User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
COVID hospitalizations climb for fourth straight week
Weekly new hospitalizations for COVID-19 have climbed for the fourth straight week.
according to newly updated Centers for Disease Control and Prevention figures. Hospitalizations reached an all-time low of about 6,300 per week in July.
The CDC stopped tracking the number of people infected by the virus earlier in 2023, and now relies on hospitalization data to gauge the current impact of COVID-19.
“We have to remember that we’re still dealing with numbers that are far less than what we’ve seen for the pandemic,” John Brownstein, PhD, a professor of biomedical informatics at Harvard Medical School, Boston, told ABC News. “We have to zoom out to look at our experience for the entire pandemic, to understand that what we’re dealing with now is far from any crisis that we’ve experienced with previous waves.”
The current predominant strain remains EG.5, and experts believe it is not more severe or more contagious than other recent variants.
Dr. Brownstein told ABC News that one reason for the concern about rising COVID metrics, despite their overall low levels, is that a surge occurred in the summer of 2021 with the dangerous Delta variant.
“But each new variant so far that has come through has subsequently had less of a population impact,” he said. “Now, is it possible we may see one in the future that is worthy, a real concern? Absolutely. But overall, we’ve seen a dampening of effect over the last several variants that have come through.”
A version of this article appeared on WebMD.com.
Weekly new hospitalizations for COVID-19 have climbed for the fourth straight week.
according to newly updated Centers for Disease Control and Prevention figures. Hospitalizations reached an all-time low of about 6,300 per week in July.
The CDC stopped tracking the number of people infected by the virus earlier in 2023, and now relies on hospitalization data to gauge the current impact of COVID-19.
“We have to remember that we’re still dealing with numbers that are far less than what we’ve seen for the pandemic,” John Brownstein, PhD, a professor of biomedical informatics at Harvard Medical School, Boston, told ABC News. “We have to zoom out to look at our experience for the entire pandemic, to understand that what we’re dealing with now is far from any crisis that we’ve experienced with previous waves.”
The current predominant strain remains EG.5, and experts believe it is not more severe or more contagious than other recent variants.
Dr. Brownstein told ABC News that one reason for the concern about rising COVID metrics, despite their overall low levels, is that a surge occurred in the summer of 2021 with the dangerous Delta variant.
“But each new variant so far that has come through has subsequently had less of a population impact,” he said. “Now, is it possible we may see one in the future that is worthy, a real concern? Absolutely. But overall, we’ve seen a dampening of effect over the last several variants that have come through.”
A version of this article appeared on WebMD.com.
Weekly new hospitalizations for COVID-19 have climbed for the fourth straight week.
according to newly updated Centers for Disease Control and Prevention figures. Hospitalizations reached an all-time low of about 6,300 per week in July.
The CDC stopped tracking the number of people infected by the virus earlier in 2023, and now relies on hospitalization data to gauge the current impact of COVID-19.
“We have to remember that we’re still dealing with numbers that are far less than what we’ve seen for the pandemic,” John Brownstein, PhD, a professor of biomedical informatics at Harvard Medical School, Boston, told ABC News. “We have to zoom out to look at our experience for the entire pandemic, to understand that what we’re dealing with now is far from any crisis that we’ve experienced with previous waves.”
The current predominant strain remains EG.5, and experts believe it is not more severe or more contagious than other recent variants.
Dr. Brownstein told ABC News that one reason for the concern about rising COVID metrics, despite their overall low levels, is that a surge occurred in the summer of 2021 with the dangerous Delta variant.
“But each new variant so far that has come through has subsequently had less of a population impact,” he said. “Now, is it possible we may see one in the future that is worthy, a real concern? Absolutely. But overall, we’ve seen a dampening of effect over the last several variants that have come through.”
A version of this article appeared on WebMD.com.
Which factors distinguish superagers from the rest of us?
Even at an advanced age, superagers have the memory of someone 20 or 30 years their junior. But why is that? A new study shows that, in superagers, However, the study also emphasizes the importance of physical and mental fitness for a healthy aging process.
“One of the most important unanswered questions with regard to superagers is: ‘Are they resistant to age-related memory loss, or do they have coping mechanisms that allow them to better offset this memory loss?’ ” wrote Marta Garo-Pascual, a PhD candidate at the Autonomous University of Madrid, Spain, and colleagues in the Lancet Healthy Longevity. “Our results indicate that superagers are resistant to these processes.”
Six years’ monitoring
From a cohort of older adults who had participated in a study aiming to identify early indicators of Alzheimer’s disease, the research group chose 64 superagers and 55 normal senior citizens. The latter served as the control group. While the superagers performed just as well in a memory test as people 30 years their junior, the control group’s performance was in line with their age and level of education.
All study participants were over age 79 years. Both the group of superagers and the control group included more females than males. On average, they were monitored for 6 years. During this period, a checkup was scheduled annually with an MRI examination, clinical tests, blood tests, and documentation of lifestyle factors.
For Alessandro Cellerino, PhD, of the Leibniz Institute on Aging–Fritz Lipmann Institute in Jena, Germany, this is the most crucial aspect of the study. “Even before this study, we knew that superagers demonstrated less atrophy in certain areas of the brain, but this was always only ever based on a single measurement.”
Memory centers protected
The MRI examinations confirmed that in superagers, gray matter atrophy in the regions responsible for memory (such as the medial temporal lobe and cholinergic forebrain), as well in regions important for movement (such as the motor thalamus), was less pronounced. In addition, the volume of gray matter in these regions, especially in the medial temporal lobe, decreased much more slowly in the superagers than in the control subjects over the study period.
Ms. Garo-Pascual and associates used a machine-learning algorithm to differentiate between superagers and normal older adults. From the 89 demographic, lifestyle, and clinical factors entered into the algorithm, two were the most important for the classification: the ability to move and mental health.
Mobility and mental health
Clinical tests such as the Timed Up-and-Go Test and the Finger Tapping Test revealed that superagers can be distinguished from the normally aging control subjects with regard to their mobility and fine motor skills. Their physical condition was better, although they, by their own admission, did not move any more than the control subjects in day-to-day life. According to Dr. Cellerino, this finding confirms that physical activity is paramount for cognitive function. “These people were over 80 years old – the fact that there was not much difference between their levels of activity is not surprising. Much more relevant is the question of how you get there – i.e., how active you are at the ages of 40, 50 or even 60 years old.”
Remaining active is important
As a matter of fact, the superagers indicated that generally they had been more active than the control subjects during their middle years. “Attempting to stay physically fit is essential; even if it just means going for a walk or taking the stairs,” said Dr. Cellerino.
On average, the superagers also fared much better in tests on physical health than the control subjects. They suffered significantly less from depression or anxiety disorders. “Earlier studies suggest that depression and anxiety disorders may influence performance in memory tests across all ages and that they are risk factors for developing dementia,” said Dr. Cellerino.
To avoid mental health issues in later life, gerontologist Dr. Cellerino recommended remaining socially engaged and involved. “Depression and anxiety are commonly also a consequence of social isolation,” he said.
Potential genetic differences
Blood sample analyses demonstrated that the superagers exhibited lower concentrations of biomarkers for neurodegenerative diseases than the control group did. In contrast, there was no difference between the two groups in the prevalence of the apo e4 allele, one of the most important genetic risk factors for Alzheimer’s disease. Nevertheless, Ms. Garo-Pascual and associates assume that genetics also play a role. They found that, despite 89 variables employed, the algorithm used could only distinguish superagers from normal older adults 66% of the time. This suggests that additional factors must be in play, such as genetic differences.
Body and mind
Since this is an observational study, whether the determined factors have a direct effect on superaging cannot be ascertained, the authors wrote. However, the results are consistent with earlier findings.
“Regarding the management of old age, we actually haven’t learned anything more than what we already knew. But it does confirm that physical and mental function are closely entwined and that we must maintain both to age healthily,” Dr. Cellerino concluded.
This article was translated from the Medscape German Edition. A version appeared on Medscape.com.
Even at an advanced age, superagers have the memory of someone 20 or 30 years their junior. But why is that? A new study shows that, in superagers, However, the study also emphasizes the importance of physical and mental fitness for a healthy aging process.
“One of the most important unanswered questions with regard to superagers is: ‘Are they resistant to age-related memory loss, or do they have coping mechanisms that allow them to better offset this memory loss?’ ” wrote Marta Garo-Pascual, a PhD candidate at the Autonomous University of Madrid, Spain, and colleagues in the Lancet Healthy Longevity. “Our results indicate that superagers are resistant to these processes.”
Six years’ monitoring
From a cohort of older adults who had participated in a study aiming to identify early indicators of Alzheimer’s disease, the research group chose 64 superagers and 55 normal senior citizens. The latter served as the control group. While the superagers performed just as well in a memory test as people 30 years their junior, the control group’s performance was in line with their age and level of education.
All study participants were over age 79 years. Both the group of superagers and the control group included more females than males. On average, they were monitored for 6 years. During this period, a checkup was scheduled annually with an MRI examination, clinical tests, blood tests, and documentation of lifestyle factors.
For Alessandro Cellerino, PhD, of the Leibniz Institute on Aging–Fritz Lipmann Institute in Jena, Germany, this is the most crucial aspect of the study. “Even before this study, we knew that superagers demonstrated less atrophy in certain areas of the brain, but this was always only ever based on a single measurement.”
Memory centers protected
The MRI examinations confirmed that in superagers, gray matter atrophy in the regions responsible for memory (such as the medial temporal lobe and cholinergic forebrain), as well in regions important for movement (such as the motor thalamus), was less pronounced. In addition, the volume of gray matter in these regions, especially in the medial temporal lobe, decreased much more slowly in the superagers than in the control subjects over the study period.
Ms. Garo-Pascual and associates used a machine-learning algorithm to differentiate between superagers and normal older adults. From the 89 demographic, lifestyle, and clinical factors entered into the algorithm, two were the most important for the classification: the ability to move and mental health.
Mobility and mental health
Clinical tests such as the Timed Up-and-Go Test and the Finger Tapping Test revealed that superagers can be distinguished from the normally aging control subjects with regard to their mobility and fine motor skills. Their physical condition was better, although they, by their own admission, did not move any more than the control subjects in day-to-day life. According to Dr. Cellerino, this finding confirms that physical activity is paramount for cognitive function. “These people were over 80 years old – the fact that there was not much difference between their levels of activity is not surprising. Much more relevant is the question of how you get there – i.e., how active you are at the ages of 40, 50 or even 60 years old.”
Remaining active is important
As a matter of fact, the superagers indicated that generally they had been more active than the control subjects during their middle years. “Attempting to stay physically fit is essential; even if it just means going for a walk or taking the stairs,” said Dr. Cellerino.
On average, the superagers also fared much better in tests on physical health than the control subjects. They suffered significantly less from depression or anxiety disorders. “Earlier studies suggest that depression and anxiety disorders may influence performance in memory tests across all ages and that they are risk factors for developing dementia,” said Dr. Cellerino.
To avoid mental health issues in later life, gerontologist Dr. Cellerino recommended remaining socially engaged and involved. “Depression and anxiety are commonly also a consequence of social isolation,” he said.
Potential genetic differences
Blood sample analyses demonstrated that the superagers exhibited lower concentrations of biomarkers for neurodegenerative diseases than the control group did. In contrast, there was no difference between the two groups in the prevalence of the apo e4 allele, one of the most important genetic risk factors for Alzheimer’s disease. Nevertheless, Ms. Garo-Pascual and associates assume that genetics also play a role. They found that, despite 89 variables employed, the algorithm used could only distinguish superagers from normal older adults 66% of the time. This suggests that additional factors must be in play, such as genetic differences.
Body and mind
Since this is an observational study, whether the determined factors have a direct effect on superaging cannot be ascertained, the authors wrote. However, the results are consistent with earlier findings.
“Regarding the management of old age, we actually haven’t learned anything more than what we already knew. But it does confirm that physical and mental function are closely entwined and that we must maintain both to age healthily,” Dr. Cellerino concluded.
This article was translated from the Medscape German Edition. A version appeared on Medscape.com.
Even at an advanced age, superagers have the memory of someone 20 or 30 years their junior. But why is that? A new study shows that, in superagers, However, the study also emphasizes the importance of physical and mental fitness for a healthy aging process.
“One of the most important unanswered questions with regard to superagers is: ‘Are they resistant to age-related memory loss, or do they have coping mechanisms that allow them to better offset this memory loss?’ ” wrote Marta Garo-Pascual, a PhD candidate at the Autonomous University of Madrid, Spain, and colleagues in the Lancet Healthy Longevity. “Our results indicate that superagers are resistant to these processes.”
Six years’ monitoring
From a cohort of older adults who had participated in a study aiming to identify early indicators of Alzheimer’s disease, the research group chose 64 superagers and 55 normal senior citizens. The latter served as the control group. While the superagers performed just as well in a memory test as people 30 years their junior, the control group’s performance was in line with their age and level of education.
All study participants were over age 79 years. Both the group of superagers and the control group included more females than males. On average, they were monitored for 6 years. During this period, a checkup was scheduled annually with an MRI examination, clinical tests, blood tests, and documentation of lifestyle factors.
For Alessandro Cellerino, PhD, of the Leibniz Institute on Aging–Fritz Lipmann Institute in Jena, Germany, this is the most crucial aspect of the study. “Even before this study, we knew that superagers demonstrated less atrophy in certain areas of the brain, but this was always only ever based on a single measurement.”
Memory centers protected
The MRI examinations confirmed that in superagers, gray matter atrophy in the regions responsible for memory (such as the medial temporal lobe and cholinergic forebrain), as well in regions important for movement (such as the motor thalamus), was less pronounced. In addition, the volume of gray matter in these regions, especially in the medial temporal lobe, decreased much more slowly in the superagers than in the control subjects over the study period.
Ms. Garo-Pascual and associates used a machine-learning algorithm to differentiate between superagers and normal older adults. From the 89 demographic, lifestyle, and clinical factors entered into the algorithm, two were the most important for the classification: the ability to move and mental health.
Mobility and mental health
Clinical tests such as the Timed Up-and-Go Test and the Finger Tapping Test revealed that superagers can be distinguished from the normally aging control subjects with regard to their mobility and fine motor skills. Their physical condition was better, although they, by their own admission, did not move any more than the control subjects in day-to-day life. According to Dr. Cellerino, this finding confirms that physical activity is paramount for cognitive function. “These people were over 80 years old – the fact that there was not much difference between their levels of activity is not surprising. Much more relevant is the question of how you get there – i.e., how active you are at the ages of 40, 50 or even 60 years old.”
