User login
Family affair: OncBrothers host oncology hangout online
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.

Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.
Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.
Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
Obesity and intestinal inflammation might influence development of IBS in children
Key clinical point: Pediatric patients with irritable bowel syndrome (IBS) and normal weight had higher levels of fecal calprotectin than those with IBS and obesity, suggesting the role of obesity and intestinal inflammation in the development and manifestations of IBS in children.
Major finding: The mean calprotectin levels were significantly higher in patients with body mass index <85th vs 85th to <95th percentile (P = .028) and ≥95th percentile (P ≥ .025), with the difference being prominent among children aged between 6 and 12 years (P = .029) but not among adolescents aged between 12 and 18 years (P = .139).
Study details: The data come from a retrospective analysis of 277 pediatric patients with IBS.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Kim JH et al. Association between body mass index and fecal calprotectin levels in children and adolescents with irritable bowel syndrome. Medicine (Baltimore). 2022;101(32):e29968 (Aug 12). Doi: 10.1097/MD.0000000000029968.
Key clinical point: Pediatric patients with irritable bowel syndrome (IBS) and normal weight had higher levels of fecal calprotectin than those with IBS and obesity, suggesting the role of obesity and intestinal inflammation in the development and manifestations of IBS in children.
Major finding: The mean calprotectin levels were significantly higher in patients with body mass index <85th vs 85th to <95th percentile (P = .028) and ≥95th percentile (P ≥ .025), with the difference being prominent among children aged between 6 and 12 years (P = .029) but not among adolescents aged between 12 and 18 years (P = .139).
Study details: The data come from a retrospective analysis of 277 pediatric patients with IBS.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Kim JH et al. Association between body mass index and fecal calprotectin levels in children and adolescents with irritable bowel syndrome. Medicine (Baltimore). 2022;101(32):e29968 (Aug 12). Doi: 10.1097/MD.0000000000029968.
Key clinical point: Pediatric patients with irritable bowel syndrome (IBS) and normal weight had higher levels of fecal calprotectin than those with IBS and obesity, suggesting the role of obesity and intestinal inflammation in the development and manifestations of IBS in children.
Major finding: The mean calprotectin levels were significantly higher in patients with body mass index <85th vs 85th to <95th percentile (P = .028) and ≥95th percentile (P ≥ .025), with the difference being prominent among children aged between 6 and 12 years (P = .029) but not among adolescents aged between 12 and 18 years (P = .139).
Study details: The data come from a retrospective analysis of 277 pediatric patients with IBS.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Kim JH et al. Association between body mass index and fecal calprotectin levels in children and adolescents with irritable bowel syndrome. Medicine (Baltimore). 2022;101(32):e29968 (Aug 12). Doi: 10.1097/MD.0000000000029968.
Meta-analysis evaluates association between Helicobacter pylori infection and IBS
Key clinical point: Meta-analysis indicated a relatively higher but nonsignificantly increased risk for Helicobacter pylori infection (HPI) in patients with irritable bowel syndrome (IBS) vs non-IBS participants; however, the association between IBS and HPI could be an underestimation, with a positive association persisting between HPI and diarrhea-type IBS (IBS-D).
Major finding: A nonsignificant positive association was observed between HPI and IBS (odds ratio [OR], 1.03 ;lt; P = .84); however, the association was significant after excluding studies with defined confounding factors (adjusted OR, 1.29; P = .03), indicating an underestimation. The positive association of HPI persisted with IBS-D (OR, 1.54; P = .0003) but not with IBS-C (P = .17) or IBS-M (P = .33).
Study details: Findings are from a systematic review and meta-analysis of 13 studies including 1,403 patients with IBS and 11,770 non-IBS participants.
Disclosures: This research was funded by the National Natural Science Foundation of China and the Natural Science Foundation of Guangdong Province. The authors declared no conflicts of interest.
Source: Wang Z et al. Helicobacterpylori infection-A risk factor for irritable bowel syndrome? An updated systematic review and meta-analysis. Medicina (Kaunas). 2022;58(8):1035 (Aug 2). Doi: 10.3390/medicina58081035.
