User login
CMS to pay more for care coordination, prevention
The Centers for Medicare & Medicaid Services plans to spend an extra $140 million on these services next year under the final physician fee schedule, released on Nov. 2 and scheduled for publication in the Federal Register on Nov. 15.

“Clinicians will additionally be able to bill and be paid more appropriately when they spend more time with their patients, serving their patients’ needs outside of the office visit, and better coordinate care,” they wrote.
CMS finalized a number of payment codes that “better identify and value primary care, care management, and cognitive services,” according to an agency fact sheet highlighting key provisions of the final physician fee schedule for 2017.
The coding changes allow for separate payments for non–face-to-face prolonged evaluation and management services; revalue existing codes for face-to-face prolonged services; separate payments for comprehensive assessment and care planning for patients with cognitive impairments such as dementia; and separate payments for chronic care management of complex patients.
“This final decision by CMS means individuals living with Alzheimer’s disease will finally have access to critical care and support services that can improve quality of life for the individual, their family, and caregivers,” Harry Johns, Alzheimer’s Association President and CEO, said in a statement. “Now that care-planning sessions will be available to them, individuals living with the disease will have access to much-needed information on treatments and services.”

“Geriatricians, internists, and family physicians provide core services for the Medicare program, including the kinds of care management and patient-centered care that are described by these new codes,” Mr. Slavitt and Dr. Conway wrote. “Over time, we estimate that the payment increases attributable to these new codes could be as much as 30% and 37%, respectively, to these specialties.”
CMS also finalized other coding changes, including:
- A separate code for moderate sedation services to account for changes in practice trends that report anesthesia separately from certain endoscopic procedures despite payment being built into the overall procedure payment.
- More payments for telehealth services, including for end-stage renal disease-related services for dialysis, advanced care planning; and critical care consultations.
The American College of Physicians applauded the final rule.
“The policies in the rule more accurately recognize the work of primary care physicians and other cognitive specialties to accommodate the changing needs of Medicare beneficiaries,” ACP President Nitin S. Damle, MD, said in a statement.
The Centers for Medicare & Medicaid Services plans to spend an extra $140 million on these services next year under the final physician fee schedule, released on Nov. 2 and scheduled for publication in the Federal Register on Nov. 15.
“Clinicians will additionally be able to bill and be paid more appropriately when they spend more time with their patients, serving their patients’ needs outside of the office visit, and better coordinate care,” they wrote.
CMS finalized a number of payment codes that “better identify and value primary care, care management, and cognitive services,” according to an agency fact sheet highlighting key provisions of the final physician fee schedule for 2017.
The coding changes allow for separate payments for non–face-to-face prolonged evaluation and management services; revalue existing codes for face-to-face prolonged services; separate payments for comprehensive assessment and care planning for patients with cognitive impairments such as dementia; and separate payments for chronic care management of complex patients.
“This final decision by CMS means individuals living with Alzheimer’s disease will finally have access to critical care and support services that can improve quality of life for the individual, their family, and caregivers,” Harry Johns, Alzheimer’s Association President and CEO, said in a statement. “Now that care-planning sessions will be available to them, individuals living with the disease will have access to much-needed information on treatments and services.”
“Geriatricians, internists, and family physicians provide core services for the Medicare program, including the kinds of care management and patient-centered care that are described by these new codes,” Mr. Slavitt and Dr. Conway wrote. “Over time, we estimate that the payment increases attributable to these new codes could be as much as 30% and 37%, respectively, to these specialties.”
CMS also finalized other coding changes, including:
- A separate code for moderate sedation services to account for changes in practice trends that report anesthesia separately from certain endoscopic procedures despite payment being built into the overall procedure payment.
- More payments for telehealth services, including for end-stage renal disease-related services for dialysis, advanced care planning; and critical care consultations.
The American College of Physicians applauded the final rule.
“The policies in the rule more accurately recognize the work of primary care physicians and other cognitive specialties to accommodate the changing needs of Medicare beneficiaries,” ACP President Nitin S. Damle, MD, said in a statement.
The Centers for Medicare & Medicaid Services plans to spend an extra $140 million on these services next year under the final physician fee schedule, released on Nov. 2 and scheduled for publication in the Federal Register on Nov. 15.
“Clinicians will additionally be able to bill and be paid more appropriately when they spend more time with their patients, serving their patients’ needs outside of the office visit, and better coordinate care,” they wrote.
CMS finalized a number of payment codes that “better identify and value primary care, care management, and cognitive services,” according to an agency fact sheet highlighting key provisions of the final physician fee schedule for 2017.
The coding changes allow for separate payments for non–face-to-face prolonged evaluation and management services; revalue existing codes for face-to-face prolonged services; separate payments for comprehensive assessment and care planning for patients with cognitive impairments such as dementia; and separate payments for chronic care management of complex patients.
“This final decision by CMS means individuals living with Alzheimer’s disease will finally have access to critical care and support services that can improve quality of life for the individual, their family, and caregivers,” Harry Johns, Alzheimer’s Association President and CEO, said in a statement. “Now that care-planning sessions will be available to them, individuals living with the disease will have access to much-needed information on treatments and services.”
“Geriatricians, internists, and family physicians provide core services for the Medicare program, including the kinds of care management and patient-centered care that are described by these new codes,” Mr. Slavitt and Dr. Conway wrote. “Over time, we estimate that the payment increases attributable to these new codes could be as much as 30% and 37%, respectively, to these specialties.”
CMS also finalized other coding changes, including:
- A separate code for moderate sedation services to account for changes in practice trends that report anesthesia separately from certain endoscopic procedures despite payment being built into the overall procedure payment.
- More payments for telehealth services, including for end-stage renal disease-related services for dialysis, advanced care planning; and critical care consultations.
The American College of Physicians applauded the final rule.
“The policies in the rule more accurately recognize the work of primary care physicians and other cognitive specialties to accommodate the changing needs of Medicare beneficiaries,” ACP President Nitin S. Damle, MD, said in a statement.
FDA’s Woodcock: Give biosimilars a chance
BOSTON – Biosimilar drugs are not identical twins of original biologic agents, but there are very strong family ties, and the newcomer is expected to look and behave very much like its older relative, said Janet Woodcock, MD, director of the Center for Drug Evaluation and Research at the Food and Drug Administration.
Although biosimilars differ from generic, small-molecule drugs, concerns about the development of biosimilars mirrors the kerfuffle over generic drugs surrounding the passage of the Hatch-Waxman (Drug Price Competition and Patent Term Restoration) Act in 1984.

She noted that clinicians today are asking the same questions about biosimilars that were asked about generics three decades ago:
- Are biosimilars as effective and as safe as the originally licensed biopharmaceuticals?
- If pharmacists substitute biosimilars for prescribed biologics, will patients be adversely affected?
- Can biosimilars reduce the high cost of biologic therapy?
“In certain specialties, this skepticism has persisted to this very day,” she said.
ACA mandate
Biosimilars owe their existence in large measure to the Biologics Price Competition and Innovation Act of 2009 (BPCI), passed as a part of the Affordable Care Act and signed into law by President Obama in 2010.
The act created an abbreviated licensure pathway for biologic products that can be shown to be either biosimilar to or interchangeable with an FDA-licensed reference drug.
A biosimilar is defined as a biological product that is highly similar to the reference product “notwithstanding minor differences in clinically inactive components,” and with no clinically meaningful differences between it and the reference product in terms of purity, safety, and potency.
To be interchangeable, a biosimilar must be expected to produce the same clinical results as the reference drug in any given patient, and “for a product that is administered more than once to an individual, the risk in terms of safety or diminished efficacy of alternating or switching between use of the product and its reference product is not greater than the risk of using the reference product without such alternation or switch.”
The definition of interchangeability includes the understanding that the prescriber’s approval is not necessary for substitution of a biosimilar for its reference product.
“If we’re going to have that kind of switching, if they are going to be interchangeable, then we have to have a very high bar,” Dr. Woodcock said.
She added that “any pressure people are feeling to push their patients to biosimilars is from the reimbursement system. There is no non-prescriber switching allowed currently; however, that doesn’t say there isn’t pressure on prescribers to write a different prescription.”
Faster track and bridge to approval
The biosimilar development and approval requires only convincing demonstration of biosimilarity to an existing agent, rather than an independent finding of safety or effectiveness, and the purpose of clinical studies in this case is to address “residual uncertainties,” Dr. Woodcock said.
Drug developers and regulatory authorities alike “are having trouble getting their mind around this concept,” she said.
The FDA requires manufacturers to provide data in their biosimilar drug license applications demonstrating biosimilarity based on analytical studies, animal studies that include toxicity assessments, and one or more clinical studies that include information on immunogenicity and pharmacokinetics (PK) or pharmacodynamics (PD) that is sufficient to demonstrate the safety, purity, and potency of the candidate biosimilar.
The FDA is also allowing manufacturers to submit data from animal studies and specified clinical studies comparing a proposed biosimilar product with a product not licensed in the United States, “as long as we are convinced that the reference product is equivalent to the U.S. product,” Dr. Woodcock said.
This “analytical bridge” process was requested by manufacturers who began development of biosimilars in Europe. The European Medicines Agency approved a biosimilar process in 2005, and gave the nod to the first biosimilar agents to existing erythropoietin products in 2007.
Current and pending
As of early October 2016, 66 programs were enrolled in FDA’s Biosimilar Product Development Program, and CDER has received requests for meetings with manufacturers to discuss what tests and documents are required for the development of biosimilars to 20 different reference products.
The FDA is prohibited from publicly discussing the existence of a pending application unless it has been previously disclosed or acknowledged publicly with the manufacturer’s permission, Dr. Woodcock noted, but as of Oct. 10, 2016, seven companies have announced a total of 10 biologic license applications for biosimilars to etanercept (Enbrel), adalimumab (Humira), pegfilgrastim (Neulasta), epoetin alfa (Epogen/Procrit), filgrastim (Neupogen), and infliximab (Remicade).
The FDA has granted licenses to four biosimilars to date (the four-letter suffix is intended to differentiate biosimilars agents from other biosimilars to the same reference product):
- Zarxio (filgrastim-sndz).
- Inflectra (infliximab-dyyb).
- Erelzi (etanercept-szzs).
- Amjevita (adalimumab-atto).
Physician perspective
“Everything I have heard suggests that biosimilars will be useful, but the scientist in me is a skeptic,” commented Donald Massenburg, MD, PhD, a rheumatologist at Wheaton Franciscan Healthcare in Franklin, Wisc., in an interview.
“I feel better now after learning that current biosimilars are not considered interchangeable, meaning that there can’t be substitutions made without the treating physician’s consent,” he said.
He acknowledged that “I wouldn’t be that excited” if a specific biosimilar was approved for interchangeability and was given to his patients without his knowledge.
Dr. Massenburg pointed to data from the NOR-SWITCH trial comparing the biosimilar Remsima to the reference product Remicade for treatment of rheumatic diseases, psoriasis, and inflammatory bowel disease. The trial showed that Remsima was noninferior to the reference product.

“I would like to be able to say whether a patient should be switched to a biosimilar or not just because of that potential risk,” Dr. Massenburg said.
A rheumatologist in private practice in New England said that what’s really needed in rheumatology is not the availability of more drugs that act like other drugs, but innovative research into therapies with better targeted mechanism of action.
“We’ve been through the ‘me-too’ hype; we did that with nonsteroidal anti-inflammatory drugs,” said J. Scott Toder, MD, director of the Toder Rheumatology and Osteoporosis Center, Providence, R.I.
“I think we need to concentrate on innovative therapies, and we may be able to do something about the escalating price of the biologics on the market by creating drugs with new mechanism of action to actually increase competition and hopefully control prices. I don’t think that having multiple drugs with the same mechanism of action is in the best interest of our patients,” he said in an interview.
Dr. Woodcock, Dr. Massenburg, and Dr. Toder reported having no relevant disclosures.
BOSTON – Biosimilar drugs are not identical twins of original biologic agents, but there are very strong family ties, and the newcomer is expected to look and behave very much like its older relative, said Janet Woodcock, MD, director of the Center for Drug Evaluation and Research at the Food and Drug Administration.
Although biosimilars differ from generic, small-molecule drugs, concerns about the development of biosimilars mirrors the kerfuffle over generic drugs surrounding the passage of the Hatch-Waxman (Drug Price Competition and Patent Term Restoration) Act in 1984.
She noted that clinicians today are asking the same questions about biosimilars that were asked about generics three decades ago:
- Are biosimilars as effective and as safe as the originally licensed biopharmaceuticals?
- If pharmacists substitute biosimilars for prescribed biologics, will patients be adversely affected?
- Can biosimilars reduce the high cost of biologic therapy?
“In certain specialties, this skepticism has persisted to this very day,” she said.
ACA mandate
Biosimilars owe their existence in large measure to the Biologics Price Competition and Innovation Act of 2009 (BPCI), passed as a part of the Affordable Care Act and signed into law by President Obama in 2010.
The act created an abbreviated licensure pathway for biologic products that can be shown to be either biosimilar to or interchangeable with an FDA-licensed reference drug.
A biosimilar is defined as a biological product that is highly similar to the reference product “notwithstanding minor differences in clinically inactive components,” and with no clinically meaningful differences between it and the reference product in terms of purity, safety, and potency.
To be interchangeable, a biosimilar must be expected to produce the same clinical results as the reference drug in any given patient, and “for a product that is administered more than once to an individual, the risk in terms of safety or diminished efficacy of alternating or switching between use of the product and its reference product is not greater than the risk of using the reference product without such alternation or switch.”
The definition of interchangeability includes the understanding that the prescriber’s approval is not necessary for substitution of a biosimilar for its reference product.
“If we’re going to have that kind of switching, if they are going to be interchangeable, then we have to have a very high bar,” Dr. Woodcock said.
She added that “any pressure people are feeling to push their patients to biosimilars is from the reimbursement system. There is no non-prescriber switching allowed currently; however, that doesn’t say there isn’t pressure on prescribers to write a different prescription.”
Faster track and bridge to approval
The biosimilar development and approval requires only convincing demonstration of biosimilarity to an existing agent, rather than an independent finding of safety or effectiveness, and the purpose of clinical studies in this case is to address “residual uncertainties,” Dr. Woodcock said.
Drug developers and regulatory authorities alike “are having trouble getting their mind around this concept,” she said.
The FDA requires manufacturers to provide data in their biosimilar drug license applications demonstrating biosimilarity based on analytical studies, animal studies that include toxicity assessments, and one or more clinical studies that include information on immunogenicity and pharmacokinetics (PK) or pharmacodynamics (PD) that is sufficient to demonstrate the safety, purity, and potency of the candidate biosimilar.
The FDA is also allowing manufacturers to submit data from animal studies and specified clinical studies comparing a proposed biosimilar product with a product not licensed in the United States, “as long as we are convinced that the reference product is equivalent to the U.S. product,” Dr. Woodcock said.
This “analytical bridge” process was requested by manufacturers who began development of biosimilars in Europe. The European Medicines Agency approved a biosimilar process in 2005, and gave the nod to the first biosimilar agents to existing erythropoietin products in 2007.
Current and pending
As of early October 2016, 66 programs were enrolled in FDA’s Biosimilar Product Development Program, and CDER has received requests for meetings with manufacturers to discuss what tests and documents are required for the development of biosimilars to 20 different reference products.
The FDA is prohibited from publicly discussing the existence of a pending application unless it has been previously disclosed or acknowledged publicly with the manufacturer’s permission, Dr. Woodcock noted, but as of Oct. 10, 2016, seven companies have announced a total of 10 biologic license applications for biosimilars to etanercept (Enbrel), adalimumab (Humira), pegfilgrastim (Neulasta), epoetin alfa (Epogen/Procrit), filgrastim (Neupogen), and infliximab (Remicade).
The FDA has granted licenses to four biosimilars to date (the four-letter suffix is intended to differentiate biosimilars agents from other biosimilars to the same reference product):
- Zarxio (filgrastim-sndz).
- Inflectra (infliximab-dyyb).
- Erelzi (etanercept-szzs).
- Amjevita (adalimumab-atto).
Physician perspective
“Everything I have heard suggests that biosimilars will be useful, but the scientist in me is a skeptic,” commented Donald Massenburg, MD, PhD, a rheumatologist at Wheaton Franciscan Healthcare in Franklin, Wisc., in an interview.
“I feel better now after learning that current biosimilars are not considered interchangeable, meaning that there can’t be substitutions made without the treating physician’s consent,” he said.
He acknowledged that “I wouldn’t be that excited” if a specific biosimilar was approved for interchangeability and was given to his patients without his knowledge.
Dr. Massenburg pointed to data from the NOR-SWITCH trial comparing the biosimilar Remsima to the reference product Remicade for treatment of rheumatic diseases, psoriasis, and inflammatory bowel disease. The trial showed that Remsima was noninferior to the reference product.
“I would like to be able to say whether a patient should be switched to a biosimilar or not just because of that potential risk,” Dr. Massenburg said.
A rheumatologist in private practice in New England said that what’s really needed in rheumatology is not the availability of more drugs that act like other drugs, but innovative research into therapies with better targeted mechanism of action.
“We’ve been through the ‘me-too’ hype; we did that with nonsteroidal anti-inflammatory drugs,” said J. Scott Toder, MD, director of the Toder Rheumatology and Osteoporosis Center, Providence, R.I.
“I think we need to concentrate on innovative therapies, and we may be able to do something about the escalating price of the biologics on the market by creating drugs with new mechanism of action to actually increase competition and hopefully control prices. I don’t think that having multiple drugs with the same mechanism of action is in the best interest of our patients,” he said in an interview.
Dr. Woodcock, Dr. Massenburg, and Dr. Toder reported having no relevant disclosures.
BOSTON – Biosimilar drugs are not identical twins of original biologic agents, but there are very strong family ties, and the newcomer is expected to look and behave very much like its older relative, said Janet Woodcock, MD, director of the Center for Drug Evaluation and Research at the Food and Drug Administration.
Although biosimilars differ from generic, small-molecule drugs, concerns about the development of biosimilars mirrors the kerfuffle over generic drugs surrounding the passage of the Hatch-Waxman (Drug Price Competition and Patent Term Restoration) Act in 1984.
She noted that clinicians today are asking the same questions about biosimilars that were asked about generics three decades ago:
- Are biosimilars as effective and as safe as the originally licensed biopharmaceuticals?
- If pharmacists substitute biosimilars for prescribed biologics, will patients be adversely affected?
- Can biosimilars reduce the high cost of biologic therapy?
“In certain specialties, this skepticism has persisted to this very day,” she said.
ACA mandate
Biosimilars owe their existence in large measure to the Biologics Price Competition and Innovation Act of 2009 (BPCI), passed as a part of the Affordable Care Act and signed into law by President Obama in 2010.
The act created an abbreviated licensure pathway for biologic products that can be shown to be either biosimilar to or interchangeable with an FDA-licensed reference drug.
A biosimilar is defined as a biological product that is highly similar to the reference product “notwithstanding minor differences in clinically inactive components,” and with no clinically meaningful differences between it and the reference product in terms of purity, safety, and potency.
To be interchangeable, a biosimilar must be expected to produce the same clinical results as the reference drug in any given patient, and “for a product that is administered more than once to an individual, the risk in terms of safety or diminished efficacy of alternating or switching between use of the product and its reference product is not greater than the risk of using the reference product without such alternation or switch.”
The definition of interchangeability includes the understanding that the prescriber’s approval is not necessary for substitution of a biosimilar for its reference product.
“If we’re going to have that kind of switching, if they are going to be interchangeable, then we have to have a very high bar,” Dr. Woodcock said.
She added that “any pressure people are feeling to push their patients to biosimilars is from the reimbursement system. There is no non-prescriber switching allowed currently; however, that doesn’t say there isn’t pressure on prescribers to write a different prescription.”
