User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
Spikes out: A COVID mystery
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.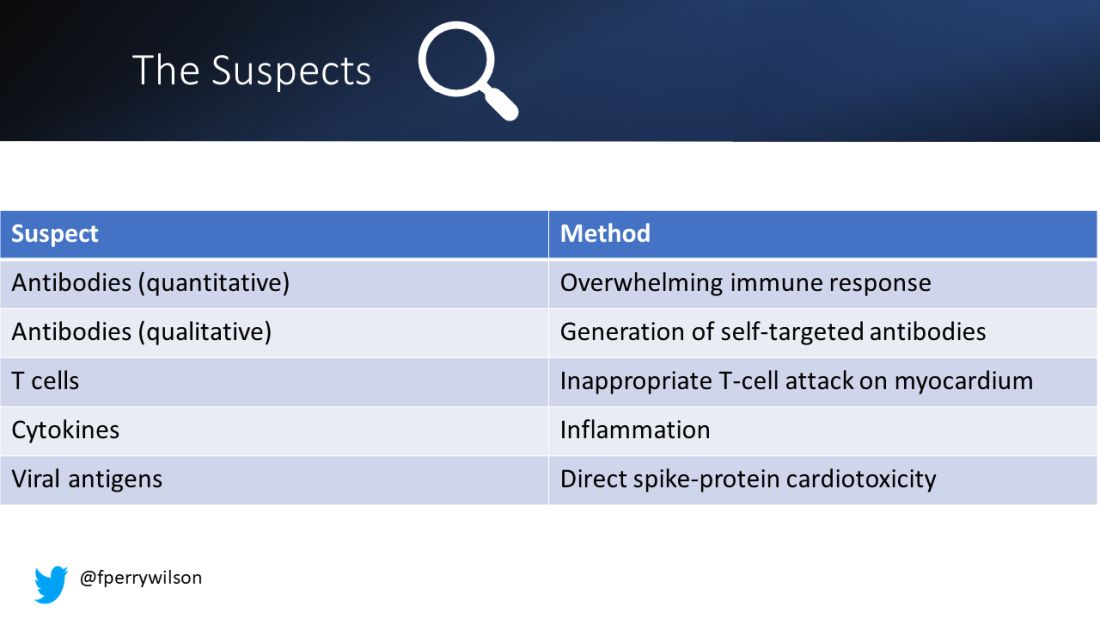
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.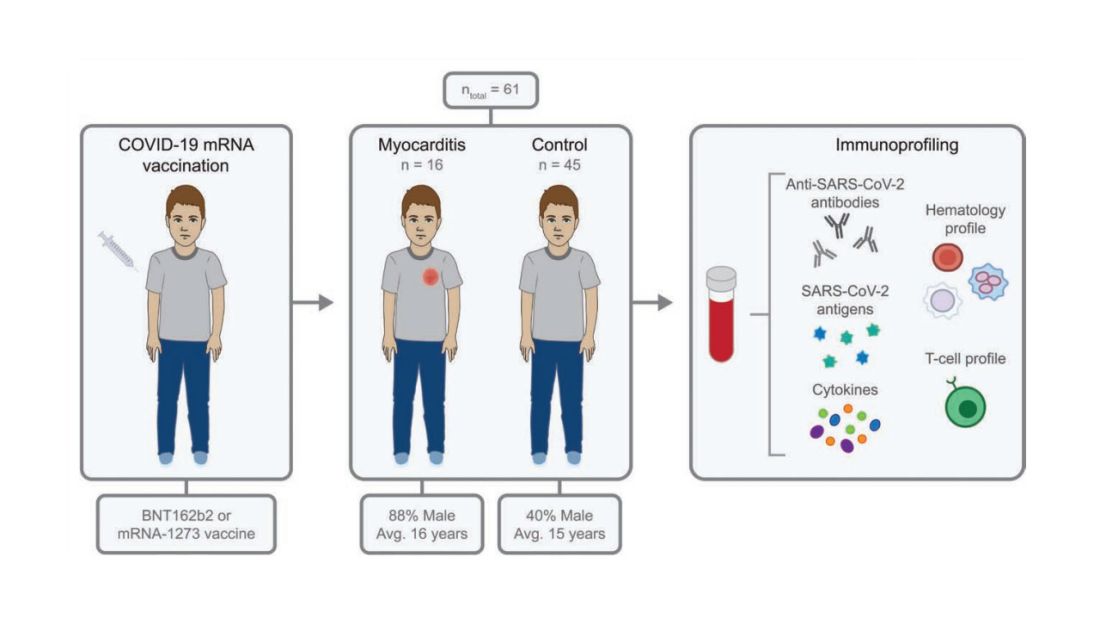
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.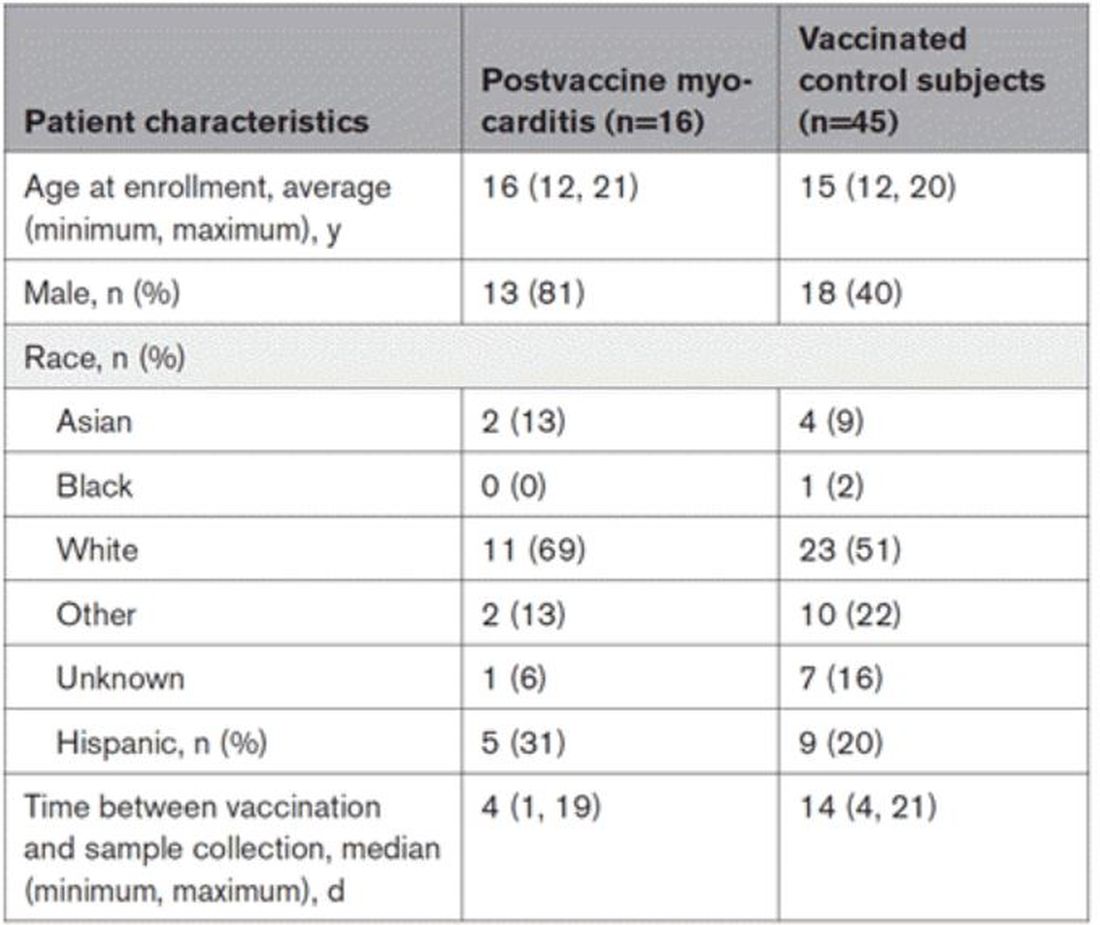
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.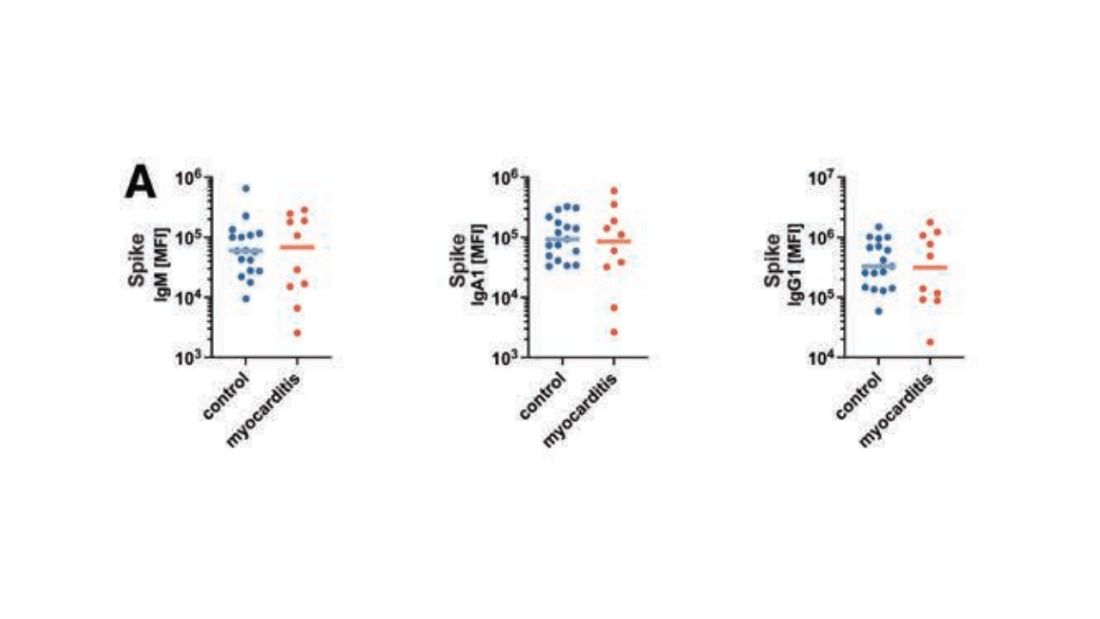
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.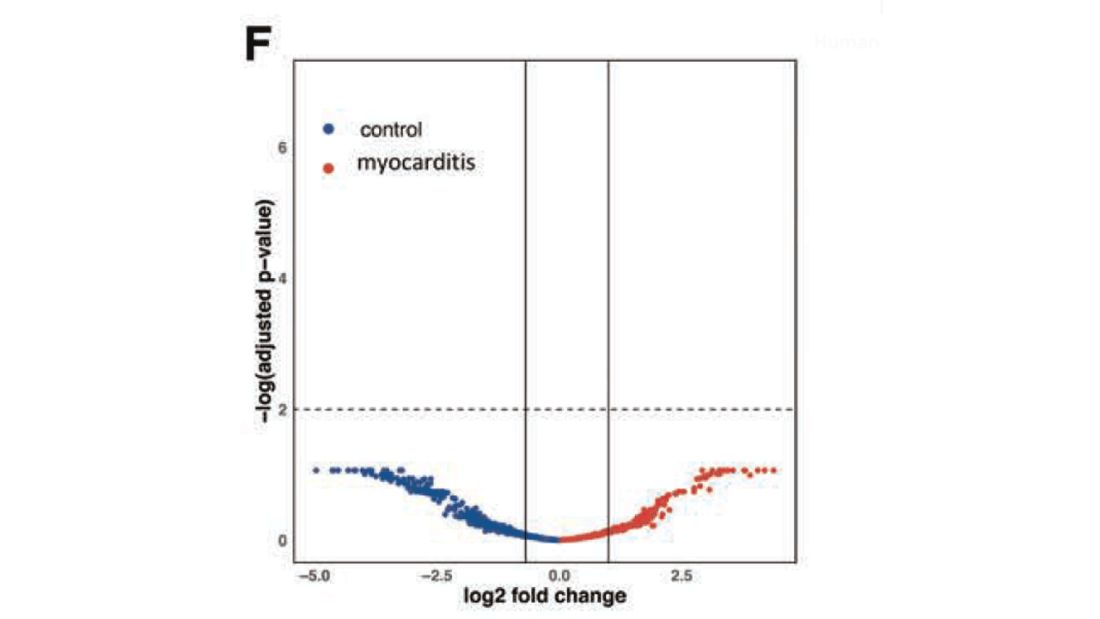
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.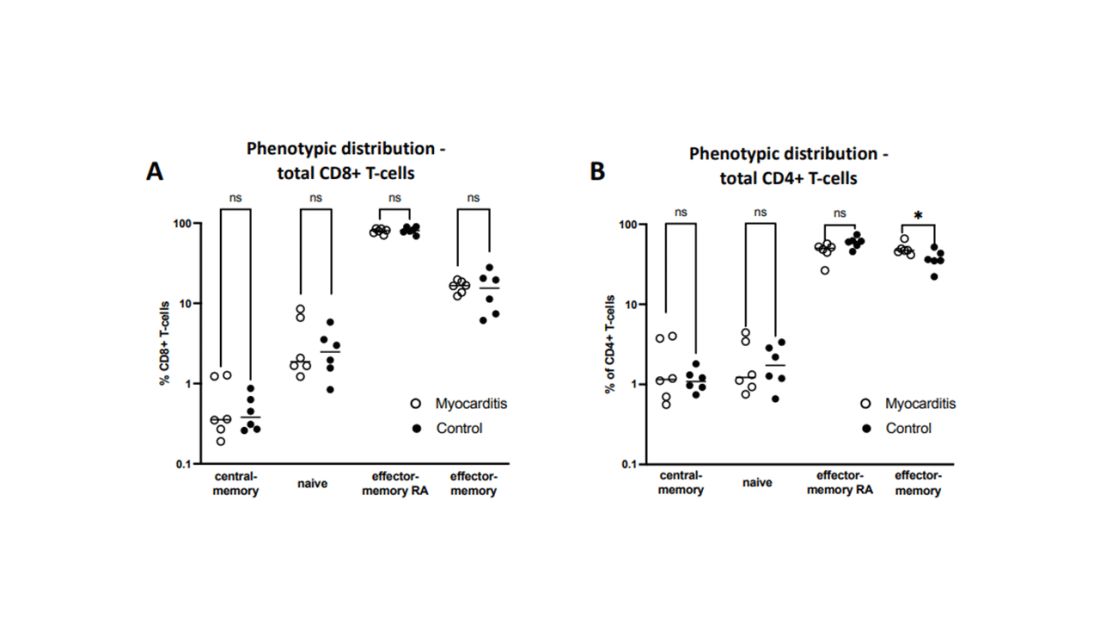
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.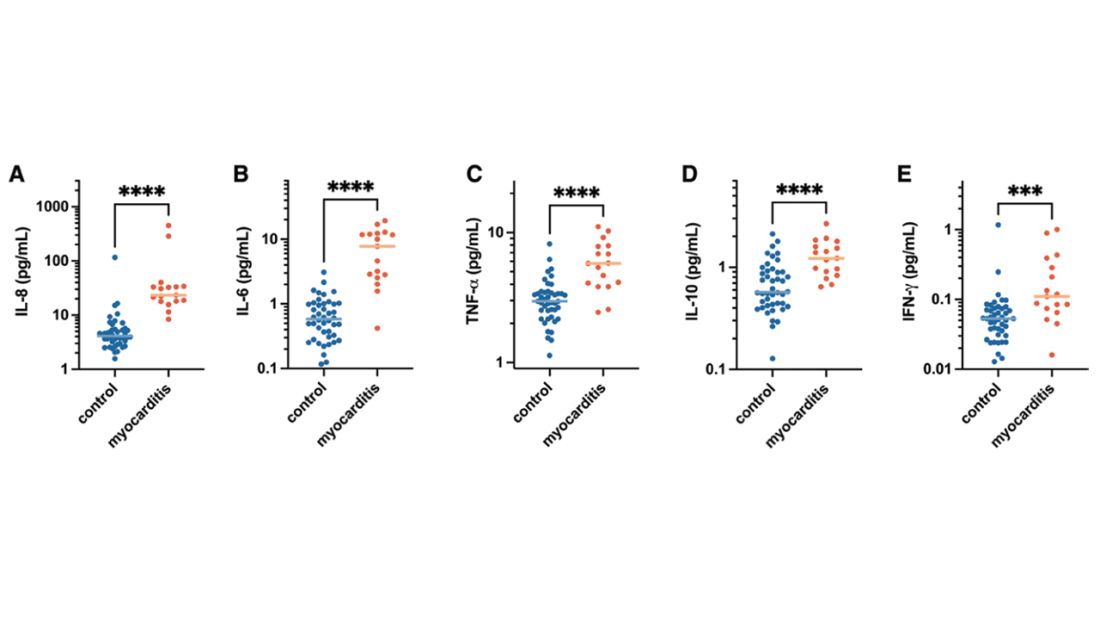
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.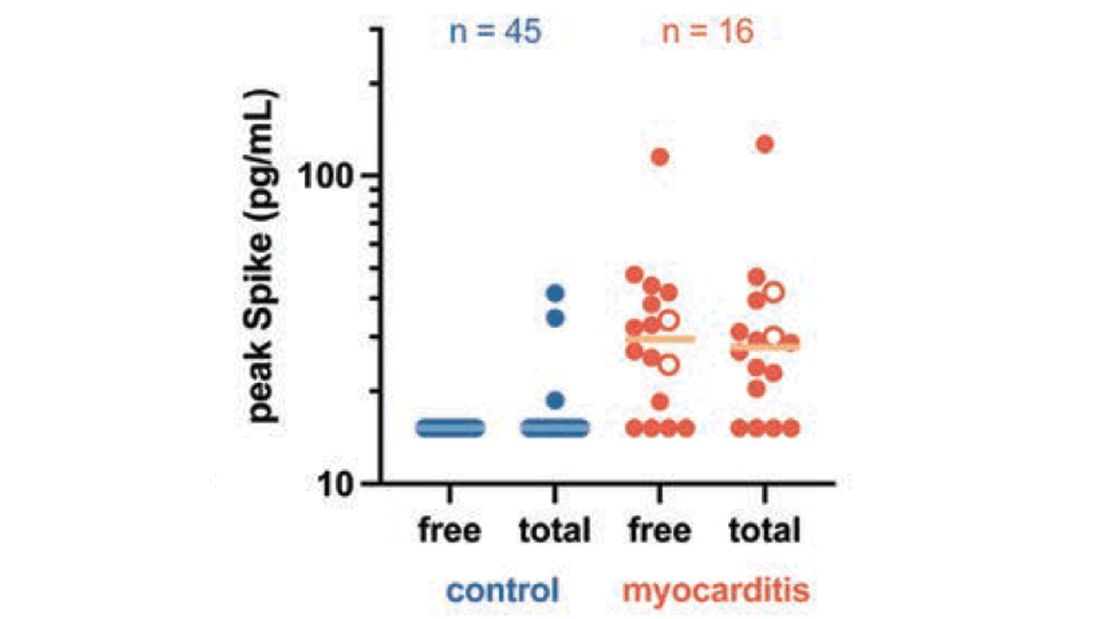
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!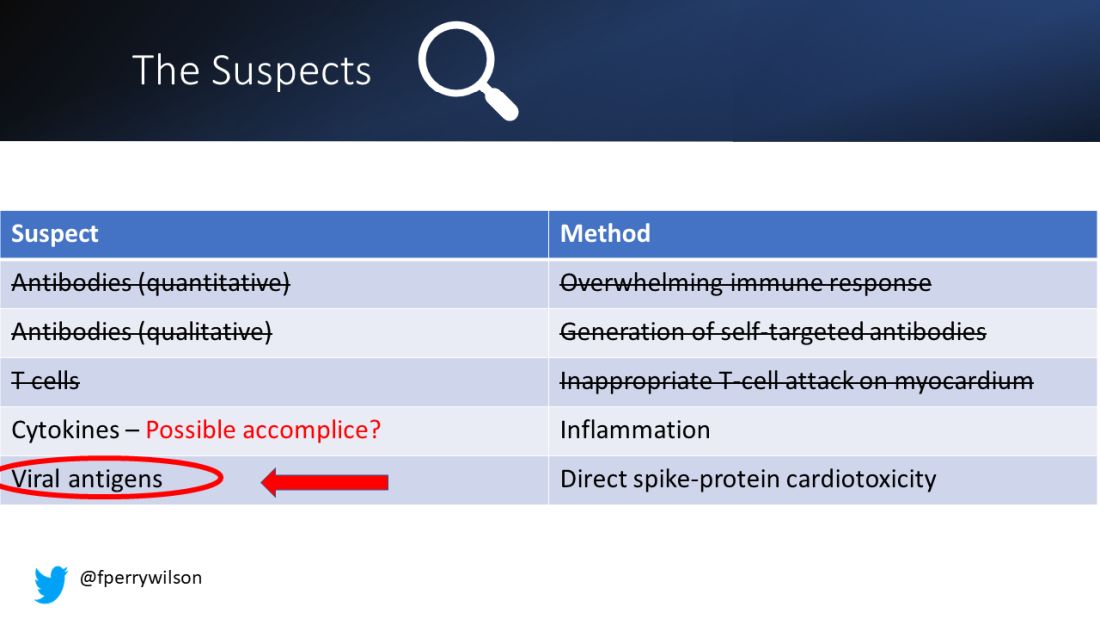
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
To date, it has been a mystery, like “Glass Onion.” And in the spirit of all the great mysteries, to get to the bottom of this, we’ll need to round up the usual suspects.
