User login
Study aims to enhance understanding of ‘tremendously understudied’ prurigo nodularis
compared with age-matched controls, as well those with atopic dermatitis and psoriasis.

Those are key findings from a retrospective analysis of claims data that was published online April 3, 2021, in the Journal of Investigative Dermatology.
“Prurigo nodularis is a tremendously understudied inflammatory skin disease,” one of the study’s cosenior authors, Shawn G. Kwatra, MD, of the department of dermatology, Johns Hopkins University, Baltimore, said in an interview. “Prurigo nodularis patients have uncontrolled itch, which leads to reduced quality of life, and the association with many disease comorbidities. We focused on better understanding in this work the unique comorbidities of prurigo nodularis, compared to other inflammatory skin diseases.”
For the study, Dr. Kwatra, cosenior author Yevgeniy R. Semenov, MD, of the department of dermatology, Massachusetts General Hospital, Boston, and colleagues evaluated nationally representative, private insurance claims data from October 2015 to December 2019 to identify prurigo nodularis (PN) patients, who were defined as individuals with two or more medical claims for PN using ICD-10-CM codes. For comparison with patients with inflammatory skin diseases, they used the same claims data to identify patients with atopic dermatitis (AD) and psoriasis as well as to select controls who were age and gender matched to PN patients. Next, they quantified the overall comorbidity burden with the Charlson Comorbidity Index (CCI).
In 2016, the claims database included 2,658 patients with PN, 21,482 patients with AD, 21,073 patients with psoriasis, and 13,290 controls. The number of patients in each category rose each subsequent year, so that by the end of 2019 there were 9,426 patients with PN, 70,298 patients with AD, 59,509 patients with psoriasis, and 47,130 controls. Between 2016 and 2019 the mean age of PN patients increased from 57.5 to 59.8 years and the percent of male patients rose from 44.5% to 46.5%.
Between 2016 and 2019, the overall PN prevalence rates rose from 18 per 100,000 to 58 per 100,000, while the PN prevalence rates among adults increased from 22 per 100,000 to 70 per 100,000, and the rates among children rose grew from 2 per 100,000 to 7 per 100,000. “Our report shows an estimated disease prevalence of around 335,000 cases of PN in the United States,” said Dr. Kwatra, who was among a group of researchers to recently report on systemic Th22-polarized inflammation in PN patients.
The researchers also found that patients with PN had the highest mean CCI in both 2016 and 2019. In 2016, their mean CCI was 1.53, compared with 0.98 among controls, 0.53 among those with AD, and 1.16 among those with psoriasis. In 2019, the mean CCI had increased in all groups of patients, to 2.32 among those with PN, 1.57 among controls, 0.75 among those with AD patients, and 1.71 among those with psoriasis.
The top five medical specialties who cared for PN patients, defined as the estimated number of visits per year per patient, were internal medicine (2.01 visits), dermatology (1.87 visits), family practice (1.60 visits), cardiology or cardiovascular disease (0.85 visits), and orthopedics or orthopedic surgery (0.49 visits).
“If you encounter a patient with prurigo nodularis, it’s important to perform a screening for chronic kidney disease, diabetes, and liver disease,” Dr. Kwatra said. “These comorbidities along with emerging studies on circulating blood biomarkers suggest prurigo nodularis is a systemic inflammatory disorder; thus systemic agents are needed for most patients as part of multimodal therapy in prurigo nodularis.”
The researchers acknowledged certain limitations of the study, including its retrospective design and the identification of patients with PN with the ICD-10-CM code, which require further validation. “Furthermore, the increase in annual prevalence estimates for PN, AD, and psoriasis observed in the study could also be a result of increasing coding of these diagnoses in the claims data along with rising awareness by the medical profession,” they wrote.
Dr. Kwatra disclosed that he is an advisory board member/consultant for AbbVie, Galderma, Incyte, Pfizer, Regeneron, and Kiniksa Pharmaceuticals, and has received grant funding from Galderma, Pfizer, and Kiniksa. He has also received a Dermatology Foundation Medical Dermatology Career Development Award, a research grant from the Skin of Color Society, and is supported by the National Institutes of Health. One coauthor has been funded by NIH grants.
compared with age-matched controls, as well those with atopic dermatitis and psoriasis.
Those are key findings from a retrospective analysis of claims data that was published online April 3, 2021, in the Journal of Investigative Dermatology.
“Prurigo nodularis is a tremendously understudied inflammatory skin disease,” one of the study’s cosenior authors, Shawn G. Kwatra, MD, of the department of dermatology, Johns Hopkins University, Baltimore, said in an interview. “Prurigo nodularis patients have uncontrolled itch, which leads to reduced quality of life, and the association with many disease comorbidities. We focused on better understanding in this work the unique comorbidities of prurigo nodularis, compared to other inflammatory skin diseases.”
For the study, Dr. Kwatra, cosenior author Yevgeniy R. Semenov, MD, of the department of dermatology, Massachusetts General Hospital, Boston, and colleagues evaluated nationally representative, private insurance claims data from October 2015 to December 2019 to identify prurigo nodularis (PN) patients, who were defined as individuals with two or more medical claims for PN using ICD-10-CM codes. For comparison with patients with inflammatory skin diseases, they used the same claims data to identify patients with atopic dermatitis (AD) and psoriasis as well as to select controls who were age and gender matched to PN patients. Next, they quantified the overall comorbidity burden with the Charlson Comorbidity Index (CCI).
In 2016, the claims database included 2,658 patients with PN, 21,482 patients with AD, 21,073 patients with psoriasis, and 13,290 controls. The number of patients in each category rose each subsequent year, so that by the end of 2019 there were 9,426 patients with PN, 70,298 patients with AD, 59,509 patients with psoriasis, and 47,130 controls. Between 2016 and 2019 the mean age of PN patients increased from 57.5 to 59.8 years and the percent of male patients rose from 44.5% to 46.5%.
Between 2016 and 2019, the overall PN prevalence rates rose from 18 per 100,000 to 58 per 100,000, while the PN prevalence rates among adults increased from 22 per 100,000 to 70 per 100,000, and the rates among children rose grew from 2 per 100,000 to 7 per 100,000. “Our report shows an estimated disease prevalence of around 335,000 cases of PN in the United States,” said Dr. Kwatra, who was among a group of researchers to recently report on systemic Th22-polarized inflammation in PN patients.
The researchers also found that patients with PN had the highest mean CCI in both 2016 and 2019. In 2016, their mean CCI was 1.53, compared with 0.98 among controls, 0.53 among those with AD, and 1.16 among those with psoriasis. In 2019, the mean CCI had increased in all groups of patients, to 2.32 among those with PN, 1.57 among controls, 0.75 among those with AD patients, and 1.71 among those with psoriasis.
The top five medical specialties who cared for PN patients, defined as the estimated number of visits per year per patient, were internal medicine (2.01 visits), dermatology (1.87 visits), family practice (1.60 visits), cardiology or cardiovascular disease (0.85 visits), and orthopedics or orthopedic surgery (0.49 visits).
“If you encounter a patient with prurigo nodularis, it’s important to perform a screening for chronic kidney disease, diabetes, and liver disease,” Dr. Kwatra said. “These comorbidities along with emerging studies on circulating blood biomarkers suggest prurigo nodularis is a systemic inflammatory disorder; thus systemic agents are needed for most patients as part of multimodal therapy in prurigo nodularis.”
