User login
High-tech pills help increase medication adherence
orlando – A digital device that patients swallow every time they take a medication may be an answer to improving compliance and disease control. An aim of this digital health system is to encourage patient engagement and provider interaction. Despite available and efficacious medicines, only slightly more than half of patients with type 2 diabetes mellitus have glycated hemoglobin (HbA1c), hypertension, or LDL cholesterol under good control. One study showed only 17% had all three under control (Endocr Pract. 2016;22:689-98).
“Important in this are the facts of medication nonadherence by the patient, poor patient engagement frequently in their care, as well as from a clinician perspective, therapeutic inertia,” said Dr. Juan Frias at the annual meeting of the American Association of Clinical Endocrinologists. Approximately half of patients with chronic diseases do not take their medications as prescribed (Circulation. 2013;128:29-41).

To improve treatment adherence, diagnose the reasons for a patient not reaching therapeutic goals, address those issues with patient education or counseling or changes in medication, and engage with the patient to reinforce adherence goals. A digital system called Proteus Discover has been designed to assist patients and clinicians with all these tasks.
Proteus uses ingestible sensor-detectable medications. Each medication and dose of medication has a unique marker. A compounding pharmacy co-encapsulates a tiny detectable chip about the size of a grain of sand with a medication as prescribed by a physician. The patient wears a Band-Aid sized skin patch sensor that transmits to a mobile device that uploads to a secure cloud server. The sensor can tell if a medication has been taken and also serves as a pedometer and activity gauge.
The information is available to the patient, who can gain insight into medication taking, activity, and rest, along with other health parameters that are entered into the system. Entering the system through a provider portal and with the patient’s permission, the clinician can see patient behavior patterns outside of the clinic, including medication adherence, which helps to determine the best treatment for that patient. The system provides a report to the clinician that can be a point of discussion when the patient visits the clinic.
Trial demonstrates better medication adherence and goal attainment
Dr. Frias, CEO and principal investigator of National Research Institute in Los Angeles, described a 12 week multicenter cluster-randomized pilot study involving 90 patients with uncontrolled hypertension and type 2 diabetes to investigate the effect of Proteus on blood pressure, HbA1c, and LDL cholesterol reduction. Other goals of the trial were to promote medication adherence and physical activity and alert providers to a need to make more medical decisions.
Cluster randomization meant that each of the 16 trial sites randomized patients to one of three treatment arms within that site. The arms were: Proteus Discover for 4 or 12 weeks or usual care. Patients had to have systolic blood pressure of 140 mm Hg or greater, have failed therapy with 2 or more antihypertensive agents, and have HbA1c at 7% or greater on metformin or a sulfonylurea. Two-thirds of the subjects also had dyslipidemia and were treated with statins. Subjects were excluded if they had a history of acute or chronic dermatitis, had a skin allergy or sensitivity to adhesive medical tape, or had secondary causes for uncontrolled hypertension or type 2 diabetes.
Usual care consisted of all standard interventions, including medication titrations, patient education, and lifestyle coaching. All subjects took medications for 12 weeks and were followed for 12 weeks after enrollment. Available medications were various doses of lisinopril, losartan, hydrochlorothiazide, amlodipine, atorvastatin, metformin, and glipizide.
All the arms were fairly well balanced as to age (58-62 years), ethnicity, employment, education, and income. About one quarter had incomes in the $20,000-$40,000 range, and about half had incomes of $20,000 or less. Body mass index was 32 kg/m2 in the Proteus and usual care arms. Total cholesterol was similar for the Proteus and usual care groups at 173-177 mg/dL, but LDL was slightly higher in the Proteus arms (103 vs. 95 mg/dL).
Better adherence and outcomes for patients using Proteus
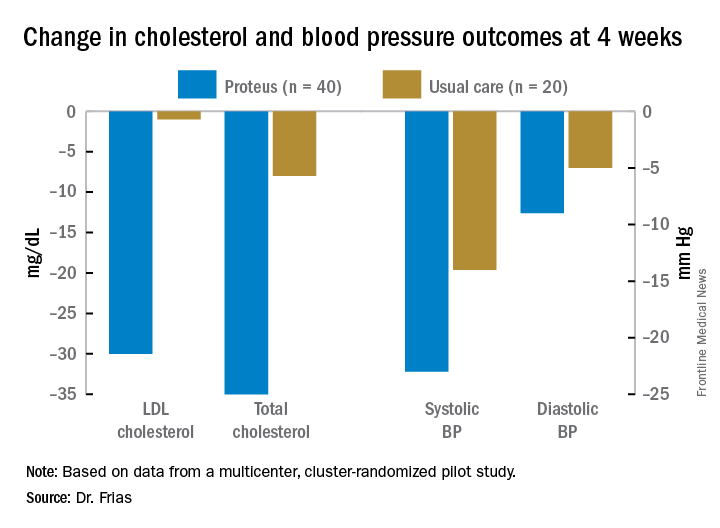
Dr. Frias presented 4-week results for blood pressure and cholesterol reduction. The 4- and 12-week Proteus arms were combined for this analysis, since up to 4 weeks they received the same intervention. Blood pressure, LDL cholesterol, and total cholesterol were all significantly reduced in the Proteus group, compared with the usual care group. At week 4, 83% of the subjects in the Proteus group had reached a blood pressure goal of less than 140/90 mm Hg vs. 33% in the usual care arm (difference of 50%; 95% confidence interval, 24%, 76%). Across all 11 medications/doses, the adherence was between 80% and 89% for every one.
The system spurred clinicians to make more treatment decisions for their patients. Providers made more changes to treatment for the Proteus patients, compared with the usual care providers (50% vs. 36%), gave more adherence counseling (28% vs. 0%), and provided more patient education (42% vs. 9%). Patients using the Proteus Discover system expressed high levels of satisfaction and acceptance of the technology (83%-100%), including ease of use in one’s daily routine, learning to use it, motivation to manage one’s health, better discussions with providers, understanding their care plan, seeing how they take their medications, and applying and wearing the sensor patch.
Safety was excellent. Twenty-seven adverse effects occurred in the Proteus arms, none of them serious, and about half were attributed to the device, mostly self-limited rashes. Seven adverse effects were attributed to the medications, mostly gastrointestinal side effects. There were four adverse effects in the usual care group, two of them serious.
Overall, compared with about 50% typical medication adherence, Proteus users had 84% adherence, which was associated with better blood pressure and LDL cholesterol control, compared with usual care.

Session moderator Dr. David Lieb, associate professor of medicine at Eastern Virginia Medical School in Norfolk, said the Proteus system may be very helpful for patients who are taking multiple medications to prompt them when to take them. “I could easily see somebody who has this system in place where they’re also able to measure their blood pressure and get that information to their provider and for their provider to make changes in their medicine dose,” he said.
This research study of 90 patients was quite manageable, but “what about when you have 300 people on this therapy and all those data are starting to come in? Who’s going to manage those data... and look at it all?” Dr. Lieb wondered. Patients may have to be taught to understand the data and make changes on their own to their medication behavior, exercise, and other factors within their control.
Half the patients in the study made $20,000 or less a year. “If you could help underserved patients with their compliance and all those other things... that would be fantastic. It’s a huge area of need,” he said. People will need internet access to upload their data to the cloud server.
Another question is how the data can interface with the various electronic health records in use and generate reports.
Proteus Discover is approved by the U.S. Food and Drug Administration and is available now.
orlando – A digital device that patients swallow every time they take a medication may be an answer to improving compliance and disease control. An aim of this digital health system is to encourage patient engagement and provider interaction. Despite available and efficacious medicines, only slightly more than half of patients with type 2 diabetes mellitus have glycated hemoglobin (HbA1c), hypertension, or LDL cholesterol under good control. One study showed only 17% had all three under control (Endocr Pract. 2016;22:689-98).
“Important in this are the facts of medication nonadherence by the patient, poor patient engagement frequently in their care, as well as from a clinician perspective, therapeutic inertia,” said Dr. Juan Frias at the annual meeting of the American Association of Clinical Endocrinologists. Approximately half of patients with chronic diseases do not take their medications as prescribed (Circulation. 2013;128:29-41).
To improve treatment adherence, diagnose the reasons for a patient not reaching therapeutic goals, address those issues with patient education or counseling or changes in medication, and engage with the patient to reinforce adherence goals. A digital system called Proteus Discover has been designed to assist patients and clinicians with all these tasks.
Proteus uses ingestible sensor-detectable medications. Each medication and dose of medication has a unique marker. A compounding pharmacy co-encapsulates a tiny detectable chip about the size of a grain of sand with a medication as prescribed by a physician. The patient wears a Band-Aid sized skin patch sensor that transmits to a mobile device that uploads to a secure cloud server. The sensor can tell if a medication has been taken and also serves as a pedometer and activity gauge.
The information is available to the patient, who can gain insight into medication taking, activity, and rest, along with other health parameters that are entered into the system. Entering the system through a provider portal and with the patient’s permission, the clinician can see patient behavior patterns outside of the clinic, including medication adherence, which helps to determine the best treatment for that patient. The system provides a report to the clinician that can be a point of discussion when the patient visits the clinic.
Trial demonstrates better medication adherence and goal attainment
Dr. Frias, CEO and principal investigator of National Research Institute in Los Angeles, described a 12 week multicenter cluster-randomized pilot study involving 90 patients with uncontrolled hypertension and type 2 diabetes to investigate the effect of Proteus on blood pressure, HbA1c, and LDL cholesterol reduction. Other goals of the trial were to promote medication adherence and physical activity and alert providers to a need to make more medical decisions.
Cluster randomization meant that each of the 16 trial sites randomized patients to one of three treatment arms within that site. The arms were: Proteus Discover for 4 or 12 weeks or usual care. Patients had to have systolic blood pressure of 140 mm Hg or greater, have failed therapy with 2 or more antihypertensive agents, and have HbA1c at 7% or greater on metformin or a sulfonylurea. Two-thirds of the subjects also had dyslipidemia and were treated with statins. Subjects were excluded if they had a history of acute or chronic dermatitis, had a skin allergy or sensitivity to adhesive medical tape, or had secondary causes for uncontrolled hypertension or type 2 diabetes.
Usual care consisted of all standard interventions, including medication titrations, patient education, and lifestyle coaching. All subjects took medications for 12 weeks and were followed for 12 weeks after enrollment. Available medications were various doses of lisinopril, losartan, hydrochlorothiazide, amlodipine, atorvastatin, metformin, and glipizide.
All the arms were fairly well balanced as to age (58-62 years), ethnicity, employment, education, and income. About one quarter had incomes in the $20,000-$40,000 range, and about half had incomes of $20,000 or less. Body mass index was 32 kg/m2 in the Proteus and usual care arms. Total cholesterol was similar for the Proteus and usual care groups at 173-177 mg/dL, but LDL was slightly higher in the Proteus arms (103 vs. 95 mg/dL).
Better adherence and outcomes for patients using Proteus
Dr. Frias presented 4-week results for blood pressure and cholesterol reduction. The 4- and 12-week Proteus arms were combined for this analysis, since up to 4 weeks they received the same intervention. Blood pressure, LDL cholesterol, and total cholesterol were all significantly reduced in the Proteus group, compared with the usual care group. At week 4, 83% of the subjects in the Proteus group had reached a blood pressure goal of less than 140/90 mm Hg vs. 33% in the usual care arm (difference of 50%; 95% confidence interval, 24%, 76%). Across all 11 medications/doses, the adherence was between 80% and 89% for every one.
The system spurred clinicians to make more treatment decisions for their patients. Providers made more changes to treatment for the Proteus patients, compared with the usual care providers (50% vs. 36%), gave more adherence counseling (28% vs. 0%), and provided more patient education (42% vs. 9%). Patients using the Proteus Discover system expressed high levels of satisfaction and acceptance of the technology (83%-100%), including ease of use in one’s daily routine, learning to use it, motivation to manage one’s health, better discussions with providers, understanding their care plan, seeing how they take their medications, and applying and wearing the sensor patch.
Safety was excellent. Twenty-seven adverse effects occurred in the Proteus arms, none of them serious, and about half were attributed to the device, mostly self-limited rashes. Seven adverse effects were attributed to the medications, mostly gastrointestinal side effects. There were four adverse effects in the usual care group, two of them serious.
Overall, compared with about 50% typical medication adherence, Proteus users had 84% adherence, which was associated with better blood pressure and LDL cholesterol control, compared with usual care.
Session moderator Dr. David Lieb, associate professor of medicine at Eastern Virginia Medical School in Norfolk, said the Proteus system may be very helpful for patients who are taking multiple medications to prompt them when to take them. “I could easily see somebody who has this system in place where they’re also able to measure their blood pressure and get that information to their provider and for their provider to make changes in their medicine dose,” he said.
This research study of 90 patients was quite manageable, but “what about when you have 300 people on this therapy and all those data are starting to come in? Who’s going to manage those data... and look at it all?” Dr. Lieb wondered. Patients may have to be taught to understand the data and make changes on their own to their medication behavior, exercise, and other factors within their control.
Half the patients in the study made $20,000 or less a year. “If you could help underserved patients with their compliance and all those other things... that would be fantastic. It’s a huge area of need,” he said. People will need internet access to upload their data to the cloud server.
Another question is how the data can interface with the various electronic health records in use and generate reports.
Proteus Discover is approved by the U.S. Food and Drug Administration and is available now.
orlando – A digital device that patients swallow every time they take a medication may be an answer to improving compliance and disease control. An aim of this digital health system is to encourage patient engagement and provider interaction. Despite available and efficacious medicines, only slightly more than half of patients with type 2 diabetes mellitus have glycated hemoglobin (HbA1c), hypertension, or LDL cholesterol under good control. One study showed only 17% had all three under control (Endocr Pract. 2016;22:689-98).
“Important in this are the facts of medication nonadherence by the patient, poor patient engagement frequently in their care, as well as from a clinician perspective, therapeutic inertia,” said Dr. Juan Frias at the annual meeting of the American Association of Clinical Endocrinologists. Approximately half of patients with chronic diseases do not take their medications as prescribed (Circulation. 2013;128:29-41).
To improve treatment adherence, diagnose the reasons for a patient not reaching therapeutic goals, address those issues with patient education or counseling or changes in medication, and engage with the patient to reinforce adherence goals. A digital system called Proteus Discover has been designed to assist patients and clinicians with all these tasks.
Proteus uses ingestible sensor-detectable medications. Each medication and dose of medication has a unique marker. A compounding pharmacy co-encapsulates a tiny detectable chip about the size of a grain of sand with a medication as prescribed by a physician. The patient wears a Band-Aid sized skin patch sensor that transmits to a mobile device that uploads to a secure cloud server. The sensor can tell if a medication has been taken and also serves as a pedometer and activity gauge.
The information is available to the patient, who can gain insight into medication taking, activity, and rest, along with other health parameters that are entered into the system. Entering the system through a provider portal and with the patient’s permission, the clinician can see patient behavior patterns outside of the clinic, including medication adherence, which helps to determine the best treatment for that patient. The system provides a report to the clinician that can be a point of discussion when the patient visits the clinic.
Trial demonstrates better medication adherence and goal attainment
Dr. Frias, CEO and principal investigator of National Research Institute in Los Angeles, described a 12 week multicenter cluster-randomized pilot study involving 90 patients with uncontrolled hypertension and type 2 diabetes to investigate the effect of Proteus on blood pressure, HbA1c, and LDL cholesterol reduction. Other goals of the trial were to promote medication adherence and physical activity and alert providers to a need to make more medical decisions.
Cluster randomization meant that each of the 16 trial sites randomized patients to one of three treatment arms within that site. The arms were: Proteus Discover for 4 or 12 weeks or usual care. Patients had to have systolic blood pressure of 140 mm Hg or greater, have failed therapy with 2 or more antihypertensive agents, and have HbA1c at 7% or greater on metformin or a sulfonylurea. Two-thirds of the subjects also had dyslipidemia and were treated with statins. Subjects were excluded if they had a history of acute or chronic dermatitis, had a skin allergy or sensitivity to adhesive medical tape, or had secondary causes for uncontrolled hypertension or type 2 diabetes.
Usual care consisted of all standard interventions, including medication titrations, patient education, and lifestyle coaching. All subjects took medications for 12 weeks and were followed for 12 weeks after enrollment. Available medications were various doses of lisinopril, losartan, hydrochlorothiazide, amlodipine, atorvastatin, metformin, and glipizide.
All the arms were fairly well balanced as to age (58-62 years), ethnicity, employment, education, and income. About one quarter had incomes in the $20,000-$40,000 range, and about half had incomes of $20,000 or less. Body mass index was 32 kg/m2 in the Proteus and usual care arms. Total cholesterol was similar for the Proteus and usual care groups at 173-177 mg/dL, but LDL was slightly higher in the Proteus arms (103 vs. 95 mg/dL).
Better adherence and outcomes for patients using Proteus
Dr. Frias presented 4-week results for blood pressure and cholesterol reduction. The 4- and 12-week Proteus arms were combined for this analysis, since up to 4 weeks they received the same intervention. Blood pressure, LDL cholesterol, and total cholesterol were all significantly reduced in the Proteus group, compared with the usual care group. At week 4, 83% of the subjects in the Proteus group had reached a blood pressure goal of less than 140/90 mm Hg vs. 33% in the usual care arm (difference of 50%; 95% confidence interval, 24%, 76%). Across all 11 medications/doses, the adherence was between 80% and 89% for every one.
The system spurred clinicians to make more treatment decisions for their patients. Providers made more changes to treatment for the Proteus patients, compared with the usual care providers (50% vs. 36%), gave more adherence counseling (28% vs. 0%), and provided more patient education (42% vs. 9%). Patients using the Proteus Discover system expressed high levels of satisfaction and acceptance of the technology (83%-100%), including ease of use in one’s daily routine, learning to use it, motivation to manage one’s health, better discussions with providers, understanding their care plan, seeing how they take their medications, and applying and wearing the sensor patch.
Safety was excellent. Twenty-seven adverse effects occurred in the Proteus arms, none of them serious, and about half were attributed to the device, mostly self-limited rashes. Seven adverse effects were attributed to the medications, mostly gastrointestinal side effects. There were four adverse effects in the usual care group, two of them serious.
Overall, compared with about 50% typical medication adherence, Proteus users had 84% adherence, which was associated with better blood pressure and LDL cholesterol control, compared with usual care.
Session moderator Dr. David Lieb, associate professor of medicine at Eastern Virginia Medical School in Norfolk, said the Proteus system may be very helpful for patients who are taking multiple medications to prompt them when to take them. “I could easily see somebody who has this system in place where they’re also able to measure their blood pressure and get that information to their provider and for their provider to make changes in their medicine dose,” he said.
This research study of 90 patients was quite manageable, but “what about when you have 300 people on this therapy and all those data are starting to come in? Who’s going to manage those data... and look at it all?” Dr. Lieb wondered. Patients may have to be taught to understand the data and make changes on their own to their medication behavior, exercise, and other factors within their control.
