User login
Scoring formula consolidates stroke, bleeding risk in atrial fib patients
ROME – A new risk-stratification formula for atrial fibrillation patients starting oral anticoagulant therapy helps sort out their potential net benefit on edoxaban, compared with warfarin.
This risk score “could help guide selection of treatment” with a vitamin K antagonist such as warfarin or a new oral anticoagulant (NOAC) such as edoxaban, Christina L. Fanola, MD, said at the annual congress of the European Society of Cardiology.
“It’s a great time to think about this type of score, because so many more patients are being diagnosed with atrial fibrillation and there is a lot of clinical equipoise” over which anticoagulant to start patients on, said Dr. Fanola, a cardiologist at Brigham and Women’s Hospital in Boston. She said she and her associates hope to externally validate the score and test it in cohorts that received other NOACs, such as apixaban (Eliquis), dabigatran (Pradaxa), or rivaroxaban (Xarelto), but it is very possible that scoring might differ from one NOAC to the next. “Each NOAC may need its own scoring formula,” Dr. Fanola said in an interview.

A Cox proportional hazards model identified 10 demographic, clinical, and laboratory features that had significant, independent correlations to a primary outcome of disabling stroke, life-threatening bleeding, or death. After weighing the point allocation for each item by the strength of its association, the researchers developed a scoring formula in a model that could account for about 69% of the three combined adverse outcomes.
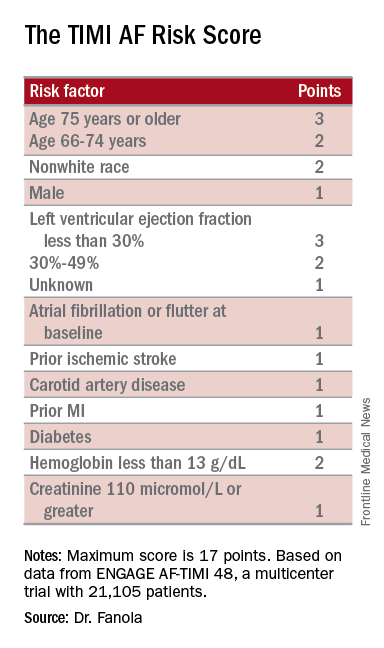
An analysis that applied the scoring formula back to the ENGAGE AF-TIMI 48 database showed that a low-risk score of 0-6 correlated with a 4% per year rate of disabling stroke, life-threatening bleed, or death; an intermediate-risk score of 7-9 correlated with a 10% per year incidence of this combined outcome, and a high-risk score of 10 or greater linked with a 21% annual event rate.
Dr. Fanola and her associates ran a further analysis that evaluated the efficacy of edoxaban, compared with warfarin, among the patients in each of these risk strata. The high-risk patients received a major benefit from edoxaban, with a 30% overall incidence of the combined endpoint during 3 years of follow-up, compared with a 51% rate among patients on warfarin, a 21-percentage-point reduction in adverse events. Intermediate-risk patients also received a significant benefit, with a 26% event rate on warfarin and an 18% rate on edoxaban. But low-risk patients had identical 10% event rates with either treatment.
These findings suggest that atrial fibrillation patients with a TIMI AF score that is high or intermediate would have a better chance for a good outcome on edoxaban, or perhaps a different NOAC, than on warfarin. Low-risk patients seem to have similar outcomes on edoxaban or warfarin, so other considerations can come into play for choosing between these drug options, such as the cost of treatment and the inconvenience of regular warfarin monitoring, Dr. Fanola said.
ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban. Dr. Fanola had no relevant financial disclosures.
[email protected]
On Twitter @mitchelzoler
ROME – A new risk-stratification formula for atrial fibrillation patients starting oral anticoagulant therapy helps sort out their potential net benefit on edoxaban, compared with warfarin.
This risk score “could help guide selection of treatment” with a vitamin K antagonist such as warfarin or a new oral anticoagulant (NOAC) such as edoxaban, Christina L. Fanola, MD, said at the annual congress of the European Society of Cardiology.
“It’s a great time to think about this type of score, because so many more patients are being diagnosed with atrial fibrillation and there is a lot of clinical equipoise” over which anticoagulant to start patients on, said Dr. Fanola, a cardiologist at Brigham and Women’s Hospital in Boston. She said she and her associates hope to externally validate the score and test it in cohorts that received other NOACs, such as apixaban (Eliquis), dabigatran (Pradaxa), or rivaroxaban (Xarelto), but it is very possible that scoring might differ from one NOAC to the next. “Each NOAC may need its own scoring formula,” Dr. Fanola said in an interview.
A Cox proportional hazards model identified 10 demographic, clinical, and laboratory features that had significant, independent correlations to a primary outcome of disabling stroke, life-threatening bleeding, or death. After weighing the point allocation for each item by the strength of its association, the researchers developed a scoring formula in a model that could account for about 69% of the three combined adverse outcomes.
An analysis that applied the scoring formula back to the ENGAGE AF-TIMI 48 database showed that a low-risk score of 0-6 correlated with a 4% per year rate of disabling stroke, life-threatening bleed, or death; an intermediate-risk score of 7-9 correlated with a 10% per year incidence of this combined outcome, and a high-risk score of 10 or greater linked with a 21% annual event rate.
Dr. Fanola and her associates ran a further analysis that evaluated the efficacy of edoxaban, compared with warfarin, among the patients in each of these risk strata. The high-risk patients received a major benefit from edoxaban, with a 30% overall incidence of the combined endpoint during 3 years of follow-up, compared with a 51% rate among patients on warfarin, a 21-percentage-point reduction in adverse events. Intermediate-risk patients also received a significant benefit, with a 26% event rate on warfarin and an 18% rate on edoxaban. But low-risk patients had identical 10% event rates with either treatment.
These findings suggest that atrial fibrillation patients with a TIMI AF score that is high or intermediate would have a better chance for a good outcome on edoxaban, or perhaps a different NOAC, than on warfarin. Low-risk patients seem to have similar outcomes on edoxaban or warfarin, so other considerations can come into play for choosing between these drug options, such as the cost of treatment and the inconvenience of regular warfarin monitoring, Dr. Fanola said.
ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban. Dr. Fanola had no relevant financial disclosures.
[email protected]
On Twitter @mitchelzoler
ROME – A new risk-stratification formula for atrial fibrillation patients starting oral anticoagulant therapy helps sort out their potential net benefit on edoxaban, compared with warfarin.
This risk score “could help guide selection of treatment” with a vitamin K antagonist such as warfarin or a new oral anticoagulant (NOAC) such as edoxaban, Christina L. Fanola, MD, said at the annual congress of the European Society of Cardiology.
“It’s a great time to think about this type of score, because so many more patients are being diagnosed with atrial fibrillation and there is a lot of clinical equipoise” over which anticoagulant to start patients on, said Dr. Fanola, a cardiologist at Brigham and Women’s Hospital in Boston. She said she and her associates hope to externally validate the score and test it in cohorts that received other NOACs, such as apixaban (Eliquis), dabigatran (Pradaxa), or rivaroxaban (Xarelto), but it is very possible that scoring might differ from one NOAC to the next. “Each NOAC may need its own scoring formula,” Dr. Fanola said in an interview.
A Cox proportional hazards model identified 10 demographic, clinical, and laboratory features that had significant, independent correlations to a primary outcome of disabling stroke, life-threatening bleeding, or death. After weighing the point allocation for each item by the strength of its association, the researchers developed a scoring formula in a model that could account for about 69% of the three combined adverse outcomes.
An analysis that applied the scoring formula back to the ENGAGE AF-TIMI 48 database showed that a low-risk score of 0-6 correlated with a 4% per year rate of disabling stroke, life-threatening bleed, or death; an intermediate-risk score of 7-9 correlated with a 10% per year incidence of this combined outcome, and a high-risk score of 10 or greater linked with a 21% annual event rate.
Dr. Fanola and her associates ran a further analysis that evaluated the efficacy of edoxaban, compared with warfarin, among the patients in each of these risk strata. The high-risk patients received a major benefit from edoxaban, with a 30% overall incidence of the combined endpoint during 3 years of follow-up, compared with a 51% rate among patients on warfarin, a 21-percentage-point reduction in adverse events. Intermediate-risk patients also received a significant benefit, with a 26% event rate on warfarin and an 18% rate on edoxaban. But low-risk patients had identical 10% event rates with either treatment.
These findings suggest that atrial fibrillation patients with a TIMI AF score that is high or intermediate would have a better chance for a good outcome on edoxaban, or perhaps a different NOAC, than on warfarin. Low-risk patients seem to have similar outcomes on edoxaban or warfarin, so other considerations can come into play for choosing between these drug options, such as the cost of treatment and the inconvenience of regular warfarin monitoring, Dr. Fanola said.
ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban. Dr. Fanola had no relevant financial disclosures.
[email protected]
On Twitter @mitchelzoler
AT THE ESC CONGRESS 2016
Key clinical point:
Major finding: Among high-risk patients, edoxaban cut adverse events by 21 percentage points, compared with warfarin.
Data source: ENGAGE AF-TIMI 48, a multicenter trial with 21,105 patients.
Disclosures: ENGAGE AF-TIMI 48 was sponsored by Daiichi Sankyo, the company that markets edoxaban (Savaysa). Dr. Fanola had no relevant financial disclosures.
Giving women HIV self-tests increases male partner testing
Providing Kenyan women attending prenatal or postpartum health care visits with HIV self-testing kits raised the rates of partner and couples testing to more than 90%, according to a report published online in PLOS Medicine.
HIV testing remains underused in many parts of sub-Saharan Africa, particularly among men, for reasons including social stigma, fear of poor prognosis, lack of awareness of HIV risk, fear that their results would be disclosed, inconvenience, and transportation costs. To assess one strategy for improving male testing rates, researchers performed a study at a hospital and two clinics in urban and suburban Kisumu, Kenya, where the HIV prevalence is approximately 20% among adult residents. 
The trial involved 600 women aged 18-39 years (mean age, 24 years) who were seeking either prenatal or postpartum health care and agreed to participate. They were randomly assigned to receive either a few HIV self-test kits plus counseling regarding HIV testing (intervention group) or counseling alone (control group) and followed for 3 months. A total of 95% of the women – 284 in the intervention group and 286 in the control group – completed the study, said Harsha Thirumurthy, PhD, of the department of health policy and management, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, and his associates.
At follow-up, 258 (90.8%) of the women in the intervention group reported that their partners had been tested for HIV, compared with 148 (51.7%) of the control group. This significant difference persisted across all subgroups of patients, regardless of study site and whether or not partners said they had been tested during the preceding year. “This result is encouraging since it suggests that the strategy of giving multiple self-tests to women can effectively increase access to HIV testing in hard-to-reach populations such as men who do not test regularly,” the investigators said (PLOS Med. 2016 Nov 8. doi: 10.1371/journal.pmed.1002166).
In three-fourths of the cases where male partners were tested for HIV, both members of the couple were tested together. This is beneficial because it helps women learn their partners’ HIV status, and because couples who test together are “more likely to adopt a range of HIV prevention and care behaviors,” Dr. Thirumurthy and his associates wrote.
Approximately one-third of the women who were eligible for this study declined to participate, often because they feared that their partners would become violent if offered an HIV self-test. Even women who did participate reported a high rate (27%) of partner violence at baseline. It is encouraging that none of the study participants reported any such incidents in response to the HIV testing, the investigators added.
The International Initiative for Impact Evaluation funded the study. Dr. Thirumurthy and his associates reported having no relevant financial disclosures.
Providing Kenyan women attending prenatal or postpartum health care visits with HIV self-testing kits raised the rates of partner and couples testing to more than 90%, according to a report published online in PLOS Medicine.
HIV testing remains underused in many parts of sub-Saharan Africa, particularly among men, for reasons including social stigma, fear of poor prognosis, lack of awareness of HIV risk, fear that their results would be disclosed, inconvenience, and transportation costs. To assess one strategy for improving male testing rates, researchers performed a study at a hospital and two clinics in urban and suburban Kisumu, Kenya, where the HIV prevalence is approximately 20% among adult residents.
The trial involved 600 women aged 18-39 years (mean age, 24 years) who were seeking either prenatal or postpartum health care and agreed to participate. They were randomly assigned to receive either a few HIV self-test kits plus counseling regarding HIV testing (intervention group) or counseling alone (control group) and followed for 3 months. A total of 95% of the women – 284 in the intervention group and 286 in the control group – completed the study, said Harsha Thirumurthy, PhD, of the department of health policy and management, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, and his associates.
At follow-up, 258 (90.8%) of the women in the intervention group reported that their partners had been tested for HIV, compared with 148 (51.7%) of the control group. This significant difference persisted across all subgroups of patients, regardless of study site and whether or not partners said they had been tested during the preceding year. “This result is encouraging since it suggests that the strategy of giving multiple self-tests to women can effectively increase access to HIV testing in hard-to-reach populations such as men who do not test regularly,” the investigators said (PLOS Med. 2016 Nov 8. doi: 10.1371/journal.pmed.1002166).
In three-fourths of the cases where male partners were tested for HIV, both members of the couple were tested together. This is beneficial because it helps women learn their partners’ HIV status, and because couples who test together are “more likely to adopt a range of HIV prevention and care behaviors,” Dr. Thirumurthy and his associates wrote.
Approximately one-third of the women who were eligible for this study declined to participate, often because they feared that their partners would become violent if offered an HIV self-test. Even women who did participate reported a high rate (27%) of partner violence at baseline. It is encouraging that none of the study participants reported any such incidents in response to the HIV testing, the investigators added.
The International Initiative for Impact Evaluation funded the study. Dr. Thirumurthy and his associates reported having no relevant financial disclosures.
Providing Kenyan women attending prenatal or postpartum health care visits with HIV self-testing kits raised the rates of partner and couples testing to more than 90%, according to a report published online in PLOS Medicine.
