User login
Get With the Guidelines propels stroke thrombolytic therapy
HOUSTON – Thrombolytic therapy for U.S. patients experiencing an acute ischemic stroke is no longer the poster child for proven, but neglected, therapies.
Long bemoaned since its introduction in the mid-1990s as an effective but woefully underused treatment, thrombolytic therapy with tissue plasminogen activator (tPA) has seen robust growth in U.S. practice recently, largely due to the promotion and quality-improvement efforts of a voluntary, non-profit program, Get With the Guidelines (GWTG)-Stroke.
“We’ve seen a dramatic increase in tPA treatment in eligible patients,” said Dr. Smith, a neurologist and medical director of the Cognitive Neurosciences Clinic at the University of Calgary (Alta.).
“This represents remarkable and clinically meaningful improvements in stroke care, overcoming substantial barriers using a systems of care approach,” Gregg C. Fonarow, MD, professor of medicine and cochief of clinical cardiology at the University of California, Los Angeles and one of the long-time leaders of GWTG-Stroke, said in an interview. “This represents one of the most transformative improvements and success stories ever observed in stroke care.”
“These data show dramatic changes in the GWTG-Stroke hospitals,” agreed Lee H. Schwamm, MD, professor of neurology at Harvard Medical School and chief of stroke services at Massachusetts General Hospital in Boston and another leader of the GWTG-Stroke program. However, “we still have work to do,” cautioned Dr. Schwamm, who notes that 68% remains significantly short of the ideal 100%. The positive is that several GWTG-Stroke participating hospitals have surged to a better than 90% rate of administering tPA to eligible patients within a 60-minute door-to-needle window.

What is GWTG-Stroke?
GWTG was launched in 2000 by the American Heart Association as a hospital-based–quality improvement initiative focused on U.S. management of acute MI. In 2003, acute stroke became another focus of the program and inspired added participation of the American Stroke Association.
“Improvements in tPA use in eligible patients were seen soon after the introduction of GWTG-Stroke in 2003, but there was minimal improvement in the percentage of patients with door-to-needle times within 60 minutes despite national guidelines,” recalled Dr. Fonarow. This slow rate of advance led him, Dr. Schwamm, and others to create a more activist program within GWTG-Stroke, Target Stroke, that not only provided resources and collected data from participating hospitals but also set acute-treatment goals that challenged participating hospitals to up their game. Target Stroke phase I asked them to try to achieve a tPA door-to-needle time within 60 minutes in at least 50% of eligible patients. By mid-2013, the program reached this goal with 53% of patients treated in the allotted time frame (JAMA. 2014 Apr 23;311[16]:1632-40).
These time-based goals lead directly to meaningful improvements in patient outcomes. “We know that, for every 15 minute reduction in tPA door-to-needle time, there is a 5% reduction of in-hospital mortality and a substantial increase in the percentage of patients who are discharged home instead of to a rehabilitation hospital or nursing home,” Dr. Schwamm said.
Dr. Smith highlighted the 11 best practices steps that Target Stroke promotes to GWTG-Stroke hospitals as their road map to achieving the performance goals. These include things such as notification of a hospital by emergency medical services that a patient showing signs of an acute ischemic stroke is on the way, transfer of the patient after hospital arrival directly to a CT or MRI scanner to get the imaging that can confirm tPA eligibility, rapid reading of the scan, premixing of the tPA, a team-based approach to acute stroke management, and quick feedback to the team regarding their performance on each stroke patient they treat.
Dr. Schwamm noted that he, Dr. Fonarow, and other program leaders are already planning a phase III for Target Stroke that will branch out to even more facets of acute stroke care, such as incorporation of goals for using endovascular thrombectomy in appropriate patients and for using telemedicine to quicken and broaden the availability of expert neurologic consults for identifying tPA- and thrombectomy-eligible patients.
Growing the program
The success of GWTG-Stroke in transforming U.S. acute stroke care has not only relied on setting aggressive performance goals but also on advancing by boosting the number of U.S. hospitals participating of more U.S. hospitals. During the Target Stroke years since the start of 2010, the number of hospitals active in GWTG-Stroke jumped from 1427 to 1,950 by mid-2016, including a 12% year-over-year jump in 2016, compared with 2015. During October 2015-October 2016, participating hospitals treated more than 570,000 acute stroke patients, or roughly 71% of the estimated 800,000 U.S. patients who have an acute stroke each year.
These numbers seem on track to continue expanding. “With the recent evidence showing that participating in GWTG-Stroke improves care and outcomes there has been even greater interest by hospitals, recently, in joining,” said Dr. Fonarow. “While many hospitals currently participate, ideally all would join and be active.”
“Hospitals now feel that they can’t afford not to focus on stroke as a quality improvement program, so they join,” said Dr. Schwamm. He believes that essentially all of the roughly 200 certified U.S. Comprehensive Stroke Centers and of the roughly 1,000 certified U.S. Primary Stroke Centers are already members of GWTG-Stroke. “We’re now in all the high-value hospitals, based on their higher numbers of patients. It’s the Acute Stroke Ready hospitals where we now have the greatest potential to penetrate, hospitals that generally treat about 20-50 stroke patients a year,” he said.
Joining GWTG-Stroke holds major attraction for hospitals because the program gives them a tool for measuring their performance, data that hospitals often now need to prove the value of the care they deliver to insurers and to avoid penalization for readmissions. However, the barrier to hospitals, especially smaller hospitals, is that data collection can be expensive. It’s something that larger hospitals now routinely do, but smaller hospitals have often balked because of the expense. To address this, the GWTG-Stroke program is trying to develop a “lighter” version of their data collection tool that involves a smaller financial burden.
“I think we can sell a trimmed down version of GWTG-Stroke to smaller hospitals that is affordable and use it to recruit another 1,000 hospitals. That’s a realistic goal,” Dr. Schwamm said.
What is also notable about GWTG-Stroke is that hospitals sign up despite the somewhat ambiguous payback they receive.

“In the past, stroke was the third-leading U.S. cause of death, but now it’s fifth,” noted Steven R. Messe, MD, a stroke neurologist at the University of Pennsylvania in Philadelphia and a member of the GWTG-Stroke steering committee. “That’s an amazing accomplishment – to drop stroke from third place to fifth – and it’s due to advances in thrombolytic use and to improved systems of care and quality improvement measures.”
Get With the Guidelines-Stroke is a program of the American Heart Association and American Stroke Association and uses funding provided by several drug companies. Dr. Smith, Dr. Fonarow, Dr. Schwamm and Dr. Messe had no relevant commercial disclosures.
[email protected]
On Twitter @mitchelzoler
HOUSTON – Thrombolytic therapy for U.S. patients experiencing an acute ischemic stroke is no longer the poster child for proven, but neglected, therapies.
Long bemoaned since its introduction in the mid-1990s as an effective but woefully underused treatment, thrombolytic therapy with tissue plasminogen activator (tPA) has seen robust growth in U.S. practice recently, largely due to the promotion and quality-improvement efforts of a voluntary, non-profit program, Get With the Guidelines (GWTG)-Stroke.
“We’ve seen a dramatic increase in tPA treatment in eligible patients,” said Dr. Smith, a neurologist and medical director of the Cognitive Neurosciences Clinic at the University of Calgary (Alta.).
“This represents remarkable and clinically meaningful improvements in stroke care, overcoming substantial barriers using a systems of care approach,” Gregg C. Fonarow, MD, professor of medicine and cochief of clinical cardiology at the University of California, Los Angeles and one of the long-time leaders of GWTG-Stroke, said in an interview. “This represents one of the most transformative improvements and success stories ever observed in stroke care.”
“These data show dramatic changes in the GWTG-Stroke hospitals,” agreed Lee H. Schwamm, MD, professor of neurology at Harvard Medical School and chief of stroke services at Massachusetts General Hospital in Boston and another leader of the GWTG-Stroke program. However, “we still have work to do,” cautioned Dr. Schwamm, who notes that 68% remains significantly short of the ideal 100%. The positive is that several GWTG-Stroke participating hospitals have surged to a better than 90% rate of administering tPA to eligible patients within a 60-minute door-to-needle window.
What is GWTG-Stroke?
GWTG was launched in 2000 by the American Heart Association as a hospital-based–quality improvement initiative focused on U.S. management of acute MI. In 2003, acute stroke became another focus of the program and inspired added participation of the American Stroke Association.
“Improvements in tPA use in eligible patients were seen soon after the introduction of GWTG-Stroke in 2003, but there was minimal improvement in the percentage of patients with door-to-needle times within 60 minutes despite national guidelines,” recalled Dr. Fonarow. This slow rate of advance led him, Dr. Schwamm, and others to create a more activist program within GWTG-Stroke, Target Stroke, that not only provided resources and collected data from participating hospitals but also set acute-treatment goals that challenged participating hospitals to up their game. Target Stroke phase I asked them to try to achieve a tPA door-to-needle time within 60 minutes in at least 50% of eligible patients. By mid-2013, the program reached this goal with 53% of patients treated in the allotted time frame (JAMA. 2014 Apr 23;311[16]:1632-40).
These time-based goals lead directly to meaningful improvements in patient outcomes. “We know that, for every 15 minute reduction in tPA door-to-needle time, there is a 5% reduction of in-hospital mortality and a substantial increase in the percentage of patients who are discharged home instead of to a rehabilitation hospital or nursing home,” Dr. Schwamm said.
Dr. Smith highlighted the 11 best practices steps that Target Stroke promotes to GWTG-Stroke hospitals as their road map to achieving the performance goals. These include things such as notification of a hospital by emergency medical services that a patient showing signs of an acute ischemic stroke is on the way, transfer of the patient after hospital arrival directly to a CT or MRI scanner to get the imaging that can confirm tPA eligibility, rapid reading of the scan, premixing of the tPA, a team-based approach to acute stroke management, and quick feedback to the team regarding their performance on each stroke patient they treat.
Dr. Schwamm noted that he, Dr. Fonarow, and other program leaders are already planning a phase III for Target Stroke that will branch out to even more facets of acute stroke care, such as incorporation of goals for using endovascular thrombectomy in appropriate patients and for using telemedicine to quicken and broaden the availability of expert neurologic consults for identifying tPA- and thrombectomy-eligible patients.
Growing the program
The success of GWTG-Stroke in transforming U.S. acute stroke care has not only relied on setting aggressive performance goals but also on advancing by boosting the number of U.S. hospitals participating of more U.S. hospitals. During the Target Stroke years since the start of 2010, the number of hospitals active in GWTG-Stroke jumped from 1427 to 1,950 by mid-2016, including a 12% year-over-year jump in 2016, compared with 2015. During October 2015-October 2016, participating hospitals treated more than 570,000 acute stroke patients, or roughly 71% of the estimated 800,000 U.S. patients who have an acute stroke each year.
These numbers seem on track to continue expanding. “With the recent evidence showing that participating in GWTG-Stroke improves care and outcomes there has been even greater interest by hospitals, recently, in joining,” said Dr. Fonarow. “While many hospitals currently participate, ideally all would join and be active.”
“Hospitals now feel that they can’t afford not to focus on stroke as a quality improvement program, so they join,” said Dr. Schwamm. He believes that essentially all of the roughly 200 certified U.S. Comprehensive Stroke Centers and of the roughly 1,000 certified U.S. Primary Stroke Centers are already members of GWTG-Stroke. “We’re now in all the high-value hospitals, based on their higher numbers of patients. It’s the Acute Stroke Ready hospitals where we now have the greatest potential to penetrate, hospitals that generally treat about 20-50 stroke patients a year,” he said.
Joining GWTG-Stroke holds major attraction for hospitals because the program gives them a tool for measuring their performance, data that hospitals often now need to prove the value of the care they deliver to insurers and to avoid penalization for readmissions. However, the barrier to hospitals, especially smaller hospitals, is that data collection can be expensive. It’s something that larger hospitals now routinely do, but smaller hospitals have often balked because of the expense. To address this, the GWTG-Stroke program is trying to develop a “lighter” version of their data collection tool that involves a smaller financial burden.
“I think we can sell a trimmed down version of GWTG-Stroke to smaller hospitals that is affordable and use it to recruit another 1,000 hospitals. That’s a realistic goal,” Dr. Schwamm said.
What is also notable about GWTG-Stroke is that hospitals sign up despite the somewhat ambiguous payback they receive.
“In the past, stroke was the third-leading U.S. cause of death, but now it’s fifth,” noted Steven R. Messe, MD, a stroke neurologist at the University of Pennsylvania in Philadelphia and a member of the GWTG-Stroke steering committee. “That’s an amazing accomplishment – to drop stroke from third place to fifth – and it’s due to advances in thrombolytic use and to improved systems of care and quality improvement measures.”
Get With the Guidelines-Stroke is a program of the American Heart Association and American Stroke Association and uses funding provided by several drug companies. Dr. Smith, Dr. Fonarow, Dr. Schwamm and Dr. Messe had no relevant commercial disclosures.
[email protected]
On Twitter @mitchelzoler
HOUSTON – Thrombolytic therapy for U.S. patients experiencing an acute ischemic stroke is no longer the poster child for proven, but neglected, therapies.
Long bemoaned since its introduction in the mid-1990s as an effective but woefully underused treatment, thrombolytic therapy with tissue plasminogen activator (tPA) has seen robust growth in U.S. practice recently, largely due to the promotion and quality-improvement efforts of a voluntary, non-profit program, Get With the Guidelines (GWTG)-Stroke.
“We’ve seen a dramatic increase in tPA treatment in eligible patients,” said Dr. Smith, a neurologist and medical director of the Cognitive Neurosciences Clinic at the University of Calgary (Alta.).
“This represents remarkable and clinically meaningful improvements in stroke care, overcoming substantial barriers using a systems of care approach,” Gregg C. Fonarow, MD, professor of medicine and cochief of clinical cardiology at the University of California, Los Angeles and one of the long-time leaders of GWTG-Stroke, said in an interview. “This represents one of the most transformative improvements and success stories ever observed in stroke care.”
“These data show dramatic changes in the GWTG-Stroke hospitals,” agreed Lee H. Schwamm, MD, professor of neurology at Harvard Medical School and chief of stroke services at Massachusetts General Hospital in Boston and another leader of the GWTG-Stroke program. However, “we still have work to do,” cautioned Dr. Schwamm, who notes that 68% remains significantly short of the ideal 100%. The positive is that several GWTG-Stroke participating hospitals have surged to a better than 90% rate of administering tPA to eligible patients within a 60-minute door-to-needle window.
What is GWTG-Stroke?
GWTG was launched in 2000 by the American Heart Association as a hospital-based–quality improvement initiative focused on U.S. management of acute MI. In 2003, acute stroke became another focus of the program and inspired added participation of the American Stroke Association.
“Improvements in tPA use in eligible patients were seen soon after the introduction of GWTG-Stroke in 2003, but there was minimal improvement in the percentage of patients with door-to-needle times within 60 minutes despite national guidelines,” recalled Dr. Fonarow. This slow rate of advance led him, Dr. Schwamm, and others to create a more activist program within GWTG-Stroke, Target Stroke, that not only provided resources and collected data from participating hospitals but also set acute-treatment goals that challenged participating hospitals to up their game. Target Stroke phase I asked them to try to achieve a tPA door-to-needle time within 60 minutes in at least 50% of eligible patients. By mid-2013, the program reached this goal with 53% of patients treated in the allotted time frame (JAMA. 2014 Apr 23;311[16]:1632-40).
These time-based goals lead directly to meaningful improvements in patient outcomes. “We know that, for every 15 minute reduction in tPA door-to-needle time, there is a 5% reduction of in-hospital mortality and a substantial increase in the percentage of patients who are discharged home instead of to a rehabilitation hospital or nursing home,” Dr. Schwamm said.
Dr. Smith highlighted the 11 best practices steps that Target Stroke promotes to GWTG-Stroke hospitals as their road map to achieving the performance goals. These include things such as notification of a hospital by emergency medical services that a patient showing signs of an acute ischemic stroke is on the way, transfer of the patient after hospital arrival directly to a CT or MRI scanner to get the imaging that can confirm tPA eligibility, rapid reading of the scan, premixing of the tPA, a team-based approach to acute stroke management, and quick feedback to the team regarding their performance on each stroke patient they treat.
Dr. Schwamm noted that he, Dr. Fonarow, and other program leaders are already planning a phase III for Target Stroke that will branch out to even more facets of acute stroke care, such as incorporation of goals for using endovascular thrombectomy in appropriate patients and for using telemedicine to quicken and broaden the availability of expert neurologic consults for identifying tPA- and thrombectomy-eligible patients.
Growing the program
The success of GWTG-Stroke in transforming U.S. acute stroke care has not only relied on setting aggressive performance goals but also on advancing by boosting the number of U.S. hospitals participating of more U.S. hospitals. During the Target Stroke years since the start of 2010, the number of hospitals active in GWTG-Stroke jumped from 1427 to 1,950 by mid-2016, including a 12% year-over-year jump in 2016, compared with 2015. During October 2015-October 2016, participating hospitals treated more than 570,000 acute stroke patients, or roughly 71% of the estimated 800,000 U.S. patients who have an acute stroke each year.
