User login
HHS proposal may limit birth control access
The Trump administration has drafted a plan that would allow more employers to opt out of offering no-cost contraception coverage to women based on religious or moral grounds, according to a leaked copy of the interim rule.
The proposed rule, first obtained by the media outlet Vox, would greatly expand the religious exemption under the Affordable Care Act for employers otherwise subject to the ACA’s contraception mandate. If approved, the rule would allow additional entities and employers that object to the mandate for religious or moral reasons to be exempt from providing coverage. The exception would apply to plans sponsored by objecting employers, whether or not they operate as a nonprofit, according to the leaked rule.

The American Congress of Obstetricians and Gynecologists denounced the rule, saying the proposal would wipe away women’s access to care and put women in all insurance plans at risk of losing coverage they have today.
“Contraception is an integral part of preventive care and a medical necessity for women during approximately 30 years of their lives. Access to contraception allows women to achieve, lead, and reach their full potentials, becoming key drivers of our Nation’s economic success,” Haywood L. Brown, MD, ACOG president, said in a statement. “Since the Affordable Care Act increased access to contraceptives, our nation has achieved a 30-year low in its unintended pregnancy rate, including among teens. Any move to decrease access to these vital services would have damaging effects on public health. Women, families, and our nation all benefit from seamless, affordable access to contraception.”
The White House has declined to comment about the leaked proposal. However, in early May, HHS Secretary Tom Price, MD, said he welcomed the chance to reexamine the ACA’s contraception mandate.

Since the ACA’s contraceptive mandate took effect, it has been the subject of multiple court challenges across the country. The mandate requires nearly all employers to provide coverage of birth control to employees, except for group health plans of “religious employers,” which are deemed exempt. Those religious employers are for the most part churches and other houses of worship.
The Obama administration later created a workaround for another group – nonprofit religious employers – to opt out of the mandate, but critics argued the process itself was a violation of their religious freedom. The issue led to the case of Zubik v. Burwell, a legal challenge over the mandate exemption that went before the U.S. Supreme Court in March 2016.
But the issue remained unresolved. In May 2016, the Supreme Court vacated the lower court rulings related to Zubik v. Burwell and remanded the case back to the four appeals courts that had originally ruled on the issue.
[email protected]
On Twitter @legal_med
The Trump administration has drafted a plan that would allow more employers to opt out of offering no-cost contraception coverage to women based on religious or moral grounds, according to a leaked copy of the interim rule.
The proposed rule, first obtained by the media outlet Vox, would greatly expand the religious exemption under the Affordable Care Act for employers otherwise subject to the ACA’s contraception mandate. If approved, the rule would allow additional entities and employers that object to the mandate for religious or moral reasons to be exempt from providing coverage. The exception would apply to plans sponsored by objecting employers, whether or not they operate as a nonprofit, according to the leaked rule.
The American Congress of Obstetricians and Gynecologists denounced the rule, saying the proposal would wipe away women’s access to care and put women in all insurance plans at risk of losing coverage they have today.
“Contraception is an integral part of preventive care and a medical necessity for women during approximately 30 years of their lives. Access to contraception allows women to achieve, lead, and reach their full potentials, becoming key drivers of our Nation’s economic success,” Haywood L. Brown, MD, ACOG president, said in a statement. “Since the Affordable Care Act increased access to contraceptives, our nation has achieved a 30-year low in its unintended pregnancy rate, including among teens. Any move to decrease access to these vital services would have damaging effects on public health. Women, families, and our nation all benefit from seamless, affordable access to contraception.”
The White House has declined to comment about the leaked proposal. However, in early May, HHS Secretary Tom Price, MD, said he welcomed the chance to reexamine the ACA’s contraception mandate.
Since the ACA’s contraceptive mandate took effect, it has been the subject of multiple court challenges across the country. The mandate requires nearly all employers to provide coverage of birth control to employees, except for group health plans of “religious employers,” which are deemed exempt. Those religious employers are for the most part churches and other houses of worship.
The Obama administration later created a workaround for another group – nonprofit religious employers – to opt out of the mandate, but critics argued the process itself was a violation of their religious freedom. The issue led to the case of Zubik v. Burwell, a legal challenge over the mandate exemption that went before the U.S. Supreme Court in March 2016.
But the issue remained unresolved. In May 2016, the Supreme Court vacated the lower court rulings related to Zubik v. Burwell and remanded the case back to the four appeals courts that had originally ruled on the issue.
[email protected]
On Twitter @legal_med
The Trump administration has drafted a plan that would allow more employers to opt out of offering no-cost contraception coverage to women based on religious or moral grounds, according to a leaked copy of the interim rule.
The proposed rule, first obtained by the media outlet Vox, would greatly expand the religious exemption under the Affordable Care Act for employers otherwise subject to the ACA’s contraception mandate. If approved, the rule would allow additional entities and employers that object to the mandate for religious or moral reasons to be exempt from providing coverage. The exception would apply to plans sponsored by objecting employers, whether or not they operate as a nonprofit, according to the leaked rule.
The American Congress of Obstetricians and Gynecologists denounced the rule, saying the proposal would wipe away women’s access to care and put women in all insurance plans at risk of losing coverage they have today.
“Contraception is an integral part of preventive care and a medical necessity for women during approximately 30 years of their lives. Access to contraception allows women to achieve, lead, and reach their full potentials, becoming key drivers of our Nation’s economic success,” Haywood L. Brown, MD, ACOG president, said in a statement. “Since the Affordable Care Act increased access to contraceptives, our nation has achieved a 30-year low in its unintended pregnancy rate, including among teens. Any move to decrease access to these vital services would have damaging effects on public health. Women, families, and our nation all benefit from seamless, affordable access to contraception.”
The White House has declined to comment about the leaked proposal. However, in early May, HHS Secretary Tom Price, MD, said he welcomed the chance to reexamine the ACA’s contraception mandate.
Since the ACA’s contraceptive mandate took effect, it has been the subject of multiple court challenges across the country. The mandate requires nearly all employers to provide coverage of birth control to employees, except for group health plans of “religious employers,” which are deemed exempt. Those religious employers are for the most part churches and other houses of worship.
The Obama administration later created a workaround for another group – nonprofit religious employers – to opt out of the mandate, but critics argued the process itself was a violation of their religious freedom. The issue led to the case of Zubik v. Burwell, a legal challenge over the mandate exemption that went before the U.S. Supreme Court in March 2016.
But the issue remained unresolved. In May 2016, the Supreme Court vacated the lower court rulings related to Zubik v. Burwell and remanded the case back to the four appeals courts that had originally ruled on the issue.
[email protected]
On Twitter @legal_med
Biomarker panel promising for early endometriosis diagnosis
VANCOUVER – Investigators at McMaster University in Hamilton, Ontario, are zeroing in on a biomarker blood test panel to diagnose endometriosis without surgery.
At the World Congress on Endometriosis, they described a decision tree incorporating blood levels of brain-derived neurotrophic factor (BDNF), glycodelin, and zinc-alpha2-glycoprotein (ZAG), quantified by enzyme-linked immunosorbent assay. ZAG levels above 91.58 ng/mL – the first cut in the decision tree, glycodelin above 39.19 ng/mL – the second cut, and BDNF above 953.9 pg/mL identified endometriosis with a sensitivity of 89.2% and a specificity of 70.0%. The combination outperformed any biomarker on its own.
BDNF is a protein involved in neurogenesis, angiogenesis, and apoptosis resistance, all hallmark pathogenic features of endometriosis. Glycodelin and ZAG are associated with secretory endometrium.
The findings come from a comparison of blood levels in 65 women undergoing endometriosis surgery with the blood levels in 14 women undergoing surgery for benign gynecological problems, and in 16 healthy controls with no history of pelvic pain.
The need is great for a noninvasive test to diagnose endometriosis. Currently, diagnosis is made during surgery and can be delayed for several years. Like investigators at other institutions, the research team at McMaster is hoping to develop an easy, accurate way to catch and treat the disease early before complications set in.
Early diagnosis has “resisted our best efforts for years, but we are slowly moving closer to the end zone,” said senior investigator Warren Foster, PhD, a professor of obstetrics and gynecology at McMaster.
Other teams have reported favorable results for microRNAs, circulating endometrial stem cells, biomarker combinations, and other approaches. “It seems to me that there is a lot of progress being made. One of the big issues that we still have to solve is reproducibility, but there’s so much coming forward,” Dr. Foster said. “It’s an exciting time to be looking for novel diagnostic markers for endometriosis.”
The McMaster team next plans to test its panel prospectively in women with suspected early stage disease.
The work was funded by the Canadian Institutes of Health Research. Dr. Foster is in talks with industry to license the algorithm.
VANCOUVER – Investigators at McMaster University in Hamilton, Ontario, are zeroing in on a biomarker blood test panel to diagnose endometriosis without surgery.
At the World Congress on Endometriosis, they described a decision tree incorporating blood levels of brain-derived neurotrophic factor (BDNF), glycodelin, and zinc-alpha2-glycoprotein (ZAG), quantified by enzyme-linked immunosorbent assay. ZAG levels above 91.58 ng/mL – the first cut in the decision tree, glycodelin above 39.19 ng/mL – the second cut, and BDNF above 953.9 pg/mL identified endometriosis with a sensitivity of 89.2% and a specificity of 70.0%. The combination outperformed any biomarker on its own.
BDNF is a protein involved in neurogenesis, angiogenesis, and apoptosis resistance, all hallmark pathogenic features of endometriosis. Glycodelin and ZAG are associated with secretory endometrium.
The findings come from a comparison of blood levels in 65 women undergoing endometriosis surgery with the blood levels in 14 women undergoing surgery for benign gynecological problems, and in 16 healthy controls with no history of pelvic pain.
The need is great for a noninvasive test to diagnose endometriosis. Currently, diagnosis is made during surgery and can be delayed for several years. Like investigators at other institutions, the research team at McMaster is hoping to develop an easy, accurate way to catch and treat the disease early before complications set in.
