User login
Evaluation of Cortical Lesions Could Improve Diagnosis of MS
LONDON—Evaluation of cortical lesions improves the specificity of the diagnostic criteria for multiple sclerosis (MS), according to research presented at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS). Assessment of cortical lesions, in concert with current McDonald criteria, also preserved a high level of diagnostic sensitivity and accuracy in a multicentric cohort of patients with clinically isolated syndrome, reported Paolo Preziosa, MD, Neuroimaging Research Unit at the Institute of Experimental Neurology and Division of Neuroscience at San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy, and his research colleagues.

Since the publication of the 2010 revised McDonald criteria, new data regarding the application of MRI for the diagnosis of MS have become available. In a single-center study, adding the assessment of cortical lesions was shown to modify the diagnostic algorithm, resulting in higher specificity.
In the present study, Dr. Preziosa and colleagues sought to test the performance of different sets of imaging criteria, including the assessment of cortical lesions, for the development of MS in a multicentric cohort of patients with clinically isolated syndrome.
The researchers analyzed brain double inversion recovery and brain and cord T2-weighted and post-contrast T1-weighted sequences acquired from 72 patients with clinically isolated syndrome from five European centers (Barcelona, Belgrade, Mainz, Milan, and Verona) within three months and after 12 months from disease onset. Patients were followed clinically for 24 or more months or until the development of clinically defined MS. Median follow-up was 24.2 months. Sensitivity, specificity, and accuracy of the different dissemination in space MRI criteria for the development of MS were tested.
At follow-up, 65 patients (90%) had clinically and/or radiologically definite MS. The sensitivity of all criteria was high (McDonald 2005, 83%; McDonald 2010, 92%; Filippi 2010, 80%). Specificity of Filippi 2010 was higher (67%), compared with the others (50% for McDonald 2005 and 2010). The accuracy of all criteria was high (McDonald 2005, 81%; McDonald 2010, 89%; Filippi 2010, 79%).
“The detection of cortical lesions in vivo using MRI should be considered in future clinical trials,” Dr. Preziosa said.
—Glenn S. Williams
Suggested Reading
Filippi M, Rocca MA, Calabrese M, et al. Intracortical lesions: relevance for new MRI diagnostic criteria for multiple sclerosis. Neurology. 2010;75(22):1988-1994.
LONDON—Evaluation of cortical lesions improves the specificity of the diagnostic criteria for multiple sclerosis (MS), according to research presented at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS). Assessment of cortical lesions, in concert with current McDonald criteria, also preserved a high level of diagnostic sensitivity and accuracy in a multicentric cohort of patients with clinically isolated syndrome, reported Paolo Preziosa, MD, Neuroimaging Research Unit at the Institute of Experimental Neurology and Division of Neuroscience at San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy, and his research colleagues.
Since the publication of the 2010 revised McDonald criteria, new data regarding the application of MRI for the diagnosis of MS have become available. In a single-center study, adding the assessment of cortical lesions was shown to modify the diagnostic algorithm, resulting in higher specificity.
In the present study, Dr. Preziosa and colleagues sought to test the performance of different sets of imaging criteria, including the assessment of cortical lesions, for the development of MS in a multicentric cohort of patients with clinically isolated syndrome.
The researchers analyzed brain double inversion recovery and brain and cord T2-weighted and post-contrast T1-weighted sequences acquired from 72 patients with clinically isolated syndrome from five European centers (Barcelona, Belgrade, Mainz, Milan, and Verona) within three months and after 12 months from disease onset. Patients were followed clinically for 24 or more months or until the development of clinically defined MS. Median follow-up was 24.2 months. Sensitivity, specificity, and accuracy of the different dissemination in space MRI criteria for the development of MS were tested.
At follow-up, 65 patients (90%) had clinically and/or radiologically definite MS. The sensitivity of all criteria was high (McDonald 2005, 83%; McDonald 2010, 92%; Filippi 2010, 80%). Specificity of Filippi 2010 was higher (67%), compared with the others (50% for McDonald 2005 and 2010). The accuracy of all criteria was high (McDonald 2005, 81%; McDonald 2010, 89%; Filippi 2010, 79%).
“The detection of cortical lesions in vivo using MRI should be considered in future clinical trials,” Dr. Preziosa said.
—Glenn S. Williams
Suggested Reading
Filippi M, Rocca MA, Calabrese M, et al. Intracortical lesions: relevance for new MRI diagnostic criteria for multiple sclerosis. Neurology. 2010;75(22):1988-1994.
LONDON—Evaluation of cortical lesions improves the specificity of the diagnostic criteria for multiple sclerosis (MS), according to research presented at the 32nd Congress of the European Committee for Treatment and Research in MS (ECTRIMS). Assessment of cortical lesions, in concert with current McDonald criteria, also preserved a high level of diagnostic sensitivity and accuracy in a multicentric cohort of patients with clinically isolated syndrome, reported Paolo Preziosa, MD, Neuroimaging Research Unit at the Institute of Experimental Neurology and Division of Neuroscience at San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy, and his research colleagues.
Since the publication of the 2010 revised McDonald criteria, new data regarding the application of MRI for the diagnosis of MS have become available. In a single-center study, adding the assessment of cortical lesions was shown to modify the diagnostic algorithm, resulting in higher specificity.
In the present study, Dr. Preziosa and colleagues sought to test the performance of different sets of imaging criteria, including the assessment of cortical lesions, for the development of MS in a multicentric cohort of patients with clinically isolated syndrome.
The researchers analyzed brain double inversion recovery and brain and cord T2-weighted and post-contrast T1-weighted sequences acquired from 72 patients with clinically isolated syndrome from five European centers (Barcelona, Belgrade, Mainz, Milan, and Verona) within three months and after 12 months from disease onset. Patients were followed clinically for 24 or more months or until the development of clinically defined MS. Median follow-up was 24.2 months. Sensitivity, specificity, and accuracy of the different dissemination in space MRI criteria for the development of MS were tested.
At follow-up, 65 patients (90%) had clinically and/or radiologically definite MS. The sensitivity of all criteria was high (McDonald 2005, 83%; McDonald 2010, 92%; Filippi 2010, 80%). Specificity of Filippi 2010 was higher (67%), compared with the others (50% for McDonald 2005 and 2010). The accuracy of all criteria was high (McDonald 2005, 81%; McDonald 2010, 89%; Filippi 2010, 79%).
“The detection of cortical lesions in vivo using MRI should be considered in future clinical trials,” Dr. Preziosa said.
—Glenn S. Williams
Suggested Reading
Filippi M, Rocca MA, Calabrese M, et al. Intracortical lesions: relevance for new MRI diagnostic criteria for multiple sclerosis. Neurology. 2010;75(22):1988-1994.
Smoking, vitamin D deficiency linked to early MS disability
LONDON – Severe vitamin D deficiency and current smoking predicted accumulated disability in patients with clinically isolated syndrome, which can be a precursor to the development of multiple sclerosis.
Prospectively collected data from the ongoing Barcelona clinically isolated syndrome (CIS) cohort, which includes more than 1,000 patients with CIS, showed that patients with a serum vitamin D below 8.0 ng/mL (9% of 503 patient samples) had more than double the risk for accumulated disability when compared with those who had higher vitamin D levels. The hazard ratio for disability with severely low vitamin D levels was 2.3 (P = .049) in an analysis adjusted for the potential confounding factors of patients’ sex and age, the number of baseline T2 lesions, receipt of disease-modifying treatment, CIS topography, and oligoclonal bands. Disability accumulation was defined as an Expanded Disability Status Scale score of 3.0 or more.

However, neither vitamin D deficiency nor current smoking predicted the conversion of CIS to clinically definite multiple sclerosis (CDMS), said María Zuluaga, MD, of the Centre d’Esclerosi Múltiple de Catalunya at Vall d’Hebron University Hospital in Barcelona.
Environmental factors such as vitamin D levels and smoking have been purported to play a role in the development of CIS to CDMS, Dr. Zuluaga explained at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Blood samples collected within 6 months of a diagnosis of CIS were examined and vitamin D deficiency defined as normal, mild, moderate, or severe based on serum 25-hydroxy vitamin D of greater than 20, 16-20, 8-15, and less that 8 ng/mL.
Levels of the nicotine metabolite cotinine in the blood were used as a proxy for current smoking. Cotinine has a half-life of around 20 hours and smokers – active or passive – have a level of 14 ng/mL or more while nonsmokers have a level of less than 14 ng/mL.
The study received no commercial funding. Dr. Zuluaga reported having no conflict of interest related to the study.
LONDON – Severe vitamin D deficiency and current smoking predicted accumulated disability in patients with clinically isolated syndrome, which can be a precursor to the development of multiple sclerosis.
Prospectively collected data from the ongoing Barcelona clinically isolated syndrome (CIS) cohort, which includes more than 1,000 patients with CIS, showed that patients with a serum vitamin D below 8.0 ng/mL (9% of 503 patient samples) had more than double the risk for accumulated disability when compared with those who had higher vitamin D levels. The hazard ratio for disability with severely low vitamin D levels was 2.3 (P = .049) in an analysis adjusted for the potential confounding factors of patients’ sex and age, the number of baseline T2 lesions, receipt of disease-modifying treatment, CIS topography, and oligoclonal bands. Disability accumulation was defined as an Expanded Disability Status Scale score of 3.0 or more.
However, neither vitamin D deficiency nor current smoking predicted the conversion of CIS to clinically definite multiple sclerosis (CDMS), said María Zuluaga, MD, of the Centre d’Esclerosi Múltiple de Catalunya at Vall d’Hebron University Hospital in Barcelona.
Environmental factors such as vitamin D levels and smoking have been purported to play a role in the development of CIS to CDMS, Dr. Zuluaga explained at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Blood samples collected within 6 months of a diagnosis of CIS were examined and vitamin D deficiency defined as normal, mild, moderate, or severe based on serum 25-hydroxy vitamin D of greater than 20, 16-20, 8-15, and less that 8 ng/mL.
Levels of the nicotine metabolite cotinine in the blood were used as a proxy for current smoking. Cotinine has a half-life of around 20 hours and smokers – active or passive – have a level of 14 ng/mL or more while nonsmokers have a level of less than 14 ng/mL.
The study received no commercial funding. Dr. Zuluaga reported having no conflict of interest related to the study.
LONDON – Severe vitamin D deficiency and current smoking predicted accumulated disability in patients with clinically isolated syndrome, which can be a precursor to the development of multiple sclerosis.
Prospectively collected data from the ongoing Barcelona clinically isolated syndrome (CIS) cohort, which includes more than 1,000 patients with CIS, showed that patients with a serum vitamin D below 8.0 ng/mL (9% of 503 patient samples) had more than double the risk for accumulated disability when compared with those who had higher vitamin D levels. The hazard ratio for disability with severely low vitamin D levels was 2.3 (P = .049) in an analysis adjusted for the potential confounding factors of patients’ sex and age, the number of baseline T2 lesions, receipt of disease-modifying treatment, CIS topography, and oligoclonal bands. Disability accumulation was defined as an Expanded Disability Status Scale score of 3.0 or more.
However, neither vitamin D deficiency nor current smoking predicted the conversion of CIS to clinically definite multiple sclerosis (CDMS), said María Zuluaga, MD, of the Centre d’Esclerosi Múltiple de Catalunya at Vall d’Hebron University Hospital in Barcelona.
Environmental factors such as vitamin D levels and smoking have been purported to play a role in the development of CIS to CDMS, Dr. Zuluaga explained at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Blood samples collected within 6 months of a diagnosis of CIS were examined and vitamin D deficiency defined as normal, mild, moderate, or severe based on serum 25-hydroxy vitamin D of greater than 20, 16-20, 8-15, and less that 8 ng/mL.
Levels of the nicotine metabolite cotinine in the blood were used as a proxy for current smoking. Cotinine has a half-life of around 20 hours and smokers – active or passive – have a level of 14 ng/mL or more while nonsmokers have a level of less than 14 ng/mL.
The study received no commercial funding. Dr. Zuluaga reported having no conflict of interest related to the study.
Key clinical point:
Major finding: Patients with a serum 25-hydroxy vitamin D level of less than 8.0 ng/mL showed an increased risk for disability in a multivariate analysis (HR, 2.3; P = .049). Nonsmokers were significantly less likely to have disability progression (HR, 0.4; P = .002).
Data source: Barcelona CIS cohort of 1,127 individuals
Disclosures: The study received no commercial funding. Dr. Zuluaga reported having no conflict of interest related to the study.
Can Treating Neuroinflammation in REM Sleep Behavior Disorder Delay Parkinson’s Disease Onset?
PORTLAND, OR—In patients with idiopathic REM sleep behavior disorder, microglial activation is increased in the substantia nigra, compared with controls, and microglial activation correlates with putamenal dopaminergic dysfunction, according to research presented at the Fourth World Parkinson Congress. These findings suggest that “anti-inflammatory agents could possibly delay progression to a manifest synucleinopathy in subjects with idiopathic REM sleep behavior disorder,” researchers said.
Longitudinal studies have found that patients with idiopathic REM sleep behavior disorder have an increased risk of Parkinson’s disease and related Lewy body disorders. “This implies that, in idiopathic REM sleep behavior disorder, the underlying pathology of developing neurodegenerative disorders can be investigated years prior to the development of manifest symptoms,” said Morten Gersel Stokholm, MD, a researcher in the Department of Clinical Medicine at Aarhus University and the Department of Nuclear Medicine & PET-Centre at Aarhus University Hospital, Denmark, and his research colleagues.

To investigate the in vivo occurrence of neuroinflammation in the brains of patients with idiopathic REM sleep behavior disorder and neuroinflammation’s temporal relationship with striatal dopamine dysfunction, Dr. Stokholm and colleagues conducted a multitracer PET study of patients with idiopathic REM sleep behavior disorder.
The investigators enrolled 15 patients with polysomnography-confirmed idiopathic REM sleep behavior disorder at Aarhus University Hospital and Hospital Clínic de Barcelona. They also enrolled 19 matched controls. Participants underwent two PET scans with 18F-DOPA and 11C-PK11195 and a structural T1 MRI scan. Parametric images of specific tracer uptake (ie, F-dopa Ki-values and PK11195 binding potential) were constructed at voxel level using Patlak graphical analysis and a supervised cluster-analysis with compartmental modeling, respectively. A region of interest analysis was performed on a priori defined regions.
Compared with controls, patients with idiopathic REM sleep behavior disorder showed significantly reduced 18F-DOPA tracer uptake in the substantia nigra. Patients with higher substantia nigra11C-PK11195 binding also had increased binding in the ipsilateral putamen. Patients with more severe reductions in putamenal 18F-DOPA uptake had significantly higher 11C-PK11195 binding in the putamen and substantia nigra.
—Jake Remaly
PORTLAND, OR—In patients with idiopathic REM sleep behavior disorder, microglial activation is increased in the substantia nigra, compared with controls, and microglial activation correlates with putamenal dopaminergic dysfunction, according to research presented at the Fourth World Parkinson Congress. These findings suggest that “anti-inflammatory agents could possibly delay progression to a manifest synucleinopathy in subjects with idiopathic REM sleep behavior disorder,” researchers said.
Longitudinal studies have found that patients with idiopathic REM sleep behavior disorder have an increased risk of Parkinson’s disease and related Lewy body disorders. “This implies that, in idiopathic REM sleep behavior disorder, the underlying pathology of developing neurodegenerative disorders can be investigated years prior to the development of manifest symptoms,” said Morten Gersel Stokholm, MD, a researcher in the Department of Clinical Medicine at Aarhus University and the Department of Nuclear Medicine & PET-Centre at Aarhus University Hospital, Denmark, and his research colleagues.
To investigate the in vivo occurrence of neuroinflammation in the brains of patients with idiopathic REM sleep behavior disorder and neuroinflammation’s temporal relationship with striatal dopamine dysfunction, Dr. Stokholm and colleagues conducted a multitracer PET study of patients with idiopathic REM sleep behavior disorder.
