User login
Half of Americans would get COVID-19 vaccine, poll shows
About half of Americans say they would get a COVID-19 vaccine if one is available, according to the Associated Press.
The poll was conducted May 14-18 and released May 27.
A massive national and international effort is underway to develop a vaccine for the coronavirus. According to the poll, 20% of Americans believe a vaccine will be available before the end of 2020. Another 61% think it will arrive in 2021, and 17% say it will take longer.
“It’s always better to under-promise and over-deliver,” William Schaffner, MD, an infectious disease specialist at Vanderbilt University Medical Center, told the AP.
Americans over age 60 were more likely to say they’ll get a coronavirus vaccine when it’s available. Those who worry that they or someone in their household could become infected with the virus were also more likely to say they’ll get a vaccine. However, Black Americans were more likely than were Hispanic or white responders to say that they don’t plan to get a vaccine.
Among those who plan to get a vaccine, 93% said they want to protect themselves, and 88% said they want to protect their family. About 72% said “life won’t go back to normal until most people are vaccinated,” and 33% said they have a chronic health condition such as asthma or diabetes and believe it’s important to receive a vaccine.
Among those who don’t plan to get a vaccine, 70% said they’re concerned about side effects. Another 42% are worried about getting the coronavirus from the vaccine. Others say they’re not concerned about getting seriously ill from the coronavirus, they don’t think vaccines work well, the COVID-19 outbreak isn’t serious, or they don’t like needles.
The National Institutes of Health says that safety is the top priority and is creating a plan to test the vaccine in thousands of people for safety and efficacy in coming months, according to the AP.
“I would not want people to think that we’re cutting corners because that would be a big mistake,” NIH director Francis Collins, MD, told AP earlier this month. “I think this is an effort to try to achieve efficiencies but not to sacrifice rigor.”
This article first appeared on WebMD.com.
About half of Americans say they would get a COVID-19 vaccine if one is available, according to the Associated Press.
The poll was conducted May 14-18 and released May 27.
A massive national and international effort is underway to develop a vaccine for the coronavirus. According to the poll, 20% of Americans believe a vaccine will be available before the end of 2020. Another 61% think it will arrive in 2021, and 17% say it will take longer.
“It’s always better to under-promise and over-deliver,” William Schaffner, MD, an infectious disease specialist at Vanderbilt University Medical Center, told the AP.
Americans over age 60 were more likely to say they’ll get a coronavirus vaccine when it’s available. Those who worry that they or someone in their household could become infected with the virus were also more likely to say they’ll get a vaccine. However, Black Americans were more likely than were Hispanic or white responders to say that they don’t plan to get a vaccine.
Among those who plan to get a vaccine, 93% said they want to protect themselves, and 88% said they want to protect their family. About 72% said “life won’t go back to normal until most people are vaccinated,” and 33% said they have a chronic health condition such as asthma or diabetes and believe it’s important to receive a vaccine.
Among those who don’t plan to get a vaccine, 70% said they’re concerned about side effects. Another 42% are worried about getting the coronavirus from the vaccine. Others say they’re not concerned about getting seriously ill from the coronavirus, they don’t think vaccines work well, the COVID-19 outbreak isn’t serious, or they don’t like needles.
The National Institutes of Health says that safety is the top priority and is creating a plan to test the vaccine in thousands of people for safety and efficacy in coming months, according to the AP.
“I would not want people to think that we’re cutting corners because that would be a big mistake,” NIH director Francis Collins, MD, told AP earlier this month. “I think this is an effort to try to achieve efficiencies but not to sacrifice rigor.”
This article first appeared on WebMD.com.
About half of Americans say they would get a COVID-19 vaccine if one is available, according to the Associated Press.
The poll was conducted May 14-18 and released May 27.
A massive national and international effort is underway to develop a vaccine for the coronavirus. According to the poll, 20% of Americans believe a vaccine will be available before the end of 2020. Another 61% think it will arrive in 2021, and 17% say it will take longer.
“It’s always better to under-promise and over-deliver,” William Schaffner, MD, an infectious disease specialist at Vanderbilt University Medical Center, told the AP.
Americans over age 60 were more likely to say they’ll get a coronavirus vaccine when it’s available. Those who worry that they or someone in their household could become infected with the virus were also more likely to say they’ll get a vaccine. However, Black Americans were more likely than were Hispanic or white responders to say that they don’t plan to get a vaccine.
Among those who plan to get a vaccine, 93% said they want to protect themselves, and 88% said they want to protect their family. About 72% said “life won’t go back to normal until most people are vaccinated,” and 33% said they have a chronic health condition such as asthma or diabetes and believe it’s important to receive a vaccine.
Among those who don’t plan to get a vaccine, 70% said they’re concerned about side effects. Another 42% are worried about getting the coronavirus from the vaccine. Others say they’re not concerned about getting seriously ill from the coronavirus, they don’t think vaccines work well, the COVID-19 outbreak isn’t serious, or they don’t like needles.
The National Institutes of Health says that safety is the top priority and is creating a plan to test the vaccine in thousands of people for safety and efficacy in coming months, according to the AP.
“I would not want people to think that we’re cutting corners because that would be a big mistake,” NIH director Francis Collins, MD, told AP earlier this month. “I think this is an effort to try to achieve efficiencies but not to sacrifice rigor.”
This article first appeared on WebMD.com.
Domestic violence amid COVID-19: Helping your patients from afar
Roger R., MD, a primary care physician from Philadelphia, set up a telemedicine appointment with a 24-year-old female patient who was experiencing headaches and was worried she might have COVID-19.

During the televisit, Dr. R. noticed that “Tonya” (not her real name) had a purplish bruise under her right eye. When asked how she got the bruise, Tonya said she had bumped into a dresser. The physician suspected abuse. He then heard a man’s voice in the background and thought it might belong to the abuser. “Is this a good time for you to talk?” he asked Tonya.
Tonya hesitated.
“When might be a better time?”
Tonya suggested an alternate time, and the physician called her then. During the visit, she shared that her fiancé, a car salesman who was also sheltering at home, was punching her.
“He always had a bad temper. Once he shoved me, but he’s never hit me before. And when he was upset, we used to go out to eat and he calmed down. Now, we’re stuck inside, we can’t even get away from each other to go to work, and he’s getting scary,” she told the doctor.
The physician asked if she would like to be connected with a domestic violence counselor. When Tonya agreed, he called Jessica DuBois Palardy, a licensed social worker and the program supervisor at STOP Intimate Partner Violence, a Philadelphia-based collaborative project of the Children’s Hospital of Philadelphia and the Lutheran Settlement House’s Bilingual Domestic Violence Program.
A ‘horrifying’ trend
Tonya’s story is not unique. A United Nations report shows that there has been a “horrifying global surge in domestic violence” linked to “lockdowns imposed by the governments responding to the COVID-19 pandemic.” The United States is no exception – 2,345 calls were placed to the National Domestic Violence Hotline during March 16–April 6, 2020.
Carole Warshaw, MD, director of the National Center on Domestic Violence, Trauma, and Mental Health in Chicago, said, “We know that intimate partner violence is increasing among people sheltering at home, and that abuse has become more severe.”
Even in nonabusive situations, being confined together at close quarters, often amid family stress and financial hardship, can be wearing, and tempers can flare. In an abusive relationship, “the main contributor to violence during shelter-in-place restrictions is that the isolation gives abusers more opportunities for controlling their partners, who have fewer options for accessing safety and support,” Dr. Warshaw said.
It is critical to “approach every clinical encounter knowing that domestic violence may be at play,” she emphasized.
Physicians might be the most important lifeline
Physicians are already facing myriad COVID-19–related challenges, and having another concern to keep in mind may be daunting.
“We’re in uncharted territory and we’re all trying to figure out how to navigate this time, how to practice medicine via phone and video conferences, and how to deal with the financial repercussions of the pandemic – not to mention concern for the health of our families,” said Peter F. Cronholm, MD, associate professor of family medicine and community health at the Hospital of the University of Pennsylvania, Philadelphia. “So maintaining vigilance is often difficult. Nevertheless, it’s important not to let this critical issue fall to the wayside.”
Marcella Nyachogo, MSW, a licensed social worker and assistant director of the Bilingual Domestic Violence Program, noted that physicians and other health care providers “may be the only people the patient interacts with, since the abuser may cut the survivor off from family and friends. And because the survivor isn’t leaving the house, he or she doesn’t have an opportunity to interact with coworkers or others – which makes health care providers the most important lifeline.”
COVID-19 as a weapon of abuse
Carey Watson, MD, regional medical director of the Family Violence Prevention Program at Kaiser Permanente in northern California, points to a disturbing trend in COVID-19–related abuse.
“Unfortunately, I’m hearing more and more accounts of how the illness itself can be one more weapon in the abuser’s arsenal,” she said.
Experts say that increasingly, abusers are claiming that their partner, who is employed in an “essential” job outside the home, is carrying the virus, and they are using this as a means of control and manipulation.
This is especially true of abusive partners of health care providers, Dr. Watson noted. She recounted the story of a divorced nurse whose husband did not allow her to have contact with their children, allegedly out of concern that she might have COVID-19, and would threaten her with a gun when she protested.
“It is important to keep this abusive tactic in mind, not only when dealing with patients but also with fellow physicians and health care professionals, and check in to see if everything is okay – especially if they seem particularly stressed out or distant,” Dr. Watson recommended.
Trust your clinical gut
How can you tell if your patients might be experiencing abuse when you’re not seeing them in person?
Pay attention to subtle signals and “trust your clinical gut when something doesn’t feel right,” Ms. Nyachogo advised.
If a patient’s demeanor is jittery or anxious or if someone next to him or her is answering all the questions or interrupting the visit, these could be red flags.
Dr. Cronholm added that telemedicine visits offer a “rare window into a patient’s home life that would not be available in an office visit.” For example, a house in disarray, the presence of broken objects, or the presence of another person hovering in the background suggests the need for further exploration.
“The main thing for all providers to keep in mind is ‘first, do no harm,’ ” Ms. Nyachogo emphasized.
“Our agency has been working for years with medical professionals in how to screen and connect folks with help most effectively and safely, and – although the specific situations posed by COVID are new – the overall approach is the same, which is to proceed with caution in how you approach the subject and how you make referrals,” she said.
Begin by asking if it is a convenient time to talk.
“This question takes the onus off the patient, who may not know how to communicate that she has no privacy or is in the middle of an argument,” explained Elsa Swenson, program manager of Home Free community program, which serves individuals experiencing domestic violence. The program is part of Minnesota-based Missions Inc. Programs, which serves those experiencing domestic abuse and chemical dependency.
If the patient indicates that it isn’t a convenient time to talk, find out when would be a better time. “This might be difficult for busy physicians and may not be what they’re accustomed to when calling a patient at home, but the patient’s circumstances are unknown to you, so it’s essential to organize around their ability to talk,” Ms. Swenson noted.
‘Are you alone?’
Another important piece of information is whether the patient has privacy – which can be tricky if the abuser is standing right there.
“You don’t want to tip the abuser off to your concerns, so you need to frame the question in a neutral way,” Dr. Watson advised.
For example, you might say that HIPAA laws require that you conduct the consultation with no one else present, and find out if there is a location in the house where the patient can have privacy.
It might be easier to talk on the phone than via video, suggests Florence Remes, a New Jersey–based licensed social worker who specializes in domestic violence. Going into another room and playing music or turning on the television might make it less obvious that a call is taking place, and the abuser would be less likely to overhear the caller’s conversation.
Dr. Watson suggested that questions about abuse might be included with other questions and asked in a simple yes/no format. “I’d like to ask you some standard questions I’m asking everyone during the pandemic. Do you have a cough or fever? Do you have any other physical symptoms? Do you have access to hand sanitizer? How is your sleep? Are you experiencing stress? Do you feel safe at home?”
The abuser, if present, will only hear the patient’s “yes” or “no” without knowing the question. If the patient indicates that she is being abused but is unable to talk, a later time can be arranged to further explore the issue.
Technology is a double-edged sword
Modern technologies have been a great boon to patients and physicians during this time of social distancing, allowing ongoing contact and health care when it would not otherwise have been possible. On the other hand, technology is fraught with potential dangers that can jeopardize the patient’s safety and compromise privacy.
Ms. Remes recounted the story of “Susan,” a client with whom she had been conducting teletherapy visits using an approved HIPAA-compliant telemedicine forum. Susan was working from home because of shelter-in-place restrictions. Her husband had been abusive, and Susan was concerned he might be “sabotaging” the household’s WiFi to isolate her from outside sources of support.
At the recommendation of Ms. Remes, Susan continued sessions either via phone calls or by using the WhatsApp program on her cellphone. Many of the requirements governing HIPAA privacy regulations have been temporarily relaxed, and clinicians can use non–encrypted forms of transmission, such as FaceTime, WhatsApp, or Skype, if no other platform is available.
But even cellphones have risks, Dr. Warshaw noted. The patient’s abuser might track texts or look at call logs – especially on unsecured platforms. It’s advisable to ask patients about who has access to their phone and computer and discuss ways to increase security.
Follow the patient’s lead
Proceed slowly and start with nonthreatening questions, Ms. Palardy advised. “I notice you have some injuries; can you tell me how you got them? Did someone hurt you? What does your relationship look like when you argue? Is there anything that makes you feel uncomfortable or unsafe?”
Emphasizing that you are asking these questions because of care and concern is reassuring and helps patients to feel they are not alone, Ms. Nyachogo pointed out.
“As your doctor, I’m worried about your health and (if relevant) your children’s safety. I can help connect you with counseling and support, legal resources, and a shelter, and everything is free and confidential. Would you be interested?” she said.
If the client acknowledges abuse, “follow their lead, but don’t push too hard,” Ms. Nyachogo warned.
“It is the client’s choice whether or not to take action,” she noted. “I’ve met survivors who said that it wasn’t until a doctor or nurse expressed concern about bruises that it even occurred to them that they were being abused. Some lied to the doctor about how they got hurt – but the question planted a seed, even though it might have taken years to follow up on the referral,” she said.
What if the patient doesn’t want to get help?
If a patient is not ready to seek help, you can create a home-safety plan. This might include setting follow-up times. If you don’t hear from him or her, you should then call the police. Or you might create a “code word,” such as “apple pie.” If the patient uses that word during a session, you know her life is in danger, Ms. Remes suggested.
Providing written information about how to get help is important but can be problematic if the abuser finds it.
Ms. Nyachogo recommends e-mailing follow-up materials that cover a variety of topics, such as keeping safe during the COVID-19 pandemic, relaxation, healthy eating, getting exercise while homebound, activities for children, and suggestions for hotlines and other resources if one is feeling suicidal or unsafe.
“If you present these as your ‘standard’ follow-up materials, the abuser is less likely to become suspicious,” Ms. Nyachogo noted.
Resources are available during COVID-19
All of the experts emphasize that resources for victims of domestic violence remain available during the COVID-19 pandemic, although some shelters may be operating at reduced capacity. Some agencies are finding alternatives to group shelters, such as hotels or Airbnb, which carry less risk of catching COVID-19.
Referring a patient to domestic violence resources is a delicate process. “You don’t want referring the patient for help to further endanger their life,” Ms. Nyachogo said.
The more you can take the burden off the patient, the better. If she is interested in getting help, you can call a domestic violence counselor or advocate while she is on the phone.
“This type of ‘warm handoff’ is what Tonya’s physician did,” Ms. Palardy recounted.
A warm handoff requires that physicians be familiar with domestic violence resources, Dr. Warshaw emphasized.
“Don’t wait until you are working with someone who needs help to find out where to refer them. Take the time to proactively research local agencies specializing in domestic violence and have their phone numbers on hand, so you can offer resources immediately if the person is interested,” she advised. The National Domestic Violence Hotline can also assist with safety planning and access to local resources.
‘Thinking on your feet’ critical for physicians
Addressing domestic violence during this unprecedented time requires “thinking on your feet” about novel forms of detection and intervention, Dr. Watson said. This involves a combination of clinical acumen, creativity, and finely honed intuition.
Ms. Nyachogo added, “Keeping an eye on domestic violence can feel like an extra burden, but don’t forget that it is lifesaving work.”
Resources
National Domestic Violence Hotline
- 800-799-SAFE (7233)
- The patient can also text LOVEIS to 22522.
National Center on Domestic Violence, Trauma, and Mental Health
- Provides resources for health care, mental health, and substance use treatment and recovery support providers on responding to domestic violence and other trauma.
- Provides resources for professionals and patients regarding access to substance use and mental health care during the COVID-1 pandemic.
- Provides support for parents, caregivers, and children during the pandemic.
- Provides resources for advocates serving families affected by domestic violence.
- A state-by-state guide to local resources
Children’s Hospital of Philadelphia Research Institute
STOP Intimate Partner Violence (IPV)
New Jersey Coalition for Domestic Violence
American Bar Association COVID-19 resources for communities
- Text HOME to 741741.
National Network to End Domestic Violence (NNEDV) COVID-19 Technology Safety
A version of this article originally appeared on Medscape.com.
Roger R., MD, a primary care physician from Philadelphia, set up a telemedicine appointment with a 24-year-old female patient who was experiencing headaches and was worried she might have COVID-19.
During the televisit, Dr. R. noticed that “Tonya” (not her real name) had a purplish bruise under her right eye. When asked how she got the bruise, Tonya said she had bumped into a dresser. The physician suspected abuse. He then heard a man’s voice in the background and thought it might belong to the abuser. “Is this a good time for you to talk?” he asked Tonya.
Tonya hesitated.
“When might be a better time?”
Tonya suggested an alternate time, and the physician called her then. During the visit, she shared that her fiancé, a car salesman who was also sheltering at home, was punching her.
“He always had a bad temper. Once he shoved me, but he’s never hit me before. And when he was upset, we used to go out to eat and he calmed down. Now, we’re stuck inside, we can’t even get away from each other to go to work, and he’s getting scary,” she told the doctor.
The physician asked if she would like to be connected with a domestic violence counselor. When Tonya agreed, he called Jessica DuBois Palardy, a licensed social worker and the program supervisor at STOP Intimate Partner Violence, a Philadelphia-based collaborative project of the Children’s Hospital of Philadelphia and the Lutheran Settlement House’s Bilingual Domestic Violence Program.
A ‘horrifying’ trend
Tonya’s story is not unique. A United Nations report shows that there has been a “horrifying global surge in domestic violence” linked to “lockdowns imposed by the governments responding to the COVID-19 pandemic.” The United States is no exception – 2,345 calls were placed to the National Domestic Violence Hotline during March 16–April 6, 2020.
Carole Warshaw, MD, director of the National Center on Domestic Violence, Trauma, and Mental Health in Chicago, said, “We know that intimate partner violence is increasing among people sheltering at home, and that abuse has become more severe.”
Even in nonabusive situations, being confined together at close quarters, often amid family stress and financial hardship, can be wearing, and tempers can flare. In an abusive relationship, “the main contributor to violence during shelter-in-place restrictions is that the isolation gives abusers more opportunities for controlling their partners, who have fewer options for accessing safety and support,” Dr. Warshaw said.
It is critical to “approach every clinical encounter knowing that domestic violence may be at play,” she emphasized.
Physicians might be the most important lifeline
Physicians are already facing myriad COVID-19–related challenges, and having another concern to keep in mind may be daunting.
“We’re in uncharted territory and we’re all trying to figure out how to navigate this time, how to practice medicine via phone and video conferences, and how to deal with the financial repercussions of the pandemic – not to mention concern for the health of our families,” said Peter F. Cronholm, MD, associate professor of family medicine and community health at the Hospital of the University of Pennsylvania, Philadelphia. “So maintaining vigilance is often difficult. Nevertheless, it’s important not to let this critical issue fall to the wayside.”
Marcella Nyachogo, MSW, a licensed social worker and assistant director of the Bilingual Domestic Violence Program, noted that physicians and other health care providers “may be the only people the patient interacts with, since the abuser may cut the survivor off from family and friends. And because the survivor isn’t leaving the house, he or she doesn’t have an opportunity to interact with coworkers or others – which makes health care providers the most important lifeline.”
COVID-19 as a weapon of abuse
Carey Watson, MD, regional medical director of the Family Violence Prevention Program at Kaiser Permanente in northern California, points to a disturbing trend in COVID-19–related abuse.
“Unfortunately, I’m hearing more and more accounts of how the illness itself can be one more weapon in the abuser’s arsenal,” she said.
Experts say that increasingly, abusers are claiming that their partner, who is employed in an “essential” job outside the home, is carrying the virus, and they are using this as a means of control and manipulation.
This is especially true of abusive partners of health care providers, Dr. Watson noted. She recounted the story of a divorced nurse whose husband did not allow her to have contact with their children, allegedly out of concern that she might have COVID-19, and would threaten her with a gun when she protested.
“It is important to keep this abusive tactic in mind, not only when dealing with patients but also with fellow physicians and health care professionals, and check in to see if everything is okay – especially if they seem particularly stressed out or distant,” Dr. Watson recommended.
Trust your clinical gut
How can you tell if your patients might be experiencing abuse when you’re not seeing them in person?
Pay attention to subtle signals and “trust your clinical gut when something doesn’t feel right,” Ms. Nyachogo advised.
If a patient’s demeanor is jittery or anxious or if someone next to him or her is answering all the questions or interrupting the visit, these could be red flags.
Dr. Cronholm added that telemedicine visits offer a “rare window into a patient’s home life that would not be available in an office visit.” For example, a house in disarray, the presence of broken objects, or the presence of another person hovering in the background suggests the need for further exploration.
“The main thing for all providers to keep in mind is ‘first, do no harm,’ ” Ms. Nyachogo emphasized.
“Our agency has been working for years with medical professionals in how to screen and connect folks with help most effectively and safely, and – although the specific situations posed by COVID are new – the overall approach is the same, which is to proceed with caution in how you approach the subject and how you make referrals,” she said.
Begin by asking if it is a convenient time to talk.
“This question takes the onus off the patient, who may not know how to communicate that she has no privacy or is in the middle of an argument,” explained Elsa Swenson, program manager of Home Free community program, which serves individuals experiencing domestic violence. The program is part of Minnesota-based Missions Inc. Programs, which serves those experiencing domestic abuse and chemical dependency.
If the patient indicates that it isn’t a convenient time to talk, find out when would be a better time. “This might be difficult for busy physicians and may not be what they’re accustomed to when calling a patient at home, but the patient’s circumstances are unknown to you, so it’s essential to organize around their ability to talk,” Ms. Swenson noted.
‘Are you alone?’
Another important piece of information is whether the patient has privacy – which can be tricky if the abuser is standing right there.
“You don’t want to tip the abuser off to your concerns, so you need to frame the question in a neutral way,” Dr. Watson advised.
For example, you might say that HIPAA laws require that you conduct the consultation with no one else present, and find out if there is a location in the house where the patient can have privacy.
It might be easier to talk on the phone than via video, suggests Florence Remes, a New Jersey–based licensed social worker who specializes in domestic violence. Going into another room and playing music or turning on the television might make it less obvious that a call is taking place, and the abuser would be less likely to overhear the caller’s conversation.
Dr. Watson suggested that questions about abuse might be included with other questions and asked in a simple yes/no format. “I’d like to ask you some standard questions I’m asking everyone during the pandemic. Do you have a cough or fever? Do you have any other physical symptoms? Do you have access to hand sanitizer? How is your sleep? Are you experiencing stress? Do you feel safe at home?”
The abuser, if present, will only hear the patient’s “yes” or “no” without knowing the question. If the patient indicates that she is being abused but is unable to talk, a later time can be arranged to further explore the issue.
Technology is a double-edged sword
Modern technologies have been a great boon to patients and physicians during this time of social distancing, allowing ongoing contact and health care when it would not otherwise have been possible. On the other hand, technology is fraught with potential dangers that can jeopardize the patient’s safety and compromise privacy.
Ms. Remes recounted the story of “Susan,” a client with whom she had been conducting teletherapy visits using an approved HIPAA-compliant telemedicine forum. Susan was working from home because of shelter-in-place restrictions. Her husband had been abusive, and Susan was concerned he might be “sabotaging” the household’s WiFi to isolate her from outside sources of support.