Appearing in Circulation, a new study does a great job of systematically evaluating multiple hypotheses linking vaccination to myocarditis, and eliminating them, Poirot-style, one by one until only one remains. We’ll get there.
But first, let’s review the suspects. Why do the mRNA vaccines cause myocarditis in a small subset of people?
There are a few leading candidates.
Number one: antibody responses. There are two flavors here. The quantitative hypothesis suggests that some people simply generate too many antibodies to the vaccine, leading to increased inflammation and heart damage.
The qualitative hypothesis suggests that maybe it’s the nature of the antibodies generated rather than the amount; they might cross-react with some protein on the surface of heart cells for instance.
Or maybe it is driven by T-cell responses, which, of course, are independent of antibody levels.
There’s the idea that myocarditis is due to excessive cytokine release – sort of like what we see in the multisystem inflammatory syndrome in children.
Or it could be due to the viral antigens themselves – the spike protein the mRNA codes for that is generated after vaccination.
To tease all these possibilities apart, researchers led by Lael Yonker at Mass General performed a case-control study. Sixteen children with postvaccine myocarditis were matched by age to 45 control children who had been vaccinated without complications.
The matching was OK, but as you can see here, there were more boys in the myocarditis group, and the time from vaccination was a bit shorter in that group as well. We’ll keep that in mind as we go through the results.
OK, let’s start eliminating suspects.
First, quantitative antibodies. Seems unlikely. Absolute antibody titers were really no different in the myocarditis vs. the control group.
What about the quality of the antibodies? Would the kids with myocarditis have more self-recognizing antibodies present? It doesn’t appear so. Autoantibody levels were similar in the two groups.
Take antibodies off the list.
T-cell responses come next, and, again, no major differences here, save for one specific T-cell subtype that was moderately elevated in the myocarditis group. Not what I would call a smoking gun, frankly.
Cytokines give us a bit more to chew on. Levels of interleukin (IL)-8, IL-6, tumor necrosis factor (TNF)-alpha, and IL-10 were all substantially higher in the kids with myocarditis.
But the thing about cytokines is that they are not particularly specific. OK, kids with myocarditis have more systemic inflammation than kids without; that’s not really surprising. It still leaves us with the question of what is causing all this inflammation? Who is the arch-villain? The kingpin? The don?
It’s the analyses of antigens – the protein products of vaccination – that may hold the key here.
In 12 out of 16 kids with myocarditis, the researchers were able to measure free spike protein in the blood – that is to say spike protein, not bound by antispike antibodies.
These free spikes were present in – wait for it – zero of the 45 control patients. That makes spike protein itself our prime suspect. J’accuse free spike protein!
Of course, all good detectives need to wrap up the case with a good story: How was it all done?
And here’s where we could use Agatha Christie’s help. How could this all work? The vaccine gets injected; mRNA is taken up into cells, where spike protein is generated and released, generating antibody and T-cell responses all the while. Those responses rapidly clear that spike protein from the system – this has been demonstrated in multiple studies – in adults, at least. But in some small number of people, apparently, spike protein is not cleared. Why? It makes no damn sense. Compels me, though. Some have suggested that inadvertent intravenous injection of vaccine, compared with the appropriate intramuscular route, might distribute the vaccine to sites with less immune surveillance. But that is definitely not proven yet.
We are on the path for sure, but this is, as Benoit Blanc would say, a twisted web – and we are not finished untangling it. Not yet.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available for preorder now. He reports no conflicts of interest.
A version of this article first appeared on Medscape.com.
Atrial fibrillation: Sex differences and modifiable risk factors
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
Is thrombolysis safe for stroke patients on DOACs?
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
From JAMA Neurology
Recount of FOURIER data finds higher mortality with evolocumab; trialists push back
Readjudication of mortality data from the FOURIER trial suggests a higher risk for cardiovascular death with evolocumab (Repatha) among patients with established atherosclerotic cardiovascular disease than originally reported for the first-in-class PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitor.
The Restoring Invisible and Abandoned Trials (RIAT) investigators launched this review in 2018, citing “significant inconsistencies and misreporting” between information in death narratives in the trial’s clinical study report (CSR) and the 2017 New England Journal of Medicine publication of the primary trial results.
“After readjudication, deaths of cardiac origin were numerically higher in the evolocumab group than in the placebo group in the FOURIER trial, suggesting possible cardiac harm,” the researchers conclude in the new report published online in BMJ Open. “At the time the trial was terminated early, a non-significantly higher risk of cardiovascular mortality was observed with evolocumab, which was numerically greater in our adjudication.
“Our findings indicate that complete restoration of all clinical outcomes from the FOURIER trial is required,” they wrote. “Meanwhile, clinicians should be skeptical about benefits vs harms of prescribing evolocumab for patients with established atherosclerotic cardiovascular disease.”
Asked to comment on the reanalysis, FOURIER lead investigator Marc Sabatine, MD, MPH, a professor of medicine at Harvard Medical School and the Lewis Dexter distinguished chair in cardiovascular medicine at Brigham and Women’s Hospital, both in Boston, said: “It’s hard to call this science. I think it lacks all scientific rigor and is fundamentally flawed and, because their process was flawed, it has led them to erroneous conclusions.”
Reached for comment, Sanjay Kaul, MD, a cardiologist and professor of medicine at Cedars-Sinai Medical Center in Los Angeles, who was not involved with either study, said: “If I were to describe this in one sentence, I would say much ado about nothing. A tempest in a teapot.”
Evaluating hard outcomes
The Food and Drug Administration approved evolocumab in 2015 for lowering LDL cholesterol levels, but without results from any trial evaluating hard outcomes.
As previously reported in 2017, FOURIER showed that adding evolocumab to high-intensity statins slashed LDL cholesterol by 59% and was associated with a 15% reduction in the primary composite cardiovascular events endpoint, compared with placebo, but numerically more all-cause and CV mortality.
The NEJM data analysis reported the risk for cardiovascular mortality was 5% (hazard ratio, 1.05; 95% confidence interval, 0.88-1.25), whereas the new review found a still nonsignificant 20% relative risk (R95% CI, 0.95-1.51).
Cardiac deaths were also numerically higher in the evolocumab group (113 vs. 88), corresponding to a 28% higher relative risk (95% CI, 0.97-1.69). Vascular deaths were similar at 37 in both groups (RR, 1.00; 95% CI, 0.63-1.58).
For 360 of the 870 deaths, the cause of death adjudicated by the FOURIER clinical events committee differs from that identified by the local clinical investigators in the CSR death narrative, the authors said.
The RIAT investigators found 11 more deaths from myocardial infarction in the evolocumab group (36 vs. 25 in NEJM) and 3 fewer deaths in the placebo group (27 vs. 30). In addition, their review indicated that deaths as a result of cardiac failure in the evolocumab group were almost double those in the placebo group, at 31 versus 16, respectively.
An ‘obvious disconnect’
Thomas L. Perry, MD, a coauthor of the BMJ Open paper and a general internist in the department of anesthesiology, pharmacology, and therapeutics at the University of British Columbia, Vancouver, said in an interview that the team repeatedly sought information from the FOURIER investigators but never received a response.
They petitioned and received the FOURIER CSR from the European Medicines Agency and Health Canada and made a similar request with the FDA but were told in October 2019 it would take up to 7 years to release the information. Case report forms were also requested but not received from all three agencies.
Dr. Perry noted that no autopsies were performed in the trial, a claim Dr. Sabatine rejected, and that their review of the death narratives in the CSR found 91 deaths classified by the local investigator as “undetermined” but subsequently adjudicated by the FOURIER clinical events committee as “sudden cardiac” deaths without any documented evidence to support the change.
At his request, Dr. Perry said they included two case examples (figures 1 and 2) in the BMJ Open paper of the “obvious disconnect” in death endpoints. Both of these were identified by the local investigator as a myocardial infarction but later “misreported” according to Dr. Perry, as a sudden cardiac death and noncardiovascular death (trauma), respectively.
“What’s so important about this is not only that it throws into doubt the reliability of what the people at Harvard and elsewhere reported in the New England Journal of Medicine in 2017, but also raises a question about any other large study like this where you rely on supposedly ethical local investigators to run the trial well and to report accurately what happens to people,” Dr. Perry said in an interview.
Although he never prescribed evolocumab after the initial results were published, Dr. Perry said he’s even less convinced of a benefit now. “Basically, I don’t believe that they are telling us the facts. I have no reason to say there’s an element of deliberately misleading us. I think it’s sloppiness, incompetence, laziness.”
Dr. Perry also favors readjudication of the mortality data in the ODYSSEY trial, which showed an all-cause mortality benefit with the PCSK9 inhibitor alirocumab (Praluent).
The ‘full picture’
Dr. Sabatine explained that when a patient had a cardiovascular event, including a death, it triggered the collection of a full dossier containing all available source documents, such as discharge summaries, laboratory and imaging data, and autopsy reports, that were independently reviewed by two board certified physicians blinded to treatment. To suggest, as the RIAT investigators have, that no autopsies were performed is “obviously ridiculous and wrong.”
In contrast, he said the new analysis was post hoc, involved unblinded individuals, and relied on serious adverse event narratives, which include a small text box that must be filled out with the site’s initial impression of the case and sent within 24 hours of the event.
Further, when the FOURIER investigators pulled the dossiers for the two more egregious examples cited in the paper, they found that the first patient died in his sleep at home. “The investigator then just said, ‘oh, I assume it’s an MI,’ but there’s no biochemical data, there’s no ECGs, there’s nothing to make the diagnosis of MI. So that’s why that is a sudden cardiac death per the FDA definition,” Dr. Sabatine said.
When the FOURIER investigators reviewed the full dossier for the second case example, they found the patient had slipped in his kitchen at home, sustained a serious head trauma, was brought into the emergency department, and died.
“That’s why we rely on the source documents. That gives the full picture,” he said. The FDA also reviewed the death narratives.
“They comment, ironically, that they were surprised at the inconsistencies between the investigator-reported causes of death and the central events committee-adjudicated ones, making it sound like something nefarious has happened. But that’s the whole point of adjudication, right? That you have a central events committee that reviews and then classifies based on all the data,” Dr. Sabatine said.
Dr. Sabatine said he sees no reason to reevaluate the ODYSSEY mortality data and that the RIAT analysis should not change the overall interpretation of FOURIER.
“I think this is in fact a disservice to the medical community because it’s not real science,” he said. “It’s just sensationalism and sends the wrong message. But I completely stand by the results that we published, as the FDA has.”
Dr. Kaul also thought the new analysis doesn’t materially change the overall benefit–risk balance. He observed that there isn’t a major difference between the reanalysis and the original evaluation. Total mortality was similar and, for cardiovascular deaths, the original NEJM paper lists 251 for evolocumab versus 240 for placebo and the reanalysis lists 150 versus 125, respectively.
Undetermined deaths were 144 for evolocumab and 164 for placebo in the reanalysis. “The conservative approach is to count them as presumed cardiovascular deaths,” Dr. Kaul said. “So, if you do the math and add those undetermined as cardiovascular deaths, we get a total of 294 (150 + 144) versus 289 (125 + 164). That’s five excess deaths with evolocumab.”
Open access
Although the RIAT group has called for the public release of the FOURIER data, commercial and legal issues will complicate that process, Steven Grover, MD, professor of medicine and director of the comprehensive health improvement program at McGill University, Montreal, said in an interview. Amgen is back in court over patent protection, filing an appeal with the Supreme Court after losing in the lower courts in a protracted battle, Reuters reported.
“One thing that’s for sure after they’ve raised questions about the results of this study [is that] somebody needs to take a good hard look at the adjudicated results,” said Dr. Grover, who coauthored several iterations of the Canadian Cardiovascular Society dyslipidemia guidelines, including the latest in 2021.
“I think the thing that got so many of us back in 2017 when the study was first published is the mortality data stuck out like a sore thumb,” he said in an interview. “It didn’t have to be statistically significant, but it did need to move in the same direction as the nonfatal coronary events. That’s what we’ve seen happen time and again and, in this case, it was going in the opposite direction.”
Dr. Sabatine said he doesn’t know whether the data will be released but that the FOURIER trialists plan to submit a rebuttal to BMJ Open to the RIAT analysis, which has caused a stir on CardioTwitter. “Now that people live with tweets of information, it necessitates then dispelling the misinformation that comes out. So yes, we will draft a rebuttal pointing out all the flaws in this analysis.”
Dr. Kaul commented that the FDA’s response not to provide the data was “rather curious” and that Dr. Sabatine and colleagues had the opportunity to address the RIAT group’s concerns, but the paper notes they did not even bother to respond. “You can’t be holier than thou in medicine. You have to treat every question with respect and humility and can’t be dismissive. ... He could have nipped the evil in the bud, so to speak.”
The study was funded by a grant from the University of Maryland, Baltimore. The authors, Dr. Kaul, and Dr. Grover reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Readjudication of mortality data from the FOURIER trial suggests a higher risk for cardiovascular death with evolocumab (Repatha) among patients with established atherosclerotic cardiovascular disease than originally reported for the first-in-class PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitor.
The Restoring Invisible and Abandoned Trials (RIAT) investigators launched this review in 2018, citing “significant inconsistencies and misreporting” between information in death narratives in the trial’s clinical study report (CSR) and the 2017 New England Journal of Medicine publication of the primary trial results.
“After readjudication, deaths of cardiac origin were numerically higher in the evolocumab group than in the placebo group in the FOURIER trial, suggesting possible cardiac harm,” the researchers conclude in the new report published online in BMJ Open. “At the time the trial was terminated early, a non-significantly higher risk of cardiovascular mortality was observed with evolocumab, which was numerically greater in our adjudication.
“Our findings indicate that complete restoration of all clinical outcomes from the FOURIER trial is required,” they wrote. “Meanwhile, clinicians should be skeptical about benefits vs harms of prescribing evolocumab for patients with established atherosclerotic cardiovascular disease.”
Asked to comment on the reanalysis, FOURIER lead investigator Marc Sabatine, MD, MPH, a professor of medicine at Harvard Medical School and the Lewis Dexter distinguished chair in cardiovascular medicine at Brigham and Women’s Hospital, both in Boston, said: “It’s hard to call this science. I think it lacks all scientific rigor and is fundamentally flawed and, because their process was flawed, it has led them to erroneous conclusions.”
Reached for comment, Sanjay Kaul, MD, a cardiologist and professor of medicine at Cedars-Sinai Medical Center in Los Angeles, who was not involved with either study, said: “If I were to describe this in one sentence, I would say much ado about nothing. A tempest in a teapot.”
Evaluating hard outcomes
The Food and Drug Administration approved evolocumab in 2015 for lowering LDL cholesterol levels, but without results from any trial evaluating hard outcomes.
As previously reported in 2017, FOURIER showed that adding evolocumab to high-intensity statins slashed LDL cholesterol by 59% and was associated with a 15% reduction in the primary composite cardiovascular events endpoint, compared with placebo, but numerically more all-cause and CV mortality.
The NEJM data analysis reported the risk for cardiovascular mortality was 5% (hazard ratio, 1.05; 95% confidence interval, 0.88-1.25), whereas the new review found a still nonsignificant 20% relative risk (R95% CI, 0.95-1.51).
Cardiac deaths were also numerically higher in the evolocumab group (113 vs. 88), corresponding to a 28% higher relative risk (95% CI, 0.97-1.69). Vascular deaths were similar at 37 in both groups (RR, 1.00; 95% CI, 0.63-1.58).
For 360 of the 870 deaths, the cause of death adjudicated by the FOURIER clinical events committee differs from that identified by the local clinical investigators in the CSR death narrative, the authors said.
The RIAT investigators found 11 more deaths from myocardial infarction in the evolocumab group (36 vs. 25 in NEJM) and 3 fewer deaths in the placebo group (27 vs. 30). In addition, their review indicated that deaths as a result of cardiac failure in the evolocumab group were almost double those in the placebo group, at 31 versus 16, respectively.
An ‘obvious disconnect’
Thomas L. Perry, MD, a coauthor of the BMJ Open paper and a general internist in the department of anesthesiology, pharmacology, and therapeutics at the University of British Columbia, Vancouver, said in an interview that the team repeatedly sought information from the FOURIER investigators but never received a response.
They petitioned and received the FOURIER CSR from the European Medicines Agency and Health Canada and made a similar request with the FDA but were told in October 2019 it would take up to 7 years to release the information. Case report forms were also requested but not received from all three agencies.
Dr. Perry noted that no autopsies were performed in the trial, a claim Dr. Sabatine rejected, and that their review of the death narratives in the CSR found 91 deaths classified by the local investigator as “undetermined” but subsequently adjudicated by the FOURIER clinical events committee as “sudden cardiac” deaths without any documented evidence to support the change.
At his request, Dr. Perry said they included two case examples (figures 1 and 2) in the BMJ Open paper of the “obvious disconnect” in death endpoints. Both of these were identified by the local investigator as a myocardial infarction but later “misreported” according to Dr. Perry, as a sudden cardiac death and noncardiovascular death (trauma), respectively.
“What’s so important about this is not only that it throws into doubt the reliability of what the people at Harvard and elsewhere reported in the New England Journal of Medicine in 2017, but also raises a question about any other large study like this where you rely on supposedly ethical local investigators to run the trial well and to report accurately what happens to people,” Dr. Perry said in an interview.
Although he never prescribed evolocumab after the initial results were published, Dr. Perry said he’s even less convinced of a benefit now. “Basically, I don’t believe that they are telling us the facts. I have no reason to say there’s an element of deliberately misleading us. I think it’s sloppiness, incompetence, laziness.”
