User login
NAVIGATOR steers uncontrolled asthma toward calmer seas
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.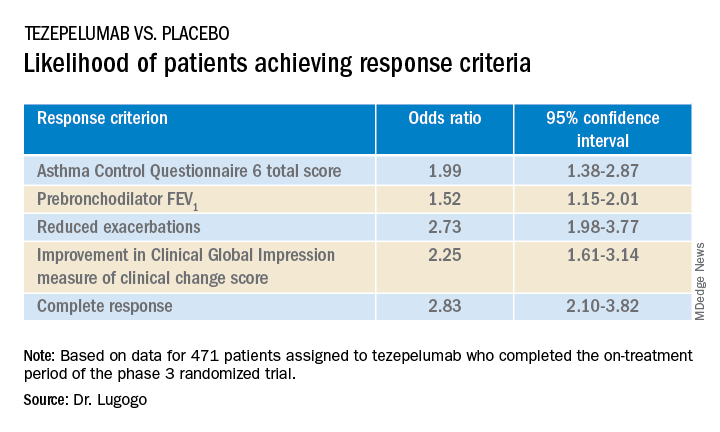
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
AT ATS 2022
Jury is in? Survival benefit with lap surgery for rectal cancer
, according to findings from a large meta-analysis.
The estimated 5-year OS rate for patients who underwent laparoscopic surgery was 76.2%, vs. 72.7% for those who had open surgery.
“The survival benefit of laparoscopic surgery is encouraging and supports the routine use of laparoscopic surgery for adult patients with rectal cancer in the era of minimally invasive surgery,” wrote the authors, led by Leping Li, MD, of the department of gastrointestinal surgery, Shandong (China) Provincial Hospital.
The article was published online in JAMA Network Open.
Surgery is an essential component in treating rectal cancer, but the benefits of laparoscopic vs. open surgery are not clear. Over the past 15 years, randomized clinical trials (RCTs) have shown comparable long-term outcomes for laparoscopic and open surgery. However, in most meta-analyses that assessed the evidence more broadly, researchers used an “inappropriate” method for the pooled analysis. Dr. Li and colleagues wanted to perform their own meta-analysis to more definitively understand whether the evidence on long-term outcomes supports or opposes the use of laparoscopic surgery for rectal cancer.
In the current study, the authors conducted an individual participant data meta-analysis using time-to-event data and focused on the long-term survival outcomes after laparoscopic or open surgery for adult patients with rectal cancer.
Ten articles involving 12 RCTs and 3,709 participants were included. In these, 2,097 patients were randomly assigned to undergo laparoscopic surgery, and 1,612 were randomly assigned to undergo open surgery. The studies covered a global population, with participants from Europe, North America, and East Asia.
In a one-stage analysis, the authors found that disease-free survival was slightly better among patients who underwent laparoscopic surgery, but the results were statistically similar (hazard ratio [HR], 0.92; P = .26).
However, when it came to OS, those who had undergone laparoscopic surgery fared significantly better (HR, 0.85; P = .02).
These results held up in the two-stage analysis for both disease-free survival (HR, 0.92; P = .25) and OS (HR, 0.85; P = .02). A sensitivity analyses conducted with large RCTs yielded similar pooled effect sizes for disease-free survival (HR, 0.91; P = .20) and OS (HR, 0.84; P = .03).
The authors highlighted several reasons why laparoscopic surgery may be associated with better survival. First, the faster recovery from the minimally invasive procedure could allow patients to begin adjuvant therapy earlier. In addition, the reduced stress responses and higher levels of immune function among patients undergoing minimally invasive surgery may contribute to a long-term survival advantage.
“These findings address concerns regarding the effectiveness of laparoscopic surgery,” the authors wrote. However, “further studies are necessary to explore the specific mechanisms underlying the positive effect of laparoscopic surgery on OS.”
No outside funding source was noted. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to findings from a large meta-analysis.
The estimated 5-year OS rate for patients who underwent laparoscopic surgery was 76.2%, vs. 72.7% for those who had open surgery.
“The survival benefit of laparoscopic surgery is encouraging and supports the routine use of laparoscopic surgery for adult patients with rectal cancer in the era of minimally invasive surgery,” wrote the authors, led by Leping Li, MD, of the department of gastrointestinal surgery, Shandong (China) Provincial Hospital.
The article was published online in JAMA Network Open.
Surgery is an essential component in treating rectal cancer, but the benefits of laparoscopic vs. open surgery are not clear. Over the past 15 years, randomized clinical trials (RCTs) have shown comparable long-term outcomes for laparoscopic and open surgery. However, in most meta-analyses that assessed the evidence more broadly, researchers used an “inappropriate” method for the pooled analysis. Dr. Li and colleagues wanted to perform their own meta-analysis to more definitively understand whether the evidence on long-term outcomes supports or opposes the use of laparoscopic surgery for rectal cancer.
In the current study, the authors conducted an individual participant data meta-analysis using time-to-event data and focused on the long-term survival outcomes after laparoscopic or open surgery for adult patients with rectal cancer.
Ten articles involving 12 RCTs and 3,709 participants were included. In these, 2,097 patients were randomly assigned to undergo laparoscopic surgery, and 1,612 were randomly assigned to undergo open surgery. The studies covered a global population, with participants from Europe, North America, and East Asia.
In a one-stage analysis, the authors found that disease-free survival was slightly better among patients who underwent laparoscopic surgery, but the results were statistically similar (hazard ratio [HR], 0.92; P = .26).
However, when it came to OS, those who had undergone laparoscopic surgery fared significantly better (HR, 0.85; P = .02).
These results held up in the two-stage analysis for both disease-free survival (HR, 0.92; P = .25) and OS (HR, 0.85; P = .02). A sensitivity analyses conducted with large RCTs yielded similar pooled effect sizes for disease-free survival (HR, 0.91; P = .20) and OS (HR, 0.84; P = .03).
The authors highlighted several reasons why laparoscopic surgery may be associated with better survival. First, the faster recovery from the minimally invasive procedure could allow patients to begin adjuvant therapy earlier. In addition, the reduced stress responses and higher levels of immune function among patients undergoing minimally invasive surgery may contribute to a long-term survival advantage.
“These findings address concerns regarding the effectiveness of laparoscopic surgery,” the authors wrote. However, “further studies are necessary to explore the specific mechanisms underlying the positive effect of laparoscopic surgery on OS.”
No outside funding source was noted. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, according to findings from a large meta-analysis.
The estimated 5-year OS rate for patients who underwent laparoscopic surgery was 76.2%, vs. 72.7% for those who had open surgery.
“The survival benefit of laparoscopic surgery is encouraging and supports the routine use of laparoscopic surgery for adult patients with rectal cancer in the era of minimally invasive surgery,” wrote the authors, led by Leping Li, MD, of the department of gastrointestinal surgery, Shandong (China) Provincial Hospital.
The article was published online in JAMA Network Open.
Surgery is an essential component in treating rectal cancer, but the benefits of laparoscopic vs. open surgery are not clear. Over the past 15 years, randomized clinical trials (RCTs) have shown comparable long-term outcomes for laparoscopic and open surgery. However, in most meta-analyses that assessed the evidence more broadly, researchers used an “inappropriate” method for the pooled analysis. Dr. Li and colleagues wanted to perform their own meta-analysis to more definitively understand whether the evidence on long-term outcomes supports or opposes the use of laparoscopic surgery for rectal cancer.
In the current study, the authors conducted an individual participant data meta-analysis using time-to-event data and focused on the long-term survival outcomes after laparoscopic or open surgery for adult patients with rectal cancer.
Ten articles involving 12 RCTs and 3,709 participants were included. In these, 2,097 patients were randomly assigned to undergo laparoscopic surgery, and 1,612 were randomly assigned to undergo open surgery. The studies covered a global population, with participants from Europe, North America, and East Asia.
In a one-stage analysis, the authors found that disease-free survival was slightly better among patients who underwent laparoscopic surgery, but the results were statistically similar (hazard ratio [HR], 0.92; P = .26).
However, when it came to OS, those who had undergone laparoscopic surgery fared significantly better (HR, 0.85; P = .02).
These results held up in the two-stage analysis for both disease-free survival (HR, 0.92; P = .25) and OS (HR, 0.85; P = .02). A sensitivity analyses conducted with large RCTs yielded similar pooled effect sizes for disease-free survival (HR, 0.91; P = .20) and OS (HR, 0.84; P = .03).
The authors highlighted several reasons why laparoscopic surgery may be associated with better survival. First, the faster recovery from the minimally invasive procedure could allow patients to begin adjuvant therapy earlier. In addition, the reduced stress responses and higher levels of immune function among patients undergoing minimally invasive surgery may contribute to a long-term survival advantage.
“These findings address concerns regarding the effectiveness of laparoscopic surgery,” the authors wrote. However, “further studies are necessary to explore the specific mechanisms underlying the positive effect of laparoscopic surgery on OS.”
No outside funding source was noted. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Male breast cancer risk linked with infertility
, according to new research funded by the charity Breast Cancer Now and published in Breast Cancer Research. The study is one of the largest ever into male breast cancer, enabling the team to show a highly statistically significant association.
A link with infertility had been suspected, since parity markedly reduces the risk of female breast cancer; there are known genetic links in both sexes, and a high risk of both breast cancer and infertility among men with Klinefelter syndrome, suggesting some sex hormone-related involvement. However, the rarity of breast cancer in men – with an annual incidence of about 370 cases and 80 deaths per year in the United Kingdom – meant that past studies were necessarily small and yielded mixed results.
“Compared with previous studies, our study of male breast cancer is large,” said study coauthor Michael Jones, PhD, of the division of genetics and epidemiology at the Institute of Cancer Research (ICR) in London. “It was carried out nationwide across England and Wales and was set in motion more than 15 years ago. Because of how rare male breast cancer is, it took us over 12 years to identify and interview the nearly 2,000 men with breast cancer who were part of this study.”
The latest research is part of the wider Breast Cancer Now Male Breast Cancer Study, launched by the charity in 2007. For the new study, the ICR team interviewed 1,998 males living in England and Wales who had been diagnosed with breast cancer between 2005 and 2017. All were aged under 80 but most 60 or older at diagnosis; 92% of their tumors were invasive, and almost all were estrogen receptor positive (98.5% of those with known status).
Their responses were compared with those of a control group of 1,597 men without breast cancer, matched by age at diagnosis and geographic region, recruited from male non-blood relatives of cases and from husbands of women participating in the Generations cohort study of breast cancer etiology.
Raised risk with history of male infertility
Overall, 112 cases (5.6%) and 80 controls (5.0%) reported that they had had infertility problems for which they or their partner had consulted a doctor or infertility clinic. This represented a raised odds ratio of 1.29 (95% confidence interval, 0.94-1.77), which was statistically not significant. However, when analyzed by outcome of the infertility consultation, there was a significant and more than doubled risk of breast cancer among men who were diagnosed as the source of the couple’s infertility (OR = 2.03 [1.18-3.49]), whereas this was not the case among men whose partner was the source (OR = 0.86 [0.51-1.45]) or for whom no source was identified (OR = 1.26 [0.71-2.24]).
In addition, proportionately fewer cases (1,615, or 80.8%) compared with controls (1,423, or 89.1%) had fathered any children, also giving a statistically significantly raised risk of breast cancer for men with no biological children (OR = 1.50 [1.21-1.86], P < .001), “congruent with infertility as a risk factor,” the authors said. The risk was statistically significant for invasive tumors but not for the much smaller number of in situ tumors.
Analysis by number of children showed a decreasing risk with increasing numbers of children, with a highly significant (P < .001) inverse trend where zero was included as a value, but a borderline significant trend (P = .04) if it was not. The team noted that number of children beyond one is difficult to interpret as an indicator of male fertility, since it may more reflect social and cultural factors than fertility per se.
