User login
November 2016 Quiz 2
Q2: Answer: B
This is likely a tapeworm infection with Diphyllobothrium latum, and most tapeworm infections are treated with praziquantel. D. latum infection can be acquired by ingesting certain forms of freshwater fish, and those who consume raw fish, including sushi, are at increased risk. Patients infected with D. latum may develop a megaloblastic anemia secondary to vitamin B12 deficiency given that D. latum competitively interferes with normal host absorption. All the other agents listed would not be used for treatment of tapeworm infection.
Reference
1. Scholz T., et al. Update on the human broad tapeworm (genus Diphyllobothrium), including clinical relevance. Clin Microbiol Rev. 2009;22:146-60.
Q2: Answer: B
This is likely a tapeworm infection with Diphyllobothrium latum, and most tapeworm infections are treated with praziquantel. D. latum infection can be acquired by ingesting certain forms of freshwater fish, and those who consume raw fish, including sushi, are at increased risk. Patients infected with D. latum may develop a megaloblastic anemia secondary to vitamin B12 deficiency given that D. latum competitively interferes with normal host absorption. All the other agents listed would not be used for treatment of tapeworm infection.
Reference
1. Scholz T., et al. Update on the human broad tapeworm (genus Diphyllobothrium), including clinical relevance. Clin Microbiol Rev. 2009;22:146-60.
Q2: Answer: B
This is likely a tapeworm infection with Diphyllobothrium latum, and most tapeworm infections are treated with praziquantel. D. latum infection can be acquired by ingesting certain forms of freshwater fish, and those who consume raw fish, including sushi, are at increased risk. Patients infected with D. latum may develop a megaloblastic anemia secondary to vitamin B12 deficiency given that D. latum competitively interferes with normal host absorption. All the other agents listed would not be used for treatment of tapeworm infection.
Reference
1. Scholz T., et al. Update on the human broad tapeworm (genus Diphyllobothrium), including clinical relevance. Clin Microbiol Rev. 2009;22:146-60.
A 40-year-old man presents to the clinic with 2 months of diarrhea and significant fatigue. He has no significant past medical history and works as a chef in a local sushi bar. He has nonbloody watery stools with nocturnal symptoms. The diarrhea is associated with abdominal cramps. His physical examination is unrevealing. His hemoglobin is 9.8 g/dL, with a mean corpuscular volume of 110 fL. Peripheral eosinophilia is noted. A stool sample is sent to the lab and is pending.
Hand Hygiene Improves Patient Safety
Clinical Question: Does improving hand hygiene compliance from a high level (>80%) to a very high level (>95%) reduce healthcare-associated infections?

Background: Hand hygiene compliance remains an elusive infection prevention parameter to master. Studies show a correlation in reduction of healthcare-associated infections with improved hand hygiene compliance from a low to medium level, but little data exist on very high rates of hand hygiene compliance.
Study Design: Prospective observational.
Setting: University of North Carolina Hospitals.
Synopsis: Researchers recruited all hospital staff to be hand hygiene monitors, thereby using the Hawthorne effect to drive hand hygiene compliance rates. Over a 17-month period, >4,000 unique observers made >140,000 observations. Data showed a significant increase in hand hygiene compliance rates of about 10% (P<0.001) and a significant decrease in overall healthcare-associated infection rates of about 6% (P=0.0066). A reduction in healthcare-associated Clostridium difficile infection of 14% was observed in association with the improved hand hygiene compliance. No association with multidrug-resistant organisms was found.
Bottom Line: There is continued correlation between improved hand hygiene compliance and reduced healthcare-associated infection rates even at very high levels (>95%) of hand hygiene compliance.
Citation: Sickbert-Bennett EE, DiBiase LM, Willis TM, Wolak ES, Weber DJ, Rutala WA. Reduction of healthcare-associated infections by exceeding high compliance with hand hygiene practices. Emerg Infect Dis. 2016;22(9):1628-1630.
Short Take
Avoid Fluoroquinolones in Acute Sinusitis, Acute Exacerbations of Bronchitis, and Uncomplicated Urinary Tract Infections If Other Treatment Options Exist
Because fluoroquinolones have been associated with potentially permanent side effects involving tendons, muscles, joints, and nerves, the FDA recently updated the boxed warning to state that the risk of use likely outweighs the benefit for uncomplicated infections.
Citation: Fluoroquinolone Antibacterial Drugs for Systemic Use: Drug Safety Communication - Warnings Updated Due to Disabling Side Effects. FDA website. Accessed September 9, 2016.
Clinical Question: Does improving hand hygiene compliance from a high level (>80%) to a very high level (>95%) reduce healthcare-associated infections?
Background: Hand hygiene compliance remains an elusive infection prevention parameter to master. Studies show a correlation in reduction of healthcare-associated infections with improved hand hygiene compliance from a low to medium level, but little data exist on very high rates of hand hygiene compliance.
Study Design: Prospective observational.
Setting: University of North Carolina Hospitals.
Synopsis: Researchers recruited all hospital staff to be hand hygiene monitors, thereby using the Hawthorne effect to drive hand hygiene compliance rates. Over a 17-month period, >4,000 unique observers made >140,000 observations. Data showed a significant increase in hand hygiene compliance rates of about 10% (P<0.001) and a significant decrease in overall healthcare-associated infection rates of about 6% (P=0.0066). A reduction in healthcare-associated Clostridium difficile infection of 14% was observed in association with the improved hand hygiene compliance. No association with multidrug-resistant organisms was found.
Bottom Line: There is continued correlation between improved hand hygiene compliance and reduced healthcare-associated infection rates even at very high levels (>95%) of hand hygiene compliance.
Citation: Sickbert-Bennett EE, DiBiase LM, Willis TM, Wolak ES, Weber DJ, Rutala WA. Reduction of healthcare-associated infections by exceeding high compliance with hand hygiene practices. Emerg Infect Dis. 2016;22(9):1628-1630.
Short Take
Avoid Fluoroquinolones in Acute Sinusitis, Acute Exacerbations of Bronchitis, and Uncomplicated Urinary Tract Infections If Other Treatment Options Exist
Because fluoroquinolones have been associated with potentially permanent side effects involving tendons, muscles, joints, and nerves, the FDA recently updated the boxed warning to state that the risk of use likely outweighs the benefit for uncomplicated infections.
Citation: Fluoroquinolone Antibacterial Drugs for Systemic Use: Drug Safety Communication - Warnings Updated Due to Disabling Side Effects. FDA website. Accessed September 9, 2016.
Clinical Question: Does improving hand hygiene compliance from a high level (>80%) to a very high level (>95%) reduce healthcare-associated infections?
Background: Hand hygiene compliance remains an elusive infection prevention parameter to master. Studies show a correlation in reduction of healthcare-associated infections with improved hand hygiene compliance from a low to medium level, but little data exist on very high rates of hand hygiene compliance.
Study Design: Prospective observational.
Setting: University of North Carolina Hospitals.
Synopsis: Researchers recruited all hospital staff to be hand hygiene monitors, thereby using the Hawthorne effect to drive hand hygiene compliance rates. Over a 17-month period, >4,000 unique observers made >140,000 observations. Data showed a significant increase in hand hygiene compliance rates of about 10% (P<0.001) and a significant decrease in overall healthcare-associated infection rates of about 6% (P=0.0066). A reduction in healthcare-associated Clostridium difficile infection of 14% was observed in association with the improved hand hygiene compliance. No association with multidrug-resistant organisms was found.
Bottom Line: There is continued correlation between improved hand hygiene compliance and reduced healthcare-associated infection rates even at very high levels (>95%) of hand hygiene compliance.
Citation: Sickbert-Bennett EE, DiBiase LM, Willis TM, Wolak ES, Weber DJ, Rutala WA. Reduction of healthcare-associated infections by exceeding high compliance with hand hygiene practices. Emerg Infect Dis. 2016;22(9):1628-1630.
Short Take
Avoid Fluoroquinolones in Acute Sinusitis, Acute Exacerbations of Bronchitis, and Uncomplicated Urinary Tract Infections If Other Treatment Options Exist
Because fluoroquinolones have been associated with potentially permanent side effects involving tendons, muscles, joints, and nerves, the FDA recently updated the boxed warning to state that the risk of use likely outweighs the benefit for uncomplicated infections.
Citation: Fluoroquinolone Antibacterial Drugs for Systemic Use: Drug Safety Communication - Warnings Updated Due to Disabling Side Effects. FDA website. Accessed September 9, 2016.

Traditional Hand Hygiene Audits Can Lead to Inaccurate Conclusions about Physician Performance
Clinical Question: Does direct observation underestimate physician compliance with hand hygiene (HH) compared to other professional groups due to the Hawthorne effect?
Background: Although it is well-known that HH is imperative to infection control, physician compliance remains suboptimal and is often reported to be below that of nurses. The Hawthorne effect may be contributing to this perceived difference because nurses, who work on the same unit consistently, may more readily recognize hospital auditors.
Study Design: Observational.
Setting: 800-bed acute-care academic hospital in Canada.
Synopsis: Two students were trained to covertly observe physician and nursing HH compliance on inpatient units. For two months, students rotated units every week to minimize risk of discovery. Their findings were compared with data gathered by hospital auditors over the same time period.
Covertly observed HH compliance was 50% (799/1,597 opportunities) compared with 83.7% (2,769/3,309) reported by hospital auditors (P<0.0002). The difference in physician compliance was 19% (73.2% compliance with overt observation versus 54.2% with covert observation). The difference was much higher for nurses at 40.7% (85.8% compliance with overt observation versus 45.1% with covert observation). Attending physician behaviors heavily influenced team behaviors—79.5% of trainees were compliant if their attending was compliant compared with 18.9% if attending was not (P<0.0002).
Bottom Line: Traditional HH audit findings that physicians are less compliant than nurses may be at least partially due to the Hawthorne effect. Nonetheless, all healthcare providers have substantial room for improvement, and attending physicians are powerful role models to effect this change.
Citation: Kovacs-Litman A, Wong K, Shojania KJ, Callery S, Vearncombe M, Leis J. Do physicians clean their hands? Insights from a covert observational study [published online ahead of print July 5, 2016]. J Hosp Med.
Clinical Question: Does direct observation underestimate physician compliance with hand hygiene (HH) compared to other professional groups due to the Hawthorne effect?
Background: Although it is well-known that HH is imperative to infection control, physician compliance remains suboptimal and is often reported to be below that of nurses. The Hawthorne effect may be contributing to this perceived difference because nurses, who work on the same unit consistently, may more readily recognize hospital auditors.
Study Design: Observational.
Setting: 800-bed acute-care academic hospital in Canada.
Synopsis: Two students were trained to covertly observe physician and nursing HH compliance on inpatient units. For two months, students rotated units every week to minimize risk of discovery. Their findings were compared with data gathered by hospital auditors over the same time period.
Covertly observed HH compliance was 50% (799/1,597 opportunities) compared with 83.7% (2,769/3,309) reported by hospital auditors (P<0.0002). The difference in physician compliance was 19% (73.2% compliance with overt observation versus 54.2% with covert observation). The difference was much higher for nurses at 40.7% (85.8% compliance with overt observation versus 45.1% with covert observation). Attending physician behaviors heavily influenced team behaviors—79.5% of trainees were compliant if their attending was compliant compared with 18.9% if attending was not (P<0.0002).
Bottom Line: Traditional HH audit findings that physicians are less compliant than nurses may be at least partially due to the Hawthorne effect. Nonetheless, all healthcare providers have substantial room for improvement, and attending physicians are powerful role models to effect this change.
Citation: Kovacs-Litman A, Wong K, Shojania KJ, Callery S, Vearncombe M, Leis J. Do physicians clean their hands? Insights from a covert observational study [published online ahead of print July 5, 2016]. J Hosp Med.
Clinical Question: Does direct observation underestimate physician compliance with hand hygiene (HH) compared to other professional groups due to the Hawthorne effect?
Background: Although it is well-known that HH is imperative to infection control, physician compliance remains suboptimal and is often reported to be below that of nurses. The Hawthorne effect may be contributing to this perceived difference because nurses, who work on the same unit consistently, may more readily recognize hospital auditors.
Study Design: Observational.
Setting: 800-bed acute-care academic hospital in Canada.
Synopsis: Two students were trained to covertly observe physician and nursing HH compliance on inpatient units. For two months, students rotated units every week to minimize risk of discovery. Their findings were compared with data gathered by hospital auditors over the same time period.
Covertly observed HH compliance was 50% (799/1,597 opportunities) compared with 83.7% (2,769/3,309) reported by hospital auditors (P<0.0002). The difference in physician compliance was 19% (73.2% compliance with overt observation versus 54.2% with covert observation). The difference was much higher for nurses at 40.7% (85.8% compliance with overt observation versus 45.1% with covert observation). Attending physician behaviors heavily influenced team behaviors—79.5% of trainees were compliant if their attending was compliant compared with 18.9% if attending was not (P<0.0002).
Bottom Line: Traditional HH audit findings that physicians are less compliant than nurses may be at least partially due to the Hawthorne effect. Nonetheless, all healthcare providers have substantial room for improvement, and attending physicians are powerful role models to effect this change.
Citation: Kovacs-Litman A, Wong K, Shojania KJ, Callery S, Vearncombe M, Leis J. Do physicians clean their hands? Insights from a covert observational study [published online ahead of print July 5, 2016]. J Hosp Med.
Vector may make gene therapy safer
Photo courtesy of Washington
State University Spokane
Using modified foamy retroviral vectors to deliver gene therapy may reduce the risk of genotoxicity, according to research published in Scientific Reports.
These vectors have demonstrated promise in vitro, and researchers believe they could be used to treat X-linked severe combined immunodeficiency, thalassemia, and other diseases.
“We’ve started to translate this in collaboration with other scientists and medical doctors into the clinic,” said study author Grant Trobridge, PhD, of Washington State University Spokane.
Dr Trobridge and his colleagues said they decided to pursue foamy retroviral vectors as a delivery system for gene therapy because these vectors are less likely than gammaretroviral vectors or lentiviral vectors to activate nearby genes, including proto-oncogenes.
Still, the researchers altered the foamy retroviral vectors to change how they interact with target stem cells in an attempt to ensure the vectors would insert themselves into safer parts of the genome.
The team said they were able to retarget the foamy retroviral vectors away from genes and into satellite regions enriched for trimethylated histone H3 at lysine 9 by modifying the foamy virus Gag and Pol proteins.
These retargeted foamy retroviral vectors integrated near genes significantly less often than unmodified foamy retroviral vectors (P<0.001).
The researchers also noted that their retargeted foamy retroviral vectors can be produced at clinically relevant titers, and engineered target cells are not needed. Any target cell can be used by using alternate foamy helper plasmids during vector production. ![]()
Photo courtesy of Washington
State University Spokane
Using modified foamy retroviral vectors to deliver gene therapy may reduce the risk of genotoxicity, according to research published in Scientific Reports.
These vectors have demonstrated promise in vitro, and researchers believe they could be used to treat X-linked severe combined immunodeficiency, thalassemia, and other diseases.
“We’ve started to translate this in collaboration with other scientists and medical doctors into the clinic,” said study author Grant Trobridge, PhD, of Washington State University Spokane.
Dr Trobridge and his colleagues said they decided to pursue foamy retroviral vectors as a delivery system for gene therapy because these vectors are less likely than gammaretroviral vectors or lentiviral vectors to activate nearby genes, including proto-oncogenes.
Still, the researchers altered the foamy retroviral vectors to change how they interact with target stem cells in an attempt to ensure the vectors would insert themselves into safer parts of the genome.
The team said they were able to retarget the foamy retroviral vectors away from genes and into satellite regions enriched for trimethylated histone H3 at lysine 9 by modifying the foamy virus Gag and Pol proteins.
These retargeted foamy retroviral vectors integrated near genes significantly less often than unmodified foamy retroviral vectors (P<0.001).
The researchers also noted that their retargeted foamy retroviral vectors can be produced at clinically relevant titers, and engineered target cells are not needed. Any target cell can be used by using alternate foamy helper plasmids during vector production. ![]()
Photo courtesy of Washington
State University Spokane
Using modified foamy retroviral vectors to deliver gene therapy may reduce the risk of genotoxicity, according to research published in Scientific Reports.
These vectors have demonstrated promise in vitro, and researchers believe they could be used to treat X-linked severe combined immunodeficiency, thalassemia, and other diseases.
“We’ve started to translate this in collaboration with other scientists and medical doctors into the clinic,” said study author Grant Trobridge, PhD, of Washington State University Spokane.
Dr Trobridge and his colleagues said they decided to pursue foamy retroviral vectors as a delivery system for gene therapy because these vectors are less likely than gammaretroviral vectors or lentiviral vectors to activate nearby genes, including proto-oncogenes.
Still, the researchers altered the foamy retroviral vectors to change how they interact with target stem cells in an attempt to ensure the vectors would insert themselves into safer parts of the genome.
The team said they were able to retarget the foamy retroviral vectors away from genes and into satellite regions enriched for trimethylated histone H3 at lysine 9 by modifying the foamy virus Gag and Pol proteins.
These retargeted foamy retroviral vectors integrated near genes significantly less often than unmodified foamy retroviral vectors (P<0.001).
The researchers also noted that their retargeted foamy retroviral vectors can be produced at clinically relevant titers, and engineered target cells are not needed. Any target cell can be used by using alternate foamy helper plasmids during vector production. ![]()
IHS Program Targets HIV/AIDs in Young Natives
More than half of the new HIV diagnoses among American Indians and Alaska Natives are estimated to be among those aged < 35 years, according to the CDC. To improve HIV prevention and care outcomes, an ongoing collaboration between IHS and the CDC is funding cooperative agreements with First Nations Community HealthSource, Albuquerque, and Inter Tribal Council of Arizona, Phoenix. The groups will receive up to $100,000 a year for up to 5 years for community health care services. “These awards increase access to culturally appropriate, high-quality HIV treatment for our American Indian and Alaska Native communities,” said Mary L. Smith, IHS principal deputy director.
First Nations, New Mexico’s urban Indian health center and a Federally Qualified Health Center, operates 2 clinic sites and 3 school-based health centers. The Inter Tribal Council of Arizona, representing 21 tribal governments, operates more than 30 projects and provides technical assistance and training to tribal governments in program planning and development, research and data collection, resource development, management and evaluation.
The awards support activities in 5 main areas:
- Increasing access to comprehensive pre-exposure prophylaxis;
- Identifying local-level priorities for HIV care needs and creating tools and resources;
- Making it easier for people living with HIV and AIDS to stay in treatment;
- Teaching people who inject drugs about reducing risks and extending access to services for medication-assisted therapies for people with opioid use disorder in accordance with federal, state, tribal, and local laws; and
- Increasing age-appropriate prevention education at the local levels.