The investigators enrolled 15 patients with polysomnography-confirmed idiopathic REM sleep behavior disorder at Aarhus University Hospital and Hospital Clínic de Barcelona. They also enrolled 19 matched controls. Participants underwent two PET scans with 18F-DOPA and 11C-PK11195 and a structural T1 MRI scan. Parametric images of specific tracer uptake (ie, F-dopa Ki-values and PK11195 binding potential) were constructed at voxel level using Patlak graphical analysis and a supervised cluster-analysis with compartmental modeling, respectively. A region of interest analysis was performed on a priori defined regions.
Compared with controls, patients with idiopathic REM sleep behavior disorder showed significantly reduced 18F-DOPA tracer uptake in the substantia nigra. Patients with higher substantia nigra11C-PK11195 binding also had increased binding in the ipsilateral putamen. Patients with more severe reductions in putamenal 18F-DOPA uptake had significantly higher 11C-PK11195 binding in the putamen and substantia nigra.
—Jake Remaly
PORTLAND, OR—In patients with idiopathic REM sleep behavior disorder, microglial activation is increased in the substantia nigra, compared with controls, and microglial activation correlates with putamenal dopaminergic dysfunction, according to research presented at the Fourth World Parkinson Congress. These findings suggest that “anti-inflammatory agents could possibly delay progression to a manifest synucleinopathy in subjects with idiopathic REM sleep behavior disorder,” researchers said.
Longitudinal studies have found that patients with idiopathic REM sleep behavior disorder have an increased risk of Parkinson’s disease and related Lewy body disorders. “This implies that, in idiopathic REM sleep behavior disorder, the underlying pathology of developing neurodegenerative disorders can be investigated years prior to the development of manifest symptoms,” said Morten Gersel Stokholm, MD, a researcher in the Department of Clinical Medicine at Aarhus University and the Department of Nuclear Medicine & PET-Centre at Aarhus University Hospital, Denmark, and his research colleagues.
To investigate the in vivo occurrence of neuroinflammation in the brains of patients with idiopathic REM sleep behavior disorder and neuroinflammation’s temporal relationship with striatal dopamine dysfunction, Dr. Stokholm and colleagues conducted a multitracer PET study of patients with idiopathic REM sleep behavior disorder.
The investigators enrolled 15 patients with polysomnography-confirmed idiopathic REM sleep behavior disorder at Aarhus University Hospital and Hospital Clínic de Barcelona. They also enrolled 19 matched controls. Participants underwent two PET scans with 18F-DOPA and 11C-PK11195 and a structural T1 MRI scan. Parametric images of specific tracer uptake (ie, F-dopa Ki-values and PK11195 binding potential) were constructed at voxel level using Patlak graphical analysis and a supervised cluster-analysis with compartmental modeling, respectively. A region of interest analysis was performed on a priori defined regions.
Compared with controls, patients with idiopathic REM sleep behavior disorder showed significantly reduced 18F-DOPA tracer uptake in the substantia nigra. Patients with higher substantia nigra11C-PK11195 binding also had increased binding in the ipsilateral putamen. Patients with more severe reductions in putamenal 18F-DOPA uptake had significantly higher 11C-PK11195 binding in the putamen and substantia nigra.
—Jake Remaly
How Do Diet, Exercise, and Supplements Affect Parkinson’s Disease Progression?
PORTLAND, OR—Among patients with Parkinson’s disease, eating foods common in a Mediterranean diet and exercising regularly are associated with reduced rates of Parkinson’s disease progression, according to the results of a natural history study described at the Fourth World Parkinson Congress.
To evaluate whether diet, exercise, and supplements are associated with rate of Parkinson’s disease progression, Laurie Mischley, ND, PhD, MPH, Assistant Research Scientist at Bastyr University Research Institute in Kenmore, Washington, and Richard Lau, MPH, a PhD student in the College of Public Health and Human Sciences at Oregon State University in Corvalis conducted an Internet-based natural history study. A total of 1,024 patients participated in the study. Participants had a mean age of 60.7 and had been diagnosed with Parkinson’s disease for an average of 6.7 years.

The researchers used the Patient-Reported Outcomes in Parkinson’s Disease (PRO-PD) scale to assess Parkinson’s disease severity. Disease progression was defined as PRO-PD score adjusted for age and years since diagnosis. They used baseline food frequency questionnaires to quantify dietary intake in the cross-sectional analysis.
Fresh fruit, fresh vegetables, nuts and seeds, olive oil, fish (non-fried), wine, eggs, and fresh herbs were associated with a statistically significant improvement in PRO-PD score, the researchers said. Fried foods, beef, diet soda, canned fruits, and canned vegetables were associated with more severe disease. Dairy consumption was not associated with disease severity.
Of the supplements and pharmaceuticals studied, oral glutathione, rasagiline, and coenzyme Q10 were associated with improved PRO-PD scores, whereas iron was associated with more severe disease. The effect of melatonin was not significant, however, when the researchers considered poor sleep. The researchers observed a dose-response curve with exercise. Exercising at least 30 minutes daily was associated with the greatest reduction in disease severity.
“Whether iron, fried foods, diet soda, or canned goods provide environmental insults that accelerate disease progression warrants immediate attention,” the researchers concluded. “This pragmatic natural history study offers the first evidence base for prescribing lifestyle modification (beyond exercise) to patients with Parkinson’s disease. Patients should ... know that they can make choices that affect outcomes.”
—Jake Remaly
PORTLAND, OR—Among patients with Parkinson’s disease, eating foods common in a Mediterranean diet and exercising regularly are associated with reduced rates of Parkinson’s disease progression, according to the results of a natural history study described at the Fourth World Parkinson Congress.
To evaluate whether diet, exercise, and supplements are associated with rate of Parkinson’s disease progression, Laurie Mischley, ND, PhD, MPH, Assistant Research Scientist at Bastyr University Research Institute in Kenmore, Washington, and Richard Lau, MPH, a PhD student in the College of Public Health and Human Sciences at Oregon State University in Corvalis conducted an Internet-based natural history study. A total of 1,024 patients participated in the study. Participants had a mean age of 60.7 and had been diagnosed with Parkinson’s disease for an average of 6.7 years.
The researchers used the Patient-Reported Outcomes in Parkinson’s Disease (PRO-PD) scale to assess Parkinson’s disease severity. Disease progression was defined as PRO-PD score adjusted for age and years since diagnosis. They used baseline food frequency questionnaires to quantify dietary intake in the cross-sectional analysis.
Fresh fruit, fresh vegetables, nuts and seeds, olive oil, fish (non-fried), wine, eggs, and fresh herbs were associated with a statistically significant improvement in PRO-PD score, the researchers said. Fried foods, beef, diet soda, canned fruits, and canned vegetables were associated with more severe disease. Dairy consumption was not associated with disease severity.
Of the supplements and pharmaceuticals studied, oral glutathione, rasagiline, and coenzyme Q10 were associated with improved PRO-PD scores, whereas iron was associated with more severe disease. The effect of melatonin was not significant, however, when the researchers considered poor sleep. The researchers observed a dose-response curve with exercise. Exercising at least 30 minutes daily was associated with the greatest reduction in disease severity.
“Whether iron, fried foods, diet soda, or canned goods provide environmental insults that accelerate disease progression warrants immediate attention,” the researchers concluded. “This pragmatic natural history study offers the first evidence base for prescribing lifestyle modification (beyond exercise) to patients with Parkinson’s disease. Patients should ... know that they can make choices that affect outcomes.”
—Jake Remaly
PORTLAND, OR—Among patients with Parkinson’s disease, eating foods common in a Mediterranean diet and exercising regularly are associated with reduced rates of Parkinson’s disease progression, according to the results of a natural history study described at the Fourth World Parkinson Congress.
To evaluate whether diet, exercise, and supplements are associated with rate of Parkinson’s disease progression, Laurie Mischley, ND, PhD, MPH, Assistant Research Scientist at Bastyr University Research Institute in Kenmore, Washington, and Richard Lau, MPH, a PhD student in the College of Public Health and Human Sciences at Oregon State University in Corvalis conducted an Internet-based natural history study. A total of 1,024 patients participated in the study. Participants had a mean age of 60.7 and had been diagnosed with Parkinson’s disease for an average of 6.7 years.
The researchers used the Patient-Reported Outcomes in Parkinson’s Disease (PRO-PD) scale to assess Parkinson’s disease severity. Disease progression was defined as PRO-PD score adjusted for age and years since diagnosis. They used baseline food frequency questionnaires to quantify dietary intake in the cross-sectional analysis.
Fresh fruit, fresh vegetables, nuts and seeds, olive oil, fish (non-fried), wine, eggs, and fresh herbs were associated with a statistically significant improvement in PRO-PD score, the researchers said. Fried foods, beef, diet soda, canned fruits, and canned vegetables were associated with more severe disease. Dairy consumption was not associated with disease severity.
Of the supplements and pharmaceuticals studied, oral glutathione, rasagiline, and coenzyme Q10 were associated with improved PRO-PD scores, whereas iron was associated with more severe disease. The effect of melatonin was not significant, however, when the researchers considered poor sleep. The researchers observed a dose-response curve with exercise. Exercising at least 30 minutes daily was associated with the greatest reduction in disease severity.
“Whether iron, fried foods, diet soda, or canned goods provide environmental insults that accelerate disease progression warrants immediate attention,” the researchers concluded. “This pragmatic natural history study offers the first evidence base for prescribing lifestyle modification (beyond exercise) to patients with Parkinson’s disease. Patients should ... know that they can make choices that affect outcomes.”
—Jake Remaly

Ceramic Femoral Heads for All Patients? An Argument for Cost Containment in Hip Surgery
Total hip arthroplasty (THA) has revolutionized the practice of orthopedic surgery. The number of primary THAs performed in the United States alone is predicted to rise to 572,000 per year by 2030.1 Increasing demand requires a tighter focus on cost-effectiveness, particularly with regard to expensive postoperative complications. Trunnionosis and taper corrosion have recently emerged as problems in THA.2-7 No longer restricted to metal-on-metal bearings, these phenomena now affect an increasing number of metal-on-polyethylene THAs and are exacerbated by modularity.8 The emergence of these complications adds complexity to the diagnostic algorithm in patients who present with painful THAs. Furthermore, the diagnosis of either trunnionosis or taper corrosion calls for revision surgery. In response to the increase in these complications, a group of orthopedic professional societies developed an algorithm for managing suspected metal toxicity issues.9 However, increases in toxicity and patient morbidity, and the added costs of toxicity surveillance and revision surgery, will place a substantial economic burden on many health systems at a time when policy makers are implementing substantial changes to health delivery in an effort to contain costs while improving patient outcomes.
Although they are more expensive than cobalt-chrome heads, ceramic femoral heads make metal toxicity a nonissue and eliminate the need for toxicity surveillance protocols. Furthermore, ceramic femoral heads are thought to have longevity advantages (this relationship needs to be confirmed in long-term studies).
In this article, we provide a theoretical framework for debating whether use of ceramic femoral heads in all THA patients could represent a more cost-effective option over the long term.
Materials and Methods
Guidelines for the diagnostic algorithm for painful THA with suspected metal toxicity were obtained from a recent orthopedic professional society consensus statement.9 The cost of this work-up was obtained from the finance department at our institution (Table 1). 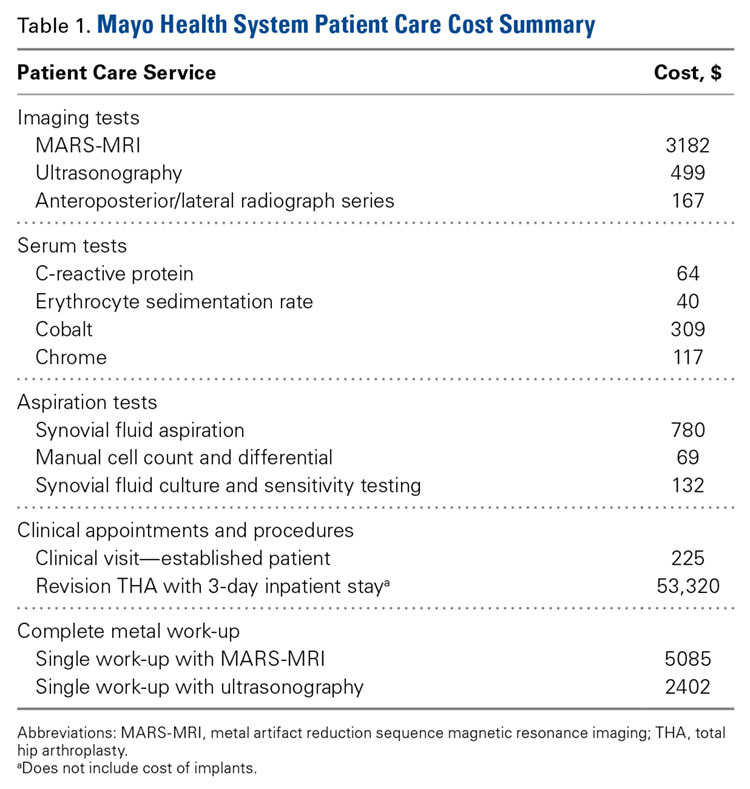
We created 2 metrics to analyze the cost difference between ceramic and cobalt-chrome femoral heads. The first metric was “ceramic surplus,” the extra cost of a ceramic femoral head above that of a cobalt-chrome femoral head, and the second was “maximum ceramic surplus,” the ceramic surplus cutoff value for which using ceramic femoral heads in all patients becomes more cost-effective than using cobalt-chrome heads. 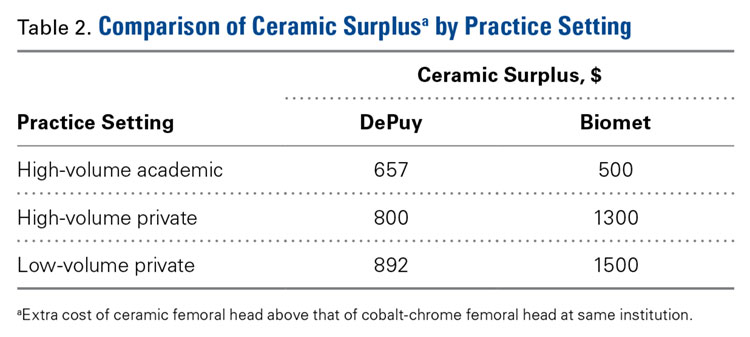
The cost of a metal work-up was determined for a single round of imaging tests (stratified by MRI and US), serum tests, aspiration tests, and clinic visit. These data were then combined with the cost of revision THA (Table 1) to create a series of maximum ceramic surplus models. In all these simulations, we assumed that about 7% of patients with metal-on-polyethylene THA would present with groin pain 1 to 2 years after surgery,10 and, working on this assumption, we applied a series of theoretical incidence ratios (12.5%, 25%, 50%) to both the percentage of patients who presented with a painful THA and received a metal toxicity work-up and the percentage of those who received the toxicity work-up and eventually needed revision surgery. For example, in the best-case scenario, the model assumes that 7% of THA patients present with pain and that 12.5% of the painful cohort receives a single work-up for metal toxicity (0.875% of all THAs). The best-case scenario then assumes that 12.5% of patients who receive a work-up for metal toxicity are eventually revised (0.11% of all THAs). By contrast, in the worst-case scenario, the model continues to assume that 7% of THA patients present with pain, but it also assumes that 50% of the painful cohort receives a single work-up for metal toxicity (3.5% of all THAs). 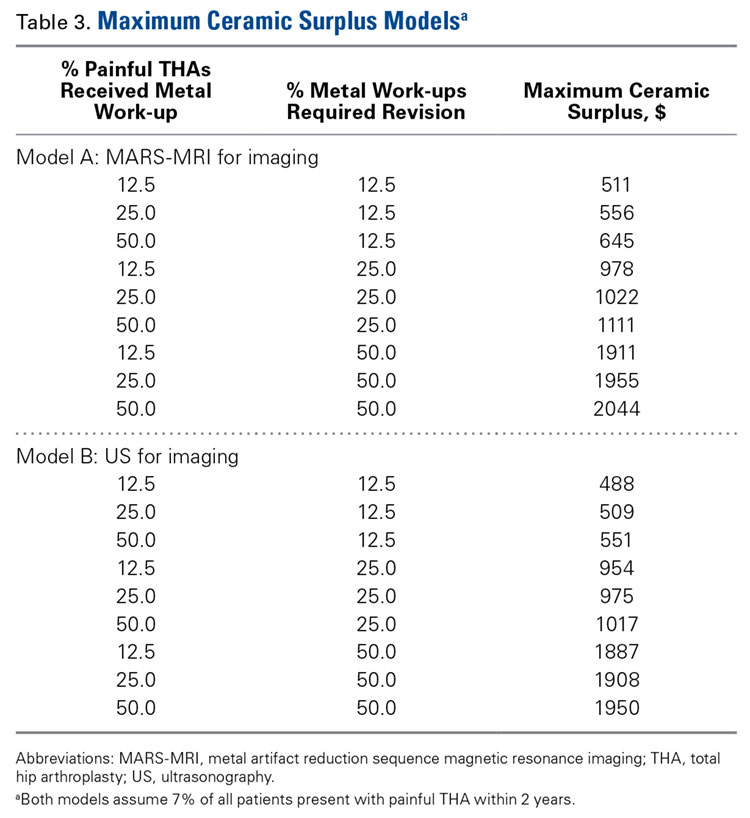
The lowest maximum ceramic surplus values were calculated from the best-case scenario, and the highest from the worst-case scenario. These steps were taken in keeping with the fact that a lower incidence of metal toxicity work-ups and revisions would require the price difference between ceramic and cobalt-chrome heads (ceramic surplus) to be small in order for ceramic heads in all patients to be cost-effective. The inverse is true for a high incidence of metal toxicity work-ups and revisions: A larger price difference between ceramic and cobalt-chrome femoral heads would be tolerable to still be cost-effective.