At the recommendation of Ms. Remes, Susan continued sessions either via phone calls or by using the WhatsApp program on her cellphone. Many of the requirements governing HIPAA privacy regulations have been temporarily relaxed, and clinicians can use non–encrypted forms of transmission, such as FaceTime, WhatsApp, or Skype, if no other platform is available.
But even cellphones have risks, Dr. Warshaw noted. The patient’s abuser might track texts or look at call logs – especially on unsecured platforms. It’s advisable to ask patients about who has access to their phone and computer and discuss ways to increase security.
Follow the patient’s lead
Proceed slowly and start with nonthreatening questions, Ms. Palardy advised. “I notice you have some injuries; can you tell me how you got them? Did someone hurt you? What does your relationship look like when you argue? Is there anything that makes you feel uncomfortable or unsafe?”
Emphasizing that you are asking these questions because of care and concern is reassuring and helps patients to feel they are not alone, Ms. Nyachogo pointed out.
“As your doctor, I’m worried about your health and (if relevant) your children’s safety. I can help connect you with counseling and support, legal resources, and a shelter, and everything is free and confidential. Would you be interested?” she said.
If the client acknowledges abuse, “follow their lead, but don’t push too hard,” Ms. Nyachogo warned.
“It is the client’s choice whether or not to take action,” she noted. “I’ve met survivors who said that it wasn’t until a doctor or nurse expressed concern about bruises that it even occurred to them that they were being abused. Some lied to the doctor about how they got hurt – but the question planted a seed, even though it might have taken years to follow up on the referral,” she said.
What if the patient doesn’t want to get help?
If a patient is not ready to seek help, you can create a home-safety plan. This might include setting follow-up times. If you don’t hear from him or her, you should then call the police. Or you might create a “code word,” such as “apple pie.” If the patient uses that word during a session, you know her life is in danger, Ms. Remes suggested.
Providing written information about how to get help is important but can be problematic if the abuser finds it.
Ms. Nyachogo recommends e-mailing follow-up materials that cover a variety of topics, such as keeping safe during the COVID-19 pandemic, relaxation, healthy eating, getting exercise while homebound, activities for children, and suggestions for hotlines and other resources if one is feeling suicidal or unsafe.
“If you present these as your ‘standard’ follow-up materials, the abuser is less likely to become suspicious,” Ms. Nyachogo noted.
Resources are available during COVID-19
All of the experts emphasize that resources for victims of domestic violence remain available during the COVID-19 pandemic, although some shelters may be operating at reduced capacity. Some agencies are finding alternatives to group shelters, such as hotels or Airbnb, which carry less risk of catching COVID-19.
Referring a patient to domestic violence resources is a delicate process. “You don’t want referring the patient for help to further endanger their life,” Ms. Nyachogo said.
The more you can take the burden off the patient, the better. If she is interested in getting help, you can call a domestic violence counselor or advocate while she is on the phone.
“This type of ‘warm handoff’ is what Tonya’s physician did,” Ms. Palardy recounted.
A warm handoff requires that physicians be familiar with domestic violence resources, Dr. Warshaw emphasized.
“Don’t wait until you are working with someone who needs help to find out where to refer them. Take the time to proactively research local agencies specializing in domestic violence and have their phone numbers on hand, so you can offer resources immediately if the person is interested,” she advised. The National Domestic Violence Hotline can also assist with safety planning and access to local resources.
‘Thinking on your feet’ critical for physicians
Addressing domestic violence during this unprecedented time requires “thinking on your feet” about novel forms of detection and intervention, Dr. Watson said. This involves a combination of clinical acumen, creativity, and finely honed intuition.
Ms. Nyachogo added, “Keeping an eye on domestic violence can feel like an extra burden, but don’t forget that it is lifesaving work.”
Resources
National Domestic Violence Hotline
- 800-799-SAFE (7233)
- The patient can also text LOVEIS to 22522.
National Center on Domestic Violence, Trauma, and Mental Health
- Provides resources for health care, mental health, and substance use treatment and recovery support providers on responding to domestic violence and other trauma.
- Provides resources for professionals and patients regarding access to substance use and mental health care during the COVID-1 pandemic.
- Provides support for parents, caregivers, and children during the pandemic.
- Provides resources for advocates serving families affected by domestic violence.
- A state-by-state guide to local resources
Children’s Hospital of Philadelphia Research Institute
STOP Intimate Partner Violence (IPV)
New Jersey Coalition for Domestic Violence
American Bar Association COVID-19 resources for communities
- Text HOME to 741741.
National Network to End Domestic Violence (NNEDV) COVID-19 Technology Safety
A version of this article originally appeared on Medscape.com.
Roger R., MD, a primary care physician from Philadelphia, set up a telemedicine appointment with a 24-year-old female patient who was experiencing headaches and was worried she might have COVID-19.
During the televisit, Dr. R. noticed that “Tonya” (not her real name) had a purplish bruise under her right eye. When asked how she got the bruise, Tonya said she had bumped into a dresser. The physician suspected abuse. He then heard a man’s voice in the background and thought it might belong to the abuser. “Is this a good time for you to talk?” he asked Tonya.
Tonya hesitated.
“When might be a better time?”
Tonya suggested an alternate time, and the physician called her then. During the visit, she shared that her fiancé, a car salesman who was also sheltering at home, was punching her.
“He always had a bad temper. Once he shoved me, but he’s never hit me before. And when he was upset, we used to go out to eat and he calmed down. Now, we’re stuck inside, we can’t even get away from each other to go to work, and he’s getting scary,” she told the doctor.
The physician asked if she would like to be connected with a domestic violence counselor. When Tonya agreed, he called Jessica DuBois Palardy, a licensed social worker and the program supervisor at STOP Intimate Partner Violence, a Philadelphia-based collaborative project of the Children’s Hospital of Philadelphia and the Lutheran Settlement House’s Bilingual Domestic Violence Program.
A ‘horrifying’ trend
Tonya’s story is not unique. A United Nations report shows that there has been a “horrifying global surge in domestic violence” linked to “lockdowns imposed by the governments responding to the COVID-19 pandemic.” The United States is no exception – 2,345 calls were placed to the National Domestic Violence Hotline during March 16–April 6, 2020.
Carole Warshaw, MD, director of the National Center on Domestic Violence, Trauma, and Mental Health in Chicago, said, “We know that intimate partner violence is increasing among people sheltering at home, and that abuse has become more severe.”
Even in nonabusive situations, being confined together at close quarters, often amid family stress and financial hardship, can be wearing, and tempers can flare. In an abusive relationship, “the main contributor to violence during shelter-in-place restrictions is that the isolation gives abusers more opportunities for controlling their partners, who have fewer options for accessing safety and support,” Dr. Warshaw said.
It is critical to “approach every clinical encounter knowing that domestic violence may be at play,” she emphasized.
Physicians might be the most important lifeline
Physicians are already facing myriad COVID-19–related challenges, and having another concern to keep in mind may be daunting.
“We’re in uncharted territory and we’re all trying to figure out how to navigate this time, how to practice medicine via phone and video conferences, and how to deal with the financial repercussions of the pandemic – not to mention concern for the health of our families,” said Peter F. Cronholm, MD, associate professor of family medicine and community health at the Hospital of the University of Pennsylvania, Philadelphia. “So maintaining vigilance is often difficult. Nevertheless, it’s important not to let this critical issue fall to the wayside.”
Marcella Nyachogo, MSW, a licensed social worker and assistant director of the Bilingual Domestic Violence Program, noted that physicians and other health care providers “may be the only people the patient interacts with, since the abuser may cut the survivor off from family and friends. And because the survivor isn’t leaving the house, he or she doesn’t have an opportunity to interact with coworkers or others – which makes health care providers the most important lifeline.”
COVID-19 as a weapon of abuse
Carey Watson, MD, regional medical director of the Family Violence Prevention Program at Kaiser Permanente in northern California, points to a disturbing trend in COVID-19–related abuse.
“Unfortunately, I’m hearing more and more accounts of how the illness itself can be one more weapon in the abuser’s arsenal,” she said.
Experts say that increasingly, abusers are claiming that their partner, who is employed in an “essential” job outside the home, is carrying the virus, and they are using this as a means of control and manipulation.
This is especially true of abusive partners of health care providers, Dr. Watson noted. She recounted the story of a divorced nurse whose husband did not allow her to have contact with their children, allegedly out of concern that she might have COVID-19, and would threaten her with a gun when she protested.
“It is important to keep this abusive tactic in mind, not only when dealing with patients but also with fellow physicians and health care professionals, and check in to see if everything is okay – especially if they seem particularly stressed out or distant,” Dr. Watson recommended.
Trust your clinical gut
How can you tell if your patients might be experiencing abuse when you’re not seeing them in person?
Pay attention to subtle signals and “trust your clinical gut when something doesn’t feel right,” Ms. Nyachogo advised.
If a patient’s demeanor is jittery or anxious or if someone next to him or her is answering all the questions or interrupting the visit, these could be red flags.
Dr. Cronholm added that telemedicine visits offer a “rare window into a patient’s home life that would not be available in an office visit.” For example, a house in disarray, the presence of broken objects, or the presence of another person hovering in the background suggests the need for further exploration.
“The main thing for all providers to keep in mind is ‘first, do no harm,’ ” Ms. Nyachogo emphasized.
“Our agency has been working for years with medical professionals in how to screen and connect folks with help most effectively and safely, and – although the specific situations posed by COVID are new – the overall approach is the same, which is to proceed with caution in how you approach the subject and how you make referrals,” she said.
Begin by asking if it is a convenient time to talk.
“This question takes the onus off the patient, who may not know how to communicate that she has no privacy or is in the middle of an argument,” explained Elsa Swenson, program manager of Home Free community program, which serves individuals experiencing domestic violence. The program is part of Minnesota-based Missions Inc. Programs, which serves those experiencing domestic abuse and chemical dependency.
If the patient indicates that it isn’t a convenient time to talk, find out when would be a better time. “This might be difficult for busy physicians and may not be what they’re accustomed to when calling a patient at home, but the patient’s circumstances are unknown to you, so it’s essential to organize around their ability to talk,” Ms. Swenson noted.
‘Are you alone?’
Another important piece of information is whether the patient has privacy – which can be tricky if the abuser is standing right there.
“You don’t want to tip the abuser off to your concerns, so you need to frame the question in a neutral way,” Dr. Watson advised.
For example, you might say that HIPAA laws require that you conduct the consultation with no one else present, and find out if there is a location in the house where the patient can have privacy.
It might be easier to talk on the phone than via video, suggests Florence Remes, a New Jersey–based licensed social worker who specializes in domestic violence. Going into another room and playing music or turning on the television might make it less obvious that a call is taking place, and the abuser would be less likely to overhear the caller’s conversation.
Dr. Watson suggested that questions about abuse might be included with other questions and asked in a simple yes/no format. “I’d like to ask you some standard questions I’m asking everyone during the pandemic. Do you have a cough or fever? Do you have any other physical symptoms? Do you have access to hand sanitizer? How is your sleep? Are you experiencing stress? Do you feel safe at home?”
The abuser, if present, will only hear the patient’s “yes” or “no” without knowing the question. If the patient indicates that she is being abused but is unable to talk, a later time can be arranged to further explore the issue.
Technology is a double-edged sword
Modern technologies have been a great boon to patients and physicians during this time of social distancing, allowing ongoing contact and health care when it would not otherwise have been possible. On the other hand, technology is fraught with potential dangers that can jeopardize the patient’s safety and compromise privacy.
Ms. Remes recounted the story of “Susan,” a client with whom she had been conducting teletherapy visits using an approved HIPAA-compliant telemedicine forum. Susan was working from home because of shelter-in-place restrictions. Her husband had been abusive, and Susan was concerned he might be “sabotaging” the household’s WiFi to isolate her from outside sources of support.
At the recommendation of Ms. Remes, Susan continued sessions either via phone calls or by using the WhatsApp program on her cellphone. Many of the requirements governing HIPAA privacy regulations have been temporarily relaxed, and clinicians can use non–encrypted forms of transmission, such as FaceTime, WhatsApp, or Skype, if no other platform is available.
But even cellphones have risks, Dr. Warshaw noted. The patient’s abuser might track texts or look at call logs – especially on unsecured platforms. It’s advisable to ask patients about who has access to their phone and computer and discuss ways to increase security.
Follow the patient’s lead
Proceed slowly and start with nonthreatening questions, Ms. Palardy advised. “I notice you have some injuries; can you tell me how you got them? Did someone hurt you? What does your relationship look like when you argue? Is there anything that makes you feel uncomfortable or unsafe?”
Emphasizing that you are asking these questions because of care and concern is reassuring and helps patients to feel they are not alone, Ms. Nyachogo pointed out.
“As your doctor, I’m worried about your health and (if relevant) your children’s safety. I can help connect you with counseling and support, legal resources, and a shelter, and everything is free and confidential. Would you be interested?” she said.
If the client acknowledges abuse, “follow their lead, but don’t push too hard,” Ms. Nyachogo warned.
“It is the client’s choice whether or not to take action,” she noted. “I’ve met survivors who said that it wasn’t until a doctor or nurse expressed concern about bruises that it even occurred to them that they were being abused. Some lied to the doctor about how they got hurt – but the question planted a seed, even though it might have taken years to follow up on the referral,” she said.
What if the patient doesn’t want to get help?
If a patient is not ready to seek help, you can create a home-safety plan. This might include setting follow-up times. If you don’t hear from him or her, you should then call the police. Or you might create a “code word,” such as “apple pie.” If the patient uses that word during a session, you know her life is in danger, Ms. Remes suggested.
Providing written information about how to get help is important but can be problematic if the abuser finds it.
Ms. Nyachogo recommends e-mailing follow-up materials that cover a variety of topics, such as keeping safe during the COVID-19 pandemic, relaxation, healthy eating, getting exercise while homebound, activities for children, and suggestions for hotlines and other resources if one is feeling suicidal or unsafe.
“If you present these as your ‘standard’ follow-up materials, the abuser is less likely to become suspicious,” Ms. Nyachogo noted.
Resources are available during COVID-19
All of the experts emphasize that resources for victims of domestic violence remain available during the COVID-19 pandemic, although some shelters may be operating at reduced capacity. Some agencies are finding alternatives to group shelters, such as hotels or Airbnb, which carry less risk of catching COVID-19.
Referring a patient to domestic violence resources is a delicate process. “You don’t want referring the patient for help to further endanger their life,” Ms. Nyachogo said.
The more you can take the burden off the patient, the better. If she is interested in getting help, you can call a domestic violence counselor or advocate while she is on the phone.
“This type of ‘warm handoff’ is what Tonya’s physician did,” Ms. Palardy recounted.
A warm handoff requires that physicians be familiar with domestic violence resources, Dr. Warshaw emphasized.
“Don’t wait until you are working with someone who needs help to find out where to refer them. Take the time to proactively research local agencies specializing in domestic violence and have their phone numbers on hand, so you can offer resources immediately if the person is interested,” she advised. The National Domestic Violence Hotline can also assist with safety planning and access to local resources.
‘Thinking on your feet’ critical for physicians
Addressing domestic violence during this unprecedented time requires “thinking on your feet” about novel forms of detection and intervention, Dr. Watson said. This involves a combination of clinical acumen, creativity, and finely honed intuition.
Ms. Nyachogo added, “Keeping an eye on domestic violence can feel like an extra burden, but don’t forget that it is lifesaving work.”
Resources
National Domestic Violence Hotline
- 800-799-SAFE (7233)
- The patient can also text LOVEIS to 22522.
National Center on Domestic Violence, Trauma, and Mental Health
- Provides resources for health care, mental health, and substance use treatment and recovery support providers on responding to domestic violence and other trauma.
- Provides resources for professionals and patients regarding access to substance use and mental health care during the COVID-1 pandemic.
- Provides support for parents, caregivers, and children during the pandemic.
- Provides resources for advocates serving families affected by domestic violence.
- A state-by-state guide to local resources
Children’s Hospital of Philadelphia Research Institute
STOP Intimate Partner Violence (IPV)
New Jersey Coalition for Domestic Violence
American Bar Association COVID-19 resources for communities
- Text HOME to 741741.
National Network to End Domestic Violence (NNEDV) COVID-19 Technology Safety
A version of this article originally appeared on Medscape.com.
Medicare will offer a $35/month insulin-cost cap in 2021
U.S. Medicare beneficiaries with diabetes will be able to cap their out-of-pocket cost for insulin at no more than $35/month starting in January 2021 under a new coverage option in the Senior Savings Model, according to program details released by the Centers for Medicare & Medicaid Services on May 26.
This facet of the Senior Savings Model for Medicare drug benefits depends on voluntary participation by insurers offering Part D (drug) coverage to Medicare beneficiaries. As of May 26, 2020, 88 insurers had agreed to participate with a total of roughly 1,750 different drug-coverage plan options with this benefit starting next year, either as part of standalone Part D policies or as part of Medicare Advantage, or “enhanced” plans with drug coverage, said Seema Verma, administrator of the CMS, during a press conference.
Beneficiaries who opt for Part D coverage with this benefit will see a cap at $35 a month for their out-of-pocket insulin costs regardless of what phase of drug coverage they are in during the course of a benefit year: the 100% responsibility phase until their annual plan deductible is met, their initial coverage phase, their coverage gap phase (which kicks in after a total of $4,020 is spent on all prescription drugs), and the catastrophic coverage phase.
A recently published analysis of average, annual, out-of-pocket insulin costs for U.S. Medicare beneficiaries with “typical” Part D plans during 2019 found that, under this four-phase pricing scheme, the 1-year total cost to patients for their insulin came to just over $1,140 (N Engl J Med. 2020 May 14;382[20]:1878-80). For 2021 participants in the new model, annual out-of-pocket cost should be no greater than $420, and could possibly be less as the $35/month rate is not set but a cost ceiling.
A written statement from CMS about the new program predicted an average, estimated out-of-pocket cost savings of $446 per beneficiary. In addition to reducing overall out-of-pocket costs, another goal of the program is to give beneficiaries month-to-month consistency in their insulin costs. Under current coverage rules, costs fluctuate from month to month depending on the phase of coverage a beneficiary qualifies for at a given time.
The change to insulin copays in 2021 for beneficiaries in participating plans will cover “all common forms of insulin,” said Ms. Verma during the press conference. “If it goes well, we’ll extend that to other drugs,” she added. “We’re starting with insulin, but depending on the progress of this, we will consider offering this flexibility to manufacturers and plans with other drugs, depending on the results. We think that this creates a foundation and a platform to fix things, some of the problems that we have in the Part D plans. It’s time for that program to be updated. A lot of the provisions just don’t work anymore, and it’s standing in the way of free-market completion and negotiation that can lower prices for seniors.”
But “only 54% of all Medicare beneficiaries are enrolled in enhanced plans that are eligible to participate in the model, and only 44% of those plans have agreed to participate,” according to a statement from Public Citizen, a consumer-rights group based in Washington. Furthermore, the statement’s author, Peter Maybarduk, director of the organizations Access to Medicines Program, cited an analysis by Public Citizen that found that the program did nothing prevent pharmaceutical corporations from setting exorbitant prices for insulin. He added that the plan leaves out younger patients with diabetes, many of whom have been forced to ration their insulin because of the “outrageous insulin price gouging.”
CMS also recently announced on May 22 that it had finalized a rule that allows for expanded use of telehealth consultations for beneficiaries in Advantage programs. The agency said that telehealth consults had become possible for a variety of medical subspecialties, including endocrinology, dermatology, cardiology, gynecology, psychiatry, and primary care. In March, CMS announced a waiver to its prior rules on use of telehealth consults effective March 6, 2020. Kellyanne Conway, a senior counselor to President Donald Trump, said during the May 26 press conference that Medicare-covered telehealth visits rose from about 12,000 per week prior to issuance of the waiver to “well into the six figures,” in recent weeks.
U.S. Medicare beneficiaries with diabetes will be able to cap their out-of-pocket cost for insulin at no more than $35/month starting in January 2021 under a new coverage option in the Senior Savings Model, according to program details released by the Centers for Medicare & Medicaid Services on May 26.
This facet of the Senior Savings Model for Medicare drug benefits depends on voluntary participation by insurers offering Part D (drug) coverage to Medicare beneficiaries. As of May 26, 2020, 88 insurers had agreed to participate with a total of roughly 1,750 different drug-coverage plan options with this benefit starting next year, either as part of standalone Part D policies or as part of Medicare Advantage, or “enhanced” plans with drug coverage, said Seema Verma, administrator of the CMS, during a press conference.
Beneficiaries who opt for Part D coverage with this benefit will see a cap at $35 a month for their out-of-pocket insulin costs regardless of what phase of drug coverage they are in during the course of a benefit year: the 100% responsibility phase until their annual plan deductible is met, their initial coverage phase, their coverage gap phase (which kicks in after a total of $4,020 is spent on all prescription drugs), and the catastrophic coverage phase.
A recently published analysis of average, annual, out-of-pocket insulin costs for U.S. Medicare beneficiaries with “typical” Part D plans during 2019 found that, under this four-phase pricing scheme, the 1-year total cost to patients for their insulin came to just over $1,140 (N Engl J Med. 2020 May 14;382[20]:1878-80). For 2021 participants in the new model, annual out-of-pocket cost should be no greater than $420, and could possibly be less as the $35/month rate is not set but a cost ceiling.
A written statement from CMS about the new program predicted an average, estimated out-of-pocket cost savings of $446 per beneficiary. In addition to reducing overall out-of-pocket costs, another goal of the program is to give beneficiaries month-to-month consistency in their insulin costs. Under current coverage rules, costs fluctuate from month to month depending on the phase of coverage a beneficiary qualifies for at a given time.
The change to insulin copays in 2021 for beneficiaries in participating plans will cover “all common forms of insulin,” said Ms. Verma during the press conference. “If it goes well, we’ll extend that to other drugs,” she added. “We’re starting with insulin, but depending on the progress of this, we will consider offering this flexibility to manufacturers and plans with other drugs, depending on the results. We think that this creates a foundation and a platform to fix things, some of the problems that we have in the Part D plans. It’s time for that program to be updated. A lot of the provisions just don’t work anymore, and it’s standing in the way of free-market completion and negotiation that can lower prices for seniors.”
But “only 54% of all Medicare beneficiaries are enrolled in enhanced plans that are eligible to participate in the model, and only 44% of those plans have agreed to participate,” according to a statement from Public Citizen, a consumer-rights group based in Washington. Furthermore, the statement’s author, Peter Maybarduk, director of the organizations Access to Medicines Program, cited an analysis by Public Citizen that found that the program did nothing prevent pharmaceutical corporations from setting exorbitant prices for insulin. He added that the plan leaves out younger patients with diabetes, many of whom have been forced to ration their insulin because of the “outrageous insulin price gouging.”
CMS also recently announced on May 22 that it had finalized a rule that allows for expanded use of telehealth consultations for beneficiaries in Advantage programs. The agency said that telehealth consults had become possible for a variety of medical subspecialties, including endocrinology, dermatology, cardiology, gynecology, psychiatry, and primary care. In March, CMS announced a waiver to its prior rules on use of telehealth consults effective March 6, 2020. Kellyanne Conway, a senior counselor to President Donald Trump, said during the May 26 press conference that Medicare-covered telehealth visits rose from about 12,000 per week prior to issuance of the waiver to “well into the six figures,” in recent weeks.
U.S. Medicare beneficiaries with diabetes will be able to cap their out-of-pocket cost for insulin at no more than $35/month starting in January 2021 under a new coverage option in the Senior Savings Model, according to program details released by the Centers for Medicare & Medicaid Services on May 26.
This facet of the Senior Savings Model for Medicare drug benefits depends on voluntary participation by insurers offering Part D (drug) coverage to Medicare beneficiaries. As of May 26, 2020, 88 insurers had agreed to participate with a total of roughly 1,750 different drug-coverage plan options with this benefit starting next year, either as part of standalone Part D policies or as part of Medicare Advantage, or “enhanced” plans with drug coverage, said Seema Verma, administrator of the CMS, during a press conference.
Beneficiaries who opt for Part D coverage with this benefit will see a cap at $35 a month for their out-of-pocket insulin costs regardless of what phase of drug coverage they are in during the course of a benefit year: the 100% responsibility phase until their annual plan deductible is met, their initial coverage phase, their coverage gap phase (which kicks in after a total of $4,020 is spent on all prescription drugs), and the catastrophic coverage phase.
