User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Large study amplifies evidence of COVID vaccine safety in pregnancy
The research team wrote in the BMJ that their reassuring findings – drawn from a registry of all births in Ontario over an 8-month period – “can inform evidence-based decision-making” about COVID vaccination during pregnancy.
Previous research has found that pregnant patients are at higher risk of severe complications and death if they become infected with COVID and that vaccination before or during pregnancy prevents such outcomes and reduces the risk of newborn infection, noted Jeffrey Ecker, chief of obstetrics and gynecology at Massachusetts General Hospital, Boston.
This new study “adds to a growing body of information arguing clearly and reassuringly that vaccination during pregnancy is not associated with complications during pregnancy,” said Dr. Ecker, who was not involved in the new study.
He added that it “should help obstetric providers further reassure those who are hesitant that vaccination is safe and best both for the pregnant patient and their pregnancy.”
Methods and results
For the new study, researchers tapped a provincial registry of all live and stillborn infants with a gestational age of at least 20 weeks or birth weight of at least 500 g. Unique health card numbers were used to link birth records to a database of COVID vaccinations.
Of 85,162 infants born from May through December of 2021, 43,099 (50.6%) were born to individuals who received at least one vaccine dose during pregnancy. Among those, 99.7% received an mRNA vaccine such as Pfizer-BioNTech or Moderna.
Vaccination during pregnancy was not associated with greater risk of overall preterm birth (6.5% among vaccinated individuals versus 6.9% among unvaccinated; hazard ratio, 1.02; 95% confidence interval, 0.96-1.08), spontaneous preterm birth (3.7% versus 4.4%; hazard ratio, 0.96; 95% CI, 0.90-1.03) or very preterm birth (0.59% versus 0.89%; hazard ratio, 0.80; 95% CI, 0.67-0.95).
Likewise, no increase was observed in the risk of an infant being small for gestational age at birth (9.1% versus 9.2%; hazard ratio, 0.98; 95% CI, 0.93-1.03).
The researchers observed a reduction in the risk of stillbirth, even after adjusting for potential confounders. Stillbirths occurred in 0.25% of vaccinated individuals, compared with 0.44% of unvaccinated individuals (hazard ratio, 0.65; 95% CI, 0.51-0.84).
A reduced risk of stillbirth – albeit to a smaller degree – was also found in a Scandinavian registry study that included 28,506 babies born to individuals who were vaccinated during pregnancy.
“Collectively, the findings from these two studies are reassuring and are consistent with no increased risk of stillbirth after COVID-19 vaccination during pregnancy. In contrast, COVID-19 disease during pregnancy has been associated with an increased risk of stillbirth,” the researchers wrote.
Findings did not vary by which mRNA vaccine a mother received, the number of doses she received, or the trimester in which a vaccine was given, the researchers reported.
Stillbirth findings will be ‘very reassuring’ for patients
The lead investigator, Deshayne Fell, PhD, said in an interview, the fact that the study comprised the entire population of pregnant people in Ontario during the study period “increases our confidence” about the validity and relevance of the findings for other geographic settings.
Dr. Fell, an associate professor in epidemiology and public health at the University of Ottawa and a scientist at the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, said the evaluation of stillbirth in particular, “a rare but devastating outcome,” will be “very reassuring and useful for clinical counseling.”
A limitation cited by the research team included a lack of data on vaccination prior to pregnancy.
In the new study, Dr, Ecker said, “Though the investigators were able to adjust for many variables they cannot be certain that some unmeasured variable that, accordingly, was not adjusted for does not hide a small risk. This seems very unlikely, however.”
The Canadian research team said similar studies of non-mRNA COVID vaccines “should be a research priority.” However, such studies are not underway in Canada, where only mRNA vaccines are used in pregnancy, Dr. Fell said.
This study was supported by the Public Health Agency of Canada.
Dr. Fell and Dr. Ecker reported no competing financial interests.
The research team wrote in the BMJ that their reassuring findings – drawn from a registry of all births in Ontario over an 8-month period – “can inform evidence-based decision-making” about COVID vaccination during pregnancy.
Previous research has found that pregnant patients are at higher risk of severe complications and death if they become infected with COVID and that vaccination before or during pregnancy prevents such outcomes and reduces the risk of newborn infection, noted Jeffrey Ecker, chief of obstetrics and gynecology at Massachusetts General Hospital, Boston.
This new study “adds to a growing body of information arguing clearly and reassuringly that vaccination during pregnancy is not associated with complications during pregnancy,” said Dr. Ecker, who was not involved in the new study.
He added that it “should help obstetric providers further reassure those who are hesitant that vaccination is safe and best both for the pregnant patient and their pregnancy.”
Methods and results
For the new study, researchers tapped a provincial registry of all live and stillborn infants with a gestational age of at least 20 weeks or birth weight of at least 500 g. Unique health card numbers were used to link birth records to a database of COVID vaccinations.
Of 85,162 infants born from May through December of 2021, 43,099 (50.6%) were born to individuals who received at least one vaccine dose during pregnancy. Among those, 99.7% received an mRNA vaccine such as Pfizer-BioNTech or Moderna.
Vaccination during pregnancy was not associated with greater risk of overall preterm birth (6.5% among vaccinated individuals versus 6.9% among unvaccinated; hazard ratio, 1.02; 95% confidence interval, 0.96-1.08), spontaneous preterm birth (3.7% versus 4.4%; hazard ratio, 0.96; 95% CI, 0.90-1.03) or very preterm birth (0.59% versus 0.89%; hazard ratio, 0.80; 95% CI, 0.67-0.95).
Likewise, no increase was observed in the risk of an infant being small for gestational age at birth (9.1% versus 9.2%; hazard ratio, 0.98; 95% CI, 0.93-1.03).
The researchers observed a reduction in the risk of stillbirth, even after adjusting for potential confounders. Stillbirths occurred in 0.25% of vaccinated individuals, compared with 0.44% of unvaccinated individuals (hazard ratio, 0.65; 95% CI, 0.51-0.84).
A reduced risk of stillbirth – albeit to a smaller degree – was also found in a Scandinavian registry study that included 28,506 babies born to individuals who were vaccinated during pregnancy.
“Collectively, the findings from these two studies are reassuring and are consistent with no increased risk of stillbirth after COVID-19 vaccination during pregnancy. In contrast, COVID-19 disease during pregnancy has been associated with an increased risk of stillbirth,” the researchers wrote.
Findings did not vary by which mRNA vaccine a mother received, the number of doses she received, or the trimester in which a vaccine was given, the researchers reported.
Stillbirth findings will be ‘very reassuring’ for patients
The lead investigator, Deshayne Fell, PhD, said in an interview, the fact that the study comprised the entire population of pregnant people in Ontario during the study period “increases our confidence” about the validity and relevance of the findings for other geographic settings.
Dr. Fell, an associate professor in epidemiology and public health at the University of Ottawa and a scientist at the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, said the evaluation of stillbirth in particular, “a rare but devastating outcome,” will be “very reassuring and useful for clinical counseling.”
A limitation cited by the research team included a lack of data on vaccination prior to pregnancy.
In the new study, Dr, Ecker said, “Though the investigators were able to adjust for many variables they cannot be certain that some unmeasured variable that, accordingly, was not adjusted for does not hide a small risk. This seems very unlikely, however.”
The Canadian research team said similar studies of non-mRNA COVID vaccines “should be a research priority.” However, such studies are not underway in Canada, where only mRNA vaccines are used in pregnancy, Dr. Fell said.
This study was supported by the Public Health Agency of Canada.
Dr. Fell and Dr. Ecker reported no competing financial interests.
The research team wrote in the BMJ that their reassuring findings – drawn from a registry of all births in Ontario over an 8-month period – “can inform evidence-based decision-making” about COVID vaccination during pregnancy.
Previous research has found that pregnant patients are at higher risk of severe complications and death if they become infected with COVID and that vaccination before or during pregnancy prevents such outcomes and reduces the risk of newborn infection, noted Jeffrey Ecker, chief of obstetrics and gynecology at Massachusetts General Hospital, Boston.
This new study “adds to a growing body of information arguing clearly and reassuringly that vaccination during pregnancy is not associated with complications during pregnancy,” said Dr. Ecker, who was not involved in the new study.
He added that it “should help obstetric providers further reassure those who are hesitant that vaccination is safe and best both for the pregnant patient and their pregnancy.”
Methods and results
For the new study, researchers tapped a provincial registry of all live and stillborn infants with a gestational age of at least 20 weeks or birth weight of at least 500 g. Unique health card numbers were used to link birth records to a database of COVID vaccinations.
Of 85,162 infants born from May through December of 2021, 43,099 (50.6%) were born to individuals who received at least one vaccine dose during pregnancy. Among those, 99.7% received an mRNA vaccine such as Pfizer-BioNTech or Moderna.
Vaccination during pregnancy was not associated with greater risk of overall preterm birth (6.5% among vaccinated individuals versus 6.9% among unvaccinated; hazard ratio, 1.02; 95% confidence interval, 0.96-1.08), spontaneous preterm birth (3.7% versus 4.4%; hazard ratio, 0.96; 95% CI, 0.90-1.03) or very preterm birth (0.59% versus 0.89%; hazard ratio, 0.80; 95% CI, 0.67-0.95).
Likewise, no increase was observed in the risk of an infant being small for gestational age at birth (9.1% versus 9.2%; hazard ratio, 0.98; 95% CI, 0.93-1.03).
The researchers observed a reduction in the risk of stillbirth, even after adjusting for potential confounders. Stillbirths occurred in 0.25% of vaccinated individuals, compared with 0.44% of unvaccinated individuals (hazard ratio, 0.65; 95% CI, 0.51-0.84).
A reduced risk of stillbirth – albeit to a smaller degree – was also found in a Scandinavian registry study that included 28,506 babies born to individuals who were vaccinated during pregnancy.
“Collectively, the findings from these two studies are reassuring and are consistent with no increased risk of stillbirth after COVID-19 vaccination during pregnancy. In contrast, COVID-19 disease during pregnancy has been associated with an increased risk of stillbirth,” the researchers wrote.
Findings did not vary by which mRNA vaccine a mother received, the number of doses she received, or the trimester in which a vaccine was given, the researchers reported.
Stillbirth findings will be ‘very reassuring’ for patients
The lead investigator, Deshayne Fell, PhD, said in an interview, the fact that the study comprised the entire population of pregnant people in Ontario during the study period “increases our confidence” about the validity and relevance of the findings for other geographic settings.
Dr. Fell, an associate professor in epidemiology and public health at the University of Ottawa and a scientist at the Children’s Hospital of Eastern Ontario Research Institute, Ottawa, said the evaluation of stillbirth in particular, “a rare but devastating outcome,” will be “very reassuring and useful for clinical counseling.”
A limitation cited by the research team included a lack of data on vaccination prior to pregnancy.
In the new study, Dr, Ecker said, “Though the investigators were able to adjust for many variables they cannot be certain that some unmeasured variable that, accordingly, was not adjusted for does not hide a small risk. This seems very unlikely, however.”
The Canadian research team said similar studies of non-mRNA COVID vaccines “should be a research priority.” However, such studies are not underway in Canada, where only mRNA vaccines are used in pregnancy, Dr. Fell said.
This study was supported by the Public Health Agency of Canada.
Dr. Fell and Dr. Ecker reported no competing financial interests.
FROM BMJ
What ketamine and psilocybin can and cannot do in depression
Recent studies with hallucinogens have raised hopes for an effective drug-based therapy to treat chronic depression. At the German Congress of Psychosomatic Medicine and Psychotherapy, Torsten Passie, MD, PhD, professor of psychiatry and psychotherapy at the Hannover (Germay) Medical School, gave a presentation on the current state of psilocybin and ketamine/esketamine research.
Dr. Passie, who also is head physician of the specialist unit for addiction and addiction prevention at the Diakonisches Werk in Hannover, has been investigating hallucinogenic substances and their application in psychotherapy for decades.
New therapies sought
In depression, gloom extends beyond the patient’s mood. For some time there has been little cause for joy with regard to chronic depression therapy. Established drug therapies hardly perform any better than placebo in meta-analyses, as a study recently confirmed. The pharmaceutical industry pulled out of psycho-pharmaceutical development more than 10 years ago. What’s more, the number of cases is rising, especially among young people, and there are long waiting times for psychotherapy appointments.
It is no wonder that some are welcoming new drug-based approaches with lysergic acid diethylamide (LSD)–like hallucinogens. In 2016, a study on psilocybin was published in The Lancet Psychiatry, although the study was unblinded and included only 24 patients.
Evoking emotions
A range of substances can be classed as hallucinogens, including psilocybin, mescaline, LSD, 3,4-methylenedioxy-methamphetamine (MDMA, also known as ecstasy), and ketamine.
Taking hallucinogens can cause a release of serotonin and dopamine, an increase in activity levels in the brain, a shift in stimulus filtering, an increase in the production of internal stimuli (inner experiences), and a change in sensory integration (for example, synesthesia).
Besides falling into a dreamlike state, patients can achieve an expansion or narrowing of consciousness if they focus on an inner experience. Internal perception increases. Perceptual routines are broken apart. Thought processes become more image-based and are more associative than normal.
Patients therefore are more capable of making new and unusual connections between different biographical or current situations. Previously unconscious ideas can become conscious. At higher doses, ego loss can occur, which can be associated with a mystical feeling of connectedness.
Hallucinogens mainly evoke and heighten emotions. Those effects may be experienced strongly as internal visions or in physical manifestations (for example, crying or laughing). In contrast, conventional antidepressants work by suppressing emotions (that is, emotional blunting).
These different mechanisms result in two contrasting management strategies. For example, SSRI antidepressants cause a patient to perceive workplace bullying as less severe and to do nothing to change the situation; the patient remains passive.
In contrast, a therapeutically guided, emotionally activating experience on hallucinogens can help the patient to try more actively to change the stressful situation.
Ketamine has a special place among hallucinogens. Unlike other hallucinogens, ketamine causes a strong clouding of consciousness, a reduction in physical sensory perception, and significant disruption in thinking and memory. It is therefore only suitable as a short-term intervention and is therapeutically impractical over the long term.
Ketamine’s effects
Ketamine, a racemic mixture of the enantiomers S-ketamine and R-ketamine, was originally used only as an analgesic and anesthetic. Owing to its rapid antidepressant effect, it has since also been used as an emergency medication for severe depression, sometimes in combination with SSRIs or serotonin noradrenaline reuptake inhibitors.
Approximately 60% of patients respond to the treatment. Whereas with conventional antidepressants, onset of action requires 10-14 days, ketamine is effective within a few hours. However, relapse always occurs, usually very quickly. After 2-3 days, the effect is usually approximately that of a placebo. An administration interval of about 2 days is optimal. However, “resistance” to the effect often develops after some time: the drug’s antidepressant effect diminishes.
Ketamine also has some unpleasant side effects, such as depersonalization, dissociation, impaired thinking, nystagmus, and psychotomimetic effects. Nausea and vomiting also occur. Interestingly, the latter does not bother the patient much, owing to the drug’s psychological effects, and it does not lead to treatment discontinuation, said Dr. Passie, who described his clinical experiences with ketamine.
Since ketamine causes a considerable clouding of consciousness, sensory disorders, and significant memory problems, it is not suitable for psychedelic-assisted psychotherapy, unlike LSD or psilocybin, he emphasized.
Ketamine 2.0?
Esketamine, the pure S-enantiomer of ketamine, has been on the market since 2019 in the form of a nasal spray (Spravato). Esketamine has been approved in combination with oral antidepressant therapy for adults with a moderate to severe episode of major depression for acute treatment of a psychiatric emergency.
A meta-analysis from 2022 concluded that the original racemic ketamine is better than the new esketamine in reducing symptoms of depression.
In his own comprehensive study, Dr. Passie concluded that the mental impairments that occur during therapy did not differ significantly between substances. The patients even felt that the side effects from esketamine therapy were much more mentally unpleasant, said Dr. Passie. He concluded that the R-enantiomer may have a kind of protective effect against some of the psychopathological effects of the S-enantiomer (esketamine).
In addition, preclinical studies have indicated that the antidepressant effects of R-enantiomer, which is not contained in esketamine, are longer lasting and stronger.
Another problem is absorption, which can be inconsistent with a nasal spray. It may differ, for example, depending on the ambient humidity or whether the patient has recently had a cold. In addition, the spray is far more expensive than the ketamine injection, said Dr. Passie. Patients must also use the nasal spray under supervision at a medical practice (as with the intravenous application) and must receive follow-up care there. It therefore offers no advantage over the ketamine injection.
According to the Institute for Quality and Efficiency in Healthcare, no additional benefit has been proven for esketamine over standard therapies for adults who have experienced a moderate to severe depressive episode when used as short-term treatment for the rapid reduction of depressive symptoms in a psychiatric emergency. The German Medical Association agreed with this evaluation in October 2021.
In the United Kingdom, the medication was never approved, owing to the fact that it was too expensive and that no studies comparing it with psychotherapy were available.
Add-on psilocybin?
What was experienced under the influence of psilocybin can also be subsequently processed and used in psychotherapy.
The acute effect of psilocybin begins after approximately 40 minutes and lasts for 4-6 hours. The antidepressant effect, if it occurs at all, is of immediate onset. Unlike ketamine/esketamine, psilocybin hardly has any physical side effects.
The neurologic mechanism of action has been investigated recently using fMRI and PET techniques. According to the investigations, the substance causes individual networks of activity in the patient’s brain to interconnect more strongly, said Dr. Passie. The thalamus, the filter station for sensory information, as well as the limbic and paralimbic structures, which generate emotions, and the cortex are all activated more strongly.
Two therapeutic settings
Psilocybin, at least in the context of studies, is used in two settings: psycholytic therapy and psychedelic therapy. Both settings originated in the 1950s and were also used with LSD as the active substance.