Early diagnosis has “resisted our best efforts for years, but we are slowly moving closer to the end zone,” said senior investigator Warren Foster, PhD, a professor of obstetrics and gynecology at McMaster.
Other teams have reported favorable results for microRNAs, circulating endometrial stem cells, biomarker combinations, and other approaches. “It seems to me that there is a lot of progress being made. One of the big issues that we still have to solve is reproducibility, but there’s so much coming forward,” Dr. Foster said. “It’s an exciting time to be looking for novel diagnostic markers for endometriosis.”
The McMaster team next plans to test its panel prospectively in women with suspected early stage disease.
The work was funded by the Canadian Institutes of Health Research. Dr. Foster is in talks with industry to license the algorithm.
VANCOUVER – Investigators at McMaster University in Hamilton, Ontario, are zeroing in on a biomarker blood test panel to diagnose endometriosis without surgery.
At the World Congress on Endometriosis, they described a decision tree incorporating blood levels of brain-derived neurotrophic factor (BDNF), glycodelin, and zinc-alpha2-glycoprotein (ZAG), quantified by enzyme-linked immunosorbent assay. ZAG levels above 91.58 ng/mL – the first cut in the decision tree, glycodelin above 39.19 ng/mL – the second cut, and BDNF above 953.9 pg/mL identified endometriosis with a sensitivity of 89.2% and a specificity of 70.0%. The combination outperformed any biomarker on its own.
BDNF is a protein involved in neurogenesis, angiogenesis, and apoptosis resistance, all hallmark pathogenic features of endometriosis. Glycodelin and ZAG are associated with secretory endometrium.
The findings come from a comparison of blood levels in 65 women undergoing endometriosis surgery with the blood levels in 14 women undergoing surgery for benign gynecological problems, and in 16 healthy controls with no history of pelvic pain.
The need is great for a noninvasive test to diagnose endometriosis. Currently, diagnosis is made during surgery and can be delayed for several years. Like investigators at other institutions, the research team at McMaster is hoping to develop an easy, accurate way to catch and treat the disease early before complications set in.
Early diagnosis has “resisted our best efforts for years, but we are slowly moving closer to the end zone,” said senior investigator Warren Foster, PhD, a professor of obstetrics and gynecology at McMaster.
Other teams have reported favorable results for microRNAs, circulating endometrial stem cells, biomarker combinations, and other approaches. “It seems to me that there is a lot of progress being made. One of the big issues that we still have to solve is reproducibility, but there’s so much coming forward,” Dr. Foster said. “It’s an exciting time to be looking for novel diagnostic markers for endometriosis.”
The McMaster team next plans to test its panel prospectively in women with suspected early stage disease.
The work was funded by the Canadian Institutes of Health Research. Dr. Foster is in talks with industry to license the algorithm.
AT WCE 2017
Key clinical point:
Major finding: Zinc-alpha2-glycoprotein levels above 91.58 ng/mL, glycodelin above 39.19 ng/mL, and brain-derived neurotrophic factor above 953.30 pg/mL identified endometriosis with a sensitivity of 89.2% and a specificity of 70.0%.
Data source: A case-control review of 95 women.
Disclosures: The work was funded by the Canadian Institutes of Health Research. The investigators are in talks with industry to license the algorithm.
Medical treatments for uterine fibroids show promise in efficacy and safety studies
Up to 80% of women who are of reproductive age have uterine fibroids that cause heavy and prolonged bleeding.1 Additional concerns include infertility and pain, says James Simon, MD, Clinical Professor at George Washington University in Washington, DC. Black women are more likely than white women to undergo hysterectomy for uterine fibroids. They also are more likely to experience severe or very severe symptoms from fibroids and report that these symptoms interfere with physical activities, relationships, and work.2
Current medical treatments include on- and off-label use of oral contraceptives, gonadotropin-releasing hormone (GnRH) receptor agonists, and progestins. Data on investigational oral GnRH antagonists and oral selective progesterone-receptor modulators (SPRMs) were presented at the 2017 Annual Clinical and Scientific Meeting of the American College of Obstetricians and Gynecologists.
Details of VENUS I
In the phase 3, randomized, controlled VENUS I trial, investigators assessed the efficacy and safety of ulipristal acetate (UPA), an SPRM, by race and body mass index (BMI) in premenopausal women (aged 18 to 50) with symptomatic uterine fibroids.1
Simon and colleagues randomly assigned participants to UPA 5 mg, UPA 10 mg, or placebo once daily for 12 weeks, followed by a 12-week treatment-free follow-up period. UPA, at 5 and 10 mg, was significantly more efficacious than placebo in rate of and time to amenorrhea (P<.0001). The superiority was observed regardless of race and BMI. In addition, women taking UPA versus placebo reported significantly less impact on activities due to uterine fibroids. The study authors concluded that “UPA treatment provides effective control of bleeding and improvement in physical and social activities for women with symptomatic uterine fibroids, regardless of race and BMI.”1
Establishing the ideal treatment period for UPA to avoid progesterone-associated endometrial changes (in this study it was 12 weeks of once-daily therapy) is a current goal, said Simon.
Details of elagolix phase 2b study
Simon also presented data on another investigational drug, elagolix, an orally administered GnRH antagonist, which has an inhibiting effect on luteinizing hormone and follicle-stimulating hormone secretion. This in turn reduces production of estradiol and progesterone. Elagolix also is being studied for the treatment of endometriosis.3
In the uterine fibroids study, a 24-week, multicenter, double-blind, randomized controlled, parallel group trial, 567 premenopausal women aged 18 to 51 with heavy menstrual bleeding of >80 mL of blood loss were assigned to placebo or elagolix 300 mg twice per day or 600 mg once per day alone or in combination with add-back therapy (with estradiol/norethindrone acetate) to prevent bone loss and menopausal symptoms.4
Compared with placebo, women treated with elagolix with or without add-back therapy had significant reductions from baseline in mean menstrual blood loss. Women treated with elagolix also had significant increases in hemoglobin concentration from baseline to month 6 compared with placebo.4
Adverse effects were similar to menopause symptoms: bone loss, hot flashes, night sweats, headaches, and disturbed sleep, said Simon. With the add-back treatments, adverse effects were mitigated in a dose-dependent fashion, he pointed out, and were most likely tolerable compared with the heavy bleeding experienced by women at the start of the study.
- Simon JA, Catherino W, Blakesley RE, Chan A, Sriukiene V, Al-Hendy A. Ulipristal acetate treatment of uterine fibroids in black and obese women. VENUS I subgroup analyses. Paper presented at: 2017 Annual Clinical and Scientific Meeting of The American College of Obstetricians and Gynecologists; May 6, 2017; San Diego, CA.
- Stewart EA, Nicholson WK, Bradley L, Borah BJ. The burden of uterine fibroids for African-American women: results of a national survey. J Womens Health (Larchmnt). 2013;22(10):807–816.
- Taylor HS, Guidice LC, Lessey BA, et al. Treatment of endometriosis-associated pain with elagolix, an oral GnRH antagonist. NEJM. doi:10.1056/NEJMoa1700089.
- Stewart EA, Owens C, Duan WR, Gao J, Chwalisz K, Simon JA. Elagolix alone and with add-back decreases heavy menstrual bleeding in women with uterine fibroids. Paper presented at: 2017 Annual Clinical and Scientific Meeting of The American College of Obstetricians and Gynecologists; May 6, 2017; San Diego, CA.
Up to 80% of women who are of reproductive age have uterine fibroids that cause heavy and prolonged bleeding.1 Additional concerns include infertility and pain, says James Simon, MD, Clinical Professor at George Washington University in Washington, DC. Black women are more likely than white women to undergo hysterectomy for uterine fibroids. They also are more likely to experience severe or very severe symptoms from fibroids and report that these symptoms interfere with physical activities, relationships, and work.2
Current medical treatments include on- and off-label use of oral contraceptives, gonadotropin-releasing hormone (GnRH) receptor agonists, and progestins. Data on investigational oral GnRH antagonists and oral selective progesterone-receptor modulators (SPRMs) were presented at the 2017 Annual Clinical and Scientific Meeting of the American College of Obstetricians and Gynecologists.
Details of VENUS I
In the phase 3, randomized, controlled VENUS I trial, investigators assessed the efficacy and safety of ulipristal acetate (UPA), an SPRM, by race and body mass index (BMI) in premenopausal women (aged 18 to 50) with symptomatic uterine fibroids.1
Simon and colleagues randomly assigned participants to UPA 5 mg, UPA 10 mg, or placebo once daily for 12 weeks, followed by a 12-week treatment-free follow-up period. UPA, at 5 and 10 mg, was significantly more efficacious than placebo in rate of and time to amenorrhea (P<.0001). The superiority was observed regardless of race and BMI. In addition, women taking UPA versus placebo reported significantly less impact on activities due to uterine fibroids. The study authors concluded that “UPA treatment provides effective control of bleeding and improvement in physical and social activities for women with symptomatic uterine fibroids, regardless of race and BMI.”1
Establishing the ideal treatment period for UPA to avoid progesterone-associated endometrial changes (in this study it was 12 weeks of once-daily therapy) is a current goal, said Simon.
Details of elagolix phase 2b study
Simon also presented data on another investigational drug, elagolix, an orally administered GnRH antagonist, which has an inhibiting effect on luteinizing hormone and follicle-stimulating hormone secretion. This in turn reduces production of estradiol and progesterone. Elagolix also is being studied for the treatment of endometriosis.3
In the uterine fibroids study, a 24-week, multicenter, double-blind, randomized controlled, parallel group trial, 567 premenopausal women aged 18 to 51 with heavy menstrual bleeding of >80 mL of blood loss were assigned to placebo or elagolix 300 mg twice per day or 600 mg once per day alone or in combination with add-back therapy (with estradiol/norethindrone acetate) to prevent bone loss and menopausal symptoms.4
Compared with placebo, women treated with elagolix with or without add-back therapy had significant reductions from baseline in mean menstrual blood loss. Women treated with elagolix also had significant increases in hemoglobin concentration from baseline to month 6 compared with placebo.4
Adverse effects were similar to menopause symptoms: bone loss, hot flashes, night sweats, headaches, and disturbed sleep, said Simon. With the add-back treatments, adverse effects were mitigated in a dose-dependent fashion, he pointed out, and were most likely tolerable compared with the heavy bleeding experienced by women at the start of the study.
