User login
Today’s top news highlights: Cancer makes COVID-19 more dangerous, treatment for heavy menstrual bleeding, and more
Here are the stories our MDedge editors across specialties think you need to know about today:
Active cancer ups death risk for patients with COVID-19
New data show that patients with COVID-19 and progressing cancer had a significantly higher risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer. Interestingly, one of the independent risk factor for death in patients with COVID-19 and cancer was treatment with hydroxychloroquine plus azithromycin. This finding, however, was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville. Read more.
Two new studies indicate that social distancing successfully flattened the curve on COVID-19 hospitalizations. One study, published in JAMA, showed significantly lower numbers of observed cases versus worst-case projections in four states: Colorado, Minnesota, Ohio, and Virginia. In Minnesota, 17 days after the order, there were 361 cumulative hospitalizations, compared with a projection of 988 had no such action been taken. In a separate study measuring COVID-19 patients occupying ICU beds in Ontario and deaths among those cases, hospitals “would have rapidly exceeded ICU capacity and observed substantially higher mortality” without any physical distancing intervention. Read more.
FDA approves treatment for heavy menstrual bleeding
The Food and Drug Administration has approved a medication for the management of heavy menstrual bleeding associated with uterine fibroids in premenopausal women. The medication, marketed as Oriahnn, is an estrogen and progestin combination product that consists of elagolix, estradiol, and norethindrone acetate capsules packaged together for oral use. The most common side effects of the drug included hot flushes, headache, fatigue, and irregular vaginal bleeding. The drug’s label includes a boxed warning about a risk of strokes and blood clots, especially in women at increased risk for these events. Read more.
Lessons from a drive-through COVID testing center
Chris Notte, MD, and Neil Skolnik, MD, were part of a team of clinicians charged with launching a drive-through COVID-19 testing center. Their task was to get the operation up and running in 2 days. It took them 3 days. While the launch was a success, the experience taught them some lessons about the limits of medical technology and the importance of personal protective equipment. “Prior to the coronavirus pandemic, I had never considered surgical masks, face shields, and nasal swabs to be critical components of medical technology. My opinion quickly changed after opening our drive-through COVID-19 site,” they wrote. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Active cancer ups death risk for patients with COVID-19
New data show that patients with COVID-19 and progressing cancer had a significantly higher risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer. Interestingly, one of the independent risk factor for death in patients with COVID-19 and cancer was treatment with hydroxychloroquine plus azithromycin. This finding, however, was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville. Read more.
Two new studies indicate that social distancing successfully flattened the curve on COVID-19 hospitalizations. One study, published in JAMA, showed significantly lower numbers of observed cases versus worst-case projections in four states: Colorado, Minnesota, Ohio, and Virginia. In Minnesota, 17 days after the order, there were 361 cumulative hospitalizations, compared with a projection of 988 had no such action been taken. In a separate study measuring COVID-19 patients occupying ICU beds in Ontario and deaths among those cases, hospitals “would have rapidly exceeded ICU capacity and observed substantially higher mortality” without any physical distancing intervention. Read more.
FDA approves treatment for heavy menstrual bleeding
The Food and Drug Administration has approved a medication for the management of heavy menstrual bleeding associated with uterine fibroids in premenopausal women. The medication, marketed as Oriahnn, is an estrogen and progestin combination product that consists of elagolix, estradiol, and norethindrone acetate capsules packaged together for oral use. The most common side effects of the drug included hot flushes, headache, fatigue, and irregular vaginal bleeding. The drug’s label includes a boxed warning about a risk of strokes and blood clots, especially in women at increased risk for these events. Read more.
Lessons from a drive-through COVID testing center
Chris Notte, MD, and Neil Skolnik, MD, were part of a team of clinicians charged with launching a drive-through COVID-19 testing center. Their task was to get the operation up and running in 2 days. It took them 3 days. While the launch was a success, the experience taught them some lessons about the limits of medical technology and the importance of personal protective equipment. “Prior to the coronavirus pandemic, I had never considered surgical masks, face shields, and nasal swabs to be critical components of medical technology. My opinion quickly changed after opening our drive-through COVID-19 site,” they wrote. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Active cancer ups death risk for patients with COVID-19
New data show that patients with COVID-19 and progressing cancer had a significantly higher risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer. Interestingly, one of the independent risk factor for death in patients with COVID-19 and cancer was treatment with hydroxychloroquine plus azithromycin. This finding, however, was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville. Read more.
Two new studies indicate that social distancing successfully flattened the curve on COVID-19 hospitalizations. One study, published in JAMA, showed significantly lower numbers of observed cases versus worst-case projections in four states: Colorado, Minnesota, Ohio, and Virginia. In Minnesota, 17 days after the order, there were 361 cumulative hospitalizations, compared with a projection of 988 had no such action been taken. In a separate study measuring COVID-19 patients occupying ICU beds in Ontario and deaths among those cases, hospitals “would have rapidly exceeded ICU capacity and observed substantially higher mortality” without any physical distancing intervention. Read more.
FDA approves treatment for heavy menstrual bleeding
The Food and Drug Administration has approved a medication for the management of heavy menstrual bleeding associated with uterine fibroids in premenopausal women. The medication, marketed as Oriahnn, is an estrogen and progestin combination product that consists of elagolix, estradiol, and norethindrone acetate capsules packaged together for oral use. The most common side effects of the drug included hot flushes, headache, fatigue, and irregular vaginal bleeding. The drug’s label includes a boxed warning about a risk of strokes and blood clots, especially in women at increased risk for these events. Read more.
Lessons from a drive-through COVID testing center
Chris Notte, MD, and Neil Skolnik, MD, were part of a team of clinicians charged with launching a drive-through COVID-19 testing center. Their task was to get the operation up and running in 2 days. It took them 3 days. While the launch was a success, the experience taught them some lessons about the limits of medical technology and the importance of personal protective equipment. “Prior to the coronavirus pandemic, I had never considered surgical masks, face shields, and nasal swabs to be critical components of medical technology. My opinion quickly changed after opening our drive-through COVID-19 site,” they wrote. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Upfront pembrolizumab doubles PFS in MSI-H/dMMR metastatic colorectal cancer
The median PFS was 16.5 months for patients who received pembrolizumab and 8.2 months for those who received investigators’ choice of chemotherapy (one of six regimens).
“In the past, no medical treatment has shown such difference in terms of improvement of PFS in metastatic colorectal cancer,” said study investigator Thierry André, MD, of Hôpital Saint Antoine in Paris.
“Today, this study demonstrates that the majority of the 5% of patients with metastatic colorectal cancer selected by MSI-high status benefited greatly from anti–PD-1 [programmed death-1] pembrolizumab, compared with standard of care,” he added.
Dr. André discussed the study in a press briefing prior to his presentation of the data as part of the American Society of Clinical Oncology virtual scientific program.
“I think this is setting a new standard of care,” said Michael J. Overman, MD, of the University of Texas MD Anderson Cancer Center in Houston. Dr. Overman, the invited discussant, commented on the KEYNOTE-177 study in an interview prior to the presentation.
Dr. Overman noted that, although the overall response rate was higher with pembrolizumab, the rate of progressive disease was higher in the pembrolizumab arm than in the chemotherapy arm. Progressive disease was the best response in 29.4% of patients on pembrolizumab and 12.3% of patients on chemotherapy.
“The only area where I think the question on pembrolizumab is still open would be in the group of patients where we’re saying ‘I care about the near future – this patient has so many symptoms and so much disease burden that I care what happens in the short term,’” Dr. Overman said. He added that, for this subgroup of patients, chemotherapy or pembrolizumab in combination with another immunotherapy, such as ipilimumab, might be more appropriate.
KEYNOTE-177 details
Investigators enrolled 307 patients with confirmed, untreated MSI-H/dMMR metastatic colorectal cancer and good performance status (Eastern Cooperative Oncology Group performance status 0 or 1).
Patients were randomized to pembrolizumab at 200 mg every 3 weeks for up to 35 cycles (n = 153) or to the investigators’ choice of chemotherapy (n = 154). Chemotherapy regimens were modified FOLFOX (5-fluorouracil, leucovorin, oxaliplatin) alone or in combination with either bevacizumab or cetuximab, or FOLFIRI (leucovorin, fluorouracil, irinotecan) alone or in combination with either bevacizumab or cetuximab.
Patients assigned to the chemotherapy arm were allowed to cross over to pembrolizumab for up to 35 cycles if they had disease progression confirmed by central review.
PFS is a coprimary endpoint with overall survival. The trial was deemed to be successful if either of the coprimary endpoints was met. Overall survival results are not yet available.
The median PFS was 16.5 months with pembrolizumab and 8.2 months with chemotherapy (hazard ratio, 0.60; P = .0002). The 12-month PFS rates were 55% and 37%, respectively. The 24-month PFS rates were 48% and 19%, respectively.
Overall response rates were 43.8% with pembrolizumab, consisting of 11.1% complete responses and 32.7% partial responses. The overall response rate with chemotherapy was 33.1%, consisting of 3.9% complete responses and 29.2% partial responses.
In all, 20.9% of patients on pembrolizumab and 42.2% of those on chemotherapy had stable disease. Rates of progressive disease were 29.4% and 12.3%, respectively.
The median duration of response was not reached in the pembrolizumab arm and was 10.6 months in the chemotherapy arm. At 2 years, 83% of patients treated with pembrolizumab and 35% treated with chemotherapy had ongoing responses.
Grade 3 or greater treatment-related adverse events occurred in 22% of patients on pembrolizumab and 66% on chemotherapy.
Immune-mediated adverse events and infusion reactions were more common with pembrolizumab than with chemotherapy (31% and 13%, respectively). Adverse events that were common with chemotherapy included gastrointestinal events, fatigue, neutropenia, and peripheral sensory neuropathy.
The study was funded by Merck. Dr. André disclosed relationships with multiple companies, including MSD Oncology. Dr. Overman disclosed consulting activities with various companies, not including Merck.
SOURCE: André T et al. ASCO 2020, Abstract LBA4.
The median PFS was 16.5 months for patients who received pembrolizumab and 8.2 months for those who received investigators’ choice of chemotherapy (one of six regimens).
“In the past, no medical treatment has shown such difference in terms of improvement of PFS in metastatic colorectal cancer,” said study investigator Thierry André, MD, of Hôpital Saint Antoine in Paris.
“Today, this study demonstrates that the majority of the 5% of patients with metastatic colorectal cancer selected by MSI-high status benefited greatly from anti–PD-1 [programmed death-1] pembrolizumab, compared with standard of care,” he added.
Dr. André discussed the study in a press briefing prior to his presentation of the data as part of the American Society of Clinical Oncology virtual scientific program.
“I think this is setting a new standard of care,” said Michael J. Overman, MD, of the University of Texas MD Anderson Cancer Center in Houston. Dr. Overman, the invited discussant, commented on the KEYNOTE-177 study in an interview prior to the presentation.
Dr. Overman noted that, although the overall response rate was higher with pembrolizumab, the rate of progressive disease was higher in the pembrolizumab arm than in the chemotherapy arm. Progressive disease was the best response in 29.4% of patients on pembrolizumab and 12.3% of patients on chemotherapy.
“The only area where I think the question on pembrolizumab is still open would be in the group of patients where we’re saying ‘I care about the near future – this patient has so many symptoms and so much disease burden that I care what happens in the short term,’” Dr. Overman said. He added that, for this subgroup of patients, chemotherapy or pembrolizumab in combination with another immunotherapy, such as ipilimumab, might be more appropriate.
KEYNOTE-177 details
Investigators enrolled 307 patients with confirmed, untreated MSI-H/dMMR metastatic colorectal cancer and good performance status (Eastern Cooperative Oncology Group performance status 0 or 1).
Patients were randomized to pembrolizumab at 200 mg every 3 weeks for up to 35 cycles (n = 153) or to the investigators’ choice of chemotherapy (n = 154). Chemotherapy regimens were modified FOLFOX (5-fluorouracil, leucovorin, oxaliplatin) alone or in combination with either bevacizumab or cetuximab, or FOLFIRI (leucovorin, fluorouracil, irinotecan) alone or in combination with either bevacizumab or cetuximab.
Patients assigned to the chemotherapy arm were allowed to cross over to pembrolizumab for up to 35 cycles if they had disease progression confirmed by central review.