Dr. Perry also favors readjudication of the mortality data in the ODYSSEY trial, which showed an all-cause mortality benefit with the PCSK9 inhibitor alirocumab (Praluent).
The ‘full picture’
Dr. Sabatine explained that when a patient had a cardiovascular event, including a death, it triggered the collection of a full dossier containing all available source documents, such as discharge summaries, laboratory and imaging data, and autopsy reports, that were independently reviewed by two board certified physicians blinded to treatment. To suggest, as the RIAT investigators have, that no autopsies were performed is “obviously ridiculous and wrong.”
In contrast, he said the new analysis was post hoc, involved unblinded individuals, and relied on serious adverse event narratives, which include a small text box that must be filled out with the site’s initial impression of the case and sent within 24 hours of the event.
Further, when the FOURIER investigators pulled the dossiers for the two more egregious examples cited in the paper, they found that the first patient died in his sleep at home. “The investigator then just said, ‘oh, I assume it’s an MI,’ but there’s no biochemical data, there’s no ECGs, there’s nothing to make the diagnosis of MI. So that’s why that is a sudden cardiac death per the FDA definition,” Dr. Sabatine said.
When the FOURIER investigators reviewed the full dossier for the second case example, they found the patient had slipped in his kitchen at home, sustained a serious head trauma, was brought into the emergency department, and died.
“That’s why we rely on the source documents. That gives the full picture,” he said. The FDA also reviewed the death narratives.
“They comment, ironically, that they were surprised at the inconsistencies between the investigator-reported causes of death and the central events committee-adjudicated ones, making it sound like something nefarious has happened. But that’s the whole point of adjudication, right? That you have a central events committee that reviews and then classifies based on all the data,” Dr. Sabatine said.
Dr. Sabatine said he sees no reason to reevaluate the ODYSSEY mortality data and that the RIAT analysis should not change the overall interpretation of FOURIER.
“I think this is in fact a disservice to the medical community because it’s not real science,” he said. “It’s just sensationalism and sends the wrong message. But I completely stand by the results that we published, as the FDA has.”
Dr. Kaul also thought the new analysis doesn’t materially change the overall benefit–risk balance. He observed that there isn’t a major difference between the reanalysis and the original evaluation. Total mortality was similar and, for cardiovascular deaths, the original NEJM paper lists 251 for evolocumab versus 240 for placebo and the reanalysis lists 150 versus 125, respectively.
Undetermined deaths were 144 for evolocumab and 164 for placebo in the reanalysis. “The conservative approach is to count them as presumed cardiovascular deaths,” Dr. Kaul said. “So, if you do the math and add those undetermined as cardiovascular deaths, we get a total of 294 (150 + 144) versus 289 (125 + 164). That’s five excess deaths with evolocumab.”
Open access
Although the RIAT group has called for the public release of the FOURIER data, commercial and legal issues will complicate that process, Steven Grover, MD, professor of medicine and director of the comprehensive health improvement program at McGill University, Montreal, said in an interview. Amgen is back in court over patent protection, filing an appeal with the Supreme Court after losing in the lower courts in a protracted battle, Reuters reported.
“One thing that’s for sure after they’ve raised questions about the results of this study [is that] somebody needs to take a good hard look at the adjudicated results,” said Dr. Grover, who coauthored several iterations of the Canadian Cardiovascular Society dyslipidemia guidelines, including the latest in 2021.
“I think the thing that got so many of us back in 2017 when the study was first published is the mortality data stuck out like a sore thumb,” he said in an interview. “It didn’t have to be statistically significant, but it did need to move in the same direction as the nonfatal coronary events. That’s what we’ve seen happen time and again and, in this case, it was going in the opposite direction.”
Dr. Sabatine said he doesn’t know whether the data will be released but that the FOURIER trialists plan to submit a rebuttal to BMJ Open to the RIAT analysis, which has caused a stir on CardioTwitter. “Now that people live with tweets of information, it necessitates then dispelling the misinformation that comes out. So yes, we will draft a rebuttal pointing out all the flaws in this analysis.”
Dr. Kaul commented that the FDA’s response not to provide the data was “rather curious” and that Dr. Sabatine and colleagues had the opportunity to address the RIAT group’s concerns, but the paper notes they did not even bother to respond. “You can’t be holier than thou in medicine. You have to treat every question with respect and humility and can’t be dismissive. ... He could have nipped the evil in the bud, so to speak.”
The study was funded by a grant from the University of Maryland, Baltimore. The authors, Dr. Kaul, and Dr. Grover reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Readjudication of mortality data from the FOURIER trial suggests a higher risk for cardiovascular death with evolocumab (Repatha) among patients with established atherosclerotic cardiovascular disease than originally reported for the first-in-class PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitor.
The Restoring Invisible and Abandoned Trials (RIAT) investigators launched this review in 2018, citing “significant inconsistencies and misreporting” between information in death narratives in the trial’s clinical study report (CSR) and the 2017 New England Journal of Medicine publication of the primary trial results.
“After readjudication, deaths of cardiac origin were numerically higher in the evolocumab group than in the placebo group in the FOURIER trial, suggesting possible cardiac harm,” the researchers conclude in the new report published online in BMJ Open. “At the time the trial was terminated early, a non-significantly higher risk of cardiovascular mortality was observed with evolocumab, which was numerically greater in our adjudication.
“Our findings indicate that complete restoration of all clinical outcomes from the FOURIER trial is required,” they wrote. “Meanwhile, clinicians should be skeptical about benefits vs harms of prescribing evolocumab for patients with established atherosclerotic cardiovascular disease.”
Asked to comment on the reanalysis, FOURIER lead investigator Marc Sabatine, MD, MPH, a professor of medicine at Harvard Medical School and the Lewis Dexter distinguished chair in cardiovascular medicine at Brigham and Women’s Hospital, both in Boston, said: “It’s hard to call this science. I think it lacks all scientific rigor and is fundamentally flawed and, because their process was flawed, it has led them to erroneous conclusions.”
Reached for comment, Sanjay Kaul, MD, a cardiologist and professor of medicine at Cedars-Sinai Medical Center in Los Angeles, who was not involved with either study, said: “If I were to describe this in one sentence, I would say much ado about nothing. A tempest in a teapot.”
Evaluating hard outcomes
The Food and Drug Administration approved evolocumab in 2015 for lowering LDL cholesterol levels, but without results from any trial evaluating hard outcomes.
As previously reported in 2017, FOURIER showed that adding evolocumab to high-intensity statins slashed LDL cholesterol by 59% and was associated with a 15% reduction in the primary composite cardiovascular events endpoint, compared with placebo, but numerically more all-cause and CV mortality.
The NEJM data analysis reported the risk for cardiovascular mortality was 5% (hazard ratio, 1.05; 95% confidence interval, 0.88-1.25), whereas the new review found a still nonsignificant 20% relative risk (R95% CI, 0.95-1.51).
Cardiac deaths were also numerically higher in the evolocumab group (113 vs. 88), corresponding to a 28% higher relative risk (95% CI, 0.97-1.69). Vascular deaths were similar at 37 in both groups (RR, 1.00; 95% CI, 0.63-1.58).
For 360 of the 870 deaths, the cause of death adjudicated by the FOURIER clinical events committee differs from that identified by the local clinical investigators in the CSR death narrative, the authors said.
The RIAT investigators found 11 more deaths from myocardial infarction in the evolocumab group (36 vs. 25 in NEJM) and 3 fewer deaths in the placebo group (27 vs. 30). In addition, their review indicated that deaths as a result of cardiac failure in the evolocumab group were almost double those in the placebo group, at 31 versus 16, respectively.
An ‘obvious disconnect’
Thomas L. Perry, MD, a coauthor of the BMJ Open paper and a general internist in the department of anesthesiology, pharmacology, and therapeutics at the University of British Columbia, Vancouver, said in an interview that the team repeatedly sought information from the FOURIER investigators but never received a response.
They petitioned and received the FOURIER CSR from the European Medicines Agency and Health Canada and made a similar request with the FDA but were told in October 2019 it would take up to 7 years to release the information. Case report forms were also requested but not received from all three agencies.
Dr. Perry noted that no autopsies were performed in the trial, a claim Dr. Sabatine rejected, and that their review of the death narratives in the CSR found 91 deaths classified by the local investigator as “undetermined” but subsequently adjudicated by the FOURIER clinical events committee as “sudden cardiac” deaths without any documented evidence to support the change.
At his request, Dr. Perry said they included two case examples (figures 1 and 2) in the BMJ Open paper of the “obvious disconnect” in death endpoints. Both of these were identified by the local investigator as a myocardial infarction but later “misreported” according to Dr. Perry, as a sudden cardiac death and noncardiovascular death (trauma), respectively.
“What’s so important about this is not only that it throws into doubt the reliability of what the people at Harvard and elsewhere reported in the New England Journal of Medicine in 2017, but also raises a question about any other large study like this where you rely on supposedly ethical local investigators to run the trial well and to report accurately what happens to people,” Dr. Perry said in an interview.
Although he never prescribed evolocumab after the initial results were published, Dr. Perry said he’s even less convinced of a benefit now. “Basically, I don’t believe that they are telling us the facts. I have no reason to say there’s an element of deliberately misleading us. I think it’s sloppiness, incompetence, laziness.”
Dr. Perry also favors readjudication of the mortality data in the ODYSSEY trial, which showed an all-cause mortality benefit with the PCSK9 inhibitor alirocumab (Praluent).
The ‘full picture’
Dr. Sabatine explained that when a patient had a cardiovascular event, including a death, it triggered the collection of a full dossier containing all available source documents, such as discharge summaries, laboratory and imaging data, and autopsy reports, that were independently reviewed by two board certified physicians blinded to treatment. To suggest, as the RIAT investigators have, that no autopsies were performed is “obviously ridiculous and wrong.”
In contrast, he said the new analysis was post hoc, involved unblinded individuals, and relied on serious adverse event narratives, which include a small text box that must be filled out with the site’s initial impression of the case and sent within 24 hours of the event.
Further, when the FOURIER investigators pulled the dossiers for the two more egregious examples cited in the paper, they found that the first patient died in his sleep at home. “The investigator then just said, ‘oh, I assume it’s an MI,’ but there’s no biochemical data, there’s no ECGs, there’s nothing to make the diagnosis of MI. So that’s why that is a sudden cardiac death per the FDA definition,” Dr. Sabatine said.
When the FOURIER investigators reviewed the full dossier for the second case example, they found the patient had slipped in his kitchen at home, sustained a serious head trauma, was brought into the emergency department, and died.
“That’s why we rely on the source documents. That gives the full picture,” he said. The FDA also reviewed the death narratives.
“They comment, ironically, that they were surprised at the inconsistencies between the investigator-reported causes of death and the central events committee-adjudicated ones, making it sound like something nefarious has happened. But that’s the whole point of adjudication, right? That you have a central events committee that reviews and then classifies based on all the data,” Dr. Sabatine said.
Dr. Sabatine said he sees no reason to reevaluate the ODYSSEY mortality data and that the RIAT analysis should not change the overall interpretation of FOURIER.
“I think this is in fact a disservice to the medical community because it’s not real science,” he said. “It’s just sensationalism and sends the wrong message. But I completely stand by the results that we published, as the FDA has.”
Dr. Kaul also thought the new analysis doesn’t materially change the overall benefit–risk balance. He observed that there isn’t a major difference between the reanalysis and the original evaluation. Total mortality was similar and, for cardiovascular deaths, the original NEJM paper lists 251 for evolocumab versus 240 for placebo and the reanalysis lists 150 versus 125, respectively.
Undetermined deaths were 144 for evolocumab and 164 for placebo in the reanalysis. “The conservative approach is to count them as presumed cardiovascular deaths,” Dr. Kaul said. “So, if you do the math and add those undetermined as cardiovascular deaths, we get a total of 294 (150 + 144) versus 289 (125 + 164). That’s five excess deaths with evolocumab.”
Open access
Although the RIAT group has called for the public release of the FOURIER data, commercial and legal issues will complicate that process, Steven Grover, MD, professor of medicine and director of the comprehensive health improvement program at McGill University, Montreal, said in an interview. Amgen is back in court over patent protection, filing an appeal with the Supreme Court after losing in the lower courts in a protracted battle, Reuters reported.
“One thing that’s for sure after they’ve raised questions about the results of this study [is that] somebody needs to take a good hard look at the adjudicated results,” said Dr. Grover, who coauthored several iterations of the Canadian Cardiovascular Society dyslipidemia guidelines, including the latest in 2021.
“I think the thing that got so many of us back in 2017 when the study was first published is the mortality data stuck out like a sore thumb,” he said in an interview. “It didn’t have to be statistically significant, but it did need to move in the same direction as the nonfatal coronary events. That’s what we’ve seen happen time and again and, in this case, it was going in the opposite direction.”
Dr. Sabatine said he doesn’t know whether the data will be released but that the FOURIER trialists plan to submit a rebuttal to BMJ Open to the RIAT analysis, which has caused a stir on CardioTwitter. “Now that people live with tweets of information, it necessitates then dispelling the misinformation that comes out. So yes, we will draft a rebuttal pointing out all the flaws in this analysis.”
Dr. Kaul commented that the FDA’s response not to provide the data was “rather curious” and that Dr. Sabatine and colleagues had the opportunity to address the RIAT group’s concerns, but the paper notes they did not even bother to respond. “You can’t be holier than thou in medicine. You have to treat every question with respect and humility and can’t be dismissive. ... He could have nipped the evil in the bud, so to speak.”
The study was funded by a grant from the University of Maryland, Baltimore. The authors, Dr. Kaul, and Dr. Grover reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM BMJ OPEN
Latest steps toward reducing U.S. insulin cost begin in 2023
As of Jan. 1, 2023, the new provision tucked into the Inflation Reduction Act, signed into law by President Biden in August 2022, means that beneficiaries who take insulin via pen or syringe, covered under Medicare part D (prescription drugs), fall under the $35/month co-pay cap.
On July 1, 2023, the same out-of-pocket limit will also apply to those who take insulin via pump, which falls under Medicare part B (durable medical equipment).
The bill originally included the co-pay cap for people with private insurance as well, but that was stripped out as part of the reconciliation process and didn’t garner the necessary 60 Senate votes to keep it in prior to passage.
However, since 2019, 22 U.S. states have passed their own co-pay caps for people with state-regulated private insurance, ranging from $25 to $100 for a 30-day supply. A few states also cap the cost of diabetes devices as well.
Moreover, federal legislation could still address co-pay caps for people with private insurance, as well as include provisions to help those without insurance to afford insulin, Niels Knutson, director of government relations for the type 1 diabetes advocacy organization JDRF, told this news organization.
“There’s a whole menu of ideas on how to address the issue of insulin affordability. Most pathways to solving this on the federal level will require 60 votes in the Senate. There is universal recognition that this is a problem. The challenge becomes: is everybody on the same page for how to fix it,” Mr. Knutson said.
JDRF is supporting the bipartisan Improving Needed Safeguards for Users of Lifesaving Insulin Now (INSULIN) Act, introduced in June 2022 by U.S. Senators Jeanne Shaheen (D-NH) and Susan Collins (R-ME), who co-chair the Senate Diabetes Caucus. The bill includes a co-pay cap and also provisions to encourage insulin manufacturers to reduce their list prices.
“The bill is unique in that it adds a pathway to reduce the cost of insulin for everybody, regardless of whether they have insurance or not ... We see the Insulin Act as being the best path forward and the most viable path to have the biggest impact for the most people,” Mr. Knutson explained.
At the same time, JDRF is also supporting a nonprofit pharmaceutical company called Civica, which plans to bring biosimilar versions of the insulin analogs glargine, lispro, and aspart to the U.S. market by 2024 at a cost of no more than $30 for a vial and $50 for a box of prefilled pens. The state of California is expected to partner with Civica as well.
“This is just another access point for insulin, especially for folks who are uninsured, that would make a big impact,” Mr. Knutson said.
Other entities that have announced intentions to bring lower-cost insulin to the United States market include the Korean firm Undbio and billionaire entrepreneur Mark Cuban, through his company Cost Plus Drugs.
“Insulin is such a clear and present crisis that we need to address,” Mr. Knutson said. “You’re seeing this problem being recognized and solutions from all different angles coming at it.”
A version of this article first appeared on Medscape.com.
As of Jan. 1, 2023, the new provision tucked into the Inflation Reduction Act, signed into law by President Biden in August 2022, means that beneficiaries who take insulin via pen or syringe, covered under Medicare part D (prescription drugs), fall under the $35/month co-pay cap.
On July 1, 2023, the same out-of-pocket limit will also apply to those who take insulin via pump, which falls under Medicare part B (durable medical equipment).
The bill originally included the co-pay cap for people with private insurance as well, but that was stripped out as part of the reconciliation process and didn’t garner the necessary 60 Senate votes to keep it in prior to passage.
However, since 2019, 22 U.S. states have passed their own co-pay caps for people with state-regulated private insurance, ranging from $25 to $100 for a 30-day supply. A few states also cap the cost of diabetes devices as well.
Moreover, federal legislation could still address co-pay caps for people with private insurance, as well as include provisions to help those without insurance to afford insulin, Niels Knutson, director of government relations for the type 1 diabetes advocacy organization JDRF, told this news organization.
“There’s a whole menu of ideas on how to address the issue of insulin affordability. Most pathways to solving this on the federal level will require 60 votes in the Senate. There is universal recognition that this is a problem. The challenge becomes: is everybody on the same page for how to fix it,” Mr. Knutson said.
JDRF is supporting the bipartisan Improving Needed Safeguards for Users of Lifesaving Insulin Now (INSULIN) Act, introduced in June 2022 by U.S. Senators Jeanne Shaheen (D-NH) and Susan Collins (R-ME), who co-chair the Senate Diabetes Caucus. The bill includes a co-pay cap and also provisions to encourage insulin manufacturers to reduce their list prices.
“The bill is unique in that it adds a pathway to reduce the cost of insulin for everybody, regardless of whether they have insurance or not ... We see the Insulin Act as being the best path forward and the most viable path to have the biggest impact for the most people,” Mr. Knutson explained.
At the same time, JDRF is also supporting a nonprofit pharmaceutical company called Civica, which plans to bring biosimilar versions of the insulin analogs glargine, lispro, and aspart to the U.S. market by 2024 at a cost of no more than $30 for a vial and $50 for a box of prefilled pens. The state of California is expected to partner with Civica as well.
“This is just another access point for insulin, especially for folks who are uninsured, that would make a big impact,” Mr. Knutson said.
Other entities that have announced intentions to bring lower-cost insulin to the United States market include the Korean firm Undbio and billionaire entrepreneur Mark Cuban, through his company Cost Plus Drugs.
“Insulin is such a clear and present crisis that we need to address,” Mr. Knutson said. “You’re seeing this problem being recognized and solutions from all different angles coming at it.”
A version of this article first appeared on Medscape.com.
As of Jan. 1, 2023, the new provision tucked into the Inflation Reduction Act, signed into law by President Biden in August 2022, means that beneficiaries who take insulin via pen or syringe, covered under Medicare part D (prescription drugs), fall under the $35/month co-pay cap.
On July 1, 2023, the same out-of-pocket limit will also apply to those who take insulin via pump, which falls under Medicare part B (durable medical equipment).
The bill originally included the co-pay cap for people with private insurance as well, but that was stripped out as part of the reconciliation process and didn’t garner the necessary 60 Senate votes to keep it in prior to passage.
However, since 2019, 22 U.S. states have passed their own co-pay caps for people with state-regulated private insurance, ranging from $25 to $100 for a 30-day supply. A few states also cap the cost of diabetes devices as well.
