User login
Children and COVID: The long goodbye continues
COVID-19 continues to be a diminishing issue for U.S. children, as the number of new cases declined for the ninth consecutive week, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. The most recently infected children brought the total number of COVID-19 cases to just over 12.8 million since the pandemic began.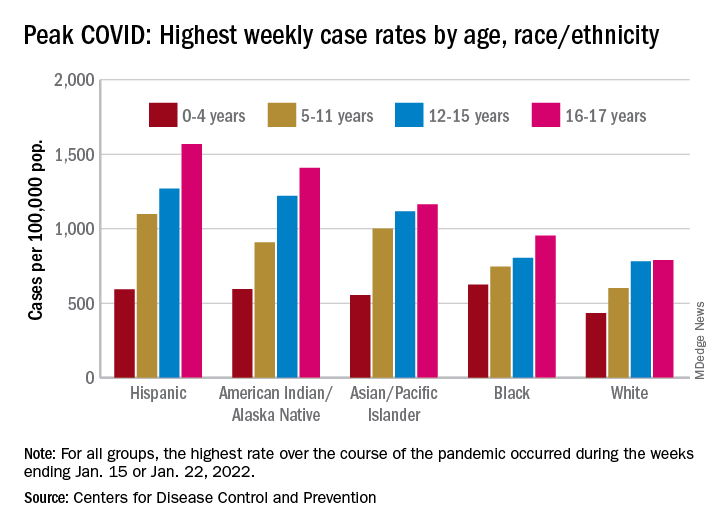
Other measures of COVID occurrence in children, such as hospital admissions and emergency department visits, also followed recent downward trends, although the sizes of the declines are beginning to decrease. Admissions dropped by 13.3% during the week ending March 26, but that followed declines of 25%, 20%, 26.5% and 24.4% for the 4 previous weeks, data from the Centers for Disease Control and Prevention show.
The slowdown in ED visits started a couple of weeks earlier, but the decline is still ongoing. As of March 25, ED visits with a confirmed COVID diagnosis represented just 0.4% of all visits for children aged 0-11 years, down from 1.1% on Feb. 25 and a peak of 14.3% on Jan. 15. For children aged 12-15, the latest figure is just 0.2%, compared with 0.5% on Feb. 25 and a peak of 14.3% on Jan. 9, the CDC reported on its COVID Data Tracker.
Although he was speaking of the nation as a whole and not specifically of children, Anthony Fauci, MD, the director of the National Institute of Allergy and Infectious Diseases, recently told the Washington Post that, “unless something changes dramatically,” another major surge isn’t on the horizon.
That sentiment, however, was not entirely shared by Moderna’s chief medical officer, Paul Burton, MD, PhD. In an interview with WebMD, he said that another COVID wave is inevitable and that it’s too soon to dismantle the vaccine infrastructure: “We’ve come so far. We’ve put so much into this to now take our foot off the gas. I think it would be a mistake for public health worldwide.”
Disparities during the Omicron surge
As the country puts Omicron in its rear view mirror, a quick look back at the CDC data shows some differences in how children were affected. At the surge’s peak in early to mid-January, Hispanic children were the most likely to get COVID-19, with incidence highest in the older groups. (See graph.)
At their peak week of Jan. 2-8, Hispanic children aged 16-17 years had a COVID rate of 1,568 cases per 100,000 population, versus 790 per 100,000 for White children, whose peak occurred a week later, from Jan. 9 to 15. Hispanic children aged 5-11 (1,098 per 100,000) and 12-15 (1,269 per 100,000) also had the highest recorded rates of the largest racial/ethnic groups, while Black children had the highest one-week rate, 625 per 100,000, among the 0- to 4-year-olds, according to the CDC.
COVID-19 continues to be a diminishing issue for U.S. children, as the number of new cases declined for the ninth consecutive week, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. The most recently infected children brought the total number of COVID-19 cases to just over 12.8 million since the pandemic began.
Other measures of COVID occurrence in children, such as hospital admissions and emergency department visits, also followed recent downward trends, although the sizes of the declines are beginning to decrease. Admissions dropped by 13.3% during the week ending March 26, but that followed declines of 25%, 20%, 26.5% and 24.4% for the 4 previous weeks, data from the Centers for Disease Control and Prevention show.
The slowdown in ED visits started a couple of weeks earlier, but the decline is still ongoing. As of March 25, ED visits with a confirmed COVID diagnosis represented just 0.4% of all visits for children aged 0-11 years, down from 1.1% on Feb. 25 and a peak of 14.3% on Jan. 15. For children aged 12-15, the latest figure is just 0.2%, compared with 0.5% on Feb. 25 and a peak of 14.3% on Jan. 9, the CDC reported on its COVID Data Tracker.
Although he was speaking of the nation as a whole and not specifically of children, Anthony Fauci, MD, the director of the National Institute of Allergy and Infectious Diseases, recently told the Washington Post that, “unless something changes dramatically,” another major surge isn’t on the horizon.
That sentiment, however, was not entirely shared by Moderna’s chief medical officer, Paul Burton, MD, PhD. In an interview with WebMD, he said that another COVID wave is inevitable and that it’s too soon to dismantle the vaccine infrastructure: “We’ve come so far. We’ve put so much into this to now take our foot off the gas. I think it would be a mistake for public health worldwide.”
Disparities during the Omicron surge
As the country puts Omicron in its rear view mirror, a quick look back at the CDC data shows some differences in how children were affected. At the surge’s peak in early to mid-January, Hispanic children were the most likely to get COVID-19, with incidence highest in the older groups. (See graph.)
At their peak week of Jan. 2-8, Hispanic children aged 16-17 years had a COVID rate of 1,568 cases per 100,000 population, versus 790 per 100,000 for White children, whose peak occurred a week later, from Jan. 9 to 15. Hispanic children aged 5-11 (1,098 per 100,000) and 12-15 (1,269 per 100,000) also had the highest recorded rates of the largest racial/ethnic groups, while Black children had the highest one-week rate, 625 per 100,000, among the 0- to 4-year-olds, according to the CDC.
COVID-19 continues to be a diminishing issue for U.S. children, as the number of new cases declined for the ninth consecutive week, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
the AAP and CHA said in their weekly COVID report. The most recently infected children brought the total number of COVID-19 cases to just over 12.8 million since the pandemic began.
Other measures of COVID occurrence in children, such as hospital admissions and emergency department visits, also followed recent downward trends, although the sizes of the declines are beginning to decrease. Admissions dropped by 13.3% during the week ending March 26, but that followed declines of 25%, 20%, 26.5% and 24.4% for the 4 previous weeks, data from the Centers for Disease Control and Prevention show.
The slowdown in ED visits started a couple of weeks earlier, but the decline is still ongoing. As of March 25, ED visits with a confirmed COVID diagnosis represented just 0.4% of all visits for children aged 0-11 years, down from 1.1% on Feb. 25 and a peak of 14.3% on Jan. 15. For children aged 12-15, the latest figure is just 0.2%, compared with 0.5% on Feb. 25 and a peak of 14.3% on Jan. 9, the CDC reported on its COVID Data Tracker.
Although he was speaking of the nation as a whole and not specifically of children, Anthony Fauci, MD, the director of the National Institute of Allergy and Infectious Diseases, recently told the Washington Post that, “unless something changes dramatically,” another major surge isn’t on the horizon.
That sentiment, however, was not entirely shared by Moderna’s chief medical officer, Paul Burton, MD, PhD. In an interview with WebMD, he said that another COVID wave is inevitable and that it’s too soon to dismantle the vaccine infrastructure: “We’ve come so far. We’ve put so much into this to now take our foot off the gas. I think it would be a mistake for public health worldwide.”
Disparities during the Omicron surge
As the country puts Omicron in its rear view mirror, a quick look back at the CDC data shows some differences in how children were affected. At the surge’s peak in early to mid-January, Hispanic children were the most likely to get COVID-19, with incidence highest in the older groups. (See graph.)
At their peak week of Jan. 2-8, Hispanic children aged 16-17 years had a COVID rate of 1,568 cases per 100,000 population, versus 790 per 100,000 for White children, whose peak occurred a week later, from Jan. 9 to 15. Hispanic children aged 5-11 (1,098 per 100,000) and 12-15 (1,269 per 100,000) also had the highest recorded rates of the largest racial/ethnic groups, while Black children had the highest one-week rate, 625 per 100,000, among the 0- to 4-year-olds, according to the CDC.
What a sleep expert thinks of sleep trackers
The pandemic not only disrupted sleep but may have also triggered an uptick in the use of wearable tech. Sleep tracking was featured at the Cardiovascular Health Tech virtual conference 2022, sponsored by the Institute of Electrical and Electronics Engineers Engineering in Medicine & Biology Society technical committee on Cardiopulmonary Systems and Physiology-Based Engineering.
This news organization interviewed presenter Kelly Glazer Baron, PhD, MPH, DBSM, an associate professor at the University of Utah, Salt Lake City, and a clinical psychologist specializing in behavioral sleep medicine.
The interview has been edited for length and clarity.
Question: Are consumer sleep trackers mainly divided into “nearables” – things that you put at the side of the bed or under the pillow – vs. wearables?
Dr. Baron: There are so many different devices these days. There are things that you put under your mattress or pillow; there are bedside recording devices; then there are headbands, rings, wrist-worn, all kinds of things.
Q: At the conference, Philip de Chazal, PhD, (University of Sydney) described the evidence on sleep tracking smartphone apps as woeful. Would you agree with that?
A: Yes. I would agree if you’re looking at how accurate they are at recording sleep, particularly compared with what we would define as the gold standard, which is a sleep study wherein you have electrodes on the scalp and you’re measuring the electrical activity directly.
They are best at detecting when you get into the bed and when you get out. But even then, there isn’t good evidence that they do that accurately when there are two people in the bed.
Overall, they may give you a general gist of what’s happening in terms of time in and out of bed, but we’re doubtful on their recording ability to tell sleep from wake time.
Q: Are the wrist-worn devices better for sleep tracking?
A: They’re getting better. We’ve used wrist activity monitors in research for years. They use an accelerometer to measure movement, and then an algorithm determines whether an interval of time is called sleep or wake.
Recently, they’ve incorporated more sensors, such as heart rate, and they can more accurately decipher rapid eye movement (REM) sleep from non-REM. They’re still not as good as doing a full sleep study. But they’re getting closer.
Q: If asked how you slept, most of us think we can answer without needing to look at a smartphone, but maybe not. Can you explain “paradoxical insomnia”?
A: You can’t really know if you’re sleeping because if you know you’re asleep, then you can’t be asleep because it’s a state of unconsciousness. How people decide whether they had a good night’s sleep probably depends on a lot of things about how they feel when they wake up in the morning or if they remember being up in the night.
Quality of sleep is not really something that people can directly ascertain. There is a selection of people who feel awake all night but they actually are sleeping. They feel that their sleep quality is poor: They’re suffering; they have insomnia, but from the objective data, they are sleeping fine.
Q: Is this related to non-REM stage 1 sleep, when you may not be aware that you’re asleep?
A: No. I’m talking about people who come into the sleep lab for an overnight study and get hooked up. And in the morning, they’ll tell the tech I was awake all night, but the tech will see that their sleep was just fine.
There is a disconnect between how people perceive their sleep and how they actually sleep. For most people it’s impossible to be completely accurate to know how much you’re sleeping. Then there are some people who perceive it very differently.
Sleep trackers don’t have the level of detail of sleep studies that use scalp electrodes. When we get into the details of sleep measurement, we’re measuring 30-second epochs (sampling periods), where we look at broad measures of electrical activity. There is even more detail there that can be pulled out using other techniques, such as analyzing the spectrum of the EEG. For example, some studies have found a beta frequency in the EEG of people with insomnia, so even though they are sleeping, they often feel awake.
Basically, the subjective experience of sleep somewhat overlaps with the objective recording of what’s happening on a sleep study, but not completely.
Q: You said that first thing in the morning might not be the best time to assess your sleep – if you wake up groggy and are already thinking, “The day is shot.”
A: In general, people really feel worst in the morning. Their circadian drive is low, especially if they’re a little sleep deprived. You shouldn’t judge the day on the first hour after waking – most people are pretty cognitively impaired. I tell people they need some boot-up time.
You feel differently as the day goes on and even at different points of the day. There’s a lull in the early afternoon because of your circadian dip and then we get a second wind in the evening. How you feel isn’t one flat line; it’s really a rhythm throughout the day
Q: Would you say that consumer sleep trackers are okay for individuals to use to see a pattern but are maybe not accurate enough to use more globally in research?
A: I think there is a huge opportunity to understand sleep at a population level. For example, if there’s been a hurricane or an earthquake or Superbowl Sunday, companies have an opportunity to look at the impact – say, daylight saving time and how it affects sleep across different countries, or men vs. women, or different age groups.
There was a paper about sleep among hospital workers in Wuhan during the outbreak of the pandemic. That was a creative use of wearable devices to look at sleep in a large population.
Now, of course, the devices are not given out randomly; the people who buy them are probably a little bit healthier, maybe a little bit younger – that sort of thing. It is a biased sample.
Q: As you note, mobile health trackers tend to be used by the “worried well.” Can you tell us about your paper that introduced the term “orthosomnia,” or “a perfectionistic quest for the ideal sleep in order to optimize daytime function”?
A: As these devices came out, more people were coming into the clinic and shoving their data in front of us saying, “I don’t feel well, and I don’t sleep 7 hours.” They were focused on this specific number. Back when we wrote this paper, the devices were primarily movement based (now the devices are a bit more accurate). Some would say, “My sleep is light, and it’s not deep.” We’d do a sleep study that showed that they have deep sleep, but they would still believe their device even though the device really wasn’t able to classify sleep accurately.
We even found people making their sleep worse because of the device. For example, trying to get the number higher by spending more time lying in bed trying to sleep which is the opposite of what you want someone with insomnia to do. These people held the data so tight and really felt that it characterized their experience, even though we sleep medicine practitioners didn’t find it very accurate and felt that it was somewhat unhelpful to their treatment.
Q: What advice would you give the harried primary care physician presented with a patient’s hypnogram or sleep pattern?
A: As someone once pointed out to me, it’s a conversation opener about their sleep. Did they buy the device because they’re worried about their sleep? It’s unlikely that you can glean anything clinically useful from the data.
I briefly look at it to see the duration of their sleep, the regularity in their sleep pattern – the pattern of awakenings during the night might suggest that they have some insomnia. But it doesn’t take the place of clinical assessment for conditions like sleep apnea: Are they snoring? Are they unrefreshed?
I had a patient in the orthosomnia study who was given a sleep tracker by a family member. He brought the data to his doctor who ordered a sleep study that found he had sleep apnea. He would say, “The device diagnosed my sleep apnea.” But that wasn’t actually the case; it just opened the conversation and the clinician said, “Well, let’s order a sleep study.”
Q: The device told him he wasn’t getting much sleep and then the sleep study told him it was apnea.
A: Right. It’s impossible to pick up sleep apnea. Some of the latest devices have some oximetry reading but it is not a clinically validated oximetry that could diagnose sleep apnea.
When these first came out I thought I’d get more referrals. So far, I haven’t had a single person come in and ask if they have sleep apnea. If you have a patient saying, “Hey, I’m worried about my oxygen level and here’s my data,” then the clinician should consider whether they need a sleep study for sleep apnea.
Q: You did a survey that suggests that clinicians are less keen on these devices than consumers. Conor Heneghan of Fitbit/Google also mentioned a study using the Fitbit Charge and a SleepLife portal. The patients were very engaged but only one physician (out of 49) logged into the portal to look at the data.
A: Our survey of sleep professionals (which we need to publish) showed that they were wary of the data. They found it frustrating in some ways because it took time out of the clinical encounter.
Some of them said that parents are putting trackers on their children and then catastrophizing their children’s sleep.
Q: Is there such a thing as an ideal hypnogram or does it vary by individual?
A: I would say that it depends on a lot of things. If you think about a hypnogram from a sleep study, the patient is not sleeping in their home environment, and it’s only one night. There’s a range of what would be considered normal, and it’s related to your sex and your age.
One night is not going to be sufficient to characterize your percentage in this or that sleep stage. Our patients come in saying, “I’m not getting enough REM.” But there isn’t a sleep disorder called lack of REM; there’s no treatment for that. It’s probably pretty normal for them or maybe they’re taking medications that suppress their REM, such as antidepressants.
The tech world is very interested to sense REM properly and to display it. But on the treatment side of things, there’s not much that we do with that data. We’re more interested in the consolidation of their sleep, the duration of their sleep, breathing-related sleep disorders, those sorts of things.
Q: Is there any reason to be concerned about the amount of REM sleep in terms of outcomes? We know that poor sleep can lead to bad cardiovascular outcomes, but has any of that correlated to sleep stage?
A: There are studies where they’ve experimentally deprived people of certain stages of sleep, but they’re not very useful in the real world. We’re looking at sleep holistically: Do you have a good sleep pattern? Any breathing-related sleep disorders? Insomnia? We don’t treat sleep by the stage.
Q: Any concern that people who are focused on a device may be ignoring the basic tenets of good sleep hygiene?
A: If people are doing things that are obviously bad for their sleep, like working too late, not exercising enough, sleeping in on weekends to compensate for being up late during the week, or probably the biggest thing contributing to insomnia – stress. A device itself won’t fix those things but it could show you the evidence.