Key clinical point: Meta-analysis indicated a relatively higher but nonsignificantly increased risk for Helicobacter pylori infection (HPI) in patients with irritable bowel syndrome (IBS) vs non-IBS participants; however, the association between IBS and HPI could be an underestimation, with a positive association persisting between HPI and diarrhea-type IBS (IBS-D).
Major finding: A nonsignificant positive association was observed between HPI and IBS (odds ratio [OR], 1.03 ;lt; P = .84); however, the association was significant after excluding studies with defined confounding factors (adjusted OR, 1.29; P = .03), indicating an underestimation. The positive association of HPI persisted with IBS-D (OR, 1.54; P = .0003) but not with IBS-C (P = .17) or IBS-M (P = .33).
Study details: Findings are from a systematic review and meta-analysis of 13 studies including 1,403 patients with IBS and 11,770 non-IBS participants.
Disclosures: This research was funded by the National Natural Science Foundation of China and the Natural Science Foundation of Guangdong Province. The authors declared no conflicts of interest.
Source: Wang Z et al. Helicobacterpylori infection-A risk factor for irritable bowel syndrome? An updated systematic review and meta-analysis. Medicina (Kaunas). 2022;58(8):1035 (Aug 2). Doi: 10.3390/medicina58081035.
Key clinical point: Meta-analysis indicated a relatively higher but nonsignificantly increased risk for Helicobacter pylori infection (HPI) in patients with irritable bowel syndrome (IBS) vs non-IBS participants; however, the association between IBS and HPI could be an underestimation, with a positive association persisting between HPI and diarrhea-type IBS (IBS-D).
Major finding: A nonsignificant positive association was observed between HPI and IBS (odds ratio [OR], 1.03 ;lt; P = .84); however, the association was significant after excluding studies with defined confounding factors (adjusted OR, 1.29; P = .03), indicating an underestimation. The positive association of HPI persisted with IBS-D (OR, 1.54; P = .0003) but not with IBS-C (P = .17) or IBS-M (P = .33).
Study details: Findings are from a systematic review and meta-analysis of 13 studies including 1,403 patients with IBS and 11,770 non-IBS participants.
Disclosures: This research was funded by the National Natural Science Foundation of China and the Natural Science Foundation of Guangdong Province. The authors declared no conflicts of interest.
Source: Wang Z et al. Helicobacterpylori infection-A risk factor for irritable bowel syndrome? An updated systematic review and meta-analysis. Medicina (Kaunas). 2022;58(8):1035 (Aug 2). Doi: 10.3390/medicina58081035.
IBS prevalence in veterans and its associations with psychological factors
Key clinical point: Irritable bowel syndrome (IBS) is prevalent among veterans and is associated with significant psychological comorbidities.
Major finding: Overall, 28.4% of veterans met Rome IV IBS criteria, and significant associations of IBS with anxiety (adjusted odds ratio [aOR], 3.47; P < .001), depression (aOR, 2.88; P < .001), post-traumatic stress disorder (aOR, 3.09; P < .001), prior infectious enteritis (aOR, 4.44; P < .001), and a history of bowel problems after antibiotics (aOR, 1.84; P = .005) were observed.
Study details: The data come from a cross-sectional survey including 858 veteran respondents (mean age, 53.6 years), of whom 244 had IBS.
Disclosures: The authors declared no conflicts of interest.
Source: Shin A et al. The prevalence, humanistic burden, and healthcare impact of irritable bowel syndrome (IBS) among United States veterans. Clin Gastroenterol Hepatol. 2022 (Aug 11). Doi: 10.1016/j.cgh.2022.08.005.
Key clinical point: Irritable bowel syndrome (IBS) is prevalent among veterans and is associated with significant psychological comorbidities.
Major finding: Overall, 28.4% of veterans met Rome IV IBS criteria, and significant associations of IBS with anxiety (adjusted odds ratio [aOR], 3.47; P < .001), depression (aOR, 2.88; P < .001), post-traumatic stress disorder (aOR, 3.09; P < .001), prior infectious enteritis (aOR, 4.44; P < .001), and a history of bowel problems after antibiotics (aOR, 1.84; P = .005) were observed.
Study details: The data come from a cross-sectional survey including 858 veteran respondents (mean age, 53.6 years), of whom 244 had IBS.
Disclosures: The authors declared no conflicts of interest.