HIV testing remains underused in many parts of sub-Saharan Africa, particularly among men, for reasons including social stigma, fear of poor prognosis, lack of awareness of HIV risk, fear that their results would be disclosed, inconvenience, and transportation costs. To assess one strategy for improving male testing rates, researchers performed a study at a hospital and two clinics in urban and suburban Kisumu, Kenya, where the HIV prevalence is approximately 20% among adult residents.
The trial involved 600 women aged 18-39 years (mean age, 24 years) who were seeking either prenatal or postpartum health care and agreed to participate. They were randomly assigned to receive either a few HIV self-test kits plus counseling regarding HIV testing (intervention group) or counseling alone (control group) and followed for 3 months. A total of 95% of the women – 284 in the intervention group and 286 in the control group – completed the study, said Harsha Thirumurthy, PhD, of the department of health policy and management, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, and his associates.
At follow-up, 258 (90.8%) of the women in the intervention group reported that their partners had been tested for HIV, compared with 148 (51.7%) of the control group. This significant difference persisted across all subgroups of patients, regardless of study site and whether or not partners said they had been tested during the preceding year. “This result is encouraging since it suggests that the strategy of giving multiple self-tests to women can effectively increase access to HIV testing in hard-to-reach populations such as men who do not test regularly,” the investigators said (PLOS Med. 2016 Nov 8. doi: 10.1371/journal.pmed.1002166).
In three-fourths of the cases where male partners were tested for HIV, both members of the couple were tested together. This is beneficial because it helps women learn their partners’ HIV status, and because couples who test together are “more likely to adopt a range of HIV prevention and care behaviors,” Dr. Thirumurthy and his associates wrote.
Approximately one-third of the women who were eligible for this study declined to participate, often because they feared that their partners would become violent if offered an HIV self-test. Even women who did participate reported a high rate (27%) of partner violence at baseline. It is encouraging that none of the study participants reported any such incidents in response to the HIV testing, the investigators added.
The International Initiative for Impact Evaluation funded the study. Dr. Thirumurthy and his associates reported having no relevant financial disclosures.
FROM PLOS MEDICINE
Key clinical point: Providing Kenyan women attending prenatal or postpartum health care visits with HIV self-testing kits raised the rates of partner and couples testing to more than 90%.
Major finding: After 3 months, 258 women (90.8%) in the intervention group reported that their partners had been tested for HIV, compared with 148 (51.7%) of the control group.
Data source: A multicenter randomized trial involving 600 women in Kenya receiving prenatal or postpartum care, and their sexual partners.
Disclosures: The International Initiative for Impact Evaluation funded the study. Dr. Thirumurthy and his associates reported having no relevant financial disclosures.
FDA addresses unmet need in drug development guidance for female sexual dysfunction
On Oct. 25, 2016, the Food and Drug Administration issued a draft guidance document titled “Low Sexual Interest, Desire, and/or Arousal in Women: Developing Drugs for Treatment.” The document outlines FDA’s current thinking about how best to design phase III trials for drugs to treat these problems. The purpose of this guidance is to provide pharmaceutical companies with a road map of what the FDA recommends should be addressed in clinical trials designed for new drug approval.
The FDA makes it clear that this guidance is only a “recommendation,” reflecting the agency’s current thinking on this important issue, and is not a requirement (unless specific regulatory or statutory requirements are cited). That may well be, but this puts me in mind of my graduate school days when my advisor used to tell me that his suggestions for my dissertation were only “recommendations.” I knew, of course, that to ignore these recommendations was folly.

Specifically, I would like to highlight several remarkable advances in this document. First, the guidance document acknowledges that there is a medical need for drugs to treat women with sexual dysfunction. Second, the guidance supports retaining the disorders of Hypoactive Sexual Desire Disorder (HSDD) and Female Sexual Arousal Disorder (FSAD) from the DSM-IV as treatment indications. Further, the guidance recognizes that the DSM-5 revisions of female sexual disorders, in this case, Female Sexual Interest and/or Arousal Disorder (FSIAD) “have not been universally accepted the scientific community.”
With regard to clinical trial design, I commend the FDA for removing Satisfying Sexual Events (SSEs) as a “required” primary endpoint and for allowing sponsors more flexibility to choose primary endpoints that will better align regulatory standards with the definition and key symptoms of HSDD (as well as FSAD and FSIAD). These endpoints include validated patient-reported outcome instruments that assess the symptoms of low desire (or arousal) and sexually related distress.
On the negative side, the guidance also reflects some carryover myths that are not in keeping with evidence or expert opinion. Specifically, the FDA cautions against the use of the Female Sexual Function Index desire (FSFI-D) subdomain as a primary endpoint in its current form. The FSFI-D has excellent construct and content validity. Furthermore, the guidance cautions against using a long recall period – 28 days/4 weeks – reflecting the FDA’s concern that women’s recall over that period of time will be inaccurate. They strongly recommend a 24-hour recall period.
Although it is certainly appropriate to evaluate on-demand treatments using more immediate and specific time frames, longer recall of desire is still appropriate as well. Longer recall periods provide a more accurate assessment of desire, which is best understood as state as of mind. A 24-hour recall (e.g., daily log of desire) is more akin to assessing one’s current hunger, whereas a 28-day look-back reflects one’s overall appetite, a concept more similar to desire.
And finally, although the FDA supports inclusion of postmenopausal women as a target population, it would be best if they not divide women into “groups” based on menopausal status unless hormonal status is relevant. This could further marginalize postmenopausal women and delay access to treatments for this population.
Once finalized, this draft guidance should serve its stated purpose to enhance discussion among FDA, pharmaceutical companies, academics, and the public.
Dr. Kingsberg is chief of the division of behavioral medicine in the department of obstetrics and gynecology at MacDonald Women’s Hospital, part of the University Hospitals Cleveland Medical Center, Ohio. She is also a professor in the departments of reproductive biology and psychiatry at Case Western Reserve University, Cleveland. Dr. Kingsberg reported being a consultant or member of the scientific advisory board for Acerus, AMAG, Bayer, Emotional Brain, Endoceutics, NovoNordisk, Palatin, Pfizer, Shionogi, Sprout, TherapeuticsMD, Sermonix, Strategic Science & Technologies, and Valeant. Valeant is the manufacturer of the HSDD drug flibanserin.
On Oct. 25, 2016, the Food and Drug Administration issued a draft guidance document titled “Low Sexual Interest, Desire, and/or Arousal in Women: Developing Drugs for Treatment.” The document outlines FDA’s current thinking about how best to design phase III trials for drugs to treat these problems. The purpose of this guidance is to provide pharmaceutical companies with a road map of what the FDA recommends should be addressed in clinical trials designed for new drug approval.
The FDA makes it clear that this guidance is only a “recommendation,” reflecting the agency’s current thinking on this important issue, and is not a requirement (unless specific regulatory or statutory requirements are cited). That may well be, but this puts me in mind of my graduate school days when my advisor used to tell me that his suggestions for my dissertation were only “recommendations.” I knew, of course, that to ignore these recommendations was folly.
Specifically, I would like to highlight several remarkable advances in this document. First, the guidance document acknowledges that there is a medical need for drugs to treat women with sexual dysfunction. Second, the guidance supports retaining the disorders of Hypoactive Sexual Desire Disorder (HSDD) and Female Sexual Arousal Disorder (FSAD) from the DSM-IV as treatment indications. Further, the guidance recognizes that the DSM-5 revisions of female sexual disorders, in this case, Female Sexual Interest and/or Arousal Disorder (FSIAD) “have not been universally accepted the scientific community.”
With regard to clinical trial design, I commend the FDA for removing Satisfying Sexual Events (SSEs) as a “required” primary endpoint and for allowing sponsors more flexibility to choose primary endpoints that will better align regulatory standards with the definition and key symptoms of HSDD (as well as FSAD and FSIAD). These endpoints include validated patient-reported outcome instruments that assess the symptoms of low desire (or arousal) and sexually related distress.
On the negative side, the guidance also reflects some carryover myths that are not in keeping with evidence or expert opinion. Specifically, the FDA cautions against the use of the Female Sexual Function Index desire (FSFI-D) subdomain as a primary endpoint in its current form. The FSFI-D has excellent construct and content validity. Furthermore, the guidance cautions against using a long recall period – 28 days/4 weeks – reflecting the FDA’s concern that women’s recall over that period of time will be inaccurate. They strongly recommend a 24-hour recall period.
Although it is certainly appropriate to evaluate on-demand treatments using more immediate and specific time frames, longer recall of desire is still appropriate as well. Longer recall periods provide a more accurate assessment of desire, which is best understood as state as of mind. A 24-hour recall (e.g., daily log of desire) is more akin to assessing one’s current hunger, whereas a 28-day look-back reflects one’s overall appetite, a concept more similar to desire.
And finally, although the FDA supports inclusion of postmenopausal women as a target population, it would be best if they not divide women into “groups” based on menopausal status unless hormonal status is relevant. This could further marginalize postmenopausal women and delay access to treatments for this population.
Once finalized, this draft guidance should serve its stated purpose to enhance discussion among FDA, pharmaceutical companies, academics, and the public.
Dr. Kingsberg is chief of the division of behavioral medicine in the department of obstetrics and gynecology at MacDonald Women’s Hospital, part of the University Hospitals Cleveland Medical Center, Ohio. She is also a professor in the departments of reproductive biology and psychiatry at Case Western Reserve University, Cleveland. Dr. Kingsberg reported being a consultant or member of the scientific advisory board for Acerus, AMAG, Bayer, Emotional Brain, Endoceutics, NovoNordisk, Palatin, Pfizer, Shionogi, Sprout, TherapeuticsMD, Sermonix, Strategic Science & Technologies, and Valeant. Valeant is the manufacturer of the HSDD drug flibanserin.
On Oct. 25, 2016, the Food and Drug Administration issued a draft guidance document titled “Low Sexual Interest, Desire, and/or Arousal in Women: Developing Drugs for Treatment.” The document outlines FDA’s current thinking about how best to design phase III trials for drugs to treat these problems. The purpose of this guidance is to provide pharmaceutical companies with a road map of what the FDA recommends should be addressed in clinical trials designed for new drug approval.
The FDA makes it clear that this guidance is only a “recommendation,” reflecting the agency’s current thinking on this important issue, and is not a requirement (unless specific regulatory or statutory requirements are cited). That may well be, but this puts me in mind of my graduate school days when my advisor used to tell me that his suggestions for my dissertation were only “recommendations.” I knew, of course, that to ignore these recommendations was folly.
Specifically, I would like to highlight several remarkable advances in this document. First, the guidance document acknowledges that there is a medical need for drugs to treat women with sexual dysfunction. Second, the guidance supports retaining the disorders of Hypoactive Sexual Desire Disorder (HSDD) and Female Sexual Arousal Disorder (FSAD) from the DSM-IV as treatment indications. Further, the guidance recognizes that the DSM-5 revisions of female sexual disorders, in this case, Female Sexual Interest and/or Arousal Disorder (FSIAD) “have not been universally accepted the scientific community.”
With regard to clinical trial design, I commend the FDA for removing Satisfying Sexual Events (SSEs) as a “required” primary endpoint and for allowing sponsors more flexibility to choose primary endpoints that will better align regulatory standards with the definition and key symptoms of HSDD (as well as FSAD and FSIAD). These endpoints include validated patient-reported outcome instruments that assess the symptoms of low desire (or arousal) and sexually related distress.
On the negative side, the guidance also reflects some carryover myths that are not in keeping with evidence or expert opinion. Specifically, the FDA cautions against the use of the Female Sexual Function Index desire (FSFI-D) subdomain as a primary endpoint in its current form. The FSFI-D has excellent construct and content validity. Furthermore, the guidance cautions against using a long recall period – 28 days/4 weeks – reflecting the FDA’s concern that women’s recall over that period of time will be inaccurate. They strongly recommend a 24-hour recall period.
Although it is certainly appropriate to evaluate on-demand treatments using more immediate and specific time frames, longer recall of desire is still appropriate as well. Longer recall periods provide a more accurate assessment of desire, which is best understood as state as of mind. A 24-hour recall (e.g., daily log of desire) is more akin to assessing one’s current hunger, whereas a 28-day look-back reflects one’s overall appetite, a concept more similar to desire.
And finally, although the FDA supports inclusion of postmenopausal women as a target population, it would be best if they not divide women into “groups” based on menopausal status unless hormonal status is relevant. This could further marginalize postmenopausal women and delay access to treatments for this population.
Once finalized, this draft guidance should serve its stated purpose to enhance discussion among FDA, pharmaceutical companies, academics, and the public.
Dr. Kingsberg is chief of the division of behavioral medicine in the department of obstetrics and gynecology at MacDonald Women’s Hospital, part of the University Hospitals Cleveland Medical Center, Ohio. She is also a professor in the departments of reproductive biology and psychiatry at Case Western Reserve University, Cleveland. Dr. Kingsberg reported being a consultant or member of the scientific advisory board for Acerus, AMAG, Bayer, Emotional Brain, Endoceutics, NovoNordisk, Palatin, Pfizer, Shionogi, Sprout, TherapeuticsMD, Sermonix, Strategic Science & Technologies, and Valeant. Valeant is the manufacturer of the HSDD drug flibanserin.
Mental health integration into pediatric primary care offers multiple benefits
SAN FRANCISCO – Integrating pediatric mental health care into your primary care office can be an effective way to ensure your patients get the care they really need – and it’s easier than you think.
That’s the message Jay Rabinowitz, MD, MPH, a clinical professor of pediatrics at the University of Colorado at Denver, Aurora, delivered to a packed room at the annual meeting of the American Academy of Pediatrics.
He noted that depression and anxiety are among the top five conditions driving overall health costs in the United States, and a 1999 Surgeon General’s Report found that one in five children have a diagnosable mental disorder – but only a fifth to a quarter of these children receive treatment. The rub is that treatment is highly successful; it’s just difficult to access for many families, so making it a part of a child’s medical home just makes sense, Dr. Rabinowitz said.
