User login
Tips for Living With Tardive Dyskinesia
Click here to download the PDF.

Click here to download the PDF.
Click here to download the PDF.

Locum tenens physicians more popular than ever
Use of locum tenens physicians reached a new high in 2016, according to an annual survey by Staff Care, a health care staffing company.
Last year, 94% of hospitals, medical groups, and other health care facilities reported using temporary physicians, compared with 91% in 2014, which was the previous high, Staff Care reported in its “2017 Survey of Temporary Physician Staffing Trends.”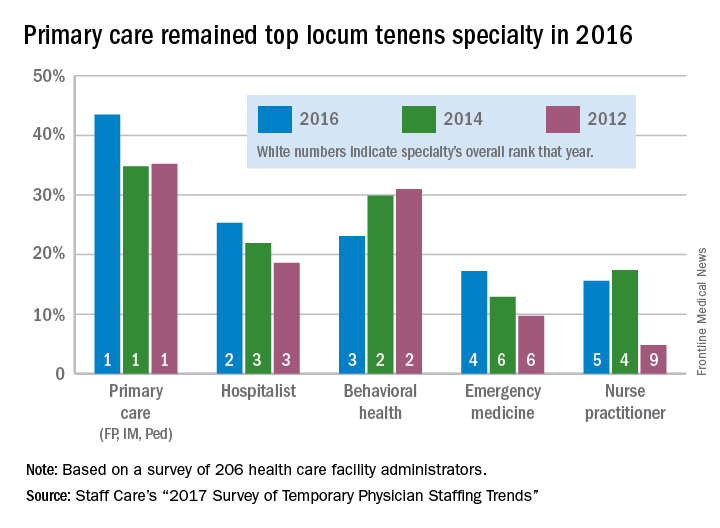
Primary care physicians (family physicians, internists, and pediatricians) were the leading locum tenens choice by specialty, with 43.5% of health care facilities reporting their use in 2016. Hospitalists were the next most popular specialists at 25%, followed by behavioral health professionals (23%), emergency physicians (17%), and nurse practitioners (16%), according to survey responses from 206 administrators of health care facilities.
Since about one-third of U.S. physicians practice primary care, “it is not particularly surprising that they are more utilized as locum tenens,” the report noted, but “only about 3.5% of all physicians are psychiatrists, [so] the fact that behavioral health professionals are the third most utilized type of locum tenens provider underlines the acute shortage of providers in this field.”
Use of locum tenens physicians reached a new high in 2016, according to an annual survey by Staff Care, a health care staffing company.
Last year, 94% of hospitals, medical groups, and other health care facilities reported using temporary physicians, compared with 91% in 2014, which was the previous high, Staff Care reported in its “2017 Survey of Temporary Physician Staffing Trends.”
Primary care physicians (family physicians, internists, and pediatricians) were the leading locum tenens choice by specialty, with 43.5% of health care facilities reporting their use in 2016. Hospitalists were the next most popular specialists at 25%, followed by behavioral health professionals (23%), emergency physicians (17%), and nurse practitioners (16%), according to survey responses from 206 administrators of health care facilities.
Since about one-third of U.S. physicians practice primary care, “it is not particularly surprising that they are more utilized as locum tenens,” the report noted, but “only about 3.5% of all physicians are psychiatrists, [so] the fact that behavioral health professionals are the third most utilized type of locum tenens provider underlines the acute shortage of providers in this field.”
Use of locum tenens physicians reached a new high in 2016, according to an annual survey by Staff Care, a health care staffing company.
Last year, 94% of hospitals, medical groups, and other health care facilities reported using temporary physicians, compared with 91% in 2014, which was the previous high, Staff Care reported in its “2017 Survey of Temporary Physician Staffing Trends.”
Primary care physicians (family physicians, internists, and pediatricians) were the leading locum tenens choice by specialty, with 43.5% of health care facilities reporting their use in 2016. Hospitalists were the next most popular specialists at 25%, followed by behavioral health professionals (23%), emergency physicians (17%), and nurse practitioners (16%), according to survey responses from 206 administrators of health care facilities.
Since about one-third of U.S. physicians practice primary care, “it is not particularly surprising that they are more utilized as locum tenens,” the report noted, but “only about 3.5% of all physicians are psychiatrists, [so] the fact that behavioral health professionals are the third most utilized type of locum tenens provider underlines the acute shortage of providers in this field.”
Subcutaneous high-dose methotrexate controls psoriasis
Subcutaneous high-dose methotrexate can be safely initiated in people with moderate to severe psoriasis, and produces a rapid and sustained response, researchers found.
Although methotrexate is a first-line agent in moderate to severe psoriasis, and is considerably cheaper than biological agents, much remains unknown about its ideal dosage and route of administration.
Authors of a 2016 systematic review noted that, despite the fact that methotrexate has been used for more than 50 years in psoriasis, high-quality trial evidence remains wanting (PLoS One 2016 May 11. doi: 10.1371/journal.pone.0153740). Recent, well-designed trials have compared methotrexate to biological drugs used in psoriasis rather than placebo. These studies also have used oral formulations of methotrexate, in a range of starting doses as low as 5 mg, rather than subcutaneous formulations.

In their 52-week, multicenter trial conducted across 13 study sites in Europe, Dr. Warren and his colleagues randomized 120 patients to subcutaneous methotrexate at a dose of 17.5 mg/week (n = 91) or sham injections (n = 29) for 16 weeks. Patients in the intervention arm who did not achieve at least 50% improvement on the baseline Psoriasis Area and Severity Index (PASI) score at 8 weeks were increased to 22.5 mg methotrexate per week; 31% received this dose increase.
The study’s primary endpoint was reduction of the PASI score by 75% or more at 16 weeks, which 41% of the intervention arm achieved, compared with 10% of patients in the placebo arm (relative risk 3.93, P = .0026). After 16 weeks, all patients in the cohort were converted to open-label methotrexate for the remainder of the trial, following the same dosing schedule of between 17.5 and 22.5 mg, depending on response at 8 weeks after initiation.
At week 52, PASI 75 response rates were 45% in the methotrexate-methotrexate group and 34% in the placebo-methotrexate group. This compared favorably, the researchers wrote, with a previous study in which the PASI 75 response rate at week 52 was 24% with oral methotrexate at doses of up to 25 mg per week.
No serious adverse events were associated with methotrexate, although gastrointestinal problems (mostly nausea) and elevated liver enzymes were more common in patients receiving the treatment.
“Our findings encourage the use of subcutaneous methotrexate for treatment of psoriasis, and suggest long-term clinical outcomes better than previously reported for oral administration, although final confirmation will be needed in a direct head-to-head trial of subcutaneous versus oral dosing. Our findings might also help to guide future recommendations for the optimum dosing of methotrexate,” the investigators wrote.
Medac Pharma funded the study. Dr. Warren and six of his coauthors disclosed financial relationships with multiple pharmaceutical firms, including the study sponsor, while three coauthors declared no financial conflicts of interest.
The results from this study compare favorably with those of a previous 52-week study of oral methotrexate in this population, suggesting that subcutaneous administration is superior to oral administration in the management of psoriasis. However, response rates for methotrexate are still lower than those reported with biological therapy, especially with infliximab, adalimumab, ustekinumab, and, more recently, the anti-interleukin-17 drugs secukinumab and ixekizumab.
The question that remains is whether methotrexate should remain the first-line systemic therapy for moderate to severe psoriasis. Because we now know that psoriasis is not just skin deep, and that many of the comorbidities – including psoriatic arthritis, metabolic syndrome, and cardiovascular events, in addition to premature death – are related to the extent of skin involvement, perhaps drugs that effectively control inflammation should be used initially. This approach could be addressed only via long-term observations of prospective studies of patients treated with methotrexate, compared with those treated with biological therapy, with collection of information not only about clinical improvement of skin disease, but also about comorbidities.
Dafna D. Gladman, MD, is director of the psoriatic arthritis program at the Centre for Prognosis Studies in The Rheumatic Diseases at Toronto Western Hospital. This comment was excerpted and modified from an editorial (Lancet. 2017;389[10068]:482-3). that accompanied the study by Warren et al. Dr. Gladman disclosed financial relationships, mostly grants and fees related to clinical trials, with several pharmaceutical manufacturers.
The results from this study compare favorably with those of a previous 52-week study of oral methotrexate in this population, suggesting that subcutaneous administration is superior to oral administration in the management of psoriasis. However, response rates for methotrexate are still lower than those reported with biological therapy, especially with infliximab, adalimumab, ustekinumab, and, more recently, the anti-interleukin-17 drugs secukinumab and ixekizumab.
The question that remains is whether methotrexate should remain the first-line systemic therapy for moderate to severe psoriasis. Because we now know that psoriasis is not just skin deep, and that many of the comorbidities – including psoriatic arthritis, metabolic syndrome, and cardiovascular events, in addition to premature death – are related to the extent of skin involvement, perhaps drugs that effectively control inflammation should be used initially. This approach could be addressed only via long-term observations of prospective studies of patients treated with methotrexate, compared with those treated with biological therapy, with collection of information not only about clinical improvement of skin disease, but also about comorbidities.
Dafna D. Gladman, MD, is director of the psoriatic arthritis program at the Centre for Prognosis Studies in The Rheumatic Diseases at Toronto Western Hospital. This comment was excerpted and modified from an editorial (Lancet. 2017;389[10068]:482-3). that accompanied the study by Warren et al. Dr. Gladman disclosed financial relationships, mostly grants and fees related to clinical trials, with several pharmaceutical manufacturers.
The results from this study compare favorably with those of a previous 52-week study of oral methotrexate in this population, suggesting that subcutaneous administration is superior to oral administration in the management of psoriasis. However, response rates for methotrexate are still lower than those reported with biological therapy, especially with infliximab, adalimumab, ustekinumab, and, more recently, the anti-interleukin-17 drugs secukinumab and ixekizumab.
