User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
COVID-19 shutdown fuels sharp rise in alcohol use
Americans sharply increased their alcohol intake last spring as many areas of the country shutdown because of the coronavirus pandemic, results of a national survey show.

The overall frequency of alcohol consumption increased by 14% among adults over age 30 in the spring of 2020 versus the same period a year earlier.
The increase was most evident in adults aged 30-59, women, and non-Hispanic Whites.
“Alcohol consumption can have significant negative health consequences, so this information suggests another way that the pandemic may be affecting the physical and mental health of Americans,” Michael Pollard, PhD, lead investigator and sociologist at Rand, said in a news release.
The results were published online as a research letter Sept. 29 in JAMA Network Open.
Booming business
After some U.S. states issued stay-at-home orders to fight the spread of SARS-CoV-2, one study noted a 54% increase in national sales of alcohol for the week ending March 21, 2020, relative to 1 year earlier and a 262% increase in online alcohol sales.
“We’ve had anecdotal information about people buying and consuming more alcohol,” Dr. Pollard said, but the Rand study provides the first survey-based information that shows how much alcohol consumption has increased during the pandemic.
The findings are based on 1,540 adults (mean age, 56.6 years; 57% women) from the Rand American Life Panel, a nationally representative sample of Americans who were surveyed about their alcohol consumption before the pandemic in the spring of 2019, and again in the spring of 2020 during the early months of the shutdown.
Overall, in spring 2020, respondents reported drinking alcohol 6.22 days in the prior month on average, a 14% increase from the monthly average of 5.48 days reported in spring 2019.
Among adults aged 30 to 59 years, the frequency of alcohol consumption increased from 4.98 days prepandemic to 5.91 days during the pandemic, a 19% increase.
Women reported drinking an average of 5.36 days in the prior month in the early pandemic period, a 17% increase from 4.58 monthly drinking days before the pandemic.
In addition, compared with spring 2019, in spring 2020 women reported a 41% increase in heavy drinking days – four or more drinks in a couple of hours.
Independent of consumption level, nearly 1 in 10 women had an increase in alcohol-related problems in the pandemic period, based on responses to the Short Inventory of Problems scale.
For non-Hispanic White individuals, the overall frequency of alcohol intake rose 10% during the early pandemic period.
“The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19,” write Dr. Pollard and colleagues.
The authors note , and whether psychological and physical well-being are subsequently affected.
The study was supported by the National Institute of Alcohol Abuse and Alcoholism. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Americans sharply increased their alcohol intake last spring as many areas of the country shutdown because of the coronavirus pandemic, results of a national survey show.
The overall frequency of alcohol consumption increased by 14% among adults over age 30 in the spring of 2020 versus the same period a year earlier.
The increase was most evident in adults aged 30-59, women, and non-Hispanic Whites.
“Alcohol consumption can have significant negative health consequences, so this information suggests another way that the pandemic may be affecting the physical and mental health of Americans,” Michael Pollard, PhD, lead investigator and sociologist at Rand, said in a news release.
The results were published online as a research letter Sept. 29 in JAMA Network Open.
Booming business
After some U.S. states issued stay-at-home orders to fight the spread of SARS-CoV-2, one study noted a 54% increase in national sales of alcohol for the week ending March 21, 2020, relative to 1 year earlier and a 262% increase in online alcohol sales.
“We’ve had anecdotal information about people buying and consuming more alcohol,” Dr. Pollard said, but the Rand study provides the first survey-based information that shows how much alcohol consumption has increased during the pandemic.
The findings are based on 1,540 adults (mean age, 56.6 years; 57% women) from the Rand American Life Panel, a nationally representative sample of Americans who were surveyed about their alcohol consumption before the pandemic in the spring of 2019, and again in the spring of 2020 during the early months of the shutdown.
Overall, in spring 2020, respondents reported drinking alcohol 6.22 days in the prior month on average, a 14% increase from the monthly average of 5.48 days reported in spring 2019.
Among adults aged 30 to 59 years, the frequency of alcohol consumption increased from 4.98 days prepandemic to 5.91 days during the pandemic, a 19% increase.
Women reported drinking an average of 5.36 days in the prior month in the early pandemic period, a 17% increase from 4.58 monthly drinking days before the pandemic.
In addition, compared with spring 2019, in spring 2020 women reported a 41% increase in heavy drinking days – four or more drinks in a couple of hours.
Independent of consumption level, nearly 1 in 10 women had an increase in alcohol-related problems in the pandemic period, based on responses to the Short Inventory of Problems scale.
For non-Hispanic White individuals, the overall frequency of alcohol intake rose 10% during the early pandemic period.
“The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19,” write Dr. Pollard and colleagues.
The authors note , and whether psychological and physical well-being are subsequently affected.
The study was supported by the National Institute of Alcohol Abuse and Alcoholism. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Americans sharply increased their alcohol intake last spring as many areas of the country shutdown because of the coronavirus pandemic, results of a national survey show.
The overall frequency of alcohol consumption increased by 14% among adults over age 30 in the spring of 2020 versus the same period a year earlier.
The increase was most evident in adults aged 30-59, women, and non-Hispanic Whites.
“Alcohol consumption can have significant negative health consequences, so this information suggests another way that the pandemic may be affecting the physical and mental health of Americans,” Michael Pollard, PhD, lead investigator and sociologist at Rand, said in a news release.
The results were published online as a research letter Sept. 29 in JAMA Network Open.
Booming business
After some U.S. states issued stay-at-home orders to fight the spread of SARS-CoV-2, one study noted a 54% increase in national sales of alcohol for the week ending March 21, 2020, relative to 1 year earlier and a 262% increase in online alcohol sales.
“We’ve had anecdotal information about people buying and consuming more alcohol,” Dr. Pollard said, but the Rand study provides the first survey-based information that shows how much alcohol consumption has increased during the pandemic.
The findings are based on 1,540 adults (mean age, 56.6 years; 57% women) from the Rand American Life Panel, a nationally representative sample of Americans who were surveyed about their alcohol consumption before the pandemic in the spring of 2019, and again in the spring of 2020 during the early months of the shutdown.
Overall, in spring 2020, respondents reported drinking alcohol 6.22 days in the prior month on average, a 14% increase from the monthly average of 5.48 days reported in spring 2019.
Among adults aged 30 to 59 years, the frequency of alcohol consumption increased from 4.98 days prepandemic to 5.91 days during the pandemic, a 19% increase.
Women reported drinking an average of 5.36 days in the prior month in the early pandemic period, a 17% increase from 4.58 monthly drinking days before the pandemic.
In addition, compared with spring 2019, in spring 2020 women reported a 41% increase in heavy drinking days – four or more drinks in a couple of hours.
Independent of consumption level, nearly 1 in 10 women had an increase in alcohol-related problems in the pandemic period, based on responses to the Short Inventory of Problems scale.
For non-Hispanic White individuals, the overall frequency of alcohol intake rose 10% during the early pandemic period.
“The population level changes for women, younger, and non-Hispanic White individuals highlight that health systems may need to educate consumers through print or online media about increased alcohol use during the pandemic and identify factors associated with susceptibility and resilience to the impacts of COVID-19,” write Dr. Pollard and colleagues.
The authors note , and whether psychological and physical well-being are subsequently affected.
The study was supported by the National Institute of Alcohol Abuse and Alcoholism. The authors have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Neoadjuvant mFOLFIRINOX improves DFS, OS effect uncertain
Adding neoadjuvant chemotherapy to standard treatment of locally advanced rectal cancer more than doubled the pathologic complete response rate and significantly improved 3-year disease-free survival (DFS) in a multicenter, phase 3 trial.
The pathologic complete response rate was 12.1% in the standard therapy arm and 27.8% with the addition of neoadjuvant chemotherapy – modified FOLFIRINOX (oxaliplatin, irinotecan, folinic acid, and 5-fluorouracil). The 3-year DFS rates were 68.5% and 75.7%, respectively.
It’s not clear if the response and DFS benefits of modified FOLFIRINOX will translate to improved overall survival (OS). Nevertheless, neoadjuvant therapy with modified FOLFIRINOX “should now be considered as a new option” for T3-T4 rectal cancer, said investigator Christophe Borg, MD, PhD, of the University of Besancon (France).
Dr. Borg presented this research at the European Society for Medical Oncology Virtual Congress 2020.
Study discussant David Sebag-Montefiore, MBBS, of the University of Leeds (England), was more cautious about these findings. Although the results were “clear” in this trial, “we have not seen any overall survival data,” Dr. Sebag-Montefiore stressed.
Study details
In explaining the trial, dubbed PRODIGE 23, Dr. Borg noted that local recurrence is minimal with modern standard treatment – chemoradiation followed by total mesorectal excision (TME) – but distant metastases occur in up to 30% of patients and remain a significant problem despite years of research. Adjuvant chemotherapy after surgery might help, but it “is still not proven” to reduce the risk, so compliance is poor, Dr. Borg said.
He and his colleagues conducted the PRODIGE 23 trial to see if neoadjuvant chemotherapy could reduce the risk of metastases.
The study enrolled 461 patients, 18-75 years old, with cT3-4 rectal cancer. Patients were randomized to receive:
- Standard therapy, consisting of chemoradiation (50.4 gy/5 weeks plus capecitabine), followed 7 weeks later by TME, then 6 months of adjuvant chemotherapy with FOLFOX (folinic acid, fluorouracil, and oxaliplatin) or XELOX (capecitabine and oxaliplatin, also known as CAPOX).
- Six cycles of modified FOLFIRINOX, followed by chemoradiation (50.4 gy/5 weeks plus capecitabine), TME, and FOLFOX/XELOX adjuvant therapy for 3 months instead of 6 months.
Overall, 119 patients in the standard therapy arm and 130 in the neoadjuvant arm completed their assigned protocol.
Results
The median follow-up was 46.5 months. The 3-year DFS, the primary endpoint, was significantly higher in the neoadjuvant arm than in the standard therapy arm (75.7% vs. 68.5%; hazard ratio = 0.69; P = .034). This correlated with a significant improvement in 3-year metastasis-free survival (78.8% vs. 71.7%; HR = 0.64; P < .02).
The rate of palliative surgery was significantly higher in the standard therapy arm (3.7% vs. 0%; P = .007), but there were no significant differences in other surgical outcomes.
A difference in 60-day postoperative mortality favored neoadjuvant therapy (0% vs. 2.8%, P = .03).
Grade 3 or 4 adverse events during adjuvant therapy were less common when subjects had neoadjuvant chemotherapy (44.4% vs. 74.1%, P < .001).
Quality of life outcomes were similar between the treatment arms, except that men in the neoadjuvant arm were significantly less likely to suffer from impotence (P = .03).
Dr. Sebag-Montefiore said these findings are “very important,” but PRODIGE 23 is not “a practice-defining or practice-changing study,” especially without OS data.
He noted that the RAPIDO trial had similar outcomes with a different neoadjuvant regimen.
RAPIDO had a standard treatment arm with capecitabine-based chemoradiotherapy followed by TME and optional CAPOX/FOLFOX, and the experimental arm consisted of short-course radiotherapy followed by CAPOX/FOLFOX then TME. The experimental arm had superior 3-year disease-related treatment failure (30.4% vs. 23.7%, P = .019) but no better OS (89.1% vs. 88.8%, P = .59).
PRODIGE 23 was funded by the French National Cancer Institute and the French National League Against Cancer. Dr. Borg disclosed relationships with Roche, Servier, Pierre Fabre, and Merck Sharp & Dohme. Dr. Sebag-Montefiore didn’t have any disclosures.
[email protected]
SOURCE: Borg C et al. ESMO 2020. Abstract LBA21.
Adding neoadjuvant chemotherapy to standard treatment of locally advanced rectal cancer more than doubled the pathologic complete response rate and significantly improved 3-year disease-free survival (DFS) in a multicenter, phase 3 trial.
The pathologic complete response rate was 12.1% in the standard therapy arm and 27.8% with the addition of neoadjuvant chemotherapy – modified FOLFIRINOX (oxaliplatin, irinotecan, folinic acid, and 5-fluorouracil). The 3-year DFS rates were 68.5% and 75.7%, respectively.
It’s not clear if the response and DFS benefits of modified FOLFIRINOX will translate to improved overall survival (OS). Nevertheless, neoadjuvant therapy with modified FOLFIRINOX “should now be considered as a new option” for T3-T4 rectal cancer, said investigator Christophe Borg, MD, PhD, of the University of Besancon (France).
Dr. Borg presented this research at the European Society for Medical Oncology Virtual Congress 2020.
Study discussant David Sebag-Montefiore, MBBS, of the University of Leeds (England), was more cautious about these findings. Although the results were “clear” in this trial, “we have not seen any overall survival data,” Dr. Sebag-Montefiore stressed.
Study details
In explaining the trial, dubbed PRODIGE 23, Dr. Borg noted that local recurrence is minimal with modern standard treatment – chemoradiation followed by total mesorectal excision (TME) – but distant metastases occur in up to 30% of patients and remain a significant problem despite years of research. Adjuvant chemotherapy after surgery might help, but it “is still not proven” to reduce the risk, so compliance is poor, Dr. Borg said.
He and his colleagues conducted the PRODIGE 23 trial to see if neoadjuvant chemotherapy could reduce the risk of metastases.
The study enrolled 461 patients, 18-75 years old, with cT3-4 rectal cancer. Patients were randomized to receive:
- Standard therapy, consisting of chemoradiation (50.4 gy/5 weeks plus capecitabine), followed 7 weeks later by TME, then 6 months of adjuvant chemotherapy with FOLFOX (folinic acid, fluorouracil, and oxaliplatin) or XELOX (capecitabine and oxaliplatin, also known as CAPOX).
- Six cycles of modified FOLFIRINOX, followed by chemoradiation (50.4 gy/5 weeks plus capecitabine), TME, and FOLFOX/XELOX adjuvant therapy for 3 months instead of 6 months.
Overall, 119 patients in the standard therapy arm and 130 in the neoadjuvant arm completed their assigned protocol.
Results
The median follow-up was 46.5 months. The 3-year DFS, the primary endpoint, was significantly higher in the neoadjuvant arm than in the standard therapy arm (75.7% vs. 68.5%; hazard ratio = 0.69; P = .034). This correlated with a significant improvement in 3-year metastasis-free survival (78.8% vs. 71.7%; HR = 0.64; P < .02).
The rate of palliative surgery was significantly higher in the standard therapy arm (3.7% vs. 0%; P = .007), but there were no significant differences in other surgical outcomes.
A difference in 60-day postoperative mortality favored neoadjuvant therapy (0% vs. 2.8%, P = .03).
Grade 3 or 4 adverse events during adjuvant therapy were less common when subjects had neoadjuvant chemotherapy (44.4% vs. 74.1%, P < .001).
Quality of life outcomes were similar between the treatment arms, except that men in the neoadjuvant arm were significantly less likely to suffer from impotence (P = .03).
Dr. Sebag-Montefiore said these findings are “very important,” but PRODIGE 23 is not “a practice-defining or practice-changing study,” especially without OS data.
He noted that the RAPIDO trial had similar outcomes with a different neoadjuvant regimen.
RAPIDO had a standard treatment arm with capecitabine-based chemoradiotherapy followed by TME and optional CAPOX/FOLFOX, and the experimental arm consisted of short-course radiotherapy followed by CAPOX/FOLFOX then TME. The experimental arm had superior 3-year disease-related treatment failure (30.4% vs. 23.7%, P = .019) but no better OS (89.1% vs. 88.8%, P = .59).
PRODIGE 23 was funded by the French National Cancer Institute and the French National League Against Cancer. Dr. Borg disclosed relationships with Roche, Servier, Pierre Fabre, and Merck Sharp & Dohme. Dr. Sebag-Montefiore didn’t have any disclosures.
[email protected]
SOURCE: Borg C et al. ESMO 2020. Abstract LBA21.
Adding neoadjuvant chemotherapy to standard treatment of locally advanced rectal cancer more than doubled the pathologic complete response rate and significantly improved 3-year disease-free survival (DFS) in a multicenter, phase 3 trial.
The pathologic complete response rate was 12.1% in the standard therapy arm and 27.8% with the addition of neoadjuvant chemotherapy – modified FOLFIRINOX (oxaliplatin, irinotecan, folinic acid, and 5-fluorouracil). The 3-year DFS rates were 68.5% and 75.7%, respectively.
It’s not clear if the response and DFS benefits of modified FOLFIRINOX will translate to improved overall survival (OS). Nevertheless, neoadjuvant therapy with modified FOLFIRINOX “should now be considered as a new option” for T3-T4 rectal cancer, said investigator Christophe Borg, MD, PhD, of the University of Besancon (France).
Dr. Borg presented this research at the European Society for Medical Oncology Virtual Congress 2020.
Study discussant David Sebag-Montefiore, MBBS, of the University of Leeds (England), was more cautious about these findings. Although the results were “clear” in this trial, “we have not seen any overall survival data,” Dr. Sebag-Montefiore stressed.
Study details
In explaining the trial, dubbed PRODIGE 23, Dr. Borg noted that local recurrence is minimal with modern standard treatment – chemoradiation followed by total mesorectal excision (TME) – but distant metastases occur in up to 30% of patients and remain a significant problem despite years of research. Adjuvant chemotherapy after surgery might help, but it “is still not proven” to reduce the risk, so compliance is poor, Dr. Borg said.
He and his colleagues conducted the PRODIGE 23 trial to see if neoadjuvant chemotherapy could reduce the risk of metastases.
The study enrolled 461 patients, 18-75 years old, with cT3-4 rectal cancer. Patients were randomized to receive:
- Standard therapy, consisting of chemoradiation (50.4 gy/5 weeks plus capecitabine), followed 7 weeks later by TME, then 6 months of adjuvant chemotherapy with FOLFOX (folinic acid, fluorouracil, and oxaliplatin) or XELOX (capecitabine and oxaliplatin, also known as CAPOX).
- Six cycles of modified FOLFIRINOX, followed by chemoradiation (50.4 gy/5 weeks plus capecitabine), TME, and FOLFOX/XELOX adjuvant therapy for 3 months instead of 6 months.
Overall, 119 patients in the standard therapy arm and 130 in the neoadjuvant arm completed their assigned protocol.
Results
The median follow-up was 46.5 months. The 3-year DFS, the primary endpoint, was significantly higher in the neoadjuvant arm than in the standard therapy arm (75.7% vs. 68.5%; hazard ratio = 0.69; P = .034). This correlated with a significant improvement in 3-year metastasis-free survival (78.8% vs. 71.7%; HR = 0.64; P < .02).
The rate of palliative surgery was significantly higher in the standard therapy arm (3.7% vs. 0%; P = .007), but there were no significant differences in other surgical outcomes.
A difference in 60-day postoperative mortality favored neoadjuvant therapy (0% vs. 2.8%, P = .03).
Grade 3 or 4 adverse events during adjuvant therapy were less common when subjects had neoadjuvant chemotherapy (44.4% vs. 74.1%, P < .001).
Quality of life outcomes were similar between the treatment arms, except that men in the neoadjuvant arm were significantly less likely to suffer from impotence (P = .03).
Dr. Sebag-Montefiore said these findings are “very important,” but PRODIGE 23 is not “a practice-defining or practice-changing study,” especially without OS data.
He noted that the RAPIDO trial had similar outcomes with a different neoadjuvant regimen.
RAPIDO had a standard treatment arm with capecitabine-based chemoradiotherapy followed by TME and optional CAPOX/FOLFOX, and the experimental arm consisted of short-course radiotherapy followed by CAPOX/FOLFOX then TME. The experimental arm had superior 3-year disease-related treatment failure (30.4% vs. 23.7%, P = .019) but no better OS (89.1% vs. 88.8%, P = .59).
PRODIGE 23 was funded by the French National Cancer Institute and the French National League Against Cancer. Dr. Borg disclosed relationships with Roche, Servier, Pierre Fabre, and Merck Sharp & Dohme. Dr. Sebag-Montefiore didn’t have any disclosures.
[email protected]
SOURCE: Borg C et al. ESMO 2020. Abstract LBA21.
FROM ESMO 2020
Children’s share of new COVID-19 cases is on the rise
The cumulative percentage of COVID-19 cases reported in children continues to climb, but “the history behind that cumulative number shows substantial change,” according to a new analysis of state health department data.
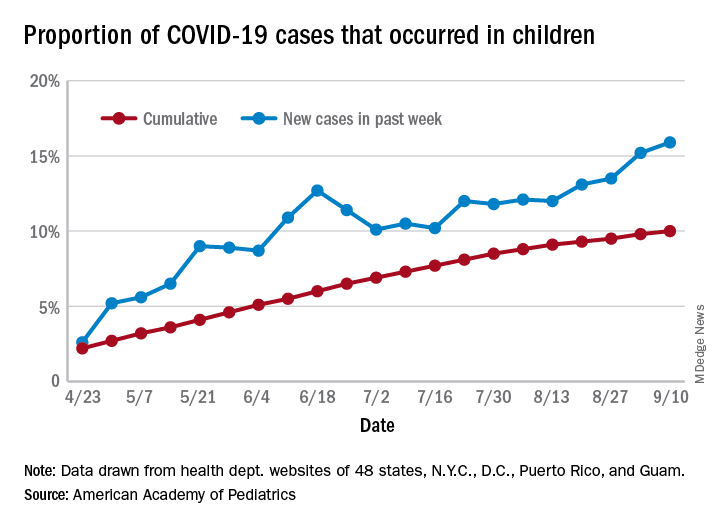
As of Sept. 10, the 549,432 cases in children represented 10.0% of all reported COVID-19 cases in the United States following a substantial rise over the course of the pandemic – the figure was 7.7% on July 16 and 3.2% on May 7, Blake Sisk, PhD, of the American Academy of Pediatrics and associates reported Sept. 29 in Pediatrics.
