User login
Malpractice issues tied to bariatric surgery explored
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.

Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.
Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
NEW ORLEANS – The first-ever analysis of medical malpractice closed claims involving bariatric surgeons spotlights key opportunities for improvement for the surgical specialty, Eric J. DeMaria, MD, declared at Obesity Week 2016.
Four of the nation’s largest medical malpractice insurance companies agreed to allow members of an American Society for Metabolic and Bariatric Surgery task force to make site visits to their corporate offices, where the surgeons sat in closed rooms to read and take notes on a total of 175 cases closed during 2010-2015. Those case notes were later shared with the full task force, which sifted through the details in order to identify common causal themes and opportunities for improvement, explained Dr. DeMaria, a bariatric surgeon in Suffolk, Va.
Among the key findings:
• The defense prevailed in 63% of cases. The mean expense for defending a lawsuit was $91,836.
• In the 37% of cases involving monetary awards, the mean figure was $293,500, ranging from $20,000 to $8 million.
• Mortality was involved in 35% of cases. Other notable complications resulting in lawsuits included leak in 18% of cases, bowel obstruction in 10%, bleeding in 5.3%, retained foreign body in 5.3%, and vascular injury from access in 4.4%.
• Preoperative issues such as informed consent and disclosure of information were rare.
• The defendant surgeon was a foreign medical graduate in 27.5% of cases, board certified in 75.9%, and only 43% of the hospitals where the surgery took place were accredited. All those figures are at odds with national norms.
• The panel determined that the cause of the complication was provider-related in 50% of cases, system-related in 29%, and intrinsic to the patient’s disease in 21%.
• In the panel’s view, the complication was preventable by the surgeon in nearly 60% of cases and not preventable by the surgeon in 20%, with the remainder of cases deemed impossible to judge.
• Better preoperative care would have prevented the complication in 20% of cases, in the panel’s view. Better postoperative care would have prevented the complication in 45%.
• Just over 5% of the malpractice claims involved nonstandard malabsorptive operations. “Some of them I’d never heard of before,” according to Dr. DeMaria.
• Care was deemed by the panel to be appropriate in roughly 21% of the malpractice cases and grossly negligent or incompetent in 8%. Twenty-three percent of lawsuits involved preventable error of such magnitude that significant coaching and instruction would be required in order to prevent a recurrence.
Dr. DeMaria observed that this analysis of closed claims suggests that in order to reduce future malpractice claims against bariatric surgeons, it makes sense to focus on a few key areas of practice where most of the serious problems occur.
“We found the same themes repeated over and over; for example, delays in diagnosis and treatment of leaks,” he said.
A substantial number of the lawsuits could have been prevented through the use of preinsufflation and optical trocars, or access away from the midline, he added.
But the number one theme to emerge from the lawsuit analysis was poor communication with the health care team and/or family. The experts on the task force considered the communication performance to be appropriate in only 20% of cases.
“I would emphasize the strong contribution of communication issues, and the strong contribution of coverage and handoff issues,” Dr. DeMaria said. “One example of an intervention that might be introduced would be to standardize the language used in the operating room just before you start to staple the stomach, very similar to what airplane pilots do in their communication. We saw cases over and over again where the anesthesia person was asked to take out the [nasogastric] tube didn’t realize that meant the esophageal stethoscope, too.
“We need to do a better job of not just making sure a coverage person has been identified, but actually communicating with that person and doing a standardized handoff procedure,” Dr. DeMaria continued. “Management of postoperative phone calls is another important area: Who answers the phone? What are they supposed to do with that information? How do you get patients to appropriate care?”
Discussant Ramsey M. Dallal, MD, congratulated Dr. DeMaria and his fellow ASMBS task force members on “the massive amount of work” entailed in this project. And he urged his colleagues to take to heart the lessons learned.
“People hear the word ‘malpractice’ and they get fearful. They think of lawyers and of being attacked. The reality is this is not a malpractice study; this is a patient safety study. A study like this is an excellent way to improve patient safety. The problem with registry data is we don’t get the details – and it’s the case details that point out problems and potential solutions,” said Dr. Dallal, director of bariatrics and vice chair of the department of surgery at the Einstein Healthcare Network in the Philadelphia area.
The closed claims analysis was conducted free of commercial support. Dr. DeMaria reported serving as a consultant to Covidien and Ethicon.
Key clinical point:
Major finding: Communication with the health care team and the patient’s family was deemed appropriate in only 20% of a large series of medical malpractice lawsuits filed against bariatric surgeons.
Data source: This analysis of malpractice insurers’ files on 175 closed malpractice claims against bariatric surgeons was conducted by an American Society for Metabolic and Bariatric Surgery task force.
Disclosures: The study was conducted free of industry support.
Insurance-mandated diet pre–bariatric surgery deemed harmful
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.

Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.
Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
NEW ORLEANS – The widespread health insurance industry practice of requiring obese patients to spend months on a physician-supervised strict weight-loss diet prior to approving coverage of bariatric surgery accomplishes nothing constructive, Charles J. Keith Jr., MD, reported at Obesity Week 2016.
“We found that insurance-mandated preoperative diets were associated with a significant delay in treatment, no improvement in postoperative complication rates, and also no improvement in weight loss outcomes. If anything, after adjusting for potential confounding variables, the outcomes were inferior to the group that wasn’t required to diet,” said Dr. Keith of the University of Alabama at Birmingham.
Dr. Keith presented a retrospective review from the prospectively collected Alabama University bariatric surgery database, which included all 284 patients who underwent laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy during 2009-2013. A total of 79% of the patients had private health insurance that required their participation in a preoperative physician-guided diet program, typically for 6 months. The other 21% did not have a mandatory preoperative diet requirement; the great majority of this group were covered under Medicare, which doesn’t require a diet program before bariatric surgery. The two groups weren’t significantly different in initial or immediately preoperative weight or body mass index, obesity-related comorbid conditions, type of bariatric surgery, or socioeconomic status.
The mean time from initial clinic visit to bariatric surgery was significantly shorter in the group with no mandated preoperative diet, at 154 vs. 218 days. In a multivariate analysis adjusted for age, sex, race, operation type, and comorbidities, the no-mandatory-diet group had a significantly greater reduction in BMI 6 months post surgery: a mean loss of 12.2 kg/m2, compared with 10.9 kg/m2 in the group required to participate in a preoperative diet. The difference was even greater at 2 years follow-up: a mean decrease of 14.9 kg/m2 in the no-diet group, vs. 10.7 kg/m2 in the mandatory diet group. The no-diet group experienced a mean 33% weight loss at 2 years, significantly better than the 25% weight loss in the mandatory diet group, Dr. Keith reported at the meeting, presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
Audience discussion showed that the insurance-mandated preoperative diet requirement is a hot button issue in the bariatric surgical community.
“I think these insurance programs are specifically designed to delay care,” one surgeon asserted.
Another bariatric surgeon commented that while Dr. Keith’s study will be helpful in advocating for removal of the mandatory preoperative diet requirement, what’s really needed are studies that demonstrate just how often this requirement results in drop out from bariatric programs by patients who’ve grown discouraged by yet-another unsuccessful attempt at nonsurgical weight loss.
Dr. Keith reported having no financial conflicts of interest regarding his study.
Key clinical point:
Major finding: At follow-up 2 years after bariatric surgery, patients who were required by their insurance company to participate in a physician-supervised preoperative diet program had an adjusted mean 25% weight loss, a significantly worse outcome than the mean 33% weight loss among patients with no such requirement.
Data source: This was a retrospective analysis of 284 patients in a prospectively collected university bariatric surgery database.
Disclosures: The study presenter reported having no relevant financial interests.
MDMA – the love drug – makes a therapeutic comeback
VIENNA – What a difference a decade can make in the world of psychiatry.
Take, for example, the case of 3,4-methylenedioxymethamphetamine, better known as MDMA or, when used recreationally, as ecstasy, the love drug.
“Ten years ago at pretty much every scientific meeting where MDMA was being discussed, people were looking to find problems with it. People were dredging around trying to vilify this drug, because there was a hope that it might cause brain damage, which would justify having made its use illicit. Ten years later, we’ve changed direction completely, from fear and hating MDMA to loving it. Now we’re talking about the possibility that MDMA might actually heal the brain, and restoring MDMA to the therapeutic armamentarium,” David Nutt, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
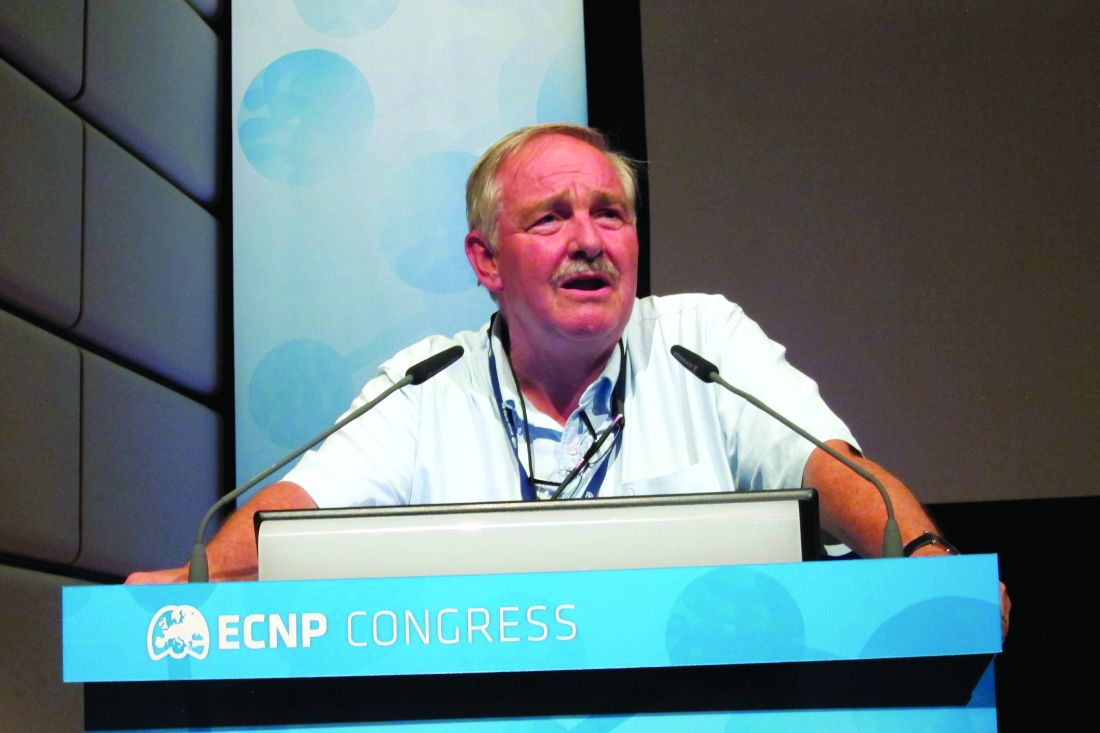
Indeed, the drug’s potential as an adjunct to psychotherapy in patients with posttraumatic stress disorder was the topic of a packed-to-the-gills session in the largest hall at the ECNP Congress, where Dr. Nutt highlighted recent insights into the psychopharmacology of MDMA and other speakers described evidence of the drug’s salutary effects on autobiographical memory and social cognition.
