User login
Inpatient Language Barriers: An Old Problem in Need of Novel Solutions
The 25 million people in the United States with limited English proficiency (LEP), which is defined as speaking English less than “very well”, are at increased risk for healthcare disparities that result in preventable harm and poor patient experiences compared with English-proficient patients.1,2 The use of trained professional interpreters is associated with improved communication, healthcare outcomes, safety, and experiences for LEP patients.3 However, underuse of professional interpreters remains common.4 Healthcare staff frequently use family members, friends, or minor children as interpreters or try to “get by” with the patient’s limited English skills or staff’s limited non-English skills.5 These practices regularly compromise patient safety and quality for LEP patients and their families.
In the article “Inpatient Communication Barriers and Drivers when Caring for Limited English Proficiency Children,” Dr. Choe and colleagues approach the problem of interpreter underuse by studying the barriers and facilitators that exist at their children’s hospital.6 The group conducted four sessions using Group Level Assessment, a structured, interactive approach to understanding a problem and identifying potential solutions. Sixty-four pediatric hospitalists and residents, bedside nurses, and staff interpreters participated. Participants identified four primary barriers to communicating effectively with LEP families: difficulty accessing interpreter services, uncertainty in communicating with LEP families, unclear roles and expectations of different team members, and unmet expectations related to family engagement. They also identified four drivers of effective communication: collaborative problem-solving between providers and interpreters, greater attention to cultural context, practicing empathy for patients and families, and using family centered communication strategies.
This study reinforces that myriad challenges remain in accessing and using an interpreter. The barriers identified fall into two major categories: systems for accessing interpretation and communication involving an interpreter. Both ultimately must be addressed to achieve equitable communication for LEP patients/families. As interpreter use is contingent upon access, optimizing delivery systems is an essential foundation. At this study site, key barriers were the opaque scheduling processes and inconsistent access to and unfamiliarity with interpreter-related technology (eg, for telephone or video interpretation). These barriers are likely generalizable to many other hospitals. Priority should be given to developing transparent, consistent, and reliable processes for interpreter access. Interventions to improve interpreter access, such as one-touch interpreter telephones at every hospital bedside, have been more successful in improving interpreter use than provider education or regulatory mandates.4
The challenges identified around communicating with LEP families via interpreter are also likely generalizable. In the current study, participants described a clear tension around the interpreters’ optimal role, in which the care team might want the interpreter to intervene or participate in the discussion more, while interpreter standards require that they remain a neutral conduit for information. This neutral-party approach, when taken to the extreme, can limit the bidirectional communication between clinical teams and interpreters necessary to address communication challenges. Fostering collaborative problem-solving between interpreters and clinicians, in both formal and informal settings, is critically needed to improve the quality of communication during encounters. In addition to the proposed presession meeting between the clinician and interpreter, incorporating a debriefing after an interpreter-mediated encounter could offer an opportunity for bidirectional feedback. Unfortunately, interpreter scheduling constraints, fueled by the lack of reimbursement for interpretation in most states, frequently limit the feasibility of such proposals.
Participating providers also reported decreased engagement with LEP families and that they spent less time with them. These observations also merit attention if we are to achieve equitable outcomes for LEP patients. A conversation via interpreter requires more time for the same content, given the time needed to interpret the message. The fact that participants reported spending less time with LEP families means that less communication occurs with those families, compared with others. There are well-established links between good communication and improved clinical outcomes, including everything from decreased glycosylated hemoglobin levels to lower inpatient narcotic use.7 Thus, it is not surprising that patients with fewer opportunities to communicate fully have worse clinical outcomes.8 Addressing this will require changing hospital culture and provider expectations. Healthcare systems could support this effort with interventions such as decreased nursing assignments, longer allocated rounding times, longer outpatient clinic visits, and additional “points” in resident patient caps, if they exist, for LEP patients. Such steps would be an important investment in improving outcomes and decreasing costs for these vulnerable patients.
For all the barriers identified by Choe and colleagues, solutions are needed. Some may be generalizable, some may be location-specific, and most will be somewhere in between, requiring context-specific tailoring. We recommend a quality improvement (QI) approach, as the evidence-based best practice for communicating with LEP patients and families is well-known, but the gap is in delivering care that meets that standard. Leveraging the growing QI expertise at many institutions to devise approaches that go beyond provider education to change the systems and culture around communicating with LEP patients holds our best promise for improving the safety and effectiveness of care for this population.
Disclosures
The authors have no financial relationships relevant to this article to disclose nor do they have any conflicts of interest relevant to this article to disclose.
Funding
Dr. Lion’s time was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, grant K23 HD078507 (PI Lion).
1. Divi C, Koss RG, Schmaltz SP, Loeb JM. Language proficiency and adverse events in US hospitals: A pilot study. Int J Qual Heal Care. 2007;19(2):60-67. https://doi.org/10.1093/intqhc/mzl069.
2. Yeheskel A, Rawal S. Exploring the “patient experience” of individuals with limited English proficiency: A scoping review. J Immigr Minor Heal. 2018. https://doi.org/10.1007/s10903-018-0816-4.
3. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Heal Serv Res. 2007;42(2):727-754. https://doi.org/10.1111/j.1475-6773.2006.00629.x.
4. Taira BR, Kim K, Mody N. Hospital and health system-level interventions to improve care for limited English proficiency patients: A systematic review. Jt Comm J Qual Patient Saf. 2019. https://doi.org/10.1016/j.jcjq.2019.02.005.
5. Diamond LC, Schenker Y, Curry L, Bradley EH, Fernandez A. Getting by: Underuse of interpreters by resident physicians. J Gen Intern Med. 2009;24(2):256-262. https://doi.org/10.1007/s11606-008-0875-7.
6. Choe A, Unaka N, Schondelmeyer A, Raglin Bignall W, Vilvens H, Thomson J. Inpatient communication barriers and drivers when caring for limited English proficiency children. J Hosp Med. 2019;14(10):607-613. https://doi.org/10.12788/jhm.3240.
7. Stewart MA. Effective physician-patient communication and health outcomes: A review. CMAJ. 1995;152(9):1423-1433. PubMed
8. Pérez-Stable EJ, El-Toukhy S. Communicating with diverse patients: How patient and clinician factors affect disparities. Patient Educ Couns. 2018;101(12):2186-2194. https://doi.org/10.1016/j.pec.2018.08.021.
The 25 million people in the United States with limited English proficiency (LEP), which is defined as speaking English less than “very well”, are at increased risk for healthcare disparities that result in preventable harm and poor patient experiences compared with English-proficient patients.1,2 The use of trained professional interpreters is associated with improved communication, healthcare outcomes, safety, and experiences for LEP patients.3 However, underuse of professional interpreters remains common.4 Healthcare staff frequently use family members, friends, or minor children as interpreters or try to “get by” with the patient’s limited English skills or staff’s limited non-English skills.5 These practices regularly compromise patient safety and quality for LEP patients and their families.
In the article “Inpatient Communication Barriers and Drivers when Caring for Limited English Proficiency Children,” Dr. Choe and colleagues approach the problem of interpreter underuse by studying the barriers and facilitators that exist at their children’s hospital.6 The group conducted four sessions using Group Level Assessment, a structured, interactive approach to understanding a problem and identifying potential solutions. Sixty-four pediatric hospitalists and residents, bedside nurses, and staff interpreters participated. Participants identified four primary barriers to communicating effectively with LEP families: difficulty accessing interpreter services, uncertainty in communicating with LEP families, unclear roles and expectations of different team members, and unmet expectations related to family engagement. They also identified four drivers of effective communication: collaborative problem-solving between providers and interpreters, greater attention to cultural context, practicing empathy for patients and families, and using family centered communication strategies.
This study reinforces that myriad challenges remain in accessing and using an interpreter. The barriers identified fall into two major categories: systems for accessing interpretation and communication involving an interpreter. Both ultimately must be addressed to achieve equitable communication for LEP patients/families. As interpreter use is contingent upon access, optimizing delivery systems is an essential foundation. At this study site, key barriers were the opaque scheduling processes and inconsistent access to and unfamiliarity with interpreter-related technology (eg, for telephone or video interpretation). These barriers are likely generalizable to many other hospitals. Priority should be given to developing transparent, consistent, and reliable processes for interpreter access. Interventions to improve interpreter access, such as one-touch interpreter telephones at every hospital bedside, have been more successful in improving interpreter use than provider education or regulatory mandates.4
The challenges identified around communicating with LEP families via interpreter are also likely generalizable. In the current study, participants described a clear tension around the interpreters’ optimal role, in which the care team might want the interpreter to intervene or participate in the discussion more, while interpreter standards require that they remain a neutral conduit for information. This neutral-party approach, when taken to the extreme, can limit the bidirectional communication between clinical teams and interpreters necessary to address communication challenges. Fostering collaborative problem-solving between interpreters and clinicians, in both formal and informal settings, is critically needed to improve the quality of communication during encounters. In addition to the proposed presession meeting between the clinician and interpreter, incorporating a debriefing after an interpreter-mediated encounter could offer an opportunity for bidirectional feedback. Unfortunately, interpreter scheduling constraints, fueled by the lack of reimbursement for interpretation in most states, frequently limit the feasibility of such proposals.
Participating providers also reported decreased engagement with LEP families and that they spent less time with them. These observations also merit attention if we are to achieve equitable outcomes for LEP patients. A conversation via interpreter requires more time for the same content, given the time needed to interpret the message. The fact that participants reported spending less time with LEP families means that less communication occurs with those families, compared with others. There are well-established links between good communication and improved clinical outcomes, including everything from decreased glycosylated hemoglobin levels to lower inpatient narcotic use.7 Thus, it is not surprising that patients with fewer opportunities to communicate fully have worse clinical outcomes.8 Addressing this will require changing hospital culture and provider expectations. Healthcare systems could support this effort with interventions such as decreased nursing assignments, longer allocated rounding times, longer outpatient clinic visits, and additional “points” in resident patient caps, if they exist, for LEP patients. Such steps would be an important investment in improving outcomes and decreasing costs for these vulnerable patients.
For all the barriers identified by Choe and colleagues, solutions are needed. Some may be generalizable, some may be location-specific, and most will be somewhere in between, requiring context-specific tailoring. We recommend a quality improvement (QI) approach, as the evidence-based best practice for communicating with LEP patients and families is well-known, but the gap is in delivering care that meets that standard. Leveraging the growing QI expertise at many institutions to devise approaches that go beyond provider education to change the systems and culture around communicating with LEP patients holds our best promise for improving the safety and effectiveness of care for this population.
Disclosures
The authors have no financial relationships relevant to this article to disclose nor do they have any conflicts of interest relevant to this article to disclose.
Funding
Dr. Lion’s time was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, grant K23 HD078507 (PI Lion).
The 25 million people in the United States with limited English proficiency (LEP), which is defined as speaking English less than “very well”, are at increased risk for healthcare disparities that result in preventable harm and poor patient experiences compared with English-proficient patients.1,2 The use of trained professional interpreters is associated with improved communication, healthcare outcomes, safety, and experiences for LEP patients.3 However, underuse of professional interpreters remains common.4 Healthcare staff frequently use family members, friends, or minor children as interpreters or try to “get by” with the patient’s limited English skills or staff’s limited non-English skills.5 These practices regularly compromise patient safety and quality for LEP patients and their families.
In the article “Inpatient Communication Barriers and Drivers when Caring for Limited English Proficiency Children,” Dr. Choe and colleagues approach the problem of interpreter underuse by studying the barriers and facilitators that exist at their children’s hospital.6 The group conducted four sessions using Group Level Assessment, a structured, interactive approach to understanding a problem and identifying potential solutions. Sixty-four pediatric hospitalists and residents, bedside nurses, and staff interpreters participated. Participants identified four primary barriers to communicating effectively with LEP families: difficulty accessing interpreter services, uncertainty in communicating with LEP families, unclear roles and expectations of different team members, and unmet expectations related to family engagement. They also identified four drivers of effective communication: collaborative problem-solving between providers and interpreters, greater attention to cultural context, practicing empathy for patients and families, and using family centered communication strategies.
This study reinforces that myriad challenges remain in accessing and using an interpreter. The barriers identified fall into two major categories: systems for accessing interpretation and communication involving an interpreter. Both ultimately must be addressed to achieve equitable communication for LEP patients/families. As interpreter use is contingent upon access, optimizing delivery systems is an essential foundation. At this study site, key barriers were the opaque scheduling processes and inconsistent access to and unfamiliarity with interpreter-related technology (eg, for telephone or video interpretation). These barriers are likely generalizable to many other hospitals. Priority should be given to developing transparent, consistent, and reliable processes for interpreter access. Interventions to improve interpreter access, such as one-touch interpreter telephones at every hospital bedside, have been more successful in improving interpreter use than provider education or regulatory mandates.4
The challenges identified around communicating with LEP families via interpreter are also likely generalizable. In the current study, participants described a clear tension around the interpreters’ optimal role, in which the care team might want the interpreter to intervene or participate in the discussion more, while interpreter standards require that they remain a neutral conduit for information. This neutral-party approach, when taken to the extreme, can limit the bidirectional communication between clinical teams and interpreters necessary to address communication challenges. Fostering collaborative problem-solving between interpreters and clinicians, in both formal and informal settings, is critically needed to improve the quality of communication during encounters. In addition to the proposed presession meeting between the clinician and interpreter, incorporating a debriefing after an interpreter-mediated encounter could offer an opportunity for bidirectional feedback. Unfortunately, interpreter scheduling constraints, fueled by the lack of reimbursement for interpretation in most states, frequently limit the feasibility of such proposals.
Participating providers also reported decreased engagement with LEP families and that they spent less time with them. These observations also merit attention if we are to achieve equitable outcomes for LEP patients. A conversation via interpreter requires more time for the same content, given the time needed to interpret the message. The fact that participants reported spending less time with LEP families means that less communication occurs with those families, compared with others. There are well-established links between good communication and improved clinical outcomes, including everything from decreased glycosylated hemoglobin levels to lower inpatient narcotic use.7 Thus, it is not surprising that patients with fewer opportunities to communicate fully have worse clinical outcomes.8 Addressing this will require changing hospital culture and provider expectations. Healthcare systems could support this effort with interventions such as decreased nursing assignments, longer allocated rounding times, longer outpatient clinic visits, and additional “points” in resident patient caps, if they exist, for LEP patients. Such steps would be an important investment in improving outcomes and decreasing costs for these vulnerable patients.
For all the barriers identified by Choe and colleagues, solutions are needed. Some may be generalizable, some may be location-specific, and most will be somewhere in between, requiring context-specific tailoring. We recommend a quality improvement (QI) approach, as the evidence-based best practice for communicating with LEP patients and families is well-known, but the gap is in delivering care that meets that standard. Leveraging the growing QI expertise at many institutions to devise approaches that go beyond provider education to change the systems and culture around communicating with LEP patients holds our best promise for improving the safety and effectiveness of care for this population.
Disclosures
The authors have no financial relationships relevant to this article to disclose nor do they have any conflicts of interest relevant to this article to disclose.
Funding
Dr. Lion’s time was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, grant K23 HD078507 (PI Lion).
1. Divi C, Koss RG, Schmaltz SP, Loeb JM. Language proficiency and adverse events in US hospitals: A pilot study. Int J Qual Heal Care. 2007;19(2):60-67. https://doi.org/10.1093/intqhc/mzl069.
2. Yeheskel A, Rawal S. Exploring the “patient experience” of individuals with limited English proficiency: A scoping review. J Immigr Minor Heal. 2018. https://doi.org/10.1007/s10903-018-0816-4.
3. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Heal Serv Res. 2007;42(2):727-754. https://doi.org/10.1111/j.1475-6773.2006.00629.x.
4. Taira BR, Kim K, Mody N. Hospital and health system-level interventions to improve care for limited English proficiency patients: A systematic review. Jt Comm J Qual Patient Saf. 2019. https://doi.org/10.1016/j.jcjq.2019.02.005.
5. Diamond LC, Schenker Y, Curry L, Bradley EH, Fernandez A. Getting by: Underuse of interpreters by resident physicians. J Gen Intern Med. 2009;24(2):256-262. https://doi.org/10.1007/s11606-008-0875-7.
6. Choe A, Unaka N, Schondelmeyer A, Raglin Bignall W, Vilvens H, Thomson J. Inpatient communication barriers and drivers when caring for limited English proficiency children. J Hosp Med. 2019;14(10):607-613. https://doi.org/10.12788/jhm.3240.
7. Stewart MA. Effective physician-patient communication and health outcomes: A review. CMAJ. 1995;152(9):1423-1433. PubMed
8. Pérez-Stable EJ, El-Toukhy S. Communicating with diverse patients: How patient and clinician factors affect disparities. Patient Educ Couns. 2018;101(12):2186-2194. https://doi.org/10.1016/j.pec.2018.08.021.
1. Divi C, Koss RG, Schmaltz SP, Loeb JM. Language proficiency and adverse events in US hospitals: A pilot study. Int J Qual Heal Care. 2007;19(2):60-67. https://doi.org/10.1093/intqhc/mzl069.
2. Yeheskel A, Rawal S. Exploring the “patient experience” of individuals with limited English proficiency: A scoping review. J Immigr Minor Heal. 2018. https://doi.org/10.1007/s10903-018-0816-4.
3. Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Heal Serv Res. 2007;42(2):727-754. https://doi.org/10.1111/j.1475-6773.2006.00629.x.
4. Taira BR, Kim K, Mody N. Hospital and health system-level interventions to improve care for limited English proficiency patients: A systematic review. Jt Comm J Qual Patient Saf. 2019. https://doi.org/10.1016/j.jcjq.2019.02.005.
5. Diamond LC, Schenker Y, Curry L, Bradley EH, Fernandez A. Getting by: Underuse of interpreters by resident physicians. J Gen Intern Med. 2009;24(2):256-262. https://doi.org/10.1007/s11606-008-0875-7.
6. Choe A, Unaka N, Schondelmeyer A, Raglin Bignall W, Vilvens H, Thomson J. Inpatient communication barriers and drivers when caring for limited English proficiency children. J Hosp Med. 2019;14(10):607-613. https://doi.org/10.12788/jhm.3240.
7. Stewart MA. Effective physician-patient communication and health outcomes: A review. CMAJ. 1995;152(9):1423-1433. PubMed
8. Pérez-Stable EJ, El-Toukhy S. Communicating with diverse patients: How patient and clinician factors affect disparities. Patient Educ Couns. 2018;101(12):2186-2194. https://doi.org/10.1016/j.pec.2018.08.021.
© 2019 Society of Hospital Medicine
Thinking Aloud: How Nurses Rationalize Responses to Monitor Alarms
In the past five years, it has become increasingly apparent that hospital physiologic monitoring systems are not functioning optimally for children. On pediatric wards, 26%-48% of children are continuously monitored, and these children generate between 42 and 155 alarms per day.1 Just 1% or fewer are considered actionable or informative, slowing nurses’ response times and placing patients at risk of delayed recognition of life-threatening events.2,3 While some factors associated with alarm response times have been elucidated,3 in order to design safe and effective monitoring systems, further work is needed to understand the complex decision-making process that nurses face when encountering alarms outside a patient’s room. It is in this area that Schondelmeyer and colleagues strive to enhance our understanding in this issue of the Journal of Hospital Medicine.4
Schondelmeyer et al. conducted a single-center, observational study using mixed methods in a general pediatric unit. Trained observers shadowed nine nurses one to four times each, during which nurses were asked to “think aloud” as they managed physiologic monitor alarms, rationalizing their decisions about how and why they might respond for the observer to document. Observers accumulated 61 patient-hours of observation before investigators halted data collection because new insights about alarm responses were no longer emerging from the data (thematic saturation).
Nurses thought aloud about 207 alarms during the study, which the investigators estimated comprised about one third of the alarms that occurred during observation periods. Most of the 207 occurred while the nurse was already in the patient’s room, where a response decision is uncomplicated. More interesting were the 45 alarms heard while outside the patient’s room, where nurses face the complex decision of whether to interrupt their current tasks and respond or delay their response and assume the associated risk of nonresponse to a potentially deteriorating patient. Of the 45 alarms, nurses went into the room to evaluate the patient 15 times and, after doing so, reported that five of the 15 warranted in-person responses to address technical issues with the monitor, clinical issues, or patients’ comfort. Reassuring clinical contexts—such as presence of the medical team or family in the room and recent patient assessments—were the reasons most commonly provided to explain alarm nonresponse.
This study has two key limitations. First, the authors designed the study to observe nurses’ responses until thematic saturation was achieved. However, the small sample size (nine nurses, 45 out-of-room alarms) could raise questions about whether sufficient data were captured to make broadly generalizable conclusions, given the diverse range of patients, families, and clinical scenarios nurses encounter on an inpatient unit. Second, by instructing nurse participants to verbalize their rationale for response or nonresponse, investigators essentially asked nurses to override the “Type 1”, heuristic-based reasoning5 that research suggests regulates nursing responses to alarms when adapting to circumstances requiring high cognitive demand or a heavy workload.3 While innovative, it is possible that this approach prevented the investigators from fully achieving their stated objective of describing how bedside nurses think about and act upon alarms.
Nonetheless, the findings by Schondelmeyer and colleagues extend our emerging understanding of why alarm responses are disconcertingly slow. Nursing staff’s dismissal of monitor alarms that are discordant with a reassuring patient evaluation underscores the imperative to reduce nuisance alarms. Furthermore, the explicit statements justifying alarm nonresponse because of the presence of family members build upon prior findings of longer response times when family members are at the bedside3 and invite a provocative question: how would family members feel if they knew that they were being entrusted as a foundational component of safety monitoring in the hospital? In their recently published study conducted at the same hospital,6 Schondelmeyer’s team elicited perceptions that families are deeply concerned about staff nonresponse to alarms—as one nurse stated, parents “wonder what’s going on when no one comes in.” While there is a valuable role for integrating families into efforts to overcome threats to patient safety, as has been achieved with family error reporting7 and communication on family-centered rounds,8 this must occur in a structured, explicit, and deliberate manner, with families engaged as key stakeholders.
In summary, while Schondelmeyer and colleagues may not have exposed the depth of implicit thinking that governs nurses’ responses to alarms, they have highlighted the high-stakes decisions that nurses confront on a daily basis in an environment with exceedingly high alarm rates and low alarm actionability. The authors cite staff education among potential solutions to improve the safety of continuous monitoring, but such an intervention cannot be effective in a system that places impossible burdens on nurses. An openly family centered and multidisciplinary approach to reengineering the system for monitoring hospitalized children is needed to enable nurses to respond quickly and accurately to patients at risk of clinical deterioration.
Disclosures
The authors report no conflicts of interest.
1. Schondelmeyer AC, Brady PW, Goel VV, et al. Physiologic monitor alarm rates at 5 children’s hospitals. J Hosp Med. 2018;13(6):396-398. https://doi.org/10.12788/jhm.2918.
2. Bonafide CP, Lin R, Zander M, et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children’s hospital. J Hosp Med. 2015;10(6):345-351. https://doi.org/10.1002/jhm.2331.
3. Bonafide CP, Localio AR, Holmes JH, et al. Video analysis of factors associated with response time to physiologic monitor alarms in a children’s hospital. JAMA Pediatr. 2017;171(6):524-531. https://doi.org/10.1001/jamapediatrics.2016.5123.
4. Schondelmeyer A, Daraiseh NM, Allison B, et al. Nurse responses to physiologic monitor alarms on a general pediatric unit. J Hosp Med. 2019;14(10):602-606. https://doi.org/10.12788/jhm.3234.
5. Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009;84(8):1022-1028. https://doi.org/10.1097/ACM.0b013e3181ace703.
6. Schondelmeyer AC, Jenkins AM, Allison B, et al. Factors influencing use of continuous physiologic monitors for hospitalized pediatric patients. Hosp Pediatr. 2019;9(6):423-428. https://doi.org/10.1542/hpeds.2019-0007.
7. Khan A, Coffey M, Litterer KP, et al. Families as partners in hospital error and adverse event surveillance. JAMA Pediatr. 2017;171(4):372-381. https://doi.org/10.1001/jamapediatrics.2016.4812.
8. Khan A, Spector ND, Baird JD, et al. Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study. BMJ. 2018;363:k4764. https://doi.org/10.1136/bmj.k4764.
In the past five years, it has become increasingly apparent that hospital physiologic monitoring systems are not functioning optimally for children. On pediatric wards, 26%-48% of children are continuously monitored, and these children generate between 42 and 155 alarms per day.1 Just 1% or fewer are considered actionable or informative, slowing nurses’ response times and placing patients at risk of delayed recognition of life-threatening events.2,3 While some factors associated with alarm response times have been elucidated,3 in order to design safe and effective monitoring systems, further work is needed to understand the complex decision-making process that nurses face when encountering alarms outside a patient’s room. It is in this area that Schondelmeyer and colleagues strive to enhance our understanding in this issue of the Journal of Hospital Medicine.4
Schondelmeyer et al. conducted a single-center, observational study using mixed methods in a general pediatric unit. Trained observers shadowed nine nurses one to four times each, during which nurses were asked to “think aloud” as they managed physiologic monitor alarms, rationalizing their decisions about how and why they might respond for the observer to document. Observers accumulated 61 patient-hours of observation before investigators halted data collection because new insights about alarm responses were no longer emerging from the data (thematic saturation).
Nurses thought aloud about 207 alarms during the study, which the investigators estimated comprised about one third of the alarms that occurred during observation periods. Most of the 207 occurred while the nurse was already in the patient’s room, where a response decision is uncomplicated. More interesting were the 45 alarms heard while outside the patient’s room, where nurses face the complex decision of whether to interrupt their current tasks and respond or delay their response and assume the associated risk of nonresponse to a potentially deteriorating patient. Of the 45 alarms, nurses went into the room to evaluate the patient 15 times and, after doing so, reported that five of the 15 warranted in-person responses to address technical issues with the monitor, clinical issues, or patients’ comfort. Reassuring clinical contexts—such as presence of the medical team or family in the room and recent patient assessments—were the reasons most commonly provided to explain alarm nonresponse.
This study has two key limitations. First, the authors designed the study to observe nurses’ responses until thematic saturation was achieved. However, the small sample size (nine nurses, 45 out-of-room alarms) could raise questions about whether sufficient data were captured to make broadly generalizable conclusions, given the diverse range of patients, families, and clinical scenarios nurses encounter on an inpatient unit. Second, by instructing nurse participants to verbalize their rationale for response or nonresponse, investigators essentially asked nurses to override the “Type 1”, heuristic-based reasoning5 that research suggests regulates nursing responses to alarms when adapting to circumstances requiring high cognitive demand or a heavy workload.3 While innovative, it is possible that this approach prevented the investigators from fully achieving their stated objective of describing how bedside nurses think about and act upon alarms.
Nonetheless, the findings by Schondelmeyer and colleagues extend our emerging understanding of why alarm responses are disconcertingly slow. Nursing staff’s dismissal of monitor alarms that are discordant with a reassuring patient evaluation underscores the imperative to reduce nuisance alarms. Furthermore, the explicit statements justifying alarm nonresponse because of the presence of family members build upon prior findings of longer response times when family members are at the bedside3 and invite a provocative question: how would family members feel if they knew that they were being entrusted as a foundational component of safety monitoring in the hospital? In their recently published study conducted at the same hospital,6 Schondelmeyer’s team elicited perceptions that families are deeply concerned about staff nonresponse to alarms—as one nurse stated, parents “wonder what’s going on when no one comes in.” While there is a valuable role for integrating families into efforts to overcome threats to patient safety, as has been achieved with family error reporting7 and communication on family-centered rounds,8 this must occur in a structured, explicit, and deliberate manner, with families engaged as key stakeholders.
In summary, while Schondelmeyer and colleagues may not have exposed the depth of implicit thinking that governs nurses’ responses to alarms, they have highlighted the high-stakes decisions that nurses confront on a daily basis in an environment with exceedingly high alarm rates and low alarm actionability. The authors cite staff education among potential solutions to improve the safety of continuous monitoring, but such an intervention cannot be effective in a system that places impossible burdens on nurses. An openly family centered and multidisciplinary approach to reengineering the system for monitoring hospitalized children is needed to enable nurses to respond quickly and accurately to patients at risk of clinical deterioration.
Disclosures
The authors report no conflicts of interest.
In the past five years, it has become increasingly apparent that hospital physiologic monitoring systems are not functioning optimally for children. On pediatric wards, 26%-48% of children are continuously monitored, and these children generate between 42 and 155 alarms per day.1 Just 1% or fewer are considered actionable or informative, slowing nurses’ response times and placing patients at risk of delayed recognition of life-threatening events.2,3 While some factors associated with alarm response times have been elucidated,3 in order to design safe and effective monitoring systems, further work is needed to understand the complex decision-making process that nurses face when encountering alarms outside a patient’s room. It is in this area that Schondelmeyer and colleagues strive to enhance our understanding in this issue of the Journal of Hospital Medicine.4
Schondelmeyer et al. conducted a single-center, observational study using mixed methods in a general pediatric unit. Trained observers shadowed nine nurses one to four times each, during which nurses were asked to “think aloud” as they managed physiologic monitor alarms, rationalizing their decisions about how and why they might respond for the observer to document. Observers accumulated 61 patient-hours of observation before investigators halted data collection because new insights about alarm responses were no longer emerging from the data (thematic saturation).
Nurses thought aloud about 207 alarms during the study, which the investigators estimated comprised about one third of the alarms that occurred during observation periods. Most of the 207 occurred while the nurse was already in the patient’s room, where a response decision is uncomplicated. More interesting were the 45 alarms heard while outside the patient’s room, where nurses face the complex decision of whether to interrupt their current tasks and respond or delay their response and assume the associated risk of nonresponse to a potentially deteriorating patient. Of the 45 alarms, nurses went into the room to evaluate the patient 15 times and, after doing so, reported that five of the 15 warranted in-person responses to address technical issues with the monitor, clinical issues, or patients’ comfort. Reassuring clinical contexts—such as presence of the medical team or family in the room and recent patient assessments—were the reasons most commonly provided to explain alarm nonresponse.
This study has two key limitations. First, the authors designed the study to observe nurses’ responses until thematic saturation was achieved. However, the small sample size (nine nurses, 45 out-of-room alarms) could raise questions about whether sufficient data were captured to make broadly generalizable conclusions, given the diverse range of patients, families, and clinical scenarios nurses encounter on an inpatient unit. Second, by instructing nurse participants to verbalize their rationale for response or nonresponse, investigators essentially asked nurses to override the “Type 1”, heuristic-based reasoning5 that research suggests regulates nursing responses to alarms when adapting to circumstances requiring high cognitive demand or a heavy workload.3 While innovative, it is possible that this approach prevented the investigators from fully achieving their stated objective of describing how bedside nurses think about and act upon alarms.
Nonetheless, the findings by Schondelmeyer and colleagues extend our emerging understanding of why alarm responses are disconcertingly slow. Nursing staff’s dismissal of monitor alarms that are discordant with a reassuring patient evaluation underscores the imperative to reduce nuisance alarms. Furthermore, the explicit statements justifying alarm nonresponse because of the presence of family members build upon prior findings of longer response times when family members are at the bedside3 and invite a provocative question: how would family members feel if they knew that they were being entrusted as a foundational component of safety monitoring in the hospital? In their recently published study conducted at the same hospital,6 Schondelmeyer’s team elicited perceptions that families are deeply concerned about staff nonresponse to alarms—as one nurse stated, parents “wonder what’s going on when no one comes in.” While there is a valuable role for integrating families into efforts to overcome threats to patient safety, as has been achieved with family error reporting7 and communication on family-centered rounds,8 this must occur in a structured, explicit, and deliberate manner, with families engaged as key stakeholders.
