User login
CMS seeks input on future of Open Payments program
The Centers for Medicare & Medicaid Services is seeking physician input on the Open Payments program.
The agency signaled its intent to gather information in its proposed Medicare Physician Fee Schedule for 2017 and will host a conference call for that purpose on August 2.

The agency already has released a slide presentation to be used during the call that highlights the information being requested, including whether the payment categories are inclusive enough; how many years of payment data is relevant; whether reporting entities should pre-vet data before reporting to the Open Payment system; the adequacy of the definition of a covered recipient teaching hospital; whether reporting entities should be able to submit data continuously throughout the calendar year; how mergers affect reporting; clarity on reporting of ownership and investment interests; clarity on the definition of physician-owned distributors; and clarity on ways to streamline the reporting process.
Details for participating in the conference call can be found here.
The Centers for Medicare & Medicaid Services is seeking physician input on the Open Payments program.
The agency signaled its intent to gather information in its proposed Medicare Physician Fee Schedule for 2017 and will host a conference call for that purpose on August 2.
The agency already has released a slide presentation to be used during the call that highlights the information being requested, including whether the payment categories are inclusive enough; how many years of payment data is relevant; whether reporting entities should pre-vet data before reporting to the Open Payment system; the adequacy of the definition of a covered recipient teaching hospital; whether reporting entities should be able to submit data continuously throughout the calendar year; how mergers affect reporting; clarity on reporting of ownership and investment interests; clarity on the definition of physician-owned distributors; and clarity on ways to streamline the reporting process.
Details for participating in the conference call can be found here.
The Centers for Medicare & Medicaid Services is seeking physician input on the Open Payments program.
The agency signaled its intent to gather information in its proposed Medicare Physician Fee Schedule for 2017 and will host a conference call for that purpose on August 2.
The agency already has released a slide presentation to be used during the call that highlights the information being requested, including whether the payment categories are inclusive enough; how many years of payment data is relevant; whether reporting entities should pre-vet data before reporting to the Open Payment system; the adequacy of the definition of a covered recipient teaching hospital; whether reporting entities should be able to submit data continuously throughout the calendar year; how mergers affect reporting; clarity on reporting of ownership and investment interests; clarity on the definition of physician-owned distributors; and clarity on ways to streamline the reporting process.
Details for participating in the conference call can be found here.

CDC reports three new cases of Zika-related birth defects
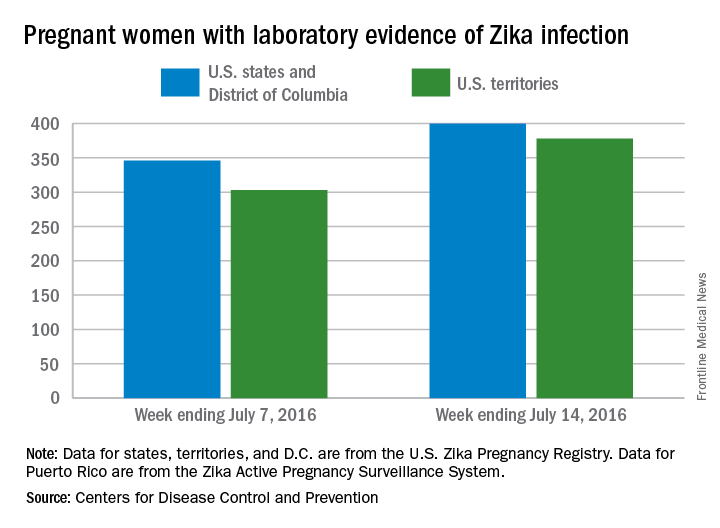
Three new cases of infants born with Zika virus–related birth defects were reported in the United States for the week ending July 14, 2016, along with 129 new infections in pregnant women, according to the Centers for Disease Control and Prevention.
The three infants were born in the 50 states and the District of Columbia, with no new pregnancy losses reported in the states or U.S. territories. Totals for the year are 12 infants with birth defects, all in the states, and seven pregnancy losses, of which six occurred in the states, the CDC reported July 21. State- or territorial-level data are not being reported to protect the privacy of affected women and children.
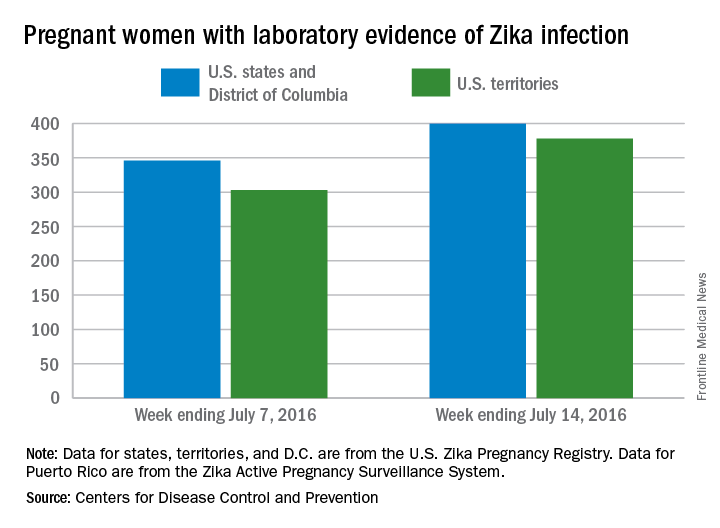
Of the 129 new infections in pregnant women for the week, 54 occurred in the states and 75 occurred in the U.S. territories. Those new cases bring the U.S. total to 778 for the year: 400 in the states and 378 in territories, the CDC also reported on July 21.
The figures for states, territories, and the District of Columbia reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Three new cases of infants born with Zika virus–related birth defects were reported in the United States for the week ending July 14, 2016, along with 129 new infections in pregnant women, according to the Centers for Disease Control and Prevention.
The three infants were born in the 50 states and the District of Columbia, with no new pregnancy losses reported in the states or U.S. territories. Totals for the year are 12 infants with birth defects, all in the states, and seven pregnancy losses, of which six occurred in the states, the CDC reported July 21. State- or territorial-level data are not being reported to protect the privacy of affected women and children.
Of the 129 new infections in pregnant women for the week, 54 occurred in the states and 75 occurred in the U.S. territories. Those new cases bring the U.S. total to 778 for the year: 400 in the states and 378 in territories, the CDC also reported on July 21.
The figures for states, territories, and the District of Columbia reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Three new cases of infants born with Zika virus–related birth defects were reported in the United States for the week ending July 14, 2016, along with 129 new infections in pregnant women, according to the Centers for Disease Control and Prevention.
The three infants were born in the 50 states and the District of Columbia, with no new pregnancy losses reported in the states or U.S. territories. Totals for the year are 12 infants with birth defects, all in the states, and seven pregnancy losses, of which six occurred in the states, the CDC reported July 21. State- or territorial-level data are not being reported to protect the privacy of affected women and children.
Of the 129 new infections in pregnant women for the week, 54 occurred in the states and 75 occurred in the U.S. territories. Those new cases bring the U.S. total to 778 for the year: 400 in the states and 378 in territories, the CDC also reported on July 21.
The figures for states, territories, and the District of Columbia reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika-related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Intermediate alleles may confer mild, late-onset Huntington-like symptoms
Asymptomatic people who carry an intermediate number (27-35) of CAG repeats on the huntingtin gene – that is, the range just below the Huntington’s disease threshold of 36 CAG repeats – may be at increased risk for mild, late-onset symptoms, according to the first report to definitely associate intermediate alleles with such symptoms.
The prevalence of this distinct category of alleles for the huntingtin (HTT) gene, termed IA (for intermediate alleles), ranges from 1.5% to 5.8% both in the general population and in affected families. The clinical manifestations of Huntington’s disease associated with IAs have remain hidden until now in part because asymptomatic family members often decline to undergo genetic testing for the disorder and so are not identified as having IAs. Emerging evidence suggests that some people with IAs are more likely than those with a smaller number of CAG repeats to develop Huntington-like neuropathologic effects, but the data are sparse, and the question is controversial, said Esther Cubo, MD, PhD, of the department of neurology, Hospital Universitario Burgos (Spain) and her associates on behalf of the European Huntington’s Disease Network (Neurology. 2016 Jul 8. doi: 10.1212/WNL.0000000000002944).
To examine this issue in a large cohort of at-risk individuals, the investigators assessed clinical and sociodemographic factors for 657 people enrolled in the European Huntington’s Disease Registry, which tracks the natural course of the disease in patients and family members treated in 1998 through 2014 at 140 medical centers in 17 European and 3 other countries. They focused on individuals who were asymptomatic at baseline: 76 (11.6%) men and women who had IAs (cases) and 581 (88.4%) who had fewer than 27 CAG repeats (controls). The two groups were similar in age, body mass index, educational background, socioeconomic status, tobacco and alcohol use, and medication use, and they scored similarly on measures of health-related quality of life, functional capacity, and the Unified Huntington’s Disease Rating Scale (UHDRS) for motor, behavioral, and cognitive status.
IA status was not associated with any significant differences between cases and controls who were younger than age 60. However, after age 60, participants with IAs had higher median total UHDRS motor scores (13.0 vs. 2.0) and were more likely to show mild gait abnormalities, chorea, and bradykinesia. In the small subgroup of patients who were followed longitudinally for up to 2 years, those with IAs showed faster cognitive decline over time; however, longer follow-up of larger groups of participants is needed to confirm this trend, the investigators said.
In addition, study participants with IAs reported lower quality of life and a greater degree of apathy than those without IAs, but these differences did not reach statistical significance. Whether apathy and poor quality of life reflect Huntington’s disease or simply correlate with normal aging could not be determined.
This study was limited by the relatively small number of participants with IAs, but the findings suggest that IAs “could produce a mild phenotype” of Huntington’s disease in some carriers after age 60. Alternatively, “clinical manifestations of Huntington’s disease in patents with IA might also be potentially accelerated by medical conditions, treatments, and environmental factors” associated with normal aging, Dr. Cubo and her associates added.
This study was supported by the European Huntington’s Disease Registry. Dr. Cubo reported receiving consulting fees from UCB, Allergan, and AbbVie.
These findings are limited by the study’s small cohort size and short follow-up, but they suggest that younger IA carriers will develop few if any signs of Huntington’s disease while older IA carriers may develop a very mild phenotype late in life.
Young IA carriers and carriers who have a low number of CAG repeats (fewer than 27) on the longer allele have “not too much to worry about.” Older IA carriers may develop some mild motor symptoms and a slightly faster cognitive decline as they age. All carriers should remain as fit and healthy as possible, as they have always been advised, and should look to their family members’ experiences as a good yardstick of what might happen to them.