Unlike the cumulative number, the weekly proportion of cases in children fell early in the summer but then started climbing again in late July. Dr. Sisk and associates wrote.
Despite the increase, however, the proportion of pediatric COVID-19 cases is still well below children’s share of the overall population (22.6%). Also, “it is unclear how much of the increase in child cases is due to increased testing capacity, although CDC data from public and commercial laboratories show the share of all tests administered to children ages 0-17 has remained stable at 5%-7% since late April,” they said.
Data for the current report were drawn from 49 state health department websites (New York state does not report ages for COVID-19 cases), along with New York City, the District of Columbia, Puerto Rico, and Guam. Alabama changed its definition of a child case in August and was not included in the trend analysis (see graph), the investigators explained.
Those data show “substantial variation in case growth by region: in April, a preponderance of cases was in the Northeast. In June, cases surged in the South and West, followed by mid-July increases in the Midwest,” Dr. Sisk and associates said.
The increase among children in Midwest states is ongoing with the number of new cases reaching its highest level yet during the week ending Sept. 10, they reported.
SOURCE: Sisk B et al. Pediatrics. 2020 Sep 29. doi: 10.1542/peds.2020-027425.
The cumulative percentage of COVID-19 cases reported in children continues to climb, but “the history behind that cumulative number shows substantial change,” according to a new analysis of state health department data.
As of Sept. 10, the 549,432 cases in children represented 10.0% of all reported COVID-19 cases in the United States following a substantial rise over the course of the pandemic – the figure was 7.7% on July 16 and 3.2% on May 7, Blake Sisk, PhD, of the American Academy of Pediatrics and associates reported Sept. 29 in Pediatrics.
Unlike the cumulative number, the weekly proportion of cases in children fell early in the summer but then started climbing again in late July. Dr. Sisk and associates wrote.
Despite the increase, however, the proportion of pediatric COVID-19 cases is still well below children’s share of the overall population (22.6%). Also, “it is unclear how much of the increase in child cases is due to increased testing capacity, although CDC data from public and commercial laboratories show the share of all tests administered to children ages 0-17 has remained stable at 5%-7% since late April,” they said.
Data for the current report were drawn from 49 state health department websites (New York state does not report ages for COVID-19 cases), along with New York City, the District of Columbia, Puerto Rico, and Guam. Alabama changed its definition of a child case in August and was not included in the trend analysis (see graph), the investigators explained.
Those data show “substantial variation in case growth by region: in April, a preponderance of cases was in the Northeast. In June, cases surged in the South and West, followed by mid-July increases in the Midwest,” Dr. Sisk and associates said.
The increase among children in Midwest states is ongoing with the number of new cases reaching its highest level yet during the week ending Sept. 10, they reported.
SOURCE: Sisk B et al. Pediatrics. 2020 Sep 29. doi: 10.1542/peds.2020-027425.
The cumulative percentage of COVID-19 cases reported in children continues to climb, but “the history behind that cumulative number shows substantial change,” according to a new analysis of state health department data.
As of Sept. 10, the 549,432 cases in children represented 10.0% of all reported COVID-19 cases in the United States following a substantial rise over the course of the pandemic – the figure was 7.7% on July 16 and 3.2% on May 7, Blake Sisk, PhD, of the American Academy of Pediatrics and associates reported Sept. 29 in Pediatrics.
Unlike the cumulative number, the weekly proportion of cases in children fell early in the summer but then started climbing again in late July. Dr. Sisk and associates wrote.
Despite the increase, however, the proportion of pediatric COVID-19 cases is still well below children’s share of the overall population (22.6%). Also, “it is unclear how much of the increase in child cases is due to increased testing capacity, although CDC data from public and commercial laboratories show the share of all tests administered to children ages 0-17 has remained stable at 5%-7% since late April,” they said.
Data for the current report were drawn from 49 state health department websites (New York state does not report ages for COVID-19 cases), along with New York City, the District of Columbia, Puerto Rico, and Guam. Alabama changed its definition of a child case in August and was not included in the trend analysis (see graph), the investigators explained.
Those data show “substantial variation in case growth by region: in April, a preponderance of cases was in the Northeast. In June, cases surged in the South and West, followed by mid-July increases in the Midwest,” Dr. Sisk and associates said.
The increase among children in Midwest states is ongoing with the number of new cases reaching its highest level yet during the week ending Sept. 10, they reported.
SOURCE: Sisk B et al. Pediatrics. 2020 Sep 29. doi: 10.1542/peds.2020-027425.
FROM PEDIATRICS
Pandemic poses new challenges for rural doctors
These include struggling with seeing patients virtually and treating patients who have politicized the virus. Additionally, the pandemic has exposed rural practices to greater financial difficulties.

Before the pandemic some rurally based primary care physicians were already working through big challenges, such as having few local medical colleagues to consult and working in small practices with lean budgets. In fact, data gathered by the National Rural Health Association showed that there are only 40 primary care physicians per 100,000 patients in rural regions, compared with 53 in urban areas – and the number of physicians overall is 13 per 10,000 in rural areas, compared with 31 in cities.
In the prepandemic world, for some doctors, the challenges were balanced by the benefits of practicing in these sparsely populated communities with scenic, low-traffic roads. Some perks of practicing in rural areas touted by doctors included having a fast commute, being able to swim in a lake near the office before work, having a low cost of living, and feeling like they are making a difference in their communities as they treat generations of the families they see around town.
But today, new hurdles to practicing medicine in rural America created by the COVID-19 pandemic have caused the hardships to feel heavier than the joys at times for some physicians interviewed by MDedge.
Many independent rural practices in need of assistance were not able to get much from the federal Provider Relief Funds, said John M. Westfall, MD, who is director of the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, in an interview.
“Rural primary care doctors function independently or in smaller critical access hospitals and community health centers,” said Dr. Westfall, who previously practiced family medicine in a small town in Colorado. “Many of these have much less financial reserves so are at risk of cutbacks and closure.”
Jacqueline W. Fincher, MD, an internist based in a tiny Georgia community along the highway between Atlanta and Augusta, said her small practice works on really thin margins and doesn’t have much cushion. At the beginning of the pandemic, all visits were down, and her practice operated at a loss. To help, Dr. Fincher and her colleagues applied for funding from the Small Business Administration’s Paycheck Protection Program (PPP) through the CARES Act.
“COVID-19 has had a tremendous impact especially on primary care practices. We live and die by volume. … Our volume in mid-March to mid-May really dropped dramatically,” explained Dr. Fincher, who is also president of the American College of Physicians. “The PPP sustained us for 2 months, enabling us to pay our staff and to remain open and get us up and running on telehealth.”
Starting up telemedicine
Experiencing spotty or no access to broadband Internet is nothing new to rural physicians, but having this problem interfere with their ability to provide care to patients is.
As much of the American health system rapidly embraced telehealth during the pandemic, obtaining access to high-speed Internet has been a major challenge for rural patients, noted Dr. Westfall.
“Some practices were able to quickly adopt some telehealth capacity with phone and video. Changes in payment for telehealth helped. But in some rural communities there was not adequate Internet bandwidth for quality video connections. And some patients did not have the means for high-speed video connections,” Dr. Westfall said.
Indeed, according to a 2019 Pew Research Center survey, 63% of rural Americans say they can access the Internet through a broadband connection at home, compared with 75% and 79% in suburban and urban areas, respectively.

In the Appalachian town of Zanesville, Ohio, for example, family physician Shelly L. Dunmyer, MD, and her colleagues discovered that many patients don’t have Internet access at home. Dr. Fincher has to go to the office to conduct telehealth visits because her own Internet access at home is unpredictable. As for patients, it may take 15 minutes for them to work out technical glitches and find good Internet reception, said Dr. Fincher. For internist Y. Ki Shin, MD, who practices in the coastal town of Montesano in Washington state, about 25% of his practice’s telehealth visits must be conducted by phone because of limitations on video, such as lack of high-speed access.
But telephone visits are often insufficient replacements for appointments via video, according to several rural physicians interviewed for this piece.
“Telehealth can be frustrating at times due to connectivity issues which can be difficult at times in the rural areas,” said Dr. Fincher. “In order for telehealth to be reasonably helpful to patients and physicians to care for people with chronic problems, the patients must have things like blood pressure monitors, glucometers, and scales to address problems like hypertension, diabetes myelitis, and congestive heart failure.”
“If you have the audio and video and the data from these devices, you’re good. If you don’t have these data, and/or don’t have the video you just can’t provide good care,” she explained.

Dr. Dunmyer and her colleagues at Medical Home Primary Care Center in Zanesville, Ohio, found a way to get around the problem of patients not being able to access Internet to participate in video visits from their homes. This involved having her patients drive into her practice’s parking lot to participate in modified telehealth visits. Staffers gave iPads to patients in their cars, and Dr. Dunmyer conducted visits from her office, about 50 yards away.
“We were even doing Medicare wellness visits: Instead of asking them to get up and move around the room, we would sit at the window and wave at them, ask them to get out, walk around the car. We were able to check mobility and all kinds of things that we’d normally do in the office,” Dr. Dunmyer explained in an interview.
The family physician noted that her practice is now conducting fewer parking lot visits since her office is allowing in-person appointments, but that they’re still an option for her patients.
Treating political adversaries
Some rural physicians have experienced strained relationships with patients for reasons other than technology – stark differences in opinion over the pandemic itself. Certain patients are following President Trump’s lead and questioning everything from the pandemic death toll to preventive measures recommended by scientists and medical experts, physicians interviewed by MDedge said.
Patients everywhere share these viewpoints, of course, but research and election results confirm that rural areas are more receptive to conservative viewpoints. In 2018, a Pew Research Center survey reported that rural and urban areas are “becoming more polarized politically,” and “rural areas tend to have a higher concentration of Republicans and Republican-leaning independents.” For example, 40% of rural respondents reported “very warm” or “somewhat warm” feelings toward Donald Trump, compared with just 19% in urban areas.
Dr. Shin has struggled to cope with patients who want to argue about pandemic safety precautions like wearing masks and seem to question whether systemic racism exists.
“We are seeing a lot more people who feel that this pandemic is not real, that it’s a political and not-true infection,” he said in an interview. “We’ve had patients who were angry at us because we made them wear masks, and some were demanding hydroxychloroquine and wanted to have an argument because we’re not going to prescribe it for them.”
In one situation, which he found especially disturbing, Dr. Shin had to leave the exam room because a patient wouldn’t stop challenging him regarding the pandemic. Things have gotten so bad that Dr. Shin has even questioned whether he wants to continue his long career in his small town because of local political attitudes such as opposition to mask-wearing and social distancing.
“Mr. Trump’s misinformation on this pandemic made my job much more difficult. As a minority, I feel less safe in my community than ever,” said Dr. Shin, who described himself as Asian American.
Despite these new stressors, Dr. Shin has experienced some joyful moments while practicing medicine in the pandemic.

He said a recent home visit to a patient who had been hospitalized for over 3 months and nearly died helped him put political disputes with his patients into perspective.
“He was discharged home but is bedbound. He had gangrene on his toes, and I could not fully examine him using video,” Dr. Shin recalled. “It was tricky to find the house, but a very large Trump sign was very helpful in locating it. It was a good visit: He was happy to see me, and I was happy to see that he was doing okay at home.”
“I need to remind myself that supporting Mr. Trump does not always mean that my patient supports Mr. Trump’s view on the pandemic and the race issues in our country,” Dr. Shin added.
The Washington-based internist said he also tells himself that, even if his patients refuse to follow his strong advice regarding pandemic precautions, it does not mean he has failed as a doctor.
“I need to continue to educate patients about the dangers of COVID infection but cannot be angry if they don’t choose to follow my recommendations,” he noted.
Dr. Fincher says her close connection with patients has allowed her to smooth over politically charged claims about the pandemic in the town of Thomson, Georgia, with a population 6,800.
“I have a sense that, even though we may differ in our understanding of some basic facts, they appreciate what I say since we have a long-term relationship built on trust,” she said. This kind of trust, Dr. Fincher suggested, may be more common than in urban areas where there’s a larger supply of physicians, and patients don’t see the same doctors for long periods of time.
“It’s more meaningful when it comes from me, rather than doctors who are [new to patients] every year when their employer changes their insurance,” she noted.
These include struggling with seeing patients virtually and treating patients who have politicized the virus. Additionally, the pandemic has exposed rural practices to greater financial difficulties.
Before the pandemic some rurally based primary care physicians were already working through big challenges, such as having few local medical colleagues to consult and working in small practices with lean budgets. In fact, data gathered by the National Rural Health Association showed that there are only 40 primary care physicians per 100,000 patients in rural regions, compared with 53 in urban areas – and the number of physicians overall is 13 per 10,000 in rural areas, compared with 31 in cities.
In the prepandemic world, for some doctors, the challenges were balanced by the benefits of practicing in these sparsely populated communities with scenic, low-traffic roads. Some perks of practicing in rural areas touted by doctors included having a fast commute, being able to swim in a lake near the office before work, having a low cost of living, and feeling like they are making a difference in their communities as they treat generations of the families they see around town.
But today, new hurdles to practicing medicine in rural America created by the COVID-19 pandemic have caused the hardships to feel heavier than the joys at times for some physicians interviewed by MDedge.
Many independent rural practices in need of assistance were not able to get much from the federal Provider Relief Funds, said John M. Westfall, MD, who is director of the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, in an interview.
“Rural primary care doctors function independently or in smaller critical access hospitals and community health centers,” said Dr. Westfall, who previously practiced family medicine in a small town in Colorado. “Many of these have much less financial reserves so are at risk of cutbacks and closure.”
Jacqueline W. Fincher, MD, an internist based in a tiny Georgia community along the highway between Atlanta and Augusta, said her small practice works on really thin margins and doesn’t have much cushion. At the beginning of the pandemic, all visits were down, and her practice operated at a loss. To help, Dr. Fincher and her colleagues applied for funding from the Small Business Administration’s Paycheck Protection Program (PPP) through the CARES Act.
“COVID-19 has had a tremendous impact especially on primary care practices. We live and die by volume. … Our volume in mid-March to mid-May really dropped dramatically,” explained Dr. Fincher, who is also president of the American College of Physicians. “The PPP sustained us for 2 months, enabling us to pay our staff and to remain open and get us up and running on telehealth.”
Starting up telemedicine
Experiencing spotty or no access to broadband Internet is nothing new to rural physicians, but having this problem interfere with their ability to provide care to patients is.
As much of the American health system rapidly embraced telehealth during the pandemic, obtaining access to high-speed Internet has been a major challenge for rural patients, noted Dr. Westfall.
“Some practices were able to quickly adopt some telehealth capacity with phone and video. Changes in payment for telehealth helped. But in some rural communities there was not adequate Internet bandwidth for quality video connections. And some patients did not have the means for high-speed video connections,” Dr. Westfall said.
Indeed, according to a 2019 Pew Research Center survey, 63% of rural Americans say they can access the Internet through a broadband connection at home, compared with 75% and 79% in suburban and urban areas, respectively.
In the Appalachian town of Zanesville, Ohio, for example, family physician Shelly L. Dunmyer, MD, and her colleagues discovered that many patients don’t have Internet access at home. Dr. Fincher has to go to the office to conduct telehealth visits because her own Internet access at home is unpredictable. As for patients, it may take 15 minutes for them to work out technical glitches and find good Internet reception, said Dr. Fincher. For internist Y. Ki Shin, MD, who practices in the coastal town of Montesano in Washington state, about 25% of his practice’s telehealth visits must be conducted by phone because of limitations on video, such as lack of high-speed access.
But telephone visits are often insufficient replacements for appointments via video, according to several rural physicians interviewed for this piece.
“Telehealth can be frustrating at times due to connectivity issues which can be difficult at times in the rural areas,” said Dr. Fincher. “In order for telehealth to be reasonably helpful to patients and physicians to care for people with chronic problems, the patients must have things like blood pressure monitors, glucometers, and scales to address problems like hypertension, diabetes myelitis, and congestive heart failure.”
“If you have the audio and video and the data from these devices, you’re good. If you don’t have these data, and/or don’t have the video you just can’t provide good care,” she explained.
Dr. Dunmyer and her colleagues at Medical Home Primary Care Center in Zanesville, Ohio, found a way to get around the problem of patients not being able to access Internet to participate in video visits from their homes. This involved having her patients drive into her practice’s parking lot to participate in modified telehealth visits. Staffers gave iPads to patients in their cars, and Dr. Dunmyer conducted visits from her office, about 50 yards away.
“We were even doing Medicare wellness visits: Instead of asking them to get up and move around the room, we would sit at the window and wave at them, ask them to get out, walk around the car. We were able to check mobility and all kinds of things that we’d normally do in the office,” Dr. Dunmyer explained in an interview.
The family physician noted that her practice is now conducting fewer parking lot visits since her office is allowing in-person appointments, but that they’re still an option for her patients.
Treating political adversaries
Some rural physicians have experienced strained relationships with patients for reasons other than technology – stark differences in opinion over the pandemic itself. Certain patients are following President Trump’s lead and questioning everything from the pandemic death toll to preventive measures recommended by scientists and medical experts, physicians interviewed by MDedge said.
Patients everywhere share these viewpoints, of course, but research and election results confirm that rural areas are more receptive to conservative viewpoints. In 2018, a Pew Research Center survey reported that rural and urban areas are “becoming more polarized politically,” and “rural areas tend to have a higher concentration of Republicans and Republican-leaning independents.” For example, 40% of rural respondents reported “very warm” or “somewhat warm” feelings toward Donald Trump, compared with just 19% in urban areas.
Dr. Shin has struggled to cope with patients who want to argue about pandemic safety precautions like wearing masks and seem to question whether systemic racism exists.
“We are seeing a lot more people who feel that this pandemic is not real, that it’s a political and not-true infection,” he said in an interview. “We’ve had patients who were angry at us because we made them wear masks, and some were demanding hydroxychloroquine and wanted to have an argument because we’re not going to prescribe it for them.”
In one situation, which he found especially disturbing, Dr. Shin had to leave the exam room because a patient wouldn’t stop challenging him regarding the pandemic. Things have gotten so bad that Dr. Shin has even questioned whether he wants to continue his long career in his small town because of local political attitudes such as opposition to mask-wearing and social distancing.
“Mr. Trump’s misinformation on this pandemic made my job much more difficult. As a minority, I feel less safe in my community than ever,” said Dr. Shin, who described himself as Asian American.
Despite these new stressors, Dr. Shin has experienced some joyful moments while practicing medicine in the pandemic.
He said a recent home visit to a patient who had been hospitalized for over 3 months and nearly died helped him put political disputes with his patients into perspective.
“He was discharged home but is bedbound. He had gangrene on his toes, and I could not fully examine him using video,” Dr. Shin recalled. “It was tricky to find the house, but a very large Trump sign was very helpful in locating it. It was a good visit: He was happy to see me, and I was happy to see that he was doing okay at home.”
“I need to remind myself that supporting Mr. Trump does not always mean that my patient supports Mr. Trump’s view on the pandemic and the race issues in our country,” Dr. Shin added.
The Washington-based internist said he also tells himself that, even if his patients refuse to follow his strong advice regarding pandemic precautions, it does not mean he has failed as a doctor.
“I need to continue to educate patients about the dangers of COVID infection but cannot be angry if they don’t choose to follow my recommendations,” he noted.
Dr. Fincher says her close connection with patients has allowed her to smooth over politically charged claims about the pandemic in the town of Thomson, Georgia, with a population 6,800.
“I have a sense that, even though we may differ in our understanding of some basic facts, they appreciate what I say since we have a long-term relationship built on trust,” she said. This kind of trust, Dr. Fincher suggested, may be more common than in urban areas where there’s a larger supply of physicians, and patients don’t see the same doctors for long periods of time.
“It’s more meaningful when it comes from me, rather than doctors who are [new to patients] every year when their employer changes their insurance,” she noted.
These include struggling with seeing patients virtually and treating patients who have politicized the virus. Additionally, the pandemic has exposed rural practices to greater financial difficulties.
Before the pandemic some rurally based primary care physicians were already working through big challenges, such as having few local medical colleagues to consult and working in small practices with lean budgets. In fact, data gathered by the National Rural Health Association showed that there are only 40 primary care physicians per 100,000 patients in rural regions, compared with 53 in urban areas – and the number of physicians overall is 13 per 10,000 in rural areas, compared with 31 in cities.
In the prepandemic world, for some doctors, the challenges were balanced by the benefits of practicing in these sparsely populated communities with scenic, low-traffic roads. Some perks of practicing in rural areas touted by doctors included having a fast commute, being able to swim in a lake near the office before work, having a low cost of living, and feeling like they are making a difference in their communities as they treat generations of the families they see around town.
But today, new hurdles to practicing medicine in rural America created by the COVID-19 pandemic have caused the hardships to feel heavier than the joys at times for some physicians interviewed by MDedge.
Many independent rural practices in need of assistance were not able to get much from the federal Provider Relief Funds, said John M. Westfall, MD, who is director of the Robert Graham Center for Policy Studies in Family Medicine and Primary Care, in an interview.
