | 20.26.6 | <0.001 |
| MS‐DRG weight | 2.92.1 | 5.96.1 | <0.001 |
| Hospital characteristics | |||
| Mean number of ICD‐9 diagnosis codes per patient per hospital | 8.51.4 | 8.61.4 | 0.280 |
| Total hospital discharges | 15,9576,553 | 16,8576,634 | <0.001 |
| HACs per 1,000 discharges | 9.83.7 | 10.23.7 | <0.001 |
| Hospital‐acquired condition | |||
| Type of HAC | <0.001 | ||
| Pressure ulcer | 334 (34.1) | 1,599 (26.4) | |
| Falls/trauma | 96 (9.8) | 440 (7.3) | |
| Catheter‐associated UTI | 19 (1.9) | 215 (3.6) | |
| Vascular catheter infection | 26 (2.7) | 1,179 (19.5) | |
| DVT/pulmonary embolism | 448 (45.7) | 2,145 (35.5) | |
| Other conditions | 57 (5.8) | 469 (7.8) | |
| HAC position | <0.001 | ||
| 2nd code | 850 (86.7) | 697 (11.5) | |
| 3rd code | 45 (4.6) | 739 (12.2) | |
| 4th code | 30 (3.1) | 641 (10.6) | |
| 5th code | 15 (1.5) | 569 (9.4) | |
| 6th code or higher | 40 (4.1) | 3,401 (56.2) | |
Withholding additional reimbursement for an HAC has been controversial. One area of debate is that the assignment of an HAC may be imprecise, in part due to the variation in how physicians document in the medical record.[1, 2, 6, 7, 8, 9] Coding is derived from documentation in physician notes and is the primary mechanism for assigning International Classification of Diseases, 9th Revision, Clinical Modification (ICD‐9) diagnosis codes to the patient's encounter. The coding process begins with health information technicians (ie, medical record coders) reviewing all medical record documentation to assign diagnosis and procedure codes using the ICD‐9 codes.[10] Primary and secondary diagnoses are determined by certain definitions in the hospital setting. Secondary diagnoses can be further separated into complications or comorbidities in the MS‐DRG system, which can affect reimbursement. The MS‐DRG is then determined using these diagnosis and procedure codes. Physician documentation is the principal source of data for hospital billing, because health information technicians (ie, medical record coders) must assign a code based on what is documented in the chart. If key medical detail is missing or language is ambiguous, then coding can be inaccurate, which may lead to inappropriate compensation.[11]
Accurate and complete ICD‐9 diagnosis and procedure coding is essential for correct MS‐DRG assignment and reimbursement.[12] Physicians may influence coding prioritization by either over‐emphasizing a patient diagnosis or by downplaying the significance of new findings. In addition, unless the physician uses specific, accurate, and accepted terminology, the diagnosis may not even appear in the list of diagnosis codes. Medical records with nonstandard abbreviations may result in coder‐omission of key diagnoses. Finally, when clinicians use qualified diagnoses such as rule‐out or probable, the final diagnosis coded may not be accurate.[10]
Although the CMS policy creates a financial incentive for hospitals to improve quality, the extent to which the policy actually impacts reimbursement across multiple HACs has not been quantified. Additionally, if HACsas a policy initiativereflect actual quality of care, then the position of the ICD‐9 code should not affect MS‐DRG assignment. In this study we evaluated the extent to which MS‐DRG assignment would have been influenced by the presence of an HAC and tested the association of the position of an HAC in the list of ICD‐9 diagnosis codes with changes in MS‐DRG assignment.
METHODS
Study Population
This study was a retrospective analysis of all patients discharged from hospital members of the University HealthSystem Consortium's (UHC) Clinical Data Base between October 2007 and April 2008. The data set was limited to patient discharge records with at least 1 of 10 HACs for which CMS no longer provides additional reimbursement (see Supporting Table 1 in the online version of this article). The presence of an HAC was indicated by the corresponding diagnosis code using the ICD‐9 diagnosis and procedure codes.
Data Source
UHC's Clinical Data Base is a database of patient discharge‐level administrative data used primarily for billing purposes. UHC's Clinical Data Base provides comparative data for in‐hospital healthcare outcomes using encounter‐level and line‐item transactional information from each member organization. UHC is a nonprofit alliance of 116 academic medical centers and 276 of their affiliated hospitals.
Dependent Variable: Change in MS‐DRG Assignment
The dependent variable was a change in MS‐DRG assignment. MS‐DRG assignment was calculated by comparing the MS‐DRG assigned when the HAC's ICD‐9 diagnosis code was considered a no‐payment event and was not included in the determination (ie, post‐policy DRG) with the MS‐DRG that would have been assigned when the HAC was not included in the determination (ie, pre‐policy DRG). The list of ICD‐9 diagnosis codes was entered into MS‐DRG grouping software with the ICD‐9 diagnosis code for each HAC in the identical position presented to CMS. Up to 29 secondary ICD‐9 diagnosis and procedure codes were entered, but the analyses of association on the position of the HAC used the first 9 diagnosis and 6 procedure codes processed by CMS, as only codes in these positions would have changed the MS‐DRG assigned during the study time period. If the 2 MS‐DRGs (pre‐policy DRG and post‐policy DRG) did not match, the case was classified as having a change in MS‐DRG assignment (MS‐DRG change).
Independent variables included in this analysis were coding variables and patient characteristics. Coding variables included the total number of ICD‐9 diagnosis codes recorded in the discharge record, absolute position of the HAC ICD‐9 diagnosis code in the order of all diagnosis codes, weight for the actual MS‐DRG, and specific type of HAC. The absolute position of the HAC was included in the analysis as a categorical variable (second position, third, fourth, fifth, and sixth position and higher). In addition, patient‐level characteristics including sociodemographic characteristics, clinical factors and severity of illness (minor, moderate, major, extreme),[6] and hospital‐level characteristics.
Statistical Analysis
Means and standard deviations or frequencies and percentages were used to describe the variables. A 2 test was used to test for differences in the absolute position of the HAC with change in MS‐DRG assignment (change/no change). In addition, 2 tests were used to test for differences in each of the other categorical independent variables with change in MS‐DRG assignment; t tests were used to test for differences in the continuous variables with change in MS‐DRG assignment.
Two multivariable binary logistic regression models were fit to test the relationship between change in MS‐DRG assignment with the absolute position of the HAC, adjusting for coding variables, patient characteristics, and hospital characteristics that were associated with change in MS‐DRG assignment in the bivariate analysis. The first model tested the relationship between change in MS‐DRG and position of the HAC, without accounting for the specific type of HAC, and the second tested the relationship including both position and the specific type of HAC. Receiver operating characteristic (ROC) curves were developed for each model to evaluate the predictive accuracy. Additionally, analyses were stratified by severity of illness, and the areas under the ROC curves for 3 models were compared to determine whether the predictive accuracy increased with the inclusion of variables other than HAC position. The first model included HAC position only, the second model added type of HAC, and the third model added other coding variables and patient‐ and hospital‐level variables.
Two sensitivity analyses were performed to test the robustness of the results. The first analysis tested the sensitivity of the results to the specification of comorbid disease burden, as measured by number of diagnosis codes. We used Elixhauser's method[13] for identifying comorbid conditions to create binary variables indicating the presence or absence of 29 distinct comorbid conditions, then calculated the total number of comorbid conditions. The binary logistic regression model was refit, with the total number of comorbid conditions in place of the number of diagnosis codes. An additional binary logistic regression model was fit that included the individual comorbid conditions that were associated with change in MS‐DRG assignment in a bivariate analysis (P<0.05). The second sensitivity analysis evaluated whether hospital‐level variation in coding practices explained change in MS‐DRG assignment using a hierarchical binary logistic regression model that included hospital as a random effect.
All statistical analyses were conducted using the SAS version 9.2 statistical software package (SAS Institute Inc., Cary, NC). The Rush University Medical Center Institutional Review Board approved the study protocol.
RESULTS
Of the 954,946 discharges from UHC academic medical centers, 7027 patients (0.7%) had an HAC. Of the patients with an HAC, 6047 did not change MS‐DRG assignment, whereas 980 patients (13.8%) had a change in MS‐DRG assignment. Patients with a change in MS‐DRG assignment were significantly different from those without a change in MS‐DRG assignment on all patient‐level characteristics and all but 1 hospital characteristic (Table 1). The variable with the largest absolute difference between those with and without a change in MS‐DRG was the actual position of the HAC; 86.7% of those with an MS‐DRG change had their HAC in the second position, whereas those without a change had only 11.5% in the second position.
After controlling for patient and hospital characteristics, an HAC in the second position in the list of ICD‐9 codes was associated with the greatest likelihood of a change in MS‐DRG assignment (P<0.001) (Table 2). Each additional ICD‐9 code decreased the odds of an MS‐DRG change (P=0.004), demonstrating that having more secondary diagnosis codes was associated with a lesser likelihood of an MS‐DRG change. After including the individual HACs in the regression model, the second position remained associated with the likelihood of a change in MS‐DRG assignment (results not shown). The predictive accuracy of our model did not improve, however, with the addition of type of HAC. The area under the ROC curve was 0.94 in both models, indicating high predictive power.
| Intercept | Odds Ratio | P Value |
|---|---|---|
| ||
| Minor severity of illness | 6.80 | <0.001 |
| Moderate severity of illness | 5.52 | <0.001 |
| Major severity of illness | 8.02 | <0.001 |
| Number of ICD‐9 diagnosis codes per patient | 0.97 | 0.004 |
| HAC ICD‐9 diagnosis code in 2nd position | 40.52 | <0.001 |
| HAC ICD‐9 diagnosis code in 3rd position | 1.82 | 0.009 |
| HAC ICD‐9 diagnosis code in 4th position | 1.72 | 0.032 |
| HAC ICD‐9 diagnosis code in 5th position | 1.15 | 0.662 |
| Area under the ROC curve | 0.94 | <0.001* |
| Area under the ROC curve, model with patient socio‐demographic characteristics only | 0.85 | |
The proportion of cases with a change in MS‐DRG by severity of illness is reported in Table 3. The largest proportion of cases with a change in MS‐DRG was in the minor severity of illness category (41.3%), whereas only 2.6% of cases with an extreme severity of illness had a change in MS‐DRG. Figure 1 shows ROC curves stratified by severity of illness. Figure 1A illustrates the ROC curves for the 121 (1.7%) patients with minor severity of illness. The area under the ROC curve for the model including HAC position only was 0.74, indicating moderate predictive power. The inclusion of HAC type increased the predictive power to 0.91, and inclusion of sociodemographic characteristics further increased the predictive power to 0.95. Figure 1BD illustrates the ROC curves for moderate, major, and extreme severities of illness. For more severe illnesses, the predictive accuracy of the models with only HAC position were similar to the full models, demonstrating that HAC position alone had a high predictive power for change in MS‐DRG assignment.
| Variable | No. | Within Category Percent With MS‐DRG Change |
|---|---|---|
| ||
| Severity of illness | ||
| Minor | 121 | 41.3 |
| Moderate | 575 | 37.6 |
| Major | 1,917 | 31.3 |
| Extreme | 4,414 | 2.6 |
In a sensitivity analysis that evaluated the robustness of our results to the specification of disease burden, inclusion of the number of comorbid conditions did not improve the predictive accuracy of the model. Although inclusion of individual comorbid conditions rather than number of diagnosis codes attenuated the odds ratio (OR) for HAC position (OR: 40.5 in the original model vs OR: 32.9 in the model with individual comorbid conditions), the improvement of the predictive accuracy of the model was small (area under the ROC curve=0.936 in the original model vs 0.943 in the model with individual conditions, P<0.001) (results not shown). In a sensitivity analysis using a hierarchical logistic regression model that included hospital random effects, hospital‐level variation in coding practices did not attenuate the relationship between HAC position and MS‐DRG change (results not shown).
DISCUSSION
This study investigated the association of a change in MS‐DRG assignment and position of the ICD‐9 diagnosis codes for HACs in a sample of patients discharged from US academic medical centers. We found that only 14% of the MS‐DRGs for patients with an HAC would have experienced a change in DRG assignment. Our results are consistent with those of Teufack et al.,[14] who estimated the economic impact of CMS' HAC policy for neurosurgery services at a single hospital to be 0.007% of overall net revenues. Nevertheless, the majority of hospitals have increased their efforts to prevent HACs that are included in CMS' policy.[15] At the same time, most hospitals have not increased their budgets for preventing HACs, and instead have reallocated resources from nontargeted HACs to those included in CMS' policy.
The low proportion of records that are impacted by the policy may be partially explained by the fact that CMS' policy only has an impact on reimbursement for MS‐DRGs with multiple levels. For example, heart failure has 3 levels of reimbursement in the MS‐DRG system (Table 4). Prior to CMS' policy, a heart failure patient with an air embolism as an HAC would have been classified in the most severe MS‐DRG (291), whereas after implementation the patient would be classified in the least severe MS‐DRG, if no other complication or comorbidity (CC) or a major complication or comorbidity (MCC) were present. Chest pain has only 1 level, and reimbursement for a patient with an HAC and classified in the chest pain MS‐DRG would not be impacted by CMS' policy. Most hospitalized patients are complicated, and the proportion of patients who are complicated will continue to increase over time as less complex care shifts to the ambulatory setting. The relative effectiveness of CMS' policy is likely to diminish with the continued shift of care to the ambulatory setting.
| Variable | MS‐DRG | DRG Weight |
|---|---|---|
| ||
| Heart failure and shock | ||
| With major complications and comorbidities (MS‐DRG 291) | 291 | 1.5062 |
| With complications and comorbidities | 292 | 0.9952 |
| Without major complications or comorbidities | 293 | 0.6718 |
| Chest pain | 313 | 0.5992 |
Patient discharges with a diagnosis code for as HAC in the second position were substantially more likely to have a change in MS‐DRG assignment compared to cases with an HAC listed lower in the final list of diagnosis codes. Perhaps it is not surprising that MS‐DRG assignment is most likely to change when the HAC is in the second position, because an ICD‐9 diagnosis code in this position is more likely to be a major complication or comorbidity. For HACs listed in a lower position of the list of ICD‐9 diagnosis codes, it is likely that the patient had another major complication or comorbidity listed in the second position that would have maintained classification in the same MS‐DRG. Our results suggest that physicians and hospitals caring for patients with lower complexity of illness will sustain a higher financial burden as a result of an HAC under CMS' policy compared to providers whose patients sustain the exact same HAC but have underlying medical care of greater complexity.
These results raise further concerns about the ability of CMS' payment policy to improve quality. One criticism of CMS' policy is that all HACs are not universally preventable. If they are not preventable, payment reductions promulgated via the policy would be punitive rather than incentivizing. In their study of central catheter‐associated bloodstream infections and catheter‐associated urinary tract infections, for example, Lee et al. found no change in infection rates after implementation of CMS' policy.[16] As such, some have suggested HACs should not be used to determine reimbursement, and CMS should abandon its current nonpayment policy.[4, 17] Our findings echo this criticism given that the financial penalty for an HAC depends on whether a patient is more or less complex.
Because coding emanates from physician documentation, a uniform documentation process must exist to ensure nonvariable coding practices.[1, 2, 7, 9] This is not the case, however, and some hospitals comanage documentation to refine or maximize the number of ICD‐9 diagnosis and procedure codes. Furthermore, there are certain differences in the documentation practices of individual physicians. If physician documentation and coding variation leads to fewer ICD‐9 codes during an encounter, the chance that an HAC will influence MS‐DRG change increases.
Another source of variation in coding practices found in this study was code sequencing. Although guidelines for appropriate ICD‐9 diagnosis coding currently exist, individual subjectivity remains. The most essential step in the coding process is identifying the principal diagnosis by extrapolating from physician documentation and clinical data. For example, when a patient is admitted for chest pain, and after some evaluation it is determined that the patient experienced a myocardial infarction, then myocardial infarction becomes the principal diagnosis. Based on that principal diagnosis, coders must select the relevant secondary diagnoses. The process involves a series of steps that must be followed exactly in order to ensure accurate coding.[12] There are no guidelines by which coding personnel must follow to sequence secondary diagnoses, with the exception of listed MCCs and CCs prior to other secondary diagnoses. Ultimately, the order by which these codes are assigned may result in unfavorable variation in MS‐DRG assignment.[1, 2, 4, 7, 8, 9, 17]
There are a number of limitations to this study. First, our cohort included only UHC‐affiliated academic medical centers, which may not represent all acute‐care hospitals and their coding practices. Although our data are for discharges prior to implementation of the policy, we were able to analyze the anticipated impact of the policy prior to any direct or indirect changes in coding that may have occurred in response to CMS' policy. Additionally, the number of diagnosis codes accepted by CMS was expanded from 9 to 25 in 2011. Future analyses that include MS‐DRG classifications with the expanded number of diagnosis codes should be conducted to validate our findings and determine whether any changes have occurred over time. It is not known whether low illness severity scores signify patient or hospital characteristics. If they represent patient characteristics, then CMS' policy will disproportionately affect hospitals taking care of less severely ill patients. Alternatively, if hospital coding practice explains more of the variation in the number of ICD‐9 codes (and thus severity of illness), then the system of adjudicating reimbursement via HACs to incentivize quality of care will be flawed, as there is no standard position for HACs on a more lengthy diagnosis list. Finally, we did not evaluate the change in DRG weight with the reassignment of MS‐DRG if the HAC had been included in the calculation. Future work should evaluate whether there is a differential impact of the policy by change in MS‐DRG weight.
CONCLUSION
Under CMS' current policy, hospitals and physicians caring for patients with lower severity of illness and have an HAC will be penalized by CMS disproportionately more than those caring for more complex, sicker patients with the identical HAC. If, in fact, HACs are indicators of a hospital's quality of care, then the CMS policy will likely do little to foster improved quality unless there is a reduction in coding practice variation and modifications to ensure that the policy impacts reimbursement, independent of severity of illness.
Disclosures
The authors acknowledge the financial support for data acquisition from the Rush University College of Health Sciences. The authors report no conflicts of interest.
- Centers for Medicare and Medicaid Services. Hospital‐acquired conditions (present on admission indicator). Available at: http://www.cms.hhs.gov/HospitalAcqCond/05_Coding.asp#TopOfPage. Updated 2012. Accessed September 20, 2012.
- Centers for Medicare and Medicaid Services. Hospital‐acquired conditions: coding. Available at: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/HospitalAcqCond/Coding.html. Updated 2012. Accessed February 2, 2012.
- ICD‐9‐CM 2009 Coders' Desk Reference for Procedures. Eden Prairie, MN: Ingenix; 2009.
- , , , . Hospital complications: linking payment reduction to preventability. Jt Comm J Qual Patient Saf. 2009;35(5):283–285.
- , , , et al. Change in MS‐DRG assignment and hospital reimbursement as a result of Centers for Medicare
- Centers for Medicare and Medicaid Services. Hospital‐acquired conditions (present on admission indicator). Available at: http://www.cms.hhs.gov/HospitalAcqCond/05_Coding.asp#TopOfPage. Updated 2012. Accessed September 20, 2012.
- Centers for Medicare and Medicaid Services. Hospital‐acquired conditions: coding. Available at: http://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/HospitalAcqCond/Coding.html. Updated 2012. Accessed February 2, 2012.
- ICD‐9‐CM 2009 Coders' Desk Reference for Procedures. Eden Prairie, MN: Ingenix; 2009.
- , , , . Hospital complications: linking payment reduction to preventability. Jt Comm J Qual Patient Saf. 2009;35(5):283–285.
- , , , et al. Change in MS‐DRG assignment and hospital reimbursement as a result of Centers for Medicare
© 2014 Society of Hospital Medicine

Hospital and Primary Care Collaboration
Poorly coordinated care between hospital and outpatient settings contributes to medical errors, poor outcomes, and high costs.[1, 2, 3] Recent policy has sought to motivate better care coordination after hospital discharge. Financial penalties for excessive hospital readmissionsa perceived marker of poorly coordinated carehave motivated hospitals to adopt transitional care programs to improve postdischarge care coordination.[4] However, the success of hospital‐initiated transitional care strategies in reducing hospital readmissions has been limited.[5] This may be due to the fact that many factors driving hospital readmissions, such as chronic medical illness, patient education, and availability of outpatient care, are outside of a hospital's control.[5, 6] Even among the most comprehensive hospital‐based transitional care intervention strategies, there is little evidence of active engagement of primary care providers or collaboration between hospitals and primary care practices in the transitional care planning process.[5] Better engagement of primary care into transitional care strategies may improve postdischarge care coordination.[7, 8]
The potential benefits of collaboration are particularly salient in healthcare safety nets.[9] The US health safety net is a patchwork of providers, funding, and programs unified by a shared missiondelivering care to patients regardless of ability to payrather than a coordinated system with shared governance.[9] Safety‐net hospitals are at risk for higher‐than‐average readmissions penalties.[10, 11] Medicaid expansion under the Affordable Care Act will likely increase demand for services in these settings, which could worsen fragmentation of care as a result of strained capacity.[12] Collaboration between hospitals and primary care clinics in the safety net could help overcome fragmentation, improve efficiencies in care, and reduce costs and readmissions.[12, 13, 14, 15]
Despite the potential benefits, we found no studies on how to enable collaboration between hospitals and primary care. We sought to understand systems‐level factors limiting and facilitating collaboration between hospitals and primary care practices around coordinating inpatient‐to‐outpatient care transitions by conducting a qualitative study, focusing on the perspective of primary care leaders in the safety net.
STUDY DATA AND METHODS
We conducted semistructured telephone interviews with primary care leaders in health safety nets across California from August 2012 through October 2012, prior to the implementation of the federal hospital readmissions penalties program. Primary care leaders were defined as clinicians or nonclinicians holding leadership positions, including chief executive officers, clinic medical directors, and local experts in care coordination or quality improvement. We defined safety‐net clinics as federally qualified health centers (FQHCs) and/or FQHC Look‐Alikes (clinics that meet eligibility requirements and receive the same benefits as FQHCs, except for Public Health Service Section 330 grants), community health centers, and public hospital‐affiliated clinics operating under a traditional fee‐for‐service model and serving a high proportion of Medicaid and uninsured patients.[9, 16] We defined public hospitals as government‐owned hospitals that provide care for individuals with limited access elsewhere.[17]
Sampling and Recruitment
We purposefully sampled participants to maximize diversity in geographic region, metropolitan status,[18] and type of county health delivery system to enable identification of common themes across different settings and contexts. Delivery systems were defined as per the Insure the Uninsured Project, a 501(c)(3) nonprofit organization that conducts research on the uninsured in California.[19] Provider systems are counties with a public hospital; payer systems are counties that contract with private hospitals to deliver uncompensated care in place of a public hospital; and County Medical Services Program is a state program that administers county health care in participating small counties, in lieu of a provider or payer system. We used the county delivery system type as a composite proxy of available county resources and market context given variations in funding, access, and eligibility by system type.
Participants were identified through online public directories, community clinic consortiums, and departments of public health websites. Additional participants were sought using snowball sampling. Potential participants were e‐mailed a recruitment letter describing the study, its purpose, topics to be covered, and confidentiality assurance. Participants who did not respond were called or e‐mailed within 1 week. When initial recruitment was unsuccessful, we attempted to recruit another participant within the same organization when possible. We recruited participants until reaching thematic saturation (i.e., no further new themes emerged from our interviews).[20] No participants were recruited through snowballing.
Data Collection and Interview Guides
We conducted in‐depth, semistructured interviews using interview guides informed by existing literature on collaboration and integration across healthcare systems[21, 22, 23] (see Supporting Information, Appendix 1, in the online version of this article). Interviews were digitally recorded and professionally transcribed verbatim.
We obtained contextual information for settings represented by each respondent, such as number of clinics and annual visits, through the California Primary Care Annual Utilization Data Report and clinic websites.[24]
Analysis
We employed thematic analysis[25] using an inductive framework to identify emergent and recurring themes. We developed and refined a coding template iteratively. Our multidisciplinary team included 2 general internists (O.K.N., L.E.G), 1 hospitalist (S.R.G.), a clinical nurse specialist with a doctorate in nursing (A.L.), and research staff with a public health background (J.K.). Two team members (O.K.N., J.K.) systematically coded all transcripts. Disagreements in coding were resolved through negotiated consensus. All investigators reviewed and discussed identified themes. We emailed summary findings to participants for confirmation to enhance the reliability of our findings.
The institutional review board at the University of California, San Francisco approved the study protocol.
RESULTS
Of 52 individuals contacted from 39 different organizations, 23 did not respond, 4 declined to participate, and 25 were scheduled for an interview. We interviewed 22 primary care leaders across 11 California counties (Table 1) and identified themes around factors influencing collaboration with hospitals (Table 2). Most respondents had prior positive experiences collaborating with hospitals on small, focused projects. However, they asserted the need for better hospitalclinic collaboration, and thought collaboration was critical to achieving high‐quality care transitions. We did not observe any differences in perspectives expressed by clinician versus nonclinician leaders. Nonparticipants were more likely than participants to be from northern rural or central counties, FQHCs, and smaller clinic settings.
| |
| Leadership position | No. (%) |
| Chief executive officer or equivalent* | 9 (41) |
| Chief medical officer or medical director | 7 (32) |
| Other | 6 (27) |
| Clinical experience | |
| Physician (MD or DO) | 15 (68) |
| Registered nurse | 1 (5) |
| Nonclinician | 6 (27) |
| Clinic setting | |
| Clinic type | |
| FQHC and FQHC Look‐Alikes | 15 (68) |
| Hospital based | 2 (9) |
| Other | 5 (23) |
| No. of clinics in system | |
| 14 | 9 (41) |
| 59 | 6 (27) |
| 10 | 7 (32) |
| Annual no. of visits | |
| <100,000 | 9 (41) |
| 100,000499,999 | 11 (50) |
| 500,000 | 2 (9) |
| County characteristics | |
| Health delivery system type | |
| Provider | 13 (59) |
| Payer | 2 (9) |
| County Medical Services Program∥ | 7 (32) |
| Rural county | 7 (32) |
| Theme | Subtheme | Quote |
|---|---|---|
| ||
| Lack of institutional financial incentives for collaboration. | Collaboration may lead to increased responsibility without reimbursement for clinic. | Where the [payment] model breaks down is that the savings is only to the hospital; and there's an expectation on our part to go ahead and take on those additional patients. If that $400,000 savings doesn't at least have a portion to the team that's going to help keep the people out of the hospital, then it won't work. (Participant 17) |
| Collaboration may lead to competition from the hospital for primary care patients. | Our biggest issues with working with the hospital[are] that we have a finite number of [Medicaid] patients [in our catchment area for whom] you get larger reimbursement. For a federally qualified health center, it is [crucial] to ensure we have a revenue stream that helps us take care of the uninsured. So you can see the natural kind of conflict when your pool of patients is very small. (Participant 10) | |
| Collaboration may lead to increased financial risk for the hospital. | 70% to 80% of our adult patients have no insurance and the fact is that none of these hospitals want those patients. They do get disproportionate hospital savings and other thingsbut they don't have a strong business model when they have uninsured patients coming in their doors. That's just the reality. (Participant 21) | |
| Collaboration may lead to decreased financial risk for the hospital. | Most of these patients either have very low reimbursement or no reimbursement, and so [the hospital doesn't] really want these people to end up in very expensive care because it's a burden on their systemphilosophically, everyone agrees that if we keep people well in the outpatient setting, that would be better for everyone. No, there is no financial incentive whatsoever for [the hospital] to not work with us. [emphasis added] (Participant 18) | |
| Competing priorities limit primary care's ability to focus on care transitions. | I wouldn't say [improving care transitions is a high priority]. It's not because we don't want to do the job. We have other priorities. [T]he big issue is access. There's a massive demand for primary care in our communityand we're just trying to make sure we have enough capacity. [There are] requirements HRSA has been asking of health centers and other priorities. We're starting up a residency program. We're recruiting more doctors. We're upping our quality improvement processes internally. We're making a reinvestment in our [electronic medical record]. It never stops. (Participant 22) | |
| The multitude of [care transitions and other quality] improvement imperatives makes it difficult to focus. It's not that any one of these things necessarily represents a flawed approach. It's just that when you have a variety of folks from the national, state, and local levels who all have different ideas about what constitutes appropriate improvement, it's very hard to respond to it all at once. (Participant 6) | ||
| Mismatched expectations about the role and capacity of primary care in care transitions limit collaboration. | Perception of primary care being undervalued by hospitals as a key stakeholder in care transitions. | They just make sure the paperwork is set up.and they have it written down, See doctor in 7 days. And I think they [the hospitals] think that's where their responsibility stops. They don't actually look at our records or talk to us. (Participant 2) |
| Perceived unrealistic expectations of primary care capacity to deliver postdischarge care. | [The hospital will] send anyone that's poor to us whether they are our patient or not. [T]hey say go to [our clinic] and they'll give you your outpatient medications. [But] we're at capacity. [W]e have a 79 month wait for a [new] primary care appointment. So then, we're stuck with the ethical dilemma of [do we send the patient back to the ER/hospital] for their medication or do we just [try to] take them in? (Participant 13) | |
| The hospitals feel every undoctored patient must be ours. [But] it's not like we're sitting on our hands. We have more than enough patients. (Participant 22) | ||
| Informal affiliations and partnerships, formed through personal relationships and interpersonal networking, facilitate collaboration. | Informal affiliations arise from existing personal relationships and/or interpersonal networking. | Our CEO [has been here] for the past 40 years, and has had very deep and ongoing relationships with the [hospital]. Those doors are very wide open. (Participant 18) |
| Informal partnerships are particularly important for FQHCs. | As an FQHC we can't have any ties financially or politically, but there's a traditional connection. (Participant 2) | |
| Increasing demands on clinical productivity lead to a loss of networking opportunities. | We're one of the few clinics that has their own inpatient service. I would say that the transitions between the hospital and [our] clinic start from a much higher level than anybody else. [However] we're about to close our hospital service. It's just too much work for our [clinic] doctors. (Participant 8) | |
| There used to be a meeting once a month where quality improvement programs and issues were discussed. Our administration eliminated these in favor of productivity, to increase our numbers of patients seen. (Participant 12) | ||
| Loss of relationships with hospital personnel amplifies challenges to collaboration. | Because the primary care docs are not visible in the hospital[quality improvement] projects [become] hospital‐based. Usually they forget that we exist. (Participant 11) | |
| External funding and support can enable opportunities for networking and relationship building. | The [national stakeholder organization] has done a lot of work with us to bring us together and figure out what we're doing [across] different counties, settings, providers. (Participant 20) | |
| Electronic health records enable collaboration by improving communication between hospitals and primary care. | Lack of timely communication between inpatient and outpatient settings is a major obstacle to postdischarge care coordination. | It's a lot of effort to get medical records back. It is often not timely. Patients are going to cycle in and out of more costly acute care because we don't know that it's happening. Communication between [outpatient and inpatient] facilities is one of the most challenging issues. (Participant 13) |
| Optimism about potential of EHRs. | A lot of people are depending on [the EHR] to make a lot of communication changes [where there was] a disconnect in the past. (Participant 7) | |
| Lack of EHR interoperability. | We have an EHR that's pieced together. The [emergency department] has their own [system]. The clinics have their own. The inpatient has their own. They're all electronic but they don't all talk to each other that well. (Participant 20) | |
| Our system has reached our maximum capacity and we've had to rely on our community partners to see the overflow. [T]he difficult communication [is] magnified. (Participant 11) | ||
| Privacy and legal concerns (nonuniform application of HIPAA standards). | There is a very different view from hospital to hospital about what it is they feel that they can share legally under HIPAA or not. It's a very strange thing and it almost depends more on the chief information officer at [each] hospital and less on what the [regulations] actually say. (Participant 21) | |
| Yes, [the EHR] does communicate with the hospitals and the hospitals [communicate] back [with us]. [T]here are some technical issues, butthe biggest impediments to making the technology work are new issues around confidentiality and access. (Participant 17) | ||
| Interpersonal contact is still needed even with robust EHRs. | I think [communication between systems is] getting better [due to the EHR], but there's still quite a few holes and a sense of the loop not being completely closed. It's like when you pick up the phoneyou don't want the automated system, you want to actually talk to somebody. (Participant 18) | |
Lack of Institutional Financial Incentives for Collaboration
Primary care leaders felt that current reimbursement strategies rewarded hospitals for reducing readmissions rather than promoting shared savings with primary care. Seeking collaboration with hospitals would potentially increase clinic responsibility for postdischarge patient care without reimbursement for additional work.
