User login
Novel Agent Curbs Alzheimer’s-Related Agitation
DENVER —
More than half of participants in the open-label extension period of the randomized clinical trial responded to the medication, which was associated with a 3.6-fold lower risk for relapse compared with placebo.
“The positive efficacy and favorable safety results with AXS-05 support its potential to fulfill a high unmet need for the treatment of Alzheimer’s disease agitation,” said Anton P. Porsteinsson, MD, director of the Alzheimer’s Disease Care, Research and Education Program, University of Rochester, New York.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology.
Common and Disruptive
Agitation is reported in up to 70% of patients with Alzheimer’s disease and is characterized by emotional distress, aggressive behaviors, disruptive irritability, and disinhibition. Alzheimer’s disease-related agitation has been associated with increased caregiver burden, decreased functioning, accelerated cognitive decline, earlier nursing home placement, and increased mortality.
A previous phase 2/3 study of AXS-05 showed that the investigative agent led to rapid and significantly improvement in Alzheimer’s disease agitation, as measured by the Cohen-Mansfield Agitation Inventory (CMAI) total score, compared with placebo.
ACCORD was a phase 3, randomized, double-blind, placebo-controlled withdrawal trial evaluating the efficacy and safety of AXS-05 in patients with Alzheimer’s disease agitation.
In the open-label period, 178 adults with probable Alzheimer’s disease and clinically significant agitation received AXS-05 (titrated to 45 mg dextromethorphan/105 mg bupropion twice daily) for up to 9 weeks.
A total of 108 (61%) patients had a sustained response, with 30% or more improvement from baseline in the CMAI total score and improvement on the Patient Global Impression of Change that were both maintained for 4 or more consecutive weeks. These patients entered the double-blind phase and were randomly allocated to receive twice-daily AXS-05 or placebo for up to 26 weeks.
In the double-blind period, AXS-05 “substantially and statistically” increased the time to relapse of agitation symptoms compared with placebo (hazard ratio [HR], 0.275; P = .014).
“The risk of relapse was 3.6-fold lower with AXS-05 compared with placebo,” Dr. Porsteinsson reported.
AXS-05 was also associated with a significantly lower relapse rate compared with placebo (7.5% vs 25.9%; P = .018).
Rates of discontinuation in the double-blind period owing to adverse events (AEs) were low (0% for AXS-05 and 1.9% for placebo). Three serious AEs were reported: one in the AXS-05 group (fecaloma), which was not related to study medication, and two in the placebo group (cardiac arrest, femur fracture).
Falls were reported in four participants in the AXS-05 group, none of which were related to study medication or associated with serious AEs, and in two participants in the placebo group, one of which was associated with femur fracture.
One death was reported in the placebo group. There was no evidence of cognitive decline with AXS-05, and treatment was not associated with sedation.
Promising Agent
Commenting on this research, Glen R. Finney, MD, director of the Geisinger Memory and Cognition Clinic in Wilkes-Barre, Pennsylvania, said the data “look promising as a safe way to help address acute agitation and reduce agitation reoccurrence.
“Agitation is a common, distressing, and sometimes safety issue for people fighting Alzheimer’s disease, and there’s very little evidence for efficacy and significant side effect issues for current medical management of agitation in Alzheimer’s disease,” said Dr. Finney, who was not part of the study.
He noted that first-line strategies for addressing agitation involve behavioral and environmental interventions.
“See if there’s a reason for the agitation and address that. Look for triggers for agitation and avoid those. Find places, things, and interactions that help people with Alzheimer’s disease avoid agitation: familiar locations, music, simple engaging activities. Reassurance, redirection, and distraction can help de-escalate agitation. Provide a safe environment that reduces safety risks,” Dr. Finney explained.
The next step, when medically appropriate, is trying acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, and then adding memantine, a weak N-methyl-D-aspartate receptor antagonist.
“These medications can help reduce the risk of agitation,” Dr. Finney said.
“Beyond that, the evidence becomes weaker for any specific treatments, and that is where treatments with emerging evidence of efficacy and safety like dextromethorphan-bupropion become important,” Dr. Finney added.
Last May, the US Food and Drug Administration (FDA) approved the antipsychotic brexpiprazole (Rexulti) for Alzheimer’s disease-related agitation, making it the first FDA-approved drug for this indication.
The drug includes a boxed warning for medications in this class that older patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk for death.
“There’s certainly a need to have multiple options for treating agitation in individuals with Alzheimer’s disease,” said Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association.
Dr. Edelmayer, who was not part of the study, noted that in the ACCORD study, AXS-05 “significantly delayed the relapse or prevented the relapse with Alzheimer’s disease agitation compared with the placebo group and it was generally well tolerated, but it will be important to make sure that there’s more thorough review of the data overall to be sure that it’s both safe and effective.”
The study was funded by Axsome Therapeutics, the manufacturer of AXS-05. Dr. Porsteinsson has disclosed no relevant conflicts of interest. Dr. Finney and Dr. Edelmayer have no relevant disclosures.
A version of this article appeared on Medscape.com.
DENVER —
More than half of participants in the open-label extension period of the randomized clinical trial responded to the medication, which was associated with a 3.6-fold lower risk for relapse compared with placebo.
“The positive efficacy and favorable safety results with AXS-05 support its potential to fulfill a high unmet need for the treatment of Alzheimer’s disease agitation,” said Anton P. Porsteinsson, MD, director of the Alzheimer’s Disease Care, Research and Education Program, University of Rochester, New York.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology.
Common and Disruptive
Agitation is reported in up to 70% of patients with Alzheimer’s disease and is characterized by emotional distress, aggressive behaviors, disruptive irritability, and disinhibition. Alzheimer’s disease-related agitation has been associated with increased caregiver burden, decreased functioning, accelerated cognitive decline, earlier nursing home placement, and increased mortality.
A previous phase 2/3 study of AXS-05 showed that the investigative agent led to rapid and significantly improvement in Alzheimer’s disease agitation, as measured by the Cohen-Mansfield Agitation Inventory (CMAI) total score, compared with placebo.
ACCORD was a phase 3, randomized, double-blind, placebo-controlled withdrawal trial evaluating the efficacy and safety of AXS-05 in patients with Alzheimer’s disease agitation.
In the open-label period, 178 adults with probable Alzheimer’s disease and clinically significant agitation received AXS-05 (titrated to 45 mg dextromethorphan/105 mg bupropion twice daily) for up to 9 weeks.
A total of 108 (61%) patients had a sustained response, with 30% or more improvement from baseline in the CMAI total score and improvement on the Patient Global Impression of Change that were both maintained for 4 or more consecutive weeks. These patients entered the double-blind phase and were randomly allocated to receive twice-daily AXS-05 or placebo for up to 26 weeks.
In the double-blind period, AXS-05 “substantially and statistically” increased the time to relapse of agitation symptoms compared with placebo (hazard ratio [HR], 0.275; P = .014).
“The risk of relapse was 3.6-fold lower with AXS-05 compared with placebo,” Dr. Porsteinsson reported.
AXS-05 was also associated with a significantly lower relapse rate compared with placebo (7.5% vs 25.9%; P = .018).
Rates of discontinuation in the double-blind period owing to adverse events (AEs) were low (0% for AXS-05 and 1.9% for placebo). Three serious AEs were reported: one in the AXS-05 group (fecaloma), which was not related to study medication, and two in the placebo group (cardiac arrest, femur fracture).
Falls were reported in four participants in the AXS-05 group, none of which were related to study medication or associated with serious AEs, and in two participants in the placebo group, one of which was associated with femur fracture.
One death was reported in the placebo group. There was no evidence of cognitive decline with AXS-05, and treatment was not associated with sedation.
Promising Agent
Commenting on this research, Glen R. Finney, MD, director of the Geisinger Memory and Cognition Clinic in Wilkes-Barre, Pennsylvania, said the data “look promising as a safe way to help address acute agitation and reduce agitation reoccurrence.
“Agitation is a common, distressing, and sometimes safety issue for people fighting Alzheimer’s disease, and there’s very little evidence for efficacy and significant side effect issues for current medical management of agitation in Alzheimer’s disease,” said Dr. Finney, who was not part of the study.
He noted that first-line strategies for addressing agitation involve behavioral and environmental interventions.
“See if there’s a reason for the agitation and address that. Look for triggers for agitation and avoid those. Find places, things, and interactions that help people with Alzheimer’s disease avoid agitation: familiar locations, music, simple engaging activities. Reassurance, redirection, and distraction can help de-escalate agitation. Provide a safe environment that reduces safety risks,” Dr. Finney explained.
The next step, when medically appropriate, is trying acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, and then adding memantine, a weak N-methyl-D-aspartate receptor antagonist.
“These medications can help reduce the risk of agitation,” Dr. Finney said.
“Beyond that, the evidence becomes weaker for any specific treatments, and that is where treatments with emerging evidence of efficacy and safety like dextromethorphan-bupropion become important,” Dr. Finney added.
Last May, the US Food and Drug Administration (FDA) approved the antipsychotic brexpiprazole (Rexulti) for Alzheimer’s disease-related agitation, making it the first FDA-approved drug for this indication.
The drug includes a boxed warning for medications in this class that older patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk for death.
“There’s certainly a need to have multiple options for treating agitation in individuals with Alzheimer’s disease,” said Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association.
Dr. Edelmayer, who was not part of the study, noted that in the ACCORD study, AXS-05 “significantly delayed the relapse or prevented the relapse with Alzheimer’s disease agitation compared with the placebo group and it was generally well tolerated, but it will be important to make sure that there’s more thorough review of the data overall to be sure that it’s both safe and effective.”
The study was funded by Axsome Therapeutics, the manufacturer of AXS-05. Dr. Porsteinsson has disclosed no relevant conflicts of interest. Dr. Finney and Dr. Edelmayer have no relevant disclosures.
A version of this article appeared on Medscape.com.
DENVER —
More than half of participants in the open-label extension period of the randomized clinical trial responded to the medication, which was associated with a 3.6-fold lower risk for relapse compared with placebo.
“The positive efficacy and favorable safety results with AXS-05 support its potential to fulfill a high unmet need for the treatment of Alzheimer’s disease agitation,” said Anton P. Porsteinsson, MD, director of the Alzheimer’s Disease Care, Research and Education Program, University of Rochester, New York.
The findings were presented at the 2024 annual meeting of the American Academy of Neurology.
Common and Disruptive
Agitation is reported in up to 70% of patients with Alzheimer’s disease and is characterized by emotional distress, aggressive behaviors, disruptive irritability, and disinhibition. Alzheimer’s disease-related agitation has been associated with increased caregiver burden, decreased functioning, accelerated cognitive decline, earlier nursing home placement, and increased mortality.
A previous phase 2/3 study of AXS-05 showed that the investigative agent led to rapid and significantly improvement in Alzheimer’s disease agitation, as measured by the Cohen-Mansfield Agitation Inventory (CMAI) total score, compared with placebo.
ACCORD was a phase 3, randomized, double-blind, placebo-controlled withdrawal trial evaluating the efficacy and safety of AXS-05 in patients with Alzheimer’s disease agitation.
In the open-label period, 178 adults with probable Alzheimer’s disease and clinically significant agitation received AXS-05 (titrated to 45 mg dextromethorphan/105 mg bupropion twice daily) for up to 9 weeks.
A total of 108 (61%) patients had a sustained response, with 30% or more improvement from baseline in the CMAI total score and improvement on the Patient Global Impression of Change that were both maintained for 4 or more consecutive weeks. These patients entered the double-blind phase and were randomly allocated to receive twice-daily AXS-05 or placebo for up to 26 weeks.
In the double-blind period, AXS-05 “substantially and statistically” increased the time to relapse of agitation symptoms compared with placebo (hazard ratio [HR], 0.275; P = .014).
“The risk of relapse was 3.6-fold lower with AXS-05 compared with placebo,” Dr. Porsteinsson reported.
AXS-05 was also associated with a significantly lower relapse rate compared with placebo (7.5% vs 25.9%; P = .018).
Rates of discontinuation in the double-blind period owing to adverse events (AEs) were low (0% for AXS-05 and 1.9% for placebo). Three serious AEs were reported: one in the AXS-05 group (fecaloma), which was not related to study medication, and two in the placebo group (cardiac arrest, femur fracture).
Falls were reported in four participants in the AXS-05 group, none of which were related to study medication or associated with serious AEs, and in two participants in the placebo group, one of which was associated with femur fracture.
One death was reported in the placebo group. There was no evidence of cognitive decline with AXS-05, and treatment was not associated with sedation.
Promising Agent
Commenting on this research, Glen R. Finney, MD, director of the Geisinger Memory and Cognition Clinic in Wilkes-Barre, Pennsylvania, said the data “look promising as a safe way to help address acute agitation and reduce agitation reoccurrence.
“Agitation is a common, distressing, and sometimes safety issue for people fighting Alzheimer’s disease, and there’s very little evidence for efficacy and significant side effect issues for current medical management of agitation in Alzheimer’s disease,” said Dr. Finney, who was not part of the study.
He noted that first-line strategies for addressing agitation involve behavioral and environmental interventions.
“See if there’s a reason for the agitation and address that. Look for triggers for agitation and avoid those. Find places, things, and interactions that help people with Alzheimer’s disease avoid agitation: familiar locations, music, simple engaging activities. Reassurance, redirection, and distraction can help de-escalate agitation. Provide a safe environment that reduces safety risks,” Dr. Finney explained.
The next step, when medically appropriate, is trying acetylcholinesterase inhibitors such as donepezil, rivastigmine, and galantamine, and then adding memantine, a weak N-methyl-D-aspartate receptor antagonist.
“These medications can help reduce the risk of agitation,” Dr. Finney said.