Patrick J. Morrison, MD, DSc, is in the department of genetic medicine at Belfast HSC Trust and the Centre for Cancer Research and Cell Biology at Queens University of Belfast (Northern Ireland). Julián Benito-León, MD, PhD, is in the department of neurology at University Hospital “12 de Octubre” and in the department of medicine at Complutense University, both in Madrid. They reported no targeted funding for this work. Dr. Morrison and Dr. Benito-León made these remarks in an editorial accompanying Dr. Cubo’s report (Neurology. 2016 Jul 8. doi: 10.1212/WNL.0000000000002958).
These findings are limited by the study’s small cohort size and short follow-up, but they suggest that younger IA carriers will develop few if any signs of Huntington’s disease while older IA carriers may develop a very mild phenotype late in life.
Young IA carriers and carriers who have a low number of CAG repeats (fewer than 27) on the longer allele have “not too much to worry about.” Older IA carriers may develop some mild motor symptoms and a slightly faster cognitive decline as they age. All carriers should remain as fit and healthy as possible, as they have always been advised, and should look to their family members’ experiences as a good yardstick of what might happen to them.
Patrick J. Morrison, MD, DSc, is in the department of genetic medicine at Belfast HSC Trust and the Centre for Cancer Research and Cell Biology at Queens University of Belfast (Northern Ireland). Julián Benito-León, MD, PhD, is in the department of neurology at University Hospital “12 de Octubre” and in the department of medicine at Complutense University, both in Madrid. They reported no targeted funding for this work. Dr. Morrison and Dr. Benito-León made these remarks in an editorial accompanying Dr. Cubo’s report (Neurology. 2016 Jul 8. doi: 10.1212/WNL.0000000000002958).
These findings are limited by the study’s small cohort size and short follow-up, but they suggest that younger IA carriers will develop few if any signs of Huntington’s disease while older IA carriers may develop a very mild phenotype late in life.
Young IA carriers and carriers who have a low number of CAG repeats (fewer than 27) on the longer allele have “not too much to worry about.” Older IA carriers may develop some mild motor symptoms and a slightly faster cognitive decline as they age. All carriers should remain as fit and healthy as possible, as they have always been advised, and should look to their family members’ experiences as a good yardstick of what might happen to them.
Patrick J. Morrison, MD, DSc, is in the department of genetic medicine at Belfast HSC Trust and the Centre for Cancer Research and Cell Biology at Queens University of Belfast (Northern Ireland). Julián Benito-León, MD, PhD, is in the department of neurology at University Hospital “12 de Octubre” and in the department of medicine at Complutense University, both in Madrid. They reported no targeted funding for this work. Dr. Morrison and Dr. Benito-León made these remarks in an editorial accompanying Dr. Cubo’s report (Neurology. 2016 Jul 8. doi: 10.1212/WNL.0000000000002958).
Asymptomatic people who carry an intermediate number (27-35) of CAG repeats on the huntingtin gene – that is, the range just below the Huntington’s disease threshold of 36 CAG repeats – may be at increased risk for mild, late-onset symptoms, according to the first report to definitely associate intermediate alleles with such symptoms.
The prevalence of this distinct category of alleles for the huntingtin (HTT) gene, termed IA (for intermediate alleles), ranges from 1.5% to 5.8% both in the general population and in affected families. The clinical manifestations of Huntington’s disease associated with IAs have remain hidden until now in part because asymptomatic family members often decline to undergo genetic testing for the disorder and so are not identified as having IAs. Emerging evidence suggests that some people with IAs are more likely than those with a smaller number of CAG repeats to develop Huntington-like neuropathologic effects, but the data are sparse, and the question is controversial, said Esther Cubo, MD, PhD, of the department of neurology, Hospital Universitario Burgos (Spain) and her associates on behalf of the European Huntington’s Disease Network (Neurology. 2016 Jul 8. doi: 10.1212/WNL.0000000000002944).
To examine this issue in a large cohort of at-risk individuals, the investigators assessed clinical and sociodemographic factors for 657 people enrolled in the European Huntington’s Disease Registry, which tracks the natural course of the disease in patients and family members treated in 1998 through 2014 at 140 medical centers in 17 European and 3 other countries. They focused on individuals who were asymptomatic at baseline: 76 (11.6%) men and women who had IAs (cases) and 581 (88.4%) who had fewer than 27 CAG repeats (controls). The two groups were similar in age, body mass index, educational background, socioeconomic status, tobacco and alcohol use, and medication use, and they scored similarly on measures of health-related quality of life, functional capacity, and the Unified Huntington’s Disease Rating Scale (UHDRS) for motor, behavioral, and cognitive status.
IA status was not associated with any significant differences between cases and controls who were younger than age 60. However, after age 60, participants with IAs had higher median total UHDRS motor scores (13.0 vs. 2.0) and were more likely to show mild gait abnormalities, chorea, and bradykinesia. In the small subgroup of patients who were followed longitudinally for up to 2 years, those with IAs showed faster cognitive decline over time; however, longer follow-up of larger groups of participants is needed to confirm this trend, the investigators said.
In addition, study participants with IAs reported lower quality of life and a greater degree of apathy than those without IAs, but these differences did not reach statistical significance. Whether apathy and poor quality of life reflect Huntington’s disease or simply correlate with normal aging could not be determined.
This study was limited by the relatively small number of participants with IAs, but the findings suggest that IAs “could produce a mild phenotype” of Huntington’s disease in some carriers after age 60. Alternatively, “clinical manifestations of Huntington’s disease in patents with IA might also be potentially accelerated by medical conditions, treatments, and environmental factors” associated with normal aging, Dr. Cubo and her associates added.
This study was supported by the European Huntington’s Disease Registry. Dr. Cubo reported receiving consulting fees from UCB, Allergan, and AbbVie.
Asymptomatic people who carry an intermediate number (27-35) of CAG repeats on the huntingtin gene – that is, the range just below the Huntington’s disease threshold of 36 CAG repeats – may be at increased risk for mild, late-onset symptoms, according to the first report to definitely associate intermediate alleles with such symptoms.
The prevalence of this distinct category of alleles for the huntingtin (HTT) gene, termed IA (for intermediate alleles), ranges from 1.5% to 5.8% both in the general population and in affected families. The clinical manifestations of Huntington’s disease associated with IAs have remain hidden until now in part because asymptomatic family members often decline to undergo genetic testing for the disorder and so are not identified as having IAs. Emerging evidence suggests that some people with IAs are more likely than those with a smaller number of CAG repeats to develop Huntington-like neuropathologic effects, but the data are sparse, and the question is controversial, said Esther Cubo, MD, PhD, of the department of neurology, Hospital Universitario Burgos (Spain) and her associates on behalf of the European Huntington’s Disease Network (Neurology. 2016 Jul 8. doi: 10.1212/WNL.0000000000002944).
To examine this issue in a large cohort of at-risk individuals, the investigators assessed clinical and sociodemographic factors for 657 people enrolled in the European Huntington’s Disease Registry, which tracks the natural course of the disease in patients and family members treated in 1998 through 2014 at 140 medical centers in 17 European and 3 other countries. They focused on individuals who were asymptomatic at baseline: 76 (11.6%) men and women who had IAs (cases) and 581 (88.4%) who had fewer than 27 CAG repeats (controls). The two groups were similar in age, body mass index, educational background, socioeconomic status, tobacco and alcohol use, and medication use, and they scored similarly on measures of health-related quality of life, functional capacity, and the Unified Huntington’s Disease Rating Scale (UHDRS) for motor, behavioral, and cognitive status.
IA status was not associated with any significant differences between cases and controls who were younger than age 60. However, after age 60, participants with IAs had higher median total UHDRS motor scores (13.0 vs. 2.0) and were more likely to show mild gait abnormalities, chorea, and bradykinesia. In the small subgroup of patients who were followed longitudinally for up to 2 years, those with IAs showed faster cognitive decline over time; however, longer follow-up of larger groups of participants is needed to confirm this trend, the investigators said.
In addition, study participants with IAs reported lower quality of life and a greater degree of apathy than those without IAs, but these differences did not reach statistical significance. Whether apathy and poor quality of life reflect Huntington’s disease or simply correlate with normal aging could not be determined.
This study was limited by the relatively small number of participants with IAs, but the findings suggest that IAs “could produce a mild phenotype” of Huntington’s disease in some carriers after age 60. Alternatively, “clinical manifestations of Huntington’s disease in patents with IA might also be potentially accelerated by medical conditions, treatments, and environmental factors” associated with normal aging, Dr. Cubo and her associates added.
This study was supported by the European Huntington’s Disease Registry. Dr. Cubo reported receiving consulting fees from UCB, Allergan, and AbbVie.
FROM NEUROLOGY
Key clinical point: Asymptomatic people who carry an intermediate number (27-35) of CAG repeats on the huntingtin gene may be at increased risk for mild symptoms after age 60.
Major finding: After age 60, people with intermediate alleles had higher median UHDRS motor scores (13.0) than did people with fewer CAG repeats (2.0).
Data source: A retrospective, international, observational study involving 76 asymptomatic adults with 27-35 CAG repeats and 581 with fewer than 27 CAG repeats.
Disclosures: This study was supported by the European Huntington’s Disease Registry. Dr. Cubo reported receiving consulting fees from UCB, Allergan, and AbbVie.
Feds sue to block mega-mergers by health insurers
The U.S. Department of Justice (DOJ) is suing to block two mega-mergers between four of the largest health insurers in the nation, claiming the alignments will harm competition and reduce patient choice.
The DOJ and a number of state attorneys general filed legal challenges July 21 in the U.S. District Court for the District of Columbia seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the two mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers, by limiting price competition, reducing benefits, decreasing incentives to provide innovative wellness programs, and lowering quality of care.

“These mergers would restrict competition for health insurance products sold in markets across the country and would give tremendous power over the nation’s health insurance industry to just three large companies,” U.S. Attorney General Loretta E. Lynch said in a statement. “Our actions seek to preserve competition that keeps premiums down and drives insurers to collaborate with doctors and hospitals to provide better health care for all Americans.”
Anthem called the lawsuit “an unfortunate and misguided step backward for access to affordable health care.
“The DOJ’s action is based on a flawed analysis and misunderstanding of the dynamic, competitive, and highly regulated health care landscape and is inconsistent with the way that the DOJ has reviewed past health care transactions,” Anthem officials said in a statement. “Anthem has an unwavering commitment to enhancing access to affordable health care, and the benefits and efficiencies from its merger with Cigna is one way that Anthem will continue its mission of improving consumer choice, quality, and affordability.”
In a statement, Cigna officials said that company is evaluating its options given the nature of the concerns raised by the DOJ. Aetna and Humana meanwhile, vowed to vigorously defend their pending merger.
“A combined company will result in a broader choice of products, access to higher quality, and more affordable care, and a better overall experience for consumers,” according to a joint statement. “Aetna and Humana look forward to making this clear in court, where a judge will review the transaction based on its merits.”
Anthem’s proposed acquisition of Cigna would be the largest merger in the history of the health insurance industry, according to the DOJ. The companies began talks of a possible merger in early 2014 and Anthem agreed to acquire Cigna for $54 billion in 2015, according to court documents.