If somebody really has a sleep disorder, then sleep hygiene alone is probably not going to be enough. They’re going to need to engage in a more extensive program to improve their sleep, such as cognitive-behavioral therapy for insomnia.
Q: Is there anything else you want to mention?
A: I don’t want to leave with a reputation of being against sleep trackers. I think they are a great opportunity for people to get excited about and learn about their sleep and try to improve it. We have a lot to learn about what people want from their data and how we can use that data to improve people’s sleep.
As providers, we can engage with our patients – sleep is an automatic process, but improving sleep takes some effort. Buying a device is not going to automatically make you sleep better. It takes work to establish a better sleep pattern; it may require some cognitive-behavioral therapy or treating a sleep disorder. That takes some work.
Dr. Baron reported no conflicts of interest.A version of this article first appeared on Medscape.com.
The pandemic not only disrupted sleep but may have also triggered an uptick in the use of wearable tech. Sleep tracking was featured at the Cardiovascular Health Tech virtual conference 2022, sponsored by the Institute of Electrical and Electronics Engineers Engineering in Medicine & Biology Society technical committee on Cardiopulmonary Systems and Physiology-Based Engineering.
This news organization interviewed presenter Kelly Glazer Baron, PhD, MPH, DBSM, an associate professor at the University of Utah, Salt Lake City, and a clinical psychologist specializing in behavioral sleep medicine.
The interview has been edited for length and clarity.
Question: Are consumer sleep trackers mainly divided into “nearables” – things that you put at the side of the bed or under the pillow – vs. wearables?
Dr. Baron: There are so many different devices these days. There are things that you put under your mattress or pillow; there are bedside recording devices; then there are headbands, rings, wrist-worn, all kinds of things.
Q: At the conference, Philip de Chazal, PhD, (University of Sydney) described the evidence on sleep tracking smartphone apps as woeful. Would you agree with that?
A: Yes. I would agree if you’re looking at how accurate they are at recording sleep, particularly compared with what we would define as the gold standard, which is a sleep study wherein you have electrodes on the scalp and you’re measuring the electrical activity directly.
They are best at detecting when you get into the bed and when you get out. But even then, there isn’t good evidence that they do that accurately when there are two people in the bed.
Overall, they may give you a general gist of what’s happening in terms of time in and out of bed, but we’re doubtful on their recording ability to tell sleep from wake time.
Q: Are the wrist-worn devices better for sleep tracking?
A: They’re getting better. We’ve used wrist activity monitors in research for years. They use an accelerometer to measure movement, and then an algorithm determines whether an interval of time is called sleep or wake.
Recently, they’ve incorporated more sensors, such as heart rate, and they can more accurately decipher rapid eye movement (REM) sleep from non-REM. They’re still not as good as doing a full sleep study. But they’re getting closer.
Q: If asked how you slept, most of us think we can answer without needing to look at a smartphone, but maybe not. Can you explain “paradoxical insomnia”?
A: You can’t really know if you’re sleeping because if you know you’re asleep, then you can’t be asleep because it’s a state of unconsciousness. How people decide whether they had a good night’s sleep probably depends on a lot of things about how they feel when they wake up in the morning or if they remember being up in the night.
Quality of sleep is not really something that people can directly ascertain. There is a selection of people who feel awake all night but they actually are sleeping. They feel that their sleep quality is poor: They’re suffering; they have insomnia, but from the objective data, they are sleeping fine.
Q: Is this related to non-REM stage 1 sleep, when you may not be aware that you’re asleep?
A: No. I’m talking about people who come into the sleep lab for an overnight study and get hooked up. And in the morning, they’ll tell the tech I was awake all night, but the tech will see that their sleep was just fine.
There is a disconnect between how people perceive their sleep and how they actually sleep. For most people it’s impossible to be completely accurate to know how much you’re sleeping. Then there are some people who perceive it very differently.
Sleep trackers don’t have the level of detail of sleep studies that use scalp electrodes. When we get into the details of sleep measurement, we’re measuring 30-second epochs (sampling periods), where we look at broad measures of electrical activity. There is even more detail there that can be pulled out using other techniques, such as analyzing the spectrum of the EEG. For example, some studies have found a beta frequency in the EEG of people with insomnia, so even though they are sleeping, they often feel awake.
Basically, the subjective experience of sleep somewhat overlaps with the objective recording of what’s happening on a sleep study, but not completely.
Q: You said that first thing in the morning might not be the best time to assess your sleep – if you wake up groggy and are already thinking, “The day is shot.”
A: In general, people really feel worst in the morning. Their circadian drive is low, especially if they’re a little sleep deprived. You shouldn’t judge the day on the first hour after waking – most people are pretty cognitively impaired. I tell people they need some boot-up time.
You feel differently as the day goes on and even at different points of the day. There’s a lull in the early afternoon because of your circadian dip and then we get a second wind in the evening. How you feel isn’t one flat line; it’s really a rhythm throughout the day
Q: Would you say that consumer sleep trackers are okay for individuals to use to see a pattern but are maybe not accurate enough to use more globally in research?
A: I think there is a huge opportunity to understand sleep at a population level. For example, if there’s been a hurricane or an earthquake or Superbowl Sunday, companies have an opportunity to look at the impact – say, daylight saving time and how it affects sleep across different countries, or men vs. women, or different age groups.
There was a paper about sleep among hospital workers in Wuhan during the outbreak of the pandemic. That was a creative use of wearable devices to look at sleep in a large population.
Now, of course, the devices are not given out randomly; the people who buy them are probably a little bit healthier, maybe a little bit younger – that sort of thing. It is a biased sample.
Q: As you note, mobile health trackers tend to be used by the “worried well.” Can you tell us about your paper that introduced the term “orthosomnia,” or “a perfectionistic quest for the ideal sleep in order to optimize daytime function”?
A: As these devices came out, more people were coming into the clinic and shoving their data in front of us saying, “I don’t feel well, and I don’t sleep 7 hours.” They were focused on this specific number. Back when we wrote this paper, the devices were primarily movement based (now the devices are a bit more accurate). Some would say, “My sleep is light, and it’s not deep.” We’d do a sleep study that showed that they have deep sleep, but they would still believe their device even though the device really wasn’t able to classify sleep accurately.
We even found people making their sleep worse because of the device. For example, trying to get the number higher by spending more time lying in bed trying to sleep which is the opposite of what you want someone with insomnia to do. These people held the data so tight and really felt that it characterized their experience, even though we sleep medicine practitioners didn’t find it very accurate and felt that it was somewhat unhelpful to their treatment.
Q: What advice would you give the harried primary care physician presented with a patient’s hypnogram or sleep pattern?
A: As someone once pointed out to me, it’s a conversation opener about their sleep. Did they buy the device because they’re worried about their sleep? It’s unlikely that you can glean anything clinically useful from the data.
I briefly look at it to see the duration of their sleep, the regularity in their sleep pattern – the pattern of awakenings during the night might suggest that they have some insomnia. But it doesn’t take the place of clinical assessment for conditions like sleep apnea: Are they snoring? Are they unrefreshed?
I had a patient in the orthosomnia study who was given a sleep tracker by a family member. He brought the data to his doctor who ordered a sleep study that found he had sleep apnea. He would say, “The device diagnosed my sleep apnea.” But that wasn’t actually the case; it just opened the conversation and the clinician said, “Well, let’s order a sleep study.”
Q: The device told him he wasn’t getting much sleep and then the sleep study told him it was apnea.
A: Right. It’s impossible to pick up sleep apnea. Some of the latest devices have some oximetry reading but it is not a clinically validated oximetry that could diagnose sleep apnea.
When these first came out I thought I’d get more referrals. So far, I haven’t had a single person come in and ask if they have sleep apnea. If you have a patient saying, “Hey, I’m worried about my oxygen level and here’s my data,” then the clinician should consider whether they need a sleep study for sleep apnea.
Q: You did a survey that suggests that clinicians are less keen on these devices than consumers. Conor Heneghan of Fitbit/Google also mentioned a study using the Fitbit Charge and a SleepLife portal. The patients were very engaged but only one physician (out of 49) logged into the portal to look at the data.
A: Our survey of sleep professionals (which we need to publish) showed that they were wary of the data. They found it frustrating in some ways because it took time out of the clinical encounter.
Some of them said that parents are putting trackers on their children and then catastrophizing their children’s sleep.
Q: Is there such a thing as an ideal hypnogram or does it vary by individual?
A: I would say that it depends on a lot of things. If you think about a hypnogram from a sleep study, the patient is not sleeping in their home environment, and it’s only one night. There’s a range of what would be considered normal, and it’s related to your sex and your age.
One night is not going to be sufficient to characterize your percentage in this or that sleep stage. Our patients come in saying, “I’m not getting enough REM.” But there isn’t a sleep disorder called lack of REM; there’s no treatment for that. It’s probably pretty normal for them or maybe they’re taking medications that suppress their REM, such as antidepressants.
The tech world is very interested to sense REM properly and to display it. But on the treatment side of things, there’s not much that we do with that data. We’re more interested in the consolidation of their sleep, the duration of their sleep, breathing-related sleep disorders, those sorts of things.
Q: Is there any reason to be concerned about the amount of REM sleep in terms of outcomes? We know that poor sleep can lead to bad cardiovascular outcomes, but has any of that correlated to sleep stage?
A: There are studies where they’ve experimentally deprived people of certain stages of sleep, but they’re not very useful in the real world. We’re looking at sleep holistically: Do you have a good sleep pattern? Any breathing-related sleep disorders? Insomnia? We don’t treat sleep by the stage.
Q: Any concern that people who are focused on a device may be ignoring the basic tenets of good sleep hygiene?
A: If people are doing things that are obviously bad for their sleep, like working too late, not exercising enough, sleeping in on weekends to compensate for being up late during the week, or probably the biggest thing contributing to insomnia – stress. A device itself won’t fix those things but it could show you the evidence.
If somebody really has a sleep disorder, then sleep hygiene alone is probably not going to be enough. They’re going to need to engage in a more extensive program to improve their sleep, such as cognitive-behavioral therapy for insomnia.
Q: Is there anything else you want to mention?
A: I don’t want to leave with a reputation of being against sleep trackers. I think they are a great opportunity for people to get excited about and learn about their sleep and try to improve it. We have a lot to learn about what people want from their data and how we can use that data to improve people’s sleep.
As providers, we can engage with our patients – sleep is an automatic process, but improving sleep takes some effort. Buying a device is not going to automatically make you sleep better. It takes work to establish a better sleep pattern; it may require some cognitive-behavioral therapy or treating a sleep disorder. That takes some work.
Dr. Baron reported no conflicts of interest.A version of this article first appeared on Medscape.com.
The pandemic not only disrupted sleep but may have also triggered an uptick in the use of wearable tech. Sleep tracking was featured at the Cardiovascular Health Tech virtual conference 2022, sponsored by the Institute of Electrical and Electronics Engineers Engineering in Medicine & Biology Society technical committee on Cardiopulmonary Systems and Physiology-Based Engineering.
This news organization interviewed presenter Kelly Glazer Baron, PhD, MPH, DBSM, an associate professor at the University of Utah, Salt Lake City, and a clinical psychologist specializing in behavioral sleep medicine.
The interview has been edited for length and clarity.
Question: Are consumer sleep trackers mainly divided into “nearables” – things that you put at the side of the bed or under the pillow – vs. wearables?
Dr. Baron: There are so many different devices these days. There are things that you put under your mattress or pillow; there are bedside recording devices; then there are headbands, rings, wrist-worn, all kinds of things.
Q: At the conference, Philip de Chazal, PhD, (University of Sydney) described the evidence on sleep tracking smartphone apps as woeful. Would you agree with that?
A: Yes. I would agree if you’re looking at how accurate they are at recording sleep, particularly compared with what we would define as the gold standard, which is a sleep study wherein you have electrodes on the scalp and you’re measuring the electrical activity directly.
They are best at detecting when you get into the bed and when you get out. But even then, there isn’t good evidence that they do that accurately when there are two people in the bed.
Overall, they may give you a general gist of what’s happening in terms of time in and out of bed, but we’re doubtful on their recording ability to tell sleep from wake time.
Q: Are the wrist-worn devices better for sleep tracking?
A: They’re getting better. We’ve used wrist activity monitors in research for years. They use an accelerometer to measure movement, and then an algorithm determines whether an interval of time is called sleep or wake.
Recently, they’ve incorporated more sensors, such as heart rate, and they can more accurately decipher rapid eye movement (REM) sleep from non-REM. They’re still not as good as doing a full sleep study. But they’re getting closer.
Q: If asked how you slept, most of us think we can answer without needing to look at a smartphone, but maybe not. Can you explain “paradoxical insomnia”?
A: You can’t really know if you’re sleeping because if you know you’re asleep, then you can’t be asleep because it’s a state of unconsciousness. How people decide whether they had a good night’s sleep probably depends on a lot of things about how they feel when they wake up in the morning or if they remember being up in the night.
Quality of sleep is not really something that people can directly ascertain. There is a selection of people who feel awake all night but they actually are sleeping. They feel that their sleep quality is poor: They’re suffering; they have insomnia, but from the objective data, they are sleeping fine.
Q: Is this related to non-REM stage 1 sleep, when you may not be aware that you’re asleep?
A: No. I’m talking about people who come into the sleep lab for an overnight study and get hooked up. And in the morning, they’ll tell the tech I was awake all night, but the tech will see that their sleep was just fine.
There is a disconnect between how people perceive their sleep and how they actually sleep. For most people it’s impossible to be completely accurate to know how much you’re sleeping. Then there are some people who perceive it very differently.
Sleep trackers don’t have the level of detail of sleep studies that use scalp electrodes. When we get into the details of sleep measurement, we’re measuring 30-second epochs (sampling periods), where we look at broad measures of electrical activity. There is even more detail there that can be pulled out using other techniques, such as analyzing the spectrum of the EEG. For example, some studies have found a beta frequency in the EEG of people with insomnia, so even though they are sleeping, they often feel awake.
Basically, the subjective experience of sleep somewhat overlaps with the objective recording of what’s happening on a sleep study, but not completely.
Q: You said that first thing in the morning might not be the best time to assess your sleep – if you wake up groggy and are already thinking, “The day is shot.”
A: In general, people really feel worst in the morning. Their circadian drive is low, especially if they’re a little sleep deprived. You shouldn’t judge the day on the first hour after waking – most people are pretty cognitively impaired. I tell people they need some boot-up time.
You feel differently as the day goes on and even at different points of the day. There’s a lull in the early afternoon because of your circadian dip and then we get a second wind in the evening. How you feel isn’t one flat line; it’s really a rhythm throughout the day
Q: Would you say that consumer sleep trackers are okay for individuals to use to see a pattern but are maybe not accurate enough to use more globally in research?
A: I think there is a huge opportunity to understand sleep at a population level. For example, if there’s been a hurricane or an earthquake or Superbowl Sunday, companies have an opportunity to look at the impact – say, daylight saving time and how it affects sleep across different countries, or men vs. women, or different age groups.
There was a paper about sleep among hospital workers in Wuhan during the outbreak of the pandemic. That was a creative use of wearable devices to look at sleep in a large population.
Now, of course, the devices are not given out randomly; the people who buy them are probably a little bit healthier, maybe a little bit younger – that sort of thing. It is a biased sample.
Q: As you note, mobile health trackers tend to be used by the “worried well.” Can you tell us about your paper that introduced the term “orthosomnia,” or “a perfectionistic quest for the ideal sleep in order to optimize daytime function”?
A: As these devices came out, more people were coming into the clinic and shoving their data in front of us saying, “I don’t feel well, and I don’t sleep 7 hours.” They were focused on this specific number. Back when we wrote this paper, the devices were primarily movement based (now the devices are a bit more accurate). Some would say, “My sleep is light, and it’s not deep.” We’d do a sleep study that showed that they have deep sleep, but they would still believe their device even though the device really wasn’t able to classify sleep accurately.
We even found people making their sleep worse because of the device. For example, trying to get the number higher by spending more time lying in bed trying to sleep which is the opposite of what you want someone with insomnia to do. These people held the data so tight and really felt that it characterized their experience, even though we sleep medicine practitioners didn’t find it very accurate and felt that it was somewhat unhelpful to their treatment.
Q: What advice would you give the harried primary care physician presented with a patient’s hypnogram or sleep pattern?
A: As someone once pointed out to me, it’s a conversation opener about their sleep. Did they buy the device because they’re worried about their sleep? It’s unlikely that you can glean anything clinically useful from the data.
I briefly look at it to see the duration of their sleep, the regularity in their sleep pattern – the pattern of awakenings during the night might suggest that they have some insomnia. But it doesn’t take the place of clinical assessment for conditions like sleep apnea: Are they snoring? Are they unrefreshed?
I had a patient in the orthosomnia study who was given a sleep tracker by a family member. He brought the data to his doctor who ordered a sleep study that found he had sleep apnea. He would say, “The device diagnosed my sleep apnea.” But that wasn’t actually the case; it just opened the conversation and the clinician said, “Well, let’s order a sleep study.”
Q: The device told him he wasn’t getting much sleep and then the sleep study told him it was apnea.