“The biggest problem with MDMA is its name,” quipped Dr. Nutt, professor of neuropsychopharmacology at Imperial College London.
“It used to be called ‘empathy,’ but when it started being used recreationally at raves and in the clubs, the dealers decided to change its name to ‘ecstasy.’ And that created havoc, because there’s nothing that aged editors of newspapers hate more than young people having ecstasy. They hated the term, and so the drug had to go,” according to the psychiatrist.
MDMA’s comeback as a potentially valuable medication in psychiatry can be traced to the first report of the drug’s impressive success when used as an adjunct to psychotherapy in a randomized, placebo-controlled pilot study. Michael C. Mithoefer, MD, a psychiatrist in private practice in South Carolina, and his coinvestigators stunned the psychiatric world by reporting that 10 of 12 patients with chronic PTSD refractory to both medications and psychotherapy showed significant clinical improvement in response to just two sessions of MDMA-assisted psychotherapy supplementing a more conventional course of psychotherapy (J Psychopharmacology. 2011 Apr;25[4]:439-52).
Moreover, the benefits proved durable: In a subsequent paper, the investigators reported the clinical benefit of this two-dose treatment program persisted at a mean 3.8 years of follow-up and no safety concerns had been seen (J Psychopharmacol. 2013 Jan;27[1]:28-39).
This study, which eventually drew the attention of military veterans’ groups with political clout, proved hugely influential, especially since PTSD is so common and often is highly treatment resistant.
“We’re now living in a very strange world where trauma has in some ways become the No. 1 problem facing many societies,” Dr. Nutt observed.
He predicted that with the Food and Drug Administration’s recent approval of clinical trials of MDMA in patients with PTSD, the drug will be licensed for that indication “within the next couple years.”
How MDMA works
The pharmacology of MDMA is complex, he continued. The drug is chiefly a serotonin-releasing agent and 5HT reuptake blocker, but it also acts as an agonist on alpha-adrenergic receptors, has muscarinic and histamine-blocking effects, and promotes release of oxytocin.
Animal studies have demonstrated that MDMA facilitates extinction of fear memories through a mechanism involving changes in levels of brain-derived neurotrophic factor. Experience in humans has shown that the drug has diverse pro-social effects: It is activating, enhances mood, promotes more flexible thinking, boosts tactile experiences, and increases empathy, which in turn aids patients in bonding with their therapists.
Dr. Nutt and his coinvestigators performed the first whole-brain study of the effects of MDMA using functional MRI. This double-blind, placebo-controlled, crossover study in healthy volunteers used measurements obtained through arterial spin labeling and analysis of blood oxygen level–dependent resting state functional connectivity. The investigators documented that the marked increase in positive mood and decreased magnitude of negative personal memories produced by MDMA was accompanied by profound reduction of cerebral blood flow in the right amygdala and hippocampus. Cerebral blood flow also was reduced in the right medial temporal lobe, thalamus, and inferior visual cortex. MDMA also resulted in decreased amygdala-cortical connectivity (Biol Psychiatry. 2015 Oct 15;78[8]:554-62; Int J Neuropsychopharmacol. 2014 Apr;17[4]:527-40).
The changes in those particular brain systems are consistent with and most likely underlie the drug’s therapeutic effects, he said. Taken together, they could serve to assist a patient in re-engaging with traumatic memories with less interference from emotional centers, thereby helping to gain executive control of the memory of the trauma.
H. Valerie Curran, PhD, a coinvestigator in the brain imaging study, cautioned the rapt audience that while there are abundant favorable anecdotal reports from psychotherapists going back as far as the 1970s, the actual evidence base for MDMA as a therapeutic adjunct to psychotherapy for PTSD is still pretty thin. She noted that in their groundbreaking study, Dr. Mithoefer and his colleagues used an unconventional form of psychotherapy modeled on the LSD therapy developed by Stanislav Grof, MD, PhD. The two MDMA-assisted sessions were each 8 hours long and included shamanistic techniques and specialized breathing to promote diminished oxygen to the brain. Also, the patient sat on a futon listening to music with a male therapist on one side and a female therapist on the other. As a clinical psychologist herself, she assured the audience that this is not standard practice in her field.
Only one other randomized, double-blind, placebo-controlled study of MDMA-assisted psychotherapy has been published to date (J Psychopharmacol. 2013 Jan;27[1]:40-52). With just 12 participants, it was too small to be conclusive. So there is a definite need for additional controlled studies on the interaction between MDMA and evidence-based forms of psychotherapy. Fortunately, additional clinical trials are ongoing, noted Dr. Curran, professor of psychopharmacology at University College London.
She presented highlights of a study she and her coinvestigators carried out to determine how MDMA affects the encoding and recall of emotional autobiographical memories, since the core of most psychotherapy for PTSD entails controlled revisiting of traumatic memories. The nonblinded study included a group of recreational MDMA users who – on two separate occasions, one under the influence of street-quality MDMA of uncertain dose and purity, the other on placebo – were tasked with responding to self-threatening scenarios, exposure to compassionate imagery, and a large series of positive and negative adjectives addressed at themselves or another person (J Psychopharmacol. 2015 Sep;29[9]:961-70).
The investigators found that MDMA enhanced the emotional intensity, vividness, and positivity of the subjects’ best autobiographical memories while modestly reducing the negativity of their worst memories. Structured ratings of compassion markedly increased while on MDMA. Overall, the drug’s effects were similar to those obtained through rigorous cognitive training methods developed in venerable Eastern contemplative practices in pursuit of a compassionate mindset, according to Dr. Curran.
The study results suggest a mechanism by which MDMA might enhance psychotherapy not only by improving the therapeutic alliance but also by reducing self-referential emotional processing without diminishing declarative memory, she added.
Findings of Swiss studies
Matthias E. Liechti, MD, head of the psychopharmacology research unit at the University of Basel, explained that at present Switzerland is the only country in the world where it’s legal to prescribe MDMA. Ditto LSD. Psychiatrists can do so on a case-by-case basis outside of a clinical trial setting in patients with treatment-resistant PTSD or anxiety disorders.
Dr. Liechti and his coinvestigators are interested in examining how MDMA affects social cognition as assessed by outcome measures, including a structured face emotion recognition test, the multifaceted empathy test, and a sexual arousal task.

In a series of studies in which they exposed subjects to MDMA, alcohol, methamphetamine, or LSD, they have established that both MDMA and LSD produce empathogenic effects that are possibly serotonin mediated. On a visual analog scale, subjects on those drugs gave high marks for feeling happy, open, trusting, and extroverted, and having a sense of well-being. MDMA impaired recognition of fearful, angry, and sad faces.
In contrast, methamphetamine, a pure stimulant that activates the norepinephrine/dopamine system, produced no empathogenic effects, but it enhanced recognition of sad or fearful faces. Alcohol slightly increased self-ratings for trust, happiness, and openness.
Methamphetamine increased ratings of sexual arousal in response to explicit sexual stimuli, while MDMA had no effect on sexual arousal.
MDMA and LSD increased oxytocin, prolactin, and cortisol levels consistent with their serotonergic effects. Methylphenidate did not, Dr. Liechti said.
A neuroscientist in the audience raised a possible safety concern regarding MDMA: If the drug has an agonist effect on serotonin receptors, couldn’t it have cardiac side effects similar to those of fenfluramine, a drug now banned because it stimulated the abundant 5HT-2b receptors present in the heart, resulting in increased risk of pulmonary hypertension and other adverse cardiovascular effects?
Dr. Nutt replied that there are multitudes of serotonin receptor subtypes, and it’s not yet known whether MDMA acts upon the 5HT-2b receptor. In any case, it shouldn’t be an issue for the drug’s medicinal use.
“Luckily, the effects of MDMA wear off quickly, and when it’s used with psychotherapy we may be giving only one or two doses in a lifetime, so it shouldn’t be a concern,” he said.
Dr. Nutt reported that the functional MRI brain imaging study was funded by a British television station and a private foundation.
“The reason for that is we’ve found it impossible to get any money from any traditional government funders to study drugs like MDMA unless you write grants to show they’re harmful,” he asserted.
Dr. Curran reported having no financial conflicts of interest regarding her studies. Dr. Liechti’s work is supported by the Swiss National Science Foundation.
VIENNA – What a difference a decade can make in the world of psychiatry.
Take, for example, the case of 3,4-methylenedioxymethamphetamine, better known as MDMA or, when used recreationally, as ecstasy, the love drug.
“Ten years ago at pretty much every scientific meeting where MDMA was being discussed, people were looking to find problems with it. People were dredging around trying to vilify this drug, because there was a hope that it might cause brain damage, which would justify having made its use illicit. Ten years later, we’ve changed direction completely, from fear and hating MDMA to loving it. Now we’re talking about the possibility that MDMA might actually heal the brain, and restoring MDMA to the therapeutic armamentarium,” David Nutt, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the drug’s potential as an adjunct to psychotherapy in patients with posttraumatic stress disorder was the topic of a packed-to-the-gills session in the largest hall at the ECNP Congress, where Dr. Nutt highlighted recent insights into the psychopharmacology of MDMA and other speakers described evidence of the drug’s salutary effects on autobiographical memory and social cognition.
“The biggest problem with MDMA is its name,” quipped Dr. Nutt, professor of neuropsychopharmacology at Imperial College London.
“It used to be called ‘empathy,’ but when it started being used recreationally at raves and in the clubs, the dealers decided to change its name to ‘ecstasy.’ And that created havoc, because there’s nothing that aged editors of newspapers hate more than young people having ecstasy. They hated the term, and so the drug had to go,” according to the psychiatrist.
MDMA’s comeback as a potentially valuable medication in psychiatry can be traced to the first report of the drug’s impressive success when used as an adjunct to psychotherapy in a randomized, placebo-controlled pilot study. Michael C. Mithoefer, MD, a psychiatrist in private practice in South Carolina, and his coinvestigators stunned the psychiatric world by reporting that 10 of 12 patients with chronic PTSD refractory to both medications and psychotherapy showed significant clinical improvement in response to just two sessions of MDMA-assisted psychotherapy supplementing a more conventional course of psychotherapy (J Psychopharmacology. 2011 Apr;25[4]:439-52).
Moreover, the benefits proved durable: In a subsequent paper, the investigators reported the clinical benefit of this two-dose treatment program persisted at a mean 3.8 years of follow-up and no safety concerns had been seen (J Psychopharmacol. 2013 Jan;27[1]:28-39).
This study, which eventually drew the attention of military veterans’ groups with political clout, proved hugely influential, especially since PTSD is so common and often is highly treatment resistant.
“We’re now living in a very strange world where trauma has in some ways become the No. 1 problem facing many societies,” Dr. Nutt observed.
He predicted that with the Food and Drug Administration’s recent approval of clinical trials of MDMA in patients with PTSD, the drug will be licensed for that indication “within the next couple years.”