Up to 80% of women who are of reproductive age have uterine fibroids that cause heavy and prolonged bleeding.1 Additional concerns include infertility and pain, says James Simon, MD, Clinical Professor at George Washington University in Washington, DC. Black women are more likely than white women to undergo hysterectomy for uterine fibroids. They also are more likely to experience severe or very severe symptoms from fibroids and report that these symptoms interfere with physical activities, relationships, and work.2
Current medical treatments include on- and off-label use of oral contraceptives, gonadotropin-releasing hormone (GnRH) receptor agonists, and progestins. Data on investigational oral GnRH antagonists and oral selective progesterone-receptor modulators (SPRMs) were presented at the 2017 Annual Clinical and Scientific Meeting of the American College of Obstetricians and Gynecologists.
Details of VENUS I
In the phase 3, randomized, controlled VENUS I trial, investigators assessed the efficacy and safety of ulipristal acetate (UPA), an SPRM, by race and body mass index (BMI) in premenopausal women (aged 18 to 50) with symptomatic uterine fibroids.1
Simon and colleagues randomly assigned participants to UPA 5 mg, UPA 10 mg, or placebo once daily for 12 weeks, followed by a 12-week treatment-free follow-up period. UPA, at 5 and 10 mg, was significantly more efficacious than placebo in rate of and time to amenorrhea (P<.0001). The superiority was observed regardless of race and BMI. In addition, women taking UPA versus placebo reported significantly less impact on activities due to uterine fibroids. The study authors concluded that “UPA treatment provides effective control of bleeding and improvement in physical and social activities for women with symptomatic uterine fibroids, regardless of race and BMI.”1
Establishing the ideal treatment period for UPA to avoid progesterone-associated endometrial changes (in this study it was 12 weeks of once-daily therapy) is a current goal, said Simon.
Details of elagolix phase 2b study
Simon also presented data on another investigational drug, elagolix, an orally administered GnRH antagonist, which has an inhibiting effect on luteinizing hormone and follicle-stimulating hormone secretion. This in turn reduces production of estradiol and progesterone. Elagolix also is being studied for the treatment of endometriosis.3
In the uterine fibroids study, a 24-week, multicenter, double-blind, randomized controlled, parallel group trial, 567 premenopausal women aged 18 to 51 with heavy menstrual bleeding of >80 mL of blood loss were assigned to placebo or elagolix 300 mg twice per day or 600 mg once per day alone or in combination with add-back therapy (with estradiol/norethindrone acetate) to prevent bone loss and menopausal symptoms.4
Compared with placebo, women treated with elagolix with or without add-back therapy had significant reductions from baseline in mean menstrual blood loss. Women treated with elagolix also had significant increases in hemoglobin concentration from baseline to month 6 compared with placebo.4
Adverse effects were similar to menopause symptoms: bone loss, hot flashes, night sweats, headaches, and disturbed sleep, said Simon. With the add-back treatments, adverse effects were mitigated in a dose-dependent fashion, he pointed out, and were most likely tolerable compared with the heavy bleeding experienced by women at the start of the study.
- Simon JA, Catherino W, Blakesley RE, Chan A, Sriukiene V, Al-Hendy A. Ulipristal acetate treatment of uterine fibroids in black and obese women. VENUS I subgroup analyses. Paper presented at: 2017 Annual Clinical and Scientific Meeting of The American College of Obstetricians and Gynecologists; May 6, 2017; San Diego, CA.
- Stewart EA, Nicholson WK, Bradley L, Borah BJ. The burden of uterine fibroids for African-American women: results of a national survey. J Womens Health (Larchmnt). 2013;22(10):807–816.
- Taylor HS, Guidice LC, Lessey BA, et al. Treatment of endometriosis-associated pain with elagolix, an oral GnRH antagonist. NEJM. doi:10.1056/NEJMoa1700089.
- Stewart EA, Owens C, Duan WR, Gao J, Chwalisz K, Simon JA. Elagolix alone and with add-back decreases heavy menstrual bleeding in women with uterine fibroids. Paper presented at: 2017 Annual Clinical and Scientific Meeting of The American College of Obstetricians and Gynecologists; May 6, 2017; San Diego, CA.
- Simon JA, Catherino W, Blakesley RE, Chan A, Sriukiene V, Al-Hendy A. Ulipristal acetate treatment of uterine fibroids in black and obese women. VENUS I subgroup analyses. Paper presented at: 2017 Annual Clinical and Scientific Meeting of The American College of Obstetricians and Gynecologists; May 6, 2017; San Diego, CA.
- Stewart EA, Nicholson WK, Bradley L, Borah BJ. The burden of uterine fibroids for African-American women: results of a national survey. J Womens Health (Larchmnt). 2013;22(10):807–816.
- Taylor HS, Guidice LC, Lessey BA, et al. Treatment of endometriosis-associated pain with elagolix, an oral GnRH antagonist. NEJM. doi:10.1056/NEJMoa1700089.
- Stewart EA, Owens C, Duan WR, Gao J, Chwalisz K, Simon JA. Elagolix alone and with add-back decreases heavy menstrual bleeding in women with uterine fibroids. Paper presented at: 2017 Annual Clinical and Scientific Meeting of The American College of Obstetricians and Gynecologists; May 6, 2017; San Diego, CA.

Minimally invasive cosmetic procedures more popular than ever
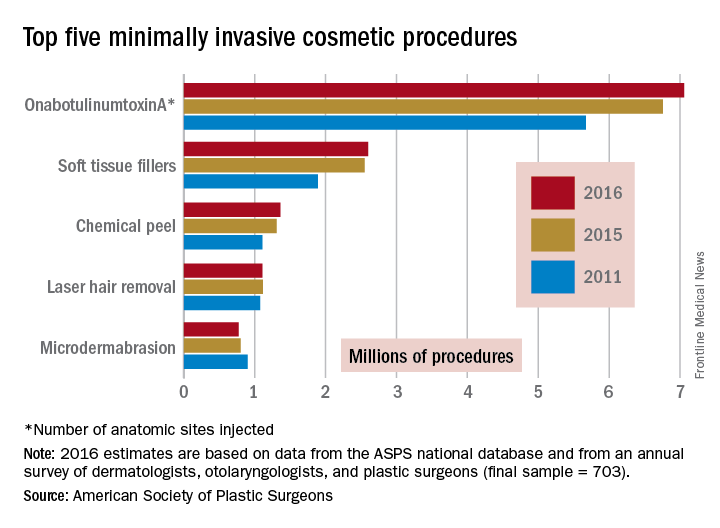
The total number of minimally invasive cosmetic procedures topped 15 million for the first time in 2016, with onabotulinumtoxinA injections leading the way, according to the American Society of Plastic Surgeons.
An estimated 15.4 million minimally invasive cosmetic procedures were performed last year, with onabotulinumtoxinA making up over 45% – approximately 7.1 million anatomic sites injected – of that total, ASPS data show.
Next in popularity was injection of soft tissue fillers, with just over 2.6 million procedures – almost 17% of the procedures performed in 2016 – followed by chemical peels with almost 1.4 million procedures, laser hair removal with 1.1 million procedures, and microdermabrasion at 775,000, the ASPS reported.
The total number of minimally invasive procedures was up 3% from the 14.96 million performed in 2015, while onabotulinumtoxinA was up 4%, soft tissue fillers were up 2%, chemical peels were up 4%, laser hair removal was down 1%, and microdermabrasion was down 3%. Larger changes were seen among some less common procedures: injection lipolysis was up 18% (55,660 procedures in 2016), fat injection was up 13% (79,208 procedures in 2016), and acellular dermal matrix procedures were down 18% (7,809 in 2016), according to the ASPS Tracking Operations and Outcomes for Plastic Surgeons database and an annual survey of board-certified dermatologists, otolaryngologists, and plastic surgeons (final sample = 703).
The total number of minimally invasive cosmetic procedures topped 15 million for the first time in 2016, with onabotulinumtoxinA injections leading the way, according to the American Society of Plastic Surgeons.
An estimated 15.4 million minimally invasive cosmetic procedures were performed last year, with onabotulinumtoxinA making up over 45% – approximately 7.1 million anatomic sites injected – of that total, ASPS data show.
Next in popularity was injection of soft tissue fillers, with just over 2.6 million procedures – almost 17% of the procedures performed in 2016 – followed by chemical peels with almost 1.4 million procedures, laser hair removal with 1.1 million procedures, and microdermabrasion at 775,000, the ASPS reported.
The total number of minimally invasive procedures was up 3% from the 14.96 million performed in 2015, while onabotulinumtoxinA was up 4%, soft tissue fillers were up 2%, chemical peels were up 4%, laser hair removal was down 1%, and microdermabrasion was down 3%. Larger changes were seen among some less common procedures: injection lipolysis was up 18% (55,660 procedures in 2016), fat injection was up 13% (79,208 procedures in 2016), and acellular dermal matrix procedures were down 18% (7,809 in 2016), according to the ASPS Tracking Operations and Outcomes for Plastic Surgeons database and an annual survey of board-certified dermatologists, otolaryngologists, and plastic surgeons (final sample = 703).
The total number of minimally invasive cosmetic procedures topped 15 million for the first time in 2016, with onabotulinumtoxinA injections leading the way, according to the American Society of Plastic Surgeons.
An estimated 15.4 million minimally invasive cosmetic procedures were performed last year, with onabotulinumtoxinA making up over 45% – approximately 7.1 million anatomic sites injected – of that total, ASPS data show.