In counties without public hospitals, leaders worried that collaboration with hospitals could lead to active loss of Medicaid patients from their practices. Developing closer relationships with local hospitals would enable those hospitals to redirect Medicaid patients to hospital‐owned primary care clinics, leading to a loss of important revenue and financial stability for their clinics.
A subset of these leaders also perceived that nonpublic hospitals were reluctant to collaborate with their clinics. They hypothesized that hospital leaders worried that collaborating with their primary care practices would lead to more uninsured patients at their hospitals, leading to an increase in uncompensated hospital care and reduced reimbursement. However, a second subset of leaders thought that nonpublic hospitals had increased financial incentives to collaborate with safety‐net clinics, because improved coordination with outpatient care could prevent uncompensated hospital care.
Competing Clinic Priorities Limit Primary Care Ability to Focus on Care Transitions
Clinic leaders struggled to balance competing priorities, including strained clinic capacity, regulatory/accreditation requirements, and financial strain. New patient‐centered medical home initiatives, which improve primary care financial incentives for postdischarge care coordination, were perceived as well intentioned but added to an overwhelming burden of ongoing quality improvement efforts.
Mismatched Expectations About the Role and Capacity of Primary Care in Care Transitions Limits Collaboration
Many leaders felt that hospitals undervalued the role of primary care as stakeholders in improving care transitions. They perceived that hospitals made little effort to directly contact primary care physicians about their patients' hospitalizations and discharges. Leaders were frustrated that hospitals had unrealistic expectations of primary care to deliver timely postdischarge care, given their strained capacity. Consequently, some were reluctant to seek opportunities to collaborate with hospitals to improve care transitions.
Informal Affiliations and Partnerships, Formed Through Personal Relationships and Interpersonal Networking, Facilitate Collaboration
Informal affiliations between hospitals and primary care clinics helped improve awareness of organizational roles and capacity and create a sense of shared mission, thus enabling collaboration in spite of other barriers. Such affiliations arose from existing, longstanding personal relationships and/or interpersonal networking between individual providers across settings. These informal affiliations were important for safety‐net clinics that were FQHCs or FQHC Look‐Alikes, because formal hospital affiliations are discouraged by federal regulations.[26]
Opportunities for building relationships and networking with hospital personnel arose when clinic physicians had hospital admitting privileges. This on‐site presence facilitated personal relationships and communication between clinic and hospital physicians, thus enabling better collaboration. However, increasing demands on outpatient clinical productivity often made a hospital presence infeasible. One health system promoted interpersonal networking through regular meetings between the clinic and the local hospital to foster collaboration on quality improvement and care delivery; however, clinical productivity demands ultimately took priority over these meetings. Although delegating inpatient care to hospitalists enabled clinics to maximize their productivity, it also decreased opportunities for networking, and consequently, clinic physicians felt their voices and opinions were not represented in improvement initiatives.
Outside funding and support, such as incentive programs and conferences sponsored by local health plans, clinic consortiums, or national stakeholder organizations, enabled the most successful networking. These successes were independent of whether the clinic staff rounded in the hospital.
Electronic Health Records Enable Collaboration By Improving Communication Between Hospitals And Primary Care
Challenges in communication and information flow were also challenges to collaboration with hospitals. No respondents reported receiving routine notification of patient hospitalizations at the time of admission. Many clinics were dedicating significant attention to implementing electronic health record (EHR) systems to receive financial incentives associated with meaningful use.[27] Implementation of EHRs helped mitigate issues with communication with hospitals, though to a lesser degree than expected. Clinics early in the process of EHR adoption were optimistic about the potential of EHRs to improve communication with hospitals. However, clinic leaders in settings with greater EHR experience were more guarded in their enthusiasm. They observed that lack of interoperability between clinic and hospital EHRs was a persistent and major issue in spite of meaningful use standards, limiting timely flow of information across settings. Even when hospitals and their associated clinics had integrated or interoperable EHRs (n=3), or were working toward EHR integration (n=5), the need to expand networks to include other community healthcare settings using different systems presented ongoing challenges to achieving seamless communication due to a lack of interoperability.
When information sharing was technically feasible, leaders noted that inconsistent understanding and application of privacy rules dictated by the Health Insurance Portability and Accountability Act (HIPAA) limited information sharing. The quality and types of information shared varied widely across settings, depending on how HIPAA regulations were interpreted.
Even with robust EHRs, interpersonal contact was still perceived as crucial to enabling collaboration. EHRs were perceived to help with information flow, but did not facilitate relationship building across settings.
DISCUSSION
We found that safety‐net primary care leaders identified several barriers to collaboration with hospitals: (1) lack of financial incentives for collaboration, (2) competing priorities, (3) mismatched expectations about the role and capacity of primary care, and (4) poor communication infrastructure. Interpersonal networking and use of EHRs helped overcome these obstacles to a limited extent.
Prior studies demonstrate that early follow‐up, timely communication, and continuity with primary care after hospital discharge are associated with improved postdischarge outcomes.[8, 28, 29, 30] Despite evidence that collaboration between primary care and hospitals may help optimize postdischarge outcomes, our study is the first to describe primary care leaders' perspectives on potential targets for improving collaboration between hospitals and primary care to improve care transitions.
Our results highlight the need to modify payment models to align financial incentives across settings for collaboration. Otherwise, it may be difficult for hospitals to engage primary care in collaborative efforts to improve care transitions. Recent pilot payment models aim to motivate improved postdischarge care coordination. The Centers for Medicare and Medicaid Services implemented two new Current Procedural Terminology Transitional Care Management codes to enable reimbursement of outpatient physicians for management of patients transitioning from the hospital to the community. This model does not require communication between accepting (outpatient) and discharging (hospital) physicians or other hospital staff.[31] Another pilot program pays primary care clinics $6 per beneficiary per month if they become level 3 patient‐centered medical homes, which have stringent requirements for communication and coordination with hospitals for postdischarge care.[32] Capitated payment models, such as expansion of Medicaid managed care, and shared‐savings models, such accountable care organizations, aim to promote shared responsibility between hospitals and primary care by creating financial incentives to prevent hospitalizations through effective use of outpatient resources. The effectiveness of these strategies to improve care transitions is not yet established.
Many tout the adoption of EHRs as a means to improve communication and collaboration across settings.[33] However, policies narrowly focused on EHR adoption fail to address broader issues regarding lack of EHR interoperability and inconsistently applied privacy regulations under HIPAA, which were substantial barriers to information sharing. Stage 2 meaningful use criteria will address some interoperability issues by implementing standards for exchange of laboratory data and summary care records for care transitions.[34] Additional regulatory policies should promote uniform application of privacy regulations to enable more fluid sharing of electronic data across various healthcare settings. Locally and regionally negotiated data sharing agreements, as well as arrangements such as regional health information exchanges, could temporize these issues until broader policies are enacted.
EHRs did not obviate the need for meaningful interpersonal communication between providers. Hospital‐based quality improvement teams could create networking opportunities to foster relationship‐building and communication across settings. Leadership should consider scheduling protected time to facilitate attendance. Colocation of outpatient staff, such as nurse coordinators and office managers, in the hospital may also improve relationship building and care coordination.[35] Such measures would bridge the perceived divide between inpatient and outpatient care, and create avenues to find mutually beneficial solutions to improving postdischarge care transitions.[36]
Our results should be interpreted in light of several limitations. This study focused on primary care practices in the California safety net; given variations in safety nets across different contexts, the transferability of our findings may be limited. Second, rural perspectives were relatively under‐represented in our study sample; there may be additional unidentified issues specific to rural areas or specific to other nonparticipants that may have not been captured in this study. For this hypothesis‐generating study, we focused on the perspectives of primary care leaders. Triangulating perspectives of other stakeholders, including hospital leadership, mental health, social services, and payer organizations, will offer a more comprehensive analysis of barriers and enablers to hospitalprimary care collaboration. We were unable to collect data on the payer mix of each facility, which may influence the perceived financial barriers to collaboration among facilities. However, we anticipate that the broader theme of lack of financial incentives for collaboration will resonate across many settings, as collaboration between inpatient and outpatient providers in general has been largely unfunded by payers.[37, 38, 39] Further, most primary care providers (PCPs) in and outside of safety‐net settings operate on slim margins that cannot support additional time by PCPs or staff to coordinate care transitions.[39, 40] Because our study was completed prior to the implementation of several new payment models motivating postdischarge care coordination, we were unable to assess their effect on clinics' collaboration with hospitals.
In conclusion, efforts to improve collaboration between clinical settings around postdischarge care transitions will require targeted policy and quality improvement efforts in 3 specific areas. Policy makers and administrators with the power to negotiate payment schemes and regulatory policies should first align financial incentives across settings to support postdischarge transitions and care coordination, and second, improve EHR interoperability and uniform application of HIPAA regulations. Third, clinic and hospital leaders, and front‐line providers should enhance opportunities for interpersonal networking between providers in hospital and primary care settings. With the expansion of insurance coverage and increased demand for primary care in the safety net and other settings, policies to promote care coordination should consider the perspective of both hospital and clinic incentives and mechanisms for coordinating care across settings.
Disclosures
Preliminary results from this study were presented at the Society of General Internal Medicine 36th Annual Meeting in Denver, Colorado, April 2013. Dr. Nguyen's work on this project was funded by a federal training grant from the National Research Service Award (NRSA T32HP19025‐07‐00). Dr. Goldman is the recipient of grants from the Agency for Health Care Research and Quality (K08 HS018090‐01). Drs. Goldman, Greysen, and Lyndon are supported by the National Institutes of Health, National Center for Research Resources, Office of the Director (UCSF‐CTSI grant no. KL2 RR024130). The authors report no conflicts of interest.
- Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , . Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;18(8):646–651.
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: Medicare Payment Advisory Commission; 2007.
- , , , , , . Hospital‐initiated transitional care interventions as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 pt 2):433–440.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , . Improving care transitions: hospitalists partnering with primary care. J Hosp Med. 2010;5(7):375–377.
- , , , , . Primary care physician communication at hospital discharge reduces medication discrepancies. J Hosp Med. 2013;8(12):672–677.
- Institute of Medicine. America's Health Care Safety Net: Intact but Endangered. Washington, DC: Institute of Medicine; 2000.
- , . Higher readmissions at safety‐net hospitals and potential policy solutions. Issue Brief (Commonw Fund). 2012;34:1–16.
- , . Characteristics of hospitals receiving penalties under the hospital readmissions reduction program. JAMA. 2013;309(4):342–343.
- , , , et al. Ensuring Equity: A Post‐Reform Framework to Achieve High Performance Health Care for Vulnerable Populations. New York, NY: The Commonwealth Fund; 2011.
- , , , , . Enhancing the Capacity of Community Centers to Achieve High Performance: Findings from the 2009 Commonwealth Fund National Survey of Federally Qualified Health Centers. New York, NY: The Commonwealth Fund; 2010.
- , , . Integration mechanisms and hospital efficiency in integrated health care delivery systems. J Med Syst. 2002;26(2):127–143.
- , , . Effect of physician collaboration network on hospitalization cost and readmission rate. Eur J Public Health. 2012;22(5):629–633.
- Health Resources and Services Administration. Health Center Look‐Alikes Program. Available at: http://bphc.hrsa.gov/about/lookalike/index.html?IsPopUp=true. Accessed on September 5, 2014.
- , , , . Public hospitals in the United States, 2008. Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb95.jsp. Published September 2010. Accessed on September 5, 2014.
- U.S. Department of Health and Human Services. Health Resources and Services Administration. Available at: http://www.hrsa.gov/shortage/. Accessed on September 5, 2014.
- , . California's Safety Net and The Need to Improve Local Collaboration in Care for the Uninsured: Counties, Clinics, Hospitals, and Local Health Plans. Available at: http://www.itup.org/Reports/Statewide/Safetynet_Report_Final.pdf. Published October 2008. Accessed on September 5, 2014.
- , . Unsatisfactory saturation: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual Res. 2013;13(2):190–197.
- . Leading successful interinstitutional collaborations using the collaboration success measurement model. Paper presented at: The Chair Academy's 16th Annual International Conference: Navigating the Future through Authentic Leadership; 2007; Jacksonville, FL. Available at http://www.chairacademy.com/conference/2007/papers/leading_successful_interinstitutional_collaborations.pdf. Accessed on September 5, 2014.
- , , , , . The difference between integration and collaboration in patient care: results from key informant interviews working in multiprofessional health care teams. J Manipulative Physiol Ther. 2009;32(9):715–722.
- , , , , , . Implementing organized delivery systems: an integration scorecard. Health Care Manag Rev. 1994;19(3):7–20.
- State of California Office of Statewide Health Planning 3(2):77–101.
- Health Resources and Services Administration Primary Care: The Health Center Program. Affiliation agreements of community 303(17):1716–1722.
- , , , , . Reducing hospital readmissions through primary care practice transformation. Journal Fam Pract. 2014;63(2):67–73.
- , , . Post‐hospitalization transitions: Examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- U.S. Department of Health and Human Services. Centers for Medicare 2009.
- , , , . Hospitalists and care transitions: the divorce of inpatient and outpatient care. Health Aff (Millwood). 2008;27(5):1315–1327.
- , , . Reducing hospital readmissions: lessons from top‐performing hospitals. Available at: http://www.commonwealthfund.org/publications/case‐studies/2011/apr/reducing‐hospital‐readmissions. Published April 2011. Accessed on September 5, 2014.
- , , . Recasting readmissions by placing the hospital role in community context. JAMA. 2013;309(4):351–352.
- . A primary care physician's ideal transitions of care—where's the evidence? J Hosp Med. 2013;8(8):472–477.
- , . Primary care: current problems and proposed solutions. Health Aff (Millwood). 2010;29(5):799–805.
Poorly coordinated care between hospital and outpatient settings contributes to medical errors, poor outcomes, and high costs.[1, 2, 3] Recent policy has sought to motivate better care coordination after hospital discharge. Financial penalties for excessive hospital readmissionsa perceived marker of poorly coordinated carehave motivated hospitals to adopt transitional care programs to improve postdischarge care coordination.[4] However, the success of hospital‐initiated transitional care strategies in reducing hospital readmissions has been limited.[5] This may be due to the fact that many factors driving hospital readmissions, such as chronic medical illness, patient education, and availability of outpatient care, are outside of a hospital's control.[5, 6] Even among the most comprehensive hospital‐based transitional care intervention strategies, there is little evidence of active engagement of primary care providers or collaboration between hospitals and primary care practices in the transitional care planning process.[5] Better engagement of primary care into transitional care strategies may improve postdischarge care coordination.[7, 8]
The potential benefits of collaboration are particularly salient in healthcare safety nets.[9] The US health safety net is a patchwork of providers, funding, and programs unified by a shared missiondelivering care to patients regardless of ability to payrather than a coordinated system with shared governance.[9] Safety‐net hospitals are at risk for higher‐than‐average readmissions penalties.[10, 11] Medicaid expansion under the Affordable Care Act will likely increase demand for services in these settings, which could worsen fragmentation of care as a result of strained capacity.[12] Collaboration between hospitals and primary care clinics in the safety net could help overcome fragmentation, improve efficiencies in care, and reduce costs and readmissions.[12, 13, 14, 15]
Despite the potential benefits, we found no studies on how to enable collaboration between hospitals and primary care. We sought to understand systems‐level factors limiting and facilitating collaboration between hospitals and primary care practices around coordinating inpatient‐to‐outpatient care transitions by conducting a qualitative study, focusing on the perspective of primary care leaders in the safety net.
STUDY DATA AND METHODS
We conducted semistructured telephone interviews with primary care leaders in health safety nets across California from August 2012 through October 2012, prior to the implementation of the federal hospital readmissions penalties program. Primary care leaders were defined as clinicians or nonclinicians holding leadership positions, including chief executive officers, clinic medical directors, and local experts in care coordination or quality improvement. We defined safety‐net clinics as federally qualified health centers (FQHCs) and/or FQHC Look‐Alikes (clinics that meet eligibility requirements and receive the same benefits as FQHCs, except for Public Health Service Section 330 grants), community health centers, and public hospital‐affiliated clinics operating under a traditional fee‐for‐service model and serving a high proportion of Medicaid and uninsured patients.[9, 16] We defined public hospitals as government‐owned hospitals that provide care for individuals with limited access elsewhere.[17]
Sampling and Recruitment
We purposefully sampled participants to maximize diversity in geographic region, metropolitan status,[18] and type of county health delivery system to enable identification of common themes across different settings and contexts. Delivery systems were defined as per the Insure the Uninsured Project, a 501(c)(3) nonprofit organization that conducts research on the uninsured in California.[19] Provider systems are counties with a public hospital; payer systems are counties that contract with private hospitals to deliver uncompensated care in place of a public hospital; and County Medical Services Program is a state program that administers county health care in participating small counties, in lieu of a provider or payer system. We used the county delivery system type as a composite proxy of available county resources and market context given variations in funding, access, and eligibility by system type.
Participants were identified through online public directories, community clinic consortiums, and departments of public health websites. Additional participants were sought using snowball sampling. Potential participants were e‐mailed a recruitment letter describing the study, its purpose, topics to be covered, and confidentiality assurance. Participants who did not respond were called or e‐mailed within 1 week. When initial recruitment was unsuccessful, we attempted to recruit another participant within the same organization when possible. We recruited participants until reaching thematic saturation (i.e., no further new themes emerged from our interviews).[20] No participants were recruited through snowballing.
Data Collection and Interview Guides
We conducted in‐depth, semistructured interviews using interview guides informed by existing literature on collaboration and integration across healthcare systems[21, 22, 23] (see Supporting Information, Appendix 1, in the online version of this article). Interviews were digitally recorded and professionally transcribed verbatim.
We obtained contextual information for settings represented by each respondent, such as number of clinics and annual visits, through the California Primary Care Annual Utilization Data Report and clinic websites.[24]
Analysis
We employed thematic analysis[25] using an inductive framework to identify emergent and recurring themes. We developed and refined a coding template iteratively. Our multidisciplinary team included 2 general internists (O.K.N., L.E.G), 1 hospitalist (S.R.G.), a clinical nurse specialist with a doctorate in nursing (A.L.), and research staff with a public health background (J.K.). Two team members (O.K.N., J.K.) systematically coded all transcripts. Disagreements in coding were resolved through negotiated consensus. All investigators reviewed and discussed identified themes. We emailed summary findings to participants for confirmation to enhance the reliability of our findings.
The institutional review board at the University of California, San Francisco approved the study protocol.
RESULTS
Of 52 individuals contacted from 39 different organizations, 23 did not respond, 4 declined to participate, and 25 were scheduled for an interview. We interviewed 22 primary care leaders across 11 California counties (Table 1) and identified themes around factors influencing collaboration with hospitals (Table 2). Most respondents had prior positive experiences collaborating with hospitals on small, focused projects. However, they asserted the need for better hospitalclinic collaboration, and thought collaboration was critical to achieving high‐quality care transitions. We did not observe any differences in perspectives expressed by clinician versus nonclinician leaders. Nonparticipants were more likely than participants to be from northern rural or central counties, FQHCs, and smaller clinic settings.
| |
| Leadership position | No. (%) |
| Chief executive officer or equivalent* | 9 (41) |
| Chief medical officer or medical director | 7 (32) |
| Other | 6 (27) |
| Clinical experience | |
| Physician (MD or DO) | 15 (68) |
| Registered nurse | 1 (5) |
| Nonclinician | 6 (27) |
| Clinic setting | |
| Clinic type | |
| FQHC and FQHC Look‐Alikes | 15 (68) |
| Hospital based | 2 (9) |
| Other | 5 (23) |
| No. of clinics in system | |
| 14 | 9 (41) |
| 59 | 6 (27) |
| 10 | 7 (32) |
| Annual no. of visits | |
| <100,000 | 9 (41) |
| 100,000499,999 | 11 (50) |
| 500,000 | 2 (9) |
| County characteristics | |
| Health delivery system type | |
| Provider | 13 (59) |
| Payer | 2 (9) |
| County Medical Services Program∥ | 7 (32) |
| Rural county | 7 (32) |
| Theme | Subtheme | Quote |
|---|---|---|
| ||
| Lack of institutional financial incentives for collaboration. | Collaboration may lead to increased responsibility without reimbursement for clinic. | Where the [payment] model breaks down is that the savings is only to the hospital; and there's an expectation on our part to go ahead and take on those additional patients. If that $400,000 savings doesn't at least have a portion to the team that's going to help keep the people out of the hospital, then it won't work. (Participant 17) |
| Collaboration may lead to competition from the hospital for primary care patients. | Our biggest issues with working with the hospital[are] that we have a finite number of [Medicaid] patients [in our catchment area for whom] you get larger reimbursement. For a federally qualified health center, it is [crucial] to ensure we have a revenue stream that helps us take care of the uninsured. So you can see the natural kind of conflict when your pool of patients is very small. (Participant 10) | |
| Collaboration may lead to increased financial risk for the hospital. | 70% to 80% of our adult patients have no insurance and the fact is that none of these hospitals want those patients. They do get disproportionate hospital savings and other thingsbut they don't have a strong business model when they have uninsured patients coming in their doors. That's just the reality. (Participant 21) | |
| Collaboration may lead to decreased financial risk for the hospital. | Most of these patients either have very low reimbursement or no reimbursement, and so [the hospital doesn't] really want these people to end up in very expensive care because it's a burden on their systemphilosophically, everyone agrees that if we keep people well in the outpatient setting, that would be better for everyone. No, there is no financial incentive whatsoever for [the hospital] to not work with us. [emphasis added] (Participant 18) | |
| Competing priorities limit primary care's ability to focus on care transitions. | I wouldn't say [improving care transitions is a high priority]. It's not because we don't want to do the job. We have other priorities. [T]he big issue is access. There's a massive demand for primary care in our communityand we're just trying to make sure we have enough capacity. [There are] requirements HRSA has been asking of health centers and other priorities. We're starting up a residency program. We're recruiting more doctors. We're upping our quality improvement processes internally. We're making a reinvestment in our [electronic medical record]. It never stops. (Participant 22) | |
| The multitude of [care transitions and other quality] improvement imperatives makes it difficult to focus. It's not that any one of these things necessarily represents a flawed approach. It's just that when you have a variety of folks from the national, state, and local levels who all have different ideas about what constitutes appropriate improvement, it's very hard to respond to it all at once. (Participant 6) | ||
| Mismatched expectations about the role and capacity of primary care in care transitions limit collaboration. | Perception of primary care being undervalued by hospitals as a key stakeholder in care transitions. | They just make sure the paperwork is set up.and they have it written down, See doctor in 7 days. And I think they [the hospitals] think that's where their responsibility stops. They don't actually look at our records or talk to us. (Participant 2) |
| Perceived unrealistic expectations of primary care capacity to deliver postdischarge care. | [The hospital will] send anyone that's poor to us whether they are our patient or not. [T]hey say go to [our clinic] and they'll give you your outpatient medications. [But] we're at capacity. [W]e have a 79 month wait for a [new] primary care appointment. So then, we're stuck with the ethical dilemma of [do we send the patient back to the ER/hospital] for their medication or do we just [try to] take them in? (Participant 13) | |
| The hospitals feel every undoctored patient must be ours. [But] it's not like we're sitting on our hands. We have more than enough patients. (Participant 22) | ||
| Informal affiliations and partnerships, formed through personal relationships and interpersonal networking, facilitate collaboration. | Informal affiliations arise from existing personal relationships and/or interpersonal networking. | Our CEO [has been here] for the past 40 years, and has had very deep and ongoing relationships with the [hospital]. Those doors are very wide open. (Participant 18) |
| Informal partnerships are particularly important for FQHCs. | As an FQHC we can't have any ties financially or politically, but there's a traditional connection. (Participant 2) | |
| Increasing demands on clinical productivity lead to a loss of networking opportunities. | We're one of the few clinics that has their own inpatient service. I would say that the transitions between the hospital and [our] clinic start from a much higher level than anybody else. [However] we're about to close our hospital service. It's just too much work for our [clinic] doctors. (Participant 8) | |
| There used to be a meeting once a month where quality improvement programs and issues were discussed. Our administration eliminated these in favor of productivity, to increase our numbers of patients seen. (Participant 12) | ||
| Loss of relationships with hospital personnel amplifies challenges to collaboration. | Because the primary care docs are not visible in the hospital[quality improvement] projects [become] hospital‐based. Usually they forget that we exist. (Participant 11) | |
| External funding and support can enable opportunities for networking and relationship building. | The [national stakeholder organization] has done a lot of work with us to bring us together and figure out what we're doing [across] different counties, settings, providers. (Participant 20) | |
| Electronic health records enable collaboration by improving communication between hospitals and primary care. | Lack of timely communication between inpatient and outpatient settings is a major obstacle to postdischarge care coordination. | It's a lot of effort to get medical records back. It is often not timely. Patients are going to cycle in and out of more costly acute care because we don't know that it's happening. Communication between [outpatient and inpatient] facilities is one of the most challenging issues. (Participant 13) |
| Optimism about potential of EHRs. | A lot of people are depending on [the EHR] to make a lot of communication changes [where there was] a disconnect in the past. (Participant 7) | |
| Lack of EHR interoperability. | We have an EHR that's pieced together. The [emergency department] has their own [system]. The clinics have their own. The inpatient has their own. They're all electronic but they don't all talk to each other that well. (Participant 20) | |
| Our system has reached our maximum capacity and we've had to rely on our community partners to see the overflow. [T]he difficult communication [is] magnified. (Participant 11) | ||
| Privacy and legal concerns (nonuniform application of HIPAA standards). | There is a very different view from hospital to hospital about what it is they feel that they can share legally under HIPAA or not. It's a very strange thing and it almost depends more on the chief information officer at [each] hospital and less on what the [regulations] actually say. (Participant 21) | |
| Yes, [the EHR] does communicate with the hospitals and the hospitals [communicate] back [with us]. [T]here are some technical issues, butthe biggest impediments to making the technology work are new issues around confidentiality and access. (Participant 17) | ||
| Interpersonal contact is still needed even with robust EHRs. | I think [communication between systems is] getting better [due to the EHR], but there's still quite a few holes and a sense of the loop not being completely closed. It's like when you pick up the phoneyou don't want the automated system, you want to actually talk to somebody. (Participant 18) | |
Lack of Institutional Financial Incentives for Collaboration
Primary care leaders felt that current reimbursement strategies rewarded hospitals for reducing readmissions rather than promoting shared savings with primary care. Seeking collaboration with hospitals would potentially increase clinic responsibility for postdischarge patient care without reimbursement for additional work.
In counties without public hospitals, leaders worried that collaboration with hospitals could lead to active loss of Medicaid patients from their practices. Developing closer relationships with local hospitals would enable those hospitals to redirect Medicaid patients to hospital‐owned primary care clinics, leading to a loss of important revenue and financial stability for their clinics.
A subset of these leaders also perceived that nonpublic hospitals were reluctant to collaborate with their clinics. They hypothesized that hospital leaders worried that collaborating with their primary care practices would lead to more uninsured patients at their hospitals, leading to an increase in uncompensated hospital care and reduced reimbursement. However, a second subset of leaders thought that nonpublic hospitals had increased financial incentives to collaborate with safety‐net clinics, because improved coordination with outpatient care could prevent uncompensated hospital care.
Competing Clinic Priorities Limit Primary Care Ability to Focus on Care Transitions
Clinic leaders struggled to balance competing priorities, including strained clinic capacity, regulatory/accreditation requirements, and financial strain. New patient‐centered medical home initiatives, which improve primary care financial incentives for postdischarge care coordination, were perceived as well intentioned but added to an overwhelming burden of ongoing quality improvement efforts.