Moreover, federal legislation could still address co-pay caps for people with private insurance, as well as include provisions to help those without insurance to afford insulin, Niels Knutson, director of government relations for the type 1 diabetes advocacy organization JDRF, told this news organization.
“There’s a whole menu of ideas on how to address the issue of insulin affordability. Most pathways to solving this on the federal level will require 60 votes in the Senate. There is universal recognition that this is a problem. The challenge becomes: is everybody on the same page for how to fix it,” Mr. Knutson said.
JDRF is supporting the bipartisan Improving Needed Safeguards for Users of Lifesaving Insulin Now (INSULIN) Act, introduced in June 2022 by U.S. Senators Jeanne Shaheen (D-NH) and Susan Collins (R-ME), who co-chair the Senate Diabetes Caucus. The bill includes a co-pay cap and also provisions to encourage insulin manufacturers to reduce their list prices.
“The bill is unique in that it adds a pathway to reduce the cost of insulin for everybody, regardless of whether they have insurance or not ... We see the Insulin Act as being the best path forward and the most viable path to have the biggest impact for the most people,” Mr. Knutson explained.
At the same time, JDRF is also supporting a nonprofit pharmaceutical company called Civica, which plans to bring biosimilar versions of the insulin analogs glargine, lispro, and aspart to the U.S. market by 2024 at a cost of no more than $30 for a vial and $50 for a box of prefilled pens. The state of California is expected to partner with Civica as well.
“This is just another access point for insulin, especially for folks who are uninsured, that would make a big impact,” Mr. Knutson said.
Other entities that have announced intentions to bring lower-cost insulin to the United States market include the Korean firm Undbio and billionaire entrepreneur Mark Cuban, through his company Cost Plus Drugs.
“Insulin is such a clear and present crisis that we need to address,” Mr. Knutson said. “You’re seeing this problem being recognized and solutions from all different angles coming at it.”
A version of this article first appeared on Medscape.com.
Five thoughts on the Damar Hamlin collapse
The obvious first statement is that it’s neither wise nor appropriate to speculate on the specifics of Damar Hamlin’s cardiac event during a football game on Jan. 2 (including the possibility of commotio cordis) or his ongoing care. The public nature of his collapse induces intense curiosity but people with illness deserve privacy. Privacy in health care is in short supply. I disagree strongly with those who say his doctors ought to be giving public updates. That’s up to the family.
But there are important general concepts to consider about this incident. These include ...
Cardiac arrest can happen to anyone
People with structural heart disease or other chronic illnesses have a higher risk of arrhythmia, but the notion that athletes are immune from cardiac arrest is wrong. This sentence almost seems too obvious to write, but to this day, I hear clinicians express surprise that an athletic person has heart disease.

Survival turns on rapid and effective intervention
In the old days of electrophysiology, we used to test implantable cardioverter-defibrillators during an implant procedure by inducing ventricular fibrillation (VF) and watching the device convert it. Thankfully, trials have shown that this is no longer necessary for most implants.
When you induce VF In the EP lab, you learn quickly that a) it causes loss of consciousness in a matter of seconds, b) rapid defibrillation restores consciousness, often without the patients knowing or remembering they passed out, and c) the failure of the shock to terminate VF results in deterioration in a matter of 1-2 minutes. Even 1 minute in VF feels so long.
Need is an appropriate word in VF treatment
Clinicians often use the verb need. As in, this patient needs this pill or this procedure. It’s rarely appropriate.
But in the case of treating VF, patients truly need rapid defibrillation. Survival of out-of-hospital cardiac arrest is low because there just aren’t enough automated external defibrillators (AEDs) or people trained to use them. A study of patients who had out-of-hospital cardiac arrest in Denmark found that 30-day survival almost doubled (28.8% vs. 16.4%), when the nearest AED was accessible.
Bystanders must act
The public messages are simple: If a person loses consciousness in front of you, and is not breathing normally, assume it is a cardiac arrest, call 911 to get professional help, and start hands-only chest compressions. Don’t spend time checking for a pulse or trying to wake the person. If this is not a cardiac arrest, they will soon tell you to stop compressing their chest. Seconds matter.
Chest compressions are important but what is really needed is defibrillation. A crucial step in CPR is to send someone to get an AED and get the pads attached. If this is a shockable rhythm, deliver the shock. Hamlin’s collapse emphasizes the importance of the AED; without it, his survival to the hospital would have been unlikely.
Widespread preparticipation screening of young athletes remains a bad idea
Whenever cardiac arrest occurs in an athlete, in such a public way, people think about prevention. Surely it is better to prevent such an event than react to it, goes the thinking. The argument against this idea has four prongs:
The incidence of cardiac disease in a young athlete is extremely low, which sets up a situation where most “positive” tests are false positive. A false positive screening ECG or echocardiogram can create harm in multiple ways. One is the risk from downstream procedures, but worse is the inappropriate disqualification from sport. Healthwise, few harms could be greater than creating long-term fear of exercise in someone.
There is also the problem of false-negative screening tests. An ECG may be normal in the setting of hypertrophic cardiomyopathy. And a normal echocardiogram does not exclude arrhythmogenic right ventricular cardiomyopathy or other genetic causes of cardiac arrest. In a 2018 study from a major sports cardiology center in London, 6 of the 8 sudden cardiac deaths in their series were in athletes who had no detectable abnormalities on screening.
Even when disease is found, it’s not clear that prohibiting participation in sports prevents sudden death. Many previous class III recommendations against participation in sport now carry class II – may be considered – designations.
Finally, screening for any disease loses value as treatments improve. Public education regarding rapid intervention with CPR and AED use is the best treatment option. A great example is the case of Christian Erikson, a Danish soccer player who suffered cardiac arrest during a match at the European Championships in 2021 and was rapidly defibrillated on the field. Therapy was so effective that he was conscious and able to wave to fans on his way out of the stadium. He has now returned to elite competition.
Proponents of screening might oppose my take by saying that National Football League players are intensely screened. But this is different from widespread screening of high school and college athletes. It might sound harsh to say, but professional teams have dualities of interests in the health of their athletes given the million-dollar contracts.
What’s more, professional teams can afford to hire expert cardiologists to perform the testing. This would likely reduce the rate of false-positive findings, compared with screening in the community setting. I often have young people referred to me because of asymptomatic bradycardia found during athletic screening – an obviously normal finding.
Conclusions
As long as there are sports, there will be athletes who suffer cardiac arrest.
We can both hope for Hamlin’s full recovery and learn lessons to help reduce the rate of death from out-of-hospital cardiac arrest. This mostly involves education on how to help fellow humans and a public health commitment to access to AEDs.
John Mandrola, MD, practices cardiac electrophysiology in Louisville, Ky. and is a writer and podcaster for Medscape. He has disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
The obvious first statement is that it’s neither wise nor appropriate to speculate on the specifics of Damar Hamlin’s cardiac event during a football game on Jan. 2 (including the possibility of commotio cordis) or his ongoing care. The public nature of his collapse induces intense curiosity but people with illness deserve privacy. Privacy in health care is in short supply. I disagree strongly with those who say his doctors ought to be giving public updates. That’s up to the family.
But there are important general concepts to consider about this incident. These include ...
Cardiac arrest can happen to anyone
People with structural heart disease or other chronic illnesses have a higher risk of arrhythmia, but the notion that athletes are immune from cardiac arrest is wrong. This sentence almost seems too obvious to write, but to this day, I hear clinicians express surprise that an athletic person has heart disease.
Survival turns on rapid and effective intervention
In the old days of electrophysiology, we used to test implantable cardioverter-defibrillators during an implant procedure by inducing ventricular fibrillation (VF) and watching the device convert it. Thankfully, trials have shown that this is no longer necessary for most implants.
When you induce VF In the EP lab, you learn quickly that a) it causes loss of consciousness in a matter of seconds, b) rapid defibrillation restores consciousness, often without the patients knowing or remembering they passed out, and c) the failure of the shock to terminate VF results in deterioration in a matter of 1-2 minutes. Even 1 minute in VF feels so long.
Need is an appropriate word in VF treatment
Clinicians often use the verb need. As in, this patient needs this pill or this procedure. It’s rarely appropriate.
But in the case of treating VF, patients truly need rapid defibrillation. Survival of out-of-hospital cardiac arrest is low because there just aren’t enough automated external defibrillators (AEDs) or people trained to use them. A study of patients who had out-of-hospital cardiac arrest in Denmark found that 30-day survival almost doubled (28.8% vs. 16.4%), when the nearest AED was accessible.
Bystanders must act
The public messages are simple: If a person loses consciousness in front of you, and is not breathing normally, assume it is a cardiac arrest, call 911 to get professional help, and start hands-only chest compressions. Don’t spend time checking for a pulse or trying to wake the person. If this is not a cardiac arrest, they will soon tell you to stop compressing their chest. Seconds matter.
Chest compressions are important but what is really needed is defibrillation. A crucial step in CPR is to send someone to get an AED and get the pads attached. If this is a shockable rhythm, deliver the shock. Hamlin’s collapse emphasizes the importance of the AED; without it, his survival to the hospital would have been unlikely.
Widespread preparticipation screening of young athletes remains a bad idea
Whenever cardiac arrest occurs in an athlete, in such a public way, people think about prevention. Surely it is better to prevent such an event than react to it, goes the thinking. The argument against this idea has four prongs:
The incidence of cardiac disease in a young athlete is extremely low, which sets up a situation where most “positive” tests are false positive. A false positive screening ECG or echocardiogram can create harm in multiple ways. One is the risk from downstream procedures, but worse is the inappropriate disqualification from sport. Healthwise, few harms could be greater than creating long-term fear of exercise in someone.
There is also the problem of false-negative screening tests. An ECG may be normal in the setting of hypertrophic cardiomyopathy. And a normal echocardiogram does not exclude arrhythmogenic right ventricular cardiomyopathy or other genetic causes of cardiac arrest. In a 2018 study from a major sports cardiology center in London, 6 of the 8 sudden cardiac deaths in their series were in athletes who had no detectable abnormalities on screening.
Even when disease is found, it’s not clear that prohibiting participation in sports prevents sudden death. Many previous class III recommendations against participation in sport now carry class II – may be considered – designations.
Finally, screening for any disease loses value as treatments improve. Public education regarding rapid intervention with CPR and AED use is the best treatment option. A great example is the case of Christian Erikson, a Danish soccer player who suffered cardiac arrest during a match at the European Championships in 2021 and was rapidly defibrillated on the field. Therapy was so effective that he was conscious and able to wave to fans on his way out of the stadium. He has now returned to elite competition.
Proponents of screening might oppose my take by saying that National Football League players are intensely screened. But this is different from widespread screening of high school and college athletes. It might sound harsh to say, but professional teams have dualities of interests in the health of their athletes given the million-dollar contracts.
What’s more, professional teams can afford to hire expert cardiologists to perform the testing. This would likely reduce the rate of false-positive findings, compared with screening in the community setting. I often have young people referred to me because of asymptomatic bradycardia found during athletic screening – an obviously normal finding.
Conclusions
As long as there are sports, there will be athletes who suffer cardiac arrest.
We can both hope for Hamlin’s full recovery and learn lessons to help reduce the rate of death from out-of-hospital cardiac arrest. This mostly involves education on how to help fellow humans and a public health commitment to access to AEDs.
John Mandrola, MD, practices cardiac electrophysiology in Louisville, Ky. and is a writer and podcaster for Medscape. He has disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
The obvious first statement is that it’s neither wise nor appropriate to speculate on the specifics of Damar Hamlin’s cardiac event during a football game on Jan. 2 (including the possibility of commotio cordis) or his ongoing care. The public nature of his collapse induces intense curiosity but people with illness deserve privacy. Privacy in health care is in short supply. I disagree strongly with those who say his doctors ought to be giving public updates. That’s up to the family.
But there are important general concepts to consider about this incident. These include ...
Cardiac arrest can happen to anyone
People with structural heart disease or other chronic illnesses have a higher risk of arrhythmia, but the notion that athletes are immune from cardiac arrest is wrong. This sentence almost seems too obvious to write, but to this day, I hear clinicians express surprise that an athletic person has heart disease.
Survival turns on rapid and effective intervention
In the old days of electrophysiology, we used to test implantable cardioverter-defibrillators during an implant procedure by inducing ventricular fibrillation (VF) and watching the device convert it. Thankfully, trials have shown that this is no longer necessary for most implants.
When you induce VF In the EP lab, you learn quickly that a) it causes loss of consciousness in a matter of seconds, b) rapid defibrillation restores consciousness, often without the patients knowing or remembering they passed out, and c) the failure of the shock to terminate VF results in deterioration in a matter of 1-2 minutes. Even 1 minute in VF feels so long.
Need is an appropriate word in VF treatment
Clinicians often use the verb need. As in, this patient needs this pill or this procedure. It’s rarely appropriate.
But in the case of treating VF, patients truly need rapid defibrillation. Survival of out-of-hospital cardiac arrest is low because there just aren’t enough automated external defibrillators (AEDs) or people trained to use them. A study of patients who had out-of-hospital cardiac arrest in Denmark found that 30-day survival almost doubled (28.8% vs. 16.4%), when the nearest AED was accessible.
Bystanders must act
The public messages are simple: If a person loses consciousness in front of you, and is not breathing normally, assume it is a cardiac arrest, call 911 to get professional help, and start hands-only chest compressions. Don’t spend time checking for a pulse or trying to wake the person. If this is not a cardiac arrest, they will soon tell you to stop compressing their chest. Seconds matter.
Chest compressions are important but what is really needed is defibrillation. A crucial step in CPR is to send someone to get an AED and get the pads attached. If this is a shockable rhythm, deliver the shock. Hamlin’s collapse emphasizes the importance of the AED; without it, his survival to the hospital would have been unlikely.
Widespread preparticipation screening of young athletes remains a bad idea
Whenever cardiac arrest occurs in an athlete, in such a public way, people think about prevention. Surely it is better to prevent such an event than react to it, goes the thinking. The argument against this idea has four prongs:
The incidence of cardiac disease in a young athlete is extremely low, which sets up a situation where most “positive” tests are false positive. A false positive screening ECG or echocardiogram can create harm in multiple ways. One is the risk from downstream procedures, but worse is the inappropriate disqualification from sport. Healthwise, few harms could be greater than creating long-term fear of exercise in someone.
There is also the problem of false-negative screening tests. An ECG may be normal in the setting of hypertrophic cardiomyopathy. And a normal echocardiogram does not exclude arrhythmogenic right ventricular cardiomyopathy or other genetic causes of cardiac arrest. In a 2018 study from a major sports cardiology center in London, 6 of the 8 sudden cardiac deaths in their series were in athletes who had no detectable abnormalities on screening.
Even when disease is found, it’s not clear that prohibiting participation in sports prevents sudden death. Many previous class III recommendations against participation in sport now carry class II – may be considered – designations.
Finally, screening for any disease loses value as treatments improve. Public education regarding rapid intervention with CPR and AED use is the best treatment option. A great example is the case of Christian Erikson, a Danish soccer player who suffered cardiac arrest during a match at the European Championships in 2021 and was rapidly defibrillated on the field. Therapy was so effective that he was conscious and able to wave to fans on his way out of the stadium. He has now returned to elite competition.
Proponents of screening might oppose my take by saying that National Football League players are intensely screened. But this is different from widespread screening of high school and college athletes. It might sound harsh to say, but professional teams have dualities of interests in the health of their athletes given the million-dollar contracts.
What’s more, professional teams can afford to hire expert cardiologists to perform the testing. This would likely reduce the rate of false-positive findings, compared with screening in the community setting. I often have young people referred to me because of asymptomatic bradycardia found during athletic screening – an obviously normal finding.
Conclusions
As long as there are sports, there will be athletes who suffer cardiac arrest.
We can both hope for Hamlin’s full recovery and learn lessons to help reduce the rate of death from out-of-hospital cardiac arrest. This mostly involves education on how to help fellow humans and a public health commitment to access to AEDs.
John Mandrola, MD, practices cardiac electrophysiology in Louisville, Ky. and is a writer and podcaster for Medscape. He has disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
One in four cardiologists worldwide report mental health issues
ranging from anxiety or anger issues to major depression or other psychiatric disorders.
Such conditions varied in prevalence by cardiology subspecialty and years in the field, were more common in women than in men, and were closely linked to enduring hostile work environments and other strains of professional life.
The survey, conducted only months before the COVID-19 pandemic and with its share of limitations, still paints a picture that’s not pretty.
For example, mental health concerns were reported by about 42% of respondents who cited a hostile work environment, defined as workplace experience of discrimination based on age, sex, religion, race or ethnicity, or emotional or sexual harassment. Conversely, the prevalence of these concerns reached only 17% among those without such workplace conditions.
The study shows substantial overlap between cardiologists reporting hostility at work and those with mental health concerns, “and that was a significant finding,” Garima Sharma, MD, Johns Hopkins University, Baltimore, said in an interview.
Still, only 31% of male and 42% of female cardiologists (P < .001) reporting mental health concerns also said they had sought professional help either within or outside their own institutions.
That means “there is a lot of silent suffering” in the field, said Dr. Sharma, who is lead author on the study, published in the Journal of the American College of Cardiology.
Bringing back the conversation
The survey findings, she added, point to at least two potential ways the cardiology community can strive to diminish what may be a major underlying cause of the mental health concerns and their consequences.
“If you work towards reducing hostility at work and making mental health a priority for your workforce, then those experiencing these types of egregious conditions based on age, gender, race, ethnicity, or sexual orientation are less likely to be harmed.”
Mental health concerns among cardiologists are seldom openly discussed, so the current study can be “a way to bring them back into the conversation,” Dr. Sharma said. Clinician mental health “is extremely important because it directly impacts patient care and productivity.”
The survey’s reported mental health conditions “are an issue across the board in medicine, and amongst our medical students as well,” senior author Laxmi S. Mehta, MD, professor of internal medicine at Ohio State University, Columbus, said in an interview. The current study provides new details about their prevalence and predictors in cardiology and, she hopes, may improve the field’s awareness of and efforts to address the problem.
“We need to support those who have underlying mental health conditions, as well as improve the work environment to reduce contributory factors to mental illnesses. And we also need to work on reducing the stigma associated with seeking treatment and on reducing the barriers to receiving treatment,” said Dr. Mehta, who chairs the Workgroup on Clinician Well-Being of the ACC, which conducted the survey in 2019.
A global perspective
Cardiologists in Africa, the Americas, Asia, Europe, the Middle East, and Oceania – 5,890 in all – responded to mental health questions on the survey, which was novel for its global reach and insights across continents and cultures.
Respondents in South America and Central America reported the highest prevalences of mental health concerns, outliers at about 39% and 33%, respectively. Rates for most other geographic regions ranged narrowly from about 20% to 26%, the lowest reported in Asia and the Middle East.
Dr. Sharma acknowledged that the countries probably varied widely in social and cultural factors likely to influence survey responses, such as interpretation of the questionnaire’s mental health terminology or the degree to which the disorders are stigmatized.
“I think it’s hard to say how people may or may not respond culturally to a certain word or metric,” she said. But on the survey results, “whether you’re practicing in rural America, in rural India, or in the United Arab Emirates, Oceania, or Eastern Europe, there is a level of consistency, across the board, in what people are recognizing as mental health conditions.”
Junior vs. senior physicians
The global perspective “is a nice positive of the study, and the high rates in Central America and South America I think were something the field was not aware of and are an important contribution,” Srijan Sen, MD, PhD, said in an interview.
The psychological toll of hostile work environments is an issue throughout medicine, “but it seems greater in certain specialties, and cardiology may be one where it’s more of a problem,” observed Dr. Sen, who studies physician mental health at the University of Michigan, Ann Arbor, and wasn’t associated with the survey.
