User login
Understanding U.S. Cardiologists’ Perspectives on Non-Valvular Atrial Fibrillation (NVAF)
A supplement to Cardiology News. This supplement was sponsored by Daiichi Sankyo Inc.

Faculty:
Hugh Calkins, MD, FHRS, Immediate Past President of The Heart Rhythm Society; Director of Cardiac Arrhythmia Service, Johns Hopkins Hospital; and Professor of Medicine at Johns Hopkins University School of Medicine, Baltimore, MD
Disclosures:
Daiichi Sankyo has provided financial support to the Heart Rhythm Society for conducting this survey. Dr. Calkins consults on behalf of Daiichi Sankyo.
A supplement to Cardiology News. This supplement was sponsored by Daiichi Sankyo Inc.
Faculty:
Hugh Calkins, MD, FHRS, Immediate Past President of The Heart Rhythm Society; Director of Cardiac Arrhythmia Service, Johns Hopkins Hospital; and Professor of Medicine at Johns Hopkins University School of Medicine, Baltimore, MD
Disclosures:
Daiichi Sankyo has provided financial support to the Heart Rhythm Society for conducting this survey. Dr. Calkins consults on behalf of Daiichi Sankyo.
A supplement to Cardiology News. This supplement was sponsored by Daiichi Sankyo Inc.
Faculty:
Hugh Calkins, MD, FHRS, Immediate Past President of The Heart Rhythm Society; Director of Cardiac Arrhythmia Service, Johns Hopkins Hospital; and Professor of Medicine at Johns Hopkins University School of Medicine, Baltimore, MD
Disclosures:
Daiichi Sankyo has provided financial support to the Heart Rhythm Society for conducting this survey. Dr. Calkins consults on behalf of Daiichi Sankyo.

Laser treatments for men
In our final segment on male dermatology, we will be focusing on laser treatments in men. There has been a steady increase in cosmetic procedures in men over the last decade, and laser procedures tend to be some of the most popular. In general, laser treatments provide faster results than topical or oral treatments and offer subtle aesthetic improvements with little to no downtime depending on the procedure. These factors appeal to male patients, who generally are generally less risk tolerant than women, and want masculinizing treatments with little downtime and natural results.
• Hair growth. Men tend to have highly pigmented, thicker hair in contrast to women, and often seek laser hair removal for excess body hair. Common sites include the back, upper arms, posterior hairline, lower beardline, and chest. Similar precautions apply to both men and women, such as proper cooling of the skin and avoidance of tanned skin. However, laser settings for male patients may need to be adjusted given the thicker, darkly pigmented hairs and often lower pain threshold. In addition, proper counseling of men is necessary with laser hair removal, because men often need more treatments than women and may need a topical anesthetic for highly sensitive areas.
• Body contouring. Men tend to deposit fat in hard-to-lose areas, such as the central abdomen and flanks. The expanding array of noninvasive devices using cold temperatures to freeze the fat, or ultrasound and radiofrequency devices to heat and thereby tighten the subcutaneous tissue have made body contouring one of the fastest growing cosmetic markets for men. Men are great candidates for these procedures given the fast results, minor discomfort, and noninvasive nature. Although many men have visceral abdominal fat that does not respond to these treatments, areas often treated with great long-term results include the upper and lower abdomen, flanks, arms, chest, and back.
• Rosacea. Men have a higher density of facial blood vessels than women, and they often seek treatment for telangiectasias and overall facial erythema. For noninflammatory erythematotelangiectatic rosacea, vascular laser treatments are the most effective treatments. Pulsed dye laser is often the best laser to target both large and small facial blood vessels and flushing erythema. Intense pulsed light (IPL) lasers are often a more popular choice for men because they involve less downtime and can treat brown spots as well. However, IPL must be used with caution in skin of color and tanned skin because of the risks of scarring and hyperpigmentation. Men may need more treatments and higher energy settings than women. Men also prefer minimal downtime and thus more frequent nonpurpuric settings are often preferred with any vascular laser. In addition, with IPL, men should be warned of the possibility of the laser temporarily stunting hair growth or causing hair to grow in patchy temporarily when using the device in the beard or mustache area.
• Laser resurfacing. Laser skin resurfacing can be performed for acne scars, rhytids, age sports, sun spots, melasma, and overall skin laxity. Options include ablative and nonablative skin resurfacing. The choice of procedure depends on the type of problem being treated, skin type, and downtime. Ablative CO2, erbium:YAG, and fractional ablative lasers provide the best results for deep rhytids, acne scars, surgical scars, and skin laxity. However, men often shy away from these procedures given the pain, postprocedure care necessary, and downtime. Nonablative lasers may be a better choice for men, particularly for fine rhytids, melasma, and sun spots. With multiple treatments, they also may be used for scars and skin laxity. Postprocedure skincare and downtime are the critical factors for men when choosing resurfacing procedures, and detailed review of the care, complexity, and side effects are essential in the care of male patients.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub.
In our final segment on male dermatology, we will be focusing on laser treatments in men. There has been a steady increase in cosmetic procedures in men over the last decade, and laser procedures tend to be some of the most popular. In general, laser treatments provide faster results than topical or oral treatments and offer subtle aesthetic improvements with little to no downtime depending on the procedure. These factors appeal to male patients, who generally are generally less risk tolerant than women, and want masculinizing treatments with little downtime and natural results.
• Hair growth. Men tend to have highly pigmented, thicker hair in contrast to women, and often seek laser hair removal for excess body hair. Common sites include the back, upper arms, posterior hairline, lower beardline, and chest. Similar precautions apply to both men and women, such as proper cooling of the skin and avoidance of tanned skin. However, laser settings for male patients may need to be adjusted given the thicker, darkly pigmented hairs and often lower pain threshold. In addition, proper counseling of men is necessary with laser hair removal, because men often need more treatments than women and may need a topical anesthetic for highly sensitive areas.
• Body contouring. Men tend to deposit fat in hard-to-lose areas, such as the central abdomen and flanks. The expanding array of noninvasive devices using cold temperatures to freeze the fat, or ultrasound and radiofrequency devices to heat and thereby tighten the subcutaneous tissue have made body contouring one of the fastest growing cosmetic markets for men. Men are great candidates for these procedures given the fast results, minor discomfort, and noninvasive nature. Although many men have visceral abdominal fat that does not respond to these treatments, areas often treated with great long-term results include the upper and lower abdomen, flanks, arms, chest, and back.
• Rosacea. Men have a higher density of facial blood vessels than women, and they often seek treatment for telangiectasias and overall facial erythema. For noninflammatory erythematotelangiectatic rosacea, vascular laser treatments are the most effective treatments. Pulsed dye laser is often the best laser to target both large and small facial blood vessels and flushing erythema. Intense pulsed light (IPL) lasers are often a more popular choice for men because they involve less downtime and can treat brown spots as well. However, IPL must be used with caution in skin of color and tanned skin because of the risks of scarring and hyperpigmentation. Men may need more treatments and higher energy settings than women. Men also prefer minimal downtime and thus more frequent nonpurpuric settings are often preferred with any vascular laser. In addition, with IPL, men should be warned of the possibility of the laser temporarily stunting hair growth or causing hair to grow in patchy temporarily when using the device in the beard or mustache area.
• Laser resurfacing. Laser skin resurfacing can be performed for acne scars, rhytids, age sports, sun spots, melasma, and overall skin laxity. Options include ablative and nonablative skin resurfacing. The choice of procedure depends on the type of problem being treated, skin type, and downtime. Ablative CO2, erbium:YAG, and fractional ablative lasers provide the best results for deep rhytids, acne scars, surgical scars, and skin laxity. However, men often shy away from these procedures given the pain, postprocedure care necessary, and downtime. Nonablative lasers may be a better choice for men, particularly for fine rhytids, melasma, and sun spots. With multiple treatments, they also may be used for scars and skin laxity. Postprocedure skincare and downtime are the critical factors for men when choosing resurfacing procedures, and detailed review of the care, complexity, and side effects are essential in the care of male patients.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub.
In our final segment on male dermatology, we will be focusing on laser treatments in men. There has been a steady increase in cosmetic procedures in men over the last decade, and laser procedures tend to be some of the most popular. In general, laser treatments provide faster results than topical or oral treatments and offer subtle aesthetic improvements with little to no downtime depending on the procedure. These factors appeal to male patients, who generally are generally less risk tolerant than women, and want masculinizing treatments with little downtime and natural results.
• Hair growth. Men tend to have highly pigmented, thicker hair in contrast to women, and often seek laser hair removal for excess body hair. Common sites include the back, upper arms, posterior hairline, lower beardline, and chest. Similar precautions apply to both men and women, such as proper cooling of the skin and avoidance of tanned skin. However, laser settings for male patients may need to be adjusted given the thicker, darkly pigmented hairs and often lower pain threshold. In addition, proper counseling of men is necessary with laser hair removal, because men often need more treatments than women and may need a topical anesthetic for highly sensitive areas.
• Body contouring. Men tend to deposit fat in hard-to-lose areas, such as the central abdomen and flanks. The expanding array of noninvasive devices using cold temperatures to freeze the fat, or ultrasound and radiofrequency devices to heat and thereby tighten the subcutaneous tissue have made body contouring one of the fastest growing cosmetic markets for men. Men are great candidates for these procedures given the fast results, minor discomfort, and noninvasive nature. Although many men have visceral abdominal fat that does not respond to these treatments, areas often treated with great long-term results include the upper and lower abdomen, flanks, arms, chest, and back.
• Rosacea. Men have a higher density of facial blood vessels than women, and they often seek treatment for telangiectasias and overall facial erythema. For noninflammatory erythematotelangiectatic rosacea, vascular laser treatments are the most effective treatments. Pulsed dye laser is often the best laser to target both large and small facial blood vessels and flushing erythema. Intense pulsed light (IPL) lasers are often a more popular choice for men because they involve less downtime and can treat brown spots as well. However, IPL must be used with caution in skin of color and tanned skin because of the risks of scarring and hyperpigmentation. Men may need more treatments and higher energy settings than women. Men also prefer minimal downtime and thus more frequent nonpurpuric settings are often preferred with any vascular laser. In addition, with IPL, men should be warned of the possibility of the laser temporarily stunting hair growth or causing hair to grow in patchy temporarily when using the device in the beard or mustache area.
• Laser resurfacing. Laser skin resurfacing can be performed for acne scars, rhytids, age sports, sun spots, melasma, and overall skin laxity. Options include ablative and nonablative skin resurfacing. The choice of procedure depends on the type of problem being treated, skin type, and downtime. Ablative CO2, erbium:YAG, and fractional ablative lasers provide the best results for deep rhytids, acne scars, surgical scars, and skin laxity. However, men often shy away from these procedures given the pain, postprocedure care necessary, and downtime. Nonablative lasers may be a better choice for men, particularly for fine rhytids, melasma, and sun spots. With multiple treatments, they also may be used for scars and skin laxity. Postprocedure skincare and downtime are the critical factors for men when choosing resurfacing procedures, and detailed review of the care, complexity, and side effects are essential in the care of male patients.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub.

Digital resource provides tips on diabetes management, treatment
More than a dozen federal agencies have banded together to create the Guiding Principles for the Care of People With or at Risk for Diabetes, a digital resource center aimed at providing clinically relevant information on diabetes management to clinicians and health care professionals.
The tool, created by the National Diabetes Education Program, is based on areas of general agreement among existing diabetes management protocols, can better inform primary care providers and health care teams on how to deliver quality care to adults with or at risk of diabetes.
The guidelines are not intended as a definitive resource for diabetes management and do not provide information on specific clinical management of diabetes.
Supporters of the guidelines include the American Diabetes Association, the Academy of Nutrition and Dietetics, the American Association of Nurse Practitioners, the Office of Minority Health, and the Agency for Healthcare Research and Quality.
The resource guide has information about the following topics:
• Identify undiagnosed diabetes and prediabetes.
• Manage prediabetes.
• Provide self-management education and support.
• Provide individualized nutrition therapy.
• Encourage regular physical activity.
• Control blood glucose.
• Reduce cardiovascular disease risk.
• Detect and monitor microvascular complications.
• Consider special populations.
• Provide patient-centered care.
To learn more about the Guiding Principles, check out the website here.
More than a dozen federal agencies have banded together to create the Guiding Principles for the Care of People With or at Risk for Diabetes, a digital resource center aimed at providing clinically relevant information on diabetes management to clinicians and health care professionals.
The tool, created by the National Diabetes Education Program, is based on areas of general agreement among existing diabetes management protocols, can better inform primary care providers and health care teams on how to deliver quality care to adults with or at risk of diabetes.
The guidelines are not intended as a definitive resource for diabetes management and do not provide information on specific clinical management of diabetes.
Supporters of the guidelines include the American Diabetes Association, the Academy of Nutrition and Dietetics, the American Association of Nurse Practitioners, the Office of Minority Health, and the Agency for Healthcare Research and Quality.
The resource guide has information about the following topics:
• Identify undiagnosed diabetes and prediabetes.
• Manage prediabetes.
• Provide self-management education and support.
• Provide individualized nutrition therapy.
• Encourage regular physical activity.
• Control blood glucose.
• Reduce cardiovascular disease risk.
• Detect and monitor microvascular complications.
• Consider special populations.
• Provide patient-centered care.
To learn more about the Guiding Principles, check out the website here.
More than a dozen federal agencies have banded together to create the Guiding Principles for the Care of People With or at Risk for Diabetes, a digital resource center aimed at providing clinically relevant information on diabetes management to clinicians and health care professionals.
The tool, created by the National Diabetes Education Program, is based on areas of general agreement among existing diabetes management protocols, can better inform primary care providers and health care teams on how to deliver quality care to adults with or at risk of diabetes.
The guidelines are not intended as a definitive resource for diabetes management and do not provide information on specific clinical management of diabetes.
Supporters of the guidelines include the American Diabetes Association, the Academy of Nutrition and Dietetics, the American Association of Nurse Practitioners, the Office of Minority Health, and the Agency for Healthcare Research and Quality.
The resource guide has information about the following topics:
• Identify undiagnosed diabetes and prediabetes.
• Manage prediabetes.
• Provide self-management education and support.
• Provide individualized nutrition therapy.
• Encourage regular physical activity.
• Control blood glucose.
• Reduce cardiovascular disease risk.
• Detect and monitor microvascular complications.
• Consider special populations.
• Provide patient-centered care.
To learn more about the Guiding Principles, check out the website here.
PODCAST: Program restores competency of defendants
CHICAGO– A competency restoration program in the District of Columbia is helping defendants with mental illness become fit to stand trial, while saving the district money. The program could serve as a model for other jurisdictions that want to improve the competency of unfit defendants, Dr. Nicole R. Johnson, director of outpatient forensic service at the district’s Department of Behavioral Health said in an interview.
The District of Columbia’s Outpatient Competency Restoration Program (OCRP) started in 2009 and receives court-ordered referrals for individuals to participate in the program. The program works to restore defendants’ competency through question and answer sessions, games, and educational lessons, among other methods, Dr. Johnson reported at the American Academy of Psychiatry and the Law meeting. Some participants have mental illness and about a third have cognitive or neurologic limitations, she said. The majority of those referred receive mental health services from separate district agencies. If such needs are being not being met, OCRP administrators refer them to a clinic for treatment.