PFS is a coprimary endpoint with overall survival. The trial was deemed to be successful if either of the coprimary endpoints was met. Overall survival results are not yet available.
The median PFS was 16.5 months with pembrolizumab and 8.2 months with chemotherapy (hazard ratio, 0.60; P = .0002). The 12-month PFS rates were 55% and 37%, respectively. The 24-month PFS rates were 48% and 19%, respectively.
Overall response rates were 43.8% with pembrolizumab, consisting of 11.1% complete responses and 32.7% partial responses. The overall response rate with chemotherapy was 33.1%, consisting of 3.9% complete responses and 29.2% partial responses.
In all, 20.9% of patients on pembrolizumab and 42.2% of those on chemotherapy had stable disease. Rates of progressive disease were 29.4% and 12.3%, respectively.
The median duration of response was not reached in the pembrolizumab arm and was 10.6 months in the chemotherapy arm. At 2 years, 83% of patients treated with pembrolizumab and 35% treated with chemotherapy had ongoing responses.
Grade 3 or greater treatment-related adverse events occurred in 22% of patients on pembrolizumab and 66% on chemotherapy.
Immune-mediated adverse events and infusion reactions were more common with pembrolizumab than with chemotherapy (31% and 13%, respectively). Adverse events that were common with chemotherapy included gastrointestinal events, fatigue, neutropenia, and peripheral sensory neuropathy.
The study was funded by Merck. Dr. André disclosed relationships with multiple companies, including MSD Oncology. Dr. Overman disclosed consulting activities with various companies, not including Merck.
SOURCE: André T et al. ASCO 2020, Abstract LBA4.
The median PFS was 16.5 months for patients who received pembrolizumab and 8.2 months for those who received investigators’ choice of chemotherapy (one of six regimens).
“In the past, no medical treatment has shown such difference in terms of improvement of PFS in metastatic colorectal cancer,” said study investigator Thierry André, MD, of Hôpital Saint Antoine in Paris.
“Today, this study demonstrates that the majority of the 5% of patients with metastatic colorectal cancer selected by MSI-high status benefited greatly from anti–PD-1 [programmed death-1] pembrolizumab, compared with standard of care,” he added.
Dr. André discussed the study in a press briefing prior to his presentation of the data as part of the American Society of Clinical Oncology virtual scientific program.
“I think this is setting a new standard of care,” said Michael J. Overman, MD, of the University of Texas MD Anderson Cancer Center in Houston. Dr. Overman, the invited discussant, commented on the KEYNOTE-177 study in an interview prior to the presentation.
Dr. Overman noted that, although the overall response rate was higher with pembrolizumab, the rate of progressive disease was higher in the pembrolizumab arm than in the chemotherapy arm. Progressive disease was the best response in 29.4% of patients on pembrolizumab and 12.3% of patients on chemotherapy.
“The only area where I think the question on pembrolizumab is still open would be in the group of patients where we’re saying ‘I care about the near future – this patient has so many symptoms and so much disease burden that I care what happens in the short term,’” Dr. Overman said. He added that, for this subgroup of patients, chemotherapy or pembrolizumab in combination with another immunotherapy, such as ipilimumab, might be more appropriate.
KEYNOTE-177 details
Investigators enrolled 307 patients with confirmed, untreated MSI-H/dMMR metastatic colorectal cancer and good performance status (Eastern Cooperative Oncology Group performance status 0 or 1).
Patients were randomized to pembrolizumab at 200 mg every 3 weeks for up to 35 cycles (n = 153) or to the investigators’ choice of chemotherapy (n = 154). Chemotherapy regimens were modified FOLFOX (5-fluorouracil, leucovorin, oxaliplatin) alone or in combination with either bevacizumab or cetuximab, or FOLFIRI (leucovorin, fluorouracil, irinotecan) alone or in combination with either bevacizumab or cetuximab.
Patients assigned to the chemotherapy arm were allowed to cross over to pembrolizumab for up to 35 cycles if they had disease progression confirmed by central review.
PFS is a coprimary endpoint with overall survival. The trial was deemed to be successful if either of the coprimary endpoints was met. Overall survival results are not yet available.
The median PFS was 16.5 months with pembrolizumab and 8.2 months with chemotherapy (hazard ratio, 0.60; P = .0002). The 12-month PFS rates were 55% and 37%, respectively. The 24-month PFS rates were 48% and 19%, respectively.
Overall response rates were 43.8% with pembrolizumab, consisting of 11.1% complete responses and 32.7% partial responses. The overall response rate with chemotherapy was 33.1%, consisting of 3.9% complete responses and 29.2% partial responses.
In all, 20.9% of patients on pembrolizumab and 42.2% of those on chemotherapy had stable disease. Rates of progressive disease were 29.4% and 12.3%, respectively.
The median duration of response was not reached in the pembrolizumab arm and was 10.6 months in the chemotherapy arm. At 2 years, 83% of patients treated with pembrolizumab and 35% treated with chemotherapy had ongoing responses.
Grade 3 or greater treatment-related adverse events occurred in 22% of patients on pembrolizumab and 66% on chemotherapy.
Immune-mediated adverse events and infusion reactions were more common with pembrolizumab than with chemotherapy (31% and 13%, respectively). Adverse events that were common with chemotherapy included gastrointestinal events, fatigue, neutropenia, and peripheral sensory neuropathy.
The study was funded by Merck. Dr. André disclosed relationships with multiple companies, including MSD Oncology. Dr. Overman disclosed consulting activities with various companies, not including Merck.
SOURCE: André T et al. ASCO 2020, Abstract LBA4.
FROM ASCO 2020
Pembrolizumab plus chemo shows benefits for PD-L1–rich triple-negative breast cancer
Adding pembrolizumab to standard chemotherapy significantly improved progression-free survival for patients with metastatic triple-negative breast cancer, but only if their tumors were enriched with comparatively high levels of the target programmed death ligand-1 (PD-L1), results of the KEYNOTE 355 trial showed.
Among 843 patients with triple-negative breast cancer (TNBC) randomized to receive either investigator’s choice of chemotherapy plus pembrolizumab (Keytruda) or placebo, patients whose tumors had a PD-L1 combined positive score (CPS) of 10 or higher had a median progression-free survival (PFS) of 9.7 months when treated with pembrolizumab and chemotherapy, compared with 5.6 months among patients treated with chemotherapy and placebo, reported Javier Cortes, MD, PhD, from the Vall d´Hebron Institute of Oncology in Madrid and Barcelona.
However, among patients with CPS between 1 and 10, there was no significant difference in PFS between the treatment arms, he said in a presentation made as a part of the 2020 American Society of Clinical Oncology virtual scientific program.
“The inclusion of taxanes and a known taxane/platinum–based regimen permits assessment of the clinical benefit of pembro in combination with several routinely used chemo partners. A trend toward improved efficacy with PD-L1 enrichment was observed in patients treated with pembro plus chemo. The improvement in progression-free survival with chemotherapy and pembrolizumab was observed across patient subgroups,” said Dr. Cortes.
In the KEYNOTE-522 study, adding pembrolizumab to chemotherapy in the neoadjuvant setting increased the likelihood that women with stage III or early node-positive TNBC would have a pathologic complete response and sustained clinical benefit.
KEYNOTE-355 examined whether pembrolizumab in combination with chemotherapy could provide additional benefit over chemotherapy alone in patients with previously untreated locally recurrent inoperable or metastatic TNBC.
Patients with previously untreated metastatic triple-negative breast cancer who had at least 6 months between definite surgery or last dose of adjuvant chemotherapy (whichever came last) and first disease recurrence were stratified by study chemotherapy received, tumor PD-L1 expression at baseline, and prior treatment with the same class of chemotherapy in the neoadjuvant and/or adjuvant setting.
The patients were then randomized in a 2:1 ratio to pembrolizumab plus chemotherapy based on the investigator’s choice of nab-paclitaxel, paclitaxel, or carboplatin-gemcitabine (562 patients) or to chemotherapy alone (281).
Pembrolizumab and placebo were administered in a double-blind fashion for up to 35 doses. Chemotherapy was given at the investigator’s discretion according to local guidelines. This trial was not powered or designed to compare differential efficacy of the various chemotherapy regimens, Dr. Cortes noted.
The trial had dual primary endpoints of PFS in patients with PD-L1–positive tumors (CPS > 10 and > 1) and in the intention-to-treat population, and overall survival both in PD-L1-positive patients and the ITT population. Overall survival results will be reported at a later date.
As noted before, the primary endpoint was met in the population of patients with CPS higher than 10, with median PFS of 9.7 among those receiving pembrolizumab versus 5.6 months among those receiving placebo, and an estimated 1 year PFS of 39.1% versus 23% for controls, translating into a hazard ratio for progression on pembrolizumab of 0.65 (P = .0012).
In the patients with CPS higher than 1, however, the median PFS was 7.6 months with pembrolizumab compared with 5.6 months with placebo, translating into a hazard ratio of 0.74. However, the results did not meet the prespecified boundary for significance. Because of this, the statistical significance in the ITT population was not tested.
“In patients with PD-L1 CPS 10 or higher tumors, the benefit of pembro/chemo on progression-free survival was generally consistent across most predefined subgroups, including eight geographic regions, ECOG performance status, on-study chemo, and prior treatment with the same class of chemo,” Dr. Cortes said.
Treatment-related adverse events occurred in 96.3% of the patients on pembrolizumab and 95% of patients on placebo. Grade 3 or greater adverse events occurred in 68.1% versus 66.9%, respectively. Two patients in the pembrolizumab arm died from a treatment-related event. There were no treatment-related deaths in the placebo arm.
The most common events were those typically associated with chemotherapy, including anemia, neutropenia, nausea, alopecia, fatigue, decreased neutrophil counts, and elevated liver transaminases. Immune-mediated adverse events of any grade occurred in 25.6% of patients in the pembrolizumab arm versus 6% of controls; none of these events were fatal.
“What is clear in this study is that again we’re seeing efficacy of pembrolizumab in combination with chemotherapy increases with increases in CPS,” according to the invited discussant Catherine M. Kelly, MB, BCh, from University College Dublin and Mater Misericordiae University Hospital in Dublin.
“The results from today’s KEYNOTE-355 appear consistent in terms of progression-free survival. However, it is ‘watch this space’ until we get overall survival data before we can make any further comparisons,” she added.
Questions that still need to be answered include which is the best test for measuring PD-L1, whether patients with CPS of 1 or more but less than 10 benefit from the treatment, which of the available chemotherapy regimens is the best partner for pembrolizumab, how to treat patients who don’t respond to the combination, and what are the implications for PD-1/PD-L1 inhibitors in late-stage disease if they are approved in the neoadjuvant or adjuvant setting, Dr. Kelly said.
The study was funded by Merck. Dr. Cortes disclosed honoraria from, a consulting/advisory role for, and institutional research funding from Merck and others. Dr. Kelly disclosed honoraria from MSD Oncology and others, and travel expenses from Pfizer and Roche.
SOURCE: Cortes J et al. ASCO 2020, Abstract 1000.
Adding pembrolizumab to standard chemotherapy significantly improved progression-free survival for patients with metastatic triple-negative breast cancer, but only if their tumors were enriched with comparatively high levels of the target programmed death ligand-1 (PD-L1), results of the KEYNOTE 355 trial showed.
Among 843 patients with triple-negative breast cancer (TNBC) randomized to receive either investigator’s choice of chemotherapy plus pembrolizumab (Keytruda) or placebo, patients whose tumors had a PD-L1 combined positive score (CPS) of 10 or higher had a median progression-free survival (PFS) of 9.7 months when treated with pembrolizumab and chemotherapy, compared with 5.6 months among patients treated with chemotherapy and placebo, reported Javier Cortes, MD, PhD, from the Vall d´Hebron Institute of Oncology in Madrid and Barcelona.
However, among patients with CPS between 1 and 10, there was no significant difference in PFS between the treatment arms, he said in a presentation made as a part of the 2020 American Society of Clinical Oncology virtual scientific program.
“The inclusion of taxanes and a known taxane/platinum–based regimen permits assessment of the clinical benefit of pembro in combination with several routinely used chemo partners. A trend toward improved efficacy with PD-L1 enrichment was observed in patients treated with pembro plus chemo. The improvement in progression-free survival with chemotherapy and pembrolizumab was observed across patient subgroups,” said Dr. Cortes.
