User login
Alcohol dependence drug the next antianxiety med?
, early research suggests.
Japanese researchers, headed by Akiyoshi Saitoh, PhD, professor in the department of pharmacy, Tokyo University of Science, compared the reactions of mice that received a classic anxiolytic agent (diazepam) to those that received disulfiram while performing a maze task and found comparable reductions in anxiety in both groups of mice.
Moreover, unlike diazepam, disulfiram caused no sedation, amnesia, or impairments in coordination.
“These results indicate that disulfiram can be used safely by elderly patients suffering from anxiety and insomnia and has the potential to become a breakthrough psychotropic drug,” Dr. Saitoh said in a press release.
The study was published online in Frontiers in Pharmacology.
Inhibitory function
Disulfiram inhibits the enzyme aldehyde dehydrogenase (ALDH), which is responsible for alcohol metabolism. Recent research suggests that disulfiram may have broader inhibitory functions.
In particular, it inhibits the cytoplasmic protein FROUNT, preventing it from interacting with two chemokine receptors (CCR2 and CCRs) that are involved in cellular signaling pathways and are associated with regulating behaviors, including anxiety, in rodents, the authors write.
“Although the functions of FROUNT-chemokines signaling in the immune system are well documented, the potential role of CNS-expressed FROUNT chemokine–related molecules as neuromodulators remains largely unknown,” they write.
The researchers had been conducting preclinical research on the secondary pharmacologic properties of disulfiram and “coincidentally discovered” its “anxiolytic-like effects.” They investigated these effects further because currently used anxiolytics – i.e., benzodiazepines – have unwanted side effects.
The researchers utilized an elevated plus-maze (EPM) test to investigate the effects of disulfiram in mice. The EPM apparatus consists of four arms set in a cross pattern and are connected to a central square. Of these, two arms are protected by vertical boundaries, while the other two have unprotected edges. Typically, mice with anxiety prefer to spend time in the closed arms. The mice also underwent other tests of coordination and the ability to navigate a Y-maze.
Some mice received disulfiram, others received a benzodiazepine, and others received merely a “vehicle,” which served as a control.
Disulfiram “significantly and dose-dependently” increased the time spent in the open arms of the EPM, compared with the vehicle-treated group, at 30 minutes after administration (F [3, 30] = 16.64; P < .0001), suggesting less anxiety. The finding was confirmed by a Bonferroni analysis that showed a significant effect of disulfiram, compared with the vehicle-treated group, at all three doses (20 mg/kg: t = 0.9894; P > .05; 40 mg/kg: t = 3.863; P < .01; 80 mg/kg: t = 6.417; P < .001).
A Student’s t-test analysis showed that diazepam likewise had a significant effect, compared to the vehicle (t = 5.038; P < .001).
Disulfiram also “significantly and dose-dependently” increased the percentage of open-arm entries (F [3, 30] = 14.24; P < .0001). The Bonferroni analysis showed this effect at all three doses (20 mg/kg: t = 0.3999; P > .05; 40 mg/kg: t = 2.693; P > .05; 80 mg/kg: t = 5.864; P < .001).
Diazepam similarly showed a significant effect, compared to the vehicle condition (t = 3.733; P < .005).
In particular, the 40 mg/kg dose of disulfiram significantly increased the percentage of time spent in the open arms at 15, 30, and 60 minutes after administration, with the peak effect occurring at 30 minutes.
The researchers examined the effect of cyanamide, another ALDH inhibitor, on the anxiety behaviors of mice and found no effect on the number of open-arm entries or percentage of time the mice spent in the open arm, compared with the vehicle condition.
In contrast to diazepam, disulfiram had no effect on the amount of spontaneous locomotor activity, time spent on the rotarod, or activity on the Y-maze test displayed by the mice, “suggesting that there were no apparent sedative effects at the dosages used.” Moreover, unlike the mice treated with diazepam, there were no increases in the number of falls the mice experienced on the rotarod.
Glutamate levels in the prelimbic-prefrontal cortex (PL-PFC) “play an important role in the development of anxiety-like behavior in mice,” the authors state. Disulfiram “significantly and completely attenuated increased extracellular glutamate levels in the PL-PFC during stress exposure” on the EPM.
“We propose that DSF inhibits FROUNT protein and the chemokine signaling pathways under its influence, which may suppress presynaptic glutamatergic transmission in the brain,” said Dr. Saitoh. “This, in turn, attenuates the levels of glutamate in the brain, reducing overall anxiety.”
Humanity’s most common affliction
Commenting for this news organization, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the mood disorders psychopharmacology unit, noted that there is a “renewed interest in psychiatry in excitatory and inhibitory balance – for example, ketamine represents a treatment that facilitates excitatory activity, while neurosteroids are candidate medicines now for inhibitory activity.”
Dr. McIntyre, who is the chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, and was not involved with the study, said it is believed “that the excitatory-inhibitory balance may be relevant to brain health and disease.”
Dr. McIntyre also pointed out that the study “highlights not only the repurposing of a well-known medicine but also exploit[s] the potential brain therapeutic effects of immune targets that indirectly affect inhibitory systems, resulting in potentially a safer treatment for anxiety – the most common affliction of humanity.”
Also commenting for this article, Wilfrid Noel Raby, MD, PhD, a psychiatrist in private practice in Teaneck, N.J., called disulfiram “grossly underused for alcohol use disorders and even more so when people use alcohol and cocaine.”
Dr. Raby, who was not involved with the study, has found that patients withdrawing from cocaine, cannabis, or stimulants “can respond very well to disulfiram [not only] in terms of their cravings but also in terms of mood stabilization and anxiolysis.”
He has also found that for patients with bipolar disorder or attention-deficit/hyperactivity disorder with depression disulfiram and low-dose lithium “can provide anxiolysis and mood stabilization, especially if a rapid effect is required, usually within a week.”
However, Dr. Raby cautioned that “it is probably not advisable to maintain patients on disulfiram for periods long than 3 months consecutively because there is a risk of neuropathy and hepatopathology that are not common but are seen often enough.” He usually interrupts treatment for a month and then resumes if necessary.
The research was partially supported by the Tsukuba Clinical Research and Development Organization from the Japan Agency for Medical Research and Development. The authors and Dr. Raby have disclosed no relevant financial relationships. Dr. McIntyre reports receiving research grant support from CIHR/GACD/National Natural Science Foundation of China; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, AbbVie, and Atai Life Sciences. Dr. McIntyre is CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
, early research suggests.
Japanese researchers, headed by Akiyoshi Saitoh, PhD, professor in the department of pharmacy, Tokyo University of Science, compared the reactions of mice that received a classic anxiolytic agent (diazepam) to those that received disulfiram while performing a maze task and found comparable reductions in anxiety in both groups of mice.
Moreover, unlike diazepam, disulfiram caused no sedation, amnesia, or impairments in coordination.
“These results indicate that disulfiram can be used safely by elderly patients suffering from anxiety and insomnia and has the potential to become a breakthrough psychotropic drug,” Dr. Saitoh said in a press release.
The study was published online in Frontiers in Pharmacology.
Inhibitory function
Disulfiram inhibits the enzyme aldehyde dehydrogenase (ALDH), which is responsible for alcohol metabolism. Recent research suggests that disulfiram may have broader inhibitory functions.
In particular, it inhibits the cytoplasmic protein FROUNT, preventing it from interacting with two chemokine receptors (CCR2 and CCRs) that are involved in cellular signaling pathways and are associated with regulating behaviors, including anxiety, in rodents, the authors write.
“Although the functions of FROUNT-chemokines signaling in the immune system are well documented, the potential role of CNS-expressed FROUNT chemokine–related molecules as neuromodulators remains largely unknown,” they write.
The researchers had been conducting preclinical research on the secondary pharmacologic properties of disulfiram and “coincidentally discovered” its “anxiolytic-like effects.” They investigated these effects further because currently used anxiolytics – i.e., benzodiazepines – have unwanted side effects.
The researchers utilized an elevated plus-maze (EPM) test to investigate the effects of disulfiram in mice. The EPM apparatus consists of four arms set in a cross pattern and are connected to a central square. Of these, two arms are protected by vertical boundaries, while the other two have unprotected edges. Typically, mice with anxiety prefer to spend time in the closed arms. The mice also underwent other tests of coordination and the ability to navigate a Y-maze.
Some mice received disulfiram, others received a benzodiazepine, and others received merely a “vehicle,” which served as a control.
Disulfiram “significantly and dose-dependently” increased the time spent in the open arms of the EPM, compared with the vehicle-treated group, at 30 minutes after administration (F [3, 30] = 16.64; P < .0001), suggesting less anxiety. The finding was confirmed by a Bonferroni analysis that showed a significant effect of disulfiram, compared with the vehicle-treated group, at all three doses (20 mg/kg: t = 0.9894; P > .05; 40 mg/kg: t = 3.863; P < .01; 80 mg/kg: t = 6.417; P < .001).
A Student’s t-test analysis showed that diazepam likewise had a significant effect, compared to the vehicle (t = 5.038; P < .001).
Disulfiram also “significantly and dose-dependently” increased the percentage of open-arm entries (F [3, 30] = 14.24; P < .0001). The Bonferroni analysis showed this effect at all three doses (20 mg/kg: t = 0.3999; P > .05; 40 mg/kg: t = 2.693; P > .05; 80 mg/kg: t = 5.864; P < .001).
Diazepam similarly showed a significant effect, compared to the vehicle condition (t = 3.733; P < .005).
In particular, the 40 mg/kg dose of disulfiram significantly increased the percentage of time spent in the open arms at 15, 30, and 60 minutes after administration, with the peak effect occurring at 30 minutes.
The researchers examined the effect of cyanamide, another ALDH inhibitor, on the anxiety behaviors of mice and found no effect on the number of open-arm entries or percentage of time the mice spent in the open arm, compared with the vehicle condition.
In contrast to diazepam, disulfiram had no effect on the amount of spontaneous locomotor activity, time spent on the rotarod, or activity on the Y-maze test displayed by the mice, “suggesting that there were no apparent sedative effects at the dosages used.” Moreover, unlike the mice treated with diazepam, there were no increases in the number of falls the mice experienced on the rotarod.
Glutamate levels in the prelimbic-prefrontal cortex (PL-PFC) “play an important role in the development of anxiety-like behavior in mice,” the authors state. Disulfiram “significantly and completely attenuated increased extracellular glutamate levels in the PL-PFC during stress exposure” on the EPM.
“We propose that DSF inhibits FROUNT protein and the chemokine signaling pathways under its influence, which may suppress presynaptic glutamatergic transmission in the brain,” said Dr. Saitoh. “This, in turn, attenuates the levels of glutamate in the brain, reducing overall anxiety.”
Humanity’s most common affliction
Commenting for this news organization, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the mood disorders psychopharmacology unit, noted that there is a “renewed interest in psychiatry in excitatory and inhibitory balance – for example, ketamine represents a treatment that facilitates excitatory activity, while neurosteroids are candidate medicines now for inhibitory activity.”
Dr. McIntyre, who is the chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, and was not involved with the study, said it is believed “that the excitatory-inhibitory balance may be relevant to brain health and disease.”
Dr. McIntyre also pointed out that the study “highlights not only the repurposing of a well-known medicine but also exploit[s] the potential brain therapeutic effects of immune targets that indirectly affect inhibitory systems, resulting in potentially a safer treatment for anxiety – the most common affliction of humanity.”
Also commenting for this article, Wilfrid Noel Raby, MD, PhD, a psychiatrist in private practice in Teaneck, N.J., called disulfiram “grossly underused for alcohol use disorders and even more so when people use alcohol and cocaine.”
Dr. Raby, who was not involved with the study, has found that patients withdrawing from cocaine, cannabis, or stimulants “can respond very well to disulfiram [not only] in terms of their cravings but also in terms of mood stabilization and anxiolysis.”
He has also found that for patients with bipolar disorder or attention-deficit/hyperactivity disorder with depression disulfiram and low-dose lithium “can provide anxiolysis and mood stabilization, especially if a rapid effect is required, usually within a week.”
However, Dr. Raby cautioned that “it is probably not advisable to maintain patients on disulfiram for periods long than 3 months consecutively because there is a risk of neuropathy and hepatopathology that are not common but are seen often enough.” He usually interrupts treatment for a month and then resumes if necessary.
The research was partially supported by the Tsukuba Clinical Research and Development Organization from the Japan Agency for Medical Research and Development. The authors and Dr. Raby have disclosed no relevant financial relationships. Dr. McIntyre reports receiving research grant support from CIHR/GACD/National Natural Science Foundation of China; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, AbbVie, and Atai Life Sciences. Dr. McIntyre is CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
, early research suggests.
Japanese researchers, headed by Akiyoshi Saitoh, PhD, professor in the department of pharmacy, Tokyo University of Science, compared the reactions of mice that received a classic anxiolytic agent (diazepam) to those that received disulfiram while performing a maze task and found comparable reductions in anxiety in both groups of mice.
Moreover, unlike diazepam, disulfiram caused no sedation, amnesia, or impairments in coordination.
“These results indicate that disulfiram can be used safely by elderly patients suffering from anxiety and insomnia and has the potential to become a breakthrough psychotropic drug,” Dr. Saitoh said in a press release.
The study was published online in Frontiers in Pharmacology.
Inhibitory function
Disulfiram inhibits the enzyme aldehyde dehydrogenase (ALDH), which is responsible for alcohol metabolism. Recent research suggests that disulfiram may have broader inhibitory functions.
In particular, it inhibits the cytoplasmic protein FROUNT, preventing it from interacting with two chemokine receptors (CCR2 and CCRs) that are involved in cellular signaling pathways and are associated with regulating behaviors, including anxiety, in rodents, the authors write.