Of 170 individuals enrolled in the OCRP from 2009 to 2013, 54 were deemed competent to stand trial after completion, said Dr. Johnson, who oversees the program.
In an interview at the meeting, Dr. Johnson discussed how much money the program has saved the district and whether other jurisdictions can feasibly start similar programs.
On Twitter @legal_med
CHICAGO– A competency restoration program in the District of Columbia is helping defendants with mental illness become fit to stand trial, while saving the district money. The program could serve as a model for other jurisdictions that want to improve the competency of unfit defendants, Dr. Nicole R. Johnson, director of outpatient forensic service at the district’s Department of Behavioral Health said in an interview.
The District of Columbia’s Outpatient Competency Restoration Program (OCRP) started in 2009 and receives court-ordered referrals for individuals to participate in the program. The program works to restore defendants’ competency through question and answer sessions, games, and educational lessons, among other methods, Dr. Johnson reported at the American Academy of Psychiatry and the Law meeting. Some participants have mental illness and about a third have cognitive or neurologic limitations, she said. The majority of those referred receive mental health services from separate district agencies. If such needs are being not being met, OCRP administrators refer them to a clinic for treatment.
Of 170 individuals enrolled in the OCRP from 2009 to 2013, 54 were deemed competent to stand trial after completion, said Dr. Johnson, who oversees the program.
In an interview at the meeting, Dr. Johnson discussed how much money the program has saved the district and whether other jurisdictions can feasibly start similar programs.
On Twitter @legal_med
CHICAGO– A competency restoration program in the District of Columbia is helping defendants with mental illness become fit to stand trial, while saving the district money. The program could serve as a model for other jurisdictions that want to improve the competency of unfit defendants, Dr. Nicole R. Johnson, director of outpatient forensic service at the district’s Department of Behavioral Health said in an interview.
The District of Columbia’s Outpatient Competency Restoration Program (OCRP) started in 2009 and receives court-ordered referrals for individuals to participate in the program. The program works to restore defendants’ competency through question and answer sessions, games, and educational lessons, among other methods, Dr. Johnson reported at the American Academy of Psychiatry and the Law meeting. Some participants have mental illness and about a third have cognitive or neurologic limitations, she said. The majority of those referred receive mental health services from separate district agencies. If such needs are being not being met, OCRP administrators refer them to a clinic for treatment.
Of 170 individuals enrolled in the OCRP from 2009 to 2013, 54 were deemed competent to stand trial after completion, said Dr. Johnson, who oversees the program.
In an interview at the meeting, Dr. Johnson discussed how much money the program has saved the district and whether other jurisdictions can feasibly start similar programs.
On Twitter @legal_med
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Blood sample storage may hinder leukemia research

Credit: Graham Colm
Storing blood samples at room temperature can induce changes that may cloud research findings, according to a group of investigators.
The team initially found that blood samples from leukemia patients had high levels of malformed RNA, a discovery they believed could explain leukemia’s origins.
But additional research showed this abnormality was a result of storing blood samples at room temperature for hours, or even days, prior to processing.
Heidi Dvinge, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, and her colleagues reported these findings in PNAS.
The investigators had searched databases to collect genomic information on leukemia patients and healthy control subjects. In all but one of the datasets they analyzed, the team found high levels of abnormal RNA in leukemia cells.
Another finding was that samples from pediatric leukemia patients had the highest levels of abnormal RNA. And this led the researchers to speculate about the cause.
They realized that pediatric leukemias are rare, so blood samples can be difficult to obtain. Therefore, the samples in the databases were collected at facilities throughout the world and shipped to where they were needed. So the samples could be stored at room temperature for days at a time.
To confirm that this practice can affect blood samples, the investigators conducted an experiment. They collected samples from 4 healthy subjects (2 men and 2 women) and looked for differences between samples that were processed immediately and samples that sat in the lab at room temperature for up to 48 hours.
Sure enough, the team observed changes in the stored samples, even if they were only stored for 4 hours. Stored samples exhibited biased activation of biological pathways and upregulation of pseudogenes, antisense RNAs, and unannotated coding isoforms.
Storage affected a number of genes that play roles in biological pathways relevant to leukemia, including cytokine production, NF-κB signaling, chromatin modification, and RNA splicing. Additionally, storage inhibited RNA surveillance, leading to the genome-wide expression of normally degraded RNAs.
The researchers said these findings coincide with the database findings, as they observed inhibited RNA surveillance in all but one of the datasets they analyzed.
The samples from that dataset were processed immediately after collection. And samples from healthy subjects were processed immediately, which explains why those samples were normal as well.
The team also noted that they did not observe inhibited RNA surveillance in lymphoma or solid tumor datasets.
These results suggest previous research utilizing these types of databases may contain errors, and future work making use of these databases could be affected as well.
Fortunately, the investigators found that putting blood samples on ice can prevent the negative effects they observed. The group also identified biomarkers that indicate prolonged storage, so researchers can look for those biomarkers if chilling blood samples is not an option.
In addition to describing these findings in PNAS, Dr Dvinge and her colleagues are planning to present their work at the upcoming ASH Annual Meeting. ![]()
Credit: Graham Colm
Storing blood samples at room temperature can induce changes that may cloud research findings, according to a group of investigators.
The team initially found that blood samples from leukemia patients had high levels of malformed RNA, a discovery they believed could explain leukemia’s origins.
But additional research showed this abnormality was a result of storing blood samples at room temperature for hours, or even days, prior to processing.
Heidi Dvinge, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, and her colleagues reported these findings in PNAS.
The investigators had searched databases to collect genomic information on leukemia patients and healthy control subjects. In all but one of the datasets they analyzed, the team found high levels of abnormal RNA in leukemia cells.
Another finding was that samples from pediatric leukemia patients had the highest levels of abnormal RNA. And this led the researchers to speculate about the cause.
They realized that pediatric leukemias are rare, so blood samples can be difficult to obtain. Therefore, the samples in the databases were collected at facilities throughout the world and shipped to where they were needed. So the samples could be stored at room temperature for days at a time.
To confirm that this practice can affect blood samples, the investigators conducted an experiment. They collected samples from 4 healthy subjects (2 men and 2 women) and looked for differences between samples that were processed immediately and samples that sat in the lab at room temperature for up to 48 hours.
Sure enough, the team observed changes in the stored samples, even if they were only stored for 4 hours. Stored samples exhibited biased activation of biological pathways and upregulation of pseudogenes, antisense RNAs, and unannotated coding isoforms.
Storage affected a number of genes that play roles in biological pathways relevant to leukemia, including cytokine production, NF-κB signaling, chromatin modification, and RNA splicing. Additionally, storage inhibited RNA surveillance, leading to the genome-wide expression of normally degraded RNAs.
The researchers said these findings coincide with the database findings, as they observed inhibited RNA surveillance in all but one of the datasets they analyzed.
The samples from that dataset were processed immediately after collection. And samples from healthy subjects were processed immediately, which explains why those samples were normal as well.
The team also noted that they did not observe inhibited RNA surveillance in lymphoma or solid tumor datasets.
These results suggest previous research utilizing these types of databases may contain errors, and future work making use of these databases could be affected as well.
Fortunately, the investigators found that putting blood samples on ice can prevent the negative effects they observed. The group also identified biomarkers that indicate prolonged storage, so researchers can look for those biomarkers if chilling blood samples is not an option.
In addition to describing these findings in PNAS, Dr Dvinge and her colleagues are planning to present their work at the upcoming ASH Annual Meeting. ![]()
Credit: Graham Colm
Storing blood samples at room temperature can induce changes that may cloud research findings, according to a group of investigators.
The team initially found that blood samples from leukemia patients had high levels of malformed RNA, a discovery they believed could explain leukemia’s origins.
But additional research showed this abnormality was a result of storing blood samples at room temperature for hours, or even days, prior to processing.
Heidi Dvinge, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, and her colleagues reported these findings in PNAS.
The investigators had searched databases to collect genomic information on leukemia patients and healthy control subjects. In all but one of the datasets they analyzed, the team found high levels of abnormal RNA in leukemia cells.
Another finding was that samples from pediatric leukemia patients had the highest levels of abnormal RNA. And this led the researchers to speculate about the cause.
They realized that pediatric leukemias are rare, so blood samples can be difficult to obtain. Therefore, the samples in the databases were collected at facilities throughout the world and shipped to where they were needed. So the samples could be stored at room temperature for days at a time.
To confirm that this practice can affect blood samples, the investigators conducted an experiment. They collected samples from 4 healthy subjects (2 men and 2 women) and looked for differences between samples that were processed immediately and samples that sat in the lab at room temperature for up to 48 hours.
Sure enough, the team observed changes in the stored samples, even if they were only stored for 4 hours. Stored samples exhibited biased activation of biological pathways and upregulation of pseudogenes, antisense RNAs, and unannotated coding isoforms.
Storage affected a number of genes that play roles in biological pathways relevant to leukemia, including cytokine production, NF-κB signaling, chromatin modification, and RNA splicing. Additionally, storage inhibited RNA surveillance, leading to the genome-wide expression of normally degraded RNAs.
The researchers said these findings coincide with the database findings, as they observed inhibited RNA surveillance in all but one of the datasets they analyzed.
The samples from that dataset were processed immediately after collection. And samples from healthy subjects were processed immediately, which explains why those samples were normal as well.
The team also noted that they did not observe inhibited RNA surveillance in lymphoma or solid tumor datasets.
These results suggest previous research utilizing these types of databases may contain errors, and future work making use of these databases could be affected as well.
Fortunately, the investigators found that putting blood samples on ice can prevent the negative effects they observed. The group also identified biomarkers that indicate prolonged storage, so researchers can look for those biomarkers if chilling blood samples is not an option.
In addition to describing these findings in PNAS, Dr Dvinge and her colleagues are planning to present their work at the upcoming ASH Annual Meeting. ![]()
Sharing research with public prompts more citations

Credit: Rhoda Baer
Academic researchers who talk to the press and use social media are more likely than their less communicative peers to have their work cited, a new study suggests.
The research revealed a connection between h-index—a measure of the quality of a researcher’s work and influence—and whether the scientists interact with reporters and get mentioned on Twitter.
The results appear in Journalism & Mass Communications Quarterly.
“I’ve been in science communication for a while now, and I am really seeing a change—especially among the younger scientists—in their willingness to share their work,” said study author Dominique Brossard, PhD, of the University of Wisconsin-Madison.
Attention from reporters is good news for h-index, Dr Brossard noted. But couple that with attention on Twitter, and you see a more pronounced spike in reputation.
“If you talk to reporters and you tweet about your research, your work is more likely to be cited than people who do one or the other,” she said.
That sort of activity hasn’t always been encouraged, Dr Brossard pointed out. Any distraction from a researcher’s work can draw criticism as a waste of a precious resource. But Dr Brossard hopes a new understanding of the relationship between research and communicating with the public can change that.
“What this shows us is that sharing your science with the public is not hurting the science by stealing time,” she said. “If the goal is to encourage people, ultimately, to be productive scientists, and if directors of labs are discouraging people from engaging in this activity, they’re actually hurting the science itself. Because people who do this are cited more often in scientific journals, [and] they’re making science accessible to broader audiences at the same time.”
Social media use is rising in other professional circles as well, according to Michael Xenos, PhD, also of the University of Wisconsin-Madison.
“As in other areas, such as politics for example, social media was once met with skepticism but is increasingly part of the culture,” he said. “Just like it became the norm there, our research shows it may one day become the norm in science.”
Even if you flip the connection between social media attention and h-index on its head, it’s still worth taking to heart, according to the researchers.
“The counter argument is that it may be just the other way around—that it may just be the big names that get mentions,” said study author Dietram A. Scheufele, PhD, also of the University of Wisconsin-Madison.
“But then, the lesson should be that the most successful people in your field are also the ones that are good at getting outside the ivory tower. That should be something to emulate.” ![]()
Credit: Rhoda Baer
Academic researchers who talk to the press and use social media are more likely than their less communicative peers to have their work cited, a new study suggests.
The research revealed a connection between h-index—a measure of the quality of a researcher’s work and influence—and whether the scientists interact with reporters and get mentioned on Twitter.
The results appear in Journalism & Mass Communications Quarterly.
“I’ve been in science communication for a while now, and I am really seeing a change—especially among the younger scientists—in their willingness to share their work,” said study author Dominique Brossard, PhD, of the University of Wisconsin-Madison.
Attention from reporters is good news for h-index, Dr Brossard noted. But couple that with attention on Twitter, and you see a more pronounced spike in reputation.
“If you talk to reporters and you tweet about your research, your work is more likely to be cited than people who do one or the other,” she said.
That sort of activity hasn’t always been encouraged, Dr Brossard pointed out. Any distraction from a researcher’s work can draw criticism as a waste of a precious resource. But Dr Brossard hopes a new understanding of the relationship between research and communicating with the public can change that.
“What this shows us is that sharing your science with the public is not hurting the science by stealing time,” she said. “If the goal is to encourage people, ultimately, to be productive scientists, and if directors of labs are discouraging people from engaging in this activity, they’re actually hurting the science itself. Because people who do this are cited more often in scientific journals, [and] they’re making science accessible to broader audiences at the same time.”
Social media use is rising in other professional circles as well, according to Michael Xenos, PhD, also of the University of Wisconsin-Madison.
“As in other areas, such as politics for example, social media was once met with skepticism but is increasingly part of the culture,” he said. “Just like it became the norm there, our research shows it may one day become the norm in science.”
Even if you flip the connection between social media attention and h-index on its head, it’s still worth taking to heart, according to the researchers.
“The counter argument is that it may be just the other way around—that it may just be the big names that get mentions,” said study author Dietram A. Scheufele, PhD, also of the University of Wisconsin-Madison.
“But then, the lesson should be that the most successful people in your field are also the ones that are good at getting outside the ivory tower. That should be something to emulate.” ![]()
Credit: Rhoda Baer
Academic researchers who talk to the press and use social media are more likely than their less communicative peers to have their work cited, a new study suggests.
The research revealed a connection between h-index—a measure of the quality of a researcher’s work and influence—and whether the scientists interact with reporters and get mentioned on Twitter.
The results appear in Journalism & Mass Communications Quarterly.
“I’ve been in science communication for a while now, and I am really seeing a change—especially among the younger scientists—in their willingness to share their work,” said study author Dominique Brossard, PhD, of the University of Wisconsin-Madison.
Attention from reporters is good news for h-index, Dr Brossard noted. But couple that with attention on Twitter, and you see a more pronounced spike in reputation.
“If you talk to reporters and you tweet about your research, your work is more likely to be cited than people who do one or the other,” she said.
That sort of activity hasn’t always been encouraged, Dr Brossard pointed out. Any distraction from a researcher’s work can draw criticism as a waste of a precious resource. But Dr Brossard hopes a new understanding of the relationship between research and communicating with the public can change that.
“What this shows us is that sharing your science with the public is not hurting the science by stealing time,” she said. “If the goal is to encourage people, ultimately, to be productive scientists, and if directors of labs are discouraging people from engaging in this activity, they’re actually hurting the science itself. Because people who do this are cited more often in scientific journals, [and] they’re making science accessible to broader audiences at the same time.”