Mental health concerns in the survey were significantly more common among women than men (33.7% vs 26.3%), and for younger cardiologists, compared with older cardiologists (32.2% for those < 40 vs. 22.1% and 16.8% for those 55-69 and 70 or older, respectively).
Those findings seem to make sense, Dr. Sen observed. “Generally, cardiology and medicine broadly are hierarchical, so being more junior can be stressful.” And if there’s more hostility in the workplace, “it might fall on junior people.”
In other studies, moreover, “a high level of work-family conflict has been a real driver of depression and burnout, and that likely is affecting younger physicians, particularly young women physicians,” who may have smaller children and a greater burden of childcare than their seniors.
He pointed to the survey’s low response rate as an important limitation of the study. Of the 71,022 cardiologists invited to participate, only 5,890 (8.3%) responded and answered the queries on mental health.
With a response rate that low, a survey “can be biased in ways that we can’t predict,” Dr. Sen noted. Also, anyone concerned about the toxicity of their own workplace might be “more likely to respond to the survey than if they worked in a more pleasant place. That would provide a skewed sense of the overall experience of cardiologists.”
Those issues might not be a concern with the current survey, however, “because the results are consistent with other studies with higher response rates.”
‘Sobering report’
An accompanying editorial said Dr. Sharm and colleagues have provided “a sobering report on the global prevalence and potential contributors to mental health concerns” in the surveyed population.
Based on its lessons, Andrew J. Sauer, MD, Saint Luke’s Mid America Heart Institute, Kansas City, Mo., proposed several potential “interventions” the field could enact.
It could “selectively promote leaders who strive to mitigate implicit bias, discrimination, and harassment while advancing diversity, equity, and inclusion within the broad ranks of cardiologists.”
Also, he continued, “we must eliminate the stigmatization of mental illness among physicians. We need to handle mental health concerns with compassion and without blaming, like how we strive to treat our veterans who suffer from posttraumatic stress disorder.”
Lastly, Dr. Sauer wrote, “mentorship programs should be formalized to assist the cardiologist in transition zones from early to mid-career, with particular attention to women and those experiencing a simultaneously increased load of family burdens that compound existing workplace contributors to burnout and psychological distress.”
Years in practice
Of the cardiologists who responded to the survey’s mental health questions, 28% reported they have experienced mental health issues that could include alcohol/drug use disorder, suicidal tendencies, psychological distress (including anxiety, irritability, or anger), “other psychiatric disorders” (such as panic disorder, posttraumatic stress, or eating disorders) or major psychiatric disorders such as major depression, bipolar disorder, or schizophrenia.
Cardiologists with 5-10 years of practice post-training were more likely than cardiologists practicing for at least 20 years to have mental health concerns (31.9% vs. 22.6%, P < .001).
Mental health concerns were cited by 42% of respondents who cited “any type of discrimination” based on age, sex, race or ethnicity, or sexual orientation, the report noted.
Among those reporting any mental health concern, 2.7% considered suicide within the past year and 2.9% considered suicide more than 12 months previously. Women were more likely than men to consider suicide within the past year (3.8% vs. 2.3%) but were also more likely to seek help (42.3% vs. 31.1%; P < .001 for both differences), the authors wrote.
In multivariate analysis, predictors of mental health concerns included emotional harassment, 2.81 (odds ratio, 2.81; 95% confidence interval, 2.46-3.20), any discrimination (OR, 1.85; 95% CI, 1.61-2.12), being divorced (OR, 1.73; 95% CI, 1.26-2.36, age less than 55 years (OR, 1.43; 95% CI, 1.24-1.66), and being mid-career versus late (OR, 1.36; 95% CI, 1.14-1.62).
Because the survey was conducted from September to October 2019, before the pandemic’s traumatic effects unfolded on health care nearly everywhere, “I think there needs to be a follow-up at some point when everything has leveled out,” Dr. Sharma said. The current study is “a baseline, and not a healthy baseline,” for the field’s state of mental health that has likely grown worse during the pandemic.
But even without such a follow-up, the current study “is actionable enough that it forces us to do something about it right now.”
Dr. Sharma, Dr. Mehta, their coauthors, Dr. Sen, and Dr. Sauer reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
ranging from anxiety or anger issues to major depression or other psychiatric disorders.
Such conditions varied in prevalence by cardiology subspecialty and years in the field, were more common in women than in men, and were closely linked to enduring hostile work environments and other strains of professional life.
The survey, conducted only months before the COVID-19 pandemic and with its share of limitations, still paints a picture that’s not pretty.
For example, mental health concerns were reported by about 42% of respondents who cited a hostile work environment, defined as workplace experience of discrimination based on age, sex, religion, race or ethnicity, or emotional or sexual harassment. Conversely, the prevalence of these concerns reached only 17% among those without such workplace conditions.
The study shows substantial overlap between cardiologists reporting hostility at work and those with mental health concerns, “and that was a significant finding,” Garima Sharma, MD, Johns Hopkins University, Baltimore, said in an interview.
Still, only 31% of male and 42% of female cardiologists (P < .001) reporting mental health concerns also said they had sought professional help either within or outside their own institutions.
That means “there is a lot of silent suffering” in the field, said Dr. Sharma, who is lead author on the study, published in the Journal of the American College of Cardiology.
Bringing back the conversation
The survey findings, she added, point to at least two potential ways the cardiology community can strive to diminish what may be a major underlying cause of the mental health concerns and their consequences.
“If you work towards reducing hostility at work and making mental health a priority for your workforce, then those experiencing these types of egregious conditions based on age, gender, race, ethnicity, or sexual orientation are less likely to be harmed.”
Mental health concerns among cardiologists are seldom openly discussed, so the current study can be “a way to bring them back into the conversation,” Dr. Sharma said. Clinician mental health “is extremely important because it directly impacts patient care and productivity.”
The survey’s reported mental health conditions “are an issue across the board in medicine, and amongst our medical students as well,” senior author Laxmi S. Mehta, MD, professor of internal medicine at Ohio State University, Columbus, said in an interview. The current study provides new details about their prevalence and predictors in cardiology and, she hopes, may improve the field’s awareness of and efforts to address the problem.
“We need to support those who have underlying mental health conditions, as well as improve the work environment to reduce contributory factors to mental illnesses. And we also need to work on reducing the stigma associated with seeking treatment and on reducing the barriers to receiving treatment,” said Dr. Mehta, who chairs the Workgroup on Clinician Well-Being of the ACC, which conducted the survey in 2019.
A global perspective
Cardiologists in Africa, the Americas, Asia, Europe, the Middle East, and Oceania – 5,890 in all – responded to mental health questions on the survey, which was novel for its global reach and insights across continents and cultures.
Respondents in South America and Central America reported the highest prevalences of mental health concerns, outliers at about 39% and 33%, respectively. Rates for most other geographic regions ranged narrowly from about 20% to 26%, the lowest reported in Asia and the Middle East.
Dr. Sharma acknowledged that the countries probably varied widely in social and cultural factors likely to influence survey responses, such as interpretation of the questionnaire’s mental health terminology or the degree to which the disorders are stigmatized.
“I think it’s hard to say how people may or may not respond culturally to a certain word or metric,” she said. But on the survey results, “whether you’re practicing in rural America, in rural India, or in the United Arab Emirates, Oceania, or Eastern Europe, there is a level of consistency, across the board, in what people are recognizing as mental health conditions.”
Junior vs. senior physicians
The global perspective “is a nice positive of the study, and the high rates in Central America and South America I think were something the field was not aware of and are an important contribution,” Srijan Sen, MD, PhD, said in an interview.
The psychological toll of hostile work environments is an issue throughout medicine, “but it seems greater in certain specialties, and cardiology may be one where it’s more of a problem,” observed Dr. Sen, who studies physician mental health at the University of Michigan, Ann Arbor, and wasn’t associated with the survey.
Mental health concerns in the survey were significantly more common among women than men (33.7% vs 26.3%), and for younger cardiologists, compared with older cardiologists (32.2% for those < 40 vs. 22.1% and 16.8% for those 55-69 and 70 or older, respectively).
Those findings seem to make sense, Dr. Sen observed. “Generally, cardiology and medicine broadly are hierarchical, so being more junior can be stressful.” And if there’s more hostility in the workplace, “it might fall on junior people.”
In other studies, moreover, “a high level of work-family conflict has been a real driver of depression and burnout, and that likely is affecting younger physicians, particularly young women physicians,” who may have smaller children and a greater burden of childcare than their seniors.
He pointed to the survey’s low response rate as an important limitation of the study. Of the 71,022 cardiologists invited to participate, only 5,890 (8.3%) responded and answered the queries on mental health.
With a response rate that low, a survey “can be biased in ways that we can’t predict,” Dr. Sen noted. Also, anyone concerned about the toxicity of their own workplace might be “more likely to respond to the survey than if they worked in a more pleasant place. That would provide a skewed sense of the overall experience of cardiologists.”
Those issues might not be a concern with the current survey, however, “because the results are consistent with other studies with higher response rates.”
‘Sobering report’
An accompanying editorial said Dr. Sharm and colleagues have provided “a sobering report on the global prevalence and potential contributors to mental health concerns” in the surveyed population.
Based on its lessons, Andrew J. Sauer, MD, Saint Luke’s Mid America Heart Institute, Kansas City, Mo., proposed several potential “interventions” the field could enact.
It could “selectively promote leaders who strive to mitigate implicit bias, discrimination, and harassment while advancing diversity, equity, and inclusion within the broad ranks of cardiologists.”
Also, he continued, “we must eliminate the stigmatization of mental illness among physicians. We need to handle mental health concerns with compassion and without blaming, like how we strive to treat our veterans who suffer from posttraumatic stress disorder.”
Lastly, Dr. Sauer wrote, “mentorship programs should be formalized to assist the cardiologist in transition zones from early to mid-career, with particular attention to women and those experiencing a simultaneously increased load of family burdens that compound existing workplace contributors to burnout and psychological distress.”
Years in practice
Of the cardiologists who responded to the survey’s mental health questions, 28% reported they have experienced mental health issues that could include alcohol/drug use disorder, suicidal tendencies, psychological distress (including anxiety, irritability, or anger), “other psychiatric disorders” (such as panic disorder, posttraumatic stress, or eating disorders) or major psychiatric disorders such as major depression, bipolar disorder, or schizophrenia.
Cardiologists with 5-10 years of practice post-training were more likely than cardiologists practicing for at least 20 years to have mental health concerns (31.9% vs. 22.6%, P < .001).
Mental health concerns were cited by 42% of respondents who cited “any type of discrimination” based on age, sex, race or ethnicity, or sexual orientation, the report noted.
Among those reporting any mental health concern, 2.7% considered suicide within the past year and 2.9% considered suicide more than 12 months previously. Women were more likely than men to consider suicide within the past year (3.8% vs. 2.3%) but were also more likely to seek help (42.3% vs. 31.1%; P < .001 for both differences), the authors wrote.
In multivariate analysis, predictors of mental health concerns included emotional harassment, 2.81 (odds ratio, 2.81; 95% confidence interval, 2.46-3.20), any discrimination (OR, 1.85; 95% CI, 1.61-2.12), being divorced (OR, 1.73; 95% CI, 1.26-2.36, age less than 55 years (OR, 1.43; 95% CI, 1.24-1.66), and being mid-career versus late (OR, 1.36; 95% CI, 1.14-1.62).
Because the survey was conducted from September to October 2019, before the pandemic’s traumatic effects unfolded on health care nearly everywhere, “I think there needs to be a follow-up at some point when everything has leveled out,” Dr. Sharma said. The current study is “a baseline, and not a healthy baseline,” for the field’s state of mental health that has likely grown worse during the pandemic.
But even without such a follow-up, the current study “is actionable enough that it forces us to do something about it right now.”
Dr. Sharma, Dr. Mehta, their coauthors, Dr. Sen, and Dr. Sauer reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
ranging from anxiety or anger issues to major depression or other psychiatric disorders.
Such conditions varied in prevalence by cardiology subspecialty and years in the field, were more common in women than in men, and were closely linked to enduring hostile work environments and other strains of professional life.
The survey, conducted only months before the COVID-19 pandemic and with its share of limitations, still paints a picture that’s not pretty.
For example, mental health concerns were reported by about 42% of respondents who cited a hostile work environment, defined as workplace experience of discrimination based on age, sex, religion, race or ethnicity, or emotional or sexual harassment. Conversely, the prevalence of these concerns reached only 17% among those without such workplace conditions.
The study shows substantial overlap between cardiologists reporting hostility at work and those with mental health concerns, “and that was a significant finding,” Garima Sharma, MD, Johns Hopkins University, Baltimore, said in an interview.
Still, only 31% of male and 42% of female cardiologists (P < .001) reporting mental health concerns also said they had sought professional help either within or outside their own institutions.
That means “there is a lot of silent suffering” in the field, said Dr. Sharma, who is lead author on the study, published in the Journal of the American College of Cardiology.
Bringing back the conversation
The survey findings, she added, point to at least two potential ways the cardiology community can strive to diminish what may be a major underlying cause of the mental health concerns and their consequences.
“If you work towards reducing hostility at work and making mental health a priority for your workforce, then those experiencing these types of egregious conditions based on age, gender, race, ethnicity, or sexual orientation are less likely to be harmed.”
Mental health concerns among cardiologists are seldom openly discussed, so the current study can be “a way to bring them back into the conversation,” Dr. Sharma said. Clinician mental health “is extremely important because it directly impacts patient care and productivity.”
The survey’s reported mental health conditions “are an issue across the board in medicine, and amongst our medical students as well,” senior author Laxmi S. Mehta, MD, professor of internal medicine at Ohio State University, Columbus, said in an interview. The current study provides new details about their prevalence and predictors in cardiology and, she hopes, may improve the field’s awareness of and efforts to address the problem.
“We need to support those who have underlying mental health conditions, as well as improve the work environment to reduce contributory factors to mental illnesses. And we also need to work on reducing the stigma associated with seeking treatment and on reducing the barriers to receiving treatment,” said Dr. Mehta, who chairs the Workgroup on Clinician Well-Being of the ACC, which conducted the survey in 2019.
A global perspective
Cardiologists in Africa, the Americas, Asia, Europe, the Middle East, and Oceania – 5,890 in all – responded to mental health questions on the survey, which was novel for its global reach and insights across continents and cultures.
Respondents in South America and Central America reported the highest prevalences of mental health concerns, outliers at about 39% and 33%, respectively. Rates for most other geographic regions ranged narrowly from about 20% to 26%, the lowest reported in Asia and the Middle East.
Dr. Sharma acknowledged that the countries probably varied widely in social and cultural factors likely to influence survey responses, such as interpretation of the questionnaire’s mental health terminology or the degree to which the disorders are stigmatized.
“I think it’s hard to say how people may or may not respond culturally to a certain word or metric,” she said. But on the survey results, “whether you’re practicing in rural America, in rural India, or in the United Arab Emirates, Oceania, or Eastern Europe, there is a level of consistency, across the board, in what people are recognizing as mental health conditions.”
Junior vs. senior physicians
The global perspective “is a nice positive of the study, and the high rates in Central America and South America I think were something the field was not aware of and are an important contribution,” Srijan Sen, MD, PhD, said in an interview.
The psychological toll of hostile work environments is an issue throughout medicine, “but it seems greater in certain specialties, and cardiology may be one where it’s more of a problem,” observed Dr. Sen, who studies physician mental health at the University of Michigan, Ann Arbor, and wasn’t associated with the survey.
Mental health concerns in the survey were significantly more common among women than men (33.7% vs 26.3%), and for younger cardiologists, compared with older cardiologists (32.2% for those < 40 vs. 22.1% and 16.8% for those 55-69 and 70 or older, respectively).
Those findings seem to make sense, Dr. Sen observed. “Generally, cardiology and medicine broadly are hierarchical, so being more junior can be stressful.” And if there’s more hostility in the workplace, “it might fall on junior people.”
In other studies, moreover, “a high level of work-family conflict has been a real driver of depression and burnout, and that likely is affecting younger physicians, particularly young women physicians,” who may have smaller children and a greater burden of childcare than their seniors.
He pointed to the survey’s low response rate as an important limitation of the study. Of the 71,022 cardiologists invited to participate, only 5,890 (8.3%) responded and answered the queries on mental health.
With a response rate that low, a survey “can be biased in ways that we can’t predict,” Dr. Sen noted. Also, anyone concerned about the toxicity of their own workplace might be “more likely to respond to the survey than if they worked in a more pleasant place. That would provide a skewed sense of the overall experience of cardiologists.”
Those issues might not be a concern with the current survey, however, “because the results are consistent with other studies with higher response rates.”
‘Sobering report’
An accompanying editorial said Dr. Sharm and colleagues have provided “a sobering report on the global prevalence and potential contributors to mental health concerns” in the surveyed population.
Based on its lessons, Andrew J. Sauer, MD, Saint Luke’s Mid America Heart Institute, Kansas City, Mo., proposed several potential “interventions” the field could enact.
It could “selectively promote leaders who strive to mitigate implicit bias, discrimination, and harassment while advancing diversity, equity, and inclusion within the broad ranks of cardiologists.”
Also, he continued, “we must eliminate the stigmatization of mental illness among physicians. We need to handle mental health concerns with compassion and without blaming, like how we strive to treat our veterans who suffer from posttraumatic stress disorder.”
Lastly, Dr. Sauer wrote, “mentorship programs should be formalized to assist the cardiologist in transition zones from early to mid-career, with particular attention to women and those experiencing a simultaneously increased load of family burdens that compound existing workplace contributors to burnout and psychological distress.”
Years in practice
Of the cardiologists who responded to the survey’s mental health questions, 28% reported they have experienced mental health issues that could include alcohol/drug use disorder, suicidal tendencies, psychological distress (including anxiety, irritability, or anger), “other psychiatric disorders” (such as panic disorder, posttraumatic stress, or eating disorders) or major psychiatric disorders such as major depression, bipolar disorder, or schizophrenia.
Cardiologists with 5-10 years of practice post-training were more likely than cardiologists practicing for at least 20 years to have mental health concerns (31.9% vs. 22.6%, P < .001).
Mental health concerns were cited by 42% of respondents who cited “any type of discrimination” based on age, sex, race or ethnicity, or sexual orientation, the report noted.
Among those reporting any mental health concern, 2.7% considered suicide within the past year and 2.9% considered suicide more than 12 months previously. Women were more likely than men to consider suicide within the past year (3.8% vs. 2.3%) but were also more likely to seek help (42.3% vs. 31.1%; P < .001 for both differences), the authors wrote.
In multivariate analysis, predictors of mental health concerns included emotional harassment, 2.81 (odds ratio, 2.81; 95% confidence interval, 2.46-3.20), any discrimination (OR, 1.85; 95% CI, 1.61-2.12), being divorced (OR, 1.73; 95% CI, 1.26-2.36, age less than 55 years (OR, 1.43; 95% CI, 1.24-1.66), and being mid-career versus late (OR, 1.36; 95% CI, 1.14-1.62).
Because the survey was conducted from September to October 2019, before the pandemic’s traumatic effects unfolded on health care nearly everywhere, “I think there needs to be a follow-up at some point when everything has leveled out,” Dr. Sharma said. The current study is “a baseline, and not a healthy baseline,” for the field’s state of mental health that has likely grown worse during the pandemic.
But even without such a follow-up, the current study “is actionable enough that it forces us to do something about it right now.”