How MDMA works
The pharmacology of MDMA is complex, he continued. The drug is chiefly a serotonin-releasing agent and 5HT reuptake blocker, but it also acts as an agonist on alpha-adrenergic receptors, has muscarinic and histamine-blocking effects, and promotes release of oxytocin.
Animal studies have demonstrated that MDMA facilitates extinction of fear memories through a mechanism involving changes in levels of brain-derived neurotrophic factor. Experience in humans has shown that the drug has diverse pro-social effects: It is activating, enhances mood, promotes more flexible thinking, boosts tactile experiences, and increases empathy, which in turn aids patients in bonding with their therapists.
Dr. Nutt and his coinvestigators performed the first whole-brain study of the effects of MDMA using functional MRI. This double-blind, placebo-controlled, crossover study in healthy volunteers used measurements obtained through arterial spin labeling and analysis of blood oxygen level–dependent resting state functional connectivity. The investigators documented that the marked increase in positive mood and decreased magnitude of negative personal memories produced by MDMA was accompanied by profound reduction of cerebral blood flow in the right amygdala and hippocampus. Cerebral blood flow also was reduced in the right medial temporal lobe, thalamus, and inferior visual cortex. MDMA also resulted in decreased amygdala-cortical connectivity (Biol Psychiatry. 2015 Oct 15;78[8]:554-62; Int J Neuropsychopharmacol. 2014 Apr;17[4]:527-40).
The changes in those particular brain systems are consistent with and most likely underlie the drug’s therapeutic effects, he said. Taken together, they could serve to assist a patient in re-engaging with traumatic memories with less interference from emotional centers, thereby helping to gain executive control of the memory of the trauma.
H. Valerie Curran, PhD, a coinvestigator in the brain imaging study, cautioned the rapt audience that while there are abundant favorable anecdotal reports from psychotherapists going back as far as the 1970s, the actual evidence base for MDMA as a therapeutic adjunct to psychotherapy for PTSD is still pretty thin. She noted that in their groundbreaking study, Dr. Mithoefer and his colleagues used an unconventional form of psychotherapy modeled on the LSD therapy developed by Stanislav Grof, MD, PhD. The two MDMA-assisted sessions were each 8 hours long and included shamanistic techniques and specialized breathing to promote diminished oxygen to the brain. Also, the patient sat on a futon listening to music with a male therapist on one side and a female therapist on the other. As a clinical psychologist herself, she assured the audience that this is not standard practice in her field.
Only one other randomized, double-blind, placebo-controlled study of MDMA-assisted psychotherapy has been published to date (J Psychopharmacol. 2013 Jan;27[1]:40-52). With just 12 participants, it was too small to be conclusive. So there is a definite need for additional controlled studies on the interaction between MDMA and evidence-based forms of psychotherapy. Fortunately, additional clinical trials are ongoing, noted Dr. Curran, professor of psychopharmacology at University College London.
She presented highlights of a study she and her coinvestigators carried out to determine how MDMA affects the encoding and recall of emotional autobiographical memories, since the core of most psychotherapy for PTSD entails controlled revisiting of traumatic memories. The nonblinded study included a group of recreational MDMA users who – on two separate occasions, one under the influence of street-quality MDMA of uncertain dose and purity, the other on placebo – were tasked with responding to self-threatening scenarios, exposure to compassionate imagery, and a large series of positive and negative adjectives addressed at themselves or another person (J Psychopharmacol. 2015 Sep;29[9]:961-70).
The investigators found that MDMA enhanced the emotional intensity, vividness, and positivity of the subjects’ best autobiographical memories while modestly reducing the negativity of their worst memories. Structured ratings of compassion markedly increased while on MDMA. Overall, the drug’s effects were similar to those obtained through rigorous cognitive training methods developed in venerable Eastern contemplative practices in pursuit of a compassionate mindset, according to Dr. Curran.
The study results suggest a mechanism by which MDMA might enhance psychotherapy not only by improving the therapeutic alliance but also by reducing self-referential emotional processing without diminishing declarative memory, she added.
Findings of Swiss studies
Matthias E. Liechti, MD, head of the psychopharmacology research unit at the University of Basel, explained that at present Switzerland is the only country in the world where it’s legal to prescribe MDMA. Ditto LSD. Psychiatrists can do so on a case-by-case basis outside of a clinical trial setting in patients with treatment-resistant PTSD or anxiety disorders.
Dr. Liechti and his coinvestigators are interested in examining how MDMA affects social cognition as assessed by outcome measures, including a structured face emotion recognition test, the multifaceted empathy test, and a sexual arousal task.
In a series of studies in which they exposed subjects to MDMA, alcohol, methamphetamine, or LSD, they have established that both MDMA and LSD produce empathogenic effects that are possibly serotonin mediated. On a visual analog scale, subjects on those drugs gave high marks for feeling happy, open, trusting, and extroverted, and having a sense of well-being. MDMA impaired recognition of fearful, angry, and sad faces.
In contrast, methamphetamine, a pure stimulant that activates the norepinephrine/dopamine system, produced no empathogenic effects, but it enhanced recognition of sad or fearful faces. Alcohol slightly increased self-ratings for trust, happiness, and openness.
Methamphetamine increased ratings of sexual arousal in response to explicit sexual stimuli, while MDMA had no effect on sexual arousal.
MDMA and LSD increased oxytocin, prolactin, and cortisol levels consistent with their serotonergic effects. Methylphenidate did not, Dr. Liechti said.
A neuroscientist in the audience raised a possible safety concern regarding MDMA: If the drug has an agonist effect on serotonin receptors, couldn’t it have cardiac side effects similar to those of fenfluramine, a drug now banned because it stimulated the abundant 5HT-2b receptors present in the heart, resulting in increased risk of pulmonary hypertension and other adverse cardiovascular effects?
Dr. Nutt replied that there are multitudes of serotonin receptor subtypes, and it’s not yet known whether MDMA acts upon the 5HT-2b receptor. In any case, it shouldn’t be an issue for the drug’s medicinal use.
“Luckily, the effects of MDMA wear off quickly, and when it’s used with psychotherapy we may be giving only one or two doses in a lifetime, so it shouldn’t be a concern,” he said.
Dr. Nutt reported that the functional MRI brain imaging study was funded by a British television station and a private foundation.
“The reason for that is we’ve found it impossible to get any money from any traditional government funders to study drugs like MDMA unless you write grants to show they’re harmful,” he asserted.
Dr. Curran reported having no financial conflicts of interest regarding her studies. Dr. Liechti’s work is supported by the Swiss National Science Foundation.
VIENNA – What a difference a decade can make in the world of psychiatry.
Take, for example, the case of 3,4-methylenedioxymethamphetamine, better known as MDMA or, when used recreationally, as ecstasy, the love drug.
“Ten years ago at pretty much every scientific meeting where MDMA was being discussed, people were looking to find problems with it. People were dredging around trying to vilify this drug, because there was a hope that it might cause brain damage, which would justify having made its use illicit. Ten years later, we’ve changed direction completely, from fear and hating MDMA to loving it. Now we’re talking about the possibility that MDMA might actually heal the brain, and restoring MDMA to the therapeutic armamentarium,” David Nutt, MD, observed at the annual congress of the European College of Neuropsychopharmacology.
Indeed, the drug’s potential as an adjunct to psychotherapy in patients with posttraumatic stress disorder was the topic of a packed-to-the-gills session in the largest hall at the ECNP Congress, where Dr. Nutt highlighted recent insights into the psychopharmacology of MDMA and other speakers described evidence of the drug’s salutary effects on autobiographical memory and social cognition.
“The biggest problem with MDMA is its name,” quipped Dr. Nutt, professor of neuropsychopharmacology at Imperial College London.
“It used to be called ‘empathy,’ but when it started being used recreationally at raves and in the clubs, the dealers decided to change its name to ‘ecstasy.’ And that created havoc, because there’s nothing that aged editors of newspapers hate more than young people having ecstasy. They hated the term, and so the drug had to go,” according to the psychiatrist.
MDMA’s comeback as a potentially valuable medication in psychiatry can be traced to the first report of the drug’s impressive success when used as an adjunct to psychotherapy in a randomized, placebo-controlled pilot study. Michael C. Mithoefer, MD, a psychiatrist in private practice in South Carolina, and his coinvestigators stunned the psychiatric world by reporting that 10 of 12 patients with chronic PTSD refractory to both medications and psychotherapy showed significant clinical improvement in response to just two sessions of MDMA-assisted psychotherapy supplementing a more conventional course of psychotherapy (J Psychopharmacology. 2011 Apr;25[4]:439-52).
Moreover, the benefits proved durable: In a subsequent paper, the investigators reported the clinical benefit of this two-dose treatment program persisted at a mean 3.8 years of follow-up and no safety concerns had been seen (J Psychopharmacol. 2013 Jan;27[1]:28-39).
This study, which eventually drew the attention of military veterans’ groups with political clout, proved hugely influential, especially since PTSD is so common and often is highly treatment resistant.
“We’re now living in a very strange world where trauma has in some ways become the No. 1 problem facing many societies,” Dr. Nutt observed.
He predicted that with the Food and Drug Administration’s recent approval of clinical trials of MDMA in patients with PTSD, the drug will be licensed for that indication “within the next couple years.”
How MDMA works
The pharmacology of MDMA is complex, he continued. The drug is chiefly a serotonin-releasing agent and 5HT reuptake blocker, but it also acts as an agonist on alpha-adrenergic receptors, has muscarinic and histamine-blocking effects, and promotes release of oxytocin.
Animal studies have demonstrated that MDMA facilitates extinction of fear memories through a mechanism involving changes in levels of brain-derived neurotrophic factor. Experience in humans has shown that the drug has diverse pro-social effects: It is activating, enhances mood, promotes more flexible thinking, boosts tactile experiences, and increases empathy, which in turn aids patients in bonding with their therapists.
Dr. Nutt and his coinvestigators performed the first whole-brain study of the effects of MDMA using functional MRI. This double-blind, placebo-controlled, crossover study in healthy volunteers used measurements obtained through arterial spin labeling and analysis of blood oxygen level–dependent resting state functional connectivity. The investigators documented that the marked increase in positive mood and decreased magnitude of negative personal memories produced by MDMA was accompanied by profound reduction of cerebral blood flow in the right amygdala and hippocampus. Cerebral blood flow also was reduced in the right medial temporal lobe, thalamus, and inferior visual cortex. MDMA also resulted in decreased amygdala-cortical connectivity (Biol Psychiatry. 2015 Oct 15;78[8]:554-62; Int J Neuropsychopharmacol. 2014 Apr;17[4]:527-40).
The changes in those particular brain systems are consistent with and most likely underlie the drug’s therapeutic effects, he said. Taken together, they could serve to assist a patient in re-engaging with traumatic memories with less interference from emotional centers, thereby helping to gain executive control of the memory of the trauma.