To drive home his point, he described a case of a depressed adolescent with cutting and suicidal ideation, and the steps he would need to take without integration: find out their insurance, get a list of covered mental health professionals, refer to someone he may or may not heard of, and then rarely receive follow-up reports, much less confirmation the patient had gone to the appointment. With integrated care, parents can make appointments on their way out, he can read the psychologist’s report immediately after the visit, and he can drop in to say hello during the child’s mental health appointment.
“Sometimes there’s a question abut a medication or something, and sometimes it’s an inopportune moment if the child is sad or crying, but generally it seems to be pretty popular,” he said.
Taking steps toward integration
If providers are interesting in exploring the possibility of integration, they need to consider and decide on several issues before taking any concrete steps, Dr. Rabinowitz said. One is the type of arrangement that would work best for your practice: hiring on mental health professionals as employees of the practice, hiring independent contractors, coordinating a space share agreement or creating an out-of-office agreement.
“In our practice, psychologists are employees of the practice, but there are other arrangements,” he said, and some may depend on what is easiest based on state law or billing procedures.
The next question is what kind of provider(s) you would hire. His office has child psychologists with a PhD and postdoctorate fellowships working with children, but other possibilities include social workers, licensed counselors, psychiatric nurse practitioners, or psychiatrists.
Another consideration is what diagnoses your office will handle because it’s not possible to see everything. His practice sees patients in-house for attention deficit/hyperactivity disorder (ADHD), depression, anxiety, drug counseling, and behavioral and adjustment disorders. They choose to refer out educational testing, autism, difficult divorce cases, and complex cases that require more than 20 sessions. They refer out divorce cases because they frequently require specialized knowledge and a lot of court time and phone calls. Aside from ADHD evaluations, his office does not see the staff’s children.
Providers also should consider options for adapting their physical space to accommodate integration. His practice converted an exam room into a consultation room, making it homier with a throw rug, soft chairs, a painted wall, and office decor.
Establishing effective protocols with integration
The next step after providers decide to integrate is to determine the office protocols that govern what forms get used, who can schedule appointments and how long they last, billing, and similar procedures.
“You need to have certain protocols, and some of these things you don’t think about it until you start doing it,” Dr. Rabinowitz said. Should mental health appointments be 50 minutes, for example, or 20 to 25 minutes? His office has gradually shrunk these appointments from 50 to 30 minutes, but they give psychologists an hour of time each day for follow-up phone calls.
Forms to consider developing include a disclosure form, notice of privacy practices, late cancel/no show policy, financial policy, and a summary of parent concerns. His office’s charting includes an extensive intake form with medical, treatment, family, and social history, an intake summary, and a progress note.
It’s with reimbursement, of course, that providers will need to do the most research, particularly with regard to their state’s laws and in looking for grants to provide funding – which is more available than many realize.
“Money is often out there if you look for it,” Dr. Rabinowitz said.” Mental health is an area where no one is really against it: You get together the NRA (National Rifle Association) and the anti-gun movement, and they are both for it.”
Planning for reimbursement challenges
Reimbursement barriers can include lack of payment if mental health codes are used instead of pediatrics ones (depending on the practice arrangement), lack of “incident to” payments, same day billing of physical and mental health appointments, reimbursement for screening, and lack of payment for non–face-to-face services. Although a concierge or fee-for-service option solves many of these, it excludes Medicaid patients and is an economic barrier for many families.
Mental health networks offer a different route, but they can involve poor reimbursement and an additional layer of administration, which makes financial integration more viable as long as providers investigate their options.
“It’s going to be a regional variation, and you need to look at state rules and regulations,” Dr. Rabinowitz said, explaining that his office then sought insurance contracts to include mental health care reimbursement through their office and then sought the same from Medicaid.
“We weren’t about to see Medicaid patients for fear of an audit unless we got written permission, but we got that,” he said. His office simply asked for it and received in writing a letter starting as follows: “Under Department policy, they (our psychologists) may submit E&M claims to Medicaid under a supervising physician’s billing ID. It is not mandatory they be credentialed into a BHO (Behavioral Healthcare Options) network…”
He also noted that his state allows inclusion of psychologists on medical malpractice insurance policies, which is far less expensive for mental health professionals, compared with medical doctors.
Ultimately, the result of mental health integration into primary care practices is greater satisfaction among patients and pediatricians as well as potentially better health outcomes, Dr. Rabinowitz said. An in-house patient satisfaction survey his office conducted found that 91% of parents felt it was convenient for their child to receive mental health services at the same location as medical care, and 90% were satisfied with their care. Only 9% cited barriers to their child seeing a psychologist at their office, and 89% found the services beneficial for their child. Similarly, providers find integration more convenient, easier for follow-up, less stressful, and more efficient while improving communication, confidence, and follow-up.
Dr. Rabinowitz reported no disclosures. No external funding was used for the presentation.
SAN FRANCISCO – Integrating pediatric mental health care into your primary care office can be an effective way to ensure your patients get the care they really need – and it’s easier than you think.
That’s the message Jay Rabinowitz, MD, MPH, a clinical professor of pediatrics at the University of Colorado at Denver, Aurora, delivered to a packed room at the annual meeting of the American Academy of Pediatrics.
He noted that depression and anxiety are among the top five conditions driving overall health costs in the United States, and a 1999 Surgeon General’s Report found that one in five children have a diagnosable mental disorder – but only a fifth to a quarter of these children receive treatment. The rub is that treatment is highly successful; it’s just difficult to access for many families, so making it a part of a child’s medical home just makes sense, Dr. Rabinowitz said.
To drive home his point, he described a case of a depressed adolescent with cutting and suicidal ideation, and the steps he would need to take without integration: find out their insurance, get a list of covered mental health professionals, refer to someone he may or may not heard of, and then rarely receive follow-up reports, much less confirmation the patient had gone to the appointment. With integrated care, parents can make appointments on their way out, he can read the psychologist’s report immediately after the visit, and he can drop in to say hello during the child’s mental health appointment.
“Sometimes there’s a question abut a medication or something, and sometimes it’s an inopportune moment if the child is sad or crying, but generally it seems to be pretty popular,” he said.
Taking steps toward integration
If providers are interesting in exploring the possibility of integration, they need to consider and decide on several issues before taking any concrete steps, Dr. Rabinowitz said. One is the type of arrangement that would work best for your practice: hiring on mental health professionals as employees of the practice, hiring independent contractors, coordinating a space share agreement or creating an out-of-office agreement.
“In our practice, psychologists are employees of the practice, but there are other arrangements,” he said, and some may depend on what is easiest based on state law or billing procedures.
The next question is what kind of provider(s) you would hire. His office has child psychologists with a PhD and postdoctorate fellowships working with children, but other possibilities include social workers, licensed counselors, psychiatric nurse practitioners, or psychiatrists.
Another consideration is what diagnoses your office will handle because it’s not possible to see everything. His practice sees patients in-house for attention deficit/hyperactivity disorder (ADHD), depression, anxiety, drug counseling, and behavioral and adjustment disorders. They choose to refer out educational testing, autism, difficult divorce cases, and complex cases that require more than 20 sessions. They refer out divorce cases because they frequently require specialized knowledge and a lot of court time and phone calls. Aside from ADHD evaluations, his office does not see the staff’s children.
Providers also should consider options for adapting their physical space to accommodate integration. His practice converted an exam room into a consultation room, making it homier with a throw rug, soft chairs, a painted wall, and office decor.
Establishing effective protocols with integration
The next step after providers decide to integrate is to determine the office protocols that govern what forms get used, who can schedule appointments and how long they last, billing, and similar procedures.
“You need to have certain protocols, and some of these things you don’t think about it until you start doing it,” Dr. Rabinowitz said. Should mental health appointments be 50 minutes, for example, or 20 to 25 minutes? His office has gradually shrunk these appointments from 50 to 30 minutes, but they give psychologists an hour of time each day for follow-up phone calls.
Forms to consider developing include a disclosure form, notice of privacy practices, late cancel/no show policy, financial policy, and a summary of parent concerns. His office’s charting includes an extensive intake form with medical, treatment, family, and social history, an intake summary, and a progress note.
It’s with reimbursement, of course, that providers will need to do the most research, particularly with regard to their state’s laws and in looking for grants to provide funding – which is more available than many realize.
“Money is often out there if you look for it,” Dr. Rabinowitz said.” Mental health is an area where no one is really against it: You get together the NRA (National Rifle Association) and the anti-gun movement, and they are both for it.”
Planning for reimbursement challenges
Reimbursement barriers can include lack of payment if mental health codes are used instead of pediatrics ones (depending on the practice arrangement), lack of “incident to” payments, same day billing of physical and mental health appointments, reimbursement for screening, and lack of payment for non–face-to-face services. Although a concierge or fee-for-service option solves many of these, it excludes Medicaid patients and is an economic barrier for many families.
Mental health networks offer a different route, but they can involve poor reimbursement and an additional layer of administration, which makes financial integration more viable as long as providers investigate their options.
“It’s going to be a regional variation, and you need to look at state rules and regulations,” Dr. Rabinowitz said, explaining that his office then sought insurance contracts to include mental health care reimbursement through their office and then sought the same from Medicaid.
“We weren’t about to see Medicaid patients for fear of an audit unless we got written permission, but we got that,” he said. His office simply asked for it and received in writing a letter starting as follows: “Under Department policy, they (our psychologists) may submit E&M claims to Medicaid under a supervising physician’s billing ID. It is not mandatory they be credentialed into a BHO (Behavioral Healthcare Options) network…”
He also noted that his state allows inclusion of psychologists on medical malpractice insurance policies, which is far less expensive for mental health professionals, compared with medical doctors.
Ultimately, the result of mental health integration into primary care practices is greater satisfaction among patients and pediatricians as well as potentially better health outcomes, Dr. Rabinowitz said. An in-house patient satisfaction survey his office conducted found that 91% of parents felt it was convenient for their child to receive mental health services at the same location as medical care, and 90% were satisfied with their care. Only 9% cited barriers to their child seeing a psychologist at their office, and 89% found the services beneficial for their child. Similarly, providers find integration more convenient, easier for follow-up, less stressful, and more efficient while improving communication, confidence, and follow-up.
Dr. Rabinowitz reported no disclosures. No external funding was used for the presentation.
SAN FRANCISCO – Integrating pediatric mental health care into your primary care office can be an effective way to ensure your patients get the care they really need – and it’s easier than you think.
That’s the message Jay Rabinowitz, MD, MPH, a clinical professor of pediatrics at the University of Colorado at Denver, Aurora, delivered to a packed room at the annual meeting of the American Academy of Pediatrics.
He noted that depression and anxiety are among the top five conditions driving overall health costs in the United States, and a 1999 Surgeon General’s Report found that one in five children have a diagnosable mental disorder – but only a fifth to a quarter of these children receive treatment. The rub is that treatment is highly successful; it’s just difficult to access for many families, so making it a part of a child’s medical home just makes sense, Dr. Rabinowitz said.
To drive home his point, he described a case of a depressed adolescent with cutting and suicidal ideation, and the steps he would need to take without integration: find out their insurance, get a list of covered mental health professionals, refer to someone he may or may not heard of, and then rarely receive follow-up reports, much less confirmation the patient had gone to the appointment. With integrated care, parents can make appointments on their way out, he can read the psychologist’s report immediately after the visit, and he can drop in to say hello during the child’s mental health appointment.
“Sometimes there’s a question abut a medication or something, and sometimes it’s an inopportune moment if the child is sad or crying, but generally it seems to be pretty popular,” he said.
Taking steps toward integration
If providers are interesting in exploring the possibility of integration, they need to consider and decide on several issues before taking any concrete steps, Dr. Rabinowitz said. One is the type of arrangement that would work best for your practice: hiring on mental health professionals as employees of the practice, hiring independent contractors, coordinating a space share agreement or creating an out-of-office agreement.
“In our practice, psychologists are employees of the practice, but there are other arrangements,” he said, and some may depend on what is easiest based on state law or billing procedures.
The next question is what kind of provider(s) you would hire. His office has child psychologists with a PhD and postdoctorate fellowships working with children, but other possibilities include social workers, licensed counselors, psychiatric nurse practitioners, or psychiatrists.
Another consideration is what diagnoses your office will handle because it’s not possible to see everything. His practice sees patients in-house for attention deficit/hyperactivity disorder (ADHD), depression, anxiety, drug counseling, and behavioral and adjustment disorders. They choose to refer out educational testing, autism, difficult divorce cases, and complex cases that require more than 20 sessions. They refer out divorce cases because they frequently require specialized knowledge and a lot of court time and phone calls. Aside from ADHD evaluations, his office does not see the staff’s children.
Providers also should consider options for adapting their physical space to accommodate integration. His practice converted an exam room into a consultation room, making it homier with a throw rug, soft chairs, a painted wall, and office decor.
Establishing effective protocols with integration
The next step after providers decide to integrate is to determine the office protocols that govern what forms get used, who can schedule appointments and how long they last, billing, and similar procedures.
“You need to have certain protocols, and some of these things you don’t think about it until you start doing it,” Dr. Rabinowitz said. Should mental health appointments be 50 minutes, for example, or 20 to 25 minutes? His office has gradually shrunk these appointments from 50 to 30 minutes, but they give psychologists an hour of time each day for follow-up phone calls.
Forms to consider developing include a disclosure form, notice of privacy practices, late cancel/no show policy, financial policy, and a summary of parent concerns. His office’s charting includes an extensive intake form with medical, treatment, family, and social history, an intake summary, and a progress note.
It’s with reimbursement, of course, that providers will need to do the most research, particularly with regard to their state’s laws and in looking for grants to provide funding – which is more available than many realize.
“Money is often out there if you look for it,” Dr. Rabinowitz said.” Mental health is an area where no one is really against it: You get together the NRA (National Rifle Association) and the anti-gun movement, and they are both for it.”