“Rural primary care doctors function independently or in smaller critical access hospitals and community health centers,” said Dr. Westfall, who previously practiced family medicine in a small town in Colorado. “Many of these have much less financial reserves so are at risk of cutbacks and closure.”
Jacqueline W. Fincher, MD, an internist based in a tiny Georgia community along the highway between Atlanta and Augusta, said her small practice works on really thin margins and doesn’t have much cushion. At the beginning of the pandemic, all visits were down, and her practice operated at a loss. To help, Dr. Fincher and her colleagues applied for funding from the Small Business Administration’s Paycheck Protection Program (PPP) through the CARES Act.
“COVID-19 has had a tremendous impact especially on primary care practices. We live and die by volume. … Our volume in mid-March to mid-May really dropped dramatically,” explained Dr. Fincher, who is also president of the American College of Physicians. “The PPP sustained us for 2 months, enabling us to pay our staff and to remain open and get us up and running on telehealth.”
Starting up telemedicine
Experiencing spotty or no access to broadband Internet is nothing new to rural physicians, but having this problem interfere with their ability to provide care to patients is.
As much of the American health system rapidly embraced telehealth during the pandemic, obtaining access to high-speed Internet has been a major challenge for rural patients, noted Dr. Westfall.
“Some practices were able to quickly adopt some telehealth capacity with phone and video. Changes in payment for telehealth helped. But in some rural communities there was not adequate Internet bandwidth for quality video connections. And some patients did not have the means for high-speed video connections,” Dr. Westfall said.
Indeed, according to a 2019 Pew Research Center survey, 63% of rural Americans say they can access the Internet through a broadband connection at home, compared with 75% and 79% in suburban and urban areas, respectively.
In the Appalachian town of Zanesville, Ohio, for example, family physician Shelly L. Dunmyer, MD, and her colleagues discovered that many patients don’t have Internet access at home. Dr. Fincher has to go to the office to conduct telehealth visits because her own Internet access at home is unpredictable. As for patients, it may take 15 minutes for them to work out technical glitches and find good Internet reception, said Dr. Fincher. For internist Y. Ki Shin, MD, who practices in the coastal town of Montesano in Washington state, about 25% of his practice’s telehealth visits must be conducted by phone because of limitations on video, such as lack of high-speed access.
But telephone visits are often insufficient replacements for appointments via video, according to several rural physicians interviewed for this piece.
“Telehealth can be frustrating at times due to connectivity issues which can be difficult at times in the rural areas,” said Dr. Fincher. “In order for telehealth to be reasonably helpful to patients and physicians to care for people with chronic problems, the patients must have things like blood pressure monitors, glucometers, and scales to address problems like hypertension, diabetes myelitis, and congestive heart failure.”
“If you have the audio and video and the data from these devices, you’re good. If you don’t have these data, and/or don’t have the video you just can’t provide good care,” she explained.
Dr. Dunmyer and her colleagues at Medical Home Primary Care Center in Zanesville, Ohio, found a way to get around the problem of patients not being able to access Internet to participate in video visits from their homes. This involved having her patients drive into her practice’s parking lot to participate in modified telehealth visits. Staffers gave iPads to patients in their cars, and Dr. Dunmyer conducted visits from her office, about 50 yards away.
“We were even doing Medicare wellness visits: Instead of asking them to get up and move around the room, we would sit at the window and wave at them, ask them to get out, walk around the car. We were able to check mobility and all kinds of things that we’d normally do in the office,” Dr. Dunmyer explained in an interview.
The family physician noted that her practice is now conducting fewer parking lot visits since her office is allowing in-person appointments, but that they’re still an option for her patients.
Treating political adversaries
Some rural physicians have experienced strained relationships with patients for reasons other than technology – stark differences in opinion over the pandemic itself. Certain patients are following President Trump’s lead and questioning everything from the pandemic death toll to preventive measures recommended by scientists and medical experts, physicians interviewed by MDedge said.
Patients everywhere share these viewpoints, of course, but research and election results confirm that rural areas are more receptive to conservative viewpoints. In 2018, a Pew Research Center survey reported that rural and urban areas are “becoming more polarized politically,” and “rural areas tend to have a higher concentration of Republicans and Republican-leaning independents.” For example, 40% of rural respondents reported “very warm” or “somewhat warm” feelings toward Donald Trump, compared with just 19% in urban areas.
Dr. Shin has struggled to cope with patients who want to argue about pandemic safety precautions like wearing masks and seem to question whether systemic racism exists.
“We are seeing a lot more people who feel that this pandemic is not real, that it’s a political and not-true infection,” he said in an interview. “We’ve had patients who were angry at us because we made them wear masks, and some were demanding hydroxychloroquine and wanted to have an argument because we’re not going to prescribe it for them.”
In one situation, which he found especially disturbing, Dr. Shin had to leave the exam room because a patient wouldn’t stop challenging him regarding the pandemic. Things have gotten so bad that Dr. Shin has even questioned whether he wants to continue his long career in his small town because of local political attitudes such as opposition to mask-wearing and social distancing.
“Mr. Trump’s misinformation on this pandemic made my job much more difficult. As a minority, I feel less safe in my community than ever,” said Dr. Shin, who described himself as Asian American.
Despite these new stressors, Dr. Shin has experienced some joyful moments while practicing medicine in the pandemic.
He said a recent home visit to a patient who had been hospitalized for over 3 months and nearly died helped him put political disputes with his patients into perspective.
“He was discharged home but is bedbound. He had gangrene on his toes, and I could not fully examine him using video,” Dr. Shin recalled. “It was tricky to find the house, but a very large Trump sign was very helpful in locating it. It was a good visit: He was happy to see me, and I was happy to see that he was doing okay at home.”
“I need to remind myself that supporting Mr. Trump does not always mean that my patient supports Mr. Trump’s view on the pandemic and the race issues in our country,” Dr. Shin added.
The Washington-based internist said he also tells himself that, even if his patients refuse to follow his strong advice regarding pandemic precautions, it does not mean he has failed as a doctor.
“I need to continue to educate patients about the dangers of COVID infection but cannot be angry if they don’t choose to follow my recommendations,” he noted.
Dr. Fincher says her close connection with patients has allowed her to smooth over politically charged claims about the pandemic in the town of Thomson, Georgia, with a population 6,800.
“I have a sense that, even though we may differ in our understanding of some basic facts, they appreciate what I say since we have a long-term relationship built on trust,” she said. This kind of trust, Dr. Fincher suggested, may be more common than in urban areas where there’s a larger supply of physicians, and patients don’t see the same doctors for long periods of time.
“It’s more meaningful when it comes from me, rather than doctors who are [new to patients] every year when their employer changes their insurance,” she noted.
Divergent findings with paclitaxel and nab-paclitaxel in TNBC
The trials, IMpassion130 and IMpassion131, both enrolled patients with metastatic or unresectable, locally advanced TNBC.
In IMpassion131, adding atezolizumab to paclitaxel did not improve progression-free survival (PFS) or overall survival (OS), regardless of programmed death–ligand 1 (PD-L1) expression.
In IMpassion130, adding atezolizumab to nab-paclitaxel did not improve OS in the intention-to-treat (ITT) population but did provide a “clinically meaningful” improvement in OS among PD-L1-positive patients, according to investigators.
IMpassion130 and IMpassion131 were presented during the same session at the European Society for Medical Oncology (ESMO) Virtual Congress 2020.
Potential reasons for the different outcomes in the two studies require further exploration, according to David Miles, MD, of Mount Vernon Cancer Centre in Northwood, England, who presented the findings from IMpassion131.
ESMO discussant Lisa A. Carey, MD, of the University of North Carolina at Chapel Hill, posited three possible explanations for the divergent findings. The steroids necessary with paclitaxel dosing may have had a negative effect on immune checkpoint inhibitor activity, differences in study populations may have played a role, or the divergent findings could be caused by chance.
Steroid use in IMpassion131 could have played a negative role because of its lympholytic activity, but other indications with steroid use have not demonstrated attenuated benefits, said Leisha A. Emens, MD, PhD, of the University of Pittsburgh Medical Center, who presented the findings from IMpassion130 at ESMO 2020.
“If I were a patient, based on the data to date, I would want nab-paclitaxel with atezolizumab,” Dr. Emens said.
Trial details
Both trials are phase 3, double-blind, placebo-controlled studies of women with metastatic or unresectable locally advanced TNBC who had received no prior therapy for advanced TNBC.
IMpassion130 included 451 patients randomized to atezolizumab plus nab-paclitaxel and 451 randomized to placebo plus nab-paclitaxel. Patients received nab-paclitaxel at a starting dose of 100 mg/m2 via IV infusion on days 1, 8, and 15 of each 28-day cycle for at least six cycles.
In both studies, patients received atezolizumab at 840 mg on days 1 and 15 of a 28-day cycle in their active treatment arms.
IMpassion131 included 651 patients randomized 2:1 to atezolizumab plus paclitaxel (n = 431) or placebo plus paclitaxel (n = 220). Patients received paclitaxel at 90 mg/m2 on days 1, 8, and 15 every 28 days until disease progression or unacceptable toxicity.
Baseline characteristics were well balanced between the treatment arms in both studies. Less than half of patients – 45% in IMpassion131 and 41% in IMpassion130 – were PD-L1 positive.
Results of IMpassion131
The primary endpoint in IMpassion131 was PFS, and there was no significant difference in PFS between the treatment arms.
“The primary objective of IMpassion131 was not met,” Dr. Miles said. “[The] addition of atezolizumab to paclitaxel did not significantly improve PFS in patients with PD-L1-positive metastatic triple-negative breast cancer.”
In the PD-L1-positive population, the median PFS was 5.7 months in the placebo arm and 6.0 months in the atezolizumab arm (stratified hazard ratio, 0.82, P = .20).
In the ITT population, the median PFS was 5.6 months in the control arm and 5.7 months in the atezolizumab arm (HR, 0.86).
In subgroup analyses, Dr. Miles noted, “There was no clue about adverse or beneficial effects in any subgroup.”
The updated OS analysis demonstrated no benefit with atezolizumab in the ITT population or the PD-L1-positive population. In fact, there was a trend toward better OS for the control group in the latter analysis.
In the PD-L1-positive population, the median OS was 28.3 months in the control arm and 22.1 months in the atezolizumab arm (HR, 1.12). The 2-year OS rates were 51% and 49%, respectively.
In the ITT population, the median OS was 22.8 months in the control arm and 19.2 months in the atezolizumab arm (HR, 1.11). The 2-year OS rates were 45% and 42%, respectively.
The safety profile of the atezolizumab-paclitaxel combination was consistent with known side effects of the individual drugs, Dr. Miles said. There were four fatal treatment-related adverse events in the atezolizumab arm.
Results of IMpassion130
Presenting the final OS analysis from IMpassion130, Dr. Emens noted that the study’s findings have led to recommendations for atezolizumab plus nab-paclitaxel as first-line treatment of PD-L1-positive TNBC in international guidelines.
The median OS in the ITT population was 18.7 months in the placebo arm and 21.0 months in the atezolizumab arm (stratified HR, 0.87, P = .077). The 3-year OS rates were 25% and 28%, respectively.
The median OS in the PD-L1-positive population was 17.9 months in the placebo arm and 25.4 months in the atezolizumab arm (HR, 0.67). The 3-year OS rates were 22% and 36%, respectively.
A P value is not available for the between-arm OS comparison in the PD-L1-positive population. OS was not formally tested in this group because the OS boundary for statistical significance was not crossed in the ITT population. However, Dr. Emens said there was a “clinically meaningful” OS benefit observed with atezolizumab in the PD-L1-positive patients.
Treatment withdrawals caused by adverse events were more common in the atezolizumab arm (19% vs. 8%). The most common of these was neuropathy, Dr. Emens said. However, she noted that atezolizumab-related adverse events were generally low grade and easily managed.
“These results support a positive benefit-risk profile for atezolizumab plus nab-paclitaxel as first-line therapy in patients with PD-L1-positive metastatic triple-negative breast cancer,” Dr. Emens concluded.
Both studies were funded by F. Hoffman–La Roche. Dr. Miles, Dr. Emens, and Dr. Carey disclosed financial relationships with Roche and other companies.
SOURCES: Miles D et al. ESMO 2020, Abstract LBA15; Emens LA et al. ESMO 2020, Abstract LBA16.
The trials, IMpassion130 and IMpassion131, both enrolled patients with metastatic or unresectable, locally advanced TNBC.
In IMpassion131, adding atezolizumab to paclitaxel did not improve progression-free survival (PFS) or overall survival (OS), regardless of programmed death–ligand 1 (PD-L1) expression.
In IMpassion130, adding atezolizumab to nab-paclitaxel did not improve OS in the intention-to-treat (ITT) population but did provide a “clinically meaningful” improvement in OS among PD-L1-positive patients, according to investigators.
IMpassion130 and IMpassion131 were presented during the same session at the European Society for Medical Oncology (ESMO) Virtual Congress 2020.
Potential reasons for the different outcomes in the two studies require further exploration, according to David Miles, MD, of Mount Vernon Cancer Centre in Northwood, England, who presented the findings from IMpassion131.
ESMO discussant Lisa A. Carey, MD, of the University of North Carolina at Chapel Hill, posited three possible explanations for the divergent findings. The steroids necessary with paclitaxel dosing may have had a negative effect on immune checkpoint inhibitor activity, differences in study populations may have played a role, or the divergent findings could be caused by chance.
Steroid use in IMpassion131 could have played a negative role because of its lympholytic activity, but other indications with steroid use have not demonstrated attenuated benefits, said Leisha A. Emens, MD, PhD, of the University of Pittsburgh Medical Center, who presented the findings from IMpassion130 at ESMO 2020.
“If I were a patient, based on the data to date, I would want nab-paclitaxel with atezolizumab,” Dr. Emens said.
Trial details
Both trials are phase 3, double-blind, placebo-controlled studies of women with metastatic or unresectable locally advanced TNBC who had received no prior therapy for advanced TNBC.
IMpassion130 included 451 patients randomized to atezolizumab plus nab-paclitaxel and 451 randomized to placebo plus nab-paclitaxel. Patients received nab-paclitaxel at a starting dose of 100 mg/m2 via IV infusion on days 1, 8, and 15 of each 28-day cycle for at least six cycles.
In both studies, patients received atezolizumab at 840 mg on days 1 and 15 of a 28-day cycle in their active treatment arms.
IMpassion131 included 651 patients randomized 2:1 to atezolizumab plus paclitaxel (n = 431) or placebo plus paclitaxel (n = 220). Patients received paclitaxel at 90 mg/m2 on days 1, 8, and 15 every 28 days until disease progression or unacceptable toxicity.
Baseline characteristics were well balanced between the treatment arms in both studies. Less than half of patients – 45% in IMpassion131 and 41% in IMpassion130 – were PD-L1 positive.
Results of IMpassion131
The primary endpoint in IMpassion131 was PFS, and there was no significant difference in PFS between the treatment arms.
“The primary objective of IMpassion131 was not met,” Dr. Miles said. “[The] addition of atezolizumab to paclitaxel did not significantly improve PFS in patients with PD-L1-positive metastatic triple-negative breast cancer.”
In the PD-L1-positive population, the median PFS was 5.7 months in the placebo arm and 6.0 months in the atezolizumab arm (stratified hazard ratio, 0.82, P = .20).
In the ITT population, the median PFS was 5.6 months in the control arm and 5.7 months in the atezolizumab arm (HR, 0.86).
In subgroup analyses, Dr. Miles noted, “There was no clue about adverse or beneficial effects in any subgroup.”
The updated OS analysis demonstrated no benefit with atezolizumab in the ITT population or the PD-L1-positive population. In fact, there was a trend toward better OS for the control group in the latter analysis.
In the PD-L1-positive population, the median OS was 28.3 months in the control arm and 22.1 months in the atezolizumab arm (HR, 1.12). The 2-year OS rates were 51% and 49%, respectively.
In the ITT population, the median OS was 22.8 months in the control arm and 19.2 months in the atezolizumab arm (HR, 1.11). The 2-year OS rates were 45% and 42%, respectively.
The safety profile of the atezolizumab-paclitaxel combination was consistent with known side effects of the individual drugs, Dr. Miles said. There were four fatal treatment-related adverse events in the atezolizumab arm.
Results of IMpassion130
Presenting the final OS analysis from IMpassion130, Dr. Emens noted that the study’s findings have led to recommendations for atezolizumab plus nab-paclitaxel as first-line treatment of PD-L1-positive TNBC in international guidelines.
The median OS in the ITT population was 18.7 months in the placebo arm and 21.0 months in the atezolizumab arm (stratified HR, 0.87, P = .077). The 3-year OS rates were 25% and 28%, respectively.
The median OS in the PD-L1-positive population was 17.9 months in the placebo arm and 25.4 months in the atezolizumab arm (HR, 0.67). The 3-year OS rates were 22% and 36%, respectively.
A P value is not available for the between-arm OS comparison in the PD-L1-positive population. OS was not formally tested in this group because the OS boundary for statistical significance was not crossed in the ITT population. However, Dr. Emens said there was a “clinically meaningful” OS benefit observed with atezolizumab in the PD-L1-positive patients.
Treatment withdrawals caused by adverse events were more common in the atezolizumab arm (19% vs. 8%). The most common of these was neuropathy, Dr. Emens said. However, she noted that atezolizumab-related adverse events were generally low grade and easily managed.
“These results support a positive benefit-risk profile for atezolizumab plus nab-paclitaxel as first-line therapy in patients with PD-L1-positive metastatic triple-negative breast cancer,” Dr. Emens concluded.
Both studies were funded by F. Hoffman–La Roche. Dr. Miles, Dr. Emens, and Dr. Carey disclosed financial relationships with Roche and other companies.
SOURCES: Miles D et al. ESMO 2020, Abstract LBA15; Emens LA et al. ESMO 2020, Abstract LBA16.
The trials, IMpassion130 and IMpassion131, both enrolled patients with metastatic or unresectable, locally advanced TNBC.
In IMpassion131, adding atezolizumab to paclitaxel did not improve progression-free survival (PFS) or overall survival (OS), regardless of programmed death–ligand 1 (PD-L1) expression.
In IMpassion130, adding atezolizumab to nab-paclitaxel did not improve OS in the intention-to-treat (ITT) population but did provide a “clinically meaningful” improvement in OS among PD-L1-positive patients, according to investigators.
IMpassion130 and IMpassion131 were presented during the same session at the European Society for Medical Oncology (ESMO) Virtual Congress 2020.
Potential reasons for the different outcomes in the two studies require further exploration, according to David Miles, MD, of Mount Vernon Cancer Centre in Northwood, England, who presented the findings from IMpassion131.
ESMO discussant Lisa A. Carey, MD, of the University of North Carolina at Chapel Hill, posited three possible explanations for the divergent findings. The steroids necessary with paclitaxel dosing may have had a negative effect on immune checkpoint inhibitor activity, differences in study populations may have played a role, or the divergent findings could be caused by chance.
Steroid use in IMpassion131 could have played a negative role because of its lympholytic activity, but other indications with steroid use have not demonstrated attenuated benefits, said Leisha A. Emens, MD, PhD, of the University of Pittsburgh Medical Center, who presented the findings from IMpassion130 at ESMO 2020.
“If I were a patient, based on the data to date, I would want nab-paclitaxel with atezolizumab,” Dr. Emens said.
Trial details
Both trials are phase 3, double-blind, placebo-controlled studies of women with metastatic or unresectable locally advanced TNBC who had received no prior therapy for advanced TNBC.
IMpassion130 included 451 patients randomized to atezolizumab plus nab-paclitaxel and 451 randomized to placebo plus nab-paclitaxel. Patients received nab-paclitaxel at a starting dose of 100 mg/m2 via IV infusion on days 1, 8, and 15 of each 28-day cycle for at least six cycles.
In both studies, patients received atezolizumab at 840 mg on days 1 and 15 of a 28-day cycle in their active treatment arms.
IMpassion131 included 651 patients randomized 2:1 to atezolizumab plus paclitaxel (n = 431) or placebo plus paclitaxel (n = 220). Patients received paclitaxel at 90 mg/m2 on days 1, 8, and 15 every 28 days until disease progression or unacceptable toxicity.
Baseline characteristics were well balanced between the treatment arms in both studies. Less than half of patients – 45% in IMpassion131 and 41% in IMpassion130 – were PD-L1 positive.
Results of IMpassion131
The primary endpoint in IMpassion131 was PFS, and there was no significant difference in PFS between the treatment arms.
“The primary objective of IMpassion131 was not met,” Dr. Miles said. “[The] addition of atezolizumab to paclitaxel did not significantly improve PFS in patients with PD-L1-positive metastatic triple-negative breast cancer.”
In the PD-L1-positive population, the median PFS was 5.7 months in the placebo arm and 6.0 months in the atezolizumab arm (stratified hazard ratio, 0.82, P = .20).
In the ITT population, the median PFS was 5.6 months in the control arm and 5.7 months in the atezolizumab arm (HR, 0.86).
In subgroup analyses, Dr. Miles noted, “There was no clue about adverse or beneficial effects in any subgroup.”
The updated OS analysis demonstrated no benefit with atezolizumab in the ITT population or the PD-L1-positive population. In fact, there was a trend toward better OS for the control group in the latter analysis.
In the PD-L1-positive population, the median OS was 28.3 months in the control arm and 22.1 months in the atezolizumab arm (HR, 1.12). The 2-year OS rates were 51% and 49%, respectively.