Psycholytic therapy with psilocybin entails multiple administrations at low doses (for example, 10-18 mg), incorporated into a longer, mostly psychodynamic therapy of around 50-100 hours (often on an inpatient basis at the beginning). It results in what is described as an extended encounter with oneself. The focus is on psychodynamic experiences, such as memories and internal conflicts. In addition, novel experiences with oneself and self-recognition are important.
Psychedelic therapy generally entails one or two sessions with a high dose (for example, 25-35 mg psilocybin). The preparation and follow-up are limited to a few sessions. These methods refer to so-called transpersonal psychology, which addresses extraordinary states of consciousness in line with religious experiences. It often leads to an intense self-confrontation as well as to new evaluations of self and world. The central element to this therapy is the experience of a mystical ego loss and the concomitant feeling of connectedness, which should help to expand one’s perspective.
Euphoria and disillusionment
The first promising studies with a few patients suffering from depression were followed by others in which the euphoria was allowed to fade away somewhat. In the first direct comparison in a methodically high-grade double-blind study, psilocybin was inferior to the SSRI antidepressant escitalopram.
“There is a great variation in response from person to person,” said Dr. Passie. “The better the study is methodically controlled, the worse the results,” he hypothesized.
“Since the method is up to 50 times more expensive in practice, compared to SSRI therapy over 6-12 weeks, the question clearly must be asked as to whether it really has any great future.”
Outlook for psilocybin
Nevertheless, Dr. Passie still sees potential in psilocybin. He considers an approach in which psilocybin therapy is more firmly incorporated into psychotherapy, with between four and 10 therapy sessions before and after administration of a lower therapeutic dose of the substance, to be more promising.
“With this kind of intensive preparation and follow-up, as well as the repeated psilocybin sessions, the patient can benefit much more than is possible with one or two high-dose sessions,” said Dr. Passie, who also is chair of the International Society for Substance-Assisted Psychotherapy. “The constant ‘in-depth work on the ego’ required for drastic therapeutic changes can be more effective and lead to permanent improvements. I have no doubt about this.”
In Dr. Passie’s opinion, the best approach would involve a dignified inpatient setting with a longer period of follow-up care and consistent posttreatment care, including group therapy. The shape of future psilocybin therapy depends on whether the rather abrupt change seen with high-dose psychedelic therapy is permanent. The answer to this question will be decisive for the method and manner of its future clinical use.
Because of the somewhat negative study results, however, the initial investors are pulling out. Dr. Passie is therefore skeptical about whether the necessary larger studies will take place and whether psilocybin will make it onto the market.
In Switzerland, which is not subject to EU restrictions, more than 30 physicians have been authorized to use psilocybin, LSD, and MDMA in psychotherapy sessions. Still, in some respects this is a special case that cannot be transferred easily to other countries, said Dr. Passie.
Possible psilocybin improvement?
Various chemical derivatives of psychoactive substances have been researched, including a psilocybin variant with the label CYB003. With CYB003, the length of the acute psychedelic experience is reduced from around 6 hours (such as with psilocybin) to 1 hour. The plasma concentration of the substance is less variable between different patients. It is assumed that its effects will also differ less from person to person.
In July, researchers began a study of the use of CYB003 in the treatment of major depression. In the randomized, double-blind, placebo-controlled study with 40 patients, multiple doses of the substance will be administered.
When asked, Dr. Passie was rather skeptical about the study. He considers the approaches with psilocybin derivatives to be the consequences of a “gold-rush atmosphere” and expects there will be no real additional benefit, especially not a reduction in the period of action.
A version of this article first appeared on Medscape.com.
Recent studies with hallucinogens have raised hopes for an effective drug-based therapy to treat chronic depression. At the German Congress of Psychosomatic Medicine and Psychotherapy, Torsten Passie, MD, PhD, professor of psychiatry and psychotherapy at the Hannover (Germay) Medical School, gave a presentation on the current state of psilocybin and ketamine/esketamine research.
Dr. Passie, who also is head physician of the specialist unit for addiction and addiction prevention at the Diakonisches Werk in Hannover, has been investigating hallucinogenic substances and their application in psychotherapy for decades.
New therapies sought
In depression, gloom extends beyond the patient’s mood. For some time there has been little cause for joy with regard to chronic depression therapy. Established drug therapies hardly perform any better than placebo in meta-analyses, as a study recently confirmed. The pharmaceutical industry pulled out of psycho-pharmaceutical development more than 10 years ago. What’s more, the number of cases is rising, especially among young people, and there are long waiting times for psychotherapy appointments.
It is no wonder that some are welcoming new drug-based approaches with lysergic acid diethylamide (LSD)–like hallucinogens. In 2016, a study on psilocybin was published in The Lancet Psychiatry, although the study was unblinded and included only 24 patients.
Evoking emotions
A range of substances can be classed as hallucinogens, including psilocybin, mescaline, LSD, 3,4-methylenedioxy-methamphetamine (MDMA, also known as ecstasy), and ketamine.
Taking hallucinogens can cause a release of serotonin and dopamine, an increase in activity levels in the brain, a shift in stimulus filtering, an increase in the production of internal stimuli (inner experiences), and a change in sensory integration (for example, synesthesia).
Besides falling into a dreamlike state, patients can achieve an expansion or narrowing of consciousness if they focus on an inner experience. Internal perception increases. Perceptual routines are broken apart. Thought processes become more image-based and are more associative than normal.
Patients therefore are more capable of making new and unusual connections between different biographical or current situations. Previously unconscious ideas can become conscious. At higher doses, ego loss can occur, which can be associated with a mystical feeling of connectedness.
Hallucinogens mainly evoke and heighten emotions. Those effects may be experienced strongly as internal visions or in physical manifestations (for example, crying or laughing). In contrast, conventional antidepressants work by suppressing emotions (that is, emotional blunting).
These different mechanisms result in two contrasting management strategies. For example, SSRI antidepressants cause a patient to perceive workplace bullying as less severe and to do nothing to change the situation; the patient remains passive.
In contrast, a therapeutically guided, emotionally activating experience on hallucinogens can help the patient to try more actively to change the stressful situation.
Ketamine has a special place among hallucinogens. Unlike other hallucinogens, ketamine causes a strong clouding of consciousness, a reduction in physical sensory perception, and significant disruption in thinking and memory. It is therefore only suitable as a short-term intervention and is therapeutically impractical over the long term.
Ketamine’s effects
Ketamine, a racemic mixture of the enantiomers S-ketamine and R-ketamine, was originally used only as an analgesic and anesthetic. Owing to its rapid antidepressant effect, it has since also been used as an emergency medication for severe depression, sometimes in combination with SSRIs or serotonin noradrenaline reuptake inhibitors.
Approximately 60% of patients respond to the treatment. Whereas with conventional antidepressants, onset of action requires 10-14 days, ketamine is effective within a few hours. However, relapse always occurs, usually very quickly. After 2-3 days, the effect is usually approximately that of a placebo. An administration interval of about 2 days is optimal. However, “resistance” to the effect often develops after some time: the drug’s antidepressant effect diminishes.
Ketamine also has some unpleasant side effects, such as depersonalization, dissociation, impaired thinking, nystagmus, and psychotomimetic effects. Nausea and vomiting also occur. Interestingly, the latter does not bother the patient much, owing to the drug’s psychological effects, and it does not lead to treatment discontinuation, said Dr. Passie, who described his clinical experiences with ketamine.
Since ketamine causes a considerable clouding of consciousness, sensory disorders, and significant memory problems, it is not suitable for psychedelic-assisted psychotherapy, unlike LSD or psilocybin, he emphasized.
Ketamine 2.0?
Esketamine, the pure S-enantiomer of ketamine, has been on the market since 2019 in the form of a nasal spray (Spravato). Esketamine has been approved in combination with oral antidepressant therapy for adults with a moderate to severe episode of major depression for acute treatment of a psychiatric emergency.
A meta-analysis from 2022 concluded that the original racemic ketamine is better than the new esketamine in reducing symptoms of depression.
In his own comprehensive study, Dr. Passie concluded that the mental impairments that occur during therapy did not differ significantly between substances. The patients even felt that the side effects from esketamine therapy were much more mentally unpleasant, said Dr. Passie. He concluded that the R-enantiomer may have a kind of protective effect against some of the psychopathological effects of the S-enantiomer (esketamine).
In addition, preclinical studies have indicated that the antidepressant effects of R-enantiomer, which is not contained in esketamine, are longer lasting and stronger.
Another problem is absorption, which can be inconsistent with a nasal spray. It may differ, for example, depending on the ambient humidity or whether the patient has recently had a cold. In addition, the spray is far more expensive than the ketamine injection, said Dr. Passie. Patients must also use the nasal spray under supervision at a medical practice (as with the intravenous application) and must receive follow-up care there. It therefore offers no advantage over the ketamine injection.
According to the Institute for Quality and Efficiency in Healthcare, no additional benefit has been proven for esketamine over standard therapies for adults who have experienced a moderate to severe depressive episode when used as short-term treatment for the rapid reduction of depressive symptoms in a psychiatric emergency. The German Medical Association agreed with this evaluation in October 2021.
In the United Kingdom, the medication was never approved, owing to the fact that it was too expensive and that no studies comparing it with psychotherapy were available.
Add-on psilocybin?
What was experienced under the influence of psilocybin can also be subsequently processed and used in psychotherapy.
The acute effect of psilocybin begins after approximately 40 minutes and lasts for 4-6 hours. The antidepressant effect, if it occurs at all, is of immediate onset. Unlike ketamine/esketamine, psilocybin hardly has any physical side effects.
The neurologic mechanism of action has been investigated recently using fMRI and PET techniques. According to the investigations, the substance causes individual networks of activity in the patient’s brain to interconnect more strongly, said Dr. Passie. The thalamus, the filter station for sensory information, as well as the limbic and paralimbic structures, which generate emotions, and the cortex are all activated more strongly.
Two therapeutic settings
Psilocybin, at least in the context of studies, is used in two settings: psycholytic therapy and psychedelic therapy. Both settings originated in the 1950s and were also used with LSD as the active substance.
Psycholytic therapy with psilocybin entails multiple administrations at low doses (for example, 10-18 mg), incorporated into a longer, mostly psychodynamic therapy of around 50-100 hours (often on an inpatient basis at the beginning). It results in what is described as an extended encounter with oneself. The focus is on psychodynamic experiences, such as memories and internal conflicts. In addition, novel experiences with oneself and self-recognition are important.
Psychedelic therapy generally entails one or two sessions with a high dose (for example, 25-35 mg psilocybin). The preparation and follow-up are limited to a few sessions. These methods refer to so-called transpersonal psychology, which addresses extraordinary states of consciousness in line with religious experiences. It often leads to an intense self-confrontation as well as to new evaluations of self and world. The central element to this therapy is the experience of a mystical ego loss and the concomitant feeling of connectedness, which should help to expand one’s perspective.
Euphoria and disillusionment
The first promising studies with a few patients suffering from depression were followed by others in which the euphoria was allowed to fade away somewhat. In the first direct comparison in a methodically high-grade double-blind study, psilocybin was inferior to the SSRI antidepressant escitalopram.
“There is a great variation in response from person to person,” said Dr. Passie. “The better the study is methodically controlled, the worse the results,” he hypothesized.
“Since the method is up to 50 times more expensive in practice, compared to SSRI therapy over 6-12 weeks, the question clearly must be asked as to whether it really has any great future.”
Outlook for psilocybin
Nevertheless, Dr. Passie still sees potential in psilocybin. He considers an approach in which psilocybin therapy is more firmly incorporated into psychotherapy, with between four and 10 therapy sessions before and after administration of a lower therapeutic dose of the substance, to be more promising.
“With this kind of intensive preparation and follow-up, as well as the repeated psilocybin sessions, the patient can benefit much more than is possible with one or two high-dose sessions,” said Dr. Passie, who also is chair of the International Society for Substance-Assisted Psychotherapy. “The constant ‘in-depth work on the ego’ required for drastic therapeutic changes can be more effective and lead to permanent improvements. I have no doubt about this.”
In Dr. Passie’s opinion, the best approach would involve a dignified inpatient setting with a longer period of follow-up care and consistent posttreatment care, including group therapy. The shape of future psilocybin therapy depends on whether the rather abrupt change seen with high-dose psychedelic therapy is permanent. The answer to this question will be decisive for the method and manner of its future clinical use.
Because of the somewhat negative study results, however, the initial investors are pulling out. Dr. Passie is therefore skeptical about whether the necessary larger studies will take place and whether psilocybin will make it onto the market.
In Switzerland, which is not subject to EU restrictions, more than 30 physicians have been authorized to use psilocybin, LSD, and MDMA in psychotherapy sessions. Still, in some respects this is a special case that cannot be transferred easily to other countries, said Dr. Passie.
Possible psilocybin improvement?
Various chemical derivatives of psychoactive substances have been researched, including a psilocybin variant with the label CYB003. With CYB003, the length of the acute psychedelic experience is reduced from around 6 hours (such as with psilocybin) to 1 hour. The plasma concentration of the substance is less variable between different patients. It is assumed that its effects will also differ less from person to person.
In July, researchers began a study of the use of CYB003 in the treatment of major depression. In the randomized, double-blind, placebo-controlled study with 40 patients, multiple doses of the substance will be administered.
When asked, Dr. Passie was rather skeptical about the study. He considers the approaches with psilocybin derivatives to be the consequences of a “gold-rush atmosphere” and expects there will be no real additional benefit, especially not a reduction in the period of action.
A version of this article first appeared on Medscape.com.
Recent studies with hallucinogens have raised hopes for an effective drug-based therapy to treat chronic depression. At the German Congress of Psychosomatic Medicine and Psychotherapy, Torsten Passie, MD, PhD, professor of psychiatry and psychotherapy at the Hannover (Germay) Medical School, gave a presentation on the current state of psilocybin and ketamine/esketamine research.
Dr. Passie, who also is head physician of the specialist unit for addiction and addiction prevention at the Diakonisches Werk in Hannover, has been investigating hallucinogenic substances and their application in psychotherapy for decades.
New therapies sought
In depression, gloom extends beyond the patient’s mood. For some time there has been little cause for joy with regard to chronic depression therapy. Established drug therapies hardly perform any better than placebo in meta-analyses, as a study recently confirmed. The pharmaceutical industry pulled out of psycho-pharmaceutical development more than 10 years ago. What’s more, the number of cases is rising, especially among young people, and there are long waiting times for psychotherapy appointments.
It is no wonder that some are welcoming new drug-based approaches with lysergic acid diethylamide (LSD)–like hallucinogens. In 2016, a study on psilocybin was published in The Lancet Psychiatry, although the study was unblinded and included only 24 patients.
Evoking emotions
A range of substances can be classed as hallucinogens, including psilocybin, mescaline, LSD, 3,4-methylenedioxy-methamphetamine (MDMA, also known as ecstasy), and ketamine.
Taking hallucinogens can cause a release of serotonin and dopamine, an increase in activity levels in the brain, a shift in stimulus filtering, an increase in the production of internal stimuli (inner experiences), and a change in sensory integration (for example, synesthesia).
Besides falling into a dreamlike state, patients can achieve an expansion or narrowing of consciousness if they focus on an inner experience. Internal perception increases. Perceptual routines are broken apart. Thought processes become more image-based and are more associative than normal.
Patients therefore are more capable of making new and unusual connections between different biographical or current situations. Previously unconscious ideas can become conscious. At higher doses, ego loss can occur, which can be associated with a mystical feeling of connectedness.
Hallucinogens mainly evoke and heighten emotions. Those effects may be experienced strongly as internal visions or in physical manifestations (for example, crying or laughing). In contrast, conventional antidepressants work by suppressing emotions (that is, emotional blunting).
These different mechanisms result in two contrasting management strategies. For example, SSRI antidepressants cause a patient to perceive workplace bullying as less severe and to do nothing to change the situation; the patient remains passive.
In contrast, a therapeutically guided, emotionally activating experience on hallucinogens can help the patient to try more actively to change the stressful situation.
Ketamine has a special place among hallucinogens. Unlike other hallucinogens, ketamine causes a strong clouding of consciousness, a reduction in physical sensory perception, and significant disruption in thinking and memory. It is therefore only suitable as a short-term intervention and is therapeutically impractical over the long term.
Ketamine’s effects
Ketamine, a racemic mixture of the enantiomers S-ketamine and R-ketamine, was originally used only as an analgesic and anesthetic. Owing to its rapid antidepressant effect, it has since also been used as an emergency medication for severe depression, sometimes in combination with SSRIs or serotonin noradrenaline reuptake inhibitors.
Approximately 60% of patients respond to the treatment. Whereas with conventional antidepressants, onset of action requires 10-14 days, ketamine is effective within a few hours. However, relapse always occurs, usually very quickly. After 2-3 days, the effect is usually approximately that of a placebo. An administration interval of about 2 days is optimal. However, “resistance” to the effect often develops after some time: the drug’s antidepressant effect diminishes.
Ketamine also has some unpleasant side effects, such as depersonalization, dissociation, impaired thinking, nystagmus, and psychotomimetic effects. Nausea and vomiting also occur. Interestingly, the latter does not bother the patient much, owing to the drug’s psychological effects, and it does not lead to treatment discontinuation, said Dr. Passie, who described his clinical experiences with ketamine.
Since ketamine causes a considerable clouding of consciousness, sensory disorders, and significant memory problems, it is not suitable for psychedelic-assisted psychotherapy, unlike LSD or psilocybin, he emphasized.
Ketamine 2.0?
Esketamine, the pure S-enantiomer of ketamine, has been on the market since 2019 in the form of a nasal spray (Spravato). Esketamine has been approved in combination with oral antidepressant therapy for adults with a moderate to severe episode of major depression for acute treatment of a psychiatric emergency.