Half the patients in the study made $20,000 or less a year. “If you could help underserved patients with their compliance and all those other things... that would be fantastic. It’s a huge area of need,” he said. People will need internet access to upload their data to the cloud server.
Another question is how the data can interface with the various electronic health records in use and generate reports.
Proteus Discover is approved by the U.S. Food and Drug Administration and is available now.
AT AACE 2016
Key clinical point: Feedback from a system of digital-enabled pills enhanced medication adherence.
Major finding: Patients using Proteus had 84% adherence and better risk control.
Data source: Randomized unblinded study of 90 patients.
Disclosures: Dr. Frias has study grants from AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Johnson & Johnson, Merck, Novo Nordisk, Pfizer, and Sanofi and has consulting relationships with Proteus Digital Health, Johnson & Johnson, AstraZeneca, CeQur, and Sanofi.

Does medical marijuana work for PTSD, other psychiatric indications?
SCOTTSDALE, ARIZ. – There’s a rapidly growing list of states that have approved marijuana for medical use, but that does not mean that there’s also an expanding body of science to support marijuana’s use for psychiatric indications, according to Dr. Deepak Cyril D’Souza.
Though moderate evidence exists to support the use of medical marijuana for nausea and vomiting in chemotherapy, HIV/AIDS cachexia, neuropathic pain, and spasticity in multiple sclerosis, there’s scant evidence for some other uses. Little evidence exists to support the use of medical marijuana in Tourette syndrome, Crohn’s disease and ulcerative colitis, and epilepsy, and the data are even weaker for Parkinson’s disease, posttraumatic stress disorder, and agitation in Alzheimer’s disease, Dr. D’Souza said at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
Even so, he said, medical marijuana has been approved in several states for all of those conditions – and more.

Different states have required widely varying standards of evidence in making decisions about whether to approve medical marijuana use, and for which conditions. These range, in some cases, from relying on mere anecdotal evidence – as when individuals provide powerful but unscientific testimony about marijuana’s efficacy for a condition – to requiring the gold standard of randomized, double-blind, placebo-controlled trials.
Dr. D’Souza and his collaborators reviewed the data supporting the use of medical marijuana for several of the most commonly approved psychiatric indications, and found many of them hampered by poor design, poor execution, and an overreliance on the subjective effects of the studied compound.
For PTSD, only one randomized controlled study was found, and only one study had an active control, so the quality of evidence was rated as “very low” or “low” by Dr. D’Souza’s group. “Most of the studies were not blinded, and the sample sizes were generally small,” said Dr. D’Souza, professor of psychiatry at Yale University, New Haven, Conn. “It’s notable that many of these studies were with dronabinol, which is a synthetic THC analog. However, one take-home is that many of these studies reported improvement with sleep and a reduction in nightmares. This is something that should be followed up.”
For Tourette syndrome, there were just two studies by the same author, both with small sample sizes and of short duration. One study was rated “low” and the other “very low” for quality; in particular, the placebo effect could not be ruled out.
Four studies, said Dr. D’Souza, examined cannabinoids for dementia, and all had low quality of evidence. One published study had a sample size of two, he said. “The point here is that the only positive finding is that people who were diagnosed with dementia ate more and gained weight. And that wasn’t the objective of the study.”
“When we’re talking about medical marijuana, we’re talking about the whole plant,” he said. The marijuana plant has at least 450 known distinct constituent chemicals; these include about 70 cannabinoids as well as terpenoids and flavonoids. This means that the whole plant as dispensed represents a much more complex compound than medical tetrahydrocannabinol, for example, Dr. D’Souza said.
“We need to think about not just efficacy but side effects,” he said. These can include tolerance, abuse, and withdrawal syndrome. Marijuana’s cognitive effects may contribute to an increased risk of motor vehicle crashes. Though acute psychotic symptoms with quick resolution have long been noted, it’s also now thought that heavy marijuana exposure in adolescence more than doubles the risk for schizophrenia and might decrease adult IQ by about 10 points.
Though cannabis is “neither necessary nor sufficient for developing psychosis” but instead is a factor in a set of complex interactions, “what’s absolutely clear is that people with a psychotic disorder or at risk for developing one are very much more vulnerable to the effects of cannabinoids,” Dr. D’Souza said.
Despite all of those concerns, he said, “public demand and legislators have usurped the [Food and Drug Administration] approval process” when it comes to state-by-state approval of medical marijuana. The current state of affairs stands in contrast to the requirements for drug approvals for new indications, which require at least two adequately powered randomized clinical trials. When it comes to marijuana, Dr. D’Souza said, “For most of the indications the evidence fails to meet FDA standards.”
However, he said, the lack of high quality evidence may reflect the difficulty of conducting medical marijuana research in the United States. If this is so, he said, the “federal and state governments need to support and encourage research to generate high quality evidence to guide decisions.”
Dr. D’Souza reported a financial relationship with Insys Therapeutics, which develops pharmaceutical cannabinoid products.
On Twitter @karioakes
SCOTTSDALE, ARIZ. – There’s a rapidly growing list of states that have approved marijuana for medical use, but that does not mean that there’s also an expanding body of science to support marijuana’s use for psychiatric indications, according to Dr. Deepak Cyril D’Souza.
Though moderate evidence exists to support the use of medical marijuana for nausea and vomiting in chemotherapy, HIV/AIDS cachexia, neuropathic pain, and spasticity in multiple sclerosis, there’s scant evidence for some other uses. Little evidence exists to support the use of medical marijuana in Tourette syndrome, Crohn’s disease and ulcerative colitis, and epilepsy, and the data are even weaker for Parkinson’s disease, posttraumatic stress disorder, and agitation in Alzheimer’s disease, Dr. D’Souza said at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
Even so, he said, medical marijuana has been approved in several states for all of those conditions – and more.
Different states have required widely varying standards of evidence in making decisions about whether to approve medical marijuana use, and for which conditions. These range, in some cases, from relying on mere anecdotal evidence – as when individuals provide powerful but unscientific testimony about marijuana’s efficacy for a condition – to requiring the gold standard of randomized, double-blind, placebo-controlled trials.
Dr. D’Souza and his collaborators reviewed the data supporting the use of medical marijuana for several of the most commonly approved psychiatric indications, and found many of them hampered by poor design, poor execution, and an overreliance on the subjective effects of the studied compound.
For PTSD, only one randomized controlled study was found, and only one study had an active control, so the quality of evidence was rated as “very low” or “low” by Dr. D’Souza’s group. “Most of the studies were not blinded, and the sample sizes were generally small,” said Dr. D’Souza, professor of psychiatry at Yale University, New Haven, Conn. “It’s notable that many of these studies were with dronabinol, which is a synthetic THC analog. However, one take-home is that many of these studies reported improvement with sleep and a reduction in nightmares. This is something that should be followed up.”
For Tourette syndrome, there were just two studies by the same author, both with small sample sizes and of short duration. One study was rated “low” and the other “very low” for quality; in particular, the placebo effect could not be ruled out.
Four studies, said Dr. D’Souza, examined cannabinoids for dementia, and all had low quality of evidence. One published study had a sample size of two, he said. “The point here is that the only positive finding is that people who were diagnosed with dementia ate more and gained weight. And that wasn’t the objective of the study.”
“When we’re talking about medical marijuana, we’re talking about the whole plant,” he said. The marijuana plant has at least 450 known distinct constituent chemicals; these include about 70 cannabinoids as well as terpenoids and flavonoids. This means that the whole plant as dispensed represents a much more complex compound than medical tetrahydrocannabinol, for example, Dr. D’Souza said.
“We need to think about not just efficacy but side effects,” he said. These can include tolerance, abuse, and withdrawal syndrome. Marijuana’s cognitive effects may contribute to an increased risk of motor vehicle crashes. Though acute psychotic symptoms with quick resolution have long been noted, it’s also now thought that heavy marijuana exposure in adolescence more than doubles the risk for schizophrenia and might decrease adult IQ by about 10 points.
Though cannabis is “neither necessary nor sufficient for developing psychosis” but instead is a factor in a set of complex interactions, “what’s absolutely clear is that people with a psychotic disorder or at risk for developing one are very much more vulnerable to the effects of cannabinoids,” Dr. D’Souza said.
Despite all of those concerns, he said, “public demand and legislators have usurped the [Food and Drug Administration] approval process” when it comes to state-by-state approval of medical marijuana. The current state of affairs stands in contrast to the requirements for drug approvals for new indications, which require at least two adequately powered randomized clinical trials. When it comes to marijuana, Dr. D’Souza said, “For most of the indications the evidence fails to meet FDA standards.”
However, he said, the lack of high quality evidence may reflect the difficulty of conducting medical marijuana research in the United States. If this is so, he said, the “federal and state governments need to support and encourage research to generate high quality evidence to guide decisions.”
Dr. D’Souza reported a financial relationship with Insys Therapeutics, which develops pharmaceutical cannabinoid products.
On Twitter @karioakes
SCOTTSDALE, ARIZ. – There’s a rapidly growing list of states that have approved marijuana for medical use, but that does not mean that there’s also an expanding body of science to support marijuana’s use for psychiatric indications, according to Dr. Deepak Cyril D’Souza.
Though moderate evidence exists to support the use of medical marijuana for nausea and vomiting in chemotherapy, HIV/AIDS cachexia, neuropathic pain, and spasticity in multiple sclerosis, there’s scant evidence for some other uses. Little evidence exists to support the use of medical marijuana in Tourette syndrome, Crohn’s disease and ulcerative colitis, and epilepsy, and the data are even weaker for Parkinson’s disease, posttraumatic stress disorder, and agitation in Alzheimer’s disease, Dr. D’Souza said at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
Even so, he said, medical marijuana has been approved in several states for all of those conditions – and more.
Different states have required widely varying standards of evidence in making decisions about whether to approve medical marijuana use, and for which conditions. These range, in some cases, from relying on mere anecdotal evidence – as when individuals provide powerful but unscientific testimony about marijuana’s efficacy for a condition – to requiring the gold standard of randomized, double-blind, placebo-controlled trials.
Dr. D’Souza and his collaborators reviewed the data supporting the use of medical marijuana for several of the most commonly approved psychiatric indications, and found many of them hampered by poor design, poor execution, and an overreliance on the subjective effects of the studied compound.
For PTSD, only one randomized controlled study was found, and only one study had an active control, so the quality of evidence was rated as “very low” or “low” by Dr. D’Souza’s group. “Most of the studies were not blinded, and the sample sizes were generally small,” said Dr. D’Souza, professor of psychiatry at Yale University, New Haven, Conn. “It’s notable that many of these studies were with dronabinol, which is a synthetic THC analog. However, one take-home is that many of these studies reported improvement with sleep and a reduction in nightmares. This is something that should be followed up.”
For Tourette syndrome, there were just two studies by the same author, both with small sample sizes and of short duration. One study was rated “low” and the other “very low” for quality; in particular, the placebo effect could not be ruled out.
Four studies, said Dr. D’Souza, examined cannabinoids for dementia, and all had low quality of evidence. One published study had a sample size of two, he said. “The point here is that the only positive finding is that people who were diagnosed with dementia ate more and gained weight. And that wasn’t the objective of the study.”
“When we’re talking about medical marijuana, we’re talking about the whole plant,” he said. The marijuana plant has at least 450 known distinct constituent chemicals; these include about 70 cannabinoids as well as terpenoids and flavonoids. This means that the whole plant as dispensed represents a much more complex compound than medical tetrahydrocannabinol, for example, Dr. D’Souza said.
“We need to think about not just efficacy but side effects,” he said. These can include tolerance, abuse, and withdrawal syndrome. Marijuana’s cognitive effects may contribute to an increased risk of motor vehicle crashes. Though acute psychotic symptoms with quick resolution have long been noted, it’s also now thought that heavy marijuana exposure in adolescence more than doubles the risk for schizophrenia and might decrease adult IQ by about 10 points.
Though cannabis is “neither necessary nor sufficient for developing psychosis” but instead is a factor in a set of complex interactions, “what’s absolutely clear is that people with a psychotic disorder or at risk for developing one are very much more vulnerable to the effects of cannabinoids,” Dr. D’Souza said.
Despite all of those concerns, he said, “public demand and legislators have usurped the [Food and Drug Administration] approval process” when it comes to state-by-state approval of medical marijuana. The current state of affairs stands in contrast to the requirements for drug approvals for new indications, which require at least two adequately powered randomized clinical trials. When it comes to marijuana, Dr. D’Souza said, “For most of the indications the evidence fails to meet FDA standards.”
However, he said, the lack of high quality evidence may reflect the difficulty of conducting medical marijuana research in the United States. If this is so, he said, the “federal and state governments need to support and encourage research to generate high quality evidence to guide decisions.”
Dr. D’Souza reported a financial relationship with Insys Therapeutics, which develops pharmaceutical cannabinoid products.
On Twitter @karioakes
EXPERT ANALYSIS FROM THE ASCP ANNUAL MEETING
Linea Aspera as Rotational Landmark for Tumor Endoprostheses: A Computed Tomography Study
The distal or proximal femur with tumor endoprosthesis is commonly replaced after segmental resections for bone tumors, complex trauma, or revision arthroplasty. In conventional joint replacements, correct rotational alignment of the component is referenced off anatomical landmarks in the proximal or distal femur. After tumor resection, however, these landmarks are often not available for rotational orientation. There are no reports of studies validating a particular method of establishing rotation in these cases.
To establish a guide for rotational alignment of tumor endoprostheses, we set out to define the natural location of the linea aspera (LA) based on axial computed tomography (CT) scans. The LA is often the most outstanding visible bony landmark on a cross-section of the femur during surgery, and it would be helpful to know its normal orientation in relation to the true anteroposterior (AP) axis of the femur and to the femoral version. We wanted to answer these 5 questions:
1. Is the prominence of the LA easily identifiable on cross-section at different levels of the femoral shaft?
2. Does an axis passing through the LA correspond to the AP axis of the femur?
3. If not, is this axis offset internally or externally and by how much?
4. Is this offset constant at all levels of the femoral shaft?
5. How does the LA axis relate to the femoral neck axis at these levels?
The answers determine if the LA can be reliably used for rotational alignment of tumor endoprostheses.
Materials and Methods
After this study received Institutional Review Board approval, we retrospectively reviewed whole-body fluorine-18-deoxyglucose (FDG) positron emission tomography–computed tomography (PET-CT) studies performed in our hospital between 2003 and 2006 to identify those with full-length bilateral femur CT scans. These scans were available on the hospital’s computerized picture archiving system (General Electric). Patients could be included in the study as long as they were at least 18 years old at time of scan and did not have any pathology that deformed the femur, broke a cortex, or otherwise caused any gross asymmetry of the femur. Of the 72 patients with full-length femur CT scans, 3 were excluded: 1 with a congenital hip dysplasia, 1 with an old, malunited femoral fracture, and 1 who was 15 years old at time of scan.
Axial Slice Selection
For each patient, scout AP films were used to measure femoral shaft length from the top of the greater trochanter to the end of the lateral femoral condyle. The levels of the proximal third, midshaft, and distal third were then calculated based on this length. The LA was studied on the axial slices nearest these levels. Next, we scrolled through the scans to identify an axial slice that best showed the femoral neck axis. The literature on CT measurement of femoral anteversion is varied. Some articles describe a technique that uses 2 superimposed axial slices, and others describe a single axial slice.1-3 We used 1 axial slice to draw the femoral neck axis because our computer software could not superimpose 2 images on 1 screen and because the CT scans were not made under specific protocols to measure anteversion but rather were part of a cancer staging work-up. Axial cuts were made at 5-mm intervals, and not all scans included a single slice capturing the head, neck, and greater trochanter. Therefore, we used a (previously described) method in which the femoral neck axis is drawn on a slice that most captured the femoral neck, usually toward its base.4 Last, in order to draw the posterior condyle (PC) axis, we selected an axial slice that showed the posterior-most aspects of the femoral condyles at the intercondylar notch.
Determining Anteroposterior and Posterior Condyle Axes of Femur
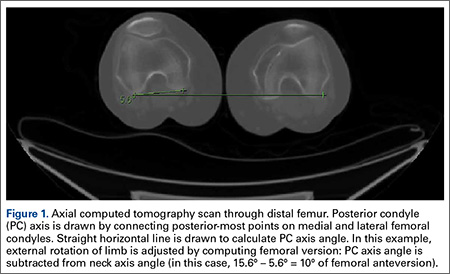
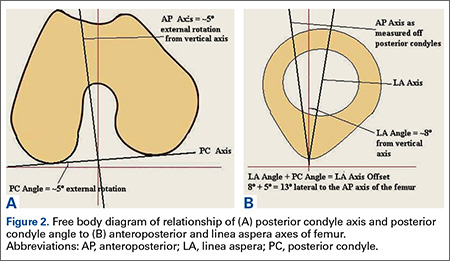
As we made all measurements for each femur off a single CT scan, we were able to use a straight horizontal line—drawn on-screen with a software tool—as a reference for measuring rotation. On a distal femur cut, the PC axis is drawn by connecting the posterior-most points of both condyles. The software calculates the angle formed—the PC angle (Figure 1). This angle, the degree to which the PC axis deviates from a straight horizontal line on-screen, can be used to account for gross rotation of the limb on comparison of images. The AP axis of the femur is the axis perpendicular to the PC axis. As such, the PC angle can also be used to determine degree of deviation of the AP axis from a straight vertical line on-screen. The AP axis was used when calculating the LA axis at the various levels of the femur (Figure 2).
Femoral Version
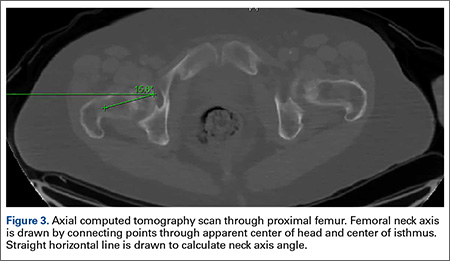
We used the software tool to draw the femoral neck axis. From the end of this line, a straight horizontal line is drawn on-screen (Figure 3). The software calculates the angle formed—the femoral neck axis angle. We assigned a positive value for a femoral head that pointed anteriorly on the image and a negative value for a head that pointed posteriorly. Adjusting for external rotation of the limb involved calculating the femoral version by subtracting the PC angle from the neck axis angle; adjusting for internal rotation involved adding these 2 angles.
Linea Aspera Morphology
After viewing the first 20 CT scans, we identified 3 types of LA morphology. Type I presents as a thickening on the posterior cortex with a sharp apex; type II presents as a flat-faced but distinct ridge of bone between the medial and lateral lips; and in type III there is no distinct cortical thickening with blunted medial and lateral lips; the latter is always more prominent.