A recently published analysis of average, annual, out-of-pocket insulin costs for U.S. Medicare beneficiaries with “typical” Part D plans during 2019 found that, under this four-phase pricing scheme, the 1-year total cost to patients for their insulin came to just over $1,140 (N Engl J Med. 2020 May 14;382[20]:1878-80). For 2021 participants in the new model, annual out-of-pocket cost should be no greater than $420, and could possibly be less as the $35/month rate is not set but a cost ceiling.
A written statement from CMS about the new program predicted an average, estimated out-of-pocket cost savings of $446 per beneficiary. In addition to reducing overall out-of-pocket costs, another goal of the program is to give beneficiaries month-to-month consistency in their insulin costs. Under current coverage rules, costs fluctuate from month to month depending on the phase of coverage a beneficiary qualifies for at a given time.
The change to insulin copays in 2021 for beneficiaries in participating plans will cover “all common forms of insulin,” said Ms. Verma during the press conference. “If it goes well, we’ll extend that to other drugs,” she added. “We’re starting with insulin, but depending on the progress of this, we will consider offering this flexibility to manufacturers and plans with other drugs, depending on the results. We think that this creates a foundation and a platform to fix things, some of the problems that we have in the Part D plans. It’s time for that program to be updated. A lot of the provisions just don’t work anymore, and it’s standing in the way of free-market completion and negotiation that can lower prices for seniors.”
But “only 54% of all Medicare beneficiaries are enrolled in enhanced plans that are eligible to participate in the model, and only 44% of those plans have agreed to participate,” according to a statement from Public Citizen, a consumer-rights group based in Washington. Furthermore, the statement’s author, Peter Maybarduk, director of the organizations Access to Medicines Program, cited an analysis by Public Citizen that found that the program did nothing prevent pharmaceutical corporations from setting exorbitant prices for insulin. He added that the plan leaves out younger patients with diabetes, many of whom have been forced to ration their insulin because of the “outrageous insulin price gouging.”
CMS also recently announced on May 22 that it had finalized a rule that allows for expanded use of telehealth consultations for beneficiaries in Advantage programs. The agency said that telehealth consults had become possible for a variety of medical subspecialties, including endocrinology, dermatology, cardiology, gynecology, psychiatry, and primary care. In March, CMS announced a waiver to its prior rules on use of telehealth consults effective March 6, 2020. Kellyanne Conway, a senior counselor to President Donald Trump, said during the May 26 press conference that Medicare-covered telehealth visits rose from about 12,000 per week prior to issuance of the waiver to “well into the six figures,” in recent weeks.
Seek safe strategies to diagnose gestational diabetes during pandemic
Clinicians and pregnant women are less likely to prescribe and undergo the oral glucose tolerance test (OGTT) to diagnose gestational diabetes in the context of the COVID-19 pandemic, according to a review by H. David McIntyre, MD, of the University of Queensland, Brisbane, Australia, and Robert G. Moses, MD, of Wollongong (Australia) Hospital.
National and international discussions of whether a one- or two-step test for gestational diabetes mellitus (GDM) is optimal, and which women should be tested are ongoing, but the potential for exposure risks to COVID-19 are impacting the test process, they wrote in a commentary published in Diabetes Care.
“Any national or local guidelines should be developed with the primary aim of being protective for pregnant women and workable in the current health crisis,” they wrote.
Key concerns expressed by women and health care providers include the need for travel to be tested, the possible need for two visits, and the several hours spent in a potentially high-risk specimen collection center.
“Further, a GDM diagnosis generally involves additional health service visits for diabetes education, glucose monitoring review, and fetal ultrasonography, all of which carry exposure risks during a pandemic,” Dr. McIntyre and Dr. Moses noted.
Professional societies in the United Kingdom, Canada, and Australia have issued guidance to clinicians for modifying GDM diagnoses criteria during the pandemic that aim to reduce the need for the oral glucose tolerance test both during and after pregnancy.
Pandemic guidelines for all three of these countries support the identification of GDM using early pregnancy hemoglobin A1c (HbA1c) of at least 41 mmol/mol (5.9%).
Then, professionals in the United Kingdom recommend testing based on risk factors and diagnosing GDM based on any of these criteria: HbA1c of at least 39 mmol/mol (5.7%), fasting venous plasma glucose of at least 5.6 mmol/L (preferred), or random VPG of at least 9.0 mmol/L.
The revised testing pathway for Canada accepts an HbA1c of at least 39 mmol/mol (5.7%) and/or random VPG of at least 11.1 mmol/L.
“The revised Australian pathway does not include HbA1c but recommends a fasting VPG with progression to OGTT only if this result is 4.7-5.0 mmol/L,” Dr. McIntyre and Dr. Moses explained.
Overall, the revised guidelines for GDM testing will likely miss some women and only identify those with higher levels of hyperglycemia, the authors wrote. In addition, “the evidence base for these revised pathways is limited and that each alternative strategy should be evaluated over the course of the current pandemic.”
Validation of new testing strategies are needed, and the pandemic may provide and opportunity to adopt an alternative to the OGTT. The World Health Organization has not issued revised guidance for other methods of testing, but fasting VPG alone may be the simplest and most cost effective, at least for the short term, they noted.
“In this ‘new COVID world,’ GDM should not be ignored but pragmatically merits a lower priority than the avoidance of exposure to the COVID-19 virus,” although no single alternative strategy applies in all countries and situations, the authors concluded. Pragmatic measures and documentation of outcomes at the local level will offer the “least worst” solution while the pandemic continues.
The authors had no relevant financial disclosures.
SOURCE: McIntyre HD, Moses RG. Diabetes Care. 2020 May. doi: 10.2337/dci20-0026.
A major concern against the backdrop of COVID-19 is ensuring long-term health while urgent care is – understandably so – being prioritized over preventive care. We can already see the impact that the decrease in primary care has had: Rates of childhood vaccination appear to have dropped; the cancellation or indefinite delay of elective medical procedures has meant a reduction in preventive cancer screenings, such as colonoscopies and mammograms; and concerns about COVID-19 may be keeping those experiencing cardiac events from seeking emergency care.
However, an outcropping of the coronavirus pandemic is an ingenuity to adapt to our new “normal.” Medical licenses have been recognized across state lines to allow much-needed professionals to practice in the hardest-hit areas. Doctors retrofitted a sleep apnea machine to be used as a makeshift ventilator. Those in the wearable device market now have a greater onus to deliver on quality, utility, security, and accuracy.
Obstetricians have had to dramatically change delivery of ante-, intra- and postpartum care. The recent commentary by Dr. McIntyre and Dr. Moses focuses on one particular area of concern: screening, diagnosis, and management of gestational diabetes mellitus (GDM).
Screening and diagnosis are mainstays to reduce the adverse maternal and neonatal outcomes of diabetes in pregnancy. Although there is no universally accepted approach to evaluating GDM, all current methods utilize an oral glucose tolerance test (OGTT), which requires significant time spent in a clinical office setting, thus increasing risk for COVID-19 exposure.
Several countries have adopted modified GDM criteria within the last months. At the time of this writing, the United States has not. Although not testing women for GDM, which is what Dr. McIntyre and Dr. Moses point out may be happening in countries with modified guidelines, seems questionable, perhaps we should think differently about our approach.
More than 20 years ago, it was reported that jelly beans could be used as an alternative to the 50-g GDM screening test (Am J Obstet Gynecol. 1999 Nov;181[5 Pt 1]:1154‐7; Am J Obstet Gynecol. 1995 Dec;173[6]:1889‐92); more recently, candy twists were used with similar results (Am J Obstet Gynecol. 2015 Apr;212[4]:522.e1-5). In addition, a number of articles have reported on the utility of capillary whole blood glucose measurements to screen for GDM in developing and resource-limited countries (Diabetes Technol Ther. 2011;13[5]:586‐91; Acta Diabetol. 2016 Feb;53[1]:91‐7; Diabetes Technol Ther. 2012 Feb;14[2]:131-4). Therefore, rather than forgo GDM screening, women could self-administer a jelly bean test at home, measure blood sugar with a glucometer, and depending on the results, have an OGTT. Importantly, this would allow ob.gyns. to maintain medical standards while managing patients via telemedicine.
We have evidence that GDM can establish poor health for generations. We know that people with underlying conditions have greater morbidity and mortality from infectious diseases. We recognize that accurate screening and diagnosis is the key to prevention and management. Rather than accept a “least worst” scenario, as Dr. McIntyre and Dr. Moses state, we must find ways to provide the best possible care under the current circumstances.
E. Albert Reece, MD, PhD, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the University of Maryland School of Medicine. He said he had no relevant financial disclosures. He is a member of the Ob.Gyn. News editorial advisory board.
A major concern against the backdrop of COVID-19 is ensuring long-term health while urgent care is – understandably so – being prioritized over preventive care. We can already see the impact that the decrease in primary care has had: Rates of childhood vaccination appear to have dropped; the cancellation or indefinite delay of elective medical procedures has meant a reduction in preventive cancer screenings, such as colonoscopies and mammograms; and concerns about COVID-19 may be keeping those experiencing cardiac events from seeking emergency care.
However, an outcropping of the coronavirus pandemic is an ingenuity to adapt to our new “normal.” Medical licenses have been recognized across state lines to allow much-needed professionals to practice in the hardest-hit areas. Doctors retrofitted a sleep apnea machine to be used as a makeshift ventilator. Those in the wearable device market now have a greater onus to deliver on quality, utility, security, and accuracy.
Obstetricians have had to dramatically change delivery of ante-, intra- and postpartum care. The recent commentary by Dr. McIntyre and Dr. Moses focuses on one particular area of concern: screening, diagnosis, and management of gestational diabetes mellitus (GDM).
Screening and diagnosis are mainstays to reduce the adverse maternal and neonatal outcomes of diabetes in pregnancy. Although there is no universally accepted approach to evaluating GDM, all current methods utilize an oral glucose tolerance test (OGTT), which requires significant time spent in a clinical office setting, thus increasing risk for COVID-19 exposure.
Several countries have adopted modified GDM criteria within the last months. At the time of this writing, the United States has not. Although not testing women for GDM, which is what Dr. McIntyre and Dr. Moses point out may be happening in countries with modified guidelines, seems questionable, perhaps we should think differently about our approach.
More than 20 years ago, it was reported that jelly beans could be used as an alternative to the 50-g GDM screening test (Am J Obstet Gynecol. 1999 Nov;181[5 Pt 1]:1154‐7; Am J Obstet Gynecol. 1995 Dec;173[6]:1889‐92); more recently, candy twists were used with similar results (Am J Obstet Gynecol. 2015 Apr;212[4]:522.e1-5). In addition, a number of articles have reported on the utility of capillary whole blood glucose measurements to screen for GDM in developing and resource-limited countries (Diabetes Technol Ther. 2011;13[5]:586‐91; Acta Diabetol. 2016 Feb;53[1]:91‐7; Diabetes Technol Ther. 2012 Feb;14[2]:131-4). Therefore, rather than forgo GDM screening, women could self-administer a jelly bean test at home, measure blood sugar with a glucometer, and depending on the results, have an OGTT. Importantly, this would allow ob.gyns. to maintain medical standards while managing patients via telemedicine.
We have evidence that GDM can establish poor health for generations. We know that people with underlying conditions have greater morbidity and mortality from infectious diseases. We recognize that accurate screening and diagnosis is the key to prevention and management. Rather than accept a “least worst” scenario, as Dr. McIntyre and Dr. Moses state, we must find ways to provide the best possible care under the current circumstances.
E. Albert Reece, MD, PhD, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the University of Maryland School of Medicine. He said he had no relevant financial disclosures. He is a member of the Ob.Gyn. News editorial advisory board.
A major concern against the backdrop of COVID-19 is ensuring long-term health while urgent care is – understandably so – being prioritized over preventive care. We can already see the impact that the decrease in primary care has had: Rates of childhood vaccination appear to have dropped; the cancellation or indefinite delay of elective medical procedures has meant a reduction in preventive cancer screenings, such as colonoscopies and mammograms; and concerns about COVID-19 may be keeping those experiencing cardiac events from seeking emergency care.
However, an outcropping of the coronavirus pandemic is an ingenuity to adapt to our new “normal.” Medical licenses have been recognized across state lines to allow much-needed professionals to practice in the hardest-hit areas. Doctors retrofitted a sleep apnea machine to be used as a makeshift ventilator. Those in the wearable device market now have a greater onus to deliver on quality, utility, security, and accuracy.
Obstetricians have had to dramatically change delivery of ante-, intra- and postpartum care. The recent commentary by Dr. McIntyre and Dr. Moses focuses on one particular area of concern: screening, diagnosis, and management of gestational diabetes mellitus (GDM).
Screening and diagnosis are mainstays to reduce the adverse maternal and neonatal outcomes of diabetes in pregnancy. Although there is no universally accepted approach to evaluating GDM, all current methods utilize an oral glucose tolerance test (OGTT), which requires significant time spent in a clinical office setting, thus increasing risk for COVID-19 exposure.
Several countries have adopted modified GDM criteria within the last months. At the time of this writing, the United States has not. Although not testing women for GDM, which is what Dr. McIntyre and Dr. Moses point out may be happening in countries with modified guidelines, seems questionable, perhaps we should think differently about our approach.
More than 20 years ago, it was reported that jelly beans could be used as an alternative to the 50-g GDM screening test (Am J Obstet Gynecol. 1999 Nov;181[5 Pt 1]:1154‐7; Am J Obstet Gynecol. 1995 Dec;173[6]:1889‐92); more recently, candy twists were used with similar results (Am J Obstet Gynecol. 2015 Apr;212[4]:522.e1-5). In addition, a number of articles have reported on the utility of capillary whole blood glucose measurements to screen for GDM in developing and resource-limited countries (Diabetes Technol Ther. 2011;13[5]:586‐91; Acta Diabetol. 2016 Feb;53[1]:91‐7; Diabetes Technol Ther. 2012 Feb;14[2]:131-4). Therefore, rather than forgo GDM screening, women could self-administer a jelly bean test at home, measure blood sugar with a glucometer, and depending on the results, have an OGTT. Importantly, this would allow ob.gyns. to maintain medical standards while managing patients via telemedicine.
We have evidence that GDM can establish poor health for generations. We know that people with underlying conditions have greater morbidity and mortality from infectious diseases. We recognize that accurate screening and diagnosis is the key to prevention and management. Rather than accept a “least worst” scenario, as Dr. McIntyre and Dr. Moses state, we must find ways to provide the best possible care under the current circumstances.
E. Albert Reece, MD, PhD, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the University of Maryland School of Medicine. He said he had no relevant financial disclosures. He is a member of the Ob.Gyn. News editorial advisory board.
Clinicians and pregnant women are less likely to prescribe and undergo the oral glucose tolerance test (OGTT) to diagnose gestational diabetes in the context of the COVID-19 pandemic, according to a review by H. David McIntyre, MD, of the University of Queensland, Brisbane, Australia, and Robert G. Moses, MD, of Wollongong (Australia) Hospital.
National and international discussions of whether a one- or two-step test for gestational diabetes mellitus (GDM) is optimal, and which women should be tested are ongoing, but the potential for exposure risks to COVID-19 are impacting the test process, they wrote in a commentary published in Diabetes Care.
“Any national or local guidelines should be developed with the primary aim of being protective for pregnant women and workable in the current health crisis,” they wrote.
Key concerns expressed by women and health care providers include the need for travel to be tested, the possible need for two visits, and the several hours spent in a potentially high-risk specimen collection center.
“Further, a GDM diagnosis generally involves additional health service visits for diabetes education, glucose monitoring review, and fetal ultrasonography, all of which carry exposure risks during a pandemic,” Dr. McIntyre and Dr. Moses noted.
Professional societies in the United Kingdom, Canada, and Australia have issued guidance to clinicians for modifying GDM diagnoses criteria during the pandemic that aim to reduce the need for the oral glucose tolerance test both during and after pregnancy.
Pandemic guidelines for all three of these countries support the identification of GDM using early pregnancy hemoglobin A1c (HbA1c) of at least 41 mmol/mol (5.9%).
Then, professionals in the United Kingdom recommend testing based on risk factors and diagnosing GDM based on any of these criteria: HbA1c of at least 39 mmol/mol (5.7%), fasting venous plasma glucose of at least 5.6 mmol/L (preferred), or random VPG of at least 9.0 mmol/L.
The revised testing pathway for Canada accepts an HbA1c of at least 39 mmol/mol (5.7%) and/or random VPG of at least 11.1 mmol/L.
“The revised Australian pathway does not include HbA1c but recommends a fasting VPG with progression to OGTT only if this result is 4.7-5.0 mmol/L,” Dr. McIntyre and Dr. Moses explained.
Overall, the revised guidelines for GDM testing will likely miss some women and only identify those with higher levels of hyperglycemia, the authors wrote. In addition, “the evidence base for these revised pathways is limited and that each alternative strategy should be evaluated over the course of the current pandemic.”
Validation of new testing strategies are needed, and the pandemic may provide and opportunity to adopt an alternative to the OGTT. The World Health Organization has not issued revised guidance for other methods of testing, but fasting VPG alone may be the simplest and most cost effective, at least for the short term, they noted.
“In this ‘new COVID world,’ GDM should not be ignored but pragmatically merits a lower priority than the avoidance of exposure to the COVID-19 virus,” although no single alternative strategy applies in all countries and situations, the authors concluded. Pragmatic measures and documentation of outcomes at the local level will offer the “least worst” solution while the pandemic continues.
The authors had no relevant financial disclosures.
SOURCE: McIntyre HD, Moses RG. Diabetes Care. 2020 May. doi: 10.2337/dci20-0026.
Clinicians and pregnant women are less likely to prescribe and undergo the oral glucose tolerance test (OGTT) to diagnose gestational diabetes in the context of the COVID-19 pandemic, according to a review by H. David McIntyre, MD, of the University of Queensland, Brisbane, Australia, and Robert G. Moses, MD, of Wollongong (Australia) Hospital.
National and international discussions of whether a one- or two-step test for gestational diabetes mellitus (GDM) is optimal, and which women should be tested are ongoing, but the potential for exposure risks to COVID-19 are impacting the test process, they wrote in a commentary published in Diabetes Care.
“Any national or local guidelines should be developed with the primary aim of being protective for pregnant women and workable in the current health crisis,” they wrote.
Key concerns expressed by women and health care providers include the need for travel to be tested, the possible need for two visits, and the several hours spent in a potentially high-risk specimen collection center.
“Further, a GDM diagnosis generally involves additional health service visits for diabetes education, glucose monitoring review, and fetal ultrasonography, all of which carry exposure risks during a pandemic,” Dr. McIntyre and Dr. Moses noted.
Professional societies in the United Kingdom, Canada, and Australia have issued guidance to clinicians for modifying GDM diagnoses criteria during the pandemic that aim to reduce the need for the oral glucose tolerance test both during and after pregnancy.
Pandemic guidelines for all three of these countries support the identification of GDM using early pregnancy hemoglobin A1c (HbA1c) of at least 41 mmol/mol (5.9%).
Then, professionals in the United Kingdom recommend testing based on risk factors and diagnosing GDM based on any of these criteria: HbA1c of at least 39 mmol/mol (5.7%), fasting venous plasma glucose of at least 5.6 mmol/L (preferred), or random VPG of at least 9.0 mmol/L.
The revised testing pathway for Canada accepts an HbA1c of at least 39 mmol/mol (5.7%) and/or random VPG of at least 11.1 mmol/L.
“The revised Australian pathway does not include HbA1c but recommends a fasting VPG with progression to OGTT only if this result is 4.7-5.0 mmol/L,” Dr. McIntyre and Dr. Moses explained.
Overall, the revised guidelines for GDM testing will likely miss some women and only identify those with higher levels of hyperglycemia, the authors wrote. In addition, “the evidence base for these revised pathways is limited and that each alternative strategy should be evaluated over the course of the current pandemic.”
Validation of new testing strategies are needed, and the pandemic may provide and opportunity to adopt an alternative to the OGTT. The World Health Organization has not issued revised guidance for other methods of testing, but fasting VPG alone may be the simplest and most cost effective, at least for the short term, they noted.
“In this ‘new COVID world,’ GDM should not be ignored but pragmatically merits a lower priority than the avoidance of exposure to the COVID-19 virus,” although no single alternative strategy applies in all countries and situations, the authors concluded. Pragmatic measures and documentation of outcomes at the local level will offer the “least worst” solution while the pandemic continues.
The authors had no relevant financial disclosures.
SOURCE: McIntyre HD, Moses RG. Diabetes Care. 2020 May. doi: 10.2337/dci20-0026.
Can you catch COVID-19 through your eyes?
You can catch COVID-19 if an infected person coughs or sneezes and contagious droplets enter your nose or mouth. But can you become ill if the virus lands in your eyes?
Virologist Joseph Fair, PhD, an NBC News contributor, raised that concern when he became critically ill with COVID-19, the disease caused by the coronavirus. From a hospital bed in his hometown of New Orleans, he told the network that he had flown on a crowded plane where flight attendants weren’t wearing masks. He wore a mask and gloves, but no eye protection.
“My best guess,” he told the interviewer, “was that it came through the eye route.”
Asked if people should start wearing eye protection, Dr. Fair replied, “In my opinion, yes.”
While Dr. Fair is convinced that eye protection helps, other experts aren’t sure. So much remains unknown about the new coronavirus, SARS-CoV-2, that researchers are still trying to establish whether infection can actually happen through the eyes.
“I don’t think we can answer that question with 100% confidence at this time,” said H. Nida Sen, MD, director of the uveitis clinic at the National Eye Institute in Bethesda, Md., and a clinical investigator who is studying the effects of COVID-19 on the eye. But, she says, “I think it is biologically plausible.”
Some research has begun pointing in that direction, according to Elia Duh, MD, a researcher and professor of ophthalmology at Johns Hopkins University in Baltimore.
The clear tissue that covers the white of the eye and lines the inside of the eyelid, known as the conjunctiva, “can be infected by other viruses, such as adenoviruses associated with the common cold and the herpes simplex virus,” he said.
There’s the same chance of infection with SARS-CoV-2, said Dr. Duh. “ just like the nasal passages are exposed. In addition, people rub and touch their eyes a lot. So there’s certainly already the vulnerability.”
To study whether SARS-CoV-2 could infect the eyes, Dr. Duh and fellow researchers at Johns Hopkins looked at whether the eye’s surface cells possess key factors that make the virus more likely to enter and infect them.
In their study (BioRxiv. 2020 May 9. doi: 10.1101/2020.05.09.086165), which is now being peer-reviewed, the team examined 10 postmortem eyes and five surgical samples of conjunctiva from patients who did not have the coronavirus. They wanted to see whether the eyes’ surface cells produced the key receptor for coronavirus, the ACE2 receptor.
For SARS-CoV-2 to enter a cell, “the cell has to have ACE2 on its surface so that the coronavirus can latch onto it and gain entry into the cell,” Dr. Duh said.
Not much research existed on ACE2 and the eye’s surface cells, he said. “We were really struck that ACE2 was clearly present in the surface cells of all of the specimens.” In addition, the researchers found that the eye’s surface cells also produce TMPRSS2, an enzyme that helps the virus enter the cell.
More research is needed for a definitive answer, Dr. Duh said. But “all of this evidence together seems to suggest that there’s a good likelihood that the ocular surface cells are susceptible to infection by coronavirus.”
If that’s the case, the virus then could be transmitted through the tear ducts that connect the eyes to the nasal cavity and subsequently infect the respiratory cells, he said.
Edward E. Manche, MD, professor of ophthalmology at Stanford (Calif.) University, said that while doctors don’t know for sure, many think eye infection can happen. “I think it’s widely believed now that you can acquire it through the eye. The way the virus works, it’s most commonly transmitted through the mouth and nasal passages. We have mucosal tissues where it can get in.”
Dr. Manche said the eyes would be “the least common mode of transmission.”
Besides looking at the eyes as an entryway, researchers are exploring whether people with SARS-CoV-2 in their eyes could infect others through their tears or eye secretions.
