User login
Isopropyl Alcohol Nasal Inhalation Effective Treatment for ED Nausea
Clinical question: Does inhaled isopropyl alcohol alleviate nausea as compared to inhaled saline solution among patients presenting to the ED with a chief complaint of nausea?

Background: Nausea and vomiting account for 4.8 million ED visits each year; however, antiemetics have not shown superiority compared to placebo. Isopropyl alcohol nasal inhalation is more effective than saline solution in treating postoperative nausea and vomiting; however, there have been no investigations of this therapy in the ED setting.
Study design: Randomized, double-blind, placebo-controlled trial.
Setting: Emergency department at the San Antonio Military Medical Center, Texas.
Synopsis: Investigators randomized a convenience sample of 80 patients in the ED presenting with nausea or vomiting to either inhaled isopropyl alcohol (37) or saline solution (43). Subjects would nasally inhale at 0, 2, and 4 minutes. Nausea outcomes were self-rated on a scale of 0–10, with 0 being no nausea and 10 being worst nausea imaginable. Responses were taken at 0, 2, 4, 6, and 10 minutes postintervention. Primary outcome was the score at 10 minutes postintervention. The minimally significant difference was two points.
Patients in the intervention arm reported lower scores during every study period than the patients in the placebo arm. Median nausea scores at 10 minutes postintervention were lower by three in the intervention arm compared to placebo arm (P<0.001). Limitations include the short (10-minute) evaluation period, which limits identification of any adverse events; limited information on duration of symptom relief and whether the isopropyl alcohol effect persisted; possible selection bias due to utilizing a convenience sample; and use of a subjective scale for the primary outcome.
Bottom line: Isopropyl alcohol inhalation is effective in reducing nausea 10 minutes after intervention as compared with placebo in the ED setting.
Citation: Beadle KL, Helbling AR, Love SL, April MD, Hunter CJ. Isopropyl alcohol nasal inhalation for nausea in the emergency department: a randomized controlled trial [published online ahead of print November 21, 2015]. Ann Emerg Med. doi:10.1016/j.annemergmed.2015.09.031.
Clinical question: Does inhaled isopropyl alcohol alleviate nausea as compared to inhaled saline solution among patients presenting to the ED with a chief complaint of nausea?
Background: Nausea and vomiting account for 4.8 million ED visits each year; however, antiemetics have not shown superiority compared to placebo. Isopropyl alcohol nasal inhalation is more effective than saline solution in treating postoperative nausea and vomiting; however, there have been no investigations of this therapy in the ED setting.
Study design: Randomized, double-blind, placebo-controlled trial.
Setting: Emergency department at the San Antonio Military Medical Center, Texas.
Synopsis: Investigators randomized a convenience sample of 80 patients in the ED presenting with nausea or vomiting to either inhaled isopropyl alcohol (37) or saline solution (43). Subjects would nasally inhale at 0, 2, and 4 minutes. Nausea outcomes were self-rated on a scale of 0–10, with 0 being no nausea and 10 being worst nausea imaginable. Responses were taken at 0, 2, 4, 6, and 10 minutes postintervention. Primary outcome was the score at 10 minutes postintervention. The minimally significant difference was two points.
Patients in the intervention arm reported lower scores during every study period than the patients in the placebo arm. Median nausea scores at 10 minutes postintervention were lower by three in the intervention arm compared to placebo arm (P<0.001). Limitations include the short (10-minute) evaluation period, which limits identification of any adverse events; limited information on duration of symptom relief and whether the isopropyl alcohol effect persisted; possible selection bias due to utilizing a convenience sample; and use of a subjective scale for the primary outcome.
Bottom line: Isopropyl alcohol inhalation is effective in reducing nausea 10 minutes after intervention as compared with placebo in the ED setting.
Citation: Beadle KL, Helbling AR, Love SL, April MD, Hunter CJ. Isopropyl alcohol nasal inhalation for nausea in the emergency department: a randomized controlled trial [published online ahead of print November 21, 2015]. Ann Emerg Med. doi:10.1016/j.annemergmed.2015.09.031.
Clinical question: Does inhaled isopropyl alcohol alleviate nausea as compared to inhaled saline solution among patients presenting to the ED with a chief complaint of nausea?
Background: Nausea and vomiting account for 4.8 million ED visits each year; however, antiemetics have not shown superiority compared to placebo. Isopropyl alcohol nasal inhalation is more effective than saline solution in treating postoperative nausea and vomiting; however, there have been no investigations of this therapy in the ED setting.
Study design: Randomized, double-blind, placebo-controlled trial.
Setting: Emergency department at the San Antonio Military Medical Center, Texas.
Synopsis: Investigators randomized a convenience sample of 80 patients in the ED presenting with nausea or vomiting to either inhaled isopropyl alcohol (37) or saline solution (43). Subjects would nasally inhale at 0, 2, and 4 minutes. Nausea outcomes were self-rated on a scale of 0–10, with 0 being no nausea and 10 being worst nausea imaginable. Responses were taken at 0, 2, 4, 6, and 10 minutes postintervention. Primary outcome was the score at 10 minutes postintervention. The minimally significant difference was two points.
Patients in the intervention arm reported lower scores during every study period than the patients in the placebo arm. Median nausea scores at 10 minutes postintervention were lower by three in the intervention arm compared to placebo arm (P<0.001). Limitations include the short (10-minute) evaluation period, which limits identification of any adverse events; limited information on duration of symptom relief and whether the isopropyl alcohol effect persisted; possible selection bias due to utilizing a convenience sample; and use of a subjective scale for the primary outcome.
Bottom line: Isopropyl alcohol inhalation is effective in reducing nausea 10 minutes after intervention as compared with placebo in the ED setting.
Citation: Beadle KL, Helbling AR, Love SL, April MD, Hunter CJ. Isopropyl alcohol nasal inhalation for nausea in the emergency department: a randomized controlled trial [published online ahead of print November 21, 2015]. Ann Emerg Med. doi:10.1016/j.annemergmed.2015.09.031.

CHMP advises against approving MM drug

multiple myeloma
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has advised the European Commission not to approve ixazomib (Ninlaro), an oral proteasome inhibitor, as a treatment for patients with relapsed and/or refractory multiple myeloma (MM).
Takeda Pharmaceutical Company Limited, the company developing ixazomib, said it intends to appeal this opinion and request a re-examination by the CHMP.
“We are disappointed by the CHMP’s opinion,” said Christophe Bianchi, MD, president of Takeda Oncology. “With the support of European key medical experts, we will continue our efforts working closely with the CHMP to make Ninlaro—the first oral proteasome inhibitor—available for patients in Europe.”
“We stand behind the TOURMALINE-MM1 trial data, which were recently published in the New England Journal of Medicine and demonstrated a significant extension in progression-free survival for Ninlaro plus lenalidomide and dexamethasone versus placebo plus lenalidomide and dexamethasone and a favorable benefit-risk profile.”
TOURMALINE-MM1
The trial enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive ixazomib, lenalidomide, and dexamethasone (IRd, n=360) or placebo, lenalidomide, and dexamethasone (Rd, n=362). Baseline patient characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival, which was significantly longer in the IRd arm than the Rd arm. The median progression-free survival was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
Adverse events (AEs) occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively; serious AEs occurred in 47% and 49%, respectively; and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia, rash, and gastrointestinal AEs were more frequent in the IRd arm than the Rd arm.
The incidence of peripheral neuropathy was similar in the 2 arms, as was the percentage patients who developed new primary malignant tumors. ![]()
multiple myeloma
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has advised the European Commission not to approve ixazomib (Ninlaro), an oral proteasome inhibitor, as a treatment for patients with relapsed and/or refractory multiple myeloma (MM).
Takeda Pharmaceutical Company Limited, the company developing ixazomib, said it intends to appeal this opinion and request a re-examination by the CHMP.
“We are disappointed by the CHMP’s opinion,” said Christophe Bianchi, MD, president of Takeda Oncology. “With the support of European key medical experts, we will continue our efforts working closely with the CHMP to make Ninlaro—the first oral proteasome inhibitor—available for patients in Europe.”
“We stand behind the TOURMALINE-MM1 trial data, which were recently published in the New England Journal of Medicine and demonstrated a significant extension in progression-free survival for Ninlaro plus lenalidomide and dexamethasone versus placebo plus lenalidomide and dexamethasone and a favorable benefit-risk profile.”
TOURMALINE-MM1
The trial enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive ixazomib, lenalidomide, and dexamethasone (IRd, n=360) or placebo, lenalidomide, and dexamethasone (Rd, n=362). Baseline patient characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival, which was significantly longer in the IRd arm than the Rd arm. The median progression-free survival was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
Adverse events (AEs) occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively; serious AEs occurred in 47% and 49%, respectively; and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia, rash, and gastrointestinal AEs were more frequent in the IRd arm than the Rd arm.
The incidence of peripheral neuropathy was similar in the 2 arms, as was the percentage patients who developed new primary malignant tumors. ![]()
multiple myeloma
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has advised the European Commission not to approve ixazomib (Ninlaro), an oral proteasome inhibitor, as a treatment for patients with relapsed and/or refractory multiple myeloma (MM).
Takeda Pharmaceutical Company Limited, the company developing ixazomib, said it intends to appeal this opinion and request a re-examination by the CHMP.
“We are disappointed by the CHMP’s opinion,” said Christophe Bianchi, MD, president of Takeda Oncology. “With the support of European key medical experts, we will continue our efforts working closely with the CHMP to make Ninlaro—the first oral proteasome inhibitor—available for patients in Europe.”
“We stand behind the TOURMALINE-MM1 trial data, which were recently published in the New England Journal of Medicine and demonstrated a significant extension in progression-free survival for Ninlaro plus lenalidomide and dexamethasone versus placebo plus lenalidomide and dexamethasone and a favorable benefit-risk profile.”
TOURMALINE-MM1
The trial enrolled 722 patients with relapsed (77%), refractory (11%), relapsed and refractory (12%), or primary refractory (6%) MM.
The patients were randomized to receive ixazomib, lenalidomide, and dexamethasone (IRd, n=360) or placebo, lenalidomide, and dexamethasone (Rd, n=362). Baseline patient characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival, which was significantly longer in the IRd arm than the Rd arm. The median progression-free survival was 20.6 months and 14.7 months, respectively. The hazard ratio was 0.74 (P=0.01).
At a median follow-up of about 23 months, the median overall survival had not been reached in either treatment arm.
Adverse events (AEs) occurred in 98% of patients in the IRd arm and 99% in the Rd arm. Grade 3 or higher AEs occurred in 74% and 69% of patients, respectively; serious AEs occurred in 47% and 49%, respectively; and on-study deaths occurred in 4% and 6%, respectively.
Grade 3 and 4 thrombocytopenia, rash, and gastrointestinal AEs were more frequent in the IRd arm than the Rd arm.
The incidence of peripheral neuropathy was similar in the 2 arms, as was the percentage patients who developed new primary malignant tumors. ![]()
Public Opinion about Healthcare Reform Becomes More Positive

Reference
1. Jacobs LR, Mettler S. Liking health reform but turned off by toxic politics [published online ahead of print April 2016]. Health Aff. doi:10.1377/hlthaff.2015.1313.