In summary, while Schondelmeyer and colleagues may not have exposed the depth of implicit thinking that governs nurses’ responses to alarms, they have highlighted the high-stakes decisions that nurses confront on a daily basis in an environment with exceedingly high alarm rates and low alarm actionability. The authors cite staff education among potential solutions to improve the safety of continuous monitoring, but such an intervention cannot be effective in a system that places impossible burdens on nurses. An openly family centered and multidisciplinary approach to reengineering the system for monitoring hospitalized children is needed to enable nurses to respond quickly and accurately to patients at risk of clinical deterioration.
Disclosures
The authors report no conflicts of interest.
1. Schondelmeyer AC, Brady PW, Goel VV, et al. Physiologic monitor alarm rates at 5 children’s hospitals. J Hosp Med. 2018;13(6):396-398. https://doi.org/10.12788/jhm.2918.
2. Bonafide CP, Lin R, Zander M, et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children’s hospital. J Hosp Med. 2015;10(6):345-351. https://doi.org/10.1002/jhm.2331.
3. Bonafide CP, Localio AR, Holmes JH, et al. Video analysis of factors associated with response time to physiologic monitor alarms in a children’s hospital. JAMA Pediatr. 2017;171(6):524-531. https://doi.org/10.1001/jamapediatrics.2016.5123.
4. Schondelmeyer A, Daraiseh NM, Allison B, et al. Nurse responses to physiologic monitor alarms on a general pediatric unit. J Hosp Med. 2019;14(10):602-606. https://doi.org/10.12788/jhm.3234.
5. Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009;84(8):1022-1028. https://doi.org/10.1097/ACM.0b013e3181ace703.
6. Schondelmeyer AC, Jenkins AM, Allison B, et al. Factors influencing use of continuous physiologic monitors for hospitalized pediatric patients. Hosp Pediatr. 2019;9(6):423-428. https://doi.org/10.1542/hpeds.2019-0007.
7. Khan A, Coffey M, Litterer KP, et al. Families as partners in hospital error and adverse event surveillance. JAMA Pediatr. 2017;171(4):372-381. https://doi.org/10.1001/jamapediatrics.2016.4812.
8. Khan A, Spector ND, Baird JD, et al. Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study. BMJ. 2018;363:k4764. https://doi.org/10.1136/bmj.k4764.
1. Schondelmeyer AC, Brady PW, Goel VV, et al. Physiologic monitor alarm rates at 5 children’s hospitals. J Hosp Med. 2018;13(6):396-398. https://doi.org/10.12788/jhm.2918.
2. Bonafide CP, Lin R, Zander M, et al. Association between exposure to nonactionable physiologic monitor alarms and response time in a children’s hospital. J Hosp Med. 2015;10(6):345-351. https://doi.org/10.1002/jhm.2331.
3. Bonafide CP, Localio AR, Holmes JH, et al. Video analysis of factors associated with response time to physiologic monitor alarms in a children’s hospital. JAMA Pediatr. 2017;171(6):524-531. https://doi.org/10.1001/jamapediatrics.2016.5123.
4. Schondelmeyer A, Daraiseh NM, Allison B, et al. Nurse responses to physiologic monitor alarms on a general pediatric unit. J Hosp Med. 2019;14(10):602-606. https://doi.org/10.12788/jhm.3234.
5. Croskerry P. A universal model of diagnostic reasoning. Acad Med. 2009;84(8):1022-1028. https://doi.org/10.1097/ACM.0b013e3181ace703.
6. Schondelmeyer AC, Jenkins AM, Allison B, et al. Factors influencing use of continuous physiologic monitors for hospitalized pediatric patients. Hosp Pediatr. 2019;9(6):423-428. https://doi.org/10.1542/hpeds.2019-0007.
7. Khan A, Coffey M, Litterer KP, et al. Families as partners in hospital error and adverse event surveillance. JAMA Pediatr. 2017;171(4):372-381. https://doi.org/10.1001/jamapediatrics.2016.4812.
8. Khan A, Spector ND, Baird JD, et al. Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study. BMJ. 2018;363:k4764. https://doi.org/10.1136/bmj.k4764.
© 2019 Society of Hospital Medicine
Collective Action and Effective Dialogue to Address Gender Bias in Medicine
In 2016, Pediatric Hospital Medicine (PHM) was recognized as a subspecialty under the American Board of Pediatrics (ABP), one of 24 certifying boards of the American Board of Medical Specialties. As with all new ABP subspecialty certification processes, a “practice pathway” with specific eligibility criteria allows individuals with expertise and sufficient practice experience within the discipline to take the certification examination. For PHM, certification via the practice pathway is permissible for the 2019, 2021, and 2023 certifying examinations.1 In this perspective, we provide an illustration of ABP leadership and the PHM community partnering to mitigate unintentional gender bias that surfaced after the practice pathway eligibility criteria were implemented. We also provide recommendations to revise these criteria to eliminate future gender bias and promote equity in medicine.
In July 2019, individuals within the PHM community began to share stories of being denied eligibility to sit for the 2019 exam.2 Some of the reported denials were due to an eligibility criterion related to “practice interruptions”, which stated that practice interruptions cannot exceed three months in the preceding four years or six months in the preceding five years. Notably, some women reported that their applications were denied because of practice interruptions due to maternity leave. These stories raised significant concerns of gender bias in the board certification process and sparked collective action to revise the board certification eligibility criteria. A petition was circulated within the PHM community and received 1,479 signatures in two weeks.
Given the magnitude of concern, leaders within the PHM community, with support from the American Academy of Pediatrics, collaboratively engaged with the ABP and members of the ABP PHM subboard to improve the transparency and equity of the eligibility process. As a result of this activism and effective dialogue, the ABP revised the PHM board certification eligibility criteria and removed the practice interruption criterion.1 Through this unique experience of advocacy and partner
Gender bias is defined as the unfair difference in the way men and women are treated.3 Maternal bias is further characterized as bias experienced by mothers related to motherhood, often involving discrimination based on pregnancy, maternity leave, or breastfeeding. Both are common in medicine. Two-thirds of physician mothers report experiencing gender bias and more than a third experience maternal bias.4 This bias may be explicit, or intentional, but often the bias is unintentional. This bias can occur even with equal representation of women and men on committees determining eligibility, and even when the committee believes it is not biased.5 Furthermore, gender or maternal bias negatively affects individuals in medicine in regards to future employment, career advancement, and compensation.6-11
Given these implications, we celebrate the removal of the practice interruptions criterion as it was unintentionally biased against women. Eligibility criteria that considered practice interruptions would have disproportionately affected women due to leaves related to pregnancy and due to discrepancies in the length of parental leave for mothers versus fathers. Though the ABP’s initial review of cases of denial did not demonstrate a significant difference in the proportion of men and women who were denied, these data may be misleading. Potential reasons why the ABP did not find significant differences in denial rates between women and men include: (1) some women who had recent maternity leaves chose not to apply because of concerns they may be denied; or (2) some women did not disclose maternity leaves on their application because they did not interpret maternity leave to be a practice interruption. This “self-censoring” may have resulted in incomplete data, making it difficult to fully understand the differential impact of this criterion on women versus men. Therefore, it is essential that we as a profession continue to identify any areas where gender bias exists in determining eligibility for certification, employment, or career advancement within medicine and eliminate it.
Despite the improvements made in the revised criteria, further revision is necessary to remove the criterion related to the “start date”, which will differentially affect women. This criterion states that an individual must have started their PHM practice on or before July of the first year of a four-year look-back period (eg, July 2015 for the 2019 cycle). We present three theoretical cases to illustrate gender bias with respect to this criterion (Table). Even though Applicants #2 and #3 accrue far more than the minimum number of hours in their first year—and more hours overall than Applicant #1—both of these women will remain ineligible under the revised criteria. While Applicant #2 could be eligible for the 2021 or 2023 cycle, Applicant #3, who is new to PHM practice in 2019 as a residency graduate, will not be eligible at all under the practice pathway due to delayed graduation from residency.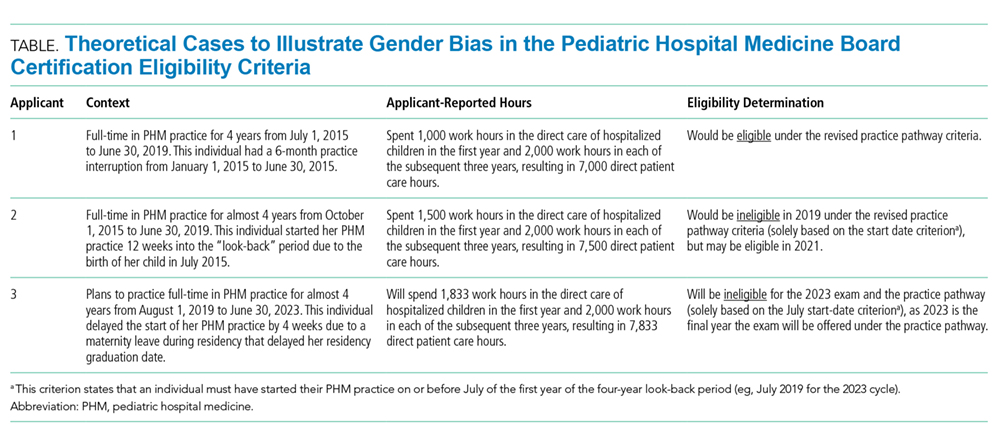
Parental leave during residency following birth of a child may result in the need to make up the time missed.12 This means that more women than men will experience delayed entry into the workforce due to late graduation from residency.13 Women who experience a gap in employment at the start of their PHM practice due to pregnancy or childbirth will also be differentially affected by this criterion. If this same type of gap were to occur later in the year, it would no longer impact a woman’s eligibility under the revised criteria. Therefore, we implore the ABP to reevaluate this criterion which results in a hidden “practice interruption” penalty. Removing eligibility criteria related to practice interruptions, wherever they may occur, will not only eliminate systematic bias against women, but may also encourage men to take paternity leave, for which the benefits to both men and women are well described.14,15
We support the ABP’s mission to maintain the public’s trust by ensuring PHM board certification is an indicator that individuals have met a high standard. We acknowledge that the ABP and PHM subboard had to draw a line to create minimum standards. The start date and four-year look-back criteria were informed by prior certification processes, and the PHM community was given the opportunity to comment on these criteria prior to final ABP approval. However, now that we have become aware of how the start date criteria can differentially impact women and men, we must reevaluate this line to ensure that women and men are treated equally. Similar to the removal of the practice interruptions criterion, we do not believe that removal of the start date criterion will in any way compromise these standards. A four-year look-back period will still be in place and individuals will still be required to accrue the minimum number of hours in the first year and each subsequent year of the four-year period.
Despite any change in the criteria, there will be individuals who remain ineligible for PHM board certification. We will need to rely on institutions and the societies that lead PHM to remember that not all individuals had the opportunity to certify as a pediatric hospitalist, and for some, this was due to maternity leave. No woman should have to worry about her future employment when considering motherhood.
We hope the lessons learned from this experience will be informative for other specialties considering a new certification. Committees designing new criteria should have proportional representation of women and men, inclusion of underrepresented minorities, and members with a range of ages, orientations, identities, and abilities. Criteria should be closely scrutinized to evaluate if a single group of people is more likely to be excluded. All application reviewers should undergo training in identifying implicit bias.16 Once eligibility criteria are determined, they should be transparent to all applicants, consistently applied, and decisions to applicants should clearly state which criteria were or were not met. Regular audits should be conducted to identify any bias. Finally, transparent and respectful dialogue between the certifying board and the physician community is paramount to ensuring continuous quality improvement in the process.
The PHM experience with this new board certification process highlights the positive impact that the PHM community had engaging with the ABP leadership, who listened to the concerns and revised the eligibility criteria. We are optimistic that this productive relationship will continue to eliminate any gender bias in the board certification process. In turn, PHM and the ABP can be leaders in ending gender inequity in medicine.
Disclosures
The authors have nothing to disclose.
1. Nichols DG, Woods SK. The American Board of Pediatrics response to the Pediatric Hospital Medicine petition. J Hosp Med. 2019;14(10):586-588. https://doi.org/10.12788/jhm.3322
2. Don’t make me choose between motherhood and my career. https://www.kevinmd.com/blog/2019/08/dont-make-me-choose-between-motherhood-and-my-career.html. Accessed September 16, 2019.
3. GENDER BIAS | definition in the Cambridge English Dictionary. April 2019. https://dictionary.cambridge.org/us/dictionary/english/gender-bias.
4. Adesoye T, Mangurian C, Choo EK, Girgis C, Sabry-Elnaggar H, Linos E. Perceived discrimination experienced by physician mothers and desired workplace changes: A cross-sectional survey. JAMA Intern Med. 2017;177(7):1033-1036. https://doi.org/10.1001/jamainternmed.2017.1394
5. Régner I, Thinus-Blanc C, Netter A, Schmader T, Huguet P. Committees with implicit biases promote fewer women when they do not believe gender bias exists. Nat Hum Behav. 2019. https://doi.org/10.1038/s41562-019-0686-3
6. Trix F, Psenka C. Exploring the color of glass: Letters of recommendation for female and male medical faculty. Discourse Soc. 2003;14(2):191-220. https://doi.org/10.1177/0957926503014002277
7. Correll SJ, Benard S, Paik I. Getting a job: Is there a motherhood penalty? Am J Sociol. 2007;112(5):1297-1339. https://doi.org/10.1086/511799
8. Aamc. Analysis in Brief - August 2009: Unconscious Bias in Faculty and Leadership Recruitment: A Literature Review; 2009. https://implicit.harvard.edu/. Accessed September 10, 2019.
9. Wright AL, Schwindt LA, Bassford TL, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500-508. https://doi.org/10.1097/00001888-200305000-00015
10. Weaver AC, Wetterneck TB, Whelan CT, Hinami K. A matter of priorities? Exploring the persistent gender pay gap in hospital medicine. J Hosp Med. 2015;10(8):486-490. https://doi.org/10.1002/jhm.2400
11. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender differences in earnings of early- and midcareer pediatricians. Pediatrics. September 2019:e20183955. https://doi.org/10.1542/peds.2018-3955
12. Section on Medical Students, Residents and Fellowship Trainees, Committee on Early Childhood. Parental leave for residents and pediatric training programs. Pediatrics. 2013;131(2):387-390. https://doi.org/10.1542/peds.2012-3542
13. Jagsi R, Tarbell NJ, Weinstein DF. Becoming a doctor, starting a family — leaves of absence from graduate medical education. N Engl J Med. 2007;357(19):1889-1891. https://doi.org/10.1056/NEJMp078163
14. Nepomnyaschy L, Waldfogel J. Paternity leave and fathers’ involvement with their young children. Community Work Fam. 2007;10(4):427-453. https://doi.org/10.1080/13668800701575077
15. Andersen SH. Paternity leave and the motherhood penalty: New causal evidence. J Marriage Fam. 2018;80(5):1125-1143. https://doi.org/10.1111/jomf.12507.
16. Girod S, Fassiotto M, Grewal D, et al. Reducing Implicit Gender Leadership Bias in Academic Medicine With an Educational Intervention. Acad Med. 2016;91(8):1143-1150. https://doi.org/10.1097/ACM.0000000000001099
In 2016, Pediatric Hospital Medicine (PHM) was recognized as a subspecialty under the American Board of Pediatrics (ABP), one of 24 certifying boards of the American Board of Medical Specialties. As with all new ABP subspecialty certification processes, a “practice pathway” with specific eligibility criteria allows individuals with expertise and sufficient practice experience within the discipline to take the certification examination. For PHM, certification via the practice pathway is permissible for the 2019, 2021, and 2023 certifying examinations.1 In this perspective, we provide an illustration of ABP leadership and the PHM community partnering to mitigate unintentional gender bias that surfaced after the practice pathway eligibility criteria were implemented. We also provide recommendations to revise these criteria to eliminate future gender bias and promote equity in medicine.
In July 2019, individuals within the PHM community began to share stories of being denied eligibility to sit for the 2019 exam.2 Some of the reported denials were due to an eligibility criterion related to “practice interruptions”, which stated that practice interruptions cannot exceed three months in the preceding four years or six months in the preceding five years. Notably, some women reported that their applications were denied because of practice interruptions due to maternity leave. These stories raised significant concerns of gender bias in the board certification process and sparked collective action to revise the board certification eligibility criteria. A petition was circulated within the PHM community and received 1,479 signatures in two weeks.
Given the magnitude of concern, leaders within the PHM community, with support from the American Academy of Pediatrics, collaboratively engaged with the ABP and members of the ABP PHM subboard to improve the transparency and equity of the eligibility process. As a result of this activism and effective dialogue, the ABP revised the PHM board certification eligibility criteria and removed the practice interruption criterion.1 Through this unique experience of advocacy and partner
Gender bias is defined as the unfair difference in the way men and women are treated.3 Maternal bias is further characterized as bias experienced by mothers related to motherhood, often involving discrimination based on pregnancy, maternity leave, or breastfeeding. Both are common in medicine. Two-thirds of physician mothers report experiencing gender bias and more than a third experience maternal bias.4 This bias may be explicit, or intentional, but often the bias is unintentional. This bias can occur even with equal representation of women and men on committees determining eligibility, and even when the committee believes it is not biased.5 Furthermore, gender or maternal bias negatively affects individuals in medicine in regards to future employment, career advancement, and compensation.6-11
Given these implications, we celebrate the removal of the practice interruptions criterion as it was unintentionally biased against women. Eligibility criteria that considered practice interruptions would have disproportionately affected women due to leaves related to pregnancy and due to discrepancies in the length of parental leave for mothers versus fathers. Though the ABP’s initial review of cases of denial did not demonstrate a significant difference in the proportion of men and women who were denied, these data may be misleading. Potential reasons why the ABP did not find significant differences in denial rates between women and men include: (1) some women who had recent maternity leaves chose not to apply because of concerns they may be denied; or (2) some women did not disclose maternity leaves on their application because they did not interpret maternity leave to be a practice interruption. This “self-censoring” may have resulted in incomplete data, making it difficult to fully understand the differential impact of this criterion on women versus men. Therefore, it is essential that we as a profession continue to identify any areas where gender bias exists in determining eligibility for certification, employment, or career advancement within medicine and eliminate it.
Despite the improvements made in the revised criteria, further revision is necessary to remove the criterion related to the “start date”, which will differentially affect women. This criterion states that an individual must have started their PHM practice on or before July of the first year of a four-year look-back period (eg, July 2015 for the 2019 cycle). We present three theoretical cases to illustrate gender bias with respect to this criterion (Table). Even though Applicants #2 and #3 accrue far more than the minimum number of hours in their first year—and more hours overall than Applicant #1—both of these women will remain ineligible under the revised criteria. While Applicant #2 could be eligible for the 2021 or 2023 cycle, Applicant #3, who is new to PHM practice in 2019 as a residency graduate, will not be eligible at all under the practice pathway due to delayed graduation from residency.
Parental leave during residency following birth of a child may result in the need to make up the time missed.12 This means that more women than men will experience delayed entry into the workforce due to late graduation from residency.13 Women who experience a gap in employment at the start of their PHM practice due to pregnancy or childbirth will also be differentially affected by this criterion. If this same type of gap were to occur later in the year, it would no longer impact a woman’s eligibility under the revised criteria. Therefore, we implore the ABP to reevaluate this criterion which results in a hidden “practice interruption” penalty. Removing eligibility criteria related to practice interruptions, wherever they may occur, will not only eliminate systematic bias against women, but may also encourage men to take paternity leave, for which the benefits to both men and women are well described.14,15
We support the ABP’s mission to maintain the public’s trust by ensuring PHM board certification is an indicator that individuals have met a high standard. We acknowledge that the ABP and PHM subboard had to draw a line to create minimum standards. The start date and four-year look-back criteria were informed by prior certification processes, and the PHM community was given the opportunity to comment on these criteria prior to final ABP approval. However, now that we have become aware of how the start date criteria can differentially impact women and men, we must reevaluate this line to ensure that women and men are treated equally. Similar to the removal of the practice interruptions criterion, we do not believe that removal of the start date criterion will in any way compromise these standards. A four-year look-back period will still be in place and individuals will still be required to accrue the minimum number of hours in the first year and each subsequent year of the four-year period.
Despite any change in the criteria, there will be individuals who remain ineligible for PHM board certification. We will need to rely on institutions and the societies that lead PHM to remember that not all individuals had the opportunity to certify as a pediatric hospitalist, and for some, this was due to maternity leave. No woman should have to worry about her future employment when considering motherhood.
We hope the lessons learned from this experience will be informative for other specialties considering a new certification. Committees designing new criteria should have proportional representation of women and men, inclusion of underrepresented minorities, and members with a range of ages, orientations, identities, and abilities. Criteria should be closely scrutinized to evaluate if a single group of people is more likely to be excluded. All application reviewers should undergo training in identifying implicit bias.16 Once eligibility criteria are determined, they should be transparent to all applicants, consistently applied, and decisions to applicants should clearly state which criteria were or were not met. Regular audits should be conducted to identify any bias. Finally, transparent and respectful dialogue between the certifying board and the physician community is paramount to ensuring continuous quality improvement in the process.
The PHM experience with this new board certification process highlights the positive impact that the PHM community had engaging with the ABP leadership, who listened to the concerns and revised the eligibility criteria. We are optimistic that this productive relationship will continue to eliminate any gender bias in the board certification process. In turn, PHM and the ABP can be leaders in ending gender inequity in medicine.
Disclosures
The authors have nothing to disclose.
In 2016, Pediatric Hospital Medicine (PHM) was recognized as a subspecialty under the American Board of Pediatrics (ABP), one of 24 certifying boards of the American Board of Medical Specialties. As with all new ABP subspecialty certification processes, a “practice pathway” with specific eligibility criteria allows individuals with expertise and sufficient practice experience within the discipline to take the certification examination. For PHM, certification via the practice pathway is permissible for the 2019, 2021, and 2023 certifying examinations.1 In this perspective, we provide an illustration of ABP leadership and the PHM community partnering to mitigate unintentional gender bias that surfaced after the practice pathway eligibility criteria were implemented. We also provide recommendations to revise these criteria to eliminate future gender bias and promote equity in medicine.
In July 2019, individuals within the PHM community began to share stories of being denied eligibility to sit for the 2019 exam.2 Some of the reported denials were due to an eligibility criterion related to “practice interruptions”, which stated that practice interruptions cannot exceed three months in the preceding four years or six months in the preceding five years. Notably, some women reported that their applications were denied because of practice interruptions due to maternity leave. These stories raised significant concerns of gender bias in the board certification process and sparked collective action to revise the board certification eligibility criteria. A petition was circulated within the PHM community and received 1,479 signatures in two weeks.
Given the magnitude of concern, leaders within the PHM community, with support from the American Academy of Pediatrics, collaboratively engaged with the ABP and members of the ABP PHM subboard to improve the transparency and equity of the eligibility process. As a result of this activism and effective dialogue, the ABP revised the PHM board certification eligibility criteria and removed the practice interruption criterion.1 Through this unique experience of advocacy and partner
Gender bias is defined as the unfair difference in the way men and women are treated.3 Maternal bias is further characterized as bias experienced by mothers related to motherhood, often involving discrimination based on pregnancy, maternity leave, or breastfeeding. Both are common in medicine. Two-thirds of physician mothers report experiencing gender bias and more than a third experience maternal bias.4 This bias may be explicit, or intentional, but often the bias is unintentional. This bias can occur even with equal representation of women and men on committees determining eligibility, and even when the committee believes it is not biased.5 Furthermore, gender or maternal bias negatively affects individuals in medicine in regards to future employment, career advancement, and compensation.6-11
Given these implications, we celebrate the removal of the practice interruptions criterion as it was unintentionally biased against women. Eligibility criteria that considered practice interruptions would have disproportionately affected women due to leaves related to pregnancy and due to discrepancies in the length of parental leave for mothers versus fathers. Though the ABP’s initial review of cases of denial did not demonstrate a significant difference in the proportion of men and women who were denied, these data may be misleading. Potential reasons why the ABP did not find significant differences in denial rates between women and men include: (1) some women who had recent maternity leaves chose not to apply because of concerns they may be denied; or (2) some women did not disclose maternity leaves on their application because they did not interpret maternity leave to be a practice interruption. This “self-censoring” may have resulted in incomplete data, making it difficult to fully understand the differential impact of this criterion on women versus men. Therefore, it is essential that we as a profession continue to identify any areas where gender bias exists in determining eligibility for certification, employment, or career advancement within medicine and eliminate it.
Despite the improvements made in the revised criteria, further revision is necessary to remove the criterion related to the “start date”, which will differentially affect women. This criterion states that an individual must have started their PHM practice on or before July of the first year of a four-year look-back period (eg, July 2015 for the 2019 cycle). We present three theoretical cases to illustrate gender bias with respect to this criterion (Table). Even though Applicants #2 and #3 accrue far more than the minimum number of hours in their first year—and more hours overall than Applicant #1—both of these women will remain ineligible under the revised criteria. While Applicant #2 could be eligible for the 2021 or 2023 cycle, Applicant #3, who is new to PHM practice in 2019 as a residency graduate, will not be eligible at all under the practice pathway due to delayed graduation from residency.
Parental leave during residency following birth of a child may result in the need to make up the time missed.12 This means that more women than men will experience delayed entry into the workforce due to late graduation from residency.13 Women who experience a gap in employment at the start of their PHM practice due to pregnancy or childbirth will also be differentially affected by this criterion. If this same type of gap were to occur later in the year, it would no longer impact a woman’s eligibility under the revised criteria. Therefore, we implore the ABP to reevaluate this criterion which results in a hidden “practice interruption” penalty. Removing eligibility criteria related to practice interruptions, wherever they may occur, will not only eliminate systematic bias against women, but may also encourage men to take paternity leave, for which the benefits to both men and women are well described.14,15
We support the ABP’s mission to maintain the public’s trust by ensuring PHM board certification is an indicator that individuals have met a high standard. We acknowledge that the ABP and PHM subboard had to draw a line to create minimum standards. The start date and four-year look-back criteria were informed by prior certification processes, and the PHM community was given the opportunity to comment on these criteria prior to final ABP approval. However, now that we have become aware of how the start date criteria can differentially impact women and men, we must reevaluate this line to ensure that women and men are treated equally. Similar to the removal of the practice interruptions criterion, we do not believe that removal of the start date criterion will in any way compromise these standards. A four-year look-back period will still be in place and individuals will still be required to accrue the minimum number of hours in the first year and each subsequent year of the four-year period.
Despite any change in the criteria, there will be individuals who remain ineligible for PHM board certification. We will need to rely on institutions and the societies that lead PHM to remember that not all individuals had the opportunity to certify as a pediatric hospitalist, and for some, this was due to maternity leave. No woman should have to worry about her future employment when considering motherhood.
We hope the lessons learned from this experience will be informative for other specialties considering a new certification. Committees designing new criteria should have proportional representation of women and men, inclusion of underrepresented minorities, and members with a range of ages, orientations, identities, and abilities. Criteria should be closely scrutinized to evaluate if a single group of people is more likely to be excluded. All application reviewers should undergo training in identifying implicit bias.16 Once eligibility criteria are determined, they should be transparent to all applicants, consistently applied, and decisions to applicants should clearly state which criteria were or were not met. Regular audits should be conducted to identify any bias. Finally, transparent and respectful dialogue between the certifying board and the physician community is paramount to ensuring continuous quality improvement in the process.
The PHM experience with this new board certification process highlights the positive impact that the PHM community had engaging with the ABP leadership, who listened to the concerns and revised the eligibility criteria. We are optimistic that this productive relationship will continue to eliminate any gender bias in the board certification process. In turn, PHM and the ABP can be leaders in ending gender inequity in medicine.
Disclosures
The authors have nothing to disclose.
1. Nichols DG, Woods SK. The American Board of Pediatrics response to the Pediatric Hospital Medicine petition. J Hosp Med. 2019;14(10):586-588. https://doi.org/10.12788/jhm.3322
2. Don’t make me choose between motherhood and my career. https://www.kevinmd.com/blog/2019/08/dont-make-me-choose-between-motherhood-and-my-career.html. Accessed September 16, 2019.
3. GENDER BIAS | definition in the Cambridge English Dictionary. April 2019. https://dictionary.cambridge.org/us/dictionary/english/gender-bias.
4. Adesoye T, Mangurian C, Choo EK, Girgis C, Sabry-Elnaggar H, Linos E. Perceived discrimination experienced by physician mothers and desired workplace changes: A cross-sectional survey. JAMA Intern Med. 2017;177(7):1033-1036. https://doi.org/10.1001/jamainternmed.2017.1394
5. Régner I, Thinus-Blanc C, Netter A, Schmader T, Huguet P. Committees with implicit biases promote fewer women when they do not believe gender bias exists. Nat Hum Behav. 2019. https://doi.org/10.1038/s41562-019-0686-3
6. Trix F, Psenka C. Exploring the color of glass: Letters of recommendation for female and male medical faculty. Discourse Soc. 2003;14(2):191-220. https://doi.org/10.1177/0957926503014002277
7. Correll SJ, Benard S, Paik I. Getting a job: Is there a motherhood penalty? Am J Sociol. 2007;112(5):1297-1339. https://doi.org/10.1086/511799
8. Aamc. Analysis in Brief - August 2009: Unconscious Bias in Faculty and Leadership Recruitment: A Literature Review; 2009. https://implicit.harvard.edu/. Accessed September 10, 2019.
9. Wright AL, Schwindt LA, Bassford TL, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500-508. https://doi.org/10.1097/00001888-200305000-00015
10. Weaver AC, Wetterneck TB, Whelan CT, Hinami K. A matter of priorities? Exploring the persistent gender pay gap in hospital medicine. J Hosp Med. 2015;10(8):486-490. https://doi.org/10.1002/jhm.2400
11. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender differences in earnings of early- and midcareer pediatricians. Pediatrics. September 2019:e20183955. https://doi.org/10.1542/peds.2018-3955
12. Section on Medical Students, Residents and Fellowship Trainees, Committee on Early Childhood. Parental leave for residents and pediatric training programs. Pediatrics. 2013;131(2):387-390. https://doi.org/10.1542/peds.2012-3542
13. Jagsi R, Tarbell NJ, Weinstein DF. Becoming a doctor, starting a family — leaves of absence from graduate medical education. N Engl J Med. 2007;357(19):1889-1891. https://doi.org/10.1056/NEJMp078163
14. Nepomnyaschy L, Waldfogel J. Paternity leave and fathers’ involvement with their young children. Community Work Fam. 2007;10(4):427-453. https://doi.org/10.1080/13668800701575077
15. Andersen SH. Paternity leave and the motherhood penalty: New causal evidence. J Marriage Fam. 2018;80(5):1125-1143. https://doi.org/10.1111/jomf.12507.