Next in popularity was injection of soft tissue fillers, with just over 2.6 million procedures – almost 17% of the procedures performed in 2016 – followed by chemical peels with almost 1.4 million procedures, laser hair removal with 1.1 million procedures, and microdermabrasion at 775,000, the ASPS reported.
The total number of minimally invasive procedures was up 3% from the 14.96 million performed in 2015, while onabotulinumtoxinA was up 4%, soft tissue fillers were up 2%, chemical peels were up 4%, laser hair removal was down 1%, and microdermabrasion was down 3%. Larger changes were seen among some less common procedures: injection lipolysis was up 18% (55,660 procedures in 2016), fat injection was up 13% (79,208 procedures in 2016), and acellular dermal matrix procedures were down 18% (7,809 in 2016), according to the ASPS Tracking Operations and Outcomes for Plastic Surgeons database and an annual survey of board-certified dermatologists, otolaryngologists, and plastic surgeons (final sample = 703).
State e-cigarette laws linked to reduced youth use
Several state regulations governing the sales or use of e-cigarettes and related products were associated with lower proportions of youth trying or regularly using vaping products, a new study found.
Restricting sales of electronic vapor products to minors, however, was not linked to a lower risk of vaping among teens.

Dr. Keim and her associates investigated possible associations between various state laws related to vaping products, all passed before 2015, and youth use of the products. They relied on 2015 data from 35 state-specific surveys of youth regarding use of vaping products and from the Youth Risk Behavior Survey from the Centers for Disease Control and Prevention, a nationally representative, biannual survey of students in grades 9-12. The Tobacco Control Laws Database of the American Nonsmokers’ Rights Foundation provided information on state laws related to electronic vapor products.
Among the 200,513 teens whose responses were included in the study, 44% had ever used any kind of electronic vapor product. Rates were similar between girls and boys for ever having tried one or currently using one, Dr. Keim reported at the Pediatric Academic Societies annual meeting.

The researchers looked at associations with each of the following types of laws:
• Statewide prohibition of vaping products on school property or in workplaces, which includes Arizona, New Hampshire, Vermont, and Virginia for schools and North Dakota for workplaces.
• Prohibition of sales to minors under age 18 years, present in 24 states.
• Prohibition or restriction of sales of e-cigarette products from vending machines, present in 17 states.
• Prohibition or restriction of self-service displays of vaping products, present in 11 states.
• Prohibition or restriction of sampling of electronic vapor products, present in Arizona, Delaware, Kentucky, Maryland, New Hampshire, North Carolina, Oklahoma, and South Carolina.
For most of the regulations, teens had a reduced likelihood of trying or currently using vaping products after adjusting for age, ethnicity, grade level, race, region, and sex. Risk of ever trying a vaping product was 12% lower in states that prohibited their use on school grounds or in workplaces, 6% lower in states that barred sales to those under age 18, and 7% lower in states that restricted or prohibited self-service vaping displays.
The risk of youth currently using electronic vapor products was 5% lower in states with the school grounds and workplace restrictions, and 13% lower in states that restricted self-service displays. Laws restricting minor sales were unrelated to the risk of current vaping among youth. Restricting vending machine sales of vaping products had no association with the risk of a teen ever trying vaping, but it was linked to a 7% lower risk of current use of the products among teens. All these associations were statistically significant based on confidence interval values.
Interestingly, a statistically significant risk increase in vaping use occurred for teens in states that restricted or outlawed sampling of vaping products. The risk was 8% higher for ever trying a product and 20% higher for current use. But those findings also could indicate the possibility of reverse causation.
“It’s possible that states that were particularly concerned about sampling had the worst problems – were the ones more likely to institute a ban on that practice, and that would generate the counterintuitive finding,” Dr. Keim said in an interview. “With the data currently available, we can’t look at teen use both before and after the restrictions, just afterwards, but with more data for 2017, it would provide a clearer picture of all of the associations we examined.”
Aside from these laws, other interventions have the potential to reduce vaping among teens as well.
“Restrictions on use in various types of public places and on school grounds may be additional helpful approaches, similar to what has been done with cigarettes,” Dr. Keim said. Although their analysis included laws that prohibited use on school grounds, only four states have one of these laws.

Several state regulations governing the sales or use of e-cigarettes and related products were associated with lower proportions of youth trying or regularly using vaping products, a new study found.
Restricting sales of electronic vapor products to minors, however, was not linked to a lower risk of vaping among teens.
Dr. Keim and her associates investigated possible associations between various state laws related to vaping products, all passed before 2015, and youth use of the products. They relied on 2015 data from 35 state-specific surveys of youth regarding use of vaping products and from the Youth Risk Behavior Survey from the Centers for Disease Control and Prevention, a nationally representative, biannual survey of students in grades 9-12. The Tobacco Control Laws Database of the American Nonsmokers’ Rights Foundation provided information on state laws related to electronic vapor products.
Among the 200,513 teens whose responses were included in the study, 44% had ever used any kind of electronic vapor product. Rates were similar between girls and boys for ever having tried one or currently using one, Dr. Keim reported at the Pediatric Academic Societies annual meeting.
The researchers looked at associations with each of the following types of laws:
• Statewide prohibition of vaping products on school property or in workplaces, which includes Arizona, New Hampshire, Vermont, and Virginia for schools and North Dakota for workplaces.
• Prohibition of sales to minors under age 18 years, present in 24 states.
• Prohibition or restriction of sales of e-cigarette products from vending machines, present in 17 states.
• Prohibition or restriction of self-service displays of vaping products, present in 11 states.
• Prohibition or restriction of sampling of electronic vapor products, present in Arizona, Delaware, Kentucky, Maryland, New Hampshire, North Carolina, Oklahoma, and South Carolina.
For most of the regulations, teens had a reduced likelihood of trying or currently using vaping products after adjusting for age, ethnicity, grade level, race, region, and sex. Risk of ever trying a vaping product was 12% lower in states that prohibited their use on school grounds or in workplaces, 6% lower in states that barred sales to those under age 18, and 7% lower in states that restricted or prohibited self-service vaping displays.
The risk of youth currently using electronic vapor products was 5% lower in states with the school grounds and workplace restrictions, and 13% lower in states that restricted self-service displays. Laws restricting minor sales were unrelated to the risk of current vaping among youth. Restricting vending machine sales of vaping products had no association with the risk of a teen ever trying vaping, but it was linked to a 7% lower risk of current use of the products among teens. All these associations were statistically significant based on confidence interval values.
Interestingly, a statistically significant risk increase in vaping use occurred for teens in states that restricted or outlawed sampling of vaping products. The risk was 8% higher for ever trying a product and 20% higher for current use. But those findings also could indicate the possibility of reverse causation.
“It’s possible that states that were particularly concerned about sampling had the worst problems – were the ones more likely to institute a ban on that practice, and that would generate the counterintuitive finding,” Dr. Keim said in an interview. “With the data currently available, we can’t look at teen use both before and after the restrictions, just afterwards, but with more data for 2017, it would provide a clearer picture of all of the associations we examined.”
Aside from these laws, other interventions have the potential to reduce vaping among teens as well.
“Restrictions on use in various types of public places and on school grounds may be additional helpful approaches, similar to what has been done with cigarettes,” Dr. Keim said. Although their analysis included laws that prohibited use on school grounds, only four states have one of these laws.
Several state regulations governing the sales or use of e-cigarettes and related products were associated with lower proportions of youth trying or regularly using vaping products, a new study found.
Restricting sales of electronic vapor products to minors, however, was not linked to a lower risk of vaping among teens.
Dr. Keim and her associates investigated possible associations between various state laws related to vaping products, all passed before 2015, and youth use of the products. They relied on 2015 data from 35 state-specific surveys of youth regarding use of vaping products and from the Youth Risk Behavior Survey from the Centers for Disease Control and Prevention, a nationally representative, biannual survey of students in grades 9-12. The Tobacco Control Laws Database of the American Nonsmokers’ Rights Foundation provided information on state laws related to electronic vapor products.
Among the 200,513 teens whose responses were included in the study, 44% had ever used any kind of electronic vapor product. Rates were similar between girls and boys for ever having tried one or currently using one, Dr. Keim reported at the Pediatric Academic Societies annual meeting.
The researchers looked at associations with each of the following types of laws:
• Statewide prohibition of vaping products on school property or in workplaces, which includes Arizona, New Hampshire, Vermont, and Virginia for schools and North Dakota for workplaces.
• Prohibition of sales to minors under age 18 years, present in 24 states.
• Prohibition or restriction of sales of e-cigarette products from vending machines, present in 17 states.
• Prohibition or restriction of self-service displays of vaping products, present in 11 states.
• Prohibition or restriction of sampling of electronic vapor products, present in Arizona, Delaware, Kentucky, Maryland, New Hampshire, North Carolina, Oklahoma, and South Carolina.
For most of the regulations, teens had a reduced likelihood of trying or currently using vaping products after adjusting for age, ethnicity, grade level, race, region, and sex. Risk of ever trying a vaping product was 12% lower in states that prohibited their use on school grounds or in workplaces, 6% lower in states that barred sales to those under age 18, and 7% lower in states that restricted or prohibited self-service vaping displays.
The risk of youth currently using electronic vapor products was 5% lower in states with the school grounds and workplace restrictions, and 13% lower in states that restricted self-service displays. Laws restricting minor sales were unrelated to the risk of current vaping among youth. Restricting vending machine sales of vaping products had no association with the risk of a teen ever trying vaping, but it was linked to a 7% lower risk of current use of the products among teens. All these associations were statistically significant based on confidence interval values.
Interestingly, a statistically significant risk increase in vaping use occurred for teens in states that restricted or outlawed sampling of vaping products. The risk was 8% higher for ever trying a product and 20% higher for current use. But those findings also could indicate the possibility of reverse causation.