Meanwhile, Aetna began inquiring about a deal with Humana in March 2015, entering into a definitive agreement to acquire Humana for $37 billion later that year. The two proposed mergers have been closely watched by the DOJ and other regulatory agencies from the start.
The DOJ’s suit against Anthem and Cigna alleges the merger would substantially reduce competition for millions of patients who receive commercial health insurance coverage, from large-group employers in at least 35 metropolitan areas and from public exchanges created by the Affordable Care Act. The elimination of Cigna also threatens competition among commercial insurers for the purchase of health care services from hospitals, physicians, and other providers, the suit alleges. Eleven states and the District of Columbia joined the department’s challenge of the Cigna acquisition.
The government’s challenge against Aetna and Humana alleges the merger would greatly reduce Medicare Advantage competition in more than 350 counties in 21 states, affecting more than 1.5 million Medicare Advantage patients. The lawsuit also claims that Aetna’s purchase of Humana would substantially reduce competition to sell commercial health insurance to individuals and families on the public exchanges in 17 counties in Florida, Georgia, and Missouri. Eight states and the District of Columbia joined the department’s challenge of the Humana acquisition.
The American Medical Association voiced support for the lawsuit, condemning the proposed transactions as moves that will lessen competition and choice. In 2015, AMA issued special analyses showing that the combined impact of the proposed Anthem/Cigna and Aetna/Humana mergers and urged the federal government to block the transactions.

“The prospect of reducing five national health insurance carriers to just three is unacceptable,” AMA President Andrew W. Gurman, MD, said in a statement. “[The] action by the DOJ acknowledges the AMA’s concern that patients’ interests can be harmed when big insurers acquire rivals and develop strangleholds on local markets. Allowing commercial health insurers to become too big and exert control over the delivery of health care would be bad for patients and vitality of the nation’s health care system.”
On Twitter @legal_med
The U.S. Department of Justice (DOJ) is suing to block two mega-mergers between four of the largest health insurers in the nation, claiming the alignments will harm competition and reduce patient choice.
The DOJ and a number of state attorneys general filed legal challenges July 21 in the U.S. District Court for the District of Columbia seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the two mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers, by limiting price competition, reducing benefits, decreasing incentives to provide innovative wellness programs, and lowering quality of care.
“These mergers would restrict competition for health insurance products sold in markets across the country and would give tremendous power over the nation’s health insurance industry to just three large companies,” U.S. Attorney General Loretta E. Lynch said in a statement. “Our actions seek to preserve competition that keeps premiums down and drives insurers to collaborate with doctors and hospitals to provide better health care for all Americans.”
Anthem called the lawsuit “an unfortunate and misguided step backward for access to affordable health care.
“The DOJ’s action is based on a flawed analysis and misunderstanding of the dynamic, competitive, and highly regulated health care landscape and is inconsistent with the way that the DOJ has reviewed past health care transactions,” Anthem officials said in a statement. “Anthem has an unwavering commitment to enhancing access to affordable health care, and the benefits and efficiencies from its merger with Cigna is one way that Anthem will continue its mission of improving consumer choice, quality, and affordability.”
In a statement, Cigna officials said that company is evaluating its options given the nature of the concerns raised by the DOJ. Aetna and Humana meanwhile, vowed to vigorously defend their pending merger.
“A combined company will result in a broader choice of products, access to higher quality, and more affordable care, and a better overall experience for consumers,” according to a joint statement. “Aetna and Humana look forward to making this clear in court, where a judge will review the transaction based on its merits.”
Anthem’s proposed acquisition of Cigna would be the largest merger in the history of the health insurance industry, according to the DOJ. The companies began talks of a possible merger in early 2014 and Anthem agreed to acquire Cigna for $54 billion in 2015, according to court documents.
Meanwhile, Aetna began inquiring about a deal with Humana in March 2015, entering into a definitive agreement to acquire Humana for $37 billion later that year. The two proposed mergers have been closely watched by the DOJ and other regulatory agencies from the start.
The DOJ’s suit against Anthem and Cigna alleges the merger would substantially reduce competition for millions of patients who receive commercial health insurance coverage, from large-group employers in at least 35 metropolitan areas and from public exchanges created by the Affordable Care Act. The elimination of Cigna also threatens competition among commercial insurers for the purchase of health care services from hospitals, physicians, and other providers, the suit alleges. Eleven states and the District of Columbia joined the department’s challenge of the Cigna acquisition.
The government’s challenge against Aetna and Humana alleges the merger would greatly reduce Medicare Advantage competition in more than 350 counties in 21 states, affecting more than 1.5 million Medicare Advantage patients. The lawsuit also claims that Aetna’s purchase of Humana would substantially reduce competition to sell commercial health insurance to individuals and families on the public exchanges in 17 counties in Florida, Georgia, and Missouri. Eight states and the District of Columbia joined the department’s challenge of the Humana acquisition.
The American Medical Association voiced support for the lawsuit, condemning the proposed transactions as moves that will lessen competition and choice. In 2015, AMA issued special analyses showing that the combined impact of the proposed Anthem/Cigna and Aetna/Humana mergers and urged the federal government to block the transactions.
“The prospect of reducing five national health insurance carriers to just three is unacceptable,” AMA President Andrew W. Gurman, MD, said in a statement. “[The] action by the DOJ acknowledges the AMA’s concern that patients’ interests can be harmed when big insurers acquire rivals and develop strangleholds on local markets. Allowing commercial health insurers to become too big and exert control over the delivery of health care would be bad for patients and vitality of the nation’s health care system.”
On Twitter @legal_med
The U.S. Department of Justice (DOJ) is suing to block two mega-mergers between four of the largest health insurers in the nation, claiming the alignments will harm competition and reduce patient choice.
The DOJ and a number of state attorneys general filed legal challenges July 21 in the U.S. District Court for the District of Columbia seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the two mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers, by limiting price competition, reducing benefits, decreasing incentives to provide innovative wellness programs, and lowering quality of care.
“These mergers would restrict competition for health insurance products sold in markets across the country and would give tremendous power over the nation’s health insurance industry to just three large companies,” U.S. Attorney General Loretta E. Lynch said in a statement. “Our actions seek to preserve competition that keeps premiums down and drives insurers to collaborate with doctors and hospitals to provide better health care for all Americans.”
Anthem called the lawsuit “an unfortunate and misguided step backward for access to affordable health care.
“The DOJ’s action is based on a flawed analysis and misunderstanding of the dynamic, competitive, and highly regulated health care landscape and is inconsistent with the way that the DOJ has reviewed past health care transactions,” Anthem officials said in a statement. “Anthem has an unwavering commitment to enhancing access to affordable health care, and the benefits and efficiencies from its merger with Cigna is one way that Anthem will continue its mission of improving consumer choice, quality, and affordability.”
In a statement, Cigna officials said that company is evaluating its options given the nature of the concerns raised by the DOJ. Aetna and Humana meanwhile, vowed to vigorously defend their pending merger.
“A combined company will result in a broader choice of products, access to higher quality, and more affordable care, and a better overall experience for consumers,” according to a joint statement. “Aetna and Humana look forward to making this clear in court, where a judge will review the transaction based on its merits.”
Anthem’s proposed acquisition of Cigna would be the largest merger in the history of the health insurance industry, according to the DOJ. The companies began talks of a possible merger in early 2014 and Anthem agreed to acquire Cigna for $54 billion in 2015, according to court documents.
Meanwhile, Aetna began inquiring about a deal with Humana in March 2015, entering into a definitive agreement to acquire Humana for $37 billion later that year. The two proposed mergers have been closely watched by the DOJ and other regulatory agencies from the start.
The DOJ’s suit against Anthem and Cigna alleges the merger would substantially reduce competition for millions of patients who receive commercial health insurance coverage, from large-group employers in at least 35 metropolitan areas and from public exchanges created by the Affordable Care Act. The elimination of Cigna also threatens competition among commercial insurers for the purchase of health care services from hospitals, physicians, and other providers, the suit alleges. Eleven states and the District of Columbia joined the department’s challenge of the Cigna acquisition.
The government’s challenge against Aetna and Humana alleges the merger would greatly reduce Medicare Advantage competition in more than 350 counties in 21 states, affecting more than 1.5 million Medicare Advantage patients. The lawsuit also claims that Aetna’s purchase of Humana would substantially reduce competition to sell commercial health insurance to individuals and families on the public exchanges in 17 counties in Florida, Georgia, and Missouri. Eight states and the District of Columbia joined the department’s challenge of the Humana acquisition.
The American Medical Association voiced support for the lawsuit, condemning the proposed transactions as moves that will lessen competition and choice. In 2015, AMA issued special analyses showing that the combined impact of the proposed Anthem/Cigna and Aetna/Humana mergers and urged the federal government to block the transactions.
“The prospect of reducing five national health insurance carriers to just three is unacceptable,” AMA President Andrew W. Gurman, MD, said in a statement. “[The] action by the DOJ acknowledges the AMA’s concern that patients’ interests can be harmed when big insurers acquire rivals and develop strangleholds on local markets. Allowing commercial health insurers to become too big and exert control over the delivery of health care would be bad for patients and vitality of the nation’s health care system.”
On Twitter @legal_med

Benefits, challenges emerge in evolution of rheumatology-dermatology clinics
MIAMI – Combined rheumatology-dermatology clinics to help people with psoriasis, psoriatic arthritis, and other relevant overlapping conditions continue to evolve, with evidence suggesting advantages and challenges for both patients and physicians.
Physicians like the improved communication and greater collaboration but still have reservations about billing and scheduling, according to preliminary results of a survey conducted by the Psoriasis and Psoriatic Arthritis Clinic Multicenter Advancement Network (PPACMAN). For patients, the advantages go beyond convenience, according to a 1-year study of outcomes at a Rhode Island Hospital–Brown University combined clinic in Providence.
“The goal of the combined clinics survey is to gauge strengths, barriers, and challenges to creating these models, to learn from one another to improve current clinical care, and to support propagation of these models,” said Joseph F. Merola, MD, at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Multiple clinic models
The clinic setups differ. In those settings where rheumatologists and dermatologists see patients on the same day, approximately three-quarters provide care together in the same room. The remaining clinics see patients through serial visits. Another 30% of respondents said dermatologists and rheumatologists generally see patients in a combined clinic on different days.

“Rheumatologists said it is a satisfying and rewarding endeavor, they form closer ties with colleagues, and it allows early, improved communication,” said Dr. Merola, a rheumatologist and dermatologist who is co-director of the Center for Skin and Related Musculoskeletal Diseases, a combined clinic at Brigham and Women’s Hospital in Boston.
Some common benefits, each cited by more than 80% of respondents, include a prompt and accurate diagnosis of psoriatic arthritis, the ability of physicians to learn from each other, and multiple training opportunities for residents and fellows. In fact, 72% said their combined clinic has rheumatology fellows, 82% have dermatology residents, and 27% incorporate internal medicine trainees.