16. Girod S, Fassiotto M, Grewal D, et al. Reducing Implicit Gender Leadership Bias in Academic Medicine With an Educational Intervention. Acad Med. 2016;91(8):1143-1150. https://doi.org/10.1097/ACM.0000000000001099
1. Nichols DG, Woods SK. The American Board of Pediatrics response to the Pediatric Hospital Medicine petition. J Hosp Med. 2019;14(10):586-588. https://doi.org/10.12788/jhm.3322
2. Don’t make me choose between motherhood and my career. https://www.kevinmd.com/blog/2019/08/dont-make-me-choose-between-motherhood-and-my-career.html. Accessed September 16, 2019.
3. GENDER BIAS | definition in the Cambridge English Dictionary. April 2019. https://dictionary.cambridge.org/us/dictionary/english/gender-bias.
4. Adesoye T, Mangurian C, Choo EK, Girgis C, Sabry-Elnaggar H, Linos E. Perceived discrimination experienced by physician mothers and desired workplace changes: A cross-sectional survey. JAMA Intern Med. 2017;177(7):1033-1036. https://doi.org/10.1001/jamainternmed.2017.1394
5. Régner I, Thinus-Blanc C, Netter A, Schmader T, Huguet P. Committees with implicit biases promote fewer women when they do not believe gender bias exists. Nat Hum Behav. 2019. https://doi.org/10.1038/s41562-019-0686-3
6. Trix F, Psenka C. Exploring the color of glass: Letters of recommendation for female and male medical faculty. Discourse Soc. 2003;14(2):191-220. https://doi.org/10.1177/0957926503014002277
7. Correll SJ, Benard S, Paik I. Getting a job: Is there a motherhood penalty? Am J Sociol. 2007;112(5):1297-1339. https://doi.org/10.1086/511799
8. Aamc. Analysis in Brief - August 2009: Unconscious Bias in Faculty and Leadership Recruitment: A Literature Review; 2009. https://implicit.harvard.edu/. Accessed September 10, 2019.
9. Wright AL, Schwindt LA, Bassford TL, et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78(5):500-508. https://doi.org/10.1097/00001888-200305000-00015
10. Weaver AC, Wetterneck TB, Whelan CT, Hinami K. A matter of priorities? Exploring the persistent gender pay gap in hospital medicine. J Hosp Med. 2015;10(8):486-490. https://doi.org/10.1002/jhm.2400
11. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender differences in earnings of early- and midcareer pediatricians. Pediatrics. September 2019:e20183955. https://doi.org/10.1542/peds.2018-3955
12. Section on Medical Students, Residents and Fellowship Trainees, Committee on Early Childhood. Parental leave for residents and pediatric training programs. Pediatrics. 2013;131(2):387-390. https://doi.org/10.1542/peds.2012-3542
13. Jagsi R, Tarbell NJ, Weinstein DF. Becoming a doctor, starting a family — leaves of absence from graduate medical education. N Engl J Med. 2007;357(19):1889-1891. https://doi.org/10.1056/NEJMp078163
14. Nepomnyaschy L, Waldfogel J. Paternity leave and fathers’ involvement with their young children. Community Work Fam. 2007;10(4):427-453. https://doi.org/10.1080/13668800701575077
15. Andersen SH. Paternity leave and the motherhood penalty: New causal evidence. J Marriage Fam. 2018;80(5):1125-1143. https://doi.org/10.1111/jomf.12507.
16. Girod S, Fassiotto M, Grewal D, et al. Reducing Implicit Gender Leadership Bias in Academic Medicine With an Educational Intervention. Acad Med. 2016;91(8):1143-1150. https://doi.org/10.1097/ACM.0000000000001099
© 2019 Society of Hospital Medicine
Leadership & Professional Development: Empowering Educators
“Better than a thousand days of diligent study is one day with a great teacher.”
—Japanese proverb
My chairman of medicine in medical school was a looming, intimidating, diagnostic genius—and one of the best teachers I have ever had. As a sub-intern it seemed I learned more in one month with him than in my prior six months of medical school. After the rotation, I asked him how he became such an effective teacher. “Simple,” he said, “I invest significant time and effort.”
But time is limited and you have to be smart with how you invest it. Here are three pearls that are a wise investment—they will make you a better teacher.
PREPARE
Those who seem to teach effortlessly do so after substantial behind-the-scenes effort. Read on your patients before rounds. Identify key teaching points and useful literature. Get some questions ready to define knowledge gaps and create “Teaching Scripts.”
Teaching Scripts are preplanned summaries of specific topics that can be used on rounds or longer talks and are “triggered” by common scenarios (eg, hypoxia). Great teaching scripts use a “hook” to engage the learner (commonly a thought-provoking question or story), two to five teaching points, and purposeful questions, mnemonics, and visual representations.
You should aim to develop at least five teaching scripts on commonly encountered topics. Eventually, you should have twenty scripts you can easily reference.
USE TECHNOLOGY
Technology significantly enhances the efficiency and impact of your teaching. For example, on rounds use your cell phone to display and teach anatomy, radiographic images, and EKGs. Use an iPad as a mobile whiteboard. Use email to collate and disseminate teaching points or send links to valuable learning resources like procedural videos. At its best, you can develop new programs and recruit team members to create resources, like I did with an online series focused on teaching to teach using graphically-enhanced TED-style talks1 and animated whiteboard videos.2
LEARN FROM OTHER DISCIPLINES
Do you easily remember the content from your medical school lectures? Likely not. But you likely remember moments from your favorite comedian or TED talk. Unlike the many PowerPoint lectures you’ve sat through, I’ll bet you stay engaged in films and documentaries. Why the difference? In short—medical educators often don’t make content engaging, readily understood, or memorable. To be most effective in teaching, learn from experts in other fields. Think how storytelling, film, theater, and graphic design contribute to learning. Don’t be afraid to be different.
All of these disciplines recognize the power of storytelling to make their points more impactful and memorable. Leverage this by mixing lessons with stories to create teaching points that stick. Lessons of character and morals can be highlighted through stories of personal struggles, prior patients, or people you admire. Clinical tips can be reinforced through sharing a “clinical story”—concise retellings of high-yield patient cases with diagnosis or management tips.
These disciplines also recognize the importance of “setting the stage” to create an optimal experience. We too can learn from this by setting the stage for our learners. Build a learning environment that is positive, collaborative, and fun by being open, curious, and enthusiastic. Treat your team to coffee rounds or lunch and get to know each learner as you walk between patients. As Teddy Roosevelt said, “people don’t care how much you know, until they know how much you care.”
My chairman taught me that exceptional teaching is not a talent of the gifted, it is a skill of the diligent. If you invest in your teaching, you can make a tremendous impact in the lives of your learners. Are you ready to be empowered?
Acknowledgments
The author wishes to thank
Disclosures
Dr. Cronin has nothing to disclose.
1. Kabeer R, Salari S, Cronin D. MENTOR Video Series: The Golden Secret. [Video]. 2019. Available at: http://mentorseries.org/FeedbackGS.
2. Kabeer R, Salari S, Cronin D. MENTOR Video Series: Effective Feedback Summary - The 5Ps. [Video]. 2019. Available at: http://mentorseries.org/Feedback5Ps.
“Better than a thousand days of diligent study is one day with a great teacher.”
—Japanese proverb
My chairman of medicine in medical school was a looming, intimidating, diagnostic genius—and one of the best teachers I have ever had. As a sub-intern it seemed I learned more in one month with him than in my prior six months of medical school. After the rotation, I asked him how he became such an effective teacher. “Simple,” he said, “I invest significant time and effort.”
But time is limited and you have to be smart with how you invest it. Here are three pearls that are a wise investment—they will make you a better teacher.
PREPARE
Those who seem to teach effortlessly do so after substantial behind-the-scenes effort. Read on your patients before rounds. Identify key teaching points and useful literature. Get some questions ready to define knowledge gaps and create “Teaching Scripts.”
Teaching Scripts are preplanned summaries of specific topics that can be used on rounds or longer talks and are “triggered” by common scenarios (eg, hypoxia). Great teaching scripts use a “hook” to engage the learner (commonly a thought-provoking question or story), two to five teaching points, and purposeful questions, mnemonics, and visual representations.
You should aim to develop at least five teaching scripts on commonly encountered topics. Eventually, you should have twenty scripts you can easily reference.
USE TECHNOLOGY
Technology significantly enhances the efficiency and impact of your teaching. For example, on rounds use your cell phone to display and teach anatomy, radiographic images, and EKGs. Use an iPad as a mobile whiteboard. Use email to collate and disseminate teaching points or send links to valuable learning resources like procedural videos. At its best, you can develop new programs and recruit team members to create resources, like I did with an online series focused on teaching to teach using graphically-enhanced TED-style talks1 and animated whiteboard videos.2
LEARN FROM OTHER DISCIPLINES
Do you easily remember the content from your medical school lectures? Likely not. But you likely remember moments from your favorite comedian or TED talk. Unlike the many PowerPoint lectures you’ve sat through, I’ll bet you stay engaged in films and documentaries. Why the difference? In short—medical educators often don’t make content engaging, readily understood, or memorable. To be most effective in teaching, learn from experts in other fields. Think how storytelling, film, theater, and graphic design contribute to learning. Don’t be afraid to be different.
All of these disciplines recognize the power of storytelling to make their points more impactful and memorable. Leverage this by mixing lessons with stories to create teaching points that stick. Lessons of character and morals can be highlighted through stories of personal struggles, prior patients, or people you admire. Clinical tips can be reinforced through sharing a “clinical story”—concise retellings of high-yield patient cases with diagnosis or management tips.
These disciplines also recognize the importance of “setting the stage” to create an optimal experience. We too can learn from this by setting the stage for our learners. Build a learning environment that is positive, collaborative, and fun by being open, curious, and enthusiastic. Treat your team to coffee rounds or lunch and get to know each learner as you walk between patients. As Teddy Roosevelt said, “people don’t care how much you know, until they know how much you care.”
My chairman taught me that exceptional teaching is not a talent of the gifted, it is a skill of the diligent. If you invest in your teaching, you can make a tremendous impact in the lives of your learners. Are you ready to be empowered?
Acknowledgments
The author wishes to thank
Disclosures
Dr. Cronin has nothing to disclose.
“Better than a thousand days of diligent study is one day with a great teacher.”
—Japanese proverb
My chairman of medicine in medical school was a looming, intimidating, diagnostic genius—and one of the best teachers I have ever had. As a sub-intern it seemed I learned more in one month with him than in my prior six months of medical school. After the rotation, I asked him how he became such an effective teacher. “Simple,” he said, “I invest significant time and effort.”
But time is limited and you have to be smart with how you invest it. Here are three pearls that are a wise investment—they will make you a better teacher.
PREPARE
Those who seem to teach effortlessly do so after substantial behind-the-scenes effort. Read on your patients before rounds. Identify key teaching points and useful literature. Get some questions ready to define knowledge gaps and create “Teaching Scripts.”
Teaching Scripts are preplanned summaries of specific topics that can be used on rounds or longer talks and are “triggered” by common scenarios (eg, hypoxia). Great teaching scripts use a “hook” to engage the learner (commonly a thought-provoking question or story), two to five teaching points, and purposeful questions, mnemonics, and visual representations.
You should aim to develop at least five teaching scripts on commonly encountered topics. Eventually, you should have twenty scripts you can easily reference.
USE TECHNOLOGY
Technology significantly enhances the efficiency and impact of your teaching. For example, on rounds use your cell phone to display and teach anatomy, radiographic images, and EKGs. Use an iPad as a mobile whiteboard. Use email to collate and disseminate teaching points or send links to valuable learning resources like procedural videos. At its best, you can develop new programs and recruit team members to create resources, like I did with an online series focused on teaching to teach using graphically-enhanced TED-style talks1 and animated whiteboard videos.2
LEARN FROM OTHER DISCIPLINES
Do you easily remember the content from your medical school lectures? Likely not. But you likely remember moments from your favorite comedian or TED talk. Unlike the many PowerPoint lectures you’ve sat through, I’ll bet you stay engaged in films and documentaries. Why the difference? In short—medical educators often don’t make content engaging, readily understood, or memorable. To be most effective in teaching, learn from experts in other fields. Think how storytelling, film, theater, and graphic design contribute to learning. Don’t be afraid to be different.
All of these disciplines recognize the power of storytelling to make their points more impactful and memorable. Leverage this by mixing lessons with stories to create teaching points that stick. Lessons of character and morals can be highlighted through stories of personal struggles, prior patients, or people you admire. Clinical tips can be reinforced through sharing a “clinical story”—concise retellings of high-yield patient cases with diagnosis or management tips.
These disciplines also recognize the importance of “setting the stage” to create an optimal experience. We too can learn from this by setting the stage for our learners. Build a learning environment that is positive, collaborative, and fun by being open, curious, and enthusiastic. Treat your team to coffee rounds or lunch and get to know each learner as you walk between patients. As Teddy Roosevelt said, “people don’t care how much you know, until they know how much you care.”
My chairman taught me that exceptional teaching is not a talent of the gifted, it is a skill of the diligent. If you invest in your teaching, you can make a tremendous impact in the lives of your learners. Are you ready to be empowered?
Acknowledgments
The author wishes to thank
Disclosures
Dr. Cronin has nothing to disclose.
1. Kabeer R, Salari S, Cronin D. MENTOR Video Series: The Golden Secret. [Video]. 2019. Available at: http://mentorseries.org/FeedbackGS.
2. Kabeer R, Salari S, Cronin D. MENTOR Video Series: Effective Feedback Summary - The 5Ps. [Video]. 2019. Available at: http://mentorseries.org/Feedback5Ps.
1. Kabeer R, Salari S, Cronin D. MENTOR Video Series: The Golden Secret. [Video]. 2019. Available at: http://mentorseries.org/FeedbackGS.
2. Kabeer R, Salari S, Cronin D. MENTOR Video Series: Effective Feedback Summary - The 5Ps. [Video]. 2019. Available at: http://mentorseries.org/Feedback5Ps.
© 2019 Society of Hospital Medicine
Psoriatic Arthritis Overview
Overview and Pathophysiology of Rheumatoid Arthritis
AGA Clinical Practice Update on the utility of endoscopic submucosal dissection in T1b esophageal cancer: Expert review
Endoscopic submucosal dissection (ESD) is a viable treatment option for patients with submucosal (T1b) esophageal cancer who have a low risk of lymph node metastasis, according to an expert review.
Among patients with T1b esophageal cancer, ideal candidates for ESD have small (less than 2 cm), well-differentiated tumors that do not invade beyond the superficial submucosa (SM1) and lack lymphovascular invasion, reported lead author Mohamed O. Othman, MD, of Baylor College of Medicine in Houston, and colleagues. The literature review was recently commissioned by the American Gastroenterological Association (AGA), because of high clinical relevance.
“[ESD] has been gaining momentum as an alternative to surgery in treating early gastrointestinal neoplasms,” the investigators wrote in Clinical Gastroenterology and Hepatology.
Most patients who undergo surgical resection develop gastroesophageal reflux, the investigators noted, and many others develop serious complications or do not survive the procedure.
“Even a high-volume center such as Mayo Clinic reported a surgical mortality of 4% for T1a esophageal cancer,” the investigators wrote. “Moreover, 34% of patients developed postoperative complications such as anastomotic leaks, anastomotic strictures, cardiopulmonary complications, and feeding jejunostomy leaks. ... Therefore, a less-invasive alternative to esophagectomy would be extremely valuable in the management of early stage [esophageal cancer] if proven effective.”
The investigators reviewed studies evaluating safety and efficacy of surgical and endoscopic techniques, as well as available data for chemoradiation and radiofrequency ablation combinations, which could potentially optimize outcomes of endoscopic resection.
They concluded that most patients with esophageal cancer that does not extend beyond the mucosa (T1a) can be cured with endoscopic resection, based on 5-year survival rates from several Japanese trials. For patients with T1b disease, however, ESD is best suited for those with a low risk of lymph node metastasis. Unfortunately, identifying these candidates can be challenging, according to the investigators.
“The risk of lymph node metastasis depends on the depth of invasion, histologic type, and molecular characterization of the tumor,” the investigators explained, noting that depth of invasion is the trickiest to discern. Although endoscopic ultrasound (EUS) is still recommended for submucosal imaging, the review showed that EUS may overstage cancer in Barrett’s esophagus. The investigators suggested that volume laser endoscopy with infrared light could be a more accurate alternative, but it is not yet a clinical reality.
The review also showed potential for combining ESD with other modalities. For example, a study by Hamada and colleagues involving 66 patients with submucosal (T1b) esophageal squamous cell carcinoma found that a combination of ESD with chemoradiation led to similar 3- and 5-year survival rates as radical esophagectomy. The investigators highlighted the importance of lymph node metastasis in this study, as none of the 30 patients lacking lymph node involvement had metastatic recurrence, compared with 6 of the 36 patients who exhibited lymph node metastasis. According to the investigators, promising data are also anticipated for this combination among those with adenocarcinoma. And for patients with intestinal metaplasia and/or dysplasia, adding radiofrequency ablation after ESD appears to be an effective option; one recent study by Sharmila Subramaniam, BMBS, and colleagues found that this strategy led to clearance rates of 85% and 96% for metaplasia and dysplasia, respectively.
“Additional treatment should be determined by factors such as tumor grade, status of lymphovascular invasion, and depth of tumor, which have a direct influence on metastatic potential,” the investigators wrote.
The investigators suggested that, in the future, better diagnostics will be needed to characterize T1b disease, as this could streamline patient selection. “Future research should focus on novel biological and immunohistochemistry markers that can aid in the prediction of tumor behavior and [lymph node metastasis] in T1b esophageal cancer,” they concluded.
The study was commissioned by the American Gastroenterological Association. The investigators disclosed additional relationships with Boston Scientific, Olympus, Lumendi, and others.
SOURCE: Othman MO et al. CGH. 2019 Jun 4. doi: 10.1016/j.cgh.2019.05.045.
Endoscopic submucosal dissection (ESD) is a viable treatment option for patients with submucosal (T1b) esophageal cancer who have a low risk of lymph node metastasis, according to an expert review.
Among patients with T1b esophageal cancer, ideal candidates for ESD have small (less than 2 cm), well-differentiated tumors that do not invade beyond the superficial submucosa (SM1) and lack lymphovascular invasion, reported lead author Mohamed O. Othman, MD, of Baylor College of Medicine in Houston, and colleagues. The literature review was recently commissioned by the American Gastroenterological Association (AGA), because of high clinical relevance.
“[ESD] has been gaining momentum as an alternative to surgery in treating early gastrointestinal neoplasms,” the investigators wrote in Clinical Gastroenterology and Hepatology.
Most patients who undergo surgical resection develop gastroesophageal reflux, the investigators noted, and many others develop serious complications or do not survive the procedure.
“Even a high-volume center such as Mayo Clinic reported a surgical mortality of 4% for T1a esophageal cancer,” the investigators wrote. “Moreover, 34% of patients developed postoperative complications such as anastomotic leaks, anastomotic strictures, cardiopulmonary complications, and feeding jejunostomy leaks. ... Therefore, a less-invasive alternative to esophagectomy would be extremely valuable in the management of early stage [esophageal cancer] if proven effective.”
The investigators reviewed studies evaluating safety and efficacy of surgical and endoscopic techniques, as well as available data for chemoradiation and radiofrequency ablation combinations, which could potentially optimize outcomes of endoscopic resection.
They concluded that most patients with esophageal cancer that does not extend beyond the mucosa (T1a) can be cured with endoscopic resection, based on 5-year survival rates from several Japanese trials. For patients with T1b disease, however, ESD is best suited for those with a low risk of lymph node metastasis. Unfortunately, identifying these candidates can be challenging, according to the investigators.
“The risk of lymph node metastasis depends on the depth of invasion, histologic type, and molecular characterization of the tumor,” the investigators explained, noting that depth of invasion is the trickiest to discern. Although endoscopic ultrasound (EUS) is still recommended for submucosal imaging, the review showed that EUS may overstage cancer in Barrett’s esophagus. The investigators suggested that volume laser endoscopy with infrared light could be a more accurate alternative, but it is not yet a clinical reality.
The review also showed potential for combining ESD with other modalities. For example, a study by Hamada and colleagues involving 66 patients with submucosal (T1b) esophageal squamous cell carcinoma found that a combination of ESD with chemoradiation led to similar 3- and 5-year survival rates as radical esophagectomy. The investigators highlighted the importance of lymph node metastasis in this study, as none of the 30 patients lacking lymph node involvement had metastatic recurrence, compared with 6 of the 36 patients who exhibited lymph node metastasis. According to the investigators, promising data are also anticipated for this combination among those with adenocarcinoma. And for patients with intestinal metaplasia and/or dysplasia, adding radiofrequency ablation after ESD appears to be an effective option; one recent study by Sharmila Subramaniam, BMBS, and colleagues found that this strategy led to clearance rates of 85% and 96% for metaplasia and dysplasia, respectively.
“Additional treatment should be determined by factors such as tumor grade, status of lymphovascular invasion, and depth of tumor, which have a direct influence on metastatic potential,” the investigators wrote.
The investigators suggested that, in the future, better diagnostics will be needed to characterize T1b disease, as this could streamline patient selection. “Future research should focus on novel biological and immunohistochemistry markers that can aid in the prediction of tumor behavior and [lymph node metastasis] in T1b esophageal cancer,” they concluded.
The study was commissioned by the American Gastroenterological Association. The investigators disclosed additional relationships with Boston Scientific, Olympus, Lumendi, and others.
SOURCE: Othman MO et al. CGH. 2019 Jun 4. doi: 10.1016/j.cgh.2019.05.045.
Endoscopic submucosal dissection (ESD) is a viable treatment option for patients with submucosal (T1b) esophageal cancer who have a low risk of lymph node metastasis, according to an expert review.
Among patients with T1b esophageal cancer, ideal candidates for ESD have small (less than 2 cm), well-differentiated tumors that do not invade beyond the superficial submucosa (SM1) and lack lymphovascular invasion, reported lead author Mohamed O. Othman, MD, of Baylor College of Medicine in Houston, and colleagues. The literature review was recently commissioned by the American Gastroenterological Association (AGA), because of high clinical relevance.
“[ESD] has been gaining momentum as an alternative to surgery in treating early gastrointestinal neoplasms,” the investigators wrote in Clinical Gastroenterology and Hepatology.
Most patients who undergo surgical resection develop gastroesophageal reflux, the investigators noted, and many others develop serious complications or do not survive the procedure.
“Even a high-volume center such as Mayo Clinic reported a surgical mortality of 4% for T1a esophageal cancer,” the investigators wrote. “Moreover, 34% of patients developed postoperative complications such as anastomotic leaks, anastomotic strictures, cardiopulmonary complications, and feeding jejunostomy leaks. ... Therefore, a less-invasive alternative to esophagectomy would be extremely valuable in the management of early stage [esophageal cancer] if proven effective.”
The investigators reviewed studies evaluating safety and efficacy of surgical and endoscopic techniques, as well as available data for chemoradiation and radiofrequency ablation combinations, which could potentially optimize outcomes of endoscopic resection.
They concluded that most patients with esophageal cancer that does not extend beyond the mucosa (T1a) can be cured with endoscopic resection, based on 5-year survival rates from several Japanese trials. For patients with T1b disease, however, ESD is best suited for those with a low risk of lymph node metastasis. Unfortunately, identifying these candidates can be challenging, according to the investigators.
“The risk of lymph node metastasis depends on the depth of invasion, histologic type, and molecular characterization of the tumor,” the investigators explained, noting that depth of invasion is the trickiest to discern. Although endoscopic ultrasound (EUS) is still recommended for submucosal imaging, the review showed that EUS may overstage cancer in Barrett’s esophagus. The investigators suggested that volume laser endoscopy with infrared light could be a more accurate alternative, but it is not yet a clinical reality.
The review also showed potential for combining ESD with other modalities. For example, a study by Hamada and colleagues involving 66 patients with submucosal (T1b) esophageal squamous cell carcinoma found that a combination of ESD with chemoradiation led to similar 3- and 5-year survival rates as radical esophagectomy. The investigators highlighted the importance of lymph node metastasis in this study, as none of the 30 patients lacking lymph node involvement had metastatic recurrence, compared with 6 of the 36 patients who exhibited lymph node metastasis. According to the investigators, promising data are also anticipated for this combination among those with adenocarcinoma. And for patients with intestinal metaplasia and/or dysplasia, adding radiofrequency ablation after ESD appears to be an effective option; one recent study by Sharmila Subramaniam, BMBS, and colleagues found that this strategy led to clearance rates of 85% and 96% for metaplasia and dysplasia, respectively.
“Additional treatment should be determined by factors such as tumor grade, status of lymphovascular invasion, and depth of tumor, which have a direct influence on metastatic potential,” the investigators wrote.
The investigators suggested that, in the future, better diagnostics will be needed to characterize T1b disease, as this could streamline patient selection. “Future research should focus on novel biological and immunohistochemistry markers that can aid in the prediction of tumor behavior and [lymph node metastasis] in T1b esophageal cancer,” they concluded.
The study was commissioned by the American Gastroenterological Association. The investigators disclosed additional relationships with Boston Scientific, Olympus, Lumendi, and others.
SOURCE: Othman MO et al. CGH. 2019 Jun 4. doi: 10.1016/j.cgh.2019.05.045.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Losing a patient to suicide: What we know
Studies have found that 1 in 2 psychiatrists,1-4 and 1 in 5 psychologists, clinical social workers, and other mental health professionals,5 will lose a patient to suicide in the course of their career. This statistic suggests that losing a patient to suicide constitutes a clear occupational hazard.6,7 Despite this, most mental health professionals continue to view suicide loss as an aberration. Consequently, there is often a lack of preparedness for such an event when it does occur.
This 2-part article summarizes what is currently known about the unique personal and professional issues experienced by clinician-survivors (clinicians who have lost patients and/or loved ones to suicide). In Part 1, I cover:
- the impact of losing a patient to suicide
- confidentiality-related constraints on the ability to discuss and process the loss
- legal and ethical issues
- colleagues’ reactions and stigma
- the effects of a suicide loss on one’s clinical work.
Part 2 will discuss the opportunities for personal growth that can result from experiencing a suicide loss, guidelines for optimal postventions, and steps clinicians can take to help support colleagues who have lost a patient to suicide.
A neglected topic
For psychiatrists and other mental health professionals, the loss of a patient to suicide is certainly not uncommon.1-5 Despite this, coping with a patient’s suicide is a “neglected topic”8 in residency and general mental health training.
There are many published articles on clinicians experiencing suicide loss (for a comprehensive bibliography, see McIntosh9), and several authors10-19 have developed suggestions, guidelines, and detailed postvention protocols to help clinicians navigate the often-complicated sequelae to such a loss. However, these resources have generally not been integrated into clinical training, and tend to be poorly disseminated. In a national survey of chief residents, Melton and Coverdale20 found that only 25% of residency training programs covered topics related to postvention, and 72% of chief residents felt this topic needed more attention. Thus, despite the existence of guidelines for optimal postvention and support, clinicians are often left to cope with the consequences of this difficult loss on their own, and under less-than-optimal conditions.
A patient’s suicide typically affects clinicians on multiple levels, both personally and professionally. In this article, I highlight the range of normative responses, as well as the factors that may facilitate or inhibit subsequent healing and growth, with the hope that this knowledge may be utilized to help current and future generations of clinician-survivors obtain optimal support, and that institutions who treat potentially suicidal individuals will develop optimal postvention responses following a suicide loss. Many aspects of what this article discusses also apply to clinicians who have experienced a suicide loss in their personal or family life, as this also tends to “spill over” into one’s professional roles and identity.
Grief and other emotional effects
In many ways, clinicians’ responses after a patient’s suicide are similar to those of other survivors after the loss of a loved one to suicide.21 Chemtob et al2 found that approximately one-half of psychiatrists who lost a patient to suicide had scores on the Impact of an Event Scale that were comparable to those of a clinical population seeking treatment after the death of a parent.
Continue to: Jordan and McIntosh have detailed...
Jordan and McIntosh22 have detailed several elements and themes that differentiate suicide loss and its associated reactions from other types of loss and grief. In general, suicide loss is considered traumatic, and is often accompanied by intense confusion and existential questioning, reflecting a negative impact on one’s core beliefs and assumptive world. The subsequent need to address the myriad of “why” questions left in its wake are often tinted with what Jordan and Baugher23 term the “tyranny of hindsight,” and take the form of implicit guilt for “sins of omission or commission” in relation to the lost individual.
Responses to suicide loss typically include initial shock, denial and numbness, intense sadness, anxiety, anger, and intense distress. Consistent with the traumatic nature of the loss, survivors are also likely to experience posttraumatic stress disorder symptoms such as intrusive thoughts, avoidance, and dissociation. Survivors also commonly experience significant guilt and shame, and this is likely to be socially reinforced by the general stigma associated with suicide as well as the actual blaming and avoidance responses of others.24-27
Clinicians’ unique reactions
For clinicians, there are additional components that may further complicate or exacerbate these reactions and extend their duration. First and foremost, such a loss affects clinicians on both personal and professional levels, a phenomenon that Plakun and Tillman13 have termed a “twin bereavement.” Thus, in addition to the personal grief and trauma reactions entailed in losing a patient to suicide, this loss is likely to impact clinicians’ professional identities, their relationships with colleagues, and their clinical work.
Clinicians’ professional identities are often predicated on generally shared assumptions and beliefs that, as trained professionals, they should have the power, aptitude, and competence to heal, or at least improve, the lives of patients, to reduce their distress, and to provide safety. In addition, such assumptions about clinicians’ responsibility and ability to prevent suicide are often reinforced in the clinical literature.28,29
These assumptions are often challenged, if not shattered, when patients take their own lives. A clinician’s sense of professional responsibility, the guilt and self-blame that may accompany this, self-doubts about one’s skills and clinical competence, the fear of (and actual) blame of colleagues and family members, and the real or imagined threat of litigation may all greatly exacerbate a clinician’s distress.11
Continue to: Hendin et al found...
Hendin et al30 found that mental health therapists have described losing a patient as “the most profoundly disturbing event of their professional careers,” noting that one-third of these clinicians experienced severe distress that lasted at least 1 year beyond the initial loss. In a 2004 study, Ruskin et al4 similarly found that one-quarter of psychiatrists and psychiatric trainees noted that losing a patient had a “profound and enduring effect on them.” In her article on surviving a patient’s suicide, Rycroft31 describes a “professional void” following the loss of her patient, in which “the world had changed, nothing was predictable any more, and it was no longer safe to assume anything.” Additionally, many clinicians experience an “acute sense of aloneness and isolation” subsequent to the loss.32
Many clinicians have noted that they considered leaving the field after such a loss,33,34 and it is hypothesized that many may have done so.35-37 Others have noted that, at least temporarily, they stopped treating patients who were potentially suicidal.29,35
Box 1
Several authors have proposed general models for describing the suicide grief trajectories of clinicians after a suicide loss. Tillman38 identified distinct groups of responses to this event: traumatic, affective, those related to the treatment, those related to interactions with colleagues, liability concerns, and the impact on one’s professional philosophy. She also found that Erikson’s stages of identity39 provided an uncannily similar trajectory to the ways in which those who participated in her research—clinicians at a mental hospital—had attempted to cope with their patients’ deaths, noting that the “suicide of a patient may provoke a revisiting of Erikson’s psychosocial crises in a telescoped and accelerated fashion.”38
Maltsberger40 offered a detailed psychoanalytic analysis of the responses clinicians may manifest in relation to a suicide loss, including the initial narcissistic injury sustained in relation to their patient’s actions; the subsequent potential for melancholic, atonement, or avoidance reactions; and the eventual capacity for the resolution of these reactions.