In the KEYNOTE-522 study, adding pembrolizumab to chemotherapy in the neoadjuvant setting increased the likelihood that women with stage III or early node-positive TNBC would have a pathologic complete response and sustained clinical benefit.
KEYNOTE-355 examined whether pembrolizumab in combination with chemotherapy could provide additional benefit over chemotherapy alone in patients with previously untreated locally recurrent inoperable or metastatic TNBC.
Patients with previously untreated metastatic triple-negative breast cancer who had at least 6 months between definite surgery or last dose of adjuvant chemotherapy (whichever came last) and first disease recurrence were stratified by study chemotherapy received, tumor PD-L1 expression at baseline, and prior treatment with the same class of chemotherapy in the neoadjuvant and/or adjuvant setting.
The patients were then randomized in a 2:1 ratio to pembrolizumab plus chemotherapy based on the investigator’s choice of nab-paclitaxel, paclitaxel, or carboplatin-gemcitabine (562 patients) or to chemotherapy alone (281).
Pembrolizumab and placebo were administered in a double-blind fashion for up to 35 doses. Chemotherapy was given at the investigator’s discretion according to local guidelines. This trial was not powered or designed to compare differential efficacy of the various chemotherapy regimens, Dr. Cortes noted.
The trial had dual primary endpoints of PFS in patients with PD-L1–positive tumors (CPS > 10 and > 1) and in the intention-to-treat population, and overall survival both in PD-L1-positive patients and the ITT population. Overall survival results will be reported at a later date.
As noted before, the primary endpoint was met in the population of patients with CPS higher than 10, with median PFS of 9.7 among those receiving pembrolizumab versus 5.6 months among those receiving placebo, and an estimated 1 year PFS of 39.1% versus 23% for controls, translating into a hazard ratio for progression on pembrolizumab of 0.65 (P = .0012).
In the patients with CPS higher than 1, however, the median PFS was 7.6 months with pembrolizumab compared with 5.6 months with placebo, translating into a hazard ratio of 0.74. However, the results did not meet the prespecified boundary for significance. Because of this, the statistical significance in the ITT population was not tested.
“In patients with PD-L1 CPS 10 or higher tumors, the benefit of pembro/chemo on progression-free survival was generally consistent across most predefined subgroups, including eight geographic regions, ECOG performance status, on-study chemo, and prior treatment with the same class of chemo,” Dr. Cortes said.
Treatment-related adverse events occurred in 96.3% of the patients on pembrolizumab and 95% of patients on placebo. Grade 3 or greater adverse events occurred in 68.1% versus 66.9%, respectively. Two patients in the pembrolizumab arm died from a treatment-related event. There were no treatment-related deaths in the placebo arm.
The most common events were those typically associated with chemotherapy, including anemia, neutropenia, nausea, alopecia, fatigue, decreased neutrophil counts, and elevated liver transaminases. Immune-mediated adverse events of any grade occurred in 25.6% of patients in the pembrolizumab arm versus 6% of controls; none of these events were fatal.
“What is clear in this study is that again we’re seeing efficacy of pembrolizumab in combination with chemotherapy increases with increases in CPS,” according to the invited discussant Catherine M. Kelly, MB, BCh, from University College Dublin and Mater Misericordiae University Hospital in Dublin.
“The results from today’s KEYNOTE-355 appear consistent in terms of progression-free survival. However, it is ‘watch this space’ until we get overall survival data before we can make any further comparisons,” she added.
Questions that still need to be answered include which is the best test for measuring PD-L1, whether patients with CPS of 1 or more but less than 10 benefit from the treatment, which of the available chemotherapy regimens is the best partner for pembrolizumab, how to treat patients who don’t respond to the combination, and what are the implications for PD-1/PD-L1 inhibitors in late-stage disease if they are approved in the neoadjuvant or adjuvant setting, Dr. Kelly said.
The study was funded by Merck. Dr. Cortes disclosed honoraria from, a consulting/advisory role for, and institutional research funding from Merck and others. Dr. Kelly disclosed honoraria from MSD Oncology and others, and travel expenses from Pfizer and Roche.
SOURCE: Cortes J et al. ASCO 2020, Abstract 1000.
Adding pembrolizumab to standard chemotherapy significantly improved progression-free survival for patients with metastatic triple-negative breast cancer, but only if their tumors were enriched with comparatively high levels of the target programmed death ligand-1 (PD-L1), results of the KEYNOTE 355 trial showed.
Among 843 patients with triple-negative breast cancer (TNBC) randomized to receive either investigator’s choice of chemotherapy plus pembrolizumab (Keytruda) or placebo, patients whose tumors had a PD-L1 combined positive score (CPS) of 10 or higher had a median progression-free survival (PFS) of 9.7 months when treated with pembrolizumab and chemotherapy, compared with 5.6 months among patients treated with chemotherapy and placebo, reported Javier Cortes, MD, PhD, from the Vall d´Hebron Institute of Oncology in Madrid and Barcelona.
However, among patients with CPS between 1 and 10, there was no significant difference in PFS between the treatment arms, he said in a presentation made as a part of the 2020 American Society of Clinical Oncology virtual scientific program.
“The inclusion of taxanes and a known taxane/platinum–based regimen permits assessment of the clinical benefit of pembro in combination with several routinely used chemo partners. A trend toward improved efficacy with PD-L1 enrichment was observed in patients treated with pembro plus chemo. The improvement in progression-free survival with chemotherapy and pembrolizumab was observed across patient subgroups,” said Dr. Cortes.
In the KEYNOTE-522 study, adding pembrolizumab to chemotherapy in the neoadjuvant setting increased the likelihood that women with stage III or early node-positive TNBC would have a pathologic complete response and sustained clinical benefit.
KEYNOTE-355 examined whether pembrolizumab in combination with chemotherapy could provide additional benefit over chemotherapy alone in patients with previously untreated locally recurrent inoperable or metastatic TNBC.
Patients with previously untreated metastatic triple-negative breast cancer who had at least 6 months between definite surgery or last dose of adjuvant chemotherapy (whichever came last) and first disease recurrence were stratified by study chemotherapy received, tumor PD-L1 expression at baseline, and prior treatment with the same class of chemotherapy in the neoadjuvant and/or adjuvant setting.
The patients were then randomized in a 2:1 ratio to pembrolizumab plus chemotherapy based on the investigator’s choice of nab-paclitaxel, paclitaxel, or carboplatin-gemcitabine (562 patients) or to chemotherapy alone (281).
Pembrolizumab and placebo were administered in a double-blind fashion for up to 35 doses. Chemotherapy was given at the investigator’s discretion according to local guidelines. This trial was not powered or designed to compare differential efficacy of the various chemotherapy regimens, Dr. Cortes noted.
The trial had dual primary endpoints of PFS in patients with PD-L1–positive tumors (CPS > 10 and > 1) and in the intention-to-treat population, and overall survival both in PD-L1-positive patients and the ITT population. Overall survival results will be reported at a later date.
As noted before, the primary endpoint was met in the population of patients with CPS higher than 10, with median PFS of 9.7 among those receiving pembrolizumab versus 5.6 months among those receiving placebo, and an estimated 1 year PFS of 39.1% versus 23% for controls, translating into a hazard ratio for progression on pembrolizumab of 0.65 (P = .0012).
In the patients with CPS higher than 1, however, the median PFS was 7.6 months with pembrolizumab compared with 5.6 months with placebo, translating into a hazard ratio of 0.74. However, the results did not meet the prespecified boundary for significance. Because of this, the statistical significance in the ITT population was not tested.
“In patients with PD-L1 CPS 10 or higher tumors, the benefit of pembro/chemo on progression-free survival was generally consistent across most predefined subgroups, including eight geographic regions, ECOG performance status, on-study chemo, and prior treatment with the same class of chemo,” Dr. Cortes said.
Treatment-related adverse events occurred in 96.3% of the patients on pembrolizumab and 95% of patients on placebo. Grade 3 or greater adverse events occurred in 68.1% versus 66.9%, respectively. Two patients in the pembrolizumab arm died from a treatment-related event. There were no treatment-related deaths in the placebo arm.
The most common events were those typically associated with chemotherapy, including anemia, neutropenia, nausea, alopecia, fatigue, decreased neutrophil counts, and elevated liver transaminases. Immune-mediated adverse events of any grade occurred in 25.6% of patients in the pembrolizumab arm versus 6% of controls; none of these events were fatal.
“What is clear in this study is that again we’re seeing efficacy of pembrolizumab in combination with chemotherapy increases with increases in CPS,” according to the invited discussant Catherine M. Kelly, MB, BCh, from University College Dublin and Mater Misericordiae University Hospital in Dublin.
“The results from today’s KEYNOTE-355 appear consistent in terms of progression-free survival. However, it is ‘watch this space’ until we get overall survival data before we can make any further comparisons,” she added.
Questions that still need to be answered include which is the best test for measuring PD-L1, whether patients with CPS of 1 or more but less than 10 benefit from the treatment, which of the available chemotherapy regimens is the best partner for pembrolizumab, how to treat patients who don’t respond to the combination, and what are the implications for PD-1/PD-L1 inhibitors in late-stage disease if they are approved in the neoadjuvant or adjuvant setting, Dr. Kelly said.
The study was funded by Merck. Dr. Cortes disclosed honoraria from, a consulting/advisory role for, and institutional research funding from Merck and others. Dr. Kelly disclosed honoraria from MSD Oncology and others, and travel expenses from Pfizer and Roche.
SOURCE: Cortes J et al. ASCO 2020, Abstract 1000.
FROM ASCO 2020
COVID-19 effect: Prescription fills mostly down for leading drugs
Prescription fills for hydroxychloroquine/chloroquine spiked right after COVID-19 was declared a national emergency in March, but use of the drugs still remains well above 2019 levels, based on data from more than 58,000 U.S. pharmacies.
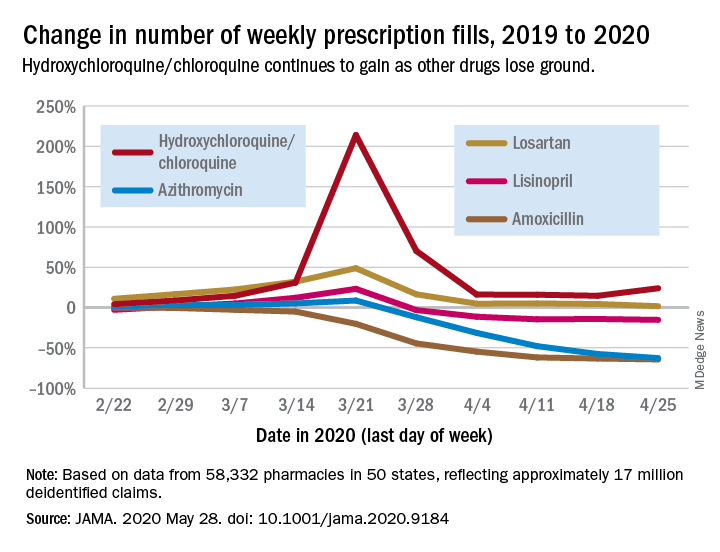
Hydroxychloroquine/chloroquine are also doing better than any of the prescription drugs in the top 10 based on total claims in 2019, Muthiah Vaduganathan, MD, MPH, of Brigham and Women’s Hospital, Boston, and associates reported May 28 in a research letter in JAMA.
Prescription fills for hydroxychloroquine/chloroquine have been above 2019 levels every week since the national emergency was declared on March 13, with the high occurring during the week of March 15-21, when fills were 214% higher than the corresponding week in 2019. The lowest level in that time came during the week of April 12-18, with growth of 14.6% over 2019, the investigators said.
The drugs occupying the top 10 – amlodipine, amoxicillin, atorvastatin, gabapentin, hydrocodone-acetaminophen, levothyroxine, lisinopril, losartan, omeprazole, and sertraline – have not done as well. Losartan, the only one that hasn’t lost ground in any week since March 13, rose by almost 49% during March 15-21, but was down to a 1.7% rise by the end of the study period, they reported.
Meanwhile, the other drug touted as a treatment for COVID-19, azithromycin, has fallen farther than most of the top 10. By April 19-25, the last week of the study period, fills for the antibiotic were down 62.7%, compared with last year, the analysis showed. Only amoxicillin had dropped more (64.4%).