“Beyond that, the evidence becomes weaker for any specific treatments, and that is where treatments with emerging evidence of efficacy and safety like dextromethorphan-bupropion become important,” Dr. Finney added.
Last May, the US Food and Drug Administration (FDA) approved the antipsychotic brexpiprazole (Rexulti) for Alzheimer’s disease-related agitation, making it the first FDA-approved drug for this indication.
The drug includes a boxed warning for medications in this class that older patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk for death.
“There’s certainly a need to have multiple options for treating agitation in individuals with Alzheimer’s disease,” said Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association.
Dr. Edelmayer, who was not part of the study, noted that in the ACCORD study, AXS-05 “significantly delayed the relapse or prevented the relapse with Alzheimer’s disease agitation compared with the placebo group and it was generally well tolerated, but it will be important to make sure that there’s more thorough review of the data overall to be sure that it’s both safe and effective.”
The study was funded by Axsome Therapeutics, the manufacturer of AXS-05. Dr. Porsteinsson has disclosed no relevant conflicts of interest. Dr. Finney and Dr. Edelmayer have no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM AAN 2024
Genetic Signatures May Predict CAR T Responders
“Our transcriptomic analysis of ZUMA-7 dataset identified novel gene expression signatures predictive of outcome with axi-cel,” the authors reported in research presented at the annual meeting of the American Association for Cancer Research earlier in April. “These gene expression signatures could support risk-stratification of LBCL patients.”
The results are from a subanalysis of the phase 3 ZUMA-7 trial in which patients with early relapsed or primary refractory LBCL were treated with axi-cel, administered as a one-time dose in the second-line setting.
Long-term results from the trial showed a 4-year overall survival of 54.6% with axi-cel versus 46.0% with the standard of care (P = .03), with a median rate of progression-free survival of 14.7 months with axi-cel versus 3.7 months in the standard-second-line treatment.
In the study, the authors noted that, “although the use of axi-cel resulted in long-term survival in more than half of treated patients, it is important to continue to strive to improve patient outcomes.”
Following up on that, senior author Simone Filosto, of Kite, a Gilead Company, of Santa Monica, California, and colleagues launched their analysis of the genetic profiles of those who did and did not have favorable responses, using data from the ZUMA-7 trial.
Using gene expression profiling with the IO-360 Nanostring gene expression panel of 769 genes, they evaluated pretreated LBCL tumor samples from 134 of the patients treated with axi-cel.
After multivariate adjustment, the results showed that those with a distinctive 6-transcript genetic expression signature, consisting of CD19, CD45RA, CCL22, KLRK1, SOX11, and SIGLEC5, had a significantly higher rate of event-free survival (hazard ratio [HR], 0.27; P = 1.82 x 10-8), as well as progression-free survival (HR, 0.27; P = 1.35 x 10-7) after treatment with axi-cel, compared with those who did not have the signature.
The authors speculated that “the 6-gene expression signature may capture lymphomas with abundant adhesion molecules, a relatively low inflammation, and abundant expression of the targeted antigen (CD19).”
Conversely, the analysis showed that increased levels of an unfavorable 17-transcript gene expression signature had a strong negative correlation with event-free survival (HR, 6.19; P = 1.51 x 10-13) and progression-free survival (HR, 7.58; P = 2.70 x 10-14).
The 17-transcript signature included CD45RO, BCL2, IL-18R1, TNFSF4 [OX40L], KLRB1 [CD161], KIR3DL2, ITGB8, DUSP5, GPC4, PSMB5, RPS6KB1, SERPINA9, NBN, GLUD1, ESR1, ARID1A, and SLC16A1.
“The 17-gene expression signature is consistent with a high level of immune infiltration and inflammation paralleled by the activation of immune-escape mechanisms, such as the upregulation of anti-apoptotic genes,” the authors explain.
Of note, the 17-gene expression signature was elevated among 18 patients who progressed after axi-cel treatment.
Importantly, the gene expression signatures were not associated with outcomes observed among patients receiving second-line standard of care in the ZUMA-7 trial. And the signatures also did not correspond with outcomes following first-line R-CHOP chemotherapy reported in two online datasets, indicating their predictive rather than prognostic value.
Commenting on the findings, Marco Ruella, MD, noted that “stratifying the [CAR T-treated] patients is extremely important given that only a subset of them, 30%-40%, will experience long-term remission.”
“In an ideal scenario, we would want to treat only the patients who would benefit from such a complex and expensive therapy,” underscored Dr. Ruella, assistant professor in the Division of Hematology/Oncology and the Center for Cellular Immunotherapies and Scientific Director of the Lymphoma Program at the Hospital of the University of Pennsylvania in Philadelphia.
A key caveat is that the results need more validation before they true gain clinical value, he noted.
“We need more data before we can use such a score in the clinic as we would need to be absolutely confident on the predictive value of such a score in additional confirmatory cohorts.”
Furthermore, caution is warranted in avoiding excluding any patients unnecessarily, he added.
“Only if there are approximately zero chances of response would we be able to exclude a patient from a treatment,” Dr. Ruella noted. “If the chance of long-term cure are minimal but still present, it might still make sense for the patient.”
Nevertheless, such findings advance the understanding of the therapy’s implication in a meaningful way, he said.
“I think this study [and similar others] are important studies that help us better understand the mechanisms of relapse,” he said.
“Translationally, we are getting closer to reaching a point where we can precisely predict outcomes and, perhaps in the future, select the patients that would benefit the most from these treatments.”
Dr. Filosto and other authors are employees of Kite, which manufactures axi-cel. Dr. Ruella treats patients with CAR T products that have been licensed to Novartis, Kite, and Vittoria Bio.
“Our transcriptomic analysis of ZUMA-7 dataset identified novel gene expression signatures predictive of outcome with axi-cel,” the authors reported in research presented at the annual meeting of the American Association for Cancer Research earlier in April. “These gene expression signatures could support risk-stratification of LBCL patients.”
The results are from a subanalysis of the phase 3 ZUMA-7 trial in which patients with early relapsed or primary refractory LBCL were treated with axi-cel, administered as a one-time dose in the second-line setting.
Long-term results from the trial showed a 4-year overall survival of 54.6% with axi-cel versus 46.0% with the standard of care (P = .03), with a median rate of progression-free survival of 14.7 months with axi-cel versus 3.7 months in the standard-second-line treatment.
In the study, the authors noted that, “although the use of axi-cel resulted in long-term survival in more than half of treated patients, it is important to continue to strive to improve patient outcomes.”
Following up on that, senior author Simone Filosto, of Kite, a Gilead Company, of Santa Monica, California, and colleagues launched their analysis of the genetic profiles of those who did and did not have favorable responses, using data from the ZUMA-7 trial.
Using gene expression profiling with the IO-360 Nanostring gene expression panel of 769 genes, they evaluated pretreated LBCL tumor samples from 134 of the patients treated with axi-cel.
After multivariate adjustment, the results showed that those with a distinctive 6-transcript genetic expression signature, consisting of CD19, CD45RA, CCL22, KLRK1, SOX11, and SIGLEC5, had a significantly higher rate of event-free survival (hazard ratio [HR], 0.27; P = 1.82 x 10-8), as well as progression-free survival (HR, 0.27; P = 1.35 x 10-7) after treatment with axi-cel, compared with those who did not have the signature.
The authors speculated that “the 6-gene expression signature may capture lymphomas with abundant adhesion molecules, a relatively low inflammation, and abundant expression of the targeted antigen (CD19).”
Conversely, the analysis showed that increased levels of an unfavorable 17-transcript gene expression signature had a strong negative correlation with event-free survival (HR, 6.19; P = 1.51 x 10-13) and progression-free survival (HR, 7.58; P = 2.70 x 10-14).
The 17-transcript signature included CD45RO, BCL2, IL-18R1, TNFSF4 [OX40L], KLRB1 [CD161], KIR3DL2, ITGB8, DUSP5, GPC4, PSMB5, RPS6KB1, SERPINA9, NBN, GLUD1, ESR1, ARID1A, and SLC16A1.
“The 17-gene expression signature is consistent with a high level of immune infiltration and inflammation paralleled by the activation of immune-escape mechanisms, such as the upregulation of anti-apoptotic genes,” the authors explain.
Of note, the 17-gene expression signature was elevated among 18 patients who progressed after axi-cel treatment.
Importantly, the gene expression signatures were not associated with outcomes observed among patients receiving second-line standard of care in the ZUMA-7 trial. And the signatures also did not correspond with outcomes following first-line R-CHOP chemotherapy reported in two online datasets, indicating their predictive rather than prognostic value.
Commenting on the findings, Marco Ruella, MD, noted that “stratifying the [CAR T-treated] patients is extremely important given that only a subset of them, 30%-40%, will experience long-term remission.”
“In an ideal scenario, we would want to treat only the patients who would benefit from such a complex and expensive therapy,” underscored Dr. Ruella, assistant professor in the Division of Hematology/Oncology and the Center for Cellular Immunotherapies and Scientific Director of the Lymphoma Program at the Hospital of the University of Pennsylvania in Philadelphia.
A key caveat is that the results need more validation before they true gain clinical value, he noted.
“We need more data before we can use such a score in the clinic as we would need to be absolutely confident on the predictive value of such a score in additional confirmatory cohorts.”
Furthermore, caution is warranted in avoiding excluding any patients unnecessarily, he added.
“Only if there are approximately zero chances of response would we be able to exclude a patient from a treatment,” Dr. Ruella noted. “If the chance of long-term cure are minimal but still present, it might still make sense for the patient.”
Nevertheless, such findings advance the understanding of the therapy’s implication in a meaningful way, he said.
“I think this study [and similar others] are important studies that help us better understand the mechanisms of relapse,” he said.
“Translationally, we are getting closer to reaching a point where we can precisely predict outcomes and, perhaps in the future, select the patients that would benefit the most from these treatments.”
Dr. Filosto and other authors are employees of Kite, which manufactures axi-cel. Dr. Ruella treats patients with CAR T products that have been licensed to Novartis, Kite, and Vittoria Bio.
“Our transcriptomic analysis of ZUMA-7 dataset identified novel gene expression signatures predictive of outcome with axi-cel,” the authors reported in research presented at the annual meeting of the American Association for Cancer Research earlier in April. “These gene expression signatures could support risk-stratification of LBCL patients.”
The results are from a subanalysis of the phase 3 ZUMA-7 trial in which patients with early relapsed or primary refractory LBCL were treated with axi-cel, administered as a one-time dose in the second-line setting.
Long-term results from the trial showed a 4-year overall survival of 54.6% with axi-cel versus 46.0% with the standard of care (P = .03), with a median rate of progression-free survival of 14.7 months with axi-cel versus 3.7 months in the standard-second-line treatment.
In the study, the authors noted that, “although the use of axi-cel resulted in long-term survival in more than half of treated patients, it is important to continue to strive to improve patient outcomes.”
Following up on that, senior author Simone Filosto, of Kite, a Gilead Company, of Santa Monica, California, and colleagues launched their analysis of the genetic profiles of those who did and did not have favorable responses, using data from the ZUMA-7 trial.
Using gene expression profiling with the IO-360 Nanostring gene expression panel of 769 genes, they evaluated pretreated LBCL tumor samples from 134 of the patients treated with axi-cel.
After multivariate adjustment, the results showed that those with a distinctive 6-transcript genetic expression signature, consisting of CD19, CD45RA, CCL22, KLRK1, SOX11, and SIGLEC5, had a significantly higher rate of event-free survival (hazard ratio [HR], 0.27; P = 1.82 x 10-8), as well as progression-free survival (HR, 0.27; P = 1.35 x 10-7) after treatment with axi-cel, compared with those who did not have the signature.
The authors speculated that “the 6-gene expression signature may capture lymphomas with abundant adhesion molecules, a relatively low inflammation, and abundant expression of the targeted antigen (CD19).”
Conversely, the analysis showed that increased levels of an unfavorable 17-transcript gene expression signature had a strong negative correlation with event-free survival (HR, 6.19; P = 1.51 x 10-13) and progression-free survival (HR, 7.58; P = 2.70 x 10-14).
The 17-transcript signature included CD45RO, BCL2, IL-18R1, TNFSF4 [OX40L], KLRB1 [CD161], KIR3DL2, ITGB8, DUSP5, GPC4, PSMB5, RPS6KB1, SERPINA9, NBN, GLUD1, ESR1, ARID1A, and SLC16A1.
“The 17-gene expression signature is consistent with a high level of immune infiltration and inflammation paralleled by the activation of immune-escape mechanisms, such as the upregulation of anti-apoptotic genes,” the authors explain.
Of note, the 17-gene expression signature was elevated among 18 patients who progressed after axi-cel treatment.
Importantly, the gene expression signatures were not associated with outcomes observed among patients receiving second-line standard of care in the ZUMA-7 trial. And the signatures also did not correspond with outcomes following first-line R-CHOP chemotherapy reported in two online datasets, indicating their predictive rather than prognostic value.
Commenting on the findings, Marco Ruella, MD, noted that “stratifying the [CAR T-treated] patients is extremely important given that only a subset of them, 30%-40%, will experience long-term remission.”
“In an ideal scenario, we would want to treat only the patients who would benefit from such a complex and expensive therapy,” underscored Dr. Ruella, assistant professor in the Division of Hematology/Oncology and the Center for Cellular Immunotherapies and Scientific Director of the Lymphoma Program at the Hospital of the University of Pennsylvania in Philadelphia.
A key caveat is that the results need more validation before they true gain clinical value, he noted.
“We need more data before we can use such a score in the clinic as we would need to be absolutely confident on the predictive value of such a score in additional confirmatory cohorts.”