These numbers seem on track to continue expanding. “With the recent evidence showing that participating in GWTG-Stroke improves care and outcomes there has been even greater interest by hospitals, recently, in joining,” said Dr. Fonarow. “While many hospitals currently participate, ideally all would join and be active.”
“Hospitals now feel that they can’t afford not to focus on stroke as a quality improvement program, so they join,” said Dr. Schwamm. He believes that essentially all of the roughly 200 certified U.S. Comprehensive Stroke Centers and of the roughly 1,000 certified U.S. Primary Stroke Centers are already members of GWTG-Stroke. “We’re now in all the high-value hospitals, based on their higher numbers of patients. It’s the Acute Stroke Ready hospitals where we now have the greatest potential to penetrate, hospitals that generally treat about 20-50 stroke patients a year,” he said.
Joining GWTG-Stroke holds major attraction for hospitals because the program gives them a tool for measuring their performance, data that hospitals often now need to prove the value of the care they deliver to insurers and to avoid penalization for readmissions. However, the barrier to hospitals, especially smaller hospitals, is that data collection can be expensive. It’s something that larger hospitals now routinely do, but smaller hospitals have often balked because of the expense. To address this, the GWTG-Stroke program is trying to develop a “lighter” version of their data collection tool that involves a smaller financial burden.
“I think we can sell a trimmed down version of GWTG-Stroke to smaller hospitals that is affordable and use it to recruit another 1,000 hospitals. That’s a realistic goal,” Dr. Schwamm said.
What is also notable about GWTG-Stroke is that hospitals sign up despite the somewhat ambiguous payback they receive.
“In the past, stroke was the third-leading U.S. cause of death, but now it’s fifth,” noted Steven R. Messe, MD, a stroke neurologist at the University of Pennsylvania in Philadelphia and a member of the GWTG-Stroke steering committee. “That’s an amazing accomplishment – to drop stroke from third place to fifth – and it’s due to advances in thrombolytic use and to improved systems of care and quality improvement measures.”
Get With the Guidelines-Stroke is a program of the American Heart Association and American Stroke Association and uses funding provided by several drug companies. Dr. Smith, Dr. Fonarow, Dr. Schwamm and Dr. Messe had no relevant commercial disclosures.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE INTERNATIONAL STROKE CONFERENCE
Hold your breath
“Exercising my ‘reasoned judgment,’ I have no doubt that the right to a climate system capable of sustaining human life is fundamental to a free and ordered society.”
– U.S. District Judge Ann Aiken in Kelsey Cascadia Rose Juliana vs. United States of America, et al.
In many areas of the world, the simple act of breathing has become hazardous to people’s health.
According to the World Health Organization, more people die every day from air pollution than from HIV/AIDS, tuberculosis, and road injuries combined. In China, more than 1 million deaths annually are linked to polluted air (76/100,000); in India the number of deaths is more than 600,000 annually (49/100,000); and in the United States, that figure comes to more than 38,000 (12/100,000).

And yet, nonpolluting, alternative options – such as sun and wind power – are readily available.
Dirty air is visible on a hot summer day – when, mixed with other substances, it forms smog. Higher temperatures can then speed up the chemical reactions that form smog. We breathe in that polluted air, especially on days when the air is stagnant or there is temperature inversion.
The health effects of climate change
Black carbon found in air pollution leads to drug-resistant bacteria and alters antibiotic tolerance.1 The pollution also is associated with multiple cancers: lung, liver, ovarian, and, possibly, breast.2,3,4,5 It causes inflammation linked to the development of coronary artery disease (seen even in children!) and plaque formation leading to heart attacks and cardiac arrhythmias – including atrial fibrillation. Air pollution causes, triggers, or worsens respiratory illnesses – chronic obstructive pulmonary disease, emphysema, asthma, infections – and is responsible for lifelong diminished lung volume in children (a reason families are leaving Beijing.) Exponentially increased rates of autism are linked to bad air quality, as are autoimmune diseases, which also are on the rise.6,7 Polluted air causes brain inflammation – living near sources of air pollution increases the risk of dementia – and other neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s, and amyotrophic lateral sclerosis.8 The blood brain barrier protects the brain from most foreign matter, but particulate matter, especially ultrafine particulate matter of less than 1 mcm such as magnetite, can cross directly into the brain via the olfactory nerve. (Magnetite has been identified in the brain tissue of residents living in areas where the substance is produced as a result of industrial waste.) While particulate matter of 2.5 mcmis measured in the United States, ultrafine particulate matter is not.
Psychiatric symptoms and chronic psychiatric disorders also are associated with polluted air: On days with poor air quality, a statistically significant increase is seen in suicide threats and visits to emergency departments for panic attacks.9,10
A rise in aggression occurs when there are abnormally high temperatures and significant changes in rainfall. More assaults, murders, suicides, domestic violence, and child abuse can be expected, and a rise in unrest around the world should come as no surprise.
As a consequence of increased CO2 in the atmosphere, temperatures have already risen by 2° F: Sixteen of the hottest years on record have occurred in the last 17 years, with 2016 as the hottest year ever recorded. In Iraq and Kuwait, the temperature last summer reached 129.2° F.
We are experiencing more frequent and extreme weather events, chronic climate conditions, and the cascading disruption of ecosystems. Drought and sea level rise are leading to physical and psychological impacts – both direct and indirect. Some regions of the world have become destabilized, triggering migrations and the refugee crisis.
Along with these psychological impacts, CO2 affects cognition: A recent study by the Harvard School of Public Health, Boston, shows that the indoor levels of CO2 to which American workers typically are exposed impair cognitive functioning, particularly in the areas of strategic thinking, information processing, and crisis management.11
What do we do about it?
As mental health professionals, we know that aggression can be overt or passive (from inaction). Overwhelming evidence shows harm to public health from burning fossil fuels, and yet, though we are making progress, resistance still exists in the transition to clean, renewable energy critical for the health of our families and communities. When political will is what stands between us and getting back on a path to breathing clean air, how can inaction be understood as anything but an act of aggression?
This issue has reached U.S. courts: In a landmark case, 21 youths aged 9-20 years represented by “Our Children’s Trust” are suing the U.S. government in the Oregon U.S. District Court for failure to act on climate. The case, heard by Judge Ann Aiken, is now headed to trial.
All of us have a duty to collectively, repeatedly, and forcefully call on policy makers to take action.
That leads me to what we can do as doctors. In this effort to quickly transition to safe, clean renewable energy, we all have a role to play. The notion that we can’t do anything as individuals is no more credible than saying “my vote doesn’t matter.” Just as our actions as voters in a democracy demonstrate the collective civic responsibility we owe one another, so too do our actions on climate. As global citizens, all actions that we take to help us live within the planet’s means are opportunities to restore balance.
What we do collectively drives markets and determines the social norms that powerfully influence the decisions of others – sometimes even unconsciously.
As doctors, we have a unique role to play in the places we work – urging hospitals, clinics, academic centers, and other organizations and facilities to lead by example, become role models for energy efficiency, and choose clean renewable energy sources over the ones harming our health. We can start by choosing wind and solar to power our homes and influencing others to do the same.
We are the voices because this is a health message.
Dr. Van Susteren is a practicing general and forensic psychiatrist in Washington. She serves on the advisory board of the Center for Health and the Global Environment at Harvard T.H. Chan School of Public Health, Boston. Dr. Van Susteren is a former member of the board of directors of the National Wildlife Federation and coauthor of group’s report, “The Psychological Effects of Global Warming on the United States – Why the U.S. Mental Health System is Not Prepared.” In 2006, Dr. Van Susteren sought the Democratic nomination for a U.S. Senate seat in Maryland. She also founded Lucky Planet Foods, a company that provides plant-based, low carbon foods.
References
1. Environ Microbiol. 2017 Feb 14. doi: 10.1111/1462-2920.13686.
2. Environ Health Perspect. 2017 Mar;125[3]:378-84.
3. J Hepatol. 2015;63[6]:1397-1404.
4. J Toxicol Environ Health A. 2012;75[3]:174-82.
5. Environ Health Perspect. 2012 Nov; 118[11]:1578-83.
6. J Child Psychol Psychiatry. 2016; 57[3]:271-92.
7. Curr Opin Pediatr. 2010;22[2]219-25.
8. Inhal Toxicol. 2008;20[5]:499-506.
9. J Psychiatr Res. 2015 Mar;62:130-5.
10. Schizophr Res. 2016 Oct 5. doi: 10.1016/j.schres.2016.10.003.
11. Environ Health Perspect. 2016 Jun;124[6]:805-12.
“Exercising my ‘reasoned judgment,’ I have no doubt that the right to a climate system capable of sustaining human life is fundamental to a free and ordered society.”
– U.S. District Judge Ann Aiken in Kelsey Cascadia Rose Juliana vs. United States of America, et al.
In many areas of the world, the simple act of breathing has become hazardous to people’s health.
According to the World Health Organization, more people die every day from air pollution than from HIV/AIDS, tuberculosis, and road injuries combined. In China, more than 1 million deaths annually are linked to polluted air (76/100,000); in India the number of deaths is more than 600,000 annually (49/100,000); and in the United States, that figure comes to more than 38,000 (12/100,000).
And yet, nonpolluting, alternative options – such as sun and wind power – are readily available.
Dirty air is visible on a hot summer day – when, mixed with other substances, it forms smog. Higher temperatures can then speed up the chemical reactions that form smog. We breathe in that polluted air, especially on days when the air is stagnant or there is temperature inversion.
The health effects of climate change
Black carbon found in air pollution leads to drug-resistant bacteria and alters antibiotic tolerance.1 The pollution also is associated with multiple cancers: lung, liver, ovarian, and, possibly, breast.2,3,4,5 It causes inflammation linked to the development of coronary artery disease (seen even in children!) and plaque formation leading to heart attacks and cardiac arrhythmias – including atrial fibrillation. Air pollution causes, triggers, or worsens respiratory illnesses – chronic obstructive pulmonary disease, emphysema, asthma, infections – and is responsible for lifelong diminished lung volume in children (a reason families are leaving Beijing.) Exponentially increased rates of autism are linked to bad air quality, as are autoimmune diseases, which also are on the rise.6,7 Polluted air causes brain inflammation – living near sources of air pollution increases the risk of dementia – and other neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s, and amyotrophic lateral sclerosis.8 The blood brain barrier protects the brain from most foreign matter, but particulate matter, especially ultrafine particulate matter of less than 1 mcm such as magnetite, can cross directly into the brain via the olfactory nerve. (Magnetite has been identified in the brain tissue of residents living in areas where the substance is produced as a result of industrial waste.) While particulate matter of 2.5 mcmis measured in the United States, ultrafine particulate matter is not.
Psychiatric symptoms and chronic psychiatric disorders also are associated with polluted air: On days with poor air quality, a statistically significant increase is seen in suicide threats and visits to emergency departments for panic attacks.9,10
A rise in aggression occurs when there are abnormally high temperatures and significant changes in rainfall. More assaults, murders, suicides, domestic violence, and child abuse can be expected, and a rise in unrest around the world should come as no surprise.
As a consequence of increased CO2 in the atmosphere, temperatures have already risen by 2° F: Sixteen of the hottest years on record have occurred in the last 17 years, with 2016 as the hottest year ever recorded. In Iraq and Kuwait, the temperature last summer reached 129.2° F.
We are experiencing more frequent and extreme weather events, chronic climate conditions, and the cascading disruption of ecosystems. Drought and sea level rise are leading to physical and psychological impacts – both direct and indirect. Some regions of the world have become destabilized, triggering migrations and the refugee crisis.
Along with these psychological impacts, CO2 affects cognition: A recent study by the Harvard School of Public Health, Boston, shows that the indoor levels of CO2 to which American workers typically are exposed impair cognitive functioning, particularly in the areas of strategic thinking, information processing, and crisis management.11
What do we do about it?
As mental health professionals, we know that aggression can be overt or passive (from inaction). Overwhelming evidence shows harm to public health from burning fossil fuels, and yet, though we are making progress, resistance still exists in the transition to clean, renewable energy critical for the health of our families and communities. When political will is what stands between us and getting back on a path to breathing clean air, how can inaction be understood as anything but an act of aggression?
This issue has reached U.S. courts: In a landmark case, 21 youths aged 9-20 years represented by “Our Children’s Trust” are suing the U.S. government in the Oregon U.S. District Court for failure to act on climate. The case, heard by Judge Ann Aiken, is now headed to trial.
All of us have a duty to collectively, repeatedly, and forcefully call on policy makers to take action.
That leads me to what we can do as doctors. In this effort to quickly transition to safe, clean renewable energy, we all have a role to play. The notion that we can’t do anything as individuals is no more credible than saying “my vote doesn’t matter.” Just as our actions as voters in a democracy demonstrate the collective civic responsibility we owe one another, so too do our actions on climate. As global citizens, all actions that we take to help us live within the planet’s means are opportunities to restore balance.
What we do collectively drives markets and determines the social norms that powerfully influence the decisions of others – sometimes even unconsciously.
As doctors, we have a unique role to play in the places we work – urging hospitals, clinics, academic centers, and other organizations and facilities to lead by example, become role models for energy efficiency, and choose clean renewable energy sources over the ones harming our health. We can start by choosing wind and solar to power our homes and influencing others to do the same.
We are the voices because this is a health message.
Dr. Van Susteren is a practicing general and forensic psychiatrist in Washington. She serves on the advisory board of the Center for Health and the Global Environment at Harvard T.H. Chan School of Public Health, Boston. Dr. Van Susteren is a former member of the board of directors of the National Wildlife Federation and coauthor of group’s report, “The Psychological Effects of Global Warming on the United States – Why the U.S. Mental Health System is Not Prepared.” In 2006, Dr. Van Susteren sought the Democratic nomination for a U.S. Senate seat in Maryland. She also founded Lucky Planet Foods, a company that provides plant-based, low carbon foods.
References
1. Environ Microbiol. 2017 Feb 14. doi: 10.1111/1462-2920.13686.
2. Environ Health Perspect. 2017 Mar;125[3]:378-84.
3. J Hepatol. 2015;63[6]:1397-1404.
4. J Toxicol Environ Health A. 2012;75[3]:174-82.
5. Environ Health Perspect. 2012 Nov; 118[11]:1578-83.
6. J Child Psychol Psychiatry. 2016; 57[3]:271-92.
7. Curr Opin Pediatr. 2010;22[2]219-25.
8. Inhal Toxicol. 2008;20[5]:499-506.
9. J Psychiatr Res. 2015 Mar;62:130-5.
10. Schizophr Res. 2016 Oct 5. doi: 10.1016/j.schres.2016.10.003.
11. Environ Health Perspect. 2016 Jun;124[6]:805-12.
“Exercising my ‘reasoned judgment,’ I have no doubt that the right to a climate system capable of sustaining human life is fundamental to a free and ordered society.”
– U.S. District Judge Ann Aiken in Kelsey Cascadia Rose Juliana vs. United States of America, et al.
In many areas of the world, the simple act of breathing has become hazardous to people’s health.
According to the World Health Organization, more people die every day from air pollution than from HIV/AIDS, tuberculosis, and road injuries combined. In China, more than 1 million deaths annually are linked to polluted air (76/100,000); in India the number of deaths is more than 600,000 annually (49/100,000); and in the United States, that figure comes to more than 38,000 (12/100,000).
And yet, nonpolluting, alternative options – such as sun and wind power – are readily available.
Dirty air is visible on a hot summer day – when, mixed with other substances, it forms smog. Higher temperatures can then speed up the chemical reactions that form smog. We breathe in that polluted air, especially on days when the air is stagnant or there is temperature inversion.
The health effects of climate change
Black carbon found in air pollution leads to drug-resistant bacteria and alters antibiotic tolerance.1 The pollution also is associated with multiple cancers: lung, liver, ovarian, and, possibly, breast.2,3,4,5 It causes inflammation linked to the development of coronary artery disease (seen even in children!) and plaque formation leading to heart attacks and cardiac arrhythmias – including atrial fibrillation. Air pollution causes, triggers, or worsens respiratory illnesses – chronic obstructive pulmonary disease, emphysema, asthma, infections – and is responsible for lifelong diminished lung volume in children (a reason families are leaving Beijing.) Exponentially increased rates of autism are linked to bad air quality, as are autoimmune diseases, which also are on the rise.6,7 Polluted air causes brain inflammation – living near sources of air pollution increases the risk of dementia – and other neurodegenerative diseases such as Alzheimer’s disease, Parkinson’s, and amyotrophic lateral sclerosis.8 The blood brain barrier protects the brain from most foreign matter, but particulate matter, especially ultrafine particulate matter of less than 1 mcm such as magnetite, can cross directly into the brain via the olfactory nerve. (Magnetite has been identified in the brain tissue of residents living in areas where the substance is produced as a result of industrial waste.) While particulate matter of 2.5 mcmis measured in the United States, ultrafine particulate matter is not.
Psychiatric symptoms and chronic psychiatric disorders also are associated with polluted air: On days with poor air quality, a statistically significant increase is seen in suicide threats and visits to emergency departments for panic attacks.9,10
A rise in aggression occurs when there are abnormally high temperatures and significant changes in rainfall. More assaults, murders, suicides, domestic violence, and child abuse can be expected, and a rise in unrest around the world should come as no surprise.