Remaining active is important
As a matter of fact, the superagers indicated that generally they had been more active than the control subjects during their middle years. “Attempting to stay physically fit is essential; even if it just means going for a walk or taking the stairs,” said Dr. Cellerino.
On average, the superagers also fared much better in tests on physical health than the control subjects. They suffered significantly less from depression or anxiety disorders. “Earlier studies suggest that depression and anxiety disorders may influence performance in memory tests across all ages and that they are risk factors for developing dementia,” said Dr. Cellerino.
To avoid mental health issues in later life, gerontologist Dr. Cellerino recommended remaining socially engaged and involved. “Depression and anxiety are commonly also a consequence of social isolation,” he said.
Potential genetic differences
Blood sample analyses demonstrated that the superagers exhibited lower concentrations of biomarkers for neurodegenerative diseases than the control group did. In contrast, there was no difference between the two groups in the prevalence of the apo e4 allele, one of the most important genetic risk factors for Alzheimer’s disease. Nevertheless, Ms. Garo-Pascual and associates assume that genetics also play a role. They found that, despite 89 variables employed, the algorithm used could only distinguish superagers from normal older adults 66% of the time. This suggests that additional factors must be in play, such as genetic differences.
Body and mind
Since this is an observational study, whether the determined factors have a direct effect on superaging cannot be ascertained, the authors wrote. However, the results are consistent with earlier findings.
“Regarding the management of old age, we actually haven’t learned anything more than what we already knew. But it does confirm that physical and mental function are closely entwined and that we must maintain both to age healthily,” Dr. Cellerino concluded.
This article was translated from the Medscape German Edition. A version appeared on Medscape.com.
FROM THE LANCET HEALTHY LONGEVITY
New COVID shots will be available in September
The updated vaccine still needs final sign-offs from the Food and Drug Administration and the CDC.
“We anticipate that they are going to be available for most folks by the third or fourth week of September,” Director Mandy Cohen, MD, MPH, said on a podcast hosted by former White House COVID adviser Andy Slavitt. “We are likely to see this as a recommendation as an annual COVID shot, just as we have an annual flu shot. I think that will give folks more clarity on whether they should get one or not.”
For people who are considering now whether they should get the currently available COVID vaccine or wait until the new one comes out, Dr. Cohen said that depends on a person’s individual risk. People who are 65 or older or who have multiple health conditions should go ahead and get the currently available shot if it’s been more than 6-8 months since their last dose. For all other people, it’s OK to wait for the new version.
Analysts expect low demand for the updated vaccine. About 240 million people in the United States got at least one dose when vaccines first became available in 2021, Reuters reported, but that number dropped to less than 50 million getting the most updated shot in the fall of 2022.
“Take a look at what happened last winter. It was 50 million in the U.S., and it seems likely to be lower than that, given that there’s less concern about COVID this year than last year,” Michael Yee, a health care industry analyst for the firm Jefferies, told Reuters.
Dr. Cohen noted during the podcast that the recent uptick in virus activity should be taken in context.
“What we’re seeing right now in August of 2023 are small increases of folks getting COVID. We are still at some of the lowest hospitalizations that we’ve been at in the past 3 years,” she said. “Even a 10% increase on a very, very small number is still very small. My level of concern continues to be low.”
A version of this article was first published on WebMD.com .
The updated vaccine still needs final sign-offs from the Food and Drug Administration and the CDC.
“We anticipate that they are going to be available for most folks by the third or fourth week of September,” Director Mandy Cohen, MD, MPH, said on a podcast hosted by former White House COVID adviser Andy Slavitt. “We are likely to see this as a recommendation as an annual COVID shot, just as we have an annual flu shot. I think that will give folks more clarity on whether they should get one or not.”
For people who are considering now whether they should get the currently available COVID vaccine or wait until the new one comes out, Dr. Cohen said that depends on a person’s individual risk. People who are 65 or older or who have multiple health conditions should go ahead and get the currently available shot if it’s been more than 6-8 months since their last dose. For all other people, it’s OK to wait for the new version.
Analysts expect low demand for the updated vaccine. About 240 million people in the United States got at least one dose when vaccines first became available in 2021, Reuters reported, but that number dropped to less than 50 million getting the most updated shot in the fall of 2022.
“Take a look at what happened last winter. It was 50 million in the U.S., and it seems likely to be lower than that, given that there’s less concern about COVID this year than last year,” Michael Yee, a health care industry analyst for the firm Jefferies, told Reuters.
Dr. Cohen noted during the podcast that the recent uptick in virus activity should be taken in context.
“What we’re seeing right now in August of 2023 are small increases of folks getting COVID. We are still at some of the lowest hospitalizations that we’ve been at in the past 3 years,” she said. “Even a 10% increase on a very, very small number is still very small. My level of concern continues to be low.”
A version of this article was first published on WebMD.com .
The updated vaccine still needs final sign-offs from the Food and Drug Administration and the CDC.
“We anticipate that they are going to be available for most folks by the third or fourth week of September,” Director Mandy Cohen, MD, MPH, said on a podcast hosted by former White House COVID adviser Andy Slavitt. “We are likely to see this as a recommendation as an annual COVID shot, just as we have an annual flu shot. I think that will give folks more clarity on whether they should get one or not.”
For people who are considering now whether they should get the currently available COVID vaccine or wait until the new one comes out, Dr. Cohen said that depends on a person’s individual risk. People who are 65 or older or who have multiple health conditions should go ahead and get the currently available shot if it’s been more than 6-8 months since their last dose. For all other people, it’s OK to wait for the new version.
Analysts expect low demand for the updated vaccine. About 240 million people in the United States got at least one dose when vaccines first became available in 2021, Reuters reported, but that number dropped to less than 50 million getting the most updated shot in the fall of 2022.
“Take a look at what happened last winter. It was 50 million in the U.S., and it seems likely to be lower than that, given that there’s less concern about COVID this year than last year,” Michael Yee, a health care industry analyst for the firm Jefferies, told Reuters.
Dr. Cohen noted during the podcast that the recent uptick in virus activity should be taken in context.
“What we’re seeing right now in August of 2023 are small increases of folks getting COVID. We are still at some of the lowest hospitalizations that we’ve been at in the past 3 years,” she said. “Even a 10% increase on a very, very small number is still very small. My level of concern continues to be low.”
A version of this article was first published on WebMD.com .
Children and long COVID: How many are affected?
Long COVID most often strikes seniors and adults, but children are also affected, even though they get less attention, new research shows.
Experts noted that the disease poses particular challenges for children and the doctors who treat them.
Parents and doctors need to be on the lookout for symptoms of long COVID in children and teens that might be easily missed or misdiagnosed, according to physicians and family groups.
Children are at lower risk for contracting COVID and often experience milder symptoms. But the virus is now widespread, and a recent study found that around 16% of pediatric patients with COVID go on to develop symptoms that last more than 3 months – the working definition of long COVID.
Parents and doctors are calling for more studies and more awareness.
Diane Sheehan, who lives outside Charlotte, N.C., says she was an active person and is now permanently disabled from long COVID. Her teenage son has it too and is still recovering.
He contracted COVID after a school event, she said. He had a mild case, but then he started experiencing dizziness and would even experience loss of consciousness when he stood up suddenly. After he contracted the virus a second time, he was bedridden for 8 months.
The staff at Hackensack Meridian Health, a pediatric long COVID clinic in New Jersey, has been working with area schools to help teachers and school nurses recognize possible long COVID in children and young people. The clinic is one of about a dozen in the United States that specializes in pediatric cases.
Katherine Clouser, MD, a pediatric hospital medicine specialist, has been with the clinic since it opened in 2021, and she’s seen a steady flow of patients. Some get better, but she sees a few new cases each week.
“We are seeing children who are having a difficult time returning to school and sports,” she said.
The clinic is having success with a mix of approaches, including intensive rehabilitation, talk therapy, and some off-label use of nirmatrelvir (Paxlovid), an antiviral now being studied as a treatment for long COVID through a National Institutes of Health clinical trials initiative that was announced last month.
Treatment depends on symptoms and is determined on a case-by-case basis, Dr. Clouser said.
Families of her patients are grateful, she added.
“We hear a lot of parents who were desperate for someone to believe them – or someone who knows about it,” she said.
A recent review of more than 30 studies with about 15,000 participants concluded that 16.2% (95% confidence interval, 8.5%-28.6%) of the pediatric participants experienced one or more persistent symptoms of long COVID at least 3 months after acute infection.
Estimates of the number of children and youth with long COVID have varied widely. A 2022 study put the number at more than 25% of cases, but the American Academy of Pediatrics notes that estimates of the percentage of children infected with SARS-CoV-2 who go on to have long COVID range from 2% to 66%.
The federal Recover Initiative has enrolled more than 10,000 children and youth – a number it plans to double – and studies of electronic health records are underway. The Recover pediatric team is also setting up a cohort that they plan to follow into 2025.
Some clinics are having luck treating young people with approaches ranging from special diets to off-label medication.
David W. Miller, MD, who runs the long COVID clinic at the UH Rainbow Babies and Children’s Hospital, Cleveland, said he’s seen about 250 patients.
A warning sign of long COVID in children is profound fatigue, he said.
“It’s the most common symptom,” Dr. Miller said. “They feel like they have the flu all the time.”
Many also experience orthostatic hypotension on standing, triggering dizziness.
He said his team targets symptom groups. Initial management consists of a diet without sugar or refined carbohydrates. Skipping pasta and sweets can be hard for young people, but Dr. Miller said sometimes the diet alone helps.
Many have vitamin D and iron deficiencies. Others need help getting a good night’s sleep. He’s treated 50 with off-label low-dose naltrexone.
Some people with long COVID – both young and old – complain about being misdiagnosed as having depression. Dr. Miller says he see a lot of anxiety – some situational and some biochemical – in pediatric patients. But he cautions doctors not to treat their illness solely as a mental health problem.
His advice: If a young person or child experiences a major change in his or her regular level of functioning or has multiple COVID symptoms that don’t go away after several months, parents and doctors should consider long COVID as a possible cause.
Dr. Miller said most of his patients get better over time with some treatments: “We see improvement in the majority of kids who can stick to the regimen,” such as a sugar-free diet, supplements, and adequate sleep. Recovery has been slow and incomplete for Diane Sheehan and her son. She was training as a permanent make-up artist, she said, but now has hand tremors that make work impossible.
She has found doctors who treat some of her symptoms with antihistamines, and her son has benefited from physical therapy.
But for now, her son is passing on a scholarship he was awarded to attend North Carolina State University this year. Instead, he’s living at home and going to a local college.
Ms. Sheehan urges parents to be on the alert for signs that their children might have long COVID, which can be confused with many other conditions.
A version of this article first appeared on Medscape.com.
Long COVID most often strikes seniors and adults, but children are also affected, even though they get less attention, new research shows.
Experts noted that the disease poses particular challenges for children and the doctors who treat them.
Parents and doctors need to be on the lookout for symptoms of long COVID in children and teens that might be easily missed or misdiagnosed, according to physicians and family groups.
Children are at lower risk for contracting COVID and often experience milder symptoms. But the virus is now widespread, and a recent study found that around 16% of pediatric patients with COVID go on to develop symptoms that last more than 3 months – the working definition of long COVID.
Parents and doctors are calling for more studies and more awareness.
Diane Sheehan, who lives outside Charlotte, N.C., says she was an active person and is now permanently disabled from long COVID. Her teenage son has it too and is still recovering.
He contracted COVID after a school event, she said. He had a mild case, but then he started experiencing dizziness and would even experience loss of consciousness when he stood up suddenly. After he contracted the virus a second time, he was bedridden for 8 months.
The staff at Hackensack Meridian Health, a pediatric long COVID clinic in New Jersey, has been working with area schools to help teachers and school nurses recognize possible long COVID in children and young people. The clinic is one of about a dozen in the United States that specializes in pediatric cases.
Katherine Clouser, MD, a pediatric hospital medicine specialist, has been with the clinic since it opened in 2021, and she’s seen a steady flow of patients. Some get better, but she sees a few new cases each week.
“We are seeing children who are having a difficult time returning to school and sports,” she said.
The clinic is having success with a mix of approaches, including intensive rehabilitation, talk therapy, and some off-label use of nirmatrelvir (Paxlovid), an antiviral now being studied as a treatment for long COVID through a National Institutes of Health clinical trials initiative that was announced last month.
Treatment depends on symptoms and is determined on a case-by-case basis, Dr. Clouser said.
Families of her patients are grateful, she added.
“We hear a lot of parents who were desperate for someone to believe them – or someone who knows about it,” she said.
A recent review of more than 30 studies with about 15,000 participants concluded that 16.2% (95% confidence interval, 8.5%-28.6%) of the pediatric participants experienced one or more persistent symptoms of long COVID at least 3 months after acute infection.
Estimates of the number of children and youth with long COVID have varied widely. A 2022 study put the number at more than 25% of cases, but the American Academy of Pediatrics notes that estimates of the percentage of children infected with SARS-CoV-2 who go on to have long COVID range from 2% to 66%.
The federal Recover Initiative has enrolled more than 10,000 children and youth – a number it plans to double – and studies of electronic health records are underway. The Recover pediatric team is also setting up a cohort that they plan to follow into 2025.
Some clinics are having luck treating young people with approaches ranging from special diets to off-label medication.
David W. Miller, MD, who runs the long COVID clinic at the UH Rainbow Babies and Children’s Hospital, Cleveland, said he’s seen about 250 patients.
A warning sign of long COVID in children is profound fatigue, he said.
“It’s the most common symptom,” Dr. Miller said. “They feel like they have the flu all the time.”
Many also experience orthostatic hypotension on standing, triggering dizziness.
He said his team targets symptom groups. Initial management consists of a diet without sugar or refined carbohydrates. Skipping pasta and sweets can be hard for young people, but Dr. Miller said sometimes the diet alone helps.
Many have vitamin D and iron deficiencies. Others need help getting a good night’s sleep. He’s treated 50 with off-label low-dose naltrexone.