Baseline demographic factors were adjusted for in the risk analyses, and results were not materially changed by sensitivity analyses adjusting additionally for alcohol consumption, smoking, liver disease, and family history of breast cancer. The association also largely remained after exclusion of patients with other preexisting potential confounders including severe obesity and testicular abnormalities, and was consistent irrespective of HER-2 status (there were too few ER-negative tumors to analyze results by ER status).
Potential underlying factors
“The causes of breast cancer in men are largely unknown, partly because it is rare and partly because previous studies have been small,” Dr. Jones said. “The evidence presented in our study suggests that the association of infertility and breast cancer should be confirmed with further research, and future investigations are needed into the potential underlying factors, such as hormone imbalances.”
Commenting on the study, Fiona Osgun, senior health information manager at Cancer Research UK, told this news organization: “Overall, there isn’t strong evidence that infertility is a risk factor for male breast cancer. This study helps to shed light onto a cancer type that is sadly still not very well understood, but much more research is needed to say that infertility is a risk factor for male breast cancer.”
She added that although male breast cancer is a rare condition, it’s still important for men to be aware of what looks and feels normal for them, and to be encouraged to seek medical advice if something is not quite right.
A spokesperson for Breast Cancer UK told this news organization: “[We] believe it’s important to understand what leads to breast cancer in men as well as women and that high quality, long-term studies such as this will help with this understanding.
The findings are consistent with an earlier study that found that U.S. men who have never fathered children are at higher risk of breast cancer. This new long-term U.K. study provides strong evidence, which supports this finding.
“As the authors note, the biological reasons are unclear, but may be associated with altered hormone levels. The ratio of circulating levels of estrogen and androgens (e.g. testosterone) is crucial in healthy functioning of breast tissue. Disruption to this, for example as a result of damage to testes, may affect both fertility and breast cancer risk.
“It is also possible that external factors, such as exposure to certain endocrine (hormone) disrupting chemicals (EDCs), which affect sex hormones, may also affect both fertility and breast cancer risk.
“More studies into breast cancer in men are needed to help us understand better all the risk factors associated with this disease including both hormonal factors and chemical exposures.”
Simon Vincent, PhD, director of research, support, and influencing at Breast Cancer Now, said: “Research has discovered different treatments directed at some features of breast cancer in women; however, breast cancer is not as well understood for men. This is why Breast Cancer Now funds the Male Breast Cancer Study, which looks at what might cause the disease in men. Discovering a link between infertility and male breast cancer is a step towards us understanding male breast cancer and how we could find more ways to diagnose and treat men – and possibly women – with this devastating disease.”
A version of this article first appeared on Medscape UK.
, according to new research funded by the charity Breast Cancer Now and published in Breast Cancer Research. The study is one of the largest ever into male breast cancer, enabling the team to show a highly statistically significant association.
A link with infertility had been suspected, since parity markedly reduces the risk of female breast cancer; there are known genetic links in both sexes, and a high risk of both breast cancer and infertility among men with Klinefelter syndrome, suggesting some sex hormone-related involvement. However, the rarity of breast cancer in men – with an annual incidence of about 370 cases and 80 deaths per year in the United Kingdom – meant that past studies were necessarily small and yielded mixed results.
“Compared with previous studies, our study of male breast cancer is large,” said study coauthor Michael Jones, PhD, of the division of genetics and epidemiology at the Institute of Cancer Research (ICR) in London. “It was carried out nationwide across England and Wales and was set in motion more than 15 years ago. Because of how rare male breast cancer is, it took us over 12 years to identify and interview the nearly 2,000 men with breast cancer who were part of this study.”
The latest research is part of the wider Breast Cancer Now Male Breast Cancer Study, launched by the charity in 2007. For the new study, the ICR team interviewed 1,998 males living in England and Wales who had been diagnosed with breast cancer between 2005 and 2017. All were aged under 80 but most 60 or older at diagnosis; 92% of their tumors were invasive, and almost all were estrogen receptor positive (98.5% of those with known status).
Their responses were compared with those of a control group of 1,597 men without breast cancer, matched by age at diagnosis and geographic region, recruited from male non-blood relatives of cases and from husbands of women participating in the Generations cohort study of breast cancer etiology.
Raised risk with history of male infertility
Overall, 112 cases (5.6%) and 80 controls (5.0%) reported that they had had infertility problems for which they or their partner had consulted a doctor or infertility clinic. This represented a raised odds ratio of 1.29 (95% confidence interval, 0.94-1.77), which was statistically not significant. However, when analyzed by outcome of the infertility consultation, there was a significant and more than doubled risk of breast cancer among men who were diagnosed as the source of the couple’s infertility (OR = 2.03 [1.18-3.49]), whereas this was not the case among men whose partner was the source (OR = 0.86 [0.51-1.45]) or for whom no source was identified (OR = 1.26 [0.71-2.24]).
In addition, proportionately fewer cases (1,615, or 80.8%) compared with controls (1,423, or 89.1%) had fathered any children, also giving a statistically significantly raised risk of breast cancer for men with no biological children (OR = 1.50 [1.21-1.86], P < .001), “congruent with infertility as a risk factor,” the authors said. The risk was statistically significant for invasive tumors but not for the much smaller number of in situ tumors.
Analysis by number of children showed a decreasing risk with increasing numbers of children, with a highly significant (P < .001) inverse trend where zero was included as a value, but a borderline significant trend (P = .04) if it was not. The team noted that number of children beyond one is difficult to interpret as an indicator of male fertility, since it may more reflect social and cultural factors than fertility per se.
Baseline demographic factors were adjusted for in the risk analyses, and results were not materially changed by sensitivity analyses adjusting additionally for alcohol consumption, smoking, liver disease, and family history of breast cancer. The association also largely remained after exclusion of patients with other preexisting potential confounders including severe obesity and testicular abnormalities, and was consistent irrespective of HER-2 status (there were too few ER-negative tumors to analyze results by ER status).
Potential underlying factors
“The causes of breast cancer in men are largely unknown, partly because it is rare and partly because previous studies have been small,” Dr. Jones said. “The evidence presented in our study suggests that the association of infertility and breast cancer should be confirmed with further research, and future investigations are needed into the potential underlying factors, such as hormone imbalances.”
Commenting on the study, Fiona Osgun, senior health information manager at Cancer Research UK, told this news organization: “Overall, there isn’t strong evidence that infertility is a risk factor for male breast cancer. This study helps to shed light onto a cancer type that is sadly still not very well understood, but much more research is needed to say that infertility is a risk factor for male breast cancer.”
She added that although male breast cancer is a rare condition, it’s still important for men to be aware of what looks and feels normal for them, and to be encouraged to seek medical advice if something is not quite right.
A spokesperson for Breast Cancer UK told this news organization: “[We] believe it’s important to understand what leads to breast cancer in men as well as women and that high quality, long-term studies such as this will help with this understanding.
The findings are consistent with an earlier study that found that U.S. men who have never fathered children are at higher risk of breast cancer. This new long-term U.K. study provides strong evidence, which supports this finding.
“As the authors note, the biological reasons are unclear, but may be associated with altered hormone levels. The ratio of circulating levels of estrogen and androgens (e.g. testosterone) is crucial in healthy functioning of breast tissue. Disruption to this, for example as a result of damage to testes, may affect both fertility and breast cancer risk.
“It is also possible that external factors, such as exposure to certain endocrine (hormone) disrupting chemicals (EDCs), which affect sex hormones, may also affect both fertility and breast cancer risk.
“More studies into breast cancer in men are needed to help us understand better all the risk factors associated with this disease including both hormonal factors and chemical exposures.”
Simon Vincent, PhD, director of research, support, and influencing at Breast Cancer Now, said: “Research has discovered different treatments directed at some features of breast cancer in women; however, breast cancer is not as well understood for men. This is why Breast Cancer Now funds the Male Breast Cancer Study, which looks at what might cause the disease in men. Discovering a link between infertility and male breast cancer is a step towards us understanding male breast cancer and how we could find more ways to diagnose and treat men – and possibly women – with this devastating disease.”
A version of this article first appeared on Medscape UK.
, according to new research funded by the charity Breast Cancer Now and published in Breast Cancer Research. The study is one of the largest ever into male breast cancer, enabling the team to show a highly statistically significant association.
A link with infertility had been suspected, since parity markedly reduces the risk of female breast cancer; there are known genetic links in both sexes, and a high risk of both breast cancer and infertility among men with Klinefelter syndrome, suggesting some sex hormone-related involvement. However, the rarity of breast cancer in men – with an annual incidence of about 370 cases and 80 deaths per year in the United Kingdom – meant that past studies were necessarily small and yielded mixed results.
“Compared with previous studies, our study of male breast cancer is large,” said study coauthor Michael Jones, PhD, of the division of genetics and epidemiology at the Institute of Cancer Research (ICR) in London. “It was carried out nationwide across England and Wales and was set in motion more than 15 years ago. Because of how rare male breast cancer is, it took us over 12 years to identify and interview the nearly 2,000 men with breast cancer who were part of this study.”
The latest research is part of the wider Breast Cancer Now Male Breast Cancer Study, launched by the charity in 2007. For the new study, the ICR team interviewed 1,998 males living in England and Wales who had been diagnosed with breast cancer between 2005 and 2017. All were aged under 80 but most 60 or older at diagnosis; 92% of their tumors were invasive, and almost all were estrogen receptor positive (98.5% of those with known status).
Their responses were compared with those of a control group of 1,597 men without breast cancer, matched by age at diagnosis and geographic region, recruited from male non-blood relatives of cases and from husbands of women participating in the Generations cohort study of breast cancer etiology.
Raised risk with history of male infertility
Overall, 112 cases (5.6%) and 80 controls (5.0%) reported that they had had infertility problems for which they or their partner had consulted a doctor or infertility clinic. This represented a raised odds ratio of 1.29 (95% confidence interval, 0.94-1.77), which was statistically not significant. However, when analyzed by outcome of the infertility consultation, there was a significant and more than doubled risk of breast cancer among men who were diagnosed as the source of the couple’s infertility (OR = 2.03 [1.18-3.49]), whereas this was not the case among men whose partner was the source (OR = 0.86 [0.51-1.45]) or for whom no source was identified (OR = 1.26 [0.71-2.24]).
In addition, proportionately fewer cases (1,615, or 80.8%) compared with controls (1,423, or 89.1%) had fathered any children, also giving a statistically significantly raised risk of breast cancer for men with no biological children (OR = 1.50 [1.21-1.86], P < .001), “congruent with infertility as a risk factor,” the authors said. The risk was statistically significant for invasive tumors but not for the much smaller number of in situ tumors.
Analysis by number of children showed a decreasing risk with increasing numbers of children, with a highly significant (P < .001) inverse trend where zero was included as a value, but a borderline significant trend (P = .04) if it was not. The team noted that number of children beyond one is difficult to interpret as an indicator of male fertility, since it may more reflect social and cultural factors than fertility per se.
Baseline demographic factors were adjusted for in the risk analyses, and results were not materially changed by sensitivity analyses adjusting additionally for alcohol consumption, smoking, liver disease, and family history of breast cancer. The association also largely remained after exclusion of patients with other preexisting potential confounders including severe obesity and testicular abnormalities, and was consistent irrespective of HER-2 status (there were too few ER-negative tumors to analyze results by ER status).
Potential underlying factors
“The causes of breast cancer in men are largely unknown, partly because it is rare and partly because previous studies have been small,” Dr. Jones said. “The evidence presented in our study suggests that the association of infertility and breast cancer should be confirmed with further research, and future investigations are needed into the potential underlying factors, such as hormone imbalances.”
Commenting on the study, Fiona Osgun, senior health information manager at Cancer Research UK, told this news organization: “Overall, there isn’t strong evidence that infertility is a risk factor for male breast cancer. This study helps to shed light onto a cancer type that is sadly still not very well understood, but much more research is needed to say that infertility is a risk factor for male breast cancer.”
She added that although male breast cancer is a rare condition, it’s still important for men to be aware of what looks and feels normal for them, and to be encouraged to seek medical advice if something is not quite right.