Furthermore, caution is warranted in avoiding excluding any patients unnecessarily, he added.
“Only if there are approximately zero chances of response would we be able to exclude a patient from a treatment,” Dr. Ruella noted. “If the chance of long-term cure are minimal but still present, it might still make sense for the patient.”
Nevertheless, such findings advance the understanding of the therapy’s implication in a meaningful way, he said.
“I think this study [and similar others] are important studies that help us better understand the mechanisms of relapse,” he said.
“Translationally, we are getting closer to reaching a point where we can precisely predict outcomes and, perhaps in the future, select the patients that would benefit the most from these treatments.”
Dr. Filosto and other authors are employees of Kite, which manufactures axi-cel. Dr. Ruella treats patients with CAR T products that have been licensed to Novartis, Kite, and Vittoria Bio.
FROM AACR 2024
Which Emergencies Are Genuine Emergencies?
WIESBADEN, GERMANY — Crowded waiting rooms, long wait times, irritable patients, and aggression toward nursing staff and doctors are increasingly the reality in German emergency rooms. Clearly, emergencies belong in the emergency room. However, “In about half of all patients in the emergency room, there is no urgent medical emergency,” Norbert Schütz, MD, director of geriatrics and rheumatology at Helios Dr. Horst Schmidt Hospital in Wiesbaden, Germany, said at a press conference for the 130th Annual Meeting of the German Society of Internal Medicine (DGIM).
“In our daily medical practice, we repeatedly experience people either accessing our emergency departments and ambulances too quickly or lingering at home for too long when they have severe symptoms,” said Dr. Schütz, who organized the Patient Day during the Internist Congress.
DGIM Educates Patients
What is an emergency? “I think the public is quite well informed about conditions associated with loss of consciousness, severe pain, chest pain, or paralysis: Think stroke or heart attack. This is undoubtedly a success of recent years. The difficulty arises with everything in between. For instance, should I go to the hospital with severe headaches?” asked Dr. Schütz.
When is a patient a case for the emergency room, the physician on-call service, or the general practitioner? At the Patient Day in Wiesbaden, DGIM aims to educate and train interested parties with a dedicated lecture. The focus is on recognizing an emergency, specifically emergencies in children and mental illnesses.
“Our Patient Day aims to contribute to making the right decisions. We want to inform, answer questions, and alleviate fears,” said Dr. Schütz. Interested parties can refresh their emergency knowledge, tour ambulances, and have the equipment explained. The public also has the opportunity to learn about resuscitation techniques theoretically and practically.
“Should, for whatever reason, the general practitioner not be reachable, the physician on-call service can be reached,” said Dr. Schütz. It may happen, however, that neither the general practitioner nor the on-call physician is immediately available.
What Are Emergencies?
In cases of severe health impairment, urgency is required, and a severe emergency should be assumed in the following cases:
- Chest pain
- Circulatory disorder
- Disorders of consciousness
- Breathing difficulties
- Sudden weakness or numbness/paralysis
- Severe bleeding
- Allergic shock
“In such cases, the emergency departments of the hospitals are available around the clock, and if necessary, an emergency doctor should be present during transportation to the hospital,” said Dr. Schütz.
Classifying emergencies is challenging, especially with children. “Children often find it difficult to clearly categorize or describe symptoms,” said Dr. Schütz. A situation is critical if, for example, the child’s breathing or consciousness is impaired.
Mental emergencies pose a particular challenge for patients and relatives because the patient and relatives are often overwhelmed by the situation. If there are suicidal thoughts, the patient should present him- or herself immediately to an emergency room.
“Patients who come to the emergency room because they cannot get appointments with their general practitioner or specialist, for whatever reason, are no emergency. We also see this in the emergency room from time to time,” said Dr. Schütz. Emergency rooms are not intended for this purpose. “And generally, these are not emergencies.”
Four of 10 Cases
The number of patients in emergency rooms has steadily increased in recent years. Statistically, only 4 out of 10 cases are genuine emergencies, as detailed surveys of patients in the emergency rooms of northern German hospitals have shown.
In the PiNo Nord cross-sectional study, Martin Scherer, MD, of University Hospital Hamburg-Eppendorf in Hamburg, Germany, and his team examined the reasons why patients visit the emergency room. They interviewed 1175 patients in five hospitals and documented the medical diagnoses. Patients classified as “immediately” or “very urgently” in need of treatment were excluded.
The surveyed patients were on average 41.8 years old, 52.9% were men, and 54.7% of the patients indicated a low urgency of treatment. About 41% of the patients visited the emergency room on their own initiative, 17% stated they were referred or entrusted by their general practitioner, and 8% were referred by a specialist in the emergency room.
The strongest predictors for low subjective treatment urgency were musculoskeletal trauma (odds ratio [OR], 2.18), skin afflictions (OR, 2.15), and the unavailability of an open general practitioner’s office (OR, 1.70).
According to Dr. Scherer and his colleagues, the reasons for visiting an emergency room are diverse and can be based on the perceived structural conditions and individual patient preferences in addition to the urgency of the health problem.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
WIESBADEN, GERMANY — Crowded waiting rooms, long wait times, irritable patients, and aggression toward nursing staff and doctors are increasingly the reality in German emergency rooms. Clearly, emergencies belong in the emergency room. However, “In about half of all patients in the emergency room, there is no urgent medical emergency,” Norbert Schütz, MD, director of geriatrics and rheumatology at Helios Dr. Horst Schmidt Hospital in Wiesbaden, Germany, said at a press conference for the 130th Annual Meeting of the German Society of Internal Medicine (DGIM).
“In our daily medical practice, we repeatedly experience people either accessing our emergency departments and ambulances too quickly or lingering at home for too long when they have severe symptoms,” said Dr. Schütz, who organized the Patient Day during the Internist Congress.
DGIM Educates Patients
What is an emergency? “I think the public is quite well informed about conditions associated with loss of consciousness, severe pain, chest pain, or paralysis: Think stroke or heart attack. This is undoubtedly a success of recent years. The difficulty arises with everything in between. For instance, should I go to the hospital with severe headaches?” asked Dr. Schütz.
When is a patient a case for the emergency room, the physician on-call service, or the general practitioner? At the Patient Day in Wiesbaden, DGIM aims to educate and train interested parties with a dedicated lecture. The focus is on recognizing an emergency, specifically emergencies in children and mental illnesses.
“Our Patient Day aims to contribute to making the right decisions. We want to inform, answer questions, and alleviate fears,” said Dr. Schütz. Interested parties can refresh their emergency knowledge, tour ambulances, and have the equipment explained. The public also has the opportunity to learn about resuscitation techniques theoretically and practically.
“Should, for whatever reason, the general practitioner not be reachable, the physician on-call service can be reached,” said Dr. Schütz. It may happen, however, that neither the general practitioner nor the on-call physician is immediately available.
What Are Emergencies?
In cases of severe health impairment, urgency is required, and a severe emergency should be assumed in the following cases:
- Chest pain
- Circulatory disorder
- Disorders of consciousness
- Breathing difficulties
- Sudden weakness or numbness/paralysis
- Severe bleeding
- Allergic shock
“In such cases, the emergency departments of the hospitals are available around the clock, and if necessary, an emergency doctor should be present during transportation to the hospital,” said Dr. Schütz.
Classifying emergencies is challenging, especially with children. “Children often find it difficult to clearly categorize or describe symptoms,” said Dr. Schütz. A situation is critical if, for example, the child’s breathing or consciousness is impaired.
Mental emergencies pose a particular challenge for patients and relatives because the patient and relatives are often overwhelmed by the situation. If there are suicidal thoughts, the patient should present him- or herself immediately to an emergency room.
“Patients who come to the emergency room because they cannot get appointments with their general practitioner or specialist, for whatever reason, are no emergency. We also see this in the emergency room from time to time,” said Dr. Schütz. Emergency rooms are not intended for this purpose. “And generally, these are not emergencies.”
Four of 10 Cases
The number of patients in emergency rooms has steadily increased in recent years. Statistically, only 4 out of 10 cases are genuine emergencies, as detailed surveys of patients in the emergency rooms of northern German hospitals have shown.
In the PiNo Nord cross-sectional study, Martin Scherer, MD, of University Hospital Hamburg-Eppendorf in Hamburg, Germany, and his team examined the reasons why patients visit the emergency room. They interviewed 1175 patients in five hospitals and documented the medical diagnoses. Patients classified as “immediately” or “very urgently” in need of treatment were excluded.
The surveyed patients were on average 41.8 years old, 52.9% were men, and 54.7% of the patients indicated a low urgency of treatment. About 41% of the patients visited the emergency room on their own initiative, 17% stated they were referred or entrusted by their general practitioner, and 8% were referred by a specialist in the emergency room.
The strongest predictors for low subjective treatment urgency were musculoskeletal trauma (odds ratio [OR], 2.18), skin afflictions (OR, 2.15), and the unavailability of an open general practitioner’s office (OR, 1.70).
According to Dr. Scherer and his colleagues, the reasons for visiting an emergency room are diverse and can be based on the perceived structural conditions and individual patient preferences in addition to the urgency of the health problem.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
WIESBADEN, GERMANY — Crowded waiting rooms, long wait times, irritable patients, and aggression toward nursing staff and doctors are increasingly the reality in German emergency rooms. Clearly, emergencies belong in the emergency room. However, “In about half of all patients in the emergency room, there is no urgent medical emergency,” Norbert Schütz, MD, director of geriatrics and rheumatology at Helios Dr. Horst Schmidt Hospital in Wiesbaden, Germany, said at a press conference for the 130th Annual Meeting of the German Society of Internal Medicine (DGIM).
“In our daily medical practice, we repeatedly experience people either accessing our emergency departments and ambulances too quickly or lingering at home for too long when they have severe symptoms,” said Dr. Schütz, who organized the Patient Day during the Internist Congress.
DGIM Educates Patients
What is an emergency? “I think the public is quite well informed about conditions associated with loss of consciousness, severe pain, chest pain, or paralysis: Think stroke or heart attack. This is undoubtedly a success of recent years. The difficulty arises with everything in between. For instance, should I go to the hospital with severe headaches?” asked Dr. Schütz.
When is a patient a case for the emergency room, the physician on-call service, or the general practitioner? At the Patient Day in Wiesbaden, DGIM aims to educate and train interested parties with a dedicated lecture. The focus is on recognizing an emergency, specifically emergencies in children and mental illnesses.
“Our Patient Day aims to contribute to making the right decisions. We want to inform, answer questions, and alleviate fears,” said Dr. Schütz. Interested parties can refresh their emergency knowledge, tour ambulances, and have the equipment explained. The public also has the opportunity to learn about resuscitation techniques theoretically and practically.
“Should, for whatever reason, the general practitioner not be reachable, the physician on-call service can be reached,” said Dr. Schütz. It may happen, however, that neither the general practitioner nor the on-call physician is immediately available.
What Are Emergencies?
In cases of severe health impairment, urgency is required, and a severe emergency should be assumed in the following cases:
- Chest pain
- Circulatory disorder
- Disorders of consciousness
- Breathing difficulties
- Sudden weakness or numbness/paralysis
- Severe bleeding
- Allergic shock
“In such cases, the emergency departments of the hospitals are available around the clock, and if necessary, an emergency doctor should be present during transportation to the hospital,” said Dr. Schütz.
Classifying emergencies is challenging, especially with children. “Children often find it difficult to clearly categorize or describe symptoms,” said Dr. Schütz. A situation is critical if, for example, the child’s breathing or consciousness is impaired.
Mental emergencies pose a particular challenge for patients and relatives because the patient and relatives are often overwhelmed by the situation. If there are suicidal thoughts, the patient should present him- or herself immediately to an emergency room.
“Patients who come to the emergency room because they cannot get appointments with their general practitioner or specialist, for whatever reason, are no emergency. We also see this in the emergency room from time to time,” said Dr. Schütz. Emergency rooms are not intended for this purpose. “And generally, these are not emergencies.”
Four of 10 Cases
The number of patients in emergency rooms has steadily increased in recent years. Statistically, only 4 out of 10 cases are genuine emergencies, as detailed surveys of patients in the emergency rooms of northern German hospitals have shown.
In the PiNo Nord cross-sectional study, Martin Scherer, MD, of University Hospital Hamburg-Eppendorf in Hamburg, Germany, and his team examined the reasons why patients visit the emergency room. They interviewed 1175 patients in five hospitals and documented the medical diagnoses. Patients classified as “immediately” or “very urgently” in need of treatment were excluded.
The surveyed patients were on average 41.8 years old, 52.9% were men, and 54.7% of the patients indicated a low urgency of treatment. About 41% of the patients visited the emergency room on their own initiative, 17% stated they were referred or entrusted by their general practitioner, and 8% were referred by a specialist in the emergency room.
The strongest predictors for low subjective treatment urgency were musculoskeletal trauma (odds ratio [OR], 2.18), skin afflictions (OR, 2.15), and the unavailability of an open general practitioner’s office (OR, 1.70).
According to Dr. Scherer and his colleagues, the reasons for visiting an emergency room are diverse and can be based on the perceived structural conditions and individual patient preferences in addition to the urgency of the health problem.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Syphilis Treatment Falls Short for Pregnant Patients
Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.
Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.
To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.
The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The findings were published in Obstetrics & Gynecology.
Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.
Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).
The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.
The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.
More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.
The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.
Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.
Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.
To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.
The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The findings were published in Obstetrics & Gynecology.
Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.
Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).
The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.
The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.
More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.
The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.
Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.
Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.
To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.
The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The findings were published in Obstetrics & Gynecology.
Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.
Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).
The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.
The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.
More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.
The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.