Social media use is rising in other professional circles as well, according to Michael Xenos, PhD, also of the University of Wisconsin-Madison.
“As in other areas, such as politics for example, social media was once met with skepticism but is increasingly part of the culture,” he said. “Just like it became the norm there, our research shows it may one day become the norm in science.”
Even if you flip the connection between social media attention and h-index on its head, it’s still worth taking to heart, according to the researchers.
“The counter argument is that it may be just the other way around—that it may just be the big names that get mentions,” said study author Dietram A. Scheufele, PhD, also of the University of Wisconsin-Madison.
“But then, the lesson should be that the most successful people in your field are also the ones that are good at getting outside the ivory tower. That should be something to emulate.” ![]()
Hospice cuts cost and use of care for cancer patients

Credit: CDC
Patients with advanced cancer receive less aggressive care and have lower healthcare costs during their last year of life if they use hospice care, according to research published in JAMA.
Patients who entered hospice had significantly lower rates of hospitalization, intensive care unit admissions, and invasive procedures, compared to patients who did not enter hospice.
Furthermore, patients who chose hospice were about 5 times less likely to die in hospitals and nursing homes.
“Our study shows very clearly that hospice matters,” said Ziad Obermeyer, MD, of Brigham and Women’s Hospital in Boston.
“Hospice and non-hospice patients had very similar patterns of healthcare utilization right up until the week of hospice enrollment. Then, the care started to look very different. Patients who didn’t enroll in hospice ended up with far more aggressive care in their last year of life, most of it related to acute complications like infections and organ failure, and not directly related to their cancer diagnosis.”
To conduct this study, Dr Obermeyer and his colleagues used data from Medicare beneficiaries with poor-prognosis cancers, including hematologic malignancies. The study included a nationally representative 20% sample of Medicare fee-for-service beneficiaries who died in 2011.
Among 86,851 patients, 51,924 (60%) entered hospice before death. Matching patients based on various criteria produced hospice and non-hospice groups, each with 18,165 patients. The median hospice duration was 11 days.
The researchers found that non-hospice patients had significantly greater healthcare utilization, largely for acute conditions not directly related to cancer.
This included rates of hospitalization (65% vs 42%), intensive care unit admissions (36% vs 15%), invasive procedures (51% vs 27%), and death in a hospital or nursing facility (74% vs 14%).
The costs of care for hospice and non-hospice patients were not significantly different before hospice care began. But they diverged sharply thereafter, contributing to a significant difference in total costs of $8697 over the last year of life—$71,517 for non-hospice patients and $62,819 for hospice patients.
“These findings highlight the importance of honest discussions between doctors and patients about our patients’ goals of their care at the end of life, relating to treatment decisions and quality of life,” Dr Obermeyer said. “This is of particular importance now, in light of the ongoing policy discussions around reimbursing providers for advance-care planning.” ![]()
Credit: CDC
Patients with advanced cancer receive less aggressive care and have lower healthcare costs during their last year of life if they use hospice care, according to research published in JAMA.
Patients who entered hospice had significantly lower rates of hospitalization, intensive care unit admissions, and invasive procedures, compared to patients who did not enter hospice.
Furthermore, patients who chose hospice were about 5 times less likely to die in hospitals and nursing homes.
“Our study shows very clearly that hospice matters,” said Ziad Obermeyer, MD, of Brigham and Women’s Hospital in Boston.
“Hospice and non-hospice patients had very similar patterns of healthcare utilization right up until the week of hospice enrollment. Then, the care started to look very different. Patients who didn’t enroll in hospice ended up with far more aggressive care in their last year of life, most of it related to acute complications like infections and organ failure, and not directly related to their cancer diagnosis.”
To conduct this study, Dr Obermeyer and his colleagues used data from Medicare beneficiaries with poor-prognosis cancers, including hematologic malignancies. The study included a nationally representative 20% sample of Medicare fee-for-service beneficiaries who died in 2011.
Among 86,851 patients, 51,924 (60%) entered hospice before death. Matching patients based on various criteria produced hospice and non-hospice groups, each with 18,165 patients. The median hospice duration was 11 days.
The researchers found that non-hospice patients had significantly greater healthcare utilization, largely for acute conditions not directly related to cancer.
This included rates of hospitalization (65% vs 42%), intensive care unit admissions (36% vs 15%), invasive procedures (51% vs 27%), and death in a hospital or nursing facility (74% vs 14%).
The costs of care for hospice and non-hospice patients were not significantly different before hospice care began. But they diverged sharply thereafter, contributing to a significant difference in total costs of $8697 over the last year of life—$71,517 for non-hospice patients and $62,819 for hospice patients.
“These findings highlight the importance of honest discussions between doctors and patients about our patients’ goals of their care at the end of life, relating to treatment decisions and quality of life,” Dr Obermeyer said. “This is of particular importance now, in light of the ongoing policy discussions around reimbursing providers for advance-care planning.” ![]()
Credit: CDC
Patients with advanced cancer receive less aggressive care and have lower healthcare costs during their last year of life if they use hospice care, according to research published in JAMA.
Patients who entered hospice had significantly lower rates of hospitalization, intensive care unit admissions, and invasive procedures, compared to patients who did not enter hospice.
Furthermore, patients who chose hospice were about 5 times less likely to die in hospitals and nursing homes.
“Our study shows very clearly that hospice matters,” said Ziad Obermeyer, MD, of Brigham and Women’s Hospital in Boston.
“Hospice and non-hospice patients had very similar patterns of healthcare utilization right up until the week of hospice enrollment. Then, the care started to look very different. Patients who didn’t enroll in hospice ended up with far more aggressive care in their last year of life, most of it related to acute complications like infections and organ failure, and not directly related to their cancer diagnosis.”
To conduct this study, Dr Obermeyer and his colleagues used data from Medicare beneficiaries with poor-prognosis cancers, including hematologic malignancies. The study included a nationally representative 20% sample of Medicare fee-for-service beneficiaries who died in 2011.
Among 86,851 patients, 51,924 (60%) entered hospice before death. Matching patients based on various criteria produced hospice and non-hospice groups, each with 18,165 patients. The median hospice duration was 11 days.
The researchers found that non-hospice patients had significantly greater healthcare utilization, largely for acute conditions not directly related to cancer.
This included rates of hospitalization (65% vs 42%), intensive care unit admissions (36% vs 15%), invasive procedures (51% vs 27%), and death in a hospital or nursing facility (74% vs 14%).
The costs of care for hospice and non-hospice patients were not significantly different before hospice care began. But they diverged sharply thereafter, contributing to a significant difference in total costs of $8697 over the last year of life—$71,517 for non-hospice patients and $62,819 for hospice patients.
“These findings highlight the importance of honest discussions between doctors and patients about our patients’ goals of their care at the end of life, relating to treatment decisions and quality of life,” Dr Obermeyer said. “This is of particular importance now, in light of the ongoing policy discussions around reimbursing providers for advance-care planning.” ![]()
NICE supports use of catheter-positioning device

The UK’s National Institute for Health and Care Excellence (NICE) has opened consultation on a draft guidance about a device designed to help healthcare professionals correctly place peripherally inserted central catheters
(PICCs).
The draft guidance supports using the Sherlock 3CG Tip Confirmation System for placing PICCs.
The standard procedure for placing PICCs is blind insertion, followed by a chest X-ray to check the catheter’s position.
In some cases, fluoroscopy is used instead of standard X-ray to assist with positioning the PICC when placing it proves difficult.
The Sherlock system, on the other hand, uses magnetic and electrocardiographic real-time tracking of a PICC to enable the person placing the catheter to detect and correct any error in how the tip is positioned.
The device’s manufacturer, C.R. Bard, says the Sherlock System eliminates the need for the patient to have an X-ray, thus preventing delays in treatment or monitoring.
“Using the technology also increases staff and patient confidence of the accuracy of the procedure during catheter insertion,” said Professor Carole Longson, director of the NICE centre for health technology evaluation.
The cost of the Sherlock 3CG TCS is stated in the manufacturer’s submission as £9990 (excluding value-added tax). The cost of consumables associated with each insertion is £189.91. Maintenance costs associated with the technology are £595 per year.
Across the whole population in which PICCs are placed, the cost of using the Sherlock system is similar to blind insertion followed by X-ray, but it can save up to £106 per patient in specific clinical situations.
In intensive care, where PICCs are more likely to be placed incorrectly using blind insertion, the savings from using the Sherlock system and a confirmatory X-ray are estimated at around £41 per patient, compared with blind insertion and standard X-ray. (In intensive care settings, staff members sometimes initially use Sherlock with confirmatory X-ray while they are becoming accustomed to the system.)
For more information on the system, see the draft guidance consultation. It is open for public comment until December 9. {HT_DN}
The UK’s National Institute for Health and Care Excellence (NICE) has opened consultation on a draft guidance about a device designed to help healthcare professionals correctly place peripherally inserted central catheters
(PICCs).
The draft guidance supports using the Sherlock 3CG Tip Confirmation System for placing PICCs.
The standard procedure for placing PICCs is blind insertion, followed by a chest X-ray to check the catheter’s position.
In some cases, fluoroscopy is used instead of standard X-ray to assist with positioning the PICC when placing it proves difficult.
The Sherlock system, on the other hand, uses magnetic and electrocardiographic real-time tracking of a PICC to enable the person placing the catheter to detect and correct any error in how the tip is positioned.
The device’s manufacturer, C.R. Bard, says the Sherlock System eliminates the need for the patient to have an X-ray, thus preventing delays in treatment or monitoring.
“Using the technology also increases staff and patient confidence of the accuracy of the procedure during catheter insertion,” said Professor Carole Longson, director of the NICE centre for health technology evaluation.
The cost of the Sherlock 3CG TCS is stated in the manufacturer’s submission as £9990 (excluding value-added tax). The cost of consumables associated with each insertion is £189.91. Maintenance costs associated with the technology are £595 per year.
Across the whole population in which PICCs are placed, the cost of using the Sherlock system is similar to blind insertion followed by X-ray, but it can save up to £106 per patient in specific clinical situations.
In intensive care, where PICCs are more likely to be placed incorrectly using blind insertion, the savings from using the Sherlock system and a confirmatory X-ray are estimated at around £41 per patient, compared with blind insertion and standard X-ray. (In intensive care settings, staff members sometimes initially use Sherlock with confirmatory X-ray while they are becoming accustomed to the system.)
For more information on the system, see the draft guidance consultation. It is open for public comment until December 9. {HT_DN}
The UK’s National Institute for Health and Care Excellence (NICE) has opened consultation on a draft guidance about a device designed to help healthcare professionals correctly place peripherally inserted central catheters
(PICCs).
The draft guidance supports using the Sherlock 3CG Tip Confirmation System for placing PICCs.
The standard procedure for placing PICCs is blind insertion, followed by a chest X-ray to check the catheter’s position.
In some cases, fluoroscopy is used instead of standard X-ray to assist with positioning the PICC when placing it proves difficult.
The Sherlock system, on the other hand, uses magnetic and electrocardiographic real-time tracking of a PICC to enable the person placing the catheter to detect and correct any error in how the tip is positioned.
The device’s manufacturer, C.R. Bard, says the Sherlock System eliminates the need for the patient to have an X-ray, thus preventing delays in treatment or monitoring.
“Using the technology also increases staff and patient confidence of the accuracy of the procedure during catheter insertion,” said Professor Carole Longson, director of the NICE centre for health technology evaluation.
The cost of the Sherlock 3CG TCS is stated in the manufacturer’s submission as £9990 (excluding value-added tax). The cost of consumables associated with each insertion is £189.91. Maintenance costs associated with the technology are £595 per year.
Across the whole population in which PICCs are placed, the cost of using the Sherlock system is similar to blind insertion followed by X-ray, but it can save up to £106 per patient in specific clinical situations.
In intensive care, where PICCs are more likely to be placed incorrectly using blind insertion, the savings from using the Sherlock system and a confirmatory X-ray are estimated at around £41 per patient, compared with blind insertion and standard X-ray. (In intensive care settings, staff members sometimes initially use Sherlock with confirmatory X-ray while they are becoming accustomed to the system.)
For more information on the system, see the draft guidance consultation. It is open for public comment until December 9. {HT_DN}
Preop risk assessment, prophylaxis for VTE
The majority of women with gynecologic cancer will undergo surgery for their disease. Deep vein thrombosis and pulmonary embolism, or venous thromboembolic events are common, serious complications. The rate of pulmonary embolism in women with gynecologic malignancy may be as high as 6.8%, with the case fatality rate being 11%-12%. Hence, one key strategy to lower the rate of fatal pulmonary embolism depends on proper prophylaxis for deep vein thrombosis prevention.
Factors associated with the development of venous thromboembolic events (VTE) include prior VTE, malignancy, older age, African American race, prolonged operative time, and prior radiation therapy (Obstet. Gynecol. 1987;69:146-50). The risk of pulmonary embolism (PE) in women undergoing gynecologic surgery is quadrupled in the presence of malignancy (Obstet. Gynecol. 2006;107:666-71) and these patients are twice as likely to die from a VTE, compared with matched controls (Gynecol. Oncol. 2007;106:439-45). In addition, cancer patients are typically older and have longer and more complex surgeries. Furthermore, the presence of a pelvic mass further contributes to venous stasis (Obstet. Gynecol. 2012;119:155-67).

Other risk factors associated with the development of VTE include hormone replacement therapy, oral contraceptives, use of tamoxifen, and inherited thrombophilias. The most common is factor V Leiden deficiency, affecting up to 20% of patients with VTE. Affected heterozygotes have a 3- to 8-fold increased risk of VTE, whereas homozygotes have a 50- to 80-fold increased risk (Blood 1995;85:1504-8).
Depending on additional risk factors, both the American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin and guidelines published by the American College of Chest Physicians (ACCP) place women with gynecologic cancers into "high" or "highest" risk categories (Obstet. Gynecol. 2007;110:429-40; Chest 2012;141:e227S-77S).
Currently, thromboprophylaxis regimens include mechanical and pharmacologic methods. Mechanical devices include graduated compression stockings and intermittent pneumatic compression, which reduce venous stasis and may promote endogenous fibrinolysis. Pharmacologic prophylaxis includes unfractionated heparin (UFH) and low-molecular weight heparin (LMWH). Prospective controlled trials have shown that UFH reduces VTE in patients with gynecologic cancer. Trials comparing LMWH with UFH have demonstrated equivalent efficacy and similar bleeding complications. The recommended prophylactic dose for LMWH is 40 mg subcutaneous injection daily. However, this dose may need to be adjusted in morbidly obese patients (body mass index greater than 40 kg/m2) as well as in women with abnormal renal clearance. UFH should be administered as a dose of 5,000 units subcutaneously three times daily. Intermittent pneumatic compression also has been shown to reduce the incidence of VTE in this patient population.