“This multiyear collaboration supports a sustained, in-depth HIV prevention program that will benefit not only tribes, but also American Indians and Alaska Natives in urban locations,” said Eugene McCray, MD, director of CDC’s Division of HIV/AIDS Prevention. “We are bringing services right to the local level, reaching American Indian and Alaska Native communities.”
More than half of the new HIV diagnoses among American Indians and Alaska Natives are estimated to be among those aged < 35 years, according to the CDC. To improve HIV prevention and care outcomes, an ongoing collaboration between IHS and the CDC is funding cooperative agreements with First Nations Community HealthSource, Albuquerque, and Inter Tribal Council of Arizona, Phoenix. The groups will receive up to $100,000 a year for up to 5 years for community health care services. “These awards increase access to culturally appropriate, high-quality HIV treatment for our American Indian and Alaska Native communities,” said Mary L. Smith, IHS principal deputy director.
First Nations, New Mexico’s urban Indian health center and a Federally Qualified Health Center, operates 2 clinic sites and 3 school-based health centers. The Inter Tribal Council of Arizona, representing 21 tribal governments, operates more than 30 projects and provides technical assistance and training to tribal governments in program planning and development, research and data collection, resource development, management and evaluation.
The awards support activities in 5 main areas:
- Increasing access to comprehensive pre-exposure prophylaxis;
- Identifying local-level priorities for HIV care needs and creating tools and resources;
- Making it easier for people living with HIV and AIDS to stay in treatment;
- Teaching people who inject drugs about reducing risks and extending access to services for medication-assisted therapies for people with opioid use disorder in accordance with federal, state, tribal, and local laws; and
- Increasing age-appropriate prevention education at the local levels.
“This multiyear collaboration supports a sustained, in-depth HIV prevention program that will benefit not only tribes, but also American Indians and Alaska Natives in urban locations,” said Eugene McCray, MD, director of CDC’s Division of HIV/AIDS Prevention. “We are bringing services right to the local level, reaching American Indian and Alaska Native communities.”
More than half of the new HIV diagnoses among American Indians and Alaska Natives are estimated to be among those aged < 35 years, according to the CDC. To improve HIV prevention and care outcomes, an ongoing collaboration between IHS and the CDC is funding cooperative agreements with First Nations Community HealthSource, Albuquerque, and Inter Tribal Council of Arizona, Phoenix. The groups will receive up to $100,000 a year for up to 5 years for community health care services. “These awards increase access to culturally appropriate, high-quality HIV treatment for our American Indian and Alaska Native communities,” said Mary L. Smith, IHS principal deputy director.
First Nations, New Mexico’s urban Indian health center and a Federally Qualified Health Center, operates 2 clinic sites and 3 school-based health centers. The Inter Tribal Council of Arizona, representing 21 tribal governments, operates more than 30 projects and provides technical assistance and training to tribal governments in program planning and development, research and data collection, resource development, management and evaluation.
The awards support activities in 5 main areas:
- Increasing access to comprehensive pre-exposure prophylaxis;
- Identifying local-level priorities for HIV care needs and creating tools and resources;
- Making it easier for people living with HIV and AIDS to stay in treatment;
- Teaching people who inject drugs about reducing risks and extending access to services for medication-assisted therapies for people with opioid use disorder in accordance with federal, state, tribal, and local laws; and
- Increasing age-appropriate prevention education at the local levels.
“This multiyear collaboration supports a sustained, in-depth HIV prevention program that will benefit not only tribes, but also American Indians and Alaska Natives in urban locations,” said Eugene McCray, MD, director of CDC’s Division of HIV/AIDS Prevention. “We are bringing services right to the local level, reaching American Indian and Alaska Native communities.”
Aromatase Inhibitor as Adjuvant Therapy for Breast Cancer: Is Longer Treatment Better?
Study Overview
Objective. To assess the effect of extending adjuvant therapy with an aromatase inhibitor beyond 5 years in postmenopausal women with breast cancer.
Design. Phase 3, randomized, double-blind, placebo-controlled trial.
Setting and participants. This was a North American Breast Cancer Group trial, coordinated by the Canadian Cancer Trials Group. The trial was originally designed as an extension of the MA.17 trial evaluating the role for 5 years of letrozole versus placebo after 5 years of tamoxifen, with re-randomization of letrozole-assigned patients to an additional 5 years of letrozole versus placebo. The trial was then extended to include additional postmenopausal women with stage I-III breast cancer who had been treated with 4.5 to 6 years of adjuvant therapy with any aromatase inhibitor with or without prior tamoxifen.
Most patients had received adjuvant treatment with tamoxifen before the aromatase inhibitor. Patients were randomized within 2 years after completing treatment with the aromatase inhibitor to either letrozole 2.5 mg or placebo orally once a day, for another 5 years. The criteria for stratification included lymph node status, prior receipt of adjuvant chemotherapy, the interval between the last dose of aromatase inhibitor and randomization, and the duration of prior use of tamoxifen. Eligibility criteria included patients who were disease-free after 4.5 to 6 years of aromatase inhibitor, hormone-positive tumors (and unknown receptor status for participants in the MA.17 trial), ECOG performance status of 0 to 2, and life expectancy of 5 or more years.
Main outcome measures. The primary endpoint was disease-free survival, defined as the time from randomization to recurrence or the development of new primary breast cancer. Secondary endpoints included overall survival, incidence of contralateral breast cancer, quality of life using the Medical Outcomes Study 36-Item Short-Form Heath Survey (SF-36) and the Menopause-Specific Quality of Life (MENQOL) questionnaire, and long-term safety. The investigators calculated that 196 events were required for the study to have 80% power to detect a 33% lower hazard of recurrence with letrozole as compared with placebo. At the 6-year point, only 176 events had been observed, and the study design was amended to have a time-based analysis instead of event-based. On 13 Nov 2015 the final database had 165 events, with 80% power to detect a hazard ratio for disease-free survival of 0.655. The analysis of time-to-event outcomes was performed utilizing a log-rank test with adjustment for stratification factors. Fisher’s exact test was used to assess binary outcomes, and Wilcoxon test, to assess continuous outcomes. Comparisons between the letrozole and the placebo groups were made using a 2-sided test with an alpha level of 5%.
Main results. A total of 1918 patients were randomized to receive either letrozole (n = 959) or placebo (n = 959). The rate of adherence to the study regimen was approximately 62% for both arms. The median duration of prior treatment with tamoxifen was 5 years; 20.7% of patients did not receive tamoxifen. The median duration of prior treatment with aromatase inhibitor was 5 years, and the median time interval between the last dose of aromatase inhibitor and randomization was less than 6 months. The median duration of the study regimen (letrozole or placebo) was 5 years, and the median follow-up was 6.3 years. Approximately 90% of patients had stage T1 or T2 tumors at diagnosis, and 94% of nodal stage were N0 or N1. Estrogen receptor, progesterone receptor or both were known to be positive in 98.8% of patients.
Disease recurrence or contralateral breast cancer occurred in 67 patients (7%) in the letrozole group and 98 patients (10.2%) in the placebo group. The hazard ratio for recurrence or occurrence of contralateral breast cancer was 0.66 (95% confidence interval [CI], 0.48–0.91, P = 0.01). In the letrozole group, 55 patients had disease recurrence and 13 patients had contralateral breast cancer. Among the patients in the placebo group, 68 had recurrence of disease and 31 had contralateral breast cancer. Both disease recurrence and contralateral breast cancer occurred in one patient in each group. Distant disease recurrence was 5.5% in the placebo group and 4.4% in the letrozole group.
Five-year disease-free survival, the primary endpoint of this study, was 95% in the letrozole group (95% CI, 93–96) and 91% in the placebo group (95% CI, 89–93). The rate of 5-year disease free-survival was higher in the letrozole group in all subgroups. A total of 200 deaths were observed, 100 in each group. The rate of 5-year overall survival was not statistically different between the 2 groups (93% in the letrozole group and 94% in the placebo group, HR 0.97, P = 0.83). The annual incidence rate of contralateral breast cancer favored the letrozole group, with a rate of 0.21% in comparison with 0.49% in the placebo group (HR 0.42, P = 0.007).
Discontinuation of treatment occurred in 5.4% of patients in the letrozole group and 3.7% in the placebo group. The majority of toxic effects had a similar incidence in both groups, however bone-related side effects were more common in the letrozole group. Bone fractures occurred in 14% of patients in the letrozole group and 9% in the placebo group (P = 0.001). New-onset osteoporosis was also more common in the letrozole group (11% versus 6%, P < 0.001). Of note, 5 patients developed a hip fracture after discontinuation of letrozole. In regards to quality of life, patients receiving letrozole had a greater reduction in scores in the role-physical subscale of the SF-36 survey, indicating worse quality of life, but the difference was less than the minimum clinically important difference. There were no differences in the MENQOL questionnaire subscales.
Conclusion. Treatment with an aromatase inhibitor for additional 4.5 to 6 years was beneficial in preventing disease recurrence. There was no difference in overall survival.
Commentary
Adjuvant endocrine therapy reduces the risk of recurrence and increases survival in women with hormone receptor–positive breast cancer. The use of tamoxifen as adjuvant therapy for women with early stage breast cancer has been extensively studied. A metanalysis performed by the Early Breast Cancer Trialists’ Collaborative Group (EBCTG) demonstrated that tamoxifen reduces breast cancer mortality by a third when given as adjuvant therapy for women with hormone positive breast cancer [1].
Two important studies published in the last decade demonstrated that extending therapy with tamoxifen beyond 5 years reduces the chance of recurrence and improves survival. In the ATLAS (Adjuvant Tamoxifen: Longer Against Shorter) trial, women with early stage breast cancer who had completed 5 years of adjuvant tamoxifen were randomized to stop therapy or to continue tamoxifen for 5 additional years. Among patients with estrogen receptor (ER)–positive disease, the results demonstrated an absolute recurrence reduction of 3.7% and an absolute mortality reduction of 2.8% in 15 years after diagnosis [2].The aTTom trial randomized 6953 women with ER-positive breast cancer to discontinue tamoxifen after 5 years or to continue to complete 10 years of treatment and confirmed a benefit in recurrence rates and breast cancer mortality with 10 years of adjuvant tamoxifen [3].
Although tamoxifen is active in both pre- and postmenopausal patients, therapy with an aromatase inhibitor either as first-line or following treatment with tamoxifen has been demonstrated to be superior to tamoxifen alone in hormone receptor–positive postmenopausal women. In the ATAC (The Arimidex, Tamoxifen, Alone or in Combination) trial, postmenopausal patients were randomized to receive 5 years of either tamoxifen or anastrozole as adjuvant therapy. The anastrozole group had higher disease-free survival, time to recurrence and time to distant recurrence [4].In the Breast Intergroup (BIG) 1-98 trial, postmenopausal women were assigned to 4 different arms: 5 years of letrozole, 5 years of tamoxifen, letrozole for 2 years followed by tamoxifen for 3 years, or tamoxifen for 2 years followed by letrozole for 3 years. The 2 groups assigned to receive letrozole initially were compared to the 2 groups assigned to receive tamoxifen initially. Compared with tamoxifen, letrozole significantly decrease the risk of recurrence [5].The MA-17 trial demonstrated a disease-free survival advantage with 5 years of letrozole compared with placebo in women who had been treated with tamoxifen for 5 years [6]. Based on these data, current guidelines for adjuvant endocrine therapy for postmenopausal women recommend an aromatase inhibitor for 5 years as primary therapy or after 2 to 3 years of tamoxifen [7].
Results from studies with extended endocrine therapy, either 10 years of tamoxifen or 5 years of aromatase inhibitor after up to 5 years of tamoxifen, provide rationale to study the effect of therapy with aromatase inhibitor beyond 5 years. The current study by Goss et al (the MA 17.R trial) addresses the relevant question of whether extended adjuvant therapy with an aromatase inhibitor in post-menopausal women beyond 5 years provides additional benefit. The design of this study has several strengths including being randomized, phase 3, placebo-controlled and double-blind. Another strength was the large number of patients enrolled. The choice of disease-free survival as the primary endpoint is in accordance with the natural course of ER-positive breast cancer, which has a prolonged rate of recurrence. The study results showed that patients who received 10 years of letrozole had a 34% lower risk of recurrence, with an absolute improvement of 4% in disease-free survival. However, no overall survival benefit was demonstrated at a median follow-up of 6.3 years. This might be a result of the fact that the highest proportional benefit was reduction in incidence of contralateral breast cancer. It is also possible that an overall survival benefit would be observed with a longer follow-up.
As highlighted by the authors, the benefit of extended adjuvant therapy is higher in the first years. Given that the majority of patients enrolled in this study had received prior tamoxifen, it is possible that patients who receive only an aromatase inhibitor for 5 years without prior tamoxifen would benefit even more from extended aromatase inhibitor therapy. On the other hand, the 1.1% numerical advantage observed in reducing distant recurrence is quite modest, with the majority of the disease-free survival advantage seen with extended aromatase inhibition being due to a reduction in local recurrence and contralateral new concerns.
The quality of life assessment enhanced this trial, since adherence to adjuvant endocrine therapy remains a challenge. It should be noted, however, that patients willing to participate in a trial of extended therapy are likely to be those who have tolerated therapy reasonably well. The increase in body pain and differences in the role-emotional subscale in the letrozole reflect side effects of aromatase inhibitors that are seen in clinical practice. The higher rates of new-onset osteoporosis and bone fractures underscore the need to balance potential benefits and risks with extended aromatase inhibitor therapy.
Results from other trials evaluating extended adjuvant therapy will be helpful. The NSABP B-42 study randomized ER-positive postmenopausal patients to receive 5 years of letrozole or placebo after completing 5 years of hormonal therapy with an aromatase inhibitor for 5 years or ≤ 3 years of tamoxifen followed by an aromatase inhibitor. This study has completed enrollment and should provide additional insight regarding duration of therapy with aromatase inhibitors.
Applications for Clinical Practice
These trial results showed a benefit with extended aromatase inhibitor therapy; however, the magnitude of benefit was relatively small, particularly with respect to impacting distant recurrence risk. Given that extended therapy has potential side effects, it is appropriate to have a detailed discussion with patients regarding potential benefits and risks. A reasonable clinical strategy is to discuss extended therapy with patients who have a higher chance of relapse and those who are motivated to continue therapy to reduce new breast cancer events.
—Leticia Varella, MD, and Halle Moore, MD,
Cleveland Clinic Taussig Cancer Institute, Cleveland, OH
1. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365:1687–717.
2. Davies C, Pan H, Godwin J, at al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013;381:805–16.
3. Gray RG, Rea D, Handley K, et al. aTTom: Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6,953 women with early breast cancer. J Clin Oncol 2013;31(suppl;abstr 5).
4. Cuzick J, Sestak I, Baum M, et al; ATAC/LATTE investigators. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol 2010;11:113541.
5. Breast International Group (BIG) 1-98 Collaborative Group, Thürlimann B, Keshaviah A, Coates AS, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005;353:2747–57.
6. Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med 2003;349:1793–802.
7. Burstein HJ, Prestrud AA, Seidenfeld J, et al; American Society of Clinical Oncology. American Society of Clinical Oncology clinical practice guideline: update on adjuvant endocrine therapy for women with hormone receptor-positive breast cancer. J Clin Oncol 2010;28:3784–96.
Study Overview
Objective. To assess the effect of extending adjuvant therapy with an aromatase inhibitor beyond 5 years in postmenopausal women with breast cancer.
Design. Phase 3, randomized, double-blind, placebo-controlled trial.
Setting and participants. This was a North American Breast Cancer Group trial, coordinated by the Canadian Cancer Trials Group. The trial was originally designed as an extension of the MA.17 trial evaluating the role for 5 years of letrozole versus placebo after 5 years of tamoxifen, with re-randomization of letrozole-assigned patients to an additional 5 years of letrozole versus placebo. The trial was then extended to include additional postmenopausal women with stage I-III breast cancer who had been treated with 4.5 to 6 years of adjuvant therapy with any aromatase inhibitor with or without prior tamoxifen.
Most patients had received adjuvant treatment with tamoxifen before the aromatase inhibitor. Patients were randomized within 2 years after completing treatment with the aromatase inhibitor to either letrozole 2.5 mg or placebo orally once a day, for another 5 years. The criteria for stratification included lymph node status, prior receipt of adjuvant chemotherapy, the interval between the last dose of aromatase inhibitor and randomization, and the duration of prior use of tamoxifen. Eligibility criteria included patients who were disease-free after 4.5 to 6 years of aromatase inhibitor, hormone-positive tumors (and unknown receptor status for participants in the MA.17 trial), ECOG performance status of 0 to 2, and life expectancy of 5 or more years.
Main outcome measures. The primary endpoint was disease-free survival, defined as the time from randomization to recurrence or the development of new primary breast cancer. Secondary endpoints included overall survival, incidence of contralateral breast cancer, quality of life using the Medical Outcomes Study 36-Item Short-Form Heath Survey (SF-36) and the Menopause-Specific Quality of Life (MENQOL) questionnaire, and long-term safety. The investigators calculated that 196 events were required for the study to have 80% power to detect a 33% lower hazard of recurrence with letrozole as compared with placebo. At the 6-year point, only 176 events had been observed, and the study design was amended to have a time-based analysis instead of event-based. On 13 Nov 2015 the final database had 165 events, with 80% power to detect a hazard ratio for disease-free survival of 0.655. The analysis of time-to-event outcomes was performed utilizing a log-rank test with adjustment for stratification factors. Fisher’s exact test was used to assess binary outcomes, and Wilcoxon test, to assess continuous outcomes. Comparisons between the letrozole and the placebo groups were made using a 2-sided test with an alpha level of 5%.
Main results. A total of 1918 patients were randomized to receive either letrozole (n = 959) or placebo (n = 959). The rate of adherence to the study regimen was approximately 62% for both arms. The median duration of prior treatment with tamoxifen was 5 years; 20.7% of patients did not receive tamoxifen. The median duration of prior treatment with aromatase inhibitor was 5 years, and the median time interval between the last dose of aromatase inhibitor and randomization was less than 6 months. The median duration of the study regimen (letrozole or placebo) was 5 years, and the median follow-up was 6.3 years. Approximately 90% of patients had stage T1 or T2 tumors at diagnosis, and 94% of nodal stage were N0 or N1. Estrogen receptor, progesterone receptor or both were known to be positive in 98.8% of patients.
