User login
Study: PDT with methyl aminolevulinate promising for severe acne
Methyl aminolevulinate plus photodynamic therapy shows promise as a treatment for severe acne vulgaris, according to a U.S. study published in the British Journal of Dermatology.
Dr. David M. Pariser of Eastern Virginia Medical School, Norfolk, and his associates conducted the randomized double-blind, vehicle-controlled trial of photodynamic therapy (PDT) with methyl aminolevulinate (MAL) as a photosensitizer in 153 males and females aged 12-35 years with severe facial acne. Inclusion criteria comprised an Investigator Global Assessment (IGA) rating score of 4, 20-100 noninflammatory lesions, and 25-75 inflammatory lesions with no more than three nodules (Br J Dermatol. 2015 December. doi: 10.1111/bjd.14345).

Participants received topical MAL 80 mg/g (100) or vehicle cream (53) and PDT every 2 weeks for four treatments, and were evaluated at each treatment and at 12 weeks. The MAL or vehicle cream was applied and covered for 1.5 hours, followed by PDT (635 nm of red light for a total dose of 37 J/cm2). Most completed the study (85% in MAL group and 91% in vehicle group).
Those in the MAL PDT group demonstrated a significant reduction in inflammatory lesions based on the percentage change at 12 weeks (a mean reduction of 37.3% vs. 16.2%; P = .003), and absolute change (a mean reduction of 15.6 lesions vs. 7.8; P = .006). However, the reduction in noninflammatory lesions was not significantly different between the two groups (a mean reduction of 11.8 lesions among those on MAL PDT vs. 10.7 with vehicle PDT) .
The rates of treatment success, defined as improvement of 2 or more IGA grades at 12 weeks, were higher among those in the MAL PDT group (44% vs. 26.4%; OR, 3.24; P = .013).
Pain scores were higher during PDT for the MAL group and remained similar with subsequent treatments. The MAL treatment was discontinued in six participants because of pain and PDT was paused briefly in 15 participants. More participants in the MAL group reported moderate erythema after the first PDT session (46% versus 15%) and three reported severe erythema.
The most commonly reported adverse events in the MAL treatment group were a sensation of skin burning and pain, mostly mild to moderate, lasting a median of 3 days. Further, 12% of those in the MAL group withdrew secondary to adverse events.
“This large, controlled randomized clinical study shows the potential of PDT using 80 mg/g MAL cream for treatment of severe acne” in patients aged 12 years and older, with all skin types, the authors concluded, noting that more follow-up data are needed on the duration of treatment response and long-term effect on scarring. “Severe acne has limited therapeutic options with problematic side effects and bacterial resistance and 80 mg/g MAL PDT could be an alternative approach with improved tolerability for these patients,” they added.
The authors noted that for severe cases of acne, treatment is limited, and while oral isotretinoin is often used, it is teratogenic, has side effects, and is associated with reimbursement difficulties.
Dr. Pariser and two colleagues disclosed receiving honoraria from Photocure ASA, which markets MAL as Visonac. The company funded the study.
Methyl aminolevulinate plus photodynamic therapy shows promise as a treatment for severe acne vulgaris, according to a U.S. study published in the British Journal of Dermatology.
Dr. David M. Pariser of Eastern Virginia Medical School, Norfolk, and his associates conducted the randomized double-blind, vehicle-controlled trial of photodynamic therapy (PDT) with methyl aminolevulinate (MAL) as a photosensitizer in 153 males and females aged 12-35 years with severe facial acne. Inclusion criteria comprised an Investigator Global Assessment (IGA) rating score of 4, 20-100 noninflammatory lesions, and 25-75 inflammatory lesions with no more than three nodules (Br J Dermatol. 2015 December. doi: 10.1111/bjd.14345).
Participants received topical MAL 80 mg/g (100) or vehicle cream (53) and PDT every 2 weeks for four treatments, and were evaluated at each treatment and at 12 weeks. The MAL or vehicle cream was applied and covered for 1.5 hours, followed by PDT (635 nm of red light for a total dose of 37 J/cm2). Most completed the study (85% in MAL group and 91% in vehicle group).
Those in the MAL PDT group demonstrated a significant reduction in inflammatory lesions based on the percentage change at 12 weeks (a mean reduction of 37.3% vs. 16.2%; P = .003), and absolute change (a mean reduction of 15.6 lesions vs. 7.8; P = .006). However, the reduction in noninflammatory lesions was not significantly different between the two groups (a mean reduction of 11.8 lesions among those on MAL PDT vs. 10.7 with vehicle PDT) .
The rates of treatment success, defined as improvement of 2 or more IGA grades at 12 weeks, were higher among those in the MAL PDT group (44% vs. 26.4%; OR, 3.24; P = .013).
Pain scores were higher during PDT for the MAL group and remained similar with subsequent treatments. The MAL treatment was discontinued in six participants because of pain and PDT was paused briefly in 15 participants. More participants in the MAL group reported moderate erythema after the first PDT session (46% versus 15%) and three reported severe erythema.
The most commonly reported adverse events in the MAL treatment group were a sensation of skin burning and pain, mostly mild to moderate, lasting a median of 3 days. Further, 12% of those in the MAL group withdrew secondary to adverse events.
“This large, controlled randomized clinical study shows the potential of PDT using 80 mg/g MAL cream for treatment of severe acne” in patients aged 12 years and older, with all skin types, the authors concluded, noting that more follow-up data are needed on the duration of treatment response and long-term effect on scarring. “Severe acne has limited therapeutic options with problematic side effects and bacterial resistance and 80 mg/g MAL PDT could be an alternative approach with improved tolerability for these patients,” they added.
The authors noted that for severe cases of acne, treatment is limited, and while oral isotretinoin is often used, it is teratogenic, has side effects, and is associated with reimbursement difficulties.
Dr. Pariser and two colleagues disclosed receiving honoraria from Photocure ASA, which markets MAL as Visonac. The company funded the study.
Methyl aminolevulinate plus photodynamic therapy shows promise as a treatment for severe acne vulgaris, according to a U.S. study published in the British Journal of Dermatology.
Dr. David M. Pariser of Eastern Virginia Medical School, Norfolk, and his associates conducted the randomized double-blind, vehicle-controlled trial of photodynamic therapy (PDT) with methyl aminolevulinate (MAL) as a photosensitizer in 153 males and females aged 12-35 years with severe facial acne. Inclusion criteria comprised an Investigator Global Assessment (IGA) rating score of 4, 20-100 noninflammatory lesions, and 25-75 inflammatory lesions with no more than three nodules (Br J Dermatol. 2015 December. doi: 10.1111/bjd.14345).
Participants received topical MAL 80 mg/g (100) or vehicle cream (53) and PDT every 2 weeks for four treatments, and were evaluated at each treatment and at 12 weeks. The MAL or vehicle cream was applied and covered for 1.5 hours, followed by PDT (635 nm of red light for a total dose of 37 J/cm2). Most completed the study (85% in MAL group and 91% in vehicle group).
