User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
‘Promising’ new txs for most common adult leukemia
The rapid rise of chimeric antigen receptor T (CAR T-cell) therapy has allowed hematologists to make great strides in treating aggressive cases of multiple myeloma and several types of lymphoma and leukemia. But patients with chronic lymphocytic leukemia (CLL), the most common leukemia in adults, have been left out.
“These are the two immunotherapies that have the most potential right now,” said Ohio State University, Columbus, hematologist Kerry A. Rogers, MD, in an interview. She went on to say that these treatments could be a boon for patients with CLL who don’t respond well to targeted therapy drugs or are so young that those medications may not retain effectiveness throughout the patients’ lifespans.
As the American Cancer Society explains, CAR T therapy is a way to get T cells “to fight cancer by changing them in the lab so they can find and destroy cancer cells.” The cells are then returned to the patient.
As the National Cancer Institute says, “If all goes as planned, the CAR T cells will continue to multiply in the patient’s body and, with guidance from their engineered receptor, recognize and kill any cancer cells that harbor the target antigen on their surfaces.”
According to Dr. Rogers, CAR T therapy is less toxic than stem cell transplantation, a related treatment. That means older people can better tolerate it, including many CLL patients in their late 60s and beyond, she said. (Side effects of CAR T therapy include cytokine release syndrome, nervous system impairment, and weakening of the immune system.)
Thus far, CAR T therapy has been approved by the U.S. Food and Drug Administration to treat lymphomas, some forms of leukemia, and multiple myeloma. “Despite the excitement around these therapies, they lead to long-term survival in fewer than half of the patients treated,” cautions the National Cancer Institute, which also notes their high cost: more than $450,000 in one case.
CAR T therapy is not FDA-approved for CLL. “There are many reasons why CAR T is less effective in patients with CLL versus other lymphomas,” said Lee Greenberger, PhD, chief scientific officer of the Leukemia & Lymphoma Society, in an interview. “For one, many patients with heavily pretreated CLL – prior to any use of CAR T – have mutations that are known to be difficult to treat. Dysfunctional T cells are also common in patients with CLL, and there’s often a lower number of available T-cells to manufacture.”
The results of a phase 1/2 trial released in August 2023 offered new insight about CAR T for CLL. In the open-label trial reported in The Lancet, 117 U.S. patients with CLL or small lymphocytic lymphoma underwent a form of CAR T therapy called lisocabtagene maraleucel after failing treatment with two lines of therapy, including a Bruton´s tyrosine kinase inhibitor. Among 49 patients at a specific dose, “the rate of complete response or remission (including with incomplete marrow recovery) was statistically significant at 18%,” the researchers reported. A total of 51 patients in the entire study died.
The rate of undetectable minimal residual disease blood was 64%. That rate is impressive, said University of Texas MD Anderson Cancer Center leukemia specialist Nitin Jain, MD, in an interview. It’s not nearly as high as researchers have seen in other disease settings, but it’s “a good, good thing for these patients. We’ll have to see in the longer follow-up how these patients fare 2, 3, or 4 years down the line.”
Dr. Rogers, the Ohio physician, said doctors had hoped durable benefit in the Lancet study would be more impressive. An important factor limiting its value may be the aggressiveness of the disease in patients who have already failed several treatments, she said. “The efficacy of CAR T might be improved by giving it as an earlier line of therapy before the CLL has become this aggressive. But it’s difficult to propose that you should use this before a Bruton´s tyrosine kinase inhibitor or venetoclax because it’s expensive and difficult.”
What’s next for CART T research in CLL? Understanding the best timing for treatment will be key, Dr. Rogers said.
The Leukemia & Lymphoma Society’s Dr. Greenberger predicted that “we will begin to see CAR T explored in CLL patients whose disease has a high risk of failing approved agents, such as Bruton´s tyrosine kinase and B cell lymphoma 2 inhibitors. However, CLL patients may still receive prior therapy with more effective Bruton’s tyrosine kinase or B cell lymphoma 2 inhibitors in the future before using CAR T. This will likely be heightened as more Bruton´s tyrosine kinase inhibitors become generic in the next 5 to 10 years and, hopefully, less expensive than CAR T therapy.”
In the big picture, he said, “treatment of CLL with CAR T is possible, but still needs significant improvements if it is to become a mainline therapy in the future.”
CAR T therapy remains available via clinical trials, and Dr. Rogers said it is “currently an important option for patients whose CLL has become resistant to standard targeted agents. We can certainly expect to extend someone’s expected survival by years if they have a favorable response.” She acknowledged that the cost is quite high, but noted that targeted therapies are also expensive, especially over the long term. They can run to $10,000-$20,000 a month. Bispecific antibodies are also being explored as potential therapy for CLL. “They’re really exciting,” Dr. Rogers said, with the potential to spur responses similar to those from CAR T therapy.
A 2022 review described these drugs as “molecules that combine antibody-directed therapies with cellular mediated immunotherapy.” The FDA explains that “by targeting two antigens or epitopes, they can cause multiple physiological or antitumor responses, which may be independent or connected.”
According to Dr. Greenberger, many bispecifics are in clinical trials now. However, “in the context of CLL, actually, the data is actually very, very limited. The development is just starting, and there are phase 1 and phase 2 trials ongoing.”
But data from lymphoma trials are encouraging, he said, and bispecifics “are actually looking as good as CAR T in some settings.”
Regimens can be a challenge for patients taking bispecifics, Dr. Greenberger said. “Repeat dosing with a step-up dosing approach to start is typically required when treating lymphoma.”
On the other hand, Dr. Rogers noted that antibody treatment can be easier for hematologists to arrange than CAR T therapy and stem cell transplants. “From an administrative side, there’s not as many things you need to have set up. So it’s able to be administered in a wider variety of settings,” she said,
Bispecific side effects include cytokine release syndrome and neurotoxicity as well as infusion reactions, Dr. Greenberger said, adding that “I would not exclude cost as a challenge.”
According to Formulary Watch, the bispecific Columvi (glofitamab-gxbm), which recently gained FDA approval to treat diffuse large B-cell lymphoma, is estimated to cost $350,000 for an 8.5-month round of treatment. Reuters reported that the bispecific Talvey (talquetamab-tgvs), which just received FDA approval to treat multiple myeloma, is estimated to cost $270,000-$360,000 for 6-8 months of treatment.
For now, bispecific trials “are mostly now reserved for patients with CLL who become resistant to our current standard targeted agents,” Dr. Rogers said. “It’s a little unclear if you can do CAR T therapy first and then bispecifics, or bispecifics and then CAR T therapy.”
What’s coming next for bispecifics? “On the horizon is better ease of administration, which is already being addressed by subcutaneous dosing for some bispecifics in lymphomas,” Dr. Greenberger said. “There’s also the possibility of combining bispecifics with conventional therapy.”
Dr. Rogers discloses ties with Genentech, AbbVie, Novartis, AstraZeneca, Janssen, Pharmacyclics, Beigene, and LOXO@Lilly. Dr. Greenberger discloses employment with the Leukemia & Lymphoma Society, which supports academic grants and a venture philanthropy via the Therapy Acceleration Program.
Dr. Jain reports ties with Pharmacyclics, AbbVie, Genentech, AstraZeneca, Pfizer, and numerous other disclosures.
The rapid rise of chimeric antigen receptor T (CAR T-cell) therapy has allowed hematologists to make great strides in treating aggressive cases of multiple myeloma and several types of lymphoma and leukemia. But patients with chronic lymphocytic leukemia (CLL), the most common leukemia in adults, have been left out.
“These are the two immunotherapies that have the most potential right now,” said Ohio State University, Columbus, hematologist Kerry A. Rogers, MD, in an interview. She went on to say that these treatments could be a boon for patients with CLL who don’t respond well to targeted therapy drugs or are so young that those medications may not retain effectiveness throughout the patients’ lifespans.
As the American Cancer Society explains, CAR T therapy is a way to get T cells “to fight cancer by changing them in the lab so they can find and destroy cancer cells.” The cells are then returned to the patient.
As the National Cancer Institute says, “If all goes as planned, the CAR T cells will continue to multiply in the patient’s body and, with guidance from their engineered receptor, recognize and kill any cancer cells that harbor the target antigen on their surfaces.”
According to Dr. Rogers, CAR T therapy is less toxic than stem cell transplantation, a related treatment. That means older people can better tolerate it, including many CLL patients in their late 60s and beyond, she said. (Side effects of CAR T therapy include cytokine release syndrome, nervous system impairment, and weakening of the immune system.)
Thus far, CAR T therapy has been approved by the U.S. Food and Drug Administration to treat lymphomas, some forms of leukemia, and multiple myeloma. “Despite the excitement around these therapies, they lead to long-term survival in fewer than half of the patients treated,” cautions the National Cancer Institute, which also notes their high cost: more than $450,000 in one case.
CAR T therapy is not FDA-approved for CLL. “There are many reasons why CAR T is less effective in patients with CLL versus other lymphomas,” said Lee Greenberger, PhD, chief scientific officer of the Leukemia & Lymphoma Society, in an interview. “For one, many patients with heavily pretreated CLL – prior to any use of CAR T – have mutations that are known to be difficult to treat. Dysfunctional T cells are also common in patients with CLL, and there’s often a lower number of available T-cells to manufacture.”
The results of a phase 1/2 trial released in August 2023 offered new insight about CAR T for CLL. In the open-label trial reported in The Lancet, 117 U.S. patients with CLL or small lymphocytic lymphoma underwent a form of CAR T therapy called lisocabtagene maraleucel after failing treatment with two lines of therapy, including a Bruton´s tyrosine kinase inhibitor. Among 49 patients at a specific dose, “the rate of complete response or remission (including with incomplete marrow recovery) was statistically significant at 18%,” the researchers reported. A total of 51 patients in the entire study died.
The rate of undetectable minimal residual disease blood was 64%. That rate is impressive, said University of Texas MD Anderson Cancer Center leukemia specialist Nitin Jain, MD, in an interview. It’s not nearly as high as researchers have seen in other disease settings, but it’s “a good, good thing for these patients. We’ll have to see in the longer follow-up how these patients fare 2, 3, or 4 years down the line.”
Dr. Rogers, the Ohio physician, said doctors had hoped durable benefit in the Lancet study would be more impressive. An important factor limiting its value may be the aggressiveness of the disease in patients who have already failed several treatments, she said. “The efficacy of CAR T might be improved by giving it as an earlier line of therapy before the CLL has become this aggressive. But it’s difficult to propose that you should use this before a Bruton´s tyrosine kinase inhibitor or venetoclax because it’s expensive and difficult.”
What’s next for CART T research in CLL? Understanding the best timing for treatment will be key, Dr. Rogers said.
The Leukemia & Lymphoma Society’s Dr. Greenberger predicted that “we will begin to see CAR T explored in CLL patients whose disease has a high risk of failing approved agents, such as Bruton´s tyrosine kinase and B cell lymphoma 2 inhibitors. However, CLL patients may still receive prior therapy with more effective Bruton’s tyrosine kinase or B cell lymphoma 2 inhibitors in the future before using CAR T. This will likely be heightened as more Bruton´s tyrosine kinase inhibitors become generic in the next 5 to 10 years and, hopefully, less expensive than CAR T therapy.”
In the big picture, he said, “treatment of CLL with CAR T is possible, but still needs significant improvements if it is to become a mainline therapy in the future.”
CAR T therapy remains available via clinical trials, and Dr. Rogers said it is “currently an important option for patients whose CLL has become resistant to standard targeted agents. We can certainly expect to extend someone’s expected survival by years if they have a favorable response.” She acknowledged that the cost is quite high, but noted that targeted therapies are also expensive, especially over the long term. They can run to $10,000-$20,000 a month. Bispecific antibodies are also being explored as potential therapy for CLL. “They’re really exciting,” Dr. Rogers said, with the potential to spur responses similar to those from CAR T therapy.
A 2022 review described these drugs as “molecules that combine antibody-directed therapies with cellular mediated immunotherapy.” The FDA explains that “by targeting two antigens or epitopes, they can cause multiple physiological or antitumor responses, which may be independent or connected.”
According to Dr. Greenberger, many bispecifics are in clinical trials now. However, “in the context of CLL, actually, the data is actually very, very limited. The development is just starting, and there are phase 1 and phase 2 trials ongoing.”
But data from lymphoma trials are encouraging, he said, and bispecifics “are actually looking as good as CAR T in some settings.”
Regimens can be a challenge for patients taking bispecifics, Dr. Greenberger said. “Repeat dosing with a step-up dosing approach to start is typically required when treating lymphoma.”
On the other hand, Dr. Rogers noted that antibody treatment can be easier for hematologists to arrange than CAR T therapy and stem cell transplants. “From an administrative side, there’s not as many things you need to have set up. So it’s able to be administered in a wider variety of settings,” she said,
Bispecific side effects include cytokine release syndrome and neurotoxicity as well as infusion reactions, Dr. Greenberger said, adding that “I would not exclude cost as a challenge.”
According to Formulary Watch, the bispecific Columvi (glofitamab-gxbm), which recently gained FDA approval to treat diffuse large B-cell lymphoma, is estimated to cost $350,000 for an 8.5-month round of treatment. Reuters reported that the bispecific Talvey (talquetamab-tgvs), which just received FDA approval to treat multiple myeloma, is estimated to cost $270,000-$360,000 for 6-8 months of treatment.