The researchers acknowledged certain limitations of the study, including its retrospective design and the identification of patients with PN with the ICD-10-CM code, which require further validation. “Furthermore, the increase in annual prevalence estimates for PN, AD, and psoriasis observed in the study could also be a result of increasing coding of these diagnoses in the claims data along with rising awareness by the medical profession,” they wrote.
Dr. Kwatra disclosed that he is an advisory board member/consultant for AbbVie, Galderma, Incyte, Pfizer, Regeneron, and Kiniksa Pharmaceuticals, and has received grant funding from Galderma, Pfizer, and Kiniksa. He has also received a Dermatology Foundation Medical Dermatology Career Development Award, a research grant from the Skin of Color Society, and is supported by the National Institutes of Health. One coauthor has been funded by NIH grants.
compared with age-matched controls, as well those with atopic dermatitis and psoriasis.
Those are key findings from a retrospective analysis of claims data that was published online April 3, 2021, in the Journal of Investigative Dermatology.
“Prurigo nodularis is a tremendously understudied inflammatory skin disease,” one of the study’s cosenior authors, Shawn G. Kwatra, MD, of the department of dermatology, Johns Hopkins University, Baltimore, said in an interview. “Prurigo nodularis patients have uncontrolled itch, which leads to reduced quality of life, and the association with many disease comorbidities. We focused on better understanding in this work the unique comorbidities of prurigo nodularis, compared to other inflammatory skin diseases.”
For the study, Dr. Kwatra, cosenior author Yevgeniy R. Semenov, MD, of the department of dermatology, Massachusetts General Hospital, Boston, and colleagues evaluated nationally representative, private insurance claims data from October 2015 to December 2019 to identify prurigo nodularis (PN) patients, who were defined as individuals with two or more medical claims for PN using ICD-10-CM codes. For comparison with patients with inflammatory skin diseases, they used the same claims data to identify patients with atopic dermatitis (AD) and psoriasis as well as to select controls who were age and gender matched to PN patients. Next, they quantified the overall comorbidity burden with the Charlson Comorbidity Index (CCI).
In 2016, the claims database included 2,658 patients with PN, 21,482 patients with AD, 21,073 patients with psoriasis, and 13,290 controls. The number of patients in each category rose each subsequent year, so that by the end of 2019 there were 9,426 patients with PN, 70,298 patients with AD, 59,509 patients with psoriasis, and 47,130 controls. Between 2016 and 2019 the mean age of PN patients increased from 57.5 to 59.8 years and the percent of male patients rose from 44.5% to 46.5%.
Between 2016 and 2019, the overall PN prevalence rates rose from 18 per 100,000 to 58 per 100,000, while the PN prevalence rates among adults increased from 22 per 100,000 to 70 per 100,000, and the rates among children rose grew from 2 per 100,000 to 7 per 100,000. “Our report shows an estimated disease prevalence of around 335,000 cases of PN in the United States,” said Dr. Kwatra, who was among a group of researchers to recently report on systemic Th22-polarized inflammation in PN patients.
The researchers also found that patients with PN had the highest mean CCI in both 2016 and 2019. In 2016, their mean CCI was 1.53, compared with 0.98 among controls, 0.53 among those with AD, and 1.16 among those with psoriasis. In 2019, the mean CCI had increased in all groups of patients, to 2.32 among those with PN, 1.57 among controls, 0.75 among those with AD patients, and 1.71 among those with psoriasis.
The top five medical specialties who cared for PN patients, defined as the estimated number of visits per year per patient, were internal medicine (2.01 visits), dermatology (1.87 visits), family practice (1.60 visits), cardiology or cardiovascular disease (0.85 visits), and orthopedics or orthopedic surgery (0.49 visits).
“If you encounter a patient with prurigo nodularis, it’s important to perform a screening for chronic kidney disease, diabetes, and liver disease,” Dr. Kwatra said. “These comorbidities along with emerging studies on circulating blood biomarkers suggest prurigo nodularis is a systemic inflammatory disorder; thus systemic agents are needed for most patients as part of multimodal therapy in prurigo nodularis.”
The researchers acknowledged certain limitations of the study, including its retrospective design and the identification of patients with PN with the ICD-10-CM code, which require further validation. “Furthermore, the increase in annual prevalence estimates for PN, AD, and psoriasis observed in the study could also be a result of increasing coding of these diagnoses in the claims data along with rising awareness by the medical profession,” they wrote.
Dr. Kwatra disclosed that he is an advisory board member/consultant for AbbVie, Galderma, Incyte, Pfizer, Regeneron, and Kiniksa Pharmaceuticals, and has received grant funding from Galderma, Pfizer, and Kiniksa. He has also received a Dermatology Foundation Medical Dermatology Career Development Award, a research grant from the Skin of Color Society, and is supported by the National Institutes of Health. One coauthor has been funded by NIH grants.
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Unique oral drug candidate designed to overcome sickle cell disease
Progress is being made in the quest for an oral treatment for sickle cell disease. In preclinical trials, a new drug has shown the ability to induce blood cells to produce fetal hemoglobin at levels predicted to prevent sickling. The new small-molecule drug could be formulated into a convenient daily oral dosage, according to researchers who presented their results at the spring meeting of the American Chemical Society, which was held virtually.
The new drug candidate, designated FTX-6058 by Fulcrum Therapeutics, was developed using a proprietary small-molecule probe and CRISPR guide RNA libraries to screen “a disease-relevant cell model that allowed us to pinpoint a treatment target,” said Ivan V. Efremov, PhD, senior director, head of medicinal chemistry at the company, who presented the research.
Even though sickle cell patients carry genes leading to defective adult hemoglobin, they still carry stem cells in their bone marrow with the potential to produce fetal hemoglobin. FTX-6058 attaches to a protein inside these bone marrow stem cells destined to become mature red blood cells and reinstates their fetal hemoglobin expression, according to Dr. Efremov.
“What is really key is FTX-6058 upregulates fetal hemoglobin across all red blood cells, a pancellular distribution,” he explained, adding that if “some red blood cells did not express this, they could still sickle and cause disease symptoms.”
The premise behind the development of the drug evolved from the example of patients with sickle cell genes who also have a mutation that causes fetal hemoglobin production. The presence of fetal hemoglobin provides significant benefits to patients with sickle cell disease. At around 5%-10% levels of fetal hemoglobin expression, mortality is reduced. By 10%-25% levels of fetal hemoglobin, recurring events including vaso-occlusive crises, acute chest syndrome, and hospitalization are reduced. When fetal hemoglobin levels reaches around 25%-30%, enough red blood cell function is restored so that these patients become asymptomatic, Dr. Efremov said.
FTX-6058 was designed to mimic this effect.
FTX-6058 inhibits the action of the polycomb repressive complex 2 (PRC2) via binding to the EED subunit. PRC2 acts as a histone methyltransferase to control gene expression. Inhibition of PRC2 leads to significant fetal hemoglobin protein expression in both cell and mouse models. Other such inhibitors are under study for the suppression of cancer progression.
Preclinical experiments comparing FTX-6058 with the fetal hemoglobin booster, hydroxyurea, approved in the 1990s, showed the new drug candidate outperforms the current treatment, Christopher Moxham, PhD, chief scientific officer of Fulcrum Therapeutics, said in a company press release. The company began a phase 1 safety trial in healthy adult volunteers last year after preclinical experiments with FTX-6058 in human-derived cell assay systems and mouse models also showed an increase in fetal hemoglobin to meet the 25%-30% asymptomatic symptom threshold level.
Ongoing studies
The researchers plan to launch phase 2 clinical trial enrolling patients with sickle cell disease by end of 2021. In addition, further characterization of the therapeutic molecule is continuing, using genomics and additional cell assay systems to expand details FTX-6058’s mode of action.