A spokesperson for Breast Cancer UK told this news organization: “[We] believe it’s important to understand what leads to breast cancer in men as well as women and that high quality, long-term studies such as this will help with this understanding.
The findings are consistent with an earlier study that found that U.S. men who have never fathered children are at higher risk of breast cancer. This new long-term U.K. study provides strong evidence, which supports this finding.
“As the authors note, the biological reasons are unclear, but may be associated with altered hormone levels. The ratio of circulating levels of estrogen and androgens (e.g. testosterone) is crucial in healthy functioning of breast tissue. Disruption to this, for example as a result of damage to testes, may affect both fertility and breast cancer risk.
“It is also possible that external factors, such as exposure to certain endocrine (hormone) disrupting chemicals (EDCs), which affect sex hormones, may also affect both fertility and breast cancer risk.
“More studies into breast cancer in men are needed to help us understand better all the risk factors associated with this disease including both hormonal factors and chemical exposures.”
Simon Vincent, PhD, director of research, support, and influencing at Breast Cancer Now, said: “Research has discovered different treatments directed at some features of breast cancer in women; however, breast cancer is not as well understood for men. This is why Breast Cancer Now funds the Male Breast Cancer Study, which looks at what might cause the disease in men. Discovering a link between infertility and male breast cancer is a step towards us understanding male breast cancer and how we could find more ways to diagnose and treat men – and possibly women – with this devastating disease.”
A version of this article first appeared on Medscape UK.
FROM BREAST CANCER RESEARCH
The psychopathic brain: New insight
Using MRI, researchers found that the striatum was about 10% larger on average in adults with psychopathic traits than in matched control persons and that this relationship was mediated by stimulation seeking and impulsivity.
The striatum is a subcortical region of the forebrain involved in the cognitive processing of reward-related information and motivational aspects of behavior.
“Our study’s results help advance our knowledge about what underlies antisocial behavior such as psychopathy,” co-author and neurocriminologist Olivia Choy, PhD, with Nanyang Technological University, Singapore, said in a news release.
“In addition to social environmental influences, it is important to consider that there can be differences in biology – in this case, the size of brain structures – between antisocial and non-antisocial individuals,” Dr. Choy added.
The study was published online in the Journal of Psychiatric Research.
Antisocial, egocentric
Individuals with psychopathic traits typically have an egocentric and antisocial personality. They generally lack remorse for their actions or empathy for others and often have criminal tendencies.
Some prior research suggests links between psychopathy and an overactive striatum, but it was unclear what role striatal volume plays in this behavior.
For the study, investigators assessed striatal volume using MRI in 120 adults living in the community, and they assessed psychopathy using the Psychopathy Checklist – Revised.
Correlational analyses showed that increased striatal volumes were associated with more psychopathic traits (P = .001) in both men and women.
Volumetric increases were found for all subregions of the striatum in psychopathic individuals, after controlling for age, substance dependence, substance abuse, antisocial personality disorder, attention-deficit/hyperactivity disorder, social adversity, and total brain volume.
An analysis of 18 psychopathic individuals showed that striatal volumes were increased 9.4%, compared with 18 propensity-matched control persons (P = .01).
Abnormal reward processing
Stimulation seeking and impulsivity partly mediated the striatal-psychopathy relationship, accounting for 49.4% of this association.
These findings “replicate and build on initial studies indicating striatal enlargement in adults with psychopathy, yielding an updated effect size of d = 0.48,” the researchers note.
The results are “consistent with the notion that striatal abnormalities in individuals with psychopathy partly reflect increased sensation-seeking and impulsivity and support the hypothesis of abnormal reward processing in psychopathy,” they add.

“We have always known that psychopaths go to extreme lengths to seek out rewards, including criminal activities that involve property, sex, and drugs,” co-author Adrian Raine, DPhil, department of criminology, psychiatry, and psychology, University of Pennsylvania, Philadelphia, said in a news release.
“We are now finding out a neurobiological underpinning of this impulsive and stimulating behavior in the form of enlargement to the striatum, a key brain area involved in rewards,” Dr. Raine added.
What causes striatal enlargement in individuals with psychopathy still needs to be determined.
In human development, the striatum typically becomes smaller as a child matures, suggesting that psychopathy is associated with differences in brain development, the researchers suggest.
“Because biological traits, such as the size of one’s striatum, can be inherited to child from parent, these findings give added support to neurodevelopmental perspectives of psychopathy – that the brains of these offenders do not develop normally throughout childhood and adolescence,” said Dr. Raine.
Larger studies needed
Commenting on the findings for this news organization, Terrie E. Moffitt, PhD, professor of psychology, Duke University, Durham, N.C., noted that there is “general consensus among brain-imaging researchers that testing brain-behavior relations requires very large samples in the thousands and also samples of research participants who represent the full extent of variation in the population as well as possible – from rich to poor, from well to unwell, from high IQ to low IQ, from strong mental health to mental illness, etc.
“It would be grand to see this study’s provocative finding replicated in a large, representative sampling design,” Dr. Moffitt said.
The study was supported in part by the National Institutes of Health. Dr. Choy, Dr. Raine, and Dr. Moffitt have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Using MRI, researchers found that the striatum was about 10% larger on average in adults with psychopathic traits than in matched control persons and that this relationship was mediated by stimulation seeking and impulsivity.
The striatum is a subcortical region of the forebrain involved in the cognitive processing of reward-related information and motivational aspects of behavior.
“Our study’s results help advance our knowledge about what underlies antisocial behavior such as psychopathy,” co-author and neurocriminologist Olivia Choy, PhD, with Nanyang Technological University, Singapore, said in a news release.
“In addition to social environmental influences, it is important to consider that there can be differences in biology – in this case, the size of brain structures – between antisocial and non-antisocial individuals,” Dr. Choy added.
The study was published online in the Journal of Psychiatric Research.
Antisocial, egocentric
Individuals with psychopathic traits typically have an egocentric and antisocial personality. They generally lack remorse for their actions or empathy for others and often have criminal tendencies.
Some prior research suggests links between psychopathy and an overactive striatum, but it was unclear what role striatal volume plays in this behavior.
For the study, investigators assessed striatal volume using MRI in 120 adults living in the community, and they assessed psychopathy using the Psychopathy Checklist – Revised.
Correlational analyses showed that increased striatal volumes were associated with more psychopathic traits (P = .001) in both men and women.
Volumetric increases were found for all subregions of the striatum in psychopathic individuals, after controlling for age, substance dependence, substance abuse, antisocial personality disorder, attention-deficit/hyperactivity disorder, social adversity, and total brain volume.
An analysis of 18 psychopathic individuals showed that striatal volumes were increased 9.4%, compared with 18 propensity-matched control persons (P = .01).
Abnormal reward processing
Stimulation seeking and impulsivity partly mediated the striatal-psychopathy relationship, accounting for 49.4% of this association.
These findings “replicate and build on initial studies indicating striatal enlargement in adults with psychopathy, yielding an updated effect size of d = 0.48,” the researchers note.
The results are “consistent with the notion that striatal abnormalities in individuals with psychopathy partly reflect increased sensation-seeking and impulsivity and support the hypothesis of abnormal reward processing in psychopathy,” they add.
“We have always known that psychopaths go to extreme lengths to seek out rewards, including criminal activities that involve property, sex, and drugs,” co-author Adrian Raine, DPhil, department of criminology, psychiatry, and psychology, University of Pennsylvania, Philadelphia, said in a news release.
“We are now finding out a neurobiological underpinning of this impulsive and stimulating behavior in the form of enlargement to the striatum, a key brain area involved in rewards,” Dr. Raine added.
What causes striatal enlargement in individuals with psychopathy still needs to be determined.
In human development, the striatum typically becomes smaller as a child matures, suggesting that psychopathy is associated with differences in brain development, the researchers suggest.
“Because biological traits, such as the size of one’s striatum, can be inherited to child from parent, these findings give added support to neurodevelopmental perspectives of psychopathy – that the brains of these offenders do not develop normally throughout childhood and adolescence,” said Dr. Raine.
Larger studies needed
Commenting on the findings for this news organization, Terrie E. Moffitt, PhD, professor of psychology, Duke University, Durham, N.C., noted that there is “general consensus among brain-imaging researchers that testing brain-behavior relations requires very large samples in the thousands and also samples of research participants who represent the full extent of variation in the population as well as possible – from rich to poor, from well to unwell, from high IQ to low IQ, from strong mental health to mental illness, etc.
“It would be grand to see this study’s provocative finding replicated in a large, representative sampling design,” Dr. Moffitt said.
The study was supported in part by the National Institutes of Health. Dr. Choy, Dr. Raine, and Dr. Moffitt have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Using MRI, researchers found that the striatum was about 10% larger on average in adults with psychopathic traits than in matched control persons and that this relationship was mediated by stimulation seeking and impulsivity.
The striatum is a subcortical region of the forebrain involved in the cognitive processing of reward-related information and motivational aspects of behavior.
“Our study’s results help advance our knowledge about what underlies antisocial behavior such as psychopathy,” co-author and neurocriminologist Olivia Choy, PhD, with Nanyang Technological University, Singapore, said in a news release.
“In addition to social environmental influences, it is important to consider that there can be differences in biology – in this case, the size of brain structures – between antisocial and non-antisocial individuals,” Dr. Choy added.
The study was published online in the Journal of Psychiatric Research.
Antisocial, egocentric
Individuals with psychopathic traits typically have an egocentric and antisocial personality. They generally lack remorse for their actions or empathy for others and often have criminal tendencies.
Some prior research suggests links between psychopathy and an overactive striatum, but it was unclear what role striatal volume plays in this behavior.
For the study, investigators assessed striatal volume using MRI in 120 adults living in the community, and they assessed psychopathy using the Psychopathy Checklist – Revised.
Correlational analyses showed that increased striatal volumes were associated with more psychopathic traits (P = .001) in both men and women.
Volumetric increases were found for all subregions of the striatum in psychopathic individuals, after controlling for age, substance dependence, substance abuse, antisocial personality disorder, attention-deficit/hyperactivity disorder, social adversity, and total brain volume.
An analysis of 18 psychopathic individuals showed that striatal volumes were increased 9.4%, compared with 18 propensity-matched control persons (P = .01).
Abnormal reward processing
Stimulation seeking and impulsivity partly mediated the striatal-psychopathy relationship, accounting for 49.4% of this association.
These findings “replicate and build on initial studies indicating striatal enlargement in adults with psychopathy, yielding an updated effect size of d = 0.48,” the researchers note.
The results are “consistent with the notion that striatal abnormalities in individuals with psychopathy partly reflect increased sensation-seeking and impulsivity and support the hypothesis of abnormal reward processing in psychopathy,” they add.
“We have always known that psychopaths go to extreme lengths to seek out rewards, including criminal activities that involve property, sex, and drugs,” co-author Adrian Raine, DPhil, department of criminology, psychiatry, and psychology, University of Pennsylvania, Philadelphia, said in a news release.
“We are now finding out a neurobiological underpinning of this impulsive and stimulating behavior in the form of enlargement to the striatum, a key brain area involved in rewards,” Dr. Raine added.
What causes striatal enlargement in individuals with psychopathy still needs to be determined.
In human development, the striatum typically becomes smaller as a child matures, suggesting that psychopathy is associated with differences in brain development, the researchers suggest.
“Because biological traits, such as the size of one’s striatum, can be inherited to child from parent, these findings give added support to neurodevelopmental perspectives of psychopathy – that the brains of these offenders do not develop normally throughout childhood and adolescence,” said Dr. Raine.
Larger studies needed
Commenting on the findings for this news organization, Terrie E. Moffitt, PhD, professor of psychology, Duke University, Durham, N.C., noted that there is “general consensus among brain-imaging researchers that testing brain-behavior relations requires very large samples in the thousands and also samples of research participants who represent the full extent of variation in the population as well as possible – from rich to poor, from well to unwell, from high IQ to low IQ, from strong mental health to mental illness, etc.