Those in the MAL PDT group demonstrated a significant reduction in inflammatory lesions based on the percentage change at 12 weeks (a mean reduction of 37.3% vs. 16.2%; P = .003), and absolute change (a mean reduction of 15.6 lesions vs. 7.8; P = .006). However, the reduction in noninflammatory lesions was not significantly different between the two groups (a mean reduction of 11.8 lesions among those on MAL PDT vs. 10.7 with vehicle PDT) .
The rates of treatment success, defined as improvement of 2 or more IGA grades at 12 weeks, were higher among those in the MAL PDT group (44% vs. 26.4%; OR, 3.24; P = .013).
Pain scores were higher during PDT for the MAL group and remained similar with subsequent treatments. The MAL treatment was discontinued in six participants because of pain and PDT was paused briefly in 15 participants. More participants in the MAL group reported moderate erythema after the first PDT session (46% versus 15%) and three reported severe erythema.
The most commonly reported adverse events in the MAL treatment group were a sensation of skin burning and pain, mostly mild to moderate, lasting a median of 3 days. Further, 12% of those in the MAL group withdrew secondary to adverse events.
“This large, controlled randomized clinical study shows the potential of PDT using 80 mg/g MAL cream for treatment of severe acne” in patients aged 12 years and older, with all skin types, the authors concluded, noting that more follow-up data are needed on the duration of treatment response and long-term effect on scarring. “Severe acne has limited therapeutic options with problematic side effects and bacterial resistance and 80 mg/g MAL PDT could be an alternative approach with improved tolerability for these patients,” they added.
The authors noted that for severe cases of acne, treatment is limited, and while oral isotretinoin is often used, it is teratogenic, has side effects, and is associated with reimbursement difficulties.
Dr. Pariser and two colleagues disclosed receiving honoraria from Photocure ASA, which markets MAL as Visonac. The company funded the study.
FROM THE BRITISH JOURNAL OF DERMATOLOGY
Key clinical point: Methyl aminolevulinate (MAL) with photodynamic therapy (PDT) shows promise as an alternative treatment for severe acne vulgaris.
Major finding: The MAL/PDT group had a significantly higher rate of treatment success compared with the vehicle/PDT group at 12 weeks (44% vs. 26.4%; P = .013).
Data source: A randomized, double-blind, vehicle-controlled study evaluating the safety and efficacy of PDT with MAL in 153 people aged 12-35 years, with severe facial acne, at 15 outpatient dermatology centers in the United States.
Disclosures: Dr. Pariser and two colleagues disclosed receiving honoraria from MAL manufacturer Photocure ASA, which funded the study.

Mutations could be therapeutic target for FL

Mutations in the RRAGC gene appear to be an “excellent candidate for therapeutic targeting” in follicular lymphoma (FL), according to investigators.
They analyzed mutations found in tumors with multiple relapses of FL without transformation to diffuse large B-cell lymphoma.
And they found that one commonly mutated gene encodes the protein RagC, which is essential for activating the amino-acid sensing mTORC1 pathway.
Although mutations in genes in the mTORC1 pathway have been associated with various cancers, this is the first time a genetic mutation in any of the 4 Rag proteins has been identified in malignancy.
“One of the mutations that we have identified allows follicular lymphoma tumors to turn on growth signals regardless of whether nutrients are available, thereby evading normal restrictions on its growth,” said study author Jessica Okosun, MB BChir, PhD, of Barts Cancer Institute at Queen Mary University of London in the UK.
“Remarkably, the mutations we have discovered have not been seen in other cancer types. However, drugs that directly target this nutrient-sensing mechanism are currently used to treat other types of cancer and may benefit patients with follicular lymphoma.”
Dr Okosun and her colleagues reported these findings in a letter to Nature Genetics.
In experiments with cell lines, the investigators found that expression of the mutated RagC proteins activate mTORC1 signaling in the absence of amino acids and increase binding to an important part of the mTORC1 complex, consistent with the established role of RagC in the mTORC1 pathway.
Because this research was performed exclusively in cell lines, the investigators have not yet deciphered the mutations’ mechanistic effect in patients. However, study author Rachel Wolfson, of the Whitehead Institute for Biomedical Research and Massachusetts Institute of Technology in Cambridge, Massachusetts, said there are clues to the mutations’ significance.
“mTORC1 is linked to cell growth, so it is not surprising that activation of the pathway could lead to some growth advantage for cancer cells,” Wolfson said. “But it leads to an interesting question: When is it a proliferative advantage versus a disadvantage to no longer be able to accurately sense amino acid levels? That is something we would need to investigate further, likely in vivo.”
The investigators would also like to know how the drug rapamycin affects FL with RagC mutations. Rapamycin binds to mTORC1 and inhibits its activity. If the drug interferes with mTORC1 dysregulation caused by RagC mutations, perhaps the drug could be used in FL treatment.
“If so, maybe these RagC mutations could be used as biomarkers to predict sensitivity to rapamycin treatment in follicular lymphoma patients,” Wolfson said. “That would be very exciting, and it’s something that should be investigated further.” ![]()
Mutations in the RRAGC gene appear to be an “excellent candidate for therapeutic targeting” in follicular lymphoma (FL), according to investigators.
They analyzed mutations found in tumors with multiple relapses of FL without transformation to diffuse large B-cell lymphoma.
And they found that one commonly mutated gene encodes the protein RagC, which is essential for activating the amino-acid sensing mTORC1 pathway.
Although mutations in genes in the mTORC1 pathway have been associated with various cancers, this is the first time a genetic mutation in any of the 4 Rag proteins has been identified in malignancy.
“One of the mutations that we have identified allows follicular lymphoma tumors to turn on growth signals regardless of whether nutrients are available, thereby evading normal restrictions on its growth,” said study author Jessica Okosun, MB BChir, PhD, of Barts Cancer Institute at Queen Mary University of London in the UK.
“Remarkably, the mutations we have discovered have not been seen in other cancer types. However, drugs that directly target this nutrient-sensing mechanism are currently used to treat other types of cancer and may benefit patients with follicular lymphoma.”
Dr Okosun and her colleagues reported these findings in a letter to Nature Genetics.
In experiments with cell lines, the investigators found that expression of the mutated RagC proteins activate mTORC1 signaling in the absence of amino acids and increase binding to an important part of the mTORC1 complex, consistent with the established role of RagC in the mTORC1 pathway.
Because this research was performed exclusively in cell lines, the investigators have not yet deciphered the mutations’ mechanistic effect in patients. However, study author Rachel Wolfson, of the Whitehead Institute for Biomedical Research and Massachusetts Institute of Technology in Cambridge, Massachusetts, said there are clues to the mutations’ significance.
“mTORC1 is linked to cell growth, so it is not surprising that activation of the pathway could lead to some growth advantage for cancer cells,” Wolfson said. “But it leads to an interesting question: When is it a proliferative advantage versus a disadvantage to no longer be able to accurately sense amino acid levels? That is something we would need to investigate further, likely in vivo.”
The investigators would also like to know how the drug rapamycin affects FL with RagC mutations. Rapamycin binds to mTORC1 and inhibits its activity. If the drug interferes with mTORC1 dysregulation caused by RagC mutations, perhaps the drug could be used in FL treatment.