The company also is looking to explore the use of FTX-6058 in patients with beta-thalassemia to supplement their reduced hemoglobin production.
The pharmacologic profile of FTX-6058 indicates that the drug has the potential to be administered as a once-a-day oral formulation, Dr. Efremov stated. Both the preclinical PK [pharmacokinetic] data and “the emerging PK from the human clinical study supports once-a-day oral administration, which obviously offers significant convenience to patients,” he added.
Fulcrum Therapeutics is funding the studies.
Progress is being made in the quest for an oral treatment for sickle cell disease. In preclinical trials, a new drug has shown the ability to induce blood cells to produce fetal hemoglobin at levels predicted to prevent sickling. The new small-molecule drug could be formulated into a convenient daily oral dosage, according to researchers who presented their results at the spring meeting of the American Chemical Society, which was held virtually.
The new drug candidate, designated FTX-6058 by Fulcrum Therapeutics, was developed using a proprietary small-molecule probe and CRISPR guide RNA libraries to screen “a disease-relevant cell model that allowed us to pinpoint a treatment target,” said Ivan V. Efremov, PhD, senior director, head of medicinal chemistry at the company, who presented the research.
Even though sickle cell patients carry genes leading to defective adult hemoglobin, they still carry stem cells in their bone marrow with the potential to produce fetal hemoglobin. FTX-6058 attaches to a protein inside these bone marrow stem cells destined to become mature red blood cells and reinstates their fetal hemoglobin expression, according to Dr. Efremov.
“What is really key is FTX-6058 upregulates fetal hemoglobin across all red blood cells, a pancellular distribution,” he explained, adding that if “some red blood cells did not express this, they could still sickle and cause disease symptoms.”
The premise behind the development of the drug evolved from the example of patients with sickle cell genes who also have a mutation that causes fetal hemoglobin production. The presence of fetal hemoglobin provides significant benefits to patients with sickle cell disease. At around 5%-10% levels of fetal hemoglobin expression, mortality is reduced. By 10%-25% levels of fetal hemoglobin, recurring events including vaso-occlusive crises, acute chest syndrome, and hospitalization are reduced. When fetal hemoglobin levels reaches around 25%-30%, enough red blood cell function is restored so that these patients become asymptomatic, Dr. Efremov said.
FTX-6058 was designed to mimic this effect.
FTX-6058 inhibits the action of the polycomb repressive complex 2 (PRC2) via binding to the EED subunit. PRC2 acts as a histone methyltransferase to control gene expression. Inhibition of PRC2 leads to significant fetal hemoglobin protein expression in both cell and mouse models. Other such inhibitors are under study for the suppression of cancer progression.
Preclinical experiments comparing FTX-6058 with the fetal hemoglobin booster, hydroxyurea, approved in the 1990s, showed the new drug candidate outperforms the current treatment, Christopher Moxham, PhD, chief scientific officer of Fulcrum Therapeutics, said in a company press release. The company began a phase 1 safety trial in healthy adult volunteers last year after preclinical experiments with FTX-6058 in human-derived cell assay systems and mouse models also showed an increase in fetal hemoglobin to meet the 25%-30% asymptomatic symptom threshold level.
Ongoing studies
The researchers plan to launch phase 2 clinical trial enrolling patients with sickle cell disease by end of 2021. In addition, further characterization of the therapeutic molecule is continuing, using genomics and additional cell assay systems to expand details FTX-6058’s mode of action.
The company also is looking to explore the use of FTX-6058 in patients with beta-thalassemia to supplement their reduced hemoglobin production.
The pharmacologic profile of FTX-6058 indicates that the drug has the potential to be administered as a once-a-day oral formulation, Dr. Efremov stated. Both the preclinical PK [pharmacokinetic] data and “the emerging PK from the human clinical study supports once-a-day oral administration, which obviously offers significant convenience to patients,” he added.
Fulcrum Therapeutics is funding the studies.
Progress is being made in the quest for an oral treatment for sickle cell disease. In preclinical trials, a new drug has shown the ability to induce blood cells to produce fetal hemoglobin at levels predicted to prevent sickling. The new small-molecule drug could be formulated into a convenient daily oral dosage, according to researchers who presented their results at the spring meeting of the American Chemical Society, which was held virtually.
The new drug candidate, designated FTX-6058 by Fulcrum Therapeutics, was developed using a proprietary small-molecule probe and CRISPR guide RNA libraries to screen “a disease-relevant cell model that allowed us to pinpoint a treatment target,” said Ivan V. Efremov, PhD, senior director, head of medicinal chemistry at the company, who presented the research.
Even though sickle cell patients carry genes leading to defective adult hemoglobin, they still carry stem cells in their bone marrow with the potential to produce fetal hemoglobin. FTX-6058 attaches to a protein inside these bone marrow stem cells destined to become mature red blood cells and reinstates their fetal hemoglobin expression, according to Dr. Efremov.
“What is really key is FTX-6058 upregulates fetal hemoglobin across all red blood cells, a pancellular distribution,” he explained, adding that if “some red blood cells did not express this, they could still sickle and cause disease symptoms.”
The premise behind the development of the drug evolved from the example of patients with sickle cell genes who also have a mutation that causes fetal hemoglobin production. The presence of fetal hemoglobin provides significant benefits to patients with sickle cell disease. At around 5%-10% levels of fetal hemoglobin expression, mortality is reduced. By 10%-25% levels of fetal hemoglobin, recurring events including vaso-occlusive crises, acute chest syndrome, and hospitalization are reduced. When fetal hemoglobin levels reaches around 25%-30%, enough red blood cell function is restored so that these patients become asymptomatic, Dr. Efremov said.
FTX-6058 was designed to mimic this effect.
FTX-6058 inhibits the action of the polycomb repressive complex 2 (PRC2) via binding to the EED subunit. PRC2 acts as a histone methyltransferase to control gene expression. Inhibition of PRC2 leads to significant fetal hemoglobin protein expression in both cell and mouse models. Other such inhibitors are under study for the suppression of cancer progression.
Preclinical experiments comparing FTX-6058 with the fetal hemoglobin booster, hydroxyurea, approved in the 1990s, showed the new drug candidate outperforms the current treatment, Christopher Moxham, PhD, chief scientific officer of Fulcrum Therapeutics, said in a company press release. The company began a phase 1 safety trial in healthy adult volunteers last year after preclinical experiments with FTX-6058 in human-derived cell assay systems and mouse models also showed an increase in fetal hemoglobin to meet the 25%-30% asymptomatic symptom threshold level.
Ongoing studies
The researchers plan to launch phase 2 clinical trial enrolling patients with sickle cell disease by end of 2021. In addition, further characterization of the therapeutic molecule is continuing, using genomics and additional cell assay systems to expand details FTX-6058’s mode of action.
The company also is looking to explore the use of FTX-6058 in patients with beta-thalassemia to supplement their reduced hemoglobin production.
The pharmacologic profile of FTX-6058 indicates that the drug has the potential to be administered as a once-a-day oral formulation, Dr. Efremov stated. Both the preclinical PK [pharmacokinetic] data and “the emerging PK from the human clinical study supports once-a-day oral administration, which obviously offers significant convenience to patients,” he added.
Fulcrum Therapeutics is funding the studies.