In the ITT population, the median OS was 22.8 months in the control arm and 19.2 months in the atezolizumab arm (HR, 1.11). The 2-year OS rates were 45% and 42%, respectively.
The safety profile of the atezolizumab-paclitaxel combination was consistent with known side effects of the individual drugs, Dr. Miles said. There were four fatal treatment-related adverse events in the atezolizumab arm.
Results of IMpassion130
Presenting the final OS analysis from IMpassion130, Dr. Emens noted that the study’s findings have led to recommendations for atezolizumab plus nab-paclitaxel as first-line treatment of PD-L1-positive TNBC in international guidelines.
The median OS in the ITT population was 18.7 months in the placebo arm and 21.0 months in the atezolizumab arm (stratified HR, 0.87, P = .077). The 3-year OS rates were 25% and 28%, respectively.
The median OS in the PD-L1-positive population was 17.9 months in the placebo arm and 25.4 months in the atezolizumab arm (HR, 0.67). The 3-year OS rates were 22% and 36%, respectively.
A P value is not available for the between-arm OS comparison in the PD-L1-positive population. OS was not formally tested in this group because the OS boundary for statistical significance was not crossed in the ITT population. However, Dr. Emens said there was a “clinically meaningful” OS benefit observed with atezolizumab in the PD-L1-positive patients.
Treatment withdrawals caused by adverse events were more common in the atezolizumab arm (19% vs. 8%). The most common of these was neuropathy, Dr. Emens said. However, she noted that atezolizumab-related adverse events were generally low grade and easily managed.
“These results support a positive benefit-risk profile for atezolizumab plus nab-paclitaxel as first-line therapy in patients with PD-L1-positive metastatic triple-negative breast cancer,” Dr. Emens concluded.
Both studies were funded by F. Hoffman–La Roche. Dr. Miles, Dr. Emens, and Dr. Carey disclosed financial relationships with Roche and other companies.
SOURCES: Miles D et al. ESMO 2020, Abstract LBA15; Emens LA et al. ESMO 2020, Abstract LBA16.
FROM ESMO 2020
Higher glycemic time in range may benefit T2D patients
Patients with type 2 or type 1 diabetes who stay in a blood glucose range of 70-180 mg/dL at least 70% of the time have the lowest rates of major adverse coronary events, severe hypoglycemic episodes, and microvascular events, according to a post hoc analysis of data collected from 5,774 patients with type 2 diabetes.

Data collected by the DEVOTE trial showed that every additional 10% of the time that a patient with type 2 diabetes (T2D) spent in their target range for blood glucose linked with a significant 6% reduced rate for developing a major adverse cardiovascular event (MACE), Richard M. Bergenstal, MD, said at the virtual annual meeting of the European Association for the Study of Diabetes.
For every 10% increase in time in range (TIR), patients showed an average 10% drop in their incidence of severe hypoglycemic episodes.
Increasing evidence from post hoc analyses
These findings confirmed a prior post hoc analysis of data collected in the DCCT trial (NCT00360815), which were published in the New England Journal of Medicine, although those results showed significant relationships between increased TIR and decreased rates of retinopathy and microalbuminuria. For every 10% drop in TIR, retinopathy rose by 64% and microalbuminuria increased by 40%, according to a post hoc analysis of the DCCT data that Dr. Bergenstal helped run and was published in Diabetes Care.
“It’s becoming clear that time in range is an important metric for diabetes management, and our new findings and those previously reported with the DCCT data make it look like time in range is becoming a good marker for clinical outcomes as well,” said Dr. Bergenstal, an endocrinologist at the Park Nicollet Clinic in Minneapolis.
“It’s a new concept, getting time-in-range data,” said Dr. Bergenstal, who was a coauthor of recommendations from Diabetes Care that were made in 2019 by an expert panel organized by the Advanced Technologies & Treatments for Diabetes Congress. “We think this will be a good marker to keep glycemia in a safe range, and the results look positive.” Patients who stay in the blood glucose range of 70-180 mg/dL (3.9-10.0 mmol/L) at least 70% of the time generally have an hemoglobin A1c of about 7%, which is what makes it a good target for patients and clinicians to focus on. Patients with a 50% TIR rate generally have an HbA1c of about 8%.
But a TIR assessment can be more informative than HbA1c, said the 2019 recommendations document. It called TIR assessments “appropriate and useful as clinical targets and outcome measurements that complement A1c for a wide range of people with diabetes.”
Data mining from DEVOTE
The analysis run by Dr. Bergenstal and his associates used data from 5,774 of the 7,637 patients enrolled in the DEVOTE trial, for whom adequate longitudinal blood glucose data were available to derive and track TIR. DEVOTE had the primary aim of comparing two different types of insulin in patients with T2D, according to its explanation in the New England Journal of Medicine. The DEVOTE patients did not undergo routine continuous blood glucose monitoring, so derivation of TIR was the only option with the dataset, Dr. Bergenstal said. “We’re trying to get continuous blood monitoring into T2D trials,” he said.
The post hoc analysis showed that, during the study’s follow-up of just under 2 years, patients who maintained a derived TIR of 70%-100% had about a 6% MACE rate, which peaked at nearly twice that in patients whose TIR was 30% or less. The analysis showed a roughly positive linear relationship between TIR and MACE rates across the range of TIR values. In an adjusted analysis, patients with at least a 70% TIR had a significant 31% lower rate of MACE events, compared with patients whose TIR was 50% or less.
A second analysis that looked for the association between TIR and incidence of hypoglycemic episodes showed a somewhat similar positive relationship, with incidence rates of severe hypoglycemia episodes of about 4%-5% among patients with a TIR of 70% or greater, and a rate of about 7% in patients with a TIR of 30% or less, spiking to 14% among patients with a TIR of 10% or less. In an adjusted analysis, patients with a TIR of at least 70% had a significant 46% lower rate of severe hypoglycemic events, compared with patients whose TIR was 50% or less. This finding belies a common misconception that the tighter glycemic control that produces a higher TIR will lead to increased episodes of severe hypoglycemia, Dr. Bergenstal noted.
He also reported less extensive data on microvascular events. In an adjusted analysis, patients with a TIR of at least 70% had a significant 40% cut in these events compared with patients with 50% or less TIR.
DEVOTE was funded by Novo Nordisk. Dr. Bergenstal has had financial relationships with Novo Nordisk and several other companies.
SOURCE: Bergenstal R et al. EASD 2020, abstract 159.
Patients with type 2 or type 1 diabetes who stay in a blood glucose range of 70-180 mg/dL at least 70% of the time have the lowest rates of major adverse coronary events, severe hypoglycemic episodes, and microvascular events, according to a post hoc analysis of data collected from 5,774 patients with type 2 diabetes.
Data collected by the DEVOTE trial showed that every additional 10% of the time that a patient with type 2 diabetes (T2D) spent in their target range for blood glucose linked with a significant 6% reduced rate for developing a major adverse cardiovascular event (MACE), Richard M. Bergenstal, MD, said at the virtual annual meeting of the European Association for the Study of Diabetes.
For every 10% increase in time in range (TIR), patients showed an average 10% drop in their incidence of severe hypoglycemic episodes.
Increasing evidence from post hoc analyses
These findings confirmed a prior post hoc analysis of data collected in the DCCT trial (NCT00360815), which were published in the New England Journal of Medicine, although those results showed significant relationships between increased TIR and decreased rates of retinopathy and microalbuminuria. For every 10% drop in TIR, retinopathy rose by 64% and microalbuminuria increased by 40%, according to a post hoc analysis of the DCCT data that Dr. Bergenstal helped run and was published in Diabetes Care.
“It’s becoming clear that time in range is an important metric for diabetes management, and our new findings and those previously reported with the DCCT data make it look like time in range is becoming a good marker for clinical outcomes as well,” said Dr. Bergenstal, an endocrinologist at the Park Nicollet Clinic in Minneapolis.
“It’s a new concept, getting time-in-range data,” said Dr. Bergenstal, who was a coauthor of recommendations from Diabetes Care that were made in 2019 by an expert panel organized by the Advanced Technologies & Treatments for Diabetes Congress. “We think this will be a good marker to keep glycemia in a safe range, and the results look positive.” Patients who stay in the blood glucose range of 70-180 mg/dL (3.9-10.0 mmol/L) at least 70% of the time generally have an hemoglobin A1c of about 7%, which is what makes it a good target for patients and clinicians to focus on. Patients with a 50% TIR rate generally have an HbA1c of about 8%.
But a TIR assessment can be more informative than HbA1c, said the 2019 recommendations document. It called TIR assessments “appropriate and useful as clinical targets and outcome measurements that complement A1c for a wide range of people with diabetes.”
Data mining from DEVOTE
The analysis run by Dr. Bergenstal and his associates used data from 5,774 of the 7,637 patients enrolled in the DEVOTE trial, for whom adequate longitudinal blood glucose data were available to derive and track TIR. DEVOTE had the primary aim of comparing two different types of insulin in patients with T2D, according to its explanation in the New England Journal of Medicine. The DEVOTE patients did not undergo routine continuous blood glucose monitoring, so derivation of TIR was the only option with the dataset, Dr. Bergenstal said. “We’re trying to get continuous blood monitoring into T2D trials,” he said.
The post hoc analysis showed that, during the study’s follow-up of just under 2 years, patients who maintained a derived TIR of 70%-100% had about a 6% MACE rate, which peaked at nearly twice that in patients whose TIR was 30% or less. The analysis showed a roughly positive linear relationship between TIR and MACE rates across the range of TIR values. In an adjusted analysis, patients with at least a 70% TIR had a significant 31% lower rate of MACE events, compared with patients whose TIR was 50% or less.
A second analysis that looked for the association between TIR and incidence of hypoglycemic episodes showed a somewhat similar positive relationship, with incidence rates of severe hypoglycemia episodes of about 4%-5% among patients with a TIR of 70% or greater, and a rate of about 7% in patients with a TIR of 30% or less, spiking to 14% among patients with a TIR of 10% or less. In an adjusted analysis, patients with a TIR of at least 70% had a significant 46% lower rate of severe hypoglycemic events, compared with patients whose TIR was 50% or less. This finding belies a common misconception that the tighter glycemic control that produces a higher TIR will lead to increased episodes of severe hypoglycemia, Dr. Bergenstal noted.
He also reported less extensive data on microvascular events. In an adjusted analysis, patients with a TIR of at least 70% had a significant 40% cut in these events compared with patients with 50% or less TIR.
DEVOTE was funded by Novo Nordisk. Dr. Bergenstal has had financial relationships with Novo Nordisk and several other companies.
SOURCE: Bergenstal R et al. EASD 2020, abstract 159.
Patients with type 2 or type 1 diabetes who stay in a blood glucose range of 70-180 mg/dL at least 70% of the time have the lowest rates of major adverse coronary events, severe hypoglycemic episodes, and microvascular events, according to a post hoc analysis of data collected from 5,774 patients with type 2 diabetes.
Data collected by the DEVOTE trial showed that every additional 10% of the time that a patient with type 2 diabetes (T2D) spent in their target range for blood glucose linked with a significant 6% reduced rate for developing a major adverse cardiovascular event (MACE), Richard M. Bergenstal, MD, said at the virtual annual meeting of the European Association for the Study of Diabetes.
For every 10% increase in time in range (TIR), patients showed an average 10% drop in their incidence of severe hypoglycemic episodes.
Increasing evidence from post hoc analyses
These findings confirmed a prior post hoc analysis of data collected in the DCCT trial (NCT00360815), which were published in the New England Journal of Medicine, although those results showed significant relationships between increased TIR and decreased rates of retinopathy and microalbuminuria. For every 10% drop in TIR, retinopathy rose by 64% and microalbuminuria increased by 40%, according to a post hoc analysis of the DCCT data that Dr. Bergenstal helped run and was published in Diabetes Care.
“It’s becoming clear that time in range is an important metric for diabetes management, and our new findings and those previously reported with the DCCT data make it look like time in range is becoming a good marker for clinical outcomes as well,” said Dr. Bergenstal, an endocrinologist at the Park Nicollet Clinic in Minneapolis.
“It’s a new concept, getting time-in-range data,” said Dr. Bergenstal, who was a coauthor of recommendations from Diabetes Care that were made in 2019 by an expert panel organized by the Advanced Technologies & Treatments for Diabetes Congress. “We think this will be a good marker to keep glycemia in a safe range, and the results look positive.” Patients who stay in the blood glucose range of 70-180 mg/dL (3.9-10.0 mmol/L) at least 70% of the time generally have an hemoglobin A1c of about 7%, which is what makes it a good target for patients and clinicians to focus on. Patients with a 50% TIR rate generally have an HbA1c of about 8%.
But a TIR assessment can be more informative than HbA1c, said the 2019 recommendations document. It called TIR assessments “appropriate and useful as clinical targets and outcome measurements that complement A1c for a wide range of people with diabetes.”
Data mining from DEVOTE
The analysis run by Dr. Bergenstal and his associates used data from 5,774 of the 7,637 patients enrolled in the DEVOTE trial, for whom adequate longitudinal blood glucose data were available to derive and track TIR. DEVOTE had the primary aim of comparing two different types of insulin in patients with T2D, according to its explanation in the New England Journal of Medicine. The DEVOTE patients did not undergo routine continuous blood glucose monitoring, so derivation of TIR was the only option with the dataset, Dr. Bergenstal said. “We’re trying to get continuous blood monitoring into T2D trials,” he said.
The post hoc analysis showed that, during the study’s follow-up of just under 2 years, patients who maintained a derived TIR of 70%-100% had about a 6% MACE rate, which peaked at nearly twice that in patients whose TIR was 30% or less. The analysis showed a roughly positive linear relationship between TIR and MACE rates across the range of TIR values. In an adjusted analysis, patients with at least a 70% TIR had a significant 31% lower rate of MACE events, compared with patients whose TIR was 50% or less.
A second analysis that looked for the association between TIR and incidence of hypoglycemic episodes showed a somewhat similar positive relationship, with incidence rates of severe hypoglycemia episodes of about 4%-5% among patients with a TIR of 70% or greater, and a rate of about 7% in patients with a TIR of 30% or less, spiking to 14% among patients with a TIR of 10% or less. In an adjusted analysis, patients with a TIR of at least 70% had a significant 46% lower rate of severe hypoglycemic events, compared with patients whose TIR was 50% or less. This finding belies a common misconception that the tighter glycemic control that produces a higher TIR will lead to increased episodes of severe hypoglycemia, Dr. Bergenstal noted.
He also reported less extensive data on microvascular events. In an adjusted analysis, patients with a TIR of at least 70% had a significant 40% cut in these events compared with patients with 50% or less TIR.
DEVOTE was funded by Novo Nordisk. Dr. Bergenstal has had financial relationships with Novo Nordisk and several other companies.
SOURCE: Bergenstal R et al. EASD 2020, abstract 159.
FROM EASD 2020
Exercise cuts diabetes death risk by a third in two studies
Type 2 diabetes patients could lower their risk for death from any cause by up to a third by exercising at a moderate to high level or by cycling, according to data from two studies reported at the virtual annual meeting of the European Association for the Study of Diabetes.

Yun-Ju Lai, MD, and colleagues from the Puli branch of Taichung Veterans General Hospital in Nantou, Taiwan, found that persons with type 2 diabetes who exercised at moderate to high intensity had a 25%-32% decreased risk for death, compared with those who did not exercise.
In a separate study, Mathias Ried-Larsen, MSc, PhD, group leader at the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and associates found that cycling was associated with a 25%-31% decreased risk for all-cause death compared to no cycling, and that cycling also reduced cardiovascular mortality.
Results fit with ADA recommendations
“There is really nothing surprising about these results as others have shown that regular participation in physical activity lowers both overall mortality rates and morbidity,” commented Sheri Colberg-Ochs, PhD, professor emerita in exercise science at Old Dominion University in Norfolk, Va., in an interview.

“Regular exercise participation lowers the risk of mortality in almost all populations with many different health conditions. It is not specific to people with type 2 diabetes,” Dr. Colberg-Ochs said. “These data add further support to the ADA [American Diabetes Association] recommendations by again suggesting that being more active leads to many health benefits for people with type 2 diabetes.”
Dr. Colberg-Ochs, who was not involved in either study, is recognized by the ADA as an Outstanding Educator in Diabetes. She was also involved in writing the ADA’s position statement on physical activity/exercise in diabetes, which advocate that adults with type 2 diabetes should reduce sedentary time and undertake both aerobic and resistance exercise training to help optimize their glycemic and general health outcomes.
Asian population understudied
In an interview Dr. Lai acknowledged that epidemiologic studies had shown that exercise reduced the risk of cardiovascular events and mortality in subjects with type 2 diabetes. “However, the dose of exercise capacity for reducing mortality risk in people with type 2 diabetes was not yet well investigated, especially in the Asian population.”
Dr. Lai and colleagues analyzed data on 4,859 subjects drawn from two Taiwanese databases – the National Health Interview Survey and the National Health Insurance research database – to study what effect exercise “capacity” had on the risk for death in those with type 2 diabetes.
“Information about physical activity during leisure time was collected by asking the questions: ‘How often do you exercise every week? What kind of exercise do you do? How long do you do the exercise?’, Dr. Lai said. “We included nearly all kinds of exercise in the analysis, such as jogging, swimming, walking, dancing, riding, and so on.”
Each exercise had an activity intensity code expressed as kilocalories per minute. This was used to determine the exercise “capacity” by multiplying it by how frequently the exercise was performed per week and for how long each time.
“I don’t think ‘capacity’ is the right word to use here. The equation they used describes their exercise ‘volume,’ not their capacity. Self-reported exercise is notoriously inaccurate,” Dr. Colberg-Ochs observed. Furthermore, “just asking people how much they exercise and at what intensity [without using a validated exercise questionnaire] gives questionable results.”
The study’s findings, however, were clear: Those who exercised at a higher level had a significantly decreased risk for all-cause mortality than did those with no exercise habits. The hazard ratio for death by any cause was 0.75 for those who undertook a moderate level of exercise, burning 0-800 kcal per week. Exercising at a higher level burned more than 800 kcal had a HR of 0.68. A significant (P < .01) trend in favor of more exercise was noted.
Cycling reduces all-cause and cardiovascular mortality
In their prospective cohort study, Dr. Ried-Larsen and associates took a more specific look at the effects of exercise on mortality in diabetes by studying a single exercise: cycling. They sampled data on more than 5,000 people collected as part of the European Prospective Investigation into Cancer and Nutrition study. First, they identified participants with diabetes – although they couldn’t distinguish type 1 from type 2 forms because this was self-reported or obtained from registries. They then identified those who reported cycling at their baseline assessment and those who reported a change in cycling habits at their second examination around 5 years later.
At baseline, 38% of participants reported that they cycled every week. The mean age was 56 years, diabetes duration was 8 years, one-fifth were smokers, and the average body mass index was 29 kg/m2.
Participants who reported cycling up to 1 hour every week at baseline had a 25% reduction in all-cause mortality, compared with those who did not cycle. The biggest reduction (31%) in all-cause mortality was seen for cycling 2.5-5 hours a week; cycling for 1-2.5 hours, and for more than 5 hours, yielded 23% and 24% risk reductions, respectively.
A reverse J–shaped relationship between cycling duration and reduction in all-cause mortality was seen, Dr. Ried-Larsen noted during a live oral session at the virtual meeting. “The maximum benefit [was at] around 5 hours per week, and the benefits persisted until around 9 hours per week.” Adjustment for the prevalence of stroke, MI, cancer, hyperlipidemia, hypertension, and central obesity did not alter the findings.
“The direction of the association was the same for cardiovascular mortality as all-cause mortality, although a bit weaker, with the maximum benefit being around 4 hours per week, and that persisted up until around 8 hours per week,” Dr. Ried-Larsen said.
The benefits of cycling on all-cause and cardiovascular mortality were lost, however, if those who cycled at baseline stopped by the second examination. Those who did not cycle at the first but did at the second examination got a benefit on both, as did those who continued cycling.
“Cycling is among one of the preferred activities for diabetes patients, so it actually may help them to achieve the recommend level of physical activity,” Dr. Ried-Larsen said.
Tailored exercise program important
Advice for exercise “should be tailored to the individual and based on starting fitness levels and activity levels,” Dr. Colberg-Ochs recommended.
“Those who are the most sedentary and the least fit have the most to gain from doing any activity. They should be advised to start out slowly and progress slowly with both aerobic activities and some resistance training,” Dr. Colberg-Ochs said.
She added: “In addition, individuals over 40 should engage in regular balance training, and all individuals should do some flexibility exercises.”
The studies received no commercial funding and all those mentioned in this article had no conflicts of interest to disclose.
SOURCE: Lai Y-J et al. EASD 2020, Poster presentation 267; Ried-Larsen M et al. EASD 2020, Oral presentation 194.
Type 2 diabetes patients could lower their risk for death from any cause by up to a third by exercising at a moderate to high level or by cycling, according to data from two studies reported at the virtual annual meeting of the European Association for the Study of Diabetes.
Yun-Ju Lai, MD, and colleagues from the Puli branch of Taichung Veterans General Hospital in Nantou, Taiwan, found that persons with type 2 diabetes who exercised at moderate to high intensity had a 25%-32% decreased risk for death, compared with those who did not exercise.
In a separate study, Mathias Ried-Larsen, MSc, PhD, group leader at the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and associates found that cycling was associated with a 25%-31% decreased risk for all-cause death compared to no cycling, and that cycling also reduced cardiovascular mortality.