Mismatched Expectations About the Role and Capacity of Primary Care in Care Transitions Limits Collaboration
Many leaders felt that hospitals undervalued the role of primary care as stakeholders in improving care transitions. They perceived that hospitals made little effort to directly contact primary care physicians about their patients' hospitalizations and discharges. Leaders were frustrated that hospitals had unrealistic expectations of primary care to deliver timely postdischarge care, given their strained capacity. Consequently, some were reluctant to seek opportunities to collaborate with hospitals to improve care transitions.
Informal Affiliations and Partnerships, Formed Through Personal Relationships and Interpersonal Networking, Facilitate Collaboration
Informal affiliations between hospitals and primary care clinics helped improve awareness of organizational roles and capacity and create a sense of shared mission, thus enabling collaboration in spite of other barriers. Such affiliations arose from existing, longstanding personal relationships and/or interpersonal networking between individual providers across settings. These informal affiliations were important for safety‐net clinics that were FQHCs or FQHC Look‐Alikes, because formal hospital affiliations are discouraged by federal regulations.[26]
Opportunities for building relationships and networking with hospital personnel arose when clinic physicians had hospital admitting privileges. This on‐site presence facilitated personal relationships and communication between clinic and hospital physicians, thus enabling better collaboration. However, increasing demands on outpatient clinical productivity often made a hospital presence infeasible. One health system promoted interpersonal networking through regular meetings between the clinic and the local hospital to foster collaboration on quality improvement and care delivery; however, clinical productivity demands ultimately took priority over these meetings. Although delegating inpatient care to hospitalists enabled clinics to maximize their productivity, it also decreased opportunities for networking, and consequently, clinic physicians felt their voices and opinions were not represented in improvement initiatives.
Outside funding and support, such as incentive programs and conferences sponsored by local health plans, clinic consortiums, or national stakeholder organizations, enabled the most successful networking. These successes were independent of whether the clinic staff rounded in the hospital.
Electronic Health Records Enable Collaboration By Improving Communication Between Hospitals And Primary Care
Challenges in communication and information flow were also challenges to collaboration with hospitals. No respondents reported receiving routine notification of patient hospitalizations at the time of admission. Many clinics were dedicating significant attention to implementing electronic health record (EHR) systems to receive financial incentives associated with meaningful use.[27] Implementation of EHRs helped mitigate issues with communication with hospitals, though to a lesser degree than expected. Clinics early in the process of EHR adoption were optimistic about the potential of EHRs to improve communication with hospitals. However, clinic leaders in settings with greater EHR experience were more guarded in their enthusiasm. They observed that lack of interoperability between clinic and hospital EHRs was a persistent and major issue in spite of meaningful use standards, limiting timely flow of information across settings. Even when hospitals and their associated clinics had integrated or interoperable EHRs (n=3), or were working toward EHR integration (n=5), the need to expand networks to include other community healthcare settings using different systems presented ongoing challenges to achieving seamless communication due to a lack of interoperability.
When information sharing was technically feasible, leaders noted that inconsistent understanding and application of privacy rules dictated by the Health Insurance Portability and Accountability Act (HIPAA) limited information sharing. The quality and types of information shared varied widely across settings, depending on how HIPAA regulations were interpreted.
Even with robust EHRs, interpersonal contact was still perceived as crucial to enabling collaboration. EHRs were perceived to help with information flow, but did not facilitate relationship building across settings.
DISCUSSION
We found that safety‐net primary care leaders identified several barriers to collaboration with hospitals: (1) lack of financial incentives for collaboration, (2) competing priorities, (3) mismatched expectations about the role and capacity of primary care, and (4) poor communication infrastructure. Interpersonal networking and use of EHRs helped overcome these obstacles to a limited extent.
Prior studies demonstrate that early follow‐up, timely communication, and continuity with primary care after hospital discharge are associated with improved postdischarge outcomes.[8, 28, 29, 30] Despite evidence that collaboration between primary care and hospitals may help optimize postdischarge outcomes, our study is the first to describe primary care leaders' perspectives on potential targets for improving collaboration between hospitals and primary care to improve care transitions.
Our results highlight the need to modify payment models to align financial incentives across settings for collaboration. Otherwise, it may be difficult for hospitals to engage primary care in collaborative efforts to improve care transitions. Recent pilot payment models aim to motivate improved postdischarge care coordination. The Centers for Medicare and Medicaid Services implemented two new Current Procedural Terminology Transitional Care Management codes to enable reimbursement of outpatient physicians for management of patients transitioning from the hospital to the community. This model does not require communication between accepting (outpatient) and discharging (hospital) physicians or other hospital staff.[31] Another pilot program pays primary care clinics $6 per beneficiary per month if they become level 3 patient‐centered medical homes, which have stringent requirements for communication and coordination with hospitals for postdischarge care.[32] Capitated payment models, such as expansion of Medicaid managed care, and shared‐savings models, such accountable care organizations, aim to promote shared responsibility between hospitals and primary care by creating financial incentives to prevent hospitalizations through effective use of outpatient resources. The effectiveness of these strategies to improve care transitions is not yet established.
Many tout the adoption of EHRs as a means to improve communication and collaboration across settings.[33] However, policies narrowly focused on EHR adoption fail to address broader issues regarding lack of EHR interoperability and inconsistently applied privacy regulations under HIPAA, which were substantial barriers to information sharing. Stage 2 meaningful use criteria will address some interoperability issues by implementing standards for exchange of laboratory data and summary care records for care transitions.[34] Additional regulatory policies should promote uniform application of privacy regulations to enable more fluid sharing of electronic data across various healthcare settings. Locally and regionally negotiated data sharing agreements, as well as arrangements such as regional health information exchanges, could temporize these issues until broader policies are enacted.
EHRs did not obviate the need for meaningful interpersonal communication between providers. Hospital‐based quality improvement teams could create networking opportunities to foster relationship‐building and communication across settings. Leadership should consider scheduling protected time to facilitate attendance. Colocation of outpatient staff, such as nurse coordinators and office managers, in the hospital may also improve relationship building and care coordination.[35] Such measures would bridge the perceived divide between inpatient and outpatient care, and create avenues to find mutually beneficial solutions to improving postdischarge care transitions.[36]
Our results should be interpreted in light of several limitations. This study focused on primary care practices in the California safety net; given variations in safety nets across different contexts, the transferability of our findings may be limited. Second, rural perspectives were relatively under‐represented in our study sample; there may be additional unidentified issues specific to rural areas or specific to other nonparticipants that may have not been captured in this study. For this hypothesis‐generating study, we focused on the perspectives of primary care leaders. Triangulating perspectives of other stakeholders, including hospital leadership, mental health, social services, and payer organizations, will offer a more comprehensive analysis of barriers and enablers to hospitalprimary care collaboration. We were unable to collect data on the payer mix of each facility, which may influence the perceived financial barriers to collaboration among facilities. However, we anticipate that the broader theme of lack of financial incentives for collaboration will resonate across many settings, as collaboration between inpatient and outpatient providers in general has been largely unfunded by payers.[37, 38, 39] Further, most primary care providers (PCPs) in and outside of safety‐net settings operate on slim margins that cannot support additional time by PCPs or staff to coordinate care transitions.[39, 40] Because our study was completed prior to the implementation of several new payment models motivating postdischarge care coordination, we were unable to assess their effect on clinics' collaboration with hospitals.
In conclusion, efforts to improve collaboration between clinical settings around postdischarge care transitions will require targeted policy and quality improvement efforts in 3 specific areas. Policy makers and administrators with the power to negotiate payment schemes and regulatory policies should first align financial incentives across settings to support postdischarge transitions and care coordination, and second, improve EHR interoperability and uniform application of HIPAA regulations. Third, clinic and hospital leaders, and front‐line providers should enhance opportunities for interpersonal networking between providers in hospital and primary care settings. With the expansion of insurance coverage and increased demand for primary care in the safety net and other settings, policies to promote care coordination should consider the perspective of both hospital and clinic incentives and mechanisms for coordinating care across settings.
Disclosures
Preliminary results from this study were presented at the Society of General Internal Medicine 36th Annual Meeting in Denver, Colorado, April 2013. Dr. Nguyen's work on this project was funded by a federal training grant from the National Research Service Award (NRSA T32HP19025‐07‐00). Dr. Goldman is the recipient of grants from the Agency for Health Care Research and Quality (K08 HS018090‐01). Drs. Goldman, Greysen, and Lyndon are supported by the National Institutes of Health, National Center for Research Resources, Office of the Director (UCSF‐CTSI grant no. KL2 RR024130). The authors report no conflicts of interest.
Poorly coordinated care between hospital and outpatient settings contributes to medical errors, poor outcomes, and high costs.[1, 2, 3] Recent policy has sought to motivate better care coordination after hospital discharge. Financial penalties for excessive hospital readmissionsa perceived marker of poorly coordinated carehave motivated hospitals to adopt transitional care programs to improve postdischarge care coordination.[4] However, the success of hospital‐initiated transitional care strategies in reducing hospital readmissions has been limited.[5] This may be due to the fact that many factors driving hospital readmissions, such as chronic medical illness, patient education, and availability of outpatient care, are outside of a hospital's control.[5, 6] Even among the most comprehensive hospital‐based transitional care intervention strategies, there is little evidence of active engagement of primary care providers or collaboration between hospitals and primary care practices in the transitional care planning process.[5] Better engagement of primary care into transitional care strategies may improve postdischarge care coordination.[7, 8]
The potential benefits of collaboration are particularly salient in healthcare safety nets.[9] The US health safety net is a patchwork of providers, funding, and programs unified by a shared missiondelivering care to patients regardless of ability to payrather than a coordinated system with shared governance.[9] Safety‐net hospitals are at risk for higher‐than‐average readmissions penalties.[10, 11] Medicaid expansion under the Affordable Care Act will likely increase demand for services in these settings, which could worsen fragmentation of care as a result of strained capacity.[12] Collaboration between hospitals and primary care clinics in the safety net could help overcome fragmentation, improve efficiencies in care, and reduce costs and readmissions.[12, 13, 14, 15]
Despite the potential benefits, we found no studies on how to enable collaboration between hospitals and primary care. We sought to understand systems‐level factors limiting and facilitating collaboration between hospitals and primary care practices around coordinating inpatient‐to‐outpatient care transitions by conducting a qualitative study, focusing on the perspective of primary care leaders in the safety net.
STUDY DATA AND METHODS
We conducted semistructured telephone interviews with primary care leaders in health safety nets across California from August 2012 through October 2012, prior to the implementation of the federal hospital readmissions penalties program. Primary care leaders were defined as clinicians or nonclinicians holding leadership positions, including chief executive officers, clinic medical directors, and local experts in care coordination or quality improvement. We defined safety‐net clinics as federally qualified health centers (FQHCs) and/or FQHC Look‐Alikes (clinics that meet eligibility requirements and receive the same benefits as FQHCs, except for Public Health Service Section 330 grants), community health centers, and public hospital‐affiliated clinics operating under a traditional fee‐for‐service model and serving a high proportion of Medicaid and uninsured patients.[9, 16] We defined public hospitals as government‐owned hospitals that provide care for individuals with limited access elsewhere.[17]
Sampling and Recruitment
We purposefully sampled participants to maximize diversity in geographic region, metropolitan status,[18] and type of county health delivery system to enable identification of common themes across different settings and contexts. Delivery systems were defined as per the Insure the Uninsured Project, a 501(c)(3) nonprofit organization that conducts research on the uninsured in California.[19] Provider systems are counties with a public hospital; payer systems are counties that contract with private hospitals to deliver uncompensated care in place of a public hospital; and County Medical Services Program is a state program that administers county health care in participating small counties, in lieu of a provider or payer system. We used the county delivery system type as a composite proxy of available county resources and market context given variations in funding, access, and eligibility by system type.
Participants were identified through online public directories, community clinic consortiums, and departments of public health websites. Additional participants were sought using snowball sampling. Potential participants were e‐mailed a recruitment letter describing the study, its purpose, topics to be covered, and confidentiality assurance. Participants who did not respond were called or e‐mailed within 1 week. When initial recruitment was unsuccessful, we attempted to recruit another participant within the same organization when possible. We recruited participants until reaching thematic saturation (i.e., no further new themes emerged from our interviews).[20] No participants were recruited through snowballing.
Data Collection and Interview Guides
We conducted in‐depth, semistructured interviews using interview guides informed by existing literature on collaboration and integration across healthcare systems[21, 22, 23] (see Supporting Information, Appendix 1, in the online version of this article). Interviews were digitally recorded and professionally transcribed verbatim.
We obtained contextual information for settings represented by each respondent, such as number of clinics and annual visits, through the California Primary Care Annual Utilization Data Report and clinic websites.[24]
Analysis
We employed thematic analysis[25] using an inductive framework to identify emergent and recurring themes. We developed and refined a coding template iteratively. Our multidisciplinary team included 2 general internists (O.K.N., L.E.G), 1 hospitalist (S.R.G.), a clinical nurse specialist with a doctorate in nursing (A.L.), and research staff with a public health background (J.K.). Two team members (O.K.N., J.K.) systematically coded all transcripts. Disagreements in coding were resolved through negotiated consensus. All investigators reviewed and discussed identified themes. We emailed summary findings to participants for confirmation to enhance the reliability of our findings.
The institutional review board at the University of California, San Francisco approved the study protocol.
RESULTS
Of 52 individuals contacted from 39 different organizations, 23 did not respond, 4 declined to participate, and 25 were scheduled for an interview. We interviewed 22 primary care leaders across 11 California counties (Table 1) and identified themes around factors influencing collaboration with hospitals (Table 2). Most respondents had prior positive experiences collaborating with hospitals on small, focused projects. However, they asserted the need for better hospitalclinic collaboration, and thought collaboration was critical to achieving high‐quality care transitions. We did not observe any differences in perspectives expressed by clinician versus nonclinician leaders. Nonparticipants were more likely than participants to be from northern rural or central counties, FQHCs, and smaller clinic settings.
| |
| Leadership position | No. (%) |
| Chief executive officer or equivalent* | 9 (41) |
| Chief medical officer or medical director | 7 (32) |
| Other | 6 (27) |
| Clinical experience | |
| Physician (MD or DO) | 15 (68) |
| Registered nurse | 1 (5) |
| Nonclinician | 6 (27) |
| Clinic setting | |
| Clinic type | |
| FQHC and FQHC Look‐Alikes | 15 (68) |
| Hospital based | 2 (9) |
| Other | 5 (23) |
| No. of clinics in system | |
| 14 | 9 (41) |
| 59 | 6 (27) |
| 10 | 7 (32) |
| Annual no. of visits | |
| <100,000 | 9 (41) |
| 100,000499,999 | 11 (50) |
| 500,000 | 2 (9) |
| County characteristics | |
| Health delivery system type | |
| Provider | 13 (59) |
| Payer | 2 (9) |
| County Medical Services Program∥ | 7 (32) |
| Rural county | 7 (32) |
| Theme | Subtheme | Quote |
|---|---|---|
| ||
| Lack of institutional financial incentives for collaboration. | Collaboration may lead to increased responsibility without reimbursement for clinic. | Where the [payment] model breaks down is that the savings is only to the hospital; and there's an expectation on our part to go ahead and take on those additional patients. If that $400,000 savings doesn't at least have a portion to the team that's going to help keep the people out of the hospital, then it won't work. (Participant 17) |
| Collaboration may lead to competition from the hospital for primary care patients. | Our biggest issues with working with the hospital[are] that we have a finite number of [Medicaid] patients [in our catchment area for whom] you get larger reimbursement. For a federally qualified health center, it is [crucial] to ensure we have a revenue stream that helps us take care of the uninsured. So you can see the natural kind of conflict when your pool of patients is very small. (Participant 10) | |
| Collaboration may lead to increased financial risk for the hospital. | 70% to 80% of our adult patients have no insurance and the fact is that none of these hospitals want those patients. They do get disproportionate hospital savings and other thingsbut they don't have a strong business model when they have uninsured patients coming in their doors. That's just the reality. (Participant 21) | |
| Collaboration may lead to decreased financial risk for the hospital. | Most of these patients either have very low reimbursement or no reimbursement, and so [the hospital doesn't] really want these people to end up in very expensive care because it's a burden on their systemphilosophically, everyone agrees that if we keep people well in the outpatient setting, that would be better for everyone. No, there is no financial incentive whatsoever for [the hospital] to not work with us. [emphasis added] (Participant 18) | |
| Competing priorities limit primary care's ability to focus on care transitions. | I wouldn't say [improving care transitions is a high priority]. It's not because we don't want to do the job. We have other priorities. [T]he big issue is access. There's a massive demand for primary care in our communityand we're just trying to make sure we have enough capacity. [There are] requirements HRSA has been asking of health centers and other priorities. We're starting up a residency program. We're recruiting more doctors. We're upping our quality improvement processes internally. We're making a reinvestment in our [electronic medical record]. It never stops. (Participant 22) | |
| The multitude of [care transitions and other quality] improvement imperatives makes it difficult to focus. It's not that any one of these things necessarily represents a flawed approach. It's just that when you have a variety of folks from the national, state, and local levels who all have different ideas about what constitutes appropriate improvement, it's very hard to respond to it all at once. (Participant 6) | ||
| Mismatched expectations about the role and capacity of primary care in care transitions limit collaboration. | Perception of primary care being undervalued by hospitals as a key stakeholder in care transitions. | They just make sure the paperwork is set up.and they have it written down, See doctor in 7 days. And I think they [the hospitals] think that's where their responsibility stops. They don't actually look at our records or talk to us. (Participant 2) |
| Perceived unrealistic expectations of primary care capacity to deliver postdischarge care. | [The hospital will] send anyone that's poor to us whether they are our patient or not. [T]hey say go to [our clinic] and they'll give you your outpatient medications. [But] we're at capacity. [W]e have a 79 month wait for a [new] primary care appointment. So then, we're stuck with the ethical dilemma of [do we send the patient back to the ER/hospital] for their medication or do we just [try to] take them in? (Participant 13) | |
| The hospitals feel every undoctored patient must be ours. [But] it's not like we're sitting on our hands. We have more than enough patients. (Participant 22) | ||
| Informal affiliations and partnerships, formed through personal relationships and interpersonal networking, facilitate collaboration. | Informal affiliations arise from existing personal relationships and/or interpersonal networking. | Our CEO [has been here] for the past 40 years, and has had very deep and ongoing relationships with the [hospital]. Those doors are very wide open. (Participant 18) |
| Informal partnerships are particularly important for FQHCs. | As an FQHC we can't have any ties financially or politically, but there's a traditional connection. (Participant 2) | |
| Increasing demands on clinical productivity lead to a loss of networking opportunities. | We're one of the few clinics that has their own inpatient service. I would say that the transitions between the hospital and [our] clinic start from a much higher level than anybody else. [However] we're about to close our hospital service. It's just too much work for our [clinic] doctors. (Participant 8) | |
| There used to be a meeting once a month where quality improvement programs and issues were discussed. Our administration eliminated these in favor of productivity, to increase our numbers of patients seen. (Participant 12) | ||
| Loss of relationships with hospital personnel amplifies challenges to collaboration. | Because the primary care docs are not visible in the hospital[quality improvement] projects [become] hospital‐based. Usually they forget that we exist. (Participant 11) | |
| External funding and support can enable opportunities for networking and relationship building. | The [national stakeholder organization] has done a lot of work with us to bring us together and figure out what we're doing [across] different counties, settings, providers. (Participant 20) | |
| Electronic health records enable collaboration by improving communication between hospitals and primary care. | Lack of timely communication between inpatient and outpatient settings is a major obstacle to postdischarge care coordination. | It's a lot of effort to get medical records back. It is often not timely. Patients are going to cycle in and out of more costly acute care because we don't know that it's happening. Communication between [outpatient and inpatient] facilities is one of the most challenging issues. (Participant 13) |
| Optimism about potential of EHRs. | A lot of people are depending on [the EHR] to make a lot of communication changes [where there was] a disconnect in the past. (Participant 7) | |
| Lack of EHR interoperability. | We have an EHR that's pieced together. The [emergency department] has their own [system]. The clinics have their own. The inpatient has their own. They're all electronic but they don't all talk to each other that well. (Participant 20) | |
| Our system has reached our maximum capacity and we've had to rely on our community partners to see the overflow. [T]he difficult communication [is] magnified. (Participant 11) | ||
| Privacy and legal concerns (nonuniform application of HIPAA standards). | There is a very different view from hospital to hospital about what it is they feel that they can share legally under HIPAA or not. It's a very strange thing and it almost depends more on the chief information officer at [each] hospital and less on what the [regulations] actually say. (Participant 21) | |
| Yes, [the EHR] does communicate with the hospitals and the hospitals [communicate] back [with us]. [T]here are some technical issues, butthe biggest impediments to making the technology work are new issues around confidentiality and access. (Participant 17) | ||
| Interpersonal contact is still needed even with robust EHRs. | I think [communication between systems is] getting better [due to the EHR], but there's still quite a few holes and a sense of the loop not being completely closed. It's like when you pick up the phoneyou don't want the automated system, you want to actually talk to somebody. (Participant 18) | |
Lack of Institutional Financial Incentives for Collaboration
Primary care leaders felt that current reimbursement strategies rewarded hospitals for reducing readmissions rather than promoting shared savings with primary care. Seeking collaboration with hospitals would potentially increase clinic responsibility for postdischarge patient care without reimbursement for additional work.
In counties without public hospitals, leaders worried that collaboration with hospitals could lead to active loss of Medicaid patients from their practices. Developing closer relationships with local hospitals would enable those hospitals to redirect Medicaid patients to hospital‐owned primary care clinics, leading to a loss of important revenue and financial stability for their clinics.
A subset of these leaders also perceived that nonpublic hospitals were reluctant to collaborate with their clinics. They hypothesized that hospital leaders worried that collaborating with their primary care practices would lead to more uninsured patients at their hospitals, leading to an increase in uncompensated hospital care and reduced reimbursement. However, a second subset of leaders thought that nonpublic hospitals had increased financial incentives to collaborate with safety‐net clinics, because improved coordination with outpatient care could prevent uncompensated hospital care.
Competing Clinic Priorities Limit Primary Care Ability to Focus on Care Transitions
Clinic leaders struggled to balance competing priorities, including strained clinic capacity, regulatory/accreditation requirements, and financial strain. New patient‐centered medical home initiatives, which improve primary care financial incentives for postdischarge care coordination, were perceived as well intentioned but added to an overwhelming burden of ongoing quality improvement efforts.
Mismatched Expectations About the Role and Capacity of Primary Care in Care Transitions Limits Collaboration
Many leaders felt that hospitals undervalued the role of primary care as stakeholders in improving care transitions. They perceived that hospitals made little effort to directly contact primary care physicians about their patients' hospitalizations and discharges. Leaders were frustrated that hospitals had unrealistic expectations of primary care to deliver timely postdischarge care, given their strained capacity. Consequently, some were reluctant to seek opportunities to collaborate with hospitals to improve care transitions.
Informal Affiliations and Partnerships, Formed Through Personal Relationships and Interpersonal Networking, Facilitate Collaboration
Informal affiliations between hospitals and primary care clinics helped improve awareness of organizational roles and capacity and create a sense of shared mission, thus enabling collaboration in spite of other barriers. Such affiliations arose from existing, longstanding personal relationships and/or interpersonal networking between individual providers across settings. These informal affiliations were important for safety‐net clinics that were FQHCs or FQHC Look‐Alikes, because formal hospital affiliations are discouraged by federal regulations.[26]
Opportunities for building relationships and networking with hospital personnel arose when clinic physicians had hospital admitting privileges. This on‐site presence facilitated personal relationships and communication between clinic and hospital physicians, thus enabling better collaboration. However, increasing demands on outpatient clinical productivity often made a hospital presence infeasible. One health system promoted interpersonal networking through regular meetings between the clinic and the local hospital to foster collaboration on quality improvement and care delivery; however, clinical productivity demands ultimately took priority over these meetings. Although delegating inpatient care to hospitalists enabled clinics to maximize their productivity, it also decreased opportunities for networking, and consequently, clinic physicians felt their voices and opinions were not represented in improvement initiatives.
Outside funding and support, such as incentive programs and conferences sponsored by local health plans, clinic consortiums, or national stakeholder organizations, enabled the most successful networking. These successes were independent of whether the clinic staff rounded in the hospital.
Electronic Health Records Enable Collaboration By Improving Communication Between Hospitals And Primary Care
Challenges in communication and information flow were also challenges to collaboration with hospitals. No respondents reported receiving routine notification of patient hospitalizations at the time of admission. Many clinics were dedicating significant attention to implementing electronic health record (EHR) systems to receive financial incentives associated with meaningful use.[27] Implementation of EHRs helped mitigate issues with communication with hospitals, though to a lesser degree than expected. Clinics early in the process of EHR adoption were optimistic about the potential of EHRs to improve communication with hospitals. However, clinic leaders in settings with greater EHR experience were more guarded in their enthusiasm. They observed that lack of interoperability between clinic and hospital EHRs was a persistent and major issue in spite of meaningful use standards, limiting timely flow of information across settings. Even when hospitals and their associated clinics had integrated or interoperable EHRs (n=3), or were working toward EHR integration (n=5), the need to expand networks to include other community healthcare settings using different systems presented ongoing challenges to achieving seamless communication due to a lack of interoperability.
When information sharing was technically feasible, leaders noted that inconsistent understanding and application of privacy rules dictated by the Health Insurance Portability and Accountability Act (HIPAA) limited information sharing. The quality and types of information shared varied widely across settings, depending on how HIPAA regulations were interpreted.
Even with robust EHRs, interpersonal contact was still perceived as crucial to enabling collaboration. EHRs were perceived to help with information flow, but did not facilitate relationship building across settings.
DISCUSSION
We found that safety‐net primary care leaders identified several barriers to collaboration with hospitals: (1) lack of financial incentives for collaboration, (2) competing priorities, (3) mismatched expectations about the role and capacity of primary care, and (4) poor communication infrastructure. Interpersonal networking and use of EHRs helped overcome these obstacles to a limited extent.
Prior studies demonstrate that early follow‐up, timely communication, and continuity with primary care after hospital discharge are associated with improved postdischarge outcomes.[8, 28, 29, 30] Despite evidence that collaboration between primary care and hospitals may help optimize postdischarge outcomes, our study is the first to describe primary care leaders' perspectives on potential targets for improving collaboration between hospitals and primary care to improve care transitions.
Our results highlight the need to modify payment models to align financial incentives across settings for collaboration. Otherwise, it may be difficult for hospitals to engage primary care in collaborative efforts to improve care transitions. Recent pilot payment models aim to motivate improved postdischarge care coordination. The Centers for Medicare and Medicaid Services implemented two new Current Procedural Terminology Transitional Care Management codes to enable reimbursement of outpatient physicians for management of patients transitioning from the hospital to the community. This model does not require communication between accepting (outpatient) and discharging (hospital) physicians or other hospital staff.[31] Another pilot program pays primary care clinics $6 per beneficiary per month if they become level 3 patient‐centered medical homes, which have stringent requirements for communication and coordination with hospitals for postdischarge care.[32] Capitated payment models, such as expansion of Medicaid managed care, and shared‐savings models, such accountable care organizations, aim to promote shared responsibility between hospitals and primary care by creating financial incentives to prevent hospitalizations through effective use of outpatient resources. The effectiveness of these strategies to improve care transitions is not yet established.
Many tout the adoption of EHRs as a means to improve communication and collaboration across settings.[33] However, policies narrowly focused on EHR adoption fail to address broader issues regarding lack of EHR interoperability and inconsistently applied privacy regulations under HIPAA, which were substantial barriers to information sharing. Stage 2 meaningful use criteria will address some interoperability issues by implementing standards for exchange of laboratory data and summary care records for care transitions.[34] Additional regulatory policies should promote uniform application of privacy regulations to enable more fluid sharing of electronic data across various healthcare settings. Locally and regionally negotiated data sharing agreements, as well as arrangements such as regional health information exchanges, could temporize these issues until broader policies are enacted.
EHRs did not obviate the need for meaningful interpersonal communication between providers. Hospital‐based quality improvement teams could create networking opportunities to foster relationship‐building and communication across settings. Leadership should consider scheduling protected time to facilitate attendance. Colocation of outpatient staff, such as nurse coordinators and office managers, in the hospital may also improve relationship building and care coordination.[35] Such measures would bridge the perceived divide between inpatient and outpatient care, and create avenues to find mutually beneficial solutions to improving postdischarge care transitions.[36]
Our results should be interpreted in light of several limitations. This study focused on primary care practices in the California safety net; given variations in safety nets across different contexts, the transferability of our findings may be limited. Second, rural perspectives were relatively under‐represented in our study sample; there may be additional unidentified issues specific to rural areas or specific to other nonparticipants that may have not been captured in this study. For this hypothesis‐generating study, we focused on the perspectives of primary care leaders. Triangulating perspectives of other stakeholders, including hospital leadership, mental health, social services, and payer organizations, will offer a more comprehensive analysis of barriers and enablers to hospitalprimary care collaboration. We were unable to collect data on the payer mix of each facility, which may influence the perceived financial barriers to collaboration among facilities. However, we anticipate that the broader theme of lack of financial incentives for collaboration will resonate across many settings, as collaboration between inpatient and outpatient providers in general has been largely unfunded by payers.[37, 38, 39] Further, most primary care providers (PCPs) in and outside of safety‐net settings operate on slim margins that cannot support additional time by PCPs or staff to coordinate care transitions.[39, 40] Because our study was completed prior to the implementation of several new payment models motivating postdischarge care coordination, we were unable to assess their effect on clinics' collaboration with hospitals.
In conclusion, efforts to improve collaboration between clinical settings around postdischarge care transitions will require targeted policy and quality improvement efforts in 3 specific areas. Policy makers and administrators with the power to negotiate payment schemes and regulatory policies should first align financial incentives across settings to support postdischarge transitions and care coordination, and second, improve EHR interoperability and uniform application of HIPAA regulations. Third, clinic and hospital leaders, and front‐line providers should enhance opportunities for interpersonal networking between providers in hospital and primary care settings. With the expansion of insurance coverage and increased demand for primary care in the safety net and other settings, policies to promote care coordination should consider the perspective of both hospital and clinic incentives and mechanisms for coordinating care across settings.