Reference
1. Jacobs LR, Mettler S. Liking health reform but turned off by toxic politics [published online ahead of print April 2016]. Health Aff. doi:10.1377/hlthaff.2015.1313.
Reference
1. Jacobs LR, Mettler S. Liking health reform but turned off by toxic politics [published online ahead of print April 2016]. Health Aff. doi:10.1377/hlthaff.2015.1313.

Tips for Improving Early Discharge Rates
Discharging patients before noon has many advantages: It creates open beds to accommodate the surge in admissions in the afternoon and helps minimize the bottleneck in system-wide patient flow, says Ragu P. Sanjeev, MD, unit-based medical director at Christiana Hospital in Newark, Del.
“Doing so can reduce ER wait times, reduce the percentage of patients leaving the ED without being seen—a safety issue for those patients—and also help to place the right patient in the right bed in a timely manner,” he says. “It’s a not just a patient flow issue; it’s a patient safety issue, as well.”
At his hospital, hospitalists developed a “Discharge by Appointment” process to address the issue systematically and completed a pilot project to test it. Their “‘Discharge by Appointment’ Improves Patient Flow, by Increasing Number of Discharges Before Noon,” was an abstract presented at HM16.1
“Giving patients that have a high predictability of being discharged next day, an appointment, and set off a series of steps to be completed the day before discharge including, notifying the transport team/family members of the appointment, helped improve the number of discharges before noon significantly,” according to the abstract.
Their successful pilot project has led to lasting changes, Dr. Sanjeev says. For about 16 months, the number of discharges before noon has been steadily increasing, helping the acute medicine service line perform better than its “Discharge by Noon” goal by 44.4% this fiscal year.
“As hospitalists, we have a great potential to positively impact the hospital-wide issues like patient flow and patient safety,” Dr. Sanjeev says. “By actively participating in important hospital committees, you can understand better and get inspired by the ongoing improvement efforts. By partnering with your care team, including bedside nurses, case managers, and social workers, we can make a big difference in early discharges. This success can be expanded to discharges throughout the day with appointments, thereby keeping the flow faucet open at all times.”
Reference
- Sanjeev R, McMillen J, Fedyk A. ‘discharge by Appointment’ Improves Patient Flow, by Increasing Number of Discharges Before Noon [abstract]. J Hosp Med. http://www.shmabstracts.com/abstract/discharge-by-appointment-improves-patient-flow-by-increasing-number-of-discharges-before-noon/. Accessed April 27, 2016.
Discharging patients before noon has many advantages: It creates open beds to accommodate the surge in admissions in the afternoon and helps minimize the bottleneck in system-wide patient flow, says Ragu P. Sanjeev, MD, unit-based medical director at Christiana Hospital in Newark, Del.
“Doing so can reduce ER wait times, reduce the percentage of patients leaving the ED without being seen—a safety issue for those patients—and also help to place the right patient in the right bed in a timely manner,” he says. “It’s a not just a patient flow issue; it’s a patient safety issue, as well.”
At his hospital, hospitalists developed a “Discharge by Appointment” process to address the issue systematically and completed a pilot project to test it. Their “‘Discharge by Appointment’ Improves Patient Flow, by Increasing Number of Discharges Before Noon,” was an abstract presented at HM16.1
“Giving patients that have a high predictability of being discharged next day, an appointment, and set off a series of steps to be completed the day before discharge including, notifying the transport team/family members of the appointment, helped improve the number of discharges before noon significantly,” according to the abstract.
Their successful pilot project has led to lasting changes, Dr. Sanjeev says. For about 16 months, the number of discharges before noon has been steadily increasing, helping the acute medicine service line perform better than its “Discharge by Noon” goal by 44.4% this fiscal year.
“As hospitalists, we have a great potential to positively impact the hospital-wide issues like patient flow and patient safety,” Dr. Sanjeev says. “By actively participating in important hospital committees, you can understand better and get inspired by the ongoing improvement efforts. By partnering with your care team, including bedside nurses, case managers, and social workers, we can make a big difference in early discharges. This success can be expanded to discharges throughout the day with appointments, thereby keeping the flow faucet open at all times.”
Reference
- Sanjeev R, McMillen J, Fedyk A. ‘discharge by Appointment’ Improves Patient Flow, by Increasing Number of Discharges Before Noon [abstract]. J Hosp Med. http://www.shmabstracts.com/abstract/discharge-by-appointment-improves-patient-flow-by-increasing-number-of-discharges-before-noon/. Accessed April 27, 2016.
Discharging patients before noon has many advantages: It creates open beds to accommodate the surge in admissions in the afternoon and helps minimize the bottleneck in system-wide patient flow, says Ragu P. Sanjeev, MD, unit-based medical director at Christiana Hospital in Newark, Del.
“Doing so can reduce ER wait times, reduce the percentage of patients leaving the ED without being seen—a safety issue for those patients—and also help to place the right patient in the right bed in a timely manner,” he says. “It’s a not just a patient flow issue; it’s a patient safety issue, as well.”
At his hospital, hospitalists developed a “Discharge by Appointment” process to address the issue systematically and completed a pilot project to test it. Their “‘Discharge by Appointment’ Improves Patient Flow, by Increasing Number of Discharges Before Noon,” was an abstract presented at HM16.1
“Giving patients that have a high predictability of being discharged next day, an appointment, and set off a series of steps to be completed the day before discharge including, notifying the transport team/family members of the appointment, helped improve the number of discharges before noon significantly,” according to the abstract.
Their successful pilot project has led to lasting changes, Dr. Sanjeev says. For about 16 months, the number of discharges before noon has been steadily increasing, helping the acute medicine service line perform better than its “Discharge by Noon” goal by 44.4% this fiscal year.
“As hospitalists, we have a great potential to positively impact the hospital-wide issues like patient flow and patient safety,” Dr. Sanjeev says. “By actively participating in important hospital committees, you can understand better and get inspired by the ongoing improvement efforts. By partnering with your care team, including bedside nurses, case managers, and social workers, we can make a big difference in early discharges. This success can be expanded to discharges throughout the day with appointments, thereby keeping the flow faucet open at all times.”
Reference
- Sanjeev R, McMillen J, Fedyk A. ‘discharge by Appointment’ Improves Patient Flow, by Increasing Number of Discharges Before Noon [abstract]. J Hosp Med. http://www.shmabstracts.com/abstract/discharge-by-appointment-improves-patient-flow-by-increasing-number-of-discharges-before-noon/. Accessed April 27, 2016.
Drug may provide benefit for VTE prevention
Results of the phase 3 APEX study suggest extended treatment with betrixaban may provide a benefit over standard-duration enoxaparin as thromboprophylaxis for patients with acute medical illnesses.
The study’s primary efficacy outcome was a composite of asymptomatic, proximal deep-vein thrombosis (DVT) and symptomatic venous thromboembolism (VTE).
Among patients with an elevated D-dimer level, there was no significant difference between the treatment arms with regard to the primary efficacy outcome.
However, there was a significant difference between the treatment arms in the entire study cohort and among a cohort of patients who either had an elevated D-dimer level or were 75 and older.
“In a pre-specified subgroup of medically ill patients who were D-dimer positive, extended-duration betrixaban demonstrated a reduction in VTE events approaching statistical significance,” explained study author C. Michael Gibson, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“In the pre-specified exploratory analyses of central lab D-dimer values and in progressively larger cohorts, including all study patients, the data demonstrated a consistent and significant reduction in VTE with betrixaban, with no statistical difference in major bleeding between the betrixaban and enoxaparin arms.”
These results were presented at the 62nd Annual International Society on Thrombosis and Haemostasis Scientific and Standardization Committee Meeting in Montpellier, France, and published simultaneously in NEJM.
This study was supported by Portola Pharmaceuticals, the company developing betrixaban.
The trial enrolled 7513 patients who were hospitalized for acute medical illnesses. The patients were randomized to receive:
- Subcutaneous enoxaparin (40 mg once daily) for 10 ± 4 days plus oral placebo for 35 to 42 days (n=3754)
- Or subcutaneous placebo for 10 ± 4 days plus oral betrixaban (80 mg once daily) for 35 to 42 days (n=3759).
Results
The researchers performed sequential analyses in 3 prespecified cohorts:
- Cohort 1—Patients with an elevated D-dimer level
- Cohort 2—Patients with an elevated D-dimer level or an age of at least 75 years
- All enrolled patients.
The statistical analysis plan specified that if the between-group difference in any of the 3 analyses was not significant, the other analyses would be considered exploratory.
In cohort 1, the primary efficacy outcome (a composite of asymptomatic proximal DVT and symptomatic VTE) occurred in 6.9% of patients receiving betrixaban and 8.5% receiving enoxaparin. The relative risk (RR) was 0.81 (95% CI, 0.65 to 1.00; P=0.054).
In cohort 2, the primary efficacy outcome occurred in 5.6% of patients receiving betrixaban and 7.1% receiving enoxaparin. The RR was 0.80 (95% CI, 0.66 to 0.98; P=0.03).
In all patients, the primary efficacy outcome occurred in 5.3% of patients receiving betrixaban and 7.0% receiving enoxaparin. The RR was 0.76 (95% CI, 0.63 to 0.92; P=0.006).
Though the differences between the treatment arms were statistically significant in the overall patient population and in cohort 2, these analyses were considered exploratory because the differences did not reach statistical significance in cohort 1.
The primary safety outcome was major bleeding. In the overall population, major bleeding occurred in 0.7% of patients receiving betrixaban and 0.6% of patients receiving enoxaparin. The RR was 1.19 (95% CI, 0.67 to 2.12; P=0.55).
The secondary safety outcome was major or clinically relevant nonmajor bleeding. It occurred in 3.1% of patients receiving betrixaban and 1.6% of patients receiving enoxaparin. The RR was 1.97 (95% CI, 1.44 to 2.68; P<0.001).
“The APEX study results show consistent evidence that VTE events can be reduced with betrixaban, with no statistical difference in major bleeding between the betrixaban and enoxaparin arms,” said study author Alexander T. Cohen, MBBS, MD, of Guy’s and St. Thomas’ Hospitals in London, UK.
“This is particularly true for the most clinically relevant symptomatic disease, where we observed a 30% to 45% reduction in events over the duration of the study. Such meaningful results in an area where there is currently no available recommended therapy offer important potential benefits for public health worldwide.” ![]()
Results of the phase 3 APEX study suggest extended treatment with betrixaban may provide a benefit over standard-duration enoxaparin as thromboprophylaxis for patients with acute medical illnesses.
The study’s primary efficacy outcome was a composite of asymptomatic, proximal deep-vein thrombosis (DVT) and symptomatic venous thromboembolism (VTE).
Among patients with an elevated D-dimer level, there was no significant difference between the treatment arms with regard to the primary efficacy outcome.
However, there was a significant difference between the treatment arms in the entire study cohort and among a cohort of patients who either had an elevated D-dimer level or were 75 and older.