“If so, maybe these RagC mutations could be used as biomarkers to predict sensitivity to rapamycin treatment in follicular lymphoma patients,” Wolfson said. “That would be very exciting, and it’s something that should be investigated further.” ![]()
Mutations in the RRAGC gene appear to be an “excellent candidate for therapeutic targeting” in follicular lymphoma (FL), according to investigators.
They analyzed mutations found in tumors with multiple relapses of FL without transformation to diffuse large B-cell lymphoma.
And they found that one commonly mutated gene encodes the protein RagC, which is essential for activating the amino-acid sensing mTORC1 pathway.
Although mutations in genes in the mTORC1 pathway have been associated with various cancers, this is the first time a genetic mutation in any of the 4 Rag proteins has been identified in malignancy.
“One of the mutations that we have identified allows follicular lymphoma tumors to turn on growth signals regardless of whether nutrients are available, thereby evading normal restrictions on its growth,” said study author Jessica Okosun, MB BChir, PhD, of Barts Cancer Institute at Queen Mary University of London in the UK.
“Remarkably, the mutations we have discovered have not been seen in other cancer types. However, drugs that directly target this nutrient-sensing mechanism are currently used to treat other types of cancer and may benefit patients with follicular lymphoma.”
Dr Okosun and her colleagues reported these findings in a letter to Nature Genetics.
In experiments with cell lines, the investigators found that expression of the mutated RagC proteins activate mTORC1 signaling in the absence of amino acids and increase binding to an important part of the mTORC1 complex, consistent with the established role of RagC in the mTORC1 pathway.
Because this research was performed exclusively in cell lines, the investigators have not yet deciphered the mutations’ mechanistic effect in patients. However, study author Rachel Wolfson, of the Whitehead Institute for Biomedical Research and Massachusetts Institute of Technology in Cambridge, Massachusetts, said there are clues to the mutations’ significance.
“mTORC1 is linked to cell growth, so it is not surprising that activation of the pathway could lead to some growth advantage for cancer cells,” Wolfson said. “But it leads to an interesting question: When is it a proliferative advantage versus a disadvantage to no longer be able to accurately sense amino acid levels? That is something we would need to investigate further, likely in vivo.”
The investigators would also like to know how the drug rapamycin affects FL with RagC mutations. Rapamycin binds to mTORC1 and inhibits its activity. If the drug interferes with mTORC1 dysregulation caused by RagC mutations, perhaps the drug could be used in FL treatment.
“If so, maybe these RagC mutations could be used as biomarkers to predict sensitivity to rapamycin treatment in follicular lymphoma patients,” Wolfson said. “That would be very exciting, and it’s something that should be investigated further.” ![]()
Studies reveal lack of transparency and poor reporting of research

Photo by Bill Branson
Two new studies suggest biomedical research may be hindered by poor reporting and a lack of transparency.
In one study, researchers analyzed more than 400 biomedical science articles and found the papers rarely provided full protocol information, complete data, and the necessary level of transparency to verify or replicate the work.
In the other study, researchers analyzed more than 500 preclinical experiments and found that most didn’t contain sufficient information on the animals used.
Both studies were published in PLOS Biology.
For the first study, Shareen Iqbal, PhD, of Emory University in Atlanta, Georgia, and her colleagues analyzed papers published between 2000 and 2014.
The team set out to determine the extent to which researchers report key information necessary for properly evaluating and replicating published research, including availability of protocols, data, and the frequency of published novel or replication studies.
Out of 441 articles drawn from across the biomedical literature, only 1 paper provided a full protocol, and none of the papers made all the data available. The majority of studies didn’t state funding or conflicts of interest, and replication studies were very rare.
Dr Iqbal and her colleagues said they hope their study will further sensitize scientists, funders, journals, and other science-related stakeholders about the need to improve these indicators.
For the second study, Ulrich Dirnagl, MD, of Charité Universitätsmedizin in Berlin, Germany, and his colleagues examined 100 papers describing preclinical research on stroke and cancer. These papers contained accounts of 316 experiments on infarct volume and 206 experiments on tumor shrinkage.
The vast majority of the reports didn’t contain sufficient information on how many animals were used in the experiments. What’s more, in many papers, animals “vanished” over the course of the study.
Using a computer model, the researchers simulated the effects of such animal loss on the validity of the experiments. They found that the more animals lost or removed, the shakier or more biased the experimental conclusions.
“The study began with an attempt to look at the robustness of findings in a handful of preclinical papers, but the sheer number of missing animals stopped us in our tracks,” said author Constance Holman, a graduate student at Charité Universitätsmedizin.
Researchers from both studies believe their findings add to the list of concerns about bias and reporting in research, but the results also establish ways in which research can become more transparent and potentially more reproducible. ![]()
Photo by Bill Branson
Two new studies suggest biomedical research may be hindered by poor reporting and a lack of transparency.
In one study, researchers analyzed more than 400 biomedical science articles and found the papers rarely provided full protocol information, complete data, and the necessary level of transparency to verify or replicate the work.
In the other study, researchers analyzed more than 500 preclinical experiments and found that most didn’t contain sufficient information on the animals used.
Both studies were published in PLOS Biology.
For the first study, Shareen Iqbal, PhD, of Emory University in Atlanta, Georgia, and her colleagues analyzed papers published between 2000 and 2014.
The team set out to determine the extent to which researchers report key information necessary for properly evaluating and replicating published research, including availability of protocols, data, and the frequency of published novel or replication studies.
Out of 441 articles drawn from across the biomedical literature, only 1 paper provided a full protocol, and none of the papers made all the data available. The majority of studies didn’t state funding or conflicts of interest, and replication studies were very rare.
Dr Iqbal and her colleagues said they hope their study will further sensitize scientists, funders, journals, and other science-related stakeholders about the need to improve these indicators.
For the second study, Ulrich Dirnagl, MD, of Charité Universitätsmedizin in Berlin, Germany, and his colleagues examined 100 papers describing preclinical research on stroke and cancer. These papers contained accounts of 316 experiments on infarct volume and 206 experiments on tumor shrinkage.
The vast majority of the reports didn’t contain sufficient information on how many animals were used in the experiments. What’s more, in many papers, animals “vanished” over the course of the study.
Using a computer model, the researchers simulated the effects of such animal loss on the validity of the experiments. They found that the more animals lost or removed, the shakier or more biased the experimental conclusions.
“The study began with an attempt to look at the robustness of findings in a handful of preclinical papers, but the sheer number of missing animals stopped us in our tracks,” said author Constance Holman, a graduate student at Charité Universitätsmedizin.
Researchers from both studies believe their findings add to the list of concerns about bias and reporting in research, but the results also establish ways in which research can become more transparent and potentially more reproducible. ![]()
Photo by Bill Branson
Two new studies suggest biomedical research may be hindered by poor reporting and a lack of transparency.
In one study, researchers analyzed more than 400 biomedical science articles and found the papers rarely provided full protocol information, complete data, and the necessary level of transparency to verify or replicate the work.
In the other study, researchers analyzed more than 500 preclinical experiments and found that most didn’t contain sufficient information on the animals used.
Both studies were published in PLOS Biology.