Disclosures
Preliminary results from this study were presented at the Society of General Internal Medicine 36th Annual Meeting in Denver, Colorado, April 2013. Dr. Nguyen's work on this project was funded by a federal training grant from the National Research Service Award (NRSA T32HP19025‐07‐00). Dr. Goldman is the recipient of grants from the Agency for Health Care Research and Quality (K08 HS018090‐01). Drs. Goldman, Greysen, and Lyndon are supported by the National Institutes of Health, National Center for Research Resources, Office of the Director (UCSF‐CTSI grant no. KL2 RR024130). The authors report no conflicts of interest.
- Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , . Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;18(8):646–651.
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: Medicare Payment Advisory Commission; 2007.
- , , , , , . Hospital‐initiated transitional care interventions as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 pt 2):433–440.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , . Improving care transitions: hospitalists partnering with primary care. J Hosp Med. 2010;5(7):375–377.
- , , , , . Primary care physician communication at hospital discharge reduces medication discrepancies. J Hosp Med. 2013;8(12):672–677.
- Institute of Medicine. America's Health Care Safety Net: Intact but Endangered. Washington, DC: Institute of Medicine; 2000.
- , . Higher readmissions at safety‐net hospitals and potential policy solutions. Issue Brief (Commonw Fund). 2012;34:1–16.
- , . Characteristics of hospitals receiving penalties under the hospital readmissions reduction program. JAMA. 2013;309(4):342–343.
- , , , et al. Ensuring Equity: A Post‐Reform Framework to Achieve High Performance Health Care for Vulnerable Populations. New York, NY: The Commonwealth Fund; 2011.
- , , , , . Enhancing the Capacity of Community Centers to Achieve High Performance: Findings from the 2009 Commonwealth Fund National Survey of Federally Qualified Health Centers. New York, NY: The Commonwealth Fund; 2010.
- , , . Integration mechanisms and hospital efficiency in integrated health care delivery systems. J Med Syst. 2002;26(2):127–143.
- , , . Effect of physician collaboration network on hospitalization cost and readmission rate. Eur J Public Health. 2012;22(5):629–633.
- Health Resources and Services Administration. Health Center Look‐Alikes Program. Available at: http://bphc.hrsa.gov/about/lookalike/index.html?IsPopUp=true. Accessed on September 5, 2014.
- , , , . Public hospitals in the United States, 2008. Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb95.jsp. Published September 2010. Accessed on September 5, 2014.
- U.S. Department of Health and Human Services. Health Resources and Services Administration. Available at: http://www.hrsa.gov/shortage/. Accessed on September 5, 2014.
- , . California's Safety Net and The Need to Improve Local Collaboration in Care for the Uninsured: Counties, Clinics, Hospitals, and Local Health Plans. Available at: http://www.itup.org/Reports/Statewide/Safetynet_Report_Final.pdf. Published October 2008. Accessed on September 5, 2014.
- , . Unsatisfactory saturation: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual Res. 2013;13(2):190–197.
- . Leading successful interinstitutional collaborations using the collaboration success measurement model. Paper presented at: The Chair Academy's 16th Annual International Conference: Navigating the Future through Authentic Leadership; 2007; Jacksonville, FL. Available at http://www.chairacademy.com/conference/2007/papers/leading_successful_interinstitutional_collaborations.pdf. Accessed on September 5, 2014.
- , , , , . The difference between integration and collaboration in patient care: results from key informant interviews working in multiprofessional health care teams. J Manipulative Physiol Ther. 2009;32(9):715–722.
- , , , , , . Implementing organized delivery systems: an integration scorecard. Health Care Manag Rev. 1994;19(3):7–20.
- State of California Office of Statewide Health Planning 3(2):77–101.
- Health Resources and Services Administration Primary Care: The Health Center Program. Affiliation agreements of community 303(17):1716–1722.
- , , , , . Reducing hospital readmissions through primary care practice transformation. Journal Fam Pract. 2014;63(2):67–73.
- , , . Post‐hospitalization transitions: Examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- U.S. Department of Health and Human Services. Centers for Medicare 2009.
- , , , . Hospitalists and care transitions: the divorce of inpatient and outpatient care. Health Aff (Millwood). 2008;27(5):1315–1327.
- , , . Reducing hospital readmissions: lessons from top‐performing hospitals. Available at: http://www.commonwealthfund.org/publications/case‐studies/2011/apr/reducing‐hospital‐readmissions. Published April 2011. Accessed on September 5, 2014.
- , , . Recasting readmissions by placing the hospital role in community context. JAMA. 2013;309(4):351–352.
- . A primary care physician's ideal transitions of care—where's the evidence? J Hosp Med. 2013;8(8):472–477.
- , . Primary care: current problems and proposed solutions. Health Aff (Millwood). 2010;29(5):799–805.
- Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: The National Academies Press; 2001.
- , , , , , . Deficits in communication and information transfer between hospital‐based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297(8):831–841.
- , , , . Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;18(8):646–651.
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare. Washington, DC: Medicare Payment Advisory Commission; 2007.
- , , , , , . Hospital‐initiated transitional care interventions as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 pt 2):433–440.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305(7):675–681.
- , . Improving care transitions: hospitalists partnering with primary care. J Hosp Med. 2010;5(7):375–377.
- , , , , . Primary care physician communication at hospital discharge reduces medication discrepancies. J Hosp Med. 2013;8(12):672–677.
- Institute of Medicine. America's Health Care Safety Net: Intact but Endangered. Washington, DC: Institute of Medicine; 2000.
- , . Higher readmissions at safety‐net hospitals and potential policy solutions. Issue Brief (Commonw Fund). 2012;34:1–16.
- , . Characteristics of hospitals receiving penalties under the hospital readmissions reduction program. JAMA. 2013;309(4):342–343.
- , , , et al. Ensuring Equity: A Post‐Reform Framework to Achieve High Performance Health Care for Vulnerable Populations. New York, NY: The Commonwealth Fund; 2011.
- , , , , . Enhancing the Capacity of Community Centers to Achieve High Performance: Findings from the 2009 Commonwealth Fund National Survey of Federally Qualified Health Centers. New York, NY: The Commonwealth Fund; 2010.
- , , . Integration mechanisms and hospital efficiency in integrated health care delivery systems. J Med Syst. 2002;26(2):127–143.
- , , . Effect of physician collaboration network on hospitalization cost and readmission rate. Eur J Public Health. 2012;22(5):629–633.
- Health Resources and Services Administration. Health Center Look‐Alikes Program. Available at: http://bphc.hrsa.gov/about/lookalike/index.html?IsPopUp=true. Accessed on September 5, 2014.
- , , , . Public hospitals in the United States, 2008. Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb95.jsp. Published September 2010. Accessed on September 5, 2014.
- U.S. Department of Health and Human Services. Health Resources and Services Administration. Available at: http://www.hrsa.gov/shortage/. Accessed on September 5, 2014.
- , . California's Safety Net and The Need to Improve Local Collaboration in Care for the Uninsured: Counties, Clinics, Hospitals, and Local Health Plans. Available at: http://www.itup.org/Reports/Statewide/Safetynet_Report_Final.pdf. Published October 2008. Accessed on September 5, 2014.
- , . Unsatisfactory saturation: a critical exploration of the notion of saturated sample sizes in qualitative research. Qual Res. 2013;13(2):190–197.
- . Leading successful interinstitutional collaborations using the collaboration success measurement model. Paper presented at: The Chair Academy's 16th Annual International Conference: Navigating the Future through Authentic Leadership; 2007; Jacksonville, FL. Available at http://www.chairacademy.com/conference/2007/papers/leading_successful_interinstitutional_collaborations.pdf. Accessed on September 5, 2014.
- , , , , . The difference between integration and collaboration in patient care: results from key informant interviews working in multiprofessional health care teams. J Manipulative Physiol Ther. 2009;32(9):715–722.
- , , , , , . Implementing organized delivery systems: an integration scorecard. Health Care Manag Rev. 1994;19(3):7–20.
- State of California Office of Statewide Health Planning 3(2):77–101.
- Health Resources and Services Administration Primary Care: The Health Center Program. Affiliation agreements of community 303(17):1716–1722.
- , , , , . Reducing hospital readmissions through primary care practice transformation. Journal Fam Pract. 2014;63(2):67–73.
- , , . Post‐hospitalization transitions: Examining the effects of timing of primary care provider follow‐up. J Hosp Med. 2010;5(7):392–397.
- U.S. Department of Health and Human Services. Centers for Medicare 2009.
- , , , . Hospitalists and care transitions: the divorce of inpatient and outpatient care. Health Aff (Millwood). 2008;27(5):1315–1327.
- , , . Reducing hospital readmissions: lessons from top‐performing hospitals. Available at: http://www.commonwealthfund.org/publications/case‐studies/2011/apr/reducing‐hospital‐readmissions. Published April 2011. Accessed on September 5, 2014.
- , , . Recasting readmissions by placing the hospital role in community context. JAMA. 2013;309(4):351–352.
- . A primary care physician's ideal transitions of care—where's the evidence? J Hosp Med. 2013;8(8):472–477.
- , . Primary care: current problems and proposed solutions. Health Aff (Millwood). 2010;29(5):799–805.
© 2014 Society of Hospital Medicine
Bedside Tools to Assess Volume Status
Clinical estimation of volume status in hospitalized medical patients is an important part of bedside examination, guiding management decisions for many common medical conditions such as heart failure, hyponatremia, and gastrointestinal bleeding. Despite the importance of bedside volume status assessment in clinical care, there are many barriers to its accurate estimation. Specific to the jugular venous pressure (JVP), estimation of its height relies on the transmission of venous pulsations to the overlying skin[1] and has been reported to not be visible in up to 80% of the time in critically ill patients.[2] Additional difficulty in its estimation may be encountered if the central venous pressure is either too high, too low, or obscured by a short or obese neck.[3] Furthermore, in medical patients with respiratory dysfunction, large variations of central venous pressures pose an additional challenge for the bedside examination.[1] Other clinical parameters, such as lung auscultation for crackles and identification of peripheral edema, are likewise equally problematic,[4] and despite training, housestaff may recognize fewer than 50% of respiratory findings at the bedside.[5]
The overall burden of volume status assessment requirements placed on housestaff is unknown. We hypothesize that housestaff are frequently asked to make volume status assessments on admitted medical patients. If this is true, we argue for the need for educating them on the use of additional bedside tools that can assist in volume status determination. An example of such a tool is the use of bedside ultrasound. The objective of this brief report was to conduct a survey to determine the frequency of clinical volume status assessments needed on medical inpatients and secondarily discuss the potential use of bedside ultrasound for volume status determination.
METHOD
Participants
All medical housestaff (medical students and residents) on the inpatient Medical Teaching Unit (MTU) at Foothills Medical Centre in Calgary, Alberta were invited to participate in the study. We randomly selected 13 study dates between February 2012 and January 2013. On study dates, all housestaff designated to be on call were invited to complete the paper‐based survey during their call shift. At our center, the majority of medical patients are admitted by family medicine. The more complex medical patients who are suitable for teaching are admitted to 1 of 3 teams on the MTU. Each team's patients (typically 1013 per team) are covered by its own team's housestaff on call, without cross‐coverage. Housestaff included residents in the internal medicine residency program (n=92), final year medical students (58 out of 163 students rotated through our center that year), and rotating off‐service residents in other residency programs (n=34 per rotation). At the start of each call shift, there was a dedicated time for handover, where information handed over was left to the discretion of the team.
This study was approved by the University of Calgary Conjoint Health Research Ethics Board.
Survey Development
After a review of key articles in the literature,[1, 6, 7, 8, 9] an initial 46‐item survey was generated by 1 investigator (D.L.), with additional input from a second investigator (I.W.Y.M.). The survey covered items on (1) impression and self‐reported certainty of impression of the patient's volume status assessment, (2) clinical parameters used to decide on volume status, and (3) self‐reported ability to perform volume status assessments. In addition to demographic information, consenting housestaff were asked to record the number of total pages or telephone requests received on patients that required a volume status assessment and the total number of pages or telephone requests received during the call shift. This survey was first piloted on 6 trainees (1 medical student, 2 postgraduate year [PGY]‐1 residents, 2 PGY‐2 residents, and 1 PGY‐3 resident), and feedback on completeness, flow, redundancy, and clarity of items was sought. Revision based on pilot data resulted in a final 25‐item survey. The final 25‐item survey was then administered to consenting participants on the selected study dates (see Supporting Information in the online version of this article for an example of the survey). Housestaff were instructed to include only pages regarding admitted inpatients. Pages regarding newly admitted patients were excluded, because all new patients require a comprehensive assessment, rather than targeted volume status assessments. Completed surveys were then returned anonymously in a designated collection folder.
Statistical Analysis
Correlations between continuous variables are reported using Pearson correlation coefficients. Data that are normally distributed are reported using meanstandard deviation, whereas data that are not normally distributed are reported using median and interquartile range (IQR). All reported P values are 2‐sided. Analyses were conducted using the SAS version 9.3 (SAS Institute Inc., Cary, NC).
RESULTS
The 13 randomly selected study dates included 10 weekdays and 3 weekend days. Of the 39 eligible housestaff who were on call during those study dates, 31 (79%) unique individuals consented to and completed the survey. The baseline characteristics of the study participants are reported in Table 1.
| Baseline Demographics | Participants (N=31) |
|---|---|
| |
| Sex | |
| Male | 16 (52%) |
| Female | 15 (48%) |
| Level of training | |
| Medical student | 12 (39%) |
| PGY‐1 | 14 (45%) |
| PGY‐2 | 2 (6%) |
| PGY‐3 | 3 (10%) |
| Specialty (excluding medical students) | |
| Internal medicine | 16 (84%) |
| Off service | 3 (16%) |
| Self‐reported competency of volume status assessment | |
| Borderline competency | 4 (13%) |
| Competent | 14 (45%) |
| Above average | 12 (39%) |
| Well above average | 1 (3%) |
A total of 455 on‐call hours were logged, with a total of 197 pages received during the study period. Median shift duration was 12 hours (IQR=1224 hours, range=724 hours) with a median of 5 pages received per shift (IQR=310). Of the 197 total pages received, 41 of these (21%) were felt by the participants to warrant a volume status assessment.
Of the 14 volume status assessment parameters considered, housestaff used a mean of 73 parameters per assessment. The most frequently used parameters in volume status assessment were the patient's history (90%), respiratory examination (76%), JVP (73%), blood pressure (71%), and heart rate (71%) (Figure 1). In 35 of these 41 assessments (85%), housestaff indicated examining the patient for JVP, respiratory examination, edema, heart sound, or abdominal jugular reflux. Of those who examined the patient, an average of 31 physical examination findings were sought. Of the 6 patients who were not examined, housestaff reported being very certain of the patients' volume status using nonphysical examination parameters.

In 24 cases (59%) the intravenous was changed (ie, type of intravenous fluid used, rate change, starting or stopping of fluids). In 9 cases (22%) a diuretic was given, and in 15 cases (37%) a chest radiograph was ordered.
Confidence in Volume Status Assessment
Overall self‐reported competency in performing volume status assessments was moderate (median score=3, IQR=34, range=25; where 1=not competent to perform independently, 3=competent to perform independently, 6=above average competence to perform independently). Overall certainty regarding the accuracy of volume status assessments on each patient during the call shift was moderate (mean score=3.5 1.4, range=15; where 1=very uncertain; 5=very certain (Table 2).
| Volume Status Assessments (N=41) | |
|---|---|
| |
| Difficulty with volume status assessment | |
| Conflicting history | 0 (0%) |
| Conflicting examination findings | 8 (20%) |
| Conflicting laboratory findings | 1 (2%) |
| Unsure of own examination skills | 3 (7%) |
| Suboptimal patient examination | 5 (12%) |
| Required help to confirm volume status assessment | 9 (22%) |
| Confidence in assessment* | 3.5 (1.4) |
In 9 of the 41 assessments (22%), there was at least 1 barrier identified in terms of conflicting history, examination findings, laboratory findings, or suboptimal patient examination. The most commonly reported barrier was conflicting physical examination findings (8 assessments, 20%). Five of the assessments (12%) were reported to be suboptimal in terms of patient examination.
In general, although none of the associations were significant, the more elements housetaff reported using, the less certainty was reported regarding the accuracy of volume status assessment (r=0.11, P=0.49); the more pages received by the housestaff during the work shift, the less the reported certainty (r=0.22, P=0.33). Finally, the higher the level of training, the higher the reported certainty (r=0.36, P=0.11).
DISCUSSION
In this brief report, we identified that over 20% of pages over a call shift regarding admitted medical patients required volume status assessments by medical housestaff. Despite moderate self‐reported competence in the ability to assess volume status, barriers to volume status determination, such as conflicting physical examination findings and suboptimal patient examinations, were present in up to 20% of the assessments.
Other studies have similarly shown trainees with difficulty regarding clinical examinations for volume status. In these studies, difficulty with findings ranged between 16% to well over 50%.[1, 2, 3, 5] To our knowledge, this is the first report on the estimated burden of volume status assessments borne by medical housestaff. Together, our results on the burden of volume status assessments and the uncertainty regarding volume status assessments argue for the need for either better education of examination skills, or alternatively, additional tools for volume status assessments.
Although future studies evaluating the effects of improving education on examination skills and accuracy would be helpful, it has been previously reported that even attending physicians' examination skills were poor.[3] Suboptimal educator's skills, coupled with less‐than‐ideal patient characteristics in some settings, such as obesity and anatomical variations, suggest that education of bedside examination skills alone is unlikely to optimally assist clinicians with volume status assessments. Therefore, we believe our results argue for the need for additional tools for determining volume status in patients.
Bedside ultrasound is a promising tool that may be of use in this setting. It can assist in volume status assessments in a number of ways. First, for example, the height of the JVP can be located on ultrasound, using a linear transducer, as the site of where the vein tapers, using either a longitudinal or transverse view.[10] This measurement can be readily obtained even in obese patients.[10] Second, pulmonary findings, such as pleural effusions and the appearance of bilateral B lines would be suggestive of volume overload.[11, 12] The presence of unilateral B lines and consolidation/hepatization, on the other hand, would be suggestive of an infective or atelectatic process.[11, 12, 13] Last, a small inferior vena cava (IVC) diameter (2 cm) or collapsibility of >50%, although more controversial, may be able to help identify patients who may benefit from intravascular fluid loading.[13, 14] Response of IVC diameter to passive leg raise may also be assessed.[13] Feasibility wise, many of these bedside skills require minimal training, even for novices. As little as 3 to 4 hours of training may suffice.[12, 15]
Although the use of bedside ultrasound holds promise, a number of important questions should be addressed. First, can trainees be taught to use ultrasound accurately and reliably? If so, can ultrasound be incorporated into clinical care or would the time required to perform these additional examinations be prohibitive? Second, how will its use impact on volume status estimation accuracy and clinical outcomes? Third, what may be some unintended consequences of introducing this tool into the existing educational curriculum? Future studies addressing these questions are needed to better assist educators in optimizing an educational curriculum that would best benefit learners and patients.
Some limitations in our study include the fact that first, this is a single‐centered study. However, as previously stated, our results regarding difficulty with clinical examination findings are in keeping with findings from other centers.[1, 2, 3, 5] Second, our results are based on what housestaff felt necessitated volume status assessments, rather than what calls truly needed volume status assessments. In addition, the number of pages received was by self‐report. However, housestaff are more likely to under‐report by forgetting to log their pages, rather than to over‐report. Thus, our results are likely a conservative estimate of the burden of volume status assessments faced by medical housestaff. Third, some parameters were not included in our survey. For example, ordering of B‐type natriuretic peptide required a cardiology consultation at our center, and thus this investigation is not readily available to us. Daily weights, urea to creatinine ratio, and fractional excretion of sodium were not included based on feedback from our pilot survey suggesting that these parameters were not commonly used or available for admitted patients. Thus, overall confidence in volume status assessments may differ should these parameters be routinely employed. Fourth, our participants were predominantly junior learners. Therefore, our results may not generalize to centers where patients are managed primarily by more senior learners. Last, our results pertain only to patients admitted to internal medicine. For patients in the intensive care unit or coronary care unit, the burden of volume status assessments is likely even higher.
These limitations notwithstanding, our results do raise a potential concern regarding the current practice by which patients' volume statuses are assessed. We urge educators to consider incorporating bedside ultrasound training for volume status into the internal medicine curriculum and to address the need for future studies on its utility for volume status assessments.
Acknowledgements
The authors thank all of the housestaff who completed the survey.
Disclosures
Dr. Kerri Novak has received a consulting fee, and support for travel and a study for an unrelated project on ultrasound imaging from AbbVie Inc. The authors report no other potential conflicts of interest.
- , . Does this patient have abnormal central venous pressure? JAMA. 1996;275:630–634.
- , . Estimation of central venous pressure by examination of jugular veins. Am Heart J. 1974;87:279–282.
- . Clinical assessment of central venous pressure in the critically ill. Am J Med Sci. 1990;299:175–178.
- . Assessment of intravascular volume: a comedy of errors. Crit Care Med. 2001;29:1635–1636.
- , . Pulmonary auscultatory skills during training in internal medicine and family practice. Am J Respir Crit Care Med. 1999;159:1119–1124.
- . Evidence Based Physical Diagnosis. 2nd ed. St. Louis, MO: Saunders; 2007.
- , , . The rational clinical examination. Is this patient hypovolemic? JAMA. 1999;281:1022–1029.
- . Physical examination of venous pressure: a critical review. Am Heart J. 1998;136:10–18.
- , , . The jugular venous pressure revisited. Cleve Clin J Med. 2013;80:638–644.
- . Estimation of central venous pressure by ultrasound of the internal jugular vein. Am J Emerg Med. 2000;18:432–434.
- , , , et al. International evidence‐based recommendations for point‐of‐care lung ultrasound. Intensive Care Med. 2012;38:577–591.
- , , , , . Impact of pocket ultrasound use by internal medicine housestaff in the diagnosis of dyspnea [published online ahead of print June 3, 2014]. J Hosp Med. doi: 10.1002/jhm.2219.
- , , , et al. International evidence‐based recommendations for focused cardiac ultrasound. J Am Soc Echocardiogr. 2014;27:683.e1–.e33.
- , , , et al. Qualitative assessment of the inferior vena cava: useful tool for the evaluation of fluid status in critically ill patients. Am Surg. 2012;78:468–470.
- , , , et al. A comparison by medicine residents of physical examination versus hand‐carried ultrasound for estimation of right atrial pressure. Am J Cardiol. 2007;99:1614–1616.
Clinical estimation of volume status in hospitalized medical patients is an important part of bedside examination, guiding management decisions for many common medical conditions such as heart failure, hyponatremia, and gastrointestinal bleeding. Despite the importance of bedside volume status assessment in clinical care, there are many barriers to its accurate estimation. Specific to the jugular venous pressure (JVP), estimation of its height relies on the transmission of venous pulsations to the overlying skin[1] and has been reported to not be visible in up to 80% of the time in critically ill patients.[2] Additional difficulty in its estimation may be encountered if the central venous pressure is either too high, too low, or obscured by a short or obese neck.[3] Furthermore, in medical patients with respiratory dysfunction, large variations of central venous pressures pose an additional challenge for the bedside examination.[1] Other clinical parameters, such as lung auscultation for crackles and identification of peripheral edema, are likewise equally problematic,[4] and despite training, housestaff may recognize fewer than 50% of respiratory findings at the bedside.[5]
The overall burden of volume status assessment requirements placed on housestaff is unknown. We hypothesize that housestaff are frequently asked to make volume status assessments on admitted medical patients. If this is true, we argue for the need for educating them on the use of additional bedside tools that can assist in volume status determination. An example of such a tool is the use of bedside ultrasound. The objective of this brief report was to conduct a survey to determine the frequency of clinical volume status assessments needed on medical inpatients and secondarily discuss the potential use of bedside ultrasound for volume status determination.
METHOD
Participants
All medical housestaff (medical students and residents) on the inpatient Medical Teaching Unit (MTU) at Foothills Medical Centre in Calgary, Alberta were invited to participate in the study. We randomly selected 13 study dates between February 2012 and January 2013. On study dates, all housestaff designated to be on call were invited to complete the paper‐based survey during their call shift. At our center, the majority of medical patients are admitted by family medicine. The more complex medical patients who are suitable for teaching are admitted to 1 of 3 teams on the MTU. Each team's patients (typically 1013 per team) are covered by its own team's housestaff on call, without cross‐coverage. Housestaff included residents in the internal medicine residency program (n=92), final year medical students (58 out of 163 students rotated through our center that year), and rotating off‐service residents in other residency programs (n=34 per rotation). At the start of each call shift, there was a dedicated time for handover, where information handed over was left to the discretion of the team.
This study was approved by the University of Calgary Conjoint Health Research Ethics Board.
Survey Development
After a review of key articles in the literature,[1, 6, 7, 8, 9] an initial 46‐item survey was generated by 1 investigator (D.L.), with additional input from a second investigator (I.W.Y.M.). The survey covered items on (1) impression and self‐reported certainty of impression of the patient's volume status assessment, (2) clinical parameters used to decide on volume status, and (3) self‐reported ability to perform volume status assessments. In addition to demographic information, consenting housestaff were asked to record the number of total pages or telephone requests received on patients that required a volume status assessment and the total number of pages or telephone requests received during the call shift. This survey was first piloted on 6 trainees (1 medical student, 2 postgraduate year [PGY]‐1 residents, 2 PGY‐2 residents, and 1 PGY‐3 resident), and feedback on completeness, flow, redundancy, and clarity of items was sought. Revision based on pilot data resulted in a final 25‐item survey. The final 25‐item survey was then administered to consenting participants on the selected study dates (see Supporting Information in the online version of this article for an example of the survey). Housestaff were instructed to include only pages regarding admitted inpatients. Pages regarding newly admitted patients were excluded, because all new patients require a comprehensive assessment, rather than targeted volume status assessments. Completed surveys were then returned anonymously in a designated collection folder.
Statistical Analysis
Correlations between continuous variables are reported using Pearson correlation coefficients. Data that are normally distributed are reported using meanstandard deviation, whereas data that are not normally distributed are reported using median and interquartile range (IQR). All reported P values are 2‐sided. Analyses were conducted using the SAS version 9.3 (SAS Institute Inc., Cary, NC).
RESULTS
The 13 randomly selected study dates included 10 weekdays and 3 weekend days. Of the 39 eligible housestaff who were on call during those study dates, 31 (79%) unique individuals consented to and completed the survey. The baseline characteristics of the study participants are reported in Table 1.
| Baseline Demographics | Participants (N=31) |
|---|---|
| |
| Sex | |
| Male | 16 (52%) |
| Female | 15 (48%) |
| Level of training | |
| Medical student | 12 (39%) |
| PGY‐1 | 14 (45%) |
| PGY‐2 | 2 (6%) |
| PGY‐3 | 3 (10%) |
| Specialty (excluding medical students) | |
| Internal medicine | 16 (84%) |
| Off service | 3 (16%) |
| Self‐reported competency of volume status assessment | |
| Borderline competency | 4 (13%) |
| Competent | 14 (45%) |
| Above average | 12 (39%) |
| Well above average | 1 (3%) |
A total of 455 on‐call hours were logged, with a total of 197 pages received during the study period. Median shift duration was 12 hours (IQR=1224 hours, range=724 hours) with a median of 5 pages received per shift (IQR=310). Of the 197 total pages received, 41 of these (21%) were felt by the participants to warrant a volume status assessment.
Of the 14 volume status assessment parameters considered, housestaff used a mean of 73 parameters per assessment. The most frequently used parameters in volume status assessment were the patient's history (90%), respiratory examination (76%), JVP (73%), blood pressure (71%), and heart rate (71%) (Figure 1). In 35 of these 41 assessments (85%), housestaff indicated examining the patient for JVP, respiratory examination, edema, heart sound, or abdominal jugular reflux. Of those who examined the patient, an average of 31 physical examination findings were sought. Of the 6 patients who were not examined, housestaff reported being very certain of the patients' volume status using nonphysical examination parameters.
In 24 cases (59%) the intravenous was changed (ie, type of intravenous fluid used, rate change, starting or stopping of fluids). In 9 cases (22%) a diuretic was given, and in 15 cases (37%) a chest radiograph was ordered.
Confidence in Volume Status Assessment
Overall self‐reported competency in performing volume status assessments was moderate (median score=3, IQR=34, range=25; where 1=not competent to perform independently, 3=competent to perform independently, 6=above average competence to perform independently). Overall certainty regarding the accuracy of volume status assessments on each patient during the call shift was moderate (mean score=3.5 1.4, range=15; where 1=very uncertain; 5=very certain (Table 2).
| Volume Status Assessments (N=41) | |
|---|---|
| |
| Difficulty with volume status assessment | |
| Conflicting history | 0 (0%) |
| Conflicting examination findings | 8 (20%) |
| Conflicting laboratory findings | 1 (2%) |
| Unsure of own examination skills | 3 (7%) |
| Suboptimal patient examination | 5 (12%) |
| Required help to confirm volume status assessment | 9 (22%) |
| Confidence in assessment* | 3.5 (1.4) |
In 9 of the 41 assessments (22%), there was at least 1 barrier identified in terms of conflicting history, examination findings, laboratory findings, or suboptimal patient examination. The most commonly reported barrier was conflicting physical examination findings (8 assessments, 20%). Five of the assessments (12%) were reported to be suboptimal in terms of patient examination.
In general, although none of the associations were significant, the more elements housetaff reported using, the less certainty was reported regarding the accuracy of volume status assessment (r=0.11, P=0.49); the more pages received by the housestaff during the work shift, the less the reported certainty (r=0.22, P=0.33). Finally, the higher the level of training, the higher the reported certainty (r=0.36, P=0.11).