Faster track and bridge to approval
The biosimilar development and approval requires only convincing demonstration of biosimilarity to an existing agent, rather than an independent finding of safety or effectiveness, and the purpose of clinical studies in this case is to address “residual uncertainties,” Dr. Woodcock said.
Drug developers and regulatory authorities alike “are having trouble getting their mind around this concept,” she said.
The FDA requires manufacturers to provide data in their biosimilar drug license applications demonstrating biosimilarity based on analytical studies, animal studies that include toxicity assessments, and one or more clinical studies that include information on immunogenicity and pharmacokinetics (PK) or pharmacodynamics (PD) that is sufficient to demonstrate the safety, purity, and potency of the candidate biosimilar.
The FDA is also allowing manufacturers to submit data from animal studies and specified clinical studies comparing a proposed biosimilar product with a product not licensed in the United States, “as long as we are convinced that the reference product is equivalent to the U.S. product,” Dr. Woodcock said.
This “analytical bridge” process was requested by manufacturers who began development of biosimilars in Europe. The European Medicines Agency approved a biosimilar process in 2005, and gave the nod to the first biosimilar agents to existing erythropoietin products in 2007.
Current and pending
As of early October 2016, 66 programs were enrolled in FDA’s Biosimilar Product Development Program, and CDER has received requests for meetings with manufacturers to discuss what tests and documents are required for the development of biosimilars to 20 different reference products.
The FDA is prohibited from publicly discussing the existence of a pending application unless it has been previously disclosed or acknowledged publicly with the manufacturer’s permission, Dr. Woodcock noted, but as of Oct. 10, 2016, seven companies have announced a total of 10 biologic license applications for biosimilars to etanercept (Enbrel), adalimumab (Humira), pegfilgrastim (Neulasta), epoetin alfa (Epogen/Procrit), filgrastim (Neupogen), and infliximab (Remicade).
The FDA has granted licenses to four biosimilars to date (the four-letter suffix is intended to differentiate biosimilars agents from other biosimilars to the same reference product):
- Zarxio (filgrastim-sndz).
- Inflectra (infliximab-dyyb).
- Erelzi (etanercept-szzs).
- Amjevita (adalimumab-atto).
Physician perspective
“Everything I have heard suggests that biosimilars will be useful, but the scientist in me is a skeptic,” commented Donald Massenburg, MD, PhD, a rheumatologist at Wheaton Franciscan Healthcare in Franklin, Wisc., in an interview.
“I feel better now after learning that current biosimilars are not considered interchangeable, meaning that there can’t be substitutions made without the treating physician’s consent,” he said.
He acknowledged that “I wouldn’t be that excited” if a specific biosimilar was approved for interchangeability and was given to his patients without his knowledge.
Dr. Massenburg pointed to data from the NOR-SWITCH trial comparing the biosimilar Remsima to the reference product Remicade for treatment of rheumatic diseases, psoriasis, and inflammatory bowel disease. The trial showed that Remsima was noninferior to the reference product.
“I would like to be able to say whether a patient should be switched to a biosimilar or not just because of that potential risk,” Dr. Massenburg said.
A rheumatologist in private practice in New England said that what’s really needed in rheumatology is not the availability of more drugs that act like other drugs, but innovative research into therapies with better targeted mechanism of action.
“We’ve been through the ‘me-too’ hype; we did that with nonsteroidal anti-inflammatory drugs,” said J. Scott Toder, MD, director of the Toder Rheumatology and Osteoporosis Center, Providence, R.I.
“I think we need to concentrate on innovative therapies, and we may be able to do something about the escalating price of the biologics on the market by creating drugs with new mechanism of action to actually increase competition and hopefully control prices. I don’t think that having multiple drugs with the same mechanism of action is in the best interest of our patients,” he said in an interview.
Dr. Woodcock, Dr. Massenburg, and Dr. Toder reported having no relevant disclosures.
EXPERT ANALYSIS FROM A BIOSIMILARS IN RHEUMATOLOGY SYMPOSIUM
Hospitalists Need to Rethink the Way They Evaluate Students
Delivering feedback is a fundamental skill in medicine. Feedback ensures trainees remain on track to meet expected goals and standards. At some point in our careers, all of us have been on the receiving end of feedback. Many of us have likely had the opportunity to provide feedback to students or junior residents during our training. Moving from the role of trainee to supervisor presents a unique set of challenges and responsibilities to the young hospitalist.

Despite an extensive amount published on feedback, translation from theory to practice remains challenging.1 When surveyed, medical students and residents commonly perceive they do not receive enough feedback.2 Conversely, attendees of faculty development courses frequently indicate their greatest need is learning how to give feedback more effectively.3 Why does this performance gap exist?
The Issues
Careful exploration of our current training model reveals several systemic barriers to effective feedback. For one, many faculty members who supervise trainees are not formally trained educators. As such, they may lack the proper skills set to deliver feedback.1 Additionally, lack of time is often cited in the pressure to complete both clinical and academic duties within a packed workday. If learners aren’t directly observed by their supervisors, the impact and quality of feedback substantially diminishes.4 Likewise, if feedback is not embedded in the local culture and expected by both educator and learner, it can be perceived as a burden rather than a valuable exercise.

Feedback can evoke deep, sometimes subconscious emotional responses in both supervisor and recipient. During verbal interactions with trainees, dialogue tends to assume positive or neutral tones regardless of content.5 To avoid bruising a young learner’s ego, a well-intentioned educator may talk around the actual problem, using indirect statements in an attempt to “soften the blow.” Fearing a negative evaluation, the student may support and reinforce the teacher’s avoidance, further obscuring the message being sent. This concept is known as “vanishing feedback” and is a common barrier to the delivery of effective feedback.4 Educators additionally may shy away from giving constructive feedback because they fear reprisal on teaching evaluations.
Mounting evidence shows physicians, as a whole, tend to overestimate their abilities, and many are not skilled at self-assessment.6 When physician-learners receive feedback incongruent with their own self-perceptions, it may trigger feelings of anger, sadness, guilt, or self-doubt, which may block the receipt of any useful information. The so-called “millennial generation effect,” describing current medical school graduates, may further compound this issue. Millennials are “raised with an emphasis on being special; a previous absence of a balanced focus on weakness may present a barrier to accepting the validity of negative feedback.”1,5 As such, certain learners may intentionally avoid feedback as a method of self-preservation.
A New Approach
Many of us were taught to use the “feedback sandwich,” in which two positive statements surround a single negative corrective comment. This model, however, has some notable weaknesses. Given the ratio of positive to negative statements, educators may concentrate too heavily on the positive, diluting any constructive criticism and leaving learners with a false impression. Alternatively, trainees may learn to ignore positive comments while waiting for the other shoe to drop. As such, any initial positivity may feel insincere and artificial.7
Instead, we advocate using the “reflective feedback conversation,” a model that begins with self-assessment and places the onus on learners to identify their strengths and weaknesses.7 For example, a trainee might remark, “I struggle with controlling my temper when I am stressed.” The educator might reinforce that comment by stating, “I noticed you raised your voice last week when talking with the nurse because she forgot to administer Lasix.” To conclude the conversation, the teacher and student discuss shared goal setting and mutually agree on future improvements. Notably, this model does not facilitate conversation about problems a learner fails to detect. Hence, the educator must be prepared to deliver feedback outside of the learner’s own assessment.
Here are our favorite tips and tricks for delivering effective feedback:
- Establish a positive learning climate. Educators must partner with learners to generate an atmosphere of mutual trust and respect.1,3,4,8 An example of how to ally with learners is to announce early on, “As a teacher, I really value feedback. As such, I plan on giving feedback throughout the rotation because I want you to be the best doctor you can possibly be.”
- Require reflection. Effective feedback hinges on learners’ ability to self-assess.2,5,7 One approach is starting each feedback session with a simple open-ended question, such as, “How do you think you are doing?” Alternatively, you could be more specific, such as, “How do you think you did in managing the patient’s electrolytes when he went into diabetic ketoacidosis?”
- Be prompt. Feedback should be timely.1,4,7,8 An important distinction between feedback and evaluation is that feedback is formative, enabling learners to make needed changes before the end of a course, whereas evaluation is summative and presents a distinct judgment.1,4 If feedback is withheld until the end of the rotation, learners will not have an opportunity to remediate behaviors.
- Take advantage of different formats. Try a brief, concrete suggestion on the fly. A statement that might occur on bedside rounds is, “Allow me to show you a better technique to measure the liver span.” Or use a teachable event, such as a medical error or a particularly challenging case. Pulling interns aside after they deliver sobering news is a great opportunity to provide feedback in a semiformal fashion. Finally, formal sit-down feedback should be scheduled halfway through each rotation to ensure learners are on track and to address any major issues, such as professionalism or an inadequate clinical performance.2
- Be specific. Focus on behaviors and examples rather than judgments.1,2,4,7,8 For example, we have all experienced the inattentive student. Instead of framing feedback as, “It seems like you don’t care about medicine because you weren’t paying attention on rounds,” one could say, “I noticed you were fidgeting and looking at your phone during Aaron’s presentation.” Feedback should be based on firsthand observations and should be descriptive, utilizing neutral language.
- Avoid information overload. Feedback is best consumed in small snacks rather than an all-you-can-eat buffet.1,7 Your goal should not be to completely overhaul a learner but rather to focus on a few observable, correctable behaviors.
- Be empathetic. To make negative feedback less threatening, take yourself off the pedestal. An example of this could be saying, “As a third-year medical student, I struggled to remember all the right questions to ask, so performing a thorough review of systems helped me to catch the things I would miss.”
- Confirm understanding. It is important to know the learner has heard the feedback and to conclude the session with an action plan.
Just as hospitals engage in continuous quality improvement, as professionals, we should all strive for continuous self-improvement. Giving and receiving feedback is critical to personal growth. It is our hope that by using these tips, all of us will improve, creating a new generation of providers who give effective and useful feedback.
References
- Anderson PA. Giving feedback on clinical skills: are we starving our young? J Grad Med Educ. 2012;4(2):154-158. doi:10.4300/JGME-D-11-000295.1.
- Branch WT, Paranjape A. Feedback and reflection: teaching methods for clinical settings. Acad Med. 2002;77(12 Pt 1):1185-1188.
- Hewson MG, Little ML. Giving feedback in medical education: verification of recommended techniques. J Gen Intern Med. 1998;13(2):111-116.
- Ende J. Feedback in clinical medical education. JAMA. 1983;250(6):777-781.
- Bing-You RG, Trowbridge RL. Why medical educators may be failing at feedback. JAMA. 2009;302(12):1330-1331.
- Davis DA, Mazmanian PE, Fordis M, Van Harrison R, Thorpe KE, Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
- Cantillon P, Sargeant J. Giving feedback in clinical settings. BMJ. 2008;337:a1961.
- Ramani S, Krackov SK. Twelve tips for giving feedback effectively in the clinical environment. Med Teach. 2012;34(10):787-791.
Delivering feedback is a fundamental skill in medicine. Feedback ensures trainees remain on track to meet expected goals and standards. At some point in our careers, all of us have been on the receiving end of feedback. Many of us have likely had the opportunity to provide feedback to students or junior residents during our training. Moving from the role of trainee to supervisor presents a unique set of challenges and responsibilities to the young hospitalist.
Despite an extensive amount published on feedback, translation from theory to practice remains challenging.1 When surveyed, medical students and residents commonly perceive they do not receive enough feedback.2 Conversely, attendees of faculty development courses frequently indicate their greatest need is learning how to give feedback more effectively.3 Why does this performance gap exist?
The Issues
Careful exploration of our current training model reveals several systemic barriers to effective feedback. For one, many faculty members who supervise trainees are not formally trained educators. As such, they may lack the proper skills set to deliver feedback.1 Additionally, lack of time is often cited in the pressure to complete both clinical and academic duties within a packed workday. If learners aren’t directly observed by their supervisors, the impact and quality of feedback substantially diminishes.4 Likewise, if feedback is not embedded in the local culture and expected by both educator and learner, it can be perceived as a burden rather than a valuable exercise.
Feedback can evoke deep, sometimes subconscious emotional responses in both supervisor and recipient. During verbal interactions with trainees, dialogue tends to assume positive or neutral tones regardless of content.5 To avoid bruising a young learner’s ego, a well-intentioned educator may talk around the actual problem, using indirect statements in an attempt to “soften the blow.” Fearing a negative evaluation, the student may support and reinforce the teacher’s avoidance, further obscuring the message being sent. This concept is known as “vanishing feedback” and is a common barrier to the delivery of effective feedback.4 Educators additionally may shy away from giving constructive feedback because they fear reprisal on teaching evaluations.
Mounting evidence shows physicians, as a whole, tend to overestimate their abilities, and many are not skilled at self-assessment.6 When physician-learners receive feedback incongruent with their own self-perceptions, it may trigger feelings of anger, sadness, guilt, or self-doubt, which may block the receipt of any useful information. The so-called “millennial generation effect,” describing current medical school graduates, may further compound this issue. Millennials are “raised with an emphasis on being special; a previous absence of a balanced focus on weakness may present a barrier to accepting the validity of negative feedback.”1,5 As such, certain learners may intentionally avoid feedback as a method of self-preservation.
A New Approach
Many of us were taught to use the “feedback sandwich,” in which two positive statements surround a single negative corrective comment. This model, however, has some notable weaknesses. Given the ratio of positive to negative statements, educators may concentrate too heavily on the positive, diluting any constructive criticism and leaving learners with a false impression. Alternatively, trainees may learn to ignore positive comments while waiting for the other shoe to drop. As such, any initial positivity may feel insincere and artificial.7
Instead, we advocate using the “reflective feedback conversation,” a model that begins with self-assessment and places the onus on learners to identify their strengths and weaknesses.7 For example, a trainee might remark, “I struggle with controlling my temper when I am stressed.” The educator might reinforce that comment by stating, “I noticed you raised your voice last week when talking with the nurse because she forgot to administer Lasix.” To conclude the conversation, the teacher and student discuss shared goal setting and mutually agree on future improvements. Notably, this model does not facilitate conversation about problems a learner fails to detect. Hence, the educator must be prepared to deliver feedback outside of the learner’s own assessment.
Here are our favorite tips and tricks for delivering effective feedback:
- Establish a positive learning climate. Educators must partner with learners to generate an atmosphere of mutual trust and respect.1,3,4,8 An example of how to ally with learners is to announce early on, “As a teacher, I really value feedback. As such, I plan on giving feedback throughout the rotation because I want you to be the best doctor you can possibly be.”
- Require reflection. Effective feedback hinges on learners’ ability to self-assess.2,5,7 One approach is starting each feedback session with a simple open-ended question, such as, “How do you think you are doing?” Alternatively, you could be more specific, such as, “How do you think you did in managing the patient’s electrolytes when he went into diabetic ketoacidosis?”
- Be prompt. Feedback should be timely.1,4,7,8 An important distinction between feedback and evaluation is that feedback is formative, enabling learners to make needed changes before the end of a course, whereas evaluation is summative and presents a distinct judgment.1,4 If feedback is withheld until the end of the rotation, learners will not have an opportunity to remediate behaviors.
- Take advantage of different formats. Try a brief, concrete suggestion on the fly. A statement that might occur on bedside rounds is, “Allow me to show you a better technique to measure the liver span.” Or use a teachable event, such as a medical error or a particularly challenging case. Pulling interns aside after they deliver sobering news is a great opportunity to provide feedback in a semiformal fashion. Finally, formal sit-down feedback should be scheduled halfway through each rotation to ensure learners are on track and to address any major issues, such as professionalism or an inadequate clinical performance.2
- Be specific. Focus on behaviors and examples rather than judgments.1,2,4,7,8 For example, we have all experienced the inattentive student. Instead of framing feedback as, “It seems like you don’t care about medicine because you weren’t paying attention on rounds,” one could say, “I noticed you were fidgeting and looking at your phone during Aaron’s presentation.” Feedback should be based on firsthand observations and should be descriptive, utilizing neutral language.
- Avoid information overload. Feedback is best consumed in small snacks rather than an all-you-can-eat buffet.1,7 Your goal should not be to completely overhaul a learner but rather to focus on a few observable, correctable behaviors.
- Be empathetic. To make negative feedback less threatening, take yourself off the pedestal. An example of this could be saying, “As a third-year medical student, I struggled to remember all the right questions to ask, so performing a thorough review of systems helped me to catch the things I would miss.”
- Confirm understanding. It is important to know the learner has heard the feedback and to conclude the session with an action plan.
Just as hospitals engage in continuous quality improvement, as professionals, we should all strive for continuous self-improvement. Giving and receiving feedback is critical to personal growth. It is our hope that by using these tips, all of us will improve, creating a new generation of providers who give effective and useful feedback.
References
- Anderson PA. Giving feedback on clinical skills: are we starving our young? J Grad Med Educ. 2012;4(2):154-158. doi:10.4300/JGME-D-11-000295.1.
- Branch WT, Paranjape A. Feedback and reflection: teaching methods for clinical settings. Acad Med. 2002;77(12 Pt 1):1185-1188.
- Hewson MG, Little ML. Giving feedback in medical education: verification of recommended techniques. J Gen Intern Med. 1998;13(2):111-116.
- Ende J. Feedback in clinical medical education. JAMA. 1983;250(6):777-781.
- Bing-You RG, Trowbridge RL. Why medical educators may be failing at feedback. JAMA. 2009;302(12):1330-1331.
- Davis DA, Mazmanian PE, Fordis M, Van Harrison R, Thorpe KE, Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
- Cantillon P, Sargeant J. Giving feedback in clinical settings. BMJ. 2008;337:a1961.
- Ramani S, Krackov SK. Twelve tips for giving feedback effectively in the clinical environment. Med Teach. 2012;34(10):787-791.
Delivering feedback is a fundamental skill in medicine. Feedback ensures trainees remain on track to meet expected goals and standards. At some point in our careers, all of us have been on the receiving end of feedback. Many of us have likely had the opportunity to provide feedback to students or junior residents during our training. Moving from the role of trainee to supervisor presents a unique set of challenges and responsibilities to the young hospitalist.
Despite an extensive amount published on feedback, translation from theory to practice remains challenging.1 When surveyed, medical students and residents commonly perceive they do not receive enough feedback.2 Conversely, attendees of faculty development courses frequently indicate their greatest need is learning how to give feedback more effectively.3 Why does this performance gap exist?
The Issues
Careful exploration of our current training model reveals several systemic barriers to effective feedback. For one, many faculty members who supervise trainees are not formally trained educators. As such, they may lack the proper skills set to deliver feedback.1 Additionally, lack of time is often cited in the pressure to complete both clinical and academic duties within a packed workday. If learners aren’t directly observed by their supervisors, the impact and quality of feedback substantially diminishes.4 Likewise, if feedback is not embedded in the local culture and expected by both educator and learner, it can be perceived as a burden rather than a valuable exercise.
Feedback can evoke deep, sometimes subconscious emotional responses in both supervisor and recipient. During verbal interactions with trainees, dialogue tends to assume positive or neutral tones regardless of content.5 To avoid bruising a young learner’s ego, a well-intentioned educator may talk around the actual problem, using indirect statements in an attempt to “soften the blow.” Fearing a negative evaluation, the student may support and reinforce the teacher’s avoidance, further obscuring the message being sent. This concept is known as “vanishing feedback” and is a common barrier to the delivery of effective feedback.4 Educators additionally may shy away from giving constructive feedback because they fear reprisal on teaching evaluations.
Mounting evidence shows physicians, as a whole, tend to overestimate their abilities, and many are not skilled at self-assessment.6 When physician-learners receive feedback incongruent with their own self-perceptions, it may trigger feelings of anger, sadness, guilt, or self-doubt, which may block the receipt of any useful information. The so-called “millennial generation effect,” describing current medical school graduates, may further compound this issue. Millennials are “raised with an emphasis on being special; a previous absence of a balanced focus on weakness may present a barrier to accepting the validity of negative feedback.”1,5 As such, certain learners may intentionally avoid feedback as a method of self-preservation.