Some people with long COVID – both young and old – complain about being misdiagnosed as having depression. Dr. Miller says he see a lot of anxiety – some situational and some biochemical – in pediatric patients. But he cautions doctors not to treat their illness solely as a mental health problem.
His advice: If a young person or child experiences a major change in his or her regular level of functioning or has multiple COVID symptoms that don’t go away after several months, parents and doctors should consider long COVID as a possible cause.
Dr. Miller said most of his patients get better over time with some treatments: “We see improvement in the majority of kids who can stick to the regimen,” such as a sugar-free diet, supplements, and adequate sleep. Recovery has been slow and incomplete for Diane Sheehan and her son. She was training as a permanent make-up artist, she said, but now has hand tremors that make work impossible.
She has found doctors who treat some of her symptoms with antihistamines, and her son has benefited from physical therapy.
But for now, her son is passing on a scholarship he was awarded to attend North Carolina State University this year. Instead, he’s living at home and going to a local college.
Ms. Sheehan urges parents to be on the alert for signs that their children might have long COVID, which can be confused with many other conditions.
A version of this article first appeared on Medscape.com.
Long COVID most often strikes seniors and adults, but children are also affected, even though they get less attention, new research shows.
Experts noted that the disease poses particular challenges for children and the doctors who treat them.
Parents and doctors need to be on the lookout for symptoms of long COVID in children and teens that might be easily missed or misdiagnosed, according to physicians and family groups.
Children are at lower risk for contracting COVID and often experience milder symptoms. But the virus is now widespread, and a recent study found that around 16% of pediatric patients with COVID go on to develop symptoms that last more than 3 months – the working definition of long COVID.
Parents and doctors are calling for more studies and more awareness.
Diane Sheehan, who lives outside Charlotte, N.C., says she was an active person and is now permanently disabled from long COVID. Her teenage son has it too and is still recovering.
He contracted COVID after a school event, she said. He had a mild case, but then he started experiencing dizziness and would even experience loss of consciousness when he stood up suddenly. After he contracted the virus a second time, he was bedridden for 8 months.
The staff at Hackensack Meridian Health, a pediatric long COVID clinic in New Jersey, has been working with area schools to help teachers and school nurses recognize possible long COVID in children and young people. The clinic is one of about a dozen in the United States that specializes in pediatric cases.
Katherine Clouser, MD, a pediatric hospital medicine specialist, has been with the clinic since it opened in 2021, and she’s seen a steady flow of patients. Some get better, but she sees a few new cases each week.
“We are seeing children who are having a difficult time returning to school and sports,” she said.
The clinic is having success with a mix of approaches, including intensive rehabilitation, talk therapy, and some off-label use of nirmatrelvir (Paxlovid), an antiviral now being studied as a treatment for long COVID through a National Institutes of Health clinical trials initiative that was announced last month.
Treatment depends on symptoms and is determined on a case-by-case basis, Dr. Clouser said.
Families of her patients are grateful, she added.
“We hear a lot of parents who were desperate for someone to believe them – or someone who knows about it,” she said.
A recent review of more than 30 studies with about 15,000 participants concluded that 16.2% (95% confidence interval, 8.5%-28.6%) of the pediatric participants experienced one or more persistent symptoms of long COVID at least 3 months after acute infection.
Estimates of the number of children and youth with long COVID have varied widely. A 2022 study put the number at more than 25% of cases, but the American Academy of Pediatrics notes that estimates of the percentage of children infected with SARS-CoV-2 who go on to have long COVID range from 2% to 66%.
The federal Recover Initiative has enrolled more than 10,000 children and youth – a number it plans to double – and studies of electronic health records are underway. The Recover pediatric team is also setting up a cohort that they plan to follow into 2025.
Some clinics are having luck treating young people with approaches ranging from special diets to off-label medication.
David W. Miller, MD, who runs the long COVID clinic at the UH Rainbow Babies and Children’s Hospital, Cleveland, said he’s seen about 250 patients.
A warning sign of long COVID in children is profound fatigue, he said.
“It’s the most common symptom,” Dr. Miller said. “They feel like they have the flu all the time.”
Many also experience orthostatic hypotension on standing, triggering dizziness.
He said his team targets symptom groups. Initial management consists of a diet without sugar or refined carbohydrates. Skipping pasta and sweets can be hard for young people, but Dr. Miller said sometimes the diet alone helps.
Many have vitamin D and iron deficiencies. Others need help getting a good night’s sleep. He’s treated 50 with off-label low-dose naltrexone.
Some people with long COVID – both young and old – complain about being misdiagnosed as having depression. Dr. Miller says he see a lot of anxiety – some situational and some biochemical – in pediatric patients. But he cautions doctors not to treat their illness solely as a mental health problem.
His advice: If a young person or child experiences a major change in his or her regular level of functioning or has multiple COVID symptoms that don’t go away after several months, parents and doctors should consider long COVID as a possible cause.
Dr. Miller said most of his patients get better over time with some treatments: “We see improvement in the majority of kids who can stick to the regimen,” such as a sugar-free diet, supplements, and adequate sleep. Recovery has been slow and incomplete for Diane Sheehan and her son. She was training as a permanent make-up artist, she said, but now has hand tremors that make work impossible.
She has found doctors who treat some of her symptoms with antihistamines, and her son has benefited from physical therapy.
But for now, her son is passing on a scholarship he was awarded to attend North Carolina State University this year. Instead, he’s living at home and going to a local college.
Ms. Sheehan urges parents to be on the alert for signs that their children might have long COVID, which can be confused with many other conditions.
A version of this article first appeared on Medscape.com.
Long COVID–induced activity limitations persist
Approximately one-quarter of adults who experience long COVID report activity limitations that do not change over time, based on data from national sample of nonhospitalized individuals.
Symptoms of long COVID, an ongoing medical condition that occurs in the wake of COVID-19 infection, include respiratory, neurologic, cardiovascular, or other complications that may last for weeks, months, or years after infection.
Current estimates of the incidence of long COVID in the United States range from 7.5% to 41%, according to Nicole D. Ford, PhD, of the Centers for Disease Control and Prevention, Atlanta, and colleagues. Long COVID has shown a significant effect on patients’ quality of life, functional status, and ability to work, but the impact on activity limitation in particular has not been examined, the researchers said.
In a study published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report (MMWR), the researchers reviewed data from surveys conducted between June 1 and 13, 2022, and June 7 and 19, 2023. The data came from the Census Bureau’s Household Pulse Survey (HPS), a cross-sectional national survey designed to measure the social and economic effects of COVID-19 on U.S. households. Surveys were conducted in 2-week cycles (2 weeks on, 2 weeks off). Questions about long COVID were added to the survey beginning on June 1, 2022, and questions about activity limitations from long COVID were added on Sept. 14, 2022, including questions about participants’ abilities to perform daily activities before and after COVID-19 infection.
Overall, the prevalence of long COVID decreased from 7.5% to 6.0% in U.S. adults aged 18 years and older during the study period. However, when stratified by age group, the decline was significant only in adults older than 60 years, and 1 in 10 adults with a history of COVID-19 reported long COVID at the end of the study period.
Among respondents with long COVID, 26.4% of respondents for time period of June 7-19, 2023, reported significant activity limitations, which remained unchanged over time, with no clear pattern in activity limitations across age groups, the researchers said.
Prevalence of long COVID was highest for individuals in middle adulthood (aged 30-39 years, 40-49 years, and 50-59 years) and lowest for younger adults (18-29 years) and older adults (aged 60 years and older). The prevalence of long COVID decreased by 1.16% per survey cycle between the June 1-13 and Jan. 4-16 cycles, but then remained stable, with a decrease of 0.01% per cycle between June 1-13, 2022, and Jan. 4-16, 2023.
Previous studies have shown that activity limitations resulting from long COVID can significantly affect quality of life and functional status, as well as the ability to work or care for others. A recent study in the United Kingdom showed that quality of life scores among long COVID patients were similar to those of individuals with advanced cancer, and more than half of the long COVID patients reported moderately severe functional impairment. “The larger economic and societal impact of long COVID could be far-reaching if working-age adults are unable to maintain employment or care for children or aging parents,” the researchers said.
The current study findings were limited by several factors including potential coverage bias in the survey sample, the relatively low survey response rate, and the inability to collect data on duration of symptoms, COVID-19 vaccination status, treatment during acute infection, and time since COVID-19 illness; any of these factors could affect the reported prevalence of long COVID, the researchers noted.
However, the results suggest the need for continued attention to COVID-19 prevention efforts, including not only staying current with recommended COVID-19 vaccination, but also planning for symptom management and health care service needs of long COVID patients, they concluded.
More data are needed to tease out patterns
“Physicians and patients are still trying to understand long COVID and its implications for the health of affected individuals,” said Noel Deep, MD, in an interview.
The current study shows a prevalence of long COVID in approximately 11% of COVID patients, which is a significant number, said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The study also was useful to illustrate a decline in the incidence of people affected by long COVID symptoms in the United States and in other countries, he said.
Dr. Deep noted that despite the persistent prevalence of long COVID symptoms overall, he was encouraged by the findings that older adults “who tend to have other underlying health conditions that could put them at a higher risk for adverse health outcomes” reported fewer long COVID symptoms than younger adults.
However, he noted that the high incidence of long COVID symptoms in able-bodied individuals in their 30s and 40s may affect their the economic situations as well as their ability to care for elderly relatives and children who might be dependent on them.
“Physicians and other clinicians should be aware of the symptoms and impacts caused by long COVID,” Dr. Deep said in an interview. “These individuals usually present with a myriad of vague and varying symptoms. Physicians should be cognizant of this situation, ask about previous infection with COVID-19, and utilize the resources of long COVID clinics where available,” he said.
Several factors can affect the assessment and management of patients with long COVID symptoms in primary care practices, said Dr. Deep. First and foremost are the time constraints of detailed evaluation and testing, he said.
Second, primary care clinicians need to be aware of the different symptoms that may be indicative of long COVID including fatigue, neurocognitive symptoms such as brain fog or memory disturbance, respiratory symptoms, and cardiovascular symptoms, as well as olfactory and gustatory symptoms. “These symptoms can be confounded by underlying health conditions, especially in elderly individuals,” he noted.
“Recommendations and guidelines are evolving regarding the evaluation and management of patients with long COVID that should help physicians and other clinicians in the future,” said Dr. Deep.
In the meantime, having a high index of suspicion, paying attention to the symptoms described by the patient, and taking a proper history with regard to previous COVID-19 infection should help overcome some of these challenges, he said.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the Editorial Advisory Board of Internal Medicine News.
Approximately one-quarter of adults who experience long COVID report activity limitations that do not change over time, based on data from national sample of nonhospitalized individuals.
Symptoms of long COVID, an ongoing medical condition that occurs in the wake of COVID-19 infection, include respiratory, neurologic, cardiovascular, or other complications that may last for weeks, months, or years after infection.
Current estimates of the incidence of long COVID in the United States range from 7.5% to 41%, according to Nicole D. Ford, PhD, of the Centers for Disease Control and Prevention, Atlanta, and colleagues. Long COVID has shown a significant effect on patients’ quality of life, functional status, and ability to work, but the impact on activity limitation in particular has not been examined, the researchers said.
In a study published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report (MMWR), the researchers reviewed data from surveys conducted between June 1 and 13, 2022, and June 7 and 19, 2023. The data came from the Census Bureau’s Household Pulse Survey (HPS), a cross-sectional national survey designed to measure the social and economic effects of COVID-19 on U.S. households. Surveys were conducted in 2-week cycles (2 weeks on, 2 weeks off). Questions about long COVID were added to the survey beginning on June 1, 2022, and questions about activity limitations from long COVID were added on Sept. 14, 2022, including questions about participants’ abilities to perform daily activities before and after COVID-19 infection.
Overall, the prevalence of long COVID decreased from 7.5% to 6.0% in U.S. adults aged 18 years and older during the study period. However, when stratified by age group, the decline was significant only in adults older than 60 years, and 1 in 10 adults with a history of COVID-19 reported long COVID at the end of the study period.
Among respondents with long COVID, 26.4% of respondents for time period of June 7-19, 2023, reported significant activity limitations, which remained unchanged over time, with no clear pattern in activity limitations across age groups, the researchers said.
Prevalence of long COVID was highest for individuals in middle adulthood (aged 30-39 years, 40-49 years, and 50-59 years) and lowest for younger adults (18-29 years) and older adults (aged 60 years and older). The prevalence of long COVID decreased by 1.16% per survey cycle between the June 1-13 and Jan. 4-16 cycles, but then remained stable, with a decrease of 0.01% per cycle between June 1-13, 2022, and Jan. 4-16, 2023.
Previous studies have shown that activity limitations resulting from long COVID can significantly affect quality of life and functional status, as well as the ability to work or care for others. A recent study in the United Kingdom showed that quality of life scores among long COVID patients were similar to those of individuals with advanced cancer, and more than half of the long COVID patients reported moderately severe functional impairment. “The larger economic and societal impact of long COVID could be far-reaching if working-age adults are unable to maintain employment or care for children or aging parents,” the researchers said.
The current study findings were limited by several factors including potential coverage bias in the survey sample, the relatively low survey response rate, and the inability to collect data on duration of symptoms, COVID-19 vaccination status, treatment during acute infection, and time since COVID-19 illness; any of these factors could affect the reported prevalence of long COVID, the researchers noted.
However, the results suggest the need for continued attention to COVID-19 prevention efforts, including not only staying current with recommended COVID-19 vaccination, but also planning for symptom management and health care service needs of long COVID patients, they concluded.
More data are needed to tease out patterns
“Physicians and patients are still trying to understand long COVID and its implications for the health of affected individuals,” said Noel Deep, MD, in an interview.
The current study shows a prevalence of long COVID in approximately 11% of COVID patients, which is a significant number, said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The study also was useful to illustrate a decline in the incidence of people affected by long COVID symptoms in the United States and in other countries, he said.
Dr. Deep noted that despite the persistent prevalence of long COVID symptoms overall, he was encouraged by the findings that older adults “who tend to have other underlying health conditions that could put them at a higher risk for adverse health outcomes” reported fewer long COVID symptoms than younger adults.
However, he noted that the high incidence of long COVID symptoms in able-bodied individuals in their 30s and 40s may affect their the economic situations as well as their ability to care for elderly relatives and children who might be dependent on them.