DISCUSSION
In this brief report, we identified that over 20% of pages over a call shift regarding admitted medical patients required volume status assessments by medical housestaff. Despite moderate self‐reported competence in the ability to assess volume status, barriers to volume status determination, such as conflicting physical examination findings and suboptimal patient examinations, were present in up to 20% of the assessments.
Other studies have similarly shown trainees with difficulty regarding clinical examinations for volume status. In these studies, difficulty with findings ranged between 16% to well over 50%.[1, 2, 3, 5] To our knowledge, this is the first report on the estimated burden of volume status assessments borne by medical housestaff. Together, our results on the burden of volume status assessments and the uncertainty regarding volume status assessments argue for the need for either better education of examination skills, or alternatively, additional tools for volume status assessments.
Although future studies evaluating the effects of improving education on examination skills and accuracy would be helpful, it has been previously reported that even attending physicians' examination skills were poor.[3] Suboptimal educator's skills, coupled with less‐than‐ideal patient characteristics in some settings, such as obesity and anatomical variations, suggest that education of bedside examination skills alone is unlikely to optimally assist clinicians with volume status assessments. Therefore, we believe our results argue for the need for additional tools for determining volume status in patients.
Bedside ultrasound is a promising tool that may be of use in this setting. It can assist in volume status assessments in a number of ways. First, for example, the height of the JVP can be located on ultrasound, using a linear transducer, as the site of where the vein tapers, using either a longitudinal or transverse view.[10] This measurement can be readily obtained even in obese patients.[10] Second, pulmonary findings, such as pleural effusions and the appearance of bilateral B lines would be suggestive of volume overload.[11, 12] The presence of unilateral B lines and consolidation/hepatization, on the other hand, would be suggestive of an infective or atelectatic process.[11, 12, 13] Last, a small inferior vena cava (IVC) diameter (2 cm) or collapsibility of >50%, although more controversial, may be able to help identify patients who may benefit from intravascular fluid loading.[13, 14] Response of IVC diameter to passive leg raise may also be assessed.[13] Feasibility wise, many of these bedside skills require minimal training, even for novices. As little as 3 to 4 hours of training may suffice.[12, 15]
Although the use of bedside ultrasound holds promise, a number of important questions should be addressed. First, can trainees be taught to use ultrasound accurately and reliably? If so, can ultrasound be incorporated into clinical care or would the time required to perform these additional examinations be prohibitive? Second, how will its use impact on volume status estimation accuracy and clinical outcomes? Third, what may be some unintended consequences of introducing this tool into the existing educational curriculum? Future studies addressing these questions are needed to better assist educators in optimizing an educational curriculum that would best benefit learners and patients.
Some limitations in our study include the fact that first, this is a single‐centered study. However, as previously stated, our results regarding difficulty with clinical examination findings are in keeping with findings from other centers.[1, 2, 3, 5] Second, our results are based on what housestaff felt necessitated volume status assessments, rather than what calls truly needed volume status assessments. In addition, the number of pages received was by self‐report. However, housestaff are more likely to under‐report by forgetting to log their pages, rather than to over‐report. Thus, our results are likely a conservative estimate of the burden of volume status assessments faced by medical housestaff. Third, some parameters were not included in our survey. For example, ordering of B‐type natriuretic peptide required a cardiology consultation at our center, and thus this investigation is not readily available to us. Daily weights, urea to creatinine ratio, and fractional excretion of sodium were not included based on feedback from our pilot survey suggesting that these parameters were not commonly used or available for admitted patients. Thus, overall confidence in volume status assessments may differ should these parameters be routinely employed. Fourth, our participants were predominantly junior learners. Therefore, our results may not generalize to centers where patients are managed primarily by more senior learners. Last, our results pertain only to patients admitted to internal medicine. For patients in the intensive care unit or coronary care unit, the burden of volume status assessments is likely even higher.
These limitations notwithstanding, our results do raise a potential concern regarding the current practice by which patients' volume statuses are assessed. We urge educators to consider incorporating bedside ultrasound training for volume status into the internal medicine curriculum and to address the need for future studies on its utility for volume status assessments.
Acknowledgements
The authors thank all of the housestaff who completed the survey.
Disclosures
Dr. Kerri Novak has received a consulting fee, and support for travel and a study for an unrelated project on ultrasound imaging from AbbVie Inc. The authors report no other potential conflicts of interest.
Clinical estimation of volume status in hospitalized medical patients is an important part of bedside examination, guiding management decisions for many common medical conditions such as heart failure, hyponatremia, and gastrointestinal bleeding. Despite the importance of bedside volume status assessment in clinical care, there are many barriers to its accurate estimation. Specific to the jugular venous pressure (JVP), estimation of its height relies on the transmission of venous pulsations to the overlying skin[1] and has been reported to not be visible in up to 80% of the time in critically ill patients.[2] Additional difficulty in its estimation may be encountered if the central venous pressure is either too high, too low, or obscured by a short or obese neck.[3] Furthermore, in medical patients with respiratory dysfunction, large variations of central venous pressures pose an additional challenge for the bedside examination.[1] Other clinical parameters, such as lung auscultation for crackles and identification of peripheral edema, are likewise equally problematic,[4] and despite training, housestaff may recognize fewer than 50% of respiratory findings at the bedside.[5]
The overall burden of volume status assessment requirements placed on housestaff is unknown. We hypothesize that housestaff are frequently asked to make volume status assessments on admitted medical patients. If this is true, we argue for the need for educating them on the use of additional bedside tools that can assist in volume status determination. An example of such a tool is the use of bedside ultrasound. The objective of this brief report was to conduct a survey to determine the frequency of clinical volume status assessments needed on medical inpatients and secondarily discuss the potential use of bedside ultrasound for volume status determination.
METHOD
Participants
All medical housestaff (medical students and residents) on the inpatient Medical Teaching Unit (MTU) at Foothills Medical Centre in Calgary, Alberta were invited to participate in the study. We randomly selected 13 study dates between February 2012 and January 2013. On study dates, all housestaff designated to be on call were invited to complete the paper‐based survey during their call shift. At our center, the majority of medical patients are admitted by family medicine. The more complex medical patients who are suitable for teaching are admitted to 1 of 3 teams on the MTU. Each team's patients (typically 1013 per team) are covered by its own team's housestaff on call, without cross‐coverage. Housestaff included residents in the internal medicine residency program (n=92), final year medical students (58 out of 163 students rotated through our center that year), and rotating off‐service residents in other residency programs (n=34 per rotation). At the start of each call shift, there was a dedicated time for handover, where information handed over was left to the discretion of the team.
This study was approved by the University of Calgary Conjoint Health Research Ethics Board.
Survey Development
After a review of key articles in the literature,[1, 6, 7, 8, 9] an initial 46‐item survey was generated by 1 investigator (D.L.), with additional input from a second investigator (I.W.Y.M.). The survey covered items on (1) impression and self‐reported certainty of impression of the patient's volume status assessment, (2) clinical parameters used to decide on volume status, and (3) self‐reported ability to perform volume status assessments. In addition to demographic information, consenting housestaff were asked to record the number of total pages or telephone requests received on patients that required a volume status assessment and the total number of pages or telephone requests received during the call shift. This survey was first piloted on 6 trainees (1 medical student, 2 postgraduate year [PGY]‐1 residents, 2 PGY‐2 residents, and 1 PGY‐3 resident), and feedback on completeness, flow, redundancy, and clarity of items was sought. Revision based on pilot data resulted in a final 25‐item survey. The final 25‐item survey was then administered to consenting participants on the selected study dates (see Supporting Information in the online version of this article for an example of the survey). Housestaff were instructed to include only pages regarding admitted inpatients. Pages regarding newly admitted patients were excluded, because all new patients require a comprehensive assessment, rather than targeted volume status assessments. Completed surveys were then returned anonymously in a designated collection folder.
Statistical Analysis
Correlations between continuous variables are reported using Pearson correlation coefficients. Data that are normally distributed are reported using meanstandard deviation, whereas data that are not normally distributed are reported using median and interquartile range (IQR). All reported P values are 2‐sided. Analyses were conducted using the SAS version 9.3 (SAS Institute Inc., Cary, NC).
RESULTS
The 13 randomly selected study dates included 10 weekdays and 3 weekend days. Of the 39 eligible housestaff who were on call during those study dates, 31 (79%) unique individuals consented to and completed the survey. The baseline characteristics of the study participants are reported in Table 1.
| Baseline Demographics | Participants (N=31) |
|---|---|
| |
| Sex | |
| Male | 16 (52%) |
| Female | 15 (48%) |
| Level of training | |
| Medical student | 12 (39%) |
| PGY‐1 | 14 (45%) |
| PGY‐2 | 2 (6%) |
| PGY‐3 | 3 (10%) |
| Specialty (excluding medical students) | |
| Internal medicine | 16 (84%) |
| Off service | 3 (16%) |
| Self‐reported competency of volume status assessment | |
| Borderline competency | 4 (13%) |
| Competent | 14 (45%) |
| Above average | 12 (39%) |
| Well above average | 1 (3%) |
A total of 455 on‐call hours were logged, with a total of 197 pages received during the study period. Median shift duration was 12 hours (IQR=1224 hours, range=724 hours) with a median of 5 pages received per shift (IQR=310). Of the 197 total pages received, 41 of these (21%) were felt by the participants to warrant a volume status assessment.
Of the 14 volume status assessment parameters considered, housestaff used a mean of 73 parameters per assessment. The most frequently used parameters in volume status assessment were the patient's history (90%), respiratory examination (76%), JVP (73%), blood pressure (71%), and heart rate (71%) (Figure 1). In 35 of these 41 assessments (85%), housestaff indicated examining the patient for JVP, respiratory examination, edema, heart sound, or abdominal jugular reflux. Of those who examined the patient, an average of 31 physical examination findings were sought. Of the 6 patients who were not examined, housestaff reported being very certain of the patients' volume status using nonphysical examination parameters.
In 24 cases (59%) the intravenous was changed (ie, type of intravenous fluid used, rate change, starting or stopping of fluids). In 9 cases (22%) a diuretic was given, and in 15 cases (37%) a chest radiograph was ordered.
Confidence in Volume Status Assessment
Overall self‐reported competency in performing volume status assessments was moderate (median score=3, IQR=34, range=25; where 1=not competent to perform independently, 3=competent to perform independently, 6=above average competence to perform independently). Overall certainty regarding the accuracy of volume status assessments on each patient during the call shift was moderate (mean score=3.5 1.4, range=15; where 1=very uncertain; 5=very certain (Table 2).
| Volume Status Assessments (N=41) | |
|---|---|
| |
| Difficulty with volume status assessment | |
| Conflicting history | 0 (0%) |
| Conflicting examination findings | 8 (20%) |
| Conflicting laboratory findings | 1 (2%) |
| Unsure of own examination skills | 3 (7%) |
| Suboptimal patient examination | 5 (12%) |
| Required help to confirm volume status assessment | 9 (22%) |
| Confidence in assessment* | 3.5 (1.4) |
In 9 of the 41 assessments (22%), there was at least 1 barrier identified in terms of conflicting history, examination findings, laboratory findings, or suboptimal patient examination. The most commonly reported barrier was conflicting physical examination findings (8 assessments, 20%). Five of the assessments (12%) were reported to be suboptimal in terms of patient examination.
In general, although none of the associations were significant, the more elements housetaff reported using, the less certainty was reported regarding the accuracy of volume status assessment (r=0.11, P=0.49); the more pages received by the housestaff during the work shift, the less the reported certainty (r=0.22, P=0.33). Finally, the higher the level of training, the higher the reported certainty (r=0.36, P=0.11).
DISCUSSION
In this brief report, we identified that over 20% of pages over a call shift regarding admitted medical patients required volume status assessments by medical housestaff. Despite moderate self‐reported competence in the ability to assess volume status, barriers to volume status determination, such as conflicting physical examination findings and suboptimal patient examinations, were present in up to 20% of the assessments.
Other studies have similarly shown trainees with difficulty regarding clinical examinations for volume status. In these studies, difficulty with findings ranged between 16% to well over 50%.[1, 2, 3, 5] To our knowledge, this is the first report on the estimated burden of volume status assessments borne by medical housestaff. Together, our results on the burden of volume status assessments and the uncertainty regarding volume status assessments argue for the need for either better education of examination skills, or alternatively, additional tools for volume status assessments.
Although future studies evaluating the effects of improving education on examination skills and accuracy would be helpful, it has been previously reported that even attending physicians' examination skills were poor.[3] Suboptimal educator's skills, coupled with less‐than‐ideal patient characteristics in some settings, such as obesity and anatomical variations, suggest that education of bedside examination skills alone is unlikely to optimally assist clinicians with volume status assessments. Therefore, we believe our results argue for the need for additional tools for determining volume status in patients.
Bedside ultrasound is a promising tool that may be of use in this setting. It can assist in volume status assessments in a number of ways. First, for example, the height of the JVP can be located on ultrasound, using a linear transducer, as the site of where the vein tapers, using either a longitudinal or transverse view.[10] This measurement can be readily obtained even in obese patients.[10] Second, pulmonary findings, such as pleural effusions and the appearance of bilateral B lines would be suggestive of volume overload.[11, 12] The presence of unilateral B lines and consolidation/hepatization, on the other hand, would be suggestive of an infective or atelectatic process.[11, 12, 13] Last, a small inferior vena cava (IVC) diameter (2 cm) or collapsibility of >50%, although more controversial, may be able to help identify patients who may benefit from intravascular fluid loading.[13, 14] Response of IVC diameter to passive leg raise may also be assessed.[13] Feasibility wise, many of these bedside skills require minimal training, even for novices. As little as 3 to 4 hours of training may suffice.[12, 15]
Although the use of bedside ultrasound holds promise, a number of important questions should be addressed. First, can trainees be taught to use ultrasound accurately and reliably? If so, can ultrasound be incorporated into clinical care or would the time required to perform these additional examinations be prohibitive? Second, how will its use impact on volume status estimation accuracy and clinical outcomes? Third, what may be some unintended consequences of introducing this tool into the existing educational curriculum? Future studies addressing these questions are needed to better assist educators in optimizing an educational curriculum that would best benefit learners and patients.
Some limitations in our study include the fact that first, this is a single‐centered study. However, as previously stated, our results regarding difficulty with clinical examination findings are in keeping with findings from other centers.[1, 2, 3, 5] Second, our results are based on what housestaff felt necessitated volume status assessments, rather than what calls truly needed volume status assessments. In addition, the number of pages received was by self‐report. However, housestaff are more likely to under‐report by forgetting to log their pages, rather than to over‐report. Thus, our results are likely a conservative estimate of the burden of volume status assessments faced by medical housestaff. Third, some parameters were not included in our survey. For example, ordering of B‐type natriuretic peptide required a cardiology consultation at our center, and thus this investigation is not readily available to us. Daily weights, urea to creatinine ratio, and fractional excretion of sodium were not included based on feedback from our pilot survey suggesting that these parameters were not commonly used or available for admitted patients. Thus, overall confidence in volume status assessments may differ should these parameters be routinely employed. Fourth, our participants were predominantly junior learners. Therefore, our results may not generalize to centers where patients are managed primarily by more senior learners. Last, our results pertain only to patients admitted to internal medicine. For patients in the intensive care unit or coronary care unit, the burden of volume status assessments is likely even higher.
These limitations notwithstanding, our results do raise a potential concern regarding the current practice by which patients' volume statuses are assessed. We urge educators to consider incorporating bedside ultrasound training for volume status into the internal medicine curriculum and to address the need for future studies on its utility for volume status assessments.
Acknowledgements
The authors thank all of the housestaff who completed the survey.
Disclosures
Dr. Kerri Novak has received a consulting fee, and support for travel and a study for an unrelated project on ultrasound imaging from AbbVie Inc. The authors report no other potential conflicts of interest.
- , . Does this patient have abnormal central venous pressure? JAMA. 1996;275:630–634.
- , . Estimation of central venous pressure by examination of jugular veins. Am Heart J. 1974;87:279–282.
- . Clinical assessment of central venous pressure in the critically ill. Am J Med Sci. 1990;299:175–178.
- . Assessment of intravascular volume: a comedy of errors. Crit Care Med. 2001;29:1635–1636.
- , . Pulmonary auscultatory skills during training in internal medicine and family practice. Am J Respir Crit Care Med. 1999;159:1119–1124.
- . Evidence Based Physical Diagnosis. 2nd ed. St. Louis, MO: Saunders; 2007.
- , , . The rational clinical examination. Is this patient hypovolemic? JAMA. 1999;281:1022–1029.
- . Physical examination of venous pressure: a critical review. Am Heart J. 1998;136:10–18.
- , , . The jugular venous pressure revisited. Cleve Clin J Med. 2013;80:638–644.
- . Estimation of central venous pressure by ultrasound of the internal jugular vein. Am J Emerg Med. 2000;18:432–434.
- , , , et al. International evidence‐based recommendations for point‐of‐care lung ultrasound. Intensive Care Med. 2012;38:577–591.
- , , , , . Impact of pocket ultrasound use by internal medicine housestaff in the diagnosis of dyspnea [published online ahead of print June 3, 2014]. J Hosp Med. doi: 10.1002/jhm.2219.
- , , , et al. International evidence‐based recommendations for focused cardiac ultrasound. J Am Soc Echocardiogr. 2014;27:683.e1–.e33.
- , , , et al. Qualitative assessment of the inferior vena cava: useful tool for the evaluation of fluid status in critically ill patients. Am Surg. 2012;78:468–470.
- , , , et al. A comparison by medicine residents of physical examination versus hand‐carried ultrasound for estimation of right atrial pressure. Am J Cardiol. 2007;99:1614–1616.
- , . Does this patient have abnormal central venous pressure? JAMA. 1996;275:630–634.
- , . Estimation of central venous pressure by examination of jugular veins. Am Heart J. 1974;87:279–282.
- . Clinical assessment of central venous pressure in the critically ill. Am J Med Sci. 1990;299:175–178.
- . Assessment of intravascular volume: a comedy of errors. Crit Care Med. 2001;29:1635–1636.
- , . Pulmonary auscultatory skills during training in internal medicine and family practice. Am J Respir Crit Care Med. 1999;159:1119–1124.
- . Evidence Based Physical Diagnosis. 2nd ed. St. Louis, MO: Saunders; 2007.
- , , . The rational clinical examination. Is this patient hypovolemic? JAMA. 1999;281:1022–1029.
- . Physical examination of venous pressure: a critical review. Am Heart J. 1998;136:10–18.
- , , . The jugular venous pressure revisited. Cleve Clin J Med. 2013;80:638–644.
- . Estimation of central venous pressure by ultrasound of the internal jugular vein. Am J Emerg Med. 2000;18:432–434.
- , , , et al. International evidence‐based recommendations for point‐of‐care lung ultrasound. Intensive Care Med. 2012;38:577–591.
- , , , , . Impact of pocket ultrasound use by internal medicine housestaff in the diagnosis of dyspnea [published online ahead of print June 3, 2014]. J Hosp Med. doi: 10.1002/jhm.2219.
- , , , et al. International evidence‐based recommendations for focused cardiac ultrasound. J Am Soc Echocardiogr. 2014;27:683.e1–.e33.
- , , , et al. Qualitative assessment of the inferior vena cava: useful tool for the evaluation of fluid status in critically ill patients. Am Surg. 2012;78:468–470.
- , , , et al. A comparison by medicine residents of physical examination versus hand‐carried ultrasound for estimation of right atrial pressure. Am J Cardiol. 2007;99:1614–1616.

Hospitalist Compensation Up 8% in Latest Survey
Annual median compensation for adult hospitalists in the U.S. rose 8% to a record high $252,996 in 2013, according to SHM's newly released 2014 State of Hospital Medicine (SOHM) report.
Hospitalists in the South region continue to earn the most, with a median compensation of $258,020—essentially static with $258,793 reported in 2012—according to data from the Medical Group Management Association Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. The MGMA compensation and productivity data are wrapped into the biennial SOHM, whose 2014 edition debuted last week.
The largest compensation jump was for hospitalists in the West region, who logged an 11.8% gain in annual median compensation to $249,894 for 2013, up from $223,574 reported in 2012. Hospitalists in the Midwest saw a 10% increase, up to $261,868 from $237,987. Practitioners in the East had both the smallest increase, 4.8%, and the lowest median compensation, $238,676 in 2013, which is up slightly from $227,656. Part of the compensation push is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) ticked up 3.3% to 4,297 in 2013 from 4,159 in the 2012 report.
Median collection-to-work RVUs rose 6.8% to 51.5 from 48.21. Production (10.5%) and performance (6.6%) in 2013 were also slightly larger portions of mean compensation than in 2012, figures many industry experts expect will increase in the future. The 2014 SOHM report also notes that academic/university hospitalists typically receive more in base pay, while hospitalists in private practice receive less.
"It is the very best survey, quantity and quality, of hospital medicine [HM] groups," says William "Tex" Landis, MD, FHM, medical director of WellSpan Hospitalists in York, Pa., and a member and former chair of SHM's Practice Analysis Committee. "And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups."
Beyond analyzing hospitalists' median compensation, the SOHM report delves into scheduling, productivity, staffing, a breakdown of payment allocations, practice models, and dozens of other topics that HM group leaders find useful. In all, 499 groups representing some 6,300 providers were included in the survey. TH
SHM will also be hosting a free webinar Oct. 14 to discuss the specifics of the report.
Visit our website for more information about SHM's 2014 State of Hospital Medicine.
Annual median compensation for adult hospitalists in the U.S. rose 8% to a record high $252,996 in 2013, according to SHM's newly released 2014 State of Hospital Medicine (SOHM) report.
Hospitalists in the South region continue to earn the most, with a median compensation of $258,020—essentially static with $258,793 reported in 2012—according to data from the Medical Group Management Association Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. The MGMA compensation and productivity data are wrapped into the biennial SOHM, whose 2014 edition debuted last week.
The largest compensation jump was for hospitalists in the West region, who logged an 11.8% gain in annual median compensation to $249,894 for 2013, up from $223,574 reported in 2012. Hospitalists in the Midwest saw a 10% increase, up to $261,868 from $237,987. Practitioners in the East had both the smallest increase, 4.8%, and the lowest median compensation, $238,676 in 2013, which is up slightly from $227,656. Part of the compensation push is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) ticked up 3.3% to 4,297 in 2013 from 4,159 in the 2012 report.
Median collection-to-work RVUs rose 6.8% to 51.5 from 48.21. Production (10.5%) and performance (6.6%) in 2013 were also slightly larger portions of mean compensation than in 2012, figures many industry experts expect will increase in the future. The 2014 SOHM report also notes that academic/university hospitalists typically receive more in base pay, while hospitalists in private practice receive less.
"It is the very best survey, quantity and quality, of hospital medicine [HM] groups," says William "Tex" Landis, MD, FHM, medical director of WellSpan Hospitalists in York, Pa., and a member and former chair of SHM's Practice Analysis Committee. "And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups."
Beyond analyzing hospitalists' median compensation, the SOHM report delves into scheduling, productivity, staffing, a breakdown of payment allocations, practice models, and dozens of other topics that HM group leaders find useful. In all, 499 groups representing some 6,300 providers were included in the survey. TH
SHM will also be hosting a free webinar Oct. 14 to discuss the specifics of the report.
Visit our website for more information about SHM's 2014 State of Hospital Medicine.
Annual median compensation for adult hospitalists in the U.S. rose 8% to a record high $252,996 in 2013, according to SHM's newly released 2014 State of Hospital Medicine (SOHM) report.
Hospitalists in the South region continue to earn the most, with a median compensation of $258,020—essentially static with $258,793 reported in 2012—according to data from the Medical Group Management Association Physician Compensation and Production Survey: 2014 Report Based on 2013 Data. The MGMA compensation and productivity data are wrapped into the biennial SOHM, whose 2014 edition debuted last week.
The largest compensation jump was for hospitalists in the West region, who logged an 11.8% gain in annual median compensation to $249,894 for 2013, up from $223,574 reported in 2012. Hospitalists in the Midwest saw a 10% increase, up to $261,868 from $237,987. Practitioners in the East had both the smallest increase, 4.8%, and the lowest median compensation, $238,676 in 2013, which is up slightly from $227,656. Part of the compensation push is tied to upward pressure on productivity. Nationwide, median relative value units (RVUs) ticked up 3.3% to 4,297 in 2013 from 4,159 in the 2012 report.
Median collection-to-work RVUs rose 6.8% to 51.5 from 48.21. Production (10.5%) and performance (6.6%) in 2013 were also slightly larger portions of mean compensation than in 2012, figures many industry experts expect will increase in the future. The 2014 SOHM report also notes that academic/university hospitalists typically receive more in base pay, while hospitalists in private practice receive less.
"It is the very best survey, quantity and quality, of hospital medicine [HM] groups," says William "Tex" Landis, MD, FHM, medical director of WellSpan Hospitalists in York, Pa., and a member and former chair of SHM's Practice Analysis Committee. "And so it becomes the best source of information to make important decisions about resourcing and operating hospital medicine groups."
Beyond analyzing hospitalists' median compensation, the SOHM report delves into scheduling, productivity, staffing, a breakdown of payment allocations, practice models, and dozens of other topics that HM group leaders find useful. In all, 499 groups representing some 6,300 providers were included in the survey. TH
SHM will also be hosting a free webinar Oct. 14 to discuss the specifics of the report.
Visit our website for more information about SHM's 2014 State of Hospital Medicine.
Improved Diet Is Recipe for Improved Inpatient Outcomes
How well is your patient eating?
How often you ask this question could improve your hospital's readmission and length-of-stay rates, says Melissa Parkhurst, MD, FHM, medical director of hospital medicine and nutrition support at the University of Kansas Hospital in Kansas City.
A recent report from the Alliance to Advance Patient Nutrition [PDF]—a partnership of four organizations, including SHM, organized to improve nutrition screening and intervention among hospitalized patients—notes that about one in three patients admitted to a hospital meets the criteria for being malnourished. If left untreated, two-thirds of these patients will become more malnourished in the hospital.
"Often patients aren't eating because of testing or because their appetites are depressed because they're ill and not feeling well," says Dr. Parkhurst, an Alliance representative. "Sometimes their medications can alter their tastes, make them nauseated, or give them diarrhea."
Released last month, the findings are included in the partnership's first progress report. It describes the group's efforts in raising awareness about hospital nutrition, such as through info booths at medical meetings and via an online resource center on SHM's Center for Hospital Innovation & Improvement website.
Dr. Parkhurst points to studies that show inpatient malnutrition can lead to higher costs and more complications, as well as make patients more prone to surgical site infections, pressure ulcers, and falls.
"Malnourished patients are more apt to come back to the hospitals and to come in with complications," she says. "That is something we all should be concerned about as clinicians and at the hospital-administration level as well."
Here are Dr. Parkhurst's tips for improving nutrition among your patients:
- Ensure that every patient is getting a nutritional assessment upon admission and that staff is available to follow up with the results;
- Incorporate nutrition into the daily scope of patient care, for example, regularly ask staff whether your patients are eating or not;
- Include information about nutrition in the discharge plan and educate the patient’s family about nutritional interventions; and
- Work with hospital leadership to see how policies and procedures compare with the patient-care models put forth by the Alliance and note areas for improvement.
TH
Visit our website for more information about the importance of inpatient nutrition.
How well is your patient eating?
How often you ask this question could improve your hospital's readmission and length-of-stay rates, says Melissa Parkhurst, MD, FHM, medical director of hospital medicine and nutrition support at the University of Kansas Hospital in Kansas City.
A recent report from the Alliance to Advance Patient Nutrition [PDF]—a partnership of four organizations, including SHM, organized to improve nutrition screening and intervention among hospitalized patients—notes that about one in three patients admitted to a hospital meets the criteria for being malnourished. If left untreated, two-thirds of these patients will become more malnourished in the hospital.
"Often patients aren't eating because of testing or because their appetites are depressed because they're ill and not feeling well," says Dr. Parkhurst, an Alliance representative. "Sometimes their medications can alter their tastes, make them nauseated, or give them diarrhea."
Released last month, the findings are included in the partnership's first progress report. It describes the group's efforts in raising awareness about hospital nutrition, such as through info booths at medical meetings and via an online resource center on SHM's Center for Hospital Innovation & Improvement website.
Dr. Parkhurst points to studies that show inpatient malnutrition can lead to higher costs and more complications, as well as make patients more prone to surgical site infections, pressure ulcers, and falls.
"Malnourished patients are more apt to come back to the hospitals and to come in with complications," she says. "That is something we all should be concerned about as clinicians and at the hospital-administration level as well."
Here are Dr. Parkhurst's tips for improving nutrition among your patients:
- Ensure that every patient is getting a nutritional assessment upon admission and that staff is available to follow up with the results;
- Incorporate nutrition into the daily scope of patient care, for example, regularly ask staff whether your patients are eating or not;
- Include information about nutrition in the discharge plan and educate the patient’s family about nutritional interventions; and
- Work with hospital leadership to see how policies and procedures compare with the patient-care models put forth by the Alliance and note areas for improvement.
TH
Visit our website for more information about the importance of inpatient nutrition.
How well is your patient eating?
How often you ask this question could improve your hospital's readmission and length-of-stay rates, says Melissa Parkhurst, MD, FHM, medical director of hospital medicine and nutrition support at the University of Kansas Hospital in Kansas City.
A recent report from the Alliance to Advance Patient Nutrition [PDF]—a partnership of four organizations, including SHM, organized to improve nutrition screening and intervention among hospitalized patients—notes that about one in three patients admitted to a hospital meets the criteria for being malnourished. If left untreated, two-thirds of these patients will become more malnourished in the hospital.
"Often patients aren't eating because of testing or because their appetites are depressed because they're ill and not feeling well," says Dr. Parkhurst, an Alliance representative. "Sometimes their medications can alter their tastes, make them nauseated, or give them diarrhea."
Released last month, the findings are included in the partnership's first progress report. It describes the group's efforts in raising awareness about hospital nutrition, such as through info booths at medical meetings and via an online resource center on SHM's Center for Hospital Innovation & Improvement website.