A New Approach
Many of us were taught to use the “feedback sandwich,” in which two positive statements surround a single negative corrective comment. This model, however, has some notable weaknesses. Given the ratio of positive to negative statements, educators may concentrate too heavily on the positive, diluting any constructive criticism and leaving learners with a false impression. Alternatively, trainees may learn to ignore positive comments while waiting for the other shoe to drop. As such, any initial positivity may feel insincere and artificial.7
Instead, we advocate using the “reflective feedback conversation,” a model that begins with self-assessment and places the onus on learners to identify their strengths and weaknesses.7 For example, a trainee might remark, “I struggle with controlling my temper when I am stressed.” The educator might reinforce that comment by stating, “I noticed you raised your voice last week when talking with the nurse because she forgot to administer Lasix.” To conclude the conversation, the teacher and student discuss shared goal setting and mutually agree on future improvements. Notably, this model does not facilitate conversation about problems a learner fails to detect. Hence, the educator must be prepared to deliver feedback outside of the learner’s own assessment.
Here are our favorite tips and tricks for delivering effective feedback:
- Establish a positive learning climate. Educators must partner with learners to generate an atmosphere of mutual trust and respect.1,3,4,8 An example of how to ally with learners is to announce early on, “As a teacher, I really value feedback. As such, I plan on giving feedback throughout the rotation because I want you to be the best doctor you can possibly be.”
- Require reflection. Effective feedback hinges on learners’ ability to self-assess.2,5,7 One approach is starting each feedback session with a simple open-ended question, such as, “How do you think you are doing?” Alternatively, you could be more specific, such as, “How do you think you did in managing the patient’s electrolytes when he went into diabetic ketoacidosis?”
- Be prompt. Feedback should be timely.1,4,7,8 An important distinction between feedback and evaluation is that feedback is formative, enabling learners to make needed changes before the end of a course, whereas evaluation is summative and presents a distinct judgment.1,4 If feedback is withheld until the end of the rotation, learners will not have an opportunity to remediate behaviors.
- Take advantage of different formats. Try a brief, concrete suggestion on the fly. A statement that might occur on bedside rounds is, “Allow me to show you a better technique to measure the liver span.” Or use a teachable event, such as a medical error or a particularly challenging case. Pulling interns aside after they deliver sobering news is a great opportunity to provide feedback in a semiformal fashion. Finally, formal sit-down feedback should be scheduled halfway through each rotation to ensure learners are on track and to address any major issues, such as professionalism or an inadequate clinical performance.2
- Be specific. Focus on behaviors and examples rather than judgments.1,2,4,7,8 For example, we have all experienced the inattentive student. Instead of framing feedback as, “It seems like you don’t care about medicine because you weren’t paying attention on rounds,” one could say, “I noticed you were fidgeting and looking at your phone during Aaron’s presentation.” Feedback should be based on firsthand observations and should be descriptive, utilizing neutral language.
- Avoid information overload. Feedback is best consumed in small snacks rather than an all-you-can-eat buffet.1,7 Your goal should not be to completely overhaul a learner but rather to focus on a few observable, correctable behaviors.
- Be empathetic. To make negative feedback less threatening, take yourself off the pedestal. An example of this could be saying, “As a third-year medical student, I struggled to remember all the right questions to ask, so performing a thorough review of systems helped me to catch the things I would miss.”
- Confirm understanding. It is important to know the learner has heard the feedback and to conclude the session with an action plan.
Just as hospitals engage in continuous quality improvement, as professionals, we should all strive for continuous self-improvement. Giving and receiving feedback is critical to personal growth. It is our hope that by using these tips, all of us will improve, creating a new generation of providers who give effective and useful feedback.
References
- Anderson PA. Giving feedback on clinical skills: are we starving our young? J Grad Med Educ. 2012;4(2):154-158. doi:10.4300/JGME-D-11-000295.1.
- Branch WT, Paranjape A. Feedback and reflection: teaching methods for clinical settings. Acad Med. 2002;77(12 Pt 1):1185-1188.
- Hewson MG, Little ML. Giving feedback in medical education: verification of recommended techniques. J Gen Intern Med. 1998;13(2):111-116.
- Ende J. Feedback in clinical medical education. JAMA. 1983;250(6):777-781.
- Bing-You RG, Trowbridge RL. Why medical educators may be failing at feedback. JAMA. 2009;302(12):1330-1331.
- Davis DA, Mazmanian PE, Fordis M, Van Harrison R, Thorpe KE, Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
- Cantillon P, Sargeant J. Giving feedback in clinical settings. BMJ. 2008;337:a1961.
- Ramani S, Krackov SK. Twelve tips for giving feedback effectively in the clinical environment. Med Teach. 2012;34(10):787-791.
Team develops multicolor electron microscopy
of endosomal uptake
of peptide proteins
Image by Adams et al/
Cell Chemical Biology 2016
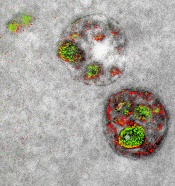
Researchers say they have found a way to image specific cellular components using multicolor electron microscopy.
With their method, which the team worked on for nearly 15 years, up to 3 colors at a time (green, red, or yellow) can be used in an image.
A detector on the microscope captures electrons lost from metal ions painted over the specimen and records the metal’s energy loss signature as a color.
A technician must add the ionized metals one at a time and then lay the full color map over the still microscopy image.
The researchers described this method in detail in Cell Chemical Biology.
“This method has many potential applications in biology,” said study author Stephen Adams, PhD, of the University of California, San Diego in La Jolla.
“In the paper, we demonstrate how it can distinguish cellular compartments or track proteins and tag cells.”
For the multicolor effect to work, the researchers needed metal complexes that are stable enough to withstand application (meaning they don’t quickly deteriorate and blur the image) and have a distinct electron energy loss signature.
The researchers used ionized lanthanum (La), cerium (Ce), and praseodymium (Pr)—all metals in the lanthanide family. Each metal complex was laid down sequentially as a precipitate onto the specimen as it sat in the microscope.
“One challenge that kept us from publishing this much earlier, because we had the chemistry and we had an instrument that worked about 4 years ago, was we needed a way to deposit the metal compounds sequentially,” said study author Mark Ellisman, PhD, of the University of California, San Diego.
“We spent an awful lot of time trying to figure out how to deposit one of the lanthanides and then clear it so that it didn’t react when we deposited a second signal on the first site.”
Once the application process had been established, the researchers illustrated the power of multicolor electron microscopy by visualizing 2 brain cells sharing a single synapse. They also showed peptides entering through a cell membrane.
The researchers said there is more chemistry to be done to perfect the metal ion application process as well as produce images with more colors. There may also be ways to increase the amount of metal ions that can be deposited, which could help with resolution.
Many in the biochemical community should be able to begin using this technique right away, as it takes advantage of tools that are already found in laboratories.
This study is one of the last that Roger Tsien, PhD, who won a 2008 Nobel Prize in Chemistry for the discovery and application of green fluorescent protein to biochemical imaging, saw accepted by a journal before his death last August.
He did the first experiments to develop the chemical compounds needed for the multicolor imaging method nearly 15 years ago.
“One theme that has gone through all of Roger’s work is the desire to peer more closely into the workings of the cell,” Dr Adams said.
“With all of the fluorescence techniques that he’s introduced, he was able to do that in live cells and make action movies of them in vivid colors. But he always wanted to look closer, and now he’s left the beginnings for a method where we can add colors to electron microscopy.”
“This is clearly an example of Roger’s brilliance at chemistry and how he saw that, if we could do this, we would be able to enjoy the advantages of electron microscopy,” Dr Ellisman added.
“The biggest advantage of electron microscopy that we saw is that you have weak contrasts by the nature of the way that staining works, so color-specific labels give context to all of the rich information in the scene of which molecules are operating.” ![]()
of endosomal uptake
of peptide proteins
Image by Adams et al/
Cell Chemical Biology 2016
Researchers say they have found a way to image specific cellular components using multicolor electron microscopy.
With their method, which the team worked on for nearly 15 years, up to 3 colors at a time (green, red, or yellow) can be used in an image.
A detector on the microscope captures electrons lost from metal ions painted over the specimen and records the metal’s energy loss signature as a color.
A technician must add the ionized metals one at a time and then lay the full color map over the still microscopy image.
The researchers described this method in detail in Cell Chemical Biology.
“This method has many potential applications in biology,” said study author Stephen Adams, PhD, of the University of California, San Diego in La Jolla.
“In the paper, we demonstrate how it can distinguish cellular compartments or track proteins and tag cells.”
For the multicolor effect to work, the researchers needed metal complexes that are stable enough to withstand application (meaning they don’t quickly deteriorate and blur the image) and have a distinct electron energy loss signature.
The researchers used ionized lanthanum (La), cerium (Ce), and praseodymium (Pr)—all metals in the lanthanide family. Each metal complex was laid down sequentially as a precipitate onto the specimen as it sat in the microscope.
“One challenge that kept us from publishing this much earlier, because we had the chemistry and we had an instrument that worked about 4 years ago, was we needed a way to deposit the metal compounds sequentially,” said study author Mark Ellisman, PhD, of the University of California, San Diego.
“We spent an awful lot of time trying to figure out how to deposit one of the lanthanides and then clear it so that it didn’t react when we deposited a second signal on the first site.”
Once the application process had been established, the researchers illustrated the power of multicolor electron microscopy by visualizing 2 brain cells sharing a single synapse. They also showed peptides entering through a cell membrane.
The researchers said there is more chemistry to be done to perfect the metal ion application process as well as produce images with more colors. There may also be ways to increase the amount of metal ions that can be deposited, which could help with resolution.
Many in the biochemical community should be able to begin using this technique right away, as it takes advantage of tools that are already found in laboratories.
This study is one of the last that Roger Tsien, PhD, who won a 2008 Nobel Prize in Chemistry for the discovery and application of green fluorescent protein to biochemical imaging, saw accepted by a journal before his death last August.
He did the first experiments to develop the chemical compounds needed for the multicolor imaging method nearly 15 years ago.
“One theme that has gone through all of Roger’s work is the desire to peer more closely into the workings of the cell,” Dr Adams said.
“With all of the fluorescence techniques that he’s introduced, he was able to do that in live cells and make action movies of them in vivid colors. But he always wanted to look closer, and now he’s left the beginnings for a method where we can add colors to electron microscopy.”
“This is clearly an example of Roger’s brilliance at chemistry and how he saw that, if we could do this, we would be able to enjoy the advantages of electron microscopy,” Dr Ellisman added.
“The biggest advantage of electron microscopy that we saw is that you have weak contrasts by the nature of the way that staining works, so color-specific labels give context to all of the rich information in the scene of which molecules are operating.” ![]()
of endosomal uptake
of peptide proteins
Image by Adams et al/
Cell Chemical Biology 2016
Researchers say they have found a way to image specific cellular components using multicolor electron microscopy.
With their method, which the team worked on for nearly 15 years, up to 3 colors at a time (green, red, or yellow) can be used in an image.
A detector on the microscope captures electrons lost from metal ions painted over the specimen and records the metal’s energy loss signature as a color.
A technician must add the ionized metals one at a time and then lay the full color map over the still microscopy image.
The researchers described this method in detail in Cell Chemical Biology.
“This method has many potential applications in biology,” said study author Stephen Adams, PhD, of the University of California, San Diego in La Jolla.
“In the paper, we demonstrate how it can distinguish cellular compartments or track proteins and tag cells.”
For the multicolor effect to work, the researchers needed metal complexes that are stable enough to withstand application (meaning they don’t quickly deteriorate and blur the image) and have a distinct electron energy loss signature.
The researchers used ionized lanthanum (La), cerium (Ce), and praseodymium (Pr)—all metals in the lanthanide family. Each metal complex was laid down sequentially as a precipitate onto the specimen as it sat in the microscope.
“One challenge that kept us from publishing this much earlier, because we had the chemistry and we had an instrument that worked about 4 years ago, was we needed a way to deposit the metal compounds sequentially,” said study author Mark Ellisman, PhD, of the University of California, San Diego.
“We spent an awful lot of time trying to figure out how to deposit one of the lanthanides and then clear it so that it didn’t react when we deposited a second signal on the first site.”
Once the application process had been established, the researchers illustrated the power of multicolor electron microscopy by visualizing 2 brain cells sharing a single synapse. They also showed peptides entering through a cell membrane.
The researchers said there is more chemistry to be done to perfect the metal ion application process as well as produce images with more colors. There may also be ways to increase the amount of metal ions that can be deposited, which could help with resolution.
Many in the biochemical community should be able to begin using this technique right away, as it takes advantage of tools that are already found in laboratories.
This study is one of the last that Roger Tsien, PhD, who won a 2008 Nobel Prize in Chemistry for the discovery and application of green fluorescent protein to biochemical imaging, saw accepted by a journal before his death last August.
He did the first experiments to develop the chemical compounds needed for the multicolor imaging method nearly 15 years ago.
“One theme that has gone through all of Roger’s work is the desire to peer more closely into the workings of the cell,” Dr Adams said.
“With all of the fluorescence techniques that he’s introduced, he was able to do that in live cells and make action movies of them in vivid colors. But he always wanted to look closer, and now he’s left the beginnings for a method where we can add colors to electron microscopy.”
“This is clearly an example of Roger’s brilliance at chemistry and how he saw that, if we could do this, we would be able to enjoy the advantages of electron microscopy,” Dr Ellisman added.
“The biggest advantage of electron microscopy that we saw is that you have weak contrasts by the nature of the way that staining works, so color-specific labels give context to all of the rich information in the scene of which molecules are operating.” ![]()
Yes, pediatric practices can provide immunizations without going broke
SAN FRANCISCO – With a little number crunching and strategizing, pediatric practices can provide immunizations to their patients without getting financially soaked, according to Chip Hart, a pediatric practice management consultant.
He discussed various pitfalls and challenges when it comes to the business aspects of providing immunizations, and offered some solutions at the annual meeting of the American Academy of Pediatrics.

His company has collected data suggesting that as of 2015, revenue from vaccine products made up fully 21% of all revenue in private pediatric practices, a near doubling from the value in 2003. As a consultant today, “I try to find out how practices manage the vaccines because, after staff, it’s your biggest expense,” he noted.
Spotting hidden costs
In its business case, the AAP determined that direct and indirect expenses for vaccine product total to 17% to 28% of the cost. In other words, “if you buy a vaccine for $100, you need to collect somewhere between $117 and $128, on average, just to break even,” Mr. Hart explained.
What accounts for that extra expense? Carrying costs that are commonly overlooked, namely, those myriad costs of providing immunizations that accrue before a child is given any vaccine and that can add up quickly.
They include the costs of the refrigerator and examination table; the sharps and waste management; insurance to cover vaccine loss; vaccine wastage and denials; and opportunity cost, that is, the cost of not being able to invest the funds tied up in vaccine sitting in the fridge – some $75,000 to $100,000 for the average practice – elsewhere.
Add to those personnel costs; costs related to activities such as ordering, inventory and storage management, registry input, and temperature monitoring; and malpractice coverage. And not to be forgotten is the inability to collect payment for some vaccines.
“You’re not paid for carrying costs. Unfortunately, society or the American health care system has given pediatricians this burden,” Mr. Hart commented.
Doing the math
Pediatricians can get a handle on the true costs to their practice of providing immunizations by spending just an hour or two crunching some key numbers, according to Mr. Hart.
They should start by ascertaining those carrying costs. For example, assuming hazardous waste costs run $3,500 per year, vaccines account for 50% of the waste, and the practice gives 13,000 vaccines annually, it averages out to $0.13 per vaccine.
Similar calculations are done to determine the costs of administering the shot (preparing, administering, counseling, billing, recording, putting it in the registry, and so on), arriving at about $12 per vaccine. The largest share here comes from clinicians, so calculations focus on their hourly wages and the percent of their time spent on vaccines.
Next is a calculation of the cost of the vaccine product. This calculation starts with the hypothetical invoiced amount of $100, factors in units that are wasted or go unpaid (at least 5%, according to AAP data), and tacks on the distributed carrying costs, arriving finally at an actual cost to the practice of about $120.
Last, all of these data are loaded into a payer-specific spreadsheet. Commonly, payers go by Red Book values and will therefore cover, for example, only $98 of that $100 invoice cost of the vaccine. But they will pay roughly $27 for its administration.
Taken together, the math suggests the practice bears a total cost of $132 for this vaccine ($120 for the product and $12 for its administration) but will collect only $125 from this payer ($98 for the product and $27 for its administration).
“You see over and over again that the payers underpay for the vaccines and pay you well for the administration, and it very often makes up the difference,” Mr. Hart noted. “But even with that boost on the admin side, this practice is losing money on this vaccine – they get $125 for something that costs them $132.”
Practices strapped for time can use some estimates in their spreadsheets instead, he said. “If you use an assumption of 25% over your invoice” – roughly the midpoint between the AAP’s 17% and 28% – “and $12 to $15 on your administration” – based on the value found in a study using time-motion analysis (Pediatrics. 2009 Dec;124 Suppl 5:S492-8) – “for your costs, all you need is your fee schedule, and you can make a spreadsheet to find out whether it makes sense to continue giving immunizations to this payer’s kids.”
Striving for profitability
“In all honesty, from what I see nationally, pediatricians break even on vaccines. It’s a break-even situation, on average,” Mr. Hart commented. “But who wants to be average? No one. We want you to actually be profitable with vaccines because it’s the only way you can continue to give them.”
Practices can take a variety of steps toward that goal. First, they should negotiate payments with payers, using the AAP’s business case and other literature. “Don’t listen to anybody” who says you can’t negotiate, he stressed. “You can negotiate. I don’t care if you’re a solo practice or you’ve just opened. If a payer says they can’t negotiate, they are fibbing to you. The only payers who don’t negotiate are the state Medicaid and Medicare. Everyone else can and does.”
Second, practices should ensure that they are using proper Current Procedural Terminology codes when submitting claims to payers to maximize payment.
“I still see too many practices who don’t bill for these properly,” Mr. Hart commented. “If you have a typical pediatric practice and you use more 90471s and 90472s than 90460s and 90461s, and frankly, if [the latter] aren’t two to three to four to five times more common… you are losing a lot of money.”
Third, practices should join or confirm that they belong to an effective group purchasing organization (GPO) to reduce their vaccine costs, with data suggesting that doing so will save the practice $10,000 to $15,000 per physician each year.
“If you are solo, out on the furthest edge of Alaska, you can see Russia from your house, and you have no leverage whatsoever, you can sign up with one of these GPOs and you are as strong as any hospital,” he said. The AAP helps here as well, by maintaining a list of GPOs on its website.
Fourth, practices should review their vaccine delivery work flow to look for money leaks, Mr. Hart advised. For example, physicians who get caught up in tasks such as ordering and inventorying are losing revenue that could come in from seeing patients.
“This is the sort of thing that affects your bottom line substantially. And it’s exactly the sort of thing that is an invisible expense: the business owners don’t consider their time as part of the expense of doing this administration,” he said.
Additionally, legacy procedures should be re-evaluated to see if they can be streamlined. Gains also may be made here from investing in better technology, such as a refrigerator with a glass door that saves time by allowing ready identification of vaccines.
Finally, practices should join the AAP’s Section on Administration and Practice Management (SOAPM) as it’s an invaluable, interactive resource in this area when questions or challenges arise, Mr. Hart recommended.
[email protected]
SAN FRANCISCO – With a little number crunching and strategizing, pediatric practices can provide immunizations to their patients without getting financially soaked, according to Chip Hart, a pediatric practice management consultant.
He discussed various pitfalls and challenges when it comes to the business aspects of providing immunizations, and offered some solutions at the annual meeting of the American Academy of Pediatrics.