“Physicians and other clinicians should be aware of the symptoms and impacts caused by long COVID,” Dr. Deep said in an interview. “These individuals usually present with a myriad of vague and varying symptoms. Physicians should be cognizant of this situation, ask about previous infection with COVID-19, and utilize the resources of long COVID clinics where available,” he said.
Several factors can affect the assessment and management of patients with long COVID symptoms in primary care practices, said Dr. Deep. First and foremost are the time constraints of detailed evaluation and testing, he said.
Second, primary care clinicians need to be aware of the different symptoms that may be indicative of long COVID including fatigue, neurocognitive symptoms such as brain fog or memory disturbance, respiratory symptoms, and cardiovascular symptoms, as well as olfactory and gustatory symptoms. “These symptoms can be confounded by underlying health conditions, especially in elderly individuals,” he noted.
“Recommendations and guidelines are evolving regarding the evaluation and management of patients with long COVID that should help physicians and other clinicians in the future,” said Dr. Deep.
In the meantime, having a high index of suspicion, paying attention to the symptoms described by the patient, and taking a proper history with regard to previous COVID-19 infection should help overcome some of these challenges, he said.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the Editorial Advisory Board of Internal Medicine News.
Approximately one-quarter of adults who experience long COVID report activity limitations that do not change over time, based on data from national sample of nonhospitalized individuals.
Symptoms of long COVID, an ongoing medical condition that occurs in the wake of COVID-19 infection, include respiratory, neurologic, cardiovascular, or other complications that may last for weeks, months, or years after infection.
Current estimates of the incidence of long COVID in the United States range from 7.5% to 41%, according to Nicole D. Ford, PhD, of the Centers for Disease Control and Prevention, Atlanta, and colleagues. Long COVID has shown a significant effect on patients’ quality of life, functional status, and ability to work, but the impact on activity limitation in particular has not been examined, the researchers said.
In a study published in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report (MMWR), the researchers reviewed data from surveys conducted between June 1 and 13, 2022, and June 7 and 19, 2023. The data came from the Census Bureau’s Household Pulse Survey (HPS), a cross-sectional national survey designed to measure the social and economic effects of COVID-19 on U.S. households. Surveys were conducted in 2-week cycles (2 weeks on, 2 weeks off). Questions about long COVID were added to the survey beginning on June 1, 2022, and questions about activity limitations from long COVID were added on Sept. 14, 2022, including questions about participants’ abilities to perform daily activities before and after COVID-19 infection.
Overall, the prevalence of long COVID decreased from 7.5% to 6.0% in U.S. adults aged 18 years and older during the study period. However, when stratified by age group, the decline was significant only in adults older than 60 years, and 1 in 10 adults with a history of COVID-19 reported long COVID at the end of the study period.
Among respondents with long COVID, 26.4% of respondents for time period of June 7-19, 2023, reported significant activity limitations, which remained unchanged over time, with no clear pattern in activity limitations across age groups, the researchers said.
Prevalence of long COVID was highest for individuals in middle adulthood (aged 30-39 years, 40-49 years, and 50-59 years) and lowest for younger adults (18-29 years) and older adults (aged 60 years and older). The prevalence of long COVID decreased by 1.16% per survey cycle between the June 1-13 and Jan. 4-16 cycles, but then remained stable, with a decrease of 0.01% per cycle between June 1-13, 2022, and Jan. 4-16, 2023.
Previous studies have shown that activity limitations resulting from long COVID can significantly affect quality of life and functional status, as well as the ability to work or care for others. A recent study in the United Kingdom showed that quality of life scores among long COVID patients were similar to those of individuals with advanced cancer, and more than half of the long COVID patients reported moderately severe functional impairment. “The larger economic and societal impact of long COVID could be far-reaching if working-age adults are unable to maintain employment or care for children or aging parents,” the researchers said.
The current study findings were limited by several factors including potential coverage bias in the survey sample, the relatively low survey response rate, and the inability to collect data on duration of symptoms, COVID-19 vaccination status, treatment during acute infection, and time since COVID-19 illness; any of these factors could affect the reported prevalence of long COVID, the researchers noted.
However, the results suggest the need for continued attention to COVID-19 prevention efforts, including not only staying current with recommended COVID-19 vaccination, but also planning for symptom management and health care service needs of long COVID patients, they concluded.
More data are needed to tease out patterns
“Physicians and patients are still trying to understand long COVID and its implications for the health of affected individuals,” said Noel Deep, MD, in an interview.
The current study shows a prevalence of long COVID in approximately 11% of COVID patients, which is a significant number, said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep also serves as chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
The study also was useful to illustrate a decline in the incidence of people affected by long COVID symptoms in the United States and in other countries, he said.
Dr. Deep noted that despite the persistent prevalence of long COVID symptoms overall, he was encouraged by the findings that older adults “who tend to have other underlying health conditions that could put them at a higher risk for adverse health outcomes” reported fewer long COVID symptoms than younger adults.
However, he noted that the high incidence of long COVID symptoms in able-bodied individuals in their 30s and 40s may affect their the economic situations as well as their ability to care for elderly relatives and children who might be dependent on them.
“Physicians and other clinicians should be aware of the symptoms and impacts caused by long COVID,” Dr. Deep said in an interview. “These individuals usually present with a myriad of vague and varying symptoms. Physicians should be cognizant of this situation, ask about previous infection with COVID-19, and utilize the resources of long COVID clinics where available,” he said.
Several factors can affect the assessment and management of patients with long COVID symptoms in primary care practices, said Dr. Deep. First and foremost are the time constraints of detailed evaluation and testing, he said.
Second, primary care clinicians need to be aware of the different symptoms that may be indicative of long COVID including fatigue, neurocognitive symptoms such as brain fog or memory disturbance, respiratory symptoms, and cardiovascular symptoms, as well as olfactory and gustatory symptoms. “These symptoms can be confounded by underlying health conditions, especially in elderly individuals,” he noted.
“Recommendations and guidelines are evolving regarding the evaluation and management of patients with long COVID that should help physicians and other clinicians in the future,” said Dr. Deep.
In the meantime, having a high index of suspicion, paying attention to the symptoms described by the patient, and taking a proper history with regard to previous COVID-19 infection should help overcome some of these challenges, he said.
The study received no outside funding. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the Editorial Advisory Board of Internal Medicine News.
FROM MMWR
It may be time to pay attention to COVID again
More than 3 years into the COVID-19 era, most Americans have settled back into their prepandemic lifestyles.
Since April, a new COVID variant has cropped up. According to recent Centers for Disease Control and Prevention data, EG.5 – from the Omicron family – now makes up 17% of all cases in the United States, up from 7.5% in the first week of July.
A summary from the Center for Infectious Disease Research and Policy at the University of Minnesota says that EG.5, nicknamed “Eris” by health trackers, is nearly the same as its parent strain, XBB.1.9.2, but has one extra spike mutation.
Along with the news of EG.5’s growing prevalence, COVID-related hospitalization rates have increased by 12.5% during the week ending on July 29 – the most significant uptick since December. Still, no connection has been made between the new variant and rising hospital admissions. And so far, experts have found no difference in the severity of illness or symptoms between Eris and the strains that came before it.
Cause for concern?
The COVID virus has a great tendency to mutate, said William Schaffner, MD, a professor of infectious diseases at Vanderbilt University, Nashville, Tenn.
“Fortunately, these are relatively minor mutations.” Even so, SARS-CoV-2, the virus that causes COVID-19, continues to be highly contagious. “There isn’t any doubt that it’s spreading – but it’s not more serious.”
So, Dr. Schaffner doesn’t think it’s time to panic. He prefers calling it an “uptick” in cases instead of a “surge,” because a surge “sounds too big.”
While the numbers are still low, compared with 2022’s summer surge, experts still urge people to stay aware of changes in the virus. “I do not think that there is any cause for alarm,” agreed Bernard Camins, MD, an infectious disease specialist at Mount Sinai Hospital, New York.
So why the higher number of cases? “There has been an increase in COVID cases this summer, probably related to travel, socializing, and dwindling masking,” said Anne Liu, MD, an allergy, immunology, and infectious disease specialist at Stanford (Calif.) University. Even so, “because of an existing level of immunity from vaccination and prior infections, it has been limited and case severity has been lower than in prior surges.”
What the official numbers say
The CDC no longer updates its COVID Data Tracker Weekly Review. They stopped in May 2023 when the federal public health emergency ended.
But the agency continues to track COVID-19 cases, hospitalizations, ED visits, and deaths in different ways. The key takeaways include 9,056 new hospitalizations reported for the week ending July 29, 2023. That is relatively low, compared with July 30, 2022, when the weekly new hospitalization numbers topped 44,000.
“Last year, we saw a summer wave with cases peaking around mid-July. In that sense, our summer wave is coming a bit later than last year,” said Pavitra Roychoudhury, PhD, an assistant professor and researcher in the vaccine and infectious disease division at the University of Washington, Seattle.
“It’s unclear how high the peak will be during this current wave. Levels of SARS-CoV-2 in wastewater, as well as the number of hospitalizations, are currently lower than this time last year.”
For part of the pandemic, the CDC recommended people monitor COVID numbers in their own communities. But the agency’s local guidance on COVID is tied to hospital admission levels, which are currently low for more than 99% of the country, even if they are increasing.
So, while it’s good news that hospitalization numbers are smaller, it means the agency’s ability to identify local outbreaks or hot spots of SARS-CoV-2 is now more limited.
It’s not just an uptick in hospitalizations nationwide, as other COVID-19 indicators, including ED visits, positive tests, and wastewater levels, are increasing across the United States.
In terms of other metrics:
- On June 19, 0.47% of ED visits resulted in a positive COVID diagnosis. On Aug. 4, that rate had more than doubled to 1.1%.
- On July 29, 8.9% of people who took a COVID test reported a positive result. The positivity rate has been increasing since June 10, when 4.1% of tests came back positive. This figure only includes test results reported to the CDC. Results of home testing remain largely unknown.
- The weekly percentage of deaths related to COVID-19 was 1% as of July 29. That’s low, compared with previous rates. For example, for the week ending July 30, 2022, it was 5.8%.
What about new COVID vaccines?
As long as the general public continue to make informed decisions and get the new Omicron vaccine or booster once it’s available, experts predict lower hospitalization rates this winter.
“Everyone should get the Omicron booster when it becomes available,” recommended Dean Winslow, MD, a professor of medicine at Stanford University.
In the meantime, “it is important to emphasize that COVID-19 is going to be with us for the foreseeable future,” he said. Since the symptoms linked to these newer Omicron subvariants are generally milder than with earlier variants, “if one has even mild cold symptoms, it is a good idea to test yourself for COVID-19 and start treatment early if one is elderly or otherwise at high risk for severe disease.”
Dr. Schaffner remains optimistic for now. “We anticipate that the vaccines we currently have available, and certainly the vaccine that is being developed for this fall, will continue to prevent severe disease associated with this virus.”
Although it’s difficult to predict an exact time line, Dr. Schaffner said they could be available by the end of September.
His predictions assume “that we don’t have a new nasty variant that crops up somewhere in the world,” he said. “[If] things continue to move the way they have been, we anticipate that this vaccine ... will be really effective and help us keep out of the hospital during this winter, when we expect more of an increase of COVID once again.”
Asked for his outlook on vaccine recommendations, Dr. Camins was less certain. “It is too soon to tell.” Guidance on COVID shots will be based on results of ongoing studies. “It would be prudent, however, for everyone to plan on getting the flu shot in September.”
Stay alert and stay realistic
Cautious optimism and a call to remain vigilant seem like the consensus at the moment. While the numbers remain low so far and the uptick in new cases and hospitalizations are relatively small, compared with past scenarios, “it makes sense to boost our anti-Omicron antibody levels with immunizations before fall and winter,” Dr. Liu said.
“It’s just advisable for everyone – especially those who are at higher risk for hospitalization or death – to be aware,” Dr. Camins said, “so they can form their own decisions to participate in activities that may put them at risk for contracting COVID-19.”
While respiratory virus work best at keeping people with the flu, COVID, or RSV out of the hospital, they’re not as good at preventing milder infections. Dr. Schaffner said: “If we don’t expect perfection, we won’t be so disappointed.”
A version of this article first appeared on WebMD.com.
More than 3 years into the COVID-19 era, most Americans have settled back into their prepandemic lifestyles.
Since April, a new COVID variant has cropped up. According to recent Centers for Disease Control and Prevention data, EG.5 – from the Omicron family – now makes up 17% of all cases in the United States, up from 7.5% in the first week of July.
A summary from the Center for Infectious Disease Research and Policy at the University of Minnesota says that EG.5, nicknamed “Eris” by health trackers, is nearly the same as its parent strain, XBB.1.9.2, but has one extra spike mutation.
Along with the news of EG.5’s growing prevalence, COVID-related hospitalization rates have increased by 12.5% during the week ending on July 29 – the most significant uptick since December. Still, no connection has been made between the new variant and rising hospital admissions. And so far, experts have found no difference in the severity of illness or symptoms between Eris and the strains that came before it.
Cause for concern?
The COVID virus has a great tendency to mutate, said William Schaffner, MD, a professor of infectious diseases at Vanderbilt University, Nashville, Tenn.
“Fortunately, these are relatively minor mutations.” Even so, SARS-CoV-2, the virus that causes COVID-19, continues to be highly contagious. “There isn’t any doubt that it’s spreading – but it’s not more serious.”
So, Dr. Schaffner doesn’t think it’s time to panic. He prefers calling it an “uptick” in cases instead of a “surge,” because a surge “sounds too big.”
While the numbers are still low, compared with 2022’s summer surge, experts still urge people to stay aware of changes in the virus. “I do not think that there is any cause for alarm,” agreed Bernard Camins, MD, an infectious disease specialist at Mount Sinai Hospital, New York.
So why the higher number of cases? “There has been an increase in COVID cases this summer, probably related to travel, socializing, and dwindling masking,” said Anne Liu, MD, an allergy, immunology, and infectious disease specialist at Stanford (Calif.) University. Even so, “because of an existing level of immunity from vaccination and prior infections, it has been limited and case severity has been lower than in prior surges.”
What the official numbers say
The CDC no longer updates its COVID Data Tracker Weekly Review. They stopped in May 2023 when the federal public health emergency ended.