Source: Shin A et al. The prevalence, humanistic burden, and healthcare impact of irritable bowel syndrome (IBS) among United States veterans. Clin Gastroenterol Hepatol. 2022 (Aug 11). Doi: 10.1016/j.cgh.2022.08.005.
Key clinical point: Irritable bowel syndrome (IBS) is prevalent among veterans and is associated with significant psychological comorbidities.
Major finding: Overall, 28.4% of veterans met Rome IV IBS criteria, and significant associations of IBS with anxiety (adjusted odds ratio [aOR], 3.47; P < .001), depression (aOR, 2.88; P < .001), post-traumatic stress disorder (aOR, 3.09; P < .001), prior infectious enteritis (aOR, 4.44; P < .001), and a history of bowel problems after antibiotics (aOR, 1.84; P = .005) were observed.
Study details: The data come from a cross-sectional survey including 858 veteran respondents (mean age, 53.6 years), of whom 244 had IBS.
Disclosures: The authors declared no conflicts of interest.
Source: Shin A et al. The prevalence, humanistic burden, and healthcare impact of irritable bowel syndrome (IBS) among United States veterans. Clin Gastroenterol Hepatol. 2022 (Aug 11). Doi: 10.1016/j.cgh.2022.08.005.
Somatization and celiac disease among primary risk factors for IBS
Key clinical point: Somatization and celiac disease are the primary risk factors associated with irritable bowel syndrome (IBS) in both men and women.
Major finding: The risk for IBS was almost 4-fold higher in men (adjusted odds ratio [aOR] 4.786; 95% CI 4.544-5.041) and women (aOR 5.326; 95% CI 4.863-5.832) experiencing somatization, with the second important influencing factor being celiac disease (men: aOR 4.107; 95% CI 3.132-5.385; women: aOR 3.783; 95% CI 3.310-4.323).
Study details: This study included 31,918 participants who met the Rome III criteria for IBS and completed the Digestive Health Questionnaire.
Disclosures: This study was supported by QW of the National Natural Science Foundation of China and the National Office for Philosophy and Social Sciences. The authors declared no potential conflicts of interest.
Source: Wang K et al. Factors related to irritable bowel syndrome and differences among subtypes: A cross-sectional study in the UK Biobank. Front Pharmacol. 2022;13:905564 (Aug 26). Doi: 10.3389/fphar.2022.905564
Key clinical point: Somatization and celiac disease are the primary risk factors associated with irritable bowel syndrome (IBS) in both men and women.
Major finding: The risk for IBS was almost 4-fold higher in men (adjusted odds ratio [aOR] 4.786; 95% CI 4.544-5.041) and women (aOR 5.326; 95% CI 4.863-5.832) experiencing somatization, with the second important influencing factor being celiac disease (men: aOR 4.107; 95% CI 3.132-5.385; women: aOR 3.783; 95% CI 3.310-4.323).
Study details: This study included 31,918 participants who met the Rome III criteria for IBS and completed the Digestive Health Questionnaire.
Disclosures: This study was supported by QW of the National Natural Science Foundation of China and the National Office for Philosophy and Social Sciences. The authors declared no potential conflicts of interest.
Source: Wang K et al. Factors related to irritable bowel syndrome and differences among subtypes: A cross-sectional study in the UK Biobank. Front Pharmacol. 2022;13:905564 (Aug 26). Doi: 10.3389/fphar.2022.905564
Key clinical point: Somatization and celiac disease are the primary risk factors associated with irritable bowel syndrome (IBS) in both men and women.
Major finding: The risk for IBS was almost 4-fold higher in men (adjusted odds ratio [aOR] 4.786; 95% CI 4.544-5.041) and women (aOR 5.326; 95% CI 4.863-5.832) experiencing somatization, with the second important influencing factor being celiac disease (men: aOR 4.107; 95% CI 3.132-5.385; women: aOR 3.783; 95% CI 3.310-4.323).
Study details: This study included 31,918 participants who met the Rome III criteria for IBS and completed the Digestive Health Questionnaire.
Disclosures: This study was supported by QW of the National Natural Science Foundation of China and the National Office for Philosophy and Social Sciences. The authors declared no potential conflicts of interest.