His company has collected data suggesting that as of 2015, revenue from vaccine products made up fully 21% of all revenue in private pediatric practices, a near doubling from the value in 2003. As a consultant today, “I try to find out how practices manage the vaccines because, after staff, it’s your biggest expense,” he noted.
Spotting hidden costs
In its business case, the AAP determined that direct and indirect expenses for vaccine product total to 17% to 28% of the cost. In other words, “if you buy a vaccine for $100, you need to collect somewhere between $117 and $128, on average, just to break even,” Mr. Hart explained.
What accounts for that extra expense? Carrying costs that are commonly overlooked, namely, those myriad costs of providing immunizations that accrue before a child is given any vaccine and that can add up quickly.
They include the costs of the refrigerator and examination table; the sharps and waste management; insurance to cover vaccine loss; vaccine wastage and denials; and opportunity cost, that is, the cost of not being able to invest the funds tied up in vaccine sitting in the fridge – some $75,000 to $100,000 for the average practice – elsewhere.
Add to those personnel costs; costs related to activities such as ordering, inventory and storage management, registry input, and temperature monitoring; and malpractice coverage. And not to be forgotten is the inability to collect payment for some vaccines.
“You’re not paid for carrying costs. Unfortunately, society or the American health care system has given pediatricians this burden,” Mr. Hart commented.
Doing the math
Pediatricians can get a handle on the true costs to their practice of providing immunizations by spending just an hour or two crunching some key numbers, according to Mr. Hart.
They should start by ascertaining those carrying costs. For example, assuming hazardous waste costs run $3,500 per year, vaccines account for 50% of the waste, and the practice gives 13,000 vaccines annually, it averages out to $0.13 per vaccine.
Similar calculations are done to determine the costs of administering the shot (preparing, administering, counseling, billing, recording, putting it in the registry, and so on), arriving at about $12 per vaccine. The largest share here comes from clinicians, so calculations focus on their hourly wages and the percent of their time spent on vaccines.
Next is a calculation of the cost of the vaccine product. This calculation starts with the hypothetical invoiced amount of $100, factors in units that are wasted or go unpaid (at least 5%, according to AAP data), and tacks on the distributed carrying costs, arriving finally at an actual cost to the practice of about $120.
Last, all of these data are loaded into a payer-specific spreadsheet. Commonly, payers go by Red Book values and will therefore cover, for example, only $98 of that $100 invoice cost of the vaccine. But they will pay roughly $27 for its administration.
Taken together, the math suggests the practice bears a total cost of $132 for this vaccine ($120 for the product and $12 for its administration) but will collect only $125 from this payer ($98 for the product and $27 for its administration).
“You see over and over again that the payers underpay for the vaccines and pay you well for the administration, and it very often makes up the difference,” Mr. Hart noted. “But even with that boost on the admin side, this practice is losing money on this vaccine – they get $125 for something that costs them $132.”
Practices strapped for time can use some estimates in their spreadsheets instead, he said. “If you use an assumption of 25% over your invoice” – roughly the midpoint between the AAP’s 17% and 28% – “and $12 to $15 on your administration” – based on the value found in a study using time-motion analysis (Pediatrics. 2009 Dec;124 Suppl 5:S492-8) – “for your costs, all you need is your fee schedule, and you can make a spreadsheet to find out whether it makes sense to continue giving immunizations to this payer’s kids.”
Striving for profitability
“In all honesty, from what I see nationally, pediatricians break even on vaccines. It’s a break-even situation, on average,” Mr. Hart commented. “But who wants to be average? No one. We want you to actually be profitable with vaccines because it’s the only way you can continue to give them.”
Practices can take a variety of steps toward that goal. First, they should negotiate payments with payers, using the AAP’s business case and other literature. “Don’t listen to anybody” who says you can’t negotiate, he stressed. “You can negotiate. I don’t care if you’re a solo practice or you’ve just opened. If a payer says they can’t negotiate, they are fibbing to you. The only payers who don’t negotiate are the state Medicaid and Medicare. Everyone else can and does.”
Second, practices should ensure that they are using proper Current Procedural Terminology codes when submitting claims to payers to maximize payment.
“I still see too many practices who don’t bill for these properly,” Mr. Hart commented. “If you have a typical pediatric practice and you use more 90471s and 90472s than 90460s and 90461s, and frankly, if [the latter] aren’t two to three to four to five times more common… you are losing a lot of money.”
Third, practices should join or confirm that they belong to an effective group purchasing organization (GPO) to reduce their vaccine costs, with data suggesting that doing so will save the practice $10,000 to $15,000 per physician each year.
“If you are solo, out on the furthest edge of Alaska, you can see Russia from your house, and you have no leverage whatsoever, you can sign up with one of these GPOs and you are as strong as any hospital,” he said. The AAP helps here as well, by maintaining a list of GPOs on its website.
Fourth, practices should review their vaccine delivery work flow to look for money leaks, Mr. Hart advised. For example, physicians who get caught up in tasks such as ordering and inventorying are losing revenue that could come in from seeing patients.
“This is the sort of thing that affects your bottom line substantially. And it’s exactly the sort of thing that is an invisible expense: the business owners don’t consider their time as part of the expense of doing this administration,” he said.
Additionally, legacy procedures should be re-evaluated to see if they can be streamlined. Gains also may be made here from investing in better technology, such as a refrigerator with a glass door that saves time by allowing ready identification of vaccines.
Finally, practices should join the AAP’s Section on Administration and Practice Management (SOAPM) as it’s an invaluable, interactive resource in this area when questions or challenges arise, Mr. Hart recommended.
[email protected]
SAN FRANCISCO – With a little number crunching and strategizing, pediatric practices can provide immunizations to their patients without getting financially soaked, according to Chip Hart, a pediatric practice management consultant.
He discussed various pitfalls and challenges when it comes to the business aspects of providing immunizations, and offered some solutions at the annual meeting of the American Academy of Pediatrics.
His company has collected data suggesting that as of 2015, revenue from vaccine products made up fully 21% of all revenue in private pediatric practices, a near doubling from the value in 2003. As a consultant today, “I try to find out how practices manage the vaccines because, after staff, it’s your biggest expense,” he noted.
Spotting hidden costs
In its business case, the AAP determined that direct and indirect expenses for vaccine product total to 17% to 28% of the cost. In other words, “if you buy a vaccine for $100, you need to collect somewhere between $117 and $128, on average, just to break even,” Mr. Hart explained.
What accounts for that extra expense? Carrying costs that are commonly overlooked, namely, those myriad costs of providing immunizations that accrue before a child is given any vaccine and that can add up quickly.
They include the costs of the refrigerator and examination table; the sharps and waste management; insurance to cover vaccine loss; vaccine wastage and denials; and opportunity cost, that is, the cost of not being able to invest the funds tied up in vaccine sitting in the fridge – some $75,000 to $100,000 for the average practice – elsewhere.
Add to those personnel costs; costs related to activities such as ordering, inventory and storage management, registry input, and temperature monitoring; and malpractice coverage. And not to be forgotten is the inability to collect payment for some vaccines.
“You’re not paid for carrying costs. Unfortunately, society or the American health care system has given pediatricians this burden,” Mr. Hart commented.
Doing the math
Pediatricians can get a handle on the true costs to their practice of providing immunizations by spending just an hour or two crunching some key numbers, according to Mr. Hart.
They should start by ascertaining those carrying costs. For example, assuming hazardous waste costs run $3,500 per year, vaccines account for 50% of the waste, and the practice gives 13,000 vaccines annually, it averages out to $0.13 per vaccine.
Similar calculations are done to determine the costs of administering the shot (preparing, administering, counseling, billing, recording, putting it in the registry, and so on), arriving at about $12 per vaccine. The largest share here comes from clinicians, so calculations focus on their hourly wages and the percent of their time spent on vaccines.
Next is a calculation of the cost of the vaccine product. This calculation starts with the hypothetical invoiced amount of $100, factors in units that are wasted or go unpaid (at least 5%, according to AAP data), and tacks on the distributed carrying costs, arriving finally at an actual cost to the practice of about $120.
Last, all of these data are loaded into a payer-specific spreadsheet. Commonly, payers go by Red Book values and will therefore cover, for example, only $98 of that $100 invoice cost of the vaccine. But they will pay roughly $27 for its administration.
Taken together, the math suggests the practice bears a total cost of $132 for this vaccine ($120 for the product and $12 for its administration) but will collect only $125 from this payer ($98 for the product and $27 for its administration).
“You see over and over again that the payers underpay for the vaccines and pay you well for the administration, and it very often makes up the difference,” Mr. Hart noted. “But even with that boost on the admin side, this practice is losing money on this vaccine – they get $125 for something that costs them $132.”
Practices strapped for time can use some estimates in their spreadsheets instead, he said. “If you use an assumption of 25% over your invoice” – roughly the midpoint between the AAP’s 17% and 28% – “and $12 to $15 on your administration” – based on the value found in a study using time-motion analysis (Pediatrics. 2009 Dec;124 Suppl 5:S492-8) – “for your costs, all you need is your fee schedule, and you can make a spreadsheet to find out whether it makes sense to continue giving immunizations to this payer’s kids.”
Striving for profitability
“In all honesty, from what I see nationally, pediatricians break even on vaccines. It’s a break-even situation, on average,” Mr. Hart commented. “But who wants to be average? No one. We want you to actually be profitable with vaccines because it’s the only way you can continue to give them.”
Practices can take a variety of steps toward that goal. First, they should negotiate payments with payers, using the AAP’s business case and other literature. “Don’t listen to anybody” who says you can’t negotiate, he stressed. “You can negotiate. I don’t care if you’re a solo practice or you’ve just opened. If a payer says they can’t negotiate, they are fibbing to you. The only payers who don’t negotiate are the state Medicaid and Medicare. Everyone else can and does.”
Second, practices should ensure that they are using proper Current Procedural Terminology codes when submitting claims to payers to maximize payment.
“I still see too many practices who don’t bill for these properly,” Mr. Hart commented. “If you have a typical pediatric practice and you use more 90471s and 90472s than 90460s and 90461s, and frankly, if [the latter] aren’t two to three to four to five times more common… you are losing a lot of money.”
Third, practices should join or confirm that they belong to an effective group purchasing organization (GPO) to reduce their vaccine costs, with data suggesting that doing so will save the practice $10,000 to $15,000 per physician each year.
“If you are solo, out on the furthest edge of Alaska, you can see Russia from your house, and you have no leverage whatsoever, you can sign up with one of these GPOs and you are as strong as any hospital,” he said. The AAP helps here as well, by maintaining a list of GPOs on its website.
Fourth, practices should review their vaccine delivery work flow to look for money leaks, Mr. Hart advised. For example, physicians who get caught up in tasks such as ordering and inventorying are losing revenue that could come in from seeing patients.
“This is the sort of thing that affects your bottom line substantially. And it’s exactly the sort of thing that is an invisible expense: the business owners don’t consider their time as part of the expense of doing this administration,” he said.
Additionally, legacy procedures should be re-evaluated to see if they can be streamlined. Gains also may be made here from investing in better technology, such as a refrigerator with a glass door that saves time by allowing ready identification of vaccines.
Finally, practices should join the AAP’s Section on Administration and Practice Management (SOAPM) as it’s an invaluable, interactive resource in this area when questions or challenges arise, Mr. Hart recommended.
[email protected]
AT AAP 16
Treating upper GI diseases: Where do we go from here?
WASHINGTON – The American Gastroenterological Association, the Food and Drug Administration, pharmaceutical companies, and patient advocacy groups came together for a first-of-its-kind meeting, a program of the AGA Center for Diagnostics and Therapeutics, to discuss new and emerging drugs for the treatment of four key GI diseases, highlighting the promise that these treatments show and the hurdles they face to gain approval.
“If we look at the AGA’s Burden of GI Disease Survey, published a few years ago in Gastroenterology, [you] can see that there are millions of visits to primary care and specialists for a variety of upper gastrointestinal symptoms, so clearly upper GI disorders still pose a major burden to our health care environment,” explained Colin W. Howden, MD, AGAF, chair of the AGA Center for Diagnostics and Therapeutics from the University of Tennessee in Memphis.

While proton pump inhibitors (PPIs) continue to be the first line of management for GERD, severe cases often require a stronger approach. Alternatives that are being investigated include potassium-competitive acid blockers, for which there have been clinical trials. However, no advantage over PPIs was demonstrated in any trials. Another alternative is bile salt binders, for which at least one trial is currently underway. Dr. Vela was unable to say when findings are expected to be published.
Another approach to managing GERD is to treat the acid pocket itself by using alginate. A randomized study by Rohof et al. investigated this in 2013, comparing Gaviscon and antacid; although the population size was small (n = 16), investigators concluded that “alginate-antacid raft localizes to the postprandial acid pocket and displaces it below the diaphragm to reduce postprandial acid reflux [making it] an appropriate therapy for postprandial acid reflux.”
Another new drug is lesogaberan, a GABA-B agonist that was examined in a 2010 randomized, double-blind crossover study by Boeckxstaens et al. While also a small trial (n = 21), the findings indicated that the drug is a good option for those with only partial response to PPIs, as it decreased the number of transient lower esophageal sphincter relaxations (TLESRs) and reflux episodes, and increased LES pressure [in] patients with reflux symptoms. Work to inhibit transient LES relaxations also is being done, but so far lesogaberan, arbaclofen, and ADX 10059 (an mGluR5 modulator) programs have all been halted because of side effects or insufficient efficacy findings.
Prokinetics are also being looked at, with drugs such as metoclopramide being examined for efficacy, although to this point, the drug has shown “no improvement in acid exposure or esophageal clearance [when] compared to placebo,” according to Dr. Vela. Other drugs that are available outside the United States include domperidone, itopride, and mosapride, but Dr. Vela, who led a 2014 report on these therapies, stated that benefits offered by these are modest, and studies investigating them are limited in number.
Also being looked at are rebamipide, which can be used a cytoprotective agent that increases prostaglandin production. A 2010 study by Yoshida et al. found that lansoprazole (15 mg/day), combined with 300 mg/day of rebamipide, was significantly better at preventing relapse within a year than was just the former medication taken on its own. Additionally, there are conceptual studies examining topical protection to maintain mucosal integrity, nociceptor blockades, and imipramine.
Regarding trials for GERD, Robyn Carson, director of health economics & outcomes research at Allergan stated that the company recently redefined what constitutes GERD in order to help refocus what its drugs were trying to do.
“I think we’ve operationalized it very recently in terms of exclusion and GERD,” she explained. “The way we define it is ‘active GERD’ with two or more episodes a week of heartburn, so it was very much focused on the heartburn and PPI use was acceptable.”
Following the GERD discussion, panelists talked about what’s coming up in the realm of EoE. Stuart J. Spechler, MD, of the University of Texas Southwestern in Dallas, discussed ongoing research into treating EoE as an antigen-driven disorder, noting that about half of all EoE patients have a history of atopic disease – such as rhinitis, asthma, and atopic dermatitis – and exhibit sensitization to food or other aeroallergens. Furthermore, about 3% of patients who undergo oral immunotherapy to treat a food allergy develop EoE.
But in terms of what to take EoE research forward, Dr. Spechler called for a shift away from trying to distinguish between EoE and GERD, arguing that GERD contributes to EoE pathogenesis, and vice versa. PPIs can and should be used in EoE for the same reasons that they’re used to treat GERD, he explained.
“We need a shift in focus [because] I don’t think it’s likely to be that productive a line of research,” Dr. Spechler said. “The two diseases often coexist.”
To attack gastroparesis, P. Jay Pasricha, MD explained that a number of trials examining several drugs have shown that they are either ineffective or “do not correlate with improvement in gastric emptying.” These drugs include cisapride, tegaserod, botulinum toxin, mitemcinal, camcinal, TZP 102, and relamorelin.
“I’m not going to talk about emerging biomarkers because there isn’t a lot to talk about with biomarkers that hasn’t already been said,” stated Dr. Pasricha of Johns Hopkins University in Baltimore adding that his focus would largely be focused on emerging therapies and treatment targets.
A 2013 study by Parkman et al. investigated the effects of nortriptyline on mitigating idiopathic gastroparesis symptoms, finding that there was no significant difference in symptoms among patients who took the drug, versus those who took a placebo. In terms of using antinauseants to alleviate symptoms, dopamine receptor antagonists continue to be commonly prescribed, but they have their limitations. Metoclopramide, though approved since 1986, can be used for only 12 weeks, has acute and chronic side effects such as mood and irreversible movement disorders, and a black box warning imposed on it by the FDA in 2009 for tardive dyskinesia. One drug approved in India, though not by the FDA, is domperidone, which has no side effects to the central nervous system but does raise cardiovascular concerns in patients with “mild hERG affinity.”
Currently, the APRON trial is investigating the efficacy of aprepitant to relieve chronic nausea and vomiting in gastroparesis patients. Those enrolled in the study are all at least 18 years old, have undergone gastric-emptying scintigraphy, and either a normal upper endoscopy or an upper GI series within the 2 years prior to enrollment, have symptoms of chronic nausea or vomiting consistent with a functional gastric disorder for at least 6 months before enrollment, and nausea defined as “significant” by a visual analog scale score of at least 25 mm.
“Continuing to focus solely on accelerating gastric emptying is a failed strategy,” said Dr. Pasricha, adding that research needs to focus on the unique aspects of the disease’s biology, including pathogenic similarities with functional dyspepsia.
To that end, the final disease covered was functional dyspepsia. In terms of ongoing or planned clinical studies, Jan Tack, MD, from the University of Leuven (Belgium), mentioned three. Two of them are multicenter controlled trials investigating acotiamide, one in Europe and the other in India, for the management of functional dyspepsia and postprandial distress syndrome, while the other is a multicenter study examining rikkunshito, a traditional Japanese medicine. Additionally, ongoing or planned mechanistic studies include single-center controlled trials in Belgium on the efficacy of acotiamide and rikkunshito for intragastric pressure, as well as another Belgian study analyzing the impact of monoacylglycerol lipase inhibitors on intragastric pressure in patients that have functional dyspepsia with “impaired accommodation.”
Meal-related symptoms, nutrient challenge tests, and intragastric pressure measurements should all become short-term pathophysiology and efficacy markers, said Dr. Tack, adding that it’s also important for new therapeutic targets to include gastric emptying, hypersensitivity, and duodenal alterations, if necessary.
Hurdles persist in getting drugs through the approval process, however. Juli Tomaino, MD, of the FDA’s Center for Drug Evaluation and Research, explained where many proposed drugs run into issues in the regulatory process.
“We really have to know what we’re diagnosing, so the regulatory pathway to any of these approvals will really depend on the independent patient population, it will depend on the mechanism of action of the drug, what the drug is able to do and not do, and how you’re going to design that trial to target whatever that drug can do,” Dr. Tomaino said.
The issue of labeling also factors in, according to her. “We know that patients with acid-mediated heartburn do well on PPIs, but if they’re having different symptoms due to different mechanisms of action, then you have to design that drug with that patient population in mind, and that’s what the labeling would look like,” she explained. “So I’m not saying that it would necessarily have to list all the enrollment criteria, all the enrichment techniques that we use in that trial, but it would be a description of the intended patient population and what the drug would do.”
Mrs. Carson also chimed in on the topic of trial difficulties, saying that “[Irritable bowel syndrome] and [chronic idiopathic constipation] became quite an impediment to recruitment, and I think as we get farther away from the complete overlapping conditions, I think that’s where in discussions with the [Qualification Review Team] at FDA, they recognize that [we should] track that and let this evidence drive the next step,” adding that “we’ll have data on that shortly.”
The AGA Center for Diagnostics and Therapeutics will be issuing white papers on each of the four upper GI disorders discussed at the meeting.