Disease recurrence or contralateral breast cancer occurred in 67 patients (7%) in the letrozole group and 98 patients (10.2%) in the placebo group. The hazard ratio for recurrence or occurrence of contralateral breast cancer was 0.66 (95% confidence interval [CI], 0.48–0.91, P = 0.01). In the letrozole group, 55 patients had disease recurrence and 13 patients had contralateral breast cancer. Among the patients in the placebo group, 68 had recurrence of disease and 31 had contralateral breast cancer. Both disease recurrence and contralateral breast cancer occurred in one patient in each group. Distant disease recurrence was 5.5% in the placebo group and 4.4% in the letrozole group.
Five-year disease-free survival, the primary endpoint of this study, was 95% in the letrozole group (95% CI, 93–96) and 91% in the placebo group (95% CI, 89–93). The rate of 5-year disease free-survival was higher in the letrozole group in all subgroups. A total of 200 deaths were observed, 100 in each group. The rate of 5-year overall survival was not statistically different between the 2 groups (93% in the letrozole group and 94% in the placebo group, HR 0.97, P = 0.83). The annual incidence rate of contralateral breast cancer favored the letrozole group, with a rate of 0.21% in comparison with 0.49% in the placebo group (HR 0.42, P = 0.007).
Discontinuation of treatment occurred in 5.4% of patients in the letrozole group and 3.7% in the placebo group. The majority of toxic effects had a similar incidence in both groups, however bone-related side effects were more common in the letrozole group. Bone fractures occurred in 14% of patients in the letrozole group and 9% in the placebo group (P = 0.001). New-onset osteoporosis was also more common in the letrozole group (11% versus 6%, P < 0.001). Of note, 5 patients developed a hip fracture after discontinuation of letrozole. In regards to quality of life, patients receiving letrozole had a greater reduction in scores in the role-physical subscale of the SF-36 survey, indicating worse quality of life, but the difference was less than the minimum clinically important difference. There were no differences in the MENQOL questionnaire subscales.
Conclusion. Treatment with an aromatase inhibitor for additional 4.5 to 6 years was beneficial in preventing disease recurrence. There was no difference in overall survival.
Commentary
Adjuvant endocrine therapy reduces the risk of recurrence and increases survival in women with hormone receptor–positive breast cancer. The use of tamoxifen as adjuvant therapy for women with early stage breast cancer has been extensively studied. A metanalysis performed by the Early Breast Cancer Trialists’ Collaborative Group (EBCTG) demonstrated that tamoxifen reduces breast cancer mortality by a third when given as adjuvant therapy for women with hormone positive breast cancer [1].
Two important studies published in the last decade demonstrated that extending therapy with tamoxifen beyond 5 years reduces the chance of recurrence and improves survival. In the ATLAS (Adjuvant Tamoxifen: Longer Against Shorter) trial, women with early stage breast cancer who had completed 5 years of adjuvant tamoxifen were randomized to stop therapy or to continue tamoxifen for 5 additional years. Among patients with estrogen receptor (ER)–positive disease, the results demonstrated an absolute recurrence reduction of 3.7% and an absolute mortality reduction of 2.8% in 15 years after diagnosis [2].The aTTom trial randomized 6953 women with ER-positive breast cancer to discontinue tamoxifen after 5 years or to continue to complete 10 years of treatment and confirmed a benefit in recurrence rates and breast cancer mortality with 10 years of adjuvant tamoxifen [3].
Although tamoxifen is active in both pre- and postmenopausal patients, therapy with an aromatase inhibitor either as first-line or following treatment with tamoxifen has been demonstrated to be superior to tamoxifen alone in hormone receptor–positive postmenopausal women. In the ATAC (The Arimidex, Tamoxifen, Alone or in Combination) trial, postmenopausal patients were randomized to receive 5 years of either tamoxifen or anastrozole as adjuvant therapy. The anastrozole group had higher disease-free survival, time to recurrence and time to distant recurrence [4].In the Breast Intergroup (BIG) 1-98 trial, postmenopausal women were assigned to 4 different arms: 5 years of letrozole, 5 years of tamoxifen, letrozole for 2 years followed by tamoxifen for 3 years, or tamoxifen for 2 years followed by letrozole for 3 years. The 2 groups assigned to receive letrozole initially were compared to the 2 groups assigned to receive tamoxifen initially. Compared with tamoxifen, letrozole significantly decrease the risk of recurrence [5].The MA-17 trial demonstrated a disease-free survival advantage with 5 years of letrozole compared with placebo in women who had been treated with tamoxifen for 5 years [6]. Based on these data, current guidelines for adjuvant endocrine therapy for postmenopausal women recommend an aromatase inhibitor for 5 years as primary therapy or after 2 to 3 years of tamoxifen [7].
Results from studies with extended endocrine therapy, either 10 years of tamoxifen or 5 years of aromatase inhibitor after up to 5 years of tamoxifen, provide rationale to study the effect of therapy with aromatase inhibitor beyond 5 years. The current study by Goss et al (the MA 17.R trial) addresses the relevant question of whether extended adjuvant therapy with an aromatase inhibitor in post-menopausal women beyond 5 years provides additional benefit. The design of this study has several strengths including being randomized, phase 3, placebo-controlled and double-blind. Another strength was the large number of patients enrolled. The choice of disease-free survival as the primary endpoint is in accordance with the natural course of ER-positive breast cancer, which has a prolonged rate of recurrence. The study results showed that patients who received 10 years of letrozole had a 34% lower risk of recurrence, with an absolute improvement of 4% in disease-free survival. However, no overall survival benefit was demonstrated at a median follow-up of 6.3 years. This might be a result of the fact that the highest proportional benefit was reduction in incidence of contralateral breast cancer. It is also possible that an overall survival benefit would be observed with a longer follow-up.
As highlighted by the authors, the benefit of extended adjuvant therapy is higher in the first years. Given that the majority of patients enrolled in this study had received prior tamoxifen, it is possible that patients who receive only an aromatase inhibitor for 5 years without prior tamoxifen would benefit even more from extended aromatase inhibitor therapy. On the other hand, the 1.1% numerical advantage observed in reducing distant recurrence is quite modest, with the majority of the disease-free survival advantage seen with extended aromatase inhibition being due to a reduction in local recurrence and contralateral new concerns.
The quality of life assessment enhanced this trial, since adherence to adjuvant endocrine therapy remains a challenge. It should be noted, however, that patients willing to participate in a trial of extended therapy are likely to be those who have tolerated therapy reasonably well. The increase in body pain and differences in the role-emotional subscale in the letrozole reflect side effects of aromatase inhibitors that are seen in clinical practice. The higher rates of new-onset osteoporosis and bone fractures underscore the need to balance potential benefits and risks with extended aromatase inhibitor therapy.
Results from other trials evaluating extended adjuvant therapy will be helpful. The NSABP B-42 study randomized ER-positive postmenopausal patients to receive 5 years of letrozole or placebo after completing 5 years of hormonal therapy with an aromatase inhibitor for 5 years or ≤ 3 years of tamoxifen followed by an aromatase inhibitor. This study has completed enrollment and should provide additional insight regarding duration of therapy with aromatase inhibitors.
Applications for Clinical Practice
These trial results showed a benefit with extended aromatase inhibitor therapy; however, the magnitude of benefit was relatively small, particularly with respect to impacting distant recurrence risk. Given that extended therapy has potential side effects, it is appropriate to have a detailed discussion with patients regarding potential benefits and risks. A reasonable clinical strategy is to discuss extended therapy with patients who have a higher chance of relapse and those who are motivated to continue therapy to reduce new breast cancer events.
—Leticia Varella, MD, and Halle Moore, MD,
Cleveland Clinic Taussig Cancer Institute, Cleveland, OH
Study Overview
Objective. To assess the effect of extending adjuvant therapy with an aromatase inhibitor beyond 5 years in postmenopausal women with breast cancer.
Design. Phase 3, randomized, double-blind, placebo-controlled trial.
Setting and participants. This was a North American Breast Cancer Group trial, coordinated by the Canadian Cancer Trials Group. The trial was originally designed as an extension of the MA.17 trial evaluating the role for 5 years of letrozole versus placebo after 5 years of tamoxifen, with re-randomization of letrozole-assigned patients to an additional 5 years of letrozole versus placebo. The trial was then extended to include additional postmenopausal women with stage I-III breast cancer who had been treated with 4.5 to 6 years of adjuvant therapy with any aromatase inhibitor with or without prior tamoxifen.
Most patients had received adjuvant treatment with tamoxifen before the aromatase inhibitor. Patients were randomized within 2 years after completing treatment with the aromatase inhibitor to either letrozole 2.5 mg or placebo orally once a day, for another 5 years. The criteria for stratification included lymph node status, prior receipt of adjuvant chemotherapy, the interval between the last dose of aromatase inhibitor and randomization, and the duration of prior use of tamoxifen. Eligibility criteria included patients who were disease-free after 4.5 to 6 years of aromatase inhibitor, hormone-positive tumors (and unknown receptor status for participants in the MA.17 trial), ECOG performance status of 0 to 2, and life expectancy of 5 or more years.
Main outcome measures. The primary endpoint was disease-free survival, defined as the time from randomization to recurrence or the development of new primary breast cancer. Secondary endpoints included overall survival, incidence of contralateral breast cancer, quality of life using the Medical Outcomes Study 36-Item Short-Form Heath Survey (SF-36) and the Menopause-Specific Quality of Life (MENQOL) questionnaire, and long-term safety. The investigators calculated that 196 events were required for the study to have 80% power to detect a 33% lower hazard of recurrence with letrozole as compared with placebo. At the 6-year point, only 176 events had been observed, and the study design was amended to have a time-based analysis instead of event-based. On 13 Nov 2015 the final database had 165 events, with 80% power to detect a hazard ratio for disease-free survival of 0.655. The analysis of time-to-event outcomes was performed utilizing a log-rank test with adjustment for stratification factors. Fisher’s exact test was used to assess binary outcomes, and Wilcoxon test, to assess continuous outcomes. Comparisons between the letrozole and the placebo groups were made using a 2-sided test with an alpha level of 5%.
Main results. A total of 1918 patients were randomized to receive either letrozole (n = 959) or placebo (n = 959). The rate of adherence to the study regimen was approximately 62% for both arms. The median duration of prior treatment with tamoxifen was 5 years; 20.7% of patients did not receive tamoxifen. The median duration of prior treatment with aromatase inhibitor was 5 years, and the median time interval between the last dose of aromatase inhibitor and randomization was less than 6 months. The median duration of the study regimen (letrozole or placebo) was 5 years, and the median follow-up was 6.3 years. Approximately 90% of patients had stage T1 or T2 tumors at diagnosis, and 94% of nodal stage were N0 or N1. Estrogen receptor, progesterone receptor or both were known to be positive in 98.8% of patients.
Disease recurrence or contralateral breast cancer occurred in 67 patients (7%) in the letrozole group and 98 patients (10.2%) in the placebo group. The hazard ratio for recurrence or occurrence of contralateral breast cancer was 0.66 (95% confidence interval [CI], 0.48–0.91, P = 0.01). In the letrozole group, 55 patients had disease recurrence and 13 patients had contralateral breast cancer. Among the patients in the placebo group, 68 had recurrence of disease and 31 had contralateral breast cancer. Both disease recurrence and contralateral breast cancer occurred in one patient in each group. Distant disease recurrence was 5.5% in the placebo group and 4.4% in the letrozole group.
Five-year disease-free survival, the primary endpoint of this study, was 95% in the letrozole group (95% CI, 93–96) and 91% in the placebo group (95% CI, 89–93). The rate of 5-year disease free-survival was higher in the letrozole group in all subgroups. A total of 200 deaths were observed, 100 in each group. The rate of 5-year overall survival was not statistically different between the 2 groups (93% in the letrozole group and 94% in the placebo group, HR 0.97, P = 0.83). The annual incidence rate of contralateral breast cancer favored the letrozole group, with a rate of 0.21% in comparison with 0.49% in the placebo group (HR 0.42, P = 0.007).
Discontinuation of treatment occurred in 5.4% of patients in the letrozole group and 3.7% in the placebo group. The majority of toxic effects had a similar incidence in both groups, however bone-related side effects were more common in the letrozole group. Bone fractures occurred in 14% of patients in the letrozole group and 9% in the placebo group (P = 0.001). New-onset osteoporosis was also more common in the letrozole group (11% versus 6%, P < 0.001). Of note, 5 patients developed a hip fracture after discontinuation of letrozole. In regards to quality of life, patients receiving letrozole had a greater reduction in scores in the role-physical subscale of the SF-36 survey, indicating worse quality of life, but the difference was less than the minimum clinically important difference. There were no differences in the MENQOL questionnaire subscales.
Conclusion. Treatment with an aromatase inhibitor for additional 4.5 to 6 years was beneficial in preventing disease recurrence. There was no difference in overall survival.
Commentary
Adjuvant endocrine therapy reduces the risk of recurrence and increases survival in women with hormone receptor–positive breast cancer. The use of tamoxifen as adjuvant therapy for women with early stage breast cancer has been extensively studied. A metanalysis performed by the Early Breast Cancer Trialists’ Collaborative Group (EBCTG) demonstrated that tamoxifen reduces breast cancer mortality by a third when given as adjuvant therapy for women with hormone positive breast cancer [1].
Two important studies published in the last decade demonstrated that extending therapy with tamoxifen beyond 5 years reduces the chance of recurrence and improves survival. In the ATLAS (Adjuvant Tamoxifen: Longer Against Shorter) trial, women with early stage breast cancer who had completed 5 years of adjuvant tamoxifen were randomized to stop therapy or to continue tamoxifen for 5 additional years. Among patients with estrogen receptor (ER)–positive disease, the results demonstrated an absolute recurrence reduction of 3.7% and an absolute mortality reduction of 2.8% in 15 years after diagnosis [2].The aTTom trial randomized 6953 women with ER-positive breast cancer to discontinue tamoxifen after 5 years or to continue to complete 10 years of treatment and confirmed a benefit in recurrence rates and breast cancer mortality with 10 years of adjuvant tamoxifen [3].
Although tamoxifen is active in both pre- and postmenopausal patients, therapy with an aromatase inhibitor either as first-line or following treatment with tamoxifen has been demonstrated to be superior to tamoxifen alone in hormone receptor–positive postmenopausal women. In the ATAC (The Arimidex, Tamoxifen, Alone or in Combination) trial, postmenopausal patients were randomized to receive 5 years of either tamoxifen or anastrozole as adjuvant therapy. The anastrozole group had higher disease-free survival, time to recurrence and time to distant recurrence [4].In the Breast Intergroup (BIG) 1-98 trial, postmenopausal women were assigned to 4 different arms: 5 years of letrozole, 5 years of tamoxifen, letrozole for 2 years followed by tamoxifen for 3 years, or tamoxifen for 2 years followed by letrozole for 3 years. The 2 groups assigned to receive letrozole initially were compared to the 2 groups assigned to receive tamoxifen initially. Compared with tamoxifen, letrozole significantly decrease the risk of recurrence [5].The MA-17 trial demonstrated a disease-free survival advantage with 5 years of letrozole compared with placebo in women who had been treated with tamoxifen for 5 years [6]. Based on these data, current guidelines for adjuvant endocrine therapy for postmenopausal women recommend an aromatase inhibitor for 5 years as primary therapy or after 2 to 3 years of tamoxifen [7].
Results from studies with extended endocrine therapy, either 10 years of tamoxifen or 5 years of aromatase inhibitor after up to 5 years of tamoxifen, provide rationale to study the effect of therapy with aromatase inhibitor beyond 5 years. The current study by Goss et al (the MA 17.R trial) addresses the relevant question of whether extended adjuvant therapy with an aromatase inhibitor in post-menopausal women beyond 5 years provides additional benefit. The design of this study has several strengths including being randomized, phase 3, placebo-controlled and double-blind. Another strength was the large number of patients enrolled. The choice of disease-free survival as the primary endpoint is in accordance with the natural course of ER-positive breast cancer, which has a prolonged rate of recurrence. The study results showed that patients who received 10 years of letrozole had a 34% lower risk of recurrence, with an absolute improvement of 4% in disease-free survival. However, no overall survival benefit was demonstrated at a median follow-up of 6.3 years. This might be a result of the fact that the highest proportional benefit was reduction in incidence of contralateral breast cancer. It is also possible that an overall survival benefit would be observed with a longer follow-up.
As highlighted by the authors, the benefit of extended adjuvant therapy is higher in the first years. Given that the majority of patients enrolled in this study had received prior tamoxifen, it is possible that patients who receive only an aromatase inhibitor for 5 years without prior tamoxifen would benefit even more from extended aromatase inhibitor therapy. On the other hand, the 1.1% numerical advantage observed in reducing distant recurrence is quite modest, with the majority of the disease-free survival advantage seen with extended aromatase inhibition being due to a reduction in local recurrence and contralateral new concerns.
The quality of life assessment enhanced this trial, since adherence to adjuvant endocrine therapy remains a challenge. It should be noted, however, that patients willing to participate in a trial of extended therapy are likely to be those who have tolerated therapy reasonably well. The increase in body pain and differences in the role-emotional subscale in the letrozole reflect side effects of aromatase inhibitors that are seen in clinical practice. The higher rates of new-onset osteoporosis and bone fractures underscore the need to balance potential benefits and risks with extended aromatase inhibitor therapy.
Results from other trials evaluating extended adjuvant therapy will be helpful. The NSABP B-42 study randomized ER-positive postmenopausal patients to receive 5 years of letrozole or placebo after completing 5 years of hormonal therapy with an aromatase inhibitor for 5 years or ≤ 3 years of tamoxifen followed by an aromatase inhibitor. This study has completed enrollment and should provide additional insight regarding duration of therapy with aromatase inhibitors.
Applications for Clinical Practice
These trial results showed a benefit with extended aromatase inhibitor therapy; however, the magnitude of benefit was relatively small, particularly with respect to impacting distant recurrence risk. Given that extended therapy has potential side effects, it is appropriate to have a detailed discussion with patients regarding potential benefits and risks. A reasonable clinical strategy is to discuss extended therapy with patients who have a higher chance of relapse and those who are motivated to continue therapy to reduce new breast cancer events.
—Leticia Varella, MD, and Halle Moore, MD,
Cleveland Clinic Taussig Cancer Institute, Cleveland, OH
1. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365:1687–717.
2. Davies C, Pan H, Godwin J, at al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013;381:805–16.
3. Gray RG, Rea D, Handley K, et al. aTTom: Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6,953 women with early breast cancer. J Clin Oncol 2013;31(suppl;abstr 5).
4. Cuzick J, Sestak I, Baum M, et al; ATAC/LATTE investigators. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol 2010;11:113541.