For the first study, Shareen Iqbal, PhD, of Emory University in Atlanta, Georgia, and her colleagues analyzed papers published between 2000 and 2014.
The team set out to determine the extent to which researchers report key information necessary for properly evaluating and replicating published research, including availability of protocols, data, and the frequency of published novel or replication studies.
Out of 441 articles drawn from across the biomedical literature, only 1 paper provided a full protocol, and none of the papers made all the data available. The majority of studies didn’t state funding or conflicts of interest, and replication studies were very rare.
Dr Iqbal and her colleagues said they hope their study will further sensitize scientists, funders, journals, and other science-related stakeholders about the need to improve these indicators.
For the second study, Ulrich Dirnagl, MD, of Charité Universitätsmedizin in Berlin, Germany, and his colleagues examined 100 papers describing preclinical research on stroke and cancer. These papers contained accounts of 316 experiments on infarct volume and 206 experiments on tumor shrinkage.
The vast majority of the reports didn’t contain sufficient information on how many animals were used in the experiments. What’s more, in many papers, animals “vanished” over the course of the study.
Using a computer model, the researchers simulated the effects of such animal loss on the validity of the experiments. They found that the more animals lost or removed, the shakier or more biased the experimental conclusions.
“The study began with an attempt to look at the robustness of findings in a handful of preclinical papers, but the sheer number of missing animals stopped us in our tracks,” said author Constance Holman, a graduate student at Charité Universitätsmedizin.
Researchers from both studies believe their findings add to the list of concerns about bias and reporting in research, but the results also establish ways in which research can become more transparent and potentially more reproducible. ![]()
Drug granted orphan designation for SCD
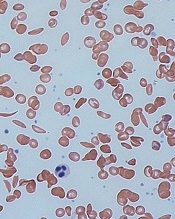
red blood cells
Image by Graham Beards
The US Food and Drug Administration (FDA) has granted orphan drug designation for the small molecule GBT440 to treat patients with sickle cell disease (SCD).
GBT440 is being developed as a potentially disease-modifying therapy for SCD. The drug works by increasing hemoglobin’s affinity for oxygen.
Since oxygenated sickle hemoglobin does not polymerize, it is believed that GBT440 blocks polymerization and the resultant sickling of red blood cells.
If GBT440 can restore normal hemoglobin function and improve oxygen delivery, the drug may be capable of modifying the progression of SCD.
“Receiving orphan drug designation, along with the previously announced fast track designation, are important milestones in our regulatory strategy for GBT440 and highlight the FDA’s agreement that the SCD community faces a critical need for new treatments,” said Ted W. Love, MD, chief executive officer of Global Blood Therapeutics, Inc., the company developing GBT440.
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US. The designation provides the drug’s sponsor with various development incentives, including opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, and 7 years of US market exclusivity if the drug is approved.
The FDA grants fast track designation to facilitate and expedite the development and review of new drugs intended to treat serious or life-threatening conditions and address unmet medical need. Through the fast track program, a drug may be eligible for priority review and rolling review, and the company developing the drug may receive additional help from the FDA to expedite development.
GBT440 trial
Early results from an ongoing phase 1/2 study of GBT440 were presented at the 2015 ASH Annual Meeting last month (abstract 542*).
The trial, which includes healthy subjects and patients with SCD, is being conducted in 2 parts: part A (single-dose administration) and part B (multiple-dose administration, daily for 15 days in healthy subjects and 28 days in SCD patients).
As of November 20, 2015, 8 SCD patients completed part A, and 30 SCD patients had either completed or were ongoing in part B.
Of the 30 SCD patients, 16 patients completed 700 mg daily dosing and follow-up (12 on GBT440 and 4 on placebo), and 14 patients completed or were ongoing at 500 mg daily dosing and follow-up (10 on GBT440 and 4 on placebo). A cohort of SCD patients on 1000 mg per day for 28 days is currently enrolling.
Thus far, GBT440 treatment has conferred several improvements from baseline to day 28.
Hemoglobin increases were evident by day 4 of treatment. And the researchers observed absolute hemoglobin increases of 0.5 and 0.7 g/dL with GBT440 at 500 and 700 mg, respectively, compared with a 0.1 g/dL decrease with placebo.
The median reticulocyte count decreased by 31% and 37% with GBT440 at 500 and 700 mg, respectively, compared with a 7% increase with placebo, indicating that the hemoglobin rise is due to decreased hemolysis.
Median erythropoietin levels decreased by 9 and 18 mU/mL with GBT440 at 500 and 700 mg, respectively, compared with an increase of 28 mU/mL with placebo.
Median unconjugated bilirubin levels decrease by 31% and 43% with GBT440 at 500 mg and 700 mg, respectively, compared with an increase of 2% with placebo.
Median lactate dehydrogenase levels decreased by 20% and 12% with GBT440 at 500 and 700 mg, respectively, compared with a decrease of 7% with placebo.
Median sickle cell counts decreased by 56% and 46% with GBT440 at 500 and 700 mg, respectively, compared with a 14% increase with placebo.
The researchers noted high inter- and intra-patient variability in circulating sickle cell counts.
They said inflammatory soluble adhesion molecules for the 700 mg dose cohort showed promising trends in improvement. The median P-selectin decreased 19%, compared with an increase of 20% with placebo. And the median ICAM-1 decreased 6%, compared with an increase of 33% in placebo. Data for the 500 mg dose cohort has not yet been analyzed.
The researchers said pharmacokinetic data demonstrated linear and dose-proportional properties, with a half-life amenable to once-daily dosing.
And GBT440 was well tolerated over the 28 days of dosing. None of the SCD patients discontinued GBT440. The most common adverse event was headache, and there have been no serious adverse events thought to be drug-related.
“We continue to believe that GBT440 has the potential to become the first mechanism-based and disease-modifying therapeutic for this grievous disease and look forward to sharing full results from our phase 1/2 trial and potentially initiating a pivotal trial in adult patients with SCD in 2016,” Dr Love said. ![]()
*Data in the abstract differ from the presentation.
red blood cells
Image by Graham Beards
The US Food and Drug Administration (FDA) has granted orphan drug designation for the small molecule GBT440 to treat patients with sickle cell disease (SCD).
GBT440 is being developed as a potentially disease-modifying therapy for SCD. The drug works by increasing hemoglobin’s affinity for oxygen.
Since oxygenated sickle hemoglobin does not polymerize, it is believed that GBT440 blocks polymerization and the resultant sickling of red blood cells.
If GBT440 can restore normal hemoglobin function and improve oxygen delivery, the drug may be capable of modifying the progression of SCD.
“Receiving orphan drug designation, along with the previously announced fast track designation, are important milestones in our regulatory strategy for GBT440 and highlight the FDA’s agreement that the SCD community faces a critical need for new treatments,” said Ted W. Love, MD, chief executive officer of Global Blood Therapeutics, Inc., the company developing GBT440.
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US. The designation provides the drug’s sponsor with various development incentives, including opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, and 7 years of US market exclusivity if the drug is approved.