A combined regimen of pharmacologic and mechanical prophylaxis may improve efficacy, especially in the highest-risk patients, such as women with gynecologic cancer. Although limited data exist to support this approach in gynecology patients, studies from other surgical disciplines suggest benefit from a combined regimen. With regards to addressing the timing of initiation, a large retrospective trial of patients undergoing hysterectomy for benign indications concluded that postoperative rather than preoperative administration of UFH or LMWH may reduce the risk of bleeding complications without apparent risk of increased VTE (Acta. Obstet. Gynecol. Scand. 2008;87:1039-47).
In summary, the majority of gynecologic oncology patients are considered to be at the highest risk for developing VTE. For this group of women, double prophylaxis with either UFH or LMWH, and a mechanical method (intermittent pneumatic compression) are recommended in the perioperative setting. In addition, ACCP further recommends that these patients receive extended postoperative prophylaxis with LMWH for 4 weeks. Further evidence is needed to determine acceptable timing for initiation of therapy in order to find a balance between adequate thromboprophylaxis and bleeding complications.
Dr. Roque is a fellow in the gynecologic oncology program at the University of North Carolina at Chapel Hill. Dr. Clarke-Pearson is the chair and the Robert A. Ross Distinguished Professor of Obstetrics and Gynecology and a professor in the division of gynecologic oncology at the university. Dr. Roque and Dr. Clarke-Pearson said they had no relevant disclosures. Scan this QR code or go to obgynnews.com to view similar columns.
The majority of women with gynecologic cancer will undergo surgery for their disease. Deep vein thrombosis and pulmonary embolism, or venous thromboembolic events are common, serious complications. The rate of pulmonary embolism in women with gynecologic malignancy may be as high as 6.8%, with the case fatality rate being 11%-12%. Hence, one key strategy to lower the rate of fatal pulmonary embolism depends on proper prophylaxis for deep vein thrombosis prevention.
Factors associated with the development of venous thromboembolic events (VTE) include prior VTE, malignancy, older age, African American race, prolonged operative time, and prior radiation therapy (Obstet. Gynecol. 1987;69:146-50). The risk of pulmonary embolism (PE) in women undergoing gynecologic surgery is quadrupled in the presence of malignancy (Obstet. Gynecol. 2006;107:666-71) and these patients are twice as likely to die from a VTE, compared with matched controls (Gynecol. Oncol. 2007;106:439-45). In addition, cancer patients are typically older and have longer and more complex surgeries. Furthermore, the presence of a pelvic mass further contributes to venous stasis (Obstet. Gynecol. 2012;119:155-67).
Other risk factors associated with the development of VTE include hormone replacement therapy, oral contraceptives, use of tamoxifen, and inherited thrombophilias. The most common is factor V Leiden deficiency, affecting up to 20% of patients with VTE. Affected heterozygotes have a 3- to 8-fold increased risk of VTE, whereas homozygotes have a 50- to 80-fold increased risk (Blood 1995;85:1504-8).
Depending on additional risk factors, both the American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin and guidelines published by the American College of Chest Physicians (ACCP) place women with gynecologic cancers into "high" or "highest" risk categories (Obstet. Gynecol. 2007;110:429-40; Chest 2012;141:e227S-77S).
Currently, thromboprophylaxis regimens include mechanical and pharmacologic methods. Mechanical devices include graduated compression stockings and intermittent pneumatic compression, which reduce venous stasis and may promote endogenous fibrinolysis. Pharmacologic prophylaxis includes unfractionated heparin (UFH) and low-molecular weight heparin (LMWH). Prospective controlled trials have shown that UFH reduces VTE in patients with gynecologic cancer. Trials comparing LMWH with UFH have demonstrated equivalent efficacy and similar bleeding complications. The recommended prophylactic dose for LMWH is 40 mg subcutaneous injection daily. However, this dose may need to be adjusted in morbidly obese patients (body mass index greater than 40 kg/m2) as well as in women with abnormal renal clearance. UFH should be administered as a dose of 5,000 units subcutaneously three times daily. Intermittent pneumatic compression also has been shown to reduce the incidence of VTE in this patient population.
A combined regimen of pharmacologic and mechanical prophylaxis may improve efficacy, especially in the highest-risk patients, such as women with gynecologic cancer. Although limited data exist to support this approach in gynecology patients, studies from other surgical disciplines suggest benefit from a combined regimen. With regards to addressing the timing of initiation, a large retrospective trial of patients undergoing hysterectomy for benign indications concluded that postoperative rather than preoperative administration of UFH or LMWH may reduce the risk of bleeding complications without apparent risk of increased VTE (Acta. Obstet. Gynecol. Scand. 2008;87:1039-47).
In summary, the majority of gynecologic oncology patients are considered to be at the highest risk for developing VTE. For this group of women, double prophylaxis with either UFH or LMWH, and a mechanical method (intermittent pneumatic compression) are recommended in the perioperative setting. In addition, ACCP further recommends that these patients receive extended postoperative prophylaxis with LMWH for 4 weeks. Further evidence is needed to determine acceptable timing for initiation of therapy in order to find a balance between adequate thromboprophylaxis and bleeding complications.
Dr. Roque is a fellow in the gynecologic oncology program at the University of North Carolina at Chapel Hill. Dr. Clarke-Pearson is the chair and the Robert A. Ross Distinguished Professor of Obstetrics and Gynecology and a professor in the division of gynecologic oncology at the university. Dr. Roque and Dr. Clarke-Pearson said they had no relevant disclosures. Scan this QR code or go to obgynnews.com to view similar columns.
The majority of women with gynecologic cancer will undergo surgery for their disease. Deep vein thrombosis and pulmonary embolism, or venous thromboembolic events are common, serious complications. The rate of pulmonary embolism in women with gynecologic malignancy may be as high as 6.8%, with the case fatality rate being 11%-12%. Hence, one key strategy to lower the rate of fatal pulmonary embolism depends on proper prophylaxis for deep vein thrombosis prevention.
Factors associated with the development of venous thromboembolic events (VTE) include prior VTE, malignancy, older age, African American race, prolonged operative time, and prior radiation therapy (Obstet. Gynecol. 1987;69:146-50). The risk of pulmonary embolism (PE) in women undergoing gynecologic surgery is quadrupled in the presence of malignancy (Obstet. Gynecol. 2006;107:666-71) and these patients are twice as likely to die from a VTE, compared with matched controls (Gynecol. Oncol. 2007;106:439-45). In addition, cancer patients are typically older and have longer and more complex surgeries. Furthermore, the presence of a pelvic mass further contributes to venous stasis (Obstet. Gynecol. 2012;119:155-67).
Other risk factors associated with the development of VTE include hormone replacement therapy, oral contraceptives, use of tamoxifen, and inherited thrombophilias. The most common is factor V Leiden deficiency, affecting up to 20% of patients with VTE. Affected heterozygotes have a 3- to 8-fold increased risk of VTE, whereas homozygotes have a 50- to 80-fold increased risk (Blood 1995;85:1504-8).
Depending on additional risk factors, both the American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin and guidelines published by the American College of Chest Physicians (ACCP) place women with gynecologic cancers into "high" or "highest" risk categories (Obstet. Gynecol. 2007;110:429-40; Chest 2012;141:e227S-77S).
Currently, thromboprophylaxis regimens include mechanical and pharmacologic methods. Mechanical devices include graduated compression stockings and intermittent pneumatic compression, which reduce venous stasis and may promote endogenous fibrinolysis. Pharmacologic prophylaxis includes unfractionated heparin (UFH) and low-molecular weight heparin (LMWH). Prospective controlled trials have shown that UFH reduces VTE in patients with gynecologic cancer. Trials comparing LMWH with UFH have demonstrated equivalent efficacy and similar bleeding complications. The recommended prophylactic dose for LMWH is 40 mg subcutaneous injection daily. However, this dose may need to be adjusted in morbidly obese patients (body mass index greater than 40 kg/m2) as well as in women with abnormal renal clearance. UFH should be administered as a dose of 5,000 units subcutaneously three times daily. Intermittent pneumatic compression also has been shown to reduce the incidence of VTE in this patient population.
A combined regimen of pharmacologic and mechanical prophylaxis may improve efficacy, especially in the highest-risk patients, such as women with gynecologic cancer. Although limited data exist to support this approach in gynecology patients, studies from other surgical disciplines suggest benefit from a combined regimen. With regards to addressing the timing of initiation, a large retrospective trial of patients undergoing hysterectomy for benign indications concluded that postoperative rather than preoperative administration of UFH or LMWH may reduce the risk of bleeding complications without apparent risk of increased VTE (Acta. Obstet. Gynecol. Scand. 2008;87:1039-47).
In summary, the majority of gynecologic oncology patients are considered to be at the highest risk for developing VTE. For this group of women, double prophylaxis with either UFH or LMWH, and a mechanical method (intermittent pneumatic compression) are recommended in the perioperative setting. In addition, ACCP further recommends that these patients receive extended postoperative prophylaxis with LMWH for 4 weeks. Further evidence is needed to determine acceptable timing for initiation of therapy in order to find a balance between adequate thromboprophylaxis and bleeding complications.
Dr. Roque is a fellow in the gynecologic oncology program at the University of North Carolina at Chapel Hill. Dr. Clarke-Pearson is the chair and the Robert A. Ross Distinguished Professor of Obstetrics and Gynecology and a professor in the division of gynecologic oncology at the university. Dr. Roque and Dr. Clarke-Pearson said they had no relevant disclosures. Scan this QR code or go to obgynnews.com to view similar columns.

Utilization of the ICF-CY for the Classification of Therapeutic Objectives in the Treatment of Spasticity in Children with Cerebral Palsy
From the IRCCS Institute of Neurological Sciences, Bellaria Hospital, Bologna, Italy.
Abstract
- Objective: To identify objectives for treatment of spasticity with botulinum toxin type A (BTX) in children with cerebral palsy (CP), standardize the objectives according to typology, and classify them according to the International Classification of Functioning for Children and Youth (ICF-CY), as well as to analyze treatment goals in relationship to CP clinical type, severity level, and age.
- Methods: 188 children were included in the study (mean age, 12 years; 42% female, 58% male). The diplegic type made up 38% of CP cases, the tetraplegic type 35%, and the hemiplegic type 24%. Children were mainly classified in the lowest and highest levels in the Gross Motor Function Classification System (GMFCS 1, 39%; GMFCS 5, 26%). Treatment objectives for individual therapies were discussed, identified, and transcribed in the therapeutic proposals. The objectives were then collected and subjected to an internal audit in order to standardize their denomination. Two trained health care providers expert in the use of the ICF-CY classification mapped the objectives to ICF-CY domains and categories. The objectives were then analyzed in relationship to CP clinical type, GMFCS level, and age.
- Results: Of the objectives, 88% (246) were in the “Body Functions” domain. In this domain, there were 28 typologies of objectives in 6 categories. Only 12% (32) of the objectives were in the “Activity” domain; there were 11 typologies in 5 categories. In diplegic and hemiplegic patients with mild disability (GMFCS 1), objectives were aimed at improving gait pattern. For quadriplegic patients with severe disability (GMFCS 5), objectives were aimed mainly at controlling deformities and improving health care provision. Objectives concerning pain treatment were proposed principally for patients with diplegic and quadriplegic type CP.
- Conclusions: The ICF-CY can be used to categorize treatment objectives proposed for patient improvement in the domains of Body Functions and Activity. Goal setting for BTX injections occurs mainly in the Body Functions domain and aims at finding changes in the gait pattern.
Botulinum toxin type A (BTX) has been used for 20 years for the focal treatment of spasticity in patients with cerebral palsy (CP) [1–3]. While numerous studies have shown the functional benefits of BTX treatment, especially if carried out in combination with other treatments (eg, physiotherapy, occupational therapy, serial casting), studies that focus on the indications for BTX use are limited.
Patients with CP require rehabilitation that involves multiple disciplines and multiprofessional therapeutic programs (eg, pharmacologic, orthotic, physiotherapeutic). The complexity of both the program and the pathology requires choosing the appropriate treatment objectives. The International Classification of Functioning for Children and Youth (ICF-CY) [4] is a unified and standard language and framework for clinical, public health, and research applications to facilitate the documentation and measurement of health and disability in child and youth populations. As such, it can be used to inform clinical thinking, practice and research in the field of cerebral palsy [5], including being used as a tool for developing treatment plans and providing a common language for defining and sharing treatment objectives with patients and families [6]. Thamar et al [7] recently pointed out the value of adopting a standardized method of writing specific and measurable goals. Goals that are specific and clear are important not only for the evaluation of efficacy but also for systematic evaluation of the quality of health services [8,9].
In the literature regarding rehabilitation (especially in adults) and, more recently, in the literature on CP [10], core sets derived from ICF that are condition- and setting-specific are increasingly being used. They are used for the evaluation of the functional profiles of patients and documentation of the results of rehabilitative treatment, and also for defining the objectives of the treatment. Some authors [11–14] have explored in detail the possibility of using the core sets for formulating treatment objectives and assessing outcomes. However, using the core sets is complicated and their use in day-to-day clinical settings is limited. In a recent study, Preston et al [15] sought to define a sub-set of functional goals and outcomes relevant to patients with CP undergoing BTX treatment that could be more appropriate for use. In this retrospective analysis, they used the ICF-CY to classify treatment goals into corresponding domains and categories. The ICF-CY contains 4 major components (Body Structure, Body Function, Activities and Participation, and Environmental Factors), which each contain hierarchically arranged chapters and category levels. The authors found that the goals were mainly in the domain of “Body Functions,” specifically “functions of joint mobility” and “functions of gait pattern.” Those in the “Activity” domain were in the “walking” and “changing body positions” categories. This study was the first to focus on CP as a pathology and on the objectives of the individual therapeutic programs; other reports in the literature deal with the entire articulation of treatment. The authors limited themselves to the identification of the domain and the category of the objectives but did not report in detail their denomination. A greater degree of specificity and standardization in the description of the objectives would be useful from a practical point of view both for comparing results and for improving communication between the health care providers, and between these professionals and the families. The authors also did not assess for the various clinical types of CP.
The aim of the present study involving patients having CP and undergoing BTX injections was to identify the treatment objectives, standardize them according to denomination, classify them according to ICF-CY domains and categories, and establish their relative frequency. A further objective of the study was to analyze treatment goals in relationship to the clinical type (eg, hemiplegia, diplegia, quadriplegia), level of severity according to the Gross Motor Function Classification System (GMFCS) [16], and age.
Methods
Our center in Bologna, Italy, specializes in the evaluation and advanced treatment of spasticity in neuromotor disability in children and young adults. Between 2010 and the first half of 2012, 217 children were admitted to our center for evaluation and BTX treatment of spasticity in the upper or lower limbs or both. Of these, 188 children who had been diagnosed with spastic CP were included in the prospective study. Twenty-nine patients with other pathologies (epileptic and degenerative encephalopathy, spastic paraparesis) were excluded. The enrolled patients and their families were informed about the study and written informed consent was obtained.