5. Breast International Group (BIG) 1-98 Collaborative Group, Thürlimann B, Keshaviah A, Coates AS, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005;353:2747–57.
6. Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med 2003;349:1793–802.
7. Burstein HJ, Prestrud AA, Seidenfeld J, et al; American Society of Clinical Oncology. American Society of Clinical Oncology clinical practice guideline: update on adjuvant endocrine therapy for women with hormone receptor-positive breast cancer. J Clin Oncol 2010;28:3784–96.
1. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365:1687–717.
2. Davies C, Pan H, Godwin J, at al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013;381:805–16.
3. Gray RG, Rea D, Handley K, et al. aTTom: Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years in 6,953 women with early breast cancer. J Clin Oncol 2013;31(suppl;abstr 5).
4. Cuzick J, Sestak I, Baum M, et al; ATAC/LATTE investigators. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol 2010;11:113541.
5. Breast International Group (BIG) 1-98 Collaborative Group, Thürlimann B, Keshaviah A, Coates AS, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 2005;353:2747–57.
6. Goss PE, Ingle JN, Martino S, et al. A randomized trial of letrozole in postmenopausal women after five years of tamoxifen therapy for early-stage breast cancer. N Engl J Med 2003;349:1793–802.
7. Burstein HJ, Prestrud AA, Seidenfeld J, et al; American Society of Clinical Oncology. American Society of Clinical Oncology clinical practice guideline: update on adjuvant endocrine therapy for women with hormone receptor-positive breast cancer. J Clin Oncol 2010;28:3784–96.
Intimate Partner and Sexual Violence Experienced by Women Serving in the Military
Study Overview
Objective. To understand how the experience of intimate partner violence and non-partner sexual assault (IPV/SA) in women in the military intersects with military service.
Design. Qualitative interviews conducted as part of a larger study focused on experiences of IPV/SA and health care needs and preferences among women veteran patients.
Setting and participants. Participants were 25 women veterans from all branches of the service, ages 22 to 58 years (mean 44.6), who were patients at the Veteran’s Medical Center in Philadelphia, PA. The sample was diverse: 56% self-identified as black or African American, 20% as white or Caucasian, 16% as Hispanic or Latina, and 8% as “other” or multiple race/ethnicity.
Interviews. Researchers conducted face-to-face interviews using a semi-structured interview guide to gather in-depth narratives related to the participants’ lives in the military and their experiences of IPV/SA. The Military Occupational Mental Health Model was used as a framework to understand the experience of IPV/SA within the cultural context of the military and how that context influences health and well-being. The model considers the unique context of the military, including the importance of the values of mission over individual well-being, hierarchy and subordination, leadership, and unit support, as well as what resources are made available.
Data analysis. The authors followed an inductive approach informed by grounded theory, with the goal of identifying themes and a unifying theory empirically grounded in the interview data. First, 2 members of the research team conducted independent, close readings of each transcript and applied open coding, then compared their coding to identify common patterns across transcripts. Through this process, they developed and refined a codebook to define a set of codes and guide application of codes to text. Research team members conducted line-by-line coding of each transcript, based on the codebook definitions. Then the authors read all coded text and met to discuss patterns within and between transcripts, leading to identification of 2 core categories pertaining to the relationship betweenIPV/SA and military service, as well as several subthemes within each core category.
Main results. The 2 core categories identified had both positive and negative influences. The first was the “experience of IPV/SA affects participation in military service, including entering and leaving military service,” and included the subthemes of coercion by the perpetrator to enter or leave military service, effects on service and work performance such as physical and mental health problems that interfered with their ability to do their job, and survival strategies that had negative repercussions on the woman’s career. The second was the “military context shapes responses to, and coping with, experiences of IPV/SA,” and included the subthemes of military sanction for IPV (but not sexual assault) if both partners were in the military, lack of accountability for and protection of service member perpetrators due to the value of unit support, military service as an opportunity to escape through relocation, even preferring a combat zone over home, and resistance to seeking help because of expectations of invulnerability related to the warrior identity.
Conclusion. The military context can provide personal and occupational resources for women who experience IPV/SA, but the institutional (ie, chain of command reporting) and cultural context can constrain women’s ability to access resources and support, negatively affecting outcomes.
Commentary
Intimate partner violence (IPV) is a widespread public health problem in the United States and women in the military are no exception. According to Black and Merrick [1], 36.3% of active duty women experienced sexual violence in their lifetime and 39.7% experienced IPV. Violence has significant health, economic, and social consequences for women in all settings, including serious short- and long-term physical and mental health problems, economic hardship, isolation, and decreased quality of life [2–5]. Women who experience IPV/SA in any setting face challenges in protecting themselves, overcoming violence, and seeking justice, however, the context in which the violence occurs can significantly influence the individual experiences of women. This study used a qualitative approach to understand how it is experienced by service women in the context of the military.
As the authors note, military culture can both facilitate and hamper women’s recovery from the physical, psychological, and economic sequelae of IPV/SA. The rigid hierarchal structure of the military and the expectation that one supports the unit and fellow soldiers above all else makes it very difficult for women to disclose IPV/SA and seek and receive protection and justice. On the other hand, military training and service provides women with the skills and means to be independent and to physically distance themselves from the perpetrator. However, the comment of one woman that facing bombs in Iraq was preferable to facing the violence at home should serve as a reminder of how devastating IPV/SA is and suggests that victims do not think there are effective institutional deterrents or protection available to them.
As the authors note, this was a small convenience sample of women at one VA medical center. This qualitative study provides a beginning understanding that should be expanded on with multisite quantitative research with large samples. Sexual assault in the military has been recognized as a significant problem, particularly for women but also for men. We need to continue to study this problem from many different perspectives to determine how to prevent violence and to ensure all victims get the resources and effective services they need.
Applications for Clinical Practice
This study has implications for all health care providers, as active duty and veteran service women seek care outside as well as within the VA. An important finding that has direct application to practice in all settings is the influence of the warrior identity. The warrior identity has been widely acknowledged as a barrier to seeking help for depression or PTSD in service men returning from combat but not as much in service women and not in the context of IPV/SA. It is important that providers consider warrior identity in assessing and treating women for IPV/SA. Not only can this affect disclosure and prevent a victim from seeking help, but the expectation that they should have been invulnerable and strong may increase feelings of self-blame and worsen psychological distress.
—Karen Roush, PhD, RN
1. Black MC, Merrick MT. Prevalence of intimate partner violence, sexual violence, and stalking among active duty women and wives of active duty men: Comparisons with women in the U.S. general population, 2010. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2013.
2. Bonomi AE, Anderson ML, Reid RJ, et al. Medical and psychosocial diagnoses in women with a history of intimate partner violence. Arch Intern Med 2009;169:1692–7.
3. Campbell J, Jones AS, Dienemann J, et al. Intimate partner violence and physical health consequences. Arch Intern Med 2002;162:1157–63.
4. Rees S, Silove D, Chey T, et al. Lifetime prevalence of gender-based violence in women and the relationship with mental disorders and psychosocial function. JAMA 2011;306:513–21.
5. Zlotnick C, Johnson DM, Kohn R. Intimate partner violence and long-term psychosocial functioning in a national sample of American women. J Interpers Violence 2006;21:
262–75.
Study Overview
Objective. To understand how the experience of intimate partner violence and non-partner sexual assault (IPV/SA) in women in the military intersects with military service.
Design. Qualitative interviews conducted as part of a larger study focused on experiences of IPV/SA and health care needs and preferences among women veteran patients.
Setting and participants. Participants were 25 women veterans from all branches of the service, ages 22 to 58 years (mean 44.6), who were patients at the Veteran’s Medical Center in Philadelphia, PA. The sample was diverse: 56% self-identified as black or African American, 20% as white or Caucasian, 16% as Hispanic or Latina, and 8% as “other” or multiple race/ethnicity.
Interviews. Researchers conducted face-to-face interviews using a semi-structured interview guide to gather in-depth narratives related to the participants’ lives in the military and their experiences of IPV/SA. The Military Occupational Mental Health Model was used as a framework to understand the experience of IPV/SA within the cultural context of the military and how that context influences health and well-being. The model considers the unique context of the military, including the importance of the values of mission over individual well-being, hierarchy and subordination, leadership, and unit support, as well as what resources are made available.
Data analysis. The authors followed an inductive approach informed by grounded theory, with the goal of identifying themes and a unifying theory empirically grounded in the interview data. First, 2 members of the research team conducted independent, close readings of each transcript and applied open coding, then compared their coding to identify common patterns across transcripts. Through this process, they developed and refined a codebook to define a set of codes and guide application of codes to text. Research team members conducted line-by-line coding of each transcript, based on the codebook definitions. Then the authors read all coded text and met to discuss patterns within and between transcripts, leading to identification of 2 core categories pertaining to the relationship betweenIPV/SA and military service, as well as several subthemes within each core category.
Main results. The 2 core categories identified had both positive and negative influences. The first was the “experience of IPV/SA affects participation in military service, including entering and leaving military service,” and included the subthemes of coercion by the perpetrator to enter or leave military service, effects on service and work performance such as physical and mental health problems that interfered with their ability to do their job, and survival strategies that had negative repercussions on the woman’s career. The second was the “military context shapes responses to, and coping with, experiences of IPV/SA,” and included the subthemes of military sanction for IPV (but not sexual assault) if both partners were in the military, lack of accountability for and protection of service member perpetrators due to the value of unit support, military service as an opportunity to escape through relocation, even preferring a combat zone over home, and resistance to seeking help because of expectations of invulnerability related to the warrior identity.
Conclusion. The military context can provide personal and occupational resources for women who experience IPV/SA, but the institutional (ie, chain of command reporting) and cultural context can constrain women’s ability to access resources and support, negatively affecting outcomes.
Commentary
Intimate partner violence (IPV) is a widespread public health problem in the United States and women in the military are no exception. According to Black and Merrick [1], 36.3% of active duty women experienced sexual violence in their lifetime and 39.7% experienced IPV. Violence has significant health, economic, and social consequences for women in all settings, including serious short- and long-term physical and mental health problems, economic hardship, isolation, and decreased quality of life [2–5]. Women who experience IPV/SA in any setting face challenges in protecting themselves, overcoming violence, and seeking justice, however, the context in which the violence occurs can significantly influence the individual experiences of women. This study used a qualitative approach to understand how it is experienced by service women in the context of the military.
As the authors note, military culture can both facilitate and hamper women’s recovery from the physical, psychological, and economic sequelae of IPV/SA. The rigid hierarchal structure of the military and the expectation that one supports the unit and fellow soldiers above all else makes it very difficult for women to disclose IPV/SA and seek and receive protection and justice. On the other hand, military training and service provides women with the skills and means to be independent and to physically distance themselves from the perpetrator. However, the comment of one woman that facing bombs in Iraq was preferable to facing the violence at home should serve as a reminder of how devastating IPV/SA is and suggests that victims do not think there are effective institutional deterrents or protection available to them.
As the authors note, this was a small convenience sample of women at one VA medical center. This qualitative study provides a beginning understanding that should be expanded on with multisite quantitative research with large samples. Sexual assault in the military has been recognized as a significant problem, particularly for women but also for men. We need to continue to study this problem from many different perspectives to determine how to prevent violence and to ensure all victims get the resources and effective services they need.
Applications for Clinical Practice
This study has implications for all health care providers, as active duty and veteran service women seek care outside as well as within the VA. An important finding that has direct application to practice in all settings is the influence of the warrior identity. The warrior identity has been widely acknowledged as a barrier to seeking help for depression or PTSD in service men returning from combat but not as much in service women and not in the context of IPV/SA. It is important that providers consider warrior identity in assessing and treating women for IPV/SA. Not only can this affect disclosure and prevent a victim from seeking help, but the expectation that they should have been invulnerable and strong may increase feelings of self-blame and worsen psychological distress.
—Karen Roush, PhD, RN
Study Overview
Objective. To understand how the experience of intimate partner violence and non-partner sexual assault (IPV/SA) in women in the military intersects with military service.
Design. Qualitative interviews conducted as part of a larger study focused on experiences of IPV/SA and health care needs and preferences among women veteran patients.
Setting and participants. Participants were 25 women veterans from all branches of the service, ages 22 to 58 years (mean 44.6), who were patients at the Veteran’s Medical Center in Philadelphia, PA. The sample was diverse: 56% self-identified as black or African American, 20% as white or Caucasian, 16% as Hispanic or Latina, and 8% as “other” or multiple race/ethnicity.
Interviews. Researchers conducted face-to-face interviews using a semi-structured interview guide to gather in-depth narratives related to the participants’ lives in the military and their experiences of IPV/SA. The Military Occupational Mental Health Model was used as a framework to understand the experience of IPV/SA within the cultural context of the military and how that context influences health and well-being. The model considers the unique context of the military, including the importance of the values of mission over individual well-being, hierarchy and subordination, leadership, and unit support, as well as what resources are made available.
Data analysis. The authors followed an inductive approach informed by grounded theory, with the goal of identifying themes and a unifying theory empirically grounded in the interview data. First, 2 members of the research team conducted independent, close readings of each transcript and applied open coding, then compared their coding to identify common patterns across transcripts. Through this process, they developed and refined a codebook to define a set of codes and guide application of codes to text. Research team members conducted line-by-line coding of each transcript, based on the codebook definitions. Then the authors read all coded text and met to discuss patterns within and between transcripts, leading to identification of 2 core categories pertaining to the relationship betweenIPV/SA and military service, as well as several subthemes within each core category.
Main results. The 2 core categories identified had both positive and negative influences. The first was the “experience of IPV/SA affects participation in military service, including entering and leaving military service,” and included the subthemes of coercion by the perpetrator to enter or leave military service, effects on service and work performance such as physical and mental health problems that interfered with their ability to do their job, and survival strategies that had negative repercussions on the woman’s career. The second was the “military context shapes responses to, and coping with, experiences of IPV/SA,” and included the subthemes of military sanction for IPV (but not sexual assault) if both partners were in the military, lack of accountability for and protection of service member perpetrators due to the value of unit support, military service as an opportunity to escape through relocation, even preferring a combat zone over home, and resistance to seeking help because of expectations of invulnerability related to the warrior identity.
Conclusion. The military context can provide personal and occupational resources for women who experience IPV/SA, but the institutional (ie, chain of command reporting) and cultural context can constrain women’s ability to access resources and support, negatively affecting outcomes.
Commentary
Intimate partner violence (IPV) is a widespread public health problem in the United States and women in the military are no exception. According to Black and Merrick [1], 36.3% of active duty women experienced sexual violence in their lifetime and 39.7% experienced IPV. Violence has significant health, economic, and social consequences for women in all settings, including serious short- and long-term physical and mental health problems, economic hardship, isolation, and decreased quality of life [2–5]. Women who experience IPV/SA in any setting face challenges in protecting themselves, overcoming violence, and seeking justice, however, the context in which the violence occurs can significantly influence the individual experiences of women. This study used a qualitative approach to understand how it is experienced by service women in the context of the military.
As the authors note, military culture can both facilitate and hamper women’s recovery from the physical, psychological, and economic sequelae of IPV/SA. The rigid hierarchal structure of the military and the expectation that one supports the unit and fellow soldiers above all else makes it very difficult for women to disclose IPV/SA and seek and receive protection and justice. On the other hand, military training and service provides women with the skills and means to be independent and to physically distance themselves from the perpetrator. However, the comment of one woman that facing bombs in Iraq was preferable to facing the violence at home should serve as a reminder of how devastating IPV/SA is and suggests that victims do not think there are effective institutional deterrents or protection available to them.
As the authors note, this was a small convenience sample of women at one VA medical center. This qualitative study provides a beginning understanding that should be expanded on with multisite quantitative research with large samples. Sexual assault in the military has been recognized as a significant problem, particularly for women but also for men. We need to continue to study this problem from many different perspectives to determine how to prevent violence and to ensure all victims get the resources and effective services they need.
Applications for Clinical Practice
This study has implications for all health care providers, as active duty and veteran service women seek care outside as well as within the VA. An important finding that has direct application to practice in all settings is the influence of the warrior identity. The warrior identity has been widely acknowledged as a barrier to seeking help for depression or PTSD in service men returning from combat but not as much in service women and not in the context of IPV/SA. It is important that providers consider warrior identity in assessing and treating women for IPV/SA. Not only can this affect disclosure and prevent a victim from seeking help, but the expectation that they should have been invulnerable and strong may increase feelings of self-blame and worsen psychological distress.
—Karen Roush, PhD, RN
1. Black MC, Merrick MT. Prevalence of intimate partner violence, sexual violence, and stalking among active duty women and wives of active duty men: Comparisons with women in the U.S. general population, 2010. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2013.
2. Bonomi AE, Anderson ML, Reid RJ, et al. Medical and psychosocial diagnoses in women with a history of intimate partner violence. Arch Intern Med 2009;169:1692–7.
3. Campbell J, Jones AS, Dienemann J, et al. Intimate partner violence and physical health consequences. Arch Intern Med 2002;162:1157–63.
4. Rees S, Silove D, Chey T, et al. Lifetime prevalence of gender-based violence in women and the relationship with mental disorders and psychosocial function. JAMA 2011;306:513–21.
5. Zlotnick C, Johnson DM, Kohn R. Intimate partner violence and long-term psychosocial functioning in a national sample of American women. J Interpers Violence 2006;21:
262–75.
1. Black MC, Merrick MT. Prevalence of intimate partner violence, sexual violence, and stalking among active duty women and wives of active duty men: Comparisons with women in the U.S. general population, 2010. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2013.
2. Bonomi AE, Anderson ML, Reid RJ, et al. Medical and psychosocial diagnoses in women with a history of intimate partner violence. Arch Intern Med 2009;169:1692–7.
3. Campbell J, Jones AS, Dienemann J, et al. Intimate partner violence and physical health consequences. Arch Intern Med 2002;162:1157–63.
4. Rees S, Silove D, Chey T, et al. Lifetime prevalence of gender-based violence in women and the relationship with mental disorders and psychosocial function. JAMA 2011;306:513–21.
5. Zlotnick C, Johnson DM, Kohn R. Intimate partner violence and long-term psychosocial functioning in a national sample of American women. J Interpers Violence 2006;21:
262–75.
A Mobile Health App for Weight Loss that Incorporates Social Networking
Study Overview
Objective. To test the efficacy of a weight loss app with incorporated social support and self-monitoring of diet, physical activity, and weight compared to a commercially available diet and PA tracking app.
Design. 2-group, randomized controlled trial.