“The virus has been detected in tears and conjunctival swab specimens from individuals with COVID-19,” Dr. Duh said. “If someone rubs their eyes and then touches someone else or touches a surface, that kind of transmission mechanism could occur.
“It again highlights how contagious the coronavirus is and how stealthy it can be in its contagiousness,” he said.
If it turns out that the coronavirus can infect the eyes, the virus could persist there as a source of contagion, Dr. Duh said. “The eyes and tears could serve as a source of infection to others for longer.” He noted a case of a COVID-infected woman with conjunctivitis who still had detectable virus in her eyes 3 weeks after her symptoms started.
Conjunctivitis, commonly called pink eye, could be a symptom of COVID-19, said Dr. Sen, who is an ophthalmologist. She recommends that people get tested for COVID-19 if they have this condition, which is marked by redness, itchiness, tearing, discharge, and a gritty sensation in the eye.
Dr. Fair, the virologist, was released from the hospital to recover at home and continued to urge eye protection. “People like to call people like me fearmongers ... but the reality is, we’re just trying to keep them safe,” he told NBC News.
The CDC hasn’t issued such advice. In an email, the agency said it “does not have specific recommendations for the public regarding eye protection. However, in health care settings, the CDC does recommend eye protection for health care workers to prevent transmission via droplets.”
Dr. Sen agrees. “For the general public, I don’t think we have enough data to suggest that they should be covering the eyes in some form,” she said.
When she goes to the grocery store, she doesn’t wear eye protection. “I am only wearing goggles when I’m seeing ophthalmology patients up close, basically because I’m 4 or 5 inches away from them.”
But fuller protection – a mask, gloves, and even eye protection, such as goggles – might help those taking care of a COVID-19 patient at home, Dr. Manche said. “If you’re caring for somebody, that’s a much higher risk because they’re shedding viral load. You lessen the chance of transmission.”
For the public, Dr. Sen stresses the continued importance of hand hygiene. “In an abundance of caution, I would still encourage handwashing and not touching the eye for many reasons, not just COVID. You can transmit simple infections to your eye. We have other viruses and bacteria that are circulating in the environment and in our bodies elsewhere, so we can easily carry those to the eyes.”
Switching from contact lenses to eyeglasses could help cut down on touching the eyes, she says. Eyeglasses can also be a “mechanical barrier” to keep hands away.
Eyeglasses might block some droplets if someone nearby sneezes or coughs, Dr. Manche said, although they “aren’t sealed around the edges. They’re not like true medical goggles that are going to keep out the virus.”
Dr. Duh agrees that health care workers must don eye protection, but he said the public doesn’t need to start wearing goggles, face shields, or other eye protection. “I still think the major mode of transmission is through the nasal passages and the respiratory system,” he said.
It’s unclear whether eye protection is warranted for airplane passengers, Dr. Manche said. “It probably wouldn’t hurt, but I think the more important thing would be to take precautions: wearing a face mask, washing your hands, cleaning the seats and tray tables in front of you, and not touching things and touching your face and eyes.”
A version of this article originally appeared on WebMD.com.
You can catch COVID-19 if an infected person coughs or sneezes and contagious droplets enter your nose or mouth. But can you become ill if the virus lands in your eyes?
Virologist Joseph Fair, PhD, an NBC News contributor, raised that concern when he became critically ill with COVID-19, the disease caused by the coronavirus. From a hospital bed in his hometown of New Orleans, he told the network that he had flown on a crowded plane where flight attendants weren’t wearing masks. He wore a mask and gloves, but no eye protection.
“My best guess,” he told the interviewer, “was that it came through the eye route.”
Asked if people should start wearing eye protection, Dr. Fair replied, “In my opinion, yes.”
While Dr. Fair is convinced that eye protection helps, other experts aren’t sure. So much remains unknown about the new coronavirus, SARS-CoV-2, that researchers are still trying to establish whether infection can actually happen through the eyes.
“I don’t think we can answer that question with 100% confidence at this time,” said H. Nida Sen, MD, director of the uveitis clinic at the National Eye Institute in Bethesda, Md., and a clinical investigator who is studying the effects of COVID-19 on the eye. But, she says, “I think it is biologically plausible.”
Some research has begun pointing in that direction, according to Elia Duh, MD, a researcher and professor of ophthalmology at Johns Hopkins University in Baltimore.
The clear tissue that covers the white of the eye and lines the inside of the eyelid, known as the conjunctiva, “can be infected by other viruses, such as adenoviruses associated with the common cold and the herpes simplex virus,” he said.
There’s the same chance of infection with SARS-CoV-2, said Dr. Duh. “ just like the nasal passages are exposed. In addition, people rub and touch their eyes a lot. So there’s certainly already the vulnerability.”
To study whether SARS-CoV-2 could infect the eyes, Dr. Duh and fellow researchers at Johns Hopkins looked at whether the eye’s surface cells possess key factors that make the virus more likely to enter and infect them.
In their study (BioRxiv. 2020 May 9. doi: 10.1101/2020.05.09.086165), which is now being peer-reviewed, the team examined 10 postmortem eyes and five surgical samples of conjunctiva from patients who did not have the coronavirus. They wanted to see whether the eyes’ surface cells produced the key receptor for coronavirus, the ACE2 receptor.
For SARS-CoV-2 to enter a cell, “the cell has to have ACE2 on its surface so that the coronavirus can latch onto it and gain entry into the cell,” Dr. Duh said.
Not much research existed on ACE2 and the eye’s surface cells, he said. “We were really struck that ACE2 was clearly present in the surface cells of all of the specimens.” In addition, the researchers found that the eye’s surface cells also produce TMPRSS2, an enzyme that helps the virus enter the cell.
More research is needed for a definitive answer, Dr. Duh said. But “all of this evidence together seems to suggest that there’s a good likelihood that the ocular surface cells are susceptible to infection by coronavirus.”
If that’s the case, the virus then could be transmitted through the tear ducts that connect the eyes to the nasal cavity and subsequently infect the respiratory cells, he said.
Edward E. Manche, MD, professor of ophthalmology at Stanford (Calif.) University, said that while doctors don’t know for sure, many think eye infection can happen. “I think it’s widely believed now that you can acquire it through the eye. The way the virus works, it’s most commonly transmitted through the mouth and nasal passages. We have mucosal tissues where it can get in.”
Dr. Manche said the eyes would be “the least common mode of transmission.”
Besides looking at the eyes as an entryway, researchers are exploring whether people with SARS-CoV-2 in their eyes could infect others through their tears or eye secretions.
“The virus has been detected in tears and conjunctival swab specimens from individuals with COVID-19,” Dr. Duh said. “If someone rubs their eyes and then touches someone else or touches a surface, that kind of transmission mechanism could occur.
“It again highlights how contagious the coronavirus is and how stealthy it can be in its contagiousness,” he said.
If it turns out that the coronavirus can infect the eyes, the virus could persist there as a source of contagion, Dr. Duh said. “The eyes and tears could serve as a source of infection to others for longer.” He noted a case of a COVID-infected woman with conjunctivitis who still had detectable virus in her eyes 3 weeks after her symptoms started.
Conjunctivitis, commonly called pink eye, could be a symptom of COVID-19, said Dr. Sen, who is an ophthalmologist. She recommends that people get tested for COVID-19 if they have this condition, which is marked by redness, itchiness, tearing, discharge, and a gritty sensation in the eye.
Dr. Fair, the virologist, was released from the hospital to recover at home and continued to urge eye protection. “People like to call people like me fearmongers ... but the reality is, we’re just trying to keep them safe,” he told NBC News.
The CDC hasn’t issued such advice. In an email, the agency said it “does not have specific recommendations for the public regarding eye protection. However, in health care settings, the CDC does recommend eye protection for health care workers to prevent transmission via droplets.”
Dr. Sen agrees. “For the general public, I don’t think we have enough data to suggest that they should be covering the eyes in some form,” she said.
When she goes to the grocery store, she doesn’t wear eye protection. “I am only wearing goggles when I’m seeing ophthalmology patients up close, basically because I’m 4 or 5 inches away from them.”
But fuller protection – a mask, gloves, and even eye protection, such as goggles – might help those taking care of a COVID-19 patient at home, Dr. Manche said. “If you’re caring for somebody, that’s a much higher risk because they’re shedding viral load. You lessen the chance of transmission.”
For the public, Dr. Sen stresses the continued importance of hand hygiene. “In an abundance of caution, I would still encourage handwashing and not touching the eye for many reasons, not just COVID. You can transmit simple infections to your eye. We have other viruses and bacteria that are circulating in the environment and in our bodies elsewhere, so we can easily carry those to the eyes.”
Switching from contact lenses to eyeglasses could help cut down on touching the eyes, she says. Eyeglasses can also be a “mechanical barrier” to keep hands away.
Eyeglasses might block some droplets if someone nearby sneezes or coughs, Dr. Manche said, although they “aren’t sealed around the edges. They’re not like true medical goggles that are going to keep out the virus.”
Dr. Duh agrees that health care workers must don eye protection, but he said the public doesn’t need to start wearing goggles, face shields, or other eye protection. “I still think the major mode of transmission is through the nasal passages and the respiratory system,” he said.
It’s unclear whether eye protection is warranted for airplane passengers, Dr. Manche said. “It probably wouldn’t hurt, but I think the more important thing would be to take precautions: wearing a face mask, washing your hands, cleaning the seats and tray tables in front of you, and not touching things and touching your face and eyes.”
A version of this article originally appeared on WebMD.com.
You can catch COVID-19 if an infected person coughs or sneezes and contagious droplets enter your nose or mouth. But can you become ill if the virus lands in your eyes?
Virologist Joseph Fair, PhD, an NBC News contributor, raised that concern when he became critically ill with COVID-19, the disease caused by the coronavirus. From a hospital bed in his hometown of New Orleans, he told the network that he had flown on a crowded plane where flight attendants weren’t wearing masks. He wore a mask and gloves, but no eye protection.
“My best guess,” he told the interviewer, “was that it came through the eye route.”
Asked if people should start wearing eye protection, Dr. Fair replied, “In my opinion, yes.”
While Dr. Fair is convinced that eye protection helps, other experts aren’t sure. So much remains unknown about the new coronavirus, SARS-CoV-2, that researchers are still trying to establish whether infection can actually happen through the eyes.
“I don’t think we can answer that question with 100% confidence at this time,” said H. Nida Sen, MD, director of the uveitis clinic at the National Eye Institute in Bethesda, Md., and a clinical investigator who is studying the effects of COVID-19 on the eye. But, she says, “I think it is biologically plausible.”
Some research has begun pointing in that direction, according to Elia Duh, MD, a researcher and professor of ophthalmology at Johns Hopkins University in Baltimore.
The clear tissue that covers the white of the eye and lines the inside of the eyelid, known as the conjunctiva, “can be infected by other viruses, such as adenoviruses associated with the common cold and the herpes simplex virus,” he said.
There’s the same chance of infection with SARS-CoV-2, said Dr. Duh. “ just like the nasal passages are exposed. In addition, people rub and touch their eyes a lot. So there’s certainly already the vulnerability.”
To study whether SARS-CoV-2 could infect the eyes, Dr. Duh and fellow researchers at Johns Hopkins looked at whether the eye’s surface cells possess key factors that make the virus more likely to enter and infect them.
In their study (BioRxiv. 2020 May 9. doi: 10.1101/2020.05.09.086165), which is now being peer-reviewed, the team examined 10 postmortem eyes and five surgical samples of conjunctiva from patients who did not have the coronavirus. They wanted to see whether the eyes’ surface cells produced the key receptor for coronavirus, the ACE2 receptor.
For SARS-CoV-2 to enter a cell, “the cell has to have ACE2 on its surface so that the coronavirus can latch onto it and gain entry into the cell,” Dr. Duh said.
Not much research existed on ACE2 and the eye’s surface cells, he said. “We were really struck that ACE2 was clearly present in the surface cells of all of the specimens.” In addition, the researchers found that the eye’s surface cells also produce TMPRSS2, an enzyme that helps the virus enter the cell.
More research is needed for a definitive answer, Dr. Duh said. But “all of this evidence together seems to suggest that there’s a good likelihood that the ocular surface cells are susceptible to infection by coronavirus.”
If that’s the case, the virus then could be transmitted through the tear ducts that connect the eyes to the nasal cavity and subsequently infect the respiratory cells, he said.
Edward E. Manche, MD, professor of ophthalmology at Stanford (Calif.) University, said that while doctors don’t know for sure, many think eye infection can happen. “I think it’s widely believed now that you can acquire it through the eye. The way the virus works, it’s most commonly transmitted through the mouth and nasal passages. We have mucosal tissues where it can get in.”
Dr. Manche said the eyes would be “the least common mode of transmission.”
Besides looking at the eyes as an entryway, researchers are exploring whether people with SARS-CoV-2 in their eyes could infect others through their tears or eye secretions.
“The virus has been detected in tears and conjunctival swab specimens from individuals with COVID-19,” Dr. Duh said. “If someone rubs their eyes and then touches someone else or touches a surface, that kind of transmission mechanism could occur.
“It again highlights how contagious the coronavirus is and how stealthy it can be in its contagiousness,” he said.
If it turns out that the coronavirus can infect the eyes, the virus could persist there as a source of contagion, Dr. Duh said. “The eyes and tears could serve as a source of infection to others for longer.” He noted a case of a COVID-infected woman with conjunctivitis who still had detectable virus in her eyes 3 weeks after her symptoms started.
Conjunctivitis, commonly called pink eye, could be a symptom of COVID-19, said Dr. Sen, who is an ophthalmologist. She recommends that people get tested for COVID-19 if they have this condition, which is marked by redness, itchiness, tearing, discharge, and a gritty sensation in the eye.
Dr. Fair, the virologist, was released from the hospital to recover at home and continued to urge eye protection. “People like to call people like me fearmongers ... but the reality is, we’re just trying to keep them safe,” he told NBC News.
The CDC hasn’t issued such advice. In an email, the agency said it “does not have specific recommendations for the public regarding eye protection. However, in health care settings, the CDC does recommend eye protection for health care workers to prevent transmission via droplets.”
Dr. Sen agrees. “For the general public, I don’t think we have enough data to suggest that they should be covering the eyes in some form,” she said.
When she goes to the grocery store, she doesn’t wear eye protection. “I am only wearing goggles when I’m seeing ophthalmology patients up close, basically because I’m 4 or 5 inches away from them.”
But fuller protection – a mask, gloves, and even eye protection, such as goggles – might help those taking care of a COVID-19 patient at home, Dr. Manche said. “If you’re caring for somebody, that’s a much higher risk because they’re shedding viral load. You lessen the chance of transmission.”
For the public, Dr. Sen stresses the continued importance of hand hygiene. “In an abundance of caution, I would still encourage handwashing and not touching the eye for many reasons, not just COVID. You can transmit simple infections to your eye. We have other viruses and bacteria that are circulating in the environment and in our bodies elsewhere, so we can easily carry those to the eyes.”
Switching from contact lenses to eyeglasses could help cut down on touching the eyes, she says. Eyeglasses can also be a “mechanical barrier” to keep hands away.
Eyeglasses might block some droplets if someone nearby sneezes or coughs, Dr. Manche said, although they “aren’t sealed around the edges. They’re not like true medical goggles that are going to keep out the virus.”
Dr. Duh agrees that health care workers must don eye protection, but he said the public doesn’t need to start wearing goggles, face shields, or other eye protection. “I still think the major mode of transmission is through the nasal passages and the respiratory system,” he said.
It’s unclear whether eye protection is warranted for airplane passengers, Dr. Manche said. “It probably wouldn’t hurt, but I think the more important thing would be to take precautions: wearing a face mask, washing your hands, cleaning the seats and tray tables in front of you, and not touching things and touching your face and eyes.”
A version of this article originally appeared on WebMD.com.
Severe disease not uncommon in children hospitalized with COVID-19
Children with COVID-19 are more likely to develop severe illness and require intensive care than previously realized, data from a single-center study suggest.
Jerry Y. Chao, MD, of the department of anesthesiology, Albert Einstein College of Medicine, New York, and colleagues reported their findings in an article published online May 11 in the Journal of Pediatrics.
“Thankfully most children with COVID-19 fare well, and some do not have any symptoms at all, but this research is a sobering reminder that children are not immune to this virus and some do require a higher level of care,” senior author Shivanand S. Medar, MD, FAAP, attending physician, Cardiac Intensive Care, Children’s Hospital at Montefiore, and assistant professor of pediatrics, Albert Einstein College of Medicine, said in a Montefiore Medical Center news release.
The study included 67 patients aged 1 month to 21 years (median, 13.1 years) who were treated for COVID-19 at a tertiary care children’s hospital between March 15 and April 13. Of those, 21 (31.3%) were treated as outpatients.
“As the number of patients screened for COVID-19 was restricted during the first weeks of the outbreak because of limited testing availability, the number of mildly symptomatic patients is not known, and therefore these 21 patients are not included in the analysis,” the authors wrote.
Of the 46 hospitalized patients, 33 (72%) were admitted to a general pediatric medical ward, and 13 (28%) were admitted to the pediatric intensive care unit (PICU).
Almost one-third (14 children; 30.4%) of the admitted patients were obese, and almost one-quarter (11 children; 24.4%) had asthma, but neither factor was associated with an increased risk for PICU admission.
“We know that in adults, obesity is a risk factor for more severe disease, however, surprisingly, our study found that children admitted to the intensive care unit did not have a higher prevalence of obesity than those on the general unit,” Dr. Chao said in the news release.
Three of the PICU patients (25%) had preexisting seizure disorders, as did one (3%) patient on the general medical unit. “There was no significant difference in the usage of ibuprofen prior to hospitalization among patients admitted to medical unit compared with those admitted to the PICU,” the authors wrote.
Platelet counts were lower in patients admitted to the PICU compared with those on the general medical unit; however, C-reactive protein, procalcitonin, and pro–brain natriuretic peptide levels were all elevated in patients admitted to the PICU compared with those admitted to the general medical unit.
Patients admitted to the PICU were more likely to need high-flow nasal cannula. Ten (77%) patients in the PICU developed acute respiratory distress syndrome (ARDS), and six (46.2%) of them needed “invasive mechanical ventilation for a median of 9 days.”
The only clinical symptom significantly linked to PICU admission was shortness of breath (92.3% vs 30.3%; P < .001).
Eight (61.5%) of the 13 patients treated in the PICU were discharged to home; four (30.7%) were still hospitalized and receiving ventilatory support on day 14. One patient had metastatic cancer and died as a result of the cancer after life-sustaining therapy was withdrawn.
Those admitted to the PICU were more likely to receive treatment with remdesivir via compassionate use compared with those treated in the general medical unit. Seven (53.8%) patients in the PICU developed severe sepsis and septic shock syndromes.
The average hospital stay was 4 days longer for the children admitted to the PICU than for the children admitted to the general medical unit.
Cough (63%) and fever (60.9%) were the most frequently reported symptoms at admission. The median duration of symptoms before admission was 3 days. None of the children had traveled to an area affected by COVID-19 before becoming ill, and only 20 (43.5%) children were confirmed to have had contact with someone with COVID-19. “The lack of a known sick contact reported in our study may have implications for how healthcare providers identify and screen for potential cases,” the authors explained.
Although children are believed to experience milder SARS-CoV-2 illness, these results and those of an earlier study suggest that some pediatric patients develop illness severe enough to require PICU admission. “This subset had significantly higher markers of inflammation (CRP, pro-BNP, procalcitonin) compared with patients in the medical unit. Inflammation likely contributed to the high rate of ARDS we observed, although serum levels of IL-6 and other cytokines linked to ARDS were not determined,” the authors wrote.
A retrospective cohort study found that of 177 children and young adults treated in a single center, patients younger than 1 year and older than 15 years were more likely to become critically ill with COVID-19 (J Pediatr. 2020 May. doi: 10.1016/j.jpeds.2020.05.007).
Each of the two age groups accounted for 32% of the hospitalized patients.
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Children with COVID-19 are more likely to develop severe illness and require intensive care than previously realized, data from a single-center study suggest.
Jerry Y. Chao, MD, of the department of anesthesiology, Albert Einstein College of Medicine, New York, and colleagues reported their findings in an article published online May 11 in the Journal of Pediatrics.
“Thankfully most children with COVID-19 fare well, and some do not have any symptoms at all, but this research is a sobering reminder that children are not immune to this virus and some do require a higher level of care,” senior author Shivanand S. Medar, MD, FAAP, attending physician, Cardiac Intensive Care, Children’s Hospital at Montefiore, and assistant professor of pediatrics, Albert Einstein College of Medicine, said in a Montefiore Medical Center news release.
The study included 67 patients aged 1 month to 21 years (median, 13.1 years) who were treated for COVID-19 at a tertiary care children’s hospital between March 15 and April 13. Of those, 21 (31.3%) were treated as outpatients.
“As the number of patients screened for COVID-19 was restricted during the first weeks of the outbreak because of limited testing availability, the number of mildly symptomatic patients is not known, and therefore these 21 patients are not included in the analysis,” the authors wrote.
Of the 46 hospitalized patients, 33 (72%) were admitted to a general pediatric medical ward, and 13 (28%) were admitted to the pediatric intensive care unit (PICU).
Almost one-third (14 children; 30.4%) of the admitted patients were obese, and almost one-quarter (11 children; 24.4%) had asthma, but neither factor was associated with an increased risk for PICU admission.
“We know that in adults, obesity is a risk factor for more severe disease, however, surprisingly, our study found that children admitted to the intensive care unit did not have a higher prevalence of obesity than those on the general unit,” Dr. Chao said in the news release.
Three of the PICU patients (25%) had preexisting seizure disorders, as did one (3%) patient on the general medical unit. “There was no significant difference in the usage of ibuprofen prior to hospitalization among patients admitted to medical unit compared with those admitted to the PICU,” the authors wrote.
Platelet counts were lower in patients admitted to the PICU compared with those on the general medical unit; however, C-reactive protein, procalcitonin, and pro–brain natriuretic peptide levels were all elevated in patients admitted to the PICU compared with those admitted to the general medical unit.
Patients admitted to the PICU were more likely to need high-flow nasal cannula. Ten (77%) patients in the PICU developed acute respiratory distress syndrome (ARDS), and six (46.2%) of them needed “invasive mechanical ventilation for a median of 9 days.”
The only clinical symptom significantly linked to PICU admission was shortness of breath (92.3% vs 30.3%; P < .001).
Eight (61.5%) of the 13 patients treated in the PICU were discharged to home; four (30.7%) were still hospitalized and receiving ventilatory support on day 14. One patient had metastatic cancer and died as a result of the cancer after life-sustaining therapy was withdrawn.
Those admitted to the PICU were more likely to receive treatment with remdesivir via compassionate use compared with those treated in the general medical unit. Seven (53.8%) patients in the PICU developed severe sepsis and septic shock syndromes.
The average hospital stay was 4 days longer for the children admitted to the PICU than for the children admitted to the general medical unit.
Cough (63%) and fever (60.9%) were the most frequently reported symptoms at admission. The median duration of symptoms before admission was 3 days. None of the children had traveled to an area affected by COVID-19 before becoming ill, and only 20 (43.5%) children were confirmed to have had contact with someone with COVID-19. “The lack of a known sick contact reported in our study may have implications for how healthcare providers identify and screen for potential cases,” the authors explained.
Although children are believed to experience milder SARS-CoV-2 illness, these results and those of an earlier study suggest that some pediatric patients develop illness severe enough to require PICU admission. “This subset had significantly higher markers of inflammation (CRP, pro-BNP, procalcitonin) compared with patients in the medical unit. Inflammation likely contributed to the high rate of ARDS we observed, although serum levels of IL-6 and other cytokines linked to ARDS were not determined,” the authors wrote.
A retrospective cohort study found that of 177 children and young adults treated in a single center, patients younger than 1 year and older than 15 years were more likely to become critically ill with COVID-19 (J Pediatr. 2020 May. doi: 10.1016/j.jpeds.2020.05.007).
Each of the two age groups accounted for 32% of the hospitalized patients.
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Children with COVID-19 are more likely to develop severe illness and require intensive care than previously realized, data from a single-center study suggest.
Jerry Y. Chao, MD, of the department of anesthesiology, Albert Einstein College of Medicine, New York, and colleagues reported their findings in an article published online May 11 in the Journal of Pediatrics.