Dr. Parkhurst points to studies that show inpatient malnutrition can lead to higher costs and more complications, as well as make patients more prone to surgical site infections, pressure ulcers, and falls.
"Malnourished patients are more apt to come back to the hospitals and to come in with complications," she says. "That is something we all should be concerned about as clinicians and at the hospital-administration level as well."
Here are Dr. Parkhurst's tips for improving nutrition among your patients:
- Ensure that every patient is getting a nutritional assessment upon admission and that staff is available to follow up with the results;
- Incorporate nutrition into the daily scope of patient care, for example, regularly ask staff whether your patients are eating or not;
- Include information about nutrition in the discharge plan and educate the patient’s family about nutritional interventions; and
- Work with hospital leadership to see how policies and procedures compare with the patient-care models put forth by the Alliance and note areas for improvement.
TH
Visit our website for more information about the importance of inpatient nutrition.
Vitiligo, alopecia more likely in GVHD when donor is female and recipient is male
The development of vitiligo or alopecia areata is not common in patients with chronic graft-versus-host disease, but it is significantly more likely to occur when the donor was female, especially when the recipient was male, according to a report published online Sept. 10 in JAMA Dermatology.
Fifteen case reports and small series in the literature have reported the development of vitiligo or alopecia areata after allogeneic hematopoietic stem cell transplantation, most often among patients who first developed chronic graft-versus-host disease (GVHD) after the procedure. To further explore the frequency of these two skin autoimmune manifestations in GVHD and to identify associated risk factors, researchers performed a retrospective cross-sectional analysis involving 282 adult and pediatric patients referred to the National Institutes of Health Clinical Center for GVHD in 2004-2013.

They identified 15 GVHD patients with vitiligo (4.9%) and 2 with alopecia areata (0.7%); one of these patients had both skin disorders. Most of the 15 patients had undergone stem-cell transplantation to treat chronic myelogenous leukemia (CML) (5 patients) or acute leukemia or myelodysplastic syndrome (5 patients), and most had had a human leukocyte antigen–identical donor. Twelve of the 15 developed the skin disorder after having GVHD for more than 1 year, said Rena C. Zuo of the National Cancer Institute’s dermatology branch and her associates.
"Notably, CML accounts for only about 300 of 7,892 (3.8%) allogeneic hematopoietic stem-cell transplantations per year in the United States, a relative minority among indicated diseases," they said.
In what they described as the first study to identify an association between donor/recipient sex mismatch and the development of concomitant autoimmunity in patients with chronic GVHD, the investigators found that 14 of the 15 patients who developed vitiligo or alopecia areata had female donors, 2 of whom had previously given birth; the gender of the donor in the 15th case was unknown. Nine of these 14 recipients were male, "resulting in a female-to-male sex mismatch in [at least] 64% of cases," Ms. Zuo and her colleagues said (JAMA Dermatol. 2014 Sept. 10 [doi:10.1001/jamadermatol.2014.1550]).
Both parous female donors and donor-recipient sex mismatch are known risk factors for GVHD. The risk of autoimmunity in female-to-male transplants "may reflect the activity of skin-homing donor T cells specific for recipient minor histocompatibility antigens encoded by Y-chromosome genes, a mechanism previously implicated in both GVHD and graft-versus-tumor responses," the investigators added.
This study was supported by the National Institutes of Health and the National Cancer Institute. Ms. Zuo and her associates reported no financial conflicts of interest.
The development of vitiligo or alopecia areata is not common in patients with chronic graft-versus-host disease, but it is significantly more likely to occur when the donor was female, especially when the recipient was male, according to a report published online Sept. 10 in JAMA Dermatology.
Fifteen case reports and small series in the literature have reported the development of vitiligo or alopecia areata after allogeneic hematopoietic stem cell transplantation, most often among patients who first developed chronic graft-versus-host disease (GVHD) after the procedure. To further explore the frequency of these two skin autoimmune manifestations in GVHD and to identify associated risk factors, researchers performed a retrospective cross-sectional analysis involving 282 adult and pediatric patients referred to the National Institutes of Health Clinical Center for GVHD in 2004-2013.
They identified 15 GVHD patients with vitiligo (4.9%) and 2 with alopecia areata (0.7%); one of these patients had both skin disorders. Most of the 15 patients had undergone stem-cell transplantation to treat chronic myelogenous leukemia (CML) (5 patients) or acute leukemia or myelodysplastic syndrome (5 patients), and most had had a human leukocyte antigen–identical donor. Twelve of the 15 developed the skin disorder after having GVHD for more than 1 year, said Rena C. Zuo of the National Cancer Institute’s dermatology branch and her associates.
"Notably, CML accounts for only about 300 of 7,892 (3.8%) allogeneic hematopoietic stem-cell transplantations per year in the United States, a relative minority among indicated diseases," they said.
In what they described as the first study to identify an association between donor/recipient sex mismatch and the development of concomitant autoimmunity in patients with chronic GVHD, the investigators found that 14 of the 15 patients who developed vitiligo or alopecia areata had female donors, 2 of whom had previously given birth; the gender of the donor in the 15th case was unknown. Nine of these 14 recipients were male, "resulting in a female-to-male sex mismatch in [at least] 64% of cases," Ms. Zuo and her colleagues said (JAMA Dermatol. 2014 Sept. 10 [doi:10.1001/jamadermatol.2014.1550]).
Both parous female donors and donor-recipient sex mismatch are known risk factors for GVHD. The risk of autoimmunity in female-to-male transplants "may reflect the activity of skin-homing donor T cells specific for recipient minor histocompatibility antigens encoded by Y-chromosome genes, a mechanism previously implicated in both GVHD and graft-versus-tumor responses," the investigators added.
This study was supported by the National Institutes of Health and the National Cancer Institute. Ms. Zuo and her associates reported no financial conflicts of interest.
The development of vitiligo or alopecia areata is not common in patients with chronic graft-versus-host disease, but it is significantly more likely to occur when the donor was female, especially when the recipient was male, according to a report published online Sept. 10 in JAMA Dermatology.
Fifteen case reports and small series in the literature have reported the development of vitiligo or alopecia areata after allogeneic hematopoietic stem cell transplantation, most often among patients who first developed chronic graft-versus-host disease (GVHD) after the procedure. To further explore the frequency of these two skin autoimmune manifestations in GVHD and to identify associated risk factors, researchers performed a retrospective cross-sectional analysis involving 282 adult and pediatric patients referred to the National Institutes of Health Clinical Center for GVHD in 2004-2013.
They identified 15 GVHD patients with vitiligo (4.9%) and 2 with alopecia areata (0.7%); one of these patients had both skin disorders. Most of the 15 patients had undergone stem-cell transplantation to treat chronic myelogenous leukemia (CML) (5 patients) or acute leukemia or myelodysplastic syndrome (5 patients), and most had had a human leukocyte antigen–identical donor. Twelve of the 15 developed the skin disorder after having GVHD for more than 1 year, said Rena C. Zuo of the National Cancer Institute’s dermatology branch and her associates.
"Notably, CML accounts for only about 300 of 7,892 (3.8%) allogeneic hematopoietic stem-cell transplantations per year in the United States, a relative minority among indicated diseases," they said.
In what they described as the first study to identify an association between donor/recipient sex mismatch and the development of concomitant autoimmunity in patients with chronic GVHD, the investigators found that 14 of the 15 patients who developed vitiligo or alopecia areata had female donors, 2 of whom had previously given birth; the gender of the donor in the 15th case was unknown. Nine of these 14 recipients were male, "resulting in a female-to-male sex mismatch in [at least] 64% of cases," Ms. Zuo and her colleagues said (JAMA Dermatol. 2014 Sept. 10 [doi:10.1001/jamadermatol.2014.1550]).
Both parous female donors and donor-recipient sex mismatch are known risk factors for GVHD. The risk of autoimmunity in female-to-male transplants "may reflect the activity of skin-homing donor T cells specific for recipient minor histocompatibility antigens encoded by Y-chromosome genes, a mechanism previously implicated in both GVHD and graft-versus-tumor responses," the investigators added.
This study was supported by the National Institutes of Health and the National Cancer Institute. Ms. Zuo and her associates reported no financial conflicts of interest.
FROM JAMA DERMATOLOGY
Key clinical point: Female-to-male stem cell donation ups the risk for vitiligo in GVHD.
Major finding: 14 of the 15 patients who developed vitiligo or alopecia areata had female donors (the gender of the 15th donor was unknown), and 9 of these 14 recipients were male.
Data source: A retrospective cross-sectional analysis involving 282 adults and children with chronic GVHD, 15 of whom developed vitiligo or alopecia areata.
Disclosures: This study was supported by the National Institutes of Health and the National Cancer Institute. Dr. Zuo and her associates reported no financial conflicts of interest.

Product News: 09 2014
Merz Licensing Agreement
Merz North America announces a licensing agreement with Brickell Biotech, Inc, for the development of a retinoid compound (BBI-3000) for the treatment of skin conditions known to be responsive to retinoid agents, such as acne and psoriasis. Under the terms of the agreement, Merz North America will assume the full cost and responsibility for future development and commercialization, initially for North America. The development of this new clinical entity demonstrates Merz’s commitment to medical dermatology. For more information, visit www.merzusa.com.
Regenica
Suneva Medical unveils a rebranded Regenica product line consisting of 3 products: Renew SPF 15 to protect skin from harmful UV rays while signaling skin’s natural repair, Replenishing Crème to hydrate skin and reverse the signs of aging, and Repair Complex to accelerate skin renewal. The rebranded line will help physicians attract patients to Multipotent Resignaling Complex (MRCx) growth factor technology. The physician-dispensed antiaging skin care line is ideal for patients looking to better target the signs of aging to see improvement in skin texture, tone, firmness, and the appearance of fine lines and wrinkles. For more information, visit www.regenica.com.
RetrinAL
Pierre Fabre Dermo-Cosmétique USA introduces Avène RetrinAL 0.05 Cream and RetrinAL 0.1 Intensive Cream to visibly reduce the signs of aging. Both products deliver 4 antiaging benefits: wrinkle reduction, radiance, skin elasticity, and skin quality (skin texture and tone). Retinaldehyde delivers a powerful and nonirritating form of vitamin A directly to the skin, boosting cell metabolism and producing an immediate corrective effect. These hypoallergenic and fragrance-free products also contain Relastide, a patented lipopeptide that helps keep collagen and elastin from becoming stiff and rigid while boosting retinaldehyde. RetrinAL 0.05 Cream treats the first signs of aging and RetrinAL 0.1 Intensive Cream delivers a higher concentration of retinaldehyde. Both RetrinAL products will be available October 2014, exclusively in physicians’ offices. For more information, visit www.aveneusa.com.
Rosaliac CC Cream
La Roche-Posay Laboratoire Dermatologique launches Rosaliac CC Cream, a daily complete tone-correcting cream with broad-spectrum sun protection factor 30 for patients with rosacea-prone skin. Rosaliac CC Cream consists of a unique blend of red, white, yellow, and black pigments to camouflage redness. The texture has been engineered to provide an optimal balance between coverage and care, providing the hydration and lightweight texture of a BB cream while delivering coverage that is comparable to a foundation. Key ingredients including Ambophenol help reduce visible redness over time. Rosaliac CC Cream is available over-the-counter at various retailers. For more information, visit www.laroche-posay.us.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at [email protected].
Merz Licensing Agreement
Merz North America announces a licensing agreement with Brickell Biotech, Inc, for the development of a retinoid compound (BBI-3000) for the treatment of skin conditions known to be responsive to retinoid agents, such as acne and psoriasis. Under the terms of the agreement, Merz North America will assume the full cost and responsibility for future development and commercialization, initially for North America. The development of this new clinical entity demonstrates Merz’s commitment to medical dermatology. For more information, visit www.merzusa.com.
Regenica
Suneva Medical unveils a rebranded Regenica product line consisting of 3 products: Renew SPF 15 to protect skin from harmful UV rays while signaling skin’s natural repair, Replenishing Crème to hydrate skin and reverse the signs of aging, and Repair Complex to accelerate skin renewal. The rebranded line will help physicians attract patients to Multipotent Resignaling Complex (MRCx) growth factor technology. The physician-dispensed antiaging skin care line is ideal for patients looking to better target the signs of aging to see improvement in skin texture, tone, firmness, and the appearance of fine lines and wrinkles. For more information, visit www.regenica.com.
RetrinAL
Pierre Fabre Dermo-Cosmétique USA introduces Avène RetrinAL 0.05 Cream and RetrinAL 0.1 Intensive Cream to visibly reduce the signs of aging. Both products deliver 4 antiaging benefits: wrinkle reduction, radiance, skin elasticity, and skin quality (skin texture and tone). Retinaldehyde delivers a powerful and nonirritating form of vitamin A directly to the skin, boosting cell metabolism and producing an immediate corrective effect. These hypoallergenic and fragrance-free products also contain Relastide, a patented lipopeptide that helps keep collagen and elastin from becoming stiff and rigid while boosting retinaldehyde. RetrinAL 0.05 Cream treats the first signs of aging and RetrinAL 0.1 Intensive Cream delivers a higher concentration of retinaldehyde. Both RetrinAL products will be available October 2014, exclusively in physicians’ offices. For more information, visit www.aveneusa.com.
Rosaliac CC Cream
La Roche-Posay Laboratoire Dermatologique launches Rosaliac CC Cream, a daily complete tone-correcting cream with broad-spectrum sun protection factor 30 for patients with rosacea-prone skin. Rosaliac CC Cream consists of a unique blend of red, white, yellow, and black pigments to camouflage redness. The texture has been engineered to provide an optimal balance between coverage and care, providing the hydration and lightweight texture of a BB cream while delivering coverage that is comparable to a foundation. Key ingredients including Ambophenol help reduce visible redness over time. Rosaliac CC Cream is available over-the-counter at various retailers. For more information, visit www.laroche-posay.us.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at [email protected].
Merz Licensing Agreement
Merz North America announces a licensing agreement with Brickell Biotech, Inc, for the development of a retinoid compound (BBI-3000) for the treatment of skin conditions known to be responsive to retinoid agents, such as acne and psoriasis. Under the terms of the agreement, Merz North America will assume the full cost and responsibility for future development and commercialization, initially for North America. The development of this new clinical entity demonstrates Merz’s commitment to medical dermatology. For more information, visit www.merzusa.com.
Regenica
Suneva Medical unveils a rebranded Regenica product line consisting of 3 products: Renew SPF 15 to protect skin from harmful UV rays while signaling skin’s natural repair, Replenishing Crème to hydrate skin and reverse the signs of aging, and Repair Complex to accelerate skin renewal. The rebranded line will help physicians attract patients to Multipotent Resignaling Complex (MRCx) growth factor technology. The physician-dispensed antiaging skin care line is ideal for patients looking to better target the signs of aging to see improvement in skin texture, tone, firmness, and the appearance of fine lines and wrinkles. For more information, visit www.regenica.com.
RetrinAL
Pierre Fabre Dermo-Cosmétique USA introduces Avène RetrinAL 0.05 Cream and RetrinAL 0.1 Intensive Cream to visibly reduce the signs of aging. Both products deliver 4 antiaging benefits: wrinkle reduction, radiance, skin elasticity, and skin quality (skin texture and tone). Retinaldehyde delivers a powerful and nonirritating form of vitamin A directly to the skin, boosting cell metabolism and producing an immediate corrective effect. These hypoallergenic and fragrance-free products also contain Relastide, a patented lipopeptide that helps keep collagen and elastin from becoming stiff and rigid while boosting retinaldehyde. RetrinAL 0.05 Cream treats the first signs of aging and RetrinAL 0.1 Intensive Cream delivers a higher concentration of retinaldehyde. Both RetrinAL products will be available October 2014, exclusively in physicians’ offices. For more information, visit www.aveneusa.com.
Rosaliac CC Cream
La Roche-Posay Laboratoire Dermatologique launches Rosaliac CC Cream, a daily complete tone-correcting cream with broad-spectrum sun protection factor 30 for patients with rosacea-prone skin. Rosaliac CC Cream consists of a unique blend of red, white, yellow, and black pigments to camouflage redness. The texture has been engineered to provide an optimal balance between coverage and care, providing the hydration and lightweight texture of a BB cream while delivering coverage that is comparable to a foundation. Key ingredients including Ambophenol help reduce visible redness over time. Rosaliac CC Cream is available over-the-counter at various retailers. For more information, visit www.laroche-posay.us.
If you would like your product included in Product News, please e-mail a press release to the Editorial Office at [email protected].

Subcutaneous Panniculitislike T-Cell Lymphoma
Subcutaneous panniculitislike T-cell lymphoma (SPTL) is a cutaneous lymphoma of α and β phenotype cytotoxic T cells in which the neoplastic cells are found almost exclusively in the subcutaneous layer and resemble a panniculitis.1 It affects males and females with equal incidence and is seen in both adults and children. Clinically, this disease presents as a nonspecific panniculitis with indurated but typically nonulcerated erythematous plaques and nodules most commonly located on the extremities. Plaques and nodules may appear on other body sites and may be generalized.1 In some cases, patients present with associated systemic symptoms including fever, malaise, weight loss, and fatigue.2
Histologically, SPTL presents as a predominantly lobular panniculitis (Figure 1) with rimming of adipocytes by neoplastic cells that appear as small and medium-sized atypical lymphocytes with hyperchromatic nuclei (Figure 2A). A less dominant septal component may be present, and neoplastic cells may encroach into the lower reticular dermis, rarely involving the papillary dermis or epidermis.2 Although rimming of adipocytes is classic, it is not specific to this entity, as rimming also can be found in other lymphomas and infectious panniculitis. Reactive lymphocytes and macrophages with ingested lipid material also are seen intermixed with neoplastic cells.2 Necrosis is a common finding, including destructive fragmentation of the nucleus, known as karyorrhexis. If necrosis is extensive, appreciation of other histologic features may be hindered.3 Histiocytes engulfing the nuclear debris known as beanbag cells also can be seen (Figure 2B). The diagnosis can be made on immunohistologic analysis demonstrating neoplastic cells with a cytotoxic α and β T-suppressor phenotype centered around and rimming the adipocytes in the subcutaneous fat.3 Immunohistochemistry reveals positive CD3, CD8 (Figure 2C), and βF1 markers, as well as T-cell intracellular antigen 1 (TIA-1), granzyme B, and perforin.1,2 The neoplastic cells often have a high proliferation index as evidenced by MIB-1 (Ki-67) labeling (Figure 2D). The neoplastic cells are negative for CD4, CD56, and CD30.1,2 Subcutaneous panniculitislike T-cell lymphoma cells are negative for Epstein-Barr virus by in situ hybridization.2
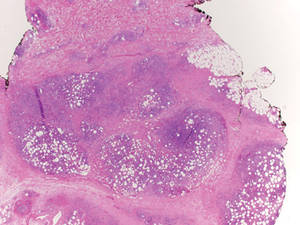
|
| Figure 1. Subcutaneous panniculitislike T-cell lymphoma showing a predominantly lobular panniculitis (H&E, original magnification ×20). |
|
| Figure 2. Rimming of adipocytes by hyperchromatic lymphocytes (A)(H&E, original magnification ×400). Arrowhead indicates a histiocyte (ie, beanbag cell) that has undergone cytophagocytosis of nuclear debris (B)(H&E, original magnification ×600). Immunohistochemistry with CD8 highlights the cells rimming the adipocytes (C)(original magnification ×600). Immunohistochemistry with MIB-1 shows an increased proliferative rate in the lymphocytes rimming the adipocytes (D)(original magnification ×600). |
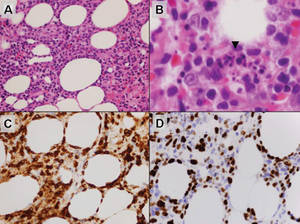
Subcutaneous panniculitislike T-cell lymphoma must be distinguished from lupus erythematosus panniculitis (LEP) and other cutaneous lymphomas. Importantly, LEP and SPTL clinically may appear similar and are not mutually exclusive diagnoses.2 On histology, they may look similar, showing T cell aggregates and necrosis; however, thickening of the basement membrane, vacuolar change at the dermoepidermal junction, plasma cells, hyaline sclerosis, mucin deposition, a lymphocytic perivascular infiltrate, and nodular aggregates of B cells are more common in LEP (Figure 3).2,4 Additionally, in LEP the T cell aggregates typically will not have a high proliferative rate as evidenced by MIB-1.3
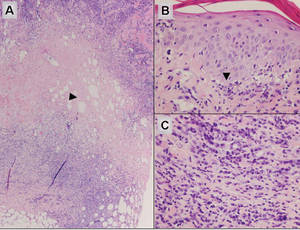
Additionally, other lobular panniculitides can be considered in the differential diagnosis, including erythema induratum (EI), α1-antitrypsin deficiency panniculitis (A1ATDP), and infectious panniculitis. Histologically, EI (Figure 4), also known as nodular vasculitis when not associated with Mycobacterium tuberculosis, has a lobular pattern of inflammation. Early in the disease process there are discrete collections of neutrophils; later, granulomas with histiocytes, giant cells, and foamy macrophages are seen.4 The reactive infiltrate of EI is more mixed than in SPTL, with small lymphocytes, plasma cells, and eosinophils. Leukocytoclastic vasculitis and extravascular caseous or fibrinoid necrosis also may be present.4,5 Substantial caseous necrosis may extend to the dermis and epidermis with EI. Importantly, EI lacks true tuberculoid granulomas and stains negative for acid-fast bacilli, as it is a reactive rather than a local infectious process, but a history of M tuberculosis exposure is common.4 α1-Antitrypsin deficiency panniculitis results from a deficiency of proteinase activity and can be distinguished from SPTL by a neutrophil-rich panniculitis (Figure 5) as well as the classic appearance of splaying of neutrophils between collagen bundles in the deep reticular dermis. Additionally, the panniculitis is characterized by focal areas of necrotic lobules and septa with an infiltrate of neutrophils and macrophages that abut areas of normal-appearing subcutaneous fat without infiltrate.6 Clinically, the A1ATDP lesions may have ulceration and express an oily substance from fat necrosis. Panniculitis with A1ATDP may precede liver and lung disease.4 Panniculitis from bacterial or fungal infection is more common in immunocompromised patients but should be considered when subcutaneous inflammation and/or necrosis is present. Depending on the responsible organism and the status of a patient’s immune system, infectious panniculitis can have variable presentations, including suppurative granulomas with mycobacterial organisms, a dermal focus of infection if the primary source is cutaneous, or a deeper reticular and subcuticular focus in the subcutaneous fat if the infectious panniculitis occurs from hematogenous spread.4 An example of an infectious panniculitis having more of a granulomatous pattern secondary to Cryptococcus can be seen in Figure 6. Ultimately, special stains to identify infectious organisms (eg, Gram, periodic acid–Schiff, Ziehl-Neelsen) can be ordered to aid in the diagnosis if a responsible organism is not visible on hematoxylin and eosin staining.
|
Figure 4. Erythema induratum is characterized by a lobular panniculitis (A and B)(both H&E, original magnifications ×40 and ×200). Vascular changes (arrowhead) are present in a majority of cases with endothelial swelling and extravasation of erythrocytes (C)(H&E, original magnification ×400). |
|
| Figure 5. Neutrophilic panniculitis that can be seen in α1-antitrypsin deficiency panniculitis (H&E, original magnification ×400). |
|
Figure 6. Infectious panniculitis secondary to Cryptococcus showing a granulomatous reaction in the subcutis (A)(H&E, original magnification ×40). Closer inspection shows a dense infiltrate of chronic inflammatory cells including numerous histiocytes and multinucleated giant cells. Some of the giant cells contain refractile organisms (arrowhead)(B)(H&E, original magnification ×400). Mucicarmine histochemical stain highlights the capsule of the organism (C)(original magnification ×400). |
Acknowledgment
The authors would like to thank Drake Poeschl, MD, St. Louis, Missouri, for proofreading the manuscript.
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3765-3785.
2. Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group study of 83 cases. Blood. 2008;111:838-845.
3. Cerroni L, Gatter K, Kerl H. Subcutaneous “panniculitis-like” T-cell lymphoma. In: Cerroni L, Gatter K, Kerl H. Skin Lymphoma: The Illustrated Guide. 3rd ed. Hoboken, NJ: Wiley-Blackwell Publishing; 2011:87-96.
4. Requena L, Sánchez Yus E. Panniculitis. part II. mostly lobular panniculitis. J Am Acad Dermatol. 2001;45:325-361.
5. Sharon V, Goodarzi H, Chambers CJ, et al. Erythema induratum of Bazin. Dermatol Online J. 2010;16:1.
6. Rajagopal R, Malik AK, Murthy PS, et al. Alpha-1 antitrypsin deficiency panniculitis. Indian J Dermatol Venereol Leprol. 2002;68:362-364.
Subcutaneous panniculitislike T-cell lymphoma (SPTL) is a cutaneous lymphoma of α and β phenotype cytotoxic T cells in which the neoplastic cells are found almost exclusively in the subcutaneous layer and resemble a panniculitis.1 It affects males and females with equal incidence and is seen in both adults and children. Clinically, this disease presents as a nonspecific panniculitis with indurated but typically nonulcerated erythematous plaques and nodules most commonly located on the extremities. Plaques and nodules may appear on other body sites and may be generalized.1 In some cases, patients present with associated systemic symptoms including fever, malaise, weight loss, and fatigue.2
Histologically, SPTL presents as a predominantly lobular panniculitis (Figure 1) with rimming of adipocytes by neoplastic cells that appear as small and medium-sized atypical lymphocytes with hyperchromatic nuclei (Figure 2A). A less dominant septal component may be present, and neoplastic cells may encroach into the lower reticular dermis, rarely involving the papillary dermis or epidermis.2 Although rimming of adipocytes is classic, it is not specific to this entity, as rimming also can be found in other lymphomas and infectious panniculitis. Reactive lymphocytes and macrophages with ingested lipid material also are seen intermixed with neoplastic cells.2 Necrosis is a common finding, including destructive fragmentation of the nucleus, known as karyorrhexis. If necrosis is extensive, appreciation of other histologic features may be hindered.3 Histiocytes engulfing the nuclear debris known as beanbag cells also can be seen (Figure 2B). The diagnosis can be made on immunohistologic analysis demonstrating neoplastic cells with a cytotoxic α and β T-suppressor phenotype centered around and rimming the adipocytes in the subcutaneous fat.3 Immunohistochemistry reveals positive CD3, CD8 (Figure 2C), and βF1 markers, as well as T-cell intracellular antigen 1 (TIA-1), granzyme B, and perforin.1,2 The neoplastic cells often have a high proliferation index as evidenced by MIB-1 (Ki-67) labeling (Figure 2D). The neoplastic cells are negative for CD4, CD56, and CD30.1,2 Subcutaneous panniculitislike T-cell lymphoma cells are negative for Epstein-Barr virus by in situ hybridization.2
|
|
| Figure 1. Subcutaneous panniculitislike T-cell lymphoma showing a predominantly lobular panniculitis (H&E, original magnification ×20). |
|
| Figure 2. Rimming of adipocytes by hyperchromatic lymphocytes (A)(H&E, original magnification ×400). Arrowhead indicates a histiocyte (ie, beanbag cell) that has undergone cytophagocytosis of nuclear debris (B)(H&E, original magnification ×600). Immunohistochemistry with CD8 highlights the cells rimming the adipocytes (C)(original magnification ×600). Immunohistochemistry with MIB-1 shows an increased proliferative rate in the lymphocytes rimming the adipocytes (D)(original magnification ×600). |
Subcutaneous panniculitislike T-cell lymphoma must be distinguished from lupus erythematosus panniculitis (LEP) and other cutaneous lymphomas. Importantly, LEP and SPTL clinically may appear similar and are not mutually exclusive diagnoses.2 On histology, they may look similar, showing T cell aggregates and necrosis; however, thickening of the basement membrane, vacuolar change at the dermoepidermal junction, plasma cells, hyaline sclerosis, mucin deposition, a lymphocytic perivascular infiltrate, and nodular aggregates of B cells are more common in LEP (Figure 3).2,4 Additionally, in LEP the T cell aggregates typically will not have a high proliferative rate as evidenced by MIB-1.3
Additionally, other lobular panniculitides can be considered in the differential diagnosis, including erythema induratum (EI), α1-antitrypsin deficiency panniculitis (A1ATDP), and infectious panniculitis. Histologically, EI (Figure 4), also known as nodular vasculitis when not associated with Mycobacterium tuberculosis, has a lobular pattern of inflammation. Early in the disease process there are discrete collections of neutrophils; later, granulomas with histiocytes, giant cells, and foamy macrophages are seen.4 The reactive infiltrate of EI is more mixed than in SPTL, with small lymphocytes, plasma cells, and eosinophils. Leukocytoclastic vasculitis and extravascular caseous or fibrinoid necrosis also may be present.4,5 Substantial caseous necrosis may extend to the dermis and epidermis with EI. Importantly, EI lacks true tuberculoid granulomas and stains negative for acid-fast bacilli, as it is a reactive rather than a local infectious process, but a history of M tuberculosis exposure is common.4 α1-Antitrypsin deficiency panniculitis results from a deficiency of proteinase activity and can be distinguished from SPTL by a neutrophil-rich panniculitis (Figure 5) as well as the classic appearance of splaying of neutrophils between collagen bundles in the deep reticular dermis. Additionally, the panniculitis is characterized by focal areas of necrotic lobules and septa with an infiltrate of neutrophils and macrophages that abut areas of normal-appearing subcutaneous fat without infiltrate.6 Clinically, the A1ATDP lesions may have ulceration and express an oily substance from fat necrosis. Panniculitis with A1ATDP may precede liver and lung disease.4 Panniculitis from bacterial or fungal infection is more common in immunocompromised patients but should be considered when subcutaneous inflammation and/or necrosis is present. Depending on the responsible organism and the status of a patient’s immune system, infectious panniculitis can have variable presentations, including suppurative granulomas with mycobacterial organisms, a dermal focus of infection if the primary source is cutaneous, or a deeper reticular and subcuticular focus in the subcutaneous fat if the infectious panniculitis occurs from hematogenous spread.4 An example of an infectious panniculitis having more of a granulomatous pattern secondary to Cryptococcus can be seen in Figure 6. Ultimately, special stains to identify infectious organisms (eg, Gram, periodic acid–Schiff, Ziehl-Neelsen) can be ordered to aid in the diagnosis if a responsible organism is not visible on hematoxylin and eosin staining.
|
|
Figure 4. Erythema induratum is characterized by a lobular panniculitis (A and B)(both H&E, original magnifications ×40 and ×200). Vascular changes (arrowhead) are present in a majority of cases with endothelial swelling and extravasation of erythrocytes (C)(H&E, original magnification ×400). |
|
|
| Figure 5. Neutrophilic panniculitis that can be seen in α1-antitrypsin deficiency panniculitis (H&E, original magnification ×400). |
|
|
Figure 6. Infectious panniculitis secondary to Cryptococcus showing a granulomatous reaction in the subcutis (A)(H&E, original magnification ×40). Closer inspection shows a dense infiltrate of chronic inflammatory cells including numerous histiocytes and multinucleated giant cells. Some of the giant cells contain refractile organisms (arrowhead)(B)(H&E, original magnification ×400). Mucicarmine histochemical stain highlights the capsule of the organism (C)(original magnification ×400). |
Acknowledgment
The authors would like to thank Drake Poeschl, MD, St. Louis, Missouri, for proofreading the manuscript.