The question that remains is whether methotrexate should remain the first-line systemic therapy for moderate to severe psoriasis. Because we now know that psoriasis is not just skin deep, and that many of the comorbidities – including psoriatic arthritis, metabolic syndrome, and cardiovascular events, in addition to premature death – are related to the extent of skin involvement, perhaps drugs that effectively control inflammation should be used initially. This approach could be addressed only via long-term observations of prospective studies of patients treated with methotrexate, compared with those treated with biological therapy, with collection of information not only about clinical improvement of skin disease, but also about comorbidities.
Dafna D. Gladman, MD, is director of the psoriatic arthritis program at the Centre for Prognosis Studies in The Rheumatic Diseases at Toronto Western Hospital. This comment was excerpted and modified from an editorial (Lancet. 2017;389[10068]:482-3). that accompanied the study by Warren et al. Dr. Gladman disclosed financial relationships, mostly grants and fees related to clinical trials, with several pharmaceutical manufacturers.
Subcutaneous high-dose methotrexate can be safely initiated in people with moderate to severe psoriasis, and produces a rapid and sustained response, researchers found.
Although methotrexate is a first-line agent in moderate to severe psoriasis, and is considerably cheaper than biological agents, much remains unknown about its ideal dosage and route of administration.
Authors of a 2016 systematic review noted that, despite the fact that methotrexate has been used for more than 50 years in psoriasis, high-quality trial evidence remains wanting (PLoS One 2016 May 11. doi: 10.1371/journal.pone.0153740). Recent, well-designed trials have compared methotrexate to biological drugs used in psoriasis rather than placebo. These studies also have used oral formulations of methotrexate, in a range of starting doses as low as 5 mg, rather than subcutaneous formulations.
In their 52-week, multicenter trial conducted across 13 study sites in Europe, Dr. Warren and his colleagues randomized 120 patients to subcutaneous methotrexate at a dose of 17.5 mg/week (n = 91) or sham injections (n = 29) for 16 weeks. Patients in the intervention arm who did not achieve at least 50% improvement on the baseline Psoriasis Area and Severity Index (PASI) score at 8 weeks were increased to 22.5 mg methotrexate per week; 31% received this dose increase.
The study’s primary endpoint was reduction of the PASI score by 75% or more at 16 weeks, which 41% of the intervention arm achieved, compared with 10% of patients in the placebo arm (relative risk 3.93, P = .0026). After 16 weeks, all patients in the cohort were converted to open-label methotrexate for the remainder of the trial, following the same dosing schedule of between 17.5 and 22.5 mg, depending on response at 8 weeks after initiation.
At week 52, PASI 75 response rates were 45% in the methotrexate-methotrexate group and 34% in the placebo-methotrexate group. This compared favorably, the researchers wrote, with a previous study in which the PASI 75 response rate at week 52 was 24% with oral methotrexate at doses of up to 25 mg per week.
No serious adverse events were associated with methotrexate, although gastrointestinal problems (mostly nausea) and elevated liver enzymes were more common in patients receiving the treatment.
“Our findings encourage the use of subcutaneous methotrexate for treatment of psoriasis, and suggest long-term clinical outcomes better than previously reported for oral administration, although final confirmation will be needed in a direct head-to-head trial of subcutaneous versus oral dosing. Our findings might also help to guide future recommendations for the optimum dosing of methotrexate,” the investigators wrote.
Medac Pharma funded the study. Dr. Warren and six of his coauthors disclosed financial relationships with multiple pharmaceutical firms, including the study sponsor, while three coauthors declared no financial conflicts of interest.
Subcutaneous high-dose methotrexate can be safely initiated in people with moderate to severe psoriasis, and produces a rapid and sustained response, researchers found.
Although methotrexate is a first-line agent in moderate to severe psoriasis, and is considerably cheaper than biological agents, much remains unknown about its ideal dosage and route of administration.
Authors of a 2016 systematic review noted that, despite the fact that methotrexate has been used for more than 50 years in psoriasis, high-quality trial evidence remains wanting (PLoS One 2016 May 11. doi: 10.1371/journal.pone.0153740). Recent, well-designed trials have compared methotrexate to biological drugs used in psoriasis rather than placebo. These studies also have used oral formulations of methotrexate, in a range of starting doses as low as 5 mg, rather than subcutaneous formulations.
In their 52-week, multicenter trial conducted across 13 study sites in Europe, Dr. Warren and his colleagues randomized 120 patients to subcutaneous methotrexate at a dose of 17.5 mg/week (n = 91) or sham injections (n = 29) for 16 weeks. Patients in the intervention arm who did not achieve at least 50% improvement on the baseline Psoriasis Area and Severity Index (PASI) score at 8 weeks were increased to 22.5 mg methotrexate per week; 31% received this dose increase.
The study’s primary endpoint was reduction of the PASI score by 75% or more at 16 weeks, which 41% of the intervention arm achieved, compared with 10% of patients in the placebo arm (relative risk 3.93, P = .0026). After 16 weeks, all patients in the cohort were converted to open-label methotrexate for the remainder of the trial, following the same dosing schedule of between 17.5 and 22.5 mg, depending on response at 8 weeks after initiation.
At week 52, PASI 75 response rates were 45% in the methotrexate-methotrexate group and 34% in the placebo-methotrexate group. This compared favorably, the researchers wrote, with a previous study in which the PASI 75 response rate at week 52 was 24% with oral methotrexate at doses of up to 25 mg per week.
No serious adverse events were associated with methotrexate, although gastrointestinal problems (mostly nausea) and elevated liver enzymes were more common in patients receiving the treatment.
“Our findings encourage the use of subcutaneous methotrexate for treatment of psoriasis, and suggest long-term clinical outcomes better than previously reported for oral administration, although final confirmation will be needed in a direct head-to-head trial of subcutaneous versus oral dosing. Our findings might also help to guide future recommendations for the optimum dosing of methotrexate,” the investigators wrote.
Medac Pharma funded the study. Dr. Warren and six of his coauthors disclosed financial relationships with multiple pharmaceutical firms, including the study sponsor, while three coauthors declared no financial conflicts of interest.
FROM THE LANCET
Key clinical point:
Major finding: At 16 weeks, 41% of patients started on methotrexate achieved a 75% reduction in psoriasis severity scores, compared with 10% of patients in the placebo arm. At 1 year of treatment, 45% of patients saw this level of response.
Data source: A multisite, placebo-controlled trial randomizing 120 patients to subcutaneous methotrexate or placebo for 16 weeks, then converting all patients to open-label subcutaneous methotrexate through week 52.
Disclosures: Medac Pharma funded the study. Dr. Warren and six of his coauthors disclosed financial relationships with multiple pharmaceutical firms, including the study sponsor, while three coauthors declared no financial conflicts of interest.
HIV research update: Late January 2017
A great volume of HIV and AIDS research enters the medical literature every month. It’s difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Researchers demonstrated the safety and activity of the HIV-neutralizing monoclonal antibody 10-1074 in humans and said their study supports the idea that antibodies targeting the V3 glycan supersite might be useful for the treatment and prevention of HIV-1 infection.
Efforts to support HIV disclosure (such as counseling) may be needed for TB-HIV coinfected patients, particularly for women and those unaware of their partners’ status, a study found.
Elevated levels of procoagulants may exert a particularly detrimental effect on neurocognitive functioning among older HIV-infected persons, according to a study in the journal AIDS.
A recent study found that a combination of the anti-HIV drugs tenofovir, lopinavir, and ritonavir in a lipid-stabilized nanosuspension enhanced and sustained intracellular drug levels and exposures in lymph node and blood cells above those in plasma.
Hepatitis B virus infection continues to be acquired in adulthood among HIV-positive Ugandans, but HBV incidence is dramatically reduced with HBV-active antiretroviral therapy, a study found.
In antiretroviral therapy-naive Ugandan children, insulin resistance changed significantly after 48 weeks of ART and correlated with monocyte activation, according to a study in the Pediatric Infectious Disease Journal.
Oxidative stress is associated with a higher risk of serious non-AIDS events in HIV patients, including non-AIDS deaths, according to a study in JAIDS. The authors said the effect is independent and additive to biomarkers of inflammation, monocyte activation and coagulation.
A study at a California teaching hospital found the yield of opt-out HIV rapid antibody screening in inpatients was comparable to the national HIV prevalence average. However, uptake of screening was markedly limited where opt-out screening was delivered by physicians during routine care, with limited time resources being the major barrier.
Variations within fat mass and the obesity-associated (FTO) gene may be predictors of fatty liver disease in HIV-infected patients independently of metabolic factors, according to a study in HIV Medicine.
After adjustment for sex, years of HIV experience, and patient caseload, providing primary care to HIV-infected patients remained associated with delivering comprehensive reproductive health counseling, according to a study in AIDS Care.
A recent study found that treatment dose nevirapine-based combination antiretroviral therapy was generally well tolerated by HIV-infected neonates, and associated with normalization of trough levels over time in most cases without dose adjustment.
Immune function may be impacted by various forms of psychological stress in HIV-positive women, a study found, and investigators said interventions that target stress reduction may be useful in improving immune parameters and quality of life.
Annual HIV incidence among men who have sex with men attending STI clinics in England is high, a study in HIV Medicine revealed, and previous STIs were predictors of HIV acquisition but accounted only for one in five infections.
A study in Public Health Reports found that the prevalence of HIV testing provision at organizations serving young people in Baltimore was low, and few organizations offered linkages to HIV testing.
A study in Hepatology found that eradication of hepatitis C virus infection in HIV/HCV coinfected patients is associated not only with a reduction in the frequency of death, HIV progression, and liver-related events, but also with a reduced hazard of diabetes mellitus and possibly of chronic renal failure.
A recent study found modest but significant improvements in self-assessed quality of life among HIV patients initiating antiretroviral therapy immediately compared to deferring treatment, supporting patient-perceived health benefits of initiating ART as soon as possible after an HIV diagnosis.
