User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
PrEP education during STI testing could boost HIV protection
TAMPA –
It comes down to numbers, said Gabriela Brito, MSN, RN, ACRN, a researcher at nonprofit CAN Community Health, headquartered in Sarasota, Fla. More people seek screening for STIs compared with those who actively seek PrEP for HIV prevention.
“One out of five individuals got tested and were diagnosed with an STI in 2021, so we can capture a huge amount of people just from STI testing and direct them to PrEP programs,” Ms. Brito said in an interview during a poster presentation here at the annual meeting of the Association of Nurses in AIDS Care (ANAC). “So our initiative is pretty much about capturing people” at the point of care.
Ms. Brito reported that as of September 30, 2022, 2,174 patients were receiving PrEP services through one of 40 CAN Community Health clinics. Nearly one-third, 32%, were initially seen for free STI screening.
Striving for better adherence
In some cases, the issue is not starting people on PrEP, it’s keeping them on the regimen over time. The study revealed that 61% of the people were still taking the medication at 6 months.
This figure might have been even lower without CAN Community Health PrEP navigators. Of the 2,174 patients, 63% work with a “PrEP navigator.” These navigators help people access the medication and check in with them on a regular basis to address any questions or reasons behind a lack of adherence.
“If we’re seeing someone’s missing their appointments, our PrEP navigator will start reaching out to them to see what’s going on,” study coauthor Cheryl Netherly, BSW, LPN, ACLPN, said in an interview.
“It could be they moved to a different area or entered a mutually monogamous relationship. They don’t realize they can continue through telehealth if they need to, because sometimes it is hard to get off of work to go [see] the doctor,” Ms. Netherly added. “So we find ways to break those barriers.”
More education needed
Greater awareness around PrEP is another issue. “I think educating people and educating professionals, it’s really crucial. It can also help diminish the stigma around PrEP,” Ms. Brito said.
An analogy is when birth control pills first came out, and some providers would not prescribe them because they were concerned women would be promiscuous, Ms. Netherly said.
“When PrEP first came out, there was a lot of that same mindset,” Ms. Netherly added. “But PrEP does not change your behavior. It’s just adding a layer of protection to the behavior, so you can understand how to keep yourself healthy.”
A primary care tenet
The strategy of identifying potential PrEP candidates during STI screening is “extremely important,” Myra L. Rutland, CPN, DNP, FNP-BC, a family nurse practitioner and director for infectious disease and community outreach at Spectrum Community Health Center in Philadelphia, said when asked to comment. Ms. Rutland was not involved in the CAN Community Health study.
“This is primary care at its most generic level. Primary care means that you intervene before there’s a problem,” Ms. Rutland said.
“We have great medications. Now if patients are adherent to the medication, they are not just a little bit effective – they are between 95% and 99% effective at preventing HIV,” she added.
The goal is to increase awareness that “if you contract any type of sexual transmitted infection ... that means that perhaps you may have come in contact with HIV,” Ms. Rutland said. “So why not offer PrEP? I do that with all of my patients.”
The study was independently supported. Ms. Brito and Ms. Rutland report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA –
It comes down to numbers, said Gabriela Brito, MSN, RN, ACRN, a researcher at nonprofit CAN Community Health, headquartered in Sarasota, Fla. More people seek screening for STIs compared with those who actively seek PrEP for HIV prevention.
“One out of five individuals got tested and were diagnosed with an STI in 2021, so we can capture a huge amount of people just from STI testing and direct them to PrEP programs,” Ms. Brito said in an interview during a poster presentation here at the annual meeting of the Association of Nurses in AIDS Care (ANAC). “So our initiative is pretty much about capturing people” at the point of care.
Ms. Brito reported that as of September 30, 2022, 2,174 patients were receiving PrEP services through one of 40 CAN Community Health clinics. Nearly one-third, 32%, were initially seen for free STI screening.
Striving for better adherence
In some cases, the issue is not starting people on PrEP, it’s keeping them on the regimen over time. The study revealed that 61% of the people were still taking the medication at 6 months.
This figure might have been even lower without CAN Community Health PrEP navigators. Of the 2,174 patients, 63% work with a “PrEP navigator.” These navigators help people access the medication and check in with them on a regular basis to address any questions or reasons behind a lack of adherence.
“If we’re seeing someone’s missing their appointments, our PrEP navigator will start reaching out to them to see what’s going on,” study coauthor Cheryl Netherly, BSW, LPN, ACLPN, said in an interview.
“It could be they moved to a different area or entered a mutually monogamous relationship. They don’t realize they can continue through telehealth if they need to, because sometimes it is hard to get off of work to go [see] the doctor,” Ms. Netherly added. “So we find ways to break those barriers.”
More education needed
Greater awareness around PrEP is another issue. “I think educating people and educating professionals, it’s really crucial. It can also help diminish the stigma around PrEP,” Ms. Brito said.
An analogy is when birth control pills first came out, and some providers would not prescribe them because they were concerned women would be promiscuous, Ms. Netherly said.
“When PrEP first came out, there was a lot of that same mindset,” Ms. Netherly added. “But PrEP does not change your behavior. It’s just adding a layer of protection to the behavior, so you can understand how to keep yourself healthy.”
A primary care tenet
The strategy of identifying potential PrEP candidates during STI screening is “extremely important,” Myra L. Rutland, CPN, DNP, FNP-BC, a family nurse practitioner and director for infectious disease and community outreach at Spectrum Community Health Center in Philadelphia, said when asked to comment. Ms. Rutland was not involved in the CAN Community Health study.
“This is primary care at its most generic level. Primary care means that you intervene before there’s a problem,” Ms. Rutland said.
“We have great medications. Now if patients are adherent to the medication, they are not just a little bit effective – they are between 95% and 99% effective at preventing HIV,” she added.
The goal is to increase awareness that “if you contract any type of sexual transmitted infection ... that means that perhaps you may have come in contact with HIV,” Ms. Rutland said. “So why not offer PrEP? I do that with all of my patients.”
The study was independently supported. Ms. Brito and Ms. Rutland report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA –
It comes down to numbers, said Gabriela Brito, MSN, RN, ACRN, a researcher at nonprofit CAN Community Health, headquartered in Sarasota, Fla. More people seek screening for STIs compared with those who actively seek PrEP for HIV prevention.
“One out of five individuals got tested and were diagnosed with an STI in 2021, so we can capture a huge amount of people just from STI testing and direct them to PrEP programs,” Ms. Brito said in an interview during a poster presentation here at the annual meeting of the Association of Nurses in AIDS Care (ANAC). “So our initiative is pretty much about capturing people” at the point of care.
Ms. Brito reported that as of September 30, 2022, 2,174 patients were receiving PrEP services through one of 40 CAN Community Health clinics. Nearly one-third, 32%, were initially seen for free STI screening.
Striving for better adherence
In some cases, the issue is not starting people on PrEP, it’s keeping them on the regimen over time. The study revealed that 61% of the people were still taking the medication at 6 months.
This figure might have been even lower without CAN Community Health PrEP navigators. Of the 2,174 patients, 63% work with a “PrEP navigator.” These navigators help people access the medication and check in with them on a regular basis to address any questions or reasons behind a lack of adherence.
“If we’re seeing someone’s missing their appointments, our PrEP navigator will start reaching out to them to see what’s going on,” study coauthor Cheryl Netherly, BSW, LPN, ACLPN, said in an interview.
“It could be they moved to a different area or entered a mutually monogamous relationship. They don’t realize they can continue through telehealth if they need to, because sometimes it is hard to get off of work to go [see] the doctor,” Ms. Netherly added. “So we find ways to break those barriers.”
More education needed
Greater awareness around PrEP is another issue. “I think educating people and educating professionals, it’s really crucial. It can also help diminish the stigma around PrEP,” Ms. Brito said.
An analogy is when birth control pills first came out, and some providers would not prescribe them because they were concerned women would be promiscuous, Ms. Netherly said.
“When PrEP first came out, there was a lot of that same mindset,” Ms. Netherly added. “But PrEP does not change your behavior. It’s just adding a layer of protection to the behavior, so you can understand how to keep yourself healthy.”
A primary care tenet
The strategy of identifying potential PrEP candidates during STI screening is “extremely important,” Myra L. Rutland, CPN, DNP, FNP-BC, a family nurse practitioner and director for infectious disease and community outreach at Spectrum Community Health Center in Philadelphia, said when asked to comment. Ms. Rutland was not involved in the CAN Community Health study.
“This is primary care at its most generic level. Primary care means that you intervene before there’s a problem,” Ms. Rutland said.
“We have great medications. Now if patients are adherent to the medication, they are not just a little bit effective – they are between 95% and 99% effective at preventing HIV,” she added.
The goal is to increase awareness that “if you contract any type of sexual transmitted infection ... that means that perhaps you may have come in contact with HIV,” Ms. Rutland said. “So why not offer PrEP? I do that with all of my patients.”
The study was independently supported. Ms. Brito and Ms. Rutland report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ANAC 2022
More vaccinated people dying of COVID as fewer get booster shots
“We can no longer say this is a pandemic of the unvaccinated,” Kaiser Family Foundation Vice President Cynthia Cox, who conducted the analysis, told The Washington Post.
People who had been vaccinated or boosted made up 58% of COVID-19 deaths in August, the analysis showed. The rate has been on the rise: 23% of coronavirus deaths were among vaccinated people in September 2021, and the vaccinated made up 42% of deaths in January and February 2022, the Post reported.
Research continues to show that people who are vaccinated or boosted have a lower risk of death. The rise in deaths among the vaccinated is the result of three factors, Ms. Cox said.
- A large majority of people in the United States have been vaccinated (267 million people, the said).
- People who are at the greatest risk of dying from COVID-19 are more likely to be vaccinated and boosted, such as the elderly.
- Vaccines lose their effectiveness over time; the virus changes to avoid vaccines; and people need to choose to get boosters to continue to be protected.
The case for the effectiveness of vaccines and boosters versus skipping the shots remains strong. People age 6 months and older who are unvaccinated are six times more likely to die of COVID-19, compared to those who got the primary series of shots, the Post reported. Survival rates were even better with additional booster shots, particularly among older people.
“I feel very confident that if people continue to get vaccinated at good numbers, if people get boosted, we can absolutely have a very safe and healthy holiday season,” Ashish Jha, White House coronavirus czar, said on Nov. 22.
The number of Americans who have gotten the most recent booster has been increasing ahead of the holidays. CDC data show that 12% of the U.S. population age 5 and older has received a booster.
A new study by a team of researchers from Harvard University and Yale University estimates that 94% of the U.S. population has been infected with COVID-19 at least once, leaving just 1 in 20 people who have never had the virus.
“Despite these high exposure numbers, there is still substantial population susceptibility to infection with an Omicron variant,” the authors wrote.
They said that if all states achieved the vaccination levels of Vermont, where 55% of people had at least one booster and 22% got a second one, there would be “an appreciable improvement in population immunity, with greater relative impact for protection against infection versus severe disease. This additional protection results from both the recovery of immunity lost due to waning and the increased effectiveness of the bivalent booster against Omicron infections.”
A version of this article first appeared on WebMD.com.
“We can no longer say this is a pandemic of the unvaccinated,” Kaiser Family Foundation Vice President Cynthia Cox, who conducted the analysis, told The Washington Post.