Results
A single metal toxicity work-up cost $5085 with MARS-MRI and $2402 with US (Table 1). Revision THA with a 3-day inpatient stay cost $53,320, and that figure does not include the cost of surgical implants or perioperative medications and devices, all of which have highly variable cost structures (Table 1). Ceramic surplus was as low as $500 in a high-volume academic practice and as high as $1500 in a low-volume private practice (Table 2). Maximum ceramic surplus ranged from $511 to $2044 in the models integrating MARS-MRI and from $488 to $1950 in the models integrating US (Table 3).
Discussion
Trunnionosis, corrosion, and metal toxicity are of increasing concern in hip implants that incorporate a cobalt-chrome femoral head, regardless of the counterpart articulation surface (metal, ceramic, polyethylene).2-8 In response to the added diagnostic challenge raised by these phenomena, a group of orthopedic professional societies developed an algorithm that can guide surgeons in the management of suspected corrosion or metal toxicity.9 In this protocol, toxicity surveillance in conjunction with potential revision surgery for metal-associated complications has the potential to increase patient morbidity and place a significant economic burden on many health systems. Given the recent emergence of trunnionosis, epidemiologic data on this complication are lacking.10 However, there is a substantial body of evidence showing devastating complications associated with adverse reactions to metal debris.11-17
Given the potential complications specific to cobalt-chrome femoral heads, we wanted to provide a theoretical framework for debating whether use of ceramic heads in all patients has the potential to be a more cost-effective option over the long term. Ceramic femoral heads are premium implants, certainly more expensive at initial point of care. One study based on a large community registry showed premium implants (eg, ceramic femoral heads) add a surplus averaging $1000.18 In our investigation, ceramic surplus varied with practice setting, from $500 to $1500. Lower costs were discovered in high-volume practice settings, indicating that a shift to increased use of ceramic femoral heads would likely decrease ceramic surplus for most institutions.
We used a series of simulations to predict maximum ceramic surplus after manipulation of theoretical incidence ratios. The main limitation of this study was our use of 7% as the incidence of painful THA within 1- to 2-year follow-up. This point estimate was derived from a manuscript that to our knowledge provides the most realistic estimate of this complication10; with use of more complete data in upcoming studies, however, the 7% figure could certainly change. As data are also lacking on the proportion of painful THAs that receive a metal work-up and on the proportion of metal work-ups that indicate revision surgery, we modeled values of 12.5%, 25%, and 50% for each of these metrics to cover a wide range of possibilities.
It is also true the model did not incorporate scenarios to account for the law of unintended consequences, which would caution that using ceramics for all patients may bring a new set of complications. Zirconia ceramic bearings have tended to fracture, with the vast majority of fractures occurring in the liner of ceramic-on-ceramic articulations. Midterm reports and laboratory data suggest this issue has largely been solved with the advent of delta ceramics, a composite containing only a small fraction of zirconia.19,20 Nevertheless, longer term in vivo data are needed to confirm the stability, longevity, and complication profile of these materials.
A final limitation of the present study is that the cost of a single metal toxicity work-up was based on just one institution. Grossly differing cost structures in other markets could alter the economic risk–benefit analysis we have described. However, we should note that the costs of tests, procedures, and appointments at our institution were uniform across a wide variety of practice settings in multiple regions of the United States, and thus are likely similar to the costs at a majority of practices.
Although our model took some liberties by necessity, it was also quite conservative in many respects. Many patients who undergo surveillance for metal toxicity undergo serial follow-ups; for this analysis, however, we considered the cost of only a single work-up. In addition, our proposed cost of revision surgery accounts only for facility and personnel costs during a 3-day inpatient stay and does not include the costs of implants, perioperative medications and devices, follow-up care, and potentially longer hospital stays or subsequent procedures, all of which can be highly variable and add considerable cost. Had any or all of these factors been incorporated into more complex modeling, the potential economic benefits of ceramic femoral heads would have been significantly greater.
After taking all these factors into account, our model found that maximum ceramic surplus ranged from $488 to $2044, depending on theoretical incidence ratio and imaging modality (Table 3). The lowest maximum ceramic surplus values ($511 for MARS-MRI protocol, $488 for US protocol) were based on the assumption that only 12.5% of patients who present with a painful THA receive a single metal work-up (0.875% of all THAs) and that only 12.5% of those patients are eventually revised (0.11% of all THAs). This outcome suggests ceramic femoral heads could be more cost-effective than cobalt-chrome femoral heads under these conservative projections when considering ceramic surplus is already as low as $500 at some high-volume centers. This figure would likely decline further in parallel with widespread growth in demand. Further study on the epidemiology of trunnionosis, corrosion, and metal toxicity in metal-on-polyethylene THA is needed to evaluate the economic validity of this proposal. Nevertheless, the superior safety profile of ceramic femoral heads with regard to metal toxicity indicates that wholesale use in THAs may in fact provide the most economical option on a societal scale.
Am J Orthop. 2016;45(6):E362-E366. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
2. Cooper HJ. The local effects of metal corrosion in total hip arthroplasty. Orthop Clin North Am. 2014;45(1):9-18.
3. Cooper HJ, Della Valle CJ, Berger RA, et al. Corrosion at the head-neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J Bone Joint Surg Am. 2012;94(18):1655-1661.
4. Cooper HJ, Urban RM, Wixson RL, Meneghini RM, Jacobs JJ. Adverse local tissue reaction arising from corrosion at the femoral neck-body junction in a dual-taper stem with a cobalt-chromium modular neck. J Bone Joint Surg Am. 2013;95(10):865-872.
5. Jacobs JJ, Cooper HJ, Urban RM, Wixson RL, Della Valle CJ. What do we know about taper corrosion in total hip arthroplasty? J Arthroplasty. 2014;29(4):668-669.
6. Pastides PS, Dodd M, Sarraf KM, Willis-Owen CA. Trunnionosis: a pain in the neck. World J Orthop. 2013;4(4):161-166.
7. Shulman RM, Zywiel MG, Gandhi R, Davey JR, Salonen DC. Trunnionosis: the latest culprit in adverse reactions to metal debris following hip arthroplasty. Skeletal Radiol. 2015;44(3):433-440.
8. Mihalko WM, Wimmer MA, Pacione CA, Laurent MP, Murphy RF, Rider C. How have alternative bearings and modularity affected revision rates in total hip arthroplasty? Clin Orthop Relat Res. 2014;472(12):3747-3758.
9. Kwon YM, Lombardi AV, Jacobs JJ, Fehring TK, Lewis CG, Cabanela ME. Risk stratification algorithm for management of patients with metal-on-metal hip arthroplasty: consensus statement of the American Association of Hip and Knee Surgeons, the American Academy of Orthopaedic Surgeons, and the Hip Society. J Bone Joint Surg Am. 2014;96(1):e4.
10. Bartelt RB, Yuan BJ, Trousdale RT, Sierra RJ. The prevalence of groin pain after metal-on-metal total hip arthroplasty and total hip resurfacing. Clin Orthop Relat Res. 2010;468(9):2346-2356.
11. Bozic KJ, Lau EC, Ong KL, Vail TP, Rubash HE, Berry DJ. Comparative effectiveness of metal-on-metal and metal-on-polyethylene bearings in Medicare total hip arthroplasty patients. J Arthroplasty. 2012;27(8 suppl):37-40.
12. Cuckler JM. Metal-on-metal surface replacement: a triumph of hope over reason: affirms. Orthopedics. 2011;34(9):e439-e441.
13. de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Bone Joint Surg Am. 2011;93(24):2287-2293.
14. Fehring TK, Odum S, Sproul R, Weathersbee J. High frequency of adverse local tissue reactions in asymptomatic patients with metal-on-metal THA. Clin Orthop Relat Res. 2014;472(2):517-522.
15. Hasegawa M, Yoshida K, Wakabayashi H, Sudo A. Prevalence of adverse reactions to metal debris following metal-on-metal THA. Orthopedics. 2013;36(5):e606-e612.
16. Melvin JS, Karthikeyan T, Cope R, Fehring TK. Early failures in total hip arthroplasty—a changing paradigm. J Arthroplasty. 2014;29(6):1285-1288.
17. Wyles CC, Van Demark RE 3rd, Sierra RJ, Trousdale RT. High rate of infection after aseptic revision of failed metal-on-metal total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):509-516.
18. Gioe TJ, Sharma A, Tatman P, Mehle S. Do “premium” joint implants add value?: Analysis of high cost joint implants in a community registry. Clin Orthop Relat Res. 2011;469(1):48-54.
19. D’Antonio JA, Capello WN, Naughton M. Ceramic bearings for total hip arthroplasty have high survivorship at 10 years. Clin Orthop Relat Res. 2012;470(2):373-381.
20. D’Antonio JA, Capello WN, Naughton M. High survivorship with a titanium-encased alumina ceramic bearing for total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):611-616.
Total hip arthroplasty (THA) has revolutionized the practice of orthopedic surgery. The number of primary THAs performed in the United States alone is predicted to rise to 572,000 per year by 2030.1 Increasing demand requires a tighter focus on cost-effectiveness, particularly with regard to expensive postoperative complications. Trunnionosis and taper corrosion have recently emerged as problems in THA.2-7 No longer restricted to metal-on-metal bearings, these phenomena now affect an increasing number of metal-on-polyethylene THAs and are exacerbated by modularity.8 The emergence of these complications adds complexity to the diagnostic algorithm in patients who present with painful THAs. Furthermore, the diagnosis of either trunnionosis or taper corrosion calls for revision surgery. In response to the increase in these complications, a group of orthopedic professional societies developed an algorithm for managing suspected metal toxicity issues.9 However, increases in toxicity and patient morbidity, and the added costs of toxicity surveillance and revision surgery, will place a substantial economic burden on many health systems at a time when policy makers are implementing substantial changes to health delivery in an effort to contain costs while improving patient outcomes.
Although they are more expensive than cobalt-chrome heads, ceramic femoral heads make metal toxicity a nonissue and eliminate the need for toxicity surveillance protocols. Furthermore, ceramic femoral heads are thought to have longevity advantages (this relationship needs to be confirmed in long-term studies).
In this article, we provide a theoretical framework for debating whether use of ceramic femoral heads in all THA patients could represent a more cost-effective option over the long term.
Materials and Methods
Guidelines for the diagnostic algorithm for painful THA with suspected metal toxicity were obtained from a recent orthopedic professional society consensus statement.9 The cost of this work-up was obtained from the finance department at our institution (Table 1).
We created 2 metrics to analyze the cost difference between ceramic and cobalt-chrome femoral heads. The first metric was “ceramic surplus,” the extra cost of a ceramic femoral head above that of a cobalt-chrome femoral head, and the second was “maximum ceramic surplus,” the ceramic surplus cutoff value for which using ceramic femoral heads in all patients becomes more cost-effective than using cobalt-chrome heads.
The cost of a metal work-up was determined for a single round of imaging tests (stratified by MRI and US), serum tests, aspiration tests, and clinic visit. These data were then combined with the cost of revision THA (Table 1) to create a series of maximum ceramic surplus models. In all these simulations, we assumed that about 7% of patients with metal-on-polyethylene THA would present with groin pain 1 to 2 years after surgery,10 and, working on this assumption, we applied a series of theoretical incidence ratios (12.5%, 25%, 50%) to both the percentage of patients who presented with a painful THA and received a metal toxicity work-up and the percentage of those who received the toxicity work-up and eventually needed revision surgery. For example, in the best-case scenario, the model assumes that 7% of THA patients present with pain and that 12.5% of the painful cohort receives a single work-up for metal toxicity (0.875% of all THAs). The best-case scenario then assumes that 12.5% of patients who receive a work-up for metal toxicity are eventually revised (0.11% of all THAs). By contrast, in the worst-case scenario, the model continues to assume that 7% of THA patients present with pain, but it also assumes that 50% of the painful cohort receives a single work-up for metal toxicity (3.5% of all THAs).
The lowest maximum ceramic surplus values were calculated from the best-case scenario, and the highest from the worst-case scenario. These steps were taken in keeping with the fact that a lower incidence of metal toxicity work-ups and revisions would require the price difference between ceramic and cobalt-chrome heads (ceramic surplus) to be small in order for ceramic heads in all patients to be cost-effective. The inverse is true for a high incidence of metal toxicity work-ups and revisions: A larger price difference between ceramic and cobalt-chrome femoral heads would be tolerable to still be cost-effective.
Results
A single metal toxicity work-up cost $5085 with MARS-MRI and $2402 with US (Table 1). Revision THA with a 3-day inpatient stay cost $53,320, and that figure does not include the cost of surgical implants or perioperative medications and devices, all of which have highly variable cost structures (Table 1). Ceramic surplus was as low as $500 in a high-volume academic practice and as high as $1500 in a low-volume private practice (Table 2). Maximum ceramic surplus ranged from $511 to $2044 in the models integrating MARS-MRI and from $488 to $1950 in the models integrating US (Table 3).
Discussion
Trunnionosis, corrosion, and metal toxicity are of increasing concern in hip implants that incorporate a cobalt-chrome femoral head, regardless of the counterpart articulation surface (metal, ceramic, polyethylene).2-8 In response to the added diagnostic challenge raised by these phenomena, a group of orthopedic professional societies developed an algorithm that can guide surgeons in the management of suspected corrosion or metal toxicity.9 In this protocol, toxicity surveillance in conjunction with potential revision surgery for metal-associated complications has the potential to increase patient morbidity and place a significant economic burden on many health systems. Given the recent emergence of trunnionosis, epidemiologic data on this complication are lacking.10 However, there is a substantial body of evidence showing devastating complications associated with adverse reactions to metal debris.11-17
Given the potential complications specific to cobalt-chrome femoral heads, we wanted to provide a theoretical framework for debating whether use of ceramic heads in all patients has the potential to be a more cost-effective option over the long term. Ceramic femoral heads are premium implants, certainly more expensive at initial point of care. One study based on a large community registry showed premium implants (eg, ceramic femoral heads) add a surplus averaging $1000.18 In our investigation, ceramic surplus varied with practice setting, from $500 to $1500. Lower costs were discovered in high-volume practice settings, indicating that a shift to increased use of ceramic femoral heads would likely decrease ceramic surplus for most institutions.