For now, bispecific trials “are mostly now reserved for patients with CLL who become resistant to our current standard targeted agents,” Dr. Rogers said. “It’s a little unclear if you can do CAR T therapy first and then bispecifics, or bispecifics and then CAR T therapy.”
What’s coming next for bispecifics? “On the horizon is better ease of administration, which is already being addressed by subcutaneous dosing for some bispecifics in lymphomas,” Dr. Greenberger said. “There’s also the possibility of combining bispecifics with conventional therapy.”
Dr. Rogers discloses ties with Genentech, AbbVie, Novartis, AstraZeneca, Janssen, Pharmacyclics, Beigene, and LOXO@Lilly. Dr. Greenberger discloses employment with the Leukemia & Lymphoma Society, which supports academic grants and a venture philanthropy via the Therapy Acceleration Program.
Dr. Jain reports ties with Pharmacyclics, AbbVie, Genentech, AstraZeneca, Pfizer, and numerous other disclosures.
The rapid rise of chimeric antigen receptor T (CAR T-cell) therapy has allowed hematologists to make great strides in treating aggressive cases of multiple myeloma and several types of lymphoma and leukemia. But patients with chronic lymphocytic leukemia (CLL), the most common leukemia in adults, have been left out.
“These are the two immunotherapies that have the most potential right now,” said Ohio State University, Columbus, hematologist Kerry A. Rogers, MD, in an interview. She went on to say that these treatments could be a boon for patients with CLL who don’t respond well to targeted therapy drugs or are so young that those medications may not retain effectiveness throughout the patients’ lifespans.
As the American Cancer Society explains, CAR T therapy is a way to get T cells “to fight cancer by changing them in the lab so they can find and destroy cancer cells.” The cells are then returned to the patient.
As the National Cancer Institute says, “If all goes as planned, the CAR T cells will continue to multiply in the patient’s body and, with guidance from their engineered receptor, recognize and kill any cancer cells that harbor the target antigen on their surfaces.”
According to Dr. Rogers, CAR T therapy is less toxic than stem cell transplantation, a related treatment. That means older people can better tolerate it, including many CLL patients in their late 60s and beyond, she said. (Side effects of CAR T therapy include cytokine release syndrome, nervous system impairment, and weakening of the immune system.)
Thus far, CAR T therapy has been approved by the U.S. Food and Drug Administration to treat lymphomas, some forms of leukemia, and multiple myeloma. “Despite the excitement around these therapies, they lead to long-term survival in fewer than half of the patients treated,” cautions the National Cancer Institute, which also notes their high cost: more than $450,000 in one case.
CAR T therapy is not FDA-approved for CLL. “There are many reasons why CAR T is less effective in patients with CLL versus other lymphomas,” said Lee Greenberger, PhD, chief scientific officer of the Leukemia & Lymphoma Society, in an interview. “For one, many patients with heavily pretreated CLL – prior to any use of CAR T – have mutations that are known to be difficult to treat. Dysfunctional T cells are also common in patients with CLL, and there’s often a lower number of available T-cells to manufacture.”
The results of a phase 1/2 trial released in August 2023 offered new insight about CAR T for CLL. In the open-label trial reported in The Lancet, 117 U.S. patients with CLL or small lymphocytic lymphoma underwent a form of CAR T therapy called lisocabtagene maraleucel after failing treatment with two lines of therapy, including a Bruton´s tyrosine kinase inhibitor. Among 49 patients at a specific dose, “the rate of complete response or remission (including with incomplete marrow recovery) was statistically significant at 18%,” the researchers reported. A total of 51 patients in the entire study died.
The rate of undetectable minimal residual disease blood was 64%. That rate is impressive, said University of Texas MD Anderson Cancer Center leukemia specialist Nitin Jain, MD, in an interview. It’s not nearly as high as researchers have seen in other disease settings, but it’s “a good, good thing for these patients. We’ll have to see in the longer follow-up how these patients fare 2, 3, or 4 years down the line.”
Dr. Rogers, the Ohio physician, said doctors had hoped durable benefit in the Lancet study would be more impressive. An important factor limiting its value may be the aggressiveness of the disease in patients who have already failed several treatments, she said. “The efficacy of CAR T might be improved by giving it as an earlier line of therapy before the CLL has become this aggressive. But it’s difficult to propose that you should use this before a Bruton´s tyrosine kinase inhibitor or venetoclax because it’s expensive and difficult.”
What’s next for CART T research in CLL? Understanding the best timing for treatment will be key, Dr. Rogers said.
The Leukemia & Lymphoma Society’s Dr. Greenberger predicted that “we will begin to see CAR T explored in CLL patients whose disease has a high risk of failing approved agents, such as Bruton´s tyrosine kinase and B cell lymphoma 2 inhibitors. However, CLL patients may still receive prior therapy with more effective Bruton’s tyrosine kinase or B cell lymphoma 2 inhibitors in the future before using CAR T. This will likely be heightened as more Bruton´s tyrosine kinase inhibitors become generic in the next 5 to 10 years and, hopefully, less expensive than CAR T therapy.”
In the big picture, he said, “treatment of CLL with CAR T is possible, but still needs significant improvements if it is to become a mainline therapy in the future.”
CAR T therapy remains available via clinical trials, and Dr. Rogers said it is “currently an important option for patients whose CLL has become resistant to standard targeted agents. We can certainly expect to extend someone’s expected survival by years if they have a favorable response.” She acknowledged that the cost is quite high, but noted that targeted therapies are also expensive, especially over the long term. They can run to $10,000-$20,000 a month. Bispecific antibodies are also being explored as potential therapy for CLL. “They’re really exciting,” Dr. Rogers said, with the potential to spur responses similar to those from CAR T therapy.
A 2022 review described these drugs as “molecules that combine antibody-directed therapies with cellular mediated immunotherapy.” The FDA explains that “by targeting two antigens or epitopes, they can cause multiple physiological or antitumor responses, which may be independent or connected.”
According to Dr. Greenberger, many bispecifics are in clinical trials now. However, “in the context of CLL, actually, the data is actually very, very limited. The development is just starting, and there are phase 1 and phase 2 trials ongoing.”
But data from lymphoma trials are encouraging, he said, and bispecifics “are actually looking as good as CAR T in some settings.”
Regimens can be a challenge for patients taking bispecifics, Dr. Greenberger said. “Repeat dosing with a step-up dosing approach to start is typically required when treating lymphoma.”
On the other hand, Dr. Rogers noted that antibody treatment can be easier for hematologists to arrange than CAR T therapy and stem cell transplants. “From an administrative side, there’s not as many things you need to have set up. So it’s able to be administered in a wider variety of settings,” she said,
Bispecific side effects include cytokine release syndrome and neurotoxicity as well as infusion reactions, Dr. Greenberger said, adding that “I would not exclude cost as a challenge.”
According to Formulary Watch, the bispecific Columvi (glofitamab-gxbm), which recently gained FDA approval to treat diffuse large B-cell lymphoma, is estimated to cost $350,000 for an 8.5-month round of treatment. Reuters reported that the bispecific Talvey (talquetamab-tgvs), which just received FDA approval to treat multiple myeloma, is estimated to cost $270,000-$360,000 for 6-8 months of treatment.
For now, bispecific trials “are mostly now reserved for patients with CLL who become resistant to our current standard targeted agents,” Dr. Rogers said. “It’s a little unclear if you can do CAR T therapy first and then bispecifics, or bispecifics and then CAR T therapy.”
What’s coming next for bispecifics? “On the horizon is better ease of administration, which is already being addressed by subcutaneous dosing for some bispecifics in lymphomas,” Dr. Greenberger said. “There’s also the possibility of combining bispecifics with conventional therapy.”
Dr. Rogers discloses ties with Genentech, AbbVie, Novartis, AstraZeneca, Janssen, Pharmacyclics, Beigene, and LOXO@Lilly. Dr. Greenberger discloses employment with the Leukemia & Lymphoma Society, which supports academic grants and a venture philanthropy via the Therapy Acceleration Program.
Dr. Jain reports ties with Pharmacyclics, AbbVie, Genentech, AstraZeneca, Pfizer, and numerous other disclosures.
AI mammogram screening is equivalent to human readers
, a radiology and biomedical imaging professor at Yale University in New Haven, Conn.
The reason is because AI is proving to be as good as humans in interpreting mammograms, at least in the research setting.
In one of the latest reports, published online in Radiology, British investigators found that the performance of a commercially available AI system (INSIGHT MMG version 1.1.7.1 – Lunit) was essentially equivalent to over 500 specialized readers. The results are in line with other recent AI studies.
Double reading – having mammograms read by two clinicians to increase cancer detection rates – is common in the United Kingdom and elsewhere in Europe.
The British team compared the performance of 552 readers with Lunit’s AI program on the Personal Performance in Mammographic Screening exam, a quality assurance test which mammogram readers in the United Kingdom are required to take twice a year. Readers assign a malignancy score to 60 challenging cases, a mix of normal breasts and breasts with benign and cancerous lesions. The study included two test sessions for a total of 120 breast screenings.
Fifty-seven percent of the readers in the study were board-certified radiologists, 37% were radiographers, and 6% were breast clinicians. Each read at least 5,000 mammograms a year.
There was no difference in overall performance between the AI program and the human readers (AUC 0.93 vs. 0.88, P = .15).
Commenting in an editorial published with the investigation, Dr. Philpotts said the results “suggest that AI could confidently act as a second reader to decrease workloads.”
As for the United States, where double reading is generally not done, she pointed out that “many U.S. radiologists interpreting mammograms are nonspecialized and do not read high volumes of mammograms. Thus, the AI system evaluated in the study “could be used as a supplemental tool to aid the performance of readers in the United States or in other countries where screening programs use a single reading.”
There was also no difference in sensitivity between AI and human readers (84% vs. 90%, P = .34), but the AI algorithm had a higher specificity (89% vs. 76%, P = .003).
Using AI recall scores that matched the average human reader performance (90% sensitivity, 76% specificity), there was no difference with AI in regard to sensitivity (91%, P = .73) or specificity (77%, P = .85), but the investigators noted the power of the analysis was limited.
Overall, “diagnostic performance of AI was comparable with that of the average human reader.” It seems “increasingly likely that AI will eventually play a part in the interpretation of screening mammograms,” said investigators led by Yan Chen, PhD, of the Nottingham Breast Institute in England.
“That the AI system was able to match the performance of the average reader in this specialized group of mammogram readers indicates the robustness of this AI algorithm,” Dr. Philpotts said.
However, there are some caveats.
For one, the system was designed for 2D mammography, the current standard of care in the United Kingdom, while digital breast tomosynthesis (DBT) is replacing 2D mammography in the United States.
In the United States, “AI algorithms specific to DBT are necessary and will need to be reliable and reproducible to be embraced by radiologists,” Dr. Philpotts said.
Also in the United Kingdom, screening is performed at 3-year intervals in women aged 50-70 years old, which means that the study population was enriched for older women with less-dense breasts. Screening generally starts earlier in the United States and includes premenopausal women with denser breasts.
A recent study from Korea, where many women have dense breasts, found that 2D mammography and supplementary ultrasound outperformed AI for cancer detection.
“This underscores the challenges of finding cancers in dense breasts, which plague both radiologists and AI alike, and provides evidence that breast density is an important factor to consider when evaluating AI performance,” Dr. Philpotts said.
The work was funded by Lunit, the maker of the AI program used in the study. The investigators and Dr. Philpotts had no disclosures.
, a radiology and biomedical imaging professor at Yale University in New Haven, Conn.
The reason is because AI is proving to be as good as humans in interpreting mammograms, at least in the research setting.
In one of the latest reports, published online in Radiology, British investigators found that the performance of a commercially available AI system (INSIGHT MMG version 1.1.7.1 – Lunit) was essentially equivalent to over 500 specialized readers. The results are in line with other recent AI studies.
Double reading – having mammograms read by two clinicians to increase cancer detection rates – is common in the United Kingdom and elsewhere in Europe.
The British team compared the performance of 552 readers with Lunit’s AI program on the Personal Performance in Mammographic Screening exam, a quality assurance test which mammogram readers in the United Kingdom are required to take twice a year. Readers assign a malignancy score to 60 challenging cases, a mix of normal breasts and breasts with benign and cancerous lesions. The study included two test sessions for a total of 120 breast screenings.
Fifty-seven percent of the readers in the study were board-certified radiologists, 37% were radiographers, and 6% were breast clinicians. Each read at least 5,000 mammograms a year.
There was no difference in overall performance between the AI program and the human readers (AUC 0.93 vs. 0.88, P = .15).
Commenting in an editorial published with the investigation, Dr. Philpotts said the results “suggest that AI could confidently act as a second reader to decrease workloads.”
As for the United States, where double reading is generally not done, she pointed out that “many U.S. radiologists interpreting mammograms are nonspecialized and do not read high volumes of mammograms. Thus, the AI system evaluated in the study “could be used as a supplemental tool to aid the performance of readers in the United States or in other countries where screening programs use a single reading.”
There was also no difference in sensitivity between AI and human readers (84% vs. 90%, P = .34), but the AI algorithm had a higher specificity (89% vs. 76%, P = .003).
Using AI recall scores that matched the average human reader performance (90% sensitivity, 76% specificity), there was no difference with AI in regard to sensitivity (91%, P = .73) or specificity (77%, P = .85), but the investigators noted the power of the analysis was limited.
