User login
Toe Nodule Obliterating the Nail Bed
The Diagnosis: Superficial Acral Fibromyxoma

Superficial acral fibromyxoma (SAF) was first described in 2001 by Fetsch et al.1 Subsequently, the term digital fibromyxoma was proposed in 2012 by Hollmann et al2 to describe a distinctive, slow-growing, soft-tissue tumor with a predilection for the periungual or subungual regions of the fingers and toes. The benign growth typically presents as a painless or tender nodule in middle-aged adults with a slight male predominance (1.3:1 ratio).1,2 In a case series (N=124) described by Hollmann et al,2 9 of 25 patients (36%) who had imaging studies showed bone involvement by an erosive or lytic lesion. Reports of SAF with bone involvement also have been described in the radiologic and orthopedic surgery literature.3,4 Radiographically, the soft-tissue invasion of the bone is demonstrated by scalloping on plain radiographs (Figure 1).3
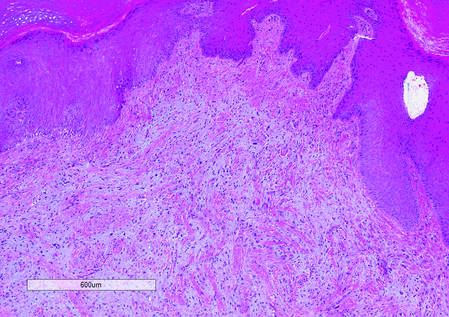
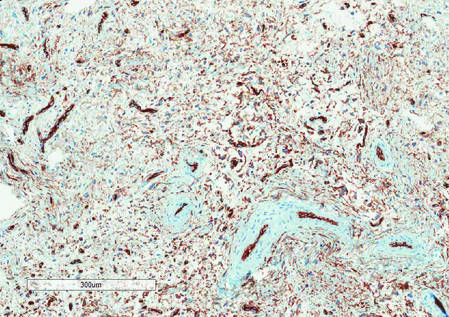
Histologically, SAFs are moderately cellular with spindled or stellate fibroblastlike cells within a myxoid or collagenous matrix (Figure 2).1 The vasculature is mildly accentuated and an increase in mast cells usually is observed. The nuclei have a low degree of atypia with few mitotic figures, and the stellate cells exhibit positive immunohistochemical staining for CD34 (Figure 3), epithelial membrane antigen, and CD99.1 Hollmann et al2 found that 66 of 95 tumors (69.5%) infiltrated the dermal collagen, 26 (27.4%) infiltrated fat, and 3 (3.2%) invaded bone. Of the 47 cases that were evaluated on follow-up, 10 tumors (21.3%) recurred locally (all near the nail unit of the fingers or toes) after a mean interval of 27 months. Although invasion of underlying tissues and recurrence of the tumor has been demonstrated, this growth is considered benign. The histologic differential diagnosis includes neurofibroma, myxoma, fibroma, low-grade fibromyxoid sarcoma, dermatofibroma, superficial angiomyxoma, and dermatofibrosarcoma protuberans.2
The primary treatment of SAF is local excision. The incidence of local recurrence found in the case series by Hollmann et al2 was directly linked to positive margins after the first excision (10/47 [21.3%] recurrent lesions had positive margins). To date, there are no known reports of metastatic disease in SAF.2 Our case manifested with a late recurrence of the tumor and bone involvement requiring surgical excision, which illustrates the role of adjuvant imaging and close follow-up following excision of any soft-tissue tumors of the fingers and toes that have been histologically confirmed as SAF, particularly those of the periungual region.
|
|
|
|
1. Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma (a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes.) Hum Pathol. 2001;32:704-714.
2. Hollmann TJ, Bovée JV, Fletcher CD. Digital fibromyxoma (superficial acral fibromyxoma): a detailed characterization of 124 cases. Am J Surg Pathol. 2012;36:789-798.
3. Varikatt W, Soper J, Simmon G, et al. Superficial acral fibromyxoma: a report of two cases with radiological findings. Skeletal Radiol. 2008;37:499-503.
4. Oteo-Alvaro A, Meizoso T, Scarpellini A, et al. Superficial acral fibromyxoma of the toe, with erosion of the distal phalanx. a clinical report. Arch Orthop Trauma Surg. 2008;128:271-274.
The Diagnosis: Superficial Acral Fibromyxoma
Superficial acral fibromyxoma (SAF) was first described in 2001 by Fetsch et al.1 Subsequently, the term digital fibromyxoma was proposed in 2012 by Hollmann et al2 to describe a distinctive, slow-growing, soft-tissue tumor with a predilection for the periungual or subungual regions of the fingers and toes. The benign growth typically presents as a painless or tender nodule in middle-aged adults with a slight male predominance (1.3:1 ratio).1,2 In a case series (N=124) described by Hollmann et al,2 9 of 25 patients (36%) who had imaging studies showed bone involvement by an erosive or lytic lesion. Reports of SAF with bone involvement also have been described in the radiologic and orthopedic surgery literature.3,4 Radiographically, the soft-tissue invasion of the bone is demonstrated by scalloping on plain radiographs (Figure 1).3
Histologically, SAFs are moderately cellular with spindled or stellate fibroblastlike cells within a myxoid or collagenous matrix (Figure 2).1 The vasculature is mildly accentuated and an increase in mast cells usually is observed. The nuclei have a low degree of atypia with few mitotic figures, and the stellate cells exhibit positive immunohistochemical staining for CD34 (Figure 3), epithelial membrane antigen, and CD99.1 Hollmann et al2 found that 66 of 95 tumors (69.5%) infiltrated the dermal collagen, 26 (27.4%) infiltrated fat, and 3 (3.2%) invaded bone. Of the 47 cases that were evaluated on follow-up, 10 tumors (21.3%) recurred locally (all near the nail unit of the fingers or toes) after a mean interval of 27 months. Although invasion of underlying tissues and recurrence of the tumor has been demonstrated, this growth is considered benign. The histologic differential diagnosis includes neurofibroma, myxoma, fibroma, low-grade fibromyxoid sarcoma, dermatofibroma, superficial angiomyxoma, and dermatofibrosarcoma protuberans.2
The primary treatment of SAF is local excision. The incidence of local recurrence found in the case series by Hollmann et al2 was directly linked to positive margins after the first excision (10/47 [21.3%] recurrent lesions had positive margins). To date, there are no known reports of metastatic disease in SAF.2 Our case manifested with a late recurrence of the tumor and bone involvement requiring surgical excision, which illustrates the role of adjuvant imaging and close follow-up following excision of any soft-tissue tumors of the fingers and toes that have been histologically confirmed as SAF, particularly those of the periungual region.
|
|
|
|
|
|
The Diagnosis: Superficial Acral Fibromyxoma
Superficial acral fibromyxoma (SAF) was first described in 2001 by Fetsch et al.1 Subsequently, the term digital fibromyxoma was proposed in 2012 by Hollmann et al2 to describe a distinctive, slow-growing, soft-tissue tumor with a predilection for the periungual or subungual regions of the fingers and toes. The benign growth typically presents as a painless or tender nodule in middle-aged adults with a slight male predominance (1.3:1 ratio).1,2 In a case series (N=124) described by Hollmann et al,2 9 of 25 patients (36%) who had imaging studies showed bone involvement by an erosive or lytic lesion. Reports of SAF with bone involvement also have been described in the radiologic and orthopedic surgery literature.3,4 Radiographically, the soft-tissue invasion of the bone is demonstrated by scalloping on plain radiographs (Figure 1).3
Histologically, SAFs are moderately cellular with spindled or stellate fibroblastlike cells within a myxoid or collagenous matrix (Figure 2).1 The vasculature is mildly accentuated and an increase in mast cells usually is observed. The nuclei have a low degree of atypia with few mitotic figures, and the stellate cells exhibit positive immunohistochemical staining for CD34 (Figure 3), epithelial membrane antigen, and CD99.1 Hollmann et al2 found that 66 of 95 tumors (69.5%) infiltrated the dermal collagen, 26 (27.4%) infiltrated fat, and 3 (3.2%) invaded bone. Of the 47 cases that were evaluated on follow-up, 10 tumors (21.3%) recurred locally (all near the nail unit of the fingers or toes) after a mean interval of 27 months. Although invasion of underlying tissues and recurrence of the tumor has been demonstrated, this growth is considered benign. The histologic differential diagnosis includes neurofibroma, myxoma, fibroma, low-grade fibromyxoid sarcoma, dermatofibroma, superficial angiomyxoma, and dermatofibrosarcoma protuberans.2
The primary treatment of SAF is local excision. The incidence of local recurrence found in the case series by Hollmann et al2 was directly linked to positive margins after the first excision (10/47 [21.3%] recurrent lesions had positive margins). To date, there are no known reports of metastatic disease in SAF.2 Our case manifested with a late recurrence of the tumor and bone involvement requiring surgical excision, which illustrates the role of adjuvant imaging and close follow-up following excision of any soft-tissue tumors of the fingers and toes that have been histologically confirmed as SAF, particularly those of the periungual region.
|
|
|
|
|
|
1. Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma (a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes.) Hum Pathol. 2001;32:704-714.
2. Hollmann TJ, Bovée JV, Fletcher CD. Digital fibromyxoma (superficial acral fibromyxoma): a detailed characterization of 124 cases. Am J Surg Pathol. 2012;36:789-798.
3. Varikatt W, Soper J, Simmon G, et al. Superficial acral fibromyxoma: a report of two cases with radiological findings. Skeletal Radiol. 2008;37:499-503.
4. Oteo-Alvaro A, Meizoso T, Scarpellini A, et al. Superficial acral fibromyxoma of the toe, with erosion of the distal phalanx. a clinical report. Arch Orthop Trauma Surg. 2008;128:271-274.
1. Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma (a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes.) Hum Pathol. 2001;32:704-714.
2. Hollmann TJ, Bovée JV, Fletcher CD. Digital fibromyxoma (superficial acral fibromyxoma): a detailed characterization of 124 cases. Am J Surg Pathol. 2012;36:789-798.
3. Varikatt W, Soper J, Simmon G, et al. Superficial acral fibromyxoma: a report of two cases with radiological findings. Skeletal Radiol. 2008;37:499-503.
4. Oteo-Alvaro A, Meizoso T, Scarpellini A, et al. Superficial acral fibromyxoma of the toe, with erosion of the distal phalanx. a clinical report. Arch Orthop Trauma Surg. 2008;128:271-274.

A generally healthy 30-year-old man presented with a 3-cm exophytic, yellowish red, subungual nodule of the left great toe of 1 year’s duration that was obliterating the nail plate. Ten years prior, a similar nodule in the same location was removed via laser by a podiatrist. Medical records were not retrievable, but the patient reported that he was told the excised lesion was a benign tumor. Plain radiographs were performed at the current presentation and demonstrated an inferior cortical lucency of the distal phalanx as well as a lucency over the nail bed region with extension of calcification to the soft tissues. Magnetic resonance imaging showed a mass with a proximal to distal maximum dimension of 2.1 cm that involved the dorsal surface of the proximal phalanx. Magnetic resonance imaging also demonstrated bone erosion from the overlying mass. A 4-mm incisional punch biopsy was performed prior to surgical excision.