“It would be grand to see this study’s provocative finding replicated in a large, representative sampling design,” Dr. Moffitt said.
The study was supported in part by the National Institutes of Health. Dr. Choy, Dr. Raine, and Dr. Moffitt have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Cluttered consciousness: The mental effects of growing up with a hoarder
Many of us are reluctant to throw things out.
We buy. We accumulate. We collect. Eventually our attics are packed with dusty heirlooms that we rarely, if ever, look at. Eventually we’re forced to pare down and head to the Goodwill.
But not all of us.
Hoarding – or the prolonged difficulty of discarding unneeded possessions – is pervasive in our culture, affecting nearly 3% of the population. This compulsive collecting, and unwillingness to part with “stuff,” is even the subject of multiple popular television series.

How do you conceptualize hoarding behavior?
The core feature of hoarding is the inability to throw things away. This can be due to many different reasons, whether there’s a strong sentimental attachment or the belief that you will need these items one day. Compulsive buying is often involved, and inevitable clutter.
How was hoarding first conceptualized among psychiatrists and psychologists? And when did the term first enter the lexicon?
It was originally conceptualized as a difficult-to-treat subtype of obsessive-compulsive disorder (OCD). A lot of that work identifying this subgroup was going on in the late 1980s and early 1990s. There was a small but growing group of researchers demonstrating that this is fundamentally different from OCD in several ways.
In terms of the clinical presentation, the comorbidity patterns are different from those for OCD. And the course is a little bit different; we see a progressive development across the lifespan, as opposed to a clear-cut diagnosis earlier in life, as is typically seen with OCD. By the time a lot of people seek treatment, they’re often being brought in by, say, family members when they’re a little bit older. With hoarding, there is also this consistent pattern of poor treatment response across the board, whether to selective serotonin reuptake inhibitors or behavioral therapy.
A lot of this work together led to advocacy for recognizing hoarding as an independent diagnosis in the DSM-5. I think official recognition by our “big book” prompted more attention to this population. Previously these patients probably would have been diagnosed with OCD, and it really isn’t appropriate to think of hoarding as purely an anxiety disorder.
Hoarding exposure and future mental health
You have a new study, published in Annals of Clinical Psychiatry, looking at mental health among adult children of parents with hoarding problems. Can you tell us what inspired you to run this study, and what you found?
There were a couple of factors.
We’d seen a lot of folks with hoarding in OCD specialty clinics, so my clinical experiences with this population certainly drew me to this general area. But then, at the same time, I have this broad training in child mental health. And childhood trauma or adverse childhood experiences, which can include being around hoarding, can be a very difficult thing to live through and deal with. And here I have to give a lot of credit to Suzanne Chabaud, PhD, of the OCD Institute of Greater New Orleans, who’s one of the coauthors on the paper. She’s been beating the drum of thinking about the family and kids of people with hoarding disorders for years. My interests came from some of those experiences, but she had the good idea of really looking at this problem in a detailed way.
Prior to your paper, had there been research on the prevalence of mental illnesses such as anxiety and depression in the children of people with hoarding behaviors?
That particular question was new to our paper. It was the first time anyone, to my knowledge, had looked at a validated assessment of anxiety and depression in this population.
How did you assess their symptoms and what did you find?
We asked study participants to think back on how they felt throughout their teenage years and gauged their responses with the Patient Health Questionnaire (PHQ), a measure of mental health disorders. I should say up front that we didn’t have a control group. But we found that among our 414 study participants, somewhere between 30% and 50% reported clinically significant anxiety or depressive symptoms, far higher than you’d expect in the normal population. So when looking back on how they were feeling as teenagers in that environment, they were struggling, and they often felt rejected by their parents.
We also found that almost 10% of participants were threatened with eviction at some point in their childhood; 15% had to live outside of their home at some point, because of the clutter; and 2% had involvement from child protective services and were removed from the home.
I know you recruited patients from online forums established by the children of hoarding parents. Presumably, these are the people most affected by this phenomenon. How does this play out in people who simply like to, say, collect something? Is this a continuum of behavior, with a breaking point at which it becomes a pathology?
I think it’s safe to conceptualize collecting and hoarding as a continuum, and you’ve got to draw a line somewhere in terms of clinical significance.
Did you assess whether the children of hoarders were more likely to hoard themselves as adults?
This is our follow-up paper; we haven’t looked at it yet.
But in looking at preliminary data, the prevalence seems pretty low, actually, at least in our sample. And as you mentioned, in our study there were folks who were seeking support specifically because they grew up in a really cluttered home.
Management
How do mental health providers typically address and treat hoarding?
To my knowledge, there are no current Food and Drug Administration–approved medications for hoarding, though psychiatrists will prescribe SSRIs and try to treat co-occurring problems such as depression and anxiety symptoms.
I can speak to cognitive-behavioral therapy (CBT) in a bit more detail. A number of randomized controlled trials support CBT for hoarding. I mentioned before that when we as a field treated hoarding akin to OCD and did exposure and response prevention therapy, we didn’t really target the specific features of hoarding. People didn’t do that well.
But now researchers are focusing on CBT interventions focused on discarding tasks that really address hoarding. You can create different categories for different items: Patients can either keep them, throw them out, or donate them. You can explore what thoughts or expectations are associated with these items and try to address them. Clinicians can help patients look at, say, different areas of their house and discuss what they might be willing to part with or at least think about parting with. You find their internal motivations for keeping things.
This sort of therapy generally takes longer than it does for, say, OCD. It can be a little bit slower, particularly if someone has a lot of stuff. And often it can involve doing home visits. In the age of Zoom this is a little bit easier because home visits aren’t always feasible.
What role does family play in managing hoarding? I imagine that including loved ones and friends in the process could be quite helpful.
Yes, absolutely. And social support, more broadly.
A colleague I worked with did a really interesting study where she looked at psychologist-delivered versus peer-delivered CBT for hoarding. They found that the biggest predictor of improved outcomes was having what they called a “clutter buddy,” which follows the Alcoholics Anonymous sponsor model. This would be somebody else struggling with the same problem who’s an accountability partner helping a patient follow through with their goals related to discarding. I think that finding underscores how important that social support is.
Any final thoughts for our audience of clinicians and researchers on how to approach hoarding?
I think there’s been a stigma – at least in psychology circles – that it’s not really treatable because of that earlier work with OCD. But on the CBT side, there’s now good reason to believe that people can live much happier lives and overcome this problem. CBT does seem to work for a lot of people with hoarding. That’s what I’d like to emphasize.
Dr. Stetka is executive editor for Medscape. A version of this article first appeared on Medscape.com.
Many of us are reluctant to throw things out.
We buy. We accumulate. We collect. Eventually our attics are packed with dusty heirlooms that we rarely, if ever, look at. Eventually we’re forced to pare down and head to the Goodwill.
But not all of us.
Hoarding – or the prolonged difficulty of discarding unneeded possessions – is pervasive in our culture, affecting nearly 3% of the population. This compulsive collecting, and unwillingness to part with “stuff,” is even the subject of multiple popular television series.
How do you conceptualize hoarding behavior?
The core feature of hoarding is the inability to throw things away. This can be due to many different reasons, whether there’s a strong sentimental attachment or the belief that you will need these items one day. Compulsive buying is often involved, and inevitable clutter.
How was hoarding first conceptualized among psychiatrists and psychologists? And when did the term first enter the lexicon?
It was originally conceptualized as a difficult-to-treat subtype of obsessive-compulsive disorder (OCD). A lot of that work identifying this subgroup was going on in the late 1980s and early 1990s. There was a small but growing group of researchers demonstrating that this is fundamentally different from OCD in several ways.
In terms of the clinical presentation, the comorbidity patterns are different from those for OCD. And the course is a little bit different; we see a progressive development across the lifespan, as opposed to a clear-cut diagnosis earlier in life, as is typically seen with OCD. By the time a lot of people seek treatment, they’re often being brought in by, say, family members when they’re a little bit older. With hoarding, there is also this consistent pattern of poor treatment response across the board, whether to selective serotonin reuptake inhibitors or behavioral therapy.
A lot of this work together led to advocacy for recognizing hoarding as an independent diagnosis in the DSM-5. I think official recognition by our “big book” prompted more attention to this population. Previously these patients probably would have been diagnosed with OCD, and it really isn’t appropriate to think of hoarding as purely an anxiety disorder.
Hoarding exposure and future mental health
You have a new study, published in Annals of Clinical Psychiatry, looking at mental health among adult children of parents with hoarding problems. Can you tell us what inspired you to run this study, and what you found?
There were a couple of factors.
We’d seen a lot of folks with hoarding in OCD specialty clinics, so my clinical experiences with this population certainly drew me to this general area. But then, at the same time, I have this broad training in child mental health. And childhood trauma or adverse childhood experiences, which can include being around hoarding, can be a very difficult thing to live through and deal with. And here I have to give a lot of credit to Suzanne Chabaud, PhD, of the OCD Institute of Greater New Orleans, who’s one of the coauthors on the paper. She’s been beating the drum of thinking about the family and kids of people with hoarding disorders for years. My interests came from some of those experiences, but she had the good idea of really looking at this problem in a detailed way.
Prior to your paper, had there been research on the prevalence of mental illnesses such as anxiety and depression in the children of people with hoarding behaviors?
That particular question was new to our paper. It was the first time anyone, to my knowledge, had looked at a validated assessment of anxiety and depression in this population.
How did you assess their symptoms and what did you find?
We asked study participants to think back on how they felt throughout their teenage years and gauged their responses with the Patient Health Questionnaire (PHQ), a measure of mental health disorders. I should say up front that we didn’t have a control group. But we found that among our 414 study participants, somewhere between 30% and 50% reported clinically significant anxiety or depressive symptoms, far higher than you’d expect in the normal population. So when looking back on how they were feeling as teenagers in that environment, they were struggling, and they often felt rejected by their parents.
We also found that almost 10% of participants were threatened with eviction at some point in their childhood; 15% had to live outside of their home at some point, because of the clutter; and 2% had involvement from child protective services and were removed from the home.
I know you recruited patients from online forums established by the children of hoarding parents. Presumably, these are the people most affected by this phenomenon. How does this play out in people who simply like to, say, collect something? Is this a continuum of behavior, with a breaking point at which it becomes a pathology?
I think it’s safe to conceptualize collecting and hoarding as a continuum, and you’ve got to draw a line somewhere in terms of clinical significance.
Did you assess whether the children of hoarders were more likely to hoard themselves as adults?
This is our follow-up paper; we haven’t looked at it yet.
But in looking at preliminary data, the prevalence seems pretty low, actually, at least in our sample. And as you mentioned, in our study there were folks who were seeking support specifically because they grew up in a really cluttered home.
Management
How do mental health providers typically address and treat hoarding?
To my knowledge, there are no current Food and Drug Administration–approved medications for hoarding, though psychiatrists will prescribe SSRIs and try to treat co-occurring problems such as depression and anxiety symptoms.
I can speak to cognitive-behavioral therapy (CBT) in a bit more detail. A number of randomized controlled trials support CBT for hoarding. I mentioned before that when we as a field treated hoarding akin to OCD and did exposure and response prevention therapy, we didn’t really target the specific features of hoarding. People didn’t do that well.
But now researchers are focusing on CBT interventions focused on discarding tasks that really address hoarding. You can create different categories for different items: Patients can either keep them, throw them out, or donate them. You can explore what thoughts or expectations are associated with these items and try to address them. Clinicians can help patients look at, say, different areas of their house and discuss what they might be willing to part with or at least think about parting with. You find their internal motivations for keeping things.
This sort of therapy generally takes longer than it does for, say, OCD. It can be a little bit slower, particularly if someone has a lot of stuff. And often it can involve doing home visits. In the age of Zoom this is a little bit easier because home visits aren’t always feasible.
What role does family play in managing hoarding? I imagine that including loved ones and friends in the process could be quite helpful.
Yes, absolutely. And social support, more broadly.