Distinct mechanisms may underlie cortical and subcortical injury in people with HIV, a study in JAIDS found, suggesting the potential importance of early initiation of HAART to protect long-term brain health.
A three-hospital study found that an EMR prompt for hospitalized patients was associated with a large increase in HIV testing, a diversification of patients tested, and an increase in diagnoses made by screening.
[email protected]
On Twitter @richpizzi
A great volume of HIV and AIDS research enters the medical literature every month. It’s difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Researchers demonstrated the safety and activity of the HIV-neutralizing monoclonal antibody 10-1074 in humans and said their study supports the idea that antibodies targeting the V3 glycan supersite might be useful for the treatment and prevention of HIV-1 infection.
Efforts to support HIV disclosure (such as counseling) may be needed for TB-HIV coinfected patients, particularly for women and those unaware of their partners’ status, a study found.
Elevated levels of procoagulants may exert a particularly detrimental effect on neurocognitive functioning among older HIV-infected persons, according to a study in the journal AIDS.
A recent study found that a combination of the anti-HIV drugs tenofovir, lopinavir, and ritonavir in a lipid-stabilized nanosuspension enhanced and sustained intracellular drug levels and exposures in lymph node and blood cells above those in plasma.
Hepatitis B virus infection continues to be acquired in adulthood among HIV-positive Ugandans, but HBV incidence is dramatically reduced with HBV-active antiretroviral therapy, a study found.
In antiretroviral therapy-naive Ugandan children, insulin resistance changed significantly after 48 weeks of ART and correlated with monocyte activation, according to a study in the Pediatric Infectious Disease Journal.
Oxidative stress is associated with a higher risk of serious non-AIDS events in HIV patients, including non-AIDS deaths, according to a study in JAIDS. The authors said the effect is independent and additive to biomarkers of inflammation, monocyte activation and coagulation.
A study at a California teaching hospital found the yield of opt-out HIV rapid antibody screening in inpatients was comparable to the national HIV prevalence average. However, uptake of screening was markedly limited where opt-out screening was delivered by physicians during routine care, with limited time resources being the major barrier.
Variations within fat mass and the obesity-associated (FTO) gene may be predictors of fatty liver disease in HIV-infected patients independently of metabolic factors, according to a study in HIV Medicine.
After adjustment for sex, years of HIV experience, and patient caseload, providing primary care to HIV-infected patients remained associated with delivering comprehensive reproductive health counseling, according to a study in AIDS Care.
A recent study found that treatment dose nevirapine-based combination antiretroviral therapy was generally well tolerated by HIV-infected neonates, and associated with normalization of trough levels over time in most cases without dose adjustment.
Immune function may be impacted by various forms of psychological stress in HIV-positive women, a study found, and investigators said interventions that target stress reduction may be useful in improving immune parameters and quality of life.
Annual HIV incidence among men who have sex with men attending STI clinics in England is high, a study in HIV Medicine revealed, and previous STIs were predictors of HIV acquisition but accounted only for one in five infections.
A study in Public Health Reports found that the prevalence of HIV testing provision at organizations serving young people in Baltimore was low, and few organizations offered linkages to HIV testing.
A study in Hepatology found that eradication of hepatitis C virus infection in HIV/HCV coinfected patients is associated not only with a reduction in the frequency of death, HIV progression, and liver-related events, but also with a reduced hazard of diabetes mellitus and possibly of chronic renal failure.
A recent study found modest but significant improvements in self-assessed quality of life among HIV patients initiating antiretroviral therapy immediately compared to deferring treatment, supporting patient-perceived health benefits of initiating ART as soon as possible after an HIV diagnosis.
Distinct mechanisms may underlie cortical and subcortical injury in people with HIV, a study in JAIDS found, suggesting the potential importance of early initiation of HAART to protect long-term brain health.
A three-hospital study found that an EMR prompt for hospitalized patients was associated with a large increase in HIV testing, a diversification of patients tested, and an increase in diagnoses made by screening.
[email protected]
On Twitter @richpizzi
A great volume of HIV and AIDS research enters the medical literature every month. It’s difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Researchers demonstrated the safety and activity of the HIV-neutralizing monoclonal antibody 10-1074 in humans and said their study supports the idea that antibodies targeting the V3 glycan supersite might be useful for the treatment and prevention of HIV-1 infection.
Efforts to support HIV disclosure (such as counseling) may be needed for TB-HIV coinfected patients, particularly for women and those unaware of their partners’ status, a study found.
Elevated levels of procoagulants may exert a particularly detrimental effect on neurocognitive functioning among older HIV-infected persons, according to a study in the journal AIDS.
A recent study found that a combination of the anti-HIV drugs tenofovir, lopinavir, and ritonavir in a lipid-stabilized nanosuspension enhanced and sustained intracellular drug levels and exposures in lymph node and blood cells above those in plasma.
Hepatitis B virus infection continues to be acquired in adulthood among HIV-positive Ugandans, but HBV incidence is dramatically reduced with HBV-active antiretroviral therapy, a study found.
In antiretroviral therapy-naive Ugandan children, insulin resistance changed significantly after 48 weeks of ART and correlated with monocyte activation, according to a study in the Pediatric Infectious Disease Journal.
Oxidative stress is associated with a higher risk of serious non-AIDS events in HIV patients, including non-AIDS deaths, according to a study in JAIDS. The authors said the effect is independent and additive to biomarkers of inflammation, monocyte activation and coagulation.
A study at a California teaching hospital found the yield of opt-out HIV rapid antibody screening in inpatients was comparable to the national HIV prevalence average. However, uptake of screening was markedly limited where opt-out screening was delivered by physicians during routine care, with limited time resources being the major barrier.
Variations within fat mass and the obesity-associated (FTO) gene may be predictors of fatty liver disease in HIV-infected patients independently of metabolic factors, according to a study in HIV Medicine.
After adjustment for sex, years of HIV experience, and patient caseload, providing primary care to HIV-infected patients remained associated with delivering comprehensive reproductive health counseling, according to a study in AIDS Care.
A recent study found that treatment dose nevirapine-based combination antiretroviral therapy was generally well tolerated by HIV-infected neonates, and associated with normalization of trough levels over time in most cases without dose adjustment.
Immune function may be impacted by various forms of psychological stress in HIV-positive women, a study found, and investigators said interventions that target stress reduction may be useful in improving immune parameters and quality of life.
Annual HIV incidence among men who have sex with men attending STI clinics in England is high, a study in HIV Medicine revealed, and previous STIs were predictors of HIV acquisition but accounted only for one in five infections.
A study in Public Health Reports found that the prevalence of HIV testing provision at organizations serving young people in Baltimore was low, and few organizations offered linkages to HIV testing.
A study in Hepatology found that eradication of hepatitis C virus infection in HIV/HCV coinfected patients is associated not only with a reduction in the frequency of death, HIV progression, and liver-related events, but also with a reduced hazard of diabetes mellitus and possibly of chronic renal failure.
A recent study found modest but significant improvements in self-assessed quality of life among HIV patients initiating antiretroviral therapy immediately compared to deferring treatment, supporting patient-perceived health benefits of initiating ART as soon as possible after an HIV diagnosis.
Distinct mechanisms may underlie cortical and subcortical injury in people with HIV, a study in JAIDS found, suggesting the potential importance of early initiation of HAART to protect long-term brain health.
A three-hospital study found that an EMR prompt for hospitalized patients was associated with a large increase in HIV testing, a diversification of patients tested, and an increase in diagnoses made by screening.
[email protected]
On Twitter @richpizzi
Hypertensive disease of pregnancy linked to earlier mortality
LAS VEGAS – Women who develop any form of hypertensive disease during pregnancy have a significantly increased mortality rate until they reach age 50, compared with women without the condition.
The findings, presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine, are based on a review of more than 2 million mothers who delivered babies in Utah during 1939-2012.
The relatively increased mortality rate linked with hypertensive disease of pregnancy (HDP) reached its peak during the first decade immediately following the index delivery and was dramatically higher in women for whom the index HDP was preceded by at least one earlier HDP. Increased mortality was especially elevated for certain types of deaths including stroke, diabetes, circulatory disease, and ischemic heart disease, said Lauren Theilen, MD, a maternal-fetal medicine researcher at the University of Utah in Salt Lake City.

She calculated that during the decade following an index case of HDP, life expectancy among mothers who had two or more HDP-affected pregnancies was about 49 years, life expectancy among women with a history of one HDP was 52 years, and postpartum women without HDP had a life expectancy of 55 years.
The data came from 2,083,331 singleton pregnancies delivered in Utah during 1939-2012 where the mother remained in Utah for at least 1 year following delivery. From this group, Dr. Theilen and her associates identified 67,384 women (3%) with HDP, including 49,598 women without a prior history of HDP and 7,786 with at least one prior HDP pregnancy. They included four different diagnoses as HDP: gestational hypertension, preeclampsia, HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count), or eclampsia.
The analysis excluded women with chronic hypertension, antiphospholipid syndrome, pregestational diabetes, or chronic kidney disease. It also excluded women who died within a year of the index delivery. For each of the included 67,384 cases with HDP, the researchers selected two controls with a delivery unaffected by HDP and matched them to a case by age, year of childbirth, and parity.
The women in the study were 26 years old on average. Gestational age at delivery among the HDP cases averaged 1 week less than among the controls, 37.8 weeks compared with 38.9 weeks, a statistically significant difference. Average birth weight also differed by a significant amount, 3,079 grams in the HDP neonates and 3,319 grams in the control newborns. During follow-up, 8% of the HDP women died, compared with 6% of the control women.
Analysis showed that relative mortality rates in HDP women were especially elevated for certain types of death: endocrine and metabolic, circulatory, genitourinary, infectious disease, and digestive. In most types of death, the increased risk linked with HDP was markedly higher in the women with recurrent HDP.