Patients were evaluated from a functional point of view by 3 expert physiatrists and 2 pediatric physiotherapists for eligibility for BTX injection according to the recommendations of Ferrari and Cioni [17]. Functional assessment included evaluation of impairments (spasticity, contractures, deformities), main motor functions (gait pattern, manipulation pattern), and capacity of carrying out the principal motor activities (walking, maintaining and changing body position, rolling, use of upper limbs), thus enabling the identification of specific and realistic objectives for treatment with BTX. The objectives were chosen by a physiatrist and a physiotherapist, shared among the health care providers and the patients and their families, and added to the written treatment proposals. For each child more than 1 treatment objective could be proposed. These proposals were then collected and audited so as to obtain a uniform denomination of the proposed therapeutic objectives. In a series of meetings among all the members of the research group, the descriptions/denominations of the therapeutic goals were standardized and shared, eliminating inexact descriptions or adding new ones as needed. Two trained health care providers expert in the use of the ICF-CY classification mapped these to the ICF-CY domains and categories (up to the 2nd level of categorization). Each interpretative disagreement was resolved by group discussion. Finally, the objectives were analyzed in relationship to clinical type, severity according to GMFCS, and age. The frequency of the individual objectives, domains, and categories was evaluated by means of descriptive statistics.
Results
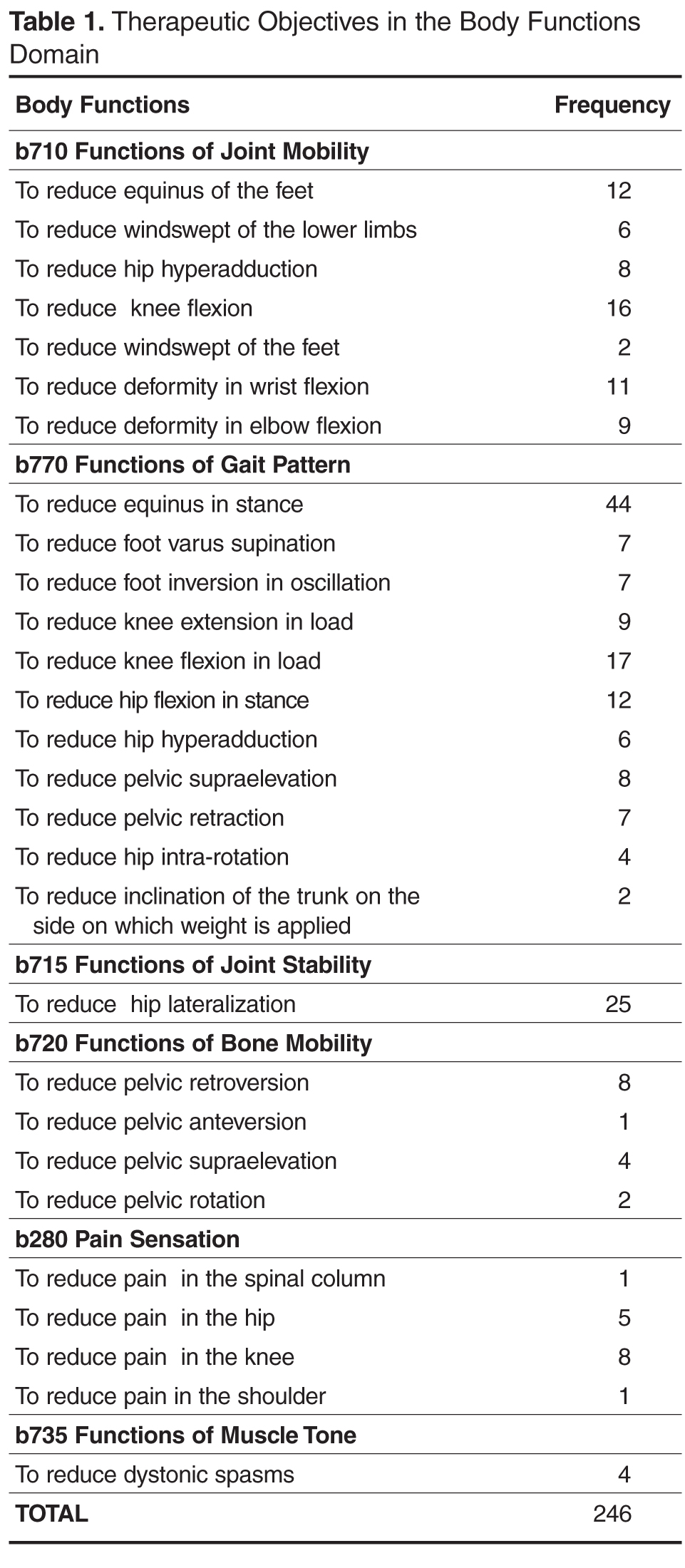
Body Functions Domain
The most represented category in the “Body Functions” domain was “b770 functions of gait pattern” (50%). There were 123 proposed objectives distributed among 11 typologies of objectives for a total of 123 proposed objectives in the functions of gait pattern category. 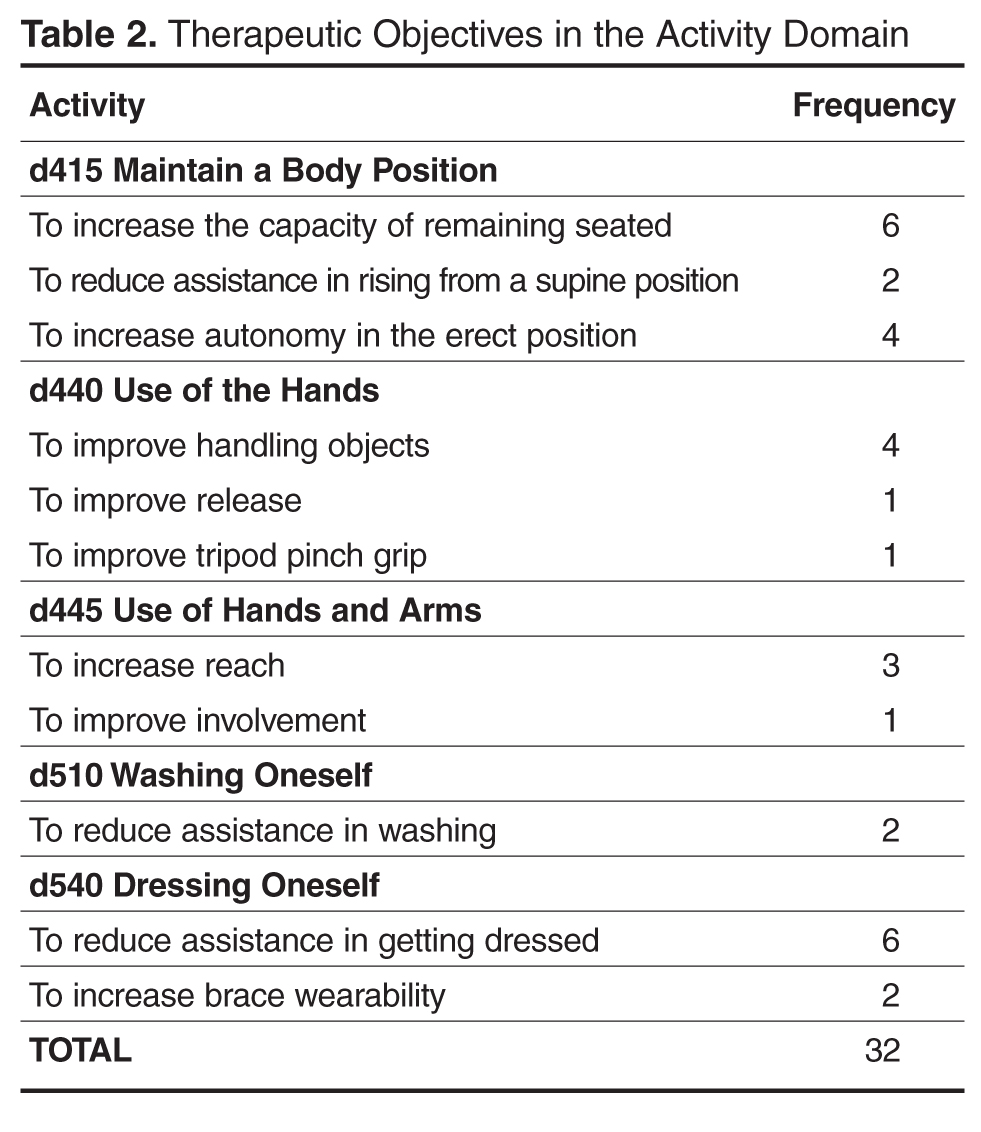
In the “b715 functions of joint stability” category, 25 objectives were proposed for controlling hip lateralization while, in the “b720 functions of bone mobility” category, 4 typologies of objectives were identified out of a total of 15 proposed objectives aimed at improving the position of the pelvis. The “b280 pain sensation” category was also used to indicate 15 objectives aiming at alleviating knee, hip and spinal column pain. Finally, 4 objectives were aimed at tone reduction.
Activity Domain
As concerns the “Activity” domain, 38% of objectives were classified into the “d415 maintain body position” category (3 typologies and a total of 12 proposals), 25% were in the “d540 dress oneself ” category (2 typologies and a total of 8 proposals), 19% were in the “d440 fine use of the hands” category (3 typologies and a total of 6 proposals), 13% were in the “d445 use of hands and arms” category (2 typologies and 4 proposals) and, 6% of cases were classified into the “d510 wash oneself” category (2 proposals) (Table 2).
Analysis by Type, Severity, and Age
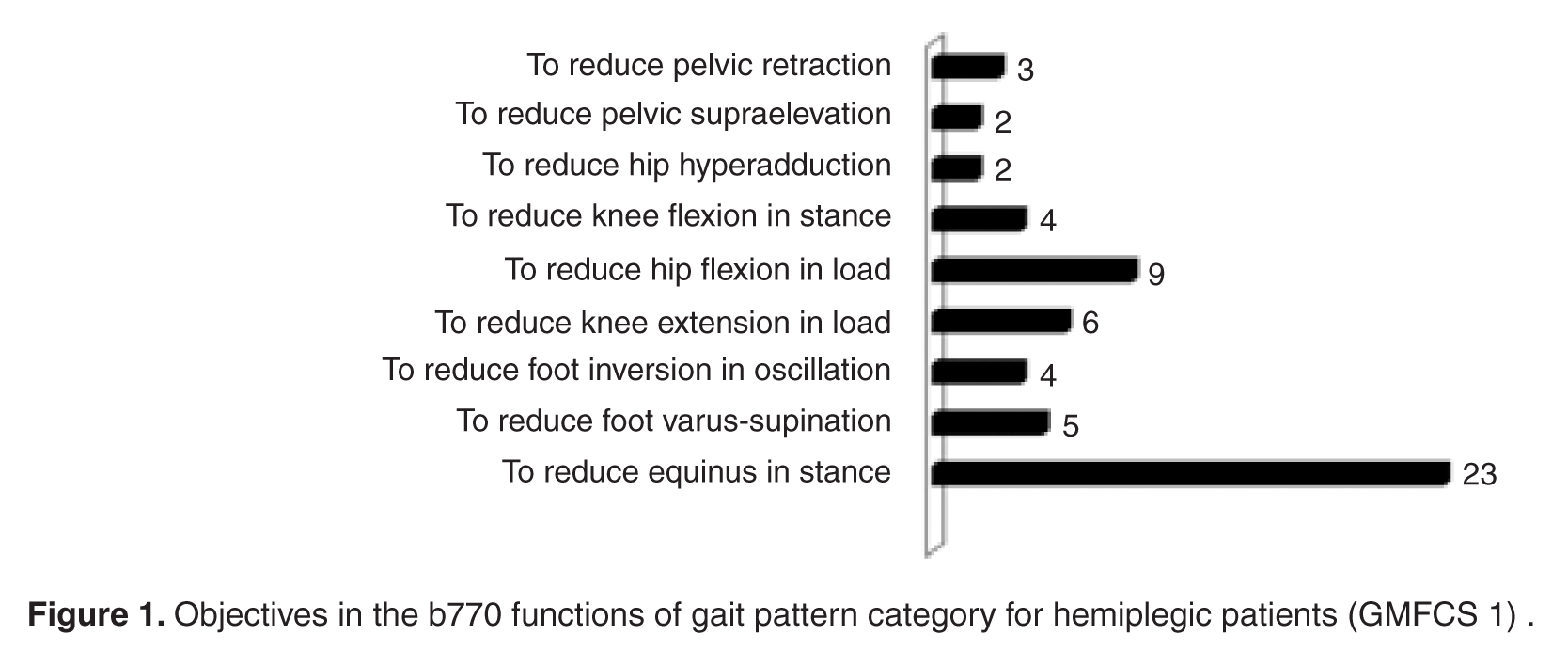
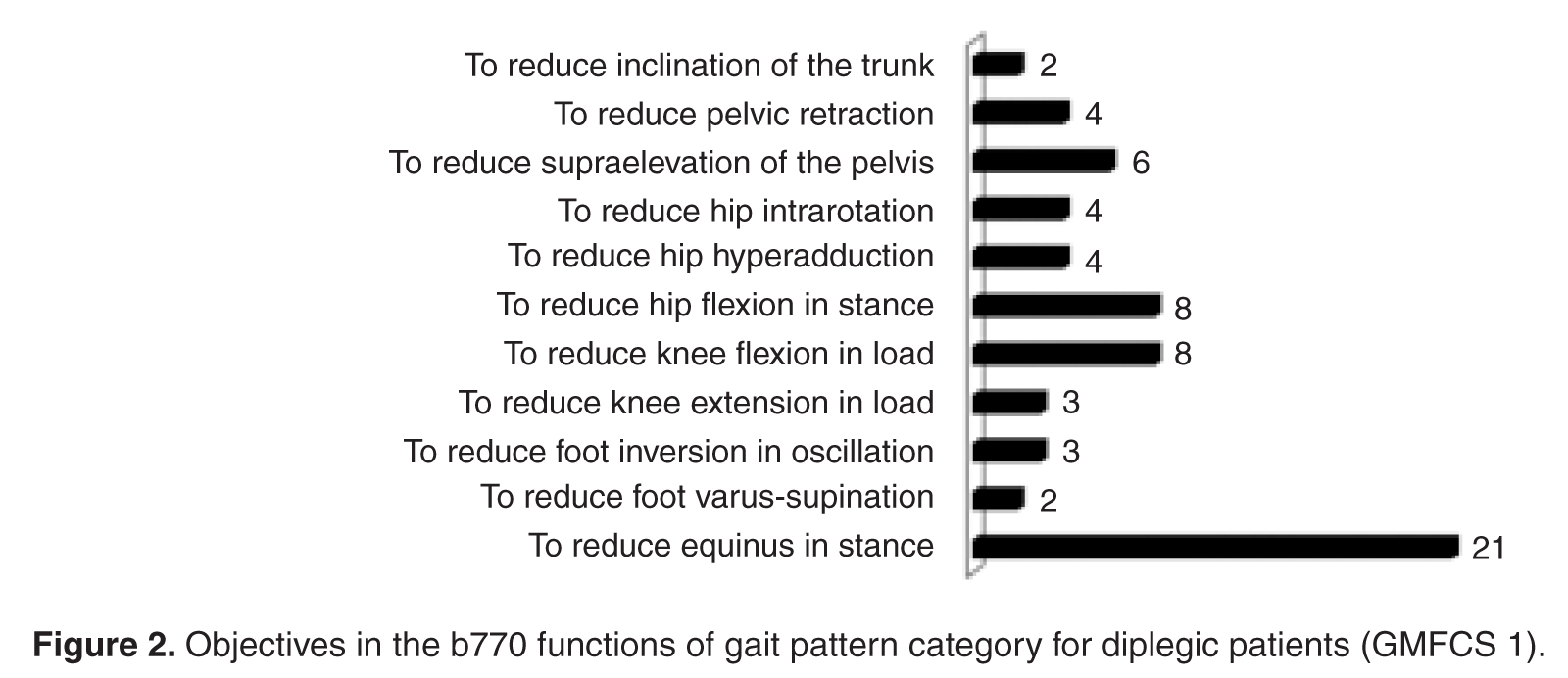
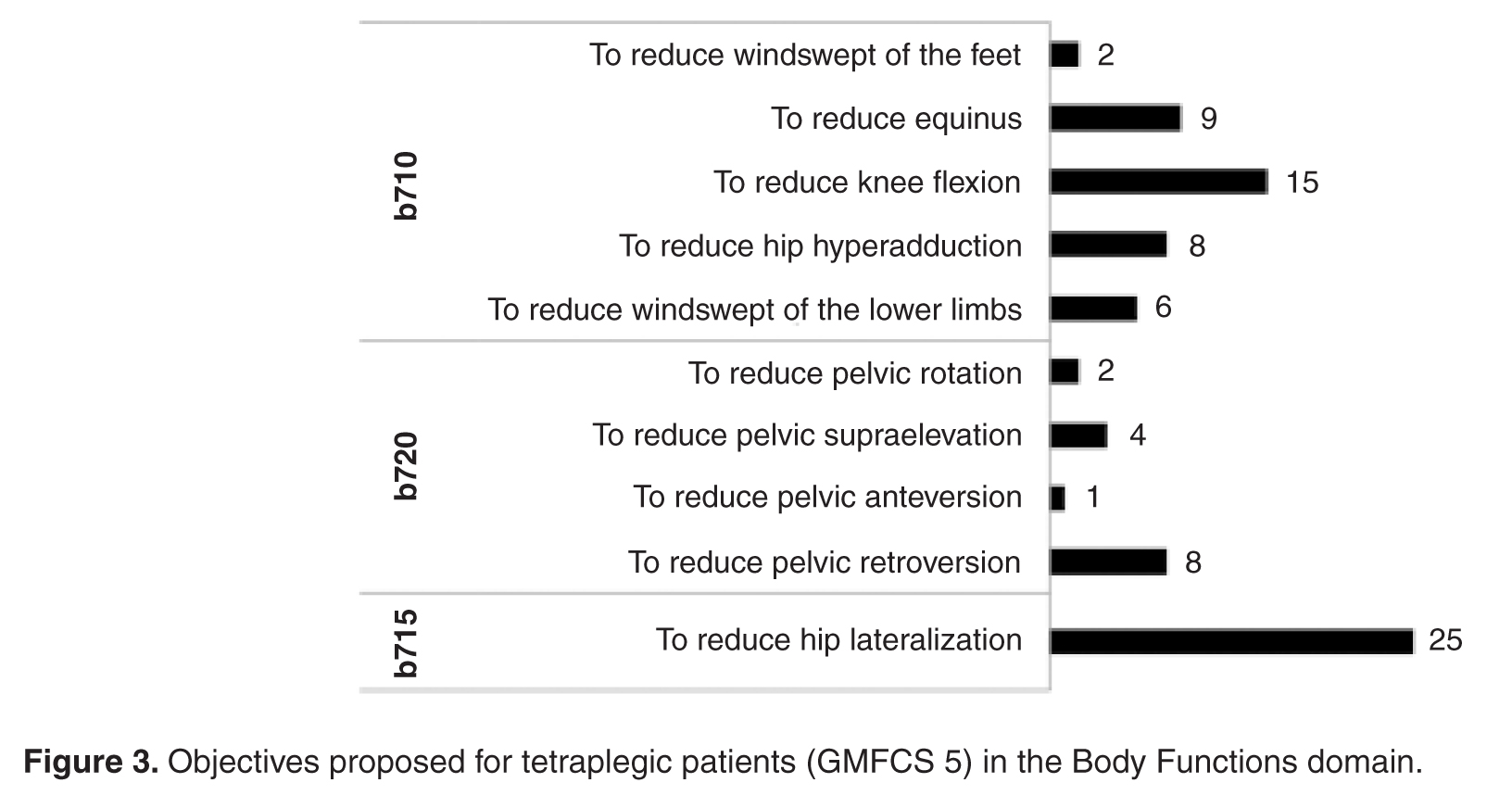
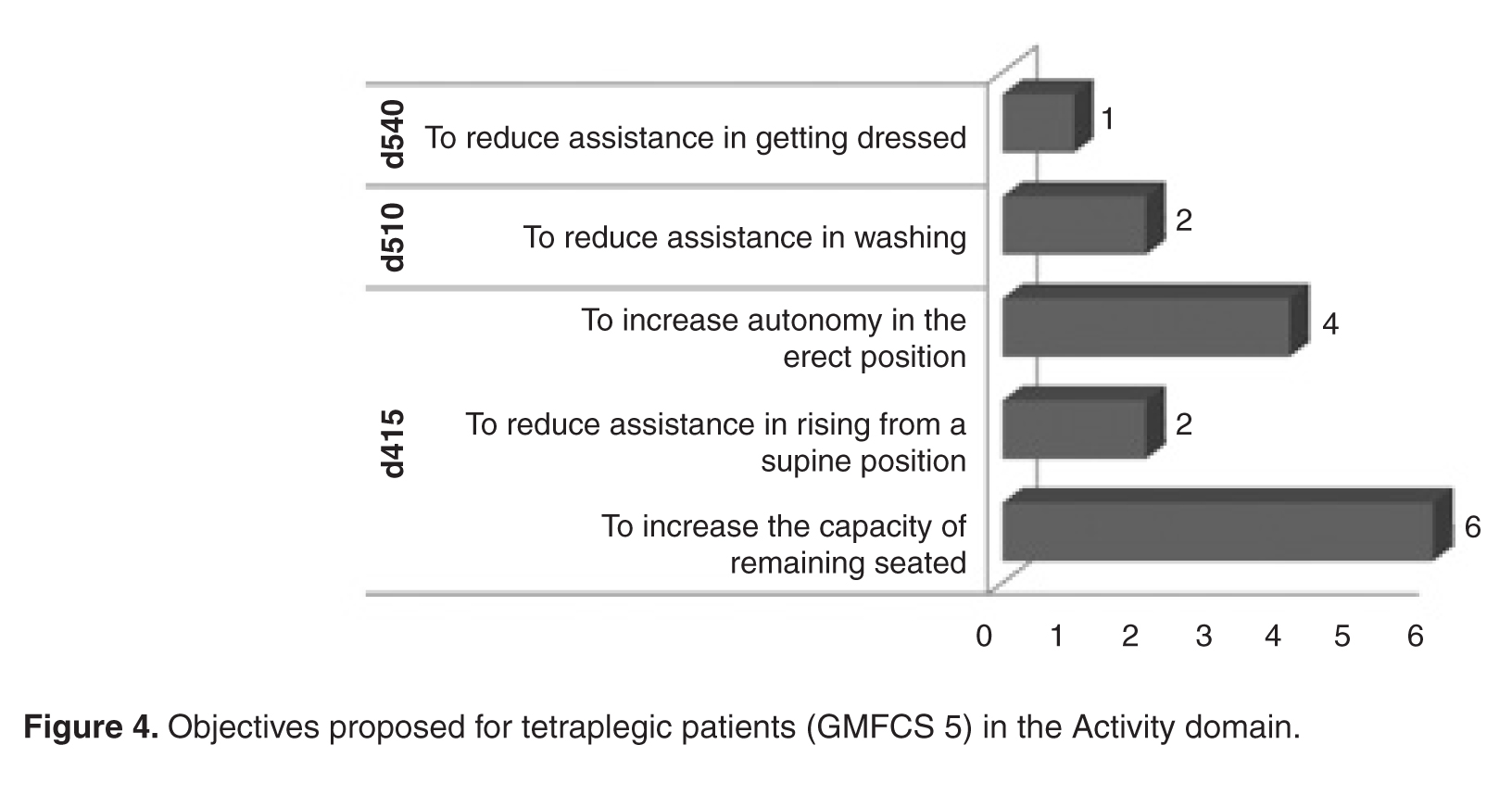
Discussion
The results show that in the majority of cases, the objectives of treatment with BTX injections proposed by our group fell within the “Body Functions” domain, in the “b770 gait pattern” and “b710 joint mobility” categories. This focus has also been reported by other authors [18]. Furthermore, these results are analogous to those reported by Preston [15]. The objectives classifiable into the “Activity” domain were more limited in our group. The most represented categories were “d415 maintain body position,” as also reported by Preston, and “d540 dressing oneself.” Preston et al reported many more objectives in the Activity domain, also utilizing the “walking” category. A possible reason is that objectives may reflect more the expectations of professionals and less those of patients. Indeed, when objectives suggested by patients and families are taken into greater consideration, goals proposed in the Activity area notably increase [19]. It is probably necessary to evaluate the objectives relevant to the professionals and those significant to the families and children separately.
The discrepancies between our data and Preston’s also most likely reflect differences in the study population. In our study, those undergoing injections aimed at improving gait pattern are, for the most part, hemiplegic and diplegic patients with mild disabilities (GMFCS 1). Their elevated degree of autonomy in mobility probably accounts for the scarcity of objectives for improving walking autonomy. In the most severe cases, such as quadriplegia, objectives are mainly aimed at controlling deformities and facilitating health care provision. Pain reduction is another important aspect and concerned quadriplegic and diplegic patients with severe disability. In contrast, objectives related to muscle tone reduction were limited, as the main objective was not a reduction but the control of muscle shortening and the subsequent deformities. However, this can become a primary objective in cases of spastic hyperactivation (eg, in adductor muscles) or in the case of dystonia, to improve patient comfort.
From a practical point of view, the use of this methodology provides for a common language that facilitates the communication and sharing of therapeutic objectives between different professionals (physiatrists and physiotherapists) and between health care providers and families and/or patients. This is important, as physiotherapy is often complementary to BTX injections and the objectives must be shared with the family. This methodology can help the clinician in the decision-making process and allows determining with greater specificity what is to be measured to document the achievement of the objectives.