Other than rheumatologists and dermatologists, 31% said their clinic has dedicated nursing, 15% have a cardiologist, and 15% have a psychiatrist.
A majority of physicians (92%) said they bill through their own department. At a subsequent roundtable discussion, Dr. Merola noted that patients pay separate copays at the combined clinic. “We’ve had some complaints from patients. They don’t like having two copayments.”
“You have to tell patients in advance,” suggested Soumya M. Reddy, MD, a rheumatologist at NYU Langone Medical Center in New York and co-director of its Psoriasis and Psoriatic Arthritis Center.
Common conditions and challenges
Not surprisingly, psoriasis and psoriatic arthritis are the most common conditions treated in these clinics, followed by lupus and dermatomyositis. Most clinics see patients either once weekly or once monthly.
A major concern expressed by 75% surrounds scheduling. More than half, 58%, worry about demonstrating value to their institution. Only a minority, 17%, responded that achieving consensus on patient management is a challenge.
In general, rheumatology evaluations take more time than dermatology assessments, presenting a challenge for scheduling and maximizing physician time. “You don’t really want the dermatologist sitting there for 20 minutes not really doing a lot,” said Alison Ehrlich, MD, professor and chair of dermatology at George Washington University in Washington.
The solution at Brigham and Women’s Hospital is to staff the clinic with two dermatologists and one rheumatologist. The two dermatologists see about 20 patients each in a half-day; the rheumatologist probably treats about 6 to 8 of those 40 patients, Dr. Merola said. At George Washington, Dr. Ehrlich sees patients along with the rheumatologist, leaves the room to treat other patients, later consults with her colleague, and they go back in together as necessary.
“The patients are incredibly appreciative” of the combined clinic, Dr. Ehrlich said. “They really love it.”
The survey is ongoing. The preliminary responses above are based on 17 responses, a 52% response rate. Of the respondents, 10 are dermatologists, 6 are rheumatologists, and 1 is dual trained. Since the meeting, Dr. Merola indicated that another two dermatologists and three rheumatologists have responded to the survey.
The Brown University experience
Charis Gn, MD, and colleagues studied outcomes for 167 patients treated at a combined clinic at Rhode Island Hospital. The ultimate goal of the clinic is “to identify patients with psoriatic arthritis early on,” Dr. Gn said at a poster presentation at the GRAPPA annual meeting. “We wanted to see what kind of outcomes [we get] for patients who see rheumatology and dermatology.”
About one-third of patients left the clinic with changes in diagnosis. About 1 in 5 patients with psoriasis were diagnosed with psoriatic arthritis as well. For the psoriasis patients newly diagnosed with psoriatic arthritis, 80% had an escalation in treatment, said Dr. Gn, an internal medicine resident.
Of the 41 patients with psoriasis, 17 (41%) had a treatment escalation. The same was true for 15 (79%) of the 19 patients with psoriatic arthritis post-evaluation.
Regarding the combined clinic, “it’s shown to be very beneficial for patients with psoriatic arthritis,” Dr. Gn said.
The record review from July 2014 to February 2016 shows the clinic also serves patients with cutaneous lupus, dermatomyositis, pyoderma gangrenosum, vasculitis, and rheumatoid arthritis, among others.
The presenters had no relevant disclosures.
MIAMI – Combined rheumatology-dermatology clinics to help people with psoriasis, psoriatic arthritis, and other relevant overlapping conditions continue to evolve, with evidence suggesting advantages and challenges for both patients and physicians.
Physicians like the improved communication and greater collaboration but still have reservations about billing and scheduling, according to preliminary results of a survey conducted by the Psoriasis and Psoriatic Arthritis Clinic Multicenter Advancement Network (PPACMAN). For patients, the advantages go beyond convenience, according to a 1-year study of outcomes at a Rhode Island Hospital–Brown University combined clinic in Providence.
“The goal of the combined clinics survey is to gauge strengths, barriers, and challenges to creating these models, to learn from one another to improve current clinical care, and to support propagation of these models,” said Joseph F. Merola, MD, at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Multiple clinic models
The clinic setups differ. In those settings where rheumatologists and dermatologists see patients on the same day, approximately three-quarters provide care together in the same room. The remaining clinics see patients through serial visits. Another 30% of respondents said dermatologists and rheumatologists generally see patients in a combined clinic on different days.
“Rheumatologists said it is a satisfying and rewarding endeavor, they form closer ties with colleagues, and it allows early, improved communication,” said Dr. Merola, a rheumatologist and dermatologist who is co-director of the Center for Skin and Related Musculoskeletal Diseases, a combined clinic at Brigham and Women’s Hospital in Boston.
Some common benefits, each cited by more than 80% of respondents, include a prompt and accurate diagnosis of psoriatic arthritis, the ability of physicians to learn from each other, and multiple training opportunities for residents and fellows. In fact, 72% said their combined clinic has rheumatology fellows, 82% have dermatology residents, and 27% incorporate internal medicine trainees.
Other than rheumatologists and dermatologists, 31% said their clinic has dedicated nursing, 15% have a cardiologist, and 15% have a psychiatrist.
A majority of physicians (92%) said they bill through their own department. At a subsequent roundtable discussion, Dr. Merola noted that patients pay separate copays at the combined clinic. “We’ve had some complaints from patients. They don’t like having two copayments.”
“You have to tell patients in advance,” suggested Soumya M. Reddy, MD, a rheumatologist at NYU Langone Medical Center in New York and co-director of its Psoriasis and Psoriatic Arthritis Center.
Common conditions and challenges
Not surprisingly, psoriasis and psoriatic arthritis are the most common conditions treated in these clinics, followed by lupus and dermatomyositis. Most clinics see patients either once weekly or once monthly.
A major concern expressed by 75% surrounds scheduling. More than half, 58%, worry about demonstrating value to their institution. Only a minority, 17%, responded that achieving consensus on patient management is a challenge.
In general, rheumatology evaluations take more time than dermatology assessments, presenting a challenge for scheduling and maximizing physician time. “You don’t really want the dermatologist sitting there for 20 minutes not really doing a lot,” said Alison Ehrlich, MD, professor and chair of dermatology at George Washington University in Washington.
The solution at Brigham and Women’s Hospital is to staff the clinic with two dermatologists and one rheumatologist. The two dermatologists see about 20 patients each in a half-day; the rheumatologist probably treats about 6 to 8 of those 40 patients, Dr. Merola said. At George Washington, Dr. Ehrlich sees patients along with the rheumatologist, leaves the room to treat other patients, later consults with her colleague, and they go back in together as necessary.
“The patients are incredibly appreciative” of the combined clinic, Dr. Ehrlich said. “They really love it.”
The survey is ongoing. The preliminary responses above are based on 17 responses, a 52% response rate. Of the respondents, 10 are dermatologists, 6 are rheumatologists, and 1 is dual trained. Since the meeting, Dr. Merola indicated that another two dermatologists and three rheumatologists have responded to the survey.
The Brown University experience
Charis Gn, MD, and colleagues studied outcomes for 167 patients treated at a combined clinic at Rhode Island Hospital. The ultimate goal of the clinic is “to identify patients with psoriatic arthritis early on,” Dr. Gn said at a poster presentation at the GRAPPA annual meeting. “We wanted to see what kind of outcomes [we get] for patients who see rheumatology and dermatology.”
About one-third of patients left the clinic with changes in diagnosis. About 1 in 5 patients with psoriasis were diagnosed with psoriatic arthritis as well. For the psoriasis patients newly diagnosed with psoriatic arthritis, 80% had an escalation in treatment, said Dr. Gn, an internal medicine resident.
Of the 41 patients with psoriasis, 17 (41%) had a treatment escalation. The same was true for 15 (79%) of the 19 patients with psoriatic arthritis post-evaluation.
Regarding the combined clinic, “it’s shown to be very beneficial for patients with psoriatic arthritis,” Dr. Gn said.
The record review from July 2014 to February 2016 shows the clinic also serves patients with cutaneous lupus, dermatomyositis, pyoderma gangrenosum, vasculitis, and rheumatoid arthritis, among others.
The presenters had no relevant disclosures.
MIAMI – Combined rheumatology-dermatology clinics to help people with psoriasis, psoriatic arthritis, and other relevant overlapping conditions continue to evolve, with evidence suggesting advantages and challenges for both patients and physicians.
Physicians like the improved communication and greater collaboration but still have reservations about billing and scheduling, according to preliminary results of a survey conducted by the Psoriasis and Psoriatic Arthritis Clinic Multicenter Advancement Network (PPACMAN). For patients, the advantages go beyond convenience, according to a 1-year study of outcomes at a Rhode Island Hospital–Brown University combined clinic in Providence.
“The goal of the combined clinics survey is to gauge strengths, barriers, and challenges to creating these models, to learn from one another to improve current clinical care, and to support propagation of these models,” said Joseph F. Merola, MD, at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
Multiple clinic models
The clinic setups differ. In those settings where rheumatologists and dermatologists see patients on the same day, approximately three-quarters provide care together in the same room. The remaining clinics see patients through serial visits. Another 30% of respondents said dermatologists and rheumatologists generally see patients in a combined clinic on different days.
“Rheumatologists said it is a satisfying and rewarding endeavor, they form closer ties with colleagues, and it allows early, improved communication,” said Dr. Merola, a rheumatologist and dermatologist who is co-director of the Center for Skin and Related Musculoskeletal Diseases, a combined clinic at Brigham and Women’s Hospital in Boston.
Some common benefits, each cited by more than 80% of respondents, include a prompt and accurate diagnosis of psoriatic arthritis, the ability of physicians to learn from each other, and multiple training opportunities for residents and fellows. In fact, 72% said their combined clinic has rheumatology fellows, 82% have dermatology residents, and 27% incorporate internal medicine trainees.
Other than rheumatologists and dermatologists, 31% said their clinic has dedicated nursing, 15% have a cardiologist, and 15% have a psychiatrist.
A majority of physicians (92%) said they bill through their own department. At a subsequent roundtable discussion, Dr. Merola noted that patients pay separate copays at the combined clinic. “We’ve had some complaints from patients. They don’t like having two copayments.”
“You have to tell patients in advance,” suggested Soumya M. Reddy, MD, a rheumatologist at NYU Langone Medical Center in New York and co-director of its Psoriasis and Psoriatic Arthritis Center.
Common conditions and challenges
Not surprisingly, psoriasis and psoriatic arthritis are the most common conditions treated in these clinics, followed by lupus and dermatomyositis. Most clinics see patients either once weekly or once monthly.
A major concern expressed by 75% surrounds scheduling. More than half, 58%, worry about demonstrating value to their institution. Only a minority, 17%, responded that achieving consensus on patient management is a challenge.