FROM OBSTETRICS & GYNECOLOGY
Federal Trade Commission Bans Noncompete Agreements, Urges More Protections for Healthcare Workers
But business groups have vowed to challenge the decision in court.
The proposed final rule passed on a 3-2 vote, with the dissenting commissioners disputing the FTC’s authority to broadly ban noncompetes.
Tensions around noncompetes have been building for years. In 2021, President Biden issued an executive order supporting measures to improve economic competition, in which he urged the FTC to consider its rulemaking authority to address noncompete clauses that unfairly limit workers’ mobility. In January 2023, per that directive, the agency proposed ending the restrictive covenants.
While the FTC estimates that the final rule will reduce healthcare costs by up to $194 billion over the next decade and increase worker earnings by $300 million annually, the ruling faces legal hurdles.
US Chamber of Commerce president and CEO Suzanne P. Clark said in a statement that the move is a “blatant power grab” that will undermine competitive business practices, adding that the Chamber will sue to block the measure.
The FTC received more than 26,000 comments on noncompetes during the public feedback period, with about 25,000 supporting the measure, said Benjamin Cady, JD, an FTC attorney.
Mr. Cady called the feedback “compelling,” citing instances of workers who were forced to commute long distances, uproot their families, or risk expensive litigation for wanting to pursue job opportunities.
For example, a comment from a physician working in Appalachia highlights the potential real-life implications of the agreements. “With hospital systems merging, providers with aggressive noncompetes must abandon the community that they serve if they [choose] to leave their employer. Healthcare providers feel trapped in their current employment situation, leading to significant burnout that can shorten their [career] longevity.”
Commissioner Alvaro Bedoya said physicians have had their lives upended by cumbersome noncompetes, often having to move out of state to practice. “A pandemic killed a million people in this country, and there are doctors who cannot work because of a noncompete,” he said.
It’s unclear whether physicians and others who work for nonprofit healthcare groups or hospitals will be covered by the new ban. FTC Commissioner Rebecca Slaughter acknowledged that the agency’s jurisdictional limitations mean that employees of “certain nonprofit organizations” may not benefit from the rule.
“We want to be transparent about the limitation and recognize there are workers, especially healthcare workers, who are bound by anticompetitive and unfair noncompete clauses, that our rule will struggle to reach,” she said. To cover nonprofit healthcare employees, Ms. Slaughter urged Congress to pass legislation banning noncompetes, such as the Workforce Mobility Act of 2021 and the Freedom to Compete Act of 2023.
The FTC final rule will take effect 120 days after it is published in the federal register, and new noncompete agreements will be banned as of this date. However, existing contracts for senior executives will remain in effect because these individuals are less likely to experience “acute harm” due to their ability to negotiate accordingly, said Mr. Cady.
States, AMA Take Aim at Noncompetes
Before the federal ban, several states had already passed legislation limiting the reach of noncompetes. According to a recent article in the Journal of the American College of Cardiology, 12 states prohibit noncompete clauses for physicians: Alabama, California, Colorado, Delaware, Massachusetts, Montana, New Hampshire, New Mexico, North Dakota, Oklahoma, Rhode Island, and South Dakota.
The remaining states allow noncompetes in some form, often excluding them for employees earning below a certain threshold. For example, in Oregon, noncompete agreements may apply to employees earning more than $113,241. Most states have provisions to adjust the threshold annually. The District of Columbia permits 2-year noncompetes for “medical specialists” earning over $250,000 annually.
Indiana employers can no longer enter into noncompete agreements with primary care providers. Other specialties may be subject to the clauses, except when the physician terminates the contract for cause or when an employer terminates the contract without cause.
Rachel Marcus, MD, a cardiologist in Washington, DC, found out how limiting her employment contract’s noncompete clause was when she wanted to leave a former position. Due to the restrictions, she told this news organization that she couldn’t work locally for a competitor for 2 years. The closest location she could seek employment without violating the agreement was Baltimore, approximately 40 miles away.
Dr. Marcus ultimately moved to another position within the same organization because of the company’s reputation for being “aggressive” in their enforcement actions.
Although the American Medical Association (AMA) does not support a total ban, its House of Delegates adopted policies last year to support the prohibition of noncompete contracts for physicians employed by for-profit or nonprofit hospitals, hospital systems, or staffing companies.
Challenges Await
The American Hospital Association, which opposed the proposed rule, called it “bad policy.” The decision “will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities,” the association said in a statement.
To ease the transition to the new rule, the FTC also released a model language for employers to use when discussing the changes with their employees. “All employers need to do to comply with the rule is to stop enforcing existing noncompetes with workers other than senior executives and provide notice to such workers,” he said.
Dr. Marcus hopes the ban improves doctors’ lives. “Your employer is going to have to treat you better because they know that you can easily go across town to a place that has a higher salary, and your patient can go with you.”
A version of this article appeared on Medscape.com.
But business groups have vowed to challenge the decision in court.
The proposed final rule passed on a 3-2 vote, with the dissenting commissioners disputing the FTC’s authority to broadly ban noncompetes.
Tensions around noncompetes have been building for years. In 2021, President Biden issued an executive order supporting measures to improve economic competition, in which he urged the FTC to consider its rulemaking authority to address noncompete clauses that unfairly limit workers’ mobility. In January 2023, per that directive, the agency proposed ending the restrictive covenants.
While the FTC estimates that the final rule will reduce healthcare costs by up to $194 billion over the next decade and increase worker earnings by $300 million annually, the ruling faces legal hurdles.
US Chamber of Commerce president and CEO Suzanne P. Clark said in a statement that the move is a “blatant power grab” that will undermine competitive business practices, adding that the Chamber will sue to block the measure.
The FTC received more than 26,000 comments on noncompetes during the public feedback period, with about 25,000 supporting the measure, said Benjamin Cady, JD, an FTC attorney.
Mr. Cady called the feedback “compelling,” citing instances of workers who were forced to commute long distances, uproot their families, or risk expensive litigation for wanting to pursue job opportunities.
For example, a comment from a physician working in Appalachia highlights the potential real-life implications of the agreements. “With hospital systems merging, providers with aggressive noncompetes must abandon the community that they serve if they [choose] to leave their employer. Healthcare providers feel trapped in their current employment situation, leading to significant burnout that can shorten their [career] longevity.”
Commissioner Alvaro Bedoya said physicians have had their lives upended by cumbersome noncompetes, often having to move out of state to practice. “A pandemic killed a million people in this country, and there are doctors who cannot work because of a noncompete,” he said.
It’s unclear whether physicians and others who work for nonprofit healthcare groups or hospitals will be covered by the new ban. FTC Commissioner Rebecca Slaughter acknowledged that the agency’s jurisdictional limitations mean that employees of “certain nonprofit organizations” may not benefit from the rule.
“We want to be transparent about the limitation and recognize there are workers, especially healthcare workers, who are bound by anticompetitive and unfair noncompete clauses, that our rule will struggle to reach,” she said. To cover nonprofit healthcare employees, Ms. Slaughter urged Congress to pass legislation banning noncompetes, such as the Workforce Mobility Act of 2021 and the Freedom to Compete Act of 2023.
The FTC final rule will take effect 120 days after it is published in the federal register, and new noncompete agreements will be banned as of this date. However, existing contracts for senior executives will remain in effect because these individuals are less likely to experience “acute harm” due to their ability to negotiate accordingly, said Mr. Cady.
States, AMA Take Aim at Noncompetes
Before the federal ban, several states had already passed legislation limiting the reach of noncompetes. According to a recent article in the Journal of the American College of Cardiology, 12 states prohibit noncompete clauses for physicians: Alabama, California, Colorado, Delaware, Massachusetts, Montana, New Hampshire, New Mexico, North Dakota, Oklahoma, Rhode Island, and South Dakota.
The remaining states allow noncompetes in some form, often excluding them for employees earning below a certain threshold. For example, in Oregon, noncompete agreements may apply to employees earning more than $113,241. Most states have provisions to adjust the threshold annually. The District of Columbia permits 2-year noncompetes for “medical specialists” earning over $250,000 annually.
Indiana employers can no longer enter into noncompete agreements with primary care providers. Other specialties may be subject to the clauses, except when the physician terminates the contract for cause or when an employer terminates the contract without cause.
Rachel Marcus, MD, a cardiologist in Washington, DC, found out how limiting her employment contract’s noncompete clause was when she wanted to leave a former position. Due to the restrictions, she told this news organization that she couldn’t work locally for a competitor for 2 years. The closest location she could seek employment without violating the agreement was Baltimore, approximately 40 miles away.
Dr. Marcus ultimately moved to another position within the same organization because of the company’s reputation for being “aggressive” in their enforcement actions.
Although the American Medical Association (AMA) does not support a total ban, its House of Delegates adopted policies last year to support the prohibition of noncompete contracts for physicians employed by for-profit or nonprofit hospitals, hospital systems, or staffing companies.
Challenges Await
The American Hospital Association, which opposed the proposed rule, called it “bad policy.” The decision “will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities,” the association said in a statement.
To ease the transition to the new rule, the FTC also released a model language for employers to use when discussing the changes with their employees. “All employers need to do to comply with the rule is to stop enforcing existing noncompetes with workers other than senior executives and provide notice to such workers,” he said.
Dr. Marcus hopes the ban improves doctors’ lives. “Your employer is going to have to treat you better because they know that you can easily go across town to a place that has a higher salary, and your patient can go with you.”
A version of this article appeared on Medscape.com.
But business groups have vowed to challenge the decision in court.
The proposed final rule passed on a 3-2 vote, with the dissenting commissioners disputing the FTC’s authority to broadly ban noncompetes.
Tensions around noncompetes have been building for years. In 2021, President Biden issued an executive order supporting measures to improve economic competition, in which he urged the FTC to consider its rulemaking authority to address noncompete clauses that unfairly limit workers’ mobility. In January 2023, per that directive, the agency proposed ending the restrictive covenants.
While the FTC estimates that the final rule will reduce healthcare costs by up to $194 billion over the next decade and increase worker earnings by $300 million annually, the ruling faces legal hurdles.
US Chamber of Commerce president and CEO Suzanne P. Clark said in a statement that the move is a “blatant power grab” that will undermine competitive business practices, adding that the Chamber will sue to block the measure.
The FTC received more than 26,000 comments on noncompetes during the public feedback period, with about 25,000 supporting the measure, said Benjamin Cady, JD, an FTC attorney.
Mr. Cady called the feedback “compelling,” citing instances of workers who were forced to commute long distances, uproot their families, or risk expensive litigation for wanting to pursue job opportunities.
For example, a comment from a physician working in Appalachia highlights the potential real-life implications of the agreements. “With hospital systems merging, providers with aggressive noncompetes must abandon the community that they serve if they [choose] to leave their employer. Healthcare providers feel trapped in their current employment situation, leading to significant burnout that can shorten their [career] longevity.”
Commissioner Alvaro Bedoya said physicians have had their lives upended by cumbersome noncompetes, often having to move out of state to practice. “A pandemic killed a million people in this country, and there are doctors who cannot work because of a noncompete,” he said.
It’s unclear whether physicians and others who work for nonprofit healthcare groups or hospitals will be covered by the new ban. FTC Commissioner Rebecca Slaughter acknowledged that the agency’s jurisdictional limitations mean that employees of “certain nonprofit organizations” may not benefit from the rule.
“We want to be transparent about the limitation and recognize there are workers, especially healthcare workers, who are bound by anticompetitive and unfair noncompete clauses, that our rule will struggle to reach,” she said. To cover nonprofit healthcare employees, Ms. Slaughter urged Congress to pass legislation banning noncompetes, such as the Workforce Mobility Act of 2021 and the Freedom to Compete Act of 2023.
The FTC final rule will take effect 120 days after it is published in the federal register, and new noncompete agreements will be banned as of this date. However, existing contracts for senior executives will remain in effect because these individuals are less likely to experience “acute harm” due to their ability to negotiate accordingly, said Mr. Cady.
States, AMA Take Aim at Noncompetes
Before the federal ban, several states had already passed legislation limiting the reach of noncompetes. According to a recent article in the Journal of the American College of Cardiology, 12 states prohibit noncompete clauses for physicians: Alabama, California, Colorado, Delaware, Massachusetts, Montana, New Hampshire, New Mexico, North Dakota, Oklahoma, Rhode Island, and South Dakota.
The remaining states allow noncompetes in some form, often excluding them for employees earning below a certain threshold. For example, in Oregon, noncompete agreements may apply to employees earning more than $113,241. Most states have provisions to adjust the threshold annually. The District of Columbia permits 2-year noncompetes for “medical specialists” earning over $250,000 annually.
Indiana employers can no longer enter into noncompete agreements with primary care providers. Other specialties may be subject to the clauses, except when the physician terminates the contract for cause or when an employer terminates the contract without cause.
Rachel Marcus, MD, a cardiologist in Washington, DC, found out how limiting her employment contract’s noncompete clause was when she wanted to leave a former position. Due to the restrictions, she told this news organization that she couldn’t work locally for a competitor for 2 years. The closest location she could seek employment without violating the agreement was Baltimore, approximately 40 miles away.
Dr. Marcus ultimately moved to another position within the same organization because of the company’s reputation for being “aggressive” in their enforcement actions.
Although the American Medical Association (AMA) does not support a total ban, its House of Delegates adopted policies last year to support the prohibition of noncompete contracts for physicians employed by for-profit or nonprofit hospitals, hospital systems, or staffing companies.
Challenges Await
The American Hospital Association, which opposed the proposed rule, called it “bad policy.” The decision “will likely be short-lived, with courts almost certain to stop it before it can do damage to hospitals’ ability to care for their patients and communities,” the association said in a statement.