The FDA grants fast track designation to facilitate and expedite the development and review of new drugs intended to treat serious or life-threatening conditions and address unmet medical need. Through the fast track program, a drug may be eligible for priority review and rolling review, and the company developing the drug may receive additional help from the FDA to expedite development.
GBT440 trial
Early results from an ongoing phase 1/2 study of GBT440 were presented at the 2015 ASH Annual Meeting last month (abstract 542*).
The trial, which includes healthy subjects and patients with SCD, is being conducted in 2 parts: part A (single-dose administration) and part B (multiple-dose administration, daily for 15 days in healthy subjects and 28 days in SCD patients).
As of November 20, 2015, 8 SCD patients completed part A, and 30 SCD patients had either completed or were ongoing in part B.
Of the 30 SCD patients, 16 patients completed 700 mg daily dosing and follow-up (12 on GBT440 and 4 on placebo), and 14 patients completed or were ongoing at 500 mg daily dosing and follow-up (10 on GBT440 and 4 on placebo). A cohort of SCD patients on 1000 mg per day for 28 days is currently enrolling.
Thus far, GBT440 treatment has conferred several improvements from baseline to day 28.
Hemoglobin increases were evident by day 4 of treatment. And the researchers observed absolute hemoglobin increases of 0.5 and 0.7 g/dL with GBT440 at 500 and 700 mg, respectively, compared with a 0.1 g/dL decrease with placebo.
The median reticulocyte count decreased by 31% and 37% with GBT440 at 500 and 700 mg, respectively, compared with a 7% increase with placebo, indicating that the hemoglobin rise is due to decreased hemolysis.
Median erythropoietin levels decreased by 9 and 18 mU/mL with GBT440 at 500 and 700 mg, respectively, compared with an increase of 28 mU/mL with placebo.
Median unconjugated bilirubin levels decrease by 31% and 43% with GBT440 at 500 mg and 700 mg, respectively, compared with an increase of 2% with placebo.
Median lactate dehydrogenase levels decreased by 20% and 12% with GBT440 at 500 and 700 mg, respectively, compared with a decrease of 7% with placebo.
Median sickle cell counts decreased by 56% and 46% with GBT440 at 500 and 700 mg, respectively, compared with a 14% increase with placebo.
The researchers noted high inter- and intra-patient variability in circulating sickle cell counts.
They said inflammatory soluble adhesion molecules for the 700 mg dose cohort showed promising trends in improvement. The median P-selectin decreased 19%, compared with an increase of 20% with placebo. And the median ICAM-1 decreased 6%, compared with an increase of 33% in placebo. Data for the 500 mg dose cohort has not yet been analyzed.
The researchers said pharmacokinetic data demonstrated linear and dose-proportional properties, with a half-life amenable to once-daily dosing.
And GBT440 was well tolerated over the 28 days of dosing. None of the SCD patients discontinued GBT440. The most common adverse event was headache, and there have been no serious adverse events thought to be drug-related.
“We continue to believe that GBT440 has the potential to become the first mechanism-based and disease-modifying therapeutic for this grievous disease and look forward to sharing full results from our phase 1/2 trial and potentially initiating a pivotal trial in adult patients with SCD in 2016,” Dr Love said. ![]()
*Data in the abstract differ from the presentation.
red blood cells
Image by Graham Beards
The US Food and Drug Administration (FDA) has granted orphan drug designation for the small molecule GBT440 to treat patients with sickle cell disease (SCD).
GBT440 is being developed as a potentially disease-modifying therapy for SCD. The drug works by increasing hemoglobin’s affinity for oxygen.
Since oxygenated sickle hemoglobin does not polymerize, it is believed that GBT440 blocks polymerization and the resultant sickling of red blood cells.
If GBT440 can restore normal hemoglobin function and improve oxygen delivery, the drug may be capable of modifying the progression of SCD.
“Receiving orphan drug designation, along with the previously announced fast track designation, are important milestones in our regulatory strategy for GBT440 and highlight the FDA’s agreement that the SCD community faces a critical need for new treatments,” said Ted W. Love, MD, chief executive officer of Global Blood Therapeutics, Inc., the company developing GBT440.
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US. The designation provides the drug’s sponsor with various development incentives, including opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, and 7 years of US market exclusivity if the drug is approved.
The FDA grants fast track designation to facilitate and expedite the development and review of new drugs intended to treat serious or life-threatening conditions and address unmet medical need. Through the fast track program, a drug may be eligible for priority review and rolling review, and the company developing the drug may receive additional help from the FDA to expedite development.
GBT440 trial
Early results from an ongoing phase 1/2 study of GBT440 were presented at the 2015 ASH Annual Meeting last month (abstract 542*).
The trial, which includes healthy subjects and patients with SCD, is being conducted in 2 parts: part A (single-dose administration) and part B (multiple-dose administration, daily for 15 days in healthy subjects and 28 days in SCD patients).
As of November 20, 2015, 8 SCD patients completed part A, and 30 SCD patients had either completed or were ongoing in part B.
Of the 30 SCD patients, 16 patients completed 700 mg daily dosing and follow-up (12 on GBT440 and 4 on placebo), and 14 patients completed or were ongoing at 500 mg daily dosing and follow-up (10 on GBT440 and 4 on placebo). A cohort of SCD patients on 1000 mg per day for 28 days is currently enrolling.
Thus far, GBT440 treatment has conferred several improvements from baseline to day 28.
Hemoglobin increases were evident by day 4 of treatment. And the researchers observed absolute hemoglobin increases of 0.5 and 0.7 g/dL with GBT440 at 500 and 700 mg, respectively, compared with a 0.1 g/dL decrease with placebo.
The median reticulocyte count decreased by 31% and 37% with GBT440 at 500 and 700 mg, respectively, compared with a 7% increase with placebo, indicating that the hemoglobin rise is due to decreased hemolysis.
Median erythropoietin levels decreased by 9 and 18 mU/mL with GBT440 at 500 and 700 mg, respectively, compared with an increase of 28 mU/mL with placebo.
Median unconjugated bilirubin levels decrease by 31% and 43% with GBT440 at 500 mg and 700 mg, respectively, compared with an increase of 2% with placebo.
Median lactate dehydrogenase levels decreased by 20% and 12% with GBT440 at 500 and 700 mg, respectively, compared with a decrease of 7% with placebo.
Median sickle cell counts decreased by 56% and 46% with GBT440 at 500 and 700 mg, respectively, compared with a 14% increase with placebo.
The researchers noted high inter- and intra-patient variability in circulating sickle cell counts.
They said inflammatory soluble adhesion molecules for the 700 mg dose cohort showed promising trends in improvement. The median P-selectin decreased 19%, compared with an increase of 20% with placebo. And the median ICAM-1 decreased 6%, compared with an increase of 33% in placebo. Data for the 500 mg dose cohort has not yet been analyzed.
The researchers said pharmacokinetic data demonstrated linear and dose-proportional properties, with a half-life amenable to once-daily dosing.
And GBT440 was well tolerated over the 28 days of dosing. None of the SCD patients discontinued GBT440. The most common adverse event was headache, and there have been no serious adverse events thought to be drug-related.