“Although the functions of FROUNT-chemokines signaling in the immune system are well documented, the potential role of CNS-expressed FROUNT chemokine–related molecules as neuromodulators remains largely unknown,” they write.
The researchers had been conducting preclinical research on the secondary pharmacologic properties of disulfiram and “coincidentally discovered” its “anxiolytic-like effects.” They investigated these effects further because currently used anxiolytics – i.e., benzodiazepines – have unwanted side effects.
The researchers utilized an elevated plus-maze (EPM) test to investigate the effects of disulfiram in mice. The EPM apparatus consists of four arms set in a cross pattern and are connected to a central square. Of these, two arms are protected by vertical boundaries, while the other two have unprotected edges. Typically, mice with anxiety prefer to spend time in the closed arms. The mice also underwent other tests of coordination and the ability to navigate a Y-maze.
Some mice received disulfiram, others received a benzodiazepine, and others received merely a “vehicle,” which served as a control.
Disulfiram “significantly and dose-dependently” increased the time spent in the open arms of the EPM, compared with the vehicle-treated group, at 30 minutes after administration (F [3, 30] = 16.64; P < .0001), suggesting less anxiety. The finding was confirmed by a Bonferroni analysis that showed a significant effect of disulfiram, compared with the vehicle-treated group, at all three doses (20 mg/kg: t = 0.9894; P > .05; 40 mg/kg: t = 3.863; P < .01; 80 mg/kg: t = 6.417; P < .001).
A Student’s t-test analysis showed that diazepam likewise had a significant effect, compared to the vehicle (t = 5.038; P < .001).
Disulfiram also “significantly and dose-dependently” increased the percentage of open-arm entries (F [3, 30] = 14.24; P < .0001). The Bonferroni analysis showed this effect at all three doses (20 mg/kg: t = 0.3999; P > .05; 40 mg/kg: t = 2.693; P > .05; 80 mg/kg: t = 5.864; P < .001).
Diazepam similarly showed a significant effect, compared to the vehicle condition (t = 3.733; P < .005).
In particular, the 40 mg/kg dose of disulfiram significantly increased the percentage of time spent in the open arms at 15, 30, and 60 minutes after administration, with the peak effect occurring at 30 minutes.
The researchers examined the effect of cyanamide, another ALDH inhibitor, on the anxiety behaviors of mice and found no effect on the number of open-arm entries or percentage of time the mice spent in the open arm, compared with the vehicle condition.
In contrast to diazepam, disulfiram had no effect on the amount of spontaneous locomotor activity, time spent on the rotarod, or activity on the Y-maze test displayed by the mice, “suggesting that there were no apparent sedative effects at the dosages used.” Moreover, unlike the mice treated with diazepam, there were no increases in the number of falls the mice experienced on the rotarod.
Glutamate levels in the prelimbic-prefrontal cortex (PL-PFC) “play an important role in the development of anxiety-like behavior in mice,” the authors state. Disulfiram “significantly and completely attenuated increased extracellular glutamate levels in the PL-PFC during stress exposure” on the EPM.
“We propose that DSF inhibits FROUNT protein and the chemokine signaling pathways under its influence, which may suppress presynaptic glutamatergic transmission in the brain,” said Dr. Saitoh. “This, in turn, attenuates the levels of glutamate in the brain, reducing overall anxiety.”
Humanity’s most common affliction
Commenting for this news organization, Roger McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the mood disorders psychopharmacology unit, noted that there is a “renewed interest in psychiatry in excitatory and inhibitory balance – for example, ketamine represents a treatment that facilitates excitatory activity, while neurosteroids are candidate medicines now for inhibitory activity.”
Dr. McIntyre, who is the chairman and executive director of the Brain and Cognitive Discover Foundation, Toronto, and was not involved with the study, said it is believed “that the excitatory-inhibitory balance may be relevant to brain health and disease.”
Dr. McIntyre also pointed out that the study “highlights not only the repurposing of a well-known medicine but also exploit[s] the potential brain therapeutic effects of immune targets that indirectly affect inhibitory systems, resulting in potentially a safer treatment for anxiety – the most common affliction of humanity.”
Also commenting for this article, Wilfrid Noel Raby, MD, PhD, a psychiatrist in private practice in Teaneck, N.J., called disulfiram “grossly underused for alcohol use disorders and even more so when people use alcohol and cocaine.”
Dr. Raby, who was not involved with the study, has found that patients withdrawing from cocaine, cannabis, or stimulants “can respond very well to disulfiram [not only] in terms of their cravings but also in terms of mood stabilization and anxiolysis.”
He has also found that for patients with bipolar disorder or attention-deficit/hyperactivity disorder with depression disulfiram and low-dose lithium “can provide anxiolysis and mood stabilization, especially if a rapid effect is required, usually within a week.”
However, Dr. Raby cautioned that “it is probably not advisable to maintain patients on disulfiram for periods long than 3 months consecutively because there is a risk of neuropathy and hepatopathology that are not common but are seen often enough.” He usually interrupts treatment for a month and then resumes if necessary.
The research was partially supported by the Tsukuba Clinical Research and Development Organization from the Japan Agency for Medical Research and Development. The authors and Dr. Raby have disclosed no relevant financial relationships. Dr. McIntyre reports receiving research grant support from CIHR/GACD/National Natural Science Foundation of China; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, AbbVie, and Atai Life Sciences. Dr. McIntyre is CEO of Braxia Scientific.
A version of this article first appeared on Medscape.com.
FROM FRONTIERS IN PHARMACOLOGY
COVID-19 accelerated psychological problems for critical care clinicians
Approximately one-third of critical care workers reported some degree of depression, anxiety, or somatic symptoms in the early phase of the COVID-19 pandemic, based on survey results from 939 health care professionals.
The emotional response of professionals in a critical care setting in the early phase of the COVID-19 pandemic has not been well studied, Robyn Branca, PhD, and Paul Branca, MD, of Carson Newman University and the University of Tennessee Medical Center, both in Knoxville, wrote in an abstract presented at the virtual Critical Care Congress sponsored by the Society of Critical Care Medicine.
The prevalence of depression, anxiety, and somatization is low in the general population overall, but the researchers predicted that these conditions increased among workers in critical care settings early in the pandemic.
To assess the prevalence of psychological problems during that time, they sent an email survey on April 7, 2020, to members of the Society of Critical Care Medicine. The survey collected data on demographics, perceived caseload, and potential course of the pandemic. The survey also collected responses to assessments for depression (using the Patient Health Questionnaire–9), anxiety (using the Generalized Anxiety Disorder [GAD] Scale–7), and symptom somatization (using the PHQ-15).
Of the 939 survey respondents, 37% were male, 61.4% were female, and 1.4% gave another or no response.
Overall, 32.3% reported encountering 0-50 COVID-19 cases, 31.1% had encountered 51-200 cases, 12.5% had encountered 201-500 cases, 9.4% had encountered 501-1000 cases, and 13.7% had encountered more than 1,000 cases.
Based on the PHQ-9 depression scale, 44.9% of the respondents had minimal symptoms, 31.1% mild symptoms, 14.3% moderate symptoms, and 9.7% met criteria for severe depressive symptoms. Based on the GAD-7 anxiety scale, 35.5% had minimal symptoms, 32.9% mild, 16.8% moderate, and 14.8% had severe symptoms. Based on the PHQ-15 somatization scale, 39.6% of respondents showed minimal symptoms, whereas 38.2% showed mild symptoms, 17.3% moderate symptoms, and 4.9% had a severe degree of somatic symptoms.
The study findings were limited by the reliance on self-reports; however, the results indicate that a high percentage of critical care workers experienced significant, diagnosable levels of depression, anxiety, and somatic symptoms, the researchers said.
The standard guidance is to pursue individual intervention for anyone with scores of moderate or severe on the scales used in the survey, the researchers said.
Therefore, the findings represent “an alarming degree of mental health impact,” they emphasized. “Immediate mitigation efforts are needed to preserve the health of our ICU workforce.”
The study is important at this time because clinician fatigue and occupational stress are at endemic levels, Bernard Chang, MD, of Columbia University Irving Medical Center, New York City, said in an interview. “It is vital that we take stock of how frontline workers in critical care settings are doing overall,” said Dr. Chang.
Dr. Chang, who was not involved with the study but has conducted research on mental health in frontline health care workers during the pandemic, said he was not surprised by the findings. “This work builds on the growing body of literature in the pandemic noting high levels of stress, fatigue, and depression/anxiety symptoms across many frontline workers, from emergency department staff, first responders and others. These are all data points highlighting the urgent need for a broad safety net, not only for patients but the providers serving them.”
The takeaway message: “Clinicians are often so focused on providing care for their patients that they may overlook the need to care for their own well-being and mental health,” said Dr. Chang.
As for additional research, “we need to now take this important data and build on creating and identifying tangible solutions to improve the morale of the acute care/health care workforce to ensure career longevity, professional satisfaction, and overall well-being,” Dr. Chang emphasized. Mental health and morale affect not only health care workers, but also the patients they care for. Well–cared for health care providers can be at their best to provide the optimal care for their patients.
The study received no outside funding. The researchers and Dr. Chang disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Approximately one-third of critical care workers reported some degree of depression, anxiety, or somatic symptoms in the early phase of the COVID-19 pandemic, based on survey results from 939 health care professionals.
The emotional response of professionals in a critical care setting in the early phase of the COVID-19 pandemic has not been well studied, Robyn Branca, PhD, and Paul Branca, MD, of Carson Newman University and the University of Tennessee Medical Center, both in Knoxville, wrote in an abstract presented at the virtual Critical Care Congress sponsored by the Society of Critical Care Medicine.
The prevalence of depression, anxiety, and somatization is low in the general population overall, but the researchers predicted that these conditions increased among workers in critical care settings early in the pandemic.
To assess the prevalence of psychological problems during that time, they sent an email survey on April 7, 2020, to members of the Society of Critical Care Medicine. The survey collected data on demographics, perceived caseload, and potential course of the pandemic. The survey also collected responses to assessments for depression (using the Patient Health Questionnaire–9), anxiety (using the Generalized Anxiety Disorder [GAD] Scale–7), and symptom somatization (using the PHQ-15).
Of the 939 survey respondents, 37% were male, 61.4% were female, and 1.4% gave another or no response.
Overall, 32.3% reported encountering 0-50 COVID-19 cases, 31.1% had encountered 51-200 cases, 12.5% had encountered 201-500 cases, 9.4% had encountered 501-1000 cases, and 13.7% had encountered more than 1,000 cases.
Based on the PHQ-9 depression scale, 44.9% of the respondents had minimal symptoms, 31.1% mild symptoms, 14.3% moderate symptoms, and 9.7% met criteria for severe depressive symptoms. Based on the GAD-7 anxiety scale, 35.5% had minimal symptoms, 32.9% mild, 16.8% moderate, and 14.8% had severe symptoms. Based on the PHQ-15 somatization scale, 39.6% of respondents showed minimal symptoms, whereas 38.2% showed mild symptoms, 17.3% moderate symptoms, and 4.9% had a severe degree of somatic symptoms.
The study findings were limited by the reliance on self-reports; however, the results indicate that a high percentage of critical care workers experienced significant, diagnosable levels of depression, anxiety, and somatic symptoms, the researchers said.
The standard guidance is to pursue individual intervention for anyone with scores of moderate or severe on the scales used in the survey, the researchers said.
Therefore, the findings represent “an alarming degree of mental health impact,” they emphasized. “Immediate mitigation efforts are needed to preserve the health of our ICU workforce.”
The study is important at this time because clinician fatigue and occupational stress are at endemic levels, Bernard Chang, MD, of Columbia University Irving Medical Center, New York City, said in an interview. “It is vital that we take stock of how frontline workers in critical care settings are doing overall,” said Dr. Chang.
Dr. Chang, who was not involved with the study but has conducted research on mental health in frontline health care workers during the pandemic, said he was not surprised by the findings. “This work builds on the growing body of literature in the pandemic noting high levels of stress, fatigue, and depression/anxiety symptoms across many frontline workers, from emergency department staff, first responders and others. These are all data points highlighting the urgent need for a broad safety net, not only for patients but the providers serving them.”
The takeaway message: “Clinicians are often so focused on providing care for their patients that they may overlook the need to care for their own well-being and mental health,” said Dr. Chang.
As for additional research, “we need to now take this important data and build on creating and identifying tangible solutions to improve the morale of the acute care/health care workforce to ensure career longevity, professional satisfaction, and overall well-being,” Dr. Chang emphasized. Mental health and morale affect not only health care workers, but also the patients they care for. Well–cared for health care providers can be at their best to provide the optimal care for their patients.
The study received no outside funding. The researchers and Dr. Chang disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Approximately one-third of critical care workers reported some degree of depression, anxiety, or somatic symptoms in the early phase of the COVID-19 pandemic, based on survey results from 939 health care professionals.
The emotional response of professionals in a critical care setting in the early phase of the COVID-19 pandemic has not been well studied, Robyn Branca, PhD, and Paul Branca, MD, of Carson Newman University and the University of Tennessee Medical Center, both in Knoxville, wrote in an abstract presented at the virtual Critical Care Congress sponsored by the Society of Critical Care Medicine.
The prevalence of depression, anxiety, and somatization is low in the general population overall, but the researchers predicted that these conditions increased among workers in critical care settings early in the pandemic.
To assess the prevalence of psychological problems during that time, they sent an email survey on April 7, 2020, to members of the Society of Critical Care Medicine. The survey collected data on demographics, perceived caseload, and potential course of the pandemic. The survey also collected responses to assessments for depression (using the Patient Health Questionnaire–9), anxiety (using the Generalized Anxiety Disorder [GAD] Scale–7), and symptom somatization (using the PHQ-15).