“In a pre-specified subgroup of medically ill patients who were D-dimer positive, extended-duration betrixaban demonstrated a reduction in VTE events approaching statistical significance,” explained study author C. Michael Gibson, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“In the pre-specified exploratory analyses of central lab D-dimer values and in progressively larger cohorts, including all study patients, the data demonstrated a consistent and significant reduction in VTE with betrixaban, with no statistical difference in major bleeding between the betrixaban and enoxaparin arms.”
These results were presented at the 62nd Annual International Society on Thrombosis and Haemostasis Scientific and Standardization Committee Meeting in Montpellier, France, and published simultaneously in NEJM.
This study was supported by Portola Pharmaceuticals, the company developing betrixaban.
The trial enrolled 7513 patients who were hospitalized for acute medical illnesses. The patients were randomized to receive:
- Subcutaneous enoxaparin (40 mg once daily) for 10 ± 4 days plus oral placebo for 35 to 42 days (n=3754)
- Or subcutaneous placebo for 10 ± 4 days plus oral betrixaban (80 mg once daily) for 35 to 42 days (n=3759).
Results
The researchers performed sequential analyses in 3 prespecified cohorts:
- Cohort 1—Patients with an elevated D-dimer level
- Cohort 2—Patients with an elevated D-dimer level or an age of at least 75 years
- All enrolled patients.
The statistical analysis plan specified that if the between-group difference in any of the 3 analyses was not significant, the other analyses would be considered exploratory.
In cohort 1, the primary efficacy outcome (a composite of asymptomatic proximal DVT and symptomatic VTE) occurred in 6.9% of patients receiving betrixaban and 8.5% receiving enoxaparin. The relative risk (RR) was 0.81 (95% CI, 0.65 to 1.00; P=0.054).
In cohort 2, the primary efficacy outcome occurred in 5.6% of patients receiving betrixaban and 7.1% receiving enoxaparin. The RR was 0.80 (95% CI, 0.66 to 0.98; P=0.03).
In all patients, the primary efficacy outcome occurred in 5.3% of patients receiving betrixaban and 7.0% receiving enoxaparin. The RR was 0.76 (95% CI, 0.63 to 0.92; P=0.006).
Though the differences between the treatment arms were statistically significant in the overall patient population and in cohort 2, these analyses were considered exploratory because the differences did not reach statistical significance in cohort 1.
The primary safety outcome was major bleeding. In the overall population, major bleeding occurred in 0.7% of patients receiving betrixaban and 0.6% of patients receiving enoxaparin. The RR was 1.19 (95% CI, 0.67 to 2.12; P=0.55).
The secondary safety outcome was major or clinically relevant nonmajor bleeding. It occurred in 3.1% of patients receiving betrixaban and 1.6% of patients receiving enoxaparin. The RR was 1.97 (95% CI, 1.44 to 2.68; P<0.001).
“The APEX study results show consistent evidence that VTE events can be reduced with betrixaban, with no statistical difference in major bleeding between the betrixaban and enoxaparin arms,” said study author Alexander T. Cohen, MBBS, MD, of Guy’s and St. Thomas’ Hospitals in London, UK.
“This is particularly true for the most clinically relevant symptomatic disease, where we observed a 30% to 45% reduction in events over the duration of the study. Such meaningful results in an area where there is currently no available recommended therapy offer important potential benefits for public health worldwide.” ![]()
Results of the phase 3 APEX study suggest extended treatment with betrixaban may provide a benefit over standard-duration enoxaparin as thromboprophylaxis for patients with acute medical illnesses.
The study’s primary efficacy outcome was a composite of asymptomatic, proximal deep-vein thrombosis (DVT) and symptomatic venous thromboembolism (VTE).
Among patients with an elevated D-dimer level, there was no significant difference between the treatment arms with regard to the primary efficacy outcome.
However, there was a significant difference between the treatment arms in the entire study cohort and among a cohort of patients who either had an elevated D-dimer level or were 75 and older.
“In a pre-specified subgroup of medically ill patients who were D-dimer positive, extended-duration betrixaban demonstrated a reduction in VTE events approaching statistical significance,” explained study author C. Michael Gibson, MD, of Beth Israel Deaconess Medical Center in Boston, Massachusetts.
“In the pre-specified exploratory analyses of central lab D-dimer values and in progressively larger cohorts, including all study patients, the data demonstrated a consistent and significant reduction in VTE with betrixaban, with no statistical difference in major bleeding between the betrixaban and enoxaparin arms.”
These results were presented at the 62nd Annual International Society on Thrombosis and Haemostasis Scientific and Standardization Committee Meeting in Montpellier, France, and published simultaneously in NEJM.
This study was supported by Portola Pharmaceuticals, the company developing betrixaban.
The trial enrolled 7513 patients who were hospitalized for acute medical illnesses. The patients were randomized to receive:
- Subcutaneous enoxaparin (40 mg once daily) for 10 ± 4 days plus oral placebo for 35 to 42 days (n=3754)
- Or subcutaneous placebo for 10 ± 4 days plus oral betrixaban (80 mg once daily) for 35 to 42 days (n=3759).
Results
The researchers performed sequential analyses in 3 prespecified cohorts:
- Cohort 1—Patients with an elevated D-dimer level
- Cohort 2—Patients with an elevated D-dimer level or an age of at least 75 years
- All enrolled patients.
The statistical analysis plan specified that if the between-group difference in any of the 3 analyses was not significant, the other analyses would be considered exploratory.
In cohort 1, the primary efficacy outcome (a composite of asymptomatic proximal DVT and symptomatic VTE) occurred in 6.9% of patients receiving betrixaban and 8.5% receiving enoxaparin. The relative risk (RR) was 0.81 (95% CI, 0.65 to 1.00; P=0.054).
In cohort 2, the primary efficacy outcome occurred in 5.6% of patients receiving betrixaban and 7.1% receiving enoxaparin. The RR was 0.80 (95% CI, 0.66 to 0.98; P=0.03).
In all patients, the primary efficacy outcome occurred in 5.3% of patients receiving betrixaban and 7.0% receiving enoxaparin. The RR was 0.76 (95% CI, 0.63 to 0.92; P=0.006).
Though the differences between the treatment arms were statistically significant in the overall patient population and in cohort 2, these analyses were considered exploratory because the differences did not reach statistical significance in cohort 1.
The primary safety outcome was major bleeding. In the overall population, major bleeding occurred in 0.7% of patients receiving betrixaban and 0.6% of patients receiving enoxaparin. The RR was 1.19 (95% CI, 0.67 to 2.12; P=0.55).
The secondary safety outcome was major or clinically relevant nonmajor bleeding. It occurred in 3.1% of patients receiving betrixaban and 1.6% of patients receiving enoxaparin. The RR was 1.97 (95% CI, 1.44 to 2.68; P<0.001).
“The APEX study results show consistent evidence that VTE events can be reduced with betrixaban, with no statistical difference in major bleeding between the betrixaban and enoxaparin arms,” said study author Alexander T. Cohen, MBBS, MD, of Guy’s and St. Thomas’ Hospitals in London, UK.
“This is particularly true for the most clinically relevant symptomatic disease, where we observed a 30% to 45% reduction in events over the duration of the study. Such meaningful results in an area where there is currently no available recommended therapy offer important potential benefits for public health worldwide.” ![]()
Clinical Challenges - May 2016: Pancreaticobiliary maljunction with bifid pancreatic ducts presenting as recurrent pancreatitis and concurrent gallbladder adenocarcinoma
What's Your Diagnosis?
The diagnosis
Figure A shows marked intrahepatic and extrahepatic biliary ductal dilation and an irregular enhancing mass along the lateral wall of the gallbladder (long arrow). Figure B shows an abnormal pancreaticobiliary junction, with the common bile duct inserting into a distal pancreatic duct to form a cystically dilated common channel (arrowhead), as well as a bifid main pancreatic duct (long arrow). Figure C shows a bifid pancreatic duct and no evidence of a pancreatic mass. Other endoscopic ultrasound images visualized an irregular gallbladder mass. Figure D shows an irregular mass in the gallbladder wall, with final pathology revealing an invasive, well-differentiated adenocarcinoma of the gallbladder (long arrow) with negative margins and no evidence of lymph node involvement (T1N0Mx). The final diagnosis was pancreaticobiliary maljunction (PBM) with bifid pancreatic ducts presenting as recurrent pancreatitis and concurrent gallbladder adenocarcinoma.
It is well established that PBM, an anomalous junction of the pancreaticobiliary ductal system, is frequently associated with carcinomas of the biliary tract. First described in 1916 by Kozumi and Kodama, PBM is a rare congenital malformation most prevalent in Asia that is defined as an anomalous junction of the pancreatic and biliary ducts located outside of the duodenal wall.1PBM often manifests clinically as intermittent abdominal pain, obstructive jaundice, and/or acute pancreatitis, although patients may be asymptomatic. The most concerning problem, however, is the close relationship of biliary tract carcinogenesis to PBM, with gallbladder carcinoma and bile duct cancers arising in 14.8% and 4.9% of patients with PBM, respectively.2 The anomalous junction is thought to preclude normal sphincter of Oddi function, thus facilitating the reciprocal reflux of bile and pancreatic juice and ultimately leading to biliary carcinogenesis. Tumor markers, such as CA 19-9 and carcinoembryonic antigen, may be of some diagnostic value in PBM and biliary tract neoplasms, although they lack sensitivity and specificity because of significant overlap with benign disease, such as pancreatitis. This particular case had the added novelty of a bifid pancreatic duct. The clinical significance of a bifid pancreatic duct is unclear, and no relationship has been demonstrated between this ductal anomaly and pancreaticobiliary disease. In this case, a pancreaticoduodenectomy with en bloc resection of the gallbladder was performed to resect the gallbladder mass with clear margins and eliminate the risk for further biliary tract carcinogenesis while simultaneously excising the anomalous junction thought to be causing the recurrent pancreatitis.
References
1. Todani T., Arima E., Eto T., et al. Diagnostic criteria of pancreaticobiliary maljunction. J Hepatobiliary Pancreat Surg. 1994;1:219-21.
2. Funabiki T., Matsubara T., Miyakawa S., et al. Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malignancy. Langenbecks Arch Surg. 2009;39:149-69.
The diagnosis
Figure A shows marked intrahepatic and extrahepatic biliary ductal dilation and an irregular enhancing mass along the lateral wall of the gallbladder (long arrow). Figure B shows an abnormal pancreaticobiliary junction, with the common bile duct inserting into a distal pancreatic duct to form a cystically dilated common channel (arrowhead), as well as a bifid main pancreatic duct (long arrow). Figure C shows a bifid pancreatic duct and no evidence of a pancreatic mass. Other endoscopic ultrasound images visualized an irregular gallbladder mass. Figure D shows an irregular mass in the gallbladder wall, with final pathology revealing an invasive, well-differentiated adenocarcinoma of the gallbladder (long arrow) with negative margins and no evidence of lymph node involvement (T1N0Mx). The final diagnosis was pancreaticobiliary maljunction (PBM) with bifid pancreatic ducts presenting as recurrent pancreatitis and concurrent gallbladder adenocarcinoma.