Overall, “diagnostic performance of AI was comparable with that of the average human reader.” It seems “increasingly likely that AI will eventually play a part in the interpretation of screening mammograms,” said investigators led by Yan Chen, PhD, of the Nottingham Breast Institute in England.
“That the AI system was able to match the performance of the average reader in this specialized group of mammogram readers indicates the robustness of this AI algorithm,” Dr. Philpotts said.
However, there are some caveats.
For one, the system was designed for 2D mammography, the current standard of care in the United Kingdom, while digital breast tomosynthesis (DBT) is replacing 2D mammography in the United States.
In the United States, “AI algorithms specific to DBT are necessary and will need to be reliable and reproducible to be embraced by radiologists,” Dr. Philpotts said.
Also in the United Kingdom, screening is performed at 3-year intervals in women aged 50-70 years old, which means that the study population was enriched for older women with less-dense breasts. Screening generally starts earlier in the United States and includes premenopausal women with denser breasts.
A recent study from Korea, where many women have dense breasts, found that 2D mammography and supplementary ultrasound outperformed AI for cancer detection.
“This underscores the challenges of finding cancers in dense breasts, which plague both radiologists and AI alike, and provides evidence that breast density is an important factor to consider when evaluating AI performance,” Dr. Philpotts said.
The work was funded by Lunit, the maker of the AI program used in the study. The investigators and Dr. Philpotts had no disclosures.
, a radiology and biomedical imaging professor at Yale University in New Haven, Conn.
The reason is because AI is proving to be as good as humans in interpreting mammograms, at least in the research setting.
In one of the latest reports, published online in Radiology, British investigators found that the performance of a commercially available AI system (INSIGHT MMG version 1.1.7.1 – Lunit) was essentially equivalent to over 500 specialized readers. The results are in line with other recent AI studies.
Double reading – having mammograms read by two clinicians to increase cancer detection rates – is common in the United Kingdom and elsewhere in Europe.
The British team compared the performance of 552 readers with Lunit’s AI program on the Personal Performance in Mammographic Screening exam, a quality assurance test which mammogram readers in the United Kingdom are required to take twice a year. Readers assign a malignancy score to 60 challenging cases, a mix of normal breasts and breasts with benign and cancerous lesions. The study included two test sessions for a total of 120 breast screenings.
Fifty-seven percent of the readers in the study were board-certified radiologists, 37% were radiographers, and 6% were breast clinicians. Each read at least 5,000 mammograms a year.
There was no difference in overall performance between the AI program and the human readers (AUC 0.93 vs. 0.88, P = .15).
Commenting in an editorial published with the investigation, Dr. Philpotts said the results “suggest that AI could confidently act as a second reader to decrease workloads.”
As for the United States, where double reading is generally not done, she pointed out that “many U.S. radiologists interpreting mammograms are nonspecialized and do not read high volumes of mammograms. Thus, the AI system evaluated in the study “could be used as a supplemental tool to aid the performance of readers in the United States or in other countries where screening programs use a single reading.”
There was also no difference in sensitivity between AI and human readers (84% vs. 90%, P = .34), but the AI algorithm had a higher specificity (89% vs. 76%, P = .003).
Using AI recall scores that matched the average human reader performance (90% sensitivity, 76% specificity), there was no difference with AI in regard to sensitivity (91%, P = .73) or specificity (77%, P = .85), but the investigators noted the power of the analysis was limited.
Overall, “diagnostic performance of AI was comparable with that of the average human reader.” It seems “increasingly likely that AI will eventually play a part in the interpretation of screening mammograms,” said investigators led by Yan Chen, PhD, of the Nottingham Breast Institute in England.
“That the AI system was able to match the performance of the average reader in this specialized group of mammogram readers indicates the robustness of this AI algorithm,” Dr. Philpotts said.
However, there are some caveats.
For one, the system was designed for 2D mammography, the current standard of care in the United Kingdom, while digital breast tomosynthesis (DBT) is replacing 2D mammography in the United States.
In the United States, “AI algorithms specific to DBT are necessary and will need to be reliable and reproducible to be embraced by radiologists,” Dr. Philpotts said.
Also in the United Kingdom, screening is performed at 3-year intervals in women aged 50-70 years old, which means that the study population was enriched for older women with less-dense breasts. Screening generally starts earlier in the United States and includes premenopausal women with denser breasts.
A recent study from Korea, where many women have dense breasts, found that 2D mammography and supplementary ultrasound outperformed AI for cancer detection.
“This underscores the challenges of finding cancers in dense breasts, which plague both radiologists and AI alike, and provides evidence that breast density is an important factor to consider when evaluating AI performance,” Dr. Philpotts said.
The work was funded by Lunit, the maker of the AI program used in the study. The investigators and Dr. Philpotts had no disclosures.
FROM RADIOLOGY
CHP/CCUS: Low blood cancer risk for most patients
The reason is that patients will inevitably “go online and see that [the conditions are] associated with lots of bad things; it can really cause patients psychosocial harm if there is no one to explain what their risk is and also provide risk-specific management,” Dr. Weeks said at the annual meeting of the Society of Hematologic Oncology in Houston.
CHIP and CCUS are precursors of myeloid malignancies but for most patients, the risk of progression is less than 1%. CHIPS and CCUS are also associated with cardiovascular, rheumatologic, hepatic, and other diseases.
CHIP is defined by somatic mutations in myeloid malignancy driver genes with a variant allele fraction of 2% or more; CCUS is when those molecular features are accompanied by an unexplained and persistent anemia, thrombocytopenia, or neutropenia.
A small 2017 study suggested that about a third of patients with otherwise unexplained cytopenias have CCUS.
With the increasing use of next generation sequencing for tissue and liquid biopsies and other uses, the incidental diagnosis of both conditions is increasing.
Fortunately, Dr. Weeks’ group recently published a tool for predicting the risk of progression to myeloid malignancy.
Their “clonal hematopoiesis risk score” (CHRS) was developed and validated in over 400,000 healthy volunteers in the UK Biobank, with additional validation in cohorts from Dana Farber and the University of Pavia, Italy.
The CHRS incorporates eight high-risk genetic and clinical prognostic factors, including the type and number of genetic mutations in blood cells, factors related to red blood cell volume, and age over 65. It’s available online.
“You just input the patient’s information and it spits out if the patient is low, intermediate, or high risk for progression to any myeloid malignancy,” Dr. Weeks told her audience.
High-risk patients have about a 50% 10-year cumulative incidence of myeloid malignancy. The large majority of patients are low risk, however, and have a 10-year cumulative incidence of less than 1%. Patients in the middle have a 10-year risk of about 8%.
The low-risk group “is the population of people who probably don’t need to see a specialist,” and can be followed with an annual CBC with their primary care doctors plus further workup with any clinical change. Patients should also be evaluated for cardiovascular and other comorbidity risks.
“It’s the high-risk group we worry most about,” Dr. Weeks said. “We see them more often and repeat the next-generation sequencing” annually with a CBC at least every 6 months and a bone marrow biopsy with any clinical change.
“This is the population we would shuttle towards a clinical trial, as this is the population most likely to benefit,” she said.
The overarching goal of the several ongoing studies in CHIP/CCUS is to find a way to prevent progression to blood cancer. They range from prospective cohorts and single arm pilot studies to randomized clinical trials. One trial is evaluating canakinumab to prevent progression. “Intervention in clonal hematopoiesis might have the dual benefit of both preventing hematologic malignancy as well as reducing [the] inflammatory comorbidities,” Dr. Weeks said.
The reason is that patients will inevitably “go online and see that [the conditions are] associated with lots of bad things; it can really cause patients psychosocial harm if there is no one to explain what their risk is and also provide risk-specific management,” Dr. Weeks said at the annual meeting of the Society of Hematologic Oncology in Houston.
CHIP and CCUS are precursors of myeloid malignancies but for most patients, the risk of progression is less than 1%. CHIPS and CCUS are also associated with cardiovascular, rheumatologic, hepatic, and other diseases.
CHIP is defined by somatic mutations in myeloid malignancy driver genes with a variant allele fraction of 2% or more; CCUS is when those molecular features are accompanied by an unexplained and persistent anemia, thrombocytopenia, or neutropenia.
A small 2017 study suggested that about a third of patients with otherwise unexplained cytopenias have CCUS.
With the increasing use of next generation sequencing for tissue and liquid biopsies and other uses, the incidental diagnosis of both conditions is increasing.
Fortunately, Dr. Weeks’ group recently published a tool for predicting the risk of progression to myeloid malignancy.
Their “clonal hematopoiesis risk score” (CHRS) was developed and validated in over 400,000 healthy volunteers in the UK Biobank, with additional validation in cohorts from Dana Farber and the University of Pavia, Italy.
The CHRS incorporates eight high-risk genetic and clinical prognostic factors, including the type and number of genetic mutations in blood cells, factors related to red blood cell volume, and age over 65. It’s available online.
“You just input the patient’s information and it spits out if the patient is low, intermediate, or high risk for progression to any myeloid malignancy,” Dr. Weeks told her audience.
High-risk patients have about a 50% 10-year cumulative incidence of myeloid malignancy. The large majority of patients are low risk, however, and have a 10-year cumulative incidence of less than 1%. Patients in the middle have a 10-year risk of about 8%.
The low-risk group “is the population of people who probably don’t need to see a specialist,” and can be followed with an annual CBC with their primary care doctors plus further workup with any clinical change. Patients should also be evaluated for cardiovascular and other comorbidity risks.
“It’s the high-risk group we worry most about,” Dr. Weeks said. “We see them more often and repeat the next-generation sequencing” annually with a CBC at least every 6 months and a bone marrow biopsy with any clinical change.
“This is the population we would shuttle towards a clinical trial, as this is the population most likely to benefit,” she said.
The overarching goal of the several ongoing studies in CHIP/CCUS is to find a way to prevent progression to blood cancer. They range from prospective cohorts and single arm pilot studies to randomized clinical trials. One trial is evaluating canakinumab to prevent progression. “Intervention in clonal hematopoiesis might have the dual benefit of both preventing hematologic malignancy as well as reducing [the] inflammatory comorbidities,” Dr. Weeks said.
The reason is that patients will inevitably “go online and see that [the conditions are] associated with lots of bad things; it can really cause patients psychosocial harm if there is no one to explain what their risk is and also provide risk-specific management,” Dr. Weeks said at the annual meeting of the Society of Hematologic Oncology in Houston.
CHIP and CCUS are precursors of myeloid malignancies but for most patients, the risk of progression is less than 1%. CHIPS and CCUS are also associated with cardiovascular, rheumatologic, hepatic, and other diseases.
CHIP is defined by somatic mutations in myeloid malignancy driver genes with a variant allele fraction of 2% or more; CCUS is when those molecular features are accompanied by an unexplained and persistent anemia, thrombocytopenia, or neutropenia.
A small 2017 study suggested that about a third of patients with otherwise unexplained cytopenias have CCUS.
With the increasing use of next generation sequencing for tissue and liquid biopsies and other uses, the incidental diagnosis of both conditions is increasing.
Fortunately, Dr. Weeks’ group recently published a tool for predicting the risk of progression to myeloid malignancy.
Their “clonal hematopoiesis risk score” (CHRS) was developed and validated in over 400,000 healthy volunteers in the UK Biobank, with additional validation in cohorts from Dana Farber and the University of Pavia, Italy.
The CHRS incorporates eight high-risk genetic and clinical prognostic factors, including the type and number of genetic mutations in blood cells, factors related to red blood cell volume, and age over 65. It’s available online.
“You just input the patient’s information and it spits out if the patient is low, intermediate, or high risk for progression to any myeloid malignancy,” Dr. Weeks told her audience.
High-risk patients have about a 50% 10-year cumulative incidence of myeloid malignancy. The large majority of patients are low risk, however, and have a 10-year cumulative incidence of less than 1%. Patients in the middle have a 10-year risk of about 8%.
The low-risk group “is the population of people who probably don’t need to see a specialist,” and can be followed with an annual CBC with their primary care doctors plus further workup with any clinical change. Patients should also be evaluated for cardiovascular and other comorbidity risks.
“It’s the high-risk group we worry most about,” Dr. Weeks said. “We see them more often and repeat the next-generation sequencing” annually with a CBC at least every 6 months and a bone marrow biopsy with any clinical change.
“This is the population we would shuttle towards a clinical trial, as this is the population most likely to benefit,” she said.
The overarching goal of the several ongoing studies in CHIP/CCUS is to find a way to prevent progression to blood cancer. They range from prospective cohorts and single arm pilot studies to randomized clinical trials. One trial is evaluating canakinumab to prevent progression. “Intervention in clonal hematopoiesis might have the dual benefit of both preventing hematologic malignancy as well as reducing [the] inflammatory comorbidities,” Dr. Weeks said.
FROM SOHO 2023
A Rare Case of Leptomeningeal Carcinomatosis From Gastroesophageal Adenocarcinoma Masquerading as Polyneuropathy
INTRODUCTION
Leptomeningeal metastasis (LM) is an extremely rare complication of gastroesophageal (GE) cancer. Diagnosis is challenging due to frequently nonspecific clinical presentations, limited sensitivity of diagnostic testing, and potential overlap with neurologic immune-related adverse events (irAE). We describe a case of metastatic gastroesophageal cancer on immunotherapy presenting with LM masquerading as polyneuropathy.