A: Right. It’s impossible to pick up sleep apnea. Some of the latest devices have some oximetry reading but it is not a clinically validated oximetry that could diagnose sleep apnea.
When these first came out I thought I’d get more referrals. So far, I haven’t had a single person come in and ask if they have sleep apnea. If you have a patient saying, “Hey, I’m worried about my oxygen level and here’s my data,” then the clinician should consider whether they need a sleep study for sleep apnea.
Q: You did a survey that suggests that clinicians are less keen on these devices than consumers. Conor Heneghan of Fitbit/Google also mentioned a study using the Fitbit Charge and a SleepLife portal. The patients were very engaged but only one physician (out of 49) logged into the portal to look at the data.
A: Our survey of sleep professionals (which we need to publish) showed that they were wary of the data. They found it frustrating in some ways because it took time out of the clinical encounter.
Some of them said that parents are putting trackers on their children and then catastrophizing their children’s sleep.
Q: Is there such a thing as an ideal hypnogram or does it vary by individual?
A: I would say that it depends on a lot of things. If you think about a hypnogram from a sleep study, the patient is not sleeping in their home environment, and it’s only one night. There’s a range of what would be considered normal, and it’s related to your sex and your age.
One night is not going to be sufficient to characterize your percentage in this or that sleep stage. Our patients come in saying, “I’m not getting enough REM.” But there isn’t a sleep disorder called lack of REM; there’s no treatment for that. It’s probably pretty normal for them or maybe they’re taking medications that suppress their REM, such as antidepressants.
The tech world is very interested to sense REM properly and to display it. But on the treatment side of things, there’s not much that we do with that data. We’re more interested in the consolidation of their sleep, the duration of their sleep, breathing-related sleep disorders, those sorts of things.
Q: Is there any reason to be concerned about the amount of REM sleep in terms of outcomes? We know that poor sleep can lead to bad cardiovascular outcomes, but has any of that correlated to sleep stage?
A: There are studies where they’ve experimentally deprived people of certain stages of sleep, but they’re not very useful in the real world. We’re looking at sleep holistically: Do you have a good sleep pattern? Any breathing-related sleep disorders? Insomnia? We don’t treat sleep by the stage.
Q: Any concern that people who are focused on a device may be ignoring the basic tenets of good sleep hygiene?
A: If people are doing things that are obviously bad for their sleep, like working too late, not exercising enough, sleeping in on weekends to compensate for being up late during the week, or probably the biggest thing contributing to insomnia – stress. A device itself won’t fix those things but it could show you the evidence.
If somebody really has a sleep disorder, then sleep hygiene alone is probably not going to be enough. They’re going to need to engage in a more extensive program to improve their sleep, such as cognitive-behavioral therapy for insomnia.
Q: Is there anything else you want to mention?
A: I don’t want to leave with a reputation of being against sleep trackers. I think they are a great opportunity for people to get excited about and learn about their sleep and try to improve it. We have a lot to learn about what people want from their data and how we can use that data to improve people’s sleep.
As providers, we can engage with our patients – sleep is an automatic process, but improving sleep takes some effort. Buying a device is not going to automatically make you sleep better. It takes work to establish a better sleep pattern; it may require some cognitive-behavioral therapy or treating a sleep disorder. That takes some work.
Dr. Baron reported no conflicts of interest.A version of this article first appeared on Medscape.com.
Oscars fight highlights for many the toll alopecia may carry
The Academy Awards ceremony on March 27 is a buzzing topic of conversation.
Troy Kotsur became the first deaf man to win an Oscar – and the highly coveted best supporting actor award, at that.
But it was what happened afterward that arguably stole the show.
Viewers and audience members alike watched in awe as actor Will Smith marched on stage and struck award presenter and comedian Chris Rock in the face after he directed a joke at Smith’s wife, Jada Pinkett Smith, for her shaved head.
and can lead to feelings of depression or mental illness.
About 700,000 people in the United States have alopecia areata, according to a 2020 study. Of them, slightly more than half are women, and more than 77% are White.
Shortly after the awards show, the Los Angeles Police Department released a statement saying it was aware of the incident and Mr. Rock had not pressed charges against Mr. Smith.
The incident set social media ablaze, and strong sentiments were heard from those who have been personally affected by alopecia.
Illness is never funny
Mr. Rock’s comment can be triggering to the millions who have been affected by hair loss, said Carolyn Goh, MD, a dermatologist at UCLA Health.
“As someone with alopecia myself, I consider it a microaggression,” Dr. Goh said. “I’ve experienced many similar comments. These build up over time and wear us down.”
One U.K.-based Instagram user, Kitty Dry, said the expression on Ms. Pinkett Smith’s face represented the hurt felt by so many with this condition.
“I want to preface this post by saying that in no way do I condone any sort of violence, but thank you Will Smith,” said Ms. Dry, 23, who was diagnosed with alopecia universalis after losing all her hair in 12 weeks.
“That slap was for anyone with alopecia who has ever been at the butt of an unwanted joke, comment or stare,” Ms. Dry said.
Others posted comments raising awareness of the tragic passing of Rio Allred, a 12-year-old girl with alopecia who recently died by suicide.
Rio Allred is said to have endured serious bullying at school, with classmates pulling off her wig and smacking her head, according to the Canadian Alopecia Areata Foundation.
It’s common for those who have hair loss conditions to feel helpless, and sometimes confused, said Amy McMichael, MD, a professor and chair of the dermatology department at Wake Forest University, Winston-Salem, N.C. That’s why it’s critical for those people to see a board-certified dermatologist, so they know they are not alone.
“As dermatologists, we can not only diagnose the type of alopecia, but we can also render treatment,” Dr. McMichael said.
Alopecia awareness
Dermatologists can also help connect patients to organizations that address the physical and emotional struggles of those who have hair loss, such as the National Alopecia Areata Foundation and the Scarring Alopecia Foundation, Dr. McMichael said.
She hopes the event shows people the “many faces of hair loss” and shows that these conditions can happen to people of all ages, ethnicities, and genders.
The National Alopecia Areata Foundation calls what happened at the Oscars a “teachable” moment.
“We encourage both our community and the broader public to learn more about alopecia areata so we can end the stigma around this disease,” the organization said in a statement.
Dr. Goh said that anyone with hair loss should feel free to explore potential medical causes and, if needed, seek out mental health treatment, too.
A version of this article first appeared on WebMD.com.
The Academy Awards ceremony on March 27 is a buzzing topic of conversation.
Troy Kotsur became the first deaf man to win an Oscar – and the highly coveted best supporting actor award, at that.
But it was what happened afterward that arguably stole the show.
Viewers and audience members alike watched in awe as actor Will Smith marched on stage and struck award presenter and comedian Chris Rock in the face after he directed a joke at Smith’s wife, Jada Pinkett Smith, for her shaved head.
and can lead to feelings of depression or mental illness.
About 700,000 people in the United States have alopecia areata, according to a 2020 study. Of them, slightly more than half are women, and more than 77% are White.
Shortly after the awards show, the Los Angeles Police Department released a statement saying it was aware of the incident and Mr. Rock had not pressed charges against Mr. Smith.
The incident set social media ablaze, and strong sentiments were heard from those who have been personally affected by alopecia.
Illness is never funny
Mr. Rock’s comment can be triggering to the millions who have been affected by hair loss, said Carolyn Goh, MD, a dermatologist at UCLA Health.
“As someone with alopecia myself, I consider it a microaggression,” Dr. Goh said. “I’ve experienced many similar comments. These build up over time and wear us down.”
One U.K.-based Instagram user, Kitty Dry, said the expression on Ms. Pinkett Smith’s face represented the hurt felt by so many with this condition.
“I want to preface this post by saying that in no way do I condone any sort of violence, but thank you Will Smith,” said Ms. Dry, 23, who was diagnosed with alopecia universalis after losing all her hair in 12 weeks.
“That slap was for anyone with alopecia who has ever been at the butt of an unwanted joke, comment or stare,” Ms. Dry said.
Others posted comments raising awareness of the tragic passing of Rio Allred, a 12-year-old girl with alopecia who recently died by suicide.
Rio Allred is said to have endured serious bullying at school, with classmates pulling off her wig and smacking her head, according to the Canadian Alopecia Areata Foundation.
It’s common for those who have hair loss conditions to feel helpless, and sometimes confused, said Amy McMichael, MD, a professor and chair of the dermatology department at Wake Forest University, Winston-Salem, N.C. That’s why it’s critical for those people to see a board-certified dermatologist, so they know they are not alone.
“As dermatologists, we can not only diagnose the type of alopecia, but we can also render treatment,” Dr. McMichael said.
Alopecia awareness
Dermatologists can also help connect patients to organizations that address the physical and emotional struggles of those who have hair loss, such as the National Alopecia Areata Foundation and the Scarring Alopecia Foundation, Dr. McMichael said.
She hopes the event shows people the “many faces of hair loss” and shows that these conditions can happen to people of all ages, ethnicities, and genders.
The National Alopecia Areata Foundation calls what happened at the Oscars a “teachable” moment.
“We encourage both our community and the broader public to learn more about alopecia areata so we can end the stigma around this disease,” the organization said in a statement.
Dr. Goh said that anyone with hair loss should feel free to explore potential medical causes and, if needed, seek out mental health treatment, too.
A version of this article first appeared on WebMD.com.
The Academy Awards ceremony on March 27 is a buzzing topic of conversation.
Troy Kotsur became the first deaf man to win an Oscar – and the highly coveted best supporting actor award, at that.
But it was what happened afterward that arguably stole the show.
Viewers and audience members alike watched in awe as actor Will Smith marched on stage and struck award presenter and comedian Chris Rock in the face after he directed a joke at Smith’s wife, Jada Pinkett Smith, for her shaved head.
and can lead to feelings of depression or mental illness.
About 700,000 people in the United States have alopecia areata, according to a 2020 study. Of them, slightly more than half are women, and more than 77% are White.
Shortly after the awards show, the Los Angeles Police Department released a statement saying it was aware of the incident and Mr. Rock had not pressed charges against Mr. Smith.
The incident set social media ablaze, and strong sentiments were heard from those who have been personally affected by alopecia.
Illness is never funny
Mr. Rock’s comment can be triggering to the millions who have been affected by hair loss, said Carolyn Goh, MD, a dermatologist at UCLA Health.
“As someone with alopecia myself, I consider it a microaggression,” Dr. Goh said. “I’ve experienced many similar comments. These build up over time and wear us down.”
One U.K.-based Instagram user, Kitty Dry, said the expression on Ms. Pinkett Smith’s face represented the hurt felt by so many with this condition.
“I want to preface this post by saying that in no way do I condone any sort of violence, but thank you Will Smith,” said Ms. Dry, 23, who was diagnosed with alopecia universalis after losing all her hair in 12 weeks.
“That slap was for anyone with alopecia who has ever been at the butt of an unwanted joke, comment or stare,” Ms. Dry said.
Others posted comments raising awareness of the tragic passing of Rio Allred, a 12-year-old girl with alopecia who recently died by suicide.
Rio Allred is said to have endured serious bullying at school, with classmates pulling off her wig and smacking her head, according to the Canadian Alopecia Areata Foundation.
It’s common for those who have hair loss conditions to feel helpless, and sometimes confused, said Amy McMichael, MD, a professor and chair of the dermatology department at Wake Forest University, Winston-Salem, N.C. That’s why it’s critical for those people to see a board-certified dermatologist, so they know they are not alone.
“As dermatologists, we can not only diagnose the type of alopecia, but we can also render treatment,” Dr. McMichael said.
Alopecia awareness
Dermatologists can also help connect patients to organizations that address the physical and emotional struggles of those who have hair loss, such as the National Alopecia Areata Foundation and the Scarring Alopecia Foundation, Dr. McMichael said.
She hopes the event shows people the “many faces of hair loss” and shows that these conditions can happen to people of all ages, ethnicities, and genders.
The National Alopecia Areata Foundation calls what happened at the Oscars a “teachable” moment.
“We encourage both our community and the broader public to learn more about alopecia areata so we can end the stigma around this disease,” the organization said in a statement.
Dr. Goh said that anyone with hair loss should feel free to explore potential medical causes and, if needed, seek out mental health treatment, too.
A version of this article first appeared on WebMD.com.
Surgery in CJD patients a potential risk factor for transmission
About one in six patients with Creutzfeldt-Jakob disease (CJD) undergo surgery, raising the risk of iatrogenic transmission of this rare but universally fatal prion disease.
In a retrospective analysis, researchers found that 26 of 121 (21%) patients with probable or definite CJD at four U.S. academic medical centers underwent a total of 55 procedures.
These included high-risk procedures for two patients with neuropathologically proven CJD. One underwent ophthalmic artery aneurysm clipping for unruptured aneurysm, and the other underwent diagnostic brain biopsy.
“The findings were definitely surprising to me and my team – particularly the high frequency with which patients with an irreversible and particularly transmissible neurologic disease underwent invasive medical procedures either just before or shortly after the emergence of symptoms later attributed to CJD,” study investigator Gregory Day, MD, with the Mayo Clinic, Jacksonville, Fla., said in an interview.
The study was published online March 9, 2022, in JAMA Network Open.
Poor infection control
The investigators noted that the majority of CJD cases are sporadic or are inherited, but research shows that prion transmission can occur via contaminated tissues or reusable medical equipment.
While the risk of iatrogenic transmission is highest following procedures involving the central nervous system, where prion burden is highest, experimental models suggest CJD transmission can occur after contact with other tissues, including nasal mucosa, lung, lymph nodes, and spleen, the researchers noted.
“If these models are accurate, surgical procedures involving these tissues may pose a risk to patients,” the investigators wrote.
To determine the potential scope of this problem, the researchers examined the frequency of invasive procedures performed in patients with CJD at four tertiary care centers.
“In several cases, these procedures were done with clear indications [such as] fixation or joint replacement following a fracture. In several others, however, the procedures were unlikely to help the patient. For instance, a hip replacement for walking difficulties that were actually due to changes in the brain due to CJD,” Dr. Day said.
“Even more surprising was the low frequency with which appropriate surgical precautions/infection control procedures were used in patients with established diagnoses of CJD,” he noted.
Only one procedure was performed with sterilization techniques adequate to prevent CJD.
Dr. Day said the findings aren’t necessarily cause for immediate alarm, but they do highlight an area for potential improvement, including better screening of patients who have new and unexplained symptoms before proceeding with surgery, especially surgery of the central nervous system, where prion burden is high.
Another potential solution is to develop and support program surveillance and to work with public health organizations such the Centers for Disease Control and Prevention and the National Prion Disease Pathology Surveillance Center to elicit a surgical history in patients diagnosed with prion disease.
“Active nationwide surveillance is needed to determine the true scope of this potential problem and to develop strategies to mitigate the potential risk of iatrogenic prion transmission to future patients,” Dr. Day said.
True prevalence unknown
The authors of an invited commentary noted that, while most CJD infections occur sporadically, iatrogenic transmission is possible. Approximately 500 such cases have been reported worldwide to date.
“Yet, reported transmission from surgical procedures remains rare, with fewer than 10 confirmed CJD cases described in the literature, although the true prevalence is difficult to quantify as confirmed diagnosis requires autopsy,” wrote Beatrice Sun, MD, and Joseph Forrester, MD, with the department of surgery, Stanford (Calif.) University.
They noted that, over a 15-year period, 19 suspected iatrogenic CJD exposures were reported to the CDC – two from ophthalmology procedures, and 17 from neurosurgical procedures.
In all 19 cases, the diagnosis of CJD was unknown before the intervention, and all surgical instruments underwent normal decontamination protocols, which are inadequate to eradicate prion disease.
For patients with suspected or confirmed CJD, the World Health Organization has published infection control guidelines to prevent transmission of spongiform encephalopathies.
The guidelines recommend proper communication with all staff involved in the surgical procedure and the sterilization of supplies to be aware of potential exposure; minimizing the number of staff in the operating room; using single-use equipment whenever possible and disposing of it by incineration; using protective coverings for all nondisposable equipment; and scheduling such procedures at the end of the day to allow adequate time for decontamination.
Funding for the study was provided by the National Institutes of Health. Dr. Day owns stock in ANI Pharmaceuticals; serves as a consultant for Parabon Nanolabs, as a topic editor (dementia) for DynaMed, and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation (uncompensated). Dr. Forrester reported receiving unrestricted research funding from Varian and has received grant funding from the Surgical Infections Society.
A version of this article first appeared on Medscape.com.
About one in six patients with Creutzfeldt-Jakob disease (CJD) undergo surgery, raising the risk of iatrogenic transmission of this rare but universally fatal prion disease.
In a retrospective analysis, researchers found that 26 of 121 (21%) patients with probable or definite CJD at four U.S. academic medical centers underwent a total of 55 procedures.
These included high-risk procedures for two patients with neuropathologically proven CJD. One underwent ophthalmic artery aneurysm clipping for unruptured aneurysm, and the other underwent diagnostic brain biopsy.
“The findings were definitely surprising to me and my team – particularly the high frequency with which patients with an irreversible and particularly transmissible neurologic disease underwent invasive medical procedures either just before or shortly after the emergence of symptoms later attributed to CJD,” study investigator Gregory Day, MD, with the Mayo Clinic, Jacksonville, Fla., said in an interview.