Linea Aspera Axis Offset
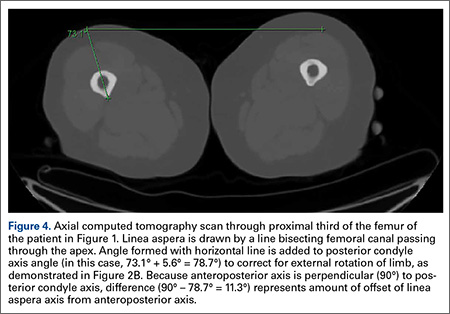
From the most posterior point of the LA, a line drawn forward bisecting the femoral canal defined the LA axis. In type I morphology, the posterior-most point was the apex; in type II, the middle of flat posterior surface was used as the starting point; in type III, the lateral lip was used, as it was sharper than the medial lip. This line is again referenced with a straight horizontal line across the image. The PC angle is then added to account for limb rotation, and the result is the LA angle. As the AP axis is perpendicular to the PC axis, the LA angle is subtracted from 90°; the difference represents the amount of offset of the LA axis from the AP axis. By convention, we assigned this a positive value for an LA lateral to the midpoint of the femur and a negative value for an LA medial to the midpoint (Figure 4).
Linea Aspera Axis and Femoral Neck Axis
The angle between the LA axis and the PC axis was measured. The femoral version angle was subtracted from that angle to obtain the arc between the LA axis and the femoral neck axis.
Statistical Analyses
All analyses were performed with SAS 9.1 (SAS Institute). All tests were 2-sided and conducted at the .05 significance level. No adjustments were made for multiple testing. Statistical analysis was performed with nonparametric tests and without making assumptions about the distribution of the study population. Univariate analyses were performed to test for significant side-to-side differences in femoral length, femoral version angle, and LA torsion angles at each level. A multivariate analysis was performed to test for interactions between sex, side, and level. In all analyses, P < .05 was used as the cutoff value for statistical significance.
Results
Femoral lengths varied by side and sex. The left side was longer than the right by a mean of 1.3 mm (P = .008). With multivariate analysis taking into account sex and age (cumulated per decade), there was still a significant effect of side on femoral length. Sex also had a significant effect on femoral length, with females’ femurs shorter by 21.7 mm (standard error, 5.0 mm). Mean (SD) anteversion of the femoral neck was 7.9° (12.7°) on the left and 13.3° (13.0°) on the right; the difference between sides was significant (P < .001). In a multivariate analysis performed to identify potential predictors of femoral version, side still had a significant (P < .001) independent effect; sex and age did not have an effect.
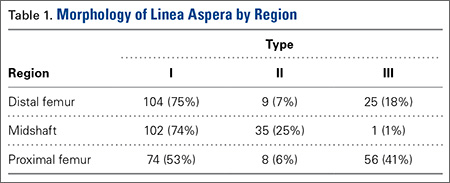
LA morphology varied according to femoral shaft level (Table 1). The morphology was type I in 75% of patients at the distal femur and 74% of patients at the midshaft femur, while only 53% of patients had a type I morphology at the proximal femur. The proportion of type III morphology was larger in the proximal femur (41%) than in the other locations.
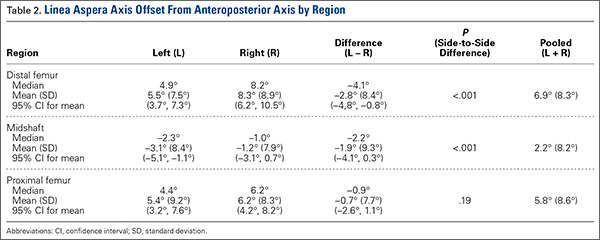
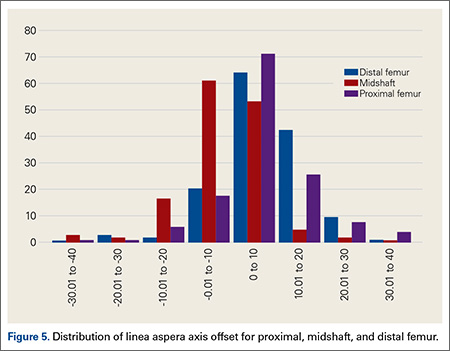
The LA axis of the femur did not correspond exactly to the AP axis at all femoral levels. At the distal femur, mean (SD) lateral offset of the LA axis was 5.5° (7.5°) on the left and 8.3° (8.9°) on the right. At the midshaft, mean (SD) medial offset of the LA axis was 3.1° (8.4°) on the left and 1.2° (7.9°) on the right. At the proximal femur, mean (SD) lateral offset of the LA axis was 5.4° (9.2°) on the left and 6.2° (8.3°) on the right. The side-to-side differences were statistically significant for the distal femur and midshaft but not the proximal femur. Table 2 lists the 95% confidence intervals for the mean values. As the range of differences was small (0.7°-2.8°), and the differences may not be clinically detected on gross inspection during surgery, we pooled both sides’ values to arrive at a single mean for each level. The LA axis was offset a mean (SD) of 6.9° (8.3°) laterally at the distal femur, 2.2° (8.2°) medially at the midshaft, and 5.8° (8.6°) laterally at the proximal femur. Figure 5 shows the frequency of distribution of LA axis offset.Offset of the LA axis from the AP axis of the femur was significantly (P < .001) different for each femoral level, even when a multivariate analysis was performed to determine the effect of sex, age, or side. Age and sex had no significant effect on mean offset of LA axis from AP axis.
We compared the mean arc between femoral neck axis and LA axis after referencing both off the PC axis. At the distal femur, mean (SD) arc between these 2 axes was 76.6° (13.1°) on the left and 68.3° (13.6°) on the right (mean difference, 8.3°); at the midshaft, mean (SD) arc was 85.2° (13.5°) on the left and 77.9° (13.1°) on the right (mean difference, 7.4°); at the proximal femur, mean (SD) arc was 76.7° (11.9°) on the left and 70.5° (12.8°) on the right (mean difference, 6.2°). The side-to-side differences were statistically significant (P < .001) for all locations.
In multivariate analysis, sex and age did not have an effect on mean arc between the 2 axes. Side and femoral level, however, had a significant effect (P < .001).
Discussion
In total hip arthroplasty, the goal is to restore femoral anteversion, usually referenced to the remaining femoral neck segment.3 In total knee arthroplasty (TKA), proper rotation preserves normal patellofemoral tracking.5 Various landmarks are used, such as the PCs or the epicondyles. After tumor resections, these landmarks are often lost.6 However, there are no reports of studies validating a particular method of achieving proper rotational orientation of tumor endoprostheses, though several methods are being used. One method involves inserting 2 drill bits before osteotomy—one proximal to the intended level of resection on the anterior femur, and the other on the anterior tibial shaft. The straight line formed can establish a plane of rotation (and length), which the surgeon must aim to restore when the components are placed. This method is useful for distal femur resections but not proximal femur resections. Another method, based on the LA’s anatomical position on the posterior aspect of the femur,4 uses the prominence of the LA to align the prosthesis. With this method, the LA is assumed to be directly posterior (6 o’clock) on the femur. However, this assumption has not been confirmed by any study. A third method, described by Heck and Carnesale,5 involves marking the anterior aspect of the femur after resection and aligning the components to it. The authors cautioned against using the LA as a landmark, saying that its course is highly variable.
The LA is a narrow, elevated length of bone, with medial and lateral lips, that serves as an attachment site for muscles in the posterior thigh. Proximally, the LA presents with lateral, medial, and intermediate lips. In the midshaft, it is often elevated by an underlying bony ridge or pilaster complex. Distally, it diverges into 2 ridges that form the triangular popliteal surface.1,7 For the LA to be a reliable landmark, first it must be clearly identifiable on viewing a femoral cross-section. The LA that presents with type I or II morphology is distinctly identifiable, and an axis from its apex and bisecting the canal can easily be constructed. In our study, the LA presented with type I or II morphology in 82% of distal femoral sections and 99% of midshaft femoral sections. Therefore, the LA is a conspicuous landmark at these levels. In the proximal femur, 59% had type I or II morphology. Type III morphology could be identified on cross-sections by the persisting prominence of the lateral lip. However, it may be difficult to appreciate the LA with this morphology at surgery.
Once the LA is identified, its normal cross-sectional position must be defined. One way to do this is to establish the relationship of its axis (LA axis) to the true AP axis. Based on mean values, the LA axis is laterally offset 7º at the distal third of the femur, medially offset 2º at the midshaft, and laterally offset 6º at the proximal third. Therefore, for ideal placement with the LA used for orientation, the component must be internally rotated 7º relative to the LA for femoral resection at the distal third, externally rotated 2º for resection at the midshaft, and internally rotated 6º for resection at the proximal third. Studies have demonstrated that joint contact forces and mechanical alignment of the lower limb can be altered with as little as 5º of femoral malrotation.8,9 Although such a small degree of malrotation is often asymptomatic, it can have long-term effects on soft-tissue tension and patellar tracking.10,11 Rotating-platform mobile-bearing TKA designs can compensate for femoral malrotation, but they may have little to no effect on patellar tracking.12 Therefore, we think aligning the components as near as possible to their natural orientation can prove beneficial in long-term patient management.
Another way of defining the normal cross-sectional position of the LA is to relate it to the femoral neck axis. We measured the difference between these 2 axes. Mean differences were 72º (distal femur), 81.5º (midshaft), and 73.5º (proximal third). Mean arc differences at all levels were larger on the left side—a reflection of the femoral neck being less anteverted on that side in our measurements. Standard deviations were smaller for measurements of LA axis offset from AP axis (range, 7.5°-9.2°) than for measurements of arc between LA axis and femoral neck axis (range, 11.9°-13.6°). This finding indicates there is less variation in the former method, making it preferable for defining the cross-sectional position of the LA.
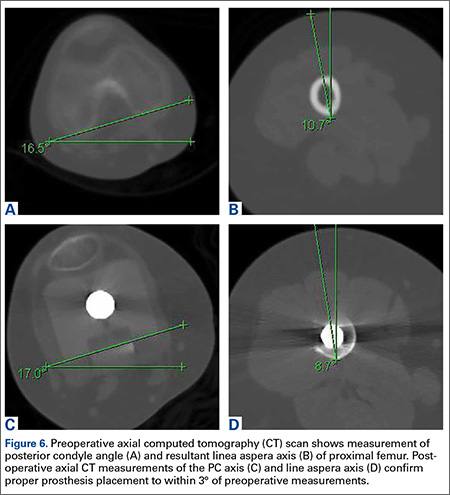
It has been said that the course of the LA is variable, and our data provide confirmation. The LA does not lie directly posterior (6 o’clock), and it does not trace a straight longitudinal course along the posterior femur, as demonstrated by the different LA axis offsets at 3 levels. However, we may still use it as a landmark if we remain aware how much the LA is offset from the AP axis at each femoral level. Figures 6A-6D, which show CT scans of a patient who underwent distal femoral resection and replacement with an endoprosthesis, illustrate how the LA axis was measured before surgery and how proper prosthesis placement was confirmed after surgery.
In hip arthroplasty, restoration of normal femoral version is the reference for endoprosthetic placement. The literature on “normal” femoral anteversion varies with the method used. In a review of studies on CT-measured adult femoral version, reported values ranged from 6.3° to 40°.2 Mean femoral version in our study ranged from 8° to 13°. Orthopedics textbooks generally put the value at 10° to 15º, and this seems to be the range that surgeons target.6 However, we found a statistically significant mean side-to-side difference of 5.4°. This finding is possibly explained by our large sample—it was larger than the samples used in other studies of CT-measured femoral version. Other studies have found mean side-to-side differences of up to 4.0º.5 Another explanation for our finding is that the studies may differ methodologically. The studies that established values for femoral anteversion were based on CT protocols—thinner slices (1-5 mm), use of foot holders to standardize limb rotation, use of 2 axial cuts in proximal femur to establish femoral neck axis2,13—designed specifically for this measurement. As the CT scans reviewed in our study are not designed for this purpose, errors in femoral version measurement may have been introduced, which may also explain why there is larger variation in measurements of the arc between the LA axis and the femoral neck axis.
Conclusion
The LA does not lie directly on the posterior surface of the femur. It deviates 6.9° laterally at the distal femur, 2.2° medially at the midshaft, and 6.9° laterally at the proximal third. As the LA is an easily identifiable structure on cross-sections of the femoral shaft at the midshaft and distal third of the femur, it may be useful as a rotational landmark for resections at these levels if these deviations are considered during tumor endoprosthetic replacements.
1. Desai SC, Willson S. Radiology of the linea aspera. Australas Radiol. 1985;29(3):273-274.
2. Kuo TY, Skedros JG, Bloebaum RD. Measurement of femoral anteversion by biplane radiography and computed tomography imaging: comparison with an anatomic reference. Invest Radiol. 2003;38(4):221-229.
3. Wines AP, McNicol D. Computed tomography measurement of the accuracy of component version in total hip arthroplasty. J Arthroplasty. 2006;21(5):696-701.
4. Gray H. Anatomy of the Human Body. Philadelphia, PA: Lea & Febiger; 1918.
5. Heck RK, Carnesale PG. General principles of tumors. In: Canale ST, ed. Campbell’s Operative Orthopaedics. Vol 1. 10th ed. St. Louis, MO: Mosby; 2003:733-791.
6. Katz, MA, Beck TD, Silber JS, Seldes RM, Lotke PA. Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques. J Arthroplasty. 2001;16(3):301-305.
7. Pitt MJ. Radiology of the femoral linea aspera–pilaster complex: the track sign. Radiology. 1982;142(1):66.
8. Bretin P, O’Loughlin PF, Suero EM, et al. Influence of femoral malrotation on knee joint alignment and intra-articular contact pressures. Arch Orthop Trauma Surg. 2011;131(8):1115-1120.
9. Zihlmann MS, Stacoff A, Romero J, Quervain IK, Stüssi E. Biomechanical background and clinical observations of rotational malalignment in TKA: literature review and consequences. Clin Biomech. 2005;20(7):661-668.
10. Ghosh KM, Merican AM, Iranpour F, Deehan DJ, Amis AA. The effect of femoral component rotation on the extensor retinaculum of the knee. J Orthop Res. 2010;28(9):1136-1141.
11. Verlinden C, Uvin P, Labey L, Luyckx JP, Bellemans J, Vandenneucker H. The influence of malrotation of the femoral component in total knee replacement on the mechanics of patellofemoral contact during gait: an in vitro biomechanical study. J Bone Joint Surg Br. 2010;92(5):737-742.
12. Kessler O, Patil S, Colwell CW Jr, D’Lima DD. The effect of femoral component malrotation on patellar biomechanics. J Biomech. 2008;41(16):3332-3339.
13. Strecker W, Keppler P, Gebhard F, Kinzl L. Length and torsion of the lower limb. J Bone Joint Surg Br. 1997;79(6):1019-1023.
The distal or proximal femur with tumor endoprosthesis is commonly replaced after segmental resections for bone tumors, complex trauma, or revision arthroplasty. In conventional joint replacements, correct rotational alignment of the component is referenced off anatomical landmarks in the proximal or distal femur. After tumor resection, however, these landmarks are often not available for rotational orientation. There are no reports of studies validating a particular method of establishing rotation in these cases.
To establish a guide for rotational alignment of tumor endoprostheses, we set out to define the natural location of the linea aspera (LA) based on axial computed tomography (CT) scans. The LA is often the most outstanding visible bony landmark on a cross-section of the femur during surgery, and it would be helpful to know its normal orientation in relation to the true anteroposterior (AP) axis of the femur and to the femoral version. We wanted to answer these 5 questions:
1. Is the prominence of the LA easily identifiable on cross-section at different levels of the femoral shaft?
2. Does an axis passing through the LA correspond to the AP axis of the femur?
3. If not, is this axis offset internally or externally and by how much?
4. Is this offset constant at all levels of the femoral shaft?
5. How does the LA axis relate to the femoral neck axis at these levels?
The answers determine if the LA can be reliably used for rotational alignment of tumor endoprostheses.
Materials and Methods
After this study received Institutional Review Board approval, we retrospectively reviewed whole-body fluorine-18-deoxyglucose (FDG) positron emission tomography–computed tomography (PET-CT) studies performed in our hospital between 2003 and 2006 to identify those with full-length bilateral femur CT scans. These scans were available on the hospital’s computerized picture archiving system (General Electric). Patients could be included in the study as long as they were at least 18 years old at time of scan and did not have any pathology that deformed the femur, broke a cortex, or otherwise caused any gross asymmetry of the femur. Of the 72 patients with full-length femur CT scans, 3 were excluded: 1 with a congenital hip dysplasia, 1 with an old, malunited femoral fracture, and 1 who was 15 years old at time of scan.
Axial Slice Selection
For each patient, scout AP films were used to measure femoral shaft length from the top of the greater trochanter to the end of the lateral femoral condyle. The levels of the proximal third, midshaft, and distal third were then calculated based on this length. The LA was studied on the axial slices nearest these levels. Next, we scrolled through the scans to identify an axial slice that best showed the femoral neck axis. The literature on CT measurement of femoral anteversion is varied. Some articles describe a technique that uses 2 superimposed axial slices, and others describe a single axial slice.1-3 We used 1 axial slice to draw the femoral neck axis because our computer software could not superimpose 2 images on 1 screen and because the CT scans were not made under specific protocols to measure anteversion but rather were part of a cancer staging work-up. Axial cuts were made at 5-mm intervals, and not all scans included a single slice capturing the head, neck, and greater trochanter. Therefore, we used a (previously described) method in which the femoral neck axis is drawn on a slice that most captured the femoral neck, usually toward its base.4 Last, in order to draw the posterior condyle (PC) axis, we selected an axial slice that showed the posterior-most aspects of the femoral condyles at the intercondylar notch.
Determining Anteroposterior and Posterior Condyle Axes of Femur
As we made all measurements for each femur off a single CT scan, we were able to use a straight horizontal line—drawn on-screen with a software tool—as a reference for measuring rotation. On a distal femur cut, the PC axis is drawn by connecting the posterior-most points of both condyles. The software calculates the angle formed—the PC angle (Figure 1). This angle, the degree to which the PC axis deviates from a straight horizontal line on-screen, can be used to account for gross rotation of the limb on comparison of images. The AP axis of the femur is the axis perpendicular to the PC axis. As such, the PC angle can also be used to determine degree of deviation of the AP axis from a straight vertical line on-screen. The AP axis was used when calculating the LA axis at the various levels of the femur (Figure 2).
Femoral Version
We used the software tool to draw the femoral neck axis. From the end of this line, a straight horizontal line is drawn on-screen (Figure 3). The software calculates the angle formed—the femoral neck axis angle. We assigned a positive value for a femoral head that pointed anteriorly on the image and a negative value for a head that pointed posteriorly. Adjusting for external rotation of the limb involved calculating the femoral version by subtracting the PC angle from the neck axis angle; adjusting for internal rotation involved adding these 2 angles.