Of the 939 survey respondents, 37% were male, 61.4% were female, and 1.4% gave another or no response.
Overall, 32.3% reported encountering 0-50 COVID-19 cases, 31.1% had encountered 51-200 cases, 12.5% had encountered 201-500 cases, 9.4% had encountered 501-1000 cases, and 13.7% had encountered more than 1,000 cases.
Based on the PHQ-9 depression scale, 44.9% of the respondents had minimal symptoms, 31.1% mild symptoms, 14.3% moderate symptoms, and 9.7% met criteria for severe depressive symptoms. Based on the GAD-7 anxiety scale, 35.5% had minimal symptoms, 32.9% mild, 16.8% moderate, and 14.8% had severe symptoms. Based on the PHQ-15 somatization scale, 39.6% of respondents showed minimal symptoms, whereas 38.2% showed mild symptoms, 17.3% moderate symptoms, and 4.9% had a severe degree of somatic symptoms.
The study findings were limited by the reliance on self-reports; however, the results indicate that a high percentage of critical care workers experienced significant, diagnosable levels of depression, anxiety, and somatic symptoms, the researchers said.
The standard guidance is to pursue individual intervention for anyone with scores of moderate or severe on the scales used in the survey, the researchers said.
Therefore, the findings represent “an alarming degree of mental health impact,” they emphasized. “Immediate mitigation efforts are needed to preserve the health of our ICU workforce.”
The study is important at this time because clinician fatigue and occupational stress are at endemic levels, Bernard Chang, MD, of Columbia University Irving Medical Center, New York City, said in an interview. “It is vital that we take stock of how frontline workers in critical care settings are doing overall,” said Dr. Chang.
Dr. Chang, who was not involved with the study but has conducted research on mental health in frontline health care workers during the pandemic, said he was not surprised by the findings. “This work builds on the growing body of literature in the pandemic noting high levels of stress, fatigue, and depression/anxiety symptoms across many frontline workers, from emergency department staff, first responders and others. These are all data points highlighting the urgent need for a broad safety net, not only for patients but the providers serving them.”
The takeaway message: “Clinicians are often so focused on providing care for their patients that they may overlook the need to care for their own well-being and mental health,” said Dr. Chang.
As for additional research, “we need to now take this important data and build on creating and identifying tangible solutions to improve the morale of the acute care/health care workforce to ensure career longevity, professional satisfaction, and overall well-being,” Dr. Chang emphasized. Mental health and morale affect not only health care workers, but also the patients they care for. Well–cared for health care providers can be at their best to provide the optimal care for their patients.
The study received no outside funding. The researchers and Dr. Chang disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SCCM 2022
Abdominal cramping and diarrhea
On the basis of the patient's history and presentation, the likely diagnosis is extensive UC. Extensive colitis is defined by the presence of disease activity proximal to the splenic flexure. Because disease activity in UC is dynamic, up to half of patients who present with proctitis and 70% of those who present with left-sided colitis go on to develop extensive colitis on follow-up.
On the basis of the workup, it appears that this patient's UC has transitioned from left-sided to extensive disease, given the loss of treatment response. Endoscopic evaluation of patients with loss of treatment response may reveal patchiness of the histologic activity, as seen in this case.
Extensive colitis is a poor prognostic factor in UC, as is systemic steroid requirement, young age at diagnosis, and an elevated C-reactive protein level or erythrocyte sedimentation rate, all of which are associated with higher rates of colectomy. Over time, patients living with extensive ulcerative colitis develop an increased risk for colorectal cancer. Routine colonoscopic screening and surveillance are recommended for these high-risk patients.
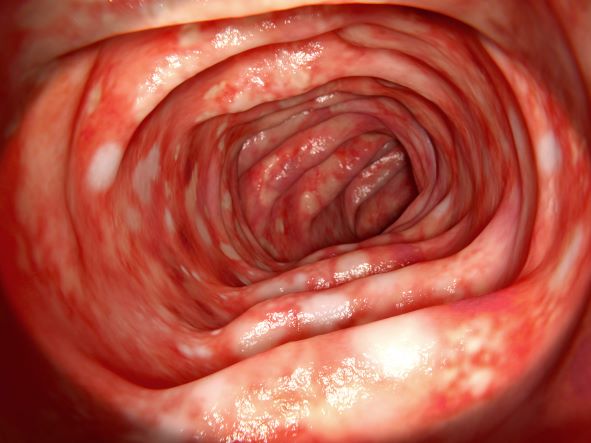
UC most often presents as a continuously inflamed segment involving the distal rectum and extending proximally. Endoscopic features of inflammation include loss of vascular markings; granularity and friability of the mucosa; erosions; and, in the setting of severe inflammation, ulcerations and spontaneous bleeding. The diagnosis of UC involves both a lower gastrointestinal endoscopic examination and histologic confirmation. In general, a complete colonoscopy including examination of the terminal ileum should be performed, allowing clinicians to assess the full extent of the disease while ruling out distal ileal involvement, which is characteristic of Crohn's disease.
Evaluation of UC during relapses should include assessment of symptom severity and potential triggers, including enteric infections, use of nonsteroidal anti-inflammatory drugs, and recent smoking cessation. Nonadherence to therapy is common in patients with UC and may lead to relapse.
To treat a patient like the one represented here, the American College of Gastroenterology guidelines recommend oral 5-ASA at a dose of at least 2 g/d to induce remission. However, because this patient lost response to this treatment, the next step in the guidelines are appropriate oral systemic corticosteroids.
Bhupinder S. Anand, MD, Professor, Department of Medicine, Baylor College of Medicine, Houston, TX
Bhupinder S. Anand, MD, has disclosed no relevant financial relationships
On the basis of the patient's history and presentation, the likely diagnosis is extensive UC. Extensive colitis is defined by the presence of disease activity proximal to the splenic flexure. Because disease activity in UC is dynamic, up to half of patients who present with proctitis and 70% of those who present with left-sided colitis go on to develop extensive colitis on follow-up.
On the basis of the workup, it appears that this patient's UC has transitioned from left-sided to extensive disease, given the loss of treatment response. Endoscopic evaluation of patients with loss of treatment response may reveal patchiness of the histologic activity, as seen in this case.
Extensive colitis is a poor prognostic factor in UC, as is systemic steroid requirement, young age at diagnosis, and an elevated C-reactive protein level or erythrocyte sedimentation rate, all of which are associated with higher rates of colectomy. Over time, patients living with extensive ulcerative colitis develop an increased risk for colorectal cancer. Routine colonoscopic screening and surveillance are recommended for these high-risk patients.
UC most often presents as a continuously inflamed segment involving the distal rectum and extending proximally. Endoscopic features of inflammation include loss of vascular markings; granularity and friability of the mucosa; erosions; and, in the setting of severe inflammation, ulcerations and spontaneous bleeding. The diagnosis of UC involves both a lower gastrointestinal endoscopic examination and histologic confirmation. In general, a complete colonoscopy including examination of the terminal ileum should be performed, allowing clinicians to assess the full extent of the disease while ruling out distal ileal involvement, which is characteristic of Crohn's disease.
Evaluation of UC during relapses should include assessment of symptom severity and potential triggers, including enteric infections, use of nonsteroidal anti-inflammatory drugs, and recent smoking cessation. Nonadherence to therapy is common in patients with UC and may lead to relapse.
To treat a patient like the one represented here, the American College of Gastroenterology guidelines recommend oral 5-ASA at a dose of at least 2 g/d to induce remission. However, because this patient lost response to this treatment, the next step in the guidelines are appropriate oral systemic corticosteroids.
Bhupinder S. Anand, MD, Professor, Department of Medicine, Baylor College of Medicine, Houston, TX
Bhupinder S. Anand, MD, has disclosed no relevant financial relationships
On the basis of the patient's history and presentation, the likely diagnosis is extensive UC. Extensive colitis is defined by the presence of disease activity proximal to the splenic flexure. Because disease activity in UC is dynamic, up to half of patients who present with proctitis and 70% of those who present with left-sided colitis go on to develop extensive colitis on follow-up.
On the basis of the workup, it appears that this patient's UC has transitioned from left-sided to extensive disease, given the loss of treatment response. Endoscopic evaluation of patients with loss of treatment response may reveal patchiness of the histologic activity, as seen in this case.
Extensive colitis is a poor prognostic factor in UC, as is systemic steroid requirement, young age at diagnosis, and an elevated C-reactive protein level or erythrocyte sedimentation rate, all of which are associated with higher rates of colectomy. Over time, patients living with extensive ulcerative colitis develop an increased risk for colorectal cancer. Routine colonoscopic screening and surveillance are recommended for these high-risk patients.
UC most often presents as a continuously inflamed segment involving the distal rectum and extending proximally. Endoscopic features of inflammation include loss of vascular markings; granularity and friability of the mucosa; erosions; and, in the setting of severe inflammation, ulcerations and spontaneous bleeding. The diagnosis of UC involves both a lower gastrointestinal endoscopic examination and histologic confirmation. In general, a complete colonoscopy including examination of the terminal ileum should be performed, allowing clinicians to assess the full extent of the disease while ruling out distal ileal involvement, which is characteristic of Crohn's disease.
Evaluation of UC during relapses should include assessment of symptom severity and potential triggers, including enteric infections, use of nonsteroidal anti-inflammatory drugs, and recent smoking cessation. Nonadherence to therapy is common in patients with UC and may lead to relapse.
To treat a patient like the one represented here, the American College of Gastroenterology guidelines recommend oral 5-ASA at a dose of at least 2 g/d to induce remission. However, because this patient lost response to this treatment, the next step in the guidelines are appropriate oral systemic corticosteroids.
Bhupinder S. Anand, MD, Professor, Department of Medicine, Baylor College of Medicine, Houston, TX
Bhupinder S. Anand, MD, has disclosed no relevant financial relationships
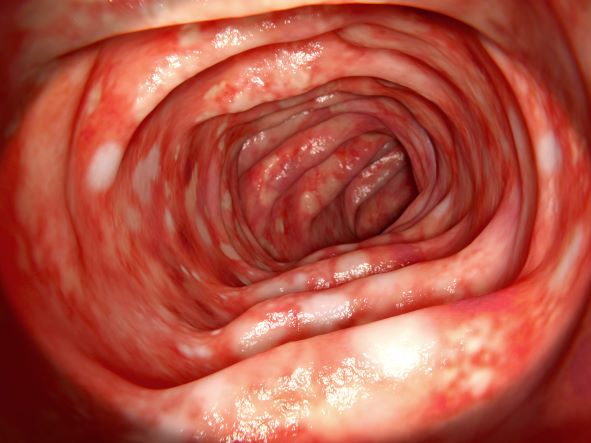
A 46-year-old man presents with abdominal cramping and diarrhea and reports about five bowel movements per day for the past 2 weeks. Height is 5 ft 9 in and weight is 157 lb (BMI, 23.2). History is significant for ulcerative colitis (UC), diagnosed about 20 years ago with proctitis and having progressed about 8 years ago to left-sided disease. He smoked "lightly" through his 20s. Until about a month ago, the patient had been able to maintain remission with oral 5-aminosalicylic acid (ASA) therapy (2 g/d). Endoscopy shows granularity and friability of the mucosa with the inflamed segment extending proximal to the splenic flexure, though there is patchiness of the histologic activity. Colonoscopy rules out distal ileal involvement. Stool culture is negative.
Which breast cancer surgery leads to better quality of life?
Women diagnosed with early breast cancer facing surgery often have a choice of having all of their breast or only a part of the breast removed.
A new study shows that a patient’s satisfaction with their breasts at 10 years after surgery is similar for both groups of women.
However, superior psychosocial and sexual well-being at 10 years after surgery was reported by women who underwent breast-conserving surgery and adjuvant radiation therapy (RT), compared with those who underwent mastectomy and reconstruction.
“These findings may inform preference-sensitive decision-making for women with early-stage breast cancer,” write the authors, led by Benjamin D. Smith, MD, department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston.
The study was published online in JAMA Surgery.
These findings have important implications for patient decision-making, given that more women eligible for breast-conserving surgery are opting for a mastectomy, say Sudheer Vemuru, MD, from the University of Colorado at Denver, Aurora, and colleagues, writing in an accompanying editorial.
“Overall, the preponderance of evidence suggests superior short-term and long-term patient-reported outcomes in patients with early-stage breast cancer undergoing breast conserving surgery compared with mastectomy,” they comment.
Study details
For their study, Dr. Smith and colleagues conducted a comparative effectiveness research study using data from the Texas Cancer Registry and identified women diagnosed with stage 0-II breast cancer and treated with breast-conserving surgery or mastectomy and reconstruction between 2006 and 2008.
A total of 647 patients were included in their analysis (40%; 356 had undergone breast-conserving surgery; 291 had undergone mastectomy and reconstruction), 551 (85.2%) confirmed treatment with breast-conserving surgery with RT (n = 315) or mastectomy and reconstruction without RT (n = 236).
The median age of the cohort was 53 years and the median time from diagnosis to survey was 10.3 years. Mastectomy and reconstruction were more common among women who were White, younger, node positive, had larger tumors, had bilateral breast cancer, received chemotherapy, and had higher income.
The primary outcome was patient satisfaction with their breasts, as measured with the BREAST-Q patient-reported outcome measure. Secondary outcomes included physical well-being, psychosocial well-being, and sexual well-being. The EuroQol Health-Related Quality of Life 5-Dimension, 3-Level gaged health utility, and local therapy decisional regret was measured via the Decisional Regret Scale.
Using breast-conserving surgery plus RT as the referent, the authors did not find any significant differences in breast satisfaction, physical well-being, health utility, or decisional regret among the study cohorts: breast satisfaction: effect size, 2.71 (P = .30); physical well-being: effect size, –1.80 (P = .36); health utility: effect size, –0.003 (P = .83); and decisional regret: effect size, 1.32 (P = .61).