As a consequence of increased CO2 in the atmosphere, temperatures have already risen by 2° F: Sixteen of the hottest years on record have occurred in the last 17 years, with 2016 as the hottest year ever recorded. In Iraq and Kuwait, the temperature last summer reached 129.2° F.
We are experiencing more frequent and extreme weather events, chronic climate conditions, and the cascading disruption of ecosystems. Drought and sea level rise are leading to physical and psychological impacts – both direct and indirect. Some regions of the world have become destabilized, triggering migrations and the refugee crisis.
Along with these psychological impacts, CO2 affects cognition: A recent study by the Harvard School of Public Health, Boston, shows that the indoor levels of CO2 to which American workers typically are exposed impair cognitive functioning, particularly in the areas of strategic thinking, information processing, and crisis management.11
What do we do about it?
As mental health professionals, we know that aggression can be overt or passive (from inaction). Overwhelming evidence shows harm to public health from burning fossil fuels, and yet, though we are making progress, resistance still exists in the transition to clean, renewable energy critical for the health of our families and communities. When political will is what stands between us and getting back on a path to breathing clean air, how can inaction be understood as anything but an act of aggression?
This issue has reached U.S. courts: In a landmark case, 21 youths aged 9-20 years represented by “Our Children’s Trust” are suing the U.S. government in the Oregon U.S. District Court for failure to act on climate. The case, heard by Judge Ann Aiken, is now headed to trial.
All of us have a duty to collectively, repeatedly, and forcefully call on policy makers to take action.
That leads me to what we can do as doctors. In this effort to quickly transition to safe, clean renewable energy, we all have a role to play. The notion that we can’t do anything as individuals is no more credible than saying “my vote doesn’t matter.” Just as our actions as voters in a democracy demonstrate the collective civic responsibility we owe one another, so too do our actions on climate. As global citizens, all actions that we take to help us live within the planet’s means are opportunities to restore balance.
What we do collectively drives markets and determines the social norms that powerfully influence the decisions of others – sometimes even unconsciously.
As doctors, we have a unique role to play in the places we work – urging hospitals, clinics, academic centers, and other organizations and facilities to lead by example, become role models for energy efficiency, and choose clean renewable energy sources over the ones harming our health. We can start by choosing wind and solar to power our homes and influencing others to do the same.
We are the voices because this is a health message.
Dr. Van Susteren is a practicing general and forensic psychiatrist in Washington. She serves on the advisory board of the Center for Health and the Global Environment at Harvard T.H. Chan School of Public Health, Boston. Dr. Van Susteren is a former member of the board of directors of the National Wildlife Federation and coauthor of group’s report, “The Psychological Effects of Global Warming on the United States – Why the U.S. Mental Health System is Not Prepared.” In 2006, Dr. Van Susteren sought the Democratic nomination for a U.S. Senate seat in Maryland. She also founded Lucky Planet Foods, a company that provides plant-based, low carbon foods.
References
1. Environ Microbiol. 2017 Feb 14. doi: 10.1111/1462-2920.13686.
2. Environ Health Perspect. 2017 Mar;125[3]:378-84.
3. J Hepatol. 2015;63[6]:1397-1404.
4. J Toxicol Environ Health A. 2012;75[3]:174-82.
5. Environ Health Perspect. 2012 Nov; 118[11]:1578-83.
6. J Child Psychol Psychiatry. 2016; 57[3]:271-92.
7. Curr Opin Pediatr. 2010;22[2]219-25.
8. Inhal Toxicol. 2008;20[5]:499-506.
9. J Psychiatr Res. 2015 Mar;62:130-5.
10. Schizophr Res. 2016 Oct 5. doi: 10.1016/j.schres.2016.10.003.
11. Environ Health Perspect. 2016 Jun;124[6]:805-12.
Pronator Teres Myotendinous Tear
Take-Home Points
- Pronator teres muscle injuries are rare.
- Injury can be mistaken for MUCL injury in athletes.
- Tenderness and weak/painful forearm pronation are common findings.
- MRI confirms the diagnosis and helps grade the muscle strain injury.
- Conservative treatment is recommended and prognosis is excellent even for high-grade strains.
Pronator teres muscle strain is a rare sporting injury reported only in cricket players, and now in a golfer whose forearm experienced an eccentric force during resisted elbow flexion and pronation.1,2 The injury occurs when the sporting club or racket strikes the ground during a swing, impeding forward progress and subjecting the pronator teres muscle to eccentric forces in excess of what it can withstand. The pronator teres, one of several muscles that comprise the flexor wad of the forearm, consists of 2 heads, originating proximally from the medical epicondyle and attaching distally to the shaft of the radius on its lateral surface and just distal to the supinator. The oblique orientation of the muscle belly allows it to serve in its primary rotatory role as the main pronator of the forearm. Injuries to the soft tissue of the medial forearm are common in both elite and recreational athletes, especially in racket and club sports.3 Often, these injuries are related to overuse and chronic fatigue of the surrounding soft tissue—caused by repetitive flexing, gripping, or swinging. Even when identified early, these injuries can result in a significant loss of training time.4 In this article, we report a case of pronator teres muscle tear at the myotendinous junction. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A right-hand–dominant 36-year-old man presented to the clinic with pain on the medial side of his right elbow after sustaining an injury to the elbow while playing golf several days earlier. The patient, an advertising executive, was playing recreational golf several times a month and had no significant medical history or previous symptoms related to the elbow. Initial pain symptoms began during a second round of play, immediately after the patient miss-hit an iron shot, making contact mostly with the ground and causing the club to forcefully stop. The pain was on the medial side of the elbow and forearm. The patient noted progressive swelling and bruising at the pain site and development of forearm weakness. Physical examination during the clinic presentation revealed ecchymosis on the anterior medial forearm, medial elbow, and medial triceps (Figure 1). 
Noncontrast magnetic resonance imaging (MRI) showed a high-grade partial tear of the pronator teres myotendinous junction (Figures 2A-2C). 
The patient was instructed to rest the elbow from strenuous activity, golf in particular, for 4 weeks. Physical therapy for ROM and forearm strengthening of the surrounding flexor wad was initiated at 2 weeks and continued for 4 weeks. The patient was advised to take over-the-counter nonsteroidal anti-inflammatory drugs as needed for comfort. On repeat examination at 4 weeks, with tenderness or weakness with pronation absent and full ROM regained, the patient was released back to full activity. He was able to return to golf and reported being symptom-free and having no sense of weakness or loss of control.
Discussion
A tear of the pronator teres is an exceedingly rare injury. Our results with conservative treatment and a full return to previous activity level are consistent with the only other case reported in the literature.5 In contrast to our patient, the previous patient sustained a tear of the pronator teres after a prolonged period of batting during a recreational cricket match.
Our patient’s pronator teres injury occurred at the myotendinous junction, a muscle-tendon transition zone often susceptible to injury. What is unusual for this athletic medial elbow injury is that the patient reported no previous symptoms, and it appears that, though the surrounding muscle may have been fatigued by overuse from the round of golf earlier that day, the pathology was caused by an acute eccentric force. During a golf swing, tremendous forces are put on the entire body, from the lower extremities to the forearm and the fingers. Successful completion of the transfer of energy from the golf club to the ball requires both proper technique and proper functioning of key muscles. Specifically, parameters such as ball positioning, club angle, and wrist control play a major role.6 Altered forearm positioning or swing arc can significantly affect club head velocity and energy transfer without putting more stress on the golfer.7 Therefore, it is easy to understand how prolonged or extended play may fatigue the surrounding elbow muscles, leading to altered technique and increased susceptibility to acute injury. Biomechanical analysis of shoulder motion can provide a helpful baseline for assessing injury-related changes in golf swing and developing specific exercise and rehabilitation programs.8,9Although injury to the pronator teres is rare, sport physicians should be aware that, after a valgus stress or force, bruising and swelling along the medial elbow do not always indicate a medial ulnar collateral ligament (MUCL) tear or medial epicondylitis. The key examination findings that differentiate this injury from a MUCL injury are the exact location of pain, the milking maneuver for MUCL incompetence, and the extensive bruising over the muscle course of the pronator teres. MRI plays a pivotal role in proper diagnosis.4 In addition, MRI allows for evaluation of any concomitant injuries that may be obscuring the clinical presentation.
Successful treatment of such injuries is important for both elite and recreational athletes. With rest and physical therapy, our patient recovered from this rare isolated injury to the pronator teres with complete resolution of symptoms and full ROM. In the literature, we found no other reports of isolated full-thickness myotendinous rupture of the pronator teres or avulsion from the medial epicondyle. Therefore, it is unclear whether the same outcome can be expected with conservative therapy. However, because of the good outcomes for partial-thickness injuries treated conservatively and the lack of robust tendinous tissue to repair at the myotendinous junction, we recommend an initial course of conservative treatment. Sports physicians should be aware of this exceedingly rare injury to the elbow and understand the large forces experienced by the soft tissues of the forearm during the golf swing.9,10
Conclusion
Pronator teres muscle strain is a rare sporting injury reported in cricket and golf players. The elbow experiences a large eccentric force during resisted elbow flexion and pronation. The injury appears to occur when the sporting club or racket strikes the ground during a forceful swing impeding forward progress of the arm. The injury can be confused with a MUCL injury, or exacerbation of medial epicondylitis. Physical examination reveals bruising and tenderness over the course of the pronator teres, often distal to the elbow. Advanced imaging confirms the diagnosis and helps grade the severity of muscle strain. Treatment is often conservative, with return to function and sport after 4 to 6 weeks of rest and restricted activities. The patient in this case report had complete return to sporting function, with no residual weakness or pain.
Am J Orthop. 2017;46(2):E105-E107. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
1. Field LD, Savoie FH. Common elbow injuries in sport. Sports Med. 1998;26(3):193-205.
2. Loomer RL. Elbow injuries in athletes. Can J Appl Sport Sci. 1982;7(3):164-166.
3. Dines JS, Bedi A, Williams PN, et al. Tennis injuries: epidemiology, pathophysiology, and treatment. J Am Acad Orthop Surg. 2015;23(3):181-189.
4. Banks KP, Ly JQ, Beall DP, Grayson DE, Bancroft LW, Tall MA. Overuse injuries of the upper extremity in the competitive athlete: magnetic resonance imaging findings associated with repetitive trauma. Curr Probl Diagn Radiol. 2005;34(4):127-142.
5. Niebulski HZ, Richardson ML. High-grade pronator teres tear in a cricket batsman. Radiol Case Rep. 2015;6(3):540.
6. Zhang X, Shan G. Where do golf drive swings go wrong? Factors influencing driver swing consistency. Scand J Med Sci Sports. 2014;24(5):749-757.
7. Nesbit SM, McGinnis RS. Kinetic constrained optimization of the golf swing hub path. J Sports Sci Med. 2014;13(4):859-873.
8. Helton MS. Conservative treatment of a proximal full-thickness biceps brachii muscle tear in a special operations soldier. Phys Ther. 2014;94(4):571-577.
9. Mitchell K, Banks S, Morgan D, Sugaya H. Shoulder motions during the golf swing in male amateur golfers. J Orthop Sports Phys Ther. 2003;33(4):196-203.
10. Grimshaw P, Giles A, Tong R, Grimmer K. Lower back and elbow injuries in golf. Sports Med. 2002;32(10):655-666.
Take-Home Points
- Pronator teres muscle injuries are rare.
- Injury can be mistaken for MUCL injury in athletes.
- Tenderness and weak/painful forearm pronation are common findings.
- MRI confirms the diagnosis and helps grade the muscle strain injury.
- Conservative treatment is recommended and prognosis is excellent even for high-grade strains.
Pronator teres muscle strain is a rare sporting injury reported only in cricket players, and now in a golfer whose forearm experienced an eccentric force during resisted elbow flexion and pronation.1,2 The injury occurs when the sporting club or racket strikes the ground during a swing, impeding forward progress and subjecting the pronator teres muscle to eccentric forces in excess of what it can withstand. The pronator teres, one of several muscles that comprise the flexor wad of the forearm, consists of 2 heads, originating proximally from the medical epicondyle and attaching distally to the shaft of the radius on its lateral surface and just distal to the supinator. The oblique orientation of the muscle belly allows it to serve in its primary rotatory role as the main pronator of the forearm. Injuries to the soft tissue of the medial forearm are common in both elite and recreational athletes, especially in racket and club sports.3 Often, these injuries are related to overuse and chronic fatigue of the surrounding soft tissue—caused by repetitive flexing, gripping, or swinging. Even when identified early, these injuries can result in a significant loss of training time.4 In this article, we report a case of pronator teres muscle tear at the myotendinous junction. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A right-hand–dominant 36-year-old man presented to the clinic with pain on the medial side of his right elbow after sustaining an injury to the elbow while playing golf several days earlier. The patient, an advertising executive, was playing recreational golf several times a month and had no significant medical history or previous symptoms related to the elbow. Initial pain symptoms began during a second round of play, immediately after the patient miss-hit an iron shot, making contact mostly with the ground and causing the club to forcefully stop. The pain was on the medial side of the elbow and forearm. The patient noted progressive swelling and bruising at the pain site and development of forearm weakness. Physical examination during the clinic presentation revealed ecchymosis on the anterior medial forearm, medial elbow, and medial triceps (Figure 1).
Noncontrast magnetic resonance imaging (MRI) showed a high-grade partial tear of the pronator teres myotendinous junction (Figures 2A-2C).
The patient was instructed to rest the elbow from strenuous activity, golf in particular, for 4 weeks. Physical therapy for ROM and forearm strengthening of the surrounding flexor wad was initiated at 2 weeks and continued for 4 weeks. The patient was advised to take over-the-counter nonsteroidal anti-inflammatory drugs as needed for comfort. On repeat examination at 4 weeks, with tenderness or weakness with pronation absent and full ROM regained, the patient was released back to full activity. He was able to return to golf and reported being symptom-free and having no sense of weakness or loss of control.
Discussion
A tear of the pronator teres is an exceedingly rare injury. Our results with conservative treatment and a full return to previous activity level are consistent with the only other case reported in the literature.5 In contrast to our patient, the previous patient sustained a tear of the pronator teres after a prolonged period of batting during a recreational cricket match.
Our patient’s pronator teres injury occurred at the myotendinous junction, a muscle-tendon transition zone often susceptible to injury. What is unusual for this athletic medial elbow injury is that the patient reported no previous symptoms, and it appears that, though the surrounding muscle may have been fatigued by overuse from the round of golf earlier that day, the pathology was caused by an acute eccentric force. During a golf swing, tremendous forces are put on the entire body, from the lower extremities to the forearm and the fingers. Successful completion of the transfer of energy from the golf club to the ball requires both proper technique and proper functioning of key muscles. Specifically, parameters such as ball positioning, club angle, and wrist control play a major role.6 Altered forearm positioning or swing arc can significantly affect club head velocity and energy transfer without putting more stress on the golfer.7 Therefore, it is easy to understand how prolonged or extended play may fatigue the surrounding elbow muscles, leading to altered technique and increased susceptibility to acute injury. Biomechanical analysis of shoulder motion can provide a helpful baseline for assessing injury-related changes in golf swing and developing specific exercise and rehabilitation programs.8,9Although injury to the pronator teres is rare, sport physicians should be aware that, after a valgus stress or force, bruising and swelling along the medial elbow do not always indicate a medial ulnar collateral ligament (MUCL) tear or medial epicondylitis. The key examination findings that differentiate this injury from a MUCL injury are the exact location of pain, the milking maneuver for MUCL incompetence, and the extensive bruising over the muscle course of the pronator teres. MRI plays a pivotal role in proper diagnosis.4 In addition, MRI allows for evaluation of any concomitant injuries that may be obscuring the clinical presentation.
Successful treatment of such injuries is important for both elite and recreational athletes. With rest and physical therapy, our patient recovered from this rare isolated injury to the pronator teres with complete resolution of symptoms and full ROM. In the literature, we found no other reports of isolated full-thickness myotendinous rupture of the pronator teres or avulsion from the medial epicondyle. Therefore, it is unclear whether the same outcome can be expected with conservative therapy. However, because of the good outcomes for partial-thickness injuries treated conservatively and the lack of robust tendinous tissue to repair at the myotendinous junction, we recommend an initial course of conservative treatment. Sports physicians should be aware of this exceedingly rare injury to the elbow and understand the large forces experienced by the soft tissues of the forearm during the golf swing.9,10
Conclusion
Pronator teres muscle strain is a rare sporting injury reported in cricket and golf players. The elbow experiences a large eccentric force during resisted elbow flexion and pronation. The injury appears to occur when the sporting club or racket strikes the ground during a forceful swing impeding forward progress of the arm. The injury can be confused with a MUCL injury, or exacerbation of medial epicondylitis. Physical examination reveals bruising and tenderness over the course of the pronator teres, often distal to the elbow. Advanced imaging confirms the diagnosis and helps grade the severity of muscle strain. Treatment is often conservative, with return to function and sport after 4 to 6 weeks of rest and restricted activities. The patient in this case report had complete return to sporting function, with no residual weakness or pain.
Am J Orthop. 2017;46(2):E105-E107. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
Take-Home Points
- Pronator teres muscle injuries are rare.
- Injury can be mistaken for MUCL injury in athletes.