Dr. Theilen reported the relative risks of death for certain specific mortality causes (Am J Obstet Gynecol. 2017 Jan;216[1][suppl]:S32-3). In women with a single index case of HDP, the mortality rate compared to women with no HDP was threefold higher for diabetes, twofold higher for ischemic heart disease, and 85% higher for stroke. In women with recurrent HDP, the relative mortality risks were fourfold higher for diabetes, threefold higher for ischemic heart disease, and fivefold higher for stroke.
For all causes of death except stroke, the increased relative risk from HDP existed only for women younger than 51 years. Once HDP women passed the age of 50, their excess mortality risk was substantially muted, even in women with recurrent HDP. But for stroke mortality, the added risk persisted among older women with a history of at least two HDPs. In this subgroup, stroke deaths were nearly fourfold higher than in the matched controls.
Dr. Theilen reported having no financial disclosures.
[email protected]
On Twitter @mitchelzoler
The findings Dr. Theilen and her associates made in this study confirm results reported several decades ago that first established a link between hypertensive disease of pregnancy (HDP) and significantly reduced life expectancy. We have known for some time that HDP identifies women with a long-term mortality risk. The real question is: Can we ameliorate the risk linked with HDP?

We know that HDP requires acute management, but we are not sure how to best manage these women once they have delivered. To address that, we need prospective studies.
Not all women who experience HDP receive appropriate follow-up after delivery. We need to ensure a better handoff of women who developed HDP from the physicians who cared for these women during pregnancy to the physicians who care for these women postpartum and during the balance of their life. Ideally, a primary care physician should closely follow and manage blood pressure and other risk factors of HDP women once they are no longer pregnant.
Mary E. D’Alton, MD , is professor and chair of ob.gyn. at Columbia University Medical Center in New York City. She is on the advisory board of Merck for Mothers. She made these comments in an interview.
The findings Dr. Theilen and her associates made in this study confirm results reported several decades ago that first established a link between hypertensive disease of pregnancy (HDP) and significantly reduced life expectancy. We have known for some time that HDP identifies women with a long-term mortality risk. The real question is: Can we ameliorate the risk linked with HDP?
We know that HDP requires acute management, but we are not sure how to best manage these women once they have delivered. To address that, we need prospective studies.
Not all women who experience HDP receive appropriate follow-up after delivery. We need to ensure a better handoff of women who developed HDP from the physicians who cared for these women during pregnancy to the physicians who care for these women postpartum and during the balance of their life. Ideally, a primary care physician should closely follow and manage blood pressure and other risk factors of HDP women once they are no longer pregnant.
Mary E. D’Alton, MD , is professor and chair of ob.gyn. at Columbia University Medical Center in New York City. She is on the advisory board of Merck for Mothers. She made these comments in an interview.
The findings Dr. Theilen and her associates made in this study confirm results reported several decades ago that first established a link between hypertensive disease of pregnancy (HDP) and significantly reduced life expectancy. We have known for some time that HDP identifies women with a long-term mortality risk. The real question is: Can we ameliorate the risk linked with HDP?
We know that HDP requires acute management, but we are not sure how to best manage these women once they have delivered. To address that, we need prospective studies.
Not all women who experience HDP receive appropriate follow-up after delivery. We need to ensure a better handoff of women who developed HDP from the physicians who cared for these women during pregnancy to the physicians who care for these women postpartum and during the balance of their life. Ideally, a primary care physician should closely follow and manage blood pressure and other risk factors of HDP women once they are no longer pregnant.
Mary E. D’Alton, MD , is professor and chair of ob.gyn. at Columbia University Medical Center in New York City. She is on the advisory board of Merck for Mothers. She made these comments in an interview.
LAS VEGAS – Women who develop any form of hypertensive disease during pregnancy have a significantly increased mortality rate until they reach age 50, compared with women without the condition.
The findings, presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine, are based on a review of more than 2 million mothers who delivered babies in Utah during 1939-2012.
The relatively increased mortality rate linked with hypertensive disease of pregnancy (HDP) reached its peak during the first decade immediately following the index delivery and was dramatically higher in women for whom the index HDP was preceded by at least one earlier HDP. Increased mortality was especially elevated for certain types of deaths including stroke, diabetes, circulatory disease, and ischemic heart disease, said Lauren Theilen, MD, a maternal-fetal medicine researcher at the University of Utah in Salt Lake City.
She calculated that during the decade following an index case of HDP, life expectancy among mothers who had two or more HDP-affected pregnancies was about 49 years, life expectancy among women with a history of one HDP was 52 years, and postpartum women without HDP had a life expectancy of 55 years.
The data came from 2,083,331 singleton pregnancies delivered in Utah during 1939-2012 where the mother remained in Utah for at least 1 year following delivery. From this group, Dr. Theilen and her associates identified 67,384 women (3%) with HDP, including 49,598 women without a prior history of HDP and 7,786 with at least one prior HDP pregnancy. They included four different diagnoses as HDP: gestational hypertension, preeclampsia, HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count), or eclampsia.
The analysis excluded women with chronic hypertension, antiphospholipid syndrome, pregestational diabetes, or chronic kidney disease. It also excluded women who died within a year of the index delivery. For each of the included 67,384 cases with HDP, the researchers selected two controls with a delivery unaffected by HDP and matched them to a case by age, year of childbirth, and parity.
The women in the study were 26 years old on average. Gestational age at delivery among the HDP cases averaged 1 week less than among the controls, 37.8 weeks compared with 38.9 weeks, a statistically significant difference. Average birth weight also differed by a significant amount, 3,079 grams in the HDP neonates and 3,319 grams in the control newborns. During follow-up, 8% of the HDP women died, compared with 6% of the control women.
Analysis showed that relative mortality rates in HDP women were especially elevated for certain types of death: endocrine and metabolic, circulatory, genitourinary, infectious disease, and digestive. In most types of death, the increased risk linked with HDP was markedly higher in the women with recurrent HDP.
Dr. Theilen reported the relative risks of death for certain specific mortality causes (Am J Obstet Gynecol. 2017 Jan;216[1][suppl]:S32-3). In women with a single index case of HDP, the mortality rate compared to women with no HDP was threefold higher for diabetes, twofold higher for ischemic heart disease, and 85% higher for stroke. In women with recurrent HDP, the relative mortality risks were fourfold higher for diabetes, threefold higher for ischemic heart disease, and fivefold higher for stroke.
For all causes of death except stroke, the increased relative risk from HDP existed only for women younger than 51 years. Once HDP women passed the age of 50, their excess mortality risk was substantially muted, even in women with recurrent HDP. But for stroke mortality, the added risk persisted among older women with a history of at least two HDPs. In this subgroup, stroke deaths were nearly fourfold higher than in the matched controls.
Dr. Theilen reported having no financial disclosures.
[email protected]
On Twitter @mitchelzoler
LAS VEGAS – Women who develop any form of hypertensive disease during pregnancy have a significantly increased mortality rate until they reach age 50, compared with women without the condition.
The findings, presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine, are based on a review of more than 2 million mothers who delivered babies in Utah during 1939-2012.
The relatively increased mortality rate linked with hypertensive disease of pregnancy (HDP) reached its peak during the first decade immediately following the index delivery and was dramatically higher in women for whom the index HDP was preceded by at least one earlier HDP. Increased mortality was especially elevated for certain types of deaths including stroke, diabetes, circulatory disease, and ischemic heart disease, said Lauren Theilen, MD, a maternal-fetal medicine researcher at the University of Utah in Salt Lake City.
She calculated that during the decade following an index case of HDP, life expectancy among mothers who had two or more HDP-affected pregnancies was about 49 years, life expectancy among women with a history of one HDP was 52 years, and postpartum women without HDP had a life expectancy of 55 years.
The data came from 2,083,331 singleton pregnancies delivered in Utah during 1939-2012 where the mother remained in Utah for at least 1 year following delivery. From this group, Dr. Theilen and her associates identified 67,384 women (3%) with HDP, including 49,598 women without a prior history of HDP and 7,786 with at least one prior HDP pregnancy. They included four different diagnoses as HDP: gestational hypertension, preeclampsia, HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count), or eclampsia.
The analysis excluded women with chronic hypertension, antiphospholipid syndrome, pregestational diabetes, or chronic kidney disease. It also excluded women who died within a year of the index delivery. For each of the included 67,384 cases with HDP, the researchers selected two controls with a delivery unaffected by HDP and matched them to a case by age, year of childbirth, and parity.
The women in the study were 26 years old on average. Gestational age at delivery among the HDP cases averaged 1 week less than among the controls, 37.8 weeks compared with 38.9 weeks, a statistically significant difference. Average birth weight also differed by a significant amount, 3,079 grams in the HDP neonates and 3,319 grams in the control newborns. During follow-up, 8% of the HDP women died, compared with 6% of the control women.
Analysis showed that relative mortality rates in HDP women were especially elevated for certain types of death: endocrine and metabolic, circulatory, genitourinary, infectious disease, and digestive. In most types of death, the increased risk linked with HDP was markedly higher in the women with recurrent HDP.
Dr. Theilen reported the relative risks of death for certain specific mortality causes (Am J Obstet Gynecol. 2017 Jan;216[1][suppl]:S32-3). In women with a single index case of HDP, the mortality rate compared to women with no HDP was threefold higher for diabetes, twofold higher for ischemic heart disease, and 85% higher for stroke. In women with recurrent HDP, the relative mortality risks were fourfold higher for diabetes, threefold higher for ischemic heart disease, and fivefold higher for stroke.
For all causes of death except stroke, the increased relative risk from HDP existed only for women younger than 51 years. Once HDP women passed the age of 50, their excess mortality risk was substantially muted, even in women with recurrent HDP. But for stroke mortality, the added risk persisted among older women with a history of at least two HDPs. In this subgroup, stroke deaths were nearly fourfold higher than in the matched controls.
Dr. Theilen reported having no financial disclosures.