CASE REPORT
A 74-year-old male with HER2+ GE junction cancer with peritoneal metastases diagnosed 6 months ago, on maintenance trastuzumab/pembrolizumab and with no previous history of cranial or spinal disease, presented with worsening ataxia, headache, and diplopia for one month with multiple negative outpatient MRIs. Examination showed left abducens nerve palsy, dysmetria and absent deep tendon reflexes in upper and lower extremities. CT head was unremarkable, and MRI showed non-specific mild enhancement of the right optic nerve, symmetrical lumbosacral nerve roots and cauda equina concerning for paraneoplastic versus immunotherapy-related polyneuropathy. He was started on empiric high-dose corticosteroids. PET-CT was negative for FDG-avid lesions. Cerebrospinal fluid (CSF) analysis revealed moderate pleocytosis with many large atypical cells, elevated protein (118 mg/dL) and LDH (28 IU/L). Immunohistochemistry was positive for CDX2, CA 19-9, CK7, and pankeratin, consistent with metastatic adenocarcinoma, negative for HER2 in contrast to the original tumor. He subsequently developed hydrocephalus requiring a ventriculoperitoneal shunt. He received ten fractions of whole brain irradiation before electing to pursue hospice care.
DISCUSSION
LM is an extremely rare complication of GE cancer with an incidence of <0.2% and carries a poor prognosis. Differentiation between LM and irAE in patients on immunotherapy can be challenging. Diagnosis relies mostly on CSF cytology, and lumbar puncture should not be delayed in patients with new neurologic symptoms. Treatment options are intrathecal chemotherapy, radiation and steroids. A recent phase II trial has shown promise for intrathecal trastuzumab in patients with HER2+ cancers, but options for HER2 negative disease remain mostly palliative.
CONCLUSIONS
Our case highlights the need for suspecting this rare metastatic site, as early diagnosis and genetic characterization allow for exploring more treatment options including targeted therapies which may improve overall survival and quality of life.
INTRODUCTION
Leptomeningeal metastasis (LM) is an extremely rare complication of gastroesophageal (GE) cancer. Diagnosis is challenging due to frequently nonspecific clinical presentations, limited sensitivity of diagnostic testing, and potential overlap with neurologic immune-related adverse events (irAE). We describe a case of metastatic gastroesophageal cancer on immunotherapy presenting with LM masquerading as polyneuropathy.
CASE REPORT
A 74-year-old male with HER2+ GE junction cancer with peritoneal metastases diagnosed 6 months ago, on maintenance trastuzumab/pembrolizumab and with no previous history of cranial or spinal disease, presented with worsening ataxia, headache, and diplopia for one month with multiple negative outpatient MRIs. Examination showed left abducens nerve palsy, dysmetria and absent deep tendon reflexes in upper and lower extremities. CT head was unremarkable, and MRI showed non-specific mild enhancement of the right optic nerve, symmetrical lumbosacral nerve roots and cauda equina concerning for paraneoplastic versus immunotherapy-related polyneuropathy. He was started on empiric high-dose corticosteroids. PET-CT was negative for FDG-avid lesions. Cerebrospinal fluid (CSF) analysis revealed moderate pleocytosis with many large atypical cells, elevated protein (118 mg/dL) and LDH (28 IU/L). Immunohistochemistry was positive for CDX2, CA 19-9, CK7, and pankeratin, consistent with metastatic adenocarcinoma, negative for HER2 in contrast to the original tumor. He subsequently developed hydrocephalus requiring a ventriculoperitoneal shunt. He received ten fractions of whole brain irradiation before electing to pursue hospice care.
DISCUSSION
LM is an extremely rare complication of GE cancer with an incidence of <0.2% and carries a poor prognosis. Differentiation between LM and irAE in patients on immunotherapy can be challenging. Diagnosis relies mostly on CSF cytology, and lumbar puncture should not be delayed in patients with new neurologic symptoms. Treatment options are intrathecal chemotherapy, radiation and steroids. A recent phase II trial has shown promise for intrathecal trastuzumab in patients with HER2+ cancers, but options for HER2 negative disease remain mostly palliative.
CONCLUSIONS
Our case highlights the need for suspecting this rare metastatic site, as early diagnosis and genetic characterization allow for exploring more treatment options including targeted therapies which may improve overall survival and quality of life.
INTRODUCTION
Leptomeningeal metastasis (LM) is an extremely rare complication of gastroesophageal (GE) cancer. Diagnosis is challenging due to frequently nonspecific clinical presentations, limited sensitivity of diagnostic testing, and potential overlap with neurologic immune-related adverse events (irAE). We describe a case of metastatic gastroesophageal cancer on immunotherapy presenting with LM masquerading as polyneuropathy.
CASE REPORT
A 74-year-old male with HER2+ GE junction cancer with peritoneal metastases diagnosed 6 months ago, on maintenance trastuzumab/pembrolizumab and with no previous history of cranial or spinal disease, presented with worsening ataxia, headache, and diplopia for one month with multiple negative outpatient MRIs. Examination showed left abducens nerve palsy, dysmetria and absent deep tendon reflexes in upper and lower extremities. CT head was unremarkable, and MRI showed non-specific mild enhancement of the right optic nerve, symmetrical lumbosacral nerve roots and cauda equina concerning for paraneoplastic versus immunotherapy-related polyneuropathy. He was started on empiric high-dose corticosteroids. PET-CT was negative for FDG-avid lesions. Cerebrospinal fluid (CSF) analysis revealed moderate pleocytosis with many large atypical cells, elevated protein (118 mg/dL) and LDH (28 IU/L). Immunohistochemistry was positive for CDX2, CA 19-9, CK7, and pankeratin, consistent with metastatic adenocarcinoma, negative for HER2 in contrast to the original tumor. He subsequently developed hydrocephalus requiring a ventriculoperitoneal shunt. He received ten fractions of whole brain irradiation before electing to pursue hospice care.
DISCUSSION
LM is an extremely rare complication of GE cancer with an incidence of <0.2% and carries a poor prognosis. Differentiation between LM and irAE in patients on immunotherapy can be challenging. Diagnosis relies mostly on CSF cytology, and lumbar puncture should not be delayed in patients with new neurologic symptoms. Treatment options are intrathecal chemotherapy, radiation and steroids. A recent phase II trial has shown promise for intrathecal trastuzumab in patients with HER2+ cancers, but options for HER2 negative disease remain mostly palliative.
CONCLUSIONS
Our case highlights the need for suspecting this rare metastatic site, as early diagnosis and genetic characterization allow for exploring more treatment options including targeted therapies which may improve overall survival and quality of life.
A Multi-Disciplinary Approach to Increasing Germline Genetic Testing for Prostate Cancer
PURPOSE
This quality improvement project aims to enhance the rate of germline genetic testing for prostate cancer at the Stratton VA Medical Center, improving risk reduction strategies and therapeutic options for patients.
BACKGROUND
Prostate cancer is prevalent at the Stratton VA Medical Center, yet the rate of genetic evaluation for prostate cancer remains suboptimal. National guidelines recommend genetic counseling and testing in specific patient populations. To address this gap, an interdisciplinary working group conducted gap analysis and root cause analysis, identifying four significant barriers.
METHODS
The working group comprised medical oncologists, urologists, primary care physicians, genetics counselors, data experts, and a LEAN coach. Interventions included implementing a prostate cancer pathway to educate staff on genetic testing indications and integrating genetic testing screening into clinic visits. After the interventions were implemented in January 2022, patient charts were reviewed for all genetic referrals and new prostate cancer diagnoses from January to December 2022.
DATA ANALYSIS
Descriptive analysis was conducted on referral rates, evaluation visit completion rates, and genetic testing outcomes among prostate cancer patients.
RESULTS
During the study period, 59 prostate cancer patients were referred for genetic evaluation. Notably, this was a large increase from no genetic referrals for prostate cancer in the previous year. Among them, 43 completed the evaluation visit, and 34 underwent genetic testing. Noteworthy findings were observed in 5 patients, including 3 variants of unknown significance and 2 pathogenic germline variants: HOXB13 and BRCA2 mutations.
IMPLICATIONS
This project highlights the power of a collaborative, multidisciplinary approach to overcome barriers and enhance the quality of care for prostate cancer patients. The team’s use of gap analysis and root cause analysis successfully identified barriers and proposed solutions, leading to increased referrals and the identification of significant genetic findings. Continued efforts to improve access to germline genetic testing are crucial for enhanced patient care and improved outcomes.
PURPOSE
This quality improvement project aims to enhance the rate of germline genetic testing for prostate cancer at the Stratton VA Medical Center, improving risk reduction strategies and therapeutic options for patients.
BACKGROUND
Prostate cancer is prevalent at the Stratton VA Medical Center, yet the rate of genetic evaluation for prostate cancer remains suboptimal. National guidelines recommend genetic counseling and testing in specific patient populations. To address this gap, an interdisciplinary working group conducted gap analysis and root cause analysis, identifying four significant barriers.
METHODS
The working group comprised medical oncologists, urologists, primary care physicians, genetics counselors, data experts, and a LEAN coach. Interventions included implementing a prostate cancer pathway to educate staff on genetic testing indications and integrating genetic testing screening into clinic visits. After the interventions were implemented in January 2022, patient charts were reviewed for all genetic referrals and new prostate cancer diagnoses from January to December 2022.
DATA ANALYSIS
Descriptive analysis was conducted on referral rates, evaluation visit completion rates, and genetic testing outcomes among prostate cancer patients.
RESULTS
During the study period, 59 prostate cancer patients were referred for genetic evaluation. Notably, this was a large increase from no genetic referrals for prostate cancer in the previous year. Among them, 43 completed the evaluation visit, and 34 underwent genetic testing. Noteworthy findings were observed in 5 patients, including 3 variants of unknown significance and 2 pathogenic germline variants: HOXB13 and BRCA2 mutations.
IMPLICATIONS
This project highlights the power of a collaborative, multidisciplinary approach to overcome barriers and enhance the quality of care for prostate cancer patients. The team’s use of gap analysis and root cause analysis successfully identified barriers and proposed solutions, leading to increased referrals and the identification of significant genetic findings. Continued efforts to improve access to germline genetic testing are crucial for enhanced patient care and improved outcomes.
PURPOSE
This quality improvement project aims to enhance the rate of germline genetic testing for prostate cancer at the Stratton VA Medical Center, improving risk reduction strategies and therapeutic options for patients.
BACKGROUND
Prostate cancer is prevalent at the Stratton VA Medical Center, yet the rate of genetic evaluation for prostate cancer remains suboptimal. National guidelines recommend genetic counseling and testing in specific patient populations. To address this gap, an interdisciplinary working group conducted gap analysis and root cause analysis, identifying four significant barriers.
METHODS
The working group comprised medical oncologists, urologists, primary care physicians, genetics counselors, data experts, and a LEAN coach. Interventions included implementing a prostate cancer pathway to educate staff on genetic testing indications and integrating genetic testing screening into clinic visits. After the interventions were implemented in January 2022, patient charts were reviewed for all genetic referrals and new prostate cancer diagnoses from January to December 2022.
DATA ANALYSIS
Descriptive analysis was conducted on referral rates, evaluation visit completion rates, and genetic testing outcomes among prostate cancer patients.
RESULTS
During the study period, 59 prostate cancer patients were referred for genetic evaluation. Notably, this was a large increase from no genetic referrals for prostate cancer in the previous year. Among them, 43 completed the evaluation visit, and 34 underwent genetic testing. Noteworthy findings were observed in 5 patients, including 3 variants of unknown significance and 2 pathogenic germline variants: HOXB13 and BRCA2 mutations.
IMPLICATIONS
This project highlights the power of a collaborative, multidisciplinary approach to overcome barriers and enhance the quality of care for prostate cancer patients. The team’s use of gap analysis and root cause analysis successfully identified barriers and proposed solutions, leading to increased referrals and the identification of significant genetic findings. Continued efforts to improve access to germline genetic testing are crucial for enhanced patient care and improved outcomes.
Pacify the Prostate, Pop Goes the Pituitary
INTRODUCTION
Excluding skin cancer, prostate cancer is the most common malignancy affecting men in the United States, accounting for ~33% of VA cancer cases. Androgen deprivation therapy (ADT) is considered standard of care in treating advanced prostate cancer. Pituitary apoplexy is a rare and morbid adverse event associated with GnRH agonist treatment. We describe a patient with advanced prostate cancer who developed pituitary apoplexy shortly after leuprolide therapy.
CASE PRESENTATION
A 70-year-old African-American male was diagnosed with a T2aN1M1 stage IVB prostate cancer, Gleason 4+5, PSA 19.5. Four hours after his first leuprolide injection, he developed vomiting, diaphoresis, myalgia, and a severe frontal headache. Brain MRI revealed a 2.4 × 1.3 × 1.3cm pituitary mass, suspicious for an adenoma with hemorrhage. Labs noted low TSH, prolactin, LH, growth hormone, ACTH, cortisol, and testosterone, consistent with pituitary apoplexy. He was treated with steroids. Three weeks later, testosterone levels remained very low. He started abiraterone and prednisone without further leuprolide.