People who had been vaccinated or boosted made up 58% of COVID-19 deaths in August, the analysis showed. The rate has been on the rise: 23% of coronavirus deaths were among vaccinated people in September 2021, and the vaccinated made up 42% of deaths in January and February 2022, the Post reported.
Research continues to show that people who are vaccinated or boosted have a lower risk of death. The rise in deaths among the vaccinated is the result of three factors, Ms. Cox said.
- A large majority of people in the United States have been vaccinated (267 million people, the said).
- People who are at the greatest risk of dying from COVID-19 are more likely to be vaccinated and boosted, such as the elderly.
- Vaccines lose their effectiveness over time; the virus changes to avoid vaccines; and people need to choose to get boosters to continue to be protected.
The case for the effectiveness of vaccines and boosters versus skipping the shots remains strong. People age 6 months and older who are unvaccinated are six times more likely to die of COVID-19, compared to those who got the primary series of shots, the Post reported. Survival rates were even better with additional booster shots, particularly among older people.
“I feel very confident that if people continue to get vaccinated at good numbers, if people get boosted, we can absolutely have a very safe and healthy holiday season,” Ashish Jha, White House coronavirus czar, said on Nov. 22.
The number of Americans who have gotten the most recent booster has been increasing ahead of the holidays. CDC data show that 12% of the U.S. population age 5 and older has received a booster.
A new study by a team of researchers from Harvard University and Yale University estimates that 94% of the U.S. population has been infected with COVID-19 at least once, leaving just 1 in 20 people who have never had the virus.
“Despite these high exposure numbers, there is still substantial population susceptibility to infection with an Omicron variant,” the authors wrote.
They said that if all states achieved the vaccination levels of Vermont, where 55% of people had at least one booster and 22% got a second one, there would be “an appreciable improvement in population immunity, with greater relative impact for protection against infection versus severe disease. This additional protection results from both the recovery of immunity lost due to waning and the increased effectiveness of the bivalent booster against Omicron infections.”
A version of this article first appeared on WebMD.com.
“We can no longer say this is a pandemic of the unvaccinated,” Kaiser Family Foundation Vice President Cynthia Cox, who conducted the analysis, told The Washington Post.
People who had been vaccinated or boosted made up 58% of COVID-19 deaths in August, the analysis showed. The rate has been on the rise: 23% of coronavirus deaths were among vaccinated people in September 2021, and the vaccinated made up 42% of deaths in January and February 2022, the Post reported.
Research continues to show that people who are vaccinated or boosted have a lower risk of death. The rise in deaths among the vaccinated is the result of three factors, Ms. Cox said.
- A large majority of people in the United States have been vaccinated (267 million people, the said).
- People who are at the greatest risk of dying from COVID-19 are more likely to be vaccinated and boosted, such as the elderly.
- Vaccines lose their effectiveness over time; the virus changes to avoid vaccines; and people need to choose to get boosters to continue to be protected.
The case for the effectiveness of vaccines and boosters versus skipping the shots remains strong. People age 6 months and older who are unvaccinated are six times more likely to die of COVID-19, compared to those who got the primary series of shots, the Post reported. Survival rates were even better with additional booster shots, particularly among older people.
“I feel very confident that if people continue to get vaccinated at good numbers, if people get boosted, we can absolutely have a very safe and healthy holiday season,” Ashish Jha, White House coronavirus czar, said on Nov. 22.
The number of Americans who have gotten the most recent booster has been increasing ahead of the holidays. CDC data show that 12% of the U.S. population age 5 and older has received a booster.
A new study by a team of researchers from Harvard University and Yale University estimates that 94% of the U.S. population has been infected with COVID-19 at least once, leaving just 1 in 20 people who have never had the virus.
“Despite these high exposure numbers, there is still substantial population susceptibility to infection with an Omicron variant,” the authors wrote.
They said that if all states achieved the vaccination levels of Vermont, where 55% of people had at least one booster and 22% got a second one, there would be “an appreciable improvement in population immunity, with greater relative impact for protection against infection versus severe disease. This additional protection results from both the recovery of immunity lost due to waning and the increased effectiveness of the bivalent booster against Omicron infections.”
A version of this article first appeared on WebMD.com.
Don’t call me ‘Dr.,’ say some physicians – but most prefer the title
When Mark Cucuzzella, MD, meets a new patient at the West Virginia Medical School clinic, he introduces himself as “Mark.” For one thing, says Dr. Cucuzzella, his last name is a mouthful. For another, the 56-year-old general practitioner asserts that getting on a first-name basis with his patients is integral to delivering the best care.
“I’m trying to break down the old paternalistic barriers of the doctor/patient relationship,” he says. “Titles create an environment where the doctors are making all the decisions and not involving the patient in any course of action.”
Aniruddh Setya, MD, has a different take on informality between patients and doctors: It’s not OK. “I am not your friend,” says the 35-year-old pediatrician from Florida-based KIDZ Medical Services. “There has to be a level of respect for the education and accomplishment of being a physician.”
published in JAMA Network Open. But that doesn’t mean most physicians support the practice. In fact, some doctors contend that it can be harmful, particularly to female physicians.
“My concern is that untitling (so termed by Amy Diehl, PhD, and Leanne Dzubinski, PhD) intrudes upon important professional boundaries and might be correlated with diminishing the value of someone’s time,” says Leah Witt, MD, a geriatrician at UCSF Health, San Francisco. Dr. Witt, along with colleague Lekshmi Santhosh, MD, a pulmonologist, offered commentary on the study results. “Studies have shown that women physicians get more patient portal messages, spend more time in the electronic health record, and have longer visits,” Dr. Witt said. “Dr. Santhosh and I wonder if untitling is a signifier of this diminished value of our time, and an assumption of increased ease of access leading to this higher workload.”
To compile the results reported in JAMA Network Open, Mayo Clinic researchers analyzed more than 90,000 emails from patients to doctors over the course of 3 years, beginning in 2018. Of those emails, more than 32% included the physician’s first name in greeting or salutation. For women physicians, the odds were twice as high that their titles would be omitted in the correspondence. The same holds true for doctors of osteopathic medicine (DOs) compared with MDs, and primary care physicians had similar odds for a title drop compared with specialists.
Dr. Witt says the findings are not surprising. “They match my experience as a woman in medicine, as Dr. Santhosh and I write in our commentary,” she says. “We think the findings could easily be replicated at other centers.”
Indeed, research on 321 speaker introductions at a medical rounds found that when female physicians introduced other physicians, they usually applied the doctor title. When the job of introducing colleagues fell to male physicians, however, the stats fell to 72.4% for male peers and only 49.2% when introducing female peers.
The Mayo Clinic study authors identified the pitfalls of patients who informally address their doctors. They wrote, “Untitling may have a negative impact on physicians, demonstrate lack of respect, and can lead to reduction in formality of the physician/patient relationship or workplace.”
Physician preferences vary
Although the results of the Mayo Clinic analysis didn’t and couldn’t address physician sentiments on patient informality, Dr. Setya observes that American culture is becoming less formal. “I’ve been practicing for over 10 years, and the number of people who consider doctors as equals is growing,” he says. “This has been particularly true over the last couple of years.”
This change was documented in 2015. Add in the pandemic and an entire society that is now accustomed to working from home in sweats, and it’s not a stretch to understand why some patients have become less formal in many settings. The 2015 article noted, however, that most physicians prefer to keep titles in the mix.
Perhaps most troublesome, says Dr. Setya, is that patients forgo asking whether it’s OK to use his first name and simply assume it’s acceptable. “It bothers me,” he says. “I became a doctor for more than the money.”
He suspects that his cultural background (Dr. Setya is of Indian descent) plays a role in how strongly he feels about patient-doctor informality. “As a British colony, Indian culture dictates that you pay respect to elders and to accomplishment,” he points out. “America is far looser when it comes to salutations.”
Dr. Cucuzzella largely agrees with Dr. Setya, but has a different view of the role culture plays in how physicians prefer to be addressed. “If your last name is difficult to pronounce, it can put the patient at ease if you give them an option,” he says. “I like my patients to feel comfortable and have a friendly conversation, so I don’t ask them to try to manage my last name.”
When patients revert to using Dr. Cucuzzella’s last name and title, this often breaks down along generational lines, Dr. Cucuzzella has found: Older patients might drop his title, whereas younger patients might keep it as a sign of respect. In some cases, Dr. Cucuzzella tries to bridge this gap, and offers the option of “Dr. Mark.” In his small West Virginia community, this is how people often refer to him.
Dr. Setya says that most of the older physicians he works with still prefer that patients and younger colleagues use their title, but he has witnessed exceptions to this. “My boss in residence hated to be called ‘Sir’ or ‘Doctor,’ ” he says. “In a situation like that, it is reasonable to ask, ‘How can I address you?’ But it has to be mutually agreed upon.”
Dr. Cucuzzella cites informality as the preferred mode for older patients. “If I have a 70-year-old patient, it seems natural they shouldn’t use my title,” he says. “They are worthy of equality in the community. If I’m talking to a retired CEO or state delegate, it’s uncomfortable if they call me doctor.”
Moreover, Dr. Cucuzzella maintains that establishing a less formal environment with patients leads to better outcomes. “Shared decision-making is a basic human right,” he says. “In 2022, doctors shouldn’t make decisions without patient input, unless it’s an emergency situation. Removing the title barriers makes that easier.”
How to handle informality
If you fall more in line with Dr. Setya, there are strategies you can use to try to keep formality in your doctor-patient relationships. Dr. Setya’s approach is indirect. “I don’t correct a patient if they use my first name, because that might seem hostile,” he says. “But I alert them in the way I address them back. A Sir, a Mrs., or a Mr. needs to go both ways.”
This particularly holds true in pediatrics, Dr. Setya has found. He has witnessed many colleagues addressing parents as “Mommy and Daddy,” something he says lacks respect and sets too informal a tone. “It’s almost universal that parents don’t like that, and we need to act accordingly.”
Dr. Witt also avoids directly correcting patients, but struggles when they drop her title. “The standard signature I use to sign every patient portal message I respond to includes my first and last name and credentials,” she says. “I maintain formality in most circumstances with that standard reply.”
Beneath the surface, however, Dr. Witt wishes it were easier. “I have struggled with answering the question, ‘Is it OK if I call you Leah?’ she says. “I want to keep our interaction anchored in professionalism without sacrificing the warmth I think is important to a productive patient-physician relationship. For this reason, I tend to say yes to this request, even though I’d rather patients didn’t make such requests.”
In the Fast Company article by Amy Diehl, PhD, and Leanne Dzubinski, PhD, on the topic of untitling professional women, the authors suggest several actions, beginning with leadership that sets expectations on the topic. They also suggest that physicians use polite corrections if patients untitle them. Supplying positive reinforcement when patients include your title can help, too. If all else fails, you can call out the offensive untitling. More often than not, especially with female physicians, the patient is demonstrating an unconscious bias rather than something deliberate.
Opinions vary on the topic of untitling, and ultimately each physician must make the decision for themselves. But creating informal cultures in an organization can have unintended consequences, especially for female peers.
Says Dr. Witt, “We all want to give our patients the best care we can, but professional boundaries are critical to time management, equitable care, and maintaining work-life balance. I would love to see a study that examines untitling by self-reported race and/or ethnicity of physicians, because we know that women of color experience higher rates of burnout and depression, and I wonder if untitling may be part of this.”