Linea Aspera Morphology
After viewing the first 20 CT scans, we identified 3 types of LA morphology. Type I presents as a thickening on the posterior cortex with a sharp apex; type II presents as a flat-faced but distinct ridge of bone between the medial and lateral lips; and in type III there is no distinct cortical thickening with blunted medial and lateral lips; the latter is always more prominent.
Linea Aspera Axis Offset
From the most posterior point of the LA, a line drawn forward bisecting the femoral canal defined the LA axis. In type I morphology, the posterior-most point was the apex; in type II, the middle of flat posterior surface was used as the starting point; in type III, the lateral lip was used, as it was sharper than the medial lip. This line is again referenced with a straight horizontal line across the image. The PC angle is then added to account for limb rotation, and the result is the LA angle. As the AP axis is perpendicular to the PC axis, the LA angle is subtracted from 90°; the difference represents the amount of offset of the LA axis from the AP axis. By convention, we assigned this a positive value for an LA lateral to the midpoint of the femur and a negative value for an LA medial to the midpoint (Figure 4).
Linea Aspera Axis and Femoral Neck Axis
The angle between the LA axis and the PC axis was measured. The femoral version angle was subtracted from that angle to obtain the arc between the LA axis and the femoral neck axis.
Statistical Analyses
All analyses were performed with SAS 9.1 (SAS Institute). All tests were 2-sided and conducted at the .05 significance level. No adjustments were made for multiple testing. Statistical analysis was performed with nonparametric tests and without making assumptions about the distribution of the study population. Univariate analyses were performed to test for significant side-to-side differences in femoral length, femoral version angle, and LA torsion angles at each level. A multivariate analysis was performed to test for interactions between sex, side, and level. In all analyses, P < .05 was used as the cutoff value for statistical significance.
Results
Femoral lengths varied by side and sex. The left side was longer than the right by a mean of 1.3 mm (P = .008). With multivariate analysis taking into account sex and age (cumulated per decade), there was still a significant effect of side on femoral length. Sex also had a significant effect on femoral length, with females’ femurs shorter by 21.7 mm (standard error, 5.0 mm). Mean (SD) anteversion of the femoral neck was 7.9° (12.7°) on the left and 13.3° (13.0°) on the right; the difference between sides was significant (P < .001). In a multivariate analysis performed to identify potential predictors of femoral version, side still had a significant (P < .001) independent effect; sex and age did not have an effect.
LA morphology varied according to femoral shaft level (Table 1). The morphology was type I in 75% of patients at the distal femur and 74% of patients at the midshaft femur, while only 53% of patients had a type I morphology at the proximal femur. The proportion of type III morphology was larger in the proximal femur (41%) than in the other locations.
The LA axis of the femur did not correspond exactly to the AP axis at all femoral levels. At the distal femur, mean (SD) lateral offset of the LA axis was 5.5° (7.5°) on the left and 8.3° (8.9°) on the right. At the midshaft, mean (SD) medial offset of the LA axis was 3.1° (8.4°) on the left and 1.2° (7.9°) on the right. At the proximal femur, mean (SD) lateral offset of the LA axis was 5.4° (9.2°) on the left and 6.2° (8.3°) on the right. The side-to-side differences were statistically significant for the distal femur and midshaft but not the proximal femur. Table 2 lists the 95% confidence intervals for the mean values. As the range of differences was small (0.7°-2.8°), and the differences may not be clinically detected on gross inspection during surgery, we pooled both sides’ values to arrive at a single mean for each level. The LA axis was offset a mean (SD) of 6.9° (8.3°) laterally at the distal femur, 2.2° (8.2°) medially at the midshaft, and 5.8° (8.6°) laterally at the proximal femur. Figure 5 shows the frequency of distribution of LA axis offset.Offset of the LA axis from the AP axis of the femur was significantly (P < .001) different for each femoral level, even when a multivariate analysis was performed to determine the effect of sex, age, or side. Age and sex had no significant effect on mean offset of LA axis from AP axis.
We compared the mean arc between femoral neck axis and LA axis after referencing both off the PC axis. At the distal femur, mean (SD) arc between these 2 axes was 76.6° (13.1°) on the left and 68.3° (13.6°) on the right (mean difference, 8.3°); at the midshaft, mean (SD) arc was 85.2° (13.5°) on the left and 77.9° (13.1°) on the right (mean difference, 7.4°); at the proximal femur, mean (SD) arc was 76.7° (11.9°) on the left and 70.5° (12.8°) on the right (mean difference, 6.2°). The side-to-side differences were statistically significant (P < .001) for all locations.
In multivariate analysis, sex and age did not have an effect on mean arc between the 2 axes. Side and femoral level, however, had a significant effect (P < .001).
Discussion
In total hip arthroplasty, the goal is to restore femoral anteversion, usually referenced to the remaining femoral neck segment.3 In total knee arthroplasty (TKA), proper rotation preserves normal patellofemoral tracking.5 Various landmarks are used, such as the PCs or the epicondyles. After tumor resections, these landmarks are often lost.6 However, there are no reports of studies validating a particular method of achieving proper rotational orientation of tumor endoprostheses, though several methods are being used. One method involves inserting 2 drill bits before osteotomy—one proximal to the intended level of resection on the anterior femur, and the other on the anterior tibial shaft. The straight line formed can establish a plane of rotation (and length), which the surgeon must aim to restore when the components are placed. This method is useful for distal femur resections but not proximal femur resections. Another method, based on the LA’s anatomical position on the posterior aspect of the femur,4 uses the prominence of the LA to align the prosthesis. With this method, the LA is assumed to be directly posterior (6 o’clock) on the femur. However, this assumption has not been confirmed by any study. A third method, described by Heck and Carnesale,5 involves marking the anterior aspect of the femur after resection and aligning the components to it. The authors cautioned against using the LA as a landmark, saying that its course is highly variable.
The LA is a narrow, elevated length of bone, with medial and lateral lips, that serves as an attachment site for muscles in the posterior thigh. Proximally, the LA presents with lateral, medial, and intermediate lips. In the midshaft, it is often elevated by an underlying bony ridge or pilaster complex. Distally, it diverges into 2 ridges that form the triangular popliteal surface.1,7 For the LA to be a reliable landmark, first it must be clearly identifiable on viewing a femoral cross-section. The LA that presents with type I or II morphology is distinctly identifiable, and an axis from its apex and bisecting the canal can easily be constructed. In our study, the LA presented with type I or II morphology in 82% of distal femoral sections and 99% of midshaft femoral sections. Therefore, the LA is a conspicuous landmark at these levels. In the proximal femur, 59% had type I or II morphology. Type III morphology could be identified on cross-sections by the persisting prominence of the lateral lip. However, it may be difficult to appreciate the LA with this morphology at surgery.
Once the LA is identified, its normal cross-sectional position must be defined. One way to do this is to establish the relationship of its axis (LA axis) to the true AP axis. Based on mean values, the LA axis is laterally offset 7º at the distal third of the femur, medially offset 2º at the midshaft, and laterally offset 6º at the proximal third. Therefore, for ideal placement with the LA used for orientation, the component must be internally rotated 7º relative to the LA for femoral resection at the distal third, externally rotated 2º for resection at the midshaft, and internally rotated 6º for resection at the proximal third. Studies have demonstrated that joint contact forces and mechanical alignment of the lower limb can be altered with as little as 5º of femoral malrotation.8,9 Although such a small degree of malrotation is often asymptomatic, it can have long-term effects on soft-tissue tension and patellar tracking.10,11 Rotating-platform mobile-bearing TKA designs can compensate for femoral malrotation, but they may have little to no effect on patellar tracking.12 Therefore, we think aligning the components as near as possible to their natural orientation can prove beneficial in long-term patient management.
Another way of defining the normal cross-sectional position of the LA is to relate it to the femoral neck axis. We measured the difference between these 2 axes. Mean differences were 72º (distal femur), 81.5º (midshaft), and 73.5º (proximal third). Mean arc differences at all levels were larger on the left side—a reflection of the femoral neck being less anteverted on that side in our measurements. Standard deviations were smaller for measurements of LA axis offset from AP axis (range, 7.5°-9.2°) than for measurements of arc between LA axis and femoral neck axis (range, 11.9°-13.6°). This finding indicates there is less variation in the former method, making it preferable for defining the cross-sectional position of the LA.
It has been said that the course of the LA is variable, and our data provide confirmation. The LA does not lie directly posterior (6 o’clock), and it does not trace a straight longitudinal course along the posterior femur, as demonstrated by the different LA axis offsets at 3 levels. However, we may still use it as a landmark if we remain aware how much the LA is offset from the AP axis at each femoral level. Figures 6A-6D, which show CT scans of a patient who underwent distal femoral resection and replacement with an endoprosthesis, illustrate how the LA axis was measured before surgery and how proper prosthesis placement was confirmed after surgery.
In hip arthroplasty, restoration of normal femoral version is the reference for endoprosthetic placement. The literature on “normal” femoral anteversion varies with the method used. In a review of studies on CT-measured adult femoral version, reported values ranged from 6.3° to 40°.2 Mean femoral version in our study ranged from 8° to 13°. Orthopedics textbooks generally put the value at 10° to 15º, and this seems to be the range that surgeons target.6 However, we found a statistically significant mean side-to-side difference of 5.4°. This finding is possibly explained by our large sample—it was larger than the samples used in other studies of CT-measured femoral version. Other studies have found mean side-to-side differences of up to 4.0º.5 Another explanation for our finding is that the studies may differ methodologically. The studies that established values for femoral anteversion were based on CT protocols—thinner slices (1-5 mm), use of foot holders to standardize limb rotation, use of 2 axial cuts in proximal femur to establish femoral neck axis2,13—designed specifically for this measurement. As the CT scans reviewed in our study are not designed for this purpose, errors in femoral version measurement may have been introduced, which may also explain why there is larger variation in measurements of the arc between the LA axis and the femoral neck axis.
Conclusion
The LA does not lie directly on the posterior surface of the femur. It deviates 6.9° laterally at the distal femur, 2.2° medially at the midshaft, and 6.9° laterally at the proximal third. As the LA is an easily identifiable structure on cross-sections of the femoral shaft at the midshaft and distal third of the femur, it may be useful as a rotational landmark for resections at these levels if these deviations are considered during tumor endoprosthetic replacements.
The distal or proximal femur with tumor endoprosthesis is commonly replaced after segmental resections for bone tumors, complex trauma, or revision arthroplasty. In conventional joint replacements, correct rotational alignment of the component is referenced off anatomical landmarks in the proximal or distal femur. After tumor resection, however, these landmarks are often not available for rotational orientation. There are no reports of studies validating a particular method of establishing rotation in these cases.
To establish a guide for rotational alignment of tumor endoprostheses, we set out to define the natural location of the linea aspera (LA) based on axial computed tomography (CT) scans. The LA is often the most outstanding visible bony landmark on a cross-section of the femur during surgery, and it would be helpful to know its normal orientation in relation to the true anteroposterior (AP) axis of the femur and to the femoral version. We wanted to answer these 5 questions:
1. Is the prominence of the LA easily identifiable on cross-section at different levels of the femoral shaft?
2. Does an axis passing through the LA correspond to the AP axis of the femur?
3. If not, is this axis offset internally or externally and by how much?
4. Is this offset constant at all levels of the femoral shaft?
5. How does the LA axis relate to the femoral neck axis at these levels?
The answers determine if the LA can be reliably used for rotational alignment of tumor endoprostheses.
Materials and Methods
After this study received Institutional Review Board approval, we retrospectively reviewed whole-body fluorine-18-deoxyglucose (FDG) positron emission tomography–computed tomography (PET-CT) studies performed in our hospital between 2003 and 2006 to identify those with full-length bilateral femur CT scans. These scans were available on the hospital’s computerized picture archiving system (General Electric). Patients could be included in the study as long as they were at least 18 years old at time of scan and did not have any pathology that deformed the femur, broke a cortex, or otherwise caused any gross asymmetry of the femur. Of the 72 patients with full-length femur CT scans, 3 were excluded: 1 with a congenital hip dysplasia, 1 with an old, malunited femoral fracture, and 1 who was 15 years old at time of scan.
Axial Slice Selection
For each patient, scout AP films were used to measure femoral shaft length from the top of the greater trochanter to the end of the lateral femoral condyle. The levels of the proximal third, midshaft, and distal third were then calculated based on this length. The LA was studied on the axial slices nearest these levels. Next, we scrolled through the scans to identify an axial slice that best showed the femoral neck axis. The literature on CT measurement of femoral anteversion is varied. Some articles describe a technique that uses 2 superimposed axial slices, and others describe a single axial slice.1-3 We used 1 axial slice to draw the femoral neck axis because our computer software could not superimpose 2 images on 1 screen and because the CT scans were not made under specific protocols to measure anteversion but rather were part of a cancer staging work-up. Axial cuts were made at 5-mm intervals, and not all scans included a single slice capturing the head, neck, and greater trochanter. Therefore, we used a (previously described) method in which the femoral neck axis is drawn on a slice that most captured the femoral neck, usually toward its base.4 Last, in order to draw the posterior condyle (PC) axis, we selected an axial slice that showed the posterior-most aspects of the femoral condyles at the intercondylar notch.
Determining Anteroposterior and Posterior Condyle Axes of Femur
As we made all measurements for each femur off a single CT scan, we were able to use a straight horizontal line—drawn on-screen with a software tool—as a reference for measuring rotation. On a distal femur cut, the PC axis is drawn by connecting the posterior-most points of both condyles. The software calculates the angle formed—the PC angle (Figure 1). This angle, the degree to which the PC axis deviates from a straight horizontal line on-screen, can be used to account for gross rotation of the limb on comparison of images. The AP axis of the femur is the axis perpendicular to the PC axis. As such, the PC angle can also be used to determine degree of deviation of the AP axis from a straight vertical line on-screen. The AP axis was used when calculating the LA axis at the various levels of the femur (Figure 2).
Femoral Version
We used the software tool to draw the femoral neck axis. From the end of this line, a straight horizontal line is drawn on-screen (Figure 3). The software calculates the angle formed—the femoral neck axis angle. We assigned a positive value for a femoral head that pointed anteriorly on the image and a negative value for a head that pointed posteriorly. Adjusting for external rotation of the limb involved calculating the femoral version by subtracting the PC angle from the neck axis angle; adjusting for internal rotation involved adding these 2 angles.
Linea Aspera Morphology
After viewing the first 20 CT scans, we identified 3 types of LA morphology. Type I presents as a thickening on the posterior cortex with a sharp apex; type II presents as a flat-faced but distinct ridge of bone between the medial and lateral lips; and in type III there is no distinct cortical thickening with blunted medial and lateral lips; the latter is always more prominent.
Linea Aspera Axis Offset
From the most posterior point of the LA, a line drawn forward bisecting the femoral canal defined the LA axis. In type I morphology, the posterior-most point was the apex; in type II, the middle of flat posterior surface was used as the starting point; in type III, the lateral lip was used, as it was sharper than the medial lip. This line is again referenced with a straight horizontal line across the image. The PC angle is then added to account for limb rotation, and the result is the LA angle. As the AP axis is perpendicular to the PC axis, the LA angle is subtracted from 90°; the difference represents the amount of offset of the LA axis from the AP axis. By convention, we assigned this a positive value for an LA lateral to the midpoint of the femur and a negative value for an LA medial to the midpoint (Figure 4).
Linea Aspera Axis and Femoral Neck Axis
The angle between the LA axis and the PC axis was measured. The femoral version angle was subtracted from that angle to obtain the arc between the LA axis and the femoral neck axis.
Statistical Analyses
All analyses were performed with SAS 9.1 (SAS Institute). All tests were 2-sided and conducted at the .05 significance level. No adjustments were made for multiple testing. Statistical analysis was performed with nonparametric tests and without making assumptions about the distribution of the study population. Univariate analyses were performed to test for significant side-to-side differences in femoral length, femoral version angle, and LA torsion angles at each level. A multivariate analysis was performed to test for interactions between sex, side, and level. In all analyses, P < .05 was used as the cutoff value for statistical significance.
Results
Femoral lengths varied by side and sex. The left side was longer than the right by a mean of 1.3 mm (P = .008). With multivariate analysis taking into account sex and age (cumulated per decade), there was still a significant effect of side on femoral length. Sex also had a significant effect on femoral length, with females’ femurs shorter by 21.7 mm (standard error, 5.0 mm). Mean (SD) anteversion of the femoral neck was 7.9° (12.7°) on the left and 13.3° (13.0°) on the right; the difference between sides was significant (P < .001). In a multivariate analysis performed to identify potential predictors of femoral version, side still had a significant (P < .001) independent effect; sex and age did not have an effect.
LA morphology varied according to femoral shaft level (Table 1). The morphology was type I in 75% of patients at the distal femur and 74% of patients at the midshaft femur, while only 53% of patients had a type I morphology at the proximal femur. The proportion of type III morphology was larger in the proximal femur (41%) than in the other locations.
The LA axis of the femur did not correspond exactly to the AP axis at all femoral levels. At the distal femur, mean (SD) lateral offset of the LA axis was 5.5° (7.5°) on the left and 8.3° (8.9°) on the right. At the midshaft, mean (SD) medial offset of the LA axis was 3.1° (8.4°) on the left and 1.2° (7.9°) on the right. At the proximal femur, mean (SD) lateral offset of the LA axis was 5.4° (9.2°) on the left and 6.2° (8.3°) on the right. The side-to-side differences were statistically significant for the distal femur and midshaft but not the proximal femur. Table 2 lists the 95% confidence intervals for the mean values. As the range of differences was small (0.7°-2.8°), and the differences may not be clinically detected on gross inspection during surgery, we pooled both sides’ values to arrive at a single mean for each level. The LA axis was offset a mean (SD) of 6.9° (8.3°) laterally at the distal femur, 2.2° (8.2°) medially at the midshaft, and 5.8° (8.6°) laterally at the proximal femur. Figure 5 shows the frequency of distribution of LA axis offset.Offset of the LA axis from the AP axis of the femur was significantly (P < .001) different for each femoral level, even when a multivariate analysis was performed to determine the effect of sex, age, or side. Age and sex had no significant effect on mean offset of LA axis from AP axis.
We compared the mean arc between femoral neck axis and LA axis after referencing both off the PC axis. At the distal femur, mean (SD) arc between these 2 axes was 76.6° (13.1°) on the left and 68.3° (13.6°) on the right (mean difference, 8.3°); at the midshaft, mean (SD) arc was 85.2° (13.5°) on the left and 77.9° (13.1°) on the right (mean difference, 7.4°); at the proximal femur, mean (SD) arc was 76.7° (11.9°) on the left and 70.5° (12.8°) on the right (mean difference, 6.2°). The side-to-side differences were statistically significant (P < .001) for all locations.
In multivariate analysis, sex and age did not have an effect on mean arc between the 2 axes. Side and femoral level, however, had a significant effect (P < .001).