To ease the transition to the new rule, the FTC also released a model language for employers to use when discussing the changes with their employees. “All employers need to do to comply with the rule is to stop enforcing existing noncompetes with workers other than senior executives and provide notice to such workers,” he said.
Dr. Marcus hopes the ban improves doctors’ lives. “Your employer is going to have to treat you better because they know that you can easily go across town to a place that has a higher salary, and your patient can go with you.”
A version of this article appeared on Medscape.com.
Getting Patients With Opioid Use Disorder Started on Buprenorphine in Primary Care
*The first thing Ann Garment, MD, wants all clinicians to know about buprenorphine is that [where state law permits] any prescriber with a DEA registration number “is able to prescribe buprenorphine and should be ready and willing to prescribe” the medication.
*A change in federal law means that for most providers “there is no longer any extra paperwork or training required to prescribe buprenorphine,” said Dr. Garment, clinical associate professor at New York University and chief of general internal medicine at Bellevue Hospital in New York City, during a presentation on April 19 at the American College of Physicians (ACP-IM) Internal Medicine Meeting 2024.
Dr. Garment, who specializes in opioid use disorder (OUD), described the current “third wave” of increasing opioid overdose deaths fueled by the increase of synthetic opioids in the drug supply. The third wave started in 2013 with the rise in use of fentanyl and tramadol. The 107,000 number of overdose deaths in the United States in 2021 was more than six times that in 1999, and 75% involved opioids.
“Now, more than ever,” Dr. Garment said, “opioid use disorder should be treated from the primary care setting.”
How to Identify OUD
“It’s less sensitive for picking up on people who have a prior opioid use disorder history or are only exhibiting risky opioid use that wouldn’t constitute opioid use disorder yet,” she said.
If someone screens positive, to verify OUD, the Diagnostic and Statistical Manual of Mental Disorders identifies criteria for any substance abuse disorder with two general themes: Loss of control and continued use despite negative consequences.
“If you have a patient who is getting prescribed opioids and they have opioid tolerance or withdrawal, that does not mean they have opioid use disorder,” she said.
Medication for OUD
Medication is the top treatment for OUD, according to Dr. Garment. Psychosocial treatments can help some but not all people with OUD, she said. “It is not a requirement for a patient to engage in psychosocial treatment in order to get a medication for opioid use disorder, so please do not let that be a barrier for your patients,” she said.
Buprenorphine has advantages over other medications for OUD, including methadone and naltrexone.
Methadone must be obtained daily at a methadone clinic instead of at a local pharmacy. And escalating doses of methadone carry an increased risk for overdose and respiratory problems and potential drug-drug interactions, Dr. Garment added.
One downside with naltrexone is loss of tolerance, she said. If a patient has been using naltrexone to treat OUD and they decide to resume taking opioids, “they no longer can use the same amount of opioids that they were using before” because they have lost their tolerance and now are at a risk for overdose with their usual amount, she said. What’s more, naltrexone has not been shown to reduce overdose deaths.
Finally, she said, buprenorphine, “is an incredibly safe medication. If anyone in this room has ever prescribed coumadin or insulin, I’m going to tell you: This is much safer.”
Dr. Garment offered three reasons for buprenorphine’s safety:
- The drug is a partial, as opposed to full, opioid agonist, so as the dose increases, the patient experiences less withdrawal and fewer opioid cravings. As a result, they will hit a ceiling effect that avoids euphoria, respiratory depression, or overdose.
- Buprenorphine is “stickier” than other OUD medications: “If I’m taking buprenorphine and I decide to use some [oxycodone], what’s going to happen is that very little of that, if any, is going to get bound to my opioid receptors because buprenorphine is so sticky and adherent, it’s not going to let other opioids on.”
- Most buprenorphine is co-formulated with naloxone, an opioid antagonist. If a patient tries to get high from buprenorphine and tries to snort or inject it, naloxone will kick in and cancel out the buprenorphine.
Dr. Garment said she obtains urine screens ideally twice a year. If other drugs show up on the test, she said, she speaks with the patient about their drug use. “It’s never a reason to discharge someone from a practice,” she said.
Dr. Garment reported no relevant financial conflicts of interest.
*This story was updated on April 29, 2024.
A version of this article appeared on Medscape.com.
*The first thing Ann Garment, MD, wants all clinicians to know about buprenorphine is that [where state law permits] any prescriber with a DEA registration number “is able to prescribe buprenorphine and should be ready and willing to prescribe” the medication.
*A change in federal law means that for most providers “there is no longer any extra paperwork or training required to prescribe buprenorphine,” said Dr. Garment, clinical associate professor at New York University and chief of general internal medicine at Bellevue Hospital in New York City, during a presentation on April 19 at the American College of Physicians (ACP-IM) Internal Medicine Meeting 2024.
Dr. Garment, who specializes in opioid use disorder (OUD), described the current “third wave” of increasing opioid overdose deaths fueled by the increase of synthetic opioids in the drug supply. The third wave started in 2013 with the rise in use of fentanyl and tramadol. The 107,000 number of overdose deaths in the United States in 2021 was more than six times that in 1999, and 75% involved opioids.
“Now, more than ever,” Dr. Garment said, “opioid use disorder should be treated from the primary care setting.”
How to Identify OUD
“It’s less sensitive for picking up on people who have a prior opioid use disorder history or are only exhibiting risky opioid use that wouldn’t constitute opioid use disorder yet,” she said.
If someone screens positive, to verify OUD, the Diagnostic and Statistical Manual of Mental Disorders identifies criteria for any substance abuse disorder with two general themes: Loss of control and continued use despite negative consequences.
“If you have a patient who is getting prescribed opioids and they have opioid tolerance or withdrawal, that does not mean they have opioid use disorder,” she said.
Medication for OUD
Medication is the top treatment for OUD, according to Dr. Garment. Psychosocial treatments can help some but not all people with OUD, she said. “It is not a requirement for a patient to engage in psychosocial treatment in order to get a medication for opioid use disorder, so please do not let that be a barrier for your patients,” she said.
Buprenorphine has advantages over other medications for OUD, including methadone and naltrexone.
Methadone must be obtained daily at a methadone clinic instead of at a local pharmacy. And escalating doses of methadone carry an increased risk for overdose and respiratory problems and potential drug-drug interactions, Dr. Garment added.
One downside with naltrexone is loss of tolerance, she said. If a patient has been using naltrexone to treat OUD and they decide to resume taking opioids, “they no longer can use the same amount of opioids that they were using before” because they have lost their tolerance and now are at a risk for overdose with their usual amount, she said. What’s more, naltrexone has not been shown to reduce overdose deaths.
Finally, she said, buprenorphine, “is an incredibly safe medication. If anyone in this room has ever prescribed coumadin or insulin, I’m going to tell you: This is much safer.”
Dr. Garment offered three reasons for buprenorphine’s safety:
- The drug is a partial, as opposed to full, opioid agonist, so as the dose increases, the patient experiences less withdrawal and fewer opioid cravings. As a result, they will hit a ceiling effect that avoids euphoria, respiratory depression, or overdose.
- Buprenorphine is “stickier” than other OUD medications: “If I’m taking buprenorphine and I decide to use some [oxycodone], what’s going to happen is that very little of that, if any, is going to get bound to my opioid receptors because buprenorphine is so sticky and adherent, it’s not going to let other opioids on.”
- Most buprenorphine is co-formulated with naloxone, an opioid antagonist. If a patient tries to get high from buprenorphine and tries to snort or inject it, naloxone will kick in and cancel out the buprenorphine.
Dr. Garment said she obtains urine screens ideally twice a year. If other drugs show up on the test, she said, she speaks with the patient about their drug use. “It’s never a reason to discharge someone from a practice,” she said.
Dr. Garment reported no relevant financial conflicts of interest.
*This story was updated on April 29, 2024.
A version of this article appeared on Medscape.com.
*The first thing Ann Garment, MD, wants all clinicians to know about buprenorphine is that [where state law permits] any prescriber with a DEA registration number “is able to prescribe buprenorphine and should be ready and willing to prescribe” the medication.
*A change in federal law means that for most providers “there is no longer any extra paperwork or training required to prescribe buprenorphine,” said Dr. Garment, clinical associate professor at New York University and chief of general internal medicine at Bellevue Hospital in New York City, during a presentation on April 19 at the American College of Physicians (ACP-IM) Internal Medicine Meeting 2024.
Dr. Garment, who specializes in opioid use disorder (OUD), described the current “third wave” of increasing opioid overdose deaths fueled by the increase of synthetic opioids in the drug supply. The third wave started in 2013 with the rise in use of fentanyl and tramadol. The 107,000 number of overdose deaths in the United States in 2021 was more than six times that in 1999, and 75% involved opioids.
“Now, more than ever,” Dr. Garment said, “opioid use disorder should be treated from the primary care setting.”
How to Identify OUD
“It’s less sensitive for picking up on people who have a prior opioid use disorder history or are only exhibiting risky opioid use that wouldn’t constitute opioid use disorder yet,” she said.
If someone screens positive, to verify OUD, the Diagnostic and Statistical Manual of Mental Disorders identifies criteria for any substance abuse disorder with two general themes: Loss of control and continued use despite negative consequences.
“If you have a patient who is getting prescribed opioids and they have opioid tolerance or withdrawal, that does not mean they have opioid use disorder,” she said.
Medication for OUD
Medication is the top treatment for OUD, according to Dr. Garment. Psychosocial treatments can help some but not all people with OUD, she said. “It is not a requirement for a patient to engage in psychosocial treatment in order to get a medication for opioid use disorder, so please do not let that be a barrier for your patients,” she said.
Buprenorphine has advantages over other medications for OUD, including methadone and naltrexone.
Methadone must be obtained daily at a methadone clinic instead of at a local pharmacy. And escalating doses of methadone carry an increased risk for overdose and respiratory problems and potential drug-drug interactions, Dr. Garment added.
One downside with naltrexone is loss of tolerance, she said. If a patient has been using naltrexone to treat OUD and they decide to resume taking opioids, “they no longer can use the same amount of opioids that they were using before” because they have lost their tolerance and now are at a risk for overdose with their usual amount, she said. What’s more, naltrexone has not been shown to reduce overdose deaths.
Finally, she said, buprenorphine, “is an incredibly safe medication. If anyone in this room has ever prescribed coumadin or insulin, I’m going to tell you: This is much safer.”
Dr. Garment offered three reasons for buprenorphine’s safety:
- The drug is a partial, as opposed to full, opioid agonist, so as the dose increases, the patient experiences less withdrawal and fewer opioid cravings. As a result, they will hit a ceiling effect that avoids euphoria, respiratory depression, or overdose.
- Buprenorphine is “stickier” than other OUD medications: “If I’m taking buprenorphine and I decide to use some [oxycodone], what’s going to happen is that very little of that, if any, is going to get bound to my opioid receptors because buprenorphine is so sticky and adherent, it’s not going to let other opioids on.”
- Most buprenorphine is co-formulated with naloxone, an opioid antagonist. If a patient tries to get high from buprenorphine and tries to snort or inject it, naloxone will kick in and cancel out the buprenorphine.
Dr. Garment said she obtains urine screens ideally twice a year. If other drugs show up on the test, she said, she speaks with the patient about their drug use. “It’s never a reason to discharge someone from a practice,” she said.
Dr. Garment reported no relevant financial conflicts of interest.
*This story was updated on April 29, 2024.
A version of this article appeared on Medscape.com.
Are Women Better Doctors Than Men?
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.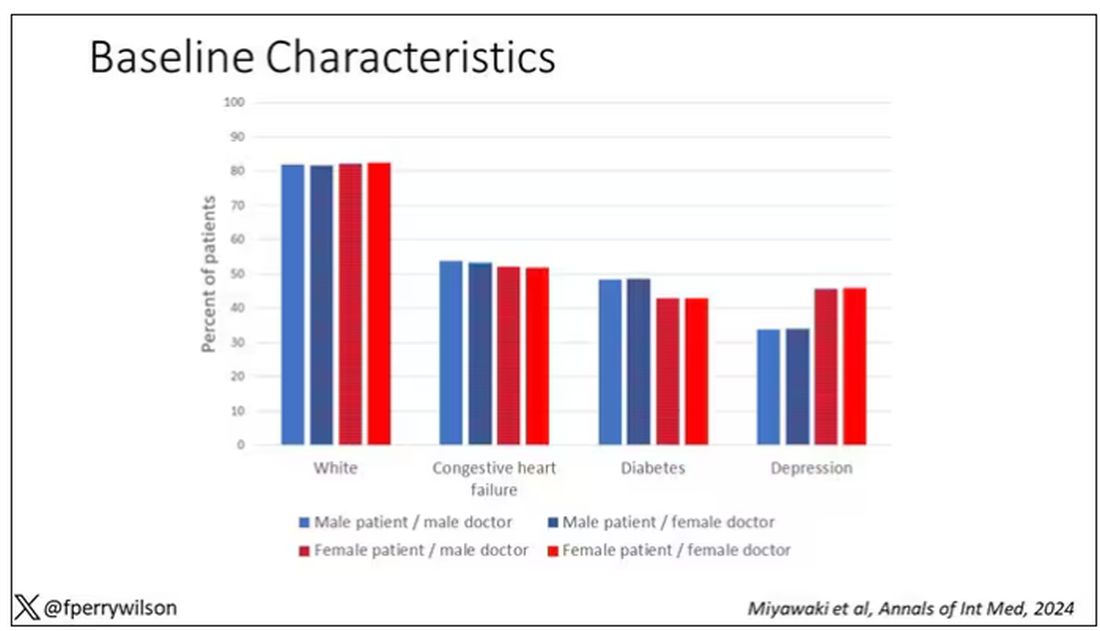
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here. 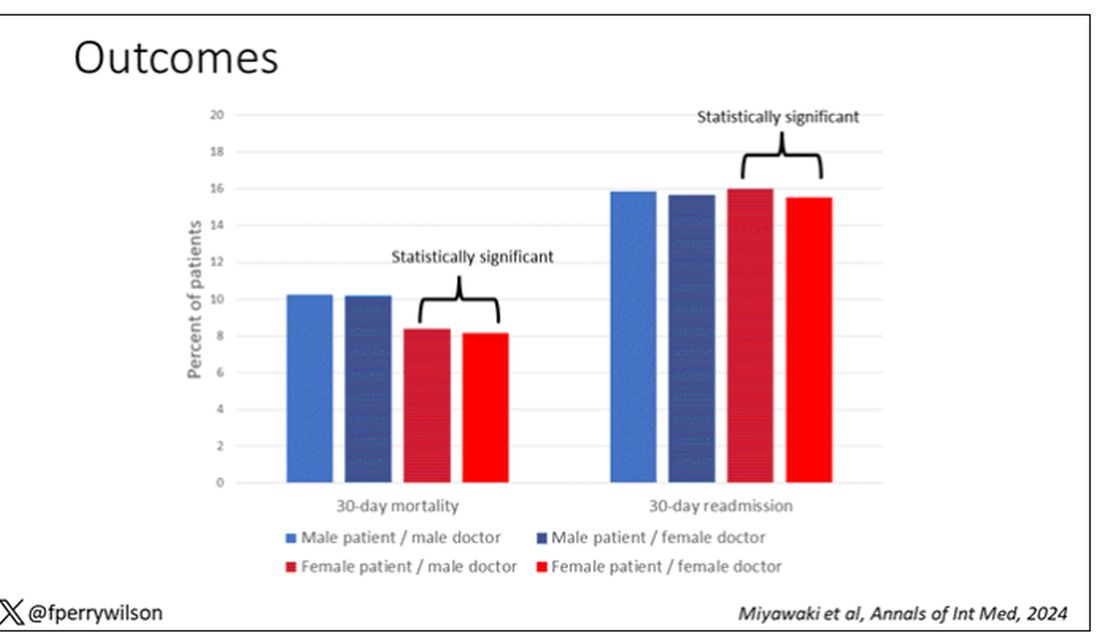
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here.