Planning for reimbursement challenges
Reimbursement barriers can include lack of payment if mental health codes are used instead of pediatrics ones (depending on the practice arrangement), lack of “incident to” payments, same day billing of physical and mental health appointments, reimbursement for screening, and lack of payment for non–face-to-face services. Although a concierge or fee-for-service option solves many of these, it excludes Medicaid patients and is an economic barrier for many families.
Mental health networks offer a different route, but they can involve poor reimbursement and an additional layer of administration, which makes financial integration more viable as long as providers investigate their options.
“It’s going to be a regional variation, and you need to look at state rules and regulations,” Dr. Rabinowitz said, explaining that his office then sought insurance contracts to include mental health care reimbursement through their office and then sought the same from Medicaid.
“We weren’t about to see Medicaid patients for fear of an audit unless we got written permission, but we got that,” he said. His office simply asked for it and received in writing a letter starting as follows: “Under Department policy, they (our psychologists) may submit E&M claims to Medicaid under a supervising physician’s billing ID. It is not mandatory they be credentialed into a BHO (Behavioral Healthcare Options) network…”
He also noted that his state allows inclusion of psychologists on medical malpractice insurance policies, which is far less expensive for mental health professionals, compared with medical doctors.
Ultimately, the result of mental health integration into primary care practices is greater satisfaction among patients and pediatricians as well as potentially better health outcomes, Dr. Rabinowitz said. An in-house patient satisfaction survey his office conducted found that 91% of parents felt it was convenient for their child to receive mental health services at the same location as medical care, and 90% were satisfied with their care. Only 9% cited barriers to their child seeing a psychologist at their office, and 89% found the services beneficial for their child. Similarly, providers find integration more convenient, easier for follow-up, less stressful, and more efficient while improving communication, confidence, and follow-up.
Dr. Rabinowitz reported no disclosures. No external funding was used for the presentation.
EXPERT ANALYSIS FROM AAP 16
Hormonal Contraceptives: Risk or Benefit in Migraine?
SAN DIEGO—Among women with migraine, low-dose combined estrogen–progestin contraceptives do not increase the risk of stroke, and continuous hormonal contraceptive use may reduce menstrual migraine, according to a lecture delivered at the 58th Annual Scientific Meeting of the American Headache Society.
High doses of combined oral contraceptives do increase stroke risk, and migraine with aura confers an independent increased risk of stroke, said Anne H. Calhoun, MD, Professor of Anesthesiology and Psychiatry at the University of North Carolina in Chapel Hill and partner and cofounder of the Carolina Headache Institute in Durham. Evidence does not suggest, however, that low-dose hormonal contraceptive use together with history of migraine confers additive risk, she said.

Over the last several decades, various combined oral contraceptive regimens (eg, triphasic, extended cycle, and continuous) with a range of estrogen doses have been developed. “They are all over the place, and we really need to know what we are dealing with,” Dr. Calhoun said. Risks of combined oral contraceptives, including myocardial infarction and stroke, are almost exclusively seen with smoking and high-dose pills, she said.
Dr. Calhoun prefers to prescribe pills that inhibit ovulation while using 20 μg or less of the synthetic estrogen ethinyl estradiol (EE) for women at increased risk of stroke. The highest dose pill in the United States contains 50 μg of estrogen. The lowest dose pill contains 10 μg.
Placebo Side Effects
In hormonal contraception, headache often develops during the placebo week. A typical contraceptive regimen includes 21 active pills and seven placebo pills. Sulak et al found that 70% of women taking birth control pills had headache during the placebo week, and peak incidence of headache was on the third day of the placebo week. “When you eliminated the placebo week, it improved mood scores, improved headache scores, there was less dysmenorrhea and pelvic pain,” Dr. Calhoun said.
When estrogen concentrations decrease upon taking placebo, 5HT concentration in the CNS declines, serotonin synthesis declines, monoamine oxidase and calcitonin gene-related peptide concentrations increase, and beta endorphins decline. “All pain is perceived as more intense,” she said. Furthermore, flow-mediated vasodilation parallels estrogen levels.
“You would think looking at all this, in a field where most of the patients are women, and the majority of them have menstrual migraine, and all of these things happen when estrogen falls, that headache specialists would be really interested in preventing estrogen from declining every month,” Dr. Calhoun said.
Reducing Migraine
In 2012, Dr. Calhoun and colleagues published a retrospective database review that identified 23 women in a subspecialty menstrual migraine clinic who had migraine with aura, a confirmed diagnosis of menstrual-related migraine, and who received treatment with extended-cycle dosing of a transvaginal ring contraceptive containing 0.120 mg of etonogestrel and 15 μg of EE for at least a month. The women were treated with the transvaginal ring for the purpose of migraine prevention, and not to prevent pregnancy. Participants were observed for an average of eight months. Women used the ultralow-dose ring contraceptive continuously. Instead of using the ring for three weeks followed by one week without the ring, women replaced the ring every three weeks. “With that, you stop ovulation with a level of estrogen that is lower than your own natural menstrual cycle. You do not have the high ovulatory peaks or even the peaks of the luteal phase,” she said.
At baseline, subjects experienced a median of 3.2 auras per month. With treatment, the median number of auras per month decreased to 0.2. Frequency of aura decreased from baseline for each participant, and menstrual migraine was eliminated in 91.3% of patients. Such use of hormonal contraceptives for the prevention of migraine is off label, Dr. Calhoun noted.
Risk of Stroke
How oral contraceptives affect risk of stroke has been studied for decades. In a 1975 study in JAMA, researchers looked at 140 cases of stroke in young women and compared them with hospital controls. There was a 4.6 times increased risk of stroke if a woman was taking high-dose oral contraceptives.
Hannaford et al in 1994 published a nested case–control analysis using data mainly from the 1970s and 1980s. They found that high-dose oral contraceptive use was associated with a sixfold increased risk of first stroke. Low-dose pills—including 30-μg and 35-μg pills, “which I do not think of as particularly low dose these days”—did not significantly increase risk, Dr. Calhoun said. However, the risk with these moderate-dose pills is usually around 1.2 to 2.5 times greater and is significant in some studies, she noted. Today’s “low-dose” pills (≤ 20 μg EE) are the best for decreasing risk.
In 1996, a study by Petitti et al looked at risk of stroke with “low-dose” (at that time meaning simply < 50 μg EE) hormonal contraceptives in the US. They identified 408 strokes in 3.6 million women-years and concluded that stroke is rare in this population. Low-dose pills did not increase the risk. At that time, 99.4% of prescriptions for hormonal contraception in the US contained less than 50 μg of estrogen.
ACOG Guideline
In 2006, however, the American College of Obstetrics and Gynecology (ACOG) recommended against using combination hormonal contraceptives in patients with migraine with aura. This guideline and some of the studies on which the recommendation was based are problematic, Dr. Calhoun said.
The recommendation stemmed in part from a concern that all women with migraine are at increased risk of stroke if they take combined hormonal contraceptives. That concern was based on a 1996 World Health Organization study that had no US sites. In the study, the majority of stroke cases were smokers and the average age was over 35. In the US, 35 tends to be the age at which physicians—in accordance with ACOG recommendations—no longer prescribe combined hormonal contraceptives for smokers, Dr. Calhoun said. In addition, the majority of the stroke cases were using high-dose pills. The authors concluded that migraine of greater than 12 years’ duration, migraine with aura, and frequent migraine with aura increased the risk of stroke. “But the authors concluded themselves, in no case did corrections for oral contraceptive use alter these observations. It was not a factor,” Dr. Calhoun said.
The ACOG guideline also was based on a Danish population-based case–control study by Lidegaard et al that found a threefold increased risk of ischemic stroke among migraineurs using oral contraceptives. In this study, however, they reported that only 6% of the control group had migraine, whereas 16% to 18% of women in Denmark have migraine—a rate similar to what was seen in the cases. That produced the threefold increased risk reported in the study, Dr. Calhoun said. A similar study in France did not find increased risk among migraineurs using oral contraceptives, but in that study, both controls and migraineurs had the normal frequency of migraine in the population.
Finally, the ACOG recommendation was based on a pooled analysis of two large US case–control studies that found a twofold increased risk of ischemic stroke among migraineurs using oral contraceptives. This finding by Schwartz et al was based on only four cases. The prevalence of migraine was virtually identical among ischemic stroke cases and controls who were using oral contraceptives (7.8% and 7.7%, respectively), but became significant after adjustment for other factors. But a key factor that was not taken into account was use of high-dose (≥ 50 μg EE) pills, Dr. Calhoun said. They were used by only 11 of the 1,564 ischemic and hemorrhagic stroke cases and controls, but accounted for four of the strokes.
Low Doses Appear Safe
Recent studies have had similar findings. A 15-year prospective population-based study by Lidegaard et al in 2012 analyzed 3,300 thrombotic strokes and 1,700 myocardial infarctions in more than 1.6 million women. The overall risk was low, and the absolute risk of thrombotic stroke and myocardial infarction was not increased with 20-μg pills. Pills with doses of 30 μg to 40 μg, however, as much as doubled the risk. “It is still better than the 4.5-times increased risk we had with the 50-μg pills, but we do not want to go there,” Dr. Calhoun said.
A 2013 study by Sidney et al compared a 20-μg oral birth control pill with a 30-μg oral birth control pill, a 20-μg patch birth control product, and a 15-μg ring birth control product. As expected, the 30-μg pill increased risk of thrombotic events, relative to the 20-μg pill, whereas the other products did not, Dr. Calhoun said.
“The argument against using combined hormonal contraceptives in migraine with aura is based on concerns that all women are at increased risk of stroke with oral contraceptives. That is false,” she said. “It is high-dose oral contraceptives that increase the risk.”
—Jake Remaly
Suggested Reading
ACOG Committee on Practice Bulletins-Gynecology. ACOG practice bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107(6):1453-1472.
Calhoun A, Ford S, Pruitt A. The impact of extended-cycle vaginal ring contraception on migraine aura: a retrospective case series. Headache. 2012;52(8):1246-1253.
Hannaford PC, Croft PR, Kay CR. Oral contraception and stroke. Evidence from the Royal College of General Practitioners’ Oral Contraception study. Stroke. 1994;25(5):935-942.
Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1996;348(9026):498-505.
Lidegaard Ø, Kreiner S. Contraceptives and cerebral thrombosis: a five-year national case-control study. Contraception. 2002;65(3):197-205.
Lidegaard Ø, Løkkegaard E, Jensen A, et al. Thrombotic stroke and myocardial infarction with hormonal contraception. N Engl J Med. 2012;366(24):2257-2266.
MacGregor EA. Contraception and headache. Headache. 2013;53(2):247-276.
Oral contraceptives and stroke in young women. Associated risk factors. JAMA. 1975;231(7):718-722.
Petitti DB, Sidney S, Bernstein A, et al. Stroke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8-15.
Schwartz SM, Petitti DB, Siscovick DS, et al. Stroke and use of low-dose oral contraceptives in young women: a pooled analysis of two US studies. Stroke. 1998;29(11):2277-2284.
Sidney S, Cheetham TC, Connell FA, et al. Recent combined hormonal contraceptives (CHCs) and the risk of thromboembolism and other cardiovascular events in new users. Contraception. 2013;87(1):93-100.
Sulak P, Willis S, Kuehl T, et al. Headaches and oral contraceptives: impact of eliminating the standard 7-day placebo interval. Headache. 2007;47(1):27-37.
Sulak PJ, Scow RD, Preece C, et al. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261-266.
SAN DIEGO—Among women with migraine, low-dose combined estrogen–progestin contraceptives do not increase the risk of stroke, and continuous hormonal contraceptive use may reduce menstrual migraine, according to a lecture delivered at the 58th Annual Scientific Meeting of the American Headache Society.
High doses of combined oral contraceptives do increase stroke risk, and migraine with aura confers an independent increased risk of stroke, said Anne H. Calhoun, MD, Professor of Anesthesiology and Psychiatry at the University of North Carolina in Chapel Hill and partner and cofounder of the Carolina Headache Institute in Durham. Evidence does not suggest, however, that low-dose hormonal contraceptive use together with history of migraine confers additive risk, she said.
Over the last several decades, various combined oral contraceptive regimens (eg, triphasic, extended cycle, and continuous) with a range of estrogen doses have been developed. “They are all over the place, and we really need to know what we are dealing with,” Dr. Calhoun said. Risks of combined oral contraceptives, including myocardial infarction and stroke, are almost exclusively seen with smoking and high-dose pills, she said.
Dr. Calhoun prefers to prescribe pills that inhibit ovulation while using 20 μg or less of the synthetic estrogen ethinyl estradiol (EE) for women at increased risk of stroke. The highest dose pill in the United States contains 50 μg of estrogen. The lowest dose pill contains 10 μg.
Placebo Side Effects
In hormonal contraception, headache often develops during the placebo week. A typical contraceptive regimen includes 21 active pills and seven placebo pills. Sulak et al found that 70% of women taking birth control pills had headache during the placebo week, and peak incidence of headache was on the third day of the placebo week. “When you eliminated the placebo week, it improved mood scores, improved headache scores, there was less dysmenorrhea and pelvic pain,” Dr. Calhoun said.
When estrogen concentrations decrease upon taking placebo, 5HT concentration in the CNS declines, serotonin synthesis declines, monoamine oxidase and calcitonin gene-related peptide concentrations increase, and beta endorphins decline. “All pain is perceived as more intense,” she said. Furthermore, flow-mediated vasodilation parallels estrogen levels.
“You would think looking at all this, in a field where most of the patients are women, and the majority of them have menstrual migraine, and all of these things happen when estrogen falls, that headache specialists would be really interested in preventing estrogen from declining every month,” Dr. Calhoun said.