“The modest decline for most common long-term therapies after peak could represent reduced contact with prescribing clinicians, restricted access to pharmacies, pharmacist rationing, loss of insurance from unemployment, or replete supplies from early stockpiling,” Dr. Vaduganathan and associates wrote.
The investigators “used all-payer U.S. pharmacy data from 58,332 chain, independent, and mail-order pharmacies across 14,421 zip codes in 50 states, reflecting approximately 17 million deidentified claims,” to estimate national prescription fills, they explained.
SOURCE: Vaduganathan M et al. JAMA 2020 May 28. doi: 10.1001/jama.2020.9184.
Prescription fills for hydroxychloroquine/chloroquine spiked right after COVID-19 was declared a national emergency in March, but use of the drugs still remains well above 2019 levels, based on data from more than 58,000 U.S. pharmacies.
Hydroxychloroquine/chloroquine are also doing better than any of the prescription drugs in the top 10 based on total claims in 2019, Muthiah Vaduganathan, MD, MPH, of Brigham and Women’s Hospital, Boston, and associates reported May 28 in a research letter in JAMA.
Prescription fills for hydroxychloroquine/chloroquine have been above 2019 levels every week since the national emergency was declared on March 13, with the high occurring during the week of March 15-21, when fills were 214% higher than the corresponding week in 2019. The lowest level in that time came during the week of April 12-18, with growth of 14.6% over 2019, the investigators said.
The drugs occupying the top 10 – amlodipine, amoxicillin, atorvastatin, gabapentin, hydrocodone-acetaminophen, levothyroxine, lisinopril, losartan, omeprazole, and sertraline – have not done as well. Losartan, the only one that hasn’t lost ground in any week since March 13, rose by almost 49% during March 15-21, but was down to a 1.7% rise by the end of the study period, they reported.
Meanwhile, the other drug touted as a treatment for COVID-19, azithromycin, has fallen farther than most of the top 10. By April 19-25, the last week of the study period, fills for the antibiotic were down 62.7%, compared with last year, the analysis showed. Only amoxicillin had dropped more (64.4%).
“The modest decline for most common long-term therapies after peak could represent reduced contact with prescribing clinicians, restricted access to pharmacies, pharmacist rationing, loss of insurance from unemployment, or replete supplies from early stockpiling,” Dr. Vaduganathan and associates wrote.
The investigators “used all-payer U.S. pharmacy data from 58,332 chain, independent, and mail-order pharmacies across 14,421 zip codes in 50 states, reflecting approximately 17 million deidentified claims,” to estimate national prescription fills, they explained.
SOURCE: Vaduganathan M et al. JAMA 2020 May 28. doi: 10.1001/jama.2020.9184.
Prescription fills for hydroxychloroquine/chloroquine spiked right after COVID-19 was declared a national emergency in March, but use of the drugs still remains well above 2019 levels, based on data from more than 58,000 U.S. pharmacies.
Hydroxychloroquine/chloroquine are also doing better than any of the prescription drugs in the top 10 based on total claims in 2019, Muthiah Vaduganathan, MD, MPH, of Brigham and Women’s Hospital, Boston, and associates reported May 28 in a research letter in JAMA.
Prescription fills for hydroxychloroquine/chloroquine have been above 2019 levels every week since the national emergency was declared on March 13, with the high occurring during the week of March 15-21, when fills were 214% higher than the corresponding week in 2019. The lowest level in that time came during the week of April 12-18, with growth of 14.6% over 2019, the investigators said.
The drugs occupying the top 10 – amlodipine, amoxicillin, atorvastatin, gabapentin, hydrocodone-acetaminophen, levothyroxine, lisinopril, losartan, omeprazole, and sertraline – have not done as well. Losartan, the only one that hasn’t lost ground in any week since March 13, rose by almost 49% during March 15-21, but was down to a 1.7% rise by the end of the study period, they reported.
Meanwhile, the other drug touted as a treatment for COVID-19, azithromycin, has fallen farther than most of the top 10. By April 19-25, the last week of the study period, fills for the antibiotic were down 62.7%, compared with last year, the analysis showed. Only amoxicillin had dropped more (64.4%).
“The modest decline for most common long-term therapies after peak could represent reduced contact with prescribing clinicians, restricted access to pharmacies, pharmacist rationing, loss of insurance from unemployment, or replete supplies from early stockpiling,” Dr. Vaduganathan and associates wrote.
The investigators “used all-payer U.S. pharmacy data from 58,332 chain, independent, and mail-order pharmacies across 14,421 zip codes in 50 states, reflecting approximately 17 million deidentified claims,” to estimate national prescription fills, they explained.
SOURCE: Vaduganathan M et al. JAMA 2020 May 28. doi: 10.1001/jama.2020.9184.
FROM JAMA
FDA approves medication to treat heavy menstrual bleeding related to fibroids
The medication, marketed as Oriahnn, is an estrogen and progestin combination product that consists of elagolix, estradiol, and norethindrone acetate capsules packaged together for oral use, according to an FDA announcement.

“Uterine fibroids are the most common benign tumors affecting premenopausal women, and one of the most common symptoms from fibroids is heavy menstrual bleeding,” Christine P. Nguyen, MD, acting director of the division of urology, obstetrics, and gynecology in the FDA’s Center for Drug Evaluation and Research, said in a news release. “Although surgical treatments, such as hysterectomy, are available, patients may not qualify for surgery or want the procedure. Various nonsurgical therapies are used to treat fibroid-related heavy menstrual bleeding, but none have been FDA approved specifically for this use. Today’s approval provides an FDA-approved medical treatment option for these patients.”
Fibroids, which occur most commonly in women aged 35-49 years, typically resolve after menopause but are a leading reason for hysterectomy in the United States, according to the release.
Researchers established the efficacy of the treatment in two clinical trials that included 591 premenopausal women with heavy menstrual bleeding. Participants received the drug or placebo for 6 months. The investigators defined heavy menstrual bleeding as at least two menstrual cycles with greater than 80 mL of menstrual blood loss. The primary endpoint was the proportion of women who achieved menstrual blood loss less than 80 mL at the final month and 50% or greater reduction in menstrual blood loss volume from baseline to the final month. In one trial, 69% of patients who received Oriahnn met this endpoint, compared with 9% of patients who received placebo. In the second study, 77% of patients who received the drug achieved this endpoint, compared with 11% of patients who received placebo.
Oriahnn may cause bone loss that may not be completely recovered after stopping treatment, so women should not take the medication for more than 24 months, according to the FDA announcement. Health care professionals may recommend bone density scans before and during treatment.
The most common side effects included hot flushes, headache, fatigue, and irregular vaginal bleeding. The drug’s label includes a boxed warning about a risk of strokes and blood clots, especially in women at increased risk for these events. Contraindications include osteoporosis, a history of breast cancer or other hormonally sensitive cancer, liver disease, and abnormal uterine bleeding. Oriahnn does not prevent pregnancy and may increase blood pressure, according to the press release. AbbVie markets the drug.
The medication, marketed as Oriahnn, is an estrogen and progestin combination product that consists of elagolix, estradiol, and norethindrone acetate capsules packaged together for oral use, according to an FDA announcement.
“Uterine fibroids are the most common benign tumors affecting premenopausal women, and one of the most common symptoms from fibroids is heavy menstrual bleeding,” Christine P. Nguyen, MD, acting director of the division of urology, obstetrics, and gynecology in the FDA’s Center for Drug Evaluation and Research, said in a news release. “Although surgical treatments, such as hysterectomy, are available, patients may not qualify for surgery or want the procedure. Various nonsurgical therapies are used to treat fibroid-related heavy menstrual bleeding, but none have been FDA approved specifically for this use. Today’s approval provides an FDA-approved medical treatment option for these patients.”
Fibroids, which occur most commonly in women aged 35-49 years, typically resolve after menopause but are a leading reason for hysterectomy in the United States, according to the release.
Researchers established the efficacy of the treatment in two clinical trials that included 591 premenopausal women with heavy menstrual bleeding. Participants received the drug or placebo for 6 months. The investigators defined heavy menstrual bleeding as at least two menstrual cycles with greater than 80 mL of menstrual blood loss. The primary endpoint was the proportion of women who achieved menstrual blood loss less than 80 mL at the final month and 50% or greater reduction in menstrual blood loss volume from baseline to the final month. In one trial, 69% of patients who received Oriahnn met this endpoint, compared with 9% of patients who received placebo. In the second study, 77% of patients who received the drug achieved this endpoint, compared with 11% of patients who received placebo.
Oriahnn may cause bone loss that may not be completely recovered after stopping treatment, so women should not take the medication for more than 24 months, according to the FDA announcement. Health care professionals may recommend bone density scans before and during treatment.
The most common side effects included hot flushes, headache, fatigue, and irregular vaginal bleeding. The drug’s label includes a boxed warning about a risk of strokes and blood clots, especially in women at increased risk for these events. Contraindications include osteoporosis, a history of breast cancer or other hormonally sensitive cancer, liver disease, and abnormal uterine bleeding. Oriahnn does not prevent pregnancy and may increase blood pressure, according to the press release. AbbVie markets the drug.
The medication, marketed as Oriahnn, is an estrogen and progestin combination product that consists of elagolix, estradiol, and norethindrone acetate capsules packaged together for oral use, according to an FDA announcement.
“Uterine fibroids are the most common benign tumors affecting premenopausal women, and one of the most common symptoms from fibroids is heavy menstrual bleeding,” Christine P. Nguyen, MD, acting director of the division of urology, obstetrics, and gynecology in the FDA’s Center for Drug Evaluation and Research, said in a news release. “Although surgical treatments, such as hysterectomy, are available, patients may not qualify for surgery or want the procedure. Various nonsurgical therapies are used to treat fibroid-related heavy menstrual bleeding, but none have been FDA approved specifically for this use. Today’s approval provides an FDA-approved medical treatment option for these patients.”
Fibroids, which occur most commonly in women aged 35-49 years, typically resolve after menopause but are a leading reason for hysterectomy in the United States, according to the release.
Researchers established the efficacy of the treatment in two clinical trials that included 591 premenopausal women with heavy menstrual bleeding. Participants received the drug or placebo for 6 months. The investigators defined heavy menstrual bleeding as at least two menstrual cycles with greater than 80 mL of menstrual blood loss. The primary endpoint was the proportion of women who achieved menstrual blood loss less than 80 mL at the final month and 50% or greater reduction in menstrual blood loss volume from baseline to the final month. In one trial, 69% of patients who received Oriahnn met this endpoint, compared with 9% of patients who received placebo. In the second study, 77% of patients who received the drug achieved this endpoint, compared with 11% of patients who received placebo.
Oriahnn may cause bone loss that may not be completely recovered after stopping treatment, so women should not take the medication for more than 24 months, according to the FDA announcement. Health care professionals may recommend bone density scans before and during treatment.
The most common side effects included hot flushes, headache, fatigue, and irregular vaginal bleeding. The drug’s label includes a boxed warning about a risk of strokes and blood clots, especially in women at increased risk for these events. Contraindications include osteoporosis, a history of breast cancer or other hormonally sensitive cancer, liver disease, and abnormal uterine bleeding. Oriahnn does not prevent pregnancy and may increase blood pressure, according to the press release. AbbVie markets the drug.
FDA recalls extended-release metformin due to NDMA impurities
The US Food and Drug Administration (FDA) has recommended voluntary recall of certain extended-release (ER) versions of metformin because testing has revealed excessive levels of N-nitrosodimethylamine (NDMA) in these products.
Metformin is the most commonly prescribed drug used to treat type 2 diabetes worldwide.
NDMA is a contaminant with the potential to be carcinogenic if there is exposure to above-acceptable levels over the long-term.
Five pharmaceutical firms in particular are being contacted by the FDA with notices (posted on the FDA website) recommending they voluntarily recall their products. At the time of writing, only one was listed, Apotex Corp and its metformin hydrochloride ER tablets, USP 500 mg.
The recall does not apply to immediate-release metformin products, the most commonly prescribed ones for diabetes, the agency stresses.
It also recommends that clinicians continue to prescribe metformin when clinically appropriate.
In late 2019, the FDA announced it had become aware of NDMA in some metformin products in other countries. The agency immediately began testing to determine whether the metformin in the US supply was at risk, as part of the ongoing investigation into nitrosamine impurities across medication types, which included recalls of hypertension and heartburn medications within the past 2 years.