“It’s possible that states that were particularly concerned about sampling had the worst problems – were the ones more likely to institute a ban on that practice, and that would generate the counterintuitive finding,” Dr. Keim said in an interview. “With the data currently available, we can’t look at teen use both before and after the restrictions, just afterwards, but with more data for 2017, it would provide a clearer picture of all of the associations we examined.”
Aside from these laws, other interventions have the potential to reduce vaping among teens as well.
“Restrictions on use in various types of public places and on school grounds may be additional helpful approaches, similar to what has been done with cigarettes,” Dr. Keim said. Although their analysis included laws that prohibited use on school grounds, only four states have one of these laws.
FROM PAS 2017
Key clinical point: The two state laws associated with lower risks of teens trying or currently using e-cigarette products were prohibiting their use at school or work and prohibiting or restricting self-service displays.
Major finding: , depending on the law.
Data source: The findings are based on an analysis of 200,513 high school students’ use of electronic vapor products and their states’ laws regarding vaping use, marketing, or sales.
Disclosures: The research did not use any external funding, and Dr. Keim had no relevant financial disclosures.
Limitations with molecular techniques in detecting onychomycosis
Real-time PCR techniques for identifying the pathogens responsible for onychomycosis can offer some advantages over conventional diagnostic approaches but also have their limitations, say the authors of a study published in Mycoses.
Anissa Z. Hafirassou of Frères-Mentouri, Constantine University, Algeria, and colleagues analyzed nail samples from 70 patients with clinical signs of onychomycosis and 15 healthy controls using four different real-time PCR assays – a panfungal, a pandermatophyte, an assay for Candida and one for Aspergillus – and conventional methods.
Most samples were of Trichophyton species and were found in patients with proven onychomycosis. In contrast, the sequencing results from the healthy samples were all negative.
The pandermatophyte analysis found dermatophyte DNA in 60% of cases – most of were proven cases of onychomycosis – representing a sensitivity of 90% compared to positive culture. This analysis showed 90% sensitivity compared to cultures, but there was no correlation between culture results and pandermatophyte RT-PCR in nine cases.
This technique also detected Trichophyton cases in 15 patients who had negative culture results, but found amplification products in three of the control subjects, two of which were Penicillium chrysogenum. However two culture-positive samples showed up as negative with both the panfungal and pandermatophyte methods.
“Due to the low sensitivity of the panfungal assay and the lack of correlation between cultures and PCR results, the possibility of the presence of environmental and colonizing species together with pathological species in nail samples, was studied,” the authors wrote.
Twenty-five fingernail samples that were negative on the panfungal analysis were also tested for Candida and Aspergillus. Candida species were detected in 76% of these samples, and Aspergillus in 60%, while 64% contained mixed populations. Ten samples contained more than one species of Candida and one had two species of Aspergillus.
“Conventional diagnostic methods have several limitations such as time-cost, low sensitivity and the need of skilled personnel,” the authors wrote, noting that the molecular methods also had limitations to their usefulness.
The panfungal method showed low sensitivity, which may have been due to the mix of fungal populations that was found even in healthy controls, the researchers added.
“The pandermatophyte assay was sensitive and specific but only detected dermatophyte species and did not allow differentiation among them,” they wrote.
The role of nondermatophyte species isolated from onychomycosis should be considered carefully, as these are also found in healthy nails, the researchers noted.
The study and one author were supported by the Spanish Fondo de Investigaciones Sanitarias of the Instituto de Salud Carlos III. No conflicts of interest were declared.
Real-time PCR techniques for identifying the pathogens responsible for onychomycosis can offer some advantages over conventional diagnostic approaches but also have their limitations, say the authors of a study published in Mycoses.
Anissa Z. Hafirassou of Frères-Mentouri, Constantine University, Algeria, and colleagues analyzed nail samples from 70 patients with clinical signs of onychomycosis and 15 healthy controls using four different real-time PCR assays – a panfungal, a pandermatophyte, an assay for Candida and one for Aspergillus – and conventional methods.
Most samples were of Trichophyton species and were found in patients with proven onychomycosis. In contrast, the sequencing results from the healthy samples were all negative.
The pandermatophyte analysis found dermatophyte DNA in 60% of cases – most of were proven cases of onychomycosis – representing a sensitivity of 90% compared to positive culture. This analysis showed 90% sensitivity compared to cultures, but there was no correlation between culture results and pandermatophyte RT-PCR in nine cases.
This technique also detected Trichophyton cases in 15 patients who had negative culture results, but found amplification products in three of the control subjects, two of which were Penicillium chrysogenum. However two culture-positive samples showed up as negative with both the panfungal and pandermatophyte methods.
“Due to the low sensitivity of the panfungal assay and the lack of correlation between cultures and PCR results, the possibility of the presence of environmental and colonizing species together with pathological species in nail samples, was studied,” the authors wrote.
Twenty-five fingernail samples that were negative on the panfungal analysis were also tested for Candida and Aspergillus. Candida species were detected in 76% of these samples, and Aspergillus in 60%, while 64% contained mixed populations. Ten samples contained more than one species of Candida and one had two species of Aspergillus.
“Conventional diagnostic methods have several limitations such as time-cost, low sensitivity and the need of skilled personnel,” the authors wrote, noting that the molecular methods also had limitations to their usefulness.
The panfungal method showed low sensitivity, which may have been due to the mix of fungal populations that was found even in healthy controls, the researchers added.
“The pandermatophyte assay was sensitive and specific but only detected dermatophyte species and did not allow differentiation among them,” they wrote.
The role of nondermatophyte species isolated from onychomycosis should be considered carefully, as these are also found in healthy nails, the researchers noted.
The study and one author were supported by the Spanish Fondo de Investigaciones Sanitarias of the Instituto de Salud Carlos III. No conflicts of interest were declared.
Real-time PCR techniques for identifying the pathogens responsible for onychomycosis can offer some advantages over conventional diagnostic approaches but also have their limitations, say the authors of a study published in Mycoses.
Anissa Z. Hafirassou of Frères-Mentouri, Constantine University, Algeria, and colleagues analyzed nail samples from 70 patients with clinical signs of onychomycosis and 15 healthy controls using four different real-time PCR assays – a panfungal, a pandermatophyte, an assay for Candida and one for Aspergillus – and conventional methods.
Most samples were of Trichophyton species and were found in patients with proven onychomycosis. In contrast, the sequencing results from the healthy samples were all negative.
The pandermatophyte analysis found dermatophyte DNA in 60% of cases – most of were proven cases of onychomycosis – representing a sensitivity of 90% compared to positive culture. This analysis showed 90% sensitivity compared to cultures, but there was no correlation between culture results and pandermatophyte RT-PCR in nine cases.
This technique also detected Trichophyton cases in 15 patients who had negative culture results, but found amplification products in three of the control subjects, two of which were Penicillium chrysogenum. However two culture-positive samples showed up as negative with both the panfungal and pandermatophyte methods.
“Due to the low sensitivity of the panfungal assay and the lack of correlation between cultures and PCR results, the possibility of the presence of environmental and colonizing species together with pathological species in nail samples, was studied,” the authors wrote.
Twenty-five fingernail samples that were negative on the panfungal analysis were also tested for Candida and Aspergillus. Candida species were detected in 76% of these samples, and Aspergillus in 60%, while 64% contained mixed populations. Ten samples contained more than one species of Candida and one had two species of Aspergillus.
“Conventional diagnostic methods have several limitations such as time-cost, low sensitivity and the need of skilled personnel,” the authors wrote, noting that the molecular methods also had limitations to their usefulness.
The panfungal method showed low sensitivity, which may have been due to the mix of fungal populations that was found even in healthy controls, the researchers added.
“The pandermatophyte assay was sensitive and specific but only detected dermatophyte species and did not allow differentiation among them,” they wrote.
The role of nondermatophyte species isolated from onychomycosis should be considered carefully, as these are also found in healthy nails, the researchers noted.
The study and one author were supported by the Spanish Fondo de Investigaciones Sanitarias of the Instituto de Salud Carlos III. No conflicts of interest were declared.
FROM MYCOSES
Key clinical point: Real-time PCR techniques for identifying the pathogens in onychomycosis have some advantages over culture but also have their limitations.
Major finding: Panfungal real-time PCR had a sensitivity of 47% and pandermatophyte RT-PCR had a sensitivity of 90% compared to positive culture.
Data source: Analysis of toenail samples from 70 patients with onychomycosis and 15 healthy controls.
Disclosures: The study and one author were supported by the Spanish Fondo de Investigaciones Sanitarias of the Instituto de Salud Carlos III. No conflicts of interest were declared.
Check Out the SVS Expanded Member Benefits Portfolio
The Society for Vascular Surgery has its very own member affinity program, offering members access to best-in-class products and services coupled with special member discounts.
The portfolio includes a number of insurance, financial and private-practice related products that will assist members in their day-to-day lives. The result: a selection of financial and practice solutions to protect and benefit your families, incomes, practices, offices and staff – even your own slice of cyberspace.
For more information, visit vsweb.org/AffinityProgram, call 855-533-1776 or email [email protected].
The Society for Vascular Surgery has its very own member affinity program, offering members access to best-in-class products and services coupled with special member discounts.
The portfolio includes a number of insurance, financial and private-practice related products that will assist members in their day-to-day lives. The result: a selection of financial and practice solutions to protect and benefit your families, incomes, practices, offices and staff – even your own slice of cyberspace.
For more information, visit vsweb.org/AffinityProgram, call 855-533-1776 or email [email protected].
The Society for Vascular Surgery has its very own member affinity program, offering members access to best-in-class products and services coupled with special member discounts.
The portfolio includes a number of insurance, financial and private-practice related products that will assist members in their day-to-day lives. The result: a selection of financial and practice solutions to protect and benefit your families, incomes, practices, offices and staff – even your own slice of cyberspace.
For more information, visit vsweb.org/AffinityProgram, call 855-533-1776 or email [email protected].