Setting and participants. From October 2014 to January 2015, potential study participants were recruited via university/worksite listserv announcements, flyers, electronic newsletters, newspaper advertisements, social media posts, and a local research fair in 2 cities in South Carolina. Exclusion criteria included body mass index (BMI) outside the range of 25.0 to 49.9 kg/m2, unable to attend required measurement sessions, unable to access a computer or internet for completing assessments, having a psychiatric illness, receiving treatment for drug or alcohol dependency, having an eating disorder, participating in another weight loss program, reporting weight loss of 10+ pounds in the past 6 months, being pregnant or planning on becoming pregnant during study, or breastfeeding, or endorsing items on the Physical Activity Readiness Questionnaire (PAR-Q) regarding having a heart condition, feeling chest pain during physical activity, experiencing chest pain, becoming dizzy/ever losing balance or consciousness, and not having a physician give consent to participate despite reporting joint problems or taking blood pressure medication. Those who were eligible were invited to an orientation to the study, signed consent, and completed baseline assessments.
Intervention. Participants were randomized to either the experimental group (theory-based podcasts plus the Social POD app) or the comparison group (theory-based podcasts plus a standard app [“Fat Secret” app]). Both groups attended a training session on how to access the podcasts and download and use their app, and also had their baseline height and weight taken by study staff. Both groups received 2 podcasts per week, tracked their diet, weight, and physical activity, completed weekly surveys to report use of their assigned tracking app, and had their weight measures taken after 3 months. Objective measures of podcast usage and app usage were collected by study staff (experimental group only).
Both apps had diet and physical activity tracking features, but the Social POD app also included notifications to track diet and physical activity, messages sent from frequent app users to re-engage infrequent app users, a newsfeed to view other participants app tracking activity, stars awarded to frequent users of the app, points awarded for tracking, and prizes for earning points distributed at the final session by study staff. The Fat Secret app did not have any social support components but included a recipe database for looking up recipes by category.
Main outcome measures. The primary outcome was between-group differences in kilograms lost at 3 months. Secondary outcomes included group change in BMI after 3 months, as well as group differences in self-reported caloric intake, caloric expenditure, social support, self-efficacy, and outcome expectations scores, controlled for baseline measures.
Main results. Of the potential participants that inquired about the study (n = 189), those found to be eligible (n = 78) were invited to an orientation. Of those that attended the orientation (n = 62), 51 were randomized after completing baseline assessments (n = 25 to experimental group with Social POD app, n = 25 to comparison group with Fat Secret app), and 42 completed final weight measurements after 3 months. Participants were mostly white (57%) females (82%) with a mean BMI of 34.7 ± 6.0 kg/m2 and mean age of 46.2 ± 12.4 years. Baseline characteristics were similar between groups except that more comparison group participants reported previously downloading an app to track their diet than experimental participants. Participation attrition was 12% (n = 3 in each group).
Experimental group participants lost significantly more weight (–5.3 kg [95% CI, –7.5 to –3.0]) than the comparison group (–2.23 kg [95% CI, –3.6 to 1.0; P = 0.02). Experimental group participants also had a greater reduction in mean BMI (–1.9 kg/m2 [95% CI, –2.6 to –1.2]) vs. the comparison group (mean –0.9 kg/m2 [95% CI, –1.4 to – 0.05], P = 0.02). While there were significant differences in positive outcome expectations between groups (P = 0.04), other secondary outcomes were not significant.
Conclusions. An intervention with theory-based podcasts, social support, and incentivized self-monitoring resulted in significantly greater weight loss than a comparison intervention with theory-based podcasts and a commercially available standard self-monitoring app. This study highlights key features to add to mobile health interventions for adult weight loss.
Commentary
Obesity prevalence rates have increased over the past several decades across all genders, ages, ethnicities, income levels, and education levels [1], and recent data show that over one-third of adults in the US are obese and over two-thirds are overweight [2,3]. Behavior or lifestyle modification, which incorporates (often tailored) diet, physical activity, and behavior therapy, is highly recommended as the first strategy for losing initial weight and sustaining weight management efforts [4,5]. Mobile health (mHealth) technologies and other web-based and technology-assisted approaches (eg, mobile applications or “apps”) to facilitate behavior change for weight loss and management have aimed to address many of the limitations posed by traditional face-to-face weight loss approaches [6–8]. Prevailing theories of health behavior change imply key intervention design features that may increase their likelihood of promoting and sustaining desired behavior changes, particularly those that impact self-efficacy, self-regulation, and social facilitation [9,10].
Despite the plethora of weight loss mobile apps available to the public, it remains unclear if these are guided by evidence-based behavior change strategies typically used in traditional programs and approaches [11,12]. Further, very few of these apps have been rigorously evaluated with scientific testing to determine true effectiveness and safety [13,14]. This study adds to the literature by evaluating a mobile app for weight loss (Social POD) that was developed by researchers and utilizes theory-based components to target specific constructs that lead to health behavior change. Additionally, while self-monitoring is commonly incorporated into most available weight loss/management apps [11], the Social POD mobile app also incorporates social support and motivational strategies, which are less often included. The findings from this study add to the limited literature that mobile phone app-based interventions may be useful tools for weight loss [13].
The authors outlined several strengths and limitations. Briefly, this study was particularly strengthened by its randomized assignment to equivalent intervention groups, the use of a researcher-developed experimental group app that targets several key theory-based constructs for behavior change, measurement of objective use of the intervention group app, a racially diverse sample (over one-third of participants in both groups identified as black), measurement of secondary psycho-social behavioral outcomes, significant efforts to ensure survey completion and compliance with the intervention (increase retention), as well efforts to decrease participation burden by limiting required in-person sessions.
However, several important aspects of the study limit the internal validity and generalizability of its findings. The study had a small sample size and included a highly educated study population. If possible, future studies should consider including a large, diverse population to enhance generalizability. Also, this study was limited to those with an Android device, and significant demographic differences between Android and iPhone users have been reported [15]. The comparison group reported significantly more prior downloading of a diet-tracking app compared to the experimental group, which may have impacted use of the comparison app. The extrinsic reward system built into the experimental group intervention could have impacted adherence to experimental app, and is likely not feasible in real-world application of the experimental group app. Findings may have been subject to recall bias and measurement error due to self-reporting of outcomes measures. Importantly, this was a short-term weight loss study, and long-term weight loss/maintenance data is needed to support findings since in the usual course of weight-loss therapy the greatest weight loss occurs within 6 months of treatment, after which weight is often regained, sometimes near original level [16].
Applications for Clinical Practice
With the increasing popularity of technology-assisted and mHealth applications for weight loss and other health behaviors, it is important for practitioners to be familiar with proven, theory-based approaches and advise patients accordingly. This study demonstrated that social support components added to self-monitoring components in a weight loss app can lead to significant weight loss compared to self-monitoring alone. Thus, those that offer obesity counseling should be mindful that tracking and controlling dietary and physical activity behaviors alone may not prove to be successful. Opportunities for social facilitation to support weight loss efforts should be discussed with patients, including sources of social influence, support and collaboration between individuals, families, and health care professionals.
—Katrina F. Mateo, MPH
1. Mitchell NS, Catenacci VA, Wyatt HR, Hill JO. Obesity: overview of an epidemic. Psychiatr Clin North Am 2011;34:717–32.
2. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303:235–41.
3. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14.
4. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology 2007;132:2226–38.
5. Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psychiatr Clin North Am 2011;34:841–59.
6. Okorodudu DE, Bosworth HB, Corsino L. Innovative interventions to promote behavioral change in overweight or obese individuals: a review of the literature. Ann Med 2015;47:179–85.
7. Taylor RW, Roy M, Jospe MR, et al. Determining how best to support overweight adults to adhere to lifestyle change: protocol for the SWIFT study. BMC Public Health 2015;15:861.
8. Laing BY, Mangione CM, Tseng C-H, et al. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: a randomized, controlled trial. Ann Intern Med 2014;161(10 Suppl):
S5–S12.
9. Teixeira PJ, Carraça E V, Marques MM, et al. Successful behavior change in obesity interventions in adults: a systematic review of self-regulation mediators. BMC Med 2015;13:84.
10. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec 2009;23:161–70.
11. Rivera J, McPherson A, Hamilton J, et al. Mobile apps for weight management: a scoping review. JMIR mHealth uHealth 2016;4:e87.
12. Pellegrini CA, Pfammatter AF, Conroy DE, Spring B. Smartphone applications to support weight loss: current perspectives. Adv Health Care Technol 2015;1:13–22.
13. Flores Mateo G, Granado-Font E, Ferré-Grau C, Montaña-Carreras X. Mobile phone apps to promote weight loss and increase physical activity: a systematic review and meta-analysis. J Med Internet Res 2015;17:e253.
14. Stephens J, Allen J. Mobile phone interventions to increase physical activity and reduce weight: a systematic review. J Cardiovasc Nurs 28:320–9.
15. Smith A. Smartphone ownership 2013. Pew Research Center.
16. Jeffery RW, Drewnowski A, Epstein LH, et al. Long-term maintenance of weight loss: current status. Health Psychol 2000;19(1 Suppl):5–16.
Study Overview
Objective. To test the efficacy of a weight loss app with incorporated social support and self-monitoring of diet, physical activity, and weight compared to a commercially available diet and PA tracking app.
Design. 2-group, randomized controlled trial.
Setting and participants. From October 2014 to January 2015, potential study participants were recruited via university/worksite listserv announcements, flyers, electronic newsletters, newspaper advertisements, social media posts, and a local research fair in 2 cities in South Carolina. Exclusion criteria included body mass index (BMI) outside the range of 25.0 to 49.9 kg/m2, unable to attend required measurement sessions, unable to access a computer or internet for completing assessments, having a psychiatric illness, receiving treatment for drug or alcohol dependency, having an eating disorder, participating in another weight loss program, reporting weight loss of 10+ pounds in the past 6 months, being pregnant or planning on becoming pregnant during study, or breastfeeding, or endorsing items on the Physical Activity Readiness Questionnaire (PAR-Q) regarding having a heart condition, feeling chest pain during physical activity, experiencing chest pain, becoming dizzy/ever losing balance or consciousness, and not having a physician give consent to participate despite reporting joint problems or taking blood pressure medication. Those who were eligible were invited to an orientation to the study, signed consent, and completed baseline assessments.
Intervention. Participants were randomized to either the experimental group (theory-based podcasts plus the Social POD app) or the comparison group (theory-based podcasts plus a standard app [“Fat Secret” app]). Both groups attended a training session on how to access the podcasts and download and use their app, and also had their baseline height and weight taken by study staff. Both groups received 2 podcasts per week, tracked their diet, weight, and physical activity, completed weekly surveys to report use of their assigned tracking app, and had their weight measures taken after 3 months. Objective measures of podcast usage and app usage were collected by study staff (experimental group only).
Both apps had diet and physical activity tracking features, but the Social POD app also included notifications to track diet and physical activity, messages sent from frequent app users to re-engage infrequent app users, a newsfeed to view other participants app tracking activity, stars awarded to frequent users of the app, points awarded for tracking, and prizes for earning points distributed at the final session by study staff. The Fat Secret app did not have any social support components but included a recipe database for looking up recipes by category.
Main outcome measures. The primary outcome was between-group differences in kilograms lost at 3 months. Secondary outcomes included group change in BMI after 3 months, as well as group differences in self-reported caloric intake, caloric expenditure, social support, self-efficacy, and outcome expectations scores, controlled for baseline measures.
Main results. Of the potential participants that inquired about the study (n = 189), those found to be eligible (n = 78) were invited to an orientation. Of those that attended the orientation (n = 62), 51 were randomized after completing baseline assessments (n = 25 to experimental group with Social POD app, n = 25 to comparison group with Fat Secret app), and 42 completed final weight measurements after 3 months. Participants were mostly white (57%) females (82%) with a mean BMI of 34.7 ± 6.0 kg/m2 and mean age of 46.2 ± 12.4 years. Baseline characteristics were similar between groups except that more comparison group participants reported previously downloading an app to track their diet than experimental participants. Participation attrition was 12% (n = 3 in each group).
Experimental group participants lost significantly more weight (–5.3 kg [95% CI, –7.5 to –3.0]) than the comparison group (–2.23 kg [95% CI, –3.6 to 1.0; P = 0.02). Experimental group participants also had a greater reduction in mean BMI (–1.9 kg/m2 [95% CI, –2.6 to –1.2]) vs. the comparison group (mean –0.9 kg/m2 [95% CI, –1.4 to – 0.05], P = 0.02). While there were significant differences in positive outcome expectations between groups (P = 0.04), other secondary outcomes were not significant.
Conclusions. An intervention with theory-based podcasts, social support, and incentivized self-monitoring resulted in significantly greater weight loss than a comparison intervention with theory-based podcasts and a commercially available standard self-monitoring app. This study highlights key features to add to mobile health interventions for adult weight loss.
Commentary
Obesity prevalence rates have increased over the past several decades across all genders, ages, ethnicities, income levels, and education levels [1], and recent data show that over one-third of adults in the US are obese and over two-thirds are overweight [2,3]. Behavior or lifestyle modification, which incorporates (often tailored) diet, physical activity, and behavior therapy, is highly recommended as the first strategy for losing initial weight and sustaining weight management efforts [4,5]. Mobile health (mHealth) technologies and other web-based and technology-assisted approaches (eg, mobile applications or “apps”) to facilitate behavior change for weight loss and management have aimed to address many of the limitations posed by traditional face-to-face weight loss approaches [6–8]. Prevailing theories of health behavior change imply key intervention design features that may increase their likelihood of promoting and sustaining desired behavior changes, particularly those that impact self-efficacy, self-regulation, and social facilitation [9,10].
Despite the plethora of weight loss mobile apps available to the public, it remains unclear if these are guided by evidence-based behavior change strategies typically used in traditional programs and approaches [11,12]. Further, very few of these apps have been rigorously evaluated with scientific testing to determine true effectiveness and safety [13,14]. This study adds to the literature by evaluating a mobile app for weight loss (Social POD) that was developed by researchers and utilizes theory-based components to target specific constructs that lead to health behavior change. Additionally, while self-monitoring is commonly incorporated into most available weight loss/management apps [11], the Social POD mobile app also incorporates social support and motivational strategies, which are less often included. The findings from this study add to the limited literature that mobile phone app-based interventions may be useful tools for weight loss [13].
The authors outlined several strengths and limitations. Briefly, this study was particularly strengthened by its randomized assignment to equivalent intervention groups, the use of a researcher-developed experimental group app that targets several key theory-based constructs for behavior change, measurement of objective use of the intervention group app, a racially diverse sample (over one-third of participants in both groups identified as black), measurement of secondary psycho-social behavioral outcomes, significant efforts to ensure survey completion and compliance with the intervention (increase retention), as well efforts to decrease participation burden by limiting required in-person sessions.
However, several important aspects of the study limit the internal validity and generalizability of its findings. The study had a small sample size and included a highly educated study population. If possible, future studies should consider including a large, diverse population to enhance generalizability. Also, this study was limited to those with an Android device, and significant demographic differences between Android and iPhone users have been reported [15]. The comparison group reported significantly more prior downloading of a diet-tracking app compared to the experimental group, which may have impacted use of the comparison app. The extrinsic reward system built into the experimental group intervention could have impacted adherence to experimental app, and is likely not feasible in real-world application of the experimental group app. Findings may have been subject to recall bias and measurement error due to self-reporting of outcomes measures. Importantly, this was a short-term weight loss study, and long-term weight loss/maintenance data is needed to support findings since in the usual course of weight-loss therapy the greatest weight loss occurs within 6 months of treatment, after which weight is often regained, sometimes near original level [16].
Applications for Clinical Practice
With the increasing popularity of technology-assisted and mHealth applications for weight loss and other health behaviors, it is important for practitioners to be familiar with proven, theory-based approaches and advise patients accordingly. This study demonstrated that social support components added to self-monitoring components in a weight loss app can lead to significant weight loss compared to self-monitoring alone. Thus, those that offer obesity counseling should be mindful that tracking and controlling dietary and physical activity behaviors alone may not prove to be successful. Opportunities for social facilitation to support weight loss efforts should be discussed with patients, including sources of social influence, support and collaboration between individuals, families, and health care professionals.
—Katrina F. Mateo, MPH
Study Overview
Objective. To test the efficacy of a weight loss app with incorporated social support and self-monitoring of diet, physical activity, and weight compared to a commercially available diet and PA tracking app.
Design. 2-group, randomized controlled trial.
Setting and participants. From October 2014 to January 2015, potential study participants were recruited via university/worksite listserv announcements, flyers, electronic newsletters, newspaper advertisements, social media posts, and a local research fair in 2 cities in South Carolina. Exclusion criteria included body mass index (BMI) outside the range of 25.0 to 49.9 kg/m2, unable to attend required measurement sessions, unable to access a computer or internet for completing assessments, having a psychiatric illness, receiving treatment for drug or alcohol dependency, having an eating disorder, participating in another weight loss program, reporting weight loss of 10+ pounds in the past 6 months, being pregnant or planning on becoming pregnant during study, or breastfeeding, or endorsing items on the Physical Activity Readiness Questionnaire (PAR-Q) regarding having a heart condition, feeling chest pain during physical activity, experiencing chest pain, becoming dizzy/ever losing balance or consciousness, and not having a physician give consent to participate despite reporting joint problems or taking blood pressure medication. Those who were eligible were invited to an orientation to the study, signed consent, and completed baseline assessments.
Intervention. Participants were randomized to either the experimental group (theory-based podcasts plus the Social POD app) or the comparison group (theory-based podcasts plus a standard app [“Fat Secret” app]). Both groups attended a training session on how to access the podcasts and download and use their app, and also had their baseline height and weight taken by study staff. Both groups received 2 podcasts per week, tracked their diet, weight, and physical activity, completed weekly surveys to report use of their assigned tracking app, and had their weight measures taken after 3 months. Objective measures of podcast usage and app usage were collected by study staff (experimental group only).
Both apps had diet and physical activity tracking features, but the Social POD app also included notifications to track diet and physical activity, messages sent from frequent app users to re-engage infrequent app users, a newsfeed to view other participants app tracking activity, stars awarded to frequent users of the app, points awarded for tracking, and prizes for earning points distributed at the final session by study staff. The Fat Secret app did not have any social support components but included a recipe database for looking up recipes by category.
Main outcome measures. The primary outcome was between-group differences in kilograms lost at 3 months. Secondary outcomes included group change in BMI after 3 months, as well as group differences in self-reported caloric intake, caloric expenditure, social support, self-efficacy, and outcome expectations scores, controlled for baseline measures.