A meta-analysis from 2022 concluded that the original racemic ketamine is better than the new esketamine in reducing symptoms of depression.
In his own comprehensive study, Dr. Passie concluded that the mental impairments that occur during therapy did not differ significantly between substances. The patients even felt that the side effects from esketamine therapy were much more mentally unpleasant, said Dr. Passie. He concluded that the R-enantiomer may have a kind of protective effect against some of the psychopathological effects of the S-enantiomer (esketamine).
In addition, preclinical studies have indicated that the antidepressant effects of R-enantiomer, which is not contained in esketamine, are longer lasting and stronger.
Another problem is absorption, which can be inconsistent with a nasal spray. It may differ, for example, depending on the ambient humidity or whether the patient has recently had a cold. In addition, the spray is far more expensive than the ketamine injection, said Dr. Passie. Patients must also use the nasal spray under supervision at a medical practice (as with the intravenous application) and must receive follow-up care there. It therefore offers no advantage over the ketamine injection.
According to the Institute for Quality and Efficiency in Healthcare, no additional benefit has been proven for esketamine over standard therapies for adults who have experienced a moderate to severe depressive episode when used as short-term treatment for the rapid reduction of depressive symptoms in a psychiatric emergency. The German Medical Association agreed with this evaluation in October 2021.
In the United Kingdom, the medication was never approved, owing to the fact that it was too expensive and that no studies comparing it with psychotherapy were available.
Add-on psilocybin?
What was experienced under the influence of psilocybin can also be subsequently processed and used in psychotherapy.
The acute effect of psilocybin begins after approximately 40 minutes and lasts for 4-6 hours. The antidepressant effect, if it occurs at all, is of immediate onset. Unlike ketamine/esketamine, psilocybin hardly has any physical side effects.
The neurologic mechanism of action has been investigated recently using fMRI and PET techniques. According to the investigations, the substance causes individual networks of activity in the patient’s brain to interconnect more strongly, said Dr. Passie. The thalamus, the filter station for sensory information, as well as the limbic and paralimbic structures, which generate emotions, and the cortex are all activated more strongly.
Two therapeutic settings
Psilocybin, at least in the context of studies, is used in two settings: psycholytic therapy and psychedelic therapy. Both settings originated in the 1950s and were also used with LSD as the active substance.
Psycholytic therapy with psilocybin entails multiple administrations at low doses (for example, 10-18 mg), incorporated into a longer, mostly psychodynamic therapy of around 50-100 hours (often on an inpatient basis at the beginning). It results in what is described as an extended encounter with oneself. The focus is on psychodynamic experiences, such as memories and internal conflicts. In addition, novel experiences with oneself and self-recognition are important.
Psychedelic therapy generally entails one or two sessions with a high dose (for example, 25-35 mg psilocybin). The preparation and follow-up are limited to a few sessions. These methods refer to so-called transpersonal psychology, which addresses extraordinary states of consciousness in line with religious experiences. It often leads to an intense self-confrontation as well as to new evaluations of self and world. The central element to this therapy is the experience of a mystical ego loss and the concomitant feeling of connectedness, which should help to expand one’s perspective.
Euphoria and disillusionment
The first promising studies with a few patients suffering from depression were followed by others in which the euphoria was allowed to fade away somewhat. In the first direct comparison in a methodically high-grade double-blind study, psilocybin was inferior to the SSRI antidepressant escitalopram.
“There is a great variation in response from person to person,” said Dr. Passie. “The better the study is methodically controlled, the worse the results,” he hypothesized.
“Since the method is up to 50 times more expensive in practice, compared to SSRI therapy over 6-12 weeks, the question clearly must be asked as to whether it really has any great future.”
Outlook for psilocybin
Nevertheless, Dr. Passie still sees potential in psilocybin. He considers an approach in which psilocybin therapy is more firmly incorporated into psychotherapy, with between four and 10 therapy sessions before and after administration of a lower therapeutic dose of the substance, to be more promising.
“With this kind of intensive preparation and follow-up, as well as the repeated psilocybin sessions, the patient can benefit much more than is possible with one or two high-dose sessions,” said Dr. Passie, who also is chair of the International Society for Substance-Assisted Psychotherapy. “The constant ‘in-depth work on the ego’ required for drastic therapeutic changes can be more effective and lead to permanent improvements. I have no doubt about this.”
In Dr. Passie’s opinion, the best approach would involve a dignified inpatient setting with a longer period of follow-up care and consistent posttreatment care, including group therapy. The shape of future psilocybin therapy depends on whether the rather abrupt change seen with high-dose psychedelic therapy is permanent. The answer to this question will be decisive for the method and manner of its future clinical use.
Because of the somewhat negative study results, however, the initial investors are pulling out. Dr. Passie is therefore skeptical about whether the necessary larger studies will take place and whether psilocybin will make it onto the market.
In Switzerland, which is not subject to EU restrictions, more than 30 physicians have been authorized to use psilocybin, LSD, and MDMA in psychotherapy sessions. Still, in some respects this is a special case that cannot be transferred easily to other countries, said Dr. Passie.
Possible psilocybin improvement?
Various chemical derivatives of psychoactive substances have been researched, including a psilocybin variant with the label CYB003. With CYB003, the length of the acute psychedelic experience is reduced from around 6 hours (such as with psilocybin) to 1 hour. The plasma concentration of the substance is less variable between different patients. It is assumed that its effects will also differ less from person to person.
In July, researchers began a study of the use of CYB003 in the treatment of major depression. In the randomized, double-blind, placebo-controlled study with 40 patients, multiple doses of the substance will be administered.
When asked, Dr. Passie was rather skeptical about the study. He considers the approaches with psilocybin derivatives to be the consequences of a “gold-rush atmosphere” and expects there will be no real additional benefit, especially not a reduction in the period of action.
A version of this article first appeared on Medscape.com.

Annual PSA screening important for Black men
, new data suggest.
The data come from a review of 45,834 veterans (aged 55-69 years) who had been diagnosed with prostate cancer. About one-third of these men self-identified as non-Hispanic Black, and the rest were White.
During the study period (2004-2017), 2,465 men (5.4%) died of the disease.
The review found that annual prostate-specific antigen (PSA) screening significantly reduced the risk of dying from prostate cancer among Black men but not White men.
The study was published online in JAMA Oncology.
“These results may be biologically plausible because a shorter screening interval may be valuable for detecting aggressive disease, which is more common in Black men,” say investigators, led by University of California, San Diego, radiation oncology resident Michael Sherer, MD.
“Given that Black men are younger at diagnosis and have worse prostate cancer survival compared with White men,” more intensive screening recommendations “may benefit Black patients,” they write.
The study “conclusions are reasonable,” said Christopher Wallis, MD, PhD, a urologic oncologist at Mount Sinai Hospital in Toronto, when asked for comment.
Annual screening may well have “a greater potential to benefit” Black men, he said. “While we would ideally see randomized data supporting this, those data are unlikely to ever be forthcoming. Thus, this study provides a strong rationale to support the recommendations from many guideline panels (including those from the American Urological Association) that Black men, in the context of shared decision-making, may benefit more from PSA-based prostate cancer screening than the population at large,” he added.
Overall, the findings could help inform screening discussions with Black men, the investigators comments. In its most recent guidance, the U.S. Preventive Services Task Force recommends shared decision-making regarding PSA screening for men aged 55-69 years.
Similar screening frequency
For their study, the team reviewed Veterans Health Administration data to assess PSA screening patterns – which they categorized as no screening, less than annual screening, or annual screening – in the 5 years leading up to diagnosis.
They then correlated screening behaviors with the subsequent risk of dying from prostate cancer.
Overall, the reduction in risk of prostate cancer–specific mortality (PCSM) associated with screening was similar among Black men (subdistribution hazard ratio, 0.56; P = .001) and White men (sHR, 0.58; P = .001).
However, on multivariable regression, annual screening, in comparison with some screening, was associated with a significant reduction in the risk of dying from prostate cancer only among Black men (sHR, 0.65; P = .02), not among White men (sHR, 0.91; P = .35).
The cumulative incidence of PCSM among Black men was 4.7% with annual screening but 7.3% with only some screening.
Among White men, the cumulative incidence of PCSM with annual screening was 5.9% vs. 6.9% with less than annual screening.
Screening frequency was similar between Black men and White men. Black men were younger on average (61.8 vs. 63.1 years) and had slightly higher PSA levels at diagnosis but were not more likely to have regional or metastatic disease.
No funding was reported for this study. The investigators have disclosed no relevant financial relationships. Dr. Wallis has received personal fees from Janssen Canada.
A version of this article first appeared on Medscape.com.
, new data suggest.
The data come from a review of 45,834 veterans (aged 55-69 years) who had been diagnosed with prostate cancer. About one-third of these men self-identified as non-Hispanic Black, and the rest were White.
During the study period (2004-2017), 2,465 men (5.4%) died of the disease.
The review found that annual prostate-specific antigen (PSA) screening significantly reduced the risk of dying from prostate cancer among Black men but not White men.
The study was published online in JAMA Oncology.
“These results may be biologically plausible because a shorter screening interval may be valuable for detecting aggressive disease, which is more common in Black men,” say investigators, led by University of California, San Diego, radiation oncology resident Michael Sherer, MD.
“Given that Black men are younger at diagnosis and have worse prostate cancer survival compared with White men,” more intensive screening recommendations “may benefit Black patients,” they write.
The study “conclusions are reasonable,” said Christopher Wallis, MD, PhD, a urologic oncologist at Mount Sinai Hospital in Toronto, when asked for comment.
Annual screening may well have “a greater potential to benefit” Black men, he said. “While we would ideally see randomized data supporting this, those data are unlikely to ever be forthcoming. Thus, this study provides a strong rationale to support the recommendations from many guideline panels (including those from the American Urological Association) that Black men, in the context of shared decision-making, may benefit more from PSA-based prostate cancer screening than the population at large,” he added.
Overall, the findings could help inform screening discussions with Black men, the investigators comments. In its most recent guidance, the U.S. Preventive Services Task Force recommends shared decision-making regarding PSA screening for men aged 55-69 years.
Similar screening frequency
For their study, the team reviewed Veterans Health Administration data to assess PSA screening patterns – which they categorized as no screening, less than annual screening, or annual screening – in the 5 years leading up to diagnosis.
They then correlated screening behaviors with the subsequent risk of dying from prostate cancer.
Overall, the reduction in risk of prostate cancer–specific mortality (PCSM) associated with screening was similar among Black men (subdistribution hazard ratio, 0.56; P = .001) and White men (sHR, 0.58; P = .001).
However, on multivariable regression, annual screening, in comparison with some screening, was associated with a significant reduction in the risk of dying from prostate cancer only among Black men (sHR, 0.65; P = .02), not among White men (sHR, 0.91; P = .35).
The cumulative incidence of PCSM among Black men was 4.7% with annual screening but 7.3% with only some screening.
Among White men, the cumulative incidence of PCSM with annual screening was 5.9% vs. 6.9% with less than annual screening.
Screening frequency was similar between Black men and White men. Black men were younger on average (61.8 vs. 63.1 years) and had slightly higher PSA levels at diagnosis but were not more likely to have regional or metastatic disease.
No funding was reported for this study. The investigators have disclosed no relevant financial relationships. Dr. Wallis has received personal fees from Janssen Canada.
A version of this article first appeared on Medscape.com.
, new data suggest.
The data come from a review of 45,834 veterans (aged 55-69 years) who had been diagnosed with prostate cancer. About one-third of these men self-identified as non-Hispanic Black, and the rest were White.
During the study period (2004-2017), 2,465 men (5.4%) died of the disease.
The review found that annual prostate-specific antigen (PSA) screening significantly reduced the risk of dying from prostate cancer among Black men but not White men.
The study was published online in JAMA Oncology.
“These results may be biologically plausible because a shorter screening interval may be valuable for detecting aggressive disease, which is more common in Black men,” say investigators, led by University of California, San Diego, radiation oncology resident Michael Sherer, MD.
“Given that Black men are younger at diagnosis and have worse prostate cancer survival compared with White men,” more intensive screening recommendations “may benefit Black patients,” they write.
The study “conclusions are reasonable,” said Christopher Wallis, MD, PhD, a urologic oncologist at Mount Sinai Hospital in Toronto, when asked for comment.
Annual screening may well have “a greater potential to benefit” Black men, he said. “While we would ideally see randomized data supporting this, those data are unlikely to ever be forthcoming. Thus, this study provides a strong rationale to support the recommendations from many guideline panels (including those from the American Urological Association) that Black men, in the context of shared decision-making, may benefit more from PSA-based prostate cancer screening than the population at large,” he added.
Overall, the findings could help inform screening discussions with Black men, the investigators comments. In its most recent guidance, the U.S. Preventive Services Task Force recommends shared decision-making regarding PSA screening for men aged 55-69 years.
Similar screening frequency
For their study, the team reviewed Veterans Health Administration data to assess PSA screening patterns – which they categorized as no screening, less than annual screening, or annual screening – in the 5 years leading up to diagnosis.
They then correlated screening behaviors with the subsequent risk of dying from prostate cancer.
Overall, the reduction in risk of prostate cancer–specific mortality (PCSM) associated with screening was similar among Black men (subdistribution hazard ratio, 0.56; P = .001) and White men (sHR, 0.58; P = .001).
However, on multivariable regression, annual screening, in comparison with some screening, was associated with a significant reduction in the risk of dying from prostate cancer only among Black men (sHR, 0.65; P = .02), not among White men (sHR, 0.91; P = .35).
The cumulative incidence of PCSM among Black men was 4.7% with annual screening but 7.3% with only some screening.
Among White men, the cumulative incidence of PCSM with annual screening was 5.9% vs. 6.9% with less than annual screening.
Screening frequency was similar between Black men and White men. Black men were younger on average (61.8 vs. 63.1 years) and had slightly higher PSA levels at diagnosis but were not more likely to have regional or metastatic disease.
No funding was reported for this study. The investigators have disclosed no relevant financial relationships. Dr. Wallis has received personal fees from Janssen Canada.
A version of this article first appeared on Medscape.com.
FROM JAMA ONCOLOGY
Mechanistic link between herpes virus, Alzheimer’s revealed?
, new research suggests.
“Our results suggest one pathway to Alzheimer’s disease, caused by a VZV infection which creates inflammatory triggers that awaken HSV in the brain,” lead author Dana Cairns, PhD, research associate, department of biomedical engineering at Tufts University, Boston, said in a news release.
The findings were published online in Journal of Alzheimer’s Disease.
‘One-two punch’
Previous research has suggested a correlation between HSV-1 and AD and involvement of VZV. However, the sequence of events that the viruses create to set the disease in motion has been unclear.
“We think we now have evidence of those events,” co–senior author David Kaplan, PhD, chair of the department of biomedical engineering at Tufts, said in the release.
Working with co–senior author Ruth Itzhaki, PhD, University of Oxford, United Kingdom, the researchers infected human-induced neural stem cells (hiNSCs) and 3D brain tissue models with HSV-1 and/or VZV. Dr. Itzhaki was one of the first to hypothesize a connection between herpes virus and AD.
The investigators found that HSV-1 infection of hiNSCs induces amyloid-beta and P-tau accumulation: the main components of AD plaques and neurofibrillary tangles, respectively.
On the other hand, VZV infection of cultured hiNSCs did not lead to amyloid-beta and P-tau accumulation but instead resulted in gliosis and increased levels of proinflammatory cytokines.
“Strikingly,” VZV infection of cells quiescently infected with HSV-1 caused reactivation of HSV-1, leading to AD-like changes, including amyloid-beta and P-tau accumulation, the investigators report.
This suggests that VZV is unlikely to be a direct cause of AD but rather acts indirectly via reactivation of HSV-1, they add.
Similar findings emerged in similar experiments using 3D human brain tissue models.
“It’s a one-two punch of two viruses that are very common and usually harmless, but the lab studies suggest that if a new exposure to VZV wakes up dormant HSV-1, they could cause trouble,” Dr. Cairns said.
The researchers note that vaccination against VZV has been shown previously to reduce risk for dementia. It is possible, they add, that the vaccine is helping to stop the cycle of viral reactivation, inflammation, and neuronal damage.
‘A first step’
Heather M. Snyder, PhD, vice president of Medical & Scientific Relations at the Alzheimer’s Association, said that the study “is using artificial systems with the goal of more clearly and more deeply understanding” the assessed associations.
She added that although it is a first step, it may provide valuable direction for follow-up research.
“This is preliminary work that first needs replication, validation, and further development to understand if any association that is uncovered between viruses and Alzheimer’s/dementia has a mechanistic link,” said Dr. Snyder.
She noted that several past studies have sought to help the research field better understand the links between different viruses and Alzheimer’s and other forms of dementia.
“There have been some challenges in evaluating these associations in our current model systems or in individuals for a number of reasons,” said Dr. Snyder.
However, “the COVID-19 pandemic has created an opportunity to examine and investigate the relationships between different viruses and Alzheimer’s and other dementias by following individuals in more common and well-established ways,” she added.
She reported that her organization is “leading and working with a large global network of studies and investigators to address some of these questions” from during and after the COVID pandemic.
“The lessons we learn and share may inform our understanding of how other viruses are, or are not, connected to Alzheimer’s and other dementia,” Dr. Snyder said.
More information on the Alzheimer’s Association International Cohort Study of Chronic Neurological Sequelae of SARS-CoV-2 is available online.
The study was funded by the National Institutes of Health. Dr. Cairns, Dr. Kaplan, Dr. Itzhaki, and Dr. Snyder have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
“Our results suggest one pathway to Alzheimer’s disease, caused by a VZV infection which creates inflammatory triggers that awaken HSV in the brain,” lead author Dana Cairns, PhD, research associate, department of biomedical engineering at Tufts University, Boston, said in a news release.