Dr. Sharma, Dr. Mehta, their coauthors, Dr. Sen, and Dr. Sauer reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
ED doctors call private equity staffing practices illegal and seek to ban them
Thirty-three states plus the District of Columbia have rules on their books against the so-called corporate practice of medicine. But over the years, critics say, companies have successfully sidestepped bans on owning medical practices by buying or establishing local staffing groups that are nominally owned by doctors and restricting the physicians’ authority so they have no direct control.
These laws and regulations, which started appearing nearly a century ago, were meant to fight the commercialization of medicine, maintain the independence and authority of physicians, and prioritize the doctor-patient relationship over the interests of investors and shareholders.
Those campaigning for stiffer enforcement of the laws say that physician-staffing firms owned by private equity investors are the most egregious offenders. Private equity-backed staffing companies manage a quarter of the nation’s emergency departments, according to a Raleigh, N.C.–based doctor who runs a job site for ED physicians. The two largest are Nashville, Tenn.–based Envision Healthcare, owned by investment giant KKR & Co., and Knoxville, Tenn.–based TeamHealth, owned by Blackstone.
Court filings in multiple states, including California, Missouri, Texas, and Tennessee, have called out Envision and TeamHealth for allegedly using doctor groups as straw men to sidestep corporate practice laws. But those filings have typically been in financial cases involving wrongful termination, breach of contract, and overbilling.
Now, physicians and consumer advocates around the country are anticipating a California lawsuit against Envision, scheduled to start in January 2024 in federal court. The plaintiff in the case, Milwaukee-based American Academy of Emergency Medicine Physician Group, alleges that Envision uses shell business structures to retain de facto ownership of ED staffing groups, and it is asking the court to declare them illegal.
“We’re not asking them to pay money, and we will not accept being paid to drop the case,” said David Millstein, lead attorney for the plaintiff. “We are simply asking the court to ban this practice model.”
‘Possibility to reverberate throughout the country’
The physician group believes a victory would lead to a prohibition of the practice across California – and not just in ERs, but for other staff provided by Envision and TeamHealth, including in anesthesiology and hospital medicine. The California Medical Association supports the lawsuit, saying it “will shape the boundaries of California’s prohibition on the corporate practice of medicine.”
The plaintiff – along with many doctors, nurses, and consumer advocates, as well as some lawmakers – hopes that success in the case will spur regulators and prosecutors in other states to take corporate medicine prohibitions more seriously. “Any decision anywhere in the country that says the corporate ownership of a medical practice is illegal has the possibility to reverberate throughout the country, absolutely – and I hope that it would,” said Julie Mayfield, a state senator in North Carolina.
But the push to reinvigorate laws restricting the corporate practice of medicine has plenty of skeptics, who view it as an effort to return to a golden era in medicine that is long gone or may never have existed to begin with. The genie is out of the bottle, they say, noting that the profit motive has penetrated every corner of health care and that nearly 70% of physicians in the United States are now employed by corporations and hospitals.
The corporate practice of medicine doctrine has “a very interesting and not a very flattering history,” said Barak Richman, a law professor at Duke University. “The medical profession was trying to assert its professional dominance that accrued a lot of benefits to itself in ways that were not terribly beneficial to patients or to the market.”
The California case involves Placentia-Linda Hospital in Orange County, where the plaintiff physician group lost its ED management contract to Envision. The complaint alleges that Envision uses the same business model at numerous hospitals around the state.
“Envision exercises profound and pervasive direct and indirect control and/or influence over the medical practice, making decisions which bear directly and indirectly on the practice of medicine, rendering physicians as mere employees, and diminishing physician independence and freedom from commercial interests,” according to the complaint.
Envision said the company is compliant with state laws and that its operating structure is common in the health care industry. “Legal challenges to that structure have proved meritless,” Envision wrote in an email. It added that “care decisions have and always will be between clinicians and patients.”
TeamHealth, an indirect target in the case, said its “world-class operating team” provides management services that “allow clinicians to focus on the practice of medicine and patient care through a structure commonly utilized by hospitals, health systems, and other providers across the country.”
State rules vary widely
State laws and regulations governing the corporate practice of medicine vary widely on multiple factors, including whether there are exceptions for nonprofit organizations, how much of doctors’ revenue outside management firms can keep, who can own the equipment, and how violations are punished. New York, Texas, and California are considered to have among the toughest restrictions, while Florida and 16 other states have none.
Kirk Ogrosky, a partner at the law firm Goodwin Procter, said this kind of management structure predates the arrival of private equity in the industry. “I would be surprised if a company that is interested in investing in this space screwed up the formation documents; it would shock me,” Mr. Ogrosky said.
Private equity–backed firms have been attracted to EDs in recent years because they are profitable and because they have been able to charge inflated amounts for out-of-network care – at least until a federal law cracked down on surprise billing. Envision and TeamHealth prioritize profits, critics say, by maximizing revenue, cutting costs, and consolidating smaller practices into ever-larger groups – to the point of regional dominance.
Envision and TeamHealth are privately owned, which makes it difficult to find reliable data on their finances and the extent of their market penetration.
Leon Adelman, MD, cofounder and CEO of Ivy Clinicians, a Raleigh, N.C.–based startup job site for emergency physicians, has spent 18 months piecing together data and found that private equity–backed staffing firms run 25% of the nation’s EDs. TeamHealth and Envision have the two largest shares, with 8.6% and 8.3%, respectively, Dr. Adelman said.
Other estimates put private equity’s penetration of ERs at closer to 40%.
Doctors push for investigations
So far, efforts by emergency physicians and others to challenge private equity staffing firms over their alleged violations have yielded frustrating results.
An advocacy group called Take Medicine Back, formed last year by a handful of ED physicians, sent a letter in July to North Carolina Attorney General Josh Stein, asking him to investigate violations of the ban on the corporate practice of medicine. And because Mr. Stein holds a senior position at the National Association of Attorneys General, the letter also asked him to take the lead in persuading his fellow AGs to “launch a multi-state investigation into the widespread lack of enforcement” of corporate practice of medicine laws.
The group’s leader, Mitchell Li, MD, said he was initially disappointed by the response he received from Mr. Stein’s office, which promised to review his request, saying it raised complex legal issues about the corporate practice of medicine in the state. But Dr. Li is now more hopeful, since he has secured a January appointment with officials in Mr. Stein’s office.
Robert McNamara, MD, a cofounder of Dr. Li’s group and chair of emergency medicine at Temple University’s Lewis Katz School of Medicine, drafted complaints to the Texas Medical Board, along with Houston physician David Hoyer, MD, asking the board to intervene against two doctors accused of fronting for professional entities controlled by Envision and TeamHealth. In both cases, the board declined to intervene.
Dr. McNamara, who serves as the chief medical officer of the physicians’ group in the California Envision case, also filed a complaint with Pennsylvania Attorney General Josh Shapiro, alleging that a group called Emergency Care Services of Pennsylvania PC, which was trying to contract with ED physicians of the Crozer Keystone Health System, was wholly owned by TeamHealth and serving as a shell to avoid scrutiny.
A senior official in Mr. Shapiro’s office responded, saying the complaint had been referred to two state agencies, but Dr. McNamara said he has heard nothing back in more than 3 years.
Differing views on private equity’s role
Proponents of private equity ownership say it has brought a lot of good to health care. Jamal Hagler, vice president of research at the American Investment Council, said private equity brings expertise to hospital systems, “whether it’s to hire new staff, grow and open up to new markets, integrate new technologies, or develop new technologies.”
But many physicians who have worked for private equity companies say their mission is not compatible with the best practice of medicine. They cite an emphasis on speed and high patient volume over safety; a preference for lesser-trained, cheaper medical providers; and treatment protocols unsuitable for certain patients.
Sean Jones, MD, an emergency physician in Asheville, N.C., said his first full-time job was at a Florida hospital, where EmCare, a subsidiary of Envision, ran the ED. Dr. Jones said EmCare, in collaboration with the hospital’s owner, pushed doctors to meet performance goals related to wait times and treatments, which were not always good for patients.
For example, if a patient came in with abnormally high heart and respiratory rates – signs of sepsis – doctors were expected to give them large amounts of fluids and antibiotics within an hour, Dr. Jones said. But those symptoms could also be caused by a panic attack or heart failure.
“You don’t want to give a patient with heart failure 2 or 3 liters of fluid, and I would get emails saying, ‘You didn’t do this,’ ” he said. “Well, no, I didn’t, because the reason they couldn’t breathe was they had too much fluid in their lungs.”
Envision said the company’s 25,000 clinicians, “like all clinicians, exercise their independent judgment to provide quality, compassionate, clinically appropriate care.”
Dr. Jones felt otherwise. “We don’t need some MBAs telling us what to do,” he said.
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Thirty-three states plus the District of Columbia have rules on their books against the so-called corporate practice of medicine. But over the years, critics say, companies have successfully sidestepped bans on owning medical practices by buying or establishing local staffing groups that are nominally owned by doctors and restricting the physicians’ authority so they have no direct control.
These laws and regulations, which started appearing nearly a century ago, were meant to fight the commercialization of medicine, maintain the independence and authority of physicians, and prioritize the doctor-patient relationship over the interests of investors and shareholders.
Those campaigning for stiffer enforcement of the laws say that physician-staffing firms owned by private equity investors are the most egregious offenders. Private equity-backed staffing companies manage a quarter of the nation’s emergency departments, according to a Raleigh, N.C.–based doctor who runs a job site for ED physicians. The two largest are Nashville, Tenn.–based Envision Healthcare, owned by investment giant KKR & Co., and Knoxville, Tenn.–based TeamHealth, owned by Blackstone.
Court filings in multiple states, including California, Missouri, Texas, and Tennessee, have called out Envision and TeamHealth for allegedly using doctor groups as straw men to sidestep corporate practice laws. But those filings have typically been in financial cases involving wrongful termination, breach of contract, and overbilling.
Now, physicians and consumer advocates around the country are anticipating a California lawsuit against Envision, scheduled to start in January 2024 in federal court. The plaintiff in the case, Milwaukee-based American Academy of Emergency Medicine Physician Group, alleges that Envision uses shell business structures to retain de facto ownership of ED staffing groups, and it is asking the court to declare them illegal.
“We’re not asking them to pay money, and we will not accept being paid to drop the case,” said David Millstein, lead attorney for the plaintiff. “We are simply asking the court to ban this practice model.”
‘Possibility to reverberate throughout the country’
The physician group believes a victory would lead to a prohibition of the practice across California – and not just in ERs, but for other staff provided by Envision and TeamHealth, including in anesthesiology and hospital medicine. The California Medical Association supports the lawsuit, saying it “will shape the boundaries of California’s prohibition on the corporate practice of medicine.”
The plaintiff – along with many doctors, nurses, and consumer advocates, as well as some lawmakers – hopes that success in the case will spur regulators and prosecutors in other states to take corporate medicine prohibitions more seriously. “Any decision anywhere in the country that says the corporate ownership of a medical practice is illegal has the possibility to reverberate throughout the country, absolutely – and I hope that it would,” said Julie Mayfield, a state senator in North Carolina.
But the push to reinvigorate laws restricting the corporate practice of medicine has plenty of skeptics, who view it as an effort to return to a golden era in medicine that is long gone or may never have existed to begin with. The genie is out of the bottle, they say, noting that the profit motive has penetrated every corner of health care and that nearly 70% of physicians in the United States are now employed by corporations and hospitals.
The corporate practice of medicine doctrine has “a very interesting and not a very flattering history,” said Barak Richman, a law professor at Duke University. “The medical profession was trying to assert its professional dominance that accrued a lot of benefits to itself in ways that were not terribly beneficial to patients or to the market.”
The California case involves Placentia-Linda Hospital in Orange County, where the plaintiff physician group lost its ED management contract to Envision. The complaint alleges that Envision uses the same business model at numerous hospitals around the state.
“Envision exercises profound and pervasive direct and indirect control and/or influence over the medical practice, making decisions which bear directly and indirectly on the practice of medicine, rendering physicians as mere employees, and diminishing physician independence and freedom from commercial interests,” according to the complaint.
Envision said the company is compliant with state laws and that its operating structure is common in the health care industry. “Legal challenges to that structure have proved meritless,” Envision wrote in an email. It added that “care decisions have and always will be between clinicians and patients.”
TeamHealth, an indirect target in the case, said its “world-class operating team” provides management services that “allow clinicians to focus on the practice of medicine and patient care through a structure commonly utilized by hospitals, health systems, and other providers across the country.”
State rules vary widely
State laws and regulations governing the corporate practice of medicine vary widely on multiple factors, including whether there are exceptions for nonprofit organizations, how much of doctors’ revenue outside management firms can keep, who can own the equipment, and how violations are punished. New York, Texas, and California are considered to have among the toughest restrictions, while Florida and 16 other states have none.
Kirk Ogrosky, a partner at the law firm Goodwin Procter, said this kind of management structure predates the arrival of private equity in the industry. “I would be surprised if a company that is interested in investing in this space screwed up the formation documents; it would shock me,” Mr. Ogrosky said.
Private equity–backed firms have been attracted to EDs in recent years because they are profitable and because they have been able to charge inflated amounts for out-of-network care – at least until a federal law cracked down on surprise billing. Envision and TeamHealth prioritize profits, critics say, by maximizing revenue, cutting costs, and consolidating smaller practices into ever-larger groups – to the point of regional dominance.
Envision and TeamHealth are privately owned, which makes it difficult to find reliable data on their finances and the extent of their market penetration.
Leon Adelman, MD, cofounder and CEO of Ivy Clinicians, a Raleigh, N.C.–based startup job site for emergency physicians, has spent 18 months piecing together data and found that private equity–backed staffing firms run 25% of the nation’s EDs. TeamHealth and Envision have the two largest shares, with 8.6% and 8.3%, respectively, Dr. Adelman said.
Other estimates put private equity’s penetration of ERs at closer to 40%.
Doctors push for investigations
So far, efforts by emergency physicians and others to challenge private equity staffing firms over their alleged violations have yielded frustrating results.
An advocacy group called Take Medicine Back, formed last year by a handful of ED physicians, sent a letter in July to North Carolina Attorney General Josh Stein, asking him to investigate violations of the ban on the corporate practice of medicine. And because Mr. Stein holds a senior position at the National Association of Attorneys General, the letter also asked him to take the lead in persuading his fellow AGs to “launch a multi-state investigation into the widespread lack of enforcement” of corporate practice of medicine laws.
The group’s leader, Mitchell Li, MD, said he was initially disappointed by the response he received from Mr. Stein’s office, which promised to review his request, saying it raised complex legal issues about the corporate practice of medicine in the state. But Dr. Li is now more hopeful, since he has secured a January appointment with officials in Mr. Stein’s office.
Robert McNamara, MD, a cofounder of Dr. Li’s group and chair of emergency medicine at Temple University’s Lewis Katz School of Medicine, drafted complaints to the Texas Medical Board, along with Houston physician David Hoyer, MD, asking the board to intervene against two doctors accused of fronting for professional entities controlled by Envision and TeamHealth. In both cases, the board declined to intervene.
Dr. McNamara, who serves as the chief medical officer of the physicians’ group in the California Envision case, also filed a complaint with Pennsylvania Attorney General Josh Shapiro, alleging that a group called Emergency Care Services of Pennsylvania PC, which was trying to contract with ED physicians of the Crozer Keystone Health System, was wholly owned by TeamHealth and serving as a shell to avoid scrutiny.
A senior official in Mr. Shapiro’s office responded, saying the complaint had been referred to two state agencies, but Dr. McNamara said he has heard nothing back in more than 3 years.
Differing views on private equity’s role
Proponents of private equity ownership say it has brought a lot of good to health care. Jamal Hagler, vice president of research at the American Investment Council, said private equity brings expertise to hospital systems, “whether it’s to hire new staff, grow and open up to new markets, integrate new technologies, or develop new technologies.”
But many physicians who have worked for private equity companies say their mission is not compatible with the best practice of medicine. They cite an emphasis on speed and high patient volume over safety; a preference for lesser-trained, cheaper medical providers; and treatment protocols unsuitable for certain patients.
Sean Jones, MD, an emergency physician in Asheville, N.C., said his first full-time job was at a Florida hospital, where EmCare, a subsidiary of Envision, ran the ED. Dr. Jones said EmCare, in collaboration with the hospital’s owner, pushed doctors to meet performance goals related to wait times and treatments, which were not always good for patients.
For example, if a patient came in with abnormally high heart and respiratory rates – signs of sepsis – doctors were expected to give them large amounts of fluids and antibiotics within an hour, Dr. Jones said. But those symptoms could also be caused by a panic attack or heart failure.
“You don’t want to give a patient with heart failure 2 or 3 liters of fluid, and I would get emails saying, ‘You didn’t do this,’ ” he said. “Well, no, I didn’t, because the reason they couldn’t breathe was they had too much fluid in their lungs.”
Envision said the company’s 25,000 clinicians, “like all clinicians, exercise their independent judgment to provide quality, compassionate, clinically appropriate care.”
Dr. Jones felt otherwise. “We don’t need some MBAs telling us what to do,” he said.
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Thirty-three states plus the District of Columbia have rules on their books against the so-called corporate practice of medicine. But over the years, critics say, companies have successfully sidestepped bans on owning medical practices by buying or establishing local staffing groups that are nominally owned by doctors and restricting the physicians’ authority so they have no direct control.
These laws and regulations, which started appearing nearly a century ago, were meant to fight the commercialization of medicine, maintain the independence and authority of physicians, and prioritize the doctor-patient relationship over the interests of investors and shareholders.
Those campaigning for stiffer enforcement of the laws say that physician-staffing firms owned by private equity investors are the most egregious offenders. Private equity-backed staffing companies manage a quarter of the nation’s emergency departments, according to a Raleigh, N.C.–based doctor who runs a job site for ED physicians. The two largest are Nashville, Tenn.–based Envision Healthcare, owned by investment giant KKR & Co., and Knoxville, Tenn.–based TeamHealth, owned by Blackstone.
Court filings in multiple states, including California, Missouri, Texas, and Tennessee, have called out Envision and TeamHealth for allegedly using doctor groups as straw men to sidestep corporate practice laws. But those filings have typically been in financial cases involving wrongful termination, breach of contract, and overbilling.
Now, physicians and consumer advocates around the country are anticipating a California lawsuit against Envision, scheduled to start in January 2024 in federal court. The plaintiff in the case, Milwaukee-based American Academy of Emergency Medicine Physician Group, alleges that Envision uses shell business structures to retain de facto ownership of ED staffing groups, and it is asking the court to declare them illegal.
“We’re not asking them to pay money, and we will not accept being paid to drop the case,” said David Millstein, lead attorney for the plaintiff. “We are simply asking the court to ban this practice model.”
‘Possibility to reverberate throughout the country’
The physician group believes a victory would lead to a prohibition of the practice across California – and not just in ERs, but for other staff provided by Envision and TeamHealth, including in anesthesiology and hospital medicine. The California Medical Association supports the lawsuit, saying it “will shape the boundaries of California’s prohibition on the corporate practice of medicine.”
The plaintiff – along with many doctors, nurses, and consumer advocates, as well as some lawmakers – hopes that success in the case will spur regulators and prosecutors in other states to take corporate medicine prohibitions more seriously. “Any decision anywhere in the country that says the corporate ownership of a medical practice is illegal has the possibility to reverberate throughout the country, absolutely – and I hope that it would,” said Julie Mayfield, a state senator in North Carolina.
But the push to reinvigorate laws restricting the corporate practice of medicine has plenty of skeptics, who view it as an effort to return to a golden era in medicine that is long gone or may never have existed to begin with. The genie is out of the bottle, they say, noting that the profit motive has penetrated every corner of health care and that nearly 70% of physicians in the United States are now employed by corporations and hospitals.