CDC: STI rates rise for sixth year in a row
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
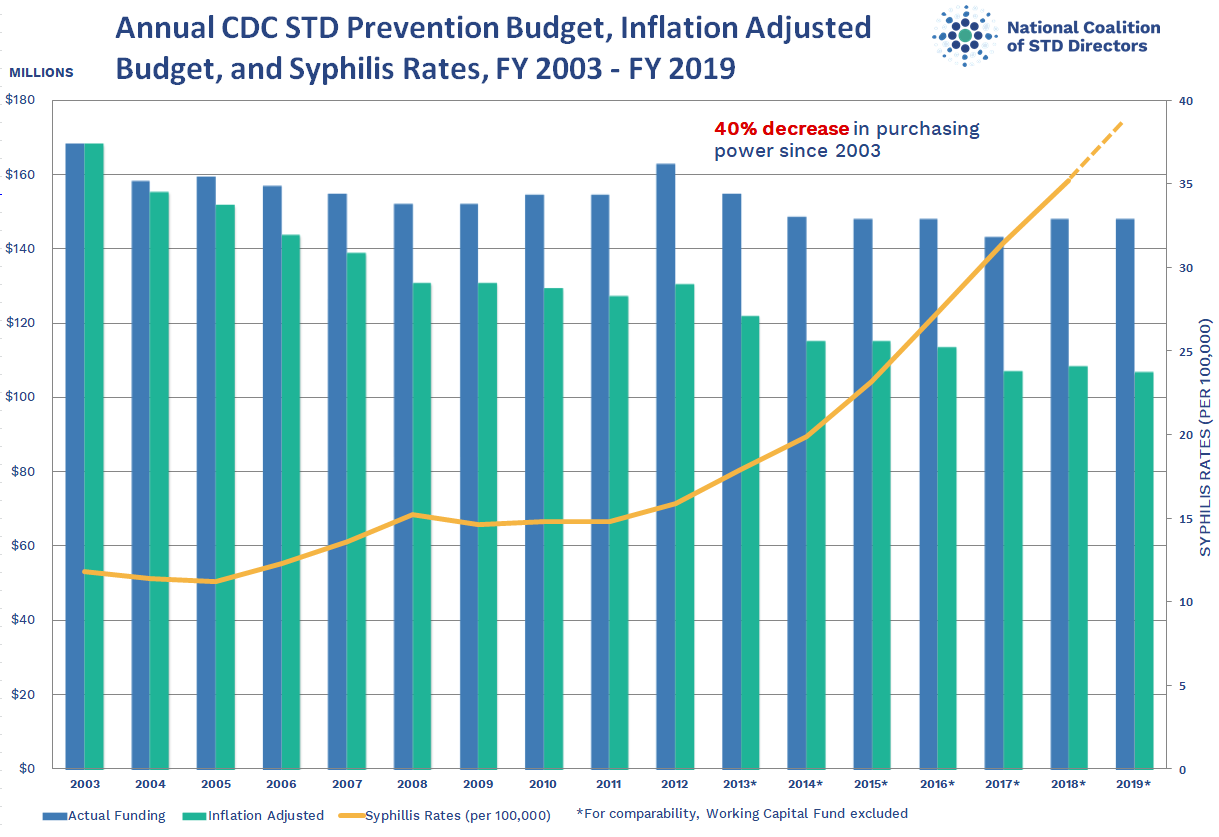
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
{kind=link}
A version of this article first appeared on Medscape.com.
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
A version of this article first appeared on Medscape.com.
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
A version of this article first appeared on Medscape.com.
COVID-19–related inflammatory syndrome tied to neurologic symptoms in children
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
About half of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) have new-onset neurologic symptoms, research shows.
These symptoms involve the central and peripheral nervous systems but do not always affect the respiratory system. In addition, neurologic symptoms appear to be more common in severe presentations of this syndrome.
“These new data consolidate the initial findings in our JAMA Neurology publication on the neurological problems that children with PIMS-TS can present with, even in the absence of respiratory systems,” study investigator Omar Abdel-Mannan, MD, clinical research fellow at University College London Institute of Neurology and senior resident at Great Ormond Street Hospital for children in London, said in an interview.
He added that the findings are in keeping with other recent research studies on PIMS-TS, which is known more commonly in the United States as multisystem inflammatory syndrome in children (MIS-C).
The findings will be presented April 18 at the American Academy of Neurology (AAN) 2021 Annual Meeting.
Neurologic manifestations common
Many children and adults with COVID-19 have developed neurologic manifestations. PIMS-TS is a severe, postinfectious, immune-mediated disorder characterized by persistent fever and extreme inflammation.
Patients may have acute diarrhea or vomiting, rash or bilateral conjunctivitis, and low blood pressure. They should be examined by a pediatric specialist, and most children with this disorder need intensive care.
To report the neurologic manifestations in children with PIMS-TS, the researchers retrospectively examined data for children and adolescents younger than 18 years who had the disorder and presented to a single center between April 4, 2020, and Sept. 1, 2020.
Forty-six patients (median age, 10.2 years) were included in the analysis. Thirty (65.2%) were male, and 37 (80.4%) were of non-White ethnicities.
Twenty-four (52.2%) patients had new-onset neurologic symptoms, which included headache (n = 24), encephalopathy (n = 14 patients), dysarthria/dysphonia (n = 6), hallucinations (n = 6), ataxia (n = 4), peripheral nerve involvement (n = 3), and seizures (n=1).
Laboratory and imaging results provided further information. One patient had 118 leukocytes in cerebrospinal fluid. Children with neurologic involvement had higher levels of peak inflammatory markers and were more likely to be ventilated and require inotropic support in the PICU (P < .05).
Four of 16 patients who underwent brain MRI had splenium signal changes. Of 15 patients who underwent electroencephalogram (EEG), 14 had an excess of slow activity. Four of 7 patients who underwent nerve conduction studies and electromyography (EMG) had myopathic and neuropathic changes.
Response to SARS-CoV-2
Central neurologic problems of the brain and peripheral nerve involvement rarely occur at the same time in children.
“This makes it highly possible that the syndrome is secondary to cytokine release in response to the SARS-CoV-2 virus, as there is significant clinical overlap with both genetic and acquired forms of another immune-mediated condition known as hemophagocytic lymphohistiocytosis,” said Dr. Abdel-Mannan.
The researchers found no demographic differences between children with neurologic involvement at presentation and those without.
“However, the numbers are small given the rarity of this condition, which makes it difficult to extrapolate associations and differences between the two groups, and will require future collaborative larger scale studies to look at what potentially makes some children more susceptible to neurologic involvement than others,” said Dr. Abdel-Mannan.
Excluding potential causes of the symptoms other than COVID-19 also is important, he added.
The preponderance of ethnic minorities in the current study population mirrors that in other PIMS-TS cohorts in other countries, said Dr. Abdel-Mannan. It reflects the higher incidence of COVID-19 in ethnic minority groups. However, presentation, investigations, and management did not differ between White and non-White children in the current study.
“Although PIMS-TS patients with neurologic involvement are initially sicker, our center’s preliminary follow-up data up to 6 months post discharge from hospital demonstrates that most of these children make an almost complete functional recovery, which is reassuring,” said Dr. Abdel-Mannan.
The data underscore how important it is that clinicians be aware that children with PIMS-TS can present with neurologic symptoms, even in the absence of respiratory involvement, he added.
The researchers will soon begin a multicenter research study that will involve longitudinal clinical and cognitive assessments and advanced neuroimaging. The objective will be to determine whether all children with PIMS-TS, or only those with neurologic symptoms, are at risk of chronic longer-term neurocognitive and psychiatric outcomes.
Unanswered questions
John B. Bodensteiner, MD, professor of neurology and pediatrics at Mayo Clinic, Rochester, Minn., said in an interview that the findings help flesh out the range of neurologic involvement that PIMS-TS entails.