The findings were published online in Journal of Alzheimer’s Disease.
‘One-two punch’
Previous research has suggested a correlation between HSV-1 and AD and involvement of VZV. However, the sequence of events that the viruses create to set the disease in motion has been unclear.
“We think we now have evidence of those events,” co–senior author David Kaplan, PhD, chair of the department of biomedical engineering at Tufts, said in the release.
Working with co–senior author Ruth Itzhaki, PhD, University of Oxford, United Kingdom, the researchers infected human-induced neural stem cells (hiNSCs) and 3D brain tissue models with HSV-1 and/or VZV. Dr. Itzhaki was one of the first to hypothesize a connection between herpes virus and AD.
The investigators found that HSV-1 infection of hiNSCs induces amyloid-beta and P-tau accumulation: the main components of AD plaques and neurofibrillary tangles, respectively.
On the other hand, VZV infection of cultured hiNSCs did not lead to amyloid-beta and P-tau accumulation but instead resulted in gliosis and increased levels of proinflammatory cytokines.
“Strikingly,” VZV infection of cells quiescently infected with HSV-1 caused reactivation of HSV-1, leading to AD-like changes, including amyloid-beta and P-tau accumulation, the investigators report.
This suggests that VZV is unlikely to be a direct cause of AD but rather acts indirectly via reactivation of HSV-1, they add.
Similar findings emerged in similar experiments using 3D human brain tissue models.
“It’s a one-two punch of two viruses that are very common and usually harmless, but the lab studies suggest that if a new exposure to VZV wakes up dormant HSV-1, they could cause trouble,” Dr. Cairns said.
The researchers note that vaccination against VZV has been shown previously to reduce risk for dementia. It is possible, they add, that the vaccine is helping to stop the cycle of viral reactivation, inflammation, and neuronal damage.
‘A first step’
Heather M. Snyder, PhD, vice president of Medical & Scientific Relations at the Alzheimer’s Association, said that the study “is using artificial systems with the goal of more clearly and more deeply understanding” the assessed associations.
She added that although it is a first step, it may provide valuable direction for follow-up research.
“This is preliminary work that first needs replication, validation, and further development to understand if any association that is uncovered between viruses and Alzheimer’s/dementia has a mechanistic link,” said Dr. Snyder.
She noted that several past studies have sought to help the research field better understand the links between different viruses and Alzheimer’s and other forms of dementia.
“There have been some challenges in evaluating these associations in our current model systems or in individuals for a number of reasons,” said Dr. Snyder.
However, “the COVID-19 pandemic has created an opportunity to examine and investigate the relationships between different viruses and Alzheimer’s and other dementias by following individuals in more common and well-established ways,” she added.
She reported that her organization is “leading and working with a large global network of studies and investigators to address some of these questions” from during and after the COVID pandemic.
“The lessons we learn and share may inform our understanding of how other viruses are, or are not, connected to Alzheimer’s and other dementia,” Dr. Snyder said.
More information on the Alzheimer’s Association International Cohort Study of Chronic Neurological Sequelae of SARS-CoV-2 is available online.
The study was funded by the National Institutes of Health. Dr. Cairns, Dr. Kaplan, Dr. Itzhaki, and Dr. Snyder have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
“Our results suggest one pathway to Alzheimer’s disease, caused by a VZV infection which creates inflammatory triggers that awaken HSV in the brain,” lead author Dana Cairns, PhD, research associate, department of biomedical engineering at Tufts University, Boston, said in a news release.
The findings were published online in Journal of Alzheimer’s Disease.
‘One-two punch’
Previous research has suggested a correlation between HSV-1 and AD and involvement of VZV. However, the sequence of events that the viruses create to set the disease in motion has been unclear.
“We think we now have evidence of those events,” co–senior author David Kaplan, PhD, chair of the department of biomedical engineering at Tufts, said in the release.
Working with co–senior author Ruth Itzhaki, PhD, University of Oxford, United Kingdom, the researchers infected human-induced neural stem cells (hiNSCs) and 3D brain tissue models with HSV-1 and/or VZV. Dr. Itzhaki was one of the first to hypothesize a connection between herpes virus and AD.
The investigators found that HSV-1 infection of hiNSCs induces amyloid-beta and P-tau accumulation: the main components of AD plaques and neurofibrillary tangles, respectively.
On the other hand, VZV infection of cultured hiNSCs did not lead to amyloid-beta and P-tau accumulation but instead resulted in gliosis and increased levels of proinflammatory cytokines.
“Strikingly,” VZV infection of cells quiescently infected with HSV-1 caused reactivation of HSV-1, leading to AD-like changes, including amyloid-beta and P-tau accumulation, the investigators report.
This suggests that VZV is unlikely to be a direct cause of AD but rather acts indirectly via reactivation of HSV-1, they add.
Similar findings emerged in similar experiments using 3D human brain tissue models.
“It’s a one-two punch of two viruses that are very common and usually harmless, but the lab studies suggest that if a new exposure to VZV wakes up dormant HSV-1, they could cause trouble,” Dr. Cairns said.
The researchers note that vaccination against VZV has been shown previously to reduce risk for dementia. It is possible, they add, that the vaccine is helping to stop the cycle of viral reactivation, inflammation, and neuronal damage.
‘A first step’
Heather M. Snyder, PhD, vice president of Medical & Scientific Relations at the Alzheimer’s Association, said that the study “is using artificial systems with the goal of more clearly and more deeply understanding” the assessed associations.
She added that although it is a first step, it may provide valuable direction for follow-up research.
“This is preliminary work that first needs replication, validation, and further development to understand if any association that is uncovered between viruses and Alzheimer’s/dementia has a mechanistic link,” said Dr. Snyder.
She noted that several past studies have sought to help the research field better understand the links between different viruses and Alzheimer’s and other forms of dementia.
“There have been some challenges in evaluating these associations in our current model systems or in individuals for a number of reasons,” said Dr. Snyder.
However, “the COVID-19 pandemic has created an opportunity to examine and investigate the relationships between different viruses and Alzheimer’s and other dementias by following individuals in more common and well-established ways,” she added.
She reported that her organization is “leading and working with a large global network of studies and investigators to address some of these questions” from during and after the COVID pandemic.
“The lessons we learn and share may inform our understanding of how other viruses are, or are not, connected to Alzheimer’s and other dementia,” Dr. Snyder said.
More information on the Alzheimer’s Association International Cohort Study of Chronic Neurological Sequelae of SARS-CoV-2 is available online.
The study was funded by the National Institutes of Health. Dr. Cairns, Dr. Kaplan, Dr. Itzhaki, and Dr. Snyder have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF ALZHEIMER’S DISEASE
Hearing aids available in October without a prescription
The White House announced today that the Food and Drug Administration will move forward with plans to make hearing aids available over the counter in pharmacies, other retail locations, and online.
This major milestone aims to make hearing aids easier to buy and more affordable, potentially saving families thousands of dollars.
An estimated 28.8 million U.S. adults could benefit from using hearing aids, according to numbers from the National Institute on Deafness and Other Communication Disorders. But only about 16% of people aged 20-69 years who could be helped by hearing aids have ever used them.
The risk for hearing loss increases with age. Among Americans ages 70 and older, only 30% who could hear better with these devices have ever used them, the institute reports.
Once the FDA final rule takes effect, Americans with mild to moderate hearing loss will be able to buy a hearing aid without a doctor’s exam, prescription, or fitting adjustment.
President Joe Biden announced in 2021 he intended to allow hearing aids to be sold over the counter without a prescription to increase competition among manufacturers. Congress also passed bipartisan legislation in 2017 requiring the FDA to create a new category for hearing aids sold directly to consumers. Some devices intended for minors or people with severe hearing loss will remain available only with a prescription.
“This action makes good on my commitment to lower costs for American families, delivering nearly $3,000 in savings to American families for a pair of hearing aids and giving people more choices to improve their health and wellbeing,” the president said in a statement announcing the news.
The new over-the-counter hearing aids will be considered medical devices. To avoid confusion, the FDA explains the differences between hearing aids and personal sound amplification products (PSAPs). For example, PSAPs are considered electronic devices designed for people with normal hearing to use in certain situations, like birdwatching or hunting.
A version of this article first appeared on WebMD.com.
The White House announced today that the Food and Drug Administration will move forward with plans to make hearing aids available over the counter in pharmacies, other retail locations, and online.
This major milestone aims to make hearing aids easier to buy and more affordable, potentially saving families thousands of dollars.
An estimated 28.8 million U.S. adults could benefit from using hearing aids, according to numbers from the National Institute on Deafness and Other Communication Disorders. But only about 16% of people aged 20-69 years who could be helped by hearing aids have ever used them.
The risk for hearing loss increases with age. Among Americans ages 70 and older, only 30% who could hear better with these devices have ever used them, the institute reports.
Once the FDA final rule takes effect, Americans with mild to moderate hearing loss will be able to buy a hearing aid without a doctor’s exam, prescription, or fitting adjustment.
President Joe Biden announced in 2021 he intended to allow hearing aids to be sold over the counter without a prescription to increase competition among manufacturers. Congress also passed bipartisan legislation in 2017 requiring the FDA to create a new category for hearing aids sold directly to consumers. Some devices intended for minors or people with severe hearing loss will remain available only with a prescription.
“This action makes good on my commitment to lower costs for American families, delivering nearly $3,000 in savings to American families for a pair of hearing aids and giving people more choices to improve their health and wellbeing,” the president said in a statement announcing the news.
The new over-the-counter hearing aids will be considered medical devices. To avoid confusion, the FDA explains the differences between hearing aids and personal sound amplification products (PSAPs). For example, PSAPs are considered electronic devices designed for people with normal hearing to use in certain situations, like birdwatching or hunting.
A version of this article first appeared on WebMD.com.
The White House announced today that the Food and Drug Administration will move forward with plans to make hearing aids available over the counter in pharmacies, other retail locations, and online.
This major milestone aims to make hearing aids easier to buy and more affordable, potentially saving families thousands of dollars.
An estimated 28.8 million U.S. adults could benefit from using hearing aids, according to numbers from the National Institute on Deafness and Other Communication Disorders. But only about 16% of people aged 20-69 years who could be helped by hearing aids have ever used them.
The risk for hearing loss increases with age. Among Americans ages 70 and older, only 30% who could hear better with these devices have ever used them, the institute reports.
Once the FDA final rule takes effect, Americans with mild to moderate hearing loss will be able to buy a hearing aid without a doctor’s exam, prescription, or fitting adjustment.
President Joe Biden announced in 2021 he intended to allow hearing aids to be sold over the counter without a prescription to increase competition among manufacturers. Congress also passed bipartisan legislation in 2017 requiring the FDA to create a new category for hearing aids sold directly to consumers. Some devices intended for minors or people with severe hearing loss will remain available only with a prescription.
“This action makes good on my commitment to lower costs for American families, delivering nearly $3,000 in savings to American families for a pair of hearing aids and giving people more choices to improve their health and wellbeing,” the president said in a statement announcing the news.
The new over-the-counter hearing aids will be considered medical devices. To avoid confusion, the FDA explains the differences between hearing aids and personal sound amplification products (PSAPs). For example, PSAPs are considered electronic devices designed for people with normal hearing to use in certain situations, like birdwatching or hunting.
A version of this article first appeared on WebMD.com.
‘Obesity paradox’ in AFib challenged as mortality climbs with BMI
The relationship between body mass index (BMI) and all-cause mortality in patients with atrial fibrillation (AFib) is U-shaped, with the risk highest in those who are underweight or severely obese and lowest in patients defined simply as obese, a registry analysis suggests. It also showed a similar relationship between BMI and risk for new or worsening heart failure (HF).
Mortality bottomed out at a BMI of about 30-35 kg/m2, which suggests that mild obesity was protective, compared even with “normal-weight” or “overweight” BMI. Still, mortality went up sharply from there with rising BMI.
But higher BMI, a surrogate for obesity, apparently didn’t worsen outcomes by itself. The risk for death from any cause at higher obesity levels was found to depend a lot on related risk factors and comorbidities when the analysis controlled for conditions such as diabetes and hypertension.
The findings suggest an inverse relationship between BMI and all-cause mortality in AFib only for patients with BMI less than about 30. They therefore argue against any “obesity paradox” in AFib that posits consistently better survival with increasing levels of obesity, say researchers, based on their analysis of patients with new-onset AFib in the GARFIELD-AF registry.
“It’s common practice now for clinicians to discuss weight within a clinic setting when they’re talking to their AFib patients,” observed Christian Fielder Camm, BM, BCh, University of Oxford (England), and Royal Berkshire NHS Foundation Trust, Reading, England. So studies suggesting an inverse association between BMI and AFib-related risk can be a concern.
Such studies “seem to suggest that once you’ve got AFib, maintaining a high or very high BMI may in some way be protective – which is contrary to what would seem to make sense and certainly contrary to what our results have shown,” Dr. Camm told this news organization.
“I think that having further evidence now to suggest, actually, that greater BMI is associated with a greater risk of all-cause mortality and heart failure helps reframe that discussion at the physician-patient interaction level more clearly, and ensures that we’re able to talk to our patients appropriately about risks associated with BMI and atrial fibrillation,” said Dr. Camm, who is lead author on the analysis published in Open Heart.
“Obesity is a cause of most cardiovascular diseases, but [these] data would support that being overweight or having mild obesity does not increase the risk,” observed Carl J. Lavie, MD, of the John Ochsner Heart and Vascular Institute, New Orleans, La., and the Ochsner Clinical School at the University of Queensland, Brisbane, Australia.
“At a BMI of 40, it’s very important for them to lose weight for their long-term prognosis,” Dr. Lavie noted, but “at a BMI of 30, the important thing would be to prevent further weight gain. And if they could keep their BMI of 30, they should have a good prognosis. Their prognosis would be particularly good if they didn’t gain weight and put themselves in a more extreme obesity class that is associated with worse risk.”

The current analysis, Dr. Lavie said, “is way better than the AFFIRM study,” which yielded an obesity-paradox report on its patients with AFib about a dozen years ago. “It’s got more data, more numbers, more statistical power,” and breaks BMI into more categories.
That previous analysis based on the influential AFFIRM randomized trial separated its 4,060 patients with AFib into normal (BMI, 18.5-25), overweight (BMI, 25-30), and obese (BMI, > 30) categories, per the convention at the time. It concluded that “obese patients with atrial fibrillation appear to have better long-term outcomes than nonobese patients.”
Bleeding risk on oral anticoagulants
Also noteworthy in the current analysis, variation in BMI didn’t seem to affect mortality or risk for major bleeding or nonhemorrhagic stroke according to choice of oral anticoagulant – whether a new oral anticoagulant (NOAC) or a vitamin K antagonist (VKA).
“We saw that even in the obese and extremely obese group, all-cause mortality was lower in the group taking NOACs, compared with taking warfarin,” Dr. Camm observed, “which goes against the idea that we would need any kind of dose adjustments for increased BMI.”
Indeed, the report notes, use of NOACs, compared with VKA, was associated with a 23% drop in risk for death among patients who were either normal weight or overweight and also in those who were obese or extremely obese.
Those findings “are basically saying that the NOACs look better than warfarin regardless of weight,” agreed Dr. Lavie. “The problem is that the study is not very powered.”
Whereas the benefits of NOACs, compared to VKA, seem similar for patients with a BMI of 30 or 34, compared with a BMI of 23, for example, “none of the studies has many people with 50 BMI.” Many clinicians “feel uncomfortable giving the same dose of NOAC to somebody who has a 60 BMI,” he said. At least with warfarin, “you can check the INR [international normalized ratio].”
The current analysis included 40,482 patients with recently diagnosed AFib and at least one other stroke risk factor from among the registry’s more than 50,000 patients from 35 countries, enrolled from 2010 to 2016. They were followed for 2 years.
The 703 patients with BMI under 18.5 at AFib diagnosis were classified per World Health Organization definitions as underweight; the 13,095 with BMI 18.5-25 as normal weight; the 15,043 with BMI 25-30 as overweight; the 7,560 with BMI 30-35 as obese; and the 4,081 with BMI above 35 as extremely obese. Their ages averaged 71 years, and 55.6% were men.
BMI effects on different outcomes
Relationships between BMI and all-cause mortality and between BMI and new or worsening HF emerged as U-shaped, the risk climbing with both increasing and decreasing BMI. The nadir BMI for risk was about 30 in the case of mortality and about 25 for new or worsening HF.
The all-cause mortality risk rose by 32% for every 5 BMI points lower than a BMI of 30, and by 16% for every 5 BMI points higher than 30, in a partially adjusted analysis. The risk for new or worsening HF rose significantly with increasing but not decreasing BMI, and the reverse was observed for the endpoint of major bleeding.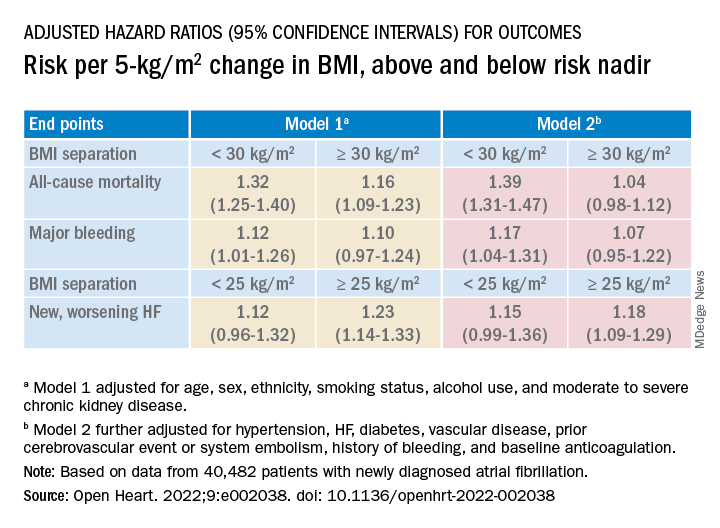
The effect of BMI on all-cause mortality was “substantially attenuated” when the analysis was further adjusted with “likely mediators of any association between BMI and outcomes,” including hypertension, diabetes, HF, cerebrovascular events, and history of bleeding, Dr. Camm said.