Patch Testing: Working With Patients to Find a Relevant Allergen

What do your patients need to know at the first visit?
Patients with chronic dermatitis are frequently referred for patch testing. An in-depth conversation reviewing the patch test procedure and the many potential causes of dermatitis (eg, endogenous, allergic, irritant, seborrheic) is needed. Patients should understand the patch test process. The testing extends over a week, requiring 3 days of visits. The patches are applied at day 1 and must be kept dry and in place for 48 hours, then they are removed and evaluated. A second follow-up visit at 96 hours to 1 week after the patches are applied is done to perform a final read, interpret, and explain the final results. The patient needs to know that we are looking for an allergen that might be causing the eruption through contact exposure with the skin. The difference between patch testing and prick testing often needs to be discussed, as patients are not always aware of the difference. Explaining the need to avoid topical steroids at the patch test site, sunburn, or systemic steroids during the patch test period is also important to obtain optimal testing conditions.
Querying all exposures including work, home, personal care products, and hobbies is important to help determine which allergen series should be tested to obtain the best results. Patients need to understand that even small intermittent exposures can cause an ongoing dermatitis. If a causative allergen(s) is identified, strict avoidance can lead to clearance and resolution.
Setting expectations is important, and therefore you should discuss the possibility that no allergen will be identified while letting the patient know that this information is also useful. Also, let patients know there are other things that can be done if patch testing is negative to try and gain control of the dermatitis including laboratory tests and biopsies, which may be needed to help direct future management.
What are your go-to treatments? What are the side effects?
The beauty of patch testing is that finding a relevant allergen and subsequent avoidance of that allergen often is sufficient to improve or clear the dermatitis. Detailed education regarding the allergen, where it is found, and how to avoid it are imperative in patient management. I provide the patient with information sheets or narratives found on the American Contact Dermatitis Society website (http://www.contactderm.org) as well as a list of safe products found on the Contact Allergen Management Program (CAMP) area of the site. These tools help in patient compliance.
Go-to treatments for relevant patch test dermatitis involve topical steroids to calm the acute dermatitis while educating and instituting a personal environment free of the identified allergens. Occasionally, systemic steroids are used to provide relief and calm down an extensive dermatitis while educating, identifying, and eliminating known allergens from the patient’s environment. Identifying and eliminating an allergen can mitigate the need for chronic steroids, and the resultant side effects of hypertension, osteoporosis, avascular necrosis, hyperglycemia, and gastrointestinal tract problems can be avoided. Likewise, avoidance of allergens can lead to the elimination of the need for chronic topical steroids and the resultant atrophy and striae.
Side effects of the patch test procedure itself include an allergic reaction to one of the chemicals tested (eg, gold), which is what you are looking for; persistent reactions; flaring of existing dermatitis; irritation; hyperpigmentation; and rarely anaphylaxis or infection at a patch test site. If no allergy is found, treatment of generalized dermatitis can include topical steroids. Topical calcineurin inhibitors can be useful as well as narrowband UV light. Several oral medications can be used for recalcitrant patch test–negative dermatitis and the selection of the right medication is based on the patient’s comorbidities and extent of dermatitis, including systemic steroids, though long-term use is not recommended. Mycophenolate mofetil, methotrexate, cyclosporine, and azathioprine all have side effects including liver and renal toxicity, immunosuppression, and risk for malignancy and therefore need to be considered on a case-by-case basis.
How do you keep the patient compliant with treatment?
Treating allergic contact dermatitis once an allergen(s) has been identified can be challenging. Education is key so that the patient understands where the allergen is found in his/her environment and how to avoid it. Teaching the patient to read labels also is important. Providing a list of safe products simplifies compliance. Reinforcing the need for ongoing vigilance in allergen avoidance is critical to resolution of the dermatitis. Reinforcing the need for continuous avoidance is imperative, as patients sometimes become less vigilant once the dermatitis resolves and the allergen can sneak back into their environment.
What do I do if a patient refuses treatment?
Sometimes patients are so attached to a product that they do not want to stop using it even though they know it is the cause of their dermatitis. If I can help them identify a comparable product, I introduce them to it, but ultimately they get to decide if they prefer to use a product that they know is the cause of their rash or if they want to avoid it and be clear of the dermatitis. For those who do not have an allergen identified through patch testing, alternative treatments can be used. If they do not want systemic medication, I try and optimize their skin care regimen with mild soaps, bland moisturizing creams, and short lukewarm showers, which often is not enough and eventually due to ongoing itch patients decide to discuss and pursue treatment options.
What do your patients need to know at the first visit?
Patients with chronic dermatitis are frequently referred for patch testing. An in-depth conversation reviewing the patch test procedure and the many potential causes of dermatitis (eg, endogenous, allergic, irritant, seborrheic) is needed. Patients should understand the patch test process. The testing extends over a week, requiring 3 days of visits. The patches are applied at day 1 and must be kept dry and in place for 48 hours, then they are removed and evaluated. A second follow-up visit at 96 hours to 1 week after the patches are applied is done to perform a final read, interpret, and explain the final results. The patient needs to know that we are looking for an allergen that might be causing the eruption through contact exposure with the skin. The difference between patch testing and prick testing often needs to be discussed, as patients are not always aware of the difference. Explaining the need to avoid topical steroids at the patch test site, sunburn, or systemic steroids during the patch test period is also important to obtain optimal testing conditions.
Querying all exposures including work, home, personal care products, and hobbies is important to help determine which allergen series should be tested to obtain the best results. Patients need to understand that even small intermittent exposures can cause an ongoing dermatitis. If a causative allergen(s) is identified, strict avoidance can lead to clearance and resolution.
Setting expectations is important, and therefore you should discuss the possibility that no allergen will be identified while letting the patient know that this information is also useful. Also, let patients know there are other things that can be done if patch testing is negative to try and gain control of the dermatitis including laboratory tests and biopsies, which may be needed to help direct future management.
What are your go-to treatments? What are the side effects?
The beauty of patch testing is that finding a relevant allergen and subsequent avoidance of that allergen often is sufficient to improve or clear the dermatitis. Detailed education regarding the allergen, where it is found, and how to avoid it are imperative in patient management. I provide the patient with information sheets or narratives found on the American Contact Dermatitis Society website (http://www.contactderm.org) as well as a list of safe products found on the Contact Allergen Management Program (CAMP) area of the site. These tools help in patient compliance.
Go-to treatments for relevant patch test dermatitis involve topical steroids to calm the acute dermatitis while educating and instituting a personal environment free of the identified allergens. Occasionally, systemic steroids are used to provide relief and calm down an extensive dermatitis while educating, identifying, and eliminating known allergens from the patient’s environment. Identifying and eliminating an allergen can mitigate the need for chronic steroids, and the resultant side effects of hypertension, osteoporosis, avascular necrosis, hyperglycemia, and gastrointestinal tract problems can be avoided. Likewise, avoidance of allergens can lead to the elimination of the need for chronic topical steroids and the resultant atrophy and striae.
Side effects of the patch test procedure itself include an allergic reaction to one of the chemicals tested (eg, gold), which is what you are looking for; persistent reactions; flaring of existing dermatitis; irritation; hyperpigmentation; and rarely anaphylaxis or infection at a patch test site. If no allergy is found, treatment of generalized dermatitis can include topical steroids. Topical calcineurin inhibitors can be useful as well as narrowband UV light. Several oral medications can be used for recalcitrant patch test–negative dermatitis and the selection of the right medication is based on the patient’s comorbidities and extent of dermatitis, including systemic steroids, though long-term use is not recommended. Mycophenolate mofetil, methotrexate, cyclosporine, and azathioprine all have side effects including liver and renal toxicity, immunosuppression, and risk for malignancy and therefore need to be considered on a case-by-case basis.
How do you keep the patient compliant with treatment?
Treating allergic contact dermatitis once an allergen(s) has been identified can be challenging. Education is key so that the patient understands where the allergen is found in his/her environment and how to avoid it. Teaching the patient to read labels also is important. Providing a list of safe products simplifies compliance. Reinforcing the need for ongoing vigilance in allergen avoidance is critical to resolution of the dermatitis. Reinforcing the need for continuous avoidance is imperative, as patients sometimes become less vigilant once the dermatitis resolves and the allergen can sneak back into their environment.
What do I do if a patient refuses treatment?
Sometimes patients are so attached to a product that they do not want to stop using it even though they know it is the cause of their dermatitis. If I can help them identify a comparable product, I introduce them to it, but ultimately they get to decide if they prefer to use a product that they know is the cause of their rash or if they want to avoid it and be clear of the dermatitis. For those who do not have an allergen identified through patch testing, alternative treatments can be used. If they do not want systemic medication, I try and optimize their skin care regimen with mild soaps, bland moisturizing creams, and short lukewarm showers, which often is not enough and eventually due to ongoing itch patients decide to discuss and pursue treatment options.
What do your patients need to know at the first visit?
Patients with chronic dermatitis are frequently referred for patch testing. An in-depth conversation reviewing the patch test procedure and the many potential causes of dermatitis (eg, endogenous, allergic, irritant, seborrheic) is needed. Patients should understand the patch test process. The testing extends over a week, requiring 3 days of visits. The patches are applied at day 1 and must be kept dry and in place for 48 hours, then they are removed and evaluated. A second follow-up visit at 96 hours to 1 week after the patches are applied is done to perform a final read, interpret, and explain the final results. The patient needs to know that we are looking for an allergen that might be causing the eruption through contact exposure with the skin. The difference between patch testing and prick testing often needs to be discussed, as patients are not always aware of the difference. Explaining the need to avoid topical steroids at the patch test site, sunburn, or systemic steroids during the patch test period is also important to obtain optimal testing conditions.
Querying all exposures including work, home, personal care products, and hobbies is important to help determine which allergen series should be tested to obtain the best results. Patients need to understand that even small intermittent exposures can cause an ongoing dermatitis. If a causative allergen(s) is identified, strict avoidance can lead to clearance and resolution.
Setting expectations is important, and therefore you should discuss the possibility that no allergen will be identified while letting the patient know that this information is also useful. Also, let patients know there are other things that can be done if patch testing is negative to try and gain control of the dermatitis including laboratory tests and biopsies, which may be needed to help direct future management.
What are your go-to treatments? What are the side effects?
The beauty of patch testing is that finding a relevant allergen and subsequent avoidance of that allergen often is sufficient to improve or clear the dermatitis. Detailed education regarding the allergen, where it is found, and how to avoid it are imperative in patient management. I provide the patient with information sheets or narratives found on the American Contact Dermatitis Society website (http://www.contactderm.org) as well as a list of safe products found on the Contact Allergen Management Program (CAMP) area of the site. These tools help in patient compliance.
Go-to treatments for relevant patch test dermatitis involve topical steroids to calm the acute dermatitis while educating and instituting a personal environment free of the identified allergens. Occasionally, systemic steroids are used to provide relief and calm down an extensive dermatitis while educating, identifying, and eliminating known allergens from the patient’s environment. Identifying and eliminating an allergen can mitigate the need for chronic steroids, and the resultant side effects of hypertension, osteoporosis, avascular necrosis, hyperglycemia, and gastrointestinal tract problems can be avoided. Likewise, avoidance of allergens can lead to the elimination of the need for chronic topical steroids and the resultant atrophy and striae.