“It’s not a surprise to us as neurologists, but it’s not been emphasized in the general literature and in the public health sector,” he said.
The study’s most important implication is that neurologic conditions are not uncommon among children with PIMS-TS, Dr. Bodensteiner added.
“We have no idea how long or what the long-term effects of that are,” he said. Not enough time has elapsed to enable a clear understanding of the syndrome’s lasting effects on cognition, he said, “but I think this certainly raises a flag that this is a real entity. This is nothing to sniff at.”
He noted that the study has the limitations of any retrospective case series. The researchers did not perform prospective and systematic evaluations of children with the syndrome
The findings also raise unanswered questions.
“They had 14 kids with encephalopathy, but not all of them got the same evaluation,” said Dr. Bodensteiner. Although the researchers mention peripheral nerve involvement in three children, they do not describe it. “They said that the EMG showed myopathic and neuropathic changes, but peripheral nerve involvement wouldn’t give you myopathic changes, so maybe there’s some direct involvement of the muscle in this inflammatory process.”
The study also focused on a select group of patients, said Dr. Bodensteiner. “These are all patients admitted to Great Ormond Street Hospital, and we don’t know what percentage of kids who get COVID are hospitalized, which is an important issue.”
It is necessary to know what proportion of children with COVID-19 develop encephalopathy and MRI changes, he added. The findings do confirm that this coronavirus-related inflammatory condition is real and may have long-term sequelae. “We should be careful about kids getting this disease,” said Dr. Bodensteiner
The study had no funding. Dr. Abdel-Mannan and Dr. Bodensteiner have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Say my name
Dr. Ben-a-bo?
Nope.
Ben-nabi?
Nope.
Ben-NO-bo?
Also no.
My surname is tricky to pronounce for some people. I sometimes exaggerate to help patients get it right: “Beh-NAAH-bee-oh.” Almost daily someone will reply: “Oh, you’re Italian!” Well, no actually, my friend Enzo who was born in Sicily and lives in Milan, he’s Italian. I’m just a Rhode Islander who knows some Italian words from his grandmother. Most times though, I just answer: ‘Yep, I’m Italian.” It’s faster.
We use names as a shortcut to identify people. In clinic, it can help to find things in common quickly, similar to asking where you’re from. (East Coast patients seem to love that I’m from New England and if they’re Italian and from New York, well then, we’re paisans right from the start.)
However, using names to guess how someone identifies can be risky. In some instances, it could even be seen as microaggressive, particularly if you got it wrong.
Like most of you I’ll bet, I’m pretty good at pronouncing names – we practice thousands of times! Other than accepting a compliment for getting a tricky one right, such as Radivojevic (I think it’s Ra-di-VOI-ye-vich), I hadn’t thought much about names until I heard a great podcast on the topic. I thought I’d share a couple tips.
First, if you’re not particularly good at names or if you struggle with certain types of names, it’s better to ask than to butcher it. Like learning the wrong way to hit a golf ball, you may never be able to do it properly once you’ve done it wrong. (Trust me, I know from both.)
If I’m feeling confident, I’ll give it a try. But if unsure, I ask the patient to pronounce it for me, then I repeat it to confirm I’ve gotten it correct. Then I say it once or twice more during the visit. Lastly, for the knotty tongue-twisting ones, I write it phonetically in their chart.
It is important because mispronouncing names can alienate patients. It might make them feel like we don’t “know” them or that we don’t care about them. and eliminating ethnic disparities in care. Just think how much harder it might be to convince skeptical patients to take their lisinopril if you can’t even get their names right.
Worse perhaps than getting the pronunciation wrong is to turn the name into an issue. Saying: “Oh, that’s hard to pronounce” could be felt as a subtly racist remark – it’s not hard for them to pronounce of course, only for you. Also, guessing a patient’s nationality from the name is risky. Asking “are you Russian?” to someone from Ukraine or “is that Chinese?” to someone from Vietnam can quickly turn a nice office visit down a road named “Awkward.” It can give the impression that they “all look the same” to you, exactly the type of exclusion we’re trying to eliminate in medicine.

Saying a patient’s name perfectly is rewarding and a super-efficient way to connect. It can make salient the truth that you care about the patient and about his or her story, even if the name happens to be Mrs. Xiomara Winyuwongse Khosrowshahi Sundararajan Ngoc. Go ahead, give it a try.
Want more on how properly pronounce names correctly? You might like this episode of NPR’s Life Kit.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]
Dr. Ben-a-bo?
Nope.
Ben-nabi?
Nope.
Ben-NO-bo?
Also no.
My surname is tricky to pronounce for some people. I sometimes exaggerate to help patients get it right: “Beh-NAAH-bee-oh.” Almost daily someone will reply: “Oh, you’re Italian!” Well, no actually, my friend Enzo who was born in Sicily and lives in Milan, he’s Italian. I’m just a Rhode Islander who knows some Italian words from his grandmother. Most times though, I just answer: ‘Yep, I’m Italian.” It’s faster.
We use names as a shortcut to identify people. In clinic, it can help to find things in common quickly, similar to asking where you’re from. (East Coast patients seem to love that I’m from New England and if they’re Italian and from New York, well then, we’re paisans right from the start.)
However, using names to guess how someone identifies can be risky. In some instances, it could even be seen as microaggressive, particularly if you got it wrong.
Like most of you I’ll bet, I’m pretty good at pronouncing names – we practice thousands of times! Other than accepting a compliment for getting a tricky one right, such as Radivojevic (I think it’s Ra-di-VOI-ye-vich), I hadn’t thought much about names until I heard a great podcast on the topic. I thought I’d share a couple tips.
First, if you’re not particularly good at names or if you struggle with certain types of names, it’s better to ask than to butcher it. Like learning the wrong way to hit a golf ball, you may never be able to do it properly once you’ve done it wrong. (Trust me, I know from both.)
If I’m feeling confident, I’ll give it a try. But if unsure, I ask the patient to pronounce it for me, then I repeat it to confirm I’ve gotten it correct. Then I say it once or twice more during the visit. Lastly, for the knotty tongue-twisting ones, I write it phonetically in their chart.
It is important because mispronouncing names can alienate patients. It might make them feel like we don’t “know” them or that we don’t care about them. and eliminating ethnic disparities in care. Just think how much harder it might be to convince skeptical patients to take their lisinopril if you can’t even get their names right.
Worse perhaps than getting the pronunciation wrong is to turn the name into an issue. Saying: “Oh, that’s hard to pronounce” could be felt as a subtly racist remark – it’s not hard for them to pronounce of course, only for you. Also, guessing a patient’s nationality from the name is risky. Asking “are you Russian?” to someone from Ukraine or “is that Chinese?” to someone from Vietnam can quickly turn a nice office visit down a road named “Awkward.” It can give the impression that they “all look the same” to you, exactly the type of exclusion we’re trying to eliminate in medicine.
Saying a patient’s name perfectly is rewarding and a super-efficient way to connect. It can make salient the truth that you care about the patient and about his or her story, even if the name happens to be Mrs. Xiomara Winyuwongse Khosrowshahi Sundararajan Ngoc. Go ahead, give it a try.
Want more on how properly pronounce names correctly? You might like this episode of NPR’s Life Kit.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]
Dr. Ben-a-bo?
Nope.
Ben-nabi?
Nope.
Ben-NO-bo?
Also no.