Future research in this field will be aimed at evaluating patient outcomes by means of the adoption of suitable instruments (measurement scales) in order to quantify results which are consistent, according to the ICF-CY classification, with the domain and the category undergoing analysis.
Conclusion
As it has already been pointed out by various authors [10–15], the ICF-CY is a useful instrument for the classification of proposed therapeutic objectives into domains and categories, in order to standardize the language and to increase the sharing of the aims between the health care providers and between providers and families/patients. The most commonly followed approach calls for the use of functional profiles at the beginning of the care planning process, in order to establish the priorities and objectives of the interventions to be carried out. In order to streamline and facilitate procedures in clinical practice, many have proposed the use of core sets, but the validation procedure is complex and not always possible in all centers. Recently, Preston et al were the first to propose using the ICF-CY for classifying the objectives of an individual program. The procedure utilized is simple, easily reproducible, and allows identifying and classifying the objectives into categories using the ICF-CY. Furthermore, it is focused on an individual program and not on the entire articulation of programs, making interpretation of the data more linear. Our proposal is similar because it is focused on the analysis of an individual therapeutic program and because it utilizes the ICF classification system to classify the objectives; however, it achieves a higher degree of detail and standardization of the objectives.
In conclusion, the classification structure of the ICF-CY furnishes a useful and recognized instrument for categorizing the objectives of the interventions to be carried out. The classification of the objectives is specific for each pathology and for each individual program. The standardization of the objectives themselves and the use of the ICF-CY categories only for classification represents a possible methodologic alternative to the use of ICF-CY individual categories and sub-categories for identifying these objectives (core sets), as proposed by other authors. This procedure offers greater detail and a greater degree of standardization, which is important for the successive and systematic evaluation of treatment results.
Corresponding author: Nicoletta Battisti, Via Altura 3, 40139 Bologna, Italy, [email protected].
1. Lukban M, Rosales RL. Effectiveness of botulinum toxin A for upper and lower limb spasticity in children with cerebral palsy: a summary of evidence. J Neural Transm 2009;116:319–31.
2. Ryll U, Bastianen C, De Bie R, Staal B. Effects of leg muscle botulinum toxin A injections on walking in children with spasticity related cerebral palsy: a systematic review. Devel Med Child Neurol 2011;53:210–6.
3. Hoare BJ, Wallen MA,Villanueva E, et al. Botulinum toxin A as an adjunct to treatment in the management of upper limb in children with spastic cerebral palsy. The Cochraine Library 2010.
4. World Health Organization. International Classification of Functioning, Disability, and Health: Children and Youth Version for Children and Youth (ICF-CY). 2007. Available at http://apps.who.int/bookorders/anglais/detart1.jsp?codlan=1&codcol=15&codcch=716#
5. Rosenbaum P, Stewart D. The World Health Organization International Classification of Functioning Disability and Health: a model to guide clinical thinking, practice, and research. Semin Pediatr Neurol 2004;11:5–10.
6. Steiner W, Ryser L, Huber E, et al. Use of the ICF model as a clinical problem solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002;82:1098–107.
7. Thamar JH, Bovend’Eerdt, Botell RE, Wade DT. Writing SMART rehabilitation goals and achieving goal attainment scaling: practical guide. Clin Rehab 2009;23:352–61.
8. Program outcome evaluations. United Way of Winnipeg; 2007.
9. Main K. Program design: a practical guide. Available at www.calgaryunitedway.org.
10. Schiariti V, Selb M, Cieza A, O’Donnel M. International classification of Functioning, Disability and Health Core sets for children and youth with cerebral palsy: a consensus meeting 1. Dev Med Child Neurol 2014 Aug 6. Epub ahead of print
11. Huber EO, Tobler A, Gloor-Juzzi T, et al. The ICF as a way to specify goals and assess the outcome of physiotherapeutic interventions in the acute hospitals Rehabil Med 2011;43:174–7.
12. Mittrach R, Grill E, Walchner-Bonjean M, et al. Goals of physiotherapy interventions can be described using the International Classification Of Functioning, Disability and Health Physiotherapy 2008;94:150–7.
13. Muller MJ, Strobl R, Grill E. Goals of patients with rehabilitation needs in acute hospitals: goal achievement is an indicator for improved functioning Rehabil Med 2011;43:145–50.
14. Grill E J, Stucki G. Criteria for validating comprehensive ICF core sets and developing brief ICF core set versions. J Rehabil Med 2011;43:87–91.
15. Preston NJ, Clarke M, Bhakta B. Development of a framework to define the functional goals and outcomes of botulinum toxin A spasticity treatment relevant to the child and family living with cerebral palsy using the international classification of functioning disability and health for children and youth (ICF-CY). J Rehabil Med 2011;43:1010–5.
16. Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;39:214–23.
17. Ferrari A, Cioni G. The spastic forms of cerebral palsy: a guide to the assessment of adaptive functions. Springer-Verlag; 2010.