- Tenderness and weak/painful forearm pronation are common findings.
- MRI confirms the diagnosis and helps grade the muscle strain injury.
- Conservative treatment is recommended and prognosis is excellent even for high-grade strains.
Pronator teres muscle strain is a rare sporting injury reported only in cricket players, and now in a golfer whose forearm experienced an eccentric force during resisted elbow flexion and pronation.1,2 The injury occurs when the sporting club or racket strikes the ground during a swing, impeding forward progress and subjecting the pronator teres muscle to eccentric forces in excess of what it can withstand. The pronator teres, one of several muscles that comprise the flexor wad of the forearm, consists of 2 heads, originating proximally from the medical epicondyle and attaching distally to the shaft of the radius on its lateral surface and just distal to the supinator. The oblique orientation of the muscle belly allows it to serve in its primary rotatory role as the main pronator of the forearm. Injuries to the soft tissue of the medial forearm are common in both elite and recreational athletes, especially in racket and club sports.3 Often, these injuries are related to overuse and chronic fatigue of the surrounding soft tissue—caused by repetitive flexing, gripping, or swinging. Even when identified early, these injuries can result in a significant loss of training time.4 In this article, we report a case of pronator teres muscle tear at the myotendinous junction. The patient provided written informed consent for print and electronic publication of this case report.
Case Report
A right-hand–dominant 36-year-old man presented to the clinic with pain on the medial side of his right elbow after sustaining an injury to the elbow while playing golf several days earlier. The patient, an advertising executive, was playing recreational golf several times a month and had no significant medical history or previous symptoms related to the elbow. Initial pain symptoms began during a second round of play, immediately after the patient miss-hit an iron shot, making contact mostly with the ground and causing the club to forcefully stop. The pain was on the medial side of the elbow and forearm. The patient noted progressive swelling and bruising at the pain site and development of forearm weakness. Physical examination during the clinic presentation revealed ecchymosis on the anterior medial forearm, medial elbow, and medial triceps (Figure 1).
Noncontrast magnetic resonance imaging (MRI) showed a high-grade partial tear of the pronator teres myotendinous junction (Figures 2A-2C).
The patient was instructed to rest the elbow from strenuous activity, golf in particular, for 4 weeks. Physical therapy for ROM and forearm strengthening of the surrounding flexor wad was initiated at 2 weeks and continued for 4 weeks. The patient was advised to take over-the-counter nonsteroidal anti-inflammatory drugs as needed for comfort. On repeat examination at 4 weeks, with tenderness or weakness with pronation absent and full ROM regained, the patient was released back to full activity. He was able to return to golf and reported being symptom-free and having no sense of weakness or loss of control.
Discussion
A tear of the pronator teres is an exceedingly rare injury. Our results with conservative treatment and a full return to previous activity level are consistent with the only other case reported in the literature.5 In contrast to our patient, the previous patient sustained a tear of the pronator teres after a prolonged period of batting during a recreational cricket match.
Our patient’s pronator teres injury occurred at the myotendinous junction, a muscle-tendon transition zone often susceptible to injury. What is unusual for this athletic medial elbow injury is that the patient reported no previous symptoms, and it appears that, though the surrounding muscle may have been fatigued by overuse from the round of golf earlier that day, the pathology was caused by an acute eccentric force. During a golf swing, tremendous forces are put on the entire body, from the lower extremities to the forearm and the fingers. Successful completion of the transfer of energy from the golf club to the ball requires both proper technique and proper functioning of key muscles. Specifically, parameters such as ball positioning, club angle, and wrist control play a major role.6 Altered forearm positioning or swing arc can significantly affect club head velocity and energy transfer without putting more stress on the golfer.7 Therefore, it is easy to understand how prolonged or extended play may fatigue the surrounding elbow muscles, leading to altered technique and increased susceptibility to acute injury. Biomechanical analysis of shoulder motion can provide a helpful baseline for assessing injury-related changes in golf swing and developing specific exercise and rehabilitation programs.8,9Although injury to the pronator teres is rare, sport physicians should be aware that, after a valgus stress or force, bruising and swelling along the medial elbow do not always indicate a medial ulnar collateral ligament (MUCL) tear or medial epicondylitis. The key examination findings that differentiate this injury from a MUCL injury are the exact location of pain, the milking maneuver for MUCL incompetence, and the extensive bruising over the muscle course of the pronator teres. MRI plays a pivotal role in proper diagnosis.4 In addition, MRI allows for evaluation of any concomitant injuries that may be obscuring the clinical presentation.
Successful treatment of such injuries is important for both elite and recreational athletes. With rest and physical therapy, our patient recovered from this rare isolated injury to the pronator teres with complete resolution of symptoms and full ROM. In the literature, we found no other reports of isolated full-thickness myotendinous rupture of the pronator teres or avulsion from the medial epicondyle. Therefore, it is unclear whether the same outcome can be expected with conservative therapy. However, because of the good outcomes for partial-thickness injuries treated conservatively and the lack of robust tendinous tissue to repair at the myotendinous junction, we recommend an initial course of conservative treatment. Sports physicians should be aware of this exceedingly rare injury to the elbow and understand the large forces experienced by the soft tissues of the forearm during the golf swing.9,10
Conclusion
Pronator teres muscle strain is a rare sporting injury reported in cricket and golf players. The elbow experiences a large eccentric force during resisted elbow flexion and pronation. The injury appears to occur when the sporting club or racket strikes the ground during a forceful swing impeding forward progress of the arm. The injury can be confused with a MUCL injury, or exacerbation of medial epicondylitis. Physical examination reveals bruising and tenderness over the course of the pronator teres, often distal to the elbow. Advanced imaging confirms the diagnosis and helps grade the severity of muscle strain. Treatment is often conservative, with return to function and sport after 4 to 6 weeks of rest and restricted activities. The patient in this case report had complete return to sporting function, with no residual weakness or pain.
Am J Orthop. 2017;46(2):E105-E107. Copyright Frontline Medical Communications Inc. 2017. All rights reserved.
1. Field LD, Savoie FH. Common elbow injuries in sport. Sports Med. 1998;26(3):193-205.
2. Loomer RL. Elbow injuries in athletes. Can J Appl Sport Sci. 1982;7(3):164-166.
3. Dines JS, Bedi A, Williams PN, et al. Tennis injuries: epidemiology, pathophysiology, and treatment. J Am Acad Orthop Surg. 2015;23(3):181-189.
4. Banks KP, Ly JQ, Beall DP, Grayson DE, Bancroft LW, Tall MA. Overuse injuries of the upper extremity in the competitive athlete: magnetic resonance imaging findings associated with repetitive trauma. Curr Probl Diagn Radiol. 2005;34(4):127-142.
5. Niebulski HZ, Richardson ML. High-grade pronator teres tear in a cricket batsman. Radiol Case Rep. 2015;6(3):540.
6. Zhang X, Shan G. Where do golf drive swings go wrong? Factors influencing driver swing consistency. Scand J Med Sci Sports. 2014;24(5):749-757.
7. Nesbit SM, McGinnis RS. Kinetic constrained optimization of the golf swing hub path. J Sports Sci Med. 2014;13(4):859-873.
8. Helton MS. Conservative treatment of a proximal full-thickness biceps brachii muscle tear in a special operations soldier. Phys Ther. 2014;94(4):571-577.
9. Mitchell K, Banks S, Morgan D, Sugaya H. Shoulder motions during the golf swing in male amateur golfers. J Orthop Sports Phys Ther. 2003;33(4):196-203.
10. Grimshaw P, Giles A, Tong R, Grimmer K. Lower back and elbow injuries in golf. Sports Med. 2002;32(10):655-666.
1. Field LD, Savoie FH. Common elbow injuries in sport. Sports Med. 1998;26(3):193-205.
2. Loomer RL. Elbow injuries in athletes. Can J Appl Sport Sci. 1982;7(3):164-166.
3. Dines JS, Bedi A, Williams PN, et al. Tennis injuries: epidemiology, pathophysiology, and treatment. J Am Acad Orthop Surg. 2015;23(3):181-189.
4. Banks KP, Ly JQ, Beall DP, Grayson DE, Bancroft LW, Tall MA. Overuse injuries of the upper extremity in the competitive athlete: magnetic resonance imaging findings associated with repetitive trauma. Curr Probl Diagn Radiol. 2005;34(4):127-142.
5. Niebulski HZ, Richardson ML. High-grade pronator teres tear in a cricket batsman. Radiol Case Rep. 2015;6(3):540.
6. Zhang X, Shan G. Where do golf drive swings go wrong? Factors influencing driver swing consistency. Scand J Med Sci Sports. 2014;24(5):749-757.
7. Nesbit SM, McGinnis RS. Kinetic constrained optimization of the golf swing hub path. J Sports Sci Med. 2014;13(4):859-873.
8. Helton MS. Conservative treatment of a proximal full-thickness biceps brachii muscle tear in a special operations soldier. Phys Ther. 2014;94(4):571-577.
9. Mitchell K, Banks S, Morgan D, Sugaya H. Shoulder motions during the golf swing in male amateur golfers. J Orthop Sports Phys Ther. 2003;33(4):196-203.
10. Grimshaw P, Giles A, Tong R, Grimmer K. Lower back and elbow injuries in golf. Sports Med. 2002;32(10):655-666.


Dupilumab improved eczema scores in children in open label trial
ORLANDO – Treatment with dupilumab in children and adolescents with moderate to severe atopic dermatitis (AD) reduced severity and pruritus scores from baseline and was well tolerated, in a multicenter, open-label trial of 78 children and adolescents.
Dupilumab’s “powerful ability” to block interleukin-4 and interleukin-13 pathways of inflammation is “especially exciting because AD is even more Th-2 cell driven in children,” said Michael J. Cork, MD, PhD, head of dermatologic research at the University of Sheffield (England), who presented the findings during a late-breaking research session at the annual meeting of the American Academy of Dermatology.
The study assessed the pharmacokinetics, safety, and efficacy of dupilumab and was conducted with 38 children, aged 6-11 years, and 40 adolescents, aged 12-17 years, with moderate to severe AD. All had failed topical corticosteroid therapy. Some of the children (16%) and adolescents (22.5%) had failed at least one systemic therapy.
Both age groups were given either a 2 mg/kg or a 4 mg/kg dose of dupilumab (administered subcutaneously), nothing for 8 weeks, followed by 4 weekly doses of their respective regimens. Mean Eczema Area and Severity Index (EASI) scores at baseline were 31.7 among the adolescents and 35.9 among the children.
At week 12, mean scores in the younger cohort given either 2 mg/kg or 4 mg/kg had improved by 76.2% and 63.4%, respectively, from baseline. In the adolescents, EASI scores at week 12 had improved by a mean of 66.4% in the 2-mg/kg group and 69.7% in the 4-mg/kg group.
Itch also improved “dramatically,” according to Dr. Cork. In the younger children, peak pruritus Numerical Rating Scale scores improved from baseline by a mean of 41.6% in the lower-dose group and 39.6% in the higher-dose group. In the older cohort, pruritus scores improved from baseline by a mean of 30.8% in the lower-dose group and 37.6% in the higher-dose group.
Treatment was well tolerated across the study, and adverse events were “mild, transient, and unrelated,” Dr. Cork said. “I would like to emphasize that these were not related to dupilumab, as they occurred during the period of time after the first dose, in weeks 6 and 7,” he commented. He attributed AD flares experienced in the study to the quick clearance of the drug in the first few weeks.
Dr. Cork reported numerous disclosures, including serving as an adviser, consultant, and investigator for Regeneron, the sponsor of the trial, and Sanofi; the companies developing dupilumab.
[email protected]
On Twitter @whitneymcknight
ORLANDO – Treatment with dupilumab in children and adolescents with moderate to severe atopic dermatitis (AD) reduced severity and pruritus scores from baseline and was well tolerated, in a multicenter, open-label trial of 78 children and adolescents.
Dupilumab’s “powerful ability” to block interleukin-4 and interleukin-13 pathways of inflammation is “especially exciting because AD is even more Th-2 cell driven in children,” said Michael J. Cork, MD, PhD, head of dermatologic research at the University of Sheffield (England), who presented the findings during a late-breaking research session at the annual meeting of the American Academy of Dermatology.
The study assessed the pharmacokinetics, safety, and efficacy of dupilumab and was conducted with 38 children, aged 6-11 years, and 40 adolescents, aged 12-17 years, with moderate to severe AD. All had failed topical corticosteroid therapy. Some of the children (16%) and adolescents (22.5%) had failed at least one systemic therapy.
Both age groups were given either a 2 mg/kg or a 4 mg/kg dose of dupilumab (administered subcutaneously), nothing for 8 weeks, followed by 4 weekly doses of their respective regimens. Mean Eczema Area and Severity Index (EASI) scores at baseline were 31.7 among the adolescents and 35.9 among the children.
At week 12, mean scores in the younger cohort given either 2 mg/kg or 4 mg/kg had improved by 76.2% and 63.4%, respectively, from baseline. In the adolescents, EASI scores at week 12 had improved by a mean of 66.4% in the 2-mg/kg group and 69.7% in the 4-mg/kg group.
Itch also improved “dramatically,” according to Dr. Cork. In the younger children, peak pruritus Numerical Rating Scale scores improved from baseline by a mean of 41.6% in the lower-dose group and 39.6% in the higher-dose group. In the older cohort, pruritus scores improved from baseline by a mean of 30.8% in the lower-dose group and 37.6% in the higher-dose group.
Treatment was well tolerated across the study, and adverse events were “mild, transient, and unrelated,” Dr. Cork said. “I would like to emphasize that these were not related to dupilumab, as they occurred during the period of time after the first dose, in weeks 6 and 7,” he commented. He attributed AD flares experienced in the study to the quick clearance of the drug in the first few weeks.
Dr. Cork reported numerous disclosures, including serving as an adviser, consultant, and investigator for Regeneron, the sponsor of the trial, and Sanofi; the companies developing dupilumab.
[email protected]
On Twitter @whitneymcknight
ORLANDO – Treatment with dupilumab in children and adolescents with moderate to severe atopic dermatitis (AD) reduced severity and pruritus scores from baseline and was well tolerated, in a multicenter, open-label trial of 78 children and adolescents.
Dupilumab’s “powerful ability” to block interleukin-4 and interleukin-13 pathways of inflammation is “especially exciting because AD is even more Th-2 cell driven in children,” said Michael J. Cork, MD, PhD, head of dermatologic research at the University of Sheffield (England), who presented the findings during a late-breaking research session at the annual meeting of the American Academy of Dermatology.
The study assessed the pharmacokinetics, safety, and efficacy of dupilumab and was conducted with 38 children, aged 6-11 years, and 40 adolescents, aged 12-17 years, with moderate to severe AD. All had failed topical corticosteroid therapy. Some of the children (16%) and adolescents (22.5%) had failed at least one systemic therapy.
Both age groups were given either a 2 mg/kg or a 4 mg/kg dose of dupilumab (administered subcutaneously), nothing for 8 weeks, followed by 4 weekly doses of their respective regimens. Mean Eczema Area and Severity Index (EASI) scores at baseline were 31.7 among the adolescents and 35.9 among the children.
At week 12, mean scores in the younger cohort given either 2 mg/kg or 4 mg/kg had improved by 76.2% and 63.4%, respectively, from baseline. In the adolescents, EASI scores at week 12 had improved by a mean of 66.4% in the 2-mg/kg group and 69.7% in the 4-mg/kg group.
Itch also improved “dramatically,” according to Dr. Cork. In the younger children, peak pruritus Numerical Rating Scale scores improved from baseline by a mean of 41.6% in the lower-dose group and 39.6% in the higher-dose group. In the older cohort, pruritus scores improved from baseline by a mean of 30.8% in the lower-dose group and 37.6% in the higher-dose group.
Treatment was well tolerated across the study, and adverse events were “mild, transient, and unrelated,” Dr. Cork said. “I would like to emphasize that these were not related to dupilumab, as they occurred during the period of time after the first dose, in weeks 6 and 7,” he commented. He attributed AD flares experienced in the study to the quick clearance of the drug in the first few weeks.
Dr. Cork reported numerous disclosures, including serving as an adviser, consultant, and investigator for Regeneron, the sponsor of the trial, and Sanofi; the companies developing dupilumab.
[email protected]
On Twitter @whitneymcknight
AT AAD 17
Key clinical point: Data on dupilumab for treating moderate to severe atopic dermatitis in children and adolescents are promising.
Major finding: At week 12, treatment with dupilumab at 2 mg/kg and 4 mg/kg doses, across 8 weeks in two pediatric cohorts improved baseline EASI scores by 69.7% and pruritus scores by a third and was well tolerated.
Data source: A phase IIa, multicenter, open label pharmacokinetics, safety, and efficacy trial evaluating two dosing regimens of dupilumab in 78 children with moderate to severe AD.
Disclosures: Dr. Cork reported numerous disclosures, including serving as an adviser, consultant, and investigator for Regeneron, the sponsor of the trial, and Sanofi – the two companies developing dupilumab.
For optimal care, consider all acne in Latinos inflammatory
ORLANDO – Postinflammatory hyperpigmentation is a common consequence of acne in Latino skin, and aggressive medical treatments or procedures can aggravate the problem.