But the agency continues to track COVID-19 cases, hospitalizations, ED visits, and deaths in different ways. The key takeaways include 9,056 new hospitalizations reported for the week ending July 29, 2023. That is relatively low, compared with July 30, 2022, when the weekly new hospitalization numbers topped 44,000.
“Last year, we saw a summer wave with cases peaking around mid-July. In that sense, our summer wave is coming a bit later than last year,” said Pavitra Roychoudhury, PhD, an assistant professor and researcher in the vaccine and infectious disease division at the University of Washington, Seattle.
“It’s unclear how high the peak will be during this current wave. Levels of SARS-CoV-2 in wastewater, as well as the number of hospitalizations, are currently lower than this time last year.”
For part of the pandemic, the CDC recommended people monitor COVID numbers in their own communities. But the agency’s local guidance on COVID is tied to hospital admission levels, which are currently low for more than 99% of the country, even if they are increasing.
So, while it’s good news that hospitalization numbers are smaller, it means the agency’s ability to identify local outbreaks or hot spots of SARS-CoV-2 is now more limited.
It’s not just an uptick in hospitalizations nationwide, as other COVID-19 indicators, including ED visits, positive tests, and wastewater levels, are increasing across the United States.
In terms of other metrics:
- On June 19, 0.47% of ED visits resulted in a positive COVID diagnosis. On Aug. 4, that rate had more than doubled to 1.1%.
- On July 29, 8.9% of people who took a COVID test reported a positive result. The positivity rate has been increasing since June 10, when 4.1% of tests came back positive. This figure only includes test results reported to the CDC. Results of home testing remain largely unknown.
- The weekly percentage of deaths related to COVID-19 was 1% as of July 29. That’s low, compared with previous rates. For example, for the week ending July 30, 2022, it was 5.8%.
What about new COVID vaccines?
As long as the general public continue to make informed decisions and get the new Omicron vaccine or booster once it’s available, experts predict lower hospitalization rates this winter.
“Everyone should get the Omicron booster when it becomes available,” recommended Dean Winslow, MD, a professor of medicine at Stanford University.
In the meantime, “it is important to emphasize that COVID-19 is going to be with us for the foreseeable future,” he said. Since the symptoms linked to these newer Omicron subvariants are generally milder than with earlier variants, “if one has even mild cold symptoms, it is a good idea to test yourself for COVID-19 and start treatment early if one is elderly or otherwise at high risk for severe disease.”
Dr. Schaffner remains optimistic for now. “We anticipate that the vaccines we currently have available, and certainly the vaccine that is being developed for this fall, will continue to prevent severe disease associated with this virus.”
Although it’s difficult to predict an exact time line, Dr. Schaffner said they could be available by the end of September.
His predictions assume “that we don’t have a new nasty variant that crops up somewhere in the world,” he said. “[If] things continue to move the way they have been, we anticipate that this vaccine ... will be really effective and help us keep out of the hospital during this winter, when we expect more of an increase of COVID once again.”
Asked for his outlook on vaccine recommendations, Dr. Camins was less certain. “It is too soon to tell.” Guidance on COVID shots will be based on results of ongoing studies. “It would be prudent, however, for everyone to plan on getting the flu shot in September.”
Stay alert and stay realistic
Cautious optimism and a call to remain vigilant seem like the consensus at the moment. While the numbers remain low so far and the uptick in new cases and hospitalizations are relatively small, compared with past scenarios, “it makes sense to boost our anti-Omicron antibody levels with immunizations before fall and winter,” Dr. Liu said.
“It’s just advisable for everyone – especially those who are at higher risk for hospitalization or death – to be aware,” Dr. Camins said, “so they can form their own decisions to participate in activities that may put them at risk for contracting COVID-19.”
While respiratory virus work best at keeping people with the flu, COVID, or RSV out of the hospital, they’re not as good at preventing milder infections. Dr. Schaffner said: “If we don’t expect perfection, we won’t be so disappointed.”
A version of this article first appeared on WebMD.com.
More than 3 years into the COVID-19 era, most Americans have settled back into their prepandemic lifestyles.
Since April, a new COVID variant has cropped up. According to recent Centers for Disease Control and Prevention data, EG.5 – from the Omicron family – now makes up 17% of all cases in the United States, up from 7.5% in the first week of July.
A summary from the Center for Infectious Disease Research and Policy at the University of Minnesota says that EG.5, nicknamed “Eris” by health trackers, is nearly the same as its parent strain, XBB.1.9.2, but has one extra spike mutation.
Along with the news of EG.5’s growing prevalence, COVID-related hospitalization rates have increased by 12.5% during the week ending on July 29 – the most significant uptick since December. Still, no connection has been made between the new variant and rising hospital admissions. And so far, experts have found no difference in the severity of illness or symptoms between Eris and the strains that came before it.
Cause for concern?
The COVID virus has a great tendency to mutate, said William Schaffner, MD, a professor of infectious diseases at Vanderbilt University, Nashville, Tenn.
“Fortunately, these are relatively minor mutations.” Even so, SARS-CoV-2, the virus that causes COVID-19, continues to be highly contagious. “There isn’t any doubt that it’s spreading – but it’s not more serious.”
So, Dr. Schaffner doesn’t think it’s time to panic. He prefers calling it an “uptick” in cases instead of a “surge,” because a surge “sounds too big.”
While the numbers are still low, compared with 2022’s summer surge, experts still urge people to stay aware of changes in the virus. “I do not think that there is any cause for alarm,” agreed Bernard Camins, MD, an infectious disease specialist at Mount Sinai Hospital, New York.
So why the higher number of cases? “There has been an increase in COVID cases this summer, probably related to travel, socializing, and dwindling masking,” said Anne Liu, MD, an allergy, immunology, and infectious disease specialist at Stanford (Calif.) University. Even so, “because of an existing level of immunity from vaccination and prior infections, it has been limited and case severity has been lower than in prior surges.”
What the official numbers say
The CDC no longer updates its COVID Data Tracker Weekly Review. They stopped in May 2023 when the federal public health emergency ended.
But the agency continues to track COVID-19 cases, hospitalizations, ED visits, and deaths in different ways. The key takeaways include 9,056 new hospitalizations reported for the week ending July 29, 2023. That is relatively low, compared with July 30, 2022, when the weekly new hospitalization numbers topped 44,000.
“Last year, we saw a summer wave with cases peaking around mid-July. In that sense, our summer wave is coming a bit later than last year,” said Pavitra Roychoudhury, PhD, an assistant professor and researcher in the vaccine and infectious disease division at the University of Washington, Seattle.
“It’s unclear how high the peak will be during this current wave. Levels of SARS-CoV-2 in wastewater, as well as the number of hospitalizations, are currently lower than this time last year.”
For part of the pandemic, the CDC recommended people monitor COVID numbers in their own communities. But the agency’s local guidance on COVID is tied to hospital admission levels, which are currently low for more than 99% of the country, even if they are increasing.
So, while it’s good news that hospitalization numbers are smaller, it means the agency’s ability to identify local outbreaks or hot spots of SARS-CoV-2 is now more limited.
It’s not just an uptick in hospitalizations nationwide, as other COVID-19 indicators, including ED visits, positive tests, and wastewater levels, are increasing across the United States.
In terms of other metrics:
- On June 19, 0.47% of ED visits resulted in a positive COVID diagnosis. On Aug. 4, that rate had more than doubled to 1.1%.
- On July 29, 8.9% of people who took a COVID test reported a positive result. The positivity rate has been increasing since June 10, when 4.1% of tests came back positive. This figure only includes test results reported to the CDC. Results of home testing remain largely unknown.
- The weekly percentage of deaths related to COVID-19 was 1% as of July 29. That’s low, compared with previous rates. For example, for the week ending July 30, 2022, it was 5.8%.
What about new COVID vaccines?
As long as the general public continue to make informed decisions and get the new Omicron vaccine or booster once it’s available, experts predict lower hospitalization rates this winter.
“Everyone should get the Omicron booster when it becomes available,” recommended Dean Winslow, MD, a professor of medicine at Stanford University.
In the meantime, “it is important to emphasize that COVID-19 is going to be with us for the foreseeable future,” he said. Since the symptoms linked to these newer Omicron subvariants are generally milder than with earlier variants, “if one has even mild cold symptoms, it is a good idea to test yourself for COVID-19 and start treatment early if one is elderly or otherwise at high risk for severe disease.”
Dr. Schaffner remains optimistic for now. “We anticipate that the vaccines we currently have available, and certainly the vaccine that is being developed for this fall, will continue to prevent severe disease associated with this virus.”
Although it’s difficult to predict an exact time line, Dr. Schaffner said they could be available by the end of September.
His predictions assume “that we don’t have a new nasty variant that crops up somewhere in the world,” he said. “[If] things continue to move the way they have been, we anticipate that this vaccine ... will be really effective and help us keep out of the hospital during this winter, when we expect more of an increase of COVID once again.”
Asked for his outlook on vaccine recommendations, Dr. Camins was less certain. “It is too soon to tell.” Guidance on COVID shots will be based on results of ongoing studies. “It would be prudent, however, for everyone to plan on getting the flu shot in September.”
Stay alert and stay realistic
Cautious optimism and a call to remain vigilant seem like the consensus at the moment. While the numbers remain low so far and the uptick in new cases and hospitalizations are relatively small, compared with past scenarios, “it makes sense to boost our anti-Omicron antibody levels with immunizations before fall and winter,” Dr. Liu said.
“It’s just advisable for everyone – especially those who are at higher risk for hospitalization or death – to be aware,” Dr. Camins said, “so they can form their own decisions to participate in activities that may put them at risk for contracting COVID-19.”
While respiratory virus work best at keeping people with the flu, COVID, or RSV out of the hospital, they’re not as good at preventing milder infections. Dr. Schaffner said: “If we don’t expect perfection, we won’t be so disappointed.”
A version of this article first appeared on WebMD.com.
U.S. has new dominant COVID variant called EG.5
Called “Eris” among avid COVID trackers, the strain EG.5 now accounts for 17% of all U.S. COVID infections, according to the latest Centers for Disease Control and Prevention estimates. That’s up from 12% the week prior.
EG.5 has been rising worldwide, just weeks after the World Health Organization added the strain to its official monitoring list. In the United Kingdom, it now accounts for 1 in 10 COVID cases, The Independent reported.
EG.5 is a descendant of the XBB strains that have dominated tracking lists in recent months. It has the same makeup as XBB.1.9.2 but carries an extra spike mutation, according to a summary published by the Center for Infectious Disease Research and Policy at the University of Minnesota. The spike protein is the part of the virus that allows it to enter human cells. But there’s no indication so far that EG.5 is more contagious or severe than other recent variants, according to the CIDRAP summary and a recent podcast from the American Medical Association. The CDC said that current vaccines protect against the variant.
U.S. hospitals saw a 12% increase in COVID admissions during the week ending on July 22, with 8,047 people being admitted because of the virus, up from an all-time low of 6,306 the week of June 24. In 17 states, the past-week increase in hospitalizations was 20% or greater. In Minnesota, the rate jumped by 50%, and in West Virginia, it jumped by 63%. Meanwhile, deaths reached their lowest weekly rate ever for the week of data ending July 29, with just 176 deaths reported by the CDC.
A version of this article first appeared on WebMD.com.
Called “Eris” among avid COVID trackers, the strain EG.5 now accounts for 17% of all U.S. COVID infections, according to the latest Centers for Disease Control and Prevention estimates. That’s up from 12% the week prior.
EG.5 has been rising worldwide, just weeks after the World Health Organization added the strain to its official monitoring list. In the United Kingdom, it now accounts for 1 in 10 COVID cases, The Independent reported.
EG.5 is a descendant of the XBB strains that have dominated tracking lists in recent months. It has the same makeup as XBB.1.9.2 but carries an extra spike mutation, according to a summary published by the Center for Infectious Disease Research and Policy at the University of Minnesota. The spike protein is the part of the virus that allows it to enter human cells. But there’s no indication so far that EG.5 is more contagious or severe than other recent variants, according to the CIDRAP summary and a recent podcast from the American Medical Association. The CDC said that current vaccines protect against the variant.
U.S. hospitals saw a 12% increase in COVID admissions during the week ending on July 22, with 8,047 people being admitted because of the virus, up from an all-time low of 6,306 the week of June 24. In 17 states, the past-week increase in hospitalizations was 20% or greater. In Minnesota, the rate jumped by 50%, and in West Virginia, it jumped by 63%. Meanwhile, deaths reached their lowest weekly rate ever for the week of data ending July 29, with just 176 deaths reported by the CDC.
A version of this article first appeared on WebMD.com.
Called “Eris” among avid COVID trackers, the strain EG.5 now accounts for 17% of all U.S. COVID infections, according to the latest Centers for Disease Control and Prevention estimates. That’s up from 12% the week prior.
EG.5 has been rising worldwide, just weeks after the World Health Organization added the strain to its official monitoring list. In the United Kingdom, it now accounts for 1 in 10 COVID cases, The Independent reported.
EG.5 is a descendant of the XBB strains that have dominated tracking lists in recent months. It has the same makeup as XBB.1.9.2 but carries an extra spike mutation, according to a summary published by the Center for Infectious Disease Research and Policy at the University of Minnesota. The spike protein is the part of the virus that allows it to enter human cells. But there’s no indication so far that EG.5 is more contagious or severe than other recent variants, according to the CIDRAP summary and a recent podcast from the American Medical Association. The CDC said that current vaccines protect against the variant.
U.S. hospitals saw a 12% increase in COVID admissions during the week ending on July 22, with 8,047 people being admitted because of the virus, up from an all-time low of 6,306 the week of June 24. In 17 states, the past-week increase in hospitalizations was 20% or greater. In Minnesota, the rate jumped by 50%, and in West Virginia, it jumped by 63%. Meanwhile, deaths reached their lowest weekly rate ever for the week of data ending July 29, with just 176 deaths reported by the CDC.
A version of this article first appeared on WebMD.com.
A new and completely different pain medicine
This transcript has been edited for clarity.
When you stub your toe or get a paper cut on your finger, you feel the pain in that part of your body. It feels like the pain is coming from that place. But, of course, that’s not really what is happening. Pain doesn’t really happen in your toe or your finger. It happens in your brain.