That blunted BMI-mortality relationship, he said, “suggests that a lot of the effect is mediated through relatively traditional risk factors like hypertension and diabetes.”
The 2010 AFFIRM analysis by BMI, Dr. Lavie noted, “didn’t even look at the underweight; they actually threw them out.” Yet, such patients with AFib, who tend to be extremely frail or have chronic diseases or conditions other than the arrhythmia, are common. A take-home of the current study is that “the underweight with atrial fibrillation have a really bad prognosis.”
That message isn’t heard as much, he observed, “but is as important as saying that BMI 30 has the best prognosis. The worst prognosis is with the underweight or the really extreme obese.”
Dr. Camm discloses research funding from the British Heart Foundation. Disclosures for the other authors are in the report. Dr. Lavie has previously disclosed serving as a speaker and consultant for PAI Health and DSM Nutritional Products and is the author of “The Obesity Paradox: When Thinner Means Sicker and Heavier Means Healthier” (Avery, 2014).
A version of this article first appeared on Medscape.com.
The relationship between body mass index (BMI) and all-cause mortality in patients with atrial fibrillation (AFib) is U-shaped, with the risk highest in those who are underweight or severely obese and lowest in patients defined simply as obese, a registry analysis suggests. It also showed a similar relationship between BMI and risk for new or worsening heart failure (HF).
Mortality bottomed out at a BMI of about 30-35 kg/m2, which suggests that mild obesity was protective, compared even with “normal-weight” or “overweight” BMI. Still, mortality went up sharply from there with rising BMI.
But higher BMI, a surrogate for obesity, apparently didn’t worsen outcomes by itself. The risk for death from any cause at higher obesity levels was found to depend a lot on related risk factors and comorbidities when the analysis controlled for conditions such as diabetes and hypertension.
The findings suggest an inverse relationship between BMI and all-cause mortality in AFib only for patients with BMI less than about 30. They therefore argue against any “obesity paradox” in AFib that posits consistently better survival with increasing levels of obesity, say researchers, based on their analysis of patients with new-onset AFib in the GARFIELD-AF registry.
“It’s common practice now for clinicians to discuss weight within a clinic setting when they’re talking to their AFib patients,” observed Christian Fielder Camm, BM, BCh, University of Oxford (England), and Royal Berkshire NHS Foundation Trust, Reading, England. So studies suggesting an inverse association between BMI and AFib-related risk can be a concern.
Such studies “seem to suggest that once you’ve got AFib, maintaining a high or very high BMI may in some way be protective – which is contrary to what would seem to make sense and certainly contrary to what our results have shown,” Dr. Camm told this news organization.
“I think that having further evidence now to suggest, actually, that greater BMI is associated with a greater risk of all-cause mortality and heart failure helps reframe that discussion at the physician-patient interaction level more clearly, and ensures that we’re able to talk to our patients appropriately about risks associated with BMI and atrial fibrillation,” said Dr. Camm, who is lead author on the analysis published in Open Heart.
“Obesity is a cause of most cardiovascular diseases, but [these] data would support that being overweight or having mild obesity does not increase the risk,” observed Carl J. Lavie, MD, of the John Ochsner Heart and Vascular Institute, New Orleans, La., and the Ochsner Clinical School at the University of Queensland, Brisbane, Australia.
“At a BMI of 40, it’s very important for them to lose weight for their long-term prognosis,” Dr. Lavie noted, but “at a BMI of 30, the important thing would be to prevent further weight gain. And if they could keep their BMI of 30, they should have a good prognosis. Their prognosis would be particularly good if they didn’t gain weight and put themselves in a more extreme obesity class that is associated with worse risk.”
The current analysis, Dr. Lavie said, “is way better than the AFFIRM study,” which yielded an obesity-paradox report on its patients with AFib about a dozen years ago. “It’s got more data, more numbers, more statistical power,” and breaks BMI into more categories.
That previous analysis based on the influential AFFIRM randomized trial separated its 4,060 patients with AFib into normal (BMI, 18.5-25), overweight (BMI, 25-30), and obese (BMI, > 30) categories, per the convention at the time. It concluded that “obese patients with atrial fibrillation appear to have better long-term outcomes than nonobese patients.”
Bleeding risk on oral anticoagulants
Also noteworthy in the current analysis, variation in BMI didn’t seem to affect mortality or risk for major bleeding or nonhemorrhagic stroke according to choice of oral anticoagulant – whether a new oral anticoagulant (NOAC) or a vitamin K antagonist (VKA).
“We saw that even in the obese and extremely obese group, all-cause mortality was lower in the group taking NOACs, compared with taking warfarin,” Dr. Camm observed, “which goes against the idea that we would need any kind of dose adjustments for increased BMI.”
Indeed, the report notes, use of NOACs, compared with VKA, was associated with a 23% drop in risk for death among patients who were either normal weight or overweight and also in those who were obese or extremely obese.
Those findings “are basically saying that the NOACs look better than warfarin regardless of weight,” agreed Dr. Lavie. “The problem is that the study is not very powered.”
Whereas the benefits of NOACs, compared to VKA, seem similar for patients with a BMI of 30 or 34, compared with a BMI of 23, for example, “none of the studies has many people with 50 BMI.” Many clinicians “feel uncomfortable giving the same dose of NOAC to somebody who has a 60 BMI,” he said. At least with warfarin, “you can check the INR [international normalized ratio].”
The current analysis included 40,482 patients with recently diagnosed AFib and at least one other stroke risk factor from among the registry’s more than 50,000 patients from 35 countries, enrolled from 2010 to 2016. They were followed for 2 years.
The 703 patients with BMI under 18.5 at AFib diagnosis were classified per World Health Organization definitions as underweight; the 13,095 with BMI 18.5-25 as normal weight; the 15,043 with BMI 25-30 as overweight; the 7,560 with BMI 30-35 as obese; and the 4,081 with BMI above 35 as extremely obese. Their ages averaged 71 years, and 55.6% were men.
BMI effects on different outcomes
Relationships between BMI and all-cause mortality and between BMI and new or worsening HF emerged as U-shaped, the risk climbing with both increasing and decreasing BMI. The nadir BMI for risk was about 30 in the case of mortality and about 25 for new or worsening HF.
The all-cause mortality risk rose by 32% for every 5 BMI points lower than a BMI of 30, and by 16% for every 5 BMI points higher than 30, in a partially adjusted analysis. The risk for new or worsening HF rose significantly with increasing but not decreasing BMI, and the reverse was observed for the endpoint of major bleeding.
The effect of BMI on all-cause mortality was “substantially attenuated” when the analysis was further adjusted with “likely mediators of any association between BMI and outcomes,” including hypertension, diabetes, HF, cerebrovascular events, and history of bleeding, Dr. Camm said.
That blunted BMI-mortality relationship, he said, “suggests that a lot of the effect is mediated through relatively traditional risk factors like hypertension and diabetes.”
The 2010 AFFIRM analysis by BMI, Dr. Lavie noted, “didn’t even look at the underweight; they actually threw them out.” Yet, such patients with AFib, who tend to be extremely frail or have chronic diseases or conditions other than the arrhythmia, are common. A take-home of the current study is that “the underweight with atrial fibrillation have a really bad prognosis.”
That message isn’t heard as much, he observed, “but is as important as saying that BMI 30 has the best prognosis. The worst prognosis is with the underweight or the really extreme obese.”
Dr. Camm discloses research funding from the British Heart Foundation. Disclosures for the other authors are in the report. Dr. Lavie has previously disclosed serving as a speaker and consultant for PAI Health and DSM Nutritional Products and is the author of “The Obesity Paradox: When Thinner Means Sicker and Heavier Means Healthier” (Avery, 2014).
A version of this article first appeared on Medscape.com.
The relationship between body mass index (BMI) and all-cause mortality in patients with atrial fibrillation (AFib) is U-shaped, with the risk highest in those who are underweight or severely obese and lowest in patients defined simply as obese, a registry analysis suggests. It also showed a similar relationship between BMI and risk for new or worsening heart failure (HF).
Mortality bottomed out at a BMI of about 30-35 kg/m2, which suggests that mild obesity was protective, compared even with “normal-weight” or “overweight” BMI. Still, mortality went up sharply from there with rising BMI.
But higher BMI, a surrogate for obesity, apparently didn’t worsen outcomes by itself. The risk for death from any cause at higher obesity levels was found to depend a lot on related risk factors and comorbidities when the analysis controlled for conditions such as diabetes and hypertension.
The findings suggest an inverse relationship between BMI and all-cause mortality in AFib only for patients with BMI less than about 30. They therefore argue against any “obesity paradox” in AFib that posits consistently better survival with increasing levels of obesity, say researchers, based on their analysis of patients with new-onset AFib in the GARFIELD-AF registry.
“It’s common practice now for clinicians to discuss weight within a clinic setting when they’re talking to their AFib patients,” observed Christian Fielder Camm, BM, BCh, University of Oxford (England), and Royal Berkshire NHS Foundation Trust, Reading, England. So studies suggesting an inverse association between BMI and AFib-related risk can be a concern.
Such studies “seem to suggest that once you’ve got AFib, maintaining a high or very high BMI may in some way be protective – which is contrary to what would seem to make sense and certainly contrary to what our results have shown,” Dr. Camm told this news organization.
“I think that having further evidence now to suggest, actually, that greater BMI is associated with a greater risk of all-cause mortality and heart failure helps reframe that discussion at the physician-patient interaction level more clearly, and ensures that we’re able to talk to our patients appropriately about risks associated with BMI and atrial fibrillation,” said Dr. Camm, who is lead author on the analysis published in Open Heart.
“Obesity is a cause of most cardiovascular diseases, but [these] data would support that being overweight or having mild obesity does not increase the risk,” observed Carl J. Lavie, MD, of the John Ochsner Heart and Vascular Institute, New Orleans, La., and the Ochsner Clinical School at the University of Queensland, Brisbane, Australia.
“At a BMI of 40, it’s very important for them to lose weight for their long-term prognosis,” Dr. Lavie noted, but “at a BMI of 30, the important thing would be to prevent further weight gain. And if they could keep their BMI of 30, they should have a good prognosis. Their prognosis would be particularly good if they didn’t gain weight and put themselves in a more extreme obesity class that is associated with worse risk.”
The current analysis, Dr. Lavie said, “is way better than the AFFIRM study,” which yielded an obesity-paradox report on its patients with AFib about a dozen years ago. “It’s got more data, more numbers, more statistical power,” and breaks BMI into more categories.
That previous analysis based on the influential AFFIRM randomized trial separated its 4,060 patients with AFib into normal (BMI, 18.5-25), overweight (BMI, 25-30), and obese (BMI, > 30) categories, per the convention at the time. It concluded that “obese patients with atrial fibrillation appear to have better long-term outcomes than nonobese patients.”
Bleeding risk on oral anticoagulants
Also noteworthy in the current analysis, variation in BMI didn’t seem to affect mortality or risk for major bleeding or nonhemorrhagic stroke according to choice of oral anticoagulant – whether a new oral anticoagulant (NOAC) or a vitamin K antagonist (VKA).
“We saw that even in the obese and extremely obese group, all-cause mortality was lower in the group taking NOACs, compared with taking warfarin,” Dr. Camm observed, “which goes against the idea that we would need any kind of dose adjustments for increased BMI.”
Indeed, the report notes, use of NOACs, compared with VKA, was associated with a 23% drop in risk for death among patients who were either normal weight or overweight and also in those who were obese or extremely obese.
Those findings “are basically saying that the NOACs look better than warfarin regardless of weight,” agreed Dr. Lavie. “The problem is that the study is not very powered.”
Whereas the benefits of NOACs, compared to VKA, seem similar for patients with a BMI of 30 or 34, compared with a BMI of 23, for example, “none of the studies has many people with 50 BMI.” Many clinicians “feel uncomfortable giving the same dose of NOAC to somebody who has a 60 BMI,” he said. At least with warfarin, “you can check the INR [international normalized ratio].”
The current analysis included 40,482 patients with recently diagnosed AFib and at least one other stroke risk factor from among the registry’s more than 50,000 patients from 35 countries, enrolled from 2010 to 2016. They were followed for 2 years.
The 703 patients with BMI under 18.5 at AFib diagnosis were classified per World Health Organization definitions as underweight; the 13,095 with BMI 18.5-25 as normal weight; the 15,043 with BMI 25-30 as overweight; the 7,560 with BMI 30-35 as obese; and the 4,081 with BMI above 35 as extremely obese. Their ages averaged 71 years, and 55.6% were men.
BMI effects on different outcomes
Relationships between BMI and all-cause mortality and between BMI and new or worsening HF emerged as U-shaped, the risk climbing with both increasing and decreasing BMI. The nadir BMI for risk was about 30 in the case of mortality and about 25 for new or worsening HF.
The all-cause mortality risk rose by 32% for every 5 BMI points lower than a BMI of 30, and by 16% for every 5 BMI points higher than 30, in a partially adjusted analysis. The risk for new or worsening HF rose significantly with increasing but not decreasing BMI, and the reverse was observed for the endpoint of major bleeding.
The effect of BMI on all-cause mortality was “substantially attenuated” when the analysis was further adjusted with “likely mediators of any association between BMI and outcomes,” including hypertension, diabetes, HF, cerebrovascular events, and history of bleeding, Dr. Camm said.
That blunted BMI-mortality relationship, he said, “suggests that a lot of the effect is mediated through relatively traditional risk factors like hypertension and diabetes.”
The 2010 AFFIRM analysis by BMI, Dr. Lavie noted, “didn’t even look at the underweight; they actually threw them out.” Yet, such patients with AFib, who tend to be extremely frail or have chronic diseases or conditions other than the arrhythmia, are common. A take-home of the current study is that “the underweight with atrial fibrillation have a really bad prognosis.”
That message isn’t heard as much, he observed, “but is as important as saying that BMI 30 has the best prognosis. The worst prognosis is with the underweight or the really extreme obese.”
Dr. Camm discloses research funding from the British Heart Foundation. Disclosures for the other authors are in the report. Dr. Lavie has previously disclosed serving as a speaker and consultant for PAI Health and DSM Nutritional Products and is the author of “The Obesity Paradox: When Thinner Means Sicker and Heavier Means Healthier” (Avery, 2014).
A version of this article first appeared on Medscape.com.
FROM OPEN HEART
On the Wisconsin-Illinois border: Clinics in neighboring states team up on abortion care
WAUKEGAN, Ill. – Around 2 days a week, Natalee Hartwig, APNP, leaves her home in Madison, Wisconsin, before her son wakes up to travel across the border into Illinois.
“Luckily it’s summer,” said Ms. Hartwig, a nurse midwife at Planned Parenthood of Wisconsin. “For now, he can sleep in. But any getting ready that has to happen will be on my spouse.”
She drives at least 2 hours each way, immersed in audiobooks and podcasts as she heads back and forth from a clinic in this northern Illinois suburb. She spends her days in the recovery room, caring for patients who have had abortions and checking their vitals before they go home. She is also licensed in Illinois and trained to provide medication abortion, something she’ll be able to do virtually through telehealth with patients across Illinois.
Ms. Hartwig is essentially working part time in Illinois because when Roe v. Wade was overturned in June, a state law immediately took effect that bans nearly all abortions in Wisconsin, except to save the life of the pregnant person. Wisconsin providers want to preserve access for patients, while those in Illinois – long an oasis for abortion rights – need more staff to help treat a surge of people arriving from across the U.S.
The Waukegan clinic is Planned Parenthood of Illinois’ busiest for out-of-state abortion patients. After Roe fell, 60% of patients came to this clinic from outside the state – mostly from Wisconsin. In fact, the organization opened in Waukegan 2 years ago with Wisconsin in mind, knowing that if Roe v. Wade did fall, access to abortion in that state would greatly diminish.
After Roe was struck down, Planned Parenthood organizations in both states announced their partnership. More than a dozen employees from Wisconsin – including doctors, nurses, and medical assistants – now commute to Waukegan to help provide care.
“It really required this perfect pairing of supply and demand,” said Kristen Schultz, Planned Parenthood of Illinois’ chief strategy and operations officer. “They had capacity without local demand, and we had the opposite.”
In the month after the U.S. Supreme Court overturned the federal landmark decision, Illinois became even more of an oasis for people seeking abortions. Dozens of clinics closed across the nation as 11 states in the South and Midwest implemented bans, according to the Guttmacher Institute, a nonprofit that supports abortion rights and tracks the issue.
The influx of patients into Illinois has had another effect. For years, abortion providers have been traveling once or twice a month to other states like Kansas, Mississippi, and Oklahoma, where their help was badly needed.
Laura Laursen, MD, an ob.gyn. in Chicago, was one of them.
“Now the script is totally flipped,” said Dr. Laursen, a fellow with Physicians for Reproductive Health. “This is where you are needed more than anywhere else.”
Anti-abortion groups oppose the Planned Parenthood partnership and are preparing for a marathon effort to restrict abortion rights in Illinois. In a statement after the organization’s announcement, Amy Gehrke, executive director of Illinois Right to Life, called it “particularly tragic.”
Some of the Wisconsin providers commute to Waukegan a few times a week; others a few days a month.
For Ms. Hartwig, associate director of clinical services at Planned Parenthood of Wisconsin, she’s able to do more in Illinois for patients than she could back home. Even as a nurse with an advanced degree, she wasn’t allowed to provide medication abortions in Wisconsin. But she can in Illinois, according to the state Department of Financial and Professional Regulation.