The study was published online March 9, 2022, in JAMA Network Open.
Poor infection control
The investigators noted that the majority of CJD cases are sporadic or are inherited, but research shows that prion transmission can occur via contaminated tissues or reusable medical equipment.
While the risk of iatrogenic transmission is highest following procedures involving the central nervous system, where prion burden is highest, experimental models suggest CJD transmission can occur after contact with other tissues, including nasal mucosa, lung, lymph nodes, and spleen, the researchers noted.
“If these models are accurate, surgical procedures involving these tissues may pose a risk to patients,” the investigators wrote.
To determine the potential scope of this problem, the researchers examined the frequency of invasive procedures performed in patients with CJD at four tertiary care centers.
“In several cases, these procedures were done with clear indications [such as] fixation or joint replacement following a fracture. In several others, however, the procedures were unlikely to help the patient. For instance, a hip replacement for walking difficulties that were actually due to changes in the brain due to CJD,” Dr. Day said.
“Even more surprising was the low frequency with which appropriate surgical precautions/infection control procedures were used in patients with established diagnoses of CJD,” he noted.
Only one procedure was performed with sterilization techniques adequate to prevent CJD.
Dr. Day said the findings aren’t necessarily cause for immediate alarm, but they do highlight an area for potential improvement, including better screening of patients who have new and unexplained symptoms before proceeding with surgery, especially surgery of the central nervous system, where prion burden is high.
Another potential solution is to develop and support program surveillance and to work with public health organizations such the Centers for Disease Control and Prevention and the National Prion Disease Pathology Surveillance Center to elicit a surgical history in patients diagnosed with prion disease.
“Active nationwide surveillance is needed to determine the true scope of this potential problem and to develop strategies to mitigate the potential risk of iatrogenic prion transmission to future patients,” Dr. Day said.
True prevalence unknown
The authors of an invited commentary noted that, while most CJD infections occur sporadically, iatrogenic transmission is possible. Approximately 500 such cases have been reported worldwide to date.
“Yet, reported transmission from surgical procedures remains rare, with fewer than 10 confirmed CJD cases described in the literature, although the true prevalence is difficult to quantify as confirmed diagnosis requires autopsy,” wrote Beatrice Sun, MD, and Joseph Forrester, MD, with the department of surgery, Stanford (Calif.) University.
They noted that, over a 15-year period, 19 suspected iatrogenic CJD exposures were reported to the CDC – two from ophthalmology procedures, and 17 from neurosurgical procedures.
In all 19 cases, the diagnosis of CJD was unknown before the intervention, and all surgical instruments underwent normal decontamination protocols, which are inadequate to eradicate prion disease.
For patients with suspected or confirmed CJD, the World Health Organization has published infection control guidelines to prevent transmission of spongiform encephalopathies.
The guidelines recommend proper communication with all staff involved in the surgical procedure and the sterilization of supplies to be aware of potential exposure; minimizing the number of staff in the operating room; using single-use equipment whenever possible and disposing of it by incineration; using protective coverings for all nondisposable equipment; and scheduling such procedures at the end of the day to allow adequate time for decontamination.
Funding for the study was provided by the National Institutes of Health. Dr. Day owns stock in ANI Pharmaceuticals; serves as a consultant for Parabon Nanolabs, as a topic editor (dementia) for DynaMed, and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation (uncompensated). Dr. Forrester reported receiving unrestricted research funding from Varian and has received grant funding from the Surgical Infections Society.
A version of this article first appeared on Medscape.com.
About one in six patients with Creutzfeldt-Jakob disease (CJD) undergo surgery, raising the risk of iatrogenic transmission of this rare but universally fatal prion disease.
In a retrospective analysis, researchers found that 26 of 121 (21%) patients with probable or definite CJD at four U.S. academic medical centers underwent a total of 55 procedures.
These included high-risk procedures for two patients with neuropathologically proven CJD. One underwent ophthalmic artery aneurysm clipping for unruptured aneurysm, and the other underwent diagnostic brain biopsy.
“The findings were definitely surprising to me and my team – particularly the high frequency with which patients with an irreversible and particularly transmissible neurologic disease underwent invasive medical procedures either just before or shortly after the emergence of symptoms later attributed to CJD,” study investigator Gregory Day, MD, with the Mayo Clinic, Jacksonville, Fla., said in an interview.
The study was published online March 9, 2022, in JAMA Network Open.
Poor infection control
The investigators noted that the majority of CJD cases are sporadic or are inherited, but research shows that prion transmission can occur via contaminated tissues or reusable medical equipment.
While the risk of iatrogenic transmission is highest following procedures involving the central nervous system, where prion burden is highest, experimental models suggest CJD transmission can occur after contact with other tissues, including nasal mucosa, lung, lymph nodes, and spleen, the researchers noted.
“If these models are accurate, surgical procedures involving these tissues may pose a risk to patients,” the investigators wrote.
To determine the potential scope of this problem, the researchers examined the frequency of invasive procedures performed in patients with CJD at four tertiary care centers.
“In several cases, these procedures were done with clear indications [such as] fixation or joint replacement following a fracture. In several others, however, the procedures were unlikely to help the patient. For instance, a hip replacement for walking difficulties that were actually due to changes in the brain due to CJD,” Dr. Day said.
“Even more surprising was the low frequency with which appropriate surgical precautions/infection control procedures were used in patients with established diagnoses of CJD,” he noted.
Only one procedure was performed with sterilization techniques adequate to prevent CJD.
Dr. Day said the findings aren’t necessarily cause for immediate alarm, but they do highlight an area for potential improvement, including better screening of patients who have new and unexplained symptoms before proceeding with surgery, especially surgery of the central nervous system, where prion burden is high.
Another potential solution is to develop and support program surveillance and to work with public health organizations such the Centers for Disease Control and Prevention and the National Prion Disease Pathology Surveillance Center to elicit a surgical history in patients diagnosed with prion disease.
“Active nationwide surveillance is needed to determine the true scope of this potential problem and to develop strategies to mitigate the potential risk of iatrogenic prion transmission to future patients,” Dr. Day said.
True prevalence unknown
The authors of an invited commentary noted that, while most CJD infections occur sporadically, iatrogenic transmission is possible. Approximately 500 such cases have been reported worldwide to date.
“Yet, reported transmission from surgical procedures remains rare, with fewer than 10 confirmed CJD cases described in the literature, although the true prevalence is difficult to quantify as confirmed diagnosis requires autopsy,” wrote Beatrice Sun, MD, and Joseph Forrester, MD, with the department of surgery, Stanford (Calif.) University.
They noted that, over a 15-year period, 19 suspected iatrogenic CJD exposures were reported to the CDC – two from ophthalmology procedures, and 17 from neurosurgical procedures.
In all 19 cases, the diagnosis of CJD was unknown before the intervention, and all surgical instruments underwent normal decontamination protocols, which are inadequate to eradicate prion disease.
For patients with suspected or confirmed CJD, the World Health Organization has published infection control guidelines to prevent transmission of spongiform encephalopathies.
The guidelines recommend proper communication with all staff involved in the surgical procedure and the sterilization of supplies to be aware of potential exposure; minimizing the number of staff in the operating room; using single-use equipment whenever possible and disposing of it by incineration; using protective coverings for all nondisposable equipment; and scheduling such procedures at the end of the day to allow adequate time for decontamination.
Funding for the study was provided by the National Institutes of Health. Dr. Day owns stock in ANI Pharmaceuticals; serves as a consultant for Parabon Nanolabs, as a topic editor (dementia) for DynaMed, and as the clinical director of the Anti-NMDA Receptor Encephalitis Foundation (uncompensated). Dr. Forrester reported receiving unrestricted research funding from Varian and has received grant funding from the Surgical Infections Society.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
As FDA OKs another COVID booster, some experts question need
, even though many top infectious disease experts questioned the need before the agency’s decision.
The FDA granted emergency use authorization for both Pfizer and Moderna to offer the second booster – and fourth shot overall – for adults over 50 as well as those over 18 with compromised immune systems.
The Centers for Control and Prevention must still sign off before those doses start reaching American arms. That approval could come at any time.
“The general consensus, certainly the CDC’s consensus, is that the current vaccines are still really quite effective against Omicron and this new BA.2 variant in keeping people out of the hospital, and preventing the development of severe disease,” William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville said prior to the FDA’s announcement March 29.
Of the 217.4 million Americans who are “fully vaccinated,” i.e., received two doses of either Pfizer or Moderna’s vaccines or one dose of the Johnson & Johnson vaccine, only 45% have also received a booster shot, according to the CDC.
“Given that, there’s no need at the moment for the general population to get a fourth inoculation,” Dr. Schaffner says. “Our current focus ought to be on making sure that as many people as possible get that [first] booster who are eligible.”
Monica Gandhi, MD, an infectious disease specialist at the University of California, San Francisco, agreed that another booster for everyone was unnecessary. The only people who would need a fourth shot (or third, if they had the Johnson & Johnson vaccine initially) are those over age 65 or 70 years, Dr. Gandhi says.
“Older people need those antibodies up high because they’re more susceptible to severe breakthroughs,” she said, also before the latest development.
To boost or not to boost
Daniel Kuritzkes, MD, chief of infectious diseases at Brigham & Women’s Hospital in Boston, said the timing of a booster and who should be eligible depends on what the nation is trying to achieve with its vaccination strategy.
“Is the goal to prevent any symptomatic infection with COVID-19, is the goal to prevent the spread of COVID-19, or is the goal to prevent severe disease that requires hospitalization?” asked Dr. Kuritzkes.
The current vaccine — with a booster — has prevented severe disease, he said.
An Israeli study showed, for instance, that a third Pfizer dose was 93% effective against hospitalization, 92% effective against severe illness, and 81% effective against death.
A just-published study in the New England Journal of Medicine found that a booster of the Pfizer vaccine was 95% effective against COVID-19 infection and that it did not raise any new safety issues.
A small Israeli study, also published in NEJM, of a fourth Pfizer dose given to health care workers found that it prevented symptomatic infection and illness, but that it was much less effective than previous doses — maybe 65% effective against symptomatic illness, the authors write.
Giving Americans another booster now — which has been shown to lose some effectiveness after about 4 months — means it might not offer protection this fall and winter, when there could be a seasonal surge of the virus, Dr. Kuritzkes says.
And, even if people receive boosters every few months, they are still likely to get a mild respiratory virus infection, he said.
“I’m pretty convinced that we cannot boost ourselves out of this pandemic,” said Dr. Kuritzkes. “We need to first of all ensure there’s global immunization so that all the people who have not been vaccinated at all get vaccinated. That’s far more important than boosting people a fourth time.”
Booster confusion
The April 6 FDA meeting of the agency’s Vaccines and Related Biological Products Advisory Committee comes as the two major COVID vaccine makers — Pfizer and Moderna — have applied for emergency use authorization for an additional booster.
Pfizer had asked for authorization for a fourth shot in patients over age 65 years, while Moderna wanted a booster to be available to all Americans over 18. The FDA instead granted authorization to both companies for those over 50 and anyone 18 or older who is immunocompromised.
What this means for the committee’s April 6 meeting is not clear. The original agenda says the committee will consider the evidence on safety and effectiveness of the additional vaccine doses and discuss how to set up a process — similar to that used for the influenza vaccine — to be able to determine the makeup of COVID vaccines as new variants emerge. That could lay the groundwork for an annual COVID shot, if needed.
The FDA advisers will not make recommendations nor vote on whether — and which — Americans should get a COVID booster. That is the job of the CDC’s Advisory Committee on Immunization Practices (ACIP).
The last time a booster was considered, CDC Director Rochelle Walensky, MD, overrode the committee and recommended that all Americans — not just older individuals — get an additional COVID shot, which became the first booster.
That past action worries Dr. Gandhi, who calls it confusing, and says it may have contributed to the fact that less than half of Americans have since chosen to get a booster.
Dr. Schaffner says he expects the FDA to authorize emergency use for fourth doses of the Pfizer and Moderna vaccines, but he doesn’t think the CDC committee will recommend routine use. As was seen before, however, the CDC director does not have to follow the committee’s advice.
The members of ACIP “might be more conservative or narrower in scope in terms of recommending who needs to be boosted and when boosting is appropriate,” Dr. Kuritzkes says.
Dr. Gandhi says she’s concerned the FDA’s deliberations could be swayed by Moderna and Pfizer’s influence and that “pharmaceutical companies are going to have more of a say than they should in the scientific process.”
There are similar worries for Dr. Schaffner. He says he’s “a bit grumpy” that the vaccine makers have been using press releases to argue for boosters.
“Press releases are no way to make vaccine recommendations,” Dr. Schaffner said, adding that he “would advise [vaccine makers] to sit down and be quiet and let the FDA and CDC advisory committee do their thing.”
Moderna Chief Medical Officer Paul Burton, MD, however, told WebMD last week that the signs point to why a fourth shot may be needed.
“We see waning of effectiveness, antibody levels come down, and certainly effectiveness against Omicron comes down in 3 to 6 months,” Burton said. “The natural history, from what we’re seeing around the world, is that BA.2 is definitely here, it’s highly transmissible, and I think we are going to get an additional wave of BA.2 here in the United States.”
Another wave is coming, he said, and “I think there will be waning of effectiveness. We need to be prepared for that, so that’s why we need the fourth dose.”
Supply issues?
Meanwhile, the United Kingdom has begun offering boosters to anyone over 75, and Sweden’s health authority has recommended a fourth shot to people over age 80.
That puts pressure on the United States — at least on its politicians and policymakers — to, in a sense, keep up, said the infectious disease specialists.
Indeed, the White House has been keeping fourth shots in the news, warning that it is running out of money to ensure that all Americans would have access to one, if recommended.
On March 23, outgoing White House COVID-19 Response Coordinator Jeff Zients said the federal government had enough vaccine for the immunocompromised to get a fourth dose “and, if authorized in the coming weeks, enough supply for fourth doses for our most vulnerable, including seniors.”
But he warned that without congressional approval of a COVID-19 funding package, “We can’t procure the necessary vaccine supply to support fourth shots for all Americans.”
Mr. Zients also noted that other countries, including Japan, Vietnam, and the Philippines had already secured future booster doses and added, “We should be securing additional supply right now.”
Dr. Schaffner says that while it would be nice to “have a booster on the shelf,” the United States needs to put more effort into creating a globally-coordinated process for ensuring that vaccines match circulating strains and that they are manufactured on a timely basis.
He says he and others “have been reminding the public that the COVID pandemic may indeed be diminishing and moving into the endemic, but that doesn’t mean COVID is over or finished or disappeared.”
Dr. Schaffner says that it may be that “perhaps we’d need a periodic reminder to our immune system to remain protected. In other words, we might have to get boosted perhaps annually like we do with influenza.”
A version of this article first appeared on WebMD.com.
, even though many top infectious disease experts questioned the need before the agency’s decision.
The FDA granted emergency use authorization for both Pfizer and Moderna to offer the second booster – and fourth shot overall – for adults over 50 as well as those over 18 with compromised immune systems.
The Centers for Control and Prevention must still sign off before those doses start reaching American arms. That approval could come at any time.
“The general consensus, certainly the CDC’s consensus, is that the current vaccines are still really quite effective against Omicron and this new BA.2 variant in keeping people out of the hospital, and preventing the development of severe disease,” William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville said prior to the FDA’s announcement March 29.
Of the 217.4 million Americans who are “fully vaccinated,” i.e., received two doses of either Pfizer or Moderna’s vaccines or one dose of the Johnson & Johnson vaccine, only 45% have also received a booster shot, according to the CDC.
“Given that, there’s no need at the moment for the general population to get a fourth inoculation,” Dr. Schaffner says. “Our current focus ought to be on making sure that as many people as possible get that [first] booster who are eligible.”
Monica Gandhi, MD, an infectious disease specialist at the University of California, San Francisco, agreed that another booster for everyone was unnecessary. The only people who would need a fourth shot (or third, if they had the Johnson & Johnson vaccine initially) are those over age 65 or 70 years, Dr. Gandhi says.
“Older people need those antibodies up high because they’re more susceptible to severe breakthroughs,” she said, also before the latest development.
To boost or not to boost
Daniel Kuritzkes, MD, chief of infectious diseases at Brigham & Women’s Hospital in Boston, said the timing of a booster and who should be eligible depends on what the nation is trying to achieve with its vaccination strategy.
“Is the goal to prevent any symptomatic infection with COVID-19, is the goal to prevent the spread of COVID-19, or is the goal to prevent severe disease that requires hospitalization?” asked Dr. Kuritzkes.
The current vaccine — with a booster — has prevented severe disease, he said.
An Israeli study showed, for instance, that a third Pfizer dose was 93% effective against hospitalization, 92% effective against severe illness, and 81% effective against death.
A just-published study in the New England Journal of Medicine found that a booster of the Pfizer vaccine was 95% effective against COVID-19 infection and that it did not raise any new safety issues.
A small Israeli study, also published in NEJM, of a fourth Pfizer dose given to health care workers found that it prevented symptomatic infection and illness, but that it was much less effective than previous doses — maybe 65% effective against symptomatic illness, the authors write.
Giving Americans another booster now — which has been shown to lose some effectiveness after about 4 months — means it might not offer protection this fall and winter, when there could be a seasonal surge of the virus, Dr. Kuritzkes says.