DISCUSSION
Prostate cancer is ubiquitous among VA patients, and ADT with GnRH agonist is vital in their care. These medications stimulate the pituitary to release LH and FSH resulting in a negative feedback loop, ultimately decreasing the levels of testosterone. Common side effects of GnRH agonists include hot flashes, diaphoresis, and sexual dysfunction. We present a patient who started leuprolide for prostate cancer. Symptoms including a severe headache led to an evaluation confirming pituitary apoplexy. Literature review reveals ~ 21 cases of pituitary apoplexy associated with GnRH agonist treatment for prostate cancer, and apoplexy can occur immediately to months later Undiagnosed pituitary adenomas are common among these patients. Treatment includes pituitary surgery or conservative management. Further prostate cancer treatment needs investigation, but we propose that GnRH modifying treatment can be withheld while testosterone levels remain low.
CONCLUSIONS
Prostate cancer is extremely common in the VA population, and treatment with leuprolide is standard. Pituitary apoplexy is a rare, but devastating complication of this treatment, and providers should be aware of the symptoms in order to intervene quickly. Further testosterone lowering treatment may be withheld if testosterone levels remain low.
INTRODUCTION
Excluding skin cancer, prostate cancer is the most common malignancy affecting men in the United States, accounting for ~33% of VA cancer cases. Androgen deprivation therapy (ADT) is considered standard of care in treating advanced prostate cancer. Pituitary apoplexy is a rare and morbid adverse event associated with GnRH agonist treatment. We describe a patient with advanced prostate cancer who developed pituitary apoplexy shortly after leuprolide therapy.
CASE PRESENTATION
A 70-year-old African-American male was diagnosed with a T2aN1M1 stage IVB prostate cancer, Gleason 4+5, PSA 19.5. Four hours after his first leuprolide injection, he developed vomiting, diaphoresis, myalgia, and a severe frontal headache. Brain MRI revealed a 2.4 × 1.3 × 1.3cm pituitary mass, suspicious for an adenoma with hemorrhage. Labs noted low TSH, prolactin, LH, growth hormone, ACTH, cortisol, and testosterone, consistent with pituitary apoplexy. He was treated with steroids. Three weeks later, testosterone levels remained very low. He started abiraterone and prednisone without further leuprolide.
DISCUSSION
Prostate cancer is ubiquitous among VA patients, and ADT with GnRH agonist is vital in their care. These medications stimulate the pituitary to release LH and FSH resulting in a negative feedback loop, ultimately decreasing the levels of testosterone. Common side effects of GnRH agonists include hot flashes, diaphoresis, and sexual dysfunction. We present a patient who started leuprolide for prostate cancer. Symptoms including a severe headache led to an evaluation confirming pituitary apoplexy. Literature review reveals ~ 21 cases of pituitary apoplexy associated with GnRH agonist treatment for prostate cancer, and apoplexy can occur immediately to months later Undiagnosed pituitary adenomas are common among these patients. Treatment includes pituitary surgery or conservative management. Further prostate cancer treatment needs investigation, but we propose that GnRH modifying treatment can be withheld while testosterone levels remain low.
CONCLUSIONS
Prostate cancer is extremely common in the VA population, and treatment with leuprolide is standard. Pituitary apoplexy is a rare, but devastating complication of this treatment, and providers should be aware of the symptoms in order to intervene quickly. Further testosterone lowering treatment may be withheld if testosterone levels remain low.
INTRODUCTION
Excluding skin cancer, prostate cancer is the most common malignancy affecting men in the United States, accounting for ~33% of VA cancer cases. Androgen deprivation therapy (ADT) is considered standard of care in treating advanced prostate cancer. Pituitary apoplexy is a rare and morbid adverse event associated with GnRH agonist treatment. We describe a patient with advanced prostate cancer who developed pituitary apoplexy shortly after leuprolide therapy.
CASE PRESENTATION
A 70-year-old African-American male was diagnosed with a T2aN1M1 stage IVB prostate cancer, Gleason 4+5, PSA 19.5. Four hours after his first leuprolide injection, he developed vomiting, diaphoresis, myalgia, and a severe frontal headache. Brain MRI revealed a 2.4 × 1.3 × 1.3cm pituitary mass, suspicious for an adenoma with hemorrhage. Labs noted low TSH, prolactin, LH, growth hormone, ACTH, cortisol, and testosterone, consistent with pituitary apoplexy. He was treated with steroids. Three weeks later, testosterone levels remained very low. He started abiraterone and prednisone without further leuprolide.
DISCUSSION
Prostate cancer is ubiquitous among VA patients, and ADT with GnRH agonist is vital in their care. These medications stimulate the pituitary to release LH and FSH resulting in a negative feedback loop, ultimately decreasing the levels of testosterone. Common side effects of GnRH agonists include hot flashes, diaphoresis, and sexual dysfunction. We present a patient who started leuprolide for prostate cancer. Symptoms including a severe headache led to an evaluation confirming pituitary apoplexy. Literature review reveals ~ 21 cases of pituitary apoplexy associated with GnRH agonist treatment for prostate cancer, and apoplexy can occur immediately to months later Undiagnosed pituitary adenomas are common among these patients. Treatment includes pituitary surgery or conservative management. Further prostate cancer treatment needs investigation, but we propose that GnRH modifying treatment can be withheld while testosterone levels remain low.
CONCLUSIONS
Prostate cancer is extremely common in the VA population, and treatment with leuprolide is standard. Pituitary apoplexy is a rare, but devastating complication of this treatment, and providers should be aware of the symptoms in order to intervene quickly. Further testosterone lowering treatment may be withheld if testosterone levels remain low.
BCR is unreliable surrogate for overall survival in prostate cancer
TOPLINE
METHODOLOGY
- In trials of localized prostate cancer, BCR remains a controversial surrogate endpoint for overall survival.
- The meta-analysis included 10,741 patients from 11 randomized clinical trials; the median follow-up was 9.2 years.
- Interventions included radiotherapy dose escalation, in which high-dose radiotherapy was compared with conventional radiotherapy (n = 3,639); short-term androgen deprivation therapy (ADT), in which radiotherapy plus short-term ADT was compared with radiotherapy alone (n = 3,930); and ADT prolongation, in which radiotherapy plus long-term ADT was compared with radiotherapy plus short-term ADT (n = 3,772).
- Prentice criteria and the two-stage meta-analytic approach were used to assess BCR as a surrogate endpoint for overall survival.
- The researchers assessed the treatment effect on BCR and on overall survival.
TAKEAWAY
- With regard to treatment effect on BCR, the three interventions significantly reduced BCR risk – dose escalation by 29%, short-term ADT by 47%, and ADT prolongation by 46%. With regard to survival, only short- and long-term ADT significantly improved overall survival, by 9% and 14%, respectively.
- At 48 months, BCR was associated with significantly increased mortality risk: 2.46-fold increased risk for dose escalation, 1.51-fold greater risk for short-term ADT, and 2.31-fold higher risk for ADT prolongation.
- However, after adjusting for BCR at 48 months, there was no significant treatment effect on overall survival (hazard ratio, 1.10; [95% confidence interval, 0.96-1.27]; HR, 0.96 [95% CI, 0.87-1.06]; HR, 1.00 [95% CI, 0.90-1.12], respectively).
- Patient-level correlation between time to BCR and overall survival was low after censoring for noncancer-related deaths. The correlation between BCR-free survival and overall survival ranged from low to moderate.
IN PRACTICE
Overall, “these results strongly suggest that BCR-based endpoints should not be the primary endpoint in randomized trials conducted for localized [prostate cancer],” the authors concluded. They added that metastasis-free survival represents a more appropriate measure.
SOURCE
The study was led by senior author Amar Kishan, MD, of the University of California, Los Angeles, and was published online in the Journal of Clinical Oncology.
LIMITATIONS
- The trials used different definitions of BCR – the older American Society of Therapeutic Radiation and Oncology definition, and the more current Phoenix criteria.
- Some trials were conducted more than 20 years ago, and a variety of factors, including patient selection, staging, diagnostic criteria, and therapeutic approaches, have evolved in that time.
- Quality of life was not captured.
DISCLOSURES
The study received support from Cancer Research UK, the UK National Health Service, the Prostate Cancer National Institutes of Health Specialized Programs of Research Excellence, the UK Department of Defense, the Prostate Cancer Foundation, and the American Society for Radiation Oncology. Authors’ relevant financial relationships are detailed in the published study.
A version of this article appeared on Medscape.com.
TOPLINE
METHODOLOGY
- In trials of localized prostate cancer, BCR remains a controversial surrogate endpoint for overall survival.
- The meta-analysis included 10,741 patients from 11 randomized clinical trials; the median follow-up was 9.2 years.
- Interventions included radiotherapy dose escalation, in which high-dose radiotherapy was compared with conventional radiotherapy (n = 3,639); short-term androgen deprivation therapy (ADT), in which radiotherapy plus short-term ADT was compared with radiotherapy alone (n = 3,930); and ADT prolongation, in which radiotherapy plus long-term ADT was compared with radiotherapy plus short-term ADT (n = 3,772).
- Prentice criteria and the two-stage meta-analytic approach were used to assess BCR as a surrogate endpoint for overall survival.
- The researchers assessed the treatment effect on BCR and on overall survival.
TAKEAWAY
- With regard to treatment effect on BCR, the three interventions significantly reduced BCR risk – dose escalation by 29%, short-term ADT by 47%, and ADT prolongation by 46%. With regard to survival, only short- and long-term ADT significantly improved overall survival, by 9% and 14%, respectively.
- At 48 months, BCR was associated with significantly increased mortality risk: 2.46-fold increased risk for dose escalation, 1.51-fold greater risk for short-term ADT, and 2.31-fold higher risk for ADT prolongation.
- However, after adjusting for BCR at 48 months, there was no significant treatment effect on overall survival (hazard ratio, 1.10; [95% confidence interval, 0.96-1.27]; HR, 0.96 [95% CI, 0.87-1.06]; HR, 1.00 [95% CI, 0.90-1.12], respectively).
- Patient-level correlation between time to BCR and overall survival was low after censoring for noncancer-related deaths. The correlation between BCR-free survival and overall survival ranged from low to moderate.
IN PRACTICE
Overall, “these results strongly suggest that BCR-based endpoints should not be the primary endpoint in randomized trials conducted for localized [prostate cancer],” the authors concluded. They added that metastasis-free survival represents a more appropriate measure.
SOURCE
The study was led by senior author Amar Kishan, MD, of the University of California, Los Angeles, and was published online in the Journal of Clinical Oncology.
LIMITATIONS
- The trials used different definitions of BCR – the older American Society of Therapeutic Radiation and Oncology definition, and the more current Phoenix criteria.
- Some trials were conducted more than 20 years ago, and a variety of factors, including patient selection, staging, diagnostic criteria, and therapeutic approaches, have evolved in that time.
- Quality of life was not captured.
DISCLOSURES
The study received support from Cancer Research UK, the UK National Health Service, the Prostate Cancer National Institutes of Health Specialized Programs of Research Excellence, the UK Department of Defense, the Prostate Cancer Foundation, and the American Society for Radiation Oncology. Authors’ relevant financial relationships are detailed in the published study.
A version of this article appeared on Medscape.com.
TOPLINE
METHODOLOGY
- In trials of localized prostate cancer, BCR remains a controversial surrogate endpoint for overall survival.
- The meta-analysis included 10,741 patients from 11 randomized clinical trials; the median follow-up was 9.2 years.
- Interventions included radiotherapy dose escalation, in which high-dose radiotherapy was compared with conventional radiotherapy (n = 3,639); short-term androgen deprivation therapy (ADT), in which radiotherapy plus short-term ADT was compared with radiotherapy alone (n = 3,930); and ADT prolongation, in which radiotherapy plus long-term ADT was compared with radiotherapy plus short-term ADT (n = 3,772).
- Prentice criteria and the two-stage meta-analytic approach were used to assess BCR as a surrogate endpoint for overall survival.
- The researchers assessed the treatment effect on BCR and on overall survival.
TAKEAWAY
- With regard to treatment effect on BCR, the three interventions significantly reduced BCR risk – dose escalation by 29%, short-term ADT by 47%, and ADT prolongation by 46%. With regard to survival, only short- and long-term ADT significantly improved overall survival, by 9% and 14%, respectively.
- At 48 months, BCR was associated with significantly increased mortality risk: 2.46-fold increased risk for dose escalation, 1.51-fold greater risk for short-term ADT, and 2.31-fold higher risk for ADT prolongation.
- However, after adjusting for BCR at 48 months, there was no significant treatment effect on overall survival (hazard ratio, 1.10; [95% confidence interval, 0.96-1.27]; HR, 0.96 [95% CI, 0.87-1.06]; HR, 1.00 [95% CI, 0.90-1.12], respectively).
- Patient-level correlation between time to BCR and overall survival was low after censoring for noncancer-related deaths. The correlation between BCR-free survival and overall survival ranged from low to moderate.
IN PRACTICE
Overall, “these results strongly suggest that BCR-based endpoints should not be the primary endpoint in randomized trials conducted for localized [prostate cancer],” the authors concluded. They added that metastasis-free survival represents a more appropriate measure.
SOURCE
The study was led by senior author Amar Kishan, MD, of the University of California, Los Angeles, and was published online in the Journal of Clinical Oncology.
LIMITATIONS
- The trials used different definitions of BCR – the older American Society of Therapeutic Radiation and Oncology definition, and the more current Phoenix criteria.