Reducing Migraine
In 2012, Dr. Calhoun and colleagues published a retrospective database review that identified 23 women in a subspecialty menstrual migraine clinic who had migraine with aura, a confirmed diagnosis of menstrual-related migraine, and who received treatment with extended-cycle dosing of a transvaginal ring contraceptive containing 0.120 mg of etonogestrel and 15 μg of EE for at least a month. The women were treated with the transvaginal ring for the purpose of migraine prevention, and not to prevent pregnancy. Participants were observed for an average of eight months. Women used the ultralow-dose ring contraceptive continuously. Instead of using the ring for three weeks followed by one week without the ring, women replaced the ring every three weeks. “With that, you stop ovulation with a level of estrogen that is lower than your own natural menstrual cycle. You do not have the high ovulatory peaks or even the peaks of the luteal phase,” she said.
At baseline, subjects experienced a median of 3.2 auras per month. With treatment, the median number of auras per month decreased to 0.2. Frequency of aura decreased from baseline for each participant, and menstrual migraine was eliminated in 91.3% of patients. Such use of hormonal contraceptives for the prevention of migraine is off label, Dr. Calhoun noted.
Risk of Stroke
How oral contraceptives affect risk of stroke has been studied for decades. In a 1975 study in JAMA, researchers looked at 140 cases of stroke in young women and compared them with hospital controls. There was a 4.6 times increased risk of stroke if a woman was taking high-dose oral contraceptives.
Hannaford et al in 1994 published a nested case–control analysis using data mainly from the 1970s and 1980s. They found that high-dose oral contraceptive use was associated with a sixfold increased risk of first stroke. Low-dose pills—including 30-μg and 35-μg pills, “which I do not think of as particularly low dose these days”—did not significantly increase risk, Dr. Calhoun said. However, the risk with these moderate-dose pills is usually around 1.2 to 2.5 times greater and is significant in some studies, she noted. Today’s “low-dose” pills (≤ 20 μg EE) are the best for decreasing risk.
In 1996, a study by Petitti et al looked at risk of stroke with “low-dose” (at that time meaning simply < 50 μg EE) hormonal contraceptives in the US. They identified 408 strokes in 3.6 million women-years and concluded that stroke is rare in this population. Low-dose pills did not increase the risk. At that time, 99.4% of prescriptions for hormonal contraception in the US contained less than 50 μg of estrogen.
ACOG Guideline
In 2006, however, the American College of Obstetrics and Gynecology (ACOG) recommended against using combination hormonal contraceptives in patients with migraine with aura. This guideline and some of the studies on which the recommendation was based are problematic, Dr. Calhoun said.
The recommendation stemmed in part from a concern that all women with migraine are at increased risk of stroke if they take combined hormonal contraceptives. That concern was based on a 1996 World Health Organization study that had no US sites. In the study, the majority of stroke cases were smokers and the average age was over 35. In the US, 35 tends to be the age at which physicians—in accordance with ACOG recommendations—no longer prescribe combined hormonal contraceptives for smokers, Dr. Calhoun said. In addition, the majority of the stroke cases were using high-dose pills. The authors concluded that migraine of greater than 12 years’ duration, migraine with aura, and frequent migraine with aura increased the risk of stroke. “But the authors concluded themselves, in no case did corrections for oral contraceptive use alter these observations. It was not a factor,” Dr. Calhoun said.
The ACOG guideline also was based on a Danish population-based case–control study by Lidegaard et al that found a threefold increased risk of ischemic stroke among migraineurs using oral contraceptives. In this study, however, they reported that only 6% of the control group had migraine, whereas 16% to 18% of women in Denmark have migraine—a rate similar to what was seen in the cases. That produced the threefold increased risk reported in the study, Dr. Calhoun said. A similar study in France did not find increased risk among migraineurs using oral contraceptives, but in that study, both controls and migraineurs had the normal frequency of migraine in the population.
Finally, the ACOG recommendation was based on a pooled analysis of two large US case–control studies that found a twofold increased risk of ischemic stroke among migraineurs using oral contraceptives. This finding by Schwartz et al was based on only four cases. The prevalence of migraine was virtually identical among ischemic stroke cases and controls who were using oral contraceptives (7.8% and 7.7%, respectively), but became significant after adjustment for other factors. But a key factor that was not taken into account was use of high-dose (≥ 50 μg EE) pills, Dr. Calhoun said. They were used by only 11 of the 1,564 ischemic and hemorrhagic stroke cases and controls, but accounted for four of the strokes.
Low Doses Appear Safe
Recent studies have had similar findings. A 15-year prospective population-based study by Lidegaard et al in 2012 analyzed 3,300 thrombotic strokes and 1,700 myocardial infarctions in more than 1.6 million women. The overall risk was low, and the absolute risk of thrombotic stroke and myocardial infarction was not increased with 20-μg pills. Pills with doses of 30 μg to 40 μg, however, as much as doubled the risk. “It is still better than the 4.5-times increased risk we had with the 50-μg pills, but we do not want to go there,” Dr. Calhoun said.
A 2013 study by Sidney et al compared a 20-μg oral birth control pill with a 30-μg oral birth control pill, a 20-μg patch birth control product, and a 15-μg ring birth control product. As expected, the 30-μg pill increased risk of thrombotic events, relative to the 20-μg pill, whereas the other products did not, Dr. Calhoun said.
“The argument against using combined hormonal contraceptives in migraine with aura is based on concerns that all women are at increased risk of stroke with oral contraceptives. That is false,” she said. “It is high-dose oral contraceptives that increase the risk.”
—Jake Remaly
Suggested Reading
ACOG Committee on Practice Bulletins-Gynecology. ACOG practice bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107(6):1453-1472.
Calhoun A, Ford S, Pruitt A. The impact of extended-cycle vaginal ring contraception on migraine aura: a retrospective case series. Headache. 2012;52(8):1246-1253.
Hannaford PC, Croft PR, Kay CR. Oral contraception and stroke. Evidence from the Royal College of General Practitioners’ Oral Contraception study. Stroke. 1994;25(5):935-942.
Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1996;348(9026):498-505.
Lidegaard Ø, Kreiner S. Contraceptives and cerebral thrombosis: a five-year national case-control study. Contraception. 2002;65(3):197-205.
Lidegaard Ø, Løkkegaard E, Jensen A, et al. Thrombotic stroke and myocardial infarction with hormonal contraception. N Engl J Med. 2012;366(24):2257-2266.
MacGregor EA. Contraception and headache. Headache. 2013;53(2):247-276.
Oral contraceptives and stroke in young women. Associated risk factors. JAMA. 1975;231(7):718-722.
Petitti DB, Sidney S, Bernstein A, et al. Stroke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8-15.
Schwartz SM, Petitti DB, Siscovick DS, et al. Stroke and use of low-dose oral contraceptives in young women: a pooled analysis of two US studies. Stroke. 1998;29(11):2277-2284.
Sidney S, Cheetham TC, Connell FA, et al. Recent combined hormonal contraceptives (CHCs) and the risk of thromboembolism and other cardiovascular events in new users. Contraception. 2013;87(1):93-100.
Sulak P, Willis S, Kuehl T, et al. Headaches and oral contraceptives: impact of eliminating the standard 7-day placebo interval. Headache. 2007;47(1):27-37.
Sulak PJ, Scow RD, Preece C, et al. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261-266.
SAN DIEGO—Among women with migraine, low-dose combined estrogen–progestin contraceptives do not increase the risk of stroke, and continuous hormonal contraceptive use may reduce menstrual migraine, according to a lecture delivered at the 58th Annual Scientific Meeting of the American Headache Society.
High doses of combined oral contraceptives do increase stroke risk, and migraine with aura confers an independent increased risk of stroke, said Anne H. Calhoun, MD, Professor of Anesthesiology and Psychiatry at the University of North Carolina in Chapel Hill and partner and cofounder of the Carolina Headache Institute in Durham. Evidence does not suggest, however, that low-dose hormonal contraceptive use together with history of migraine confers additive risk, she said.
Over the last several decades, various combined oral contraceptive regimens (eg, triphasic, extended cycle, and continuous) with a range of estrogen doses have been developed. “They are all over the place, and we really need to know what we are dealing with,” Dr. Calhoun said. Risks of combined oral contraceptives, including myocardial infarction and stroke, are almost exclusively seen with smoking and high-dose pills, she said.
Dr. Calhoun prefers to prescribe pills that inhibit ovulation while using 20 μg or less of the synthetic estrogen ethinyl estradiol (EE) for women at increased risk of stroke. The highest dose pill in the United States contains 50 μg of estrogen. The lowest dose pill contains 10 μg.
Placebo Side Effects
In hormonal contraception, headache often develops during the placebo week. A typical contraceptive regimen includes 21 active pills and seven placebo pills. Sulak et al found that 70% of women taking birth control pills had headache during the placebo week, and peak incidence of headache was on the third day of the placebo week. “When you eliminated the placebo week, it improved mood scores, improved headache scores, there was less dysmenorrhea and pelvic pain,” Dr. Calhoun said.
When estrogen concentrations decrease upon taking placebo, 5HT concentration in the CNS declines, serotonin synthesis declines, monoamine oxidase and calcitonin gene-related peptide concentrations increase, and beta endorphins decline. “All pain is perceived as more intense,” she said. Furthermore, flow-mediated vasodilation parallels estrogen levels.
“You would think looking at all this, in a field where most of the patients are women, and the majority of them have menstrual migraine, and all of these things happen when estrogen falls, that headache specialists would be really interested in preventing estrogen from declining every month,” Dr. Calhoun said.
Reducing Migraine
In 2012, Dr. Calhoun and colleagues published a retrospective database review that identified 23 women in a subspecialty menstrual migraine clinic who had migraine with aura, a confirmed diagnosis of menstrual-related migraine, and who received treatment with extended-cycle dosing of a transvaginal ring contraceptive containing 0.120 mg of etonogestrel and 15 μg of EE for at least a month. The women were treated with the transvaginal ring for the purpose of migraine prevention, and not to prevent pregnancy. Participants were observed for an average of eight months. Women used the ultralow-dose ring contraceptive continuously. Instead of using the ring for three weeks followed by one week without the ring, women replaced the ring every three weeks. “With that, you stop ovulation with a level of estrogen that is lower than your own natural menstrual cycle. You do not have the high ovulatory peaks or even the peaks of the luteal phase,” she said.
At baseline, subjects experienced a median of 3.2 auras per month. With treatment, the median number of auras per month decreased to 0.2. Frequency of aura decreased from baseline for each participant, and menstrual migraine was eliminated in 91.3% of patients. Such use of hormonal contraceptives for the prevention of migraine is off label, Dr. Calhoun noted.
Risk of Stroke
How oral contraceptives affect risk of stroke has been studied for decades. In a 1975 study in JAMA, researchers looked at 140 cases of stroke in young women and compared them with hospital controls. There was a 4.6 times increased risk of stroke if a woman was taking high-dose oral contraceptives.
Hannaford et al in 1994 published a nested case–control analysis using data mainly from the 1970s and 1980s. They found that high-dose oral contraceptive use was associated with a sixfold increased risk of first stroke. Low-dose pills—including 30-μg and 35-μg pills, “which I do not think of as particularly low dose these days”—did not significantly increase risk, Dr. Calhoun said. However, the risk with these moderate-dose pills is usually around 1.2 to 2.5 times greater and is significant in some studies, she noted. Today’s “low-dose” pills (≤ 20 μg EE) are the best for decreasing risk.
In 1996, a study by Petitti et al looked at risk of stroke with “low-dose” (at that time meaning simply < 50 μg EE) hormonal contraceptives in the US. They identified 408 strokes in 3.6 million women-years and concluded that stroke is rare in this population. Low-dose pills did not increase the risk. At that time, 99.4% of prescriptions for hormonal contraception in the US contained less than 50 μg of estrogen.
ACOG Guideline
In 2006, however, the American College of Obstetrics and Gynecology (ACOG) recommended against using combination hormonal contraceptives in patients with migraine with aura. This guideline and some of the studies on which the recommendation was based are problematic, Dr. Calhoun said.
The recommendation stemmed in part from a concern that all women with migraine are at increased risk of stroke if they take combined hormonal contraceptives. That concern was based on a 1996 World Health Organization study that had no US sites. In the study, the majority of stroke cases were smokers and the average age was over 35. In the US, 35 tends to be the age at which physicians—in accordance with ACOG recommendations—no longer prescribe combined hormonal contraceptives for smokers, Dr. Calhoun said. In addition, the majority of the stroke cases were using high-dose pills. The authors concluded that migraine of greater than 12 years’ duration, migraine with aura, and frequent migraine with aura increased the risk of stroke. “But the authors concluded themselves, in no case did corrections for oral contraceptive use alter these observations. It was not a factor,” Dr. Calhoun said.
The ACOG guideline also was based on a Danish population-based case–control study by Lidegaard et al that found a threefold increased risk of ischemic stroke among migraineurs using oral contraceptives. In this study, however, they reported that only 6% of the control group had migraine, whereas 16% to 18% of women in Denmark have migraine—a rate similar to what was seen in the cases. That produced the threefold increased risk reported in the study, Dr. Calhoun said. A similar study in France did not find increased risk among migraineurs using oral contraceptives, but in that study, both controls and migraineurs had the normal frequency of migraine in the population.
Finally, the ACOG recommendation was based on a pooled analysis of two large US case–control studies that found a twofold increased risk of ischemic stroke among migraineurs using oral contraceptives. This finding by Schwartz et al was based on only four cases. The prevalence of migraine was virtually identical among ischemic stroke cases and controls who were using oral contraceptives (7.8% and 7.7%, respectively), but became significant after adjustment for other factors. But a key factor that was not taken into account was use of high-dose (≥ 50 μg EE) pills, Dr. Calhoun said. They were used by only 11 of the 1,564 ischemic and hemorrhagic stroke cases and controls, but accounted for four of the strokes.