“Thankfully most children with COVID-19 fare well, and some do not have any symptoms at all, but this research is a sobering reminder that children are not immune to this virus and some do require a higher level of care,” senior author Shivanand S. Medar, MD, FAAP, attending physician, Cardiac Intensive Care, Children’s Hospital at Montefiore, and assistant professor of pediatrics, Albert Einstein College of Medicine, said in a Montefiore Medical Center news release.
The study included 67 patients aged 1 month to 21 years (median, 13.1 years) who were treated for COVID-19 at a tertiary care children’s hospital between March 15 and April 13. Of those, 21 (31.3%) were treated as outpatients.
“As the number of patients screened for COVID-19 was restricted during the first weeks of the outbreak because of limited testing availability, the number of mildly symptomatic patients is not known, and therefore these 21 patients are not included in the analysis,” the authors wrote.
Of the 46 hospitalized patients, 33 (72%) were admitted to a general pediatric medical ward, and 13 (28%) were admitted to the pediatric intensive care unit (PICU).
Almost one-third (14 children; 30.4%) of the admitted patients were obese, and almost one-quarter (11 children; 24.4%) had asthma, but neither factor was associated with an increased risk for PICU admission.
“We know that in adults, obesity is a risk factor for more severe disease, however, surprisingly, our study found that children admitted to the intensive care unit did not have a higher prevalence of obesity than those on the general unit,” Dr. Chao said in the news release.
Three of the PICU patients (25%) had preexisting seizure disorders, as did one (3%) patient on the general medical unit. “There was no significant difference in the usage of ibuprofen prior to hospitalization among patients admitted to medical unit compared with those admitted to the PICU,” the authors wrote.
Platelet counts were lower in patients admitted to the PICU compared with those on the general medical unit; however, C-reactive protein, procalcitonin, and pro–brain natriuretic peptide levels were all elevated in patients admitted to the PICU compared with those admitted to the general medical unit.
Patients admitted to the PICU were more likely to need high-flow nasal cannula. Ten (77%) patients in the PICU developed acute respiratory distress syndrome (ARDS), and six (46.2%) of them needed “invasive mechanical ventilation for a median of 9 days.”
The only clinical symptom significantly linked to PICU admission was shortness of breath (92.3% vs 30.3%; P < .001).
Eight (61.5%) of the 13 patients treated in the PICU were discharged to home; four (30.7%) were still hospitalized and receiving ventilatory support on day 14. One patient had metastatic cancer and died as a result of the cancer after life-sustaining therapy was withdrawn.
Those admitted to the PICU were more likely to receive treatment with remdesivir via compassionate use compared with those treated in the general medical unit. Seven (53.8%) patients in the PICU developed severe sepsis and septic shock syndromes.
The average hospital stay was 4 days longer for the children admitted to the PICU than for the children admitted to the general medical unit.
Cough (63%) and fever (60.9%) were the most frequently reported symptoms at admission. The median duration of symptoms before admission was 3 days. None of the children had traveled to an area affected by COVID-19 before becoming ill, and only 20 (43.5%) children were confirmed to have had contact with someone with COVID-19. “The lack of a known sick contact reported in our study may have implications for how healthcare providers identify and screen for potential cases,” the authors explained.
Although children are believed to experience milder SARS-CoV-2 illness, these results and those of an earlier study suggest that some pediatric patients develop illness severe enough to require PICU admission. “This subset had significantly higher markers of inflammation (CRP, pro-BNP, procalcitonin) compared with patients in the medical unit. Inflammation likely contributed to the high rate of ARDS we observed, although serum levels of IL-6 and other cytokines linked to ARDS were not determined,” the authors wrote.
A retrospective cohort study found that of 177 children and young adults treated in a single center, patients younger than 1 year and older than 15 years were more likely to become critically ill with COVID-19 (J Pediatr. 2020 May. doi: 10.1016/j.jpeds.2020.05.007).
Each of the two age groups accounted for 32% of the hospitalized patients.
The authors have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Cutaneous Metastatic Breast Adenocarcinoma
To the Editor:
Cutaneous metastases occur more often in the setting of breast carcinoma than other malignancies in women.1 Although interventions are aimed at halting disease progression, cutaneous metastases indicate widespread disease and are associated with poor prognosis. We present the case of a patient with metastatic breast adenocarcinoma who developed cutaneous metastasis on the trunk after a double mastectomy. The widespread distribution and wide range of clinical manifestations are unique.
An 81-year-old woman presented to the dermatology office for evaluation of a skin eruption that started along a mastectomy scar on the left breast a few months postoperatively. She had a history of stage IV breast adenocarcinoma metastatic to the chest wall that was treated with a double mastectomy 2 years prior. The patient denied associated pain or pruritus and mainly was concerned with the cosmetic appearance. At the time of the initial diagnosis of breast adenocarcinoma, the patient was offered chemotherapy, which she did not tolerate. The patient opted against radiation therapy, as she preferred a more natural approach, such as anticancer shakes, which she was taking from a homeopathic source. She was unaware of the ingredients used in the shakes.
Physical examination revealed multiple grouped, firm, purpuric papules, nodules, and pseudovesicles on a background of violaceous erythema on the chest, abdomen, and flank (Figure 1). The background erythema had a mosaic pattern that extended toward the central back (Figure 2). A scoop shave biopsy of one of the purpuric nodules revealed highly atypical cells with abundant cytoplasm, large nuclei, and prominent nucleoli (Figure 3). Focally, the cells appeared to form glandular structures. Numerous atypical mitotic figures were present. Lymphatic invasion and microcalcifications were identified (Figure 3 [inset]). Immunohistochemical staining for cytokeratin 7 and gross cystic disease fluid protein 15 were strongly positive (Figure 4). Based on the histopathologic and immunohistochemical findings, a diagnosis of cutaneous metastatic breast adenocarcinoma was made. The patient opted to continue the homeopathic anticancer shakes and was subsequently lost to follow-up.
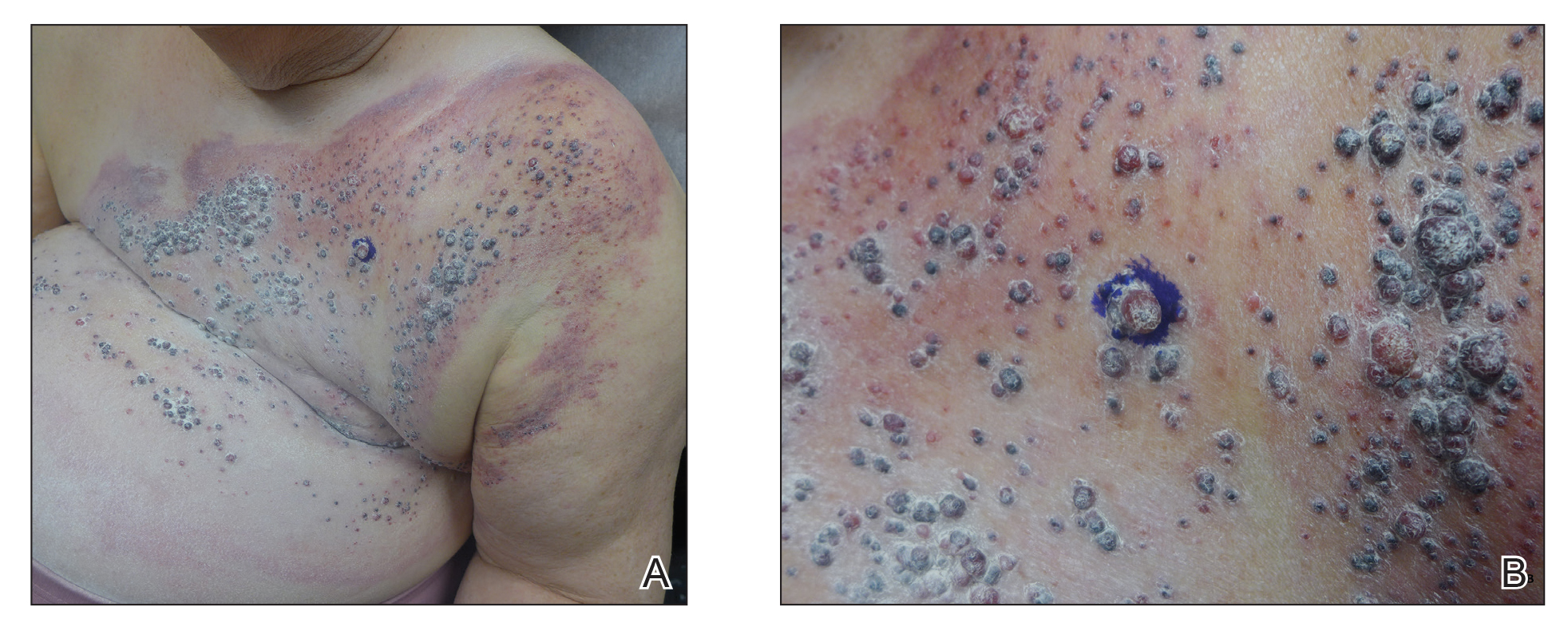

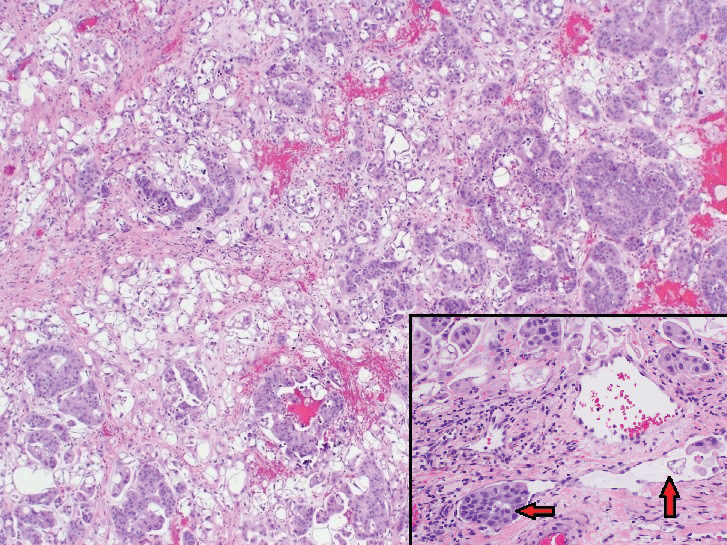
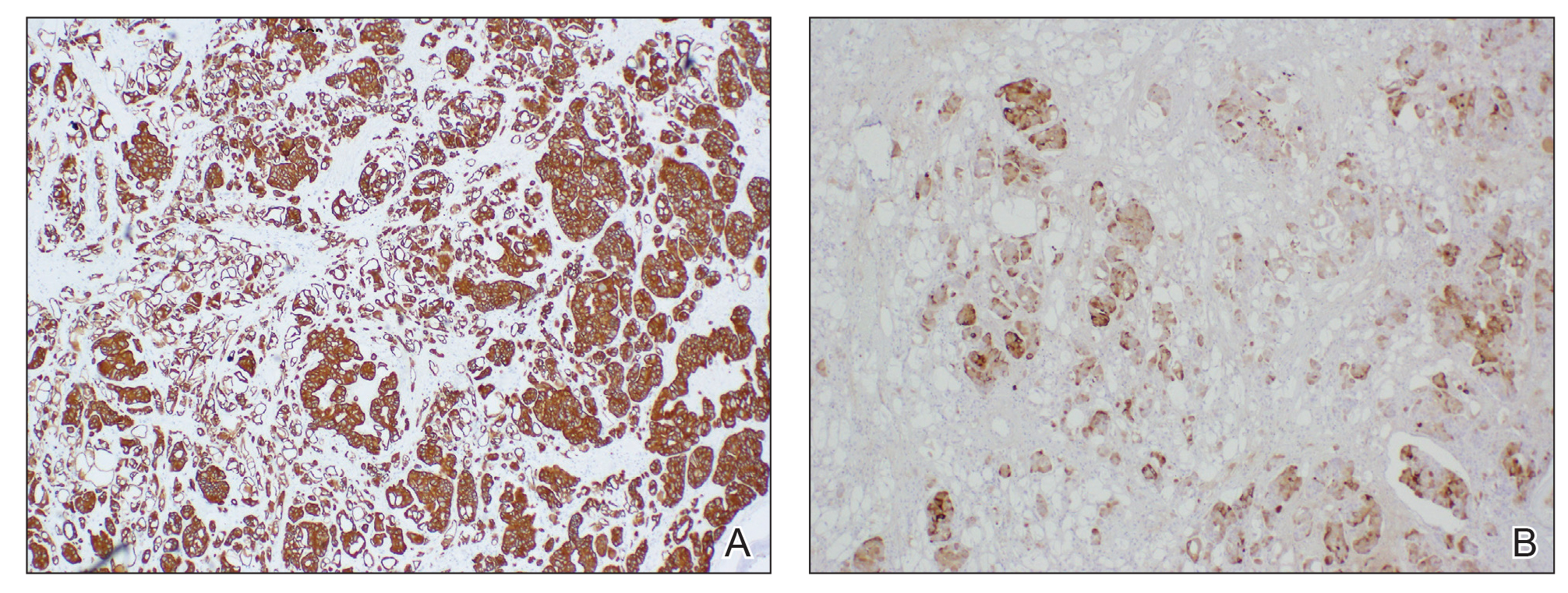
Cutaneous metastases of internal malignancies make up only 2% of all skin tumors,1 making them relatively uncommon in the dermatologic setting. However, cutaneous metastasis occurs in 23.9% of patients with breast carcinoma, making it the most common tumor after malignant melanoma to metastasize to the skin.2 The most common sites for breast carcinoma cutaneous metastasis (BCCM) are the chest wall and abdomen; other sites include the head/neck region and the extremities. The clinical presentation of BCCM varies depending on the mode of dissemination—lymphatic, hematogenous, contiguous growth, or iatrogenic implantation. The most common presentation is nodular carcinoma (47%–80%).2,3 Other presentations include carcinoma telangiectoides (8%–11%),2,3 alopecia neoplastica (2%–12%),2,3 and carcinoma erysipeloides (3%–6%).2,3 Carcinoma en cuirasse is rare.3
Nodular BCCM may present as firm solitary or grouped papules and nodules that are painless and range in color from flesh colored or pink to red-brown. Histologically, they are composed of atypical neoplastic cells arranged in small nests and cords, usually in a single-file line within the collagen bundles of the dermis.4 Carcinoma telangiectoides is characterized by its violaceous hue due to the dilated vascular channels. The lesions are purpuric papules and pseudovesicles appearing on an erythematous base, most commonly contiguous with the surgical scar. Histologically, collections of atypical tumor cells and erythrocytes are present along with dilated blood vessels in the papillary dermis.2 Alopecia neoplastica presents as singular or grouped cicatricial patches of hair loss. Lesions of carcinoma erysipeloides present as warm, erythematous, tender, well-defined patches or plaques. Carcinoma en cuirasse is characterized by an erythematous sclerodermoid plaque on the chest wall.2
Our patient’s presentation was unique due to the widespread distribution, unusual pattern, and variable clinical morphologies of the cutaneous metastases. Our patient had findings of both carcinoma telangiectoides and nodular carcinoma. The mosaic violaceous erythema extending toward the mid-back rarely is reported in the literature and indicates extensive intravascular spread of tumor cells in the dermis.
Metastatic breast cancer is associated with a poor prognosis because it typically occurs in advanced stages and often does not respond to treatment.5 Although chemotherapy, hormonal therapy, and/or radiation therapy may improve survival, the choice in regimen is guided by cancer histology as well as prior treatments. In our case, the patient chose to continue her homeopathic therapy.
- Nashan D, Meiss F, Braun-Falco M, et al. Cutaneous metastasis from internal malignancies. Dermatol Ther. 2010;23:567-580.
- De Giorgi V, Grazzini M, Alfaioli B, et al. Cutaneous manifestations of breast carcinoma. Dermatol Ther. 2010;23:581-589.
- Mordenti C, Peris K, Concetta Fargnoli M, et al. Cutaneous metastatic breast carcinoma. Acta Dermatovenerologica. 2000;9:143-148.
- Nava G, Greer K, Patterson J, et al. Metastatic cutaneous breast carcinoma: a case report and review of the literature. Can J Plast Surg. 2009;17:25-27.
- Kalmykow B, Walker S. Cutaneous metastasis in breast cancer. Clin J Oncol Nurs. 2001;15:99-101.
To the Editor:
Cutaneous metastases occur more often in the setting of breast carcinoma than other malignancies in women.1 Although interventions are aimed at halting disease progression, cutaneous metastases indicate widespread disease and are associated with poor prognosis. We present the case of a patient with metastatic breast adenocarcinoma who developed cutaneous metastasis on the trunk after a double mastectomy. The widespread distribution and wide range of clinical manifestations are unique.
An 81-year-old woman presented to the dermatology office for evaluation of a skin eruption that started along a mastectomy scar on the left breast a few months postoperatively. She had a history of stage IV breast adenocarcinoma metastatic to the chest wall that was treated with a double mastectomy 2 years prior. The patient denied associated pain or pruritus and mainly was concerned with the cosmetic appearance. At the time of the initial diagnosis of breast adenocarcinoma, the patient was offered chemotherapy, which she did not tolerate. The patient opted against radiation therapy, as she preferred a more natural approach, such as anticancer shakes, which she was taking from a homeopathic source. She was unaware of the ingredients used in the shakes.
Physical examination revealed multiple grouped, firm, purpuric papules, nodules, and pseudovesicles on a background of violaceous erythema on the chest, abdomen, and flank (Figure 1). The background erythema had a mosaic pattern that extended toward the central back (Figure 2). A scoop shave biopsy of one of the purpuric nodules revealed highly atypical cells with abundant cytoplasm, large nuclei, and prominent nucleoli (Figure 3). Focally, the cells appeared to form glandular structures. Numerous atypical mitotic figures were present. Lymphatic invasion and microcalcifications were identified (Figure 3 [inset]). Immunohistochemical staining for cytokeratin 7 and gross cystic disease fluid protein 15 were strongly positive (Figure 4). Based on the histopathologic and immunohistochemical findings, a diagnosis of cutaneous metastatic breast adenocarcinoma was made. The patient opted to continue the homeopathic anticancer shakes and was subsequently lost to follow-up.
Cutaneous metastases of internal malignancies make up only 2% of all skin tumors,1 making them relatively uncommon in the dermatologic setting. However, cutaneous metastasis occurs in 23.9% of patients with breast carcinoma, making it the most common tumor after malignant melanoma to metastasize to the skin.2 The most common sites for breast carcinoma cutaneous metastasis (BCCM) are the chest wall and abdomen; other sites include the head/neck region and the extremities. The clinical presentation of BCCM varies depending on the mode of dissemination—lymphatic, hematogenous, contiguous growth, or iatrogenic implantation. The most common presentation is nodular carcinoma (47%–80%).2,3 Other presentations include carcinoma telangiectoides (8%–11%),2,3 alopecia neoplastica (2%–12%),2,3 and carcinoma erysipeloides (3%–6%).2,3 Carcinoma en cuirasse is rare.3
Nodular BCCM may present as firm solitary or grouped papules and nodules that are painless and range in color from flesh colored or pink to red-brown. Histologically, they are composed of atypical neoplastic cells arranged in small nests and cords, usually in a single-file line within the collagen bundles of the dermis.4 Carcinoma telangiectoides is characterized by its violaceous hue due to the dilated vascular channels. The lesions are purpuric papules and pseudovesicles appearing on an erythematous base, most commonly contiguous with the surgical scar. Histologically, collections of atypical tumor cells and erythrocytes are present along with dilated blood vessels in the papillary dermis.2 Alopecia neoplastica presents as singular or grouped cicatricial patches of hair loss. Lesions of carcinoma erysipeloides present as warm, erythematous, tender, well-defined patches or plaques. Carcinoma en cuirasse is characterized by an erythematous sclerodermoid plaque on the chest wall.2
Our patient’s presentation was unique due to the widespread distribution, unusual pattern, and variable clinical morphologies of the cutaneous metastases. Our patient had findings of both carcinoma telangiectoides and nodular carcinoma. The mosaic violaceous erythema extending toward the mid-back rarely is reported in the literature and indicates extensive intravascular spread of tumor cells in the dermis.
Metastatic breast cancer is associated with a poor prognosis because it typically occurs in advanced stages and often does not respond to treatment.5 Although chemotherapy, hormonal therapy, and/or radiation therapy may improve survival, the choice in regimen is guided by cancer histology as well as prior treatments. In our case, the patient chose to continue her homeopathic therapy.
To the Editor:
Cutaneous metastases occur more often in the setting of breast carcinoma than other malignancies in women.1 Although interventions are aimed at halting disease progression, cutaneous metastases indicate widespread disease and are associated with poor prognosis. We present the case of a patient with metastatic breast adenocarcinoma who developed cutaneous metastasis on the trunk after a double mastectomy. The widespread distribution and wide range of clinical manifestations are unique.
An 81-year-old woman presented to the dermatology office for evaluation of a skin eruption that started along a mastectomy scar on the left breast a few months postoperatively. She had a history of stage IV breast adenocarcinoma metastatic to the chest wall that was treated with a double mastectomy 2 years prior. The patient denied associated pain or pruritus and mainly was concerned with the cosmetic appearance. At the time of the initial diagnosis of breast adenocarcinoma, the patient was offered chemotherapy, which she did not tolerate. The patient opted against radiation therapy, as she preferred a more natural approach, such as anticancer shakes, which she was taking from a homeopathic source. She was unaware of the ingredients used in the shakes.
Physical examination revealed multiple grouped, firm, purpuric papules, nodules, and pseudovesicles on a background of violaceous erythema on the chest, abdomen, and flank (Figure 1). The background erythema had a mosaic pattern that extended toward the central back (Figure 2). A scoop shave biopsy of one of the purpuric nodules revealed highly atypical cells with abundant cytoplasm, large nuclei, and prominent nucleoli (Figure 3). Focally, the cells appeared to form glandular structures. Numerous atypical mitotic figures were present. Lymphatic invasion and microcalcifications were identified (Figure 3 [inset]). Immunohistochemical staining for cytokeratin 7 and gross cystic disease fluid protein 15 were strongly positive (Figure 4). Based on the histopathologic and immunohistochemical findings, a diagnosis of cutaneous metastatic breast adenocarcinoma was made. The patient opted to continue the homeopathic anticancer shakes and was subsequently lost to follow-up.
Cutaneous metastases of internal malignancies make up only 2% of all skin tumors,1 making them relatively uncommon in the dermatologic setting. However, cutaneous metastasis occurs in 23.9% of patients with breast carcinoma, making it the most common tumor after malignant melanoma to metastasize to the skin.2 The most common sites for breast carcinoma cutaneous metastasis (BCCM) are the chest wall and abdomen; other sites include the head/neck region and the extremities. The clinical presentation of BCCM varies depending on the mode of dissemination—lymphatic, hematogenous, contiguous growth, or iatrogenic implantation. The most common presentation is nodular carcinoma (47%–80%).2,3 Other presentations include carcinoma telangiectoides (8%–11%),2,3 alopecia neoplastica (2%–12%),2,3 and carcinoma erysipeloides (3%–6%).2,3 Carcinoma en cuirasse is rare.3
Nodular BCCM may present as firm solitary or grouped papules and nodules that are painless and range in color from flesh colored or pink to red-brown. Histologically, they are composed of atypical neoplastic cells arranged in small nests and cords, usually in a single-file line within the collagen bundles of the dermis.4 Carcinoma telangiectoides is characterized by its violaceous hue due to the dilated vascular channels. The lesions are purpuric papules and pseudovesicles appearing on an erythematous base, most commonly contiguous with the surgical scar. Histologically, collections of atypical tumor cells and erythrocytes are present along with dilated blood vessels in the papillary dermis.2 Alopecia neoplastica presents as singular or grouped cicatricial patches of hair loss. Lesions of carcinoma erysipeloides present as warm, erythematous, tender, well-defined patches or plaques. Carcinoma en cuirasse is characterized by an erythematous sclerodermoid plaque on the chest wall.2
Our patient’s presentation was unique due to the widespread distribution, unusual pattern, and variable clinical morphologies of the cutaneous metastases. Our patient had findings of both carcinoma telangiectoides and nodular carcinoma. The mosaic violaceous erythema extending toward the mid-back rarely is reported in the literature and indicates extensive intravascular spread of tumor cells in the dermis.