It is well established that PBM, an anomalous junction of the pancreaticobiliary ductal system, is frequently associated with carcinomas of the biliary tract. First described in 1916 by Kozumi and Kodama, PBM is a rare congenital malformation most prevalent in Asia that is defined as an anomalous junction of the pancreatic and biliary ducts located outside of the duodenal wall.1PBM often manifests clinically as intermittent abdominal pain, obstructive jaundice, and/or acute pancreatitis, although patients may be asymptomatic. The most concerning problem, however, is the close relationship of biliary tract carcinogenesis to PBM, with gallbladder carcinoma and bile duct cancers arising in 14.8% and 4.9% of patients with PBM, respectively.2 The anomalous junction is thought to preclude normal sphincter of Oddi function, thus facilitating the reciprocal reflux of bile and pancreatic juice and ultimately leading to biliary carcinogenesis. Tumor markers, such as CA 19-9 and carcinoembryonic antigen, may be of some diagnostic value in PBM and biliary tract neoplasms, although they lack sensitivity and specificity because of significant overlap with benign disease, such as pancreatitis. This particular case had the added novelty of a bifid pancreatic duct. The clinical significance of a bifid pancreatic duct is unclear, and no relationship has been demonstrated between this ductal anomaly and pancreaticobiliary disease. In this case, a pancreaticoduodenectomy with en bloc resection of the gallbladder was performed to resect the gallbladder mass with clear margins and eliminate the risk for further biliary tract carcinogenesis while simultaneously excising the anomalous junction thought to be causing the recurrent pancreatitis.
References
1. Todani T., Arima E., Eto T., et al. Diagnostic criteria of pancreaticobiliary maljunction. J Hepatobiliary Pancreat Surg. 1994;1:219-21.
2. Funabiki T., Matsubara T., Miyakawa S., et al. Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malignancy. Langenbecks Arch Surg. 2009;39:149-69.
The diagnosis
Figure A shows marked intrahepatic and extrahepatic biliary ductal dilation and an irregular enhancing mass along the lateral wall of the gallbladder (long arrow). Figure B shows an abnormal pancreaticobiliary junction, with the common bile duct inserting into a distal pancreatic duct to form a cystically dilated common channel (arrowhead), as well as a bifid main pancreatic duct (long arrow). Figure C shows a bifid pancreatic duct and no evidence of a pancreatic mass. Other endoscopic ultrasound images visualized an irregular gallbladder mass. Figure D shows an irregular mass in the gallbladder wall, with final pathology revealing an invasive, well-differentiated adenocarcinoma of the gallbladder (long arrow) with negative margins and no evidence of lymph node involvement (T1N0Mx). The final diagnosis was pancreaticobiliary maljunction (PBM) with bifid pancreatic ducts presenting as recurrent pancreatitis and concurrent gallbladder adenocarcinoma.
It is well established that PBM, an anomalous junction of the pancreaticobiliary ductal system, is frequently associated with carcinomas of the biliary tract. First described in 1916 by Kozumi and Kodama, PBM is a rare congenital malformation most prevalent in Asia that is defined as an anomalous junction of the pancreatic and biliary ducts located outside of the duodenal wall.1PBM often manifests clinically as intermittent abdominal pain, obstructive jaundice, and/or acute pancreatitis, although patients may be asymptomatic. The most concerning problem, however, is the close relationship of biliary tract carcinogenesis to PBM, with gallbladder carcinoma and bile duct cancers arising in 14.8% and 4.9% of patients with PBM, respectively.2 The anomalous junction is thought to preclude normal sphincter of Oddi function, thus facilitating the reciprocal reflux of bile and pancreatic juice and ultimately leading to biliary carcinogenesis. Tumor markers, such as CA 19-9 and carcinoembryonic antigen, may be of some diagnostic value in PBM and biliary tract neoplasms, although they lack sensitivity and specificity because of significant overlap with benign disease, such as pancreatitis. This particular case had the added novelty of a bifid pancreatic duct. The clinical significance of a bifid pancreatic duct is unclear, and no relationship has been demonstrated between this ductal anomaly and pancreaticobiliary disease. In this case, a pancreaticoduodenectomy with en bloc resection of the gallbladder was performed to resect the gallbladder mass with clear margins and eliminate the risk for further biliary tract carcinogenesis while simultaneously excising the anomalous junction thought to be causing the recurrent pancreatitis.
References
1. Todani T., Arima E., Eto T., et al. Diagnostic criteria of pancreaticobiliary maljunction. J Hepatobiliary Pancreat Surg. 1994;1:219-21.
2. Funabiki T., Matsubara T., Miyakawa S., et al. Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malignancy. Langenbecks Arch Surg. 2009;39:149-69.
What's Your Diagnosis?
What's Your Diagnosis?
By Dr. Katherine Albutt, Dr. Laurence Bailen, and Dr. Carlos Fernandez-del Castillo. Published previously in Gastroenterology (2012;143:896, 1121-2).
A 63-year-old African American woman with a history of recurrent pancreatitis was admitted with severe right upper quadrant pain radiating to the back. Her medical history was notable for three prior episodes of pancreatitis that required hospitalization in 2000, 2006, and 2007.

On the day of admission, physical examination revealed a soft abdomen that was tender to palpation in the right upper quadrant with a positive Murphy’s sign. Laboratory data were notable for an amylase level of 1,203 U/L and a lipase level of 2,091 U/L in the setting of normal liver function tests (LFTs) and a normal leukocyte count. The cancer antigen (CA) 19-9 level at this time was 299 U/mL.

The patient then underwent abdominal sonography and computed tomography (Figure A). Magnetic resonance cholangiopancreatography was also performed (Figure B). Because of rising LFTs, endoscopic retrograde cholangiopancreatography was performed, and a biliary stent was placed. An endoscopic ultrasound was performed at the time of endoscopic retrograde cholangiopancreatography (Figure C).
Once the acute pancreatitis resolved and the patient was tolerating a regular diet, she was discharged home. At this time, the level of CA 19-9 was 35 U/mL. She was subsequently taken to the operating room for a planned pancreaticoduodenectomy, cholecystectomy, and dissection of periportal lymph nodes. The Whipple specimen was removed en bloc with the gallbladder (Figure D).
The patient’s postoperative course was uneventful, and she was discharged home on postoperative day 7. Postoperative laboratory values were notable for a CA 19-9 of 23 U/mL and carcinoembryonic antigen of 3.3 ng/mL. What is the diagnosis?
Register for Pediatric Hospital Medicine 2016

PHM16 will provide in-depth review and challenge participants in various areas, including clinical practice, medical education, quality improvement, and professional development. Time will also be dedicated to networking and meeting with leaders in the field.
Register, book your hotel, and see the full course schedule at www.phmmeeting.org.
Brett Radler is SHM’s communications coordinator.
PHM16 will provide in-depth review and challenge participants in various areas, including clinical practice, medical education, quality improvement, and professional development. Time will also be dedicated to networking and meeting with leaders in the field.
Register, book your hotel, and see the full course schedule at www.phmmeeting.org.
Brett Radler is SHM’s communications coordinator.
PHM16 will provide in-depth review and challenge participants in various areas, including clinical practice, medical education, quality improvement, and professional development. Time will also be dedicated to networking and meeting with leaders in the field.
Register, book your hotel, and see the full course schedule at www.phmmeeting.org.
Brett Radler is SHM’s communications coordinator.
New SHM Members – June 2016
B. Abdalsm, MD, MPH, Alabama
A. Aboutalib, Alabama
D. Adams, MD, Arkansas
A. Afzal, MD, FACP, Arizona
J. Aheam, MD, California
S. Ahluwalia, MBBS, California
A. Alhusseini, MD, FAACP, MBchB, California
L. Anderson, MD, California
K. Arunachalam, MD, California
B. Asalone, California
L. Atkins, MD, California
T. Aultman, MD, California
T. Ayangade, MD, California
A. Azizi, MD, California
F. Azizi, MD, California
S. Balu, MD, California
K. Basra, APRN, FNP, California
N. Bassi, California
C. Batchelor, MD, California
K. Beinlich, MD, California
S. Bhat, MD, MBBS, California
H. Bilal, MBBS, California
G. Bismack, MD, California
M. Bokhari, MD, California
M. Brandenbug, MD, Colorado
H. Briggs, MD, PhD, Colorado
E. Burgh, MD, Colorado
M. Cabrera, BC, Delaware
J. Camden, BA, Delaware
P. Chandra Mohan, MD, Delaware
D. Chau, MD, Delaware
M. Chen, Florida
V. Chennamaneni, Florida
L. Cler, Florida
D. Cooks, Florida
S. Crenshaw, Florida
K. Cunningham, MD, FACP, Florida
V. De Guzman, APRN, MSN, NP, Florida
M. Del Rosario, MD, Florida
D. DeVere, MD, Florida
S. Dharmapuri, Florida
P. Dodson, MD, Florida
A. Domaoal, Georgia
J. Duncan, MD, Georgia
B. Dyck, BSC, MD, PhD, Georgia
J. Dzundza, MD, Georgia