Dr. Howden disclosed that he is a consultant for Aralez, Ironwood, Allergan, Otsuka, and SynteractHCR; an expert witness for Allergan; and coeditor of Alimentary Pharmacology & Therapeutics. Dr. Spechler disclosed that he is a consultant for Interpace Diagnostics, Takeda Pharmaceuticals, and Ironwood Pharmaceuticals. Dr. Pasricha disclosed that he is the cofounder of Neurogastrx, OrphoMed, and ETX Pharma, and is a consultant for Vanda and Allergan. Dr. Tack disclosed that he is a consultant for Abide, Allergan, AstraZeneca, Danone, El Pharma, Menarini, Novartis, Ono, Shire, Takeda, Theravance, Tsumura, and Zeria, as well as being on several of their advisory boards and speakers bureaus. Dr. Vela is a consultant for Medtronic and Torax.*
*Additions were made to the story on 11/8/2016 and 11/18/2016.
WASHINGTON – The American Gastroenterological Association, the Food and Drug Administration, pharmaceutical companies, and patient advocacy groups came together for a first-of-its-kind meeting, a program of the AGA Center for Diagnostics and Therapeutics, to discuss new and emerging drugs for the treatment of four key GI diseases, highlighting the promise that these treatments show and the hurdles they face to gain approval.
“If we look at the AGA’s Burden of GI Disease Survey, published a few years ago in Gastroenterology, [you] can see that there are millions of visits to primary care and specialists for a variety of upper gastrointestinal symptoms, so clearly upper GI disorders still pose a major burden to our health care environment,” explained Colin W. Howden, MD, AGAF, chair of the AGA Center for Diagnostics and Therapeutics from the University of Tennessee in Memphis.
While proton pump inhibitors (PPIs) continue to be the first line of management for GERD, severe cases often require a stronger approach. Alternatives that are being investigated include potassium-competitive acid blockers, for which there have been clinical trials. However, no advantage over PPIs was demonstrated in any trials. Another alternative is bile salt binders, for which at least one trial is currently underway. Dr. Vela was unable to say when findings are expected to be published.
Another approach to managing GERD is to treat the acid pocket itself by using alginate. A randomized study by Rohof et al. investigated this in 2013, comparing Gaviscon and antacid; although the population size was small (n = 16), investigators concluded that “alginate-antacid raft localizes to the postprandial acid pocket and displaces it below the diaphragm to reduce postprandial acid reflux [making it] an appropriate therapy for postprandial acid reflux.”
Another new drug is lesogaberan, a GABA-B agonist that was examined in a 2010 randomized, double-blind crossover study by Boeckxstaens et al. While also a small trial (n = 21), the findings indicated that the drug is a good option for those with only partial response to PPIs, as it decreased the number of transient lower esophageal sphincter relaxations (TLESRs) and reflux episodes, and increased LES pressure [in] patients with reflux symptoms. Work to inhibit transient LES relaxations also is being done, but so far lesogaberan, arbaclofen, and ADX 10059 (an mGluR5 modulator) programs have all been halted because of side effects or insufficient efficacy findings.
Prokinetics are also being looked at, with drugs such as metoclopramide being examined for efficacy, although to this point, the drug has shown “no improvement in acid exposure or esophageal clearance [when] compared to placebo,” according to Dr. Vela. Other drugs that are available outside the United States include domperidone, itopride, and mosapride, but Dr. Vela, who led a 2014 report on these therapies, stated that benefits offered by these are modest, and studies investigating them are limited in number.
Also being looked at are rebamipide, which can be used a cytoprotective agent that increases prostaglandin production. A 2010 study by Yoshida et al. found that lansoprazole (15 mg/day), combined with 300 mg/day of rebamipide, was significantly better at preventing relapse within a year than was just the former medication taken on its own. Additionally, there are conceptual studies examining topical protection to maintain mucosal integrity, nociceptor blockades, and imipramine.
Regarding trials for GERD, Robyn Carson, director of health economics & outcomes research at Allergan stated that the company recently redefined what constitutes GERD in order to help refocus what its drugs were trying to do.
“I think we’ve operationalized it very recently in terms of exclusion and GERD,” she explained. “The way we define it is ‘active GERD’ with two or more episodes a week of heartburn, so it was very much focused on the heartburn and PPI use was acceptable.”
Following the GERD discussion, panelists talked about what’s coming up in the realm of EoE. Stuart J. Spechler, MD, of the University of Texas Southwestern in Dallas, discussed ongoing research into treating EoE as an antigen-driven disorder, noting that about half of all EoE patients have a history of atopic disease – such as rhinitis, asthma, and atopic dermatitis – and exhibit sensitization to food or other aeroallergens. Furthermore, about 3% of patients who undergo oral immunotherapy to treat a food allergy develop EoE.
But in terms of what to take EoE research forward, Dr. Spechler called for a shift away from trying to distinguish between EoE and GERD, arguing that GERD contributes to EoE pathogenesis, and vice versa. PPIs can and should be used in EoE for the same reasons that they’re used to treat GERD, he explained.
“We need a shift in focus [because] I don’t think it’s likely to be that productive a line of research,” Dr. Spechler said. “The two diseases often coexist.”
To attack gastroparesis, P. Jay Pasricha, MD explained that a number of trials examining several drugs have shown that they are either ineffective or “do not correlate with improvement in gastric emptying.” These drugs include cisapride, tegaserod, botulinum toxin, mitemcinal, camcinal, TZP 102, and relamorelin.
“I’m not going to talk about emerging biomarkers because there isn’t a lot to talk about with biomarkers that hasn’t already been said,” stated Dr. Pasricha of Johns Hopkins University in Baltimore adding that his focus would largely be focused on emerging therapies and treatment targets.
A 2013 study by Parkman et al. investigated the effects of nortriptyline on mitigating idiopathic gastroparesis symptoms, finding that there was no significant difference in symptoms among patients who took the drug, versus those who took a placebo. In terms of using antinauseants to alleviate symptoms, dopamine receptor antagonists continue to be commonly prescribed, but they have their limitations. Metoclopramide, though approved since 1986, can be used for only 12 weeks, has acute and chronic side effects such as mood and irreversible movement disorders, and a black box warning imposed on it by the FDA in 2009 for tardive dyskinesia. One drug approved in India, though not by the FDA, is domperidone, which has no side effects to the central nervous system but does raise cardiovascular concerns in patients with “mild hERG affinity.”
Currently, the APRON trial is investigating the efficacy of aprepitant to relieve chronic nausea and vomiting in gastroparesis patients. Those enrolled in the study are all at least 18 years old, have undergone gastric-emptying scintigraphy, and either a normal upper endoscopy or an upper GI series within the 2 years prior to enrollment, have symptoms of chronic nausea or vomiting consistent with a functional gastric disorder for at least 6 months before enrollment, and nausea defined as “significant” by a visual analog scale score of at least 25 mm.
“Continuing to focus solely on accelerating gastric emptying is a failed strategy,” said Dr. Pasricha, adding that research needs to focus on the unique aspects of the disease’s biology, including pathogenic similarities with functional dyspepsia.
To that end, the final disease covered was functional dyspepsia. In terms of ongoing or planned clinical studies, Jan Tack, MD, from the University of Leuven (Belgium), mentioned three. Two of them are multicenter controlled trials investigating acotiamide, one in Europe and the other in India, for the management of functional dyspepsia and postprandial distress syndrome, while the other is a multicenter study examining rikkunshito, a traditional Japanese medicine. Additionally, ongoing or planned mechanistic studies include single-center controlled trials in Belgium on the efficacy of acotiamide and rikkunshito for intragastric pressure, as well as another Belgian study analyzing the impact of monoacylglycerol lipase inhibitors on intragastric pressure in patients that have functional dyspepsia with “impaired accommodation.”
Meal-related symptoms, nutrient challenge tests, and intragastric pressure measurements should all become short-term pathophysiology and efficacy markers, said Dr. Tack, adding that it’s also important for new therapeutic targets to include gastric emptying, hypersensitivity, and duodenal alterations, if necessary.
Hurdles persist in getting drugs through the approval process, however. Juli Tomaino, MD, of the FDA’s Center for Drug Evaluation and Research, explained where many proposed drugs run into issues in the regulatory process.
“We really have to know what we’re diagnosing, so the regulatory pathway to any of these approvals will really depend on the independent patient population, it will depend on the mechanism of action of the drug, what the drug is able to do and not do, and how you’re going to design that trial to target whatever that drug can do,” Dr. Tomaino said.
The issue of labeling also factors in, according to her. “We know that patients with acid-mediated heartburn do well on PPIs, but if they’re having different symptoms due to different mechanisms of action, then you have to design that drug with that patient population in mind, and that’s what the labeling would look like,” she explained. “So I’m not saying that it would necessarily have to list all the enrollment criteria, all the enrichment techniques that we use in that trial, but it would be a description of the intended patient population and what the drug would do.”
Mrs. Carson also chimed in on the topic of trial difficulties, saying that “[Irritable bowel syndrome] and [chronic idiopathic constipation] became quite an impediment to recruitment, and I think as we get farther away from the complete overlapping conditions, I think that’s where in discussions with the [Qualification Review Team] at FDA, they recognize that [we should] track that and let this evidence drive the next step,” adding that “we’ll have data on that shortly.”
The AGA Center for Diagnostics and Therapeutics will be issuing white papers on each of the four upper GI disorders discussed at the meeting.
Dr. Howden disclosed that he is a consultant for Aralez, Ironwood, Allergan, Otsuka, and SynteractHCR; an expert witness for Allergan; and coeditor of Alimentary Pharmacology & Therapeutics. Dr. Spechler disclosed that he is a consultant for Interpace Diagnostics, Takeda Pharmaceuticals, and Ironwood Pharmaceuticals. Dr. Pasricha disclosed that he is the cofounder of Neurogastrx, OrphoMed, and ETX Pharma, and is a consultant for Vanda and Allergan. Dr. Tack disclosed that he is a consultant for Abide, Allergan, AstraZeneca, Danone, El Pharma, Menarini, Novartis, Ono, Shire, Takeda, Theravance, Tsumura, and Zeria, as well as being on several of their advisory boards and speakers bureaus. Dr. Vela is a consultant for Medtronic and Torax.*
*Additions were made to the story on 11/8/2016 and 11/18/2016.
WASHINGTON – The American Gastroenterological Association, the Food and Drug Administration, pharmaceutical companies, and patient advocacy groups came together for a first-of-its-kind meeting, a program of the AGA Center for Diagnostics and Therapeutics, to discuss new and emerging drugs for the treatment of four key GI diseases, highlighting the promise that these treatments show and the hurdles they face to gain approval.
“If we look at the AGA’s Burden of GI Disease Survey, published a few years ago in Gastroenterology, [you] can see that there are millions of visits to primary care and specialists for a variety of upper gastrointestinal symptoms, so clearly upper GI disorders still pose a major burden to our health care environment,” explained Colin W. Howden, MD, AGAF, chair of the AGA Center for Diagnostics and Therapeutics from the University of Tennessee in Memphis.
While proton pump inhibitors (PPIs) continue to be the first line of management for GERD, severe cases often require a stronger approach. Alternatives that are being investigated include potassium-competitive acid blockers, for which there have been clinical trials. However, no advantage over PPIs was demonstrated in any trials. Another alternative is bile salt binders, for which at least one trial is currently underway. Dr. Vela was unable to say when findings are expected to be published.
Another approach to managing GERD is to treat the acid pocket itself by using alginate. A randomized study by Rohof et al. investigated this in 2013, comparing Gaviscon and antacid; although the population size was small (n = 16), investigators concluded that “alginate-antacid raft localizes to the postprandial acid pocket and displaces it below the diaphragm to reduce postprandial acid reflux [making it] an appropriate therapy for postprandial acid reflux.”
Another new drug is lesogaberan, a GABA-B agonist that was examined in a 2010 randomized, double-blind crossover study by Boeckxstaens et al. While also a small trial (n = 21), the findings indicated that the drug is a good option for those with only partial response to PPIs, as it decreased the number of transient lower esophageal sphincter relaxations (TLESRs) and reflux episodes, and increased LES pressure [in] patients with reflux symptoms. Work to inhibit transient LES relaxations also is being done, but so far lesogaberan, arbaclofen, and ADX 10059 (an mGluR5 modulator) programs have all been halted because of side effects or insufficient efficacy findings.
Prokinetics are also being looked at, with drugs such as metoclopramide being examined for efficacy, although to this point, the drug has shown “no improvement in acid exposure or esophageal clearance [when] compared to placebo,” according to Dr. Vela. Other drugs that are available outside the United States include domperidone, itopride, and mosapride, but Dr. Vela, who led a 2014 report on these therapies, stated that benefits offered by these are modest, and studies investigating them are limited in number.
Also being looked at are rebamipide, which can be used a cytoprotective agent that increases prostaglandin production. A 2010 study by Yoshida et al. found that lansoprazole (15 mg/day), combined with 300 mg/day of rebamipide, was significantly better at preventing relapse within a year than was just the former medication taken on its own. Additionally, there are conceptual studies examining topical protection to maintain mucosal integrity, nociceptor blockades, and imipramine.
Regarding trials for GERD, Robyn Carson, director of health economics & outcomes research at Allergan stated that the company recently redefined what constitutes GERD in order to help refocus what its drugs were trying to do.
“I think we’ve operationalized it very recently in terms of exclusion and GERD,” she explained. “The way we define it is ‘active GERD’ with two or more episodes a week of heartburn, so it was very much focused on the heartburn and PPI use was acceptable.”
Following the GERD discussion, panelists talked about what’s coming up in the realm of EoE. Stuart J. Spechler, MD, of the University of Texas Southwestern in Dallas, discussed ongoing research into treating EoE as an antigen-driven disorder, noting that about half of all EoE patients have a history of atopic disease – such as rhinitis, asthma, and atopic dermatitis – and exhibit sensitization to food or other aeroallergens. Furthermore, about 3% of patients who undergo oral immunotherapy to treat a food allergy develop EoE.
But in terms of what to take EoE research forward, Dr. Spechler called for a shift away from trying to distinguish between EoE and GERD, arguing that GERD contributes to EoE pathogenesis, and vice versa. PPIs can and should be used in EoE for the same reasons that they’re used to treat GERD, he explained.
“We need a shift in focus [because] I don’t think it’s likely to be that productive a line of research,” Dr. Spechler said. “The two diseases often coexist.”
To attack gastroparesis, P. Jay Pasricha, MD explained that a number of trials examining several drugs have shown that they are either ineffective or “do not correlate with improvement in gastric emptying.” These drugs include cisapride, tegaserod, botulinum toxin, mitemcinal, camcinal, TZP 102, and relamorelin.
“I’m not going to talk about emerging biomarkers because there isn’t a lot to talk about with biomarkers that hasn’t already been said,” stated Dr. Pasricha of Johns Hopkins University in Baltimore adding that his focus would largely be focused on emerging therapies and treatment targets.
A 2013 study by Parkman et al. investigated the effects of nortriptyline on mitigating idiopathic gastroparesis symptoms, finding that there was no significant difference in symptoms among patients who took the drug, versus those who took a placebo. In terms of using antinauseants to alleviate symptoms, dopamine receptor antagonists continue to be commonly prescribed, but they have their limitations. Metoclopramide, though approved since 1986, can be used for only 12 weeks, has acute and chronic side effects such as mood and irreversible movement disorders, and a black box warning imposed on it by the FDA in 2009 for tardive dyskinesia. One drug approved in India, though not by the FDA, is domperidone, which has no side effects to the central nervous system but does raise cardiovascular concerns in patients with “mild hERG affinity.”
Currently, the APRON trial is investigating the efficacy of aprepitant to relieve chronic nausea and vomiting in gastroparesis patients. Those enrolled in the study are all at least 18 years old, have undergone gastric-emptying scintigraphy, and either a normal upper endoscopy or an upper GI series within the 2 years prior to enrollment, have symptoms of chronic nausea or vomiting consistent with a functional gastric disorder for at least 6 months before enrollment, and nausea defined as “significant” by a visual analog scale score of at least 25 mm.
“Continuing to focus solely on accelerating gastric emptying is a failed strategy,” said Dr. Pasricha, adding that research needs to focus on the unique aspects of the disease’s biology, including pathogenic similarities with functional dyspepsia.
To that end, the final disease covered was functional dyspepsia. In terms of ongoing or planned clinical studies, Jan Tack, MD, from the University of Leuven (Belgium), mentioned three. Two of them are multicenter controlled trials investigating acotiamide, one in Europe and the other in India, for the management of functional dyspepsia and postprandial distress syndrome, while the other is a multicenter study examining rikkunshito, a traditional Japanese medicine. Additionally, ongoing or planned mechanistic studies include single-center controlled trials in Belgium on the efficacy of acotiamide and rikkunshito for intragastric pressure, as well as another Belgian study analyzing the impact of monoacylglycerol lipase inhibitors on intragastric pressure in patients that have functional dyspepsia with “impaired accommodation.”
Meal-related symptoms, nutrient challenge tests, and intragastric pressure measurements should all become short-term pathophysiology and efficacy markers, said Dr. Tack, adding that it’s also important for new therapeutic targets to include gastric emptying, hypersensitivity, and duodenal alterations, if necessary.
Hurdles persist in getting drugs through the approval process, however. Juli Tomaino, MD, of the FDA’s Center for Drug Evaluation and Research, explained where many proposed drugs run into issues in the regulatory process.
“We really have to know what we’re diagnosing, so the regulatory pathway to any of these approvals will really depend on the independent patient population, it will depend on the mechanism of action of the drug, what the drug is able to do and not do, and how you’re going to design that trial to target whatever that drug can do,” Dr. Tomaino said.
The issue of labeling also factors in, according to her. “We know that patients with acid-mediated heartburn do well on PPIs, but if they’re having different symptoms due to different mechanisms of action, then you have to design that drug with that patient population in mind, and that’s what the labeling would look like,” she explained. “So I’m not saying that it would necessarily have to list all the enrollment criteria, all the enrichment techniques that we use in that trial, but it would be a description of the intended patient population and what the drug would do.”
Mrs. Carson also chimed in on the topic of trial difficulties, saying that “[Irritable bowel syndrome] and [chronic idiopathic constipation] became quite an impediment to recruitment, and I think as we get farther away from the complete overlapping conditions, I think that’s where in discussions with the [Qualification Review Team] at FDA, they recognize that [we should] track that and let this evidence drive the next step,” adding that “we’ll have data on that shortly.”
The AGA Center for Diagnostics and Therapeutics will be issuing white papers on each of the four upper GI disorders discussed at the meeting.
Dr. Howden disclosed that he is a consultant for Aralez, Ironwood, Allergan, Otsuka, and SynteractHCR; an expert witness for Allergan; and coeditor of Alimentary Pharmacology & Therapeutics. Dr. Spechler disclosed that he is a consultant for Interpace Diagnostics, Takeda Pharmaceuticals, and Ironwood Pharmaceuticals. Dr. Pasricha disclosed that he is the cofounder of Neurogastrx, OrphoMed, and ETX Pharma, and is a consultant for Vanda and Allergan. Dr. Tack disclosed that he is a consultant for Abide, Allergan, AstraZeneca, Danone, El Pharma, Menarini, Novartis, Ono, Shire, Takeda, Theravance, Tsumura, and Zeria, as well as being on several of their advisory boards and speakers bureaus. Dr. Vela is a consultant for Medtronic and Torax.*
*Additions were made to the story on 11/8/2016 and 11/18/2016.
AT THE AGA DRUG DEVELOPMENT CONFERENCE
Shared medical appointment model shows potential for fibromyalgia patients
Fibromyalgia patients who participated in shared medical appointments staffed by an interdisciplinary team at a rural academic medical center reported high satisfaction with the new care model, according to Nicole M. Orzechowski, DO, and her colleagues in the department of rheumatology at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The study of 67 referred patients, who were evaluated during a 1-year period with the shared medical appointment (SMA) model, revealed in post-session surveys that not only did all patients agree that the care model would assist in managing their condition, but 95% also thought that the peer-to-peer interaction was “extremely helpful.”