We used a series of simulations to predict maximum ceramic surplus after manipulation of theoretical incidence ratios. The main limitation of this study was our use of 7% as the incidence of painful THA within 1- to 2-year follow-up. This point estimate was derived from a manuscript that to our knowledge provides the most realistic estimate of this complication10; with use of more complete data in upcoming studies, however, the 7% figure could certainly change. As data are also lacking on the proportion of painful THAs that receive a metal work-up and on the proportion of metal work-ups that indicate revision surgery, we modeled values of 12.5%, 25%, and 50% for each of these metrics to cover a wide range of possibilities.
It is also true the model did not incorporate scenarios to account for the law of unintended consequences, which would caution that using ceramics for all patients may bring a new set of complications. Zirconia ceramic bearings have tended to fracture, with the vast majority of fractures occurring in the liner of ceramic-on-ceramic articulations. Midterm reports and laboratory data suggest this issue has largely been solved with the advent of delta ceramics, a composite containing only a small fraction of zirconia.19,20 Nevertheless, longer term in vivo data are needed to confirm the stability, longevity, and complication profile of these materials.
A final limitation of the present study is that the cost of a single metal toxicity work-up was based on just one institution. Grossly differing cost structures in other markets could alter the economic risk–benefit analysis we have described. However, we should note that the costs of tests, procedures, and appointments at our institution were uniform across a wide variety of practice settings in multiple regions of the United States, and thus are likely similar to the costs at a majority of practices.
Although our model took some liberties by necessity, it was also quite conservative in many respects. Many patients who undergo surveillance for metal toxicity undergo serial follow-ups; for this analysis, however, we considered the cost of only a single work-up. In addition, our proposed cost of revision surgery accounts only for facility and personnel costs during a 3-day inpatient stay and does not include the costs of implants, perioperative medications and devices, follow-up care, and potentially longer hospital stays or subsequent procedures, all of which can be highly variable and add considerable cost. Had any or all of these factors been incorporated into more complex modeling, the potential economic benefits of ceramic femoral heads would have been significantly greater.
After taking all these factors into account, our model found that maximum ceramic surplus ranged from $488 to $2044, depending on theoretical incidence ratio and imaging modality (Table 3). The lowest maximum ceramic surplus values ($511 for MARS-MRI protocol, $488 for US protocol) were based on the assumption that only 12.5% of patients who present with a painful THA receive a single metal work-up (0.875% of all THAs) and that only 12.5% of those patients are eventually revised (0.11% of all THAs). This outcome suggests ceramic femoral heads could be more cost-effective than cobalt-chrome femoral heads under these conservative projections when considering ceramic surplus is already as low as $500 at some high-volume centers. This figure would likely decline further in parallel with widespread growth in demand. Further study on the epidemiology of trunnionosis, corrosion, and metal toxicity in metal-on-polyethylene THA is needed to evaluate the economic validity of this proposal. Nevertheless, the superior safety profile of ceramic femoral heads with regard to metal toxicity indicates that wholesale use in THAs may in fact provide the most economical option on a societal scale.
Am J Orthop. 2016;45(6):E362-E366. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
Total hip arthroplasty (THA) has revolutionized the practice of orthopedic surgery. The number of primary THAs performed in the United States alone is predicted to rise to 572,000 per year by 2030.1 Increasing demand requires a tighter focus on cost-effectiveness, particularly with regard to expensive postoperative complications. Trunnionosis and taper corrosion have recently emerged as problems in THA.2-7 No longer restricted to metal-on-metal bearings, these phenomena now affect an increasing number of metal-on-polyethylene THAs and are exacerbated by modularity.8 The emergence of these complications adds complexity to the diagnostic algorithm in patients who present with painful THAs. Furthermore, the diagnosis of either trunnionosis or taper corrosion calls for revision surgery. In response to the increase in these complications, a group of orthopedic professional societies developed an algorithm for managing suspected metal toxicity issues.9 However, increases in toxicity and patient morbidity, and the added costs of toxicity surveillance and revision surgery, will place a substantial economic burden on many health systems at a time when policy makers are implementing substantial changes to health delivery in an effort to contain costs while improving patient outcomes.
Although they are more expensive than cobalt-chrome heads, ceramic femoral heads make metal toxicity a nonissue and eliminate the need for toxicity surveillance protocols. Furthermore, ceramic femoral heads are thought to have longevity advantages (this relationship needs to be confirmed in long-term studies).
In this article, we provide a theoretical framework for debating whether use of ceramic femoral heads in all THA patients could represent a more cost-effective option over the long term.
Materials and Methods
Guidelines for the diagnostic algorithm for painful THA with suspected metal toxicity were obtained from a recent orthopedic professional society consensus statement.9 The cost of this work-up was obtained from the finance department at our institution (Table 1).
We created 2 metrics to analyze the cost difference between ceramic and cobalt-chrome femoral heads. The first metric was “ceramic surplus,” the extra cost of a ceramic femoral head above that of a cobalt-chrome femoral head, and the second was “maximum ceramic surplus,” the ceramic surplus cutoff value for which using ceramic femoral heads in all patients becomes more cost-effective than using cobalt-chrome heads.
The cost of a metal work-up was determined for a single round of imaging tests (stratified by MRI and US), serum tests, aspiration tests, and clinic visit. These data were then combined with the cost of revision THA (Table 1) to create a series of maximum ceramic surplus models. In all these simulations, we assumed that about 7% of patients with metal-on-polyethylene THA would present with groin pain 1 to 2 years after surgery,10 and, working on this assumption, we applied a series of theoretical incidence ratios (12.5%, 25%, 50%) to both the percentage of patients who presented with a painful THA and received a metal toxicity work-up and the percentage of those who received the toxicity work-up and eventually needed revision surgery. For example, in the best-case scenario, the model assumes that 7% of THA patients present with pain and that 12.5% of the painful cohort receives a single work-up for metal toxicity (0.875% of all THAs). The best-case scenario then assumes that 12.5% of patients who receive a work-up for metal toxicity are eventually revised (0.11% of all THAs). By contrast, in the worst-case scenario, the model continues to assume that 7% of THA patients present with pain, but it also assumes that 50% of the painful cohort receives a single work-up for metal toxicity (3.5% of all THAs).
The lowest maximum ceramic surplus values were calculated from the best-case scenario, and the highest from the worst-case scenario. These steps were taken in keeping with the fact that a lower incidence of metal toxicity work-ups and revisions would require the price difference between ceramic and cobalt-chrome heads (ceramic surplus) to be small in order for ceramic heads in all patients to be cost-effective. The inverse is true for a high incidence of metal toxicity work-ups and revisions: A larger price difference between ceramic and cobalt-chrome femoral heads would be tolerable to still be cost-effective.
Results
A single metal toxicity work-up cost $5085 with MARS-MRI and $2402 with US (Table 1). Revision THA with a 3-day inpatient stay cost $53,320, and that figure does not include the cost of surgical implants or perioperative medications and devices, all of which have highly variable cost structures (Table 1). Ceramic surplus was as low as $500 in a high-volume academic practice and as high as $1500 in a low-volume private practice (Table 2). Maximum ceramic surplus ranged from $511 to $2044 in the models integrating MARS-MRI and from $488 to $1950 in the models integrating US (Table 3).
Discussion
Trunnionosis, corrosion, and metal toxicity are of increasing concern in hip implants that incorporate a cobalt-chrome femoral head, regardless of the counterpart articulation surface (metal, ceramic, polyethylene).2-8 In response to the added diagnostic challenge raised by these phenomena, a group of orthopedic professional societies developed an algorithm that can guide surgeons in the management of suspected corrosion or metal toxicity.9 In this protocol, toxicity surveillance in conjunction with potential revision surgery for metal-associated complications has the potential to increase patient morbidity and place a significant economic burden on many health systems. Given the recent emergence of trunnionosis, epidemiologic data on this complication are lacking.10 However, there is a substantial body of evidence showing devastating complications associated with adverse reactions to metal debris.11-17
Given the potential complications specific to cobalt-chrome femoral heads, we wanted to provide a theoretical framework for debating whether use of ceramic heads in all patients has the potential to be a more cost-effective option over the long term. Ceramic femoral heads are premium implants, certainly more expensive at initial point of care. One study based on a large community registry showed premium implants (eg, ceramic femoral heads) add a surplus averaging $1000.18 In our investigation, ceramic surplus varied with practice setting, from $500 to $1500. Lower costs were discovered in high-volume practice settings, indicating that a shift to increased use of ceramic femoral heads would likely decrease ceramic surplus for most institutions.
We used a series of simulations to predict maximum ceramic surplus after manipulation of theoretical incidence ratios. The main limitation of this study was our use of 7% as the incidence of painful THA within 1- to 2-year follow-up. This point estimate was derived from a manuscript that to our knowledge provides the most realistic estimate of this complication10; with use of more complete data in upcoming studies, however, the 7% figure could certainly change. As data are also lacking on the proportion of painful THAs that receive a metal work-up and on the proportion of metal work-ups that indicate revision surgery, we modeled values of 12.5%, 25%, and 50% for each of these metrics to cover a wide range of possibilities.
It is also true the model did not incorporate scenarios to account for the law of unintended consequences, which would caution that using ceramics for all patients may bring a new set of complications. Zirconia ceramic bearings have tended to fracture, with the vast majority of fractures occurring in the liner of ceramic-on-ceramic articulations. Midterm reports and laboratory data suggest this issue has largely been solved with the advent of delta ceramics, a composite containing only a small fraction of zirconia.19,20 Nevertheless, longer term in vivo data are needed to confirm the stability, longevity, and complication profile of these materials.
A final limitation of the present study is that the cost of a single metal toxicity work-up was based on just one institution. Grossly differing cost structures in other markets could alter the economic risk–benefit analysis we have described. However, we should note that the costs of tests, procedures, and appointments at our institution were uniform across a wide variety of practice settings in multiple regions of the United States, and thus are likely similar to the costs at a majority of practices.
Although our model took some liberties by necessity, it was also quite conservative in many respects. Many patients who undergo surveillance for metal toxicity undergo serial follow-ups; for this analysis, however, we considered the cost of only a single work-up. In addition, our proposed cost of revision surgery accounts only for facility and personnel costs during a 3-day inpatient stay and does not include the costs of implants, perioperative medications and devices, follow-up care, and potentially longer hospital stays or subsequent procedures, all of which can be highly variable and add considerable cost. Had any or all of these factors been incorporated into more complex modeling, the potential economic benefits of ceramic femoral heads would have been significantly greater.
After taking all these factors into account, our model found that maximum ceramic surplus ranged from $488 to $2044, depending on theoretical incidence ratio and imaging modality (Table 3). The lowest maximum ceramic surplus values ($511 for MARS-MRI protocol, $488 for US protocol) were based on the assumption that only 12.5% of patients who present with a painful THA receive a single metal work-up (0.875% of all THAs) and that only 12.5% of those patients are eventually revised (0.11% of all THAs). This outcome suggests ceramic femoral heads could be more cost-effective than cobalt-chrome femoral heads under these conservative projections when considering ceramic surplus is already as low as $500 at some high-volume centers. This figure would likely decline further in parallel with widespread growth in demand. Further study on the epidemiology of trunnionosis, corrosion, and metal toxicity in metal-on-polyethylene THA is needed to evaluate the economic validity of this proposal. Nevertheless, the superior safety profile of ceramic femoral heads with regard to metal toxicity indicates that wholesale use in THAs may in fact provide the most economical option on a societal scale.
Am J Orthop. 2016;45(6):E362-E366. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
2. Cooper HJ. The local effects of metal corrosion in total hip arthroplasty. Orthop Clin North Am. 2014;45(1):9-18.
3. Cooper HJ, Della Valle CJ, Berger RA, et al. Corrosion at the head-neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J Bone Joint Surg Am. 2012;94(18):1655-1661.
4. Cooper HJ, Urban RM, Wixson RL, Meneghini RM, Jacobs JJ. Adverse local tissue reaction arising from corrosion at the femoral neck-body junction in a dual-taper stem with a cobalt-chromium modular neck. J Bone Joint Surg Am. 2013;95(10):865-872.
5. Jacobs JJ, Cooper HJ, Urban RM, Wixson RL, Della Valle CJ. What do we know about taper corrosion in total hip arthroplasty? J Arthroplasty. 2014;29(4):668-669.
6. Pastides PS, Dodd M, Sarraf KM, Willis-Owen CA. Trunnionosis: a pain in the neck. World J Orthop. 2013;4(4):161-166.
7. Shulman RM, Zywiel MG, Gandhi R, Davey JR, Salonen DC. Trunnionosis: the latest culprit in adverse reactions to metal debris following hip arthroplasty. Skeletal Radiol. 2015;44(3):433-440.
8. Mihalko WM, Wimmer MA, Pacione CA, Laurent MP, Murphy RF, Rider C. How have alternative bearings and modularity affected revision rates in total hip arthroplasty? Clin Orthop Relat Res. 2014;472(12):3747-3758.
9. Kwon YM, Lombardi AV, Jacobs JJ, Fehring TK, Lewis CG, Cabanela ME. Risk stratification algorithm for management of patients with metal-on-metal hip arthroplasty: consensus statement of the American Association of Hip and Knee Surgeons, the American Academy of Orthopaedic Surgeons, and the Hip Society. J Bone Joint Surg Am. 2014;96(1):e4.
10. Bartelt RB, Yuan BJ, Trousdale RT, Sierra RJ. The prevalence of groin pain after metal-on-metal total hip arthroplasty and total hip resurfacing. Clin Orthop Relat Res. 2010;468(9):2346-2356.
11. Bozic KJ, Lau EC, Ong KL, Vail TP, Rubash HE, Berry DJ. Comparative effectiveness of metal-on-metal and metal-on-polyethylene bearings in Medicare total hip arthroplasty patients. J Arthroplasty. 2012;27(8 suppl):37-40.
12. Cuckler JM. Metal-on-metal surface replacement: a triumph of hope over reason: affirms. Orthopedics. 2011;34(9):e439-e441.
13. de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Bone Joint Surg Am. 2011;93(24):2287-2293.
14. Fehring TK, Odum S, Sproul R, Weathersbee J. High frequency of adverse local tissue reactions in asymptomatic patients with metal-on-metal THA. Clin Orthop Relat Res. 2014;472(2):517-522.
15. Hasegawa M, Yoshida K, Wakabayashi H, Sudo A. Prevalence of adverse reactions to metal debris following metal-on-metal THA. Orthopedics. 2013;36(5):e606-e612.
16. Melvin JS, Karthikeyan T, Cope R, Fehring TK. Early failures in total hip arthroplasty—a changing paradigm. J Arthroplasty. 2014;29(6):1285-1288.
17. Wyles CC, Van Demark RE 3rd, Sierra RJ, Trousdale RT. High rate of infection after aseptic revision of failed metal-on-metal total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):509-516.
18. Gioe TJ, Sharma A, Tatman P, Mehle S. Do “premium” joint implants add value?: Analysis of high cost joint implants in a community registry. Clin Orthop Relat Res. 2011;469(1):48-54.
19. D’Antonio JA, Capello WN, Naughton M. Ceramic bearings for total hip arthroplasty have high survivorship at 10 years. Clin Orthop Relat Res. 2012;470(2):373-381.
20. D’Antonio JA, Capello WN, Naughton M. High survivorship with a titanium-encased alumina ceramic bearing for total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):611-616.
1. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780-785.