However, psychosocial well-being (effect size, –8.61; P < .001) and sexual well-being (effect size, –10.68; P < .001) were significantly worse among women who had undergone mastectomy and reconstruction without RT.
They noted that interactions of race and ethnicity and age by treatment group were not significant for reported satisfaction with breast outcomes. But the findings “indicated that the burden of poor long-term QOL outcomes was greater among younger individuals, those with lower educational attainment and income, and certain racial and ethnic minority populations,” they write. “These findings suggest that opportunities exist to enhance equity in the long-term QOL of individuals with breast cancer.”
The editorialists note that previous studies have also found diminished quality of life following mastectomy compared with breast-conserving surgery. However, most of these prior studies included patients undergoing breast-conserving surgery without RT, patients undergoing mastectomy without reconstruction, and patients undergoing mastectomy with RT.
In contrast, this latest study “directly compared breast-conserving surgery with RT vs. mastectomy and reconstruction without RT to avoid those potential confounders,” they point out.
The study was supported by grants from the National Cancer Institute and other bodies. Several of the study authors disclosed relationships with industry and/or with nonprofit organizations. The full list can be found with the original article. Editorialist Clara Lee, MD, reported receiving grants from the Agency for Healthcare Research and Quality during the conduct of the study.
A version of this article first appeared on Medscape.com.
Women diagnosed with early breast cancer facing surgery often have a choice of having all of their breast or only a part of the breast removed.
A new study shows that a patient’s satisfaction with their breasts at 10 years after surgery is similar for both groups of women.
However, superior psychosocial and sexual well-being at 10 years after surgery was reported by women who underwent breast-conserving surgery and adjuvant radiation therapy (RT), compared with those who underwent mastectomy and reconstruction.
“These findings may inform preference-sensitive decision-making for women with early-stage breast cancer,” write the authors, led by Benjamin D. Smith, MD, department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston.
The study was published online in JAMA Surgery.
These findings have important implications for patient decision-making, given that more women eligible for breast-conserving surgery are opting for a mastectomy, say Sudheer Vemuru, MD, from the University of Colorado at Denver, Aurora, and colleagues, writing in an accompanying editorial.
“Overall, the preponderance of evidence suggests superior short-term and long-term patient-reported outcomes in patients with early-stage breast cancer undergoing breast conserving surgery compared with mastectomy,” they comment.
Study details
For their study, Dr. Smith and colleagues conducted a comparative effectiveness research study using data from the Texas Cancer Registry and identified women diagnosed with stage 0-II breast cancer and treated with breast-conserving surgery or mastectomy and reconstruction between 2006 and 2008.
A total of 647 patients were included in their analysis (40%; 356 had undergone breast-conserving surgery; 291 had undergone mastectomy and reconstruction), 551 (85.2%) confirmed treatment with breast-conserving surgery with RT (n = 315) or mastectomy and reconstruction without RT (n = 236).
The median age of the cohort was 53 years and the median time from diagnosis to survey was 10.3 years. Mastectomy and reconstruction were more common among women who were White, younger, node positive, had larger tumors, had bilateral breast cancer, received chemotherapy, and had higher income.
The primary outcome was patient satisfaction with their breasts, as measured with the BREAST-Q patient-reported outcome measure. Secondary outcomes included physical well-being, psychosocial well-being, and sexual well-being. The EuroQol Health-Related Quality of Life 5-Dimension, 3-Level gaged health utility, and local therapy decisional regret was measured via the Decisional Regret Scale.
Using breast-conserving surgery plus RT as the referent, the authors did not find any significant differences in breast satisfaction, physical well-being, health utility, or decisional regret among the study cohorts: breast satisfaction: effect size, 2.71 (P = .30); physical well-being: effect size, –1.80 (P = .36); health utility: effect size, –0.003 (P = .83); and decisional regret: effect size, 1.32 (P = .61).
However, psychosocial well-being (effect size, –8.61; P < .001) and sexual well-being (effect size, –10.68; P < .001) were significantly worse among women who had undergone mastectomy and reconstruction without RT.
They noted that interactions of race and ethnicity and age by treatment group were not significant for reported satisfaction with breast outcomes. But the findings “indicated that the burden of poor long-term QOL outcomes was greater among younger individuals, those with lower educational attainment and income, and certain racial and ethnic minority populations,” they write. “These findings suggest that opportunities exist to enhance equity in the long-term QOL of individuals with breast cancer.”
The editorialists note that previous studies have also found diminished quality of life following mastectomy compared with breast-conserving surgery. However, most of these prior studies included patients undergoing breast-conserving surgery without RT, patients undergoing mastectomy without reconstruction, and patients undergoing mastectomy with RT.
In contrast, this latest study “directly compared breast-conserving surgery with RT vs. mastectomy and reconstruction without RT to avoid those potential confounders,” they point out.
The study was supported by grants from the National Cancer Institute and other bodies. Several of the study authors disclosed relationships with industry and/or with nonprofit organizations. The full list can be found with the original article. Editorialist Clara Lee, MD, reported receiving grants from the Agency for Healthcare Research and Quality during the conduct of the study.
A version of this article first appeared on Medscape.com.
Women diagnosed with early breast cancer facing surgery often have a choice of having all of their breast or only a part of the breast removed.
A new study shows that a patient’s satisfaction with their breasts at 10 years after surgery is similar for both groups of women.
However, superior psychosocial and sexual well-being at 10 years after surgery was reported by women who underwent breast-conserving surgery and adjuvant radiation therapy (RT), compared with those who underwent mastectomy and reconstruction.
“These findings may inform preference-sensitive decision-making for women with early-stage breast cancer,” write the authors, led by Benjamin D. Smith, MD, department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston.
The study was published online in JAMA Surgery.
These findings have important implications for patient decision-making, given that more women eligible for breast-conserving surgery are opting for a mastectomy, say Sudheer Vemuru, MD, from the University of Colorado at Denver, Aurora, and colleagues, writing in an accompanying editorial.
“Overall, the preponderance of evidence suggests superior short-term and long-term patient-reported outcomes in patients with early-stage breast cancer undergoing breast conserving surgery compared with mastectomy,” they comment.
Study details
For their study, Dr. Smith and colleagues conducted a comparative effectiveness research study using data from the Texas Cancer Registry and identified women diagnosed with stage 0-II breast cancer and treated with breast-conserving surgery or mastectomy and reconstruction between 2006 and 2008.
A total of 647 patients were included in their analysis (40%; 356 had undergone breast-conserving surgery; 291 had undergone mastectomy and reconstruction), 551 (85.2%) confirmed treatment with breast-conserving surgery with RT (n = 315) or mastectomy and reconstruction without RT (n = 236).
The median age of the cohort was 53 years and the median time from diagnosis to survey was 10.3 years. Mastectomy and reconstruction were more common among women who were White, younger, node positive, had larger tumors, had bilateral breast cancer, received chemotherapy, and had higher income.
The primary outcome was patient satisfaction with their breasts, as measured with the BREAST-Q patient-reported outcome measure. Secondary outcomes included physical well-being, psychosocial well-being, and sexual well-being. The EuroQol Health-Related Quality of Life 5-Dimension, 3-Level gaged health utility, and local therapy decisional regret was measured via the Decisional Regret Scale.
Using breast-conserving surgery plus RT as the referent, the authors did not find any significant differences in breast satisfaction, physical well-being, health utility, or decisional regret among the study cohorts: breast satisfaction: effect size, 2.71 (P = .30); physical well-being: effect size, –1.80 (P = .36); health utility: effect size, –0.003 (P = .83); and decisional regret: effect size, 1.32 (P = .61).
However, psychosocial well-being (effect size, –8.61; P < .001) and sexual well-being (effect size, –10.68; P < .001) were significantly worse among women who had undergone mastectomy and reconstruction without RT.
They noted that interactions of race and ethnicity and age by treatment group were not significant for reported satisfaction with breast outcomes. But the findings “indicated that the burden of poor long-term QOL outcomes was greater among younger individuals, those with lower educational attainment and income, and certain racial and ethnic minority populations,” they write. “These findings suggest that opportunities exist to enhance equity in the long-term QOL of individuals with breast cancer.”
The editorialists note that previous studies have also found diminished quality of life following mastectomy compared with breast-conserving surgery. However, most of these prior studies included patients undergoing breast-conserving surgery without RT, patients undergoing mastectomy without reconstruction, and patients undergoing mastectomy with RT.
In contrast, this latest study “directly compared breast-conserving surgery with RT vs. mastectomy and reconstruction without RT to avoid those potential confounders,” they point out.
The study was supported by grants from the National Cancer Institute and other bodies. Several of the study authors disclosed relationships with industry and/or with nonprofit organizations. The full list can be found with the original article. Editorialist Clara Lee, MD, reported receiving grants from the Agency for Healthcare Research and Quality during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM JAMA SURGERY
Recent unintended weight loss
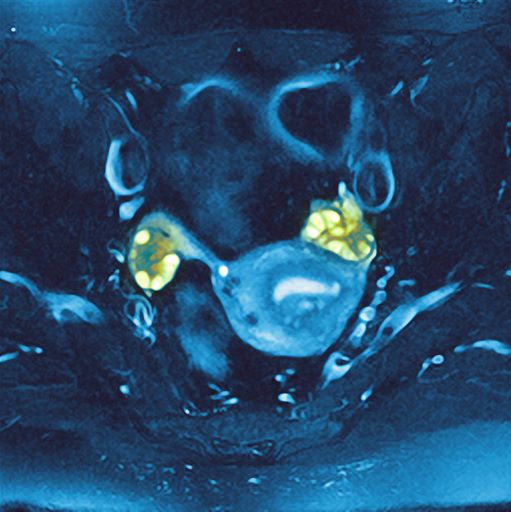
PCOS is most often defined according to the Rotterdam criteria, which stipulate that at least two of the following be present: irregular ovulation, biochemical/clinical hyperandrogenism, and polycystic ovaries (seen in the MRI scan above). Insulin resistance is part of the pathogenesis of PCOS, and insulin resistance is associated with T2D in PCOS.
In fact, PCOS is an independent risk factor for T2D, even after adjustment for BMI and obesity. Even normal-weight women with PCOS have an increased risk for T2D. More than half of women with PCOS develop T2D by age 40.
Even though family history and obesity are major contributors in the development of diabetes in patients with PCOS, diabetes can still occur in lean patients with PCOS who have no family history, mainly secondary to insulin resistance.
The Endocrine Society recommends that all individuals with PCOS undergo an oral glucose tolerance test every 3-5 years, with more frequent screening for those who develop symptoms of T2D, significant weight gain, or central adiposity. In guidelines published in 2015 by the American Association of Clinical Endocrinologists, the American College of Endocrinology, and the Androgen Excess and PCOS Society, an annual oral glucose tolerance test is recommended for patients with PCOS and impaired glucose tolerance, whereas those with a family history of T2D or a BMI above 30 should be screened every 1-2 years.
Management of T2D with PCOS is similar to that of T2D without PCOS. Accordingly, metformin and lifestyle changes are the treatments of choice; any antidiabetic agent may be added in patients who do not achieve glycemic targets despite treatment with metformin.
Romesh K. Khardori, MD, PhD, Professor, Department of Internal Medicine, Division of Diabetes, Endocrine, and Metabolic Disorders, Eastern Virginia Medical School; EVMS Medical Group, Norfolk, Virginia
Romesh K. Khardori, MD, PhD, has disclosed no relevant financial relationships
PCOS is most often defined according to the Rotterdam criteria, which stipulate that at least two of the following be present: irregular ovulation, biochemical/clinical hyperandrogenism, and polycystic ovaries (seen in the MRI scan above). Insulin resistance is part of the pathogenesis of PCOS, and insulin resistance is associated with T2D in PCOS.
In fact, PCOS is an independent risk factor for T2D, even after adjustment for BMI and obesity. Even normal-weight women with PCOS have an increased risk for T2D. More than half of women with PCOS develop T2D by age 40.
Even though family history and obesity are major contributors in the development of diabetes in patients with PCOS, diabetes can still occur in lean patients with PCOS who have no family history, mainly secondary to insulin resistance.
The Endocrine Society recommends that all individuals with PCOS undergo an oral glucose tolerance test every 3-5 years, with more frequent screening for those who develop symptoms of T2D, significant weight gain, or central adiposity. In guidelines published in 2015 by the American Association of Clinical Endocrinologists, the American College of Endocrinology, and the Androgen Excess and PCOS Society, an annual oral glucose tolerance test is recommended for patients with PCOS and impaired glucose tolerance, whereas those with a family history of T2D or a BMI above 30 should be screened every 1-2 years.
Management of T2D with PCOS is similar to that of T2D without PCOS. Accordingly, metformin and lifestyle changes are the treatments of choice; any antidiabetic agent may be added in patients who do not achieve glycemic targets despite treatment with metformin.
Romesh K. Khardori, MD, PhD, Professor, Department of Internal Medicine, Division of Diabetes, Endocrine, and Metabolic Disorders, Eastern Virginia Medical School; EVMS Medical Group, Norfolk, Virginia
Romesh K. Khardori, MD, PhD, has disclosed no relevant financial relationships
PCOS is most often defined according to the Rotterdam criteria, which stipulate that at least two of the following be present: irregular ovulation, biochemical/clinical hyperandrogenism, and polycystic ovaries (seen in the MRI scan above). Insulin resistance is part of the pathogenesis of PCOS, and insulin resistance is associated with T2D in PCOS.
In fact, PCOS is an independent risk factor for T2D, even after adjustment for BMI and obesity. Even normal-weight women with PCOS have an increased risk for T2D. More than half of women with PCOS develop T2D by age 40.