A. Ellis, FNP, Georgia
R. Erickson, Idaho
A. Faraj, Idaho
S. Fernandez, MD, Illinois
G. Ferrari, MD, Illinois
W. Folad, MD, Illinois
L. Fowler, ACNP, APRN, MBA, Illinois
J. Golderberg, MD, Illinois
G. Goldman, MD, Illinois
L. Gonzales, MD, Indiana
A. Gonzalez, Kansas
W. Griffo, MD, Kansas
R. Guzman, Kansas
L. Guzman Vinasco, MD, Kansas
K. Hageman, DO, Kentucky
M. Haggerty, PA-C, Kentucky
B. Hammond, Louisiana
G. Harris, MD, Louisiana
J. Hasan-Jones, RN, FACHE, Louisiana
J. Herring, Louisiana
L. Hsu, MD, Massachusetts
A. C. Hunag, DO, Massachusetts
M. Huq, Massachusetts
M. Jandrin, PA-C, Massachusetts
C. Janish, MD, Maryland
J. Jarin, MD, Maine
A. Jenkins, Maine
S. Jindal, MD, Michigan
M. Johl, Michigan
T. John, Michigan
N. Kapadia, MD, Michigan
L. Katona, Michigan
K. Kaye, Michigan
M. Keating, Michigan
L. Keeton, MD, Michigan
L. Kendall, Michigan
M. Kerlin, Michigan
A. Kia, MD, Minnesota
R. Klett, Minnesota
L. Knapp, DO, Minnesota
K. Knox, Missouri
M. Kraynak, MD, Missouri
P. Kuppireddy, MBBS, Missouri
W. Landrum, MD, Missouri
C. Larion, ACNP, Missouri
E. Latcheva, MD, Mississippi
D. Leforce, North Carolina
V. Leigh, DO, North Carolina
C. Leon, North Carolina
T. Li, MD, North Dakota
X. Li, MD, Nebraska
Y. Li, New Hampshire
J. Liu, New Hampshire
L. Lu, DO, New Jersey
S. Mathapathi, New Jersey
L. McGann, New Jersey
S. Melkaveri, MD, Nevada
R. Mercado Garcia, New York
S. Merry, MD, New York
P. Meyer, DO, New York
J. Mikulca, PharmD, New York
Z. Moyenda, MD, MBA, New York
K. Murphy, DO, MPH, New York
J. Musenze, New York
P. Mutungi, New York
G. Nanna, USA, New York
I. Nasir, New York
U. Nazario-Vidah, MD, New York
D. Nguyen, New York
C. Ojha, MBBS, New York
K. Olson, MD, Ohio
V. Paulson, MD, Ohio
R. Pearson, DO, PhD, Ohio
A. Peel, MD, Ohio
S. Pettis, PA-C, Ohio
E. Picloglou, MD, Ohio
H. Pokhrel, MD, Ohio
H. Bush, Oklahoma
R. Porter, PA, Oklahoma
P. Prabhakar, Oklahoma
U. Qamar, Oklahoma
R. Quansah, MD, Oklahoma
M. Rahman, Oklahoma
R. Rajeshwar, Oregon
E. Randal, Oregon
A. Ray, Oregon
V. Reddy, Oregon
J. Reed, MD, RN, Oregon
R. Regidor, Oregon
A. Reitsma-Mathias, MD, Oregon
R. Reyes, MD, Oregon
T. Richardson, NP, Oregon
T. Ringer, Oregon
L. Rivera-Crespo, Pennsylvania
T. Rothwell, PA, Pennsylvania
E. Sacolick, MD, Pennsylvania
E. Saluke, MD, Pennsylvania
M. Santinelli, NP, Pennsylvania
M. Sapon-Amoah, FNP, Pennsylvania
D. Scarine, NP, Pennsylvania
K. Seger, Pennsylvania
A. Shah, Pennsylvania
K. Shah, MD, Pennsylvania
S. Shah, MD, Pennsylvania
G. Sharma, MD, Pennsylvania
K. Shaukat, MD, Pennsylvania
E. Sheindler, Rhode Island
D. Sheps, South Carolina
J. Shipe-Spotloe, South Carolina
S. Sim, South Carolina
M. Simon, MD, MMM, CPE, South Carolina
A. Singh, South Carolina
S. Singh-Patel, PO, South Dakota
M. Snyder, South Dakota
A. Srikanth, MBBS, Tennessee
B. Staats, Tennessee
C. Standley, Texas
R. Stanhiser, Texas
M. Stevens, Texas
K. Stuart, Texas
A. Summers, Texas
E. Taylo, Texas
L. Taylor, PA-C, Texas
L. Theaker, Texas
M. Thieman, Texas
J. Tong, Texas
N. Trivedi, MD, Texas
L. Tuazon, MD, FACP, Texas
S. Tummalapalli, Texas
A. Ufferman, MD, Virginia
R. Urrea, MD, Virginia
N. Van Groningen, Virginia
D. Vaughn, MD, Vermont
R. Vento, MD, MPH, Washington
Y. Villaran, MD, Washington
L. Viscome, DO, Washington
K. Vo, Washington
H. Vu, MD, Washington
T. Washko, MD, Washington
T. Waters, DO, Wisconsin
L. Weisberger, USA, Wisconsin
A. Whitehead, Wisconsin
A. Workman, West Virginia
F. Yasin, MD, West Virginia
A. Yoon, MD, West Virginia
M. Yu, West Virginia
A. Yuen, DO, West Virginia
K. Zwieg, West Virginia
B. Abdalsm, MD, MPH, Alabama
A. Aboutalib, Alabama
D. Adams, MD, Arkansas
A. Afzal, MD, FACP, Arizona
J. Aheam, MD, California
S. Ahluwalia, MBBS, California
A. Alhusseini, MD, FAACP, MBchB, California
L. Anderson, MD, California
K. Arunachalam, MD, California
B. Asalone, California
L. Atkins, MD, California
T. Aultman, MD, California
T. Ayangade, MD, California
A. Azizi, MD, California
F. Azizi, MD, California
S. Balu, MD, California
K. Basra, APRN, FNP, California
N. Bassi, California
C. Batchelor, MD, California
K. Beinlich, MD, California
S. Bhat, MD, MBBS, California
H. Bilal, MBBS, California
G. Bismack, MD, California
M. Bokhari, MD, California
M. Brandenbug, MD, Colorado
H. Briggs, MD, PhD, Colorado
E. Burgh, MD, Colorado
M. Cabrera, BC, Delaware
J. Camden, BA, Delaware
P. Chandra Mohan, MD, Delaware
D. Chau, MD, Delaware
M. Chen, Florida
V. Chennamaneni, Florida
L. Cler, Florida
D. Cooks, Florida
S. Crenshaw, Florida
K. Cunningham, MD, FACP, Florida
V. De Guzman, APRN, MSN, NP, Florida
M. Del Rosario, MD, Florida
D. DeVere, MD, Florida
S. Dharmapuri, Florida
P. Dodson, MD, Florida
A. Domaoal, Georgia
J. Duncan, MD, Georgia
B. Dyck, BSC, MD, PhD, Georgia
J. Dzundza, MD, Georgia
A. Ellis, FNP, Georgia
R. Erickson, Idaho
A. Faraj, Idaho
S. Fernandez, MD, Illinois
G. Ferrari, MD, Illinois
W. Folad, MD, Illinois
L. Fowler, ACNP, APRN, MBA, Illinois
J. Golderberg, MD, Illinois
G. Goldman, MD, Illinois
L. Gonzales, MD, Indiana
A. Gonzalez, Kansas
W. Griffo, MD, Kansas
R. Guzman, Kansas
L. Guzman Vinasco, MD, Kansas
K. Hageman, DO, Kentucky
M. Haggerty, PA-C, Kentucky
B. Hammond, Louisiana
G. Harris, MD, Louisiana
J. Hasan-Jones, RN, FACHE, Louisiana
J. Herring, Louisiana
L. Hsu, MD, Massachusetts
A. C. Hunag, DO, Massachusetts
M. Huq, Massachusetts
M. Jandrin, PA-C, Massachusetts
C. Janish, MD, Maryland
J. Jarin, MD, Maine
A. Jenkins, Maine
S. Jindal, MD, Michigan
M. Johl, Michigan
T. John, Michigan
N. Kapadia, MD, Michigan
L. Katona, Michigan
K. Kaye, Michigan
M. Keating, Michigan
L. Keeton, MD, Michigan
L. Kendall, Michigan
M. Kerlin, Michigan
A. Kia, MD, Minnesota
R. Klett, Minnesota
L. Knapp, DO, Minnesota
K. Knox, Missouri
M. Kraynak, MD, Missouri
P. Kuppireddy, MBBS, Missouri
W. Landrum, MD, Missouri
C. Larion, ACNP, Missouri
E. Latcheva, MD, Mississippi
D. Leforce, North Carolina
V. Leigh, DO, North Carolina
C. Leon, North Carolina
T. Li, MD, North Dakota
X. Li, MD, Nebraska
Y. Li, New Hampshire
J. Liu, New Hampshire
L. Lu, DO, New Jersey
S. Mathapathi, New Jersey
L. McGann, New Jersey
S. Melkaveri, MD, Nevada
R. Mercado Garcia, New York
S. Merry, MD, New York
P. Meyer, DO, New York
J. Mikulca, PharmD, New York
Z. Moyenda, MD, MBA, New York
K. Murphy, DO, MPH, New York
J. Musenze, New York
P. Mutungi, New York
G. Nanna, USA, New York
I. Nasir, New York
U. Nazario-Vidah, MD, New York
D. Nguyen, New York
C. Ojha, MBBS, New York
K. Olson, MD, Ohio
V. Paulson, MD, Ohio
R. Pearson, DO, PhD, Ohio
A. Peel, MD, Ohio
S. Pettis, PA-C, Ohio
E. Picloglou, MD, Ohio
H. Pokhrel, MD, Ohio
H. Bush, Oklahoma
R. Porter, PA, Oklahoma
P. Prabhakar, Oklahoma
U. Qamar, Oklahoma
R. Quansah, MD, Oklahoma
M. Rahman, Oklahoma
R. Rajeshwar, Oregon
E. Randal, Oregon
A. Ray, Oregon
V. Reddy, Oregon
J. Reed, MD, RN, Oregon
R. Regidor, Oregon
A. Reitsma-Mathias, MD, Oregon
R. Reyes, MD, Oregon
T. Richardson, NP, Oregon
T. Ringer, Oregon
L. Rivera-Crespo, Pennsylvania
T. Rothwell, PA, Pennsylvania
E. Sacolick, MD, Pennsylvania
E. Saluke, MD, Pennsylvania
M. Santinelli, NP, Pennsylvania
M. Sapon-Amoah, FNP, Pennsylvania
D. Scarine, NP, Pennsylvania
K. Seger, Pennsylvania
A. Shah, Pennsylvania
K. Shah, MD, Pennsylvania
S. Shah, MD, Pennsylvania
G. Sharma, MD, Pennsylvania
K. Shaukat, MD, Pennsylvania
E. Sheindler, Rhode Island
D. Sheps, South Carolina
J. Shipe-Spotloe, South Carolina
S. Sim, South Carolina
M. Simon, MD, MMM, CPE, South Carolina
A. Singh, South Carolina
S. Singh-Patel, PO, South Dakota
M. Snyder, South Dakota
A. Srikanth, MBBS, Tennessee
B. Staats, Tennessee
C. Standley, Texas
R. Stanhiser, Texas
M. Stevens, Texas
K. Stuart, Texas
A. Summers, Texas
E. Taylo, Texas
L. Taylor, PA-C, Texas
L. Theaker, Texas
M. Thieman, Texas
J. Tong, Texas
N. Trivedi, MD, Texas
L. Tuazon, MD, FACP, Texas
S. Tummalapalli, Texas
A. Ufferman, MD, Virginia
R. Urrea, MD, Virginia
N. Van Groningen, Virginia
D. Vaughn, MD, Vermont
R. Vento, MD, MPH, Washington
Y. Villaran, MD, Washington
L. Viscome, DO, Washington
K. Vo, Washington
H. Vu, MD, Washington
T. Washko, MD, Washington
T. Waters, DO, Wisconsin
L. Weisberger, USA, Wisconsin
A. Whitehead, Wisconsin
A. Workman, West Virginia
F. Yasin, MD, West Virginia
A. Yoon, MD, West Virginia
M. Yu, West Virginia
A. Yuen, DO, West Virginia
K. Zwieg, West Virginia
B. Abdalsm, MD, MPH, Alabama
A. Aboutalib, Alabama
D. Adams, MD, Arkansas
A. Afzal, MD, FACP, Arizona
J. Aheam, MD, California
S. Ahluwalia, MBBS, California
A. Alhusseini, MD, FAACP, MBchB, California
L. Anderson, MD, California
K. Arunachalam, MD, California
B. Asalone, California
L. Atkins, MD, California
T. Aultman, MD, California
T. Ayangade, MD, California
A. Azizi, MD, California
F. Azizi, MD, California
S. Balu, MD, California
K. Basra, APRN, FNP, California
N. Bassi, California
C. Batchelor, MD, California
K. Beinlich, MD, California
S. Bhat, MD, MBBS, California
H. Bilal, MBBS, California
G. Bismack, MD, California
M. Bokhari, MD, California
M. Brandenbug, MD, Colorado
H. Briggs, MD, PhD, Colorado
E. Burgh, MD, Colorado
M. Cabrera, BC, Delaware
J. Camden, BA, Delaware
P. Chandra Mohan, MD, Delaware
D. Chau, MD, Delaware
M. Chen, Florida
V. Chennamaneni, Florida
L. Cler, Florida
D. Cooks, Florida
S. Crenshaw, Florida
K. Cunningham, MD, FACP, Florida
V. De Guzman, APRN, MSN, NP, Florida
M. Del Rosario, MD, Florida
D. DeVere, MD, Florida
S. Dharmapuri, Florida
P. Dodson, MD, Florida