2. Cooper HJ. The local effects of metal corrosion in total hip arthroplasty. Orthop Clin North Am. 2014;45(1):9-18.
3. Cooper HJ, Della Valle CJ, Berger RA, et al. Corrosion at the head-neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J Bone Joint Surg Am. 2012;94(18):1655-1661.
4. Cooper HJ, Urban RM, Wixson RL, Meneghini RM, Jacobs JJ. Adverse local tissue reaction arising from corrosion at the femoral neck-body junction in a dual-taper stem with a cobalt-chromium modular neck. J Bone Joint Surg Am. 2013;95(10):865-872.
5. Jacobs JJ, Cooper HJ, Urban RM, Wixson RL, Della Valle CJ. What do we know about taper corrosion in total hip arthroplasty? J Arthroplasty. 2014;29(4):668-669.
6. Pastides PS, Dodd M, Sarraf KM, Willis-Owen CA. Trunnionosis: a pain in the neck. World J Orthop. 2013;4(4):161-166.
7. Shulman RM, Zywiel MG, Gandhi R, Davey JR, Salonen DC. Trunnionosis: the latest culprit in adverse reactions to metal debris following hip arthroplasty. Skeletal Radiol. 2015;44(3):433-440.
8. Mihalko WM, Wimmer MA, Pacione CA, Laurent MP, Murphy RF, Rider C. How have alternative bearings and modularity affected revision rates in total hip arthroplasty? Clin Orthop Relat Res. 2014;472(12):3747-3758.
9. Kwon YM, Lombardi AV, Jacobs JJ, Fehring TK, Lewis CG, Cabanela ME. Risk stratification algorithm for management of patients with metal-on-metal hip arthroplasty: consensus statement of the American Association of Hip and Knee Surgeons, the American Academy of Orthopaedic Surgeons, and the Hip Society. J Bone Joint Surg Am. 2014;96(1):e4.
10. Bartelt RB, Yuan BJ, Trousdale RT, Sierra RJ. The prevalence of groin pain after metal-on-metal total hip arthroplasty and total hip resurfacing. Clin Orthop Relat Res. 2010;468(9):2346-2356.
11. Bozic KJ, Lau EC, Ong KL, Vail TP, Rubash HE, Berry DJ. Comparative effectiveness of metal-on-metal and metal-on-polyethylene bearings in Medicare total hip arthroplasty patients. J Arthroplasty. 2012;27(8 suppl):37-40.
12. Cuckler JM. Metal-on-metal surface replacement: a triumph of hope over reason: affirms. Orthopedics. 2011;34(9):e439-e441.
13. de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: an analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J Bone Joint Surg Am. 2011;93(24):2287-2293.
14. Fehring TK, Odum S, Sproul R, Weathersbee J. High frequency of adverse local tissue reactions in asymptomatic patients with metal-on-metal THA. Clin Orthop Relat Res. 2014;472(2):517-522.
15. Hasegawa M, Yoshida K, Wakabayashi H, Sudo A. Prevalence of adverse reactions to metal debris following metal-on-metal THA. Orthopedics. 2013;36(5):e606-e612.
16. Melvin JS, Karthikeyan T, Cope R, Fehring TK. Early failures in total hip arthroplasty—a changing paradigm. J Arthroplasty. 2014;29(6):1285-1288.
17. Wyles CC, Van Demark RE 3rd, Sierra RJ, Trousdale RT. High rate of infection after aseptic revision of failed metal-on-metal total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):509-516.
18. Gioe TJ, Sharma A, Tatman P, Mehle S. Do “premium” joint implants add value?: Analysis of high cost joint implants in a community registry. Clin Orthop Relat Res. 2011;469(1):48-54.
19. D’Antonio JA, Capello WN, Naughton M. Ceramic bearings for total hip arthroplasty have high survivorship at 10 years. Clin Orthop Relat Res. 2012;470(2):373-381.
20. D’Antonio JA, Capello WN, Naughton M. High survivorship with a titanium-encased alumina ceramic bearing for total hip arthroplasty. Clin Orthop Relat Res. 2014;472(2):611-616.
Fluoxetine fails to slow progressive multiple sclerosis
LONDON – Contrary to expectation of a neuroprotective benefit, fluoxetine does not slow down the progressive phase of multiple sclerosis, according to the results of a randomized, double-blind, multicenter trial.
The first results of the FLUOX-PMS trial, reported by Melissa Cambron, MD, of University Hospital Brussels (Belgium), showed no statistically significant difference between fluoxetine and placebo for improving the primary endpoint of the time to confirmed disease progression.

“The progressive phase of MS remains an ill-understood part of the disease and it is a holy grail to find a drug that can stop this progression,” Dr. Cambron said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
The rationale for looking at whether fluoxetine, a well-studied antidepressant drug, could be such a drug, was that it had several neuroprotective features – it has been shown to stimulate the release of brain-derived neurotrophic factor, stimulate metabolism in astrocytes, and lower glutamatergic toxicity, she said. All of these could potentially help prevent axonal degeneration.
The FLUOX-PMS (Fluoxetine in Progressive Multiple Sclerosis) trial (Trials. 2014;15:37) ran from 2012 to June 2016 and enrolled patients with primary progressive MS (PPMS) or secondary progressive MS (SPMS), as defined by the 2010 McDonald criteria. A total of 137 patients were enrolled, and 69 were randomized to treatment with fluoxetine 40 mg/day and 68 were randomized to placebo. Fluoxetine treatment was started at a dose of 20 mg and titrated to the full 40-mg dose by 12 weeks.
Patient demographics were mostly similar between the groups. Around 44% of patients in the fluoxetine and placebo groups were female; roughly 40% had PPMS and 60% had SPMS in both groups; the mean Expanded Disability Status Scale score was 5.2 in both groups; the mean age was 54 and 51 years, respectively; and the disease duration was between 18 and 20 years.
Dr. Cambron also reported that the trials’ secondary endpoints showed no advantage of using fluoxetine over placebo. The proportion of patients without sustained progression during the trial was similar among the fluoxetine- and placebo-treated patients, at a respective 69.6% and 61.8% (P = .434). The proportion of patients with a stable Hauser Ambulation Index was also similar (P = .371).
The primary and secondary endpoints were assessed every 3 months in the trial. Patients also underwent cognitive testing, completed the Beck Depression Inventory-II, and Modified Fatigue Impact Scale before treatment and at 48 and 108 weeks after treatment with fluoxetine or placebo. Brain MRI was also performed at baseline and at week 108. The results of these measurements have yet to be analyzed.
Although patients in the fluoxetine group versus the placebo arm experienced more side effects, there was no evidence of an excess of severe adverse events.
“Unfortunately, our study was inconclusive because we failed to show a statistical significant difference between the placebo arm and the fluoxetine group, although I’m convinced that there’s a trend that can certainly not be ignored,” Dr. Cambron maintained. “Probably there was not enough progression in the study and possibly the study duration was too short, she suggested, “but it remains challenging to study these patients for a long period of time, especially with a placebo-controlled design.”
The trial was funded by IWT, the Government Agency for Innovation by Science and Technology in Flanders (Belgium). Dr. Cambron had no relevant financial disclosures.
LONDON – Contrary to expectation of a neuroprotective benefit, fluoxetine does not slow down the progressive phase of multiple sclerosis, according to the results of a randomized, double-blind, multicenter trial.
The first results of the FLUOX-PMS trial, reported by Melissa Cambron, MD, of University Hospital Brussels (Belgium), showed no statistically significant difference between fluoxetine and placebo for improving the primary endpoint of the time to confirmed disease progression.
“The progressive phase of MS remains an ill-understood part of the disease and it is a holy grail to find a drug that can stop this progression,” Dr. Cambron said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
The rationale for looking at whether fluoxetine, a well-studied antidepressant drug, could be such a drug, was that it had several neuroprotective features – it has been shown to stimulate the release of brain-derived neurotrophic factor, stimulate metabolism in astrocytes, and lower glutamatergic toxicity, she said. All of these could potentially help prevent axonal degeneration.
The FLUOX-PMS (Fluoxetine in Progressive Multiple Sclerosis) trial (Trials. 2014;15:37) ran from 2012 to June 2016 and enrolled patients with primary progressive MS (PPMS) or secondary progressive MS (SPMS), as defined by the 2010 McDonald criteria. A total of 137 patients were enrolled, and 69 were randomized to treatment with fluoxetine 40 mg/day and 68 were randomized to placebo. Fluoxetine treatment was started at a dose of 20 mg and titrated to the full 40-mg dose by 12 weeks.
Patient demographics were mostly similar between the groups. Around 44% of patients in the fluoxetine and placebo groups were female; roughly 40% had PPMS and 60% had SPMS in both groups; the mean Expanded Disability Status Scale score was 5.2 in both groups; the mean age was 54 and 51 years, respectively; and the disease duration was between 18 and 20 years.
Dr. Cambron also reported that the trials’ secondary endpoints showed no advantage of using fluoxetine over placebo. The proportion of patients without sustained progression during the trial was similar among the fluoxetine- and placebo-treated patients, at a respective 69.6% and 61.8% (P = .434). The proportion of patients with a stable Hauser Ambulation Index was also similar (P = .371).
The primary and secondary endpoints were assessed every 3 months in the trial. Patients also underwent cognitive testing, completed the Beck Depression Inventory-II, and Modified Fatigue Impact Scale before treatment and at 48 and 108 weeks after treatment with fluoxetine or placebo. Brain MRI was also performed at baseline and at week 108. The results of these measurements have yet to be analyzed.
Although patients in the fluoxetine group versus the placebo arm experienced more side effects, there was no evidence of an excess of severe adverse events.
“Unfortunately, our study was inconclusive because we failed to show a statistical significant difference between the placebo arm and the fluoxetine group, although I’m convinced that there’s a trend that can certainly not be ignored,” Dr. Cambron maintained. “Probably there was not enough progression in the study and possibly the study duration was too short, she suggested, “but it remains challenging to study these patients for a long period of time, especially with a placebo-controlled design.”
The trial was funded by IWT, the Government Agency for Innovation by Science and Technology in Flanders (Belgium). Dr. Cambron had no relevant financial disclosures.
LONDON – Contrary to expectation of a neuroprotective benefit, fluoxetine does not slow down the progressive phase of multiple sclerosis, according to the results of a randomized, double-blind, multicenter trial.
The first results of the FLUOX-PMS trial, reported by Melissa Cambron, MD, of University Hospital Brussels (Belgium), showed no statistically significant difference between fluoxetine and placebo for improving the primary endpoint of the time to confirmed disease progression.
“The progressive phase of MS remains an ill-understood part of the disease and it is a holy grail to find a drug that can stop this progression,” Dr. Cambron said at the annual congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
The rationale for looking at whether fluoxetine, a well-studied antidepressant drug, could be such a drug, was that it had several neuroprotective features – it has been shown to stimulate the release of brain-derived neurotrophic factor, stimulate metabolism in astrocytes, and lower glutamatergic toxicity, she said. All of these could potentially help prevent axonal degeneration.
The FLUOX-PMS (Fluoxetine in Progressive Multiple Sclerosis) trial (Trials. 2014;15:37) ran from 2012 to June 2016 and enrolled patients with primary progressive MS (PPMS) or secondary progressive MS (SPMS), as defined by the 2010 McDonald criteria. A total of 137 patients were enrolled, and 69 were randomized to treatment with fluoxetine 40 mg/day and 68 were randomized to placebo. Fluoxetine treatment was started at a dose of 20 mg and titrated to the full 40-mg dose by 12 weeks.
Patient demographics were mostly similar between the groups. Around 44% of patients in the fluoxetine and placebo groups were female; roughly 40% had PPMS and 60% had SPMS in both groups; the mean Expanded Disability Status Scale score was 5.2 in both groups; the mean age was 54 and 51 years, respectively; and the disease duration was between 18 and 20 years.
Dr. Cambron also reported that the trials’ secondary endpoints showed no advantage of using fluoxetine over placebo. The proportion of patients without sustained progression during the trial was similar among the fluoxetine- and placebo-treated patients, at a respective 69.6% and 61.8% (P = .434). The proportion of patients with a stable Hauser Ambulation Index was also similar (P = .371).
The primary and secondary endpoints were assessed every 3 months in the trial. Patients also underwent cognitive testing, completed the Beck Depression Inventory-II, and Modified Fatigue Impact Scale before treatment and at 48 and 108 weeks after treatment with fluoxetine or placebo. Brain MRI was also performed at baseline and at week 108. The results of these measurements have yet to be analyzed.
Although patients in the fluoxetine group versus the placebo arm experienced more side effects, there was no evidence of an excess of severe adverse events.
“Unfortunately, our study was inconclusive because we failed to show a statistical significant difference between the placebo arm and the fluoxetine group, although I’m convinced that there’s a trend that can certainly not be ignored,” Dr. Cambron maintained. “Probably there was not enough progression in the study and possibly the study duration was too short, she suggested, “but it remains challenging to study these patients for a long period of time, especially with a placebo-controlled design.”
The trial was funded by IWT, the Government Agency for Innovation by Science and Technology in Flanders (Belgium). Dr. Cambron had no relevant financial disclosures.
Key clinical point:
Major finding: There was no difference in the time to confirmed disease progression between fluoxetine- and placebo-treated patients (P = .07).
Data source: FLUOX-PMS, a multicenter, randomized, double-blind, placebo-controlled clinical study of 137 patients with primary or secondary progressive multiple sclerosis treated with fluoxetine or placebo.
Disclosures: The trial was funded by IWT, the Government Agency for Innovation by Science and Technology in Flanders (Belgium). Dr. Cambron had no relevant financial disclosures.
Zika virus shows no signs of slowing down
Zika virus transmission continues at a rapid clip as the number of new cases among pregnant women topped 200 again for the week ending Sept. 22, according to the Centers for Disease Control and Prevention.
After setting a new high of 210 the previous week, there were 201 new cases of pregnant women with laboratory-confirmed Zika infection for the week ending Sept. 22. There were 59 new cases in the 50 states and the District of Columbia and 142 new cases in the U.S. territories, the CDC reported Sept. 29. In the United States this year, there have been 2,298 reported cases of Zika-infected pregnant women: 808 in the states and D.C. and 1,490 in the territories.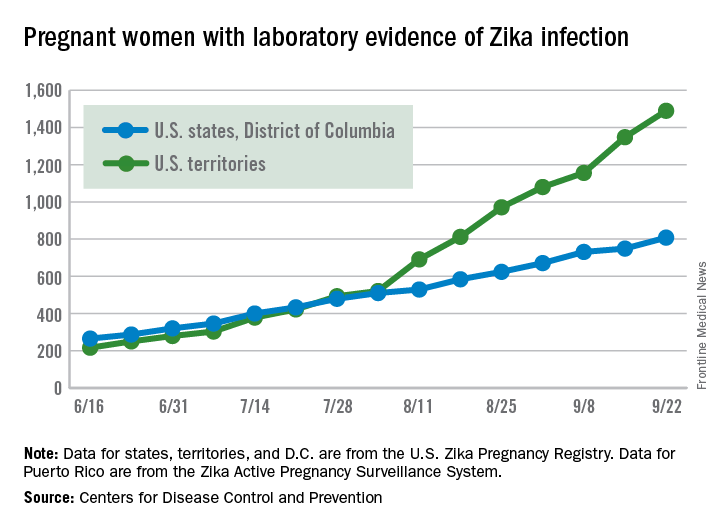
Among all Americans, there were 2,559 new cases of Zika infection as of Sept. 28 – 267 in the states/D.C. and 2,292 in the territories – although Puerto Rico continues to retroactively report cases, which has been pushing the numbers higher in recent weeks. There have been 25,694 total cases of Zika infection in 2015-2016, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika virus transmission continues at a rapid clip as the number of new cases among pregnant women topped 200 again for the week ending Sept. 22, according to the Centers for Disease Control and Prevention.