A colleague I worked with did a really interesting study where she looked at psychologist-delivered versus peer-delivered CBT for hoarding. They found that the biggest predictor of improved outcomes was having what they called a “clutter buddy,” which follows the Alcoholics Anonymous sponsor model. This would be somebody else struggling with the same problem who’s an accountability partner helping a patient follow through with their goals related to discarding. I think that finding underscores how important that social support is.
Any final thoughts for our audience of clinicians and researchers on how to approach hoarding?
I think there’s been a stigma – at least in psychology circles – that it’s not really treatable because of that earlier work with OCD. But on the CBT side, there’s now good reason to believe that people can live much happier lives and overcome this problem. CBT does seem to work for a lot of people with hoarding. That’s what I’d like to emphasize.
Dr. Stetka is executive editor for Medscape. A version of this article first appeared on Medscape.com.
Many of us are reluctant to throw things out.
We buy. We accumulate. We collect. Eventually our attics are packed with dusty heirlooms that we rarely, if ever, look at. Eventually we’re forced to pare down and head to the Goodwill.
But not all of us.
Hoarding – or the prolonged difficulty of discarding unneeded possessions – is pervasive in our culture, affecting nearly 3% of the population. This compulsive collecting, and unwillingness to part with “stuff,” is even the subject of multiple popular television series.
How do you conceptualize hoarding behavior?
The core feature of hoarding is the inability to throw things away. This can be due to many different reasons, whether there’s a strong sentimental attachment or the belief that you will need these items one day. Compulsive buying is often involved, and inevitable clutter.
How was hoarding first conceptualized among psychiatrists and psychologists? And when did the term first enter the lexicon?
It was originally conceptualized as a difficult-to-treat subtype of obsessive-compulsive disorder (OCD). A lot of that work identifying this subgroup was going on in the late 1980s and early 1990s. There was a small but growing group of researchers demonstrating that this is fundamentally different from OCD in several ways.
In terms of the clinical presentation, the comorbidity patterns are different from those for OCD. And the course is a little bit different; we see a progressive development across the lifespan, as opposed to a clear-cut diagnosis earlier in life, as is typically seen with OCD. By the time a lot of people seek treatment, they’re often being brought in by, say, family members when they’re a little bit older. With hoarding, there is also this consistent pattern of poor treatment response across the board, whether to selective serotonin reuptake inhibitors or behavioral therapy.
A lot of this work together led to advocacy for recognizing hoarding as an independent diagnosis in the DSM-5. I think official recognition by our “big book” prompted more attention to this population. Previously these patients probably would have been diagnosed with OCD, and it really isn’t appropriate to think of hoarding as purely an anxiety disorder.
Hoarding exposure and future mental health
You have a new study, published in Annals of Clinical Psychiatry, looking at mental health among adult children of parents with hoarding problems. Can you tell us what inspired you to run this study, and what you found?
There were a couple of factors.
We’d seen a lot of folks with hoarding in OCD specialty clinics, so my clinical experiences with this population certainly drew me to this general area. But then, at the same time, I have this broad training in child mental health. And childhood trauma or adverse childhood experiences, which can include being around hoarding, can be a very difficult thing to live through and deal with. And here I have to give a lot of credit to Suzanne Chabaud, PhD, of the OCD Institute of Greater New Orleans, who’s one of the coauthors on the paper. She’s been beating the drum of thinking about the family and kids of people with hoarding disorders for years. My interests came from some of those experiences, but she had the good idea of really looking at this problem in a detailed way.
Prior to your paper, had there been research on the prevalence of mental illnesses such as anxiety and depression in the children of people with hoarding behaviors?
That particular question was new to our paper. It was the first time anyone, to my knowledge, had looked at a validated assessment of anxiety and depression in this population.
How did you assess their symptoms and what did you find?
We asked study participants to think back on how they felt throughout their teenage years and gauged their responses with the Patient Health Questionnaire (PHQ), a measure of mental health disorders. I should say up front that we didn’t have a control group. But we found that among our 414 study participants, somewhere between 30% and 50% reported clinically significant anxiety or depressive symptoms, far higher than you’d expect in the normal population. So when looking back on how they were feeling as teenagers in that environment, they were struggling, and they often felt rejected by their parents.
We also found that almost 10% of participants were threatened with eviction at some point in their childhood; 15% had to live outside of their home at some point, because of the clutter; and 2% had involvement from child protective services and were removed from the home.
I know you recruited patients from online forums established by the children of hoarding parents. Presumably, these are the people most affected by this phenomenon. How does this play out in people who simply like to, say, collect something? Is this a continuum of behavior, with a breaking point at which it becomes a pathology?
I think it’s safe to conceptualize collecting and hoarding as a continuum, and you’ve got to draw a line somewhere in terms of clinical significance.
Did you assess whether the children of hoarders were more likely to hoard themselves as adults?
This is our follow-up paper; we haven’t looked at it yet.
But in looking at preliminary data, the prevalence seems pretty low, actually, at least in our sample. And as you mentioned, in our study there were folks who were seeking support specifically because they grew up in a really cluttered home.
Management
How do mental health providers typically address and treat hoarding?
To my knowledge, there are no current Food and Drug Administration–approved medications for hoarding, though psychiatrists will prescribe SSRIs and try to treat co-occurring problems such as depression and anxiety symptoms.
I can speak to cognitive-behavioral therapy (CBT) in a bit more detail. A number of randomized controlled trials support CBT for hoarding. I mentioned before that when we as a field treated hoarding akin to OCD and did exposure and response prevention therapy, we didn’t really target the specific features of hoarding. People didn’t do that well.
But now researchers are focusing on CBT interventions focused on discarding tasks that really address hoarding. You can create different categories for different items: Patients can either keep them, throw them out, or donate them. You can explore what thoughts or expectations are associated with these items and try to address them. Clinicians can help patients look at, say, different areas of their house and discuss what they might be willing to part with or at least think about parting with. You find their internal motivations for keeping things.
This sort of therapy generally takes longer than it does for, say, OCD. It can be a little bit slower, particularly if someone has a lot of stuff. And often it can involve doing home visits. In the age of Zoom this is a little bit easier because home visits aren’t always feasible.
What role does family play in managing hoarding? I imagine that including loved ones and friends in the process could be quite helpful.
Yes, absolutely. And social support, more broadly.
A colleague I worked with did a really interesting study where she looked at psychologist-delivered versus peer-delivered CBT for hoarding. They found that the biggest predictor of improved outcomes was having what they called a “clutter buddy,” which follows the Alcoholics Anonymous sponsor model. This would be somebody else struggling with the same problem who’s an accountability partner helping a patient follow through with their goals related to discarding. I think that finding underscores how important that social support is.
Any final thoughts for our audience of clinicians and researchers on how to approach hoarding?
I think there’s been a stigma – at least in psychology circles – that it’s not really treatable because of that earlier work with OCD. But on the CBT side, there’s now good reason to believe that people can live much happier lives and overcome this problem. CBT does seem to work for a lot of people with hoarding. That’s what I’d like to emphasize.
Dr. Stetka is executive editor for Medscape. A version of this article first appeared on Medscape.com.
Cancer patients unaware of their increased thrombosis risk
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
FROM CANCER TREATMENT AND RESEARCH COMMUNICATIONS
Doc faces U.S. federal charges for hacking, ransomware
According to a statement from the U.S. Department of Justice, 55-year-old Moises Luis Zagala Gonzalez, MD, is charged with creating and distributing ransomware with a “doomsday” clock and sharing in profits from ransomware attacks.
Dr. Zagala, also known as “Nosophoros,” “Aesculapius,” and “Nebuchadnezzar,” is a citizen of France and Venezuela who currently lives in Ciudad Bolivar, Venezuela.
Breon Peace, U.S. attorney for the Eastern District of New York, and Michael J. Driscoll, assistant director in charge of the Federal Bureau of Investigaton’s New York Field Office, announced the charges.
“As alleged, the multitasking doctor treated patients, created and named his cyber tool after death, profited from a global ransomware ecosystem in which he sold the tools for conducting ransomware attacks, trained the attackers about how to extort victims, and then boasted about successful attacks, including by malicious actors associated with the government of Iran,” Mr. Peace said in the news release from the DOJ.
“We allege Zagala not only created and sold ransomware products to hackers, but also trained them in their use. Our actions today will prevent Zagala from further victimizing users,” Mr. Driscoll said. “However, many other malicious criminals are searching for businesses and organizations that haven’t taken steps to protect their systems – which is an incredibly vital step in stopping the next ransomware attack.”
Ransomware tools are malicious software that cybercriminals use to extort money from companies, nonprofits, and other institutions by encrypting their files and then demanding a ransom for the decryption keys.
One of Dr. Zagala’s early ransomware tools, called “Jigsaw v. 2,” had what Dr. Zagala described as a doomsday counter that kept track of how many times the user tried to remove the ransomware. “If the user kills the ransomware too many times, then it’s clear he won’t pay so better erase the whole hard drive,” Dr. Zagala wrote.
According to the DOJ, beginning in late 2019, Dr. Zagala began advertising a new tool as a “private ransomware builder,” which he called Thanos. The name appears to be in reference to a fictional villain responsible for destroying half of all life in the universe and to “Thanatos” from Greek mythology, who is associated with death.
Dr. Zagala’s Thanos software allows users to create their own unique ransomware software for personal use or to rent to other cybercriminals.
Dr. Zagala allegedly not only sold or rented out his ransomware tools to cybercriminals, but he also taught users how to deploy the tools, steal passwords from victim computers, and set up a Bitcoin address for ransom payments.
Dr. Zagala’s customers were happy with his products, the DOJ release noted. In a message posted in July 2020, one user said the ransomware was “very powerful” and claimed that he had used it to infect a network of roughly 3,000 computers.
In December 2020, another user wrote a post in Russian: “We have been working with this product for over a month now, we have a good profit! Best support I’ve met.”
Earlier in May, law enforcement agents interviewed a relative of Dr. Zagala who lives in Florida and whose PayPal account was used by Dr. Zagala to receive illicit proceeds.
According to the DOJ, the relative confirmed that Dr. Zagala lives in Venezuela and had taught himself computer programming. The relative also showed agents contact information for Dr. Zagala that matched the registered email for malicious infrastructure associated with the Thanos ransomware.
Dr. Zagala, who remains in Venezuela, faces up to 10 years in prison for attempted computer intrusions and conspiracy charges if brought to justice in the United States.
A version of this article first appeared on Medscape.com.
According to a statement from the U.S. Department of Justice, 55-year-old Moises Luis Zagala Gonzalez, MD, is charged with creating and distributing ransomware with a “doomsday” clock and sharing in profits from ransomware attacks.
Dr. Zagala, also known as “Nosophoros,” “Aesculapius,” and “Nebuchadnezzar,” is a citizen of France and Venezuela who currently lives in Ciudad Bolivar, Venezuela.
Breon Peace, U.S. attorney for the Eastern District of New York, and Michael J. Driscoll, assistant director in charge of the Federal Bureau of Investigaton’s New York Field Office, announced the charges.
“As alleged, the multitasking doctor treated patients, created and named his cyber tool after death, profited from a global ransomware ecosystem in which he sold the tools for conducting ransomware attacks, trained the attackers about how to extort victims, and then boasted about successful attacks, including by malicious actors associated with the government of Iran,” Mr. Peace said in the news release from the DOJ.
“We allege Zagala not only created and sold ransomware products to hackers, but also trained them in their use. Our actions today will prevent Zagala from further victimizing users,” Mr. Driscoll said. “However, many other malicious criminals are searching for businesses and organizations that haven’t taken steps to protect their systems – which is an incredibly vital step in stopping the next ransomware attack.”
Ransomware tools are malicious software that cybercriminals use to extort money from companies, nonprofits, and other institutions by encrypting their files and then demanding a ransom for the decryption keys.