A version of this article first appeared on Medscape.com.
When Mark Cucuzzella, MD, meets a new patient at the West Virginia Medical School clinic, he introduces himself as “Mark.” For one thing, says Dr. Cucuzzella, his last name is a mouthful. For another, the 56-year-old general practitioner asserts that getting on a first-name basis with his patients is integral to delivering the best care.
“I’m trying to break down the old paternalistic barriers of the doctor/patient relationship,” he says. “Titles create an environment where the doctors are making all the decisions and not involving the patient in any course of action.”
Aniruddh Setya, MD, has a different take on informality between patients and doctors: It’s not OK. “I am not your friend,” says the 35-year-old pediatrician from Florida-based KIDZ Medical Services. “There has to be a level of respect for the education and accomplishment of being a physician.”
published in JAMA Network Open. But that doesn’t mean most physicians support the practice. In fact, some doctors contend that it can be harmful, particularly to female physicians.
“My concern is that untitling (so termed by Amy Diehl, PhD, and Leanne Dzubinski, PhD) intrudes upon important professional boundaries and might be correlated with diminishing the value of someone’s time,” says Leah Witt, MD, a geriatrician at UCSF Health, San Francisco. Dr. Witt, along with colleague Lekshmi Santhosh, MD, a pulmonologist, offered commentary on the study results. “Studies have shown that women physicians get more patient portal messages, spend more time in the electronic health record, and have longer visits,” Dr. Witt said. “Dr. Santhosh and I wonder if untitling is a signifier of this diminished value of our time, and an assumption of increased ease of access leading to this higher workload.”
To compile the results reported in JAMA Network Open, Mayo Clinic researchers analyzed more than 90,000 emails from patients to doctors over the course of 3 years, beginning in 2018. Of those emails, more than 32% included the physician’s first name in greeting or salutation. For women physicians, the odds were twice as high that their titles would be omitted in the correspondence. The same holds true for doctors of osteopathic medicine (DOs) compared with MDs, and primary care physicians had similar odds for a title drop compared with specialists.
Dr. Witt says the findings are not surprising. “They match my experience as a woman in medicine, as Dr. Santhosh and I write in our commentary,” she says. “We think the findings could easily be replicated at other centers.”
Indeed, research on 321 speaker introductions at a medical rounds found that when female physicians introduced other physicians, they usually applied the doctor title. When the job of introducing colleagues fell to male physicians, however, the stats fell to 72.4% for male peers and only 49.2% when introducing female peers.
The Mayo Clinic study authors identified the pitfalls of patients who informally address their doctors. They wrote, “Untitling may have a negative impact on physicians, demonstrate lack of respect, and can lead to reduction in formality of the physician/patient relationship or workplace.”
Physician preferences vary
Although the results of the Mayo Clinic analysis didn’t and couldn’t address physician sentiments on patient informality, Dr. Setya observes that American culture is becoming less formal. “I’ve been practicing for over 10 years, and the number of people who consider doctors as equals is growing,” he says. “This has been particularly true over the last couple of years.”
This change was documented in 2015. Add in the pandemic and an entire society that is now accustomed to working from home in sweats, and it’s not a stretch to understand why some patients have become less formal in many settings. The 2015 article noted, however, that most physicians prefer to keep titles in the mix.
Perhaps most troublesome, says Dr. Setya, is that patients forgo asking whether it’s OK to use his first name and simply assume it’s acceptable. “It bothers me,” he says. “I became a doctor for more than the money.”
He suspects that his cultural background (Dr. Setya is of Indian descent) plays a role in how strongly he feels about patient-doctor informality. “As a British colony, Indian culture dictates that you pay respect to elders and to accomplishment,” he points out. “America is far looser when it comes to salutations.”
Dr. Cucuzzella largely agrees with Dr. Setya, but has a different view of the role culture plays in how physicians prefer to be addressed. “If your last name is difficult to pronounce, it can put the patient at ease if you give them an option,” he says. “I like my patients to feel comfortable and have a friendly conversation, so I don’t ask them to try to manage my last name.”
When patients revert to using Dr. Cucuzzella’s last name and title, this often breaks down along generational lines, Dr. Cucuzzella has found: Older patients might drop his title, whereas younger patients might keep it as a sign of respect. In some cases, Dr. Cucuzzella tries to bridge this gap, and offers the option of “Dr. Mark.” In his small West Virginia community, this is how people often refer to him.
Dr. Setya says that most of the older physicians he works with still prefer that patients and younger colleagues use their title, but he has witnessed exceptions to this. “My boss in residence hated to be called ‘Sir’ or ‘Doctor,’ ” he says. “In a situation like that, it is reasonable to ask, ‘How can I address you?’ But it has to be mutually agreed upon.”
Dr. Cucuzzella cites informality as the preferred mode for older patients. “If I have a 70-year-old patient, it seems natural they shouldn’t use my title,” he says. “They are worthy of equality in the community. If I’m talking to a retired CEO or state delegate, it’s uncomfortable if they call me doctor.”
Moreover, Dr. Cucuzzella maintains that establishing a less formal environment with patients leads to better outcomes. “Shared decision-making is a basic human right,” he says. “In 2022, doctors shouldn’t make decisions without patient input, unless it’s an emergency situation. Removing the title barriers makes that easier.”
How to handle informality
If you fall more in line with Dr. Setya, there are strategies you can use to try to keep formality in your doctor-patient relationships. Dr. Setya’s approach is indirect. “I don’t correct a patient if they use my first name, because that might seem hostile,” he says. “But I alert them in the way I address them back. A Sir, a Mrs., or a Mr. needs to go both ways.”
This particularly holds true in pediatrics, Dr. Setya has found. He has witnessed many colleagues addressing parents as “Mommy and Daddy,” something he says lacks respect and sets too informal a tone. “It’s almost universal that parents don’t like that, and we need to act accordingly.”
Dr. Witt also avoids directly correcting patients, but struggles when they drop her title. “The standard signature I use to sign every patient portal message I respond to includes my first and last name and credentials,” she says. “I maintain formality in most circumstances with that standard reply.”
Beneath the surface, however, Dr. Witt wishes it were easier. “I have struggled with answering the question, ‘Is it OK if I call you Leah?’ she says. “I want to keep our interaction anchored in professionalism without sacrificing the warmth I think is important to a productive patient-physician relationship. For this reason, I tend to say yes to this request, even though I’d rather patients didn’t make such requests.”
In the Fast Company article by Amy Diehl, PhD, and Leanne Dzubinski, PhD, on the topic of untitling professional women, the authors suggest several actions, beginning with leadership that sets expectations on the topic. They also suggest that physicians use polite corrections if patients untitle them. Supplying positive reinforcement when patients include your title can help, too. If all else fails, you can call out the offensive untitling. More often than not, especially with female physicians, the patient is demonstrating an unconscious bias rather than something deliberate.
Opinions vary on the topic of untitling, and ultimately each physician must make the decision for themselves. But creating informal cultures in an organization can have unintended consequences, especially for female peers.
Says Dr. Witt, “We all want to give our patients the best care we can, but professional boundaries are critical to time management, equitable care, and maintaining work-life balance. I would love to see a study that examines untitling by self-reported race and/or ethnicity of physicians, because we know that women of color experience higher rates of burnout and depression, and I wonder if untitling may be part of this.”
A version of this article first appeared on Medscape.com.
When Mark Cucuzzella, MD, meets a new patient at the West Virginia Medical School clinic, he introduces himself as “Mark.” For one thing, says Dr. Cucuzzella, his last name is a mouthful. For another, the 56-year-old general practitioner asserts that getting on a first-name basis with his patients is integral to delivering the best care.
“I’m trying to break down the old paternalistic barriers of the doctor/patient relationship,” he says. “Titles create an environment where the doctors are making all the decisions and not involving the patient in any course of action.”
Aniruddh Setya, MD, has a different take on informality between patients and doctors: It’s not OK. “I am not your friend,” says the 35-year-old pediatrician from Florida-based KIDZ Medical Services. “There has to be a level of respect for the education and accomplishment of being a physician.”
published in JAMA Network Open. But that doesn’t mean most physicians support the practice. In fact, some doctors contend that it can be harmful, particularly to female physicians.
“My concern is that untitling (so termed by Amy Diehl, PhD, and Leanne Dzubinski, PhD) intrudes upon important professional boundaries and might be correlated with diminishing the value of someone’s time,” says Leah Witt, MD, a geriatrician at UCSF Health, San Francisco. Dr. Witt, along with colleague Lekshmi Santhosh, MD, a pulmonologist, offered commentary on the study results. “Studies have shown that women physicians get more patient portal messages, spend more time in the electronic health record, and have longer visits,” Dr. Witt said. “Dr. Santhosh and I wonder if untitling is a signifier of this diminished value of our time, and an assumption of increased ease of access leading to this higher workload.”
To compile the results reported in JAMA Network Open, Mayo Clinic researchers analyzed more than 90,000 emails from patients to doctors over the course of 3 years, beginning in 2018. Of those emails, more than 32% included the physician’s first name in greeting or salutation. For women physicians, the odds were twice as high that their titles would be omitted in the correspondence. The same holds true for doctors of osteopathic medicine (DOs) compared with MDs, and primary care physicians had similar odds for a title drop compared with specialists.
Dr. Witt says the findings are not surprising. “They match my experience as a woman in medicine, as Dr. Santhosh and I write in our commentary,” she says. “We think the findings could easily be replicated at other centers.”
Indeed, research on 321 speaker introductions at a medical rounds found that when female physicians introduced other physicians, they usually applied the doctor title. When the job of introducing colleagues fell to male physicians, however, the stats fell to 72.4% for male peers and only 49.2% when introducing female peers.
The Mayo Clinic study authors identified the pitfalls of patients who informally address their doctors. They wrote, “Untitling may have a negative impact on physicians, demonstrate lack of respect, and can lead to reduction in formality of the physician/patient relationship or workplace.”
Physician preferences vary
Although the results of the Mayo Clinic analysis didn’t and couldn’t address physician sentiments on patient informality, Dr. Setya observes that American culture is becoming less formal. “I’ve been practicing for over 10 years, and the number of people who consider doctors as equals is growing,” he says. “This has been particularly true over the last couple of years.”
This change was documented in 2015. Add in the pandemic and an entire society that is now accustomed to working from home in sweats, and it’s not a stretch to understand why some patients have become less formal in many settings. The 2015 article noted, however, that most physicians prefer to keep titles in the mix.
Perhaps most troublesome, says Dr. Setya, is that patients forgo asking whether it’s OK to use his first name and simply assume it’s acceptable. “It bothers me,” he says. “I became a doctor for more than the money.”
He suspects that his cultural background (Dr. Setya is of Indian descent) plays a role in how strongly he feels about patient-doctor informality. “As a British colony, Indian culture dictates that you pay respect to elders and to accomplishment,” he points out. “America is far looser when it comes to salutations.”
Dr. Cucuzzella largely agrees with Dr. Setya, but has a different view of the role culture plays in how physicians prefer to be addressed. “If your last name is difficult to pronounce, it can put the patient at ease if you give them an option,” he says. “I like my patients to feel comfortable and have a friendly conversation, so I don’t ask them to try to manage my last name.”