Side effects of the patch test procedure itself include an allergic reaction to one of the chemicals tested (eg, gold), which is what you are looking for; persistent reactions; flaring of existing dermatitis; irritation; hyperpigmentation; and rarely anaphylaxis or infection at a patch test site. If no allergy is found, treatment of generalized dermatitis can include topical steroids. Topical calcineurin inhibitors can be useful as well as narrowband UV light. Several oral medications can be used for recalcitrant patch test–negative dermatitis and the selection of the right medication is based on the patient’s comorbidities and extent of dermatitis, including systemic steroids, though long-term use is not recommended. Mycophenolate mofetil, methotrexate, cyclosporine, and azathioprine all have side effects including liver and renal toxicity, immunosuppression, and risk for malignancy and therefore need to be considered on a case-by-case basis.
How do you keep the patient compliant with treatment?
Treating allergic contact dermatitis once an allergen(s) has been identified can be challenging. Education is key so that the patient understands where the allergen is found in his/her environment and how to avoid it. Teaching the patient to read labels also is important. Providing a list of safe products simplifies compliance. Reinforcing the need for ongoing vigilance in allergen avoidance is critical to resolution of the dermatitis. Reinforcing the need for continuous avoidance is imperative, as patients sometimes become less vigilant once the dermatitis resolves and the allergen can sneak back into their environment.
What do I do if a patient refuses treatment?
Sometimes patients are so attached to a product that they do not want to stop using it even though they know it is the cause of their dermatitis. If I can help them identify a comparable product, I introduce them to it, but ultimately they get to decide if they prefer to use a product that they know is the cause of their rash or if they want to avoid it and be clear of the dermatitis. For those who do not have an allergen identified through patch testing, alternative treatments can be used. If they do not want systemic medication, I try and optimize their skin care regimen with mild soaps, bland moisturizing creams, and short lukewarm showers, which often is not enough and eventually due to ongoing itch patients decide to discuss and pursue treatment options.

IBD and the Risk of Oral Cancer
Patients with inflammatory bowel disease (IBD) may have a higher risk of oral cancer, according to a study at Mount Sinai Medical Center. Researchers collected data on 7,294 patients from 2000 through 2011. The results were published in the March issue of Clinical Gastroenterology and Hepatology.
Related: Exercise and Inflammatory Bowel Disease
In the study, the expected incidence of oral cancer was calculated for the patients who were stratified by gender and age using the Surveillance, Epidemiology and End Results (SEER) 18 registry data. Seven men and 4 women had biopsy-proven oral cancer. Six had cancer of the tongue, 2 had cancer of the hard palate, and 3 had tonsillar, buccal, or mandibular sarcoma. Seven patients had been treated for IBD before the cancer diagnosis.
Women had a higher risk of oral cancer. Adjusted for age and sex, the incidence ratio for oral cancer in patients with IBD was 9.77:12.07 for women12.07 and 9.77:8.49 for men. The age-adjusted incidence ratio for tongue cancer was 18.91: 17.06 for men, 22.10 for women.
Related: More Illnesses Linked to Camp Lejeune Water
The authors concluded that, “we found patients with IBD to be at increased risk for oral cancers, especially tongue cancer. Women are at higher risk than men.”
Source:
Katsanos KH, Roda G, McBride RB, Cohen B, Colombel JF. Clin Gastroenterol Hepatol. 2016;14(3):413-420
doi: 10.1016/j.cgh.2015.09.041.
Patients with inflammatory bowel disease (IBD) may have a higher risk of oral cancer, according to a study at Mount Sinai Medical Center. Researchers collected data on 7,294 patients from 2000 through 2011. The results were published in the March issue of Clinical Gastroenterology and Hepatology.
Related: Exercise and Inflammatory Bowel Disease
In the study, the expected incidence of oral cancer was calculated for the patients who were stratified by gender and age using the Surveillance, Epidemiology and End Results (SEER) 18 registry data. Seven men and 4 women had biopsy-proven oral cancer. Six had cancer of the tongue, 2 had cancer of the hard palate, and 3 had tonsillar, buccal, or mandibular sarcoma. Seven patients had been treated for IBD before the cancer diagnosis.
Women had a higher risk of oral cancer. Adjusted for age and sex, the incidence ratio for oral cancer in patients with IBD was 9.77:12.07 for women12.07 and 9.77:8.49 for men. The age-adjusted incidence ratio for tongue cancer was 18.91: 17.06 for men, 22.10 for women.
Related: More Illnesses Linked to Camp Lejeune Water
The authors concluded that, “we found patients with IBD to be at increased risk for oral cancers, especially tongue cancer. Women are at higher risk than men.”
Source:
Katsanos KH, Roda G, McBride RB, Cohen B, Colombel JF. Clin Gastroenterol Hepatol. 2016;14(3):413-420
doi: 10.1016/j.cgh.2015.09.041.
Patients with inflammatory bowel disease (IBD) may have a higher risk of oral cancer, according to a study at Mount Sinai Medical Center. Researchers collected data on 7,294 patients from 2000 through 2011. The results were published in the March issue of Clinical Gastroenterology and Hepatology.
Related: Exercise and Inflammatory Bowel Disease
In the study, the expected incidence of oral cancer was calculated for the patients who were stratified by gender and age using the Surveillance, Epidemiology and End Results (SEER) 18 registry data. Seven men and 4 women had biopsy-proven oral cancer. Six had cancer of the tongue, 2 had cancer of the hard palate, and 3 had tonsillar, buccal, or mandibular sarcoma. Seven patients had been treated for IBD before the cancer diagnosis.
Women had a higher risk of oral cancer. Adjusted for age and sex, the incidence ratio for oral cancer in patients with IBD was 9.77:12.07 for women12.07 and 9.77:8.49 for men. The age-adjusted incidence ratio for tongue cancer was 18.91: 17.06 for men, 22.10 for women.
Related: More Illnesses Linked to Camp Lejeune Water
The authors concluded that, “we found patients with IBD to be at increased risk for oral cancers, especially tongue cancer. Women are at higher risk than men.”
Source:
Katsanos KH, Roda G, McBride RB, Cohen B, Colombel JF. Clin Gastroenterol Hepatol. 2016;14(3):413-420
doi: 10.1016/j.cgh.2015.09.041.
Prelabor cesarean delivery linked to increased risk of childhood ALL
An increased risk of acute lymphoblastic leukemia (ALL) was seen in young children born by prelabor cesarean delivery, in a pooled analysis of 13 case-control studies from nine countries.
The odds ratio was significant at 1.23 for an association between prelabor cesarean delivery and ALL (P = .018); there was not a significant association between ALL and all indications of cesarean delivery nor was there an association with emergency cesarean delivery. Further, the risk for childhood AML was not associated with cesarean delivery, prelabor cesarean delivery, or emergency cesarean delivery, reported Erin L. Marcotte, Ph.D., of the University of Minnesota, Minneapolis, and her associates.

The association between ALL and prelabor cesarean delivery is based on 13 case-control studies from the Childhood Leukemia International Consortium. Birth delivery method was known for 97%-99% of 8,780 ALL cases, 1,332 AML cases, and 23,459 controls in those studies. In four of the studies, the indications for cesarean delivery were known for 1,061 of 4,313 ALL cases, 138 of 664 AML cases, and 1,401 of 5,884 controls. The multivariable logistic regression models used for the analysis were adjusted for birth weight, sex, age, ethnic origin, parental education, maternal age, and study.
If the association proves to be causal, “maladaptive immune activation due to an absence of stress response before birth in children born by prelabor caesarean delivery could be considered as a potential mechanism,” the researchers wrote (Lancet Haematol. 2016;3[4]:e176–e185).
ALL involves genetic and developmental aberrations that are probably modified by exposure and response to infectious agents. Early exposure to a variety of infections seems to decrease risk, and a vigorous response to infections (quantified by physician visits for infections) increases risk. During vaginal birth, the newborn is exposed to commensal bacteria that modulate immune development, Joseph Weimels, Ph.D., of the University of California at San Francisco, and Xiaomei Ma, Ph.D., of the Yale School of Public Health, New Haven, Conn., wrote in an editorial published in the same issue of The Lancet Haematology. Children delivered vaginally have different gut microbiomes and T-cell reactivity persisting up to age 2 years compared with children born by cesarean, they wrote.
The National Cancer Institute funded the study. The researchers had no relevant disclosures.
On Twitter @maryjodales
An increased risk of acute lymphoblastic leukemia (ALL) was seen in young children born by prelabor cesarean delivery, in a pooled analysis of 13 case-control studies from nine countries.
The odds ratio was significant at 1.23 for an association between prelabor cesarean delivery and ALL (P = .018); there was not a significant association between ALL and all indications of cesarean delivery nor was there an association with emergency cesarean delivery. Further, the risk for childhood AML was not associated with cesarean delivery, prelabor cesarean delivery, or emergency cesarean delivery, reported Erin L. Marcotte, Ph.D., of the University of Minnesota, Minneapolis, and her associates.
The association between ALL and prelabor cesarean delivery is based on 13 case-control studies from the Childhood Leukemia International Consortium. Birth delivery method was known for 97%-99% of 8,780 ALL cases, 1,332 AML cases, and 23,459 controls in those studies. In four of the studies, the indications for cesarean delivery were known for 1,061 of 4,313 ALL cases, 138 of 664 AML cases, and 1,401 of 5,884 controls. The multivariable logistic regression models used for the analysis were adjusted for birth weight, sex, age, ethnic origin, parental education, maternal age, and study.
If the association proves to be causal, “maladaptive immune activation due to an absence of stress response before birth in children born by prelabor caesarean delivery could be considered as a potential mechanism,” the researchers wrote (Lancet Haematol. 2016;3[4]:e176–e185).
ALL involves genetic and developmental aberrations that are probably modified by exposure and response to infectious agents. Early exposure to a variety of infections seems to decrease risk, and a vigorous response to infections (quantified by physician visits for infections) increases risk. During vaginal birth, the newborn is exposed to commensal bacteria that modulate immune development, Joseph Weimels, Ph.D., of the University of California at San Francisco, and Xiaomei Ma, Ph.D., of the Yale School of Public Health, New Haven, Conn., wrote in an editorial published in the same issue of The Lancet Haematology. Children delivered vaginally have different gut microbiomes and T-cell reactivity persisting up to age 2 years compared with children born by cesarean, they wrote.
The National Cancer Institute funded the study. The researchers had no relevant disclosures.
On Twitter @maryjodales
An increased risk of acute lymphoblastic leukemia (ALL) was seen in young children born by prelabor cesarean delivery, in a pooled analysis of 13 case-control studies from nine countries.
The odds ratio was significant at 1.23 for an association between prelabor cesarean delivery and ALL (P = .018); there was not a significant association between ALL and all indications of cesarean delivery nor was there an association with emergency cesarean delivery. Further, the risk for childhood AML was not associated with cesarean delivery, prelabor cesarean delivery, or emergency cesarean delivery, reported Erin L. Marcotte, Ph.D., of the University of Minnesota, Minneapolis, and her associates.