After setting a new high of 210 the previous week, there were 201 new cases of pregnant women with laboratory-confirmed Zika infection for the week ending Sept. 22. There were 59 new cases in the 50 states and the District of Columbia and 142 new cases in the U.S. territories, the CDC reported Sept. 29. In the United States this year, there have been 2,298 reported cases of Zika-infected pregnant women: 808 in the states and D.C. and 1,490 in the territories.
Among all Americans, there were 2,559 new cases of Zika infection as of Sept. 28 – 267 in the states/D.C. and 2,292 in the territories – although Puerto Rico continues to retroactively report cases, which has been pushing the numbers higher in recent weeks. There have been 25,694 total cases of Zika infection in 2015-2016, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika virus transmission continues at a rapid clip as the number of new cases among pregnant women topped 200 again for the week ending Sept. 22, according to the Centers for Disease Control and Prevention.
After setting a new high of 210 the previous week, there were 201 new cases of pregnant women with laboratory-confirmed Zika infection for the week ending Sept. 22. There were 59 new cases in the 50 states and the District of Columbia and 142 new cases in the U.S. territories, the CDC reported Sept. 29. In the United States this year, there have been 2,298 reported cases of Zika-infected pregnant women: 808 in the states and D.C. and 1,490 in the territories.
Among all Americans, there were 2,559 new cases of Zika infection as of Sept. 28 – 267 in the states/D.C. and 2,292 in the territories – although Puerto Rico continues to retroactively report cases, which has been pushing the numbers higher in recent weeks. There have been 25,694 total cases of Zika infection in 2015-2016, the CDC reported.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Sentinel lymph node technique in endometrial cancer, Part 2
As reviewed in Part 1, surgery is indicated for the staging and treatment of endometrial cancer. Lymph node status is one of the most important factors in determining prognosis and the need for adjuvant treatment. The extent of lymph node evaluation is controversial as full lymphadenectomy carries risks, including increased operative time, blood loss, nerve injury, and lymphedema.
Two trials have found no survival benefit from lymphadenectomy for endometrial cancer; however, other evidence suggests that women without known nodal status may be more likely to receive radiotherapy.1,2,3

Given these issues, the sentinel lymph node technique strikes a balance between the risks and benefits of lymph node evaluation in endometrial cancer.
Sentinel lymph nodes (SLN) are the first nodes to drain a tumor site, and thus, are typically the first to demonstrate occult malignancy. The use of the SLN technique as an alternative to complete lymphadenectomy in endometrial cancer has been well described, although its accuracy and the validity of its use are still debated.
The viability of the SLN technique is predicated on the ability to achieve mapping of dye or tracer from the tumor to the first lymph node to drain the tumor. The lymphatic drainage of the endometrium is complex and unlike vulvar or breast cancer, endometrial cancer is less accessible for peritumoral injection. Several injection techniques have been described; cervical injection is the easiest to achieve and has been found to have similar or higher SLN detection than hysteroscopic or fundal injections.4,5
There are a number of techniques for SLN detection, each with unique benefits and risks. Visual identification of blue dye, most frequently isosulfan blue, is the “colorimetric method” and has been used most commonly with cervical injection for endometrial cancer. Injection of isosulfan blue does not require specialized equipment, however visualization in obese patients is inferior.6
Technetium sulfur colloid (Tc) is a radioactive tracer that can be detected by gamma probes. A preoperative lymphoscintigraphy and a handheld gamma probe are used to map lymphatics. This technique has limitations, including the additional time and coordination of procedures, as well as some evidence of poor correlation between lymphoscintigraphy and surgical SLN mapping.7
Indocyanine green (ICG) is a fluorescent dye that has excellent signal penetration and allows for real-time visual identification using near-infrared fluorescence imaging. The bilateral detection rate with ICG appears comparable or better than blue dye.8 Combinations of dye, either ICG plus Tc or Tc plus blue dye, may be also used to increase SLN detection.

The accuracy of the SLN technique is the cornerstone to its success. In a prospective multicenter study – Senti-Endo – patients with early-stage disease underwent pelvic SLN assessment with cervical injection of a combination of dyes followed by systematic pelvic node dissection. The overall negative predictive value was 97% with three patients who had positive lymph nodes that were not detected, all of whom had a type 2 endometrial cancer.9
With the uptake of the SLN technique, many institutions have protocols surrounding the technique to ensure appropriate SLN detection and evaluation. Physicians using this technique should adhere to protocols supported by National Comprehensive Cancer Network guidelines, taking care to remove any suspicious lymph nodes and perform a full side-specific lymphadenectomy if bilateral mapping is not achieved.
The extent of lymphadenectomy and application of the SLN technique in high-risk endometrial cancer remains controversial. These patients are at higher risk for unsuccessful mapping and isolated para-aortic metastasis. Retrospective series have suggested equivalent oncologic outcomes for women with high-grade cancers who have been staged by SLN biopsy, compared with selective or complete lymphadenectomy.10,11
We await the results of a large prospective trial in which patients undergo comprehensive lymphadenectomy in addition to SLN biopsy to assess the accuracy of the technique (NCT01673022).
Pathologic evaluation of SLNs is frequently done with ultrastaging, which describes additional sectioning and staining of the node. This technique frequently identifies isolated tumor cells and micrometastasis (collectively called low-volume disease) in addition to macrometastasis. The clinical and prognostic significance of low-volume disease is unknown and additional investigation is urgently needed to determine appropriate adjuvant therapy and follow-up for these patients.
The SLN technique is an acceptable approach to assess clinical stage I endometrial cancer. Physicians should consider adding the SLN biopsy to their routine staging techniques prior to exclusively adopting the new technique. They should take care to adhere to SLN algorithms and monitor outcomes.
References
1. J Natl Cancer Inst. 2008;100(23):1707-16.
2. Lancet. 2009 Jan;373(9658):125-36.
3. Am J Obstet Gynecol. 2011 Dec;205(6):562.e1–9.
4. Gynecol Oncol. 2013 Nov;131(2):299-303.
5. Int J Gynecol Cancer. 2013 Nov;23(9):1704-11.
6. Gynecol Oncol 2014 Aug;134(2):281-6.
7. Gynecol Oncol. 2009 Feb;112(2):348-352.
8. Gynecol Oncol. 2014 May;133(2):274-7.
9. Lancet Oncol. 2011 May;12(5):469-76.
10. Ann Surg Oncol. 2016 Jan;23(1):196-202.
11. Gynecol Oncol. 2016 Mar;140(3):394-9.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. Dr. Sullivan is a clinical fellow in the division of gynecologic oncology at UNC, Chapel Hill. Dr. Rossi and Dr. Sullivan reported having no relevant financial disclosures.
As reviewed in Part 1, surgery is indicated for the staging and treatment of endometrial cancer. Lymph node status is one of the most important factors in determining prognosis and the need for adjuvant treatment. The extent of lymph node evaluation is controversial as full lymphadenectomy carries risks, including increased operative time, blood loss, nerve injury, and lymphedema.
Two trials have found no survival benefit from lymphadenectomy for endometrial cancer; however, other evidence suggests that women without known nodal status may be more likely to receive radiotherapy.1,2,3
Given these issues, the sentinel lymph node technique strikes a balance between the risks and benefits of lymph node evaluation in endometrial cancer.
Sentinel lymph nodes (SLN) are the first nodes to drain a tumor site, and thus, are typically the first to demonstrate occult malignancy. The use of the SLN technique as an alternative to complete lymphadenectomy in endometrial cancer has been well described, although its accuracy and the validity of its use are still debated.
The viability of the SLN technique is predicated on the ability to achieve mapping of dye or tracer from the tumor to the first lymph node to drain the tumor. The lymphatic drainage of the endometrium is complex and unlike vulvar or breast cancer, endometrial cancer is less accessible for peritumoral injection. Several injection techniques have been described; cervical injection is the easiest to achieve and has been found to have similar or higher SLN detection than hysteroscopic or fundal injections.4,5
There are a number of techniques for SLN detection, each with unique benefits and risks. Visual identification of blue dye, most frequently isosulfan blue, is the “colorimetric method” and has been used most commonly with cervical injection for endometrial cancer. Injection of isosulfan blue does not require specialized equipment, however visualization in obese patients is inferior.6
Technetium sulfur colloid (Tc) is a radioactive tracer that can be detected by gamma probes. A preoperative lymphoscintigraphy and a handheld gamma probe are used to map lymphatics. This technique has limitations, including the additional time and coordination of procedures, as well as some evidence of poor correlation between lymphoscintigraphy and surgical SLN mapping.7
Indocyanine green (ICG) is a fluorescent dye that has excellent signal penetration and allows for real-time visual identification using near-infrared fluorescence imaging. The bilateral detection rate with ICG appears comparable or better than blue dye.8 Combinations of dye, either ICG plus Tc or Tc plus blue dye, may be also used to increase SLN detection.
The accuracy of the SLN technique is the cornerstone to its success. In a prospective multicenter study – Senti-Endo – patients with early-stage disease underwent pelvic SLN assessment with cervical injection of a combination of dyes followed by systematic pelvic node dissection. The overall negative predictive value was 97% with three patients who had positive lymph nodes that were not detected, all of whom had a type 2 endometrial cancer.9
With the uptake of the SLN technique, many institutions have protocols surrounding the technique to ensure appropriate SLN detection and evaluation. Physicians using this technique should adhere to protocols supported by National Comprehensive Cancer Network guidelines, taking care to remove any suspicious lymph nodes and perform a full side-specific lymphadenectomy if bilateral mapping is not achieved.
The extent of lymphadenectomy and application of the SLN technique in high-risk endometrial cancer remains controversial. These patients are at higher risk for unsuccessful mapping and isolated para-aortic metastasis. Retrospective series have suggested equivalent oncologic outcomes for women with high-grade cancers who have been staged by SLN biopsy, compared with selective or complete lymphadenectomy.10,11
We await the results of a large prospective trial in which patients undergo comprehensive lymphadenectomy in addition to SLN biopsy to assess the accuracy of the technique (NCT01673022).
Pathologic evaluation of SLNs is frequently done with ultrastaging, which describes additional sectioning and staining of the node. This technique frequently identifies isolated tumor cells and micrometastasis (collectively called low-volume disease) in addition to macrometastasis. The clinical and prognostic significance of low-volume disease is unknown and additional investigation is urgently needed to determine appropriate adjuvant therapy and follow-up for these patients.
The SLN technique is an acceptable approach to assess clinical stage I endometrial cancer. Physicians should consider adding the SLN biopsy to their routine staging techniques prior to exclusively adopting the new technique. They should take care to adhere to SLN algorithms and monitor outcomes.
References
1. J Natl Cancer Inst. 2008;100(23):1707-16.
2. Lancet. 2009 Jan;373(9658):125-36.
3. Am J Obstet Gynecol. 2011 Dec;205(6):562.e1–9.
4. Gynecol Oncol. 2013 Nov;131(2):299-303.
5. Int J Gynecol Cancer. 2013 Nov;23(9):1704-11.
6. Gynecol Oncol 2014 Aug;134(2):281-6.
7. Gynecol Oncol. 2009 Feb;112(2):348-352.
8. Gynecol Oncol. 2014 May;133(2):274-7.
9. Lancet Oncol. 2011 May;12(5):469-76.
10. Ann Surg Oncol. 2016 Jan;23(1):196-202.
11. Gynecol Oncol. 2016 Mar;140(3):394-9.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. Dr. Sullivan is a clinical fellow in the division of gynecologic oncology at UNC, Chapel Hill. Dr. Rossi and Dr. Sullivan reported having no relevant financial disclosures.
As reviewed in Part 1, surgery is indicated for the staging and treatment of endometrial cancer. Lymph node status is one of the most important factors in determining prognosis and the need for adjuvant treatment. The extent of lymph node evaluation is controversial as full lymphadenectomy carries risks, including increased operative time, blood loss, nerve injury, and lymphedema.
Two trials have found no survival benefit from lymphadenectomy for endometrial cancer; however, other evidence suggests that women without known nodal status may be more likely to receive radiotherapy.1,2,3
Given these issues, the sentinel lymph node technique strikes a balance between the risks and benefits of lymph node evaluation in endometrial cancer.
Sentinel lymph nodes (SLN) are the first nodes to drain a tumor site, and thus, are typically the first to demonstrate occult malignancy. The use of the SLN technique as an alternative to complete lymphadenectomy in endometrial cancer has been well described, although its accuracy and the validity of its use are still debated.
The viability of the SLN technique is predicated on the ability to achieve mapping of dye or tracer from the tumor to the first lymph node to drain the tumor. The lymphatic drainage of the endometrium is complex and unlike vulvar or breast cancer, endometrial cancer is less accessible for peritumoral injection. Several injection techniques have been described; cervical injection is the easiest to achieve and has been found to have similar or higher SLN detection than hysteroscopic or fundal injections.4,5
There are a number of techniques for SLN detection, each with unique benefits and risks. Visual identification of blue dye, most frequently isosulfan blue, is the “colorimetric method” and has been used most commonly with cervical injection for endometrial cancer. Injection of isosulfan blue does not require specialized equipment, however visualization in obese patients is inferior.6
Technetium sulfur colloid (Tc) is a radioactive tracer that can be detected by gamma probes. A preoperative lymphoscintigraphy and a handheld gamma probe are used to map lymphatics. This technique has limitations, including the additional time and coordination of procedures, as well as some evidence of poor correlation between lymphoscintigraphy and surgical SLN mapping.7
Indocyanine green (ICG) is a fluorescent dye that has excellent signal penetration and allows for real-time visual identification using near-infrared fluorescence imaging. The bilateral detection rate with ICG appears comparable or better than blue dye.8 Combinations of dye, either ICG plus Tc or Tc plus blue dye, may be also used to increase SLN detection.
The accuracy of the SLN technique is the cornerstone to its success. In a prospective multicenter study – Senti-Endo – patients with early-stage disease underwent pelvic SLN assessment with cervical injection of a combination of dyes followed by systematic pelvic node dissection. The overall negative predictive value was 97% with three patients who had positive lymph nodes that were not detected, all of whom had a type 2 endometrial cancer.9
With the uptake of the SLN technique, many institutions have protocols surrounding the technique to ensure appropriate SLN detection and evaluation. Physicians using this technique should adhere to protocols supported by National Comprehensive Cancer Network guidelines, taking care to remove any suspicious lymph nodes and perform a full side-specific lymphadenectomy if bilateral mapping is not achieved.
The extent of lymphadenectomy and application of the SLN technique in high-risk endometrial cancer remains controversial. These patients are at higher risk for unsuccessful mapping and isolated para-aortic metastasis. Retrospective series have suggested equivalent oncologic outcomes for women with high-grade cancers who have been staged by SLN biopsy, compared with selective or complete lymphadenectomy.10,11
We await the results of a large prospective trial in which patients undergo comprehensive lymphadenectomy in addition to SLN biopsy to assess the accuracy of the technique (NCT01673022).
Pathologic evaluation of SLNs is frequently done with ultrastaging, which describes additional sectioning and staining of the node. This technique frequently identifies isolated tumor cells and micrometastasis (collectively called low-volume disease) in addition to macrometastasis. The clinical and prognostic significance of low-volume disease is unknown and additional investigation is urgently needed to determine appropriate adjuvant therapy and follow-up for these patients.
The SLN technique is an acceptable approach to assess clinical stage I endometrial cancer. Physicians should consider adding the SLN biopsy to their routine staging techniques prior to exclusively adopting the new technique. They should take care to adhere to SLN algorithms and monitor outcomes.