When patients revert to using Dr. Cucuzzella’s last name and title, this often breaks down along generational lines, Dr. Cucuzzella has found: Older patients might drop his title, whereas younger patients might keep it as a sign of respect. In some cases, Dr. Cucuzzella tries to bridge this gap, and offers the option of “Dr. Mark.” In his small West Virginia community, this is how people often refer to him.
Dr. Setya says that most of the older physicians he works with still prefer that patients and younger colleagues use their title, but he has witnessed exceptions to this. “My boss in residence hated to be called ‘Sir’ or ‘Doctor,’ ” he says. “In a situation like that, it is reasonable to ask, ‘How can I address you?’ But it has to be mutually agreed upon.”
Dr. Cucuzzella cites informality as the preferred mode for older patients. “If I have a 70-year-old patient, it seems natural they shouldn’t use my title,” he says. “They are worthy of equality in the community. If I’m talking to a retired CEO or state delegate, it’s uncomfortable if they call me doctor.”
Moreover, Dr. Cucuzzella maintains that establishing a less formal environment with patients leads to better outcomes. “Shared decision-making is a basic human right,” he says. “In 2022, doctors shouldn’t make decisions without patient input, unless it’s an emergency situation. Removing the title barriers makes that easier.”
How to handle informality
If you fall more in line with Dr. Setya, there are strategies you can use to try to keep formality in your doctor-patient relationships. Dr. Setya’s approach is indirect. “I don’t correct a patient if they use my first name, because that might seem hostile,” he says. “But I alert them in the way I address them back. A Sir, a Mrs., or a Mr. needs to go both ways.”
This particularly holds true in pediatrics, Dr. Setya has found. He has witnessed many colleagues addressing parents as “Mommy and Daddy,” something he says lacks respect and sets too informal a tone. “It’s almost universal that parents don’t like that, and we need to act accordingly.”
Dr. Witt also avoids directly correcting patients, but struggles when they drop her title. “The standard signature I use to sign every patient portal message I respond to includes my first and last name and credentials,” she says. “I maintain formality in most circumstances with that standard reply.”
Beneath the surface, however, Dr. Witt wishes it were easier. “I have struggled with answering the question, ‘Is it OK if I call you Leah?’ she says. “I want to keep our interaction anchored in professionalism without sacrificing the warmth I think is important to a productive patient-physician relationship. For this reason, I tend to say yes to this request, even though I’d rather patients didn’t make such requests.”
In the Fast Company article by Amy Diehl, PhD, and Leanne Dzubinski, PhD, on the topic of untitling professional women, the authors suggest several actions, beginning with leadership that sets expectations on the topic. They also suggest that physicians use polite corrections if patients untitle them. Supplying positive reinforcement when patients include your title can help, too. If all else fails, you can call out the offensive untitling. More often than not, especially with female physicians, the patient is demonstrating an unconscious bias rather than something deliberate.
Opinions vary on the topic of untitling, and ultimately each physician must make the decision for themselves. But creating informal cultures in an organization can have unintended consequences, especially for female peers.
Says Dr. Witt, “We all want to give our patients the best care we can, but professional boundaries are critical to time management, equitable care, and maintaining work-life balance. I would love to see a study that examines untitling by self-reported race and/or ethnicity of physicians, because we know that women of color experience higher rates of burnout and depression, and I wonder if untitling may be part of this.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Opt-out HIV testing in EDs can help identify undiagnosed cases
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
in populations with an HIV positivity rate greater than 0.2%.
On implementation of opt-out testing of patients aged 18-59 years admitted to the ED at St. George’s University Hospital in London, the proportion of tests performed increased from 57.9% to 69%. Upon increasing the age range to those 16 and older and implementing notional consent, overall testing coverage improved to 74.2%.
“An opt-out HIV testing program in the emergency department provides an excellent opportunity to diagnose patients who do not perceive themselves to be at risk or who have never tested before,” lead author Rebecca Marchant, MBBS, of St. George’s Hospital, said in an interview.
The study was published online in HIV Medicine.
She continued, “I think this take-away message would be applicable to other countries with prevalence of HIV greater than 2 per 1,000 people, as routine HIV testing in areas of high prevalence removes the need to target testing of specific populations, potentially preventing stigmatization.”
Despite excellent uptake of HIV testing in antenatal and sexual health services, 6% of people living in the United Kingdom are unaware of their status, and up to 42% of people living with HIV are diagnosed at a late stage of infection. Because blood is routinely drawn in EDs, it’s an excellent opportunity for increased testing. Late-stage diagnosis carries an increased risk of developing an AIDS-related illness, a sevenfold increase in risk for death in the first year after diagnosis, and increased rates of HIV transmission and health care costs.
The study was conducted in a region of London that has an HIV prevalence of 5.4 cases per 1,000 residents aged 15-59 years. Opt-out HIV testing was implemented in February 2019 for people aged 18-59, and in March 2021, this was changed to include those aged 16-plus years along with a move to notional consent.
Out of 78,333 HIV tests, there were 1054 reactive results. Of these, 728 (69%) were known people living with HIV, 8 (0.8%) were not contactable, 2 (0.2%) retested elsewhere and 3 (0.3%) declined a retest. A total of 259 false positives were determined by follow-up testing.
Of those who received a confirmed HIV diagnosis, 50 (4.8%) were newly diagnosed. HIV was suspected in only 22% of these people, and 48% had never previously tested for the virus. New diagnoses were 80% male with a median age of 42 years. CD4 counts varied widely (3 cells/mcL to 1,344 cells/mcL), with 60% diagnosed at a late stage (CD4 < 350 cells/mcL) and 40% with advanced immunosuppression (CD4 < 200 cells/mcL).
“It did not surprise me that heterosexuals made up 62% of all new diagnoses,” Dr. Marchant noted. “This is because routine opt-out testing in the ED offers the opportunity to test people who don’t perceive themselves to be at risk or who have never tested before, and I believe heterosexual people are more likely to fit into those categories. In London, new HIV diagnoses amongst men who have sex with men have fallen year on year likely due to pre-exposure prophylaxis being more readily available and a generally good awareness of HIV and testing amongst MSM.”
Michael D. Levine, MD, associate professor of emergency medicine at the University of California, Los Angeles, agreed with its main findings.
“Doing widespread screening of patients in the emergency department is a feasible option,” Dr. Levine, who was not involved with this study, said in an interview. “But it only makes sense to do this in a population with some prevalence of HIV. With some forms of testing, like rapid HIV tests, you only get a presumptive positive and you then have a confirmatory test. The presumptive positives do have false positives associated with them. So if you’re in a population with very few cases of HIV, and you have a significant number of false positives, that’s going to be problematic. It’s going to add a tremendous amount of stress to the patient.”
A version of this article first appeared on Medscape.com.
FROM HIV MEDICINE
HIV prevention: Clinician attitudes may be curtailing PrEP use
Taking an antiretroviral tablet daily for preexposure prophylaxis (PrEP) has been shown to be a safe and effective method of HIV prevention. However, low and variable uptake of PrEP among men who have sex with men (MSM) remains concerning.
Lead author Samuel R. Bunting, MD, and colleagues explored whether the attitudes of prescribing clinicians are impeding access to PrEP among MSM in the United States. They sought to understand whether clinician biases and expectations about race, HIV risk, adherence, and condom use might be affecting willingness to prescribe PrEP to a patient who specifically requests it.
They reached out to 16 U.S. medical schools (allopathic and osteopathic) with a combined total of 12,660 students. A total of 1,592 students indicated interest in participating in the study, and 600 completed it accurately.
Researchers simulated an electronic medical record for a fictional patient: a sexually active cisgender MSM presenting to a primary care physician and directly requesting access to PrEP for the first time. The simulated record included an uncomplicated medical history and lab results indicating that the patient was negative for HIV and other STIs.
Researchers systematically varied key aspects of the fictional patient, including his race (White or Black) and his intentions for future condom use if prescribed PrEP (continue using, unlikely to begin using, or will stop using). They asked the medical students a series of questions about their hypothetical patient interaction, including assessing patient HIV risk and provider willingness to prescribe PrEP.
The simulated medical records randomly included Black and White patients.
Dr. Bunting and coauthors found that the medical students were significantly less likely to indicate that they would prescribe PrEP to a patient described as “intending to discontinue” condom use were he to be prescribed PrEP, compared with patients “intending to continue” former practices of condom use or nonuse. On a scale from 1 (least likely to prescribe) to 7 (most likely to prescribe), willingness to prescribe was highest for the continued-nonuse group (mean score 6.35; 95% confidence interval, 6.18-6.52) and was lower for the planned-discontinuation group (mean score 5.91; 95% CI, 5.75-6.08; P = .001).
This finding reflects a prevailing fear of “risk compensation” – the concern that an individual on PrEP may start to take additional compensatory risks in his HIV exposures, including discontinuing condom use or increasing number of sexual partners.
In an interview with this news organization, Julia Marcus, PhD, MPH, an associate professor in the department of population medicine at Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, said: “These provider concerns [about risk compensation] are missing the mark. Just like oral contraception, the whole point of a prevention tool like PrEP is to allow people to engage in certain behaviors more safely. Rather than an unwanted consequence, behavior change may be the intended goal.” Dr. Marcus was not involved in the study.
Prior research has shown that uptake of PrEP among Black MSM is significantly lower than among White MSM in the United States. But this study showed no associations with patient race. However, Dr. Bunting and his coauthors found a troubling association with the personal attitudes of the medical students toward sexual activity: The more likely the medical students were to disapprove of nonmonogamy, the more likely they were to assume the possibility of future nonadherence to PrEP and to hesitate before prescribing PrEP.
Were the medical students making assumptions about patients’ ability to be faithful and consistent, whether to a partner or to a drug regimen? Either way, provider hesitancy to prescribe PrEP to a patient on the basis of their stated intention to discontinue condom use or because of the clinician’s own internalized biases about nonmonogamous relationships both represent troubling barriers to accessing clinical care, reinforcing the clinician’s role as gatekeeper to PrEP.
“It’s frustrating that these biases are still in play and potentially contributing to slow and inequitable PrEP uptake” Dr. Marcus commented. “Every sexually active primary care patient should be informed about PrEP, in accordance with CDC guidance, but providers often feel constrained by time ... We need tools that can normalize PrEP in primary care and help limit the potential effect of biases on PrEP prescribing decisions.”
In an interview, Dr. Bunting, resident physician in the department of psychiatry and behavioral neuroscience at University of Chicago Medicine, said in an interview, “Condom use has long been a stalwart prevention mechanism, but PrEP offers superior protection and patients who are seeking PrEP are exhibiting agency and informed risk mitigation ... When a patient is seeking additional protection, it is less about what is the right way to experience a sexual relationship, and more about what is the right way to be safe from HIV.”
Although this study has a number of limitations, including the fact that it is based on a controlled and hypothetical scenario and study participants are still medical students not yet licensed to prescribe, its results have important implications: It underscores the need to train clinicians to recognize and set aside their own social biases during clinical interactions.
Bunting suggested that provider training should support clinicians to evaluate patient requests in a nonjudgmental, pragmatic, and realistic manner appropriately reflecting patient informed agency and knowledge of their own risk factors.
And Dr. Marcus concurred, noting that standardizing the delivery of PrEP through a screening algorithm presents an alternative pathway for eliminating the role of stigmatizing clinician biases and working toward equitable access to PrEP.