And, even if people receive boosters every few months, they are still likely to get a mild respiratory virus infection, he said.
“I’m pretty convinced that we cannot boost ourselves out of this pandemic,” said Dr. Kuritzkes. “We need to first of all ensure there’s global immunization so that all the people who have not been vaccinated at all get vaccinated. That’s far more important than boosting people a fourth time.”
Booster confusion
The April 6 FDA meeting of the agency’s Vaccines and Related Biological Products Advisory Committee comes as the two major COVID vaccine makers — Pfizer and Moderna — have applied for emergency use authorization for an additional booster.
Pfizer had asked for authorization for a fourth shot in patients over age 65 years, while Moderna wanted a booster to be available to all Americans over 18. The FDA instead granted authorization to both companies for those over 50 and anyone 18 or older who is immunocompromised.
What this means for the committee’s April 6 meeting is not clear. The original agenda says the committee will consider the evidence on safety and effectiveness of the additional vaccine doses and discuss how to set up a process — similar to that used for the influenza vaccine — to be able to determine the makeup of COVID vaccines as new variants emerge. That could lay the groundwork for an annual COVID shot, if needed.
The FDA advisers will not make recommendations nor vote on whether — and which — Americans should get a COVID booster. That is the job of the CDC’s Advisory Committee on Immunization Practices (ACIP).
The last time a booster was considered, CDC Director Rochelle Walensky, MD, overrode the committee and recommended that all Americans — not just older individuals — get an additional COVID shot, which became the first booster.
That past action worries Dr. Gandhi, who calls it confusing, and says it may have contributed to the fact that less than half of Americans have since chosen to get a booster.
Dr. Schaffner says he expects the FDA to authorize emergency use for fourth doses of the Pfizer and Moderna vaccines, but he doesn’t think the CDC committee will recommend routine use. As was seen before, however, the CDC director does not have to follow the committee’s advice.
The members of ACIP “might be more conservative or narrower in scope in terms of recommending who needs to be boosted and when boosting is appropriate,” Dr. Kuritzkes says.
Dr. Gandhi says she’s concerned the FDA’s deliberations could be swayed by Moderna and Pfizer’s influence and that “pharmaceutical companies are going to have more of a say than they should in the scientific process.”
There are similar worries for Dr. Schaffner. He says he’s “a bit grumpy” that the vaccine makers have been using press releases to argue for boosters.
“Press releases are no way to make vaccine recommendations,” Dr. Schaffner said, adding that he “would advise [vaccine makers] to sit down and be quiet and let the FDA and CDC advisory committee do their thing.”
Moderna Chief Medical Officer Paul Burton, MD, however, told WebMD last week that the signs point to why a fourth shot may be needed.
“We see waning of effectiveness, antibody levels come down, and certainly effectiveness against Omicron comes down in 3 to 6 months,” Burton said. “The natural history, from what we’re seeing around the world, is that BA.2 is definitely here, it’s highly transmissible, and I think we are going to get an additional wave of BA.2 here in the United States.”
Another wave is coming, he said, and “I think there will be waning of effectiveness. We need to be prepared for that, so that’s why we need the fourth dose.”
Supply issues?
Meanwhile, the United Kingdom has begun offering boosters to anyone over 75, and Sweden’s health authority has recommended a fourth shot to people over age 80.
That puts pressure on the United States — at least on its politicians and policymakers — to, in a sense, keep up, said the infectious disease specialists.
Indeed, the White House has been keeping fourth shots in the news, warning that it is running out of money to ensure that all Americans would have access to one, if recommended.
On March 23, outgoing White House COVID-19 Response Coordinator Jeff Zients said the federal government had enough vaccine for the immunocompromised to get a fourth dose “and, if authorized in the coming weeks, enough supply for fourth doses for our most vulnerable, including seniors.”
But he warned that without congressional approval of a COVID-19 funding package, “We can’t procure the necessary vaccine supply to support fourth shots for all Americans.”
Mr. Zients also noted that other countries, including Japan, Vietnam, and the Philippines had already secured future booster doses and added, “We should be securing additional supply right now.”
Dr. Schaffner says that while it would be nice to “have a booster on the shelf,” the United States needs to put more effort into creating a globally-coordinated process for ensuring that vaccines match circulating strains and that they are manufactured on a timely basis.
He says he and others “have been reminding the public that the COVID pandemic may indeed be diminishing and moving into the endemic, but that doesn’t mean COVID is over or finished or disappeared.”
Dr. Schaffner says that it may be that “perhaps we’d need a periodic reminder to our immune system to remain protected. In other words, we might have to get boosted perhaps annually like we do with influenza.”
A version of this article first appeared on WebMD.com.
, even though many top infectious disease experts questioned the need before the agency’s decision.
The FDA granted emergency use authorization for both Pfizer and Moderna to offer the second booster – and fourth shot overall – for adults over 50 as well as those over 18 with compromised immune systems.
The Centers for Control and Prevention must still sign off before those doses start reaching American arms. That approval could come at any time.
“The general consensus, certainly the CDC’s consensus, is that the current vaccines are still really quite effective against Omicron and this new BA.2 variant in keeping people out of the hospital, and preventing the development of severe disease,” William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville said prior to the FDA’s announcement March 29.
Of the 217.4 million Americans who are “fully vaccinated,” i.e., received two doses of either Pfizer or Moderna’s vaccines or one dose of the Johnson & Johnson vaccine, only 45% have also received a booster shot, according to the CDC.
“Given that, there’s no need at the moment for the general population to get a fourth inoculation,” Dr. Schaffner says. “Our current focus ought to be on making sure that as many people as possible get that [first] booster who are eligible.”
Monica Gandhi, MD, an infectious disease specialist at the University of California, San Francisco, agreed that another booster for everyone was unnecessary. The only people who would need a fourth shot (or third, if they had the Johnson & Johnson vaccine initially) are those over age 65 or 70 years, Dr. Gandhi says.
“Older people need those antibodies up high because they’re more susceptible to severe breakthroughs,” she said, also before the latest development.
To boost or not to boost
Daniel Kuritzkes, MD, chief of infectious diseases at Brigham & Women’s Hospital in Boston, said the timing of a booster and who should be eligible depends on what the nation is trying to achieve with its vaccination strategy.
“Is the goal to prevent any symptomatic infection with COVID-19, is the goal to prevent the spread of COVID-19, or is the goal to prevent severe disease that requires hospitalization?” asked Dr. Kuritzkes.
The current vaccine — with a booster — has prevented severe disease, he said.
An Israeli study showed, for instance, that a third Pfizer dose was 93% effective against hospitalization, 92% effective against severe illness, and 81% effective against death.
A just-published study in the New England Journal of Medicine found that a booster of the Pfizer vaccine was 95% effective against COVID-19 infection and that it did not raise any new safety issues.
A small Israeli study, also published in NEJM, of a fourth Pfizer dose given to health care workers found that it prevented symptomatic infection and illness, but that it was much less effective than previous doses — maybe 65% effective against symptomatic illness, the authors write.
Giving Americans another booster now — which has been shown to lose some effectiveness after about 4 months — means it might not offer protection this fall and winter, when there could be a seasonal surge of the virus, Dr. Kuritzkes says.
And, even if people receive boosters every few months, they are still likely to get a mild respiratory virus infection, he said.
“I’m pretty convinced that we cannot boost ourselves out of this pandemic,” said Dr. Kuritzkes. “We need to first of all ensure there’s global immunization so that all the people who have not been vaccinated at all get vaccinated. That’s far more important than boosting people a fourth time.”
Booster confusion
The April 6 FDA meeting of the agency’s Vaccines and Related Biological Products Advisory Committee comes as the two major COVID vaccine makers — Pfizer and Moderna — have applied for emergency use authorization for an additional booster.
Pfizer had asked for authorization for a fourth shot in patients over age 65 years, while Moderna wanted a booster to be available to all Americans over 18. The FDA instead granted authorization to both companies for those over 50 and anyone 18 or older who is immunocompromised.
What this means for the committee’s April 6 meeting is not clear. The original agenda says the committee will consider the evidence on safety and effectiveness of the additional vaccine doses and discuss how to set up a process — similar to that used for the influenza vaccine — to be able to determine the makeup of COVID vaccines as new variants emerge. That could lay the groundwork for an annual COVID shot, if needed.
The FDA advisers will not make recommendations nor vote on whether — and which — Americans should get a COVID booster. That is the job of the CDC’s Advisory Committee on Immunization Practices (ACIP).
The last time a booster was considered, CDC Director Rochelle Walensky, MD, overrode the committee and recommended that all Americans — not just older individuals — get an additional COVID shot, which became the first booster.
That past action worries Dr. Gandhi, who calls it confusing, and says it may have contributed to the fact that less than half of Americans have since chosen to get a booster.
Dr. Schaffner says he expects the FDA to authorize emergency use for fourth doses of the Pfizer and Moderna vaccines, but he doesn’t think the CDC committee will recommend routine use. As was seen before, however, the CDC director does not have to follow the committee’s advice.
The members of ACIP “might be more conservative or narrower in scope in terms of recommending who needs to be boosted and when boosting is appropriate,” Dr. Kuritzkes says.
Dr. Gandhi says she’s concerned the FDA’s deliberations could be swayed by Moderna and Pfizer’s influence and that “pharmaceutical companies are going to have more of a say than they should in the scientific process.”
There are similar worries for Dr. Schaffner. He says he’s “a bit grumpy” that the vaccine makers have been using press releases to argue for boosters.
“Press releases are no way to make vaccine recommendations,” Dr. Schaffner said, adding that he “would advise [vaccine makers] to sit down and be quiet and let the FDA and CDC advisory committee do their thing.”
Moderna Chief Medical Officer Paul Burton, MD, however, told WebMD last week that the signs point to why a fourth shot may be needed.
“We see waning of effectiveness, antibody levels come down, and certainly effectiveness against Omicron comes down in 3 to 6 months,” Burton said. “The natural history, from what we’re seeing around the world, is that BA.2 is definitely here, it’s highly transmissible, and I think we are going to get an additional wave of BA.2 here in the United States.”
Another wave is coming, he said, and “I think there will be waning of effectiveness. We need to be prepared for that, so that’s why we need the fourth dose.”
Supply issues?
Meanwhile, the United Kingdom has begun offering boosters to anyone over 75, and Sweden’s health authority has recommended a fourth shot to people over age 80.
That puts pressure on the United States — at least on its politicians and policymakers — to, in a sense, keep up, said the infectious disease specialists.
Indeed, the White House has been keeping fourth shots in the news, warning that it is running out of money to ensure that all Americans would have access to one, if recommended.
On March 23, outgoing White House COVID-19 Response Coordinator Jeff Zients said the federal government had enough vaccine for the immunocompromised to get a fourth dose “and, if authorized in the coming weeks, enough supply for fourth doses for our most vulnerable, including seniors.”
But he warned that without congressional approval of a COVID-19 funding package, “We can’t procure the necessary vaccine supply to support fourth shots for all Americans.”
Mr. Zients also noted that other countries, including Japan, Vietnam, and the Philippines had already secured future booster doses and added, “We should be securing additional supply right now.”
Dr. Schaffner says that while it would be nice to “have a booster on the shelf,” the United States needs to put more effort into creating a globally-coordinated process for ensuring that vaccines match circulating strains and that they are manufactured on a timely basis.
He says he and others “have been reminding the public that the COVID pandemic may indeed be diminishing and moving into the endemic, but that doesn’t mean COVID is over or finished or disappeared.”
Dr. Schaffner says that it may be that “perhaps we’d need a periodic reminder to our immune system to remain protected. In other words, we might have to get boosted perhaps annually like we do with influenza.”
A version of this article first appeared on WebMD.com.
‘Staggeringly high’ rates of psychiatric symptoms after COVID-19
DENVER – Neurocognitive and psychiatric symptoms of mental illness, including posttraumatic stress disorder, are alarmingly high among patients who have previously had COVID-19 – even among those who were not hospitalized with the virus, new research shows.
The findings are from an online survey of more than 800 respondents.
“Regardless of how long ago they had been infected with COVID-19, all respondents had persistent symptoms,” co-investigator Beth Patterson, MSc, adjunct clinical professor at McMaster University, MacAnxiety Research Centre, Hamilton, Ont., told this news organization.
“The take-home message for clinicians is to be aware that if you have patients who had COVID-19, it’s quite likely that they may also experience a psychiatric issue and that they may have reduced resilience and lower quality-of-life [issues],” Ms. Patterson said.
The survey results were presented here at the Anxiety and Depression Association of America (ADAA) Conference 2022.
100% report symptoms
The study included 827 respondents (81% women) to an online survey who had contracted COVID.
Using validated symptom severity scores, respondents were assessed for mental health and neurocognitive issues, as well as some physical and quality-of-life factors.
Remarkably, all participants (100%) reported having current, persistent symptoms of COVID. In addition, 88% (n = 729) reported persistent neurocognitive symptoms, even though only 15.5% reported they had been hospitalized for COVID.
Of those hospitalized, 28.9% were treated in the intensive care unit; 42.2% stayed in hospital for less than 1 week; and 13.3% remained hospitalized for at least 3 weeks.
Data were not available on how long it had been since the patients were diagnosed or hospitalized, but most participants (68%) said they had not returned to normal functioning since contracting COVID.
The most common persistent symptoms were fatigue (75.9%), brain fog (67.9%), difficulty concentrating (61%), and weakness (51.2%).
More than half of respondents reported neurocognitive symptoms, including poor memory (57.4%) and word-finding problems in processing information (46.9%). Only 11% reported no persistent neurocognitive symptoms.
A total of 41.7% of respondents reported anxiety using the Generalized Anxiety Disorder-7 (GAD-7) scale, and rates of depression were 61.4% as assessed with the Patient Health Questionnaire (PHQ-9).
Rates of probable posttraumatic stress disorder were 40.5% as assessed via the PTSD checklist (PCL-5).
Although it wasn’t possible to use diagnostic screens, the assessment scores suggest strikingly high rates of mental health disorders among the respondents, Ms. Patterson said.
“When we look at the mean scores on the validated scales, we see percentages of probable diagnoses that are staggeringly higher than you would find in the population,” she added.
Of note, about 44% of respondents reported having had mental health treatment in the past, and 33.7% were receiving current mental health treatment.
Although the study had no control group, the findings are consistent with larger studies that have had comparator groups, including research recently published in the BMJ.
Poor understanding of COVID’s fallout
In an editorial accompanying the BMJ study, Scott Weich, MD, Mental Health Research Unit, School of Health and Related Research, University of Sheffield, United Kingdom, emphasized the need to better understand the lingering mental health aspects of COVID-19 infection.
“Our attachment to syndromal phenotypes means that we have learned remarkably little about the causes of mental ill health – in this case psychopathology associated with a viral pandemic,” Dr. Weich writes.
Dr. Weich called for improved efforts to understanding long COVID, as well as the establishment of more effective responses to the mental health fallout from the pandemic.
Commenting on the current study, Dr. Weich elaborated on the challenges in disentangling the causes of mental health effects in illness.
“In terms of other viruses, etc., there is a long history of debate and pitched battles between those that attribute mental health effects to predominantly biological processes, [involving] immunological and other responses, and those who understand these responses are mediated by psychological and social processes,” he noted.
“The story of myalgic encephalomyelitis/chronic fatigue syndrome speaks volumes about these different positions, and how difficult it can be to find a middle ground,” he said.
“This has been going on for centuries and may never be fully resolved, at least until we have clearer and more definitive evidence of pathophysiology, though this seems incredibly elusive,” Dr. Weich said.
The authors and Dr. Weich have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DENVER – Neurocognitive and psychiatric symptoms of mental illness, including posttraumatic stress disorder, are alarmingly high among patients who have previously had COVID-19 – even among those who were not hospitalized with the virus, new research shows.
The findings are from an online survey of more than 800 respondents.
“Regardless of how long ago they had been infected with COVID-19, all respondents had persistent symptoms,” co-investigator Beth Patterson, MSc, adjunct clinical professor at McMaster University, MacAnxiety Research Centre, Hamilton, Ont., told this news organization.
“The take-home message for clinicians is to be aware that if you have patients who had COVID-19, it’s quite likely that they may also experience a psychiatric issue and that they may have reduced resilience and lower quality-of-life [issues],” Ms. Patterson said.
The survey results were presented here at the Anxiety and Depression Association of America (ADAA) Conference 2022.
100% report symptoms
The study included 827 respondents (81% women) to an online survey who had contracted COVID.
Using validated symptom severity scores, respondents were assessed for mental health and neurocognitive issues, as well as some physical and quality-of-life factors.
Remarkably, all participants (100%) reported having current, persistent symptoms of COVID. In addition, 88% (n = 729) reported persistent neurocognitive symptoms, even though only 15.5% reported they had been hospitalized for COVID.
Of those hospitalized, 28.9% were treated in the intensive care unit; 42.2% stayed in hospital for less than 1 week; and 13.3% remained hospitalized for at least 3 weeks.
Data were not available on how long it had been since the patients were diagnosed or hospitalized, but most participants (68%) said they had not returned to normal functioning since contracting COVID.
The most common persistent symptoms were fatigue (75.9%), brain fog (67.9%), difficulty concentrating (61%), and weakness (51.2%).