In general, rheumatology evaluations take more time than dermatology assessments, presenting a challenge for scheduling and maximizing physician time. “You don’t really want the dermatologist sitting there for 20 minutes not really doing a lot,” said Alison Ehrlich, MD, professor and chair of dermatology at George Washington University in Washington.
The solution at Brigham and Women’s Hospital is to staff the clinic with two dermatologists and one rheumatologist. The two dermatologists see about 20 patients each in a half-day; the rheumatologist probably treats about 6 to 8 of those 40 patients, Dr. Merola said. At George Washington, Dr. Ehrlich sees patients along with the rheumatologist, leaves the room to treat other patients, later consults with her colleague, and they go back in together as necessary.
“The patients are incredibly appreciative” of the combined clinic, Dr. Ehrlich said. “They really love it.”
The survey is ongoing. The preliminary responses above are based on 17 responses, a 52% response rate. Of the respondents, 10 are dermatologists, 6 are rheumatologists, and 1 is dual trained. Since the meeting, Dr. Merola indicated that another two dermatologists and three rheumatologists have responded to the survey.
The Brown University experience
Charis Gn, MD, and colleagues studied outcomes for 167 patients treated at a combined clinic at Rhode Island Hospital. The ultimate goal of the clinic is “to identify patients with psoriatic arthritis early on,” Dr. Gn said at a poster presentation at the GRAPPA annual meeting. “We wanted to see what kind of outcomes [we get] for patients who see rheumatology and dermatology.”
About one-third of patients left the clinic with changes in diagnosis. About 1 in 5 patients with psoriasis were diagnosed with psoriatic arthritis as well. For the psoriasis patients newly diagnosed with psoriatic arthritis, 80% had an escalation in treatment, said Dr. Gn, an internal medicine resident.
Of the 41 patients with psoriasis, 17 (41%) had a treatment escalation. The same was true for 15 (79%) of the 19 patients with psoriatic arthritis post-evaluation.
Regarding the combined clinic, “it’s shown to be very beneficial for patients with psoriatic arthritis,” Dr. Gn said.
The record review from July 2014 to February 2016 shows the clinic also serves patients with cutaneous lupus, dermatomyositis, pyoderma gangrenosum, vasculitis, and rheumatoid arthritis, among others.
The presenters had no relevant disclosures.
AT 2016 GRAPPA ANNUAL MEETING

Belonging and grieving: Lessons from Orlando
We belong in our family, in our group, and in our community. Belonging is a basic human need, and we work throughout our lives to seek or create safe places where we can belong. For the LGBTQ+ community, the Pulse nightclub was one of those rare places where they could feel like they truly belonged. It was a place where they did not need to pretend to be someone else or to keep their guard up against insults or criticism. For survivors of the shooting, the families, and the LGBTQ+ community, that sense of belonging is now fractured.
Pulse reportedly represented every LGBTQ+’s queer bar, where a safe environment is sought – an environment in which to grow and express identity. For the LGBTQ+ community, the June 12 massacre threatened all safe havens – where few currently exist – especially in the night scene, where the increased risk of violence is a constant factor in deciding where to party. There are few gay bars.

What must psychiatrists understand about the impact of the event, besides the regular work of grieving? Some specifics pertinent to this attack must be understood: the preponderance of Latinos1, the youthfulness of most victims, and the impact and reverberations throughout the LGBTQ+ community. This column highlights the unique aspects of this tragedy, and the complexity of the grieving that will take place in these families and communities.
Grief, illness, and resilience: What do we know?
Grieving after sudden and violent deaths, compared with natural deaths, is more likely to be associated with mental health disorders and a slower recovery (Psychiatry. 2012 Spring;75[1]:76-97). Traumatic loss can cause incapacitating grief and a search for meaning that can continue for years, especially in those who identify closely with the victims (J Trauma Stress. 2016 Feb;29[1]41-8).
The LGBTQ+ community identifies strongly with the victims of the Orlando shooting, and so is more likely to have a prolonged and difficult grieving process. Feelings of “it could have been me” or “this might happen to me or my loved ones,” can result in symptoms of anxiety and survivor guilt. The LGBTQ+ community also is grieving the loss of a safe place and that associated sense of belonging. Loss of safety and feelings of reduced control over one’s life result in a more difficult grieving process, irrespective of the cause of death (Death Stud. 2006;30[5]:403-28). It is as if the loss provides further evidence of life’s injustices and unpredictability, provoking feelings of helplessness and fear.
Being able to make sense or make meaning after a disaster is a key component of developing resilience (J Clin Psychol. 2016 Feb 22. doi: 10.1002/jclp.22270). To make meaning out of a loss, people inevitably will examine their own lives for meaning and purpose. Meaning-making also can result in post-traumatic growth, such as an increased appreciation for life, stronger connections with family and friends, or greater awareness of one’s strengths.
The meaning-making process, often facilitated by psychotherapy, plays a critical role in recovery. Meaning-making takes different forms. For some people, the record-breaking turnout at NYC Pride, in which the owner of Pulse and others rode on a float and received great support, was a significant event. Meanwhile, another person who might be scared might want to see his family, regardless of whether or not the family is fully accepting.
Grief as a social process
Coping with grief is the working out of “the meaning of the loss,” both personally and in community. Grieving is a social process, and eulogies, grief accounts in popular literature, and elegies help construct the identity of the loved one and the meaning of the event. Grieving involves reviewing the relationship to the lost loved one and establishing a sense of continuity between life before and life after the loss (Death Stud. 2014 Jul-Dec; 38[6-10]:485-98).
One challenge for the LGBTQ+ community is how to direct the meaning of the loss. What is the meaning of this loss and how will the dead be remembered? The outpouring of support across the world is heartwarming and reflects how the LGBTQ+ community has become more accepted in the world at large.
The LGBTQ+ community experiences much less stigma than 50 years ago. In 1973, after the firebombing of a club in New Orleans, some relatives reportedly refused to claim the bodies of their gay sons. However, there remains much variation in how communities/societies view LGBTQ+ individuals and relationships.
Cultural considerations of being LGBTQ+
Nonbinary gender identity is recognized in several cultures around the world. The word “Mahu” in Polynesian culture and the concept of being Two-Spirit in some Native American cultures describe those who do not identify as their assigned sex at birth, play out gender roles opposite their assigned sex, or are attracted to same-sex partners, according to biologist Joan Roughgarden, PhD, (“Evolution’s Rainbow: Diversity, Gender and Sexuality in Nature and People” Los Angeles: University of California Press, 2004). In Dr. Roughgarden’s 2010 book, “The Genial Gene” (Los Angeles: University of California Press), she promotes social-selection theory as an alternative to the Darwinian selfish gene theory. She lists 26 phenomena, not explained by current sexual-selection theory, that are better explained by social selection, a population-based explanation of partner selection. Those ideas are beginning to reach a wider audience in mainstream culture, although for many communities and religions, those ideas are seen as “wrong” or “blasphemous.”
For all minority groups, the importance of belonging to a safe, accepting community ranks highly. The pressure for all minority group members to conform to mainstream society is strong and persistent. A good parallel is found when thinking about race and the pressure of dark-skinned individuals to conform to white society. Skin bleaching remains a common practice; some people turn dark skin whiter in order to conform to a societal ideal. Similarly, in order to fit in and avoid discrimination or persecution, many LGBTQ+ individuals work hard to keep their gender conforming face forward. Pulse offered an opportunity for LGBTQ+ individuals and couples to feel like they could be themselves, express themselves, and forget about the societal pressures of conformity. Belonging to a safe community is, therefore, vital to maintaining a sense of self and self-worth.
The acknowledgment of LGBTQ+ status varies by culture. Ninety percent of the Pulse shooting victims reportedly were gay Latino men; a group that expresses its gender identity differently from gay white men. Verbal disclosure benefits gay white men’s well-being but doesn’t affect gay Latino men’s well-being, either positively or negatively. For gay white men, the more they verbally disclose their gay identity to others, the more they feel they are showing their true, feelings of authenticity, research shows). Additionally, LGBTQ+ members may be out in English but not in their Spanish-speaking church, according to Marianne Duddy-Burke, executive director of Dignity/USA, the largest national lay movement of LGBTQ Catholics, their families, and friends. Sadly, many of the Latino families of the Pulse shooting victims are Spanish-speaking only and reportedly had difficulty finding someone to explain what had happened.
Family considerations of being LGBTQ+.
Some families may know privately that they have an LGBTQ member but do not publicly acknowledge the fact. Family members may say things like “being married is maybe not for you, and that’s OK,” or “People should be allowed to be whoever they are.” This communication, while masked, is supportive and illustrates “an understanding” in the family. It may be some time before a family can say “we support our child, regardless” or “I know you are gay, and that’s OK.”
Gender identity can, therefore, be communicated nonverbally and behaviorally. For example, gay Puerto Rican and gay Dominican men in New York City discussed how they disclosed their gender identity by bringing their same-sex partner to family functions without the direct verbalization of a romantic relationship. This strategy, by which gay identity is implied and unspoken, is known as “tacit subjectivity,” or “tacitness.” The authors of this study postulated that for gay Latino men, their relationships in the family and Latino community are more important than the acknowledgment of individual difference and the expression of authenticity.
This perspective is consistent with the importance of community and family identity, a common aspect of non-Western cultures. At the extreme, some communities are very hostile to LGBTQ+ individuals, including in the United States. After sending “thoughts and prayers” to Orlando, the GOP House chair blocked legislation aimed at making sure that federal contractors cannot discriminate based on gender identity or sexual orientation.
Meanwhile, in Pakistani Muslim families, an LGBTQ+ member threatens the marriage prospects of the girls and may place the family in danger of being killed. Yet, 50 top Pakistani clerics recently issued a religious decree, or fatwa, declaring that transgender people have full marriage, inheritance, and funeral rights under Islamic law. The fatwa stated that a female-born transgender person having “visible signs of being a male” may marry a woman or a male-born transgender with “visible signs of being a female,” and vice versa. However, it ruled that a transgender person carrying “visible signs of both genders” – or intersex – may not marry anyone.
Currently in Pakistan, gay marriage is punishable by life imprisonment. The new fatwa also declared that any act intended to “humiliate, insult, or tease” the community was “haraam” (forbidden). The fatwa also states that transgender people should not be deprived of family inheritances, nor the right to be buried in Muslim ceremonies and that parents who deprived their transgender sons or daughters of inheritances were “inviting the wrath of God.”
Complexity of grieving after Pulse
The unique cultural and family aspects of the Pulse shooting makes the process of grieving complex. The cultural aspects of LGBTQ+ identity, both within that community and within Latino culture, bring new variables to the grieving process. Many of the previously held truths about grieving may turn out to be unimportant in this tragedy, and new factors may emerge.
Previously held findings on complex grief include:
• The importance of personal risk factors, such as female gender and preexisting psychiatric difficulties, in increasing the probability for mental distress.
• Interpersonal risk factors, such as kinship and social support, especially the loss of a child.
• Low perceived social support associated with depression after disaster-related bereavement.