Discussion
In total hip arthroplasty, the goal is to restore femoral anteversion, usually referenced to the remaining femoral neck segment.3 In total knee arthroplasty (TKA), proper rotation preserves normal patellofemoral tracking.5 Various landmarks are used, such as the PCs or the epicondyles. After tumor resections, these landmarks are often lost.6 However, there are no reports of studies validating a particular method of achieving proper rotational orientation of tumor endoprostheses, though several methods are being used. One method involves inserting 2 drill bits before osteotomy—one proximal to the intended level of resection on the anterior femur, and the other on the anterior tibial shaft. The straight line formed can establish a plane of rotation (and length), which the surgeon must aim to restore when the components are placed. This method is useful for distal femur resections but not proximal femur resections. Another method, based on the LA’s anatomical position on the posterior aspect of the femur,4 uses the prominence of the LA to align the prosthesis. With this method, the LA is assumed to be directly posterior (6 o’clock) on the femur. However, this assumption has not been confirmed by any study. A third method, described by Heck and Carnesale,5 involves marking the anterior aspect of the femur after resection and aligning the components to it. The authors cautioned against using the LA as a landmark, saying that its course is highly variable.
The LA is a narrow, elevated length of bone, with medial and lateral lips, that serves as an attachment site for muscles in the posterior thigh. Proximally, the LA presents with lateral, medial, and intermediate lips. In the midshaft, it is often elevated by an underlying bony ridge or pilaster complex. Distally, it diverges into 2 ridges that form the triangular popliteal surface.1,7 For the LA to be a reliable landmark, first it must be clearly identifiable on viewing a femoral cross-section. The LA that presents with type I or II morphology is distinctly identifiable, and an axis from its apex and bisecting the canal can easily be constructed. In our study, the LA presented with type I or II morphology in 82% of distal femoral sections and 99% of midshaft femoral sections. Therefore, the LA is a conspicuous landmark at these levels. In the proximal femur, 59% had type I or II morphology. Type III morphology could be identified on cross-sections by the persisting prominence of the lateral lip. However, it may be difficult to appreciate the LA with this morphology at surgery.
Once the LA is identified, its normal cross-sectional position must be defined. One way to do this is to establish the relationship of its axis (LA axis) to the true AP axis. Based on mean values, the LA axis is laterally offset 7º at the distal third of the femur, medially offset 2º at the midshaft, and laterally offset 6º at the proximal third. Therefore, for ideal placement with the LA used for orientation, the component must be internally rotated 7º relative to the LA for femoral resection at the distal third, externally rotated 2º for resection at the midshaft, and internally rotated 6º for resection at the proximal third. Studies have demonstrated that joint contact forces and mechanical alignment of the lower limb can be altered with as little as 5º of femoral malrotation.8,9 Although such a small degree of malrotation is often asymptomatic, it can have long-term effects on soft-tissue tension and patellar tracking.10,11 Rotating-platform mobile-bearing TKA designs can compensate for femoral malrotation, but they may have little to no effect on patellar tracking.12 Therefore, we think aligning the components as near as possible to their natural orientation can prove beneficial in long-term patient management.
Another way of defining the normal cross-sectional position of the LA is to relate it to the femoral neck axis. We measured the difference between these 2 axes. Mean differences were 72º (distal femur), 81.5º (midshaft), and 73.5º (proximal third). Mean arc differences at all levels were larger on the left side—a reflection of the femoral neck being less anteverted on that side in our measurements. Standard deviations were smaller for measurements of LA axis offset from AP axis (range, 7.5°-9.2°) than for measurements of arc between LA axis and femoral neck axis (range, 11.9°-13.6°). This finding indicates there is less variation in the former method, making it preferable for defining the cross-sectional position of the LA.
It has been said that the course of the LA is variable, and our data provide confirmation. The LA does not lie directly posterior (6 o’clock), and it does not trace a straight longitudinal course along the posterior femur, as demonstrated by the different LA axis offsets at 3 levels. However, we may still use it as a landmark if we remain aware how much the LA is offset from the AP axis at each femoral level. Figures 6A-6D, which show CT scans of a patient who underwent distal femoral resection and replacement with an endoprosthesis, illustrate how the LA axis was measured before surgery and how proper prosthesis placement was confirmed after surgery.
In hip arthroplasty, restoration of normal femoral version is the reference for endoprosthetic placement. The literature on “normal” femoral anteversion varies with the method used. In a review of studies on CT-measured adult femoral version, reported values ranged from 6.3° to 40°.2 Mean femoral version in our study ranged from 8° to 13°. Orthopedics textbooks generally put the value at 10° to 15º, and this seems to be the range that surgeons target.6 However, we found a statistically significant mean side-to-side difference of 5.4°. This finding is possibly explained by our large sample—it was larger than the samples used in other studies of CT-measured femoral version. Other studies have found mean side-to-side differences of up to 4.0º.5 Another explanation for our finding is that the studies may differ methodologically. The studies that established values for femoral anteversion were based on CT protocols—thinner slices (1-5 mm), use of foot holders to standardize limb rotation, use of 2 axial cuts in proximal femur to establish femoral neck axis2,13—designed specifically for this measurement. As the CT scans reviewed in our study are not designed for this purpose, errors in femoral version measurement may have been introduced, which may also explain why there is larger variation in measurements of the arc between the LA axis and the femoral neck axis.
Conclusion
The LA does not lie directly on the posterior surface of the femur. It deviates 6.9° laterally at the distal femur, 2.2° medially at the midshaft, and 6.9° laterally at the proximal third. As the LA is an easily identifiable structure on cross-sections of the femoral shaft at the midshaft and distal third of the femur, it may be useful as a rotational landmark for resections at these levels if these deviations are considered during tumor endoprosthetic replacements.
1. Desai SC, Willson S. Radiology of the linea aspera. Australas Radiol. 1985;29(3):273-274.
2. Kuo TY, Skedros JG, Bloebaum RD. Measurement of femoral anteversion by biplane radiography and computed tomography imaging: comparison with an anatomic reference. Invest Radiol. 2003;38(4):221-229.
3. Wines AP, McNicol D. Computed tomography measurement of the accuracy of component version in total hip arthroplasty. J Arthroplasty. 2006;21(5):696-701.
4. Gray H. Anatomy of the Human Body. Philadelphia, PA: Lea & Febiger; 1918.
5. Heck RK, Carnesale PG. General principles of tumors. In: Canale ST, ed. Campbell’s Operative Orthopaedics. Vol 1. 10th ed. St. Louis, MO: Mosby; 2003:733-791.
6. Katz, MA, Beck TD, Silber JS, Seldes RM, Lotke PA. Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques. J Arthroplasty. 2001;16(3):301-305.
7. Pitt MJ. Radiology of the femoral linea aspera–pilaster complex: the track sign. Radiology. 1982;142(1):66.
8. Bretin P, O’Loughlin PF, Suero EM, et al. Influence of femoral malrotation on knee joint alignment and intra-articular contact pressures. Arch Orthop Trauma Surg. 2011;131(8):1115-1120.
9. Zihlmann MS, Stacoff A, Romero J, Quervain IK, Stüssi E. Biomechanical background and clinical observations of rotational malalignment in TKA: literature review and consequences. Clin Biomech. 2005;20(7):661-668.
10. Ghosh KM, Merican AM, Iranpour F, Deehan DJ, Amis AA. The effect of femoral component rotation on the extensor retinaculum of the knee. J Orthop Res. 2010;28(9):1136-1141.
11. Verlinden C, Uvin P, Labey L, Luyckx JP, Bellemans J, Vandenneucker H. The influence of malrotation of the femoral component in total knee replacement on the mechanics of patellofemoral contact during gait: an in vitro biomechanical study. J Bone Joint Surg Br. 2010;92(5):737-742.
12. Kessler O, Patil S, Colwell CW Jr, D’Lima DD. The effect of femoral component malrotation on patellar biomechanics. J Biomech. 2008;41(16):3332-3339.
13. Strecker W, Keppler P, Gebhard F, Kinzl L. Length and torsion of the lower limb. J Bone Joint Surg Br. 1997;79(6):1019-1023.
1. Desai SC, Willson S. Radiology of the linea aspera. Australas Radiol. 1985;29(3):273-274.
2. Kuo TY, Skedros JG, Bloebaum RD. Measurement of femoral anteversion by biplane radiography and computed tomography imaging: comparison with an anatomic reference. Invest Radiol. 2003;38(4):221-229.
3. Wines AP, McNicol D. Computed tomography measurement of the accuracy of component version in total hip arthroplasty. J Arthroplasty. 2006;21(5):696-701.
4. Gray H. Anatomy of the Human Body. Philadelphia, PA: Lea & Febiger; 1918.
5. Heck RK, Carnesale PG. General principles of tumors. In: Canale ST, ed. Campbell’s Operative Orthopaedics. Vol 1. 10th ed. St. Louis, MO: Mosby; 2003:733-791.
6. Katz, MA, Beck TD, Silber JS, Seldes RM, Lotke PA. Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques. J Arthroplasty. 2001;16(3):301-305.
7. Pitt MJ. Radiology of the femoral linea aspera–pilaster complex: the track sign. Radiology. 1982;142(1):66.
8. Bretin P, O’Loughlin PF, Suero EM, et al. Influence of femoral malrotation on knee joint alignment and intra-articular contact pressures. Arch Orthop Trauma Surg. 2011;131(8):1115-1120.
9. Zihlmann MS, Stacoff A, Romero J, Quervain IK, Stüssi E. Biomechanical background and clinical observations of rotational malalignment in TKA: literature review and consequences. Clin Biomech. 2005;20(7):661-668.
10. Ghosh KM, Merican AM, Iranpour F, Deehan DJ, Amis AA. The effect of femoral component rotation on the extensor retinaculum of the knee. J Orthop Res. 2010;28(9):1136-1141.
11. Verlinden C, Uvin P, Labey L, Luyckx JP, Bellemans J, Vandenneucker H. The influence of malrotation of the femoral component in total knee replacement on the mechanics of patellofemoral contact during gait: an in vitro biomechanical study. J Bone Joint Surg Br. 2010;92(5):737-742.
12. Kessler O, Patil S, Colwell CW Jr, D’Lima DD. The effect of femoral component malrotation on patellar biomechanics. J Biomech. 2008;41(16):3332-3339.
13. Strecker W, Keppler P, Gebhard F, Kinzl L. Length and torsion of the lower limb. J Bone Joint Surg Br. 1997;79(6):1019-1023.
Liquid biopsies prove useful alternative to tissue biopsies
CHICAGO – Liquid biopsy, the testing of the blood for circulating tumor DNA (ctDNA), identified cancer mutations useful as biomarkers in 85% of all advanced cancer cases in the largest-ever genomic analysis performed using such technology.
In nearly half of those (49%), the biomarkers were associated with an approved targeted drug, Philip C. Mack, Ph.D., reported at the annual meeting of the American Society of Clinical Oncology.
The patterns of genetic changes detected in the 17,628 blood specimens analyzed for the study using a highly sensitive next-generation sequencing technique closely mirrored those identified using traditional tumor biopsies, suggesting that liquid biopsy provides a non-invasive alternative to tissue biopsy in certain cases, Dr. Mack, professor and director of molecular pharmacology at the University of California, Davis Comprehensive Cancer Center, said during a press briefing at the meeting.
Overall, taking into account FDA-approved drugs and eligibility for clinical trials, the ctDNA testing revealed a possible treatment option for 63.6% of the 15,191 patients who provided samples.
Further, the commercially available liquid biopsy assay used in the study (Guardant360) identified the presence of resistance alterations that could guide new therapy in patients with tumors that acquire resistance to an effective treatment, he said, noting that these resistance mutations are not typically present at the time of initial tissue-biopsy.
Of the patients included in the study, 37% had lung cancer, 14% had breast cancer, 10% had colorectal cancer, and 39% had other cancers. A comparison of genomic changes in ctDNA in 398 patients with available tumor tissue genetic test results showed that when ctDNA was positive for key abnormalities associated with tumor growth, the same mutations were reported in tissue 94% to 100% of the time.

Most of the ctDNA alterations were found at very low levels – with half occurring at a frequency below 0.4% of the total DNA in circulation; even at such low levels, the accuracy of the liquid biopsy assay remained high, Dr. Mack noted.
The ctDNA findings also compared well with those from publicly available population-scale sequencing projects, most notably the Cancer Genome Atlas, he said.
Alterations observed at ctDNA fractions as low as 0.06% responded to treatment, which highlights the importance of assay sensitivity.
Interest in comprehensive tumor genetic profiling to guide patients toward appropriate targeted therapies based on the molecular makeup of their tumors has been increasing, and the current findings underscore its potential value. Advantages of plasma testing include ease of use in any clinic setting, avoidance of biopsy-related complications, ability to monitor changes in disease over time, potential identification of mutations in metastatic lesions not observed in the original tumor biopsy (as genetic changes driving tumor growth often differ in different parts of the tumor), and the opportunity to identify treatment-induced resistance mechanisms, Dr. Mack said.
Additionally, liquid biopsy could be particularly helpful in cases involving tumors for which a traditional biopsy is difficult to obtain.
In fact, the clinical utility of liquid biopsy was evident among 362 lung cancer cases in the study. Tissue was insufficient for traditional biopsy in 63% of the cases, and ctDNA testing identified key genetic mutations at frequencies consistent with their prevalence in the published literature. Thus, ctDNA provided these patients with their only source of an actionable target, Dr. Mack noted.
As for whether liquid biopsy could or should replace tissue biopsy, he explained that it should be viewed more as an additional tool.
“I think there is always going to be a role for tissue-based biopsy,” he said, explaining that a tissue biopsy allows the pathologist to assess the morphological features of the cancer to diagnose it and determine what the tumor type is and where it originated. “That will always be required.”
Leftover tissue should be used for mutational testing, and this is the gold standard. It is in cases when the tissue is of insufficient quality or quantity to allow a broader array of testing that liquid biopsy can provide a complementary source of information, he said.
Further, while it would be ideal to have biopsies of any progressing lesion in a patient who initially had a great response to treatment, that is not feasible, he said.
“So probably, the biggest role for plasma analysis will be occurring down the road as patients are progressing on therapies, as their tumors are evolving, as a way to monitor progression of those cancers,” he said.
Dr. Sumanta Kumar Pal, an ASCO spokesperson and a panel member at the press briefing, noted that “the data that Dr. Mack reported provides key insights into the feasibility of the so-called liquid biopsy.”
“We’re increasingly using genomic data from day-to-day in our clinics to guide therapies,” he said, reiterating that tests such as this provide a useful alternative to tissue-based testing, particularly for the many patients in clinics who have tumors that are challenging to access, such as tumors on bone or near the brain.
“The authors have demonstrated not only the feasibility of the test in detecting alterations, but that the results are often potentially actionable as well ... As oncologists obtain this assay, it’s important to keep in mind trials such as the ASCO-led TAPUR study. TAPUR can potentially link patients with selected genomic alterations to relevant therapies that would otherwise be challenging to access,” he said.
Dr. Pal also noted that there are several other blood-based genomic tests emerging, and it will be important to “rigorously define which of these platforms deliver optimal results.”
Going forward, Dr. Mack and his colleagues will be working to increase the sensitivity of the Gaurdant360 assay to detect mutations at extremely low ctDNA level, as some tumors – glioblastomas, for example – diminish the ability to detect ctDNA. Improved sensitivity could also enable the use of the assay in earlier-stage cancers, he said.
This study was supported by funding from Guardant Health.
CHICAGO – Liquid biopsy, the testing of the blood for circulating tumor DNA (ctDNA), identified cancer mutations useful as biomarkers in 85% of all advanced cancer cases in the largest-ever genomic analysis performed using such technology.
In nearly half of those (49%), the biomarkers were associated with an approved targeted drug, Philip C. Mack, Ph.D., reported at the annual meeting of the American Society of Clinical Oncology.
The patterns of genetic changes detected in the 17,628 blood specimens analyzed for the study using a highly sensitive next-generation sequencing technique closely mirrored those identified using traditional tumor biopsies, suggesting that liquid biopsy provides a non-invasive alternative to tissue biopsy in certain cases, Dr. Mack, professor and director of molecular pharmacology at the University of California, Davis Comprehensive Cancer Center, said during a press briefing at the meeting.
Overall, taking into account FDA-approved drugs and eligibility for clinical trials, the ctDNA testing revealed a possible treatment option for 63.6% of the 15,191 patients who provided samples.
Further, the commercially available liquid biopsy assay used in the study (Guardant360) identified the presence of resistance alterations that could guide new therapy in patients with tumors that acquire resistance to an effective treatment, he said, noting that these resistance mutations are not typically present at the time of initial tissue-biopsy.
Of the patients included in the study, 37% had lung cancer, 14% had breast cancer, 10% had colorectal cancer, and 39% had other cancers. A comparison of genomic changes in ctDNA in 398 patients with available tumor tissue genetic test results showed that when ctDNA was positive for key abnormalities associated with tumor growth, the same mutations were reported in tissue 94% to 100% of the time.
Most of the ctDNA alterations were found at very low levels – with half occurring at a frequency below 0.4% of the total DNA in circulation; even at such low levels, the accuracy of the liquid biopsy assay remained high, Dr. Mack noted.
The ctDNA findings also compared well with those from publicly available population-scale sequencing projects, most notably the Cancer Genome Atlas, he said.
Alterations observed at ctDNA fractions as low as 0.06% responded to treatment, which highlights the importance of assay sensitivity.
Interest in comprehensive tumor genetic profiling to guide patients toward appropriate targeted therapies based on the molecular makeup of their tumors has been increasing, and the current findings underscore its potential value. Advantages of plasma testing include ease of use in any clinic setting, avoidance of biopsy-related complications, ability to monitor changes in disease over time, potential identification of mutations in metastatic lesions not observed in the original tumor biopsy (as genetic changes driving tumor growth often differ in different parts of the tumor), and the opportunity to identify treatment-induced resistance mechanisms, Dr. Mack said.
Additionally, liquid biopsy could be particularly helpful in cases involving tumors for which a traditional biopsy is difficult to obtain.
In fact, the clinical utility of liquid biopsy was evident among 362 lung cancer cases in the study. Tissue was insufficient for traditional biopsy in 63% of the cases, and ctDNA testing identified key genetic mutations at frequencies consistent with their prevalence in the published literature. Thus, ctDNA provided these patients with their only source of an actionable target, Dr. Mack noted.
As for whether liquid biopsy could or should replace tissue biopsy, he explained that it should be viewed more as an additional tool.
“I think there is always going to be a role for tissue-based biopsy,” he said, explaining that a tissue biopsy allows the pathologist to assess the morphological features of the cancer to diagnose it and determine what the tumor type is and where it originated. “That will always be required.”
Leftover tissue should be used for mutational testing, and this is the gold standard. It is in cases when the tissue is of insufficient quality or quantity to allow a broader array of testing that liquid biopsy can provide a complementary source of information, he said.