“This was really just what I was always supposed to do,” Ms. Hartwig said. “There’s nothing that’s going to keep me from helping our patients.”
Kathy King, MD, Planned Parenthood of Wisconsin’s medical director, said that while her staff is dedicated to providing these services, it comes at a cost.
“It is a burden on our clinicians and nurses and medical assistants who have young children at home,” Dr. King said. “It sounds great. Sure, we’ll all just travel down to Waukegan 5 days a week. But the logistics of that and the sacrifice of doing that on just people’s day-to-day lives takes a toll.”
Still, this sacrifice has helped. With staff from Wisconsin, the Waukegan clinic has doubled the number of abortion appointments available, and it is still ramping up. The support frees up other staffers to treat patients with different needs, like birth control and cancer screenings.
There has been a surge of patients from Wisconsin for abortion appointments at all Planned Parenthood of Illinois clinics – a tenfold increase in the month after Roe was overturned, from about 35 patients a month to 350, Dr. King said. That doesn’t include Wisconsin residents who might have sought abortions with other providers.
The partnership at the Waukegan clinic has ignited interest from abortion providers in other nearby states. Planned Parenthood of Illinois is fielding calls from Indiana, Kentucky, and Ohio, for example, Ms. Schultz said.
What Illinois needs is more staff to treat more patients. The commute from Wisconsin to Waukegan is relatively short compared with abortion providers in Ohio, for example, who’d have to cross Indiana to help relieve the staffing need.
Across the nation, other conversations are happening among providers. The National Abortion Federation, which has about 500 facility members including independent abortion clinics and hospitals, is pairing up people looking for jobs at clinics with those that need workers, said Melissa Fowler, chief program officer at the federation.
Still, she acknowledged moving isn’t a realistic option for everyone.
“People have lives,” Ms. Fowler said. “They have families. They’re deeply rooted in their communities. ... And so a situation like you’re seeing in Illinois and Wisconsin is great because people are able to stay connected to their community, not have to move their family, and still be able to provide care.”
This story is part of a partnership that includes WBEZ Chicago, NPR, and KHN.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
WAUKEGAN, Ill. – Around 2 days a week, Natalee Hartwig, APNP, leaves her home in Madison, Wisconsin, before her son wakes up to travel across the border into Illinois.
“Luckily it’s summer,” said Ms. Hartwig, a nurse midwife at Planned Parenthood of Wisconsin. “For now, he can sleep in. But any getting ready that has to happen will be on my spouse.”
She drives at least 2 hours each way, immersed in audiobooks and podcasts as she heads back and forth from a clinic in this northern Illinois suburb. She spends her days in the recovery room, caring for patients who have had abortions and checking their vitals before they go home. She is also licensed in Illinois and trained to provide medication abortion, something she’ll be able to do virtually through telehealth with patients across Illinois.
Ms. Hartwig is essentially working part time in Illinois because when Roe v. Wade was overturned in June, a state law immediately took effect that bans nearly all abortions in Wisconsin, except to save the life of the pregnant person. Wisconsin providers want to preserve access for patients, while those in Illinois – long an oasis for abortion rights – need more staff to help treat a surge of people arriving from across the U.S.
The Waukegan clinic is Planned Parenthood of Illinois’ busiest for out-of-state abortion patients. After Roe fell, 60% of patients came to this clinic from outside the state – mostly from Wisconsin. In fact, the organization opened in Waukegan 2 years ago with Wisconsin in mind, knowing that if Roe v. Wade did fall, access to abortion in that state would greatly diminish.
After Roe was struck down, Planned Parenthood organizations in both states announced their partnership. More than a dozen employees from Wisconsin – including doctors, nurses, and medical assistants – now commute to Waukegan to help provide care.
“It really required this perfect pairing of supply and demand,” said Kristen Schultz, Planned Parenthood of Illinois’ chief strategy and operations officer. “They had capacity without local demand, and we had the opposite.”
In the month after the U.S. Supreme Court overturned the federal landmark decision, Illinois became even more of an oasis for people seeking abortions. Dozens of clinics closed across the nation as 11 states in the South and Midwest implemented bans, according to the Guttmacher Institute, a nonprofit that supports abortion rights and tracks the issue.
The influx of patients into Illinois has had another effect. For years, abortion providers have been traveling once or twice a month to other states like Kansas, Mississippi, and Oklahoma, where their help was badly needed.
Laura Laursen, MD, an ob.gyn. in Chicago, was one of them.
“Now the script is totally flipped,” said Dr. Laursen, a fellow with Physicians for Reproductive Health. “This is where you are needed more than anywhere else.”
Anti-abortion groups oppose the Planned Parenthood partnership and are preparing for a marathon effort to restrict abortion rights in Illinois. In a statement after the organization’s announcement, Amy Gehrke, executive director of Illinois Right to Life, called it “particularly tragic.”
Some of the Wisconsin providers commute to Waukegan a few times a week; others a few days a month.
For Ms. Hartwig, associate director of clinical services at Planned Parenthood of Wisconsin, she’s able to do more in Illinois for patients than she could back home. Even as a nurse with an advanced degree, she wasn’t allowed to provide medication abortions in Wisconsin. But she can in Illinois, according to the state Department of Financial and Professional Regulation.
“This was really just what I was always supposed to do,” Ms. Hartwig said. “There’s nothing that’s going to keep me from helping our patients.”
Kathy King, MD, Planned Parenthood of Wisconsin’s medical director, said that while her staff is dedicated to providing these services, it comes at a cost.
“It is a burden on our clinicians and nurses and medical assistants who have young children at home,” Dr. King said. “It sounds great. Sure, we’ll all just travel down to Waukegan 5 days a week. But the logistics of that and the sacrifice of doing that on just people’s day-to-day lives takes a toll.”
Still, this sacrifice has helped. With staff from Wisconsin, the Waukegan clinic has doubled the number of abortion appointments available, and it is still ramping up. The support frees up other staffers to treat patients with different needs, like birth control and cancer screenings.
There has been a surge of patients from Wisconsin for abortion appointments at all Planned Parenthood of Illinois clinics – a tenfold increase in the month after Roe was overturned, from about 35 patients a month to 350, Dr. King said. That doesn’t include Wisconsin residents who might have sought abortions with other providers.
The partnership at the Waukegan clinic has ignited interest from abortion providers in other nearby states. Planned Parenthood of Illinois is fielding calls from Indiana, Kentucky, and Ohio, for example, Ms. Schultz said.
What Illinois needs is more staff to treat more patients. The commute from Wisconsin to Waukegan is relatively short compared with abortion providers in Ohio, for example, who’d have to cross Indiana to help relieve the staffing need.
Across the nation, other conversations are happening among providers. The National Abortion Federation, which has about 500 facility members including independent abortion clinics and hospitals, is pairing up people looking for jobs at clinics with those that need workers, said Melissa Fowler, chief program officer at the federation.
Still, she acknowledged moving isn’t a realistic option for everyone.
“People have lives,” Ms. Fowler said. “They have families. They’re deeply rooted in their communities. ... And so a situation like you’re seeing in Illinois and Wisconsin is great because people are able to stay connected to their community, not have to move their family, and still be able to provide care.”
This story is part of a partnership that includes WBEZ Chicago, NPR, and KHN.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
WAUKEGAN, Ill. – Around 2 days a week, Natalee Hartwig, APNP, leaves her home in Madison, Wisconsin, before her son wakes up to travel across the border into Illinois.
“Luckily it’s summer,” said Ms. Hartwig, a nurse midwife at Planned Parenthood of Wisconsin. “For now, he can sleep in. But any getting ready that has to happen will be on my spouse.”
She drives at least 2 hours each way, immersed in audiobooks and podcasts as she heads back and forth from a clinic in this northern Illinois suburb. She spends her days in the recovery room, caring for patients who have had abortions and checking their vitals before they go home. She is also licensed in Illinois and trained to provide medication abortion, something she’ll be able to do virtually through telehealth with patients across Illinois.
Ms. Hartwig is essentially working part time in Illinois because when Roe v. Wade was overturned in June, a state law immediately took effect that bans nearly all abortions in Wisconsin, except to save the life of the pregnant person. Wisconsin providers want to preserve access for patients, while those in Illinois – long an oasis for abortion rights – need more staff to help treat a surge of people arriving from across the U.S.
The Waukegan clinic is Planned Parenthood of Illinois’ busiest for out-of-state abortion patients. After Roe fell, 60% of patients came to this clinic from outside the state – mostly from Wisconsin. In fact, the organization opened in Waukegan 2 years ago with Wisconsin in mind, knowing that if Roe v. Wade did fall, access to abortion in that state would greatly diminish.
After Roe was struck down, Planned Parenthood organizations in both states announced their partnership. More than a dozen employees from Wisconsin – including doctors, nurses, and medical assistants – now commute to Waukegan to help provide care.
“It really required this perfect pairing of supply and demand,” said Kristen Schultz, Planned Parenthood of Illinois’ chief strategy and operations officer. “They had capacity without local demand, and we had the opposite.”
In the month after the U.S. Supreme Court overturned the federal landmark decision, Illinois became even more of an oasis for people seeking abortions. Dozens of clinics closed across the nation as 11 states in the South and Midwest implemented bans, according to the Guttmacher Institute, a nonprofit that supports abortion rights and tracks the issue.
The influx of patients into Illinois has had another effect. For years, abortion providers have been traveling once or twice a month to other states like Kansas, Mississippi, and Oklahoma, where their help was badly needed.
Laura Laursen, MD, an ob.gyn. in Chicago, was one of them.
“Now the script is totally flipped,” said Dr. Laursen, a fellow with Physicians for Reproductive Health. “This is where you are needed more than anywhere else.”
Anti-abortion groups oppose the Planned Parenthood partnership and are preparing for a marathon effort to restrict abortion rights in Illinois. In a statement after the organization’s announcement, Amy Gehrke, executive director of Illinois Right to Life, called it “particularly tragic.”
Some of the Wisconsin providers commute to Waukegan a few times a week; others a few days a month.
For Ms. Hartwig, associate director of clinical services at Planned Parenthood of Wisconsin, she’s able to do more in Illinois for patients than she could back home. Even as a nurse with an advanced degree, she wasn’t allowed to provide medication abortions in Wisconsin. But she can in Illinois, according to the state Department of Financial and Professional Regulation.
“This was really just what I was always supposed to do,” Ms. Hartwig said. “There’s nothing that’s going to keep me from helping our patients.”
Kathy King, MD, Planned Parenthood of Wisconsin’s medical director, said that while her staff is dedicated to providing these services, it comes at a cost.
“It is a burden on our clinicians and nurses and medical assistants who have young children at home,” Dr. King said. “It sounds great. Sure, we’ll all just travel down to Waukegan 5 days a week. But the logistics of that and the sacrifice of doing that on just people’s day-to-day lives takes a toll.”
Still, this sacrifice has helped. With staff from Wisconsin, the Waukegan clinic has doubled the number of abortion appointments available, and it is still ramping up. The support frees up other staffers to treat patients with different needs, like birth control and cancer screenings.
There has been a surge of patients from Wisconsin for abortion appointments at all Planned Parenthood of Illinois clinics – a tenfold increase in the month after Roe was overturned, from about 35 patients a month to 350, Dr. King said. That doesn’t include Wisconsin residents who might have sought abortions with other providers.
The partnership at the Waukegan clinic has ignited interest from abortion providers in other nearby states. Planned Parenthood of Illinois is fielding calls from Indiana, Kentucky, and Ohio, for example, Ms. Schultz said.
What Illinois needs is more staff to treat more patients. The commute from Wisconsin to Waukegan is relatively short compared with abortion providers in Ohio, for example, who’d have to cross Indiana to help relieve the staffing need.
Across the nation, other conversations are happening among providers. The National Abortion Federation, which has about 500 facility members including independent abortion clinics and hospitals, is pairing up people looking for jobs at clinics with those that need workers, said Melissa Fowler, chief program officer at the federation.
Still, she acknowledged moving isn’t a realistic option for everyone.
“People have lives,” Ms. Fowler said. “They have families. They’re deeply rooted in their communities. ... And so a situation like you’re seeing in Illinois and Wisconsin is great because people are able to stay connected to their community, not have to move their family, and still be able to provide care.”
This story is part of a partnership that includes WBEZ Chicago, NPR, and KHN.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Strength training overcomes bone effects of vegan diet
People who maintain a vegan diet show significant deficits in bone microarchitecture, compared with omnivores; however, resistance training not only appears to improve those deficits but may have a stronger effect in vegans, suggesting an important strategy in maintaining bone health with a vegan diet.
“We expected better bone structure in both vegans and omnivores who reported resistance training,” first author Robert Wakolbinger-Habel, MD, PhD, of St. Vincent Hospital Vienna and the Medical University of Vienna, said in an interview.
“However, we expected [there would still be] differences in structure between vegans and omnivores [who practiced resistance training], as previous literature reported higher fracture rates in vegans,” he said. “Still, the positive message is that ‘pumping iron’ could counterbalance these differences between vegans and omnivores.”
The research was published online in The Endocrine Society’s Journal of Clinical Endocrinology & Metabolism.
Exercise significantly impacts bone health in vegans
The potential effects of the plant-based vegan diet on bone health have been reported in studies linking the diet to an increased risk of fractures and lower bone mineral density (BMD), with common theories including lower bone- and muscle-building protein in vegan diets.
However, most previous studies have not considered other key factors, such as the effects of exercise, the authors noted.
“While previous studies on bone health in vegans only took BMD, biochemical and nutritional parameters into account, they did not consider the significant effects of physical activity,” they wrote.
“By ignoring these effects, important factors influencing bone health are neglected.”
For the study, 88 participants were enrolled in Vienna, with vegan participants recruited with the help of the Austrian Vegan Society.
Importantly, the study documented participants’ bone microarchitecture, a key measure of bone strength that has also not been previously investigated in vegans, using high-resolution peripheral quantitative CT.
Inclusion criteria included maintaining an omnivore diet of meat and plant-based foods or a vegan diet for at least 5 years, not being underweight or obese (body mass index [BMI], 18.5-30 kg/m2), being age 30-50 years, and being premenopausal.
Of the participants, 43 were vegan and 45 were omnivores, with generally equal ratios of men and women.
Vegan bone deficits disappear with strength training
Overall, compared with omnivores, the vegan group showed significant deficits in 7 of 14 measures of BMI-adjusted trabecular and cortical structure (all P < .05).
Among participants who reported no resistance training, vegans still showed significant decreases in bone microarchitecture, compared with omnivores, including radius trabecular BMD, radius trabecular bone volume fraction, and other tibial and cortical bone microarchitecture measures.
However, among those who did report progressive resistant training (20 vegans and 25 omnivores), defined as using machines, free weights, or bodyweight resistance exercises at least once a week, those differences disappeared and there were no significant differences in BMI-adjusted bone microarchitecture between vegans and omnivores after the 5 years.
Of note, no significant differences in bone microarchitecture were observed between those who performed exclusively aerobic activities and those who reported no sports activities in the vegan or omnivore group.
Based on the findings, “other types of exercise such as aerobics, cycling, etc, would not be sufficient for a similar positive effect on bone [as resistance training],” Dr. Wakolbinger-Habel said.
Although the findings suggest that resistance training seemed to allow vegans to “catch up” with omnivores in terms of bone microarchitecture, Dr. Wakolbinger-Habel cautioned that a study limitation is the relatively low number of participants.
“The absolute numbers suggest that in vegans the differences, and the relative effect, respectively of resistance training might be larger,” he said. “However, the number of participants in the subgroups is small and it is still an observational study, so we need to be careful in drawing causal conclusions.”
Serum bone markers were within normal ranges across all subgroups. And although there were some correlations between nutrient intake and bone microarchitecture among vegans who did and did not practice resistance training, no conclusions could be drawn from that data, the authors noted.
“Based on our data, the structural [differences between vegans and omnivores] cannot solely be explained by deficits in certain nutrients according to lifestyle,” the authors concluded.
Mechanisms
The mechanisms by which progressive resistance training could result in the benefits include that mechanical loads trigger stimulation of key pathways involved in bone formation, or mechanotransduction, the authors explained.
The unique effects have been observed in other studies, including one study showing that, among young adult runners, the addition of resistance training once a week was associated with significantly greater BMD.
“Veganism is a global trend with strongly increasing numbers of people worldwide adhering to a purely plant-based diet,” first author Christian Muschitz, MD, also of St. Vincent Hospital Vienna and the Medical University of Vienna, said in a press statement.
“Our study showed resistance training offsets diminished bone structure in vegan people when compared to omnivores,” he said.
Dr. Wakolbinger-Habel recommended that, based on the findings, “exercise, including resistance training, should be strongly advocated [for vegans], I would say, at least two times per week.”
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People who maintain a vegan diet show significant deficits in bone microarchitecture, compared with omnivores; however, resistance training not only appears to improve those deficits but may have a stronger effect in vegans, suggesting an important strategy in maintaining bone health with a vegan diet.
“We expected better bone structure in both vegans and omnivores who reported resistance training,” first author Robert Wakolbinger-Habel, MD, PhD, of St. Vincent Hospital Vienna and the Medical University of Vienna, said in an interview.
“However, we expected [there would still be] differences in structure between vegans and omnivores [who practiced resistance training], as previous literature reported higher fracture rates in vegans,” he said. “Still, the positive message is that ‘pumping iron’ could counterbalance these differences between vegans and omnivores.”
The research was published online in The Endocrine Society’s Journal of Clinical Endocrinology & Metabolism.
Exercise significantly impacts bone health in vegans
The potential effects of the plant-based vegan diet on bone health have been reported in studies linking the diet to an increased risk of fractures and lower bone mineral density (BMD), with common theories including lower bone- and muscle-building protein in vegan diets.