In fact, the hyperpigmentation that remains after acne is treated can be even more upsetting than the acne itself, according to Mercedes Florez-White, MD.
“Most of the time, the postinflammatory hyperpigmentation [PIH] has much more impact on the patient’s quality of life even than the disease itself, so you need to be very careful when treating these patients,” said Dr. Florez-White of Florida International University, Miami.
Every Fitzpatrick phototype can be observed in the Latino population, but one feature seems to link them: inflammation linked with all types of acne, even comedonal. “Even patients with very pale skin can show, at the periphery of the comedone, a little darkness signaling inflammation. The skin of a mestizo [a person of mixed Spanish/Native American ancestry] is especially prone to this,” she said at the annual meeting of the American Academy of Dermatology.
There is a paucity of research on the treatment of acne in people with skin of color, Dr. Florez-White said. Even the most recent acne treatment guidelines, published in 2016 by the AAD, acknowledge the area as a “research gap” that needs to be addressed.
In the meantime, she offered what she called “pearls of acne wisdom” gleaned from 35 years of treating Latino patients in South America and the United States.
Overview and diagnosis
Nodulocystic acne is the most common type in this population, followed by comedonal acne. Although the comedonal type is not generally considered inflammatory acne, it should be in Latino patients, given their sensitivity to skin inflammation and its outcome. “There is inflammation there from the beginning – treat it as an inflammatory disease for the best results.”
• Acne in Latino patients occurs most commonly, but not exclusively, on the lower face. “We have also seen this on the neck and chest,” she noted.
• A thorough history – including a rundown of hair and skin products the patient is using – is critical. “You never know when something you think is acne is really something else,” like an allergic reaction, she said.
Treatment
There are no AAD-generated treatment guidelines for acne in Latino patients. Dr. Florez-White manages her patients according to a treatment algorithm published by the Ibero-Latin American College of Dermatology and a paper published in the Journal of Dermatologic Treatment (2010 May;21[3]:206-11), as well as her own clinical experience.
Topical therapy
• Start topical retinoids at a lower concentration, two to three times a week, and gradually increase the dose and frequency until the desired effect is reached. Also, start benzoyl peroxide at lower doses.
• For a patient with very proinflammatory cystic acne, initiate a short course of corticosteroids to decrease inflammation – this will reduce the risk of PIH.
• Add azelaic acid in a 20% cream or 15% gel. “It’s an anti-inflammatory and antibacterial, and it really does help reduce the chance of PIH. This is used all over Latin American and Asia, but it is an off-label use in the U.S.” she said.
• For adult women, consider 5% dapsone gel, but not in combination with benzoyl peroxide.
Oral therapy
• Doxycycline is first-line treatment for moderate to severe papulopustular or nodulocystic acne. Other primary agents could be minocycline or tetracycline. Second-line antibiotic choices include erythromycin, azithromycin, and sulfamethoxazole/trimethoprim. Antibiotics should be given with benzoyl peroxide to reduce the chance of bacterial resistance.
• For nonresponsive cases, use oral isotretinoin, started at half the recommended dose. Increase gradually to treatment response.
For women with hormonally mediated acne, give a trial of oral contraceptives with antiandrogen properties, or spironolactone. “I like to combine oral contraceptive pills with isotretinoin. You can give this because the absorption of isotretinoin is very superficial. You won’t have any problems with that,” she noted.
Skin care
Good skin care will help promote healing and generally increase patient compliance with medication, Dr. Florez-White said.
• A noncomedogenic broad-spectrum sunscreen should be used daily. Consider one with mineral oxides, especially iron oxide, as only these preparations scatter both visible light and infrared radiation, which both increase the risk of PIH.
• Cleanse with a synthetic detergent or lipid-free cleanser.
• Recommend daily use of a salicylic, lactic, or glycolic acid.
Camouflage is very important for some patients, especially teens. “I always recommend a noncomedogenic fluid makeup,” she said.
Procedures
• Comedo extraction is an essential part of a comprehensive acne treatment program, but hold off until after a month of retinoid treatment. Removing the lesions significantly decreases the chance of PIH.
• Very superficial chemical peels with salicylic acid alone, or in combination with mandelic acid, may improve outcome faster and decrease PIH that already exists. These can be used in conjunction with oral agents, including isotretinoin.
Dr. Florez-White had no financial disclosures.
[email protected]
On Twitter @alz_gal
ORLANDO – Postinflammatory hyperpigmentation is a common consequence of acne in Latino skin, and aggressive medical treatments or procedures can aggravate the problem.
In fact, the hyperpigmentation that remains after acne is treated can be even more upsetting than the acne itself, according to Mercedes Florez-White, MD.
“Most of the time, the postinflammatory hyperpigmentation [PIH] has much more impact on the patient’s quality of life even than the disease itself, so you need to be very careful when treating these patients,” said Dr. Florez-White of Florida International University, Miami.
Every Fitzpatrick phototype can be observed in the Latino population, but one feature seems to link them: inflammation linked with all types of acne, even comedonal. “Even patients with very pale skin can show, at the periphery of the comedone, a little darkness signaling inflammation. The skin of a mestizo [a person of mixed Spanish/Native American ancestry] is especially prone to this,” she said at the annual meeting of the American Academy of Dermatology.
There is a paucity of research on the treatment of acne in people with skin of color, Dr. Florez-White said. Even the most recent acne treatment guidelines, published in 2016 by the AAD, acknowledge the area as a “research gap” that needs to be addressed.
In the meantime, she offered what she called “pearls of acne wisdom” gleaned from 35 years of treating Latino patients in South America and the United States.
Overview and diagnosis
Nodulocystic acne is the most common type in this population, followed by comedonal acne. Although the comedonal type is not generally considered inflammatory acne, it should be in Latino patients, given their sensitivity to skin inflammation and its outcome. “There is inflammation there from the beginning – treat it as an inflammatory disease for the best results.”
• Acne in Latino patients occurs most commonly, but not exclusively, on the lower face. “We have also seen this on the neck and chest,” she noted.
• A thorough history – including a rundown of hair and skin products the patient is using – is critical. “You never know when something you think is acne is really something else,” like an allergic reaction, she said.
Treatment
There are no AAD-generated treatment guidelines for acne in Latino patients. Dr. Florez-White manages her patients according to a treatment algorithm published by the Ibero-Latin American College of Dermatology and a paper published in the Journal of Dermatologic Treatment (2010 May;21[3]:206-11), as well as her own clinical experience.
Topical therapy
• Start topical retinoids at a lower concentration, two to three times a week, and gradually increase the dose and frequency until the desired effect is reached. Also, start benzoyl peroxide at lower doses.
• For a patient with very proinflammatory cystic acne, initiate a short course of corticosteroids to decrease inflammation – this will reduce the risk of PIH.
• Add azelaic acid in a 20% cream or 15% gel. “It’s an anti-inflammatory and antibacterial, and it really does help reduce the chance of PIH. This is used all over Latin American and Asia, but it is an off-label use in the U.S.” she said.
• For adult women, consider 5% dapsone gel, but not in combination with benzoyl peroxide.
Oral therapy
• Doxycycline is first-line treatment for moderate to severe papulopustular or nodulocystic acne. Other primary agents could be minocycline or tetracycline. Second-line antibiotic choices include erythromycin, azithromycin, and sulfamethoxazole/trimethoprim. Antibiotics should be given with benzoyl peroxide to reduce the chance of bacterial resistance.
• For nonresponsive cases, use oral isotretinoin, started at half the recommended dose. Increase gradually to treatment response.
For women with hormonally mediated acne, give a trial of oral contraceptives with antiandrogen properties, or spironolactone. “I like to combine oral contraceptive pills with isotretinoin. You can give this because the absorption of isotretinoin is very superficial. You won’t have any problems with that,” she noted.
Skin care
Good skin care will help promote healing and generally increase patient compliance with medication, Dr. Florez-White said.
• A noncomedogenic broad-spectrum sunscreen should be used daily. Consider one with mineral oxides, especially iron oxide, as only these preparations scatter both visible light and infrared radiation, which both increase the risk of PIH.
• Cleanse with a synthetic detergent or lipid-free cleanser.
• Recommend daily use of a salicylic, lactic, or glycolic acid.
Camouflage is very important for some patients, especially teens. “I always recommend a noncomedogenic fluid makeup,” she said.
Procedures
• Comedo extraction is an essential part of a comprehensive acne treatment program, but hold off until after a month of retinoid treatment. Removing the lesions significantly decreases the chance of PIH.
• Very superficial chemical peels with salicylic acid alone, or in combination with mandelic acid, may improve outcome faster and decrease PIH that already exists. These can be used in conjunction with oral agents, including isotretinoin.
Dr. Florez-White had no financial disclosures.
[email protected]
On Twitter @alz_gal
ORLANDO – Postinflammatory hyperpigmentation is a common consequence of acne in Latino skin, and aggressive medical treatments or procedures can aggravate the problem.
In fact, the hyperpigmentation that remains after acne is treated can be even more upsetting than the acne itself, according to Mercedes Florez-White, MD.
“Most of the time, the postinflammatory hyperpigmentation [PIH] has much more impact on the patient’s quality of life even than the disease itself, so you need to be very careful when treating these patients,” said Dr. Florez-White of Florida International University, Miami.
Every Fitzpatrick phototype can be observed in the Latino population, but one feature seems to link them: inflammation linked with all types of acne, even comedonal. “Even patients with very pale skin can show, at the periphery of the comedone, a little darkness signaling inflammation. The skin of a mestizo [a person of mixed Spanish/Native American ancestry] is especially prone to this,” she said at the annual meeting of the American Academy of Dermatology.
There is a paucity of research on the treatment of acne in people with skin of color, Dr. Florez-White said. Even the most recent acne treatment guidelines, published in 2016 by the AAD, acknowledge the area as a “research gap” that needs to be addressed.
In the meantime, she offered what she called “pearls of acne wisdom” gleaned from 35 years of treating Latino patients in South America and the United States.
Overview and diagnosis
Nodulocystic acne is the most common type in this population, followed by comedonal acne. Although the comedonal type is not generally considered inflammatory acne, it should be in Latino patients, given their sensitivity to skin inflammation and its outcome. “There is inflammation there from the beginning – treat it as an inflammatory disease for the best results.”
• Acne in Latino patients occurs most commonly, but not exclusively, on the lower face. “We have also seen this on the neck and chest,” she noted.
• A thorough history – including a rundown of hair and skin products the patient is using – is critical. “You never know when something you think is acne is really something else,” like an allergic reaction, she said.
Treatment
There are no AAD-generated treatment guidelines for acne in Latino patients. Dr. Florez-White manages her patients according to a treatment algorithm published by the Ibero-Latin American College of Dermatology and a paper published in the Journal of Dermatologic Treatment (2010 May;21[3]:206-11), as well as her own clinical experience.
Topical therapy
• Start topical retinoids at a lower concentration, two to three times a week, and gradually increase the dose and frequency until the desired effect is reached. Also, start benzoyl peroxide at lower doses.
• For a patient with very proinflammatory cystic acne, initiate a short course of corticosteroids to decrease inflammation – this will reduce the risk of PIH.
• Add azelaic acid in a 20% cream or 15% gel. “It’s an anti-inflammatory and antibacterial, and it really does help reduce the chance of PIH. This is used all over Latin American and Asia, but it is an off-label use in the U.S.” she said.
• For adult women, consider 5% dapsone gel, but not in combination with benzoyl peroxide.
Oral therapy
• Doxycycline is first-line treatment for moderate to severe papulopustular or nodulocystic acne. Other primary agents could be minocycline or tetracycline. Second-line antibiotic choices include erythromycin, azithromycin, and sulfamethoxazole/trimethoprim. Antibiotics should be given with benzoyl peroxide to reduce the chance of bacterial resistance.
• For nonresponsive cases, use oral isotretinoin, started at half the recommended dose. Increase gradually to treatment response.
For women with hormonally mediated acne, give a trial of oral contraceptives with antiandrogen properties, or spironolactone. “I like to combine oral contraceptive pills with isotretinoin. You can give this because the absorption of isotretinoin is very superficial. You won’t have any problems with that,” she noted.
Skin care
Good skin care will help promote healing and generally increase patient compliance with medication, Dr. Florez-White said.
• A noncomedogenic broad-spectrum sunscreen should be used daily. Consider one with mineral oxides, especially iron oxide, as only these preparations scatter both visible light and infrared radiation, which both increase the risk of PIH.
• Cleanse with a synthetic detergent or lipid-free cleanser.
• Recommend daily use of a salicylic, lactic, or glycolic acid.
Camouflage is very important for some patients, especially teens. “I always recommend a noncomedogenic fluid makeup,” she said.
Procedures
• Comedo extraction is an essential part of a comprehensive acne treatment program, but hold off until after a month of retinoid treatment. Removing the lesions significantly decreases the chance of PIH.
• Very superficial chemical peels with salicylic acid alone, or in combination with mandelic acid, may improve outcome faster and decrease PIH that already exists. These can be used in conjunction with oral agents, including isotretinoin.
Dr. Florez-White had no financial disclosures.
[email protected]
On Twitter @alz_gal
EXPERT ANALYSIS FROM AAD 17
Education: Register Now for the 2017 VAM
The topic is vascular care. The subjects to be covered are nearly too numerous to count. And the clock is ticking for signing up.
Registration and housing will open in early March for the 2017 Vascular Annual Meeting, set for May 31 to June 3 in San Diego, Calif., with plenaries and exhibits from June 1 to 3. This premier meeting of vascular specialists will be held at the San Diego Convention Center. The headquarters hotel, the Marriott Marquis San Diego Marina Hotel, adjoins the center.
There is plenty going on.
Additional programming: Expanded programming begins Wednesday and continues through Saturday. Be sure to plan your travel to attend these informative sessions. This year’s meeting includes more concurrent sessions, and the number of joint society programs has doubled from last year.
Free postgraduate courses for SVS members: Once again, all SVS member-registrants receive free admittance to the six Wednesday postgraduate courses, a savings of $300. Non-members plus anyone registering only for the postgraduate courses must pay the appropriate registration fee. Self-assessment credit is available to all physician attendees.
SVS/STS Aortic Summit: New this year, and a highlight for Saturday, is the SVS/STS Summit: Advances and Controversies in the Management of Complex Thoracoabdominal Aneurysmal Diseases and Type B Aortic Dissection. This program will take place from 1 to 5 p.m. and is co-sponsored by the Society of Thoracic Surgeons. An additional fee is required. ![]()
Revamped workshops: Wednesday’s workshops will feature a new format, with four separate two-hour timeslots, and the opportunity to rotate between sessions in each time period. Cost is $100 for each timeslot and registration is required. Attendance is limited to 25 registrants per workshop; register early for the best selection.
Expanded international programming: A new session has been added to Wednesday’s International program: “International Consortium of Vascular Registries: Quality Improvement in Vascular Surgery Goes Global.” This presentation will be held from 8 to 10 a.m. and kicks off a full day of international events.
VQI @ VAM – VQI’s Second Annual Meeting: Vascular Quality Initiative’s second Annual Meeting has expanded to 1 ½ days, beginning Tuesday afternoon, May 30, and continuing all day Wednesday. Also new this year are a poster session and networking reception. Registration and a separate $200 fee are required.
Exhibit Hall: Learn first-hand from our industry partners about the latest devices, products and services. The Exhibit Hall also hosts the Opening Reception, box lunches and coffee breaks Thursday through Saturday. Industry participation in the exhibits underwrites a signification portion of VAM – allowing us to keep registration fees at lower rates than other industry meetings – so please support our industry partners.
And more: VAM also will include: breakfast sessions; a discount for the On-Demand Library; texting of questions; Interactive Poster Session, programming for fellows, residents and students; the Physician Vascular Interpretation Examination Review course; SVS Member Business Luncheon, with the election of officers plus the presentation of SVS and SVS Foundation awards; Vascular Live sessions highlighting the latest products and developments; plus socializing, with alumni receptions and other events.
For information and to register, visit vsweb.org/VAM17.
The topic is vascular care. The subjects to be covered are nearly too numerous to count. And the clock is ticking for signing up.
Registration and housing will open in early March for the 2017 Vascular Annual Meeting, set for May 31 to June 3 in San Diego, Calif., with plenaries and exhibits from June 1 to 3. This premier meeting of vascular specialists will be held at the San Diego Convention Center. The headquarters hotel, the Marriott Marquis San Diego Marina Hotel, adjoins the center.
There is plenty going on.
Additional programming: Expanded programming begins Wednesday and continues through Saturday. Be sure to plan your travel to attend these informative sessions. This year’s meeting includes more concurrent sessions, and the number of joint society programs has doubled from last year.
Free postgraduate courses for SVS members: Once again, all SVS member-registrants receive free admittance to the six Wednesday postgraduate courses, a savings of $300. Non-members plus anyone registering only for the postgraduate courses must pay the appropriate registration fee. Self-assessment credit is available to all physician attendees.
SVS/STS Aortic Summit: New this year, and a highlight for Saturday, is the SVS/STS Summit: Advances and Controversies in the Management of Complex Thoracoabdominal Aneurysmal Diseases and Type B Aortic Dissection. This program will take place from 1 to 5 p.m. and is co-sponsored by the Society of Thoracic Surgeons. An additional fee is required. ![]()
Revamped workshops: Wednesday’s workshops will feature a new format, with four separate two-hour timeslots, and the opportunity to rotate between sessions in each time period. Cost is $100 for each timeslot and registration is required. Attendance is limited to 25 registrants per workshop; register early for the best selection.