Al-Mateen et al33 described 3 phases of the clinician’s reaction after losing a patient who was a child to suicide:
- initial, which includes trauma and shock
- turmoil, which includes emotional flooding and functional impairments
- new growth, in which clinicians are able to reflect on their experiences and implications for training and policy.
For each phase, they also described staff activities that would foster forward movement through the trajectory.
In a 1981 study, Bissell41 found that psychiatric nurses who had experienced patient completed suicides progressed through several developmental stages (naïveté, recognition, responsibility, individual choice) that enabled them to come to terms with their personal reactions and place the ultimate responsibility for the suicide with the patient.
After losing a patient to suicide, a clinician may experience grief that proceeds through specific stages (Box 133,38-41). Box 22-4,6,16,24,29,30,33,34,40,42-45 describes a wide range of factors that affect each clinician’s unique response to losing a patient to suicide.
Box 2
There are many factors that make the experience of losing a patient to suicide unique and variable for individual clinicians. These include the amount of a clinician’s professional training and experience, both in general and in working with potentially suicidal individuals. Chemtob et al2 found that trainees were more likely to experience patient suicide loss than more seasoned clinicians, and to experience more distress.4,30,42 Brown24 noted that many training programs were likely to assign the most “extraordinarily sick patients to inexperienced trainees.” He noted that because the skill level of trainees has not yet tempered their personal aspirations, they are likely to experience a patient’s suicide as a personal failure. However, in contrast to the findings of Kleespies,42 Hendin,30 Ruskin et al,4 and Brown24 suggested that the overall impact of a patient’s suicide may be greater for seasoned clinicians, when the “protective advantage” or “explanation” of being in training is no longer applicable. This appears consistent with Munson’s study,43 which found that a greater number of years of clinical experience prior to a suicide loss was negatively correlated with posttraumatic growth.
Other factors affecting a clinician’s grief response include the context in which the treatment occurred, such as inpatient, outpatient, clinic, private practice, etc.44; the presence and involvement of supportive mentors or supervisors16; the length and intensity of the clinical relationship6,29; countertransference issues40; whether the patient was a child33; and the time elapsed since the suicide occurred.
In addition, each clinician’s set of personal and life experiences can affect the way he/ she moves through the grieving process. Any previous trauma or losses, particularly prior exposure to suicide, will likely impact a clinician’s reaction to his/her current loss, as will any susceptibility to anxiety or depression. Gorkin45 has suggested that the degree of omnipotence in the clinician’s therapeutic strivings will affect his/her ability to accept the inherent ambiguity involved in suicide loss. Gender may also play a role: Henry et al34 found that female clinicians had higher levels of stress reactions, and Grad et al3 found that female clinicians felt more shame and guilt and professed more doubts about their professional competence than male clinicians, and were more than twice as likely as men to identify talking with colleagues as an effective coping strategy.
Continue to: Implications of confidentiality restrictions
Implications of confidentiality restrictions
Confidentiality issues, as well as advice from attorneys to limit the disclosure of information about a patient, are likely to preclude a clinician’s ability to talk freely about the patient, the therapeutic relationship, and his/her reactions to the loss, all of which are known to facilitate movement through the grief process.46
The development of trust and the sharing of pain are just 2 factors that can make the clinical encounter an intense emotional experience for both parties. Recent trends in the psychodynamic literature acknowledge the profundity and depth of the personal impact that patients have on the clinician, an impact that is neither pathological nor an indication of poor boundaries in the therapy dyad, but instead a recognition of how all aspects of the clinician’s person, whether consciously or not, are used within the context of a therapeutic relationship. Yet when clinicians lose a patient, confidentiality restrictions often leave them wondering if and where any aspects of their experiences can be shared. Legal counsel may advise a clinician against speaking to consultants or supervisors or even surviving family members for fear that these non-privileged communications are subject to discovery should any legal proceedings ensue. Furthermore, the usual grief rituals that facilitate the healing of loss and the processing of grief (eg, gathering with others who knew the deceased, sharing feelings and memories, attending memorials) are usually denied to the clinician, and are often compounded by the reactions of one’s professional colleagues, who tend not to view the therapist’s grief as “legitimate.” Thus, clinician-survivors, despite having experienced a profound and traumatic loss, have very few places where this may be processed or even validated. As one clinician in a clinician-survivors support group stated, “I felt like I was grieving in a vacuum, that I wasn’t allowed to talk about how much my patient meant to me or how I’m feeling about it.” The isolation of grieving alone is likely to be compounded by the general lack of resources for supporting clinicians after such a loss. In contrast to the general suicide “survivor” network of support groups for family members who have experienced a suicide loss, there is an almost complete lack of supportive resources for clinicians following such a loss, and most clinicians are not aware of the resources that are available, such as the Clinician Survivor Task Force of the American Association of Suicidology (Box 312).
Box 3
Frank Jones and Judy Meade founded the Clinician Survivor Task Force (CSTF) of the American Association of Suicidology (AAS) in 1987. As Jones noted, “clinicians who have lost patients to suicide need a place to acknowledge and carry forward their personal loss … to benefit both personally and professionally from the opportunity to talk with other therapists who have survived the loss of a patient through suicide.”12
Nina Gutin, PhD, and Vanessa McGann, PhD, have co-chaired the CSTF since 2003. It now supports clinicians who have lost patients and/or loved ones, with the recognition that both types of losses carry implications within clinical and professional domains. The CSTF provides a listserve, opportunities to participate in video support groups, and a web site (www. cliniciansurvivor.org) that provides information about the clinician-survivor experience, the opportunity to read and post narratives about one’s experience with suicide loss, an updated bibliography maintained by John McIntosh, PhD, a list of clinical contacts, and a link to several excellent postvention protocols. In addition, Drs. Gutin and McGann conduct clinician-survivor support activities at the annual AAS conference, and in their respective geographic areas.
Continue to: Doka has described...
Doka47 has described “disenfranchised grief” in which the bereaved person does not receive the type and quality of support accorded to other bereaved persons, and thus is likely to internalize the view that his/her grief is not legitimate, and to believe that sharing related distress is a shame-ridden liability. This clearly relates to the sense of profound isolation and distress often described by clinician-survivors.
Other legal/ethical issues
The clinician-survivor’s concern about litigation, or an actual lawsuit, is likely to produce intense anxiety. This common fear is both understandable and credible. According to Bongar,48 the most common malpractice lawsuits filed against clinicians are those that involve a patient’s suicide. Peterson et al49 found that 34% of surviving family members considered bringing a lawsuit against the clinician, and of these, 57% consulted a lawyer.
In addition, an institution’s concern about protecting itself from liability may compromise its ability to support the clinician or trainee who sustained the loss. As noted above, the potential prohibitions around discussing the case can compromise the grief process. Additionally, the fear of (or actual) legal reprisals against supervisors and the larger institution may engender angry and blaming responses toward the treating clinician. In a personal communication (April 2008), Quinnett described an incident in which a supervising psychologist stomped into the grieving therapist’s office unannounced and shouted, “Now look what you’ve done! You’re going to get me sued!”
Other studies29,50,51 note that clinician-survivors fear losing their job, and that their colleagues and supervisors will be reluctant to assign new patients to them. Spiegleman and Werth17 also note that trainees grapple with additional concerns over negative evaluations, suspension or termination from clinical sites or training programs, and a potential interruption of obtaining a degree. Such supervisory and institutional reactions are likely to intensify a clinician’s sense of shame and distress, and are antithetical to postvention responses that promote optimal personal and professional growth. Such negative reactions are also likely to contribute to a clinician or trainee’s subsequent reluctance to work with suicidal individuals, or their decision to discontinue their clinical work altogether. Lastly, other ethical issues, such as contact with the patient’s family following the suicide, attending the funeral, etc., are likely to be a source of additional anxiety and distress, particularly if the clinician needs to address these issues in isolation.
Professional relationships/colleagues’ reactions
Many clinician-survivors have described reactions from colleagues and supervisors that are hurtful and unsupportive. According to Jobes and Maltsberger,52 “the suicide death of a patient in active treatment is commonly taken as prima facie evidence that the therapist, somehow or another, has mismanaged the case,” and thus the clinician often faces unwarranted blame and censure from colleagues and supervisors. Hendin et al30 noted that many trainees found reactions by their institutions to be insensitive and unsupportive, one noting that the department’s review of the case “felt more like a tribunal or inquest.” In a personal communication (April 2008), Quinnett noted that many clinicians he interviewed following a suicide loss reported a pattern of isolation and interpersonal discomfort with their colleagues, who implicitly or explicitly expressed concerns about their competence. He described how a respected colleague received “no understanding, no support, only abuse” from her supervisors. Such responses, while perhaps surprising from mental health professionals, probably reflect the long-standing cultural attitude of social condemnation of suicide, and of those who are associated with it.
Continue to: Negative reactions from professional colleagues...
Negative reactions from professional colleagues are most likely to occur immediately after the suicide loss and/or during the course of a subsequent investigation or psychological autopsy. Castelli-Dransart et al53 found that the lack of institutional support after a clinician experiences a suicide loss contributed to significantly higher stress responses for impacted clinicians, and may lead to a well-founded ambivalence about disclosure to colleagues, and consequent resistance to seeking out optimal supervision/consultation or even personal therapy that could help the clinician gain clarity on the effects of these issues. Many mental health professionals have described how, after the distressing experience of losing a patient to suicide, they moved through this process in relative isolation and loneliness, feeling abandoned by their colleagues and by their own hopes and expectations for support.
Stigmatization. In clinical settings, when a patient in treatment completes suicide, the treating clinician becomes an easy scapegoat for family members and colleagues. To the extent that mental health professionals are not immune from the effects and imposition of stigma, this might also affect their previously mentioned tendency to project judgment, overtly or covertly, onto the treating clinician.
Stigma around suicide is well documented.25 In The Surgeon General’s Call to Action to Prevent Suicide,54 former Surgeon General David Satcher specifically described stigma around suicide as one of the biggest barriers to prevention. Studies have shown that individuals bereaved by suicide are also stigmatized, and that those who were in caregiving roles (parents, clinicians) are believed to be more psychologically disturbed, less likable, more blameworthy, and less worthy of receiving support than other bereaved individuals.25,55-63 These judgments often mirror survivors’ self-punitive assessments, which then become exacerbated by and intertwined with both externally imposed and internalized stigma. Hence, it is not uncommon for suicide survivors to question their own right to grieve, to report low expectations of social support, and to feel compelled to deny or hide the mode of death. Feigelman et al26 found that stigmatization after a suicide loss was specifically associated with ongoing grief difficulties, depression, and suicidal thinking.
In my long-term work with clinician-survivors, I’ve come to believe that in addition to stigma around suicide, there may also be stigma projected by colleagues in relation to a clinician’s perceived emotional vulnerability. A traumatized clinician potentially challenges the notion of the implicit dichotomy/power imbalance between professionals and the patients we treat: “Us”—the professional, competent, healthy, and benevolent clinicians who have the care to offer, and “Them”—our patients, being needy, pathological, looking to us for care. This “us/them” distinction may serve to bolster a clinician’s professional esteem and identity. But when one of “us” becomes one of “them”—when a professional colleague is perceived as being emotionally vulnerable—this can be threatening to the predicates of this distinction, leading to the need to put the affected clinician firmly into the “them” camp. Thus, unwarranted condemnations of the clinician-survivor’s handling of the case, and/or the pathologizing of their normative grief reactions after the suicide loss, can seem justified.
Stigma associated both with suicide and with professional vulnerability is likely to be internalized and to have a profound effect on the clinician’s decisions about disclosure, asking for support, and ultimately on one’s ability to integrate the loss. When this occurs, it is likely to lead to even more isolation, shame, and self-blame. It is not surprising that many clinicians consider leaving the profession after this type of experience.
Continue to: Effects on clinical work
Effects on clinical work
A suicide loss is also likely to affect a clinician’s therapeutic work. Many authors12,52,64-67 have found that this commonly leads therapists to question their abilities as clinicians, and to experience a sharp loss of confidence in their work with patients. The shattered beliefs and assumptions around the efficacy of the therapeutic process, a sense of guilt or self-blame, and any perceived or actual negative judgment from colleagues can dramatically compromise a clinician’s sense of competence. Hendin et al30 noted that even the most experienced therapists expressed difficulty in trusting their own clinical judgment, or accurately assessing risk after a suicide loss.
In addition, the common grief and trauma-related responses to a suicide loss (including shock, numbness, sadness, anxiety, and generalized distress) are likely to result in at least some temporary disruption of a clinician’s optimal functioning. If trauma-related symptoms are more pronounced, the effect and longevity of such impairment may be exacerbated, and are likely to “impair clinical response and therapeutic judgment.”15 In addition, because such symptoms and states may be triggered by exposure to other potentially suicidal patients, they are more likely to impact clinical functioning when the clinician works with suicidal individuals. Thus, the normative responses to a suicide loss are likely to impact a clinician’s work, just as they are likely to impact the personal and occupational functioning of any survivor of suicide loss.
In clinician-survivor discussions and support groups I’ve led, participants have identified many common areas of clinical impact. Perhaps one of the most common early responses reported by clinician-survivors who continued to work with potentially suicidal individuals was to become hypervigilant in relation to any perceived suicide risk, to interpret such risk in such a way as to warrant more conservative interventions than are necessary, and to consequently minimize the patient’s own capacities for self-care.68 Conversely, others reported a tendency to minimize or deny suicidal potential by, for example, avoiding asking patients directly about suicidal ideation, even when they later realized that such questioning was indicated.69
Suicide loss may also lead to more subtle clinical reactions that have been observed not only with suicidal patients, but also in relation to patients who struggle with loss or grief. These include avoidant or even dissociative reactions in relation to their patient’s pain, which in turn can impact the clinician’s ability to “be fully present” or empathic in clinical encounters.50,69 Still, other clinicians noted that they tended to project residual feelings of anger onto their current suicidal patients, or envied patients who seemed to have mastered their grief. Consistent with Maltsberger’s description of “atonement reactions,”40 some clinicians found themselves doing more than should be expected for their patients, even losing their sense of professional boundaries in the process. Anderson70 noted that in pushing herself beyond what she knew were her optimal clinical boundaries, she was “punishing herself” for failing to prevent her patient’s suicide because, as she realized, “doing ‘penance’ was better than feeling helpless and powerless.” And Schultz16 described how therapists may have subsequent difficulty in trusting other patients, especially if patients who completed suicide did not disclose or denied their suicidal intent.
Working toward a supportive solution
In summary, unless clinicians who lose a patient to suicide have more supportive experiences, the combination of confidentiality-related restrictions, confusion about legal/ethical repercussions, unsupportive reactions from colleagues, and unexpected impairments in clinical work are likely to lead to intensified distress, isolation, the perceived need to “hide” the impact in professional settings, and consideration of leaving the profession. However, as I will describe in Part 2 (
Bottom Line
For mental health clinicians, losing a patient to suicide is a clear occupational hazard. After a suicide loss, clinicians often experience unique personal and professional challenges, including the impact of the loss on clinical work and professional identity, legal/ethical issues, and confidentiality-related constraints on the ability to discuss and process the loss.
Related Resources
- American Association of Suicidology Clinician Survivor Task Force. www.cliniciansurvivor.org.
- Gutin N. Helping survivors in the aftermath of suicide loss. Current Psychiatry. 2018;17(8):27-33.
1. Alexander D, Klein S, Gray NM, et al. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ. 2000;320(7249):1571-1574.
2. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry. 1988;145(2):224-228.
3. Grad OT, Zavasnik A, Groleger U. Suicide of a patient: gender differences in bereavement reactions of therapists. Suicide Life Threat Behav. 1997;27(4):379-386.
4. Ruskin R, Sakinofsky I, Bagby RM, et al. Impact of patient suicide on psychiatrists and psychiatric trainees. Acad Psychiatry. 2004;28(2):104-110.
5. Bersoff DN. Ethical conflicts in psychology, 2nd ed. Washington, DC: American Psychological Association; 1999.
6. Chemtob CM, Bauer GB, Hamada RS, et al. Patient suicide: occupational hazard for psychologists and psychiatrists. Prof Psychol Res Pr. 1989;20(5):294-300.
7. Rubin HL. Surviving a suicide in your practice. In: Blumenthal SJ, Kupfer DJ, eds. Suicide over the life cycle: risk factors, assessment, and treatment of suicidal patients. Washington, DC: American Psychiatric Press; 1990:619-636.
8. Kaye NS, Soreff SM. The psychiatrist’s role, responses, and responsibilities when a patient commits suicide. Am J Psychiatry. 1991;148(6):739-743.
9. McIntosh JL. Clinicians as survivors of suicide: bibliography. American Association of Suicidology Clinician Survivor Task Force. http://pages.iu.edu/~jmcintos/Surv.Ther.bib.htm. Updated May 19, 2019. Accessed August 26, 2019.
10. Douglas J, Brown HN. Suicide: understanding and responding: Harvard Medical School perspectives. Madison, CT: International Universities Press; 1989.
11. Farberow NL. The mental health professional as suicide survivor. Clin Neuropsychiatry. 2005;2(1):13-20.
12. Jones FA Jr. Therapists as survivors of patient suicide. In: Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: W.W. Norton; 1987;126-141.
13. Plakun EM, Tillman JG. Responding to clinicians after loss of a patient to suicide. Dir Psychiatry. 2005;25:301-310.
14. Prabhakar D, Anzia JM, Balon R, et al. “Collateral damages”: preparing residents for coping with patient suicide. Acad Psychiatry. 2013;37(6):429-30.
15. Quinnett P. QPR: for suicide prevention. QPR Institute, Inc. http://pages.iu.edu/~jmcintos/postvention.htm. Published September 21, 2009. Accessed August 26, 2019.
16. Schultz, D. Suggestions for supervisors when a therapist experiences a client’s suicide. Women Ther. 2005;28(1):59-69.
17. Spiegelman JS Jr, Werth JL Jr. Don’t forget about me: the experiences of therapists-in-training after a patient has attempted or died by suicide. Women Ther. 2005;28(1):35-57.
18. American Association of Suicidology. Clinician Survivor Task Force. Clinicians as survivors of suicide: postvention information.
19. Whitmore CA, Cook J, Salg L. Supporting residents in the wake of patient suicide. The American Journal of Psychiatry Residents’ Journal. 2017;12(1):5-7.
20. Melton B, Coverdale J. What do we teach psychiatric residents about suicide? A national survey of chief residents. Acad Psychiatry. 2009;33(1):47-50.
21. Valente SM. Psychotherapist reactions to the suicide of a patient. Am J Orthopsychiatry. 1994;64(4):614-621.
22. Jordan JR, McIntosh JL. Is suicide bereavement different? A framework for rethinking the question. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge; 2011:19-42.
23. Jordan JR, Baugher B. After suicide loss: coping with your grief, 2nd ed. Newcastle, WA: Caring People Press; 2016.
24. Brown HB. The impact of suicide on therapists in training. Compr Psychiatry. 1987;28(2):101-112.
25. Cvinar JG. Do suicide survivors suffer social stigma: a review of the literature. Perspect Psychiatr Care. 2005;41(1):14-21.
26. Feigelman W, Gorman BS, Jordan JR. Stigmatization and suicide bereavement. Death Stud. 2009;33(7):591-608.
27. Goffman E. Stigma: notes on the management of spoiled identity. New York, NY: Simon & Schuster; 1963.
28. Goldney RD. The privilege and responsibility of suicide prevention. Crisis. 2000;21(1):8-15.
29. Litman RE. When patients commit suicide. Am J Psychother. 1965;19(4):570-576.
30. Hendin H, Lipschitz A, Maltsberger JT, et al. Therapists’ reactions to patients’ suicides. Am J Psychiatry. 2000;157(12):2022-2027.
31. Rycroft P. Touching the heart and soul of therapy: surviving client suicide. Women Ther. 2004;28(1):83-94.
32. Ellis TE, Patel AB. Client suicide: what now? Cogn Behav Pract. 2012;19(2):277-287.
33. Al-Mateen CS, Jones K, Linker J, et al. Clinician response to a child who completes suicide. Child Adolesc Psychiatric Clin N Am. 2018;27(4):621-635.
34. Henry M, Séguin M, Drouin M-S. Mental health professionals’ response to the suicide of their patients [in French]. Revue Québécoise de Psychologie. 2004;25:241-257.
35. Carter RE. Some effects of client suicide on the therapist. Psychother Theory Res Practice. 1971;8(4):287-289.
36. Dewar I, Eagles J, Klein S, et al. Psychiatric trainees’ experiences of, and reactions to, patient suicide. Psychiatr Bull. 2000;24(1):20-23.
37. Gitlin M. Aftermath of a tragedy: reaction of psychiatrists to patient suicides. Psychiatr Ann. 2007;37(10):684-687.
38. Tillman JG. When a patient commits suicide: an empirical study of psychoanalytic clinicians. Inter J Psychoanal. 2006;87(1):159-177.
39. Erikson EH. Identity and the life cycle. New York, NY: International Universities Press, Inc.; 1959.
40. Maltsberger JT. The implications of patient suicide for the surviving psychotherapist. In: Jacobs D, ed. Suicide and clinical practice. Washington, DC: American Psychiatric Press; 1992:169-182.
41. Bissell BPH. The experience of the nurse therapist working with suicidal cases: a developmental study [dissertation]. Boston, MA: Boston University School of Education; 1981.
42. Kleespies PM. The stress of patient suicidal behavior: Implications for interns and training programs in psychology. Prof Psychol Res Pract. 1993;24(4):477-482.
43. Munson JS. Impact of client suicide on practitioner posttraumatic growth [dissertation]. Gainsville, Florida: University of Florida; 2009.
44. Hodgkinson PE. Responding to in-patient suicide. Br J Med Psychol. 1987;60(4):387-392.
45. Gorkin M. On the suicide of one’s patient. Bull Menninger Clin. 1985;49(1):1-9.
46. Fuentes MA, Cruz D. Posttraumatic growth: positive psychological changes after trauma. Mental Health News. 2009;11(1):31,37.
47. Doka KJ. Disenfranchised grief: new Directions, challenges, and strategies for practice. Champaign, IL: Research Press; 2002.
48. Bongar B. The suicidal patient: clinical and legal standards of care, 2nd ed. Washington, DC: American Psychological Association; 2002.
49. Peterson EM, Luoma JB, Dunne E. Suicide survivors’ perceptions of the treating clinician. Suicide Life Threat Behav. 2002;32(2):158-166.
50. Kolodny S, Binder RL, Bronstein AA, et al. The working through of patients’ suicides by four therapists. Suicide Life Threat Behav. 1979;9(1):33-46.
51. Marshall KA. When a patient commits suicide. Suicide Life Threat Behav. 1980;10(1):29-40.
52. Jobes DA, Maltsberger JT. The hazards of treating suicidal patients. In: Sussman MB, ed. A perilous calling: the hazards of psychotherapy practice. New York, NY: Wiley & Sons; 1995:200-214.
53. Castelli-Dransart DA, Gutjahr E, Gulfi A, et al. Patient suicide in institutions: emotional responses and traumatic impact on Swiss mental health professionals. Death Stud. 2014;38(1-5):315-321.
54. US Public Health Service. The Surgeon General’s call to action to prevent suicide. Washington, DC: Department of Health and Human Services; 1999.
55. Armour M. Violent death: understanding the context of traumatic and stigmatized grief. J Hum Behav Soc Environ. 2006;14(4):53-90.
56. Calhoun, LG, Allen BG. Social reactions to the survivor of a suicide in the family: a review of the literature. Omega (Westport). 1991;23(2):95-107.
57. Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: WW Norton & Co; 1987.
58. Harwood D, Hawton K, Hope J, et al. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: a descriptive and case-control study. J Affect Disord. 2002;72(2):185-194.
59. Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31(1):91-102.
60. McIntosh JL. Control group studies of suicide survivors: a review and critique. Suicide Life Threat Behav. 2003;23(2):146-161.
61. Range LM. When a loss is due to suicide: unique aspects of bereavement. In: Harvey JH, ed. Perspectives on loss: a sourcebook. Philadelphia, PA: Brunner/Mazel; 1998:213-220.
62. Sveen CA, Walby FA. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat Behav. 2008;38(1):13-29.
63. Van Dongen CJ. Social context of postsuicide bereavement. Death Stud. 1993;17(2):125-141.
64. Bultema JK. The healing process for the multidisciplinary team: recovering post-inpatient suicide. J Psychosoc Nurs. 1994;32(2):19-24.
65. Cooper C. Patient suicide and assault: their impact on psychiatric hospital staff. J Psychosoc Nurs Ment Health Serv. 1995;33(6):26-29.
66. Foster VA, McAdams CR III. The impact of client suicide in counselor training: Implications for counselor education and supervision. Counselor Educ Supervision. 1999;39(1):22-33.
67. Little JD. Staff response to inpatient and outpatient suicide: what happened and what do we do? Aust N Z J Psychiatry. 1992;26(2):162-167.
68. Horn PJ. Therapists’ psychological adaptation to client suicidal behavior. Chicago, IL: Loyola University of Chicago; 1995.
69. Gutin N, McGann VM, Jordan JR. The impact of suicide on professional caregivers. In: Jordan J, McIntosh J, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge; 2011:93-111.
70. Anderson GO. Who, what, when, where, how, and mostly why? A therapist’s grief over the suicide of a client. Women Ther. 2004;28(1):25-34.
Studies have found that 1 in 2 psychiatrists,1-4 and 1 in 5 psychologists, clinical social workers, and other mental health professionals,5 will lose a patient to suicide in the course of their career. This statistic suggests that losing a patient to suicide constitutes a clear occupational hazard.6,7 Despite this, most mental health professionals continue to view suicide loss as an aberration. Consequently, there is often a lack of preparedness for such an event when it does occur.
This 2-part article summarizes what is currently known about the unique personal and professional issues experienced by clinician-survivors (clinicians who have lost patients and/or loved ones to suicide). In Part 1, I cover:
- the impact of losing a patient to suicide
- confidentiality-related constraints on the ability to discuss and process the loss
- legal and ethical issues
- colleagues’ reactions and stigma
- the effects of a suicide loss on one’s clinical work.
Part 2 will discuss the opportunities for personal growth that can result from experiencing a suicide loss, guidelines for optimal postventions, and steps clinicians can take to help support colleagues who have lost a patient to suicide.
A neglected topic
For psychiatrists and other mental health professionals, the loss of a patient to suicide is certainly not uncommon.1-5 Despite this, coping with a patient’s suicide is a “neglected topic”8 in residency and general mental health training.
There are many published articles on clinicians experiencing suicide loss (for a comprehensive bibliography, see McIntosh9), and several authors10-19 have developed suggestions, guidelines, and detailed postvention protocols to help clinicians navigate the often-complicated sequelae to such a loss. However, these resources have generally not been integrated into clinical training, and tend to be poorly disseminated. In a national survey of chief residents, Melton and Coverdale20 found that only 25% of residency training programs covered topics related to postvention, and 72% of chief residents felt this topic needed more attention. Thus, despite the existence of guidelines for optimal postvention and support, clinicians are often left to cope with the consequences of this difficult loss on their own, and under less-than-optimal conditions.
A patient’s suicide typically affects clinicians on multiple levels, both personally and professionally. In this article, I highlight the range of normative responses, as well as the factors that may facilitate or inhibit subsequent healing and growth, with the hope that this knowledge may be utilized to help current and future generations of clinician-survivors obtain optimal support, and that institutions who treat potentially suicidal individuals will develop optimal postvention responses following a suicide loss. Many aspects of what this article discusses also apply to clinicians who have experienced a suicide loss in their personal or family life, as this also tends to “spill over” into one’s professional roles and identity.
Grief and other emotional effects
In many ways, clinicians’ responses after a patient’s suicide are similar to those of other survivors after the loss of a loved one to suicide.21 Chemtob et al2 found that approximately one-half of psychiatrists who lost a patient to suicide had scores on the Impact of an Event Scale that were comparable to those of a clinical population seeking treatment after the death of a parent.
Continue to: Jordan and McIntosh have detailed...
Jordan and McIntosh22 have detailed several elements and themes that differentiate suicide loss and its associated reactions from other types of loss and grief. In general, suicide loss is considered traumatic, and is often accompanied by intense confusion and existential questioning, reflecting a negative impact on one’s core beliefs and assumptive world. The subsequent need to address the myriad of “why” questions left in its wake are often tinted with what Jordan and Baugher23 term the “tyranny of hindsight,” and take the form of implicit guilt for “sins of omission or commission” in relation to the lost individual.
Responses to suicide loss typically include initial shock, denial and numbness, intense sadness, anxiety, anger, and intense distress. Consistent with the traumatic nature of the loss, survivors are also likely to experience posttraumatic stress disorder symptoms such as intrusive thoughts, avoidance, and dissociation. Survivors also commonly experience significant guilt and shame, and this is likely to be socially reinforced by the general stigma associated with suicide as well as the actual blaming and avoidance responses of others.24-27
Clinicians’ unique reactions
For clinicians, there are additional components that may further complicate or exacerbate these reactions and extend their duration. First and foremost, such a loss affects clinicians on both personal and professional levels, a phenomenon that Plakun and Tillman13 have termed a “twin bereavement.” Thus, in addition to the personal grief and trauma reactions entailed in losing a patient to suicide, this loss is likely to impact clinicians’ professional identities, their relationships with colleagues, and their clinical work.
Clinicians’ professional identities are often predicated on generally shared assumptions and beliefs that, as trained professionals, they should have the power, aptitude, and competence to heal, or at least improve, the lives of patients, to reduce their distress, and to provide safety. In addition, such assumptions about clinicians’ responsibility and ability to prevent suicide are often reinforced in the clinical literature.28,29
These assumptions are often challenged, if not shattered, when patients take their own lives. A clinician’s sense of professional responsibility, the guilt and self-blame that may accompany this, self-doubts about one’s skills and clinical competence, the fear of (and actual) blame of colleagues and family members, and the real or imagined threat of litigation may all greatly exacerbate a clinician’s distress.11
Continue to: Hendin et al found...