In the study, which Dr. Orzechowski will report at the annual meeting of the American College of Rheumatology in Washington, she and her associates noted that the 2.5-hour visits conducted by a rheumatologist, two nurse practitioners, a chaplain, and a secretary led to “clinical efficiency in assessing multiple new patients in a defined period of time,” improved wait times for fibromyalgia patients from 3 months to 1 month, and also freed up new patient consultation slots for other conditions. The investigators estimated that the SMA has generated an additional 113 work relative value units since its inception.
Prior to the SMA, each patient received a medical history questionnaire in the mail, and the investigators informed primary care physicians about the SMA and its format and asked them to perform specific labs if they had not been done already. Besides individual exams for confirming the diagnosis, measuring vital signs, and reconciling medications, the SMA consisted of a facilitated discussion by a trained chaplain, followed by a short presentation by the clinician (with time for discussion and questions), and then concluded with the chaplain’s demonstration of mindfulness techniques for managing chronic pain.
In the future, the investigators said that they hope to enhance and optimize the visit, expand its use, address referring provider satisfaction, and examine post-visit resource utilization.
None of the authors had disclosures to report.
Fibromyalgia patients who participated in shared medical appointments staffed by an interdisciplinary team at a rural academic medical center reported high satisfaction with the new care model, according to Nicole M. Orzechowski, DO, and her colleagues in the department of rheumatology at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The study of 67 referred patients, who were evaluated during a 1-year period with the shared medical appointment (SMA) model, revealed in post-session surveys that not only did all patients agree that the care model would assist in managing their condition, but 95% also thought that the peer-to-peer interaction was “extremely helpful.”
In the study, which Dr. Orzechowski will report at the annual meeting of the American College of Rheumatology in Washington, she and her associates noted that the 2.5-hour visits conducted by a rheumatologist, two nurse practitioners, a chaplain, and a secretary led to “clinical efficiency in assessing multiple new patients in a defined period of time,” improved wait times for fibromyalgia patients from 3 months to 1 month, and also freed up new patient consultation slots for other conditions. The investigators estimated that the SMA has generated an additional 113 work relative value units since its inception.
Prior to the SMA, each patient received a medical history questionnaire in the mail, and the investigators informed primary care physicians about the SMA and its format and asked them to perform specific labs if they had not been done already. Besides individual exams for confirming the diagnosis, measuring vital signs, and reconciling medications, the SMA consisted of a facilitated discussion by a trained chaplain, followed by a short presentation by the clinician (with time for discussion and questions), and then concluded with the chaplain’s demonstration of mindfulness techniques for managing chronic pain.
In the future, the investigators said that they hope to enhance and optimize the visit, expand its use, address referring provider satisfaction, and examine post-visit resource utilization.
None of the authors had disclosures to report.
Fibromyalgia patients who participated in shared medical appointments staffed by an interdisciplinary team at a rural academic medical center reported high satisfaction with the new care model, according to Nicole M. Orzechowski, DO, and her colleagues in the department of rheumatology at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The study of 67 referred patients, who were evaluated during a 1-year period with the shared medical appointment (SMA) model, revealed in post-session surveys that not only did all patients agree that the care model would assist in managing their condition, but 95% also thought that the peer-to-peer interaction was “extremely helpful.”
In the study, which Dr. Orzechowski will report at the annual meeting of the American College of Rheumatology in Washington, she and her associates noted that the 2.5-hour visits conducted by a rheumatologist, two nurse practitioners, a chaplain, and a secretary led to “clinical efficiency in assessing multiple new patients in a defined period of time,” improved wait times for fibromyalgia patients from 3 months to 1 month, and also freed up new patient consultation slots for other conditions. The investigators estimated that the SMA has generated an additional 113 work relative value units since its inception.
Prior to the SMA, each patient received a medical history questionnaire in the mail, and the investigators informed primary care physicians about the SMA and its format and asked them to perform specific labs if they had not been done already. Besides individual exams for confirming the diagnosis, measuring vital signs, and reconciling medications, the SMA consisted of a facilitated discussion by a trained chaplain, followed by a short presentation by the clinician (with time for discussion and questions), and then concluded with the chaplain’s demonstration of mindfulness techniques for managing chronic pain.
In the future, the investigators said that they hope to enhance and optimize the visit, expand its use, address referring provider satisfaction, and examine post-visit resource utilization.
None of the authors had disclosures to report.
FROM THE ACR ANNUAL MEETING
Liletta gets a new inserter: Steps for successful placement
A new single-handed inserter (SHI) for placement of Liletta has been introduced and is currently available (FIGURE 1). Liletta is a levonorgestrel 52-mg intrauterine system (IUS) that is currently approved for 3 years of use as a contraceptive in the United States. The same product in Europe, known as Levosert, is approved for both contraception and the treatment of heavy menstrual bleeding. Liletta, as a branded contraceptive, is being studied through a large Phase 3 clinical trial called ACCESS IUS, which will continue to evaluate the contraceptive efficacy of Liletta for at least 7 years of use.1 A recent publication from the study showed that the levonorgestrel release rates from Liletta are almost identical to the rates reported for the other levonorgestrel 52-mg IUS on the market (Mirena) through 5 years and supports the continued study of the IUS for at least 7 years.2
Related article:
Benefit of self-administered vaginal lidocaine gel in IUD placement
The initial marketing and distribution of Liletta used a two-handed inserter that allowed for successful placement but required multiple steps. The SHI will make loading and placement of Liletta easier for all clinicians. Features of the new SHI include:
- A double-slider mechanism in which the first slider moves into the second slider during IUS placement, providing a tactile sense for the user during the insertion process
- The ability to reload the inserter if needed before placement
- A firm but bendable tube (that is 2 cm longer than other IUS inserters on the market). This length can be helpful for obese patients or postprocedure placements.
- Depth markings to 12 cm on both sides of the insertion tube.
Related article:
2016 Update on contraception
Liletta is an important and unique product in the US market. For most public sector providers and clinics, Liletta costs only $50, significantly less than other long-acting reversible contraceptives. The price of the IUS is only one aspect of its overall cost, however, as women still need to pay for any office visit or insertion fees. Liletta is unique in its pricing. Sales of Liletta in the private sector support the low price in the public sector. As a health care community, even if we do not directly care for women in public-sector settings, we all can help poor women access affordable, effective contraception. For providers, Liletta is a highly effective and lower-cost alternative to currently available hormonal IUS products.
How to insert Liletta
Insertion can be performed using a no-touch technique. The loading and placement technique outlined below should occur after speculum and tenaculum placement, sounding of the uterus, and vaginal preparation as would be performed for any intrauterine contraceptive insertion. Never force the uterine sound or insertion tube through the cervix; if necessary, stop and dilate the cervical canal. The steps below are the main points for successful Liletta placement; see the full product label for more details.3
Related article:
In which clinical situations can the use of the 52-mg levonorgestrel-releasing IUD (Mirena) and the TCu380A copper-IUD (ParaGard) be extended?
The key steps to remember are firm-gentle-firm
- Load the device. While pushing forward firmly on the blue slider (with the number 1), load Liletta by pulling down evenly on the threads. The IUS should be laid on a flat surface in the sterile tray to keep the arms parallel to the floor while pulling on the threads. Once loaded, the threads can be pulled up or down to be locked in the cleft. The tip of the IUS will form a hemispheric dome at the top of the insertion tube.
- Adjust the flange to the measured uterine depth based on sounding using the notch in the tray.
- Place inserter into the cervix. Apply gentle traction on the tenaculum to align the cervical canal and uterine cavity. While still holding firm forward pressure on the blue slider, place the tube through the cervical canal until the flange is approximately 1.5 to 2 cm from the cervix. (FIGURE 2.) Gently slide the blue slider downward until it is flush with the green slider (with the number 2; FIGURE 3). This step will allow the IUS arms to open in the lower uterine segment; wait 10 to 15 seconds for the arms to fully unfold. By sliding gently, you will feel when to stop moving the slider.
 Image copyright Medicines360.
Image copyright Medicines360.Figure 2. Placing the inserter through the cervix  Image copyright Medicines360.
Image copyright Medicines360.Figure 3. Merging the blue and green sliders together to release the IUS arms - Advance the inserter. While holding traction on the tenaculum, advance the inserter to the fundus. You will feel slight resistance when the IUS is at the fundus and the flange should be flush against the cervix.
- Firmly slide both sliders together downward until a click is heard (FIGURE 4). A green indicator will be visible at the bottom of the handle to show that the threads have been ejected from the cleft.
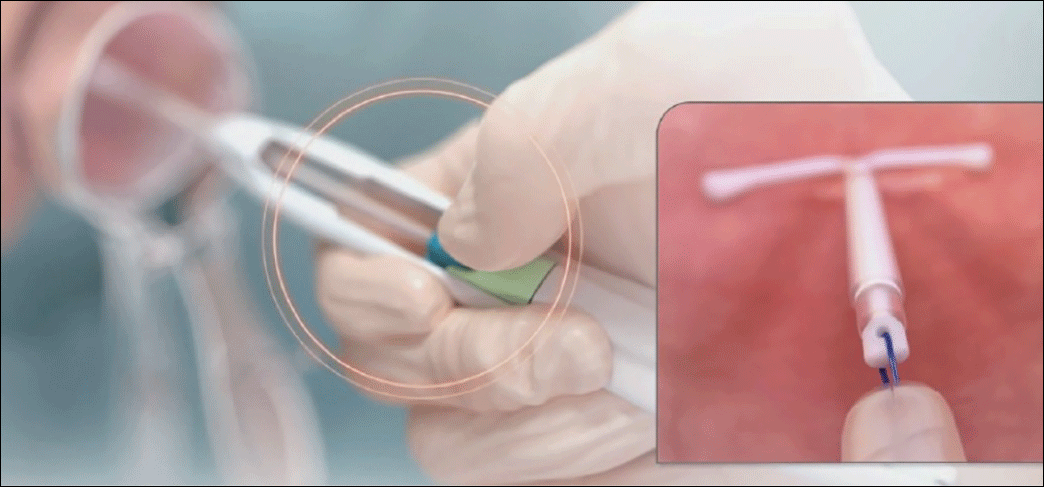 Image copyright Medicines360.
Image copyright Medicines360.Figure 4. Moving the blue and green sliders downward together to release the IUS - Withdraw the inserter from the uterus and cut the threads with blunt tipped scissors approximately 3 cm from the cervical os.
Technique video
Allergan and Medicines360 offer a video demonstrating proper Liletta insertion technique at www.lilettahcp.com. The video includes proper loading of the inserter as well as correct uterine depth measurement and release of Liletta from the inserter. Clinicians are reminded to use aseptic technique during the entire insertion procedure.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Eisenberg DL, Schreiber CA, Turok DK, Teal SB, Westhoff CL, Creinin MD. Three year efficacy and safety of a new 52-mg levonorgestrel-releasing intrauterine system. Contraception. 2015;92(1):10-16.
- Creinin MD, Jansen R, Starr R, Gobburu J, Gopalakrishnan M, Olariu A. Levonorgestrel release rates over 5 years with the Liletta® 52 mg intrauterine system. Contraception. 2016;94(4):353-356.
- Liletta [package insert]. Irvine, California: Allergan USA, Inc., and San Francisco, California: Medicines360; 2016.
A new single-handed inserter (SHI) for placement of Liletta has been introduced and is currently available (FIGURE 1). Liletta is a levonorgestrel 52-mg intrauterine system (IUS) that is currently approved for 3 years of use as a contraceptive in the United States. The same product in Europe, known as Levosert, is approved for both contraception and the treatment of heavy menstrual bleeding. Liletta, as a branded contraceptive, is being studied through a large Phase 3 clinical trial called ACCESS IUS, which will continue to evaluate the contraceptive efficacy of Liletta for at least 7 years of use.1 A recent publication from the study showed that the levonorgestrel release rates from Liletta are almost identical to the rates reported for the other levonorgestrel 52-mg IUS on the market (Mirena) through 5 years and supports the continued study of the IUS for at least 7 years.2
Related article:
Benefit of self-administered vaginal lidocaine gel in IUD placement
The initial marketing and distribution of Liletta used a two-handed inserter that allowed for successful placement but required multiple steps. The SHI will make loading and placement of Liletta easier for all clinicians. Features of the new SHI include:
- A double-slider mechanism in which the first slider moves into the second slider during IUS placement, providing a tactile sense for the user during the insertion process
- The ability to reload the inserter if needed before placement
- A firm but bendable tube (that is 2 cm longer than other IUS inserters on the market). This length can be helpful for obese patients or postprocedure placements.
- Depth markings to 12 cm on both sides of the insertion tube.
Related article:
2016 Update on contraception
Liletta is an important and unique product in the US market. For most public sector providers and clinics, Liletta costs only $50, significantly less than other long-acting reversible contraceptives. The price of the IUS is only one aspect of its overall cost, however, as women still need to pay for any office visit or insertion fees. Liletta is unique in its pricing. Sales of Liletta in the private sector support the low price in the public sector. As a health care community, even if we do not directly care for women in public-sector settings, we all can help poor women access affordable, effective contraception. For providers, Liletta is a highly effective and lower-cost alternative to currently available hormonal IUS products.
How to insert Liletta
Insertion can be performed using a no-touch technique. The loading and placement technique outlined below should occur after speculum and tenaculum placement, sounding of the uterus, and vaginal preparation as would be performed for any intrauterine contraceptive insertion. Never force the uterine sound or insertion tube through the cervix; if necessary, stop and dilate the cervical canal. The steps below are the main points for successful Liletta placement; see the full product label for more details.3
Related article:
In which clinical situations can the use of the 52-mg levonorgestrel-releasing IUD (Mirena) and the TCu380A copper-IUD (ParaGard) be extended?
The key steps to remember are firm-gentle-firm
- Load the device. While pushing forward firmly on the blue slider (with the number 1), load Liletta by pulling down evenly on the threads. The IUS should be laid on a flat surface in the sterile tray to keep the arms parallel to the floor while pulling on the threads. Once loaded, the threads can be pulled up or down to be locked in the cleft. The tip of the IUS will form a hemispheric dome at the top of the insertion tube.
- Adjust the flange to the measured uterine depth based on sounding using the notch in the tray.
- Place inserter into the cervix. Apply gentle traction on the tenaculum to align the cervical canal and uterine cavity. While still holding firm forward pressure on the blue slider, place the tube through the cervical canal until the flange is approximately 1.5 to 2 cm from the cervix. (FIGURE 2.) Gently slide the blue slider downward until it is flush with the green slider (with the number 2; FIGURE 3). This step will allow the IUS arms to open in the lower uterine segment; wait 10 to 15 seconds for the arms to fully unfold. By sliding gently, you will feel when to stop moving the slider.
Image copyright Medicines360.
Figure 2. Placing the inserter through the cervix
Image copyright Medicines360.Figure 3. Merging the blue and green sliders together to release the IUS arms - Advance the inserter. While holding traction on the tenaculum, advance the inserter to the fundus. You will feel slight resistance when the IUS is at the fundus and the flange should be flush against the cervix.
- Firmly slide both sliders together downward until a click is heard (FIGURE 4). A green indicator will be visible at the bottom of the handle to show that the threads have been ejected from the cleft.
Image copyright Medicines360.
Figure 4. Moving the blue and green sliders downward together to release the IUS - Withdraw the inserter from the uterus and cut the threads with blunt tipped scissors approximately 3 cm from the cervical os.
Technique video
Allergan and Medicines360 offer a video demonstrating proper Liletta insertion technique at www.lilettahcp.com. The video includes proper loading of the inserter as well as correct uterine depth measurement and release of Liletta from the inserter. Clinicians are reminded to use aseptic technique during the entire insertion procedure.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
A new single-handed inserter (SHI) for placement of Liletta has been introduced and is currently available (FIGURE 1). Liletta is a levonorgestrel 52-mg intrauterine system (IUS) that is currently approved for 3 years of use as a contraceptive in the United States. The same product in Europe, known as Levosert, is approved for both contraception and the treatment of heavy menstrual bleeding. Liletta, as a branded contraceptive, is being studied through a large Phase 3 clinical trial called ACCESS IUS, which will continue to evaluate the contraceptive efficacy of Liletta for at least 7 years of use.1 A recent publication from the study showed that the levonorgestrel release rates from Liletta are almost identical to the rates reported for the other levonorgestrel 52-mg IUS on the market (Mirena) through 5 years and supports the continued study of the IUS for at least 7 years.2
Related article:
Benefit of self-administered vaginal lidocaine gel in IUD placement
The initial marketing and distribution of Liletta used a two-handed inserter that allowed for successful placement but required multiple steps. The SHI will make loading and placement of Liletta easier for all clinicians. Features of the new SHI include:
- A double-slider mechanism in which the first slider moves into the second slider during IUS placement, providing a tactile sense for the user during the insertion process
- The ability to reload the inserter if needed before placement
- A firm but bendable tube (that is 2 cm longer than other IUS inserters on the market). This length can be helpful for obese patients or postprocedure placements.
- Depth markings to 12 cm on both sides of the insertion tube.
Related article:
2016 Update on contraception
Liletta is an important and unique product in the US market. For most public sector providers and clinics, Liletta costs only $50, significantly less than other long-acting reversible contraceptives. The price of the IUS is only one aspect of its overall cost, however, as women still need to pay for any office visit or insertion fees. Liletta is unique in its pricing. Sales of Liletta in the private sector support the low price in the public sector. As a health care community, even if we do not directly care for women in public-sector settings, we all can help poor women access affordable, effective contraception. For providers, Liletta is a highly effective and lower-cost alternative to currently available hormonal IUS products.
How to insert Liletta
Insertion can be performed using a no-touch technique. The loading and placement technique outlined below should occur after speculum and tenaculum placement, sounding of the uterus, and vaginal preparation as would be performed for any intrauterine contraceptive insertion. Never force the uterine sound or insertion tube through the cervix; if necessary, stop and dilate the cervical canal. The steps below are the main points for successful Liletta placement; see the full product label for more details.3
Related article:
In which clinical situations can the use of the 52-mg levonorgestrel-releasing IUD (Mirena) and the TCu380A copper-IUD (ParaGard) be extended?
The key steps to remember are firm-gentle-firm
- Load the device. While pushing forward firmly on the blue slider (with the number 1), load Liletta by pulling down evenly on the threads. The IUS should be laid on a flat surface in the sterile tray to keep the arms parallel to the floor while pulling on the threads. Once loaded, the threads can be pulled up or down to be locked in the cleft. The tip of the IUS will form a hemispheric dome at the top of the insertion tube.
- Adjust the flange to the measured uterine depth based on sounding using the notch in the tray.
- Place inserter into the cervix. Apply gentle traction on the tenaculum to align the cervical canal and uterine cavity. While still holding firm forward pressure on the blue slider, place the tube through the cervical canal until the flange is approximately 1.5 to 2 cm from the cervix. (FIGURE 2.) Gently slide the blue slider downward until it is flush with the green slider (with the number 2; FIGURE 3). This step will allow the IUS arms to open in the lower uterine segment; wait 10 to 15 seconds for the arms to fully unfold. By sliding gently, you will feel when to stop moving the slider.
Image copyright Medicines360.
Figure 2. Placing the inserter through the cervix
Image copyright Medicines360.Figure 3. Merging the blue and green sliders together to release the IUS arms - Advance the inserter. While holding traction on the tenaculum, advance the inserter to the fundus. You will feel slight resistance when the IUS is at the fundus and the flange should be flush against the cervix.
- Firmly slide both sliders together downward until a click is heard (FIGURE 4). A green indicator will be visible at the bottom of the handle to show that the threads have been ejected from the cleft.
Image copyright Medicines360.