Subcutaneous panniculitislike T-cell lymphoma (SPTL) is a cutaneous lymphoma of α and β phenotype cytotoxic T cells in which the neoplastic cells are found almost exclusively in the subcutaneous layer and resemble a panniculitis.1 It affects males and females with equal incidence and is seen in both adults and children. Clinically, this disease presents as a nonspecific panniculitis with indurated but typically nonulcerated erythematous plaques and nodules most commonly located on the extremities. Plaques and nodules may appear on other body sites and may be generalized.1 In some cases, patients present with associated systemic symptoms including fever, malaise, weight loss, and fatigue.2
Histologically, SPTL presents as a predominantly lobular panniculitis (Figure 1) with rimming of adipocytes by neoplastic cells that appear as small and medium-sized atypical lymphocytes with hyperchromatic nuclei (Figure 2A). A less dominant septal component may be present, and neoplastic cells may encroach into the lower reticular dermis, rarely involving the papillary dermis or epidermis.2 Although rimming of adipocytes is classic, it is not specific to this entity, as rimming also can be found in other lymphomas and infectious panniculitis. Reactive lymphocytes and macrophages with ingested lipid material also are seen intermixed with neoplastic cells.2 Necrosis is a common finding, including destructive fragmentation of the nucleus, known as karyorrhexis. If necrosis is extensive, appreciation of other histologic features may be hindered.3 Histiocytes engulfing the nuclear debris known as beanbag cells also can be seen (Figure 2B). The diagnosis can be made on immunohistologic analysis demonstrating neoplastic cells with a cytotoxic α and β T-suppressor phenotype centered around and rimming the adipocytes in the subcutaneous fat.3 Immunohistochemistry reveals positive CD3, CD8 (Figure 2C), and βF1 markers, as well as T-cell intracellular antigen 1 (TIA-1), granzyme B, and perforin.1,2 The neoplastic cells often have a high proliferation index as evidenced by MIB-1 (Ki-67) labeling (Figure 2D). The neoplastic cells are negative for CD4, CD56, and CD30.1,2 Subcutaneous panniculitislike T-cell lymphoma cells are negative for Epstein-Barr virus by in situ hybridization.2
|
|
| Figure 1. Subcutaneous panniculitislike T-cell lymphoma showing a predominantly lobular panniculitis (H&E, original magnification ×20). |
|
| Figure 2. Rimming of adipocytes by hyperchromatic lymphocytes (A)(H&E, original magnification ×400). Arrowhead indicates a histiocyte (ie, beanbag cell) that has undergone cytophagocytosis of nuclear debris (B)(H&E, original magnification ×600). Immunohistochemistry with CD8 highlights the cells rimming the adipocytes (C)(original magnification ×600). Immunohistochemistry with MIB-1 shows an increased proliferative rate in the lymphocytes rimming the adipocytes (D)(original magnification ×600). |
Subcutaneous panniculitislike T-cell lymphoma must be distinguished from lupus erythematosus panniculitis (LEP) and other cutaneous lymphomas. Importantly, LEP and SPTL clinically may appear similar and are not mutually exclusive diagnoses.2 On histology, they may look similar, showing T cell aggregates and necrosis; however, thickening of the basement membrane, vacuolar change at the dermoepidermal junction, plasma cells, hyaline sclerosis, mucin deposition, a lymphocytic perivascular infiltrate, and nodular aggregates of B cells are more common in LEP (Figure 3).2,4 Additionally, in LEP the T cell aggregates typically will not have a high proliferative rate as evidenced by MIB-1.3
Additionally, other lobular panniculitides can be considered in the differential diagnosis, including erythema induratum (EI), α1-antitrypsin deficiency panniculitis (A1ATDP), and infectious panniculitis. Histologically, EI (Figure 4), also known as nodular vasculitis when not associated with Mycobacterium tuberculosis, has a lobular pattern of inflammation. Early in the disease process there are discrete collections of neutrophils; later, granulomas with histiocytes, giant cells, and foamy macrophages are seen.4 The reactive infiltrate of EI is more mixed than in SPTL, with small lymphocytes, plasma cells, and eosinophils. Leukocytoclastic vasculitis and extravascular caseous or fibrinoid necrosis also may be present.4,5 Substantial caseous necrosis may extend to the dermis and epidermis with EI. Importantly, EI lacks true tuberculoid granulomas and stains negative for acid-fast bacilli, as it is a reactive rather than a local infectious process, but a history of M tuberculosis exposure is common.4 α1-Antitrypsin deficiency panniculitis results from a deficiency of proteinase activity and can be distinguished from SPTL by a neutrophil-rich panniculitis (Figure 5) as well as the classic appearance of splaying of neutrophils between collagen bundles in the deep reticular dermis. Additionally, the panniculitis is characterized by focal areas of necrotic lobules and septa with an infiltrate of neutrophils and macrophages that abut areas of normal-appearing subcutaneous fat without infiltrate.6 Clinically, the A1ATDP lesions may have ulceration and express an oily substance from fat necrosis. Panniculitis with A1ATDP may precede liver and lung disease.4 Panniculitis from bacterial or fungal infection is more common in immunocompromised patients but should be considered when subcutaneous inflammation and/or necrosis is present. Depending on the responsible organism and the status of a patient’s immune system, infectious panniculitis can have variable presentations, including suppurative granulomas with mycobacterial organisms, a dermal focus of infection if the primary source is cutaneous, or a deeper reticular and subcuticular focus in the subcutaneous fat if the infectious panniculitis occurs from hematogenous spread.4 An example of an infectious panniculitis having more of a granulomatous pattern secondary to Cryptococcus can be seen in Figure 6. Ultimately, special stains to identify infectious organisms (eg, Gram, periodic acid–Schiff, Ziehl-Neelsen) can be ordered to aid in the diagnosis if a responsible organism is not visible on hematoxylin and eosin staining.
|
|
Figure 4. Erythema induratum is characterized by a lobular panniculitis (A and B)(both H&E, original magnifications ×40 and ×200). Vascular changes (arrowhead) are present in a majority of cases with endothelial swelling and extravasation of erythrocytes (C)(H&E, original magnification ×400). |
|
|
| Figure 5. Neutrophilic panniculitis that can be seen in α1-antitrypsin deficiency panniculitis (H&E, original magnification ×400). |
|
|
Figure 6. Infectious panniculitis secondary to Cryptococcus showing a granulomatous reaction in the subcutis (A)(H&E, original magnification ×40). Closer inspection shows a dense infiltrate of chronic inflammatory cells including numerous histiocytes and multinucleated giant cells. Some of the giant cells contain refractile organisms (arrowhead)(B)(H&E, original magnification ×400). Mucicarmine histochemical stain highlights the capsule of the organism (C)(original magnification ×400). |
Acknowledgment
The authors would like to thank Drake Poeschl, MD, St. Louis, Missouri, for proofreading the manuscript.
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3765-3785.
2. Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group study of 83 cases. Blood. 2008;111:838-845.
3. Cerroni L, Gatter K, Kerl H. Subcutaneous “panniculitis-like” T-cell lymphoma. In: Cerroni L, Gatter K, Kerl H. Skin Lymphoma: The Illustrated Guide. 3rd ed. Hoboken, NJ: Wiley-Blackwell Publishing; 2011:87-96.
4. Requena L, Sánchez Yus E. Panniculitis. part II. mostly lobular panniculitis. J Am Acad Dermatol. 2001;45:325-361.
5. Sharon V, Goodarzi H, Chambers CJ, et al. Erythema induratum of Bazin. Dermatol Online J. 2010;16:1.
6. Rajagopal R, Malik AK, Murthy PS, et al. Alpha-1 antitrypsin deficiency panniculitis. Indian J Dermatol Venereol Leprol. 2002;68:362-364.
1. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3765-3785.
2. Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group study of 83 cases. Blood. 2008;111:838-845.
3. Cerroni L, Gatter K, Kerl H. Subcutaneous “panniculitis-like” T-cell lymphoma. In: Cerroni L, Gatter K, Kerl H. Skin Lymphoma: The Illustrated Guide. 3rd ed. Hoboken, NJ: Wiley-Blackwell Publishing; 2011:87-96.
4. Requena L, Sánchez Yus E. Panniculitis. part II. mostly lobular panniculitis. J Am Acad Dermatol. 2001;45:325-361.
5. Sharon V, Goodarzi H, Chambers CJ, et al. Erythema induratum of Bazin. Dermatol Online J. 2010;16:1.
6. Rajagopal R, Malik AK, Murthy PS, et al. Alpha-1 antitrypsin deficiency panniculitis. Indian J Dermatol Venereol Leprol. 2002;68:362-364.
Five reasons physicians will use mobile health for patient care
Mobile health technologies will become a part of the health care landscape for all stakeholders at some point. Other sectors of society currently cannot function without mobile; for example, retail and financial services consider mobile a vital component of their business models.
There are many reasons for lag in adoption of mobile technologies by health care. Regulatory issues, the need for a digital cultural shift, lack of business models, and lack of proof of efficacy are certainly barriers.

But what is underappreciated by app developers and industry analysts is the fact that physicians will be key players in the future of mobile health. Physicians are the most trusted stakeholder by patients with regard to care planning. Issues that are important to consider from a clinician’s standpoint are reimbursement for coordinating digital care; the fresh, negative experience of poorly performing electronic health records (which should not be the face of other digital tech); the present lack of commitment to the philosophy of participatory medicine and that most health apps are consumer (not patient) oriented, with little proof of efficacy via clinical studies.
That said, there remain fundamental reasons that mobile health app prescribing will occur:
• Patients are mobile. According to the Pew Research Center’s Internet and American Life Project, 91% of adults in the United States own a cell phone. Few older adults use smart phones (18% in 2013), but effective mobile health can take the form of text messages, as has been proven with prenatal care and smoking cessation, as well as more sophisticated disease management apps such as WellDoc. Even though older patients might not be smart phone users now, a baby boomer turns 65 every 8 seconds. Many in the sandwich generation today and all in the future will be mobile health tech ready.
• There is a perfect storm of necessity and opportunity. The number of patients participating in health care has increased because of the Affordable Care Act. There is a well-recognized physician shortage, especially in primary care. Americans today do not want to live out their last years in an institutional setting as 70% of them do today. Digital technology will be required for this aging at home. Sensor technology, whether environmental or wearable, will be fundamental. Mobile technology not only will facilitate new care models, but will create them.
• Useful information and data will be at patients’ fingertips. New technologies – such as IBM’s Watson and Apple’s HealthKit – will hopefully serve as frameworks for many disease-specific apps. EHRs are repositories of huge amounts of data. The key to better health care lies in applying analytics to harness the power of this data and make it useful for better care on both population and individualized patient levels. Analytics will improve patient safety, proscribe therapy based on individual and population data, and increase efficiency.
• It is how patient content will be delivered. Physicians and health policy experts recognize the need for better patient education with regard to their diagnoses and medications. A research2guidance report on the disappointing diabetes app market illustrates the pharmaceutical industry’s heretofore slow uptake of mobile health. In general, the pharmaceutical and medical device industries (with 250 of the approximately 100,000 health and fitness apps) have so far concentrated on disease-specific content. The challenge remains to design apps that center on the clinician-patient interaction, not just the disease state. Interoperability with EHRs via more robust patient portals will help close this loop.
• It will create the engaged patient. "Patient engagement" is as overused as "innovation" when discussing technology in health care today. However, the concept is paramount to improving health and promoting wellness. I like a definition of patient engagement from the Center for Advanced Health: "Actions individuals must take to obtain the greatest benefit from the health care services available to them."
I believe that the basis of patient engagement is the combination of an informed patient (and caregiver) and shared decision making. It is not surprising that a significant percentage of patients leave the hospital or physician’s office not knowing their diagnosis or why a medication was prescribed. Mobile health is the potential holy grail of patient engagement. Behavioral change by both patients and providers in the broad sense (which includes payers, clinicians, and institutions) is imperative to affect patient engagement.
Health care must, for the first time, be approached as a rightful partnership between the patient and physician. I believe that mobile technology can utilize trending patient-derived data, transforming it into a useful actionable tool, and create a multidirectional (patient, provider, caregiver) platform of communication leading to better shared decision making.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.
Mobile health technologies will become a part of the health care landscape for all stakeholders at some point. Other sectors of society currently cannot function without mobile; for example, retail and financial services consider mobile a vital component of their business models.
There are many reasons for lag in adoption of mobile technologies by health care. Regulatory issues, the need for a digital cultural shift, lack of business models, and lack of proof of efficacy are certainly barriers.
But what is underappreciated by app developers and industry analysts is the fact that physicians will be key players in the future of mobile health. Physicians are the most trusted stakeholder by patients with regard to care planning. Issues that are important to consider from a clinician’s standpoint are reimbursement for coordinating digital care; the fresh, negative experience of poorly performing electronic health records (which should not be the face of other digital tech); the present lack of commitment to the philosophy of participatory medicine and that most health apps are consumer (not patient) oriented, with little proof of efficacy via clinical studies.
That said, there remain fundamental reasons that mobile health app prescribing will occur:
• Patients are mobile. According to the Pew Research Center’s Internet and American Life Project, 91% of adults in the United States own a cell phone. Few older adults use smart phones (18% in 2013), but effective mobile health can take the form of text messages, as has been proven with prenatal care and smoking cessation, as well as more sophisticated disease management apps such as WellDoc. Even though older patients might not be smart phone users now, a baby boomer turns 65 every 8 seconds. Many in the sandwich generation today and all in the future will be mobile health tech ready.
• There is a perfect storm of necessity and opportunity. The number of patients participating in health care has increased because of the Affordable Care Act. There is a well-recognized physician shortage, especially in primary care. Americans today do not want to live out their last years in an institutional setting as 70% of them do today. Digital technology will be required for this aging at home. Sensor technology, whether environmental or wearable, will be fundamental. Mobile technology not only will facilitate new care models, but will create them.
• Useful information and data will be at patients’ fingertips. New technologies – such as IBM’s Watson and Apple’s HealthKit – will hopefully serve as frameworks for many disease-specific apps. EHRs are repositories of huge amounts of data. The key to better health care lies in applying analytics to harness the power of this data and make it useful for better care on both population and individualized patient levels. Analytics will improve patient safety, proscribe therapy based on individual and population data, and increase efficiency.
• It is how patient content will be delivered. Physicians and health policy experts recognize the need for better patient education with regard to their diagnoses and medications. A research2guidance report on the disappointing diabetes app market illustrates the pharmaceutical industry’s heretofore slow uptake of mobile health. In general, the pharmaceutical and medical device industries (with 250 of the approximately 100,000 health and fitness apps) have so far concentrated on disease-specific content. The challenge remains to design apps that center on the clinician-patient interaction, not just the disease state. Interoperability with EHRs via more robust patient portals will help close this loop.
• It will create the engaged patient. "Patient engagement" is as overused as "innovation" when discussing technology in health care today. However, the concept is paramount to improving health and promoting wellness. I like a definition of patient engagement from the Center for Advanced Health: "Actions individuals must take to obtain the greatest benefit from the health care services available to them."
I believe that the basis of patient engagement is the combination of an informed patient (and caregiver) and shared decision making. It is not surprising that a significant percentage of patients leave the hospital or physician’s office not knowing their diagnosis or why a medication was prescribed. Mobile health is the potential holy grail of patient engagement. Behavioral change by both patients and providers in the broad sense (which includes payers, clinicians, and institutions) is imperative to affect patient engagement.
Health care must, for the first time, be approached as a rightful partnership between the patient and physician. I believe that mobile technology can utilize trending patient-derived data, transforming it into a useful actionable tool, and create a multidirectional (patient, provider, caregiver) platform of communication leading to better shared decision making.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.
Mobile health technologies will become a part of the health care landscape for all stakeholders at some point. Other sectors of society currently cannot function without mobile; for example, retail and financial services consider mobile a vital component of their business models.
There are many reasons for lag in adoption of mobile technologies by health care. Regulatory issues, the need for a digital cultural shift, lack of business models, and lack of proof of efficacy are certainly barriers.
But what is underappreciated by app developers and industry analysts is the fact that physicians will be key players in the future of mobile health. Physicians are the most trusted stakeholder by patients with regard to care planning. Issues that are important to consider from a clinician’s standpoint are reimbursement for coordinating digital care; the fresh, negative experience of poorly performing electronic health records (which should not be the face of other digital tech); the present lack of commitment to the philosophy of participatory medicine and that most health apps are consumer (not patient) oriented, with little proof of efficacy via clinical studies.
That said, there remain fundamental reasons that mobile health app prescribing will occur:
• Patients are mobile. According to the Pew Research Center’s Internet and American Life Project, 91% of adults in the United States own a cell phone. Few older adults use smart phones (18% in 2013), but effective mobile health can take the form of text messages, as has been proven with prenatal care and smoking cessation, as well as more sophisticated disease management apps such as WellDoc. Even though older patients might not be smart phone users now, a baby boomer turns 65 every 8 seconds. Many in the sandwich generation today and all in the future will be mobile health tech ready.
• There is a perfect storm of necessity and opportunity. The number of patients participating in health care has increased because of the Affordable Care Act. There is a well-recognized physician shortage, especially in primary care. Americans today do not want to live out their last years in an institutional setting as 70% of them do today. Digital technology will be required for this aging at home. Sensor technology, whether environmental or wearable, will be fundamental. Mobile technology not only will facilitate new care models, but will create them.
• Useful information and data will be at patients’ fingertips. New technologies – such as IBM’s Watson and Apple’s HealthKit – will hopefully serve as frameworks for many disease-specific apps. EHRs are repositories of huge amounts of data. The key to better health care lies in applying analytics to harness the power of this data and make it useful for better care on both population and individualized patient levels. Analytics will improve patient safety, proscribe therapy based on individual and population data, and increase efficiency.
• It is how patient content will be delivered. Physicians and health policy experts recognize the need for better patient education with regard to their diagnoses and medications. A research2guidance report on the disappointing diabetes app market illustrates the pharmaceutical industry’s heretofore slow uptake of mobile health. In general, the pharmaceutical and medical device industries (with 250 of the approximately 100,000 health and fitness apps) have so far concentrated on disease-specific content. The challenge remains to design apps that center on the clinician-patient interaction, not just the disease state. Interoperability with EHRs via more robust patient portals will help close this loop.
• It will create the engaged patient. "Patient engagement" is as overused as "innovation" when discussing technology in health care today. However, the concept is paramount to improving health and promoting wellness. I like a definition of patient engagement from the Center for Advanced Health: "Actions individuals must take to obtain the greatest benefit from the health care services available to them."
I believe that the basis of patient engagement is the combination of an informed patient (and caregiver) and shared decision making. It is not surprising that a significant percentage of patients leave the hospital or physician’s office not knowing their diagnosis or why a medication was prescribed. Mobile health is the potential holy grail of patient engagement. Behavioral change by both patients and providers in the broad sense (which includes payers, clinicians, and institutions) is imperative to affect patient engagement.
Health care must, for the first time, be approached as a rightful partnership between the patient and physician. I believe that mobile technology can utilize trending patient-derived data, transforming it into a useful actionable tool, and create a multidirectional (patient, provider, caregiver) platform of communication leading to better shared decision making.
Dr. Scher is an electrophysiologist with the Heart Group of Lancaster (Pa.) General Health. He is also director of DLS Healthcare Consulting, Harrisburg, Pa., and clinical associate professor of medicine at the Pennsylvania State University, Hershey.

Calcipotriene–Betamethasone Dipropionate Topical Suspension in the Management of Psoriasis: A Status Report on Available Data With an Overview of Practical Clinical Application
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
What data are available on the efficacy and safety of C/Bd-TS?
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.
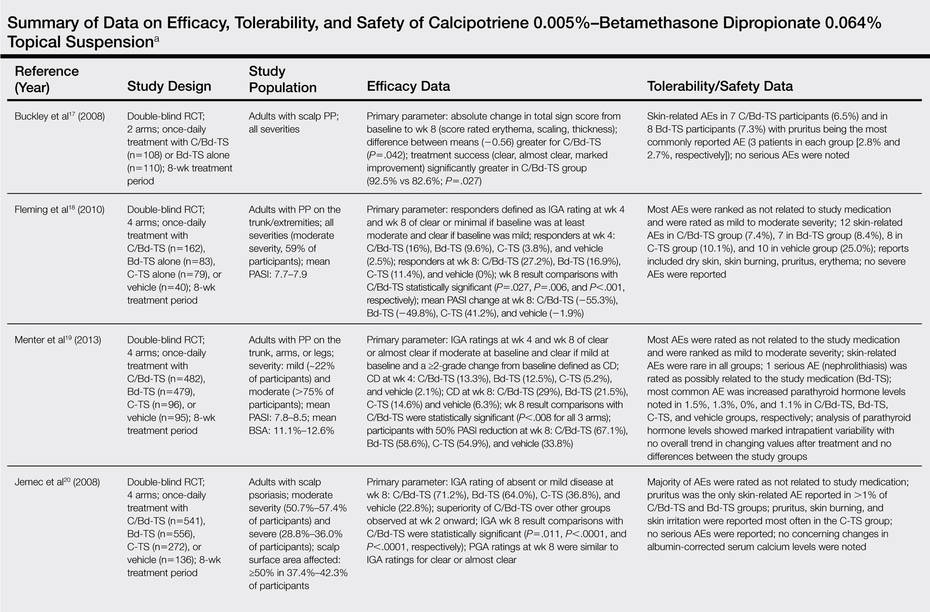
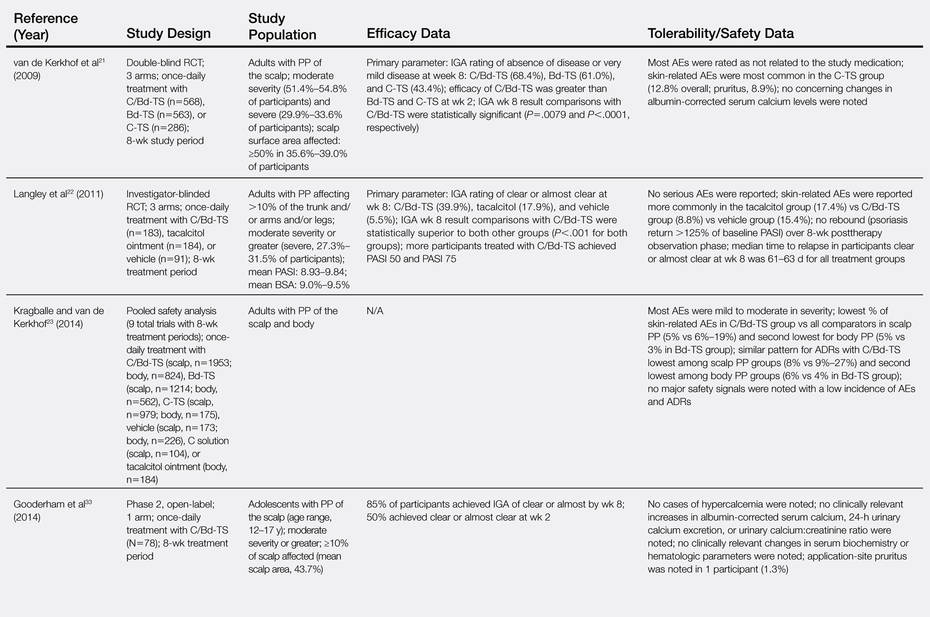
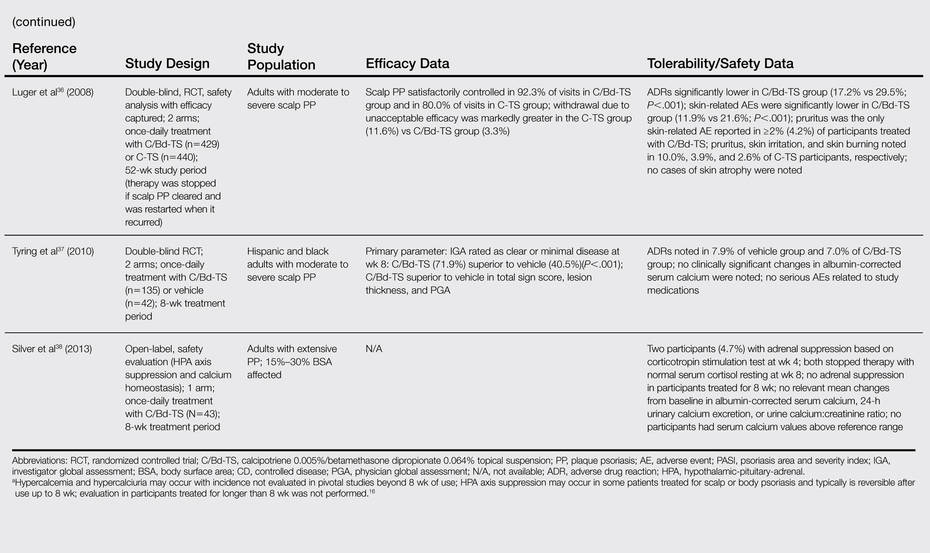
What practical recommendations can be made regarding the use of C/Bd-TS for PP?
Calcipotriene 0.005%–Bd 0.064% topical suspension applied once daily provides a formulation that allows for treatment of PP involving both the scalp and body using a single product, which provides an element of convenience and is likely to enhance compliance and reduce costs compared with the use of 2 separate products. The efficacy and safety of C/Bd-TS has been well established in several studies,16-23,37 including a 52-week trial in patients with scalp psoriasis.36 The combination of calcipotriene and Bd appears to favorably address the pathophysiologic pathways involved in psoriasis.29,30 Calcipotriene 0.005%–Bd 0.064% topical suspension is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP.6-9,14,15 Appropriate use of C/Bd-TS is likely to achieve favorable efficacy with a low risk of tolerability reactions and a very low risk of major adverse drug reactions.16-23,36-38
1. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol. 2007;157:1103-1115.
2. Menter MA. An overview of psoriasis. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:1-21.
3. Sandoval LF, Feldman SR. General approach to psoriasis treatment. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:3-8.
4. Zeichner JA, Lebwohl MG, Menter A, et al. Optimizing topical therapies for treating psoriasis: a consensus conference. Cutis. 2010;(3 suppl):5-31.
5. American Academy of Dermatology Work Group, Menter A, Korman NJ, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions [published online ahead of print February 8, 2011]. J Am Acad Dermatol. 2011;65:137-174.
6. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1, suppl 1):S50-S58.
7. Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis. section 3. guidelines of care for the management and treatment of psoriasis with topical therapies [published online ahead of print February 13, 2009]. J Am Acad Dermatol. 2009;60:643-659.
8. Koo J. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10:1-4.
9. Mason AR, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis. Cochrane Database Syst Rev. 2009;2:CD005028.
10. Belge K, Brück J, Ghoreschi K. Advances in treating psoriasis. F1000Prime Rep. 2014;6:4.
11. Mease PJ, Armstrong AW. Managing patients with psoriatic disease: the diagnosis and pharmacologic treatment of psoriatic arthritis in patients with psoriasis. Drugs. 2014;74:423-441.
12. Boehncke WH, Qureshi A, Merola JF, et al. Diagnosing and treating psoriatic arthritis: an update. Br J Dermatol. 2014;170:772-786.
13. Feldman SR. Effectiveness of clobetasol propionate spray 0.05% added to other stable treatments: add-on therapy in the COBRA trial. Cutis. 2007;80(suppl 5):20-28.
14. Feldman SR, Gelfand JM, Stein Gold L, et al. The role of topical therapy for patients with extensive psoriasis. Cutis. 2007;79(suppl 1[ii]):18-31.
15. Kircik L. Topical calcipotriene 0.005% and betamethasone dipropionate 0.064% maintains efficacy of etanercept after step-down dose in patients with moderate-to-severe plaque psoriasis: results of an open label trial. J Drugs Dermatol. 2011;10:878-882.
16. Taclonex [product insert]. Parsippany, NJ: LEO Pharma Inc; 2014.
17. Buckley C, Hoffmann V, Shapiro J, et al. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology. 2008;217:107-113.
18. Fleming C, Ganslandt C, Guenther L, et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomized, parallel group, double-blind, exploratory study. Eur J Dermatol. 2010;20:465-471.
19. Menter A, Stein Gold L, Bukhalo M, et al. Calcipotriene plus betamethasone dipropionate topical suspension for the treatment of mild to moderate psoriasis vulgaris on the body: a randomized, double-blind, vehicle-controlled trial. J Drugs Dermatol. 2013;12:92-98.
20. Jemec GBE, Ganslandt C, Ortonne JP, et al. A new scalp formulation of calcipotriene plus betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2008;59:455-463.