Source: Wang K et al. Factors related to irritable bowel syndrome and differences among subtypes: A cross-sectional study in the UK Biobank. Front Pharmacol. 2022;13:905564 (Aug 26). Doi: 10.3389/fphar.2022.905564
Supplementation with a multistrain probiotic improves leaky gut in patients with IBS-D
Key clinical point: Supplementation with a multistrain probiotic for 30 days improved intestinal permeability, stool consistency, and health-related quality-of-life (QoL) in a considerable proportion of patients with diarrhea-predominant irritable bowel syndrome (IBS-D).
Major finding: On day 30, the intestinal permeability improved or normalized in 81.5% of patients, with the intestinal permeability decreasing by 3.4 units (P = .0005), the Bristol Stool Scale score decreasing by 0.9 units (P = .0057), and the IBS-QoL total score increasing by 8.0 points (95% CI 3.0-12.9). The multistrain probiotic was well tolerated.
Study details: The data come from a pilot, open-label, prospective, phase 4 study including 30 patients with IBS-D and leaky gut who received 2 capsules of multistrain probiotic daily for 30 days.
Disclosures: This study was sponsored by PiLeJe Laboratoire. SA Abdellah and C Gal declared being employees of PiLeJe Laboratoire. L Laterza and A Gasbarrini reported ties with various sources.
Source: Ait Abdellah S et al. Effect of a multistrain probiotic on leaky gut in patients with diarrhea-predominant irritable bowel syndrome (IBS-D): A pilot study. Dig Dis. 2022 (Aug 25). Doi: 10.1159/000526712
Key clinical point: Supplementation with a multistrain probiotic for 30 days improved intestinal permeability, stool consistency, and health-related quality-of-life (QoL) in a considerable proportion of patients with diarrhea-predominant irritable bowel syndrome (IBS-D).
Major finding: On day 30, the intestinal permeability improved or normalized in 81.5% of patients, with the intestinal permeability decreasing by 3.4 units (P = .0005), the Bristol Stool Scale score decreasing by 0.9 units (P = .0057), and the IBS-QoL total score increasing by 8.0 points (95% CI 3.0-12.9). The multistrain probiotic was well tolerated.
Study details: The data come from a pilot, open-label, prospective, phase 4 study including 30 patients with IBS-D and leaky gut who received 2 capsules of multistrain probiotic daily for 30 days.
Disclosures: This study was sponsored by PiLeJe Laboratoire. SA Abdellah and C Gal declared being employees of PiLeJe Laboratoire. L Laterza and A Gasbarrini reported ties with various sources.
Source: Ait Abdellah S et al. Effect of a multistrain probiotic on leaky gut in patients with diarrhea-predominant irritable bowel syndrome (IBS-D): A pilot study. Dig Dis. 2022 (Aug 25). Doi: 10.1159/000526712
Key clinical point: Supplementation with a multistrain probiotic for 30 days improved intestinal permeability, stool consistency, and health-related quality-of-life (QoL) in a considerable proportion of patients with diarrhea-predominant irritable bowel syndrome (IBS-D).
Major finding: On day 30, the intestinal permeability improved or normalized in 81.5% of patients, with the intestinal permeability decreasing by 3.4 units (P = .0005), the Bristol Stool Scale score decreasing by 0.9 units (P = .0057), and the IBS-QoL total score increasing by 8.0 points (95% CI 3.0-12.9). The multistrain probiotic was well tolerated.
Study details: The data come from a pilot, open-label, prospective, phase 4 study including 30 patients with IBS-D and leaky gut who received 2 capsules of multistrain probiotic daily for 30 days.
Disclosures: This study was sponsored by PiLeJe Laboratoire. SA Abdellah and C Gal declared being employees of PiLeJe Laboratoire. L Laterza and A Gasbarrini reported ties with various sources.
Source: Ait Abdellah S et al. Effect of a multistrain probiotic on leaky gut in patients with diarrhea-predominant irritable bowel syndrome (IBS-D): A pilot study. Dig Dis. 2022 (Aug 25). Doi: 10.1159/000526712
Increased risk for IBS among women with endometriosis
Key clinical point: Endometriosis is associated with a 3-fold increase in the risk for irritable bowel syndrome (IBS), with 1 in every 5 women with endometriosis having IBS.