One of Dr. Zagala’s early ransomware tools, called “Jigsaw v. 2,” had what Dr. Zagala described as a doomsday counter that kept track of how many times the user tried to remove the ransomware. “If the user kills the ransomware too many times, then it’s clear he won’t pay so better erase the whole hard drive,” Dr. Zagala wrote.
According to the DOJ, beginning in late 2019, Dr. Zagala began advertising a new tool as a “private ransomware builder,” which he called Thanos. The name appears to be in reference to a fictional villain responsible for destroying half of all life in the universe and to “Thanatos” from Greek mythology, who is associated with death.
Dr. Zagala’s Thanos software allows users to create their own unique ransomware software for personal use or to rent to other cybercriminals.
Dr. Zagala allegedly not only sold or rented out his ransomware tools to cybercriminals, but he also taught users how to deploy the tools, steal passwords from victim computers, and set up a Bitcoin address for ransom payments.
Dr. Zagala’s customers were happy with his products, the DOJ release noted. In a message posted in July 2020, one user said the ransomware was “very powerful” and claimed that he had used it to infect a network of roughly 3,000 computers.
In December 2020, another user wrote a post in Russian: “We have been working with this product for over a month now, we have a good profit! Best support I’ve met.”
Earlier in May, law enforcement agents interviewed a relative of Dr. Zagala who lives in Florida and whose PayPal account was used by Dr. Zagala to receive illicit proceeds.
According to the DOJ, the relative confirmed that Dr. Zagala lives in Venezuela and had taught himself computer programming. The relative also showed agents contact information for Dr. Zagala that matched the registered email for malicious infrastructure associated with the Thanos ransomware.
Dr. Zagala, who remains in Venezuela, faces up to 10 years in prison for attempted computer intrusions and conspiracy charges if brought to justice in the United States.
A version of this article first appeared on Medscape.com.
According to a statement from the U.S. Department of Justice, 55-year-old Moises Luis Zagala Gonzalez, MD, is charged with creating and distributing ransomware with a “doomsday” clock and sharing in profits from ransomware attacks.
Dr. Zagala, also known as “Nosophoros,” “Aesculapius,” and “Nebuchadnezzar,” is a citizen of France and Venezuela who currently lives in Ciudad Bolivar, Venezuela.
Breon Peace, U.S. attorney for the Eastern District of New York, and Michael J. Driscoll, assistant director in charge of the Federal Bureau of Investigaton’s New York Field Office, announced the charges.
“As alleged, the multitasking doctor treated patients, created and named his cyber tool after death, profited from a global ransomware ecosystem in which he sold the tools for conducting ransomware attacks, trained the attackers about how to extort victims, and then boasted about successful attacks, including by malicious actors associated with the government of Iran,” Mr. Peace said in the news release from the DOJ.
“We allege Zagala not only created and sold ransomware products to hackers, but also trained them in their use. Our actions today will prevent Zagala from further victimizing users,” Mr. Driscoll said. “However, many other malicious criminals are searching for businesses and organizations that haven’t taken steps to protect their systems – which is an incredibly vital step in stopping the next ransomware attack.”
Ransomware tools are malicious software that cybercriminals use to extort money from companies, nonprofits, and other institutions by encrypting their files and then demanding a ransom for the decryption keys.
One of Dr. Zagala’s early ransomware tools, called “Jigsaw v. 2,” had what Dr. Zagala described as a doomsday counter that kept track of how many times the user tried to remove the ransomware. “If the user kills the ransomware too many times, then it’s clear he won’t pay so better erase the whole hard drive,” Dr. Zagala wrote.
According to the DOJ, beginning in late 2019, Dr. Zagala began advertising a new tool as a “private ransomware builder,” which he called Thanos. The name appears to be in reference to a fictional villain responsible for destroying half of all life in the universe and to “Thanatos” from Greek mythology, who is associated with death.
Dr. Zagala’s Thanos software allows users to create their own unique ransomware software for personal use or to rent to other cybercriminals.
Dr. Zagala allegedly not only sold or rented out his ransomware tools to cybercriminals, but he also taught users how to deploy the tools, steal passwords from victim computers, and set up a Bitcoin address for ransom payments.
Dr. Zagala’s customers were happy with his products, the DOJ release noted. In a message posted in July 2020, one user said the ransomware was “very powerful” and claimed that he had used it to infect a network of roughly 3,000 computers.
In December 2020, another user wrote a post in Russian: “We have been working with this product for over a month now, we have a good profit! Best support I’ve met.”
Earlier in May, law enforcement agents interviewed a relative of Dr. Zagala who lives in Florida and whose PayPal account was used by Dr. Zagala to receive illicit proceeds.
According to the DOJ, the relative confirmed that Dr. Zagala lives in Venezuela and had taught himself computer programming. The relative also showed agents contact information for Dr. Zagala that matched the registered email for malicious infrastructure associated with the Thanos ransomware.
Dr. Zagala, who remains in Venezuela, faces up to 10 years in prison for attempted computer intrusions and conspiracy charges if brought to justice in the United States.
A version of this article first appeared on Medscape.com.
Does suicide risk show up in the blood?
Investigators found patients with MDD who died by suicide had a gene expression signature in blood distinct from patients with MDD who died by other means.
The signature included genes involved in stress response changes, including polyamine metabolism, circadian rhythm, immune dysregulation, and telomere maintenance.
“These blood biomarkers are an important step toward developing blood tests to identify patients with imminent risk of ending their lives,” study investigator Adolfo Sequeira, PhD, associate researcher in the department of psychiatry and human behavior, University of California, Irvine, said in a news release.
“To our knowledge, this is the first study to analyze blood and brain samples in a well-defined population of MDDs demonstrating significant differences in gene expression associated with completed suicide,” Dr. Sequeira added.
The findings were published online in Translational Psychiatry.
A pressing challenge
Suicide rates in the United States have jumped by more than 35% over the past 2 decades, with more than 48,000 deaths by suicide occurring just last year. MDD is the most common diagnosis among completed suicides, and identifying individuals at the highest risk for suicide remains a “pressing challenge,” the researchers noted.
They looked for changes in gene expression associated with suicide in archived postmortem blood and brain samples from adults with MDD who died by suicide (MDD-S) or by other means (MDD-NS), as well as a group of controls with no psychiatric illness.
In total, there were blood and brain samples for 45 adults, including 53 blood samples and 69 dorsolateral prefrontal cortex (DLPFC) tissue samples.
In blood, investigators identified 14 genes that significantly differentiated MDD-S from MDD-NS. The top six genes differentially expressed in blood were PER3, MTPAP, SLC25A26, CD19, SOX9, and GAR1.
In addition, four genes showed significant changes in brain and blood between the MDD-S and MDD-NS groups. SOX9 was decreased and PER3 was increased in MDD-S in both blood and brain samples, while CD19 and TERF1 were increased in blood but decreased in DLPFC.
SOX9, an astrocytic marker in the brain and B-cell marker in blood, has been shown to be decreased in MDD-S compared with controls in the prefrontal cortex.
In the current study, researchers found that SOX9 expression was significantly reduced both in blood and brain in MDD-S compared with MDD-NS, “suggesting similar immune/astrocytic dysregulations in suicide that could be further investigated.”
Potential signatures, potential targets
PER3 is a circadian rhythm gene implicated in sleep disorders associated with shifts in circadian rhythms and is thought to increase susceptibility to MDD.
Mutations in PER3 have been shown previously to alter multiple systems, including response to antidepressants; and increased blood expression of PER1 has been linked to suicidality in women, the researchers noted.
There also were significantly higher levels of two inflammatory markers (CD19 and CD6 genes) in blood of MDD-S patients compared to MDD-NS patients.
Another “significant” finding was the involvement of several mitochondrial genes in suicide, the researchers said.
Two nuclear genes coding for mitochondria-located proteins MTPAP (a mitochondrial poly(A) polymerase) and the mitochondrial polyamine transporter SLC25A26 were increased in blood in MDD-S compared with MDD-NS and controls, suggesting that “mitochondrial alterations could be used as potential signatures to differentiate MDD-S from MDD-NS patients and also from controls.”
The researchers added that the genes found to be dysregulated in suicide represent potential targets for future drug therapies to prevent suicide and could also be used to develop a molecular test to identify individuals at high risk for suicide.
The study was funded by the National Institute of Mental Health, the American Society for Suicide Prevention, and the Pritzker Family Philanthropic Fund. The investigators have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found patients with MDD who died by suicide had a gene expression signature in blood distinct from patients with MDD who died by other means.
The signature included genes involved in stress response changes, including polyamine metabolism, circadian rhythm, immune dysregulation, and telomere maintenance.
“These blood biomarkers are an important step toward developing blood tests to identify patients with imminent risk of ending their lives,” study investigator Adolfo Sequeira, PhD, associate researcher in the department of psychiatry and human behavior, University of California, Irvine, said in a news release.
“To our knowledge, this is the first study to analyze blood and brain samples in a well-defined population of MDDs demonstrating significant differences in gene expression associated with completed suicide,” Dr. Sequeira added.
The findings were published online in Translational Psychiatry.
A pressing challenge
Suicide rates in the United States have jumped by more than 35% over the past 2 decades, with more than 48,000 deaths by suicide occurring just last year. MDD is the most common diagnosis among completed suicides, and identifying individuals at the highest risk for suicide remains a “pressing challenge,” the researchers noted.
They looked for changes in gene expression associated with suicide in archived postmortem blood and brain samples from adults with MDD who died by suicide (MDD-S) or by other means (MDD-NS), as well as a group of controls with no psychiatric illness.
In total, there were blood and brain samples for 45 adults, including 53 blood samples and 69 dorsolateral prefrontal cortex (DLPFC) tissue samples.
In blood, investigators identified 14 genes that significantly differentiated MDD-S from MDD-NS. The top six genes differentially expressed in blood were PER3, MTPAP, SLC25A26, CD19, SOX9, and GAR1.
In addition, four genes showed significant changes in brain and blood between the MDD-S and MDD-NS groups. SOX9 was decreased and PER3 was increased in MDD-S in both blood and brain samples, while CD19 and TERF1 were increased in blood but decreased in DLPFC.
SOX9, an astrocytic marker in the brain and B-cell marker in blood, has been shown to be decreased in MDD-S compared with controls in the prefrontal cortex.
In the current study, researchers found that SOX9 expression was significantly reduced both in blood and brain in MDD-S compared with MDD-NS, “suggesting similar immune/astrocytic dysregulations in suicide that could be further investigated.”
Potential signatures, potential targets
PER3 is a circadian rhythm gene implicated in sleep disorders associated with shifts in circadian rhythms and is thought to increase susceptibility to MDD.
Mutations in PER3 have been shown previously to alter multiple systems, including response to antidepressants; and increased blood expression of PER1 has been linked to suicidality in women, the researchers noted.
There also were significantly higher levels of two inflammatory markers (CD19 and CD6 genes) in blood of MDD-S patients compared to MDD-NS patients.
Another “significant” finding was the involvement of several mitochondrial genes in suicide, the researchers said.
Two nuclear genes coding for mitochondria-located proteins MTPAP (a mitochondrial poly(A) polymerase) and the mitochondrial polyamine transporter SLC25A26 were increased in blood in MDD-S compared with MDD-NS and controls, suggesting that “mitochondrial alterations could be used as potential signatures to differentiate MDD-S from MDD-NS patients and also from controls.”
The researchers added that the genes found to be dysregulated in suicide represent potential targets for future drug therapies to prevent suicide and could also be used to develop a molecular test to identify individuals at high risk for suicide.
The study was funded by the National Institute of Mental Health, the American Society for Suicide Prevention, and the Pritzker Family Philanthropic Fund. The investigators have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found patients with MDD who died by suicide had a gene expression signature in blood distinct from patients with MDD who died by other means.
The signature included genes involved in stress response changes, including polyamine metabolism, circadian rhythm, immune dysregulation, and telomere maintenance.
“These blood biomarkers are an important step toward developing blood tests to identify patients with imminent risk of ending their lives,” study investigator Adolfo Sequeira, PhD, associate researcher in the department of psychiatry and human behavior, University of California, Irvine, said in a news release.