Even though family history and obesity are major contributors in the development of diabetes in patients with PCOS, diabetes can still occur in lean patients with PCOS who have no family history, mainly secondary to insulin resistance.
The Endocrine Society recommends that all individuals with PCOS undergo an oral glucose tolerance test every 3-5 years, with more frequent screening for those who develop symptoms of T2D, significant weight gain, or central adiposity. In guidelines published in 2015 by the American Association of Clinical Endocrinologists, the American College of Endocrinology, and the Androgen Excess and PCOS Society, an annual oral glucose tolerance test is recommended for patients with PCOS and impaired glucose tolerance, whereas those with a family history of T2D or a BMI above 30 should be screened every 1-2 years.
Management of T2D with PCOS is similar to that of T2D without PCOS. Accordingly, metformin and lifestyle changes are the treatments of choice; any antidiabetic agent may be added in patients who do not achieve glycemic targets despite treatment with metformin.
Romesh K. Khardori, MD, PhD, Professor, Department of Internal Medicine, Division of Diabetes, Endocrine, and Metabolic Disorders, Eastern Virginia Medical School; EVMS Medical Group, Norfolk, Virginia
Romesh K. Khardori, MD, PhD, has disclosed no relevant financial relationships
A 36-year-old woman presents with recent unintended weight loss of 12 lb in 2 months. Currently, she weighs 153 lb (BMI 24.7). She complains of increased thirst, increased urination, lack of energy, and fatigue.
Metabolic workup reveals that A1c is 7.1%, fasting blood glucose level is 131 mg/dL, oral glucose tolerance test level is 210 mg/dL, and random blood glucose level is 215 mg/dL, all of which are diagnostic for type 2 diabetes (T2D). She has no family history of diabetes.
A lipid panel shows a low-density lipoprotein cholesterol of 140 mg/dL, high-density lipoprotein cholesterol 38 mg/dL, and triglycerides 210 mg/dL. Blood pressure is 150/95 mm Hg.
The patient had been diagnosed with polycystic ovary syndrome (PCOS) at age 33, during a workup for infertility. At the time of her PCOS diagnosis, she weighed 190 lb (BMI, 30.7). She gave birth to an 8-lb son 14 months ago.

Mental illness tied to COVID-19 breakthrough infection
“Psychiatric disorders remained significantly associated with incident breakthrough infections above and beyond sociodemographic and medical factors, suggesting that mental health is important to consider in conjunction with other risk factors,” wrote the investigators, led by Aoife O’Donovan, PhD, University of California, San Francisco.
Individuals with psychiatric disorders “should be prioritized for booster vaccinations and other critical preventive efforts, including increased SARS-CoV-2 screening, public health campaigns, or COVID-19 discussions during clinical care,” they added.
The study was published online in JAMA Network Open.
Elderly most vulnerable
The researchers reviewed the records of 263,697 veterans who were fully vaccinated against COVID-19.
Just over a half (51.4%) had one or more psychiatric diagnoses within the last 5 years and 14.8% developed breakthrough COVID-19 infections, confirmed by a positive SARS-CoV-2 test.
Psychiatric diagnoses among the veterans included depression, posttraumatic stress, anxiety, adjustment disorder, substance use disorder, bipolar disorder, psychosis, ADHD, dissociation, and eating disorders.
In the overall sample, a history of any psychiatric disorder was associated with a 7% higher incidence of breakthrough COVID-19 infection in models adjusted for potential confounders (adjusted relative risk, 1.07; 95% confidence interval, 1.05-1.09) and a 3% higher incidence in models additionally adjusted for underlying medical comorbidities and smoking (aRR, 1.03; 95% CI, 1.01-1.05).
Most psychiatric disorders were associated with a higher incidence of breakthrough infection, with the highest relative risk observed for substance use disorders (aRR, 1.16; 95% CI, 1.12 -1.21) and adjustment disorder (aRR, 1.13; 95% CI, 1.10-1.16) in fully adjusted models.
Older vaccinated veterans with psychiatric illnesses appear to be most vulnerable to COVID-19 reinfection.
In veterans aged 65 and older, all psychiatric disorders were associated with an increased incidence of breakthrough infection, with increases in the incidence rate ranging from 3% to 24% in fully adjusted models.
In the younger veterans, in contrast, only anxiety, adjustment, and substance use disorders were associated with an increased incidence of breakthrough infection in fully adjusted models.
Psychotic disorders were associated with a 10% lower incidence of breakthrough infection among younger veterans, perhaps because of greater social isolation, the researchers said.
Risky behavior or impaired immunity?
“Although some of the larger observed effect sizes are compelling at an individual level, even the relatively modest effect sizes may have a large effect at the population level when considering the high prevalence of psychiatric disorders and the global reach and scale of the pandemic,” Dr. O’Donovan and colleagues wrote.
They noted that psychiatric disorders, including depression, schizophrenia, and bipolar disorders, have been associated with impaired cellular immunity and blunted response to vaccines. Therefore, it’s possible that those with psychiatric disorders have poorer responses to COVID-19 vaccination.
It’s also possible that immunity following vaccination wanes more quickly or more strongly in people with psychiatric disorders and they could have less protection against new variants, they added.
Patients with psychiatric disorders could be more apt to engage in risky behaviors for contracting COVID-19, which could also increase the risk for breakthrough infection, they said.
The study was supported by a UCSF Department of Psychiatry Rapid Award and UCSF Faculty Resource Fund Award. Dr. O’Donovan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
“Psychiatric disorders remained significantly associated with incident breakthrough infections above and beyond sociodemographic and medical factors, suggesting that mental health is important to consider in conjunction with other risk factors,” wrote the investigators, led by Aoife O’Donovan, PhD, University of California, San Francisco.
Individuals with psychiatric disorders “should be prioritized for booster vaccinations and other critical preventive efforts, including increased SARS-CoV-2 screening, public health campaigns, or COVID-19 discussions during clinical care,” they added.
The study was published online in JAMA Network Open.
Elderly most vulnerable
The researchers reviewed the records of 263,697 veterans who were fully vaccinated against COVID-19.
Just over a half (51.4%) had one or more psychiatric diagnoses within the last 5 years and 14.8% developed breakthrough COVID-19 infections, confirmed by a positive SARS-CoV-2 test.
Psychiatric diagnoses among the veterans included depression, posttraumatic stress, anxiety, adjustment disorder, substance use disorder, bipolar disorder, psychosis, ADHD, dissociation, and eating disorders.
In the overall sample, a history of any psychiatric disorder was associated with a 7% higher incidence of breakthrough COVID-19 infection in models adjusted for potential confounders (adjusted relative risk, 1.07; 95% confidence interval, 1.05-1.09) and a 3% higher incidence in models additionally adjusted for underlying medical comorbidities and smoking (aRR, 1.03; 95% CI, 1.01-1.05).
Most psychiatric disorders were associated with a higher incidence of breakthrough infection, with the highest relative risk observed for substance use disorders (aRR, 1.16; 95% CI, 1.12 -1.21) and adjustment disorder (aRR, 1.13; 95% CI, 1.10-1.16) in fully adjusted models.
Older vaccinated veterans with psychiatric illnesses appear to be most vulnerable to COVID-19 reinfection.
In veterans aged 65 and older, all psychiatric disorders were associated with an increased incidence of breakthrough infection, with increases in the incidence rate ranging from 3% to 24% in fully adjusted models.
In the younger veterans, in contrast, only anxiety, adjustment, and substance use disorders were associated with an increased incidence of breakthrough infection in fully adjusted models.
Psychotic disorders were associated with a 10% lower incidence of breakthrough infection among younger veterans, perhaps because of greater social isolation, the researchers said.
Risky behavior or impaired immunity?
“Although some of the larger observed effect sizes are compelling at an individual level, even the relatively modest effect sizes may have a large effect at the population level when considering the high prevalence of psychiatric disorders and the global reach and scale of the pandemic,” Dr. O’Donovan and colleagues wrote.
They noted that psychiatric disorders, including depression, schizophrenia, and bipolar disorders, have been associated with impaired cellular immunity and blunted response to vaccines. Therefore, it’s possible that those with psychiatric disorders have poorer responses to COVID-19 vaccination.
It’s also possible that immunity following vaccination wanes more quickly or more strongly in people with psychiatric disorders and they could have less protection against new variants, they added.
Patients with psychiatric disorders could be more apt to engage in risky behaviors for contracting COVID-19, which could also increase the risk for breakthrough infection, they said.
The study was supported by a UCSF Department of Psychiatry Rapid Award and UCSF Faculty Resource Fund Award. Dr. O’Donovan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
“Psychiatric disorders remained significantly associated with incident breakthrough infections above and beyond sociodemographic and medical factors, suggesting that mental health is important to consider in conjunction with other risk factors,” wrote the investigators, led by Aoife O’Donovan, PhD, University of California, San Francisco.
Individuals with psychiatric disorders “should be prioritized for booster vaccinations and other critical preventive efforts, including increased SARS-CoV-2 screening, public health campaigns, or COVID-19 discussions during clinical care,” they added.
The study was published online in JAMA Network Open.
Elderly most vulnerable
The researchers reviewed the records of 263,697 veterans who were fully vaccinated against COVID-19.
Just over a half (51.4%) had one or more psychiatric diagnoses within the last 5 years and 14.8% developed breakthrough COVID-19 infections, confirmed by a positive SARS-CoV-2 test.
Psychiatric diagnoses among the veterans included depression, posttraumatic stress, anxiety, adjustment disorder, substance use disorder, bipolar disorder, psychosis, ADHD, dissociation, and eating disorders.
In the overall sample, a history of any psychiatric disorder was associated with a 7% higher incidence of breakthrough COVID-19 infection in models adjusted for potential confounders (adjusted relative risk, 1.07; 95% confidence interval, 1.05-1.09) and a 3% higher incidence in models additionally adjusted for underlying medical comorbidities and smoking (aRR, 1.03; 95% CI, 1.01-1.05).
Most psychiatric disorders were associated with a higher incidence of breakthrough infection, with the highest relative risk observed for substance use disorders (aRR, 1.16; 95% CI, 1.12 -1.21) and adjustment disorder (aRR, 1.13; 95% CI, 1.10-1.16) in fully adjusted models.
Older vaccinated veterans with psychiatric illnesses appear to be most vulnerable to COVID-19 reinfection.
In veterans aged 65 and older, all psychiatric disorders were associated with an increased incidence of breakthrough infection, with increases in the incidence rate ranging from 3% to 24% in fully adjusted models.
In the younger veterans, in contrast, only anxiety, adjustment, and substance use disorders were associated with an increased incidence of breakthrough infection in fully adjusted models.
Psychotic disorders were associated with a 10% lower incidence of breakthrough infection among younger veterans, perhaps because of greater social isolation, the researchers said.
Risky behavior or impaired immunity?
“Although some of the larger observed effect sizes are compelling at an individual level, even the relatively modest effect sizes may have a large effect at the population level when considering the high prevalence of psychiatric disorders and the global reach and scale of the pandemic,” Dr. O’Donovan and colleagues wrote.
They noted that psychiatric disorders, including depression, schizophrenia, and bipolar disorders, have been associated with impaired cellular immunity and blunted response to vaccines. Therefore, it’s possible that those with psychiatric disorders have poorer responses to COVID-19 vaccination.
It’s also possible that immunity following vaccination wanes more quickly or more strongly in people with psychiatric disorders and they could have less protection against new variants, they added.
Patients with psychiatric disorders could be more apt to engage in risky behaviors for contracting COVID-19, which could also increase the risk for breakthrough infection, they said.
The study was supported by a UCSF Department of Psychiatry Rapid Award and UCSF Faculty Resource Fund Award. Dr. O’Donovan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
International group identifies actions to improve lung cancer survival
The International Cancer Benchmarking Partnership, a collaboration of physicians, clinicians, researchers, policy makers, and data experts, has reached a consensus on key actions designed to standardize and homogenize lung cancer care that includes early diagnosis and access to care for all patients.
This consensus, reported at the 2022 European Lung Cancer Congress, is an effort to address disparities in care recognized by the group’s in-house research team. The team identified significantly different survival rates in early stage lung cancer patients from a group of countries with similar health care metrics, such as health care expenditure and universal access to health care.
“This group of countries is very comparable, but we saw a 20% difference in survival in localized, stage I and II cancers. When you consider that lung cancer is a bigger killer than any other cancer –more than breast, prostate, and colon cancer combined – that’s thousands of people,” said the project’s lead clinician, Christian Finley, MD, a thoracic surgeon with St. Joseph’s Healthcare Hamilton (Ont.).
Founded in 2009, the ICBP includes about 500 experts in its core countries of Sweden, Norway, Denmark, Australia, the United Kingdom, and Canada; New Zealand and Ireland have also participated. The goal of the partnership is to benchmark survival and other outcomes in cancer and to research why disparities between countries exist.
“That’s why we keep the membership fairly small, so that we can actually make more meaningful research projects to get into depth in factors beyond benchmarking survival and mortality,” said study author Charlotte Lynch, MSc, a senior researcher with Cancer Research UK in London.
To help narrow the disparity gap, Ms. Lynch, Dr. Finley and colleagues brought together nine key informants from ICBP countries to discuss local clinical insights and best practices, and ultimately came up a list of five recommendations considered most crucial: implementing cost-effective, equitable, and effective screening; ensuring diagnoses of lung cancer within 30 days of referral; developing thoracic centers of excellence; launching an international audit of lung cancer care; and prioritizing the recognition of improvements in lung cancer care and outcomes.
“For example, points supporting the screening call to action focus on timely access to cross-sectional imaging and availability and development of patient and health care practitioner lung cancer awareness materials,” Ms. Lynch said.