References
1. J Natl Cancer Inst. 2008;100(23):1707-16.
2. Lancet. 2009 Jan;373(9658):125-36.
3. Am J Obstet Gynecol. 2011 Dec;205(6):562.e1–9.
4. Gynecol Oncol. 2013 Nov;131(2):299-303.
5. Int J Gynecol Cancer. 2013 Nov;23(9):1704-11.
6. Gynecol Oncol 2014 Aug;134(2):281-6.
7. Gynecol Oncol. 2009 Feb;112(2):348-352.
8. Gynecol Oncol. 2014 May;133(2):274-7.
9. Lancet Oncol. 2011 May;12(5):469-76.
10. Ann Surg Oncol. 2016 Jan;23(1):196-202.
11. Gynecol Oncol. 2016 Mar;140(3):394-9.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. Dr. Sullivan is a clinical fellow in the division of gynecologic oncology at UNC, Chapel Hill. Dr. Rossi and Dr. Sullivan reported having no relevant financial disclosures.

Well-woman care: Reshaping the routine visit
From her vantage point in medical education, Christine M. Peterson, MD, is acutely aware that well-woman care is at a turning point.
“We’re at an interesting crossroads between tradition and evidence-based practice,” said Dr. Peterson, who practiced obstetrics and gynecology in the 1980s and now serves as associate professor of ob.gyn. and assistant dean for student affairs at the University of Virginia’s School of Medicine in Charlottesville.

“Even young trainees are aware of the traditions for the annual well-woman visit – the Pap, the pelvic, the breast exam,” she said. “But the evidence is pointing us in a different direction ... toward doing only those things that are effective for prevention and early detection of disease, or that have [demonstrated] value in one way or another.”
If all goes as planned at a national level, Dr. Peterson’s students who become ob.gyns., family physicians, and general internists will practice under a reshaped and well-defined umbrella of well-woman care – one that includes a broad array of insurer-covered screening and counseling services.
That umbrella already includes HPV testing, and screening and/or counseling on intimate partner violence, sexually transmitted infections, and HIV, in addition to contraception counseling. These preventive services were described in the Women’s Preventive Services Guidelines and adopted as covered benefits by the Department of Health & Human Services in 2011.
And more change is on the way. In March, the American College of Obstetricians and Gynecologists (ACOG) launched the Women’s Preventive Services Initiative (WPSI) – a broad coalition tasked with recommending updates to the 2011 guidelines and developing new recommendations for the scope and implementation of women’s preventive health care services.
The effort is funded through a 5-year cooperative agreement with the Health Resources & Services Administration (HRSA). It’s similar to the American Academy of Pediatrics’ approach in developing the HRSA-supported Bright Futures guidelines almost 25 years ago. Under the Affordable Care Act, all HRSA-recommended preventive services must be covered by most private insurers without patient cost sharing.

“Over the years, we’ve gone from an emphasis on the Pap and pelvic to well-woman care that assesses the whole woman,” said Jeanne A. Conry, MD, assistant physician-in-chief at the Permanente Medical Group in Roseville, Calif., and a past president of ACOG.
Ob.gyns. have long provided preventive care, but today more than ever before, Dr. Conry said, “my emphasis is on helping women to get well and stay well.”
The evolution
Fifty years ago, in 1966, use of the Pap test was being widely promoted, modern mammography techniques were on the cusp of advancement, and ob.gyns. were prescribing the first birth control pill approved by the Food and Drug Administration. ACOG’s main practice guidance book, “Standards for Obstetric-Gynecologic Hospital Services,” addressed the general physical examination but otherwise focused on obstetrics and reproductive health.
Thirty years later, women’s health care as described in the first edition of ACOG’s “Guidelines for Women’s Health Care” (1996) had grown to include distinct categories of “primary and preventive care” and “evaluation and counseling” that were separate from gynecologic services and broken down by age.
What was referred to as the “women’s health exam” through the 1990s gradually took on the “well-woman” label in the 2000s. Ob.gyns. were encouraged to address a growing range of preventive issues, but the annual Pap test remained a focus and, in many ways, drove women’s visits.
“Women would say, ‘I’m going for my Pap,’” Dr. Conry said.
Most recently, new technology and evidence-based reviews have changed the framework for well-woman visits to one with longer intervals for cervical cancer screening (every 3-5 years) and a move away from performing internal pelvic exams in all women (ACOG recommends pelvic exams annually for patients aged 21 and older but advises shared decision making for complete pelvic exams in asymptomatic patients).
Recent evidence reviews have also added some uncertainty about the role of annual breast exams in all women, as well as the role of breast self-exams, particularly for women not at high risk.
Maintaining patient relationships
One of the biggest and most immediate challenges for ob.gyns in the face of changing guidelines lies in maintaining the physician-patient relationship and “continuing communication” about the importance of regular well-woman visits, said Jill Rabin, MD, cochief of the division of ambulatory care, women’s health programs–prenatal care assistance program services at Northwell Health, New Hyde Park, N.Y.
“We want patients to understand that, even though they no longer need the Pap every year, they still should see us for good, comprehensive care ... that we can help them achieve their health care goals,” she said.
How often well-woman visits should occur has been a subject of much discussion. The HRSA-supported preventive services guidelines call for well-woman preventive care annually but note that “several visits may be needed to obtain all the necessary recommended services.”
And, in its first set of draft recommendations for HRSA, WPSI offered clarifications, saying there’s a need for “at least one annual preventive care visit for women beginning in adolescence and continuing across the lifespan to ensure that women obtain recommended preventive services” as determined by age and risk factors.
The draft recommendations, aimed at reviewing and updating the 2011 HRSA-sponsored guidelines, will be finalized by the end of 2016. WPSI will submit additional recommendations over the next 4 years.

Carol S. Weisman, PhD, a sociologist and health services researcher who sat on the Institute of Medicine committee that wrote the Women’s Preventive Services Guidelines, said the IOM’s recommendation for well-women visits – “in plural” form – recognizes “that historically many women have patched together their well-woman care from multiple providers, getting some of their preventive care from their generalist, and some from their ob.gyn.”
What’s more, the current list of preventive services covered under the Affordable Care Act is “enormous” – too long to address in one visit for many patients, said Dr. Weisman of the Penn State Center for Women’s Health Research in Hershey.
In addition to the women’s preventive services, the Affordable Care Act requires plans to cover services recommended with a grade A or B rating by the U.S. Preventive Services Task Force (counseling and screening for cancer, cardiovascular disease, and more) as well as vaccines recommended by the Advisory Committee on Immunization Practices, and HRSA’s Bright Futures services (for adolescents as well as children).
Beyond gynecology
How much further ob.gyns. will reach outside the gynecologic realm to offer additional preventive care services is an open question, but it’s likely to be based mainly on comfort levels, sources said.
“The changing needs of the gynecologic visit enable us to spend more time on other things,” said Hal C. Lawrence III, MD, ACOG’s executive vice president and chief executive officer. “But within the specialty, there’s going to be variation as to what level of expanded services ob.gyns. provide. Some will provide a lot of what women need, others not as much.”
Heather Johnson, MD, practices with a large ob.gyn. group in Chevy Chase, Md. and provides well-woman care largely to women in their 50s and 60s, whose children she delivered. She’s comfortable, she said, with screening for and treating osteoporosis and mild depression, for instance. She regularly performs lipid testing but refers out for management of high cholesterol levels or high blood pressure.
“I encourage all my patients to have a primary care physician of record,” she said, “but I still am happy to discuss the issues with them.”
What’s key, according to Dr. Lawrence and Dr. Conry, is coordination.
“We know there will be different individuals providing different components [of well-woman care],” Dr. Conry said. “I may see a woman for various things. Then she may go to her internist. But we should be able to collaborate to hit all the preventive health goals for her.”
Dr. Conry emphasized that the ob.gyn.’s expertise in reproductive health is critical to well-woman care planning, especially given medicine’s growing knowledge of how obstetric health and pregnancy complications can have long-term impacts on cardiovascular disease and other conditions. “It’s important for all providers to realize this,” she said.
Primary care status?
Intertwined with the future of well-women care is the issue of primary care status for ob.gyns. ACOG continues to advocate for ob.gyns. to be listed as primary care providers and part of primary care payment policies. Leaders are also pushing for projects on ob.gyn.–led medical homes.
At the same time, ACOG has been taking a broad collaborative approach to shaping well-woman care, aiming to develop comprehensive, age-specific recommendations for use by any provider who cares for adolescent girls and women.
Representatives of the American Academy of Family Physicians, the American College of Physicians, and the National Association of Nurse Practitioners in Women’s Health were involved in a Well-Woman Task Force that Dr. Conry appointed while serving as ACOG president in 2013-2014. These organizations now sit on WPSI’s advisory panel with ACOG.
Representatives from the American Academy of Pediatrics have also been close partners, as ACOG officials view the HRSA-sponsored Bright Futures guidelines (which includes the “Periodicity Schedule”) as a potential model for well-woman care. The guidelines are comprehensive, well-organized, and user-friendly, ACOG officials said.
At the University of Virginia, in the meantime, Dr. Peterson is arming the next generation of ob.gyns. with the skills needed for a team-based approach to well-woman visits. She said nurse practitioners and physician assistants will provide much more of the education and “more of the truly individualized conversations with patients” that will increasingly be part of well-woman care.
This is already happening. All of the nurse practitioners in Dr. Johnson’s group practice perform well-woman visits, “referring to the gynecologists for complicated gyn problems and out to the patient’s primary care physician for complicated medical problems,” Dr. Johnson said.
Even as the tools and recommendations for women’s preventive care become more evidence-based, the scope of well-woman visits will be based on risk factors, shared decision making, and other issues, Dr. Peterson said. “We will be telling patients, this is your path for your well-woman care,” she said.
Throughout 2016, Ob.Gyn. News is celebrating its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of contraception, changes in gynecologic surgery, and whether the practice environment is better or worse.
From her vantage point in medical education, Christine M. Peterson, MD, is acutely aware that well-woman care is at a turning point.
“We’re at an interesting crossroads between tradition and evidence-based practice,” said Dr. Peterson, who practiced obstetrics and gynecology in the 1980s and now serves as associate professor of ob.gyn. and assistant dean for student affairs at the University of Virginia’s School of Medicine in Charlottesville.
“Even young trainees are aware of the traditions for the annual well-woman visit – the Pap, the pelvic, the breast exam,” she said. “But the evidence is pointing us in a different direction ... toward doing only those things that are effective for prevention and early detection of disease, or that have [demonstrated] value in one way or another.”
If all goes as planned at a national level, Dr. Peterson’s students who become ob.gyns., family physicians, and general internists will practice under a reshaped and well-defined umbrella of well-woman care – one that includes a broad array of insurer-covered screening and counseling services.
That umbrella already includes HPV testing, and screening and/or counseling on intimate partner violence, sexually transmitted infections, and HIV, in addition to contraception counseling. These preventive services were described in the Women’s Preventive Services Guidelines and adopted as covered benefits by the Department of Health & Human Services in 2011.
And more change is on the way. In March, the American College of Obstetricians and Gynecologists (ACOG) launched the Women’s Preventive Services Initiative (WPSI) – a broad coalition tasked with recommending updates to the 2011 guidelines and developing new recommendations for the scope and implementation of women’s preventive health care services.
The effort is funded through a 5-year cooperative agreement with the Health Resources & Services Administration (HRSA). It’s similar to the American Academy of Pediatrics’ approach in developing the HRSA-supported Bright Futures guidelines almost 25 years ago. Under the Affordable Care Act, all HRSA-recommended preventive services must be covered by most private insurers without patient cost sharing.
“Over the years, we’ve gone from an emphasis on the Pap and pelvic to well-woman care that assesses the whole woman,” said Jeanne A. Conry, MD, assistant physician-in-chief at the Permanente Medical Group in Roseville, Calif., and a past president of ACOG.
Ob.gyns. have long provided preventive care, but today more than ever before, Dr. Conry said, “my emphasis is on helping women to get well and stay well.”
The evolution
Fifty years ago, in 1966, use of the Pap test was being widely promoted, modern mammography techniques were on the cusp of advancement, and ob.gyns. were prescribing the first birth control pill approved by the Food and Drug Administration. ACOG’s main practice guidance book, “Standards for Obstetric-Gynecologic Hospital Services,” addressed the general physical examination but otherwise focused on obstetrics and reproductive health.
Thirty years later, women’s health care as described in the first edition of ACOG’s “Guidelines for Women’s Health Care” (1996) had grown to include distinct categories of “primary and preventive care” and “evaluation and counseling” that were separate from gynecologic services and broken down by age.
What was referred to as the “women’s health exam” through the 1990s gradually took on the “well-woman” label in the 2000s. Ob.gyns. were encouraged to address a growing range of preventive issues, but the annual Pap test remained a focus and, in many ways, drove women’s visits.
“Women would say, ‘I’m going for my Pap,’” Dr. Conry said.
Most recently, new technology and evidence-based reviews have changed the framework for well-woman visits to one with longer intervals for cervical cancer screening (every 3-5 years) and a move away from performing internal pelvic exams in all women (ACOG recommends pelvic exams annually for patients aged 21 and older but advises shared decision making for complete pelvic exams in asymptomatic patients).
Recent evidence reviews have also added some uncertainty about the role of annual breast exams in all women, as well as the role of breast self-exams, particularly for women not at high risk.
Maintaining patient relationships
One of the biggest and most immediate challenges for ob.gyns in the face of changing guidelines lies in maintaining the physician-patient relationship and “continuing communication” about the importance of regular well-woman visits, said Jill Rabin, MD, cochief of the division of ambulatory care, women’s health programs–prenatal care assistance program services at Northwell Health, New Hyde Park, N.Y.
“We want patients to understand that, even though they no longer need the Pap every year, they still should see us for good, comprehensive care ... that we can help them achieve their health care goals,” she said.
How often well-woman visits should occur has been a subject of much discussion. The HRSA-supported preventive services guidelines call for well-woman preventive care annually but note that “several visits may be needed to obtain all the necessary recommended services.”
And, in its first set of draft recommendations for HRSA, WPSI offered clarifications, saying there’s a need for “at least one annual preventive care visit for women beginning in adolescence and continuing across the lifespan to ensure that women obtain recommended preventive services” as determined by age and risk factors.
The draft recommendations, aimed at reviewing and updating the 2011 HRSA-sponsored guidelines, will be finalized by the end of 2016. WPSI will submit additional recommendations over the next 4 years.
Carol S. Weisman, PhD, a sociologist and health services researcher who sat on the Institute of Medicine committee that wrote the Women’s Preventive Services Guidelines, said the IOM’s recommendation for well-women visits – “in plural” form – recognizes “that historically many women have patched together their well-woman care from multiple providers, getting some of their preventive care from their generalist, and some from their ob.gyn.”
What’s more, the current list of preventive services covered under the Affordable Care Act is “enormous” – too long to address in one visit for many patients, said Dr. Weisman of the Penn State Center for Women’s Health Research in Hershey.
In addition to the women’s preventive services, the Affordable Care Act requires plans to cover services recommended with a grade A or B rating by the U.S. Preventive Services Task Force (counseling and screening for cancer, cardiovascular disease, and more) as well as vaccines recommended by the Advisory Committee on Immunization Practices, and HRSA’s Bright Futures services (for adolescents as well as children).
Beyond gynecology
How much further ob.gyns. will reach outside the gynecologic realm to offer additional preventive care services is an open question, but it’s likely to be based mainly on comfort levels, sources said.
“The changing needs of the gynecologic visit enable us to spend more time on other things,” said Hal C. Lawrence III, MD, ACOG’s executive vice president and chief executive officer. “But within the specialty, there’s going to be variation as to what level of expanded services ob.gyns. provide. Some will provide a lot of what women need, others not as much.”
Heather Johnson, MD, practices with a large ob.gyn. group in Chevy Chase, Md. and provides well-woman care largely to women in their 50s and 60s, whose children she delivered. She’s comfortable, she said, with screening for and treating osteoporosis and mild depression, for instance. She regularly performs lipid testing but refers out for management of high cholesterol levels or high blood pressure.
“I encourage all my patients to have a primary care physician of record,” she said, “but I still am happy to discuss the issues with them.”
What’s key, according to Dr. Lawrence and Dr. Conry, is coordination.