This study was supported by unrestricted research funding from Gilead Sciences. The funder had no input into research design, implementation, analysis, interpretation, or publication decisions. Coauthor Brian A. Feinstein’s time was supported by a grant from the National Institute on Drug Abuse. No additional funding was received to support this research.
A version of this article first appeared on Medscape.com.
Taking an antiretroviral tablet daily for preexposure prophylaxis (PrEP) has been shown to be a safe and effective method of HIV prevention. However, low and variable uptake of PrEP among men who have sex with men (MSM) remains concerning.
Lead author Samuel R. Bunting, MD, and colleagues explored whether the attitudes of prescribing clinicians are impeding access to PrEP among MSM in the United States. They sought to understand whether clinician biases and expectations about race, HIV risk, adherence, and condom use might be affecting willingness to prescribe PrEP to a patient who specifically requests it.
They reached out to 16 U.S. medical schools (allopathic and osteopathic) with a combined total of 12,660 students. A total of 1,592 students indicated interest in participating in the study, and 600 completed it accurately.
Researchers simulated an electronic medical record for a fictional patient: a sexually active cisgender MSM presenting to a primary care physician and directly requesting access to PrEP for the first time. The simulated record included an uncomplicated medical history and lab results indicating that the patient was negative for HIV and other STIs.
Researchers systematically varied key aspects of the fictional patient, including his race (White or Black) and his intentions for future condom use if prescribed PrEP (continue using, unlikely to begin using, or will stop using). They asked the medical students a series of questions about their hypothetical patient interaction, including assessing patient HIV risk and provider willingness to prescribe PrEP.
The simulated medical records randomly included Black and White patients.
Dr. Bunting and coauthors found that the medical students were significantly less likely to indicate that they would prescribe PrEP to a patient described as “intending to discontinue” condom use were he to be prescribed PrEP, compared with patients “intending to continue” former practices of condom use or nonuse. On a scale from 1 (least likely to prescribe) to 7 (most likely to prescribe), willingness to prescribe was highest for the continued-nonuse group (mean score 6.35; 95% confidence interval, 6.18-6.52) and was lower for the planned-discontinuation group (mean score 5.91; 95% CI, 5.75-6.08; P = .001).
This finding reflects a prevailing fear of “risk compensation” – the concern that an individual on PrEP may start to take additional compensatory risks in his HIV exposures, including discontinuing condom use or increasing number of sexual partners.
In an interview with this news organization, Julia Marcus, PhD, MPH, an associate professor in the department of population medicine at Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, said: “These provider concerns [about risk compensation] are missing the mark. Just like oral contraception, the whole point of a prevention tool like PrEP is to allow people to engage in certain behaviors more safely. Rather than an unwanted consequence, behavior change may be the intended goal.” Dr. Marcus was not involved in the study.
Prior research has shown that uptake of PrEP among Black MSM is significantly lower than among White MSM in the United States. But this study showed no associations with patient race. However, Dr. Bunting and his coauthors found a troubling association with the personal attitudes of the medical students toward sexual activity: The more likely the medical students were to disapprove of nonmonogamy, the more likely they were to assume the possibility of future nonadherence to PrEP and to hesitate before prescribing PrEP.
Were the medical students making assumptions about patients’ ability to be faithful and consistent, whether to a partner or to a drug regimen? Either way, provider hesitancy to prescribe PrEP to a patient on the basis of their stated intention to discontinue condom use or because of the clinician’s own internalized biases about nonmonogamous relationships both represent troubling barriers to accessing clinical care, reinforcing the clinician’s role as gatekeeper to PrEP.
“It’s frustrating that these biases are still in play and potentially contributing to slow and inequitable PrEP uptake” Dr. Marcus commented. “Every sexually active primary care patient should be informed about PrEP, in accordance with CDC guidance, but providers often feel constrained by time ... We need tools that can normalize PrEP in primary care and help limit the potential effect of biases on PrEP prescribing decisions.”
In an interview, Dr. Bunting, resident physician in the department of psychiatry and behavioral neuroscience at University of Chicago Medicine, said in an interview, “Condom use has long been a stalwart prevention mechanism, but PrEP offers superior protection and patients who are seeking PrEP are exhibiting agency and informed risk mitigation ... When a patient is seeking additional protection, it is less about what is the right way to experience a sexual relationship, and more about what is the right way to be safe from HIV.”
Although this study has a number of limitations, including the fact that it is based on a controlled and hypothetical scenario and study participants are still medical students not yet licensed to prescribe, its results have important implications: It underscores the need to train clinicians to recognize and set aside their own social biases during clinical interactions.
Bunting suggested that provider training should support clinicians to evaluate patient requests in a nonjudgmental, pragmatic, and realistic manner appropriately reflecting patient informed agency and knowledge of their own risk factors.
And Dr. Marcus concurred, noting that standardizing the delivery of PrEP through a screening algorithm presents an alternative pathway for eliminating the role of stigmatizing clinician biases and working toward equitable access to PrEP.
This study was supported by unrestricted research funding from Gilead Sciences. The funder had no input into research design, implementation, analysis, interpretation, or publication decisions. Coauthor Brian A. Feinstein’s time was supported by a grant from the National Institute on Drug Abuse. No additional funding was received to support this research.
A version of this article first appeared on Medscape.com.
Taking an antiretroviral tablet daily for preexposure prophylaxis (PrEP) has been shown to be a safe and effective method of HIV prevention. However, low and variable uptake of PrEP among men who have sex with men (MSM) remains concerning.
Lead author Samuel R. Bunting, MD, and colleagues explored whether the attitudes of prescribing clinicians are impeding access to PrEP among MSM in the United States. They sought to understand whether clinician biases and expectations about race, HIV risk, adherence, and condom use might be affecting willingness to prescribe PrEP to a patient who specifically requests it.
They reached out to 16 U.S. medical schools (allopathic and osteopathic) with a combined total of 12,660 students. A total of 1,592 students indicated interest in participating in the study, and 600 completed it accurately.
Researchers simulated an electronic medical record for a fictional patient: a sexually active cisgender MSM presenting to a primary care physician and directly requesting access to PrEP for the first time. The simulated record included an uncomplicated medical history and lab results indicating that the patient was negative for HIV and other STIs.
Researchers systematically varied key aspects of the fictional patient, including his race (White or Black) and his intentions for future condom use if prescribed PrEP (continue using, unlikely to begin using, or will stop using). They asked the medical students a series of questions about their hypothetical patient interaction, including assessing patient HIV risk and provider willingness to prescribe PrEP.
The simulated medical records randomly included Black and White patients.
Dr. Bunting and coauthors found that the medical students were significantly less likely to indicate that they would prescribe PrEP to a patient described as “intending to discontinue” condom use were he to be prescribed PrEP, compared with patients “intending to continue” former practices of condom use or nonuse. On a scale from 1 (least likely to prescribe) to 7 (most likely to prescribe), willingness to prescribe was highest for the continued-nonuse group (mean score 6.35; 95% confidence interval, 6.18-6.52) and was lower for the planned-discontinuation group (mean score 5.91; 95% CI, 5.75-6.08; P = .001).
This finding reflects a prevailing fear of “risk compensation” – the concern that an individual on PrEP may start to take additional compensatory risks in his HIV exposures, including discontinuing condom use or increasing number of sexual partners.
In an interview with this news organization, Julia Marcus, PhD, MPH, an associate professor in the department of population medicine at Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, said: “These provider concerns [about risk compensation] are missing the mark. Just like oral contraception, the whole point of a prevention tool like PrEP is to allow people to engage in certain behaviors more safely. Rather than an unwanted consequence, behavior change may be the intended goal.” Dr. Marcus was not involved in the study.
Prior research has shown that uptake of PrEP among Black MSM is significantly lower than among White MSM in the United States. But this study showed no associations with patient race. However, Dr. Bunting and his coauthors found a troubling association with the personal attitudes of the medical students toward sexual activity: The more likely the medical students were to disapprove of nonmonogamy, the more likely they were to assume the possibility of future nonadherence to PrEP and to hesitate before prescribing PrEP.
Were the medical students making assumptions about patients’ ability to be faithful and consistent, whether to a partner or to a drug regimen? Either way, provider hesitancy to prescribe PrEP to a patient on the basis of their stated intention to discontinue condom use or because of the clinician’s own internalized biases about nonmonogamous relationships both represent troubling barriers to accessing clinical care, reinforcing the clinician’s role as gatekeeper to PrEP.
“It’s frustrating that these biases are still in play and potentially contributing to slow and inequitable PrEP uptake” Dr. Marcus commented. “Every sexually active primary care patient should be informed about PrEP, in accordance with CDC guidance, but providers often feel constrained by time ... We need tools that can normalize PrEP in primary care and help limit the potential effect of biases on PrEP prescribing decisions.”
In an interview, Dr. Bunting, resident physician in the department of psychiatry and behavioral neuroscience at University of Chicago Medicine, said in an interview, “Condom use has long been a stalwart prevention mechanism, but PrEP offers superior protection and patients who are seeking PrEP are exhibiting agency and informed risk mitigation ... When a patient is seeking additional protection, it is less about what is the right way to experience a sexual relationship, and more about what is the right way to be safe from HIV.”
Although this study has a number of limitations, including the fact that it is based on a controlled and hypothetical scenario and study participants are still medical students not yet licensed to prescribe, its results have important implications: It underscores the need to train clinicians to recognize and set aside their own social biases during clinical interactions.
Bunting suggested that provider training should support clinicians to evaluate patient requests in a nonjudgmental, pragmatic, and realistic manner appropriately reflecting patient informed agency and knowledge of their own risk factors.
And Dr. Marcus concurred, noting that standardizing the delivery of PrEP through a screening algorithm presents an alternative pathway for eliminating the role of stigmatizing clinician biases and working toward equitable access to PrEP.
This study was supported by unrestricted research funding from Gilead Sciences. The funder had no input into research design, implementation, analysis, interpretation, or publication decisions. Coauthor Brian A. Feinstein’s time was supported by a grant from the National Institute on Drug Abuse. No additional funding was received to support this research.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF ACQUIRED IMMUNE DEFICIENCY SYNDROME
The right indoor relative humidity could ward off COVID
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
The “sweet spot” associated with reduced COVID-19 cases and deaths is 40%-60% indoor relative humidity, an MIT news release said. People who maintained indoor relative humidity outside those parameters had higher rates of catching COVID-19.
Most people are comfortable with 30%-50% relative humidity, researchers said. An airplane cabin has about 20% relative humidity.
Relative humidity is the amount of moisture in the air, compared with the total moisture the air can hold at a given temperature before saturating and forming condensation.
The study was published in The Journal of the Royal Society Interface. Researchers examined COVID-19 data and meteorological measurements from 121 countries from January 2020 through August 2020, before vaccines became available to the public.
“When outdoor temperatures were below the typical human comfort range, they assumed indoor spaces were heated to reach that comfort range. Based on the added heating, they calculated the associated drop in indoor relative humidity,” the MIT news release said.
The research teams found that when a region reported a rise in COVID-19 cases and deaths, the region’s estimated indoor relative humidity was either lower than 40% or higher than 60%, the release said.
“There’s potentially a protective effect of this intermediate indoor relative humidity,” said Connor Verheyen, the lead author and a PhD student in medical engineering and medical physics in the Harvard-MIT Program in Health Sciences and Technology.
Widespread use of the 40%-60% indoor humidity range could reduce the need for lockdowns and other widespread restrictions, the study concluded.