The association between ALL and prelabor cesarean delivery is based on 13 case-control studies from the Childhood Leukemia International Consortium. Birth delivery method was known for 97%-99% of 8,780 ALL cases, 1,332 AML cases, and 23,459 controls in those studies. In four of the studies, the indications for cesarean delivery were known for 1,061 of 4,313 ALL cases, 138 of 664 AML cases, and 1,401 of 5,884 controls. The multivariable logistic regression models used for the analysis were adjusted for birth weight, sex, age, ethnic origin, parental education, maternal age, and study.
If the association proves to be causal, “maladaptive immune activation due to an absence of stress response before birth in children born by prelabor caesarean delivery could be considered as a potential mechanism,” the researchers wrote (Lancet Haematol. 2016;3[4]:e176–e185).
ALL involves genetic and developmental aberrations that are probably modified by exposure and response to infectious agents. Early exposure to a variety of infections seems to decrease risk, and a vigorous response to infections (quantified by physician visits for infections) increases risk. During vaginal birth, the newborn is exposed to commensal bacteria that modulate immune development, Joseph Weimels, Ph.D., of the University of California at San Francisco, and Xiaomei Ma, Ph.D., of the Yale School of Public Health, New Haven, Conn., wrote in an editorial published in the same issue of The Lancet Haematology. Children delivered vaginally have different gut microbiomes and T-cell reactivity persisting up to age 2 years compared with children born by cesarean, they wrote.
The National Cancer Institute funded the study. The researchers had no relevant disclosures.
On Twitter @maryjodales
THE LANCET HAEMATOLOGY
Key clinical point: Prelabor cesarean delivery was associated with an increased risk of childhood ALL, but not AML.
Major finding: The odds ratio was significant at 1.23 for an association between prelabor cesarean delivery and ALL (P = .018).
Data source: Thirteen case-control studies from the Childhood Leukemia International Consortium.
Disclosures: The National Cancer Institute funded the study. The researchers had no relevant disclosures.

Physical therapy underused for knee osteoarthritis
AMSTERDAM – Physical therapy is underused as a first conservative treatment option for knee osteoarthritis, according to a review of data of more than 130,000 men and women serving in the U.S. military.
Data from the Military Health System Data Repository (MDR) show that clinical practice is often out of step with guidelines, as many patients are treated with intra-articular corticosteroid injections rather than physical therapy.

Within a week of an initial episode of knee OA, patients were four times more likely to be given steroid injections than receive physical therapy (14,290 vs. 3,177 patients), although a similar number of patients received injections or physical therapy within 30 days (8,228 vs. 8,407) and 90 days (9,125 vs. 10,059). Of the patients given injections early, 12,311 received them on the day of the index episode.
“What was interesting, anecdotally, was how few patients had been to physical therapy prior to surgery and how many of them had had injections before physical therapy,” Dr. Dan Rhon, director of physical therapy at Brooke Army Medical Center, Houston, said in an interview at the World Congress on Osteoarthritis.
“We wanted to look at the practice patterns because guidelines generally say that you should try physical therapy before surgery and that invasive procedures such as injections should be utilized further down the road,” he said at the meeting, which was sponsored by Osteoarthritis Research Society International.
Dr. Rhon noted that in a study of clinical practice patterns over a 5-year period from the United Healthcare Database, researchers found that physical rehabilitation was used in about one-quarter of patients, with 10% of those who went on to have surgery receiving physical therapy specific for OA, and 16% had been given intra-articular injections (Arthroscopy. 2014;30:65-71).
Results from the MDR data, which considered records from 2008 to 2013 and 1 year of follow-up, now show similar findings with 29% of patients receiving physical rehabilitation, 17.5% prior to knee arthroplasty, and 36% of patients receiving corticosteroid injections first.
What this shows, Dr. Rhon said, is that clinical practice patterns in the Military Health System do not appear to be following established guidelines. “It’s a little bit worrisome because most of these patients should at least have a trial of conservative management.” Perhaps there is some confusion over what constitutes conservative management, but when there is a choice between physical therapy and corticosteroid injections, it seems that the latter is more commonly being selected. Patients themselves could also be opting for injections over physical rehabilitation, so there may be a need for education on what options are available before surgical intervention.
Further research is needed to examine the clinical outcomes of this and perhaps look at how cost savings could be made if clinical practice more closely adhered to the OA guidelines. Looking at a longer follow-up period, say 2-5 years post diagnosis, might also give a better reflection of the use of physical therapy before surgery.
Dr. Rhon had no financial disclosures.
AMSTERDAM – Physical therapy is underused as a first conservative treatment option for knee osteoarthritis, according to a review of data of more than 130,000 men and women serving in the U.S. military.
Data from the Military Health System Data Repository (MDR) show that clinical practice is often out of step with guidelines, as many patients are treated with intra-articular corticosteroid injections rather than physical therapy.
Within a week of an initial episode of knee OA, patients were four times more likely to be given steroid injections than receive physical therapy (14,290 vs. 3,177 patients), although a similar number of patients received injections or physical therapy within 30 days (8,228 vs. 8,407) and 90 days (9,125 vs. 10,059). Of the patients given injections early, 12,311 received them on the day of the index episode.
“What was interesting, anecdotally, was how few patients had been to physical therapy prior to surgery and how many of them had had injections before physical therapy,” Dr. Dan Rhon, director of physical therapy at Brooke Army Medical Center, Houston, said in an interview at the World Congress on Osteoarthritis.
“We wanted to look at the practice patterns because guidelines generally say that you should try physical therapy before surgery and that invasive procedures such as injections should be utilized further down the road,” he said at the meeting, which was sponsored by Osteoarthritis Research Society International.
Dr. Rhon noted that in a study of clinical practice patterns over a 5-year period from the United Healthcare Database, researchers found that physical rehabilitation was used in about one-quarter of patients, with 10% of those who went on to have surgery receiving physical therapy specific for OA, and 16% had been given intra-articular injections (Arthroscopy. 2014;30:65-71).
Results from the MDR data, which considered records from 2008 to 2013 and 1 year of follow-up, now show similar findings with 29% of patients receiving physical rehabilitation, 17.5% prior to knee arthroplasty, and 36% of patients receiving corticosteroid injections first.
What this shows, Dr. Rhon said, is that clinical practice patterns in the Military Health System do not appear to be following established guidelines. “It’s a little bit worrisome because most of these patients should at least have a trial of conservative management.” Perhaps there is some confusion over what constitutes conservative management, but when there is a choice between physical therapy and corticosteroid injections, it seems that the latter is more commonly being selected. Patients themselves could also be opting for injections over physical rehabilitation, so there may be a need for education on what options are available before surgical intervention.
Further research is needed to examine the clinical outcomes of this and perhaps look at how cost savings could be made if clinical practice more closely adhered to the OA guidelines. Looking at a longer follow-up period, say 2-5 years post diagnosis, might also give a better reflection of the use of physical therapy before surgery.
Dr. Rhon had no financial disclosures.
AMSTERDAM – Physical therapy is underused as a first conservative treatment option for knee osteoarthritis, according to a review of data of more than 130,000 men and women serving in the U.S. military.
Data from the Military Health System Data Repository (MDR) show that clinical practice is often out of step with guidelines, as many patients are treated with intra-articular corticosteroid injections rather than physical therapy.
Within a week of an initial episode of knee OA, patients were four times more likely to be given steroid injections than receive physical therapy (14,290 vs. 3,177 patients), although a similar number of patients received injections or physical therapy within 30 days (8,228 vs. 8,407) and 90 days (9,125 vs. 10,059). Of the patients given injections early, 12,311 received them on the day of the index episode.
“What was interesting, anecdotally, was how few patients had been to physical therapy prior to surgery and how many of them had had injections before physical therapy,” Dr. Dan Rhon, director of physical therapy at Brooke Army Medical Center, Houston, said in an interview at the World Congress on Osteoarthritis.
“We wanted to look at the practice patterns because guidelines generally say that you should try physical therapy before surgery and that invasive procedures such as injections should be utilized further down the road,” he said at the meeting, which was sponsored by Osteoarthritis Research Society International.
Dr. Rhon noted that in a study of clinical practice patterns over a 5-year period from the United Healthcare Database, researchers found that physical rehabilitation was used in about one-quarter of patients, with 10% of those who went on to have surgery receiving physical therapy specific for OA, and 16% had been given intra-articular injections (Arthroscopy. 2014;30:65-71).
Results from the MDR data, which considered records from 2008 to 2013 and 1 year of follow-up, now show similar findings with 29% of patients receiving physical rehabilitation, 17.5% prior to knee arthroplasty, and 36% of patients receiving corticosteroid injections first.
What this shows, Dr. Rhon said, is that clinical practice patterns in the Military Health System do not appear to be following established guidelines. “It’s a little bit worrisome because most of these patients should at least have a trial of conservative management.” Perhaps there is some confusion over what constitutes conservative management, but when there is a choice between physical therapy and corticosteroid injections, it seems that the latter is more commonly being selected. Patients themselves could also be opting for injections over physical rehabilitation, so there may be a need for education on what options are available before surgical intervention.
Further research is needed to examine the clinical outcomes of this and perhaps look at how cost savings could be made if clinical practice more closely adhered to the OA guidelines. Looking at a longer follow-up period, say 2-5 years post diagnosis, might also give a better reflection of the use of physical therapy before surgery.
Dr. Rhon had no financial disclosures.
AT OARSI 2016
Key clinical point: Contrary to guidelines, physical therapy is being underused as a first treatment option for osteoarthritis.
Major finding: Only 29% of patients received physical rehabilitation while 36% were given intra-articular steroid injections first.
Data source: Retrospective review of data from the U.S. Military Health Care System Data Repository from 2008 to 2013 on more than 130,000 patients with OA.
Disclosures: Dr. Rhon had no financial disclosures.

TKI trial leaves questions unanswered

Image by Difu Wu
The phase 3 EPIC trial, a comparison of tyrosine kinase inhibitors (TKIs), has left some questions unanswered.
The trial did not determine whether the third-generation TKI ponatinib is more effective than the first-generation TKI imatinib for patients with previously untreated chronic myeloid leukemia (CML).
The study was terminated early due to safety concerns associated with ponatinib, so the primary endpoint could only be analyzed in a small number of patients.
Results in these patients showed no significant difference in that endpoint—major molecular response (MMR) at 12 months—between the imatinib and ponatinib arms.
Results in the entire study cohort suggested that, overall, ponatinib was more toxic than imatinib. In particular, ponatinib produced more arterial occlusive events.
However, the trial’s investigators have questioned whether reducing the dose of ponatinib might change that.
Jeffrey H. Lipton, MD, of Princess Margaret Cancer Centre in Toronto, Ontario, Canada, and his colleagues reported results from the EPIC trial in The Lancet Oncology. The trial was supported by Ariad Pharmaceuticals.
Problems with ponatinib
Ponatinib was approved by the US Food and Drug Administration (FDA) in December 2012 to treat adults with CML or Philadelphia chromosome-positive acute lymphoblastic leukemia that is resistant to or intolerant of other TKIs.