Main results. Of the potential participants that inquired about the study (n = 189), those found to be eligible (n = 78) were invited to an orientation. Of those that attended the orientation (n = 62), 51 were randomized after completing baseline assessments (n = 25 to experimental group with Social POD app, n = 25 to comparison group with Fat Secret app), and 42 completed final weight measurements after 3 months. Participants were mostly white (57%) females (82%) with a mean BMI of 34.7 ± 6.0 kg/m2 and mean age of 46.2 ± 12.4 years. Baseline characteristics were similar between groups except that more comparison group participants reported previously downloading an app to track their diet than experimental participants. Participation attrition was 12% (n = 3 in each group).
Experimental group participants lost significantly more weight (–5.3 kg [95% CI, –7.5 to –3.0]) than the comparison group (–2.23 kg [95% CI, –3.6 to 1.0; P = 0.02). Experimental group participants also had a greater reduction in mean BMI (–1.9 kg/m2 [95% CI, –2.6 to –1.2]) vs. the comparison group (mean –0.9 kg/m2 [95% CI, –1.4 to – 0.05], P = 0.02). While there were significant differences in positive outcome expectations between groups (P = 0.04), other secondary outcomes were not significant.
Conclusions. An intervention with theory-based podcasts, social support, and incentivized self-monitoring resulted in significantly greater weight loss than a comparison intervention with theory-based podcasts and a commercially available standard self-monitoring app. This study highlights key features to add to mobile health interventions for adult weight loss.
Commentary
Obesity prevalence rates have increased over the past several decades across all genders, ages, ethnicities, income levels, and education levels [1], and recent data show that over one-third of adults in the US are obese and over two-thirds are overweight [2,3]. Behavior or lifestyle modification, which incorporates (often tailored) diet, physical activity, and behavior therapy, is highly recommended as the first strategy for losing initial weight and sustaining weight management efforts [4,5]. Mobile health (mHealth) technologies and other web-based and technology-assisted approaches (eg, mobile applications or “apps”) to facilitate behavior change for weight loss and management have aimed to address many of the limitations posed by traditional face-to-face weight loss approaches [6–8]. Prevailing theories of health behavior change imply key intervention design features that may increase their likelihood of promoting and sustaining desired behavior changes, particularly those that impact self-efficacy, self-regulation, and social facilitation [9,10].
Despite the plethora of weight loss mobile apps available to the public, it remains unclear if these are guided by evidence-based behavior change strategies typically used in traditional programs and approaches [11,12]. Further, very few of these apps have been rigorously evaluated with scientific testing to determine true effectiveness and safety [13,14]. This study adds to the literature by evaluating a mobile app for weight loss (Social POD) that was developed by researchers and utilizes theory-based components to target specific constructs that lead to health behavior change. Additionally, while self-monitoring is commonly incorporated into most available weight loss/management apps [11], the Social POD mobile app also incorporates social support and motivational strategies, which are less often included. The findings from this study add to the limited literature that mobile phone app-based interventions may be useful tools for weight loss [13].
The authors outlined several strengths and limitations. Briefly, this study was particularly strengthened by its randomized assignment to equivalent intervention groups, the use of a researcher-developed experimental group app that targets several key theory-based constructs for behavior change, measurement of objective use of the intervention group app, a racially diverse sample (over one-third of participants in both groups identified as black), measurement of secondary psycho-social behavioral outcomes, significant efforts to ensure survey completion and compliance with the intervention (increase retention), as well efforts to decrease participation burden by limiting required in-person sessions.
However, several important aspects of the study limit the internal validity and generalizability of its findings. The study had a small sample size and included a highly educated study population. If possible, future studies should consider including a large, diverse population to enhance generalizability. Also, this study was limited to those with an Android device, and significant demographic differences between Android and iPhone users have been reported [15]. The comparison group reported significantly more prior downloading of a diet-tracking app compared to the experimental group, which may have impacted use of the comparison app. The extrinsic reward system built into the experimental group intervention could have impacted adherence to experimental app, and is likely not feasible in real-world application of the experimental group app. Findings may have been subject to recall bias and measurement error due to self-reporting of outcomes measures. Importantly, this was a short-term weight loss study, and long-term weight loss/maintenance data is needed to support findings since in the usual course of weight-loss therapy the greatest weight loss occurs within 6 months of treatment, after which weight is often regained, sometimes near original level [16].
Applications for Clinical Practice
With the increasing popularity of technology-assisted and mHealth applications for weight loss and other health behaviors, it is important for practitioners to be familiar with proven, theory-based approaches and advise patients accordingly. This study demonstrated that social support components added to self-monitoring components in a weight loss app can lead to significant weight loss compared to self-monitoring alone. Thus, those that offer obesity counseling should be mindful that tracking and controlling dietary and physical activity behaviors alone may not prove to be successful. Opportunities for social facilitation to support weight loss efforts should be discussed with patients, including sources of social influence, support and collaboration between individuals, families, and health care professionals.
—Katrina F. Mateo, MPH
1. Mitchell NS, Catenacci VA, Wyatt HR, Hill JO. Obesity: overview of an epidemic. Psychiatr Clin North Am 2011;34:717–32.
2. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303:235–41.
3. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14.
4. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology 2007;132:2226–38.
5. Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psychiatr Clin North Am 2011;34:841–59.
6. Okorodudu DE, Bosworth HB, Corsino L. Innovative interventions to promote behavioral change in overweight or obese individuals: a review of the literature. Ann Med 2015;47:179–85.
7. Taylor RW, Roy M, Jospe MR, et al. Determining how best to support overweight adults to adhere to lifestyle change: protocol for the SWIFT study. BMC Public Health 2015;15:861.
8. Laing BY, Mangione CM, Tseng C-H, et al. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: a randomized, controlled trial. Ann Intern Med 2014;161(10 Suppl):
S5–S12.
9. Teixeira PJ, Carraça E V, Marques MM, et al. Successful behavior change in obesity interventions in adults: a systematic review of self-regulation mediators. BMC Med 2015;13:84.
10. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec 2009;23:161–70.
11. Rivera J, McPherson A, Hamilton J, et al. Mobile apps for weight management: a scoping review. JMIR mHealth uHealth 2016;4:e87.
12. Pellegrini CA, Pfammatter AF, Conroy DE, Spring B. Smartphone applications to support weight loss: current perspectives. Adv Health Care Technol 2015;1:13–22.
13. Flores Mateo G, Granado-Font E, Ferré-Grau C, Montaña-Carreras X. Mobile phone apps to promote weight loss and increase physical activity: a systematic review and meta-analysis. J Med Internet Res 2015;17:e253.
14. Stephens J, Allen J. Mobile phone interventions to increase physical activity and reduce weight: a systematic review. J Cardiovasc Nurs 28:320–9.
15. Smith A. Smartphone ownership 2013. Pew Research Center.
16. Jeffery RW, Drewnowski A, Epstein LH, et al. Long-term maintenance of weight loss: current status. Health Psychol 2000;19(1 Suppl):5–16.
1. Mitchell NS, Catenacci VA, Wyatt HR, Hill JO. Obesity: overview of an epidemic. Psychiatr Clin North Am 2011;34:717–32.
2. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303:235–41.
3. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14.
4. Wadden TA, Butryn ML, Wilson C. Lifestyle modification for the management of obesity. Gastroenterology 2007;132:2226–38.
5. Butryn ML, Webb V, Wadden TA. Behavioral treatment of obesity. Psychiatr Clin North Am 2011;34:841–59.
6. Okorodudu DE, Bosworth HB, Corsino L. Innovative interventions to promote behavioral change in overweight or obese individuals: a review of the literature. Ann Med 2015;47:179–85.
7. Taylor RW, Roy M, Jospe MR, et al. Determining how best to support overweight adults to adhere to lifestyle change: protocol for the SWIFT study. BMC Public Health 2015;15:861.
8. Laing BY, Mangione CM, Tseng C-H, et al. Effectiveness of a smartphone application for weight loss compared with usual care in overweight primary care patients: a randomized, controlled trial. Ann Intern Med 2014;161(10 Suppl):
S5–S12.
9. Teixeira PJ, Carraça E V, Marques MM, et al. Successful behavior change in obesity interventions in adults: a systematic review of self-regulation mediators. BMC Med 2015;13:84.
10. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec 2009;23:161–70.
11. Rivera J, McPherson A, Hamilton J, et al. Mobile apps for weight management: a scoping review. JMIR mHealth uHealth 2016;4:e87.
12. Pellegrini CA, Pfammatter AF, Conroy DE, Spring B. Smartphone applications to support weight loss: current perspectives. Adv Health Care Technol 2015;1:13–22.
13. Flores Mateo G, Granado-Font E, Ferré-Grau C, Montaña-Carreras X. Mobile phone apps to promote weight loss and increase physical activity: a systematic review and meta-analysis. J Med Internet Res 2015;17:e253.
14. Stephens J, Allen J. Mobile phone interventions to increase physical activity and reduce weight: a systematic review. J Cardiovasc Nurs 28:320–9.
15. Smith A. Smartphone ownership 2013. Pew Research Center.
16. Jeffery RW, Drewnowski A, Epstein LH, et al. Long-term maintenance of weight loss: current status. Health Psychol 2000;19(1 Suppl):5–16.
Hypotension Prevalence Among Treated Hypertensive Patients
Study Overview
Objective. To determine the prevalence of hypotension using both clinic and ambulatory blood pressure monitoring (ABPM) in treated hypertensive patients and the factors associated with its presence.
Design. Registry-based study.
Setting and participants. Researchers studied patients in the Spanish Society of Hypertension ABPM Registry, which was established to evaluate the utility of the wider use of ABPM with the distribution of >1000 ambulatory BP monitors for routine use by primary care physicians and physicians from specialist units across Spain. The registry continues to expand since the first patient was recruited in June 2004. In June 2015, a total of 135,500 hypertensive patients were in the registry.
Measurements. Blood pressure readings in the clinic were taken according to current recommendations, with the patients in a seated position and their backs supported, after a 5-minute rest, using calibrated sphygmomanometers or validated automatic devices. The visit BP was the average of 2 separate readings. Validated devices (Spacelabs) were used for ABPM, which was performed during a working day with measurements taken every 30 minutes. Patients were told to keep their activity normal and to extend the arm without any movement during BP measurements. ABPM was considered successful in ≥ 80% systolic and diastolic BP valid readings. Patients were classified into 3 categories: hypotension, adequate BP control, or poor BP control for each type of blood pressure (office, daytime, nighttime, and 24-hour). The definitions for hypotension for each BP type were mainly based of the PROVE IT-TIMI study, ie, < 110 and/or 70 mm Hg for office, < 105 and/or 65 mm Hg for daytime ABPM, < 90 and or 50 mm Hg for nightime ABPM, and < 100 and/or 60 mm Hg for 24-hr ABPM.
Results. Of the 135,500 patients in the registry, only data from treated hypertensive patients were analyzed (n = 70,997). Mean age was 61.8 ± 12.8 years and 52.5% were men. The prevalence of hypotension was 8.2% with office BP, 12.2% with daytime ABPM, 3.9% with nightime ABPM, and 6.8% with 24-hour ABPM. Low diastolic BP values were responsible for the majority of hypotension. More than 68% of patients with hypotension detected with ABPM did not have hypotension according to office BP. Patients with hypotension were older, more likely to be female, and more likely to have high pulse pressue, lower heart rate, ischemic heart disease, and renal insufficiency. They were also more likely to be taking 3 or more drugs for hypertension.
Conclusion. The prevalence of hypotension is relatively high in treated hypertensive patients, and two-thirds are not identified with office BP measurement. Prevalence was higher in patients who were very elderly or with coronary or renal disease.
Commentary
Hypertension is a major public health concern worldwide [1]. In 2011–12 among US adults with hypertension, only 51.9% had their blood pressure controlled [2]. High blood pressure can effectively be reduced with antihypertensive treatment, and efforts are needed to improve clinical management of hypertension. However, excessive BP reduction may lead to patient harm.
In this study, researchers aimed to determine the prevalence of hypotension using both clinic and ABPM in hypertensive-treated patients and the factors associated with its presence, using descriptive statistics and multivariate analysis. The results highlight the need for health care providers to be aware of the individual response to antihypertensives in patients with high blood pressure and to individualize treatment to avoid complications of hypotension. A strength of this study was it large sample size.
Adherence to treatment recommendations was not a variable taken into consideration for this study and could be considered a confounder. Diet and behavioral interventions can have a significantly beneficial effect on hypertension and can reduce the need for drug therapy [3]. If patients were highly engaged and adopted lifestyle habits that can contribute to better blood pressure levels along with taking prescribed medications, this could have contributed to levels of hypotension.
Hypotension among hypertensive patients can be difficult to identify during clinical consultations due the “white coat effect.” This syndrome is characterized by a peak of high blood pressure caused by the stress of the individual in the presence of a healthcare provider or in a stressful medical environment [4]. This study showed that more than half of the patients in the sample with detected hypotension in the ABPM did not show hypotension during consultation at the medical office. This finding highlights the challenge in identifying hypotension and making adjustments to antihypertensive medication regimens as needed.
Women, patients with low body weight, and elderly patients were the groups more likely to develop hypo-tension. Thus, strategies specifically targeting these vulnerable groups are required. As suggested by the authors of this study, further longitudinal research is needed in order to identify gaps in the state of science in regards this topic and changes in the prevalence this population. The replication of this study in different populations is also encouraged.
Applications for Clinical Practice
The prevalence of hypotension is relatively high and may not be detected during office BP measurement. In patients with a higher risk of hypotension, such as the elderly those with cardiovascular disease, the use of ABPM should be considered.
—Paloma Cesar de Sales, BS, RN, MS
1. Kantachuvessiri A. Hypertension in public health. Southeast Asian J Trop Med Public Health 2002;33:425–31.
2. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief 2013;1–8.
3. Nicoll R, Henein MY. Hypertension and lifestyle modification: how useful are the guidelines? Br J Gen Pract 2010; 60:879–80.
4. Celis H, Fagard RH. White-coat hypertension: a clinical review. Eur J Intern Med 2004;15:348–57.
Study Overview
Objective. To determine the prevalence of hypotension using both clinic and ambulatory blood pressure monitoring (ABPM) in treated hypertensive patients and the factors associated with its presence.
Design. Registry-based study.
Setting and participants. Researchers studied patients in the Spanish Society of Hypertension ABPM Registry, which was established to evaluate the utility of the wider use of ABPM with the distribution of >1000 ambulatory BP monitors for routine use by primary care physicians and physicians from specialist units across Spain. The registry continues to expand since the first patient was recruited in June 2004. In June 2015, a total of 135,500 hypertensive patients were in the registry.
Measurements. Blood pressure readings in the clinic were taken according to current recommendations, with the patients in a seated position and their backs supported, after a 5-minute rest, using calibrated sphygmomanometers or validated automatic devices. The visit BP was the average of 2 separate readings. Validated devices (Spacelabs) were used for ABPM, which was performed during a working day with measurements taken every 30 minutes. Patients were told to keep their activity normal and to extend the arm without any movement during BP measurements. ABPM was considered successful in ≥ 80% systolic and diastolic BP valid readings. Patients were classified into 3 categories: hypotension, adequate BP control, or poor BP control for each type of blood pressure (office, daytime, nighttime, and 24-hour). The definitions for hypotension for each BP type were mainly based of the PROVE IT-TIMI study, ie, < 110 and/or 70 mm Hg for office, < 105 and/or 65 mm Hg for daytime ABPM, < 90 and or 50 mm Hg for nightime ABPM, and < 100 and/or 60 mm Hg for 24-hr ABPM.
Results. Of the 135,500 patients in the registry, only data from treated hypertensive patients were analyzed (n = 70,997). Mean age was 61.8 ± 12.8 years and 52.5% were men. The prevalence of hypotension was 8.2% with office BP, 12.2% with daytime ABPM, 3.9% with nightime ABPM, and 6.8% with 24-hour ABPM. Low diastolic BP values were responsible for the majority of hypotension. More than 68% of patients with hypotension detected with ABPM did not have hypotension according to office BP. Patients with hypotension were older, more likely to be female, and more likely to have high pulse pressue, lower heart rate, ischemic heart disease, and renal insufficiency. They were also more likely to be taking 3 or more drugs for hypertension.
Conclusion. The prevalence of hypotension is relatively high in treated hypertensive patients, and two-thirds are not identified with office BP measurement. Prevalence was higher in patients who were very elderly or with coronary or renal disease.
Commentary
Hypertension is a major public health concern worldwide [1]. In 2011–12 among US adults with hypertension, only 51.9% had their blood pressure controlled [2]. High blood pressure can effectively be reduced with antihypertensive treatment, and efforts are needed to improve clinical management of hypertension. However, excessive BP reduction may lead to patient harm.
In this study, researchers aimed to determine the prevalence of hypotension using both clinic and ABPM in hypertensive-treated patients and the factors associated with its presence, using descriptive statistics and multivariate analysis. The results highlight the need for health care providers to be aware of the individual response to antihypertensives in patients with high blood pressure and to individualize treatment to avoid complications of hypotension. A strength of this study was it large sample size.
Adherence to treatment recommendations was not a variable taken into consideration for this study and could be considered a confounder. Diet and behavioral interventions can have a significantly beneficial effect on hypertension and can reduce the need for drug therapy [3]. If patients were highly engaged and adopted lifestyle habits that can contribute to better blood pressure levels along with taking prescribed medications, this could have contributed to levels of hypotension.
Hypotension among hypertensive patients can be difficult to identify during clinical consultations due the “white coat effect.” This syndrome is characterized by a peak of high blood pressure caused by the stress of the individual in the presence of a healthcare provider or in a stressful medical environment [4]. This study showed that more than half of the patients in the sample with detected hypotension in the ABPM did not show hypotension during consultation at the medical office. This finding highlights the challenge in identifying hypotension and making adjustments to antihypertensive medication regimens as needed.
Women, patients with low body weight, and elderly patients were the groups more likely to develop hypo-tension. Thus, strategies specifically targeting these vulnerable groups are required. As suggested by the authors of this study, further longitudinal research is needed in order to identify gaps in the state of science in regards this topic and changes in the prevalence this population. The replication of this study in different populations is also encouraged.
Applications for Clinical Practice
The prevalence of hypotension is relatively high and may not be detected during office BP measurement. In patients with a higher risk of hypotension, such as the elderly those with cardiovascular disease, the use of ABPM should be considered.
—Paloma Cesar de Sales, BS, RN, MS
Study Overview
Objective. To determine the prevalence of hypotension using both clinic and ambulatory blood pressure monitoring (ABPM) in treated hypertensive patients and the factors associated with its presence.
Design. Registry-based study.