By February 2020, the agency had identified very low levels of NDMA in some samples, but at that time, no FDA-tested sample of metformin exceeded the acceptable intake limit for NDMA, as reported by Medscape Medical News.
“Now that we have identified some metformin products that do not meet our standards, we’re taking action. As we have been doing since this impurity was first identified, we will communicate as new scientific information becomes available and will take further action, if appropriate,” Patrizia Cavazzoni, MD, acting director of the FDA Center for Drug Evaluation and Research, said in a press release.
Requests for recall apply only to affected products
The recall was instigated after the FDA became aware of reports of higher levels of NDMA in certain ER formulations of metformin through a citizen petition filed by a private laboratory. The agency confirmed unacceptable NDMA levels in some, but not all, of those lots.
“In other instances, our laboratory detected NDMA in lots that the private laboratory did not,” it notes.
The FDA says it is working closely with manufacturers of the recalled tablets to identify the source of the NDMA impurity and ensure appropriate testing is carried out.
Elevated levels of NDMA have been found in some finished-dose tablets of the ER formulations but NDMA has not been detected in samples of the metformin active pharmaceutical ingredient.
The FDA also stresses there are many other additional manufacturers that supply metformin ER products to much of the US market, and they are not being asked to recall their products.
Work is also ongoing to determine whether the drug recalls will result in shortages, and if so, the agency says it will collaborate with manufacturers to prevent or reduce any impact of shortages.
“We understand that patients may have concerns about possible impurities in their medicines and want to assure the public that we have been looking closely at this problem over many months in order to provide patients and healthcare professionals with clear and accurate answers,” Cavazzoni said.
For more information about NDMA, visit the FDA nitrosamines web page.
This article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has recommended voluntary recall of certain extended-release (ER) versions of metformin because testing has revealed excessive levels of N-nitrosodimethylamine (NDMA) in these products.
Metformin is the most commonly prescribed drug used to treat type 2 diabetes worldwide.
NDMA is a contaminant with the potential to be carcinogenic if there is exposure to above-acceptable levels over the long-term.
Five pharmaceutical firms in particular are being contacted by the FDA with notices (posted on the FDA website) recommending they voluntarily recall their products. At the time of writing, only one was listed, Apotex Corp and its metformin hydrochloride ER tablets, USP 500 mg.
The recall does not apply to immediate-release metformin products, the most commonly prescribed ones for diabetes, the agency stresses.
It also recommends that clinicians continue to prescribe metformin when clinically appropriate.
In late 2019, the FDA announced it had become aware of NDMA in some metformin products in other countries. The agency immediately began testing to determine whether the metformin in the US supply was at risk, as part of the ongoing investigation into nitrosamine impurities across medication types, which included recalls of hypertension and heartburn medications within the past 2 years.
By February 2020, the agency had identified very low levels of NDMA in some samples, but at that time, no FDA-tested sample of metformin exceeded the acceptable intake limit for NDMA, as reported by Medscape Medical News.
“Now that we have identified some metformin products that do not meet our standards, we’re taking action. As we have been doing since this impurity was first identified, we will communicate as new scientific information becomes available and will take further action, if appropriate,” Patrizia Cavazzoni, MD, acting director of the FDA Center for Drug Evaluation and Research, said in a press release.
Requests for recall apply only to affected products
The recall was instigated after the FDA became aware of reports of higher levels of NDMA in certain ER formulations of metformin through a citizen petition filed by a private laboratory. The agency confirmed unacceptable NDMA levels in some, but not all, of those lots.
“In other instances, our laboratory detected NDMA in lots that the private laboratory did not,” it notes.
The FDA says it is working closely with manufacturers of the recalled tablets to identify the source of the NDMA impurity and ensure appropriate testing is carried out.
Elevated levels of NDMA have been found in some finished-dose tablets of the ER formulations but NDMA has not been detected in samples of the metformin active pharmaceutical ingredient.
The FDA also stresses there are many other additional manufacturers that supply metformin ER products to much of the US market, and they are not being asked to recall their products.
Work is also ongoing to determine whether the drug recalls will result in shortages, and if so, the agency says it will collaborate with manufacturers to prevent or reduce any impact of shortages.
“We understand that patients may have concerns about possible impurities in their medicines and want to assure the public that we have been looking closely at this problem over many months in order to provide patients and healthcare professionals with clear and accurate answers,” Cavazzoni said.
For more information about NDMA, visit the FDA nitrosamines web page.
This article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has recommended voluntary recall of certain extended-release (ER) versions of metformin because testing has revealed excessive levels of N-nitrosodimethylamine (NDMA) in these products.
Metformin is the most commonly prescribed drug used to treat type 2 diabetes worldwide.
NDMA is a contaminant with the potential to be carcinogenic if there is exposure to above-acceptable levels over the long-term.
Five pharmaceutical firms in particular are being contacted by the FDA with notices (posted on the FDA website) recommending they voluntarily recall their products. At the time of writing, only one was listed, Apotex Corp and its metformin hydrochloride ER tablets, USP 500 mg.
The recall does not apply to immediate-release metformin products, the most commonly prescribed ones for diabetes, the agency stresses.
It also recommends that clinicians continue to prescribe metformin when clinically appropriate.
In late 2019, the FDA announced it had become aware of NDMA in some metformin products in other countries. The agency immediately began testing to determine whether the metformin in the US supply was at risk, as part of the ongoing investigation into nitrosamine impurities across medication types, which included recalls of hypertension and heartburn medications within the past 2 years.
By February 2020, the agency had identified very low levels of NDMA in some samples, but at that time, no FDA-tested sample of metformin exceeded the acceptable intake limit for NDMA, as reported by Medscape Medical News.
“Now that we have identified some metformin products that do not meet our standards, we’re taking action. As we have been doing since this impurity was first identified, we will communicate as new scientific information becomes available and will take further action, if appropriate,” Patrizia Cavazzoni, MD, acting director of the FDA Center for Drug Evaluation and Research, said in a press release.
Requests for recall apply only to affected products
The recall was instigated after the FDA became aware of reports of higher levels of NDMA in certain ER formulations of metformin through a citizen petition filed by a private laboratory. The agency confirmed unacceptable NDMA levels in some, but not all, of those lots.
“In other instances, our laboratory detected NDMA in lots that the private laboratory did not,” it notes.
The FDA says it is working closely with manufacturers of the recalled tablets to identify the source of the NDMA impurity and ensure appropriate testing is carried out.
Elevated levels of NDMA have been found in some finished-dose tablets of the ER formulations but NDMA has not been detected in samples of the metformin active pharmaceutical ingredient.
The FDA also stresses there are many other additional manufacturers that supply metformin ER products to much of the US market, and they are not being asked to recall their products.
Work is also ongoing to determine whether the drug recalls will result in shortages, and if so, the agency says it will collaborate with manufacturers to prevent or reduce any impact of shortages.
“We understand that patients may have concerns about possible impurities in their medicines and want to assure the public that we have been looking closely at this problem over many months in order to provide patients and healthcare professionals with clear and accurate answers,” Cavazzoni said.
For more information about NDMA, visit the FDA nitrosamines web page.
This article first appeared on Medscape.com.
FDA okays first tau radiotracer to aid Alzheimer’s disease diagnosis
to estimate the density and distribution of aggregated tau neurofibrillary tangles (NFTs) in adults with cognitive impairment who are being evaluated for Alzheimer disease.
“While there are FDA-approved imaging drugs for amyloid pathology, this is the first drug approved for imaging tau pathology, one of the two neuropathological hallmarks of Alzheimer’s disease, and represents a major advance for patients with cognitive impairment being evaluated for the condition,” Charles Ganley, MD, director of the Office of Specialty Medicine at the Center for Drug Evaluation and Research, said in an FDA news release.
“The use of diagnostic imaging can help patients and their families plan for the future and make informed choices about their health and well-being, in addition to facilitating appropriate patient management for physicians,” Reisa Sperling, MD, director of the Center for Alzheimer Research and Treatment at Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, said in a company news release.
“Determining the anatomic distribution and density of tau NFTs in the brain was previously possible only at autopsy. Now we have a way to obtain this important information in patients,” said Dr. Sperling.
Clinical trial results
Following intravenous administration, flortaucipir F18 binds to tau pathology in the brain and can be seen on a PET scan.
The safety and effectiveness of the tau tracer were demonstrated in two clinical studies. In each study, five evaluators, blinded to clinical information, interpreted the flortaucipir F18 PET scan results as positive or negative.
The first study included 156 terminally ill patients who agreed to undergo flortaucipir F18 PET imaging and to donate their brains after death. Of these patients, 64 died within 9 months of undergoing brain scanning. The evaluators’ readings of these scans were compared with postmortem readings from independent pathologists blinded to scan results.
Evaluators reading the flortaucipir F18 PET scans had a “high probability” of correctly evaluating patients with tau pathology and had an “average to high probability” of correctly evaluating patients without tau pathology, the FDA said in the release.
According to the company, reader sensitivity ranged from 92% (95% confidence interval, 80%-97%) to 100% (95% CI, 91%-100%). Specificity ranged from 52% (95% CI, 34%-70%) to 92% (95% CI, 75%-98%).
Initial limited availability
The second study included the same patients with terminal illness as the first study, plus 18 additional patients who had terminal illness and 159 patients who had cognitive impairment and were being evaluated for Alzheimer’s disease (the indicated population).
The study gauged how well evaluators’ readings of flortaucipir F18 PET scans agreed with each other’s assessments of the readings. In this study, reader agreement was 0.87 (perfect agreement was indicated as 1) across all 241 patients.
In a separate subgroup analysis that included the 82 terminally ill patients who were diagnosed after death and the 159 patients with cognitive impairment, reader agreement was 0.90 for the patients in the indicated population and 0.82 in the terminally ill patients.
The FDA noted that the ability of flortaucipir F18 PET scans to detect tau pathology was assessed in patients with generally severe stages of dementia and may be lower in patients with cognitive decline of earlier stages.
The most common adverse reactions among patients who received flortaucipir F18 injection were headache, injection site pain, and an increase in blood pressure. The tau radiotracer is not indicated for use in the evaluation of patients for chronic traumatic encephalopathy.
The FDA granted flortaucipir F18 priority review, in which the FDA aims to take action on an application within 6 months of the time the agency determines that the drug, if approved, would significantly improve the safety or effectiveness of treating, diagnosing, or preventing a serious condition.
The company said that the availability of flortaucipir F18 will initially be “limited and will expand in response to commercial demand and payor reimbursement.”
Alzheimer’s disease is among the top 10 leading causes of death in the United States. In 2014, 5 million Americans were living with the disease, according to federal health officials. That number is projected to nearly triple to 14 million by 2060.
A version of this article originally appeared on Medscape.com.
to estimate the density and distribution of aggregated tau neurofibrillary tangles (NFTs) in adults with cognitive impairment who are being evaluated for Alzheimer disease.
“While there are FDA-approved imaging drugs for amyloid pathology, this is the first drug approved for imaging tau pathology, one of the two neuropathological hallmarks of Alzheimer’s disease, and represents a major advance for patients with cognitive impairment being evaluated for the condition,” Charles Ganley, MD, director of the Office of Specialty Medicine at the Center for Drug Evaluation and Research, said in an FDA news release.
“The use of diagnostic imaging can help patients and their families plan for the future and make informed choices about their health and well-being, in addition to facilitating appropriate patient management for physicians,” Reisa Sperling, MD, director of the Center for Alzheimer Research and Treatment at Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, said in a company news release.
“Determining the anatomic distribution and density of tau NFTs in the brain was previously possible only at autopsy. Now we have a way to obtain this important information in patients,” said Dr. Sperling.
Clinical trial results
Following intravenous administration, flortaucipir F18 binds to tau pathology in the brain and can be seen on a PET scan.
The safety and effectiveness of the tau tracer were demonstrated in two clinical studies. In each study, five evaluators, blinded to clinical information, interpreted the flortaucipir F18 PET scan results as positive or negative.
The first study included 156 terminally ill patients who agreed to undergo flortaucipir F18 PET imaging and to donate their brains after death. Of these patients, 64 died within 9 months of undergoing brain scanning. The evaluators’ readings of these scans were compared with postmortem readings from independent pathologists blinded to scan results.