Further, while it would be ideal to have biopsies of any progressing lesion in a patient who initially had a great response to treatment, that is not feasible, he said.
“So probably, the biggest role for plasma analysis will be occurring down the road as patients are progressing on therapies, as their tumors are evolving, as a way to monitor progression of those cancers,” he said.
Dr. Sumanta Kumar Pal, an ASCO spokesperson and a panel member at the press briefing, noted that “the data that Dr. Mack reported provides key insights into the feasibility of the so-called liquid biopsy.”
“We’re increasingly using genomic data from day-to-day in our clinics to guide therapies,” he said, reiterating that tests such as this provide a useful alternative to tissue-based testing, particularly for the many patients in clinics who have tumors that are challenging to access, such as tumors on bone or near the brain.
“The authors have demonstrated not only the feasibility of the test in detecting alterations, but that the results are often potentially actionable as well ... As oncologists obtain this assay, it’s important to keep in mind trials such as the ASCO-led TAPUR study. TAPUR can potentially link patients with selected genomic alterations to relevant therapies that would otherwise be challenging to access,” he said.
Dr. Pal also noted that there are several other blood-based genomic tests emerging, and it will be important to “rigorously define which of these platforms deliver optimal results.”
Going forward, Dr. Mack and his colleagues will be working to increase the sensitivity of the Gaurdant360 assay to detect mutations at extremely low ctDNA level, as some tumors – glioblastomas, for example – diminish the ability to detect ctDNA. Improved sensitivity could also enable the use of the assay in earlier-stage cancers, he said.
This study was supported by funding from Guardant Health.
CHICAGO – Liquid biopsy, the testing of the blood for circulating tumor DNA (ctDNA), identified cancer mutations useful as biomarkers in 85% of all advanced cancer cases in the largest-ever genomic analysis performed using such technology.
In nearly half of those (49%), the biomarkers were associated with an approved targeted drug, Philip C. Mack, Ph.D., reported at the annual meeting of the American Society of Clinical Oncology.
The patterns of genetic changes detected in the 17,628 blood specimens analyzed for the study using a highly sensitive next-generation sequencing technique closely mirrored those identified using traditional tumor biopsies, suggesting that liquid biopsy provides a non-invasive alternative to tissue biopsy in certain cases, Dr. Mack, professor and director of molecular pharmacology at the University of California, Davis Comprehensive Cancer Center, said during a press briefing at the meeting.
Overall, taking into account FDA-approved drugs and eligibility for clinical trials, the ctDNA testing revealed a possible treatment option for 63.6% of the 15,191 patients who provided samples.
Further, the commercially available liquid biopsy assay used in the study (Guardant360) identified the presence of resistance alterations that could guide new therapy in patients with tumors that acquire resistance to an effective treatment, he said, noting that these resistance mutations are not typically present at the time of initial tissue-biopsy.
Of the patients included in the study, 37% had lung cancer, 14% had breast cancer, 10% had colorectal cancer, and 39% had other cancers. A comparison of genomic changes in ctDNA in 398 patients with available tumor tissue genetic test results showed that when ctDNA was positive for key abnormalities associated with tumor growth, the same mutations were reported in tissue 94% to 100% of the time.
Most of the ctDNA alterations were found at very low levels – with half occurring at a frequency below 0.4% of the total DNA in circulation; even at such low levels, the accuracy of the liquid biopsy assay remained high, Dr. Mack noted.
The ctDNA findings also compared well with those from publicly available population-scale sequencing projects, most notably the Cancer Genome Atlas, he said.
Alterations observed at ctDNA fractions as low as 0.06% responded to treatment, which highlights the importance of assay sensitivity.
Interest in comprehensive tumor genetic profiling to guide patients toward appropriate targeted therapies based on the molecular makeup of their tumors has been increasing, and the current findings underscore its potential value. Advantages of plasma testing include ease of use in any clinic setting, avoidance of biopsy-related complications, ability to monitor changes in disease over time, potential identification of mutations in metastatic lesions not observed in the original tumor biopsy (as genetic changes driving tumor growth often differ in different parts of the tumor), and the opportunity to identify treatment-induced resistance mechanisms, Dr. Mack said.
Additionally, liquid biopsy could be particularly helpful in cases involving tumors for which a traditional biopsy is difficult to obtain.
In fact, the clinical utility of liquid biopsy was evident among 362 lung cancer cases in the study. Tissue was insufficient for traditional biopsy in 63% of the cases, and ctDNA testing identified key genetic mutations at frequencies consistent with their prevalence in the published literature. Thus, ctDNA provided these patients with their only source of an actionable target, Dr. Mack noted.
As for whether liquid biopsy could or should replace tissue biopsy, he explained that it should be viewed more as an additional tool.
“I think there is always going to be a role for tissue-based biopsy,” he said, explaining that a tissue biopsy allows the pathologist to assess the morphological features of the cancer to diagnose it and determine what the tumor type is and where it originated. “That will always be required.”
Leftover tissue should be used for mutational testing, and this is the gold standard. It is in cases when the tissue is of insufficient quality or quantity to allow a broader array of testing that liquid biopsy can provide a complementary source of information, he said.
Further, while it would be ideal to have biopsies of any progressing lesion in a patient who initially had a great response to treatment, that is not feasible, he said.
“So probably, the biggest role for plasma analysis will be occurring down the road as patients are progressing on therapies, as their tumors are evolving, as a way to monitor progression of those cancers,” he said.
Dr. Sumanta Kumar Pal, an ASCO spokesperson and a panel member at the press briefing, noted that “the data that Dr. Mack reported provides key insights into the feasibility of the so-called liquid biopsy.”
“We’re increasingly using genomic data from day-to-day in our clinics to guide therapies,” he said, reiterating that tests such as this provide a useful alternative to tissue-based testing, particularly for the many patients in clinics who have tumors that are challenging to access, such as tumors on bone or near the brain.
“The authors have demonstrated not only the feasibility of the test in detecting alterations, but that the results are often potentially actionable as well ... As oncologists obtain this assay, it’s important to keep in mind trials such as the ASCO-led TAPUR study. TAPUR can potentially link patients with selected genomic alterations to relevant therapies that would otherwise be challenging to access,” he said.
Dr. Pal also noted that there are several other blood-based genomic tests emerging, and it will be important to “rigorously define which of these platforms deliver optimal results.”
Going forward, Dr. Mack and his colleagues will be working to increase the sensitivity of the Gaurdant360 assay to detect mutations at extremely low ctDNA level, as some tumors – glioblastomas, for example – diminish the ability to detect ctDNA. Improved sensitivity could also enable the use of the assay in earlier-stage cancers, he said.
This study was supported by funding from Guardant Health.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Liquid biopsy, the testing of the blood for circulating tumor DNA (ctDNA), identified cancer mutations useful as biomarkers – many associated with an approved targeted drug – in 85% of all advanced cancer cases in a large genomic analysis.
Major finding: A comparison of genomic changes in ctDNA in 398 patients with available tumor tissue genetic test results showed that when ctDNA was positive for key abnormalities associated with tumor growth, the same mutations were reported in tissue 94% to 100% of the time.
Data source: A genomic analysis of 17,628 blood specimens from 15,191 patients.
Disclosures: This study was supported by funding from Guardant Health.

Connecting Health Care Providers With Patients Through Mobile Technology
NATIONAL HARBOR, MD—The Multiple Sclerosis @Point of Care clinician app, powered by IBM Watson, and the Multiple Sclerosis Association of America (MSAA) patient app My MS Manager facilitate the interface of clinicians and patients with multiple sclerosis (MS) and can lead to changes in MS management and improved patient outcomes, according to a presentation at the 2016 CMSC Annual Meeting. “A growing number of patients are using the My MS Manager app to enter their data, track their MS management, and share this data with their clinicians,” said lead author Elaine Rudell, PhD, CHCP, from @Point of Care in Livingston, New Jersey, and colleagues.
Multiple Sclerosis @Point of Care, powered by IBM Watson, and the patient app, the Multiple Sclerosis Association of America’s My MS Manager, use a HIPAA-compliant mobile platform to provide practice-based tools designed to enable shared decision-making. “These tools provide clinicians with access to evidence-based answers at the point of care while incorporating patient-reported outcomes,” said Dr. Rudell. The clinician platform contains up-to-date information about the etiology, epidemiology, pathophysiology, diagnosis, treatment, and management of MS. A cognitive learning tool answers specific questions clinicians pose to improve patient outcomes. The patient app provides patients with the ability to collect and track data (eg, activities of daily living, fatigue scale records, and medications) as well as utilize their personalized data for follow-up discussion with their health care provider.
In the present study, Dr. Rudell and colleagues sought to assess how clinicians utilize and value Multiple Sclerosis @Point of Care and the companion patient app. Data were collected and analyzed from clinicians caring for patients with MS and their participating patients. Data included demographic information, clinicians’ questions posed to the Ask Watson cognitive learning tool, clinicians’ self-reported impact of content on their patients’ health outcomes, number of registered patient app users, average active users/month, patient access frequency, patient record entries, and proprietary patient survey findings that further assess how patients use and value the app.
Currently, 10,627 clinicians use the platform. These providers spend an average of eight minutes per visit on the Multiple Sclerosis @Point of Care platform. Of these users, 77% are repeat users. Nearly 80% of learners posing questions on demand were neurologists, internists, general practitioners, or family practitioners treating patients with MS.
The patient app had 6,880 registered users at the time of the study, with an average of 1,022 active users per month. Active use of the app by patients with MS in this study resulted in 28,794 journal records for activities of daily living, 1,897 fatigue scale journal records, and 3,640 adherence journal records.
Patients accessed the patient app daily (31%), weekly (46%), and monthly (23%). Nearly 80% of patients reported that the app helps them better track how they are doing. Nearly 80% also agreed that regular use of the patient app improved their ability to discuss and manage their MS. Almost 90% of patient users agreed that the app motivated them to talk with clinicians about MS management. Nearly 75% of patient users shared their records with their clinicians. More than 70% of patients agreed that sharing records with their clinician has improved their MS management and sense of well-being.
Regarding the fatigue scale results, patients also agreed that clinicians are more aware of fatigue’s impact on their daily lives (80% of patient respondents), improved fatigue management (75%), and improved management of fatigue-related cognitive function (65%).
After reviewing patient records, clinicians changed medications (14%), changed other aspects of treatment plans (10%), suggested lifestyle changes (6%), requested more tests (1%), or concurred that treatment was on track (no changes, 69%).
This study was funded by @Point of Care.
—Glenn S. Williams
NATIONAL HARBOR, MD—The Multiple Sclerosis @Point of Care clinician app, powered by IBM Watson, and the Multiple Sclerosis Association of America (MSAA) patient app My MS Manager facilitate the interface of clinicians and patients with multiple sclerosis (MS) and can lead to changes in MS management and improved patient outcomes, according to a presentation at the 2016 CMSC Annual Meeting. “A growing number of patients are using the My MS Manager app to enter their data, track their MS management, and share this data with their clinicians,” said lead author Elaine Rudell, PhD, CHCP, from @Point of Care in Livingston, New Jersey, and colleagues.
Multiple Sclerosis @Point of Care, powered by IBM Watson, and the patient app, the Multiple Sclerosis Association of America’s My MS Manager, use a HIPAA-compliant mobile platform to provide practice-based tools designed to enable shared decision-making. “These tools provide clinicians with access to evidence-based answers at the point of care while incorporating patient-reported outcomes,” said Dr. Rudell. The clinician platform contains up-to-date information about the etiology, epidemiology, pathophysiology, diagnosis, treatment, and management of MS. A cognitive learning tool answers specific questions clinicians pose to improve patient outcomes. The patient app provides patients with the ability to collect and track data (eg, activities of daily living, fatigue scale records, and medications) as well as utilize their personalized data for follow-up discussion with their health care provider.
In the present study, Dr. Rudell and colleagues sought to assess how clinicians utilize and value Multiple Sclerosis @Point of Care and the companion patient app. Data were collected and analyzed from clinicians caring for patients with MS and their participating patients. Data included demographic information, clinicians’ questions posed to the Ask Watson cognitive learning tool, clinicians’ self-reported impact of content on their patients’ health outcomes, number of registered patient app users, average active users/month, patient access frequency, patient record entries, and proprietary patient survey findings that further assess how patients use and value the app.
Currently, 10,627 clinicians use the platform. These providers spend an average of eight minutes per visit on the Multiple Sclerosis @Point of Care platform. Of these users, 77% are repeat users. Nearly 80% of learners posing questions on demand were neurologists, internists, general practitioners, or family practitioners treating patients with MS.
The patient app had 6,880 registered users at the time of the study, with an average of 1,022 active users per month. Active use of the app by patients with MS in this study resulted in 28,794 journal records for activities of daily living, 1,897 fatigue scale journal records, and 3,640 adherence journal records.
Patients accessed the patient app daily (31%), weekly (46%), and monthly (23%). Nearly 80% of patients reported that the app helps them better track how they are doing. Nearly 80% also agreed that regular use of the patient app improved their ability to discuss and manage their MS. Almost 90% of patient users agreed that the app motivated them to talk with clinicians about MS management. Nearly 75% of patient users shared their records with their clinicians. More than 70% of patients agreed that sharing records with their clinician has improved their MS management and sense of well-being.
Regarding the fatigue scale results, patients also agreed that clinicians are more aware of fatigue’s impact on their daily lives (80% of patient respondents), improved fatigue management (75%), and improved management of fatigue-related cognitive function (65%).
After reviewing patient records, clinicians changed medications (14%), changed other aspects of treatment plans (10%), suggested lifestyle changes (6%), requested more tests (1%), or concurred that treatment was on track (no changes, 69%).
This study was funded by @Point of Care.
—Glenn S. Williams
NATIONAL HARBOR, MD—The Multiple Sclerosis @Point of Care clinician app, powered by IBM Watson, and the Multiple Sclerosis Association of America (MSAA) patient app My MS Manager facilitate the interface of clinicians and patients with multiple sclerosis (MS) and can lead to changes in MS management and improved patient outcomes, according to a presentation at the 2016 CMSC Annual Meeting. “A growing number of patients are using the My MS Manager app to enter their data, track their MS management, and share this data with their clinicians,” said lead author Elaine Rudell, PhD, CHCP, from @Point of Care in Livingston, New Jersey, and colleagues.
Multiple Sclerosis @Point of Care, powered by IBM Watson, and the patient app, the Multiple Sclerosis Association of America’s My MS Manager, use a HIPAA-compliant mobile platform to provide practice-based tools designed to enable shared decision-making. “These tools provide clinicians with access to evidence-based answers at the point of care while incorporating patient-reported outcomes,” said Dr. Rudell. The clinician platform contains up-to-date information about the etiology, epidemiology, pathophysiology, diagnosis, treatment, and management of MS. A cognitive learning tool answers specific questions clinicians pose to improve patient outcomes. The patient app provides patients with the ability to collect and track data (eg, activities of daily living, fatigue scale records, and medications) as well as utilize their personalized data for follow-up discussion with their health care provider.
In the present study, Dr. Rudell and colleagues sought to assess how clinicians utilize and value Multiple Sclerosis @Point of Care and the companion patient app. Data were collected and analyzed from clinicians caring for patients with MS and their participating patients. Data included demographic information, clinicians’ questions posed to the Ask Watson cognitive learning tool, clinicians’ self-reported impact of content on their patients’ health outcomes, number of registered patient app users, average active users/month, patient access frequency, patient record entries, and proprietary patient survey findings that further assess how patients use and value the app.
Currently, 10,627 clinicians use the platform. These providers spend an average of eight minutes per visit on the Multiple Sclerosis @Point of Care platform. Of these users, 77% are repeat users. Nearly 80% of learners posing questions on demand were neurologists, internists, general practitioners, or family practitioners treating patients with MS.
The patient app had 6,880 registered users at the time of the study, with an average of 1,022 active users per month. Active use of the app by patients with MS in this study resulted in 28,794 journal records for activities of daily living, 1,897 fatigue scale journal records, and 3,640 adherence journal records.
Patients accessed the patient app daily (31%), weekly (46%), and monthly (23%). Nearly 80% of patients reported that the app helps them better track how they are doing. Nearly 80% also agreed that regular use of the patient app improved their ability to discuss and manage their MS. Almost 90% of patient users agreed that the app motivated them to talk with clinicians about MS management. Nearly 75% of patient users shared their records with their clinicians. More than 70% of patients agreed that sharing records with their clinician has improved their MS management and sense of well-being.
Regarding the fatigue scale results, patients also agreed that clinicians are more aware of fatigue’s impact on their daily lives (80% of patient respondents), improved fatigue management (75%), and improved management of fatigue-related cognitive function (65%).
After reviewing patient records, clinicians changed medications (14%), changed other aspects of treatment plans (10%), suggested lifestyle changes (6%), requested more tests (1%), or concurred that treatment was on track (no changes, 69%).
This study was funded by @Point of Care.
—Glenn S. Williams
New heart failure interventions face outcomes test
A history of trials where a well-reasoned heart failure intervention did not have the expected results is now coloring the way some clinicians view potential new treatments.
A couple of examples of this cautious, skeptical mindset cropped up during the annual meeting of the Heart Failure Association of the European Society of Cardiology in Florence, Italy, in May.

I previously reported on one of the major talks at the sessions, results from a pivotal trial of a phrenic nerve stimulation device in 151 patients with some type of cardiovascular disease (more than half had heart failure) and central sleep apnea. These patients generally had significant improvement in their apnea-hypopnea index while on active treatment with the phrenic nerve stimulator, designed to produce rhythmic contractions of the diaphragm to create negative chest pressure and enhance breathing in a way that mimics natural respiration and avoids the apparent danger from a positive-pressure intervention in patients with central sleep apnea and heart failure with reduced ejection fraction (HFrEF).
The positive-pressure danger in such patients occurred unexpectedly and dramatically in the form of significantly increased mortality among HFrEF patients with central sleep apnea enrolled in the SERVE-HF trial. Based on that chilling experience, “our understanding of central sleep apnea is imperfect,” said Dr. Martin R. Cowie, lead investigator of SERVE-HF, who rehashed his experience with that study during the recent meeting. “A really important message was that just because patients say they feel better [with the adaptive servo-ventilation tested in SERVE-HF], that doesn’t necessarily translate into benefit,” Dr. Cowie noted.
Dr. Mariell L. Jessup, a leading U.S. heart failure expert, had a similar reaction when I spoke with her during the meeting.
“A lot of things made a lot of sense, including treating central sleep apnea in a patient with HFrEF with positive air pressure that made them feel better,” she said, also invoking the specter of SERVE-HF. “We have to now demand that sleep trials show benefit in clinical outcomes,” such as reduced mortality or a cut in heart failure hospitalizations, and certainly no increase in mortality. Until that’s shown for phrenic nerve stimulation she’ll stay a skeptic, she told me.