“We continue to believe that GBT440 has the potential to become the first mechanism-based and disease-modifying therapeutic for this grievous disease and look forward to sharing full results from our phase 1/2 trial and potentially initiating a pivotal trial in adult patients with SCD in 2016,” Dr Love said. ![]()
*Data in the abstract differ from the presentation.
Docs’ body language may convey racial bias

Doctors may convey racial bias with their body language, according to research published in The Journal of Pain and Symptom Management.
In this small study, a group of physicians, most of whom were white males, gave less compassionate nonverbal cues when interacting with black actors portraying seriously ill patients than when interacting with white actors portraying seriously ill patients.
“Although we found that physicians said the same things to their black and white patients, communication is not just the spoken word. It also involves nonverbal cues, such as eye contact, body positioning, and touch,” said study author Amber Barnato, MD, of the University of Pittsburg in Pennsylvania.
“Poor nonverbal communication—something the physician may not even be aware he or she is doing—could explain why many black patients perceive discrimination in the healthcare setting.”
For this study, Dr Barnato and her colleagues recruited 33 hospital-based attending emergency medicine physicians, hospitalists, and intensivists from Allegheny County, Pennsylvania, and put them in realistic simulations where actors portrayed dying black and white patients accompanied by a family member.
The actors portrayed comparable medical conditions—plummeting vital signs related to either metastatic gastric or pancreatic cancer—and read from matching scripts. The physicians were unaware of what the trial was testing.
The majority of the physicians were white men, so the researchers could not derive any statistically significant conclusions about whether a physician’s race impacted his or her actions.
Physicians were scored on a point system for both their verbal and nonverbal communication skills when interacting with the patient and family member. The physicians averaged 7% lower scores for their nonverbal interactions with the black patients than with the white patients.
“When explaining what was happening and what the next steps for care could be, with the white patients, the physicians were more likely to stand right at the patient’s bedside and touch them in a sympathetic manner,” Dr Barnato said.
She explained that something as simple as a physician staying near the door and holding a binder in front of his body could be perceived by the patient and family as defensive or disengaged. This could lead to a cascade of misunderstandings that result in patients and their families requesting extraordinary life-saving measures because they don’t trust the doctor has their best interests in mind when suggesting gentler, end-of-life care options.
“When you survey people in the community about their feelings on end-of-life care, blacks are only slightly more likely than whites to say they want aggressive, life-sustaining measures when terminally ill,” Dr Barnato said.
“However, blacks are much more likely than whites to request such care when they are faced with making the decision in the hospital. Body language is a significant tool in building trust—or mistrust—and physicians need to ensure that their body language isn’t contributing to that decision.”
“To help black patients and their families feel welcome and encouraged to be partners in medical decision-making, it is critical that doctors be aware of their verbal and nonverbal communication and any unintentional biases.” ![]()
Doctors may convey racial bias with their body language, according to research published in The Journal of Pain and Symptom Management.
In this small study, a group of physicians, most of whom were white males, gave less compassionate nonverbal cues when interacting with black actors portraying seriously ill patients than when interacting with white actors portraying seriously ill patients.
“Although we found that physicians said the same things to their black and white patients, communication is not just the spoken word. It also involves nonverbal cues, such as eye contact, body positioning, and touch,” said study author Amber Barnato, MD, of the University of Pittsburg in Pennsylvania.
“Poor nonverbal communication—something the physician may not even be aware he or she is doing—could explain why many black patients perceive discrimination in the healthcare setting.”
For this study, Dr Barnato and her colleagues recruited 33 hospital-based attending emergency medicine physicians, hospitalists, and intensivists from Allegheny County, Pennsylvania, and put them in realistic simulations where actors portrayed dying black and white patients accompanied by a family member.
The actors portrayed comparable medical conditions—plummeting vital signs related to either metastatic gastric or pancreatic cancer—and read from matching scripts. The physicians were unaware of what the trial was testing.
The majority of the physicians were white men, so the researchers could not derive any statistically significant conclusions about whether a physician’s race impacted his or her actions.
Physicians were scored on a point system for both their verbal and nonverbal communication skills when interacting with the patient and family member. The physicians averaged 7% lower scores for their nonverbal interactions with the black patients than with the white patients.
“When explaining what was happening and what the next steps for care could be, with the white patients, the physicians were more likely to stand right at the patient’s bedside and touch them in a sympathetic manner,” Dr Barnato said.
She explained that something as simple as a physician staying near the door and holding a binder in front of his body could be perceived by the patient and family as defensive or disengaged. This could lead to a cascade of misunderstandings that result in patients and their families requesting extraordinary life-saving measures because they don’t trust the doctor has their best interests in mind when suggesting gentler, end-of-life care options.
“When you survey people in the community about their feelings on end-of-life care, blacks are only slightly more likely than whites to say they want aggressive, life-sustaining measures when terminally ill,” Dr Barnato said.
“However, blacks are much more likely than whites to request such care when they are faced with making the decision in the hospital. Body language is a significant tool in building trust—or mistrust—and physicians need to ensure that their body language isn’t contributing to that decision.”
“To help black patients and their families feel welcome and encouraged to be partners in medical decision-making, it is critical that doctors be aware of their verbal and nonverbal communication and any unintentional biases.” ![]()
Doctors may convey racial bias with their body language, according to research published in The Journal of Pain and Symptom Management.
In this small study, a group of physicians, most of whom were white males, gave less compassionate nonverbal cues when interacting with black actors portraying seriously ill patients than when interacting with white actors portraying seriously ill patients.
“Although we found that physicians said the same things to their black and white patients, communication is not just the spoken word. It also involves nonverbal cues, such as eye contact, body positioning, and touch,” said study author Amber Barnato, MD, of the University of Pittsburg in Pennsylvania.
“Poor nonverbal communication—something the physician may not even be aware he or she is doing—could explain why many black patients perceive discrimination in the healthcare setting.”
For this study, Dr Barnato and her colleagues recruited 33 hospital-based attending emergency medicine physicians, hospitalists, and intensivists from Allegheny County, Pennsylvania, and put them in realistic simulations where actors portrayed dying black and white patients accompanied by a family member.
The actors portrayed comparable medical conditions—plummeting vital signs related to either metastatic gastric or pancreatic cancer—and read from matching scripts. The physicians were unaware of what the trial was testing.
The majority of the physicians were white men, so the researchers could not derive any statistically significant conclusions about whether a physician’s race impacted his or her actions.
Physicians were scored on a point system for both their verbal and nonverbal communication skills when interacting with the patient and family member. The physicians averaged 7% lower scores for their nonverbal interactions with the black patients than with the white patients.
“When explaining what was happening and what the next steps for care could be, with the white patients, the physicians were more likely to stand right at the patient’s bedside and touch them in a sympathetic manner,” Dr Barnato said.
She explained that something as simple as a physician staying near the door and holding a binder in front of his body could be perceived by the patient and family as defensive or disengaged. This could lead to a cascade of misunderstandings that result in patients and their families requesting extraordinary life-saving measures because they don’t trust the doctor has their best interests in mind when suggesting gentler, end-of-life care options.