Low Doses Appear Safe
Recent studies have had similar findings. A 15-year prospective population-based study by Lidegaard et al in 2012 analyzed 3,300 thrombotic strokes and 1,700 myocardial infarctions in more than 1.6 million women. The overall risk was low, and the absolute risk of thrombotic stroke and myocardial infarction was not increased with 20-μg pills. Pills with doses of 30 μg to 40 μg, however, as much as doubled the risk. “It is still better than the 4.5-times increased risk we had with the 50-μg pills, but we do not want to go there,” Dr. Calhoun said.
A 2013 study by Sidney et al compared a 20-μg oral birth control pill with a 30-μg oral birth control pill, a 20-μg patch birth control product, and a 15-μg ring birth control product. As expected, the 30-μg pill increased risk of thrombotic events, relative to the 20-μg pill, whereas the other products did not, Dr. Calhoun said.
“The argument against using combined hormonal contraceptives in migraine with aura is based on concerns that all women are at increased risk of stroke with oral contraceptives. That is false,” she said. “It is high-dose oral contraceptives that increase the risk.”
—Jake Remaly
Suggested Reading
ACOG Committee on Practice Bulletins-Gynecology. ACOG practice bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107(6):1453-1472.
Calhoun A, Ford S, Pruitt A. The impact of extended-cycle vaginal ring contraception on migraine aura: a retrospective case series. Headache. 2012;52(8):1246-1253.
Hannaford PC, Croft PR, Kay CR. Oral contraception and stroke. Evidence from the Royal College of General Practitioners’ Oral Contraception study. Stroke. 1994;25(5):935-942.
Ischaemic stroke and combined oral contraceptives: results of an international, multicentre, case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1996;348(9026):498-505.
Lidegaard Ø, Kreiner S. Contraceptives and cerebral thrombosis: a five-year national case-control study. Contraception. 2002;65(3):197-205.
Lidegaard Ø, Løkkegaard E, Jensen A, et al. Thrombotic stroke and myocardial infarction with hormonal contraception. N Engl J Med. 2012;366(24):2257-2266.
MacGregor EA. Contraception and headache. Headache. 2013;53(2):247-276.
Oral contraceptives and stroke in young women. Associated risk factors. JAMA. 1975;231(7):718-722.
Petitti DB, Sidney S, Bernstein A, et al. Stroke in users of low-dose oral contraceptives. N Engl J Med. 1996;335(1):8-15.
Schwartz SM, Petitti DB, Siscovick DS, et al. Stroke and use of low-dose oral contraceptives in young women: a pooled analysis of two US studies. Stroke. 1998;29(11):2277-2284.
Sidney S, Cheetham TC, Connell FA, et al. Recent combined hormonal contraceptives (CHCs) and the risk of thromboembolism and other cardiovascular events in new users. Contraception. 2013;87(1):93-100.
Sulak P, Willis S, Kuehl T, et al. Headaches and oral contraceptives: impact of eliminating the standard 7-day placebo interval. Headache. 2007;47(1):27-37.
Sulak PJ, Scow RD, Preece C, et al. Hormone withdrawal symptoms in oral contraceptive users. Obstet Gynecol. 2000;95(2):261-266.

Is regional anesthesia safer in CEA?
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.

Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.
Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
COLUMBUS, OHIO – General anesthesia during carotid endarterectomy carries almost twice the risk of complications and unplanned intubation as regional anesthesia, but the latter approach, which is not available in all hospitals, has its own issues, an analysis of procedures from a statewide database in Michigan found.
“This study is timely because of CMS [Center for Medicare & Medicaid Services] initiatives tying reimbursement to specific quality measures,” Ahmad S Hussain, MD, of Wayne State University in Detroit said in reporting the study results at the annual meeting of the Midwestern Vascular Surgery Society.
Regional anesthesia in CEA emerged in the 1990s, Dr. Hussain said, and allows for more reliable neurologic monitoring and more direct evaluation of the need for stenting during CEA than general anesthesia, which requires continuous monitoring of cerebral perfusion with carotid stump pressures, electroencephalogram, and transcranial doppler.
The researchers retrospectively analyzed 4,558 patients who had CEA at hospitals participating in the Michigan Surgical Quality Cooperative from 2012 to 2014 – 4,008 of whom had general anesthesia and 550 regional anesthesia.
“Advocates for carotid endarterectomy with regional anesthesia cite a reduction in hemodynamic instability and the ability for neurological monitoring, but many still prefer general anesthesia because the benefits of regional anesthesia have not been clearly demonstrated, allowing that regional anesthesia may not be available in all centers and allowing that a certain amount of patient movement during the procedure may not be uniformly tolerated,” Dr. Hussain said.
General anesthesia patients in the study had more than twice the rate of any morbidity at 30 days than those who had regional, 8.7% vs. 4.2%, and significantly higher rates of unplanned intervention, 2.1% vs. 0.6%. Dr. Hussain said. However, the study could not determine differences in 30-day mortality or other key outcomes, such as rates of pneumonia, sepsis, deep vein thrombosis, or pulmonary embolism, becauseof insufficient sample sizes, Dr. Hussain said
The study found less significant differences between general and regional anesthesia techniques, respectively, in rates of extended length of stay, 12.1% vs. 9.5%; readmissions, 9.2% vs. 6.1%; and reoperation, 4.5% vs. 3%.
The retrospective study used two models to analyze odds ratios: Model 1 adjusted for case mix; and model 2 adjusted for case mix as fixed effects and site as a random effect. While the retrospective nature of the study may be a limitation, the findings support the use of regional anesthesia for CEA when available, Dr. Hussain said.
Dr. Hussain had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: General anesthesia for carotid endarterectomy carries a higher risk of complications and readmissions than regional anesthesia.
Major finding: Any morbidity after CEA with general anesthesia was 8.7% vs. 4.2% for regional anesthesia, and readmissions rates were 9.2% vs. 6.1%.
Data source: Retrospective analysis of 4,558 patients who had CEA between 2012 and 2014 at hospitals participating in the Michigan Surgical Quality Collaborative database.
Disclosures: Dr. Hussain reported having no financial disclosures.
Another Zika vaccine heads to Phase I trials
Scientists with the U.S. Department of Defense have launched a Phase I clinical trial to test an investigational Zika vaccine that relies on inactivated virus.
The candidate vaccine is known as the Zika Purified Inactivated Virus (ZPIV) vaccine and contains whole but inactivated Zika virus particles to stimulate an immune system response without replicating and causing illness.
“We urgently need a safe and effective vaccine to protect people from Zika virus infection as the virus continues to spread and cause serious public health consequences, particularly for pregnant women and their babies,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases (NIAID), said in a statement. “We are pleased to be part of the collaborative effort to advance this promising candidate vaccine into clinical trials.”
The NIAID helped support the preclinical development of the vaccine candidate and is part of a joint research agreement with the Department of Defense and other federal agencies to develop the vaccine for use in humans.
The trial at Walter Reed will enroll 75 individuals, ranging in age from 18-49 years, all of whom should have no history of a flavivirus infection. Twenty-five subjects will be given a pair of either intramuscular ZPIV injections, or a placebo (saline), with 28 days between injections.
The remaining 50 subjects will be divided into two groups of 25, with one group receiving two doses of a Japanese encephalitis virus vaccine and the other getting one dose of a yellow fever vaccine, before they both receive the two-dose ZPIV vaccine regimen.
A subgroup of 30 patients will then receive a third ZPIV dose 1 year later. Across all cohorts, the ZPIV dosage will be 5 micrograms.
In addition to the testing of the ZPIV vaccine, there are Phase I trials of a DNA-based Zika vaccine ongoing at the National Institutes of Health Clinical Center in Bethesda, Md., the Center for Vaccine Development at the University of Maryland in Baltimore, Md., and at Emory University in Atlanta, Ga. Those trials were launched in August 2016.
Scientists with the U.S. Department of Defense have launched a Phase I clinical trial to test an investigational Zika vaccine that relies on inactivated virus.
The candidate vaccine is known as the Zika Purified Inactivated Virus (ZPIV) vaccine and contains whole but inactivated Zika virus particles to stimulate an immune system response without replicating and causing illness.
“We urgently need a safe and effective vaccine to protect people from Zika virus infection as the virus continues to spread and cause serious public health consequences, particularly for pregnant women and their babies,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases (NIAID), said in a statement. “We are pleased to be part of the collaborative effort to advance this promising candidate vaccine into clinical trials.”
The NIAID helped support the preclinical development of the vaccine candidate and is part of a joint research agreement with the Department of Defense and other federal agencies to develop the vaccine for use in humans.
The trial at Walter Reed will enroll 75 individuals, ranging in age from 18-49 years, all of whom should have no history of a flavivirus infection. Twenty-five subjects will be given a pair of either intramuscular ZPIV injections, or a placebo (saline), with 28 days between injections.
The remaining 50 subjects will be divided into two groups of 25, with one group receiving two doses of a Japanese encephalitis virus vaccine and the other getting one dose of a yellow fever vaccine, before they both receive the two-dose ZPIV vaccine regimen.
A subgroup of 30 patients will then receive a third ZPIV dose 1 year later. Across all cohorts, the ZPIV dosage will be 5 micrograms.
In addition to the testing of the ZPIV vaccine, there are Phase I trials of a DNA-based Zika vaccine ongoing at the National Institutes of Health Clinical Center in Bethesda, Md., the Center for Vaccine Development at the University of Maryland in Baltimore, Md., and at Emory University in Atlanta, Ga. Those trials were launched in August 2016.
Scientists with the U.S. Department of Defense have launched a Phase I clinical trial to test an investigational Zika vaccine that relies on inactivated virus.
The candidate vaccine is known as the Zika Purified Inactivated Virus (ZPIV) vaccine and contains whole but inactivated Zika virus particles to stimulate an immune system response without replicating and causing illness.
“We urgently need a safe and effective vaccine to protect people from Zika virus infection as the virus continues to spread and cause serious public health consequences, particularly for pregnant women and their babies,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases (NIAID), said in a statement. “We are pleased to be part of the collaborative effort to advance this promising candidate vaccine into clinical trials.”
The NIAID helped support the preclinical development of the vaccine candidate and is part of a joint research agreement with the Department of Defense and other federal agencies to develop the vaccine for use in humans.
The trial at Walter Reed will enroll 75 individuals, ranging in age from 18-49 years, all of whom should have no history of a flavivirus infection. Twenty-five subjects will be given a pair of either intramuscular ZPIV injections, or a placebo (saline), with 28 days between injections.
The remaining 50 subjects will be divided into two groups of 25, with one group receiving two doses of a Japanese encephalitis virus vaccine and the other getting one dose of a yellow fever vaccine, before they both receive the two-dose ZPIV vaccine regimen.
A subgroup of 30 patients will then receive a third ZPIV dose 1 year later. Across all cohorts, the ZPIV dosage will be 5 micrograms.
In addition to the testing of the ZPIV vaccine, there are Phase I trials of a DNA-based Zika vaccine ongoing at the National Institutes of Health Clinical Center in Bethesda, Md., the Center for Vaccine Development at the University of Maryland in Baltimore, Md., and at Emory University in Atlanta, Ga. Those trials were launched in August 2016.
Low parental confidence in HPV vaccine stymies adolescent vaccination rates
More than a quarter of U.S. parents surveyed refused human papillomavirus (HPV) vaccination for their adolescents because of a lack of overall trust in adolescent vaccination programs and higher levels of perceived harm, a study found.
In an online survey of 1,484 U.S. parents, 28% of respondents reported they had refused the HPV vaccine on behalf of their children aged 11-17 years at least once. Another 8% responded they had elected to delay vaccination. The remaining two-thirds of respondents said they had neither refused nor delayed the vaccination, reported Melissa B. Gilkey, PhD, of Harvard Medical School, Boston, and her associates (Hum Vaccin Immunother. 2016. doi: 10.1080/21645515.2016.1247134).
Compared with parents who reported neither refusal nor delay, refusal was associated with lower confidence in adolescent vaccination (relative risk ratio = 0.66, 95% CI, 0.48-0.91), lower perceived HPV vaccine effectiveness (RRR = 0.68, 95% CI, 0.50-0.91), and higher perceived harms (RRR = 3.49, 95% CI, 2.65-4.60). Parents who reported delaying vaccination were more likely to endorse insufficient information as the reason (RRR = 1.76, 95% CI, 1.08-2.85). While 79% of parents who had delayed HPV vaccination said talking with a physician would help them with their decision, 61% of parents who refused the vaccination said it would. In addition, nearly half of parents who delayed vaccination said they did so out of a preference to wait until their children were older.
In adolescents whose parents had ever refused the vaccine, only 27% had received one HPV vaccine vs. 59% in those whose parents had elected to delay vaccination. Among adolescents whose parents responded they had neither refused nor delayed the vaccine, 56% had received one HPV vaccine.
Although the investigators did not find race, ethnicity, nor educational attainment were drivers of whether a parent chose to vaccinate, families with higher income levels tended to refuse the HPV vaccine more often than did other parents (RRR: 1.48, 95% confidence interval, 1.02-2.15).
Merck and the National Cancer Institute funded the study. Coauthor Noel T. Brewer, PhD, has received HPV vaccine-related grants from, or been on paid advisory boards for, Merck, GlaxoSmithKline, and Pfizer; he served on the National Vaccine Advisory Committee Working Group on HPV Vaccine and is chair of the National HPV Vaccination Roundtable.
[email protected]
On Twitter @whitneymcknight
More than a quarter of U.S. parents surveyed refused human papillomavirus (HPV) vaccination for their adolescents because of a lack of overall trust in adolescent vaccination programs and higher levels of perceived harm, a study found.
In an online survey of 1,484 U.S. parents, 28% of respondents reported they had refused the HPV vaccine on behalf of their children aged 11-17 years at least once. Another 8% responded they had elected to delay vaccination. The remaining two-thirds of respondents said they had neither refused nor delayed the vaccination, reported Melissa B. Gilkey, PhD, of Harvard Medical School, Boston, and her associates (Hum Vaccin Immunother. 2016. doi: 10.1080/21645515.2016.1247134).