Expanded international programming: A new session has been added to Wednesday’s International program: “International Consortium of Vascular Registries: Quality Improvement in Vascular Surgery Goes Global.” This presentation will be held from 8 to 10 a.m. and kicks off a full day of international events.
VQI @ VAM – VQI’s Second Annual Meeting: Vascular Quality Initiative’s second Annual Meeting has expanded to 1 ½ days, beginning Tuesday afternoon, May 30, and continuing all day Wednesday. Also new this year are a poster session and networking reception. Registration and a separate $200 fee are required.
Exhibit Hall: Learn first-hand from our industry partners about the latest devices, products and services. The Exhibit Hall also hosts the Opening Reception, box lunches and coffee breaks Thursday through Saturday. Industry participation in the exhibits underwrites a signification portion of VAM – allowing us to keep registration fees at lower rates than other industry meetings – so please support our industry partners.
And more: VAM also will include: breakfast sessions; a discount for the On-Demand Library; texting of questions; Interactive Poster Session, programming for fellows, residents and students; the Physician Vascular Interpretation Examination Review course; SVS Member Business Luncheon, with the election of officers plus the presentation of SVS and SVS Foundation awards; Vascular Live sessions highlighting the latest products and developments; plus socializing, with alumni receptions and other events.
For information and to register, visit vsweb.org/VAM17.
The topic is vascular care. The subjects to be covered are nearly too numerous to count. And the clock is ticking for signing up.
Registration and housing will open in early March for the 2017 Vascular Annual Meeting, set for May 31 to June 3 in San Diego, Calif., with plenaries and exhibits from June 1 to 3. This premier meeting of vascular specialists will be held at the San Diego Convention Center. The headquarters hotel, the Marriott Marquis San Diego Marina Hotel, adjoins the center.
There is plenty going on.
Additional programming: Expanded programming begins Wednesday and continues through Saturday. Be sure to plan your travel to attend these informative sessions. This year’s meeting includes more concurrent sessions, and the number of joint society programs has doubled from last year.
Free postgraduate courses for SVS members: Once again, all SVS member-registrants receive free admittance to the six Wednesday postgraduate courses, a savings of $300. Non-members plus anyone registering only for the postgraduate courses must pay the appropriate registration fee. Self-assessment credit is available to all physician attendees.
SVS/STS Aortic Summit: New this year, and a highlight for Saturday, is the SVS/STS Summit: Advances and Controversies in the Management of Complex Thoracoabdominal Aneurysmal Diseases and Type B Aortic Dissection. This program will take place from 1 to 5 p.m. and is co-sponsored by the Society of Thoracic Surgeons. An additional fee is required. ![]()
Revamped workshops: Wednesday’s workshops will feature a new format, with four separate two-hour timeslots, and the opportunity to rotate between sessions in each time period. Cost is $100 for each timeslot and registration is required. Attendance is limited to 25 registrants per workshop; register early for the best selection.
Expanded international programming: A new session has been added to Wednesday’s International program: “International Consortium of Vascular Registries: Quality Improvement in Vascular Surgery Goes Global.” This presentation will be held from 8 to 10 a.m. and kicks off a full day of international events.
VQI @ VAM – VQI’s Second Annual Meeting: Vascular Quality Initiative’s second Annual Meeting has expanded to 1 ½ days, beginning Tuesday afternoon, May 30, and continuing all day Wednesday. Also new this year are a poster session and networking reception. Registration and a separate $200 fee are required.
Exhibit Hall: Learn first-hand from our industry partners about the latest devices, products and services. The Exhibit Hall also hosts the Opening Reception, box lunches and coffee breaks Thursday through Saturday. Industry participation in the exhibits underwrites a signification portion of VAM – allowing us to keep registration fees at lower rates than other industry meetings – so please support our industry partners.
And more: VAM also will include: breakfast sessions; a discount for the On-Demand Library; texting of questions; Interactive Poster Session, programming for fellows, residents and students; the Physician Vascular Interpretation Examination Review course; SVS Member Business Luncheon, with the election of officers plus the presentation of SVS and SVS Foundation awards; Vascular Live sessions highlighting the latest products and developments; plus socializing, with alumni receptions and other events.
For information and to register, visit vsweb.org/VAM17.
Preoperative variables can predict prolonged air leak
Prolonged air leak is a well-known complication after lung cancer surgery that can worsen patient outcomes and drive up costs, and while international authors have developed tools to calculate the risk of PAL, their use has been limited in the United States for various reasons. Researchers at the University of Pittsburgh have reported on a predictive model that uses easy-to-obtain patient factors, such as forced expiratory volume and smoking history, to help surgeons identify patients at greatest risk for complications and implement preventative measures.
Adam Attaar and his coauthors reported that their nomogram had an accuracy rate of 76%, with a 95% confidence interval, for predicting PAL after surgery (J Thorac Cardiovasc Surg. 2017 March;153[3]:690-9). “Using readily available candidate variables, our nomogram predicts increasing risk of prolonged air leak with good discriminatory ability,” noted Mr. Attaar, a student at University of Pittsburgh, and his coauthors.
Previously published reports put the incidence of PAL complications at 6%-18%, they noted. In the University of Pittsburgh series of 2,317 patients who had pulmonary resection for lung cancer or nodules from January 2009 to June 2014, the incidence was 8.6%.
In this series, patients with PAL were more likely to be older, men, and smokers, and to have a lower body mass index, peripheral vascular disease, chronic obstructive pulmonary disease, a history of steroid use, a high Zubrod score and lower forced expiratory volume.“They were less likely to have diabetes or to be hospitalized before surgery,” the researchers said. Surgical factors that characterized patients with PAL were resection for primary lung cancer rather than benign or metastatic tumors; lobectomy/segmentectomy or bilobectomy rather than wedge resection; a right-sided resection; thoracotomy; and a surgeon with higher annual caseloads.
Not all those factors made it into the nomogram, however. The nomogram scores each of these 10 variables to calculate the risk of PAL, in order of their weighting: lower forced expiratory volume, procedure type, BMI, right-sided thoracotomy, preoperative hospitalization, annual surgeon caseload, wedge resection by thoracotomy, reoperation, smoking history, and Zubrod score. A second nomogram drops out surgeon volume to make it more generalizable to other institutions.
In explaining higher surgeon volume as a risk factor for PAL, the researchers said that high-volume surgeons may be operating on patients with variables not accounted for in the Society of Thoracic Surgeons General Thoracic Surgery Database. “These unmeasured variables … could reveal modifiable technical factors to reduce the incidence of PAL and require further study,” the researchers said.
Fast-track discharge has gained acceptance in recent years as a way to spare patients a prolonged hospital stay and cut costs, but in this series the median hospital stay for patients with PAL was 10 days vs. 4 days for non-PAL patients (P less than 0.001).
“An accurate and generalizable PAL risk stratification tool could facilitate surgical decision making and patient-specific care” and aid in the design of trials to evaluate air-leak reduction methods such as sealants, buttressed staple lines, and pneumoperitoneum the researchers wrote.
Going forward, further development of the model would involve a multicenter study and inclusion of risk factors not accounted for in the thoracic surgery database, they noted.
The researchers had no relevant financial relationships to disclose.
The authors of this study “have performed a rigorous set of analyses to create this model,” Chi-Fu Jeffrey Yang, MD, of Duke University, Durham, N.C., noted in his invited commentary (J Thorac Cardiovasc Surg. 2017 March;53[3]:700-1). “The strengths of this study include its sound statistical analysis and study design,” Dr. Yang wrote. He gave the authors credit for using bootstrapping to internally validate the model.
However, Dr. Yang said that the database used by the researchers did not account for “numerous important variables,” including presence of pleural adhesions and emphysema status. The analysis also grouped lobectomy and segmentectomy together, and did not consider intraoperative variables such as sealant use, or postoperative management.
While Dr. Yang commended the study authors for developing a “reliable nomogram,” getting it implemented in the clinic is another hurdle. “It is commonly cited that it takes approximately 17 years for research evidence to translate into daily practice,” he said. To shorten that time line, he suggested the authors take a cue from various tech groups: Develop an app that surgeons can use.
Dr. Yang had no relevant financial relationships to disclose.
The authors of this study “have performed a rigorous set of analyses to create this model,” Chi-Fu Jeffrey Yang, MD, of Duke University, Durham, N.C., noted in his invited commentary (J Thorac Cardiovasc Surg. 2017 March;53[3]:700-1). “The strengths of this study include its sound statistical analysis and study design,” Dr. Yang wrote. He gave the authors credit for using bootstrapping to internally validate the model.
However, Dr. Yang said that the database used by the researchers did not account for “numerous important variables,” including presence of pleural adhesions and emphysema status. The analysis also grouped lobectomy and segmentectomy together, and did not consider intraoperative variables such as sealant use, or postoperative management.
While Dr. Yang commended the study authors for developing a “reliable nomogram,” getting it implemented in the clinic is another hurdle. “It is commonly cited that it takes approximately 17 years for research evidence to translate into daily practice,” he said. To shorten that time line, he suggested the authors take a cue from various tech groups: Develop an app that surgeons can use.
Dr. Yang had no relevant financial relationships to disclose.
The authors of this study “have performed a rigorous set of analyses to create this model,” Chi-Fu Jeffrey Yang, MD, of Duke University, Durham, N.C., noted in his invited commentary (J Thorac Cardiovasc Surg. 2017 March;53[3]:700-1). “The strengths of this study include its sound statistical analysis and study design,” Dr. Yang wrote. He gave the authors credit for using bootstrapping to internally validate the model.
However, Dr. Yang said that the database used by the researchers did not account for “numerous important variables,” including presence of pleural adhesions and emphysema status. The analysis also grouped lobectomy and segmentectomy together, and did not consider intraoperative variables such as sealant use, or postoperative management.
While Dr. Yang commended the study authors for developing a “reliable nomogram,” getting it implemented in the clinic is another hurdle. “It is commonly cited that it takes approximately 17 years for research evidence to translate into daily practice,” he said. To shorten that time line, he suggested the authors take a cue from various tech groups: Develop an app that surgeons can use.
Dr. Yang had no relevant financial relationships to disclose.
Prolonged air leak is a well-known complication after lung cancer surgery that can worsen patient outcomes and drive up costs, and while international authors have developed tools to calculate the risk of PAL, their use has been limited in the United States for various reasons. Researchers at the University of Pittsburgh have reported on a predictive model that uses easy-to-obtain patient factors, such as forced expiratory volume and smoking history, to help surgeons identify patients at greatest risk for complications and implement preventative measures.
Adam Attaar and his coauthors reported that their nomogram had an accuracy rate of 76%, with a 95% confidence interval, for predicting PAL after surgery (J Thorac Cardiovasc Surg. 2017 March;153[3]:690-9). “Using readily available candidate variables, our nomogram predicts increasing risk of prolonged air leak with good discriminatory ability,” noted Mr. Attaar, a student at University of Pittsburgh, and his coauthors.
Previously published reports put the incidence of PAL complications at 6%-18%, they noted. In the University of Pittsburgh series of 2,317 patients who had pulmonary resection for lung cancer or nodules from January 2009 to June 2014, the incidence was 8.6%.
In this series, patients with PAL were more likely to be older, men, and smokers, and to have a lower body mass index, peripheral vascular disease, chronic obstructive pulmonary disease, a history of steroid use, a high Zubrod score and lower forced expiratory volume.“They were less likely to have diabetes or to be hospitalized before surgery,” the researchers said. Surgical factors that characterized patients with PAL were resection for primary lung cancer rather than benign or metastatic tumors; lobectomy/segmentectomy or bilobectomy rather than wedge resection; a right-sided resection; thoracotomy; and a surgeon with higher annual caseloads.
Not all those factors made it into the nomogram, however. The nomogram scores each of these 10 variables to calculate the risk of PAL, in order of their weighting: lower forced expiratory volume, procedure type, BMI, right-sided thoracotomy, preoperative hospitalization, annual surgeon caseload, wedge resection by thoracotomy, reoperation, smoking history, and Zubrod score. A second nomogram drops out surgeon volume to make it more generalizable to other institutions.
In explaining higher surgeon volume as a risk factor for PAL, the researchers said that high-volume surgeons may be operating on patients with variables not accounted for in the Society of Thoracic Surgeons General Thoracic Surgery Database. “These unmeasured variables … could reveal modifiable technical factors to reduce the incidence of PAL and require further study,” the researchers said.
Fast-track discharge has gained acceptance in recent years as a way to spare patients a prolonged hospital stay and cut costs, but in this series the median hospital stay for patients with PAL was 10 days vs. 4 days for non-PAL patients (P less than 0.001).
“An accurate and generalizable PAL risk stratification tool could facilitate surgical decision making and patient-specific care” and aid in the design of trials to evaluate air-leak reduction methods such as sealants, buttressed staple lines, and pneumoperitoneum the researchers wrote.
Going forward, further development of the model would involve a multicenter study and inclusion of risk factors not accounted for in the thoracic surgery database, they noted.
The researchers had no relevant financial relationships to disclose.
Prolonged air leak is a well-known complication after lung cancer surgery that can worsen patient outcomes and drive up costs, and while international authors have developed tools to calculate the risk of PAL, their use has been limited in the United States for various reasons. Researchers at the University of Pittsburgh have reported on a predictive model that uses easy-to-obtain patient factors, such as forced expiratory volume and smoking history, to help surgeons identify patients at greatest risk for complications and implement preventative measures.
Adam Attaar and his coauthors reported that their nomogram had an accuracy rate of 76%, with a 95% confidence interval, for predicting PAL after surgery (J Thorac Cardiovasc Surg. 2017 March;153[3]:690-9). “Using readily available candidate variables, our nomogram predicts increasing risk of prolonged air leak with good discriminatory ability,” noted Mr. Attaar, a student at University of Pittsburgh, and his coauthors.
Previously published reports put the incidence of PAL complications at 6%-18%, they noted. In the University of Pittsburgh series of 2,317 patients who had pulmonary resection for lung cancer or nodules from January 2009 to June 2014, the incidence was 8.6%.
In this series, patients with PAL were more likely to be older, men, and smokers, and to have a lower body mass index, peripheral vascular disease, chronic obstructive pulmonary disease, a history of steroid use, a high Zubrod score and lower forced expiratory volume.“They were less likely to have diabetes or to be hospitalized before surgery,” the researchers said. Surgical factors that characterized patients with PAL were resection for primary lung cancer rather than benign or metastatic tumors; lobectomy/segmentectomy or bilobectomy rather than wedge resection; a right-sided resection; thoracotomy; and a surgeon with higher annual caseloads.
Not all those factors made it into the nomogram, however. The nomogram scores each of these 10 variables to calculate the risk of PAL, in order of their weighting: lower forced expiratory volume, procedure type, BMI, right-sided thoracotomy, preoperative hospitalization, annual surgeon caseload, wedge resection by thoracotomy, reoperation, smoking history, and Zubrod score. A second nomogram drops out surgeon volume to make it more generalizable to other institutions.
In explaining higher surgeon volume as a risk factor for PAL, the researchers said that high-volume surgeons may be operating on patients with variables not accounted for in the Society of Thoracic Surgeons General Thoracic Surgery Database. “These unmeasured variables … could reveal modifiable technical factors to reduce the incidence of PAL and require further study,” the researchers said.
Fast-track discharge has gained acceptance in recent years as a way to spare patients a prolonged hospital stay and cut costs, but in this series the median hospital stay for patients with PAL was 10 days vs. 4 days for non-PAL patients (P less than 0.001).
“An accurate and generalizable PAL risk stratification tool could facilitate surgical decision making and patient-specific care” and aid in the design of trials to evaluate air-leak reduction methods such as sealants, buttressed staple lines, and pneumoperitoneum the researchers wrote.
Going forward, further development of the model would involve a multicenter study and inclusion of risk factors not accounted for in the thoracic surgery database, they noted.
The researchers had no relevant financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Preoperative variables can be evaluated to determine patient risk for prolonged air leak (PAL) in lung resection for cancer.
Major finding: A nomogram demonstrated 76% discriminatory accuracy in predicting PAL after lung resection.
Data source: Analysis of 2,522 pulmonary resections performed at eight hospitals within the University of Pittsburgh health system from January 2009 to June 2014.
Disclosures: The researchers had no conflicts of interest to disclose.
Colonic Diaphragm Disease: An Important NSAID Complication to Know
Colonic diaphragm disease (CDD) is a rare but serious complication of nonsteroidal anti‐inflammatory drug (NSAID) use in which diaphragm‐like strictures develop in the large and/or small intestines. There have been about 100 reported cases of CDD since this finding was first reported in the medical literature in 1989.1,2 However, given the frequency of NSAID use, providers should consider this diagnosis.