• Social isolation related to difficulties in adjustment after the sudden and violent loss of a child.
• Finding meaning in the loss is related to lower mental distress and grief after violent losses.
• Social support has shown nonconclusive results in the general bereavement literature. Still, some studies suggest that social support may exert a protective effect on mental health adversities after sudden and violent losses.
After the Pulse shooting, these variables need to be reanalyzed. Specific personal risk factors are likely to emerge, such as a victim’s comfort with LGBTQ+ identity and their feelings of connection with the victims. Interpersonal factors will relate to the acceptance of their families and the presence of other safe places. The social status of LGBTQ+ community vis-à-vis the mainstream culture also will have an impact. Meaning-finding is a universal need that may be more difficult to reach for the LGBTQ+ community.
An assumption that likely will be upheld is that sudden, unexpected, and violent losses, compared with losses from natural deaths, are followed by a more difficult grieving process. This has been confirmed in several empirical studies that show a heightened risk for prolonged grief disorder (PGD), major depressive disorder, and posttraumatic stress disorder (PTSD) after violent losses.
In a study measuring PGD in 1,723 college students who had experienced either sudden and violent or natural losses, Joseph Currier, PhD, and his colleagues found that the violence of the loss, not the suddenness, predicted the increased PGD risk (Death Stud. 2006;30:403-28).
Also, it was more difficult to make sense of violent losses, and those students spent more time talking about the loss. In line with studies of PGD, the violence of the loss – not the suddenness – has been shown to account for the increased PTSD risk in the bereaved (J Anxiety Disord. 2003; 17[2]131-47).
DSM-5 diagnosis of persistent complex bereavement disorder
How to make a diagnosis? There is controversy surrounding the accuracy of DSM-5 proposed criteria for persistent complex bereavement disorder (PCBD). In a study of family members of U.S. military service members who died of any cause since Sept. 11, 2001 (n = 1,732), the DSM-5 PCBD criteria accurately excluded nonclinical, normative grief, but also excluded nearly half of clinical cases (Am J Psychiatry. 2016 May 24. [doi: 10.1176/appi.ajp.2016.15111442]).
PCBD previously has been referred to in the literature as complicated grief and prolonged grief disorder. However, those three labels refer to the same syndrome of clinically impairing grief, which affects approximately 7%-15% of bereaved individuals. This syndrome is diagnosed when persistent and severe grief symptoms continue beyond 6-12 months after the death of a loved one and are associated with functional impairment.
Typical symptoms include difficulty accepting the death or a strong sense of disbelief about the death, intense yearning and longing for the deceased, anger and bitterness, distressing and intrusive thoughts related to the death, and excessive avoidance of reminders of the painful loss. In recognition of their lack of validation, PCBD criteria were included in section 3 of DSM-5 Conditions for Further Study.
In summary, the Pulse shooting highlights the importance of assessing grief from a variety of new perspectives. First, assess the patient’s own personal sense of identity and how much she identifies with the victims. Second, assess the cultural and family aspects pertinent to the patient’s expression of gender identity. Third, assess the degree of acceptance the person feels and her ability to access a safe community. Assess the degree of persecution she feels in society at large. This assessment includes identifying where the patient experiences a true sense of belonging. Lastly, the path forward is always a meaning-making endeavor.
Summary of proposed PCBD in DSM-5
• Criterion A requires that the individual has experienced the death of a loved one.
• Criterion B requires the presence of 1 of 4 symptoms related to yearning, longing, and sorrow.
• Criterion C requires 6 of 12 symptoms demonstrating reactive distress to the death or social/identity disruption.
• Criterion D requires clinically significant distress or functional impairment.
• Criterion E requires that distress or impairment is outside of sociocultural norms.
Symptoms present for at least 12 months and that are not better accounted for by major depressive disorder, generalized anxiety disorder, or posttraumatic stress disorder.
Source: Dr. Heru
Thank you to Shiona Heru, JD, for her comments.
References
1. Gender-inclusive version is to use either Latinx (the x symbol represents the absence of o/a) or Latin@ (using the @ symbol mixes the o and @).
2. For more on “The Singular Experience of the Queer Latin Nightclub”: http://www.theatlantic.com/entertainment/archive/2016/06/orlando-shooting-pulse-latin-queer-gay-nightclub-ramon-rivera-servera-intrerview/487442/
Dr. Heru is with the department of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals (New York: Routledge, 2013). She has no conflicts of interest to disclose. .
We belong in our family, in our group, and in our community. Belonging is a basic human need, and we work throughout our lives to seek or create safe places where we can belong. For the LGBTQ+ community, the Pulse nightclub was one of those rare places where they could feel like they truly belonged. It was a place where they did not need to pretend to be someone else or to keep their guard up against insults or criticism. For survivors of the shooting, the families, and the LGBTQ+ community, that sense of belonging is now fractured.
Pulse reportedly represented every LGBTQ+’s queer bar, where a safe environment is sought – an environment in which to grow and express identity. For the LGBTQ+ community, the June 12 massacre threatened all safe havens – where few currently exist – especially in the night scene, where the increased risk of violence is a constant factor in deciding where to party. There are few gay bars.
What must psychiatrists understand about the impact of the event, besides the regular work of grieving? Some specifics pertinent to this attack must be understood: the preponderance of Latinos1, the youthfulness of most victims, and the impact and reverberations throughout the LGBTQ+ community. This column highlights the unique aspects of this tragedy, and the complexity of the grieving that will take place in these families and communities.
Grief, illness, and resilience: What do we know?
Grieving after sudden and violent deaths, compared with natural deaths, is more likely to be associated with mental health disorders and a slower recovery (Psychiatry. 2012 Spring;75[1]:76-97). Traumatic loss can cause incapacitating grief and a search for meaning that can continue for years, especially in those who identify closely with the victims (J Trauma Stress. 2016 Feb;29[1]41-8).
The LGBTQ+ community identifies strongly with the victims of the Orlando shooting, and so is more likely to have a prolonged and difficult grieving process. Feelings of “it could have been me” or “this might happen to me or my loved ones,” can result in symptoms of anxiety and survivor guilt. The LGBTQ+ community also is grieving the loss of a safe place and that associated sense of belonging. Loss of safety and feelings of reduced control over one’s life result in a more difficult grieving process, irrespective of the cause of death (Death Stud. 2006;30[5]:403-28). It is as if the loss provides further evidence of life’s injustices and unpredictability, provoking feelings of helplessness and fear.
Being able to make sense or make meaning after a disaster is a key component of developing resilience (J Clin Psychol. 2016 Feb 22. doi: 10.1002/jclp.22270). To make meaning out of a loss, people inevitably will examine their own lives for meaning and purpose. Meaning-making also can result in post-traumatic growth, such as an increased appreciation for life, stronger connections with family and friends, or greater awareness of one’s strengths.
The meaning-making process, often facilitated by psychotherapy, plays a critical role in recovery. Meaning-making takes different forms. For some people, the record-breaking turnout at NYC Pride, in which the owner of Pulse and others rode on a float and received great support, was a significant event. Meanwhile, another person who might be scared might want to see his family, regardless of whether or not the family is fully accepting.
Grief as a social process
Coping with grief is the working out of “the meaning of the loss,” both personally and in community. Grieving is a social process, and eulogies, grief accounts in popular literature, and elegies help construct the identity of the loved one and the meaning of the event. Grieving involves reviewing the relationship to the lost loved one and establishing a sense of continuity between life before and life after the loss (Death Stud. 2014 Jul-Dec; 38[6-10]:485-98).
One challenge for the LGBTQ+ community is how to direct the meaning of the loss. What is the meaning of this loss and how will the dead be remembered? The outpouring of support across the world is heartwarming and reflects how the LGBTQ+ community has become more accepted in the world at large.
The LGBTQ+ community experiences much less stigma than 50 years ago. In 1973, after the firebombing of a club in New Orleans, some relatives reportedly refused to claim the bodies of their gay sons. However, there remains much variation in how communities/societies view LGBTQ+ individuals and relationships.
Cultural considerations of being LGBTQ+
Nonbinary gender identity is recognized in several cultures around the world. The word “Mahu” in Polynesian culture and the concept of being Two-Spirit in some Native American cultures describe those who do not identify as their assigned sex at birth, play out gender roles opposite their assigned sex, or are attracted to same-sex partners, according to biologist Joan Roughgarden, PhD, (“Evolution’s Rainbow: Diversity, Gender and Sexuality in Nature and People” Los Angeles: University of California Press, 2004). In Dr. Roughgarden’s 2010 book, “The Genial Gene” (Los Angeles: University of California Press), she promotes social-selection theory as an alternative to the Darwinian selfish gene theory. She lists 26 phenomena, not explained by current sexual-selection theory, that are better explained by social selection, a population-based explanation of partner selection. Those ideas are beginning to reach a wider audience in mainstream culture, although for many communities and religions, those ideas are seen as “wrong” or “blasphemous.”
For all minority groups, the importance of belonging to a safe, accepting community ranks highly. The pressure for all minority group members to conform to mainstream society is strong and persistent. A good parallel is found when thinking about race and the pressure of dark-skinned individuals to conform to white society. Skin bleaching remains a common practice; some people turn dark skin whiter in order to conform to a societal ideal. Similarly, in order to fit in and avoid discrimination or persecution, many LGBTQ+ individuals work hard to keep their gender conforming face forward. Pulse offered an opportunity for LGBTQ+ individuals and couples to feel like they could be themselves, express themselves, and forget about the societal pressures of conformity. Belonging to a safe community is, therefore, vital to maintaining a sense of self and self-worth.
The acknowledgment of LGBTQ+ status varies by culture. Ninety percent of the Pulse shooting victims reportedly were gay Latino men; a group that expresses its gender identity differently from gay white men. Verbal disclosure benefits gay white men’s well-being but doesn’t affect gay Latino men’s well-being, either positively or negatively. For gay white men, the more they verbally disclose their gay identity to others, the more they feel they are showing their true, feelings of authenticity, research shows). Additionally, LGBTQ+ members may be out in English but not in their Spanish-speaking church, according to Marianne Duddy-Burke, executive director of Dignity/USA, the largest national lay movement of LGBTQ Catholics, their families, and friends. Sadly, many of the Latino families of the Pulse shooting victims are Spanish-speaking only and reportedly had difficulty finding someone to explain what had happened.
Family considerations of being LGBTQ+.
Some families may know privately that they have an LGBTQ member but do not publicly acknowledge the fact. Family members may say things like “being married is maybe not for you, and that’s OK,” or “People should be allowed to be whoever they are.” This communication, while masked, is supportive and illustrates “an understanding” in the family. It may be some time before a family can say “we support our child, regardless” or “I know you are gay, and that’s OK.”