“We know there will be different individuals providing different components [of well-woman care],” Dr. Conry said. “I may see a woman for various things. Then she may go to her internist. But we should be able to collaborate to hit all the preventive health goals for her.”
Dr. Conry emphasized that the ob.gyn.’s expertise in reproductive health is critical to well-woman care planning, especially given medicine’s growing knowledge of how obstetric health and pregnancy complications can have long-term impacts on cardiovascular disease and other conditions. “It’s important for all providers to realize this,” she said.
Primary care status?
Intertwined with the future of well-women care is the issue of primary care status for ob.gyns. ACOG continues to advocate for ob.gyns. to be listed as primary care providers and part of primary care payment policies. Leaders are also pushing for projects on ob.gyn.–led medical homes.
At the same time, ACOG has been taking a broad collaborative approach to shaping well-woman care, aiming to develop comprehensive, age-specific recommendations for use by any provider who cares for adolescent girls and women.
Representatives of the American Academy of Family Physicians, the American College of Physicians, and the National Association of Nurse Practitioners in Women’s Health were involved in a Well-Woman Task Force that Dr. Conry appointed while serving as ACOG president in 2013-2014. These organizations now sit on WPSI’s advisory panel with ACOG.
Representatives from the American Academy of Pediatrics have also been close partners, as ACOG officials view the HRSA-sponsored Bright Futures guidelines (which includes the “Periodicity Schedule”) as a potential model for well-woman care. The guidelines are comprehensive, well-organized, and user-friendly, ACOG officials said.
At the University of Virginia, in the meantime, Dr. Peterson is arming the next generation of ob.gyns. with the skills needed for a team-based approach to well-woman visits. She said nurse practitioners and physician assistants will provide much more of the education and “more of the truly individualized conversations with patients” that will increasingly be part of well-woman care.
This is already happening. All of the nurse practitioners in Dr. Johnson’s group practice perform well-woman visits, “referring to the gynecologists for complicated gyn problems and out to the patient’s primary care physician for complicated medical problems,” Dr. Johnson said.
Even as the tools and recommendations for women’s preventive care become more evidence-based, the scope of well-woman visits will be based on risk factors, shared decision making, and other issues, Dr. Peterson said. “We will be telling patients, this is your path for your well-woman care,” she said.
Throughout 2016, Ob.Gyn. News is celebrating its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of contraception, changes in gynecologic surgery, and whether the practice environment is better or worse.
From her vantage point in medical education, Christine M. Peterson, MD, is acutely aware that well-woman care is at a turning point.
“We’re at an interesting crossroads between tradition and evidence-based practice,” said Dr. Peterson, who practiced obstetrics and gynecology in the 1980s and now serves as associate professor of ob.gyn. and assistant dean for student affairs at the University of Virginia’s School of Medicine in Charlottesville.
“Even young trainees are aware of the traditions for the annual well-woman visit – the Pap, the pelvic, the breast exam,” she said. “But the evidence is pointing us in a different direction ... toward doing only those things that are effective for prevention and early detection of disease, or that have [demonstrated] value in one way or another.”
If all goes as planned at a national level, Dr. Peterson’s students who become ob.gyns., family physicians, and general internists will practice under a reshaped and well-defined umbrella of well-woman care – one that includes a broad array of insurer-covered screening and counseling services.
That umbrella already includes HPV testing, and screening and/or counseling on intimate partner violence, sexually transmitted infections, and HIV, in addition to contraception counseling. These preventive services were described in the Women’s Preventive Services Guidelines and adopted as covered benefits by the Department of Health & Human Services in 2011.
And more change is on the way. In March, the American College of Obstetricians and Gynecologists (ACOG) launched the Women’s Preventive Services Initiative (WPSI) – a broad coalition tasked with recommending updates to the 2011 guidelines and developing new recommendations for the scope and implementation of women’s preventive health care services.
The effort is funded through a 5-year cooperative agreement with the Health Resources & Services Administration (HRSA). It’s similar to the American Academy of Pediatrics’ approach in developing the HRSA-supported Bright Futures guidelines almost 25 years ago. Under the Affordable Care Act, all HRSA-recommended preventive services must be covered by most private insurers without patient cost sharing.
“Over the years, we’ve gone from an emphasis on the Pap and pelvic to well-woman care that assesses the whole woman,” said Jeanne A. Conry, MD, assistant physician-in-chief at the Permanente Medical Group in Roseville, Calif., and a past president of ACOG.
Ob.gyns. have long provided preventive care, but today more than ever before, Dr. Conry said, “my emphasis is on helping women to get well and stay well.”
The evolution
Fifty years ago, in 1966, use of the Pap test was being widely promoted, modern mammography techniques were on the cusp of advancement, and ob.gyns. were prescribing the first birth control pill approved by the Food and Drug Administration. ACOG’s main practice guidance book, “Standards for Obstetric-Gynecologic Hospital Services,” addressed the general physical examination but otherwise focused on obstetrics and reproductive health.
Thirty years later, women’s health care as described in the first edition of ACOG’s “Guidelines for Women’s Health Care” (1996) had grown to include distinct categories of “primary and preventive care” and “evaluation and counseling” that were separate from gynecologic services and broken down by age.
What was referred to as the “women’s health exam” through the 1990s gradually took on the “well-woman” label in the 2000s. Ob.gyns. were encouraged to address a growing range of preventive issues, but the annual Pap test remained a focus and, in many ways, drove women’s visits.
“Women would say, ‘I’m going for my Pap,’” Dr. Conry said.
Most recently, new technology and evidence-based reviews have changed the framework for well-woman visits to one with longer intervals for cervical cancer screening (every 3-5 years) and a move away from performing internal pelvic exams in all women (ACOG recommends pelvic exams annually for patients aged 21 and older but advises shared decision making for complete pelvic exams in asymptomatic patients).
Recent evidence reviews have also added some uncertainty about the role of annual breast exams in all women, as well as the role of breast self-exams, particularly for women not at high risk.
Maintaining patient relationships
One of the biggest and most immediate challenges for ob.gyns in the face of changing guidelines lies in maintaining the physician-patient relationship and “continuing communication” about the importance of regular well-woman visits, said Jill Rabin, MD, cochief of the division of ambulatory care, women’s health programs–prenatal care assistance program services at Northwell Health, New Hyde Park, N.Y.
“We want patients to understand that, even though they no longer need the Pap every year, they still should see us for good, comprehensive care ... that we can help them achieve their health care goals,” she said.
How often well-woman visits should occur has been a subject of much discussion. The HRSA-supported preventive services guidelines call for well-woman preventive care annually but note that “several visits may be needed to obtain all the necessary recommended services.”
And, in its first set of draft recommendations for HRSA, WPSI offered clarifications, saying there’s a need for “at least one annual preventive care visit for women beginning in adolescence and continuing across the lifespan to ensure that women obtain recommended preventive services” as determined by age and risk factors.
The draft recommendations, aimed at reviewing and updating the 2011 HRSA-sponsored guidelines, will be finalized by the end of 2016. WPSI will submit additional recommendations over the next 4 years.
Carol S. Weisman, PhD, a sociologist and health services researcher who sat on the Institute of Medicine committee that wrote the Women’s Preventive Services Guidelines, said the IOM’s recommendation for well-women visits – “in plural” form – recognizes “that historically many women have patched together their well-woman care from multiple providers, getting some of their preventive care from their generalist, and some from their ob.gyn.”
What’s more, the current list of preventive services covered under the Affordable Care Act is “enormous” – too long to address in one visit for many patients, said Dr. Weisman of the Penn State Center for Women’s Health Research in Hershey.
In addition to the women’s preventive services, the Affordable Care Act requires plans to cover services recommended with a grade A or B rating by the U.S. Preventive Services Task Force (counseling and screening for cancer, cardiovascular disease, and more) as well as vaccines recommended by the Advisory Committee on Immunization Practices, and HRSA’s Bright Futures services (for adolescents as well as children).
Beyond gynecology
How much further ob.gyns. will reach outside the gynecologic realm to offer additional preventive care services is an open question, but it’s likely to be based mainly on comfort levels, sources said.
“The changing needs of the gynecologic visit enable us to spend more time on other things,” said Hal C. Lawrence III, MD, ACOG’s executive vice president and chief executive officer. “But within the specialty, there’s going to be variation as to what level of expanded services ob.gyns. provide. Some will provide a lot of what women need, others not as much.”
Heather Johnson, MD, practices with a large ob.gyn. group in Chevy Chase, Md. and provides well-woman care largely to women in their 50s and 60s, whose children she delivered. She’s comfortable, she said, with screening for and treating osteoporosis and mild depression, for instance. She regularly performs lipid testing but refers out for management of high cholesterol levels or high blood pressure.
“I encourage all my patients to have a primary care physician of record,” she said, “but I still am happy to discuss the issues with them.”
What’s key, according to Dr. Lawrence and Dr. Conry, is coordination.
“We know there will be different individuals providing different components [of well-woman care],” Dr. Conry said. “I may see a woman for various things. Then she may go to her internist. But we should be able to collaborate to hit all the preventive health goals for her.”
Dr. Conry emphasized that the ob.gyn.’s expertise in reproductive health is critical to well-woman care planning, especially given medicine’s growing knowledge of how obstetric health and pregnancy complications can have long-term impacts on cardiovascular disease and other conditions. “It’s important for all providers to realize this,” she said.
Primary care status?
Intertwined with the future of well-women care is the issue of primary care status for ob.gyns. ACOG continues to advocate for ob.gyns. to be listed as primary care providers and part of primary care payment policies. Leaders are also pushing for projects on ob.gyn.–led medical homes.
At the same time, ACOG has been taking a broad collaborative approach to shaping well-woman care, aiming to develop comprehensive, age-specific recommendations for use by any provider who cares for adolescent girls and women.
Representatives of the American Academy of Family Physicians, the American College of Physicians, and the National Association of Nurse Practitioners in Women’s Health were involved in a Well-Woman Task Force that Dr. Conry appointed while serving as ACOG president in 2013-2014. These organizations now sit on WPSI’s advisory panel with ACOG.
Representatives from the American Academy of Pediatrics have also been close partners, as ACOG officials view the HRSA-sponsored Bright Futures guidelines (which includes the “Periodicity Schedule”) as a potential model for well-woman care. The guidelines are comprehensive, well-organized, and user-friendly, ACOG officials said.
At the University of Virginia, in the meantime, Dr. Peterson is arming the next generation of ob.gyns. with the skills needed for a team-based approach to well-woman visits. She said nurse practitioners and physician assistants will provide much more of the education and “more of the truly individualized conversations with patients” that will increasingly be part of well-woman care.
This is already happening. All of the nurse practitioners in Dr. Johnson’s group practice perform well-woman visits, “referring to the gynecologists for complicated gyn problems and out to the patient’s primary care physician for complicated medical problems,” Dr. Johnson said.
Even as the tools and recommendations for women’s preventive care become more evidence-based, the scope of well-woman visits will be based on risk factors, shared decision making, and other issues, Dr. Peterson said. “We will be telling patients, this is your path for your well-woman care,” she said.
Throughout 2016, Ob.Gyn. News is celebrating its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of contraception, changes in gynecologic surgery, and whether the practice environment is better or worse.

U.S. Falls Short on Protecting Against Vehicular Deaths
The U.S. has more motor vehicle crash deaths than do other high-income countries. Iin fact, the rate in the U.S. is roughly double the nearest countries in line: 10 deaths per 100,000 people, vs 5 to 6 in New Zealand, Canada, and France.
About one-third of deaths are due to drunk driving, and speeding contributes to another third. More than 9,500 of the deaths were due to passengers not using seat belts, car seats, or booster seats. Seat belts saved 12,500 plus lives in 2013, the CDC says, but about half of drivers or passengers who died in crashes weren’t buckled up. By contrast, 99% of drivers and passengers use front seat belts in France, and the average of the 19 countries studied is 94%—vs 87% in the U.S.
Although U.S. crash deaths fell 31% between 2000 and 2013, losing 90 people a day to crashes is still far too high, says the CDC. According to a Vital Signs report, more than 18,000 of the 32,000 lives lost each year could be saved if the U.S. took some safety tips from the other countries, the report says. Enforcing seat belt laws that cover everyone in every seat would be a good step, for instance. As would redefining blood alcohol concentration (BAC) limits—all the comparison countries use BAC levels at 0.02% to 0.05%, vs 0.08% in the U.S., Canada, and the United Kingdom. The report also urges using advanced engineering and technology, such as ignition interlocks for people convicted of drunk driving.
In the meantime, the CDC says, health care providers can help by reminding patients about using a seat belt on every trip, no matter how short; counseling parents on age- and size-appropriate seats for children; talking to patients about the dangers of impaired driving and “distracted” driving (eg, using cell phones or texting); and giving parents and caregivers of teens resources on safe teen driving.
The U.S. has more motor vehicle crash deaths than do other high-income countries. Iin fact, the rate in the U.S. is roughly double the nearest countries in line: 10 deaths per 100,000 people, vs 5 to 6 in New Zealand, Canada, and France.
About one-third of deaths are due to drunk driving, and speeding contributes to another third. More than 9,500 of the deaths were due to passengers not using seat belts, car seats, or booster seats. Seat belts saved 12,500 plus lives in 2013, the CDC says, but about half of drivers or passengers who died in crashes weren’t buckled up. By contrast, 99% of drivers and passengers use front seat belts in France, and the average of the 19 countries studied is 94%—vs 87% in the U.S.
Although U.S. crash deaths fell 31% between 2000 and 2013, losing 90 people a day to crashes is still far too high, says the CDC. According to a Vital Signs report, more than 18,000 of the 32,000 lives lost each year could be saved if the U.S. took some safety tips from the other countries, the report says. Enforcing seat belt laws that cover everyone in every seat would be a good step, for instance. As would redefining blood alcohol concentration (BAC) limits—all the comparison countries use BAC levels at 0.02% to 0.05%, vs 0.08% in the U.S., Canada, and the United Kingdom. The report also urges using advanced engineering and technology, such as ignition interlocks for people convicted of drunk driving.
In the meantime, the CDC says, health care providers can help by reminding patients about using a seat belt on every trip, no matter how short; counseling parents on age- and size-appropriate seats for children; talking to patients about the dangers of impaired driving and “distracted” driving (eg, using cell phones or texting); and giving parents and caregivers of teens resources on safe teen driving.
The U.S. has more motor vehicle crash deaths than do other high-income countries. Iin fact, the rate in the U.S. is roughly double the nearest countries in line: 10 deaths per 100,000 people, vs 5 to 6 in New Zealand, Canada, and France.
About one-third of deaths are due to drunk driving, and speeding contributes to another third. More than 9,500 of the deaths were due to passengers not using seat belts, car seats, or booster seats. Seat belts saved 12,500 plus lives in 2013, the CDC says, but about half of drivers or passengers who died in crashes weren’t buckled up. By contrast, 99% of drivers and passengers use front seat belts in France, and the average of the 19 countries studied is 94%—vs 87% in the U.S.
Although U.S. crash deaths fell 31% between 2000 and 2013, losing 90 people a day to crashes is still far too high, says the CDC. According to a Vital Signs report, more than 18,000 of the 32,000 lives lost each year could be saved if the U.S. took some safety tips from the other countries, the report says. Enforcing seat belt laws that cover everyone in every seat would be a good step, for instance. As would redefining blood alcohol concentration (BAC) limits—all the comparison countries use BAC levels at 0.02% to 0.05%, vs 0.08% in the U.S., Canada, and the United Kingdom. The report also urges using advanced engineering and technology, such as ignition interlocks for people convicted of drunk driving.
In the meantime, the CDC says, health care providers can help by reminding patients about using a seat belt on every trip, no matter how short; counseling parents on age- and size-appropriate seats for children; talking to patients about the dangers of impaired driving and “distracted” driving (eg, using cell phones or texting); and giving parents and caregivers of teens resources on safe teen driving.