Compared with parents who reported neither refusal nor delay, refusal was associated with lower confidence in adolescent vaccination (relative risk ratio = 0.66, 95% CI, 0.48-0.91), lower perceived HPV vaccine effectiveness (RRR = 0.68, 95% CI, 0.50-0.91), and higher perceived harms (RRR = 3.49, 95% CI, 2.65-4.60). Parents who reported delaying vaccination were more likely to endorse insufficient information as the reason (RRR = 1.76, 95% CI, 1.08-2.85). While 79% of parents who had delayed HPV vaccination said talking with a physician would help them with their decision, 61% of parents who refused the vaccination said it would. In addition, nearly half of parents who delayed vaccination said they did so out of a preference to wait until their children were older.
In adolescents whose parents had ever refused the vaccine, only 27% had received one HPV vaccine vs. 59% in those whose parents had elected to delay vaccination. Among adolescents whose parents responded they had neither refused nor delayed the vaccine, 56% had received one HPV vaccine.
Although the investigators did not find race, ethnicity, nor educational attainment were drivers of whether a parent chose to vaccinate, families with higher income levels tended to refuse the HPV vaccine more often than did other parents (RRR: 1.48, 95% confidence interval, 1.02-2.15).
Merck and the National Cancer Institute funded the study. Coauthor Noel T. Brewer, PhD, has received HPV vaccine-related grants from, or been on paid advisory boards for, Merck, GlaxoSmithKline, and Pfizer; he served on the National Vaccine Advisory Committee Working Group on HPV Vaccine and is chair of the National HPV Vaccination Roundtable.
[email protected]
On Twitter @whitneymcknight
More than a quarter of U.S. parents surveyed refused human papillomavirus (HPV) vaccination for their adolescents because of a lack of overall trust in adolescent vaccination programs and higher levels of perceived harm, a study found.
In an online survey of 1,484 U.S. parents, 28% of respondents reported they had refused the HPV vaccine on behalf of their children aged 11-17 years at least once. Another 8% responded they had elected to delay vaccination. The remaining two-thirds of respondents said they had neither refused nor delayed the vaccination, reported Melissa B. Gilkey, PhD, of Harvard Medical School, Boston, and her associates (Hum Vaccin Immunother. 2016. doi: 10.1080/21645515.2016.1247134).
Compared with parents who reported neither refusal nor delay, refusal was associated with lower confidence in adolescent vaccination (relative risk ratio = 0.66, 95% CI, 0.48-0.91), lower perceived HPV vaccine effectiveness (RRR = 0.68, 95% CI, 0.50-0.91), and higher perceived harms (RRR = 3.49, 95% CI, 2.65-4.60). Parents who reported delaying vaccination were more likely to endorse insufficient information as the reason (RRR = 1.76, 95% CI, 1.08-2.85). While 79% of parents who had delayed HPV vaccination said talking with a physician would help them with their decision, 61% of parents who refused the vaccination said it would. In addition, nearly half of parents who delayed vaccination said they did so out of a preference to wait until their children were older.
In adolescents whose parents had ever refused the vaccine, only 27% had received one HPV vaccine vs. 59% in those whose parents had elected to delay vaccination. Among adolescents whose parents responded they had neither refused nor delayed the vaccine, 56% had received one HPV vaccine.
Although the investigators did not find race, ethnicity, nor educational attainment were drivers of whether a parent chose to vaccinate, families with higher income levels tended to refuse the HPV vaccine more often than did other parents (RRR: 1.48, 95% confidence interval, 1.02-2.15).
Merck and the National Cancer Institute funded the study. Coauthor Noel T. Brewer, PhD, has received HPV vaccine-related grants from, or been on paid advisory boards for, Merck, GlaxoSmithKline, and Pfizer; he served on the National Vaccine Advisory Committee Working Group on HPV Vaccine and is chair of the National HPV Vaccination Roundtable.
[email protected]
On Twitter @whitneymcknight
Key clinical point:
Major finding: HPV vaccine refusal rate was 28% in parents of teens and preteens; the rate of vaccine delay was 8%.
Data source: Online survey conducted in 2014-2015 of 1,484 U.S. parents with children between ages of 11 and 17 years.
Disclosures: Merck and the National Cancer Institute funded the study. Coauthor Noel T. Brewer, PhD, has received HPV vaccine-related grants from, or been on paid advisory boards for, Merck, GlaxoSmithKline, and Pfizer; he served on the National Vaccine Advisory Committee Working Group on HPV Vaccine and is chair of the National HPV Vaccination Roundtable.
Malpractice Counsel: Missed Nodule
Case
A 48-year-old man presented to the ED with a 2-day history of cough and congestion. He described the cough as gradual in onset and, though initially nonproductive, it was now productive of green sputum. He denied fevers or chills, chest pain, nausea, vomiting, or diarrhea, and complained of only mild shortness of breath. His medical history was significant for hypertension, which was well managed with daily lisinopril-hydrochlorothiazide. He admitted to smoking one pack of cigarettes per day for the past 25 years, but denied alcohol or illicit drug use.
On physical examination, the patient’s vital signs were: blood pressure, 112/64 mm Hg; heart rate, 84 beats/min; respiratory rate, 20 breaths/min; and temperature, 98oF. Oxygen saturation was 97% on room air. The head, eyes, ears, nose, and throat examination was normal. Auscultation of the lungs revealed bilateral breath sounds with scattered, faint expiratory wheezing; the heart had a regular rate and rhythm, without murmurs, rubs, or gallops.
The emergency physician (EP) ordered posteroanterior and lateral chest X-rays (CXR), which he interpreted as normal. He also ordered an albuterol handheld nebulizer treatment for the patient. After the albuterol treatment, the patient felt he was breathing more easily. The frequency of his cough had also decreased following treatment and, on re-examination, he exhibited no wheezing and was given azithromycin 500 mg orally in the ED. The EP diagnosed the patient with acute bronchitis and discharged him home with an albuterol metered dose inhaler with a spacer, and a 4-day course of azithromycin. He also encouraged the patient to quit smoking.
The next day the radiologist’s official reading of the patient’s radiographs included the finding of a very small pulmonary nodule, which was seen only on the lateral X-ray. The radiologist recommended a repeat CXR or a computed tomography (CT) scan of the chest in 6 months.
Unfortunately, the EP never saw this information, and the patient was not contacted regarding the abnormal radiology finding and the need for follow-up. Approximately 20 months later, the patient was diagnosed with lung cancer with metastasis to the thoracic spine and liver. Despite chemotherapy and radiation treatment, he died from the cancer.
The patient’s family brought a malpractice suit against the EP, stating that the cancer could have been successfully treated prior to any metastasis if the patient had been informed of the abnormal radiology findings at his ED visit 20 months prior. The EP argued that he never saw the official radiology report, and therefore had no knowledge of the need for follow-up. At trial, a jury verdict was returned in favor of the defendant.
Discussion
Unfortunately, some version of this scenario occurs on a frequent basis. While imaging studies account for the majority of such cases, the same situation can occur with abnormal laboratory results, body-fluid cultures, or pathology reports in which an abnormality is identified (eg, positive blood culture, missed fracture) but, for a myriad of reasons, the critical information does not get related to the patient.
Because of the episodic nature of the practice of emergency medicine (EM), a process must be in place to ensure any “positive” test results or findings discovered after patient discharge are reviewed and compared to the ED diagnosis, and that any “misses” result in notifying the patient and/or his or her primary care physician and arranging follow-up. In cases such as the one presented here, a system issue existed—one that was not due to any fault or oversight of the EP. Ideally, EM leadership should work closely with leadership from radiology and laboratory services and hospital risk management to develop such a process—one that will be effective every day, including weekends and holidays.
Missed fractures on radiographs are a common cause of malpractice litigation against EPs. In one review by Kachalia et al1 examining malpractice claims involving EPs, missed fractures on radiographs accounted for 19% (the most common) of the 79 missed diagnoses identified in their study.In a similar study by Karcz et al,2 missed fractures ranked second in frequency and dollars lost in malpractice cases against EPs in Massachusetts.
While missed lesions on CXR do not occur with the same frequency as missed fractures, the results are much more devastating when the lesion turns out to be malignant. Three common areas where such lesions are missed on CXR include: the apex of the lung, obscured by overlying clavicle and ribs; the retrocardiac region (as in the patient in this case); and the lung bases obscured by the diaphragm.
Emergency physicians are neither trained nor expected to identify every single abnormality—especially subtle radiographic abnormalities. This is why there are radiology overreads, and a system or process must be in place to ensure patients are informed of any positive findings and to arrange proper follow-up.
1. Kachalia A, Gandhi TK, Puopolo AL, et al. Missed and delayed diagnoses in the emergency department: a study of closed malpractice claims from 4 liability insurers. Ann Emerg Med. 2007;49(2):196-205.
2. Karcz A, Korn R, Burke MC, et al. Malpractice claims against emergency physicians in Massachusetts: 1975-1993. Am J Emerg Med. 1996;14(4):341-345.
Case
A 48-year-old man presented to the ED with a 2-day history of cough and congestion. He described the cough as gradual in onset and, though initially nonproductive, it was now productive of green sputum. He denied fevers or chills, chest pain, nausea, vomiting, or diarrhea, and complained of only mild shortness of breath. His medical history was significant for hypertension, which was well managed with daily lisinopril-hydrochlorothiazide. He admitted to smoking one pack of cigarettes per day for the past 25 years, but denied alcohol or illicit drug use.
On physical examination, the patient’s vital signs were: blood pressure, 112/64 mm Hg; heart rate, 84 beats/min; respiratory rate, 20 breaths/min; and temperature, 98oF. Oxygen saturation was 97% on room air. The head, eyes, ears, nose, and throat examination was normal. Auscultation of the lungs revealed bilateral breath sounds with scattered, faint expiratory wheezing; the heart had a regular rate and rhythm, without murmurs, rubs, or gallops.
The emergency physician (EP) ordered posteroanterior and lateral chest X-rays (CXR), which he interpreted as normal. He also ordered an albuterol handheld nebulizer treatment for the patient. After the albuterol treatment, the patient felt he was breathing more easily. The frequency of his cough had also decreased following treatment and, on re-examination, he exhibited no wheezing and was given azithromycin 500 mg orally in the ED. The EP diagnosed the patient with acute bronchitis and discharged him home with an albuterol metered dose inhaler with a spacer, and a 4-day course of azithromycin. He also encouraged the patient to quit smoking.
The next day the radiologist’s official reading of the patient’s radiographs included the finding of a very small pulmonary nodule, which was seen only on the lateral X-ray. The radiologist recommended a repeat CXR or a computed tomography (CT) scan of the chest in 6 months.
Unfortunately, the EP never saw this information, and the patient was not contacted regarding the abnormal radiology finding and the need for follow-up. Approximately 20 months later, the patient was diagnosed with lung cancer with metastasis to the thoracic spine and liver. Despite chemotherapy and radiation treatment, he died from the cancer.
The patient’s family brought a malpractice suit against the EP, stating that the cancer could have been successfully treated prior to any metastasis if the patient had been informed of the abnormal radiology findings at his ED visit 20 months prior. The EP argued that he never saw the official radiology report, and therefore had no knowledge of the need for follow-up. At trial, a jury verdict was returned in favor of the defendant.
Discussion
Unfortunately, some version of this scenario occurs on a frequent basis. While imaging studies account for the majority of such cases, the same situation can occur with abnormal laboratory results, body-fluid cultures, or pathology reports in which an abnormality is identified (eg, positive blood culture, missed fracture) but, for a myriad of reasons, the critical information does not get related to the patient.
Because of the episodic nature of the practice of emergency medicine (EM), a process must be in place to ensure any “positive” test results or findings discovered after patient discharge are reviewed and compared to the ED diagnosis, and that any “misses” result in notifying the patient and/or his or her primary care physician and arranging follow-up. In cases such as the one presented here, a system issue existed—one that was not due to any fault or oversight of the EP. Ideally, EM leadership should work closely with leadership from radiology and laboratory services and hospital risk management to develop such a process—one that will be effective every day, including weekends and holidays.
Missed fractures on radiographs are a common cause of malpractice litigation against EPs. In one review by Kachalia et al1 examining malpractice claims involving EPs, missed fractures on radiographs accounted for 19% (the most common) of the 79 missed diagnoses identified in their study.In a similar study by Karcz et al,2 missed fractures ranked second in frequency and dollars lost in malpractice cases against EPs in Massachusetts.
While missed lesions on CXR do not occur with the same frequency as missed fractures, the results are much more devastating when the lesion turns out to be malignant. Three common areas where such lesions are missed on CXR include: the apex of the lung, obscured by overlying clavicle and ribs; the retrocardiac region (as in the patient in this case); and the lung bases obscured by the diaphragm.
Emergency physicians are neither trained nor expected to identify every single abnormality—especially subtle radiographic abnormalities. This is why there are radiology overreads, and a system or process must be in place to ensure patients are informed of any positive findings and to arrange proper follow-up.
Case
A 48-year-old man presented to the ED with a 2-day history of cough and congestion. He described the cough as gradual in onset and, though initially nonproductive, it was now productive of green sputum. He denied fevers or chills, chest pain, nausea, vomiting, or diarrhea, and complained of only mild shortness of breath. His medical history was significant for hypertension, which was well managed with daily lisinopril-hydrochlorothiazide. He admitted to smoking one pack of cigarettes per day for the past 25 years, but denied alcohol or illicit drug use.
On physical examination, the patient’s vital signs were: blood pressure, 112/64 mm Hg; heart rate, 84 beats/min; respiratory rate, 20 breaths/min; and temperature, 98oF. Oxygen saturation was 97% on room air. The head, eyes, ears, nose, and throat examination was normal. Auscultation of the lungs revealed bilateral breath sounds with scattered, faint expiratory wheezing; the heart had a regular rate and rhythm, without murmurs, rubs, or gallops.