Evaluators reading the flortaucipir F18 PET scans had a “high probability” of correctly evaluating patients with tau pathology and had an “average to high probability” of correctly evaluating patients without tau pathology, the FDA said in the release.
According to the company, reader sensitivity ranged from 92% (95% confidence interval, 80%-97%) to 100% (95% CI, 91%-100%). Specificity ranged from 52% (95% CI, 34%-70%) to 92% (95% CI, 75%-98%).
Initial limited availability
The second study included the same patients with terminal illness as the first study, plus 18 additional patients who had terminal illness and 159 patients who had cognitive impairment and were being evaluated for Alzheimer’s disease (the indicated population).
The study gauged how well evaluators’ readings of flortaucipir F18 PET scans agreed with each other’s assessments of the readings. In this study, reader agreement was 0.87 (perfect agreement was indicated as 1) across all 241 patients.
In a separate subgroup analysis that included the 82 terminally ill patients who were diagnosed after death and the 159 patients with cognitive impairment, reader agreement was 0.90 for the patients in the indicated population and 0.82 in the terminally ill patients.
The FDA noted that the ability of flortaucipir F18 PET scans to detect tau pathology was assessed in patients with generally severe stages of dementia and may be lower in patients with cognitive decline of earlier stages.
The most common adverse reactions among patients who received flortaucipir F18 injection were headache, injection site pain, and an increase in blood pressure. The tau radiotracer is not indicated for use in the evaluation of patients for chronic traumatic encephalopathy.
The FDA granted flortaucipir F18 priority review, in which the FDA aims to take action on an application within 6 months of the time the agency determines that the drug, if approved, would significantly improve the safety or effectiveness of treating, diagnosing, or preventing a serious condition.
The company said that the availability of flortaucipir F18 will initially be “limited and will expand in response to commercial demand and payor reimbursement.”
Alzheimer’s disease is among the top 10 leading causes of death in the United States. In 2014, 5 million Americans were living with the disease, according to federal health officials. That number is projected to nearly triple to 14 million by 2060.
A version of this article originally appeared on Medscape.com.
to estimate the density and distribution of aggregated tau neurofibrillary tangles (NFTs) in adults with cognitive impairment who are being evaluated for Alzheimer disease.
“While there are FDA-approved imaging drugs for amyloid pathology, this is the first drug approved for imaging tau pathology, one of the two neuropathological hallmarks of Alzheimer’s disease, and represents a major advance for patients with cognitive impairment being evaluated for the condition,” Charles Ganley, MD, director of the Office of Specialty Medicine at the Center for Drug Evaluation and Research, said in an FDA news release.
“The use of diagnostic imaging can help patients and their families plan for the future and make informed choices about their health and well-being, in addition to facilitating appropriate patient management for physicians,” Reisa Sperling, MD, director of the Center for Alzheimer Research and Treatment at Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, said in a company news release.
“Determining the anatomic distribution and density of tau NFTs in the brain was previously possible only at autopsy. Now we have a way to obtain this important information in patients,” said Dr. Sperling.
Clinical trial results
Following intravenous administration, flortaucipir F18 binds to tau pathology in the brain and can be seen on a PET scan.
The safety and effectiveness of the tau tracer were demonstrated in two clinical studies. In each study, five evaluators, blinded to clinical information, interpreted the flortaucipir F18 PET scan results as positive or negative.
The first study included 156 terminally ill patients who agreed to undergo flortaucipir F18 PET imaging and to donate their brains after death. Of these patients, 64 died within 9 months of undergoing brain scanning. The evaluators’ readings of these scans were compared with postmortem readings from independent pathologists blinded to scan results.
Evaluators reading the flortaucipir F18 PET scans had a “high probability” of correctly evaluating patients with tau pathology and had an “average to high probability” of correctly evaluating patients without tau pathology, the FDA said in the release.
According to the company, reader sensitivity ranged from 92% (95% confidence interval, 80%-97%) to 100% (95% CI, 91%-100%). Specificity ranged from 52% (95% CI, 34%-70%) to 92% (95% CI, 75%-98%).
Initial limited availability
The second study included the same patients with terminal illness as the first study, plus 18 additional patients who had terminal illness and 159 patients who had cognitive impairment and were being evaluated for Alzheimer’s disease (the indicated population).
The study gauged how well evaluators’ readings of flortaucipir F18 PET scans agreed with each other’s assessments of the readings. In this study, reader agreement was 0.87 (perfect agreement was indicated as 1) across all 241 patients.
In a separate subgroup analysis that included the 82 terminally ill patients who were diagnosed after death and the 159 patients with cognitive impairment, reader agreement was 0.90 for the patients in the indicated population and 0.82 in the terminally ill patients.
The FDA noted that the ability of flortaucipir F18 PET scans to detect tau pathology was assessed in patients with generally severe stages of dementia and may be lower in patients with cognitive decline of earlier stages.
The most common adverse reactions among patients who received flortaucipir F18 injection were headache, injection site pain, and an increase in blood pressure. The tau radiotracer is not indicated for use in the evaluation of patients for chronic traumatic encephalopathy.
The FDA granted flortaucipir F18 priority review, in which the FDA aims to take action on an application within 6 months of the time the agency determines that the drug, if approved, would significantly improve the safety or effectiveness of treating, diagnosing, or preventing a serious condition.
The company said that the availability of flortaucipir F18 will initially be “limited and will expand in response to commercial demand and payor reimbursement.”
Alzheimer’s disease is among the top 10 leading causes of death in the United States. In 2014, 5 million Americans were living with the disease, according to federal health officials. That number is projected to nearly triple to 14 million by 2060.
A version of this article originally appeared on Medscape.com.
APA, others lobby to make COVID-19 telehealth waivers permanent
The American Psychiatric Association (APA) is calling on Congress to permanently lift restrictions that have allowed unfettered delivery of telehealth services during the COVID-19 pandemic, which experts say has been a boon to patients and physicians alike.

“We ask Congress to extend the telehealth waiver authority under COVID-19 beyond the emergency and to study its impact while doing so,” said APA President Jeffrey Geller, MD, in a May 27 video briefing with congressional staff and reporters.
The APA is also seeking to make permanent certain waivers granted by the Centers for Medicare & Medicaid Services on April 30, including elimination of geographic restrictions on behavioral health and allowing patients be seen at home, said Dr. Geller.
The APA also is asking for the elimination of the rule that requires clinicians to have an initial face-to-face meeting with patients before they can prescribe controlled substances, Dr. Geller said. The Drug Enforcement Administration waived that requirement, known as the Ryan Haight Act, on March 17 for the duration of the national emergency.
Telemedicine has supporters on both sides of the aisle in Congress, including Rep. Paul Tonko (D-N.Y.) who said at the APA briefing he would fight to make the waivers permanent.
“The expanded use of telehealth has enormous potential during normal times as well, especially in behavioral health,” said Mr. Tonko. “I am pushing fiercely for these current flexibilities to be extended for a reasonable time after the public health emergency so that we can have time to evaluate which should be made permanent,” he said.
Dr. Geller, other clinicians, and advocates in the briefing praised CMS for facilitating telepsychiatry for Medicare. That follows in the footsteps of most private insurers, who have also relaxed requirements into the summer, according to the Medical Group Management Association.
Game changer
The Medicare waivers “have dramatically changed the entire scene for someone like myself as a clinician to allow me to see my patients in a much easier way,” said Peter Yellowlees, MBBS, MD, chief wellness officer, University of California Davis Health. Within 2 weeks in March, the health system converted almost all of its regular outpatient visits to telemedicine, he said.
Dr. Yellowlees added government still needs to address, what he called, outdated HIPAA regulations that ban certain technologies.
“It makes no sense that I can talk to someone on an iPhone, but the moment I talk to them on FaceTime, it’s illegal,” said Dr. Yellowlees, a former president of the American Telemedicine Association.
Dr. Geller said that “psychiatric care provided by telehealth is as effective as in-person psychiatric services,” adding that “some patients prefer telepsychiatry because of its convenience and as a means of reducing stigma associated with seeking help for mental health.”
Shabana Khan, MD, a child psychiatrist and director of telepsychiatry at New York University Langone Health, said audio and video conferencing are helping address a shortage and maldistribution of child and adolescent psychiatrists.
Americans’ mental health is suffering during the pandemic. The U.S. Census Bureau recently released data showing that half of those surveyed reported depressed mood and that one-third are reporting anxiety, depression, or both, as reported by the Washington Post.
“At this very time that anxiety, depression, substance use, and other mental health problems are rising, our nation’s already strained mental health system is really being pushed to the brink,” said Jodi Kwarciany, manager for mental health policy for the National Alliance on Mental Illness, during the briefing.
Telemedicine can help “by connecting people to providers at the time and the place and using the technology that works best for them,” she said, adding that NAMI would press policymakers to address barriers to access.
The clinicians on the briefing said they’ve observed that some patients are more comfortable with video or audio interactions than with in-person visits.
Increased access to care
Telepsychiatry seems to be convincing some to reconsider therapy, since they can do it at home, said Dr. Yellowlees. he said.
For instance, he said, he has been able to consult by phone and video with several patients who receive care through the Indian Health Service who had not be able to get into the physical clinic.
Dr. Yellowlees said video sessions also may encourage patients to be more, not less, talkative. “Video is actually counterintuitively a very intimate experience,” he said, in part because of the perceived distance and people’s tendency to be less inhibited on technology platforms.“It’s less embarrassing,” he said. “If you’ve got really dramatic, difficult, traumatic things to talk about, it’s slightly easier to talk to someone who’s slightly further apart from you on video,” said Dr. Yellowlees.
“Individuals who have a significant amount of anxiety may actually feel more comfortable with the distance that this technology affords,” agreed Dr. Khan. She said telemedicine had made sessions more comfortable for some of her patients with autism spectrum disorder.
Dr. Geller said audio and video have been important to his practice during the pandemic. One of his patients never leaves the house and does not use computers. “He spends his time sequestered at home listening to records on his record player,” said Dr. Geller. But he’s been amenable to phone sessions. “What I’ve found with him, and I’ve found with several other patients, is that they actually talk more easily when they’re not face to face,” he said.
Far fewer no-shows
Another plus for his New England–based practice during the last few months: patients have not been anxious about missing sessions because of the weather. The clinicians all noted that telepsychiatry seemed to reduce missed visits.
Dr. Yellowlees said that no-show rates had decreased by half at UC Davis. “That means no significant loss of income,” during the pandemic, he said.
“The no-show rate is incredibly low, particularly because when you call the patients and they don’t remember they had an appointment, you have the appointment anyway, most of the time,” said Dr. Geller.
For Dr. Khan, being able to conduct audio and video sessions during the pandemic has meant keeping up continuity of care.
As a result of the pandemic, many college students in New York City had to go home – often to another state. The waivers granted by New York’s Medicaid program and other insurers have allowed Dr. Khan to continue care for these patients.
The NYU clinic also operates day programs in rural areas 5 hours from the city. Dr. Khan recently evaluated a 12-year-old girl with significant anxiety and low mood, both of which had worsened.
“She would not have been able to access care otherwise,” said Dr. Khan. And for rural patients who do not have access to broadband or smartphones, audio visits “have been immensely helpful,” she said.
Dr. Khan, Dr. Geller, and Dr. Yellowlees have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The American Psychiatric Association (APA) is calling on Congress to permanently lift restrictions that have allowed unfettered delivery of telehealth services during the COVID-19 pandemic, which experts say has been a boon to patients and physicians alike.
“We ask Congress to extend the telehealth waiver authority under COVID-19 beyond the emergency and to study its impact while doing so,” said APA President Jeffrey Geller, MD, in a May 27 video briefing with congressional staff and reporters.
The APA is also seeking to make permanent certain waivers granted by the Centers for Medicare & Medicaid Services on April 30, including elimination of geographic restrictions on behavioral health and allowing patients be seen at home, said Dr. Geller.
The APA also is asking for the elimination of the rule that requires clinicians to have an initial face-to-face meeting with patients before they can prescribe controlled substances, Dr. Geller said. The Drug Enforcement Administration waived that requirement, known as the Ryan Haight Act, on March 17 for the duration of the national emergency.
Telemedicine has supporters on both sides of the aisle in Congress, including Rep. Paul Tonko (D-N.Y.) who said at the APA briefing he would fight to make the waivers permanent.