The corporate practice of medicine doctrine has “a very interesting and not a very flattering history,” said Barak Richman, a law professor at Duke University. “The medical profession was trying to assert its professional dominance that accrued a lot of benefits to itself in ways that were not terribly beneficial to patients or to the market.”
The California case involves Placentia-Linda Hospital in Orange County, where the plaintiff physician group lost its ED management contract to Envision. The complaint alleges that Envision uses the same business model at numerous hospitals around the state.
“Envision exercises profound and pervasive direct and indirect control and/or influence over the medical practice, making decisions which bear directly and indirectly on the practice of medicine, rendering physicians as mere employees, and diminishing physician independence and freedom from commercial interests,” according to the complaint.
Envision said the company is compliant with state laws and that its operating structure is common in the health care industry. “Legal challenges to that structure have proved meritless,” Envision wrote in an email. It added that “care decisions have and always will be between clinicians and patients.”
TeamHealth, an indirect target in the case, said its “world-class operating team” provides management services that “allow clinicians to focus on the practice of medicine and patient care through a structure commonly utilized by hospitals, health systems, and other providers across the country.”
State rules vary widely
State laws and regulations governing the corporate practice of medicine vary widely on multiple factors, including whether there are exceptions for nonprofit organizations, how much of doctors’ revenue outside management firms can keep, who can own the equipment, and how violations are punished. New York, Texas, and California are considered to have among the toughest restrictions, while Florida and 16 other states have none.
Kirk Ogrosky, a partner at the law firm Goodwin Procter, said this kind of management structure predates the arrival of private equity in the industry. “I would be surprised if a company that is interested in investing in this space screwed up the formation documents; it would shock me,” Mr. Ogrosky said.
Private equity–backed firms have been attracted to EDs in recent years because they are profitable and because they have been able to charge inflated amounts for out-of-network care – at least until a federal law cracked down on surprise billing. Envision and TeamHealth prioritize profits, critics say, by maximizing revenue, cutting costs, and consolidating smaller practices into ever-larger groups – to the point of regional dominance.
Envision and TeamHealth are privately owned, which makes it difficult to find reliable data on their finances and the extent of their market penetration.
Leon Adelman, MD, cofounder and CEO of Ivy Clinicians, a Raleigh, N.C.–based startup job site for emergency physicians, has spent 18 months piecing together data and found that private equity–backed staffing firms run 25% of the nation’s EDs. TeamHealth and Envision have the two largest shares, with 8.6% and 8.3%, respectively, Dr. Adelman said.
Other estimates put private equity’s penetration of ERs at closer to 40%.
Doctors push for investigations
So far, efforts by emergency physicians and others to challenge private equity staffing firms over their alleged violations have yielded frustrating results.
An advocacy group called Take Medicine Back, formed last year by a handful of ED physicians, sent a letter in July to North Carolina Attorney General Josh Stein, asking him to investigate violations of the ban on the corporate practice of medicine. And because Mr. Stein holds a senior position at the National Association of Attorneys General, the letter also asked him to take the lead in persuading his fellow AGs to “launch a multi-state investigation into the widespread lack of enforcement” of corporate practice of medicine laws.
The group’s leader, Mitchell Li, MD, said he was initially disappointed by the response he received from Mr. Stein’s office, which promised to review his request, saying it raised complex legal issues about the corporate practice of medicine in the state. But Dr. Li is now more hopeful, since he has secured a January appointment with officials in Mr. Stein’s office.
Robert McNamara, MD, a cofounder of Dr. Li’s group and chair of emergency medicine at Temple University’s Lewis Katz School of Medicine, drafted complaints to the Texas Medical Board, along with Houston physician David Hoyer, MD, asking the board to intervene against two doctors accused of fronting for professional entities controlled by Envision and TeamHealth. In both cases, the board declined to intervene.
Dr. McNamara, who serves as the chief medical officer of the physicians’ group in the California Envision case, also filed a complaint with Pennsylvania Attorney General Josh Shapiro, alleging that a group called Emergency Care Services of Pennsylvania PC, which was trying to contract with ED physicians of the Crozer Keystone Health System, was wholly owned by TeamHealth and serving as a shell to avoid scrutiny.
A senior official in Mr. Shapiro’s office responded, saying the complaint had been referred to two state agencies, but Dr. McNamara said he has heard nothing back in more than 3 years.
Differing views on private equity’s role
Proponents of private equity ownership say it has brought a lot of good to health care. Jamal Hagler, vice president of research at the American Investment Council, said private equity brings expertise to hospital systems, “whether it’s to hire new staff, grow and open up to new markets, integrate new technologies, or develop new technologies.”
But many physicians who have worked for private equity companies say their mission is not compatible with the best practice of medicine. They cite an emphasis on speed and high patient volume over safety; a preference for lesser-trained, cheaper medical providers; and treatment protocols unsuitable for certain patients.
Sean Jones, MD, an emergency physician in Asheville, N.C., said his first full-time job was at a Florida hospital, where EmCare, a subsidiary of Envision, ran the ED. Dr. Jones said EmCare, in collaboration with the hospital’s owner, pushed doctors to meet performance goals related to wait times and treatments, which were not always good for patients.
For example, if a patient came in with abnormally high heart and respiratory rates – signs of sepsis – doctors were expected to give them large amounts of fluids and antibiotics within an hour, Dr. Jones said. But those symptoms could also be caused by a panic attack or heart failure.
“You don’t want to give a patient with heart failure 2 or 3 liters of fluid, and I would get emails saying, ‘You didn’t do this,’ ” he said. “Well, no, I didn’t, because the reason they couldn’t breathe was they had too much fluid in their lungs.”
Envision said the company’s 25,000 clinicians, “like all clinicians, exercise their independent judgment to provide quality, compassionate, clinically appropriate care.”
Dr. Jones felt otherwise. “We don’t need some MBAs telling us what to do,” he said.
This story was produced by KHN, which publishes California Healthline, an editorially independent service of the California Health Care Foundation. Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
What’s next for COVID? Here’s what to know
As holiday celebrations wind down in the United States, COVID is on the rise.
Will there be another winter surge? If so, can we minimize it? How big a role might the boosters play in that? Are more mandates coming, along with a return to closed offices and businesses? Read on for a look at the latest info.
Cases, hospitalizations, deaths
As of Dec. 27, the latest statistics, the Centers for Disease Control and Prevention reports more than 487,000 weekly cases, compared to about 265,000 for the week ending Oct. 12. On average, 4,938 people were admitted to the hospital daily from Dec. 19 to 25, down about 6% from the 5,257 admitted daily the week before.
Deaths totaled 2,952 weekly as of Dec. 21, up from 2,699 on Dec. 14.
“What’s sobering overall is still seeing about 400 deaths a day in the U.S.,” said Peter Chin-Hong, MD, professor of medicine and infectious disease specialist at the University of California, San Francisco. “It’s still very high.”
As of Dec. 17, the variants predominating are BQ.1, BQ.1.1, and XBB. Experts said they are paying close attention to XBB, which is increasing quickly in the Northeast.
Predicting a winter surge
Experts tracking the pandemic agree there will be a surge.
“We are in the midst of it now,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape (MDedge’s sister site). “It’s not nearly like what we’ve had in Omicron or other waves; it’s not as severe. But it’s being particularly felt by seniors.”
One bit of good news: “Outside of that group it doesn’t look like – so far – it is going to be as bad a wave [as in the past],” Dr. Topol said.
Predicting the extent of the post-holiday surge “is the billion-dollar question right now,” said Katelyn Jetelina, PhD, a San Diego epidemiologist and author of the newsletter Your Local Epidemiologist.
“Much of these waves are not being driven by subvariants of concern but rather behavior,” she said.
People are opening up their social networks to gather for celebrations and family time. That’s unique to this winter, she said.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
Others point out that the surge doesn’t involve just COVID.
“We are expecting a Christmas surge and we are concerned it might be a triple surge,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University, Nashville, Tenn., referring to the rising cases of flu and RSV (respiratory syncytial virus).
Dr. Jetelina shares that concern, worrying that those illnesses may be what overwhelms hospital capacity.
Another wild card is the situation in China. With the easing of China’s “zero COVID” policies, cases there are rising dramatically. Some models are predicting up to 1 million COVID deaths could occur in China in 2023. (The United States is now requiring travelers from China to show a negative COVID test before entering. Italy and Japan have taken similar measures.)
“The suffering that is going to occur in China is not good news at all,” Dr. Topol said. “We are going to be seeing that for many weeks if not months ahead.”
Theoretically, uncontained spread such as what is expected there could generate a whole new family of variants, he said. But “the main hit is going to be in China,” he predicted. “But it’s hard to project with accuracy.”
“China is 20% of the global population, so we can’t ignore it,” Dr. Jetelina said. “The question is, what’s the probability of a subvariant of concern coming from China? I think the probability is pretty low, but the possibility is there.”
What happens with cases in China may “throw a wrench” in the transition from pandemic to endemic, Dr. Chin-Hong said. But even if the rising cases in China do result in a new variant, “there’s so much T cell and B cell immunity [here], your average person is still not going to get seriously ill, even if the variant looks really scary.”
Minimizing the damage
Experts echo the same advice on stemming the surge, especially for adults who are 65 or older: Get the bivalent booster, and get it now.
“The same with the influenza vaccine,” Dr. Schaffner said.
Both the booster vaccine and the flu vaccine have been underused this year, he said. “It’s part of the general vaccine fatigue.”
The low uptake of the booster vaccine is concerning, Dr. Topol said, especially among adults aged 65 and older, the age group most vulnerable to severe disease. Just 35.7% of U.S. adults 65 and older have gotten the booster, according to the CDC. Dr. Topol calls that a tragedy.
Younger people have not taken to the booster, either. Overall, only 14.1% of people aged 5 and up have gotten an updated booster dose, according to the CDC.
Recent studies find value in the boosters. One study looked only at adults age 65 or older, finding that the bivalent booster reduced the risk of hospitalization by 84% compared to someone not vaccinated, and 73% compared to someone who had received only the monovalent vaccine. Another study of adults found those who had gotten the bivalent were less likely to need COVID-related emergency room care or urgent care.
In a Dec. 21 report in the New England Journal of Medicine, researchers took plasma samples from people who had gotten either one or two monovalent boosters or the bivalent to determine how well they worked against the circulating Omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB. The bivalent worked better than the monovalent against all the Omicron subvariants, but especially against BA.2.75.2, BQ.1.1, and XBB.
Rapid testing can help minimize transmission. On Dec. 15, the Biden administration announced its Winter Preparedness Plan, urging Americans to test before and after travel as well as indoor visiting with vulnerable individuals, providing another round of free at-home tests, continuing to make community testing available and continuing to provide vaccines.
Besides the general precautions, Dr. Schaffner suggested: “Look at yourself. Who are you? If you are older than 65, or have underlying illness or are immunocompromised, or are pregnant, please put your mask back on. And think about social distancing. It might be time to worship at home and stream a movie,” instead of going to the theaters, he said.
Back to mandates?
On Dec. 9, the New York City Commissioner of Health and Mental Hygiene urged a return to masking indoors, saying people “should” mask up, including in schools, stores, offices, and when in crowded outdoor settings.
On the same date, the County of Los Angeles Public Health urged a return to masking for everyone aged 2 and older when indoors, including at schools, in transit, or in work sites when around others.
While the CDC order requiring masks on public transportation is no longer in effect, the agency continues to recommend that those using public transportation do so.
But some are taking that further. In Philadelphia, for example, School Superintendent Tony B. Watlington Sr., EdD, announced before the winter break that indoor masking would be required for all students and staff for the first 2 weeks of school return, through Jan. 13, citing guidance from the Philadelphia Department of Public Health.
Universal masking in schools does reduce COVID transmission, as a study published in late November suggests. After Massachusetts dropped the statewide universal masking policy in public schools in February 2022, researchers compared the incidence of COVID in 70 school districts there that dropped the mandate with two school districts that kept it. In the 15 weeks after the policy was rescinded, the lifting of the mandate was linked with an additional 44.9 cases of COVID per 1,000 students and staff. That corresponded to an estimated 11,901 cases and to nearly 30% of the cases in all districts during that time.
That said, experts see mandates as the exception rather than the rule, at least for now, citing public backlash against mandates to mask or follow other restrictions.
“Mandating, we know, it shuts people off,” Dr. Topol said. “It’s unenforceable. If you have a very strong recommendation, that’s probably as good as you’re going to be able to do right now.”
There may be communities where mandates go over better than others, Dr. Schaffner said, such as communities where people have confidence in their public health authorities.
Glimmers of hope
Despite uncertainties, experts offered some not-so-dismal perspectives as well.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
A version of this article first appeared on WebMD.com.
As holiday celebrations wind down in the United States, COVID is on the rise.
Will there be another winter surge? If so, can we minimize it? How big a role might the boosters play in that? Are more mandates coming, along with a return to closed offices and businesses? Read on for a look at the latest info.
Cases, hospitalizations, deaths
As of Dec. 27, the latest statistics, the Centers for Disease Control and Prevention reports more than 487,000 weekly cases, compared to about 265,000 for the week ending Oct. 12. On average, 4,938 people were admitted to the hospital daily from Dec. 19 to 25, down about 6% from the 5,257 admitted daily the week before.
Deaths totaled 2,952 weekly as of Dec. 21, up from 2,699 on Dec. 14.
“What’s sobering overall is still seeing about 400 deaths a day in the U.S.,” said Peter Chin-Hong, MD, professor of medicine and infectious disease specialist at the University of California, San Francisco. “It’s still very high.”
As of Dec. 17, the variants predominating are BQ.1, BQ.1.1, and XBB. Experts said they are paying close attention to XBB, which is increasing quickly in the Northeast.
Predicting a winter surge
Experts tracking the pandemic agree there will be a surge.
“We are in the midst of it now,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape (MDedge’s sister site). “It’s not nearly like what we’ve had in Omicron or other waves; it’s not as severe. But it’s being particularly felt by seniors.”
One bit of good news: “Outside of that group it doesn’t look like – so far – it is going to be as bad a wave [as in the past],” Dr. Topol said.
Predicting the extent of the post-holiday surge “is the billion-dollar question right now,” said Katelyn Jetelina, PhD, a San Diego epidemiologist and author of the newsletter Your Local Epidemiologist.
“Much of these waves are not being driven by subvariants of concern but rather behavior,” she said.
People are opening up their social networks to gather for celebrations and family time. That’s unique to this winter, she said.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
Others point out that the surge doesn’t involve just COVID.
“We are expecting a Christmas surge and we are concerned it might be a triple surge,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University, Nashville, Tenn., referring to the rising cases of flu and RSV (respiratory syncytial virus).
Dr. Jetelina shares that concern, worrying that those illnesses may be what overwhelms hospital capacity.
Another wild card is the situation in China. With the easing of China’s “zero COVID” policies, cases there are rising dramatically. Some models are predicting up to 1 million COVID deaths could occur in China in 2023. (The United States is now requiring travelers from China to show a negative COVID test before entering. Italy and Japan have taken similar measures.)
“The suffering that is going to occur in China is not good news at all,” Dr. Topol said. “We are going to be seeing that for many weeks if not months ahead.”
Theoretically, uncontained spread such as what is expected there could generate a whole new family of variants, he said. But “the main hit is going to be in China,” he predicted. “But it’s hard to project with accuracy.”
“China is 20% of the global population, so we can’t ignore it,” Dr. Jetelina said. “The question is, what’s the probability of a subvariant of concern coming from China? I think the probability is pretty low, but the possibility is there.”
What happens with cases in China may “throw a wrench” in the transition from pandemic to endemic, Dr. Chin-Hong said. But even if the rising cases in China do result in a new variant, “there’s so much T cell and B cell immunity [here], your average person is still not going to get seriously ill, even if the variant looks really scary.”
Minimizing the damage
Experts echo the same advice on stemming the surge, especially for adults who are 65 or older: Get the bivalent booster, and get it now.
“The same with the influenza vaccine,” Dr. Schaffner said.
Both the booster vaccine and the flu vaccine have been underused this year, he said. “It’s part of the general vaccine fatigue.”
The low uptake of the booster vaccine is concerning, Dr. Topol said, especially among adults aged 65 and older, the age group most vulnerable to severe disease. Just 35.7% of U.S. adults 65 and older have gotten the booster, according to the CDC. Dr. Topol calls that a tragedy.
Younger people have not taken to the booster, either. Overall, only 14.1% of people aged 5 and up have gotten an updated booster dose, according to the CDC.
Recent studies find value in the boosters. One study looked only at adults age 65 or older, finding that the bivalent booster reduced the risk of hospitalization by 84% compared to someone not vaccinated, and 73% compared to someone who had received only the monovalent vaccine. Another study of adults found those who had gotten the bivalent were less likely to need COVID-related emergency room care or urgent care.
In a Dec. 21 report in the New England Journal of Medicine, researchers took plasma samples from people who had gotten either one or two monovalent boosters or the bivalent to determine how well they worked against the circulating Omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB. The bivalent worked better than the monovalent against all the Omicron subvariants, but especially against BA.2.75.2, BQ.1.1, and XBB.
Rapid testing can help minimize transmission. On Dec. 15, the Biden administration announced its Winter Preparedness Plan, urging Americans to test before and after travel as well as indoor visiting with vulnerable individuals, providing another round of free at-home tests, continuing to make community testing available and continuing to provide vaccines.
Besides the general precautions, Dr. Schaffner suggested: “Look at yourself. Who are you? If you are older than 65, or have underlying illness or are immunocompromised, or are pregnant, please put your mask back on. And think about social distancing. It might be time to worship at home and stream a movie,” instead of going to the theaters, he said.
Back to mandates?
On Dec. 9, the New York City Commissioner of Health and Mental Hygiene urged a return to masking indoors, saying people “should” mask up, including in schools, stores, offices, and when in crowded outdoor settings.
On the same date, the County of Los Angeles Public Health urged a return to masking for everyone aged 2 and older when indoors, including at schools, in transit, or in work sites when around others.
While the CDC order requiring masks on public transportation is no longer in effect, the agency continues to recommend that those using public transportation do so.
But some are taking that further. In Philadelphia, for example, School Superintendent Tony B. Watlington Sr., EdD, announced before the winter break that indoor masking would be required for all students and staff for the first 2 weeks of school return, through Jan. 13, citing guidance from the Philadelphia Department of Public Health.
Universal masking in schools does reduce COVID transmission, as a study published in late November suggests. After Massachusetts dropped the statewide universal masking policy in public schools in February 2022, researchers compared the incidence of COVID in 70 school districts there that dropped the mandate with two school districts that kept it. In the 15 weeks after the policy was rescinded, the lifting of the mandate was linked with an additional 44.9 cases of COVID per 1,000 students and staff. That corresponded to an estimated 11,901 cases and to nearly 30% of the cases in all districts during that time.
That said, experts see mandates as the exception rather than the rule, at least for now, citing public backlash against mandates to mask or follow other restrictions.
“Mandating, we know, it shuts people off,” Dr. Topol said. “It’s unenforceable. If you have a very strong recommendation, that’s probably as good as you’re going to be able to do right now.”
There may be communities where mandates go over better than others, Dr. Schaffner said, such as communities where people have confidence in their public health authorities.
Glimmers of hope
Despite uncertainties, experts offered some not-so-dismal perspectives as well.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
A version of this article first appeared on WebMD.com.
As holiday celebrations wind down in the United States, COVID is on the rise.
Will there be another winter surge? If so, can we minimize it? How big a role might the boosters play in that? Are more mandates coming, along with a return to closed offices and businesses? Read on for a look at the latest info.