In October 2013, follow-up results from the phase 2 PACE trial suggested ponatinib can increase a patient’s risk of arterial and venous thrombotic events. So all trials of the drug were placed on partial clinical hold, with the exception of the EPIC trial, which was terminated.
That November, the FDA suspended sales and marketing of ponatinib, pending results of a safety evaluation. In December, the agency decided ponatinib could return to the market if new safety measures were implemented. In January 2014, ponatinib was put back on the market in the US.
EPIC trial
The trial enrolled 307 patients with newly diagnosed, chronic-phase CML. Patients were randomized to receive ponatinib at 45 mg (n=155) or imatinib at 400 mg (n=152) once daily until progression, unacceptable toxicity, or other criteria for withdrawal were met.
The median age was 55 (range, 18-89) in the ponatinib arm and 52 (range, 18-86) in the imatinib arm. Most patients were male—63% and 61%, respectively—and most had an ECOG performance status of 0—75% and 78%, respectively.
Patients were randomized between August 14, 2012, and October 9, 2013, and the trial was terminated on October 17, 2013.
Because of the early termination, only 10 patients in the ponatinib arm and 13 in the imatinib arm were evaluable for the primary endpoint—MMR at 12 months. Eighty percent (8/10) of the evaluable patients in the ponatinib arm and 38% (5/13) of those in the imatinib arm achieved an MMR at 12 months (P=0.074).
The investigators also evaluated the incidence of MMR at any time in patients with any post-baseline molecular response assessment. This time, the incidence of MMR was significantly higher in the ponatinib arm than the imatinib arm—41% (61/149) and 18% (25/142), respectively (P<0.0001).
All of the patients were evaluable for safety—154 in the ponatinib arm and 152 in the imatinib arm.
Arterial occlusive events occurred in 7% (n=11) of patients in the ponatinib arm and 2% (n=3) in the imatinib arm (P=0.052). These events were considered serious in 6% (n=10) and 1% (n=1), respectively (P=0.010).
Common grade 3/4 adverse events—in the ponatinib and imatinib arms, respectively—were increased lipase (14% vs 2%), thrombocytopenia (12% vs 7%), rash (6% vs 1%), and neutropenia (3% vs 8%).
Serious adverse events that occurred in 3 or more patients in the ponatinib arm were pancreatitis (n=5), atrial fibrillation (n=3), and thrombocytopenia (n=3). There were no serious adverse events that occurred in 3 or more patients in the imatinib arm.
Dr Lipton and his colleagues said the premature termination of the EPIC trial restricts the interpretation of its results, but the available data provide some insight into the activity and safety of ponatinib in previously untreated CML.
The investigators also noted that data from this trial and the clinical development program for ponatinib suggest that lowering doses of the drug could improve its vascular safety profile and, therefore, the benefit-risk balance.
Two ongoing trials (NCT02467270 and NCT02627677) may provide more insight. Both are investigating starting doses of ponatinib at 15 mg or 30 mg. ![]()
Image by Difu Wu
The phase 3 EPIC trial, a comparison of tyrosine kinase inhibitors (TKIs), has left some questions unanswered.
The trial did not determine whether the third-generation TKI ponatinib is more effective than the first-generation TKI imatinib for patients with previously untreated chronic myeloid leukemia (CML).
The study was terminated early due to safety concerns associated with ponatinib, so the primary endpoint could only be analyzed in a small number of patients.
Results in these patients showed no significant difference in that endpoint—major molecular response (MMR) at 12 months—between the imatinib and ponatinib arms.
Results in the entire study cohort suggested that, overall, ponatinib was more toxic than imatinib. In particular, ponatinib produced more arterial occlusive events.
However, the trial’s investigators have questioned whether reducing the dose of ponatinib might change that.
Jeffrey H. Lipton, MD, of Princess Margaret Cancer Centre in Toronto, Ontario, Canada, and his colleagues reported results from the EPIC trial in The Lancet Oncology. The trial was supported by Ariad Pharmaceuticals.
Problems with ponatinib
Ponatinib was approved by the US Food and Drug Administration (FDA) in December 2012 to treat adults with CML or Philadelphia chromosome-positive acute lymphoblastic leukemia that is resistant to or intolerant of other TKIs.
In October 2013, follow-up results from the phase 2 PACE trial suggested ponatinib can increase a patient’s risk of arterial and venous thrombotic events. So all trials of the drug were placed on partial clinical hold, with the exception of the EPIC trial, which was terminated.
That November, the FDA suspended sales and marketing of ponatinib, pending results of a safety evaluation. In December, the agency decided ponatinib could return to the market if new safety measures were implemented. In January 2014, ponatinib was put back on the market in the US.
EPIC trial
The trial enrolled 307 patients with newly diagnosed, chronic-phase CML. Patients were randomized to receive ponatinib at 45 mg (n=155) or imatinib at 400 mg (n=152) once daily until progression, unacceptable toxicity, or other criteria for withdrawal were met.
The median age was 55 (range, 18-89) in the ponatinib arm and 52 (range, 18-86) in the imatinib arm. Most patients were male—63% and 61%, respectively—and most had an ECOG performance status of 0—75% and 78%, respectively.
Patients were randomized between August 14, 2012, and October 9, 2013, and the trial was terminated on October 17, 2013.
Because of the early termination, only 10 patients in the ponatinib arm and 13 in the imatinib arm were evaluable for the primary endpoint—MMR at 12 months. Eighty percent (8/10) of the evaluable patients in the ponatinib arm and 38% (5/13) of those in the imatinib arm achieved an MMR at 12 months (P=0.074).
The investigators also evaluated the incidence of MMR at any time in patients with any post-baseline molecular response assessment. This time, the incidence of MMR was significantly higher in the ponatinib arm than the imatinib arm—41% (61/149) and 18% (25/142), respectively (P<0.0001).
All of the patients were evaluable for safety—154 in the ponatinib arm and 152 in the imatinib arm.
Arterial occlusive events occurred in 7% (n=11) of patients in the ponatinib arm and 2% (n=3) in the imatinib arm (P=0.052). These events were considered serious in 6% (n=10) and 1% (n=1), respectively (P=0.010).
Common grade 3/4 adverse events—in the ponatinib and imatinib arms, respectively—were increased lipase (14% vs 2%), thrombocytopenia (12% vs 7%), rash (6% vs 1%), and neutropenia (3% vs 8%).
Serious adverse events that occurred in 3 or more patients in the ponatinib arm were pancreatitis (n=5), atrial fibrillation (n=3), and thrombocytopenia (n=3). There were no serious adverse events that occurred in 3 or more patients in the imatinib arm.
Dr Lipton and his colleagues said the premature termination of the EPIC trial restricts the interpretation of its results, but the available data provide some insight into the activity and safety of ponatinib in previously untreated CML.
The investigators also noted that data from this trial and the clinical development program for ponatinib suggest that lowering doses of the drug could improve its vascular safety profile and, therefore, the benefit-risk balance.
Two ongoing trials (NCT02467270 and NCT02627677) may provide more insight. Both are investigating starting doses of ponatinib at 15 mg or 30 mg. ![]()
Image by Difu Wu
The phase 3 EPIC trial, a comparison of tyrosine kinase inhibitors (TKIs), has left some questions unanswered.
The trial did not determine whether the third-generation TKI ponatinib is more effective than the first-generation TKI imatinib for patients with previously untreated chronic myeloid leukemia (CML).
The study was terminated early due to safety concerns associated with ponatinib, so the primary endpoint could only be analyzed in a small number of patients.
Results in these patients showed no significant difference in that endpoint—major molecular response (MMR) at 12 months—between the imatinib and ponatinib arms.
Results in the entire study cohort suggested that, overall, ponatinib was more toxic than imatinib. In particular, ponatinib produced more arterial occlusive events.
However, the trial’s investigators have questioned whether reducing the dose of ponatinib might change that.
Jeffrey H. Lipton, MD, of Princess Margaret Cancer Centre in Toronto, Ontario, Canada, and his colleagues reported results from the EPIC trial in The Lancet Oncology. The trial was supported by Ariad Pharmaceuticals.
Problems with ponatinib
Ponatinib was approved by the US Food and Drug Administration (FDA) in December 2012 to treat adults with CML or Philadelphia chromosome-positive acute lymphoblastic leukemia that is resistant to or intolerant of other TKIs.
In October 2013, follow-up results from the phase 2 PACE trial suggested ponatinib can increase a patient’s risk of arterial and venous thrombotic events. So all trials of the drug were placed on partial clinical hold, with the exception of the EPIC trial, which was terminated.
That November, the FDA suspended sales and marketing of ponatinib, pending results of a safety evaluation. In December, the agency decided ponatinib could return to the market if new safety measures were implemented. In January 2014, ponatinib was put back on the market in the US.
EPIC trial
The trial enrolled 307 patients with newly diagnosed, chronic-phase CML. Patients were randomized to receive ponatinib at 45 mg (n=155) or imatinib at 400 mg (n=152) once daily until progression, unacceptable toxicity, or other criteria for withdrawal were met.
The median age was 55 (range, 18-89) in the ponatinib arm and 52 (range, 18-86) in the imatinib arm. Most patients were male—63% and 61%, respectively—and most had an ECOG performance status of 0—75% and 78%, respectively.
Patients were randomized between August 14, 2012, and October 9, 2013, and the trial was terminated on October 17, 2013.
Because of the early termination, only 10 patients in the ponatinib arm and 13 in the imatinib arm were evaluable for the primary endpoint—MMR at 12 months. Eighty percent (8/10) of the evaluable patients in the ponatinib arm and 38% (5/13) of those in the imatinib arm achieved an MMR at 12 months (P=0.074).
The investigators also evaluated the incidence of MMR at any time in patients with any post-baseline molecular response assessment. This time, the incidence of MMR was significantly higher in the ponatinib arm than the imatinib arm—41% (61/149) and 18% (25/142), respectively (P<0.0001).
All of the patients were evaluable for safety—154 in the ponatinib arm and 152 in the imatinib arm.
Arterial occlusive events occurred in 7% (n=11) of patients in the ponatinib arm and 2% (n=3) in the imatinib arm (P=0.052). These events were considered serious in 6% (n=10) and 1% (n=1), respectively (P=0.010).
Common grade 3/4 adverse events—in the ponatinib and imatinib arms, respectively—were increased lipase (14% vs 2%), thrombocytopenia (12% vs 7%), rash (6% vs 1%), and neutropenia (3% vs 8%).
Serious adverse events that occurred in 3 or more patients in the ponatinib arm were pancreatitis (n=5), atrial fibrillation (n=3), and thrombocytopenia (n=3). There were no serious adverse events that occurred in 3 or more patients in the imatinib arm.
Dr Lipton and his colleagues said the premature termination of the EPIC trial restricts the interpretation of its results, but the available data provide some insight into the activity and safety of ponatinib in previously untreated CML.
The investigators also noted that data from this trial and the clinical development program for ponatinib suggest that lowering doses of the drug could improve its vascular safety profile and, therefore, the benefit-risk balance.