Another example would be the point that describes the need for a minimum data set to evaluate lung cancer patients’ diagnosis, treatment, and aftercare.
“I think we all work in a very disrupted system right now. Screening programs really took a hit during the pandemic, and I think people coming out of those disruptions are trying to imagine a more effective system using tools like information technologies, mobile clinics and having a better understanding of equity,” Dr. Finley said.
Ms. Lynch said the ICBP intends to use the consensus to generate concrete actions. “We’re thinking about how we can get everyone in the room to share lessons learned and best practices to push things forward rather than saying, ‘this is what should be done,’ making sure we do the next steps, collaborative thinking, and moving forward.”
In a press release, Antonio Passaro, MD, a lung cancer expert from the European Institute of Oncology in Milan, said there is a need to prioritize primary and secondary prevention of lung cancer.
“Although a much-debated topic in recent years, a strong body of research has now shown that lung cancer screening through annual computed tomography scans in individuals with a history of smoking can improve detection rates. Targeting the right populations with these interventions will be crucial to implementing screening approaches that are both efficacious and cost effective,” he stated.
The authors declared no conflicts of interest and this study was not funded.
The International Cancer Benchmarking Partnership, a collaboration of physicians, clinicians, researchers, policy makers, and data experts, has reached a consensus on key actions designed to standardize and homogenize lung cancer care that includes early diagnosis and access to care for all patients.
This consensus, reported at the 2022 European Lung Cancer Congress, is an effort to address disparities in care recognized by the group’s in-house research team. The team identified significantly different survival rates in early stage lung cancer patients from a group of countries with similar health care metrics, such as health care expenditure and universal access to health care.
“This group of countries is very comparable, but we saw a 20% difference in survival in localized, stage I and II cancers. When you consider that lung cancer is a bigger killer than any other cancer –more than breast, prostate, and colon cancer combined – that’s thousands of people,” said the project’s lead clinician, Christian Finley, MD, a thoracic surgeon with St. Joseph’s Healthcare Hamilton (Ont.).
Founded in 2009, the ICBP includes about 500 experts in its core countries of Sweden, Norway, Denmark, Australia, the United Kingdom, and Canada; New Zealand and Ireland have also participated. The goal of the partnership is to benchmark survival and other outcomes in cancer and to research why disparities between countries exist.
“That’s why we keep the membership fairly small, so that we can actually make more meaningful research projects to get into depth in factors beyond benchmarking survival and mortality,” said study author Charlotte Lynch, MSc, a senior researcher with Cancer Research UK in London.
To help narrow the disparity gap, Ms. Lynch, Dr. Finley and colleagues brought together nine key informants from ICBP countries to discuss local clinical insights and best practices, and ultimately came up a list of five recommendations considered most crucial: implementing cost-effective, equitable, and effective screening; ensuring diagnoses of lung cancer within 30 days of referral; developing thoracic centers of excellence; launching an international audit of lung cancer care; and prioritizing the recognition of improvements in lung cancer care and outcomes.
“For example, points supporting the screening call to action focus on timely access to cross-sectional imaging and availability and development of patient and health care practitioner lung cancer awareness materials,” Ms. Lynch said.
Another example would be the point that describes the need for a minimum data set to evaluate lung cancer patients’ diagnosis, treatment, and aftercare.
“I think we all work in a very disrupted system right now. Screening programs really took a hit during the pandemic, and I think people coming out of those disruptions are trying to imagine a more effective system using tools like information technologies, mobile clinics and having a better understanding of equity,” Dr. Finley said.
Ms. Lynch said the ICBP intends to use the consensus to generate concrete actions. “We’re thinking about how we can get everyone in the room to share lessons learned and best practices to push things forward rather than saying, ‘this is what should be done,’ making sure we do the next steps, collaborative thinking, and moving forward.”
In a press release, Antonio Passaro, MD, a lung cancer expert from the European Institute of Oncology in Milan, said there is a need to prioritize primary and secondary prevention of lung cancer.
“Although a much-debated topic in recent years, a strong body of research has now shown that lung cancer screening through annual computed tomography scans in individuals with a history of smoking can improve detection rates. Targeting the right populations with these interventions will be crucial to implementing screening approaches that are both efficacious and cost effective,” he stated.
The authors declared no conflicts of interest and this study was not funded.
The International Cancer Benchmarking Partnership, a collaboration of physicians, clinicians, researchers, policy makers, and data experts, has reached a consensus on key actions designed to standardize and homogenize lung cancer care that includes early diagnosis and access to care for all patients.
This consensus, reported at the 2022 European Lung Cancer Congress, is an effort to address disparities in care recognized by the group’s in-house research team. The team identified significantly different survival rates in early stage lung cancer patients from a group of countries with similar health care metrics, such as health care expenditure and universal access to health care.
“This group of countries is very comparable, but we saw a 20% difference in survival in localized, stage I and II cancers. When you consider that lung cancer is a bigger killer than any other cancer –more than breast, prostate, and colon cancer combined – that’s thousands of people,” said the project’s lead clinician, Christian Finley, MD, a thoracic surgeon with St. Joseph’s Healthcare Hamilton (Ont.).
Founded in 2009, the ICBP includes about 500 experts in its core countries of Sweden, Norway, Denmark, Australia, the United Kingdom, and Canada; New Zealand and Ireland have also participated. The goal of the partnership is to benchmark survival and other outcomes in cancer and to research why disparities between countries exist.
“That’s why we keep the membership fairly small, so that we can actually make more meaningful research projects to get into depth in factors beyond benchmarking survival and mortality,” said study author Charlotte Lynch, MSc, a senior researcher with Cancer Research UK in London.
To help narrow the disparity gap, Ms. Lynch, Dr. Finley and colleagues brought together nine key informants from ICBP countries to discuss local clinical insights and best practices, and ultimately came up a list of five recommendations considered most crucial: implementing cost-effective, equitable, and effective screening; ensuring diagnoses of lung cancer within 30 days of referral; developing thoracic centers of excellence; launching an international audit of lung cancer care; and prioritizing the recognition of improvements in lung cancer care and outcomes.
“For example, points supporting the screening call to action focus on timely access to cross-sectional imaging and availability and development of patient and health care practitioner lung cancer awareness materials,” Ms. Lynch said.
Another example would be the point that describes the need for a minimum data set to evaluate lung cancer patients’ diagnosis, treatment, and aftercare.
“I think we all work in a very disrupted system right now. Screening programs really took a hit during the pandemic, and I think people coming out of those disruptions are trying to imagine a more effective system using tools like information technologies, mobile clinics and having a better understanding of equity,” Dr. Finley said.
Ms. Lynch said the ICBP intends to use the consensus to generate concrete actions. “We’re thinking about how we can get everyone in the room to share lessons learned and best practices to push things forward rather than saying, ‘this is what should be done,’ making sure we do the next steps, collaborative thinking, and moving forward.”
In a press release, Antonio Passaro, MD, a lung cancer expert from the European Institute of Oncology in Milan, said there is a need to prioritize primary and secondary prevention of lung cancer.
“Although a much-debated topic in recent years, a strong body of research has now shown that lung cancer screening through annual computed tomography scans in individuals with a history of smoking can improve detection rates. Targeting the right populations with these interventions will be crucial to implementing screening approaches that are both efficacious and cost effective,” he stated.
The authors declared no conflicts of interest and this study was not funded.
FROM ELCC 2022
Are free lunches back? Docs start seeing drug reps again
In their heyday, drug reps had big expense budgets and would wine and dine physicians, golf with them, and give gifts to their potential physician clients.
But in 2002, pressure from Congress and increased scrutiny from the American Medical Association prompted the Pharmaceutical Research and Manufacturers of America to adopt a set of voluntary ethical codes to regulate the gifts given to physicians. Now, physicians must report even small gifts or meals to the National Practitioner Data Bank.
Before the restrictions, physician/pharmaceutical rep relationships relied on face-to-face meetings. These included lunches with a limited budget or sharing a cup of coffee during a morning visit to a practice. The parties got to know each other, which led to trust and long-term relationships.
During the COVID-19 pandemic, everything changed. “It was culture shock for us,” admitted Craig F, a career pharmaceutical rep. “We didn’t know what we were going to do.”
The pharmaceutical industry pivoted and quickly got up to speed with Zoom, Microsoft Teams, and the like. “We began by reaching out to doctors via email and cell phones to set up virtual meetings,” Craig said. “Most of the doctors were working from home, doing telehealth whenever possible. For new sales reps, this was particularly difficult, because they couldn’t visit offices and get to know doctors.”
Many physicians didn’t want to devote time to Zoom meetings with pharma reps. “We worked around their schedules, and sometimes this even looked like Sunday calls,” he said.
As vaccination levels increased and medical offices began to reopen, so too did some of the old-school, face-to-face pharma rep/doctor meetings. But most proceeded with caution. “Some pharmaceutical companies didn’t put reps back into the field until the fall of 2020,” said Craig. “If we weren’t welcome in an office, we didn’t push it.”
Once much of the population was vaccinated, the thaw began in earnest, although the drug reps continued to tread cautiously, mask up, and respect the wishes of physicians. Today, Craig estimated that about two-thirds of his appointments are in person.
Still, it’s unlikely that the drug rep–supplied “free staff lunch” will ever regain its former popularity. Medical office staff are still keeping distance, owing to COVID; office schedules may be more crowded and may not allow the time; and many physicians are still nervous about having to report “gifts” or “paid lunches” from pharma.
The post-COVID paradigm shift
The pandemic put a dent in the pharma rep/doctor relationship, said Suzy Jackson, managing director of life sciences at Accenture and an author of The “New” Rules of Healthcare Provider Engagement . “COVID started moving power away from reps because they lost the ability to simply wander into a building and have a conversation with a health care provider. We’re seeing the pandemic evolve the meeting model into a hybrid in-person and virtual.”
“Many doctors are operating in a slower fashion because they’re balancing a hybrid model with patients, as well,” said Craig. “Some of my visits now involve talking to nurses or front-office staff, not getting in to see the doctors.”
The push from some doctors to see reps virtually as opposed to in person is a challenge for the pharma companies. “We get more done in person, so virtual is not our favorite way to do business,” said Craig. “But we’re thankful for any time we can get with doctors, so when they ask to do virtual, we agree.”
Still, the Accenture survey offered good news for pharma reps: Only 4% of respondents didn’t want to continue with in-person meetings at all. “I think of this as a positive,” Ms. Jackson said. “It shows that physicians value these relationships, if they’re done in the right way.”
But a survey by Boston Consulting Group confirms that virtual visits are likely to continue. BCG’s Doctors’ Changing Expectations of Pharma Are Here to Stay revealed that three-quarters of respondent physicians prefer to maintain or increase the amount of virtual engagements with pharma reps after becoming accustomed to the practice during the pandemic.
Under these changing scenarios, said Ms. Jackson, pharma reps have to think about more meaningful ways to engage with doctors.
“I feel that doctors are more crunched for time now, managing hybrid environments,” Craig said. “They have less time and want more patient-specific information that leads to fewer calls back to their offices.”
More physicians now value webinars, virtual training, and speaker programs. Virtual channels, the survey found, “give physicians access to the information they need in an easy and convenient manner.”
Still, physicians have noted that the survey indicated that email communications from pharma reps had increased. Often, physicians found the useful information buried in irrelevant “clutter.”
Restrictions on drug reps became tighter
In the 20 years since the guidelines came into existence, PhRMA has continued to strengthen the codes. In 2009, PhRMA issued new recommendations surrounding noneducational gifts and placed a cap of $100 for meals, drug samples, and other items. In 2022, they added layers to the code that focus on speaker programs. For instance, while companies can provide “modest” meals to attendees as an incidental courtesy, pharma reps can no longer pay for or provide alcohol in conjunction with these programs.
The rules vary from state to state. In Minnesota, for instance, gifts from pharma companies cannot exceed $50 per year. Some institutions – such as the Cleveland Clinic – have even stricter rules. “When we have conventions, we put up signage reminding doctors from the strictest states that they can’t even accept a cup of coffee from a rep,” said Craig.
However, COVID hasn’t completely changed doctor/pharma relationships. In Ms. Jackson’s words, “In spite of the shift to a more hybrid model, this is a very human relationship yielding real human results.”
A version of this article first appeared on Medscape.com.
In their heyday, drug reps had big expense budgets and would wine and dine physicians, golf with them, and give gifts to their potential physician clients.
But in 2002, pressure from Congress and increased scrutiny from the American Medical Association prompted the Pharmaceutical Research and Manufacturers of America to adopt a set of voluntary ethical codes to regulate the gifts given to physicians. Now, physicians must report even small gifts or meals to the National Practitioner Data Bank.
Before the restrictions, physician/pharmaceutical rep relationships relied on face-to-face meetings. These included lunches with a limited budget or sharing a cup of coffee during a morning visit to a practice. The parties got to know each other, which led to trust and long-term relationships.
During the COVID-19 pandemic, everything changed. “It was culture shock for us,” admitted Craig F, a career pharmaceutical rep. “We didn’t know what we were going to do.”
The pharmaceutical industry pivoted and quickly got up to speed with Zoom, Microsoft Teams, and the like. “We began by reaching out to doctors via email and cell phones to set up virtual meetings,” Craig said. “Most of the doctors were working from home, doing telehealth whenever possible. For new sales reps, this was particularly difficult, because they couldn’t visit offices and get to know doctors.”
Many physicians didn’t want to devote time to Zoom meetings with pharma reps. “We worked around their schedules, and sometimes this even looked like Sunday calls,” he said.