[email protected]
On Twitter @mitchelzoler
AT THE PREGNANCY MEETING
Key clinical point:
Major finding: Postpartum life expectancy was 49 years in women with two or more hypertensive pregnancies and 55 years in women without hypertension.
Data source: Retrospective, case-control study of 2,083,331 singleton pregnancies delivered in Utah during 1939-2012.
Disclosures: Dr. Theilen reported having no financial disclosures.
Obinutuzumab approved to treat FL in Canada

Health Canada has approved the use of obinutuzumab (Gazyva®), an anti-CD20 monoclonal antibody, in patients with follicular lymphoma (FL).
The approval means obinutuzumab can be given, first in combination with bendamustine and then alone as maintenance therapy, to FL patients who relapsed after, or are refractory to, a rituximab-containing regimen.
Obinutuzumab is also approved in Canada for use in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia.
Obinutuzumab is a product of Roche.
Health Canada’s approval of obinutuzumab in FL is based on results from the phase 3 GADOLIN trial.
The study included 413 patients with rituximab-refractory non-Hodgkin lymphoma, including 321 patients with FL, 46 with marginal zone lymphoma, and 28 with small lymphocytic lymphoma.
The patients were randomized to receive bendamustine alone (control arm) or a combination of bendamustine and obinutuzumab followed by obinutuzumab maintenance (every 2 months for 2 years or until progression).
The primary endpoint of the study was progression-free survival (PFS), as assessed by an independent review committee (IRC). The secondary endpoints were PFS assessed by investigator review, best overall response, complete response (CR), partial response (PR), duration of response, overall survival, and safety profile.
Among patients with FL, the obinutuzumab regimen improved PFS compared to bendamustine alone, as assessed by the IRC (hazard ratio [HR]=0.48, P<0.0001). The median PFS was not reached in patients receiving the obinutuzumab regimen but was 13.8 months in those receiving bendamustine alone.
Investigator-assessed PFS was consistent with IRC-assessed PFS. Investigators said the median PFS with the obinutuzumab regimen was more than double that with bendamustine alone—29.2 months vs 13.7 months (HR=0.48, P<0.0001).
The best overall response for patients receiving the obinutuzumab regimen was 78.7% (15.5% CR, 63.2% PR), compared to 74.7% (18.7% CR, 56% PR) for those receiving bendamustine alone, as assessed by the IRC.
The median duration of response was not reached for patients receiving the obinutuzumab regimen and was 11.6 months for those receiving bendamustine alone.
At last follow-up, the median overall survival had not been reached in either study arm.
The most common grade 3/4 adverse events observed in patients receiving the obinutuzumab regimen were neutropenia (33%), infusion reactions (11%), and thrombocytopenia (10%).
The most common adverse events of any grade were infusion reactions (69%), neutropenia (35%), nausea (54%), fatigue (39%), cough (26%), diarrhea (27%), constipation (19%), fever (18%), thrombocytopenia (15%), vomiting (22%), upper respiratory tract infection (13%), decreased appetite (18%), joint or muscle pain (12%), sinusitis (12%), anemia (12%), general weakness (11%), and urinary tract infection (10%). ![]()
Health Canada has approved the use of obinutuzumab (Gazyva®), an anti-CD20 monoclonal antibody, in patients with follicular lymphoma (FL).
The approval means obinutuzumab can be given, first in combination with bendamustine and then alone as maintenance therapy, to FL patients who relapsed after, or are refractory to, a rituximab-containing regimen.
Obinutuzumab is also approved in Canada for use in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia.
Obinutuzumab is a product of Roche.
Health Canada’s approval of obinutuzumab in FL is based on results from the phase 3 GADOLIN trial.
The study included 413 patients with rituximab-refractory non-Hodgkin lymphoma, including 321 patients with FL, 46 with marginal zone lymphoma, and 28 with small lymphocytic lymphoma.
The patients were randomized to receive bendamustine alone (control arm) or a combination of bendamustine and obinutuzumab followed by obinutuzumab maintenance (every 2 months for 2 years or until progression).
The primary endpoint of the study was progression-free survival (PFS), as assessed by an independent review committee (IRC). The secondary endpoints were PFS assessed by investigator review, best overall response, complete response (CR), partial response (PR), duration of response, overall survival, and safety profile.
Among patients with FL, the obinutuzumab regimen improved PFS compared to bendamustine alone, as assessed by the IRC (hazard ratio [HR]=0.48, P<0.0001). The median PFS was not reached in patients receiving the obinutuzumab regimen but was 13.8 months in those receiving bendamustine alone.
Investigator-assessed PFS was consistent with IRC-assessed PFS. Investigators said the median PFS with the obinutuzumab regimen was more than double that with bendamustine alone—29.2 months vs 13.7 months (HR=0.48, P<0.0001).
The best overall response for patients receiving the obinutuzumab regimen was 78.7% (15.5% CR, 63.2% PR), compared to 74.7% (18.7% CR, 56% PR) for those receiving bendamustine alone, as assessed by the IRC.
The median duration of response was not reached for patients receiving the obinutuzumab regimen and was 11.6 months for those receiving bendamustine alone.
At last follow-up, the median overall survival had not been reached in either study arm.
The most common grade 3/4 adverse events observed in patients receiving the obinutuzumab regimen were neutropenia (33%), infusion reactions (11%), and thrombocytopenia (10%).
The most common adverse events of any grade were infusion reactions (69%), neutropenia (35%), nausea (54%), fatigue (39%), cough (26%), diarrhea (27%), constipation (19%), fever (18%), thrombocytopenia (15%), vomiting (22%), upper respiratory tract infection (13%), decreased appetite (18%), joint or muscle pain (12%), sinusitis (12%), anemia (12%), general weakness (11%), and urinary tract infection (10%). ![]()
Health Canada has approved the use of obinutuzumab (Gazyva®), an anti-CD20 monoclonal antibody, in patients with follicular lymphoma (FL).
The approval means obinutuzumab can be given, first in combination with bendamustine and then alone as maintenance therapy, to FL patients who relapsed after, or are refractory to, a rituximab-containing regimen.
Obinutuzumab is also approved in Canada for use in combination with chlorambucil to treat patients with previously untreated chronic lymphocytic leukemia.
Obinutuzumab is a product of Roche.
Health Canada’s approval of obinutuzumab in FL is based on results from the phase 3 GADOLIN trial.
The study included 413 patients with rituximab-refractory non-Hodgkin lymphoma, including 321 patients with FL, 46 with marginal zone lymphoma, and 28 with small lymphocytic lymphoma.
The patients were randomized to receive bendamustine alone (control arm) or a combination of bendamustine and obinutuzumab followed by obinutuzumab maintenance (every 2 months for 2 years or until progression).
The primary endpoint of the study was progression-free survival (PFS), as assessed by an independent review committee (IRC). The secondary endpoints were PFS assessed by investigator review, best overall response, complete response (CR), partial response (PR), duration of response, overall survival, and safety profile.
Among patients with FL, the obinutuzumab regimen improved PFS compared to bendamustine alone, as assessed by the IRC (hazard ratio [HR]=0.48, P<0.0001). The median PFS was not reached in patients receiving the obinutuzumab regimen but was 13.8 months in those receiving bendamustine alone.
Investigator-assessed PFS was consistent with IRC-assessed PFS. Investigators said the median PFS with the obinutuzumab regimen was more than double that with bendamustine alone—29.2 months vs 13.7 months (HR=0.48, P<0.0001).
The best overall response for patients receiving the obinutuzumab regimen was 78.7% (15.5% CR, 63.2% PR), compared to 74.7% (18.7% CR, 56% PR) for those receiving bendamustine alone, as assessed by the IRC.
The median duration of response was not reached for patients receiving the obinutuzumab regimen and was 11.6 months for those receiving bendamustine alone.
At last follow-up, the median overall survival had not been reached in either study arm.
The most common grade 3/4 adverse events observed in patients receiving the obinutuzumab regimen were neutropenia (33%), infusion reactions (11%), and thrombocytopenia (10%).
The most common adverse events of any grade were infusion reactions (69%), neutropenia (35%), nausea (54%), fatigue (39%), cough (26%), diarrhea (27%), constipation (19%), fever (18%), thrombocytopenia (15%), vomiting (22%), upper respiratory tract infection (13%), decreased appetite (18%), joint or muscle pain (12%), sinusitis (12%), anemia (12%), general weakness (11%), and urinary tract infection (10%). ![]()
US-trained docs have higher patient death rate

Photo courtesy of the CDC
A large study has revealed a lower death rate among US patients treated by internationally trained doctors rather than US-trained doctors.
Researchers
analyzed data on more than 1.2 million US hospital admissions and found
a slight but statistically significant difference in 30-day mortality
for patients treated by internationally trained doctors and US-trained
doctors—11.2% and
11.6%, respectively (P<0.001).
These findings were published in The BMJ.
Yusuke Tsugawa, MD, PhD, of Harvard T H Chan School of Public Health in Boston, Massachusetts, and his colleagues conducted this research.
The team wanted to determine whether patient outcomes differ between general internists who graduated from a medical school outside the US and those who graduated from a US medical school.
The researchers analyzed data on the treatment of Medicare beneficiaries (age 65 and older) who were admitted to a hospital with a medical condition from 2011 through 2014. This included 1,215,490 hospital admissions and 44,227 general internists.
The primary outcome was 30-day patient mortality. Secondary outcomes were 30-day readmission rates and costs of care.
Compared with patients treated by US graduates, patients treated by international graduates had slightly more chronic conditions.
After adjusting for factors that could have affected the results (including patient characteristics, physician characteristics, and hospital fixed effects), the researchers found that patients cared for by international graduates had a lower rate of 30-day mortality than patients cared for by US graduates (11.2% and
11.6%, respectively, P<0.001).
The researchers said that for every 250 patients treated by US medical graduates, 1 patient’s life would be saved if the quality of care were equivalent between the international graduates and US graduates.
Thirty-day readmission rates did not differ significantly between the 2 types of graduates—15.4% for international graduates and 15.5% for US graduates (P=0.54).