Gender identity can, therefore, be communicated nonverbally and behaviorally. For example, gay Puerto Rican and gay Dominican men in New York City discussed how they disclosed their gender identity by bringing their same-sex partner to family functions without the direct verbalization of a romantic relationship. This strategy, by which gay identity is implied and unspoken, is known as “tacit subjectivity,” or “tacitness.” The authors of this study postulated that for gay Latino men, their relationships in the family and Latino community are more important than the acknowledgment of individual difference and the expression of authenticity.
This perspective is consistent with the importance of community and family identity, a common aspect of non-Western cultures. At the extreme, some communities are very hostile to LGBTQ+ individuals, including in the United States. After sending “thoughts and prayers” to Orlando, the GOP House chair blocked legislation aimed at making sure that federal contractors cannot discriminate based on gender identity or sexual orientation.
Meanwhile, in Pakistani Muslim families, an LGBTQ+ member threatens the marriage prospects of the girls and may place the family in danger of being killed. Yet, 50 top Pakistani clerics recently issued a religious decree, or fatwa, declaring that transgender people have full marriage, inheritance, and funeral rights under Islamic law. The fatwa stated that a female-born transgender person having “visible signs of being a male” may marry a woman or a male-born transgender with “visible signs of being a female,” and vice versa. However, it ruled that a transgender person carrying “visible signs of both genders” – or intersex – may not marry anyone.
Currently in Pakistan, gay marriage is punishable by life imprisonment. The new fatwa also declared that any act intended to “humiliate, insult, or tease” the community was “haraam” (forbidden). The fatwa also states that transgender people should not be deprived of family inheritances, nor the right to be buried in Muslim ceremonies and that parents who deprived their transgender sons or daughters of inheritances were “inviting the wrath of God.”
Complexity of grieving after Pulse
The unique cultural and family aspects of the Pulse shooting makes the process of grieving complex. The cultural aspects of LGBTQ+ identity, both within that community and within Latino culture, bring new variables to the grieving process. Many of the previously held truths about grieving may turn out to be unimportant in this tragedy, and new factors may emerge.
Previously held findings on complex grief include:
• The importance of personal risk factors, such as female gender and preexisting psychiatric difficulties, in increasing the probability for mental distress.
• Interpersonal risk factors, such as kinship and social support, especially the loss of a child.
• Low perceived social support associated with depression after disaster-related bereavement.
• Social isolation related to difficulties in adjustment after the sudden and violent loss of a child.
• Finding meaning in the loss is related to lower mental distress and grief after violent losses.
• Social support has shown nonconclusive results in the general bereavement literature. Still, some studies suggest that social support may exert a protective effect on mental health adversities after sudden and violent losses.
After the Pulse shooting, these variables need to be reanalyzed. Specific personal risk factors are likely to emerge, such as a victim’s comfort with LGBTQ+ identity and their feelings of connection with the victims. Interpersonal factors will relate to the acceptance of their families and the presence of other safe places. The social status of LGBTQ+ community vis-à-vis the mainstream culture also will have an impact. Meaning-finding is a universal need that may be more difficult to reach for the LGBTQ+ community.
An assumption that likely will be upheld is that sudden, unexpected, and violent losses, compared with losses from natural deaths, are followed by a more difficult grieving process. This has been confirmed in several empirical studies that show a heightened risk for prolonged grief disorder (PGD), major depressive disorder, and posttraumatic stress disorder (PTSD) after violent losses.
In a study measuring PGD in 1,723 college students who had experienced either sudden and violent or natural losses, Joseph Currier, PhD, and his colleagues found that the violence of the loss, not the suddenness, predicted the increased PGD risk (Death Stud. 2006;30:403-28).
Also, it was more difficult to make sense of violent losses, and those students spent more time talking about the loss. In line with studies of PGD, the violence of the loss – not the suddenness – has been shown to account for the increased PTSD risk in the bereaved (J Anxiety Disord. 2003; 17[2]131-47).
DSM-5 diagnosis of persistent complex bereavement disorder
How to make a diagnosis? There is controversy surrounding the accuracy of DSM-5 proposed criteria for persistent complex bereavement disorder (PCBD). In a study of family members of U.S. military service members who died of any cause since Sept. 11, 2001 (n = 1,732), the DSM-5 PCBD criteria accurately excluded nonclinical, normative grief, but also excluded nearly half of clinical cases (Am J Psychiatry. 2016 May 24. [doi: 10.1176/appi.ajp.2016.15111442]).
PCBD previously has been referred to in the literature as complicated grief and prolonged grief disorder. However, those three labels refer to the same syndrome of clinically impairing grief, which affects approximately 7%-15% of bereaved individuals. This syndrome is diagnosed when persistent and severe grief symptoms continue beyond 6-12 months after the death of a loved one and are associated with functional impairment.
Typical symptoms include difficulty accepting the death or a strong sense of disbelief about the death, intense yearning and longing for the deceased, anger and bitterness, distressing and intrusive thoughts related to the death, and excessive avoidance of reminders of the painful loss. In recognition of their lack of validation, PCBD criteria were included in section 3 of DSM-5 Conditions for Further Study.
In summary, the Pulse shooting highlights the importance of assessing grief from a variety of new perspectives. First, assess the patient’s own personal sense of identity and how much she identifies with the victims. Second, assess the cultural and family aspects pertinent to the patient’s expression of gender identity. Third, assess the degree of acceptance the person feels and her ability to access a safe community. Assess the degree of persecution she feels in society at large. This assessment includes identifying where the patient experiences a true sense of belonging. Lastly, the path forward is always a meaning-making endeavor.
Summary of proposed PCBD in DSM-5
• Criterion A requires that the individual has experienced the death of a loved one.
• Criterion B requires the presence of 1 of 4 symptoms related to yearning, longing, and sorrow.
• Criterion C requires 6 of 12 symptoms demonstrating reactive distress to the death or social/identity disruption.
• Criterion D requires clinically significant distress or functional impairment.
• Criterion E requires that distress or impairment is outside of sociocultural norms.
Symptoms present for at least 12 months and that are not better accounted for by major depressive disorder, generalized anxiety disorder, or posttraumatic stress disorder.
Source: Dr. Heru
Thank you to Shiona Heru, JD, for her comments.
References
1. Gender-inclusive version is to use either Latinx (the x symbol represents the absence of o/a) or Latin@ (using the @ symbol mixes the o and @).
2. For more on “The Singular Experience of the Queer Latin Nightclub”: http://www.theatlantic.com/entertainment/archive/2016/06/orlando-shooting-pulse-latin-queer-gay-nightclub-ramon-rivera-servera-intrerview/487442/
Dr. Heru is with the department of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals (New York: Routledge, 2013). She has no conflicts of interest to disclose. .
We belong in our family, in our group, and in our community. Belonging is a basic human need, and we work throughout our lives to seek or create safe places where we can belong. For the LGBTQ+ community, the Pulse nightclub was one of those rare places where they could feel like they truly belonged. It was a place where they did not need to pretend to be someone else or to keep their guard up against insults or criticism. For survivors of the shooting, the families, and the LGBTQ+ community, that sense of belonging is now fractured.
Pulse reportedly represented every LGBTQ+’s queer bar, where a safe environment is sought – an environment in which to grow and express identity. For the LGBTQ+ community, the June 12 massacre threatened all safe havens – where few currently exist – especially in the night scene, where the increased risk of violence is a constant factor in deciding where to party. There are few gay bars.
What must psychiatrists understand about the impact of the event, besides the regular work of grieving? Some specifics pertinent to this attack must be understood: the preponderance of Latinos1, the youthfulness of most victims, and the impact and reverberations throughout the LGBTQ+ community. This column highlights the unique aspects of this tragedy, and the complexity of the grieving that will take place in these families and communities.
Grief, illness, and resilience: What do we know?
Grieving after sudden and violent deaths, compared with natural deaths, is more likely to be associated with mental health disorders and a slower recovery (Psychiatry. 2012 Spring;75[1]:76-97). Traumatic loss can cause incapacitating grief and a search for meaning that can continue for years, especially in those who identify closely with the victims (J Trauma Stress. 2016 Feb;29[1]41-8).
The LGBTQ+ community identifies strongly with the victims of the Orlando shooting, and so is more likely to have a prolonged and difficult grieving process. Feelings of “it could have been me” or “this might happen to me or my loved ones,” can result in symptoms of anxiety and survivor guilt. The LGBTQ+ community also is grieving the loss of a safe place and that associated sense of belonging. Loss of safety and feelings of reduced control over one’s life result in a more difficult grieving process, irrespective of the cause of death (Death Stud. 2006;30[5]:403-28). It is as if the loss provides further evidence of life’s injustices and unpredictability, provoking feelings of helplessness and fear.
Being able to make sense or make meaning after a disaster is a key component of developing resilience (J Clin Psychol. 2016 Feb 22. doi: 10.1002/jclp.22270). To make meaning out of a loss, people inevitably will examine their own lives for meaning and purpose. Meaning-making also can result in post-traumatic growth, such as an increased appreciation for life, stronger connections with family and friends, or greater awareness of one’s strengths.
The meaning-making process, often facilitated by psychotherapy, plays a critical role in recovery. Meaning-making takes different forms. For some people, the record-breaking turnout at NYC Pride, in which the owner of Pulse and others rode on a float and received great support, was a significant event. Meanwhile, another person who might be scared might want to see his family, regardless of whether or not the family is fully accepting.
Grief as a social process
Coping with grief is the working out of “the meaning of the loss,” both personally and in community. Grieving is a social process, and eulogies, grief accounts in popular literature, and elegies help construct the identity of the loved one and the meaning of the event. Grieving involves reviewing the relationship to the lost loved one and establishing a sense of continuity between life before and life after the loss (Death Stud. 2014 Jul-Dec; 38[6-10]:485-98).
One challenge for the LGBTQ+ community is how to direct the meaning of the loss. What is the meaning of this loss and how will the dead be remembered? The outpouring of support across the world is heartwarming and reflects how the LGBTQ+ community has become more accepted in the world at large.
The LGBTQ+ community experiences much less stigma than 50 years ago. In 1973, after the firebombing of a club in New Orleans, some relatives reportedly refused to claim the bodies of their gay sons. However, there remains much variation in how communities/societies view LGBTQ+ individuals and relationships.
Cultural considerations of being LGBTQ+
Nonbinary gender identity is recognized in several cultures around the world. The word “Mahu” in Polynesian culture and the concept of being Two-Spirit in some Native American cultures describe those who do not identify as their assigned sex at birth, play out gender roles opposite their assigned sex, or are attracted to same-sex partners, according to biologist Joan Roughgarden, PhD, (“Evolution’s Rainbow: Diversity, Gender and Sexuality in Nature and People” Los Angeles: University of California Press, 2004). In Dr. Roughgarden’s 2010 book, “The Genial Gene” (Los Angeles: University of California Press), she promotes social-selection theory as an alternative to the Darwinian selfish gene theory. She lists 26 phenomena, not explained by current sexual-selection theory, that are better explained by social selection, a population-based explanation of partner selection. Those ideas are beginning to reach a wider audience in mainstream culture, although for many communities and religions, those ideas are seen as “wrong” or “blasphemous.”