“To our knowledge, this is the first study to analyze blood and brain samples in a well-defined population of MDDs demonstrating significant differences in gene expression associated with completed suicide,” Dr. Sequeira added.
The findings were published online in Translational Psychiatry.
A pressing challenge
Suicide rates in the United States have jumped by more than 35% over the past 2 decades, with more than 48,000 deaths by suicide occurring just last year. MDD is the most common diagnosis among completed suicides, and identifying individuals at the highest risk for suicide remains a “pressing challenge,” the researchers noted.
They looked for changes in gene expression associated with suicide in archived postmortem blood and brain samples from adults with MDD who died by suicide (MDD-S) or by other means (MDD-NS), as well as a group of controls with no psychiatric illness.
In total, there were blood and brain samples for 45 adults, including 53 blood samples and 69 dorsolateral prefrontal cortex (DLPFC) tissue samples.
In blood, investigators identified 14 genes that significantly differentiated MDD-S from MDD-NS. The top six genes differentially expressed in blood were PER3, MTPAP, SLC25A26, CD19, SOX9, and GAR1.
In addition, four genes showed significant changes in brain and blood between the MDD-S and MDD-NS groups. SOX9 was decreased and PER3 was increased in MDD-S in both blood and brain samples, while CD19 and TERF1 were increased in blood but decreased in DLPFC.
SOX9, an astrocytic marker in the brain and B-cell marker in blood, has been shown to be decreased in MDD-S compared with controls in the prefrontal cortex.
In the current study, researchers found that SOX9 expression was significantly reduced both in blood and brain in MDD-S compared with MDD-NS, “suggesting similar immune/astrocytic dysregulations in suicide that could be further investigated.”
Potential signatures, potential targets
PER3 is a circadian rhythm gene implicated in sleep disorders associated with shifts in circadian rhythms and is thought to increase susceptibility to MDD.
Mutations in PER3 have been shown previously to alter multiple systems, including response to antidepressants; and increased blood expression of PER1 has been linked to suicidality in women, the researchers noted.
There also were significantly higher levels of two inflammatory markers (CD19 and CD6 genes) in blood of MDD-S patients compared to MDD-NS patients.
Another “significant” finding was the involvement of several mitochondrial genes in suicide, the researchers said.
Two nuclear genes coding for mitochondria-located proteins MTPAP (a mitochondrial poly(A) polymerase) and the mitochondrial polyamine transporter SLC25A26 were increased in blood in MDD-S compared with MDD-NS and controls, suggesting that “mitochondrial alterations could be used as potential signatures to differentiate MDD-S from MDD-NS patients and also from controls.”
The researchers added that the genes found to be dysregulated in suicide represent potential targets for future drug therapies to prevent suicide and could also be used to develop a molecular test to identify individuals at high risk for suicide.
The study was funded by the National Institute of Mental Health, the American Society for Suicide Prevention, and the Pritzker Family Philanthropic Fund. The investigators have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM TRANSLATIONAL PSYCHIATRY
New guideline gives active surveillance a boost
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Experts hailed the new guidelines, released May 10 by the American Urological Association (AUA) and the American Society for Radiation Oncology (ASTRO) as a boon for patients with low-risk to favorable intermediate-risk prostate cancers.
“The guideline is unequivocal that AS is the preferred management option for the majority of men with low-risk prostate cancer,” panel chair James A. Eastham, MD, Peter T. Scardino Chair in Oncology and chief of urology at Memorial Sloan Kettering Cancer Center, New York, said in an interview.
The new guideline is the first guideline for localized prostate cancer since 2017.
In the new document, guideline writers merged low-risk patients and very-low-risk patients into a single category of “low-risk.” Dr. Eastham said a distinction between very-low-risk and low-risk is inconsequential since the treatment for the two groups of patients is identical.
The 2022 guideline for the first time makes AS the recommended treatment for select patients with favorable intermediate-risk Gleason 3+4 prostate cancer, he said. The document also provides guidance on how such patients should be selected for AS.
Most research suggests that as many as 40% of patients newly diagnosed with prostate cancer have low-risk disease. Favorable intermediate-risk cancer represents 10%-15% of newly diagnosed patients, said Todd Morgan, MD, the Jack Lapides, MD, Research Professor and chief of urologic oncology at Michigan Medicine, Ann Arbor.
Dr. Morgan, who was not on the AUA/ASTRO panel, called the new recommendations “a very strong update compared to the guideline from 5 years ago.”
The guideline has been pared back some from 2017 to include fewer statements, but it covers several key clinical trials that have appeared over the past 6 years to strengthen the evidence base for the document, he said.
“I would say that we still have to acknowledge that many statements are based on ‘expert opinion’ rather than high-level evidence, which highlights the continued need for well-conducted studies that prove or disprove some of these statements,” Dr. Morgan added.
Patients weighed in
This year, AUA’s advocacy group urged patients to comment on the proposed guideline.
Rick Davis, founder of the AnCan Foundation, a virtual support network for prostate cancer and other diseases, thanked the groups for acknowledging the value of peer support and virtual support groups.
“AnCan congratulates the AUA/ASTRO on endorsing the proper role for the Active Surveillance protocol to manage early low-risk and favorable intermediate-risk prostate cancer and also their qualified and well-supported warnings against focal therapy,” Mr. Davis, who reviewed the guideline, said in an email. “We are, however, disappointed at the lack of a recommendation to provide comprehensive counseling when hormone therapy is prescribed.”
James Schraidt, another patient reviewer for AnCan, said that on balance, the 2022 guideline was an improvement over 2017 and will benefit patients.
He praised AUA/ASTRO for, at the urging of patient reviewers, introducing the “cribriform” and “intraductal” pathology patterns into the guideline for the first time as risk factors.
But he criticized the doctor groups for “a less than fulsome and orderly discussion of the use of MRI. It is not mentioned as a tool that should be used prior to initial biopsy, leaving the door wide open to random biopsies. The recommended role of MRI in AS monitoring was unclear.” He also said the panel should have reviewed micro-ultrasound, an emerging technology, that can be used by itself or to complement MRIs.
Many of the AUA/ASTRO guideline changes involve semantic issues – but which experts said nevertheless were important nuances.
Dr. Eastham said the AUA/ASTRO panel debated and finally settled on the word “preferred” for AS rather than “recommended” or “strongly recommended.”
“This is a very strong statement from the AUA/ASTRO,” Dr. Morgan said. “The semantics are definitely important, but ... ’preferred’ is actually a strong word. For the AUA, what’s really important is the ‘strong recommendation’ and Grade A level of evidence.”
Dr. Morgan also observed that the AS recommendations for patients with low-risk prostate cancer are stronger in the new AUA guideline than those in the latest recommendations from the National Comprehensive Cancer Network (NCCN), which he helped write.
The AUA/ASTRO guideline states that AS is preferred for patients with low-risk cancer, whereas in the NCCN guideline the language is: “preferred for most patients with low-risk disease cancer,” Dr. Morgan said.
“All of these statements ultimately acknowledge what I think that the vast majority of experts agree on – a small proportion of patients with low-risk prostate cancer may appropriately be recommended to undergo primary therapy,” he said.
Dr. Eastham said the goal of the guideline is to persuade surgeons to emphasize that AS is the best choice for most patients with low-risk prostate cancer: “The hope is that surgeons read the guideline. The guideline is definitive in recommending AS in low-risk prostate cancer.”
Dr. Eastham said the new guideline also does the following:
- Further endorses shared decisionmaking, with the understanding that for a decision to be made, both patient and physician need appropriate information regarding the risk posed by the cancer and the risk posed by treatment;
- Endorses selective use of somatic genetic testing when the data are needed for shared decisionmaking;
- Updates a section on genetic testing in patients considered to be at high risk for a germline mutation;
- Updates pretreatment evaluation for patients opting for treatment, primarily the role of imaging and how the evolution of next-generation imaging – such as , a new type of nuclear medicine procedure, in clinically localized prostate cancer;
- Addresses aspects of both radiotherapy and surgery, including nerve sparing, pelvic lymph node dissection, and adjuvant/neoadjuvant therapy, such as chemotherapy or hormone therapy delivered before or after the primary treatment. Dr. Eastham said the “significant evolution” in how best to provide radiotherapy resulted in several changes to this section.
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF UROLOGY
Finding ‘bright lights’: Why family physician continues to love practicing mid-career
A few years ago I tracked down my medical school interviewer to thank him for giving me the opportunity to do what I felt I was called to do. I was surprised that, after 15 years, he actually remembered me and remembered details like walking to the courtyard to meet my father who’d driven me to the interview.
Sharing my gratitude and letting him know I was happy felt important to me.

Choosing to practice family medicine has a lot to do with why I am happy in my career today.
One of my frustrations with health care had been its emphasis on treatment of sickness, rather than a broader one that incorporated prevention of sickness. During my third year of medical school, I was following a family and sports medicine faculty member who was focusing on aspects of lifestyle medicine to help a patient remain active and age gracefully. Seeing opportunities to practice preventative medicine in family medicine made me realize the specialty was the perfect fit for me.
Food as medicine
While participating in rotations I also realized you can find a subspecialty within family medicine.
During my fourth year of medical school, I followed an attending who was seeing a patient for hypertension, prediabetes and hypercholesterolemia. The attending told the patient to eat “healthier,” gave her a handout, and scheduled a follow up appointment for 6 months later.
My thoughts were: “That’s it? That’s how we counsel patients to improve their dietary habits?”
As the patient was leaving the exam room, I asked her what type of oil she cooked with, and I proceeded to share culinary tips from my mother – who was a self-taught and early adopter of the food-as-medicine movement.
Once I started my residency, I knew I’d want to incorporate lifestyle and dietary approaches at many of my patient visits.
I scheduled patients every month to monitor their weight, follow up on chronic conditions, but more importantly, to engage them in their health and empower them to make small lifestyle changes each month and report their efforts. I felt like I was their health coach and cheerleader.
My career in family medicine
Entering the job market allowed me to form my philosophy of treating patients with a mind, body, and spirit approach. I chose to practice value-based care, which aligns with my lifestyle and preventative medicine approach .
I currently practice in a small family medicine–only clinic that is part of a larger multispecialty system. Primary care specialties in my organization are valued, respected and central to a patient’s well being and care. We are encouraged to spend time with patients, assess barriers to care and work collaboratively with our healthcare team, so that preventative medicine approaches take the lead in a patient’s health. This supportive culture and environment is one where my passion for food as medicine has thrived.
One day I forgot to pack a lunch and instead brought a grocery bag of items to make a salad. When I realized I made too much, I sent an email to my staff to get some “free salad in my office.” This serendipitous moment started an informal office “salad club” each week. Continued support from my staff and leadership, allowed me to consider further extending this teaching to my patients and my colleagues.
Three years ago, I helped adopt a sustainable plant-forward menu for our physician meetings, complete with a recipe from the menu for physicians to replicate at home or give to their patients.
I also pursued adoption of shared medical appointments for our medical group. These appointments apply the “see one, do one, teach one” model in medicine, but with culinary medicine as the focus.
Knowing that my patients are all connected to their families through food, I sought this as an opportunity to dive in further with wellness opportunities at their next meal. After almost 2 years of working on this project, I was able to host my first shared medical appointment with a group of patients on March 12, 2020. The next day schools closed, lockdowns occurred, and the world changed.
Opportunities highlighted by the pandemic
We always knew health care was broken but adding the increasingly longer hours and COVID vaccine–hesitant patients that the pandemic brought made everything look dark at times. What has helped me stay hopeful and energetic for system changes is feeling gratitude and seeking bright lights.
My experiences seeing patients in telehealth visits are examples of some of the bright lights I found in the pandemic. During these visits, patients showed me something from their pantry, and we’d go over nutritional labels together.
Additionally, my patients became engaged with their own conditions and wanted to improve them because of news articles highlighting risk factors for COVID-19, such as obesity. I had an active audience when it came to talking about food-as-medicine approaches to improving risk factors and immunity. And since everyone was listening, I didn’t stop at food. I also talked about physical health, stress resiliency, planetary diets, sleep, connections, and lastly vaccines!
Once the vaccines were distributed, I naturally gravitated to having those conversations with patients and colleagues and on social media. Plus, the pandemic gave us moments of simple times to slow down, take more rests, be less overscheduled, consider work-life priorities, and, lastly, to be okay with not being totally okay.
In practicing primary care, we have a unique role in seeing medicine from a whole body, whole person, whole family perspective. There is an opportunity to highlight what is broken in medicine and aim to make it whole.
I’m currently looking at shared medical appointments as a new standard way to provide care to all patients, because it improves access, provides better quality visits and aligns my values, mission, and purpose.
In the midst of the pandemic, I helped advocate for a sustainable plant-forward menu that was launched throughout four different hospitals in the Sharp HealthCare system, in California, in 2020. Knowing that patients were served a menu I played a role in, gave me solace.
As part of the hospital food and nutrition team, I am grateful for the opportunity I have to work on a broader mission to address social determinants of health and seek opportunities to help the system work for our patients.
Public health communication has been lacking in the pandemic, but another bright light is that we were still the trusted messengers to our patients and our communities. I’m continually honored and humbled to be trusted with a whole family’s health.
Dr. Neison practices family medicine and culinary medicine at Sharp Rees-Stealy Medical Group in San Diego, and is cochair of climate and planetary health for SRS Medical Group. You can follow her on Instagram, LinkedIn, and Facebook @Flavors4WellnessMD.
A few years ago I tracked down my medical school interviewer to thank him for giving me the opportunity to do what I felt I was called to do. I was surprised that, after 15 years, he actually remembered me and remembered details like walking to the courtyard to meet my father who’d driven me to the interview.
Sharing my gratitude and letting him know I was happy felt important to me.
Choosing to practice family medicine has a lot to do with why I am happy in my career today.
One of my frustrations with health care had been its emphasis on treatment of sickness, rather than a broader one that incorporated prevention of sickness. During my third year of medical school, I was following a family and sports medicine faculty member who was focusing on aspects of lifestyle medicine to help a patient remain active and age gracefully. Seeing opportunities to practice preventative medicine in family medicine made me realize the specialty was the perfect fit for me.
Food as medicine
While participating in rotations I also realized you can find a subspecialty within family medicine.
During my fourth year of medical school, I followed an attending who was seeing a patient for hypertension, prediabetes and hypercholesterolemia. The attending told the patient to eat “healthier,” gave her a handout, and scheduled a follow up appointment for 6 months later.
My thoughts were: “That’s it? That’s how we counsel patients to improve their dietary habits?”
As the patient was leaving the exam room, I asked her what type of oil she cooked with, and I proceeded to share culinary tips from my mother – who was a self-taught and early adopter of the food-as-medicine movement.
Once I started my residency, I knew I’d want to incorporate lifestyle and dietary approaches at many of my patient visits.
I scheduled patients every month to monitor their weight, follow up on chronic conditions, but more importantly, to engage them in their health and empower them to make small lifestyle changes each month and report their efforts. I felt like I was their health coach and cheerleader.
My career in family medicine
Entering the job market allowed me to form my philosophy of treating patients with a mind, body, and spirit approach. I chose to practice value-based care, which aligns with my lifestyle and preventative medicine approach .
I currently practice in a small family medicine–only clinic that is part of a larger multispecialty system. Primary care specialties in my organization are valued, respected and central to a patient’s well being and care. We are encouraged to spend time with patients, assess barriers to care and work collaboratively with our healthcare team, so that preventative medicine approaches take the lead in a patient’s health. This supportive culture and environment is one where my passion for food as medicine has thrived.
One day I forgot to pack a lunch and instead brought a grocery bag of items to make a salad. When I realized I made too much, I sent an email to my staff to get some “free salad in my office.” This serendipitous moment started an informal office “salad club” each week. Continued support from my staff and leadership, allowed me to consider further extending this teaching to my patients and my colleagues.
Three years ago, I helped adopt a sustainable plant-forward menu for our physician meetings, complete with a recipe from the menu for physicians to replicate at home or give to their patients.
I also pursued adoption of shared medical appointments for our medical group. These appointments apply the “see one, do one, teach one” model in medicine, but with culinary medicine as the focus.
Knowing that my patients are all connected to their families through food, I sought this as an opportunity to dive in further with wellness opportunities at their next meal. After almost 2 years of working on this project, I was able to host my first shared medical appointment with a group of patients on March 12, 2020. The next day schools closed, lockdowns occurred, and the world changed.
Opportunities highlighted by the pandemic
We always knew health care was broken but adding the increasingly longer hours and COVID vaccine–hesitant patients that the pandemic brought made everything look dark at times. What has helped me stay hopeful and energetic for system changes is feeling gratitude and seeking bright lights.
My experiences seeing patients in telehealth visits are examples of some of the bright lights I found in the pandemic. During these visits, patients showed me something from their pantry, and we’d go over nutritional labels together.
Additionally, my patients became engaged with their own conditions and wanted to improve them because of news articles highlighting risk factors for COVID-19, such as obesity. I had an active audience when it came to talking about food-as-medicine approaches to improving risk factors and immunity. And since everyone was listening, I didn’t stop at food. I also talked about physical health, stress resiliency, planetary diets, sleep, connections, and lastly vaccines!
Once the vaccines were distributed, I naturally gravitated to having those conversations with patients and colleagues and on social media. Plus, the pandemic gave us moments of simple times to slow down, take more rests, be less overscheduled, consider work-life priorities, and, lastly, to be okay with not being totally okay.
In practicing primary care, we have a unique role in seeing medicine from a whole body, whole person, whole family perspective. There is an opportunity to highlight what is broken in medicine and aim to make it whole.
I’m currently looking at shared medical appointments as a new standard way to provide care to all patients, because it improves access, provides better quality visits and aligns my values, mission, and purpose.
In the midst of the pandemic, I helped advocate for a sustainable plant-forward menu that was launched throughout four different hospitals in the Sharp HealthCare system, in California, in 2020. Knowing that patients were served a menu I played a role in, gave me solace.
As part of the hospital food and nutrition team, I am grateful for the opportunity I have to work on a broader mission to address social determinants of health and seek opportunities to help the system work for our patients.
Public health communication has been lacking in the pandemic, but another bright light is that we were still the trusted messengers to our patients and our communities. I’m continually honored and humbled to be trusted with a whole family’s health.
Dr. Neison practices family medicine and culinary medicine at Sharp Rees-Stealy Medical Group in San Diego, and is cochair of climate and planetary health for SRS Medical Group. You can follow her on Instagram, LinkedIn, and Facebook @Flavors4WellnessMD.
A few years ago I tracked down my medical school interviewer to thank him for giving me the opportunity to do what I felt I was called to do. I was surprised that, after 15 years, he actually remembered me and remembered details like walking to the courtyard to meet my father who’d driven me to the interview.
Sharing my gratitude and letting him know I was happy felt important to me.
Choosing to practice family medicine has a lot to do with why I am happy in my career today.
One of my frustrations with health care had been its emphasis on treatment of sickness, rather than a broader one that incorporated prevention of sickness. During my third year of medical school, I was following a family and sports medicine faculty member who was focusing on aspects of lifestyle medicine to help a patient remain active and age gracefully. Seeing opportunities to practice preventative medicine in family medicine made me realize the specialty was the perfect fit for me.
Food as medicine
While participating in rotations I also realized you can find a subspecialty within family medicine.
During my fourth year of medical school, I followed an attending who was seeing a patient for hypertension, prediabetes and hypercholesterolemia. The attending told the patient to eat “healthier,” gave her a handout, and scheduled a follow up appointment for 6 months later.
My thoughts were: “That’s it? That’s how we counsel patients to improve their dietary habits?”
As the patient was leaving the exam room, I asked her what type of oil she cooked with, and I proceeded to share culinary tips from my mother – who was a self-taught and early adopter of the food-as-medicine movement.
Once I started my residency, I knew I’d want to incorporate lifestyle and dietary approaches at many of my patient visits.
I scheduled patients every month to monitor their weight, follow up on chronic conditions, but more importantly, to engage them in their health and empower them to make small lifestyle changes each month and report their efforts. I felt like I was their health coach and cheerleader.
My career in family medicine
Entering the job market allowed me to form my philosophy of treating patients with a mind, body, and spirit approach. I chose to practice value-based care, which aligns with my lifestyle and preventative medicine approach .
I currently practice in a small family medicine–only clinic that is part of a larger multispecialty system. Primary care specialties in my organization are valued, respected and central to a patient’s well being and care. We are encouraged to spend time with patients, assess barriers to care and work collaboratively with our healthcare team, so that preventative medicine approaches take the lead in a patient’s health. This supportive culture and environment is one where my passion for food as medicine has thrived.
One day I forgot to pack a lunch and instead brought a grocery bag of items to make a salad. When I realized I made too much, I sent an email to my staff to get some “free salad in my office.” This serendipitous moment started an informal office “salad club” each week. Continued support from my staff and leadership, allowed me to consider further extending this teaching to my patients and my colleagues.
Three years ago, I helped adopt a sustainable plant-forward menu for our physician meetings, complete with a recipe from the menu for physicians to replicate at home or give to their patients.
I also pursued adoption of shared medical appointments for our medical group. These appointments apply the “see one, do one, teach one” model in medicine, but with culinary medicine as the focus.
Knowing that my patients are all connected to their families through food, I sought this as an opportunity to dive in further with wellness opportunities at their next meal. After almost 2 years of working on this project, I was able to host my first shared medical appointment with a group of patients on March 12, 2020. The next day schools closed, lockdowns occurred, and the world changed.
Opportunities highlighted by the pandemic
We always knew health care was broken but adding the increasingly longer hours and COVID vaccine–hesitant patients that the pandemic brought made everything look dark at times. What has helped me stay hopeful and energetic for system changes is feeling gratitude and seeking bright lights.
My experiences seeing patients in telehealth visits are examples of some of the bright lights I found in the pandemic. During these visits, patients showed me something from their pantry, and we’d go over nutritional labels together.
Additionally, my patients became engaged with their own conditions and wanted to improve them because of news articles highlighting risk factors for COVID-19, such as obesity. I had an active audience when it came to talking about food-as-medicine approaches to improving risk factors and immunity. And since everyone was listening, I didn’t stop at food. I also talked about physical health, stress resiliency, planetary diets, sleep, connections, and lastly vaccines!
Once the vaccines were distributed, I naturally gravitated to having those conversations with patients and colleagues and on social media. Plus, the pandemic gave us moments of simple times to slow down, take more rests, be less overscheduled, consider work-life priorities, and, lastly, to be okay with not being totally okay.
In practicing primary care, we have a unique role in seeing medicine from a whole body, whole person, whole family perspective. There is an opportunity to highlight what is broken in medicine and aim to make it whole.
I’m currently looking at shared medical appointments as a new standard way to provide care to all patients, because it improves access, provides better quality visits and aligns my values, mission, and purpose.
In the midst of the pandemic, I helped advocate for a sustainable plant-forward menu that was launched throughout four different hospitals in the Sharp HealthCare system, in California, in 2020. Knowing that patients were served a menu I played a role in, gave me solace.
As part of the hospital food and nutrition team, I am grateful for the opportunity I have to work on a broader mission to address social determinants of health and seek opportunities to help the system work for our patients.
Public health communication has been lacking in the pandemic, but another bright light is that we were still the trusted messengers to our patients and our communities. I’m continually honored and humbled to be trusted with a whole family’s health.
Dr. Neison practices family medicine and culinary medicine at Sharp Rees-Stealy Medical Group in San Diego, and is cochair of climate and planetary health for SRS Medical Group. You can follow her on Instagram, LinkedIn, and Facebook @Flavors4WellnessMD.