However, the cost of care per admission was higher for international medical graduates—$1145 vs $1098 (P<0.001).
Further analysis to test the strength of these results made no difference to the overall findings.
One possible explanation for these findings, according to the researchers, is that the current approach for allowing international medical graduates to practice in the US may select for, on average, better physicians.
The team stressed that this is an observational study, so no firm conclusions can be drawn about cause and effect. Nevertheless, they said their findings “should reassure policymakers and the public that our current approach to licensing international medical graduates in the US is sufficiently rigorous to ensure high quality care.” ![]()
Photo courtesy of the CDC
A large study has revealed a lower death rate among US patients treated by internationally trained doctors rather than US-trained doctors.
Researchers
analyzed data on more than 1.2 million US hospital admissions and found
a slight but statistically significant difference in 30-day mortality
for patients treated by internationally trained doctors and US-trained
doctors—11.2% and
11.6%, respectively (P<0.001).
These findings were published in The BMJ.
Yusuke Tsugawa, MD, PhD, of Harvard T H Chan School of Public Health in Boston, Massachusetts, and his colleagues conducted this research.
The team wanted to determine whether patient outcomes differ between general internists who graduated from a medical school outside the US and those who graduated from a US medical school.
The researchers analyzed data on the treatment of Medicare beneficiaries (age 65 and older) who were admitted to a hospital with a medical condition from 2011 through 2014. This included 1,215,490 hospital admissions and 44,227 general internists.
The primary outcome was 30-day patient mortality. Secondary outcomes were 30-day readmission rates and costs of care.
Compared with patients treated by US graduates, patients treated by international graduates had slightly more chronic conditions.
After adjusting for factors that could have affected the results (including patient characteristics, physician characteristics, and hospital fixed effects), the researchers found that patients cared for by international graduates had a lower rate of 30-day mortality than patients cared for by US graduates (11.2% and
11.6%, respectively, P<0.001).
The researchers said that for every 250 patients treated by US medical graduates, 1 patient’s life would be saved if the quality of care were equivalent between the international graduates and US graduates.
Thirty-day readmission rates did not differ significantly between the 2 types of graduates—15.4% for international graduates and 15.5% for US graduates (P=0.54).
However, the cost of care per admission was higher for international medical graduates—$1145 vs $1098 (P<0.001).
Further analysis to test the strength of these results made no difference to the overall findings.
One possible explanation for these findings, according to the researchers, is that the current approach for allowing international medical graduates to practice in the US may select for, on average, better physicians.
The team stressed that this is an observational study, so no firm conclusions can be drawn about cause and effect. Nevertheless, they said their findings “should reassure policymakers and the public that our current approach to licensing international medical graduates in the US is sufficiently rigorous to ensure high quality care.” ![]()
Photo courtesy of the CDC
A large study has revealed a lower death rate among US patients treated by internationally trained doctors rather than US-trained doctors.
Researchers
analyzed data on more than 1.2 million US hospital admissions and found
a slight but statistically significant difference in 30-day mortality
for patients treated by internationally trained doctors and US-trained
doctors—11.2% and
11.6%, respectively (P<0.001).
These findings were published in The BMJ.
Yusuke Tsugawa, MD, PhD, of Harvard T H Chan School of Public Health in Boston, Massachusetts, and his colleagues conducted this research.
The team wanted to determine whether patient outcomes differ between general internists who graduated from a medical school outside the US and those who graduated from a US medical school.
The researchers analyzed data on the treatment of Medicare beneficiaries (age 65 and older) who were admitted to a hospital with a medical condition from 2011 through 2014. This included 1,215,490 hospital admissions and 44,227 general internists.
The primary outcome was 30-day patient mortality. Secondary outcomes were 30-day readmission rates and costs of care.
Compared with patients treated by US graduates, patients treated by international graduates had slightly more chronic conditions.
After adjusting for factors that could have affected the results (including patient characteristics, physician characteristics, and hospital fixed effects), the researchers found that patients cared for by international graduates had a lower rate of 30-day mortality than patients cared for by US graduates (11.2% and
11.6%, respectively, P<0.001).
The researchers said that for every 250 patients treated by US medical graduates, 1 patient’s life would be saved if the quality of care were equivalent between the international graduates and US graduates.
Thirty-day readmission rates did not differ significantly between the 2 types of graduates—15.4% for international graduates and 15.5% for US graduates (P=0.54).
However, the cost of care per admission was higher for international medical graduates—$1145 vs $1098 (P<0.001).
Further analysis to test the strength of these results made no difference to the overall findings.
One possible explanation for these findings, according to the researchers, is that the current approach for allowing international medical graduates to practice in the US may select for, on average, better physicians.
The team stressed that this is an observational study, so no firm conclusions can be drawn about cause and effect. Nevertheless, they said their findings “should reassure policymakers and the public that our current approach to licensing international medical graduates in the US is sufficiently rigorous to ensure high quality care.” ![]()
Sickle cell trait may confound blood sugar readings

Photo by Juan D. Alfonso
A new study suggests that hemoglobin A1c (HbA1c), a biomarker used to measure blood sugar over time, may not perform as accurately among African-Americans with sickle cell trait (SCT) and could be leading to a systemic underestimation of blood sugar control in that population.
Researchers analyzed data from more than 4600 people and found that HbA1c readings were significantly lower in individuals with SCT than in those without it, even after accounting for several possible confounding factors.
The team reported these findings in JAMA.
“We found that HbA1c was systematically lower in African-Americans with sickle cell trait than those without sickle cell trait, despite similar blood sugar measurements using other tests,” said study author Mary Lacy, a doctoral candidate at the Brown University School of Public Health in Providence, Rhode Island.
“We might be missing an opportunity for diagnosis and treatment of a serious disease.”
Lacy and her co-authors found that using standard clinical HbA1c cutoffs resulted in identifying 40% fewer potential cases of prediabetes and 48% fewer potential cases of diabetes in people with SCT than in people without SCT.
However, when the researchers used other blood glucose measures as the diagnostic criteria, they found no significant difference in the likelihood of diabetes and prediabetes among patients with or without SCT.
The questions the study raises about using HbA1c among SCT carriers matter for treatment as well as diagnosis, said study author Wen-Chih Wu, MD, of Brown University.
“The clinical implications of these results are highly relevant,” Dr Wu said. “For patients with diabetes, HbA1c is often used as a marker of how well they are managing their diabetes, so having an underestimation of their blood sugars is problematic because they might have a false sense of security, thinking they are doing okay when they are not.”
Study details
For this study, the researchers analyzed data from 2 major public health studies—the Coronary Artery Risk Development in Young Adults (CARDIA) study and the Jackson Heart Study (JHS). Of the 4620 participants included in the analysis, 367 had SCT.
Among all the patients included in the analysis, HbA1c readings came from either of 2 widely used, clinically accepted assays made by Tosoh Bioscience Inc. that rely on a process called high-performance liquid chromatography.
In addition to those measures, the researchers also compared fasting and 2-hour blood glucose and statistically controlled for demographic and medical factors, such as gender, age, body-mass index, whether diabetes had already been diagnosed, and whether it was being treated.
Study author Gregory Wellenius, ScD, of Brown University, said the study’s scale and breadth allowed for the most definitive comparison to date of HbA1c readings in patients with and without SCT. Two previous, smaller studies had not detected a similar discrepancy.
“The strengths of the study are that it’s the largest sample size ever used, it’s across 2 different studies with somewhat different populations, and it’s a more thorough evaluation than prior studies,” Dr Wellenius said.
While the study showed that HbA1c readings were significantly different between people with and without SCT, it also showed that blood glucose readings were not, suggesting that glucose metabolism is not necessarily different between the 2 groups, as the HbA1c readings alone would suggest.
Implications for practice
The study does not explain why the HbA1c readings differ. While it could be related to the assay method, which is approved by the NGSP (formerly National Glycohemoglobin Standardization Program) for use in patients with SCT, it could also be a consequence of the underlying biology of SCT.
Hypothetically, according to the researchers, if the hemoglobin variant of the trait endows red blood cells with a shorter lifespan, the cells’ hemoglobin would carry less accumulated blood glucose, leading to falsely low HbA1c readings.
“Irrespective of the reason of the underestimation, the underestimation is very real, and clinicians should consider screening for sickle cell trait and account for the difference in HbA1c,” Dr Wu said.
Yet not many people with SCT in the US know they carry the variant, especially those born before routine screenings at birth began, Lacy said.
The researchers therefore recommend that practitioners following African-American patients whose HbA1c levels are within 0.3 percentage points of a diagnostic cutoff also consider using additional blood glucose measures. Current diagnostic thresholds for A1C are ≥5.7% for prediabetes and ≥6.5% for diabetes. ![]()
Photo by Juan D. Alfonso
A new study suggests that hemoglobin A1c (HbA1c), a biomarker used to measure blood sugar over time, may not perform as accurately among African-Americans with sickle cell trait (SCT) and could be leading to a systemic underestimation of blood sugar control in that population.
Researchers analyzed data from more than 4600 people and found that HbA1c readings were significantly lower in individuals with SCT than in those without it, even after accounting for several possible confounding factors.
The team reported these findings in JAMA.
“We found that HbA1c was systematically lower in African-Americans with sickle cell trait than those without sickle cell trait, despite similar blood sugar measurements using other tests,” said study author Mary Lacy, a doctoral candidate at the Brown University School of Public Health in Providence, Rhode Island.
“We might be missing an opportunity for diagnosis and treatment of a serious disease.”
Lacy and her co-authors found that using standard clinical HbA1c cutoffs resulted in identifying 40% fewer potential cases of prediabetes and 48% fewer potential cases of diabetes in people with SCT than in people without SCT.
However, when the researchers used other blood glucose measures as the diagnostic criteria, they found no significant difference in the likelihood of diabetes and prediabetes among patients with or without SCT.