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s a battle of the sexes today as we dive into a paper that makes you say, “Wow, what an interesting study” and also “Boy, am I glad I didn’t do that study.” That’s because studies like this are always somewhat fraught; they say something about medicine but also something about society — and that makes this a bit precarious. But that’s never stopped us before. So, let’s go ahead and try to answer the question: Do women make better doctors than men?
On the surface, this question seems nearly impossible to answer. It’s too broad; what does it mean to be a “better” doctor? At first blush it seems that there are just too many variables to control for here: the type of doctor, the type of patient, the clinical scenario, and so on.
But this study, “Comparison of hospital mortality and readmission rates by physician and patient sex,” which appears in Annals of Internal Medicine, uses a fairly ingenious method to cut through all the bias by leveraging two simple facts: First, hospital medicine is largely conducted by hospitalists these days; second, due to the shift-based nature of hospitalist work, the hospitalist you get when you are admitted to the hospital is pretty much random.
In other words, if you are admitted to the hospital for an acute illness and get a hospitalist as your attending, you have no control over whether it is a man or a woman. Is this a randomized trial? No, but it’s not bad.
Researchers used Medicare claims data to identify adults over age 65 who had nonelective hospital admissions throughout the United States. The claims revealed the sex of the patient and the name of the attending physician. By linking to a medical provider database, they could determine the sex of the provider.
The goal was to look at outcomes across four dyads:
- Male patient – male doctor
- Male patient – female doctor
- Female patient – male doctor
- Female patient – female doctor
The primary outcome was 30-day mortality.
I told you that focusing on hospitalists produces some pseudorandomization, but let’s look at the data to be sure. Just under a million patients were treated by approximately 50,000 physicians, 30% of whom were female. And, though female patients and male patients differed, they did not differ with respect to the sex of their hospitalist. So, by physician sex, patients were similar in mean age, race, ethnicity, household income, eligibility for Medicaid, and comorbid conditions. The authors even created a “predicted mortality” score which was similar across the groups as well.
Now, the female physicians were a bit different from the male physicians. The female hospitalists were slightly more likely to have an osteopathic degree, had slightly fewer admissions per year, and were a bit younger.
So, we have broadly similar patients regardless of who their hospitalist was, but hospitalists differ by factors other than their sex. Fine.
I’ve graphed the results here.
This is a relatively small effect, to be sure, but if you multiply it across the millions of hospitalist admissions per year, you can start to put up some real numbers.
So, what is going on here? I see four broad buckets of possibilities.
Let’s start with the obvious explanation: Women, on average, are better doctors than men. I am married to a woman doctor, and based on my personal experience, this explanation is undoubtedly true. But why would that be?
The authors cite data that suggest that female physicians are less likely than male physicians to dismiss patient concerns — and in particular, the concerns of female patients — perhaps leading to fewer missed diagnoses. But this is impossible to measure with administrative data, so this study can no more tell us whether these female hospitalists are more attentive than their male counterparts than it can suggest that the benefit is mediated by the shorter average height of female physicians. Perhaps the key is being closer to the patient?
The second possibility here is that this has nothing to do with the sex of the physician at all; it has to do with those other things that associate with the sex of the physician. We know, for example, that the female physicians saw fewer patients per year than the male physicians, but the study authors adjusted for this in the statistical models. Still, other unmeasured factors (confounders) could be present. By the way, confounders wouldn’t necessarily change the primary finding — you are better off being cared for by female physicians. It’s just not because they are female; it’s a convenient marker for some other quality, such as age.
The third possibility is that the study represents a phenomenon called collider bias. The idea here is that physicians only get into the study if they are hospitalists, and the quality of physicians who choose to become a hospitalist may differ by sex. When deciding on a specialty, a talented resident considering certain lifestyle issues may find hospital medicine particularly attractive — and that draw toward a more lifestyle-friendly specialty may differ by sex, as some prior studies have shown. If true, the pool of women hospitalists may be better than their male counterparts because male physicians of that caliber don’t become hospitalists.
Okay, don’t write in. I’m just trying to cite examples of how to think about collider bias. I can’t prove that this is the case, and in fact the authors do a sensitivity analysis of all physicians, not just hospitalists, and show the same thing. So this is probably not true, but epidemiology is fun, right?
And the fourth possibility: This is nothing but statistical noise. The effect size is incredibly small and just on the border of statistical significance. Especially when you’re working with very large datasets like this, you’ve got to be really careful about overinterpreting statistically significant findings that are nevertheless of small magnitude.
Regardless, it’s an interesting study, one that made me think and, of course, worry a bit about how I would present it. Forgive me if I’ve been indelicate in handling the complex issues of sex, gender, and society here. But I’m not sure what you expect; after all, I’m only a male doctor.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Avoidance Predicts Worse Long-term Outcomes From Intensive OCD Treatment
BOSTON — , a new analysis shows.
Although avoidant patients with OCD reported symptom improvement immediately after treatment, baseline avoidance was associated with significantly worse outcomes 1 year later.
“Avoidance is often overlooked in OCD,” said lead investigator Michael Wheaton, PhD, an assistant professor of psychology at Barnard College in New York. “It’s really important clinically to focus on that.”
The findings were presented at the Anxiety and Depression Association of America (ADAA) annual conference and published online in the Journal of Obsessive-Compulsive and Related Disorders.
The Avoidance Question
Although ERP is often included in treatment for OCD, between 38% and 60% of patients have residual symptoms after treatment and as many as a quarter don’t respond at all, Dr. Wheaton said.
Severe pretreatment avoidance could affect the efficacy of ERP, which involves exposing patients to situations and stimuli they may usually avoid. But prior research to identify predictors of ERP outcomes have largely excluded severity of pretreatment avoidance as a factor.
The new study analyzed data from 161 Norwegian adults with treatment-resistant OCD who participated in a concentrated ERP therapy called the Bergen 4-day Exposure and Response Prevention (B4DT) treatment. This method delivers intensive treatment over 4 consecutive days in small groups with a 1:1 ratio of therapists to patients.
B4DT is common throughout Norway, with the treatment offered at 55 clinics, and has been trialed in other countries including the United States, Nepal, Ecuador, and Kenya.
Symptom severity was measured using the Yale-Brown Obsessive Compulsive Scale (YBOCS) at baseline, immediately after treatment, and 3 and 12 months later. Functional impairment was measured 12 months after treatment using the Work and Social Adjustment Scale.
Although the formal scoring of the YBOCS does not include any questions about avoidance, one question in the auxiliary items does: “Have you been avoiding doing anything, going anyplace or being with anyone because of obsessional thoughts or out of a need to perform compulsions?”
Dr. Wheaton used this response, which is rated on a five-point scale, to measure avoidance. Overall, 18.8% of participants had no deliberate avoidance, 15% were rated as having mild avoidance, 36% moderate, 23% severe, and 6.8% extreme.
Long-Term Outcomes
Overall, 84% of participants responded to treatment, with a change in mean YBOCS scores from 26.98 at baseline to 12.28 immediately after treatment. Acute outcomes were similar between avoidant and nonavoidant patients.
But at 12-month follow-up, even after controlling for pretreatment OCD severity, patients with more extensive avoidance at baseline had worse long-term outcomes — both more severe OCD symptoms (P = .031) and greater functional impairment (P = .002).
Across all patients, average avoidance decreased significantly immediately after the concentrated ERP treatment. Average avoidance increased somewhat at 3- and 12-month follow-up but remained significantly improved from pretreatment.
Interestingly, patients’ change in avoidance immediately post-treatment to 3 months post-treatment predicted worsening of OCD severity at 12 months. This change could potentially identify people at risk of relapse, Dr. Wheaton said.
Previous research has shown that pretreatment OCD severity, measured using the YBOCS, does not significantly predict ERP outcomes, and this study found the same.
Relapse Prevention
“The fact that they did equally well in the short run I think was great,” Dr. Wheaton said.
Previous research, including 2018 and 2023 papers from Wheaton’s team, has shown that more avoidant patients have worse outcomes from standard 12-week ERP programs.
One possible explanation for this difference is that in the Bergen treatment, most exposures happen during face-to-face time with a therapist instead of as homework, which may be easier to avoid, he said.
“But then the finding was that their symptoms were worsening over time — their avoidance was sliding back into old habits,” said Dr. Wheaton.
He would like to see the study replicated in diverse populations outside Norway and in treatment-naive people. Dr. Wheaton also noted that the study assessed avoidance with only a single item.
Future work is needed to test ways to improve relapse prevention. For example, clinicians may be able to monitor for avoidance behaviors post-treatment, which could be the start of a relapse, said Dr. Wheaton.
Although clinicians consider avoidance when treating phobias, social anxiety disorder, and panic disorder, “somehow avoidance got relegated to item 11 on the YBOCS that isn’t scored,” Helen Blair Simpson, MD, PhD, director of the Center for OCD and Related Disorders at Columbia University, New York, New York, said during the presentation.
A direct implication of Dr. Wheaton’s findings to clinical practice is to “talk to people about their avoidance right up front,” said Dr. Simpson, who was not part of the study.
Clinicians who deliver ERP in their practices “can apply this tomorrow,” Dr. Simpson added.
Dr. Wheaton reported no disclosures. Dr. Simpson reported a stipend from the American Medical Association for serving as associate editor of JAMA Psychiatry and royalties from UpToDate, Inc for articles on OCD and from Cambridge University Press for editing a book on anxiety disorders.
A version of this article appeared on Medscape.com.
BOSTON — , a new analysis shows.
Although avoidant patients with OCD reported symptom improvement immediately after treatment, baseline avoidance was associated with significantly worse outcomes 1 year later.
“Avoidance is often overlooked in OCD,” said lead investigator Michael Wheaton, PhD, an assistant professor of psychology at Barnard College in New York. “It’s really important clinically to focus on that.”
The findings were presented at the Anxiety and Depression Association of America (ADAA) annual conference and published online in the Journal of Obsessive-Compulsive and Related Disorders.
The Avoidance Question
Although ERP is often included in treatment for OCD, between 38% and 60% of patients have residual symptoms after treatment and as many as a quarter don’t respond at all, Dr. Wheaton said.
Severe pretreatment avoidance could affect the efficacy of ERP, which involves exposing patients to situations and stimuli they may usually avoid. But prior research to identify predictors of ERP outcomes have largely excluded severity of pretreatment avoidance as a factor.
The new study analyzed data from 161 Norwegian adults with treatment-resistant OCD who participated in a concentrated ERP therapy called the Bergen 4-day Exposure and Response Prevention (B4DT) treatment. This method delivers intensive treatment over 4 consecutive days in small groups with a 1:1 ratio of therapists to patients.
B4DT is common throughout Norway, with the treatment offered at 55 clinics, and has been trialed in other countries including the United States, Nepal, Ecuador, and Kenya.
Symptom severity was measured using the Yale-Brown Obsessive Compulsive Scale (YBOCS) at baseline, immediately after treatment, and 3 and 12 months later. Functional impairment was measured 12 months after treatment using the Work and Social Adjustment Scale.
Although the formal scoring of the YBOCS does not include any questions about avoidance, one question in the auxiliary items does: “Have you been avoiding doing anything, going anyplace or being with anyone because of obsessional thoughts or out of a need to perform compulsions?”
Dr. Wheaton used this response, which is rated on a five-point scale, to measure avoidance. Overall, 18.8% of participants had no deliberate avoidance, 15% were rated as having mild avoidance, 36% moderate, 23% severe, and 6.8% extreme.