Major finding: The odds of IBS were significantly higher in women with endometriosis compared with healthy controls (odds ratio 2.97; 95% CI 2.17-4.06), and the pooled prevalence of IBS among women with endometriosis was 23.4% (95% CI 9.7%-37.2%).
Study details: This study evaluated the prevalence of IBS in endometriosis (meta-analysis of 6 studies) and association between endometriosis and IBS (meta-analysis of 11 studies involving 18,887 patients with endometriosis and 77,171 healthy controls).
Disclosures: This study did not report any source of funding. The authors declared no conflicts of interest.
Source: Nabi MY et al. Endometriosis and irritable bowel syndrome: A systematic review and meta-analyses. Front Med (Lausanne). 2022;9:914356 (Jul 25). Doi: 10.3389/fmed.2022.914356
Key clinical point: Endometriosis is associated with a 3-fold increase in the risk for irritable bowel syndrome (IBS), with 1 in every 5 women with endometriosis having IBS.
Major finding: The odds of IBS were significantly higher in women with endometriosis compared with healthy controls (odds ratio 2.97; 95% CI 2.17-4.06), and the pooled prevalence of IBS among women with endometriosis was 23.4% (95% CI 9.7%-37.2%).
Study details: This study evaluated the prevalence of IBS in endometriosis (meta-analysis of 6 studies) and association between endometriosis and IBS (meta-analysis of 11 studies involving 18,887 patients with endometriosis and 77,171 healthy controls).
Disclosures: This study did not report any source of funding. The authors declared no conflicts of interest.
Source: Nabi MY et al. Endometriosis and irritable bowel syndrome: A systematic review and meta-analyses. Front Med (Lausanne). 2022;9:914356 (Jul 25). Doi: 10.3389/fmed.2022.914356
Key clinical point: Endometriosis is associated with a 3-fold increase in the risk for irritable bowel syndrome (IBS), with 1 in every 5 women with endometriosis having IBS.
Major finding: The odds of IBS were significantly higher in women with endometriosis compared with healthy controls (odds ratio 2.97; 95% CI 2.17-4.06), and the pooled prevalence of IBS among women with endometriosis was 23.4% (95% CI 9.7%-37.2%).
Study details: This study evaluated the prevalence of IBS in endometriosis (meta-analysis of 6 studies) and association between endometriosis and IBS (meta-analysis of 11 studies involving 18,887 patients with endometriosis and 77,171 healthy controls).
Disclosures: This study did not report any source of funding. The authors declared no conflicts of interest.
Source: Nabi MY et al. Endometriosis and irritable bowel syndrome: A systematic review and meta-analyses. Front Med (Lausanne). 2022;9:914356 (Jul 25). Doi: 10.3389/fmed.2022.914356
IBS symptoms affecting more than two-thirds of patients with IBD
Key clinical point: More than two-thirds of patients with inflammatory bowel disease (IBD) were affected by irritable bowel syndrome (IBS)-type symptoms, which were associated with worse depression, anxiety, somatoform symptoms, and quality-of-life scores.
Major finding: Overall, 67.2% of patients reported IBS-type symptoms at least once during the follow-up, with anxiety, depression, and somatoform symptom scores being worse in patients with vs without IBS-type symptoms (P < .001).
Study details: The data come from a 6-year longitudinal follow-up study including 760 individuals with well-characterized IBD.
Disclosures: This study was funded by The Leeds Teaching Hospitals Charitable Foundation and Tillotts Pharma U.K. Ltd. The authors declared no conflicts of interest.
Source: Fairbrass KM et al. Natural history and impact of irritable bowel syndrome-type symptoms in inflammatory bowel disease during 6 years of longitudinal follow-up. Aliment Pharmacol Ther. 2022 (Aug 22). Doi: 10.1111/apt.17193
Key clinical point: More than two-thirds of patients with inflammatory bowel disease (IBD) were affected by irritable bowel syndrome (IBS)-type symptoms, which were associated with worse depression, anxiety, somatoform symptoms, and quality-of-life scores.
Major finding: Overall, 67.2% of patients reported IBS-type symptoms at least once during the follow-up, with anxiety, depression, and somatoform symptom scores being worse in patients with vs without IBS-type symptoms (P < .001).