Figure 4. Moving the blue and green sliders downward together to release the IUS - Withdraw the inserter from the uterus and cut the threads with blunt tipped scissors approximately 3 cm from the cervical os.
Technique video
Allergan and Medicines360 offer a video demonstrating proper Liletta insertion technique at www.lilettahcp.com. The video includes proper loading of the inserter as well as correct uterine depth measurement and release of Liletta from the inserter. Clinicians are reminded to use aseptic technique during the entire insertion procedure.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Eisenberg DL, Schreiber CA, Turok DK, Teal SB, Westhoff CL, Creinin MD. Three year efficacy and safety of a new 52-mg levonorgestrel-releasing intrauterine system. Contraception. 2015;92(1):10-16.
- Creinin MD, Jansen R, Starr R, Gobburu J, Gopalakrishnan M, Olariu A. Levonorgestrel release rates over 5 years with the Liletta® 52 mg intrauterine system. Contraception. 2016;94(4):353-356.
- Liletta [package insert]. Irvine, California: Allergan USA, Inc., and San Francisco, California: Medicines360; 2016.
- Eisenberg DL, Schreiber CA, Turok DK, Teal SB, Westhoff CL, Creinin MD. Three year efficacy and safety of a new 52-mg levonorgestrel-releasing intrauterine system. Contraception. 2015;92(1):10-16.
- Creinin MD, Jansen R, Starr R, Gobburu J, Gopalakrishnan M, Olariu A. Levonorgestrel release rates over 5 years with the Liletta® 52 mg intrauterine system. Contraception. 2016;94(4):353-356.
- Liletta [package insert]. Irvine, California: Allergan USA, Inc., and San Francisco, California: Medicines360; 2016.
In this article
Obese IVF patients need higher HCG trigger dose
SALT LAKE CITY – Women who are obese should receive more than 5,000 IU of human chorionic gonadotropin (HCG) to trigger final oocyte maturation during in vitro fertilization, findings of a retrospective cohort study suggest.
Fully 23% of obese women had low beta-HCG levels the day after receiving a 5,000 IU HCG trigger dose, compared with 1% of non-obese women (odds ratio, 21.4; 95% confidence interval, 15.0-30.4), reported Mohamad Irani, MD, and his associates from Cornell University, New York. In contrast, 10,000 IU HCG triggered adequate beta-HCG levels in 81% of obese patients with a BMI of 30-40 kg/m2, and in 90% of those whose BMI exceeded 40 kg/m2.
Low beta-HCG levels decreased the chances of oocyte maturation, fertilization, and live birth in the study. “Patients’ BMI should be taken into consideration when determining the dose of HCG trigger,” the investigators concluded in a poster presented at the annual meeting of the American Society for Reproductive Medicine.
Patients with hypothalamic amenorrhea or who are undergoing stimulation with a gonadotropin-releasing hormone (GnRH) agonist are not candidates for a GnRH-agonist trigger and therefore need to receive HCG instead, the researchers noted. To understand how the dose of HCG affects the chances of final oocyte maturation, they studied 19,084 HCG trigger recipients at their center between 2004 and 2013.
By protocol, patients received 10,000 IU HCG if their serum estradiol (E2) level was less than 1,500 pg/mL on the day of trigger; 5,000 IU if it measured 1,501-2,500 pg/mL; 4,000 IU if it was 2,501-3,000 pg/mL; and 3,300 IU if it exceeded 3,000 pg/mL.
The day after HCG trigger, 18,666 patients had beta-HCG levels of at least 50 mIU/mL, while 418 patients had low beta-HCG levels of less than 50 mIU/mL. A comparison of the two groups showed that low beta-HCG was associated with significantly lower rates of oocyte maturation (77% vs. 81%; P less than .001) and fertilization (63% vs. 72%; P less than .001). It was also associated with more than a 30% lower chance of a live birth (adjusted OR, 0.67; 95% CI, 0.5-0.8), even after accounting for age, and the stage and number of embryos transferred.
The researchers also examined response to HCG trigger among non-obese patients. Among patients who were overweight (BMI 25 to 30 kg/m2), the chances of a low beta-HCG level the day after trigger were 14% when the HCG dose was 3,300 IU, 12.5% when it was 4,000 IU, 4.3% when it was 5,000 IU, and 0.4% when it was 10,000 IU.
Among healthy-weight patients (BMI 18.5-25 kg/m2), low beta-HCG levels occurred 3.6% of the time when the HCG dose was 3,300 IU, 2.3% of the time when it was 4,000 IU, 0.6% of the time when it was 5,000 IU, and 0.08% of the time when it was 10,000 IU. Notably, these same doses triggered adequate beta-HCG levels in all 660 patients who were underweight (BMI less than 18.5 kg/m2), the researchers reported.
Dr. Irani reported having no relevant financial disclosures.
SALT LAKE CITY – Women who are obese should receive more than 5,000 IU of human chorionic gonadotropin (HCG) to trigger final oocyte maturation during in vitro fertilization, findings of a retrospective cohort study suggest.
Fully 23% of obese women had low beta-HCG levels the day after receiving a 5,000 IU HCG trigger dose, compared with 1% of non-obese women (odds ratio, 21.4; 95% confidence interval, 15.0-30.4), reported Mohamad Irani, MD, and his associates from Cornell University, New York. In contrast, 10,000 IU HCG triggered adequate beta-HCG levels in 81% of obese patients with a BMI of 30-40 kg/m2, and in 90% of those whose BMI exceeded 40 kg/m2.
Low beta-HCG levels decreased the chances of oocyte maturation, fertilization, and live birth in the study. “Patients’ BMI should be taken into consideration when determining the dose of HCG trigger,” the investigators concluded in a poster presented at the annual meeting of the American Society for Reproductive Medicine.
Patients with hypothalamic amenorrhea or who are undergoing stimulation with a gonadotropin-releasing hormone (GnRH) agonist are not candidates for a GnRH-agonist trigger and therefore need to receive HCG instead, the researchers noted. To understand how the dose of HCG affects the chances of final oocyte maturation, they studied 19,084 HCG trigger recipients at their center between 2004 and 2013.
By protocol, patients received 10,000 IU HCG if their serum estradiol (E2) level was less than 1,500 pg/mL on the day of trigger; 5,000 IU if it measured 1,501-2,500 pg/mL; 4,000 IU if it was 2,501-3,000 pg/mL; and 3,300 IU if it exceeded 3,000 pg/mL.
The day after HCG trigger, 18,666 patients had beta-HCG levels of at least 50 mIU/mL, while 418 patients had low beta-HCG levels of less than 50 mIU/mL. A comparison of the two groups showed that low beta-HCG was associated with significantly lower rates of oocyte maturation (77% vs. 81%; P less than .001) and fertilization (63% vs. 72%; P less than .001). It was also associated with more than a 30% lower chance of a live birth (adjusted OR, 0.67; 95% CI, 0.5-0.8), even after accounting for age, and the stage and number of embryos transferred.
The researchers also examined response to HCG trigger among non-obese patients. Among patients who were overweight (BMI 25 to 30 kg/m2), the chances of a low beta-HCG level the day after trigger were 14% when the HCG dose was 3,300 IU, 12.5% when it was 4,000 IU, 4.3% when it was 5,000 IU, and 0.4% when it was 10,000 IU.
Among healthy-weight patients (BMI 18.5-25 kg/m2), low beta-HCG levels occurred 3.6% of the time when the HCG dose was 3,300 IU, 2.3% of the time when it was 4,000 IU, 0.6% of the time when it was 5,000 IU, and 0.08% of the time when it was 10,000 IU. Notably, these same doses triggered adequate beta-HCG levels in all 660 patients who were underweight (BMI less than 18.5 kg/m2), the researchers reported.
Dr. Irani reported having no relevant financial disclosures.
SALT LAKE CITY – Women who are obese should receive more than 5,000 IU of human chorionic gonadotropin (HCG) to trigger final oocyte maturation during in vitro fertilization, findings of a retrospective cohort study suggest.
Fully 23% of obese women had low beta-HCG levels the day after receiving a 5,000 IU HCG trigger dose, compared with 1% of non-obese women (odds ratio, 21.4; 95% confidence interval, 15.0-30.4), reported Mohamad Irani, MD, and his associates from Cornell University, New York. In contrast, 10,000 IU HCG triggered adequate beta-HCG levels in 81% of obese patients with a BMI of 30-40 kg/m2, and in 90% of those whose BMI exceeded 40 kg/m2.
Low beta-HCG levels decreased the chances of oocyte maturation, fertilization, and live birth in the study. “Patients’ BMI should be taken into consideration when determining the dose of HCG trigger,” the investigators concluded in a poster presented at the annual meeting of the American Society for Reproductive Medicine.
Patients with hypothalamic amenorrhea or who are undergoing stimulation with a gonadotropin-releasing hormone (GnRH) agonist are not candidates for a GnRH-agonist trigger and therefore need to receive HCG instead, the researchers noted. To understand how the dose of HCG affects the chances of final oocyte maturation, they studied 19,084 HCG trigger recipients at their center between 2004 and 2013.
By protocol, patients received 10,000 IU HCG if their serum estradiol (E2) level was less than 1,500 pg/mL on the day of trigger; 5,000 IU if it measured 1,501-2,500 pg/mL; 4,000 IU if it was 2,501-3,000 pg/mL; and 3,300 IU if it exceeded 3,000 pg/mL.
The day after HCG trigger, 18,666 patients had beta-HCG levels of at least 50 mIU/mL, while 418 patients had low beta-HCG levels of less than 50 mIU/mL. A comparison of the two groups showed that low beta-HCG was associated with significantly lower rates of oocyte maturation (77% vs. 81%; P less than .001) and fertilization (63% vs. 72%; P less than .001). It was also associated with more than a 30% lower chance of a live birth (adjusted OR, 0.67; 95% CI, 0.5-0.8), even after accounting for age, and the stage and number of embryos transferred.
The researchers also examined response to HCG trigger among non-obese patients. Among patients who were overweight (BMI 25 to 30 kg/m2), the chances of a low beta-HCG level the day after trigger were 14% when the HCG dose was 3,300 IU, 12.5% when it was 4,000 IU, 4.3% when it was 5,000 IU, and 0.4% when it was 10,000 IU.
Among healthy-weight patients (BMI 18.5-25 kg/m2), low beta-HCG levels occurred 3.6% of the time when the HCG dose was 3,300 IU, 2.3% of the time when it was 4,000 IU, 0.6% of the time when it was 5,000 IU, and 0.08% of the time when it was 10,000 IU. Notably, these same doses triggered adequate beta-HCG levels in all 660 patients who were underweight (BMI less than 18.5 kg/m2), the researchers reported.
Dr. Irani reported having no relevant financial disclosures.
AT 2016 ASRM
Key clinical point:
Major finding: Fully 23% of obese individuals had low beta-HCG levels the day after receiving a 5,000 IU HCG trigger, compared with 1% of non-obese patients (OR, 21.4).
Data source: A retrospective cohort study of 18,666 patients with beta-HCG levels of at least 50 mIU/mL and 418 patients with “low” levels of less than 50 mIU/mL the day after HCG trigger.
Disclosures: Dr. Irani reported having no relevant financial disclosures.
Acute Localized Exanthematous Pustulosis Caused by Flurbiprofen
To the Editor:
Acute generalized exanthematous pustulosis (AGEP) is an acute skin reaction that is characterized by generalized, nonfollicular, pinhead-sized, sterile pustules on an erythematous and edematous background. The eruption can be accompanied by fever and neutrophilic leukocytosis. Skin symptoms arise quickly (within a few hours), most commonly following drug administration. The medications most frequently responsible are beta-lactam antibiotics, macrolides, calcium channel blockers, and antimalarials. Pustules spontaneously resolve in 15 days and generalized desquamation occurs approximately 2 weeks later. The estimated incidence rate of AGEP is approximately 1 to 5 cases per million per year. Acute localized exanthematous pustulosis (ALEP) is a less common form of AGEP. We report a case of ALEP localized on the face that was caused by flurbiprofen, a propionic acid derivative from the family of nonsteroidal anti-inflammatory drugs (NSAIDs).
A 40-year-old woman was referred to the dermatology department due to the sudden onset of multiple pustules on the face. One week earlier she started oral flurbiprofen (8.75 mg daily) for a sore throat. After 3 days of therapy, multiple pruritic, erythematous and edematous lesions appeared abruptly on the face with associated multiple small nonfollicular pustules. At presentation the patient was febrile (temperature, 38.2°C) and presented with bilateral ocular edema and superficial small nonfollicular pustules on an erythematous background over the face, scalp, and oral mucosa (Figure 1). The rest of the body was not involved. The patient denied prior adverse reactions to other drugs. The white blood cell count was 15,000/μL (reference range, 4500–11,000/μL), with an increased neutrophil count (12,000/μL [reference range, 1800–7800/μL]). The erythrocyte sedimentation rate and C-reactive protein level was elevated (erythrocyte sedimentation rate, 53 mm/h [reference range, 0–20 mm/h]; C-reactive protein, 98 mg/dL [reference range, 0–5 mg/dL]). Bacterial and fungal cultures of skin lesions were negative. The results of a viral polymerase chain reaction analysis proved the absence of varicella-zoster virus or herpes simplex virus. Histopathology of a skin biopsy specimen showed subcorneal pustules composed of neutrophils and eosinophils, epidermal spongiosis, some necrotic keratinocytes, vacuolization of the basal layer, papillary edema, and a perivascular neutrophil and lymphocyte infiltrate (Figure 2). A leukocytoclastic infiltrate within and around the walls of blood vessels at the superficial level of the dermis and red cell extravasation in the epidermis was present. She discontinued use of flurbiprofen and was treated with a systemic corticosteroid (methylprednisolone 0.5 mg/kg daily). The pustules rapidly resolved within 7 days after discontinuation of flurbiprofen and were followed by transient scaling and discrete residual hyperpigmentation.

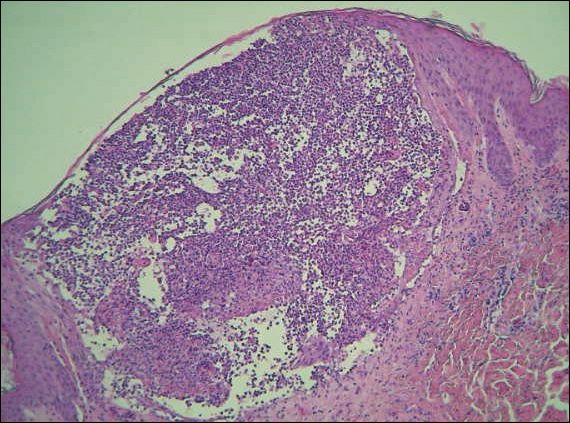
Acute localized exanthematous pustulosis is a less common form of a pustular drug eruption in which lesions are consistent with AGEP but typically are localized to the face, neck, or chest. The definition of ALEP was introduced by Prange et al1 to describe a woman who was diagnosed with a localized pustular eruption on the face without a generalized distribution as in AGEP. In the past, this localized eruption was described under different names (eg, localized pustular eruption, localized toxin follicular pustuloderma, nongeneralized acute exanthematic pustulosis).2-5 According to a PubMed search of articles indexed for MEDLINE using the terms localized pustulosis, localized pustular eruption, and localized pustuloderma, only 16 separate cases of ALEP have been documented since the report by Prange et al.1 The medications most frequently responsible are antibiotics. Three cases developed following administration of amoxicillin2,5,6; 2 cases of amoxicillin–clavulanic acid7,8; 1 of penicillin1; 1 of azithromycin9; 1 of levofloxacin10; and 1 of combination of cephalosporin, sulfamethoxazole-trimethoprim, and vancomycin.11 Other nonantibiotic causative drugs include sulfamethoxazole-trimethoprim,12 infliximab,13 sorafenib,14 docetaxel,15 finasteride,16 ibuprofen,17 and paracetamol.18 In reported cases, the lesions are consistent with the characteristics of AGEP both clinically and histopathologically but are localized typically to the face, neck, or chest. In the majority of patients with ALEP, the absence of fever has been observed, but it does not appear distinctive for diagnosis. Our patient represents another case of ALEP with flurbiprofen as the causative drug. The close relationship between the administration of the drug and the development of the pustules, the rapid acute resolution as soon as treatment was interrupted, and the histologic findings all supported the diagnosis of ALEP following administration of flurbiprofen. This NSAID—2-fluoro-α-methyl-(1,1'-biphenyl)-4-acetic acid—is a prostaglandin synthetase inhibitor with anti-inflammatory activity. It is a propionic acid derivative that is similar to ibuprofen, which was once involved in the occurrence of ALEP.17 In 2009, Rastogi et al17 reported a case of a 64-year-old woman with an acute outbreak of multiple pustular lesions and underlying erythema affecting the cheeks and chin without fever who had been taking ibuprofen for a toothache. The case is similar to ours and confirms that NSAIDs can induce ALEP. Compared with other NSAIDs, propionic acid derivatives are usually well tolerated and serious adverse reactions rarely have been documented.19
The physiopathologic mechanisms of ALEP are unknown but likely are similar to AGEP. The demonstration of drug-specific positive patch test responses and in vitro lymphocyte proliferative responses in patients with a history of AGEP strongly suggests that this adverse cutaneous reaction occurs via a drug-specific T cell–mediated process.20
Further study is needed to understand the etiopathogenesis of the localized form of the disease and to facilitate a correct diagnosis of this rare disorder.
- Prange B, Marini A, Kalke A, et al. Acute localized exanthematous pustulosis (ALEP). J Dtsch Dermatol Ges. 2005;3:210-212.
- Shuttleworth D. A localized, recurrent pustular eruption following amoxycillin administration. Clin Exp Dermatol. 1989;14:367-368.
- De Argila D, Ortiz-Frutos J, Rodriguez-Peralto JL, et al. An atypical case of non-generalized acute exanthematic pustulosis. Actas Dermosifiliogr. 1996;87:475-478.
- Corbalan-Velez R, Peon G, Ara M, et al. Localized toxic follicular pustuloderma. Int J Dermatol. 2000;39:209-211.
- Prieto A, de Barrio M, López-Sáez P, et al. Recurrent localized pustular eruption induced by amoxicillin. Allergy. 1997;52:777-778.
- Vickers JL, Matherne RJ, Mainous EG, et al. Acute localized exanthematous pustulosis: a cutaneous drug reaction in a dental setting. J Am Dent Assoc. 2008;139:1200-1203.
- Betto P, Germi L, Bonoldi E, et al. Acute localized exanthematous pustulosis (ALEP) caused by amoxicillin-clavulanic acid. Int J Dermatol. 2008;47:295-296.
- Ozkaya-Parlakay A, Azkur D, Kara A, et al. Localized acute generalized exanthematous pustulosis with amoxicillin and clavulanic acid. Turk J Pediatr. 2011;53:229-232.
- Zweegers J, Bovenschen HJ. A woman with skin abnormalities around the mouth [in Dutch]. Ned Tijdschr Geneeskd. 2012;156:A4613.
- Corral de la Calle M, Martín Díaz MA, Flores CR, et al. Acute localized exanthematous pustulosis secondary to levofloxacin. Br J Dermatol. 2005;152:1076-1077.
- Sim HS, Seol JE, Chun JS, et al. Acute localized exanthematous pustulosis on the face. Ann Dermatol. 2011;23(suppl 3):S3368-S3370.
- Lee I, Turner M, Lee CC. Acute patchy exanthematous pustulosis caused by sulfamethoxazole-trimethoprim. J Am Acad Dermatol. 2010;63:e41-e43.
- Lee HY, Pelivani N, Beltraminelli H, et al. Amicrobial pustulosis-like rash in a patient with Crohn’s disease under anti-TNF-alpha blocker. Dermatology. 2011;222:304-310.
- Liang CP, Yang CS, Shen JL, et al. Sorafenib-induced acute localized exanthematous pustulosis in a patient with hepatocellular carcinoma. Br J Dermatol. 2011;165:443-445.