As vaccination levels increased and medical offices began to reopen, so too did some of the old-school, face-to-face pharma rep/doctor meetings. But most proceeded with caution. “Some pharmaceutical companies didn’t put reps back into the field until the fall of 2020,” said Craig. “If we weren’t welcome in an office, we didn’t push it.”
Once much of the population was vaccinated, the thaw began in earnest, although the drug reps continued to tread cautiously, mask up, and respect the wishes of physicians. Today, Craig estimated that about two-thirds of his appointments are in person.
Still, it’s unlikely that the drug rep–supplied “free staff lunch” will ever regain its former popularity. Medical office staff are still keeping distance, owing to COVID; office schedules may be more crowded and may not allow the time; and many physicians are still nervous about having to report “gifts” or “paid lunches” from pharma.
The post-COVID paradigm shift
The pandemic put a dent in the pharma rep/doctor relationship, said Suzy Jackson, managing director of life sciences at Accenture and an author of The “New” Rules of Healthcare Provider Engagement . “COVID started moving power away from reps because they lost the ability to simply wander into a building and have a conversation with a health care provider. We’re seeing the pandemic evolve the meeting model into a hybrid in-person and virtual.”
“Many doctors are operating in a slower fashion because they’re balancing a hybrid model with patients, as well,” said Craig. “Some of my visits now involve talking to nurses or front-office staff, not getting in to see the doctors.”
The push from some doctors to see reps virtually as opposed to in person is a challenge for the pharma companies. “We get more done in person, so virtual is not our favorite way to do business,” said Craig. “But we’re thankful for any time we can get with doctors, so when they ask to do virtual, we agree.”
Still, the Accenture survey offered good news for pharma reps: Only 4% of respondents didn’t want to continue with in-person meetings at all. “I think of this as a positive,” Ms. Jackson said. “It shows that physicians value these relationships, if they’re done in the right way.”
But a survey by Boston Consulting Group confirms that virtual visits are likely to continue. BCG’s Doctors’ Changing Expectations of Pharma Are Here to Stay revealed that three-quarters of respondent physicians prefer to maintain or increase the amount of virtual engagements with pharma reps after becoming accustomed to the practice during the pandemic.
Under these changing scenarios, said Ms. Jackson, pharma reps have to think about more meaningful ways to engage with doctors.
“I feel that doctors are more crunched for time now, managing hybrid environments,” Craig said. “They have less time and want more patient-specific information that leads to fewer calls back to their offices.”
More physicians now value webinars, virtual training, and speaker programs. Virtual channels, the survey found, “give physicians access to the information they need in an easy and convenient manner.”
Still, physicians have noted that the survey indicated that email communications from pharma reps had increased. Often, physicians found the useful information buried in irrelevant “clutter.”
Restrictions on drug reps became tighter
In the 20 years since the guidelines came into existence, PhRMA has continued to strengthen the codes. In 2009, PhRMA issued new recommendations surrounding noneducational gifts and placed a cap of $100 for meals, drug samples, and other items. In 2022, they added layers to the code that focus on speaker programs. For instance, while companies can provide “modest” meals to attendees as an incidental courtesy, pharma reps can no longer pay for or provide alcohol in conjunction with these programs.
The rules vary from state to state. In Minnesota, for instance, gifts from pharma companies cannot exceed $50 per year. Some institutions – such as the Cleveland Clinic – have even stricter rules. “When we have conventions, we put up signage reminding doctors from the strictest states that they can’t even accept a cup of coffee from a rep,” said Craig.
However, COVID hasn’t completely changed doctor/pharma relationships. In Ms. Jackson’s words, “In spite of the shift to a more hybrid model, this is a very human relationship yielding real human results.”
A version of this article first appeared on Medscape.com.
In their heyday, drug reps had big expense budgets and would wine and dine physicians, golf with them, and give gifts to their potential physician clients.
But in 2002, pressure from Congress and increased scrutiny from the American Medical Association prompted the Pharmaceutical Research and Manufacturers of America to adopt a set of voluntary ethical codes to regulate the gifts given to physicians. Now, physicians must report even small gifts or meals to the National Practitioner Data Bank.
Before the restrictions, physician/pharmaceutical rep relationships relied on face-to-face meetings. These included lunches with a limited budget or sharing a cup of coffee during a morning visit to a practice. The parties got to know each other, which led to trust and long-term relationships.
During the COVID-19 pandemic, everything changed. “It was culture shock for us,” admitted Craig F, a career pharmaceutical rep. “We didn’t know what we were going to do.”
The pharmaceutical industry pivoted and quickly got up to speed with Zoom, Microsoft Teams, and the like. “We began by reaching out to doctors via email and cell phones to set up virtual meetings,” Craig said. “Most of the doctors were working from home, doing telehealth whenever possible. For new sales reps, this was particularly difficult, because they couldn’t visit offices and get to know doctors.”
Many physicians didn’t want to devote time to Zoom meetings with pharma reps. “We worked around their schedules, and sometimes this even looked like Sunday calls,” he said.
As vaccination levels increased and medical offices began to reopen, so too did some of the old-school, face-to-face pharma rep/doctor meetings. But most proceeded with caution. “Some pharmaceutical companies didn’t put reps back into the field until the fall of 2020,” said Craig. “If we weren’t welcome in an office, we didn’t push it.”
Once much of the population was vaccinated, the thaw began in earnest, although the drug reps continued to tread cautiously, mask up, and respect the wishes of physicians. Today, Craig estimated that about two-thirds of his appointments are in person.
Still, it’s unlikely that the drug rep–supplied “free staff lunch” will ever regain its former popularity. Medical office staff are still keeping distance, owing to COVID; office schedules may be more crowded and may not allow the time; and many physicians are still nervous about having to report “gifts” or “paid lunches” from pharma.
The post-COVID paradigm shift
The pandemic put a dent in the pharma rep/doctor relationship, said Suzy Jackson, managing director of life sciences at Accenture and an author of The “New” Rules of Healthcare Provider Engagement . “COVID started moving power away from reps because they lost the ability to simply wander into a building and have a conversation with a health care provider. We’re seeing the pandemic evolve the meeting model into a hybrid in-person and virtual.”
“Many doctors are operating in a slower fashion because they’re balancing a hybrid model with patients, as well,” said Craig. “Some of my visits now involve talking to nurses or front-office staff, not getting in to see the doctors.”
The push from some doctors to see reps virtually as opposed to in person is a challenge for the pharma companies. “We get more done in person, so virtual is not our favorite way to do business,” said Craig. “But we’re thankful for any time we can get with doctors, so when they ask to do virtual, we agree.”
Still, the Accenture survey offered good news for pharma reps: Only 4% of respondents didn’t want to continue with in-person meetings at all. “I think of this as a positive,” Ms. Jackson said. “It shows that physicians value these relationships, if they’re done in the right way.”
But a survey by Boston Consulting Group confirms that virtual visits are likely to continue. BCG’s Doctors’ Changing Expectations of Pharma Are Here to Stay revealed that three-quarters of respondent physicians prefer to maintain or increase the amount of virtual engagements with pharma reps after becoming accustomed to the practice during the pandemic.
Under these changing scenarios, said Ms. Jackson, pharma reps have to think about more meaningful ways to engage with doctors.
“I feel that doctors are more crunched for time now, managing hybrid environments,” Craig said. “They have less time and want more patient-specific information that leads to fewer calls back to their offices.”
More physicians now value webinars, virtual training, and speaker programs. Virtual channels, the survey found, “give physicians access to the information they need in an easy and convenient manner.”
Still, physicians have noted that the survey indicated that email communications from pharma reps had increased. Often, physicians found the useful information buried in irrelevant “clutter.”
Restrictions on drug reps became tighter
In the 20 years since the guidelines came into existence, PhRMA has continued to strengthen the codes. In 2009, PhRMA issued new recommendations surrounding noneducational gifts and placed a cap of $100 for meals, drug samples, and other items. In 2022, they added layers to the code that focus on speaker programs. For instance, while companies can provide “modest” meals to attendees as an incidental courtesy, pharma reps can no longer pay for or provide alcohol in conjunction with these programs.
The rules vary from state to state. In Minnesota, for instance, gifts from pharma companies cannot exceed $50 per year. Some institutions – such as the Cleveland Clinic – have even stricter rules. “When we have conventions, we put up signage reminding doctors from the strictest states that they can’t even accept a cup of coffee from a rep,” said Craig.
However, COVID hasn’t completely changed doctor/pharma relationships. In Ms. Jackson’s words, “In spite of the shift to a more hybrid model, this is a very human relationship yielding real human results.”
A version of this article first appeared on Medscape.com.
CDC panel lists reasons to get second COVID booster
The Centers for Disease Control and Prevention is considering what to tell the public about second booster shots with mRNA vaccinations for COVID-19.
The U.S. Food and Drug Administration in March authorized a second booster dose of either the Pfizer-BioNTech or the Moderna COVID-19 vaccines for people aged 50 and older and certain immunocompromised adults, even though many top infectious disease experts questioned the need before the agency’s decision.
In a meeting April 20, the CDC asked its Advisory Committee on Immunization Practices to discuss second booster shots, but did not ask the group of experts to vote on formal recommendations.
Instead,
ACIP member Beth Bell, MD, MPH, of the University of Washington, Seattle, said she’s concerned about the potential for “booster fatigue.”
“A vaccination program that’s going to require boosting large proportions of the population every 4-6 months is really not sustainable and probably not something that most people want to participate in,” she said.
The benefit of additional COVID-19 shots for now appears to be smaller than what people get from the initial doses, Dr. Bell said.
Earlier in the meeting, CDC staff presented estimates about how well the COVID-19 vaccines work to prevent one case of hospitalization from the disease over 4 months among people aged 50 and older.
The major gain in preventing hospitalizations occurs with the first vaccination series and then wanes, the CDC said.
It appears that one hospitalization is prevented for every 135 people who get the first round of COVID-19 vaccinations. But it takes 674 people getting a first booster dose to prevent one hospitalization. A second booster prevents one hospitalization for every 1,205 people vaccinated.
Dr. Bell said she’s concerned about considering additional doses for “smaller and smaller return and creating an impression that we don’t have a very effective vaccination program,” even though the CDC’s data show a clear benefit.
Reasons to get a second booster
Elisha Hall, PhD, RD, of the CDC presented slides with some factors to help determine the urgency for a person to get a second booster:
- Having certain underlying medical conditions that increase the risk of severe COVID-19 illness.
- Being moderately or severely immunocompromised.
- Living with someone who is immunocompromised, at increased risk for severe disease, or who cannot be vaccinated because of age or contraindication.
- Being at increased risk of exposure to SARS-CoV-2, the virus that causes COVID-19, such as through occupational, institutional, or other activities (e.g., travel or large gatherings).
- Living or working in an area where there is a medium or high level of COVID-19 in the community.
In contrast, people might want to wait if they had been infected with SARS-CoV-2 within the past 3 months, Dr. Hall said in her presentation. Another reason for delay might be a concern that a booster dose may be more important later in the year.
The experts also addressed public confusion over boosters. For the Pfizer and Moderna mRNA vaccines, a second booster is a fourth dose, but for those who received the one-shot J&J vaccine, the second booster is a third dose.
Going forward, it may be easier to refer to subsequent doses as “annual boosters,” the CDC’s Sara Oliver, MD, MSPH, told the panel. It will be important to keep language about subsequent vaccinations clear and easy for the public to follow, she said.
Dr. Oliver also said there’s already been a drop-off in the acceptance of second rounds of COVID-19 vaccinations. CDC data show that 77% of people in the United States have had at least one dose of a COVID-19 vaccine, but only 66% of the population is fully vaccinated, and only 45% have had a first booster dose.
In her presentation, Dr. Oliver said the top priority in COVID-19 vaccination efforts remains initial vaccinations for people who haven’t gotten them.
Kids younger than 5
During the public comment session of the CDC meeting, several people called on the FDA to move quickly to expand authorization of COVID-19 vaccines to children aged 5 years and younger.
“We know that many parents and caregivers and health care providers are anxious to have COVID vaccines available” for young children, said Doran Fink, MD, PhD, a deputy director of the FDA’s vaccines division.
He said the agency is working to be ready to authorize the shots for young children while it awaits research results from the manufacturers.
A version of this article first appeared on WebMD.com.
The Centers for Disease Control and Prevention is considering what to tell the public about second booster shots with mRNA vaccinations for COVID-19.
The U.S. Food and Drug Administration in March authorized a second booster dose of either the Pfizer-BioNTech or the Moderna COVID-19 vaccines for people aged 50 and older and certain immunocompromised adults, even though many top infectious disease experts questioned the need before the agency’s decision.
In a meeting April 20, the CDC asked its Advisory Committee on Immunization Practices to discuss second booster shots, but did not ask the group of experts to vote on formal recommendations.
Instead,
ACIP member Beth Bell, MD, MPH, of the University of Washington, Seattle, said she’s concerned about the potential for “booster fatigue.”
“A vaccination program that’s going to require boosting large proportions of the population every 4-6 months is really not sustainable and probably not something that most people want to participate in,” she said.
The benefit of additional COVID-19 shots for now appears to be smaller than what people get from the initial doses, Dr. Bell said.
Earlier in the meeting, CDC staff presented estimates about how well the COVID-19 vaccines work to prevent one case of hospitalization from the disease over 4 months among people aged 50 and older.
The major gain in preventing hospitalizations occurs with the first vaccination series and then wanes, the CDC said.
It appears that one hospitalization is prevented for every 135 people who get the first round of COVID-19 vaccinations. But it takes 674 people getting a first booster dose to prevent one hospitalization. A second booster prevents one hospitalization for every 1,205 people vaccinated.
Dr. Bell said she’s concerned about considering additional doses for “smaller and smaller return and creating an impression that we don’t have a very effective vaccination program,” even though the CDC’s data show a clear benefit.