My surname is tricky to pronounce for some people. I sometimes exaggerate to help patients get it right: “Beh-NAAH-bee-oh.” Almost daily someone will reply: “Oh, you’re Italian!” Well, no actually, my friend Enzo who was born in Sicily and lives in Milan, he’s Italian. I’m just a Rhode Islander who knows some Italian words from his grandmother. Most times though, I just answer: ‘Yep, I’m Italian.” It’s faster.
We use names as a shortcut to identify people. In clinic, it can help to find things in common quickly, similar to asking where you’re from. (East Coast patients seem to love that I’m from New England and if they’re Italian and from New York, well then, we’re paisans right from the start.)
However, using names to guess how someone identifies can be risky. In some instances, it could even be seen as microaggressive, particularly if you got it wrong.
Like most of you I’ll bet, I’m pretty good at pronouncing names – we practice thousands of times! Other than accepting a compliment for getting a tricky one right, such as Radivojevic (I think it’s Ra-di-VOI-ye-vich), I hadn’t thought much about names until I heard a great podcast on the topic. I thought I’d share a couple tips.
First, if you’re not particularly good at names or if you struggle with certain types of names, it’s better to ask than to butcher it. Like learning the wrong way to hit a golf ball, you may never be able to do it properly once you’ve done it wrong. (Trust me, I know from both.)
If I’m feeling confident, I’ll give it a try. But if unsure, I ask the patient to pronounce it for me, then I repeat it to confirm I’ve gotten it correct. Then I say it once or twice more during the visit. Lastly, for the knotty tongue-twisting ones, I write it phonetically in their chart.
It is important because mispronouncing names can alienate patients. It might make them feel like we don’t “know” them or that we don’t care about them. and eliminating ethnic disparities in care. Just think how much harder it might be to convince skeptical patients to take their lisinopril if you can’t even get their names right.
Worse perhaps than getting the pronunciation wrong is to turn the name into an issue. Saying: “Oh, that’s hard to pronounce” could be felt as a subtly racist remark – it’s not hard for them to pronounce of course, only for you. Also, guessing a patient’s nationality from the name is risky. Asking “are you Russian?” to someone from Ukraine or “is that Chinese?” to someone from Vietnam can quickly turn a nice office visit down a road named “Awkward.” It can give the impression that they “all look the same” to you, exactly the type of exclusion we’re trying to eliminate in medicine.
Saying a patient’s name perfectly is rewarding and a super-efficient way to connect. It can make salient the truth that you care about the patient and about his or her story, even if the name happens to be Mrs. Xiomara Winyuwongse Khosrowshahi Sundararajan Ngoc. Go ahead, give it a try.
Want more on how properly pronounce names correctly? You might like this episode of NPR’s Life Kit.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected]
Preventing the psychosocial effects of adult ADHD during the pandemic
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2

The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4

Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2
The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4
Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
As some countries brace for yet another possible surge in the COVID-19 pandemic – particularly among young adults who have not yet been vaccinated – clinicians should remain wary of the cardinal symptoms of adult ADHD.
Research from an Israeli study shows that individuals with unmedicated ADHD are 52% more likely to test positive for the virus.1,2
The symptoms of ADHD, including impulsiveness and inability to follow directions, combined with the tendency to leave adults with ADHD on their own to sort out COVID-19–related protocols – make these individuals susceptible to exposure.
As we know, ADHD is a condition characterized by a pervasive pattern of impulsivity and/or inattention, which greatly reduces organizational capabilities by interfering at the developmental level.3 Other key symptoms include short attention span, hyperactivity, restlessness, difficulty in prioritizing tasks, and an absence of time awareness. Symptom presentation of ADHD is contingent upon the nature of the individual’s overall mental health and etiologic issues that may be traced back to the brain’s development.4
Diagnosing ADHD in adults is relatively difficult, because a formal diagnosis generally requires symptoms to show up between the ages of 6 and 12.5 Also, clinicians can interview parents and family members to assess whether the classical features of ADHD were present in childhood for those suspected of having the condition.
Early vs. late presentation
Among the preschool population, it has been observed that emerging ADHD symptoms may progress with time or remain relatively constant with respect to the activities that children partake in. In some instances, impulsive behavior, especially compared with other symptoms, might be identified quickly by the attentive parent or caregiver. However, when ADHD appears in adulthood, it is possible that prior ADHD symptoms escaped detection – only to be diagnosed later in life because of varying presentations and the increased organizational demands of adulthood.
Meanwhile, diagnosis in adolescence can bring a different set of challenges to the forefront as teenagers face problems with self-management and responsibilities of daily living. These young people must cope with academic6 and social pressures – and a host of new societal expectations.
It is essential to understand how all of those societal factors have affected ADHD and its aspects, especially within the context of COVID-19. The coronavirus has introduced myriad challenges at the global level. Individuals with ADHD exhibit neurodevelopmental and corollary attention deficit issues that make them more susceptible to environmental stressors. Physical distancing practices might aggravate existing behavioral problems.
Distance forced by pandemic offers challenges
Despite the widespread adoption of telemedicine during the pandemic, some physicians think that the delivery of optimal care and the ability to adequately address patients’ health-related concerns have been compromised. Certainly, in the case of addressing the needs of patients with ADHD or related learning disorders, in-person examinations and clinical visits are best.
That is also the case for ADHD patients with comorbid sleep disorders. For those patients, it might be prudent to explore lifestyle changes (for example, improvements in sleep hygiene practices) before resorting to the use of pharmacologic agents such as hypnotics and melatonin. Along similar lines, the European ADHD Guideline Group (EAGG) advises the use of pharmacotherapy after the successful completion of a physical exam; patients already adhering to a treatment plan should continue therapy without interruption. Clinicians caring for patients with adult ADHD have faced a dilemma because treatment breaks increase the likelihood of illnesses resulting from the pandemic. Also, the inability to conduct treatment in person because of the pandemic raises concerns about pharmacotherapy.
The pandemic has affected the course of pediatric care and also has presented new challenges for adolescents as they begin to tackle unique problems related to their health concerns. In prepandemic times, teachers played integral roles in the diagnostic process, because they were able to readily identify children and teenagers with mental and physical challenges. In stark contrast, connecting with students online may not allow teachers to identify skill deficits in young patients or in adults with ADHD.
Furthermore, adults with ADHD and medical comorbidities may be at increased risk of disease exposure directly resulting from an inability to address their social and/or emotional well-being adequately. The social distancing and other mitigation measures advised by public health experts ensure safety and protection but also can present numerous hurdles for children, teenagers, adults – and their respective families.
Individuals with adult ADHD and other psychiatric disorders may downplay their psychological distress7 [for example, sleep dysfunction, issues concerning activities of daily living], and view it as being the natural product of the COVID-19 environment. As a result of their misconceptions, they may avoid increasing their medication dose to control emergent symptoms of hyperactivity and impulsivity, instead opting to manage stress without aid from health care professionals. The absence of patient-provider interactivity and the integration of telemedicine has introduced unnecessary obstacles with respect to medication management and therapy as well as general access to expert advice. It is of utmost importance for clinicians to identify at-risk patients and reeducate the adult ADHD patient on issues concerning medication intake and psychological wellness.
Individuals with developmental disorders may experience numerous setbacks when trying to navigate their environments. The lack of correct feedback, supervision, and guidance may adversely affect adults with ADHD, contributing toward a lack of self-esteem and social awareness.
Individuals with adult ADHD are more likely than are their younger counterparts to have medical comorbidities, such as cardiovascular disease8 and type 2 diabetes,9 so it is crucial to prescribe dietary instructions to patients. Sometimes patients with adult ADHD lack support in the form of acceptance by family and peers, so it is critical for the patient to come to terms with his/her condition and seek professional help, incorporating effective strategies wherever needed to maintain day-to-day functioning.