H. Valerie Curran, PhD, a coinvestigator in the brain imaging study, cautioned the rapt audience that while there are abundant favorable anecdotal reports from psychotherapists going back as far as the 1970s, the actual evidence base for MDMA as a therapeutic adjunct to psychotherapy for PTSD is still pretty thin. She noted that in their groundbreaking study, Dr. Mithoefer and his colleagues used an unconventional form of psychotherapy modeled on the LSD therapy developed by Stanislav Grof, MD, PhD. The two MDMA-assisted sessions were each 8 hours long and included shamanistic techniques and specialized breathing to promote diminished oxygen to the brain. Also, the patient sat on a futon listening to music with a male therapist on one side and a female therapist on the other. As a clinical psychologist herself, she assured the audience that this is not standard practice in her field.
Only one other randomized, double-blind, placebo-controlled study of MDMA-assisted psychotherapy has been published to date (J Psychopharmacol. 2013 Jan;27[1]:40-52). With just 12 participants, it was too small to be conclusive. So there is a definite need for additional controlled studies on the interaction between MDMA and evidence-based forms of psychotherapy. Fortunately, additional clinical trials are ongoing, noted Dr. Curran, professor of psychopharmacology at University College London.
She presented highlights of a study she and her coinvestigators carried out to determine how MDMA affects the encoding and recall of emotional autobiographical memories, since the core of most psychotherapy for PTSD entails controlled revisiting of traumatic memories. The nonblinded study included a group of recreational MDMA users who – on two separate occasions, one under the influence of street-quality MDMA of uncertain dose and purity, the other on placebo – were tasked with responding to self-threatening scenarios, exposure to compassionate imagery, and a large series of positive and negative adjectives addressed at themselves or another person (J Psychopharmacol. 2015 Sep;29[9]:961-70).
The investigators found that MDMA enhanced the emotional intensity, vividness, and positivity of the subjects’ best autobiographical memories while modestly reducing the negativity of their worst memories. Structured ratings of compassion markedly increased while on MDMA. Overall, the drug’s effects were similar to those obtained through rigorous cognitive training methods developed in venerable Eastern contemplative practices in pursuit of a compassionate mindset, according to Dr. Curran.
The study results suggest a mechanism by which MDMA might enhance psychotherapy not only by improving the therapeutic alliance but also by reducing self-referential emotional processing without diminishing declarative memory, she added.
Findings of Swiss studies
Matthias E. Liechti, MD, head of the psychopharmacology research unit at the University of Basel, explained that at present Switzerland is the only country in the world where it’s legal to prescribe MDMA. Ditto LSD. Psychiatrists can do so on a case-by-case basis outside of a clinical trial setting in patients with treatment-resistant PTSD or anxiety disorders.
Dr. Liechti and his coinvestigators are interested in examining how MDMA affects social cognition as assessed by outcome measures, including a structured face emotion recognition test, the multifaceted empathy test, and a sexual arousal task.
In a series of studies in which they exposed subjects to MDMA, alcohol, methamphetamine, or LSD, they have established that both MDMA and LSD produce empathogenic effects that are possibly serotonin mediated. On a visual analog scale, subjects on those drugs gave high marks for feeling happy, open, trusting, and extroverted, and having a sense of well-being. MDMA impaired recognition of fearful, angry, and sad faces.
In contrast, methamphetamine, a pure stimulant that activates the norepinephrine/dopamine system, produced no empathogenic effects, but it enhanced recognition of sad or fearful faces. Alcohol slightly increased self-ratings for trust, happiness, and openness.
Methamphetamine increased ratings of sexual arousal in response to explicit sexual stimuli, while MDMA had no effect on sexual arousal.
MDMA and LSD increased oxytocin, prolactin, and cortisol levels consistent with their serotonergic effects. Methylphenidate did not, Dr. Liechti said.
A neuroscientist in the audience raised a possible safety concern regarding MDMA: If the drug has an agonist effect on serotonin receptors, couldn’t it have cardiac side effects similar to those of fenfluramine, a drug now banned because it stimulated the abundant 5HT-2b receptors present in the heart, resulting in increased risk of pulmonary hypertension and other adverse cardiovascular effects?
Dr. Nutt replied that there are multitudes of serotonin receptor subtypes, and it’s not yet known whether MDMA acts upon the 5HT-2b receptor. In any case, it shouldn’t be an issue for the drug’s medicinal use.
“Luckily, the effects of MDMA wear off quickly, and when it’s used with psychotherapy we may be giving only one or two doses in a lifetime, so it shouldn’t be a concern,” he said.
Dr. Nutt reported that the functional MRI brain imaging study was funded by a British television station and a private foundation.
“The reason for that is we’ve found it impossible to get any money from any traditional government funders to study drugs like MDMA unless you write grants to show they’re harmful,” he asserted.
Dr. Curran reported having no financial conflicts of interest regarding her studies. Dr. Liechti’s work is supported by the Swiss National Science Foundation.
Teens see marijuana as less harmful after legalization
The legalization of recreational marijuana use is associated with an increase in use of the drug among adolescents, who also perceive it as being less harmful, a new study published online suggests.
In the study, Magdalena Cerdá, DrPH, MPH, and her associates used data from the Monitoring the Future study – a national, annual, cross-sectional survey conducted by the University of Michigan, Ann Arbor, that looks at attitudes about drug use among students in 8th, 10th, and 12th grade. The investigators analyzed the data gathered from 2010 to 2015 in an effort to compare attitudes about marijuana and its use before and after legalization in Washington and Colorado, and in states that did not legalize.
“While the increase in marijuana use among 8th graders in Washington was not significantly greater than zero, the significant decrease in use among 8th graders in states [with no recreational marijuana laws] suggests that if there had been no legalization in Washington, then marijuana use among 8th graders in this state would decrease rather than remain stable, as it did,” wrote Dr. Cerdà of the emergency medicine department at the University of California, Davis, in Sacramento, and her coauthors. “Specifically, the prevalence of regular users of marijuana increased and the prevalence of nonusers decreased; no change was observed among occasional users.”
Legalization, however, did not appear to significantly affect perceived harmfulness or use among 12th graders in any states, nor were there any significant changes after legalization among adolescents in all three grades surveyed in Colorado.
The authors noted that Colorado had a well-developed medical marijuana program in place, with substantial advertising, which might account for the lack of apparent impact of legalization for recreational use.
Commenting on the overall impact of legalization on use, the authors suggested that, besides reducing stigma and perceptions of risk, the legalization of recreational marijuana might have increased availability and potentially decreased the price, which might have led to the increase in use.
Given this, they cautiously proposed increased investment in evidence-based adolescent substance use prevention programs in states that choose to legalize recreational marijuana.
Dr. Cerdá and her associates cited several limitations. For example, the use of marijuana was self reported, and the Monitoring the Future results might have missed adolescents who were either absent from school when the survey was taken or had dropped out.
The study was supported by the National Institute on Drug Abuse, the National Institutes of Health, the National Institute on Alcohol Abuse and Alcoholism, and the New York State Psychiatric Institute. No conflicts of interest were declared.
The legalization of marijuana complicates efforts to prevent use of the drug by young people, Wayne Hall, PhD, and Megan Weier wrote in an accompanying editorial (JAMA Pediatr. 2016 Dec 27. doi: 10.1001/jamapediatrics.2016.3917).
“The challenge for health educators will be in acknowledging that the acute adverse effects of marijuana use are modest by comparison with those of alcohol or heroin, while persuading young people that they can experience adverse effects, especially if they begin use in their teens and use daily throughout young adult life,” Dr. Hall and Ms. Weir wrote.
Users of the drug, they said, should be told that the risk of a collision while driving while intoxicated doubles, “especially if they use both alcohol and marijuana.” In addition, Dr. Hall and Ms. Weier said, people who use the drug regularly should be informed that they can become dependent. “The risk for dependence is about 1 in 10 for those who ever use marijuana and 1 in 6 for those who first use in adolescence. Marijuana users also need to know that dependent users have more anxiety, depression, and psychotic disorders and are more likely to leave school early, to be unemployed as adults, and experience downward social mobility in mid-adulthood,” they wrote.
Dr. Hall and Ms. Weier are affiliated with the Centre for Youth Substance Abuse Research at Royal Brisbane and Women’s Hospital in Herston, Australia. They reported no conflicts of interest.
The legalization of marijuana complicates efforts to prevent use of the drug by young people, Wayne Hall, PhD, and Megan Weier wrote in an accompanying editorial (JAMA Pediatr. 2016 Dec 27. doi: 10.1001/jamapediatrics.2016.3917).
“The challenge for health educators will be in acknowledging that the acute adverse effects of marijuana use are modest by comparison with those of alcohol or heroin, while persuading young people that they can experience adverse effects, especially if they begin use in their teens and use daily throughout young adult life,” Dr. Hall and Ms. Weir wrote.
Users of the drug, they said, should be told that the risk of a collision while driving while intoxicated doubles, “especially if they use both alcohol and marijuana.” In addition, Dr. Hall and Ms. Weier said, people who use the drug regularly should be informed that they can become dependent. “The risk for dependence is about 1 in 10 for those who ever use marijuana and 1 in 6 for those who first use in adolescence. Marijuana users also need to know that dependent users have more anxiety, depression, and psychotic disorders and are more likely to leave school early, to be unemployed as adults, and experience downward social mobility in mid-adulthood,” they wrote.
Dr. Hall and Ms. Weier are affiliated with the Centre for Youth Substance Abuse Research at Royal Brisbane and Women’s Hospital in Herston, Australia. They reported no conflicts of interest.
The legalization of marijuana complicates efforts to prevent use of the drug by young people, Wayne Hall, PhD, and Megan Weier wrote in an accompanying editorial (JAMA Pediatr. 2016 Dec 27. doi: 10.1001/jamapediatrics.2016.3917).
“The challenge for health educators will be in acknowledging that the acute adverse effects of marijuana use are modest by comparison with those of alcohol or heroin, while persuading young people that they can experience adverse effects, especially if they begin use in their teens and use daily throughout young adult life,” Dr. Hall and Ms. Weir wrote.
Users of the drug, they said, should be told that the risk of a collision while driving while intoxicated doubles, “especially if they use both alcohol and marijuana.” In addition, Dr. Hall and Ms. Weier said, people who use the drug regularly should be informed that they can become dependent. “The risk for dependence is about 1 in 10 for those who ever use marijuana and 1 in 6 for those who first use in adolescence. Marijuana users also need to know that dependent users have more anxiety, depression, and psychotic disorders and are more likely to leave school early, to be unemployed as adults, and experience downward social mobility in mid-adulthood,” they wrote.
Dr. Hall and Ms. Weier are affiliated with the Centre for Youth Substance Abuse Research at Royal Brisbane and Women’s Hospital in Herston, Australia. They reported no conflicts of interest.
The legalization of recreational marijuana use is associated with an increase in use of the drug among adolescents, who also perceive it as being less harmful, a new study published online suggests.
In the study, Magdalena Cerdá, DrPH, MPH, and her associates used data from the Monitoring the Future study – a national, annual, cross-sectional survey conducted by the University of Michigan, Ann Arbor, that looks at attitudes about drug use among students in 8th, 10th, and 12th grade. The investigators analyzed the data gathered from 2010 to 2015 in an effort to compare attitudes about marijuana and its use before and after legalization in Washington and Colorado, and in states that did not legalize.