It’s a game of telephone, really. The afferent nerve fiber detects the noxious stimulus, passing that signal to the second-order neuron in the dorsal root ganglia of the spinal cord, which runs it up to the thalamus to be passed to the third-order neuron which brings it to the cortex for localization and conscious perception. It’s not even a very good game of telephone. It takes about 100 ms for a pain signal to get from the hand to the brain – longer from the feet, given the greater distance. You see your foot hit the corner of the coffee table and have just enough time to think: “Oh no!” before the pain hits.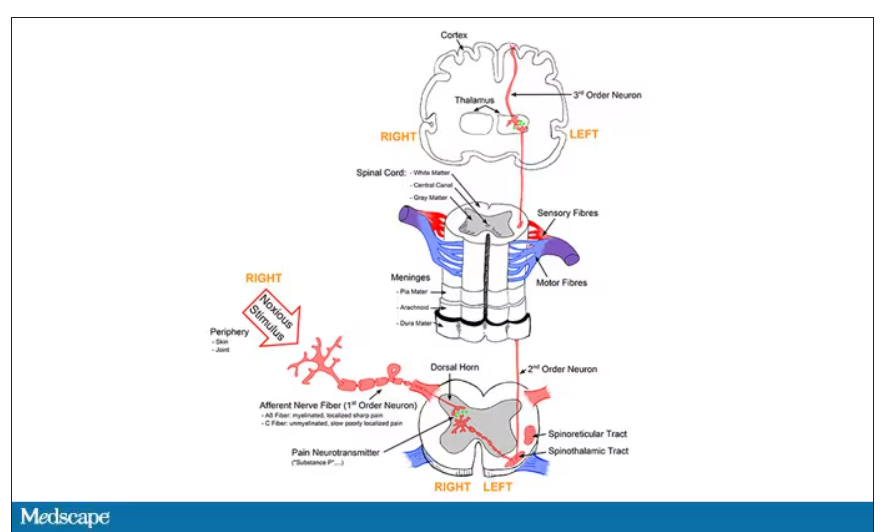
Given the Rube Goldberg nature of the process, it would seem like there are any number of places we could stop pain sensation. And sure, local anesthetics at the site of injury, or even spinal anesthetics, are powerful – if temporary and hard to administer – solutions to acute pain.
But in our everyday armamentarium, let’s be honest – we essentially have three options: opiates and opioids, which activate the mu-receptors in the brain to dull pain (and cause a host of other nasty side effects); NSAIDs, which block prostaglandin synthesis and thus limit the ability for pain-conducting neurons to get excited; and acetaminophen, which, despite being used for a century, is poorly understood.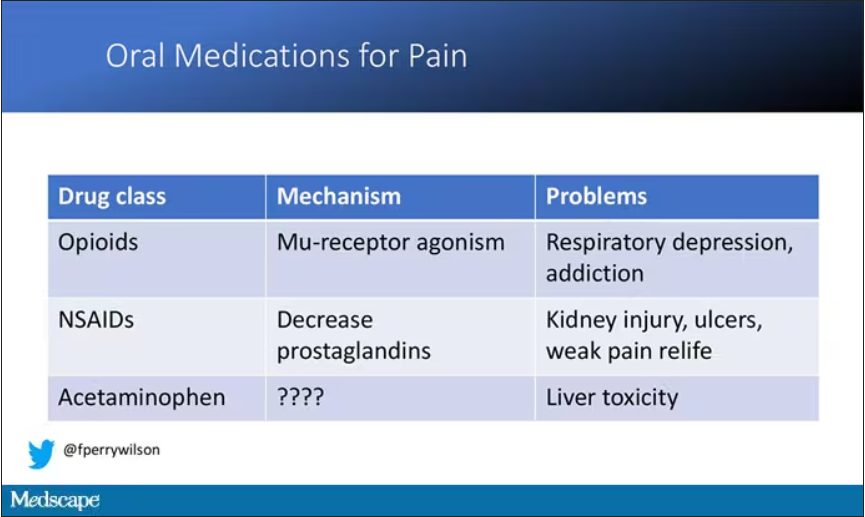
But
If you were to zoom in on the connection between that first afferent pain fiber and the secondary nerve in the spinal cord dorsal root ganglion, you would see a receptor called Nav1.8, a voltage-gated sodium channel.
This receptor is a key part of the apparatus that passes information from nerve 1 to nerve 2, but only for fibers that transmit pain signals. In fact, humans with mutations in this receptor that leave it always in the “open” state have a severe pain syndrome. Blocking the receptor, therefore, might reduce pain.
In preclinical work, researchers identified VX-548, which doesn’t have a brand name yet, as a potent blocker of that channel even in nanomolar concentrations. Importantly, the compound was highly selective for that particular channel – about 30,000 times more selective than it was for the other sodium channels in that family.
Of course, a highly selective and specific drug does not a blockbuster analgesic make. To determine how this drug would work on humans in pain, they turned to two populations: 303 individuals undergoing abdominoplasty and 274 undergoing bunionectomy, as reported in a new paper in the New England Journal of Medicine.
I know this seems a bit random, but abdominoplasty is quite painful and a good model for soft-tissue pain. Bunionectomy is also quite a painful procedure and a useful model of bone pain. After the surgeries, patients were randomized to several different doses of VX-548, hydrocodone plus acetaminophen, or placebo for 48 hours.
At 19 time points over that 48-hour period, participants were asked to rate their pain on a scale from 0 to 10. The primary outcome was the cumulative pain experienced over the 48 hours. So, higher pain would be worse here, but longer duration of pain would also be worse.
The story of the study is really told in this chart.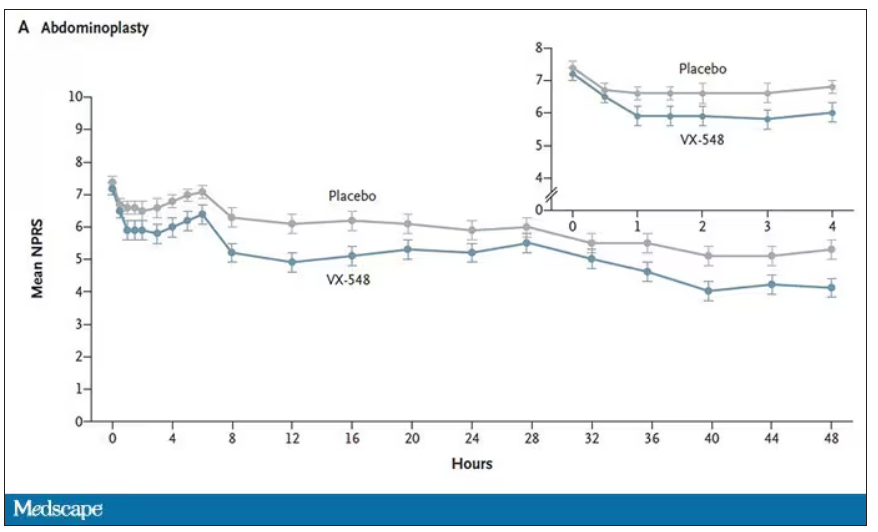
Yes, those assigned to the highest dose of VX-548 had a statistically significant lower cumulative amount of pain in the 48 hours after surgery. But the picture is really worth more than the stats here. You can see that the onset of pain relief was fairly quick, and that pain relief was sustained over time. You can also see that this is not a miracle drug. Pain scores were a bit better 48 hours out, but only by about a point and a half.
Placebo isn’t really the fair comparison here; few of us treat our postabdominoplasty patients with placebo, after all. The authors do not formally compare the effect of VX-548 with that of the opioid hydrocodone, for instance. But that doesn’t stop us.
This graph, which I put together from data in the paper, shows pain control across the four randomization categories, with higher numbers indicating more (cumulative) control. While all the active agents do a bit better than placebo, VX-548 at the higher dose appears to do the best. But I should note that 5 mg of hydrocodone may not be an adequate dose for most people.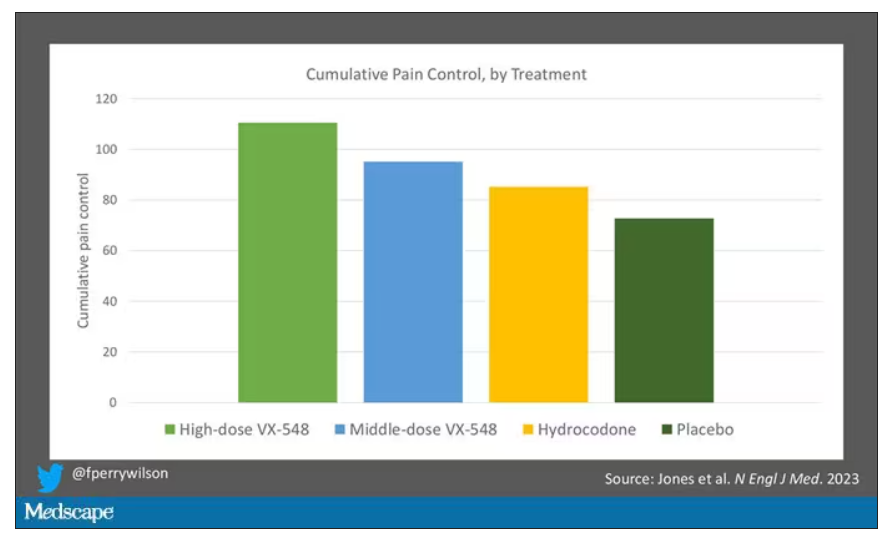
Yes, I would really have killed for an NSAID arm in this trial. Its absence, given that NSAIDs are a staple of postoperative care, is ... well, let’s just say, notable.
Although not a pain-destroying machine, VX-548 has some other things to recommend it. The receptor is really not found in the brain at all, which suggests that the drug should not carry much risk for dependency, though that has not been formally studied.
The side effects were generally mild – headache was the most common – and less prevalent than what you see even in the placebo arm.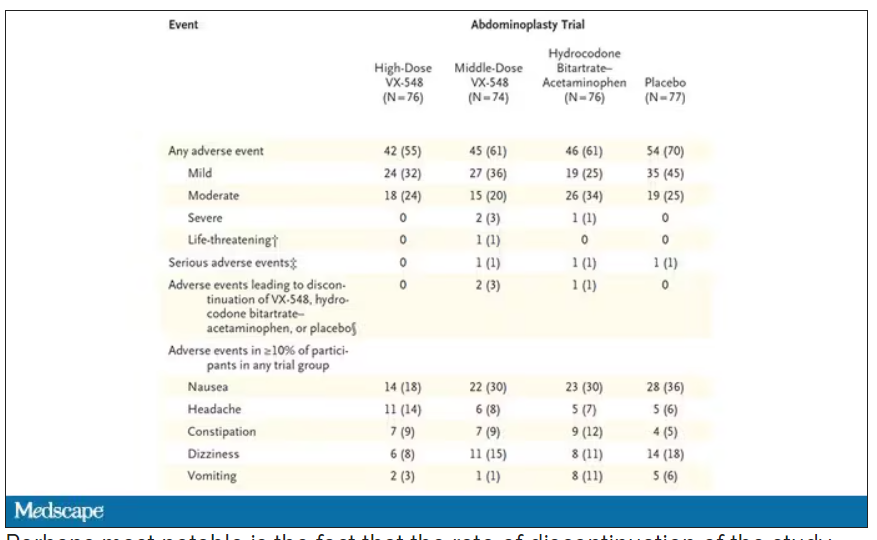
Perhaps most notable is the fact that the rate of discontinuation of the study drug was lowest in the VX-548 arm. Patients could stop taking the pill they were assigned for any reason, ranging from perceived lack of efficacy to side effects. A low discontinuation rate indicates to me a sort of “voting with your feet” that suggests this might be a well-tolerated and reasonably effective drug.
VX-548 isn’t on the market yet; phase 3 trials are ongoing. But whether it is this particular drug or another in this class, I’m happy to see researchers trying to find new ways to target that most primeval form of suffering: pain.
Dr. Wilson is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
When you stub your toe or get a paper cut on your finger, you feel the pain in that part of your body. It feels like the pain is coming from that place. But, of course, that’s not really what is happening. Pain doesn’t really happen in your toe or your finger. It happens in your brain.
It’s a game of telephone, really. The afferent nerve fiber detects the noxious stimulus, passing that signal to the second-order neuron in the dorsal root ganglia of the spinal cord, which runs it up to the thalamus to be passed to the third-order neuron which brings it to the cortex for localization and conscious perception. It’s not even a very good game of telephone. It takes about 100 ms for a pain signal to get from the hand to the brain – longer from the feet, given the greater distance. You see your foot hit the corner of the coffee table and have just enough time to think: “Oh no!” before the pain hits.
Given the Rube Goldberg nature of the process, it would seem like there are any number of places we could stop pain sensation. And sure, local anesthetics at the site of injury, or even spinal anesthetics, are powerful – if temporary and hard to administer – solutions to acute pain.
But in our everyday armamentarium, let’s be honest – we essentially have three options: opiates and opioids, which activate the mu-receptors in the brain to dull pain (and cause a host of other nasty side effects); NSAIDs, which block prostaglandin synthesis and thus limit the ability for pain-conducting neurons to get excited; and acetaminophen, which, despite being used for a century, is poorly understood.
But
If you were to zoom in on the connection between that first afferent pain fiber and the secondary nerve in the spinal cord dorsal root ganglion, you would see a receptor called Nav1.8, a voltage-gated sodium channel.
This receptor is a key part of the apparatus that passes information from nerve 1 to nerve 2, but only for fibers that transmit pain signals. In fact, humans with mutations in this receptor that leave it always in the “open” state have a severe pain syndrome. Blocking the receptor, therefore, might reduce pain.
In preclinical work, researchers identified VX-548, which doesn’t have a brand name yet, as a potent blocker of that channel even in nanomolar concentrations. Importantly, the compound was highly selective for that particular channel – about 30,000 times more selective than it was for the other sodium channels in that family.
Of course, a highly selective and specific drug does not a blockbuster analgesic make. To determine how this drug would work on humans in pain, they turned to two populations: 303 individuals undergoing abdominoplasty and 274 undergoing bunionectomy, as reported in a new paper in the New England Journal of Medicine.
