User login
Glucocorticoids linked to damage accrual in SLE regardless of disease activity
, according to recent findings published in The Lancet Rheumatology.
“Disentangling the potential contribution of glucocorticoid use to organ damage in SLE is confounded, in most studies, by the fact that glucocorticoid use is usually associated with active disease. Our study showed that organ damage accrual occurred in a similar proportion of patients without disease activity as in the overall cohort, and that glucocorticoid use was a significant risk factor for damage,” wrote Diane Apostolopoulos, MBBS, of Monash University, Melbourne, and colleagues.
The longitudinal cohort study prospectively enrolled 1,707 patients with SLE from May 2013 to December 2016. Study participants were recruited from 13 institutions throughout Australia and Asia. The researchers defined glucocorticoid use as any exposure and cumulative exposure to prednisolone, in addition to mean time-adjusted daily prednisolone dose. Follow-up assessment occurred at least once every 6 months and varied depending on clinical necessity. At baseline, the researchers collected various demographic information, including smoking status, age, and education level, among others. The primary endpoint measured was organ damage accrual, which was assessed at baseline and annually thereafter. In addition, disease activity was evaluated in two multivariable models using Physician Global Assessment (PGA) and Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) scores.
After a median duration of 2.2 years, the researchers found that 82.3% of patients were exposed to prednisolone, and 14.9% of patients had experienced a damage accrual event. In the PGA model, mean time-adjusted PGA score (based on a 0- to 1-unit increase) was associated with damage accrual independent of clinical or serologic disease activity (hazard ratio, 1.05; P = .0012).
In the SLEDAI-2K model, baseline damage scores were independently associated with damage accrual (hazard ratio, 1.32; P = .0427).
In both models, ethnicity (Asian vs. non-Asian), age at study enrollment, and mean time-adjusted prednisolone dose were parameters independently associated with damage accrual.
“Novel findings from this study were that Asian ethnicity was protective when compared with any non-Asian ethnicity, and that antimalarial usage was not protective for damage accrual,” the researchers wrote.
Despite the novel results, the researchers acknowledged that the protective effects of antimalarials could have gone undetected because of the short duration of follow-up.
In a related editorial, Guillermo Ruiz-Irastorza, MD, PhD, of University of the Basque Country in Bizkaia, Spain, said that the study provides novel data highlighting that glucocorticoid use has the potential to negatively affect the clinical progression of patients with SLE (Lancet Rheumatol. 2019 Nov 25. doi: 10.1016/S2665-9913(19)30132-8).
One question that remains from the current study is how to effectively reduce glucocorticoid-related adverse events, while still managing the disease, he further explained.
“These findings suggest that unnecessary use of glucocorticoids should be avoided in the management of the disease where possible,” the investigators concluded.
The study was funded by UCB Pharma, GlaxoSmithKline, Janssen, Bristol-Myers Squibb, and AstraZeneca. The authors reported financial affiliations with Abbott, AbbVie, Astellas, Ayumi Pharmaceutical, Bristol-Myers Squibb, Novartis, Pfizer, and several others.
SOURCE: Apostolopoulos D et al. Lancet Rheumatol. 2019 Nov 25. doi: 10.1016/S2665-9913(19)30105-5.
, according to recent findings published in The Lancet Rheumatology.
“Disentangling the potential contribution of glucocorticoid use to organ damage in SLE is confounded, in most studies, by the fact that glucocorticoid use is usually associated with active disease. Our study showed that organ damage accrual occurred in a similar proportion of patients without disease activity as in the overall cohort, and that glucocorticoid use was a significant risk factor for damage,” wrote Diane Apostolopoulos, MBBS, of Monash University, Melbourne, and colleagues.
The longitudinal cohort study prospectively enrolled 1,707 patients with SLE from May 2013 to December 2016. Study participants were recruited from 13 institutions throughout Australia and Asia. The researchers defined glucocorticoid use as any exposure and cumulative exposure to prednisolone, in addition to mean time-adjusted daily prednisolone dose. Follow-up assessment occurred at least once every 6 months and varied depending on clinical necessity. At baseline, the researchers collected various demographic information, including smoking status, age, and education level, among others. The primary endpoint measured was organ damage accrual, which was assessed at baseline and annually thereafter. In addition, disease activity was evaluated in two multivariable models using Physician Global Assessment (PGA) and Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) scores.
After a median duration of 2.2 years, the researchers found that 82.3% of patients were exposed to prednisolone, and 14.9% of patients had experienced a damage accrual event. In the PGA model, mean time-adjusted PGA score (based on a 0- to 1-unit increase) was associated with damage accrual independent of clinical or serologic disease activity (hazard ratio, 1.05; P = .0012).
In the SLEDAI-2K model, baseline damage scores were independently associated with damage accrual (hazard ratio, 1.32; P = .0427).
In both models, ethnicity (Asian vs. non-Asian), age at study enrollment, and mean time-adjusted prednisolone dose were parameters independently associated with damage accrual.
“Novel findings from this study were that Asian ethnicity was protective when compared with any non-Asian ethnicity, and that antimalarial usage was not protective for damage accrual,” the researchers wrote.
Despite the novel results, the researchers acknowledged that the protective effects of antimalarials could have gone undetected because of the short duration of follow-up.
In a related editorial, Guillermo Ruiz-Irastorza, MD, PhD, of University of the Basque Country in Bizkaia, Spain, said that the study provides novel data highlighting that glucocorticoid use has the potential to negatively affect the clinical progression of patients with SLE (Lancet Rheumatol. 2019 Nov 25. doi: 10.1016/S2665-9913(19)30132-8).
One question that remains from the current study is how to effectively reduce glucocorticoid-related adverse events, while still managing the disease, he further explained.
“These findings suggest that unnecessary use of glucocorticoids should be avoided in the management of the disease where possible,” the investigators concluded.
The study was funded by UCB Pharma, GlaxoSmithKline, Janssen, Bristol-Myers Squibb, and AstraZeneca. The authors reported financial affiliations with Abbott, AbbVie, Astellas, Ayumi Pharmaceutical, Bristol-Myers Squibb, Novartis, Pfizer, and several others.
SOURCE: Apostolopoulos D et al. Lancet Rheumatol. 2019 Nov 25. doi: 10.1016/S2665-9913(19)30105-5.
, according to recent findings published in The Lancet Rheumatology.
“Disentangling the potential contribution of glucocorticoid use to organ damage in SLE is confounded, in most studies, by the fact that glucocorticoid use is usually associated with active disease. Our study showed that organ damage accrual occurred in a similar proportion of patients without disease activity as in the overall cohort, and that glucocorticoid use was a significant risk factor for damage,” wrote Diane Apostolopoulos, MBBS, of Monash University, Melbourne, and colleagues.
The longitudinal cohort study prospectively enrolled 1,707 patients with SLE from May 2013 to December 2016. Study participants were recruited from 13 institutions throughout Australia and Asia. The researchers defined glucocorticoid use as any exposure and cumulative exposure to prednisolone, in addition to mean time-adjusted daily prednisolone dose. Follow-up assessment occurred at least once every 6 months and varied depending on clinical necessity. At baseline, the researchers collected various demographic information, including smoking status, age, and education level, among others. The primary endpoint measured was organ damage accrual, which was assessed at baseline and annually thereafter. In addition, disease activity was evaluated in two multivariable models using Physician Global Assessment (PGA) and Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) scores.
After a median duration of 2.2 years, the researchers found that 82.3% of patients were exposed to prednisolone, and 14.9% of patients had experienced a damage accrual event. In the PGA model, mean time-adjusted PGA score (based on a 0- to 1-unit increase) was associated with damage accrual independent of clinical or serologic disease activity (hazard ratio, 1.05; P = .0012).
In the SLEDAI-2K model, baseline damage scores were independently associated with damage accrual (hazard ratio, 1.32; P = .0427).
In both models, ethnicity (Asian vs. non-Asian), age at study enrollment, and mean time-adjusted prednisolone dose were parameters independently associated with damage accrual.
“Novel findings from this study were that Asian ethnicity was protective when compared with any non-Asian ethnicity, and that antimalarial usage was not protective for damage accrual,” the researchers wrote.
Despite the novel results, the researchers acknowledged that the protective effects of antimalarials could have gone undetected because of the short duration of follow-up.
In a related editorial, Guillermo Ruiz-Irastorza, MD, PhD, of University of the Basque Country in Bizkaia, Spain, said that the study provides novel data highlighting that glucocorticoid use has the potential to negatively affect the clinical progression of patients with SLE (Lancet Rheumatol. 2019 Nov 25. doi: 10.1016/S2665-9913(19)30132-8).
One question that remains from the current study is how to effectively reduce glucocorticoid-related adverse events, while still managing the disease, he further explained.
“These findings suggest that unnecessary use of glucocorticoids should be avoided in the management of the disease where possible,” the investigators concluded.
The study was funded by UCB Pharma, GlaxoSmithKline, Janssen, Bristol-Myers Squibb, and AstraZeneca. The authors reported financial affiliations with Abbott, AbbVie, Astellas, Ayumi Pharmaceutical, Bristol-Myers Squibb, Novartis, Pfizer, and several others.