21. van de Kerkhof PC, Hoffmann V, Anstey A, et al. A new scalp formulation of calcipotriol plus betamethasone dipropionate compared with each of its active ingredients in the same vehicle for the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. Br J Dermatol. 2009;160:170-176.
22. Langley RG, Gupta A, Papp K, et al. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology. 2011;222:148-156.
23. Kragballe K, van de Kerkhof P. Pooled safety analysis of calcipotriol plus betamethasone dipropionate gel for the treatment of psoriasis on the body and scalp. J Eur Acad Dermatol Venereol. 2014;28:10-21.
24. Lebwohl MG, Corvari L. Compatibility of topical therapies for psoriasis: challenges and innovations. Cutis. 2007;79(suppl 1[ii]):5-10.
25. Patel B, Siskin S, Krazmien R, et al. Compatibility of calcipotriene with other topical medications. J Am Acad Dermatol. 1998;38(6, pt 1):1010-1011.
26. Traulsen J. Bioavailability of betamethasone dipropionate when combined with calcipotriol. Int J Dermatol. 2004;43:611-617.
27. Sandoval LF, Feldman SR. Topical corticosteroids. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:21-36.
28. deShazo R, Krueger GG, Duffin KC. Topical agents. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:41-65.
29. Hegyi Z, Zwicker S, Bureik D, et al. Vitamin D analog calcipotriol suppresses the Th17 cytokine-induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J Invest Dermatol. 2012;132:1416-1424.
30. Lovato P, Norsgaard H, Ropke M. Key immunomodulatory effects exerted by calcipotriol in combination with corticosteroid on human cells. Poster presented at: 21st European Academy of Dermatology and Venereology Congress; September 27-30, 2012; Prague, Czech Republic.
31. Renton C. Diagnosis and treatment of adults with scalp psoriasis. Nurs Stand. 2014;28:35-39.
32. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221-224.
33. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriene plus betamethasone dipropionate topical suspension in adolescents with scalp psoriasis: an open, non-controlled, 8-week trial. Poster presented at: American Academy of Dermatology 72nd Annual Meeting; March 21-25, 2014; Denver, CO.
34. Ortonne JP, Tan J, Nordin P, et al. Quality of life of patients with scalp psoriasis treated with calcipotriene plus betamethasone dipropionate gel compared to calcipotriene solution. J Am Academy Dermatol. 2008;58(2, suppl 2):AB134.
35. Mrowietz U, Macheleidt O, Eicke C. Effective treatment and improvement of quality of life in patients with scalp psoriasis by topical use of calcipotriol/betamethasone (Xamiol®-gel): results [in German]. J Dtsch Dermatol Ges. 2011;9:825-831.
36. Luger TA, Cambazard F, Larsen FG, et al. A study of the safety and efficacy of calcipotriol and betamethasone dipropionate scalp formulation in the long-term management of scalp psoriasis. Dermatology. 2008;217:321-328.
37. Tyring S, Mendoza N, Appell M, et al. A calcipotriene/betamethasone dipropionate two-compound scalp formulation in the treatment of scalp psoriasis in Hispanic/Latino and Black/African American patients: results of the randomized, 8-week, double-blind phase of a clinical trial. Int J Dermatol. 2010;49:1328-1333.
38. Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12:882-888.
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
What data are available on the efficacy and safety of C/Bd-TS?
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.
What practical recommendations can be made regarding the use of C/Bd-TS for PP?
Calcipotriene 0.005%–Bd 0.064% topical suspension applied once daily provides a formulation that allows for treatment of PP involving both the scalp and body using a single product, which provides an element of convenience and is likely to enhance compliance and reduce costs compared with the use of 2 separate products. The efficacy and safety of C/Bd-TS has been well established in several studies,16-23,37 including a 52-week trial in patients with scalp psoriasis.36 The combination of calcipotriene and Bd appears to favorably address the pathophysiologic pathways involved in psoriasis.29,30 Calcipotriene 0.005%–Bd 0.064% topical suspension is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP.6-9,14,15 Appropriate use of C/Bd-TS is likely to achieve favorable efficacy with a low risk of tolerability reactions and a very low risk of major adverse drug reactions.16-23,36-38
Psoriasis is a common inflammatory skin disorder that appears to be induced by multifactorial pathophysiologic processes associated with immunologic dysregulation.1 It can affect patients of any age, gender, and ethnicity, and it presents clinically with a variety of visible manifestations. The disease course and severity of psoriasis varies among affected patients.1 Chronic plaque psoriasis (PP), also referred to as psoriasis vulgaris, is the most common clinical presentation.1,2 Although many patients are affected by psoriasis that is widespread and in some cases severe, the majority of affected patients exhibit localized involvement that usually affects less than 2% to 5% of the body surface area. Although the skin at any anatomic location can be affected, commonly involved sites are described by the mnemonic term SNAKES (scalp, nails, anogenital region, knees, elbows, sacral region).2,3
Because the majority of patients with PP present with localized disease, topical therapy is the foundation of treatment in most cases. Topical corticosteroids (TCs) are the most commonly utilized agents, supported by a long track record of favorable efficacy and safety over approximately 6 decades.4,5 However, optimal management of PP with TCs requires use of a formulation that is of adequate potency, is adaptable for application to the affected body sites, and is properly monitored and adjusted to avoid potential TC-induced adverse effects.4-6 Nonsteroidal topical therapies such as vitamin D analogues (eg, calcipotriene) and retinoids (eg, tazarotene) are commonly integrated into topical regimens to reduce the application frequency and duration of TC use as well as to sustain efficacy.5,7,8 Plaque psoriasis is characteristically a chronic disease associated with periods of persistence and episodes of flaring; therefore, intermittent use of TC therapy along with concurrent or sequential use of a nonsteroidal topical agent are commonly employed to achieve and sustain control of the disorder.7-9
In the last decade, several advances have revolutionized the management of psoriasis, especially for PP patients with extensive involvement who require systemic therapy and/or phototherapy as well as for those with psoriatic arthritis.10,11 The availability of biologic agents such as tumor necrosis factor a inhibitors and certain interleukin inhibitors (eg, IL-12/IL-23) have been at the forefront of major advances in PP treatment, with some agents also blocking the progression of joint destruction associated with psoriatic arthritis.10-12 However, even when patients with PP respond favorably to biologic therapy, it is not uncommon for them to still be affected by some persistent PP. In these cases, although much of the chronic PP may clear with use of the biologic agent, persistence of psoriatic plaques may involve the lower extremities, scalp, and/or trunk, with topical therapy often added to augment the therapeutic response.13-15
This article provides a review of a patented topical suspension combination formulation that contains calcipotriene hydrate 0.005%, a vitamin D analogue, and betamethasone dipropio-nate (Bd) 0.064%, a high-potency TC. In 2008, the US Food and Drug Administration approved the once-daily application of calcipotriene 0.005%–Bd 0.064% topical suspension (C/Bd-TS) for the treatment of PP; this formulation is approved for use on the scalp and body in patients 18 years of age and older. According to the product insert, the recommended maximum duration of treatment with C/Bd-TS once daily is 8 weeks, and patients may not exceed a maximum weekly dose of 100 g.16 It is important to note that the terms calcipotriene and calcipotriol refer to the same molecule and are used interchangeably in the literature. Formulation characteristics of C/Bd-TS, perspectives on modes of action, outcomes from pivotal trials, and efficacy and safety data reported from additional studies are discussed in this article.
What are the formulation characteristics of C/Bd-TS?
Each gram of C/Bd-TS contains 52.18 mg of calcipotriene hydrate (equivalent to 50 µg of calcipotriene) and 0.643 µg of Bd (equivalent to 0.5 mg of betamethasone), formulated together in a viscous, nearly odorless, almost clear to slightly off-white suspension. The excipients are hydrogenated castor oil, polypropylene glycol 11 stearyl ether, α-tocopherol, butylhydroxytoluene, and mineral oil, collectively producing a gel base in which both active ingredients are suspended.16 Although the viscous quality of the suspension warrants some additional effort for removal during hair washing, the tenacious gel-like viscosity assists in removing scale on psoriatic plaques, which is often adherent, especially on the scalp. Additionally, it is important that C/Bd-TS be shaken well before use.16 Initially, C/Bd-TS was studied and marketed in the United States for treatment of scalp psoriasis; however, the indication was expanded to include treatment of PP on the rest of the body, supported by evidence from randomized controlled trials (RCTs).16-23
Vitamin D analogues (eg, calcipotriene/calcitriol) have been shown to be photolabile when exposed to UV light, especially UVA. They also have been shown to be chemically incompatible and less stable when admixed with a variety of other active ingredients and/or vehicles used to treat PP, including hydrocortisone valerate ointment 0.2%, ammonium lactate lotion 12%, and salicylic acid compound ointment 6%.24-26 As a result, it is important for clinicians to consider avoidance of concomitant topical calcipotriene application with use of a TC unless the stability of the active ingredients has been tested when the formulations are combined. Calcipotriene 0.005%/Bd 0.064% topical suspension utilizes vehicle technology that maintains the stability and activity of both calcipotriene and Bd within the suspension formulation.16,26
What is the rationale behind combining calcipotriene and Bd in a single formulation for the treatment of PP?
The potential advantages of C/Bd-TS include the combined modes of action of 2 different active ingredients used for treatment of PP, complementary immunomodulatory effects as compared to use of a TC or vitamin D analogue alone, ease of use with a single product applied once daily, adaptability of the vehicle for use on scalp and/or body skin, and improvement in quality-of-life (QOL) measures.27-34
Combined Modes of Action
Calcipotriene 0.005%–Bd 0.064% topical suspension combines the modes of action of a high-potency topical suspension and a vitamin D analogue for the treatment of PP in a single stable gel formulation that is approved in the United States for treatment of PP in adults.16 The multiple anti-inflammatory properties of corticosteroids as well as the efficacy and safety of TC therapy for psoriasis have been well described.4,6,7,9,27 The antiproliferative and anti-inflammatory properties of vitamin D analogues that appear to correlate with therapeutic effects in the treatment of PP also have been discussed in the literature.28
Complementary Immunomodulatory Effects
More recent studies using various research assays have provided further evidence supporting relevant immunomodulatory properties of calcipotriene alone and in combination with Bd that favorably modify immune dysregulation pathways described more recently in the pathogenesis of PP.1,29,30 Treatment of psoriatic plaques with calcipotriene has been shown to suppress the increased production of peptide alarmins (psoriasin and koebnerisin) in psoriatic skin and their TH17-mediated regulation in epidermal ke-ratinocytes, thus interfering with the S100 amplification loop that appears to produce inflammation in psoriasis.29 In T-lymphocyte cultures evaluating exposure to calcipotriene and Bd both alone and as a combined therapy, calcipotriene inhibited IFN-g, IL-8, IL-17, and IL-22 expression, and it reversed the corticosteroid-induced suppression of IL-4, IL-5, IL-10, and IL-13; Bd inhibited both IL-6 and tumor necrosis factor α expression. The outcomes demonstrated that the combination of calcipotriene and Bd inhibited the endogenous release of TH1- and TH17-associated cytokines that are associated with psoriatic inflammation and together induced a more favorable anti-inflammatory cytokine profile.30 Although the broad range of anti-inflammatory effects provided by a TC of adequate potency, such as Bd, can clear or markedly improve PP, the concurrent use of calcipotriene was shown to provide additional immunomodulatory effects that suppressed the key TH17/TH1 pathophysiologic mediators of psoriatic inflammation and simultaneously induced a TH2/T regulatory response that is believed to provide therapeutic benefit.29,30
Ease of Use and Vehicle Adaptability
A once-daily regimen and a vehicle formulation adaptable for use on both the scalp and body are advantageous in enhancing the potential for greater patient adherence.31,32 The adaptability of the C/Bd-TS for use on the scalp and/or body is supported by several studies encompassing a large number of actively treated subjects. Calcipotriene 0.005%–Bd 0.064% topical suspension has been extensively studied in patients with PP on the scalp and/or body as evidenced by a pooled analysis of 9 eight-week RCTs (scalp, n=6; body, n=3) that encompassed 2777 total subjects treated once daily for PP (scalp, n=1953; body, n=824).23 Additionally, C/Bd-TS applied once daily was evaluated in an open-label, single-arm, 8-week, phase 2 study of adolescents (N=78; age range, 12–17 years [mean age, 14.6 years]) with scalp psoriasis (mean affected scalp area, 43.7%). The investigator global assessment of treatment success (clear or almost clear) and the patient global assessment of treatment success (clear or very mild) were essentially identical among participants and investigators with 85% and 87% reported after 8 weeks, respectively; approximately 50% of participants achieved treatment success after 2 weeks based on both the investigator global assessment and patient global assessment.33
Improvement in QOL Measures
Quality-of-life measures were compared in an 8-week RCT of participants with at least moderate scalp psoriasis treated with C/Bd-TS once daily (n=207) or calcipotriene solution twice daily (n=107). Significantly greater improvement in QOL scores compared to baseline were noted at all time points using the Skindex-16 questionnaire in participants treated with C/Bd-TS compared to calcipotriene solution (total score, P<.001 at weeks 2 and 4 and P=.008 at week 8; symptoms score, P<.001 at weeks 2 and 4 and P=.004 at week 8; emotions score, P<.001 at weeks 2 and 4 and P=.005 at week 8).34 A 4-week, open-label, noninterventional cohort, postmarketing (“real life”) study of 721 patients treated at 333 dermatology centers with C/Bd-TS showed a 69.5% improvement in the scalp life quality index score compared to baseline (P<.0001), with 89.5% and 90.4% of participants reporting that C/Bd-TS was better/much better than previously used therapies for scalp psoriasis and easy/very easy to use, respectively.35 An 8-week RCT trial evaluated C/Bd-TS once daily compared to calcipotriene alone, betamethasone dipropionate alone, and vehicle in 1152 participants with mild to moderate PP involving the trunk and extremities. Participants treated with C/Bd-TS (n=442) demonstrated superior reductions in QOL scores using the dermatology life quality index at weeks 4 and 8 compared to those treated with Bd alone (n=418) or vehicle (n=77) but not compared to calcipotriene alone (n=80).19
What data are available on the efficacy and safety of C/Bd-TS?
Several clinical studies have evaluated the efficacy, tolerability, and safety of C/Bd-TS applied once daily for PP of the scalp and body (ie, trunk, extremities). Most studies were completed over a duration of 8 weeks in adults16-23; however, studies also have been performed in adolescents,33 in adults treated for up to 52 weeks,36 and in a subgroup of Hispanic/Latino and black/African American patients with scalp psoriasis.37 The Table provides a detailed summary of primary efficacy data along with important tolerability and safety considerations based on study outcomes.
What practical recommendations can be made regarding the use of C/Bd-TS for PP?
Calcipotriene 0.005%–Bd 0.064% topical suspension applied once daily provides a formulation that allows for treatment of PP involving both the scalp and body using a single product, which provides an element of convenience and is likely to enhance compliance and reduce costs compared with the use of 2 separate products. The efficacy and safety of C/Bd-TS has been well established in several studies,16-23,37 including a 52-week trial in patients with scalp psoriasis.36 The combination of calcipotriene and Bd appears to favorably address the pathophysiologic pathways involved in psoriasis.29,30 Calcipotriene 0.005%–Bd 0.064% topical suspension is a rational option for the treatment of PP in patients with localized disease or in patients treated systemically or with phototherapy for more extensive disease who exhibit persistence or recurrence of scattered areas of PP.6-9,14,15 Appropriate use of C/Bd-TS is likely to achieve favorable efficacy with a low risk of tolerability reactions and a very low risk of major adverse drug reactions.16-23,36-38
1. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol. 2007;157:1103-1115.
2. Menter MA. An overview of psoriasis. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:1-21.
3. Sandoval LF, Feldman SR. General approach to psoriasis treatment. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:3-8.
4. Zeichner JA, Lebwohl MG, Menter A, et al. Optimizing topical therapies for treating psoriasis: a consensus conference. Cutis. 2010;(3 suppl):5-31.
5. American Academy of Dermatology Work Group, Menter A, Korman NJ, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions [published online ahead of print February 8, 2011]. J Am Acad Dermatol. 2011;65:137-174.
6. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1, suppl 1):S50-S58.
7. Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis. section 3. guidelines of care for the management and treatment of psoriasis with topical therapies [published online ahead of print February 13, 2009]. J Am Acad Dermatol. 2009;60:643-659.
8. Koo J. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10:1-4.
9. Mason AR, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis. Cochrane Database Syst Rev. 2009;2:CD005028.
10. Belge K, Brück J, Ghoreschi K. Advances in treating psoriasis. F1000Prime Rep. 2014;6:4.
11. Mease PJ, Armstrong AW. Managing patients with psoriatic disease: the diagnosis and pharmacologic treatment of psoriatic arthritis in patients with psoriasis. Drugs. 2014;74:423-441.
12. Boehncke WH, Qureshi A, Merola JF, et al. Diagnosing and treating psoriatic arthritis: an update. Br J Dermatol. 2014;170:772-786.
13. Feldman SR. Effectiveness of clobetasol propionate spray 0.05% added to other stable treatments: add-on therapy in the COBRA trial. Cutis. 2007;80(suppl 5):20-28.
14. Feldman SR, Gelfand JM, Stein Gold L, et al. The role of topical therapy for patients with extensive psoriasis. Cutis. 2007;79(suppl 1[ii]):18-31.
15. Kircik L. Topical calcipotriene 0.005% and betamethasone dipropionate 0.064% maintains efficacy of etanercept after step-down dose in patients with moderate-to-severe plaque psoriasis: results of an open label trial. J Drugs Dermatol. 2011;10:878-882.
16. Taclonex [product insert]. Parsippany, NJ: LEO Pharma Inc; 2014.
17. Buckley C, Hoffmann V, Shapiro J, et al. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology. 2008;217:107-113.
18. Fleming C, Ganslandt C, Guenther L, et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomized, parallel group, double-blind, exploratory study. Eur J Dermatol. 2010;20:465-471.
19. Menter A, Stein Gold L, Bukhalo M, et al. Calcipotriene plus betamethasone dipropionate topical suspension for the treatment of mild to moderate psoriasis vulgaris on the body: a randomized, double-blind, vehicle-controlled trial. J Drugs Dermatol. 2013;12:92-98.
20. Jemec GBE, Ganslandt C, Ortonne JP, et al. A new scalp formulation of calcipotriene plus betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2008;59:455-463.
21. van de Kerkhof PC, Hoffmann V, Anstey A, et al. A new scalp formulation of calcipotriol plus betamethasone dipropionate compared with each of its active ingredients in the same vehicle for the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. Br J Dermatol. 2009;160:170-176.
22. Langley RG, Gupta A, Papp K, et al. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology. 2011;222:148-156.
23. Kragballe K, van de Kerkhof P. Pooled safety analysis of calcipotriol plus betamethasone dipropionate gel for the treatment of psoriasis on the body and scalp. J Eur Acad Dermatol Venereol. 2014;28:10-21.
24. Lebwohl MG, Corvari L. Compatibility of topical therapies for psoriasis: challenges and innovations. Cutis. 2007;79(suppl 1[ii]):5-10.
25. Patel B, Siskin S, Krazmien R, et al. Compatibility of calcipotriene with other topical medications. J Am Acad Dermatol. 1998;38(6, pt 1):1010-1011.
26. Traulsen J. Bioavailability of betamethasone dipropionate when combined with calcipotriol. Int J Dermatol. 2004;43:611-617.
27. Sandoval LF, Feldman SR. Topical corticosteroids. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:21-36.
28. deShazo R, Krueger GG, Duffin KC. Topical agents. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:41-65.
29. Hegyi Z, Zwicker S, Bureik D, et al. Vitamin D analog calcipotriol suppresses the Th17 cytokine-induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J Invest Dermatol. 2012;132:1416-1424.
30. Lovato P, Norsgaard H, Ropke M. Key immunomodulatory effects exerted by calcipotriol in combination with corticosteroid on human cells. Poster presented at: 21st European Academy of Dermatology and Venereology Congress; September 27-30, 2012; Prague, Czech Republic.
31. Renton C. Diagnosis and treatment of adults with scalp psoriasis. Nurs Stand. 2014;28:35-39.
32. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221-224.
33. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriene plus betamethasone dipropionate topical suspension in adolescents with scalp psoriasis: an open, non-controlled, 8-week trial. Poster presented at: American Academy of Dermatology 72nd Annual Meeting; March 21-25, 2014; Denver, CO.
34. Ortonne JP, Tan J, Nordin P, et al. Quality of life of patients with scalp psoriasis treated with calcipotriene plus betamethasone dipropionate gel compared to calcipotriene solution. J Am Academy Dermatol. 2008;58(2, suppl 2):AB134.
35. Mrowietz U, Macheleidt O, Eicke C. Effective treatment and improvement of quality of life in patients with scalp psoriasis by topical use of calcipotriol/betamethasone (Xamiol®-gel): results [in German]. J Dtsch Dermatol Ges. 2011;9:825-831.
36. Luger TA, Cambazard F, Larsen FG, et al. A study of the safety and efficacy of calcipotriol and betamethasone dipropionate scalp formulation in the long-term management of scalp psoriasis. Dermatology. 2008;217:321-328.
37. Tyring S, Mendoza N, Appell M, et al. A calcipotriene/betamethasone dipropionate two-compound scalp formulation in the treatment of scalp psoriasis in Hispanic/Latino and Black/African American patients: results of the randomized, 8-week, double-blind phase of a clinical trial. Int J Dermatol. 2010;49:1328-1333.
38. Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12:882-888.
1. Guttman-Yassky E, Krueger JG. Psoriasis: evolution of pathogenic concepts and new therapies through phases of translational research. Br J Dermatol. 2007;157:1103-1115.
2. Menter MA. An overview of psoriasis. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:1-21.
3. Sandoval LF, Feldman SR. General approach to psoriasis treatment. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:3-8.
4. Zeichner JA, Lebwohl MG, Menter A, et al. Optimizing topical therapies for treating psoriasis: a consensus conference. Cutis. 2010;(3 suppl):5-31.
5. American Academy of Dermatology Work Group, Menter A, Korman NJ, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions [published online ahead of print February 8, 2011]. J Am Acad Dermatol. 2011;65:137-174.
6. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53(1, suppl 1):S50-S58.
7. Menter A, Korman NJ, Elmets CA, et al; American Academy of Dermatology. Guidelines of care for the management of psoriasis and psoriatic arthritis. section 3. guidelines of care for the management and treatment of psoriasis with topical therapies [published online ahead of print February 13, 2009]. J Am Acad Dermatol. 2009;60:643-659.
8. Koo J. New developments in topical sequential therapy for psoriasis. Skin Therapy Lett. 2005;10:1-4.
9. Mason AR, Mason J, Cork M, et al. Topical treatments for chronic plaque psoriasis. Cochrane Database Syst Rev. 2009;2:CD005028.
10. Belge K, Brück J, Ghoreschi K. Advances in treating psoriasis. F1000Prime Rep. 2014;6:4.
11. Mease PJ, Armstrong AW. Managing patients with psoriatic disease: the diagnosis and pharmacologic treatment of psoriatic arthritis in patients with psoriasis. Drugs. 2014;74:423-441.
12. Boehncke WH, Qureshi A, Merola JF, et al. Diagnosing and treating psoriatic arthritis: an update. Br J Dermatol. 2014;170:772-786.
13. Feldman SR. Effectiveness of clobetasol propionate spray 0.05% added to other stable treatments: add-on therapy in the COBRA trial. Cutis. 2007;80(suppl 5):20-28.
14. Feldman SR, Gelfand JM, Stein Gold L, et al. The role of topical therapy for patients with extensive psoriasis. Cutis. 2007;79(suppl 1[ii]):18-31.
15. Kircik L. Topical calcipotriene 0.005% and betamethasone dipropionate 0.064% maintains efficacy of etanercept after step-down dose in patients with moderate-to-severe plaque psoriasis: results of an open label trial. J Drugs Dermatol. 2011;10:878-882.
16. Taclonex [product insert]. Parsippany, NJ: LEO Pharma Inc; 2014.
17. Buckley C, Hoffmann V, Shapiro J, et al. Calcipotriol plus betamethasone dipropionate scalp formulation is effective and well tolerated in the treatment of scalp psoriasis: a phase II study. Dermatology. 2008;217:107-113.
18. Fleming C, Ganslandt C, Guenther L, et al. Calcipotriol plus betamethasone dipropionate gel compared with its active components in the same vehicle and the vehicle alone in the treatment of psoriasis vulgaris: a randomized, parallel group, double-blind, exploratory study. Eur J Dermatol. 2010;20:465-471.
19. Menter A, Stein Gold L, Bukhalo M, et al. Calcipotriene plus betamethasone dipropionate topical suspension for the treatment of mild to moderate psoriasis vulgaris on the body: a randomized, double-blind, vehicle-controlled trial. J Drugs Dermatol. 2013;12:92-98.
20. Jemec GBE, Ganslandt C, Ortonne JP, et al. A new scalp formulation of calcipotriene plus betamethasone compared with its active ingredients and the vehicle in the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. J Am Acad Dermatol. 2008;59:455-463.
21. van de Kerkhof PC, Hoffmann V, Anstey A, et al. A new scalp formulation of calcipotriol plus betamethasone dipropionate compared with each of its active ingredients in the same vehicle for the treatment of scalp psoriasis: a randomized, double-blind, controlled trial. Br J Dermatol. 2009;160:170-176.
22. Langley RG, Gupta A, Papp K, et al. Calcipotriol plus betamethasone dipropionate gel compared with tacalcitol ointment and the gel vehicle alone in patients with psoriasis vulgaris: a randomized, controlled clinical trial. Dermatology. 2011;222:148-156.
23. Kragballe K, van de Kerkhof P. Pooled safety analysis of calcipotriol plus betamethasone dipropionate gel for the treatment of psoriasis on the body and scalp. J Eur Acad Dermatol Venereol. 2014;28:10-21.
24. Lebwohl MG, Corvari L. Compatibility of topical therapies for psoriasis: challenges and innovations. Cutis. 2007;79(suppl 1[ii]):5-10.
25. Patel B, Siskin S, Krazmien R, et al. Compatibility of calcipotriene with other topical medications. J Am Acad Dermatol. 1998;38(6, pt 1):1010-1011.
26. Traulsen J. Bioavailability of betamethasone dipropionate when combined with calcipotriol. Int J Dermatol. 2004;43:611-617.
27. Sandoval LF, Feldman SR. Topical corticosteroids. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:21-36.
28. deShazo R, Krueger GG, Duffin KC. Topical agents. In: Koo JYM, Levin EC, Leon A, et al, eds. Moderate to Severe Psoriasis. 4th ed. Boca Raton, FL: CRC Press Taylor & Francis Group; 2014:41-65.
29. Hegyi Z, Zwicker S, Bureik D, et al. Vitamin D analog calcipotriol suppresses the Th17 cytokine-induced proinflammatory S100 “alarmins” psoriasin (S100A7) and koebnerisin (S100A15) in psoriasis. J Invest Dermatol. 2012;132:1416-1424.
30. Lovato P, Norsgaard H, Ropke M. Key immunomodulatory effects exerted by calcipotriol in combination with corticosteroid on human cells. Poster presented at: 21st European Academy of Dermatology and Venereology Congress; September 27-30, 2012; Prague, Czech Republic.
31. Renton C. Diagnosis and treatment of adults with scalp psoriasis. Nurs Stand. 2014;28:35-39.
32. Feldman SR, Housman TS. Patients’ vehicle preference for corticosteroid treatments of scalp psoriasis. Am J Clin Dermatol. 2003;4:221-224.
33. Gooderham M, Debarre JM, Keddy-Grant J, et al. Safety and efficacy of calcipotriene plus betamethasone dipropionate topical suspension in adolescents with scalp psoriasis: an open, non-controlled, 8-week trial. Poster presented at: American Academy of Dermatology 72nd Annual Meeting; March 21-25, 2014; Denver, CO.
34. Ortonne JP, Tan J, Nordin P, et al. Quality of life of patients with scalp psoriasis treated with calcipotriene plus betamethasone dipropionate gel compared to calcipotriene solution. J Am Academy Dermatol. 2008;58(2, suppl 2):AB134.
35. Mrowietz U, Macheleidt O, Eicke C. Effective treatment and improvement of quality of life in patients with scalp psoriasis by topical use of calcipotriol/betamethasone (Xamiol®-gel): results [in German]. J Dtsch Dermatol Ges. 2011;9:825-831.
36. Luger TA, Cambazard F, Larsen FG, et al. A study of the safety and efficacy of calcipotriol and betamethasone dipropionate scalp formulation in the long-term management of scalp psoriasis. Dermatology. 2008;217:321-328.
37. Tyring S, Mendoza N, Appell M, et al. A calcipotriene/betamethasone dipropionate two-compound scalp formulation in the treatment of scalp psoriasis in Hispanic/Latino and Black/African American patients: results of the randomized, 8-week, double-blind phase of a clinical trial. Int J Dermatol. 2010;49:1328-1333.
38. Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12:882-888.
Practice Points
- Calcipotriene 0.005%–betamethasone dipropionate 0.064% topical suspension (C/Bd-TS) applied once daily has been shown in multiple studies to be effective, well tolerated, and safe for the treatment of plaque psoriasis (PP) involving the scalp and/or other body sites such as the trunk and extremities. Studies have included all severities of PP, with both investigator and subject assessments shown to be favorable overall.
- Most studies were completed in adults over a duration of 8 weeks; however, clinical trials also have been performed with C/Bd-TS in adults treated for up to 52 weeks for scalp psoriasis, in a subgroup of Hispanic/Latino and black/African American adult patients with scalp psoriasis, and in adolescents with scalp psoriasis.
- Studies evaluating application of C/Bd-TS once daily for PP affecting nonscalp sites have primarily involved use on the trunk and extremities.
- The adaptability for scalp and body application allows for use in many cases of a single topical product without needing to prescribe a second leave-on medication specifically for use on the scalp.