Metastatic breast cancer is associated with a poor prognosis because it typically occurs in advanced stages and often does not respond to treatment.5 Although chemotherapy, hormonal therapy, and/or radiation therapy may improve survival, the choice in regimen is guided by cancer histology as well as prior treatments. In our case, the patient chose to continue her homeopathic therapy.
- Nashan D, Meiss F, Braun-Falco M, et al. Cutaneous metastasis from internal malignancies. Dermatol Ther. 2010;23:567-580.
- De Giorgi V, Grazzini M, Alfaioli B, et al. Cutaneous manifestations of breast carcinoma. Dermatol Ther. 2010;23:581-589.
- Mordenti C, Peris K, Concetta Fargnoli M, et al. Cutaneous metastatic breast carcinoma. Acta Dermatovenerologica. 2000;9:143-148.
- Nava G, Greer K, Patterson J, et al. Metastatic cutaneous breast carcinoma: a case report and review of the literature. Can J Plast Surg. 2009;17:25-27.
- Kalmykow B, Walker S. Cutaneous metastasis in breast cancer. Clin J Oncol Nurs. 2001;15:99-101.
- Nashan D, Meiss F, Braun-Falco M, et al. Cutaneous metastasis from internal malignancies. Dermatol Ther. 2010;23:567-580.
- De Giorgi V, Grazzini M, Alfaioli B, et al. Cutaneous manifestations of breast carcinoma. Dermatol Ther. 2010;23:581-589.
- Mordenti C, Peris K, Concetta Fargnoli M, et al. Cutaneous metastatic breast carcinoma. Acta Dermatovenerologica. 2000;9:143-148.
- Nava G, Greer K, Patterson J, et al. Metastatic cutaneous breast carcinoma: a case report and review of the literature. Can J Plast Surg. 2009;17:25-27.
- Kalmykow B, Walker S. Cutaneous metastasis in breast cancer. Clin J Oncol Nurs. 2001;15:99-101.
Practice Points
- Breast carcinoma is one of the most common malignancies to metastasize to the skin in women.
- Although interventions are aimed at halting disease progression, cutaneous metastases indicate widespread disease and are associated with a poor prognosis.

Penile Paraffinoma: Dramatic Recurrence After Surgical Resection
To the Editor:
The term paraffinoma refers to a chronic granulomatous response to injection of paraffin, silicone, or other mineral oils into skin and soft tissue. Paraffinomas develop when the material is injected into the skin for cosmetic purposes to augment or enhance one’s appearance. Although they may occur in any location, the most common sites include the breasts and buttocks. The penis is a rare but emerging site for paraffinomas.1-3 We present a rare case of recurrence of a penile paraffinoma following surgical resection.
A 26-year-old uncircumcised Trinidadian man presented with a 5-cm, exquisitely tender tumor involving the penile shaft and median raphe that rapidly evolved over the course of 3 weeks (Figure 1). He presented with inability to urinate, attain an erection, or ambulate without notable tenderness. Additionally, he developed swelling of the penis and surrounding tissue. He had no other medical comorbidities; however, 1 year prior he presented to a urologist with a 1-cm nodule involving the median raphe that was surgically resected and required circumcision. Biopsy at the time of his surgical procedure revealed an exuberant foreign body giant cell reaction with surrounding empty spaces in the dermis resembling Swiss cheese, consistent with a paraffinoma (Figure 2). The recurrent tumor, which was 5 times the size of the initial nodule, was biopsied. Again, histopathologic findings were consistent with a paraffinoma with extensive dermal fibrosis and absence of polarizable material.

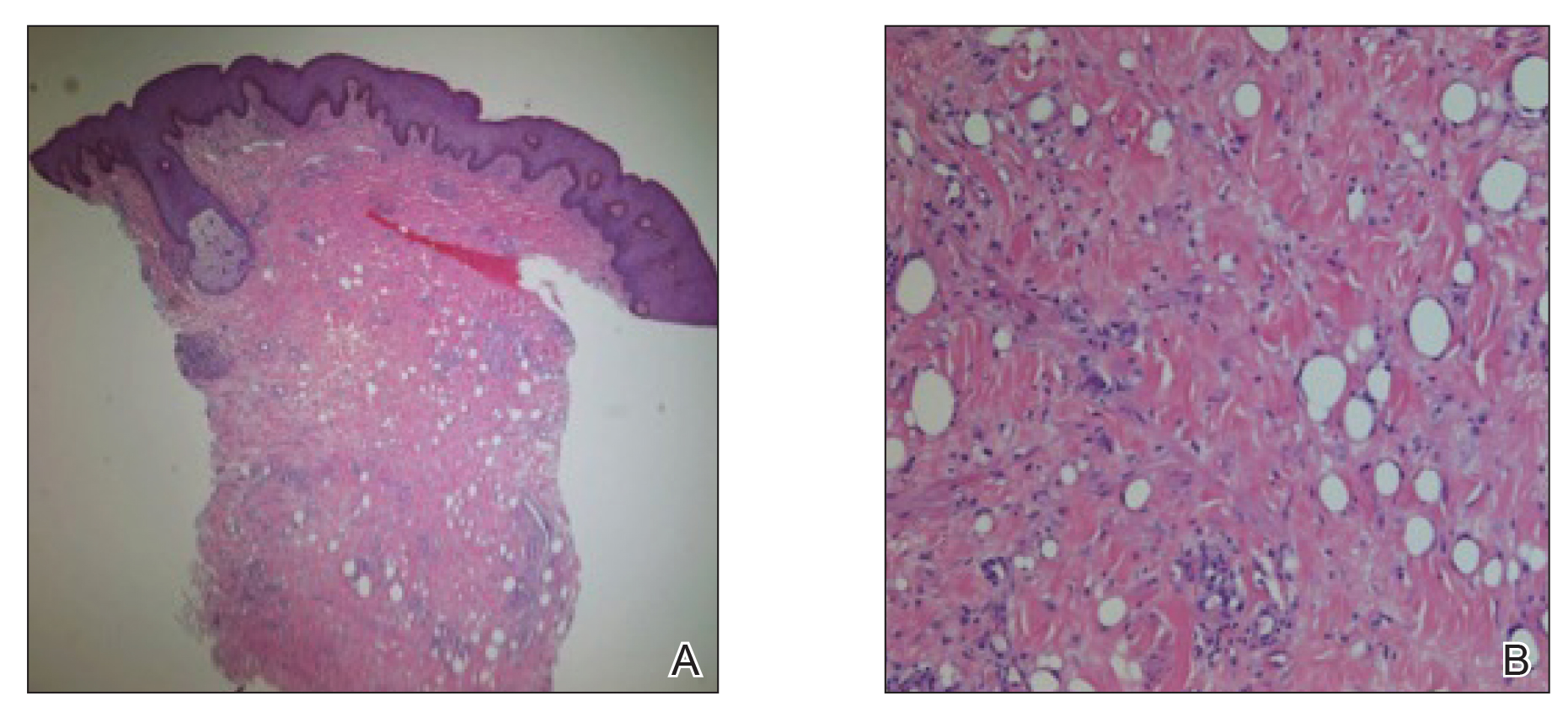
The patient underwent extensive reconstructive surgery requiring skin grafting to the penile shaft. Given the size and location of this recurrent tumor with the ability to destroy vital urologic and reproductive function, consideration for prevention of recurrent episodes included novel therapeutic treatment options to suppress inflammation and fibrosis with doxycycline and nicotinamide.
Paraffin injections are used for cosmetic enhancement and most often occur in a nonclinical setting without medical supervision, as they are not US Food and Drug Administration–approved medical injectable materials. Examples of oils injected include paraffin, camphorated oil, cottonseed or sesame oil, mineral oil, petroleum jelly, and beeswax. These oils are not hydrolyzed by tissue lipases but are instead treated as a foreign body substance with subsequent granuloma formation (also known as sclerosing lipogranuloma), which can occur many years after injection.4 The granulomatous response may be observed months to years after injection. The paraffinoma normally affects the injection site; however, regional lymphadenopathy and systemic disease has been reported.2 Histopathologic findings are characteristic and consist of a foreign body giant cell reaction, variably sized round to oval cavities within the dermis, and varying degrees of dermal fibrosis.5
In 1899, mineral oil was first injected into male genitalia to restore architecture in a patient’s testicles following bilateral orchiectomy. After the success of this endeavor, mineral oil injections were used as filler for other defects.3 However, by 1906 the complications of these injections became public knowledge when 2 patients developed subcutaneous nodules after receiving injections for facial wrinkles.2 Despite public knowledge of these complications, penile paraffin injections continued to occur both in medical and eventually nonmedical settings.
In 1947, Quérnu and Pérol6 described 6 penile paraffinoma cases outside the United States. Patients had petroleum jelly injections that eventuated in penile paraffinomas, and all of them lost the ability to attain an erection.6 Four years later, Bradley and Ehrgott7 described a case of penile paraffinoma likely caused by application of paraffin in association with occupational exposure. In 1956, May and Pickering8 cited a case of penile paraffinoma affecting the entire penile shaft in which the patient had undergone paraffin injection 7 years prior to treat premature ejaculation. Unfortunately, the injection resulted in a painful and unsatisfactory erection without resolution of premature ejaculation.8 Lee et al9 analyzed 26 cases of penile paraffinomas that occurred from 1981 to 1993. They found that all patients underwent injections of paraffin or petroleum jelly performed by nonmedical personnel with the predominant goal of enhancing penis size. Within 18.5 months of injection, 19 patients already experienced tenderness at the injection site. The remaining 7 patients experienced penile skin discoloration and abnormal contouring of the penis. Biopsy specimens revealed hyaline necrosis of subcutaneous adipose septa, cystlike spaces throughout involved tissue, and macrophages engulfing adipose tissue were found near blood vessels.9 In 2007, Eandi et al4 reported a case of penile paraffinoma with a 40-year delay of onset. Four years later, Manny et al10 reported penile paraffinomas in 3 Laotian men who injected a mineral oil.
Currently, paraffin injections are uncommon but still are being performed in some countries in Eastern Europe and the Far East11; they rarely are reported in the United States. Injections can occur in unusual sites such as the knee, and paraffinomas can develop many years after the procedure.12 Additionally, paraffinomas can obscure proper diagnosis of carcinomas, as described by Lee et al13 in a case in which a cervical paraffin injection confounded the diagnosis of a thyroid tumor. Furthermore, these injections usually are performed by nonmedical personnel and typically are repeated multiple times to reach cosmetic goals, rendering the patient vulnerable to early complications including allergic reactions, paraphimosis, infection, and inflammation.3
The clinical presentation of a penile paraffinoma may be a mimicker of several different entities, which are important to consider in the evaluation of a presenting patient. Infectious etiologies must be considered including lymphogranuloma venereum, granuloma inguinale, atypical mycobacteria, lupus vulgaris, and sexually transmitted infections. Importantly, neoplasms must be ruled out including squamous cell carcinoma, soft tissue sarcomas, melanoma, adenocarcinoma, or metastasis. Lymphedema, prior surgical procedures, trauma, and inflammatory etiologies also are in the differential diagnosis.14 Nonetheless, physicians must have a high clinical suspicion in the evaluation of a possible paraffinoma, as patients may not be forthcoming with relevant clinical history regarding a prior injection to the affected site, particularly if the injection occurred many years ago. As such, the patient may not consider this history relevant or may not even remember the event occurred, as was observed in our case. Furthermore, embarrassment, social taboo, and stigma may be associated with the behavior of undergoing injections in nonclinical settings without medical supervision.15
Patients may be motivated to undergo dangerous procedures to potentially alter their appearance due to perceived enhanced sexual ability, influence by loved ones, cultural rituals, and societal pressure.15,16 Furthermore, patients may not be aware of the material being injected or the volume. Given that these injections often are used with the goal of cosmetic enhancement, biopsies in cosmetically sensitive areas must be given careful consideration, and a thorough clinical history must support the decision to pursue a biopsy to obtain a definitive diagnosis.
The definitive diagnosis of a paraffinoma is determined by histopathology. However, the use of imaging modalities such as magnetic resonance imaging and computed tomography have been employed to delineate the extent of involvement. Imaging studies allow for surgical planning and may assist in narrowing a differential diagnosis.17 Currently, wide and complete surgical resection is the only definitive treatment of paraffinomas, including penile paraffinomas, as there is no evidence of spontaneous regression.3 A report of a reconstructive surgery involving penile resurfacing without T-style anastomosis has been found effective at preventing necrosis of the ventral penile skin. Not all paraffinomas behave similarly, and there is no reliable method to determine which paraffinoma may possess a more aggressive clinical course compared to those which have a more indolent course.18 As such, early detection is critical in the management of paraffinomas, especially in anatomic locations where tissue preservation is of utmost importance. In the case of a large penile paraffinoma with the ability to destroy vital urologic and reproductive function, physicians must consider prevention of recurrent episodes through suppression of inflammation and fibrosis with doxycycline and nicotinamide.19 Other medical treatments reported with varying success include corticosteroids, imiquimod, and isotretinoin.19-24 Employing adjunctive medical treatment may decrease the size of the mass, reducing the surgical defect size and preserving tissue vitality. Ultimately, the most crucial aspect in treatment is prevention, as injection of foreign materials elicits a foreign body response and can lead to notable morbidity.
- De Siati M, Selvaggio O, Di Fino G, et al. An unusual delayed complication of paraffin self-injection for penile girth augmentation. BMC Urol. 2013;13:66.
- Sejben I, Rácz A, Svébis M, et al. Petroleum jelly-induced penile paraffinoma with inguinal lymphadenitis mimicking incarcerated inguinal hernia. Can Urol Assoc J. 2012;6:E137-E139.
- Bayraktar N, Basar I. Penile paraffinoma [published online September 17, 2012]. Case Rep Urol. 2012;2012:202840.
- Eandi JA, Yao AP, Javidan J. Penile paraffinoma: the delayed presentation. Int Urol Nephrol. 2007;29:553-555.
- HirshBCJohnsonWC. Pathology of granulomatous diseases. foreign body granulomas. Int J Dermatol. 1984;23:531-538.
- Quérnu J, Pérol E. Paraffinomas of the penis. J Chir Par. 1947;63:345.
- Bradley, RH, Ehrgott WA. Paraffinoma of the penis: case report. J Urol. 1951;65:453.
- May JA, Pickering PP. Paraffinoma of the penis. Calif Med. 1956;85:42-44.
Yonsei Med J. 1994;35:344-348. - Lee T, Choi HR, Lee YT, et al. Paraffinoma of the penis.
- Manny T, Pettus J, Hemal A, et al. Penile sclerosing lipogranulomas and disfigurement from use of “1Super Extenze” among Laotian immigrants. J Sex Med. 2011;8:3505-3510.
- Akkus E Paraffinoma and ulcer of the external genitalia after self-injection of vaseline. J Sex Med. 2006;3:170-172.
- Grassetti L, Lazzeri D, Torresetti M, et al. Paraffinoma of the knee 60 years after primary infection. Arch Plast Surg. 2013;40:789-790.
- Lee YS, Son EJ, Kim BW, et al. Difficult evaluation of thyroid cancer due to cervical paraffin injection. J Korean Surg Soc. 2011;81(suppl 1):S17-S20.
- Gómez-Armayones S, Penín R, Marcoval J. Penile paraffinoma [in Spanish]. Actas Dermosifiliogr. 2014;105:957-959.
- Moon DG, Yoo JW, Bae JH, et al. Sexual function and psychological characteristics of penile paraffinoma. Asian J Androl. 2003;5:191-194.
- Pehlivanov G, Kavaklieva S, Kazandjieva J, et al. Foreign-body granuloma of the penis in sexually active individuals (penile paraffinoma). J Eur Acad Dermatol Venereol. 2008;22:845-851.
- Cormio L, Di Fino G, Scavone C, et al. Magnetic resonance imaging of penile paraffinoma: case report. BMC Med Imaging. 2014;14:39.
- Shin YS, Zhao C, Park JK. New reconstructive surgery for penile paraffinoma to prevent necrosis of ventral penile skin. Urology. 2013;81:437-441.
- Feldmann R, Harms M, Chavaz P, et al. Orbital and palpebral paraffinoma. J Am Acad Dermatol. 1992;26:833-835.
- MastruserioDNPesqueiraMJCobbMW. Severe granulomatous reaction and facial ulceration occurring after subcutaneous silicone injection. J Am Acad Dermatol. 1996;34:849-852.
- HoWS Management of paraffinoma of the breast. Br J Plast Surg. 2001;54:232-234.
- LloretPSuccessful treatment of granulomatous reactions secondary to injection of esthetic implants. Dermatol Surg. 2005;31:486-490.
- RosenbergEThree cases of penile paraffinoma. Urology. 2007;70:372.
- Baumann LS, Halem ML. Lip silicone granulomatous foreign body reaction treated with Aldara (imiquimod 5%). Dermatol Surg. 2003;29:429-432.
To the Editor:
The term paraffinoma refers to a chronic granulomatous response to injection of paraffin, silicone, or other mineral oils into skin and soft tissue. Paraffinomas develop when the material is injected into the skin for cosmetic purposes to augment or enhance one’s appearance. Although they may occur in any location, the most common sites include the breasts and buttocks. The penis is a rare but emerging site for paraffinomas.1-3 We present a rare case of recurrence of a penile paraffinoma following surgical resection.
A 26-year-old uncircumcised Trinidadian man presented with a 5-cm, exquisitely tender tumor involving the penile shaft and median raphe that rapidly evolved over the course of 3 weeks (Figure 1). He presented with inability to urinate, attain an erection, or ambulate without notable tenderness. Additionally, he developed swelling of the penis and surrounding tissue. He had no other medical comorbidities; however, 1 year prior he presented to a urologist with a 1-cm nodule involving the median raphe that was surgically resected and required circumcision. Biopsy at the time of his surgical procedure revealed an exuberant foreign body giant cell reaction with surrounding empty spaces in the dermis resembling Swiss cheese, consistent with a paraffinoma (Figure 2). The recurrent tumor, which was 5 times the size of the initial nodule, was biopsied. Again, histopathologic findings were consistent with a paraffinoma with extensive dermal fibrosis and absence of polarizable material.
The patient underwent extensive reconstructive surgery requiring skin grafting to the penile shaft. Given the size and location of this recurrent tumor with the ability to destroy vital urologic and reproductive function, consideration for prevention of recurrent episodes included novel therapeutic treatment options to suppress inflammation and fibrosis with doxycycline and nicotinamide.
Paraffin injections are used for cosmetic enhancement and most often occur in a nonclinical setting without medical supervision, as they are not US Food and Drug Administration–approved medical injectable materials. Examples of oils injected include paraffin, camphorated oil, cottonseed or sesame oil, mineral oil, petroleum jelly, and beeswax. These oils are not hydrolyzed by tissue lipases but are instead treated as a foreign body substance with subsequent granuloma formation (also known as sclerosing lipogranuloma), which can occur many years after injection.4 The granulomatous response may be observed months to years after injection. The paraffinoma normally affects the injection site; however, regional lymphadenopathy and systemic disease has been reported.2 Histopathologic findings are characteristic and consist of a foreign body giant cell reaction, variably sized round to oval cavities within the dermis, and varying degrees of dermal fibrosis.5
In 1899, mineral oil was first injected into male genitalia to restore architecture in a patient’s testicles following bilateral orchiectomy. After the success of this endeavor, mineral oil injections were used as filler for other defects.3 However, by 1906 the complications of these injections became public knowledge when 2 patients developed subcutaneous nodules after receiving injections for facial wrinkles.2 Despite public knowledge of these complications, penile paraffin injections continued to occur both in medical and eventually nonmedical settings.
In 1947, Quérnu and Pérol6 described 6 penile paraffinoma cases outside the United States. Patients had petroleum jelly injections that eventuated in penile paraffinomas, and all of them lost the ability to attain an erection.6 Four years later, Bradley and Ehrgott7 described a case of penile paraffinoma likely caused by application of paraffin in association with occupational exposure. In 1956, May and Pickering8 cited a case of penile paraffinoma affecting the entire penile shaft in which the patient had undergone paraffin injection 7 years prior to treat premature ejaculation. Unfortunately, the injection resulted in a painful and unsatisfactory erection without resolution of premature ejaculation.8 Lee et al9 analyzed 26 cases of penile paraffinomas that occurred from 1981 to 1993. They found that all patients underwent injections of paraffin or petroleum jelly performed by nonmedical personnel with the predominant goal of enhancing penis size. Within 18.5 months of injection, 19 patients already experienced tenderness at the injection site. The remaining 7 patients experienced penile skin discoloration and abnormal contouring of the penis. Biopsy specimens revealed hyaline necrosis of subcutaneous adipose septa, cystlike spaces throughout involved tissue, and macrophages engulfing adipose tissue were found near blood vessels.9 In 2007, Eandi et al4 reported a case of penile paraffinoma with a 40-year delay of onset. Four years later, Manny et al10 reported penile paraffinomas in 3 Laotian men who injected a mineral oil.
Currently, paraffin injections are uncommon but still are being performed in some countries in Eastern Europe and the Far East11; they rarely are reported in the United States. Injections can occur in unusual sites such as the knee, and paraffinomas can develop many years after the procedure.12 Additionally, paraffinomas can obscure proper diagnosis of carcinomas, as described by Lee et al13 in a case in which a cervical paraffin injection confounded the diagnosis of a thyroid tumor. Furthermore, these injections usually are performed by nonmedical personnel and typically are repeated multiple times to reach cosmetic goals, rendering the patient vulnerable to early complications including allergic reactions, paraphimosis, infection, and inflammation.3
The clinical presentation of a penile paraffinoma may be a mimicker of several different entities, which are important to consider in the evaluation of a presenting patient. Infectious etiologies must be considered including lymphogranuloma venereum, granuloma inguinale, atypical mycobacteria, lupus vulgaris, and sexually transmitted infections. Importantly, neoplasms must be ruled out including squamous cell carcinoma, soft tissue sarcomas, melanoma, adenocarcinoma, or metastasis. Lymphedema, prior surgical procedures, trauma, and inflammatory etiologies also are in the differential diagnosis.14 Nonetheless, physicians must have a high clinical suspicion in the evaluation of a possible paraffinoma, as patients may not be forthcoming with relevant clinical history regarding a prior injection to the affected site, particularly if the injection occurred many years ago. As such, the patient may not consider this history relevant or may not even remember the event occurred, as was observed in our case. Furthermore, embarrassment, social taboo, and stigma may be associated with the behavior of undergoing injections in nonclinical settings without medical supervision.15
Patients may be motivated to undergo dangerous procedures to potentially alter their appearance due to perceived enhanced sexual ability, influence by loved ones, cultural rituals, and societal pressure.15,16 Furthermore, patients may not be aware of the material being injected or the volume. Given that these injections often are used with the goal of cosmetic enhancement, biopsies in cosmetically sensitive areas must be given careful consideration, and a thorough clinical history must support the decision to pursue a biopsy to obtain a definitive diagnosis.
The definitive diagnosis of a paraffinoma is determined by histopathology. However, the use of imaging modalities such as magnetic resonance imaging and computed tomography have been employed to delineate the extent of involvement. Imaging studies allow for surgical planning and may assist in narrowing a differential diagnosis.17 Currently, wide and complete surgical resection is the only definitive treatment of paraffinomas, including penile paraffinomas, as there is no evidence of spontaneous regression.3 A report of a reconstructive surgery involving penile resurfacing without T-style anastomosis has been found effective at preventing necrosis of the ventral penile skin. Not all paraffinomas behave similarly, and there is no reliable method to determine which paraffinoma may possess a more aggressive clinical course compared to those which have a more indolent course.18 As such, early detection is critical in the management of paraffinomas, especially in anatomic locations where tissue preservation is of utmost importance. In the case of a large penile paraffinoma with the ability to destroy vital urologic and reproductive function, physicians must consider prevention of recurrent episodes through suppression of inflammation and fibrosis with doxycycline and nicotinamide.19 Other medical treatments reported with varying success include corticosteroids, imiquimod, and isotretinoin.19-24 Employing adjunctive medical treatment may decrease the size of the mass, reducing the surgical defect size and preserving tissue vitality. Ultimately, the most crucial aspect in treatment is prevention, as injection of foreign materials elicits a foreign body response and can lead to notable morbidity.