Results fit with ADA recommendations
“There is really nothing surprising about these results as others have shown that regular participation in physical activity lowers both overall mortality rates and morbidity,” commented Sheri Colberg-Ochs, PhD, professor emerita in exercise science at Old Dominion University in Norfolk, Va., in an interview.
“Regular exercise participation lowers the risk of mortality in almost all populations with many different health conditions. It is not specific to people with type 2 diabetes,” Dr. Colberg-Ochs said. “These data add further support to the ADA [American Diabetes Association] recommendations by again suggesting that being more active leads to many health benefits for people with type 2 diabetes.”
Dr. Colberg-Ochs, who was not involved in either study, is recognized by the ADA as an Outstanding Educator in Diabetes. She was also involved in writing the ADA’s position statement on physical activity/exercise in diabetes, which advocate that adults with type 2 diabetes should reduce sedentary time and undertake both aerobic and resistance exercise training to help optimize their glycemic and general health outcomes.
Asian population understudied
In an interview Dr. Lai acknowledged that epidemiologic studies had shown that exercise reduced the risk of cardiovascular events and mortality in subjects with type 2 diabetes. “However, the dose of exercise capacity for reducing mortality risk in people with type 2 diabetes was not yet well investigated, especially in the Asian population.”
Dr. Lai and colleagues analyzed data on 4,859 subjects drawn from two Taiwanese databases – the National Health Interview Survey and the National Health Insurance research database – to study what effect exercise “capacity” had on the risk for death in those with type 2 diabetes.
“Information about physical activity during leisure time was collected by asking the questions: ‘How often do you exercise every week? What kind of exercise do you do? How long do you do the exercise?’, Dr. Lai said. “We included nearly all kinds of exercise in the analysis, such as jogging, swimming, walking, dancing, riding, and so on.”
Each exercise had an activity intensity code expressed as kilocalories per minute. This was used to determine the exercise “capacity” by multiplying it by how frequently the exercise was performed per week and for how long each time.
“I don’t think ‘capacity’ is the right word to use here. The equation they used describes their exercise ‘volume,’ not their capacity. Self-reported exercise is notoriously inaccurate,” Dr. Colberg-Ochs observed. Furthermore, “just asking people how much they exercise and at what intensity [without using a validated exercise questionnaire] gives questionable results.”
The study’s findings, however, were clear: Those who exercised at a higher level had a significantly decreased risk for all-cause mortality than did those with no exercise habits. The hazard ratio for death by any cause was 0.75 for those who undertook a moderate level of exercise, burning 0-800 kcal per week. Exercising at a higher level burned more than 800 kcal had a HR of 0.68. A significant (P < .01) trend in favor of more exercise was noted.
Cycling reduces all-cause and cardiovascular mortality
In their prospective cohort study, Dr. Ried-Larsen and associates took a more specific look at the effects of exercise on mortality in diabetes by studying a single exercise: cycling. They sampled data on more than 5,000 people collected as part of the European Prospective Investigation into Cancer and Nutrition study. First, they identified participants with diabetes – although they couldn’t distinguish type 1 from type 2 forms because this was self-reported or obtained from registries. They then identified those who reported cycling at their baseline assessment and those who reported a change in cycling habits at their second examination around 5 years later.
At baseline, 38% of participants reported that they cycled every week. The mean age was 56 years, diabetes duration was 8 years, one-fifth were smokers, and the average body mass index was 29 kg/m2.
Participants who reported cycling up to 1 hour every week at baseline had a 25% reduction in all-cause mortality, compared with those who did not cycle. The biggest reduction (31%) in all-cause mortality was seen for cycling 2.5-5 hours a week; cycling for 1-2.5 hours, and for more than 5 hours, yielded 23% and 24% risk reductions, respectively.
A reverse J–shaped relationship between cycling duration and reduction in all-cause mortality was seen, Dr. Ried-Larsen noted during a live oral session at the virtual meeting. “The maximum benefit [was at] around 5 hours per week, and the benefits persisted until around 9 hours per week.” Adjustment for the prevalence of stroke, MI, cancer, hyperlipidemia, hypertension, and central obesity did not alter the findings.
“The direction of the association was the same for cardiovascular mortality as all-cause mortality, although a bit weaker, with the maximum benefit being around 4 hours per week, and that persisted up until around 8 hours per week,” Dr. Ried-Larsen said.
The benefits of cycling on all-cause and cardiovascular mortality were lost, however, if those who cycled at baseline stopped by the second examination. Those who did not cycle at the first but did at the second examination got a benefit on both, as did those who continued cycling.
“Cycling is among one of the preferred activities for diabetes patients, so it actually may help them to achieve the recommend level of physical activity,” Dr. Ried-Larsen said.
Tailored exercise program important
Advice for exercise “should be tailored to the individual and based on starting fitness levels and activity levels,” Dr. Colberg-Ochs recommended.
“Those who are the most sedentary and the least fit have the most to gain from doing any activity. They should be advised to start out slowly and progress slowly with both aerobic activities and some resistance training,” Dr. Colberg-Ochs said.
She added: “In addition, individuals over 40 should engage in regular balance training, and all individuals should do some flexibility exercises.”
The studies received no commercial funding and all those mentioned in this article had no conflicts of interest to disclose.
SOURCE: Lai Y-J et al. EASD 2020, Poster presentation 267; Ried-Larsen M et al. EASD 2020, Oral presentation 194.
Type 2 diabetes patients could lower their risk for death from any cause by up to a third by exercising at a moderate to high level or by cycling, according to data from two studies reported at the virtual annual meeting of the European Association for the Study of Diabetes.
Yun-Ju Lai, MD, and colleagues from the Puli branch of Taichung Veterans General Hospital in Nantou, Taiwan, found that persons with type 2 diabetes who exercised at moderate to high intensity had a 25%-32% decreased risk for death, compared with those who did not exercise.
In a separate study, Mathias Ried-Larsen, MSc, PhD, group leader at the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and associates found that cycling was associated with a 25%-31% decreased risk for all-cause death compared to no cycling, and that cycling also reduced cardiovascular mortality.
Results fit with ADA recommendations
“There is really nothing surprising about these results as others have shown that regular participation in physical activity lowers both overall mortality rates and morbidity,” commented Sheri Colberg-Ochs, PhD, professor emerita in exercise science at Old Dominion University in Norfolk, Va., in an interview.
“Regular exercise participation lowers the risk of mortality in almost all populations with many different health conditions. It is not specific to people with type 2 diabetes,” Dr. Colberg-Ochs said. “These data add further support to the ADA [American Diabetes Association] recommendations by again suggesting that being more active leads to many health benefits for people with type 2 diabetes.”
Dr. Colberg-Ochs, who was not involved in either study, is recognized by the ADA as an Outstanding Educator in Diabetes. She was also involved in writing the ADA’s position statement on physical activity/exercise in diabetes, which advocate that adults with type 2 diabetes should reduce sedentary time and undertake both aerobic and resistance exercise training to help optimize their glycemic and general health outcomes.
Asian population understudied
In an interview Dr. Lai acknowledged that epidemiologic studies had shown that exercise reduced the risk of cardiovascular events and mortality in subjects with type 2 diabetes. “However, the dose of exercise capacity for reducing mortality risk in people with type 2 diabetes was not yet well investigated, especially in the Asian population.”
Dr. Lai and colleagues analyzed data on 4,859 subjects drawn from two Taiwanese databases – the National Health Interview Survey and the National Health Insurance research database – to study what effect exercise “capacity” had on the risk for death in those with type 2 diabetes.
“Information about physical activity during leisure time was collected by asking the questions: ‘How often do you exercise every week? What kind of exercise do you do? How long do you do the exercise?’, Dr. Lai said. “We included nearly all kinds of exercise in the analysis, such as jogging, swimming, walking, dancing, riding, and so on.”
Each exercise had an activity intensity code expressed as kilocalories per minute. This was used to determine the exercise “capacity” by multiplying it by how frequently the exercise was performed per week and for how long each time.
“I don’t think ‘capacity’ is the right word to use here. The equation they used describes their exercise ‘volume,’ not their capacity. Self-reported exercise is notoriously inaccurate,” Dr. Colberg-Ochs observed. Furthermore, “just asking people how much they exercise and at what intensity [without using a validated exercise questionnaire] gives questionable results.”
The study’s findings, however, were clear: Those who exercised at a higher level had a significantly decreased risk for all-cause mortality than did those with no exercise habits. The hazard ratio for death by any cause was 0.75 for those who undertook a moderate level of exercise, burning 0-800 kcal per week. Exercising at a higher level burned more than 800 kcal had a HR of 0.68. A significant (P < .01) trend in favor of more exercise was noted.
Cycling reduces all-cause and cardiovascular mortality
In their prospective cohort study, Dr. Ried-Larsen and associates took a more specific look at the effects of exercise on mortality in diabetes by studying a single exercise: cycling. They sampled data on more than 5,000 people collected as part of the European Prospective Investigation into Cancer and Nutrition study. First, they identified participants with diabetes – although they couldn’t distinguish type 1 from type 2 forms because this was self-reported or obtained from registries. They then identified those who reported cycling at their baseline assessment and those who reported a change in cycling habits at their second examination around 5 years later.
At baseline, 38% of participants reported that they cycled every week. The mean age was 56 years, diabetes duration was 8 years, one-fifth were smokers, and the average body mass index was 29 kg/m2.
Participants who reported cycling up to 1 hour every week at baseline had a 25% reduction in all-cause mortality, compared with those who did not cycle. The biggest reduction (31%) in all-cause mortality was seen for cycling 2.5-5 hours a week; cycling for 1-2.5 hours, and for more than 5 hours, yielded 23% and 24% risk reductions, respectively.
A reverse J–shaped relationship between cycling duration and reduction in all-cause mortality was seen, Dr. Ried-Larsen noted during a live oral session at the virtual meeting. “The maximum benefit [was at] around 5 hours per week, and the benefits persisted until around 9 hours per week.” Adjustment for the prevalence of stroke, MI, cancer, hyperlipidemia, hypertension, and central obesity did not alter the findings.
“The direction of the association was the same for cardiovascular mortality as all-cause mortality, although a bit weaker, with the maximum benefit being around 4 hours per week, and that persisted up until around 8 hours per week,” Dr. Ried-Larsen said.
The benefits of cycling on all-cause and cardiovascular mortality were lost, however, if those who cycled at baseline stopped by the second examination. Those who did not cycle at the first but did at the second examination got a benefit on both, as did those who continued cycling.
“Cycling is among one of the preferred activities for diabetes patients, so it actually may help them to achieve the recommend level of physical activity,” Dr. Ried-Larsen said.
Tailored exercise program important
Advice for exercise “should be tailored to the individual and based on starting fitness levels and activity levels,” Dr. Colberg-Ochs recommended.
“Those who are the most sedentary and the least fit have the most to gain from doing any activity. They should be advised to start out slowly and progress slowly with both aerobic activities and some resistance training,” Dr. Colberg-Ochs said.
She added: “In addition, individuals over 40 should engage in regular balance training, and all individuals should do some flexibility exercises.”
The studies received no commercial funding and all those mentioned in this article had no conflicts of interest to disclose.
SOURCE: Lai Y-J et al. EASD 2020, Poster presentation 267; Ried-Larsen M et al. EASD 2020, Oral presentation 194.
FROM EASD 2020
Landmark sickle cell report targets massive failures, calls for action
The National Academies of Science, Engineering, and Medicine have just released a 522-page report, but it’s not the usual compilation of guidelines for treatment of a disease. Instead, the authors of “Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action” argue in stark terms that the American society has colossally failed individuals living with sickle cell disease (SCD), who are mostly Black or Brown. A dramatic overhaul of the country’s medical and societal priorities is needed to turn things around to improve health and longevity among this rare disease population.
The findings from the NASEM report are explicit: “There has been substantial success in increasing the survival of children with SCD, but this success had not been translated to similar success as they become adults.” One factor posited to contribute to the slow progress in the improvement of quality and quantity of life for adults living with this disease is the fact that “SCD is largely a disease of African Americans, and as such exists in a context of racial discrimination, health and other societal disparities, mistrust of the health care system, and the effects of poverty.” The report also cites the substantial evidence that those with SCD may receive poorer quality of care.
The report’s 14 authors were made up of an ad hoc committee formed at the request of the Department of Health & Human Services’ Office of Minority Health. The office asked NASEM to convene the committee to develop a strategic plan and blueprint for the United States and others regarding SCD.
The NASEM SCD committee members “realized that we can’t address the medical components of SCD if we don’t explore societal issues and why it’s been so hard to get good care for people with sickle cell disease,” hematologist and report coauthor Ifeyinwa (Ify) Osunkwo, MD, professor of medicine and pediatrics at Atrium Health and director of the Sickle Cell Disease Enterprise, Levine Cancer Institute, Charlotte, N.C., said in an interview. Dr. Osunkwo is also the medical editor of Hematology News.
“After almost a year of meetings and digging into the background and history of SCD care, we came out with very comprehensive summary of where we were and where we want to be,” she said. “The report provides short-, intermediate- and long-term recommendations and identifies which entity and organization should be responsible for implementing them.”
The report authors, led by pediatrician and committee chair Marie Clare McCormick, MD, of the Harvard School of Public Health, Boston, stated that about 100,000 people in the United States and millions worldwide live with SCD. The disease kills more than 700 people per year in the United States, and treatment costs an estimated $2 billion a year.
When judged by disability-adjusted life-years lost – a measurement of expected healthy years of life without an illness – the impact of SCD on individuals is estimated to be greater than a long list of other diseases such as Alzheimer’s disease, breast cancer, type 1 diabetes, and AIDS/HIV, the report noted.
“The health care needs of individuals living with SCD have been neglected by the U.S. and global health care systems, causing them and their families to suffer,” the report said. “Many of the complications that afflict individuals with SCD, particularly pain, are invisible. Pain is only diagnosed by self-reports, and in SCD there are few to no external indicators of the pain experience. Nevertheless, the pain can be excruciatingly severe and requires treatment with strong analgesics.”
There’s even more misery to the story of SCD, the report said, and Dr. Osunkwo agreed. “It’s not just about pain. These individuals suffer from multiple organ-system complications that are physical but also psychological and societal. They experience a lot of disparities in every aspect of their lives. You’re sick, so then you can’t get a job or health insurance, you can’t get Social Security benefits. You can’t get the type of health care you need nor can you access the other forms of support you need and often you are judged as a drug seeker for complaining of pain or repeatedly seeking acute care for unresolved pain.”
Multiple factors exacerbate the experience of people living with SCD in America, the report said. “Because of systemic racism, unconscious bias, and the stigma associated with the diagnosis, the disease brings with it a much broader burden.”

Dr. Osunkwo put it this way: “SCD is a disease that mostly affects Brown and Black people, and that gets layered into the whole discrimination issues that Black and Brown people face compounding the health burden from their disease.”
The report added that “the SCD community has developed a significant lack of trust in the health care system due to the nearly universal stigma and lack of belief in their reports of pain, a lack of trust that has been further reinforced by historical events, such as the Tuskegee experiment.”
The report highlighted research that finds that Blacks “are more likely to receive a lower quality of pain management than white patients and may be perceived as having drug-seeking behavior.”
The report also identified gaps in treatment, noting that “many SCD complications are not restricted to any one organ system, and the impact of the disease on [quality of life] can be profound but hard to define and compartmentalize.”
Dr. Osunkwo said medical professionals often fail to understand the full breadth of the disease. “There’s no particular look to SCD. When you have cancer, you come in, and you look like you’re sick because you’re bald. Everyone clues into that cancer look and knows it’s lethal, that you’re may likely die early. We don’t have that “look that generates empathy” for SCD, and people don’t understand the burden on those affected. They don’t understand or appreciate that SCD shortens your lifespan as well ... that people living with SCD die 3 decades earlier than their ethnically matched peers. Also, SCD is associated with a lot of pain, and pain and the treatment of pain with opioids makes people [health care providers] uncomfortable unless it’s cancer pain.”
She added: “People also assume that, if it’s not pain, it’s not SCD even though SCD can cause leg ulcers and blood clots and even affect the tonsils, or lead to a stroke. When a disease complexity is too difficult for providers to understand, they either avoid it or don’t do anything for the patient.”
Screening and surveillance for SCD and sickle cell trait is insufficient, the report said, and the potential cost of missed childhood cases is large. Detecting the condition at birth allows the implementation of appropriate comprehensive care and treatment to prevent early death from infections and strokes. As the authors noted, “tremendous strides have been made in the past few decades in the care of children with SCD, which have led to almost all children in high-income settings surviving to adulthood.” However, there remains gaps in care coordination and follow-up of babies screened at birth and even bigger gaps in translating these life span gains to adults particularly around the period of transition from pediatrics to adult care when there appears to be a spike in morbidity and mortality.
The report summarized current treatments for SCD and noted “an influx of pipeline products” after years of little progress and identifies “a need for targeted SCD therapies that address the underlying cause of the disease.”
While treatment recommendations exist, Dr. Osunkwo said, “the evidence for them is very poor and many SCD complications have no evidence-based guidelines for providers to follow. We need more research to provide high quality evidence to make guidelines for SCD treatment stronger and more robust.”
In its final section, the report offers a “strategic plan and blueprint for sickle cell disease action.” It offers several strategies to achieve the vision of “long healthy productive lives for those living with sickle cell disease and sickle cell trait”:
- Establish and fund a research agenda to inform effective programs and policies across the life span.
- Implement efforts to advance understanding of the full impact of sickle cell trait on individuals and society.
- Address barriers to accessing current and pipeline therapies for SCD.
- Improve SCD awareness and strengthen advocacy efforts.
- Increase the number of qualified health professionals providing SCD care.
- Strengthen the evidence base for interventions and disease management and implement widespread efforts to monitor the quality of SCD care.
- Establish organized systems of care assuring both clinical and nonclinical supportive services to all persons living with SCD.
- Establish a national system to collect and link data to characterize the burden of disease, outcomes, and the needs of those with SCD across the life span.
“Right now, the average lifespan for SCD is in the mid-40s to mid-50s,” Dr. Osunkwo said. “That’s a horrible statistic. Even if we just take up half of these recommendations, people will live longer with SCD, and they’ll be more productive and contribute more to society. If we value a cancer life the same as a sickle cell life, we’ll be halfway across the finish line. But the stigma of SCD being a Black and Brown problem is going to be the hardest to confront as it requires a systemic change in our culture as a country and a health care system.”
Still, she said, the commissioning of the report “shows that there is a desire to understand the issue in better detail and try to mitigate it.”
Dr. Osunkwo and Dr. McCormick had no relevant disclosures.
SOURCE: National Academies of Sciences, Engineering, and Medicine. Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action. Washington, D.C.: National Academies Press, 2020.
The National Academies of Science, Engineering, and Medicine have just released a 522-page report, but it’s not the usual compilation of guidelines for treatment of a disease. Instead, the authors of “Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action” argue in stark terms that the American society has colossally failed individuals living with sickle cell disease (SCD), who are mostly Black or Brown. A dramatic overhaul of the country’s medical and societal priorities is needed to turn things around to improve health and longevity among this rare disease population.
The findings from the NASEM report are explicit: “There has been substantial success in increasing the survival of children with SCD, but this success had not been translated to similar success as they become adults.” One factor posited to contribute to the slow progress in the improvement of quality and quantity of life for adults living with this disease is the fact that “SCD is largely a disease of African Americans, and as such exists in a context of racial discrimination, health and other societal disparities, mistrust of the health care system, and the effects of poverty.” The report also cites the substantial evidence that those with SCD may receive poorer quality of care.
The report’s 14 authors were made up of an ad hoc committee formed at the request of the Department of Health & Human Services’ Office of Minority Health. The office asked NASEM to convene the committee to develop a strategic plan and blueprint for the United States and others regarding SCD.
The NASEM SCD committee members “realized that we can’t address the medical components of SCD if we don’t explore societal issues and why it’s been so hard to get good care for people with sickle cell disease,” hematologist and report coauthor Ifeyinwa (Ify) Osunkwo, MD, professor of medicine and pediatrics at Atrium Health and director of the Sickle Cell Disease Enterprise, Levine Cancer Institute, Charlotte, N.C., said in an interview. Dr. Osunkwo is also the medical editor of Hematology News.
“After almost a year of meetings and digging into the background and history of SCD care, we came out with very comprehensive summary of where we were and where we want to be,” she said. “The report provides short-, intermediate- and long-term recommendations and identifies which entity and organization should be responsible for implementing them.”
The report authors, led by pediatrician and committee chair Marie Clare McCormick, MD, of the Harvard School of Public Health, Boston, stated that about 100,000 people in the United States and millions worldwide live with SCD. The disease kills more than 700 people per year in the United States, and treatment costs an estimated $2 billion a year.
When judged by disability-adjusted life-years lost – a measurement of expected healthy years of life without an illness – the impact of SCD on individuals is estimated to be greater than a long list of other diseases such as Alzheimer’s disease, breast cancer, type 1 diabetes, and AIDS/HIV, the report noted.
“The health care needs of individuals living with SCD have been neglected by the U.S. and global health care systems, causing them and their families to suffer,” the report said. “Many of the complications that afflict individuals with SCD, particularly pain, are invisible. Pain is only diagnosed by self-reports, and in SCD there are few to no external indicators of the pain experience. Nevertheless, the pain can be excruciatingly severe and requires treatment with strong analgesics.”