“Unlike measures that depend on individual compliance (for example, masking or hand-washing), indoor RH optimization would achieve high compliance because all occupants of a common indoor space would be exposed to similar ambient conditions,” the study said. “Compared to the long timelines and high costs of vaccine production and distribution, humidity control systems could potentially be implemented more quickly and cheaply in certain indoor settings.”
A version of this article first appeared on WebMD.com.
FROM THE JOURNAL OF THE ROYAL SOCIETY INTERFACE
Children and COVID: Weekly cases maintain a low-level plateau
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.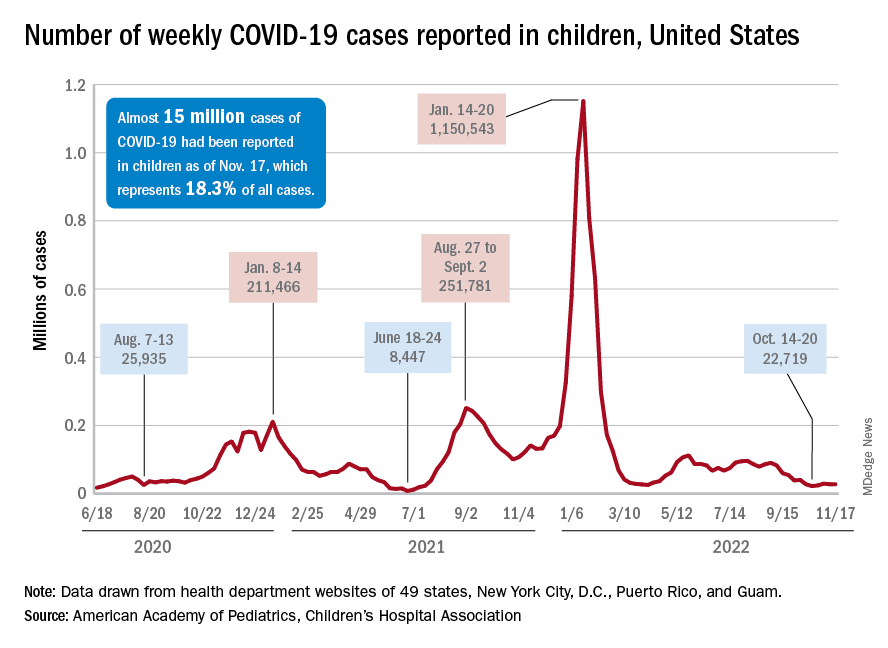
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
A less-than-1% decrease in weekly COVID-19 cases in children demonstrated continued stability in the pandemic situation as the nation heads into the holiday season.
the American Academy of Pediatrics and the Children’s Hospital Association said in the latest edition of their joint COVID report.
New cases for the week of Nov. 11-17 totaled 27,899, down by 0.9% from the previous week and just 4 weeks removed from the lowest total of the year: 22,719 for Oct. 14-20. There have been just under 15 million cases of COVID-19 in children since the pandemic began, and children represent 18.3% of cases in all ages, the AAP and CHA reported.
Conditions look favorable for that plateau to continue, despite the upcoming holidays, White House COVID-19 coordinator Ashish Jha said recently. “We are in a very different place and we will remain in a different place,” Dr. Jha said, according to STAT News. “We are now at a point where I believe if you’re up to date on your vaccines, you have access to treatments ... there really should be no restrictions on people’s activities.”
One possible spoiler, an apparent spike in COVID-related hospitalizations in children we reported last week, seems to have been a false alarm. The rate of new admissions for Nov. 11, which preliminary data suggested was 0.48 per 100,000 population, has now been revised with more solid data to 0.20 per 100,000, according to the Centers for Disease Control and Prevention.
“We continue to monitor the recent increases in admissions among children. Some of these may be admissions with COVID-19, not because of COVID-19. Co-infections are being noted in our surveillance systems for hospitalizations among children; as much as 10% of admissions or higher have viruses codetected (RSV, influenza, enterovirus/rhinovirus, and other respiratory viruses),” a CDC spokesperson told this news organization.
For children aged 0-17 years, the current 7-day (Nov. 13-19) average number of new admissions with confirmed COVID is 129 per day, down from 147 for the previous 7-day average. Emergency department visits with diagnosed COVID, measured as a percentage of all ED visits, are largely holding steady. The latest 7-day averages available (Nov. 18) – 1.0% for children aged 0-11 years, 0.7% for 12- to 15-year-olds, and 0.8% in 16- to 17-year-olds – are the same or within a tenth of a percent of the rates recorded on Oct. 18, CDC data show.
New vaccinations for the week of Nov. 10-16 were down just slightly for children under age 5 years and for those aged 5-11 years, with a larger drop seen among 12- to 17-year-olds, the AAP said in its weekly vaccination report. So far, 7.9% of all children under age 5 have received at least one dose of COVID vaccine, as have 39.1% of 5 to 11-year-olds and 71.5% of those aged 12-17years, the CDC said on its COVID Data Tracker.
Nurse practitioner fined $20k for advertising herself as ‘Doctor Sarah’
Last month, the San Luis Obispo County, California, District Attorney Dan Dow filed a complaint against Sarah Erny, RN, NP, citing unfair business practices and unprofessional conduct.
According to court documents, California’s Medical Practice Act does not permit individuals to refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
In addition to the fine, Ms. Erny agreed to refrain from referring to herself as a doctor in her practice and on social media. She has already deleted her Twitter account.
The case underscores tensions between physicians fighting to preserve their scope of practice and the allied professionals that U.S. lawmakers increasingly see as a less expensive way to improve access to health care.
The American Medical Association and specialty groups strongly oppose a new bill, the Improving Care and Access to Nurses Act, that would expand the scope of practice for nurse practitioners and physician assistants.
Court records show that Ms. Erny earned a doctor of nursing practice (DNP) degree from Vanderbilt University, Nashville, Tenn., and that she met the state requirements to obtain licensure as a registered nurse and nurse practitioner. In 2018, she opened a practice in Arroyo Grande, California, called Holistic Women’s Healing, where she provided medical services and drug supplements to patients.
She also entered a collaborative agreement with ob.gyn. Anika Moore, MD, for approximately 3 years. Dr. Moore’s medical practice was in another county and state, and the physician returned every 2 to 3 months to review a portion of Ms. Erny’s patient files.
Ms. Erny and Dr. Moore terminated the collaborative agreement in March, according to court documents.
However, Mr. Dow alleged that Ms. Erny regularly referred to herself as “Dr. Sarah” or “Dr. Sarah Erny” in her online advertising and social media accounts. Her patients “were so proud of her” that they called her doctor, and her supervising physician instructed staff to do the same.
Mr. Dow said Ms. Erny did not clearly advise the public that she was not a medical doctor and failed to identify her supervising physician. “Simply put, there is a great need for health care providers to state their level of training and licensing clearly and honestly in all of their advertising and marketing materials,” he said in a press release.
In California, nurse practitioners who have been certified by the Board of Registered Nursing may use the following titles: Advanced Practice Registered Nurse; Certified Nurse Practitioner; APRN-CNP; RN and NP; or a combination of other letters or words to identify specialization, such as adult nurse practitioner, pediatric nurse practitioner, obstetrical-gynecological nurse practitioner, and family nurse practitioner.
As educational requirements shift for advanced practice clinicians, similar cases will likely emerge, said Grant Martsolf, PhD, MPH, RN, FAAN, professor at the University of Pittsburgh School of Nursing.
“Scope of practice is governed by states, [so they] will have to figure [it] out as more professional disciplines move to clinical doctorates as the entry to practice. Pharma, [physical therapy], and [occupational therapy] have already done this, and advanced practice nursing is on its way. [Certified registered nurse anesthetists] are already required to get a DNP to sit for certification,” he said.
More guidance is needed, especially when considering other professions like dentists, clinical psychologists, and individuals with clinical or research doctorates who often call themselves doctors, Dr. Martsolf said.
“It seems that the honorific of ‘Dr.’ emerges from the degree, not from being a physician or surgeon,” he said.
Beyond the false advertising, Mr. Dow alleged that Ms. Erny did not file a fictitious business name statement for 2020 and 2021 – a requirement under the California Business and Professions Code to identify who is operating the business.
A version of this article first appeared on Medscape.com.
Last month, the San Luis Obispo County, California, District Attorney Dan Dow filed a complaint against Sarah Erny, RN, NP, citing unfair business practices and unprofessional conduct.
According to court documents, California’s Medical Practice Act does not permit individuals to refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
In addition to the fine, Ms. Erny agreed to refrain from referring to herself as a doctor in her practice and on social media. She has already deleted her Twitter account.
The case underscores tensions between physicians fighting to preserve their scope of practice and the allied professionals that U.S. lawmakers increasingly see as a less expensive way to improve access to health care.
The American Medical Association and specialty groups strongly oppose a new bill, the Improving Care and Access to Nurses Act, that would expand the scope of practice for nurse practitioners and physician assistants.
Court records show that Ms. Erny earned a doctor of nursing practice (DNP) degree from Vanderbilt University, Nashville, Tenn., and that she met the state requirements to obtain licensure as a registered nurse and nurse practitioner. In 2018, she opened a practice in Arroyo Grande, California, called Holistic Women’s Healing, where she provided medical services and drug supplements to patients.
She also entered a collaborative agreement with ob.gyn. Anika Moore, MD, for approximately 3 years. Dr. Moore’s medical practice was in another county and state, and the physician returned every 2 to 3 months to review a portion of Ms. Erny’s patient files.
Ms. Erny and Dr. Moore terminated the collaborative agreement in March, according to court documents.
However, Mr. Dow alleged that Ms. Erny regularly referred to herself as “Dr. Sarah” or “Dr. Sarah Erny” in her online advertising and social media accounts. Her patients “were so proud of her” that they called her doctor, and her supervising physician instructed staff to do the same.
Mr. Dow said Ms. Erny did not clearly advise the public that she was not a medical doctor and failed to identify her supervising physician. “Simply put, there is a great need for health care providers to state their level of training and licensing clearly and honestly in all of their advertising and marketing materials,” he said in a press release.
In California, nurse practitioners who have been certified by the Board of Registered Nursing may use the following titles: Advanced Practice Registered Nurse; Certified Nurse Practitioner; APRN-CNP; RN and NP; or a combination of other letters or words to identify specialization, such as adult nurse practitioner, pediatric nurse practitioner, obstetrical-gynecological nurse practitioner, and family nurse practitioner.
As educational requirements shift for advanced practice clinicians, similar cases will likely emerge, said Grant Martsolf, PhD, MPH, RN, FAAN, professor at the University of Pittsburgh School of Nursing.
“Scope of practice is governed by states, [so they] will have to figure [it] out as more professional disciplines move to clinical doctorates as the entry to practice. Pharma, [physical therapy], and [occupational therapy] have already done this, and advanced practice nursing is on its way. [Certified registered nurse anesthetists] are already required to get a DNP to sit for certification,” he said.
More guidance is needed, especially when considering other professions like dentists, clinical psychologists, and individuals with clinical or research doctorates who often call themselves doctors, Dr. Martsolf said.
“It seems that the honorific of ‘Dr.’ emerges from the degree, not from being a physician or surgeon,” he said.