Setting and participants. Researchers studied patients in the Spanish Society of Hypertension ABPM Registry, which was established to evaluate the utility of the wider use of ABPM with the distribution of >1000 ambulatory BP monitors for routine use by primary care physicians and physicians from specialist units across Spain. The registry continues to expand since the first patient was recruited in June 2004. In June 2015, a total of 135,500 hypertensive patients were in the registry.
Measurements. Blood pressure readings in the clinic were taken according to current recommendations, with the patients in a seated position and their backs supported, after a 5-minute rest, using calibrated sphygmomanometers or validated automatic devices. The visit BP was the average of 2 separate readings. Validated devices (Spacelabs) were used for ABPM, which was performed during a working day with measurements taken every 30 minutes. Patients were told to keep their activity normal and to extend the arm without any movement during BP measurements. ABPM was considered successful in ≥ 80% systolic and diastolic BP valid readings. Patients were classified into 3 categories: hypotension, adequate BP control, or poor BP control for each type of blood pressure (office, daytime, nighttime, and 24-hour). The definitions for hypotension for each BP type were mainly based of the PROVE IT-TIMI study, ie, < 110 and/or 70 mm Hg for office, < 105 and/or 65 mm Hg for daytime ABPM, < 90 and or 50 mm Hg for nightime ABPM, and < 100 and/or 60 mm Hg for 24-hr ABPM.
Results. Of the 135,500 patients in the registry, only data from treated hypertensive patients were analyzed (n = 70,997). Mean age was 61.8 ± 12.8 years and 52.5% were men. The prevalence of hypotension was 8.2% with office BP, 12.2% with daytime ABPM, 3.9% with nightime ABPM, and 6.8% with 24-hour ABPM. Low diastolic BP values were responsible for the majority of hypotension. More than 68% of patients with hypotension detected with ABPM did not have hypotension according to office BP. Patients with hypotension were older, more likely to be female, and more likely to have high pulse pressue, lower heart rate, ischemic heart disease, and renal insufficiency. They were also more likely to be taking 3 or more drugs for hypertension.
Conclusion. The prevalence of hypotension is relatively high in treated hypertensive patients, and two-thirds are not identified with office BP measurement. Prevalence was higher in patients who were very elderly or with coronary or renal disease.
Commentary
Hypertension is a major public health concern worldwide [1]. In 2011–12 among US adults with hypertension, only 51.9% had their blood pressure controlled [2]. High blood pressure can effectively be reduced with antihypertensive treatment, and efforts are needed to improve clinical management of hypertension. However, excessive BP reduction may lead to patient harm.
In this study, researchers aimed to determine the prevalence of hypotension using both clinic and ABPM in hypertensive-treated patients and the factors associated with its presence, using descriptive statistics and multivariate analysis. The results highlight the need for health care providers to be aware of the individual response to antihypertensives in patients with high blood pressure and to individualize treatment to avoid complications of hypotension. A strength of this study was it large sample size.
Adherence to treatment recommendations was not a variable taken into consideration for this study and could be considered a confounder. Diet and behavioral interventions can have a significantly beneficial effect on hypertension and can reduce the need for drug therapy [3]. If patients were highly engaged and adopted lifestyle habits that can contribute to better blood pressure levels along with taking prescribed medications, this could have contributed to levels of hypotension.
Hypotension among hypertensive patients can be difficult to identify during clinical consultations due the “white coat effect.” This syndrome is characterized by a peak of high blood pressure caused by the stress of the individual in the presence of a healthcare provider or in a stressful medical environment [4]. This study showed that more than half of the patients in the sample with detected hypotension in the ABPM did not show hypotension during consultation at the medical office. This finding highlights the challenge in identifying hypotension and making adjustments to antihypertensive medication regimens as needed.
Women, patients with low body weight, and elderly patients were the groups more likely to develop hypo-tension. Thus, strategies specifically targeting these vulnerable groups are required. As suggested by the authors of this study, further longitudinal research is needed in order to identify gaps in the state of science in regards this topic and changes in the prevalence this population. The replication of this study in different populations is also encouraged.
Applications for Clinical Practice
The prevalence of hypotension is relatively high and may not be detected during office BP measurement. In patients with a higher risk of hypotension, such as the elderly those with cardiovascular disease, the use of ABPM should be considered.
—Paloma Cesar de Sales, BS, RN, MS
1. Kantachuvessiri A. Hypertension in public health. Southeast Asian J Trop Med Public Health 2002;33:425–31.
2. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief 2013;1–8.
3. Nicoll R, Henein MY. Hypertension and lifestyle modification: how useful are the guidelines? Br J Gen Pract 2010; 60:879–80.
4. Celis H, Fagard RH. White-coat hypertension: a clinical review. Eur J Intern Med 2004;15:348–57.
1. Kantachuvessiri A. Hypertension in public health. Southeast Asian J Trop Med Public Health 2002;33:425–31.
2. Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief 2013;1–8.
3. Nicoll R, Henein MY. Hypertension and lifestyle modification: how useful are the guidelines? Br J Gen Pract 2010; 60:879–80.
4. Celis H, Fagard RH. White-coat hypertension: a clinical review. Eur J Intern Med 2004;15:348–57.
A Computer-Assisted Process to Reduce Discharge of Emergency Department Patients with Abnormal Vital Signs
From Case Western Reserve University, MetroHealth Medical Center, Cleveland, OH.
Abstract
- Objective: To describe a computer-assisted process for reducing the number of patients discharged from the emergency department with abnormal vital signs.
- Methods: We devised a best practice alert in the Epic electronic medical record that triggers when the clinician attempts to print an after visit summary (discharge paperwork) at the time of discharge from the emergency department.
- Results: We saw no change in the percentage of patients discharged with elevated blood pressures, consistent with national recommendations. Removing that category of patients, we saw a decrease in the percentage of patients discharged with abnormal vital signs, primarily driven by a decrease in the percentage of patients discharged with tachycardia.
- Conclusion: A computer-assisted process can reduce the percentage of patients discharged with abnormal vital signs. Since based on national recommendations ED physicians do not address most elevated blood pressures in the ED, hypertension should not trigger an alert.
Abnormal vital signs in the emergency department (ED) have been associated with adverse outcomes [1,2]. While most patients discharged from the ED do well, some studies have found that the death rate within days to weeks post–ED discharge may be as high as 200 per 100,000 visits, although other studies have found a much lower rate [1]. A study by Sklar et al, although not specifically focused on vital signs at discharge, found that unexpected death within 7 days of ED discharge occurred at a rate of 30 per 100,000 patients. Abnormal vital signs, most commonly tachycardia, were present in 83% of cases [2].
In busy EDs, the combination of patient volume, frequent interruptions, and the intensity of tasks can result in deficiencies in vital sign monitoring [3–5] as well as abnormal vital signs not being recognized by the clinician at the time of patient discharge [6]. The importance of addressing this quality problem has been recognized. Prior efforts to address the problem have included nurses using manual methods to alert the physician to the presence of abnormal vital signs at the time of discharge [7]. Recommendations have been made to use electronic medical record (EMR) functions for prospectively addressing the problem of ED discharge with abnormal vital signs [8]. The utility of the EMR to identify potentially septic patients earlier and reduce mortality from sepsis via an algorithm that incorporated vital signs and other clinical crieria has been demonstrated [9,10]. In addition, automated vital signs advisories have been associated with increased survival on general hospital wards [11].
An adverse event that occurred at our institution prompted us to review this issue for our ED. We designed an EMR-assisted intervention to reduce the rate of patients discharged from the ED with abnormal vital signs.
Methods
Setting
Our ED is a busy, urban, Level 1 trauma center within a teaching facility. It sees over 100,000 patients per year and is segmented into resuscitation, high acuity, moderate acuity, and fast tract areas, in addition to the observation unit. Our organization uses the Epic (Madison, Wisconsin) electronic health record, which we have been using for over a decade.
Discharge Instructions—Old Process
In our ED, providers, attending physicians, residents and advance practice nurses enter and print their own discharge instructions, which are given to nursing staff to review with patients. Prior to the project, nurses were expected to notify a physician if they thought a vital sign was abnormal. Each nurse made independent decisions on what constituted a vital sign abnormality based on the patient’s condition and could communicate that to the provider at their discretion prior to discharge. This process created inconsistencies in care.
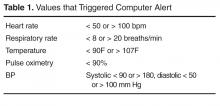
Development of Alert
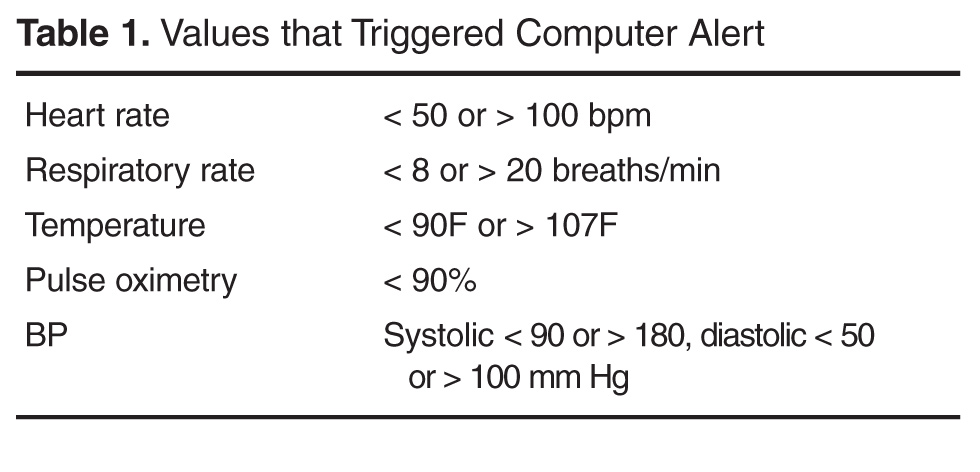
We created an alert that appears within the provider workflow at the time the provider attempts to print discharge instructions. Based on literature review and operational leadership consensus, we set the parameters for abnormal vital signs (Table 1). We chose parameters to identify abnormalities important to 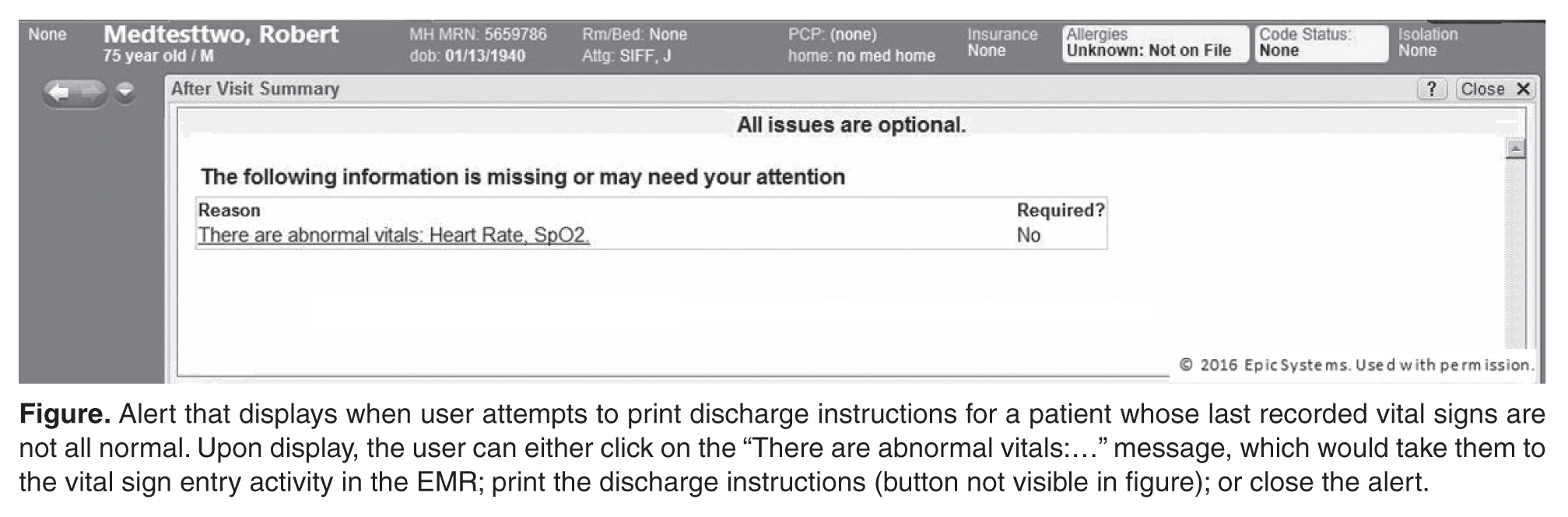
The alert displays when a user attempts to print discharge instructions on a patient whose last recorded vital signs are not all normal. The display informs that there are abnormal vital signs (Figure). Upon display of the alert, the user can click on the message, which would take them to the vital sign entry activity in the EMR, or they can proceed with printing by clicking the print button (not visible in the Figure). The alert is not a forcing function; the user can proceed with printing the discharge instructions without addressing the abnormality that triggered the alert.
Pre-Post Evaluation
We would have liked to have determined how often the abnormal vital signs alert triggered, how it was responded to, and whether the patient was subsequently discharged with normal vital signs; however, our system does not record these events. Instead, we used the system to compare the percentage of adult patients who were discharged with abnormal vital signs for 2 time periods: the period prior to our December 2014 implementation (1 Oct to 1 Dec 2014) and the post implementation period (15 Dec 2014 to 15 Feb 2015). Our presumption was that the use of the alert system would reduce the percentage of patients discharged with abnormal vital signs, including an abnormal pulse oximetry.
To conduct our analysis, we identified adult patients seen during the 2 time periods. We eliminated those patients who died, left without being seen, eloped, were admitted or were transferred to other institutions. This resulted in 3664 patients, with 2179 in the pre-implementation group and 1485 in the post-implementation group. The higher volume in the pre group reflects the early occurrence of influenza season in our area during the study period, along with our generally busier time in late fall compared to winter.
The analysis was performed as a likelihood ratio chi-square analysis using SAS (Cary, NC) software.
Results
The analysis demonstrated that physicians were, by and large, following recommendations consistent with policies of the American College of Emergency Physicians regarding the management of elevated blood pressures, which do not mandate that patients with asymptomatic elevations of blood pressure receive medical intervention in the ED [12]. In our analysis, the percentage of patients discharged with elevated blood pressures actually increased from 7.5% to 9.9% following the intervention. Importantly, however, the percentage of patients discharged with low blood pressures decreased from 6.9% to 5.0% (P < 0.01).Tthe percent of patients discharged with an elevated heart rate, decreased from 58% in the pre alert group to 42% in the post alert group (P < 0.02). 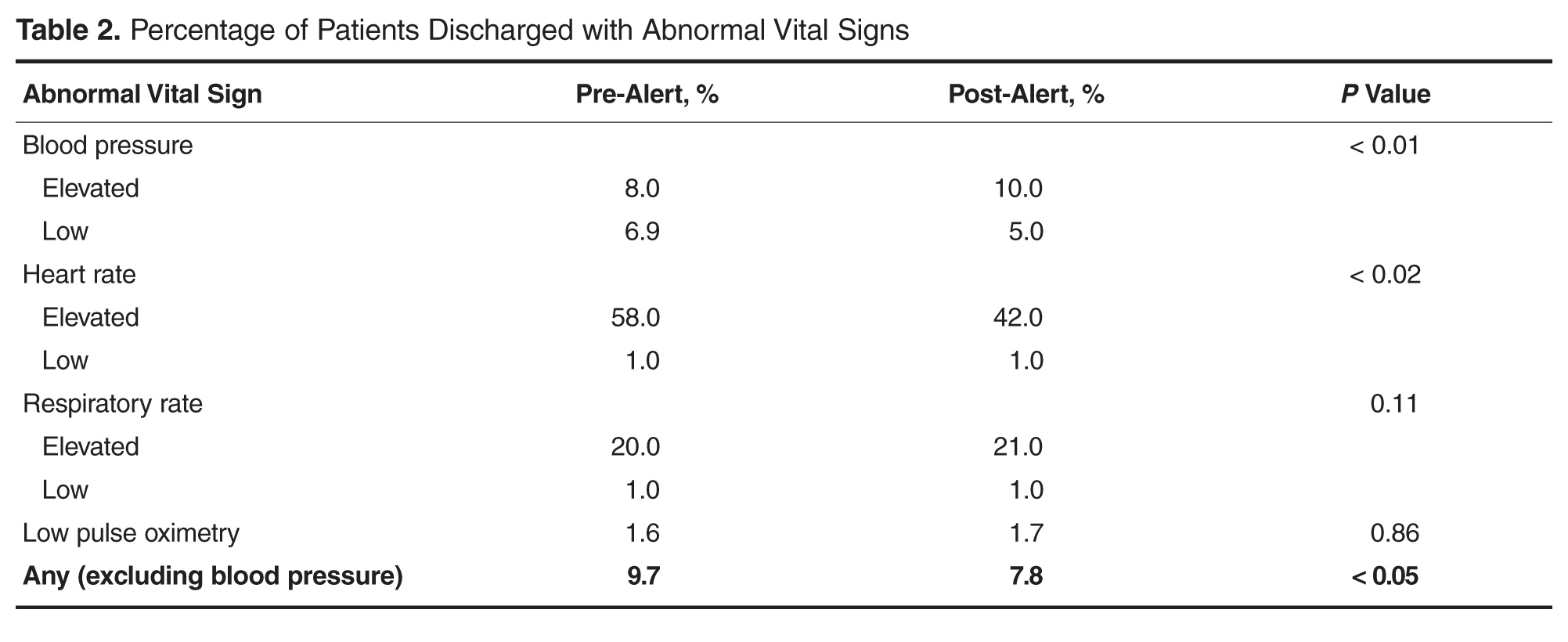
Discussion
In our study, we used features of the EMR prospectively to affect discharge and then used the database functions of the EMR to assess the effectiveness of those efforts. Previous studies that have looked at the incidence of abnormal vital signs at discharge have been manual, retrospective reviews of records. We are not aware of any studies reporting the results of introducing an EMR alert to prospectively identify patients with abnormal vital signs prior to discharge
While we found that this intervention was successful in reducing clinically relevant abnormal vital signs at discharge, we have realized that the elevated blood pressure alert was unnecessary and we have eliminated it from the programming. We will revisit our strategy to determine if further reducing the high blood pressure alerts can lead to greater improvements in reducing the percentage of patients discharged with abnormal vital signs.
Future plans include a review of the re-visit or hospitalization rate for patients discharged with abnormal vital signs. A companion study evaluating a similar approach to the care of children is under consideration. We are also considering including a field in the EMR for the clinician to document why they discharged a patient with abnormal vital signs.