For all minority groups, the importance of belonging to a safe, accepting community ranks highly. The pressure for all minority group members to conform to mainstream society is strong and persistent. A good parallel is found when thinking about race and the pressure of dark-skinned individuals to conform to white society. Skin bleaching remains a common practice; some people turn dark skin whiter in order to conform to a societal ideal. Similarly, in order to fit in and avoid discrimination or persecution, many LGBTQ+ individuals work hard to keep their gender conforming face forward. Pulse offered an opportunity for LGBTQ+ individuals and couples to feel like they could be themselves, express themselves, and forget about the societal pressures of conformity. Belonging to a safe community is, therefore, vital to maintaining a sense of self and self-worth.
The acknowledgment of LGBTQ+ status varies by culture. Ninety percent of the Pulse shooting victims reportedly were gay Latino men; a group that expresses its gender identity differently from gay white men. Verbal disclosure benefits gay white men’s well-being but doesn’t affect gay Latino men’s well-being, either positively or negatively. For gay white men, the more they verbally disclose their gay identity to others, the more they feel they are showing their true, feelings of authenticity, research shows). Additionally, LGBTQ+ members may be out in English but not in their Spanish-speaking church, according to Marianne Duddy-Burke, executive director of Dignity/USA, the largest national lay movement of LGBTQ Catholics, their families, and friends. Sadly, many of the Latino families of the Pulse shooting victims are Spanish-speaking only and reportedly had difficulty finding someone to explain what had happened.
Family considerations of being LGBTQ+.
Some families may know privately that they have an LGBTQ member but do not publicly acknowledge the fact. Family members may say things like “being married is maybe not for you, and that’s OK,” or “People should be allowed to be whoever they are.” This communication, while masked, is supportive and illustrates “an understanding” in the family. It may be some time before a family can say “we support our child, regardless” or “I know you are gay, and that’s OK.”
Gender identity can, therefore, be communicated nonverbally and behaviorally. For example, gay Puerto Rican and gay Dominican men in New York City discussed how they disclosed their gender identity by bringing their same-sex partner to family functions without the direct verbalization of a romantic relationship. This strategy, by which gay identity is implied and unspoken, is known as “tacit subjectivity,” or “tacitness.” The authors of this study postulated that for gay Latino men, their relationships in the family and Latino community are more important than the acknowledgment of individual difference and the expression of authenticity.
This perspective is consistent with the importance of community and family identity, a common aspect of non-Western cultures. At the extreme, some communities are very hostile to LGBTQ+ individuals, including in the United States. After sending “thoughts and prayers” to Orlando, the GOP House chair blocked legislation aimed at making sure that federal contractors cannot discriminate based on gender identity or sexual orientation.
Meanwhile, in Pakistani Muslim families, an LGBTQ+ member threatens the marriage prospects of the girls and may place the family in danger of being killed. Yet, 50 top Pakistani clerics recently issued a religious decree, or fatwa, declaring that transgender people have full marriage, inheritance, and funeral rights under Islamic law. The fatwa stated that a female-born transgender person having “visible signs of being a male” may marry a woman or a male-born transgender with “visible signs of being a female,” and vice versa. However, it ruled that a transgender person carrying “visible signs of both genders” – or intersex – may not marry anyone.
Currently in Pakistan, gay marriage is punishable by life imprisonment. The new fatwa also declared that any act intended to “humiliate, insult, or tease” the community was “haraam” (forbidden). The fatwa also states that transgender people should not be deprived of family inheritances, nor the right to be buried in Muslim ceremonies and that parents who deprived their transgender sons or daughters of inheritances were “inviting the wrath of God.”
Complexity of grieving after Pulse
The unique cultural and family aspects of the Pulse shooting makes the process of grieving complex. The cultural aspects of LGBTQ+ identity, both within that community and within Latino culture, bring new variables to the grieving process. Many of the previously held truths about grieving may turn out to be unimportant in this tragedy, and new factors may emerge.
Previously held findings on complex grief include:
• The importance of personal risk factors, such as female gender and preexisting psychiatric difficulties, in increasing the probability for mental distress.
• Interpersonal risk factors, such as kinship and social support, especially the loss of a child.
• Low perceived social support associated with depression after disaster-related bereavement.
• Social isolation related to difficulties in adjustment after the sudden and violent loss of a child.
• Finding meaning in the loss is related to lower mental distress and grief after violent losses.
• Social support has shown nonconclusive results in the general bereavement literature. Still, some studies suggest that social support may exert a protective effect on mental health adversities after sudden and violent losses.
After the Pulse shooting, these variables need to be reanalyzed. Specific personal risk factors are likely to emerge, such as a victim’s comfort with LGBTQ+ identity and their feelings of connection with the victims. Interpersonal factors will relate to the acceptance of their families and the presence of other safe places. The social status of LGBTQ+ community vis-à-vis the mainstream culture also will have an impact. Meaning-finding is a universal need that may be more difficult to reach for the LGBTQ+ community.
An assumption that likely will be upheld is that sudden, unexpected, and violent losses, compared with losses from natural deaths, are followed by a more difficult grieving process. This has been confirmed in several empirical studies that show a heightened risk for prolonged grief disorder (PGD), major depressive disorder, and posttraumatic stress disorder (PTSD) after violent losses.
In a study measuring PGD in 1,723 college students who had experienced either sudden and violent or natural losses, Joseph Currier, PhD, and his colleagues found that the violence of the loss, not the suddenness, predicted the increased PGD risk (Death Stud. 2006;30:403-28).
Also, it was more difficult to make sense of violent losses, and those students spent more time talking about the loss. In line with studies of PGD, the violence of the loss – not the suddenness – has been shown to account for the increased PTSD risk in the bereaved (J Anxiety Disord. 2003; 17[2]131-47).
DSM-5 diagnosis of persistent complex bereavement disorder
How to make a diagnosis? There is controversy surrounding the accuracy of DSM-5 proposed criteria for persistent complex bereavement disorder (PCBD). In a study of family members of U.S. military service members who died of any cause since Sept. 11, 2001 (n = 1,732), the DSM-5 PCBD criteria accurately excluded nonclinical, normative grief, but also excluded nearly half of clinical cases (Am J Psychiatry. 2016 May 24. [doi: 10.1176/appi.ajp.2016.15111442]).
PCBD previously has been referred to in the literature as complicated grief and prolonged grief disorder. However, those three labels refer to the same syndrome of clinically impairing grief, which affects approximately 7%-15% of bereaved individuals. This syndrome is diagnosed when persistent and severe grief symptoms continue beyond 6-12 months after the death of a loved one and are associated with functional impairment.
Typical symptoms include difficulty accepting the death or a strong sense of disbelief about the death, intense yearning and longing for the deceased, anger and bitterness, distressing and intrusive thoughts related to the death, and excessive avoidance of reminders of the painful loss. In recognition of their lack of validation, PCBD criteria were included in section 3 of DSM-5 Conditions for Further Study.
In summary, the Pulse shooting highlights the importance of assessing grief from a variety of new perspectives. First, assess the patient’s own personal sense of identity and how much she identifies with the victims. Second, assess the cultural and family aspects pertinent to the patient’s expression of gender identity. Third, assess the degree of acceptance the person feels and her ability to access a safe community. Assess the degree of persecution she feels in society at large. This assessment includes identifying where the patient experiences a true sense of belonging. Lastly, the path forward is always a meaning-making endeavor.
Summary of proposed PCBD in DSM-5
• Criterion A requires that the individual has experienced the death of a loved one.
• Criterion B requires the presence of 1 of 4 symptoms related to yearning, longing, and sorrow.
• Criterion C requires 6 of 12 symptoms demonstrating reactive distress to the death or social/identity disruption.
• Criterion D requires clinically significant distress or functional impairment.
• Criterion E requires that distress or impairment is outside of sociocultural norms.
Symptoms present for at least 12 months and that are not better accounted for by major depressive disorder, generalized anxiety disorder, or posttraumatic stress disorder.
Source: Dr. Heru
Thank you to Shiona Heru, JD, for her comments.
References
1. Gender-inclusive version is to use either Latinx (the x symbol represents the absence of o/a) or Latin@ (using the @ symbol mixes the o and @).
2. For more on “The Singular Experience of the Queer Latin Nightclub”: http://www.theatlantic.com/entertainment/archive/2016/06/orlando-shooting-pulse-latin-queer-gay-nightclub-ramon-rivera-servera-intrerview/487442/
Dr. Heru is with the department of psychiatry at the University of Colorado Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals (New York: Routledge, 2013). She has no conflicts of interest to disclose. .

Pitt Hopkins Scientific Symposium to Take Place in November
The Pitt Hopkins Research Foundation Scientific Symposium and Family Conference will take place November 3-5 in Dallas, Texas.
The Pitt Hopkins Research Foundation Scientific Symposium and Family Conference will take place November 3-5 in Dallas, Texas.
The Pitt Hopkins Research Foundation Scientific Symposium and Family Conference will take place November 3-5 in Dallas, Texas.

HCU Network Australia Develops Q & A Video With Homocystinuria Expert
Clinician Andrew Morris of the UK is interviewed about the importance of timely diagnosis of homocystinuria in a brief video published recently by the HCU Network Australia.
Clinician Andrew Morris of the UK is interviewed about the importance of timely diagnosis of homocystinuria in a brief video published recently by the HCU Network Australia.
Clinician Andrew Morris of the UK is interviewed about the importance of timely diagnosis of homocystinuria in a brief video published recently by the HCU Network Australia.

Foundation Seeks Proposals to Improve Care of Children With Chronic and Complex Diseases
The Lucile Packard Foundation for Children’s Health seeks applications for grants to develop single-topic issue briefs that describe goals and processes to improve aspects of the systems of care for children with chronic and complex health conditions in the US. Proposals are due September 15.
The Lucile Packard Foundation for Children’s Health seeks applications for grants to develop single-topic issue briefs that describe goals and processes to improve aspects of the systems of care for children with chronic and complex health conditions in the US. Proposals are due September 15.
The Lucile Packard Foundation for Children’s Health seeks applications for grants to develop single-topic issue briefs that describe goals and processes to improve aspects of the systems of care for children with chronic and complex health conditions in the US. Proposals are due September 15.

ACP Develops Toolkit for Transition From Pediatric to Adult Care
The American College of Physicians Initiative has developed a toolkit to facilitate more effective transition of young adults from pediatric to adult care. The kit includes a major focus on providing a framework for the adult care provider.
The American College of Physicians Initiative has developed a toolkit to facilitate more effective transition of young adults from pediatric to adult care. The kit includes a major focus on providing a framework for the adult care provider.
The American College of Physicians Initiative has developed a toolkit to facilitate more effective transition of young adults from pediatric to adult care. The kit includes a major focus on providing a framework for the adult care provider.