Gastrointestinal healing in treated celiac patients can vary
CHICAGO – A gluten-free diet is the cornerstone of treatment for celiac disease, but healing of the gut may take longer in some patients than in others.
New findings presented at the annual Digestive Disease Week suggest that, even though patients treated with a gluten-free diet generally experience clinical improvement during the first few weeks or months of making dietary changes, serologic and especially histologic normalization may take longer – and it is not always certain that it will occur.
As many as 45% of patients exhibit substantial differences in the degree of intestinal injury in separate biopsies. Thus, caution is needed when interpreting the results of individual biopsies when assessing healing in patients who are on gluten-free diets, explained Dr. Choung. Evaluating multiple biopsies “may give a more accurate picture of the mucosal healing,” he noted.
The degree of intestinal damage varies considerably in individuals with celiac disease, and this variability can affect accurate assessments of both recovery and residual injury in patients who continue to have persistent symptoms despite adherence to a gluten-free diet.
The goal of the current study was to evaluate uniformity versus patchiness of mucosal damage in a large cohort of patients with celiac disease who were being treated but who still experienced symptoms.
The study included 1,352 patients with celiac disease who had been on a gluten-free diet for at least 1 year and who had undergone four biopsies from the distal duodenum. Each biopsy was processed separately, and, in each one, the villous height (Vh) and crypt depth (Cd) were measured in up to three different, well-oriented crypts.
The mucosal patchiness of villous atrophy was then defined as a variation in Vh:Cd ratio between biopsies from the same patient that was greater than two standard deviations of the Vh:Cd variations of the study population (mean of Vh:Cd, 2.13; standard deviation, 0.67).
Of the 1,125 patients who had at least five crypts that were measured from all four biopsies, 45% met the criteria for histological patchiness of mucosal healing in the small intestine. The authors found that several factors, including a younger age at diagnosis, female gender, and a higher average Vh:Cd ratio, were positively associated with mucosal patchiness.
However, there were no significant associations observed between mucosal patchiness and the duration of a gluten-free diet or of any gastrointestinal symptoms.
When the analysis was restricted to the population with a Vh:Cd no greater than 2, Dr. Choung and his colleagues found that human leukocyte antigen typing and tissue transglutaminase–immunoglobulin A did not predict mucosal patchiness. However, patients who were positive for deamidated gliadin peptide–IgA or deamidated gliadin peptide–IgG were less likely to exhibit patchiness but had more uniform intestinal injury (odds ratio, 0.4 and 0.4, respectively).
Digestive Disease Week is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE) and the Society for Surgery of the Alimentary Tract (SSAT). Dr. Choung declared no relevant disclosures.
CHICAGO – A gluten-free diet is the cornerstone of treatment for celiac disease, but healing of the gut may take longer in some patients than in others.
New findings presented at the annual Digestive Disease Week suggest that, even though patients treated with a gluten-free diet generally experience clinical improvement during the first few weeks or months of making dietary changes, serologic and especially histologic normalization may take longer – and it is not always certain that it will occur.
As many as 45% of patients exhibit substantial differences in the degree of intestinal injury in separate biopsies. Thus, caution is needed when interpreting the results of individual biopsies when assessing healing in patients who are on gluten-free diets, explained Dr. Choung. Evaluating multiple biopsies “may give a more accurate picture of the mucosal healing,” he noted.
The degree of intestinal damage varies considerably in individuals with celiac disease, and this variability can affect accurate assessments of both recovery and residual injury in patients who continue to have persistent symptoms despite adherence to a gluten-free diet.
The goal of the current study was to evaluate uniformity versus patchiness of mucosal damage in a large cohort of patients with celiac disease who were being treated but who still experienced symptoms.
The study included 1,352 patients with celiac disease who had been on a gluten-free diet for at least 1 year and who had undergone four biopsies from the distal duodenum. Each biopsy was processed separately, and, in each one, the villous height (Vh) and crypt depth (Cd) were measured in up to three different, well-oriented crypts.
The mucosal patchiness of villous atrophy was then defined as a variation in Vh:Cd ratio between biopsies from the same patient that was greater than two standard deviations of the Vh:Cd variations of the study population (mean of Vh:Cd, 2.13; standard deviation, 0.67).
Of the 1,125 patients who had at least five crypts that were measured from all four biopsies, 45% met the criteria for histological patchiness of mucosal healing in the small intestine. The authors found that several factors, including a younger age at diagnosis, female gender, and a higher average Vh:Cd ratio, were positively associated with mucosal patchiness.
However, there were no significant associations observed between mucosal patchiness and the duration of a gluten-free diet or of any gastrointestinal symptoms.
When the analysis was restricted to the population with a Vh:Cd no greater than 2, Dr. Choung and his colleagues found that human leukocyte antigen typing and tissue transglutaminase–immunoglobulin A did not predict mucosal patchiness. However, patients who were positive for deamidated gliadin peptide–IgA or deamidated gliadin peptide–IgG were less likely to exhibit patchiness but had more uniform intestinal injury (odds ratio, 0.4 and 0.4, respectively).
Digestive Disease Week is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE) and the Society for Surgery of the Alimentary Tract (SSAT). Dr. Choung declared no relevant disclosures.
CHICAGO – A gluten-free diet is the cornerstone of treatment for celiac disease, but healing of the gut may take longer in some patients than in others.
New findings presented at the annual Digestive Disease Week suggest that, even though patients treated with a gluten-free diet generally experience clinical improvement during the first few weeks or months of making dietary changes, serologic and especially histologic normalization may take longer – and it is not always certain that it will occur.
As many as 45% of patients exhibit substantial differences in the degree of intestinal injury in separate biopsies. Thus, caution is needed when interpreting the results of individual biopsies when assessing healing in patients who are on gluten-free diets, explained Dr. Choung. Evaluating multiple biopsies “may give a more accurate picture of the mucosal healing,” he noted.
The degree of intestinal damage varies considerably in individuals with celiac disease, and this variability can affect accurate assessments of both recovery and residual injury in patients who continue to have persistent symptoms despite adherence to a gluten-free diet.
The goal of the current study was to evaluate uniformity versus patchiness of mucosal damage in a large cohort of patients with celiac disease who were being treated but who still experienced symptoms.
The study included 1,352 patients with celiac disease who had been on a gluten-free diet for at least 1 year and who had undergone four biopsies from the distal duodenum. Each biopsy was processed separately, and, in each one, the villous height (Vh) and crypt depth (Cd) were measured in up to three different, well-oriented crypts.
The mucosal patchiness of villous atrophy was then defined as a variation in Vh:Cd ratio between biopsies from the same patient that was greater than two standard deviations of the Vh:Cd variations of the study population (mean of Vh:Cd, 2.13; standard deviation, 0.67).
Of the 1,125 patients who had at least five crypts that were measured from all four biopsies, 45% met the criteria for histological patchiness of mucosal healing in the small intestine. The authors found that several factors, including a younger age at diagnosis, female gender, and a higher average Vh:Cd ratio, were positively associated with mucosal patchiness.
However, there were no significant associations observed between mucosal patchiness and the duration of a gluten-free diet or of any gastrointestinal symptoms.
When the analysis was restricted to the population with a Vh:Cd no greater than 2, Dr. Choung and his colleagues found that human leukocyte antigen typing and tissue transglutaminase–immunoglobulin A did not predict mucosal patchiness. However, patients who were positive for deamidated gliadin peptide–IgA or deamidated gliadin peptide–IgG were less likely to exhibit patchiness but had more uniform intestinal injury (odds ratio, 0.4 and 0.4, respectively).
Digestive Disease Week is jointly sponsored by the American Association for the Study of Liver Diseases (AASLD), the American Gastroenterological Association (AGA) Institute, the American Society for Gastrointestinal Endoscopy (ASGE) and the Society for Surgery of the Alimentary Tract (SSAT). Dr. Choung declared no relevant disclosures.
AT DDW
Key clinical point:
Major finding: Patients positive for DGP-IgA or DGP-IgG were less likely to exhibit patchiness but had more uniform intestinal injury (odds ratio, 0.4 and 0.4, respectively).
Data source: 1,352 patients with celiac disease who had been on a gluten-free diet for at least 1 year and who had undergone four biopsies from the distal duodenum.
Disclosures: Dr. Choung declared no relevant disclosures.
Waiving screening copayments could cut colorectal cancer deaths
CHICAGO – Out-of-pocket costs may present a barrier to colorectal screening, and removing those costs could reduce colorectal cancer deaths, according to new data presented at the annual Digestive Disease Week.
These data imply that removing copayments could result in a 16% decrease in colorectal cancer–related deaths among Medicare beneficiaries, explained lead author Elisabeth Peterse, PhD, of the department of public health, Erasmus Medical Center, Rotterdam, the Netherlands.
The research also demonstrated that waiving copayments is cost effective, she added.
Despite the effectiveness of colorectal cancer screening, only 58% of eligible individuals adhere to current screening recommendations, Dr. Peterse noted. Financial barriers may play a role in the lack of adherence, as studies have found that removing out-of-pocket costs is one of the most effective interventions for increasing screening.
“But despite the fact that the Affordable Care Act has been successful in partially eliminating cost sharing for colorectal screening, Medicare beneficiaries may still face unexpected out-of-pocket liabilities,” said Dr. Peterse.
Out-of-pocket costs can be complicated, given that they can depend largely on how a procedure is coded. A screening colonoscopy or fecal immunochemical test (FIT) is completely covered if it is coded as a screening test, but follow-up colonoscopies come with 20% copayments.
A screening colonoscopy with polypectomy and a follow-up colonoscopy that is done after a positive fecal immunochemical test are coded as diagnostic rather than screening, so the patient has out-of-pocket costs, she explained.
To explore how waiving the cost of screening could impact colorectal cancer–related mortality and cost effectiveness, the researchers conducted an analysis using a microsimulation model for a cohort composed of 65-year-old individuals.