“When you survey people in the community about their feelings on end-of-life care, blacks are only slightly more likely than whites to say they want aggressive, life-sustaining measures when terminally ill,” Dr Barnato said.
“However, blacks are much more likely than whites to request such care when they are faced with making the decision in the hospital. Body language is a significant tool in building trust—or mistrust—and physicians need to ensure that their body language isn’t contributing to that decision.”
“To help black patients and their families feel welcome and encouraged to be partners in medical decision-making, it is critical that doctors be aware of their verbal and nonverbal communication and any unintentional biases.” ![]()
Antiepileptic Drugs and Hyponatremia
Call for abstracts: Gut Microbiota for Health World Summit 2016
Share your research at the Gut Microbiota for Health World Summit 2016 with an international audience of researchers and clinicians.
Students, medical residents, trainees, postdoctoral fellows and junior faculty (within 3 years of their first appointment) are invited to submit an abstract for oral or poster presentation. Only a select number of abstracts will be accepted for oral presentation.
If selected, presenters will receive discounted registration and a travel grant to help cover the cost of airfare and accommodations. Abstracts must be submitted to Sandra Megally at [email protected] no later than Sunday, Jan. 17, 2016.
The summit is cosponsored by AGA Institute, European Society of Neurogastroenterology and Motility, European Society for Pediatric Gastroenterology, Hepatology and Nutrition, European Crohn’s and Colitis Organization, and the European Association for the Study of Liver.
Gut Microbiota for Health World Summit 2016 is supported by grants from Danone Dairy and Biocodex.
Share your research at the Gut Microbiota for Health World Summit 2016 with an international audience of researchers and clinicians.
Students, medical residents, trainees, postdoctoral fellows and junior faculty (within 3 years of their first appointment) are invited to submit an abstract for oral or poster presentation. Only a select number of abstracts will be accepted for oral presentation.
If selected, presenters will receive discounted registration and a travel grant to help cover the cost of airfare and accommodations. Abstracts must be submitted to Sandra Megally at [email protected] no later than Sunday, Jan. 17, 2016.
The summit is cosponsored by AGA Institute, European Society of Neurogastroenterology and Motility, European Society for Pediatric Gastroenterology, Hepatology and Nutrition, European Crohn’s and Colitis Organization, and the European Association for the Study of Liver.
Gut Microbiota for Health World Summit 2016 is supported by grants from Danone Dairy and Biocodex.
Share your research at the Gut Microbiota for Health World Summit 2016 with an international audience of researchers and clinicians.
Students, medical residents, trainees, postdoctoral fellows and junior faculty (within 3 years of their first appointment) are invited to submit an abstract for oral or poster presentation. Only a select number of abstracts will be accepted for oral presentation.
If selected, presenters will receive discounted registration and a travel grant to help cover the cost of airfare and accommodations. Abstracts must be submitted to Sandra Megally at [email protected] no later than Sunday, Jan. 17, 2016.
The summit is cosponsored by AGA Institute, European Society of Neurogastroenterology and Motility, European Society for Pediatric Gastroenterology, Hepatology and Nutrition, European Crohn’s and Colitis Organization, and the European Association for the Study of Liver.
Gut Microbiota for Health World Summit 2016 is supported by grants from Danone Dairy and Biocodex.
Help your patients manage chronic constipation
AGA has published the latest in a series of guideline-based resources for members to provide their patients. Based on the published AGA guideline on constipation, the new patient guide explains how a gastroenterologist can help when diet and lifestyle modifications fail.
The guide also explains defecatory disorders, slow-transit and normal-transit constipation, as well as information about tests and medication options in language that is accessible to patients.
AGA’s evidence-based patient guides can help improve the efficiency of office visits and the value you provide patients.
If your patients are suffering from chronic constipation, make sure to let them know about this helpful AGA patient guide.
AGA has published the latest in a series of guideline-based resources for members to provide their patients. Based on the published AGA guideline on constipation, the new patient guide explains how a gastroenterologist can help when diet and lifestyle modifications fail.
The guide also explains defecatory disorders, slow-transit and normal-transit constipation, as well as information about tests and medication options in language that is accessible to patients.
AGA’s evidence-based patient guides can help improve the efficiency of office visits and the value you provide patients.
If your patients are suffering from chronic constipation, make sure to let them know about this helpful AGA patient guide.
AGA has published the latest in a series of guideline-based resources for members to provide their patients. Based on the published AGA guideline on constipation, the new patient guide explains how a gastroenterologist can help when diet and lifestyle modifications fail.
The guide also explains defecatory disorders, slow-transit and normal-transit constipation, as well as information about tests and medication options in language that is accessible to patients.
AGA’s evidence-based patient guides can help improve the efficiency of office visits and the value you provide patients.
If your patients are suffering from chronic constipation, make sure to let them know about this helpful AGA patient guide.
Apply for 2016 research grants
Six grant deadlines are approaching in January 2016; make sure you’re prepared to submit your application by the deadline. Awards are available for both established and young investigators.
AGA is now accepting online applications through the new Grants Management System, which streamlines the application submission process and will be used to facilitate grant reviews.
Apply now for:
• The AGA-Elsevier Gut Microbiome Pilot Research Award. It will provide $25,000 to support pilot research projects pertaining to the gut microbiome. The application deadline is Jan. 15.
• The AGA-Elsevier Pilot Research Award. This is a 1-year grant providing young investigators, instructors, research associates, or equivalents $25,000 to support pilot research projects in gastroenterology- or hepatology-related areas. Two award recipients will be selected. The deadline is Jan. 15.
• The AGA–Rome Foundation Functional GI and Motility Disorders Pilot Research Award. This research initiative grant for $50,000 for 1 year is offered to early-stage investigators to support pilot research projects pertaining to functional GI and motility disorders. This award is jointly sponsored by the Rome Foundation and AGA. The deadline is Jan. 15.
• The AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer. One award of $40,000 will support a young investigator, instructor, research associate, or equivalent who currently holds a federal or nonfederal career development award devoted to conducting research related to digestive cancer. The deadline is Jan. 29.
• The AGA–Covidien Research & Development Pilot Award in Technology. This $30,000 research initiative is offered to investigators to support the research and development of novel devices or technologies that will potentially impact the diagnosis or treatment of digestive disease. The award also includes a $1,000 travel stipend to attend the 2016 AGA Technology Summit. The deadline is Jan. 29.
• The 16th AGA–June & Donald O. Castell, M.D., Esophageal Clinical Research Award. This is a $25,000 grant, which provides research and/or salary support for junior faculty involved in clinical research in esophageal diseases. The deadline is Jan. 29.
We are also now accepting applications for the AGA Investing in the Future Student Research Fellowship. This provides 12 awards at $5,000 for underrepresented minority undergraduate and medical school students to perform 8-10 weeks of research related to digestive diseases or nutrition. The deadline to apply is Feb. 5.
Complete information about these and other research awards is available on www.gastro.org. All recipients will be acknowledged at the Research Recognition Celebration at Digestive Disease Week® 2016 in San Diego.
Six grant deadlines are approaching in January 2016; make sure you’re prepared to submit your application by the deadline. Awards are available for both established and young investigators.