There’s even more misery to the story of SCD, the report said, and Dr. Osunkwo agreed. “It’s not just about pain. These individuals suffer from multiple organ-system complications that are physical but also psychological and societal. They experience a lot of disparities in every aspect of their lives. You’re sick, so then you can’t get a job or health insurance, you can’t get Social Security benefits. You can’t get the type of health care you need nor can you access the other forms of support you need and often you are judged as a drug seeker for complaining of pain or repeatedly seeking acute care for unresolved pain.”
Multiple factors exacerbate the experience of people living with SCD in America, the report said. “Because of systemic racism, unconscious bias, and the stigma associated with the diagnosis, the disease brings with it a much broader burden.”
Dr. Osunkwo put it this way: “SCD is a disease that mostly affects Brown and Black people, and that gets layered into the whole discrimination issues that Black and Brown people face compounding the health burden from their disease.”
The report added that “the SCD community has developed a significant lack of trust in the health care system due to the nearly universal stigma and lack of belief in their reports of pain, a lack of trust that has been further reinforced by historical events, such as the Tuskegee experiment.”
The report highlighted research that finds that Blacks “are more likely to receive a lower quality of pain management than white patients and may be perceived as having drug-seeking behavior.”
The report also identified gaps in treatment, noting that “many SCD complications are not restricted to any one organ system, and the impact of the disease on [quality of life] can be profound but hard to define and compartmentalize.”
Dr. Osunkwo said medical professionals often fail to understand the full breadth of the disease. “There’s no particular look to SCD. When you have cancer, you come in, and you look like you’re sick because you’re bald. Everyone clues into that cancer look and knows it’s lethal, that you’re may likely die early. We don’t have that “look that generates empathy” for SCD, and people don’t understand the burden on those affected. They don’t understand or appreciate that SCD shortens your lifespan as well ... that people living with SCD die 3 decades earlier than their ethnically matched peers. Also, SCD is associated with a lot of pain, and pain and the treatment of pain with opioids makes people [health care providers] uncomfortable unless it’s cancer pain.”
She added: “People also assume that, if it’s not pain, it’s not SCD even though SCD can cause leg ulcers and blood clots and even affect the tonsils, or lead to a stroke. When a disease complexity is too difficult for providers to understand, they either avoid it or don’t do anything for the patient.”
Screening and surveillance for SCD and sickle cell trait is insufficient, the report said, and the potential cost of missed childhood cases is large. Detecting the condition at birth allows the implementation of appropriate comprehensive care and treatment to prevent early death from infections and strokes. As the authors noted, “tremendous strides have been made in the past few decades in the care of children with SCD, which have led to almost all children in high-income settings surviving to adulthood.” However, there remains gaps in care coordination and follow-up of babies screened at birth and even bigger gaps in translating these life span gains to adults particularly around the period of transition from pediatrics to adult care when there appears to be a spike in morbidity and mortality.
The report summarized current treatments for SCD and noted “an influx of pipeline products” after years of little progress and identifies “a need for targeted SCD therapies that address the underlying cause of the disease.”
While treatment recommendations exist, Dr. Osunkwo said, “the evidence for them is very poor and many SCD complications have no evidence-based guidelines for providers to follow. We need more research to provide high quality evidence to make guidelines for SCD treatment stronger and more robust.”
In its final section, the report offers a “strategic plan and blueprint for sickle cell disease action.” It offers several strategies to achieve the vision of “long healthy productive lives for those living with sickle cell disease and sickle cell trait”:
- Establish and fund a research agenda to inform effective programs and policies across the life span.
- Implement efforts to advance understanding of the full impact of sickle cell trait on individuals and society.
- Address barriers to accessing current and pipeline therapies for SCD.
- Improve SCD awareness and strengthen advocacy efforts.
- Increase the number of qualified health professionals providing SCD care.
- Strengthen the evidence base for interventions and disease management and implement widespread efforts to monitor the quality of SCD care.
- Establish organized systems of care assuring both clinical and nonclinical supportive services to all persons living with SCD.
- Establish a national system to collect and link data to characterize the burden of disease, outcomes, and the needs of those with SCD across the life span.
“Right now, the average lifespan for SCD is in the mid-40s to mid-50s,” Dr. Osunkwo said. “That’s a horrible statistic. Even if we just take up half of these recommendations, people will live longer with SCD, and they’ll be more productive and contribute more to society. If we value a cancer life the same as a sickle cell life, we’ll be halfway across the finish line. But the stigma of SCD being a Black and Brown problem is going to be the hardest to confront as it requires a systemic change in our culture as a country and a health care system.”
Still, she said, the commissioning of the report “shows that there is a desire to understand the issue in better detail and try to mitigate it.”
Dr. Osunkwo and Dr. McCormick had no relevant disclosures.
SOURCE: National Academies of Sciences, Engineering, and Medicine. Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action. Washington, D.C.: National Academies Press, 2020.
The National Academies of Science, Engineering, and Medicine have just released a 522-page report, but it’s not the usual compilation of guidelines for treatment of a disease. Instead, the authors of “Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action” argue in stark terms that the American society has colossally failed individuals living with sickle cell disease (SCD), who are mostly Black or Brown. A dramatic overhaul of the country’s medical and societal priorities is needed to turn things around to improve health and longevity among this rare disease population.
The findings from the NASEM report are explicit: “There has been substantial success in increasing the survival of children with SCD, but this success had not been translated to similar success as they become adults.” One factor posited to contribute to the slow progress in the improvement of quality and quantity of life for adults living with this disease is the fact that “SCD is largely a disease of African Americans, and as such exists in a context of racial discrimination, health and other societal disparities, mistrust of the health care system, and the effects of poverty.” The report also cites the substantial evidence that those with SCD may receive poorer quality of care.
The report’s 14 authors were made up of an ad hoc committee formed at the request of the Department of Health & Human Services’ Office of Minority Health. The office asked NASEM to convene the committee to develop a strategic plan and blueprint for the United States and others regarding SCD.
The NASEM SCD committee members “realized that we can’t address the medical components of SCD if we don’t explore societal issues and why it’s been so hard to get good care for people with sickle cell disease,” hematologist and report coauthor Ifeyinwa (Ify) Osunkwo, MD, professor of medicine and pediatrics at Atrium Health and director of the Sickle Cell Disease Enterprise, Levine Cancer Institute, Charlotte, N.C., said in an interview. Dr. Osunkwo is also the medical editor of Hematology News.
“After almost a year of meetings and digging into the background and history of SCD care, we came out with very comprehensive summary of where we were and where we want to be,” she said. “The report provides short-, intermediate- and long-term recommendations and identifies which entity and organization should be responsible for implementing them.”
The report authors, led by pediatrician and committee chair Marie Clare McCormick, MD, of the Harvard School of Public Health, Boston, stated that about 100,000 people in the United States and millions worldwide live with SCD. The disease kills more than 700 people per year in the United States, and treatment costs an estimated $2 billion a year.
When judged by disability-adjusted life-years lost – a measurement of expected healthy years of life without an illness – the impact of SCD on individuals is estimated to be greater than a long list of other diseases such as Alzheimer’s disease, breast cancer, type 1 diabetes, and AIDS/HIV, the report noted.
“The health care needs of individuals living with SCD have been neglected by the U.S. and global health care systems, causing them and their families to suffer,” the report said. “Many of the complications that afflict individuals with SCD, particularly pain, are invisible. Pain is only diagnosed by self-reports, and in SCD there are few to no external indicators of the pain experience. Nevertheless, the pain can be excruciatingly severe and requires treatment with strong analgesics.”
There’s even more misery to the story of SCD, the report said, and Dr. Osunkwo agreed. “It’s not just about pain. These individuals suffer from multiple organ-system complications that are physical but also psychological and societal. They experience a lot of disparities in every aspect of their lives. You’re sick, so then you can’t get a job or health insurance, you can’t get Social Security benefits. You can’t get the type of health care you need nor can you access the other forms of support you need and often you are judged as a drug seeker for complaining of pain or repeatedly seeking acute care for unresolved pain.”
Multiple factors exacerbate the experience of people living with SCD in America, the report said. “Because of systemic racism, unconscious bias, and the stigma associated with the diagnosis, the disease brings with it a much broader burden.”
Dr. Osunkwo put it this way: “SCD is a disease that mostly affects Brown and Black people, and that gets layered into the whole discrimination issues that Black and Brown people face compounding the health burden from their disease.”
The report added that “the SCD community has developed a significant lack of trust in the health care system due to the nearly universal stigma and lack of belief in their reports of pain, a lack of trust that has been further reinforced by historical events, such as the Tuskegee experiment.”
The report highlighted research that finds that Blacks “are more likely to receive a lower quality of pain management than white patients and may be perceived as having drug-seeking behavior.”
The report also identified gaps in treatment, noting that “many SCD complications are not restricted to any one organ system, and the impact of the disease on [quality of life] can be profound but hard to define and compartmentalize.”
Dr. Osunkwo said medical professionals often fail to understand the full breadth of the disease. “There’s no particular look to SCD. When you have cancer, you come in, and you look like you’re sick because you’re bald. Everyone clues into that cancer look and knows it’s lethal, that you’re may likely die early. We don’t have that “look that generates empathy” for SCD, and people don’t understand the burden on those affected. They don’t understand or appreciate that SCD shortens your lifespan as well ... that people living with SCD die 3 decades earlier than their ethnically matched peers. Also, SCD is associated with a lot of pain, and pain and the treatment of pain with opioids makes people [health care providers] uncomfortable unless it’s cancer pain.”
She added: “People also assume that, if it’s not pain, it’s not SCD even though SCD can cause leg ulcers and blood clots and even affect the tonsils, or lead to a stroke. When a disease complexity is too difficult for providers to understand, they either avoid it or don’t do anything for the patient.”
Screening and surveillance for SCD and sickle cell trait is insufficient, the report said, and the potential cost of missed childhood cases is large. Detecting the condition at birth allows the implementation of appropriate comprehensive care and treatment to prevent early death from infections and strokes. As the authors noted, “tremendous strides have been made in the past few decades in the care of children with SCD, which have led to almost all children in high-income settings surviving to adulthood.” However, there remains gaps in care coordination and follow-up of babies screened at birth and even bigger gaps in translating these life span gains to adults particularly around the period of transition from pediatrics to adult care when there appears to be a spike in morbidity and mortality.
The report summarized current treatments for SCD and noted “an influx of pipeline products” after years of little progress and identifies “a need for targeted SCD therapies that address the underlying cause of the disease.”
While treatment recommendations exist, Dr. Osunkwo said, “the evidence for them is very poor and many SCD complications have no evidence-based guidelines for providers to follow. We need more research to provide high quality evidence to make guidelines for SCD treatment stronger and more robust.”
In its final section, the report offers a “strategic plan and blueprint for sickle cell disease action.” It offers several strategies to achieve the vision of “long healthy productive lives for those living with sickle cell disease and sickle cell trait”:
- Establish and fund a research agenda to inform effective programs and policies across the life span.
- Implement efforts to advance understanding of the full impact of sickle cell trait on individuals and society.
- Address barriers to accessing current and pipeline therapies for SCD.
- Improve SCD awareness and strengthen advocacy efforts.
- Increase the number of qualified health professionals providing SCD care.
- Strengthen the evidence base for interventions and disease management and implement widespread efforts to monitor the quality of SCD care.
- Establish organized systems of care assuring both clinical and nonclinical supportive services to all persons living with SCD.
- Establish a national system to collect and link data to characterize the burden of disease, outcomes, and the needs of those with SCD across the life span.
“Right now, the average lifespan for SCD is in the mid-40s to mid-50s,” Dr. Osunkwo said. “That’s a horrible statistic. Even if we just take up half of these recommendations, people will live longer with SCD, and they’ll be more productive and contribute more to society. If we value a cancer life the same as a sickle cell life, we’ll be halfway across the finish line. But the stigma of SCD being a Black and Brown problem is going to be the hardest to confront as it requires a systemic change in our culture as a country and a health care system.”
Still, she said, the commissioning of the report “shows that there is a desire to understand the issue in better detail and try to mitigate it.”
Dr. Osunkwo and Dr. McCormick had no relevant disclosures.
SOURCE: National Academies of Sciences, Engineering, and Medicine. Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action. Washington, D.C.: National Academies Press, 2020.
Novel schizophrenia drugs advance through pipeline
Two oral agents with novel mechanisms of action in schizophrenia generated considerable audience interest after acing large phase 2 clinical trials presented at the virtual congress of the European College of Neuropsychopharmacology.
The two successful drugs moving on to definitive phase 3 studies after their performance at ECNP 2020 are KarXT, a proprietary combination of xanomeline and trospium chloride, and an inhibitor of glycine transporter 1 (Gly-T1) known for now as BI 425809.
Pimavanserin, an oral selective serotonin inverse agonist with a high affinity for 5-HT2A receptors and low affinity for 5-HT2C receptors, has taken a more convoluted path through the developmental pipeline for schizophrenia. It recently failed to outperform placebo as adjunctive treatment for schizophrenia on the primary endpoint of improvement in Positive And Negative Syndrome Scale (PANSS) total score in the 6-week, phase 3 ENHANCE (Efficacy and Safety of Adjunctive Pimavanserin for the Treatment of Schizophrenia) study. The drug did, however, show significant benefit on secondary endpoints involving negative symptoms.
And in the 400-patient, 26-week, placebo-controlled, phase 2 ADVANCE trial, adjunctive pimavanserin was positive for the primary endpoint of improvement in the Negative Symptom Assessment-16 (NSA-16) score. A phase 3 program evaluating the drug specifically for negative symptoms is underway.
Another novel therapy, an investigational selective estrogen receptor beta agonist, proved reassuringly safe but completely ineffective in men with schizophrenia in a study presented at ECNP 2020.
“The results, unfortunately, were disappointing. We saw no signal on cognition, no change on brain imaging with fMRI, and no improvement in negative symptoms or PANSS total score,” reported Alan Breier, MD, professor and vice chair of the department of psychiatry at Indiana University in Indianapolis.

Broad agreement exists that current antipsychotics targeting D2 dopamine and serotonin receptors in schizophrenia leave much to be desired. They’re ineffective for two of the three major symptom categories that define schizophrenia: cognitive impairment and negative symptoms, such as apathy and social withdrawal. And even for the current antipsychotics’ forte – treatment of positive symptoms, including hallucinations and delusions – effectiveness is often only modest to moderate and accompanied by limiting side effects.
KarXT
KarXT combines xanomeline, a selective M1/M4 muscarinic receptor agonist exclusively licensed from Lilly to Karuna Therapeutics, with trospium chloride, a muscarinic antagonist approved for more than a decade in the United States and Europe for treatment of overactive bladder. Xanomeline was synthesized in the 1990s. It showed promising evidence of antipsychotic efficacy in schizophrenia and Alzheimer’s disease in yearlong clinical trials totaling more than 800 patients, but interest in further developing the drug cooled because of limiting GI and other cholinergic adverse events. KarXT, Karuna’s lead product candidate, is designed to maintain the efficacy of xanomeline while trospium, which doesn’t cross the blood-brain barrier, cancels out its side effects, explained Stephen Brannan, MD, a psychiatrist and chief medical officer at the company.
He presented the results of the phase 2 study, a multicenter, randomized, double-blind, placebo-controlled, 5-week trial conducted with 182 schizophrenia inpatients experiencing an acute psychotic exacerbation. All other antipsychotics were washed out before randomization to KarXT at 50 mg xanomeline/20 mg trospium twice daily, titrated to 100/20 twice daily on days 3-7 and 100/20 b.i.d. thereafter, with an optional increase to 125/30 twice daily.
The primary study endpoint was change from baseline to week 5 in PANSS total score. The results were positive at the P < .0001 level, with a mean 17.4-point reduction in the KarXT group, compared with a 5.9-point improvement in placebo-treated controls. The between-group difference was significant by the first assessment at week 2.
Four of five prespecified secondary endpoints were also positive in rapid and sustained fashion: improvement in the PANSS positive subscore, PANSS negative subscore, Marder PANSS negative subscore, and Clinical Global Impressions-Severity. The fifth secondary endpoint – the proportion of patients with a Clinical Global Impressions rating of 1 or 2, meaning normal or only mildly mentally ill – wasn’t significantly different with KarXT, compared with placebo, but Dr. Brannan shrugged that off.
“In hindsight, it was probably a little overly optimistic to think that after 5 weeks [patients with schizophrenia] would be either well or almost well,” he quipped.
An exploratory analysis of participants’ before-and-after scores on a battery of six cognitive tests showed an encouraging trend: Patients on KarXT performed numerically better than did controls on five of the six tests, albeit not significantly so. Moreover, in a further analysis stratified by baseline impairment, patients in the most impaired tertile showed a larger, statistically significant benefit in response to KarXT.
“We’re interested enough that we plan to continue to look at this in our upcoming larger and longer-term trials,” Dr. Brannan said.
As for safety and tolerability, he continued: “We were pleasantly surprised. We certainly see more side effects with KarXT than with placebo, but not by that much, and they’re much, much better than with xanomeline alone.”
The side effects, mostly cholinergic and anticholinergic, occurred 2-4 times more frequently than in controls. Notably, the rates of nausea, vomiting, and dry mouth – three of the five most common treatment-related adverse events in patients on KarXT – decreased over time to levels similar to placebo by week 5. In contrast, rates of constipation and dyspepsia remained stable over time. All side effects were mild to moderate, and none led to study discontinuation.
A key point was that the KarXT-related side effects were not the same ones that are commonly problematic and limiting with current antipsychotics. There was no weight gain or other metabolic changes, sleepiness or sedation, or extrapyramidal symptoms.
“These results show KarXT has the potential to offer patients a novel mechanism-of-action antipsychotic with a different efficacy and/or tolerability profile than current antipsychotic medications,” Dr. Brannan said.
BI 425809
BI 425809 is a once-daily oral inhibitor of glycine transporter 1 (Gly-T1) specifically designed to alleviate cognitive impairment in people with schizophrenia. Underactivity by the NMDA (N-methyl-D-aspartic acid) receptor has been implicated in this cognitive dysfunction. Glycine is an NMDA cotransmitter. By blocking glutamatergic presynaptic and astrocyte reuptake of glycine, BI 425809 results in increased glycine levels in the synaptic cleft, facilitating neurotransmission, explained W. Wolfgang Fleischhacker, MD, president of the Medical University of Innsbruck (Austria), where he is also professor of psychiatry.
He presented the results of a phase 2, randomized, double-blind, 11-country study in which 509 adults with stable schizophrenia on no more than two antipsychotics were placed on add-on BI 425809 at 2, 5, 10, or 25 mg once daily or placebo for 12 weeks.
The primary endpoint was change from baseline to 12 weeks in the MATRICS (Measurement and Treatment Research to Improve Cognition in Schizophrenia) Consensus Cognitive Battery (MCCB) score. The results were strongly positive, with patients on the two top doses of BI 425809 – 10 and 25 mg/day – showing roughly a 2-point greater improvement in MCCB overall composite T-score compared with controls. Dr. Fleischhacker drew attention to the high study completion rates in the various study arms, ranging from a low of 91% to 97.6% in the 25 mg/day group.
“That’s a very nice but also an unusual finding for a trial of this length,” he observed.
The high study completion rate was a reflection of the drug’s high-level tolerability. Indeed, the rate of adverse events leading to treatment discontinuation was 0% with BI 425809 at 10 mg/day, 2.4% at 25 mg/day, and identical at 2.4% with placebo. No increase was found in psychiatric adverse events such as suicidal ideation or behavior.
“This is a first very promising result,” Dr. Fleischhacker concluded. “Basically, this is the first study that has really shown in a convincing fashion an effect of any novel compound on cognitive impairment in people suffering from schizophrenia.”
A separate ongoing phase 2 study is evaluating BI 425809 in combination with adjunctive computerized cognitive training in an effort to increase cognitive stimulation. The company is awaiting those study results before designing its phase 3 program.
Pimavanserin
It has been a busy year for pimavanserin, with both successes and disappointments in clinical trials addressing a range of psychotic disorders, according to Dragana Bugarski-Kirola, MD, MBA, MSc, vice president for clinical development at Acadia Pharmaceuticals in San Diego.

At present, pimavanserin is Food and Drug Administration–approved as Nuplazid only for treatment of hallucinations and delusions associated with Parkinson’s disease psychosis. But in July 2020, on the strength of the positive results of the pivotal phase 3 HARMONY trial, Acadia filed an application with the FDA for marketing approval of the drug for treatment of dementia-related psychosis. In HARMONY, patients on placebo proved to be 2.8-fold more likely to experience a relapse of delusions or hallucinations than with pimavanserin.
A big recent disappointment was that pimavanserin failed to meet its primary endpoint in the phase 3 CLARITY I and CLARITY II trials as adjunctive therapy for major depressive disorder inadequately responsive to a selective serotonin reuptake inhibitor or serotonin norepinephrine reuptake inhibitor. The change in Hamilton Depression Rating Scale–17 scores in patients on the atypical antipsychotic wasn’t significantly better than with placebo. However, pimavanserin did outperform placebo on the secondary endpoint of Clinical Global Impression–Severity. Additional clinical trials of the drug for treatment of major depression are planned, Dr. Bugarski-Kirola said.
LY500307
Although schizophrenia is equally common in men and women, the disease has a later onset and more benign course in women. This suggests a possible protective effect of estrogen, and indeed, extensive literature supports the use of exogenous estrogen in schizophrenia, where it reduces relapses and improves cognitive impairment and negative symptoms.