In the simulation, they estimated colorectal cancer–related mortality, quality-adjusted life-years, and total cost of screening and treatment using the current Medicare copayment schedule. These were then compared with outcomes for alternative situations.
The study was conducted in two parts, explained Dr. Peterse. In the first part, the researchers looked at five scenarios: one in which the 20% copayment was intact. In the second, the copayment was waived without having any impact on adherence. In the third, the investigators looked at a 5% increase in adherence but only at diagnostic follow-up.
In the fourth and fifth scenarios, the investigators looked at 5% and 10% increases in adherence, in both first screening and diagnostic follow-up, she added.
In the study’s second part, the researchers also estimated the threshold increase in participation at which copayment removal would be cost effective, using a $50,000 willingness-to-pay threshold.
They found that without screening, the expected mortality would be 25 colorectal deaths per 1,000 people in a population of 65-year-old individuals. With screening, the number was reduced to 12.8 deaths per 1,000 65-year-olds for colonoscopy, and 14.9 deaths per 1,000 for FIT screening. The total associated costs for screening and treatment for the two modalities were $3.02 million and $2.87 million.
If waiving the copayments had no impact in increasing screening levels, the cost of screening was estimated to increase to $3.1 million (2.8% increase) for colonoscopy and $2.9 million (1.6% increase) for FIT.
But if copayments were removed and there were a 5% increase in adherence, colorectal cancer deaths were estimated to decline to 11.7 (–8.3%) and 13.9 (–6.3%) per 1,000 for colonoscopy and FIT, respectively. That would result in cost-effectiveness ratios of $19,288 and $7,894 for no copayment versus having a copayment. Increasing adherence to 10% would result in an even lower ratio, noted Dr. Peterse.
The threshold increase for participating in screening programs – the point where removing a copayment becomes cost effective – was a 1.8% increase in colonoscopy screening and a 0.8% increase for FIT.
The conclusion is that waiving copayments is cost effective, Dr. Peterse said.
Dr. Peterse added that a limitation to the analysis is that the study authors don’t know to what extent patients are even aware of the copayments. “So, we don’t know if it is a barrier, and we didn’t take other insurance scenarios into account,” she said.
Dr. Peterse declared no relevant disclosures.
CHICAGO – Out-of-pocket costs may present a barrier to colorectal screening, and removing those costs could reduce colorectal cancer deaths, according to new data presented at the annual Digestive Disease Week.
These data imply that removing copayments could result in a 16% decrease in colorectal cancer–related deaths among Medicare beneficiaries, explained lead author Elisabeth Peterse, PhD, of the department of public health, Erasmus Medical Center, Rotterdam, the Netherlands.
The research also demonstrated that waiving copayments is cost effective, she added.
Despite the effectiveness of colorectal cancer screening, only 58% of eligible individuals adhere to current screening recommendations, Dr. Peterse noted. Financial barriers may play a role in the lack of adherence, as studies have found that removing out-of-pocket costs is one of the most effective interventions for increasing screening.
“But despite the fact that the Affordable Care Act has been successful in partially eliminating cost sharing for colorectal screening, Medicare beneficiaries may still face unexpected out-of-pocket liabilities,” said Dr. Peterse.
Out-of-pocket costs can be complicated, given that they can depend largely on how a procedure is coded. A screening colonoscopy or fecal immunochemical test (FIT) is completely covered if it is coded as a screening test, but follow-up colonoscopies come with 20% copayments.
A screening colonoscopy with polypectomy and a follow-up colonoscopy that is done after a positive fecal immunochemical test are coded as diagnostic rather than screening, so the patient has out-of-pocket costs, she explained.
To explore how waiving the cost of screening could impact colorectal cancer–related mortality and cost effectiveness, the researchers conducted an analysis using a microsimulation model for a cohort composed of 65-year-old individuals.
In the simulation, they estimated colorectal cancer–related mortality, quality-adjusted life-years, and total cost of screening and treatment using the current Medicare copayment schedule. These were then compared with outcomes for alternative situations.
The study was conducted in two parts, explained Dr. Peterse. In the first part, the researchers looked at five scenarios: one in which the 20% copayment was intact. In the second, the copayment was waived without having any impact on adherence. In the third, the investigators looked at a 5% increase in adherence but only at diagnostic follow-up.
In the fourth and fifth scenarios, the investigators looked at 5% and 10% increases in adherence, in both first screening and diagnostic follow-up, she added.
In the study’s second part, the researchers also estimated the threshold increase in participation at which copayment removal would be cost effective, using a $50,000 willingness-to-pay threshold.
They found that without screening, the expected mortality would be 25 colorectal deaths per 1,000 people in a population of 65-year-old individuals. With screening, the number was reduced to 12.8 deaths per 1,000 65-year-olds for colonoscopy, and 14.9 deaths per 1,000 for FIT screening. The total associated costs for screening and treatment for the two modalities were $3.02 million and $2.87 million.
If waiving the copayments had no impact in increasing screening levels, the cost of screening was estimated to increase to $3.1 million (2.8% increase) for colonoscopy and $2.9 million (1.6% increase) for FIT.
But if copayments were removed and there were a 5% increase in adherence, colorectal cancer deaths were estimated to decline to 11.7 (–8.3%) and 13.9 (–6.3%) per 1,000 for colonoscopy and FIT, respectively. That would result in cost-effectiveness ratios of $19,288 and $7,894 for no copayment versus having a copayment. Increasing adherence to 10% would result in an even lower ratio, noted Dr. Peterse.
The threshold increase for participating in screening programs – the point where removing a copayment becomes cost effective – was a 1.8% increase in colonoscopy screening and a 0.8% increase for FIT.
The conclusion is that waiving copayments is cost effective, Dr. Peterse said.
Dr. Peterse added that a limitation to the analysis is that the study authors don’t know to what extent patients are even aware of the copayments. “So, we don’t know if it is a barrier, and we didn’t take other insurance scenarios into account,” she said.
Dr. Peterse declared no relevant disclosures.
CHICAGO – Out-of-pocket costs may present a barrier to colorectal screening, and removing those costs could reduce colorectal cancer deaths, according to new data presented at the annual Digestive Disease Week.
These data imply that removing copayments could result in a 16% decrease in colorectal cancer–related deaths among Medicare beneficiaries, explained lead author Elisabeth Peterse, PhD, of the department of public health, Erasmus Medical Center, Rotterdam, the Netherlands.
The research also demonstrated that waiving copayments is cost effective, she added.
Despite the effectiveness of colorectal cancer screening, only 58% of eligible individuals adhere to current screening recommendations, Dr. Peterse noted. Financial barriers may play a role in the lack of adherence, as studies have found that removing out-of-pocket costs is one of the most effective interventions for increasing screening.
“But despite the fact that the Affordable Care Act has been successful in partially eliminating cost sharing for colorectal screening, Medicare beneficiaries may still face unexpected out-of-pocket liabilities,” said Dr. Peterse.
Out-of-pocket costs can be complicated, given that they can depend largely on how a procedure is coded. A screening colonoscopy or fecal immunochemical test (FIT) is completely covered if it is coded as a screening test, but follow-up colonoscopies come with 20% copayments.
A screening colonoscopy with polypectomy and a follow-up colonoscopy that is done after a positive fecal immunochemical test are coded as diagnostic rather than screening, so the patient has out-of-pocket costs, she explained.
To explore how waiving the cost of screening could impact colorectal cancer–related mortality and cost effectiveness, the researchers conducted an analysis using a microsimulation model for a cohort composed of 65-year-old individuals.
In the simulation, they estimated colorectal cancer–related mortality, quality-adjusted life-years, and total cost of screening and treatment using the current Medicare copayment schedule. These were then compared with outcomes for alternative situations.
The study was conducted in two parts, explained Dr. Peterse. In the first part, the researchers looked at five scenarios: one in which the 20% copayment was intact. In the second, the copayment was waived without having any impact on adherence. In the third, the investigators looked at a 5% increase in adherence but only at diagnostic follow-up.
In the fourth and fifth scenarios, the investigators looked at 5% and 10% increases in adherence, in both first screening and diagnostic follow-up, she added.
In the study’s second part, the researchers also estimated the threshold increase in participation at which copayment removal would be cost effective, using a $50,000 willingness-to-pay threshold.
They found that without screening, the expected mortality would be 25 colorectal deaths per 1,000 people in a population of 65-year-old individuals. With screening, the number was reduced to 12.8 deaths per 1,000 65-year-olds for colonoscopy, and 14.9 deaths per 1,000 for FIT screening. The total associated costs for screening and treatment for the two modalities were $3.02 million and $2.87 million.
If waiving the copayments had no impact in increasing screening levels, the cost of screening was estimated to increase to $3.1 million (2.8% increase) for colonoscopy and $2.9 million (1.6% increase) for FIT.
But if copayments were removed and there were a 5% increase in adherence, colorectal cancer deaths were estimated to decline to 11.7 (–8.3%) and 13.9 (–6.3%) per 1,000 for colonoscopy and FIT, respectively. That would result in cost-effectiveness ratios of $19,288 and $7,894 for no copayment versus having a copayment. Increasing adherence to 10% would result in an even lower ratio, noted Dr. Peterse.
The threshold increase for participating in screening programs – the point where removing a copayment becomes cost effective – was a 1.8% increase in colonoscopy screening and a 0.8% increase for FIT.
The conclusion is that waiving copayments is cost effective, Dr. Peterse said.
Dr. Peterse added that a limitation to the analysis is that the study authors don’t know to what extent patients are even aware of the copayments. “So, we don’t know if it is a barrier, and we didn’t take other insurance scenarios into account,” she said.
Dr. Peterse declared no relevant disclosures.
AT DDW
Key clinical point:
Major finding: Removing copayments for routine screening could reduce deaths from colorectal cancer by up to 16% in Medicare beneficiaries.
Data source: A simulation model that looked at five scenarios to assess how increased adherence to colorectal cancer screening would reduce mortality and cost.