SOURCE: Apostolopoulos D et al. Lancet Rheumatol. 2019 Nov 25. doi: 10.1016/S2665-9913(19)30105-5.
FROM THE LANCET RHEUMATOLOGY
OnabotA Treatment Cycles Too Short for Migraine
Key clinical point: The 12-week injection cycle of Onabotulinumtoxin A (OnabotA) may need to be reconsidered.
Major finding: The study of 98 patients and 471 treatment cycles found that 43 patients experienced one or more wearing-off-effect (WOE) events (worsening headaches and neck pain). Of those patients, 24 reported 1 WOE event and 19 patients reported 2 or more WOEs. Almost 32% of patients used abortive therapy to manage their WOEs.
Study details: This was a retrospective review of patients with worsening headache variables and neck pain who received OnabotA for their chronic migraine in treatment cycles.
Disclosures: Dr. Khan received honorarium for Depomed, Inc. and Promius Pharma while conducting the study.
Citation: Khan FA, et al. Headache. 2019 Nov 22. doi: 10.1111/head.13713. [Epub ahead of print].
Key clinical point: The 12-week injection cycle of Onabotulinumtoxin A (OnabotA) may need to be reconsidered.
Major finding: The study of 98 patients and 471 treatment cycles found that 43 patients experienced one or more wearing-off-effect (WOE) events (worsening headaches and neck pain). Of those patients, 24 reported 1 WOE event and 19 patients reported 2 or more WOEs. Almost 32% of patients used abortive therapy to manage their WOEs.
Study details: This was a retrospective review of patients with worsening headache variables and neck pain who received OnabotA for their chronic migraine in treatment cycles.
Disclosures: Dr. Khan received honorarium for Depomed, Inc. and Promius Pharma while conducting the study.
Citation: Khan FA, et al. Headache. 2019 Nov 22. doi: 10.1111/head.13713. [Epub ahead of print].
Key clinical point: The 12-week injection cycle of Onabotulinumtoxin A (OnabotA) may need to be reconsidered.
Major finding: The study of 98 patients and 471 treatment cycles found that 43 patients experienced one or more wearing-off-effect (WOE) events (worsening headaches and neck pain). Of those patients, 24 reported 1 WOE event and 19 patients reported 2 or more WOEs. Almost 32% of patients used abortive therapy to manage their WOEs.
Study details: This was a retrospective review of patients with worsening headache variables and neck pain who received OnabotA for their chronic migraine in treatment cycles.
Disclosures: Dr. Khan received honorarium for Depomed, Inc. and Promius Pharma while conducting the study.
Citation: Khan FA, et al. Headache. 2019 Nov 22. doi: 10.1111/head.13713. [Epub ahead of print].
OnabotA Found to Decrease Migraine Days
Key clinical point: Onabotulinumtoxin A (OnabotA) may decrease migraine days by 50% or more.
Major finding: Of 112 patients with chronic migraine (100 female), 96 responded positively to OnabotA, resulting in decreased migraine days by at least 50%. Having a dependent personality trait was linked to treatment nonresponse.
Study details: This was a case-control observational study of chronic migraine patients that received two or more treatment cycles of OnabotA.
Disclosures: None.
Citation: Gonzalez-Martinez A, et al. Headache. 2019 Nov 6. doi: 10.1111/head.13693. [Epub ahead of print].
Key clinical point: Onabotulinumtoxin A (OnabotA) may decrease migraine days by 50% or more.
Major finding: Of 112 patients with chronic migraine (100 female), 96 responded positively to OnabotA, resulting in decreased migraine days by at least 50%. Having a dependent personality trait was linked to treatment nonresponse.
Study details: This was a case-control observational study of chronic migraine patients that received two or more treatment cycles of OnabotA.
Disclosures: None.
Citation: Gonzalez-Martinez A, et al. Headache. 2019 Nov 6. doi: 10.1111/head.13693. [Epub ahead of print].
Key clinical point: Onabotulinumtoxin A (OnabotA) may decrease migraine days by 50% or more.
Major finding: Of 112 patients with chronic migraine (100 female), 96 responded positively to OnabotA, resulting in decreased migraine days by at least 50%. Having a dependent personality trait was linked to treatment nonresponse.
Study details: This was a case-control observational study of chronic migraine patients that received two or more treatment cycles of OnabotA.
Disclosures: None.
Citation: Gonzalez-Martinez A, et al. Headache. 2019 Nov 6. doi: 10.1111/head.13693. [Epub ahead of print].
Vitamin D May Decrease Migraine Severity
Key clinical point: Vitamin D supplementation may decrease the frequency, severity, and duration of migraines.
Major finding: Significantly lower 25 (OH)-vitamin D levels were found in patients with migraine, compared with healthy controls. Migraine patients with low vitamin D levels had a higher incidence of aura, phonophobia/photophobia, autonomic manifestations, allodynia, and medication resistance.
Study details: This was a case-control study of 40 patients with migraine, compared with 40 healthy control patients. Patient history was taken including headache characteristics, MIGSEV, and HIT-6 scores. Each patient’s serum 25 (OH)-vitamin D level was measured.
Disclosures: None.
Citation: Hussein M, et al. J Pain Res. 2019 Aug 20;12:2529-36. doi: 10.2147/JPR.S216314. eCollection 2019.
Key clinical point: Vitamin D supplementation may decrease the frequency, severity, and duration of migraines.
Major finding: Significantly lower 25 (OH)-vitamin D levels were found in patients with migraine, compared with healthy controls. Migraine patients with low vitamin D levels had a higher incidence of aura, phonophobia/photophobia, autonomic manifestations, allodynia, and medication resistance.
Study details: This was a case-control study of 40 patients with migraine, compared with 40 healthy control patients. Patient history was taken including headache characteristics, MIGSEV, and HIT-6 scores. Each patient’s serum 25 (OH)-vitamin D level was measured.
Disclosures: None.
Citation: Hussein M, et al. J Pain Res. 2019 Aug 20;12:2529-36. doi: 10.2147/JPR.S216314. eCollection 2019.
Key clinical point: Vitamin D supplementation may decrease the frequency, severity, and duration of migraines.
Major finding: Significantly lower 25 (OH)-vitamin D levels were found in patients with migraine, compared with healthy controls. Migraine patients with low vitamin D levels had a higher incidence of aura, phonophobia/photophobia, autonomic manifestations, allodynia, and medication resistance.
Study details: This was a case-control study of 40 patients with migraine, compared with 40 healthy control patients. Patient history was taken including headache characteristics, MIGSEV, and HIT-6 scores. Each patient’s serum 25 (OH)-vitamin D level was measured.
Disclosures: None.
Citation: Hussein M, et al. J Pain Res. 2019 Aug 20;12:2529-36. doi: 10.2147/JPR.S216314. eCollection 2019.
Antibiotic use may increase the risk of Parkinson’s disease
according to a report published in Movement Disorders. Associations were found for broad-spectrum antibiotics and those that act against anaerobic bacteria and fungi. The timing of antibiotic exposure also seemed to matter.
In a nationwide case-control study, Finnish researchers compared data on antibiotic use in 13,976 individuals diagnosed with Parkinson’s disease between 1998 and 2014 with antibiotic-use data from 40,697 controls. The strongest connection with Parkinson’s disease risk was found for oral exposure to macrolides and lincosamides (adjusted odds ratio up to 1.416). After correction for multiple comparisons, exposure to antianaerobics and tetracyclines 10-15 years before the index date, and antifungal medications 1-5 years before the index date were positively associated with Parkinson’s disease risk. In post hoc analyses, further positive associations were found for broad-spectrum antibiotics.
Tuomas H. Mertsalmi, MD, from the Helsinki University Hospital and coauthors reported that this was the first study to explore a possible connection between antimicrobial use and Parkinson’s disease.
“In Parkinson’s disease, several studies have described alterations of gut microbiota composition, and changes in fecal microbiota abundance have been found to be associated with gastrointestinal and motor symptoms,” they wrote.
Commenting on the delay between the exposure and diagnosis for the most strongly associated antimicrobials, the authors noted that this 10-15 year lag was comparable with what has been found between the peripheral initiation of Parkinson’s disease and its motor manifestation.
“This would also explain the lack of association between antibiotic exposure 1-5 years before index date – if antibiotic exposure could induce or contribute to the pathogenesis of Parkinson’s disease in the gastrointestinal tract, it would probably take several years before the clinical manifestation of Parkinson’s disease,” they wrote.
With regards to the association seen for sulfonamides and trimethoprim – which was 1-5 years before the index date – they speculated this could reflect treatment for urinary tract infections, which individuals with Parkinson’s disease might be more susceptible to in the prodromal phase of the disease.
The authors noted that infectious disease has also been associated with Parkinson’s disease, and that their analysis did not include information about why the antimicrobial agents were prescribed. However, they pointed out that the associations were only for certain antibiotic classes, which makes it unlikely that the association was related to greater burden of infectious disease among individuals with Parkinson’s disease.