- Some trials were conducted more than 20 years ago, and a variety of factors, including patient selection, staging, diagnostic criteria, and therapeutic approaches, have evolved in that time.
- Quality of life was not captured.
DISCLOSURES
The study received support from Cancer Research UK, the UK National Health Service, the Prostate Cancer National Institutes of Health Specialized Programs of Research Excellence, the UK Department of Defense, the Prostate Cancer Foundation, and the American Society for Radiation Oncology. Authors’ relevant financial relationships are detailed in the published study.
A version of this article appeared on Medscape.com.
Predicting prostate cancer risk: Are polygenic risk scores ready for prime time?
DNA testing for prostate cancer – of the patients’ inherited DNA and their tumors’ somatic DNA – is increasingly used in the U.S. to determine whether and how to treat low-grade, localized prostate cancers.
Another genetic approach, known as the polygenic risk score (PRS), is emerging as a third genetic approach for sorting out prostate cancer risks.
PRS aims to stratify a person’s disease risk by going beyond rare variants in genes, such as BRCA2, and compiling a weighted score that integrates thousands of common variants whose role in cancer may be unknown but are found more frequently in men with prostate cancer. Traditional germline testing, by contrast, looks for about 30 specific genes directly linked to prostate cancer.
Essentially, “a polygenic risk score estimates your risk by adding together the number of bad cards you were dealt by the impact of each card, such as an ace versus a deuce,” said William Catalona, MD, a urologist at Northwestern University Feinberg School of Medicine, Chicago, known as the father of prostate-specific antigen (PSA) screening.
In combination, these variants can have powerful predictive value.
Having a tool that can mine the depths of a person’s genetic makeup and help doctors devise a nuanced risk assessment for prostate cancer seems like a winning proposition.
Despite its promise, PRS testing is not yet used routinely in practice. The central uncertainty regarding its use lies in whether the risk score can accurately predict who will develop aggressive prostate cancer that needs to be treated and who won’t. The research to date has been mixed, and experts remain polarized.
“PRS absolutely, irrefutably can distinguish between the probability of somebody developing prostate cancer or not. Nobody could look at the data and argue with that,” said Todd Morgan, MD, a genomics researcher from the University of Michigan, Ann Arbor. “What [the data] so far haven’t really been able to do is distinguish whether somebody is likely to have clinically significant prostate cancer versus lower-risk prostate cancer.”
The promise of PRS in prostate cancer?
, according to Burcu Darst, PhD, a genetic epidemiologist at Fred Hutchinson Cancer Center, Seattle.
Research in the area has intensified in recent years as genome-wide association studies (GWAS) have become more affordable and the genetic information from these studies has been increasingly aggregated in biobanks.
“Because the sample sizes now are so much bigger than they used to be for GWAS studies, we’re able to develop much better polygenic risk scores than we were before,” said Dr. Darst.
Dr. Darst is lead author on the largest, most diverse prostate GWAS analysis, which led to the development of a PRS that is highly predictive of prostate cancer risk across diverse populations.
In the 2021 meta-analysis, which included 107,247 case patients and 127,006 control patients, Dr. Darst and colleagues identified 86 new genetic risk variants independently associated with prostate cancer risk, bringing the total to 269 known risk variants.
Compared with men at average genetic risk for prostate cancer – those in the 40%-60% genetic risk score category – men in the top 10% of the risk score (90%-100%) had between a 3.74-fold to fivefold higher risk for prostate cancer. However, the team did not find evidence that the genetic risk score could differentiate a person’s risk for aggressive versus nonaggressive disease.
As Dr. Darst’s team continues to improve the PRS, Dr. Darst says it will get better at predicting aggressive disease. One recent analysis from Dr. Darst and colleagues found that “although the PRS generally did not differentiate aggressive versus nonaggressive prostate cancer,” about 40% of men who will develop aggressive disease have a PRS in the top 20%, whereas only about 7% of men who will develop aggressive tumors have a PRS in the bottom 20%. Another recent study from Dr. Darst and colleagues found that PRS can distinguish between aggressive and nonaggressive disease in men of African ancestry.
These findings highlight “the potential clinical utility of the polygenic risk score,” Dr. Darst said.
Although the growing body of research makes Dr. Catalona, Dr. Darst, and others optimistic about PRS, the landscape is also littered with critics and studies showcasing its limitations.
An analysis, published in JAMA Internal Medicine, found that, compared with a contemporary clinical risk predictor, PRS did not improve prediction of aggressive prostate cancers. Another recent study, which used a 6.6 million–variant PRS to predict the risk of incident prostate cancer among 5,701 healthy men of European descent older than age 69, found that men in the top 20% of the PRS distribution “had an almost three times higher risk of prostate cancer,” compared with men in the lowest quintile; however, a higher PRS was not associated with a higher Gleason grade group, indicative of more aggressive disease.
“While a PRS for prostate cancer is strongly associated with incident risk” in the cohort, “the clinical utility of the PRS as a biomarker is currently limited by its inability to select for clinically significant disease,” the authors concluded.
Utility in practice?
Although PRS has been billed as a predictive test, Dr. Catalona believes PRS could have a range of uses both before and after diagnosis.
PRS may, for instance, guide treatment choices for men diagnosed with prostate cancer, Dr. Catalona noted. For men with a PRS that signals a higher risk for aggressive disease, a positive prostate biopsy result could help them decide whether to seek active treatment with surgery or radiation or go on active surveillance.
PRS could also help inform cancer screening. If a PRS test found a patient’s risk for prostate cancer was high, that person could decide to seek PSA screening before age 50 – the recommended age for average-risk men.
However, Aroon Hingorani, MD, a professor of genetic epidemiology at the University College London, expressed concern over using PRS to inform cancer screenings.
Part of the issue, Dr. Hingorani and colleagues explained in a recent article in the BMJ, is that “risk is notoriously difficult to communicate.”
PRS estimates a person’s relative risk for a disease but does not factor in the underlying population risk. Risk prediction should include both, Dr. Hingorani said.
People with high-risk scores may, for instance, discuss earlier screening with their clinician, even if their absolute risk for the disease – which accounts for both relative risk and underlying population disease risk – is still small, Dr. Hingorani and colleagues said. “Conversely, people who do not have ‘high risk’ polygenic scores might be less likely to seek medical attention for concerning symptoms, or their clinicians might be less inclined to investigate.”
Given this, Dr. Hingorani and colleagues believe polygenic scores “will always be limited in their ability to predict disease” and “will always remain one of many risk factors,” such as environmental influences.
Another caveat is that PRS generally is based on data collected from European populations, said Eric Klein, MD, chairman emeritus of urology at the Cleveland Clinic and now a scientist at the biotechnology company Grail, which developed the Galleri blood test that screens for 50 types of cancer. While a valid concern, “that’s easy to fix ultimately,” he said, as the diversity of inputs from various ethnicities increases over time.
Although several companies offer PRS products, moving PRS into the clinic would require an infrastructure for testing which does not yet exist in the U.S., said Dr. Catalona.
Giordano Botta, PhD, CEO of New York–based PRS software start-up Alleica, which bills itself as the Polygenic Risk Score Company, said “test demand is growing rapidly.” His company offers PRS scores that integrate up to 700,000 markers for prostate cancer depending on ancestry and charges patients $250 out of pocket for testing.
Dr. Botta noted that thousands of American patients have undergone PRS testing through his company. Several health systems, including Penn Medicine, Brigham and Women’s Hospital, and the University of Alabama at Birmingham, have been using the test to help “see beyond what traditional risk factors allow,” he said.
However, this and other PRS tests are not yet widely used in the primary care setting.
A major barrier to wider adoption is that experts remain divided on its clinical utility. “People either say it’s ready, and it should be implemented, or they say it’s never going to work,” said Sowmiya Moorthie, PhD, a senior policy analyst with the PHG Foundation, a Cambridge University–associated think tank.
Dr. Klein sits in the optimistic camp. He envisions a day soon when patients will undergo whole-genome testing to collect data on risk scores and incorporate the full genome into the electronic record. At a certain age, primary care physicians would then query the data to determine the patient’s germline risk for a variety of diseases.
“At age 45, if I were a primary care physician seeing a male, I would query the PRS for prostate cancer, and if the risks were low, I would say, ‘You don’t need your first PSA probably until you’re 50,’ ” Dr. Klein said. “If your risk is high, I’d say, ‘Let’s do a baseline PSA now.’ ”
We would then have the data to watch these patients a little more closely, he said.
Dr. Moorthie, however, remains more reserved about the future of PRS. “I take the middle ground and say, I think there is some value because it’s an additional data point,” Dr. Moorthie said. “And I can see it having value in certain scenarios, but we still don’t have a clear picture of what these are and how best to use and communicate this information.”
A version of this article first appeared on Medscape.com.
DNA testing for prostate cancer – of the patients’ inherited DNA and their tumors’ somatic DNA – is increasingly used in the U.S. to determine whether and how to treat low-grade, localized prostate cancers.
Another genetic approach, known as the polygenic risk score (PRS), is emerging as a third genetic approach for sorting out prostate cancer risks.
PRS aims to stratify a person’s disease risk by going beyond rare variants in genes, such as BRCA2, and compiling a weighted score that integrates thousands of common variants whose role in cancer may be unknown but are found more frequently in men with prostate cancer. Traditional germline testing, by contrast, looks for about 30 specific genes directly linked to prostate cancer.
Essentially, “a polygenic risk score estimates your risk by adding together the number of bad cards you were dealt by the impact of each card, such as an ace versus a deuce,” said William Catalona, MD, a urologist at Northwestern University Feinberg School of Medicine, Chicago, known as the father of prostate-specific antigen (PSA) screening.
In combination, these variants can have powerful predictive value.
Having a tool that can mine the depths of a person’s genetic makeup and help doctors devise a nuanced risk assessment for prostate cancer seems like a winning proposition.
Despite its promise, PRS testing is not yet used routinely in practice. The central uncertainty regarding its use lies in whether the risk score can accurately predict who will develop aggressive prostate cancer that needs to be treated and who won’t. The research to date has been mixed, and experts remain polarized.
“PRS absolutely, irrefutably can distinguish between the probability of somebody developing prostate cancer or not. Nobody could look at the data and argue with that,” said Todd Morgan, MD, a genomics researcher from the University of Michigan, Ann Arbor. “What [the data] so far haven’t really been able to do is distinguish whether somebody is likely to have clinically significant prostate cancer versus lower-risk prostate cancer.”
The promise of PRS in prostate cancer?
, according to Burcu Darst, PhD, a genetic epidemiologist at Fred Hutchinson Cancer Center, Seattle.
Research in the area has intensified in recent years as genome-wide association studies (GWAS) have become more affordable and the genetic information from these studies has been increasingly aggregated in biobanks.
“Because the sample sizes now are so much bigger than they used to be for GWAS studies, we’re able to develop much better polygenic risk scores than we were before,” said Dr. Darst.
Dr. Darst is lead author on the largest, most diverse prostate GWAS analysis, which led to the development of a PRS that is highly predictive of prostate cancer risk across diverse populations.
In the 2021 meta-analysis, which included 107,247 case patients and 127,006 control patients, Dr. Darst and colleagues identified 86 new genetic risk variants independently associated with prostate cancer risk, bringing the total to 269 known risk variants.
Compared with men at average genetic risk for prostate cancer – those in the 40%-60% genetic risk score category – men in the top 10% of the risk score (90%-100%) had between a 3.74-fold to fivefold higher risk for prostate cancer. However, the team did not find evidence that the genetic risk score could differentiate a person’s risk for aggressive versus nonaggressive disease.
As Dr. Darst’s team continues to improve the PRS, Dr. Darst says it will get better at predicting aggressive disease. One recent analysis from Dr. Darst and colleagues found that “although the PRS generally did not differentiate aggressive versus nonaggressive prostate cancer,” about 40% of men who will develop aggressive disease have a PRS in the top 20%, whereas only about 7% of men who will develop aggressive tumors have a PRS in the bottom 20%. Another recent study from Dr. Darst and colleagues found that PRS can distinguish between aggressive and nonaggressive disease in men of African ancestry.
These findings highlight “the potential clinical utility of the polygenic risk score,” Dr. Darst said.
Although the growing body of research makes Dr. Catalona, Dr. Darst, and others optimistic about PRS, the landscape is also littered with critics and studies showcasing its limitations.
An analysis, published in JAMA Internal Medicine, found that, compared with a contemporary clinical risk predictor, PRS did not improve prediction of aggressive prostate cancers. Another recent study, which used a 6.6 million–variant PRS to predict the risk of incident prostate cancer among 5,701 healthy men of European descent older than age 69, found that men in the top 20% of the PRS distribution “had an almost three times higher risk of prostate cancer,” compared with men in the lowest quintile; however, a higher PRS was not associated with a higher Gleason grade group, indicative of more aggressive disease.
“While a PRS for prostate cancer is strongly associated with incident risk” in the cohort, “the clinical utility of the PRS as a biomarker is currently limited by its inability to select for clinically significant disease,” the authors concluded.
Utility in practice?
Although PRS has been billed as a predictive test, Dr. Catalona believes PRS could have a range of uses both before and after diagnosis.
PRS may, for instance, guide treatment choices for men diagnosed with prostate cancer, Dr. Catalona noted. For men with a PRS that signals a higher risk for aggressive disease, a positive prostate biopsy result could help them decide whether to seek active treatment with surgery or radiation or go on active surveillance.