Beyond the false advertising, Mr. Dow alleged that Ms. Erny did not file a fictitious business name statement for 2020 and 2021 – a requirement under the California Business and Professions Code to identify who is operating the business.
A version of this article first appeared on Medscape.com.
Last month, the San Luis Obispo County, California, District Attorney Dan Dow filed a complaint against Sarah Erny, RN, NP, citing unfair business practices and unprofessional conduct.
According to court documents, California’s Medical Practice Act does not permit individuals to refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
In addition to the fine, Ms. Erny agreed to refrain from referring to herself as a doctor in her practice and on social media. She has already deleted her Twitter account.
The case underscores tensions between physicians fighting to preserve their scope of practice and the allied professionals that U.S. lawmakers increasingly see as a less expensive way to improve access to health care.
The American Medical Association and specialty groups strongly oppose a new bill, the Improving Care and Access to Nurses Act, that would expand the scope of practice for nurse practitioners and physician assistants.
Court records show that Ms. Erny earned a doctor of nursing practice (DNP) degree from Vanderbilt University, Nashville, Tenn., and that she met the state requirements to obtain licensure as a registered nurse and nurse practitioner. In 2018, she opened a practice in Arroyo Grande, California, called Holistic Women’s Healing, where she provided medical services and drug supplements to patients.
She also entered a collaborative agreement with ob.gyn. Anika Moore, MD, for approximately 3 years. Dr. Moore’s medical practice was in another county and state, and the physician returned every 2 to 3 months to review a portion of Ms. Erny’s patient files.
Ms. Erny and Dr. Moore terminated the collaborative agreement in March, according to court documents.
However, Mr. Dow alleged that Ms. Erny regularly referred to herself as “Dr. Sarah” or “Dr. Sarah Erny” in her online advertising and social media accounts. Her patients “were so proud of her” that they called her doctor, and her supervising physician instructed staff to do the same.
Mr. Dow said Ms. Erny did not clearly advise the public that she was not a medical doctor and failed to identify her supervising physician. “Simply put, there is a great need for health care providers to state their level of training and licensing clearly and honestly in all of their advertising and marketing materials,” he said in a press release.
In California, nurse practitioners who have been certified by the Board of Registered Nursing may use the following titles: Advanced Practice Registered Nurse; Certified Nurse Practitioner; APRN-CNP; RN and NP; or a combination of other letters or words to identify specialization, such as adult nurse practitioner, pediatric nurse practitioner, obstetrical-gynecological nurse practitioner, and family nurse practitioner.
As educational requirements shift for advanced practice clinicians, similar cases will likely emerge, said Grant Martsolf, PhD, MPH, RN, FAAN, professor at the University of Pittsburgh School of Nursing.
“Scope of practice is governed by states, [so they] will have to figure [it] out as more professional disciplines move to clinical doctorates as the entry to practice. Pharma, [physical therapy], and [occupational therapy] have already done this, and advanced practice nursing is on its way. [Certified registered nurse anesthetists] are already required to get a DNP to sit for certification,” he said.
More guidance is needed, especially when considering other professions like dentists, clinical psychologists, and individuals with clinical or research doctorates who often call themselves doctors, Dr. Martsolf said.
“It seems that the honorific of ‘Dr.’ emerges from the degree, not from being a physician or surgeon,” he said.
Beyond the false advertising, Mr. Dow alleged that Ms. Erny did not file a fictitious business name statement for 2020 and 2021 – a requirement under the California Business and Professions Code to identify who is operating the business.
A version of this article first appeared on Medscape.com.
AAP issues guidelines to combat rise in respiratory illness
Updated guidance from the group outlines measures to optimize resources to manage a surge of patients filling hospital beds, emergency departments, and physicians’ practices.
A separate document from the AAP endorses giving extra doses of palivizumab, a monoclonal antibody used to prevent severe infection in infants at high risk of respiratory syncytial virus (RSV), as long as the illness is prevalent in the community.
Upticks in rates of RSV and influenza, along with a crisis in children’s mental health, prompted the AAP and the Children’s Hospital Association to petition the Biden administration on Nov. 14 to declare an emergency. Such a move would free up extra funding and waivers to allow physicians and hospitals to pool resources, the organizations said.
Despite those challenges, the AAP stressed in its new guidance that routine care, such as immunizations and chronic disease management, “cannot be neglected.”
Shifting resources
Officials at some children’s hospitals said that they have already implemented many of the AAP’s recommended measures for providing care during a surge, such as cross-training staff who usually treat adults, expanding telehealth and urgent care, and optimizing the use of ancillary care spaces.
“A lot of this is just reinforcing the things that I think children’s hospitals have been doing,” Lindsay Ragsdale, MD, chief medical officer for Kentucky Children’s Hospital, Lexington, said. “Can we shift adults around? Can we use an adult unit? Can we use an occupied space creatively? We’re really thinking outside the box.”
Andrew Pavia, MD, chief of the division of pediatric infectious diseases at University of Utah Health, Salt Lake City, said large children’s hospitals have been actively sharing practices for handling a surge through various channels, but the new guidance could be a useful “checklist” for small hospitals and physician practices that lack well-developed plans.
The AAP’s suggestions for pediatricians in outpatient settings include stocking up on personal protective equipment, using social media and office staff to increase communication with families, and keeping abreast of wait times at local emergency departments.
Addressing a subset of kids
In updated guidance for palivizumab, the AAP noted that earlier-than-usual circulation of RSV prompted pediatricians in some areas to begin administering the drug in the summer and early fall.
Palivizumab is typically given in five consecutive monthly intramuscular injections during RSV season, starting in November. Eligible infants and young children include those born prematurely or who have conditions such as chronic lung disease, hemodynamically significant congenital heart disease, or a suppressed immune system.
The AAP said it supports giving extra doses if RSV activity “persists at high levels in a given region through the fall and winter.” Published studies are sparse but contain “no evidence of increased frequency or severity of adverse events with later doses in a five-dose series nor with doses beyond five doses,” the group added.
The guidance may encourage payers to pick up the tab for extra doses, which are priced at more than $1,800 for cash customers, Dr. Pavia said. However, that recommendation addresses “a pretty small part of the problem overall because the injections are used for a very small subset of kids who are at the highest risk, and more than 80% of hospitalizations for RSV are among healthy kids,” he added.
Dr. Ragsdale and Dr. Pavia have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Updated guidance from the group outlines measures to optimize resources to manage a surge of patients filling hospital beds, emergency departments, and physicians’ practices.
A separate document from the AAP endorses giving extra doses of palivizumab, a monoclonal antibody used to prevent severe infection in infants at high risk of respiratory syncytial virus (RSV), as long as the illness is prevalent in the community.
Upticks in rates of RSV and influenza, along with a crisis in children’s mental health, prompted the AAP and the Children’s Hospital Association to petition the Biden administration on Nov. 14 to declare an emergency. Such a move would free up extra funding and waivers to allow physicians and hospitals to pool resources, the organizations said.
Despite those challenges, the AAP stressed in its new guidance that routine care, such as immunizations and chronic disease management, “cannot be neglected.”
Shifting resources
Officials at some children’s hospitals said that they have already implemented many of the AAP’s recommended measures for providing care during a surge, such as cross-training staff who usually treat adults, expanding telehealth and urgent care, and optimizing the use of ancillary care spaces.
“A lot of this is just reinforcing the things that I think children’s hospitals have been doing,” Lindsay Ragsdale, MD, chief medical officer for Kentucky Children’s Hospital, Lexington, said. “Can we shift adults around? Can we use an adult unit? Can we use an occupied space creatively? We’re really thinking outside the box.”
Andrew Pavia, MD, chief of the division of pediatric infectious diseases at University of Utah Health, Salt Lake City, said large children’s hospitals have been actively sharing practices for handling a surge through various channels, but the new guidance could be a useful “checklist” for small hospitals and physician practices that lack well-developed plans.
The AAP’s suggestions for pediatricians in outpatient settings include stocking up on personal protective equipment, using social media and office staff to increase communication with families, and keeping abreast of wait times at local emergency departments.
Addressing a subset of kids
In updated guidance for palivizumab, the AAP noted that earlier-than-usual circulation of RSV prompted pediatricians in some areas to begin administering the drug in the summer and early fall.
Palivizumab is typically given in five consecutive monthly intramuscular injections during RSV season, starting in November. Eligible infants and young children include those born prematurely or who have conditions such as chronic lung disease, hemodynamically significant congenital heart disease, or a suppressed immune system.
The AAP said it supports giving extra doses if RSV activity “persists at high levels in a given region through the fall and winter.” Published studies are sparse but contain “no evidence of increased frequency or severity of adverse events with later doses in a five-dose series nor with doses beyond five doses,” the group added.
The guidance may encourage payers to pick up the tab for extra doses, which are priced at more than $1,800 for cash customers, Dr. Pavia said. However, that recommendation addresses “a pretty small part of the problem overall because the injections are used for a very small subset of kids who are at the highest risk, and more than 80% of hospitalizations for RSV are among healthy kids,” he added.
Dr. Ragsdale and Dr. Pavia have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Updated guidance from the group outlines measures to optimize resources to manage a surge of patients filling hospital beds, emergency departments, and physicians’ practices.
A separate document from the AAP endorses giving extra doses of palivizumab, a monoclonal antibody used to prevent severe infection in infants at high risk of respiratory syncytial virus (RSV), as long as the illness is prevalent in the community.
Upticks in rates of RSV and influenza, along with a crisis in children’s mental health, prompted the AAP and the Children’s Hospital Association to petition the Biden administration on Nov. 14 to declare an emergency. Such a move would free up extra funding and waivers to allow physicians and hospitals to pool resources, the organizations said.
Despite those challenges, the AAP stressed in its new guidance that routine care, such as immunizations and chronic disease management, “cannot be neglected.”
Shifting resources
Officials at some children’s hospitals said that they have already implemented many of the AAP’s recommended measures for providing care during a surge, such as cross-training staff who usually treat adults, expanding telehealth and urgent care, and optimizing the use of ancillary care spaces.
“A lot of this is just reinforcing the things that I think children’s hospitals have been doing,” Lindsay Ragsdale, MD, chief medical officer for Kentucky Children’s Hospital, Lexington, said. “Can we shift adults around? Can we use an adult unit? Can we use an occupied space creatively? We’re really thinking outside the box.”
Andrew Pavia, MD, chief of the division of pediatric infectious diseases at University of Utah Health, Salt Lake City, said large children’s hospitals have been actively sharing practices for handling a surge through various channels, but the new guidance could be a useful “checklist” for small hospitals and physician practices that lack well-developed plans.
The AAP’s suggestions for pediatricians in outpatient settings include stocking up on personal protective equipment, using social media and office staff to increase communication with families, and keeping abreast of wait times at local emergency departments.
Addressing a subset of kids
In updated guidance for palivizumab, the AAP noted that earlier-than-usual circulation of RSV prompted pediatricians in some areas to begin administering the drug in the summer and early fall.
Palivizumab is typically given in five consecutive monthly intramuscular injections during RSV season, starting in November. Eligible infants and young children include those born prematurely or who have conditions such as chronic lung disease, hemodynamically significant congenital heart disease, or a suppressed immune system.
The AAP said it supports giving extra doses if RSV activity “persists at high levels in a given region through the fall and winter.” Published studies are sparse but contain “no evidence of increased frequency or severity of adverse events with later doses in a five-dose series nor with doses beyond five doses,” the group added.