Corresponding author: Jonathan E. Siff, MD 2500 MetroHealth Drive BG3-65 Cleveland, Ohio 44109 [email protected].
Financial disclosures: None.
1. Gunnarsdottir OS, Rafnsson V. Death within 8 days after discharge to home from the emergency department. Eur J of Public Health 2008;18:522–6.
2. Sklar DP, Crandall CS, Loeliger E, et al. Unanticipated death after discharge home from the emergency department. Ann Emerg Med 2007;49:735–45.
3. Johnson KD, Winkelman C, Burant CJ, et al. The factors that affect the frequency of vital sign monitoring in the emergency department. J Emerg Nurs 2014;40:27–35.
4. Gravel J, Opatrny L, Gouin S. High rate of missing vital signs data at triage in a paediatric emergency department. Paediatr Child Health 2006;11:211–5.
5. Depinet HE, Iyer SB, Hornung R, et al. The effect of emergency department crowding on reassessment of children with critically abnormal vital signs. Acad Emerg Med 2014;21:1116–20.
6. Hafner JW, Parrish SE, Hubler JR, et al. Repeat assessment of abnormal vital signs and patient re-examination in us emergency department patients. Ann Emerg Med 2006;48(4 Suppl):S66.
7. Domagala SE. Discharge vital signs: an enhancement to ED quality and patient outcomes. J Emerg Nursing 2009;35:138–40.
8. Welch S. Red flags: abnormal vital signs at discharge.Emerg Med News 2011:33;7–8.
9. Nguyen SQ, Mwakalindile E, Booth JS, et al. Automated electronic medical record sepsis detection in the emergency department. PeerJ 2014;2:e343.
10. Narayanan N, Gross AK, Pintens M, et al. Effect of an electronic medical record alert for severe sepsis among ED patients. Am J Emerg Med 2016;34:185–8.
11. Bellomo R, Ackerman M, Bailey M, et al. A controlled trial of electronic automated advisory vital signs monitoring in general hospital wards. Crit Care Med 2012;40:2349–61.
12. Wolf SJ, Lo B, Smith MD, et al. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med 2013:62;59–68.
From Case Western Reserve University, MetroHealth Medical Center, Cleveland, OH.
Abstract
- Objective: To describe a computer-assisted process for reducing the number of patients discharged from the emergency department with abnormal vital signs.
- Methods: We devised a best practice alert in the Epic electronic medical record that triggers when the clinician attempts to print an after visit summary (discharge paperwork) at the time of discharge from the emergency department.
- Results: We saw no change in the percentage of patients discharged with elevated blood pressures, consistent with national recommendations. Removing that category of patients, we saw a decrease in the percentage of patients discharged with abnormal vital signs, primarily driven by a decrease in the percentage of patients discharged with tachycardia.
- Conclusion: A computer-assisted process can reduce the percentage of patients discharged with abnormal vital signs. Since based on national recommendations ED physicians do not address most elevated blood pressures in the ED, hypertension should not trigger an alert.
Abnormal vital signs in the emergency department (ED) have been associated with adverse outcomes [1,2]. While most patients discharged from the ED do well, some studies have found that the death rate within days to weeks post–ED discharge may be as high as 200 per 100,000 visits, although other studies have found a much lower rate [1]. A study by Sklar et al, although not specifically focused on vital signs at discharge, found that unexpected death within 7 days of ED discharge occurred at a rate of 30 per 100,000 patients. Abnormal vital signs, most commonly tachycardia, were present in 83% of cases [2].
In busy EDs, the combination of patient volume, frequent interruptions, and the intensity of tasks can result in deficiencies in vital sign monitoring [3–5] as well as abnormal vital signs not being recognized by the clinician at the time of patient discharge [6]. The importance of addressing this quality problem has been recognized. Prior efforts to address the problem have included nurses using manual methods to alert the physician to the presence of abnormal vital signs at the time of discharge [7]. Recommendations have been made to use electronic medical record (EMR) functions for prospectively addressing the problem of ED discharge with abnormal vital signs [8]. The utility of the EMR to identify potentially septic patients earlier and reduce mortality from sepsis via an algorithm that incorporated vital signs and other clinical crieria has been demonstrated [9,10]. In addition, automated vital signs advisories have been associated with increased survival on general hospital wards [11].
An adverse event that occurred at our institution prompted us to review this issue for our ED. We designed an EMR-assisted intervention to reduce the rate of patients discharged from the ED with abnormal vital signs.
Methods
Setting
Our ED is a busy, urban, Level 1 trauma center within a teaching facility. It sees over 100,000 patients per year and is segmented into resuscitation, high acuity, moderate acuity, and fast tract areas, in addition to the observation unit. Our organization uses the Epic (Madison, Wisconsin) electronic health record, which we have been using for over a decade.
Discharge Instructions—Old Process
In our ED, providers, attending physicians, residents and advance practice nurses enter and print their own discharge instructions, which are given to nursing staff to review with patients. Prior to the project, nurses were expected to notify a physician if they thought a vital sign was abnormal. Each nurse made independent decisions on what constituted a vital sign abnormality based on the patient’s condition and could communicate that to the provider at their discretion prior to discharge. This process created inconsistencies in care.
Development of Alert
We created an alert that appears within the provider workflow at the time the provider attempts to print discharge instructions. Based on literature review and operational leadership consensus, we set the parameters for abnormal vital signs (Table 1). We chose parameters to identify abnormalities important to
The alert displays when a user attempts to print discharge instructions on a patient whose last recorded vital signs are not all normal. The display informs that there are abnormal vital signs (Figure). Upon display of the alert, the user can click on the message, which would take them to the vital sign entry activity in the EMR, or they can proceed with printing by clicking the print button (not visible in the Figure). The alert is not a forcing function; the user can proceed with printing the discharge instructions without addressing the abnormality that triggered the alert.
Pre-Post Evaluation
We would have liked to have determined how often the abnormal vital signs alert triggered, how it was responded to, and whether the patient was subsequently discharged with normal vital signs; however, our system does not record these events. Instead, we used the system to compare the percentage of adult patients who were discharged with abnormal vital signs for 2 time periods: the period prior to our December 2014 implementation (1 Oct to 1 Dec 2014) and the post implementation period (15 Dec 2014 to 15 Feb 2015). Our presumption was that the use of the alert system would reduce the percentage of patients discharged with abnormal vital signs, including an abnormal pulse oximetry.
To conduct our analysis, we identified adult patients seen during the 2 time periods. We eliminated those patients who died, left without being seen, eloped, were admitted or were transferred to other institutions. This resulted in 3664 patients, with 2179 in the pre-implementation group and 1485 in the post-implementation group. The higher volume in the pre group reflects the early occurrence of influenza season in our area during the study period, along with our generally busier time in late fall compared to winter.
The analysis was performed as a likelihood ratio chi-square analysis using SAS (Cary, NC) software.
Results
The analysis demonstrated that physicians were, by and large, following recommendations consistent with policies of the American College of Emergency Physicians regarding the management of elevated blood pressures, which do not mandate that patients with asymptomatic elevations of blood pressure receive medical intervention in the ED [12]. In our analysis, the percentage of patients discharged with elevated blood pressures actually increased from 7.5% to 9.9% following the intervention. Importantly, however, the percentage of patients discharged with low blood pressures decreased from 6.9% to 5.0% (P < 0.01).Tthe percent of patients discharged with an elevated heart rate, decreased from 58% in the pre alert group to 42% in the post alert group (P < 0.02).
Discussion
In our study, we used features of the EMR prospectively to affect discharge and then used the database functions of the EMR to assess the effectiveness of those efforts. Previous studies that have looked at the incidence of abnormal vital signs at discharge have been manual, retrospective reviews of records. We are not aware of any studies reporting the results of introducing an EMR alert to prospectively identify patients with abnormal vital signs prior to discharge
While we found that this intervention was successful in reducing clinically relevant abnormal vital signs at discharge, we have realized that the elevated blood pressure alert was unnecessary and we have eliminated it from the programming. We will revisit our strategy to determine if further reducing the high blood pressure alerts can lead to greater improvements in reducing the percentage of patients discharged with abnormal vital signs.
Future plans include a review of the re-visit or hospitalization rate for patients discharged with abnormal vital signs. A companion study evaluating a similar approach to the care of children is under consideration. We are also considering including a field in the EMR for the clinician to document why they discharged a patient with abnormal vital signs.
Corresponding author: Jonathan E. Siff, MD 2500 MetroHealth Drive BG3-65 Cleveland, Ohio 44109 [email protected].
Financial disclosures: None.
From Case Western Reserve University, MetroHealth Medical Center, Cleveland, OH.
Abstract
- Objective: To describe a computer-assisted process for reducing the number of patients discharged from the emergency department with abnormal vital signs.
- Methods: We devised a best practice alert in the Epic electronic medical record that triggers when the clinician attempts to print an after visit summary (discharge paperwork) at the time of discharge from the emergency department.
- Results: We saw no change in the percentage of patients discharged with elevated blood pressures, consistent with national recommendations. Removing that category of patients, we saw a decrease in the percentage of patients discharged with abnormal vital signs, primarily driven by a decrease in the percentage of patients discharged with tachycardia.
- Conclusion: A computer-assisted process can reduce the percentage of patients discharged with abnormal vital signs. Since based on national recommendations ED physicians do not address most elevated blood pressures in the ED, hypertension should not trigger an alert.
Abnormal vital signs in the emergency department (ED) have been associated with adverse outcomes [1,2]. While most patients discharged from the ED do well, some studies have found that the death rate within days to weeks post–ED discharge may be as high as 200 per 100,000 visits, although other studies have found a much lower rate [1]. A study by Sklar et al, although not specifically focused on vital signs at discharge, found that unexpected death within 7 days of ED discharge occurred at a rate of 30 per 100,000 patients. Abnormal vital signs, most commonly tachycardia, were present in 83% of cases [2].
In busy EDs, the combination of patient volume, frequent interruptions, and the intensity of tasks can result in deficiencies in vital sign monitoring [3–5] as well as abnormal vital signs not being recognized by the clinician at the time of patient discharge [6]. The importance of addressing this quality problem has been recognized. Prior efforts to address the problem have included nurses using manual methods to alert the physician to the presence of abnormal vital signs at the time of discharge [7]. Recommendations have been made to use electronic medical record (EMR) functions for prospectively addressing the problem of ED discharge with abnormal vital signs [8]. The utility of the EMR to identify potentially septic patients earlier and reduce mortality from sepsis via an algorithm that incorporated vital signs and other clinical crieria has been demonstrated [9,10]. In addition, automated vital signs advisories have been associated with increased survival on general hospital wards [11].
An adverse event that occurred at our institution prompted us to review this issue for our ED. We designed an EMR-assisted intervention to reduce the rate of patients discharged from the ED with abnormal vital signs.
Methods
Setting
Our ED is a busy, urban, Level 1 trauma center within a teaching facility. It sees over 100,000 patients per year and is segmented into resuscitation, high acuity, moderate acuity, and fast tract areas, in addition to the observation unit. Our organization uses the Epic (Madison, Wisconsin) electronic health record, which we have been using for over a decade.
Discharge Instructions—Old Process
In our ED, providers, attending physicians, residents and advance practice nurses enter and print their own discharge instructions, which are given to nursing staff to review with patients. Prior to the project, nurses were expected to notify a physician if they thought a vital sign was abnormal. Each nurse made independent decisions on what constituted a vital sign abnormality based on the patient’s condition and could communicate that to the provider at their discretion prior to discharge. This process created inconsistencies in care.
Development of Alert
We created an alert that appears within the provider workflow at the time the provider attempts to print discharge instructions. Based on literature review and operational leadership consensus, we set the parameters for abnormal vital signs (Table 1). We chose parameters to identify abnormalities important to
The alert displays when a user attempts to print discharge instructions on a patient whose last recorded vital signs are not all normal. The display informs that there are abnormal vital signs (Figure). Upon display of the alert, the user can click on the message, which would take them to the vital sign entry activity in the EMR, or they can proceed with printing by clicking the print button (not visible in the Figure). The alert is not a forcing function; the user can proceed with printing the discharge instructions without addressing the abnormality that triggered the alert.
Pre-Post Evaluation
We would have liked to have determined how often the abnormal vital signs alert triggered, how it was responded to, and whether the patient was subsequently discharged with normal vital signs; however, our system does not record these events. Instead, we used the system to compare the percentage of adult patients who were discharged with abnormal vital signs for 2 time periods: the period prior to our December 2014 implementation (1 Oct to 1 Dec 2014) and the post implementation period (15 Dec 2014 to 15 Feb 2015). Our presumption was that the use of the alert system would reduce the percentage of patients discharged with abnormal vital signs, including an abnormal pulse oximetry.
To conduct our analysis, we identified adult patients seen during the 2 time periods. We eliminated those patients who died, left without being seen, eloped, were admitted or were transferred to other institutions. This resulted in 3664 patients, with 2179 in the pre-implementation group and 1485 in the post-implementation group. The higher volume in the pre group reflects the early occurrence of influenza season in our area during the study period, along with our generally busier time in late fall compared to winter.
The analysis was performed as a likelihood ratio chi-square analysis using SAS (Cary, NC) software.
Results
The analysis demonstrated that physicians were, by and large, following recommendations consistent with policies of the American College of Emergency Physicians regarding the management of elevated blood pressures, which do not mandate that patients with asymptomatic elevations of blood pressure receive medical intervention in the ED [12]. In our analysis, the percentage of patients discharged with elevated blood pressures actually increased from 7.5% to 9.9% following the intervention. Importantly, however, the percentage of patients discharged with low blood pressures decreased from 6.9% to 5.0% (P < 0.01).Tthe percent of patients discharged with an elevated heart rate, decreased from 58% in the pre alert group to 42% in the post alert group (P < 0.02).
Discussion
In our study, we used features of the EMR prospectively to affect discharge and then used the database functions of the EMR to assess the effectiveness of those efforts. Previous studies that have looked at the incidence of abnormal vital signs at discharge have been manual, retrospective reviews of records. We are not aware of any studies reporting the results of introducing an EMR alert to prospectively identify patients with abnormal vital signs prior to discharge
While we found that this intervention was successful in reducing clinically relevant abnormal vital signs at discharge, we have realized that the elevated blood pressure alert was unnecessary and we have eliminated it from the programming. We will revisit our strategy to determine if further reducing the high blood pressure alerts can lead to greater improvements in reducing the percentage of patients discharged with abnormal vital signs.
Future plans include a review of the re-visit or hospitalization rate for patients discharged with abnormal vital signs. A companion study evaluating a similar approach to the care of children is under consideration. We are also considering including a field in the EMR for the clinician to document why they discharged a patient with abnormal vital signs.
Corresponding author: Jonathan E. Siff, MD 2500 MetroHealth Drive BG3-65 Cleveland, Ohio 44109 [email protected].
Financial disclosures: None.
1. Gunnarsdottir OS, Rafnsson V. Death within 8 days after discharge to home from the emergency department. Eur J of Public Health 2008;18:522–6.
2. Sklar DP, Crandall CS, Loeliger E, et al. Unanticipated death after discharge home from the emergency department. Ann Emerg Med 2007;49:735–45.
3. Johnson KD, Winkelman C, Burant CJ, et al. The factors that affect the frequency of vital sign monitoring in the emergency department. J Emerg Nurs 2014;40:27–35.
4. Gravel J, Opatrny L, Gouin S. High rate of missing vital signs data at triage in a paediatric emergency department. Paediatr Child Health 2006;11:211–5.
5. Depinet HE, Iyer SB, Hornung R, et al. The effect of emergency department crowding on reassessment of children with critically abnormal vital signs. Acad Emerg Med 2014;21:1116–20.
6. Hafner JW, Parrish SE, Hubler JR, et al. Repeat assessment of abnormal vital signs and patient re-examination in us emergency department patients. Ann Emerg Med 2006;48(4 Suppl):S66.
7. Domagala SE. Discharge vital signs: an enhancement to ED quality and patient outcomes. J Emerg Nursing 2009;35:138–40.
8. Welch S. Red flags: abnormal vital signs at discharge.Emerg Med News 2011:33;7–8.
9. Nguyen SQ, Mwakalindile E, Booth JS, et al. Automated electronic medical record sepsis detection in the emergency department. PeerJ 2014;2:e343.
10. Narayanan N, Gross AK, Pintens M, et al. Effect of an electronic medical record alert for severe sepsis among ED patients. Am J Emerg Med 2016;34:185–8.
11. Bellomo R, Ackerman M, Bailey M, et al. A controlled trial of electronic automated advisory vital signs monitoring in general hospital wards. Crit Care Med 2012;40:2349–61.
12. Wolf SJ, Lo B, Smith MD, et al. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med 2013:62;59–68.
1. Gunnarsdottir OS, Rafnsson V. Death within 8 days after discharge to home from the emergency department. Eur J of Public Health 2008;18:522–6.
2. Sklar DP, Crandall CS, Loeliger E, et al. Unanticipated death after discharge home from the emergency department. Ann Emerg Med 2007;49:735–45.
3. Johnson KD, Winkelman C, Burant CJ, et al. The factors that affect the frequency of vital sign monitoring in the emergency department. J Emerg Nurs 2014;40:27–35.
4. Gravel J, Opatrny L, Gouin S. High rate of missing vital signs data at triage in a paediatric emergency department. Paediatr Child Health 2006;11:211–5.
5. Depinet HE, Iyer SB, Hornung R, et al. The effect of emergency department crowding on reassessment of children with critically abnormal vital signs. Acad Emerg Med 2014;21:1116–20.
6. Hafner JW, Parrish SE, Hubler JR, et al. Repeat assessment of abnormal vital signs and patient re-examination in us emergency department patients. Ann Emerg Med 2006;48(4 Suppl):S66.
7. Domagala SE. Discharge vital signs: an enhancement to ED quality and patient outcomes. J Emerg Nursing 2009;35:138–40.
8. Welch S. Red flags: abnormal vital signs at discharge.Emerg Med News 2011:33;7–8.
9. Nguyen SQ, Mwakalindile E, Booth JS, et al. Automated electronic medical record sepsis detection in the emergency department. PeerJ 2014;2:e343.
10. Narayanan N, Gross AK, Pintens M, et al. Effect of an electronic medical record alert for severe sepsis among ED patients. Am J Emerg Med 2016;34:185–8.
11. Bellomo R, Ackerman M, Bailey M, et al. A controlled trial of electronic automated advisory vital signs monitoring in general hospital wards. Crit Care Med 2012;40:2349–61.
12. Wolf SJ, Lo B, Smith MD, et al. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med 2013:62;59–68.