Case Report
An 85-year‐old woman presented to the emergency department (ED) with generalized weakness, occult positive stool, and severe anemia requiring blood transfusions. Eight months prior, she had presented to her primary care physician (PCP) for a routine visit and was found to have anemia. She was referred to gastroenterology by her PCP for an upper endoscopy but refused the referral despite clear warnings of the potential for serious complications. She was started on ferrous sulfate 325 mg po tid at that time. The patient’s hemoglobin (Hbg) levels ranged from 10.8 to 11.2 g/dL prior to her ED presentation, and random fecal occult blood testing had been negative.
In the ED, the patient reported no abdominal pain, nausea emesis or constipation. Her past medical history was significant for compensated diastolic heart failure, paroxysmal atrial fibrillation controlled by medication, and chronic lumbago. The patient had been prescribed NSAIDs for 10 years for the chronic lumbago diagnosis; however, she was inconsistent in taking this medication until more recent years. Surgical history included a hysterectomy and back surgeries in the distant past. She had no symptoms or history of inflammatory bowel disease. The patient’s medications included both the oral and topical forms of diclofenac, conjugated estrogen, nitroglycerin, amlodipine, hydrocodone bitartrate and acetaminophen 5 mg once daily, amiodarone, diazepam, valsartan, furosemide, oxycodone 5 mg nightly prn for severe pain, and ferrous sulfate 325 mg.
Significant laboratory results in the ED included a Hbg level of 8.3 g/dL; a ferritin level of 11.9 ng/mL, and a serum iron level of 12 mg/dL. A computerized tomography scan of the abdomen and pelvis was normal. The patient was admitted, received a blood transfusion, and a gastroenterology consult was obtained for an upper and lower endoscopy. Although copy was normal, the colonoscopy revealed evidence of CDD of the ascending colon.
Colonic Diaphragm Disease
The gross findings seen on this patient’s colonoscopy showed evidence of the development of an internal colonic stricture from the fibrous overgrowth of the diaphragm (Figures A, B, & C). The narrow lumen is exhibited particularly well in Figure A in the upper left image. The external surface of the intestine appears normal.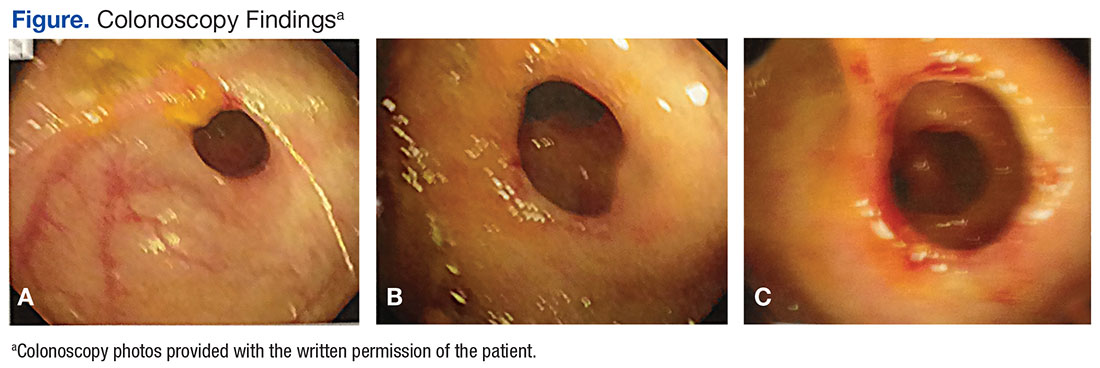
Presentation and Evaluation
The presenting symptoms of CDD can vary and include abdominal pain, vomiting, lower gastrointestinal bleeding, anemia, and intestinal obstruction/perforation. Evidence seems to suggest a greater association with use of the oxicams (meloxicam, piroxicam) or diclofenac.1,2 Some researchers have suggested an association with long‐acting NSAID formulations.1 The use of misoprostol or proton pump inhibitors does not seem to lessen the chance of stricture formulation.2 Cox‐2 inhibitors are less likely players in the development of CDD.2 Most diaphragms in the large colon have been noted in the cecum, ascending and transverse colon, though descending colonic lesions have been documented as well.1
The incidence of CDD is higher among women and occurs most often in the seventh decade of life. Correlation with the duration of NSAID use prior to disease onset varies widely, with studies documenting disease onset from 3 months to 5 years after initiating consistent NSAID use.1 The patient in this case study was prescribed NSAIDs for almost 10 years, although she had poor adherence. One study also notes a possible association of CYP2C9*3 genetic polymorphism with the propensity to develop CDD. This finding is particularly interesting since NSAIDs are principally metabolized by CYP2C9 in the liver. CYP2C9 polymorphisms are thought to induce higher plasma concentrations of NSAIDs over time, which may lead to the formation of colonic diaphragms.2
Endoscopy with biopsy is the diagnostic modality of choice. Use of capsule endoscopy is limited because the capsule may not be able to pass through narrow stricture walls.
Pathology and Histology
The mechanism by which NSAIDs induce the formation of colonic diaphragms may be related to these medications’ effects on mucosal integrity, vasoconstriction, and vascular spasm. These effects may lead to “erosions, ulceration, and diaphragm-like strictures.”3
The primary histologic feature of these strictures is submucosal fibrosis with an intact muscularis propria. Prominent features also include areas of ulceration and granulation.1 The widened submucosa results in annular constriction of the intestinal lumen with disorganized bundles of smooth muscle, unmyelinated nerve bundles, scattered ganglion cells, and blood vessels. This morphology can resemble a node or mass.4 The mucosa is typically normal.5 Conditions such as vascular and neuromuscular hamartoma can resemble CDD. Interestingly, the fibrous changes in CDD have been noted apart from NSAID use, leading to speculation that diaphragm formation may be a result of injury and not exclusively a reaction to NSAID use.5
Treatment
Recommendations include NSAID withdrawal, endoscopic/fluoroscopic dilatation, and surgical resection. Outcomes with these treatment approaches have been highly variable. For some patients, NSAID withdrawal alone or following resection has resulted in success. However, even with withdrawal of NSAIDs, symptoms may improve, although the histologic findings of CDD may not be reversed.3,6 In one case report, a colonic stricture persisted endoscopically after NSAID withdrawal but resolved after a 20-week course of prednisone.7
Conclusion
Despite NSAID cessation, the patient in this case study presented a month later with an acute bowel obstruction. The bowel obstruction responded to conservative treatment, and the patient declined surgical intervention. The patient was readmitted again 4 months later with an acute bowel obstruction, and underwent an emergent colonic resection. The pathology report was consistent with CDD. In the 3 years since the resection, the patient has had no recurrences and continues to avoid all NSAIDs. She has refused a follow-up postresection colonoscopy.
1. Munipalle PC, Garud T, Light D. Diaphragmatic disease of the colon: systematic review. Colorectal Dis. 2013;15(9):1063-1069.
2. Ishihara M, Ohmiya N, Nakamura M, et al. Risk factors of symptomatic NSAID-induced small intestinal injury and diaphragm disease. Aliment Pharmacol Ther. 2014;40(5):538-547.
3. Keeling AN, Davis JL, Williams A, Sabharwal T, Adam A. Fluoroscopically guided balloon dilation of NSAID-induced colonic diaphragm. J Vasc Interv Radiol. 2007;18(8):1060-1062.
4. Yousfi MM, De Petris G, Leighton JA, et al. Diaphragm disease after use of nonsteroidal anti-inflammatory agents: first report of diagnosis with capsule endoscopy. J Clin Gastroenterol. 2004;38(8):686-691.
5. Pilgrim S, Velchuru V, Waters G, Tsiamis A, Lal R. Diaphragm disease and small bowel enteropathy due to nonsteroidal anti-inflammatory drugs: a surgical perspective. Colorectal Dis. 2011;13(4):463-466.
6. Munipalle PC, Little M, Garud T, Henderson D. NSAID-induced diaphragmatic disease of the colon. BMJ Case Rep. 2013;2013:pii:bcr2012008448.
7. Penner RM, Williams CN. Resolution of multiple severe nonsteroidal anti-inflammatory drug-induced colonic strictures with prednisone therapy: a case report and review of the literature. Can J Gastroenterol. 2003;17(8):497-500.
Colonic diaphragm disease (CDD) is a rare but serious complication of nonsteroidal anti‐inflammatory drug (NSAID) use in which diaphragm‐like strictures develop in the large and/or small intestines. There have been about 100 reported cases of CDD since this finding was first reported in the medical literature in 1989.1,2 However, given the frequency of NSAID use, providers should consider this diagnosis.
Case Report
An 85-year‐old woman presented to the emergency department (ED) with generalized weakness, occult positive stool, and severe anemia requiring blood transfusions. Eight months prior, she had presented to her primary care physician (PCP) for a routine visit and was found to have anemia. She was referred to gastroenterology by her PCP for an upper endoscopy but refused the referral despite clear warnings of the potential for serious complications. She was started on ferrous sulfate 325 mg po tid at that time. The patient’s hemoglobin (Hbg) levels ranged from 10.8 to 11.2 g/dL prior to her ED presentation, and random fecal occult blood testing had been negative.
In the ED, the patient reported no abdominal pain, nausea emesis or constipation. Her past medical history was significant for compensated diastolic heart failure, paroxysmal atrial fibrillation controlled by medication, and chronic lumbago. The patient had been prescribed NSAIDs for 10 years for the chronic lumbago diagnosis; however, she was inconsistent in taking this medication until more recent years. Surgical history included a hysterectomy and back surgeries in the distant past. She had no symptoms or history of inflammatory bowel disease. The patient’s medications included both the oral and topical forms of diclofenac, conjugated estrogen, nitroglycerin, amlodipine, hydrocodone bitartrate and acetaminophen 5 mg once daily, amiodarone, diazepam, valsartan, furosemide, oxycodone 5 mg nightly prn for severe pain, and ferrous sulfate 325 mg.
Significant laboratory results in the ED included a Hbg level of 8.3 g/dL; a ferritin level of 11.9 ng/mL, and a serum iron level of 12 mg/dL. A computerized tomography scan of the abdomen and pelvis was normal. The patient was admitted, received a blood transfusion, and a gastroenterology consult was obtained for an upper and lower endoscopy. Although copy was normal, the colonoscopy revealed evidence of CDD of the ascending colon.
Colonic Diaphragm Disease
The gross findings seen on this patient’s colonoscopy showed evidence of the development of an internal colonic stricture from the fibrous overgrowth of the diaphragm (Figures A, B, & C). The narrow lumen is exhibited particularly well in Figure A in the upper left image. The external surface of the intestine appears normal.
Presentation and Evaluation
The presenting symptoms of CDD can vary and include abdominal pain, vomiting, lower gastrointestinal bleeding, anemia, and intestinal obstruction/perforation. Evidence seems to suggest a greater association with use of the oxicams (meloxicam, piroxicam) or diclofenac.1,2 Some researchers have suggested an association with long‐acting NSAID formulations.1 The use of misoprostol or proton pump inhibitors does not seem to lessen the chance of stricture formulation.2 Cox‐2 inhibitors are less likely players in the development of CDD.2 Most diaphragms in the large colon have been noted in the cecum, ascending and transverse colon, though descending colonic lesions have been documented as well.1
The incidence of CDD is higher among women and occurs most often in the seventh decade of life. Correlation with the duration of NSAID use prior to disease onset varies widely, with studies documenting disease onset from 3 months to 5 years after initiating consistent NSAID use.1 The patient in this case study was prescribed NSAIDs for almost 10 years, although she had poor adherence. One study also notes a possible association of CYP2C9*3 genetic polymorphism with the propensity to develop CDD. This finding is particularly interesting since NSAIDs are principally metabolized by CYP2C9 in the liver. CYP2C9 polymorphisms are thought to induce higher plasma concentrations of NSAIDs over time, which may lead to the formation of colonic diaphragms.2
Endoscopy with biopsy is the diagnostic modality of choice. Use of capsule endoscopy is limited because the capsule may not be able to pass through narrow stricture walls.
Pathology and Histology
The mechanism by which NSAIDs induce the formation of colonic diaphragms may be related to these medications’ effects on mucosal integrity, vasoconstriction, and vascular spasm. These effects may lead to “erosions, ulceration, and diaphragm-like strictures.”3
The primary histologic feature of these strictures is submucosal fibrosis with an intact muscularis propria. Prominent features also include areas of ulceration and granulation.1 The widened submucosa results in annular constriction of the intestinal lumen with disorganized bundles of smooth muscle, unmyelinated nerve bundles, scattered ganglion cells, and blood vessels. This morphology can resemble a node or mass.4 The mucosa is typically normal.5 Conditions such as vascular and neuromuscular hamartoma can resemble CDD. Interestingly, the fibrous changes in CDD have been noted apart from NSAID use, leading to speculation that diaphragm formation may be a result of injury and not exclusively a reaction to NSAID use.5
Treatment
Recommendations include NSAID withdrawal, endoscopic/fluoroscopic dilatation, and surgical resection. Outcomes with these treatment approaches have been highly variable. For some patients, NSAID withdrawal alone or following resection has resulted in success. However, even with withdrawal of NSAIDs, symptoms may improve, although the histologic findings of CDD may not be reversed.3,6 In one case report, a colonic stricture persisted endoscopically after NSAID withdrawal but resolved after a 20-week course of prednisone.7
Conclusion
Despite NSAID cessation, the patient in this case study presented a month later with an acute bowel obstruction. The bowel obstruction responded to conservative treatment, and the patient declined surgical intervention. The patient was readmitted again 4 months later with an acute bowel obstruction, and underwent an emergent colonic resection. The pathology report was consistent with CDD. In the 3 years since the resection, the patient has had no recurrences and continues to avoid all NSAIDs. She has refused a follow-up postresection colonoscopy.
Colonic diaphragm disease (CDD) is a rare but serious complication of nonsteroidal anti‐inflammatory drug (NSAID) use in which diaphragm‐like strictures develop in the large and/or small intestines. There have been about 100 reported cases of CDD since this finding was first reported in the medical literature in 1989.1,2 However, given the frequency of NSAID use, providers should consider this diagnosis.
Case Report
An 85-year‐old woman presented to the emergency department (ED) with generalized weakness, occult positive stool, and severe anemia requiring blood transfusions. Eight months prior, she had presented to her primary care physician (PCP) for a routine visit and was found to have anemia. She was referred to gastroenterology by her PCP for an upper endoscopy but refused the referral despite clear warnings of the potential for serious complications. She was started on ferrous sulfate 325 mg po tid at that time. The patient’s hemoglobin (Hbg) levels ranged from 10.8 to 11.2 g/dL prior to her ED presentation, and random fecal occult blood testing had been negative.
In the ED, the patient reported no abdominal pain, nausea emesis or constipation. Her past medical history was significant for compensated diastolic heart failure, paroxysmal atrial fibrillation controlled by medication, and chronic lumbago. The patient had been prescribed NSAIDs for 10 years for the chronic lumbago diagnosis; however, she was inconsistent in taking this medication until more recent years. Surgical history included a hysterectomy and back surgeries in the distant past. She had no symptoms or history of inflammatory bowel disease. The patient’s medications included both the oral and topical forms of diclofenac, conjugated estrogen, nitroglycerin, amlodipine, hydrocodone bitartrate and acetaminophen 5 mg once daily, amiodarone, diazepam, valsartan, furosemide, oxycodone 5 mg nightly prn for severe pain, and ferrous sulfate 325 mg.
Significant laboratory results in the ED included a Hbg level of 8.3 g/dL; a ferritin level of 11.9 ng/mL, and a serum iron level of 12 mg/dL. A computerized tomography scan of the abdomen and pelvis was normal. The patient was admitted, received a blood transfusion, and a gastroenterology consult was obtained for an upper and lower endoscopy. Although copy was normal, the colonoscopy revealed evidence of CDD of the ascending colon.
Colonic Diaphragm Disease
The gross findings seen on this patient’s colonoscopy showed evidence of the development of an internal colonic stricture from the fibrous overgrowth of the diaphragm (Figures A, B, & C). The narrow lumen is exhibited particularly well in Figure A in the upper left image. The external surface of the intestine appears normal.
Presentation and Evaluation
The presenting symptoms of CDD can vary and include abdominal pain, vomiting, lower gastrointestinal bleeding, anemia, and intestinal obstruction/perforation. Evidence seems to suggest a greater association with use of the oxicams (meloxicam, piroxicam) or diclofenac.1,2 Some researchers have suggested an association with long‐acting NSAID formulations.1 The use of misoprostol or proton pump inhibitors does not seem to lessen the chance of stricture formulation.2 Cox‐2 inhibitors are less likely players in the development of CDD.2 Most diaphragms in the large colon have been noted in the cecum, ascending and transverse colon, though descending colonic lesions have been documented as well.1
The incidence of CDD is higher among women and occurs most often in the seventh decade of life. Correlation with the duration of NSAID use prior to disease onset varies widely, with studies documenting disease onset from 3 months to 5 years after initiating consistent NSAID use.1 The patient in this case study was prescribed NSAIDs for almost 10 years, although she had poor adherence. One study also notes a possible association of CYP2C9*3 genetic polymorphism with the propensity to develop CDD. This finding is particularly interesting since NSAIDs are principally metabolized by CYP2C9 in the liver. CYP2C9 polymorphisms are thought to induce higher plasma concentrations of NSAIDs over time, which may lead to the formation of colonic diaphragms.2
Endoscopy with biopsy is the diagnostic modality of choice. Use of capsule endoscopy is limited because the capsule may not be able to pass through narrow stricture walls.