Study details: The data come from a 6-year longitudinal follow-up study including 760 individuals with well-characterized IBD.
Disclosures: This study was funded by The Leeds Teaching Hospitals Charitable Foundation and Tillotts Pharma U.K. Ltd. The authors declared no conflicts of interest.
Source: Fairbrass KM et al. Natural history and impact of irritable bowel syndrome-type symptoms in inflammatory bowel disease during 6 years of longitudinal follow-up. Aliment Pharmacol Ther. 2022 (Aug 22). Doi: 10.1111/apt.17193
Key clinical point: More than two-thirds of patients with inflammatory bowel disease (IBD) were affected by irritable bowel syndrome (IBS)-type symptoms, which were associated with worse depression, anxiety, somatoform symptoms, and quality-of-life scores.
Major finding: Overall, 67.2% of patients reported IBS-type symptoms at least once during the follow-up, with anxiety, depression, and somatoform symptom scores being worse in patients with vs without IBS-type symptoms (P < .001).
Study details: The data come from a 6-year longitudinal follow-up study including 760 individuals with well-characterized IBD.
Disclosures: This study was funded by The Leeds Teaching Hospitals Charitable Foundation and Tillotts Pharma U.K. Ltd. The authors declared no conflicts of interest.
Source: Fairbrass KM et al. Natural history and impact of irritable bowel syndrome-type symptoms in inflammatory bowel disease during 6 years of longitudinal follow-up. Aliment Pharmacol Ther. 2022 (Aug 22). Doi: 10.1111/apt.17193
High degree of fatty liver and NAFLD tied to increased incident IBS risk
Key clinical point: The risk for incident irritable bowel syndrome (IBS) was significantly higher in individuals in the highest vs lowest quartile of nonalcoholic fatty liver index and in those with a diagnosis of nonalcoholic fatty liver disease (NAFLD).
Major finding: The risk of developing IBS was 21% higher among individuals in the highest vs lowest quartile of fatty liver index (hazard ratio [HR] 1.21; Ptrend < .001) and 13% higher among patients with vs without NAFLD (HR 1.13; 95% CI 1.05-1.17).
Study details: Findings are from an analysis of 396,838 participants from a large-scale prospective cohort who were free from IBS, any cancer, inflammatory bowel disease, alcoholic liver disease, and celiac disease, of which 38.6% had an NAFLD diagnosis.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflicts of interest.
Source: Wu S et al. Non-alcoholic fatty liver is associated with increased risk of irritable bowel syndrome: A prospective cohort study. BMC Med. 2022;20(1):262 (Aug 22). Doi: 10.1186/s12916-022-02460-8
Key clinical point: The risk for incident irritable bowel syndrome (IBS) was significantly higher in individuals in the highest vs lowest quartile of nonalcoholic fatty liver index and in those with a diagnosis of nonalcoholic fatty liver disease (NAFLD).
Major finding: The risk of developing IBS was 21% higher among individuals in the highest vs lowest quartile of fatty liver index (hazard ratio [HR] 1.21; Ptrend < .001) and 13% higher among patients with vs without NAFLD (HR 1.13; 95% CI 1.05-1.17).
Study details: Findings are from an analysis of 396,838 participants from a large-scale prospective cohort who were free from IBS, any cancer, inflammatory bowel disease, alcoholic liver disease, and celiac disease, of which 38.6% had an NAFLD diagnosis.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflicts of interest.
Source: Wu S et al. Non-alcoholic fatty liver is associated with increased risk of irritable bowel syndrome: A prospective cohort study. BMC Med. 2022;20(1):262 (Aug 22). Doi: 10.1186/s12916-022-02460-8
Key clinical point: The risk for incident irritable bowel syndrome (IBS) was significantly higher in individuals in the highest vs lowest quartile of nonalcoholic fatty liver index and in those with a diagnosis of nonalcoholic fatty liver disease (NAFLD).
Major finding: The risk of developing IBS was 21% higher among individuals in the highest vs lowest quartile of fatty liver index (hazard ratio [HR] 1.21; Ptrend < .001) and 13% higher among patients with vs without NAFLD (HR 1.13; 95% CI 1.05-1.17).