PRS could also help inform cancer screening. If a PRS test found a patient’s risk for prostate cancer was high, that person could decide to seek PSA screening before age 50 – the recommended age for average-risk men.
However, Aroon Hingorani, MD, a professor of genetic epidemiology at the University College London, expressed concern over using PRS to inform cancer screenings.
Part of the issue, Dr. Hingorani and colleagues explained in a recent article in the BMJ, is that “risk is notoriously difficult to communicate.”
PRS estimates a person’s relative risk for a disease but does not factor in the underlying population risk. Risk prediction should include both, Dr. Hingorani said.
People with high-risk scores may, for instance, discuss earlier screening with their clinician, even if their absolute risk for the disease – which accounts for both relative risk and underlying population disease risk – is still small, Dr. Hingorani and colleagues said. “Conversely, people who do not have ‘high risk’ polygenic scores might be less likely to seek medical attention for concerning symptoms, or their clinicians might be less inclined to investigate.”
Given this, Dr. Hingorani and colleagues believe polygenic scores “will always be limited in their ability to predict disease” and “will always remain one of many risk factors,” such as environmental influences.
Another caveat is that PRS generally is based on data collected from European populations, said Eric Klein, MD, chairman emeritus of urology at the Cleveland Clinic and now a scientist at the biotechnology company Grail, which developed the Galleri blood test that screens for 50 types of cancer. While a valid concern, “that’s easy to fix ultimately,” he said, as the diversity of inputs from various ethnicities increases over time.
Although several companies offer PRS products, moving PRS into the clinic would require an infrastructure for testing which does not yet exist in the U.S., said Dr. Catalona.
Giordano Botta, PhD, CEO of New York–based PRS software start-up Alleica, which bills itself as the Polygenic Risk Score Company, said “test demand is growing rapidly.” His company offers PRS scores that integrate up to 700,000 markers for prostate cancer depending on ancestry and charges patients $250 out of pocket for testing.
Dr. Botta noted that thousands of American patients have undergone PRS testing through his company. Several health systems, including Penn Medicine, Brigham and Women’s Hospital, and the University of Alabama at Birmingham, have been using the test to help “see beyond what traditional risk factors allow,” he said.
However, this and other PRS tests are not yet widely used in the primary care setting.
A major barrier to wider adoption is that experts remain divided on its clinical utility. “People either say it’s ready, and it should be implemented, or they say it’s never going to work,” said Sowmiya Moorthie, PhD, a senior policy analyst with the PHG Foundation, a Cambridge University–associated think tank.
Dr. Klein sits in the optimistic camp. He envisions a day soon when patients will undergo whole-genome testing to collect data on risk scores and incorporate the full genome into the electronic record. At a certain age, primary care physicians would then query the data to determine the patient’s germline risk for a variety of diseases.
“At age 45, if I were a primary care physician seeing a male, I would query the PRS for prostate cancer, and if the risks were low, I would say, ‘You don’t need your first PSA probably until you’re 50,’ ” Dr. Klein said. “If your risk is high, I’d say, ‘Let’s do a baseline PSA now.’ ”
We would then have the data to watch these patients a little more closely, he said.
Dr. Moorthie, however, remains more reserved about the future of PRS. “I take the middle ground and say, I think there is some value because it’s an additional data point,” Dr. Moorthie said. “And I can see it having value in certain scenarios, but we still don’t have a clear picture of what these are and how best to use and communicate this information.”
A version of this article first appeared on Medscape.com.
DNA testing for prostate cancer – of the patients’ inherited DNA and their tumors’ somatic DNA – is increasingly used in the U.S. to determine whether and how to treat low-grade, localized prostate cancers.
Another genetic approach, known as the polygenic risk score (PRS), is emerging as a third genetic approach for sorting out prostate cancer risks.
PRS aims to stratify a person’s disease risk by going beyond rare variants in genes, such as BRCA2, and compiling a weighted score that integrates thousands of common variants whose role in cancer may be unknown but are found more frequently in men with prostate cancer. Traditional germline testing, by contrast, looks for about 30 specific genes directly linked to prostate cancer.
Essentially, “a polygenic risk score estimates your risk by adding together the number of bad cards you were dealt by the impact of each card, such as an ace versus a deuce,” said William Catalona, MD, a urologist at Northwestern University Feinberg School of Medicine, Chicago, known as the father of prostate-specific antigen (PSA) screening.
In combination, these variants can have powerful predictive value.
Having a tool that can mine the depths of a person’s genetic makeup and help doctors devise a nuanced risk assessment for prostate cancer seems like a winning proposition.
Despite its promise, PRS testing is not yet used routinely in practice. The central uncertainty regarding its use lies in whether the risk score can accurately predict who will develop aggressive prostate cancer that needs to be treated and who won’t. The research to date has been mixed, and experts remain polarized.
“PRS absolutely, irrefutably can distinguish between the probability of somebody developing prostate cancer or not. Nobody could look at the data and argue with that,” said Todd Morgan, MD, a genomics researcher from the University of Michigan, Ann Arbor. “What [the data] so far haven’t really been able to do is distinguish whether somebody is likely to have clinically significant prostate cancer versus lower-risk prostate cancer.”
The promise of PRS in prostate cancer?
, according to Burcu Darst, PhD, a genetic epidemiologist at Fred Hutchinson Cancer Center, Seattle.
Research in the area has intensified in recent years as genome-wide association studies (GWAS) have become more affordable and the genetic information from these studies has been increasingly aggregated in biobanks.
“Because the sample sizes now are so much bigger than they used to be for GWAS studies, we’re able to develop much better polygenic risk scores than we were before,” said Dr. Darst.
Dr. Darst is lead author on the largest, most diverse prostate GWAS analysis, which led to the development of a PRS that is highly predictive of prostate cancer risk across diverse populations.
In the 2021 meta-analysis, which included 107,247 case patients and 127,006 control patients, Dr. Darst and colleagues identified 86 new genetic risk variants independently associated with prostate cancer risk, bringing the total to 269 known risk variants.
Compared with men at average genetic risk for prostate cancer – those in the 40%-60% genetic risk score category – men in the top 10% of the risk score (90%-100%) had between a 3.74-fold to fivefold higher risk for prostate cancer. However, the team did not find evidence that the genetic risk score could differentiate a person’s risk for aggressive versus nonaggressive disease.
As Dr. Darst’s team continues to improve the PRS, Dr. Darst says it will get better at predicting aggressive disease. One recent analysis from Dr. Darst and colleagues found that “although the PRS generally did not differentiate aggressive versus nonaggressive prostate cancer,” about 40% of men who will develop aggressive disease have a PRS in the top 20%, whereas only about 7% of men who will develop aggressive tumors have a PRS in the bottom 20%. Another recent study from Dr. Darst and colleagues found that PRS can distinguish between aggressive and nonaggressive disease in men of African ancestry.
These findings highlight “the potential clinical utility of the polygenic risk score,” Dr. Darst said.
Although the growing body of research makes Dr. Catalona, Dr. Darst, and others optimistic about PRS, the landscape is also littered with critics and studies showcasing its limitations.
An analysis, published in JAMA Internal Medicine, found that, compared with a contemporary clinical risk predictor, PRS did not improve prediction of aggressive prostate cancers. Another recent study, which used a 6.6 million–variant PRS to predict the risk of incident prostate cancer among 5,701 healthy men of European descent older than age 69, found that men in the top 20% of the PRS distribution “had an almost three times higher risk of prostate cancer,” compared with men in the lowest quintile; however, a higher PRS was not associated with a higher Gleason grade group, indicative of more aggressive disease.
“While a PRS for prostate cancer is strongly associated with incident risk” in the cohort, “the clinical utility of the PRS as a biomarker is currently limited by its inability to select for clinically significant disease,” the authors concluded.
Utility in practice?
Although PRS has been billed as a predictive test, Dr. Catalona believes PRS could have a range of uses both before and after diagnosis.
PRS may, for instance, guide treatment choices for men diagnosed with prostate cancer, Dr. Catalona noted. For men with a PRS that signals a higher risk for aggressive disease, a positive prostate biopsy result could help them decide whether to seek active treatment with surgery or radiation or go on active surveillance.
PRS could also help inform cancer screening. If a PRS test found a patient’s risk for prostate cancer was high, that person could decide to seek PSA screening before age 50 – the recommended age for average-risk men.
However, Aroon Hingorani, MD, a professor of genetic epidemiology at the University College London, expressed concern over using PRS to inform cancer screenings.
Part of the issue, Dr. Hingorani and colleagues explained in a recent article in the BMJ, is that “risk is notoriously difficult to communicate.”
PRS estimates a person’s relative risk for a disease but does not factor in the underlying population risk. Risk prediction should include both, Dr. Hingorani said.
People with high-risk scores may, for instance, discuss earlier screening with their clinician, even if their absolute risk for the disease – which accounts for both relative risk and underlying population disease risk – is still small, Dr. Hingorani and colleagues said. “Conversely, people who do not have ‘high risk’ polygenic scores might be less likely to seek medical attention for concerning symptoms, or their clinicians might be less inclined to investigate.”
Given this, Dr. Hingorani and colleagues believe polygenic scores “will always be limited in their ability to predict disease” and “will always remain one of many risk factors,” such as environmental influences.
Another caveat is that PRS generally is based on data collected from European populations, said Eric Klein, MD, chairman emeritus of urology at the Cleveland Clinic and now a scientist at the biotechnology company Grail, which developed the Galleri blood test that screens for 50 types of cancer. While a valid concern, “that’s easy to fix ultimately,” he said, as the diversity of inputs from various ethnicities increases over time.
Although several companies offer PRS products, moving PRS into the clinic would require an infrastructure for testing which does not yet exist in the U.S., said Dr. Catalona.
Giordano Botta, PhD, CEO of New York–based PRS software start-up Alleica, which bills itself as the Polygenic Risk Score Company, said “test demand is growing rapidly.” His company offers PRS scores that integrate up to 700,000 markers for prostate cancer depending on ancestry and charges patients $250 out of pocket for testing.
Dr. Botta noted that thousands of American patients have undergone PRS testing through his company. Several health systems, including Penn Medicine, Brigham and Women’s Hospital, and the University of Alabama at Birmingham, have been using the test to help “see beyond what traditional risk factors allow,” he said.
However, this and other PRS tests are not yet widely used in the primary care setting.
A major barrier to wider adoption is that experts remain divided on its clinical utility. “People either say it’s ready, and it should be implemented, or they say it’s never going to work,” said Sowmiya Moorthie, PhD, a senior policy analyst with the PHG Foundation, a Cambridge University–associated think tank.
Dr. Klein sits in the optimistic camp. He envisions a day soon when patients will undergo whole-genome testing to collect data on risk scores and incorporate the full genome into the electronic record. At a certain age, primary care physicians would then query the data to determine the patient’s germline risk for a variety of diseases.
“At age 45, if I were a primary care physician seeing a male, I would query the PRS for prostate cancer, and if the risks were low, I would say, ‘You don’t need your first PSA probably until you’re 50,’ ” Dr. Klein said. “If your risk is high, I’d say, ‘Let’s do a baseline PSA now.’ ”
We would then have the data to watch these patients a little more closely, he said.
Dr. Moorthie, however, remains more reserved about the future of PRS. “I take the middle ground and say, I think there is some value because it’s an additional data point,” Dr. Moorthie said. “And I can see it having value in certain scenarios, but we still don’t have a clear picture of what these are and how best to use and communicate this information.”
A version of this article first appeared on Medscape.com.
Improving Germline Genetic Testing Among Veterans With High Risk, Very High Risk and Metastatic Prostate Cancer
PURPOSE
To improve germline genetic testing among Veterans with high risk, very high risk and metastatic prostate cancer.
BACKGROUND
During our Commission on Cancer survey in 2021, it was noted that the Detroit VA’s referrals for germline genetic testing and counseling were extremely low. In 2020, only 1 Veteran was referred for prostate germline genetic testing and counseling and only 8 Veterans were referred in 2021. It was felt that the need to refer Veterans outside of the Detroit VA may have contributed to these low numbers. Our Cancer Committee chose prostate cancer as a disease to focus on. We chose a timeline of one year to implement our process.
METHODS
We made testing and counseling locally accessible to Veterans and encouraged medical oncology providers to make it part of the care of Veterans with high risk, very high risk and metastatic prostate cancer. We sought the assistance of the VA’s National Precision Oncology Program and were able to secure financial and logistical support to perform germline molecular prostate panel testing at the Detroit VA. We were also able to identify a cancer genetic specialist at the Ann Arbor VA that would perform genetic counseling among this group of patients based on their test results. Our medical oncology providers identified Veterans meeting the criteria for testing. Education regarding germline testing, its benefits and implications were conducted with Veterans, and performed after obtaining their informed consent in collaboration with our pathology department. The specimen is then sent to a VA central laboratory for processing. Detroit VA providers are alerted by the local laboratory once results are available. Veterans are then referred to the genetic counseling specialist based on the results. Some of these counseling visits are done virtually for the Veteran’s convenience.
DATA ANALYSIS
A retrospective chart analysis was used to collect the data.
RESULTS
After the implementation of our initiative, 97 Veterans with high risk, very high risk or metastatic prostate cancer were educated on the benefits of germline genetic testing, 87 of whom agreed to be tested. As of 4/2/23, 48 tests have already been performed. Pathogenic variants were recorded on 2 Veterans so far. One was for BRCA2 and KDM6A, and the other was for ATM. Data collection and recording is on-going.