However, most previous studies have not considered other key factors, such as the effects of exercise, the authors noted.
“While previous studies on bone health in vegans only took BMD, biochemical and nutritional parameters into account, they did not consider the significant effects of physical activity,” they wrote.
“By ignoring these effects, important factors influencing bone health are neglected.”
For the study, 88 participants were enrolled in Vienna, with vegan participants recruited with the help of the Austrian Vegan Society.
Importantly, the study documented participants’ bone microarchitecture, a key measure of bone strength that has also not been previously investigated in vegans, using high-resolution peripheral quantitative CT.
Inclusion criteria included maintaining an omnivore diet of meat and plant-based foods or a vegan diet for at least 5 years, not being underweight or obese (body mass index [BMI], 18.5-30 kg/m2), being age 30-50 years, and being premenopausal.
Of the participants, 43 were vegan and 45 were omnivores, with generally equal ratios of men and women.
Vegan bone deficits disappear with strength training
Overall, compared with omnivores, the vegan group showed significant deficits in 7 of 14 measures of BMI-adjusted trabecular and cortical structure (all P < .05).
Among participants who reported no resistance training, vegans still showed significant decreases in bone microarchitecture, compared with omnivores, including radius trabecular BMD, radius trabecular bone volume fraction, and other tibial and cortical bone microarchitecture measures.
However, among those who did report progressive resistant training (20 vegans and 25 omnivores), defined as using machines, free weights, or bodyweight resistance exercises at least once a week, those differences disappeared and there were no significant differences in BMI-adjusted bone microarchitecture between vegans and omnivores after the 5 years.
Of note, no significant differences in bone microarchitecture were observed between those who performed exclusively aerobic activities and those who reported no sports activities in the vegan or omnivore group.
Based on the findings, “other types of exercise such as aerobics, cycling, etc, would not be sufficient for a similar positive effect on bone [as resistance training],” Dr. Wakolbinger-Habel said.
Although the findings suggest that resistance training seemed to allow vegans to “catch up” with omnivores in terms of bone microarchitecture, Dr. Wakolbinger-Habel cautioned that a study limitation is the relatively low number of participants.
“The absolute numbers suggest that in vegans the differences, and the relative effect, respectively of resistance training might be larger,” he said. “However, the number of participants in the subgroups is small and it is still an observational study, so we need to be careful in drawing causal conclusions.”
Serum bone markers were within normal ranges across all subgroups. And although there were some correlations between nutrient intake and bone microarchitecture among vegans who did and did not practice resistance training, no conclusions could be drawn from that data, the authors noted.
“Based on our data, the structural [differences between vegans and omnivores] cannot solely be explained by deficits in certain nutrients according to lifestyle,” the authors concluded.
Mechanisms
The mechanisms by which progressive resistance training could result in the benefits include that mechanical loads trigger stimulation of key pathways involved in bone formation, or mechanotransduction, the authors explained.
The unique effects have been observed in other studies, including one study showing that, among young adult runners, the addition of resistance training once a week was associated with significantly greater BMD.
“Veganism is a global trend with strongly increasing numbers of people worldwide adhering to a purely plant-based diet,” first author Christian Muschitz, MD, also of St. Vincent Hospital Vienna and the Medical University of Vienna, said in a press statement.
“Our study showed resistance training offsets diminished bone structure in vegan people when compared to omnivores,” he said.
Dr. Wakolbinger-Habel recommended that, based on the findings, “exercise, including resistance training, should be strongly advocated [for vegans], I would say, at least two times per week.”
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
People who maintain a vegan diet show significant deficits in bone microarchitecture, compared with omnivores; however, resistance training not only appears to improve those deficits but may have a stronger effect in vegans, suggesting an important strategy in maintaining bone health with a vegan diet.
“We expected better bone structure in both vegans and omnivores who reported resistance training,” first author Robert Wakolbinger-Habel, MD, PhD, of St. Vincent Hospital Vienna and the Medical University of Vienna, said in an interview.
“However, we expected [there would still be] differences in structure between vegans and omnivores [who practiced resistance training], as previous literature reported higher fracture rates in vegans,” he said. “Still, the positive message is that ‘pumping iron’ could counterbalance these differences between vegans and omnivores.”
The research was published online in The Endocrine Society’s Journal of Clinical Endocrinology & Metabolism.
Exercise significantly impacts bone health in vegans
The potential effects of the plant-based vegan diet on bone health have been reported in studies linking the diet to an increased risk of fractures and lower bone mineral density (BMD), with common theories including lower bone- and muscle-building protein in vegan diets.
However, most previous studies have not considered other key factors, such as the effects of exercise, the authors noted.
“While previous studies on bone health in vegans only took BMD, biochemical and nutritional parameters into account, they did not consider the significant effects of physical activity,” they wrote.
“By ignoring these effects, important factors influencing bone health are neglected.”
For the study, 88 participants were enrolled in Vienna, with vegan participants recruited with the help of the Austrian Vegan Society.
Importantly, the study documented participants’ bone microarchitecture, a key measure of bone strength that has also not been previously investigated in vegans, using high-resolution peripheral quantitative CT.
Inclusion criteria included maintaining an omnivore diet of meat and plant-based foods or a vegan diet for at least 5 years, not being underweight or obese (body mass index [BMI], 18.5-30 kg/m2), being age 30-50 years, and being premenopausal.
Of the participants, 43 were vegan and 45 were omnivores, with generally equal ratios of men and women.
Vegan bone deficits disappear with strength training
Overall, compared with omnivores, the vegan group showed significant deficits in 7 of 14 measures of BMI-adjusted trabecular and cortical structure (all P < .05).
Among participants who reported no resistance training, vegans still showed significant decreases in bone microarchitecture, compared with omnivores, including radius trabecular BMD, radius trabecular bone volume fraction, and other tibial and cortical bone microarchitecture measures.
However, among those who did report progressive resistant training (20 vegans and 25 omnivores), defined as using machines, free weights, or bodyweight resistance exercises at least once a week, those differences disappeared and there were no significant differences in BMI-adjusted bone microarchitecture between vegans and omnivores after the 5 years.
Of note, no significant differences in bone microarchitecture were observed between those who performed exclusively aerobic activities and those who reported no sports activities in the vegan or omnivore group.
Based on the findings, “other types of exercise such as aerobics, cycling, etc, would not be sufficient for a similar positive effect on bone [as resistance training],” Dr. Wakolbinger-Habel said.
Although the findings suggest that resistance training seemed to allow vegans to “catch up” with omnivores in terms of bone microarchitecture, Dr. Wakolbinger-Habel cautioned that a study limitation is the relatively low number of participants.
“The absolute numbers suggest that in vegans the differences, and the relative effect, respectively of resistance training might be larger,” he said. “However, the number of participants in the subgroups is small and it is still an observational study, so we need to be careful in drawing causal conclusions.”
Serum bone markers were within normal ranges across all subgroups. And although there were some correlations between nutrient intake and bone microarchitecture among vegans who did and did not practice resistance training, no conclusions could be drawn from that data, the authors noted.
“Based on our data, the structural [differences between vegans and omnivores] cannot solely be explained by deficits in certain nutrients according to lifestyle,” the authors concluded.
Mechanisms
The mechanisms by which progressive resistance training could result in the benefits include that mechanical loads trigger stimulation of key pathways involved in bone formation, or mechanotransduction, the authors explained.
The unique effects have been observed in other studies, including one study showing that, among young adult runners, the addition of resistance training once a week was associated with significantly greater BMD.
“Veganism is a global trend with strongly increasing numbers of people worldwide adhering to a purely plant-based diet,” first author Christian Muschitz, MD, also of St. Vincent Hospital Vienna and the Medical University of Vienna, said in a press statement.
“Our study showed resistance training offsets diminished bone structure in vegan people when compared to omnivores,” he said.
Dr. Wakolbinger-Habel recommended that, based on the findings, “exercise, including resistance training, should be strongly advocated [for vegans], I would say, at least two times per week.”
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM
Mindfulness ‘changes the biology’ of pain
In a randomized trial, more than 100 healthy individuals were assigned to an 8-week mindfulness-based stress reduction (MBSR) program, a health improvement program (HEP) of the same length, or a waiting list.
Scanning participants’ brains during a heat-based stimulus pain task showed those who completed the MBSR had a reduction in a brain signature linked to the sensory intensity of pain.

“Our finding supports the idea that for new practitioners, mindfulness training directly affects how sensory signals from the body are converted into a brain response,” lead investigator Joseph Wielgosz, PhD, of the Center for Healthy Minds, University of Wisconsin–Madison, said in a release.
Further analysis in long-term meditation practitioners showed the total time spent on intensive retreats was associated with neural changes associated with the perceived stress of pain.
“Just like an experienced athlete plays a sport differently than a first-timer, experienced mindfulness practitioners seem to use their mental ‘muscles’ differently in response to pain than first-time meditators,” Dr. Wielgosz noted.
The findings were published online in the American Journal of Psychiatry.
A complex condition
Dr. Wielgosz told this news organization that pain is “complex,” with multiple stages and several phases between the time signals are sent from pain receptors and the experience of pain.
“The way that mindfulness affects pain processing has more to do with the way the brain interprets pain signals.”
The investigators note that understanding the neurocognitive mechanisms underlying the efficacy of nonpharmacologic pain interventions is a “high-priority objective for improving pain treatment.”
Evidence from brief laboratory interventions and cross-sectional studies suggests that mindfulness training is associated with alterations in both sensory processing and cognitive-emotional regulatory networks, the investigators note.
“However, no such study has yet been conducted on a standardized, full-length, and widely used clinical intervention, such as MBSR,” they add.
Thermal pain task
The randomized, active-control trial included 115 healthy, meditation-naive individuals (61.7% women; average age, 48.3 years). Just over half (58%) had a graduate degree and their mean score on the Hollingshead index was 58.3, indicting a higher socioeconomic status.
All were randomly assigned to an 8-week MBSR course, an 8-week HEP course as an active control group, or a waiting-list control group with no intervention.
The MBSR involved instruction and practice in continuous focused attention on the breath, bodily sensations, and mental content while in seated postures, walking, and doing yoga.
The HEP matched the MBSR in terms of its length, structure, and nonspecific therapeutic elements, which included a supportive group atmosphere, expert instruction, and positive expectancy for benefit.
To examine the interventions’ effect on the pain experience, participants underwent a pain task in which they had 20 thermal stimuli applied to the inside of the left wrist for 12 seconds, including 8 seconds at peak temperature.
The stimuli were separated by a distractor task and intervals for cued anticipation, recovery, and subjective ratings of intensity and unpleasantness on a scale of 0-20.
During the task, participants underwent MRI to assess the neurologic pain signature (NPS) and the stimulus intensity independent pain signature-1 (SIIPS-1) within the brain.
The NPS is activated by various types of pain stimuli, while responding minimally or not at all to “emotionally evocative stimuli” relating to pain or to placebo treatment, the researchers note.
In contrast, the SIIPS-1 is activated in response to aspects of pain unrelated to the stimulus itself. It incorporates a “broader range of cognitive and emotional modulatory circuits,” including those related to expectancy and cognitive processes to modulate the pain experience.
Neural signatures
Results showed that in all groups, age was significantly negatively associated with both NPS (P = .001) and SIIPS-1 response (P < .001), although not subjective pain reports, and was subsequently included in all analyses of neural signatures.
Persons in the MBSR group had a significant decrease in the NPS, compared with those in the HEP group (P = .05), and from pre- to postintervention assessments (P = .023).
Those in the MBSR group also had “marginal” decreases in the NPS vs. the waiting list group (P = .096), and in the SIIPS-1 relative to both the HEP (P = .089) and waiting list groups (P = .087).
In subjective pain ratings, the MBSR group showed a marginal decrease, compared with the waiting list group (P = .078), and from the pre- to postintervention assessments (P = .028).
The HEP group also had marginal decreases in pain unpleasantness vs. the waiting list group (P = .043), and from the pre- to postintervention assessments for pain intensity (P = .046) and unpleasantness (P = .007).
The researchers also assessed 30 long-term meditators who had undertaken at least 3 years of formal experience with meditation, including participating in multiple intensive retreats and ongoing daily practice, and compared them with meditation-naive individuals.
Long-term meditators reported significantly less pain intensity and unpleasantness than those who had not undergone the training (P < .001).
In addition, a higher number of practice hours during a retreat was linked to a greater reduction in pain ratings. This association remained even after adjustment for gender and respiration rate.
However, the number of daily practice hours was not significantly associated with pain ratings among long-term meditators.
Although there were no average differences in neural signature responses between long-term meditators and individuals who were naive to the technique, there was an inverse relationship between hours on retreat and SIIPS-1 response (P = .027).
‘We’re seeing the biology change’
Commenting for this news organization, Fadel Zeidan, PhD, associate professor of anesthesiology, University of California, San Diego, said that in attenuating the experience of pain, mindfulness engages “very novel” mechanisms.

However, the “most remarkable thing about this study” is that the pain effect occurred when the participants were not meditating, “which gives rise to the notion that mental training is just like physical training,” said Dr. Zeidan, who was not involved with the research.
He noted that the notion was not appreciated previously, “because we weren’t able to see the changes,” as they were based on self-report alone.
However, combining those reports with brain imaging and other objective methods means that “we’re actually seeing the biology change,” Dr. Zeidan said.
He added that mindfulness is different from other techniques for modulating the pain experience, because it is self-facilitated.
“People can learn this technique, ideally, for free online. They can learn the recipe, and it’s one of the only techniques out there that can be used immediately to assuage one’s own pain,” he said.
“There’s nothing else out there on this planet that could immediately reduce one’s own pain. You have to wait 45 minutes for Tylenol, distraction can only work for so long, and you can’t really placebo yourself,” Dr. Zeidan added.
The study was funded by a National Center for Complementary and Alternative Medicine grant, National Institute of Mental Health grants, a Fetzer Institute grant, and a John Templeton Foundation grant, as well as a core grant to the Waisman Center from the National Institute of Child Health and Human Development to Albee Messing. Dr. Wielgosz and Dr. Zeidan have reported no relevant financial relationships. Disclosures for the coinvestigators are listed in the original article.
A version of this article first appeared on Medscape.com.
In a randomized trial, more than 100 healthy individuals were assigned to an 8-week mindfulness-based stress reduction (MBSR) program, a health improvement program (HEP) of the same length, or a waiting list.
Scanning participants’ brains during a heat-based stimulus pain task showed those who completed the MBSR had a reduction in a brain signature linked to the sensory intensity of pain.
“Our finding supports the idea that for new practitioners, mindfulness training directly affects how sensory signals from the body are converted into a brain response,” lead investigator Joseph Wielgosz, PhD, of the Center for Healthy Minds, University of Wisconsin–Madison, said in a release.
Further analysis in long-term meditation practitioners showed the total time spent on intensive retreats was associated with neural changes associated with the perceived stress of pain.
“Just like an experienced athlete plays a sport differently than a first-timer, experienced mindfulness practitioners seem to use their mental ‘muscles’ differently in response to pain than first-time meditators,” Dr. Wielgosz noted.
The findings were published online in the American Journal of Psychiatry.
A complex condition
Dr. Wielgosz told this news organization that pain is “complex,” with multiple stages and several phases between the time signals are sent from pain receptors and the experience of pain.
“The way that mindfulness affects pain processing has more to do with the way the brain interprets pain signals.”
The investigators note that understanding the neurocognitive mechanisms underlying the efficacy of nonpharmacologic pain interventions is a “high-priority objective for improving pain treatment.”
Evidence from brief laboratory interventions and cross-sectional studies suggests that mindfulness training is associated with alterations in both sensory processing and cognitive-emotional regulatory networks, the investigators note.
“However, no such study has yet been conducted on a standardized, full-length, and widely used clinical intervention, such as MBSR,” they add.
Thermal pain task
The randomized, active-control trial included 115 healthy, meditation-naive individuals (61.7% women; average age, 48.3 years). Just over half (58%) had a graduate degree and their mean score on the Hollingshead index was 58.3, indicting a higher socioeconomic status.
All were randomly assigned to an 8-week MBSR course, an 8-week HEP course as an active control group, or a waiting-list control group with no intervention.
The MBSR involved instruction and practice in continuous focused attention on the breath, bodily sensations, and mental content while in seated postures, walking, and doing yoga.
The HEP matched the MBSR in terms of its length, structure, and nonspecific therapeutic elements, which included a supportive group atmosphere, expert instruction, and positive expectancy for benefit.
To examine the interventions’ effect on the pain experience, participants underwent a pain task in which they had 20 thermal stimuli applied to the inside of the left wrist for 12 seconds, including 8 seconds at peak temperature.
The stimuli were separated by a distractor task and intervals for cued anticipation, recovery, and subjective ratings of intensity and unpleasantness on a scale of 0-20.
During the task, participants underwent MRI to assess the neurologic pain signature (NPS) and the stimulus intensity independent pain signature-1 (SIIPS-1) within the brain.
The NPS is activated by various types of pain stimuli, while responding minimally or not at all to “emotionally evocative stimuli” relating to pain or to placebo treatment, the researchers note.
In contrast, the SIIPS-1 is activated in response to aspects of pain unrelated to the stimulus itself. It incorporates a “broader range of cognitive and emotional modulatory circuits,” including those related to expectancy and cognitive processes to modulate the pain experience.
Neural signatures
Results showed that in all groups, age was significantly negatively associated with both NPS (P = .001) and SIIPS-1 response (P < .001), although not subjective pain reports, and was subsequently included in all analyses of neural signatures.
Persons in the MBSR group had a significant decrease in the NPS, compared with those in the HEP group (P = .05), and from pre- to postintervention assessments (P = .023).