Hendin et al30 found that mental health therapists have described losing a patient as “the most profoundly disturbing event of their professional careers,” noting that one-third of these clinicians experienced severe distress that lasted at least 1 year beyond the initial loss. In a 2004 study, Ruskin et al4 similarly found that one-quarter of psychiatrists and psychiatric trainees noted that losing a patient had a “profound and enduring effect on them.” In her article on surviving a patient’s suicide, Rycroft31 describes a “professional void” following the loss of her patient, in which “the world had changed, nothing was predictable any more, and it was no longer safe to assume anything.” Additionally, many clinicians experience an “acute sense of aloneness and isolation” subsequent to the loss.32
Many clinicians have noted that they considered leaving the field after such a loss,33,34 and it is hypothesized that many may have done so.35-37 Others have noted that, at least temporarily, they stopped treating patients who were potentially suicidal.29,35
Box 1
Several authors have proposed general models for describing the suicide grief trajectories of clinicians after a suicide loss. Tillman38 identified distinct groups of responses to this event: traumatic, affective, those related to the treatment, those related to interactions with colleagues, liability concerns, and the impact on one’s professional philosophy. She also found that Erikson’s stages of identity39 provided an uncannily similar trajectory to the ways in which those who participated in her research—clinicians at a mental hospital—had attempted to cope with their patients’ deaths, noting that the “suicide of a patient may provoke a revisiting of Erikson’s psychosocial crises in a telescoped and accelerated fashion.”38
Maltsberger40 offered a detailed psychoanalytic analysis of the responses clinicians may manifest in relation to a suicide loss, including the initial narcissistic injury sustained in relation to their patient’s actions; the subsequent potential for melancholic, atonement, or avoidance reactions; and the eventual capacity for the resolution of these reactions.
Al-Mateen et al33 described 3 phases of the clinician’s reaction after losing a patient who was a child to suicide:
- initial, which includes trauma and shock
- turmoil, which includes emotional flooding and functional impairments
- new growth, in which clinicians are able to reflect on their experiences and implications for training and policy.
For each phase, they also described staff activities that would foster forward movement through the trajectory.
In a 1981 study, Bissell41 found that psychiatric nurses who had experienced patient completed suicides progressed through several developmental stages (naïveté, recognition, responsibility, individual choice) that enabled them to come to terms with their personal reactions and place the ultimate responsibility for the suicide with the patient.
After losing a patient to suicide, a clinician may experience grief that proceeds through specific stages (Box 133,38-41). Box 22-4,6,16,24,29,30,33,34,40,42-45 describes a wide range of factors that affect each clinician’s unique response to losing a patient to suicide.
Box 2
There are many factors that make the experience of losing a patient to suicide unique and variable for individual clinicians. These include the amount of a clinician’s professional training and experience, both in general and in working with potentially suicidal individuals. Chemtob et al2 found that trainees were more likely to experience patient suicide loss than more seasoned clinicians, and to experience more distress.4,30,42 Brown24 noted that many training programs were likely to assign the most “extraordinarily sick patients to inexperienced trainees.” He noted that because the skill level of trainees has not yet tempered their personal aspirations, they are likely to experience a patient’s suicide as a personal failure. However, in contrast to the findings of Kleespies,42 Hendin,30 Ruskin et al,4 and Brown24 suggested that the overall impact of a patient’s suicide may be greater for seasoned clinicians, when the “protective advantage” or “explanation” of being in training is no longer applicable. This appears consistent with Munson’s study,43 which found that a greater number of years of clinical experience prior to a suicide loss was negatively correlated with posttraumatic growth.
Other factors affecting a clinician’s grief response include the context in which the treatment occurred, such as inpatient, outpatient, clinic, private practice, etc.44; the presence and involvement of supportive mentors or supervisors16; the length and intensity of the clinical relationship6,29; countertransference issues40; whether the patient was a child33; and the time elapsed since the suicide occurred.
In addition, each clinician’s set of personal and life experiences can affect the way he/ she moves through the grieving process. Any previous trauma or losses, particularly prior exposure to suicide, will likely impact a clinician’s reaction to his/her current loss, as will any susceptibility to anxiety or depression. Gorkin45 has suggested that the degree of omnipotence in the clinician’s therapeutic strivings will affect his/her ability to accept the inherent ambiguity involved in suicide loss. Gender may also play a role: Henry et al34 found that female clinicians had higher levels of stress reactions, and Grad et al3 found that female clinicians felt more shame and guilt and professed more doubts about their professional competence than male clinicians, and were more than twice as likely as men to identify talking with colleagues as an effective coping strategy.
Continue to: Implications of confidentiality restrictions
Implications of confidentiality restrictions
Confidentiality issues, as well as advice from attorneys to limit the disclosure of information about a patient, are likely to preclude a clinician’s ability to talk freely about the patient, the therapeutic relationship, and his/her reactions to the loss, all of which are known to facilitate movement through the grief process.46
The development of trust and the sharing of pain are just 2 factors that can make the clinical encounter an intense emotional experience for both parties. Recent trends in the psychodynamic literature acknowledge the profundity and depth of the personal impact that patients have on the clinician, an impact that is neither pathological nor an indication of poor boundaries in the therapy dyad, but instead a recognition of how all aspects of the clinician’s person, whether consciously or not, are used within the context of a therapeutic relationship. Yet when clinicians lose a patient, confidentiality restrictions often leave them wondering if and where any aspects of their experiences can be shared. Legal counsel may advise a clinician against speaking to consultants or supervisors or even surviving family members for fear that these non-privileged communications are subject to discovery should any legal proceedings ensue. Furthermore, the usual grief rituals that facilitate the healing of loss and the processing of grief (eg, gathering with others who knew the deceased, sharing feelings and memories, attending memorials) are usually denied to the clinician, and are often compounded by the reactions of one’s professional colleagues, who tend not to view the therapist’s grief as “legitimate.” Thus, clinician-survivors, despite having experienced a profound and traumatic loss, have very few places where this may be processed or even validated. As one clinician in a clinician-survivors support group stated, “I felt like I was grieving in a vacuum, that I wasn’t allowed to talk about how much my patient meant to me or how I’m feeling about it.” The isolation of grieving alone is likely to be compounded by the general lack of resources for supporting clinicians after such a loss. In contrast to the general suicide “survivor” network of support groups for family members who have experienced a suicide loss, there is an almost complete lack of supportive resources for clinicians following such a loss, and most clinicians are not aware of the resources that are available, such as the Clinician Survivor Task Force of the American Association of Suicidology (Box 312).
Box 3
Frank Jones and Judy Meade founded the Clinician Survivor Task Force (CSTF) of the American Association of Suicidology (AAS) in 1987. As Jones noted, “clinicians who have lost patients to suicide need a place to acknowledge and carry forward their personal loss … to benefit both personally and professionally from the opportunity to talk with other therapists who have survived the loss of a patient through suicide.”12
Nina Gutin, PhD, and Vanessa McGann, PhD, have co-chaired the CSTF since 2003. It now supports clinicians who have lost patients and/or loved ones, with the recognition that both types of losses carry implications within clinical and professional domains. The CSTF provides a listserve, opportunities to participate in video support groups, and a web site (www. cliniciansurvivor.org) that provides information about the clinician-survivor experience, the opportunity to read and post narratives about one’s experience with suicide loss, an updated bibliography maintained by John McIntosh, PhD, a list of clinical contacts, and a link to several excellent postvention protocols. In addition, Drs. Gutin and McGann conduct clinician-survivor support activities at the annual AAS conference, and in their respective geographic areas.
Continue to: Doka has described...
Doka47 has described “disenfranchised grief” in which the bereaved person does not receive the type and quality of support accorded to other bereaved persons, and thus is likely to internalize the view that his/her grief is not legitimate, and to believe that sharing related distress is a shame-ridden liability. This clearly relates to the sense of profound isolation and distress often described by clinician-survivors.
Other legal/ethical issues
The clinician-survivor’s concern about litigation, or an actual lawsuit, is likely to produce intense anxiety. This common fear is both understandable and credible. According to Bongar,48 the most common malpractice lawsuits filed against clinicians are those that involve a patient’s suicide. Peterson et al49 found that 34% of surviving family members considered bringing a lawsuit against the clinician, and of these, 57% consulted a lawyer.
In addition, an institution’s concern about protecting itself from liability may compromise its ability to support the clinician or trainee who sustained the loss. As noted above, the potential prohibitions around discussing the case can compromise the grief process. Additionally, the fear of (or actual) legal reprisals against supervisors and the larger institution may engender angry and blaming responses toward the treating clinician. In a personal communication (April 2008), Quinnett described an incident in which a supervising psychologist stomped into the grieving therapist’s office unannounced and shouted, “Now look what you’ve done! You’re going to get me sued!”
Other studies29,50,51 note that clinician-survivors fear losing their job, and that their colleagues and supervisors will be reluctant to assign new patients to them. Spiegleman and Werth17 also note that trainees grapple with additional concerns over negative evaluations, suspension or termination from clinical sites or training programs, and a potential interruption of obtaining a degree. Such supervisory and institutional reactions are likely to intensify a clinician’s sense of shame and distress, and are antithetical to postvention responses that promote optimal personal and professional growth. Such negative reactions are also likely to contribute to a clinician or trainee’s subsequent reluctance to work with suicidal individuals, or their decision to discontinue their clinical work altogether. Lastly, other ethical issues, such as contact with the patient’s family following the suicide, attending the funeral, etc., are likely to be a source of additional anxiety and distress, particularly if the clinician needs to address these issues in isolation.
Professional relationships/colleagues’ reactions
Many clinician-survivors have described reactions from colleagues and supervisors that are hurtful and unsupportive. According to Jobes and Maltsberger,52 “the suicide death of a patient in active treatment is commonly taken as prima facie evidence that the therapist, somehow or another, has mismanaged the case,” and thus the clinician often faces unwarranted blame and censure from colleagues and supervisors. Hendin et al30 noted that many trainees found reactions by their institutions to be insensitive and unsupportive, one noting that the department’s review of the case “felt more like a tribunal or inquest.” In a personal communication (April 2008), Quinnett noted that many clinicians he interviewed following a suicide loss reported a pattern of isolation and interpersonal discomfort with their colleagues, who implicitly or explicitly expressed concerns about their competence. He described how a respected colleague received “no understanding, no support, only abuse” from her supervisors. Such responses, while perhaps surprising from mental health professionals, probably reflect the long-standing cultural attitude of social condemnation of suicide, and of those who are associated with it.
Continue to: Negative reactions from professional colleagues...
Negative reactions from professional colleagues are most likely to occur immediately after the suicide loss and/or during the course of a subsequent investigation or psychological autopsy. Castelli-Dransart et al53 found that the lack of institutional support after a clinician experiences a suicide loss contributed to significantly higher stress responses for impacted clinicians, and may lead to a well-founded ambivalence about disclosure to colleagues, and consequent resistance to seeking out optimal supervision/consultation or even personal therapy that could help the clinician gain clarity on the effects of these issues. Many mental health professionals have described how, after the distressing experience of losing a patient to suicide, they moved through this process in relative isolation and loneliness, feeling abandoned by their colleagues and by their own hopes and expectations for support.
Stigmatization. In clinical settings, when a patient in treatment completes suicide, the treating clinician becomes an easy scapegoat for family members and colleagues. To the extent that mental health professionals are not immune from the effects and imposition of stigma, this might also affect their previously mentioned tendency to project judgment, overtly or covertly, onto the treating clinician.
Stigma around suicide is well documented.25 In The Surgeon General’s Call to Action to Prevent Suicide,54 former Surgeon General David Satcher specifically described stigma around suicide as one of the biggest barriers to prevention. Studies have shown that individuals bereaved by suicide are also stigmatized, and that those who were in caregiving roles (parents, clinicians) are believed to be more psychologically disturbed, less likable, more blameworthy, and less worthy of receiving support than other bereaved individuals.25,55-63 These judgments often mirror survivors’ self-punitive assessments, which then become exacerbated by and intertwined with both externally imposed and internalized stigma. Hence, it is not uncommon for suicide survivors to question their own right to grieve, to report low expectations of social support, and to feel compelled to deny or hide the mode of death. Feigelman et al26 found that stigmatization after a suicide loss was specifically associated with ongoing grief difficulties, depression, and suicidal thinking.
In my long-term work with clinician-survivors, I’ve come to believe that in addition to stigma around suicide, there may also be stigma projected by colleagues in relation to a clinician’s perceived emotional vulnerability. A traumatized clinician potentially challenges the notion of the implicit dichotomy/power imbalance between professionals and the patients we treat: “Us”—the professional, competent, healthy, and benevolent clinicians who have the care to offer, and “Them”—our patients, being needy, pathological, looking to us for care. This “us/them” distinction may serve to bolster a clinician’s professional esteem and identity. But when one of “us” becomes one of “them”—when a professional colleague is perceived as being emotionally vulnerable—this can be threatening to the predicates of this distinction, leading to the need to put the affected clinician firmly into the “them” camp. Thus, unwarranted condemnations of the clinician-survivor’s handling of the case, and/or the pathologizing of their normative grief reactions after the suicide loss, can seem justified.
Stigma associated both with suicide and with professional vulnerability is likely to be internalized and to have a profound effect on the clinician’s decisions about disclosure, asking for support, and ultimately on one’s ability to integrate the loss. When this occurs, it is likely to lead to even more isolation, shame, and self-blame. It is not surprising that many clinicians consider leaving the profession after this type of experience.
Continue to: Effects on clinical work
Effects on clinical work
A suicide loss is also likely to affect a clinician’s therapeutic work. Many authors12,52,64-67 have found that this commonly leads therapists to question their abilities as clinicians, and to experience a sharp loss of confidence in their work with patients. The shattered beliefs and assumptions around the efficacy of the therapeutic process, a sense of guilt or self-blame, and any perceived or actual negative judgment from colleagues can dramatically compromise a clinician’s sense of competence. Hendin et al30 noted that even the most experienced therapists expressed difficulty in trusting their own clinical judgment, or accurately assessing risk after a suicide loss.
In addition, the common grief and trauma-related responses to a suicide loss (including shock, numbness, sadness, anxiety, and generalized distress) are likely to result in at least some temporary disruption of a clinician’s optimal functioning. If trauma-related symptoms are more pronounced, the effect and longevity of such impairment may be exacerbated, and are likely to “impair clinical response and therapeutic judgment.”15 In addition, because such symptoms and states may be triggered by exposure to other potentially suicidal patients, they are more likely to impact clinical functioning when the clinician works with suicidal individuals. Thus, the normative responses to a suicide loss are likely to impact a clinician’s work, just as they are likely to impact the personal and occupational functioning of any survivor of suicide loss.
In clinician-survivor discussions and support groups I’ve led, participants have identified many common areas of clinical impact. Perhaps one of the most common early responses reported by clinician-survivors who continued to work with potentially suicidal individuals was to become hypervigilant in relation to any perceived suicide risk, to interpret such risk in such a way as to warrant more conservative interventions than are necessary, and to consequently minimize the patient’s own capacities for self-care.68 Conversely, others reported a tendency to minimize or deny suicidal potential by, for example, avoiding asking patients directly about suicidal ideation, even when they later realized that such questioning was indicated.69
Suicide loss may also lead to more subtle clinical reactions that have been observed not only with suicidal patients, but also in relation to patients who struggle with loss or grief. These include avoidant or even dissociative reactions in relation to their patient’s pain, which in turn can impact the clinician’s ability to “be fully present” or empathic in clinical encounters.50,69 Still, other clinicians noted that they tended to project residual feelings of anger onto their current suicidal patients, or envied patients who seemed to have mastered their grief. Consistent with Maltsberger’s description of “atonement reactions,”40 some clinicians found themselves doing more than should be expected for their patients, even losing their sense of professional boundaries in the process. Anderson70 noted that in pushing herself beyond what she knew were her optimal clinical boundaries, she was “punishing herself” for failing to prevent her patient’s suicide because, as she realized, “doing ‘penance’ was better than feeling helpless and powerless.” And Schultz16 described how therapists may have subsequent difficulty in trusting other patients, especially if patients who completed suicide did not disclose or denied their suicidal intent.
Working toward a supportive solution
In summary, unless clinicians who lose a patient to suicide have more supportive experiences, the combination of confidentiality-related restrictions, confusion about legal/ethical repercussions, unsupportive reactions from colleagues, and unexpected impairments in clinical work are likely to lead to intensified distress, isolation, the perceived need to “hide” the impact in professional settings, and consideration of leaving the profession. However, as I will describe in Part 2 (
Bottom Line
For mental health clinicians, losing a patient to suicide is a clear occupational hazard. After a suicide loss, clinicians often experience unique personal and professional challenges, including the impact of the loss on clinical work and professional identity, legal/ethical issues, and confidentiality-related constraints on the ability to discuss and process the loss.
Related Resources
- American Association of Suicidology Clinician Survivor Task Force. www.cliniciansurvivor.org.
- Gutin N. Helping survivors in the aftermath of suicide loss. Current Psychiatry. 2018;17(8):27-33.
Studies have found that 1 in 2 psychiatrists,1-4 and 1 in 5 psychologists, clinical social workers, and other mental health professionals,5 will lose a patient to suicide in the course of their career. This statistic suggests that losing a patient to suicide constitutes a clear occupational hazard.6,7 Despite this, most mental health professionals continue to view suicide loss as an aberration. Consequently, there is often a lack of preparedness for such an event when it does occur.
This 2-part article summarizes what is currently known about the unique personal and professional issues experienced by clinician-survivors (clinicians who have lost patients and/or loved ones to suicide). In Part 1, I cover:
- the impact of losing a patient to suicide
- confidentiality-related constraints on the ability to discuss and process the loss
- legal and ethical issues
- colleagues’ reactions and stigma
- the effects of a suicide loss on one’s clinical work.
Part 2 will discuss the opportunities for personal growth that can result from experiencing a suicide loss, guidelines for optimal postventions, and steps clinicians can take to help support colleagues who have lost a patient to suicide.
A neglected topic
For psychiatrists and other mental health professionals, the loss of a patient to suicide is certainly not uncommon.1-5 Despite this, coping with a patient’s suicide is a “neglected topic”8 in residency and general mental health training.
There are many published articles on clinicians experiencing suicide loss (for a comprehensive bibliography, see McIntosh9), and several authors10-19 have developed suggestions, guidelines, and detailed postvention protocols to help clinicians navigate the often-complicated sequelae to such a loss. However, these resources have generally not been integrated into clinical training, and tend to be poorly disseminated. In a national survey of chief residents, Melton and Coverdale20 found that only 25% of residency training programs covered topics related to postvention, and 72% of chief residents felt this topic needed more attention. Thus, despite the existence of guidelines for optimal postvention and support, clinicians are often left to cope with the consequences of this difficult loss on their own, and under less-than-optimal conditions.
A patient’s suicide typically affects clinicians on multiple levels, both personally and professionally. In this article, I highlight the range of normative responses, as well as the factors that may facilitate or inhibit subsequent healing and growth, with the hope that this knowledge may be utilized to help current and future generations of clinician-survivors obtain optimal support, and that institutions who treat potentially suicidal individuals will develop optimal postvention responses following a suicide loss. Many aspects of what this article discusses also apply to clinicians who have experienced a suicide loss in their personal or family life, as this also tends to “spill over” into one’s professional roles and identity.
Grief and other emotional effects
In many ways, clinicians’ responses after a patient’s suicide are similar to those of other survivors after the loss of a loved one to suicide.21 Chemtob et al2 found that approximately one-half of psychiatrists who lost a patient to suicide had scores on the Impact of an Event Scale that were comparable to those of a clinical population seeking treatment after the death of a parent.
Continue to: Jordan and McIntosh have detailed...
Jordan and McIntosh22 have detailed several elements and themes that differentiate suicide loss and its associated reactions from other types of loss and grief. In general, suicide loss is considered traumatic, and is often accompanied by intense confusion and existential questioning, reflecting a negative impact on one’s core beliefs and assumptive world. The subsequent need to address the myriad of “why” questions left in its wake are often tinted with what Jordan and Baugher23 term the “tyranny of hindsight,” and take the form of implicit guilt for “sins of omission or commission” in relation to the lost individual.
Responses to suicide loss typically include initial shock, denial and numbness, intense sadness, anxiety, anger, and intense distress. Consistent with the traumatic nature of the loss, survivors are also likely to experience posttraumatic stress disorder symptoms such as intrusive thoughts, avoidance, and dissociation. Survivors also commonly experience significant guilt and shame, and this is likely to be socially reinforced by the general stigma associated with suicide as well as the actual blaming and avoidance responses of others.24-27
Clinicians’ unique reactions
For clinicians, there are additional components that may further complicate or exacerbate these reactions and extend their duration. First and foremost, such a loss affects clinicians on both personal and professional levels, a phenomenon that Plakun and Tillman13 have termed a “twin bereavement.” Thus, in addition to the personal grief and trauma reactions entailed in losing a patient to suicide, this loss is likely to impact clinicians’ professional identities, their relationships with colleagues, and their clinical work.
Clinicians’ professional identities are often predicated on generally shared assumptions and beliefs that, as trained professionals, they should have the power, aptitude, and competence to heal, or at least improve, the lives of patients, to reduce their distress, and to provide safety. In addition, such assumptions about clinicians’ responsibility and ability to prevent suicide are often reinforced in the clinical literature.28,29
These assumptions are often challenged, if not shattered, when patients take their own lives. A clinician’s sense of professional responsibility, the guilt and self-blame that may accompany this, self-doubts about one’s skills and clinical competence, the fear of (and actual) blame of colleagues and family members, and the real or imagined threat of litigation may all greatly exacerbate a clinician’s distress.11
Continue to: Hendin et al found...
Hendin et al30 found that mental health therapists have described losing a patient as “the most profoundly disturbing event of their professional careers,” noting that one-third of these clinicians experienced severe distress that lasted at least 1 year beyond the initial loss. In a 2004 study, Ruskin et al4 similarly found that one-quarter of psychiatrists and psychiatric trainees noted that losing a patient had a “profound and enduring effect on them.” In her article on surviving a patient’s suicide, Rycroft31 describes a “professional void” following the loss of her patient, in which “the world had changed, nothing was predictable any more, and it was no longer safe to assume anything.” Additionally, many clinicians experience an “acute sense of aloneness and isolation” subsequent to the loss.32
Many clinicians have noted that they considered leaving the field after such a loss,33,34 and it is hypothesized that many may have done so.35-37 Others have noted that, at least temporarily, they stopped treating patients who were potentially suicidal.29,35
Box 1
Several authors have proposed general models for describing the suicide grief trajectories of clinicians after a suicide loss. Tillman38 identified distinct groups of responses to this event: traumatic, affective, those related to the treatment, those related to interactions with colleagues, liability concerns, and the impact on one’s professional philosophy. She also found that Erikson’s stages of identity39 provided an uncannily similar trajectory to the ways in which those who participated in her research—clinicians at a mental hospital—had attempted to cope with their patients’ deaths, noting that the “suicide of a patient may provoke a revisiting of Erikson’s psychosocial crises in a telescoped and accelerated fashion.”38
Maltsberger40 offered a detailed psychoanalytic analysis of the responses clinicians may manifest in relation to a suicide loss, including the initial narcissistic injury sustained in relation to their patient’s actions; the subsequent potential for melancholic, atonement, or avoidance reactions; and the eventual capacity for the resolution of these reactions.
Al-Mateen et al33 described 3 phases of the clinician’s reaction after losing a patient who was a child to suicide:
- initial, which includes trauma and shock
- turmoil, which includes emotional flooding and functional impairments
- new growth, in which clinicians are able to reflect on their experiences and implications for training and policy.
For each phase, they also described staff activities that would foster forward movement through the trajectory.
In a 1981 study, Bissell41 found that psychiatric nurses who had experienced patient completed suicides progressed through several developmental stages (naïveté, recognition, responsibility, individual choice) that enabled them to come to terms with their personal reactions and place the ultimate responsibility for the suicide with the patient.
After losing a patient to suicide, a clinician may experience grief that proceeds through specific stages (Box 133,38-41). Box 22-4,6,16,24,29,30,33,34,40,42-45 describes a wide range of factors that affect each clinician’s unique response to losing a patient to suicide.
Box 2
There are many factors that make the experience of losing a patient to suicide unique and variable for individual clinicians. These include the amount of a clinician’s professional training and experience, both in general and in working with potentially suicidal individuals. Chemtob et al2 found that trainees were more likely to experience patient suicide loss than more seasoned clinicians, and to experience more distress.4,30,42 Brown24 noted that many training programs were likely to assign the most “extraordinarily sick patients to inexperienced trainees.” He noted that because the skill level of trainees has not yet tempered their personal aspirations, they are likely to experience a patient’s suicide as a personal failure. However, in contrast to the findings of Kleespies,42 Hendin,30 Ruskin et al,4 and Brown24 suggested that the overall impact of a patient’s suicide may be greater for seasoned clinicians, when the “protective advantage” or “explanation” of being in training is no longer applicable. This appears consistent with Munson’s study,43 which found that a greater number of years of clinical experience prior to a suicide loss was negatively correlated with posttraumatic growth.
Other factors affecting a clinician’s grief response include the context in which the treatment occurred, such as inpatient, outpatient, clinic, private practice, etc.44; the presence and involvement of supportive mentors or supervisors16; the length and intensity of the clinical relationship6,29; countertransference issues40; whether the patient was a child33; and the time elapsed since the suicide occurred.
In addition, each clinician’s set of personal and life experiences can affect the way he/ she moves through the grieving process. Any previous trauma or losses, particularly prior exposure to suicide, will likely impact a clinician’s reaction to his/her current loss, as will any susceptibility to anxiety or depression. Gorkin45 has suggested that the degree of omnipotence in the clinician’s therapeutic strivings will affect his/her ability to accept the inherent ambiguity involved in suicide loss. Gender may also play a role: Henry et al34 found that female clinicians had higher levels of stress reactions, and Grad et al3 found that female clinicians felt more shame and guilt and professed more doubts about their professional competence than male clinicians, and were more than twice as likely as men to identify talking with colleagues as an effective coping strategy.
Continue to: Implications of confidentiality restrictions
Implications of confidentiality restrictions
Confidentiality issues, as well as advice from attorneys to limit the disclosure of information about a patient, are likely to preclude a clinician’s ability to talk freely about the patient, the therapeutic relationship, and his/her reactions to the loss, all of which are known to facilitate movement through the grief process.46
The development of trust and the sharing of pain are just 2 factors that can make the clinical encounter an intense emotional experience for both parties. Recent trends in the psychodynamic literature acknowledge the profundity and depth of the personal impact that patients have on the clinician, an impact that is neither pathological nor an indication of poor boundaries in the therapy dyad, but instead a recognition of how all aspects of the clinician’s person, whether consciously or not, are used within the context of a therapeutic relationship. Yet when clinicians lose a patient, confidentiality restrictions often leave them wondering if and where any aspects of their experiences can be shared. Legal counsel may advise a clinician against speaking to consultants or supervisors or even surviving family members for fear that these non-privileged communications are subject to discovery should any legal proceedings ensue. Furthermore, the usual grief rituals that facilitate the healing of loss and the processing of grief (eg, gathering with others who knew the deceased, sharing feelings and memories, attending memorials) are usually denied to the clinician, and are often compounded by the reactions of one’s professional colleagues, who tend not to view the therapist’s grief as “legitimate.” Thus, clinician-survivors, despite having experienced a profound and traumatic loss, have very few places where this may be processed or even validated. As one clinician in a clinician-survivors support group stated, “I felt like I was grieving in a vacuum, that I wasn’t allowed to talk about how much my patient meant to me or how I’m feeling about it.” The isolation of grieving alone is likely to be compounded by the general lack of resources for supporting clinicians after such a loss. In contrast to the general suicide “survivor” network of support groups for family members who have experienced a suicide loss, there is an almost complete lack of supportive resources for clinicians following such a loss, and most clinicians are not aware of the resources that are available, such as the Clinician Survivor Task Force of the American Association of Suicidology (Box 312).
Box 3
Frank Jones and Judy Meade founded the Clinician Survivor Task Force (CSTF) of the American Association of Suicidology (AAS) in 1987. As Jones noted, “clinicians who have lost patients to suicide need a place to acknowledge and carry forward their personal loss … to benefit both personally and professionally from the opportunity to talk with other therapists who have survived the loss of a patient through suicide.”12
Nina Gutin, PhD, and Vanessa McGann, PhD, have co-chaired the CSTF since 2003. It now supports clinicians who have lost patients and/or loved ones, with the recognition that both types of losses carry implications within clinical and professional domains. The CSTF provides a listserve, opportunities to participate in video support groups, and a web site (www. cliniciansurvivor.org) that provides information about the clinician-survivor experience, the opportunity to read and post narratives about one’s experience with suicide loss, an updated bibliography maintained by John McIntosh, PhD, a list of clinical contacts, and a link to several excellent postvention protocols. In addition, Drs. Gutin and McGann conduct clinician-survivor support activities at the annual AAS conference, and in their respective geographic areas.
Continue to: Doka has described...
Doka47 has described “disenfranchised grief” in which the bereaved person does not receive the type and quality of support accorded to other bereaved persons, and thus is likely to internalize the view that his/her grief is not legitimate, and to believe that sharing related distress is a shame-ridden liability. This clearly relates to the sense of profound isolation and distress often described by clinician-survivors.
Other legal/ethical issues
The clinician-survivor’s concern about litigation, or an actual lawsuit, is likely to produce intense anxiety. This common fear is both understandable and credible. According to Bongar,48 the most common malpractice lawsuits filed against clinicians are those that involve a patient’s suicide. Peterson et al49 found that 34% of surviving family members considered bringing a lawsuit against the clinician, and of these, 57% consulted a lawyer.
In addition, an institution’s concern about protecting itself from liability may compromise its ability to support the clinician or trainee who sustained the loss. As noted above, the potential prohibitions around discussing the case can compromise the grief process. Additionally, the fear of (or actual) legal reprisals against supervisors and the larger institution may engender angry and blaming responses toward the treating clinician. In a personal communication (April 2008), Quinnett described an incident in which a supervising psychologist stomped into the grieving therapist’s office unannounced and shouted, “Now look what you’ve done! You’re going to get me sued!”
Other studies29,50,51 note that clinician-survivors fear losing their job, and that their colleagues and supervisors will be reluctant to assign new patients to them. Spiegleman and Werth17 also note that trainees grapple with additional concerns over negative evaluations, suspension or termination from clinical sites or training programs, and a potential interruption of obtaining a degree. Such supervisory and institutional reactions are likely to intensify a clinician’s sense of shame and distress, and are antithetical to postvention responses that promote optimal personal and professional growth. Such negative reactions are also likely to contribute to a clinician or trainee’s subsequent reluctance to work with suicidal individuals, or their decision to discontinue their clinical work altogether. Lastly, other ethical issues, such as contact with the patient’s family following the suicide, attending the funeral, etc., are likely to be a source of additional anxiety and distress, particularly if the clinician needs to address these issues in isolation.
Professional relationships/colleagues’ reactions
Many clinician-survivors have described reactions from colleagues and supervisors that are hurtful and unsupportive. According to Jobes and Maltsberger,52 “the suicide death of a patient in active treatment is commonly taken as prima facie evidence that the therapist, somehow or another, has mismanaged the case,” and thus the clinician often faces unwarranted blame and censure from colleagues and supervisors. Hendin et al30 noted that many trainees found reactions by their institutions to be insensitive and unsupportive, one noting that the department’s review of the case “felt more like a tribunal or inquest.” In a personal communication (April 2008), Quinnett noted that many clinicians he interviewed following a suicide loss reported a pattern of isolation and interpersonal discomfort with their colleagues, who implicitly or explicitly expressed concerns about their competence. He described how a respected colleague received “no understanding, no support, only abuse” from her supervisors. Such responses, while perhaps surprising from mental health professionals, probably reflect the long-standing cultural attitude of social condemnation of suicide, and of those who are associated with it.