“While the increase in marijuana use among 8th graders in Washington was not significantly greater than zero, the significant decrease in use among 8th graders in states [with no recreational marijuana laws] suggests that if there had been no legalization in Washington, then marijuana use among 8th graders in this state would decrease rather than remain stable, as it did,” wrote Dr. Cerdà of the emergency medicine department at the University of California, Davis, in Sacramento, and her coauthors. “Specifically, the prevalence of regular users of marijuana increased and the prevalence of nonusers decreased; no change was observed among occasional users.”
Legalization, however, did not appear to significantly affect perceived harmfulness or use among 12th graders in any states, nor were there any significant changes after legalization among adolescents in all three grades surveyed in Colorado.
The authors noted that Colorado had a well-developed medical marijuana program in place, with substantial advertising, which might account for the lack of apparent impact of legalization for recreational use.
Commenting on the overall impact of legalization on use, the authors suggested that, besides reducing stigma and perceptions of risk, the legalization of recreational marijuana might have increased availability and potentially decreased the price, which might have led to the increase in use.
Given this, they cautiously proposed increased investment in evidence-based adolescent substance use prevention programs in states that choose to legalize recreational marijuana.
Dr. Cerdá and her associates cited several limitations. For example, the use of marijuana was self reported, and the Monitoring the Future results might have missed adolescents who were either absent from school when the survey was taken or had dropped out.
The study was supported by the National Institute on Drug Abuse, the National Institutes of Health, the National Institute on Alcohol Abuse and Alcoholism, and the New York State Psychiatric Institute. No conflicts of interest were declared.
The legalization of recreational marijuana use is associated with an increase in use of the drug among adolescents, who also perceive it as being less harmful, a new study published online suggests.
In the study, Magdalena Cerdá, DrPH, MPH, and her associates used data from the Monitoring the Future study – a national, annual, cross-sectional survey conducted by the University of Michigan, Ann Arbor, that looks at attitudes about drug use among students in 8th, 10th, and 12th grade. The investigators analyzed the data gathered from 2010 to 2015 in an effort to compare attitudes about marijuana and its use before and after legalization in Washington and Colorado, and in states that did not legalize.
“While the increase in marijuana use among 8th graders in Washington was not significantly greater than zero, the significant decrease in use among 8th graders in states [with no recreational marijuana laws] suggests that if there had been no legalization in Washington, then marijuana use among 8th graders in this state would decrease rather than remain stable, as it did,” wrote Dr. Cerdà of the emergency medicine department at the University of California, Davis, in Sacramento, and her coauthors. “Specifically, the prevalence of regular users of marijuana increased and the prevalence of nonusers decreased; no change was observed among occasional users.”
Legalization, however, did not appear to significantly affect perceived harmfulness or use among 12th graders in any states, nor were there any significant changes after legalization among adolescents in all three grades surveyed in Colorado.
The authors noted that Colorado had a well-developed medical marijuana program in place, with substantial advertising, which might account for the lack of apparent impact of legalization for recreational use.
Commenting on the overall impact of legalization on use, the authors suggested that, besides reducing stigma and perceptions of risk, the legalization of recreational marijuana might have increased availability and potentially decreased the price, which might have led to the increase in use.
Given this, they cautiously proposed increased investment in evidence-based adolescent substance use prevention programs in states that choose to legalize recreational marijuana.
Dr. Cerdá and her associates cited several limitations. For example, the use of marijuana was self reported, and the Monitoring the Future results might have missed adolescents who were either absent from school when the survey was taken or had dropped out.
The study was supported by the National Institute on Drug Abuse, the National Institutes of Health, the National Institute on Alcohol Abuse and Alcoholism, and the New York State Psychiatric Institute. No conflicts of interest were declared.
Key clinical point: The legalization of recreational marijuana use is associated with an increase in its use among adolescents, who also perceive it as being less harmful.
Major finding: The perceived harmfulness of marijuana declined by 14.2% among 8th graders and 16.1% among 10th graders after legalization in Washington, compared with 4.9% and 7.1% decreases among 8th and 10th graders in states that did not legalize.
Data source: The Monitoring the Future study is a national, annual, cross-sectional survey of 253,902 students in the 8th, 10th, and 12th grades.
Disclosures: The study was supported by the National Institute on Drug Abuse, the National Institutes of Health, the National Institute on Alcohol Abuse and Alcoholism, and the New York State Psychiatric Institute. No conflicts of interest were declared.
Combo improves survival in newly diagnosed MM

Photo courtesy of
Millenium Pharmaceuticals
Results of a phase 3 trial suggest a 3-drug combination improves survival in newly diagnosed multiple myeloma (MM).
The trial showed that bortezomib, lenalidomide, and dexamethasone (VRd) could significantly
improve progression-free and overall survival when compared to lenalidomide and dexamethasone (Rd).
In addition, investigators said the risk-benefit profile of VRd was acceptable.
The team noted, however, that grade 3 or higher neurologic adverse events (AEs) were more common with VRd than with Rd.
“Our results are clear,” said principal investigator Brian G.M. Durie, MD, of Cedars-Sinai Outpatient Cancer Center in Los Angeles, California.
“Using bortezomib in combination with lenalidomide and dexamethasone in frontline treatment—hitting the disease early and hard—makes a meaningful difference for myeloma patients. Our results represent a potential new standard of care.”
Dr Durie and his colleagues reported the results of this trial in The Lancet.
The research was funded by Millennium Pharmaceuticals, Takeda Oncology Company, Celgene Corporation, the National Institutes of Health, the National Cancer Institute, and the National Clinical Trial Network.
The trial enrolled 525 adults with MM. The patients ranged in age from 28 to 87, had active MM, and had not had any prior treatment for their disease.
The patients were randomized to 2 treatment groups. One group received Rd for 6 cycles over 6 months. The other group received VRd for 8 cycles over 6 months.
Results
The median follow-up was 55 months. In the VRd group, 241 patients were evaluable for safety and 216 for response. In the Rd group, 226 patients were evaluable for safety and 214 for response.
The overall response rate was 82% (176/216) in the VRd group and 72% (153/214) in the Rd group. The complete response rates were 16% (34/216) and 8% (18/214), respectively.
The median progression-free survival was 43 months in the VRd group and 30 months in the Rd group. The hazard ratio was 0.712 (P=0.0018).
The median overall survival was 75 months in the VRd group and 64 months in the Rd group. The hazard ratio was 0.709 (P=0.025).
The rate of grade 3 or higher AEs was 82% in the VRd group and 75% in the Rd group. The rate of discontinuation due to AEs was 23% and 10%, respectively.
Grade 3 or higher neurologic AEs were more frequent in the VRd group than in the Rd group—33% and 11%, respectively (P<0.0001).
There were 2 treatment-related deaths in the VRd group but none in the Rd group. And 10 patients in each group had a second primary malignancy.
“This is a landmark study that lends clarity to frontline therapy of myeloma,” said study author S. Vincent Rajkumar, MD, of Mayo Clinic in Rochester, Minnesota.
“Newer alternatives to VRd may be more expensive, cumbersome, or toxic. These regimens will therefore need to show superiority over VRd in randomized trials.”
Also worth noting, Dr Rajkumar said, is that the VRd regimen will become even more cost-effective as the drugs in this combination become generic over time. ![]()
Photo courtesy of
Millenium Pharmaceuticals
Results of a phase 3 trial suggest a 3-drug combination improves survival in newly diagnosed multiple myeloma (MM).
The trial showed that bortezomib, lenalidomide, and dexamethasone (VRd) could significantly
improve progression-free and overall survival when compared to lenalidomide and dexamethasone (Rd).
In addition, investigators said the risk-benefit profile of VRd was acceptable.
The team noted, however, that grade 3 or higher neurologic adverse events (AEs) were more common with VRd than with Rd.
“Our results are clear,” said principal investigator Brian G.M. Durie, MD, of Cedars-Sinai Outpatient Cancer Center in Los Angeles, California.
“Using bortezomib in combination with lenalidomide and dexamethasone in frontline treatment—hitting the disease early and hard—makes a meaningful difference for myeloma patients. Our results represent a potential new standard of care.”
Dr Durie and his colleagues reported the results of this trial in The Lancet.
The research was funded by Millennium Pharmaceuticals, Takeda Oncology Company, Celgene Corporation, the National Institutes of Health, the National Cancer Institute, and the National Clinical Trial Network.
The trial enrolled 525 adults with MM. The patients ranged in age from 28 to 87, had active MM, and had not had any prior treatment for their disease.
The patients were randomized to 2 treatment groups. One group received Rd for 6 cycles over 6 months. The other group received VRd for 8 cycles over 6 months.
Results
The median follow-up was 55 months. In the VRd group, 241 patients were evaluable for safety and 216 for response. In the Rd group, 226 patients were evaluable for safety and 214 for response.
The overall response rate was 82% (176/216) in the VRd group and 72% (153/214) in the Rd group. The complete response rates were 16% (34/216) and 8% (18/214), respectively.
The median progression-free survival was 43 months in the VRd group and 30 months in the Rd group. The hazard ratio was 0.712 (P=0.0018).
The median overall survival was 75 months in the VRd group and 64 months in the Rd group. The hazard ratio was 0.709 (P=0.025).
The rate of grade 3 or higher AEs was 82% in the VRd group and 75% in the Rd group. The rate of discontinuation due to AEs was 23% and 10%, respectively.
Grade 3 or higher neurologic AEs were more frequent in the VRd group than in the Rd group—33% and 11%, respectively (P<0.0001).
There were 2 treatment-related deaths in the VRd group but none in the Rd group. And 10 patients in each group had a second primary malignancy.
“This is a landmark study that lends clarity to frontline therapy of myeloma,” said study author S. Vincent Rajkumar, MD, of Mayo Clinic in Rochester, Minnesota.
“Newer alternatives to VRd may be more expensive, cumbersome, or toxic. These regimens will therefore need to show superiority over VRd in randomized trials.”
Also worth noting, Dr Rajkumar said, is that the VRd regimen will become even more cost-effective as the drugs in this combination become generic over time. ![]()
Photo courtesy of
Millenium Pharmaceuticals
Results of a phase 3 trial suggest a 3-drug combination improves survival in newly diagnosed multiple myeloma (MM).
The trial showed that bortezomib, lenalidomide, and dexamethasone (VRd) could significantly
improve progression-free and overall survival when compared to lenalidomide and dexamethasone (Rd).
In addition, investigators said the risk-benefit profile of VRd was acceptable.
The team noted, however, that grade 3 or higher neurologic adverse events (AEs) were more common with VRd than with Rd.
“Our results are clear,” said principal investigator Brian G.M. Durie, MD, of Cedars-Sinai Outpatient Cancer Center in Los Angeles, California.
“Using bortezomib in combination with lenalidomide and dexamethasone in frontline treatment—hitting the disease early and hard—makes a meaningful difference for myeloma patients. Our results represent a potential new standard of care.”
Dr Durie and his colleagues reported the results of this trial in The Lancet.
The research was funded by Millennium Pharmaceuticals, Takeda Oncology Company, Celgene Corporation, the National Institutes of Health, the National Cancer Institute, and the National Clinical Trial Network.