IMPLICATIONS
Improving accessibility and incorporating genetic testing and counseling in cancer care can improve their utilization.
PURPOSE
To improve germline genetic testing among Veterans with high risk, very high risk and metastatic prostate cancer.
BACKGROUND
During our Commission on Cancer survey in 2021, it was noted that the Detroit VA’s referrals for germline genetic testing and counseling were extremely low. In 2020, only 1 Veteran was referred for prostate germline genetic testing and counseling and only 8 Veterans were referred in 2021. It was felt that the need to refer Veterans outside of the Detroit VA may have contributed to these low numbers. Our Cancer Committee chose prostate cancer as a disease to focus on. We chose a timeline of one year to implement our process.
METHODS
We made testing and counseling locally accessible to Veterans and encouraged medical oncology providers to make it part of the care of Veterans with high risk, very high risk and metastatic prostate cancer. We sought the assistance of the VA’s National Precision Oncology Program and were able to secure financial and logistical support to perform germline molecular prostate panel testing at the Detroit VA. We were also able to identify a cancer genetic specialist at the Ann Arbor VA that would perform genetic counseling among this group of patients based on their test results. Our medical oncology providers identified Veterans meeting the criteria for testing. Education regarding germline testing, its benefits and implications were conducted with Veterans, and performed after obtaining their informed consent in collaboration with our pathology department. The specimen is then sent to a VA central laboratory for processing. Detroit VA providers are alerted by the local laboratory once results are available. Veterans are then referred to the genetic counseling specialist based on the results. Some of these counseling visits are done virtually for the Veteran’s convenience.
DATA ANALYSIS
A retrospective chart analysis was used to collect the data.
RESULTS
After the implementation of our initiative, 97 Veterans with high risk, very high risk or metastatic prostate cancer were educated on the benefits of germline genetic testing, 87 of whom agreed to be tested. As of 4/2/23, 48 tests have already been performed. Pathogenic variants were recorded on 2 Veterans so far. One was for BRCA2 and KDM6A, and the other was for ATM. Data collection and recording is on-going.
IMPLICATIONS
Improving accessibility and incorporating genetic testing and counseling in cancer care can improve their utilization.
PURPOSE
To improve germline genetic testing among Veterans with high risk, very high risk and metastatic prostate cancer.
BACKGROUND
During our Commission on Cancer survey in 2021, it was noted that the Detroit VA’s referrals for germline genetic testing and counseling were extremely low. In 2020, only 1 Veteran was referred for prostate germline genetic testing and counseling and only 8 Veterans were referred in 2021. It was felt that the need to refer Veterans outside of the Detroit VA may have contributed to these low numbers. Our Cancer Committee chose prostate cancer as a disease to focus on. We chose a timeline of one year to implement our process.
METHODS
We made testing and counseling locally accessible to Veterans and encouraged medical oncology providers to make it part of the care of Veterans with high risk, very high risk and metastatic prostate cancer. We sought the assistance of the VA’s National Precision Oncology Program and were able to secure financial and logistical support to perform germline molecular prostate panel testing at the Detroit VA. We were also able to identify a cancer genetic specialist at the Ann Arbor VA that would perform genetic counseling among this group of patients based on their test results. Our medical oncology providers identified Veterans meeting the criteria for testing. Education regarding germline testing, its benefits and implications were conducted with Veterans, and performed after obtaining their informed consent in collaboration with our pathology department. The specimen is then sent to a VA central laboratory for processing. Detroit VA providers are alerted by the local laboratory once results are available. Veterans are then referred to the genetic counseling specialist based on the results. Some of these counseling visits are done virtually for the Veteran’s convenience.
DATA ANALYSIS
A retrospective chart analysis was used to collect the data.
RESULTS
After the implementation of our initiative, 97 Veterans with high risk, very high risk or metastatic prostate cancer were educated on the benefits of germline genetic testing, 87 of whom agreed to be tested. As of 4/2/23, 48 tests have already been performed. Pathogenic variants were recorded on 2 Veterans so far. One was for BRCA2 and KDM6A, and the other was for ATM. Data collection and recording is on-going.
IMPLICATIONS
Improving accessibility and incorporating genetic testing and counseling in cancer care can improve their utilization.
Mammography breast density reporting: What it means for clinicians
This transcript has been edited for clarity.
Today, I’m going to talk about the 2023 Food and Drug Administration regulation that requires breast density to be reported on all mammogram results nationwide, and for that report to go to both clinicians and patients. Previously this was the rule in some states, but not in others. This is important because 40%-50% of women have dense breasts. I’m going to discuss what that means for you, and for our patients.
First
Breast density describes the appearance of the breast on mammography. Appearance varies on the basis of breast tissue composition, with fibroglandular tissue being more dense than fatty tissue. Breast density is important because it relates to both the risk for cancer and the ability of mammography to detect cancer.
Breast density is defined and classified according to the American College of Radiology’s BI-RADS four-category scale. Categories 1 and 2 refer to breast tissue that is not dense, accounting for about 50% of the population. Categories 3 and 4 describe heterogeneously dense and extremely dense breast tissue, which occur in approximately 40% and 50% of women, respectively. When speaking about dense breast tissue readings on mammography, we are referring to categories 3 and 4.
Women with dense breast tissue have an increased risk of developing breast cancer and are less likely to have early breast cancer detected on mammography.
Let’s go over the details by category:
For women in categories 1 and 2 (considered not dense breast tissue), the sensitivity of mammography for detecting early breast cancer is 80%-90%. In categories 3 and 4, the sensitivity of mammography drops to 60%-70%.
Compared with women with average breast density, the risk of developing breast cancer is 20% higher in women with BI-RADS category 3 breasts, and more than twice as high (relative risk, 2.1) in those with BI-RADS category 4 breasts. Thus, the risk of developing breast cancer is higher, but the sensitivity of the test is lower.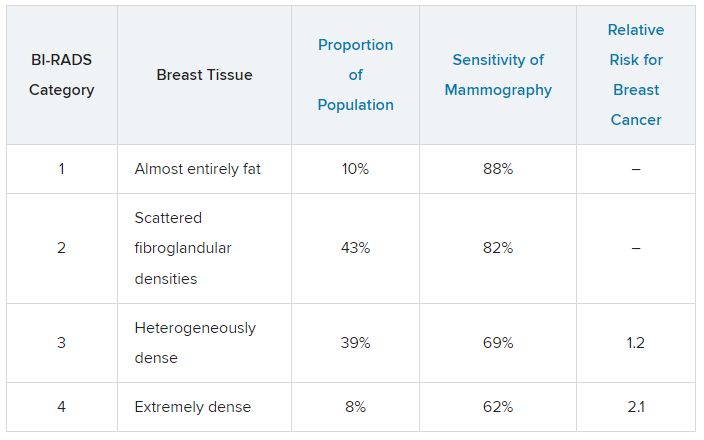
The clinical question is, what should we do about this? For women who have a normal mammogram with dense breasts, should follow-up testing be done, and if so, what test? The main follow-up testing options are either ultrasound or MRI, usually ultrasound. Additional testing will detect additional cancers that were not picked up on the initial mammogram and will also lead to additional biopsies for false-positive tests from the additional testing.
An American College of Gynecology and Obstetrics practice advisory nicely summarizes the evidence and clarifies that this decision is made in the context of a lack of published evidence demonstrating improved outcomes, specifically no reduction in breast cancer mortality, with supplemental testing. The official ACOG stance is that they “do not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
This is an area where it is important to understand the data. We are all going to be getting test results back that indicate level of breast density, and those test results will also be sent to our patients, so we are going to be asked about this by interested patients. Should this be something that we talk to patients about, utilizing shared decision-making to decide about whether follow-up testing is necessary in women with dense breasts? That is something each clinician will need to decide, and knowing the data is a critically important step in that decision.
Neil Skolnik, MD, is a professor, department of family medicine, at Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director, department of family medicine, Abington (Pennsylvania) Jefferson Health.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Today, I’m going to talk about the 2023 Food and Drug Administration regulation that requires breast density to be reported on all mammogram results nationwide, and for that report to go to both clinicians and patients. Previously this was the rule in some states, but not in others. This is important because 40%-50% of women have dense breasts. I’m going to discuss what that means for you, and for our patients.
First
Breast density describes the appearance of the breast on mammography. Appearance varies on the basis of breast tissue composition, with fibroglandular tissue being more dense than fatty tissue. Breast density is important because it relates to both the risk for cancer and the ability of mammography to detect cancer.
Breast density is defined and classified according to the American College of Radiology’s BI-RADS four-category scale. Categories 1 and 2 refer to breast tissue that is not dense, accounting for about 50% of the population. Categories 3 and 4 describe heterogeneously dense and extremely dense breast tissue, which occur in approximately 40% and 50% of women, respectively. When speaking about dense breast tissue readings on mammography, we are referring to categories 3 and 4.
Women with dense breast tissue have an increased risk of developing breast cancer and are less likely to have early breast cancer detected on mammography.
Let’s go over the details by category:
For women in categories 1 and 2 (considered not dense breast tissue), the sensitivity of mammography for detecting early breast cancer is 80%-90%. In categories 3 and 4, the sensitivity of mammography drops to 60%-70%.
Compared with women with average breast density, the risk of developing breast cancer is 20% higher in women with BI-RADS category 3 breasts, and more than twice as high (relative risk, 2.1) in those with BI-RADS category 4 breasts. Thus, the risk of developing breast cancer is higher, but the sensitivity of the test is lower.
The clinical question is, what should we do about this? For women who have a normal mammogram with dense breasts, should follow-up testing be done, and if so, what test? The main follow-up testing options are either ultrasound or MRI, usually ultrasound. Additional testing will detect additional cancers that were not picked up on the initial mammogram and will also lead to additional biopsies for false-positive tests from the additional testing.
An American College of Gynecology and Obstetrics practice advisory nicely summarizes the evidence and clarifies that this decision is made in the context of a lack of published evidence demonstrating improved outcomes, specifically no reduction in breast cancer mortality, with supplemental testing. The official ACOG stance is that they “do not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
This is an area where it is important to understand the data. We are all going to be getting test results back that indicate level of breast density, and those test results will also be sent to our patients, so we are going to be asked about this by interested patients. Should this be something that we talk to patients about, utilizing shared decision-making to decide about whether follow-up testing is necessary in women with dense breasts? That is something each clinician will need to decide, and knowing the data is a critically important step in that decision.
Neil Skolnik, MD, is a professor, department of family medicine, at Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director, department of family medicine, Abington (Pennsylvania) Jefferson Health.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Today, I’m going to talk about the 2023 Food and Drug Administration regulation that requires breast density to be reported on all mammogram results nationwide, and for that report to go to both clinicians and patients. Previously this was the rule in some states, but not in others. This is important because 40%-50% of women have dense breasts. I’m going to discuss what that means for you, and for our patients.
First
Breast density describes the appearance of the breast on mammography. Appearance varies on the basis of breast tissue composition, with fibroglandular tissue being more dense than fatty tissue. Breast density is important because it relates to both the risk for cancer and the ability of mammography to detect cancer.
Breast density is defined and classified according to the American College of Radiology’s BI-RADS four-category scale. Categories 1 and 2 refer to breast tissue that is not dense, accounting for about 50% of the population. Categories 3 and 4 describe heterogeneously dense and extremely dense breast tissue, which occur in approximately 40% and 50% of women, respectively. When speaking about dense breast tissue readings on mammography, we are referring to categories 3 and 4.
Women with dense breast tissue have an increased risk of developing breast cancer and are less likely to have early breast cancer detected on mammography.
Let’s go over the details by category:
For women in categories 1 and 2 (considered not dense breast tissue), the sensitivity of mammography for detecting early breast cancer is 80%-90%. In categories 3 and 4, the sensitivity of mammography drops to 60%-70%.
Compared with women with average breast density, the risk of developing breast cancer is 20% higher in women with BI-RADS category 3 breasts, and more than twice as high (relative risk, 2.1) in those with BI-RADS category 4 breasts. Thus, the risk of developing breast cancer is higher, but the sensitivity of the test is lower.
The clinical question is, what should we do about this? For women who have a normal mammogram with dense breasts, should follow-up testing be done, and if so, what test? The main follow-up testing options are either ultrasound or MRI, usually ultrasound. Additional testing will detect additional cancers that were not picked up on the initial mammogram and will also lead to additional biopsies for false-positive tests from the additional testing.
An American College of Gynecology and Obstetrics practice advisory nicely summarizes the evidence and clarifies that this decision is made in the context of a lack of published evidence demonstrating improved outcomes, specifically no reduction in breast cancer mortality, with supplemental testing. The official ACOG stance is that they “do not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
This is an area where it is important to understand the data. We are all going to be getting test results back that indicate level of breast density, and those test results will also be sent to our patients, so we are going to be asked about this by interested patients. Should this be something that we talk to patients about, utilizing shared decision-making to decide about whether follow-up testing is necessary in women with dense breasts? That is something each clinician will need to decide, and knowing the data is a critically important step in that decision.
Neil Skolnik, MD, is a professor, department of family medicine, at Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director, department of family medicine, Abington (Pennsylvania) Jefferson Health.
A version of this article first appeared on Medscape.com.