Continue to: Negative reactions from professional colleagues...
Negative reactions from professional colleagues are most likely to occur immediately after the suicide loss and/or during the course of a subsequent investigation or psychological autopsy. Castelli-Dransart et al53 found that the lack of institutional support after a clinician experiences a suicide loss contributed to significantly higher stress responses for impacted clinicians, and may lead to a well-founded ambivalence about disclosure to colleagues, and consequent resistance to seeking out optimal supervision/consultation or even personal therapy that could help the clinician gain clarity on the effects of these issues. Many mental health professionals have described how, after the distressing experience of losing a patient to suicide, they moved through this process in relative isolation and loneliness, feeling abandoned by their colleagues and by their own hopes and expectations for support.
Stigmatization. In clinical settings, when a patient in treatment completes suicide, the treating clinician becomes an easy scapegoat for family members and colleagues. To the extent that mental health professionals are not immune from the effects and imposition of stigma, this might also affect their previously mentioned tendency to project judgment, overtly or covertly, onto the treating clinician.
Stigma around suicide is well documented.25 In The Surgeon General’s Call to Action to Prevent Suicide,54 former Surgeon General David Satcher specifically described stigma around suicide as one of the biggest barriers to prevention. Studies have shown that individuals bereaved by suicide are also stigmatized, and that those who were in caregiving roles (parents, clinicians) are believed to be more psychologically disturbed, less likable, more blameworthy, and less worthy of receiving support than other bereaved individuals.25,55-63 These judgments often mirror survivors’ self-punitive assessments, which then become exacerbated by and intertwined with both externally imposed and internalized stigma. Hence, it is not uncommon for suicide survivors to question their own right to grieve, to report low expectations of social support, and to feel compelled to deny or hide the mode of death. Feigelman et al26 found that stigmatization after a suicide loss was specifically associated with ongoing grief difficulties, depression, and suicidal thinking.
In my long-term work with clinician-survivors, I’ve come to believe that in addition to stigma around suicide, there may also be stigma projected by colleagues in relation to a clinician’s perceived emotional vulnerability. A traumatized clinician potentially challenges the notion of the implicit dichotomy/power imbalance between professionals and the patients we treat: “Us”—the professional, competent, healthy, and benevolent clinicians who have the care to offer, and “Them”—our patients, being needy, pathological, looking to us for care. This “us/them” distinction may serve to bolster a clinician’s professional esteem and identity. But when one of “us” becomes one of “them”—when a professional colleague is perceived as being emotionally vulnerable—this can be threatening to the predicates of this distinction, leading to the need to put the affected clinician firmly into the “them” camp. Thus, unwarranted condemnations of the clinician-survivor’s handling of the case, and/or the pathologizing of their normative grief reactions after the suicide loss, can seem justified.
Stigma associated both with suicide and with professional vulnerability is likely to be internalized and to have a profound effect on the clinician’s decisions about disclosure, asking for support, and ultimately on one’s ability to integrate the loss. When this occurs, it is likely to lead to even more isolation, shame, and self-blame. It is not surprising that many clinicians consider leaving the profession after this type of experience.
Continue to: Effects on clinical work
Effects on clinical work
A suicide loss is also likely to affect a clinician’s therapeutic work. Many authors12,52,64-67 have found that this commonly leads therapists to question their abilities as clinicians, and to experience a sharp loss of confidence in their work with patients. The shattered beliefs and assumptions around the efficacy of the therapeutic process, a sense of guilt or self-blame, and any perceived or actual negative judgment from colleagues can dramatically compromise a clinician’s sense of competence. Hendin et al30 noted that even the most experienced therapists expressed difficulty in trusting their own clinical judgment, or accurately assessing risk after a suicide loss.
In addition, the common grief and trauma-related responses to a suicide loss (including shock, numbness, sadness, anxiety, and generalized distress) are likely to result in at least some temporary disruption of a clinician’s optimal functioning. If trauma-related symptoms are more pronounced, the effect and longevity of such impairment may be exacerbated, and are likely to “impair clinical response and therapeutic judgment.”15 In addition, because such symptoms and states may be triggered by exposure to other potentially suicidal patients, they are more likely to impact clinical functioning when the clinician works with suicidal individuals. Thus, the normative responses to a suicide loss are likely to impact a clinician’s work, just as they are likely to impact the personal and occupational functioning of any survivor of suicide loss.
In clinician-survivor discussions and support groups I’ve led, participants have identified many common areas of clinical impact. Perhaps one of the most common early responses reported by clinician-survivors who continued to work with potentially suicidal individuals was to become hypervigilant in relation to any perceived suicide risk, to interpret such risk in such a way as to warrant more conservative interventions than are necessary, and to consequently minimize the patient’s own capacities for self-care.68 Conversely, others reported a tendency to minimize or deny suicidal potential by, for example, avoiding asking patients directly about suicidal ideation, even when they later realized that such questioning was indicated.69
Suicide loss may also lead to more subtle clinical reactions that have been observed not only with suicidal patients, but also in relation to patients who struggle with loss or grief. These include avoidant or even dissociative reactions in relation to their patient’s pain, which in turn can impact the clinician’s ability to “be fully present” or empathic in clinical encounters.50,69 Still, other clinicians noted that they tended to project residual feelings of anger onto their current suicidal patients, or envied patients who seemed to have mastered their grief. Consistent with Maltsberger’s description of “atonement reactions,”40 some clinicians found themselves doing more than should be expected for their patients, even losing their sense of professional boundaries in the process. Anderson70 noted that in pushing herself beyond what she knew were her optimal clinical boundaries, she was “punishing herself” for failing to prevent her patient’s suicide because, as she realized, “doing ‘penance’ was better than feeling helpless and powerless.” And Schultz16 described how therapists may have subsequent difficulty in trusting other patients, especially if patients who completed suicide did not disclose or denied their suicidal intent.
Working toward a supportive solution
In summary, unless clinicians who lose a patient to suicide have more supportive experiences, the combination of confidentiality-related restrictions, confusion about legal/ethical repercussions, unsupportive reactions from colleagues, and unexpected impairments in clinical work are likely to lead to intensified distress, isolation, the perceived need to “hide” the impact in professional settings, and consideration of leaving the profession. However, as I will describe in Part 2 (
Bottom Line
For mental health clinicians, losing a patient to suicide is a clear occupational hazard. After a suicide loss, clinicians often experience unique personal and professional challenges, including the impact of the loss on clinical work and professional identity, legal/ethical issues, and confidentiality-related constraints on the ability to discuss and process the loss.
Related Resources
- American Association of Suicidology Clinician Survivor Task Force. www.cliniciansurvivor.org.
- Gutin N. Helping survivors in the aftermath of suicide loss. Current Psychiatry. 2018;17(8):27-33.
1. Alexander D, Klein S, Gray NM, et al. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ. 2000;320(7249):1571-1574.
2. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry. 1988;145(2):224-228.
3. Grad OT, Zavasnik A, Groleger U. Suicide of a patient: gender differences in bereavement reactions of therapists. Suicide Life Threat Behav. 1997;27(4):379-386.
4. Ruskin R, Sakinofsky I, Bagby RM, et al. Impact of patient suicide on psychiatrists and psychiatric trainees. Acad Psychiatry. 2004;28(2):104-110.
5. Bersoff DN. Ethical conflicts in psychology, 2nd ed. Washington, DC: American Psychological Association; 1999.
6. Chemtob CM, Bauer GB, Hamada RS, et al. Patient suicide: occupational hazard for psychologists and psychiatrists. Prof Psychol Res Pr. 1989;20(5):294-300.
7. Rubin HL. Surviving a suicide in your practice. In: Blumenthal SJ, Kupfer DJ, eds. Suicide over the life cycle: risk factors, assessment, and treatment of suicidal patients. Washington, DC: American Psychiatric Press; 1990:619-636.
8. Kaye NS, Soreff SM. The psychiatrist’s role, responses, and responsibilities when a patient commits suicide. Am J Psychiatry. 1991;148(6):739-743.
9. McIntosh JL. Clinicians as survivors of suicide: bibliography. American Association of Suicidology Clinician Survivor Task Force. http://pages.iu.edu/~jmcintos/Surv.Ther.bib.htm. Updated May 19, 2019. Accessed August 26, 2019.
10. Douglas J, Brown HN. Suicide: understanding and responding: Harvard Medical School perspectives. Madison, CT: International Universities Press; 1989.
11. Farberow NL. The mental health professional as suicide survivor. Clin Neuropsychiatry. 2005;2(1):13-20.
12. Jones FA Jr. Therapists as survivors of patient suicide. In: Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: W.W. Norton; 1987;126-141.
13. Plakun EM, Tillman JG. Responding to clinicians after loss of a patient to suicide. Dir Psychiatry. 2005;25:301-310.
14. Prabhakar D, Anzia JM, Balon R, et al. “Collateral damages”: preparing residents for coping with patient suicide. Acad Psychiatry. 2013;37(6):429-30.
15. Quinnett P. QPR: for suicide prevention. QPR Institute, Inc. http://pages.iu.edu/~jmcintos/postvention.htm. Published September 21, 2009. Accessed August 26, 2019.
16. Schultz, D. Suggestions for supervisors when a therapist experiences a client’s suicide. Women Ther. 2005;28(1):59-69.
17. Spiegelman JS Jr, Werth JL Jr. Don’t forget about me: the experiences of therapists-in-training after a patient has attempted or died by suicide. Women Ther. 2005;28(1):35-57.
18. American Association of Suicidology. Clinician Survivor Task Force. Clinicians as survivors of suicide: postvention information.
19. Whitmore CA, Cook J, Salg L. Supporting residents in the wake of patient suicide. The American Journal of Psychiatry Residents’ Journal. 2017;12(1):5-7.
20. Melton B, Coverdale J. What do we teach psychiatric residents about suicide? A national survey of chief residents. Acad Psychiatry. 2009;33(1):47-50.
21. Valente SM. Psychotherapist reactions to the suicide of a patient. Am J Orthopsychiatry. 1994;64(4):614-621.
22. Jordan JR, McIntosh JL. Is suicide bereavement different? A framework for rethinking the question. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge; 2011:19-42.
23. Jordan JR, Baugher B. After suicide loss: coping with your grief, 2nd ed. Newcastle, WA: Caring People Press; 2016.
24. Brown HB. The impact of suicide on therapists in training. Compr Psychiatry. 1987;28(2):101-112.
25. Cvinar JG. Do suicide survivors suffer social stigma: a review of the literature. Perspect Psychiatr Care. 2005;41(1):14-21.
26. Feigelman W, Gorman BS, Jordan JR. Stigmatization and suicide bereavement. Death Stud. 2009;33(7):591-608.
27. Goffman E. Stigma: notes on the management of spoiled identity. New York, NY: Simon & Schuster; 1963.
28. Goldney RD. The privilege and responsibility of suicide prevention. Crisis. 2000;21(1):8-15.
29. Litman RE. When patients commit suicide. Am J Psychother. 1965;19(4):570-576.
30. Hendin H, Lipschitz A, Maltsberger JT, et al. Therapists’ reactions to patients’ suicides. Am J Psychiatry. 2000;157(12):2022-2027.
31. Rycroft P. Touching the heart and soul of therapy: surviving client suicide. Women Ther. 2004;28(1):83-94.
32. Ellis TE, Patel AB. Client suicide: what now? Cogn Behav Pract. 2012;19(2):277-287.
33. Al-Mateen CS, Jones K, Linker J, et al. Clinician response to a child who completes suicide. Child Adolesc Psychiatric Clin N Am. 2018;27(4):621-635.
34. Henry M, Séguin M, Drouin M-S. Mental health professionals’ response to the suicide of their patients [in French]. Revue Québécoise de Psychologie. 2004;25:241-257.
35. Carter RE. Some effects of client suicide on the therapist. Psychother Theory Res Practice. 1971;8(4):287-289.
36. Dewar I, Eagles J, Klein S, et al. Psychiatric trainees’ experiences of, and reactions to, patient suicide. Psychiatr Bull. 2000;24(1):20-23.
37. Gitlin M. Aftermath of a tragedy: reaction of psychiatrists to patient suicides. Psychiatr Ann. 2007;37(10):684-687.
38. Tillman JG. When a patient commits suicide: an empirical study of psychoanalytic clinicians. Inter J Psychoanal. 2006;87(1):159-177.
39. Erikson EH. Identity and the life cycle. New York, NY: International Universities Press, Inc.; 1959.
40. Maltsberger JT. The implications of patient suicide for the surviving psychotherapist. In: Jacobs D, ed. Suicide and clinical practice. Washington, DC: American Psychiatric Press; 1992:169-182.
41. Bissell BPH. The experience of the nurse therapist working with suicidal cases: a developmental study [dissertation]. Boston, MA: Boston University School of Education; 1981.
42. Kleespies PM. The stress of patient suicidal behavior: Implications for interns and training programs in psychology. Prof Psychol Res Pract. 1993;24(4):477-482.
43. Munson JS. Impact of client suicide on practitioner posttraumatic growth [dissertation]. Gainsville, Florida: University of Florida; 2009.
44. Hodgkinson PE. Responding to in-patient suicide. Br J Med Psychol. 1987;60(4):387-392.
45. Gorkin M. On the suicide of one’s patient. Bull Menninger Clin. 1985;49(1):1-9.
46. Fuentes MA, Cruz D. Posttraumatic growth: positive psychological changes after trauma. Mental Health News. 2009;11(1):31,37.
47. Doka KJ. Disenfranchised grief: new Directions, challenges, and strategies for practice. Champaign, IL: Research Press; 2002.
48. Bongar B. The suicidal patient: clinical and legal standards of care, 2nd ed. Washington, DC: American Psychological Association; 2002.
49. Peterson EM, Luoma JB, Dunne E. Suicide survivors’ perceptions of the treating clinician. Suicide Life Threat Behav. 2002;32(2):158-166.
50. Kolodny S, Binder RL, Bronstein AA, et al. The working through of patients’ suicides by four therapists. Suicide Life Threat Behav. 1979;9(1):33-46.
51. Marshall KA. When a patient commits suicide. Suicide Life Threat Behav. 1980;10(1):29-40.
52. Jobes DA, Maltsberger JT. The hazards of treating suicidal patients. In: Sussman MB, ed. A perilous calling: the hazards of psychotherapy practice. New York, NY: Wiley & Sons; 1995:200-214.
53. Castelli-Dransart DA, Gutjahr E, Gulfi A, et al. Patient suicide in institutions: emotional responses and traumatic impact on Swiss mental health professionals. Death Stud. 2014;38(1-5):315-321.
54. US Public Health Service. The Surgeon General’s call to action to prevent suicide. Washington, DC: Department of Health and Human Services; 1999.
55. Armour M. Violent death: understanding the context of traumatic and stigmatized grief. J Hum Behav Soc Environ. 2006;14(4):53-90.
56. Calhoun, LG, Allen BG. Social reactions to the survivor of a suicide in the family: a review of the literature. Omega (Westport). 1991;23(2):95-107.
57. Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: WW Norton & Co; 1987.
58. Harwood D, Hawton K, Hope J, et al. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: a descriptive and case-control study. J Affect Disord. 2002;72(2):185-194.
59. Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31(1):91-102.
60. McIntosh JL. Control group studies of suicide survivors: a review and critique. Suicide Life Threat Behav. 2003;23(2):146-161.
61. Range LM. When a loss is due to suicide: unique aspects of bereavement. In: Harvey JH, ed. Perspectives on loss: a sourcebook. Philadelphia, PA: Brunner/Mazel; 1998:213-220.
62. Sveen CA, Walby FA. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat Behav. 2008;38(1):13-29.
63. Van Dongen CJ. Social context of postsuicide bereavement. Death Stud. 1993;17(2):125-141.
64. Bultema JK. The healing process for the multidisciplinary team: recovering post-inpatient suicide. J Psychosoc Nurs. 1994;32(2):19-24.
65. Cooper C. Patient suicide and assault: their impact on psychiatric hospital staff. J Psychosoc Nurs Ment Health Serv. 1995;33(6):26-29.
66. Foster VA, McAdams CR III. The impact of client suicide in counselor training: Implications for counselor education and supervision. Counselor Educ Supervision. 1999;39(1):22-33.
67. Little JD. Staff response to inpatient and outpatient suicide: what happened and what do we do? Aust N Z J Psychiatry. 1992;26(2):162-167.
68. Horn PJ. Therapists’ psychological adaptation to client suicidal behavior. Chicago, IL: Loyola University of Chicago; 1995.
69. Gutin N, McGann VM, Jordan JR. The impact of suicide on professional caregivers. In: Jordan J, McIntosh J, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge; 2011:93-111.
70. Anderson GO. Who, what, when, where, how, and mostly why? A therapist’s grief over the suicide of a client. Women Ther. 2004;28(1):25-34.
1. Alexander D, Klein S, Gray NM, et al. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ. 2000;320(7249):1571-1574.
2. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry. 1988;145(2):224-228.
3. Grad OT, Zavasnik A, Groleger U. Suicide of a patient: gender differences in bereavement reactions of therapists. Suicide Life Threat Behav. 1997;27(4):379-386.
4. Ruskin R, Sakinofsky I, Bagby RM, et al. Impact of patient suicide on psychiatrists and psychiatric trainees. Acad Psychiatry. 2004;28(2):104-110.
5. Bersoff DN. Ethical conflicts in psychology, 2nd ed. Washington, DC: American Psychological Association; 1999.
6. Chemtob CM, Bauer GB, Hamada RS, et al. Patient suicide: occupational hazard for psychologists and psychiatrists. Prof Psychol Res Pr. 1989;20(5):294-300.
7. Rubin HL. Surviving a suicide in your practice. In: Blumenthal SJ, Kupfer DJ, eds. Suicide over the life cycle: risk factors, assessment, and treatment of suicidal patients. Washington, DC: American Psychiatric Press; 1990:619-636.
8. Kaye NS, Soreff SM. The psychiatrist’s role, responses, and responsibilities when a patient commits suicide. Am J Psychiatry. 1991;148(6):739-743.
9. McIntosh JL. Clinicians as survivors of suicide: bibliography. American Association of Suicidology Clinician Survivor Task Force. http://pages.iu.edu/~jmcintos/Surv.Ther.bib.htm. Updated May 19, 2019. Accessed August 26, 2019.
10. Douglas J, Brown HN. Suicide: understanding and responding: Harvard Medical School perspectives. Madison, CT: International Universities Press; 1989.
11. Farberow NL. The mental health professional as suicide survivor. Clin Neuropsychiatry. 2005;2(1):13-20.
12. Jones FA Jr. Therapists as survivors of patient suicide. In: Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: W.W. Norton; 1987;126-141.
13. Plakun EM, Tillman JG. Responding to clinicians after loss of a patient to suicide. Dir Psychiatry. 2005;25:301-310.
14. Prabhakar D, Anzia JM, Balon R, et al. “Collateral damages”: preparing residents for coping with patient suicide. Acad Psychiatry. 2013;37(6):429-30.
15. Quinnett P. QPR: for suicide prevention. QPR Institute, Inc. http://pages.iu.edu/~jmcintos/postvention.htm. Published September 21, 2009. Accessed August 26, 2019.
16. Schultz, D. Suggestions for supervisors when a therapist experiences a client’s suicide. Women Ther. 2005;28(1):59-69.
17. Spiegelman JS Jr, Werth JL Jr. Don’t forget about me: the experiences of therapists-in-training after a patient has attempted or died by suicide. Women Ther. 2005;28(1):35-57.
18. American Association of Suicidology. Clinician Survivor Task Force. Clinicians as survivors of suicide: postvention information.
19. Whitmore CA, Cook J, Salg L. Supporting residents in the wake of patient suicide. The American Journal of Psychiatry Residents’ Journal. 2017;12(1):5-7.
20. Melton B, Coverdale J. What do we teach psychiatric residents about suicide? A national survey of chief residents. Acad Psychiatry. 2009;33(1):47-50.
21. Valente SM. Psychotherapist reactions to the suicide of a patient. Am J Orthopsychiatry. 1994;64(4):614-621.
22. Jordan JR, McIntosh JL. Is suicide bereavement different? A framework for rethinking the question. In: Jordan JR, McIntosh JL, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge; 2011:19-42.
23. Jordan JR, Baugher B. After suicide loss: coping with your grief, 2nd ed. Newcastle, WA: Caring People Press; 2016.
24. Brown HB. The impact of suicide on therapists in training. Compr Psychiatry. 1987;28(2):101-112.
25. Cvinar JG. Do suicide survivors suffer social stigma: a review of the literature. Perspect Psychiatr Care. 2005;41(1):14-21.
26. Feigelman W, Gorman BS, Jordan JR. Stigmatization and suicide bereavement. Death Stud. 2009;33(7):591-608.
27. Goffman E. Stigma: notes on the management of spoiled identity. New York, NY: Simon & Schuster; 1963.
28. Goldney RD. The privilege and responsibility of suicide prevention. Crisis. 2000;21(1):8-15.
29. Litman RE. When patients commit suicide. Am J Psychother. 1965;19(4):570-576.
30. Hendin H, Lipschitz A, Maltsberger JT, et al. Therapists’ reactions to patients’ suicides. Am J Psychiatry. 2000;157(12):2022-2027.
31. Rycroft P. Touching the heart and soul of therapy: surviving client suicide. Women Ther. 2004;28(1):83-94.
32. Ellis TE, Patel AB. Client suicide: what now? Cogn Behav Pract. 2012;19(2):277-287.
33. Al-Mateen CS, Jones K, Linker J, et al. Clinician response to a child who completes suicide. Child Adolesc Psychiatric Clin N Am. 2018;27(4):621-635.
34. Henry M, Séguin M, Drouin M-S. Mental health professionals’ response to the suicide of their patients [in French]. Revue Québécoise de Psychologie. 2004;25:241-257.
35. Carter RE. Some effects of client suicide on the therapist. Psychother Theory Res Practice. 1971;8(4):287-289.
36. Dewar I, Eagles J, Klein S, et al. Psychiatric trainees’ experiences of, and reactions to, patient suicide. Psychiatr Bull. 2000;24(1):20-23.
37. Gitlin M. Aftermath of a tragedy: reaction of psychiatrists to patient suicides. Psychiatr Ann. 2007;37(10):684-687.
38. Tillman JG. When a patient commits suicide: an empirical study of psychoanalytic clinicians. Inter J Psychoanal. 2006;87(1):159-177.
39. Erikson EH. Identity and the life cycle. New York, NY: International Universities Press, Inc.; 1959.
40. Maltsberger JT. The implications of patient suicide for the surviving psychotherapist. In: Jacobs D, ed. Suicide and clinical practice. Washington, DC: American Psychiatric Press; 1992:169-182.
41. Bissell BPH. The experience of the nurse therapist working with suicidal cases: a developmental study [dissertation]. Boston, MA: Boston University School of Education; 1981.
42. Kleespies PM. The stress of patient suicidal behavior: Implications for interns and training programs in psychology. Prof Psychol Res Pract. 1993;24(4):477-482.
43. Munson JS. Impact of client suicide on practitioner posttraumatic growth [dissertation]. Gainsville, Florida: University of Florida; 2009.
44. Hodgkinson PE. Responding to in-patient suicide. Br J Med Psychol. 1987;60(4):387-392.
45. Gorkin M. On the suicide of one’s patient. Bull Menninger Clin. 1985;49(1):1-9.
46. Fuentes MA, Cruz D. Posttraumatic growth: positive psychological changes after trauma. Mental Health News. 2009;11(1):31,37.
47. Doka KJ. Disenfranchised grief: new Directions, challenges, and strategies for practice. Champaign, IL: Research Press; 2002.
48. Bongar B. The suicidal patient: clinical and legal standards of care, 2nd ed. Washington, DC: American Psychological Association; 2002.
49. Peterson EM, Luoma JB, Dunne E. Suicide survivors’ perceptions of the treating clinician. Suicide Life Threat Behav. 2002;32(2):158-166.
50. Kolodny S, Binder RL, Bronstein AA, et al. The working through of patients’ suicides by four therapists. Suicide Life Threat Behav. 1979;9(1):33-46.
51. Marshall KA. When a patient commits suicide. Suicide Life Threat Behav. 1980;10(1):29-40.
52. Jobes DA, Maltsberger JT. The hazards of treating suicidal patients. In: Sussman MB, ed. A perilous calling: the hazards of psychotherapy practice. New York, NY: Wiley & Sons; 1995:200-214.
53. Castelli-Dransart DA, Gutjahr E, Gulfi A, et al. Patient suicide in institutions: emotional responses and traumatic impact on Swiss mental health professionals. Death Stud. 2014;38(1-5):315-321.
54. US Public Health Service. The Surgeon General’s call to action to prevent suicide. Washington, DC: Department of Health and Human Services; 1999.
55. Armour M. Violent death: understanding the context of traumatic and stigmatized grief. J Hum Behav Soc Environ. 2006;14(4):53-90.
56. Calhoun, LG, Allen BG. Social reactions to the survivor of a suicide in the family: a review of the literature. Omega (Westport). 1991;23(2):95-107.
57. Dunne EJ, McIntosh JL, Dunne-Maxim K, eds. Suicide and its aftermath: understanding and counseling the survivors. New York, NY: WW Norton & Co; 1987.
58. Harwood D, Hawton K, Hope J, et al. The grief experiences and needs of bereaved relatives and friends of older people dying through suicide: a descriptive and case-control study. J Affect Disord. 2002;72(2):185-194.
59. Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31(1):91-102.
60. McIntosh JL. Control group studies of suicide survivors: a review and critique. Suicide Life Threat Behav. 2003;23(2):146-161.
61. Range LM. When a loss is due to suicide: unique aspects of bereavement. In: Harvey JH, ed. Perspectives on loss: a sourcebook. Philadelphia, PA: Brunner/Mazel; 1998:213-220.
62. Sveen CA, Walby FA. Suicide survivors’ mental health and grief reactions: a systematic review of controlled studies. Suicide Life Threat Behav. 2008;38(1):13-29.
63. Van Dongen CJ. Social context of postsuicide bereavement. Death Stud. 1993;17(2):125-141.
64. Bultema JK. The healing process for the multidisciplinary team: recovering post-inpatient suicide. J Psychosoc Nurs. 1994;32(2):19-24.
65. Cooper C. Patient suicide and assault: their impact on psychiatric hospital staff. J Psychosoc Nurs Ment Health Serv. 1995;33(6):26-29.
66. Foster VA, McAdams CR III. The impact of client suicide in counselor training: Implications for counselor education and supervision. Counselor Educ Supervision. 1999;39(1):22-33.
67. Little JD. Staff response to inpatient and outpatient suicide: what happened and what do we do? Aust N Z J Psychiatry. 1992;26(2):162-167.
68. Horn PJ. Therapists’ psychological adaptation to client suicidal behavior. Chicago, IL: Loyola University of Chicago; 1995.
69. Gutin N, McGann VM, Jordan JR. The impact of suicide on professional caregivers. In: Jordan J, McIntosh J, eds. Grief after suicide: understanding the consequences and caring for the survivors. New York, NY: Routledge; 2011:93-111.
70. Anderson GO. Who, what, when, where, how, and mostly why? A therapist’s grief over the suicide of a client. Women Ther. 2004;28(1):25-34.

Assessing decisional capacity in patients with substance use disorders
Ms. B, age 31, is brought to the emergency department (ED) via ambulance after emergency medical technicians used naloxone nasal spray to revive her following an overdose on heroin. She reports daily IV heroin use for the last 4 years as well as frequent use of other illicit substances, including marijuana and alprazolam, for which she does not have
How can you determine if Ms. B has the capacity to make decisions regarding her care?
Decisional capacity is defined as a patient’s ability to use information about an illness and the proposed treatment options to make a choice that is congruent with one’s own values and preferences.1 Determining whether a patient has adequate capacity to make decisions regarding their care is an inherent aspect of all clinician-patient interactions.
Published reports have focused on the challenges clinicians face when assessing decisional capacity in patients with psychiatric and cognitive disorders. However, there is little evidence about assessing decisional capacity in patients with substance use disorders (SUDs), even though increasing numbers of patients with SUDs are presenting to EDs2 and being admitted as inpatients in general hospitals.3 In this article, I discuss:
- the biologic basis for impaired decision-making in patients with SUDs
- common substance use–related conditions that may impact a patient’s decisional capacity
- the clinical challenges and legal considerations clinicians face when assessing decisional capacity in patients with SUDs
- how to assess decisional capacity in such patients.
Decisional capacity vs competence
“Capacity” and “competence” are not the same. Decisional capacity, which refers to the ability to make decisions, is a clinical construct that is determined by clinicians and is generally used in the acute clinical setting. Because cognition is the main determinant of capacity, conditions or treatments that affect cognition can impair an individual’s decision-making capacity.1 Decisional capacity is not a global concept but a decision-specific one, subject to fluctuations depending on the time and the nature of the decision at hand. Therefore, requests for determination of decisional capacity in the clinical setting should be specific to an individual decision or set of decisions.
In contrast, competence is an enduring legal determination of incapacitation, typically made by a probate judge. It refers to the ability of an individual to perform actions needed to put decisions into effect. Decisional capacity as assessed by a clinician often serves as the basis for petitions submitted for the purpose of competency adjudication by the judicial system.
A biologic basis for impaired decision-making?
Jeste and Saks4 suggested that addiction itself is characterized by impaired decision-making because individuals keep using a substance despite experiencing recurrent physical, psychologic, or social problems caused or worsened by the substance. Several studies suggest there may be a biologic basis for impaired decision-making in these patients, even in the absence of severe psychiatric or cognitive disorders.
Continue to: Bechara and Damasio found...
Bechara and Damasio5 found that the decision-making impairment seen in some patients with SUDs was similar to that observed in patients who have lesions of the ventromedial prefrontal cortex. In both groups of patients, the impaired decision-making was characterized by a preference to opt for high immediate reward despite even higher future losses.
These deficits were also observed by Grant et al.6 In this study, patients with SUDs displayed markedly impaired performance on the Gambling Task, which examines decisions that result in long-term losses that exceed short-term gains. However, patients with SUDs performed similarly to controls on the Wisconsin Card Sorting Test, which evaluates the ability to form abstract concepts and to shift from established response sets.
MacDonald et al7 used a laboratory experiment and 2 field studies to test the hypothesis that alcohol affects attitudes and intentions toward drinking and driving. Their findings support the concept that alcohol intoxication decreases cognitive capacity such that people are more likely to attend to only the most salient cues.7
Whether the impairment documented in such studies is a contributing factor in addiction or is a result of addiction remains uncertain. While individuals with SUDs may have some level of impairment in decision-making in general, particularly in regard to their substance use, their decisional capacity on specific clinical decisions should be assessed carefully. In a study of 300 consecutive psychiatric consultations for decisional capacity at an urban hospital, Boettger et al8 found that 41% were related to SUDs. Of these, 37% were found to have impaired decisional capacity.
Impaired decision-making in patients with SUDs may specifically pertain to choices related to their addiction, including9:
- consent for addiction treatment
- consistency in maintaining a choice of recovery
- changing values regarding treatment over time
- capacity to participate in addiction research involving the use of addictive substances.
Continue to: It is important to recognize...
It is important to recognize that this impairment may not necessarily translate into altered decisional capacity regarding other health care decisions, such as consenting to surgery or other necessary medical interventions.9
Substance-related disorders that affect decisional capacity
Substance-related syndromes can affect mood, reality testing, and/or cognitive function, thereby directly impacting a patient’s decisional capacity. Substance-related syndromes can be divided into 2 categories: 1) disorders resulting from the direct effects of the substance, and 2) secondary disorders resulting from/or associated with substance use.
Disorders resulting from the direct effects of the substance
Temporary/reversible incapacitation
- Acute intoxication or intoxication delirium may be the most frequent type of temporary incapacitation. It can result from toxic levels of licit or illicit substances; alcohol is likely the most frequent offending agent. Although some individuals who are intoxicated may appear to be alert, oriented, and able to engage in lengthy conversations, the majority do not possess adequate decisional capacity.10
- Withdrawal delirium, associated with longstanding alcohol, sedative-hypnotic, or barbiturate dependence, is typically prolonged, but usually resolves, either spontaneously or with treatment. Although most deliria resolve once the underlying etiology is corrected, vulnerable individuals may experience irreversible cognitive impairment and permanent decisional incapacitation.11,12
- Severe substance-induced depressive disorders, especially if accompanied by frank psychotic symptoms or severe depressive distortions of reality, may result in decisional incapacity. Substance abuse treatment that incorporates multiple strategies, sometimes in conjunction with pharmacotherapy to manage depression, should lead to sufficient recovery and restoration of decisional capacity.
- Transient psychotic disorders such as those associated with the use of stimulants are often treatable. Patients may recover decisional capacity spontaneously or with treatment.
Permanent incapacitation
- Dementia is associated with substance use, particularly alcohol use.13 For a patient who develops dementia, no appreciable recovery can be expected, even with prolonged abstinence.
- Persistent amnestic disorders (eg, Korsakoff syndrome) resulting from undiagnosed or untreated severe thiamine deficiency (Wernicke’s encephalopathy). Although an isolated Korsakoff syndrome consists primarily of anterograde amnesia, these patients may experience additional cognitive impairment resulting from years of alcohol consumption or associated with other neurodegenerative processes, and therefore are sufficiently impaired and lack decisional capacity. Even in the absence of such concomitant cognitive deficits, a very severe anterograde amnestic disorder directly impacts a patient’s capacity to perform the necessary tasks required to give informed consent. The inability to consolidate information about new medical developments, treatments, and procedures, even when they are thoroughly explained by the medical team, can pose serious challenges. For example, a patient may protest to being taken to surgery because he/she does not recall signing a consent form the previous day.
- Enduring severe and treatment-refractory psychotic disorders associated with drug use, specifically stimulants, can result in permanent incapacitation similar to that seen in severe primary psychotic disorders (such as treatment-resistant schizophrenia).
- Hepatic encephalopathy may be seen in patients with advanced cirrhosis of the liver (due to hepatitis C resulting from IV drug use, and/or alcohol use). In late stages of cirrhosis, the confusional state patients experience may become severe and may no longer be reversible unless liver transplantation is available and successful. This would therefore constitute a basis for permanent decisional incapacitation.
- Human immunodeficiency virus encephalitis or dementia can result from IV drug use.
Continue to: Clinical challenges
Clinical challenges
In intensive care settings, where a patient with a SUD may be treated for acute life-threatening intoxication or severe withdrawal delirium, an assumption of decisional incapacitation often exists as a result of medical acuity and impaired mentation. In these situations, treatment usually proceeds with consent obtained from next-of-kin, a guardian, or an administrative (hospital) authority when other substitute decision makers are unavailable or unwilling. In such cases, psychiatric consultation can play a dual role in documenting the patient’s decisional capacity and also in contributing to the care of patients with SUDs.
It is critical to perform a cognitive evaluation and mental status examination in a medically compromised patient with an SUD. Unfortunately, serious cognitive disorders can often be concealed by a superficially jovial or verbally skilled patient, or by an uncooperative individual who refuses to engage in a thorough conversation with his/her clinicians. These scenarios present significant challenges and may result in missed opportunities for care or premature discharges. Negative countertransference by clinicians toward patients with SUDs may also promote poor outcomes. For difficult cases, legal and ethical consultations may help mitigate risk and guide management approaches (Box14).
Box
The legal system rarely views patients with substance use disorders (SUDs) as lacking decisional capacity in the absence of overt psychiatric or cognitive deficits. The penal system offers little if any mitigation of liability on account of addiction in civil or criminal cases. On the contrary, intoxication is an aggravating factor in such settings. Despite extensive literature that questions the “free will,” accountability, and responsibility of patients with SUDs, the legal system takes an “all-or-none” approach to this issue. It assumes free choice and accountability for patients with SUDs, except when a clear superimposed psychiatric or cognitive disorder (such as psychosis or dementia) exists. Rarely, some jurisdictions may allow for mental health commitments on account of severe and persistent addictive behaviors that clearly pose a risk to the individual or to society, implicitly recognizing that incapacitation can result from severe addiction. Nevertheless, a finding of imminent or impending dangerousness is generally required for such commitments to be justified.
In other situations, individual health care settings may resort to local hospital policies that allow impaired patients with SUDs with a clearly altered mental status to be detained for the purpose of completing medical treatment. Presumably, discharge would occur when the medical and psychiatric acuity has resolved (often under the umbrella of a “Medical Hold” policy). Jain et al14 suggested that although such commitment laws for patients with SUDs may be appealing to some people, especially family members, specific statutes and their implementation are highly variable; the deprivation of liberty raises ethical concerns; and outcome data are limited. Conversely, most states either do not have such legislation, or rarely enforce it.
How to assess decisional capacity
A direct conclusion of incapacity in an individual cannot be determined solely on the knowledge of the patient having a SUD-related clinical condition. (The possible exception to this may be a patient with severe dementia.)
- understand the decision at hand
- discuss its benefits and risks
- describe alternatives
- demonstrate an appreciation of the implications of treatment or lack thereof
- communicate a clear and consistent choice.
Continue to: While most clinicians...
While most clinicians rely on a psychiatric interview (with or without a cognitive examination) to make these determinations, several instruments have been developed to aid these evaluations, such as the MacArthur Competence Assessment Tool for Treatment (Mac-CAT-T).15 In patients with potentially reversible incapacitating conditions, serial examinations over time, especially re-evaluation when a patient has achieved and maintained sobriety, may be necessary and helpful.

The Table offers a guide to assessing decisional capacity in a patient with an SUD.
Who should conduct the assessment?
Mental health professionals—usually psychiatrists or psychologists—are consulted when there is uncertainty about a patient’s decisional capacity, and when a more thorough mental status examination is warranted to formulate an informed opinion.16 Unfortunately, this typically occurs only if a patient refuses treatment or demands to be discharged before treatment has been completed, or there is a high level of risk to the patient or others after discharge.
In acute settings, when a patient consents to treatment, a psychiatric consultation regarding decisional capacity is rarely requested. While it is often tempting for medical or surgical teams to proceed with an intervention in a cooperative patient who willingly signs a consent form without a formal assessment of his/her decisional capacity, doing so raises challenging ethical and legal questions in the event of an adverse outcome. It is therefore prudent to strongly recommend that medical and surgical colleagues obtain a psychiatric consultation when an individual’s decisional capacity is uncertain, especially when a patient is known to have a psychiatric or neurocognitive disorder, or exhibits evidence of recent mental status changes. In cases of potentially reversible impairment (eg, delirium, psychosis, or acute anxiety), targeted interventions may help restore capacity and allow treatment to proceed.
No jurisdictions mandate that the determination of decisional capacity should be made exclusively by a mental health professional. Any treating health care professional (usually the attending physician) can make a determination of decisional capacity in scenarios where there is no overt evidence the patient has a mental or cognitive disorder and the patient is communicating clear and reasoned choices, or when a patient is profoundly impaired and no meaningful communication can take place.
Continue to: CASE CONTINUED
CASE CONTINUED
The emergency physician requests a psychiatric consultation. You assess Ms. B’s decisional capacity using the Mac-CAT-T along with a standard psychiatric evaluation. Her score of 14 reflects that she is able to understand the risks associated with her opioid use, and although irritated by engaging in such a discussion, is capable of reasoning through the various medical and psychosocial aspects of her addiction, and shows moderate appreciation of the impact of her choices on her future and that of significant others. The psychiatric evaluation fails to elicit any substantial mood, anxiety, or psychotic disorders associated with/or resulting from her addiction, and her cognitive examination is within normal limits. She does not exhibit severe withdrawal and is not delirious on examination. Finally, she did not harbor thoughts of intentional harm to self or others and is not deemed imminently dangerous.
You document that in your opinion, despite Ms. B’s unfortunate choices and questionable judgment, she does have the capacity to make informed decisions regarding her care and could be released against medical advice if she so chooses, while providing her with information about available resources should she decide to seek rehabilitation in the future.
An increasingly common scenario
Decisional capacity assessment in patients with SUDs is an increasingly common reason for psychiatric consultations. Primary and secondary conditions related to substance use can affect a patient’s decisional capacity on a temporary or permanent basis. The same principles that guide the assessment of decisional capacity in patients with other psychiatric or cognitive disorders should be applied to compromised individuals with SUDs. In challenging cases, a skilled psychiatric evaluation that is supported by a thorough cognitive examination and, when required, complemented by a legal or ethical consultation, can help clinicians make safe and judicious decisions.
Bottom Line
Assessing the decisional capacity of a patient with a substance use disorder can be challenging. Primary or secondary conditions related to substance use can affect a patient’s decisional capacity on a temporary or permanent basis. A skilled psychiatric evaluation that includes a thorough cognitive examination and is complemented by legal or ethical consultation can help in making judicious decisions.
Related Resources
- Tan SY. Determining patients’ decisional capacity. Clinical Psychiatry News. https://www.mdedge.com/psychiatry/article/137939/practice-management/determining-patients-decisional-capacity. Published May 10, 2017.
- Sorrentino R. Performing capacity evaluations: What’s expected from your consult. Current Psychiatry. 2014;13(1):41-44.
Drug Brand Names
Alprazolam • Xanax
Naloxone nasal spray • Narcan
1. Karlawish K. Assessment of decision-making capacity in adults. UpToDate. https://www.uptodate.com/contents/assessment-of-decision-making-capacity-in-adults. Updated July 2019. Accessed August 19, 2019.
2. Owens PL, Mutter R, Stocks C. Mental health and substance abuse-related emergency department visits among adults, 2007. HCUP Statistical Brief #92. https://www.ncbi.nlm.nih.gov/books/NBK52659/pdf/Bookshelf_NBK52659.pdf. Published July 2010. Accessed August 19, 2019.
3. Smothers BA, Yahr HT. Alcohol use disorder and illicit drug use in admissions to general hospitals in the United States. Am J Addict. 2005;14(3):256-267.
4. Jeste DV, Saks E. Decisional capacity in mental illness and substance use disorders: empirical database and policy implications. Behav Sci Law. 2006;24(4):607-628.
5. Bechara A, Damasio H. Decision-making and addiction (part I): impaired activation of somatic states in substance dependent individuals when pondering decisions with negative future consequences. Neuropsychologia. 2002;40(10):1675-1689.
6. Grant S, Contoreggi C, London ED. Drug abusers show impaired performance in a laboratory test of decision making. Neuropsychologia. 2000;38(8):1180-1187.
7. MacDonald TK, Zanna MP, Fong GT. Decision making in altered states: effects of alcohol on attitudes toward drinking and driving. J Pers Soc Psychol. 1995;68(6):973-985.
8. Boettger S, Bergman M, Jenewein J, et al. Assessment of decisional capacity: prevalence of medical illness and psychiatric comorbidities. Palliat Support Care. 2015;13(5):1275-1281.
9. Charland LC. Chapter 6: Decision-making capacity and responsibility in addiction. In: Poland J, Graham G. Addiction and responsibility. Cambridge, MA: MIT Press Scholarship Online; 2011:139-158.
10. Martel ML, Klein LR, Miner JR, et al. A brief assessment of capacity to consent instrument in acutely intoxicated emergency department patients. Am J Emerg Med. 2018;36(1):18-23.
11. MacLullich AM, Beaglehole A, Hall RJ, et al. Delirium and long-term cognitive impairment. Int Rev Psychiatry. 2009;21(1):30-42.
12. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306-1316.
13. Rehm J, Hasan OSM, Black SE, et al. Alcohol use and dementia: a systematic scoping review. Alzheimers Res Ther. 2019;11(1):1.
14. Jain A, Christopher P, Appelbaum PS. Civil commitment for opioid and other substance use disorders: does it work? Psychiatr Serv. 2018;69(4):374-376.
15. Grisso T, Appelbaum PS. Chapter 6: Using the MacArthur competence assessment tool – treatment. In: Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. New York, NY: Oxford University Press; 1998:101-126.
16. Hazelton LD, Sterns GL, Chisholm T. Decision-making capacity and alcohol abuse: clinical and ethical considerations in personal care choices. Gen Hosp Psychiatry. 2003;25(2):130-135.
Ms. B, age 31, is brought to the emergency department (ED) via ambulance after emergency medical technicians used naloxone nasal spray to revive her following an overdose on heroin. She reports daily IV heroin use for the last 4 years as well as frequent use of other illicit substances, including marijuana and alprazolam, for which she does not have
How can you determine if Ms. B has the capacity to make decisions regarding her care?
Decisional capacity is defined as a patient’s ability to use information about an illness and the proposed treatment options to make a choice that is congruent with one’s own values and preferences.1 Determining whether a patient has adequate capacity to make decisions regarding their care is an inherent aspect of all clinician-patient interactions.
Published reports have focused on the challenges clinicians face when assessing decisional capacity in patients with psychiatric and cognitive disorders. However, there is little evidence about assessing decisional capacity in patients with substance use disorders (SUDs), even though increasing numbers of patients with SUDs are presenting to EDs2 and being admitted as inpatients in general hospitals.3 In this article, I discuss:
- the biologic basis for impaired decision-making in patients with SUDs
- common substance use–related conditions that may impact a patient’s decisional capacity
- the clinical challenges and legal considerations clinicians face when assessing decisional capacity in patients with SUDs
- how to assess decisional capacity in such patients.
Decisional capacity vs competence
“Capacity” and “competence” are not the same. Decisional capacity, which refers to the ability to make decisions, is a clinical construct that is determined by clinicians and is generally used in the acute clinical setting. Because cognition is the main determinant of capacity, conditions or treatments that affect cognition can impair an individual’s decision-making capacity.1 Decisional capacity is not a global concept but a decision-specific one, subject to fluctuations depending on the time and the nature of the decision at hand. Therefore, requests for determination of decisional capacity in the clinical setting should be specific to an individual decision or set of decisions.
In contrast, competence is an enduring legal determination of incapacitation, typically made by a probate judge. It refers to the ability of an individual to perform actions needed to put decisions into effect. Decisional capacity as assessed by a clinician often serves as the basis for petitions submitted for the purpose of competency adjudication by the judicial system.
A biologic basis for impaired decision-making?
Jeste and Saks4 suggested that addiction itself is characterized by impaired decision-making because individuals keep using a substance despite experiencing recurrent physical, psychologic, or social problems caused or worsened by the substance. Several studies suggest there may be a biologic basis for impaired decision-making in these patients, even in the absence of severe psychiatric or cognitive disorders.
Continue to: Bechara and Damasio found...
Bechara and Damasio5 found that the decision-making impairment seen in some patients with SUDs was similar to that observed in patients who have lesions of the ventromedial prefrontal cortex. In both groups of patients, the impaired decision-making was characterized by a preference to opt for high immediate reward despite even higher future losses.
These deficits were also observed by Grant et al.6 In this study, patients with SUDs displayed markedly impaired performance on the Gambling Task, which examines decisions that result in long-term losses that exceed short-term gains. However, patients with SUDs performed similarly to controls on the Wisconsin Card Sorting Test, which evaluates the ability to form abstract concepts and to shift from established response sets.
MacDonald et al7 used a laboratory experiment and 2 field studies to test the hypothesis that alcohol affects attitudes and intentions toward drinking and driving. Their findings support the concept that alcohol intoxication decreases cognitive capacity such that people are more likely to attend to only the most salient cues.7
Whether the impairment documented in such studies is a contributing factor in addiction or is a result of addiction remains uncertain. While individuals with SUDs may have some level of impairment in decision-making in general, particularly in regard to their substance use, their decisional capacity on specific clinical decisions should be assessed carefully. In a study of 300 consecutive psychiatric consultations for decisional capacity at an urban hospital, Boettger et al8 found that 41% were related to SUDs. Of these, 37% were found to have impaired decisional capacity.
Impaired decision-making in patients with SUDs may specifically pertain to choices related to their addiction, including9:
- consent for addiction treatment
- consistency in maintaining a choice of recovery
- changing values regarding treatment over time
- capacity to participate in addiction research involving the use of addictive substances.
Continue to: It is important to recognize...
It is important to recognize that this impairment may not necessarily translate into altered decisional capacity regarding other health care decisions, such as consenting to surgery or other necessary medical interventions.9
Substance-related disorders that affect decisional capacity
Substance-related syndromes can affect mood, reality testing, and/or cognitive function, thereby directly impacting a patient’s decisional capacity. Substance-related syndromes can be divided into 2 categories: 1) disorders resulting from the direct effects of the substance, and 2) secondary disorders resulting from/or associated with substance use.
Disorders resulting from the direct effects of the substance
Temporary/reversible incapacitation
- Acute intoxication or intoxication delirium may be the most frequent type of temporary incapacitation. It can result from toxic levels of licit or illicit substances; alcohol is likely the most frequent offending agent. Although some individuals who are intoxicated may appear to be alert, oriented, and able to engage in lengthy conversations, the majority do not possess adequate decisional capacity.10
- Withdrawal delirium, associated with longstanding alcohol, sedative-hypnotic, or barbiturate dependence, is typically prolonged, but usually resolves, either spontaneously or with treatment. Although most deliria resolve once the underlying etiology is corrected, vulnerable individuals may experience irreversible cognitive impairment and permanent decisional incapacitation.11,12
- Severe substance-induced depressive disorders, especially if accompanied by frank psychotic symptoms or severe depressive distortions of reality, may result in decisional incapacity. Substance abuse treatment that incorporates multiple strategies, sometimes in conjunction with pharmacotherapy to manage depression, should lead to sufficient recovery and restoration of decisional capacity.
- Transient psychotic disorders such as those associated with the use of stimulants are often treatable. Patients may recover decisional capacity spontaneously or with treatment.
Permanent incapacitation
- Dementia is associated with substance use, particularly alcohol use.13 For a patient who develops dementia, no appreciable recovery can be expected, even with prolonged abstinence.
- Persistent amnestic disorders (eg, Korsakoff syndrome) resulting from undiagnosed or untreated severe thiamine deficiency (Wernicke’s encephalopathy). Although an isolated Korsakoff syndrome consists primarily of anterograde amnesia, these patients may experience additional cognitive impairment resulting from years of alcohol consumption or associated with other neurodegenerative processes, and therefore are sufficiently impaired and lack decisional capacity. Even in the absence of such concomitant cognitive deficits, a very severe anterograde amnestic disorder directly impacts a patient’s capacity to perform the necessary tasks required to give informed consent. The inability to consolidate information about new medical developments, treatments, and procedures, even when they are thoroughly explained by the medical team, can pose serious challenges. For example, a patient may protest to being taken to surgery because he/she does not recall signing a consent form the previous day.
- Enduring severe and treatment-refractory psychotic disorders associated with drug use, specifically stimulants, can result in permanent incapacitation similar to that seen in severe primary psychotic disorders (such as treatment-resistant schizophrenia).
- Hepatic encephalopathy may be seen in patients with advanced cirrhosis of the liver (due to hepatitis C resulting from IV drug use, and/or alcohol use). In late stages of cirrhosis, the confusional state patients experience may become severe and may no longer be reversible unless liver transplantation is available and successful. This would therefore constitute a basis for permanent decisional incapacitation.
- Human immunodeficiency virus encephalitis or dementia can result from IV drug use.
Continue to: Clinical challenges
Clinical challenges
In intensive care settings, where a patient with a SUD may be treated for acute life-threatening intoxication or severe withdrawal delirium, an assumption of decisional incapacitation often exists as a result of medical acuity and impaired mentation. In these situations, treatment usually proceeds with consent obtained from next-of-kin, a guardian, or an administrative (hospital) authority when other substitute decision makers are unavailable or unwilling. In such cases, psychiatric consultation can play a dual role in documenting the patient’s decisional capacity and also in contributing to the care of patients with SUDs.
It is critical to perform a cognitive evaluation and mental status examination in a medically compromised patient with an SUD. Unfortunately, serious cognitive disorders can often be concealed by a superficially jovial or verbally skilled patient, or by an uncooperative individual who refuses to engage in a thorough conversation with his/her clinicians. These scenarios present significant challenges and may result in missed opportunities for care or premature discharges. Negative countertransference by clinicians toward patients with SUDs may also promote poor outcomes. For difficult cases, legal and ethical consultations may help mitigate risk and guide management approaches (Box14).
Box
The legal system rarely views patients with substance use disorders (SUDs) as lacking decisional capacity in the absence of overt psychiatric or cognitive deficits. The penal system offers little if any mitigation of liability on account of addiction in civil or criminal cases. On the contrary, intoxication is an aggravating factor in such settings. Despite extensive literature that questions the “free will,” accountability, and responsibility of patients with SUDs, the legal system takes an “all-or-none” approach to this issue. It assumes free choice and accountability for patients with SUDs, except when a clear superimposed psychiatric or cognitive disorder (such as psychosis or dementia) exists. Rarely, some jurisdictions may allow for mental health commitments on account of severe and persistent addictive behaviors that clearly pose a risk to the individual or to society, implicitly recognizing that incapacitation can result from severe addiction. Nevertheless, a finding of imminent or impending dangerousness is generally required for such commitments to be justified.
In other situations, individual health care settings may resort to local hospital policies that allow impaired patients with SUDs with a clearly altered mental status to be detained for the purpose of completing medical treatment. Presumably, discharge would occur when the medical and psychiatric acuity has resolved (often under the umbrella of a “Medical Hold” policy). Jain et al14 suggested that although such commitment laws for patients with SUDs may be appealing to some people, especially family members, specific statutes and their implementation are highly variable; the deprivation of liberty raises ethical concerns; and outcome data are limited. Conversely, most states either do not have such legislation, or rarely enforce it.
How to assess decisional capacity
A direct conclusion of incapacity in an individual cannot be determined solely on the knowledge of the patient having a SUD-related clinical condition. (The possible exception to this may be a patient with severe dementia.)
- understand the decision at hand
- discuss its benefits and risks
- describe alternatives
- demonstrate an appreciation of the implications of treatment or lack thereof
- communicate a clear and consistent choice.
Continue to: While most clinicians...
While most clinicians rely on a psychiatric interview (with or without a cognitive examination) to make these determinations, several instruments have been developed to aid these evaluations, such as the MacArthur Competence Assessment Tool for Treatment (Mac-CAT-T).15 In patients with potentially reversible incapacitating conditions, serial examinations over time, especially re-evaluation when a patient has achieved and maintained sobriety, may be necessary and helpful.
The Table offers a guide to assessing decisional capacity in a patient with an SUD.
Who should conduct the assessment?
Mental health professionals—usually psychiatrists or psychologists—are consulted when there is uncertainty about a patient’s decisional capacity, and when a more thorough mental status examination is warranted to formulate an informed opinion.16 Unfortunately, this typically occurs only if a patient refuses treatment or demands to be discharged before treatment has been completed, or there is a high level of risk to the patient or others after discharge.
In acute settings, when a patient consents to treatment, a psychiatric consultation regarding decisional capacity is rarely requested. While it is often tempting for medical or surgical teams to proceed with an intervention in a cooperative patient who willingly signs a consent form without a formal assessment of his/her decisional capacity, doing so raises challenging ethical and legal questions in the event of an adverse outcome. It is therefore prudent to strongly recommend that medical and surgical colleagues obtain a psychiatric consultation when an individual’s decisional capacity is uncertain, especially when a patient is known to have a psychiatric or neurocognitive disorder, or exhibits evidence of recent mental status changes. In cases of potentially reversible impairment (eg, delirium, psychosis, or acute anxiety), targeted interventions may help restore capacity and allow treatment to proceed.
No jurisdictions mandate that the determination of decisional capacity should be made exclusively by a mental health professional. Any treating health care professional (usually the attending physician) can make a determination of decisional capacity in scenarios where there is no overt evidence the patient has a mental or cognitive disorder and the patient is communicating clear and reasoned choices, or when a patient is profoundly impaired and no meaningful communication can take place.
Continue to: CASE CONTINUED
CASE CONTINUED
The emergency physician requests a psychiatric consultation. You assess Ms. B’s decisional capacity using the Mac-CAT-T along with a standard psychiatric evaluation. Her score of 14 reflects that she is able to understand the risks associated with her opioid use, and although irritated by engaging in such a discussion, is capable of reasoning through the various medical and psychosocial aspects of her addiction, and shows moderate appreciation of the impact of her choices on her future and that of significant others. The psychiatric evaluation fails to elicit any substantial mood, anxiety, or psychotic disorders associated with/or resulting from her addiction, and her cognitive examination is within normal limits. She does not exhibit severe withdrawal and is not delirious on examination. Finally, she did not harbor thoughts of intentional harm to self or others and is not deemed imminently dangerous.
You document that in your opinion, despite Ms. B’s unfortunate choices and questionable judgment, she does have the capacity to make informed decisions regarding her care and could be released against medical advice if she so chooses, while providing her with information about available resources should she decide to seek rehabilitation in the future.
An increasingly common scenario
Decisional capacity assessment in patients with SUDs is an increasingly common reason for psychiatric consultations. Primary and secondary conditions related to substance use can affect a patient’s decisional capacity on a temporary or permanent basis. The same principles that guide the assessment of decisional capacity in patients with other psychiatric or cognitive disorders should be applied to compromised individuals with SUDs. In challenging cases, a skilled psychiatric evaluation that is supported by a thorough cognitive examination and, when required, complemented by a legal or ethical consultation, can help clinicians make safe and judicious decisions.
Bottom Line
Assessing the decisional capacity of a patient with a substance use disorder can be challenging. Primary or secondary conditions related to substance use can affect a patient’s decisional capacity on a temporary or permanent basis. A skilled psychiatric evaluation that includes a thorough cognitive examination and is complemented by legal or ethical consultation can help in making judicious decisions.
Related Resources
- Tan SY. Determining patients’ decisional capacity. Clinical Psychiatry News. https://www.mdedge.com/psychiatry/article/137939/practice-management/determining-patients-decisional-capacity. Published May 10, 2017.
- Sorrentino R. Performing capacity evaluations: What’s expected from your consult. Current Psychiatry. 2014;13(1):41-44.
Drug Brand Names
Alprazolam • Xanax
Naloxone nasal spray • Narcan
Ms. B, age 31, is brought to the emergency department (ED) via ambulance after emergency medical technicians used naloxone nasal spray to revive her following an overdose on heroin. She reports daily IV heroin use for the last 4 years as well as frequent use of other illicit substances, including marijuana and alprazolam, for which she does not have
How can you determine if Ms. B has the capacity to make decisions regarding her care?
Decisional capacity is defined as a patient’s ability to use information about an illness and the proposed treatment options to make a choice that is congruent with one’s own values and preferences.1 Determining whether a patient has adequate capacity to make decisions regarding their care is an inherent aspect of all clinician-patient interactions.
Published reports have focused on the challenges clinicians face when assessing decisional capacity in patients with psychiatric and cognitive disorders. However, there is little evidence about assessing decisional capacity in patients with substance use disorders (SUDs), even though increasing numbers of patients with SUDs are presenting to EDs2 and being admitted as inpatients in general hospitals.3 In this article, I discuss:
- the biologic basis for impaired decision-making in patients with SUDs
- common substance use–related conditions that may impact a patient’s decisional capacity
- the clinical challenges and legal considerations clinicians face when assessing decisional capacity in patients with SUDs
- how to assess decisional capacity in such patients.
Decisional capacity vs competence
“Capacity” and “competence” are not the same. Decisional capacity, which refers to the ability to make decisions, is a clinical construct that is determined by clinicians and is generally used in the acute clinical setting. Because cognition is the main determinant of capacity, conditions or treatments that affect cognition can impair an individual’s decision-making capacity.1 Decisional capacity is not a global concept but a decision-specific one, subject to fluctuations depending on the time and the nature of the decision at hand. Therefore, requests for determination of decisional capacity in the clinical setting should be specific to an individual decision or set of decisions.
In contrast, competence is an enduring legal determination of incapacitation, typically made by a probate judge. It refers to the ability of an individual to perform actions needed to put decisions into effect. Decisional capacity as assessed by a clinician often serves as the basis for petitions submitted for the purpose of competency adjudication by the judicial system.
A biologic basis for impaired decision-making?
Jeste and Saks4 suggested that addiction itself is characterized by impaired decision-making because individuals keep using a substance despite experiencing recurrent physical, psychologic, or social problems caused or worsened by the substance. Several studies suggest there may be a biologic basis for impaired decision-making in these patients, even in the absence of severe psychiatric or cognitive disorders.
Continue to: Bechara and Damasio found...
Bechara and Damasio5 found that the decision-making impairment seen in some patients with SUDs was similar to that observed in patients who have lesions of the ventromedial prefrontal cortex. In both groups of patients, the impaired decision-making was characterized by a preference to opt for high immediate reward despite even higher future losses.
These deficits were also observed by Grant et al.6 In this study, patients with SUDs displayed markedly impaired performance on the Gambling Task, which examines decisions that result in long-term losses that exceed short-term gains. However, patients with SUDs performed similarly to controls on the Wisconsin Card Sorting Test, which evaluates the ability to form abstract concepts and to shift from established response sets.
MacDonald et al7 used a laboratory experiment and 2 field studies to test the hypothesis that alcohol affects attitudes and intentions toward drinking and driving. Their findings support the concept that alcohol intoxication decreases cognitive capacity such that people are more likely to attend to only the most salient cues.7
Whether the impairment documented in such studies is a contributing factor in addiction or is a result of addiction remains uncertain. While individuals with SUDs may have some level of impairment in decision-making in general, particularly in regard to their substance use, their decisional capacity on specific clinical decisions should be assessed carefully. In a study of 300 consecutive psychiatric consultations for decisional capacity at an urban hospital, Boettger et al8 found that 41% were related to SUDs. Of these, 37% were found to have impaired decisional capacity.
Impaired decision-making in patients with SUDs may specifically pertain to choices related to their addiction, including9:
- consent for addiction treatment
- consistency in maintaining a choice of recovery
- changing values regarding treatment over time
- capacity to participate in addiction research involving the use of addictive substances.
Continue to: It is important to recognize...
It is important to recognize that this impairment may not necessarily translate into altered decisional capacity regarding other health care decisions, such as consenting to surgery or other necessary medical interventions.9
Substance-related disorders that affect decisional capacity
Substance-related syndromes can affect mood, reality testing, and/or cognitive function, thereby directly impacting a patient’s decisional capacity. Substance-related syndromes can be divided into 2 categories: 1) disorders resulting from the direct effects of the substance, and 2) secondary disorders resulting from/or associated with substance use.
Disorders resulting from the direct effects of the substance
Temporary/reversible incapacitation
- Acute intoxication or intoxication delirium may be the most frequent type of temporary incapacitation. It can result from toxic levels of licit or illicit substances; alcohol is likely the most frequent offending agent. Although some individuals who are intoxicated may appear to be alert, oriented, and able to engage in lengthy conversations, the majority do not possess adequate decisional capacity.10
- Withdrawal delirium, associated with longstanding alcohol, sedative-hypnotic, or barbiturate dependence, is typically prolonged, but usually resolves, either spontaneously or with treatment. Although most deliria resolve once the underlying etiology is corrected, vulnerable individuals may experience irreversible cognitive impairment and permanent decisional incapacitation.11,12
- Severe substance-induced depressive disorders, especially if accompanied by frank psychotic symptoms or severe depressive distortions of reality, may result in decisional incapacity. Substance abuse treatment that incorporates multiple strategies, sometimes in conjunction with pharmacotherapy to manage depression, should lead to sufficient recovery and restoration of decisional capacity.
- Transient psychotic disorders such as those associated with the use of stimulants are often treatable. Patients may recover decisional capacity spontaneously or with treatment.
Permanent incapacitation
- Dementia is associated with substance use, particularly alcohol use.13 For a patient who develops dementia, no appreciable recovery can be expected, even with prolonged abstinence.
- Persistent amnestic disorders (eg, Korsakoff syndrome) resulting from undiagnosed or untreated severe thiamine deficiency (Wernicke’s encephalopathy). Although an isolated Korsakoff syndrome consists primarily of anterograde amnesia, these patients may experience additional cognitive impairment resulting from years of alcohol consumption or associated with other neurodegenerative processes, and therefore are sufficiently impaired and lack decisional capacity. Even in the absence of such concomitant cognitive deficits, a very severe anterograde amnestic disorder directly impacts a patient’s capacity to perform the necessary tasks required to give informed consent. The inability to consolidate information about new medical developments, treatments, and procedures, even when they are thoroughly explained by the medical team, can pose serious challenges. For example, a patient may protest to being taken to surgery because he/she does not recall signing a consent form the previous day.
- Enduring severe and treatment-refractory psychotic disorders associated with drug use, specifically stimulants, can result in permanent incapacitation similar to that seen in severe primary psychotic disorders (such as treatment-resistant schizophrenia).
- Hepatic encephalopathy may be seen in patients with advanced cirrhosis of the liver (due to hepatitis C resulting from IV drug use, and/or alcohol use). In late stages of cirrhosis, the confusional state patients experience may become severe and may no longer be reversible unless liver transplantation is available and successful. This would therefore constitute a basis for permanent decisional incapacitation.
- Human immunodeficiency virus encephalitis or dementia can result from IV drug use.
Continue to: Clinical challenges
Clinical challenges
In intensive care settings, where a patient with a SUD may be treated for acute life-threatening intoxication or severe withdrawal delirium, an assumption of decisional incapacitation often exists as a result of medical acuity and impaired mentation. In these situations, treatment usually proceeds with consent obtained from next-of-kin, a guardian, or an administrative (hospital) authority when other substitute decision makers are unavailable or unwilling. In such cases, psychiatric consultation can play a dual role in documenting the patient’s decisional capacity and also in contributing to the care of patients with SUDs.
It is critical to perform a cognitive evaluation and mental status examination in a medically compromised patient with an SUD. Unfortunately, serious cognitive disorders can often be concealed by a superficially jovial or verbally skilled patient, or by an uncooperative individual who refuses to engage in a thorough conversation with his/her clinicians. These scenarios present significant challenges and may result in missed opportunities for care or premature discharges. Negative countertransference by clinicians toward patients with SUDs may also promote poor outcomes. For difficult cases, legal and ethical consultations may help mitigate risk and guide management approaches (Box14).
Box
The legal system rarely views patients with substance use disorders (SUDs) as lacking decisional capacity in the absence of overt psychiatric or cognitive deficits. The penal system offers little if any mitigation of liability on account of addiction in civil or criminal cases. On the contrary, intoxication is an aggravating factor in such settings. Despite extensive literature that questions the “free will,” accountability, and responsibility of patients with SUDs, the legal system takes an “all-or-none” approach to this issue. It assumes free choice and accountability for patients with SUDs, except when a clear superimposed psychiatric or cognitive disorder (such as psychosis or dementia) exists. Rarely, some jurisdictions may allow for mental health commitments on account of severe and persistent addictive behaviors that clearly pose a risk to the individual or to society, implicitly recognizing that incapacitation can result from severe addiction. Nevertheless, a finding of imminent or impending dangerousness is generally required for such commitments to be justified.
In other situations, individual health care settings may resort to local hospital policies that allow impaired patients with SUDs with a clearly altered mental status to be detained for the purpose of completing medical treatment. Presumably, discharge would occur when the medical and psychiatric acuity has resolved (often under the umbrella of a “Medical Hold” policy). Jain et al14 suggested that although such commitment laws for patients with SUDs may be appealing to some people, especially family members, specific statutes and their implementation are highly variable; the deprivation of liberty raises ethical concerns; and outcome data are limited. Conversely, most states either do not have such legislation, or rarely enforce it.
How to assess decisional capacity
A direct conclusion of incapacity in an individual cannot be determined solely on the knowledge of the patient having a SUD-related clinical condition. (The possible exception to this may be a patient with severe dementia.)
- understand the decision at hand
- discuss its benefits and risks
- describe alternatives
- demonstrate an appreciation of the implications of treatment or lack thereof
- communicate a clear and consistent choice.
Continue to: While most clinicians...
While most clinicians rely on a psychiatric interview (with or without a cognitive examination) to make these determinations, several instruments have been developed to aid these evaluations, such as the MacArthur Competence Assessment Tool for Treatment (Mac-CAT-T).15 In patients with potentially reversible incapacitating conditions, serial examinations over time, especially re-evaluation when a patient has achieved and maintained sobriety, may be necessary and helpful.
The Table offers a guide to assessing decisional capacity in a patient with an SUD.
Who should conduct the assessment?
Mental health professionals—usually psychiatrists or psychologists—are consulted when there is uncertainty about a patient’s decisional capacity, and when a more thorough mental status examination is warranted to formulate an informed opinion.16 Unfortunately, this typically occurs only if a patient refuses treatment or demands to be discharged before treatment has been completed, or there is a high level of risk to the patient or others after discharge.
In acute settings, when a patient consents to treatment, a psychiatric consultation regarding decisional capacity is rarely requested. While it is often tempting for medical or surgical teams to proceed with an intervention in a cooperative patient who willingly signs a consent form without a formal assessment of his/her decisional capacity, doing so raises challenging ethical and legal questions in the event of an adverse outcome. It is therefore prudent to strongly recommend that medical and surgical colleagues obtain a psychiatric consultation when an individual’s decisional capacity is uncertain, especially when a patient is known to have a psychiatric or neurocognitive disorder, or exhibits evidence of recent mental status changes. In cases of potentially reversible impairment (eg, delirium, psychosis, or acute anxiety), targeted interventions may help restore capacity and allow treatment to proceed.
No jurisdictions mandate that the determination of decisional capacity should be made exclusively by a mental health professional. Any treating health care professional (usually the attending physician) can make a determination of decisional capacity in scenarios where there is no overt evidence the patient has a mental or cognitive disorder and the patient is communicating clear and reasoned choices, or when a patient is profoundly impaired and no meaningful communication can take place.
Continue to: CASE CONTINUED
CASE CONTINUED
The emergency physician requests a psychiatric consultation. You assess Ms. B’s decisional capacity using the Mac-CAT-T along with a standard psychiatric evaluation. Her score of 14 reflects that she is able to understand the risks associated with her opioid use, and although irritated by engaging in such a discussion, is capable of reasoning through the various medical and psychosocial aspects of her addiction, and shows moderate appreciation of the impact of her choices on her future and that of significant others. The psychiatric evaluation fails to elicit any substantial mood, anxiety, or psychotic disorders associated with/or resulting from her addiction, and her cognitive examination is within normal limits. She does not exhibit severe withdrawal and is not delirious on examination. Finally, she did not harbor thoughts of intentional harm to self or others and is not deemed imminently dangerous.
You document that in your opinion, despite Ms. B’s unfortunate choices and questionable judgment, she does have the capacity to make informed decisions regarding her care and could be released against medical advice if she so chooses, while providing her with information about available resources should she decide to seek rehabilitation in the future.
An increasingly common scenario
Decisional capacity assessment in patients with SUDs is an increasingly common reason for psychiatric consultations. Primary and secondary conditions related to substance use can affect a patient’s decisional capacity on a temporary or permanent basis. The same principles that guide the assessment of decisional capacity in patients with other psychiatric or cognitive disorders should be applied to compromised individuals with SUDs. In challenging cases, a skilled psychiatric evaluation that is supported by a thorough cognitive examination and, when required, complemented by a legal or ethical consultation, can help clinicians make safe and judicious decisions.
Bottom Line
Assessing the decisional capacity of a patient with a substance use disorder can be challenging. Primary or secondary conditions related to substance use can affect a patient’s decisional capacity on a temporary or permanent basis. A skilled psychiatric evaluation that includes a thorough cognitive examination and is complemented by legal or ethical consultation can help in making judicious decisions.
Related Resources
- Tan SY. Determining patients’ decisional capacity. Clinical Psychiatry News. https://www.mdedge.com/psychiatry/article/137939/practice-management/determining-patients-decisional-capacity. Published May 10, 2017.
- Sorrentino R. Performing capacity evaluations: What’s expected from your consult. Current Psychiatry. 2014;13(1):41-44.
Drug Brand Names
Alprazolam • Xanax
Naloxone nasal spray • Narcan
1. Karlawish K. Assessment of decision-making capacity in adults. UpToDate. https://www.uptodate.com/contents/assessment-of-decision-making-capacity-in-adults. Updated July 2019. Accessed August 19, 2019.
2. Owens PL, Mutter R, Stocks C. Mental health and substance abuse-related emergency department visits among adults, 2007. HCUP Statistical Brief #92. https://www.ncbi.nlm.nih.gov/books/NBK52659/pdf/Bookshelf_NBK52659.pdf. Published July 2010. Accessed August 19, 2019.
3. Smothers BA, Yahr HT. Alcohol use disorder and illicit drug use in admissions to general hospitals in the United States. Am J Addict. 2005;14(3):256-267.
4. Jeste DV, Saks E. Decisional capacity in mental illness and substance use disorders: empirical database and policy implications. Behav Sci Law. 2006;24(4):607-628.
5. Bechara A, Damasio H. Decision-making and addiction (part I): impaired activation of somatic states in substance dependent individuals when pondering decisions with negative future consequences. Neuropsychologia. 2002;40(10):1675-1689.
6. Grant S, Contoreggi C, London ED. Drug abusers show impaired performance in a laboratory test of decision making. Neuropsychologia. 2000;38(8):1180-1187.
7. MacDonald TK, Zanna MP, Fong GT. Decision making in altered states: effects of alcohol on attitudes toward drinking and driving. J Pers Soc Psychol. 1995;68(6):973-985.
8. Boettger S, Bergman M, Jenewein J, et al. Assessment of decisional capacity: prevalence of medical illness and psychiatric comorbidities. Palliat Support Care. 2015;13(5):1275-1281.
9. Charland LC. Chapter 6: Decision-making capacity and responsibility in addiction. In: Poland J, Graham G. Addiction and responsibility. Cambridge, MA: MIT Press Scholarship Online; 2011:139-158.
10. Martel ML, Klein LR, Miner JR, et al. A brief assessment of capacity to consent instrument in acutely intoxicated emergency department patients. Am J Emerg Med. 2018;36(1):18-23.
11. MacLullich AM, Beaglehole A, Hall RJ, et al. Delirium and long-term cognitive impairment. Int Rev Psychiatry. 2009;21(1):30-42.
12. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306-1316.
13. Rehm J, Hasan OSM, Black SE, et al. Alcohol use and dementia: a systematic scoping review. Alzheimers Res Ther. 2019;11(1):1.
14. Jain A, Christopher P, Appelbaum PS. Civil commitment for opioid and other substance use disorders: does it work? Psychiatr Serv. 2018;69(4):374-376.
15. Grisso T, Appelbaum PS. Chapter 6: Using the MacArthur competence assessment tool – treatment. In: Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. New York, NY: Oxford University Press; 1998:101-126.
16. Hazelton LD, Sterns GL, Chisholm T. Decision-making capacity and alcohol abuse: clinical and ethical considerations in personal care choices. Gen Hosp Psychiatry. 2003;25(2):130-135.
1. Karlawish K. Assessment of decision-making capacity in adults. UpToDate. https://www.uptodate.com/contents/assessment-of-decision-making-capacity-in-adults. Updated July 2019. Accessed August 19, 2019.
2. Owens PL, Mutter R, Stocks C. Mental health and substance abuse-related emergency department visits among adults, 2007. HCUP Statistical Brief #92. https://www.ncbi.nlm.nih.gov/books/NBK52659/pdf/Bookshelf_NBK52659.pdf. Published July 2010. Accessed August 19, 2019.
3. Smothers BA, Yahr HT. Alcohol use disorder and illicit drug use in admissions to general hospitals in the United States. Am J Addict. 2005;14(3):256-267.
4. Jeste DV, Saks E. Decisional capacity in mental illness and substance use disorders: empirical database and policy implications. Behav Sci Law. 2006;24(4):607-628.
5. Bechara A, Damasio H. Decision-making and addiction (part I): impaired activation of somatic states in substance dependent individuals when pondering decisions with negative future consequences. Neuropsychologia. 2002;40(10):1675-1689.
6. Grant S, Contoreggi C, London ED. Drug abusers show impaired performance in a laboratory test of decision making. Neuropsychologia. 2000;38(8):1180-1187.
7. MacDonald TK, Zanna MP, Fong GT. Decision making in altered states: effects of alcohol on attitudes toward drinking and driving. J Pers Soc Psychol. 1995;68(6):973-985.
8. Boettger S, Bergman M, Jenewein J, et al. Assessment of decisional capacity: prevalence of medical illness and psychiatric comorbidities. Palliat Support Care. 2015;13(5):1275-1281.
9. Charland LC. Chapter 6: Decision-making capacity and responsibility in addiction. In: Poland J, Graham G. Addiction and responsibility. Cambridge, MA: MIT Press Scholarship Online; 2011:139-158.
10. Martel ML, Klein LR, Miner JR, et al. A brief assessment of capacity to consent instrument in acutely intoxicated emergency department patients. Am J Emerg Med. 2018;36(1):18-23.
11. MacLullich AM, Beaglehole A, Hall RJ, et al. Delirium and long-term cognitive impairment. Int Rev Psychiatry. 2009;21(1):30-42.
12. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306-1316.
13. Rehm J, Hasan OSM, Black SE, et al. Alcohol use and dementia: a systematic scoping review. Alzheimers Res Ther. 2019;11(1):1.
14. Jain A, Christopher P, Appelbaum PS. Civil commitment for opioid and other substance use disorders: does it work? Psychiatr Serv. 2018;69(4):374-376.
15. Grisso T, Appelbaum PS. Chapter 6: Using the MacArthur competence assessment tool – treatment. In: Grisso T, Appelbaum PS. Assessing competence to consent to treatment: a guide for physicians and other health professionals. New York, NY: Oxford University Press; 1998:101-126.
16. Hazelton LD, Sterns GL, Chisholm T. Decision-making capacity and alcohol abuse: clinical and ethical considerations in personal care choices. Gen Hosp Psychiatry. 2003;25(2):130-135.

The challenges of caring for a physician with a mental illness
A physician’s mental health is important for the delivery of quality health care to his/her patients. Early identification and treatment of physicians with mental illnesses is challenging because physicians may neglect their own mental health due to the associated stigma, time constraints, or uncertainty regarding where to seek help. Physicians often worry about whom to confide in and harbor a fear that others will doubt his/her competence after recovery.1 Physicians have higher rates of suicide than the general population.2 According to data from the National Violent Death Reporting System, a diagnosed mental illness or a job problem significantly contribute to suicide among physicians.3 Additionally, physicians also have high rates of substance use and affective disorders.1,4
Here, we present the case of a physician we treated on an inpatient psychiatry unit who stirred profound emotions in us as trainees, and discuss how we managed this complicated scenario.
CASE REPORT
Dr. P, a 35-year-old male endocrinologist, was admitted to our inpatient psychiatry unit with a diagnosis of bipolar disorder, manic, severe, with psychotic features. Earlier that day, Dr. P had walked out of his private outpatient practice where he still had several appointments. After he had been missing for several hours, he was picked up by the police. Dr. P had 2 prior psychiatric admissions; the last one had occurred >10 years ago. A few weeks before this admission, he stopped taking lithium, while continuing escitalopram. He had not been keeping his appointments with his outpatient psychiatrist.
At admission, Dr. P had pressured speech, grandiose delusions, an expansive affect, and aggressive behavior. He was responding to internal stimuli with no insight into his illness. He was evasive when asked about hallucinations. Dr. P believed he was superior in intelligence and physical prowess to everyone in the emergency department (ED), and for that reason, the ED staff was persecuting him. His urine toxicology was negative.
On the inpatient unit, because Dr. P exhibited posturing, mutism, and negativism, catatonia associated with bipolar disorder was added to his diagnosis. For the first 2 days, his catatonia was managed with oral lorazepam, 2 mg twice daily. Dr. P was also observed giving medical advice to other patients on the unit, and was told to stop. Throughout his hospitalization, he dictated his own treatment and would frequently debate with his treatment team on the pharmacologic basis for treatment decisions, asserting his expertise as a physician and claiming to have a general clinical knowledge of the acute management of bipolar disorder.
Dr. P was eventually stabilized on oral lithium, 450 mg twice daily, and aripiprazole, 10 mg/d. He also received oral clonazepam, as needed for acute agitation, which was eventually tapered and discontinued. He gradually responded to treatment, and demonstrated improved insight. The treatment team met with Dr. P’s parents, who also were physicians, to discuss treatment goals, management considerations, and an aftercare plan. After spending 8 days in the hospital, Dr. P was discharged home to the care of his immediate family, and instructed to follow up with his outpatient psychiatrist. We do not know if he resumed clinical duties.
Managing an extremely knowledgeable patient
During his hospitalization, Dr. P frequently challenged our clinical knowledge; he would repeatedly remind us that he was a physician and that we were still trainees, which caused us to second-guess ourselves. Eventually, the attending physician on our team was able to impress upon Dr. P the clearly established roles of the treatment team and the patient. It was also important to maintain open communication channels with Dr. P and his family, and to address his anxiety by discussing the treatment plan in detail.5
Continue to: Although his queries on medication...
Although his queries on medication pharmacodynamics and pharmacokinetics were daunting, we empathized with him, recognizing that his knowledge invariably contributed to his anxiety. We engaged with Dr. P and his parents and elaborated on the rationale behind treatment decisions. This earned his trust and tremendously facilitated his recovery.
We were also cautious about using benzodiazepines to treat Dr. P’s catatonia because we were concerned that his knowledge could aid him in feigning symptoms to obtain these medications. Physicians have a high rate of prescription medication abuse, mainly opiates and benzodiazepines.2 The abuse of prescription medications by physicians is related to several psychological and psychiatric factors, including anxiety, depression, stress at work, personality problems, loss of loved ones, and pain. While treating physician patients, treatment decisions that include the use of opiates and benzodiazepines should be carefully considered.
A complicated scenario
Managing a physician patient can be a rewarding experience; however, there are several factors that can impact the experience, including:
- The treating physicians’ anxiety and countertransference/transference dynamics. We repeatedly imagined ourselves in Dr. P’s position and thought long and hard about how this scenario could happen to anyone in the medical profession; these thoughts induced significant anxiety in each of us. Further, interacting with Dr. P was reminiscent of our training under senior residents and attendings. Dr. P viewed us—his treatment team—as his trainees and challenged our clinical knowledge and actions.
- The physician-patient’s emotional responses, which may include anxiety, despair, denial, and an inability to accept role reversal.
Our medical culture needs a paradigm shift. We need a model designed to encourage early self-disclosure and treatment-seeking among physicians with mental illness. This will reduce the stigma towards mental illness in our profession.
1. Bianchi EF, Bhattacharyya MR, Meakin R. Exploring senior doctors’ beliefs and attitudes regarding mental illness within the medical profession: a qualitative study. BMJ Open. 2016;6(9):e012598. doi: 10.1136/bmjopen-2016 012598.
2. Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302.
3. Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. Gen Hosp Psychiatry. 2013;35(1):45-49.
4. Schneck SA. “Doctoring” doctors and their families. JAMA. 1998;280(23):2039-2042.
5. Marshall EJ. Doctors’ health and fitness to practise: treating addicted doctors. Occup Med (Lond). 2008;58(5):334-340.
A physician’s mental health is important for the delivery of quality health care to his/her patients. Early identification and treatment of physicians with mental illnesses is challenging because physicians may neglect their own mental health due to the associated stigma, time constraints, or uncertainty regarding where to seek help. Physicians often worry about whom to confide in and harbor a fear that others will doubt his/her competence after recovery.1 Physicians have higher rates of suicide than the general population.2 According to data from the National Violent Death Reporting System, a diagnosed mental illness or a job problem significantly contribute to suicide among physicians.3 Additionally, physicians also have high rates of substance use and affective disorders.1,4
Here, we present the case of a physician we treated on an inpatient psychiatry unit who stirred profound emotions in us as trainees, and discuss how we managed this complicated scenario.
CASE REPORT
Dr. P, a 35-year-old male endocrinologist, was admitted to our inpatient psychiatry unit with a diagnosis of bipolar disorder, manic, severe, with psychotic features. Earlier that day, Dr. P had walked out of his private outpatient practice where he still had several appointments. After he had been missing for several hours, he was picked up by the police. Dr. P had 2 prior psychiatric admissions; the last one had occurred >10 years ago. A few weeks before this admission, he stopped taking lithium, while continuing escitalopram. He had not been keeping his appointments with his outpatient psychiatrist.
At admission, Dr. P had pressured speech, grandiose delusions, an expansive affect, and aggressive behavior. He was responding to internal stimuli with no insight into his illness. He was evasive when asked about hallucinations. Dr. P believed he was superior in intelligence and physical prowess to everyone in the emergency department (ED), and for that reason, the ED staff was persecuting him. His urine toxicology was negative.
On the inpatient unit, because Dr. P exhibited posturing, mutism, and negativism, catatonia associated with bipolar disorder was added to his diagnosis. For the first 2 days, his catatonia was managed with oral lorazepam, 2 mg twice daily. Dr. P was also observed giving medical advice to other patients on the unit, and was told to stop. Throughout his hospitalization, he dictated his own treatment and would frequently debate with his treatment team on the pharmacologic basis for treatment decisions, asserting his expertise as a physician and claiming to have a general clinical knowledge of the acute management of bipolar disorder.
Dr. P was eventually stabilized on oral lithium, 450 mg twice daily, and aripiprazole, 10 mg/d. He also received oral clonazepam, as needed for acute agitation, which was eventually tapered and discontinued. He gradually responded to treatment, and demonstrated improved insight. The treatment team met with Dr. P’s parents, who also were physicians, to discuss treatment goals, management considerations, and an aftercare plan. After spending 8 days in the hospital, Dr. P was discharged home to the care of his immediate family, and instructed to follow up with his outpatient psychiatrist. We do not know if he resumed clinical duties.
Managing an extremely knowledgeable patient
During his hospitalization, Dr. P frequently challenged our clinical knowledge; he would repeatedly remind us that he was a physician and that we were still trainees, which caused us to second-guess ourselves. Eventually, the attending physician on our team was able to impress upon Dr. P the clearly established roles of the treatment team and the patient. It was also important to maintain open communication channels with Dr. P and his family, and to address his anxiety by discussing the treatment plan in detail.5
Continue to: Although his queries on medication...
Although his queries on medication pharmacodynamics and pharmacokinetics were daunting, we empathized with him, recognizing that his knowledge invariably contributed to his anxiety. We engaged with Dr. P and his parents and elaborated on the rationale behind treatment decisions. This earned his trust and tremendously facilitated his recovery.
We were also cautious about using benzodiazepines to treat Dr. P’s catatonia because we were concerned that his knowledge could aid him in feigning symptoms to obtain these medications. Physicians have a high rate of prescription medication abuse, mainly opiates and benzodiazepines.2 The abuse of prescription medications by physicians is related to several psychological and psychiatric factors, including anxiety, depression, stress at work, personality problems, loss of loved ones, and pain. While treating physician patients, treatment decisions that include the use of opiates and benzodiazepines should be carefully considered.
A complicated scenario
Managing a physician patient can be a rewarding experience; however, there are several factors that can impact the experience, including:
- The treating physicians’ anxiety and countertransference/transference dynamics. We repeatedly imagined ourselves in Dr. P’s position and thought long and hard about how this scenario could happen to anyone in the medical profession; these thoughts induced significant anxiety in each of us. Further, interacting with Dr. P was reminiscent of our training under senior residents and attendings. Dr. P viewed us—his treatment team—as his trainees and challenged our clinical knowledge and actions.
- The physician-patient’s emotional responses, which may include anxiety, despair, denial, and an inability to accept role reversal.
Our medical culture needs a paradigm shift. We need a model designed to encourage early self-disclosure and treatment-seeking among physicians with mental illness. This will reduce the stigma towards mental illness in our profession.
A physician’s mental health is important for the delivery of quality health care to his/her patients. Early identification and treatment of physicians with mental illnesses is challenging because physicians may neglect their own mental health due to the associated stigma, time constraints, or uncertainty regarding where to seek help. Physicians often worry about whom to confide in and harbor a fear that others will doubt his/her competence after recovery.1 Physicians have higher rates of suicide than the general population.2 According to data from the National Violent Death Reporting System, a diagnosed mental illness or a job problem significantly contribute to suicide among physicians.3 Additionally, physicians also have high rates of substance use and affective disorders.1,4
Here, we present the case of a physician we treated on an inpatient psychiatry unit who stirred profound emotions in us as trainees, and discuss how we managed this complicated scenario.
CASE REPORT
Dr. P, a 35-year-old male endocrinologist, was admitted to our inpatient psychiatry unit with a diagnosis of bipolar disorder, manic, severe, with psychotic features. Earlier that day, Dr. P had walked out of his private outpatient practice where he still had several appointments. After he had been missing for several hours, he was picked up by the police. Dr. P had 2 prior psychiatric admissions; the last one had occurred >10 years ago. A few weeks before this admission, he stopped taking lithium, while continuing escitalopram. He had not been keeping his appointments with his outpatient psychiatrist.
At admission, Dr. P had pressured speech, grandiose delusions, an expansive affect, and aggressive behavior. He was responding to internal stimuli with no insight into his illness. He was evasive when asked about hallucinations. Dr. P believed he was superior in intelligence and physical prowess to everyone in the emergency department (ED), and for that reason, the ED staff was persecuting him. His urine toxicology was negative.
On the inpatient unit, because Dr. P exhibited posturing, mutism, and negativism, catatonia associated with bipolar disorder was added to his diagnosis. For the first 2 days, his catatonia was managed with oral lorazepam, 2 mg twice daily. Dr. P was also observed giving medical advice to other patients on the unit, and was told to stop. Throughout his hospitalization, he dictated his own treatment and would frequently debate with his treatment team on the pharmacologic basis for treatment decisions, asserting his expertise as a physician and claiming to have a general clinical knowledge of the acute management of bipolar disorder.
Dr. P was eventually stabilized on oral lithium, 450 mg twice daily, and aripiprazole, 10 mg/d. He also received oral clonazepam, as needed for acute agitation, which was eventually tapered and discontinued. He gradually responded to treatment, and demonstrated improved insight. The treatment team met with Dr. P’s parents, who also were physicians, to discuss treatment goals, management considerations, and an aftercare plan. After spending 8 days in the hospital, Dr. P was discharged home to the care of his immediate family, and instructed to follow up with his outpatient psychiatrist. We do not know if he resumed clinical duties.
Managing an extremely knowledgeable patient
During his hospitalization, Dr. P frequently challenged our clinical knowledge; he would repeatedly remind us that he was a physician and that we were still trainees, which caused us to second-guess ourselves. Eventually, the attending physician on our team was able to impress upon Dr. P the clearly established roles of the treatment team and the patient. It was also important to maintain open communication channels with Dr. P and his family, and to address his anxiety by discussing the treatment plan in detail.5
Continue to: Although his queries on medication...
Although his queries on medication pharmacodynamics and pharmacokinetics were daunting, we empathized with him, recognizing that his knowledge invariably contributed to his anxiety. We engaged with Dr. P and his parents and elaborated on the rationale behind treatment decisions. This earned his trust and tremendously facilitated his recovery.
We were also cautious about using benzodiazepines to treat Dr. P’s catatonia because we were concerned that his knowledge could aid him in feigning symptoms to obtain these medications. Physicians have a high rate of prescription medication abuse, mainly opiates and benzodiazepines.2 The abuse of prescription medications by physicians is related to several psychological and psychiatric factors, including anxiety, depression, stress at work, personality problems, loss of loved ones, and pain. While treating physician patients, treatment decisions that include the use of opiates and benzodiazepines should be carefully considered.
A complicated scenario
Managing a physician patient can be a rewarding experience; however, there are several factors that can impact the experience, including:
- The treating physicians’ anxiety and countertransference/transference dynamics. We repeatedly imagined ourselves in Dr. P’s position and thought long and hard about how this scenario could happen to anyone in the medical profession; these thoughts induced significant anxiety in each of us. Further, interacting with Dr. P was reminiscent of our training under senior residents and attendings. Dr. P viewed us—his treatment team—as his trainees and challenged our clinical knowledge and actions.
- The physician-patient’s emotional responses, which may include anxiety, despair, denial, and an inability to accept role reversal.
Our medical culture needs a paradigm shift. We need a model designed to encourage early self-disclosure and treatment-seeking among physicians with mental illness. This will reduce the stigma towards mental illness in our profession.
1. Bianchi EF, Bhattacharyya MR, Meakin R. Exploring senior doctors’ beliefs and attitudes regarding mental illness within the medical profession: a qualitative study. BMJ Open. 2016;6(9):e012598. doi: 10.1136/bmjopen-2016 012598.
2. Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302.
3. Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. Gen Hosp Psychiatry. 2013;35(1):45-49.
4. Schneck SA. “Doctoring” doctors and their families. JAMA. 1998;280(23):2039-2042.
5. Marshall EJ. Doctors’ health and fitness to practise: treating addicted doctors. Occup Med (Lond). 2008;58(5):334-340.
1. Bianchi EF, Bhattacharyya MR, Meakin R. Exploring senior doctors’ beliefs and attitudes regarding mental illness within the medical profession: a qualitative study. BMJ Open. 2016;6(9):e012598. doi: 10.1136/bmjopen-2016 012598.
2. Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161(12):2295-2302.
3. Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. Gen Hosp Psychiatry. 2013;35(1):45-49.
4. Schneck SA. “Doctoring” doctors and their families. JAMA. 1998;280(23):2039-2042.
5. Marshall EJ. Doctors’ health and fitness to practise: treating addicted doctors. Occup Med (Lond). 2008;58(5):334-340.