“The expanded use of telehealth has enormous potential during normal times as well, especially in behavioral health,” said Mr. Tonko. “I am pushing fiercely for these current flexibilities to be extended for a reasonable time after the public health emergency so that we can have time to evaluate which should be made permanent,” he said.
Dr. Geller, other clinicians, and advocates in the briefing praised CMS for facilitating telepsychiatry for Medicare. That follows in the footsteps of most private insurers, who have also relaxed requirements into the summer, according to the Medical Group Management Association.
Game changer
The Medicare waivers “have dramatically changed the entire scene for someone like myself as a clinician to allow me to see my patients in a much easier way,” said Peter Yellowlees, MBBS, MD, chief wellness officer, University of California Davis Health. Within 2 weeks in March, the health system converted almost all of its regular outpatient visits to telemedicine, he said.
Dr. Yellowlees added government still needs to address, what he called, outdated HIPAA regulations that ban certain technologies.
“It makes no sense that I can talk to someone on an iPhone, but the moment I talk to them on FaceTime, it’s illegal,” said Dr. Yellowlees, a former president of the American Telemedicine Association.
Dr. Geller said that “psychiatric care provided by telehealth is as effective as in-person psychiatric services,” adding that “some patients prefer telepsychiatry because of its convenience and as a means of reducing stigma associated with seeking help for mental health.”
Shabana Khan, MD, a child psychiatrist and director of telepsychiatry at New York University Langone Health, said audio and video conferencing are helping address a shortage and maldistribution of child and adolescent psychiatrists.
Americans’ mental health is suffering during the pandemic. The U.S. Census Bureau recently released data showing that half of those surveyed reported depressed mood and that one-third are reporting anxiety, depression, or both, as reported by the Washington Post.
“At this very time that anxiety, depression, substance use, and other mental health problems are rising, our nation’s already strained mental health system is really being pushed to the brink,” said Jodi Kwarciany, manager for mental health policy for the National Alliance on Mental Illness, during the briefing.
Telemedicine can help “by connecting people to providers at the time and the place and using the technology that works best for them,” she said, adding that NAMI would press policymakers to address barriers to access.
The clinicians on the briefing said they’ve observed that some patients are more comfortable with video or audio interactions than with in-person visits.
Increased access to care
Telepsychiatry seems to be convincing some to reconsider therapy, since they can do it at home, said Dr. Yellowlees. he said.
For instance, he said, he has been able to consult by phone and video with several patients who receive care through the Indian Health Service who had not be able to get into the physical clinic.
Dr. Yellowlees said video sessions also may encourage patients to be more, not less, talkative. “Video is actually counterintuitively a very intimate experience,” he said, in part because of the perceived distance and people’s tendency to be less inhibited on technology platforms.“It’s less embarrassing,” he said. “If you’ve got really dramatic, difficult, traumatic things to talk about, it’s slightly easier to talk to someone who’s slightly further apart from you on video,” said Dr. Yellowlees.
“Individuals who have a significant amount of anxiety may actually feel more comfortable with the distance that this technology affords,” agreed Dr. Khan. She said telemedicine had made sessions more comfortable for some of her patients with autism spectrum disorder.
Dr. Geller said audio and video have been important to his practice during the pandemic. One of his patients never leaves the house and does not use computers. “He spends his time sequestered at home listening to records on his record player,” said Dr. Geller. But he’s been amenable to phone sessions. “What I’ve found with him, and I’ve found with several other patients, is that they actually talk more easily when they’re not face to face,” he said.
Far fewer no-shows
Another plus for his New England–based practice during the last few months: patients have not been anxious about missing sessions because of the weather. The clinicians all noted that telepsychiatry seemed to reduce missed visits.
Dr. Yellowlees said that no-show rates had decreased by half at UC Davis. “That means no significant loss of income,” during the pandemic, he said.
“The no-show rate is incredibly low, particularly because when you call the patients and they don’t remember they had an appointment, you have the appointment anyway, most of the time,” said Dr. Geller.
For Dr. Khan, being able to conduct audio and video sessions during the pandemic has meant keeping up continuity of care.
As a result of the pandemic, many college students in New York City had to go home – often to another state. The waivers granted by New York’s Medicaid program and other insurers have allowed Dr. Khan to continue care for these patients.
The NYU clinic also operates day programs in rural areas 5 hours from the city. Dr. Khan recently evaluated a 12-year-old girl with significant anxiety and low mood, both of which had worsened.
“She would not have been able to access care otherwise,” said Dr. Khan. And for rural patients who do not have access to broadband or smartphones, audio visits “have been immensely helpful,” she said.
Dr. Khan, Dr. Geller, and Dr. Yellowlees have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The American Psychiatric Association (APA) is calling on Congress to permanently lift restrictions that have allowed unfettered delivery of telehealth services during the COVID-19 pandemic, which experts say has been a boon to patients and physicians alike.
“We ask Congress to extend the telehealth waiver authority under COVID-19 beyond the emergency and to study its impact while doing so,” said APA President Jeffrey Geller, MD, in a May 27 video briefing with congressional staff and reporters.
The APA is also seeking to make permanent certain waivers granted by the Centers for Medicare & Medicaid Services on April 30, including elimination of geographic restrictions on behavioral health and allowing patients be seen at home, said Dr. Geller.
The APA also is asking for the elimination of the rule that requires clinicians to have an initial face-to-face meeting with patients before they can prescribe controlled substances, Dr. Geller said. The Drug Enforcement Administration waived that requirement, known as the Ryan Haight Act, on March 17 for the duration of the national emergency.
Telemedicine has supporters on both sides of the aisle in Congress, including Rep. Paul Tonko (D-N.Y.) who said at the APA briefing he would fight to make the waivers permanent.
“The expanded use of telehealth has enormous potential during normal times as well, especially in behavioral health,” said Mr. Tonko. “I am pushing fiercely for these current flexibilities to be extended for a reasonable time after the public health emergency so that we can have time to evaluate which should be made permanent,” he said.
Dr. Geller, other clinicians, and advocates in the briefing praised CMS for facilitating telepsychiatry for Medicare. That follows in the footsteps of most private insurers, who have also relaxed requirements into the summer, according to the Medical Group Management Association.
Game changer
The Medicare waivers “have dramatically changed the entire scene for someone like myself as a clinician to allow me to see my patients in a much easier way,” said Peter Yellowlees, MBBS, MD, chief wellness officer, University of California Davis Health. Within 2 weeks in March, the health system converted almost all of its regular outpatient visits to telemedicine, he said.
Dr. Yellowlees added government still needs to address, what he called, outdated HIPAA regulations that ban certain technologies.
“It makes no sense that I can talk to someone on an iPhone, but the moment I talk to them on FaceTime, it’s illegal,” said Dr. Yellowlees, a former president of the American Telemedicine Association.
Dr. Geller said that “psychiatric care provided by telehealth is as effective as in-person psychiatric services,” adding that “some patients prefer telepsychiatry because of its convenience and as a means of reducing stigma associated with seeking help for mental health.”
Shabana Khan, MD, a child psychiatrist and director of telepsychiatry at New York University Langone Health, said audio and video conferencing are helping address a shortage and maldistribution of child and adolescent psychiatrists.
Americans’ mental health is suffering during the pandemic. The U.S. Census Bureau recently released data showing that half of those surveyed reported depressed mood and that one-third are reporting anxiety, depression, or both, as reported by the Washington Post.
“At this very time that anxiety, depression, substance use, and other mental health problems are rising, our nation’s already strained mental health system is really being pushed to the brink,” said Jodi Kwarciany, manager for mental health policy for the National Alliance on Mental Illness, during the briefing.
Telemedicine can help “by connecting people to providers at the time and the place and using the technology that works best for them,” she said, adding that NAMI would press policymakers to address barriers to access.
The clinicians on the briefing said they’ve observed that some patients are more comfortable with video or audio interactions than with in-person visits.
Increased access to care
Telepsychiatry seems to be convincing some to reconsider therapy, since they can do it at home, said Dr. Yellowlees. he said.
For instance, he said, he has been able to consult by phone and video with several patients who receive care through the Indian Health Service who had not be able to get into the physical clinic.
Dr. Yellowlees said video sessions also may encourage patients to be more, not less, talkative. “Video is actually counterintuitively a very intimate experience,” he said, in part because of the perceived distance and people’s tendency to be less inhibited on technology platforms.“It’s less embarrassing,” he said. “If you’ve got really dramatic, difficult, traumatic things to talk about, it’s slightly easier to talk to someone who’s slightly further apart from you on video,” said Dr. Yellowlees.
“Individuals who have a significant amount of anxiety may actually feel more comfortable with the distance that this technology affords,” agreed Dr. Khan. She said telemedicine had made sessions more comfortable for some of her patients with autism spectrum disorder.
Dr. Geller said audio and video have been important to his practice during the pandemic. One of his patients never leaves the house and does not use computers. “He spends his time sequestered at home listening to records on his record player,” said Dr. Geller. But he’s been amenable to phone sessions. “What I’ve found with him, and I’ve found with several other patients, is that they actually talk more easily when they’re not face to face,” he said.
Far fewer no-shows
Another plus for his New England–based practice during the last few months: patients have not been anxious about missing sessions because of the weather. The clinicians all noted that telepsychiatry seemed to reduce missed visits.
Dr. Yellowlees said that no-show rates had decreased by half at UC Davis. “That means no significant loss of income,” during the pandemic, he said.
“The no-show rate is incredibly low, particularly because when you call the patients and they don’t remember they had an appointment, you have the appointment anyway, most of the time,” said Dr. Geller.
For Dr. Khan, being able to conduct audio and video sessions during the pandemic has meant keeping up continuity of care.
As a result of the pandemic, many college students in New York City had to go home – often to another state. The waivers granted by New York’s Medicaid program and other insurers have allowed Dr. Khan to continue care for these patients.
The NYU clinic also operates day programs in rural areas 5 hours from the city. Dr. Khan recently evaluated a 12-year-old girl with significant anxiety and low mood, both of which had worsened.
“She would not have been able to access care otherwise,” said Dr. Khan. And for rural patients who do not have access to broadband or smartphones, audio visits “have been immensely helpful,” she said.
Dr. Khan, Dr. Geller, and Dr. Yellowlees have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
‘Loss-frame’ approach makes psoriasis patients more agreeable to treatment
, held virtually.
“We typically explain to patients the benefits of treatment,” Ari A. Kassardjian, BS, of the University of Southern California, Los Angeles, said in his presentation. “However, explaining to them the harmful effects on their skin and joint diseases, such as exacerbation of psoriasis and/or psoriatic arthritis, could offer some patients a new perspective that may influence their treatment preferences; and ultimately, better communication may lead to better medication adherence in patients.”
In the study he presented, explaining to patients possible outcomes without treatment was more effective in getting them to agree to treatment than was messaging that focused on the positive effects of a therapy (reducing disease severity and pain, and improved health).
He noted that the impact of framing choices in terms of gain or loss on decision-making has been measured in other areas of medicine, including in patients with multiple sclerosis where medication adherence is an issue (J Health Commun. 2017 Jun;22[6]:523-31). “Gain-framed” messages focus on the benefits of taking a medication, while “loss-framed” messages highlight the potential consequences of not agreeing or adhering to treatment.
In the study, Mr. Kassardjian and coinvestigators evaluated 90 patients with psoriasis who were randomized to receive a gain-framed or loss-framed message about a hypothetical new biologic injectable medication for psoriasis and psoriatic arthritis (PsA). More than half were male (64.4%), white (53.3%), and non-Hispanic or Latino (55.6%); and about one-fourth of the participants (27.8%) also had psoriatic arthritis (PsA).
The gain-framed message emphasized “the chance to reduce psoriasis severity, reduce joint pain, and improve how you feel overall,” while the loss-framed message described the downsides of not taking medication – missing out “on the chance to improve your skin, your joints, and your overall health,” with the possibility that psoriasis may get worse, “with worsening pain in your joints from psoriatic arthritis,” and feeling “worse overall.” Both messages included the side effects of the theoretical injectable, a small risk of injection-site pain and skin infections. After receiving the message, participants ranked their likelihood of taking the medication on an 11-point Likert scale, with a score of 0 indicating that they would “definitely” not use the medication and a score of 10 indicating that they would “definitely” use the medication.