Two ongoing trials (NCT02467270 and NCT02627677) may provide more insight. Both are investigating starting doses of ponatinib at 15 mg or 30 mg. ![]()
Ten-Year Results Find that Bypass Lowers the Odds of Cardiovascular Death
NEW YORK (Reuters Health) - Ten-year results from a comparison of coronary-artery bypass grafting (CABG) with medical therapy alone has found that bypass lowers the odds of cardiovascular death by about nine percentage points in people with ischemic cardiomyopathy.
The 16% reduction in the death rate meant volunteers who received bypass grafting typically lived nearly a year and a half longer than those who received optimal nonsurgical therapy.
The findings are based on a study population of 1,212 patients with an ejection fraction of 35% or less who received bypass grafts between 2002 and 2007.
Death from any cause, the primary endpoint, occurred in 66.1% of the control patients and 58.9% of the bypass recipients (p=0.02).
When the researchers looked exclusively at cardiovascular deaths, the rates were 49.3% in the medical-therapy group and 40.5% in the group receiving bypass in addition to standard medical care (p=0.006).
The combined odds of hospitalization or death from any cause were also lower with bypass.
For death or hospitalization for cardiovascular causes, there was a 10.4 percentage point difference (p<0.001). For death or hospitalization for heart failure, the difference was 8.6 points (p<0.002). It was for 6.4 percentage points for death or hospitalization for any cause (p=0.001).
Results from the study, known as STICHES, were released April 3 at the American College of Cardiology annual scientific session in Chicago and online by the New England Journal of Medicine.
Bypass grafting "was associated with more favorable results than medical therapy alone across all clinically relevant long-term outcomes we evaluated," said the team, led by Dr. Eric Velazquez of the Duke Clinical Research Institute at Duke University, Durham, North Carolina.
The trends "resulted from a persistent and perhaps increasing effect size over time," they said. "Thus, it appears that the operative risk associated with CABG is offset by a durable effect that translates into increasing clinical benefit to at least 10 years."
Coronary artery disease kills more than 538,000 people in the United States each year. Most of the studies establishing the benefits of bypass grafting were done more than 40 years ago.
The initial version of the new study was known as STICH and it followed patients at 99 sites in 22 countries for a median of just over four and a half years. It found no significant difference between the two treatments when it came to the rate of death from any cause. However, bypass recipients were less likely to die from a cardiovascular event or to die from any cause or be hospitalized for cardiovascular causes.
STICHES extends those results to 10 years and found that any-cause death became significant.
Median survival was 7.73 years with bypass and 6.29 years without. The researchers calculated that the number needed to treat to prevent one death was 14 patients. The number needed to prevent one death from a cardiovascular cause was 11.
Other secondary measures were the rates of death combined with specific cardiovascular events. Once again, they consistently found a benefit for bypass.
There was a 15.8 percentage point difference for any cause of death or revascularization (p<0.001). For death or nonfatal myocardial infarction the difference was 6.3 points and it was for 7.2 percentage points for death or nonfatal stroke (both p=0.03).
Among the 610 people originally assigned to the bypass group, 9% did not receive a graft before the end of the trial. In the 602 assigned to medical therapy alone, 19.8% underwent bypass surgery. Eleven percent had it within the first year.
In an accompanying editorial, Drs. Robert Guyton and Andrew Smith of Emory University in Atlanta, wrote, "The STICHES 10-year results firmly extend the survival benefit of CABG in patients with advanced coronary artery disease to patients with heart failure and severe ischemic cardiomyopathy. These findings should prompt strong consideration of coronary bypass as an addition to medical therapy in shared decision making with these patients."
The National Heart Lung and Blood Institute funded this research. Two coauthors reported disclosures.
NEW YORK (Reuters Health) - Ten-year results from a comparison of coronary-artery bypass grafting (CABG) with medical therapy alone has found that bypass lowers the odds of cardiovascular death by about nine percentage points in people with ischemic cardiomyopathy.
The 16% reduction in the death rate meant volunteers who received bypass grafting typically lived nearly a year and a half longer than those who received optimal nonsurgical therapy.
The findings are based on a study population of 1,212 patients with an ejection fraction of 35% or less who received bypass grafts between 2002 and 2007.
Death from any cause, the primary endpoint, occurred in 66.1% of the control patients and 58.9% of the bypass recipients (p=0.02).
When the researchers looked exclusively at cardiovascular deaths, the rates were 49.3% in the medical-therapy group and 40.5% in the group receiving bypass in addition to standard medical care (p=0.006).
The combined odds of hospitalization or death from any cause were also lower with bypass.
For death or hospitalization for cardiovascular causes, there was a 10.4 percentage point difference (p<0.001). For death or hospitalization for heart failure, the difference was 8.6 points (p<0.002). It was for 6.4 percentage points for death or hospitalization for any cause (p=0.001).
Results from the study, known as STICHES, were released April 3 at the American College of Cardiology annual scientific session in Chicago and online by the New England Journal of Medicine.
Bypass grafting "was associated with more favorable results than medical therapy alone across all clinically relevant long-term outcomes we evaluated," said the team, led by Dr. Eric Velazquez of the Duke Clinical Research Institute at Duke University, Durham, North Carolina.
The trends "resulted from a persistent and perhaps increasing effect size over time," they said. "Thus, it appears that the operative risk associated with CABG is offset by a durable effect that translates into increasing clinical benefit to at least 10 years."
Coronary artery disease kills more than 538,000 people in the United States each year. Most of the studies establishing the benefits of bypass grafting were done more than 40 years ago.
The initial version of the new study was known as STICH and it followed patients at 99 sites in 22 countries for a median of just over four and a half years. It found no significant difference between the two treatments when it came to the rate of death from any cause. However, bypass recipients were less likely to die from a cardiovascular event or to die from any cause or be hospitalized for cardiovascular causes.
STICHES extends those results to 10 years and found that any-cause death became significant.
Median survival was 7.73 years with bypass and 6.29 years without. The researchers calculated that the number needed to treat to prevent one death was 14 patients. The number needed to prevent one death from a cardiovascular cause was 11.
Other secondary measures were the rates of death combined with specific cardiovascular events. Once again, they consistently found a benefit for bypass.
There was a 15.8 percentage point difference for any cause of death or revascularization (p<0.001). For death or nonfatal myocardial infarction the difference was 6.3 points and it was for 7.2 percentage points for death or nonfatal stroke (both p=0.03).
Among the 610 people originally assigned to the bypass group, 9% did not receive a graft before the end of the trial. In the 602 assigned to medical therapy alone, 19.8% underwent bypass surgery. Eleven percent had it within the first year.
In an accompanying editorial, Drs. Robert Guyton and Andrew Smith of Emory University in Atlanta, wrote, "The STICHES 10-year results firmly extend the survival benefit of CABG in patients with advanced coronary artery disease to patients with heart failure and severe ischemic cardiomyopathy. These findings should prompt strong consideration of coronary bypass as an addition to medical therapy in shared decision making with these patients."
The National Heart Lung and Blood Institute funded this research. Two coauthors reported disclosures.
NEW YORK (Reuters Health) - Ten-year results from a comparison of coronary-artery bypass grafting (CABG) with medical therapy alone has found that bypass lowers the odds of cardiovascular death by about nine percentage points in people with ischemic cardiomyopathy.
The 16% reduction in the death rate meant volunteers who received bypass grafting typically lived nearly a year and a half longer than those who received optimal nonsurgical therapy.
The findings are based on a study population of 1,212 patients with an ejection fraction of 35% or less who received bypass grafts between 2002 and 2007.
Death from any cause, the primary endpoint, occurred in 66.1% of the control patients and 58.9% of the bypass recipients (p=0.02).
When the researchers looked exclusively at cardiovascular deaths, the rates were 49.3% in the medical-therapy group and 40.5% in the group receiving bypass in addition to standard medical care (p=0.006).
The combined odds of hospitalization or death from any cause were also lower with bypass.
For death or hospitalization for cardiovascular causes, there was a 10.4 percentage point difference (p<0.001). For death or hospitalization for heart failure, the difference was 8.6 points (p<0.002). It was for 6.4 percentage points for death or hospitalization for any cause (p=0.001).
Results from the study, known as STICHES, were released April 3 at the American College of Cardiology annual scientific session in Chicago and online by the New England Journal of Medicine.
Bypass grafting "was associated with more favorable results than medical therapy alone across all clinically relevant long-term outcomes we evaluated," said the team, led by Dr. Eric Velazquez of the Duke Clinical Research Institute at Duke University, Durham, North Carolina.
The trends "resulted from a persistent and perhaps increasing effect size over time," they said. "Thus, it appears that the operative risk associated with CABG is offset by a durable effect that translates into increasing clinical benefit to at least 10 years."
Coronary artery disease kills more than 538,000 people in the United States each year. Most of the studies establishing the benefits of bypass grafting were done more than 40 years ago.
The initial version of the new study was known as STICH and it followed patients at 99 sites in 22 countries for a median of just over four and a half years. It found no significant difference between the two treatments when it came to the rate of death from any cause. However, bypass recipients were less likely to die from a cardiovascular event or to die from any cause or be hospitalized for cardiovascular causes.
STICHES extends those results to 10 years and found that any-cause death became significant.
Median survival was 7.73 years with bypass and 6.29 years without. The researchers calculated that the number needed to treat to prevent one death was 14 patients. The number needed to prevent one death from a cardiovascular cause was 11.
Other secondary measures were the rates of death combined with specific cardiovascular events. Once again, they consistently found a benefit for bypass.
There was a 15.8 percentage point difference for any cause of death or revascularization (p<0.001). For death or nonfatal myocardial infarction the difference was 6.3 points and it was for 7.2 percentage points for death or nonfatal stroke (both p=0.03).
Among the 610 people originally assigned to the bypass group, 9% did not receive a graft before the end of the trial. In the 602 assigned to medical therapy alone, 19.8% underwent bypass surgery. Eleven percent had it within the first year.
In an accompanying editorial, Drs. Robert Guyton and Andrew Smith of Emory University in Atlanta, wrote, "The STICHES 10-year results firmly extend the survival benefit of CABG in patients with advanced coronary artery disease to patients with heart failure and severe ischemic cardiomyopathy. These findings should prompt strong consideration of coronary bypass as an addition to medical therapy in shared decision making with these patients."
The National Heart Lung and Blood Institute funded this research. Two coauthors reported disclosures.
CDC says Zika causes microcephaly, other birth defects

Photo by Nina Matthews
After reviewing existing evidence, scientists from the US Centers for Disease Control and Prevention (CDC) have concluded that Zika virus causes
microcephaly and other severe fetal brain defects.
“This study marks a turning point in the Zika outbreak,” said Tom Frieden, MD, director of the CDC.
“It is now clear that the virus causes microcephaly. We’ve now confirmed what mounting evidence has suggested.”
Details on the CDC’s review were published in NEJM.
The report notes that no single piece of evidence provides conclusive proof that Zika virus infection is a cause of microcephaly and other fetal brain defects. Rather, increasing evidence from a number of recently published studies and a careful evaluation using established scientific criteria support the authors’ conclusions.
The finding that Zika virus infection can cause microcephaly and other severe fetal brain defects means that a woman who is infected with Zika during pregnancy has an increased risk of having a baby with these health problems.