Other possible comorbidities
There can be risk factors associated with isolation of adults who have depression and/or anxiety, poor eating habits, and maladaptive behaviors. Other adverse health-related issues may include substance use disorder.10 Drug use suppresses developmental growth and may induce ADHD symptom exacerbation. Consistent with Khantzian’s self-medication hypothesis, among individuals with ADHD, including those who lack a formal diagnosis, there is a tendency to gravitate toward illicit substances, in particular, stimulants.11
We also know that adolescents are known to engage in normal risk-taking and social experimentation. Given that, the notion of boundary setting becomes a complicated affair during a pandemic. Adults may no longer be involved in the same types of risk-taking behaviors, but enforced self-isolation coupled with unchecked consumption of various social medial platforms continue to take a toll on personal development. Socialization plays an enormous role in maintaining psychological health, and social media is no substitute for in-person interactions. Such platforms can reduce mental growth opportunities and affect ADHD adults unfavorably.
For instance, it has been reported that women with adult ADHD are more likely to present with negative cognitive biases and symptoms of anxiety as a function of social media use.12,13 As clinicians, we should recommend introducing activities with the aim of enhancing self-acceptance, mindfulness, and the ability to engage in healthy lifestyles. A holistic framework that focuses on psychological wellness and physical fitness will ensure treatment success. Medication management may prove to be a challenge because of differences in dosing, response schedules, and agreed-upon diagnostic criteria used for young patients, compared with those needed for adults.
Treatment strategies
Before the pandemic, researchers were observing an increase globally in the ADHD diagnosis,14 and clinicians have been exploring the efficacy of select medications, sometimes with limited success.15 Stimulant medication, combined with behavioral interventions, is supported by evidenced-based medicine and is the treatment of choice for childhood ADHD.
The stimulant remedy considered to be the most efficacious for adult ADHD is methylphenidate or dextroamphetamine.
However, be sure to proceed with caution and prepare a thorough work-up, because there can be cardiovascular risk factors associated with these medications with a pronounced increase in heart rate and blood pressure.
Stimulant medications are known to increase the risk of stroke or myocardial infarction for individuals with preexisting cardiovascular anomalies or structural anomalies. The American Heart Association no longer recommends a baseline EKG before commencing stimulant therapy with the exception of preexisting cardiac risk. Nonstimulant medications such as atomoxetine are available as alternatives.
The process of finding therapies that will reduce symptoms of ADHD takes considerable time, and individuals may fail to notice improvements, at least initially.
Before prescribing any medicine or therapies, it is important to evaluate for factors that are specific to ADHD and rule out the presence of other learning or developmental disorders, to prevent negative consequences.
Health care professionals can introduce nonspecific interventions as a means of tackling complicated cases of adult ADHD, especially those that coincide with underlying medical conditions (for example, cardiovascular disease, seizure disorders, and/or eating disorders). In such cases, stimulant medications may lead to symptom exacerbation, and the health care professional should carry out a systematic evaluation (risks vs. benefits of drug classes), despite the limitations of online appointments over the course of the pandemic.
Moreover, ADHD symptoms can take on a more severe form within the context of preexisting mood and anxiety disorders. Unfortunately, these comorbidities may have a negative prognostic outcome, too, thereby increasing other health-related risk factors. Psychological interventions can be implemented via online assessments because of recent technological advances worldwide, providing a new level of confidence and social engagement. EEG-assisted biofeedback is an example of new technological modalities that may help improve the overall performance and functionality of individuals with adult ADHD.16 Numerous services and resources are available to patients and their families that can improve mental health and well-being.
Other nonpharmacologic choices also play an instrumental role in bringing harmony and organization into a patient’s life through the use of daily planners, alarms, and to-do lists. In addition, therapists can provide treatment that helps individuals get motivated and reduce their anxiety levels. Behavioral therapies support patient initiatives by increasing their productivity, activity management, and satisfaction. Cognitive-behavioral therapy (CBT), and marriage counseling and family therapy are modalities that may help adults with ADHD change underlying thoughts and perceptions and develop coping skills and self-esteem.
Appropriate to the pandemic situation is another treatment, e-therapy, which includes text-based communication, video calling, and phone calls. It is a low-cost and convenient alternative for people. For some patients, traveling to a particular clinic or counseling center can be difficult, and there is a shortage of counselors worldwide, so it is beneficial to talk with a counselor on a video/phone call or through social media. It is crucial for the ADHD coach to be trained with relevant knowledge to make plans, set goals, and manage a patient’s schedule of activities. For the counselor, sharing tips based on personal experience and making the appropriate suggestions allows adults with ADHD to stay motivated and focus on the task at hand. It should be noted that counselors play an important role in reducing stress levels for those diagnosed with ADHD, allowing patients to lead productive lives and achieve career goals.
Various online support communities can provide patients and their parents with educational resources, to address issues connected to ADHD in a professional manner.17
The road to treatment success
Any delays in treating adults with ADHD can lead to a frustrating situation in which the entire family will be affected. As stated earlier, numerous support groups are available to adults with ADHD, and some of those groups can offer valuable tips about addressing stress management and the diverse roles that parents and family members may play in patient care.18 These groups provide a network for people to exchange ideas and recommend strategies. Online support groups may connect patients directly with key opinion leaders and health care providers.
Individuals with ADHD often experience problems with organization and concentration – especially within the context of the pandemic – and receiving guidance from counselors will provide an opportunity to learn valuable coping strategies and manage symptoms, recognizing and mitigating any mood swings associated with anxiety or depression that emerge alongside their ADHD. Psychotherapy is instrumental in patient care, and individuals with adult ADHD should be taught to acknowledge the role of medications (for example, neglect, divert, or self-medicate). A holistic approach to managing ADHD symptoms is necessary for optimal functioning and independence.
Dr. Aman is a faculty member in the biology department of City Colleges of Chicago. She is a postdoctoral researcher at the International Maternal and Child Health Foundation (IMCHF), Montreal; a fellow, medical staff development, from the American Academy of Medical Management; and a Masters Online Teacher, University of Illinois at Chicago. Dr. Aman disclosed no relevant financial relationships. Dr. Islam is a medical adviser for the IMCHF, Montreal, and is based in New York. He is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships. Dr. Karama is a psychiatrist at the Douglas Mental Health University Institute, Montreal. He is an assistant professor at the department of psychiatry, McGill University, also in Montreal. He has no disclosures. Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the IMCHF. He has no disclosures.
References
1. J Atten Disord. 2020. doi: 10.1177/1087054720943271.
2. ADDitude Magazine. 2020 Jul 23.
3. Management of ADHD in Adults: What the Science Says. 2007 Oct 9. Guilford Press.
4. N Engl J Med. 2013 Nov 14;369(20):1935-44.
5. J Clin Psychiatry. 2002;63 Suppl 12:29-35.
6. J Atten Dis. 2015 Jan 12. doi: 10.1177/1087054144566076.
7. Psychiatry Res. 2020 Oct;292. doi: 10.1016/j.psychres.2020.113345.
8. Case Rep Cardiol. 2016. doi: 10.1155/2016/2343691.
9. Curr Diab Rep. 2019 Jun 27;19(8):46. doi: 10.1007/s11892-019-1174-x.
10. Curr Psychiatry Rep. 2014 Mar;16(3):436. doi: 10.1007/s/11920-013-0436-6.
11. Current Psychiatry. 2014 Dec;13(12):e3-4.
12. BMC Psychiatry. 2020;20(40). doi: 10.1186/s/12888-020-02707-9.
13. Psychol Addict Behav. 2016 Mar;30(2):252–62.
14. ADDitude Magazine. 2017 Apr 6.
15. Harv Mental Health Letter. 2009 Nov.
16. MGM J Med Sci. 2020 Jul 17(3):161-2.
17. J Child Psychol Psychiatry. 2020 Jul 7.
18. Int J Disaster Risk Reduct. 2020 Dec;51. doi: 10.1016/j.ijdrr.2020.101845.
Antipsychotics protective against COVID-19?