Study details: Findings are from an analysis of 396,838 participants from a large-scale prospective cohort who were free from IBS, any cancer, inflammatory bowel disease, alcoholic liver disease, and celiac disease, of which 38.6% had an NAFLD diagnosis.
Disclosures: This study was funded by the National Natural Science Foundation of China. The authors declared no conflicts of interest.
Source: Wu S et al. Non-alcoholic fatty liver is associated with increased risk of irritable bowel syndrome: A prospective cohort study. BMC Med. 2022;20(1):262 (Aug 22). Doi: 10.1186/s12916-022-02460-8
Home BP monitoring in older adults falls short of recommendations
Just over 51% of older hypertensive adults regularly check their own blood pressure, compared with 48% of those with blood pressure–related health conditions (BPHCs), based on a 2021 survey of individuals aged 50-80 years.
“Guidelines recommend that patients use self-measured blood pressure monitoring (SBPM) outside the clinic to diagnose and manage hypertension,” but just 61% of respondents with a BPHC and 68% of those with hypertension said that they had received such a recommendation from a physician, nurse, or other health care professional, Melanie V. Springer, MD, and associates said in JAMA Network Open.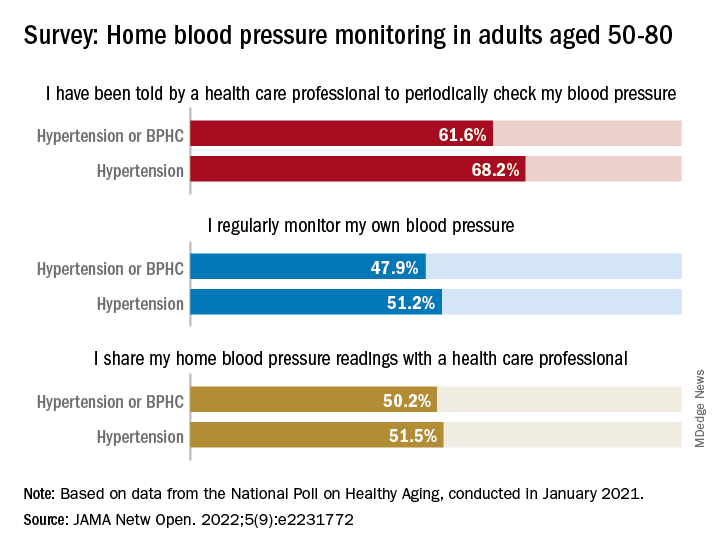
The prevalence of regular monitoring among those with hypertension, 51.2%, does, however, compare favorably with an earlier study showing that 43% of adults aged 18 and older regularly monitored their BP in 2005 and 2008, “which is perhaps associated with our sample’s older age,” said Dr. Springer and associates of the University of Michigan, Ann Arbor.
The current study, they noted, is the first to report “SBPM prevalence in adults ages 50 to 80 years with hypertension or BPHCs, who have a higher risk of adverse outcomes from uncontrolled BP than younger adults.” The analysis is based on data from the National Poll on Healthy Aging, conducted by the University of Michigan in January 2021 and completed by 2,023 individuals.
The frequency of home monitoring varied among adults with BPHCs, as just under 15% reported daily checks and the largest proportion, about 28%, used their device one to three times per month. The results of home monitoring were shared with health care professionals by 50.2% of respondents with a BPHC and by 51.5% of those with hypertension, they said in the research letter.
Home monitoring’s less-than-universal recommendation by providers and use by patients “suggest that protocols should be developed to educate patients about the importance of SBPM and sharing readings with clinicians and the frequency that SBPM should be performed,” Dr. Springer and associates wrote.
The study was funded by AARP, Michigan Medicine, the National Institute of Neurological Disorders and Stroke, and the Department of Veterans Affairs. One investigator has received consulting fees or honoraria from SeeChange Health, HealthMine, the Kaiser Permanente Washington Health Research Institute, the Robert Wood Johnson Foundation, AbilTo, Kansas City Area Life Sciences Institute, American Diabetes Association, Donaghue Foundation, and Luxembourg National Research Fund.
Just over 51% of older hypertensive adults regularly check their own blood pressure, compared with 48% of those with blood pressure–related health conditions (BPHCs), based on a 2021 survey of individuals aged 50-80 years.