To the Editor:
The term paraffinoma refers to a chronic granulomatous response to injection of paraffin, silicone, or other mineral oils into skin and soft tissue. Paraffinomas develop when the material is injected into the skin for cosmetic purposes to augment or enhance one’s appearance. Although they may occur in any location, the most common sites include the breasts and buttocks. The penis is a rare but emerging site for paraffinomas.1-3 We present a rare case of recurrence of a penile paraffinoma following surgical resection.
A 26-year-old uncircumcised Trinidadian man presented with a 5-cm, exquisitely tender tumor involving the penile shaft and median raphe that rapidly evolved over the course of 3 weeks (Figure 1). He presented with inability to urinate, attain an erection, or ambulate without notable tenderness. Additionally, he developed swelling of the penis and surrounding tissue. He had no other medical comorbidities; however, 1 year prior he presented to a urologist with a 1-cm nodule involving the median raphe that was surgically resected and required circumcision. Biopsy at the time of his surgical procedure revealed an exuberant foreign body giant cell reaction with surrounding empty spaces in the dermis resembling Swiss cheese, consistent with a paraffinoma (Figure 2). The recurrent tumor, which was 5 times the size of the initial nodule, was biopsied. Again, histopathologic findings were consistent with a paraffinoma with extensive dermal fibrosis and absence of polarizable material.
The patient underwent extensive reconstructive surgery requiring skin grafting to the penile shaft. Given the size and location of this recurrent tumor with the ability to destroy vital urologic and reproductive function, consideration for prevention of recurrent episodes included novel therapeutic treatment options to suppress inflammation and fibrosis with doxycycline and nicotinamide.
Paraffin injections are used for cosmetic enhancement and most often occur in a nonclinical setting without medical supervision, as they are not US Food and Drug Administration–approved medical injectable materials. Examples of oils injected include paraffin, camphorated oil, cottonseed or sesame oil, mineral oil, petroleum jelly, and beeswax. These oils are not hydrolyzed by tissue lipases but are instead treated as a foreign body substance with subsequent granuloma formation (also known as sclerosing lipogranuloma), which can occur many years after injection.4 The granulomatous response may be observed months to years after injection. The paraffinoma normally affects the injection site; however, regional lymphadenopathy and systemic disease has been reported.2 Histopathologic findings are characteristic and consist of a foreign body giant cell reaction, variably sized round to oval cavities within the dermis, and varying degrees of dermal fibrosis.5
In 1899, mineral oil was first injected into male genitalia to restore architecture in a patient’s testicles following bilateral orchiectomy. After the success of this endeavor, mineral oil injections were used as filler for other defects.3 However, by 1906 the complications of these injections became public knowledge when 2 patients developed subcutaneous nodules after receiving injections for facial wrinkles.2 Despite public knowledge of these complications, penile paraffin injections continued to occur both in medical and eventually nonmedical settings.
In 1947, Quérnu and Pérol6 described 6 penile paraffinoma cases outside the United States. Patients had petroleum jelly injections that eventuated in penile paraffinomas, and all of them lost the ability to attain an erection.6 Four years later, Bradley and Ehrgott7 described a case of penile paraffinoma likely caused by application of paraffin in association with occupational exposure. In 1956, May and Pickering8 cited a case of penile paraffinoma affecting the entire penile shaft in which the patient had undergone paraffin injection 7 years prior to treat premature ejaculation. Unfortunately, the injection resulted in a painful and unsatisfactory erection without resolution of premature ejaculation.8 Lee et al9 analyzed 26 cases of penile paraffinomas that occurred from 1981 to 1993. They found that all patients underwent injections of paraffin or petroleum jelly performed by nonmedical personnel with the predominant goal of enhancing penis size. Within 18.5 months of injection, 19 patients already experienced tenderness at the injection site. The remaining 7 patients experienced penile skin discoloration and abnormal contouring of the penis. Biopsy specimens revealed hyaline necrosis of subcutaneous adipose septa, cystlike spaces throughout involved tissue, and macrophages engulfing adipose tissue were found near blood vessels.9 In 2007, Eandi et al4 reported a case of penile paraffinoma with a 40-year delay of onset. Four years later, Manny et al10 reported penile paraffinomas in 3 Laotian men who injected a mineral oil.
Currently, paraffin injections are uncommon but still are being performed in some countries in Eastern Europe and the Far East11; they rarely are reported in the United States. Injections can occur in unusual sites such as the knee, and paraffinomas can develop many years after the procedure.12 Additionally, paraffinomas can obscure proper diagnosis of carcinomas, as described by Lee et al13 in a case in which a cervical paraffin injection confounded the diagnosis of a thyroid tumor. Furthermore, these injections usually are performed by nonmedical personnel and typically are repeated multiple times to reach cosmetic goals, rendering the patient vulnerable to early complications including allergic reactions, paraphimosis, infection, and inflammation.3
The clinical presentation of a penile paraffinoma may be a mimicker of several different entities, which are important to consider in the evaluation of a presenting patient. Infectious etiologies must be considered including lymphogranuloma venereum, granuloma inguinale, atypical mycobacteria, lupus vulgaris, and sexually transmitted infections. Importantly, neoplasms must be ruled out including squamous cell carcinoma, soft tissue sarcomas, melanoma, adenocarcinoma, or metastasis. Lymphedema, prior surgical procedures, trauma, and inflammatory etiologies also are in the differential diagnosis.14 Nonetheless, physicians must have a high clinical suspicion in the evaluation of a possible paraffinoma, as patients may not be forthcoming with relevant clinical history regarding a prior injection to the affected site, particularly if the injection occurred many years ago. As such, the patient may not consider this history relevant or may not even remember the event occurred, as was observed in our case. Furthermore, embarrassment, social taboo, and stigma may be associated with the behavior of undergoing injections in nonclinical settings without medical supervision.15
Patients may be motivated to undergo dangerous procedures to potentially alter their appearance due to perceived enhanced sexual ability, influence by loved ones, cultural rituals, and societal pressure.15,16 Furthermore, patients may not be aware of the material being injected or the volume. Given that these injections often are used with the goal of cosmetic enhancement, biopsies in cosmetically sensitive areas must be given careful consideration, and a thorough clinical history must support the decision to pursue a biopsy to obtain a definitive diagnosis.
The definitive diagnosis of a paraffinoma is determined by histopathology. However, the use of imaging modalities such as magnetic resonance imaging and computed tomography have been employed to delineate the extent of involvement. Imaging studies allow for surgical planning and may assist in narrowing a differential diagnosis.17 Currently, wide and complete surgical resection is the only definitive treatment of paraffinomas, including penile paraffinomas, as there is no evidence of spontaneous regression.3 A report of a reconstructive surgery involving penile resurfacing without T-style anastomosis has been found effective at preventing necrosis of the ventral penile skin. Not all paraffinomas behave similarly, and there is no reliable method to determine which paraffinoma may possess a more aggressive clinical course compared to those which have a more indolent course.18 As such, early detection is critical in the management of paraffinomas, especially in anatomic locations where tissue preservation is of utmost importance. In the case of a large penile paraffinoma with the ability to destroy vital urologic and reproductive function, physicians must consider prevention of recurrent episodes through suppression of inflammation and fibrosis with doxycycline and nicotinamide.19 Other medical treatments reported with varying success include corticosteroids, imiquimod, and isotretinoin.19-24 Employing adjunctive medical treatment may decrease the size of the mass, reducing the surgical defect size and preserving tissue vitality. Ultimately, the most crucial aspect in treatment is prevention, as injection of foreign materials elicits a foreign body response and can lead to notable morbidity.
- De Siati M, Selvaggio O, Di Fino G, et al. An unusual delayed complication of paraffin self-injection for penile girth augmentation. BMC Urol. 2013;13:66.
- Sejben I, Rácz A, Svébis M, et al. Petroleum jelly-induced penile paraffinoma with inguinal lymphadenitis mimicking incarcerated inguinal hernia. Can Urol Assoc J. 2012;6:E137-E139.
- Bayraktar N, Basar I. Penile paraffinoma [published online September 17, 2012]. Case Rep Urol. 2012;2012:202840.
- Eandi JA, Yao AP, Javidan J. Penile paraffinoma: the delayed presentation. Int Urol Nephrol. 2007;29:553-555.
- HirshBCJohnsonWC. Pathology of granulomatous diseases. foreign body granulomas. Int J Dermatol. 1984;23:531-538.
- Quérnu J, Pérol E. Paraffinomas of the penis. J Chir Par. 1947;63:345.
- Bradley, RH, Ehrgott WA. Paraffinoma of the penis: case report. J Urol. 1951;65:453.
- May JA, Pickering PP. Paraffinoma of the penis. Calif Med. 1956;85:42-44.
Yonsei Med J. 1994;35:344-348. - Lee T, Choi HR, Lee YT, et al. Paraffinoma of the penis.
- Manny T, Pettus J, Hemal A, et al. Penile sclerosing lipogranulomas and disfigurement from use of “1Super Extenze” among Laotian immigrants. J Sex Med. 2011;8:3505-3510.
- Akkus E Paraffinoma and ulcer of the external genitalia after self-injection of vaseline. J Sex Med. 2006;3:170-172.
- Grassetti L, Lazzeri D, Torresetti M, et al. Paraffinoma of the knee 60 years after primary infection. Arch Plast Surg. 2013;40:789-790.
- Lee YS, Son EJ, Kim BW, et al. Difficult evaluation of thyroid cancer due to cervical paraffin injection. J Korean Surg Soc. 2011;81(suppl 1):S17-S20.
- Gómez-Armayones S, Penín R, Marcoval J. Penile paraffinoma [in Spanish]. Actas Dermosifiliogr. 2014;105:957-959.
- Moon DG, Yoo JW, Bae JH, et al. Sexual function and psychological characteristics of penile paraffinoma. Asian J Androl. 2003;5:191-194.
- Pehlivanov G, Kavaklieva S, Kazandjieva J, et al. Foreign-body granuloma of the penis in sexually active individuals (penile paraffinoma). J Eur Acad Dermatol Venereol. 2008;22:845-851.
- Cormio L, Di Fino G, Scavone C, et al. Magnetic resonance imaging of penile paraffinoma: case report. BMC Med Imaging. 2014;14:39.
- Shin YS, Zhao C, Park JK. New reconstructive surgery for penile paraffinoma to prevent necrosis of ventral penile skin. Urology. 2013;81:437-441.
- Feldmann R, Harms M, Chavaz P, et al. Orbital and palpebral paraffinoma. J Am Acad Dermatol. 1992;26:833-835.
- MastruserioDNPesqueiraMJCobbMW. Severe granulomatous reaction and facial ulceration occurring after subcutaneous silicone injection. J Am Acad Dermatol. 1996;34:849-852.
- HoWS Management of paraffinoma of the breast. Br J Plast Surg. 2001;54:232-234.
- LloretPSuccessful treatment of granulomatous reactions secondary to injection of esthetic implants. Dermatol Surg. 2005;31:486-490.
- RosenbergEThree cases of penile paraffinoma. Urology. 2007;70:372.
- Baumann LS, Halem ML. Lip silicone granulomatous foreign body reaction treated with Aldara (imiquimod 5%). Dermatol Surg. 2003;29:429-432.
- De Siati M, Selvaggio O, Di Fino G, et al. An unusual delayed complication of paraffin self-injection for penile girth augmentation. BMC Urol. 2013;13:66.
- Sejben I, Rácz A, Svébis M, et al. Petroleum jelly-induced penile paraffinoma with inguinal lymphadenitis mimicking incarcerated inguinal hernia. Can Urol Assoc J. 2012;6:E137-E139.
- Bayraktar N, Basar I. Penile paraffinoma [published online September 17, 2012]. Case Rep Urol. 2012;2012:202840.
- Eandi JA, Yao AP, Javidan J. Penile paraffinoma: the delayed presentation. Int Urol Nephrol. 2007;29:553-555.
- HirshBCJohnsonWC. Pathology of granulomatous diseases. foreign body granulomas. Int J Dermatol. 1984;23:531-538.
- Quérnu J, Pérol E. Paraffinomas of the penis. J Chir Par. 1947;63:345.
- Bradley, RH, Ehrgott WA. Paraffinoma of the penis: case report. J Urol. 1951;65:453.
- May JA, Pickering PP. Paraffinoma of the penis. Calif Med. 1956;85:42-44.
Yonsei Med J. 1994;35:344-348. - Lee T, Choi HR, Lee YT, et al. Paraffinoma of the penis.
- Manny T, Pettus J, Hemal A, et al. Penile sclerosing lipogranulomas and disfigurement from use of “1Super Extenze” among Laotian immigrants. J Sex Med. 2011;8:3505-3510.
- Akkus E Paraffinoma and ulcer of the external genitalia after self-injection of vaseline. J Sex Med. 2006;3:170-172.
- Grassetti L, Lazzeri D, Torresetti M, et al. Paraffinoma of the knee 60 years after primary infection. Arch Plast Surg. 2013;40:789-790.
- Lee YS, Son EJ, Kim BW, et al. Difficult evaluation of thyroid cancer due to cervical paraffin injection. J Korean Surg Soc. 2011;81(suppl 1):S17-S20.
- Gómez-Armayones S, Penín R, Marcoval J. Penile paraffinoma [in Spanish]. Actas Dermosifiliogr. 2014;105:957-959.
- Moon DG, Yoo JW, Bae JH, et al. Sexual function and psychological characteristics of penile paraffinoma. Asian J Androl. 2003;5:191-194.
- Pehlivanov G, Kavaklieva S, Kazandjieva J, et al. Foreign-body granuloma of the penis in sexually active individuals (penile paraffinoma). J Eur Acad Dermatol Venereol. 2008;22:845-851.
- Cormio L, Di Fino G, Scavone C, et al. Magnetic resonance imaging of penile paraffinoma: case report. BMC Med Imaging. 2014;14:39.
- Shin YS, Zhao C, Park JK. New reconstructive surgery for penile paraffinoma to prevent necrosis of ventral penile skin. Urology. 2013;81:437-441.
- Feldmann R, Harms M, Chavaz P, et al. Orbital and palpebral paraffinoma. J Am Acad Dermatol. 1992;26:833-835.
- MastruserioDNPesqueiraMJCobbMW. Severe granulomatous reaction and facial ulceration occurring after subcutaneous silicone injection. J Am Acad Dermatol. 1996;34:849-852.
- HoWS Management of paraffinoma of the breast. Br J Plast Surg. 2001;54:232-234.
- LloretPSuccessful treatment of granulomatous reactions secondary to injection of esthetic implants. Dermatol Surg. 2005;31:486-490.
- RosenbergEThree cases of penile paraffinoma. Urology. 2007;70:372.
- Baumann LS, Halem ML. Lip silicone granulomatous foreign body reaction treated with Aldara (imiquimod 5%). Dermatol Surg. 2003;29:429-432.
Practice Points
- Taking a thorough history in patients with possible paraffinomas is vital, including a history of injectables even in the genital region.
- Biopsies in cosmetically sensitive areas must be given careful consideration. Clinical history must support the decision to pursue a definitive diagnosis.
- Early detection is critical in the management of paraffinomas, especially in anatomic locations where tissue preservation is of utmost importance.

FDA approves apomorphine sublingual film for ‘off’ episodes in Parkinson’s disease
, the manufacturer has announced. This marks the first approval for a sublingual therapy for this indication, which is defined as the re-emergence or worsening of Parkinson’s disease symptoms that have otherwise been controlled with standard care of levodopa/carbidopa, Sunovion reports. Almost 60% of patients with Parkinson’s disease experience off episodes.
The approval “affords healthcare providers with a needed option that can be added to their patients’ medication regimen to adequately address off episodes as their Parkinson’s disease progresses,” Stewart Factor, DO, professor of neurology and director of the Movement Disorders Program at Emory University School of Medicine, Atlanta, Georgia, said in a press release from the manufacturer.
“We know from our research and discussion with the Parkinson’s community that off episodes can significantly disrupt a patient’s daily life,” Todd Sherer, PhD, CEO of the Michael J. Fox Foundation for Parkinson’s Research, said in the same release. He added that the Fox Foundation “supported early clinical development of sublingual apomorphine.”
The treatment is expected to be available in US pharmacies in September.
Disruptive symptoms
Off episodes can include periods of tremor, slowed movement, and stiffness and occur during daytime hours.
“Several years after a person is diagnosed with [Parkinson’s disease] they may notice problems such as having trouble getting out of bed in the morning or having difficulty getting out of a chair, or that they feel frozen while trying to walk as the effect of their maintenance medication diminishes,” Dr. Factor noted.
Subcutaneous infusion of the dopamine agonist apomorphine previously has shown benefit in treating persistent motor fluctuations in patients with Parkinson’s disease.
Apomorphine hydrochloride sublingual film is a novel formulation of apomorphine. It dissolves under the tongue to help improve off episode symptoms as needed up to five times per day.
A phase 3 study of 109 patients that was published in December in Lancet Neurology showed that those who received the sublingual film therapy had a mean reduction of 11.1 points on the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III 30 minutes after dosing at the 12-week assessment. This was a significant improvement in motor symptoms versus those who received placebo (mean difference, -7.6 points; P = .0002).
In addition, initial clinical improvement was found 15 minutes after dosing.
The most frequently reported treatment-emergent adverse events in the study population were oropharyngeal reactions, followed by nausea, somnolence, and dizziness.
Long-term safety?
“The availability of this new apomorphine sublingual formulation, along with an inhaled formulation under development, will broaden the treatment options for off periods,” Angelo Antonini, MD, PhD, from University of Padua, Italy, wrote in an accompanying editorial in The Lancet Neurology.
Although the results were encouraging, he noted some caution should be heeded.
Because of “the high rate of oropharyngeal adverse events, long-term safety needs to be monitored once the product is registered and available for chronic use in patients with Parkinson’s disease,” Dr. Antonini wrote.
Other safety information issued by the manufacturer includes a warning that patients who take the 5HT3 antagonists ondansetron, dolasetron, palonosetron, granisetron, or alosetron for nausea should not also use apomorphine hydrochloride sublingual film.
“People taking ondansetron together with apomorphine, the active ingredient in Kynmobi, have had very low blood pressure and lost consciousness or ‘blacked out,’ “ the warning notes.
It also should not be taken by individuals who are allergic to the ingredients in the medication, including sodium metabisulfite.
This article first appeared on Medscape.com.
, the manufacturer has announced. This marks the first approval for a sublingual therapy for this indication, which is defined as the re-emergence or worsening of Parkinson’s disease symptoms that have otherwise been controlled with standard care of levodopa/carbidopa, Sunovion reports. Almost 60% of patients with Parkinson’s disease experience off episodes.
The approval “affords healthcare providers with a needed option that can be added to their patients’ medication regimen to adequately address off episodes as their Parkinson’s disease progresses,” Stewart Factor, DO, professor of neurology and director of the Movement Disorders Program at Emory University School of Medicine, Atlanta, Georgia, said in a press release from the manufacturer.
“We know from our research and discussion with the Parkinson’s community that off episodes can significantly disrupt a patient’s daily life,” Todd Sherer, PhD, CEO of the Michael J. Fox Foundation for Parkinson’s Research, said in the same release. He added that the Fox Foundation “supported early clinical development of sublingual apomorphine.”
The treatment is expected to be available in US pharmacies in September.
Disruptive symptoms
Off episodes can include periods of tremor, slowed movement, and stiffness and occur during daytime hours.
“Several years after a person is diagnosed with [Parkinson’s disease] they may notice problems such as having trouble getting out of bed in the morning or having difficulty getting out of a chair, or that they feel frozen while trying to walk as the effect of their maintenance medication diminishes,” Dr. Factor noted.
Subcutaneous infusion of the dopamine agonist apomorphine previously has shown benefit in treating persistent motor fluctuations in patients with Parkinson’s disease.
Apomorphine hydrochloride sublingual film is a novel formulation of apomorphine. It dissolves under the tongue to help improve off episode symptoms as needed up to five times per day.
A phase 3 study of 109 patients that was published in December in Lancet Neurology showed that those who received the sublingual film therapy had a mean reduction of 11.1 points on the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III 30 minutes after dosing at the 12-week assessment. This was a significant improvement in motor symptoms versus those who received placebo (mean difference, -7.6 points; P = .0002).
In addition, initial clinical improvement was found 15 minutes after dosing.
The most frequently reported treatment-emergent adverse events in the study population were oropharyngeal reactions, followed by nausea, somnolence, and dizziness.
Long-term safety?
“The availability of this new apomorphine sublingual formulation, along with an inhaled formulation under development, will broaden the treatment options for off periods,” Angelo Antonini, MD, PhD, from University of Padua, Italy, wrote in an accompanying editorial in The Lancet Neurology.
Although the results were encouraging, he noted some caution should be heeded.
Because of “the high rate of oropharyngeal adverse events, long-term safety needs to be monitored once the product is registered and available for chronic use in patients with Parkinson’s disease,” Dr. Antonini wrote.
Other safety information issued by the manufacturer includes a warning that patients who take the 5HT3 antagonists ondansetron, dolasetron, palonosetron, granisetron, or alosetron for nausea should not also use apomorphine hydrochloride sublingual film.
“People taking ondansetron together with apomorphine, the active ingredient in Kynmobi, have had very low blood pressure and lost consciousness or ‘blacked out,’ “ the warning notes.
It also should not be taken by individuals who are allergic to the ingredients in the medication, including sodium metabisulfite.
This article first appeared on Medscape.com.
, the manufacturer has announced. This marks the first approval for a sublingual therapy for this indication, which is defined as the re-emergence or worsening of Parkinson’s disease symptoms that have otherwise been controlled with standard care of levodopa/carbidopa, Sunovion reports. Almost 60% of patients with Parkinson’s disease experience off episodes.
The approval “affords healthcare providers with a needed option that can be added to their patients’ medication regimen to adequately address off episodes as their Parkinson’s disease progresses,” Stewart Factor, DO, professor of neurology and director of the Movement Disorders Program at Emory University School of Medicine, Atlanta, Georgia, said in a press release from the manufacturer.
“We know from our research and discussion with the Parkinson’s community that off episodes can significantly disrupt a patient’s daily life,” Todd Sherer, PhD, CEO of the Michael J. Fox Foundation for Parkinson’s Research, said in the same release. He added that the Fox Foundation “supported early clinical development of sublingual apomorphine.”
The treatment is expected to be available in US pharmacies in September.
Disruptive symptoms
Off episodes can include periods of tremor, slowed movement, and stiffness and occur during daytime hours.
“Several years after a person is diagnosed with [Parkinson’s disease] they may notice problems such as having trouble getting out of bed in the morning or having difficulty getting out of a chair, or that they feel frozen while trying to walk as the effect of their maintenance medication diminishes,” Dr. Factor noted.
Subcutaneous infusion of the dopamine agonist apomorphine previously has shown benefit in treating persistent motor fluctuations in patients with Parkinson’s disease.
Apomorphine hydrochloride sublingual film is a novel formulation of apomorphine. It dissolves under the tongue to help improve off episode symptoms as needed up to five times per day.
A phase 3 study of 109 patients that was published in December in Lancet Neurology showed that those who received the sublingual film therapy had a mean reduction of 11.1 points on the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III 30 minutes after dosing at the 12-week assessment. This was a significant improvement in motor symptoms versus those who received placebo (mean difference, -7.6 points; P = .0002).
In addition, initial clinical improvement was found 15 minutes after dosing.
The most frequently reported treatment-emergent adverse events in the study population were oropharyngeal reactions, followed by nausea, somnolence, and dizziness.
Long-term safety?
“The availability of this new apomorphine sublingual formulation, along with an inhaled formulation under development, will broaden the treatment options for off periods,” Angelo Antonini, MD, PhD, from University of Padua, Italy, wrote in an accompanying editorial in The Lancet Neurology.
Although the results were encouraging, he noted some caution should be heeded.