A. Domaoal, Georgia
J. Duncan, MD, Georgia
B. Dyck, BSC, MD, PhD, Georgia
J. Dzundza, MD, Georgia
A. Ellis, FNP, Georgia
R. Erickson, Idaho
A. Faraj, Idaho
S. Fernandez, MD, Illinois
G. Ferrari, MD, Illinois
W. Folad, MD, Illinois
L. Fowler, ACNP, APRN, MBA, Illinois
J. Golderberg, MD, Illinois
G. Goldman, MD, Illinois
L. Gonzales, MD, Indiana
A. Gonzalez, Kansas
W. Griffo, MD, Kansas
R. Guzman, Kansas
L. Guzman Vinasco, MD, Kansas
K. Hageman, DO, Kentucky
M. Haggerty, PA-C, Kentucky
B. Hammond, Louisiana
G. Harris, MD, Louisiana
J. Hasan-Jones, RN, FACHE, Louisiana
J. Herring, Louisiana
L. Hsu, MD, Massachusetts
A. C. Hunag, DO, Massachusetts
M. Huq, Massachusetts
M. Jandrin, PA-C, Massachusetts
C. Janish, MD, Maryland
J. Jarin, MD, Maine
A. Jenkins, Maine
S. Jindal, MD, Michigan
M. Johl, Michigan
T. John, Michigan
N. Kapadia, MD, Michigan
L. Katona, Michigan
K. Kaye, Michigan
M. Keating, Michigan
L. Keeton, MD, Michigan
L. Kendall, Michigan
M. Kerlin, Michigan
A. Kia, MD, Minnesota
R. Klett, Minnesota
L. Knapp, DO, Minnesota
K. Knox, Missouri
M. Kraynak, MD, Missouri
P. Kuppireddy, MBBS, Missouri
W. Landrum, MD, Missouri
C. Larion, ACNP, Missouri
E. Latcheva, MD, Mississippi
D. Leforce, North Carolina
V. Leigh, DO, North Carolina
C. Leon, North Carolina
T. Li, MD, North Dakota
X. Li, MD, Nebraska
Y. Li, New Hampshire
J. Liu, New Hampshire
L. Lu, DO, New Jersey
S. Mathapathi, New Jersey
L. McGann, New Jersey
S. Melkaveri, MD, Nevada
R. Mercado Garcia, New York
S. Merry, MD, New York
P. Meyer, DO, New York
J. Mikulca, PharmD, New York
Z. Moyenda, MD, MBA, New York
K. Murphy, DO, MPH, New York
J. Musenze, New York
P. Mutungi, New York
G. Nanna, USA, New York
I. Nasir, New York
U. Nazario-Vidah, MD, New York
D. Nguyen, New York
C. Ojha, MBBS, New York
K. Olson, MD, Ohio
V. Paulson, MD, Ohio
R. Pearson, DO, PhD, Ohio
A. Peel, MD, Ohio
S. Pettis, PA-C, Ohio
E. Picloglou, MD, Ohio
H. Pokhrel, MD, Ohio
H. Bush, Oklahoma
R. Porter, PA, Oklahoma
P. Prabhakar, Oklahoma
U. Qamar, Oklahoma
R. Quansah, MD, Oklahoma
M. Rahman, Oklahoma
R. Rajeshwar, Oregon
E. Randal, Oregon
A. Ray, Oregon
V. Reddy, Oregon
J. Reed, MD, RN, Oregon
R. Regidor, Oregon
A. Reitsma-Mathias, MD, Oregon
R. Reyes, MD, Oregon
T. Richardson, NP, Oregon
T. Ringer, Oregon
L. Rivera-Crespo, Pennsylvania
T. Rothwell, PA, Pennsylvania
E. Sacolick, MD, Pennsylvania
E. Saluke, MD, Pennsylvania
M. Santinelli, NP, Pennsylvania
M. Sapon-Amoah, FNP, Pennsylvania
D. Scarine, NP, Pennsylvania
K. Seger, Pennsylvania
A. Shah, Pennsylvania
K. Shah, MD, Pennsylvania
S. Shah, MD, Pennsylvania
G. Sharma, MD, Pennsylvania
K. Shaukat, MD, Pennsylvania
E. Sheindler, Rhode Island
D. Sheps, South Carolina
J. Shipe-Spotloe, South Carolina
S. Sim, South Carolina
M. Simon, MD, MMM, CPE, South Carolina
A. Singh, South Carolina
S. Singh-Patel, PO, South Dakota
M. Snyder, South Dakota
A. Srikanth, MBBS, Tennessee
B. Staats, Tennessee
C. Standley, Texas
R. Stanhiser, Texas
M. Stevens, Texas
K. Stuart, Texas
A. Summers, Texas
E. Taylo, Texas
L. Taylor, PA-C, Texas
L. Theaker, Texas
M. Thieman, Texas
J. Tong, Texas
N. Trivedi, MD, Texas
L. Tuazon, MD, FACP, Texas
S. Tummalapalli, Texas
A. Ufferman, MD, Virginia
R. Urrea, MD, Virginia
N. Van Groningen, Virginia
D. Vaughn, MD, Vermont
R. Vento, MD, MPH, Washington
Y. Villaran, MD, Washington
L. Viscome, DO, Washington
K. Vo, Washington
H. Vu, MD, Washington
T. Washko, MD, Washington
T. Waters, DO, Wisconsin
L. Weisberger, USA, Wisconsin
A. Whitehead, Wisconsin
A. Workman, West Virginia
F. Yasin, MD, West Virginia
A. Yoon, MD, West Virginia
M. Yu, West Virginia
A. Yuen, DO, West Virginia
K. Zwieg, West Virginia
CHMP recommends extending brentuximab approval

Photo from Business Wire
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended extending the current conditional approval of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) at increased risk of relapse or progression following autologous stem cell transplant (ASCT).
The CHMP’s recommendation will now be reviewed by the European Commission (EC).
If the recommendation is formally adopted by the EC, brentuximab vedotin will be approved for the aforementioned indication in the 28 member states of the European Union as well as Norway, Liechtenstein, and Iceland.
Brentuximab vedotin already has conditional marketing authorization from the EC for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The CHMP’s recommendation to extend the approval of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended extending the current conditional approval of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) at increased risk of relapse or progression following autologous stem cell transplant (ASCT).
The CHMP’s recommendation will now be reviewed by the European Commission (EC).
If the recommendation is formally adopted by the EC, brentuximab vedotin will be approved for the aforementioned indication in the 28 member states of the European Union as well as Norway, Liechtenstein, and Iceland.
Brentuximab vedotin already has conditional marketing authorization from the EC for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The CHMP’s recommendation to extend the approval of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Photo from Business Wire
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended extending the current conditional approval of brentuximab vedotin (Adcetris) to include the treatment of adults with CD30+ Hodgkin lymphoma (HL) at increased risk of relapse or progression following autologous stem cell transplant (ASCT).
The CHMP’s recommendation will now be reviewed by the European Commission (EC).
If the recommendation is formally adopted by the EC, brentuximab vedotin will be approved for the aforementioned indication in the 28 member states of the European Union as well as Norway, Liechtenstein, and Iceland.
Brentuximab vedotin already has conditional marketing authorization from the EC for 2 indications:
- To treat adults with relapsed or refractory CD30+ HL after ASCT or following at least 2 prior therapies when ASCT or multi-agent chemotherapy is not a treatment option
- To treat adults with relapsed or refractory systemic anaplastic large-cell lymphoma (sALCL).
In January 2016, the EC approved a Type II variation to include data on the retreatment of adult patients with HL or sALCL who previously responded to brentuximab vedotin and later relapsed.
Brentuximab vedotin is under joint development by Seattle Genetics and Takeda Pharmaceutical Company Limited.
AETHERA trial
The CHMP’s recommendation to extend the approval of brentuximab vedotin is based on results from the phase 3 AETHERA trial.
The trial was designed to compare brentuximab vedotin to placebo, both administered for up to 16 cycles (approximately 1 year) every 3 weeks following ASCT. Results from the trial were published in The Lancet in March 2015 and presented at the 2014 ASH Annual Meeting.
The study enrolled 329 HL patients at risk of relapse or progression, including 165 on the brentuximab vedotin arm and 164 on the placebo arm.
Patients were eligible for enrollment if they had a history of primary refractory HL, relapsed within a year of receiving frontline chemotherapy, and/or had disease outside of the lymph nodes at the time of pre-ASCT relapse.
Brentuximab vedotin conferred a significant increase in progression-free survival over placebo, with a hazard ratio of 0.57 (P=0.001). The median progression-free survival was 43 months for patients who received brentuximab vedotin and 24 months for those who received placebo.
The most common adverse events (≥20%), of any grade and regardless of causality, in the brentuximab vedotin arm were neutropenia (78%), peripheral sensory neuropathy (56%), thrombocytopenia (41%), anemia (27%), upper respiratory tract infection (26%), fatigue (24%), peripheral motor neuropathy (23%), nausea (22%), cough (21%), and diarrhea (20%).
The most common adverse events (≥20%), of any grade and regardless of causality, in the placebo arm were neutropenia (34%), upper respiratory tract infection (23%), and thrombocytopenia (20%).
In all, 67% of patients on the brentuximab vedotin arm experienced peripheral neuropathy. Of those patients, 85% had resolution (59%) or partial improvement (26%) in symptoms at the time of their last evaluation, with a median time to improvement of 23 weeks (range, 0.1-138). ![]()
Monitor Alarms in a Children's Hospital
Physiologic monitor alarms are an inescapable part of the soundtrack for hospitals. Data from primarily adult hospitals have shown that alarms occur at high rates, and most alarms are not actionable.[1] Small studies have suggested that high alarm rates can lead to alarm fatigue.[2, 3] To prioritize alarm types to target in future intervention studies, in this study we aimed to investigate the alarm rates on all inpatient units and the most common causes of alarms at a children's hospital.
METHODS
This was a cross‐sectional study of audible physiologic monitor alarms at Cincinnati Children's Hospital Medical Center (CCHMC) over 7 consecutive days during August 2014. CCHMC is a 522‐bed free‐standing children's hospital. Inpatient beds are equipped with GE Healthcare (Little Chalfont, United Kingdom) bedside monitors (models Dash 3000, 4000, and 5000, and Solar 8000). Age‐specific vital sign parameters were employed for monitors on all units.