Scores among those who received the loss-framed message were a mean of 8.84, compared with 7.11 among patients who received the gain-framed message (between-group difference; 1.73; P less than .0001). When comparing patients with and without PsA, the between-group difference was 1.90 for patients with PsA (P less than .0001) and 1.08 for patients who did not have PsA (P = .002). Comparing the responses of those with PsA and those without PsA, the between-group difference was 1.08 (P = .03). While PsA and non-PsA patients favored the loss-framed messages, “regardless of the framing type, PsA patients always responded with a greater preference for the therapy,” Mr. Kassardjian said.
Gender also had an effect on responsiveness to gain-framed or loss-framed messaging. Both men and women ranked the loss-framed messaging as making them more likely to use the medication, but the between-group difference for women (2.00; P = .008) was higher than in men (1.49; P = .003). However, the total men compared with total women between-group differences were not significant.
“In clinical practice, physicians regularly weigh the benefits and risks of treatment. In order to communicate this information to patients, it is important to understand how framing these benefits and risks impacts patient preferences for therapy,” Mr. Kassardjian said. “While most available biologics are effective and have tolerable safety profiles, many psoriasis patients may be hesitant to initiate these therapies. Thus, it is important to convey the benefits and risks of these systemic agents in ways that resonate with patients.”
Mr. Kassardjian reports receiving the Dean’s Research Scholarship at the University of Southern California, funded by the Wright Foundation at the time of the study. Senior author April Armstrong, MD, disclosed serving as an investigator and/or consultant for AbbVie, BMS, Dermavant, Dermira, Eli Lilly, Janssen, Leo Pharma, Kyowa Hakko Kirin, Modernizing Medicine, Novartis, Ortho Dermatologics, Regeneron, Sanofi, Sun Pharma, and UCB.
SOURCE: Kassardjian A. SID 2020, Abstract 489.
, held virtually.
“We typically explain to patients the benefits of treatment,” Ari A. Kassardjian, BS, of the University of Southern California, Los Angeles, said in his presentation. “However, explaining to them the harmful effects on their skin and joint diseases, such as exacerbation of psoriasis and/or psoriatic arthritis, could offer some patients a new perspective that may influence their treatment preferences; and ultimately, better communication may lead to better medication adherence in patients.”
In the study he presented, explaining to patients possible outcomes without treatment was more effective in getting them to agree to treatment than was messaging that focused on the positive effects of a therapy (reducing disease severity and pain, and improved health).
He noted that the impact of framing choices in terms of gain or loss on decision-making has been measured in other areas of medicine, including in patients with multiple sclerosis where medication adherence is an issue (J Health Commun. 2017 Jun;22[6]:523-31). “Gain-framed” messages focus on the benefits of taking a medication, while “loss-framed” messages highlight the potential consequences of not agreeing or adhering to treatment.
In the study, Mr. Kassardjian and coinvestigators evaluated 90 patients with psoriasis who were randomized to receive a gain-framed or loss-framed message about a hypothetical new biologic injectable medication for psoriasis and psoriatic arthritis (PsA). More than half were male (64.4%), white (53.3%), and non-Hispanic or Latino (55.6%); and about one-fourth of the participants (27.8%) also had psoriatic arthritis (PsA).
The gain-framed message emphasized “the chance to reduce psoriasis severity, reduce joint pain, and improve how you feel overall,” while the loss-framed message described the downsides of not taking medication – missing out “on the chance to improve your skin, your joints, and your overall health,” with the possibility that psoriasis may get worse, “with worsening pain in your joints from psoriatic arthritis,” and feeling “worse overall.” Both messages included the side effects of the theoretical injectable, a small risk of injection-site pain and skin infections. After receiving the message, participants ranked their likelihood of taking the medication on an 11-point Likert scale, with a score of 0 indicating that they would “definitely” not use the medication and a score of 10 indicating that they would “definitely” use the medication.
Scores among those who received the loss-framed message were a mean of 8.84, compared with 7.11 among patients who received the gain-framed message (between-group difference; 1.73; P less than .0001). When comparing patients with and without PsA, the between-group difference was 1.90 for patients with PsA (P less than .0001) and 1.08 for patients who did not have PsA (P = .002). Comparing the responses of those with PsA and those without PsA, the between-group difference was 1.08 (P = .03). While PsA and non-PsA patients favored the loss-framed messages, “regardless of the framing type, PsA patients always responded with a greater preference for the therapy,” Mr. Kassardjian said.
Gender also had an effect on responsiveness to gain-framed or loss-framed messaging. Both men and women ranked the loss-framed messaging as making them more likely to use the medication, but the between-group difference for women (2.00; P = .008) was higher than in men (1.49; P = .003). However, the total men compared with total women between-group differences were not significant.
“In clinical practice, physicians regularly weigh the benefits and risks of treatment. In order to communicate this information to patients, it is important to understand how framing these benefits and risks impacts patient preferences for therapy,” Mr. Kassardjian said. “While most available biologics are effective and have tolerable safety profiles, many psoriasis patients may be hesitant to initiate these therapies. Thus, it is important to convey the benefits and risks of these systemic agents in ways that resonate with patients.”
Mr. Kassardjian reports receiving the Dean’s Research Scholarship at the University of Southern California, funded by the Wright Foundation at the time of the study. Senior author April Armstrong, MD, disclosed serving as an investigator and/or consultant for AbbVie, BMS, Dermavant, Dermira, Eli Lilly, Janssen, Leo Pharma, Kyowa Hakko Kirin, Modernizing Medicine, Novartis, Ortho Dermatologics, Regeneron, Sanofi, Sun Pharma, and UCB.
SOURCE: Kassardjian A. SID 2020, Abstract 489.
, held virtually.
“We typically explain to patients the benefits of treatment,” Ari A. Kassardjian, BS, of the University of Southern California, Los Angeles, said in his presentation. “However, explaining to them the harmful effects on their skin and joint diseases, such as exacerbation of psoriasis and/or psoriatic arthritis, could offer some patients a new perspective that may influence their treatment preferences; and ultimately, better communication may lead to better medication adherence in patients.”
In the study he presented, explaining to patients possible outcomes without treatment was more effective in getting them to agree to treatment than was messaging that focused on the positive effects of a therapy (reducing disease severity and pain, and improved health).
He noted that the impact of framing choices in terms of gain or loss on decision-making has been measured in other areas of medicine, including in patients with multiple sclerosis where medication adherence is an issue (J Health Commun. 2017 Jun;22[6]:523-31). “Gain-framed” messages focus on the benefits of taking a medication, while “loss-framed” messages highlight the potential consequences of not agreeing or adhering to treatment.
In the study, Mr. Kassardjian and coinvestigators evaluated 90 patients with psoriasis who were randomized to receive a gain-framed or loss-framed message about a hypothetical new biologic injectable medication for psoriasis and psoriatic arthritis (PsA). More than half were male (64.4%), white (53.3%), and non-Hispanic or Latino (55.6%); and about one-fourth of the participants (27.8%) also had psoriatic arthritis (PsA).
The gain-framed message emphasized “the chance to reduce psoriasis severity, reduce joint pain, and improve how you feel overall,” while the loss-framed message described the downsides of not taking medication – missing out “on the chance to improve your skin, your joints, and your overall health,” with the possibility that psoriasis may get worse, “with worsening pain in your joints from psoriatic arthritis,” and feeling “worse overall.” Both messages included the side effects of the theoretical injectable, a small risk of injection-site pain and skin infections. After receiving the message, participants ranked their likelihood of taking the medication on an 11-point Likert scale, with a score of 0 indicating that they would “definitely” not use the medication and a score of 10 indicating that they would “definitely” use the medication.
Scores among those who received the loss-framed message were a mean of 8.84, compared with 7.11 among patients who received the gain-framed message (between-group difference; 1.73; P less than .0001). When comparing patients with and without PsA, the between-group difference was 1.90 for patients with PsA (P less than .0001) and 1.08 for patients who did not have PsA (P = .002). Comparing the responses of those with PsA and those without PsA, the between-group difference was 1.08 (P = .03). While PsA and non-PsA patients favored the loss-framed messages, “regardless of the framing type, PsA patients always responded with a greater preference for the therapy,” Mr. Kassardjian said.
Gender also had an effect on responsiveness to gain-framed or loss-framed messaging. Both men and women ranked the loss-framed messaging as making them more likely to use the medication, but the between-group difference for women (2.00; P = .008) was higher than in men (1.49; P = .003). However, the total men compared with total women between-group differences were not significant.
“In clinical practice, physicians regularly weigh the benefits and risks of treatment. In order to communicate this information to patients, it is important to understand how framing these benefits and risks impacts patient preferences for therapy,” Mr. Kassardjian said. “While most available biologics are effective and have tolerable safety profiles, many psoriasis patients may be hesitant to initiate these therapies. Thus, it is important to convey the benefits and risks of these systemic agents in ways that resonate with patients.”
Mr. Kassardjian reports receiving the Dean’s Research Scholarship at the University of Southern California, funded by the Wright Foundation at the time of the study. Senior author April Armstrong, MD, disclosed serving as an investigator and/or consultant for AbbVie, BMS, Dermavant, Dermira, Eli Lilly, Janssen, Leo Pharma, Kyowa Hakko Kirin, Modernizing Medicine, Novartis, Ortho Dermatologics, Regeneron, Sanofi, Sun Pharma, and UCB.
SOURCE: Kassardjian A. SID 2020, Abstract 489.
FROM SID 2020
COVID-19 crushers: An appreciation of hospitalists
The hospitalist team at Overlake Medical Center and Clinics in Bellevue, Wash., has been a major partner of our Clinical Documentation Integrity Department in achieving its goal of accurately capturing the quality care patients receive on their records.
For many years, we have been witnesses of our hospitalists’ hard work, and the unique challenges of this pandemic further showed their tenacity and resilience. I thought that the best way to tell this story is through the poster accompanying this article.
To the viewer, this demonstrates the fierce battle raging between our hospitalists and the invisible foe, COVID-19. To my hospitalist colleagues, this is a constant reminder, albeit visually, that you are appreciated, admired and valued – not only by the CDI Department but by the whole organization as well.
Beyond my local colleagues, I would like to also thank the hospitalists working around the globe for their dedication and resolve in fighting this pandemic.
Mr. Valentin is a nurse and Certified Clinical Documentation Integrity Specialist at Overlake Medical Center and Clinics, Bellevue, Wash. His clinical specialties within nursing practice are in the OR, acute inpatient psychiatry, and the AIDS Unit.
The hospitalist team at Overlake Medical Center and Clinics in Bellevue, Wash., has been a major partner of our Clinical Documentation Integrity Department in achieving its goal of accurately capturing the quality care patients receive on their records.
For many years, we have been witnesses of our hospitalists’ hard work, and the unique challenges of this pandemic further showed their tenacity and resilience. I thought that the best way to tell this story is through the poster accompanying this article.
To the viewer, this demonstrates the fierce battle raging between our hospitalists and the invisible foe, COVID-19. To my hospitalist colleagues, this is a constant reminder, albeit visually, that you are appreciated, admired and valued – not only by the CDI Department but by the whole organization as well.
Beyond my local colleagues, I would like to also thank the hospitalists working around the globe for their dedication and resolve in fighting this pandemic.
Mr. Valentin is a nurse and Certified Clinical Documentation Integrity Specialist at Overlake Medical Center and Clinics, Bellevue, Wash. His clinical specialties within nursing practice are in the OR, acute inpatient psychiatry, and the AIDS Unit.
The hospitalist team at Overlake Medical Center and Clinics in Bellevue, Wash., has been a major partner of our Clinical Documentation Integrity Department in achieving its goal of accurately capturing the quality care patients receive on their records.
For many years, we have been witnesses of our hospitalists’ hard work, and the unique challenges of this pandemic further showed their tenacity and resilience. I thought that the best way to tell this story is through the poster accompanying this article.
To the viewer, this demonstrates the fierce battle raging between our hospitalists and the invisible foe, COVID-19. To my hospitalist colleagues, this is a constant reminder, albeit visually, that you are appreciated, admired and valued – not only by the CDI Department but by the whole organization as well.
Beyond my local colleagues, I would like to also thank the hospitalists working around the globe for their dedication and resolve in fighting this pandemic.
Mr. Valentin is a nurse and Certified Clinical Documentation Integrity Specialist at Overlake Medical Center and Clinics, Bellevue, Wash. His clinical specialties within nursing practice are in the OR, acute inpatient psychiatry, and the AIDS Unit.