- Kim SW, Lee UH, Jang SJ, et al. Acute localized exanthematous pustulosis induced by docetaxel. J Am Acad Dermatol. 2010;63:e44-e46.
- Tresch S, Cozzio A, Kamarashev J, et al. T cell-mediated acute localized exanthematous pustulosis caused by finasteride. J Allergy Clin Immunol. 2012;129:589-594.
- Rastogi S, Modi M, Dhawan V. Acute localized exanthematous pustulosis (ALEP) caused by Ibuprofen. a case report. Br J Oral Maxillofac Surg. 2009;47:132-134.
- Wohl Y, Goldberg I, Sharazi I, et al. A case of paracetamol-induced acute generalized exanthematous pustulosis in a pregnant woman localized in the neck region. Skinmed. 2004;3:47-49.
- Mehra KK, Rupawala AH, Gogtay NJ. Immediate hypersensitivity reaction to a single oral dose of flurbiprofen. J Postgrad Med. 2010;56:36-37.
- Girardi M, Duncan KO, Tigelaar RE, et al. Cross comparison of patch-test and lymphocyte proliferation responses in patients with a history of acute generalized exanthematous pustulosis. Am J Dermatopathol. 2005;27:343-346.
To the Editor:
Acute generalized exanthematous pustulosis (AGEP) is an acute skin reaction that is characterized by generalized, nonfollicular, pinhead-sized, sterile pustules on an erythematous and edematous background. The eruption can be accompanied by fever and neutrophilic leukocytosis. Skin symptoms arise quickly (within a few hours), most commonly following drug administration. The medications most frequently responsible are beta-lactam antibiotics, macrolides, calcium channel blockers, and antimalarials. Pustules spontaneously resolve in 15 days and generalized desquamation occurs approximately 2 weeks later. The estimated incidence rate of AGEP is approximately 1 to 5 cases per million per year. Acute localized exanthematous pustulosis (ALEP) is a less common form of AGEP. We report a case of ALEP localized on the face that was caused by flurbiprofen, a propionic acid derivative from the family of nonsteroidal anti-inflammatory drugs (NSAIDs).
A 40-year-old woman was referred to the dermatology department due to the sudden onset of multiple pustules on the face. One week earlier she started oral flurbiprofen (8.75 mg daily) for a sore throat. After 3 days of therapy, multiple pruritic, erythematous and edematous lesions appeared abruptly on the face with associated multiple small nonfollicular pustules. At presentation the patient was febrile (temperature, 38.2°C) and presented with bilateral ocular edema and superficial small nonfollicular pustules on an erythematous background over the face, scalp, and oral mucosa (Figure 1). The rest of the body was not involved. The patient denied prior adverse reactions to other drugs. The white blood cell count was 15,000/μL (reference range, 4500–11,000/μL), with an increased neutrophil count (12,000/μL [reference range, 1800–7800/μL]). The erythrocyte sedimentation rate and C-reactive protein level was elevated (erythrocyte sedimentation rate, 53 mm/h [reference range, 0–20 mm/h]; C-reactive protein, 98 mg/dL [reference range, 0–5 mg/dL]). Bacterial and fungal cultures of skin lesions were negative. The results of a viral polymerase chain reaction analysis proved the absence of varicella-zoster virus or herpes simplex virus. Histopathology of a skin biopsy specimen showed subcorneal pustules composed of neutrophils and eosinophils, epidermal spongiosis, some necrotic keratinocytes, vacuolization of the basal layer, papillary edema, and a perivascular neutrophil and lymphocyte infiltrate (Figure 2). A leukocytoclastic infiltrate within and around the walls of blood vessels at the superficial level of the dermis and red cell extravasation in the epidermis was present. She discontinued use of flurbiprofen and was treated with a systemic corticosteroid (methylprednisolone 0.5 mg/kg daily). The pustules rapidly resolved within 7 days after discontinuation of flurbiprofen and were followed by transient scaling and discrete residual hyperpigmentation.
Acute localized exanthematous pustulosis is a less common form of a pustular drug eruption in which lesions are consistent with AGEP but typically are localized to the face, neck, or chest. The definition of ALEP was introduced by Prange et al1 to describe a woman who was diagnosed with a localized pustular eruption on the face without a generalized distribution as in AGEP. In the past, this localized eruption was described under different names (eg, localized pustular eruption, localized toxin follicular pustuloderma, nongeneralized acute exanthematic pustulosis).2-5 According to a PubMed search of articles indexed for MEDLINE using the terms localized pustulosis, localized pustular eruption, and localized pustuloderma, only 16 separate cases of ALEP have been documented since the report by Prange et al.1 The medications most frequently responsible are antibiotics. Three cases developed following administration of amoxicillin2,5,6; 2 cases of amoxicillin–clavulanic acid7,8; 1 of penicillin1; 1 of azithromycin9; 1 of levofloxacin10; and 1 of combination of cephalosporin, sulfamethoxazole-trimethoprim, and vancomycin.11 Other nonantibiotic causative drugs include sulfamethoxazole-trimethoprim,12 infliximab,13 sorafenib,14 docetaxel,15 finasteride,16 ibuprofen,17 and paracetamol.18 In reported cases, the lesions are consistent with the characteristics of AGEP both clinically and histopathologically but are localized typically to the face, neck, or chest. In the majority of patients with ALEP, the absence of fever has been observed, but it does not appear distinctive for diagnosis. Our patient represents another case of ALEP with flurbiprofen as the causative drug. The close relationship between the administration of the drug and the development of the pustules, the rapid acute resolution as soon as treatment was interrupted, and the histologic findings all supported the diagnosis of ALEP following administration of flurbiprofen. This NSAID—2-fluoro-α-methyl-(1,1'-biphenyl)-4-acetic acid—is a prostaglandin synthetase inhibitor with anti-inflammatory activity. It is a propionic acid derivative that is similar to ibuprofen, which was once involved in the occurrence of ALEP.17 In 2009, Rastogi et al17 reported a case of a 64-year-old woman with an acute outbreak of multiple pustular lesions and underlying erythema affecting the cheeks and chin without fever who had been taking ibuprofen for a toothache. The case is similar to ours and confirms that NSAIDs can induce ALEP. Compared with other NSAIDs, propionic acid derivatives are usually well tolerated and serious adverse reactions rarely have been documented.19
The physiopathologic mechanisms of ALEP are unknown but likely are similar to AGEP. The demonstration of drug-specific positive patch test responses and in vitro lymphocyte proliferative responses in patients with a history of AGEP strongly suggests that this adverse cutaneous reaction occurs via a drug-specific T cell–mediated process.20
Further study is needed to understand the etiopathogenesis of the localized form of the disease and to facilitate a correct diagnosis of this rare disorder.
To the Editor:
Acute generalized exanthematous pustulosis (AGEP) is an acute skin reaction that is characterized by generalized, nonfollicular, pinhead-sized, sterile pustules on an erythematous and edematous background. The eruption can be accompanied by fever and neutrophilic leukocytosis. Skin symptoms arise quickly (within a few hours), most commonly following drug administration. The medications most frequently responsible are beta-lactam antibiotics, macrolides, calcium channel blockers, and antimalarials. Pustules spontaneously resolve in 15 days and generalized desquamation occurs approximately 2 weeks later. The estimated incidence rate of AGEP is approximately 1 to 5 cases per million per year. Acute localized exanthematous pustulosis (ALEP) is a less common form of AGEP. We report a case of ALEP localized on the face that was caused by flurbiprofen, a propionic acid derivative from the family of nonsteroidal anti-inflammatory drugs (NSAIDs).
A 40-year-old woman was referred to the dermatology department due to the sudden onset of multiple pustules on the face. One week earlier she started oral flurbiprofen (8.75 mg daily) for a sore throat. After 3 days of therapy, multiple pruritic, erythematous and edematous lesions appeared abruptly on the face with associated multiple small nonfollicular pustules. At presentation the patient was febrile (temperature, 38.2°C) and presented with bilateral ocular edema and superficial small nonfollicular pustules on an erythematous background over the face, scalp, and oral mucosa (Figure 1). The rest of the body was not involved. The patient denied prior adverse reactions to other drugs. The white blood cell count was 15,000/μL (reference range, 4500–11,000/μL), with an increased neutrophil count (12,000/μL [reference range, 1800–7800/μL]). The erythrocyte sedimentation rate and C-reactive protein level was elevated (erythrocyte sedimentation rate, 53 mm/h [reference range, 0–20 mm/h]; C-reactive protein, 98 mg/dL [reference range, 0–5 mg/dL]). Bacterial and fungal cultures of skin lesions were negative. The results of a viral polymerase chain reaction analysis proved the absence of varicella-zoster virus or herpes simplex virus. Histopathology of a skin biopsy specimen showed subcorneal pustules composed of neutrophils and eosinophils, epidermal spongiosis, some necrotic keratinocytes, vacuolization of the basal layer, papillary edema, and a perivascular neutrophil and lymphocyte infiltrate (Figure 2). A leukocytoclastic infiltrate within and around the walls of blood vessels at the superficial level of the dermis and red cell extravasation in the epidermis was present. She discontinued use of flurbiprofen and was treated with a systemic corticosteroid (methylprednisolone 0.5 mg/kg daily). The pustules rapidly resolved within 7 days after discontinuation of flurbiprofen and were followed by transient scaling and discrete residual hyperpigmentation.
Acute localized exanthematous pustulosis is a less common form of a pustular drug eruption in which lesions are consistent with AGEP but typically are localized to the face, neck, or chest. The definition of ALEP was introduced by Prange et al1 to describe a woman who was diagnosed with a localized pustular eruption on the face without a generalized distribution as in AGEP. In the past, this localized eruption was described under different names (eg, localized pustular eruption, localized toxin follicular pustuloderma, nongeneralized acute exanthematic pustulosis).2-5 According to a PubMed search of articles indexed for MEDLINE using the terms localized pustulosis, localized pustular eruption, and localized pustuloderma, only 16 separate cases of ALEP have been documented since the report by Prange et al.1 The medications most frequently responsible are antibiotics. Three cases developed following administration of amoxicillin2,5,6; 2 cases of amoxicillin–clavulanic acid7,8; 1 of penicillin1; 1 of azithromycin9; 1 of levofloxacin10; and 1 of combination of cephalosporin, sulfamethoxazole-trimethoprim, and vancomycin.11 Other nonantibiotic causative drugs include sulfamethoxazole-trimethoprim,12 infliximab,13 sorafenib,14 docetaxel,15 finasteride,16 ibuprofen,17 and paracetamol.18 In reported cases, the lesions are consistent with the characteristics of AGEP both clinically and histopathologically but are localized typically to the face, neck, or chest. In the majority of patients with ALEP, the absence of fever has been observed, but it does not appear distinctive for diagnosis. Our patient represents another case of ALEP with flurbiprofen as the causative drug. The close relationship between the administration of the drug and the development of the pustules, the rapid acute resolution as soon as treatment was interrupted, and the histologic findings all supported the diagnosis of ALEP following administration of flurbiprofen. This NSAID—2-fluoro-α-methyl-(1,1'-biphenyl)-4-acetic acid—is a prostaglandin synthetase inhibitor with anti-inflammatory activity. It is a propionic acid derivative that is similar to ibuprofen, which was once involved in the occurrence of ALEP.17 In 2009, Rastogi et al17 reported a case of a 64-year-old woman with an acute outbreak of multiple pustular lesions and underlying erythema affecting the cheeks and chin without fever who had been taking ibuprofen for a toothache. The case is similar to ours and confirms that NSAIDs can induce ALEP. Compared with other NSAIDs, propionic acid derivatives are usually well tolerated and serious adverse reactions rarely have been documented.19
The physiopathologic mechanisms of ALEP are unknown but likely are similar to AGEP. The demonstration of drug-specific positive patch test responses and in vitro lymphocyte proliferative responses in patients with a history of AGEP strongly suggests that this adverse cutaneous reaction occurs via a drug-specific T cell–mediated process.20
Further study is needed to understand the etiopathogenesis of the localized form of the disease and to facilitate a correct diagnosis of this rare disorder.
- Prange B, Marini A, Kalke A, et al. Acute localized exanthematous pustulosis (ALEP). J Dtsch Dermatol Ges. 2005;3:210-212.
- Shuttleworth D. A localized, recurrent pustular eruption following amoxycillin administration. Clin Exp Dermatol. 1989;14:367-368.
- De Argila D, Ortiz-Frutos J, Rodriguez-Peralto JL, et al. An atypical case of non-generalized acute exanthematic pustulosis. Actas Dermosifiliogr. 1996;87:475-478.
- Corbalan-Velez R, Peon G, Ara M, et al. Localized toxic follicular pustuloderma. Int J Dermatol. 2000;39:209-211.
- Prieto A, de Barrio M, López-Sáez P, et al. Recurrent localized pustular eruption induced by amoxicillin. Allergy. 1997;52:777-778.
- Vickers JL, Matherne RJ, Mainous EG, et al. Acute localized exanthematous pustulosis: a cutaneous drug reaction in a dental setting. J Am Dent Assoc. 2008;139:1200-1203.
- Betto P, Germi L, Bonoldi E, et al. Acute localized exanthematous pustulosis (ALEP) caused by amoxicillin-clavulanic acid. Int J Dermatol. 2008;47:295-296.
- Ozkaya-Parlakay A, Azkur D, Kara A, et al. Localized acute generalized exanthematous pustulosis with amoxicillin and clavulanic acid. Turk J Pediatr. 2011;53:229-232.
- Zweegers J, Bovenschen HJ. A woman with skin abnormalities around the mouth [in Dutch]. Ned Tijdschr Geneeskd. 2012;156:A4613.
- Corral de la Calle M, Martín Díaz MA, Flores CR, et al. Acute localized exanthematous pustulosis secondary to levofloxacin. Br J Dermatol. 2005;152:1076-1077.
- Sim HS, Seol JE, Chun JS, et al. Acute localized exanthematous pustulosis on the face. Ann Dermatol. 2011;23(suppl 3):S3368-S3370.
- Lee I, Turner M, Lee CC. Acute patchy exanthematous pustulosis caused by sulfamethoxazole-trimethoprim. J Am Acad Dermatol. 2010;63:e41-e43.
- Lee HY, Pelivani N, Beltraminelli H, et al. Amicrobial pustulosis-like rash in a patient with Crohn’s disease under anti-TNF-alpha blocker. Dermatology. 2011;222:304-310.
- Liang CP, Yang CS, Shen JL, et al. Sorafenib-induced acute localized exanthematous pustulosis in a patient with hepatocellular carcinoma. Br J Dermatol. 2011;165:443-445.
- Kim SW, Lee UH, Jang SJ, et al. Acute localized exanthematous pustulosis induced by docetaxel. J Am Acad Dermatol. 2010;63:e44-e46.
- Tresch S, Cozzio A, Kamarashev J, et al. T cell-mediated acute localized exanthematous pustulosis caused by finasteride. J Allergy Clin Immunol. 2012;129:589-594.
- Rastogi S, Modi M, Dhawan V. Acute localized exanthematous pustulosis (ALEP) caused by Ibuprofen. a case report. Br J Oral Maxillofac Surg. 2009;47:132-134.
- Wohl Y, Goldberg I, Sharazi I, et al. A case of paracetamol-induced acute generalized exanthematous pustulosis in a pregnant woman localized in the neck region. Skinmed. 2004;3:47-49.
- Mehra KK, Rupawala AH, Gogtay NJ. Immediate hypersensitivity reaction to a single oral dose of flurbiprofen. J Postgrad Med. 2010;56:36-37.
- Girardi M, Duncan KO, Tigelaar RE, et al. Cross comparison of patch-test and lymphocyte proliferation responses in patients with a history of acute generalized exanthematous pustulosis. Am J Dermatopathol. 2005;27:343-346.
- Prange B, Marini A, Kalke A, et al. Acute localized exanthematous pustulosis (ALEP). J Dtsch Dermatol Ges. 2005;3:210-212.
- Shuttleworth D. A localized, recurrent pustular eruption following amoxycillin administration. Clin Exp Dermatol. 1989;14:367-368.
- De Argila D, Ortiz-Frutos J, Rodriguez-Peralto JL, et al. An atypical case of non-generalized acute exanthematic pustulosis. Actas Dermosifiliogr. 1996;87:475-478.
- Corbalan-Velez R, Peon G, Ara M, et al. Localized toxic follicular pustuloderma. Int J Dermatol. 2000;39:209-211.
- Prieto A, de Barrio M, López-Sáez P, et al. Recurrent localized pustular eruption induced by amoxicillin. Allergy. 1997;52:777-778.
- Vickers JL, Matherne RJ, Mainous EG, et al. Acute localized exanthematous pustulosis: a cutaneous drug reaction in a dental setting. J Am Dent Assoc. 2008;139:1200-1203.
- Betto P, Germi L, Bonoldi E, et al. Acute localized exanthematous pustulosis (ALEP) caused by amoxicillin-clavulanic acid. Int J Dermatol. 2008;47:295-296.
- Ozkaya-Parlakay A, Azkur D, Kara A, et al. Localized acute generalized exanthematous pustulosis with amoxicillin and clavulanic acid. Turk J Pediatr. 2011;53:229-232.
- Zweegers J, Bovenschen HJ. A woman with skin abnormalities around the mouth [in Dutch]. Ned Tijdschr Geneeskd. 2012;156:A4613.
- Corral de la Calle M, Martín Díaz MA, Flores CR, et al. Acute localized exanthematous pustulosis secondary to levofloxacin. Br J Dermatol. 2005;152:1076-1077.
- Sim HS, Seol JE, Chun JS, et al. Acute localized exanthematous pustulosis on the face. Ann Dermatol. 2011;23(suppl 3):S3368-S3370.
- Lee I, Turner M, Lee CC. Acute patchy exanthematous pustulosis caused by sulfamethoxazole-trimethoprim. J Am Acad Dermatol. 2010;63:e41-e43.
- Lee HY, Pelivani N, Beltraminelli H, et al. Amicrobial pustulosis-like rash in a patient with Crohn’s disease under anti-TNF-alpha blocker. Dermatology. 2011;222:304-310.
- Liang CP, Yang CS, Shen JL, et al. Sorafenib-induced acute localized exanthematous pustulosis in a patient with hepatocellular carcinoma. Br J Dermatol. 2011;165:443-445.
- Kim SW, Lee UH, Jang SJ, et al. Acute localized exanthematous pustulosis induced by docetaxel. J Am Acad Dermatol. 2010;63:e44-e46.
- Tresch S, Cozzio A, Kamarashev J, et al. T cell-mediated acute localized exanthematous pustulosis caused by finasteride. J Allergy Clin Immunol. 2012;129:589-594.
- Rastogi S, Modi M, Dhawan V. Acute localized exanthematous pustulosis (ALEP) caused by Ibuprofen. a case report. Br J Oral Maxillofac Surg. 2009;47:132-134.
- Wohl Y, Goldberg I, Sharazi I, et al. A case of paracetamol-induced acute generalized exanthematous pustulosis in a pregnant woman localized in the neck region. Skinmed. 2004;3:47-49.
- Mehra KK, Rupawala AH, Gogtay NJ. Immediate hypersensitivity reaction to a single oral dose of flurbiprofen. J Postgrad Med. 2010;56:36-37.
- Girardi M, Duncan KO, Tigelaar RE, et al. Cross comparison of patch-test and lymphocyte proliferation responses in patients with a history of acute generalized exanthematous pustulosis. Am J Dermatopathol. 2005;27:343-346.
Practice Points
- Acute localized exanthematous pustulosis is a form of a pustular drug eruption in which lesions are consistent with acute generalized exanthematous pustulosis but typically localized in a single area.
- The medications most frequently responsible are antibiotics. Flurbiprofen, a propionic acid derivative, could be a rare causative agent of this disease.