Cases, hospitalizations, deaths
As of Dec. 27, the latest statistics, the Centers for Disease Control and Prevention reports more than 487,000 weekly cases, compared to about 265,000 for the week ending Oct. 12. On average, 4,938 people were admitted to the hospital daily from Dec. 19 to 25, down about 6% from the 5,257 admitted daily the week before.
Deaths totaled 2,952 weekly as of Dec. 21, up from 2,699 on Dec. 14.
“What’s sobering overall is still seeing about 400 deaths a day in the U.S.,” said Peter Chin-Hong, MD, professor of medicine and infectious disease specialist at the University of California, San Francisco. “It’s still very high.”
As of Dec. 17, the variants predominating are BQ.1, BQ.1.1, and XBB. Experts said they are paying close attention to XBB, which is increasing quickly in the Northeast.
Predicting a winter surge
Experts tracking the pandemic agree there will be a surge.
“We are in the midst of it now,” said Eric Topol, MD, founder and director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape (MDedge’s sister site). “It’s not nearly like what we’ve had in Omicron or other waves; it’s not as severe. But it’s being particularly felt by seniors.”
One bit of good news: “Outside of that group it doesn’t look like – so far – it is going to be as bad a wave [as in the past],” Dr. Topol said.
Predicting the extent of the post-holiday surge “is the billion-dollar question right now,” said Katelyn Jetelina, PhD, a San Diego epidemiologist and author of the newsletter Your Local Epidemiologist.
“Much of these waves are not being driven by subvariants of concern but rather behavior,” she said.
People are opening up their social networks to gather for celebrations and family time. That’s unique to this winter, she said.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
Others point out that the surge doesn’t involve just COVID.
“We are expecting a Christmas surge and we are concerned it might be a triple surge,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University, Nashville, Tenn., referring to the rising cases of flu and RSV (respiratory syncytial virus).
Dr. Jetelina shares that concern, worrying that those illnesses may be what overwhelms hospital capacity.
Another wild card is the situation in China. With the easing of China’s “zero COVID” policies, cases there are rising dramatically. Some models are predicting up to 1 million COVID deaths could occur in China in 2023. (The United States is now requiring travelers from China to show a negative COVID test before entering. Italy and Japan have taken similar measures.)
“The suffering that is going to occur in China is not good news at all,” Dr. Topol said. “We are going to be seeing that for many weeks if not months ahead.”
Theoretically, uncontained spread such as what is expected there could generate a whole new family of variants, he said. But “the main hit is going to be in China,” he predicted. “But it’s hard to project with accuracy.”
“China is 20% of the global population, so we can’t ignore it,” Dr. Jetelina said. “The question is, what’s the probability of a subvariant of concern coming from China? I think the probability is pretty low, but the possibility is there.”
What happens with cases in China may “throw a wrench” in the transition from pandemic to endemic, Dr. Chin-Hong said. But even if the rising cases in China do result in a new variant, “there’s so much T cell and B cell immunity [here], your average person is still not going to get seriously ill, even if the variant looks really scary.”
Minimizing the damage
Experts echo the same advice on stemming the surge, especially for adults who are 65 or older: Get the bivalent booster, and get it now.
“The same with the influenza vaccine,” Dr. Schaffner said.
Both the booster vaccine and the flu vaccine have been underused this year, he said. “It’s part of the general vaccine fatigue.”
The low uptake of the booster vaccine is concerning, Dr. Topol said, especially among adults aged 65 and older, the age group most vulnerable to severe disease. Just 35.7% of U.S. adults 65 and older have gotten the booster, according to the CDC. Dr. Topol calls that a tragedy.
Younger people have not taken to the booster, either. Overall, only 14.1% of people aged 5 and up have gotten an updated booster dose, according to the CDC.
Recent studies find value in the boosters. One study looked only at adults age 65 or older, finding that the bivalent booster reduced the risk of hospitalization by 84% compared to someone not vaccinated, and 73% compared to someone who had received only the monovalent vaccine. Another study of adults found those who had gotten the bivalent were less likely to need COVID-related emergency room care or urgent care.
In a Dec. 21 report in the New England Journal of Medicine, researchers took plasma samples from people who had gotten either one or two monovalent boosters or the bivalent to determine how well they worked against the circulating Omicron subvariants BA.1, BA.5, BA.2.75.2, BQ.1.1, and XBB. The bivalent worked better than the monovalent against all the Omicron subvariants, but especially against BA.2.75.2, BQ.1.1, and XBB.
Rapid testing can help minimize transmission. On Dec. 15, the Biden administration announced its Winter Preparedness Plan, urging Americans to test before and after travel as well as indoor visiting with vulnerable individuals, providing another round of free at-home tests, continuing to make community testing available and continuing to provide vaccines.
Besides the general precautions, Dr. Schaffner suggested: “Look at yourself. Who are you? If you are older than 65, or have underlying illness or are immunocompromised, or are pregnant, please put your mask back on. And think about social distancing. It might be time to worship at home and stream a movie,” instead of going to the theaters, he said.
Back to mandates?
On Dec. 9, the New York City Commissioner of Health and Mental Hygiene urged a return to masking indoors, saying people “should” mask up, including in schools, stores, offices, and when in crowded outdoor settings.
On the same date, the County of Los Angeles Public Health urged a return to masking for everyone aged 2 and older when indoors, including at schools, in transit, or in work sites when around others.
While the CDC order requiring masks on public transportation is no longer in effect, the agency continues to recommend that those using public transportation do so.
But some are taking that further. In Philadelphia, for example, School Superintendent Tony B. Watlington Sr., EdD, announced before the winter break that indoor masking would be required for all students and staff for the first 2 weeks of school return, through Jan. 13, citing guidance from the Philadelphia Department of Public Health.
Universal masking in schools does reduce COVID transmission, as a study published in late November suggests. After Massachusetts dropped the statewide universal masking policy in public schools in February 2022, researchers compared the incidence of COVID in 70 school districts there that dropped the mandate with two school districts that kept it. In the 15 weeks after the policy was rescinded, the lifting of the mandate was linked with an additional 44.9 cases of COVID per 1,000 students and staff. That corresponded to an estimated 11,901 cases and to nearly 30% of the cases in all districts during that time.
That said, experts see mandates as the exception rather than the rule, at least for now, citing public backlash against mandates to mask or follow other restrictions.
“Mandating, we know, it shuts people off,” Dr. Topol said. “It’s unenforceable. If you have a very strong recommendation, that’s probably as good as you’re going to be able to do right now.”
There may be communities where mandates go over better than others, Dr. Schaffner said, such as communities where people have confidence in their public health authorities.
Glimmers of hope
Despite uncertainties, experts offered some not-so-dismal perspectives as well.
“I think our numbers will continue to go up, but certainly not like 2021 or 2020,” Dr. Chin-Hong said.
A version of this article first appeared on WebMD.com.
Medical practice gave 8,000 patients cancer for Christmas
We wish you a merry Christmas and a happy heart failure
Does anyone really like it when places of business send out cards or messages for the holidays? A card from a truly small family business is one thing, but when you start getting emails from multibillion dollar corporations, it feels a bit dishonest. And that’s not even mentioning the potential blowback when things go wrong.

Now, you may wonder how a company could possibly mess up something so simple. “We wish you a merry Christmas and a happy New Year.” Not that difficult. Unless you’re Askern Medical Practice in Doncaster, England. Instead of expressing a simple expression of joy for the holiday season, Askern informed all 8,000 of its patients that they had aggressive lung cancer with metastases and they needed to fill out a DS1500 form, which entitles terminal patients to certain benefits.
It only took an hour for Askern to recognize its mistake and send a second text apologizing and adding in the appropriate season’s greetings, but obviously the damage was done. Presumably patients who were last at the doctor to have their cold treated were able to shrug off the text, or simply didn’t see it before the correction came through, but obviously many patients had concerns directly related to cancer and panicked. They called in but were by and large unable to reach anyone at the practice. Some patients close by even went to center itself to clear things up.
One patient, Mr. Carl Chegwin, raised an excellent point about the debacle: “What if that message was meant for someone, and then they are told it’s a Christmas message, then again told, ‘Oh no, that was actually meant for you?’ ” The old double backtrack into yes, you actually do have cancer has got to be a candidate for worst Christmas gift of all. Yes, even worse than socks.
Genes know it: You are when you eat
There’s been a lot of recent research on intermittent fasting and what it can and can’t do for one’s health. Much of it has focused on participants’ metabolic rates, but a study just published in Cell Metabolism shows how time-restricted feeding (TRF) has an impact on gene expression, the process through which genes are activated and respond to their environment by creating proteins.

The research conducted by Satchidananda Panda, PhD, of the Salk Institute and his team involved two groups of mice, one with free access to food and the other with a daily 9-hour feeding window. Analysis of tissue samples collected from 22 organ groups revealed that nearly 80% of mouse genes responded to TRF. Interestingly, 40% of the genes in the hypothalamus, adrenal gland, and pancreas, which handle hormone regulation, were affected, suggesting that TRF could potentially aid in diabetes and stress disorder management, the investigators said in a written statement.
The researchers also found that TRF aligned the circadian rhythms of multiple organs of the body, which brings sleep into the picture. “Time-restricted eating synchronized the circadian rhythms to have two major waves: one during fasting, and another just after eating. We suspect this allows the body to coordinate different processes,” said Dr. Panda, whose previous research looked at TRF in firefighters, who typically work on shift schedules.
Time-restricted eating, it appears, affects gene expression throughout the body and allows interconnected organ systems to work smoothly. It’s not just about eating. Go figure.
This group practice reduced stress for everyone
It’s been awhile since we checked in on the good folks at Maharishi International University in Fairfield, Iowa – fictional home of the Fighting Transcendentalists [MAHARISHI RULES!] – but we just have to mention their long-term effort to reduce the national stress.

Way back in the year 2000, a group from MIU began practicing transcendental meditation. The size of the group increased over the next few years and eventually reached 1,725 in 2006. That number is important because it represents the square root of 1% of the U.S. population. When that “transition threshold was achieved,” the university explained in a written statement, “all stress indicators immediately started decreasing.”
By stress indicators they mean the U.S. stress index, the mean of eight variables – murder, rape, assault, robbery, infant mortality, drug deaths, vehicle fatalities, and child deaths by injuries – that the study investigators used to track the effectiveness of the meditation program, they said in the World Journal of Social Science.
After 2011, “when the size of the group size began to decline the rate of decrease in stress slowed and then it reversed and began to increase,” MIU reported.
Coauthor Dr. Kenneth Cavanaugh of MIU explained the process: “This study used state-of-the-art methods of time series regression analysis for eliminating potential alternative explanations due to intrinsic preexisting trends and fluctuations in the data. We carefully studied potential alternative explanations in terms of changes in economic conditions, political leadership, population demographics, and policing strategies. None of these factors could account for the results.”
Since we here at LOTME are serious professional journalists, the use of quotes means we are not making this up. Here’s one more thing in quotes: “A grant for 75 million dollars from the Howard and Alice Settle Foundation provided stipends for participants to be in the group and provided funding to bring several hundred visiting [meditation] experts from India to further augment the MIU group.”
Who needs to make up stuff? Not us.
We wish you a merry Christmas and a happy heart failure
Does anyone really like it when places of business send out cards or messages for the holidays? A card from a truly small family business is one thing, but when you start getting emails from multibillion dollar corporations, it feels a bit dishonest. And that’s not even mentioning the potential blowback when things go wrong.
Now, you may wonder how a company could possibly mess up something so simple. “We wish you a merry Christmas and a happy New Year.” Not that difficult. Unless you’re Askern Medical Practice in Doncaster, England. Instead of expressing a simple expression of joy for the holiday season, Askern informed all 8,000 of its patients that they had aggressive lung cancer with metastases and they needed to fill out a DS1500 form, which entitles terminal patients to certain benefits.
It only took an hour for Askern to recognize its mistake and send a second text apologizing and adding in the appropriate season’s greetings, but obviously the damage was done. Presumably patients who were last at the doctor to have their cold treated were able to shrug off the text, or simply didn’t see it before the correction came through, but obviously many patients had concerns directly related to cancer and panicked. They called in but were by and large unable to reach anyone at the practice. Some patients close by even went to center itself to clear things up.
One patient, Mr. Carl Chegwin, raised an excellent point about the debacle: “What if that message was meant for someone, and then they are told it’s a Christmas message, then again told, ‘Oh no, that was actually meant for you?’ ” The old double backtrack into yes, you actually do have cancer has got to be a candidate for worst Christmas gift of all. Yes, even worse than socks.
Genes know it: You are when you eat
There’s been a lot of recent research on intermittent fasting and what it can and can’t do for one’s health. Much of it has focused on participants’ metabolic rates, but a study just published in Cell Metabolism shows how time-restricted feeding (TRF) has an impact on gene expression, the process through which genes are activated and respond to their environment by creating proteins.
The research conducted by Satchidananda Panda, PhD, of the Salk Institute and his team involved two groups of mice, one with free access to food and the other with a daily 9-hour feeding window. Analysis of tissue samples collected from 22 organ groups revealed that nearly 80% of mouse genes responded to TRF. Interestingly, 40% of the genes in the hypothalamus, adrenal gland, and pancreas, which handle hormone regulation, were affected, suggesting that TRF could potentially aid in diabetes and stress disorder management, the investigators said in a written statement.
The researchers also found that TRF aligned the circadian rhythms of multiple organs of the body, which brings sleep into the picture. “Time-restricted eating synchronized the circadian rhythms to have two major waves: one during fasting, and another just after eating. We suspect this allows the body to coordinate different processes,” said Dr. Panda, whose previous research looked at TRF in firefighters, who typically work on shift schedules.
Time-restricted eating, it appears, affects gene expression throughout the body and allows interconnected organ systems to work smoothly. It’s not just about eating. Go figure.
This group practice reduced stress for everyone
It’s been awhile since we checked in on the good folks at Maharishi International University in Fairfield, Iowa – fictional home of the Fighting Transcendentalists [MAHARISHI RULES!] – but we just have to mention their long-term effort to reduce the national stress.
Way back in the year 2000, a group from MIU began practicing transcendental meditation. The size of the group increased over the next few years and eventually reached 1,725 in 2006. That number is important because it represents the square root of 1% of the U.S. population. When that “transition threshold was achieved,” the university explained in a written statement, “all stress indicators immediately started decreasing.”
By stress indicators they mean the U.S. stress index, the mean of eight variables – murder, rape, assault, robbery, infant mortality, drug deaths, vehicle fatalities, and child deaths by injuries – that the study investigators used to track the effectiveness of the meditation program, they said in the World Journal of Social Science.
After 2011, “when the size of the group size began to decline the rate of decrease in stress slowed and then it reversed and began to increase,” MIU reported.
Coauthor Dr. Kenneth Cavanaugh of MIU explained the process: “This study used state-of-the-art methods of time series regression analysis for eliminating potential alternative explanations due to intrinsic preexisting trends and fluctuations in the data. We carefully studied potential alternative explanations in terms of changes in economic conditions, political leadership, population demographics, and policing strategies. None of these factors could account for the results.”
Since we here at LOTME are serious professional journalists, the use of quotes means we are not making this up. Here’s one more thing in quotes: “A grant for 75 million dollars from the Howard and Alice Settle Foundation provided stipends for participants to be in the group and provided funding to bring several hundred visiting [meditation] experts from India to further augment the MIU group.”
Who needs to make up stuff? Not us.
We wish you a merry Christmas and a happy heart failure
Does anyone really like it when places of business send out cards or messages for the holidays? A card from a truly small family business is one thing, but when you start getting emails from multibillion dollar corporations, it feels a bit dishonest. And that’s not even mentioning the potential blowback when things go wrong.
Now, you may wonder how a company could possibly mess up something so simple. “We wish you a merry Christmas and a happy New Year.” Not that difficult. Unless you’re Askern Medical Practice in Doncaster, England. Instead of expressing a simple expression of joy for the holiday season, Askern informed all 8,000 of its patients that they had aggressive lung cancer with metastases and they needed to fill out a DS1500 form, which entitles terminal patients to certain benefits.
It only took an hour for Askern to recognize its mistake and send a second text apologizing and adding in the appropriate season’s greetings, but obviously the damage was done. Presumably patients who were last at the doctor to have their cold treated were able to shrug off the text, or simply didn’t see it before the correction came through, but obviously many patients had concerns directly related to cancer and panicked. They called in but were by and large unable to reach anyone at the practice. Some patients close by even went to center itself to clear things up.
One patient, Mr. Carl Chegwin, raised an excellent point about the debacle: “What if that message was meant for someone, and then they are told it’s a Christmas message, then again told, ‘Oh no, that was actually meant for you?’ ” The old double backtrack into yes, you actually do have cancer has got to be a candidate for worst Christmas gift of all. Yes, even worse than socks.
Genes know it: You are when you eat
There’s been a lot of recent research on intermittent fasting and what it can and can’t do for one’s health. Much of it has focused on participants’ metabolic rates, but a study just published in Cell Metabolism shows how time-restricted feeding (TRF) has an impact on gene expression, the process through which genes are activated and respond to their environment by creating proteins.
The research conducted by Satchidananda Panda, PhD, of the Salk Institute and his team involved two groups of mice, one with free access to food and the other with a daily 9-hour feeding window. Analysis of tissue samples collected from 22 organ groups revealed that nearly 80% of mouse genes responded to TRF. Interestingly, 40% of the genes in the hypothalamus, adrenal gland, and pancreas, which handle hormone regulation, were affected, suggesting that TRF could potentially aid in diabetes and stress disorder management, the investigators said in a written statement.
The researchers also found that TRF aligned the circadian rhythms of multiple organs of the body, which brings sleep into the picture. “Time-restricted eating synchronized the circadian rhythms to have two major waves: one during fasting, and another just after eating. We suspect this allows the body to coordinate different processes,” said Dr. Panda, whose previous research looked at TRF in firefighters, who typically work on shift schedules.
Time-restricted eating, it appears, affects gene expression throughout the body and allows interconnected organ systems to work smoothly. It’s not just about eating. Go figure.
This group practice reduced stress for everyone
It’s been awhile since we checked in on the good folks at Maharishi International University in Fairfield, Iowa – fictional home of the Fighting Transcendentalists [MAHARISHI RULES!] – but we just have to mention their long-term effort to reduce the national stress.
Way back in the year 2000, a group from MIU began practicing transcendental meditation. The size of the group increased over the next few years and eventually reached 1,725 in 2006. That number is important because it represents the square root of 1% of the U.S. population. When that “transition threshold was achieved,” the university explained in a written statement, “all stress indicators immediately started decreasing.”
By stress indicators they mean the U.S. stress index, the mean of eight variables – murder, rape, assault, robbery, infant mortality, drug deaths, vehicle fatalities, and child deaths by injuries – that the study investigators used to track the effectiveness of the meditation program, they said in the World Journal of Social Science.
After 2011, “when the size of the group size began to decline the rate of decrease in stress slowed and then it reversed and began to increase,” MIU reported.
Coauthor Dr. Kenneth Cavanaugh of MIU explained the process: “This study used state-of-the-art methods of time series regression analysis for eliminating potential alternative explanations due to intrinsic preexisting trends and fluctuations in the data. We carefully studied potential alternative explanations in terms of changes in economic conditions, political leadership, population demographics, and policing strategies. None of these factors could account for the results.”
Since we here at LOTME are serious professional journalists, the use of quotes means we are not making this up. Here’s one more thing in quotes: “A grant for 75 million dollars from the Howard and Alice Settle Foundation provided stipends for participants to be in the group and provided funding to bring several hundred visiting [meditation] experts from India to further augment the MIU group.”
Who needs to make up stuff? Not us.