“We have no other agents that do that,” noted Dr. Breier, also chief of the psychotic disorders program and director of the Prevention and Recovery Center at Indiana University.
What he considers the best-executed clinical trial of estradiol in schizophrenia, an 8-week, double-blind, randomized study of a 200-mcg estradiol patch or placebo in 200 women aged 19-46 on antipsychotics, was published last year (JAMA Psychiatry. 2019 Jul 31;76[10]:1-9).
The results were impressive. However, estrogen may not be a viable treatment for men and premenopausal women because of its side effects, including feminization, and increased thrombotic and malignancy risks.
This was the impetus for the placebo-controlled randomized trial of LY500307, a highly selective estrogen receptor beta agonist originally developed by Eli Lilly as a potential treatment for benign prostatic hypertrophy, for which it proved ineffective. In animal models, estrogen receptor beta is responsible for a range of effects, including enhanced cognition, social behavior, and an anxiolytic action, whereas the alpha receptor affects the sex organs, skeletal and metabolic homeostasis, and is responsible for estrogen’s problematic side effects.
All three doses studied in the phase 2 randomized trial, which included 94 men with schizophrenia, proved safe, well-tolerated – and ineffective.
“I think one potential conclusion one could consider from these data is that estrogen receptor alpha engagement may be necessary for the estrogenic therapeutics in schizophrenia,” Dr. Breier said.
He reported having no financial conflicts regarding the trial, funded by Indiana University. Outside the scope of the study, he serves as a consultant to Karuna Therapeutics, BioXcel, and Perception Neuroscience.
Dr. Fleischhacker serves as a consultant to Boehringer Ingelheim, which sponsored the phase 2 study of BI 425809, as well as to Angelini, Richter, and Recordati.
SOURCE: ECNP 2020, Session S.12.
Two oral agents with novel mechanisms of action in schizophrenia generated considerable audience interest after acing large phase 2 clinical trials presented at the virtual congress of the European College of Neuropsychopharmacology.
The two successful drugs moving on to definitive phase 3 studies after their performance at ECNP 2020 are KarXT, a proprietary combination of xanomeline and trospium chloride, and an inhibitor of glycine transporter 1 (Gly-T1) known for now as BI 425809.
Pimavanserin, an oral selective serotonin inverse agonist with a high affinity for 5-HT2A receptors and low affinity for 5-HT2C receptors, has taken a more convoluted path through the developmental pipeline for schizophrenia. It recently failed to outperform placebo as adjunctive treatment for schizophrenia on the primary endpoint of improvement in Positive And Negative Syndrome Scale (PANSS) total score in the 6-week, phase 3 ENHANCE (Efficacy and Safety of Adjunctive Pimavanserin for the Treatment of Schizophrenia) study. The drug did, however, show significant benefit on secondary endpoints involving negative symptoms.
And in the 400-patient, 26-week, placebo-controlled, phase 2 ADVANCE trial, adjunctive pimavanserin was positive for the primary endpoint of improvement in the Negative Symptom Assessment-16 (NSA-16) score. A phase 3 program evaluating the drug specifically for negative symptoms is underway.
Another novel therapy, an investigational selective estrogen receptor beta agonist, proved reassuringly safe but completely ineffective in men with schizophrenia in a study presented at ECNP 2020.
“The results, unfortunately, were disappointing. We saw no signal on cognition, no change on brain imaging with fMRI, and no improvement in negative symptoms or PANSS total score,” reported Alan Breier, MD, professor and vice chair of the department of psychiatry at Indiana University in Indianapolis.
Broad agreement exists that current antipsychotics targeting D2 dopamine and serotonin receptors in schizophrenia leave much to be desired. They’re ineffective for two of the three major symptom categories that define schizophrenia: cognitive impairment and negative symptoms, such as apathy and social withdrawal. And even for the current antipsychotics’ forte – treatment of positive symptoms, including hallucinations and delusions – effectiveness is often only modest to moderate and accompanied by limiting side effects.
KarXT
KarXT combines xanomeline, a selective M1/M4 muscarinic receptor agonist exclusively licensed from Lilly to Karuna Therapeutics, with trospium chloride, a muscarinic antagonist approved for more than a decade in the United States and Europe for treatment of overactive bladder. Xanomeline was synthesized in the 1990s. It showed promising evidence of antipsychotic efficacy in schizophrenia and Alzheimer’s disease in yearlong clinical trials totaling more than 800 patients, but interest in further developing the drug cooled because of limiting GI and other cholinergic adverse events. KarXT, Karuna’s lead product candidate, is designed to maintain the efficacy of xanomeline while trospium, which doesn’t cross the blood-brain barrier, cancels out its side effects, explained Stephen Brannan, MD, a psychiatrist and chief medical officer at the company.
He presented the results of the phase 2 study, a multicenter, randomized, double-blind, placebo-controlled, 5-week trial conducted with 182 schizophrenia inpatients experiencing an acute psychotic exacerbation. All other antipsychotics were washed out before randomization to KarXT at 50 mg xanomeline/20 mg trospium twice daily, titrated to 100/20 twice daily on days 3-7 and 100/20 b.i.d. thereafter, with an optional increase to 125/30 twice daily.
The primary study endpoint was change from baseline to week 5 in PANSS total score. The results were positive at the P < .0001 level, with a mean 17.4-point reduction in the KarXT group, compared with a 5.9-point improvement in placebo-treated controls. The between-group difference was significant by the first assessment at week 2.
Four of five prespecified secondary endpoints were also positive in rapid and sustained fashion: improvement in the PANSS positive subscore, PANSS negative subscore, Marder PANSS negative subscore, and Clinical Global Impressions-Severity. The fifth secondary endpoint – the proportion of patients with a Clinical Global Impressions rating of 1 or 2, meaning normal or only mildly mentally ill – wasn’t significantly different with KarXT, compared with placebo, but Dr. Brannan shrugged that off.
“In hindsight, it was probably a little overly optimistic to think that after 5 weeks [patients with schizophrenia] would be either well or almost well,” he quipped.
An exploratory analysis of participants’ before-and-after scores on a battery of six cognitive tests showed an encouraging trend: Patients on KarXT performed numerically better than did controls on five of the six tests, albeit not significantly so. Moreover, in a further analysis stratified by baseline impairment, patients in the most impaired tertile showed a larger, statistically significant benefit in response to KarXT.
“We’re interested enough that we plan to continue to look at this in our upcoming larger and longer-term trials,” Dr. Brannan said.
As for safety and tolerability, he continued: “We were pleasantly surprised. We certainly see more side effects with KarXT than with placebo, but not by that much, and they’re much, much better than with xanomeline alone.”
The side effects, mostly cholinergic and anticholinergic, occurred 2-4 times more frequently than in controls. Notably, the rates of nausea, vomiting, and dry mouth – three of the five most common treatment-related adverse events in patients on KarXT – decreased over time to levels similar to placebo by week 5. In contrast, rates of constipation and dyspepsia remained stable over time. All side effects were mild to moderate, and none led to study discontinuation.
A key point was that the KarXT-related side effects were not the same ones that are commonly problematic and limiting with current antipsychotics. There was no weight gain or other metabolic changes, sleepiness or sedation, or extrapyramidal symptoms.
“These results show KarXT has the potential to offer patients a novel mechanism-of-action antipsychotic with a different efficacy and/or tolerability profile than current antipsychotic medications,” Dr. Brannan said.
BI 425809
BI 425809 is a once-daily oral inhibitor of glycine transporter 1 (Gly-T1) specifically designed to alleviate cognitive impairment in people with schizophrenia. Underactivity by the NMDA (N-methyl-D-aspartic acid) receptor has been implicated in this cognitive dysfunction. Glycine is an NMDA cotransmitter. By blocking glutamatergic presynaptic and astrocyte reuptake of glycine, BI 425809 results in increased glycine levels in the synaptic cleft, facilitating neurotransmission, explained W. Wolfgang Fleischhacker, MD, president of the Medical University of Innsbruck (Austria), where he is also professor of psychiatry.
He presented the results of a phase 2, randomized, double-blind, 11-country study in which 509 adults with stable schizophrenia on no more than two antipsychotics were placed on add-on BI 425809 at 2, 5, 10, or 25 mg once daily or placebo for 12 weeks.
The primary endpoint was change from baseline to 12 weeks in the MATRICS (Measurement and Treatment Research to Improve Cognition in Schizophrenia) Consensus Cognitive Battery (MCCB) score. The results were strongly positive, with patients on the two top doses of BI 425809 – 10 and 25 mg/day – showing roughly a 2-point greater improvement in MCCB overall composite T-score compared with controls. Dr. Fleischhacker drew attention to the high study completion rates in the various study arms, ranging from a low of 91% to 97.6% in the 25 mg/day group.
“That’s a very nice but also an unusual finding for a trial of this length,” he observed.
The high study completion rate was a reflection of the drug’s high-level tolerability. Indeed, the rate of adverse events leading to treatment discontinuation was 0% with BI 425809 at 10 mg/day, 2.4% at 25 mg/day, and identical at 2.4% with placebo. No increase was found in psychiatric adverse events such as suicidal ideation or behavior.
“This is a first very promising result,” Dr. Fleischhacker concluded. “Basically, this is the first study that has really shown in a convincing fashion an effect of any novel compound on cognitive impairment in people suffering from schizophrenia.”
A separate ongoing phase 2 study is evaluating BI 425809 in combination with adjunctive computerized cognitive training in an effort to increase cognitive stimulation. The company is awaiting those study results before designing its phase 3 program.
Pimavanserin
It has been a busy year for pimavanserin, with both successes and disappointments in clinical trials addressing a range of psychotic disorders, according to Dragana Bugarski-Kirola, MD, MBA, MSc, vice president for clinical development at Acadia Pharmaceuticals in San Diego.
At present, pimavanserin is Food and Drug Administration–approved as Nuplazid only for treatment of hallucinations and delusions associated with Parkinson’s disease psychosis. But in July 2020, on the strength of the positive results of the pivotal phase 3 HARMONY trial, Acadia filed an application with the FDA for marketing approval of the drug for treatment of dementia-related psychosis. In HARMONY, patients on placebo proved to be 2.8-fold more likely to experience a relapse of delusions or hallucinations than with pimavanserin.
A big recent disappointment was that pimavanserin failed to meet its primary endpoint in the phase 3 CLARITY I and CLARITY II trials as adjunctive therapy for major depressive disorder inadequately responsive to a selective serotonin reuptake inhibitor or serotonin norepinephrine reuptake inhibitor. The change in Hamilton Depression Rating Scale–17 scores in patients on the atypical antipsychotic wasn’t significantly better than with placebo. However, pimavanserin did outperform placebo on the secondary endpoint of Clinical Global Impression–Severity. Additional clinical trials of the drug for treatment of major depression are planned, Dr. Bugarski-Kirola said.
LY500307
Although schizophrenia is equally common in men and women, the disease has a later onset and more benign course in women. This suggests a possible protective effect of estrogen, and indeed, extensive literature supports the use of exogenous estrogen in schizophrenia, where it reduces relapses and improves cognitive impairment and negative symptoms.
“We have no other agents that do that,” noted Dr. Breier, also chief of the psychotic disorders program and director of the Prevention and Recovery Center at Indiana University.
What he considers the best-executed clinical trial of estradiol in schizophrenia, an 8-week, double-blind, randomized study of a 200-mcg estradiol patch or placebo in 200 women aged 19-46 on antipsychotics, was published last year (JAMA Psychiatry. 2019 Jul 31;76[10]:1-9).
The results were impressive. However, estrogen may not be a viable treatment for men and premenopausal women because of its side effects, including feminization, and increased thrombotic and malignancy risks.
This was the impetus for the placebo-controlled randomized trial of LY500307, a highly selective estrogen receptor beta agonist originally developed by Eli Lilly as a potential treatment for benign prostatic hypertrophy, for which it proved ineffective. In animal models, estrogen receptor beta is responsible for a range of effects, including enhanced cognition, social behavior, and an anxiolytic action, whereas the alpha receptor affects the sex organs, skeletal and metabolic homeostasis, and is responsible for estrogen’s problematic side effects.
All three doses studied in the phase 2 randomized trial, which included 94 men with schizophrenia, proved safe, well-tolerated – and ineffective.
“I think one potential conclusion one could consider from these data is that estrogen receptor alpha engagement may be necessary for the estrogenic therapeutics in schizophrenia,” Dr. Breier said.
He reported having no financial conflicts regarding the trial, funded by Indiana University. Outside the scope of the study, he serves as a consultant to Karuna Therapeutics, BioXcel, and Perception Neuroscience.
Dr. Fleischhacker serves as a consultant to Boehringer Ingelheim, which sponsored the phase 2 study of BI 425809, as well as to Angelini, Richter, and Recordati.
SOURCE: ECNP 2020, Session S.12.
Two oral agents with novel mechanisms of action in schizophrenia generated considerable audience interest after acing large phase 2 clinical trials presented at the virtual congress of the European College of Neuropsychopharmacology.
The two successful drugs moving on to definitive phase 3 studies after their performance at ECNP 2020 are KarXT, a proprietary combination of xanomeline and trospium chloride, and an inhibitor of glycine transporter 1 (Gly-T1) known for now as BI 425809.
Pimavanserin, an oral selective serotonin inverse agonist with a high affinity for 5-HT2A receptors and low affinity for 5-HT2C receptors, has taken a more convoluted path through the developmental pipeline for schizophrenia. It recently failed to outperform placebo as adjunctive treatment for schizophrenia on the primary endpoint of improvement in Positive And Negative Syndrome Scale (PANSS) total score in the 6-week, phase 3 ENHANCE (Efficacy and Safety of Adjunctive Pimavanserin for the Treatment of Schizophrenia) study. The drug did, however, show significant benefit on secondary endpoints involving negative symptoms.
And in the 400-patient, 26-week, placebo-controlled, phase 2 ADVANCE trial, adjunctive pimavanserin was positive for the primary endpoint of improvement in the Negative Symptom Assessment-16 (NSA-16) score. A phase 3 program evaluating the drug specifically for negative symptoms is underway.
Another novel therapy, an investigational selective estrogen receptor beta agonist, proved reassuringly safe but completely ineffective in men with schizophrenia in a study presented at ECNP 2020.
“The results, unfortunately, were disappointing. We saw no signal on cognition, no change on brain imaging with fMRI, and no improvement in negative symptoms or PANSS total score,” reported Alan Breier, MD, professor and vice chair of the department of psychiatry at Indiana University in Indianapolis.
Broad agreement exists that current antipsychotics targeting D2 dopamine and serotonin receptors in schizophrenia leave much to be desired. They’re ineffective for two of the three major symptom categories that define schizophrenia: cognitive impairment and negative symptoms, such as apathy and social withdrawal. And even for the current antipsychotics’ forte – treatment of positive symptoms, including hallucinations and delusions – effectiveness is often only modest to moderate and accompanied by limiting side effects.
KarXT
KarXT combines xanomeline, a selective M1/M4 muscarinic receptor agonist exclusively licensed from Lilly to Karuna Therapeutics, with trospium chloride, a muscarinic antagonist approved for more than a decade in the United States and Europe for treatment of overactive bladder. Xanomeline was synthesized in the 1990s. It showed promising evidence of antipsychotic efficacy in schizophrenia and Alzheimer’s disease in yearlong clinical trials totaling more than 800 patients, but interest in further developing the drug cooled because of limiting GI and other cholinergic adverse events. KarXT, Karuna’s lead product candidate, is designed to maintain the efficacy of xanomeline while trospium, which doesn’t cross the blood-brain barrier, cancels out its side effects, explained Stephen Brannan, MD, a psychiatrist and chief medical officer at the company.
He presented the results of the phase 2 study, a multicenter, randomized, double-blind, placebo-controlled, 5-week trial conducted with 182 schizophrenia inpatients experiencing an acute psychotic exacerbation. All other antipsychotics were washed out before randomization to KarXT at 50 mg xanomeline/20 mg trospium twice daily, titrated to 100/20 twice daily on days 3-7 and 100/20 b.i.d. thereafter, with an optional increase to 125/30 twice daily.
The primary study endpoint was change from baseline to week 5 in PANSS total score. The results were positive at the P < .0001 level, with a mean 17.4-point reduction in the KarXT group, compared with a 5.9-point improvement in placebo-treated controls. The between-group difference was significant by the first assessment at week 2.
Four of five prespecified secondary endpoints were also positive in rapid and sustained fashion: improvement in the PANSS positive subscore, PANSS negative subscore, Marder PANSS negative subscore, and Clinical Global Impressions-Severity. The fifth secondary endpoint – the proportion of patients with a Clinical Global Impressions rating of 1 or 2, meaning normal or only mildly mentally ill – wasn’t significantly different with KarXT, compared with placebo, but Dr. Brannan shrugged that off.
“In hindsight, it was probably a little overly optimistic to think that after 5 weeks [patients with schizophrenia] would be either well or almost well,” he quipped.
An exploratory analysis of participants’ before-and-after scores on a battery of six cognitive tests showed an encouraging trend: Patients on KarXT performed numerically better than did controls on five of the six tests, albeit not significantly so. Moreover, in a further analysis stratified by baseline impairment, patients in the most impaired tertile showed a larger, statistically significant benefit in response to KarXT.
“We’re interested enough that we plan to continue to look at this in our upcoming larger and longer-term trials,” Dr. Brannan said.
As for safety and tolerability, he continued: “We were pleasantly surprised. We certainly see more side effects with KarXT than with placebo, but not by that much, and they’re much, much better than with xanomeline alone.”
The side effects, mostly cholinergic and anticholinergic, occurred 2-4 times more frequently than in controls. Notably, the rates of nausea, vomiting, and dry mouth – three of the five most common treatment-related adverse events in patients on KarXT – decreased over time to levels similar to placebo by week 5. In contrast, rates of constipation and dyspepsia remained stable over time. All side effects were mild to moderate, and none led to study discontinuation.
A key point was that the KarXT-related side effects were not the same ones that are commonly problematic and limiting with current antipsychotics. There was no weight gain or other metabolic changes, sleepiness or sedation, or extrapyramidal symptoms.
“These results show KarXT has the potential to offer patients a novel mechanism-of-action antipsychotic with a different efficacy and/or tolerability profile than current antipsychotic medications,” Dr. Brannan said.
BI 425809
BI 425809 is a once-daily oral inhibitor of glycine transporter 1 (Gly-T1) specifically designed to alleviate cognitive impairment in people with schizophrenia. Underactivity by the NMDA (N-methyl-D-aspartic acid) receptor has been implicated in this cognitive dysfunction. Glycine is an NMDA cotransmitter. By blocking glutamatergic presynaptic and astrocyte reuptake of glycine, BI 425809 results in increased glycine levels in the synaptic cleft, facilitating neurotransmission, explained W. Wolfgang Fleischhacker, MD, president of the Medical University of Innsbruck (Austria), where he is also professor of psychiatry.
He presented the results of a phase 2, randomized, double-blind, 11-country study in which 509 adults with stable schizophrenia on no more than two antipsychotics were placed on add-on BI 425809 at 2, 5, 10, or 25 mg once daily or placebo for 12 weeks.
The primary endpoint was change from baseline to 12 weeks in the MATRICS (Measurement and Treatment Research to Improve Cognition in Schizophrenia) Consensus Cognitive Battery (MCCB) score. The results were strongly positive, with patients on the two top doses of BI 425809 – 10 and 25 mg/day – showing roughly a 2-point greater improvement in MCCB overall composite T-score compared with controls. Dr. Fleischhacker drew attention to the high study completion rates in the various study arms, ranging from a low of 91% to 97.6% in the 25 mg/day group.
“That’s a very nice but also an unusual finding for a trial of this length,” he observed.
The high study completion rate was a reflection of the drug’s high-level tolerability. Indeed, the rate of adverse events leading to treatment discontinuation was 0% with BI 425809 at 10 mg/day, 2.4% at 25 mg/day, and identical at 2.4% with placebo. No increase was found in psychiatric adverse events such as suicidal ideation or behavior.
“This is a first very promising result,” Dr. Fleischhacker concluded. “Basically, this is the first study that has really shown in a convincing fashion an effect of any novel compound on cognitive impairment in people suffering from schizophrenia.”
A separate ongoing phase 2 study is evaluating BI 425809 in combination with adjunctive computerized cognitive training in an effort to increase cognitive stimulation. The company is awaiting those study results before designing its phase 3 program.
Pimavanserin
It has been a busy year for pimavanserin, with both successes and disappointments in clinical trials addressing a range of psychotic disorders, according to Dragana Bugarski-Kirola, MD, MBA, MSc, vice president for clinical development at Acadia Pharmaceuticals in San Diego.
At present, pimavanserin is Food and Drug Administration–approved as Nuplazid only for treatment of hallucinations and delusions associated with Parkinson’s disease psychosis. But in July 2020, on the strength of the positive results of the pivotal phase 3 HARMONY trial, Acadia filed an application with the FDA for marketing approval of the drug for treatment of dementia-related psychosis. In HARMONY, patients on placebo proved to be 2.8-fold more likely to experience a relapse of delusions or hallucinations than with pimavanserin.
A big recent disappointment was that pimavanserin failed to meet its primary endpoint in the phase 3 CLARITY I and CLARITY II trials as adjunctive therapy for major depressive disorder inadequately responsive to a selective serotonin reuptake inhibitor or serotonin norepinephrine reuptake inhibitor. The change in Hamilton Depression Rating Scale–17 scores in patients on the atypical antipsychotic wasn’t significantly better than with placebo. However, pimavanserin did outperform placebo on the secondary endpoint of Clinical Global Impression–Severity. Additional clinical trials of the drug for treatment of major depression are planned, Dr. Bugarski-Kirola said.