Pathology and Histology
The mechanism by which NSAIDs induce the formation of colonic diaphragms may be related to these medications’ effects on mucosal integrity, vasoconstriction, and vascular spasm. These effects may lead to “erosions, ulceration, and diaphragm-like strictures.”3
The primary histologic feature of these strictures is submucosal fibrosis with an intact muscularis propria. Prominent features also include areas of ulceration and granulation.1 The widened submucosa results in annular constriction of the intestinal lumen with disorganized bundles of smooth muscle, unmyelinated nerve bundles, scattered ganglion cells, and blood vessels. This morphology can resemble a node or mass.4 The mucosa is typically normal.5 Conditions such as vascular and neuromuscular hamartoma can resemble CDD. Interestingly, the fibrous changes in CDD have been noted apart from NSAID use, leading to speculation that diaphragm formation may be a result of injury and not exclusively a reaction to NSAID use.5
Treatment
Recommendations include NSAID withdrawal, endoscopic/fluoroscopic dilatation, and surgical resection. Outcomes with these treatment approaches have been highly variable. For some patients, NSAID withdrawal alone or following resection has resulted in success. However, even with withdrawal of NSAIDs, symptoms may improve, although the histologic findings of CDD may not be reversed.3,6 In one case report, a colonic stricture persisted endoscopically after NSAID withdrawal but resolved after a 20-week course of prednisone.7
Conclusion
Despite NSAID cessation, the patient in this case study presented a month later with an acute bowel obstruction. The bowel obstruction responded to conservative treatment, and the patient declined surgical intervention. The patient was readmitted again 4 months later with an acute bowel obstruction, and underwent an emergent colonic resection. The pathology report was consistent with CDD. In the 3 years since the resection, the patient has had no recurrences and continues to avoid all NSAIDs. She has refused a follow-up postresection colonoscopy.
1. Munipalle PC, Garud T, Light D. Diaphragmatic disease of the colon: systematic review. Colorectal Dis. 2013;15(9):1063-1069.
2. Ishihara M, Ohmiya N, Nakamura M, et al. Risk factors of symptomatic NSAID-induced small intestinal injury and diaphragm disease. Aliment Pharmacol Ther. 2014;40(5):538-547.
3. Keeling AN, Davis JL, Williams A, Sabharwal T, Adam A. Fluoroscopically guided balloon dilation of NSAID-induced colonic diaphragm. J Vasc Interv Radiol. 2007;18(8):1060-1062.
4. Yousfi MM, De Petris G, Leighton JA, et al. Diaphragm disease after use of nonsteroidal anti-inflammatory agents: first report of diagnosis with capsule endoscopy. J Clin Gastroenterol. 2004;38(8):686-691.
5. Pilgrim S, Velchuru V, Waters G, Tsiamis A, Lal R. Diaphragm disease and small bowel enteropathy due to nonsteroidal anti-inflammatory drugs: a surgical perspective. Colorectal Dis. 2011;13(4):463-466.
6. Munipalle PC, Little M, Garud T, Henderson D. NSAID-induced diaphragmatic disease of the colon. BMJ Case Rep. 2013;2013:pii:bcr2012008448.
7. Penner RM, Williams CN. Resolution of multiple severe nonsteroidal anti-inflammatory drug-induced colonic strictures with prednisone therapy: a case report and review of the literature. Can J Gastroenterol. 2003;17(8):497-500.
1. Munipalle PC, Garud T, Light D. Diaphragmatic disease of the colon: systematic review. Colorectal Dis. 2013;15(9):1063-1069.
2. Ishihara M, Ohmiya N, Nakamura M, et al. Risk factors of symptomatic NSAID-induced small intestinal injury and diaphragm disease. Aliment Pharmacol Ther. 2014;40(5):538-547.
3. Keeling AN, Davis JL, Williams A, Sabharwal T, Adam A. Fluoroscopically guided balloon dilation of NSAID-induced colonic diaphragm. J Vasc Interv Radiol. 2007;18(8):1060-1062.
4. Yousfi MM, De Petris G, Leighton JA, et al. Diaphragm disease after use of nonsteroidal anti-inflammatory agents: first report of diagnosis with capsule endoscopy. J Clin Gastroenterol. 2004;38(8):686-691.
5. Pilgrim S, Velchuru V, Waters G, Tsiamis A, Lal R. Diaphragm disease and small bowel enteropathy due to nonsteroidal anti-inflammatory drugs: a surgical perspective. Colorectal Dis. 2011;13(4):463-466.
6. Munipalle PC, Little M, Garud T, Henderson D. NSAID-induced diaphragmatic disease of the colon. BMJ Case Rep. 2013;2013:pii:bcr2012008448.
7. Penner RM, Williams CN. Resolution of multiple severe nonsteroidal anti-inflammatory drug-induced colonic strictures with prednisone therapy: a case report and review of the literature. Can J Gastroenterol. 2003;17(8):497-500.
Apixaban bests warfarin in real-world analysis

WASHINGTON, DC—An analysis of real-world data suggests elderly patients with non-valvular atrial fibrillation (NVAF) have a lower risk of stroke or systemic embolism and a lower risk of major bleeding if they receive apixaban rather than warfarin.
The study also indicates that elderly NVAF patients who receive dabigatran have a similar risk of stroke/systemic embolism as those on warfarin, but the risk of major bleeding is lower with dabigatran.
And rivaroxaban poses a lower risk of stroke/systemic embolism than warfarin but a higher risk of major bleeding.
However, the researchers who conducted this analysis stressed that it cannot be used as stand-alone evidence to validate the efficacy and/or safety of any of the drugs studied.
The results of the analysis were presented at the American College of Cardiology’s 66th Annual Scientific Session (abstract 1134M-13).
The researchers also presented data on the financial costs of major bleeding associated with apixaban, dabigatran, rivaroxaban, and warfarin (abstract 1189-085/085).
The research was conducted by employees from Bristol-Myers Squibb Company and Pfizer Inc., the companies marketing apixaban, as well as other researchers who have relationships with the companies.
The team evaluated medical and pharmacy claims from the US Medicare fee-for-service database. They looked at NVAF patients age 65 and older who were newly prescribed apixaban, dabigatran, rivaroxaban, or warfarin between January 1, 2013, and December 31, 2014.
The researchers compared each of the direct oral anticoagulants to warfarin using 1:1 propensity score matching methodology to balance select demographic and clinical characteristics between the groups.
The team used Cox proportional hazards models to estimate the hazard ratio (HR) of stroke/systemic embolism and major bleeding.
Results
In a comparison of apixaban and warfarin (20,803 patients in each treatment group), apixaban was associated with a significantly lower risk of stroke or systemic embolism than warfarin (HR: 0.40, 95% CI: 0.31-0.53; P<0.0001).
Apixaban was also associated with a significantly lower risk of major bleeding than warfarin (HR: 0.51, 95% CI: 0.44-0.58; P<0.0001). The cost of major bleeding per patient per month was $286 with apixaban and $537 with warfarin (P<0.0001).
In a comparison of dabigatran and warfarin (16,731 patients in each treatment group), the risk of stroke or systemic embolism was similar between the cohorts (HR: 0.94, 95% CI: 0.74-1.21; P=0.647).
However, the risk of major bleeding was significantly lower with dabigatran than with warfarin (HR: 0.79, 95% CI: 0.69-0.91; P=0.001). The cost of major bleeding per patient per month was $367 with dabigatran and $452 with warfarin (P=0.032).
In a comparison of rivaroxaban and warfarin (52,476 patients in each group), rivaroxaban was associated with a significantly lower risk of stroke or systemic embolism than warfarin (HR: 0.72, 95% CI: 0.63-0.83; P<0.0001).
However, the risk of major bleeding was significantly higher with rivaroxaban than with warfarin (HR: 1.17, 95% CI: 1.10-1.26; P<0.0001). The cost of major bleeding per patient per month was $524 with rivaroxaban and $500 with warfarin (P=0.154).
Limitations
The researchers noted that this analysis has several limitations. For instance, information on laboratory results and time in therapeutic range were not available. Diagnoses were identified through ICD-9 codes, and drug prescriptions were identified through prescription claims.
Propensity score matching was used to mimic randomization by balancing pre-defined demographic and clinical characteristics at baseline for both treatment cohorts. However, unobserved confounders (such as laboratory values and patient preferences) may exist.
As with any real-world data analysis, missing values, coding errors, and a lack of clinical accuracy may have introduced bias.
The researchers stressed that, due to such limitations, real-world data analyses cannot be used as stand-alone evidence to validate the efficacy and/or safety of a treatment. However, these analyses add to information provided by randomized clinical trials.
“Studies such as this large US Medicare database analysis supplement pivotal trials by broadening and deepening our scientific knowledge of how patients respond to direct oral anticoagulants in everyday clinical practice,” said Alpesh Amin, MD, principal investigator and professor of medicine at the University of California, Irvine.
“Given the diversity of patients with non-valvular atrial fibrillation, analyses of real-world data provide further information that adds to data generated in randomized clinical trials.” ![]()
WASHINGTON, DC—An analysis of real-world data suggests elderly patients with non-valvular atrial fibrillation (NVAF) have a lower risk of stroke or systemic embolism and a lower risk of major bleeding if they receive apixaban rather than warfarin.
The study also indicates that elderly NVAF patients who receive dabigatran have a similar risk of stroke/systemic embolism as those on warfarin, but the risk of major bleeding is lower with dabigatran.
And rivaroxaban poses a lower risk of stroke/systemic embolism than warfarin but a higher risk of major bleeding.
However, the researchers who conducted this analysis stressed that it cannot be used as stand-alone evidence to validate the efficacy and/or safety of any of the drugs studied.
The results of the analysis were presented at the American College of Cardiology’s 66th Annual Scientific Session (abstract 1134M-13).
The researchers also presented data on the financial costs of major bleeding associated with apixaban, dabigatran, rivaroxaban, and warfarin (abstract 1189-085/085).
The research was conducted by employees from Bristol-Myers Squibb Company and Pfizer Inc., the companies marketing apixaban, as well as other researchers who have relationships with the companies.
The team evaluated medical and pharmacy claims from the US Medicare fee-for-service database. They looked at NVAF patients age 65 and older who were newly prescribed apixaban, dabigatran, rivaroxaban, or warfarin between January 1, 2013, and December 31, 2014.
The researchers compared each of the direct oral anticoagulants to warfarin using 1:1 propensity score matching methodology to balance select demographic and clinical characteristics between the groups.
The team used Cox proportional hazards models to estimate the hazard ratio (HR) of stroke/systemic embolism and major bleeding.
Results
In a comparison of apixaban and warfarin (20,803 patients in each treatment group), apixaban was associated with a significantly lower risk of stroke or systemic embolism than warfarin (HR: 0.40, 95% CI: 0.31-0.53; P<0.0001).
Apixaban was also associated with a significantly lower risk of major bleeding than warfarin (HR: 0.51, 95% CI: 0.44-0.58; P<0.0001). The cost of major bleeding per patient per month was $286 with apixaban and $537 with warfarin (P<0.0001).
In a comparison of dabigatran and warfarin (16,731 patients in each treatment group), the risk of stroke or systemic embolism was similar between the cohorts (HR: 0.94, 95% CI: 0.74-1.21; P=0.647).
However, the risk of major bleeding was significantly lower with dabigatran than with warfarin (HR: 0.79, 95% CI: 0.69-0.91; P=0.001). The cost of major bleeding per patient per month was $367 with dabigatran and $452 with warfarin (P=0.032).
In a comparison of rivaroxaban and warfarin (52,476 patients in each group), rivaroxaban was associated with a significantly lower risk of stroke or systemic embolism than warfarin (HR: 0.72, 95% CI: 0.63-0.83; P<0.0001).
However, the risk of major bleeding was significantly higher with rivaroxaban than with warfarin (HR: 1.17, 95% CI: 1.10-1.26; P<0.0001). The cost of major bleeding per patient per month was $524 with rivaroxaban and $500 with warfarin (P=0.154).
Limitations
The researchers noted that this analysis has several limitations. For instance, information on laboratory results and time in therapeutic range were not available. Diagnoses were identified through ICD-9 codes, and drug prescriptions were identified through prescription claims.
Propensity score matching was used to mimic randomization by balancing pre-defined demographic and clinical characteristics at baseline for both treatment cohorts. However, unobserved confounders (such as laboratory values and patient preferences) may exist.
As with any real-world data analysis, missing values, coding errors, and a lack of clinical accuracy may have introduced bias.
The researchers stressed that, due to such limitations, real-world data analyses cannot be used as stand-alone evidence to validate the efficacy and/or safety of a treatment. However, these analyses add to information provided by randomized clinical trials.
“Studies such as this large US Medicare database analysis supplement pivotal trials by broadening and deepening our scientific knowledge of how patients respond to direct oral anticoagulants in everyday clinical practice,” said Alpesh Amin, MD, principal investigator and professor of medicine at the University of California, Irvine.
“Given the diversity of patients with non-valvular atrial fibrillation, analyses of real-world data provide further information that adds to data generated in randomized clinical trials.” ![]()
WASHINGTON, DC—An analysis of real-world data suggests elderly patients with non-valvular atrial fibrillation (NVAF) have a lower risk of stroke or systemic embolism and a lower risk of major bleeding if they receive apixaban rather than warfarin.
The study also indicates that elderly NVAF patients who receive dabigatran have a similar risk of stroke/systemic embolism as those on warfarin, but the risk of major bleeding is lower with dabigatran.
And rivaroxaban poses a lower risk of stroke/systemic embolism than warfarin but a higher risk of major bleeding.
However, the researchers who conducted this analysis stressed that it cannot be used as stand-alone evidence to validate the efficacy and/or safety of any of the drugs studied.
The results of the analysis were presented at the American College of Cardiology’s 66th Annual Scientific Session (abstract 1134M-13).
The researchers also presented data on the financial costs of major bleeding associated with apixaban, dabigatran, rivaroxaban, and warfarin (abstract 1189-085/085).
The research was conducted by employees from Bristol-Myers Squibb Company and Pfizer Inc., the companies marketing apixaban, as well as other researchers who have relationships with the companies.
The team evaluated medical and pharmacy claims from the US Medicare fee-for-service database. They looked at NVAF patients age 65 and older who were newly prescribed apixaban, dabigatran, rivaroxaban, or warfarin between January 1, 2013, and December 31, 2014.
The researchers compared each of the direct oral anticoagulants to warfarin using 1:1 propensity score matching methodology to balance select demographic and clinical characteristics between the groups.
The team used Cox proportional hazards models to estimate the hazard ratio (HR) of stroke/systemic embolism and major bleeding.
Results
In a comparison of apixaban and warfarin (20,803 patients in each treatment group), apixaban was associated with a significantly lower risk of stroke or systemic embolism than warfarin (HR: 0.40, 95% CI: 0.31-0.53; P<0.0001).
Apixaban was also associated with a significantly lower risk of major bleeding than warfarin (HR: 0.51, 95% CI: 0.44-0.58; P<0.0001). The cost of major bleeding per patient per month was $286 with apixaban and $537 with warfarin (P<0.0001).
In a comparison of dabigatran and warfarin (16,731 patients in each treatment group), the risk of stroke or systemic embolism was similar between the cohorts (HR: 0.94, 95% CI: 0.74-1.21; P=0.647).
However, the risk of major bleeding was significantly lower with dabigatran than with warfarin (HR: 0.79, 95% CI: 0.69-0.91; P=0.001). The cost of major bleeding per patient per month was $367 with dabigatran and $452 with warfarin (P=0.032).
In a comparison of rivaroxaban and warfarin (52,476 patients in each group), rivaroxaban was associated with a significantly lower risk of stroke or systemic embolism than warfarin (HR: 0.72, 95% CI: 0.63-0.83; P<0.0001).
However, the risk of major bleeding was significantly higher with rivaroxaban than with warfarin (HR: 1.17, 95% CI: 1.10-1.26; P<0.0001). The cost of major bleeding per patient per month was $524 with rivaroxaban and $500 with warfarin (P=0.154).
Limitations
The researchers noted that this analysis has several limitations. For instance, information on laboratory results and time in therapeutic range were not available. Diagnoses were identified through ICD-9 codes, and drug prescriptions were identified through prescription claims.
Propensity score matching was used to mimic randomization by balancing pre-defined demographic and clinical characteristics at baseline for both treatment cohorts. However, unobserved confounders (such as laboratory values and patient preferences) may exist.
As with any real-world data analysis, missing values, coding errors, and a lack of clinical accuracy may have introduced bias.
The researchers stressed that, due to such limitations, real-world data analyses cannot be used as stand-alone evidence to validate the efficacy and/or safety of a treatment. However, these analyses add to information provided by randomized clinical trials.
“Studies such as this large US Medicare database analysis supplement pivotal trials by broadening and deepening our scientific knowledge of how patients respond to direct oral anticoagulants in everyday clinical practice,” said Alpesh Amin, MD, principal investigator and professor of medicine at the University of California, Irvine.
“Given the diversity of patients with non-valvular atrial fibrillation, analyses of real-world data provide further information that adds to data generated in randomized clinical trials.” ![]()