Reasons to get a second booster
Elisha Hall, PhD, RD, of the CDC presented slides with some factors to help determine the urgency for a person to get a second booster:
- Having certain underlying medical conditions that increase the risk of severe COVID-19 illness.
- Being moderately or severely immunocompromised.
- Living with someone who is immunocompromised, at increased risk for severe disease, or who cannot be vaccinated because of age or contraindication.
- Being at increased risk of exposure to SARS-CoV-2, the virus that causes COVID-19, such as through occupational, institutional, or other activities (e.g., travel or large gatherings).
- Living or working in an area where there is a medium or high level of COVID-19 in the community.
In contrast, people might want to wait if they had been infected with SARS-CoV-2 within the past 3 months, Dr. Hall said in her presentation. Another reason for delay might be a concern that a booster dose may be more important later in the year.
The experts also addressed public confusion over boosters. For the Pfizer and Moderna mRNA vaccines, a second booster is a fourth dose, but for those who received the one-shot J&J vaccine, the second booster is a third dose.
Going forward, it may be easier to refer to subsequent doses as “annual boosters,” the CDC’s Sara Oliver, MD, MSPH, told the panel. It will be important to keep language about subsequent vaccinations clear and easy for the public to follow, she said.
Dr. Oliver also said there’s already been a drop-off in the acceptance of second rounds of COVID-19 vaccinations. CDC data show that 77% of people in the United States have had at least one dose of a COVID-19 vaccine, but only 66% of the population is fully vaccinated, and only 45% have had a first booster dose.
In her presentation, Dr. Oliver said the top priority in COVID-19 vaccination efforts remains initial vaccinations for people who haven’t gotten them.
Kids younger than 5
During the public comment session of the CDC meeting, several people called on the FDA to move quickly to expand authorization of COVID-19 vaccines to children aged 5 years and younger.
“We know that many parents and caregivers and health care providers are anxious to have COVID vaccines available” for young children, said Doran Fink, MD, PhD, a deputy director of the FDA’s vaccines division.
He said the agency is working to be ready to authorize the shots for young children while it awaits research results from the manufacturers.
A version of this article first appeared on WebMD.com.
The Centers for Disease Control and Prevention is considering what to tell the public about second booster shots with mRNA vaccinations for COVID-19.
The U.S. Food and Drug Administration in March authorized a second booster dose of either the Pfizer-BioNTech or the Moderna COVID-19 vaccines for people aged 50 and older and certain immunocompromised adults, even though many top infectious disease experts questioned the need before the agency’s decision.
In a meeting April 20, the CDC asked its Advisory Committee on Immunization Practices to discuss second booster shots, but did not ask the group of experts to vote on formal recommendations.
Instead,
ACIP member Beth Bell, MD, MPH, of the University of Washington, Seattle, said she’s concerned about the potential for “booster fatigue.”
“A vaccination program that’s going to require boosting large proportions of the population every 4-6 months is really not sustainable and probably not something that most people want to participate in,” she said.
The benefit of additional COVID-19 shots for now appears to be smaller than what people get from the initial doses, Dr. Bell said.
Earlier in the meeting, CDC staff presented estimates about how well the COVID-19 vaccines work to prevent one case of hospitalization from the disease over 4 months among people aged 50 and older.
The major gain in preventing hospitalizations occurs with the first vaccination series and then wanes, the CDC said.
It appears that one hospitalization is prevented for every 135 people who get the first round of COVID-19 vaccinations. But it takes 674 people getting a first booster dose to prevent one hospitalization. A second booster prevents one hospitalization for every 1,205 people vaccinated.
Dr. Bell said she’s concerned about considering additional doses for “smaller and smaller return and creating an impression that we don’t have a very effective vaccination program,” even though the CDC’s data show a clear benefit.
Reasons to get a second booster
Elisha Hall, PhD, RD, of the CDC presented slides with some factors to help determine the urgency for a person to get a second booster:
- Having certain underlying medical conditions that increase the risk of severe COVID-19 illness.
- Being moderately or severely immunocompromised.
- Living with someone who is immunocompromised, at increased risk for severe disease, or who cannot be vaccinated because of age or contraindication.
- Being at increased risk of exposure to SARS-CoV-2, the virus that causes COVID-19, such as through occupational, institutional, or other activities (e.g., travel or large gatherings).
- Living or working in an area where there is a medium or high level of COVID-19 in the community.
In contrast, people might want to wait if they had been infected with SARS-CoV-2 within the past 3 months, Dr. Hall said in her presentation. Another reason for delay might be a concern that a booster dose may be more important later in the year.
The experts also addressed public confusion over boosters. For the Pfizer and Moderna mRNA vaccines, a second booster is a fourth dose, but for those who received the one-shot J&J vaccine, the second booster is a third dose.
Going forward, it may be easier to refer to subsequent doses as “annual boosters,” the CDC’s Sara Oliver, MD, MSPH, told the panel. It will be important to keep language about subsequent vaccinations clear and easy for the public to follow, she said.
Dr. Oliver also said there’s already been a drop-off in the acceptance of second rounds of COVID-19 vaccinations. CDC data show that 77% of people in the United States have had at least one dose of a COVID-19 vaccine, but only 66% of the population is fully vaccinated, and only 45% have had a first booster dose.
In her presentation, Dr. Oliver said the top priority in COVID-19 vaccination efforts remains initial vaccinations for people who haven’t gotten them.
Kids younger than 5
During the public comment session of the CDC meeting, several people called on the FDA to move quickly to expand authorization of COVID-19 vaccines to children aged 5 years and younger.
“We know that many parents and caregivers and health care providers are anxious to have COVID vaccines available” for young children, said Doran Fink, MD, PhD, a deputy director of the FDA’s vaccines division.
He said the agency is working to be ready to authorize the shots for young children while it awaits research results from the manufacturers.
A version of this article first appeared on WebMD.com.
Retro-orbital headache and nausea
On the basis of his presentation, this patient is probably experiencing migraine with visual aura. Migraine is a condition in children and adolescents whose prevalence increases with age: 1%-3% between age 3 and 7 years, 4%-11% between age 7 and 11 years, and 8%-23% by age 15 years. Although migraine without aura is relatively uncommon in the pediatric population, visual aura is a hallmark sign of migraine headache and excludes the other headache types in the differential diagnosis. Basilar migraine is unlikely because the patient has not experienced symptoms that suggest occipital or brainstem area dysfunction post-aura.
The diagnosis of migraine is largely clinical, but the American Academy of Neurology (AAN) guidelines for the acute treatment of pediatric migraine recommend that when assessing children and adolescents with headache, clinicians should diagnose a specific headache type: primary, secondary, or other headache syndrome. Migraine in pediatric patients is often related to triggering factors such as infection, physical or psychological stress, or dietary choices, but on the basis of the patient's history, this headache appears to be primary in nature.
Most pediatric patients can achieve control of their migraines with acute treatments and benefit from nonprescription oral analgesics, including acetaminophen, ibuprofen, and naproxen. Clinicians should prescribe ibuprofen orally (10 mg/kg) as an initial treatment for children and adolescents with migraine. The US Food and Drug Administration has only approved certain triptans for pediatric patients: almotriptan, sumatriptan-naproxen, and zolmitriptan nasal spray for patients aged 12 years or older and rizatriptan for patients aged 6-17 years.
The AAN guidelines for the pharmacologic treatment of pediatric migraine prevention report that for those who experience migraine with aura, taking a triptan during the aura is safe, though it may be more effective when taken at the onset of head pain, as is the case with other acute treatments.
In pediatric patients, avoidance of known headache triggers is generally sufficient for migraine prevention. This includes managing anxiety, depression, attention-deficit/hyperactivity disorder, and other psychiatric comorbidities that can exacerbate headache. Lifestyle management also includes ensuring adequate sleep, exercise, hydration, and stress management.
The guidelines conclude that although the majority of randomized controlled trials exploring the efficacy of preventive medications in the pediatric population fail to demonstrate superiority to placebo, migraine prophylaxis should be considered when headaches occur with high frequency and severity and cause migraine-related disability based on the Pediatric Migraine Disability Assessment (PedMIDAS).
Jasmin Harpe, MD, MPH, Headache Fellow, Department of Neurology, Harvard University, John R. Graham Headache Center, Mass General Brigham, Boston, MA
Jasmin Harpe, MD, MPH, has disclosed no relevant financial relationships
On the basis of his presentation, this patient is probably experiencing migraine with visual aura. Migraine is a condition in children and adolescents whose prevalence increases with age: 1%-3% between age 3 and 7 years, 4%-11% between age 7 and 11 years, and 8%-23% by age 15 years. Although migraine without aura is relatively uncommon in the pediatric population, visual aura is a hallmark sign of migraine headache and excludes the other headache types in the differential diagnosis. Basilar migraine is unlikely because the patient has not experienced symptoms that suggest occipital or brainstem area dysfunction post-aura.
The diagnosis of migraine is largely clinical, but the American Academy of Neurology (AAN) guidelines for the acute treatment of pediatric migraine recommend that when assessing children and adolescents with headache, clinicians should diagnose a specific headache type: primary, secondary, or other headache syndrome. Migraine in pediatric patients is often related to triggering factors such as infection, physical or psychological stress, or dietary choices, but on the basis of the patient's history, this headache appears to be primary in nature.
Most pediatric patients can achieve control of their migraines with acute treatments and benefit from nonprescription oral analgesics, including acetaminophen, ibuprofen, and naproxen. Clinicians should prescribe ibuprofen orally (10 mg/kg) as an initial treatment for children and adolescents with migraine. The US Food and Drug Administration has only approved certain triptans for pediatric patients: almotriptan, sumatriptan-naproxen, and zolmitriptan nasal spray for patients aged 12 years or older and rizatriptan for patients aged 6-17 years.
The AAN guidelines for the pharmacologic treatment of pediatric migraine prevention report that for those who experience migraine with aura, taking a triptan during the aura is safe, though it may be more effective when taken at the onset of head pain, as is the case with other acute treatments.
In pediatric patients, avoidance of known headache triggers is generally sufficient for migraine prevention. This includes managing anxiety, depression, attention-deficit/hyperactivity disorder, and other psychiatric comorbidities that can exacerbate headache. Lifestyle management also includes ensuring adequate sleep, exercise, hydration, and stress management.
The guidelines conclude that although the majority of randomized controlled trials exploring the efficacy of preventive medications in the pediatric population fail to demonstrate superiority to placebo, migraine prophylaxis should be considered when headaches occur with high frequency and severity and cause migraine-related disability based on the Pediatric Migraine Disability Assessment (PedMIDAS).
Jasmin Harpe, MD, MPH, Headache Fellow, Department of Neurology, Harvard University, John R. Graham Headache Center, Mass General Brigham, Boston, MA
Jasmin Harpe, MD, MPH, has disclosed no relevant financial relationships
On the basis of his presentation, this patient is probably experiencing migraine with visual aura. Migraine is a condition in children and adolescents whose prevalence increases with age: 1%-3% between age 3 and 7 years, 4%-11% between age 7 and 11 years, and 8%-23% by age 15 years. Although migraine without aura is relatively uncommon in the pediatric population, visual aura is a hallmark sign of migraine headache and excludes the other headache types in the differential diagnosis. Basilar migraine is unlikely because the patient has not experienced symptoms that suggest occipital or brainstem area dysfunction post-aura.
The diagnosis of migraine is largely clinical, but the American Academy of Neurology (AAN) guidelines for the acute treatment of pediatric migraine recommend that when assessing children and adolescents with headache, clinicians should diagnose a specific headache type: primary, secondary, or other headache syndrome. Migraine in pediatric patients is often related to triggering factors such as infection, physical or psychological stress, or dietary choices, but on the basis of the patient's history, this headache appears to be primary in nature.
Most pediatric patients can achieve control of their migraines with acute treatments and benefit from nonprescription oral analgesics, including acetaminophen, ibuprofen, and naproxen. Clinicians should prescribe ibuprofen orally (10 mg/kg) as an initial treatment for children and adolescents with migraine. The US Food and Drug Administration has only approved certain triptans for pediatric patients: almotriptan, sumatriptan-naproxen, and zolmitriptan nasal spray for patients aged 12 years or older and rizatriptan for patients aged 6-17 years.
The AAN guidelines for the pharmacologic treatment of pediatric migraine prevention report that for those who experience migraine with aura, taking a triptan during the aura is safe, though it may be more effective when taken at the onset of head pain, as is the case with other acute treatments.
In pediatric patients, avoidance of known headache triggers is generally sufficient for migraine prevention. This includes managing anxiety, depression, attention-deficit/hyperactivity disorder, and other psychiatric comorbidities that can exacerbate headache. Lifestyle management also includes ensuring adequate sleep, exercise, hydration, and stress management.
The guidelines conclude that although the majority of randomized controlled trials exploring the efficacy of preventive medications in the pediatric population fail to demonstrate superiority to placebo, migraine prophylaxis should be considered when headaches occur with high frequency and severity and cause migraine-related disability based on the Pediatric Migraine Disability Assessment (PedMIDAS).
Jasmin Harpe, MD, MPH, Headache Fellow, Department of Neurology, Harvard University, John R. Graham Headache Center, Mass General Brigham, Boston, MA
Jasmin Harpe, MD, MPH, has disclosed no relevant financial relationships

A 7-year-old boy presents with a retro-orbital headache, nausea, and photophobia. Height is 4 ft 2 in and weight is 70 lb (BMI 19.7). The patient's mother reports that he described seeing "rainbow shapes" in his line of vision about 20 minutes before the onset of head pain and notes that she herself has a history of headache. The patient is nonfebrile but sweating and drowsy. Physical examination is unrevealing. The patient has no known allergies and is not currently on medication.