The trial enrolled 525 adults with MM. The patients ranged in age from 28 to 87, had active MM, and had not had any prior treatment for their disease.
The patients were randomized to 2 treatment groups. One group received Rd for 6 cycles over 6 months. The other group received VRd for 8 cycles over 6 months.
Results
The median follow-up was 55 months. In the VRd group, 241 patients were evaluable for safety and 216 for response. In the Rd group, 226 patients were evaluable for safety and 214 for response.
The overall response rate was 82% (176/216) in the VRd group and 72% (153/214) in the Rd group. The complete response rates were 16% (34/216) and 8% (18/214), respectively.
The median progression-free survival was 43 months in the VRd group and 30 months in the Rd group. The hazard ratio was 0.712 (P=0.0018).
The median overall survival was 75 months in the VRd group and 64 months in the Rd group. The hazard ratio was 0.709 (P=0.025).
The rate of grade 3 or higher AEs was 82% in the VRd group and 75% in the Rd group. The rate of discontinuation due to AEs was 23% and 10%, respectively.
Grade 3 or higher neurologic AEs were more frequent in the VRd group than in the Rd group—33% and 11%, respectively (P<0.0001).
There were 2 treatment-related deaths in the VRd group but none in the Rd group. And 10 patients in each group had a second primary malignancy.
“This is a landmark study that lends clarity to frontline therapy of myeloma,” said study author S. Vincent Rajkumar, MD, of Mayo Clinic in Rochester, Minnesota.
“Newer alternatives to VRd may be more expensive, cumbersome, or toxic. These regimens will therefore need to show superiority over VRd in randomized trials.”
Also worth noting, Dr Rajkumar said, is that the VRd regimen will become even more cost-effective as the drugs in this combination become generic over time. ![]()
Company withdraws MAA for biosimilar pegfilgrastim

Image by Volker Brinkmann
Gedeon Richter Plc. has withdrawn its marketing authorization application (MAA) for the biosimilar pegfilgrastim product Cavoley from the European Medicines Agency (EMA).
Richter was seeking approval of Cavoley for the same indications as the reference product, Neulasta, a pegylated recombinant granulocyte-colony stimulating factor used to reduce the duration of neutropenia and the occurrence of febrile neutropenia in adults receiving cytotoxic chemotherapy to treat malignancies (except chronic myeloid leukemia and myelodysplastic syndromes).
The MAA filing for Cavoley was based on data from Richter’s completed biosimilar development program.
The company presented to the EMA results of studies in healthy volunteers designed to show that Cavoley is highly similar to Neulasta in terms of chemical structure, purity, the way it works, and how the body handles the drug.
Richter also presented results of a study comparing the safety and effectiveness of Cavoley and Neulasta in breast cancer patients receiving cytotoxic chemotherapy (EudraCT 2013-003166-14).
Richter withdrew the MAA for Cavoley after the EMA’s Committee for Medicinal Products for Human Use (CHMP) evaluated the documentation provided by the company and formulated lists of questions.
After the CHMP had assessed the company’s responses to the last round of questions, there were still some unresolved issues.
Based on the review of the data and Richter’s response to the CHMP’s list of questions, at the time of the withdrawal, the CHMP had some concerns and was of the provisional opinion that Cavoley could not have been approved.
The CHMP said the company had not demonstrated that Cavoley is highly similar to Neulasta.
In its letter notifying the EMA of the MAA withdrawal, Richter said it would continue developing Cavoley and follow the CHMP’s advice to eliminate the remaining uncertainty that Cavoley is highly similar to Neulasta. ![]()
Image by Volker Brinkmann
Gedeon Richter Plc. has withdrawn its marketing authorization application (MAA) for the biosimilar pegfilgrastim product Cavoley from the European Medicines Agency (EMA).
Richter was seeking approval of Cavoley for the same indications as the reference product, Neulasta, a pegylated recombinant granulocyte-colony stimulating factor used to reduce the duration of neutropenia and the occurrence of febrile neutropenia in adults receiving cytotoxic chemotherapy to treat malignancies (except chronic myeloid leukemia and myelodysplastic syndromes).
The MAA filing for Cavoley was based on data from Richter’s completed biosimilar development program.
The company presented to the EMA results of studies in healthy volunteers designed to show that Cavoley is highly similar to Neulasta in terms of chemical structure, purity, the way it works, and how the body handles the drug.
Richter also presented results of a study comparing the safety and effectiveness of Cavoley and Neulasta in breast cancer patients receiving cytotoxic chemotherapy (EudraCT 2013-003166-14).
Richter withdrew the MAA for Cavoley after the EMA’s Committee for Medicinal Products for Human Use (CHMP) evaluated the documentation provided by the company and formulated lists of questions.
After the CHMP had assessed the company’s responses to the last round of questions, there were still some unresolved issues.
Based on the review of the data and Richter’s response to the CHMP’s list of questions, at the time of the withdrawal, the CHMP had some concerns and was of the provisional opinion that Cavoley could not have been approved.
The CHMP said the company had not demonstrated that Cavoley is highly similar to Neulasta.
In its letter notifying the EMA of the MAA withdrawal, Richter said it would continue developing Cavoley and follow the CHMP’s advice to eliminate the remaining uncertainty that Cavoley is highly similar to Neulasta. ![]()
Image by Volker Brinkmann
Gedeon Richter Plc. has withdrawn its marketing authorization application (MAA) for the biosimilar pegfilgrastim product Cavoley from the European Medicines Agency (EMA).
Richter was seeking approval of Cavoley for the same indications as the reference product, Neulasta, a pegylated recombinant granulocyte-colony stimulating factor used to reduce the duration of neutropenia and the occurrence of febrile neutropenia in adults receiving cytotoxic chemotherapy to treat malignancies (except chronic myeloid leukemia and myelodysplastic syndromes).
The MAA filing for Cavoley was based on data from Richter’s completed biosimilar development program.
The company presented to the EMA results of studies in healthy volunteers designed to show that Cavoley is highly similar to Neulasta in terms of chemical structure, purity, the way it works, and how the body handles the drug.
Richter also presented results of a study comparing the safety and effectiveness of Cavoley and Neulasta in breast cancer patients receiving cytotoxic chemotherapy (EudraCT 2013-003166-14).
Richter withdrew the MAA for Cavoley after the EMA’s Committee for Medicinal Products for Human Use (CHMP) evaluated the documentation provided by the company and formulated lists of questions.
After the CHMP had assessed the company’s responses to the last round of questions, there were still some unresolved issues.
Based on the review of the data and Richter’s response to the CHMP’s list of questions, at the time of the withdrawal, the CHMP had some concerns and was of the provisional opinion that Cavoley could not have been approved.
The CHMP said the company had not demonstrated that Cavoley is highly similar to Neulasta.
In its letter notifying the EMA of the MAA withdrawal, Richter said it would continue developing Cavoley and follow the CHMP’s advice to eliminate the remaining uncertainty that Cavoley is highly similar to Neulasta. ![]()
Drug can improve upon chelation therapy in thalassemia major

An anti-hypertensive drug can improve the effects of chelation therapy in patients with thalassemia major and cardiac iron overload, according to research published in Blood.
Researchers found that administering the drug, amlodipine, in conjunction with conventional chelation therapy significantly reduced myocardial iron concentration (MIC) in patients with cardiac iron overload at baseline, when compared to chelation therapy alone.
In addition, amlodipine did not cause any serious adverse events.
“The drug has been used clinically for decades and is considered safe for adults and children,” said study author Juliano de Lara Fernandes, MD, PhD, of José Michel Kalaf Research Institute in Campinas, São Paulo State, Brazil.
“As an adjunct to standard treatment, it can be greatly beneficial to patients and has few side effects.”
Dr Fernandes said he and his colleagues decided to test amlodipine in patients with thalassemia major because although chelation therapy works well in peripheral organs, it’s difficult to remove iron from the heart.
“Myocardial dysfunctions are currently the main cause of death among patients with thalassemia and can emerge in children from the age of 10,” Dr Fernandes said.
The most serious problem of all, he added, is caused by an accumulation of non-transferrin bound iron (NTBI) in myocardial cells. NTBI enters and leaves the liver without causing much damage to the organ, but it enters the heart via a channel whose main role is to carry calcium into cells.
“It occurred to us that drugs capable of blocking the calcium channel could also prevent NTBI from entering the heart and therefore increase the efficacy of chelation therapy,” Dr Fernandes said.
He and his colleagues tested this hypothesis in 62 patients with thalassemia major. The patients were divided into 2 treatment groups. One group received conventional chelation therapy along with amlodipine (5 mg/day), and the other received chelation therapy plus oral placebo.
Patients were further divided according to cardiac iron levels at baseline. Cardiac iron overload was defined as T2* < 35 ms. Fifty percent of patients in the amlodipine arm and 52% of those in the placebo arm had cardiac iron overload at baseline.
Results
The study’s main outcome was change in MIC, as determined by magnetic resonance imaging at 12 months.
At that point, among patients with cardiac iron overload at baseline, there was a significant decrease in MIC in the amlodipine arm but not the placebo arm. The median change in MIC was -0.26 mg/g and 0.01 mg/g, respectively (P=0.02).
The median MIC in the amlodipine arm went from 1.31 mg/g at baseline to 1.05 mg/g at 12 months (P=0.02). The median MIC in the placebo arm went from 0.77 mg/g at baseline to 0.75 at 12 months (P=0.76).
“Myocardial iron concentration fell 21% in patients with initial iron overload who were treated with chelation plus amlodipine, whereas it increased by 2% in those with initial overload who were treated with chelation plus placebo,” Dr Fernandes said.
On the other hand, there were no significant differences in MIC from baseline to 12 months among patients who received amlodipine but did not have cardiac iron overload at baseline.
For patients without cardiac iron overload at baseline, the median change in MIC was +0.04 mg/g in the amlodipine arm and -0.01 in the placebo arm (P=0.07).
The median MIC in the amlodipine arm went from 0.54 mg/g at baseline to 0.55 mg/g at 12 months. The median MIC in the placebo arm went from 0.55 mg/g at baseline to 0.52 mg/g at 12 months.
“Perhaps we would have needed to monitor these patients for a longer period to see the benefits of preventive therapy with amlodipine for people who don’t have excess iron in their organs,” Dr Fernandes said.
“For those who do, however, the results show it’s worth using amlodipine. There’s no need to change the existing therapy. It’s enough to administer the anti-hypertensive orally every day.”
There were 4 mild adverse events in the amlodipine arm but none in the placebo arm (13% vs 0%, P=0.11).
Three patients (10%) in the amlodipine arm had their initial dose of 5 mg/day reduced to 2.5 mg/day because of mild ankle edema (n=2) and dizziness (n=1). One patient had a mild cutaneous allergic reaction and stopped receiving amlodipine after 15 days but continued on study.
There were no deaths or hospital admissions due to cardiovascular complications during the trial. ![]()
An anti-hypertensive drug can improve the effects of chelation therapy in patients with thalassemia major and cardiac iron overload, according to research published in Blood.