Long-Term Outcomes
Overall, 84% of participants responded to treatment, with a change in mean YBOCS scores from 26.98 at baseline to 12.28 immediately after treatment. Acute outcomes were similar between avoidant and nonavoidant patients.
But at 12-month follow-up, even after controlling for pretreatment OCD severity, patients with more extensive avoidance at baseline had worse long-term outcomes — both more severe OCD symptoms (P = .031) and greater functional impairment (P = .002).
Across all patients, average avoidance decreased significantly immediately after the concentrated ERP treatment. Average avoidance increased somewhat at 3- and 12-month follow-up but remained significantly improved from pretreatment.
Interestingly, patients’ change in avoidance immediately post-treatment to 3 months post-treatment predicted worsening of OCD severity at 12 months. This change could potentially identify people at risk of relapse, Dr. Wheaton said.
Previous research has shown that pretreatment OCD severity, measured using the YBOCS, does not significantly predict ERP outcomes, and this study found the same.
Relapse Prevention
“The fact that they did equally well in the short run I think was great,” Dr. Wheaton said.
Previous research, including 2018 and 2023 papers from Wheaton’s team, has shown that more avoidant patients have worse outcomes from standard 12-week ERP programs.
One possible explanation for this difference is that in the Bergen treatment, most exposures happen during face-to-face time with a therapist instead of as homework, which may be easier to avoid, he said.
“But then the finding was that their symptoms were worsening over time — their avoidance was sliding back into old habits,” said Dr. Wheaton.
He would like to see the study replicated in diverse populations outside Norway and in treatment-naive people. Dr. Wheaton also noted that the study assessed avoidance with only a single item.
Future work is needed to test ways to improve relapse prevention. For example, clinicians may be able to monitor for avoidance behaviors post-treatment, which could be the start of a relapse, said Dr. Wheaton.
Although clinicians consider avoidance when treating phobias, social anxiety disorder, and panic disorder, “somehow avoidance got relegated to item 11 on the YBOCS that isn’t scored,” Helen Blair Simpson, MD, PhD, director of the Center for OCD and Related Disorders at Columbia University, New York, New York, said during the presentation.
A direct implication of Dr. Wheaton’s findings to clinical practice is to “talk to people about their avoidance right up front,” said Dr. Simpson, who was not part of the study.
Clinicians who deliver ERP in their practices “can apply this tomorrow,” Dr. Simpson added.
Dr. Wheaton reported no disclosures. Dr. Simpson reported a stipend from the American Medical Association for serving as associate editor of JAMA Psychiatry and royalties from UpToDate, Inc for articles on OCD and from Cambridge University Press for editing a book on anxiety disorders.
A version of this article appeared on Medscape.com.
BOSTON — , a new analysis shows.
Although avoidant patients with OCD reported symptom improvement immediately after treatment, baseline avoidance was associated with significantly worse outcomes 1 year later.
“Avoidance is often overlooked in OCD,” said lead investigator Michael Wheaton, PhD, an assistant professor of psychology at Barnard College in New York. “It’s really important clinically to focus on that.”
The findings were presented at the Anxiety and Depression Association of America (ADAA) annual conference and published online in the Journal of Obsessive-Compulsive and Related Disorders.
The Avoidance Question
Although ERP is often included in treatment for OCD, between 38% and 60% of patients have residual symptoms after treatment and as many as a quarter don’t respond at all, Dr. Wheaton said.
Severe pretreatment avoidance could affect the efficacy of ERP, which involves exposing patients to situations and stimuli they may usually avoid. But prior research to identify predictors of ERP outcomes have largely excluded severity of pretreatment avoidance as a factor.
The new study analyzed data from 161 Norwegian adults with treatment-resistant OCD who participated in a concentrated ERP therapy called the Bergen 4-day Exposure and Response Prevention (B4DT) treatment. This method delivers intensive treatment over 4 consecutive days in small groups with a 1:1 ratio of therapists to patients.
B4DT is common throughout Norway, with the treatment offered at 55 clinics, and has been trialed in other countries including the United States, Nepal, Ecuador, and Kenya.
Symptom severity was measured using the Yale-Brown Obsessive Compulsive Scale (YBOCS) at baseline, immediately after treatment, and 3 and 12 months later. Functional impairment was measured 12 months after treatment using the Work and Social Adjustment Scale.
Although the formal scoring of the YBOCS does not include any questions about avoidance, one question in the auxiliary items does: “Have you been avoiding doing anything, going anyplace or being with anyone because of obsessional thoughts or out of a need to perform compulsions?”
Dr. Wheaton used this response, which is rated on a five-point scale, to measure avoidance. Overall, 18.8% of participants had no deliberate avoidance, 15% were rated as having mild avoidance, 36% moderate, 23% severe, and 6.8% extreme.
Long-Term Outcomes
Overall, 84% of participants responded to treatment, with a change in mean YBOCS scores from 26.98 at baseline to 12.28 immediately after treatment. Acute outcomes were similar between avoidant and nonavoidant patients.
But at 12-month follow-up, even after controlling for pretreatment OCD severity, patients with more extensive avoidance at baseline had worse long-term outcomes — both more severe OCD symptoms (P = .031) and greater functional impairment (P = .002).
Across all patients, average avoidance decreased significantly immediately after the concentrated ERP treatment. Average avoidance increased somewhat at 3- and 12-month follow-up but remained significantly improved from pretreatment.
Interestingly, patients’ change in avoidance immediately post-treatment to 3 months post-treatment predicted worsening of OCD severity at 12 months. This change could potentially identify people at risk of relapse, Dr. Wheaton said.
Previous research has shown that pretreatment OCD severity, measured using the YBOCS, does not significantly predict ERP outcomes, and this study found the same.
Relapse Prevention
“The fact that they did equally well in the short run I think was great,” Dr. Wheaton said.
Previous research, including 2018 and 2023 papers from Wheaton’s team, has shown that more avoidant patients have worse outcomes from standard 12-week ERP programs.
One possible explanation for this difference is that in the Bergen treatment, most exposures happen during face-to-face time with a therapist instead of as homework, which may be easier to avoid, he said.
“But then the finding was that their symptoms were worsening over time — their avoidance was sliding back into old habits,” said Dr. Wheaton.
He would like to see the study replicated in diverse populations outside Norway and in treatment-naive people. Dr. Wheaton also noted that the study assessed avoidance with only a single item.
Future work is needed to test ways to improve relapse prevention. For example, clinicians may be able to monitor for avoidance behaviors post-treatment, which could be the start of a relapse, said Dr. Wheaton.
Although clinicians consider avoidance when treating phobias, social anxiety disorder, and panic disorder, “somehow avoidance got relegated to item 11 on the YBOCS that isn’t scored,” Helen Blair Simpson, MD, PhD, director of the Center for OCD and Related Disorders at Columbia University, New York, New York, said during the presentation.
A direct implication of Dr. Wheaton’s findings to clinical practice is to “talk to people about their avoidance right up front,” said Dr. Simpson, who was not part of the study.
Clinicians who deliver ERP in their practices “can apply this tomorrow,” Dr. Simpson added.
Dr. Wheaton reported no disclosures. Dr. Simpson reported a stipend from the American Medical Association for serving as associate editor of JAMA Psychiatry and royalties from UpToDate, Inc for articles on OCD and from Cambridge University Press for editing a book on anxiety disorders.
A version of this article appeared on Medscape.com.
FROM ADAA 2024
GLP-1 Receptor Agonists: Which Drug for Which Patient?
With all the excitement about GLP-1 agonists,
Of course, we want to make sure that we’re treating the right condition. If the patient has type 2 diabetes, we tend to give them medication that is indicated for type 2 diabetes. Many GLP-1 agonists are available in a diabetes version and a chronic weight management or obesity version. If a patient has diabetes and obesity, they can receive either one. If a patient has only diabetes but not obesity, they should be prescribed the diabetes version. For obesity without diabetes, we tend to stick with the drugs that are indicated for chronic weight management.
Let’s go through them.
Exenatide. In chronological order of approval, the first GLP-1 drug that was used for diabetes dates back to exenatide (Bydureon). Bydureon had a partner called Byetta (also exenatide), both of which are still on the market but infrequently used. Some patients reported that these medications were inconvenient because they required twice-daily injections and caused painful injection-site nodules.
Diabetes drugs in more common use include liraglutide (Victoza) for type 2 diabetes. It is a daily injection and has various doses. We always start low and increase with tolerance and desired effect for A1c.
Liraglutide. Victoza has an antiobesity counterpart called Saxenda. The Saxenda pen looks very similar to the Victoza pen. It is a daily GLP-1 agonist for chronic weight management. The SCALE trial demonstrated 8%-12% weight loss with Saxenda.
Those are the daily injections: Victoza for diabetes and Saxenda for weight loss.
Our patients are very excited about the advent of weekly injections for diabetes and weight management. Ozempic is very popular. It is a weekly GLP-1 agonist for type 2 diabetes. Many patients come in asking for Ozempic, and we must make sure that we’re moving them in the right direction depending on their condition.
Semaglutide. Ozempic has a few different doses. It is a weekly injection and has been found to be quite efficacious for treating diabetes. The drug’s weight loss counterpart is called Wegovy, which comes in a different pen. Both forms contain the compound semaglutide. While all of these GLP-1 agonists are indicated to treat type 2 diabetes or for weight management, Wegovy has a special indication that none of the others have. In March 2024, Wegovy acquired an indication to decrease cardiac risk in those with a BMI ≥ 27 and a previous cardiac history. This will really change the accessibility of this medication because patients with heart conditions who are on Medicare are expected to have access to Wegovy.
Tirzepatide. Another weekly injection for treatment of type 2 diabetes is called Mounjaro. Its counterpart for weight management is called Zepbound, which was found to have about 20.9% weight loss over 72 weeks. These medications have similar side effects in differing degrees, but the most-often reported are nausea, stool changes, abdominal pain, and reflux. There are some other potential side effects; I recommend that you read the individual prescribing information available for each drug to have more clarity about that.
It is important that we stay on label for using the GLP-1 receptor agonists, for many reasons. One, it increases our patients’ accessibility to the right medication for them, and we can also make sure that we’re treating the patient with the right drug according to the clinical trials. When the clinical trials are done, the study populations demonstrate safety and efficacy for that population. But if we’re prescribing a GLP-1 for a different population, it is considered off-label use.
Dr. Lofton, an obesity medicine specialist, is clinical associate professor of surgery and medicine at NYU Grossman School of Medicine, and director of the medical weight management program at NYU Langone Weight Management Center, New York. She disclosed ties to Novo Nordisk and Eli Lilly. This transcript has been edited for clarity.
A version of this article appeared on Medscape.com.
With all the excitement about GLP-1 agonists,
Of course, we want to make sure that we’re treating the right condition. If the patient has type 2 diabetes, we tend to give them medication that is indicated for type 2 diabetes. Many GLP-1 agonists are available in a diabetes version and a chronic weight management or obesity version. If a patient has diabetes and obesity, they can receive either one. If a patient has only diabetes but not obesity, they should be prescribed the diabetes version. For obesity without diabetes, we tend to stick with the drugs that are indicated for chronic weight management.
Let’s go through them.
Exenatide. In chronological order of approval, the first GLP-1 drug that was used for diabetes dates back to exenatide (Bydureon). Bydureon had a partner called Byetta (also exenatide), both of which are still on the market but infrequently used. Some patients reported that these medications were inconvenient because they required twice-daily injections and caused painful injection-site nodules.
Diabetes drugs in more common use include liraglutide (Victoza) for type 2 diabetes. It is a daily injection and has various doses. We always start low and increase with tolerance and desired effect for A1c.
Liraglutide. Victoza has an antiobesity counterpart called Saxenda. The Saxenda pen looks very similar to the Victoza pen. It is a daily GLP-1 agonist for chronic weight management. The SCALE trial demonstrated 8%-12% weight loss with Saxenda.
Those are the daily injections: Victoza for diabetes and Saxenda for weight loss.
Our patients are very excited about the advent of weekly injections for diabetes and weight management. Ozempic is very popular. It is a weekly GLP-1 agonist for type 2 diabetes. Many patients come in asking for Ozempic, and we must make sure that we’re moving them in the right direction depending on their condition.
Semaglutide. Ozempic has a few different doses. It is a weekly injection and has been found to be quite efficacious for treating diabetes. The drug’s weight loss counterpart is called Wegovy, which comes in a different pen. Both forms contain the compound semaglutide. While all of these GLP-1 agonists are indicated to treat type 2 diabetes or for weight management, Wegovy has a special indication that none of the others have. In March 2024, Wegovy acquired an indication to decrease cardiac risk in those with a BMI ≥ 27 and a previous cardiac history. This will really change the accessibility of this medication because patients with heart conditions who are on Medicare are expected to have access to Wegovy.
Tirzepatide. Another weekly injection for treatment of type 2 diabetes is called Mounjaro. Its counterpart for weight management is called Zepbound, which was found to have about 20.9% weight loss over 72 weeks. These medications have similar side effects in differing degrees, but the most-often reported are nausea, stool changes, abdominal pain, and reflux. There are some other potential side effects; I recommend that you read the individual prescribing information available for each drug to have more clarity about that.
It is important that we stay on label for using the GLP-1 receptor agonists, for many reasons. One, it increases our patients’ accessibility to the right medication for them, and we can also make sure that we’re treating the patient with the right drug according to the clinical trials. When the clinical trials are done, the study populations demonstrate safety and efficacy for that population. But if we’re prescribing a GLP-1 for a different population, it is considered off-label use.