The questions the study raises about using HbA1c among SCT carriers matter for treatment as well as diagnosis, said study author Wen-Chih Wu, MD, of Brown University.
“The clinical implications of these results are highly relevant,” Dr Wu said. “For patients with diabetes, HbA1c is often used as a marker of how well they are managing their diabetes, so having an underestimation of their blood sugars is problematic because they might have a false sense of security, thinking they are doing okay when they are not.”
Study details
For this study, the researchers analyzed data from 2 major public health studies—the Coronary Artery Risk Development in Young Adults (CARDIA) study and the Jackson Heart Study (JHS). Of the 4620 participants included in the analysis, 367 had SCT.
Among all the patients included in the analysis, HbA1c readings came from either of 2 widely used, clinically accepted assays made by Tosoh Bioscience Inc. that rely on a process called high-performance liquid chromatography.
In addition to those measures, the researchers also compared fasting and 2-hour blood glucose and statistically controlled for demographic and medical factors, such as gender, age, body-mass index, whether diabetes had already been diagnosed, and whether it was being treated.
Study author Gregory Wellenius, ScD, of Brown University, said the study’s scale and breadth allowed for the most definitive comparison to date of HbA1c readings in patients with and without SCT. Two previous, smaller studies had not detected a similar discrepancy.
“The strengths of the study are that it’s the largest sample size ever used, it’s across 2 different studies with somewhat different populations, and it’s a more thorough evaluation than prior studies,” Dr Wellenius said.
While the study showed that HbA1c readings were significantly different between people with and without SCT, it also showed that blood glucose readings were not, suggesting that glucose metabolism is not necessarily different between the 2 groups, as the HbA1c readings alone would suggest.
Implications for practice
The study does not explain why the HbA1c readings differ. While it could be related to the assay method, which is approved by the NGSP (formerly National Glycohemoglobin Standardization Program) for use in patients with SCT, it could also be a consequence of the underlying biology of SCT.
Hypothetically, according to the researchers, if the hemoglobin variant of the trait endows red blood cells with a shorter lifespan, the cells’ hemoglobin would carry less accumulated blood glucose, leading to falsely low HbA1c readings.
“Irrespective of the reason of the underestimation, the underestimation is very real, and clinicians should consider screening for sickle cell trait and account for the difference in HbA1c,” Dr Wu said.
Yet not many people with SCT in the US know they carry the variant, especially those born before routine screenings at birth began, Lacy said.
The researchers therefore recommend that practitioners following African-American patients whose HbA1c levels are within 0.3 percentage points of a diagnostic cutoff also consider using additional blood glucose measures. Current diagnostic thresholds for A1C are ≥5.7% for prediabetes and ≥6.5% for diabetes. ![]()
Photo by Juan D. Alfonso
A new study suggests that hemoglobin A1c (HbA1c), a biomarker used to measure blood sugar over time, may not perform as accurately among African-Americans with sickle cell trait (SCT) and could be leading to a systemic underestimation of blood sugar control in that population.
Researchers analyzed data from more than 4600 people and found that HbA1c readings were significantly lower in individuals with SCT than in those without it, even after accounting for several possible confounding factors.
The team reported these findings in JAMA.
“We found that HbA1c was systematically lower in African-Americans with sickle cell trait than those without sickle cell trait, despite similar blood sugar measurements using other tests,” said study author Mary Lacy, a doctoral candidate at the Brown University School of Public Health in Providence, Rhode Island.
“We might be missing an opportunity for diagnosis and treatment of a serious disease.”
Lacy and her co-authors found that using standard clinical HbA1c cutoffs resulted in identifying 40% fewer potential cases of prediabetes and 48% fewer potential cases of diabetes in people with SCT than in people without SCT.
However, when the researchers used other blood glucose measures as the diagnostic criteria, they found no significant difference in the likelihood of diabetes and prediabetes among patients with or without SCT.
The questions the study raises about using HbA1c among SCT carriers matter for treatment as well as diagnosis, said study author Wen-Chih Wu, MD, of Brown University.
“The clinical implications of these results are highly relevant,” Dr Wu said. “For patients with diabetes, HbA1c is often used as a marker of how well they are managing their diabetes, so having an underestimation of their blood sugars is problematic because they might have a false sense of security, thinking they are doing okay when they are not.”
Study details
For this study, the researchers analyzed data from 2 major public health studies—the Coronary Artery Risk Development in Young Adults (CARDIA) study and the Jackson Heart Study (JHS). Of the 4620 participants included in the analysis, 367 had SCT.
Among all the patients included in the analysis, HbA1c readings came from either of 2 widely used, clinically accepted assays made by Tosoh Bioscience Inc. that rely on a process called high-performance liquid chromatography.
In addition to those measures, the researchers also compared fasting and 2-hour blood glucose and statistically controlled for demographic and medical factors, such as gender, age, body-mass index, whether diabetes had already been diagnosed, and whether it was being treated.
Study author Gregory Wellenius, ScD, of Brown University, said the study’s scale and breadth allowed for the most definitive comparison to date of HbA1c readings in patients with and without SCT. Two previous, smaller studies had not detected a similar discrepancy.
“The strengths of the study are that it’s the largest sample size ever used, it’s across 2 different studies with somewhat different populations, and it’s a more thorough evaluation than prior studies,” Dr Wellenius said.
While the study showed that HbA1c readings were significantly different between people with and without SCT, it also showed that blood glucose readings were not, suggesting that glucose metabolism is not necessarily different between the 2 groups, as the HbA1c readings alone would suggest.
Implications for practice
The study does not explain why the HbA1c readings differ. While it could be related to the assay method, which is approved by the NGSP (formerly National Glycohemoglobin Standardization Program) for use in patients with SCT, it could also be a consequence of the underlying biology of SCT.
Hypothetically, according to the researchers, if the hemoglobin variant of the trait endows red blood cells with a shorter lifespan, the cells’ hemoglobin would carry less accumulated blood glucose, leading to falsely low HbA1c readings.
“Irrespective of the reason of the underestimation, the underestimation is very real, and clinicians should consider screening for sickle cell trait and account for the difference in HbA1c,” Dr Wu said.
Yet not many people with SCT in the US know they carry the variant, especially those born before routine screenings at birth began, Lacy said.
The researchers therefore recommend that practitioners following African-American patients whose HbA1c levels are within 0.3 percentage points of a diagnostic cutoff also consider using additional blood glucose measures. Current diagnostic thresholds for A1C are ≥5.7% for prediabetes and ≥6.5% for diabetes. ![]()
‘Alternative’ BMT deemed ‘promising’ for SAA

Photo by Chad McNeeley
Researchers have reported a “promising” treatment approach for
refractory, severe aplastic anemia (SAA).
The
regimen consists of nonmyeloablative conditioning, bone marrow
transplants (BMTs) from “alternative” donors, and graft-vs-host disease
(GVHD) prophylaxis.
All 16 SAA patients who received this treatment
achieved engraftment and were completely cleared of disease.
There were 2 cases of acute and chronic GVHD, but they resolved.
All patients were ultimately able to stop immunosuppressive therapy.
Robert Brodsky, MD, of Sidney Kimmel Cancer Center in Baltimore, Maryland, and his colleagues reported these findings in Biology of Blood and Marrow Transplantation.
“Our findings have the potential to greatly widen treatment options for the vast majority of severe aplastic anemia patients,” Dr Brodsky said.
He and his colleagues tested their approach in 16 SAA patients between 11 and 69 years of age. Each of the patients had failed to respond to immunosuppressive therapy and other treatments.
The patients received conditioning with antithymocyte globulin, fludarabine, low-dose cyclophosphamide, and total body irradiation.
They then received BMTs. Thirteen of the donors were haploidentical related, 2 were fully matched unrelated, and 1 was mismatched unrelated.
Three and 4 days after BMT, the patients received cyclophosphamide at 50 mg/kg/day as GVHD prophylaxis. They then received mycophenolate mofetil on days 5 through 35 and tacrolimus from day 5 through 1 year.
The median time to neutrophil recovery (over 1000 × 103/mm3 for 3 consecutive days) was 19 days (range, 16 to 27). The median time to red cell engraftment was 25 days (range, 2 to 58). And the median time to the last platelet transfusion (to keep platelet counts over 50 × 103/mm3) was 27.5 days (range, 22 to 108).
At a median follow-up of 21 months (range, 3 to 64), all 16 patients were still alive, disease-free, and no longer required transfusions.
Two patients did develop grade 1/2 acute skin GVHD. They also had mild chronic GVHD of the skin/mouth, which required systemic steroids.
One of these patients was able to come off all immunosuppressive therapy by 15 months, and the other was able to do so by 17 months. All of the other patients stopped immunosuppressive therapy at 1 year.
Ending all therapy related to their disease has been life-changing for these patients, said study author Amy DeZern, MD, also of the Sidney Kimmel Cancer Center.
“It’s like night and day,” she said. “They go from not knowing if they have a future to hoping for what they’d hoped for before they got sick. It’s that transformative.”
Successful BMTs using partially matched donors open up the transplant option to nearly all patients with SAA, especially minority patients, added Dr Brodsky.
“Now, a therapy that used to be available to 25% to 30% of patients with severe aplastic anemia is potentially available to more than 95%,” he said. ![]()
Photo by Chad McNeeley
Researchers have reported a “promising” treatment approach for
refractory, severe aplastic anemia (SAA).
The
regimen consists of nonmyeloablative conditioning, bone marrow
transplants (BMTs) from “alternative” donors, and graft-vs-host disease
(GVHD) prophylaxis.
All 16 SAA patients who received this treatment
achieved engraftment and were completely cleared of disease.
There were 2 cases of acute and chronic GVHD, but they resolved.
All patients were ultimately able to stop immunosuppressive therapy.
Robert Brodsky, MD, of Sidney Kimmel Cancer Center in Baltimore, Maryland, and his colleagues reported these findings in Biology of Blood and Marrow Transplantation.