18. Franki I, De Cat J, Deschepper E, et al. A clinical decision framework for the identification of main problems and treatment goals for ambulant children with bilateral spastic cerebral palsy. Res Dev Disabil 2014;35:1160–76.
19. Lohmann S, Decker J, Müller M, et al. The ICF forms a useful framework for classifying individual patients goals in post-acute rehabilitation. Rehabil Med 2011;43:151–5.
From the IRCCS Institute of Neurological Sciences, Bellaria Hospital, Bologna, Italy.
Abstract
- Objective: To identify objectives for treatment of spasticity with botulinum toxin type A (BTX) in children with cerebral palsy (CP), standardize the objectives according to typology, and classify them according to the International Classification of Functioning for Children and Youth (ICF-CY), as well as to analyze treatment goals in relationship to CP clinical type, severity level, and age.
- Methods: 188 children were included in the study (mean age, 12 years; 42% female, 58% male). The diplegic type made up 38% of CP cases, the tetraplegic type 35%, and the hemiplegic type 24%. Children were mainly classified in the lowest and highest levels in the Gross Motor Function Classification System (GMFCS 1, 39%; GMFCS 5, 26%). Treatment objectives for individual therapies were discussed, identified, and transcribed in the therapeutic proposals. The objectives were then collected and subjected to an internal audit in order to standardize their denomination. Two trained health care providers expert in the use of the ICF-CY classification mapped the objectives to ICF-CY domains and categories. The objectives were then analyzed in relationship to CP clinical type, GMFCS level, and age.
- Results: Of the objectives, 88% (246) were in the “Body Functions” domain. In this domain, there were 28 typologies of objectives in 6 categories. Only 12% (32) of the objectives were in the “Activity” domain; there were 11 typologies in 5 categories. In diplegic and hemiplegic patients with mild disability (GMFCS 1), objectives were aimed at improving gait pattern. For quadriplegic patients with severe disability (GMFCS 5), objectives were aimed mainly at controlling deformities and improving health care provision. Objectives concerning pain treatment were proposed principally for patients with diplegic and quadriplegic type CP.
- Conclusions: The ICF-CY can be used to categorize treatment objectives proposed for patient improvement in the domains of Body Functions and Activity. Goal setting for BTX injections occurs mainly in the Body Functions domain and aims at finding changes in the gait pattern.
Botulinum toxin type A (BTX) has been used for 20 years for the focal treatment of spasticity in patients with cerebral palsy (CP) [1–3]. While numerous studies have shown the functional benefits of BTX treatment, especially if carried out in combination with other treatments (eg, physiotherapy, occupational therapy, serial casting), studies that focus on the indications for BTX use are limited.
Patients with CP require rehabilitation that involves multiple disciplines and multiprofessional therapeutic programs (eg, pharmacologic, orthotic, physiotherapeutic). The complexity of both the program and the pathology requires choosing the appropriate treatment objectives. The International Classification of Functioning for Children and Youth (ICF-CY) [4] is a unified and standard language and framework for clinical, public health, and research applications to facilitate the documentation and measurement of health and disability in child and youth populations. As such, it can be used to inform clinical thinking, practice and research in the field of cerebral palsy [5], including being used as a tool for developing treatment plans and providing a common language for defining and sharing treatment objectives with patients and families [6]. Thamar et al [7] recently pointed out the value of adopting a standardized method of writing specific and measurable goals. Goals that are specific and clear are important not only for the evaluation of efficacy but also for systematic evaluation of the quality of health services [8,9].
In the literature regarding rehabilitation (especially in adults) and, more recently, in the literature on CP [10], core sets derived from ICF that are condition- and setting-specific are increasingly being used. They are used for the evaluation of the functional profiles of patients and documentation of the results of rehabilitative treatment, and also for defining the objectives of the treatment. Some authors [11–14] have explored in detail the possibility of using the core sets for formulating treatment objectives and assessing outcomes. However, using the core sets is complicated and their use in day-to-day clinical settings is limited. In a recent study, Preston et al [15] sought to define a sub-set of functional goals and outcomes relevant to patients with CP undergoing BTX treatment that could be more appropriate for use. In this retrospective analysis, they used the ICF-CY to classify treatment goals into corresponding domains and categories. The ICF-CY contains 4 major components (Body Structure, Body Function, Activities and Participation, and Environmental Factors), which each contain hierarchically arranged chapters and category levels. The authors found that the goals were mainly in the domain of “Body Functions,” specifically “functions of joint mobility” and “functions of gait pattern.” Those in the “Activity” domain were in the “walking” and “changing body positions” categories. This study was the first to focus on CP as a pathology and on the objectives of the individual therapeutic programs; other reports in the literature deal with the entire articulation of treatment. The authors limited themselves to the identification of the domain and the category of the objectives but did not report in detail their denomination. A greater degree of specificity and standardization in the description of the objectives would be useful from a practical point of view both for comparing results and for improving communication between the health care providers, and between these professionals and the families. The authors also did not assess for the various clinical types of CP.
The aim of the present study involving patients having CP and undergoing BTX injections was to identify the treatment objectives, standardize them according to denomination, classify them according to ICF-CY domains and categories, and establish their relative frequency. A further objective of the study was to analyze treatment goals in relationship to the clinical type (eg, hemiplegia, diplegia, quadriplegia), level of severity according to the Gross Motor Function Classification System (GMFCS) [16], and age.
Methods
Our center in Bologna, Italy, specializes in the evaluation and advanced treatment of spasticity in neuromotor disability in children and young adults. Between 2010 and the first half of 2012, 217 children were admitted to our center for evaluation and BTX treatment of spasticity in the upper or lower limbs or both. Of these, 188 children who had been diagnosed with spastic CP were included in the prospective study. Twenty-nine patients with other pathologies (epileptic and degenerative encephalopathy, spastic paraparesis) were excluded. The enrolled patients and their families were informed about the study and written informed consent was obtained.
Patients were evaluated from a functional point of view by 3 expert physiatrists and 2 pediatric physiotherapists for eligibility for BTX injection according to the recommendations of Ferrari and Cioni [17]. Functional assessment included evaluation of impairments (spasticity, contractures, deformities), main motor functions (gait pattern, manipulation pattern), and capacity of carrying out the principal motor activities (walking, maintaining and changing body position, rolling, use of upper limbs), thus enabling the identification of specific and realistic objectives for treatment with BTX. The objectives were chosen by a physiatrist and a physiotherapist, shared among the health care providers and the patients and their families, and added to the written treatment proposals. For each child more than 1 treatment objective could be proposed. These proposals were then collected and audited so as to obtain a uniform denomination of the proposed therapeutic objectives. In a series of meetings among all the members of the research group, the descriptions/denominations of the therapeutic goals were standardized and shared, eliminating inexact descriptions or adding new ones as needed. Two trained health care providers expert in the use of the ICF-CY classification mapped these to the ICF-CY domains and categories (up to the 2nd level of categorization). Each interpretative disagreement was resolved by group discussion. Finally, the objectives were analyzed in relationship to clinical type, severity according to GMFCS, and age. The frequency of the individual objectives, domains, and categories was evaluated by means of descriptive statistics.
Results
Body Functions Domain
The most represented category in the “Body Functions” domain was “b770 functions of gait pattern” (50%). There were 123 proposed objectives distributed among 11 typologies of objectives for a total of 123 proposed objectives in the functions of gait pattern category.
In the “b715 functions of joint stability” category, 25 objectives were proposed for controlling hip lateralization while, in the “b720 functions of bone mobility” category, 4 typologies of objectives were identified out of a total of 15 proposed objectives aimed at improving the position of the pelvis. The “b280 pain sensation” category was also used to indicate 15 objectives aiming at alleviating knee, hip and spinal column pain. Finally, 4 objectives were aimed at tone reduction.
Activity Domain
As concerns the “Activity” domain, 38% of objectives were classified into the “d415 maintain body position” category (3 typologies and a total of 12 proposals), 25% were in the “d540 dress oneself ” category (2 typologies and a total of 8 proposals), 19% were in the “d440 fine use of the hands” category (3 typologies and a total of 6 proposals), 13% were in the “d445 use of hands and arms” category (2 typologies and 4 proposals) and, 6% of cases were classified into the “d510 wash oneself” category (2 proposals) (Table 2).
Analysis by Type, Severity, and Age
Discussion
The results show that in the majority of cases, the objectives of treatment with BTX injections proposed by our group fell within the “Body Functions” domain, in the “b770 gait pattern” and “b710 joint mobility” categories. This focus has also been reported by other authors [18]. Furthermore, these results are analogous to those reported by Preston [15]. The objectives classifiable into the “Activity” domain were more limited in our group. The most represented categories were “d415 maintain body position,” as also reported by Preston, and “d540 dressing oneself.” Preston et al reported many more objectives in the Activity domain, also utilizing the “walking” category. A possible reason is that objectives may reflect more the expectations of professionals and less those of patients. Indeed, when objectives suggested by patients and families are taken into greater consideration, goals proposed in the Activity area notably increase [19]. It is probably necessary to evaluate the objectives relevant to the professionals and those significant to the families and children separately.
The discrepancies between our data and Preston’s also most likely reflect differences in the study population. In our study, those undergoing injections aimed at improving gait pattern are, for the most part, hemiplegic and diplegic patients with mild disabilities (GMFCS 1). Their elevated degree of autonomy in mobility probably accounts for the scarcity of objectives for improving walking autonomy. In the most severe cases, such as quadriplegia, objectives are mainly aimed at controlling deformities and facilitating health care provision. Pain reduction is another important aspect and concerned quadriplegic and diplegic patients with severe disability. In contrast, objectives related to muscle tone reduction were limited, as the main objective was not a reduction but the control of muscle shortening and the subsequent deformities. However, this can become a primary objective in cases of spastic hyperactivation (eg, in adductor muscles) or in the case of dystonia, to improve patient comfort.
From a practical point of view, the use of this methodology provides for a common language that facilitates the communication and sharing of therapeutic objectives between different professionals (physiatrists and physiotherapists) and between health care providers and families and/or patients. This is important, as physiotherapy is often complementary to BTX injections and the objectives must be shared with the family. This methodology can help the clinician in the decision-making process and allows determining with greater specificity what is to be measured to document the achievement of the objectives.
Future research in this field will be aimed at evaluating patient outcomes by means of the adoption of suitable instruments (measurement scales) in order to quantify results which are consistent, according to the ICF-CY classification, with the domain and the category undergoing analysis.
Conclusion
As it has already been pointed out by various authors [10–15], the ICF-CY is a useful instrument for the classification of proposed therapeutic objectives into domains and categories, in order to standardize the language and to increase the sharing of the aims between the health care providers and between providers and families/patients. The most commonly followed approach calls for the use of functional profiles at the beginning of the care planning process, in order to establish the priorities and objectives of the interventions to be carried out. In order to streamline and facilitate procedures in clinical practice, many have proposed the use of core sets, but the validation procedure is complex and not always possible in all centers. Recently, Preston et al were the first to propose using the ICF-CY for classifying the objectives of an individual program. The procedure utilized is simple, easily reproducible, and allows identifying and classifying the objectives into categories using the ICF-CY. Furthermore, it is focused on an individual program and not on the entire articulation of programs, making interpretation of the data more linear. Our proposal is similar because it is focused on the analysis of an individual therapeutic program and because it utilizes the ICF classification system to classify the objectives; however, it achieves a higher degree of detail and standardization of the objectives.
In conclusion, the classification structure of the ICF-CY furnishes a useful and recognized instrument for categorizing the objectives of the interventions to be carried out. The classification of the objectives is specific for each pathology and for each individual program. The standardization of the objectives themselves and the use of the ICF-CY categories only for classification represents a possible methodologic alternative to the use of ICF-CY individual categories and sub-categories for identifying these objectives (core sets), as proposed by other authors. This procedure offers greater detail and a greater degree of standardization, which is important for the successive and systematic evaluation of treatment results.
Corresponding author: Nicoletta Battisti, Via Altura 3, 40139 Bologna, Italy, [email protected].
From the IRCCS Institute of Neurological Sciences, Bellaria Hospital, Bologna, Italy.
Abstract
- Objective: To identify objectives for treatment of spasticity with botulinum toxin type A (BTX) in children with cerebral palsy (CP), standardize the objectives according to typology, and classify them according to the International Classification of Functioning for Children and Youth (ICF-CY), as well as to analyze treatment goals in relationship to CP clinical type, severity level, and age.
- Methods: 188 children were included in the study (mean age, 12 years; 42% female, 58% male). The diplegic type made up 38% of CP cases, the tetraplegic type 35%, and the hemiplegic type 24%. Children were mainly classified in the lowest and highest levels in the Gross Motor Function Classification System (GMFCS 1, 39%; GMFCS 5, 26%). Treatment objectives for individual therapies were discussed, identified, and transcribed in the therapeutic proposals. The objectives were then collected and subjected to an internal audit in order to standardize their denomination. Two trained health care providers expert in the use of the ICF-CY classification mapped the objectives to ICF-CY domains and categories. The objectives were then analyzed in relationship to CP clinical type, GMFCS level, and age.
- Results: Of the objectives, 88% (246) were in the “Body Functions” domain. In this domain, there were 28 typologies of objectives in 6 categories. Only 12% (32) of the objectives were in the “Activity” domain; there were 11 typologies in 5 categories. In diplegic and hemiplegic patients with mild disability (GMFCS 1), objectives were aimed at improving gait pattern. For quadriplegic patients with severe disability (GMFCS 5), objectives were aimed mainly at controlling deformities and improving health care provision. Objectives concerning pain treatment were proposed principally for patients with diplegic and quadriplegic type CP.
- Conclusions: The ICF-CY can be used to categorize treatment objectives proposed for patient improvement in the domains of Body Functions and Activity. Goal setting for BTX injections occurs mainly in the Body Functions domain and aims at finding changes in the gait pattern.
Botulinum toxin type A (BTX) has been used for 20 years for the focal treatment of spasticity in patients with cerebral palsy (CP) [1–3]. While numerous studies have shown the functional benefits of BTX treatment, especially if carried out in combination with other treatments (eg, physiotherapy, occupational therapy, serial casting), studies that focus on the indications for BTX use are limited.
Patients with CP require rehabilitation that involves multiple disciplines and multiprofessional therapeutic programs (eg, pharmacologic, orthotic, physiotherapeutic). The complexity of both the program and the pathology requires choosing the appropriate treatment objectives. The International Classification of Functioning for Children and Youth (ICF-CY) [4] is a unified and standard language and framework for clinical, public health, and research applications to facilitate the documentation and measurement of health and disability in child and youth populations. As such, it can be used to inform clinical thinking, practice and research in the field of cerebral palsy [5], including being used as a tool for developing treatment plans and providing a common language for defining and sharing treatment objectives with patients and families [6]. Thamar et al [7] recently pointed out the value of adopting a standardized method of writing specific and measurable goals. Goals that are specific and clear are important not only for the evaluation of efficacy but also for systematic evaluation of the quality of health services [8,9].