Disclosures: Dr. Peterse declared no relevant disclosures.
Emergency Care When the Music Stops
In this issue of Emergency Medicine (EM), emergency physician (EP) Christopher Hunter, MD, and his colleagues from Orlando Regional Medical Center (ORMC) share their first-person experiences planning for and dealing with the medical issues presented by an estimated 40,000 people attending an annual outdoor electronic dance music festival on each of 2 days in November 2016. Reacting to the overwhelming burden that had been placed on their ED and hospital by the same event the year before, the ORMC EPs demonstrate how a coordinated approach to planning and execution by EPs, the local emergency medical services system, festival organizers, and disaster response groups can accurately anticipate and effectively deal with the myriad of urgent and emergent needs presented by this type of event. In recent years, the number of such events throughout the country has been increasing rapidly.
This same group of skilled and dedicated ORMC EPs authored a first-person account in the August 2016 issue of EM (The Orlando Nightclub Shooting: Firsthand Accounts and Lessons Learned. Emerg Med. 2016;48(8):348-356), describing how they handled the aftermath of the Pulse Nightclub mass casualty incident (MCI), which also occurred in close proximity to ORMC.
Tragically, as this issue of EM was going to press, the world was shocked by yet another terrorist MCI, this time at a concert venue in Manchester, England. The lethal explosives were detonated in Manchester by a suicide bomber just outside the arena as the exiting crowd was heading to the nearby railroad station. This latest MCI claimed the lives of at least 22 children, parents, and young adults, and is of great concern to all who participate in concerts and large outdoor events: We must now consider the possibility of incidents combining the problems described in both of the first-person accounts mentioned above.
The most recent wave of terrorist MCIs, including the 2016 Orlando Pulse Nightclub shootings (49 deaths, 53 injuries, all but four victims were under the age of 40 years); the November 2015 terrorist incidents in Paris, including the Bataclan theatre rock concert massacre (89 deaths); and the April 15, 2013 Boston Marathon bombing (three deaths—ages 8, 23, 29 years—and 264 injuries), have all targeted mostly children and young adults.
In contrast, the victims of previous terrorist MCIs were mostly working adults. Of the almost 3,000 people who died in the 9/11 World Trade Center (WTC) and Pentagon attacks, almost all were between 35 and 39 years old, with the youngest WTC tower victim 18 years of age and the oldest 79. Terrorist activities in trains such as the March 11, 2004 Madrid commuter train bombings (192 deaths, about 2,000 injuries), and the March 20, 1995 Tokyo subway sarin gas release (12 deaths, over 1,000 severe injuries) also appeared to have targeted adults traveling to work during rush hours.
Clearly, EPs have an important role to play in providing urgent and emergent care at large outdoor gatherings, and emergent care and resuscitation of victims after natural and man-made MCIs. But the prospect of both types of events occurring in rapid succession at the same venue underlines the importance of preserving hospital-based ED resources during large gatherings by treating and releasing the majority of patients with festival-related illnesses and minor injuries on-site, as described in this month’s cover article.
The proliferation of EP-staffed urgent care centers and freestanding EDs (FSEDs) in recent years has demonstrated the ability of EPs to provide expert, needed emergency care outside of the walls of traditional, hospital-based EDs—a healthy trend for the future of emergency medicine. Like “pop-up” seasonal retail stores, the “pop-up FSED” described here by the ORMC EPs will become an increasingly important means of delivering urgent and emergent care in the future.
In this issue of Emergency Medicine (EM), emergency physician (EP) Christopher Hunter, MD, and his colleagues from Orlando Regional Medical Center (ORMC) share their first-person experiences planning for and dealing with the medical issues presented by an estimated 40,000 people attending an annual outdoor electronic dance music festival on each of 2 days in November 2016. Reacting to the overwhelming burden that had been placed on their ED and hospital by the same event the year before, the ORMC EPs demonstrate how a coordinated approach to planning and execution by EPs, the local emergency medical services system, festival organizers, and disaster response groups can accurately anticipate and effectively deal with the myriad of urgent and emergent needs presented by this type of event. In recent years, the number of such events throughout the country has been increasing rapidly.
This same group of skilled and dedicated ORMC EPs authored a first-person account in the August 2016 issue of EM (The Orlando Nightclub Shooting: Firsthand Accounts and Lessons Learned. Emerg Med. 2016;48(8):348-356), describing how they handled the aftermath of the Pulse Nightclub mass casualty incident (MCI), which also occurred in close proximity to ORMC.
Tragically, as this issue of EM was going to press, the world was shocked by yet another terrorist MCI, this time at a concert venue in Manchester, England. The lethal explosives were detonated in Manchester by a suicide bomber just outside the arena as the exiting crowd was heading to the nearby railroad station. This latest MCI claimed the lives of at least 22 children, parents, and young adults, and is of great concern to all who participate in concerts and large outdoor events: We must now consider the possibility of incidents combining the problems described in both of the first-person accounts mentioned above.
The most recent wave of terrorist MCIs, including the 2016 Orlando Pulse Nightclub shootings (49 deaths, 53 injuries, all but four victims were under the age of 40 years); the November 2015 terrorist incidents in Paris, including the Bataclan theatre rock concert massacre (89 deaths); and the April 15, 2013 Boston Marathon bombing (three deaths—ages 8, 23, 29 years—and 264 injuries), have all targeted mostly children and young adults.
In contrast, the victims of previous terrorist MCIs were mostly working adults. Of the almost 3,000 people who died in the 9/11 World Trade Center (WTC) and Pentagon attacks, almost all were between 35 and 39 years old, with the youngest WTC tower victim 18 years of age and the oldest 79. Terrorist activities in trains such as the March 11, 2004 Madrid commuter train bombings (192 deaths, about 2,000 injuries), and the March 20, 1995 Tokyo subway sarin gas release (12 deaths, over 1,000 severe injuries) also appeared to have targeted adults traveling to work during rush hours.
Clearly, EPs have an important role to play in providing urgent and emergent care at large outdoor gatherings, and emergent care and resuscitation of victims after natural and man-made MCIs. But the prospect of both types of events occurring in rapid succession at the same venue underlines the importance of preserving hospital-based ED resources during large gatherings by treating and releasing the majority of patients with festival-related illnesses and minor injuries on-site, as described in this month’s cover article.
The proliferation of EP-staffed urgent care centers and freestanding EDs (FSEDs) in recent years has demonstrated the ability of EPs to provide expert, needed emergency care outside of the walls of traditional, hospital-based EDs—a healthy trend for the future of emergency medicine. Like “pop-up” seasonal retail stores, the “pop-up FSED” described here by the ORMC EPs will become an increasingly important means of delivering urgent and emergent care in the future.
In this issue of Emergency Medicine (EM), emergency physician (EP) Christopher Hunter, MD, and his colleagues from Orlando Regional Medical Center (ORMC) share their first-person experiences planning for and dealing with the medical issues presented by an estimated 40,000 people attending an annual outdoor electronic dance music festival on each of 2 days in November 2016. Reacting to the overwhelming burden that had been placed on their ED and hospital by the same event the year before, the ORMC EPs demonstrate how a coordinated approach to planning and execution by EPs, the local emergency medical services system, festival organizers, and disaster response groups can accurately anticipate and effectively deal with the myriad of urgent and emergent needs presented by this type of event. In recent years, the number of such events throughout the country has been increasing rapidly.
This same group of skilled and dedicated ORMC EPs authored a first-person account in the August 2016 issue of EM (The Orlando Nightclub Shooting: Firsthand Accounts and Lessons Learned. Emerg Med. 2016;48(8):348-356), describing how they handled the aftermath of the Pulse Nightclub mass casualty incident (MCI), which also occurred in close proximity to ORMC.
Tragically, as this issue of EM was going to press, the world was shocked by yet another terrorist MCI, this time at a concert venue in Manchester, England. The lethal explosives were detonated in Manchester by a suicide bomber just outside the arena as the exiting crowd was heading to the nearby railroad station. This latest MCI claimed the lives of at least 22 children, parents, and young adults, and is of great concern to all who participate in concerts and large outdoor events: We must now consider the possibility of incidents combining the problems described in both of the first-person accounts mentioned above.
The most recent wave of terrorist MCIs, including the 2016 Orlando Pulse Nightclub shootings (49 deaths, 53 injuries, all but four victims were under the age of 40 years); the November 2015 terrorist incidents in Paris, including the Bataclan theatre rock concert massacre (89 deaths); and the April 15, 2013 Boston Marathon bombing (three deaths—ages 8, 23, 29 years—and 264 injuries), have all targeted mostly children and young adults.
In contrast, the victims of previous terrorist MCIs were mostly working adults. Of the almost 3,000 people who died in the 9/11 World Trade Center (WTC) and Pentagon attacks, almost all were between 35 and 39 years old, with the youngest WTC tower victim 18 years of age and the oldest 79. Terrorist activities in trains such as the March 11, 2004 Madrid commuter train bombings (192 deaths, about 2,000 injuries), and the March 20, 1995 Tokyo subway sarin gas release (12 deaths, over 1,000 severe injuries) also appeared to have targeted adults traveling to work during rush hours.
Clearly, EPs have an important role to play in providing urgent and emergent care at large outdoor gatherings, and emergent care and resuscitation of victims after natural and man-made MCIs. But the prospect of both types of events occurring in rapid succession at the same venue underlines the importance of preserving hospital-based ED resources during large gatherings by treating and releasing the majority of patients with festival-related illnesses and minor injuries on-site, as described in this month’s cover article.
The proliferation of EP-staffed urgent care centers and freestanding EDs (FSEDs) in recent years has demonstrated the ability of EPs to provide expert, needed emergency care outside of the walls of traditional, hospital-based EDs—a healthy trend for the future of emergency medicine. Like “pop-up” seasonal retail stores, the “pop-up FSED” described here by the ORMC EPs will become an increasingly important means of delivering urgent and emergent care in the future.