More than half of respondents reported neurocognitive symptoms, including poor memory (57.4%) and word-finding problems in processing information (46.9%). Only 11% reported no persistent neurocognitive symptoms.
A total of 41.7% of respondents reported anxiety using the Generalized Anxiety Disorder-7 (GAD-7) scale, and rates of depression were 61.4% as assessed with the Patient Health Questionnaire (PHQ-9).
Rates of probable posttraumatic stress disorder were 40.5% as assessed via the PTSD checklist (PCL-5).
Although it wasn’t possible to use diagnostic screens, the assessment scores suggest strikingly high rates of mental health disorders among the respondents, Ms. Patterson said.
“When we look at the mean scores on the validated scales, we see percentages of probable diagnoses that are staggeringly higher than you would find in the population,” she added.
Of note, about 44% of respondents reported having had mental health treatment in the past, and 33.7% were receiving current mental health treatment.
Although the study had no control group, the findings are consistent with larger studies that have had comparator groups, including research recently published in the BMJ.
Poor understanding of COVID’s fallout
In an editorial accompanying the BMJ study, Scott Weich, MD, Mental Health Research Unit, School of Health and Related Research, University of Sheffield, United Kingdom, emphasized the need to better understand the lingering mental health aspects of COVID-19 infection.
“Our attachment to syndromal phenotypes means that we have learned remarkably little about the causes of mental ill health – in this case psychopathology associated with a viral pandemic,” Dr. Weich writes.
Dr. Weich called for improved efforts to understanding long COVID, as well as the establishment of more effective responses to the mental health fallout from the pandemic.
Commenting on the current study, Dr. Weich elaborated on the challenges in disentangling the causes of mental health effects in illness.
“In terms of other viruses, etc., there is a long history of debate and pitched battles between those that attribute mental health effects to predominantly biological processes, [involving] immunological and other responses, and those who understand these responses are mediated by psychological and social processes,” he noted.
“The story of myalgic encephalomyelitis/chronic fatigue syndrome speaks volumes about these different positions, and how difficult it can be to find a middle ground,” he said.
“This has been going on for centuries and may never be fully resolved, at least until we have clearer and more definitive evidence of pathophysiology, though this seems incredibly elusive,” Dr. Weich said.
The authors and Dr. Weich have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
DENVER – Neurocognitive and psychiatric symptoms of mental illness, including posttraumatic stress disorder, are alarmingly high among patients who have previously had COVID-19 – even among those who were not hospitalized with the virus, new research shows.
The findings are from an online survey of more than 800 respondents.
“Regardless of how long ago they had been infected with COVID-19, all respondents had persistent symptoms,” co-investigator Beth Patterson, MSc, adjunct clinical professor at McMaster University, MacAnxiety Research Centre, Hamilton, Ont., told this news organization.
“The take-home message for clinicians is to be aware that if you have patients who had COVID-19, it’s quite likely that they may also experience a psychiatric issue and that they may have reduced resilience and lower quality-of-life [issues],” Ms. Patterson said.
The survey results were presented here at the Anxiety and Depression Association of America (ADAA) Conference 2022.
100% report symptoms
The study included 827 respondents (81% women) to an online survey who had contracted COVID.
Using validated symptom severity scores, respondents were assessed for mental health and neurocognitive issues, as well as some physical and quality-of-life factors.
Remarkably, all participants (100%) reported having current, persistent symptoms of COVID. In addition, 88% (n = 729) reported persistent neurocognitive symptoms, even though only 15.5% reported they had been hospitalized for COVID.
Of those hospitalized, 28.9% were treated in the intensive care unit; 42.2% stayed in hospital for less than 1 week; and 13.3% remained hospitalized for at least 3 weeks.
Data were not available on how long it had been since the patients were diagnosed or hospitalized, but most participants (68%) said they had not returned to normal functioning since contracting COVID.
The most common persistent symptoms were fatigue (75.9%), brain fog (67.9%), difficulty concentrating (61%), and weakness (51.2%).
More than half of respondents reported neurocognitive symptoms, including poor memory (57.4%) and word-finding problems in processing information (46.9%). Only 11% reported no persistent neurocognitive symptoms.
A total of 41.7% of respondents reported anxiety using the Generalized Anxiety Disorder-7 (GAD-7) scale, and rates of depression were 61.4% as assessed with the Patient Health Questionnaire (PHQ-9).
Rates of probable posttraumatic stress disorder were 40.5% as assessed via the PTSD checklist (PCL-5).
Although it wasn’t possible to use diagnostic screens, the assessment scores suggest strikingly high rates of mental health disorders among the respondents, Ms. Patterson said.
“When we look at the mean scores on the validated scales, we see percentages of probable diagnoses that are staggeringly higher than you would find in the population,” she added.
Of note, about 44% of respondents reported having had mental health treatment in the past, and 33.7% were receiving current mental health treatment.
Although the study had no control group, the findings are consistent with larger studies that have had comparator groups, including research recently published in the BMJ.
Poor understanding of COVID’s fallout
In an editorial accompanying the BMJ study, Scott Weich, MD, Mental Health Research Unit, School of Health and Related Research, University of Sheffield, United Kingdom, emphasized the need to better understand the lingering mental health aspects of COVID-19 infection.
“Our attachment to syndromal phenotypes means that we have learned remarkably little about the causes of mental ill health – in this case psychopathology associated with a viral pandemic,” Dr. Weich writes.
Dr. Weich called for improved efforts to understanding long COVID, as well as the establishment of more effective responses to the mental health fallout from the pandemic.
Commenting on the current study, Dr. Weich elaborated on the challenges in disentangling the causes of mental health effects in illness.
“In terms of other viruses, etc., there is a long history of debate and pitched battles between those that attribute mental health effects to predominantly biological processes, [involving] immunological and other responses, and those who understand these responses are mediated by psychological and social processes,” he noted.
“The story of myalgic encephalomyelitis/chronic fatigue syndrome speaks volumes about these different positions, and how difficult it can be to find a middle ground,” he said.
“This has been going on for centuries and may never be fully resolved, at least until we have clearer and more definitive evidence of pathophysiology, though this seems incredibly elusive,” Dr. Weich said.
The authors and Dr. Weich have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ADAA 2022
Suicide attempts in kids ages 10-12 quadrupled over 20 years
Suicide attempts spurring calls to poison control centers more than quadrupled among U.S. children aged 10-12 years from 2000 to 2020, according to research published in JAMA Pediatrics.
The reasons for the increase in suicide attempts isn’t clear from the new study, but the researchers note that popular social media networks launched during the 20-year period, and other studies have linked spending time on social media with depression in adolescence. The COVID-19 pandemic, which began in the last year the researchers looked at, also disrupted normal life and routines for children.
For all children older than age 9, the proportion of incidents in which kids ate or drank something harmful that were deemed suicide attempts increased, while those classified as misuse or abuse of potentially poisonous substances declined. Children aged 6-9 did not have an increase in suicide attempts, the study found.
“It’s a huge problem we’re seeing in [ERs]. It’s exponentially blowing up numbers across the nation,” says David Sheridan, MD, an ER pediatric doctor at the Oregon Health and Science University, Portland, who led the study.
Adolescents or preteens who have attempted suicide can sit in ERs “for days or weeks” as they wait to be moved elsewhere in the hospital or to an outpatient facility for treatment, Dr. Sheridan says. The delays are not only unpleasant for the children, he says, but they also strain hospitals by leaving less space available for other patients coming to the ER.
“It’s really tough on the entire health care system, and most importantly, it’s really rough on the families who are going through a crisis,” Dr. Sheridan says. He noted that young people often attempt suicide by taking excessive quantities of common over-the-counter products found in many medicine cabinets – acetaminophen, ibuprofen, diphenhydramine – not items marked “poison.”
Twenty-year trend
The researchers examined phone calls to poison control centers about kids age 6 and up taking in potentially harmful substances from 2000-2020 recorded in the National Poison Data System, which is maintained by the American Association of Poison Control Centers.
Of more than 1.2 million total calls, 854,000 involved girls. A poison control data analyst determined if the call involved attempted suicide or the deliberate misuse or abuse of a potentially poisonous substance.
The researchers identified 1,005 deaths. About 70% of the total cases had either no effect or a minor effect on the child’s health.
Over the 20-year period, more than 90% of the calls involved children aged at least 13 years, with approximately 72,000 (5.7%) about children aged 10-12. Most calls for children 13 and older were for suicide attempts.
Suspected suicide attempts accounted for about 50% of the total calls to poison control centers among children aged 10-12 in 2000 – a figure that ballooned to 80% in 2020, the researchers found.
Both the number of calls and the proportion related to suicide attempts increased among children aged 10-12, Dr. Sheridan says. By 2020, the researchers found, poison control centers were fielding 4.5 times as many suicide-related calls among kids of this age group as they had in 2000. This jump was the largest such increase for any age group in the study, he says.
The reasons for such a large increase of suicide-related calls among preadolescents are unclear, the researchers note.
The increase became apparent around 2013, at the time many popular social media networks launched. Dr. Sheridan and his colleagues cite studies showing an association between spending more time on social media or watching television and depression in adolescence but said further research is needed to understand the root causes of this increase.
The latest study did not look specifically at the effect of the COVID-19 pandemic on suicide among young people. The Centers for Disease Control and Prevention earlier reported a sharp rise in suicide attempts among youth during the early months of the pandemic, especially among girls aged 12-17 years. By February 2021, suicide attempts within this group had climbed by 50%, compared with 2 years earlier.
Although suicide attempts are concerning enough, deaths by suicide are even more worrisome, experts said.
The researchers’ findings are consistent with overall recent trends in youth suicide deaths, says Jeff Bridge, PhD, an epidemiologist at Nationwide Children’s Hospital, Columbus. From 2010-2020, suicide rates increased by 50% among 13- to 18-year-olds, Dr. Bridge said, and more than doubled in children aged 10-12.
The latest study captured only calls to poison control centers, so it did not count suicide attempts that did not result in a call for help. Another limitation of the study is that poison control data are not categorized by race or ethnicity, prompting Dr. Bridge to urge researchers to look specifically at the effect of race and ethnicity on these trends.
“This study supports screening for suicide risk as young as 10 years old,” Dr. Bridge says.
Dr. Sheridan agrees that prevention is essential: “The ER is where kids come when they’re in crisis. Trying to be more preventative by diagnosing or picking up on this earlier, I think, is really important.”
A version of this article first appeared on WebMD.com.
Suicide attempts spurring calls to poison control centers more than quadrupled among U.S. children aged 10-12 years from 2000 to 2020, according to research published in JAMA Pediatrics.
The reasons for the increase in suicide attempts isn’t clear from the new study, but the researchers note that popular social media networks launched during the 20-year period, and other studies have linked spending time on social media with depression in adolescence. The COVID-19 pandemic, which began in the last year the researchers looked at, also disrupted normal life and routines for children.
For all children older than age 9, the proportion of incidents in which kids ate or drank something harmful that were deemed suicide attempts increased, while those classified as misuse or abuse of potentially poisonous substances declined. Children aged 6-9 did not have an increase in suicide attempts, the study found.
“It’s a huge problem we’re seeing in [ERs]. It’s exponentially blowing up numbers across the nation,” says David Sheridan, MD, an ER pediatric doctor at the Oregon Health and Science University, Portland, who led the study.
Adolescents or preteens who have attempted suicide can sit in ERs “for days or weeks” as they wait to be moved elsewhere in the hospital or to an outpatient facility for treatment, Dr. Sheridan says. The delays are not only unpleasant for the children, he says, but they also strain hospitals by leaving less space available for other patients coming to the ER.
“It’s really tough on the entire health care system, and most importantly, it’s really rough on the families who are going through a crisis,” Dr. Sheridan says. He noted that young people often attempt suicide by taking excessive quantities of common over-the-counter products found in many medicine cabinets – acetaminophen, ibuprofen, diphenhydramine – not items marked “poison.”
Twenty-year trend
The researchers examined phone calls to poison control centers about kids age 6 and up taking in potentially harmful substances from 2000-2020 recorded in the National Poison Data System, which is maintained by the American Association of Poison Control Centers.
Of more than 1.2 million total calls, 854,000 involved girls. A poison control data analyst determined if the call involved attempted suicide or the deliberate misuse or abuse of a potentially poisonous substance.
The researchers identified 1,005 deaths. About 70% of the total cases had either no effect or a minor effect on the child’s health.
Over the 20-year period, more than 90% of the calls involved children aged at least 13 years, with approximately 72,000 (5.7%) about children aged 10-12. Most calls for children 13 and older were for suicide attempts.
Suspected suicide attempts accounted for about 50% of the total calls to poison control centers among children aged 10-12 in 2000 – a figure that ballooned to 80% in 2020, the researchers found.
Both the number of calls and the proportion related to suicide attempts increased among children aged 10-12, Dr. Sheridan says. By 2020, the researchers found, poison control centers were fielding 4.5 times as many suicide-related calls among kids of this age group as they had in 2000. This jump was the largest such increase for any age group in the study, he says.
The reasons for such a large increase of suicide-related calls among preadolescents are unclear, the researchers note.
The increase became apparent around 2013, at the time many popular social media networks launched. Dr. Sheridan and his colleagues cite studies showing an association between spending more time on social media or watching television and depression in adolescence but said further research is needed to understand the root causes of this increase.
The latest study did not look specifically at the effect of the COVID-19 pandemic on suicide among young people. The Centers for Disease Control and Prevention earlier reported a sharp rise in suicide attempts among youth during the early months of the pandemic, especially among girls aged 12-17 years. By February 2021, suicide attempts within this group had climbed by 50%, compared with 2 years earlier.
Although suicide attempts are concerning enough, deaths by suicide are even more worrisome, experts said.
The researchers’ findings are consistent with overall recent trends in youth suicide deaths, says Jeff Bridge, PhD, an epidemiologist at Nationwide Children’s Hospital, Columbus. From 2010-2020, suicide rates increased by 50% among 13- to 18-year-olds, Dr. Bridge said, and more than doubled in children aged 10-12.
The latest study captured only calls to poison control centers, so it did not count suicide attempts that did not result in a call for help. Another limitation of the study is that poison control data are not categorized by race or ethnicity, prompting Dr. Bridge to urge researchers to look specifically at the effect of race and ethnicity on these trends.
“This study supports screening for suicide risk as young as 10 years old,” Dr. Bridge says.
Dr. Sheridan agrees that prevention is essential: “The ER is where kids come when they’re in crisis. Trying to be more preventative by diagnosing or picking up on this earlier, I think, is really important.”
A version of this article first appeared on WebMD.com.
Suicide attempts spurring calls to poison control centers more than quadrupled among U.S. children aged 10-12 years from 2000 to 2020, according to research published in JAMA Pediatrics.
The reasons for the increase in suicide attempts isn’t clear from the new study, but the researchers note that popular social media networks launched during the 20-year period, and other studies have linked spending time on social media with depression in adolescence. The COVID-19 pandemic, which began in the last year the researchers looked at, also disrupted normal life and routines for children.
For all children older than age 9, the proportion of incidents in which kids ate or drank something harmful that were deemed suicide attempts increased, while those classified as misuse or abuse of potentially poisonous substances declined. Children aged 6-9 did not have an increase in suicide attempts, the study found.
“It’s a huge problem we’re seeing in [ERs]. It’s exponentially blowing up numbers across the nation,” says David Sheridan, MD, an ER pediatric doctor at the Oregon Health and Science University, Portland, who led the study.
Adolescents or preteens who have attempted suicide can sit in ERs “for days or weeks” as they wait to be moved elsewhere in the hospital or to an outpatient facility for treatment, Dr. Sheridan says. The delays are not only unpleasant for the children, he says, but they also strain hospitals by leaving less space available for other patients coming to the ER.
“It’s really tough on the entire health care system, and most importantly, it’s really rough on the families who are going through a crisis,” Dr. Sheridan says. He noted that young people often attempt suicide by taking excessive quantities of common over-the-counter products found in many medicine cabinets – acetaminophen, ibuprofen, diphenhydramine – not items marked “poison.”
Twenty-year trend
The researchers examined phone calls to poison control centers about kids age 6 and up taking in potentially harmful substances from 2000-2020 recorded in the National Poison Data System, which is maintained by the American Association of Poison Control Centers.
Of more than 1.2 million total calls, 854,000 involved girls. A poison control data analyst determined if the call involved attempted suicide or the deliberate misuse or abuse of a potentially poisonous substance.
The researchers identified 1,005 deaths. About 70% of the total cases had either no effect or a minor effect on the child’s health.
Over the 20-year period, more than 90% of the calls involved children aged at least 13 years, with approximately 72,000 (5.7%) about children aged 10-12. Most calls for children 13 and older were for suicide attempts.
Suspected suicide attempts accounted for about 50% of the total calls to poison control centers among children aged 10-12 in 2000 – a figure that ballooned to 80% in 2020, the researchers found.
Both the number of calls and the proportion related to suicide attempts increased among children aged 10-12, Dr. Sheridan says. By 2020, the researchers found, poison control centers were fielding 4.5 times as many suicide-related calls among kids of this age group as they had in 2000. This jump was the largest such increase for any age group in the study, he says.