Those in the MBSR group also had “marginal” decreases in the NPS vs. the waiting list group (P = .096), and in the SIIPS-1 relative to both the HEP (P = .089) and waiting list groups (P = .087).
In subjective pain ratings, the MBSR group showed a marginal decrease, compared with the waiting list group (P = .078), and from the pre- to postintervention assessments (P = .028).
The HEP group also had marginal decreases in pain unpleasantness vs. the waiting list group (P = .043), and from the pre- to postintervention assessments for pain intensity (P = .046) and unpleasantness (P = .007).
The researchers also assessed 30 long-term meditators who had undertaken at least 3 years of formal experience with meditation, including participating in multiple intensive retreats and ongoing daily practice, and compared them with meditation-naive individuals.
Long-term meditators reported significantly less pain intensity and unpleasantness than those who had not undergone the training (P < .001).
In addition, a higher number of practice hours during a retreat was linked to a greater reduction in pain ratings. This association remained even after adjustment for gender and respiration rate.
However, the number of daily practice hours was not significantly associated with pain ratings among long-term meditators.
Although there were no average differences in neural signature responses between long-term meditators and individuals who were naive to the technique, there was an inverse relationship between hours on retreat and SIIPS-1 response (P = .027).
‘We’re seeing the biology change’
Commenting for this news organization, Fadel Zeidan, PhD, associate professor of anesthesiology, University of California, San Diego, said that in attenuating the experience of pain, mindfulness engages “very novel” mechanisms.
However, the “most remarkable thing about this study” is that the pain effect occurred when the participants were not meditating, “which gives rise to the notion that mental training is just like physical training,” said Dr. Zeidan, who was not involved with the research.
He noted that the notion was not appreciated previously, “because we weren’t able to see the changes,” as they were based on self-report alone.
However, combining those reports with brain imaging and other objective methods means that “we’re actually seeing the biology change,” Dr. Zeidan said.
He added that mindfulness is different from other techniques for modulating the pain experience, because it is self-facilitated.
“People can learn this technique, ideally, for free online. They can learn the recipe, and it’s one of the only techniques out there that can be used immediately to assuage one’s own pain,” he said.
“There’s nothing else out there on this planet that could immediately reduce one’s own pain. You have to wait 45 minutes for Tylenol, distraction can only work for so long, and you can’t really placebo yourself,” Dr. Zeidan added.
The study was funded by a National Center for Complementary and Alternative Medicine grant, National Institute of Mental Health grants, a Fetzer Institute grant, and a John Templeton Foundation grant, as well as a core grant to the Waisman Center from the National Institute of Child Health and Human Development to Albee Messing. Dr. Wielgosz and Dr. Zeidan have reported no relevant financial relationships. Disclosures for the coinvestigators are listed in the original article.
A version of this article first appeared on Medscape.com.
In a randomized trial, more than 100 healthy individuals were assigned to an 8-week mindfulness-based stress reduction (MBSR) program, a health improvement program (HEP) of the same length, or a waiting list.
Scanning participants’ brains during a heat-based stimulus pain task showed those who completed the MBSR had a reduction in a brain signature linked to the sensory intensity of pain.
“Our finding supports the idea that for new practitioners, mindfulness training directly affects how sensory signals from the body are converted into a brain response,” lead investigator Joseph Wielgosz, PhD, of the Center for Healthy Minds, University of Wisconsin–Madison, said in a release.
Further analysis in long-term meditation practitioners showed the total time spent on intensive retreats was associated with neural changes associated with the perceived stress of pain.
“Just like an experienced athlete plays a sport differently than a first-timer, experienced mindfulness practitioners seem to use their mental ‘muscles’ differently in response to pain than first-time meditators,” Dr. Wielgosz noted.
The findings were published online in the American Journal of Psychiatry.
A complex condition
Dr. Wielgosz told this news organization that pain is “complex,” with multiple stages and several phases between the time signals are sent from pain receptors and the experience of pain.
“The way that mindfulness affects pain processing has more to do with the way the brain interprets pain signals.”
The investigators note that understanding the neurocognitive mechanisms underlying the efficacy of nonpharmacologic pain interventions is a “high-priority objective for improving pain treatment.”
Evidence from brief laboratory interventions and cross-sectional studies suggests that mindfulness training is associated with alterations in both sensory processing and cognitive-emotional regulatory networks, the investigators note.
“However, no such study has yet been conducted on a standardized, full-length, and widely used clinical intervention, such as MBSR,” they add.
Thermal pain task
The randomized, active-control trial included 115 healthy, meditation-naive individuals (61.7% women; average age, 48.3 years). Just over half (58%) had a graduate degree and their mean score on the Hollingshead index was 58.3, indicting a higher socioeconomic status.
All were randomly assigned to an 8-week MBSR course, an 8-week HEP course as an active control group, or a waiting-list control group with no intervention.
The MBSR involved instruction and practice in continuous focused attention on the breath, bodily sensations, and mental content while in seated postures, walking, and doing yoga.
The HEP matched the MBSR in terms of its length, structure, and nonspecific therapeutic elements, which included a supportive group atmosphere, expert instruction, and positive expectancy for benefit.
To examine the interventions’ effect on the pain experience, participants underwent a pain task in which they had 20 thermal stimuli applied to the inside of the left wrist for 12 seconds, including 8 seconds at peak temperature.
The stimuli were separated by a distractor task and intervals for cued anticipation, recovery, and subjective ratings of intensity and unpleasantness on a scale of 0-20.
During the task, participants underwent MRI to assess the neurologic pain signature (NPS) and the stimulus intensity independent pain signature-1 (SIIPS-1) within the brain.
The NPS is activated by various types of pain stimuli, while responding minimally or not at all to “emotionally evocative stimuli” relating to pain or to placebo treatment, the researchers note.
In contrast, the SIIPS-1 is activated in response to aspects of pain unrelated to the stimulus itself. It incorporates a “broader range of cognitive and emotional modulatory circuits,” including those related to expectancy and cognitive processes to modulate the pain experience.
Neural signatures
Results showed that in all groups, age was significantly negatively associated with both NPS (P = .001) and SIIPS-1 response (P < .001), although not subjective pain reports, and was subsequently included in all analyses of neural signatures.
Persons in the MBSR group had a significant decrease in the NPS, compared with those in the HEP group (P = .05), and from pre- to postintervention assessments (P = .023).
Those in the MBSR group also had “marginal” decreases in the NPS vs. the waiting list group (P = .096), and in the SIIPS-1 relative to both the HEP (P = .089) and waiting list groups (P = .087).
In subjective pain ratings, the MBSR group showed a marginal decrease, compared with the waiting list group (P = .078), and from the pre- to postintervention assessments (P = .028).
The HEP group also had marginal decreases in pain unpleasantness vs. the waiting list group (P = .043), and from the pre- to postintervention assessments for pain intensity (P = .046) and unpleasantness (P = .007).
The researchers also assessed 30 long-term meditators who had undertaken at least 3 years of formal experience with meditation, including participating in multiple intensive retreats and ongoing daily practice, and compared them with meditation-naive individuals.
Long-term meditators reported significantly less pain intensity and unpleasantness than those who had not undergone the training (P < .001).
In addition, a higher number of practice hours during a retreat was linked to a greater reduction in pain ratings. This association remained even after adjustment for gender and respiration rate.
However, the number of daily practice hours was not significantly associated with pain ratings among long-term meditators.
Although there were no average differences in neural signature responses between long-term meditators and individuals who were naive to the technique, there was an inverse relationship between hours on retreat and SIIPS-1 response (P = .027).
‘We’re seeing the biology change’
Commenting for this news organization, Fadel Zeidan, PhD, associate professor of anesthesiology, University of California, San Diego, said that in attenuating the experience of pain, mindfulness engages “very novel” mechanisms.
However, the “most remarkable thing about this study” is that the pain effect occurred when the participants were not meditating, “which gives rise to the notion that mental training is just like physical training,” said Dr. Zeidan, who was not involved with the research.
He noted that the notion was not appreciated previously, “because we weren’t able to see the changes,” as they were based on self-report alone.
However, combining those reports with brain imaging and other objective methods means that “we’re actually seeing the biology change,” Dr. Zeidan said.
He added that mindfulness is different from other techniques for modulating the pain experience, because it is self-facilitated.
“People can learn this technique, ideally, for free online. They can learn the recipe, and it’s one of the only techniques out there that can be used immediately to assuage one’s own pain,” he said.
“There’s nothing else out there on this planet that could immediately reduce one’s own pain. You have to wait 45 minutes for Tylenol, distraction can only work for so long, and you can’t really placebo yourself,” Dr. Zeidan added.
The study was funded by a National Center for Complementary and Alternative Medicine grant, National Institute of Mental Health grants, a Fetzer Institute grant, and a John Templeton Foundation grant, as well as a core grant to the Waisman Center from the National Institute of Child Health and Human Development to Albee Messing. Dr. Wielgosz and Dr. Zeidan have reported no relevant financial relationships. Disclosures for the coinvestigators are listed in the original article.
A version of this article first appeared on Medscape.com.
FROM AMERICAN JOURNAL OF PSYCHIATRY
Ultrasound on par with CT for evaluating sarcopenia in patients with cirrhosis
Using ultrasound (US) to evaluate sarcopenic obesity in patients with cirrhosis may offer accuracy on par with computed tomography (CT), according to investigators.
US-based assessment presents a more affordable point-of-care strategy that limits radiation exposure, which enables sequential monitoring, reported lead author Sukhpal Dhariwal, MBBS, MD, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India.
“Preliminary data in patients with liver disease ... suggest that US muscle assessment–derived indices, especially thigh muscle thickness, identify sarcopenia CT-skeletal muscle index (SMI) and also predict hospitalization and mortality,” the investigators wrote in Journal of Clinical Gastroenterology. “However, the applicability of US-based techniques to measure muscle mass in the high-risk group of patients with cirrhosis and sarcopenic obesity has not been evaluated.”
To address this knowledge gap, the investigators performed both US- and CT-based muscle assessments in 52 patients with obesity and evidence of cirrhosis; 40 patients were male and the mean age was 50.9 years. In all, 20 (38.5%) were diagnosed with sarcopenia based on CT-determined SMI scores of less than 39 cm2/m2 for women and 50 cm2/m2 for men.
US showed that it was similarly capable of categorizing patients. The modality significantly differentiated individuals with or without sarcopenia based on high area under the curve values in four muscle indices: quadriceps muscle thickness (0.98), quadriceps muscle feather index (0.95), forearm muscle thickness (0.85), and forearm feather index (0.80).
Direct comparison of US-based assessment against CT-based SMI revealed positive correlations, with significant r values ranging from 0.40 to 0.58. These correlations were stronger in a male-only subgroup analysis, in which r values ranged from 0.52 to 0.70. R values were not calculated in the female subgroup because of the small sample size (n = 12).
The investigators adjusted indices for height, which may pose bias for overestimating muscle mass. Another limitation is the small sample size.
“US-based assessment of sarcopenia has excellent diagnostic accuracy and correlates highly with cross-sectional imaging-based SMI in cirrhosis patients with sarcopenic obesity,” the investigators concluded. “US may serve as an easy-to-use, point-of-care tool for assessing sarcopenia in sarcopenic obesity with the advantage of repeated sequential assessment.”
According to Jamile Wakim-Fleming, MD, of the Cleveland Clinic, “US-based muscle mass assessment seems to be reliable, reproducible, and simple to perform and should be encouraged along with nutrition assessments in all patients with cirrhosis and obesity.”

In a written comment, Dr. Wakim-Fleming noted the importance of timely monitoring and intervention in this patient population.
“Considering the morbidity and the poor outcomes associated with sarcopenic obesity and its frequency in cirrhosis, it is important to make early diagnosis and institute a management plan to improve muscle mass and function,” she said.
The study was supported the Patient-Centered Outcomes Research Institute, the American Medical Association, and the American Heart Association. The investigators disclosed additional relationships with Pfizer, Bristol Myers Squibb, and Novartis. Dr. Wakim-Fleming reported no relevant conflicts of interest.
Using ultrasound (US) to evaluate sarcopenic obesity in patients with cirrhosis may offer accuracy on par with computed tomography (CT), according to investigators.
US-based assessment presents a more affordable point-of-care strategy that limits radiation exposure, which enables sequential monitoring, reported lead author Sukhpal Dhariwal, MBBS, MD, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India.
“Preliminary data in patients with liver disease ... suggest that US muscle assessment–derived indices, especially thigh muscle thickness, identify sarcopenia CT-skeletal muscle index (SMI) and also predict hospitalization and mortality,” the investigators wrote in Journal of Clinical Gastroenterology. “However, the applicability of US-based techniques to measure muscle mass in the high-risk group of patients with cirrhosis and sarcopenic obesity has not been evaluated.”
To address this knowledge gap, the investigators performed both US- and CT-based muscle assessments in 52 patients with obesity and evidence of cirrhosis; 40 patients were male and the mean age was 50.9 years. In all, 20 (38.5%) were diagnosed with sarcopenia based on CT-determined SMI scores of less than 39 cm2/m2 for women and 50 cm2/m2 for men.
US showed that it was similarly capable of categorizing patients. The modality significantly differentiated individuals with or without sarcopenia based on high area under the curve values in four muscle indices: quadriceps muscle thickness (0.98), quadriceps muscle feather index (0.95), forearm muscle thickness (0.85), and forearm feather index (0.80).
Direct comparison of US-based assessment against CT-based SMI revealed positive correlations, with significant r values ranging from 0.40 to 0.58. These correlations were stronger in a male-only subgroup analysis, in which r values ranged from 0.52 to 0.70. R values were not calculated in the female subgroup because of the small sample size (n = 12).
The investigators adjusted indices for height, which may pose bias for overestimating muscle mass. Another limitation is the small sample size.
“US-based assessment of sarcopenia has excellent diagnostic accuracy and correlates highly with cross-sectional imaging-based SMI in cirrhosis patients with sarcopenic obesity,” the investigators concluded. “US may serve as an easy-to-use, point-of-care tool for assessing sarcopenia in sarcopenic obesity with the advantage of repeated sequential assessment.”
According to Jamile Wakim-Fleming, MD, of the Cleveland Clinic, “US-based muscle mass assessment seems to be reliable, reproducible, and simple to perform and should be encouraged along with nutrition assessments in all patients with cirrhosis and obesity.”
In a written comment, Dr. Wakim-Fleming noted the importance of timely monitoring and intervention in this patient population.
“Considering the morbidity and the poor outcomes associated with sarcopenic obesity and its frequency in cirrhosis, it is important to make early diagnosis and institute a management plan to improve muscle mass and function,” she said.
The study was supported the Patient-Centered Outcomes Research Institute, the American Medical Association, and the American Heart Association. The investigators disclosed additional relationships with Pfizer, Bristol Myers Squibb, and Novartis. Dr. Wakim-Fleming reported no relevant conflicts of interest.
Using ultrasound (US) to evaluate sarcopenic obesity in patients with cirrhosis may offer accuracy on par with computed tomography (CT), according to investigators.
US-based assessment presents a more affordable point-of-care strategy that limits radiation exposure, which enables sequential monitoring, reported lead author Sukhpal Dhariwal, MBBS, MD, of the Postgraduate Institute of Medical Education and Research, Chandigarh, India.
“Preliminary data in patients with liver disease ... suggest that US muscle assessment–derived indices, especially thigh muscle thickness, identify sarcopenia CT-skeletal muscle index (SMI) and also predict hospitalization and mortality,” the investigators wrote in Journal of Clinical Gastroenterology. “However, the applicability of US-based techniques to measure muscle mass in the high-risk group of patients with cirrhosis and sarcopenic obesity has not been evaluated.”
To address this knowledge gap, the investigators performed both US- and CT-based muscle assessments in 52 patients with obesity and evidence of cirrhosis; 40 patients were male and the mean age was 50.9 years. In all, 20 (38.5%) were diagnosed with sarcopenia based on CT-determined SMI scores of less than 39 cm2/m2 for women and 50 cm2/m2 for men.
US showed that it was similarly capable of categorizing patients. The modality significantly differentiated individuals with or without sarcopenia based on high area under the curve values in four muscle indices: quadriceps muscle thickness (0.98), quadriceps muscle feather index (0.95), forearm muscle thickness (0.85), and forearm feather index (0.80).
Direct comparison of US-based assessment against CT-based SMI revealed positive correlations, with significant r values ranging from 0.40 to 0.58. These correlations were stronger in a male-only subgroup analysis, in which r values ranged from 0.52 to 0.70. R values were not calculated in the female subgroup because of the small sample size (n = 12).
The investigators adjusted indices for height, which may pose bias for overestimating muscle mass. Another limitation is the small sample size.
“US-based assessment of sarcopenia has excellent diagnostic accuracy and correlates highly with cross-sectional imaging-based SMI in cirrhosis patients with sarcopenic obesity,” the investigators concluded. “US may serve as an easy-to-use, point-of-care tool for assessing sarcopenia in sarcopenic obesity with the advantage of repeated sequential assessment.”
According to Jamile Wakim-Fleming, MD, of the Cleveland Clinic, “US-based muscle mass assessment seems to be reliable, reproducible, and simple to perform and should be encouraged along with nutrition assessments in all patients with cirrhosis and obesity.”
In a written comment, Dr. Wakim-Fleming noted the importance of timely monitoring and intervention in this patient population.
“Considering the morbidity and the poor outcomes associated with sarcopenic obesity and its frequency in cirrhosis, it is important to make early diagnosis and institute a management plan to improve muscle mass and function,” she said.
The study was supported the Patient-Centered Outcomes Research Institute, the American Medical Association, and the American Heart Association. The investigators disclosed additional relationships with Pfizer, Bristol Myers Squibb, and Novartis. Dr. Wakim-Fleming reported no relevant conflicts of interest.
FROM JAMA INTERNAL MEDICINE