However, as we’ve seen during the current Zika outbreak, some infected women deliver babies that appear to be healthy.
The CDC said establishing the causal relationship between Zika and fetal brain defects is an important step in driving additional prevention efforts, focusing research activities, and reinforcing the need for direct communication about the risks of Zika.
However, the agency noted that many questions about the Zika virus remain. And answering these questions will be the focus of ongoing research.
The CDC also said it is not changing its current recommendations regarding the Zika virus. Pregnant women should continue to avoid travel to areas where Zika is actively spreading.
If a pregnant woman travels to or lives in an area with active Zika virus transmission, she should talk with her healthcare provider and take steps to prevent mosquito bites and sexual transmission of the virus.
The CDC also encourages women and their partners in areas with active Zika transmission to engage in pregnancy planning and counseling with their healthcare providers so they know the risks and the ways to mitigate them. ![]()
Photo by Nina Matthews
After reviewing existing evidence, scientists from the US Centers for Disease Control and Prevention (CDC) have concluded that Zika virus causes
microcephaly and other severe fetal brain defects.
“This study marks a turning point in the Zika outbreak,” said Tom Frieden, MD, director of the CDC.
“It is now clear that the virus causes microcephaly. We’ve now confirmed what mounting evidence has suggested.”
Details on the CDC’s review were published in NEJM.
The report notes that no single piece of evidence provides conclusive proof that Zika virus infection is a cause of microcephaly and other fetal brain defects. Rather, increasing evidence from a number of recently published studies and a careful evaluation using established scientific criteria support the authors’ conclusions.
The finding that Zika virus infection can cause microcephaly and other severe fetal brain defects means that a woman who is infected with Zika during pregnancy has an increased risk of having a baby with these health problems.
However, as we’ve seen during the current Zika outbreak, some infected women deliver babies that appear to be healthy.
The CDC said establishing the causal relationship between Zika and fetal brain defects is an important step in driving additional prevention efforts, focusing research activities, and reinforcing the need for direct communication about the risks of Zika.
However, the agency noted that many questions about the Zika virus remain. And answering these questions will be the focus of ongoing research.
The CDC also said it is not changing its current recommendations regarding the Zika virus. Pregnant women should continue to avoid travel to areas where Zika is actively spreading.
If a pregnant woman travels to or lives in an area with active Zika virus transmission, she should talk with her healthcare provider and take steps to prevent mosquito bites and sexual transmission of the virus.
The CDC also encourages women and their partners in areas with active Zika transmission to engage in pregnancy planning and counseling with their healthcare providers so they know the risks and the ways to mitigate them. ![]()
Photo by Nina Matthews
After reviewing existing evidence, scientists from the US Centers for Disease Control and Prevention (CDC) have concluded that Zika virus causes
microcephaly and other severe fetal brain defects.
“This study marks a turning point in the Zika outbreak,” said Tom Frieden, MD, director of the CDC.
“It is now clear that the virus causes microcephaly. We’ve now confirmed what mounting evidence has suggested.”
Details on the CDC’s review were published in NEJM.
The report notes that no single piece of evidence provides conclusive proof that Zika virus infection is a cause of microcephaly and other fetal brain defects. Rather, increasing evidence from a number of recently published studies and a careful evaluation using established scientific criteria support the authors’ conclusions.
The finding that Zika virus infection can cause microcephaly and other severe fetal brain defects means that a woman who is infected with Zika during pregnancy has an increased risk of having a baby with these health problems.
However, as we’ve seen during the current Zika outbreak, some infected women deliver babies that appear to be healthy.
The CDC said establishing the causal relationship between Zika and fetal brain defects is an important step in driving additional prevention efforts, focusing research activities, and reinforcing the need for direct communication about the risks of Zika.
However, the agency noted that many questions about the Zika virus remain. And answering these questions will be the focus of ongoing research.
The CDC also said it is not changing its current recommendations regarding the Zika virus. Pregnant women should continue to avoid travel to areas where Zika is actively spreading.
If a pregnant woman travels to or lives in an area with active Zika virus transmission, she should talk with her healthcare provider and take steps to prevent mosquito bites and sexual transmission of the virus.
The CDC also encourages women and their partners in areas with active Zika transmission to engage in pregnancy planning and counseling with their healthcare providers so they know the risks and the ways to mitigate them. ![]()
Drug appears safe, effective for ocular GVHD

Photo courtesy of
Massachusetts Eye and Ear
A topical immunosuppressant may be a feasible treatment option for ocular graft-versus-host-disease (GVHD), according to a phase 1/2 study.
The immunosuppressant, tacrolimus, proved equally as effective as the steroid methylprednisolone.
And although tacrolimus was significantly more likely to produce a burning sensation, the drug did not significantly increase intraocular pressure (IOP) the way methylprednisolone did.
These results were published in Ophthalmology. The study was supported by the National Eye Institute, National Institutes of Health, and Research to Prevent Blindness.
“We found tacrolimus to be very effective—just as good as the steroid, in the reduction of ocular symptoms of GVHD,” said study author Reza Dana, MD, of Massachusetts Eye and Ear Infirmary in Boston.
“We saw this improvement without any of the negative effects, such as a rise in pressure in the eye, as we saw with the steroid.”
The trial included 40 patients with ocular GVHD. They had received a hematopoietic stem cell transplant to treat leukemias, lymphomas, multiple myeloma, myelodysplastic syndromes, and thrombocytopenia.
The patients were randomized to receive topical tacrolimus 0.05% (n=24) or topical methylprednisolone 0.5% (n=16). Their median ages were 54±12 and 58±11, respectively. And the mean baseline ocular GVHD duration was 27±34 months and 28±33 months, respectively.
The patients received treatment for 10 weeks. Three patients were lost to follow-up in the tacrolimus group, 3 withdrew from the study because of a burning sensation when applying tacrolimus, and 1 patient from the methylprednisolone group was withdrawn due to a geographic corneal epithelial defect.
Safety/tolerability
There were no major adverse events in either treatment group, and there was no significant difference in the composite tolerability scores between the groups (P=0.06).
Tolerability scores were calculated based on patients’ reports of burning sensation, discharge, redness, itchiness, and foreign body sensation (scale, 0-4 for each variable).
The burning sensation score was higher in the tacrolimus group than the methylprednisolone group. At week 5, the scores were 3.6 and 1.6, respectively (P<0.001). At week 10, they were 3.5 and 2.2, respectively (P=0.002).
There was no significant change from baseline in the mean IOP in the tacrolimus group at week 5 (P=0.50) or week 10 (P=0.20). But there was a significant change in the methylprednisolone group at both time points (P=0.04 for both).
Still, this did not amount to a significant difference between the treatment groups. In the tacrolimus group, the mean IOP was 15.6 mmHg at baseline, 16 mmHg at week 5, and 16.5 at week 10. In the methylprednisolone group the mean IOPs were 15.3 mmHg, 17.5 mmHg, and 17 mmHg, respectively.
Efficacy
The main efficacy endpoints were corneal fluorescein staining (CFS), tear film break-up time (TBUT), Schirmer test results, and expression of the ocular surface inflammatory markers human leukocyte antigen-DR (HLA-DR) and intercellular adhesion molecule-1 (ICAM-1).
Topical tacrolimus was more effective than methylprednisolone in reducing the CFS score from baseline to week 10. CFS scores were reduced by 55% and 23%, respectively (P=0.01).
There was a significant increase in TBUT from baseline to week 10 in the tacrolimus group (0.7-2.6 seconds, P=0.003) but not in the methylprednisolone group (0.6-1.0 seconds, P=0.42). However, there was no significant difference in TBUT changes between the treatment groups (P=0.06).
Schirmer test scores did not change significantly in either treatment group.
ICAM-1 expression decreased significantly from baseline in both the tacrolimus group (39% reduction, P=0.003) and the methylprednisolone group (40% reduction, P=0.008).
HLA-DR expression decreased significantly in the tacrolimus group (46% reduction, P=0.03) but not the methylprednisolone group (24% reduction, P=0.09).
“The problem with steroid treatment for ocular GVHD is that it can cause the pressure in the eye to rise, and it can also cause cataracts,” Dr Dana noted.
“The results of this trial give us reassurance that [tacrolimus] is another effective treatment for GVHD, without the negative side effects of steroids. This is a game-changer in terms of managing their care.” ![]()
Photo courtesy of
Massachusetts Eye and Ear
A topical immunosuppressant may be a feasible treatment option for ocular graft-versus-host-disease (GVHD), according to a phase 1/2 study.
The immunosuppressant, tacrolimus, proved equally as effective as the steroid methylprednisolone.
And although tacrolimus was significantly more likely to produce a burning sensation, the drug did not significantly increase intraocular pressure (IOP) the way methylprednisolone did.
These results were published in Ophthalmology. The study was supported by the National Eye Institute, National Institutes of Health, and Research to Prevent Blindness.
“We found tacrolimus to be very effective—just as good as the steroid, in the reduction of ocular symptoms of GVHD,” said study author Reza Dana, MD, of Massachusetts Eye and Ear Infirmary in Boston.
“We saw this improvement without any of the negative effects, such as a rise in pressure in the eye, as we saw with the steroid.”
The trial included 40 patients with ocular GVHD. They had received a hematopoietic stem cell transplant to treat leukemias, lymphomas, multiple myeloma, myelodysplastic syndromes, and thrombocytopenia.
The patients were randomized to receive topical tacrolimus 0.05% (n=24) or topical methylprednisolone 0.5% (n=16). Their median ages were 54±12 and 58±11, respectively. And the mean baseline ocular GVHD duration was 27±34 months and 28±33 months, respectively.
The patients received treatment for 10 weeks. Three patients were lost to follow-up in the tacrolimus group, 3 withdrew from the study because of a burning sensation when applying tacrolimus, and 1 patient from the methylprednisolone group was withdrawn due to a geographic corneal epithelial defect.
Safety/tolerability
There were no major adverse events in either treatment group, and there was no significant difference in the composite tolerability scores between the groups (P=0.06).
Tolerability scores were calculated based on patients’ reports of burning sensation, discharge, redness, itchiness, and foreign body sensation (scale, 0-4 for each variable).
The burning sensation score was higher in the tacrolimus group than the methylprednisolone group. At week 5, the scores were 3.6 and 1.6, respectively (P<0.001). At week 10, they were 3.5 and 2.2, respectively (P=0.002).
There was no significant change from baseline in the mean IOP in the tacrolimus group at week 5 (P=0.50) or week 10 (P=0.20). But there was a significant change in the methylprednisolone group at both time points (P=0.04 for both).
Still, this did not amount to a significant difference between the treatment groups. In the tacrolimus group, the mean IOP was 15.6 mmHg at baseline, 16 mmHg at week 5, and 16.5 at week 10. In the methylprednisolone group the mean IOPs were 15.3 mmHg, 17.5 mmHg, and 17 mmHg, respectively.
Efficacy
The main efficacy endpoints were corneal fluorescein staining (CFS), tear film break-up time (TBUT), Schirmer test results, and expression of the ocular surface inflammatory markers human leukocyte antigen-DR (HLA-DR) and intercellular adhesion molecule-1 (ICAM-1).