We obtained date, time, and type of alarm from bedside physiologic monitors using Connexall middleware (GlobeStar Systems, Toronto, Ontario, Canada).
We determined unit census using the electronic health records for the time period concurrent with the alarm data collection. Given previously described variation in hospital census over the day,[4] we used 4 daily census measurements (6:00 am, 12:00 pm, 6:00 pm, and 11:00 pm) rather than 1 single measurement to more accurately reflect the hospital census.
The CCHMC Institutional Review Board determined this work to be not human subjects research.
Statistical Analysis
For each unit and each census time interval, we generated a rate based on the number of occupied beds (alarms per patient‐day) resulting in a total of 28 rates (4 census measurement periods per/day 7 days) for each unit over the study period. We used descriptive statistics to summarize alarms per patient‐day by unit. Analysis of variance was used to compare alarm rates between units. For significant main effects, we used Tukey's multiple comparisons tests for all pairwise comparisons to control the type I experiment‐wise error rate. Alarms were then classified by alarm cause (eg, high heart rate). We summarized the cause for all alarms using counts and percentages.
RESULTS
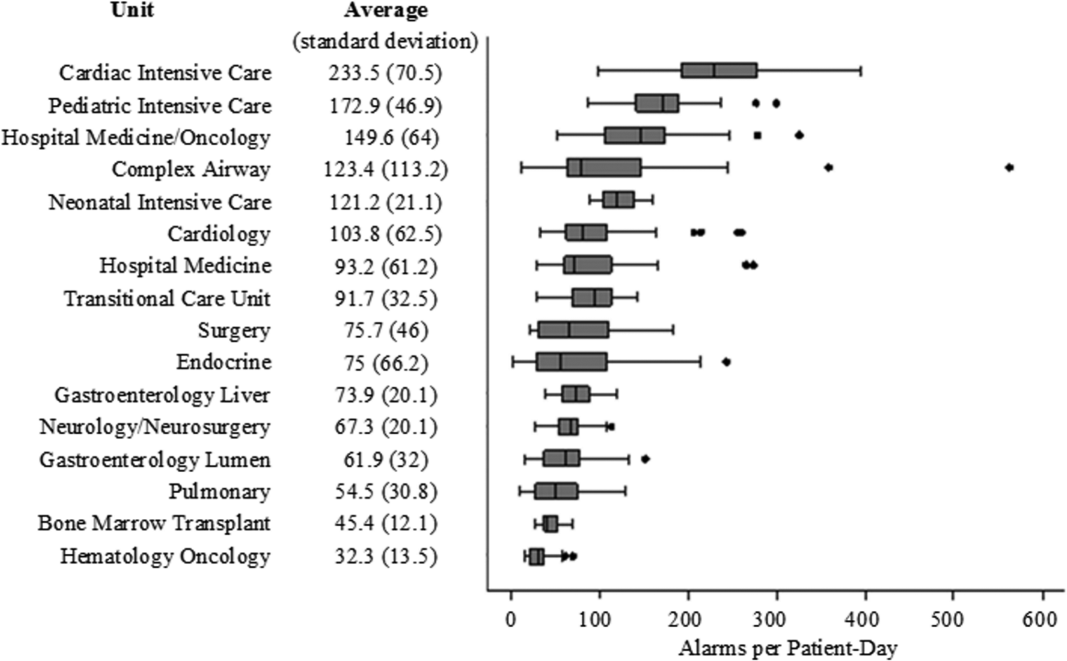
There were a total of 220,813 audible alarms over 1 week. Median alarm rate per patient‐day by unit ranged from 30.4 to 228.5; the highest alarm rates occurred in the cardiac intensive care unit, with a median of 228.5 (interquartile range [IQR], 193275) followed by the pediatric intensive care unit (172.4; IQR, 141188) (Figure 1). The average alarm rate was significantly different among the units (P 0.01).
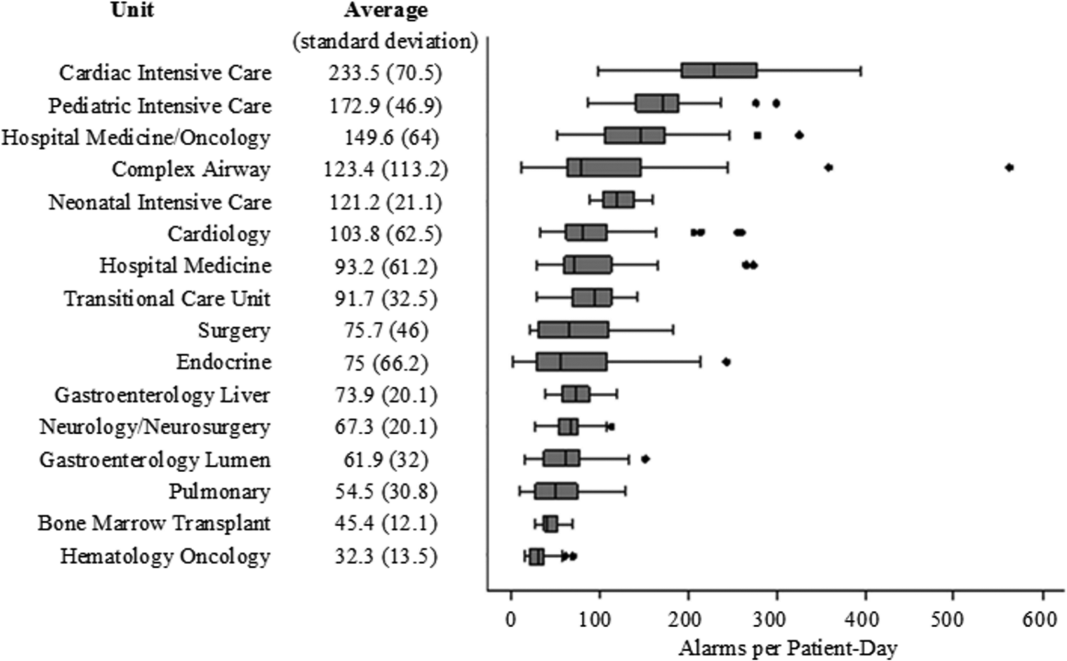
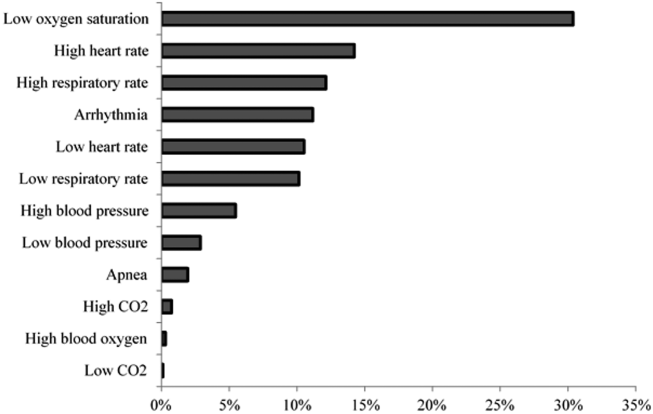
Technical alarms (eg, alarms for artifact, lead failure), comprised 33% of the total number of alarms. The remaining 67% of alarms were for clinical conditions, the most common of which was low oxygen saturation (30% of clinical alarms) (Figure 2).
DISCUSSION
We described alarm rates and causes over multiple units at a large children's hospital. To our knowledge, this is the first description of alarm rates across multiple pediatric inpatient units. Alarm counts were high even for the general units, indicating that a nurse taking care of 4 monitored patients would need to process a physiologic monitor alarm every 4 minutes on average, in addition to other sources of alarms such as infusion pumps.
Alarm rates were highest in the intensive care unit areas, which may be attributable to both higher rates of monitoring and sicker patients. Importantly, however, alarms were quite high and variable on the acute care units. This suggests that factors other than patient acuity may have substantial influence on alarm rates.
Technical alarms, alarms that do not indicate a change in patient condition, accounted for the largest percentage of alarms during the study period. This is consistent with prior literature that has suggested that regular electrode replacement, which decreases technical alarms, can be effective in reducing alarm rates.[5, 6] The most common vital sign change to cause alarms was low oxygen saturation, followed by elevated heart rate and elevated respiratory rate. Whereas in most healthy patients, certain low oxygen levels would prompt initiation of supplemental oxygen, there are many conditions in which elevated heart rate and respiratory rate may not require titration of any particular therapy. These may be potential intervention targets for hospitals trying to improve alarm rates.
Limitations
There are several limitations to our study. First, our results are not necessarily generalizable to other types of hospitals or those utilizing monitors from other vendors. Second, we were unable to include other sources of alarms such as infusion pumps and ventilators. However, given the high alarm rates from physiologic monitors alone, these data add urgency to the need for further investigation in the pediatric setting.
CONCLUSION
Alarm rates at a single children's hospital varied depending on the unit. Strategies targeted at reducing technical alarms and reducing nonactionable clinical alarms for low oxygen saturation, high heart rate, and high respiratory rate may offer the greatest opportunity to reduce alarm rates.
Acknowledgements
The authors acknowledge Melinda Egan for her assistance in obtaining data for this study and Ting Sa for her assistance with data management.
Disclosures: Dr. Bonafide is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL116427. Dr. Bonafide also holds a Young Investigator Award grant from the Academic Pediatric Association evaluating the impact of a data‐driven monitor alarm reduction strategy implemented in safety huddles. Dr. Brady is supported by the Agency for Healthcare Research and Quality under award number K08HS23827. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Agency for Healthcare Research and Quality. This study was funded by the Arnold W. Strauss Fellow Grant, Cincinnati Children's Hospital Medical Center. The authors have no conflicts of interest to disclose.
- , , , et al. Systematic review of physiologic monitor alarm characteristics and pragmatic interventions to reduce alarm frequency. J Hosp Med. 2016;11(2):136–144.
- , , , et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children's hospital. J Hosp Med. 2015;10(6):345–351.
- , , , et al. Pulse oximetry desaturation alarms on a general postoperative adult unit: a prospective observational study of nurse response time. Int J Nurs Stud. 2013;50(10):1351–1358.
- , , , , . Traditional measures of hospital utilization may not accurately reflect dynamic patient demand: findings from a children's hospital. Hosp Pediatr. 2012;2(1):10–18.
- , , , et al. A team‐based approach to reducing cardiac monitor alarms. Pediatrics. 2014;134(6):e1686–e1694.
- , , , . Daily electrode change and effect on cardiac monitor alarms: an evidence‐based practice approach. J Nurs Care Qual. 2013;28(3):265–271.
Physiologic monitor alarms are an inescapable part of the soundtrack for hospitals. Data from primarily adult hospitals have shown that alarms occur at high rates, and most alarms are not actionable.[1] Small studies have suggested that high alarm rates can lead to alarm fatigue.[2, 3] To prioritize alarm types to target in future intervention studies, in this study we aimed to investigate the alarm rates on all inpatient units and the most common causes of alarms at a children's hospital.