Another intervention recently available for U.S. heart failure patients that seems on track to confront this “show-me-the-outcomes” attitude involves new drugs that cut serum potassium levels by binding to potassium in the gastrointestinal tract. This class includes patiromer (Veltassa), approved by the Food and Drug Administration in October 2015. Another potassium binder, sodium zirconium cyclosilicate (ZS-9), seems on track to soon receive FDA approval.
Several speakers at the meeting spoke of the potential to use these drugs to control the hyperkalemia that often complicates treatment of heart failure patients with an ACE inhibitor, angiotensin receptor blocker, or a mineralocorticoid receptor antagonist, especially heart failure patients with concomitant renal disease. Study results showed treatment with patiromer or ZS-9 reversed hyperkalemia, thereby allowing patients to remain on these drugs that are known to significantly cut rates of mortality and heart failure hospitalizations in heart failure patients.

“Right now, a lot of patients don’t get these lifesaving drugs” because of hyperkalemia, noted Dr. Bertram Pitt, a University of Michigan cardiologist who has been involved in several patiromer trials (and is a consultant to Relypsa, the company that markets patiromer).
The problem is that no studies of patiromer or ZS-9 treatment have so far shown that these drugs lead to reduced mortality or heart failure hospitalizations in heart failure patients. All that’s been shown is that patiromer and ZS-9 are effective at lowering potassium levels in patients with hyperkalemia out of the danger zone, levels above 5 mEq/L.
“I want to see outcome trials,” said Dr. Jessup.
Dr. Pitt agreed that outcomes data would be ideal, but also noted that currently no studies aimed at collecting these data are underway.
Without these data, clinicians need to decide whether they believe proven potassium lowering alone is a good enough reason to prescribe patiromer or ZS-9, or whether they need to see proof that these drugs give patients clinically meaningful benefits.
If they demand outcomes evidence they may need to wait quite a while.
On Twitter @mitchelzoler
A history of trials where a well-reasoned heart failure intervention did not have the expected results is now coloring the way some clinicians view potential new treatments.
A couple of examples of this cautious, skeptical mindset cropped up during the annual meeting of the Heart Failure Association of the European Society of Cardiology in Florence, Italy, in May.
I previously reported on one of the major talks at the sessions, results from a pivotal trial of a phrenic nerve stimulation device in 151 patients with some type of cardiovascular disease (more than half had heart failure) and central sleep apnea. These patients generally had significant improvement in their apnea-hypopnea index while on active treatment with the phrenic nerve stimulator, designed to produce rhythmic contractions of the diaphragm to create negative chest pressure and enhance breathing in a way that mimics natural respiration and avoids the apparent danger from a positive-pressure intervention in patients with central sleep apnea and heart failure with reduced ejection fraction (HFrEF).
The positive-pressure danger in such patients occurred unexpectedly and dramatically in the form of significantly increased mortality among HFrEF patients with central sleep apnea enrolled in the SERVE-HF trial. Based on that chilling experience, “our understanding of central sleep apnea is imperfect,” said Dr. Martin R. Cowie, lead investigator of SERVE-HF, who rehashed his experience with that study during the recent meeting. “A really important message was that just because patients say they feel better [with the adaptive servo-ventilation tested in SERVE-HF], that doesn’t necessarily translate into benefit,” Dr. Cowie noted.
Dr. Mariell L. Jessup, a leading U.S. heart failure expert, had a similar reaction when I spoke with her during the meeting.
“A lot of things made a lot of sense, including treating central sleep apnea in a patient with HFrEF with positive air pressure that made them feel better,” she said, also invoking the specter of SERVE-HF. “We have to now demand that sleep trials show benefit in clinical outcomes,” such as reduced mortality or a cut in heart failure hospitalizations, and certainly no increase in mortality. Until that’s shown for phrenic nerve stimulation she’ll stay a skeptic, she told me.
Another intervention recently available for U.S. heart failure patients that seems on track to confront this “show-me-the-outcomes” attitude involves new drugs that cut serum potassium levels by binding to potassium in the gastrointestinal tract. This class includes patiromer (Veltassa), approved by the Food and Drug Administration in October 2015. Another potassium binder, sodium zirconium cyclosilicate (ZS-9), seems on track to soon receive FDA approval.
Several speakers at the meeting spoke of the potential to use these drugs to control the hyperkalemia that often complicates treatment of heart failure patients with an ACE inhibitor, angiotensin receptor blocker, or a mineralocorticoid receptor antagonist, especially heart failure patients with concomitant renal disease. Study results showed treatment with patiromer or ZS-9 reversed hyperkalemia, thereby allowing patients to remain on these drugs that are known to significantly cut rates of mortality and heart failure hospitalizations in heart failure patients.
“Right now, a lot of patients don’t get these lifesaving drugs” because of hyperkalemia, noted Dr. Bertram Pitt, a University of Michigan cardiologist who has been involved in several patiromer trials (and is a consultant to Relypsa, the company that markets patiromer).
The problem is that no studies of patiromer or ZS-9 treatment have so far shown that these drugs lead to reduced mortality or heart failure hospitalizations in heart failure patients. All that’s been shown is that patiromer and ZS-9 are effective at lowering potassium levels in patients with hyperkalemia out of the danger zone, levels above 5 mEq/L.
“I want to see outcome trials,” said Dr. Jessup.
Dr. Pitt agreed that outcomes data would be ideal, but also noted that currently no studies aimed at collecting these data are underway.
Without these data, clinicians need to decide whether they believe proven potassium lowering alone is a good enough reason to prescribe patiromer or ZS-9, or whether they need to see proof that these drugs give patients clinically meaningful benefits.
If they demand outcomes evidence they may need to wait quite a while.
On Twitter @mitchelzoler
A history of trials where a well-reasoned heart failure intervention did not have the expected results is now coloring the way some clinicians view potential new treatments.
A couple of examples of this cautious, skeptical mindset cropped up during the annual meeting of the Heart Failure Association of the European Society of Cardiology in Florence, Italy, in May.
I previously reported on one of the major talks at the sessions, results from a pivotal trial of a phrenic nerve stimulation device in 151 patients with some type of cardiovascular disease (more than half had heart failure) and central sleep apnea. These patients generally had significant improvement in their apnea-hypopnea index while on active treatment with the phrenic nerve stimulator, designed to produce rhythmic contractions of the diaphragm to create negative chest pressure and enhance breathing in a way that mimics natural respiration and avoids the apparent danger from a positive-pressure intervention in patients with central sleep apnea and heart failure with reduced ejection fraction (HFrEF).
The positive-pressure danger in such patients occurred unexpectedly and dramatically in the form of significantly increased mortality among HFrEF patients with central sleep apnea enrolled in the SERVE-HF trial. Based on that chilling experience, “our understanding of central sleep apnea is imperfect,” said Dr. Martin R. Cowie, lead investigator of SERVE-HF, who rehashed his experience with that study during the recent meeting. “A really important message was that just because patients say they feel better [with the adaptive servo-ventilation tested in SERVE-HF], that doesn’t necessarily translate into benefit,” Dr. Cowie noted.
Dr. Mariell L. Jessup, a leading U.S. heart failure expert, had a similar reaction when I spoke with her during the meeting.
“A lot of things made a lot of sense, including treating central sleep apnea in a patient with HFrEF with positive air pressure that made them feel better,” she said, also invoking the specter of SERVE-HF. “We have to now demand that sleep trials show benefit in clinical outcomes,” such as reduced mortality or a cut in heart failure hospitalizations, and certainly no increase in mortality. Until that’s shown for phrenic nerve stimulation she’ll stay a skeptic, she told me.
Another intervention recently available for U.S. heart failure patients that seems on track to confront this “show-me-the-outcomes” attitude involves new drugs that cut serum potassium levels by binding to potassium in the gastrointestinal tract. This class includes patiromer (Veltassa), approved by the Food and Drug Administration in October 2015. Another potassium binder, sodium zirconium cyclosilicate (ZS-9), seems on track to soon receive FDA approval.
Several speakers at the meeting spoke of the potential to use these drugs to control the hyperkalemia that often complicates treatment of heart failure patients with an ACE inhibitor, angiotensin receptor blocker, or a mineralocorticoid receptor antagonist, especially heart failure patients with concomitant renal disease. Study results showed treatment with patiromer or ZS-9 reversed hyperkalemia, thereby allowing patients to remain on these drugs that are known to significantly cut rates of mortality and heart failure hospitalizations in heart failure patients.
“Right now, a lot of patients don’t get these lifesaving drugs” because of hyperkalemia, noted Dr. Bertram Pitt, a University of Michigan cardiologist who has been involved in several patiromer trials (and is a consultant to Relypsa, the company that markets patiromer).
The problem is that no studies of patiromer or ZS-9 treatment have so far shown that these drugs lead to reduced mortality or heart failure hospitalizations in heart failure patients. All that’s been shown is that patiromer and ZS-9 are effective at lowering potassium levels in patients with hyperkalemia out of the danger zone, levels above 5 mEq/L.
“I want to see outcome trials,” said Dr. Jessup.
Dr. Pitt agreed that outcomes data would be ideal, but also noted that currently no studies aimed at collecting these data are underway.
Without these data, clinicians need to decide whether they believe proven potassium lowering alone is a good enough reason to prescribe patiromer or ZS-9, or whether they need to see proof that these drugs give patients clinically meaningful benefits.
If they demand outcomes evidence they may need to wait quite a while.
On Twitter @mitchelzoler

Obesity continues to trend up among women over the past decade
Four in 10 women in the United States are obese, 1 in 10 women has a body mass index above 40 kg/m2, and significantly more women are obese than a decade ago, according to a large study published June 7 in JAMA.
In contrast, obesity rates among men in the United States have remained stable since 2005, said Dr. Katherine Flegal of the National Center for Health Statistics. “Other studies are needed to determine the reasons for these trends,” she and her associates wrote.

Between 1980 and 2000, obesity rates in the United States rose significantly among both men and women. Between 2000 and 2004, rates rose significantly for men, but not women. Rates then leveled off for both sexes through 2012. To further explore these trends, Dr. Flegal and her associates calculated the prevalence of obesity (BMI greater than 30 kg/m2) and class 3 obesity (BMI greater than 40 kg/m2) for 2,638 men and 2,817 women aged 20 and up during 2013-2014, the most recently available 2-year data period from the National Health and Nutrition Examination Survey (NHANES). The researchers also examined trends in obesity since 2005, based on NHANES data from 21,013 adults (JAMA. 2016 Jun 7. doi: 10.1001/jama.2016.6458).
About 38% of adults in the United States were obese during 2013-2014 (95% confidence interval, 36%-40%), including about 40% of women and 35% of men, the researchers found. A total of 7.7% of adults had a BMI of at least 40, including 5.5 % of men and 9.9% of women.
During the decade from 2005 through 2014, the prevalence of obesity among women rose significantly from 35.6% to 41.1% (P = .004), even after the investigators adjusted for age, race and Hispanic origin, smoking status, and education. Among men, the adjusted prevalence of obesity remained about 35% during this time period. Likewise, the adjusted prevalence of class 3 obesity (BMI of at least 40) rose significantly for women (P = .01), but not for men.
Black women also were significantly more likely to be obese or severely obese, compared with non-Hispanic white women in the study, the investigators found. Among men, current smokers were less likely to be obese than never smokers, and women with education beyond high school were less likely to be obese than women who had not finished high school.
The investigators reported no funding sources and had no disclosures.
Much research and attention have been directed toward the treatment of obesity, but the development of new drugs and procedures will not solve the problem. Perhaps genetics will unlock some of the mysteries of obesity, but this will take time, and more immediate solutions are needed. The emphasis has to be on prevention, despite evidence that school- and community-based prevention programs and education campaigns by local governments and professional societies have not been highly successful.
The obesity epidemic in the United States is now 3 decades old, and huge investments have been made in research, clinical care, and development of various programs to counteract obesity. However, few data suggest the epidemic is diminishing. Perhaps it is time for an entirely different approach, one that emphasizes collaboration with the food and restaurant industries that are in part responsible for putting food on our dinner tables.
Dr. Jody W. Zylke is deputy editor of JAMA. Dr. Howard Bauchner is editor in chief of JAMA. These comments are from their accompanying editorial (JAMA. 2016 Jun 7. doi: 10.1001/jama.2016.6190).
Much research and attention have been directed toward the treatment of obesity, but the development of new drugs and procedures will not solve the problem. Perhaps genetics will unlock some of the mysteries of obesity, but this will take time, and more immediate solutions are needed. The emphasis has to be on prevention, despite evidence that school- and community-based prevention programs and education campaigns by local governments and professional societies have not been highly successful.
The obesity epidemic in the United States is now 3 decades old, and huge investments have been made in research, clinical care, and development of various programs to counteract obesity. However, few data suggest the epidemic is diminishing. Perhaps it is time for an entirely different approach, one that emphasizes collaboration with the food and restaurant industries that are in part responsible for putting food on our dinner tables.
Dr. Jody W. Zylke is deputy editor of JAMA. Dr. Howard Bauchner is editor in chief of JAMA. These comments are from their accompanying editorial (JAMA. 2016 Jun 7. doi: 10.1001/jama.2016.6190).
Much research and attention have been directed toward the treatment of obesity, but the development of new drugs and procedures will not solve the problem. Perhaps genetics will unlock some of the mysteries of obesity, but this will take time, and more immediate solutions are needed. The emphasis has to be on prevention, despite evidence that school- and community-based prevention programs and education campaigns by local governments and professional societies have not been highly successful.
The obesity epidemic in the United States is now 3 decades old, and huge investments have been made in research, clinical care, and development of various programs to counteract obesity. However, few data suggest the epidemic is diminishing. Perhaps it is time for an entirely different approach, one that emphasizes collaboration with the food and restaurant industries that are in part responsible for putting food on our dinner tables.
Dr. Jody W. Zylke is deputy editor of JAMA. Dr. Howard Bauchner is editor in chief of JAMA. These comments are from their accompanying editorial (JAMA. 2016 Jun 7. doi: 10.1001/jama.2016.6190).
Four in 10 women in the United States are obese, 1 in 10 women has a body mass index above 40 kg/m2, and significantly more women are obese than a decade ago, according to a large study published June 7 in JAMA.
In contrast, obesity rates among men in the United States have remained stable since 2005, said Dr. Katherine Flegal of the National Center for Health Statistics. “Other studies are needed to determine the reasons for these trends,” she and her associates wrote.
Between 1980 and 2000, obesity rates in the United States rose significantly among both men and women. Between 2000 and 2004, rates rose significantly for men, but not women. Rates then leveled off for both sexes through 2012. To further explore these trends, Dr. Flegal and her associates calculated the prevalence of obesity (BMI greater than 30 kg/m2) and class 3 obesity (BMI greater than 40 kg/m2) for 2,638 men and 2,817 women aged 20 and up during 2013-2014, the most recently available 2-year data period from the National Health and Nutrition Examination Survey (NHANES). The researchers also examined trends in obesity since 2005, based on NHANES data from 21,013 adults (JAMA. 2016 Jun 7. doi: 10.1001/jama.2016.6458).
About 38% of adults in the United States were obese during 2013-2014 (95% confidence interval, 36%-40%), including about 40% of women and 35% of men, the researchers found. A total of 7.7% of adults had a BMI of at least 40, including 5.5 % of men and 9.9% of women.
During the decade from 2005 through 2014, the prevalence of obesity among women rose significantly from 35.6% to 41.1% (P = .004), even after the investigators adjusted for age, race and Hispanic origin, smoking status, and education. Among men, the adjusted prevalence of obesity remained about 35% during this time period. Likewise, the adjusted prevalence of class 3 obesity (BMI of at least 40) rose significantly for women (P = .01), but not for men.
Black women also were significantly more likely to be obese or severely obese, compared with non-Hispanic white women in the study, the investigators found. Among men, current smokers were less likely to be obese than never smokers, and women with education beyond high school were less likely to be obese than women who had not finished high school.
The investigators reported no funding sources and had no disclosures.
Four in 10 women in the United States are obese, 1 in 10 women has a body mass index above 40 kg/m2, and significantly more women are obese than a decade ago, according to a large study published June 7 in JAMA.
In contrast, obesity rates among men in the United States have remained stable since 2005, said Dr. Katherine Flegal of the National Center for Health Statistics. “Other studies are needed to determine the reasons for these trends,” she and her associates wrote.
Between 1980 and 2000, obesity rates in the United States rose significantly among both men and women. Between 2000 and 2004, rates rose significantly for men, but not women. Rates then leveled off for both sexes through 2012. To further explore these trends, Dr. Flegal and her associates calculated the prevalence of obesity (BMI greater than 30 kg/m2) and class 3 obesity (BMI greater than 40 kg/m2) for 2,638 men and 2,817 women aged 20 and up during 2013-2014, the most recently available 2-year data period from the National Health and Nutrition Examination Survey (NHANES). The researchers also examined trends in obesity since 2005, based on NHANES data from 21,013 adults (JAMA. 2016 Jun 7. doi: 10.1001/jama.2016.6458).
About 38% of adults in the United States were obese during 2013-2014 (95% confidence interval, 36%-40%), including about 40% of women and 35% of men, the researchers found. A total of 7.7% of adults had a BMI of at least 40, including 5.5 % of men and 9.9% of women.
During the decade from 2005 through 2014, the prevalence of obesity among women rose significantly from 35.6% to 41.1% (P = .004), even after the investigators adjusted for age, race and Hispanic origin, smoking status, and education. Among men, the adjusted prevalence of obesity remained about 35% during this time period. Likewise, the adjusted prevalence of class 3 obesity (BMI of at least 40) rose significantly for women (P = .01), but not for men.
Black women also were significantly more likely to be obese or severely obese, compared with non-Hispanic white women in the study, the investigators found. Among men, current smokers were less likely to be obese than never smokers, and women with education beyond high school were less likely to be obese than women who had not finished high school.
The investigators reported no funding sources and had no disclosures.
FROM JAMA
Key clinical point: Significantly more women in the United States are obese now than a decade ago, while obesity rates among men have leveled off.
Major finding: During 2005 through 2014, the adjusted prevalence of obesity among women rose from 35.6% to 41.1% (P = .004).
Data source: An analysis of the body mass index for 26,468 adults from the National Health and Nutrition Examination Survey.
Disclosures: The researchers reported no funding sources and had no disclosures.

Charting the Benefits of AAA Screening in England
The United Kingdom’s National Health Service (NHS) in England has invited around 1.3 million 65-year-old men for abdominal aortic aneurysm (AAA) screening since 2009. Dr. Jonothan Earnshaw and his colleagues performed a study to examine the results of this screening and the safety of the men in surveillance.

The NHS AAA Screening Programme (NAAASP) conducted ultrasound scans to look for AAAs, according to Dr. Earnshaw.
A total of 1,019,480 of those invited were scanned (79.5%). The prevalence of an AAA greater than 2.9 cm diameter was 1.3% (falling from 1.7% in 2009 and 2010 to 1.1% in 2015).