Researchers found that administering the drug, amlodipine, in conjunction with conventional chelation therapy significantly reduced myocardial iron concentration (MIC) in patients with cardiac iron overload at baseline, when compared to chelation therapy alone.
In addition, amlodipine did not cause any serious adverse events.
“The drug has been used clinically for decades and is considered safe for adults and children,” said study author Juliano de Lara Fernandes, MD, PhD, of José Michel Kalaf Research Institute in Campinas, São Paulo State, Brazil.
“As an adjunct to standard treatment, it can be greatly beneficial to patients and has few side effects.”
Dr Fernandes said he and his colleagues decided to test amlodipine in patients with thalassemia major because although chelation therapy works well in peripheral organs, it’s difficult to remove iron from the heart.
“Myocardial dysfunctions are currently the main cause of death among patients with thalassemia and can emerge in children from the age of 10,” Dr Fernandes said.
The most serious problem of all, he added, is caused by an accumulation of non-transferrin bound iron (NTBI) in myocardial cells. NTBI enters and leaves the liver without causing much damage to the organ, but it enters the heart via a channel whose main role is to carry calcium into cells.
“It occurred to us that drugs capable of blocking the calcium channel could also prevent NTBI from entering the heart and therefore increase the efficacy of chelation therapy,” Dr Fernandes said.
He and his colleagues tested this hypothesis in 62 patients with thalassemia major. The patients were divided into 2 treatment groups. One group received conventional chelation therapy along with amlodipine (5 mg/day), and the other received chelation therapy plus oral placebo.
Patients were further divided according to cardiac iron levels at baseline. Cardiac iron overload was defined as T2* < 35 ms. Fifty percent of patients in the amlodipine arm and 52% of those in the placebo arm had cardiac iron overload at baseline.
Results
The study’s main outcome was change in MIC, as determined by magnetic resonance imaging at 12 months.
At that point, among patients with cardiac iron overload at baseline, there was a significant decrease in MIC in the amlodipine arm but not the placebo arm. The median change in MIC was -0.26 mg/g and 0.01 mg/g, respectively (P=0.02).
The median MIC in the amlodipine arm went from 1.31 mg/g at baseline to 1.05 mg/g at 12 months (P=0.02). The median MIC in the placebo arm went from 0.77 mg/g at baseline to 0.75 at 12 months (P=0.76).
“Myocardial iron concentration fell 21% in patients with initial iron overload who were treated with chelation plus amlodipine, whereas it increased by 2% in those with initial overload who were treated with chelation plus placebo,” Dr Fernandes said.
On the other hand, there were no significant differences in MIC from baseline to 12 months among patients who received amlodipine but did not have cardiac iron overload at baseline.
For patients without cardiac iron overload at baseline, the median change in MIC was +0.04 mg/g in the amlodipine arm and -0.01 in the placebo arm (P=0.07).
The median MIC in the amlodipine arm went from 0.54 mg/g at baseline to 0.55 mg/g at 12 months. The median MIC in the placebo arm went from 0.55 mg/g at baseline to 0.52 mg/g at 12 months.
“Perhaps we would have needed to monitor these patients for a longer period to see the benefits of preventive therapy with amlodipine for people who don’t have excess iron in their organs,” Dr Fernandes said.
“For those who do, however, the results show it’s worth using amlodipine. There’s no need to change the existing therapy. It’s enough to administer the anti-hypertensive orally every day.”
There were 4 mild adverse events in the amlodipine arm but none in the placebo arm (13% vs 0%, P=0.11).
Three patients (10%) in the amlodipine arm had their initial dose of 5 mg/day reduced to 2.5 mg/day because of mild ankle edema (n=2) and dizziness (n=1). One patient had a mild cutaneous allergic reaction and stopped receiving amlodipine after 15 days but continued on study.
There were no deaths or hospital admissions due to cardiovascular complications during the trial. ![]()
An anti-hypertensive drug can improve the effects of chelation therapy in patients with thalassemia major and cardiac iron overload, according to research published in Blood.
Researchers found that administering the drug, amlodipine, in conjunction with conventional chelation therapy significantly reduced myocardial iron concentration (MIC) in patients with cardiac iron overload at baseline, when compared to chelation therapy alone.
In addition, amlodipine did not cause any serious adverse events.
“The drug has been used clinically for decades and is considered safe for adults and children,” said study author Juliano de Lara Fernandes, MD, PhD, of José Michel Kalaf Research Institute in Campinas, São Paulo State, Brazil.
“As an adjunct to standard treatment, it can be greatly beneficial to patients and has few side effects.”
Dr Fernandes said he and his colleagues decided to test amlodipine in patients with thalassemia major because although chelation therapy works well in peripheral organs, it’s difficult to remove iron from the heart.
“Myocardial dysfunctions are currently the main cause of death among patients with thalassemia and can emerge in children from the age of 10,” Dr Fernandes said.
The most serious problem of all, he added, is caused by an accumulation of non-transferrin bound iron (NTBI) in myocardial cells. NTBI enters and leaves the liver without causing much damage to the organ, but it enters the heart via a channel whose main role is to carry calcium into cells.
“It occurred to us that drugs capable of blocking the calcium channel could also prevent NTBI from entering the heart and therefore increase the efficacy of chelation therapy,” Dr Fernandes said.
He and his colleagues tested this hypothesis in 62 patients with thalassemia major. The patients were divided into 2 treatment groups. One group received conventional chelation therapy along with amlodipine (5 mg/day), and the other received chelation therapy plus oral placebo.
Patients were further divided according to cardiac iron levels at baseline. Cardiac iron overload was defined as T2* < 35 ms. Fifty percent of patients in the amlodipine arm and 52% of those in the placebo arm had cardiac iron overload at baseline.
Results
The study’s main outcome was change in MIC, as determined by magnetic resonance imaging at 12 months.
At that point, among patients with cardiac iron overload at baseline, there was a significant decrease in MIC in the amlodipine arm but not the placebo arm. The median change in MIC was -0.26 mg/g and 0.01 mg/g, respectively (P=0.02).
The median MIC in the amlodipine arm went from 1.31 mg/g at baseline to 1.05 mg/g at 12 months (P=0.02). The median MIC in the placebo arm went from 0.77 mg/g at baseline to 0.75 at 12 months (P=0.76).
“Myocardial iron concentration fell 21% in patients with initial iron overload who were treated with chelation plus amlodipine, whereas it increased by 2% in those with initial overload who were treated with chelation plus placebo,” Dr Fernandes said.
On the other hand, there were no significant differences in MIC from baseline to 12 months among patients who received amlodipine but did not have cardiac iron overload at baseline.
For patients without cardiac iron overload at baseline, the median change in MIC was +0.04 mg/g in the amlodipine arm and -0.01 in the placebo arm (P=0.07).
The median MIC in the amlodipine arm went from 0.54 mg/g at baseline to 0.55 mg/g at 12 months. The median MIC in the placebo arm went from 0.55 mg/g at baseline to 0.52 mg/g at 12 months.
“Perhaps we would have needed to monitor these patients for a longer period to see the benefits of preventive therapy with amlodipine for people who don’t have excess iron in their organs,” Dr Fernandes said.
“For those who do, however, the results show it’s worth using amlodipine. There’s no need to change the existing therapy. It’s enough to administer the anti-hypertensive orally every day.”
There were 4 mild adverse events in the amlodipine arm but none in the placebo arm (13% vs 0%, P=0.11).
Three patients (10%) in the amlodipine arm had their initial dose of 5 mg/day reduced to 2.5 mg/day because of mild ankle edema (n=2) and dizziness (n=1). One patient had a mild cutaneous allergic reaction and stopped receiving amlodipine after 15 days but continued on study.
There were no deaths or hospital admissions due to cardiovascular complications during the trial. ![]()
Rash on top of feet

The FP suspected that contact dermatitis was to blame for the rash on the dorsum of the patient’s feet. This would have been an unlikely location for tinea pedis and the patient had already tried topical antifungal medications without any benefit. The FP asked the patient if he had purchased any new shoes or boots before the rash started, and the patient indicated that he’d purchased new running shoes about a year earlier.
The FP prescribed 0.1% triamcinolone cream to be applied twice daily. The FP recognized that patch testing might be indicated, but did not perform this in her office. She also recommended that the patient stay away from the running shoes at this time. One month later, the rash was 95% better, except for some postinflammatory hyperpigmentation that was likely to take months to fade. The patient was happy with the results, but wanted to know the cause of his allergy and what shoes would be safe to wear.
The FP offered the patient a referral to a local dermatologist who performed patch testing. The patient went for patch testing and learned he was allergic to chromates found in many types of leather. Statistically, the most likely offending allergens for a rash in this location would be formaldehyde or a chromate. Both are found in leather and are common allergens that cause contact dermatitis on the feet.
Allergic contact dermatitis to chromate in leather shoes may be seasonal as a result of the allergen being leached out by perspiration in warmer months. There are leather shoes that are made free of chromates for people who suffer from allergic contact dermatitis due to this allergen.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Reppa R. Tinea pedis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:799-804.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP suspected that contact dermatitis was to blame for the rash on the dorsum of the patient’s feet. This would have been an unlikely location for tinea pedis and the patient had already tried topical antifungal medications without any benefit. The FP asked the patient if he had purchased any new shoes or boots before the rash started, and the patient indicated that he’d purchased new running shoes about a year earlier.
The FP prescribed 0.1% triamcinolone cream to be applied twice daily. The FP recognized that patch testing might be indicated, but did not perform this in her office. She also recommended that the patient stay away from the running shoes at this time. One month later, the rash was 95% better, except for some postinflammatory hyperpigmentation that was likely to take months to fade. The patient was happy with the results, but wanted to know the cause of his allergy and what shoes would be safe to wear.
The FP offered the patient a referral to a local dermatologist who performed patch testing. The patient went for patch testing and learned he was allergic to chromates found in many types of leather. Statistically, the most likely offending allergens for a rash in this location would be formaldehyde or a chromate. Both are found in leather and are common allergens that cause contact dermatitis on the feet.
Allergic contact dermatitis to chromate in leather shoes may be seasonal as a result of the allergen being leached out by perspiration in warmer months. There are leather shoes that are made free of chromates for people who suffer from allergic contact dermatitis due to this allergen.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Reppa R. Tinea pedis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:799-804.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP suspected that contact dermatitis was to blame for the rash on the dorsum of the patient’s feet. This would have been an unlikely location for tinea pedis and the patient had already tried topical antifungal medications without any benefit. The FP asked the patient if he had purchased any new shoes or boots before the rash started, and the patient indicated that he’d purchased new running shoes about a year earlier.
The FP prescribed 0.1% triamcinolone cream to be applied twice daily. The FP recognized that patch testing might be indicated, but did not perform this in her office. She also recommended that the patient stay away from the running shoes at this time. One month later, the rash was 95% better, except for some postinflammatory hyperpigmentation that was likely to take months to fade. The patient was happy with the results, but wanted to know the cause of his allergy and what shoes would be safe to wear.
The FP offered the patient a referral to a local dermatologist who performed patch testing. The patient went for patch testing and learned he was allergic to chromates found in many types of leather. Statistically, the most likely offending allergens for a rash in this location would be formaldehyde or a chromate. Both are found in leather and are common allergens that cause contact dermatitis on the feet.