I know this seems a bit random, but abdominoplasty is quite painful and a good model for soft-tissue pain. Bunionectomy is also quite a painful procedure and a useful model of bone pain. After the surgeries, patients were randomized to several different doses of VX-548, hydrocodone plus acetaminophen, or placebo for 48 hours.
At 19 time points over that 48-hour period, participants were asked to rate their pain on a scale from 0 to 10. The primary outcome was the cumulative pain experienced over the 48 hours. So, higher pain would be worse here, but longer duration of pain would also be worse.
The story of the study is really told in this chart.
Yes, those assigned to the highest dose of VX-548 had a statistically significant lower cumulative amount of pain in the 48 hours after surgery. But the picture is really worth more than the stats here. You can see that the onset of pain relief was fairly quick, and that pain relief was sustained over time. You can also see that this is not a miracle drug. Pain scores were a bit better 48 hours out, but only by about a point and a half.
Placebo isn’t really the fair comparison here; few of us treat our postabdominoplasty patients with placebo, after all. The authors do not formally compare the effect of VX-548 with that of the opioid hydrocodone, for instance. But that doesn’t stop us.
This graph, which I put together from data in the paper, shows pain control across the four randomization categories, with higher numbers indicating more (cumulative) control. While all the active agents do a bit better than placebo, VX-548 at the higher dose appears to do the best. But I should note that 5 mg of hydrocodone may not be an adequate dose for most people.
Yes, I would really have killed for an NSAID arm in this trial. Its absence, given that NSAIDs are a staple of postoperative care, is ... well, let’s just say, notable.
Although not a pain-destroying machine, VX-548 has some other things to recommend it. The receptor is really not found in the brain at all, which suggests that the drug should not carry much risk for dependency, though that has not been formally studied.
The side effects were generally mild – headache was the most common – and less prevalent than what you see even in the placebo arm.
Perhaps most notable is the fact that the rate of discontinuation of the study drug was lowest in the VX-548 arm. Patients could stop taking the pill they were assigned for any reason, ranging from perceived lack of efficacy to side effects. A low discontinuation rate indicates to me a sort of “voting with your feet” that suggests this might be a well-tolerated and reasonably effective drug.
VX-548 isn’t on the market yet; phase 3 trials are ongoing. But whether it is this particular drug or another in this class, I’m happy to see researchers trying to find new ways to target that most primeval form of suffering: pain.
Dr. Wilson is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
When you stub your toe or get a paper cut on your finger, you feel the pain in that part of your body. It feels like the pain is coming from that place. But, of course, that’s not really what is happening. Pain doesn’t really happen in your toe or your finger. It happens in your brain.
It’s a game of telephone, really. The afferent nerve fiber detects the noxious stimulus, passing that signal to the second-order neuron in the dorsal root ganglia of the spinal cord, which runs it up to the thalamus to be passed to the third-order neuron which brings it to the cortex for localization and conscious perception. It’s not even a very good game of telephone. It takes about 100 ms for a pain signal to get from the hand to the brain – longer from the feet, given the greater distance. You see your foot hit the corner of the coffee table and have just enough time to think: “Oh no!” before the pain hits.
Given the Rube Goldberg nature of the process, it would seem like there are any number of places we could stop pain sensation. And sure, local anesthetics at the site of injury, or even spinal anesthetics, are powerful – if temporary and hard to administer – solutions to acute pain.
But in our everyday armamentarium, let’s be honest – we essentially have three options: opiates and opioids, which activate the mu-receptors in the brain to dull pain (and cause a host of other nasty side effects); NSAIDs, which block prostaglandin synthesis and thus limit the ability for pain-conducting neurons to get excited; and acetaminophen, which, despite being used for a century, is poorly understood.
But
If you were to zoom in on the connection between that first afferent pain fiber and the secondary nerve in the spinal cord dorsal root ganglion, you would see a receptor called Nav1.8, a voltage-gated sodium channel.
This receptor is a key part of the apparatus that passes information from nerve 1 to nerve 2, but only for fibers that transmit pain signals. In fact, humans with mutations in this receptor that leave it always in the “open” state have a severe pain syndrome. Blocking the receptor, therefore, might reduce pain.
In preclinical work, researchers identified VX-548, which doesn’t have a brand name yet, as a potent blocker of that channel even in nanomolar concentrations. Importantly, the compound was highly selective for that particular channel – about 30,000 times more selective than it was for the other sodium channels in that family.
Of course, a highly selective and specific drug does not a blockbuster analgesic make. To determine how this drug would work on humans in pain, they turned to two populations: 303 individuals undergoing abdominoplasty and 274 undergoing bunionectomy, as reported in a new paper in the New England Journal of Medicine.
I know this seems a bit random, but abdominoplasty is quite painful and a good model for soft-tissue pain. Bunionectomy is also quite a painful procedure and a useful model of bone pain. After the surgeries, patients were randomized to several different doses of VX-548, hydrocodone plus acetaminophen, or placebo for 48 hours.
At 19 time points over that 48-hour period, participants were asked to rate their pain on a scale from 0 to 10. The primary outcome was the cumulative pain experienced over the 48 hours. So, higher pain would be worse here, but longer duration of pain would also be worse.
The story of the study is really told in this chart.
Yes, those assigned to the highest dose of VX-548 had a statistically significant lower cumulative amount of pain in the 48 hours after surgery. But the picture is really worth more than the stats here. You can see that the onset of pain relief was fairly quick, and that pain relief was sustained over time. You can also see that this is not a miracle drug. Pain scores were a bit better 48 hours out, but only by about a point and a half.
Placebo isn’t really the fair comparison here; few of us treat our postabdominoplasty patients with placebo, after all. The authors do not formally compare the effect of VX-548 with that of the opioid hydrocodone, for instance. But that doesn’t stop us.
This graph, which I put together from data in the paper, shows pain control across the four randomization categories, with higher numbers indicating more (cumulative) control. While all the active agents do a bit better than placebo, VX-548 at the higher dose appears to do the best. But I should note that 5 mg of hydrocodone may not be an adequate dose for most people.
Yes, I would really have killed for an NSAID arm in this trial. Its absence, given that NSAIDs are a staple of postoperative care, is ... well, let’s just say, notable.
Although not a pain-destroying machine, VX-548 has some other things to recommend it. The receptor is really not found in the brain at all, which suggests that the drug should not carry much risk for dependency, though that has not been formally studied.
The side effects were generally mild – headache was the most common – and less prevalent than what you see even in the placebo arm.
Perhaps most notable is the fact that the rate of discontinuation of the study drug was lowest in the VX-548 arm. Patients could stop taking the pill they were assigned for any reason, ranging from perceived lack of efficacy to side effects. A low discontinuation rate indicates to me a sort of “voting with your feet” that suggests this might be a well-tolerated and reasonably effective drug.
VX-548 isn’t on the market yet; phase 3 trials are ongoing. But whether it is this particular drug or another in this class, I’m happy to see researchers trying to find new ways to target that most primeval form of suffering: pain.
Dr. Wilson is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Depression at any stage of life tied to increased dementia risk
Adults with depression have more than double the risk of developing dementia and the risk persists regardless of when in life depression is diagnosed, a large population-based study shows.
That the association between depression and dementia persisted even among individuals first diagnosed with depression in early or mid-life provides “strong evidence that depression is not only an early symptom of dementia, but also that depression increases dementia risk,” study investigator Holly Elser, MD, PhD, epidemiologist and resident physician, University of Pennsylvania, Philadelphia, told this news organization.
The study was published online in JAMA Neurology.
Double the risk
Several prior studies that have examined the relationship between depression and dementia over the life course have consistently shown depression later in life is associated with subsequent dementia.
“Late-life depression is generally thought to be an early symptom of dementia or a reaction to subclinical cognitive decline,” said Dr. Elser.
The investigators wanted to examine whether the association between depression and dementia persists even when depression is diagnosed earlier in life, which may suggest it increases the risk of dementia.
“To my knowledge, ours is the largest study on this topic to date, leveraging routinely and prospectively collected data from more than 1.4 million Danish citizens followed from 1977 to 2018,” Dr. Elser noted.
The cohort included 246,499 individuals diagnosed with depression and 1,190,302 individuals without depression.
In both groups, the median age was 50 years and 65% were women. Roughly two-thirds (68%) of those diagnosed with depression were diagnosed before age 60 years.
In Cox proportional hazards regression models, the overall hazard of dementia was more than doubled in those diagnosed with depression (hazard ratio [HR] 2.41). The risk of dementia with depression was more pronounced for men (HR, 2.98) than in women (HR, 2.21).
This association persisted even when the time elapsed from depression diagnosis was between 20 and 39 years (HR, 1.79) and whether depression was diagnosed in early life (18-44 years: HR, 3.08), mid-life (45-59 years: HR, 2.95), or late life (≥ 60 years: HR, 2.31).
It remains unclear whether effective treatment of depression modifies the risk of dementia, as the current study explored the role of antidepressants in a “very limited fashion,” Dr. Elser said.
Specifically, the researchers considered whether an individual was treated with an antidepressant within 6 months of the initial depression diagnosis and found no evidence of a difference in dementia risk between the treated and untreated groups.
“Research that explores implications of the timing and duration of treatment with antidepressants for dementia, treatment with cognitive behavioral therapy, and is able to evaluate the effectiveness of those treatments will be extremely important,” Dr. Elser said.
‘An assault on the brain’
Reached for comment, John Showalter, MD, chief product officer at Linus Health, said one of the most “intriguing” findings of the study is that a depression diagnosis earlier in adulthood conferred a greater risk of developing vascular dementia (HR, 3.28) than did dementia due to Alzheimer’s disease (HR, 1.73).
“The difference in risk for subtypes of dementia is a meaningful addition to our understanding of depression’s connection to dementia,” said Dr. Showalter, who was not involved in the study.
Also weighing in, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said the findings from this “far-reaching investigation leave little room for doubt – depression unleashes a devastating storm within the brain, wreaking havoc on the lives of those ensnared by its grip.
“This massive, multi-decade, and high-data quality registry study adds another brick to the growing edifice of evidence attesting to the profound connection between psychiatric health and the very essence of brain health,” said Dr. Lakhan, who was not involved in the study.
“In a resounding declaration, this research underscores that psychiatric health should be perceived as an integral component of overall health – a paradigm shift that challenges long-standing misconceptions and stigmas surrounding mental disorders. Depression, once marginalized, now claims its rightful place on the pedestal of health concerns that must be addressed with unwavering resolve,” said Dr. Lakhan.
He noted that depression is “not just a mental battle, it’s a profound assault on the very fabric of the brain, leaving lives in turmoil and hearts in search of hope. No longer shrouded in silence, depression demands society’s attention.”
The study had no specific funding. Dr. Elser, Dr. Showalter, and Dr. Lakhan have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Adults with depression have more than double the risk of developing dementia and the risk persists regardless of when in life depression is diagnosed, a large population-based study shows.
That the association between depression and dementia persisted even among individuals first diagnosed with depression in early or mid-life provides “strong evidence that depression is not only an early symptom of dementia, but also that depression increases dementia risk,” study investigator Holly Elser, MD, PhD, epidemiologist and resident physician, University of Pennsylvania, Philadelphia, told this news organization.
The study was published online in JAMA Neurology.
Double the risk
Several prior studies that have examined the relationship between depression and dementia over the life course have consistently shown depression later in life is associated with subsequent dementia.
“Late-life depression is generally thought to be an early symptom of dementia or a reaction to subclinical cognitive decline,” said Dr. Elser.
The investigators wanted to examine whether the association between depression and dementia persists even when depression is diagnosed earlier in life, which may suggest it increases the risk of dementia.
“To my knowledge, ours is the largest study on this topic to date, leveraging routinely and prospectively collected data from more than 1.4 million Danish citizens followed from 1977 to 2018,” Dr. Elser noted.
The cohort included 246,499 individuals diagnosed with depression and 1,190,302 individuals without depression.
In both groups, the median age was 50 years and 65% were women. Roughly two-thirds (68%) of those diagnosed with depression were diagnosed before age 60 years.
In Cox proportional hazards regression models, the overall hazard of dementia was more than doubled in those diagnosed with depression (hazard ratio [HR] 2.41). The risk of dementia with depression was more pronounced for men (HR, 2.98) than in women (HR, 2.21).
This association persisted even when the time elapsed from depression diagnosis was between 20 and 39 years (HR, 1.79) and whether depression was diagnosed in early life (18-44 years: HR, 3.08), mid-life (45-59 years: HR, 2.95), or late life (≥ 60 years: HR, 2.31).
It remains unclear whether effective treatment of depression modifies the risk of dementia, as the current study explored the role of antidepressants in a “very limited fashion,” Dr. Elser said.
Specifically, the researchers considered whether an individual was treated with an antidepressant within 6 months of the initial depression diagnosis and found no evidence of a difference in dementia risk between the treated and untreated groups.
“Research that explores implications of the timing and duration of treatment with antidepressants for dementia, treatment with cognitive behavioral therapy, and is able to evaluate the effectiveness of those treatments will be extremely important,” Dr. Elser said.
‘An assault on the brain’
Reached for comment, John Showalter, MD, chief product officer at Linus Health, said one of the most “intriguing” findings of the study is that a depression diagnosis earlier in adulthood conferred a greater risk of developing vascular dementia (HR, 3.28) than did dementia due to Alzheimer’s disease (HR, 1.73).
“The difference in risk for subtypes of dementia is a meaningful addition to our understanding of depression’s connection to dementia,” said Dr. Showalter, who was not involved in the study.
Also weighing in, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said the findings from this “far-reaching investigation leave little room for doubt – depression unleashes a devastating storm within the brain, wreaking havoc on the lives of those ensnared by its grip.
“This massive, multi-decade, and high-data quality registry study adds another brick to the growing edifice of evidence attesting to the profound connection between psychiatric health and the very essence of brain health,” said Dr. Lakhan, who was not involved in the study.
“In a resounding declaration, this research underscores that psychiatric health should be perceived as an integral component of overall health – a paradigm shift that challenges long-standing misconceptions and stigmas surrounding mental disorders. Depression, once marginalized, now claims its rightful place on the pedestal of health concerns that must be addressed with unwavering resolve,” said Dr. Lakhan.
He noted that depression is “not just a mental battle, it’s a profound assault on the very fabric of the brain, leaving lives in turmoil and hearts in search of hope. No longer shrouded in silence, depression demands society’s attention.”