“Guidelines recommend that patients use self-measured blood pressure monitoring (SBPM) outside the clinic to diagnose and manage hypertension,” but just 61% of respondents with a BPHC and 68% of those with hypertension said that they had received such a recommendation from a physician, nurse, or other health care professional, Melanie V. Springer, MD, and associates said in JAMA Network Open.
The prevalence of regular monitoring among those with hypertension, 51.2%, does, however, compare favorably with an earlier study showing that 43% of adults aged 18 and older regularly monitored their BP in 2005 and 2008, “which is perhaps associated with our sample’s older age,” said Dr. Springer and associates of the University of Michigan, Ann Arbor.
The current study, they noted, is the first to report “SBPM prevalence in adults ages 50 to 80 years with hypertension or BPHCs, who have a higher risk of adverse outcomes from uncontrolled BP than younger adults.” The analysis is based on data from the National Poll on Healthy Aging, conducted by the University of Michigan in January 2021 and completed by 2,023 individuals.
The frequency of home monitoring varied among adults with BPHCs, as just under 15% reported daily checks and the largest proportion, about 28%, used their device one to three times per month. The results of home monitoring were shared with health care professionals by 50.2% of respondents with a BPHC and by 51.5% of those with hypertension, they said in the research letter.
Home monitoring’s less-than-universal recommendation by providers and use by patients “suggest that protocols should be developed to educate patients about the importance of SBPM and sharing readings with clinicians and the frequency that SBPM should be performed,” Dr. Springer and associates wrote.
The study was funded by AARP, Michigan Medicine, the National Institute of Neurological Disorders and Stroke, and the Department of Veterans Affairs. One investigator has received consulting fees or honoraria from SeeChange Health, HealthMine, the Kaiser Permanente Washington Health Research Institute, the Robert Wood Johnson Foundation, AbilTo, Kansas City Area Life Sciences Institute, American Diabetes Association, Donaghue Foundation, and Luxembourg National Research Fund.
Just over 51% of older hypertensive adults regularly check their own blood pressure, compared with 48% of those with blood pressure–related health conditions (BPHCs), based on a 2021 survey of individuals aged 50-80 years.
“Guidelines recommend that patients use self-measured blood pressure monitoring (SBPM) outside the clinic to diagnose and manage hypertension,” but just 61% of respondents with a BPHC and 68% of those with hypertension said that they had received such a recommendation from a physician, nurse, or other health care professional, Melanie V. Springer, MD, and associates said in JAMA Network Open.
The prevalence of regular monitoring among those with hypertension, 51.2%, does, however, compare favorably with an earlier study showing that 43% of adults aged 18 and older regularly monitored their BP in 2005 and 2008, “which is perhaps associated with our sample’s older age,” said Dr. Springer and associates of the University of Michigan, Ann Arbor.
The current study, they noted, is the first to report “SBPM prevalence in adults ages 50 to 80 years with hypertension or BPHCs, who have a higher risk of adverse outcomes from uncontrolled BP than younger adults.” The analysis is based on data from the National Poll on Healthy Aging, conducted by the University of Michigan in January 2021 and completed by 2,023 individuals.
The frequency of home monitoring varied among adults with BPHCs, as just under 15% reported daily checks and the largest proportion, about 28%, used their device one to three times per month. The results of home monitoring were shared with health care professionals by 50.2% of respondents with a BPHC and by 51.5% of those with hypertension, they said in the research letter.
Home monitoring’s less-than-universal recommendation by providers and use by patients “suggest that protocols should be developed to educate patients about the importance of SBPM and sharing readings with clinicians and the frequency that SBPM should be performed,” Dr. Springer and associates wrote.
The study was funded by AARP, Michigan Medicine, the National Institute of Neurological Disorders and Stroke, and the Department of Veterans Affairs. One investigator has received consulting fees or honoraria from SeeChange Health, HealthMine, the Kaiser Permanente Washington Health Research Institute, the Robert Wood Johnson Foundation, AbilTo, Kansas City Area Life Sciences Institute, American Diabetes Association, Donaghue Foundation, and Luxembourg National Research Fund.
FROM JAMA NETWORK OPEN