Allergic contact dermatitis to chromate in leather shoes may be seasonal as a result of the allergen being leached out by perspiration in warmer months. There are leather shoes that are made free of chromates for people who suffer from allergic contact dermatitis due to this allergen.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R, Reppa R. Tinea pedis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013:799-804.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Hawaii continues to top ‘America’s Health Rankings’
2016 has been a year full of surprises, but not when it comes to the state leading “America’s Health Rankings.” For the fifth consecutive year, Hawaii has been named the healthiest state by the United Health Foundation’s annual report.
Also not a surprise was Mississippi’s 50th-place finish. The Magnolia State most recently finished last in 2014 and has never finished out of the bottom three in the annual ranking. Hawaii, on the other hand, has finished first eight times in the 27 years of the rankings – more than any other state – and has never finished out of the top six, according to the foundation’s 2016 report.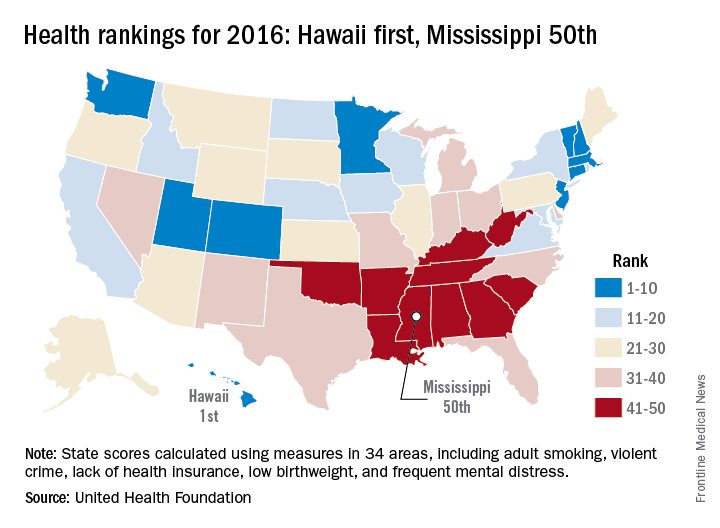
The other states ranked in the top five were well behind Hawaii’s score of 0.905 (representing the weighted standard deviation relative to the U.S. value): Massachusetts was second at 0.760, followed by Connecticut (0.747), Minnesota (0.727), and Vermont (0.709). Just above Mississippi’s score of –1.123 were Louisiana (–1.043), Arkansas (–0.834), Alabama (–0.793), and Oklahoma (–0.691), the foundation reported.
The report ranks states using 34 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. Measures include drug death rate, air pollution, child immunization rate, preventable hospitalization rate, and premature death rate.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
2016 has been a year full of surprises, but not when it comes to the state leading “America’s Health Rankings.” For the fifth consecutive year, Hawaii has been named the healthiest state by the United Health Foundation’s annual report.
Also not a surprise was Mississippi’s 50th-place finish. The Magnolia State most recently finished last in 2014 and has never finished out of the bottom three in the annual ranking. Hawaii, on the other hand, has finished first eight times in the 27 years of the rankings – more than any other state – and has never finished out of the top six, according to the foundation’s 2016 report.
The other states ranked in the top five were well behind Hawaii’s score of 0.905 (representing the weighted standard deviation relative to the U.S. value): Massachusetts was second at 0.760, followed by Connecticut (0.747), Minnesota (0.727), and Vermont (0.709). Just above Mississippi’s score of –1.123 were Louisiana (–1.043), Arkansas (–0.834), Alabama (–0.793), and Oklahoma (–0.691), the foundation reported.
The report ranks states using 34 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. Measures include drug death rate, air pollution, child immunization rate, preventable hospitalization rate, and premature death rate.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
2016 has been a year full of surprises, but not when it comes to the state leading “America’s Health Rankings.” For the fifth consecutive year, Hawaii has been named the healthiest state by the United Health Foundation’s annual report.
Also not a surprise was Mississippi’s 50th-place finish. The Magnolia State most recently finished last in 2014 and has never finished out of the bottom three in the annual ranking. Hawaii, on the other hand, has finished first eight times in the 27 years of the rankings – more than any other state – and has never finished out of the top six, according to the foundation’s 2016 report.
The other states ranked in the top five were well behind Hawaii’s score of 0.905 (representing the weighted standard deviation relative to the U.S. value): Massachusetts was second at 0.760, followed by Connecticut (0.747), Minnesota (0.727), and Vermont (0.709). Just above Mississippi’s score of –1.123 were Louisiana (–1.043), Arkansas (–0.834), Alabama (–0.793), and Oklahoma (–0.691), the foundation reported.
The report ranks states using 34 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. Measures include drug death rate, air pollution, child immunization rate, preventable hospitalization rate, and premature death rate.
“America’s Health Rankings” is a joint effort by the United Health Foundation and the American Public Health Association. It is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
Which Patients With Epilepsy Can Safely Drive?
HOUSTON—Seizure duration and impaired consciousness may be important factors that affect driving performance, according to a study presented at the 70th Annual Meeting of the American Epilepsy Society. “With further work, we hope to … determine whether specific seizure types or localizations present a greater driving risk, with the goal of providing improved guidance to physicians and patients with epilepsy,” researchers said.
A lack of data about driving performance during ictal and postictal periods can make it difficult for physicians to determine whether patients can safely drive.
To study driving impairment during seizures, Hal Blumenfeld, MD, PhD, Director of the Yale Clinical Neuroscience Imaging Center in New Haven, Connecticut, and colleagues asked patients to perform a driving simulation test during inpatient video EEG monitoring. Dr. Blumenfeld, the study’s lead author, is the Mark Loughridge and Michele Williams Professor of Neurology and a Professor of Neuroscience and Neurosurgery at Yale University.

The study included 20 patients who were observed in the epilepsy monitoring unit at Yale New Haven Hospital. Investigators analyzed ictal and interictal driving data captured prospectively from the driving simulator. A total of 33 seizures were analyzed. The investigators compared interictal and ictal driving performance through quantitative analysis. Variables included car velocity, steering wheel movement, braking, and crash occurrence.
Patients drove between one and 10 hours, with an average driving duration of about three hours. Patients had variable impairment during ictal and postictal periods and during subclinical epileptiform discharges. Some seizures showed obvious impairment, and others showed no change in driving performance. Seizures with driving impairment had significantly greater duration and were more likely to involve impaired consciousness than seizures without driving impairment. Seven of the seizures resulted in crashes. Seizures lasted an average of 75 seconds in patients who crashed, compared with an average of 30 seconds in patients who did not crash.
Driving simulations during inpatient video-EEG monitoring may be a useful way to determine factors that influence driving safety, the researchers concluded.
“It is going to take a lot more data to come up with a reliable way of predicting which people with epilepsy should drive and which should not,” said Dr. Blumenfeld. “We want to unearth more detail to learn if there are people with epilepsy who are driving who shouldn’t be, as well those who are not driving who can safely drive.”
HOUSTON—Seizure duration and impaired consciousness may be important factors that affect driving performance, according to a study presented at the 70th Annual Meeting of the American Epilepsy Society. “With further work, we hope to … determine whether specific seizure types or localizations present a greater driving risk, with the goal of providing improved guidance to physicians and patients with epilepsy,” researchers said.
A lack of data about driving performance during ictal and postictal periods can make it difficult for physicians to determine whether patients can safely drive.
To study driving impairment during seizures, Hal Blumenfeld, MD, PhD, Director of the Yale Clinical Neuroscience Imaging Center in New Haven, Connecticut, and colleagues asked patients to perform a driving simulation test during inpatient video EEG monitoring. Dr. Blumenfeld, the study’s lead author, is the Mark Loughridge and Michele Williams Professor of Neurology and a Professor of Neuroscience and Neurosurgery at Yale University.
The study included 20 patients who were observed in the epilepsy monitoring unit at Yale New Haven Hospital. Investigators analyzed ictal and interictal driving data captured prospectively from the driving simulator. A total of 33 seizures were analyzed. The investigators compared interictal and ictal driving performance through quantitative analysis. Variables included car velocity, steering wheel movement, braking, and crash occurrence.
Patients drove between one and 10 hours, with an average driving duration of about three hours. Patients had variable impairment during ictal and postictal periods and during subclinical epileptiform discharges. Some seizures showed obvious impairment, and others showed no change in driving performance. Seizures with driving impairment had significantly greater duration and were more likely to involve impaired consciousness than seizures without driving impairment. Seven of the seizures resulted in crashes. Seizures lasted an average of 75 seconds in patients who crashed, compared with an average of 30 seconds in patients who did not crash.
Driving simulations during inpatient video-EEG monitoring may be a useful way to determine factors that influence driving safety, the researchers concluded.
“It is going to take a lot more data to come up with a reliable way of predicting which people with epilepsy should drive and which should not,” said Dr. Blumenfeld. “We want to unearth more detail to learn if there are people with epilepsy who are driving who shouldn’t be, as well those who are not driving who can safely drive.”
HOUSTON—Seizure duration and impaired consciousness may be important factors that affect driving performance, according to a study presented at the 70th Annual Meeting of the American Epilepsy Society. “With further work, we hope to … determine whether specific seizure types or localizations present a greater driving risk, with the goal of providing improved guidance to physicians and patients with epilepsy,” researchers said.
A lack of data about driving performance during ictal and postictal periods can make it difficult for physicians to determine whether patients can safely drive.
To study driving impairment during seizures, Hal Blumenfeld, MD, PhD, Director of the Yale Clinical Neuroscience Imaging Center in New Haven, Connecticut, and colleagues asked patients to perform a driving simulation test during inpatient video EEG monitoring. Dr. Blumenfeld, the study’s lead author, is the Mark Loughridge and Michele Williams Professor of Neurology and a Professor of Neuroscience and Neurosurgery at Yale University.
The study included 20 patients who were observed in the epilepsy monitoring unit at Yale New Haven Hospital. Investigators analyzed ictal and interictal driving data captured prospectively from the driving simulator. A total of 33 seizures were analyzed. The investigators compared interictal and ictal driving performance through quantitative analysis. Variables included car velocity, steering wheel movement, braking, and crash occurrence.
Patients drove between one and 10 hours, with an average driving duration of about three hours. Patients had variable impairment during ictal and postictal periods and during subclinical epileptiform discharges. Some seizures showed obvious impairment, and others showed no change in driving performance. Seizures with driving impairment had significantly greater duration and were more likely to involve impaired consciousness than seizures without driving impairment. Seven of the seizures resulted in crashes. Seizures lasted an average of 75 seconds in patients who crashed, compared with an average of 30 seconds in patients who did not crash.
Driving simulations during inpatient video-EEG monitoring may be a useful way to determine factors that influence driving safety, the researchers concluded.
“It is going to take a lot more data to come up with a reliable way of predicting which people with epilepsy should drive and which should not,” said Dr. Blumenfeld. “We want to unearth more detail to learn if there are people with epilepsy who are driving who shouldn’t be, as well those who are not driving who can safely drive.”