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.

While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.
While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Antipsychotics may protect against SARS-CoV-2 infection or lead to a milder course of illness, new research suggests.
“Counterintuitively,” the investigators noted, vulnerable people with severe mental illness “on antipsychotic treatment showed a lower risk of SARS-CoV-2 infection and a likely better COVID-19 prognosis.”
“These are very interesting findings that reflect a clinical reality where we see few patients with severe COVID-19, despite the presence of various risk factors,” study investigator Manuel Canal-Rivero, PhD, clinical psychologist, Virgen del Rocio University Hospital, Sevilla, Spain, said in a news release.
“The number of COVID-19 patients is lower than expected among this group of people and in cases where a proven infection does occur, the evolution is benign and does not reach a life-threatening clinical situation. These data as a whole seem to point to the protective effect of the medication,” Dr. Canal-Rivero added.
The study was published online as a letter to the editor February 19, 2021, in Schizophrenia Research.
A ‘striking’ finding
The researchers assessed the prevalence and prognosis of COVID-19 in 698 patients with serious mental disorders (SMDs) receiving treatment with long-acting injectable antipsychotic medication. The non-SMD population included the catchment area population of 557,576 individuals.
From February to November 2020, 4.1% of the non-SMD population were infected with SARS-CoV-2 versus just 1.3% of the SMD population (9 of 698 patients). All but one patient with SMD had asymptomatic illness (8 of 9, 89%). Accurate information on asymptomatic illness in the non-SMD population was not available.
There were also fewer hospital admissions in the SMD population (0% vs. 8.5%), ICU admissions (0% vs. 0.9%) and deaths because of COVID-19 (0% vs. 1.1%), although the differences were not statistically significant.
In related research, the same investigators found that many of the genes whose expression is altered by SARS-CoV-2 infection are significantly down-regulated by antipsychotic drugs.
“In a striking way, we have shown how antipsychotics reduce the activation of genes involved in many of the inflammatory and immunological pathways associated with the severity of COVID-19 infection,” Benedicto Crespo-Facorro, MD, PhD, University of Sevilla, who led the study, said in the news release.
“Although this finding requires replication, the discovery could be very significant because the treatment of COVID-19 with drugs originally indicated for unrelated clinical situations, that is to say drug repositioning, has been shown to be an interesting source of effective treatments for COVID-19 patients,” he added.
Antiviral properties?
In a comment, Samoon Ahmad, MD, professor, department of psychiatry, New York University, said the findings are “fascinating” and should be explored further.
While the findings on long-acting injectable antipsychotic treatment “seem counterintuitive at first, they are in line with other studies,” said Dr. Ahmad, who heads the inpatient psychiatry unit at Bellevue Hospital Center and is founder of the Integrative Center for Wellness in New York.
“ and antidepressant medications appear to activate key cellular proteins that the SARS-CoV-2 virus uses for replication,” explained Dr. Ahmad, who was not associated with the study.
For example, as reported by this news organization, a preliminary study published in 2020 showed that early treatment with the antidepressant fluvoxamine prevented clinical deterioration in adult outpatients with confirmed COVID-19.
The antipsychotic aripiprazole has also shown potential to treat severe COVID-19 infection.
“Consequently, there appears to be a possible explanation as to why these drugs afford patients with severe mental disorders increased protection against the SARS-CoV-2 virus,” Dr. Ahmad said in an interview.
However, he cautioned, there are several factors at play that could influence the results. Therefore, more research is needed before drawing any firm conclusions.
“Still, the possibility that psychiatric medications may have antiviral properties is a tremendous development and I really hope that additional studies confirm the preliminary findings,” Dr. Ahmad said.
The study had no specific funding. The authors and Dr. Ahmad disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Poor sleep and stress linked to higher headache recurrence in episodic migraine
Key clinical point: Poor sleep and higher stress level is associated with a higher rate of headache recurrence over next 6 weeks in patients with episodic migraine.
Major finding: Poor sleep quality was associated with a 22% higher rate of headache recurrence (adjusted hazard ratio [aHR], 1.22; 95% confidence interval [95% CI], 1.02-1.46), and the combination of poor sleep and moderate/high stress vs. good sleep and low stress was associated with a 31% higher rate of headache recurrence (aHR, 1.31; 95% CI, 1.05-1.65).
Study details: Findings are from a priori secondary analysis of a prospective cohort study of 98 patients with episodic migraine.
Disclosures: The work was funded by the National Institute of Neurological Disorders and Stroke, the American Sleep Medicine Foundation, the Harvard Clinical and Translational Science Center, and Harvard University and its affiliated academic health care centers. Dr. SM Bertisch reported receiving research support from and serving as a consultant for various sources. All other authors declared no financial conflicts of interest.
Source: Vgontzas A et al. Headache. 2021 Mar 22. doi: 10.1111/head.14105.
Key clinical point: Poor sleep and higher stress level is associated with a higher rate of headache recurrence over next 6 weeks in patients with episodic migraine.
Major finding: Poor sleep quality was associated with a 22% higher rate of headache recurrence (adjusted hazard ratio [aHR], 1.22; 95% confidence interval [95% CI], 1.02-1.46), and the combination of poor sleep and moderate/high stress vs. good sleep and low stress was associated with a 31% higher rate of headache recurrence (aHR, 1.31; 95% CI, 1.05-1.65).
Study details: Findings are from a priori secondary analysis of a prospective cohort study of 98 patients with episodic migraine.
Disclosures: The work was funded by the National Institute of Neurological Disorders and Stroke, the American Sleep Medicine Foundation, the Harvard Clinical and Translational Science Center, and Harvard University and its affiliated academic health care centers. Dr. SM Bertisch reported receiving research support from and serving as a consultant for various sources. All other authors declared no financial conflicts of interest.
Source: Vgontzas A et al. Headache. 2021 Mar 22. doi: 10.1111/head.14105.
Key clinical point: Poor sleep and higher stress level is associated with a higher rate of headache recurrence over next 6 weeks in patients with episodic migraine.
Major finding: Poor sleep quality was associated with a 22% higher rate of headache recurrence (adjusted hazard ratio [aHR], 1.22; 95% confidence interval [95% CI], 1.02-1.46), and the combination of poor sleep and moderate/high stress vs. good sleep and low stress was associated with a 31% higher rate of headache recurrence (aHR, 1.31; 95% CI, 1.05-1.65).
Study details: Findings are from a priori secondary analysis of a prospective cohort study of 98 patients with episodic migraine.
Disclosures: The work was funded by the National Institute of Neurological Disorders and Stroke, the American Sleep Medicine Foundation, the Harvard Clinical and Translational Science Center, and Harvard University and its affiliated academic health care centers. Dr. SM Bertisch reported receiving research support from and serving as a consultant for various sources. All other authors declared no financial conflicts of interest.
Source: Vgontzas A et al. Headache. 2021 Mar 22. doi: 10.1111/head.14105.