LY500307
Although schizophrenia is equally common in men and women, the disease has a later onset and more benign course in women. This suggests a possible protective effect of estrogen, and indeed, extensive literature supports the use of exogenous estrogen in schizophrenia, where it reduces relapses and improves cognitive impairment and negative symptoms.
“We have no other agents that do that,” noted Dr. Breier, also chief of the psychotic disorders program and director of the Prevention and Recovery Center at Indiana University.
What he considers the best-executed clinical trial of estradiol in schizophrenia, an 8-week, double-blind, randomized study of a 200-mcg estradiol patch or placebo in 200 women aged 19-46 on antipsychotics, was published last year (JAMA Psychiatry. 2019 Jul 31;76[10]:1-9).
The results were impressive. However, estrogen may not be a viable treatment for men and premenopausal women because of its side effects, including feminization, and increased thrombotic and malignancy risks.
This was the impetus for the placebo-controlled randomized trial of LY500307, a highly selective estrogen receptor beta agonist originally developed by Eli Lilly as a potential treatment for benign prostatic hypertrophy, for which it proved ineffective. In animal models, estrogen receptor beta is responsible for a range of effects, including enhanced cognition, social behavior, and an anxiolytic action, whereas the alpha receptor affects the sex organs, skeletal and metabolic homeostasis, and is responsible for estrogen’s problematic side effects.
All three doses studied in the phase 2 randomized trial, which included 94 men with schizophrenia, proved safe, well-tolerated – and ineffective.
“I think one potential conclusion one could consider from these data is that estrogen receptor alpha engagement may be necessary for the estrogenic therapeutics in schizophrenia,” Dr. Breier said.
He reported having no financial conflicts regarding the trial, funded by Indiana University. Outside the scope of the study, he serves as a consultant to Karuna Therapeutics, BioXcel, and Perception Neuroscience.
Dr. Fleischhacker serves as a consultant to Boehringer Ingelheim, which sponsored the phase 2 study of BI 425809, as well as to Angelini, Richter, and Recordati.
SOURCE: ECNP 2020, Session S.12.
FROM ECNP 2020
Global stomach cancer deaths decline as colorectal cancer deaths stagnate, rise
The data suggest fewer people are dying from stomach cancer, but in some countries, the risk of colorectal cancer death is increasing or declining much more slowly than other causes of premature death.
As for other cancers, in more than half of the countries analyzed, the risk of liver and prostate cancer death is on the rise in men, and the risk of lung cancer death is on the rise in women.
The global decrease in the risk of stomach cancer death may be explained by the fact that stomach cancer’s main cause is Helicobacter pylori infection, which correlates with general food hygiene, the study’s corresponding author Majid Ezzati, PhD, professor of global environmental health at Imperial College London, said in an interview.
“Factors such as more widespread electrification and refrigeration tend to drive the rates down,” he explained.
Dr. Ezzati and colleagues detailed their findings in the second edition of the NCD Countdown 2030 report, recently published in The Lancet.
The report revolves around the Sustainable Development Goal (SDG) target 3.4, which is to reduce premature deaths from NCDs by one-third between 2015 and 2030. The causes of death include cancer, cardiovascular disease, chronic respiratory disease, and diabetes, which are collectively known as NCD4. “Premature” deaths are defined as deaths in people aged 30-70 years.
SDG target 3.4 is still attainable, according to Dr. Ezzati and colleagues. However, their report showed that many countries are falling short of this goal.
The findings come from an analysis of 2016 World Health Organization global estimate data on age-, sex-, and cause-specific mortality for 176 countries and territories with at least 200,000 inhabitants. Mathematical modeling was used to assess the number of approaches countries used to accelerate declines in mortality.
Results of the analysis
“Trends in the risk of death from 2010 to 2016 varied considerably among NCD4 causes of death,” Dr. Ezzati and colleagues wrote.
Stomach cancer, ischemic and hemorrhagic stroke, ischemic heart disease, and chronic respiratory diseases had the fastest rates of decline among risks of premature death.
In fact, stomach cancer was the fastest declining cause of death in 45 countries (25.6%) among men and in 40 countries (22.7%) among women.
On the other hand, the risk of premature death from colorectal, liver, breast, prostate, and other cancers declined more slowly than the risk of premature death from other NCDs.
The risk of death from colorectal, liver, and prostate cancers in men and lung cancer in women rose in more than 50% of the countries surveyed.
“The median annual rate of change in the probability of dying prematurely from various causes ranged from +0.2% per year for lung cancer to –2.5% per year for hemorrhagic stroke in women, and from +0.5% per year for colorectal cancer to –1.8% per year for hemorrhagic stroke in men,” the investigators summarized.
Explaining the GI cancer results
“There are dramatic differences between the upper and lower GI tract, both in terms of anatomy/embryologic origin but also in terms of exposures,” observed Mark Lewis, MD, medical director of the gastrointestinal oncology program at Intermountain Healthcare in Salt Lake City, in an interview.
H. pylori infection, family history, and diet factor into stomach cancer risk, Dr. Lewis said.
While family history isn’t modifiable, “we are much better now at identifying and eradicating the potentially carcinogenic H. pylori bacterium. In terms of diet, the advent of modern refrigeration has made the prevalence of heavily salted/preserved foods decline,” he added.
A 14-day course of treatment (with a proton pump inhibitor and antibiotics) can eliminate H. pylori, Dr. Lewis continued. “The prophylactic effect against gastric cancer is massive, cutting risk by roughly half,” he said.
At least in the United States, colorectal cancer rates have declined in people 50 years and older, but rates have risen sharply in younger age groups, increasing by 2% annually in the last decade, according to statistics in CA: A Cancer Journal for Clinicians.
“One prevailing theory is prior antibiotic prescriptions [even in childhood] might perturb the microbiome of the lower GI tract and predispose to cancer,” Dr. Lewis said, pointing to a recent study in the British Journal of Cancer that identified an association between repeated antibiotic use and colorectal cancer.
Reducing NCD deaths
Dr. Ezzati and colleagues said six high-income countries – Denmark, Luxembourg, New Zealand, Norway, Singapore, and South Korea – are likely to meet SDG target 3.4 if they maintain or exceed average rates of decline seen during 2010-2016. Seventeen countries are on track to reach the target for women, and 15 countries are on track for men.
High-income countries in Asia-Pacific, western Europe, Australasia, and Canada have seen the lowest NCD4 mortality risk, whereas low- and middle-income countries in sub-Saharan Africa and men in central Asia and eastern Europe have seen the highest risk.
“To move forward, we must learn from those countries that are doing well and replicate their strategies to NCD prevention and healthcare,” Dr. Ezzati said in a statement. “Our analysis shows that every country still has options to achieve SDG target 3.4, but they need to address multiple diseases and have strong health systems.”
Increasing access to effective cancer screening and diagnosing and treating cancers earlier could help reduce long-term health consequences and premature deaths from cancer, according to Dr. Ezzati and colleagues. Screening would help even the playing field on cancer diagnosis and survival rates between higher-income countries and low- and middle-income countries.
“This approach will allow earlier diagnosis during precancerous or early stages of disease, followed by treatment of those cancers with effective treatment,” the authors stated.
Tobacco and alcohol interventions and increasing access to quality primary care would also help tamp down on NCD-related deaths.
The authors acknowledged that low-income countries, which may be struggling with other health crises such as COVID-19 and Ebola, may find it a challenge to stage such interventions.
“COVID-19 has exposed how a failure to invest in effective public health to prevent NCDs and provide health care for people living with NCDs can come back to bite us,” said Katie Dain, CEO of the NCD Alliance.
“The good news is that all countries can still meet the 2030 targets, with sound policies and smart investments. NCD prevention and treatment can no longer be seen a ‘nice to have.’ It must be considered as part of pandemic preparedness,” she added.
COVID-19 should serve as an impetus for governments to invest in healthier lifestyle and diet habits and curb alcohol and tobacco use, according to an editorial in The Lancet related to the analysis.
The current report updates 2018’s first NCD Countdown Report, which linked NCD4 conditions to approximately 32 million or 80% of NCD deaths. Unlike the recent report, 2018’s data didn’t focus on specific diseases.
The current report was funded by Research England. Dr. Ezzati received a charitable grant from the AstraZeneca Young Health Programme and personal fees from Prudential and Scor, outside of this report. None of the other authors reported competing interests. Dr. Lewis has no relevant disclosures except that he is a commentator for Medscape, which is owned by the same parent company as MDedge.
SOURCE: Bennett JE et al. Lancet. 2020 Sep 3. doi: 10.1016/S0140-6736(20)31761-X.
The data suggest fewer people are dying from stomach cancer, but in some countries, the risk of colorectal cancer death is increasing or declining much more slowly than other causes of premature death.
As for other cancers, in more than half of the countries analyzed, the risk of liver and prostate cancer death is on the rise in men, and the risk of lung cancer death is on the rise in women.
The global decrease in the risk of stomach cancer death may be explained by the fact that stomach cancer’s main cause is Helicobacter pylori infection, which correlates with general food hygiene, the study’s corresponding author Majid Ezzati, PhD, professor of global environmental health at Imperial College London, said in an interview.
“Factors such as more widespread electrification and refrigeration tend to drive the rates down,” he explained.
Dr. Ezzati and colleagues detailed their findings in the second edition of the NCD Countdown 2030 report, recently published in The Lancet.
The report revolves around the Sustainable Development Goal (SDG) target 3.4, which is to reduce premature deaths from NCDs by one-third between 2015 and 2030. The causes of death include cancer, cardiovascular disease, chronic respiratory disease, and diabetes, which are collectively known as NCD4. “Premature” deaths are defined as deaths in people aged 30-70 years.
SDG target 3.4 is still attainable, according to Dr. Ezzati and colleagues. However, their report showed that many countries are falling short of this goal.
The findings come from an analysis of 2016 World Health Organization global estimate data on age-, sex-, and cause-specific mortality for 176 countries and territories with at least 200,000 inhabitants. Mathematical modeling was used to assess the number of approaches countries used to accelerate declines in mortality.
Results of the analysis
“Trends in the risk of death from 2010 to 2016 varied considerably among NCD4 causes of death,” Dr. Ezzati and colleagues wrote.
Stomach cancer, ischemic and hemorrhagic stroke, ischemic heart disease, and chronic respiratory diseases had the fastest rates of decline among risks of premature death.
In fact, stomach cancer was the fastest declining cause of death in 45 countries (25.6%) among men and in 40 countries (22.7%) among women.
On the other hand, the risk of premature death from colorectal, liver, breast, prostate, and other cancers declined more slowly than the risk of premature death from other NCDs.
The risk of death from colorectal, liver, and prostate cancers in men and lung cancer in women rose in more than 50% of the countries surveyed.
“The median annual rate of change in the probability of dying prematurely from various causes ranged from +0.2% per year for lung cancer to –2.5% per year for hemorrhagic stroke in women, and from +0.5% per year for colorectal cancer to –1.8% per year for hemorrhagic stroke in men,” the investigators summarized.
Explaining the GI cancer results
“There are dramatic differences between the upper and lower GI tract, both in terms of anatomy/embryologic origin but also in terms of exposures,” observed Mark Lewis, MD, medical director of the gastrointestinal oncology program at Intermountain Healthcare in Salt Lake City, in an interview.
H. pylori infection, family history, and diet factor into stomach cancer risk, Dr. Lewis said.
While family history isn’t modifiable, “we are much better now at identifying and eradicating the potentially carcinogenic H. pylori bacterium. In terms of diet, the advent of modern refrigeration has made the prevalence of heavily salted/preserved foods decline,” he added.
A 14-day course of treatment (with a proton pump inhibitor and antibiotics) can eliminate H. pylori, Dr. Lewis continued. “The prophylactic effect against gastric cancer is massive, cutting risk by roughly half,” he said.
At least in the United States, colorectal cancer rates have declined in people 50 years and older, but rates have risen sharply in younger age groups, increasing by 2% annually in the last decade, according to statistics in CA: A Cancer Journal for Clinicians.
“One prevailing theory is prior antibiotic prescriptions [even in childhood] might perturb the microbiome of the lower GI tract and predispose to cancer,” Dr. Lewis said, pointing to a recent study in the British Journal of Cancer that identified an association between repeated antibiotic use and colorectal cancer.
Reducing NCD deaths
Dr. Ezzati and colleagues said six high-income countries – Denmark, Luxembourg, New Zealand, Norway, Singapore, and South Korea – are likely to meet SDG target 3.4 if they maintain or exceed average rates of decline seen during 2010-2016. Seventeen countries are on track to reach the target for women, and 15 countries are on track for men.
High-income countries in Asia-Pacific, western Europe, Australasia, and Canada have seen the lowest NCD4 mortality risk, whereas low- and middle-income countries in sub-Saharan Africa and men in central Asia and eastern Europe have seen the highest risk.
“To move forward, we must learn from those countries that are doing well and replicate their strategies to NCD prevention and healthcare,” Dr. Ezzati said in a statement. “Our analysis shows that every country still has options to achieve SDG target 3.4, but they need to address multiple diseases and have strong health systems.”
Increasing access to effective cancer screening and diagnosing and treating cancers earlier could help reduce long-term health consequences and premature deaths from cancer, according to Dr. Ezzati and colleagues. Screening would help even the playing field on cancer diagnosis and survival rates between higher-income countries and low- and middle-income countries.
“This approach will allow earlier diagnosis during precancerous or early stages of disease, followed by treatment of those cancers with effective treatment,” the authors stated.
Tobacco and alcohol interventions and increasing access to quality primary care would also help tamp down on NCD-related deaths.
The authors acknowledged that low-income countries, which may be struggling with other health crises such as COVID-19 and Ebola, may find it a challenge to stage such interventions.
“COVID-19 has exposed how a failure to invest in effective public health to prevent NCDs and provide health care for people living with NCDs can come back to bite us,” said Katie Dain, CEO of the NCD Alliance.
“The good news is that all countries can still meet the 2030 targets, with sound policies and smart investments. NCD prevention and treatment can no longer be seen a ‘nice to have.’ It must be considered as part of pandemic preparedness,” she added.
COVID-19 should serve as an impetus for governments to invest in healthier lifestyle and diet habits and curb alcohol and tobacco use, according to an editorial in The Lancet related to the analysis.
The current report updates 2018’s first NCD Countdown Report, which linked NCD4 conditions to approximately 32 million or 80% of NCD deaths. Unlike the recent report, 2018’s data didn’t focus on specific diseases.
The current report was funded by Research England. Dr. Ezzati received a charitable grant from the AstraZeneca Young Health Programme and personal fees from Prudential and Scor, outside of this report. None of the other authors reported competing interests. Dr. Lewis has no relevant disclosures except that he is a commentator for Medscape, which is owned by the same parent company as MDedge.
SOURCE: Bennett JE et al. Lancet. 2020 Sep 3. doi: 10.1016/S0140-6736(20)31761-X.
The data suggest fewer people are dying from stomach cancer, but in some countries, the risk of colorectal cancer death is increasing or declining much more slowly than other causes of premature death.
As for other cancers, in more than half of the countries analyzed, the risk of liver and prostate cancer death is on the rise in men, and the risk of lung cancer death is on the rise in women.
The global decrease in the risk of stomach cancer death may be explained by the fact that stomach cancer’s main cause is Helicobacter pylori infection, which correlates with general food hygiene, the study’s corresponding author Majid Ezzati, PhD, professor of global environmental health at Imperial College London, said in an interview.
“Factors such as more widespread electrification and refrigeration tend to drive the rates down,” he explained.
Dr. Ezzati and colleagues detailed their findings in the second edition of the NCD Countdown 2030 report, recently published in The Lancet.
The report revolves around the Sustainable Development Goal (SDG) target 3.4, which is to reduce premature deaths from NCDs by one-third between 2015 and 2030. The causes of death include cancer, cardiovascular disease, chronic respiratory disease, and diabetes, which are collectively known as NCD4. “Premature” deaths are defined as deaths in people aged 30-70 years.
SDG target 3.4 is still attainable, according to Dr. Ezzati and colleagues. However, their report showed that many countries are falling short of this goal.
The findings come from an analysis of 2016 World Health Organization global estimate data on age-, sex-, and cause-specific mortality for 176 countries and territories with at least 200,000 inhabitants. Mathematical modeling was used to assess the number of approaches countries used to accelerate declines in mortality.
Results of the analysis
“Trends in the risk of death from 2010 to 2016 varied considerably among NCD4 causes of death,” Dr. Ezzati and colleagues wrote.
Stomach cancer, ischemic and hemorrhagic stroke, ischemic heart disease, and chronic respiratory diseases had the fastest rates of decline among risks of premature death.
In fact, stomach cancer was the fastest declining cause of death in 45 countries (25.6%) among men and in 40 countries (22.7%) among women.
On the other hand, the risk of premature death from colorectal, liver, breast, prostate, and other cancers declined more slowly than the risk of premature death from other NCDs.
The risk of death from colorectal, liver, and prostate cancers in men and lung cancer in women rose in more than 50% of the countries surveyed.
“The median annual rate of change in the probability of dying prematurely from various causes ranged from +0.2% per year for lung cancer to –2.5% per year for hemorrhagic stroke in women, and from +0.5% per year for colorectal cancer to –1.8% per year for hemorrhagic stroke in men,” the investigators summarized.
Explaining the GI cancer results
“There are dramatic differences between the upper and lower GI tract, both in terms of anatomy/embryologic origin but also in terms of exposures,” observed Mark Lewis, MD, medical director of the gastrointestinal oncology program at Intermountain Healthcare in Salt Lake City, in an interview.
H. pylori infection, family history, and diet factor into stomach cancer risk, Dr. Lewis said.
While family history isn’t modifiable, “we are much better now at identifying and eradicating the potentially carcinogenic H. pylori bacterium. In terms of diet, the advent of modern refrigeration has made the prevalence of heavily salted/preserved foods decline,” he added.
A 14-day course of treatment (with a proton pump inhibitor and antibiotics) can eliminate H. pylori, Dr. Lewis continued. “The prophylactic effect against gastric cancer is massive, cutting risk by roughly half,” he said.
At least in the United States, colorectal cancer rates have declined in people 50 years and older, but rates have risen sharply in younger age groups, increasing by 2% annually in the last decade, according to statistics in CA: A Cancer Journal for Clinicians.
“One prevailing theory is prior antibiotic prescriptions [even in childhood] might perturb the microbiome of the lower GI tract and predispose to cancer,” Dr. Lewis said, pointing to a recent study in the British Journal of Cancer that identified an association between repeated antibiotic use and colorectal cancer.
Reducing NCD deaths
Dr. Ezzati and colleagues said six high-income countries – Denmark, Luxembourg, New Zealand, Norway, Singapore, and South Korea – are likely to meet SDG target 3.4 if they maintain or exceed average rates of decline seen during 2010-2016. Seventeen countries are on track to reach the target for women, and 15 countries are on track for men.
High-income countries in Asia-Pacific, western Europe, Australasia, and Canada have seen the lowest NCD4 mortality risk, whereas low- and middle-income countries in sub-Saharan Africa and men in central Asia and eastern Europe have seen the highest risk.
“To move forward, we must learn from those countries that are doing well and replicate their strategies to NCD prevention and healthcare,” Dr. Ezzati said in a statement. “Our analysis shows that every country still has options to achieve SDG target 3.4, but they need to address multiple diseases and have strong health systems.”
Increasing access to effective cancer screening and diagnosing and treating cancers earlier could help reduce long-term health consequences and premature deaths from cancer, according to Dr. Ezzati and colleagues. Screening would help even the playing field on cancer diagnosis and survival rates between higher-income countries and low- and middle-income countries.
“This approach will allow earlier diagnosis during precancerous or early stages of disease, followed by treatment of those cancers with effective treatment,” the authors stated.
Tobacco and alcohol interventions and increasing access to quality primary care would also help tamp down on NCD-related deaths.
The authors acknowledged that low-income countries, which may be struggling with other health crises such as COVID-19 and Ebola, may find it a challenge to stage such interventions.
“COVID-19 has exposed how a failure to invest in effective public health to prevent NCDs and provide health care for people living with NCDs can come back to bite us,” said Katie Dain, CEO of the NCD Alliance.
“The good news is that all countries can still meet the 2030 targets, with sound policies and smart investments. NCD prevention and treatment can no longer be seen a ‘nice to have.’ It must be considered as part of pandemic preparedness,” she added.
COVID-19 should serve as an impetus for governments to invest in healthier lifestyle and diet habits and curb alcohol and tobacco use, according to an editorial in The Lancet related to the analysis.
The current report updates 2018’s first NCD Countdown Report, which linked NCD4 conditions to approximately 32 million or 80% of NCD deaths. Unlike the recent report, 2018’s data didn’t focus on specific diseases.
The current report was funded by Research England. Dr. Ezzati received a charitable grant from the AstraZeneca Young Health Programme and personal fees from Prudential and Scor, outside of this report. None of the other authors reported competing interests. Dr. Lewis has no relevant disclosures except that he is a commentator for Medscape, which is owned by the same parent company as MDedge.
SOURCE: Bennett JE et al. Lancet. 2020 Sep 3. doi: 10.1016/S0140-6736(20)31761-X.
FROM THE LANCET