The guidance may encourage payers to pick up the tab for extra doses, which are priced at more than $1,800 for cash customers, Dr. Pavia said. However, that recommendation addresses “a pretty small part of the problem overall because the injections are used for a very small subset of kids who are at the highest risk, and more than 80% of hospitalizations for RSV are among healthy kids,” he added.
Dr. Ragsdale and Dr. Pavia have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HIV: Treating ‘symptom clusters’ could help improve QOL
TAMPA – People living with HIV experience many symptoms that can be grouped into “clusters” to help guide therapy and ideally treat more than one symptom at a time in an effort to improve quality of life, according to a study presented at the annual meeting of the Association of Nurses in AIDS Care.
Interestingly, these symptoms were more common among people living with HIV who are older than 45 years versus those who are younger, with one exception.
“In HIV, with exception of anxiety, we saw older people had more symptoms than younger ones,” said Natalie Wilson, PhD, assistant professor of community health systems at the University of California, San Francisco.
Dr. Wilson and colleagues performed a study that also suggests the older group experienced more distress from their symptoms than the younger cohort, again with the exception of anxiety.
Symptom clusters are two or more related symptoms that occur together with or without the same etiology. “Imagine you can’t sleep and the next day you’re tired and have no energy, you have trouble remembering someone’s name ... and then the next night you get so anxious about not getting sleep that it keeps you from sleeping.” That’s an example of a symptom cluster, Dr. Wilson said.
A high burden
“Why should we even evaluate symptom clusters?” Dr. Wilson asked. “The symptom burden is still high in people living with HIV. The medications got better but the symptoms remain.”
A high symptom burden also is linked to lower adherence to antiretrovirals. Also, considering groups of symptoms together could lead to targeted interventions that treat multiple symptoms, she said, “instead of treating one symptom at a time and increasing the pill burden for people living with HIV.”
Accelerated aging concerns
In addition, people living with HIV can experience accelerated aging, which is one reason Dr. Wilson and colleagues chose the 45-year-old cutoff in the study. Living with inflammation from HIV and the toxicity of earlier treatments likely contribute.
“Those over age 45 have higher rates of age-associated noncommunicable comorbidities developing at an earlier age than uninfected people with comparable lifestyles and demographics,” Dr. Wilson said.
In the full study, published in the Journal of Pain and Symptom Management, a total 2,000 people living with HIV completed the 20-item HIV Symptom Index. The participants reported their symptoms on their first visit to one of six national HIV Centers of Excellence. People were asked to report presence or absence of a particular symptom, and if they had it, how distressing it was on a scale of 1 “doesn’t bother me” to 4 “bothers me a lot.”
Younger people not only reported more anxiety but were also more distressed by it, Dr. Wilson said. The older group was more likely to be distressed by muscle aches and joint pain, trouble remembering things, and more.
The mean age in the younger group was 35 years, and it was 55 years in the older group. A total of 86% in the younger group and 87% in the older were men, and there were some differences by race, Dr. Wilson said.
More research needed
“These findings warrant further confirmation,” Dr. Wilson added. Future work could evaluate whether symptom clusters share etiology and how symptom clusters change over time. “We need to look at outcomes over time. Can we predict poorer outcomes, such as cardiac events, over time based on symptom clusters?”
Also, as part of HIV treatment success in recent years, “Our guidelines are moving people out further – if you’re undetectable sometimes you can come back at 6 months or 1 year.” The question, she said, is then: “Do we need to watch people with certain symptom clusters more closely?”
Limitations of the study include a lack of information on symptom causes and severity and its cross-sectional design.
‘Absolutely useful’
The study is “absolutely useful,” said session moderator Cheryl Netherly, an HIV nurse and clinical educator for CAN Community Health headquartered in Sarasota, Fla.
“One of the things that she mentioned was people with HIV, especially long-term HIV, they’re aging faster than the population without HIV. So, that is really important to look at.”
People living with HIV and dying from age-related comorbidities is something “we never thought would happen,” Ms. Netherly said. “Unfortunately, we’re now losing them to the different things like kidney issues, heart disease, and diabetes.”
The study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Wilson and Ms. Netherly disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA – People living with HIV experience many symptoms that can be grouped into “clusters” to help guide therapy and ideally treat more than one symptom at a time in an effort to improve quality of life, according to a study presented at the annual meeting of the Association of Nurses in AIDS Care.
Interestingly, these symptoms were more common among people living with HIV who are older than 45 years versus those who are younger, with one exception.
“In HIV, with exception of anxiety, we saw older people had more symptoms than younger ones,” said Natalie Wilson, PhD, assistant professor of community health systems at the University of California, San Francisco.
Dr. Wilson and colleagues performed a study that also suggests the older group experienced more distress from their symptoms than the younger cohort, again with the exception of anxiety.
Symptom clusters are two or more related symptoms that occur together with or without the same etiology. “Imagine you can’t sleep and the next day you’re tired and have no energy, you have trouble remembering someone’s name ... and then the next night you get so anxious about not getting sleep that it keeps you from sleeping.” That’s an example of a symptom cluster, Dr. Wilson said.
A high burden
“Why should we even evaluate symptom clusters?” Dr. Wilson asked. “The symptom burden is still high in people living with HIV. The medications got better but the symptoms remain.”
A high symptom burden also is linked to lower adherence to antiretrovirals. Also, considering groups of symptoms together could lead to targeted interventions that treat multiple symptoms, she said, “instead of treating one symptom at a time and increasing the pill burden for people living with HIV.”
Accelerated aging concerns
In addition, people living with HIV can experience accelerated aging, which is one reason Dr. Wilson and colleagues chose the 45-year-old cutoff in the study. Living with inflammation from HIV and the toxicity of earlier treatments likely contribute.
“Those over age 45 have higher rates of age-associated noncommunicable comorbidities developing at an earlier age than uninfected people with comparable lifestyles and demographics,” Dr. Wilson said.
In the full study, published in the Journal of Pain and Symptom Management, a total 2,000 people living with HIV completed the 20-item HIV Symptom Index. The participants reported their symptoms on their first visit to one of six national HIV Centers of Excellence. People were asked to report presence or absence of a particular symptom, and if they had it, how distressing it was on a scale of 1 “doesn’t bother me” to 4 “bothers me a lot.”
Younger people not only reported more anxiety but were also more distressed by it, Dr. Wilson said. The older group was more likely to be distressed by muscle aches and joint pain, trouble remembering things, and more.
The mean age in the younger group was 35 years, and it was 55 years in the older group. A total of 86% in the younger group and 87% in the older were men, and there were some differences by race, Dr. Wilson said.
More research needed
“These findings warrant further confirmation,” Dr. Wilson added. Future work could evaluate whether symptom clusters share etiology and how symptom clusters change over time. “We need to look at outcomes over time. Can we predict poorer outcomes, such as cardiac events, over time based on symptom clusters?”
Also, as part of HIV treatment success in recent years, “Our guidelines are moving people out further – if you’re undetectable sometimes you can come back at 6 months or 1 year.” The question, she said, is then: “Do we need to watch people with certain symptom clusters more closely?”
Limitations of the study include a lack of information on symptom causes and severity and its cross-sectional design.
‘Absolutely useful’
The study is “absolutely useful,” said session moderator Cheryl Netherly, an HIV nurse and clinical educator for CAN Community Health headquartered in Sarasota, Fla.
“One of the things that she mentioned was people with HIV, especially long-term HIV, they’re aging faster than the population without HIV. So, that is really important to look at.”
People living with HIV and dying from age-related comorbidities is something “we never thought would happen,” Ms. Netherly said. “Unfortunately, we’re now losing them to the different things like kidney issues, heart disease, and diabetes.”
The study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Wilson and Ms. Netherly disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TAMPA – People living with HIV experience many symptoms that can be grouped into “clusters” to help guide therapy and ideally treat more than one symptom at a time in an effort to improve quality of life, according to a study presented at the annual meeting of the Association of Nurses in AIDS Care.
Interestingly, these symptoms were more common among people living with HIV who are older than 45 years versus those who are younger, with one exception.
“In HIV, with exception of anxiety, we saw older people had more symptoms than younger ones,” said Natalie Wilson, PhD, assistant professor of community health systems at the University of California, San Francisco.
Dr. Wilson and colleagues performed a study that also suggests the older group experienced more distress from their symptoms than the younger cohort, again with the exception of anxiety.
Symptom clusters are two or more related symptoms that occur together with or without the same etiology. “Imagine you can’t sleep and the next day you’re tired and have no energy, you have trouble remembering someone’s name ... and then the next night you get so anxious about not getting sleep that it keeps you from sleeping.” That’s an example of a symptom cluster, Dr. Wilson said.
A high burden
“Why should we even evaluate symptom clusters?” Dr. Wilson asked. “The symptom burden is still high in people living with HIV. The medications got better but the symptoms remain.”
A high symptom burden also is linked to lower adherence to antiretrovirals. Also, considering groups of symptoms together could lead to targeted interventions that treat multiple symptoms, she said, “instead of treating one symptom at a time and increasing the pill burden for people living with HIV.”
Accelerated aging concerns
In addition, people living with HIV can experience accelerated aging, which is one reason Dr. Wilson and colleagues chose the 45-year-old cutoff in the study. Living with inflammation from HIV and the toxicity of earlier treatments likely contribute.
“Those over age 45 have higher rates of age-associated noncommunicable comorbidities developing at an earlier age than uninfected people with comparable lifestyles and demographics,” Dr. Wilson said.
In the full study, published in the Journal of Pain and Symptom Management, a total 2,000 people living with HIV completed the 20-item HIV Symptom Index. The participants reported their symptoms on their first visit to one of six national HIV Centers of Excellence. People were asked to report presence or absence of a particular symptom, and if they had it, how distressing it was on a scale of 1 “doesn’t bother me” to 4 “bothers me a lot.”
Younger people not only reported more anxiety but were also more distressed by it, Dr. Wilson said. The older group was more likely to be distressed by muscle aches and joint pain, trouble remembering things, and more.
The mean age in the younger group was 35 years, and it was 55 years in the older group. A total of 86% in the younger group and 87% in the older were men, and there were some differences by race, Dr. Wilson said.
More research needed
“These findings warrant further confirmation,” Dr. Wilson added. Future work could evaluate whether symptom clusters share etiology and how symptom clusters change over time. “We need to look at outcomes over time. Can we predict poorer outcomes, such as cardiac events, over time based on symptom clusters?”
Also, as part of HIV treatment success in recent years, “Our guidelines are moving people out further – if you’re undetectable sometimes you can come back at 6 months or 1 year.” The question, she said, is then: “Do we need to watch people with certain symptom clusters more closely?”
Limitations of the study include a lack of information on symptom causes and severity and its cross-sectional design.
‘Absolutely useful’
The study is “absolutely useful,” said session moderator Cheryl Netherly, an HIV nurse and clinical educator for CAN Community Health headquartered in Sarasota, Fla.
“One of the things that she mentioned was people with HIV, especially long-term HIV, they’re aging faster than the population without HIV. So, that is really important to look at.”
People living with HIV and dying from age-related comorbidities is something “we never thought would happen,” Ms. Netherly said. “Unfortunately, we’re now losing them to the different things like kidney issues, heart disease, and diabetes.”
The study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Wilson and Ms. Netherly disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.