The reasons for such a large increase of suicide-related calls among preadolescents are unclear, the researchers note.
The increase became apparent around 2013, at the time many popular social media networks launched. Dr. Sheridan and his colleagues cite studies showing an association between spending more time on social media or watching television and depression in adolescence but said further research is needed to understand the root causes of this increase.
The latest study did not look specifically at the effect of the COVID-19 pandemic on suicide among young people. The Centers for Disease Control and Prevention earlier reported a sharp rise in suicide attempts among youth during the early months of the pandemic, especially among girls aged 12-17 years. By February 2021, suicide attempts within this group had climbed by 50%, compared with 2 years earlier.
Although suicide attempts are concerning enough, deaths by suicide are even more worrisome, experts said.
The researchers’ findings are consistent with overall recent trends in youth suicide deaths, says Jeff Bridge, PhD, an epidemiologist at Nationwide Children’s Hospital, Columbus. From 2010-2020, suicide rates increased by 50% among 13- to 18-year-olds, Dr. Bridge said, and more than doubled in children aged 10-12.
The latest study captured only calls to poison control centers, so it did not count suicide attempts that did not result in a call for help. Another limitation of the study is that poison control data are not categorized by race or ethnicity, prompting Dr. Bridge to urge researchers to look specifically at the effect of race and ethnicity on these trends.
“This study supports screening for suicide risk as young as 10 years old,” Dr. Bridge says.
Dr. Sheridan agrees that prevention is essential: “The ER is where kids come when they’re in crisis. Trying to be more preventative by diagnosing or picking up on this earlier, I think, is really important.”
A version of this article first appeared on WebMD.com.
FROM JAMA PEDIATRICS
Virtual and in-person pediatric visits get similar family ratings
CHICAGO – Satisfaction ratings for virtual outpatient visits for pediatric orthopedic patients were similar to those for in-person office visits across most categories in an analysis of postencounter surveys completed by patients at the Cleveland Clinic.
Satisfaction ratings for both virtual and office visits were consistently higher than 85% across all measured parameters, according to the data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
Ahmed Emara, MD, a clinical research fellow in adult joint reconstruction at the Cleveland Clinic, led the study, which included data from all patients or guardians at the clinic who experienced such visits from March 2020 to March 2021.
A total of 1,686 responses were received, of which 226 (13.4%) involved virtual visits and 1,460 (86.6%) involved in-office visits. The primary endpoint was a patient-reported satisfaction score of good or excellent.
Analysis included ratings for access, care provider, telemedicine technology, and overall assessment/perception of satisfaction.
Target areas for improvement
In some areas, the virtual visits were less satisfactory than the in-office visits.
Patients had lower odds of reporting good/excellent satisfaction regarding their ability to schedule at a particularly convenient time (odds ratio, 0.1; 95% confidence interval, 0.08-0.18; P < .001). The study authors said scheduling more virtual time slots may help increase satisfaction in that area.
Satisfaction was also lower than with in-office visits with respect to providers’ explanations of patients’ conditions (OR, 0.4; 95% CI, 0.17-0.91; P = .03). Providers may need to find ways to better provide educational material in addition to the virtual consultation, the authors wrote.
No significant differences in categories of satisfaction
The researchers accounted for age, sex, traumatic etiology, and anatomic location of the complaint in multivariate regression analysis and found no significant differences between the two types of visits in the odds of getting a good/excellent rating for the following areas: patient inclusion in treatment decision (P = .562), discussion of proposed treatment (P = .222), concern by the provider (P = .189), degree of care for the patient as a person (P = .208), adequacy of teamwork in care provision (P = .053), likelihood of recommending the practice to others (P = .108), ease of receiving care at a particular practice (P = .109), ease of contacting the clinic (P = .177), and likelihood of recommending a particular provider (P = .218).
Anna Dimitriovna Vergun, MD, a pediatric orthopedist at the University of North Carolina at Chapel Hill, who was not involved in the study, said in an interview she had been conducting virtual visits even before the pandemic, when she worked for several years at a Shriner’s children’s hospital in Los Angeles, before coming to UNC. The virtual visits were necessary because the hospital offered charity care and covered an area that included several states.
She said that during the height of the pandemic, 80% of her visits at UNC were virtual; it is down to about 5% now.
Some consultations don’t need physical visits at all, Dr. Vergun noted. For example, UNC is starting a clinic for prenatal counseling in cases in which ultrasound detects a limb deformity. Without a virtual option, she said, pregnant mothers in all parts of the state may have to drive long distances when no physical exam is necessary.
And sometimes, a visit simply involves checking in with families to see whether pain is being controlled, which is done well virtually.
“Those are particularly useful for telemedicine,” Dr. Vergun said. “There’s a lot of space for this to be useful. You sometimes don’t realize it until you start doing it and getting feedback from the families that they like it.”
Other exams may be better suited to office visits, she said. These include spine and hip exams and exams in which providers need to check reflexes.
She said she sees many cases of club feet, for which an in-person exam is needed to determine flexibility.
Expert says virtual misses nuances
Ryan Fitzgerald, MD, an orthopedic expert with Children’s Orthopaedic and Scoliosis Surgery Associates in St. Petersburg, Fla., who also was not involved in the study, said in an interview he doesn’t offer the virtual option now because he thinks those visits usually miss too much.
COSSA is a private practice that provides orthopedic services for Johns Hopkins All Children’s Hospital.
“I think physicians’ perspective versus the families’ perspective may be quite a bit different,” he said.
While families like the convenience, “a lot of what we do is watching the patient walk, looking at their hip range of motion, and virtually, that’s a really difficult thing to do,” he said.
You can instruct a family on how to turn a camera on the patient, but “it doesn’t always translate,” he said.
He said virtual visits also highlight disparities in access, because many families don’t own the hardware needed for such visits, and internet connections can be spotty or images pixelated.
Dr. Fitzgerald said virtual visits were helpful during the pandemic and would be beneficial for yearly checkups “if you know [the patient] well and it’s a fairly run-of-the-mill thing.”
However, he said, “everything we do is about human interaction, and I think that’s a downfall of the virtual platform right now. While it is helpful in situations like COVID and where it is a very basic follow-up, it still has a ways to go.”
Dr. Fitzgerald is a consultant for OrthoPediatrics, Medtronic, and Depuy Synthes. Dr. Vergun disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Satisfaction ratings for virtual outpatient visits for pediatric orthopedic patients were similar to those for in-person office visits across most categories in an analysis of postencounter surveys completed by patients at the Cleveland Clinic.
Satisfaction ratings for both virtual and office visits were consistently higher than 85% across all measured parameters, according to the data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
Ahmed Emara, MD, a clinical research fellow in adult joint reconstruction at the Cleveland Clinic, led the study, which included data from all patients or guardians at the clinic who experienced such visits from March 2020 to March 2021.
A total of 1,686 responses were received, of which 226 (13.4%) involved virtual visits and 1,460 (86.6%) involved in-office visits. The primary endpoint was a patient-reported satisfaction score of good or excellent.
Analysis included ratings for access, care provider, telemedicine technology, and overall assessment/perception of satisfaction.
Target areas for improvement
In some areas, the virtual visits were less satisfactory than the in-office visits.
Patients had lower odds of reporting good/excellent satisfaction regarding their ability to schedule at a particularly convenient time (odds ratio, 0.1; 95% confidence interval, 0.08-0.18; P < .001). The study authors said scheduling more virtual time slots may help increase satisfaction in that area.
Satisfaction was also lower than with in-office visits with respect to providers’ explanations of patients’ conditions (OR, 0.4; 95% CI, 0.17-0.91; P = .03). Providers may need to find ways to better provide educational material in addition to the virtual consultation, the authors wrote.
No significant differences in categories of satisfaction
The researchers accounted for age, sex, traumatic etiology, and anatomic location of the complaint in multivariate regression analysis and found no significant differences between the two types of visits in the odds of getting a good/excellent rating for the following areas: patient inclusion in treatment decision (P = .562), discussion of proposed treatment (P = .222), concern by the provider (P = .189), degree of care for the patient as a person (P = .208), adequacy of teamwork in care provision (P = .053), likelihood of recommending the practice to others (P = .108), ease of receiving care at a particular practice (P = .109), ease of contacting the clinic (P = .177), and likelihood of recommending a particular provider (P = .218).
Anna Dimitriovna Vergun, MD, a pediatric orthopedist at the University of North Carolina at Chapel Hill, who was not involved in the study, said in an interview she had been conducting virtual visits even before the pandemic, when she worked for several years at a Shriner’s children’s hospital in Los Angeles, before coming to UNC. The virtual visits were necessary because the hospital offered charity care and covered an area that included several states.
She said that during the height of the pandemic, 80% of her visits at UNC were virtual; it is down to about 5% now.
Some consultations don’t need physical visits at all, Dr. Vergun noted. For example, UNC is starting a clinic for prenatal counseling in cases in which ultrasound detects a limb deformity. Without a virtual option, she said, pregnant mothers in all parts of the state may have to drive long distances when no physical exam is necessary.
And sometimes, a visit simply involves checking in with families to see whether pain is being controlled, which is done well virtually.
“Those are particularly useful for telemedicine,” Dr. Vergun said. “There’s a lot of space for this to be useful. You sometimes don’t realize it until you start doing it and getting feedback from the families that they like it.”
Other exams may be better suited to office visits, she said. These include spine and hip exams and exams in which providers need to check reflexes.
She said she sees many cases of club feet, for which an in-person exam is needed to determine flexibility.
Expert says virtual misses nuances
Ryan Fitzgerald, MD, an orthopedic expert with Children’s Orthopaedic and Scoliosis Surgery Associates in St. Petersburg, Fla., who also was not involved in the study, said in an interview he doesn’t offer the virtual option now because he thinks those visits usually miss too much.
COSSA is a private practice that provides orthopedic services for Johns Hopkins All Children’s Hospital.
“I think physicians’ perspective versus the families’ perspective may be quite a bit different,” he said.
While families like the convenience, “a lot of what we do is watching the patient walk, looking at their hip range of motion, and virtually, that’s a really difficult thing to do,” he said.
You can instruct a family on how to turn a camera on the patient, but “it doesn’t always translate,” he said.
He said virtual visits also highlight disparities in access, because many families don’t own the hardware needed for such visits, and internet connections can be spotty or images pixelated.
Dr. Fitzgerald said virtual visits were helpful during the pandemic and would be beneficial for yearly checkups “if you know [the patient] well and it’s a fairly run-of-the-mill thing.”
However, he said, “everything we do is about human interaction, and I think that’s a downfall of the virtual platform right now. While it is helpful in situations like COVID and where it is a very basic follow-up, it still has a ways to go.”
Dr. Fitzgerald is a consultant for OrthoPediatrics, Medtronic, and Depuy Synthes. Dr. Vergun disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
CHICAGO – Satisfaction ratings for virtual outpatient visits for pediatric orthopedic patients were similar to those for in-person office visits across most categories in an analysis of postencounter surveys completed by patients at the Cleveland Clinic.
Satisfaction ratings for both virtual and office visits were consistently higher than 85% across all measured parameters, according to the data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
Ahmed Emara, MD, a clinical research fellow in adult joint reconstruction at the Cleveland Clinic, led the study, which included data from all patients or guardians at the clinic who experienced such visits from March 2020 to March 2021.
A total of 1,686 responses were received, of which 226 (13.4%) involved virtual visits and 1,460 (86.6%) involved in-office visits. The primary endpoint was a patient-reported satisfaction score of good or excellent.
Analysis included ratings for access, care provider, telemedicine technology, and overall assessment/perception of satisfaction.
Target areas for improvement
In some areas, the virtual visits were less satisfactory than the in-office visits.
Patients had lower odds of reporting good/excellent satisfaction regarding their ability to schedule at a particularly convenient time (odds ratio, 0.1; 95% confidence interval, 0.08-0.18; P < .001). The study authors said scheduling more virtual time slots may help increase satisfaction in that area.
Satisfaction was also lower than with in-office visits with respect to providers’ explanations of patients’ conditions (OR, 0.4; 95% CI, 0.17-0.91; P = .03). Providers may need to find ways to better provide educational material in addition to the virtual consultation, the authors wrote.
No significant differences in categories of satisfaction
The researchers accounted for age, sex, traumatic etiology, and anatomic location of the complaint in multivariate regression analysis and found no significant differences between the two types of visits in the odds of getting a good/excellent rating for the following areas: patient inclusion in treatment decision (P = .562), discussion of proposed treatment (P = .222), concern by the provider (P = .189), degree of care for the patient as a person (P = .208), adequacy of teamwork in care provision (P = .053), likelihood of recommending the practice to others (P = .108), ease of receiving care at a particular practice (P = .109), ease of contacting the clinic (P = .177), and likelihood of recommending a particular provider (P = .218).
Anna Dimitriovna Vergun, MD, a pediatric orthopedist at the University of North Carolina at Chapel Hill, who was not involved in the study, said in an interview she had been conducting virtual visits even before the pandemic, when she worked for several years at a Shriner’s children’s hospital in Los Angeles, before coming to UNC. The virtual visits were necessary because the hospital offered charity care and covered an area that included several states.
She said that during the height of the pandemic, 80% of her visits at UNC were virtual; it is down to about 5% now.
Some consultations don’t need physical visits at all, Dr. Vergun noted. For example, UNC is starting a clinic for prenatal counseling in cases in which ultrasound detects a limb deformity. Without a virtual option, she said, pregnant mothers in all parts of the state may have to drive long distances when no physical exam is necessary.
And sometimes, a visit simply involves checking in with families to see whether pain is being controlled, which is done well virtually.
“Those are particularly useful for telemedicine,” Dr. Vergun said. “There’s a lot of space for this to be useful. You sometimes don’t realize it until you start doing it and getting feedback from the families that they like it.”
Other exams may be better suited to office visits, she said. These include spine and hip exams and exams in which providers need to check reflexes.
She said she sees many cases of club feet, for which an in-person exam is needed to determine flexibility.
Expert says virtual misses nuances
Ryan Fitzgerald, MD, an orthopedic expert with Children’s Orthopaedic and Scoliosis Surgery Associates in St. Petersburg, Fla., who also was not involved in the study, said in an interview he doesn’t offer the virtual option now because he thinks those visits usually miss too much.
COSSA is a private practice that provides orthopedic services for Johns Hopkins All Children’s Hospital.
“I think physicians’ perspective versus the families’ perspective may be quite a bit different,” he said.
While families like the convenience, “a lot of what we do is watching the patient walk, looking at their hip range of motion, and virtually, that’s a really difficult thing to do,” he said.
You can instruct a family on how to turn a camera on the patient, but “it doesn’t always translate,” he said.
He said virtual visits also highlight disparities in access, because many families don’t own the hardware needed for such visits, and internet connections can be spotty or images pixelated.
Dr. Fitzgerald said virtual visits were helpful during the pandemic and would be beneficial for yearly checkups “if you know [the patient] well and it’s a fairly run-of-the-mill thing.”
However, he said, “everything we do is about human interaction, and I think that’s a downfall of the virtual platform right now. While it is helpful in situations like COVID and where it is a very basic follow-up, it still has a ways to go.”
Dr. Fitzgerald is a consultant for OrthoPediatrics, Medtronic, and Depuy Synthes. Dr. Vergun disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AAOS 2022
Medical cannabis may cut opioid use for back pain, OA
CHICAGO – Access to medical cannabis (MC) cut opioid prescriptions for patients with chronic noncancer back pain and patients with osteoarthritis, according to preliminary data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
For those with chronic back pain, the average morphine milligram equivalents (MME) per day dropped from 15.1 to 11.0 (n = 186; P < .01). More than one-third of the patients (38.7%) stopped taking morphine after they filled prescriptions for medical cannabis.
Opioid prescriptions were filled 6 months before access to MC and then were compared with 6 months after access to MC.
In analyzing subgroups, the researchers found that patients who started at less than 15 MME/day and more than 15 MME/day showed significant decreases after filling the MC prescription.
Almost half (48.5%) of the patients in the group that started at less than 15 MME daily dropped to 0 MME/day, and 13.5% of patients who were getting more than 15 MME/day stopped using opioids.
Data on filled opioid prescriptions were gathered from a Prescription Drug Monitoring Program (PDMP) system for patients diagnosed with chronic musculoskeletal noncancer back pain who were eligible for MC access between February 2018 and July 2019.
Medical cannabis has shown benefit in treating chronic pain, but evidence has been limited on whether it can reduce opioid use, which can lead to substance abuse, addiction, overdose, and death, the researchers noted.
Researchers found that using MC via multiple routes of administration seemed to be important.
Patients who used only a single administration route showed a statistically insignificant decrease in MME/day from 20.0 to 15.1 (n = 68; P = .054), whereas patients who used two or more routes showed a significant decrease from 13.2 to 9.5 (n = 76; P < .01).
“We have many patients who are benefiting from a single route of delivery for chronic orthopedic pain,” Ari Greis, DO, a physical medicine and rehabilitation specialist in Bryn Mawr, Pa., and a coauthor of the MC studies for both back pain and OA, said in an interview. “However, our data shows a greater reduction in opioid consumption in patients using more than one route of delivery.”

He said delivery modes in the studies included vaporized cannabis oil or flower; sublingual tinctures; capsules or tablets; and topical lotions, creams, and salves.