The pattern of associations supports the hypothesis that effects on gut microbiota could link antibiotics to Parkinson’s disease. “The link between antibiotic exposure and Parkinson’s disease fits the current view that in a significant proportion of patients the pathology of Parkinson’s disease may originate in the gut, possibly related to microbial changes, years before the onset of typical Parkinson’s disease motor symptoms such as slowness, muscle stiffness, and shaking of the extremities. It was known that bacterial composition of the intestine in patients with Parkinson’s disease is abnormal, but the cause is unclear. Our results suggest that some commonly used antibiotics, which are known to strongly influence the gut microbiota, could be a predisposing factor,” said lead investigator Filip Scheperjans, MD, PhD, from the department of neurology at Helsinki University Hospital.
The findings may have implications for antibiotic prescribing practices in the future, said Dr. Scheperjans. “In addition to the problem of antibiotic resistance, antimicrobial prescribing should also take into account their potentially long-lasting effects on the gut microbiome and the development of certain diseases.”
The study was funded by the Finnish Parkinson Foundation, the Finnish Medical Foundation, the Maire Taponen Foundation, and the Academy of Finland. One author declared relevant patents and his position as founder and chief executive of a private company. No other conflicts of interest were declared.
SOURCE: Mertsalmi TH et al. Mov Disord. 2019 Nov 18. doi: 10.1002/mds.27924.
according to a report published in Movement Disorders. Associations were found for broad-spectrum antibiotics and those that act against anaerobic bacteria and fungi. The timing of antibiotic exposure also seemed to matter.
In a nationwide case-control study, Finnish researchers compared data on antibiotic use in 13,976 individuals diagnosed with Parkinson’s disease between 1998 and 2014 with antibiotic-use data from 40,697 controls. The strongest connection with Parkinson’s disease risk was found for oral exposure to macrolides and lincosamides (adjusted odds ratio up to 1.416). After correction for multiple comparisons, exposure to antianaerobics and tetracyclines 10-15 years before the index date, and antifungal medications 1-5 years before the index date were positively associated with Parkinson’s disease risk. In post hoc analyses, further positive associations were found for broad-spectrum antibiotics.
Tuomas H. Mertsalmi, MD, from the Helsinki University Hospital and coauthors reported that this was the first study to explore a possible connection between antimicrobial use and Parkinson’s disease.
“In Parkinson’s disease, several studies have described alterations of gut microbiota composition, and changes in fecal microbiota abundance have been found to be associated with gastrointestinal and motor symptoms,” they wrote.
Commenting on the delay between the exposure and diagnosis for the most strongly associated antimicrobials, the authors noted that this 10-15 year lag was comparable with what has been found between the peripheral initiation of Parkinson’s disease and its motor manifestation.
“This would also explain the lack of association between antibiotic exposure 1-5 years before index date – if antibiotic exposure could induce or contribute to the pathogenesis of Parkinson’s disease in the gastrointestinal tract, it would probably take several years before the clinical manifestation of Parkinson’s disease,” they wrote.
With regards to the association seen for sulfonamides and trimethoprim – which was 1-5 years before the index date – they speculated this could reflect treatment for urinary tract infections, which individuals with Parkinson’s disease might be more susceptible to in the prodromal phase of the disease.
The authors noted that infectious disease has also been associated with Parkinson’s disease, and that their analysis did not include information about why the antimicrobial agents were prescribed. However, they pointed out that the associations were only for certain antibiotic classes, which makes it unlikely that the association was related to greater burden of infectious disease among individuals with Parkinson’s disease.
The pattern of associations supports the hypothesis that effects on gut microbiota could link antibiotics to Parkinson’s disease. “The link between antibiotic exposure and Parkinson’s disease fits the current view that in a significant proportion of patients the pathology of Parkinson’s disease may originate in the gut, possibly related to microbial changes, years before the onset of typical Parkinson’s disease motor symptoms such as slowness, muscle stiffness, and shaking of the extremities. It was known that bacterial composition of the intestine in patients with Parkinson’s disease is abnormal, but the cause is unclear. Our results suggest that some commonly used antibiotics, which are known to strongly influence the gut microbiota, could be a predisposing factor,” said lead investigator Filip Scheperjans, MD, PhD, from the department of neurology at Helsinki University Hospital.
The findings may have implications for antibiotic prescribing practices in the future, said Dr. Scheperjans. “In addition to the problem of antibiotic resistance, antimicrobial prescribing should also take into account their potentially long-lasting effects on the gut microbiome and the development of certain diseases.”
The study was funded by the Finnish Parkinson Foundation, the Finnish Medical Foundation, the Maire Taponen Foundation, and the Academy of Finland. One author declared relevant patents and his position as founder and chief executive of a private company. No other conflicts of interest were declared.
SOURCE: Mertsalmi TH et al. Mov Disord. 2019 Nov 18. doi: 10.1002/mds.27924.
according to a report published in Movement Disorders. Associations were found for broad-spectrum antibiotics and those that act against anaerobic bacteria and fungi. The timing of antibiotic exposure also seemed to matter.
In a nationwide case-control study, Finnish researchers compared data on antibiotic use in 13,976 individuals diagnosed with Parkinson’s disease between 1998 and 2014 with antibiotic-use data from 40,697 controls. The strongest connection with Parkinson’s disease risk was found for oral exposure to macrolides and lincosamides (adjusted odds ratio up to 1.416). After correction for multiple comparisons, exposure to antianaerobics and tetracyclines 10-15 years before the index date, and antifungal medications 1-5 years before the index date were positively associated with Parkinson’s disease risk. In post hoc analyses, further positive associations were found for broad-spectrum antibiotics.
Tuomas H. Mertsalmi, MD, from the Helsinki University Hospital and coauthors reported that this was the first study to explore a possible connection between antimicrobial use and Parkinson’s disease.
“In Parkinson’s disease, several studies have described alterations of gut microbiota composition, and changes in fecal microbiota abundance have been found to be associated with gastrointestinal and motor symptoms,” they wrote.
Commenting on the delay between the exposure and diagnosis for the most strongly associated antimicrobials, the authors noted that this 10-15 year lag was comparable with what has been found between the peripheral initiation of Parkinson’s disease and its motor manifestation.
“This would also explain the lack of association between antibiotic exposure 1-5 years before index date – if antibiotic exposure could induce or contribute to the pathogenesis of Parkinson’s disease in the gastrointestinal tract, it would probably take several years before the clinical manifestation of Parkinson’s disease,” they wrote.
With regards to the association seen for sulfonamides and trimethoprim – which was 1-5 years before the index date – they speculated this could reflect treatment for urinary tract infections, which individuals with Parkinson’s disease might be more susceptible to in the prodromal phase of the disease.
The authors noted that infectious disease has also been associated with Parkinson’s disease, and that their analysis did not include information about why the antimicrobial agents were prescribed. However, they pointed out that the associations were only for certain antibiotic classes, which makes it unlikely that the association was related to greater burden of infectious disease among individuals with Parkinson’s disease.
The pattern of associations supports the hypothesis that effects on gut microbiota could link antibiotics to Parkinson’s disease. “The link between antibiotic exposure and Parkinson’s disease fits the current view that in a significant proportion of patients the pathology of Parkinson’s disease may originate in the gut, possibly related to microbial changes, years before the onset of typical Parkinson’s disease motor symptoms such as slowness, muscle stiffness, and shaking of the extremities. It was known that bacterial composition of the intestine in patients with Parkinson’s disease is abnormal, but the cause is unclear. Our results suggest that some commonly used antibiotics, which are known to strongly influence the gut microbiota, could be a predisposing factor,” said lead investigator Filip Scheperjans, MD, PhD, from the department of neurology at Helsinki University Hospital.
The findings may have implications for antibiotic prescribing practices in the future, said Dr. Scheperjans. “In addition to the problem of antibiotic resistance, antimicrobial prescribing should also take into account their potentially long-lasting effects on the gut microbiome and the development of certain diseases.”
The study was funded by the Finnish Parkinson Foundation, the Finnish Medical Foundation, the Maire Taponen Foundation, and the Academy of Finland. One author declared relevant patents and his position as founder and chief executive of a private company. No other conflicts of interest were declared.
SOURCE: Mertsalmi TH et al. Mov Disord. 2019 Nov 18. doi: 10.1002/mds.27924.
FROM MOVEMENT DISORDERS
High recurrence, shortening cycle length in bipolar disorder associated with several biomarkers
Several potential biomarkers may indicate whether patients with bipolar disorder may have high-recurrence disease with a cycle length that progressively shortens, according to Erik Smedler, MD, PhD, of the department of psychiatry and neurochemistry at Gothenburg (Sweden) University.
For the analysis, published in European Neuropsychopharmacology, A total of 745 patients had serum samples available; assays for 203 different protein biomarkers were performed on those samples.
The investigators clustered patients according to frequency – with low-frequency recurrence defined as a maximum of one inpatient episode per year – and by cycle length – with sensitized patients having progressively shorter periods between inpatient episodes. No difference in biomarkers or clinical features were seen between high- and low-frequency recurrence patients, but sensitized patients were significantly more ill and were more likely to be treated with antidepressants.
In addition, in a specific cohort of patients who were both sensitized and had a high recurrence rate (at least five inpatient episodes), four proteins were expressed at a significantly lower level than that of nonsensitized patients: tumor necrosis factor receptor-2, tumor necrosis factor receptor superfamily member 4, placenta growth factor, and adrenomedullin. Sensitization also was associated with a single nucleotide polymorphism near the calcium channel gene CACNA2D3.
“These results suggest the potential for translational research aimed at preventive actions,” the investigators wrote.
The authors reported that they had no conflicts of interest.
SOURCE: Smedler E et al. Eur Neuropsychopharmacol. 2019 Aug 1. doi: 10.1016/j.euroneuro.2019.07.132.
Several potential biomarkers may indicate whether patients with bipolar disorder may have high-recurrence disease with a cycle length that progressively shortens, according to Erik Smedler, MD, PhD, of the department of psychiatry and neurochemistry at Gothenburg (Sweden) University.
For the analysis, published in European Neuropsychopharmacology, A total of 745 patients had serum samples available; assays for 203 different protein biomarkers were performed on those samples.
The investigators clustered patients according to frequency – with low-frequency recurrence defined as a maximum of one inpatient episode per year – and by cycle length – with sensitized patients having progressively shorter periods between inpatient episodes. No difference in biomarkers or clinical features were seen between high- and low-frequency recurrence patients, but sensitized patients were significantly more ill and were more likely to be treated with antidepressants.
In addition, in a specific cohort of patients who were both sensitized and had a high recurrence rate (at least five inpatient episodes), four proteins were expressed at a significantly lower level than that of nonsensitized patients: tumor necrosis factor receptor-2, tumor necrosis factor receptor superfamily member 4, placenta growth factor, and adrenomedullin. Sensitization also was associated with a single nucleotide polymorphism near the calcium channel gene CACNA2D3.
“These results suggest the potential for translational research aimed at preventive actions,” the investigators wrote.
The authors reported that they had no conflicts of interest.
SOURCE: Smedler E et al. Eur Neuropsychopharmacol. 2019 Aug 1. doi: 10.1016/j.euroneuro.2019.07.132.
Several potential biomarkers may indicate whether patients with bipolar disorder may have high-recurrence disease with a cycle length that progressively shortens, according to Erik Smedler, MD, PhD, of the department of psychiatry and neurochemistry at Gothenburg (Sweden) University.
For the analysis, published in European Neuropsychopharmacology, A total of 745 patients had serum samples available; assays for 203 different protein biomarkers were performed on those samples.
The investigators clustered patients according to frequency – with low-frequency recurrence defined as a maximum of one inpatient episode per year – and by cycle length – with sensitized patients having progressively shorter periods between inpatient episodes. No difference in biomarkers or clinical features were seen between high- and low-frequency recurrence patients, but sensitized patients were significantly more ill and were more likely to be treated with antidepressants.
In addition, in a specific cohort of patients who were both sensitized and had a high recurrence rate (at least five inpatient episodes), four proteins were expressed at a significantly lower level than that of nonsensitized patients: tumor necrosis factor receptor-2, tumor necrosis factor receptor superfamily member 4, placenta growth factor, and adrenomedullin. Sensitization also was associated with a single nucleotide polymorphism near the calcium channel gene CACNA2D3.
“These results suggest the potential for translational research aimed at preventive actions,” the investigators wrote.
The authors reported that they had no conflicts of interest.
SOURCE: Smedler E et al. Eur Neuropsychopharmacol. 2019 Aug 1. doi: 10.1016/j.euroneuro.2019.07.132.
FROM EUROPEAN NEUROPSYCHOPHARMACOLOGY
Ob.Gyn. News welcomes Dr. Angela Martin to the board
Dr. Martin is an assistant professor of gynecology and obstetrics in the division of maternal-fetal medicine at the University of Kansas Medical Center in Kansas City, where she is the director of ultrasound training for the residency program. She also serves on the Pharmacy and Therapeutics Committee at the university.

Dr. Martin has been a primary author or coauthor of many articles published and accepted in refereed medical publications on topics including influenza infection during pregnancy, maternal and fetal risk associated with assisted reproductive technology, hepatitis B in pregnancy, umbilical cord blood banking, pregnancy and obesity, and cell-free fetal DNA. She currently is involved in research on resident operative delivery training, chorionic villus sampling, and preterm birth.
Graduating summa cum laude from Drake University in Des Moines, Iowa, with a bachelor of science degree in biology and a minor in psychology, Dr. Martin received her doctorate of medicine at the University of Missouri, Columbia. She completed her postgraduate training at Emory University in Atlanta with an internship and residency in the department of gynecology and obstetrics, followed by a fellowship in the maternal-fetal medicine division.
Dr. Martin has won numerous honors and awards, including Outstanding Research Proposal by a fellow at Emory University, Excellence in Teaching awards for a fellow for several consecutive years at the university, and a National Faculty Award from the American College of Obstetricians and Gynecologists.*
*This article was updated 2/7/2020.
Dr. Martin is an assistant professor of gynecology and obstetrics in the division of maternal-fetal medicine at the University of Kansas Medical Center in Kansas City, where she is the director of ultrasound training for the residency program. She also serves on the Pharmacy and Therapeutics Committee at the university.
Dr. Martin has been a primary author or coauthor of many articles published and accepted in refereed medical publications on topics including influenza infection during pregnancy, maternal and fetal risk associated with assisted reproductive technology, hepatitis B in pregnancy, umbilical cord blood banking, pregnancy and obesity, and cell-free fetal DNA. She currently is involved in research on resident operative delivery training, chorionic villus sampling, and preterm birth.
Graduating summa cum laude from Drake University in Des Moines, Iowa, with a bachelor of science degree in biology and a minor in psychology, Dr. Martin received her doctorate of medicine at the University of Missouri, Columbia. She completed her postgraduate training at Emory University in Atlanta with an internship and residency in the department of gynecology and obstetrics, followed by a fellowship in the maternal-fetal medicine division.
Dr. Martin has won numerous honors and awards, including Outstanding Research Proposal by a fellow at Emory University, Excellence in Teaching awards for a fellow for several consecutive years at the university, and a National Faculty Award from the American College of Obstetricians and Gynecologists.*
*This article was updated 2/7/2020.
Dr. Martin is an assistant professor of gynecology and obstetrics in the division of maternal-fetal medicine at the University of Kansas Medical Center in Kansas City, where she is the director of ultrasound training for the residency program. She also serves on the Pharmacy and Therapeutics Committee at the university.
Dr. Martin has been a primary author or coauthor of many articles published and accepted in refereed medical publications on topics including influenza infection during pregnancy, maternal and fetal risk associated with assisted reproductive technology, hepatitis B in pregnancy, umbilical cord blood banking, pregnancy and obesity, and cell-free fetal DNA. She currently is involved in research on resident operative delivery training, chorionic villus sampling, and preterm birth.
Graduating summa cum laude from Drake University in Des Moines, Iowa, with a bachelor of science degree in biology and a minor in psychology, Dr. Martin received her doctorate of medicine at the University of Missouri, Columbia. She completed her postgraduate training at Emory University in Atlanta with an internship and residency in the department of gynecology and obstetrics, followed by a fellowship in the maternal-fetal medicine division.
Dr. Martin has won numerous honors and awards, including Outstanding Research Proposal by a fellow at Emory University, Excellence in Teaching awards for a fellow for several consecutive years at the university, and a National Faculty Award from the American College of Obstetricians and Gynecologists.*
*This article was updated 2/7/2020.
Antidepressant Tx for Anxiety Disorders: How Long?
PRACTICE CHANGER
Keep patients on antidepressant therapy for anxiety disorders for a year or longer before considering a taper.1
STRENGTH OF RECOMMENDATION
A: Based on a systematic review/meta-analysis of several good-quality randomized controlled trials.
A 42-year-old woman with generalized anxiety disorder (GAD) and panic attacks has been treated with sertraline (100 mg/d) for the past 8 months. She has also engaged in cognitive behavioral therapy (CBT) for 6 months. Her Generalized Anxiety Disorder-7 score has decreased from 19 prior to treatment to 5 at present. Now she would like to stop her antidepressant medication because she feels better. Would you recommend that she discontinue her medication at this point?
Anxiety disorders are common and often chronic and can cause significant morbidity and impairment.2,3 Firstline treatments for anxiety disorders include CBT and antidepressants, particularly selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors.4-6
There is limited evidence regarding duration of antidepressant therapy for anxiety disorders. Previous studies have shown a high risk for relapse after discontinuation of antidepressants.6 A review of current practice patterns regarding pharmacologic treatment of depression and anxiety indicates an uptick in longer term antidepressant use for up to 2 years.7 However, long-term studies to guide treatment decisions are lacking.
STUDY SUMMARY
Clear benefit of continuing treatment
This systematic review and meta-analysis evaluated studies that looked at relapse rates and time to relapse in patients treated for anxiety disorders.1 The authors used PubMed, Cochrane, and Embase to identify studies involving patients treated for a variety of psychiatric disorders, including GAD, posttraumatic stress disorder (PTSD), panic disorder (PD), obsessive compulsive disorder (OCD), and social phobia. Eligible studies enrolled patients with anxiety disorders who had a positive response to an antidepressant and then randomized them in a double-blind fashion to either discontinuation of antidepressants and commencement of placebo (stopping group) or continuation of antidepressants (continuation group) for a duration of 8 to 52 weeks. The primary outcomes were relapse rate and time to relapse.
Twenty-eight studies met the inclusion criteria for the meta-analysis, with a total of 5233 patients (2625 patients in the continuation group and 2608 patients in the stopping group). A breakdown of the trials by indication included OCD (7), PD (6), GAD (6), social phobia (5), and PTSD (4). The authors graded the overall risk for bias to be low but noted that attrition bias was present in most studies.
Continue to: Results
Results. Relapse was more likely in the stopping group (odds ratio [OR], 3.11; n = 28 studies). Heterogeneity for relapse rate was low (I2 = 8.07%). Subgroup analyses by type of antidepressant, mode of discontinuation, and exclusion of patient comorbidities yielded similar results. Relapse prevalence was 16.4% in the continuation group and 36.4% in the stopping group. Additionally, time to relapse was shorter when antidepressants were discontinued (hazard ratio [HR], 3.63; n = 11 studies). Again, the heterogeneity for relapse rate was low (I2 = 0%). The original publications did not consistently report medication tolerance or withdrawal symptoms, preventing analysis of these. Dropout rates were higher in the stopping group (OR, 1.31; n = 27 studies).
WHAT’S NEW
No more guessing about how long to treat
Previously, there was limited evidence to guide decisions about the duration of antidepressant treatment for anxiety disorders. This study provides evidence that stopping antidepressants before completing 1 year of treatment increases the risk for relapse.
CAVEATS
In a word: Bias
While the authors used standard and appropriate methodologies for this type of study, some significant threats to validity remained. All but 2 studies in the analysis were industry funded. Publication bias is another potential issue, even though the authors identified and included 6 unpublished studies, 4 of which had negative results.
Additionally, the authors graded 11 of 28 trials as having a high likelihood of selective reporting bias, meaning that important portions of the original studies’ results may not have been published. Most studies were at high risk for attrition bias, resulting in loss of information when patients dropped out of the study. While this happened more often in the stopping groups, it is still possible that there are unidentified harms or unexpected outcomes in the medication groups.
While PTSD and OCD are no longer considered anxiety disorders, subgroup analyses found no difference in relapse rates between these diagnoses and the others included in the studies. Finally, a treatment duration longer than 52 weeks has not been studied, so the optimal treatment duration is unknown.
Continue to: CHALLENGES TO IMPLEMENTATION
CHALLENGES TO IMPLEMENTATION
Patient resistance to continuing treatment
Some patients may want to discontinue antidepressant treatment if their anxiety symptoms improve before completing 1 year. It may be difficult to convince them that continuing treatment will prevent relapse of their condition. Providing patients with information about the increased relapse rate associated with stopping their antidepressant early (with an estimated number needed to treat of 5) may help patients make a more informed decision.
ACKNOWLEDGMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2019. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2019;68[7]:409-410).
1. Batelaan NM, Bosman RC, Muntingh A, et al. Risk of relapse after antidepressant discontinuation in anxiety disorders, obsessive-compulsive disorder, and post-traumatic stress disorder: systematic review and meta-analysis of relapse prevention trials. BMJ. 2017;358:j3927. Erratum in: BMJ. 2017;358:j4461.
2. National Institute of Mental Health. Prevalence of any anxiety disorder among adults. www.nimh.nih.gov/health/statistics/any-anxiety-disorder.shtml#part_155094. Updated November 2017. Accessed November 26, 2019.
3. Kessler RC, Petukhova M, Sampson NA, et al. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. 2012;21:169-184.
4. Bandelow B, Sher L, Bunevicius R, et al. Guidelines for the pharmacological treatment of anxiety disorders, obsessive-compulsive disorder and posttraumatic stress disorder in primary care. Int J Psychiatry Clin Pract. 2012;16:77-84.
5. Kaczkurkin AN, Foa EB. Cognitive-behavioral therapy for anxiety disorders: an update on the empirical evidence. Dialogues Clin Neurosci. 2015;17:337-346.
6. Donovan MR, Glue P, Kolluri S, et al. Comparative efficacy of antidepressants in preventing relapse in anxiety disorders—a meta-analysis. J Affect Disord. 2010;123:9-16.
7. Mojtabai R, Olfson M. National trends in long-term use of antidepressant medications: results from the U.S. National Health and Nutrition Examination Survey. J Clin Psychiatry. 2014;75:169-177.
PRACTICE CHANGER
Keep patients on antidepressant therapy for anxiety disorders for a year or longer before considering a taper.1
STRENGTH OF RECOMMENDATION
A: Based on a systematic review/meta-analysis of several good-quality randomized controlled trials.
A 42-year-old woman with generalized anxiety disorder (GAD) and panic attacks has been treated with sertraline (100 mg/d) for the past 8 months. She has also engaged in cognitive behavioral therapy (CBT) for 6 months. Her Generalized Anxiety Disorder-7 score has decreased from 19 prior to treatment to 5 at present. Now she would like to stop her antidepressant medication because she feels better. Would you recommend that she discontinue her medication at this point?
Anxiety disorders are common and often chronic and can cause significant morbidity and impairment.2,3 Firstline treatments for anxiety disorders include CBT and antidepressants, particularly selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors.4-6
There is limited evidence regarding duration of antidepressant therapy for anxiety disorders. Previous studies have shown a high risk for relapse after discontinuation of antidepressants.6 A review of current practice patterns regarding pharmacologic treatment of depression and anxiety indicates an uptick in longer term antidepressant use for up to 2 years.7 However, long-term studies to guide treatment decisions are lacking.
STUDY SUMMARY
Clear benefit of continuing treatment
This systematic review and meta-analysis evaluated studies that looked at relapse rates and time to relapse in patients treated for anxiety disorders.1 The authors used PubMed, Cochrane, and Embase to identify studies involving patients treated for a variety of psychiatric disorders, including GAD, posttraumatic stress disorder (PTSD), panic disorder (PD), obsessive compulsive disorder (OCD), and social phobia. Eligible studies enrolled patients with anxiety disorders who had a positive response to an antidepressant and then randomized them in a double-blind fashion to either discontinuation of antidepressants and commencement of placebo (stopping group) or continuation of antidepressants (continuation group) for a duration of 8 to 52 weeks. The primary outcomes were relapse rate and time to relapse.
Twenty-eight studies met the inclusion criteria for the meta-analysis, with a total of 5233 patients (2625 patients in the continuation group and 2608 patients in the stopping group). A breakdown of the trials by indication included OCD (7), PD (6), GAD (6), social phobia (5), and PTSD (4). The authors graded the overall risk for bias to be low but noted that attrition bias was present in most studies.
Continue to: Results
Results. Relapse was more likely in the stopping group (odds ratio [OR], 3.11; n = 28 studies). Heterogeneity for relapse rate was low (I2 = 8.07%). Subgroup analyses by type of antidepressant, mode of discontinuation, and exclusion of patient comorbidities yielded similar results. Relapse prevalence was 16.4% in the continuation group and 36.4% in the stopping group. Additionally, time to relapse was shorter when antidepressants were discontinued (hazard ratio [HR], 3.63; n = 11 studies). Again, the heterogeneity for relapse rate was low (I2 = 0%). The original publications did not consistently report medication tolerance or withdrawal symptoms, preventing analysis of these. Dropout rates were higher in the stopping group (OR, 1.31; n = 27 studies).
WHAT’S NEW
No more guessing about how long to treat
Previously, there was limited evidence to guide decisions about the duration of antidepressant treatment for anxiety disorders. This study provides evidence that stopping antidepressants before completing 1 year of treatment increases the risk for relapse.
CAVEATS
In a word: Bias
While the authors used standard and appropriate methodologies for this type of study, some significant threats to validity remained. All but 2 studies in the analysis were industry funded. Publication bias is another potential issue, even though the authors identified and included 6 unpublished studies, 4 of which had negative results.
Additionally, the authors graded 11 of 28 trials as having a high likelihood of selective reporting bias, meaning that important portions of the original studies’ results may not have been published. Most studies were at high risk for attrition bias, resulting in loss of information when patients dropped out of the study. While this happened more often in the stopping groups, it is still possible that there are unidentified harms or unexpected outcomes in the medication groups.
While PTSD and OCD are no longer considered anxiety disorders, subgroup analyses found no difference in relapse rates between these diagnoses and the others included in the studies. Finally, a treatment duration longer than 52 weeks has not been studied, so the optimal treatment duration is unknown.
Continue to: CHALLENGES TO IMPLEMENTATION
CHALLENGES TO IMPLEMENTATION
Patient resistance to continuing treatment
Some patients may want to discontinue antidepressant treatment if their anxiety symptoms improve before completing 1 year. It may be difficult to convince them that continuing treatment will prevent relapse of their condition. Providing patients with information about the increased relapse rate associated with stopping their antidepressant early (with an estimated number needed to treat of 5) may help patients make a more informed decision.
ACKNOWLEDGMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2019. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2019;68[7]:409-410).
PRACTICE CHANGER
Keep patients on antidepressant therapy for anxiety disorders for a year or longer before considering a taper.1
STRENGTH OF RECOMMENDATION
A: Based on a systematic review/meta-analysis of several good-quality randomized controlled trials.
A 42-year-old woman with generalized anxiety disorder (GAD) and panic attacks has been treated with sertraline (100 mg/d) for the past 8 months. She has also engaged in cognitive behavioral therapy (CBT) for 6 months. Her Generalized Anxiety Disorder-7 score has decreased from 19 prior to treatment to 5 at present. Now she would like to stop her antidepressant medication because she feels better. Would you recommend that she discontinue her medication at this point?
Anxiety disorders are common and often chronic and can cause significant morbidity and impairment.2,3 Firstline treatments for anxiety disorders include CBT and antidepressants, particularly selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors.4-6
There is limited evidence regarding duration of antidepressant therapy for anxiety disorders. Previous studies have shown a high risk for relapse after discontinuation of antidepressants.6 A review of current practice patterns regarding pharmacologic treatment of depression and anxiety indicates an uptick in longer term antidepressant use for up to 2 years.7 However, long-term studies to guide treatment decisions are lacking.
STUDY SUMMARY
Clear benefit of continuing treatment
This systematic review and meta-analysis evaluated studies that looked at relapse rates and time to relapse in patients treated for anxiety disorders.1 The authors used PubMed, Cochrane, and Embase to identify studies involving patients treated for a variety of psychiatric disorders, including GAD, posttraumatic stress disorder (PTSD), panic disorder (PD), obsessive compulsive disorder (OCD), and social phobia. Eligible studies enrolled patients with anxiety disorders who had a positive response to an antidepressant and then randomized them in a double-blind fashion to either discontinuation of antidepressants and commencement of placebo (stopping group) or continuation of antidepressants (continuation group) for a duration of 8 to 52 weeks. The primary outcomes were relapse rate and time to relapse.
Twenty-eight studies met the inclusion criteria for the meta-analysis, with a total of 5233 patients (2625 patients in the continuation group and 2608 patients in the stopping group). A breakdown of the trials by indication included OCD (7), PD (6), GAD (6), social phobia (5), and PTSD (4). The authors graded the overall risk for bias to be low but noted that attrition bias was present in most studies.
Continue to: Results
Results. Relapse was more likely in the stopping group (odds ratio [OR], 3.11; n = 28 studies). Heterogeneity for relapse rate was low (I2 = 8.07%). Subgroup analyses by type of antidepressant, mode of discontinuation, and exclusion of patient comorbidities yielded similar results. Relapse prevalence was 16.4% in the continuation group and 36.4% in the stopping group. Additionally, time to relapse was shorter when antidepressants were discontinued (hazard ratio [HR], 3.63; n = 11 studies). Again, the heterogeneity for relapse rate was low (I2 = 0%). The original publications did not consistently report medication tolerance or withdrawal symptoms, preventing analysis of these. Dropout rates were higher in the stopping group (OR, 1.31; n = 27 studies).
WHAT’S NEW
No more guessing about how long to treat
Previously, there was limited evidence to guide decisions about the duration of antidepressant treatment for anxiety disorders. This study provides evidence that stopping antidepressants before completing 1 year of treatment increases the risk for relapse.
CAVEATS
In a word: Bias
While the authors used standard and appropriate methodologies for this type of study, some significant threats to validity remained. All but 2 studies in the analysis were industry funded. Publication bias is another potential issue, even though the authors identified and included 6 unpublished studies, 4 of which had negative results.
Additionally, the authors graded 11 of 28 trials as having a high likelihood of selective reporting bias, meaning that important portions of the original studies’ results may not have been published. Most studies were at high risk for attrition bias, resulting in loss of information when patients dropped out of the study. While this happened more often in the stopping groups, it is still possible that there are unidentified harms or unexpected outcomes in the medication groups.
While PTSD and OCD are no longer considered anxiety disorders, subgroup analyses found no difference in relapse rates between these diagnoses and the others included in the studies. Finally, a treatment duration longer than 52 weeks has not been studied, so the optimal treatment duration is unknown.
Continue to: CHALLENGES TO IMPLEMENTATION
CHALLENGES TO IMPLEMENTATION
Patient resistance to continuing treatment
Some patients may want to discontinue antidepressant treatment if their anxiety symptoms improve before completing 1 year. It may be difficult to convince them that continuing treatment will prevent relapse of their condition. Providing patients with information about the increased relapse rate associated with stopping their antidepressant early (with an estimated number needed to treat of 5) may help patients make a more informed decision.
ACKNOWLEDGMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2019. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2019;68[7]:409-410).
1. Batelaan NM, Bosman RC, Muntingh A, et al. Risk of relapse after antidepressant discontinuation in anxiety disorders, obsessive-compulsive disorder, and post-traumatic stress disorder: systematic review and meta-analysis of relapse prevention trials. BMJ. 2017;358:j3927. Erratum in: BMJ. 2017;358:j4461.
2. National Institute of Mental Health. Prevalence of any anxiety disorder among adults. www.nimh.nih.gov/health/statistics/any-anxiety-disorder.shtml#part_155094. Updated November 2017. Accessed November 26, 2019.
3. Kessler RC, Petukhova M, Sampson NA, et al. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. 2012;21:169-184.
4. Bandelow B, Sher L, Bunevicius R, et al. Guidelines for the pharmacological treatment of anxiety disorders, obsessive-compulsive disorder and posttraumatic stress disorder in primary care. Int J Psychiatry Clin Pract. 2012;16:77-84.
5. Kaczkurkin AN, Foa EB. Cognitive-behavioral therapy for anxiety disorders: an update on the empirical evidence. Dialogues Clin Neurosci. 2015;17:337-346.
6. Donovan MR, Glue P, Kolluri S, et al. Comparative efficacy of antidepressants in preventing relapse in anxiety disorders—a meta-analysis. J Affect Disord. 2010;123:9-16.
7. Mojtabai R, Olfson M. National trends in long-term use of antidepressant medications: results from the U.S. National Health and Nutrition Examination Survey. J Clin Psychiatry. 2014;75:169-177.
1. Batelaan NM, Bosman RC, Muntingh A, et al. Risk of relapse after antidepressant discontinuation in anxiety disorders, obsessive-compulsive disorder, and post-traumatic stress disorder: systematic review and meta-analysis of relapse prevention trials. BMJ. 2017;358:j3927. Erratum in: BMJ. 2017;358:j4461.
2. National Institute of Mental Health. Prevalence of any anxiety disorder among adults. www.nimh.nih.gov/health/statistics/any-anxiety-disorder.shtml#part_155094. Updated November 2017. Accessed November 26, 2019.
3. Kessler RC, Petukhova M, Sampson NA, et al. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. 2012;21:169-184.
4. Bandelow B, Sher L, Bunevicius R, et al. Guidelines for the pharmacological treatment of anxiety disorders, obsessive-compulsive disorder and posttraumatic stress disorder in primary care. Int J Psychiatry Clin Pract. 2012;16:77-84.
5. Kaczkurkin AN, Foa EB. Cognitive-behavioral therapy for anxiety disorders: an update on the empirical evidence. Dialogues Clin Neurosci. 2015;17:337-346.
6. Donovan MR, Glue P, Kolluri S, et al. Comparative efficacy of antidepressants in preventing relapse in anxiety disorders—a meta-analysis. J Affect Disord. 2010;123:9-16.
7. Mojtabai R, Olfson M. National trends in long-term use of antidepressant medications: results from the U.S. National Health and Nutrition Examination Survey. J Clin Psychiatry. 2014;75:169-177.

Bethesda system underpredicts malignancy in pediatric thyroid tumors
CHICAGO –
Especially for nodules that fall into indeterminate categories, “the rate of malignancy in thyroid nodules is higher [in pediatric patients] than that reported in adults,” said Wen Jiang, MD, of the University of California San Diego and Rady Children’s Hospital, also in San Diego.
Current pediatric guidelines recommend that thyroid fine-needle aspiration (FNA) be performed only under ultrasound guidance, noted Dr. Jiang, a pediatric otolaryngologist, at the annual meeting of the American Thyroid Association. In addition, the Bethesda thyroid cytopathology system should be used to report FNA cytology results, and when cytopathology of FNA for a thyroid nodule is indeterminate, thyroid lobectomy is preferred over repeat FNA for most children with thyroid nodules.
To assess how well pediatric patients fared using the Bethesda system for thyroid cytopathology, Dr. Jiang and colleagues performed a retrospective review of children with thyroid nodules who received FNA at Rady Children’s Hospital during 2002-2018. The investigators used the Bethesda system to classify FNA results.
In addition to collecting the initial cytologic findings and demographic data, Dr. Jiang and colleagues also tracked repeat cytology and histopathology, as well as any radiographic and clinical follow-up data that were available.
A total of 203 cytologic samples were available from 171 patients. In all, 50 patients (29.2%) had malignancy. The mean age was about 15 years (range, 6-18 years), and the ratio of 140 female to 31 male participants was 4.5:1.
All but 21 of the samples were performed under ultrasound guidance. The nondiagnostic rate for ultrasound-guided samples was 11.5%, and for those obtained without use of ultrasound – which occurred in older cases – the nondiagnostic rate was 38.5%. “Ultrasound guidance improves the diagnostic rate,” said Dr. Jiang, adding that incorporation of on-site adequacy testing also “significantly decreased the nondiagnostic rate over the study period.”
The Bethesda system has the following six diagnostic categories, with each accompanied by follow-up recommendations in the adult population.
- Category I is nondiagnostic, and a repeat ultrasound-guided FNA is recommended for adults in this category.
- Category II is benign. Patients with these nodules should receive clinical follow-up and repeat ultrasound examination.
- Category III nodules may show atypia of undetermined significance or be judged a follicular lesion of undetermined significance. Here, adult management options include repeat FNA, molecular testing, or thyroid lobectomy.
- Category IV nodules may be assessed as follicular neoplasm or as suspicious for follicular neoplasm. Molecular testing or lobectomy are the adult management options.
- Category V describes nodules suspicious for malignancy. Either lobectomy or total thyroidectomy are options for adult management.
- Category VI is reserved for clearly malignant nodules. Again, lobectomy or total thyroidectomy are the adult management options.
In terms of the real-world outcomes in this cohort of pediatric patients with nodules, 14.8% of the 29 nodules with Bethesda category I – nondiagnostic – status were later found to be malignant, a higher rate than the 5%-10% expected in adults. Of 106 Bethesda category II – benign – nodules, 4% were malignant. In adults, 0%-3% of category II nodules turn out to be malignant.
Cytopathology from FNA of 22 nodules fell into the Bethesda category III, and 25% were malignant, which was within the expected range of 10%-30% for adults. “Bethesda class II accurately identified benign nodules with low risk of subsequent malignancy,” said Dr. Jiang.
Fourteen nodules were Bethesda category IV, and of those, 42.9% were malignant, again slightly higher than the 25%-40% expected in adults.
Just six nodules had FNA results falling into Bethesda category V, of which 83.3% were malignant, a higher rate than the 50%-75% expected for adult category V cytopathology results. All category V nodules were papillary thyroid carcinoma.
All 26 Bethesda category VI nodules were malignant; in adult category VI nodules, 97%-99% are expected to be malignant. All but four of the cases were found to be papillary thyroid carcinoma.
Dr. Jiang explained that at Rady Children’s Hospital, all FNA cytology slides received a second-opinion assessment by pathologists at the University of California San Diego. Of all the samples assessed in the study, there was disagreement about one slide, with a difference of one Bethesda category. “Malignant class cytology is quite reliable,” she said, adding the caveat that “second-opinion confirmation adds additional confidence to the cytologic diagnosis.”
She emphasized again that the initiation of on-site testing for sample adequacy significantly decreased the nondiagnostic rate seen over the course of the study.
Dr. Jiang reported no relevant conflicts of interest and no outside sources of funding.
SOURCE: Jiang W et al. ATA 2019, Oral Abstract 34.
CHICAGO –
Especially for nodules that fall into indeterminate categories, “the rate of malignancy in thyroid nodules is higher [in pediatric patients] than that reported in adults,” said Wen Jiang, MD, of the University of California San Diego and Rady Children’s Hospital, also in San Diego.
Current pediatric guidelines recommend that thyroid fine-needle aspiration (FNA) be performed only under ultrasound guidance, noted Dr. Jiang, a pediatric otolaryngologist, at the annual meeting of the American Thyroid Association. In addition, the Bethesda thyroid cytopathology system should be used to report FNA cytology results, and when cytopathology of FNA for a thyroid nodule is indeterminate, thyroid lobectomy is preferred over repeat FNA for most children with thyroid nodules.
To assess how well pediatric patients fared using the Bethesda system for thyroid cytopathology, Dr. Jiang and colleagues performed a retrospective review of children with thyroid nodules who received FNA at Rady Children’s Hospital during 2002-2018. The investigators used the Bethesda system to classify FNA results.
In addition to collecting the initial cytologic findings and demographic data, Dr. Jiang and colleagues also tracked repeat cytology and histopathology, as well as any radiographic and clinical follow-up data that were available.
A total of 203 cytologic samples were available from 171 patients. In all, 50 patients (29.2%) had malignancy. The mean age was about 15 years (range, 6-18 years), and the ratio of 140 female to 31 male participants was 4.5:1.
All but 21 of the samples were performed under ultrasound guidance. The nondiagnostic rate for ultrasound-guided samples was 11.5%, and for those obtained without use of ultrasound – which occurred in older cases – the nondiagnostic rate was 38.5%. “Ultrasound guidance improves the diagnostic rate,” said Dr. Jiang, adding that incorporation of on-site adequacy testing also “significantly decreased the nondiagnostic rate over the study period.”
The Bethesda system has the following six diagnostic categories, with each accompanied by follow-up recommendations in the adult population.
- Category I is nondiagnostic, and a repeat ultrasound-guided FNA is recommended for adults in this category.
- Category II is benign. Patients with these nodules should receive clinical follow-up and repeat ultrasound examination.
- Category III nodules may show atypia of undetermined significance or be judged a follicular lesion of undetermined significance. Here, adult management options include repeat FNA, molecular testing, or thyroid lobectomy.
- Category IV nodules may be assessed as follicular neoplasm or as suspicious for follicular neoplasm. Molecular testing or lobectomy are the adult management options.
- Category V describes nodules suspicious for malignancy. Either lobectomy or total thyroidectomy are options for adult management.
- Category VI is reserved for clearly malignant nodules. Again, lobectomy or total thyroidectomy are the adult management options.
In terms of the real-world outcomes in this cohort of pediatric patients with nodules, 14.8% of the 29 nodules with Bethesda category I – nondiagnostic – status were later found to be malignant, a higher rate than the 5%-10% expected in adults. Of 106 Bethesda category II – benign – nodules, 4% were malignant. In adults, 0%-3% of category II nodules turn out to be malignant.
Cytopathology from FNA of 22 nodules fell into the Bethesda category III, and 25% were malignant, which was within the expected range of 10%-30% for adults. “Bethesda class II accurately identified benign nodules with low risk of subsequent malignancy,” said Dr. Jiang.
Fourteen nodules were Bethesda category IV, and of those, 42.9% were malignant, again slightly higher than the 25%-40% expected in adults.
Just six nodules had FNA results falling into Bethesda category V, of which 83.3% were malignant, a higher rate than the 50%-75% expected for adult category V cytopathology results. All category V nodules were papillary thyroid carcinoma.
All 26 Bethesda category VI nodules were malignant; in adult category VI nodules, 97%-99% are expected to be malignant. All but four of the cases were found to be papillary thyroid carcinoma.
Dr. Jiang explained that at Rady Children’s Hospital, all FNA cytology slides received a second-opinion assessment by pathologists at the University of California San Diego. Of all the samples assessed in the study, there was disagreement about one slide, with a difference of one Bethesda category. “Malignant class cytology is quite reliable,” she said, adding the caveat that “second-opinion confirmation adds additional confidence to the cytologic diagnosis.”
She emphasized again that the initiation of on-site testing for sample adequacy significantly decreased the nondiagnostic rate seen over the course of the study.
Dr. Jiang reported no relevant conflicts of interest and no outside sources of funding.
SOURCE: Jiang W et al. ATA 2019, Oral Abstract 34.
CHICAGO –
Especially for nodules that fall into indeterminate categories, “the rate of malignancy in thyroid nodules is higher [in pediatric patients] than that reported in adults,” said Wen Jiang, MD, of the University of California San Diego and Rady Children’s Hospital, also in San Diego.
Current pediatric guidelines recommend that thyroid fine-needle aspiration (FNA) be performed only under ultrasound guidance, noted Dr. Jiang, a pediatric otolaryngologist, at the annual meeting of the American Thyroid Association. In addition, the Bethesda thyroid cytopathology system should be used to report FNA cytology results, and when cytopathology of FNA for a thyroid nodule is indeterminate, thyroid lobectomy is preferred over repeat FNA for most children with thyroid nodules.
To assess how well pediatric patients fared using the Bethesda system for thyroid cytopathology, Dr. Jiang and colleagues performed a retrospective review of children with thyroid nodules who received FNA at Rady Children’s Hospital during 2002-2018. The investigators used the Bethesda system to classify FNA results.
In addition to collecting the initial cytologic findings and demographic data, Dr. Jiang and colleagues also tracked repeat cytology and histopathology, as well as any radiographic and clinical follow-up data that were available.
A total of 203 cytologic samples were available from 171 patients. In all, 50 patients (29.2%) had malignancy. The mean age was about 15 years (range, 6-18 years), and the ratio of 140 female to 31 male participants was 4.5:1.
All but 21 of the samples were performed under ultrasound guidance. The nondiagnostic rate for ultrasound-guided samples was 11.5%, and for those obtained without use of ultrasound – which occurred in older cases – the nondiagnostic rate was 38.5%. “Ultrasound guidance improves the diagnostic rate,” said Dr. Jiang, adding that incorporation of on-site adequacy testing also “significantly decreased the nondiagnostic rate over the study period.”
The Bethesda system has the following six diagnostic categories, with each accompanied by follow-up recommendations in the adult population.
- Category I is nondiagnostic, and a repeat ultrasound-guided FNA is recommended for adults in this category.
- Category II is benign. Patients with these nodules should receive clinical follow-up and repeat ultrasound examination.
- Category III nodules may show atypia of undetermined significance or be judged a follicular lesion of undetermined significance. Here, adult management options include repeat FNA, molecular testing, or thyroid lobectomy.
- Category IV nodules may be assessed as follicular neoplasm or as suspicious for follicular neoplasm. Molecular testing or lobectomy are the adult management options.
- Category V describes nodules suspicious for malignancy. Either lobectomy or total thyroidectomy are options for adult management.
- Category VI is reserved for clearly malignant nodules. Again, lobectomy or total thyroidectomy are the adult management options.
In terms of the real-world outcomes in this cohort of pediatric patients with nodules, 14.8% of the 29 nodules with Bethesda category I – nondiagnostic – status were later found to be malignant, a higher rate than the 5%-10% expected in adults. Of 106 Bethesda category II – benign – nodules, 4% were malignant. In adults, 0%-3% of category II nodules turn out to be malignant.
Cytopathology from FNA of 22 nodules fell into the Bethesda category III, and 25% were malignant, which was within the expected range of 10%-30% for adults. “Bethesda class II accurately identified benign nodules with low risk of subsequent malignancy,” said Dr. Jiang.
Fourteen nodules were Bethesda category IV, and of those, 42.9% were malignant, again slightly higher than the 25%-40% expected in adults.
Just six nodules had FNA results falling into Bethesda category V, of which 83.3% were malignant, a higher rate than the 50%-75% expected for adult category V cytopathology results. All category V nodules were papillary thyroid carcinoma.
All 26 Bethesda category VI nodules were malignant; in adult category VI nodules, 97%-99% are expected to be malignant. All but four of the cases were found to be papillary thyroid carcinoma.
Dr. Jiang explained that at Rady Children’s Hospital, all FNA cytology slides received a second-opinion assessment by pathologists at the University of California San Diego. Of all the samples assessed in the study, there was disagreement about one slide, with a difference of one Bethesda category. “Malignant class cytology is quite reliable,” she said, adding the caveat that “second-opinion confirmation adds additional confidence to the cytologic diagnosis.”
She emphasized again that the initiation of on-site testing for sample adequacy significantly decreased the nondiagnostic rate seen over the course of the study.
Dr. Jiang reported no relevant conflicts of interest and no outside sources of funding.
SOURCE: Jiang W et al. ATA 2019, Oral Abstract 34.
REPORTING FROM ATA 2019
Key clinical point: Pediatric thyroid nodule cytopathology classified according to the Bethesda system showed a higher rate of malignancy than that reported in adults.
Major finding: Of 203 nodules, 14 were Bethesda category IV (follicular neoplasm or suspicious for neoplasm), and 42.9% of those were malignant, compared with the 25%-40% expected in adults.
Study details: Retrospective, single-center review of 203 fine needle–aspirated samples from 171 pediatric patients with thyroid nodules tracked over a 16-year period.
Disclosures: Dr. Jiang reported no relevant conflicts of interest and no outside sources of funding.
Source: Johnson T et al. ATA 2019, Oral Abstract 34.
2019-2020 flu season starts off full throttle
For the week ending Nov. 23, there were five states, along with Puerto Rico, at the highest level of the Centers for Disease Control and Prevention’s 1-10 scale of flu activity. That’s more than any year since 2012, including the pandemic season of 2017-2018, according to CDC data, and may suggest either an early peak or the beginning of a particularly bad winter.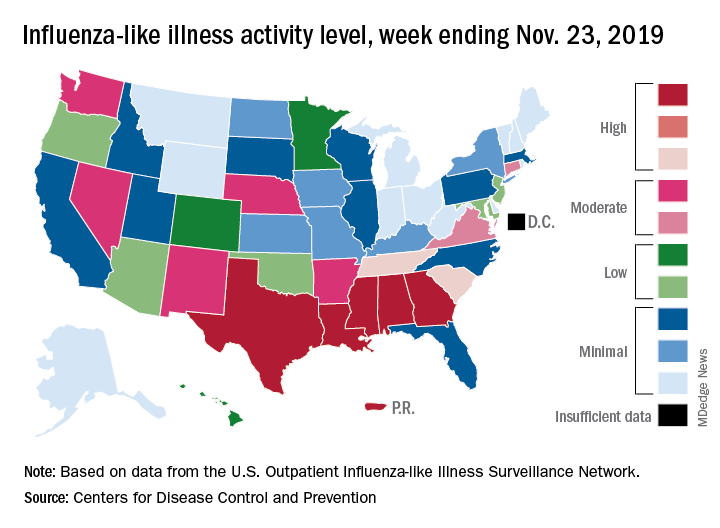
“Nationally, ILI [influenza-like illness] activity has been at or above baseline for 3 weeks; however, the amount of influenza activity across the country varies with the south and parts of the west seeing elevated activity while other parts of the country are still seeing low activity,” the CDC’s influenza division said in its weekly FluView report.
The five highest-activity states – Alabama, Georgia, Louisiana, Mississippi, and Texas – are all at level 10, and they join two others – South Carolina and Tennessee, which are at level 8 – in the “high” range from 8-10 on the ILI activity scale; Puerto Rico also is at level 10. ILI is defined as “fever (temperature of 100° F [37.8° C] or greater) and a cough and/or a sore throat without a known cause other than influenza,” the CDC said.
The activity scale is based on the percentage of outpatient visits for ILI in each state, which is reported to the CDC’s Outpatient Influenza-like Illness Surveillance Network (ILINet) each week. The national rate for the week ending Nov. 23 was 2.9%, which is above the new-for-this-season baseline rate of 2.4%. For the three previous flu seasons, the national baseline was 2.2%, having been raised from its previous level of 2.1% in 2015-2016, CDC data show.
The peak month of flu activity occurs most often in February – 15 times from 1982-1983 to 2017-2018 – but there were seven peaks in December and six each in January and March over that time period, along with one peak each in October and November, the CDC said. The October peak occurred during the H1N1 pandemic year of 2009, when the national outpatient ILI rate climbed to just over 7.7%.
For the week ending Nov. 23, there were five states, along with Puerto Rico, at the highest level of the Centers for Disease Control and Prevention’s 1-10 scale of flu activity. That’s more than any year since 2012, including the pandemic season of 2017-2018, according to CDC data, and may suggest either an early peak or the beginning of a particularly bad winter.
“Nationally, ILI [influenza-like illness] activity has been at or above baseline for 3 weeks; however, the amount of influenza activity across the country varies with the south and parts of the west seeing elevated activity while other parts of the country are still seeing low activity,” the CDC’s influenza division said in its weekly FluView report.
The five highest-activity states – Alabama, Georgia, Louisiana, Mississippi, and Texas – are all at level 10, and they join two others – South Carolina and Tennessee, which are at level 8 – in the “high” range from 8-10 on the ILI activity scale; Puerto Rico also is at level 10. ILI is defined as “fever (temperature of 100° F [37.8° C] or greater) and a cough and/or a sore throat without a known cause other than influenza,” the CDC said.
The activity scale is based on the percentage of outpatient visits for ILI in each state, which is reported to the CDC’s Outpatient Influenza-like Illness Surveillance Network (ILINet) each week. The national rate for the week ending Nov. 23 was 2.9%, which is above the new-for-this-season baseline rate of 2.4%. For the three previous flu seasons, the national baseline was 2.2%, having been raised from its previous level of 2.1% in 2015-2016, CDC data show.
The peak month of flu activity occurs most often in February – 15 times from 1982-1983 to 2017-2018 – but there were seven peaks in December and six each in January and March over that time period, along with one peak each in October and November, the CDC said. The October peak occurred during the H1N1 pandemic year of 2009, when the national outpatient ILI rate climbed to just over 7.7%.
For the week ending Nov. 23, there were five states, along with Puerto Rico, at the highest level of the Centers for Disease Control and Prevention’s 1-10 scale of flu activity. That’s more than any year since 2012, including the pandemic season of 2017-2018, according to CDC data, and may suggest either an early peak or the beginning of a particularly bad winter.
“Nationally, ILI [influenza-like illness] activity has been at or above baseline for 3 weeks; however, the amount of influenza activity across the country varies with the south and parts of the west seeing elevated activity while other parts of the country are still seeing low activity,” the CDC’s influenza division said in its weekly FluView report.
The five highest-activity states – Alabama, Georgia, Louisiana, Mississippi, and Texas – are all at level 10, and they join two others – South Carolina and Tennessee, which are at level 8 – in the “high” range from 8-10 on the ILI activity scale; Puerto Rico also is at level 10. ILI is defined as “fever (temperature of 100° F [37.8° C] or greater) and a cough and/or a sore throat without a known cause other than influenza,” the CDC said.
The activity scale is based on the percentage of outpatient visits for ILI in each state, which is reported to the CDC’s Outpatient Influenza-like Illness Surveillance Network (ILINet) each week. The national rate for the week ending Nov. 23 was 2.9%, which is above the new-for-this-season baseline rate of 2.4%. For the three previous flu seasons, the national baseline was 2.2%, having been raised from its previous level of 2.1% in 2015-2016, CDC data show.
The peak month of flu activity occurs most often in February – 15 times from 1982-1983 to 2017-2018 – but there were seven peaks in December and six each in January and March over that time period, along with one peak each in October and November, the CDC said. The October peak occurred during the H1N1 pandemic year of 2009, when the national outpatient ILI rate climbed to just over 7.7%.