The emergency physician (EP) ordered posteroanterior and lateral chest X-rays (CXR), which he interpreted as normal. He also ordered an albuterol handheld nebulizer treatment for the patient. After the albuterol treatment, the patient felt he was breathing more easily. The frequency of his cough had also decreased following treatment and, on re-examination, he exhibited no wheezing and was given azithromycin 500 mg orally in the ED. The EP diagnosed the patient with acute bronchitis and discharged him home with an albuterol metered dose inhaler with a spacer, and a 4-day course of azithromycin. He also encouraged the patient to quit smoking.
The next day the radiologist’s official reading of the patient’s radiographs included the finding of a very small pulmonary nodule, which was seen only on the lateral X-ray. The radiologist recommended a repeat CXR or a computed tomography (CT) scan of the chest in 6 months.
Unfortunately, the EP never saw this information, and the patient was not contacted regarding the abnormal radiology finding and the need for follow-up. Approximately 20 months later, the patient was diagnosed with lung cancer with metastasis to the thoracic spine and liver. Despite chemotherapy and radiation treatment, he died from the cancer.
The patient’s family brought a malpractice suit against the EP, stating that the cancer could have been successfully treated prior to any metastasis if the patient had been informed of the abnormal radiology findings at his ED visit 20 months prior. The EP argued that he never saw the official radiology report, and therefore had no knowledge of the need for follow-up. At trial, a jury verdict was returned in favor of the defendant.
Discussion
Unfortunately, some version of this scenario occurs on a frequent basis. While imaging studies account for the majority of such cases, the same situation can occur with abnormal laboratory results, body-fluid cultures, or pathology reports in which an abnormality is identified (eg, positive blood culture, missed fracture) but, for a myriad of reasons, the critical information does not get related to the patient.
Because of the episodic nature of the practice of emergency medicine (EM), a process must be in place to ensure any “positive” test results or findings discovered after patient discharge are reviewed and compared to the ED diagnosis, and that any “misses” result in notifying the patient and/or his or her primary care physician and arranging follow-up. In cases such as the one presented here, a system issue existed—one that was not due to any fault or oversight of the EP. Ideally, EM leadership should work closely with leadership from radiology and laboratory services and hospital risk management to develop such a process—one that will be effective every day, including weekends and holidays.
Missed fractures on radiographs are a common cause of malpractice litigation against EPs. In one review by Kachalia et al1 examining malpractice claims involving EPs, missed fractures on radiographs accounted for 19% (the most common) of the 79 missed diagnoses identified in their study.In a similar study by Karcz et al,2 missed fractures ranked second in frequency and dollars lost in malpractice cases against EPs in Massachusetts.
While missed lesions on CXR do not occur with the same frequency as missed fractures, the results are much more devastating when the lesion turns out to be malignant. Three common areas where such lesions are missed on CXR include: the apex of the lung, obscured by overlying clavicle and ribs; the retrocardiac region (as in the patient in this case); and the lung bases obscured by the diaphragm.
Emergency physicians are neither trained nor expected to identify every single abnormality—especially subtle radiographic abnormalities. This is why there are radiology overreads, and a system or process must be in place to ensure patients are informed of any positive findings and to arrange proper follow-up.
1. Kachalia A, Gandhi TK, Puopolo AL, et al. Missed and delayed diagnoses in the emergency department: a study of closed malpractice claims from 4 liability insurers. Ann Emerg Med. 2007;49(2):196-205.
2. Karcz A, Korn R, Burke MC, et al. Malpractice claims against emergency physicians in Massachusetts: 1975-1993. Am J Emerg Med. 1996;14(4):341-345.
1. Kachalia A, Gandhi TK, Puopolo AL, et al. Missed and delayed diagnoses in the emergency department: a study of closed malpractice claims from 4 liability insurers. Ann Emerg Med. 2007;49(2):196-205.
2. Karcz A, Korn R, Burke MC, et al. Malpractice claims against emergency physicians in Massachusetts: 1975-1993. Am J Emerg Med. 1996;14(4):341-345.
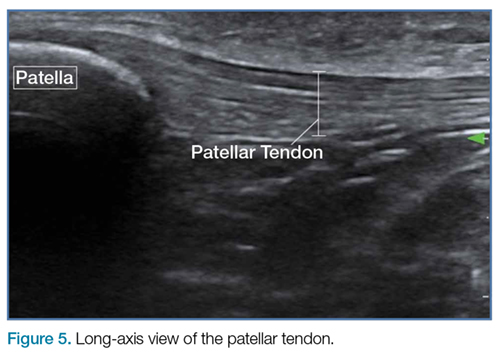
Emergency Ultrasound: Ultrasound-Guided Femoral Nerve Block
Case Scenario
A young man presented to the ED for evaluation of a large laceration to the anterior thigh that resulted from an industrial accident (Figure 1). 
Femoral nerve blocks are useful in a variety of clinical scenarios, including fractures of the femur or hip1 and laceration repairs (Figure 2). 
Identifying the Femoral Nerve on Ultrasound
To perform this nerve block, one must recall the anatomy of femoral central-line placement. The femoral nerve lies lateral to the femoral artery and vein. The high-frequency probe should be placed over the femoral crease (Figure 3). 

Performing the Block
An ultrasound-guided femoral nerve block can be performed using a 22-gauge blunt tip spinal needle, and an in-plane or out-of-plane technique can be employed. We prefer using an in-plane technique because the entire shaft of the needle can be visualized as it approaches the nerve. Anatomically, the femoral nerve lies in a separate fascial plane from the artery and vein, beneath the fascia iliaca (Figure 4). You can use this anatomic location of the femoral nerve to your advantage when performing the block. The needle can be advanced to a target slightly lateral to the nerve until it pops beneath the fascia iliaca. On the ultrasound, you can monitor the spread of anesthetic as it is injected. If the needle is in the right location, the hypoechoic fluid will spread medially toward the nerve, but will not track around the artery or vein. At least 15 cc to 20 cc of local anesthetic is typically required.2,3 If you prefer, the anesthetic can be diluted in normal saline, in a 1:1 ratio, to achieve adequate volume.
If you do not see the anesthetic spread during the injection, you should stop and check the needle placement, as it may be intravascular. Using a more lateral approach, targeting the injection at the fascial plane, rather than the nerve, helps to avoid direct intraneural injection or contact with the nerve—and it keeps the needle far away from the femoral vascular bundle.
Safety Considerations
As with any technique, prior to the procedure, aseptic measures should be taken, including the use of a sterile probe cover and sterile gloves. All patients undergoing ultrasound-guided nerve blocks proximal to the wrist or ankle should be placed on a cardiac monitor. In addition, intralipid emulsion should be readily available for administration in the unlikely event there is inadvertent intravascular injection of local anesthetic and cardiovascular collapse occurs.
Summary
With practice, ultrasound guidance can improve the procedural success of femoral nerve blocks and decrease the risk of nerve injury compared to blind nerve blocks
1. Dickman E, Pushkar I, Likourezos A, et al. Ultrasound-guided nerve blocks for intracapsular and extracapsular hip fractures. Am J Emerg Med. 2016;34(3):586-589.
2. Femoral nerve block. In: Hadzic A, Carrera A, Clark T, et al, eds. Hadzic’s Peripheral Nerve Blocks: An Anatomy for Ultrasound-Guided Regional Anesthesia. 2nd ed. New York, NY: The McGraw Hill Companies, Inc; 2012:267-279.
3. Ultrasound-guided femoral nerve block. In: Hadzic A, Carrera A, Clark T, et al, eds. Hadzic’s Peripheral Nerve Blocks: An Anatomy for Ultrasound-Guided Regional Anesthesia. 2nd ed. New York, NY: The McGraw Hill Companies, Inc; 2012:397-404.
Case Scenario
A young man presented to the ED for evaluation of a large laceration to the anterior thigh that resulted from an industrial accident (Figure 1).
Femoral nerve blocks are useful in a variety of clinical scenarios, including fractures of the femur or hip1 and laceration repairs (Figure 2).
Identifying the Femoral Nerve on Ultrasound
To perform this nerve block, one must recall the anatomy of femoral central-line placement. The femoral nerve lies lateral to the femoral artery and vein. The high-frequency probe should be placed over the femoral crease (Figure 3).
Performing the Block
An ultrasound-guided femoral nerve block can be performed using a 22-gauge blunt tip spinal needle, and an in-plane or out-of-plane technique can be employed. We prefer using an in-plane technique because the entire shaft of the needle can be visualized as it approaches the nerve. Anatomically, the femoral nerve lies in a separate fascial plane from the artery and vein, beneath the fascia iliaca (Figure 4). You can use this anatomic location of the femoral nerve to your advantage when performing the block. The needle can be advanced to a target slightly lateral to the nerve until it pops beneath the fascia iliaca. On the ultrasound, you can monitor the spread of anesthetic as it is injected. If the needle is in the right location, the hypoechoic fluid will spread medially toward the nerve, but will not track around the artery or vein. At least 15 cc to 20 cc of local anesthetic is typically required.2,3 If you prefer, the anesthetic can be diluted in normal saline, in a 1:1 ratio, to achieve adequate volume.
If you do not see the anesthetic spread during the injection, you should stop and check the needle placement, as it may be intravascular. Using a more lateral approach, targeting the injection at the fascial plane, rather than the nerve, helps to avoid direct intraneural injection or contact with the nerve—and it keeps the needle far away from the femoral vascular bundle.
Safety Considerations
As with any technique, prior to the procedure, aseptic measures should be taken, including the use of a sterile probe cover and sterile gloves. All patients undergoing ultrasound-guided nerve blocks proximal to the wrist or ankle should be placed on a cardiac monitor. In addition, intralipid emulsion should be readily available for administration in the unlikely event there is inadvertent intravascular injection of local anesthetic and cardiovascular collapse occurs.
Summary
With practice, ultrasound guidance can improve the procedural success of femoral nerve blocks and decrease the risk of nerve injury compared to blind nerve blocks
Case Scenario
A young man presented to the ED for evaluation of a large laceration to the anterior thigh that resulted from an industrial accident (Figure 1).
Femoral nerve blocks are useful in a variety of clinical scenarios, including fractures of the femur or hip1 and laceration repairs (Figure 2).
Identifying the Femoral Nerve on Ultrasound
To perform this nerve block, one must recall the anatomy of femoral central-line placement. The femoral nerve lies lateral to the femoral artery and vein. The high-frequency probe should be placed over the femoral crease (Figure 3).
Performing the Block
An ultrasound-guided femoral nerve block can be performed using a 22-gauge blunt tip spinal needle, and an in-plane or out-of-plane technique can be employed. We prefer using an in-plane technique because the entire shaft of the needle can be visualized as it approaches the nerve. Anatomically, the femoral nerve lies in a separate fascial plane from the artery and vein, beneath the fascia iliaca (Figure 4). You can use this anatomic location of the femoral nerve to your advantage when performing the block. The needle can be advanced to a target slightly lateral to the nerve until it pops beneath the fascia iliaca. On the ultrasound, you can monitor the spread of anesthetic as it is injected. If the needle is in the right location, the hypoechoic fluid will spread medially toward the nerve, but will not track around the artery or vein. At least 15 cc to 20 cc of local anesthetic is typically required.2,3 If you prefer, the anesthetic can be diluted in normal saline, in a 1:1 ratio, to achieve adequate volume.
If you do not see the anesthetic spread during the injection, you should stop and check the needle placement, as it may be intravascular. Using a more lateral approach, targeting the injection at the fascial plane, rather than the nerve, helps to avoid direct intraneural injection or contact with the nerve—and it keeps the needle far away from the femoral vascular bundle.
Safety Considerations
As with any technique, prior to the procedure, aseptic measures should be taken, including the use of a sterile probe cover and sterile gloves. All patients undergoing ultrasound-guided nerve blocks proximal to the wrist or ankle should be placed on a cardiac monitor. In addition, intralipid emulsion should be readily available for administration in the unlikely event there is inadvertent intravascular injection of local anesthetic and cardiovascular collapse occurs.
Summary
With practice, ultrasound guidance can improve the procedural success of femoral nerve blocks and decrease the risk of nerve injury compared to blind nerve blocks
1. Dickman E, Pushkar I, Likourezos A, et al. Ultrasound-guided nerve blocks for intracapsular and extracapsular hip fractures. Am J Emerg Med. 2016;34(3):586-589.
2. Femoral nerve block. In: Hadzic A, Carrera A, Clark T, et al, eds. Hadzic’s Peripheral Nerve Blocks: An Anatomy for Ultrasound-Guided Regional Anesthesia. 2nd ed. New York, NY: The McGraw Hill Companies, Inc; 2012:267-279.
3. Ultrasound-guided femoral nerve block. In: Hadzic A, Carrera A, Clark T, et al, eds. Hadzic’s Peripheral Nerve Blocks: An Anatomy for Ultrasound-Guided Regional Anesthesia. 2nd ed. New York, NY: The McGraw Hill Companies, Inc; 2012:397-404.
1. Dickman E, Pushkar I, Likourezos A, et al. Ultrasound-guided nerve blocks for intracapsular and extracapsular hip fractures. Am J Emerg Med. 2016;34(3):586-589.
2. Femoral nerve block. In: Hadzic A, Carrera A, Clark T, et al, eds. Hadzic’s Peripheral Nerve Blocks: An Anatomy for Ultrasound-Guided Regional Anesthesia. 2nd ed. New York, NY: The McGraw Hill Companies, Inc; 2012:267-279.
3. Ultrasound-guided femoral nerve block. In: Hadzic A, Carrera A, Clark T, et al, eds. Hadzic’s Peripheral Nerve Blocks: An Anatomy for Ultrasound-Guided Regional Anesthesia. 2nd ed. New York, NY: The McGraw Hill Companies, Inc; 2012:397-404.