The study had no specific funding. Dr. Elser, Dr. Showalter, and Dr. Lakhan have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Adults with depression have more than double the risk of developing dementia and the risk persists regardless of when in life depression is diagnosed, a large population-based study shows.
That the association between depression and dementia persisted even among individuals first diagnosed with depression in early or mid-life provides “strong evidence that depression is not only an early symptom of dementia, but also that depression increases dementia risk,” study investigator Holly Elser, MD, PhD, epidemiologist and resident physician, University of Pennsylvania, Philadelphia, told this news organization.
The study was published online in JAMA Neurology.
Double the risk
Several prior studies that have examined the relationship between depression and dementia over the life course have consistently shown depression later in life is associated with subsequent dementia.
“Late-life depression is generally thought to be an early symptom of dementia or a reaction to subclinical cognitive decline,” said Dr. Elser.
The investigators wanted to examine whether the association between depression and dementia persists even when depression is diagnosed earlier in life, which may suggest it increases the risk of dementia.
“To my knowledge, ours is the largest study on this topic to date, leveraging routinely and prospectively collected data from more than 1.4 million Danish citizens followed from 1977 to 2018,” Dr. Elser noted.
The cohort included 246,499 individuals diagnosed with depression and 1,190,302 individuals without depression.
In both groups, the median age was 50 years and 65% were women. Roughly two-thirds (68%) of those diagnosed with depression were diagnosed before age 60 years.
In Cox proportional hazards regression models, the overall hazard of dementia was more than doubled in those diagnosed with depression (hazard ratio [HR] 2.41). The risk of dementia with depression was more pronounced for men (HR, 2.98) than in women (HR, 2.21).
This association persisted even when the time elapsed from depression diagnosis was between 20 and 39 years (HR, 1.79) and whether depression was diagnosed in early life (18-44 years: HR, 3.08), mid-life (45-59 years: HR, 2.95), or late life (≥ 60 years: HR, 2.31).
It remains unclear whether effective treatment of depression modifies the risk of dementia, as the current study explored the role of antidepressants in a “very limited fashion,” Dr. Elser said.
Specifically, the researchers considered whether an individual was treated with an antidepressant within 6 months of the initial depression diagnosis and found no evidence of a difference in dementia risk between the treated and untreated groups.
“Research that explores implications of the timing and duration of treatment with antidepressants for dementia, treatment with cognitive behavioral therapy, and is able to evaluate the effectiveness of those treatments will be extremely important,” Dr. Elser said.
‘An assault on the brain’
Reached for comment, John Showalter, MD, chief product officer at Linus Health, said one of the most “intriguing” findings of the study is that a depression diagnosis earlier in adulthood conferred a greater risk of developing vascular dementia (HR, 3.28) than did dementia due to Alzheimer’s disease (HR, 1.73).
“The difference in risk for subtypes of dementia is a meaningful addition to our understanding of depression’s connection to dementia,” said Dr. Showalter, who was not involved in the study.
Also weighing in, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said the findings from this “far-reaching investigation leave little room for doubt – depression unleashes a devastating storm within the brain, wreaking havoc on the lives of those ensnared by its grip.
“This massive, multi-decade, and high-data quality registry study adds another brick to the growing edifice of evidence attesting to the profound connection between psychiatric health and the very essence of brain health,” said Dr. Lakhan, who was not involved in the study.
“In a resounding declaration, this research underscores that psychiatric health should be perceived as an integral component of overall health – a paradigm shift that challenges long-standing misconceptions and stigmas surrounding mental disorders. Depression, once marginalized, now claims its rightful place on the pedestal of health concerns that must be addressed with unwavering resolve,” said Dr. Lakhan.
He noted that depression is “not just a mental battle, it’s a profound assault on the very fabric of the brain, leaving lives in turmoil and hearts in search of hope. No longer shrouded in silence, depression demands society’s attention.”
The study had no specific funding. Dr. Elser, Dr. Showalter, and Dr. Lakhan have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Medicare to pay for at-home dementia care coordination
Under a new Medicare pilot program that will begin in 2024, the federal government will pay clinicians to coordinate at-home dementia support services, including respite care for family members.
A Department of Health & Human Services initiative, part of the aim of the Guiding an Improved Dementia Experience (GUIDE) program is to help Medicare beneficiaries with dementia stay in the community for as long as possible. It is estimated that there are 6.7 million Americans living with Alzheimer’s disease or some other form of dementia, said HHS.
The program is voluntary and will be open to Medicare-enrolled clinicians and other providers who can assemble an interdisciplinary care team and meet the program’s participation criteria.
“Our new GUIDE Model has the potential to improve the quality of life for people with dementia and alleviate the significant strain on our families,” said HHS Secretary Xavier Becerra, in a statement.
“Not only is dementia care management a proven way to improve the quality of care and quality of life for those living with Alzheimer’s and other dementia, but now we know that it would also save the federal government billions of dollars,” Robert Egge, Alzheimer’s Association chief public policy officer and Alzheimer’s Impact Movement (AIM) executive director, said in a statement.
Mr. Egge cited a recent analysis commissioned by AIM that found that dementia care management would save the federal government nearly $21 billion over 10 years.
“People living with dementia and their caregivers too often struggle to manage their health care and connect with key supports that can allow them to remain in their homes and communities,” said Centers for Medicare & Medicaid Services Administrator Chiquita Brooks-LaSure, in the HHS statement.
“Fragmented care contributes to the mental and physical health strain of caring for someone with dementia, as well as the substantial financial burden,” she said, adding that Black, Hispanic, Asian American, Native Hawaiian, and Pacific Islander populations have been especially disadvantaged.
The GUIDE Model will provide new resources and greater access to specialty care to those communities, said Ms. Brooks-LaSure.
Care teams that seek to participate in the GUIDE model must have a care navigator who has received required training in dementia, assessment, and care planning.
The teams also must have a clinician with dementia proficiency as recognized by experience caring for adults with cognitive impairment; experience caring for patients aged 65 years old or older; or specialty designation in neurology, psychiatry, geriatrics, geriatric psychiatry, behavioral neurology, or geriatric neurology.
Medicare beneficiaries will be eligible if they are not residing in a nursing home; are not enrolled in hospice; and have a confirmed dementia diagnosis.
Beneficiaries who receive care from GUIDE participants will be placed in one of five “tiers,” based on a combination of disease stage and caregiver status. Beneficiary needs, and care intensity and payment, increase by tier.
GUIDE teams will receive a monthly, per-beneficiary amount for providing care management and coordination and caregiver education and support services. They can also bill for respite services – up to an annual cap – for Medicare beneficiaries who have an unpaid caregiver.
Clinicians seeking to participate in GUIDE can apply beginning in the fall. The program will run for 8 years beginning July 1, 2024.
Alzheimer’s Association President and CEO Joanne Pike, DrPH, said in a statement that the organization had “advocated for this approach for years, believing it [to be] the key to addressing systemic challenges faced by those with dementia, their families and those who provide them with care and support.”
The John A. Hartford Foundation noted that it also had long pushed for a comprehensive dementia care program. “Comprehensive dementia care supports both the medical and nonmedical needs of patients and their family caregivers,” said Foundation President Terry Fulmer, PhD, RN, FAAN, in a statement.
“Notably and necessarily, the model will help improve equity in access to care for underserved communities by addressing unpaid caregiver needs, including respite services and screening for health-related social needs,” added Dr. Fulmer.
A version of this article first appeared on Medscape.com.
Under a new Medicare pilot program that will begin in 2024, the federal government will pay clinicians to coordinate at-home dementia support services, including respite care for family members.
A Department of Health & Human Services initiative, part of the aim of the Guiding an Improved Dementia Experience (GUIDE) program is to help Medicare beneficiaries with dementia stay in the community for as long as possible. It is estimated that there are 6.7 million Americans living with Alzheimer’s disease or some other form of dementia, said HHS.
The program is voluntary and will be open to Medicare-enrolled clinicians and other providers who can assemble an interdisciplinary care team and meet the program’s participation criteria.
“Our new GUIDE Model has the potential to improve the quality of life for people with dementia and alleviate the significant strain on our families,” said HHS Secretary Xavier Becerra, in a statement.
“Not only is dementia care management a proven way to improve the quality of care and quality of life for those living with Alzheimer’s and other dementia, but now we know that it would also save the federal government billions of dollars,” Robert Egge, Alzheimer’s Association chief public policy officer and Alzheimer’s Impact Movement (AIM) executive director, said in a statement.
Mr. Egge cited a recent analysis commissioned by AIM that found that dementia care management would save the federal government nearly $21 billion over 10 years.
“People living with dementia and their caregivers too often struggle to manage their health care and connect with key supports that can allow them to remain in their homes and communities,” said Centers for Medicare & Medicaid Services Administrator Chiquita Brooks-LaSure, in the HHS statement.
“Fragmented care contributes to the mental and physical health strain of caring for someone with dementia, as well as the substantial financial burden,” she said, adding that Black, Hispanic, Asian American, Native Hawaiian, and Pacific Islander populations have been especially disadvantaged.
The GUIDE Model will provide new resources and greater access to specialty care to those communities, said Ms. Brooks-LaSure.
Care teams that seek to participate in the GUIDE model must have a care navigator who has received required training in dementia, assessment, and care planning.
The teams also must have a clinician with dementia proficiency as recognized by experience caring for adults with cognitive impairment; experience caring for patients aged 65 years old or older; or specialty designation in neurology, psychiatry, geriatrics, geriatric psychiatry, behavioral neurology, or geriatric neurology.
Medicare beneficiaries will be eligible if they are not residing in a nursing home; are not enrolled in hospice; and have a confirmed dementia diagnosis.
Beneficiaries who receive care from GUIDE participants will be placed in one of five “tiers,” based on a combination of disease stage and caregiver status. Beneficiary needs, and care intensity and payment, increase by tier.
GUIDE teams will receive a monthly, per-beneficiary amount for providing care management and coordination and caregiver education and support services. They can also bill for respite services – up to an annual cap – for Medicare beneficiaries who have an unpaid caregiver.
Clinicians seeking to participate in GUIDE can apply beginning in the fall. The program will run for 8 years beginning July 1, 2024.
Alzheimer’s Association President and CEO Joanne Pike, DrPH, said in a statement that the organization had “advocated for this approach for years, believing it [to be] the key to addressing systemic challenges faced by those with dementia, their families and those who provide them with care and support.”
The John A. Hartford Foundation noted that it also had long pushed for a comprehensive dementia care program. “Comprehensive dementia care supports both the medical and nonmedical needs of patients and their family caregivers,” said Foundation President Terry Fulmer, PhD, RN, FAAN, in a statement.
“Notably and necessarily, the model will help improve equity in access to care for underserved communities by addressing unpaid caregiver needs, including respite services and screening for health-related social needs,” added Dr. Fulmer.
A version of this article first appeared on Medscape.com.
Under a new Medicare pilot program that will begin in 2024, the federal government will pay clinicians to coordinate at-home dementia support services, including respite care for family members.
A Department of Health & Human Services initiative, part of the aim of the Guiding an Improved Dementia Experience (GUIDE) program is to help Medicare beneficiaries with dementia stay in the community for as long as possible. It is estimated that there are 6.7 million Americans living with Alzheimer’s disease or some other form of dementia, said HHS.
The program is voluntary and will be open to Medicare-enrolled clinicians and other providers who can assemble an interdisciplinary care team and meet the program’s participation criteria.
“Our new GUIDE Model has the potential to improve the quality of life for people with dementia and alleviate the significant strain on our families,” said HHS Secretary Xavier Becerra, in a statement.
“Not only is dementia care management a proven way to improve the quality of care and quality of life for those living with Alzheimer’s and other dementia, but now we know that it would also save the federal government billions of dollars,” Robert Egge, Alzheimer’s Association chief public policy officer and Alzheimer’s Impact Movement (AIM) executive director, said in a statement.
Mr. Egge cited a recent analysis commissioned by AIM that found that dementia care management would save the federal government nearly $21 billion over 10 years.
“People living with dementia and their caregivers too often struggle to manage their health care and connect with key supports that can allow them to remain in their homes and communities,” said Centers for Medicare & Medicaid Services Administrator Chiquita Brooks-LaSure, in the HHS statement.
“Fragmented care contributes to the mental and physical health strain of caring for someone with dementia, as well as the substantial financial burden,” she said, adding that Black, Hispanic, Asian American, Native Hawaiian, and Pacific Islander populations have been especially disadvantaged.
The GUIDE Model will provide new resources and greater access to specialty care to those communities, said Ms. Brooks-LaSure.
Care teams that seek to participate in the GUIDE model must have a care navigator who has received required training in dementia, assessment, and care planning.
The teams also must have a clinician with dementia proficiency as recognized by experience caring for adults with cognitive impairment; experience caring for patients aged 65 years old or older; or specialty designation in neurology, psychiatry, geriatrics, geriatric psychiatry, behavioral neurology, or geriatric neurology.
Medicare beneficiaries will be eligible if they are not residing in a nursing home; are not enrolled in hospice; and have a confirmed dementia diagnosis.
Beneficiaries who receive care from GUIDE participants will be placed in one of five “tiers,” based on a combination of disease stage and caregiver status. Beneficiary needs, and care intensity and payment, increase by tier.
GUIDE teams will receive a monthly, per-beneficiary amount for providing care management and coordination and caregiver education and support services. They can also bill for respite services – up to an annual cap – for Medicare beneficiaries who have an unpaid caregiver.
Clinicians seeking to participate in GUIDE can apply beginning in the fall. The program will run for 8 years beginning July 1, 2024.
Alzheimer’s Association President and CEO Joanne Pike, DrPH, said in a statement that the organization had “advocated for this approach for years, believing it [to be] the key to addressing systemic challenges faced by those with dementia, their families and those who provide them with care and support.”
The John A. Hartford Foundation noted that it also had long pushed for a comprehensive dementia care program. “Comprehensive dementia care supports both the medical and nonmedical needs of patients and their family caregivers,” said Foundation President Terry Fulmer, PhD, RN, FAAN, in a statement.
“Notably and necessarily, the model will help improve equity in access to care for underserved communities by addressing unpaid caregiver needs, including respite services and screening for health-related social needs,” added Dr. Fulmer.
A version of this article first appeared on Medscape.com.