AGA is now accepting online applications through the new Grants Management System, which streamlines the application submission process and will be used to facilitate grant reviews.
Apply now for:
• The AGA-Elsevier Gut Microbiome Pilot Research Award. It will provide $25,000 to support pilot research projects pertaining to the gut microbiome. The application deadline is Jan. 15.
• The AGA-Elsevier Pilot Research Award. This is a 1-year grant providing young investigators, instructors, research associates, or equivalents $25,000 to support pilot research projects in gastroenterology- or hepatology-related areas. Two award recipients will be selected. The deadline is Jan. 15.
• The AGA–Rome Foundation Functional GI and Motility Disorders Pilot Research Award. This research initiative grant for $50,000 for 1 year is offered to early-stage investigators to support pilot research projects pertaining to functional GI and motility disorders. This award is jointly sponsored by the Rome Foundation and AGA. The deadline is Jan. 15.
• The AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer. One award of $40,000 will support a young investigator, instructor, research associate, or equivalent who currently holds a federal or nonfederal career development award devoted to conducting research related to digestive cancer. The deadline is Jan. 29.
• The AGA–Covidien Research & Development Pilot Award in Technology. This $30,000 research initiative is offered to investigators to support the research and development of novel devices or technologies that will potentially impact the diagnosis or treatment of digestive disease. The award also includes a $1,000 travel stipend to attend the 2016 AGA Technology Summit. The deadline is Jan. 29.
• The 16th AGA–June & Donald O. Castell, M.D., Esophageal Clinical Research Award. This is a $25,000 grant, which provides research and/or salary support for junior faculty involved in clinical research in esophageal diseases. The deadline is Jan. 29.
We are also now accepting applications for the AGA Investing in the Future Student Research Fellowship. This provides 12 awards at $5,000 for underrepresented minority undergraduate and medical school students to perform 8-10 weeks of research related to digestive diseases or nutrition. The deadline to apply is Feb. 5.
Complete information about these and other research awards is available on www.gastro.org. All recipients will be acknowledged at the Research Recognition Celebration at Digestive Disease Week® 2016 in San Diego.
Six grant deadlines are approaching in January 2016; make sure you’re prepared to submit your application by the deadline. Awards are available for both established and young investigators.
AGA is now accepting online applications through the new Grants Management System, which streamlines the application submission process and will be used to facilitate grant reviews.
Apply now for:
• The AGA-Elsevier Gut Microbiome Pilot Research Award. It will provide $25,000 to support pilot research projects pertaining to the gut microbiome. The application deadline is Jan. 15.
• The AGA-Elsevier Pilot Research Award. This is a 1-year grant providing young investigators, instructors, research associates, or equivalents $25,000 to support pilot research projects in gastroenterology- or hepatology-related areas. Two award recipients will be selected. The deadline is Jan. 15.
• The AGA–Rome Foundation Functional GI and Motility Disorders Pilot Research Award. This research initiative grant for $50,000 for 1 year is offered to early-stage investigators to support pilot research projects pertaining to functional GI and motility disorders. This award is jointly sponsored by the Rome Foundation and AGA. The deadline is Jan. 15.
• The AGA–Caroline Craig Augustyn & Damian Augustyn Award in Digestive Cancer. One award of $40,000 will support a young investigator, instructor, research associate, or equivalent who currently holds a federal or nonfederal career development award devoted to conducting research related to digestive cancer. The deadline is Jan. 29.
• The AGA–Covidien Research & Development Pilot Award in Technology. This $30,000 research initiative is offered to investigators to support the research and development of novel devices or technologies that will potentially impact the diagnosis or treatment of digestive disease. The award also includes a $1,000 travel stipend to attend the 2016 AGA Technology Summit. The deadline is Jan. 29.
• The 16th AGA–June & Donald O. Castell, M.D., Esophageal Clinical Research Award. This is a $25,000 grant, which provides research and/or salary support for junior faculty involved in clinical research in esophageal diseases. The deadline is Jan. 29.
We are also now accepting applications for the AGA Investing in the Future Student Research Fellowship. This provides 12 awards at $5,000 for underrepresented minority undergraduate and medical school students to perform 8-10 weeks of research related to digestive diseases or nutrition. The deadline to apply is Feb. 5.
Complete information about these and other research awards is available on www.gastro.org. All recipients will be acknowledged at the Research Recognition Celebration at Digestive Disease Week® 2016 in San Diego.
Learn how to avoid a reimbursement loss
The Physician Quality Reporting System (PQRS) will apply a negative 2% payment adjustment in 2017 if practices do not report data on quality measures for covered professional services furnished to Medicare beneficiaries in 2015. By participating in AGA’s Digestive Health Recognition Program™ (www.agarecognition.org), or DHRP, members can report on quality measures and work to avoid this negative payment adjustment.
To learn more about DHRP, register for a free, 30-minute webinar taking place during these two dates (attendee.gotowebinar.com/rt/2452555612218433025):
• Jan 28, 2016, 5 p.m. ET
• Feb. 25, 2016, noon ET
The deadline to enroll for the 2015 PQRS year through DHRP is Feb. 26, 2016. Members pay $300 to enroll.
DHRP is made possible by support from AbbVie; Gilead Science, Inc.; Janssen Biotech, Inc. and Janssen Therapeutics, Division of Janssen Products, LLP; and Shire Pharmaceuticals.
The Physician Quality Reporting System (PQRS) will apply a negative 2% payment adjustment in 2017 if practices do not report data on quality measures for covered professional services furnished to Medicare beneficiaries in 2015. By participating in AGA’s Digestive Health Recognition Program™ (www.agarecognition.org), or DHRP, members can report on quality measures and work to avoid this negative payment adjustment.
To learn more about DHRP, register for a free, 30-minute webinar taking place during these two dates (attendee.gotowebinar.com/rt/2452555612218433025):
• Jan 28, 2016, 5 p.m. ET
• Feb. 25, 2016, noon ET
The deadline to enroll for the 2015 PQRS year through DHRP is Feb. 26, 2016. Members pay $300 to enroll.
DHRP is made possible by support from AbbVie; Gilead Science, Inc.; Janssen Biotech, Inc. and Janssen Therapeutics, Division of Janssen Products, LLP; and Shire Pharmaceuticals.
The Physician Quality Reporting System (PQRS) will apply a negative 2% payment adjustment in 2017 if practices do not report data on quality measures for covered professional services furnished to Medicare beneficiaries in 2015. By participating in AGA’s Digestive Health Recognition Program™ (www.agarecognition.org), or DHRP, members can report on quality measures and work to avoid this negative payment adjustment.
To learn more about DHRP, register for a free, 30-minute webinar taking place during these two dates (attendee.gotowebinar.com/rt/2452555612218433025):
• Jan 28, 2016, 5 p.m. ET
• Feb. 25, 2016, noon ET
The deadline to enroll for the 2015 PQRS year through DHRP is Feb. 26, 2016. Members pay $300 to enroll.
DHRP is made possible by support from AbbVie; Gilead Science, Inc.; Janssen Biotech, Inc. and Janssen Therapeutics, Division of Janssen Products, LLP; and Shire Pharmaceuticals.