In the literature regarding rehabilitation (especially in adults) and, more recently, in the literature on CP [10], core sets derived from ICF that are condition- and setting-specific are increasingly being used. They are used for the evaluation of the functional profiles of patients and documentation of the results of rehabilitative treatment, and also for defining the objectives of the treatment. Some authors [11–14] have explored in detail the possibility of using the core sets for formulating treatment objectives and assessing outcomes. However, using the core sets is complicated and their use in day-to-day clinical settings is limited. In a recent study, Preston et al [15] sought to define a sub-set of functional goals and outcomes relevant to patients with CP undergoing BTX treatment that could be more appropriate for use. In this retrospective analysis, they used the ICF-CY to classify treatment goals into corresponding domains and categories. The ICF-CY contains 4 major components (Body Structure, Body Function, Activities and Participation, and Environmental Factors), which each contain hierarchically arranged chapters and category levels. The authors found that the goals were mainly in the domain of “Body Functions,” specifically “functions of joint mobility” and “functions of gait pattern.” Those in the “Activity” domain were in the “walking” and “changing body positions” categories. This study was the first to focus on CP as a pathology and on the objectives of the individual therapeutic programs; other reports in the literature deal with the entire articulation of treatment. The authors limited themselves to the identification of the domain and the category of the objectives but did not report in detail their denomination. A greater degree of specificity and standardization in the description of the objectives would be useful from a practical point of view both for comparing results and for improving communication between the health care providers, and between these professionals and the families. The authors also did not assess for the various clinical types of CP.
The aim of the present study involving patients having CP and undergoing BTX injections was to identify the treatment objectives, standardize them according to denomination, classify them according to ICF-CY domains and categories, and establish their relative frequency. A further objective of the study was to analyze treatment goals in relationship to the clinical type (eg, hemiplegia, diplegia, quadriplegia), level of severity according to the Gross Motor Function Classification System (GMFCS) [16], and age.
Methods
Our center in Bologna, Italy, specializes in the evaluation and advanced treatment of spasticity in neuromotor disability in children and young adults. Between 2010 and the first half of 2012, 217 children were admitted to our center for evaluation and BTX treatment of spasticity in the upper or lower limbs or both. Of these, 188 children who had been diagnosed with spastic CP were included in the prospective study. Twenty-nine patients with other pathologies (epileptic and degenerative encephalopathy, spastic paraparesis) were excluded. The enrolled patients and their families were informed about the study and written informed consent was obtained.
Patients were evaluated from a functional point of view by 3 expert physiatrists and 2 pediatric physiotherapists for eligibility for BTX injection according to the recommendations of Ferrari and Cioni [17]. Functional assessment included evaluation of impairments (spasticity, contractures, deformities), main motor functions (gait pattern, manipulation pattern), and capacity of carrying out the principal motor activities (walking, maintaining and changing body position, rolling, use of upper limbs), thus enabling the identification of specific and realistic objectives for treatment with BTX. The objectives were chosen by a physiatrist and a physiotherapist, shared among the health care providers and the patients and their families, and added to the written treatment proposals. For each child more than 1 treatment objective could be proposed. These proposals were then collected and audited so as to obtain a uniform denomination of the proposed therapeutic objectives. In a series of meetings among all the members of the research group, the descriptions/denominations of the therapeutic goals were standardized and shared, eliminating inexact descriptions or adding new ones as needed. Two trained health care providers expert in the use of the ICF-CY classification mapped these to the ICF-CY domains and categories (up to the 2nd level of categorization). Each interpretative disagreement was resolved by group discussion. Finally, the objectives were analyzed in relationship to clinical type, severity according to GMFCS, and age. The frequency of the individual objectives, domains, and categories was evaluated by means of descriptive statistics.
Results
Body Functions Domain
The most represented category in the “Body Functions” domain was “b770 functions of gait pattern” (50%). There were 123 proposed objectives distributed among 11 typologies of objectives for a total of 123 proposed objectives in the functions of gait pattern category.
In the “b715 functions of joint stability” category, 25 objectives were proposed for controlling hip lateralization while, in the “b720 functions of bone mobility” category, 4 typologies of objectives were identified out of a total of 15 proposed objectives aimed at improving the position of the pelvis. The “b280 pain sensation” category was also used to indicate 15 objectives aiming at alleviating knee, hip and spinal column pain. Finally, 4 objectives were aimed at tone reduction.
Activity Domain
As concerns the “Activity” domain, 38% of objectives were classified into the “d415 maintain body position” category (3 typologies and a total of 12 proposals), 25% were in the “d540 dress oneself ” category (2 typologies and a total of 8 proposals), 19% were in the “d440 fine use of the hands” category (3 typologies and a total of 6 proposals), 13% were in the “d445 use of hands and arms” category (2 typologies and 4 proposals) and, 6% of cases were classified into the “d510 wash oneself” category (2 proposals) (Table 2).
Analysis by Type, Severity, and Age
Discussion
The results show that in the majority of cases, the objectives of treatment with BTX injections proposed by our group fell within the “Body Functions” domain, in the “b770 gait pattern” and “b710 joint mobility” categories. This focus has also been reported by other authors [18]. Furthermore, these results are analogous to those reported by Preston [15]. The objectives classifiable into the “Activity” domain were more limited in our group. The most represented categories were “d415 maintain body position,” as also reported by Preston, and “d540 dressing oneself.” Preston et al reported many more objectives in the Activity domain, also utilizing the “walking” category. A possible reason is that objectives may reflect more the expectations of professionals and less those of patients. Indeed, when objectives suggested by patients and families are taken into greater consideration, goals proposed in the Activity area notably increase [19]. It is probably necessary to evaluate the objectives relevant to the professionals and those significant to the families and children separately.
The discrepancies between our data and Preston’s also most likely reflect differences in the study population. In our study, those undergoing injections aimed at improving gait pattern are, for the most part, hemiplegic and diplegic patients with mild disabilities (GMFCS 1). Their elevated degree of autonomy in mobility probably accounts for the scarcity of objectives for improving walking autonomy. In the most severe cases, such as quadriplegia, objectives are mainly aimed at controlling deformities and facilitating health care provision. Pain reduction is another important aspect and concerned quadriplegic and diplegic patients with severe disability. In contrast, objectives related to muscle tone reduction were limited, as the main objective was not a reduction but the control of muscle shortening and the subsequent deformities. However, this can become a primary objective in cases of spastic hyperactivation (eg, in adductor muscles) or in the case of dystonia, to improve patient comfort.
From a practical point of view, the use of this methodology provides for a common language that facilitates the communication and sharing of therapeutic objectives between different professionals (physiatrists and physiotherapists) and between health care providers and families and/or patients. This is important, as physiotherapy is often complementary to BTX injections and the objectives must be shared with the family. This methodology can help the clinician in the decision-making process and allows determining with greater specificity what is to be measured to document the achievement of the objectives.
Future research in this field will be aimed at evaluating patient outcomes by means of the adoption of suitable instruments (measurement scales) in order to quantify results which are consistent, according to the ICF-CY classification, with the domain and the category undergoing analysis.
Conclusion
As it has already been pointed out by various authors [10–15], the ICF-CY is a useful instrument for the classification of proposed therapeutic objectives into domains and categories, in order to standardize the language and to increase the sharing of the aims between the health care providers and between providers and families/patients. The most commonly followed approach calls for the use of functional profiles at the beginning of the care planning process, in order to establish the priorities and objectives of the interventions to be carried out. In order to streamline and facilitate procedures in clinical practice, many have proposed the use of core sets, but the validation procedure is complex and not always possible in all centers. Recently, Preston et al were the first to propose using the ICF-CY for classifying the objectives of an individual program. The procedure utilized is simple, easily reproducible, and allows identifying and classifying the objectives into categories using the ICF-CY. Furthermore, it is focused on an individual program and not on the entire articulation of programs, making interpretation of the data more linear. Our proposal is similar because it is focused on the analysis of an individual therapeutic program and because it utilizes the ICF classification system to classify the objectives; however, it achieves a higher degree of detail and standardization of the objectives.
In conclusion, the classification structure of the ICF-CY furnishes a useful and recognized instrument for categorizing the objectives of the interventions to be carried out. The classification of the objectives is specific for each pathology and for each individual program. The standardization of the objectives themselves and the use of the ICF-CY categories only for classification represents a possible methodologic alternative to the use of ICF-CY individual categories and sub-categories for identifying these objectives (core sets), as proposed by other authors. This procedure offers greater detail and a greater degree of standardization, which is important for the successive and systematic evaluation of treatment results.
Corresponding author: Nicoletta Battisti, Via Altura 3, 40139 Bologna, Italy, [email protected].
1. Lukban M, Rosales RL. Effectiveness of botulinum toxin A for upper and lower limb spasticity in children with cerebral palsy: a summary of evidence. J Neural Transm 2009;116:319–31.
2. Ryll U, Bastianen C, De Bie R, Staal B. Effects of leg muscle botulinum toxin A injections on walking in children with spasticity related cerebral palsy: a systematic review. Devel Med Child Neurol 2011;53:210–6.
3. Hoare BJ, Wallen MA,Villanueva E, et al. Botulinum toxin A as an adjunct to treatment in the management of upper limb in children with spastic cerebral palsy. The Cochraine Library 2010.
4. World Health Organization. International Classification of Functioning, Disability, and Health: Children and Youth Version for Children and Youth (ICF-CY). 2007. Available at http://apps.who.int/bookorders/anglais/detart1.jsp?codlan=1&codcol=15&codcch=716#
5. Rosenbaum P, Stewart D. The World Health Organization International Classification of Functioning Disability and Health: a model to guide clinical thinking, practice, and research. Semin Pediatr Neurol 2004;11:5–10.
6. Steiner W, Ryser L, Huber E, et al. Use of the ICF model as a clinical problem solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002;82:1098–107.
7. Thamar JH, Bovend’Eerdt, Botell RE, Wade DT. Writing SMART rehabilitation goals and achieving goal attainment scaling: practical guide. Clin Rehab 2009;23:352–61.
8. Program outcome evaluations. United Way of Winnipeg; 2007.
9. Main K. Program design: a practical guide. Available at www.calgaryunitedway.org.
10. Schiariti V, Selb M, Cieza A, O’Donnel M. International classification of Functioning, Disability and Health Core sets for children and youth with cerebral palsy: a consensus meeting 1. Dev Med Child Neurol 2014 Aug 6. Epub ahead of print
11. Huber EO, Tobler A, Gloor-Juzzi T, et al. The ICF as a way to specify goals and assess the outcome of physiotherapeutic interventions in the acute hospitals Rehabil Med 2011;43:174–7.
12. Mittrach R, Grill E, Walchner-Bonjean M, et al. Goals of physiotherapy interventions can be described using the International Classification Of Functioning, Disability and Health Physiotherapy 2008;94:150–7.
13. Muller MJ, Strobl R, Grill E. Goals of patients with rehabilitation needs in acute hospitals: goal achievement is an indicator for improved functioning Rehabil Med 2011;43:145–50.
14. Grill E J, Stucki G. Criteria for validating comprehensive ICF core sets and developing brief ICF core set versions. J Rehabil Med 2011;43:87–91.
15. Preston NJ, Clarke M, Bhakta B. Development of a framework to define the functional goals and outcomes of botulinum toxin A spasticity treatment relevant to the child and family living with cerebral palsy using the international classification of functioning disability and health for children and youth (ICF-CY). J Rehabil Med 2011;43:1010–5.
16. Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;39:214–23.
17. Ferrari A, Cioni G. The spastic forms of cerebral palsy: a guide to the assessment of adaptive functions. Springer-Verlag; 2010.
18. Franki I, De Cat J, Deschepper E, et al. A clinical decision framework for the identification of main problems and treatment goals for ambulant children with bilateral spastic cerebral palsy. Res Dev Disabil 2014;35:1160–76.
19. Lohmann S, Decker J, Müller M, et al. The ICF forms a useful framework for classifying individual patients goals in post-acute rehabilitation. Rehabil Med 2011;43:151–5.
1. Lukban M, Rosales RL. Effectiveness of botulinum toxin A for upper and lower limb spasticity in children with cerebral palsy: a summary of evidence. J Neural Transm 2009;116:319–31.
2. Ryll U, Bastianen C, De Bie R, Staal B. Effects of leg muscle botulinum toxin A injections on walking in children with spasticity related cerebral palsy: a systematic review. Devel Med Child Neurol 2011;53:210–6.
3. Hoare BJ, Wallen MA,Villanueva E, et al. Botulinum toxin A as an adjunct to treatment in the management of upper limb in children with spastic cerebral palsy. The Cochraine Library 2010.
4. World Health Organization. International Classification of Functioning, Disability, and Health: Children and Youth Version for Children and Youth (ICF-CY). 2007. Available at http://apps.who.int/bookorders/anglais/detart1.jsp?codlan=1&codcol=15&codcch=716#
5. Rosenbaum P, Stewart D. The World Health Organization International Classification of Functioning Disability and Health: a model to guide clinical thinking, practice, and research. Semin Pediatr Neurol 2004;11:5–10.
6. Steiner W, Ryser L, Huber E, et al. Use of the ICF model as a clinical problem solving tool in physical therapy and rehabilitation medicine. Phys Ther 2002;82:1098–107.
7. Thamar JH, Bovend’Eerdt, Botell RE, Wade DT. Writing SMART rehabilitation goals and achieving goal attainment scaling: practical guide. Clin Rehab 2009;23:352–61.
8. Program outcome evaluations. United Way of Winnipeg; 2007.
9. Main K. Program design: a practical guide. Available at www.calgaryunitedway.org.
10. Schiariti V, Selb M, Cieza A, O’Donnel M. International classification of Functioning, Disability and Health Core sets for children and youth with cerebral palsy: a consensus meeting 1. Dev Med Child Neurol 2014 Aug 6. Epub ahead of print
11. Huber EO, Tobler A, Gloor-Juzzi T, et al. The ICF as a way to specify goals and assess the outcome of physiotherapeutic interventions in the acute hospitals Rehabil Med 2011;43:174–7.
12. Mittrach R, Grill E, Walchner-Bonjean M, et al. Goals of physiotherapy interventions can be described using the International Classification Of Functioning, Disability and Health Physiotherapy 2008;94:150–7.
13. Muller MJ, Strobl R, Grill E. Goals of patients with rehabilitation needs in acute hospitals: goal achievement is an indicator for improved functioning Rehabil Med 2011;43:145–50.
14. Grill E J, Stucki G. Criteria for validating comprehensive ICF core sets and developing brief ICF core set versions. J Rehabil Med 2011;43:87–91.
15. Preston NJ, Clarke M, Bhakta B. Development of a framework to define the functional goals and outcomes of botulinum toxin A spasticity treatment relevant to the child and family living with cerebral palsy using the international classification of functioning disability and health for children and youth (ICF-CY). J Rehabil Med 2011;43:1010–5.
16. Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol 1997;39:214–23.
17. Ferrari A, Cioni G. The spastic forms of cerebral palsy: a guide to the assessment of adaptive functions. Springer-Verlag; 2010.
18. Franki I, De Cat J, Deschepper E, et al. A clinical decision framework for the identification of main problems and treatment goals for ambulant children with bilateral spastic cerebral palsy. Res Dev Disabil 2014;35:1160–76.
19. Lohmann S, Decker J, Müller M, et al. The ICF forms a useful framework for classifying individual patients goals in post-acute rehabilitation. Rehabil Med 2011;43:151–5.