Dr. Greis is the director of the medical cannabis department at Rothman Orthopaedic Institute in Bryn Mawr, and is a senior fellow in the Institute of Emerging Health Professions and the Lambert Center for the Study of Medicinal Cannabis and Hemp, both in Philadelphia.
Medical cannabis also reduces opioids for OA
The same team of researchers, using the data from the PDMP system, showed that medical cannabis also helped reduce opioid use for osteoarthritis.
For patients using opioids for OA, there was a significant decrease in average MME/day of prescriptions filled by patients following MC access – from 18.2 to 9.8 (n = 40; P < .05). The average drop in MME/day was 46.3%. The percentage of patients who stopped using opioids was 37.5%. Pain score on a 0-10 visual analog scale decreased significantly from 6.6 (n = 36) to 5.0 (n = 26; P < .01) at 3 months and 5.4 (n = 16; P < .05) at 6 months.
Gary Stewart, MD, an orthopedic surgeon in Morrow, Ga., who was not part of the studies, told this news organization that the studies offer good preliminary data to offer help with the opioid issue.

“I sometimes feel that we, as orthopedic surgeons and physicians in general, are working with one hand behind our back. We’re taking something that is a heroin or morphine derivative and giving it to our patients when we know it has a high risk of building tolerance and addiction. But at the same time, we have no alternative,” he said.
He said it’s important to remember the results from the relatively small study are preliminary and observational. People used different forms and amounts of MC and the data show only that prescriptions were filled, but not whether the cannabis was used. Prospective, controlled studies where opioids go head-to-head with MC are needed, he said.
“Still, this can lead us to more studies to give us an option [apart from] an opioid that we know is highly addictive,” he said.
Dr. Stewart is a member of the AAOS Opioid Task Force. Dr. Greis and several coauthors have disclosed no relevant financial relationships, and other coauthors report financial ties to companies unrelated to the research presented.
A version of this article first appeared on Medscape.com.
CHICAGO – Access to medical cannabis (MC) cut opioid prescriptions for patients with chronic noncancer back pain and patients with osteoarthritis, according to preliminary data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
For those with chronic back pain, the average morphine milligram equivalents (MME) per day dropped from 15.1 to 11.0 (n = 186; P < .01). More than one-third of the patients (38.7%) stopped taking morphine after they filled prescriptions for medical cannabis.
Opioid prescriptions were filled 6 months before access to MC and then were compared with 6 months after access to MC.
In analyzing subgroups, the researchers found that patients who started at less than 15 MME/day and more than 15 MME/day showed significant decreases after filling the MC prescription.
Almost half (48.5%) of the patients in the group that started at less than 15 MME daily dropped to 0 MME/day, and 13.5% of patients who were getting more than 15 MME/day stopped using opioids.
Data on filled opioid prescriptions were gathered from a Prescription Drug Monitoring Program (PDMP) system for patients diagnosed with chronic musculoskeletal noncancer back pain who were eligible for MC access between February 2018 and July 2019.
Medical cannabis has shown benefit in treating chronic pain, but evidence has been limited on whether it can reduce opioid use, which can lead to substance abuse, addiction, overdose, and death, the researchers noted.
Researchers found that using MC via multiple routes of administration seemed to be important.
Patients who used only a single administration route showed a statistically insignificant decrease in MME/day from 20.0 to 15.1 (n = 68; P = .054), whereas patients who used two or more routes showed a significant decrease from 13.2 to 9.5 (n = 76; P < .01).
“We have many patients who are benefiting from a single route of delivery for chronic orthopedic pain,” Ari Greis, DO, a physical medicine and rehabilitation specialist in Bryn Mawr, Pa., and a coauthor of the MC studies for both back pain and OA, said in an interview. “However, our data shows a greater reduction in opioid consumption in patients using more than one route of delivery.”
He said delivery modes in the studies included vaporized cannabis oil or flower; sublingual tinctures; capsules or tablets; and topical lotions, creams, and salves.
Dr. Greis is the director of the medical cannabis department at Rothman Orthopaedic Institute in Bryn Mawr, and is a senior fellow in the Institute of Emerging Health Professions and the Lambert Center for the Study of Medicinal Cannabis and Hemp, both in Philadelphia.
Medical cannabis also reduces opioids for OA
The same team of researchers, using the data from the PDMP system, showed that medical cannabis also helped reduce opioid use for osteoarthritis.
For patients using opioids for OA, there was a significant decrease in average MME/day of prescriptions filled by patients following MC access – from 18.2 to 9.8 (n = 40; P < .05). The average drop in MME/day was 46.3%. The percentage of patients who stopped using opioids was 37.5%. Pain score on a 0-10 visual analog scale decreased significantly from 6.6 (n = 36) to 5.0 (n = 26; P < .01) at 3 months and 5.4 (n = 16; P < .05) at 6 months.
Gary Stewart, MD, an orthopedic surgeon in Morrow, Ga., who was not part of the studies, told this news organization that the studies offer good preliminary data to offer help with the opioid issue.
“I sometimes feel that we, as orthopedic surgeons and physicians in general, are working with one hand behind our back. We’re taking something that is a heroin or morphine derivative and giving it to our patients when we know it has a high risk of building tolerance and addiction. But at the same time, we have no alternative,” he said.
He said it’s important to remember the results from the relatively small study are preliminary and observational. People used different forms and amounts of MC and the data show only that prescriptions were filled, but not whether the cannabis was used. Prospective, controlled studies where opioids go head-to-head with MC are needed, he said.
“Still, this can lead us to more studies to give us an option [apart from] an opioid that we know is highly addictive,” he said.
Dr. Stewart is a member of the AAOS Opioid Task Force. Dr. Greis and several coauthors have disclosed no relevant financial relationships, and other coauthors report financial ties to companies unrelated to the research presented.
A version of this article first appeared on Medscape.com.
CHICAGO – Access to medical cannabis (MC) cut opioid prescriptions for patients with chronic noncancer back pain and patients with osteoarthritis, according to preliminary data presented at the annual meeting of the American Academy of Orthopaedic Surgeons.
For those with chronic back pain, the average morphine milligram equivalents (MME) per day dropped from 15.1 to 11.0 (n = 186; P < .01). More than one-third of the patients (38.7%) stopped taking morphine after they filled prescriptions for medical cannabis.
Opioid prescriptions were filled 6 months before access to MC and then were compared with 6 months after access to MC.
In analyzing subgroups, the researchers found that patients who started at less than 15 MME/day and more than 15 MME/day showed significant decreases after filling the MC prescription.
Almost half (48.5%) of the patients in the group that started at less than 15 MME daily dropped to 0 MME/day, and 13.5% of patients who were getting more than 15 MME/day stopped using opioids.
Data on filled opioid prescriptions were gathered from a Prescription Drug Monitoring Program (PDMP) system for patients diagnosed with chronic musculoskeletal noncancer back pain who were eligible for MC access between February 2018 and July 2019.
Medical cannabis has shown benefit in treating chronic pain, but evidence has been limited on whether it can reduce opioid use, which can lead to substance abuse, addiction, overdose, and death, the researchers noted.
Researchers found that using MC via multiple routes of administration seemed to be important.
Patients who used only a single administration route showed a statistically insignificant decrease in MME/day from 20.0 to 15.1 (n = 68; P = .054), whereas patients who used two or more routes showed a significant decrease from 13.2 to 9.5 (n = 76; P < .01).
“We have many patients who are benefiting from a single route of delivery for chronic orthopedic pain,” Ari Greis, DO, a physical medicine and rehabilitation specialist in Bryn Mawr, Pa., and a coauthor of the MC studies for both back pain and OA, said in an interview. “However, our data shows a greater reduction in opioid consumption in patients using more than one route of delivery.”
He said delivery modes in the studies included vaporized cannabis oil or flower; sublingual tinctures; capsules or tablets; and topical lotions, creams, and salves.
Dr. Greis is the director of the medical cannabis department at Rothman Orthopaedic Institute in Bryn Mawr, and is a senior fellow in the Institute of Emerging Health Professions and the Lambert Center for the Study of Medicinal Cannabis and Hemp, both in Philadelphia.
Medical cannabis also reduces opioids for OA
The same team of researchers, using the data from the PDMP system, showed that medical cannabis also helped reduce opioid use for osteoarthritis.
For patients using opioids for OA, there was a significant decrease in average MME/day of prescriptions filled by patients following MC access – from 18.2 to 9.8 (n = 40; P < .05). The average drop in MME/day was 46.3%. The percentage of patients who stopped using opioids was 37.5%. Pain score on a 0-10 visual analog scale decreased significantly from 6.6 (n = 36) to 5.0 (n = 26; P < .01) at 3 months and 5.4 (n = 16; P < .05) at 6 months.
Gary Stewart, MD, an orthopedic surgeon in Morrow, Ga., who was not part of the studies, told this news organization that the studies offer good preliminary data to offer help with the opioid issue.
“I sometimes feel that we, as orthopedic surgeons and physicians in general, are working with one hand behind our back. We’re taking something that is a heroin or morphine derivative and giving it to our patients when we know it has a high risk of building tolerance and addiction. But at the same time, we have no alternative,” he said.
He said it’s important to remember the results from the relatively small study are preliminary and observational. People used different forms and amounts of MC and the data show only that prescriptions were filled, but not whether the cannabis was used. Prospective, controlled studies where opioids go head-to-head with MC are needed, he said.
“Still, this can lead us to more studies to give us an option [apart from] an opioid that we know is highly addictive,” he said.
Dr. Stewart is a member of the AAOS Opioid Task Force. Dr. Greis and several coauthors have disclosed no relevant financial relationships, and other coauthors report financial ties to companies unrelated to the research presented.
A version of this article first appeared on Medscape.com.
AT AAOS 2022
Metformin use linked to birth defects in boys
researchers have found.
The association appears to involve the effects of metformin on the development of sperm during a critical window prior to conception. Female offspring were not affected. Although previous studies have linked diabetes with fertility problems in men, the latest study is the first to show that these problems can result from treatment rather than the disease itself, according to the researchers, whose findings appear in Annals of Internal Medicine.
“This is the first data to suggest that paternal metformin [use] may be associated with birth defects in children. As such, it would be early to begin to alter clinical practice,” Michael Eisenberg, MD, director of male reproductive medicine and surgery, department of urology, Stanford (Calif.) University, who is a coauthor of the study, said in an interview. “However, if it is confirmed in other populations, then it may begin to enter counseling discussions.”
Dr. Eisenberg added that eating a nutritious diet, exercising, and maintaining a healthy body weight “can improve a man’s health and likely his fertility as well.”
For the new study, Dr. Eisenberg and colleagues analyzed records in a registry of all 1.25 million births that occurred in Denmark between 1997 and 2016. The registry included information on birth defects and parental drug prescriptions.
Offspring were considered exposed to a diabetes drug if a father had filled one or more prescriptions for the medications during the 3 months prior to conception, when the fertilizing sperm would have been produced.
The final analysis included 1,116,779 offspring – all singleton births to women without a history of diabetes or essential hypertension – of whom 7,029 were exposed to diabetes drugs via the father, and 3.3% (n = 36,585) had one or more major birth defects.
Among male offspring whose fathers had taken metformin (n = 1,451), there was a 3.4-fold greater incidence of major genitourinary birth defects, according to the researchers. The study failed to find associations between birth defects and the use of insulin. Although a signal did emerge for sulfonylurea-based drugs, it did not reach statistical significance.
The risk associated with metformin did not appear for men who were prescribed the drug in the year before or after sperm development. Nor was it evident in siblings of the boys with birth defects who were not considered to have been exposed to the medication, the researchers reported.
In an editorial accompanying the journal article, Germaine Buck Louis, PhD, a reproductive and perinatal epidemiologist, wrote: “Given the prevalence of metformin use as first-line therapy for type 2 diabetes, corroboration of these findings is urgently needed.”
Dr. Louis, dean of the College of Health and Human Services at George Mason University, Washington, said a key limitation of the research is the lack of data on how well men in the study adhered to their diabetes treatment. Nevertheless, “clinical guidance is needed to help couples planning pregnancy weigh the risks and benefits of paternal metformin use relative to other medications.”
The researchers received funding from the National Institutes of Health and the Centers for Disease Control and Prevention.
A version of this article first appeared on Medscape.com.
researchers have found.
The association appears to involve the effects of metformin on the development of sperm during a critical window prior to conception. Female offspring were not affected. Although previous studies have linked diabetes with fertility problems in men, the latest study is the first to show that these problems can result from treatment rather than the disease itself, according to the researchers, whose findings appear in Annals of Internal Medicine.
“This is the first data to suggest that paternal metformin [use] may be associated with birth defects in children. As such, it would be early to begin to alter clinical practice,” Michael Eisenberg, MD, director of male reproductive medicine and surgery, department of urology, Stanford (Calif.) University, who is a coauthor of the study, said in an interview. “However, if it is confirmed in other populations, then it may begin to enter counseling discussions.”
Dr. Eisenberg added that eating a nutritious diet, exercising, and maintaining a healthy body weight “can improve a man’s health and likely his fertility as well.”
For the new study, Dr. Eisenberg and colleagues analyzed records in a registry of all 1.25 million births that occurred in Denmark between 1997 and 2016. The registry included information on birth defects and parental drug prescriptions.
Offspring were considered exposed to a diabetes drug if a father had filled one or more prescriptions for the medications during the 3 months prior to conception, when the fertilizing sperm would have been produced.
The final analysis included 1,116,779 offspring – all singleton births to women without a history of diabetes or essential hypertension – of whom 7,029 were exposed to diabetes drugs via the father, and 3.3% (n = 36,585) had one or more major birth defects.
Among male offspring whose fathers had taken metformin (n = 1,451), there was a 3.4-fold greater incidence of major genitourinary birth defects, according to the researchers. The study failed to find associations between birth defects and the use of insulin. Although a signal did emerge for sulfonylurea-based drugs, it did not reach statistical significance.
The risk associated with metformin did not appear for men who were prescribed the drug in the year before or after sperm development. Nor was it evident in siblings of the boys with birth defects who were not considered to have been exposed to the medication, the researchers reported.
In an editorial accompanying the journal article, Germaine Buck Louis, PhD, a reproductive and perinatal epidemiologist, wrote: “Given the prevalence of metformin use as first-line therapy for type 2 diabetes, corroboration of these findings is urgently needed.”
Dr. Louis, dean of the College of Health and Human Services at George Mason University, Washington, said a key limitation of the research is the lack of data on how well men in the study adhered to their diabetes treatment. Nevertheless, “clinical guidance is needed to help couples planning pregnancy weigh the risks and benefits of paternal metformin use relative to other medications.”
The researchers received funding from the National Institutes of Health and the Centers for Disease Control and Prevention.
A version of this article first appeared on Medscape.com.
researchers have found.
The association appears to involve the effects of metformin on the development of sperm during a critical window prior to conception. Female offspring were not affected. Although previous studies have linked diabetes with fertility problems in men, the latest study is the first to show that these problems can result from treatment rather than the disease itself, according to the researchers, whose findings appear in Annals of Internal Medicine.
“This is the first data to suggest that paternal metformin [use] may be associated with birth defects in children. As such, it would be early to begin to alter clinical practice,” Michael Eisenberg, MD, director of male reproductive medicine and surgery, department of urology, Stanford (Calif.) University, who is a coauthor of the study, said in an interview. “However, if it is confirmed in other populations, then it may begin to enter counseling discussions.”
Dr. Eisenberg added that eating a nutritious diet, exercising, and maintaining a healthy body weight “can improve a man’s health and likely his fertility as well.”
For the new study, Dr. Eisenberg and colleagues analyzed records in a registry of all 1.25 million births that occurred in Denmark between 1997 and 2016. The registry included information on birth defects and parental drug prescriptions.
Offspring were considered exposed to a diabetes drug if a father had filled one or more prescriptions for the medications during the 3 months prior to conception, when the fertilizing sperm would have been produced.
The final analysis included 1,116,779 offspring – all singleton births to women without a history of diabetes or essential hypertension – of whom 7,029 were exposed to diabetes drugs via the father, and 3.3% (n = 36,585) had one or more major birth defects.
Among male offspring whose fathers had taken metformin (n = 1,451), there was a 3.4-fold greater incidence of major genitourinary birth defects, according to the researchers. The study failed to find associations between birth defects and the use of insulin. Although a signal did emerge for sulfonylurea-based drugs, it did not reach statistical significance.
The risk associated with metformin did not appear for men who were prescribed the drug in the year before or after sperm development. Nor was it evident in siblings of the boys with birth defects who were not considered to have been exposed to the medication, the researchers reported.
In an editorial accompanying the journal article, Germaine Buck Louis, PhD, a reproductive and perinatal epidemiologist, wrote: “Given the prevalence of metformin use as first-line therapy for type 2 diabetes, corroboration of these findings is urgently needed.”
Dr. Louis, dean of the College of Health and Human Services at George Mason University, Washington, said a key limitation of the research is the lack of data on how well men in the study adhered to their diabetes treatment. Nevertheless, “clinical guidance is needed to help couples planning pregnancy weigh the risks and benefits of paternal metformin use relative to other medications.”
The researchers received funding from the National Institutes of Health and the Centers for Disease Control and Prevention.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE