User login
The mother’s double jeopardy
Jamestown, Colo., is a small mountain town several miles up through Lefthand Canyon out of Boulder, in the Rocky Mountains. The canyon roads are steep, winding, and narrow, and peopled by brightly clad cyclists struggling up the hill and flying down faster than the cars. The road through Jamestown is dusty in the summer with brightly colored oil barrels strategically placed in the middle of the single road through town. Slashed across their sides: “SLOW DOWN! Watch out for our feral children!”
Wild child or hothouse child? What is the best choice? Women bear the brunt of this deciding, whether they are working outside of the home, or stay-at-home caregivers, or both. Women know they will be blamed if they get it wrong.

Society has exacted a tall order on women who choose to have children. Patriarchal norms ask (White) women who choose both to work and have children, if they are really a “stay-at-home” mother who must work, or a “working” mother who prefers work over their children. The underlying attitude can be read as: “Are you someone who prioritizes paid work over caregiving, or are you someone who prioritizes caregiving over work?” You may be seen as a bad mother if you prioritize work over the welfare of your child. If you prioritize your child over your work, then you are not a reliable, dedicated worker. The working mother can’t win.
Woman’s central question is what kind of mother should I be? Mothers struggle with this question all their lives; when their child has difficulties, society’s question is what did you do wrong with your child? Mothers internalize the standard of the “good mother” and are aware of each minor transgression that depicts them as the “bad mother.” It is hard to escape the impossible perfectionistic standard of the good mother. But perhaps it has come time to push back on the moral imbalance.
Internalized sexism
As women move out of the home into the workplace, the societal pressures to maintain the status quo bear down on women, trying to keep them in their place.
Social pressures employ subtle “technologies of the self,” so that women – as any oppressed group – learn to internalize these technologies, and monitor themselves.1 This is now widely accepted as internalized sexism, whereby women feel that they are not good enough, do not have the right qualifications, and are “less” than the dominant group (men). This phenomenon is also recognized when racial and ethnic biases are assimilated unconsciously, as internalized racism. Should we also have internalized “momism”?
Women are caught between trying to claim their individualism as well as feeling the responsibility to be the self-denying mother. Everyone has an opinion about the place of women. Conservative activist Phyllis Schlafly considered “women’s lib” to be un-American, citing women in the military and the establishment of federal day care centers as actions of a communist state. A similar ideology helped form the antifeminist organization Concerned Women for America, which self-reports that it is the largest American public policy women’s organization. Formed in opposition to the National Organization for Women, CWA is focused on maintaining the traditional family, as understood by (White) evangelical Christians.
An example similar to CWA is the Council of Biblical Manhood and Womanhood. It was established to help evangelical Christian churches defend themselves against an accommodation of secular feminism and also against evangelical feminism (which pushes for more equality in the church). It promotes complementarianism – the idea that masculinity and femininity are ordained by God and that men and women are created to complement each other.
At the other extreme, the most radical of feminists believe in the need to create a women-only society where women would be free from the patriarchy. Less angry but decidedly weirder are the feminists called “FEMEN” who once staged a protest at the Vatican where topless women feigned intercourse with crucifixes, chanting slogans against the pope and religion.
Most women tread a path between extremes, a path which is difficult and lonely. Without a firm ideology, this path is strewn with doubts and pitfalls. Some career-oriented women who have delayed motherhood, knowing that they will soon be biologically past their peak and possibly also without a partner, wonder if they should become single mothers using sperm donation. For many women, the workplace does not offer much help with maternity leave or childcare. Even when maternity leave is available, there is a still a lack of understanding about what is needed.
“Think of it as caregiver bias. If you just extend maternity leave, what is implied is that you’re still expecting me to be the primary source of care for my child, when in fact my partner wants to share the load and will need support to do so as well,” said Pamela Culpepper, an expert in corporate diversity and inclusion.2
Intensive mothering
When the glamor of the workplace wears off and/or when the misogyny and the harassment become too much, women who have the financial stability may decide to return to the role of the stay-at-home mother. Perhaps, in the home, she can feel fulfilled. Yet, young American urban and suburban mothers now parent under a new name – “intensive mothering.”
Conducting in-depth interviews of 38 women of diverse backgrounds in the United States, Sharon Hays found women describing their 2- to 4-year-old children as innocent and priceless, and believing that they – the mothers – should be primarily responsible for rearing their children, using “child-rearing methods that are child centered, expert guided, emotionally absorbing, labor intensive, and financially expensive.”3 Ms. Hays clarified four beliefs that were common to all the women in the study: mothers are more suitable caregivers than fathers; mothering should be child centered; parenting consists of a set of skills that need to be learned; and parenting is labor-intensive but an emotionally fulfilling activity.
Hays wondered if this type of mothering developed as the last defense against “the impoverishment of social ties, communal obligations and unremunerated commitments.”3 She suggested that women succumbing to social pressures to return to the home is yet another example of how society is set up to benefit men, capitalism, political leaders, and those who try to maintain a “traditional” form of family life.3 Ms. Hays concluded that the practice of intensive mothering is a class-based practice of privileged white women, entangled with capitalism in that the buying of “essential” baby products is equated with good mothering. She found this ideology to be oppressive of all women, regardless of their social class, ethnic background, household composition, and financial situation. Ms. Hays noted that many women experience guilt for not matching up to these ideals.
In “Dead End Feminism,” Elisabeth Badinter asks if the upheaval in the role of women has caused so much uncertainty that it is easier for women to regress to a time when they were in the home and knew themselves as mothers. They ask if this has been reinforced by the movement to embrace all things natural, eschewing the falseness of chemicals and other things that threaten Mother Earth.4
There is no escaping the power of the mother: she will continue to symbolize all that is good and bad as the embodiment of the Mother Archetype. All of this is the background against which you will see the new mother in the family. She will not articulate her dilemma, that is your role as the family psychiatrist.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose. Contact Dr. Heru at [email protected].
References
1. Martin LH et al (eds.). Technologies of the Self: A Seminar with Michel Foucault. University of Massachusetts Press: Amherst, Mass.: University of Massachusetts Press, 2022.
2. How Pamela Culpepper Is Changing The Narrative Of Women In The Workplace. Huffpost. 2020 Mar 6. https://www.huffpost.com/entry/pamela-culpepper-diversity-inclusion-empowerment_n_5e56b6ffc5b62e9dc7dbc307.
3. Hays S. Cultural Contradictions of Motherhood. Yale University Press: New Haven, Conn.: Yale University Press, 1996.
4. Badinter E. (translated by Borossa J). Dead End Feminism. Malden, Mass.: Polity Press, 2006.
Jamestown, Colo., is a small mountain town several miles up through Lefthand Canyon out of Boulder, in the Rocky Mountains. The canyon roads are steep, winding, and narrow, and peopled by brightly clad cyclists struggling up the hill and flying down faster than the cars. The road through Jamestown is dusty in the summer with brightly colored oil barrels strategically placed in the middle of the single road through town. Slashed across their sides: “SLOW DOWN! Watch out for our feral children!”
Wild child or hothouse child? What is the best choice? Women bear the brunt of this deciding, whether they are working outside of the home, or stay-at-home caregivers, or both. Women know they will be blamed if they get it wrong.
Society has exacted a tall order on women who choose to have children. Patriarchal norms ask (White) women who choose both to work and have children, if they are really a “stay-at-home” mother who must work, or a “working” mother who prefers work over their children. The underlying attitude can be read as: “Are you someone who prioritizes paid work over caregiving, or are you someone who prioritizes caregiving over work?” You may be seen as a bad mother if you prioritize work over the welfare of your child. If you prioritize your child over your work, then you are not a reliable, dedicated worker. The working mother can’t win.
Woman’s central question is what kind of mother should I be? Mothers struggle with this question all their lives; when their child has difficulties, society’s question is what did you do wrong with your child? Mothers internalize the standard of the “good mother” and are aware of each minor transgression that depicts them as the “bad mother.” It is hard to escape the impossible perfectionistic standard of the good mother. But perhaps it has come time to push back on the moral imbalance.
Internalized sexism
As women move out of the home into the workplace, the societal pressures to maintain the status quo bear down on women, trying to keep them in their place.
Social pressures employ subtle “technologies of the self,” so that women – as any oppressed group – learn to internalize these technologies, and monitor themselves.1 This is now widely accepted as internalized sexism, whereby women feel that they are not good enough, do not have the right qualifications, and are “less” than the dominant group (men). This phenomenon is also recognized when racial and ethnic biases are assimilated unconsciously, as internalized racism. Should we also have internalized “momism”?
Women are caught between trying to claim their individualism as well as feeling the responsibility to be the self-denying mother. Everyone has an opinion about the place of women. Conservative activist Phyllis Schlafly considered “women’s lib” to be un-American, citing women in the military and the establishment of federal day care centers as actions of a communist state. A similar ideology helped form the antifeminist organization Concerned Women for America, which self-reports that it is the largest American public policy women’s organization. Formed in opposition to the National Organization for Women, CWA is focused on maintaining the traditional family, as understood by (White) evangelical Christians.
An example similar to CWA is the Council of Biblical Manhood and Womanhood. It was established to help evangelical Christian churches defend themselves against an accommodation of secular feminism and also against evangelical feminism (which pushes for more equality in the church). It promotes complementarianism – the idea that masculinity and femininity are ordained by God and that men and women are created to complement each other.
At the other extreme, the most radical of feminists believe in the need to create a women-only society where women would be free from the patriarchy. Less angry but decidedly weirder are the feminists called “FEMEN” who once staged a protest at the Vatican where topless women feigned intercourse with crucifixes, chanting slogans against the pope and religion.
Most women tread a path between extremes, a path which is difficult and lonely. Without a firm ideology, this path is strewn with doubts and pitfalls. Some career-oriented women who have delayed motherhood, knowing that they will soon be biologically past their peak and possibly also without a partner, wonder if they should become single mothers using sperm donation. For many women, the workplace does not offer much help with maternity leave or childcare. Even when maternity leave is available, there is a still a lack of understanding about what is needed.
“Think of it as caregiver bias. If you just extend maternity leave, what is implied is that you’re still expecting me to be the primary source of care for my child, when in fact my partner wants to share the load and will need support to do so as well,” said Pamela Culpepper, an expert in corporate diversity and inclusion.2
Intensive mothering
When the glamor of the workplace wears off and/or when the misogyny and the harassment become too much, women who have the financial stability may decide to return to the role of the stay-at-home mother. Perhaps, in the home, she can feel fulfilled. Yet, young American urban and suburban mothers now parent under a new name – “intensive mothering.”
Conducting in-depth interviews of 38 women of diverse backgrounds in the United States, Sharon Hays found women describing their 2- to 4-year-old children as innocent and priceless, and believing that they – the mothers – should be primarily responsible for rearing their children, using “child-rearing methods that are child centered, expert guided, emotionally absorbing, labor intensive, and financially expensive.”3 Ms. Hays clarified four beliefs that were common to all the women in the study: mothers are more suitable caregivers than fathers; mothering should be child centered; parenting consists of a set of skills that need to be learned; and parenting is labor-intensive but an emotionally fulfilling activity.
Hays wondered if this type of mothering developed as the last defense against “the impoverishment of social ties, communal obligations and unremunerated commitments.”3 She suggested that women succumbing to social pressures to return to the home is yet another example of how society is set up to benefit men, capitalism, political leaders, and those who try to maintain a “traditional” form of family life.3 Ms. Hays concluded that the practice of intensive mothering is a class-based practice of privileged white women, entangled with capitalism in that the buying of “essential” baby products is equated with good mothering. She found this ideology to be oppressive of all women, regardless of their social class, ethnic background, household composition, and financial situation. Ms. Hays noted that many women experience guilt for not matching up to these ideals.
In “Dead End Feminism,” Elisabeth Badinter asks if the upheaval in the role of women has caused so much uncertainty that it is easier for women to regress to a time when they were in the home and knew themselves as mothers. They ask if this has been reinforced by the movement to embrace all things natural, eschewing the falseness of chemicals and other things that threaten Mother Earth.4
There is no escaping the power of the mother: she will continue to symbolize all that is good and bad as the embodiment of the Mother Archetype. All of this is the background against which you will see the new mother in the family. She will not articulate her dilemma, that is your role as the family psychiatrist.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose. Contact Dr. Heru at [email protected].
References
1. Martin LH et al (eds.). Technologies of the Self: A Seminar with Michel Foucault. University of Massachusetts Press: Amherst, Mass.: University of Massachusetts Press, 2022.
2. How Pamela Culpepper Is Changing The Narrative Of Women In The Workplace. Huffpost. 2020 Mar 6. https://www.huffpost.com/entry/pamela-culpepper-diversity-inclusion-empowerment_n_5e56b6ffc5b62e9dc7dbc307.
3. Hays S. Cultural Contradictions of Motherhood. Yale University Press: New Haven, Conn.: Yale University Press, 1996.
4. Badinter E. (translated by Borossa J). Dead End Feminism. Malden, Mass.: Polity Press, 2006.
Jamestown, Colo., is a small mountain town several miles up through Lefthand Canyon out of Boulder, in the Rocky Mountains. The canyon roads are steep, winding, and narrow, and peopled by brightly clad cyclists struggling up the hill and flying down faster than the cars. The road through Jamestown is dusty in the summer with brightly colored oil barrels strategically placed in the middle of the single road through town. Slashed across their sides: “SLOW DOWN! Watch out for our feral children!”
Wild child or hothouse child? What is the best choice? Women bear the brunt of this deciding, whether they are working outside of the home, or stay-at-home caregivers, or both. Women know they will be blamed if they get it wrong.
Society has exacted a tall order on women who choose to have children. Patriarchal norms ask (White) women who choose both to work and have children, if they are really a “stay-at-home” mother who must work, or a “working” mother who prefers work over their children. The underlying attitude can be read as: “Are you someone who prioritizes paid work over caregiving, or are you someone who prioritizes caregiving over work?” You may be seen as a bad mother if you prioritize work over the welfare of your child. If you prioritize your child over your work, then you are not a reliable, dedicated worker. The working mother can’t win.
Woman’s central question is what kind of mother should I be? Mothers struggle with this question all their lives; when their child has difficulties, society’s question is what did you do wrong with your child? Mothers internalize the standard of the “good mother” and are aware of each minor transgression that depicts them as the “bad mother.” It is hard to escape the impossible perfectionistic standard of the good mother. But perhaps it has come time to push back on the moral imbalance.
Internalized sexism
As women move out of the home into the workplace, the societal pressures to maintain the status quo bear down on women, trying to keep them in their place.
Social pressures employ subtle “technologies of the self,” so that women – as any oppressed group – learn to internalize these technologies, and monitor themselves.1 This is now widely accepted as internalized sexism, whereby women feel that they are not good enough, do not have the right qualifications, and are “less” than the dominant group (men). This phenomenon is also recognized when racial and ethnic biases are assimilated unconsciously, as internalized racism. Should we also have internalized “momism”?
Women are caught between trying to claim their individualism as well as feeling the responsibility to be the self-denying mother. Everyone has an opinion about the place of women. Conservative activist Phyllis Schlafly considered “women’s lib” to be un-American, citing women in the military and the establishment of federal day care centers as actions of a communist state. A similar ideology helped form the antifeminist organization Concerned Women for America, which self-reports that it is the largest American public policy women’s organization. Formed in opposition to the National Organization for Women, CWA is focused on maintaining the traditional family, as understood by (White) evangelical Christians.
An example similar to CWA is the Council of Biblical Manhood and Womanhood. It was established to help evangelical Christian churches defend themselves against an accommodation of secular feminism and also against evangelical feminism (which pushes for more equality in the church). It promotes complementarianism – the idea that masculinity and femininity are ordained by God and that men and women are created to complement each other.
At the other extreme, the most radical of feminists believe in the need to create a women-only society where women would be free from the patriarchy. Less angry but decidedly weirder are the feminists called “FEMEN” who once staged a protest at the Vatican where topless women feigned intercourse with crucifixes, chanting slogans against the pope and religion.
Most women tread a path between extremes, a path which is difficult and lonely. Without a firm ideology, this path is strewn with doubts and pitfalls. Some career-oriented women who have delayed motherhood, knowing that they will soon be biologically past their peak and possibly also without a partner, wonder if they should become single mothers using sperm donation. For many women, the workplace does not offer much help with maternity leave or childcare. Even when maternity leave is available, there is a still a lack of understanding about what is needed.
“Think of it as caregiver bias. If you just extend maternity leave, what is implied is that you’re still expecting me to be the primary source of care for my child, when in fact my partner wants to share the load and will need support to do so as well,” said Pamela Culpepper, an expert in corporate diversity and inclusion.2
Intensive mothering
When the glamor of the workplace wears off and/or when the misogyny and the harassment become too much, women who have the financial stability may decide to return to the role of the stay-at-home mother. Perhaps, in the home, she can feel fulfilled. Yet, young American urban and suburban mothers now parent under a new name – “intensive mothering.”
Conducting in-depth interviews of 38 women of diverse backgrounds in the United States, Sharon Hays found women describing their 2- to 4-year-old children as innocent and priceless, and believing that they – the mothers – should be primarily responsible for rearing their children, using “child-rearing methods that are child centered, expert guided, emotionally absorbing, labor intensive, and financially expensive.”3 Ms. Hays clarified four beliefs that were common to all the women in the study: mothers are more suitable caregivers than fathers; mothering should be child centered; parenting consists of a set of skills that need to be learned; and parenting is labor-intensive but an emotionally fulfilling activity.
Hays wondered if this type of mothering developed as the last defense against “the impoverishment of social ties, communal obligations and unremunerated commitments.”3 She suggested that women succumbing to social pressures to return to the home is yet another example of how society is set up to benefit men, capitalism, political leaders, and those who try to maintain a “traditional” form of family life.3 Ms. Hays concluded that the practice of intensive mothering is a class-based practice of privileged white women, entangled with capitalism in that the buying of “essential” baby products is equated with good mothering. She found this ideology to be oppressive of all women, regardless of their social class, ethnic background, household composition, and financial situation. Ms. Hays noted that many women experience guilt for not matching up to these ideals.
In “Dead End Feminism,” Elisabeth Badinter asks if the upheaval in the role of women has caused so much uncertainty that it is easier for women to regress to a time when they were in the home and knew themselves as mothers. They ask if this has been reinforced by the movement to embrace all things natural, eschewing the falseness of chemicals and other things that threaten Mother Earth.4
There is no escaping the power of the mother: she will continue to symbolize all that is good and bad as the embodiment of the Mother Archetype. All of this is the background against which you will see the new mother in the family. She will not articulate her dilemma, that is your role as the family psychiatrist.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose. Contact Dr. Heru at [email protected].
References
1. Martin LH et al (eds.). Technologies of the Self: A Seminar with Michel Foucault. University of Massachusetts Press: Amherst, Mass.: University of Massachusetts Press, 2022.
2. How Pamela Culpepper Is Changing The Narrative Of Women In The Workplace. Huffpost. 2020 Mar 6. https://www.huffpost.com/entry/pamela-culpepper-diversity-inclusion-empowerment_n_5e56b6ffc5b62e9dc7dbc307.
3. Hays S. Cultural Contradictions of Motherhood. Yale University Press: New Haven, Conn.: Yale University Press, 1996.
4. Badinter E. (translated by Borossa J). Dead End Feminism. Malden, Mass.: Polity Press, 2006.
Pediatricians’ incomes rose faster than most specialties in 2021: Survey
In an unprecedented year when income increased for all specialties, pediatricians did better than most, according to a recent survey by Medscape.
. Medscape also noted that, for the first time in the 11 years it’s been conducting these physician compensation surveys, “all specialties have seen an increase in income.”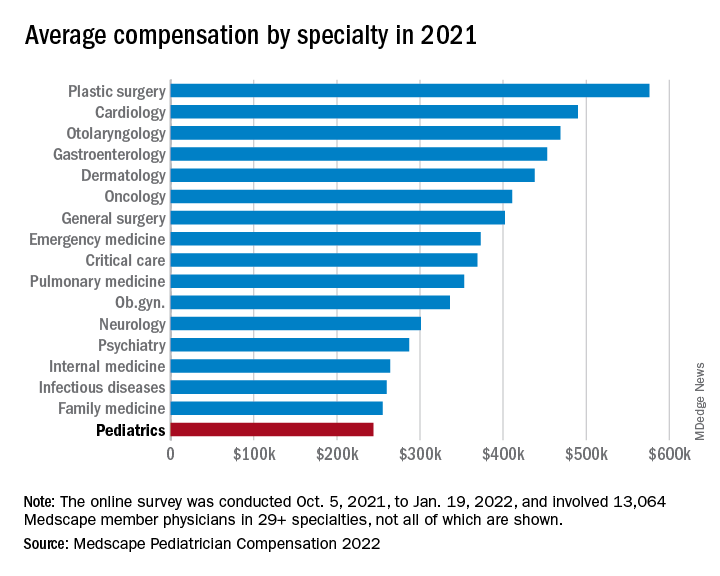
At least some of that positive news can be traced back to the reduced impact of COVID-19. “Compensation for most physicians is trending back up as demand for physicians accelerates. The market for physicians has done a complete 180 over just 7 or 8 months,” James Taylor of AMN Healthcare’s physician and leadership solutions division said in Medscape Pediatrician Compensation Report 2022.
The 10% increase in pediatricians’ income, however, was not enough to reach the average for primary care physicians, $260,000, which was up by 7.4% over 2020. It was enough, though, to move pediatricians from the bottom of the earnings-by-specialty list, where they were last year, to next-to-last this year (public health/preventive medicine, with average earnings of $243,000 in 2021, is not shown in the graph).
The gender gap in earnings left male pediatricians’ income 26% higher than their female counterparts, slightly above the gap of 25% for primary care physicians and 24% for all physicians. For specialists, the gap was 31% in favor of men, based on data from 13,064 Medscape member physicians who participated in the survey, which was conducted online from Oct. 5, 2021, to Jan. 19, 2022. For the record, 57% of the pediatricians who responded were women.
The gaps and low income averages were enough, it seems, to keep pediatricians fairly negative regarding their feelings on compensation. Only 47% think they were fairly compensated in 2021, higher only than diabetes/endocrinology and nephrology. Among the other primary care specialties, internal medicine and ob.gyn. were slightly higher at 49% and family medicine was 55% – still just middle of the pack, compared with public health/preventive medicine at 72%, Medscape said in the report.
Would you do it again?
Moving to the less-economic aspects of the survey, respondents also were asked if they would choose medicine again as a career. Once more pediatricians were low on the scale, as only 70% said that they would enter medicine again, down from 77% last year and lower than this year’s average of 73% average for all physicians.
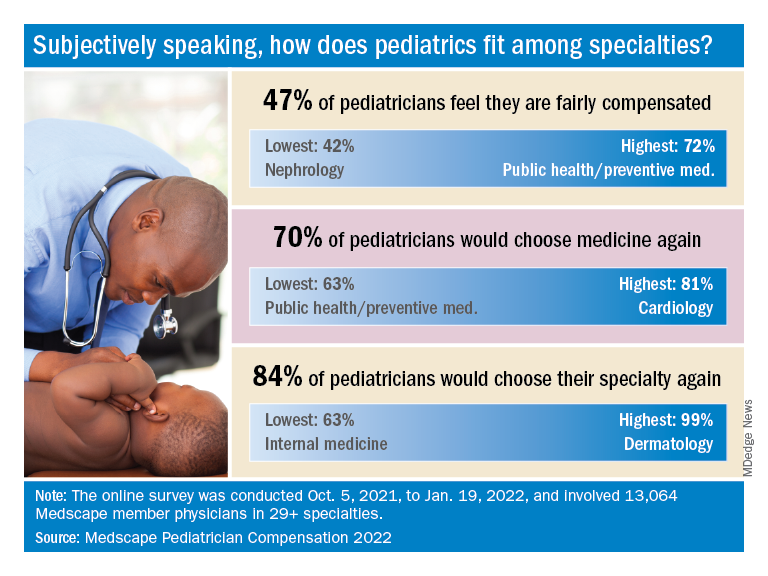
When they were asked if they would choose pediatrics again as a specialty, the response was a bit more positive: 84% said yes. That middle-of-the-pack showing was well ahead of internal medicine (63%) and family medicine (68%), but well below dermatology (99%) and orthopedics (97%), which are “among the top groups in our survey year after year,” Medscape said.
Did the administrative challenges of medical practice have an effect on those answers? Pediatrician respondents said that they spend 14.9 hours per week on paperwork and administration, close to the average of 15.5 hours for all physicians. The internists, who are least likely to choose their original specialty again, spend 18.7 hours on paperwork each week, while dermatologists, the most likely to repeat their first choice, have just 11.9 hours of paperwork per week.
The exact number of pediatricians involved in the survey was not provided, but they made up about 8% of the total cohort, which works out to somewhere between 1,000 and 1,100 individuals. All respondents had to be practicing in the United States, and compensation was analyzed for full-time physicians only. The sampling error is ±0.86% at a 95% confidence level.
In an unprecedented year when income increased for all specialties, pediatricians did better than most, according to a recent survey by Medscape.
. Medscape also noted that, for the first time in the 11 years it’s been conducting these physician compensation surveys, “all specialties have seen an increase in income.”
At least some of that positive news can be traced back to the reduced impact of COVID-19. “Compensation for most physicians is trending back up as demand for physicians accelerates. The market for physicians has done a complete 180 over just 7 or 8 months,” James Taylor of AMN Healthcare’s physician and leadership solutions division said in Medscape Pediatrician Compensation Report 2022.
The 10% increase in pediatricians’ income, however, was not enough to reach the average for primary care physicians, $260,000, which was up by 7.4% over 2020. It was enough, though, to move pediatricians from the bottom of the earnings-by-specialty list, where they were last year, to next-to-last this year (public health/preventive medicine, with average earnings of $243,000 in 2021, is not shown in the graph).
The gender gap in earnings left male pediatricians’ income 26% higher than their female counterparts, slightly above the gap of 25% for primary care physicians and 24% for all physicians. For specialists, the gap was 31% in favor of men, based on data from 13,064 Medscape member physicians who participated in the survey, which was conducted online from Oct. 5, 2021, to Jan. 19, 2022. For the record, 57% of the pediatricians who responded were women.
The gaps and low income averages were enough, it seems, to keep pediatricians fairly negative regarding their feelings on compensation. Only 47% think they were fairly compensated in 2021, higher only than diabetes/endocrinology and nephrology. Among the other primary care specialties, internal medicine and ob.gyn. were slightly higher at 49% and family medicine was 55% – still just middle of the pack, compared with public health/preventive medicine at 72%, Medscape said in the report.
Would you do it again?
Moving to the less-economic aspects of the survey, respondents also were asked if they would choose medicine again as a career. Once more pediatricians were low on the scale, as only 70% said that they would enter medicine again, down from 77% last year and lower than this year’s average of 73% average for all physicians.
When they were asked if they would choose pediatrics again as a specialty, the response was a bit more positive: 84% said yes. That middle-of-the-pack showing was well ahead of internal medicine (63%) and family medicine (68%), but well below dermatology (99%) and orthopedics (97%), which are “among the top groups in our survey year after year,” Medscape said.
Did the administrative challenges of medical practice have an effect on those answers? Pediatrician respondents said that they spend 14.9 hours per week on paperwork and administration, close to the average of 15.5 hours for all physicians. The internists, who are least likely to choose their original specialty again, spend 18.7 hours on paperwork each week, while dermatologists, the most likely to repeat their first choice, have just 11.9 hours of paperwork per week.
The exact number of pediatricians involved in the survey was not provided, but they made up about 8% of the total cohort, which works out to somewhere between 1,000 and 1,100 individuals. All respondents had to be practicing in the United States, and compensation was analyzed for full-time physicians only. The sampling error is ±0.86% at a 95% confidence level.
In an unprecedented year when income increased for all specialties, pediatricians did better than most, according to a recent survey by Medscape.
. Medscape also noted that, for the first time in the 11 years it’s been conducting these physician compensation surveys, “all specialties have seen an increase in income.”
At least some of that positive news can be traced back to the reduced impact of COVID-19. “Compensation for most physicians is trending back up as demand for physicians accelerates. The market for physicians has done a complete 180 over just 7 or 8 months,” James Taylor of AMN Healthcare’s physician and leadership solutions division said in Medscape Pediatrician Compensation Report 2022.
The 10% increase in pediatricians’ income, however, was not enough to reach the average for primary care physicians, $260,000, which was up by 7.4% over 2020. It was enough, though, to move pediatricians from the bottom of the earnings-by-specialty list, where they were last year, to next-to-last this year (public health/preventive medicine, with average earnings of $243,000 in 2021, is not shown in the graph).
The gender gap in earnings left male pediatricians’ income 26% higher than their female counterparts, slightly above the gap of 25% for primary care physicians and 24% for all physicians. For specialists, the gap was 31% in favor of men, based on data from 13,064 Medscape member physicians who participated in the survey, which was conducted online from Oct. 5, 2021, to Jan. 19, 2022. For the record, 57% of the pediatricians who responded were women.
The gaps and low income averages were enough, it seems, to keep pediatricians fairly negative regarding their feelings on compensation. Only 47% think they were fairly compensated in 2021, higher only than diabetes/endocrinology and nephrology. Among the other primary care specialties, internal medicine and ob.gyn. were slightly higher at 49% and family medicine was 55% – still just middle of the pack, compared with public health/preventive medicine at 72%, Medscape said in the report.
Would you do it again?
Moving to the less-economic aspects of the survey, respondents also were asked if they would choose medicine again as a career. Once more pediatricians were low on the scale, as only 70% said that they would enter medicine again, down from 77% last year and lower than this year’s average of 73% average for all physicians.
When they were asked if they would choose pediatrics again as a specialty, the response was a bit more positive: 84% said yes. That middle-of-the-pack showing was well ahead of internal medicine (63%) and family medicine (68%), but well below dermatology (99%) and orthopedics (97%), which are “among the top groups in our survey year after year,” Medscape said.
Did the administrative challenges of medical practice have an effect on those answers? Pediatrician respondents said that they spend 14.9 hours per week on paperwork and administration, close to the average of 15.5 hours for all physicians. The internists, who are least likely to choose their original specialty again, spend 18.7 hours on paperwork each week, while dermatologists, the most likely to repeat their first choice, have just 11.9 hours of paperwork per week.
The exact number of pediatricians involved in the survey was not provided, but they made up about 8% of the total cohort, which works out to somewhere between 1,000 and 1,100 individuals. All respondents had to be practicing in the United States, and compensation was analyzed for full-time physicians only. The sampling error is ±0.86% at a 95% confidence level.
Hormone therapy and breast cancer: An overview
It is projected that by 2050, 1.6 billion women in the world will have reached menopause or the postmenopausal period, a significant increase, compared with a billion women in 2020. Of all menopausal women, around 75% are affected by troublesome menopause symptoms, such as hot flashes and night sweats.
Around 84% of postmenopausal women experience genitourinary symptoms, such as vulvovaginal atrophy and incontinence.
Menopausal hormone therapy (MHT) is the most effective treatment for managing these symptoms; however, its effects on numerous aspects of female health remain uncertain, in particular with regard to breast cancer. The influence of MHT on breast cancer remains unsettled, with discordant findings from observational studies and randomized clinical trials, a factor that affects the decisions made by doctors concerning hormone therapy in menopausal women.
Background
Conjugated equine estrogens (CEEs) were introduced into clinical practice in the 1940s. For decades, MHT was the main treatment in conventional medicine for the symptoms of menopause. MHT was used in Western countries for about 600 million women starting from 1970, and it progressively increased during the 1990s. Professional organizations recommended MHT for the prevention of osteoporosis and chronic heart disease (CHD), and a third of prescriptions were for women older than 60 years.
Against this background, the National Institutes of Health launched randomized trials of MHT through the Women’s Health Initiative (WHI) to test whether the association with reduced risk for CHD found in observational studies was real and to obtain reliable information on the overall risks and benefits regarding the prevention of chronic disease for postmenopausal women aged 50-79 years.
The WHI trials tested standard-dose oral CEEs with and without standard-dose continuous medroxyprogesterone acetate (EPT). In 2002, the results of the WHI studies raised a series of concerns about the long-term safety of MHT, in particular the finding of an increased risk of breast cancer for women undergoing therapy. That risk exceeded the benefits from reductions in hip fractures and colorectal cancer.
The WHI findings received wide attention. Prescriptions for MHT dropped precipitously after 2002 and continued to decline in subsequent years. Declines were most marked for standard-dose EPT and in older women. The results of the CEE study were less negative, compared with those for EPT, as they showed no effect on CHD, a nonsignificant reduction in the risk of breast cancer, and a more favorable risk-benefit ratio for younger women, compared with older women. A decade later, it had become widely accepted that MHT should not be used for the prevention of chronic disease in older women; however, short-term use for treatment of vasomotor symptoms remains an accepted indication.
Risks and outcomes
Emerging from a series of WHI reports are complex models on the effect of hormonal therapy on the risk and outcome of breast cancer. In one study, women with an intact uterus received CEEs plus medroxyprogesterone acetate (MPA). An increase in the risk of breast cancer was observed over a median of 5.6 years of treatment, followed by a moderate reduction, with the risk increasing after 13 years of cumulative follow-up. For women treated with CEE alone, the reduction in risk observed over an average of 7.2 years of treatment was maintained for 13 years of follow-up.
Results from observational studies contrast with those from randomized controlled trials, particularly those concerning the use of estrogens only. A meta-analysis by the Collaborative Group on Hormonal Factors in Breast Cancer showed that both EPT and CEE were associated with a higher risk of breast neoplasia. Results of the Million Women Study showed a higher death rate.
Treatment methods and duration
Information from prospective studies on the effects of commencing MHT at various ages between 40 and 59 years show that for women who commenced treatment at any time within this age range, the relative risk was similar and was highly significant for all ages. Few women had started MHT treatment well after menopause at ages 60-69 years, and their excess risks during years 5-14 of current use were significant for estrogen-progestogen but not for estrogen-only MHT.
If these associations are largely causal, then for women of average weight in developed countries, 5 years of MHT, starting at age 50 years, would increase breast cancer incidence at ages 50-69 years by about 1 in every 50 users of estrogen plus daily progestogen preparations; 1 in every 70 users of estrogen plus intermittent progestogen preparations; and 1 in every 200 users of estrogen-only preparations. The corresponding excesses from 10 years of MHT would be about twice as great.
During 5-14 years of MHT use, the RRs were similarly increased if MHT use had started at ages 40-44 years, 45-49 years, 50-54 years, and 55-59 years; RRs appeared to be attenuated if MHT use had started after age 60 years. They were also attenuated by adiposity, particularly for estrogen-only MHT (which had little effect in obese women). After MHT use ceased, some excess risk of breast cancer persisted for more than a decade; this is directly correlated with the duration of treatment.
Therefore, it can be expected that the effects of MHT may vary between participants on the basis of age or time since menopause, as well as treatments (MHT type, dose, formulation, duration of use, and route of administration). Regarding formulation effects on the risk of breast cancer, new evidence shows an increased risk of 28%. Progestogens appeared to be differentially associated with breast cancer (micronized progesterone: odds ratio, 0.99; 95% confidence interval 0.55-1.79; synthetic progestin: OR, 1.28; 95% CI, 1.22-1.35). When prescribing MHT, micronized progesterone may be the safer progestogen to use.
In conclusion, MHT has a complex balance of benefits and risk on various health outcomes. Some effects differ qualitatively between ET and EPT. Regarding use of MHT, consideration should be given to the full range of effects, along with patients’ values and preferences. The overall quality of existing systematic reviews is moderate to poor. Clinicians should evaluate their scientific strength before considering applying their results in clinical practice. Regarding use of any hormone therapy regimen, consideration should be given to the full range of risk and benefits and should involve shared decisionmaking with the patient. It should be recognized that risk-benefit balance is altered by factors such as age, time from menopause, oophorectomy status, and prior hysterectomy and that some outcomes persist and there is some attenuation after stopping use.
This article was translated from Univadis Italy.
A version of the article appeared on Medscape.com.
It is projected that by 2050, 1.6 billion women in the world will have reached menopause or the postmenopausal period, a significant increase, compared with a billion women in 2020. Of all menopausal women, around 75% are affected by troublesome menopause symptoms, such as hot flashes and night sweats.
Around 84% of postmenopausal women experience genitourinary symptoms, such as vulvovaginal atrophy and incontinence.
Menopausal hormone therapy (MHT) is the most effective treatment for managing these symptoms; however, its effects on numerous aspects of female health remain uncertain, in particular with regard to breast cancer. The influence of MHT on breast cancer remains unsettled, with discordant findings from observational studies and randomized clinical trials, a factor that affects the decisions made by doctors concerning hormone therapy in menopausal women.
Background
Conjugated equine estrogens (CEEs) were introduced into clinical practice in the 1940s. For decades, MHT was the main treatment in conventional medicine for the symptoms of menopause. MHT was used in Western countries for about 600 million women starting from 1970, and it progressively increased during the 1990s. Professional organizations recommended MHT for the prevention of osteoporosis and chronic heart disease (CHD), and a third of prescriptions were for women older than 60 years.
Against this background, the National Institutes of Health launched randomized trials of MHT through the Women’s Health Initiative (WHI) to test whether the association with reduced risk for CHD found in observational studies was real and to obtain reliable information on the overall risks and benefits regarding the prevention of chronic disease for postmenopausal women aged 50-79 years.
The WHI trials tested standard-dose oral CEEs with and without standard-dose continuous medroxyprogesterone acetate (EPT). In 2002, the results of the WHI studies raised a series of concerns about the long-term safety of MHT, in particular the finding of an increased risk of breast cancer for women undergoing therapy. That risk exceeded the benefits from reductions in hip fractures and colorectal cancer.
The WHI findings received wide attention. Prescriptions for MHT dropped precipitously after 2002 and continued to decline in subsequent years. Declines were most marked for standard-dose EPT and in older women. The results of the CEE study were less negative, compared with those for EPT, as they showed no effect on CHD, a nonsignificant reduction in the risk of breast cancer, and a more favorable risk-benefit ratio for younger women, compared with older women. A decade later, it had become widely accepted that MHT should not be used for the prevention of chronic disease in older women; however, short-term use for treatment of vasomotor symptoms remains an accepted indication.
Risks and outcomes
Emerging from a series of WHI reports are complex models on the effect of hormonal therapy on the risk and outcome of breast cancer. In one study, women with an intact uterus received CEEs plus medroxyprogesterone acetate (MPA). An increase in the risk of breast cancer was observed over a median of 5.6 years of treatment, followed by a moderate reduction, with the risk increasing after 13 years of cumulative follow-up. For women treated with CEE alone, the reduction in risk observed over an average of 7.2 years of treatment was maintained for 13 years of follow-up.
Results from observational studies contrast with those from randomized controlled trials, particularly those concerning the use of estrogens only. A meta-analysis by the Collaborative Group on Hormonal Factors in Breast Cancer showed that both EPT and CEE were associated with a higher risk of breast neoplasia. Results of the Million Women Study showed a higher death rate.
Treatment methods and duration
Information from prospective studies on the effects of commencing MHT at various ages between 40 and 59 years show that for women who commenced treatment at any time within this age range, the relative risk was similar and was highly significant for all ages. Few women had started MHT treatment well after menopause at ages 60-69 years, and their excess risks during years 5-14 of current use were significant for estrogen-progestogen but not for estrogen-only MHT.
If these associations are largely causal, then for women of average weight in developed countries, 5 years of MHT, starting at age 50 years, would increase breast cancer incidence at ages 50-69 years by about 1 in every 50 users of estrogen plus daily progestogen preparations; 1 in every 70 users of estrogen plus intermittent progestogen preparations; and 1 in every 200 users of estrogen-only preparations. The corresponding excesses from 10 years of MHT would be about twice as great.
During 5-14 years of MHT use, the RRs were similarly increased if MHT use had started at ages 40-44 years, 45-49 years, 50-54 years, and 55-59 years; RRs appeared to be attenuated if MHT use had started after age 60 years. They were also attenuated by adiposity, particularly for estrogen-only MHT (which had little effect in obese women). After MHT use ceased, some excess risk of breast cancer persisted for more than a decade; this is directly correlated with the duration of treatment.
Therefore, it can be expected that the effects of MHT may vary between participants on the basis of age or time since menopause, as well as treatments (MHT type, dose, formulation, duration of use, and route of administration). Regarding formulation effects on the risk of breast cancer, new evidence shows an increased risk of 28%. Progestogens appeared to be differentially associated with breast cancer (micronized progesterone: odds ratio, 0.99; 95% confidence interval 0.55-1.79; synthetic progestin: OR, 1.28; 95% CI, 1.22-1.35). When prescribing MHT, micronized progesterone may be the safer progestogen to use.
In conclusion, MHT has a complex balance of benefits and risk on various health outcomes. Some effects differ qualitatively between ET and EPT. Regarding use of MHT, consideration should be given to the full range of effects, along with patients’ values and preferences. The overall quality of existing systematic reviews is moderate to poor. Clinicians should evaluate their scientific strength before considering applying their results in clinical practice. Regarding use of any hormone therapy regimen, consideration should be given to the full range of risk and benefits and should involve shared decisionmaking with the patient. It should be recognized that risk-benefit balance is altered by factors such as age, time from menopause, oophorectomy status, and prior hysterectomy and that some outcomes persist and there is some attenuation after stopping use.
This article was translated from Univadis Italy.
A version of the article appeared on Medscape.com.
It is projected that by 2050, 1.6 billion women in the world will have reached menopause or the postmenopausal period, a significant increase, compared with a billion women in 2020. Of all menopausal women, around 75% are affected by troublesome menopause symptoms, such as hot flashes and night sweats.
Around 84% of postmenopausal women experience genitourinary symptoms, such as vulvovaginal atrophy and incontinence.
Menopausal hormone therapy (MHT) is the most effective treatment for managing these symptoms; however, its effects on numerous aspects of female health remain uncertain, in particular with regard to breast cancer. The influence of MHT on breast cancer remains unsettled, with discordant findings from observational studies and randomized clinical trials, a factor that affects the decisions made by doctors concerning hormone therapy in menopausal women.
Background
Conjugated equine estrogens (CEEs) were introduced into clinical practice in the 1940s. For decades, MHT was the main treatment in conventional medicine for the symptoms of menopause. MHT was used in Western countries for about 600 million women starting from 1970, and it progressively increased during the 1990s. Professional organizations recommended MHT for the prevention of osteoporosis and chronic heart disease (CHD), and a third of prescriptions were for women older than 60 years.
Against this background, the National Institutes of Health launched randomized trials of MHT through the Women’s Health Initiative (WHI) to test whether the association with reduced risk for CHD found in observational studies was real and to obtain reliable information on the overall risks and benefits regarding the prevention of chronic disease for postmenopausal women aged 50-79 years.
The WHI trials tested standard-dose oral CEEs with and without standard-dose continuous medroxyprogesterone acetate (EPT). In 2002, the results of the WHI studies raised a series of concerns about the long-term safety of MHT, in particular the finding of an increased risk of breast cancer for women undergoing therapy. That risk exceeded the benefits from reductions in hip fractures and colorectal cancer.
The WHI findings received wide attention. Prescriptions for MHT dropped precipitously after 2002 and continued to decline in subsequent years. Declines were most marked for standard-dose EPT and in older women. The results of the CEE study were less negative, compared with those for EPT, as they showed no effect on CHD, a nonsignificant reduction in the risk of breast cancer, and a more favorable risk-benefit ratio for younger women, compared with older women. A decade later, it had become widely accepted that MHT should not be used for the prevention of chronic disease in older women; however, short-term use for treatment of vasomotor symptoms remains an accepted indication.
Risks and outcomes
Emerging from a series of WHI reports are complex models on the effect of hormonal therapy on the risk and outcome of breast cancer. In one study, women with an intact uterus received CEEs plus medroxyprogesterone acetate (MPA). An increase in the risk of breast cancer was observed over a median of 5.6 years of treatment, followed by a moderate reduction, with the risk increasing after 13 years of cumulative follow-up. For women treated with CEE alone, the reduction in risk observed over an average of 7.2 years of treatment was maintained for 13 years of follow-up.
Results from observational studies contrast with those from randomized controlled trials, particularly those concerning the use of estrogens only. A meta-analysis by the Collaborative Group on Hormonal Factors in Breast Cancer showed that both EPT and CEE were associated with a higher risk of breast neoplasia. Results of the Million Women Study showed a higher death rate.
Treatment methods and duration
Information from prospective studies on the effects of commencing MHT at various ages between 40 and 59 years show that for women who commenced treatment at any time within this age range, the relative risk was similar and was highly significant for all ages. Few women had started MHT treatment well after menopause at ages 60-69 years, and their excess risks during years 5-14 of current use were significant for estrogen-progestogen but not for estrogen-only MHT.
If these associations are largely causal, then for women of average weight in developed countries, 5 years of MHT, starting at age 50 years, would increase breast cancer incidence at ages 50-69 years by about 1 in every 50 users of estrogen plus daily progestogen preparations; 1 in every 70 users of estrogen plus intermittent progestogen preparations; and 1 in every 200 users of estrogen-only preparations. The corresponding excesses from 10 years of MHT would be about twice as great.
During 5-14 years of MHT use, the RRs were similarly increased if MHT use had started at ages 40-44 years, 45-49 years, 50-54 years, and 55-59 years; RRs appeared to be attenuated if MHT use had started after age 60 years. They were also attenuated by adiposity, particularly for estrogen-only MHT (which had little effect in obese women). After MHT use ceased, some excess risk of breast cancer persisted for more than a decade; this is directly correlated with the duration of treatment.
Therefore, it can be expected that the effects of MHT may vary between participants on the basis of age or time since menopause, as well as treatments (MHT type, dose, formulation, duration of use, and route of administration). Regarding formulation effects on the risk of breast cancer, new evidence shows an increased risk of 28%. Progestogens appeared to be differentially associated with breast cancer (micronized progesterone: odds ratio, 0.99; 95% confidence interval 0.55-1.79; synthetic progestin: OR, 1.28; 95% CI, 1.22-1.35). When prescribing MHT, micronized progesterone may be the safer progestogen to use.
In conclusion, MHT has a complex balance of benefits and risk on various health outcomes. Some effects differ qualitatively between ET and EPT. Regarding use of MHT, consideration should be given to the full range of effects, along with patients’ values and preferences. The overall quality of existing systematic reviews is moderate to poor. Clinicians should evaluate their scientific strength before considering applying their results in clinical practice. Regarding use of any hormone therapy regimen, consideration should be given to the full range of risk and benefits and should involve shared decisionmaking with the patient. It should be recognized that risk-benefit balance is altered by factors such as age, time from menopause, oophorectomy status, and prior hysterectomy and that some outcomes persist and there is some attenuation after stopping use.
This article was translated from Univadis Italy.
A version of the article appeared on Medscape.com.
Can dietary tweaks improve some skin diseases?
Since 1950, the terms “diet and skin” in the medical literature have markedly increased, said Vivian Shi, MD associate professor of dermatology at the University of Arkansas for Medical Sciences, Little Rock, who talked about nutritional approaches for select skin diseases at MedscapeLive’s Women’s and Pediatric Dermatology Seminar.
Myths abound, but some associations of diet with skin diseases hold water, and she said.
Acne
What’s known, Dr. Shi said, is that the prevalence of acne is substantially lower in non-Westernized countries, and that diets in those countries generally have a low glycemic load, which decreases IGF-1 insulinlike growth factor 1 (IGF-1) concentrations, an accepted risk factor for acne. The Western diet also includes the hormonal effects of cow’s milk products.
Whey protein, which is popular as a supplement, isn’t good for acne, Dr. Shi said. It takes a couple of hours to digest, while casein protein digests more slowly, over 5-7 hours. If casein protein isn’t acceptable, good alternatives to whey protein are hemp seed, plant protein blends (peas, seeds, berries), egg white, brown rice isolate, and soy isolate protein.
Dairy products increase IGF-1 levels, hormonal mediators that can make acne worse. In addition, industrial cow’s milk can contain anabolic steroids and growth factor, leading to sebogenesis, Dr. Shi said. As for the type of milk, skim milk tends to be the most acnegenic and associated with the highest blood levels of IGF-1.
Supplementing with omega-3 fatty acids and gamma-linolenic acid improved mild to moderate acne in a double-blind, controlled study. Researchers randomized 45 patients with mild to moderate acne to an omega-3 fatty acid group (2,000 mg of eicosapentaenoic acid and docosahexaenoic acid), a gamma-linolenic acid group (borage oil with 400 mg gamma-linolenic acid) or a control group. After 10 weeks in both treatment groups, there was a significant reduction in inflammatory and noninflammatory lesions.
Those with acne are more likely to be deficient in Vitamin D, research suggests. Researchers also found that among those who had vitamin D deficiency, supplementing with 1,000 IU daily for 2 months reduced inflammatory lesions by 35% after 8 weeks, compared with a 6% reduction in the control group.
Other research has found that those with a low serum zinc level had more severe acne and that 30-200 mg of zinc orally for 2-4 months reduced inflammatory acne. However, Dr. Shi cautioned that those taking zinc for more than 2 months also need a copper supplement, as zinc reduces the amount of copper absorbed by the body.
Dr. Shi’s “do’s” diet list for acne patients is a follows: Paleolithic and Mediterranean diets, omega-3 fatty acids, gamma-linolenic acids, Vitamin D, zinc, tubers, legumes, vegetables, fruits, and fish.
Unknowns, she said, include chocolate, caffeine, green tea, and high salt.
Hidradenitis suppurativa
Patents with HS who follow a Mediterranean diet most closely have less severe disease, research has found. In this study, those patients with HS with the lowest adherence had a Sartorius HS score of 59.38, while those who followed it the most closely had a score of 39 (of 80).
In another study, patients with HS reported the following foods as exacerbating HS: sweets, bread/pasta/rice, dairy, and high-fat foods. Alleviating foods included vegetables, fruit, chicken, and fish.
Dr. Shi’s dietary recommendations for patients with HS: Follow a Mediterranean diet, avoid high fat foods and highly processed foods, and focus on eating more vegetables, fresh fruit, corn-based cereal, white meat, and fish.
A retrospective study of patients with Hurley stage 1 and 2 found that oral zinc gluconate, 90 mg a day, combined with 2% topical triclosan twice a day, resulted in significantly decreased HS scores and nodules and improved quality of life after 3 months. Expect vitamin D deficiency, she added.
Lastly, Dr. Shi recommended, if necessary, “weight loss to reduce the inflammatory burden.”
Rosacea
Dietary triggers for rosacea are thought to include high-fat foods, dairy foods, spicy foods, hot drinks, cinnamon, and vanilla.
A population-based case-control study in China, which evaluated 1,347 rosacea patients and 1,290 healthy controls, found that a high intake of fatty foods positively correlated with erythematotelangiectatic rosacea (ETR) and phymatous rosacea. High-frequency dairy intake negatively correlated with ETR and papulopustular rosacea, which was a surprise, she said. And in this study, no significant correlations were found between sweets, coffee, and spicy foods. That goes against the traditional thinking, she said, but this was a Chinese cohort and their diet is probably vastly different than those in the United States.
Other rosacea triggers, Dr. Shi said, are niacin-containing foods such as turkey, chicken breast, crustaceans, dried Shiitake mushrooms, peanuts, tuna, and liver, as well as cold drinks, and formalin-containing foods (fish, squid, tofu, wet noodles).
As the field of nutrigenics – how genes affect how the body responds to food – evolves, more answers about the impact of diet on these diseases will be forthcoming, Dr. Shi said.
In an interactive panel discussion, she was asked if she talks about diet with all her patients with acne, rosacea, and HS, or just those not responding to traditional therapy.
“I think it’s an important conversation to have,” Dr. Shi responded. “When I’m done with the medication [instructions], I say: ‘There is something else you can do to augment what I just told you.’ ” That’s when she explains the dietary information. She also has a handout on diet and routinely refers patients for dietary counseling.
MedscapeLive and this news organization are owned by the same parent company. Dr. Shi disclosed consulting, investigative and research funding from several sources, but not directly related to the content of her talk.
Since 1950, the terms “diet and skin” in the medical literature have markedly increased, said Vivian Shi, MD associate professor of dermatology at the University of Arkansas for Medical Sciences, Little Rock, who talked about nutritional approaches for select skin diseases at MedscapeLive’s Women’s and Pediatric Dermatology Seminar.
Myths abound, but some associations of diet with skin diseases hold water, and she said.
Acne
What’s known, Dr. Shi said, is that the prevalence of acne is substantially lower in non-Westernized countries, and that diets in those countries generally have a low glycemic load, which decreases IGF-1 insulinlike growth factor 1 (IGF-1) concentrations, an accepted risk factor for acne. The Western diet also includes the hormonal effects of cow’s milk products.
Whey protein, which is popular as a supplement, isn’t good for acne, Dr. Shi said. It takes a couple of hours to digest, while casein protein digests more slowly, over 5-7 hours. If casein protein isn’t acceptable, good alternatives to whey protein are hemp seed, plant protein blends (peas, seeds, berries), egg white, brown rice isolate, and soy isolate protein.
Dairy products increase IGF-1 levels, hormonal mediators that can make acne worse. In addition, industrial cow’s milk can contain anabolic steroids and growth factor, leading to sebogenesis, Dr. Shi said. As for the type of milk, skim milk tends to be the most acnegenic and associated with the highest blood levels of IGF-1.
Supplementing with omega-3 fatty acids and gamma-linolenic acid improved mild to moderate acne in a double-blind, controlled study. Researchers randomized 45 patients with mild to moderate acne to an omega-3 fatty acid group (2,000 mg of eicosapentaenoic acid and docosahexaenoic acid), a gamma-linolenic acid group (borage oil with 400 mg gamma-linolenic acid) or a control group. After 10 weeks in both treatment groups, there was a significant reduction in inflammatory and noninflammatory lesions.
Those with acne are more likely to be deficient in Vitamin D, research suggests. Researchers also found that among those who had vitamin D deficiency, supplementing with 1,000 IU daily for 2 months reduced inflammatory lesions by 35% after 8 weeks, compared with a 6% reduction in the control group.
Other research has found that those with a low serum zinc level had more severe acne and that 30-200 mg of zinc orally for 2-4 months reduced inflammatory acne. However, Dr. Shi cautioned that those taking zinc for more than 2 months also need a copper supplement, as zinc reduces the amount of copper absorbed by the body.
Dr. Shi’s “do’s” diet list for acne patients is a follows: Paleolithic and Mediterranean diets, omega-3 fatty acids, gamma-linolenic acids, Vitamin D, zinc, tubers, legumes, vegetables, fruits, and fish.
Unknowns, she said, include chocolate, caffeine, green tea, and high salt.
Hidradenitis suppurativa
Patents with HS who follow a Mediterranean diet most closely have less severe disease, research has found. In this study, those patients with HS with the lowest adherence had a Sartorius HS score of 59.38, while those who followed it the most closely had a score of 39 (of 80).
In another study, patients with HS reported the following foods as exacerbating HS: sweets, bread/pasta/rice, dairy, and high-fat foods. Alleviating foods included vegetables, fruit, chicken, and fish.
Dr. Shi’s dietary recommendations for patients with HS: Follow a Mediterranean diet, avoid high fat foods and highly processed foods, and focus on eating more vegetables, fresh fruit, corn-based cereal, white meat, and fish.
A retrospective study of patients with Hurley stage 1 and 2 found that oral zinc gluconate, 90 mg a day, combined with 2% topical triclosan twice a day, resulted in significantly decreased HS scores and nodules and improved quality of life after 3 months. Expect vitamin D deficiency, she added.
Lastly, Dr. Shi recommended, if necessary, “weight loss to reduce the inflammatory burden.”
Rosacea
Dietary triggers for rosacea are thought to include high-fat foods, dairy foods, spicy foods, hot drinks, cinnamon, and vanilla.
A population-based case-control study in China, which evaluated 1,347 rosacea patients and 1,290 healthy controls, found that a high intake of fatty foods positively correlated with erythematotelangiectatic rosacea (ETR) and phymatous rosacea. High-frequency dairy intake negatively correlated with ETR and papulopustular rosacea, which was a surprise, she said. And in this study, no significant correlations were found between sweets, coffee, and spicy foods. That goes against the traditional thinking, she said, but this was a Chinese cohort and their diet is probably vastly different than those in the United States.
Other rosacea triggers, Dr. Shi said, are niacin-containing foods such as turkey, chicken breast, crustaceans, dried Shiitake mushrooms, peanuts, tuna, and liver, as well as cold drinks, and formalin-containing foods (fish, squid, tofu, wet noodles).
As the field of nutrigenics – how genes affect how the body responds to food – evolves, more answers about the impact of diet on these diseases will be forthcoming, Dr. Shi said.
In an interactive panel discussion, she was asked if she talks about diet with all her patients with acne, rosacea, and HS, or just those not responding to traditional therapy.
“I think it’s an important conversation to have,” Dr. Shi responded. “When I’m done with the medication [instructions], I say: ‘There is something else you can do to augment what I just told you.’ ” That’s when she explains the dietary information. She also has a handout on diet and routinely refers patients for dietary counseling.
MedscapeLive and this news organization are owned by the same parent company. Dr. Shi disclosed consulting, investigative and research funding from several sources, but not directly related to the content of her talk.
Since 1950, the terms “diet and skin” in the medical literature have markedly increased, said Vivian Shi, MD associate professor of dermatology at the University of Arkansas for Medical Sciences, Little Rock, who talked about nutritional approaches for select skin diseases at MedscapeLive’s Women’s and Pediatric Dermatology Seminar.
Myths abound, but some associations of diet with skin diseases hold water, and she said.
Acne
What’s known, Dr. Shi said, is that the prevalence of acne is substantially lower in non-Westernized countries, and that diets in those countries generally have a low glycemic load, which decreases IGF-1 insulinlike growth factor 1 (IGF-1) concentrations, an accepted risk factor for acne. The Western diet also includes the hormonal effects of cow’s milk products.
Whey protein, which is popular as a supplement, isn’t good for acne, Dr. Shi said. It takes a couple of hours to digest, while casein protein digests more slowly, over 5-7 hours. If casein protein isn’t acceptable, good alternatives to whey protein are hemp seed, plant protein blends (peas, seeds, berries), egg white, brown rice isolate, and soy isolate protein.
Dairy products increase IGF-1 levels, hormonal mediators that can make acne worse. In addition, industrial cow’s milk can contain anabolic steroids and growth factor, leading to sebogenesis, Dr. Shi said. As for the type of milk, skim milk tends to be the most acnegenic and associated with the highest blood levels of IGF-1.
Supplementing with omega-3 fatty acids and gamma-linolenic acid improved mild to moderate acne in a double-blind, controlled study. Researchers randomized 45 patients with mild to moderate acne to an omega-3 fatty acid group (2,000 mg of eicosapentaenoic acid and docosahexaenoic acid), a gamma-linolenic acid group (borage oil with 400 mg gamma-linolenic acid) or a control group. After 10 weeks in both treatment groups, there was a significant reduction in inflammatory and noninflammatory lesions.
Those with acne are more likely to be deficient in Vitamin D, research suggests. Researchers also found that among those who had vitamin D deficiency, supplementing with 1,000 IU daily for 2 months reduced inflammatory lesions by 35% after 8 weeks, compared with a 6% reduction in the control group.
Other research has found that those with a low serum zinc level had more severe acne and that 30-200 mg of zinc orally for 2-4 months reduced inflammatory acne. However, Dr. Shi cautioned that those taking zinc for more than 2 months also need a copper supplement, as zinc reduces the amount of copper absorbed by the body.
Dr. Shi’s “do’s” diet list for acne patients is a follows: Paleolithic and Mediterranean diets, omega-3 fatty acids, gamma-linolenic acids, Vitamin D, zinc, tubers, legumes, vegetables, fruits, and fish.
Unknowns, she said, include chocolate, caffeine, green tea, and high salt.
Hidradenitis suppurativa
Patents with HS who follow a Mediterranean diet most closely have less severe disease, research has found. In this study, those patients with HS with the lowest adherence had a Sartorius HS score of 59.38, while those who followed it the most closely had a score of 39 (of 80).
In another study, patients with HS reported the following foods as exacerbating HS: sweets, bread/pasta/rice, dairy, and high-fat foods. Alleviating foods included vegetables, fruit, chicken, and fish.
Dr. Shi’s dietary recommendations for patients with HS: Follow a Mediterranean diet, avoid high fat foods and highly processed foods, and focus on eating more vegetables, fresh fruit, corn-based cereal, white meat, and fish.
A retrospective study of patients with Hurley stage 1 and 2 found that oral zinc gluconate, 90 mg a day, combined with 2% topical triclosan twice a day, resulted in significantly decreased HS scores and nodules and improved quality of life after 3 months. Expect vitamin D deficiency, she added.
Lastly, Dr. Shi recommended, if necessary, “weight loss to reduce the inflammatory burden.”
Rosacea
Dietary triggers for rosacea are thought to include high-fat foods, dairy foods, spicy foods, hot drinks, cinnamon, and vanilla.
A population-based case-control study in China, which evaluated 1,347 rosacea patients and 1,290 healthy controls, found that a high intake of fatty foods positively correlated with erythematotelangiectatic rosacea (ETR) and phymatous rosacea. High-frequency dairy intake negatively correlated with ETR and papulopustular rosacea, which was a surprise, she said. And in this study, no significant correlations were found between sweets, coffee, and spicy foods. That goes against the traditional thinking, she said, but this was a Chinese cohort and their diet is probably vastly different than those in the United States.
Other rosacea triggers, Dr. Shi said, are niacin-containing foods such as turkey, chicken breast, crustaceans, dried Shiitake mushrooms, peanuts, tuna, and liver, as well as cold drinks, and formalin-containing foods (fish, squid, tofu, wet noodles).
As the field of nutrigenics – how genes affect how the body responds to food – evolves, more answers about the impact of diet on these diseases will be forthcoming, Dr. Shi said.
In an interactive panel discussion, she was asked if she talks about diet with all her patients with acne, rosacea, and HS, or just those not responding to traditional therapy.
“I think it’s an important conversation to have,” Dr. Shi responded. “When I’m done with the medication [instructions], I say: ‘There is something else you can do to augment what I just told you.’ ” That’s when she explains the dietary information. She also has a handout on diet and routinely refers patients for dietary counseling.
MedscapeLive and this news organization are owned by the same parent company. Dr. Shi disclosed consulting, investigative and research funding from several sources, but not directly related to the content of her talk.
FROM MEDSCAPELIVE WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
Finding HBV ‘cure’ may mean going ‘back to the drawing board’
LONDON – Achieving a functional cure for hepatitis B virus (HBV) is not going to be easily achieved with the drugs that are currently in development, according to a presentation at the annual International Liver Congress sponsored by the European Association for the Study of the Liver.
“Intriguing results have been presented at ILC 2022 that must be carefully interpreted,” said Jean-Michel Pawlotsky, MD, PhD, of Henri Mondor Hospital in Créteil, France, during the viral hepatitis highlights session on the closing day of the meeting.
“New HBV drug development looks more complicated than initially expected and its goals and strategies need to be redefined and refocused,” he added

“This is really something that came from the discussions we had during the sessions but also in the corridors,” Dr. Pawlotsky added. “We know it’s going to be difficult; we have to reset, restart – not from zero, but from not much – and revise our strategy,” he suggested.
There are many new drugs under investigation for HBV, Dr. Pawlotsky said, noting that the number of studies being presented at the meeting was reminiscent of the flurry of activity before a functional cure for hepatitis C had been found. “It’s good to see that this is happening again for HBV,” he said.
Indeed, there are many new direct-acting antiviral agents, immunomodulatory, or other approaches being tested, and some of the more advanced studies are “teaching us a few things and probably raising more questions than getting answers,” Dr. Pawlotsky said.
The B-CLEAR study
One these studies is the phase 2b B-CLEAR study presented during the late-breaker session. This study involved bepirovirsen, an antisense oligonucleotide, and tested its efficacy and safety in patients with chronic hepatitis B virus infection who were either on or off stable nucleos(t)ide analogue (NA/NUC) therapy.
A similar proportion (28% and 29%, respectively) of patients achieved an hepatitis B surface antigen (HBsAg) level below the lower limit of quantification at the end of 24 weeks treatment. However, the effect on HBsAg varied according to the treatment arm, with changes to the dosing or switching to placebo indicating that the effect might wane when the treatment is stopped or if the dose is reduced.
“Interestingly, ALT elevations were observed in association with most HBsAg declines,” Dr. Pawlotsky pointed out. “I think we still have to determine whether this is good flare/bad flare, good sign/bad sign, of what is going to happen afterward.”
The REEF studies
Another approach highlighted was the combination of the silencing or small interfering RNA (siRNA) JNJ-3989 with the capsid assembly modulator (CAM) JNJ-6379 in the phase 2 REEF-1 and REEF-2 studies.
REEF-1, conducted in patients who were either hepatitis B e antigen (HBeAg) positive or negative who were not treated with NA/NUC or were NA/NUC suppressed, showed a dose-dependent, but variable effect among individual patients as might be expected at the end of 48 weeks’ treatment. This was sustained at week 72, which was 24 weeks’ follow-up after stopping treatment.
However, pointed out Dr. Pawlotsky “I think the most important part of this is that if you add a CAM on top of the siRNA, you do not improve the effect on HBsAg levels.”
Then there is the REEF-2 study, testing the same combination but in only patients who were NA suppressed or HBeAg negative alongside standard NA/NUC therapy. As well as being the first novel combination treatment trial to report, this was essentially a stopping trial, Kosh Agarwal, BMedSci (Hons), MBBS, MD, one of the study’s investigators explained separately at a media briefing.
Patients (n = 130) were treated for 48 weeks, then all treatment – including NA/NUC – was discontinued, with 48 weeks of follow-up after discontinuation, said Dr. Agarwal, who is a consultant hepatologist based at the Institute of Liver Studies at King’s College Hospital, London. He presented data from the first 24 week period after treatment had ended.
At the end of treatment, the combination had resulted in a mean reduction in HBsAg of 1.89 log10 IU/mL versus a reduction of 0.06 for the NA/NUC-only group, which acted as the control group in this trial. But “no patient in this study lost their surface antigen, i.e., were cured of their hepatitis B in the active arm or in the control arm,” Dr. Agarwal said.
“We didn’t achieve a cure, but a significant proportion were in a ‘controlled’ viral stage,” said Dr. Agarwal. Indeed, during his presentation of the findings, he showed that HBsAg inhibition was maintained in the majority (72%) of patients after stopping the combination.
While the trial’s primary endpoint wasn’t met, “it’s a really important study,” said Dr. Agarwal. “This [study] was fulfilled and delivered in the COVID era, so a lot of patients were looked after very carefully by sites in Europe,” he observed.
Further follow-up from the trial is expected, and Dr. Agarwal said that the subsequent discussion will “take us back to the drawing board to think about whether we need better antiviral treatments or whether we need to think about different combinations, and whether actually stopping treatment with every treatment is the right strategy to take.”
Both Dr. Agarwal and Dr. Pawlotsky flagged up the case of one patient in the trial who had been in the control arm and had experienced severe HBV reactivation that required a liver transplant.
“This patient is a warning signal,” Dr. Pawlotsky suggested in his talk. “When we think about NUC stopping, we have to think about the potential benefit in terms of HbsAg loss but also the potential risks.”
While Dr. Agarwal had noted that it highlights that “careful design of retreatment criteria is important in studies assessing the NA/NUC-stopping concept”.
Monoclonal antibody shows promise
Other combinations could involve an siRNA and an immunomodulatory agent and, during the poster sessions at the meeting, Dr. Agarwal also presented data from an ongoing phase 1 study with a novel, neutralizing monoclonal antibody called VIR-3434.
This monoclonal antibody is novel because it is thought to have several modes of action, first by binding to HBV and affecting its entry into liver cells, then by presenting the virus to T cells and stimulating a ‘vaccinal’ or immune effect, and then by helping the with the clearance of HBsAg and delivery of the virus to dendritic cells.
In the study, single doses of VIR-3434 were found to be well tolerated and to produce rapid reductions in HBsAg, with the highest dose used (300 mg) producing the greatest and most durable effect up to week 8.
VIR-3434 is also being tested in combination with other drugs in the phase 2 MARCH trial. One of these combinations is VIR-3434 together with an investigational siRNA dubbed VIR-2218. Preclinical work presented at ILC 2022 suggests that this combination appears to be capable of reducing HBsAg to a greater extent than using either agent alone.
Rethinking the strategy to get to a cure
Of course, VIR-3434 is one of several immunomodulatory compounds in development. There are therapeutic vaccines, drugs targeting the innate immune response, other monoclonal antibodies, T-cell receptors, checkpoint inhibitors and PD-L1 inhibitors. Then there are other compounds such as entry inhibitors, apoptosis inducers, and farnesoid X receptor agonists.
“I finish this meeting with more questions than answers,” Dr. Pawlotsky said. “What is the right target to enhance specific anti-HBV immunity? Does in vivo induction of immune responses translate into any beneficial effect on HBV infection? Will therapeutic vaccines every work in a viral infection?”
Moreover, he asked, “how can we avoid the side effect of enhancing multiple and complex nonspecific immune responses? Are treatment-induced flares good flares or bad flares? All of these are questions that are really unanswered and that we’ll have to get answers to in the near future.”
The B-CLEAR study was sponsored by GlaxoSmithKline. The REEF-2 study was sponsored by Janssen Research & Development. The VIR-3434 studies were funded by Vir Biotechnology. Dr. Pawlotsky has received grant and research support, acted as a consultant, adviser, or speaker, and participated in advisory boards for multiple pharmaceutical and biotechnology companies. This news organization was unable to verify Dr. Agarwal’s ties to Vir Biotechnology, but he presented one of the posters on VIR-3434 at the meeting and has been involved in the phase 1 study that was reported.
LONDON – Achieving a functional cure for hepatitis B virus (HBV) is not going to be easily achieved with the drugs that are currently in development, according to a presentation at the annual International Liver Congress sponsored by the European Association for the Study of the Liver.
“Intriguing results have been presented at ILC 2022 that must be carefully interpreted,” said Jean-Michel Pawlotsky, MD, PhD, of Henri Mondor Hospital in Créteil, France, during the viral hepatitis highlights session on the closing day of the meeting.
“New HBV drug development looks more complicated than initially expected and its goals and strategies need to be redefined and refocused,” he added
“This is really something that came from the discussions we had during the sessions but also in the corridors,” Dr. Pawlotsky added. “We know it’s going to be difficult; we have to reset, restart – not from zero, but from not much – and revise our strategy,” he suggested.
There are many new drugs under investigation for HBV, Dr. Pawlotsky said, noting that the number of studies being presented at the meeting was reminiscent of the flurry of activity before a functional cure for hepatitis C had been found. “It’s good to see that this is happening again for HBV,” he said.
Indeed, there are many new direct-acting antiviral agents, immunomodulatory, or other approaches being tested, and some of the more advanced studies are “teaching us a few things and probably raising more questions than getting answers,” Dr. Pawlotsky said.
The B-CLEAR study
One these studies is the phase 2b B-CLEAR study presented during the late-breaker session. This study involved bepirovirsen, an antisense oligonucleotide, and tested its efficacy and safety in patients with chronic hepatitis B virus infection who were either on or off stable nucleos(t)ide analogue (NA/NUC) therapy.
A similar proportion (28% and 29%, respectively) of patients achieved an hepatitis B surface antigen (HBsAg) level below the lower limit of quantification at the end of 24 weeks treatment. However, the effect on HBsAg varied according to the treatment arm, with changes to the dosing or switching to placebo indicating that the effect might wane when the treatment is stopped or if the dose is reduced.
“Interestingly, ALT elevations were observed in association with most HBsAg declines,” Dr. Pawlotsky pointed out. “I think we still have to determine whether this is good flare/bad flare, good sign/bad sign, of what is going to happen afterward.”
The REEF studies
Another approach highlighted was the combination of the silencing or small interfering RNA (siRNA) JNJ-3989 with the capsid assembly modulator (CAM) JNJ-6379 in the phase 2 REEF-1 and REEF-2 studies.
REEF-1, conducted in patients who were either hepatitis B e antigen (HBeAg) positive or negative who were not treated with NA/NUC or were NA/NUC suppressed, showed a dose-dependent, but variable effect among individual patients as might be expected at the end of 48 weeks’ treatment. This was sustained at week 72, which was 24 weeks’ follow-up after stopping treatment.
However, pointed out Dr. Pawlotsky “I think the most important part of this is that if you add a CAM on top of the siRNA, you do not improve the effect on HBsAg levels.”
Then there is the REEF-2 study, testing the same combination but in only patients who were NA suppressed or HBeAg negative alongside standard NA/NUC therapy. As well as being the first novel combination treatment trial to report, this was essentially a stopping trial, Kosh Agarwal, BMedSci (Hons), MBBS, MD, one of the study’s investigators explained separately at a media briefing.
Patients (n = 130) were treated for 48 weeks, then all treatment – including NA/NUC – was discontinued, with 48 weeks of follow-up after discontinuation, said Dr. Agarwal, who is a consultant hepatologist based at the Institute of Liver Studies at King’s College Hospital, London. He presented data from the first 24 week period after treatment had ended.
At the end of treatment, the combination had resulted in a mean reduction in HBsAg of 1.89 log10 IU/mL versus a reduction of 0.06 for the NA/NUC-only group, which acted as the control group in this trial. But “no patient in this study lost their surface antigen, i.e., were cured of their hepatitis B in the active arm or in the control arm,” Dr. Agarwal said.
“We didn’t achieve a cure, but a significant proportion were in a ‘controlled’ viral stage,” said Dr. Agarwal. Indeed, during his presentation of the findings, he showed that HBsAg inhibition was maintained in the majority (72%) of patients after stopping the combination.
While the trial’s primary endpoint wasn’t met, “it’s a really important study,” said Dr. Agarwal. “This [study] was fulfilled and delivered in the COVID era, so a lot of patients were looked after very carefully by sites in Europe,” he observed.
Further follow-up from the trial is expected, and Dr. Agarwal said that the subsequent discussion will “take us back to the drawing board to think about whether we need better antiviral treatments or whether we need to think about different combinations, and whether actually stopping treatment with every treatment is the right strategy to take.”
Both Dr. Agarwal and Dr. Pawlotsky flagged up the case of one patient in the trial who had been in the control arm and had experienced severe HBV reactivation that required a liver transplant.
“This patient is a warning signal,” Dr. Pawlotsky suggested in his talk. “When we think about NUC stopping, we have to think about the potential benefit in terms of HbsAg loss but also the potential risks.”
While Dr. Agarwal had noted that it highlights that “careful design of retreatment criteria is important in studies assessing the NA/NUC-stopping concept”.
Monoclonal antibody shows promise
Other combinations could involve an siRNA and an immunomodulatory agent and, during the poster sessions at the meeting, Dr. Agarwal also presented data from an ongoing phase 1 study with a novel, neutralizing monoclonal antibody called VIR-3434.
This monoclonal antibody is novel because it is thought to have several modes of action, first by binding to HBV and affecting its entry into liver cells, then by presenting the virus to T cells and stimulating a ‘vaccinal’ or immune effect, and then by helping the with the clearance of HBsAg and delivery of the virus to dendritic cells.
In the study, single doses of VIR-3434 were found to be well tolerated and to produce rapid reductions in HBsAg, with the highest dose used (300 mg) producing the greatest and most durable effect up to week 8.
VIR-3434 is also being tested in combination with other drugs in the phase 2 MARCH trial. One of these combinations is VIR-3434 together with an investigational siRNA dubbed VIR-2218. Preclinical work presented at ILC 2022 suggests that this combination appears to be capable of reducing HBsAg to a greater extent than using either agent alone.
Rethinking the strategy to get to a cure
Of course, VIR-3434 is one of several immunomodulatory compounds in development. There are therapeutic vaccines, drugs targeting the innate immune response, other monoclonal antibodies, T-cell receptors, checkpoint inhibitors and PD-L1 inhibitors. Then there are other compounds such as entry inhibitors, apoptosis inducers, and farnesoid X receptor agonists.
“I finish this meeting with more questions than answers,” Dr. Pawlotsky said. “What is the right target to enhance specific anti-HBV immunity? Does in vivo induction of immune responses translate into any beneficial effect on HBV infection? Will therapeutic vaccines every work in a viral infection?”
Moreover, he asked, “how can we avoid the side effect of enhancing multiple and complex nonspecific immune responses? Are treatment-induced flares good flares or bad flares? All of these are questions that are really unanswered and that we’ll have to get answers to in the near future.”
The B-CLEAR study was sponsored by GlaxoSmithKline. The REEF-2 study was sponsored by Janssen Research & Development. The VIR-3434 studies were funded by Vir Biotechnology. Dr. Pawlotsky has received grant and research support, acted as a consultant, adviser, or speaker, and participated in advisory boards for multiple pharmaceutical and biotechnology companies. This news organization was unable to verify Dr. Agarwal’s ties to Vir Biotechnology, but he presented one of the posters on VIR-3434 at the meeting and has been involved in the phase 1 study that was reported.
LONDON – Achieving a functional cure for hepatitis B virus (HBV) is not going to be easily achieved with the drugs that are currently in development, according to a presentation at the annual International Liver Congress sponsored by the European Association for the Study of the Liver.
“Intriguing results have been presented at ILC 2022 that must be carefully interpreted,” said Jean-Michel Pawlotsky, MD, PhD, of Henri Mondor Hospital in Créteil, France, during the viral hepatitis highlights session on the closing day of the meeting.
“New HBV drug development looks more complicated than initially expected and its goals and strategies need to be redefined and refocused,” he added
“This is really something that came from the discussions we had during the sessions but also in the corridors,” Dr. Pawlotsky added. “We know it’s going to be difficult; we have to reset, restart – not from zero, but from not much – and revise our strategy,” he suggested.
There are many new drugs under investigation for HBV, Dr. Pawlotsky said, noting that the number of studies being presented at the meeting was reminiscent of the flurry of activity before a functional cure for hepatitis C had been found. “It’s good to see that this is happening again for HBV,” he said.
Indeed, there are many new direct-acting antiviral agents, immunomodulatory, or other approaches being tested, and some of the more advanced studies are “teaching us a few things and probably raising more questions than getting answers,” Dr. Pawlotsky said.
The B-CLEAR study
One these studies is the phase 2b B-CLEAR study presented during the late-breaker session. This study involved bepirovirsen, an antisense oligonucleotide, and tested its efficacy and safety in patients with chronic hepatitis B virus infection who were either on or off stable nucleos(t)ide analogue (NA/NUC) therapy.
A similar proportion (28% and 29%, respectively) of patients achieved an hepatitis B surface antigen (HBsAg) level below the lower limit of quantification at the end of 24 weeks treatment. However, the effect on HBsAg varied according to the treatment arm, with changes to the dosing or switching to placebo indicating that the effect might wane when the treatment is stopped or if the dose is reduced.
“Interestingly, ALT elevations were observed in association with most HBsAg declines,” Dr. Pawlotsky pointed out. “I think we still have to determine whether this is good flare/bad flare, good sign/bad sign, of what is going to happen afterward.”
The REEF studies
Another approach highlighted was the combination of the silencing or small interfering RNA (siRNA) JNJ-3989 with the capsid assembly modulator (CAM) JNJ-6379 in the phase 2 REEF-1 and REEF-2 studies.
REEF-1, conducted in patients who were either hepatitis B e antigen (HBeAg) positive or negative who were not treated with NA/NUC or were NA/NUC suppressed, showed a dose-dependent, but variable effect among individual patients as might be expected at the end of 48 weeks’ treatment. This was sustained at week 72, which was 24 weeks’ follow-up after stopping treatment.
However, pointed out Dr. Pawlotsky “I think the most important part of this is that if you add a CAM on top of the siRNA, you do not improve the effect on HBsAg levels.”
Then there is the REEF-2 study, testing the same combination but in only patients who were NA suppressed or HBeAg negative alongside standard NA/NUC therapy. As well as being the first novel combination treatment trial to report, this was essentially a stopping trial, Kosh Agarwal, BMedSci (Hons), MBBS, MD, one of the study’s investigators explained separately at a media briefing.
Patients (n = 130) were treated for 48 weeks, then all treatment – including NA/NUC – was discontinued, with 48 weeks of follow-up after discontinuation, said Dr. Agarwal, who is a consultant hepatologist based at the Institute of Liver Studies at King’s College Hospital, London. He presented data from the first 24 week period after treatment had ended.
At the end of treatment, the combination had resulted in a mean reduction in HBsAg of 1.89 log10 IU/mL versus a reduction of 0.06 for the NA/NUC-only group, which acted as the control group in this trial. But “no patient in this study lost their surface antigen, i.e., were cured of their hepatitis B in the active arm or in the control arm,” Dr. Agarwal said.
“We didn’t achieve a cure, but a significant proportion were in a ‘controlled’ viral stage,” said Dr. Agarwal. Indeed, during his presentation of the findings, he showed that HBsAg inhibition was maintained in the majority (72%) of patients after stopping the combination.
While the trial’s primary endpoint wasn’t met, “it’s a really important study,” said Dr. Agarwal. “This [study] was fulfilled and delivered in the COVID era, so a lot of patients were looked after very carefully by sites in Europe,” he observed.
Further follow-up from the trial is expected, and Dr. Agarwal said that the subsequent discussion will “take us back to the drawing board to think about whether we need better antiviral treatments or whether we need to think about different combinations, and whether actually stopping treatment with every treatment is the right strategy to take.”
Both Dr. Agarwal and Dr. Pawlotsky flagged up the case of one patient in the trial who had been in the control arm and had experienced severe HBV reactivation that required a liver transplant.
“This patient is a warning signal,” Dr. Pawlotsky suggested in his talk. “When we think about NUC stopping, we have to think about the potential benefit in terms of HbsAg loss but also the potential risks.”
While Dr. Agarwal had noted that it highlights that “careful design of retreatment criteria is important in studies assessing the NA/NUC-stopping concept”.
Monoclonal antibody shows promise
Other combinations could involve an siRNA and an immunomodulatory agent and, during the poster sessions at the meeting, Dr. Agarwal also presented data from an ongoing phase 1 study with a novel, neutralizing monoclonal antibody called VIR-3434.
This monoclonal antibody is novel because it is thought to have several modes of action, first by binding to HBV and affecting its entry into liver cells, then by presenting the virus to T cells and stimulating a ‘vaccinal’ or immune effect, and then by helping the with the clearance of HBsAg and delivery of the virus to dendritic cells.
In the study, single doses of VIR-3434 were found to be well tolerated and to produce rapid reductions in HBsAg, with the highest dose used (300 mg) producing the greatest and most durable effect up to week 8.
VIR-3434 is also being tested in combination with other drugs in the phase 2 MARCH trial. One of these combinations is VIR-3434 together with an investigational siRNA dubbed VIR-2218. Preclinical work presented at ILC 2022 suggests that this combination appears to be capable of reducing HBsAg to a greater extent than using either agent alone.
Rethinking the strategy to get to a cure
Of course, VIR-3434 is one of several immunomodulatory compounds in development. There are therapeutic vaccines, drugs targeting the innate immune response, other monoclonal antibodies, T-cell receptors, checkpoint inhibitors and PD-L1 inhibitors. Then there are other compounds such as entry inhibitors, apoptosis inducers, and farnesoid X receptor agonists.
“I finish this meeting with more questions than answers,” Dr. Pawlotsky said. “What is the right target to enhance specific anti-HBV immunity? Does in vivo induction of immune responses translate into any beneficial effect on HBV infection? Will therapeutic vaccines every work in a viral infection?”
Moreover, he asked, “how can we avoid the side effect of enhancing multiple and complex nonspecific immune responses? Are treatment-induced flares good flares or bad flares? All of these are questions that are really unanswered and that we’ll have to get answers to in the near future.”
The B-CLEAR study was sponsored by GlaxoSmithKline. The REEF-2 study was sponsored by Janssen Research & Development. The VIR-3434 studies were funded by Vir Biotechnology. Dr. Pawlotsky has received grant and research support, acted as a consultant, adviser, or speaker, and participated in advisory boards for multiple pharmaceutical and biotechnology companies. This news organization was unable to verify Dr. Agarwal’s ties to Vir Biotechnology, but he presented one of the posters on VIR-3434 at the meeting and has been involved in the phase 1 study that was reported.
AT ILC 2022
Innovations in Dermatology Spring Abstract Compendium

How much health insurers pay for almost everything is about to go public
perhaps helping answer a question that has long dogged those who buy insurance: Are we getting the best deal we can?
As of July 1, health insurers and self-insured employers must post on websites just about every price they’ve negotiated with providers for health care services, item by item. About the only thing excluded are the prices paid for prescription drugs, except those administered in hospitals or doctors’ offices.
The federally required data release could affect future prices or even how employers contract for health care. Many will see for the first time how well their insurers are doing, compared with others.
The new rules are far broader than those that went into effect in 2021 requiring hospitals to post their negotiated rates for the public to see. Now insurers must post the amounts paid for “every physician in network, every hospital, every surgery center, every nursing facility,” said Jeffrey Leibach, a partner at the consulting firm Guidehouse.
“When you start doing the math, you’re talking trillions of records,” he said. The fines the federal government could impose for noncompliance are also heftier than the penalties that hospitals face.
Federal officials learned from the hospital experience and gave insurers more direction on what was expected, said Mr. Leibach. Insurers or self-insured employers could be fined as much as $100 a day for each violation, for each affected enrollee if they fail to provide the data.
“Get your calculator out: All of a sudden you are in the millions pretty fast,” Mr. Leibach said.
Determined consumers, especially those with high-deductible health plans, may try to dig in right away and use the data to try comparing what they will have to pay at different hospitals, clinics, or doctor offices for specific services.
But each database’s enormous size may mean that most people “will find it very hard to use the data in a nuanced way,” said Katherine Baicker, dean of the University of Chicago Harris School of Public Policy.
At least at first.
Entrepreneurs are expected to quickly translate the information into more user-friendly formats so it can be incorporated into new or existing services that estimate costs for patients. And starting Jan. 1, the rules require insurers to provide online tools that will help people get up-front cost estimates for about 500 so-called “shoppable” services, meaning medical care they can schedule ahead of time.
Once those things happen, “you’ll at least have the options in front of you,” said Chris Severn, CEO of Turquoise Health, an online company that has posted price information made available under the rules for hospitals, although many hospitals have yet to comply.
With the addition of the insurers’ data, sites like his will be able to drill down further into cost variation from one place to another or among insurers.
“If you’re going to get an x-ray, you will be able to see that you can do it for $250 at this hospital, $75 at the imaging center down the road, or your specialist can do it in office for $25,” he said.
Everyone will know everyone else’s business: for example, how much insurers Aetna and Humana pay the same surgery center for a knee replacement.
The requirements stem from the Affordable Care Act and a 2019 executive order by then-President Donald Trump.
“These plans are supposed to be acting on behalf of employers in negotiating good rates, and the little insight we have on that shows it has not happened,” said Elizabeth Mitchell, president and CEO of the Purchaser Business Group on Health, an affiliation of employers who offer job-based health benefits to workers. “I do believe the dynamics are going to change.”
Other observers are more circumspect.
“Maybe at best this will reduce the wide variance of prices out there,” said Zack Cooper, director of health policy at the Yale University Institution for Social and Policy Studies, New Haven, Conn. “But it won’t be unleashing a consumer revolution.”
Still, the biggest value of the July data release may well be to shed light on how successful insurers have been at negotiating prices. It comes on the heels of research that has shown tremendous variation in what is paid for health care. A recent study by Rand, for example, shows that employers that offer job-based insurance plans paid, on average, 224% more than Medicare for the same services.
Tens of thousands of employers who buy insurance coverage for their workers will get this more-complete pricing picture – and may not like what they see.
“What we’re learning from the hospital data is that insurers are really bad at negotiating,” said Gerard Anderson, a professor in the department of health policy at the Johns Hopkins Bloomberg, Baltimore, citing research that found that negotiated rates for hospital care can be higher than what the facilities accept from patients who are not using insurance and are paying cash.
That could add to the frustration that Ms. Mitchell and others say employers have with the current health insurance system. More might try to contract with providers directly, only using insurance companies for claims processing.
Other employers may bring their insurers back to the bargaining table.
“For the first time, an employer will be able to go to an insurance company and say: ‘You have not negotiated a good-enough deal, and we know that because we can see the same provider has negotiated a better deal with another company,’ ” said James Gelfand, president of the ERISA Industry Committee, a trade group of self-insured employers.
If that happens, he added, “patients will be able to save money.”
That’s not necessarily a given, however.
Because this kind of public release of pricing data hasn’t been tried widely in health care before, how it will affect future spending remains uncertain. If insurers are pushed back to the bargaining table or providers see where they stand relative to their peers, prices could drop. However, some providers could raise their prices if they see they are charging less than their peers.
“Downward pressure may not be a given,” said Kelley Schultz, vice president of commercial policy for AHIP, the industry’s trade lobby.
Ms. Baicker said that, even after the data is out, rates will continue to be heavily influenced by local conditions, such as the size of an insurer or employer – providers often give bigger discounts, for example, to the insurers or self-insured employers that can send them the most patients. The number of hospitals in a region also matters – if an area has only one, for instance, that usually means the facility can demand higher rates.
Another unknown: Will insurers meet the deadline and provide usable data?
Ms. Schultz, at AHIP, said the industry is well on the way, partly because the original deadline was extended by 6 months. She expects insurers to do better than the hospital industry. “We saw a lot of hospitals that just decided not to post files or make them difficult to find,” she said.
So far, more than 300 noncompliant hospitals received warning letters from the government. But they could face fines of $300 a day fines for failing to comply, which is less than what insurers potentially face, although the federal government has recently upped the ante to up to $5,500 a day for the largest facilities.
Even after the pricing data is public, “I don’t think things will change overnight,” said Mr. Leibach. “Patients are still going to make care decisions based on their doctors and referrals, a lot of reasons other than price.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
perhaps helping answer a question that has long dogged those who buy insurance: Are we getting the best deal we can?
As of July 1, health insurers and self-insured employers must post on websites just about every price they’ve negotiated with providers for health care services, item by item. About the only thing excluded are the prices paid for prescription drugs, except those administered in hospitals or doctors’ offices.
The federally required data release could affect future prices or even how employers contract for health care. Many will see for the first time how well their insurers are doing, compared with others.
The new rules are far broader than those that went into effect in 2021 requiring hospitals to post their negotiated rates for the public to see. Now insurers must post the amounts paid for “every physician in network, every hospital, every surgery center, every nursing facility,” said Jeffrey Leibach, a partner at the consulting firm Guidehouse.
“When you start doing the math, you’re talking trillions of records,” he said. The fines the federal government could impose for noncompliance are also heftier than the penalties that hospitals face.
Federal officials learned from the hospital experience and gave insurers more direction on what was expected, said Mr. Leibach. Insurers or self-insured employers could be fined as much as $100 a day for each violation, for each affected enrollee if they fail to provide the data.
“Get your calculator out: All of a sudden you are in the millions pretty fast,” Mr. Leibach said.
Determined consumers, especially those with high-deductible health plans, may try to dig in right away and use the data to try comparing what they will have to pay at different hospitals, clinics, or doctor offices for specific services.
But each database’s enormous size may mean that most people “will find it very hard to use the data in a nuanced way,” said Katherine Baicker, dean of the University of Chicago Harris School of Public Policy.
At least at first.
Entrepreneurs are expected to quickly translate the information into more user-friendly formats so it can be incorporated into new or existing services that estimate costs for patients. And starting Jan. 1, the rules require insurers to provide online tools that will help people get up-front cost estimates for about 500 so-called “shoppable” services, meaning medical care they can schedule ahead of time.
Once those things happen, “you’ll at least have the options in front of you,” said Chris Severn, CEO of Turquoise Health, an online company that has posted price information made available under the rules for hospitals, although many hospitals have yet to comply.
With the addition of the insurers’ data, sites like his will be able to drill down further into cost variation from one place to another or among insurers.
“If you’re going to get an x-ray, you will be able to see that you can do it for $250 at this hospital, $75 at the imaging center down the road, or your specialist can do it in office for $25,” he said.
Everyone will know everyone else’s business: for example, how much insurers Aetna and Humana pay the same surgery center for a knee replacement.
The requirements stem from the Affordable Care Act and a 2019 executive order by then-President Donald Trump.
“These plans are supposed to be acting on behalf of employers in negotiating good rates, and the little insight we have on that shows it has not happened,” said Elizabeth Mitchell, president and CEO of the Purchaser Business Group on Health, an affiliation of employers who offer job-based health benefits to workers. “I do believe the dynamics are going to change.”
Other observers are more circumspect.
“Maybe at best this will reduce the wide variance of prices out there,” said Zack Cooper, director of health policy at the Yale University Institution for Social and Policy Studies, New Haven, Conn. “But it won’t be unleashing a consumer revolution.”
Still, the biggest value of the July data release may well be to shed light on how successful insurers have been at negotiating prices. It comes on the heels of research that has shown tremendous variation in what is paid for health care. A recent study by Rand, for example, shows that employers that offer job-based insurance plans paid, on average, 224% more than Medicare for the same services.
Tens of thousands of employers who buy insurance coverage for their workers will get this more-complete pricing picture – and may not like what they see.
“What we’re learning from the hospital data is that insurers are really bad at negotiating,” said Gerard Anderson, a professor in the department of health policy at the Johns Hopkins Bloomberg, Baltimore, citing research that found that negotiated rates for hospital care can be higher than what the facilities accept from patients who are not using insurance and are paying cash.
That could add to the frustration that Ms. Mitchell and others say employers have with the current health insurance system. More might try to contract with providers directly, only using insurance companies for claims processing.
Other employers may bring their insurers back to the bargaining table.
“For the first time, an employer will be able to go to an insurance company and say: ‘You have not negotiated a good-enough deal, and we know that because we can see the same provider has negotiated a better deal with another company,’ ” said James Gelfand, president of the ERISA Industry Committee, a trade group of self-insured employers.
If that happens, he added, “patients will be able to save money.”
That’s not necessarily a given, however.
Because this kind of public release of pricing data hasn’t been tried widely in health care before, how it will affect future spending remains uncertain. If insurers are pushed back to the bargaining table or providers see where they stand relative to their peers, prices could drop. However, some providers could raise their prices if they see they are charging less than their peers.
“Downward pressure may not be a given,” said Kelley Schultz, vice president of commercial policy for AHIP, the industry’s trade lobby.
Ms. Baicker said that, even after the data is out, rates will continue to be heavily influenced by local conditions, such as the size of an insurer or employer – providers often give bigger discounts, for example, to the insurers or self-insured employers that can send them the most patients. The number of hospitals in a region also matters – if an area has only one, for instance, that usually means the facility can demand higher rates.
Another unknown: Will insurers meet the deadline and provide usable data?
Ms. Schultz, at AHIP, said the industry is well on the way, partly because the original deadline was extended by 6 months. She expects insurers to do better than the hospital industry. “We saw a lot of hospitals that just decided not to post files or make them difficult to find,” she said.
So far, more than 300 noncompliant hospitals received warning letters from the government. But they could face fines of $300 a day fines for failing to comply, which is less than what insurers potentially face, although the federal government has recently upped the ante to up to $5,500 a day for the largest facilities.
Even after the pricing data is public, “I don’t think things will change overnight,” said Mr. Leibach. “Patients are still going to make care decisions based on their doctors and referrals, a lot of reasons other than price.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
perhaps helping answer a question that has long dogged those who buy insurance: Are we getting the best deal we can?
As of July 1, health insurers and self-insured employers must post on websites just about every price they’ve negotiated with providers for health care services, item by item. About the only thing excluded are the prices paid for prescription drugs, except those administered in hospitals or doctors’ offices.
The federally required data release could affect future prices or even how employers contract for health care. Many will see for the first time how well their insurers are doing, compared with others.
The new rules are far broader than those that went into effect in 2021 requiring hospitals to post their negotiated rates for the public to see. Now insurers must post the amounts paid for “every physician in network, every hospital, every surgery center, every nursing facility,” said Jeffrey Leibach, a partner at the consulting firm Guidehouse.
“When you start doing the math, you’re talking trillions of records,” he said. The fines the federal government could impose for noncompliance are also heftier than the penalties that hospitals face.
Federal officials learned from the hospital experience and gave insurers more direction on what was expected, said Mr. Leibach. Insurers or self-insured employers could be fined as much as $100 a day for each violation, for each affected enrollee if they fail to provide the data.
“Get your calculator out: All of a sudden you are in the millions pretty fast,” Mr. Leibach said.
Determined consumers, especially those with high-deductible health plans, may try to dig in right away and use the data to try comparing what they will have to pay at different hospitals, clinics, or doctor offices for specific services.
But each database’s enormous size may mean that most people “will find it very hard to use the data in a nuanced way,” said Katherine Baicker, dean of the University of Chicago Harris School of Public Policy.
At least at first.
Entrepreneurs are expected to quickly translate the information into more user-friendly formats so it can be incorporated into new or existing services that estimate costs for patients. And starting Jan. 1, the rules require insurers to provide online tools that will help people get up-front cost estimates for about 500 so-called “shoppable” services, meaning medical care they can schedule ahead of time.
Once those things happen, “you’ll at least have the options in front of you,” said Chris Severn, CEO of Turquoise Health, an online company that has posted price information made available under the rules for hospitals, although many hospitals have yet to comply.
With the addition of the insurers’ data, sites like his will be able to drill down further into cost variation from one place to another or among insurers.
“If you’re going to get an x-ray, you will be able to see that you can do it for $250 at this hospital, $75 at the imaging center down the road, or your specialist can do it in office for $25,” he said.
Everyone will know everyone else’s business: for example, how much insurers Aetna and Humana pay the same surgery center for a knee replacement.
The requirements stem from the Affordable Care Act and a 2019 executive order by then-President Donald Trump.
“These plans are supposed to be acting on behalf of employers in negotiating good rates, and the little insight we have on that shows it has not happened,” said Elizabeth Mitchell, president and CEO of the Purchaser Business Group on Health, an affiliation of employers who offer job-based health benefits to workers. “I do believe the dynamics are going to change.”
Other observers are more circumspect.
“Maybe at best this will reduce the wide variance of prices out there,” said Zack Cooper, director of health policy at the Yale University Institution for Social and Policy Studies, New Haven, Conn. “But it won’t be unleashing a consumer revolution.”
Still, the biggest value of the July data release may well be to shed light on how successful insurers have been at negotiating prices. It comes on the heels of research that has shown tremendous variation in what is paid for health care. A recent study by Rand, for example, shows that employers that offer job-based insurance plans paid, on average, 224% more than Medicare for the same services.
Tens of thousands of employers who buy insurance coverage for their workers will get this more-complete pricing picture – and may not like what they see.
“What we’re learning from the hospital data is that insurers are really bad at negotiating,” said Gerard Anderson, a professor in the department of health policy at the Johns Hopkins Bloomberg, Baltimore, citing research that found that negotiated rates for hospital care can be higher than what the facilities accept from patients who are not using insurance and are paying cash.
That could add to the frustration that Ms. Mitchell and others say employers have with the current health insurance system. More might try to contract with providers directly, only using insurance companies for claims processing.
Other employers may bring their insurers back to the bargaining table.
“For the first time, an employer will be able to go to an insurance company and say: ‘You have not negotiated a good-enough deal, and we know that because we can see the same provider has negotiated a better deal with another company,’ ” said James Gelfand, president of the ERISA Industry Committee, a trade group of self-insured employers.
If that happens, he added, “patients will be able to save money.”
That’s not necessarily a given, however.
Because this kind of public release of pricing data hasn’t been tried widely in health care before, how it will affect future spending remains uncertain. If insurers are pushed back to the bargaining table or providers see where they stand relative to their peers, prices could drop. However, some providers could raise their prices if they see they are charging less than their peers.
“Downward pressure may not be a given,” said Kelley Schultz, vice president of commercial policy for AHIP, the industry’s trade lobby.
Ms. Baicker said that, even after the data is out, rates will continue to be heavily influenced by local conditions, such as the size of an insurer or employer – providers often give bigger discounts, for example, to the insurers or self-insured employers that can send them the most patients. The number of hospitals in a region also matters – if an area has only one, for instance, that usually means the facility can demand higher rates.
Another unknown: Will insurers meet the deadline and provide usable data?
Ms. Schultz, at AHIP, said the industry is well on the way, partly because the original deadline was extended by 6 months. She expects insurers to do better than the hospital industry. “We saw a lot of hospitals that just decided not to post files or make them difficult to find,” she said.
So far, more than 300 noncompliant hospitals received warning letters from the government. But they could face fines of $300 a day fines for failing to comply, which is less than what insurers potentially face, although the federal government has recently upped the ante to up to $5,500 a day for the largest facilities.
Even after the pricing data is public, “I don’t think things will change overnight,” said Mr. Leibach. “Patients are still going to make care decisions based on their doctors and referrals, a lot of reasons other than price.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
New biomarker data add to concerns over REDUCE-IT trial
A new analysis of the REDUCE-IT study has reignited concerns that the benefit shown by the high-dose fish oil product in the study, icosapent ethyl (Vascepa, Amarin), may have been related to harms caused by the placebo mineral oil.
Results show that allocation to icosapent ethyl had minimal effects on a series of biomarkers associated with atherosclerotic disease, whereas levels of these biomarkers increased among those allocated to mineral oil.
At 12 months, the median percent increases from baseline in the mineral oil group were 1.5% for homocysteine, 2.2% for lipoprotein(a), 10.9% for oxidized low-density-lipoprotein (LDL) cholesterol, 16.2% for interleukin (IL)-6, 18.5% for lipoprotein-associated phospholipase A2, 21.9% for high-sensitivity C-reactive protein (hsCRP), and 28.9% for IL-1β. The changes were similar at 24 months. However, in the icosapent ethyl group, there were minimal changes in these biomarkers at 12 and 24 months.
The study was published online in Circulation.
The authors, led by Paul Ridker, MD, Brigham & Women’s Hospital, Boston, do not voice much opinion on what the results mean, concluding that “the effect of these findings on the interpretation of the REDUCE-IT trial results remains unclear and will require further investigation.”
They also say that a second icosapent ethyl trial using a nonmineral oil comparator “would help resolve ongoing controversy.”
However, the authors are a mixed group; Dr. Ridker and some of his coauthors were not part of the original REDUCE-IT trial, whereas other coauthors were members of the REDUCE-IT steering committee, and one was an employee of Amarin.
Lead investigator of the REDUCE-IT trial, Deepak Bhatt, MD, also from Brigham & Women’s Hospital, who is the senior author of the current study, played down the new findings, saying they did not offer much new incremental information on mechanistic insight.

“These are small degrees of biomarker increases on an absolute level we are seeing with the placebo that would not be expected to produce harm,” Dr. Bhatt told this news organization. He also said the Circulation peer-review process had removed some of the discussion, which could lead to some “misinterpretation” of the authors’ views.
Dr. Ridker was unavailable for further comment.
The publication of this study has inevitably poured fuel on the fire regarding the controversy that has long dogged the REDUCE-IT trial, with questions about the large reduction in event rates seen with icosapent ethyl without an obvious mechanistic explanation.
‘Smoking gun’
One of the loudest critics of the study, Steve Nissen, MD, Cleveland Clinic, described the new findings as “the closest thing I’ve seen to a smoking gun in medicine for a long, long time.”

“The result of this new analysis shows that mineral oil increases virtually every inflammatory and lipid marker that they measured,” he commented.
“There are a lot of theories, but the bottom line is that something really bad happened in the mineral-oil group, which makes icosapent ethyl look efficacious. In my view, this needs to be reviewed by the FDA for consideration of removing the label claim for cardiovascular benefit.”
Other experts in the field not directly involved in the study voiced concern about these new findings, adding to calls for another trial.
In a Twitter thread on the issue, Harlan Krumholz, MD, describes the Circulation publication as “an exceptionally important article,” adding that it is “time to rethink this drug.”
“My point is ... once you know you have non-neutral comparator and the effect on risk biomarkers is far from trivial ... then you have introduced substantial uncertainty about the trial result, as conveyed by the authors ... and no one can say what would happen with a neutral comparator,” Dr. Krumholz writes.
In an accompanying editorial in Circulation, Robert Harrington, MD, professor of medicine at Stanford (Calif.) University, concludes that “the hard reality is that we are left with uncertainties and the questions raised by use of the mineral oil as placebo can only be answered by another randomized controlled trial.”

“My main points are that the chosen placebo was not inert (an essential characteristic for an active control–placebo comparison), that the biomarker data show elevations in multiple markers involved with inflammatory pathways associated with atherosclerosis, and that these data create enough uncertainty in the trial interpretation that the best recourse to answer the criticisms is to do another trial with a truly inert placebo,” Dr. Harrington said in an interview.
He added that Dr. Bhatt’s point that the changes in biomarkers are too small to really matter clinically may be right. “But for me, the uncertainties mean that I have less confidence in the true magnitude of the treatment effect than I would have if there were no changes in the inflammatory markers.”
In Circulation, the authors say it is unclear why multiple biomarkers increased over time among REDUCE-IT participants allocated to mineral oil. They note that no substantive changes in these biomarkers were observed in the placebo groups over periods of 3-5 years in other trials, including JUPITER, CIRT, CANTOS, SPIRE, and the STRENGTH trials, which evaluated a different high-dose omega-3 oil product but used corn oil as the placebo.
“The core design of REDUCE-IT does not make it possible to resolve convincingly whether any adverse effects associated with mineral oil use as a comparator may have affected clinical outcomes,” they write.
They point out that regulatory agencies evaluating REDUCE-IT estimated that approximately 3% of the net clinical benefit observed with icosapent ethyl might have been a consequence of adverse biomarker effects on LDL cholesterol and hsCRP attributable to mineral oil. But in the context of an overall 25% relative risk reduction in first events and a 30% reduction in total ischemic events observed, a potential bias of this magnitude, even if doubled in size, would be unlikely to fully attenuate the overall benefit of icosapent ethyl observed.
They add that they are not aware of a method to assess what the potential magnitude might be of a combination of the multiple effects.
New data do not change the debate
“We did a large, well-powered randomized trial, and this paper shouldn’t change anything in how that trial should be interpreted,” Dr. Bhatt said in an interview.
He claims the new biomarkers evaluated in the study are correlated with LDL and CRP, data which have already been reported and analyzed so have limited relevance.
“It’s not really independent biomarker information; this is what we would expect to see when we see small increases in LDL and CRP. So, I don’t think this new information fundamentally changes the debate,” he said.
Dr. Bhatt also pointed out that the study highlights relative increases rather than absolute increases in the biomarkers, making it seem more alarming than is actually the case.
“The paper makes it seem like that there are large increases in these other biomarkers, but the values reported are relative increases and the absolute increases were actually rather small. In many cases, the changes reported are less than the lower limit of quantification of the assay used,” he noted.
He added: “Even if one is unable to get around the placebo issue in the REDUCE-IT trial, there will always be the JELIS trial – a randomized trial with no placebo showing a 19% relative risk reduction. While the biomarker data may be interesting, what really matters in the end is clinical events. And significant reductions in two independent trials should be enough.”
Dr. Bhatt says the REDUCE-IT steering committee does not believe another trial is needed. “Maybe a different population would be good – such as primary prevention, patients without elevated triglycerides – but just repeating REDUCE- IT with a different placebo would be a waste of resources,” he commented.
But Dr. Nissen refuted Dr. Bhatt’s claims.
“These biomarkers are not in the same pathways as LDL and CRP, and these are not small increases. In the CANTOS trial, a monoclonal antibody against interleukin-1β beta showed a significant benefit. The increase in interleukin-1β now reported in REDUCE-IT is exactly the opposite of CANTOS,” he pointed out.
“The FDA did not know about these additional biomarkers when it reviewed the data on LDL and CRP. Now we have new information. It needs to be looked at again,” Dr. Nissen added.
Funding for the study was provided by Amarin Pharma. Dr. Bhatt was the lead investigator of the REDUCE-IT trial. Dr. Nissen was the lead investigator the STRENGTH trial. Further disclosures of the authors can be found in Circulation.
A version of this article first appeared on Medscape.com.
A new analysis of the REDUCE-IT study has reignited concerns that the benefit shown by the high-dose fish oil product in the study, icosapent ethyl (Vascepa, Amarin), may have been related to harms caused by the placebo mineral oil.
Results show that allocation to icosapent ethyl had minimal effects on a series of biomarkers associated with atherosclerotic disease, whereas levels of these biomarkers increased among those allocated to mineral oil.
At 12 months, the median percent increases from baseline in the mineral oil group were 1.5% for homocysteine, 2.2% for lipoprotein(a), 10.9% for oxidized low-density-lipoprotein (LDL) cholesterol, 16.2% for interleukin (IL)-6, 18.5% for lipoprotein-associated phospholipase A2, 21.9% for high-sensitivity C-reactive protein (hsCRP), and 28.9% for IL-1β. The changes were similar at 24 months. However, in the icosapent ethyl group, there were minimal changes in these biomarkers at 12 and 24 months.
The study was published online in Circulation.
The authors, led by Paul Ridker, MD, Brigham & Women’s Hospital, Boston, do not voice much opinion on what the results mean, concluding that “the effect of these findings on the interpretation of the REDUCE-IT trial results remains unclear and will require further investigation.”
They also say that a second icosapent ethyl trial using a nonmineral oil comparator “would help resolve ongoing controversy.”
However, the authors are a mixed group; Dr. Ridker and some of his coauthors were not part of the original REDUCE-IT trial, whereas other coauthors were members of the REDUCE-IT steering committee, and one was an employee of Amarin.
Lead investigator of the REDUCE-IT trial, Deepak Bhatt, MD, also from Brigham & Women’s Hospital, who is the senior author of the current study, played down the new findings, saying they did not offer much new incremental information on mechanistic insight.
“These are small degrees of biomarker increases on an absolute level we are seeing with the placebo that would not be expected to produce harm,” Dr. Bhatt told this news organization. He also said the Circulation peer-review process had removed some of the discussion, which could lead to some “misinterpretation” of the authors’ views.
Dr. Ridker was unavailable for further comment.
The publication of this study has inevitably poured fuel on the fire regarding the controversy that has long dogged the REDUCE-IT trial, with questions about the large reduction in event rates seen with icosapent ethyl without an obvious mechanistic explanation.
‘Smoking gun’
One of the loudest critics of the study, Steve Nissen, MD, Cleveland Clinic, described the new findings as “the closest thing I’ve seen to a smoking gun in medicine for a long, long time.”
“The result of this new analysis shows that mineral oil increases virtually every inflammatory and lipid marker that they measured,” he commented.
“There are a lot of theories, but the bottom line is that something really bad happened in the mineral-oil group, which makes icosapent ethyl look efficacious. In my view, this needs to be reviewed by the FDA for consideration of removing the label claim for cardiovascular benefit.”
Other experts in the field not directly involved in the study voiced concern about these new findings, adding to calls for another trial.
In a Twitter thread on the issue, Harlan Krumholz, MD, describes the Circulation publication as “an exceptionally important article,” adding that it is “time to rethink this drug.”
“My point is ... once you know you have non-neutral comparator and the effect on risk biomarkers is far from trivial ... then you have introduced substantial uncertainty about the trial result, as conveyed by the authors ... and no one can say what would happen with a neutral comparator,” Dr. Krumholz writes.
In an accompanying editorial in Circulation, Robert Harrington, MD, professor of medicine at Stanford (Calif.) University, concludes that “the hard reality is that we are left with uncertainties and the questions raised by use of the mineral oil as placebo can only be answered by another randomized controlled trial.”
“My main points are that the chosen placebo was not inert (an essential characteristic for an active control–placebo comparison), that the biomarker data show elevations in multiple markers involved with inflammatory pathways associated with atherosclerosis, and that these data create enough uncertainty in the trial interpretation that the best recourse to answer the criticisms is to do another trial with a truly inert placebo,” Dr. Harrington said in an interview.
He added that Dr. Bhatt’s point that the changes in biomarkers are too small to really matter clinically may be right. “But for me, the uncertainties mean that I have less confidence in the true magnitude of the treatment effect than I would have if there were no changes in the inflammatory markers.”
In Circulation, the authors say it is unclear why multiple biomarkers increased over time among REDUCE-IT participants allocated to mineral oil. They note that no substantive changes in these biomarkers were observed in the placebo groups over periods of 3-5 years in other trials, including JUPITER, CIRT, CANTOS, SPIRE, and the STRENGTH trials, which evaluated a different high-dose omega-3 oil product but used corn oil as the placebo.
“The core design of REDUCE-IT does not make it possible to resolve convincingly whether any adverse effects associated with mineral oil use as a comparator may have affected clinical outcomes,” they write.
They point out that regulatory agencies evaluating REDUCE-IT estimated that approximately 3% of the net clinical benefit observed with icosapent ethyl might have been a consequence of adverse biomarker effects on LDL cholesterol and hsCRP attributable to mineral oil. But in the context of an overall 25% relative risk reduction in first events and a 30% reduction in total ischemic events observed, a potential bias of this magnitude, even if doubled in size, would be unlikely to fully attenuate the overall benefit of icosapent ethyl observed.
They add that they are not aware of a method to assess what the potential magnitude might be of a combination of the multiple effects.
New data do not change the debate
“We did a large, well-powered randomized trial, and this paper shouldn’t change anything in how that trial should be interpreted,” Dr. Bhatt said in an interview.
He claims the new biomarkers evaluated in the study are correlated with LDL and CRP, data which have already been reported and analyzed so have limited relevance.
“It’s not really independent biomarker information; this is what we would expect to see when we see small increases in LDL and CRP. So, I don’t think this new information fundamentally changes the debate,” he said.
Dr. Bhatt also pointed out that the study highlights relative increases rather than absolute increases in the biomarkers, making it seem more alarming than is actually the case.
“The paper makes it seem like that there are large increases in these other biomarkers, but the values reported are relative increases and the absolute increases were actually rather small. In many cases, the changes reported are less than the lower limit of quantification of the assay used,” he noted.
He added: “Even if one is unable to get around the placebo issue in the REDUCE-IT trial, there will always be the JELIS trial – a randomized trial with no placebo showing a 19% relative risk reduction. While the biomarker data may be interesting, what really matters in the end is clinical events. And significant reductions in two independent trials should be enough.”
Dr. Bhatt says the REDUCE-IT steering committee does not believe another trial is needed. “Maybe a different population would be good – such as primary prevention, patients without elevated triglycerides – but just repeating REDUCE- IT with a different placebo would be a waste of resources,” he commented.
But Dr. Nissen refuted Dr. Bhatt’s claims.
“These biomarkers are not in the same pathways as LDL and CRP, and these are not small increases. In the CANTOS trial, a monoclonal antibody against interleukin-1β beta showed a significant benefit. The increase in interleukin-1β now reported in REDUCE-IT is exactly the opposite of CANTOS,” he pointed out.
“The FDA did not know about these additional biomarkers when it reviewed the data on LDL and CRP. Now we have new information. It needs to be looked at again,” Dr. Nissen added.
Funding for the study was provided by Amarin Pharma. Dr. Bhatt was the lead investigator of the REDUCE-IT trial. Dr. Nissen was the lead investigator the STRENGTH trial. Further disclosures of the authors can be found in Circulation.
A version of this article first appeared on Medscape.com.
A new analysis of the REDUCE-IT study has reignited concerns that the benefit shown by the high-dose fish oil product in the study, icosapent ethyl (Vascepa, Amarin), may have been related to harms caused by the placebo mineral oil.
Results show that allocation to icosapent ethyl had minimal effects on a series of biomarkers associated with atherosclerotic disease, whereas levels of these biomarkers increased among those allocated to mineral oil.
At 12 months, the median percent increases from baseline in the mineral oil group were 1.5% for homocysteine, 2.2% for lipoprotein(a), 10.9% for oxidized low-density-lipoprotein (LDL) cholesterol, 16.2% for interleukin (IL)-6, 18.5% for lipoprotein-associated phospholipase A2, 21.9% for high-sensitivity C-reactive protein (hsCRP), and 28.9% for IL-1β. The changes were similar at 24 months. However, in the icosapent ethyl group, there were minimal changes in these biomarkers at 12 and 24 months.
The study was published online in Circulation.
The authors, led by Paul Ridker, MD, Brigham & Women’s Hospital, Boston, do not voice much opinion on what the results mean, concluding that “the effect of these findings on the interpretation of the REDUCE-IT trial results remains unclear and will require further investigation.”
They also say that a second icosapent ethyl trial using a nonmineral oil comparator “would help resolve ongoing controversy.”
However, the authors are a mixed group; Dr. Ridker and some of his coauthors were not part of the original REDUCE-IT trial, whereas other coauthors were members of the REDUCE-IT steering committee, and one was an employee of Amarin.
Lead investigator of the REDUCE-IT trial, Deepak Bhatt, MD, also from Brigham & Women’s Hospital, who is the senior author of the current study, played down the new findings, saying they did not offer much new incremental information on mechanistic insight.
“These are small degrees of biomarker increases on an absolute level we are seeing with the placebo that would not be expected to produce harm,” Dr. Bhatt told this news organization. He also said the Circulation peer-review process had removed some of the discussion, which could lead to some “misinterpretation” of the authors’ views.
Dr. Ridker was unavailable for further comment.
The publication of this study has inevitably poured fuel on the fire regarding the controversy that has long dogged the REDUCE-IT trial, with questions about the large reduction in event rates seen with icosapent ethyl without an obvious mechanistic explanation.
‘Smoking gun’
One of the loudest critics of the study, Steve Nissen, MD, Cleveland Clinic, described the new findings as “the closest thing I’ve seen to a smoking gun in medicine for a long, long time.”
“The result of this new analysis shows that mineral oil increases virtually every inflammatory and lipid marker that they measured,” he commented.
“There are a lot of theories, but the bottom line is that something really bad happened in the mineral-oil group, which makes icosapent ethyl look efficacious. In my view, this needs to be reviewed by the FDA for consideration of removing the label claim for cardiovascular benefit.”
Other experts in the field not directly involved in the study voiced concern about these new findings, adding to calls for another trial.
In a Twitter thread on the issue, Harlan Krumholz, MD, describes the Circulation publication as “an exceptionally important article,” adding that it is “time to rethink this drug.”
“My point is ... once you know you have non-neutral comparator and the effect on risk biomarkers is far from trivial ... then you have introduced substantial uncertainty about the trial result, as conveyed by the authors ... and no one can say what would happen with a neutral comparator,” Dr. Krumholz writes.
In an accompanying editorial in Circulation, Robert Harrington, MD, professor of medicine at Stanford (Calif.) University, concludes that “the hard reality is that we are left with uncertainties and the questions raised by use of the mineral oil as placebo can only be answered by another randomized controlled trial.”
“My main points are that the chosen placebo was not inert (an essential characteristic for an active control–placebo comparison), that the biomarker data show elevations in multiple markers involved with inflammatory pathways associated with atherosclerosis, and that these data create enough uncertainty in the trial interpretation that the best recourse to answer the criticisms is to do another trial with a truly inert placebo,” Dr. Harrington said in an interview.
He added that Dr. Bhatt’s point that the changes in biomarkers are too small to really matter clinically may be right. “But for me, the uncertainties mean that I have less confidence in the true magnitude of the treatment effect than I would have if there were no changes in the inflammatory markers.”
In Circulation, the authors say it is unclear why multiple biomarkers increased over time among REDUCE-IT participants allocated to mineral oil. They note that no substantive changes in these biomarkers were observed in the placebo groups over periods of 3-5 years in other trials, including JUPITER, CIRT, CANTOS, SPIRE, and the STRENGTH trials, which evaluated a different high-dose omega-3 oil product but used corn oil as the placebo.
“The core design of REDUCE-IT does not make it possible to resolve convincingly whether any adverse effects associated with mineral oil use as a comparator may have affected clinical outcomes,” they write.
They point out that regulatory agencies evaluating REDUCE-IT estimated that approximately 3% of the net clinical benefit observed with icosapent ethyl might have been a consequence of adverse biomarker effects on LDL cholesterol and hsCRP attributable to mineral oil. But in the context of an overall 25% relative risk reduction in first events and a 30% reduction in total ischemic events observed, a potential bias of this magnitude, even if doubled in size, would be unlikely to fully attenuate the overall benefit of icosapent ethyl observed.
They add that they are not aware of a method to assess what the potential magnitude might be of a combination of the multiple effects.
New data do not change the debate
“We did a large, well-powered randomized trial, and this paper shouldn’t change anything in how that trial should be interpreted,” Dr. Bhatt said in an interview.
He claims the new biomarkers evaluated in the study are correlated with LDL and CRP, data which have already been reported and analyzed so have limited relevance.
“It’s not really independent biomarker information; this is what we would expect to see when we see small increases in LDL and CRP. So, I don’t think this new information fundamentally changes the debate,” he said.
Dr. Bhatt also pointed out that the study highlights relative increases rather than absolute increases in the biomarkers, making it seem more alarming than is actually the case.
“The paper makes it seem like that there are large increases in these other biomarkers, but the values reported are relative increases and the absolute increases were actually rather small. In many cases, the changes reported are less than the lower limit of quantification of the assay used,” he noted.
He added: “Even if one is unable to get around the placebo issue in the REDUCE-IT trial, there will always be the JELIS trial – a randomized trial with no placebo showing a 19% relative risk reduction. While the biomarker data may be interesting, what really matters in the end is clinical events. And significant reductions in two independent trials should be enough.”
Dr. Bhatt says the REDUCE-IT steering committee does not believe another trial is needed. “Maybe a different population would be good – such as primary prevention, patients without elevated triglycerides – but just repeating REDUCE- IT with a different placebo would be a waste of resources,” he commented.
But Dr. Nissen refuted Dr. Bhatt’s claims.
“These biomarkers are not in the same pathways as LDL and CRP, and these are not small increases. In the CANTOS trial, a monoclonal antibody against interleukin-1β beta showed a significant benefit. The increase in interleukin-1β now reported in REDUCE-IT is exactly the opposite of CANTOS,” he pointed out.
“The FDA did not know about these additional biomarkers when it reviewed the data on LDL and CRP. Now we have new information. It needs to be looked at again,” Dr. Nissen added.
Funding for the study was provided by Amarin Pharma. Dr. Bhatt was the lead investigator of the REDUCE-IT trial. Dr. Nissen was the lead investigator the STRENGTH trial. Further disclosures of the authors can be found in Circulation.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
What are the benefits of a fourth vaccination against COVID?
The fourth vaccination against COVID-19 is the subject of intense discussion. Immunity against new Omicron variants (currently BA.4 and BA.5) is getting weaker and weaker. Is another vaccination with the available vaccines worth it?
For Leif Erik Sander, MD, director of infectious diseases and pneumology at Charité University Medicine, Berlin, the latest data send a clear message. “The COVID-19 vaccination is still effective against Omicron. After three doses of the vaccine, it continues to prevent severe diseases, respiratory failures, and death,” he reported at the 62nd Congress of the German Pneumology and Respiratory Medicine Society in Leipzig.
The most recent data from the United Kingdom show that the vaccine’s effectiveness against Omicron decreases after just a few months, which speaks in favor of a fourth vaccination. “Omicron is a development that we did not anticipate occurring so early on,” said Dr. Sander.
In terms of phylogenetics, Omicron is far removed from the previous variants of concern. More than 30 mutations to the spike protein (the antigen that is vaccinated against) foster the loss of immunity.
Boosters broaden immunity
“The booster makes all the difference here,” emphasized Dr. Sander. Experiments at Charité Berlin show that after double vaccination, the vaccination sera from healthy young people no longer neutralizes Omicron.
“The third vaccination broadens the humoral immune response against the spike protein so that conserved epitopes that are unchanged, even in Omicron, are addressed, with the result that you have neutralization capacity again,” the infectious diseases specialist explained.
Continued protection
However, data from the United Kingdom on vaccine effectiveness show where the limit lies. Initially, after three doses, vaccine effectiveness against symptomatic disease after Omicron infection is very good. This effectiveness decreases significantly over the course of the next few months. “Lots of people experience an Omicron infection despite the booster,” said Mr. Sander.
Nonetheless, the high incidence of Omicron infections in the recent past has not overwhelmed the health care system. “This is because the vaccine’s effectiveness against severe diseases that require hospitalization and against respiratory failure is still good in the at-risk population over the age of 65, once they have had their three vaccinations,” said Dr. Sander. The data also show that there is good protection of over 90%, even against mortality.
Waning observed
It could be said that currently, vaccination even continues to work against Omicron, says Dr. Sander. It prevents severe disease, respiratory failure, and death. Nonetheless, after just 3 months, a slight waning of immune protection can be observed in all three endpoints.
Therefore, the question arises as to whether a fourth vaccination is worthwhile. In Israel, “Delta was successfully eradicated with the third vaccination,” and now they are trying this again for Omicron with a fourth vaccination, reported Dr. Sander.
Fourth vaccination protective
The first investigations show that protection against severe disease can be increased once more. “For the over-60s, protection is almost quadrupled through the fourth vaccination,” says Dr. Sander. “However, this is still plagued with a lot of uncertainty; it is still not known how stable it is.”
There is hope on the basis of results of an as yet non–peer-reviewed study from Sweden, which is currently available only as a preprint. That study shows that a fourth vaccination in a high-risk population of care-home residents and people older than 80 years can halve overall mortality. “If this can be confirmed and replicated, it must be recommended quite extensively for this high-risk group,” said Dr. Sander. The Standing Committee on Vaccination in Germany is currently recommending that high-risk groups be vaccinated against COVID-19 for the fourth time. To date, though, this has only been implemented halfheartedly.
Propensity for mutation
Omicron keeps developing. Following BA.1 and the more infectious subvariant BA.2, BA.4 and BA.5 are spreading in Germany. “To date, there is no evidence that vaccine protection against severe diseases has changed as a result of BA.2 emerging,” said Dr. Sander.
However, the loss of immunity against BA.4 and BA.5 is more strongly pronounced. “If you were infected with BA.1, you are not immune to BA.5,” says Dr. Sander. Lessened immunity from BA.4 and BA.5 is even more pronounced. “Anyone who was infected with BA.1 is not immune to BA.5,” says Dr. Sander. The two clades not only have spike protein mutations shared by BA.2 but also additional spike protein mutations. According to the expert, it could well be that these strains will prevail because they are best able to avoid the immunity of the population.
Adapted vaccines feasible?
“Vaccines adapted to BA.1 were developed very early on and were also part of clinical research,” said Dr. Sander. The initial data indicate that additional antibody responses are being mobilized that may neutralize the new variants.
It was deduced from trials on monkeys that the available vaccines were so good that only small improvements were to be expected, said Dr. Sander.
Moderna’s adapted vaccine
The U.S. pharmaceutical company Moderna recently submitted the first results regarding its bivalent Omicron vaccine mRNA-1273.214, which is adapted to Omicron BA.1. Data from BioNTech are expected soon.
Moderna tested a booster that contains both the spike mRNA from the original vaccine and a new mRNA adapted to the Omicron variant BA.1. The experimental vaccine mRNA-1273.214 exhibited an eightfold increase in geometric mean neutralization titer against Omicron in study participants who were seronegative at the start, compared with the already-approved vaccine.
In its latest notice, Moderna did not publish any data on how effective the updated vaccine is against the virus variants BA.4 or BA.5. Data on clinical endpoints, such as hospitalization or mortality, are also not available.
Conservative epitopes
Should it be assumed that the development of vaccines will always lag the emergence of new subvariants? In this respect, Dr. Sander appears optimistic. “The immunological mechanism is clear, that various B cells and antibodies will be formed that are directed against conservative epitopes that have various variants. This is good news, since we do not want to protect against BA.1 now, just for BA.8 to emerge when the vaccine goes to market. We want to protect ourselves as broadly as possible, and it seems like it may be possible to do so with this vaccine.”
Double vaccination?
Dr. Sander anticipates that a fourth vaccination against COVID-19 will occur with the next wave of the coronavirus in September or October. He remarked that coupling it with the influenza vaccination should be considered.
The coronavirus pandemic has led to shifts in other seasonal waves of pathogens. In the summer, pediatric departments were unexpectedly inundated with children suffering from RSV infections. And while the flu season over the past 2 years has been almost absent, the influenza wave may occur significantly earlier than usual this year.
“In Australia, the influenza wave arrived much earlier this year than usual, which may of course also be fruitful for us,” said Dr. Sander. “Perhaps we will also get influenza as early as in September or October. I would then plead for vaccine centers to be allowed to vaccinate against both influenza and COVID-19 at the same time. Maybe then we will also have a reasonable influenza vaccination rate,” he added.
This article was translated from the Medscape German edition.
A version of this article first appeared on Medscape.com.
The fourth vaccination against COVID-19 is the subject of intense discussion. Immunity against new Omicron variants (currently BA.4 and BA.5) is getting weaker and weaker. Is another vaccination with the available vaccines worth it?
For Leif Erik Sander, MD, director of infectious diseases and pneumology at Charité University Medicine, Berlin, the latest data send a clear message. “The COVID-19 vaccination is still effective against Omicron. After three doses of the vaccine, it continues to prevent severe diseases, respiratory failures, and death,” he reported at the 62nd Congress of the German Pneumology and Respiratory Medicine Society in Leipzig.
The most recent data from the United Kingdom show that the vaccine’s effectiveness against Omicron decreases after just a few months, which speaks in favor of a fourth vaccination. “Omicron is a development that we did not anticipate occurring so early on,” said Dr. Sander.
In terms of phylogenetics, Omicron is far removed from the previous variants of concern. More than 30 mutations to the spike protein (the antigen that is vaccinated against) foster the loss of immunity.
Boosters broaden immunity
“The booster makes all the difference here,” emphasized Dr. Sander. Experiments at Charité Berlin show that after double vaccination, the vaccination sera from healthy young people no longer neutralizes Omicron.
“The third vaccination broadens the humoral immune response against the spike protein so that conserved epitopes that are unchanged, even in Omicron, are addressed, with the result that you have neutralization capacity again,” the infectious diseases specialist explained.
Continued protection
However, data from the United Kingdom on vaccine effectiveness show where the limit lies. Initially, after three doses, vaccine effectiveness against symptomatic disease after Omicron infection is very good. This effectiveness decreases significantly over the course of the next few months. “Lots of people experience an Omicron infection despite the booster,” said Mr. Sander.
Nonetheless, the high incidence of Omicron infections in the recent past has not overwhelmed the health care system. “This is because the vaccine’s effectiveness against severe diseases that require hospitalization and against respiratory failure is still good in the at-risk population over the age of 65, once they have had their three vaccinations,” said Dr. Sander. The data also show that there is good protection of over 90%, even against mortality.
Waning observed
It could be said that currently, vaccination even continues to work against Omicron, says Dr. Sander. It prevents severe disease, respiratory failure, and death. Nonetheless, after just 3 months, a slight waning of immune protection can be observed in all three endpoints.
Therefore, the question arises as to whether a fourth vaccination is worthwhile. In Israel, “Delta was successfully eradicated with the third vaccination,” and now they are trying this again for Omicron with a fourth vaccination, reported Dr. Sander.
Fourth vaccination protective
The first investigations show that protection against severe disease can be increased once more. “For the over-60s, protection is almost quadrupled through the fourth vaccination,” says Dr. Sander. “However, this is still plagued with a lot of uncertainty; it is still not known how stable it is.”
There is hope on the basis of results of an as yet non–peer-reviewed study from Sweden, which is currently available only as a preprint. That study shows that a fourth vaccination in a high-risk population of care-home residents and people older than 80 years can halve overall mortality. “If this can be confirmed and replicated, it must be recommended quite extensively for this high-risk group,” said Dr. Sander. The Standing Committee on Vaccination in Germany is currently recommending that high-risk groups be vaccinated against COVID-19 for the fourth time. To date, though, this has only been implemented halfheartedly.
Propensity for mutation
Omicron keeps developing. Following BA.1 and the more infectious subvariant BA.2, BA.4 and BA.5 are spreading in Germany. “To date, there is no evidence that vaccine protection against severe diseases has changed as a result of BA.2 emerging,” said Dr. Sander.
However, the loss of immunity against BA.4 and BA.5 is more strongly pronounced. “If you were infected with BA.1, you are not immune to BA.5,” says Dr. Sander. Lessened immunity from BA.4 and BA.5 is even more pronounced. “Anyone who was infected with BA.1 is not immune to BA.5,” says Dr. Sander. The two clades not only have spike protein mutations shared by BA.2 but also additional spike protein mutations. According to the expert, it could well be that these strains will prevail because they are best able to avoid the immunity of the population.
Adapted vaccines feasible?
“Vaccines adapted to BA.1 were developed very early on and were also part of clinical research,” said Dr. Sander. The initial data indicate that additional antibody responses are being mobilized that may neutralize the new variants.
It was deduced from trials on monkeys that the available vaccines were so good that only small improvements were to be expected, said Dr. Sander.
Moderna’s adapted vaccine
The U.S. pharmaceutical company Moderna recently submitted the first results regarding its bivalent Omicron vaccine mRNA-1273.214, which is adapted to Omicron BA.1. Data from BioNTech are expected soon.
Moderna tested a booster that contains both the spike mRNA from the original vaccine and a new mRNA adapted to the Omicron variant BA.1. The experimental vaccine mRNA-1273.214 exhibited an eightfold increase in geometric mean neutralization titer against Omicron in study participants who were seronegative at the start, compared with the already-approved vaccine.
In its latest notice, Moderna did not publish any data on how effective the updated vaccine is against the virus variants BA.4 or BA.5. Data on clinical endpoints, such as hospitalization or mortality, are also not available.
Conservative epitopes
Should it be assumed that the development of vaccines will always lag the emergence of new subvariants? In this respect, Dr. Sander appears optimistic. “The immunological mechanism is clear, that various B cells and antibodies will be formed that are directed against conservative epitopes that have various variants. This is good news, since we do not want to protect against BA.1 now, just for BA.8 to emerge when the vaccine goes to market. We want to protect ourselves as broadly as possible, and it seems like it may be possible to do so with this vaccine.”
Double vaccination?
Dr. Sander anticipates that a fourth vaccination against COVID-19 will occur with the next wave of the coronavirus in September or October. He remarked that coupling it with the influenza vaccination should be considered.
The coronavirus pandemic has led to shifts in other seasonal waves of pathogens. In the summer, pediatric departments were unexpectedly inundated with children suffering from RSV infections. And while the flu season over the past 2 years has been almost absent, the influenza wave may occur significantly earlier than usual this year.
“In Australia, the influenza wave arrived much earlier this year than usual, which may of course also be fruitful for us,” said Dr. Sander. “Perhaps we will also get influenza as early as in September or October. I would then plead for vaccine centers to be allowed to vaccinate against both influenza and COVID-19 at the same time. Maybe then we will also have a reasonable influenza vaccination rate,” he added.
This article was translated from the Medscape German edition.
A version of this article first appeared on Medscape.com.
The fourth vaccination against COVID-19 is the subject of intense discussion. Immunity against new Omicron variants (currently BA.4 and BA.5) is getting weaker and weaker. Is another vaccination with the available vaccines worth it?
For Leif Erik Sander, MD, director of infectious diseases and pneumology at Charité University Medicine, Berlin, the latest data send a clear message. “The COVID-19 vaccination is still effective against Omicron. After three doses of the vaccine, it continues to prevent severe diseases, respiratory failures, and death,” he reported at the 62nd Congress of the German Pneumology and Respiratory Medicine Society in Leipzig.
The most recent data from the United Kingdom show that the vaccine’s effectiveness against Omicron decreases after just a few months, which speaks in favor of a fourth vaccination. “Omicron is a development that we did not anticipate occurring so early on,” said Dr. Sander.
In terms of phylogenetics, Omicron is far removed from the previous variants of concern. More than 30 mutations to the spike protein (the antigen that is vaccinated against) foster the loss of immunity.
Boosters broaden immunity
“The booster makes all the difference here,” emphasized Dr. Sander. Experiments at Charité Berlin show that after double vaccination, the vaccination sera from healthy young people no longer neutralizes Omicron.
“The third vaccination broadens the humoral immune response against the spike protein so that conserved epitopes that are unchanged, even in Omicron, are addressed, with the result that you have neutralization capacity again,” the infectious diseases specialist explained.
Continued protection
However, data from the United Kingdom on vaccine effectiveness show where the limit lies. Initially, after three doses, vaccine effectiveness against symptomatic disease after Omicron infection is very good. This effectiveness decreases significantly over the course of the next few months. “Lots of people experience an Omicron infection despite the booster,” said Mr. Sander.
Nonetheless, the high incidence of Omicron infections in the recent past has not overwhelmed the health care system. “This is because the vaccine’s effectiveness against severe diseases that require hospitalization and against respiratory failure is still good in the at-risk population over the age of 65, once they have had their three vaccinations,” said Dr. Sander. The data also show that there is good protection of over 90%, even against mortality.
Waning observed
It could be said that currently, vaccination even continues to work against Omicron, says Dr. Sander. It prevents severe disease, respiratory failure, and death. Nonetheless, after just 3 months, a slight waning of immune protection can be observed in all three endpoints.
Therefore, the question arises as to whether a fourth vaccination is worthwhile. In Israel, “Delta was successfully eradicated with the third vaccination,” and now they are trying this again for Omicron with a fourth vaccination, reported Dr. Sander.
Fourth vaccination protective
The first investigations show that protection against severe disease can be increased once more. “For the over-60s, protection is almost quadrupled through the fourth vaccination,” says Dr. Sander. “However, this is still plagued with a lot of uncertainty; it is still not known how stable it is.”
There is hope on the basis of results of an as yet non–peer-reviewed study from Sweden, which is currently available only as a preprint. That study shows that a fourth vaccination in a high-risk population of care-home residents and people older than 80 years can halve overall mortality. “If this can be confirmed and replicated, it must be recommended quite extensively for this high-risk group,” said Dr. Sander. The Standing Committee on Vaccination in Germany is currently recommending that high-risk groups be vaccinated against COVID-19 for the fourth time. To date, though, this has only been implemented halfheartedly.
Propensity for mutation
Omicron keeps developing. Following BA.1 and the more infectious subvariant BA.2, BA.4 and BA.5 are spreading in Germany. “To date, there is no evidence that vaccine protection against severe diseases has changed as a result of BA.2 emerging,” said Dr. Sander.
However, the loss of immunity against BA.4 and BA.5 is more strongly pronounced. “If you were infected with BA.1, you are not immune to BA.5,” says Dr. Sander. Lessened immunity from BA.4 and BA.5 is even more pronounced. “Anyone who was infected with BA.1 is not immune to BA.5,” says Dr. Sander. The two clades not only have spike protein mutations shared by BA.2 but also additional spike protein mutations. According to the expert, it could well be that these strains will prevail because they are best able to avoid the immunity of the population.
Adapted vaccines feasible?
“Vaccines adapted to BA.1 were developed very early on and were also part of clinical research,” said Dr. Sander. The initial data indicate that additional antibody responses are being mobilized that may neutralize the new variants.
It was deduced from trials on monkeys that the available vaccines were so good that only small improvements were to be expected, said Dr. Sander.
Moderna’s adapted vaccine
The U.S. pharmaceutical company Moderna recently submitted the first results regarding its bivalent Omicron vaccine mRNA-1273.214, which is adapted to Omicron BA.1. Data from BioNTech are expected soon.
Moderna tested a booster that contains both the spike mRNA from the original vaccine and a new mRNA adapted to the Omicron variant BA.1. The experimental vaccine mRNA-1273.214 exhibited an eightfold increase in geometric mean neutralization titer against Omicron in study participants who were seronegative at the start, compared with the already-approved vaccine.
In its latest notice, Moderna did not publish any data on how effective the updated vaccine is against the virus variants BA.4 or BA.5. Data on clinical endpoints, such as hospitalization or mortality, are also not available.
Conservative epitopes
Should it be assumed that the development of vaccines will always lag the emergence of new subvariants? In this respect, Dr. Sander appears optimistic. “The immunological mechanism is clear, that various B cells and antibodies will be formed that are directed against conservative epitopes that have various variants. This is good news, since we do not want to protect against BA.1 now, just for BA.8 to emerge when the vaccine goes to market. We want to protect ourselves as broadly as possible, and it seems like it may be possible to do so with this vaccine.”
Double vaccination?
Dr. Sander anticipates that a fourth vaccination against COVID-19 will occur with the next wave of the coronavirus in September or October. He remarked that coupling it with the influenza vaccination should be considered.
The coronavirus pandemic has led to shifts in other seasonal waves of pathogens. In the summer, pediatric departments were unexpectedly inundated with children suffering from RSV infections. And while the flu season over the past 2 years has been almost absent, the influenza wave may occur significantly earlier than usual this year.
“In Australia, the influenza wave arrived much earlier this year than usual, which may of course also be fruitful for us,” said Dr. Sander. “Perhaps we will also get influenza as early as in September or October. I would then plead for vaccine centers to be allowed to vaccinate against both influenza and COVID-19 at the same time. Maybe then we will also have a reasonable influenza vaccination rate,” he added.
This article was translated from the Medscape German edition.
A version of this article first appeared on Medscape.com.
Menstrual phase impacts exercise effects in type 1 diabetes
Women with type 1 diabetes may need additional glucose after exercise during the luteal phase of the menstrual cycle, compared with other times, according to a study in nine women.
“We know that exercise is very beneficial for people with type 1 diabetes; we also know that fear of hypoglycemia is a major barrier to exercise in this population,” said Jane E. Yardley, PhD, in a presentation at the annual scientific sessions of the American Diabetes Association, New Orleans. Women with type 1 diabetes (T1D) perceive more barriers, compared with men, she added.
The menstrual cycle could be an additional barrier to exercise for women with T1D because it increases glucose fluctuations that have not been well documented in the literature to date, said Dr. Yardley, of the University of Alberta, Augustana.
The follicular phase of the menstrual cycle lasts from menses to the midcycle, about 14 days later. This is followed by the luteal phase, which lasts until approximately day 28, Dr. Yardley explained. Data on insulin sensitivity have shown that the late luteal phase is associated with “a little less insulin sensitivity” in women with T1D, she noted.
To assess the relationship between menstrual cycle, glucose control, and exercise, Dr. Yardley and colleagues compared the effects of a moderate aerobic exercise on glycemic responses between the early follicular and late luteal phases of the menstrual cycle in nine female participants with T1D.
The exercise involved 45 minutes of aerobic cycling at 50% of predetermined peak oxygen uptake (VO2peak) for 45 min. The mean age of the participants was 30.2 years, the mean hemoglobin A1C was 7.4%, and the mean VO2peak was 32.5 mL/kg per min. The women reported regular menstrual cycles, and none were using oral contraceptives.
Blood samples were collected before and immediately after exercise and after an hour of recovery. Participants wore continuous glucose monitors for at least 1 hour before and after exercise.
Menstrual cycle was confirmed via estrogen, estradiol, and progesterone.
Insulin levels varied greatly among the study participants, but the differences were not significant, Dr. Yardley said. Glucose levels consistently decreased during exercise and increased after exercise, she noted.
No significant difference in glucose was observed between the follicular and luteal phases.
However, “this needs to be interpreted in the context of the safety profiles that are in place in our lab,” which include carbohydrate supplements for individuals whose blood glucose levels drop below 4.5 mmol/L, she said.
In the current study, 6 of 9 participants required additional carbohydrates during the luteal phase, but only 1 participant needed additional carbohydrates during the follicular phase, she noted. For this reason, no differences were noted. “We actually prevented changes,” she said.
No significant differences were noted in mean glucose levels or number of hypoglycemic episodes at any of the time points between the two phases.
“One place where we did see a difference was in hyperglycemia 24 hours after exercise,” Dr. Yardley said. Level 1 hyperglycemia 24 hours after exercise was significantly more frequent in the follicular phase, compared with the luteal phase (P = .028).
The study findings were limited by the small sample size and homogenous population, and more research is needed to interpret the data, said Dr. Yardley.
However, the need for more glucose supplementation to prevent hypoglycemia during the luteal phase suggests a higher hypoglycemic risk associated with aerobic exercise during this time, she said.
In addition, the results suggest that the menstrual cycle should be taken into consideration when female participants are involved in exercise studies, she noted.
Study supports personalized exercise plans
“It is important to evaluate effects of exercise in people with type 1 diabetes and evaluate whether there is a difference those effects in men and women,” said Helena W. Rodbard, MD, an endocrinologist in private practice in Rockville, Md., in an interview. “There is also a need to evaluate to what extent the changes in blood glucose patterns in women in response to exercise differ depending on the phase of the ovarian cycle,” said Dr. Rodbard, who was not involved in the study.

In the current study, “the researchers observed a decline in glucose during a 45-minute period of moderate aerobic exercise, cycling at 50% VO2peak followed by an increase during a 60-minute recovery period. There was a suggestive finding, in the nine subjects, that more carbohydrate supplementation was needed during the late luteal phase of the menstrual cycle than during the follicular phase,” Dr. Rodbard noted. “In contrast, the authors reported a significantly increased degree of hyperglycemia during the recovery phase for subjects during the follicular phase. These findings are consistent with and extend several recent studies from Dr. Yardley and coworkers, who have been focused on this area of research,” she said.
“This study provides provocative evidence that glucose responses to aerobic exercise in women may depend on the timing in relationship to their ovarian cycle,” said Dr. Rodbard. “These findings are based on a small group of subjects and were present in some but not all subjects. Clinicians should encourage women to evaluate and record their experiences during and after exercise in terms of need for carbohydrate supplementation for documented or symptomatic hypoglycemia and in terms of glucose changes as recorded using continuous glucose monitoring (CGM), both in relation to type of exercise and in relation to time in the menstrual cycle,” she said.
The findings also highlight the importance of individualized therapy that is “based on subjective inputs combined with analysis of CGM data during and following exercise,” said Dr. Rodbard. “It is likely that use of Automated Insulin Delivery (AID) will be helpful in achieving this level of individualization in view of the wide range of types, intensity, and duration of physical activity and exercise in which people with T1D engage and the myriad factors that can influence the glycemic response,” she said.
Looking ahead, “the authors and others should expand the present series of subjects using aerobic exercise and examine other types of exercise as well,” Dr. Rodbard noted. “It will be important to evaluate the consistency of these changes in glucose patterns within individuals on multiple occasions, and it would be helpful to repeat the studies in women using oral contraceptives.”
Dr. Yardley disclosed research support from Abbott, Dexcom, and LifeScan and disclosed serving on the speaker’s bureau for Abbott Diabetes. Dr. Rodbard had no financial conflicts to disclose. She serves on the Editorial Advisory Board of Clinical Endocrinology News.
Women with type 1 diabetes may need additional glucose after exercise during the luteal phase of the menstrual cycle, compared with other times, according to a study in nine women.
“We know that exercise is very beneficial for people with type 1 diabetes; we also know that fear of hypoglycemia is a major barrier to exercise in this population,” said Jane E. Yardley, PhD, in a presentation at the annual scientific sessions of the American Diabetes Association, New Orleans. Women with type 1 diabetes (T1D) perceive more barriers, compared with men, she added.
The menstrual cycle could be an additional barrier to exercise for women with T1D because it increases glucose fluctuations that have not been well documented in the literature to date, said Dr. Yardley, of the University of Alberta, Augustana.
The follicular phase of the menstrual cycle lasts from menses to the midcycle, about 14 days later. This is followed by the luteal phase, which lasts until approximately day 28, Dr. Yardley explained. Data on insulin sensitivity have shown that the late luteal phase is associated with “a little less insulin sensitivity” in women with T1D, she noted.
To assess the relationship between menstrual cycle, glucose control, and exercise, Dr. Yardley and colleagues compared the effects of a moderate aerobic exercise on glycemic responses between the early follicular and late luteal phases of the menstrual cycle in nine female participants with T1D.
The exercise involved 45 minutes of aerobic cycling at 50% of predetermined peak oxygen uptake (VO2peak) for 45 min. The mean age of the participants was 30.2 years, the mean hemoglobin A1C was 7.4%, and the mean VO2peak was 32.5 mL/kg per min. The women reported regular menstrual cycles, and none were using oral contraceptives.
Blood samples were collected before and immediately after exercise and after an hour of recovery. Participants wore continuous glucose monitors for at least 1 hour before and after exercise.
Menstrual cycle was confirmed via estrogen, estradiol, and progesterone.
Insulin levels varied greatly among the study participants, but the differences were not significant, Dr. Yardley said. Glucose levels consistently decreased during exercise and increased after exercise, she noted.
No significant difference in glucose was observed between the follicular and luteal phases.
However, “this needs to be interpreted in the context of the safety profiles that are in place in our lab,” which include carbohydrate supplements for individuals whose blood glucose levels drop below 4.5 mmol/L, she said.
In the current study, 6 of 9 participants required additional carbohydrates during the luteal phase, but only 1 participant needed additional carbohydrates during the follicular phase, she noted. For this reason, no differences were noted. “We actually prevented changes,” she said.
No significant differences were noted in mean glucose levels or number of hypoglycemic episodes at any of the time points between the two phases.
“One place where we did see a difference was in hyperglycemia 24 hours after exercise,” Dr. Yardley said. Level 1 hyperglycemia 24 hours after exercise was significantly more frequent in the follicular phase, compared with the luteal phase (P = .028).
The study findings were limited by the small sample size and homogenous population, and more research is needed to interpret the data, said Dr. Yardley.
However, the need for more glucose supplementation to prevent hypoglycemia during the luteal phase suggests a higher hypoglycemic risk associated with aerobic exercise during this time, she said.
In addition, the results suggest that the menstrual cycle should be taken into consideration when female participants are involved in exercise studies, she noted.
Study supports personalized exercise plans
“It is important to evaluate effects of exercise in people with type 1 diabetes and evaluate whether there is a difference those effects in men and women,” said Helena W. Rodbard, MD, an endocrinologist in private practice in Rockville, Md., in an interview. “There is also a need to evaluate to what extent the changes in blood glucose patterns in women in response to exercise differ depending on the phase of the ovarian cycle,” said Dr. Rodbard, who was not involved in the study.
In the current study, “the researchers observed a decline in glucose during a 45-minute period of moderate aerobic exercise, cycling at 50% VO2peak followed by an increase during a 60-minute recovery period. There was a suggestive finding, in the nine subjects, that more carbohydrate supplementation was needed during the late luteal phase of the menstrual cycle than during the follicular phase,” Dr. Rodbard noted. “In contrast, the authors reported a significantly increased degree of hyperglycemia during the recovery phase for subjects during the follicular phase. These findings are consistent with and extend several recent studies from Dr. Yardley and coworkers, who have been focused on this area of research,” she said.
“This study provides provocative evidence that glucose responses to aerobic exercise in women may depend on the timing in relationship to their ovarian cycle,” said Dr. Rodbard. “These findings are based on a small group of subjects and were present in some but not all subjects. Clinicians should encourage women to evaluate and record their experiences during and after exercise in terms of need for carbohydrate supplementation for documented or symptomatic hypoglycemia and in terms of glucose changes as recorded using continuous glucose monitoring (CGM), both in relation to type of exercise and in relation to time in the menstrual cycle,” she said.
The findings also highlight the importance of individualized therapy that is “based on subjective inputs combined with analysis of CGM data during and following exercise,” said Dr. Rodbard. “It is likely that use of Automated Insulin Delivery (AID) will be helpful in achieving this level of individualization in view of the wide range of types, intensity, and duration of physical activity and exercise in which people with T1D engage and the myriad factors that can influence the glycemic response,” she said.
Looking ahead, “the authors and others should expand the present series of subjects using aerobic exercise and examine other types of exercise as well,” Dr. Rodbard noted. “It will be important to evaluate the consistency of these changes in glucose patterns within individuals on multiple occasions, and it would be helpful to repeat the studies in women using oral contraceptives.”
Dr. Yardley disclosed research support from Abbott, Dexcom, and LifeScan and disclosed serving on the speaker’s bureau for Abbott Diabetes. Dr. Rodbard had no financial conflicts to disclose. She serves on the Editorial Advisory Board of Clinical Endocrinology News.
Women with type 1 diabetes may need additional glucose after exercise during the luteal phase of the menstrual cycle, compared with other times, according to a study in nine women.
“We know that exercise is very beneficial for people with type 1 diabetes; we also know that fear of hypoglycemia is a major barrier to exercise in this population,” said Jane E. Yardley, PhD, in a presentation at the annual scientific sessions of the American Diabetes Association, New Orleans. Women with type 1 diabetes (T1D) perceive more barriers, compared with men, she added.
The menstrual cycle could be an additional barrier to exercise for women with T1D because it increases glucose fluctuations that have not been well documented in the literature to date, said Dr. Yardley, of the University of Alberta, Augustana.
The follicular phase of the menstrual cycle lasts from menses to the midcycle, about 14 days later. This is followed by the luteal phase, which lasts until approximately day 28, Dr. Yardley explained. Data on insulin sensitivity have shown that the late luteal phase is associated with “a little less insulin sensitivity” in women with T1D, she noted.
To assess the relationship between menstrual cycle, glucose control, and exercise, Dr. Yardley and colleagues compared the effects of a moderate aerobic exercise on glycemic responses between the early follicular and late luteal phases of the menstrual cycle in nine female participants with T1D.
The exercise involved 45 minutes of aerobic cycling at 50% of predetermined peak oxygen uptake (VO2peak) for 45 min. The mean age of the participants was 30.2 years, the mean hemoglobin A1C was 7.4%, and the mean VO2peak was 32.5 mL/kg per min. The women reported regular menstrual cycles, and none were using oral contraceptives.
Blood samples were collected before and immediately after exercise and after an hour of recovery. Participants wore continuous glucose monitors for at least 1 hour before and after exercise.
Menstrual cycle was confirmed via estrogen, estradiol, and progesterone.
Insulin levels varied greatly among the study participants, but the differences were not significant, Dr. Yardley said. Glucose levels consistently decreased during exercise and increased after exercise, she noted.
No significant difference in glucose was observed between the follicular and luteal phases.
However, “this needs to be interpreted in the context of the safety profiles that are in place in our lab,” which include carbohydrate supplements for individuals whose blood glucose levels drop below 4.5 mmol/L, she said.
In the current study, 6 of 9 participants required additional carbohydrates during the luteal phase, but only 1 participant needed additional carbohydrates during the follicular phase, she noted. For this reason, no differences were noted. “We actually prevented changes,” she said.
No significant differences were noted in mean glucose levels or number of hypoglycemic episodes at any of the time points between the two phases.
“One place where we did see a difference was in hyperglycemia 24 hours after exercise,” Dr. Yardley said. Level 1 hyperglycemia 24 hours after exercise was significantly more frequent in the follicular phase, compared with the luteal phase (P = .028).
The study findings were limited by the small sample size and homogenous population, and more research is needed to interpret the data, said Dr. Yardley.
However, the need for more glucose supplementation to prevent hypoglycemia during the luteal phase suggests a higher hypoglycemic risk associated with aerobic exercise during this time, she said.
In addition, the results suggest that the menstrual cycle should be taken into consideration when female participants are involved in exercise studies, she noted.
Study supports personalized exercise plans
“It is important to evaluate effects of exercise in people with type 1 diabetes and evaluate whether there is a difference those effects in men and women,” said Helena W. Rodbard, MD, an endocrinologist in private practice in Rockville, Md., in an interview. “There is also a need to evaluate to what extent the changes in blood glucose patterns in women in response to exercise differ depending on the phase of the ovarian cycle,” said Dr. Rodbard, who was not involved in the study.
In the current study, “the researchers observed a decline in glucose during a 45-minute period of moderate aerobic exercise, cycling at 50% VO2peak followed by an increase during a 60-minute recovery period. There was a suggestive finding, in the nine subjects, that more carbohydrate supplementation was needed during the late luteal phase of the menstrual cycle than during the follicular phase,” Dr. Rodbard noted. “In contrast, the authors reported a significantly increased degree of hyperglycemia during the recovery phase for subjects during the follicular phase. These findings are consistent with and extend several recent studies from Dr. Yardley and coworkers, who have been focused on this area of research,” she said.
“This study provides provocative evidence that glucose responses to aerobic exercise in women may depend on the timing in relationship to their ovarian cycle,” said Dr. Rodbard. “These findings are based on a small group of subjects and were present in some but not all subjects. Clinicians should encourage women to evaluate and record their experiences during and after exercise in terms of need for carbohydrate supplementation for documented or symptomatic hypoglycemia and in terms of glucose changes as recorded using continuous glucose monitoring (CGM), both in relation to type of exercise and in relation to time in the menstrual cycle,” she said.
The findings also highlight the importance of individualized therapy that is “based on subjective inputs combined with analysis of CGM data during and following exercise,” said Dr. Rodbard. “It is likely that use of Automated Insulin Delivery (AID) will be helpful in achieving this level of individualization in view of the wide range of types, intensity, and duration of physical activity and exercise in which people with T1D engage and the myriad factors that can influence the glycemic response,” she said.
Looking ahead, “the authors and others should expand the present series of subjects using aerobic exercise and examine other types of exercise as well,” Dr. Rodbard noted. “It will be important to evaluate the consistency of these changes in glucose patterns within individuals on multiple occasions, and it would be helpful to repeat the studies in women using oral contraceptives.”
Dr. Yardley disclosed research support from Abbott, Dexcom, and LifeScan and disclosed serving on the speaker’s bureau for Abbott Diabetes. Dr. Rodbard had no financial conflicts to disclose. She serves on the Editorial Advisory Board of Clinical Endocrinology News.
FROM ADA 2022