“Our findings have the potential to greatly widen treatment options for the vast majority of severe aplastic anemia patients,” Dr Brodsky said.
He and his colleagues tested their approach in 16 SAA patients between 11 and 69 years of age. Each of the patients had failed to respond to immunosuppressive therapy and other treatments.
The patients received conditioning with antithymocyte globulin, fludarabine, low-dose cyclophosphamide, and total body irradiation.
They then received BMTs. Thirteen of the donors were haploidentical related, 2 were fully matched unrelated, and 1 was mismatched unrelated.
Three and 4 days after BMT, the patients received cyclophosphamide at 50 mg/kg/day as GVHD prophylaxis. They then received mycophenolate mofetil on days 5 through 35 and tacrolimus from day 5 through 1 year.
The median time to neutrophil recovery (over 1000 × 103/mm3 for 3 consecutive days) was 19 days (range, 16 to 27). The median time to red cell engraftment was 25 days (range, 2 to 58). And the median time to the last platelet transfusion (to keep platelet counts over 50 × 103/mm3) was 27.5 days (range, 22 to 108).
At a median follow-up of 21 months (range, 3 to 64), all 16 patients were still alive, disease-free, and no longer required transfusions.
Two patients did develop grade 1/2 acute skin GVHD. They also had mild chronic GVHD of the skin/mouth, which required systemic steroids.
One of these patients was able to come off all immunosuppressive therapy by 15 months, and the other was able to do so by 17 months. All of the other patients stopped immunosuppressive therapy at 1 year.
Ending all therapy related to their disease has been life-changing for these patients, said study author Amy DeZern, MD, also of the Sidney Kimmel Cancer Center.
“It’s like night and day,” she said. “They go from not knowing if they have a future to hoping for what they’d hoped for before they got sick. It’s that transformative.”
Successful BMTs using partially matched donors open up the transplant option to nearly all patients with SAA, especially minority patients, added Dr Brodsky.
“Now, a therapy that used to be available to 25% to 30% of patients with severe aplastic anemia is potentially available to more than 95%,” he said. ![]()
Photo by Chad McNeeley
Researchers have reported a “promising” treatment approach for
refractory, severe aplastic anemia (SAA).
The
regimen consists of nonmyeloablative conditioning, bone marrow
transplants (BMTs) from “alternative” donors, and graft-vs-host disease
(GVHD) prophylaxis.
All 16 SAA patients who received this treatment
achieved engraftment and were completely cleared of disease.
There were 2 cases of acute and chronic GVHD, but they resolved.
All patients were ultimately able to stop immunosuppressive therapy.
Robert Brodsky, MD, of Sidney Kimmel Cancer Center in Baltimore, Maryland, and his colleagues reported these findings in Biology of Blood and Marrow Transplantation.
“Our findings have the potential to greatly widen treatment options for the vast majority of severe aplastic anemia patients,” Dr Brodsky said.
He and his colleagues tested their approach in 16 SAA patients between 11 and 69 years of age. Each of the patients had failed to respond to immunosuppressive therapy and other treatments.
The patients received conditioning with antithymocyte globulin, fludarabine, low-dose cyclophosphamide, and total body irradiation.
They then received BMTs. Thirteen of the donors were haploidentical related, 2 were fully matched unrelated, and 1 was mismatched unrelated.
Three and 4 days after BMT, the patients received cyclophosphamide at 50 mg/kg/day as GVHD prophylaxis. They then received mycophenolate mofetil on days 5 through 35 and tacrolimus from day 5 through 1 year.
The median time to neutrophil recovery (over 1000 × 103/mm3 for 3 consecutive days) was 19 days (range, 16 to 27). The median time to red cell engraftment was 25 days (range, 2 to 58). And the median time to the last platelet transfusion (to keep platelet counts over 50 × 103/mm3) was 27.5 days (range, 22 to 108).
At a median follow-up of 21 months (range, 3 to 64), all 16 patients were still alive, disease-free, and no longer required transfusions.
Two patients did develop grade 1/2 acute skin GVHD. They also had mild chronic GVHD of the skin/mouth, which required systemic steroids.
One of these patients was able to come off all immunosuppressive therapy by 15 months, and the other was able to do so by 17 months. All of the other patients stopped immunosuppressive therapy at 1 year.
Ending all therapy related to their disease has been life-changing for these patients, said study author Amy DeZern, MD, also of the Sidney Kimmel Cancer Center.
“It’s like night and day,” she said. “They go from not knowing if they have a future to hoping for what they’d hoped for before they got sick. It’s that transformative.”
Successful BMTs using partially matched donors open up the transplant option to nearly all patients with SAA, especially minority patients, added Dr Brodsky.
“Now, a therapy that used to be available to 25% to 30% of patients with severe aplastic anemia is potentially available to more than 95%,” he said. ![]()
Food Insecurity Among Veterans
Nearly half of a group of homeless and formerly homeless veterans reported experiencing food insecurity, according to VA researchers. More than one-quarter of those said they’d averaged only 1 meal a day.
Researchers screened 270 new patients who enrolled in 1 of 6 VA primary care clinics. Screening began with a single question: “In the past month, were there times when the food for you just did not last, and there was no money to buy more?” Patients who answered yes were then asked where they got their food, how many meals per day they ate, whether they prepared their meals, whether they received food stamps, whether they had diabetes, and whether they had symptoms of hypoglycemia.
Of the respondents, 63% were living in their own apartment, and 26% were in a transitional housing program where they were responsible for some of their meals. Of the patients who reported food insecurity, 87% prepared their meals, with half relying on food they bought, 23% on food from soup kitchens and food pantries, 15% from shelters, 19% from family and friends. About half (47%) were receiving food stamps.
One-fifth of the patients had diabetes or prediabetes, and 44% reported hypoglycemia symptoms when without food. The researchers point out that the consequences of food insecurity are “significant and potentially life threatening.” They cite another study that found risk for hospital admissions for hypoglycemia rose 27% in the last week of the month among low-income populations, typically when food stamps and supplies at food pantries ran low or were exhausted.
The study revealed that asking about only food insecurity was not enough, the researchers say. “The additional context provided by the follow-up questions and the breadth of different responses underscored that the needs of these patients extend beyond those available from 1 health care provider or 1 health care discipline.”
Both patients and health care providers endorsed the screening program. One staff member, for instance, called the program a good rapport builder. No team found the questions burdensome, the researchers say. In fact,4 teams said the follow-up questions highlighted the complexity of issues underlying food insecurity and the need for a well-integrated, multidisciplinary approach to the problem.
Nearly half of a group of homeless and formerly homeless veterans reported experiencing food insecurity, according to VA researchers. More than one-quarter of those said they’d averaged only 1 meal a day.
Researchers screened 270 new patients who enrolled in 1 of 6 VA primary care clinics. Screening began with a single question: “In the past month, were there times when the food for you just did not last, and there was no money to buy more?” Patients who answered yes were then asked where they got their food, how many meals per day they ate, whether they prepared their meals, whether they received food stamps, whether they had diabetes, and whether they had symptoms of hypoglycemia.
Of the respondents, 63% were living in their own apartment, and 26% were in a transitional housing program where they were responsible for some of their meals. Of the patients who reported food insecurity, 87% prepared their meals, with half relying on food they bought, 23% on food from soup kitchens and food pantries, 15% from shelters, 19% from family and friends. About half (47%) were receiving food stamps.
One-fifth of the patients had diabetes or prediabetes, and 44% reported hypoglycemia symptoms when without food. The researchers point out that the consequences of food insecurity are “significant and potentially life threatening.” They cite another study that found risk for hospital admissions for hypoglycemia rose 27% in the last week of the month among low-income populations, typically when food stamps and supplies at food pantries ran low or were exhausted.
The study revealed that asking about only food insecurity was not enough, the researchers say. “The additional context provided by the follow-up questions and the breadth of different responses underscored that the needs of these patients extend beyond those available from 1 health care provider or 1 health care discipline.”
Both patients and health care providers endorsed the screening program. One staff member, for instance, called the program a good rapport builder. No team found the questions burdensome, the researchers say. In fact,4 teams said the follow-up questions highlighted the complexity of issues underlying food insecurity and the need for a well-integrated, multidisciplinary approach to the problem.
Nearly half of a group of homeless and formerly homeless veterans reported experiencing food insecurity, according to VA researchers. More than one-quarter of those said they’d averaged only 1 meal a day.
Researchers screened 270 new patients who enrolled in 1 of 6 VA primary care clinics. Screening began with a single question: “In the past month, were there times when the food for you just did not last, and there was no money to buy more?” Patients who answered yes were then asked where they got their food, how many meals per day they ate, whether they prepared their meals, whether they received food stamps, whether they had diabetes, and whether they had symptoms of hypoglycemia.
Of the respondents, 63% were living in their own apartment, and 26% were in a transitional housing program where they were responsible for some of their meals. Of the patients who reported food insecurity, 87% prepared their meals, with half relying on food they bought, 23% on food from soup kitchens and food pantries, 15% from shelters, 19% from family and friends. About half (47%) were receiving food stamps.
One-fifth of the patients had diabetes or prediabetes, and 44% reported hypoglycemia symptoms when without food. The researchers point out that the consequences of food insecurity are “significant and potentially life threatening.” They cite another study that found risk for hospital admissions for hypoglycemia rose 27% in the last week of the month among low-income populations, typically when food stamps and supplies at food pantries ran low or were exhausted.
The study revealed that asking about only food insecurity was not enough, the researchers say. “The additional context provided by the follow-up questions and the breadth of different responses underscored that the needs of these patients extend beyond those available from 1 health care provider or 1 health care discipline.”
Both patients and health care providers endorsed the screening program. One staff member, for instance, called the program a good rapport builder. No team found the questions burdensome, the researchers say. In fact,4 teams said the follow-up questions highlighted the complexity of issues underlying food insecurity and the need for a well-integrated, multidisciplinary approach to the problem.