METHODS
This was a cross‐sectional study of audible physiologic monitor alarms at Cincinnati Children's Hospital Medical Center (CCHMC) over 7 consecutive days during August 2014. CCHMC is a 522‐bed free‐standing children's hospital. Inpatient beds are equipped with GE Healthcare (Little Chalfont, United Kingdom) bedside monitors (models Dash 3000, 4000, and 5000, and Solar 8000). Age‐specific vital sign parameters were employed for monitors on all units.
We obtained date, time, and type of alarm from bedside physiologic monitors using Connexall middleware (GlobeStar Systems, Toronto, Ontario, Canada).
We determined unit census using the electronic health records for the time period concurrent with the alarm data collection. Given previously described variation in hospital census over the day,[4] we used 4 daily census measurements (6:00 am, 12:00 pm, 6:00 pm, and 11:00 pm) rather than 1 single measurement to more accurately reflect the hospital census.
The CCHMC Institutional Review Board determined this work to be not human subjects research.
Statistical Analysis
For each unit and each census time interval, we generated a rate based on the number of occupied beds (alarms per patient‐day) resulting in a total of 28 rates (4 census measurement periods per/day 7 days) for each unit over the study period. We used descriptive statistics to summarize alarms per patient‐day by unit. Analysis of variance was used to compare alarm rates between units. For significant main effects, we used Tukey's multiple comparisons tests for all pairwise comparisons to control the type I experiment‐wise error rate. Alarms were then classified by alarm cause (eg, high heart rate). We summarized the cause for all alarms using counts and percentages.
RESULTS
There were a total of 220,813 audible alarms over 1 week. Median alarm rate per patient‐day by unit ranged from 30.4 to 228.5; the highest alarm rates occurred in the cardiac intensive care unit, with a median of 228.5 (interquartile range [IQR], 193275) followed by the pediatric intensive care unit (172.4; IQR, 141188) (Figure 1). The average alarm rate was significantly different among the units (P 0.01).
Technical alarms (eg, alarms for artifact, lead failure), comprised 33% of the total number of alarms. The remaining 67% of alarms were for clinical conditions, the most common of which was low oxygen saturation (30% of clinical alarms) (Figure 2).
DISCUSSION
We described alarm rates and causes over multiple units at a large children's hospital. To our knowledge, this is the first description of alarm rates across multiple pediatric inpatient units. Alarm counts were high even for the general units, indicating that a nurse taking care of 4 monitored patients would need to process a physiologic monitor alarm every 4 minutes on average, in addition to other sources of alarms such as infusion pumps.
Alarm rates were highest in the intensive care unit areas, which may be attributable to both higher rates of monitoring and sicker patients. Importantly, however, alarms were quite high and variable on the acute care units. This suggests that factors other than patient acuity may have substantial influence on alarm rates.
Technical alarms, alarms that do not indicate a change in patient condition, accounted for the largest percentage of alarms during the study period. This is consistent with prior literature that has suggested that regular electrode replacement, which decreases technical alarms, can be effective in reducing alarm rates.[5, 6] The most common vital sign change to cause alarms was low oxygen saturation, followed by elevated heart rate and elevated respiratory rate. Whereas in most healthy patients, certain low oxygen levels would prompt initiation of supplemental oxygen, there are many conditions in which elevated heart rate and respiratory rate may not require titration of any particular therapy. These may be potential intervention targets for hospitals trying to improve alarm rates.
Limitations
There are several limitations to our study. First, our results are not necessarily generalizable to other types of hospitals or those utilizing monitors from other vendors. Second, we were unable to include other sources of alarms such as infusion pumps and ventilators. However, given the high alarm rates from physiologic monitors alone, these data add urgency to the need for further investigation in the pediatric setting.
CONCLUSION
Alarm rates at a single children's hospital varied depending on the unit. Strategies targeted at reducing technical alarms and reducing nonactionable clinical alarms for low oxygen saturation, high heart rate, and high respiratory rate may offer the greatest opportunity to reduce alarm rates.
Acknowledgements
The authors acknowledge Melinda Egan for her assistance in obtaining data for this study and Ting Sa for her assistance with data management.
Disclosures: Dr. Bonafide is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL116427. Dr. Bonafide also holds a Young Investigator Award grant from the Academic Pediatric Association evaluating the impact of a data‐driven monitor alarm reduction strategy implemented in safety huddles. Dr. Brady is supported by the Agency for Healthcare Research and Quality under award number K08HS23827. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Agency for Healthcare Research and Quality. This study was funded by the Arnold W. Strauss Fellow Grant, Cincinnati Children's Hospital Medical Center. The authors have no conflicts of interest to disclose.
Physiologic monitor alarms are an inescapable part of the soundtrack for hospitals. Data from primarily adult hospitals have shown that alarms occur at high rates, and most alarms are not actionable.[1] Small studies have suggested that high alarm rates can lead to alarm fatigue.[2, 3] To prioritize alarm types to target in future intervention studies, in this study we aimed to investigate the alarm rates on all inpatient units and the most common causes of alarms at a children's hospital.
METHODS
This was a cross‐sectional study of audible physiologic monitor alarms at Cincinnati Children's Hospital Medical Center (CCHMC) over 7 consecutive days during August 2014. CCHMC is a 522‐bed free‐standing children's hospital. Inpatient beds are equipped with GE Healthcare (Little Chalfont, United Kingdom) bedside monitors (models Dash 3000, 4000, and 5000, and Solar 8000). Age‐specific vital sign parameters were employed for monitors on all units.
We obtained date, time, and type of alarm from bedside physiologic monitors using Connexall middleware (GlobeStar Systems, Toronto, Ontario, Canada).
We determined unit census using the electronic health records for the time period concurrent with the alarm data collection. Given previously described variation in hospital census over the day,[4] we used 4 daily census measurements (6:00 am, 12:00 pm, 6:00 pm, and 11:00 pm) rather than 1 single measurement to more accurately reflect the hospital census.
The CCHMC Institutional Review Board determined this work to be not human subjects research.
Statistical Analysis
For each unit and each census time interval, we generated a rate based on the number of occupied beds (alarms per patient‐day) resulting in a total of 28 rates (4 census measurement periods per/day 7 days) for each unit over the study period. We used descriptive statistics to summarize alarms per patient‐day by unit. Analysis of variance was used to compare alarm rates between units. For significant main effects, we used Tukey's multiple comparisons tests for all pairwise comparisons to control the type I experiment‐wise error rate. Alarms were then classified by alarm cause (eg, high heart rate). We summarized the cause for all alarms using counts and percentages.
RESULTS
There were a total of 220,813 audible alarms over 1 week. Median alarm rate per patient‐day by unit ranged from 30.4 to 228.5; the highest alarm rates occurred in the cardiac intensive care unit, with a median of 228.5 (interquartile range [IQR], 193275) followed by the pediatric intensive care unit (172.4; IQR, 141188) (Figure 1). The average alarm rate was significantly different among the units (P 0.01).
Technical alarms (eg, alarms for artifact, lead failure), comprised 33% of the total number of alarms. The remaining 67% of alarms were for clinical conditions, the most common of which was low oxygen saturation (30% of clinical alarms) (Figure 2).
DISCUSSION
We described alarm rates and causes over multiple units at a large children's hospital. To our knowledge, this is the first description of alarm rates across multiple pediatric inpatient units. Alarm counts were high even for the general units, indicating that a nurse taking care of 4 monitored patients would need to process a physiologic monitor alarm every 4 minutes on average, in addition to other sources of alarms such as infusion pumps.
Alarm rates were highest in the intensive care unit areas, which may be attributable to both higher rates of monitoring and sicker patients. Importantly, however, alarms were quite high and variable on the acute care units. This suggests that factors other than patient acuity may have substantial influence on alarm rates.
Technical alarms, alarms that do not indicate a change in patient condition, accounted for the largest percentage of alarms during the study period. This is consistent with prior literature that has suggested that regular electrode replacement, which decreases technical alarms, can be effective in reducing alarm rates.[5, 6] The most common vital sign change to cause alarms was low oxygen saturation, followed by elevated heart rate and elevated respiratory rate. Whereas in most healthy patients, certain low oxygen levels would prompt initiation of supplemental oxygen, there are many conditions in which elevated heart rate and respiratory rate may not require titration of any particular therapy. These may be potential intervention targets for hospitals trying to improve alarm rates.
Limitations
There are several limitations to our study. First, our results are not necessarily generalizable to other types of hospitals or those utilizing monitors from other vendors. Second, we were unable to include other sources of alarms such as infusion pumps and ventilators. However, given the high alarm rates from physiologic monitors alone, these data add urgency to the need for further investigation in the pediatric setting.
CONCLUSION
Alarm rates at a single children's hospital varied depending on the unit. Strategies targeted at reducing technical alarms and reducing nonactionable clinical alarms for low oxygen saturation, high heart rate, and high respiratory rate may offer the greatest opportunity to reduce alarm rates.
Acknowledgements
The authors acknowledge Melinda Egan for her assistance in obtaining data for this study and Ting Sa for her assistance with data management.
Disclosures: Dr. Bonafide is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL116427. Dr. Bonafide also holds a Young Investigator Award grant from the Academic Pediatric Association evaluating the impact of a data‐driven monitor alarm reduction strategy implemented in safety huddles. Dr. Brady is supported by the Agency for Healthcare Research and Quality under award number K08HS23827. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Agency for Healthcare Research and Quality. This study was funded by the Arnold W. Strauss Fellow Grant, Cincinnati Children's Hospital Medical Center. The authors have no conflicts of interest to disclose.
- , , , et al. Systematic review of physiologic monitor alarm characteristics and pragmatic interventions to reduce alarm frequency. J Hosp Med. 2016;11(2):136–144.
- , , , et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children's hospital. J Hosp Med. 2015;10(6):345–351.
- , , , et al. Pulse oximetry desaturation alarms on a general postoperative adult unit: a prospective observational study of nurse response time. Int J Nurs Stud. 2013;50(10):1351–1358.
- , , , , . Traditional measures of hospital utilization may not accurately reflect dynamic patient demand: findings from a children's hospital. Hosp Pediatr. 2012;2(1):10–18.
- , , , et al. A team‐based approach to reducing cardiac monitor alarms. Pediatrics. 2014;134(6):e1686–e1694.
- , , , . Daily electrode change and effect on cardiac monitor alarms: an evidence‐based practice approach. J Nurs Care Qual. 2013;28(3):265–271.
- , , , et al. Systematic review of physiologic monitor alarm characteristics and pragmatic interventions to reduce alarm frequency. J Hosp Med. 2016;11(2):136–144.
- , , , et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children's hospital. J Hosp Med. 2015;10(6):345–351.
- , , , et al. Pulse oximetry desaturation alarms on a general postoperative adult unit: a prospective observational study of nurse response time. Int J Nurs Stud. 2013;50(10):1351–1358.
- , , , , . Traditional measures of hospital utilization may not accurately reflect dynamic patient demand: findings from a children's hospital. Hosp Pediatr. 2012;2(1):10–18.
- , , , et al. A team‐based approach to reducing cardiac monitor alarms. Pediatrics. 2014;134(6):e1686–e1694.
- , , , . Daily electrode change and effect on cardiac monitor alarms: an evidence‐based practice approach. J Nurs Care Qual. 2013;28(3):265–271.