Dr. Lofton, an obesity medicine specialist, is clinical associate professor of surgery and medicine at NYU Grossman School of Medicine, and director of the medical weight management program at NYU Langone Weight Management Center, New York. She disclosed ties to Novo Nordisk and Eli Lilly. This transcript has been edited for clarity.
A version of this article appeared on Medscape.com.
With all the excitement about GLP-1 agonists,
Of course, we want to make sure that we’re treating the right condition. If the patient has type 2 diabetes, we tend to give them medication that is indicated for type 2 diabetes. Many GLP-1 agonists are available in a diabetes version and a chronic weight management or obesity version. If a patient has diabetes and obesity, they can receive either one. If a patient has only diabetes but not obesity, they should be prescribed the diabetes version. For obesity without diabetes, we tend to stick with the drugs that are indicated for chronic weight management.
Let’s go through them.
Exenatide. In chronological order of approval, the first GLP-1 drug that was used for diabetes dates back to exenatide (Bydureon). Bydureon had a partner called Byetta (also exenatide), both of which are still on the market but infrequently used. Some patients reported that these medications were inconvenient because they required twice-daily injections and caused painful injection-site nodules.
Diabetes drugs in more common use include liraglutide (Victoza) for type 2 diabetes. It is a daily injection and has various doses. We always start low and increase with tolerance and desired effect for A1c.
Liraglutide. Victoza has an antiobesity counterpart called Saxenda. The Saxenda pen looks very similar to the Victoza pen. It is a daily GLP-1 agonist for chronic weight management. The SCALE trial demonstrated 8%-12% weight loss with Saxenda.
Those are the daily injections: Victoza for diabetes and Saxenda for weight loss.
Our patients are very excited about the advent of weekly injections for diabetes and weight management. Ozempic is very popular. It is a weekly GLP-1 agonist for type 2 diabetes. Many patients come in asking for Ozempic, and we must make sure that we’re moving them in the right direction depending on their condition.
Semaglutide. Ozempic has a few different doses. It is a weekly injection and has been found to be quite efficacious for treating diabetes. The drug’s weight loss counterpart is called Wegovy, which comes in a different pen. Both forms contain the compound semaglutide. While all of these GLP-1 agonists are indicated to treat type 2 diabetes or for weight management, Wegovy has a special indication that none of the others have. In March 2024, Wegovy acquired an indication to decrease cardiac risk in those with a BMI ≥ 27 and a previous cardiac history. This will really change the accessibility of this medication because patients with heart conditions who are on Medicare are expected to have access to Wegovy.
Tirzepatide. Another weekly injection for treatment of type 2 diabetes is called Mounjaro. Its counterpart for weight management is called Zepbound, which was found to have about 20.9% weight loss over 72 weeks. These medications have similar side effects in differing degrees, but the most-often reported are nausea, stool changes, abdominal pain, and reflux. There are some other potential side effects; I recommend that you read the individual prescribing information available for each drug to have more clarity about that.
It is important that we stay on label for using the GLP-1 receptor agonists, for many reasons. One, it increases our patients’ accessibility to the right medication for them, and we can also make sure that we’re treating the patient with the right drug according to the clinical trials. When the clinical trials are done, the study populations demonstrate safety and efficacy for that population. But if we’re prescribing a GLP-1 for a different population, it is considered off-label use.
Dr. Lofton, an obesity medicine specialist, is clinical associate professor of surgery and medicine at NYU Grossman School of Medicine, and director of the medical weight management program at NYU Langone Weight Management Center, New York. She disclosed ties to Novo Nordisk and Eli Lilly. This transcript has been edited for clarity.
A version of this article appeared on Medscape.com.
Is Osimertinib Better Alone or With Chemotherapy in Non–Small Cell Lung Cancer?
SAN DIEGO —
That is a question brewing among some oncologists now that the US Food and Drug Administration (FDA) has approved osimertinib (Tagrisso, AstraZeneca) for both indications in patients with epidermal growth factor receptor (EGFR) mutations.
An answer began to emerge in research presented at the American Association for Cancer Research annual meeting.
An exploratory analysis of the FLAURA2 trial found that, when patients have EGFR mutations on baseline circulating tumor DNA (ctDNA) testing, the combination treatment can extend progression-free survival (PFS). In this patient group, those receiving osimertinib alongside pemetrexed plus cisplatin or carboplatin had a 9-month PFS advantage compared with those who received osimertinib alone.
Conversely, when patients do not have EGFR mutations following baseline ctDNA testing, osimertinib alone appears to offer similar PFS outcomes to the combination therapy, but with less toxicity.
“Baseline detection of plasma EGFR mutations may identify a subgroup of patients who derive most benefit from the addition of platinum-pemetrexed to osimertinib as first-line treatment of EGFR-mutated advance non–small cell lung cancer,” investigator Pasi A. Jänne, MD, PhD, a lung cancer oncologist at the Dana-Farber Cancer Institute, Boston, said during his presentation.
The FLAURA2 trial randomized 557 patients equally to daily osimertinib either alone or with pemetrexed plus cisplatin or carboplatin every 3 weeks for four cycles followed by pemetrexed every 3 weeks until disease progression or unacceptable toxicity.
Patients were tested for Ex19del or L858R EGFR mutations at baseline and at 3 and 6 weeks; baseline mutations were found in 73% of evaluable patients.
In patients with baseline mutations, the median PFS was 24.8 months with the combination therapy vs 13.9 months with osimertinib alone (hazard ratio [HR], 0.60).
In patients without baseline mutations, the median PFS was similar in both groups — 33.3 months with the combination vs 30.3 months with monotherapy (HR, 0.93; 95% CI, 0.51-1.72).
The investigators also found that having baseline mutations was associated with worse outcomes regardless of study arm, and mutation clearance was associated with improved outcomes. Clearance occurred more quickly among patients receiving the combination treatment, but almost 90% of patients in both arms cleared their mutations by week 6.
“As we move forward and think about which of our patients we would treat with the combination ... the presence of baseline EGFR mutations in ctDNA may be one of the features that goes into the conversation,” Dr. Jänne said.
Study discussant Marina Chiara Garassino, MD, a thoracic oncologist at the University of Chicago, agreed that this trial can help oncologists make this kind of treatment decision.
Patients with baseline EGFR mutations also tended to have larger tumors, more brain metastases, and worse performance scores; the combination therapy makes sense when such factors are present in patients with baseline EGFR mutations, Dr. Garassino said.
The wrinkle in the findings is that the study used digital droplet polymerase chain reaction (Biodesix) to test for EGFR mutations, which is not commonly used. Clinicians often use next-generation sequencing, which is less sensitive and can lead to false negatives.
It makes it difficult to know how to apply the findings to everyday practice, but Janne hopes a study will be done to correlate next-generation sequencing detection with outcomes.
The study was funded by AstraZeneca, maker of osimertinib, and researchers included AstraZeneca employees. Dr. Jänne is a consultant for and reported research funding from the company. He is a co-inventor on an EGFR mutations patent. Dr. Garassino is also an AstraZeneca consultant and reported institutional financial interests in the company.
A version of this article appeared on Medscape.com.
SAN DIEGO —
That is a question brewing among some oncologists now that the US Food and Drug Administration (FDA) has approved osimertinib (Tagrisso, AstraZeneca) for both indications in patients with epidermal growth factor receptor (EGFR) mutations.
An answer began to emerge in research presented at the American Association for Cancer Research annual meeting.
An exploratory analysis of the FLAURA2 trial found that, when patients have EGFR mutations on baseline circulating tumor DNA (ctDNA) testing, the combination treatment can extend progression-free survival (PFS). In this patient group, those receiving osimertinib alongside pemetrexed plus cisplatin or carboplatin had a 9-month PFS advantage compared with those who received osimertinib alone.
Conversely, when patients do not have EGFR mutations following baseline ctDNA testing, osimertinib alone appears to offer similar PFS outcomes to the combination therapy, but with less toxicity.
“Baseline detection of plasma EGFR mutations may identify a subgroup of patients who derive most benefit from the addition of platinum-pemetrexed to osimertinib as first-line treatment of EGFR-mutated advance non–small cell lung cancer,” investigator Pasi A. Jänne, MD, PhD, a lung cancer oncologist at the Dana-Farber Cancer Institute, Boston, said during his presentation.
The FLAURA2 trial randomized 557 patients equally to daily osimertinib either alone or with pemetrexed plus cisplatin or carboplatin every 3 weeks for four cycles followed by pemetrexed every 3 weeks until disease progression or unacceptable toxicity.
Patients were tested for Ex19del or L858R EGFR mutations at baseline and at 3 and 6 weeks; baseline mutations were found in 73% of evaluable patients.
In patients with baseline mutations, the median PFS was 24.8 months with the combination therapy vs 13.9 months with osimertinib alone (hazard ratio [HR], 0.60).
In patients without baseline mutations, the median PFS was similar in both groups — 33.3 months with the combination vs 30.3 months with monotherapy (HR, 0.93; 95% CI, 0.51-1.72).
The investigators also found that having baseline mutations was associated with worse outcomes regardless of study arm, and mutation clearance was associated with improved outcomes. Clearance occurred more quickly among patients receiving the combination treatment, but almost 90% of patients in both arms cleared their mutations by week 6.
“As we move forward and think about which of our patients we would treat with the combination ... the presence of baseline EGFR mutations in ctDNA may be one of the features that goes into the conversation,” Dr. Jänne said.
Study discussant Marina Chiara Garassino, MD, a thoracic oncologist at the University of Chicago, agreed that this trial can help oncologists make this kind of treatment decision.
Patients with baseline EGFR mutations also tended to have larger tumors, more brain metastases, and worse performance scores; the combination therapy makes sense when such factors are present in patients with baseline EGFR mutations, Dr. Garassino said.
The wrinkle in the findings is that the study used digital droplet polymerase chain reaction (Biodesix) to test for EGFR mutations, which is not commonly used. Clinicians often use next-generation sequencing, which is less sensitive and can lead to false negatives.
It makes it difficult to know how to apply the findings to everyday practice, but Janne hopes a study will be done to correlate next-generation sequencing detection with outcomes.
The study was funded by AstraZeneca, maker of osimertinib, and researchers included AstraZeneca employees. Dr. Jänne is a consultant for and reported research funding from the company. He is a co-inventor on an EGFR mutations patent. Dr. Garassino is also an AstraZeneca consultant and reported institutional financial interests in the company.
A version of this article appeared on Medscape.com.
SAN DIEGO —
That is a question brewing among some oncologists now that the US Food and Drug Administration (FDA) has approved osimertinib (Tagrisso, AstraZeneca) for both indications in patients with epidermal growth factor receptor (EGFR) mutations.
An answer began to emerge in research presented at the American Association for Cancer Research annual meeting.
An exploratory analysis of the FLAURA2 trial found that, when patients have EGFR mutations on baseline circulating tumor DNA (ctDNA) testing, the combination treatment can extend progression-free survival (PFS). In this patient group, those receiving osimertinib alongside pemetrexed plus cisplatin or carboplatin had a 9-month PFS advantage compared with those who received osimertinib alone.
Conversely, when patients do not have EGFR mutations following baseline ctDNA testing, osimertinib alone appears to offer similar PFS outcomes to the combination therapy, but with less toxicity.
“Baseline detection of plasma EGFR mutations may identify a subgroup of patients who derive most benefit from the addition of platinum-pemetrexed to osimertinib as first-line treatment of EGFR-mutated advance non–small cell lung cancer,” investigator Pasi A. Jänne, MD, PhD, a lung cancer oncologist at the Dana-Farber Cancer Institute, Boston, said during his presentation.
The FLAURA2 trial randomized 557 patients equally to daily osimertinib either alone or with pemetrexed plus cisplatin or carboplatin every 3 weeks for four cycles followed by pemetrexed every 3 weeks until disease progression or unacceptable toxicity.
Patients were tested for Ex19del or L858R EGFR mutations at baseline and at 3 and 6 weeks; baseline mutations were found in 73% of evaluable patients.
In patients with baseline mutations, the median PFS was 24.8 months with the combination therapy vs 13.9 months with osimertinib alone (hazard ratio [HR], 0.60).
In patients without baseline mutations, the median PFS was similar in both groups — 33.3 months with the combination vs 30.3 months with monotherapy (HR, 0.93; 95% CI, 0.51-1.72).
The investigators also found that having baseline mutations was associated with worse outcomes regardless of study arm, and mutation clearance was associated with improved outcomes. Clearance occurred more quickly among patients receiving the combination treatment, but almost 90% of patients in both arms cleared their mutations by week 6.
“As we move forward and think about which of our patients we would treat with the combination ... the presence of baseline EGFR mutations in ctDNA may be one of the features that goes into the conversation,” Dr. Jänne said.
Study discussant Marina Chiara Garassino, MD, a thoracic oncologist at the University of Chicago, agreed that this trial can help oncologists make this kind of treatment decision.
Patients with baseline EGFR mutations also tended to have larger tumors, more brain metastases, and worse performance scores; the combination therapy makes sense when such factors are present in patients with baseline EGFR mutations, Dr. Garassino said.
The wrinkle in the findings is that the study used digital droplet polymerase chain reaction (Biodesix) to test for EGFR mutations, which is not commonly used. Clinicians often use next-generation sequencing, which is less sensitive and can lead to false negatives.
It makes it difficult to know how to apply the findings to everyday practice, but Janne hopes a study will be done to correlate next-generation sequencing detection with outcomes.
The study was funded by AstraZeneca, maker of osimertinib, and researchers included AstraZeneca employees. Dr. Jänne is a consultant for and reported research funding from the company. He is a co-inventor on an EGFR mutations patent. Dr. Garassino is also an AstraZeneca consultant and reported institutional financial interests in the company.
A version of this article appeared on Medscape.com.
FROM AACR