A total of 11,972 men had small (3-4.5 cm) or medium (4.5-5.4 cm) AAAs and were monitored via surveillance, with 13 deaths from AAA rupture.
Some 1,025 men with initial aortic diameter greater than 5.4 cm, and a further 898 men whose AAA grew during surveillance were referred for consideration of elective AAA repair. Mortality in those men who were electively treated was 0.91%.
“Although the prevalence of AAA in 65-year-old men is lower than expected and may be falling, the NAAASP remains cost-effective and is finding large numbers of AAA,” according to Dr. Earnshaw.
“It remains on course to prevent up to half of deaths from ruptured AAA by the end of the decade,” he concluded.
International Forum
3:00 - 6:00 p.m. Thursday
Potomac Ballroom A/B
The United Kingdom’s National Health Service (NHS) in England has invited around 1.3 million 65-year-old men for abdominal aortic aneurysm (AAA) screening since 2009. Dr. Jonothan Earnshaw and his colleagues performed a study to examine the results of this screening and the safety of the men in surveillance.
The NHS AAA Screening Programme (NAAASP) conducted ultrasound scans to look for AAAs, according to Dr. Earnshaw.
A total of 1,019,480 of those invited were scanned (79.5%). The prevalence of an AAA greater than 2.9 cm diameter was 1.3% (falling from 1.7% in 2009 and 2010 to 1.1% in 2015).
A total of 11,972 men had small (3-4.5 cm) or medium (4.5-5.4 cm) AAAs and were monitored via surveillance, with 13 deaths from AAA rupture.
Some 1,025 men with initial aortic diameter greater than 5.4 cm, and a further 898 men whose AAA grew during surveillance were referred for consideration of elective AAA repair. Mortality in those men who were electively treated was 0.91%.
“Although the prevalence of AAA in 65-year-old men is lower than expected and may be falling, the NAAASP remains cost-effective and is finding large numbers of AAA,” according to Dr. Earnshaw.
“It remains on course to prevent up to half of deaths from ruptured AAA by the end of the decade,” he concluded.
International Forum
3:00 - 6:00 p.m. Thursday
Potomac Ballroom A/B
The United Kingdom’s National Health Service (NHS) in England has invited around 1.3 million 65-year-old men for abdominal aortic aneurysm (AAA) screening since 2009. Dr. Jonothan Earnshaw and his colleagues performed a study to examine the results of this screening and the safety of the men in surveillance.
The NHS AAA Screening Programme (NAAASP) conducted ultrasound scans to look for AAAs, according to Dr. Earnshaw.
A total of 1,019,480 of those invited were scanned (79.5%). The prevalence of an AAA greater than 2.9 cm diameter was 1.3% (falling from 1.7% in 2009 and 2010 to 1.1% in 2015).
A total of 11,972 men had small (3-4.5 cm) or medium (4.5-5.4 cm) AAAs and were monitored via surveillance, with 13 deaths from AAA rupture.
Some 1,025 men with initial aortic diameter greater than 5.4 cm, and a further 898 men whose AAA grew during surveillance were referred for consideration of elective AAA repair. Mortality in those men who were electively treated was 0.91%.
“Although the prevalence of AAA in 65-year-old men is lower than expected and may be falling, the NAAASP remains cost-effective and is finding large numbers of AAA,” according to Dr. Earnshaw.
“It remains on course to prevent up to half of deaths from ruptured AAA by the end of the decade,” he concluded.
International Forum
3:00 - 6:00 p.m. Thursday
Potomac Ballroom A/B

Tracking Endovascular Treatment of the Femoral Arteries
Dr. Jeffrey Siracuse will report on the study he and his colleagues performed to analyze practice patterns and outcomes from endovascular treatment of the common femoral (CFA) and deep femoral arteries (DFA). The Vascular Quality Initiative (2010-2015) was queried for all endovascular interventions on the CFA and DFA. They identified 3,960 endovascular CFA/DFA interventions; 1296 (nearly 33%) were isolated to the CFA/DFA. The average age of this isolated cohort was 68 years and 59% were men.
Indications for treatment were claudication (62%), rest pain (18%), and tissue loss (19%). Stents and atherectomy were used in about 28% and 18% of cases, respectively. The intervention was a technical success in nearly 92% of cases.
Perioperative complications included embolization, perforation, access hematoma, and dissection.
They found that thirty-day mortality was 1.6%, with survival of 93% and 87% at 1 and 3 years.
Dr. Siracuse, from the Boston University School of Medicine, will detail their results showing that the significant predictors of mortality were end-stage renal disease (hazard ratio [HR], 3.21, tissue loss, HR, 2.59), combined CFA/DFA intervention (HR, 1.88), chronic obstructive pulmonary disease (HR, 1.73), and nonambulatory status (HR, 1.61).
Freedom from loss of patency/death was 83% at 1 year, according to the researchers. Predictors of patency loss/death were tissue loss (HR, 2.67) and nonambulatory status (HR, 2.17). Freedom from reintervention/death was 83%. Signficant predictors of reintervention or death were tissue loss (HR, 3.52),and stenting (HR, 1.73); with P2Y12 antagonists (HR, 0.62) being signficantly protective.
Amputation-free survival at 1 year was 92%. Significant predictors of amputation/death were tissue loss (HR, 18.9), rest pain (HR, 5.47), previous major amputation (HR, 4.02), and stenting (HR, 2.83), with aspirin use (HR, 0.42) and P2Y12 antagonists (HR, 0.25) being protective.
“Endovascular interventions of the CFA/DFA have a low rate of perioperative morbidity and mortality. One-year patency is lower than historical controls of CFA endarterectomy. Stent use is associated with reinterventions and amputation and should be avoided if possible. Longer-term analysis is needed to better assess durability,” Dr. Siracuse concluded.
VON LIEBIG FORUM
8:30 – 10:00 a.m. Thursday
Potomac Ballroom A/B
Dr. Jeffrey Siracuse will report on the study he and his colleagues performed to analyze practice patterns and outcomes from endovascular treatment of the common femoral (CFA) and deep femoral arteries (DFA). The Vascular Quality Initiative (2010-2015) was queried for all endovascular interventions on the CFA and DFA. They identified 3,960 endovascular CFA/DFA interventions; 1296 (nearly 33%) were isolated to the CFA/DFA. The average age of this isolated cohort was 68 years and 59% were men.
Indications for treatment were claudication (62%), rest pain (18%), and tissue loss (19%). Stents and atherectomy were used in about 28% and 18% of cases, respectively. The intervention was a technical success in nearly 92% of cases.
Perioperative complications included embolization, perforation, access hematoma, and dissection.
They found that thirty-day mortality was 1.6%, with survival of 93% and 87% at 1 and 3 years.
Dr. Siracuse, from the Boston University School of Medicine, will detail their results showing that the significant predictors of mortality were end-stage renal disease (hazard ratio [HR], 3.21, tissue loss, HR, 2.59), combined CFA/DFA intervention (HR, 1.88), chronic obstructive pulmonary disease (HR, 1.73), and nonambulatory status (HR, 1.61).
Freedom from loss of patency/death was 83% at 1 year, according to the researchers. Predictors of patency loss/death were tissue loss (HR, 2.67) and nonambulatory status (HR, 2.17). Freedom from reintervention/death was 83%. Signficant predictors of reintervention or death were tissue loss (HR, 3.52),and stenting (HR, 1.73); with P2Y12 antagonists (HR, 0.62) being signficantly protective.
Amputation-free survival at 1 year was 92%. Significant predictors of amputation/death were tissue loss (HR, 18.9), rest pain (HR, 5.47), previous major amputation (HR, 4.02), and stenting (HR, 2.83), with aspirin use (HR, 0.42) and P2Y12 antagonists (HR, 0.25) being protective.
“Endovascular interventions of the CFA/DFA have a low rate of perioperative morbidity and mortality. One-year patency is lower than historical controls of CFA endarterectomy. Stent use is associated with reinterventions and amputation and should be avoided if possible. Longer-term analysis is needed to better assess durability,” Dr. Siracuse concluded.
VON LIEBIG FORUM
8:30 – 10:00 a.m. Thursday
Potomac Ballroom A/B
Dr. Jeffrey Siracuse will report on the study he and his colleagues performed to analyze practice patterns and outcomes from endovascular treatment of the common femoral (CFA) and deep femoral arteries (DFA). The Vascular Quality Initiative (2010-2015) was queried for all endovascular interventions on the CFA and DFA. They identified 3,960 endovascular CFA/DFA interventions; 1296 (nearly 33%) were isolated to the CFA/DFA. The average age of this isolated cohort was 68 years and 59% were men.
Indications for treatment were claudication (62%), rest pain (18%), and tissue loss (19%). Stents and atherectomy were used in about 28% and 18% of cases, respectively. The intervention was a technical success in nearly 92% of cases.
Perioperative complications included embolization, perforation, access hematoma, and dissection.
They found that thirty-day mortality was 1.6%, with survival of 93% and 87% at 1 and 3 years.
Dr. Siracuse, from the Boston University School of Medicine, will detail their results showing that the significant predictors of mortality were end-stage renal disease (hazard ratio [HR], 3.21, tissue loss, HR, 2.59), combined CFA/DFA intervention (HR, 1.88), chronic obstructive pulmonary disease (HR, 1.73), and nonambulatory status (HR, 1.61).
Freedom from loss of patency/death was 83% at 1 year, according to the researchers. Predictors of patency loss/death were tissue loss (HR, 2.67) and nonambulatory status (HR, 2.17). Freedom from reintervention/death was 83%. Signficant predictors of reintervention or death were tissue loss (HR, 3.52),and stenting (HR, 1.73); with P2Y12 antagonists (HR, 0.62) being signficantly protective.
Amputation-free survival at 1 year was 92%. Significant predictors of amputation/death were tissue loss (HR, 18.9), rest pain (HR, 5.47), previous major amputation (HR, 4.02), and stenting (HR, 2.83), with aspirin use (HR, 0.42) and P2Y12 antagonists (HR, 0.25) being protective.
“Endovascular interventions of the CFA/DFA have a low rate of perioperative morbidity and mortality. One-year patency is lower than historical controls of CFA endarterectomy. Stent use is associated with reinterventions and amputation and should be avoided if possible. Longer-term analysis is needed to better assess durability,” Dr. Siracuse concluded.
VON LIEBIG FORUM
8:30 – 10:00 a.m. Thursday
Potomac Ballroom A/B
How Does DMT Initiation Affect Health Care Costs?
NATIONAL HARBOR, MD—Total health care costs increase following initiation of a disease-modifying therapy for multiple sclerosis (MS), but a subsequent overall decrease in health care resource utilization may partially offset the increased costs, according to data presented at the 2016 CMSC Annual Meeting. Upon initiation of disease-modifying therapy, total health care costs increase by $38,561 for patients receiving dimethyl fumarate and by $53,626 for patients receiving fingolimod.
There are limited real-world data on comparative health care resource utilization and costs associated with disease-modifying therapy use in routine clinical practice. Researchers decided to further investigate the effect of the initiation of disease-modifying therapy (ie, dimethyl fumarate, interferon β, glatiramer acetate, teriflunomide, or fingolimod) on health care resource utilization. Jacqueline Nicholas, MD, MPH, a neuroimmunologist at OhioHealth in Columbus, and her colleagues conducted this study.
Researchers used data collected between January 2012 and December 2014 from the Truven MarketScan Commercial Claims Databases, which included administrative claims and eligibility records of 80 million commercially insured people from the United States. Demographic information included age at index date, sex, type of health plan, and region of residence. The mean patient age was 43.2 for patients who initiated glatiramer acetate and 48.6 for patients who initiated teriflunomide. Between 76.9% and 84.1% of patients were female.

Jacqueline Nicholas, MD, MPH
Patients with MS who initiated a disease-modifying therapy in 2013 were analyzed. The index date was defined as the first claim for the disease-modifying therapy. Only patients with no disease-modifying therapy exposure in the year before the index date were included in this study. Researchers evaluated baseline clinical characteristics based on claims dated within one year before the index date and included chronic disease burden (measured using Charlson Comorbidity Index and MS-related symptoms).
Health care resource utilization was defined as the proportion of patients who were hospitalized or who had visited the emergency room during one year before and one year after the index date. Total health care costs were estimated for one year before and one year after the index date. Costs of prescriptions were not included, and costs were adjusted to the 2014 values based on the Consumer Price Index Medical Component.
There was a significant increase in health care costs in the post-index period for all disease-modifying therapies. Patients receiving dimethyl fumarate had a lower increase in their health care costs, compared with patients receiving interferon β, glatiramer acetate, or fingolimod. Following the initiation of disease-modifying therapy, medical costs decreased significantly among patients receiving dimethyl fumarate or interferon β.
Medical cost reductions (excluding prescription medicine costs) were highly dependent on a decreased use of outpatient services and hospital stays, which suggests that the increased costs of disease-modifying therapies are partially offset by reduced health resource utilization and costs.
One limitation of this study was that it focused on health resource utilization and costs only one year before and one year after initiation of disease-modifying therapy. Researchers recommend that future studies assess outcomes over a longer period of time. In addition, the claims data were not collected specifically for clinical research and did not provide the clinical information needed to assess disease severity.
This study was supported by Biogen.
—Erica Robinson
NATIONAL HARBOR, MD—Total health care costs increase following initiation of a disease-modifying therapy for multiple sclerosis (MS), but a subsequent overall decrease in health care resource utilization may partially offset the increased costs, according to data presented at the 2016 CMSC Annual Meeting. Upon initiation of disease-modifying therapy, total health care costs increase by $38,561 for patients receiving dimethyl fumarate and by $53,626 for patients receiving fingolimod.
There are limited real-world data on comparative health care resource utilization and costs associated with disease-modifying therapy use in routine clinical practice. Researchers decided to further investigate the effect of the initiation of disease-modifying therapy (ie, dimethyl fumarate, interferon β, glatiramer acetate, teriflunomide, or fingolimod) on health care resource utilization. Jacqueline Nicholas, MD, MPH, a neuroimmunologist at OhioHealth in Columbus, and her colleagues conducted this study.
Researchers used data collected between January 2012 and December 2014 from the Truven MarketScan Commercial Claims Databases, which included administrative claims and eligibility records of 80 million commercially insured people from the United States. Demographic information included age at index date, sex, type of health plan, and region of residence. The mean patient age was 43.2 for patients who initiated glatiramer acetate and 48.6 for patients who initiated teriflunomide. Between 76.9% and 84.1% of patients were female.
Jacqueline Nicholas, MD, MPH
Patients with MS who initiated a disease-modifying therapy in 2013 were analyzed. The index date was defined as the first claim for the disease-modifying therapy. Only patients with no disease-modifying therapy exposure in the year before the index date were included in this study. Researchers evaluated baseline clinical characteristics based on claims dated within one year before the index date and included chronic disease burden (measured using Charlson Comorbidity Index and MS-related symptoms).
Health care resource utilization was defined as the proportion of patients who were hospitalized or who had visited the emergency room during one year before and one year after the index date. Total health care costs were estimated for one year before and one year after the index date. Costs of prescriptions were not included, and costs were adjusted to the 2014 values based on the Consumer Price Index Medical Component.
There was a significant increase in health care costs in the post-index period for all disease-modifying therapies. Patients receiving dimethyl fumarate had a lower increase in their health care costs, compared with patients receiving interferon β, glatiramer acetate, or fingolimod. Following the initiation of disease-modifying therapy, medical costs decreased significantly among patients receiving dimethyl fumarate or interferon β.
Medical cost reductions (excluding prescription medicine costs) were highly dependent on a decreased use of outpatient services and hospital stays, which suggests that the increased costs of disease-modifying therapies are partially offset by reduced health resource utilization and costs.
One limitation of this study was that it focused on health resource utilization and costs only one year before and one year after initiation of disease-modifying therapy. Researchers recommend that future studies assess outcomes over a longer period of time. In addition, the claims data were not collected specifically for clinical research and did not provide the clinical information needed to assess disease severity.
This study was supported by Biogen.
—Erica Robinson
NATIONAL HARBOR, MD—Total health care costs increase following initiation of a disease-modifying therapy for multiple sclerosis (MS), but a subsequent overall decrease in health care resource utilization may partially offset the increased costs, according to data presented at the 2016 CMSC Annual Meeting. Upon initiation of disease-modifying therapy, total health care costs increase by $38,561 for patients receiving dimethyl fumarate and by $53,626 for patients receiving fingolimod.
There are limited real-world data on comparative health care resource utilization and costs associated with disease-modifying therapy use in routine clinical practice. Researchers decided to further investigate the effect of the initiation of disease-modifying therapy (ie, dimethyl fumarate, interferon β, glatiramer acetate, teriflunomide, or fingolimod) on health care resource utilization. Jacqueline Nicholas, MD, MPH, a neuroimmunologist at OhioHealth in Columbus, and her colleagues conducted this study.
Researchers used data collected between January 2012 and December 2014 from the Truven MarketScan Commercial Claims Databases, which included administrative claims and eligibility records of 80 million commercially insured people from the United States. Demographic information included age at index date, sex, type of health plan, and region of residence. The mean patient age was 43.2 for patients who initiated glatiramer acetate and 48.6 for patients who initiated teriflunomide. Between 76.9% and 84.1% of patients were female.
Jacqueline Nicholas, MD, MPH
Patients with MS who initiated a disease-modifying therapy in 2013 were analyzed. The index date was defined as the first claim for the disease-modifying therapy. Only patients with no disease-modifying therapy exposure in the year before the index date were included in this study. Researchers evaluated baseline clinical characteristics based on claims dated within one year before the index date and included chronic disease burden (measured using Charlson Comorbidity Index and MS-related symptoms).
Health care resource utilization was defined as the proportion of patients who were hospitalized or who had visited the emergency room during one year before and one year after the index date. Total health care costs were estimated for one year before and one year after the index date. Costs of prescriptions were not included, and costs were adjusted to the 2014 values based on the Consumer Price Index Medical Component.
There was a significant increase in health care costs in the post-index period for all disease-modifying therapies. Patients receiving dimethyl fumarate had a lower increase in their health care costs, compared with patients receiving interferon β, glatiramer acetate, or fingolimod. Following the initiation of disease-modifying therapy, medical costs decreased significantly among patients receiving dimethyl fumarate or interferon β.
Medical cost reductions (excluding prescription medicine costs) were highly dependent on a decreased use of outpatient services and hospital stays, which suggests that the increased costs of disease-modifying therapies are partially offset by reduced health resource utilization and costs.
One limitation of this study was that it focused on health resource utilization and costs only one year before and one year after initiation of disease-modifying therapy. Researchers recommend that future studies assess outcomes over a longer period of time. In addition, the claims data were not collected specifically for clinical research and did not provide the clinical information needed to assess disease severity.
This study was supported by Biogen.
—Erica Robinson