Because of “the high rate of oropharyngeal adverse events, long-term safety needs to be monitored once the product is registered and available for chronic use in patients with Parkinson’s disease,” Dr. Antonini wrote.
Other safety information issued by the manufacturer includes a warning that patients who take the 5HT3 antagonists ondansetron, dolasetron, palonosetron, granisetron, or alosetron for nausea should not also use apomorphine hydrochloride sublingual film.
“People taking ondansetron together with apomorphine, the active ingredient in Kynmobi, have had very low blood pressure and lost consciousness or ‘blacked out,’ “ the warning notes.
It also should not be taken by individuals who are allergic to the ingredients in the medication, including sodium metabisulfite.
This article first appeared on Medscape.com.
Complex Regional Pain Syndrome Type II After a Brachial Plexus and C6 Nerve Root Injury
To the Editor:
A 62-year-old man presented with an atrophied painful left arm of 17 years’ duration that began when he was hit by a car as a pedestrian. He sustained severe multisystem injuries from the accident, including left brachial plexus and C6 nerve root avulsion injury. When he regained consciousness after 6 weeks in the intensive care unit, he immediately noted diffuse pain throughout the body, especially in the left arm. Since the accident, the patient continued to have diminished sensation to touch and temperature in the left arm. He also had burning, throbbing, and electrical pain in the left arm with light touch as well as spontaneously. He was thoroughly evaluated by a neurologist and was diagnosed with complex regional pain syndrome (CRPS) type II. For the treatment of pain, dorsal column stimulation and hemilaminectomy with exploration of the avulsed nerve root were attempted, both of which had minimal effect. He was maintained on hydromorphone, methadone, and oxazepam. He reported that for many years he was unable move out of bed due to the unbearable pain. With pain medications, he was able to regain most of his independence in his daily life, though the pain and other clinical aspects of CRPS still completely limited his use of the left arm.
Physical examination revealed glossy, cold, hairless skin with hypohidrosis of the left arm, forearm, and hand (Figures 1 and 2A). The left arm was conspicuously atrophied, with the forearm and hand erythematous. The fingers were taut, contracted, and edematous (Figure 2B), and the skin was unable to be pinched. The fingernails on the left hand had dystrophic changes including yellow color and brittleness with longitudinal ridges (Figure 3). The patient could activate the left bicep and tricep muscles against gravity but had minimal function of the deltoid muscle. He also had minimal movement of the left index finger and was unable to move any other digits of the left hand. The patient was continued on pain management treatments and physical therapy for his condition.


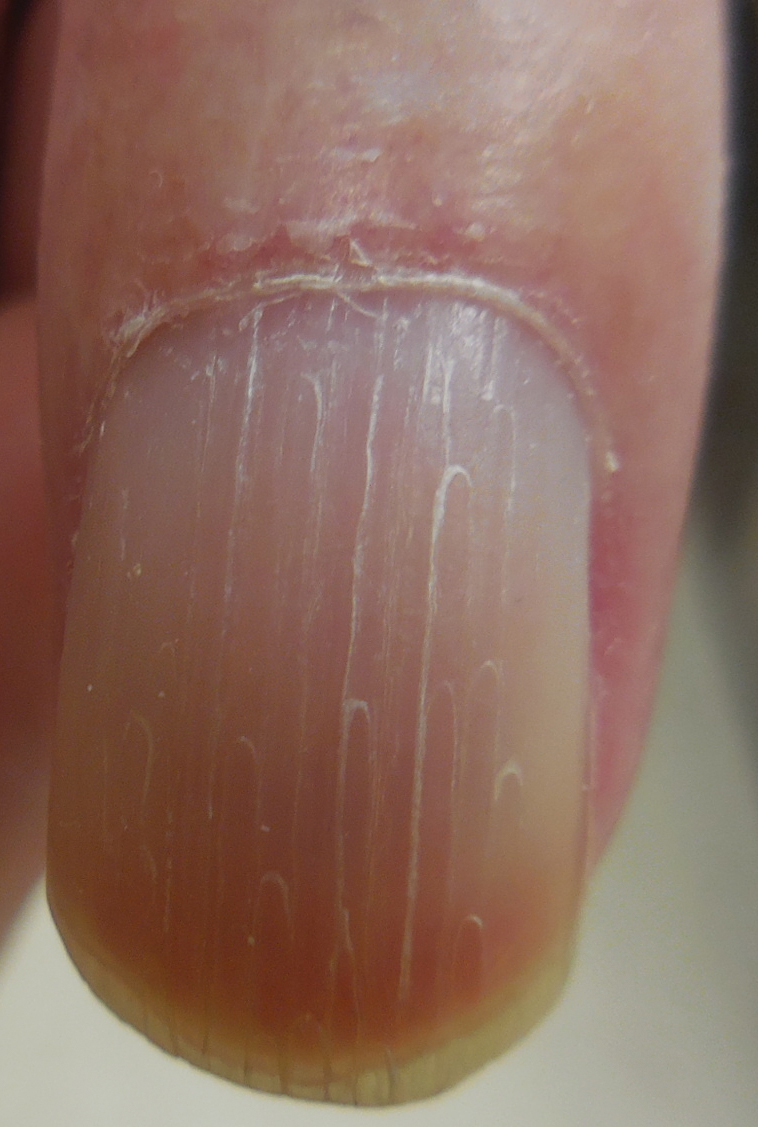
Complex regional pain syndrome is a neuropathic disorder of the extremities characterized by pain and a variety of autonomic and motor disturbances such as local edema, limited active range of motion, and vasomotor and trophic skin changes. There are 2 types of CRPS: type II is marked by explicit nerve injury and type I is not. The pathophysiology of CRPS is unknown.1-3
There is no definite set of diagnostic criteria for CRPS. The lack of any gold-standard diagnostic test for CRPS has made arriving at one valid, widely accepted set of diagnostic criteria impossible.1 There are 4 widely used sets of diagnostic criteria. One is the International Association for the Study of Pain diagnostic criteria defined in 1994.4 However, the criteria rely entirely on subjective symptoms and have been under great scrutiny due to their questionable validity.2 Veldman et al5 presented other widely used CRPS diagnostic criteria in their prospective study of 829 reflex sympathetic dystrophy patients, which paid particular attention to the early clinical manifestations of CRPS. In 1999, Bruehl et al2 proposed their own modified diagnostic criteria, which required physician-assessed signs in 2 of 4 categories to avoid the practice of exclusively relying on subjective symptoms. In addition, during a consensus meeting in Budapest, Hungary, a modified version of the Bruehl criteria was proposed.6 All 4 criteria rely solely on detailed history and physical examination, and the choice of diagnostic criteria remains subjective.
The pathophysiology of CRPS also remains unclear. There are several proposed mechanisms such as sympathetic nervous system dysfunction, abnormal inflammatory response, and central nervous system involvement.1 Psychologic factors, sequelae of nerve injury, and genetic predisposition also have been implicated in the pathophysiology of CRPS.1 It is likely that several mechanisms variably contribute to each presentation of CRPS.
Many dermatologic findings, in addition to neuromuscular symptoms, accompany CRPS and serve as important clues to making the clinical diagnosis. Complex regional pain syndrome has been thought to have 3 distinct sequential stages of CRPS.1,3,7 Stage 1—the acute stage—is marked by hyperalgesia, allodynia, sudomotor disturbances, and prominent edema. Stage 2—the dystrophic stage—is characterized by more marked pain and sensory dysfunction, vasomotor dysfunction, development of motor dysfunction, soft tissue edema, skin and articular soft tissue thickening, and development of dystrophic nail changes. Stage 3—the atrophic stage—is marked by decreased pain and sensory disturbances, markedly increased motor dysfunction, waxy atrophic skin changes, progression of dystrophic nail changes, and skeletal cystic and subchondral erosions with diffuse osteoporosis.1,3,7
The staging model, however, has been called into question.3 In a cluster analysis, Bruehl et al3 arrived at 3 relatively consistent CRPS patient subgroups that did not have notably different pain duration, suggesting the existence of 3 CRPS subtypes, not stages. Their study found that one of the subgroups best represented the clinical presentation of CRPS type II. This subgroup had the greatest pain and sensory abnormalities and the least vasomotor dysfunction of all 3 subgroups. Nonetheless, this study has not settled the discussion, as it only included 113 patients.3 Thus, with future studies, our understanding of CRPS in stages may change, which likely will impact how the clinical diagnosis is made.
There is a lack of high-quality evidence for most treatment interventions for CRPS8; however, the current practice is to use an interdisciplinary approach.1,9,10 The main therapeutic arm of this approach is rehabilitation; physical and occupational therapy can help improve range of motion, contracture, and atrophy. The other 2 arms of the approach are psychologic therapy to improve quality of life and pain management with pharmacologic therapy and/or invasive interventions. The choice of therapy remains empirical; trial and error should be expected in developing an adequate treatment plan for each individual patient.
Many aspects of CRPS remain unclear, and even our current understanding of the disease will inevitably change over time. The syndrome can cause life-changing morbidities in patients, and late diagnosis and treatment are associated with poor prognosis. Because there are many dermatologic findings associated with the disorder, it is crucial for dermatologists to clinically recognize the disorder and to refer patients to appropriate channels so that treatment can be started as soon as possible.
- Borchers A, Gershwin M. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014;13:242-265.
- Bruehl S, Harden RN, Galer BS, et al. External validation of IASP diagnostic criteria for complex regional pain syndrome and proposed research diagnostic criteria. International Association for the Study of Pain. Pain. 1999;81:147-154.
- Bruehl S, Harden RN, Gaker BS, et al. Complex regional pain syndrome: are there distinct subtypes and sequential stages of the syndrome? Pain. 2002;95:119-124.
- Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 2nd ed. Seattle, WA: IASP Press; 1994.
- Veldman PH, Reynen HM, Arntz IE, et al. Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet. 1993;342:1012-1016.
- Harden RN, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150:268-274.
- Sebastin SJ. Complex regional pain syndrome. Indian J Plast Surg. 2011;44:298-307.
- O’Connell NE, Wand BM, McAuley J, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome. Cochrane Database Syst Rev. 2013;4:CD009416.
- Hsu ES. Practical management of complex regional pain syndrome. Am J Ther. 2009;16:147-154.
- Stanton-Hicks MD, Burton AW, Bruehl SP, et al. An updated interdisciplinary clinical pathway for CRPS: report of an expert panel. Pain Pract. 2002;2:1-16.
To the Editor:
A 62-year-old man presented with an atrophied painful left arm of 17 years’ duration that began when he was hit by a car as a pedestrian. He sustained severe multisystem injuries from the accident, including left brachial plexus and C6 nerve root avulsion injury. When he regained consciousness after 6 weeks in the intensive care unit, he immediately noted diffuse pain throughout the body, especially in the left arm. Since the accident, the patient continued to have diminished sensation to touch and temperature in the left arm. He also had burning, throbbing, and electrical pain in the left arm with light touch as well as spontaneously. He was thoroughly evaluated by a neurologist and was diagnosed with complex regional pain syndrome (CRPS) type II. For the treatment of pain, dorsal column stimulation and hemilaminectomy with exploration of the avulsed nerve root were attempted, both of which had minimal effect. He was maintained on hydromorphone, methadone, and oxazepam. He reported that for many years he was unable move out of bed due to the unbearable pain. With pain medications, he was able to regain most of his independence in his daily life, though the pain and other clinical aspects of CRPS still completely limited his use of the left arm.
Physical examination revealed glossy, cold, hairless skin with hypohidrosis of the left arm, forearm, and hand (Figures 1 and 2A). The left arm was conspicuously atrophied, with the forearm and hand erythematous. The fingers were taut, contracted, and edematous (Figure 2B), and the skin was unable to be pinched. The fingernails on the left hand had dystrophic changes including yellow color and brittleness with longitudinal ridges (Figure 3). The patient could activate the left bicep and tricep muscles against gravity but had minimal function of the deltoid muscle. He also had minimal movement of the left index finger and was unable to move any other digits of the left hand. The patient was continued on pain management treatments and physical therapy for his condition.
Complex regional pain syndrome is a neuropathic disorder of the extremities characterized by pain and a variety of autonomic and motor disturbances such as local edema, limited active range of motion, and vasomotor and trophic skin changes. There are 2 types of CRPS: type II is marked by explicit nerve injury and type I is not. The pathophysiology of CRPS is unknown.1-3
There is no definite set of diagnostic criteria for CRPS. The lack of any gold-standard diagnostic test for CRPS has made arriving at one valid, widely accepted set of diagnostic criteria impossible.1 There are 4 widely used sets of diagnostic criteria. One is the International Association for the Study of Pain diagnostic criteria defined in 1994.4 However, the criteria rely entirely on subjective symptoms and have been under great scrutiny due to their questionable validity.2 Veldman et al5 presented other widely used CRPS diagnostic criteria in their prospective study of 829 reflex sympathetic dystrophy patients, which paid particular attention to the early clinical manifestations of CRPS. In 1999, Bruehl et al2 proposed their own modified diagnostic criteria, which required physician-assessed signs in 2 of 4 categories to avoid the practice of exclusively relying on subjective symptoms. In addition, during a consensus meeting in Budapest, Hungary, a modified version of the Bruehl criteria was proposed.6 All 4 criteria rely solely on detailed history and physical examination, and the choice of diagnostic criteria remains subjective.
The pathophysiology of CRPS also remains unclear. There are several proposed mechanisms such as sympathetic nervous system dysfunction, abnormal inflammatory response, and central nervous system involvement.1 Psychologic factors, sequelae of nerve injury, and genetic predisposition also have been implicated in the pathophysiology of CRPS.1 It is likely that several mechanisms variably contribute to each presentation of CRPS.
Many dermatologic findings, in addition to neuromuscular symptoms, accompany CRPS and serve as important clues to making the clinical diagnosis. Complex regional pain syndrome has been thought to have 3 distinct sequential stages of CRPS.1,3,7 Stage 1—the acute stage—is marked by hyperalgesia, allodynia, sudomotor disturbances, and prominent edema. Stage 2—the dystrophic stage—is characterized by more marked pain and sensory dysfunction, vasomotor dysfunction, development of motor dysfunction, soft tissue edema, skin and articular soft tissue thickening, and development of dystrophic nail changes. Stage 3—the atrophic stage—is marked by decreased pain and sensory disturbances, markedly increased motor dysfunction, waxy atrophic skin changes, progression of dystrophic nail changes, and skeletal cystic and subchondral erosions with diffuse osteoporosis.1,3,7
The staging model, however, has been called into question.3 In a cluster analysis, Bruehl et al3 arrived at 3 relatively consistent CRPS patient subgroups that did not have notably different pain duration, suggesting the existence of 3 CRPS subtypes, not stages. Their study found that one of the subgroups best represented the clinical presentation of CRPS type II. This subgroup had the greatest pain and sensory abnormalities and the least vasomotor dysfunction of all 3 subgroups. Nonetheless, this study has not settled the discussion, as it only included 113 patients.3 Thus, with future studies, our understanding of CRPS in stages may change, which likely will impact how the clinical diagnosis is made.
There is a lack of high-quality evidence for most treatment interventions for CRPS8; however, the current practice is to use an interdisciplinary approach.1,9,10 The main therapeutic arm of this approach is rehabilitation; physical and occupational therapy can help improve range of motion, contracture, and atrophy. The other 2 arms of the approach are psychologic therapy to improve quality of life and pain management with pharmacologic therapy and/or invasive interventions. The choice of therapy remains empirical; trial and error should be expected in developing an adequate treatment plan for each individual patient.
Many aspects of CRPS remain unclear, and even our current understanding of the disease will inevitably change over time. The syndrome can cause life-changing morbidities in patients, and late diagnosis and treatment are associated with poor prognosis. Because there are many dermatologic findings associated with the disorder, it is crucial for dermatologists to clinically recognize the disorder and to refer patients to appropriate channels so that treatment can be started as soon as possible.
To the Editor:
A 62-year-old man presented with an atrophied painful left arm of 17 years’ duration that began when he was hit by a car as a pedestrian. He sustained severe multisystem injuries from the accident, including left brachial plexus and C6 nerve root avulsion injury. When he regained consciousness after 6 weeks in the intensive care unit, he immediately noted diffuse pain throughout the body, especially in the left arm. Since the accident, the patient continued to have diminished sensation to touch and temperature in the left arm. He also had burning, throbbing, and electrical pain in the left arm with light touch as well as spontaneously. He was thoroughly evaluated by a neurologist and was diagnosed with complex regional pain syndrome (CRPS) type II. For the treatment of pain, dorsal column stimulation and hemilaminectomy with exploration of the avulsed nerve root were attempted, both of which had minimal effect. He was maintained on hydromorphone, methadone, and oxazepam. He reported that for many years he was unable move out of bed due to the unbearable pain. With pain medications, he was able to regain most of his independence in his daily life, though the pain and other clinical aspects of CRPS still completely limited his use of the left arm.
Physical examination revealed glossy, cold, hairless skin with hypohidrosis of the left arm, forearm, and hand (Figures 1 and 2A). The left arm was conspicuously atrophied, with the forearm and hand erythematous. The fingers were taut, contracted, and edematous (Figure 2B), and the skin was unable to be pinched. The fingernails on the left hand had dystrophic changes including yellow color and brittleness with longitudinal ridges (Figure 3). The patient could activate the left bicep and tricep muscles against gravity but had minimal function of the deltoid muscle. He also had minimal movement of the left index finger and was unable to move any other digits of the left hand. The patient was continued on pain management treatments and physical therapy for his condition.
Complex regional pain syndrome is a neuropathic disorder of the extremities characterized by pain and a variety of autonomic and motor disturbances such as local edema, limited active range of motion, and vasomotor and trophic skin changes. There are 2 types of CRPS: type II is marked by explicit nerve injury and type I is not. The pathophysiology of CRPS is unknown.1-3
There is no definite set of diagnostic criteria for CRPS. The lack of any gold-standard diagnostic test for CRPS has made arriving at one valid, widely accepted set of diagnostic criteria impossible.1 There are 4 widely used sets of diagnostic criteria. One is the International Association for the Study of Pain diagnostic criteria defined in 1994.4 However, the criteria rely entirely on subjective symptoms and have been under great scrutiny due to their questionable validity.2 Veldman et al5 presented other widely used CRPS diagnostic criteria in their prospective study of 829 reflex sympathetic dystrophy patients, which paid particular attention to the early clinical manifestations of CRPS. In 1999, Bruehl et al2 proposed their own modified diagnostic criteria, which required physician-assessed signs in 2 of 4 categories to avoid the practice of exclusively relying on subjective symptoms. In addition, during a consensus meeting in Budapest, Hungary, a modified version of the Bruehl criteria was proposed.6 All 4 criteria rely solely on detailed history and physical examination, and the choice of diagnostic criteria remains subjective.
The pathophysiology of CRPS also remains unclear. There are several proposed mechanisms such as sympathetic nervous system dysfunction, abnormal inflammatory response, and central nervous system involvement.1 Psychologic factors, sequelae of nerve injury, and genetic predisposition also have been implicated in the pathophysiology of CRPS.1 It is likely that several mechanisms variably contribute to each presentation of CRPS.
Many dermatologic findings, in addition to neuromuscular symptoms, accompany CRPS and serve as important clues to making the clinical diagnosis. Complex regional pain syndrome has been thought to have 3 distinct sequential stages of CRPS.1,3,7 Stage 1—the acute stage—is marked by hyperalgesia, allodynia, sudomotor disturbances, and prominent edema. Stage 2—the dystrophic stage—is characterized by more marked pain and sensory dysfunction, vasomotor dysfunction, development of motor dysfunction, soft tissue edema, skin and articular soft tissue thickening, and development of dystrophic nail changes. Stage 3—the atrophic stage—is marked by decreased pain and sensory disturbances, markedly increased motor dysfunction, waxy atrophic skin changes, progression of dystrophic nail changes, and skeletal cystic and subchondral erosions with diffuse osteoporosis.1,3,7
The staging model, however, has been called into question.3 In a cluster analysis, Bruehl et al3 arrived at 3 relatively consistent CRPS patient subgroups that did not have notably different pain duration, suggesting the existence of 3 CRPS subtypes, not stages. Their study found that one of the subgroups best represented the clinical presentation of CRPS type II. This subgroup had the greatest pain and sensory abnormalities and the least vasomotor dysfunction of all 3 subgroups. Nonetheless, this study has not settled the discussion, as it only included 113 patients.3 Thus, with future studies, our understanding of CRPS in stages may change, which likely will impact how the clinical diagnosis is made.
There is a lack of high-quality evidence for most treatment interventions for CRPS8; however, the current practice is to use an interdisciplinary approach.1,9,10 The main therapeutic arm of this approach is rehabilitation; physical and occupational therapy can help improve range of motion, contracture, and atrophy. The other 2 arms of the approach are psychologic therapy to improve quality of life and pain management with pharmacologic therapy and/or invasive interventions. The choice of therapy remains empirical; trial and error should be expected in developing an adequate treatment plan for each individual patient.
Many aspects of CRPS remain unclear, and even our current understanding of the disease will inevitably change over time. The syndrome can cause life-changing morbidities in patients, and late diagnosis and treatment are associated with poor prognosis. Because there are many dermatologic findings associated with the disorder, it is crucial for dermatologists to clinically recognize the disorder and to refer patients to appropriate channels so that treatment can be started as soon as possible.
- Borchers A, Gershwin M. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014;13:242-265.
- Bruehl S, Harden RN, Galer BS, et al. External validation of IASP diagnostic criteria for complex regional pain syndrome and proposed research diagnostic criteria. International Association for the Study of Pain. Pain. 1999;81:147-154.
- Bruehl S, Harden RN, Gaker BS, et al. Complex regional pain syndrome: are there distinct subtypes and sequential stages of the syndrome? Pain. 2002;95:119-124.
- Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 2nd ed. Seattle, WA: IASP Press; 1994.
- Veldman PH, Reynen HM, Arntz IE, et al. Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet. 1993;342:1012-1016.
- Harden RN, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150:268-274.
- Sebastin SJ. Complex regional pain syndrome. Indian J Plast Surg. 2011;44:298-307.
- O’Connell NE, Wand BM, McAuley J, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome. Cochrane Database Syst Rev. 2013;4:CD009416.
- Hsu ES. Practical management of complex regional pain syndrome. Am J Ther. 2009;16:147-154.
- Stanton-Hicks MD, Burton AW, Bruehl SP, et al. An updated interdisciplinary clinical pathway for CRPS: report of an expert panel. Pain Pract. 2002;2:1-16.
- Borchers A, Gershwin M. Complex regional pain syndrome: a comprehensive and critical review. Autoimmun Rev. 2014;13:242-265.
- Bruehl S, Harden RN, Galer BS, et al. External validation of IASP diagnostic criteria for complex regional pain syndrome and proposed research diagnostic criteria. International Association for the Study of Pain. Pain. 1999;81:147-154.
- Bruehl S, Harden RN, Gaker BS, et al. Complex regional pain syndrome: are there distinct subtypes and sequential stages of the syndrome? Pain. 2002;95:119-124.
- Merskey H, Bogduk N. Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. 2nd ed. Seattle, WA: IASP Press; 1994.
- Veldman PH, Reynen HM, Arntz IE, et al. Signs and symptoms of reflex sympathetic dystrophy: prospective study of 829 patients. Lancet. 1993;342:1012-1016.
- Harden RN, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150:268-274.
- Sebastin SJ. Complex regional pain syndrome. Indian J Plast Surg. 2011;44:298-307.
- O’Connell NE, Wand BM, McAuley J, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome. Cochrane Database Syst Rev. 2013;4:CD009416.
- Hsu ES. Practical management of complex regional pain syndrome. Am J Ther. 2009;16:147-154.
- Stanton-Hicks MD, Burton AW, Bruehl SP, et al. An updated interdisciplinary clinical pathway for CRPS: report of an expert panel. Pain Pract. 2002;2:1-16.
Practice Points
- Complex regional pain syndrome (CRPS) is a neuropathic disorder of the extremities characterized by pain, a variety of autonomic and motor disturbances, and dermatologic findings.
- Early recognition of CRPS is critical, as it presents life-changing morbidities to patients.
- A multidisciplinary treatment approach with physical therapy, occupational therapy, psychological support, and pain control is needed for the management of CRPS.