Topical tacrolimus was more effective than methylprednisolone in reducing the CFS score from baseline to week 10. CFS scores were reduced by 55% and 23%, respectively (P=0.01).
There was a significant increase in TBUT from baseline to week 10 in the tacrolimus group (0.7-2.6 seconds, P=0.003) but not in the methylprednisolone group (0.6-1.0 seconds, P=0.42). However, there was no significant difference in TBUT changes between the treatment groups (P=0.06).
Schirmer test scores did not change significantly in either treatment group.
ICAM-1 expression decreased significantly from baseline in both the tacrolimus group (39% reduction, P=0.003) and the methylprednisolone group (40% reduction, P=0.008).
HLA-DR expression decreased significantly in the tacrolimus group (46% reduction, P=0.03) but not the methylprednisolone group (24% reduction, P=0.09).
“The problem with steroid treatment for ocular GVHD is that it can cause the pressure in the eye to rise, and it can also cause cataracts,” Dr Dana noted.
“The results of this trial give us reassurance that [tacrolimus] is another effective treatment for GVHD, without the negative side effects of steroids. This is a game-changer in terms of managing their care.” ![]()
Photo courtesy of
Massachusetts Eye and Ear
A topical immunosuppressant may be a feasible treatment option for ocular graft-versus-host-disease (GVHD), according to a phase 1/2 study.
The immunosuppressant, tacrolimus, proved equally as effective as the steroid methylprednisolone.
And although tacrolimus was significantly more likely to produce a burning sensation, the drug did not significantly increase intraocular pressure (IOP) the way methylprednisolone did.
These results were published in Ophthalmology. The study was supported by the National Eye Institute, National Institutes of Health, and Research to Prevent Blindness.
“We found tacrolimus to be very effective—just as good as the steroid, in the reduction of ocular symptoms of GVHD,” said study author Reza Dana, MD, of Massachusetts Eye and Ear Infirmary in Boston.
“We saw this improvement without any of the negative effects, such as a rise in pressure in the eye, as we saw with the steroid.”
The trial included 40 patients with ocular GVHD. They had received a hematopoietic stem cell transplant to treat leukemias, lymphomas, multiple myeloma, myelodysplastic syndromes, and thrombocytopenia.
The patients were randomized to receive topical tacrolimus 0.05% (n=24) or topical methylprednisolone 0.5% (n=16). Their median ages were 54±12 and 58±11, respectively. And the mean baseline ocular GVHD duration was 27±34 months and 28±33 months, respectively.
The patients received treatment for 10 weeks. Three patients were lost to follow-up in the tacrolimus group, 3 withdrew from the study because of a burning sensation when applying tacrolimus, and 1 patient from the methylprednisolone group was withdrawn due to a geographic corneal epithelial defect.
Safety/tolerability
There were no major adverse events in either treatment group, and there was no significant difference in the composite tolerability scores between the groups (P=0.06).
Tolerability scores were calculated based on patients’ reports of burning sensation, discharge, redness, itchiness, and foreign body sensation (scale, 0-4 for each variable).
The burning sensation score was higher in the tacrolimus group than the methylprednisolone group. At week 5, the scores were 3.6 and 1.6, respectively (P<0.001). At week 10, they were 3.5 and 2.2, respectively (P=0.002).
There was no significant change from baseline in the mean IOP in the tacrolimus group at week 5 (P=0.50) or week 10 (P=0.20). But there was a significant change in the methylprednisolone group at both time points (P=0.04 for both).
Still, this did not amount to a significant difference between the treatment groups. In the tacrolimus group, the mean IOP was 15.6 mmHg at baseline, 16 mmHg at week 5, and 16.5 at week 10. In the methylprednisolone group the mean IOPs were 15.3 mmHg, 17.5 mmHg, and 17 mmHg, respectively.
Efficacy
The main efficacy endpoints were corneal fluorescein staining (CFS), tear film break-up time (TBUT), Schirmer test results, and expression of the ocular surface inflammatory markers human leukocyte antigen-DR (HLA-DR) and intercellular adhesion molecule-1 (ICAM-1).
Topical tacrolimus was more effective than methylprednisolone in reducing the CFS score from baseline to week 10. CFS scores were reduced by 55% and 23%, respectively (P=0.01).
There was a significant increase in TBUT from baseline to week 10 in the tacrolimus group (0.7-2.6 seconds, P=0.003) but not in the methylprednisolone group (0.6-1.0 seconds, P=0.42). However, there was no significant difference in TBUT changes between the treatment groups (P=0.06).
Schirmer test scores did not change significantly in either treatment group.
ICAM-1 expression decreased significantly from baseline in both the tacrolimus group (39% reduction, P=0.003) and the methylprednisolone group (40% reduction, P=0.008).
HLA-DR expression decreased significantly in the tacrolimus group (46% reduction, P=0.03) but not the methylprednisolone group (24% reduction, P=0.09).
“The problem with steroid treatment for ocular GVHD is that it can cause the pressure in the eye to rise, and it can also cause cataracts,” Dr Dana noted.
“The results of this trial give us reassurance that [tacrolimus] is another effective treatment for GVHD, without the negative side effects of steroids. This is a game-changer in terms of managing their care.” ![]()
Alternative splicing regulates activity of MALT1

Photo courtesy of
Helmholtz Zentrum München
Researchers say they have gained new insights into the workings of MALT1, a protein that controls the activation of lymphocytes.
The team found that, through alternative splicing, two variants of MALT1 may arise, and one has a stronger effect than the other.
The researchers say understanding this process is important because previous research has suggested MALT1 may be a therapeutic
target for lymphomas and other diseases.
Isabel Meininger, a doctoral student at Helmholtz Zentrum München in Neuherberg, Germany, and her colleagues described their MALT1-related findings in Nature Communications.
“To our surprise, we showed that MALT1 is regulated by post-transcriptional splicing,” Meininger said. “Depending on which MALT1 variant is expressed, the immune system is activated more or less.”
The researchers explained that most pre-messenger RNAs in mammals are prone to alternative splicing, which results in the generation of multiple transcripts and proteins with diverse functions.
In the case of MALT1, the variants MALT1A and MALT1B differ only through the presence of exon 7, a short sequence that encodes 11 amino acids.
If exon 7 is missing, as in the case of MALT1B, the protein’s ability to stimulate T cells is impaired. So MALT1A has a stronger effect on T cells than MALT1B.
The researchers also found that a molecule called hnRNP U (heterogeneous nuclear ribonucleoprotein U) regulates which of the two variants is preferably expressed.
If hnRNP U is present in small amounts, higher levels of MALT1A are expressed, resulting in stronger activation of T cells. With higher levels of hnRNP U, higher levels of MALT1B are expressed, and the response of the T cells is weaker.
“Our findings contribute to a better understanding of the function of MALT1 and enable us to better assess the potential impact of a pharmacological effect on this promising drug candidate,” said study author Daniel Krappmann, PhD, of Helmholtz Zentrum München.
In a previous study, Dr Krappmann and his team identified small molecules that can inhibit MALT1 to treat diffuse large B-cell lymphoma.
In future studies, the researchers want to confirm, in a preclinical model, the effects of MALT1 splicing on the immune system and disease development. ![]()
Photo courtesy of
Helmholtz Zentrum München
Researchers say they have gained new insights into the workings of MALT1, a protein that controls the activation of lymphocytes.
The team found that, through alternative splicing, two variants of MALT1 may arise, and one has a stronger effect than the other.
The researchers say understanding this process is important because previous research has suggested MALT1 may be a therapeutic
target for lymphomas and other diseases.
Isabel Meininger, a doctoral student at Helmholtz Zentrum München in Neuherberg, Germany, and her colleagues described their MALT1-related findings in Nature Communications.
“To our surprise, we showed that MALT1 is regulated by post-transcriptional splicing,” Meininger said. “Depending on which MALT1 variant is expressed, the immune system is activated more or less.”
The researchers explained that most pre-messenger RNAs in mammals are prone to alternative splicing, which results in the generation of multiple transcripts and proteins with diverse functions.
In the case of MALT1, the variants MALT1A and MALT1B differ only through the presence of exon 7, a short sequence that encodes 11 amino acids.
If exon 7 is missing, as in the case of MALT1B, the protein’s ability to stimulate T cells is impaired. So MALT1A has a stronger effect on T cells than MALT1B.
The researchers also found that a molecule called hnRNP U (heterogeneous nuclear ribonucleoprotein U) regulates which of the two variants is preferably expressed.
If hnRNP U is present in small amounts, higher levels of MALT1A are expressed, resulting in stronger activation of T cells. With higher levels of hnRNP U, higher levels of MALT1B are expressed, and the response of the T cells is weaker.
“Our findings contribute to a better understanding of the function of MALT1 and enable us to better assess the potential impact of a pharmacological effect on this promising drug candidate,” said study author Daniel Krappmann, PhD, of Helmholtz Zentrum München.
In a previous study, Dr Krappmann and his team identified small molecules that can inhibit MALT1 to treat diffuse large B-cell lymphoma.
In future studies, the researchers want to confirm, in a preclinical model, the effects of MALT1 splicing on the immune system and disease development. ![]()
Photo courtesy of
Helmholtz Zentrum München
Researchers say they have gained new insights into the workings of MALT1, a protein that controls the activation of lymphocytes.
The team found that, through alternative splicing, two variants of MALT1 may arise, and one has a stronger effect than the other.
The researchers say understanding this process is important because previous research has suggested MALT1 may be a therapeutic
target for lymphomas and other diseases.
Isabel Meininger, a doctoral student at Helmholtz Zentrum München in Neuherberg, Germany, and her colleagues described their MALT1-related findings in Nature Communications.
“To our surprise, we showed that MALT1 is regulated by post-transcriptional splicing,” Meininger said. “Depending on which MALT1 variant is expressed, the immune system is activated more or less.”
The researchers explained that most pre-messenger RNAs in mammals are prone to alternative splicing, which results in the generation of multiple transcripts and proteins with diverse functions.
In the case of MALT1, the variants MALT1A and MALT1B differ only through the presence of exon 7, a short sequence that encodes 11 amino acids.
If exon 7 is missing, as in the case of MALT1B, the protein’s ability to stimulate T cells is impaired. So MALT1A has a stronger effect on T cells than MALT1B.
The researchers also found that a molecule called hnRNP U (heterogeneous nuclear ribonucleoprotein U) regulates which of the two variants is preferably expressed.
If hnRNP U is present in small amounts, higher levels of MALT1A are expressed, resulting in stronger activation of T cells. With higher levels of hnRNP U, higher levels of MALT1B are expressed, and the response of the T cells is weaker.
“Our findings contribute to a better understanding of the function of MALT1 and enable us to better assess the potential impact of a pharmacological effect on this promising drug candidate,” said study author Daniel Krappmann, PhD, of Helmholtz Zentrum München.
In a previous study, Dr Krappmann and his team identified small molecules that can inhibit MALT1 to treat diffuse large B-cell lymphoma.
In future studies, the researchers want to confirm, in a preclinical model, the effects of MALT1 splicing on the immune system and disease development. ![]()